turkish journal of physiotherapy and rehabilitation
TRANSCRIPT

Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17617
A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF
MASHA TAILA AND KARPASASTHYADI TAILA NASYA IN THE
MANAGEMENT OF PAKSHAGHATA.
Dr. Shipra Raheja1, Dr. Maitree Patel2, Dr. Ravi Pandya3, Dr.Dhimant Bhatta4 1Assi. Proof of Mahayogi Gorakhnath Vishva Vidhyalay, Gorakhpur 2Assi.Proff of Parul Ayurveda Hospital ,Parul university, Vadodara 3Assi.Proff of Parul Ayurveda Hospital ,Parul university, Vadodara
4Assi.Proff. G.J Patel Ayurveda Hospital, New Vvvngr.
ABSTRACT
Pakshaghatha is included under the Mahagadha and is an intricate disease to cure. According to National Stroke
Association, Stroke is one of the leading causes of long term disability in the elderly. An effective treatment
for the same is being searched for even today. Nasya is one of the treatment modality in Pakshaghatha. Nasya
is a simple method of treatment mentioned for many disorders and is considered effective in Vatavyadhi. Same
is being tried with sincere effort herein.
Objective of the study:
1. To evaluate the efficacy of Masha Taila Nasya in management of Pakshaghata.
2. To evaluate the efficacy of Karpasasthi Taila Nasya in management of Pakshaghata.
3. To study the comparative effect of Masha Taila over Karpasthyadi Taila.
The method followed was a randomized study. A special Performa was prepared with all points of history
taking, examination to confirm the diagnosis as mentioned in our classics and allied sciences. Patients were
randomly selected. Nasya is a therapy in which the medicinal oil is instilled in both the nostrils. The oil was
prepared in the Parul Ayurved pharmacy with the decoction method. Significant improvement was seen in
terms of gross movements. The study revealed that Nasya will help immensely to the patients suffering from
Pakshaghatha.
Key words: Pakshaghatha, Nasya, Masha, Karpasasthyadi.
I. INTRODUCTION:
Health and ailing, pleasure and pain, ease and disease are inborn properties of human life, centuries and centuries
succeeded in struggle between man and disease.
Ayurveda is a rich storehouse of time tested and effective methods for the treatment of several obstinate and
incurable diseases. Ayurveda has its own independent and practicable principles which can never be substituted by
other systems of medicines. Ayurveda is one among the most ancient medical sciences of the world. It conceives
and describes the basis & applied aspect of life process, health, disease & its management in terms of its own
principles & approaches.
Panchakarma is the most effectual and confirmatory therapy which ensuresthe disease does not persist. In Ayurveda
Pakshaghata is considered as one among the Vata vyadhi, which is considered Mahagada or Duschikitsya. Hence
an energetic and step by step approach towards the management of this disease is taken up in the classics like-
“Snehana, Swedana, Mrudu virechana, Basti, Nasya, Mastiskya”.
Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17618
Globally, Cerebrovascular disease (stroke) is the second leading cause of death.1 It is a disease that predominantly
occurs in mid-age and older adults. WHO estimated that in 2005, stroke accounted for 5.7 million deaths
worldwide, equivalent to 9.9 % of all death. Over 85% of these deaths will have occurred in people living in low
and middle income countries and one third will be in people aged less than 70 years. (www.WHO.htm). It is
surprising that (for stroke) no treatment exists that has been conclusively shown to reduce the risk of death or
disability. Despite a massive worldwide effort to rectify this early results are disappointing (Philip MW Bath, 1995).
The rate of recovery of all impairments is maximal in the first few weeks, slows down after 2 or 3 months, and
probably stops at about 6-12 months post stroke (Meerwald 1983; Wade, Wood and Langdon Hewer 1985; Wade
and Langdon Hewer 1987; Wade, Wood and Langdon Hewer 1988).Being a Vatavyadhi Pakshaghata is a
Maharoga. Its Samprapti evolves in Shira (head), which is a Mahamarma. Due to this devastating and refractory
nature of Pakshaghata a minimum course of three months of appropriate treatment is recommended by Sushruta
(Chi.4).
Aacharya Charaka, declared Pakshaghata incurable if not intervened in the early stage (Ch.Chi.28/73).
Shosha of Sira and Snayu, which is the most important event in the Samprapti, denotes craving for Brihana therapy.
Being an obstinate Vata disorder Pakshaghata demands a pioneer treatment of Vata.Pakshaghata, most of the times
is presented when it ventures in Yapya or Asadhya stage. This makes it difficult to treat it with the anticipation of
complete cure.
II. MATERIALS AND METHODS:
Aim of the study:
To evaluate the efficacy of Masha taila and Karpasasthyadi taila Nasya in the management of Pakshaghata.
Inclusion Criteria
Diagnosed case of Pakshaghata Patients between age group of 18 to 70 years.
Patients from both gender.
Patients presenting with clinical signs and symptoms of Pakshaghata.
Ischaemic patients with stable vitals and up to 5years.
Exclusion Criteria:
Patients with uncontrolled metabolic disorders and other systemic disorders.
Unconscious patients.
Paralysis complicated with heart disease.
Intracranial infections.
Hemorrhagic patients also if in acute condition.
Laboratry Investigations:
Hb, TLC, DLC, ESR (before treatment)
Urine (routine & micro)
Design:
It is a randomized clinical study with a pre-test and post-test design. In this study 30 patients diagnosed with
Pakshaghata of either gender were subjected to clinical study.
Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17619
PLAN OF TREATMENT:
Purva Karma – Abyanga of neck, face with tila taila, Tapa Sveda(mrudu) with cloth dipped in hot water will be
done for 10 minutes.
Pradhana Karma –
Position of the Patient:- supine with head endlowered.
Taila is slightly warmed indirectly with the help of hot waterbath.
8 drops of selected Taila is instilled in eachnostril.
Soles, palms, neck and ears aremassaged
Secretions are spittedout.
Paschat Karma – Haridra dhumapana and kavala with sukhoshna jala.
Total Duration – 21 consecutive Days.
Follow up Study: 15 days after completion of Nasya Karma
ASSESSMENT CRITERIA
Subjective & Objective Parameters include the clinical grading and standard scoring method of signs and symptoms
of the condition. These data were collected before the initiation of the treatment & after the completion of 21 days
of treatment.
Subjective Parameters:
Dakshin or Vama Paksha Chesta Nivriti (Hemiplegia)
Hasta Pada Sankoch (Stiffness of extremities)
Vak Stambha (Utter voice)
Objective Criteria (Hemispheric stroke scale)
Motor Dysfunction
Sensory Dysfunction
Cranial Nerve Dysfunction.
Autonomic Nerve Dysfunction
Visual fields
Test clinically and score hemi-field loss as:
3 = Severe loss; inability to recognize moving hand, no response to threat
2 = Moderate loss; inability to recognize stationary finger, sees moving finger
1 = Mild loss: defect to double simultaneous stimulation
0 = Normal
Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17620
Facial expression
Score movement:
3 = Severe weakness;drooling
2 = Moderate loss; asymmetry at rest
1 = Mild weakness; asymmetry on smiling
0 = Normal
MOTOR FUNCTION
Arm, proximal
Arm, distal
Leg, proximal
Leg, distal
All scored 0-7 as:
7 = No movement (MRC 0)
6 = Trace movement only (MRC 1)
5 = Motion without gravity only (MRC 2)
4 = Moves against gravity but not against resistance (MRC 3)
3 = Moderate weakness (MRC 4 -)
2 = Mild weakness (MRC 4)
1 = Positive drift of arm/leg (MRC 4 +)
0 = Normal (MRC 5)
Deep tendon reflexes
2 = Hypoactive or hyperactive
0 = Normal
Pathologic reflexes
2 = Babinski (plantar) and another abnormal
1 = Babinski (plantar) or another abnormal
0 = Normal
Muscle tone
2 = Increased or decreased
0 = Normal
Gait
Test ability to stand and walk, and score:
Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17621
6 = Unable to stand unsupported or cannot evaluate
5 = Can stand with support but cannot walk
4 = Severely abnormal; walking distance limited even with support (from aid or person)
3 = Moderately abnormal; no assistance required (apart from a stick/cane), but distance limited
2 = Mildly abnormal (weak, uncoordinated); can walk independently but slowly
1 = Minimally abnormal, no reduction in speed or distance
0 = Normal
SENSORY
Primary modalities (of affected side only),
Test touch, pain and score as
4 = Anesthesia
3 = Severe hypaesthesia
2 = Moderate hypaesthesia or deficit only; or extinction to double simultaneous stimulation
1 = Mild hypaesthesia or dysaesthesia
0 = Normal
(Reference: Hemispheric stroke scale.)
Assessment of NasyaKarma:
Samyak Yoga, Ayoga & Atiyoga Yoga Lakshanas of NasyaKarma were assessed daily after the procedure.
Lakshana Day 1 7 14 21 FU
Shiro laghva
Sukha swapn
Vikara prash
Sukhucchwas
Swapnabodha
III. OBSERVATION:
A total of known case of 30 patients of Pakshaghata, fulfilling the inclusion criteria were taken for
thestudy.Observations as well as results of the therapy are analyzed below.
1. Age wise distribution: The minimum age of the patient of this study was 20 years & maximum was 70 years.
Table shows that nature of distribution of patients in every 4-years age group. The maximum percentage of
patients i.e. (26.7%) was between 36-40 age groups and minimum 3.3% was between 20-25 age groups. And
5 (i.e. 16.7%) were between 51-65 years of age and 13.3% were between the age group of 41-45.
2. Religion wise distribution of the patients: The maximum no. of patients were from Hindu community i.e.
90% and minimum no. of patients were from Muslim community i.e. 3 (10%)
3. Education wise distribution of the patients: Among all the selected 30 patients maximum percentage of
patients were uneducated (46.7%), where as only 3.3% of patient has done graduation and 20% of patients have
completed their middle school education. 5 out of 30 i.e. 16.7% have done high schooling.
Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17622
4. Gender wise distribution of the patients: Out of the selected 30 patients, maximum no. of patients were male
i.e. 24(80%) and 20% of the patients were female.
5. Marital status wise distribution of the patients:Out of the total 30 patients 80 % of the patients were married
and 6 out of 30 were unmarried i.e. 20% of the total no. of patients.
6. Socio economic status wise distribution of the patients :Maximum no. of patients were poor i.e. 50%
patients were poor and 16.7% of the patients were from very poor socioeconomic status. 10 out of 30 patients
(33.3%) were middle class
7. Residential status wise distribution of the patients: Maximum no. of patients was from urban residential
area i.e. 18 out of 30 (60%). Minimum no. of patients was from rural area, 12 patients out of 30 (40%)
8. Occupation wise distribution of the Patients:Maximum patients were from the labor class and from
agriculture field i.e.30% of the total patients and 8 out of 30 patients were house holder i.e. 26.7% and 13.3%
of the patients were professional or employee.
9. Part of the body affected wise distribution:Maximum no. of patients were having the complaint of right side
hemiplegia i.e. 36.7% and 63.3% of patients were having the complaint of lt. side hemiplegia.
10. Classification according to vaka stambha:33.3% of the patients were having normal speech while 66.7 % of
the patients had difficulty in utring words
11. Classification according to Karma Hani:33.3% of the patients had complete loss of function and 66.7 % of
the patients had partial loss of function.
12. Classification according to facial expressions :Out of 30 patients 1 patient had normal facial expression
i.e.3.3% and 13.3% of the patients had mild weakness, 66.7% of the patients had moderate weakness while
16.7% of the patients had severe weakness with drooling.
13. Classification according to Dysarthria:40% of the patients had moderate dysarthria , 40% had severe
dysarthria , 20% of the patients were normal.
14. Distribution according to range of motion Arm (Proximal movement) 6.7% of the patients had mild
weakness of the hands, 26.7% of the patients had moderate weakness, 30% of the patients can move the arm
against the gravity and 16.7% cannot move against the gravity, 10% of the patients had trace movement of the
arm and 10% had no movement.
15. (Distal movement):20% of the patients had mild weakness in the distal movement of arm, 16.7% had moderate
weakness, 33.3 % can move the arm against gravity and 13.3% can move without gravity, 6.7% patients had
trace movement only and 10% had no movement.
16. Movement of leg:(Proximal movement) 20 % of the patients had mild weakness in the proximal movement of
leg and 50% had moderate weakness, 13.3% can move the leg against gravity and 6.7% cannot move without
gravity. 10% patients had no movement.
17. Pathological reflex :13.3% patients had normal reflexes, 10% patients had Babinski or other reflexes normal
and 23% had Babinski and other reflexes abnormal.
18. Muscle tone :100% of the patients had increased or decreased muscle tone.
19. Gait wise distribution:40 % patients had mildly abnormal gait i.e. they can walk independently but slowly,
33.3% patients had moderately abnormal gait, walking distance was limited even with support, 13.3% can walk
limited distance even with support, 3.3% patients can stand with support but cannot walk, 10% of the patients
were unable to stand.
20. Koshta wise distribution of the patients:Out of 30 patients 3 were of mridu kostha i.e. 10%patients were of
mridu koshtha, and 53.3% pts were of madhyama koshta and 36.7% were of kroora koshta.
Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17623
21. Distribution of patients according to family history:Out of total no. of 30 patients 26.7% were having the
family history of hypertension and 73.3% patients were having the family history of diabetes.
22. Distribution of patients according to the Aahara:The present study shows that maximum no. of patients
were having vegetarian diet (73.3%) whereas 26.7% of the patients were having mixed diet.
23. Classification of patients based on bowel :Study shows that maximum patients (66.7%) were having regular
bowel habits, 23.3% patients were having irregular bowel habits. 3 out of 30 patients i.e.10% were having the
problem of constipation.
24. Classification of patients according to addiction:The study shows that 60% of patients were not having any
addiction. 13.3% of the patients were having the addiction of smoking. 5 out of 30 patients i.e. 16.7% of patients
were alcoholic, 10% patients were addicted to tobacco chewing.
25. Classification of patients according to the treatment history:Study shows that maximum patients were
taking antihypertensive drugs 83.3% and 16.7% of patients were taking Ayurvedic medicine, Ayurvedic
medicine were stopped during the course of treatment.
26. Vyayam shakti wise distribution of the patients :3.3% of the patients had pravara vyayam shakti, 56.7% had
madhyama vyayam shakti, 40.3% had avara vyayam shakti.
27. Classification of patients according to the shabad pariksha:Study shows that 60% patients were having
vaikrut swara and 40% patients were having prakrut swara.
28. Classification of patients according to the sparsha pariksha :Study shows that 53.3% patients were having
ushna sparsha and 46.7% patients were having sheeta.
