transoral laser microsurgery as primary treatment for advanced-stage oropharyngeal cancer: a united...
TRANSCRIPT

ORIGINAL ARTICLE
TRANSORAL LASER MICROSURGERY AS PRIMARYTREATMENT FOR ADVANCED-STAGE OROPHARYNGEALCANCER: A UNITED STATES MULTICENTER STUDY
Bruce H. Haughey, MBChB,1 Michael L. Hinni, MD,2 John R. Salassa, MD,3
Richard E. Hayden, MD,2 David G. Grant, MBChB,3 Jason T. Rich, MD,1
Simon Milov, MD,1 James S. Lewis, Jr, MD,4 Murli Krishna, MD5
1Department of Otolaryngology–Head and Neck Surgery Washington University School of Medicine,St. Louis, Missouri. E-mail: [email protected]
2Department of Otolaryngology–Head and Neck Surgery, Mayo Clinic, Scottsdale, Arizona3Department of Otolaryngology, Mayo Clinic, Jacksonville, Florida4Department of Pathology and Immunology, Washington University School of Medicine, St. Louis, Missouri5Department of Laboratory Medicine and Pathology, Mayo Clinic, Jacksonville, Florida
Accepted 4 October 2010Published online 31 January 2011 in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/hed.21669
Abstract: Background. Nonsurgical modalities are some-
times advocated as the standard of care for advanced oropha-
ryngeal tumors. Oncologic and functional results have been
modest. The aim of our study was to evaluate outcomes of a
minimally invasive approach, using transoral laser microsur-
gery (TLM) as the primary treatment for advanced oropharyn-
geal carcinoma.
Methods. A prospectively assembled database of 204
patients with American Joint Committee on Cancer (AJCC)
stages III and IV tonsil or tongue base cancer, treated primar-
ily with TLM during 1996–2006 at 3 centers with minimum 2-
year follow-up was analyzed. Survival, locoregional control,
and swallowing status were recorded.
Results. Mean follow-up was 49 months and 79.4% of
patients were alive. Three-year overall survival, disease-spe-
cific survival, and disease-free survival were 86%, 88%, and
82%, respectively. Local control was 97%, and 87% of patients
had normal swallowing or episodic dysphagia.
Conclusions. TLM as a primary treatment for advanced
oropharyngeal malignancy confers excellent survival and swal-
lowing proficiency. VVC 2011 Wiley Periodicals, Inc. Head Neck
33: 1683–1694, 2011
Keywords: tonsil cancer; base of tongue cancer; minimally
invasive; human papillomavirus; laser
Over the past decade, the recorded incidence of oro-pharyngeal cancer has increased, attributed mainlyto the human papillomavirus (HPV).1,2 Nonsurgicaltherapies that use varied combinations and timing ofradiotherapy (RT) and chemotherapy are currentlypopular for advanced-stage oropharyngeal cancers.3,4
Although the available literature on RT versus RT
with chemotherapy reports improvement in survivaland locoregional control with chemoradiotherapy(CRT) compared with RT alone, absolute survival anddisease control rates using this treatment approachhave remained modest.5,6 For example, a multicenterphase III trial reported 3-year overall survival (OS),disease-free survival (DFS), and locoregional controlrates of 51%, 42%, and 66%, respectively.6 Anotherrecent study comprising 1681 patients documented anoverall recurrence rate of 25.8% for early and latestages and a local recurrence rate of 11.8% using anonsurgical, primary treatment policy.7 Salvage sur-gery was performed in 24% of locally recurrent cases(41/168) and two thirds of this salvage cohort (67%)developed subsequent rerecurrence.7
Furthermore, RT to the head and neck with con-
current chemotherapy is associated with a high rate
of severe acute toxicities8 in the majority of patients,
treatment-related mortality, swallowing dysfunction,
and late toxic effects such as pharyngeal fibrosis and
severe xerostomia, necessitating nonoral feeding.6,8–11
In the past, conventional surgical intervention foradvanced oropharyngeal cancer has been open en blocsurgery to the pharynx and neck with free flap recon-struction, a major procedure that requires the surgeonto dismantle and repair normal musculoskeletal struc-tures of the neck and maxillofacial skeleton foraccess.12 This en bloc approach often precludes adetailed, magnified view of the invasive front of the tu-mor and the required flaps incur donor wounds. Withthis approach, survivorship has been modest, althoughrecent surgical reports document that p16þ patientshave a favorable prognosis maintained under surgicaltreatment.13,14
Transoral approaches to the oropharynx are, bycontrast, less invasive. Transoral laser microsurgery
Correspondence to: Bruce H. HaugheyThis work was presented orally at the Meeting of the American Headand Neck Society on May 31, 2009, in Phoenix, Arizona.VVC 2011 Wiley Periodicals, Inc.