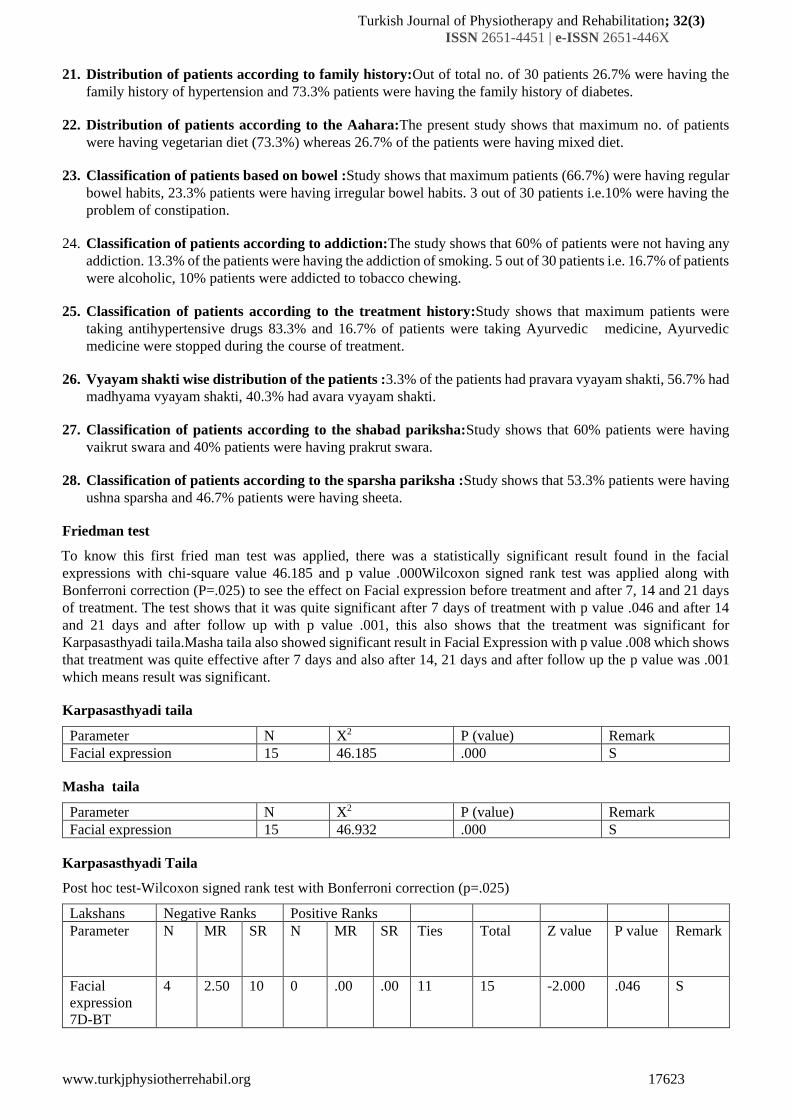
Friedman test
To know this first fried man test was applied, there was a statistically significant result found in the facial
expressions with chi-square value 46.185 and p value .000Wilcoxon signed rank test was applied along with
Bonferroni correction (P=.025) to see the effect on Facial expression before treatment and after 7, 14 and 21 days
of treatment. The test shows that it was quite significant after 7 days of treatment with p value .046 and after 14
and 21 days and after follow up with p value .001, this also shows that the treatment was significant for
Karpasasthyadi taila.Masha taila also showed significant result in Facial Expression with p value .008 which shows
that treatment was quite effective after 7 days and also after 14, 21 days and after follow up the p value was .001
which means result was significant.
Karpasasthyadi taila
Parameter N X2 P (value) Remark
Facial expression 15 46.185 .000 S
Masha taila
Parameter N X2 P (value) Remark
Facial expression 15 46.932 .000 S
Karpasasthyadi Taila
Post hoc test-Wilcoxon signed rank test with Bonferroni correction (p=.025)
Lakshans Negative Ranks Positive Ranks
Parameter N MR SR N MR SR Ties Total Z value P value Remark
Facial
expression
7D-BT
4 2.50 10 0 .00 .00 11 15 -2.000 .046 S
Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17624
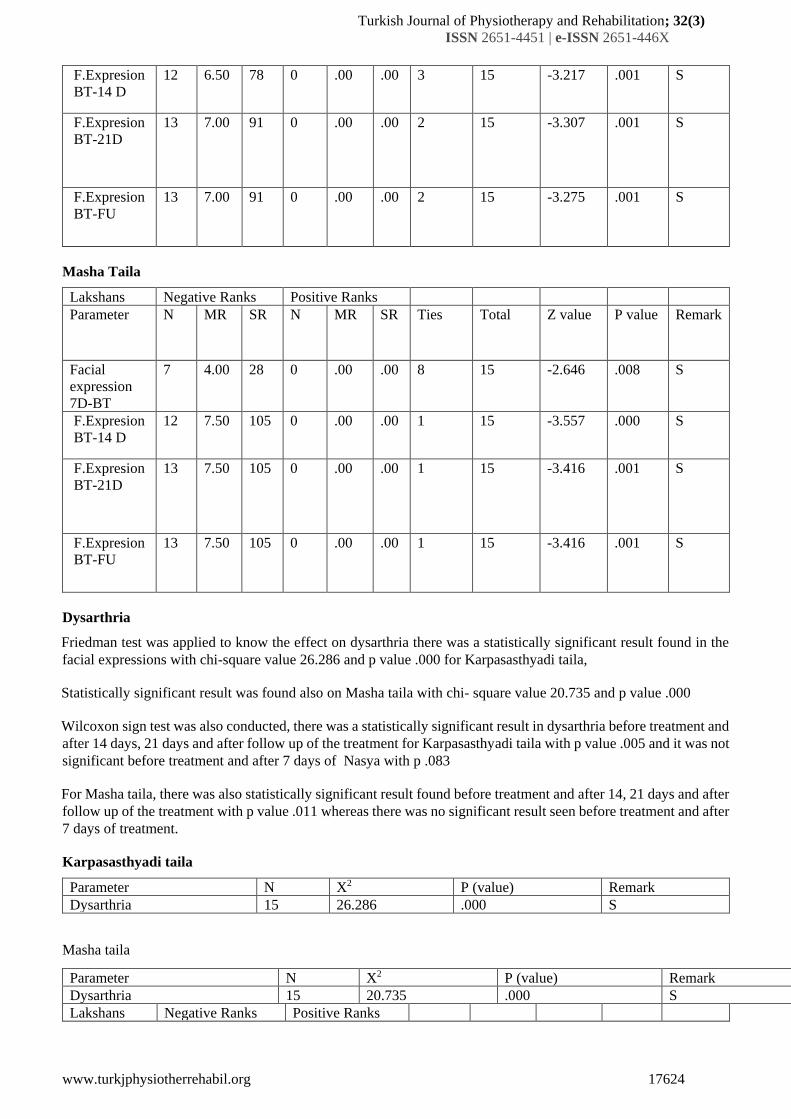
F.Expresion
BT-14 D
12 6.50 78 0 .00 .00 3 15 -3.217 .001 S
F.Expresion
BT-21D
13 7.00 91 0 .00 .00 2 15 -3.307 .001 S
F.Expresion
BT-FU
13 7.00 91 0 .00 .00 2 15 -3.275 .001 S
Masha Taila
Lakshans Negative Ranks Positive Ranks
Parameter N MR SR N MR SR Ties Total Z value P value Remark
Facial
expression
7D-BT
7 4.00 28 0 .00 .00 8 15 -2.646 .008 S
F.Expresion
BT-14 D
12 7.50 105 0 .00 .00 1 15 -3.557 .000 S
F.Expresion
BT-21D
13 7.50 105 0 .00 .00 1 15 -3.416 .001 S
F.Expresion
BT-FU
13 7.50 105 0 .00 .00 1 15 -3.416 .001 S
Dysarthria
Friedman test was applied to know the effect on dysarthria there was a statistically significant result found in the
facial expressions with chi-square value 26.286 and p value .000 for Karpasasthyadi taila,
Statistically significant result was found also on Masha taila with chi- square value 20.735 and p value .000
Wilcoxon sign test was also conducted, there was a statistically significant result in dysarthria before treatment and
after 14 days, 21 days and after follow up of the treatment for Karpasasthyadi taila with p value .005 and it was not
significant before treatment and after 7 days of Nasya with p .083
For Masha taila, there was also statistically significant result found before treatment and after 14, 21 days and after
follow up of the treatment with p value .011 whereas there was no significant result seen before treatment and after
7 days of treatment.
Karpasasthyadi taila
Parameter N X2 P (value) Remark
Dysarthria 15 26.286 .000 S
Masha taila
Parameter N X2 P (value) Remark
Dysarthria 15 20.735 .000 S
Lakshans Negative Ranks Positive Ranks
Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17625
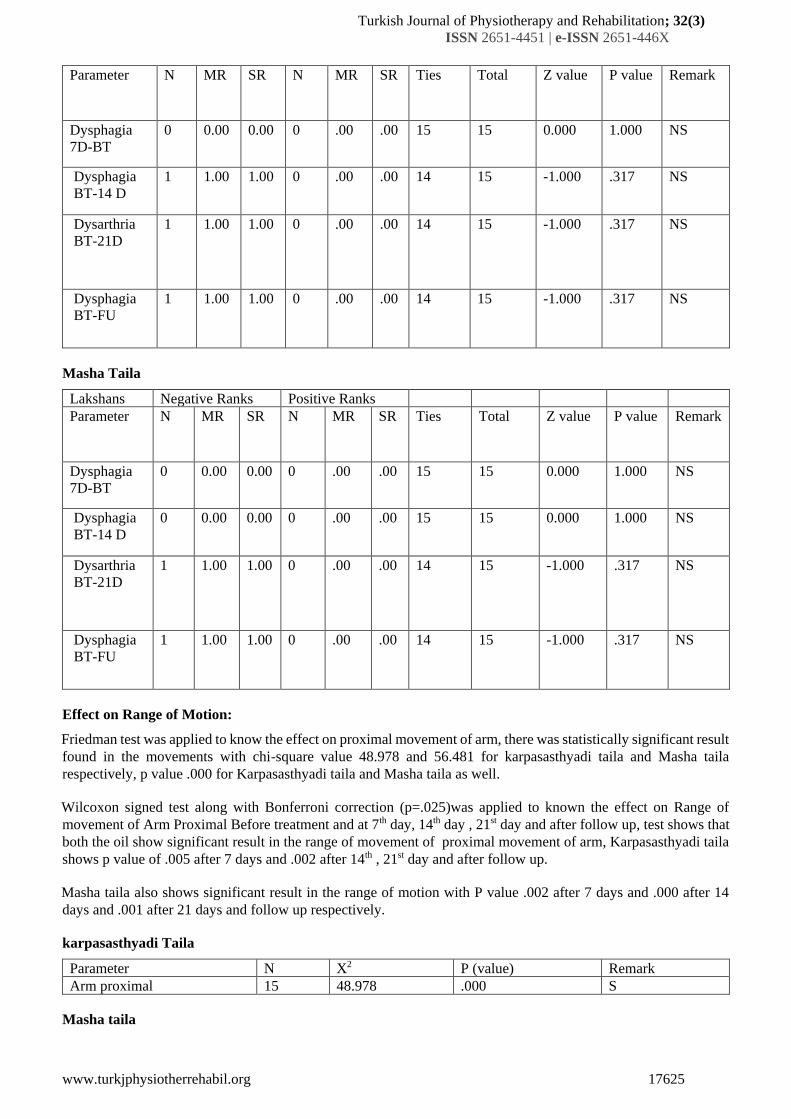
Parameter N MR SR N MR SR Ties Total Z value P value Remark
Dysphagia
7D-BT
0 0.00 0.00 0 .00 .00 15 15 0.000 1.000 NS
Dysphagia
BT-14 D
1 1.00 1.00 0 .00 .00 14 15 -1.000 .317 NS
Dysarthria
BT-21D
1 1.00 1.00 0 .00 .00 14 15 -1.000 .317 NS
Dysphagia
BT-FU
1 1.00 1.00 0 .00 .00 14 15 -1.000 .317 NS
Masha Taila
Lakshans Negative Ranks Positive Ranks
Parameter N MR SR N MR SR Ties Total Z value P value Remark
Dysphagia
7D-BT
0 0.00 0.00 0 .00 .00 15 15 0.000 1.000 NS
Dysphagia
BT-14 D
0 0.00 0.00 0 .00 .00 15 15 0.000 1.000 NS
Dysarthria
BT-21D
1 1.00 1.00 0 .00 .00 14 15 -1.000 .317 NS
Dysphagia
BT-FU
1 1.00 1.00 0 .00 .00 14 15 -1.000 .317 NS
Effect on Range of Motion:
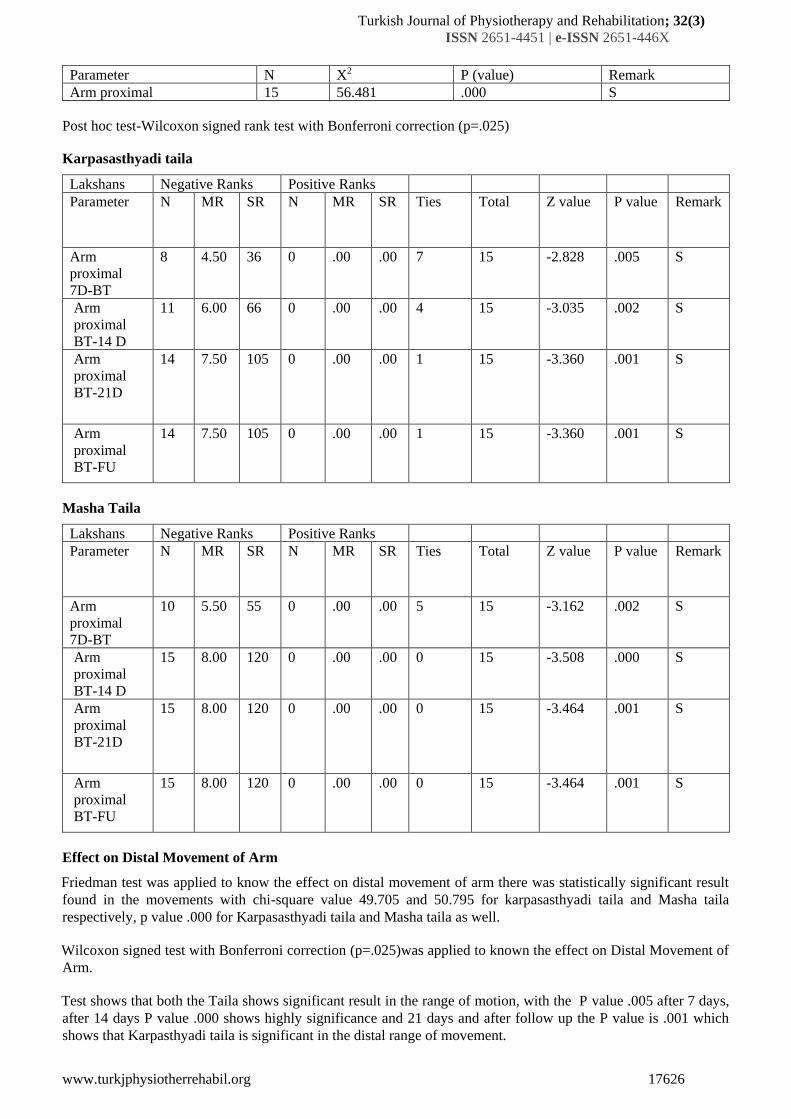
Friedman test was applied to know the effect on proximal movement of arm, there was statistically significant result
found in the movements with chi-square value 48.978 and 56.481 for karpasasthyadi taila and Masha taila
respectively, p value .000 for Karpasasthyadi taila and Masha taila as well.
Wilcoxon signed test along with Bonferroni correction (p=.025)was applied to known the effect on Range of
movement of Arm Proximal Before treatment and at 7th day, 14th day , 21st day and after follow up, test shows that
both the oil show significant result in the range of movement of proximal movement of arm, Karpasasthyadi taila
shows p value of .005 after 7 days and .002 after 14th , 21st day and after follow up.