TLM for Advanced-Stage Oropharyngeal Cancer HEAD & NECK—DOI 10.1002/hed December 2011 1683

(TLM) is a minimally invasive endoscopic surgicaltechnique that offers tumor-targeted treatment, rela-tively rapid recovery, and a low long-term toxicityprofile.15 Starting as a treatment for limited head andneck malignancies,16 its scope has now broadened toinclude advanced T-classification disease at a varietyof sites in the upper aerodigestive tract.17,18 Thus far,the majority of published studies investigating therole of TLM in treating oropharyngeal cancer haverecruited modest numbers with limited follow-up.19 Asingle-center study of 84 patients was recently per-formed to exclusively address American JointCommittee on Cancer (AJCC) stages III and IV, or‘‘advanced’’ oropharyngeal cancer, now one of themost common groups presenting to head and neckcancer treatment centers.20
To document the generalizability of TLM techni-ques for advanced oropharyngeal cancer and to fur-ther analyze prognostic factors such as the role ofadjuvant treatment, which were not discernable inthe previous smaller study,20 this single-center data-base is now pooled with 2 other centers, creating amulticenter, multisurgeon study with a large samplesize and mature follow-up. Our multicenter studyinvestigates the long-term survival, functional out-comes, and relevant prognostic variables, includingp16 and human papillomavirus (HPV) in situ hybrid-ization (ISH) status in patients treated with TLM �postoperative adjuvant therapy.
MATERIALS AND METHODS
Study Design, Population, and Entry Criteria/Patient
Selection. A prospective, computerized databasecomprising head and neck cancer patients (Excel soft-ware; Microsoft Corp., Redmond, WA) was searched foradvanced-stage oropharyngeal cases treated with TLMat 3 tertiary centers: Mayo Clinic Jacksonville, FL;Mayo Clinic Scottsdale, AZ; and Washington Univer-sity School of Medicine/Siteman Cancer Center, St.Louis, MO (a National Cancer Institute–designatedComprehensive Cancer Center). The Human StudiesCommittees at all 3 centers approved the database,plus this specific research protocol. Patients were con-sented individually. Staging, treatments, outcomes,and any complications for each patient were recordedreal time in the database. Information from these pro-spectively gathered data was further verified and con-firmed for this study by careful review of electronic andpaper medical records, national death registries, anddirect telephone contact with patients.
Entry criteria for this study included patients man-aged with TLM þ neck dissection(s) as primary man-agement, with curative intent between September1996 and November 2006, for a biopsy-proven, AJCCstage III or stage IV oropharyngeal squamous carci-noma (T3N0, T1–3N1, T4aN0–1, T1–4aN2, T4a, N3,hereafter referred to as ‘‘advanced oropharyngeal can-cer’’). Three cases of basaloid squamous cell carcinoma
and 1 case of adenosquamous carcinoma were includedgiven that these are variants of squamous cell carci-noma (SCC). All had been followed for a minimum of 2years, or to death. Patients were included who had al-ready undergone diagnostic procedures up to a tonsil-lectomy or neck node biopsy, and who weresubsequently referred to 1 of the centers for definitiveTLM management. Patients were excluded who had aprior history of head and neck aerodigestive tract can-cer or evidence of distant metastasis at presentation.After these exclusions we identified 204 patients whomet criteria and who became the subjects of this study.