Masha taila also shows significant result in the range of motion with P value .002 after 7 days and .000 after 14
days and .001 after 21 days and follow up respectively.
karpasasthyadi Taila
Parameter N X2 P (value) Remark
Arm proximal 15 48.978 .000 S
Masha taila
Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17626
Parameter N X2 P (value) Remark
Arm proximal 15 56.481 .000 S
Post hoc test-Wilcoxon signed rank test with Bonferroni correction (p=.025)
Karpasasthyadi taila
Lakshans Negative Ranks Positive Ranks
Parameter N MR SR N MR SR Ties Total Z value P value Remark
Arm
proximal
7D-BT
8 4.50 36 0 .00 .00 7 15 -2.828 .005 S
Arm
proximal
BT-14 D
11 6.00 66 0 .00 .00 4 15 -3.035 .002 S
Arm
proximal
BT-21D
14 7.50 105 0 .00 .00 1 15 -3.360 .001 S
Arm
proximal
BT-FU
14 7.50 105 0 .00 .00 1 15 -3.360 .001 S
Masha Taila
Lakshans Negative Ranks Positive Ranks
Parameter N MR SR N MR SR Ties Total Z value P value Remark
Arm
proximal
7D-BT
10 5.50 55 0 .00 .00 5 15 -3.162 .002 S
Arm
proximal
BT-14 D
15 8.00 120 0 .00 .00 0 15 -3.508 .000 S
Arm
proximal
BT-21D
15 8.00 120 0 .00 .00 0 15 -3.464 .001 S
Arm
proximal
BT-FU
15 8.00 120 0 .00 .00 0 15 -3.464 .001 S
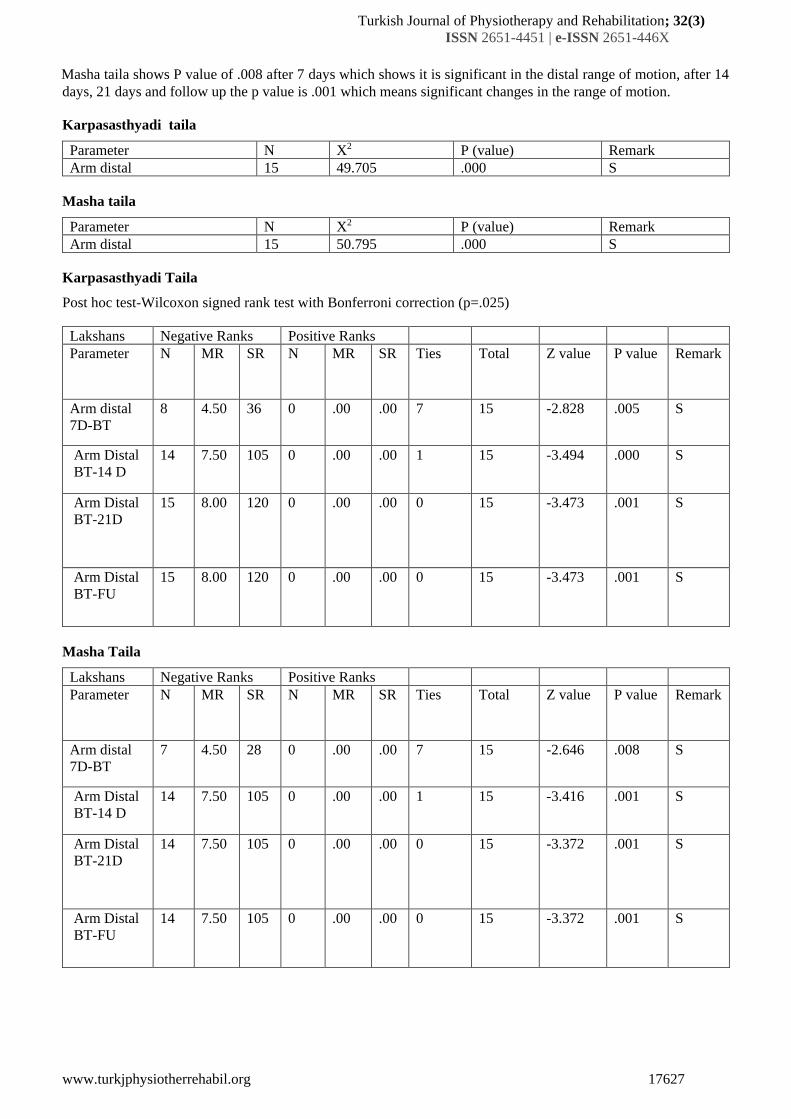
Effect on Distal Movement of Arm
Friedman test was applied to know the effect on distal movement of arm there was statistically significant result
found in the movements with chi-square value 49.705 and 50.795 for karpasasthyadi taila and Masha taila
respectively, p value .000 for Karpasasthyadi taila and Masha taila as well.
Wilcoxon signed test with Bonferroni correction (p=.025)was applied to known the effect on Distal Movement of
Arm.
Test shows that both the Taila shows significant result in the range of motion, with the P value .005 after 7 days,
after 14 days P value .000 shows highly significance and 21 days and after follow up the P value is .001 which
shows that Karpasthyadi taila is significant in the distal range of movement.
Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17627
Masha taila shows P value of .008 after 7 days which shows it is significant in the distal range of motion, after 14
days, 21 days and follow up the p value is .001 which means significant changes in the range of motion.
Karpasasthyadi taila
Parameter N X2 P (value) Remark
Arm distal 15 49.705 .000 S
Masha taila
Parameter N X2 P (value) Remark
Arm distal 15 50.795 .000 S
Karpasasthyadi Taila
Post hoc test-Wilcoxon signed rank test with Bonferroni correction (p=.025)
Lakshans Negative Ranks Positive Ranks
Parameter N MR SR N MR SR Ties Total Z value P value Remark
Arm distal
7D-BT
8 4.50 36 0 .00 .00 7 15 -2.828 .005 S
Arm Distal
BT-14 D
14 7.50 105 0 .00 .00 1 15 -3.494 .000 S
Arm Distal
BT-21D
15 8.00 120 0 .00 .00 0 15 -3.473 .001 S
Arm Distal
BT-FU
15 8.00 120 0 .00 .00 0 15 -3.473 .001 S
Masha Taila
Lakshans Negative Ranks Positive Ranks
Parameter N MR SR N MR SR Ties Total Z value P value Remark
Arm distal
7D-BT
7 4.50 28 0 .00 .00 7 15 -2.646 .008 S
Arm Distal
BT-14 D
14 7.50 105 0 .00 .00 1 15 -3.416 .001 S
Arm Distal
BT-21D
14 7.50 105 0 .00 .00 0 15 -3.372 .001 S
Arm Distal
BT-FU
14 7.50 105 0 .00 .00 0 15 -3.372 .001 S
Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17628
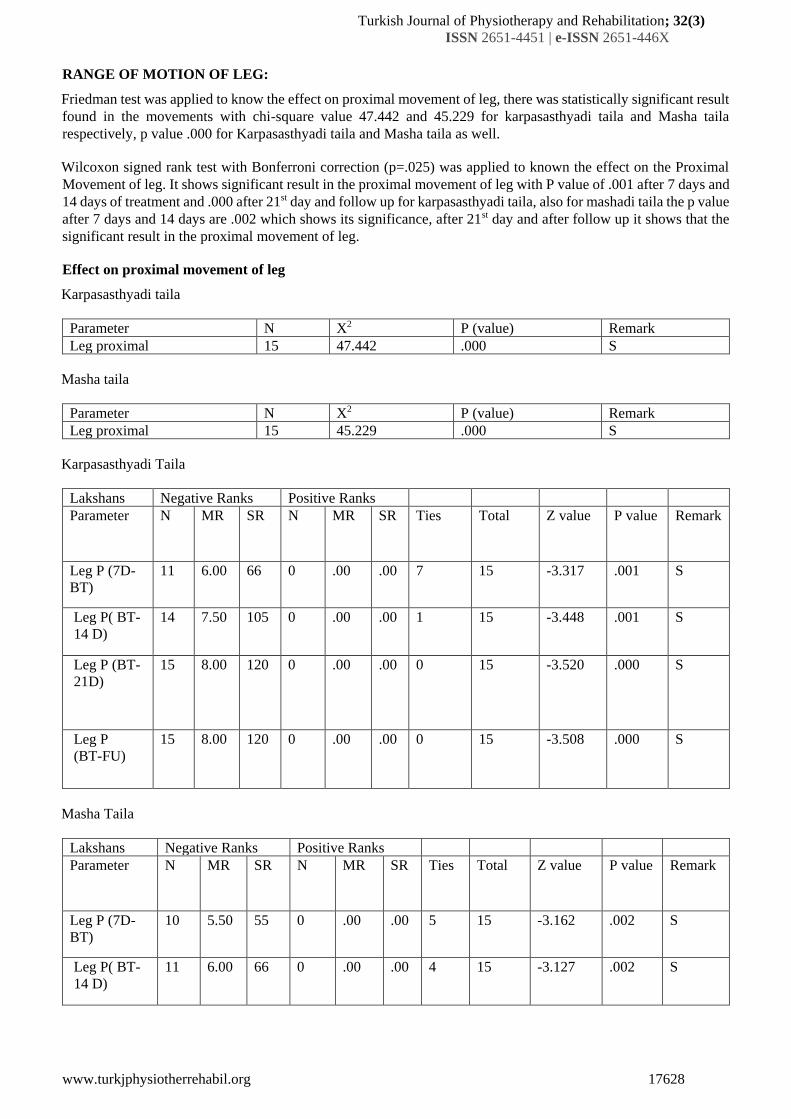
RANGE OF MOTION OF LEG:
Friedman test was applied to know the effect on proximal movement of leg, there was statistically significant result
found in the movements with chi-square value 47.442 and 45.229 for karpasasthyadi taila and Masha taila
respectively, p value .000 for Karpasasthyadi taila and Masha taila as well.
Wilcoxon signed rank test with Bonferroni correction (p=.025) was applied to known the effect on the Proximal
Movement of leg. It shows significant result in the proximal movement of leg with P value of .001 after 7 days and
14 days of treatment and .000 after 21st day and follow up for karpasasthyadi taila, also for mashadi taila the p value
after 7 days and 14 days are .002 which shows its significance, after 21st day and after follow up it shows that the
significant result in the proximal movement of leg.
Effect on proximal movement of leg
Karpasasthyadi taila
Parameter N X2 P (value) Remark
Leg proximal 15 47.442 .000 S
Masha taila
Parameter N X2 P (value) Remark
Leg proximal 15 45.229 .000 S
Karpasasthyadi Taila
Lakshans Negative Ranks Positive Ranks
Parameter N MR SR N MR SR Ties Total Z value P value Remark
Leg P (7D-
BT)
11 6.00 66 0 .00 .00 7 15 -3.317 .001 S
Leg P( BT-
14 D)
14 7.50 105 0 .00 .00 1 15 -3.448 .001 S
Leg P (BT-
21D)
15 8.00 120 0 .00 .00 0 15 -3.520 .000 S
Leg P
(BT-FU)
15 8.00 120 0 .00 .00 0 15 -3.508 .000 S
Masha Taila
Lakshans Negative Ranks Positive Ranks
Parameter N MR SR N MR SR Ties Total Z value P value Remark
Leg P (7D-
BT)
10 5.50 55 0 .00 .00 5 15 -3.162 .002 S
Leg P( BT-
14 D)
11 6.00 66 0 .00 .00 4 15 -3.127 .002 S
Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17629
Leg P (BT-
21D)
13 7.00 91 0 .00 .00 2 15 -3.307 .001 S
Leg P ( BT-
FU)
13 7.00 91 0 .00 .00 2 15 -3.307 .001 S
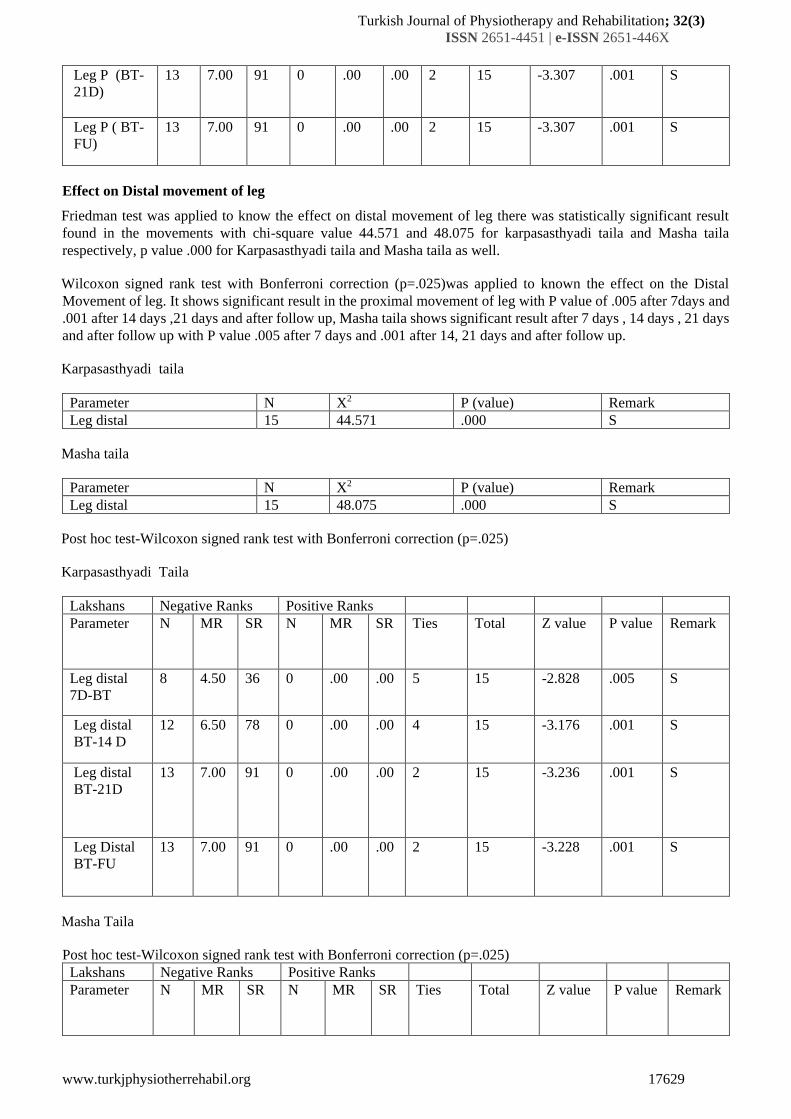
Effect on Distal movement of leg
Friedman test was applied to know the effect on distal movement of leg there was statistically significant result
found in the movements with chi-square value 44.571 and 48.075 for karpasasthyadi taila and Masha taila
respectively, p value .000 for Karpasasthyadi taila and Masha taila as well.
Wilcoxon signed rank test with Bonferroni correction (p=.025)was applied to known the effect on the Distal
Movement of leg. It shows significant result in the proximal movement of leg with P value of .005 after 7days and
.001 after 14 days ,21 days and after follow up, Masha taila shows significant result after 7 days , 14 days , 21 days
and after follow up with P value .005 after 7 days and .001 after 14, 21 days and after follow up.
Karpasasthyadi taila
Parameter N X2 P (value) Remark
Leg distal 15 44.571 .000 S
Masha taila
Parameter N X2 P (value) Remark
Leg distal 15 48.075 .000 S
Post hoc test-Wilcoxon signed rank test with Bonferroni correction (p=.025)
Karpasasthyadi Taila
Lakshans Negative Ranks Positive Ranks
Parameter N MR SR N MR SR Ties Total Z value P value Remark
Leg distal
7D-BT
8 4.50 36 0 .00 .00 5 15 -2.828 .005 S
Leg distal
BT-14 D
12 6.50 78 0 .00 .00 4 15 -3.176 .001 S
Leg distal
BT-21D
13 7.00 91 0 .00 .00 2 15 -3.236 .001 S
Leg Distal
BT-FU
13 7.00 91 0 .00 .00 2 15 -3.228 .001 S
Masha Taila
Post hoc test-Wilcoxon signed rank test with Bonferroni correction (p=.025)
Lakshans Negative Ranks Positive Ranks
Parameter N MR SR N MR SR Ties Total Z value P value Remark
Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17630
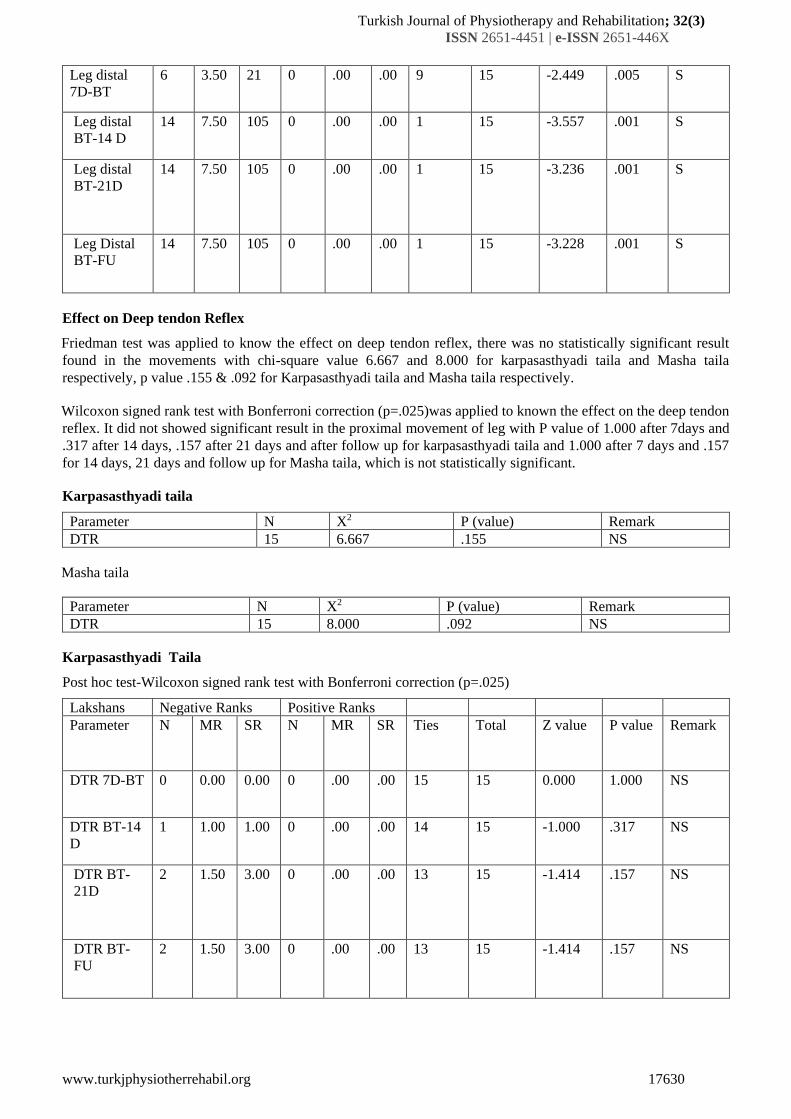
Leg distal
7D-BT
6 3.50 21 0 .00 .00 9 15 -2.449 .005 S
Leg distal
BT-14 D
14 7.50 105 0 .00 .00 1 15 -3.557 .001 S
Leg distal
BT-21D
14 7.50 105 0 .00 .00 1 15 -3.236 .001 S
Leg Distal
BT-FU
14 7.50 105 0 .00 .00 1 15 -3.228 .001 S
Effect on Deep tendon Reflex
Friedman test was applied to know the effect on deep tendon reflex, there was no statistically significant result
found in the movements with chi-square value 6.667 and 8.000 for karpasasthyadi taila and Masha taila
respectively, p value .155 & .092 for Karpasasthyadi taila and Masha taila respectively.
Wilcoxon signed rank test with Bonferroni correction (p=.025)was applied to known the effect on the deep tendon
reflex. It did not showed significant result in the proximal movement of leg with P value of 1.000 after 7days and
.317 after 14 days, .157 after 21 days and after follow up for karpasasthyadi taila and 1.000 after 7 days and .157
for 14 days, 21 days and follow up for Masha taila, which is not statistically significant.
Karpasasthyadi taila
Parameter N X2 P (value) Remark
DTR 15 6.667 .155 NS
Masha taila
Parameter N X2 P (value) Remark
DTR 15 8.000 .092 NS
Karpasasthyadi Taila
Post hoc test-Wilcoxon signed rank test with Bonferroni correction (p=.025)
Lakshans Negative Ranks Positive Ranks
Parameter N MR SR N MR SR Ties Total Z value P value Remark
DTR 7D-BT 0 0.00 0.00 0 .00 .00 15 15 0.000 1.000 NS
DTR BT-14
D
1 1.00 1.00 0 .00 .00 14 15 -1.000 .317 NS
DTR BT-
21D
2 1.50 3.00 0 .00 .00 13 15 -1.414 .157 NS
DTR BT-
FU
2 1.50 3.00 0 .00 .00 13 15 -1.414 .157 NS
Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17631
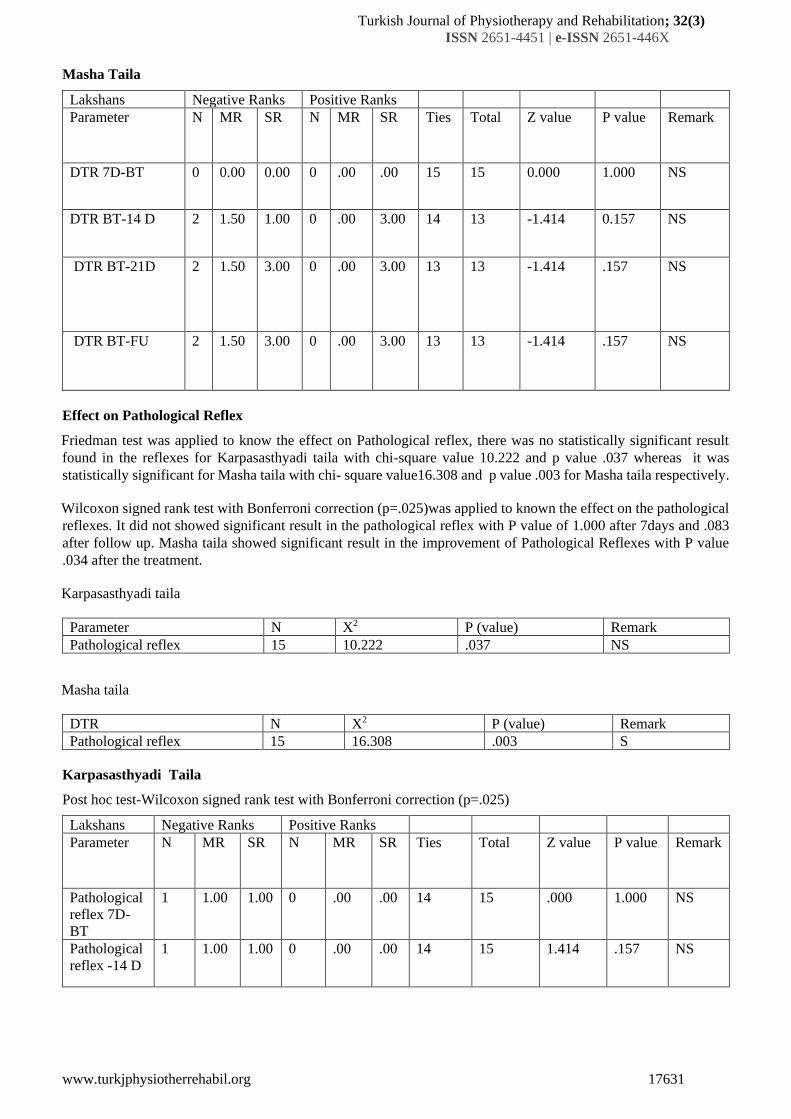
Masha Taila
Lakshans Negative Ranks Positive Ranks
Parameter N MR SR N MR SR Ties Total Z value P value Remark
DTR 7D-BT 0 0.00 0.00 0 .00 .00 15 15 0.000 1.000 NS
DTR BT-14 D 2 1.50 1.00 0 .00 3.00 14 13 -1.414 0.157 NS
DTR BT-21D 2 1.50 3.00 0 .00 3.00 13 13 -1.414 .157 NS
DTR BT-FU 2 1.50 3.00 0 .00 3.00 13 13 -1.414 .157 NS
Effect on Pathological Reflex
Friedman test was applied to know the effect on Pathological reflex, there was no statistically significant result
found in the reflexes for Karpasasthyadi taila with chi-square value 10.222 and p value .037 whereas it was
statistically significant for Masha taila with chi- square value16.308 and p value .003 for Masha taila respectively.
Wilcoxon signed rank test with Bonferroni correction (p=.025)was applied to known the effect on the pathological
reflexes. It did not showed significant result in the pathological reflex with P value of 1.000 after 7days and .083
after follow up. Masha taila showed significant result in the improvement of Pathological Reflexes with P value
.034 after the treatment.
Karpasasthyadi taila
Parameter N X2 P (value) Remark
Pathological reflex 15 10.222 .037 NS
Masha taila
DTR N X2 P (value) Remark
Pathological reflex 15 16.308 .003 S
Karpasasthyadi Taila
Post hoc test-Wilcoxon signed rank test with Bonferroni correction (p=.025)
Lakshans Negative Ranks Positive Ranks
Parameter N MR SR N MR SR Ties Total Z value P value Remark
Pathological
reflex 7D-
BT
1 1.00 1.00 0 .00 .00 14 15 .000 1.000 NS
Pathological
reflex -14 D
1 1.00 1.00 0 .00 .00 14 15 1.414 .157 NS
Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17632
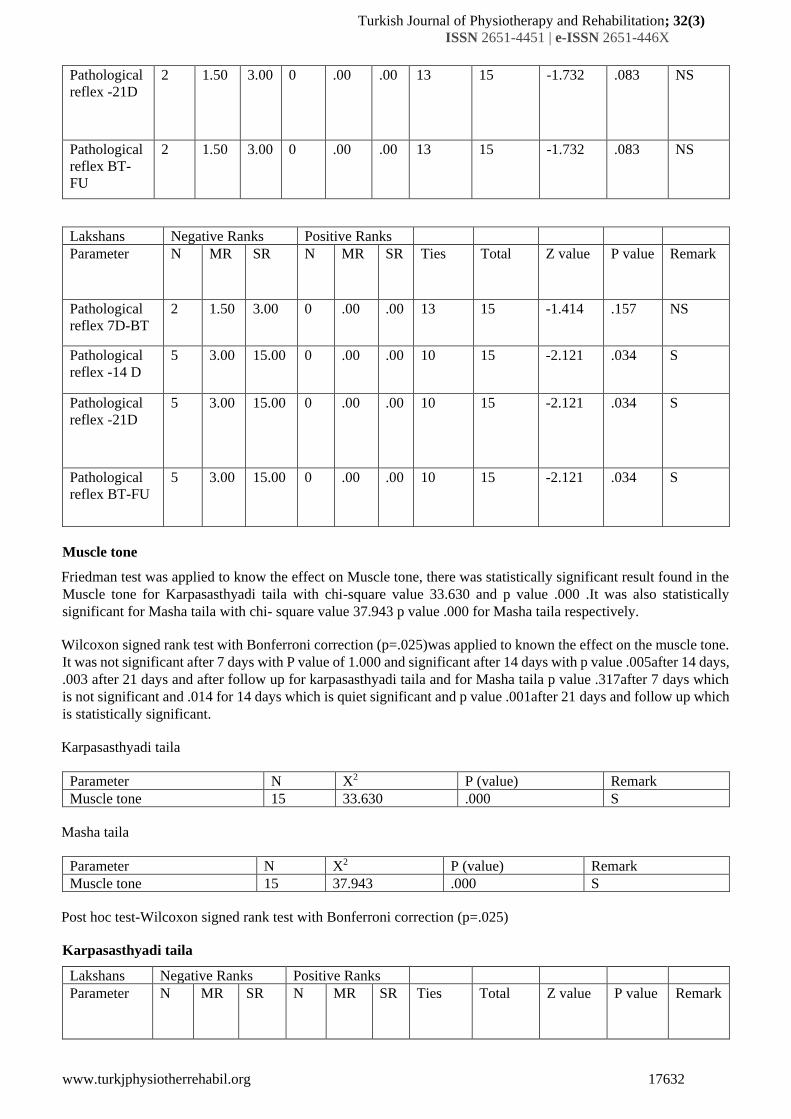
Pathological
reflex -21D
2 1.50 3.00 0 .00 .00 13 15 -1.732 .083 NS
Pathological
reflex BT-
FU
2 1.50 3.00 0 .00 .00 13 15 -1.732 .083 NS
Lakshans Negative Ranks Positive Ranks
Parameter N MR SR N MR SR Ties Total Z value P value Remark
Pathological
reflex 7D-BT
2 1.50 3.00 0 .00 .00 13 15 -1.414 .157 NS
Pathological
reflex -14 D
5 3.00 15.00 0 .00 .00 10 15 -2.121 .034 S
Pathological
reflex -21D
5 3.00 15.00 0 .00 .00 10 15 -2.121 .034 S
Pathological
reflex BT-FU
5 3.00 15.00 0 .00 .00 10 15 -2.121 .034 S
Muscle tone
Friedman test was applied to know the effect on Muscle tone, there was statistically significant result found in the
Muscle tone for Karpasasthyadi taila with chi-square value 33.630 and p value .000 .It was also statistically
significant for Masha taila with chi- square value 37.943 p value .000 for Masha taila respectively.
Wilcoxon signed rank test with Bonferroni correction (p=.025)was applied to known the effect on the muscle tone.
It was not significant after 7 days with P value of 1.000 and significant after 14 days with p value .005after 14 days,
.003 after 21 days and after follow up for karpasasthyadi taila and for Masha taila p value .317after 7 days which
is not significant and .014 for 14 days which is quiet significant and p value .001after 21 days and follow up which
is statistically significant.