Patients were not selected in accord with HPVstatus, since in the majority of the decade of thisstudy the contribution of HPV to oropharyngeal can-cer was unsuspected and there is no known distinc-tive or validated clinical ‘‘phenotype’’ of HPV ISH orp16þ tumors by which to select these tumors. Fur-thermore, the pathologists’ testing for HPV in thisstudy was entirely post hoc, not in any case on pre-treatment biopsies. During this study there was norecord of how many patients were not considered eli-gible for TLM but by surgeon report a few wereexcluded for poor transoral access.
N classification was determined and recordedfrom pathologic results of neck dissections, and Tclassification was determined primarily by clinicalstaging, unless operative findings upstaged the dis-ease (eg, extension to the extrinsic tongue muscula-ture or pterygoid muscles).
Treatment
Primary Tumor/TLM. Attending surgeons at the MayoCenters, attendings, and fellows at Washington Uni-versity performed all TLM procedures, following theprinciples of TLM set forth by Steiner andAmbrosch.17 The role of TLM in this patient cohortwas to completely eliminate all known primary siteoropharyngeal disease to a negative microscopic mar-gin. For tonsil and base of tongue primaries, a modi-fied mouth gag and/or a modified expandablelaryngoscope is used to expose the primary tumor. Anoperating microscope or rod telescope is used to illu-minate and magnify the operative field and to discernclearly between healthy versus tumor tissue at theperimeter of the resection bed as the tumor is trans-ected and excised segmentally with a CO2 laser. Verybulky tumors are expeditiously cored out and reducedin size, so that a ‘‘rind’’ of tumor remains that is thenmanaged using series of transtumoral cuts.
The tumor is deliberately transected at a series oflocations to map deep extension along the invadingfront. A reasonable margin of normal tissue, usually 1to 1.5 cm, is excised beyond the invading front of the tu-mor. The specimen is removed in 2 or more pieces as amultibloc resection. Margins of the resected tissue aredetermined by the surgeon, inked in the operatingroom to allow orientation, and then analyzed by
1684 TLM for Advanced-Stage Oropharyngeal Cancer HEAD & NECK—DOI 10.1002/hed December 2011

pathologists. Frozen sections are used to direct furtherlaser resection of any invisible residual microscopic dis-ease, such as around and along the styloid apparatus inlarge tonsil tumors that invade into the pterygoids(T4a), and the floor of mouth/submandibular glandstructures anteriorly, in a large base of tongue tumors.TLM thus allows for controlled and complete primarytumor excision in nearly all cases, with maximal pres-ervation of normal tissue and function.
Defects from these resections can be large enoughto expose the mandible, large vessels including the in-ternal carotid, and/or result in full thickness defects ofthe soft palate. Such large wounds can be slow to heal,especially when resection extends well into the para-pharyngeal space. Each of the above-cited criteriaserves as a potential indication for endoscopic tissuegrafting or flap reconstruction (see Figure 1).
Neck Dissection and Adjuvant Therapy. Neck dissectionsremoving level II through IV lymph nodes were per-formed in a single surgical session with TLM, basedon the presence of cervical lymphadenopathy or riskof occult metastasis. Dissection was extended to levelIB if the primary tumor invaded the floor of mouthfrom the tongue base. Administration of adjuvanttherapy was based on pathology reports of extracap-sular spread (ECS) from nodal metastasis, �2 posi-tive, or contralateral lymph nodes, positive margins,patient preference for chemotherapy, surgeon recom-mendation, and an array of hematologic, biochemical,and performance status criteria. Use of adjuvant CRTversus RT varied between centers in accord with localtreatment policy, and over time of the study, withmore cases receiving CRT in later years due to evolv-ing ‘‘high risk’’ criteria.
Pathology Review and HPV Testing. To detect HPV indiceswe used immunohistochemical staining (IHC) for p16and ISH for HPV DNA. p16, a tumor suppressor gene,is aberrantly overexpressed secondary to action of theHPV E7 oncogene effect on the retinoblastoma gene,making it a surrogate marker of HPV presence.21,22 Wealso classified the histomorphology of the tumors into 3groups, as previously reported.23 Type 1, or keratiniz-ing SCC, was defined as entirely composed of maturesquamous cells without areas demonstrating NK SCCmorphology. Type 2, or ‘‘hybrid’’ SCC, showed convinc-ing nonkeratinizing morphology, but with significantareas of squamous maturation. Type 3, or nonkeratiniz-ing SCC, was defined as forming sheets, nests, or tra-beculae with pushing borders, little stromal response,and having ovoid to spindled, hyperchromatic cells thatlack prominent nucleoli, but indistinct cell borders.