Karpasasthyadi taila
Parameter N X2 P (value) Remark
Muscle tone 15 33.630 .000 S
Masha taila
Parameter N X2 P (value) Remark
Muscle tone 15 37.943 .000 S
Post hoc test-Wilcoxon signed rank test with Bonferroni correction (p=.025)
Karpasasthyadi taila
Lakshans Negative Ranks Positive Ranks
Parameter N MR SR N MR SR Ties Total Z value P value Remark
Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17633
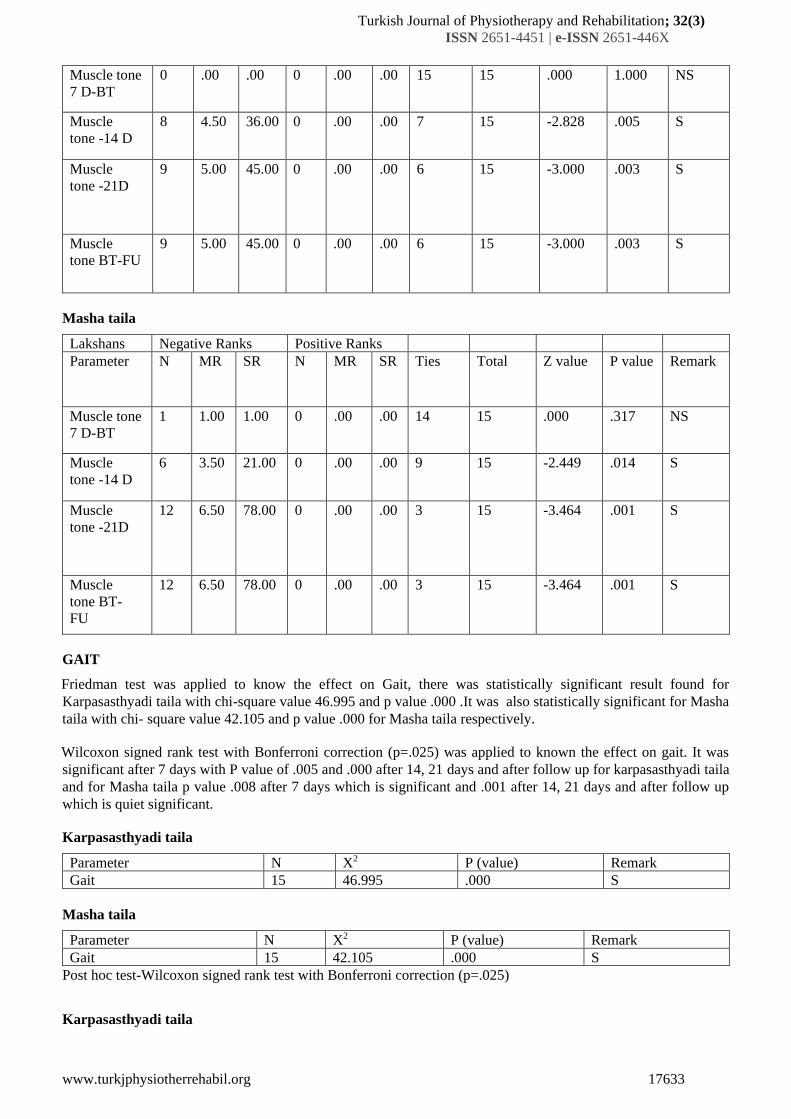
Muscle tone
7 D-BT
0 .00 .00 0 .00 .00 15 15 .000 1.000 NS
Muscle
tone -14 D
8 4.50 36.00 0 .00 .00 7 15 -2.828 .005 S
Muscle
tone -21D
9 5.00 45.00 0 .00 .00 6 15 -3.000 .003 S
Muscle
tone BT-FU
9 5.00 45.00 0 .00 .00 6 15 -3.000 .003 S
Masha taila
Lakshans Negative Ranks Positive Ranks
Parameter N MR SR N MR SR Ties Total Z value P value Remark
Muscle tone
7 D-BT
1 1.00 1.00 0 .00 .00 14 15 .000 .317 NS
Muscle
tone -14 D
6 3.50 21.00 0 .00 .00 9 15 -2.449 .014 S
Muscle
tone -21D
12 6.50 78.00 0 .00 .00 3 15 -3.464 .001 S
Muscle
tone BT-
FU
12 6.50 78.00 0 .00 .00 3 15 -3.464 .001 S
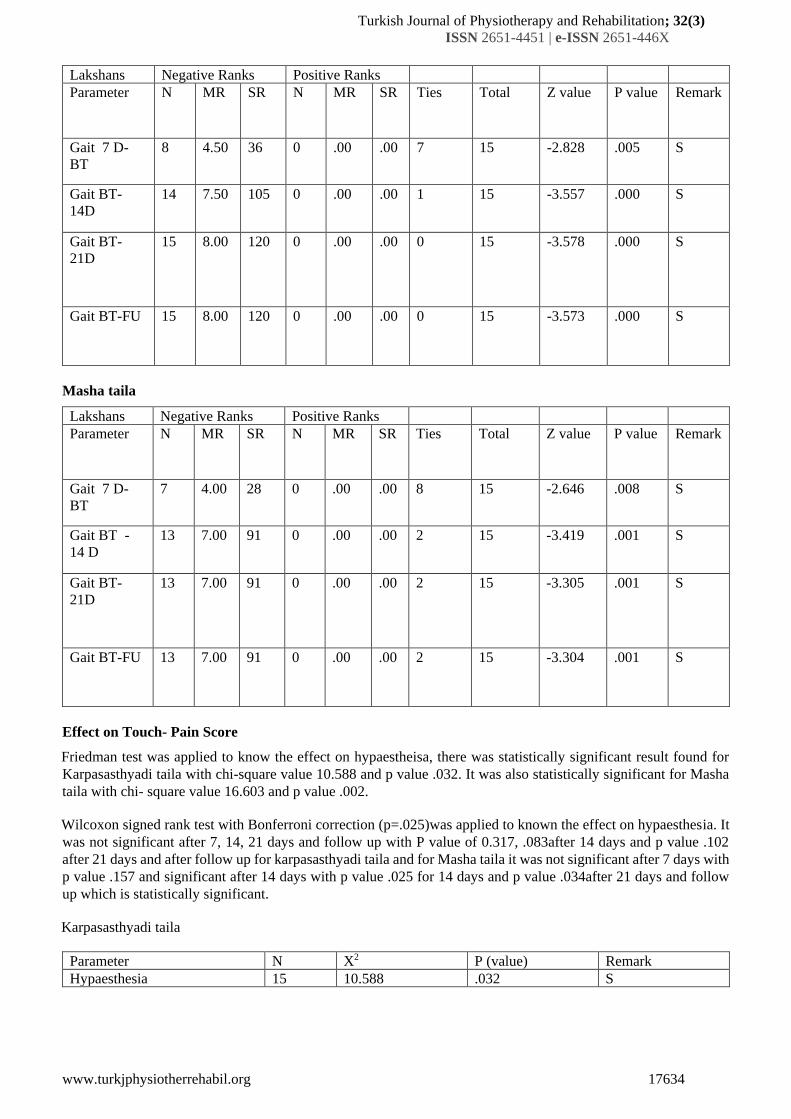
GAIT
Friedman test was applied to know the effect on Gait, there was statistically significant result found for
Karpasasthyadi taila with chi-square value 46.995 and p value .000 .It was also statistically significant for Masha
taila with chi- square value 42.105 and p value .000 for Masha taila respectively.
Wilcoxon signed rank test with Bonferroni correction (p=.025) was applied to known the effect on gait. It was
significant after 7 days with P value of .005 and .000 after 14, 21 days and after follow up for karpasasthyadi taila
and for Masha taila p value .008 after 7 days which is significant and .001 after 14, 21 days and after follow up
which is quiet significant.
Karpasasthyadi taila
Parameter N X2 P (value) Remark
Gait 15 46.995 .000 S
Masha taila
Parameter N X2 P (value) Remark
Gait 15 42.105 .000 S
Post hoc test-Wilcoxon signed rank test with Bonferroni correction (p=.025)
Karpasasthyadi taila
Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17634
Lakshans Negative Ranks Positive Ranks
Parameter N MR SR N MR SR Ties Total Z value P value Remark
Gait 7 D-
BT
8 4.50 36 0 .00 .00 7 15 -2.828 .005 S
Gait BT-
14D
14 7.50 105 0 .00 .00 1 15 -3.557 .000 S
Gait BT-
21D
15 8.00 120 0 .00 .00 0 15 -3.578 .000 S
Gait BT-FU 15 8.00 120 0 .00 .00 0 15 -3.573 .000 S
Masha taila
Lakshans Negative Ranks Positive Ranks
Parameter N MR SR N MR SR Ties Total Z value P value Remark
Gait 7 D-
BT
7 4.00 28 0 .00 .00 8 15 -2.646 .008 S
Gait BT -
14 D
13 7.00 91 0 .00 .00 2 15 -3.419 .001 S
Gait BT-
21D
13 7.00 91 0 .00 .00 2 15 -3.305 .001 S
Gait BT-FU 13 7.00 91 0 .00 .00 2 15 -3.304 .001 S
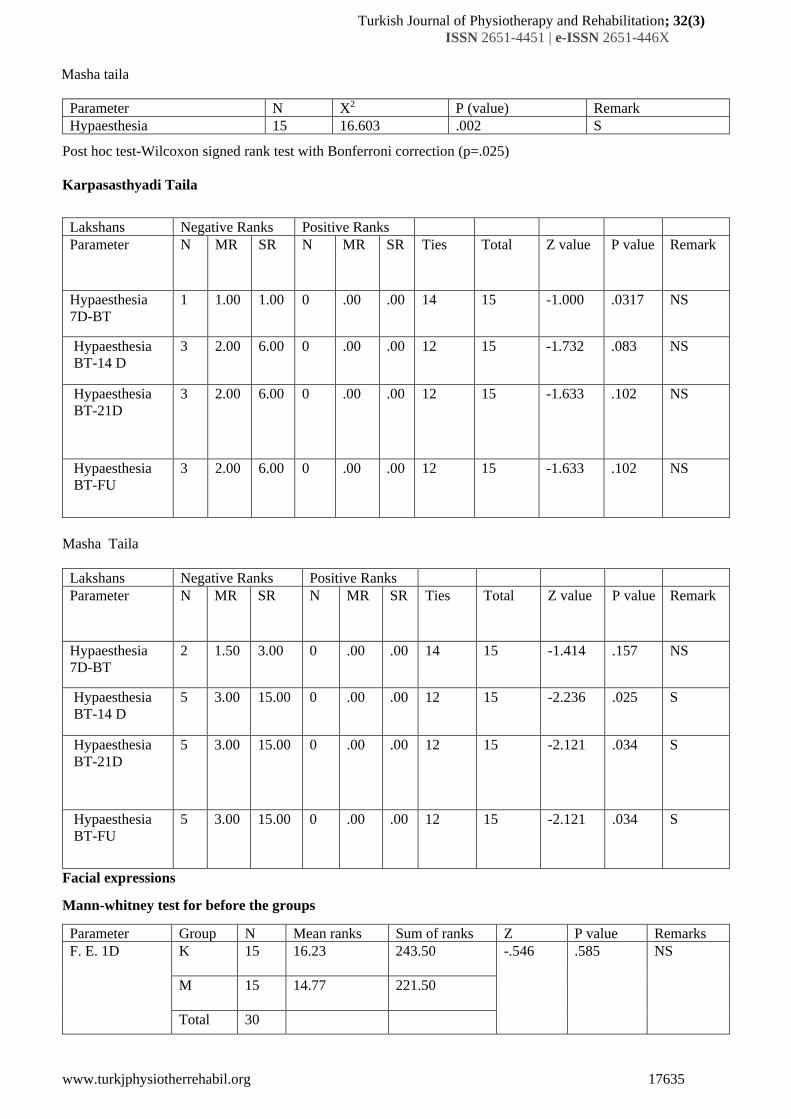
Effect on Touch- Pain Score
Friedman test was applied to know the effect on hypaestheisa, there was statistically significant result found for
Karpasasthyadi taila with chi-square value 10.588 and p value .032. It was also statistically significant for Masha
taila with chi- square value 16.603 and p value .002.
Wilcoxon signed rank test with Bonferroni correction (p=.025)was applied to known the effect on hypaesthesia. It
was not significant after 7, 14, 21 days and follow up with P value of 0.317, .083after 14 days and p value .102
after 21 days and after follow up for karpasasthyadi taila and for Masha taila it was not significant after 7 days with
p value .157 and significant after 14 days with p value .025 for 14 days and p value .034after 21 days and follow
up which is statistically significant.
Karpasasthyadi taila
Parameter N X2 P (value) Remark
Hypaesthesia 15 10.588 .032 S
Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17635
Masha taila
Parameter N X2 P (value) Remark
Hypaesthesia 15 16.603 .002 S
Post hoc test-Wilcoxon signed rank test with Bonferroni correction (p=.025)
Karpasasthyadi Taila
Lakshans Negative Ranks Positive Ranks
Parameter N MR SR N MR SR Ties Total Z value P value Remark
Hypaesthesia
7D-BT
1 1.00 1.00 0 .00 .00 14 15 -1.000 .0317 NS
Hypaesthesia
BT-14 D
3 2.00 6.00 0 .00 .00 12 15 -1.732 .083 NS
Hypaesthesia
BT-21D
3 2.00 6.00 0 .00 .00 12 15 -1.633 .102 NS
Hypaesthesia
BT-FU
3 2.00 6.00 0 .00 .00 12 15 -1.633 .102 NS
Masha Taila
Lakshans Negative Ranks Positive Ranks
Parameter N MR SR N MR SR Ties Total Z value P value Remark
Hypaesthesia
7D-BT
2 1.50 3.00 0 .00 .00 14 15 -1.414 .157 NS
Hypaesthesia
BT-14 D
5 3.00 15.00 0 .00 .00 12 15 -2.236 .025 S
Hypaesthesia
BT-21D
5 3.00 15.00 0 .00 .00 12 15 -2.121 .034 S
Hypaesthesia
BT-FU
5 3.00 15.00 0 .00 .00 12 15 -2.121 .034 S
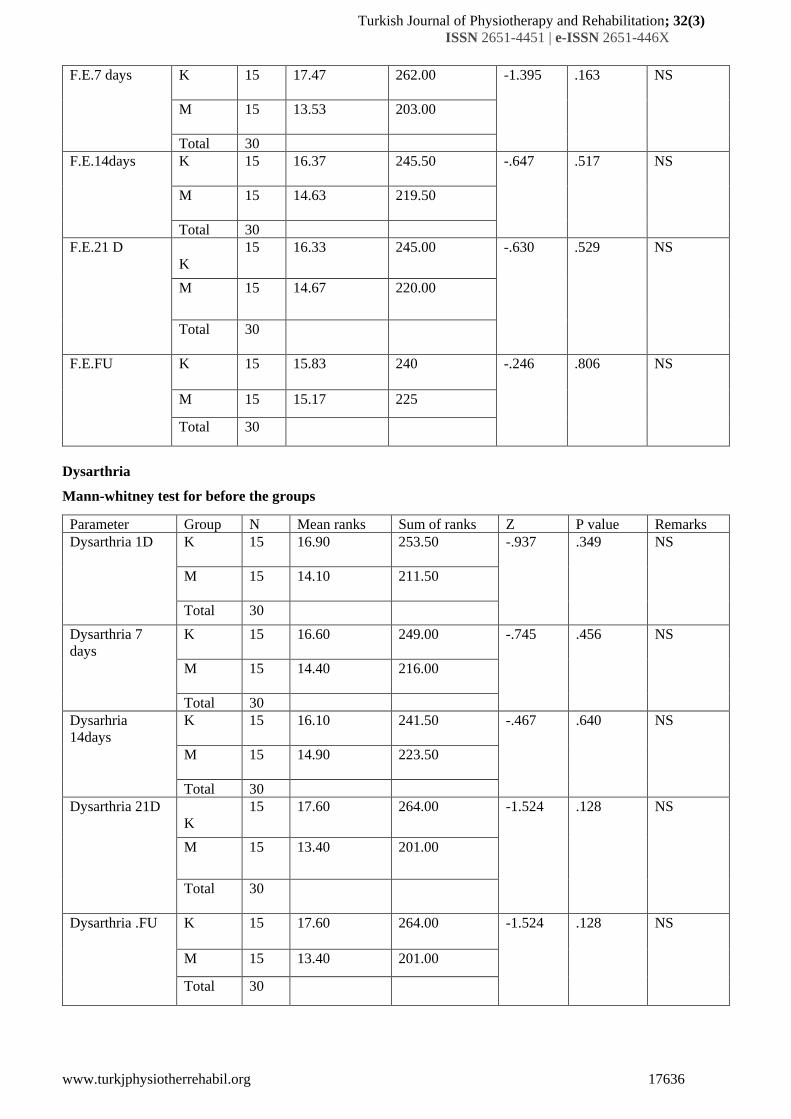
Facial expressions
Mann-whitney test for before the groups
Parameter Group N Mean ranks Sum of ranks Z P value Remarks
F. E. 1D K
15 16.23 243.50 -.546 .585 NS
M
15 14.77 221.50
Total 30
Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17636
F.E.7 days K
15 17.47 262.00 -1.395 .163 NS
M
15 13.53 203.00
Total 30
F.E.14days K
15 16.37 245.50 -.647 .517 NS
M
15 14.63 219.50
Total 30
F.E.21 D
K
15 16.33 245.00 -.630 .529 NS
M
15 14.67 220.00
Total
30
F.E.FU
K 15 15.83 240 -.246 .806 NS
M 15 15.17 225
Total 30
Dysarthria
Mann-whitney test for before the groups
Parameter Group N Mean ranks Sum of ranks Z P value Remarks
Dysarthria 1D K
15 16.90 253.50 -.937 .349 NS
M
15 14.10 211.50
Total 30
Dysarthria 7
days
K
15 16.60 249.00 -.745 .456 NS
M
15 14.40 216.00
Total 30
Dysarhria
14days
K
15 16.10 241.50 -.467 .640 NS
M
15 14.90 223.50
Total 30
Dysarthria 21D
K
15 17.60 264.00 -1.524 .128 NS
M
15 13.40 201.00
Total
30
Dysarthria .FU
K 15 17.60 264.00 -1.524 .128 NS
M 15 13.40 201.00
Total 30
Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17637
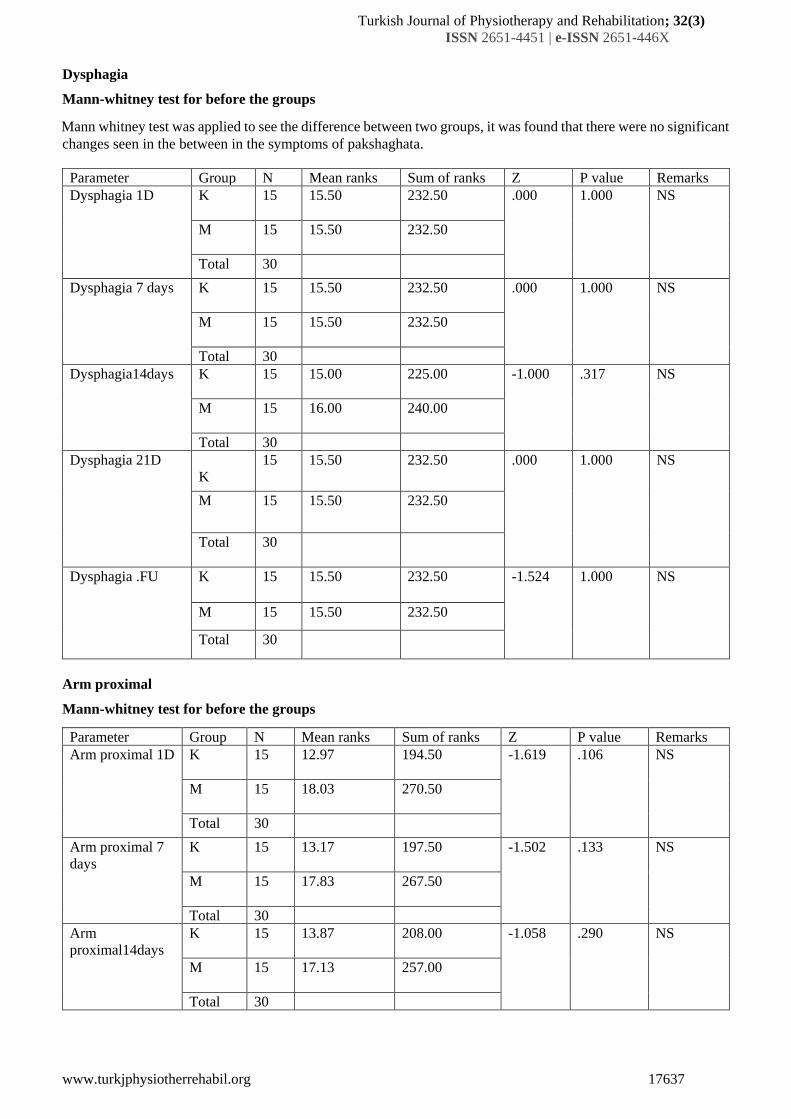
Dysphagia
Mann-whitney test for before the groups
Mann whitney test was applied to see the difference between two groups, it was found that there were no significant
changes seen in the between in the symptoms of pakshaghata.
Parameter Group N Mean ranks Sum of ranks Z P value Remarks
Dysphagia 1D K
15 15.50 232.50 .000 1.000 NS
M
15 15.50 232.50
Total 30
Dysphagia 7 days K
15 15.50 232.50 .000 1.000 NS
M
15 15.50 232.50
Total 30
Dysphagia14days K
15 15.00 225.00 -1.000 .317 NS
M
15 16.00 240.00
Total 30
Dysphagia 21D
K
15 15.50 232.50 .000 1.000 NS
M
15 15.50 232.50
Total
30
Dysphagia .FU
K 15 15.50 232.50 -1.524 1.000 NS
M 15 15.50 232.50
Total 30
Arm proximal
Mann-whitney test for before the groups
Parameter Group N Mean ranks Sum of ranks Z P value Remarks
Arm proximal 1D K
15 12.97 194.50 -1.619 .106 NS
M
15 18.03 270.50
Total 30
Arm proximal 7
days
K
15 13.17 197.50 -1.502 .133 NS
M
15 17.83 267.50
Total 30
Arm
proximal14days
K
15 13.87 208.00 -1.058 .290 NS
M
15 17.13 257.00
Total 30
Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17638
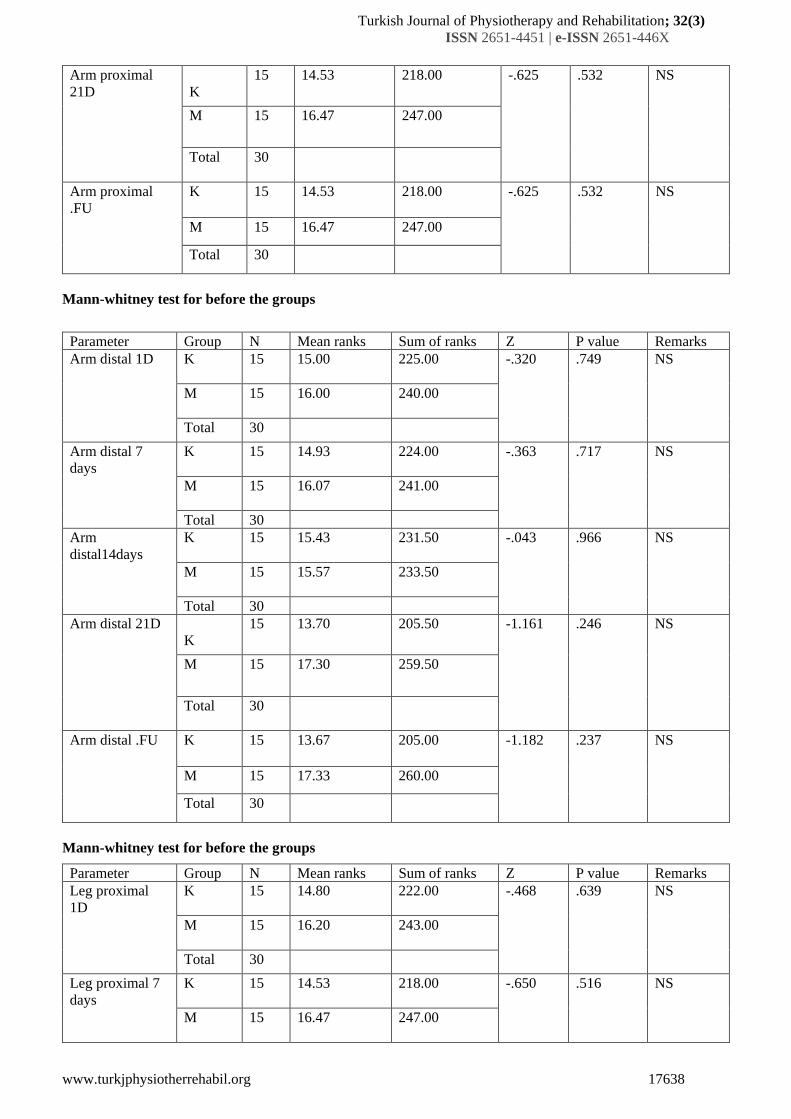
Arm proximal
21D
K
15 14.53 218.00 -.625 .532 NS
M
15 16.47 247.00
Total
30
Arm proximal
.FU
K 15 14.53 218.00 -.625 .532 NS
M 15 16.47 247.00
Total 30
Mann-whitney test for before the groups
Parameter Group N Mean ranks Sum of ranks Z P value Remarks
Arm distal 1D K
15 15.00 225.00 -.320 .749 NS
M
15 16.00 240.00
Total 30
Arm distal 7
days
K
15 14.93 224.00 -.363 .717 NS
M
15 16.07 241.00
Total 30
Arm
distal14days
K
15 15.43 231.50 -.043 .966 NS
M
15 15.57 233.50
Total 30
Arm distal 21D
K
15 13.70 205.50 -1.161 .246 NS
M
15 17.30 259.50
Total
30
Arm distal .FU
K 15 13.67 205.00 -1.182 .237 NS
M 15 17.33 260.00
Total 30
Mann-whitney test for before the groups
Parameter Group N Mean ranks Sum of ranks Z P value Remarks
Leg proximal
1D
K
15 14.80 222.00 -.468 .639 NS
M
15 16.20 243.00
Total 30
Leg proximal 7
days
K
15 14.53 218.00 -.650 .516 NS
M
15 16.47 247.00
Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17639
Total 30
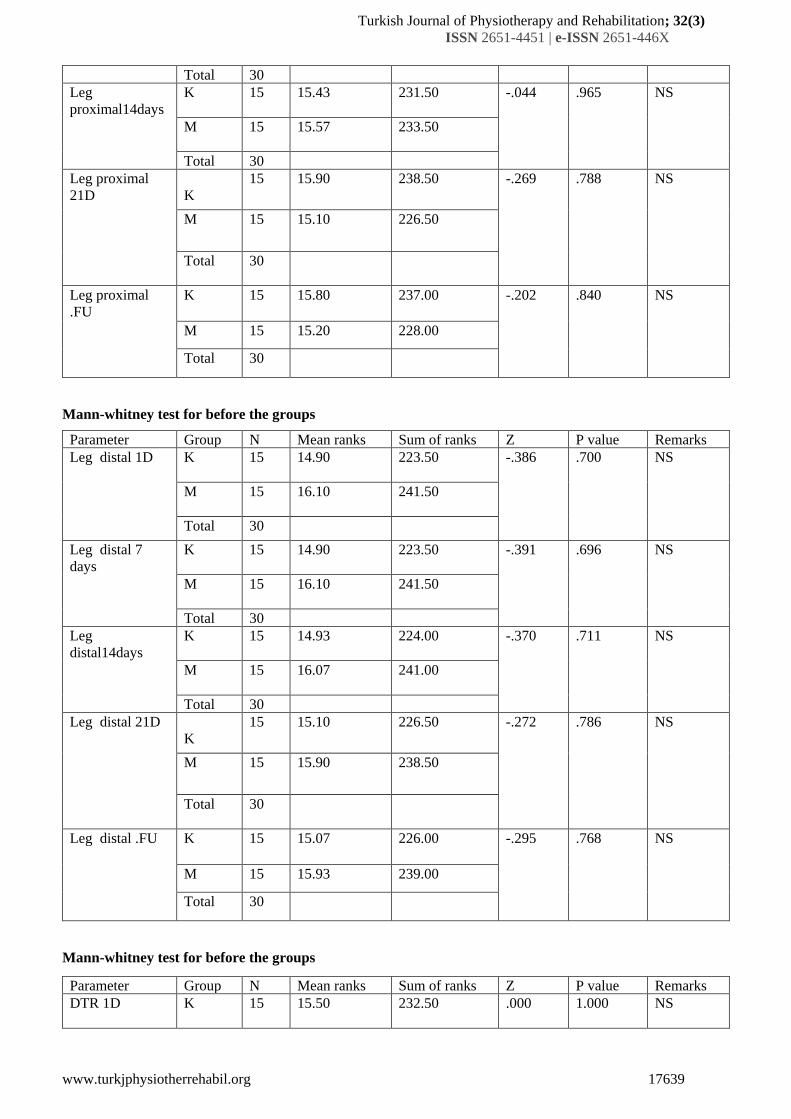
Leg
proximal14days
K
15 15.43 231.50 -.044 .965 NS
M
15 15.57 233.50
Total 30
Leg proximal
21D
K
15 15.90 238.50 -.269 .788 NS
M
15 15.10 226.50
Total
30
Leg proximal
.FU
K 15 15.80 237.00 -.202 .840 NS
M 15 15.20 228.00
Total 30
Mann-whitney test for before the groups
Parameter Group N Mean ranks Sum of ranks Z P value Remarks
Leg distal 1D K
15 14.90 223.50 -.386 .700 NS
M
15 16.10 241.50
Total 30
Leg distal 7
days
K
15 14.90 223.50 -.391 .696 NS
M
15 16.10 241.50
Total 30
Leg
distal14days
K
15 14.93 224.00 -.370 .711 NS
M
15 16.07 241.00
Total 30
Leg distal 21D
K
15 15.10 226.50 -.272 .786 NS
M
15 15.90 238.50
Total
30
Leg distal .FU
K 15 15.07 226.00 -.295 .768 NS
M 15 15.93 239.00
Total 30
Mann-whitney test for before the groups
Parameter Group N Mean ranks Sum of ranks Z P value Remarks
DTR 1D K
15 15.50 232.50 .000 1.000 NS
Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17640
M
15 15.50 232.50
Total 30
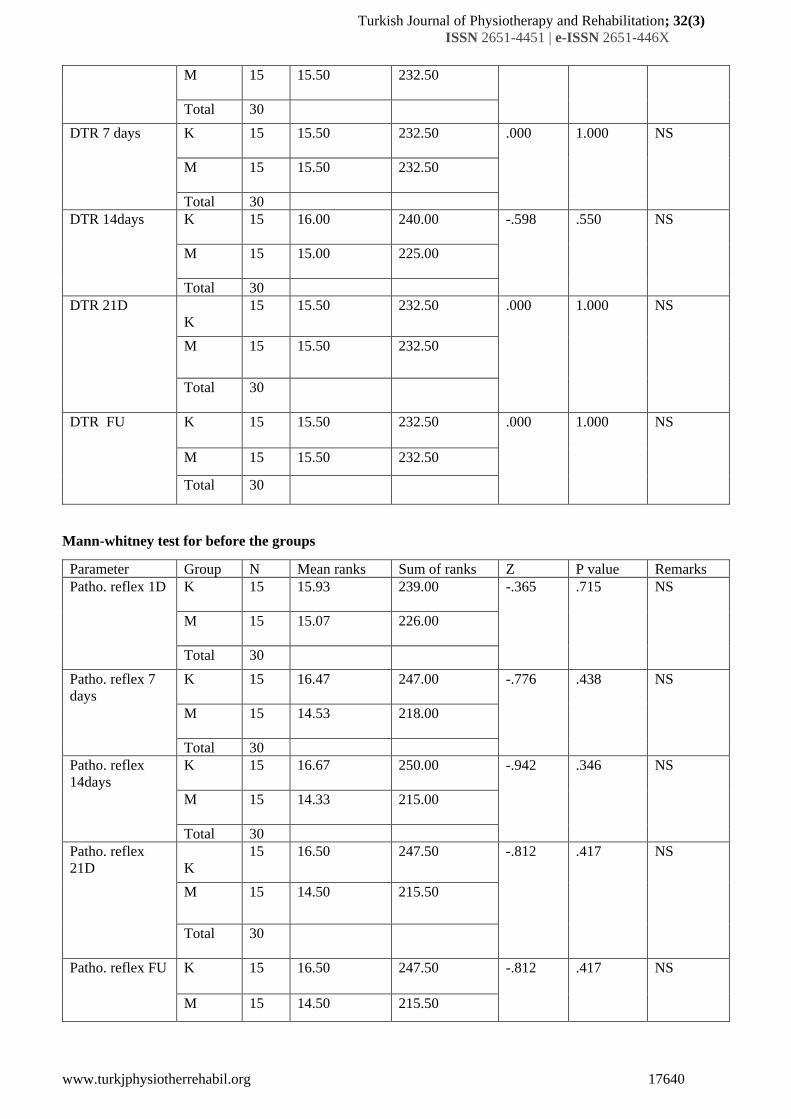
DTR 7 days K
15 15.50 232.50 .000 1.000 NS
M
15 15.50 232.50
Total 30
DTR 14days K
15 16.00 240.00 -.598 .550 NS
M
15 15.00 225.00
Total 30
DTR 21D
K
15 15.50 232.50 .000 1.000 NS
M
15 15.50 232.50
Total
30
DTR FU
K 15 15.50 232.50 .000 1.000 NS
M 15 15.50 232.50
Total 30
Mann-whitney test for before the groups
Parameter Group N Mean ranks Sum of ranks Z P value Remarks
Patho. reflex 1D K
15 15.93 239.00 -.365 .715 NS
M
15 15.07 226.00
Total 30
Patho. reflex 7
days
K
15 16.47 247.00 -.776 .438 NS
M
15 14.53 218.00
Total 30
Patho. reflex
14days
K
15 16.67 250.00 -.942 .346 NS
M
15 14.33 215.00
Total 30
Patho. reflex
21D
K
15 16.50 247.50 -.812 .417 NS
M
15 14.50 215.50
Total
30
Patho. reflex FU
K 15 16.50 247.50 -.812 .417 NS
M 15 14.50 215.50
Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17641
Total 30
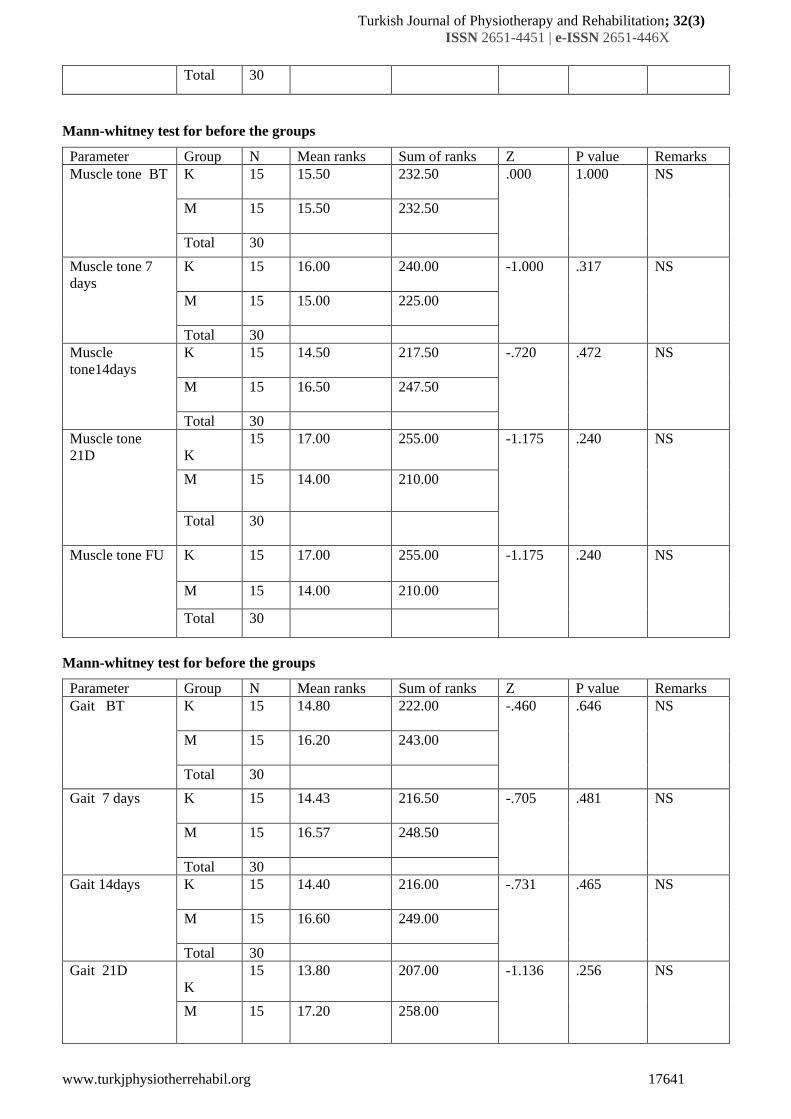
Mann-whitney test for before the groups
Parameter Group N Mean ranks Sum of ranks Z P value Remarks
Muscle tone BT K
15 15.50 232.50 .000 1.000 NS
M
15 15.50 232.50
Total 30
Muscle tone 7
days
K
15 16.00 240.00 -1.000 .317 NS
M
15 15.00 225.00
Total 30
Muscle
tone14days
K
15 14.50 217.50 -.720 .472 NS
M
15 16.50 247.50
Total 30
Muscle tone
21D
K
15 17.00 255.00 -1.175 .240 NS
M
15 14.00 210.00
Total
30
Muscle tone FU
K 15 17.00 255.00 -1.175 .240 NS
M 15 14.00 210.00
Total 30
Mann-whitney test for before the groups
Parameter Group N Mean ranks Sum of ranks Z P value Remarks
Gait BT K
15 14.80 222.00 -.460 .646 NS
M
15 16.20 243.00
Total 30
Gait 7 days K
15 14.43 216.50 -.705 .481 NS
M
15 16.57 248.50
Total 30
Gait 14days K
15 14.40 216.00 -.731 .465 NS
M
15 16.60 249.00
Total 30
Gait 21D
K
15 13.80 207.00 -1.136 .256 NS
M
15 17.20 258.00
Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17642
Total
30
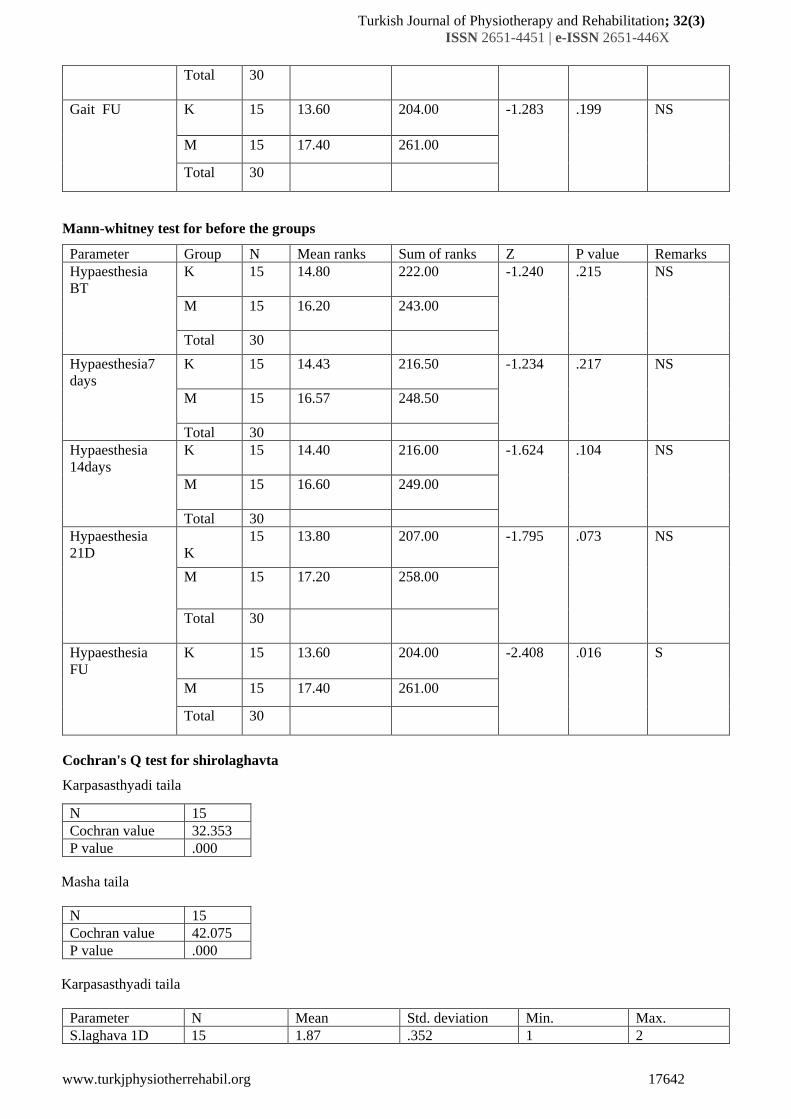
Gait FU
K 15 13.60 204.00 -1.283 .199 NS
M 15 17.40 261.00
Total 30
Mann-whitney test for before the groups
Parameter Group N Mean ranks Sum of ranks Z P value Remarks
Hypaesthesia
BT
K
15 14.80 222.00 -1.240 .215 NS
M
15 16.20 243.00
Total 30
Hypaesthesia7
days
K
15 14.43 216.50 -1.234 .217 NS
M
15 16.57 248.50
Total 30
Hypaesthesia
14days
K
15 14.40 216.00 -1.624 .104 NS
M
15 16.60 249.00
Total 30
Hypaesthesia
21D
K
15 13.80 207.00 -1.795 .073 NS
M
15 17.20 258.00
Total
30
Hypaesthesia
FU
K 15 13.60 204.00 -2.408 .016 S
M 15 17.40 261.00
Total 30
Cochran's Q test for shirolaghavta
Karpasasthyadi taila
N 15
Cochran value 32.353
P value .000
Masha taila
N 15
Cochran value 42.075
P value .000
Karpasasthyadi taila
Parameter N Mean Std. deviation Min. Max.
S.laghava 1D 15 1.87 .352 1 2
Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17643
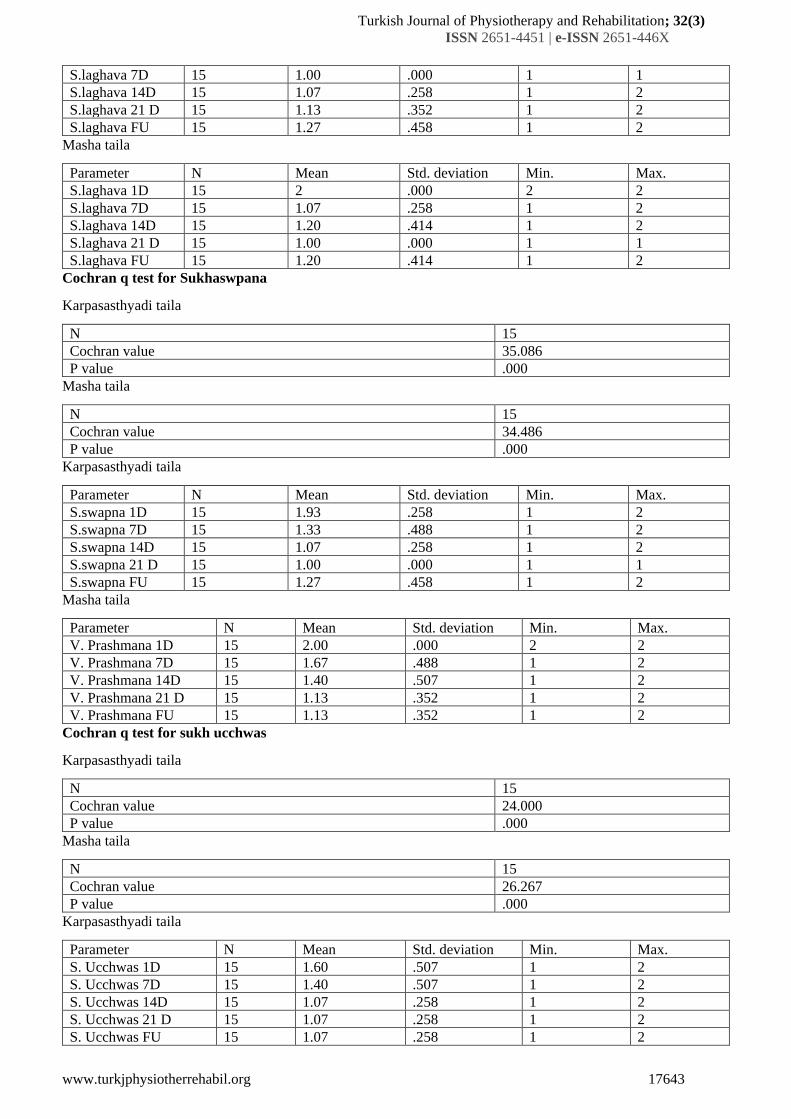
S.laghava 7D 15 1.00 .000 1 1
S.laghava 14D 15 1.07 .258 1 2
S.laghava 21 D 15 1.13 .352 1 2
S.laghava FU 15 1.27 .458 1 2
Masha taila
Parameter N Mean Std. deviation Min. Max.
S.laghava 1D 15 2 .000 2 2
S.laghava 7D 15 1.07 .258 1 2
S.laghava 14D 15 1.20 .414 1 2
S.laghava 21 D 15 1.00 .000 1 1
S.laghava FU 15 1.20 .414 1 2
Cochran q test for Sukhaswpana
Karpasasthyadi taila
N 15
Cochran value 35.086
P value .000
Masha taila
N 15
Cochran value 34.486
P value .000
Karpasasthyadi taila
Parameter N Mean Std. deviation Min. Max.
S.swapna 1D 15 1.93 .258 1 2
S.swapna 7D 15 1.33 .488 1 2
S.swapna 14D 15 1.07 .258 1 2
S.swapna 21 D 15 1.00 .000 1 1
S.swapna FU 15 1.27 .458 1 2
Masha taila
Parameter N Mean Std. deviation Min. Max.
V. Prashmana 1D 15 2.00 .000 2 2
V. Prashmana 7D 15 1.67 .488 1 2
V. Prashmana 14D 15 1.40 .507 1 2
V. Prashmana 21 D 15 1.13 .352 1 2
V. Prashmana FU 15 1.13 .352 1 2
Cochran q test for sukh ucchwas
Karpasasthyadi taila
N 15
Cochran value 24.000
P value .000
Masha taila
N 15
Cochran value 26.267
P value .000
Karpasasthyadi taila
Parameter N Mean Std. deviation Min. Max.
S. Ucchwas 1D 15 1.60 .507 1 2
S. Ucchwas 7D 15 1.40 .507 1 2
S. Ucchwas 14D 15 1.07 .258 1 2
S. Ucchwas 21 D 15 1.07 .258 1 2
S. Ucchwas FU 15 1.07 .258 1 2
Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17644
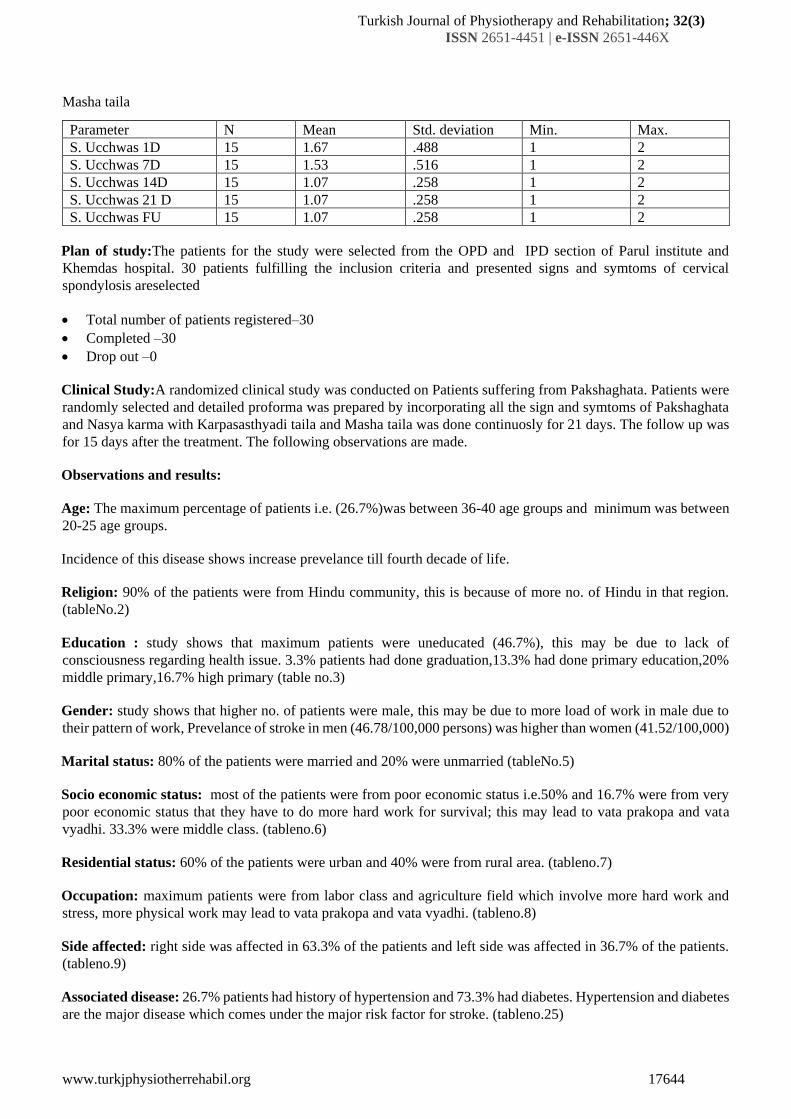
Masha taila
Parameter N Mean Std. deviation Min. Max.
S. Ucchwas 1D 15 1.67 .488 1 2
S. Ucchwas 7D 15 1.53 .516 1 2
S. Ucchwas 14D 15 1.07 .258 1 2
S. Ucchwas 21 D 15 1.07 .258 1 2
S. Ucchwas FU 15 1.07 .258 1 2
Plan of study:The patients for the study were selected from the OPD and IPD section of Parul institute and
Khemdas hospital. 30 patients fulfilling the inclusion criteria and presented signs and symtoms of cervical
spondylosis areselected
• Total number of patients registered–30
• Completed –30
• Drop out –0
Clinical Study:A randomized clinical study was conducted on Patients suffering from Pakshaghata. Patients were
randomly selected and detailed proforma was prepared by incorporating all the sign and symtoms of Pakshaghata
and Nasya karma with Karpasasthyadi taila and Masha taila was done continuosly for 21 days. The follow up was
for 15 days after the treatment. The following observations are made.
Observations and results:
Age: The maximum percentage of patients i.e. (26.7%)was between 36-40 age groups and minimum was between
20-25 age groups.
Incidence of this disease shows increase prevelance till fourth decade of life.
Religion: 90% of the patients were from Hindu community, this is because of more no. of Hindu in that region.
(tableNo.2)
Education : study shows that maximum patients were uneducated (46.7%), this may be due to lack of
consciousness regarding health issue. 3.3% patients had done graduation,13.3% had done primary education,20%
middle primary,16.7% high primary (table no.3)
Gender: study shows that higher no. of patients were male, this may be due to more load of work in male due to
their pattern of work, Prevelance of stroke in men (46.78/100,000 persons) was higher than women (41.52/100,000)
Marital status: 80% of the patients were married and 20% were unmarried (tableNo.5)
Socio economic status: most of the patients were from poor economic status i.e.50% and 16.7% were from very
poor economic status that they have to do more hard work for survival; this may lead to vata prakopa and vata
vyadhi. 33.3% were middle class. (tableno.6)
Residential status: 60% of the patients were urban and 40% were from rural area. (tableno.7)
Occupation: maximum patients were from labor class and agriculture field which involve more hard work and
stress, more physical work may lead to vata prakopa and vata vyadhi. (tableno.8)
Side affected: right side was affected in 63.3% of the patients and left side was affected in 36.7% of the patients.
(tableno.9)
Associated disease: 26.7% patients had history of hypertension and 73.3% had diabetes. Hypertension and diabetes
are the major disease which comes under the major risk factor for stroke. (tableno.25)
Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17645
Diet: 73.3% patients were vegetarian and 26.7% were having mixed diet. (tableno.26)
Bowel habits: 66.7% patients were having regular bowel and 23.3% had irregular bowel habits and 10% patients
had constipation. (tableno.27)
Habits: 16.7% patients were alcoholic, 10% patients were having the habit of tobacco chewing, 13.3% patients
were smoker. These are the risk factors of Cerebro vascular accidents.(tableno.28)
Vyayam shakti: 40.3% patients were having Avara Vyayam shakti, 56.7% had Madhyama Vyayam Shakti and
3.3% patients had Pravra Vyayam Shakti.(tableno.30)
Koshta: 53.3% patients were Mridu koshthi, 36.7% of the patients were having Kroor koshta and 10% patients
were Mridu koshthi. (tableno.24)
Shabad: 60% of the patients were having vaikrut swara, 40% of the patients were having prakrut swara.(tableno.31)
Duration of illness: maximum patients were having less than 6 months of history of illness i.e.40% of the patients,
30% patients were having history of less than one year of illness,10% patients had history of illness between one
to one and half year,6.7% patients had the history of illness between 1to 1and half yrs,3% pts had the illness from
2 to 2and half yrs, 2and half to 3,3yrs to 3and half yrs, 3and half to 4, 4yrs to 4 and half yrs.(tableno.23)
Lakshana of Nasya Karma: in this clinical study, most patients showed the samyaka nasya lakshana, 93.3%
patients achieved the lakshana of shirolaghava, 96.7% got the lakshana of sukhaswapna, 93.3% got the lakshana
sukhaucchwas, 90% patients got the lakshana of swapnabodha, 80% patients achieved the lakshan of
vikarprashmana upto some extent.
IV. EFFECT OF THERAPIES
The present clinical study was conducted to evaluate the efficacy of Nasya in two groups, each group had 15
patients, course of nasya was for 21 days.
1. Effect on Facial Expressions:
Effect on the Facial Expressions: Both the taila show significant result in the facial expressions with p value .000,
so we can conclude that both the Nasya has significant result in the facial expressions. The p value was .046 before
the treatment changed to .001 after the treatment for Karpasasthyadi taila and for Masha taila thep value was .008
before the treatment and changed to .000 after 7 days of Nasya, which was quiet significant and later on p value
was .001 after 14 and 21 days, the change that occurred with the treatment was statistically significant. (p=.001)
2. Effect on Dysarthria:
Both the taila show significant result in dysarthria with mean value p value .000 after the treatment, p value was
.083 after 7 days of treatment and after 14 days it was .005 which was quiet significant statistically for
karpasasthyadi taila, this shows that there was marked improvement in dysarthria after 14 days of treatment. For
Masha taila the p value was .157 after 7 days of treatment and changed to .025 after 14 days and .011 after 21 days
and after follow up which shows good improvement significantally.
3. Effect on Dysphagia:
Both the taila doesnot show any significant result in dysphagia with p value .046 which was not significant
statistically.
4. Effect on Range Of Motion:
ARM: (Proximal movement)
Both the taila shows significant result in the proximal movement with p value .000 for both the taila, the p value
was .005 after 7 days of treatment and changed to .002 after 14 days of treatment and changed to .001 after 21 days
of treatment for Karpasasthyadi taila.
Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17646
For Masha taila the p value was quiet significant after 7 days of treatment i.e. .002 and changed to .000 after 14
days which was quiet significant and .000 after 21 days which shows that it shows significant result in the treatment.
Arm: (Distal movement)
Both the taila shows significant result in the distal movement with p value .000
The p value for karpasthyadi taila was .005 after seven days of treatment and .000 after 14 days which was quiet
significant statistically, the p value was .001 after 21days and after follow up of the treatment which shows the
treatment was significant.
For Masha taila, p value was .008 after 7 days of treatment and later on it was .001 after 14 days of treatment and
upto follow up which means that it is significant statistically.
V. LEG MOVEMENTS
Leg (proximal)
Both the taila shows significant results in the movement of the affected leg, with p value .000 for both the taila.
The p value for karpasasthyadi taila was .001after 7 days and 14 days of the treatment and .000 after 21 days and
follow up and .002 after 7 and 14 days for Masha taila and .001 after 21 days and after follow up,which means that
both the taila are showing significant results in the proximal movements.
Leg (distal)
Both the taila shows significant results in the distal movement of the affected leg, with p value .000 for both the
taila which is quiet significant.
The p value for karpasasthyadi taila and Masha taila as well was .005 after 7 days of treatment and .001 after 14,
21 days and after follow up, which is significant statistically.
Effect on DTR
Both the taila doesnot show any significant result in the deep tendon reflex with p value .155 for karpasasthyadi
taila and .092 for Masha taila.
Effect on Pathological Reflex
Masha taila shows significant result in the management of pathological reflex, Karpasasthyadi taila did not show
any significant results in the reflexes. The p value is .034 after 7 days and upto follow up which proves that its role
is significant in the management of reflexes.
Effect on Muscle Tone
Both the taila shows significant result in the muscle tone with p value .00 for both the taila means both are
significant in the management. The change that occurred with the treatment is greater than expected, there is
statstically significant change (p=.000)
The p value is .003 after 14 days for karpasasthyadi and .001 for Masha. The change that occurred with the treatment
is greater than expected.
Effect on Gait:
Both the taila shows significant result in the gait with p value .000 for both the taila. The change that occurred with
the treatment is greater than expected.
The p value is .000 after 14 days for group 1 and .001 for group 2
VI. OVERALL EFFECT OF THE THERAPY
Out of 15 patients of Pakshaghata treated with two schedule of Nasya Karma, all patients got marked improvement.
Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17647
Effect on Facial expressions:
The herb Bala strengthens the Nerves and the Muscles. Ashwagandha is an exceptional nervine tonic and nourishes
the nerves and improves nerve function. It helps in providing progressive, long lasting results for various health
concerns like aging, slow growth. Clinical trials and animal research support the role of Ashwagandha for anxiety,
cognitive and neurological disorders. The total alkaloids of Ashwagandha showed relaxant effect against several
spasmogens on intestinal, uterine and blood vascular muscles. The pattern of smooth muscle activity of the alkaloid
was similar to that of papaverine which suggests a direct musculotrophic action. Masha is described as
Paramvatahara in Charaka, Sutrasthana having Guru, Brimhana, Tarpana, Balya and Snigdha properties which
control vitiated vata and Dhatukshaya. Generally it is recommended in degenerative nervine disorders and it is
considered as nervine tonic.
Effect on speech: Eranda is Madhur, Katu, Kshaya Rasa, Ushna Virya and Madhur Vipaka and it helps to treat
Stambha, Sankoch.it may help to reduce Vakastambha.
Effect on leg and arm movements:
Atmagupta (mucuna puriens), supports a healthy central and peripheral nervous system, it supports the body ability
to handle stress, it promotes healthy motor skills and coordination.
Effect on gait:
Atmagupta supports physical balance and postures. It contains naturally occurring levodopa which is an essential
precursor of the neurotransmitter dopamine, it has many function in the brain and nervous system, it plays an
important role in cognition, voluntary movement, sleep. L-dopa reaches the central nervous system more readily.
Effect on Muscle Tone:
Ashwagandha has revitalizing action on nerves, bone marrow. Regular consumption is believed to rectify the
abnormalities of the sense organs and hypertrophy of muscles. It is also useful in stress, weakness, nervous
exhaustion, memory loss, muscular weakness. In Dhanwantar Nighantu and Raj Nighantu, Bala is considered as
tridoshanut, a nervine stimulant, Balya, Ojovardhaka, Dhatuvardhaka, Pushtikara and Vatanulomana. It is having
Laghu, snigdha and Picchila guna, Madhura Rasa and Madhura Vipaka, it is said to restore muscular function and
body strength. kapikacchu may help increase lean mucle mass by stimulating human growth hormone production.
Dopamine has been shown to increase protein synthesis and help stimulating muscle growth.
Effect on Touch Pain Score:
Effect on dysarthria:
Both the group shows marked improvement in dysarthria, it can be said that Nasya has checked the dushti of vitiated
vata especially Prana and Udana, it also effect on Indriya i.e.Vagindrya as it is mainly attached to Murdha, the
overall effect of Nasya with Masha Taila, a potent Vatashamaka, Kaphashamka, Swarakar property.
FOLLOW UP OF THE STUDY
In the recent study, 1 follow up was done after 15 days of the therapy. The effect of nasya karma in both the
groups were assessed in both the groups, relief is sustained, further improved and no changes were assessed.
Data of follow up shows that most of the patients attained sustained relief.
PROBABLE MODE OF ACTION OF NASYA:
The mode of administration of Aushada through Nasya Karma is having several advantages. The rich vascular
plexus of the nasal cavity provides a direct route into the blood stream for medications that easily cross
mucousmembranes.This direct absorption into the blood stream avoids gastrointestinal destruction and hepatic
first pass metabolism (destruction of drugs by liver enzymes) allowing more drug to be cost-effectively, rapidly,
and predictably bioavailable than if it were administered orally. The probable mode of action of Nasya Karma
can be assed under many aspects, these are:
Turkish Journal of Physiotherapy and Rehabilitation; 32(3)
ISSN 2651-4451 | e-ISSN 2651-446X
www.turkjphysiotherrehabil.org 17648
According to Anatomical Aspects:
The Sringataka Marma has been explained by recent authors as the middle cephalic fossa of the skull consisting of
meningial vessels, paranasal sinuses and nerves. One can see the truth of the narration made by Vagbhata here -
the drug administered enters the paranasal sinuses, that is, the Sringataka, where the ophthalmic vein and the other
veins spread out. The sphenoidal sinuses are in close relation with the intracranial structures. The mentioning of
the Sringataka in this context seems to be more reasonable. As the procedure of Nasya involves Mukhabhyanga
and Sveda over many Marmas existing on the face and head, these also help in allievation of Marmaksobha and
Vatashamana. Brumhana Nasya provides nourishment to the Shiras and other Supra clavicular organs there by
alleviates the vitiated Vata. Hence, it is useful in Vatajanyaailments.
According to Absorption in Nasal Epithelium:The richly supplied vascular nature of the nasal mucosa coupled with
its high drug permeation makes the nasal route of administration attractive for many drugs, especially lipids, and
lipid soluble drugs. Lipid soluble substances have grater affinity for passive absorption through the cell walls of
nasal mucosa, thus Navana Nasya may be superior to all the varieties. The cilia of the olfactory cells and perhaps
the portions of the body of the olfactory cells contain relatively large quantities of lipid materials;
thiscouldexplainwhy asubstancemustbe lipidsolubletocausestimulationof olfactory cell and further the
Mukhabhyanga and Svedana helps in vasodilatation and there by increases the rate and area of absorption.
The absorption of drugs is influenced by the residence (contact) time between the drug and the epithelial tissue.
The mucociliary clearance is inversely related to the residence time and therefore inversely proportional to the
absorption of drugs administered. A prolonged residence time in the nasal cavity may also be achieved by properties
of Viscosity. In this study Masha Taila is taken for the Nasya Karma and it is highly viscous.
The Specific gravity of Mashadi Taila, taken for the study was 0.9209 at 250C [API]. The pH of the drug has got
very important role in the Nasal delivery, why because the Nasal epithelium is very thin and heavily vascularised.
So the drug is of high pH, i.e. highly alkaline or acidic (5-14), it will be toxic. The pH of Mashadi Taila is 2, and
there by it will not cause any harm to the nasal epithelium, it will help in better absorptiononly.Thus Mashadi Taila
is having high viscosity and Specific Gravity and non-toxic pH; it will get more time for muco ciliary clearance,
and will retain for more time in the nasal cavity and will help in the better absorption.
According to the Aushadha:Ayurveda has mentioned medicated Sneha Dravya in a majority of the Nasya Karmas,
because nose is a highly vascular structure and its mucous membrane provides a good absorbing surface. Hence,
Siddha Sneha, on their administration, spread along the nasal mucous membrane. An active principle along with
Sneha gets absorbed inside the olfactory and respiratory mucosa. The networks of lymph vessels have
communications with the subdural and subarachnoid spaces. This fact is one of the important factors contributing
to the extension of the mentioned drugs from the nose into the cranial cavity. Therefore, these substances can pass
easily through the blood- brain barrier and can exert their actions. Certain lipids are used for providing energy to
the nervous tissue.
Masha Taila:
It contains many dravya having the qualities like Guru, Snigdha, Picchilaetc. and is Vata Shamaka. Tila Taila
(Sesamum indicum) is considered best among the oils. It is having the qualities like Snigdha, Ushna etc. Tailam
kapha sa vate cha”, if the disease is caused by vata along with kapha.Taila has got both the action of Brumhana and
Karshana. By these properties Taila will help in Brumhana in Vataja condition of Pakshaghata.
The lipid contents of the 'Masha taila' may pass through the blood-brain barrier easily due to their transport. Some
of the active principles may reach certain levels in the nervous system where they can exert their Vataghna property.
Masha Taila provides nourishment to the nervous system on its nasal administration; it reaches different Shirogata
Indriya and causes Vatashamana and Brumhana. On the basis of the foregoing observations we can state that the
procedures, properties & conducts explained for Masha Taila in Nasya Karma are of vital importance in drug
absorption & transportation. To conclude, Nasya Karma helps in Pakshaghata by its Vatashamana and Brumhana
Karma.