After assembly of the study population from ourdatabase, p16 and HPV status of tumors were ana-lyzed exclusively by a single, study pathologist(J.S.L.) without knowledge of clinical status, follow-up, or outcome. A representative block was chosen at
each center, but the analyses were done at the pathol-ogy study center, Washington University.
IHC for p16 was performed using monoclonal anti-body (MTM Laboratories CINTEC, Westborough, MA)and either DAKO LSAB2 horseradish peroxidase sys-tem (DAKO Corp., Carpenteria, CA) or Ventana Autos-tainer (Ventana Medical Systems Inc., Tucson, AZ). p16IHC for all cases showed either no staining or >75% oftumor cells positivity. Results were classified in a bi-nary manner as negative or positive, with positive indi-cating >75% presence of p16 gene overexpression. ISHfor HPV was performed using ISH I View Blue PlusDetection Kit (Ventana Medical Systems), whichhybridizes with high-risk HPV genotypes 16, 18, 33, 35,45, 51, 52, 56, and 66. Any definitive nuclear stainingin the tumor cells was considered positive.
Information about other pathologic variables,including extracapsular extension in cervical lymphnode metastases, was gleaned from the patients’ sur-gical pathology reports and not by central review.Final margin status was defined by the specific sur-geon after integrating operative findings with finalhistopathologic analysis.
Statistical Analysis. Primary endpoints for thisstudy were overall survival (OS), disease-specific sur-vival (DSS), and disease-free survival (DFS). Second-ary endpoints were HPV status (p16, ISH,histopathology), patterns of failure (local, regional,distant), ECS from neck nodes, tracheostomy rates,days of hospitalization, and swallowing function asdetermined by gastrostomy tube (G-tube) placement(single-center study) and Functional Outcome Swal-lowing Scale (FOSS).24 The FOSS ranks swallowingfunction from 0 to 5, with 0 being normal function
FIGURE 1. Endoscopic view of left oropharyngeal wall recon-
struction with an anterolateral thigh (ALT) flap, healed following
transoral laser microsurgery (TLM), and endoscopic flap inset.
(i) ALT flap, (ii) tongue base, (iii) epiglottis, and (iv) native pha-
ryngeal wall. [Color figure can be viewed in the online issue,
which is available at wileyonlinelibrary.com.]
TLM for Advanced-Stage Oropharyngeal Cancer HEAD & NECK—DOI 10.1002/hed December 2011 1685

and 4 to 5 being gastrostomy tube (G-tube) dependent(Table 1). OS was defined as the time from surgery tothe date of death resulting from any cause. DSS wasdefined as the time from surgery to the date of deathfrom oropharyngeal cancer or the direct effects of itstreatment. DFS was defined as the time from surgeryto the date of death or recurrence of disease. A vari-ety of prognostic variables, including patient demo-graphics, site and stage of tumor, margins, HPVbiomarkers, and treatment modality (Tables 2 and 3)were stratified and tested for significance of effects onthe 3 survival outcomes calculated in this study. Sur-vival data were expressed as crude rates, as well asby the Kaplan–Meier method, and statistical signifi-cance was determined by log-rank testing.
To adjust for covariate effects and calculate haz-ard ratios (HRs), Cox proportional hazards modelswere developed when appropriate. In the multivariateanalysis, Cox proportional hazards model was used toadjust for variables that were likely on clinicalgrounds to have an effect, or were statistically signifi-cant from the univariate analyses. All statistical testswere 2-sided, and values of p � .05 was consideredsignificant. All analyses were performed using SAS9.1.3 software (SAS Institute Inc., Cary, NC). A logis-tic regression model was performed to assess theFOSS scores for adjuvant RT and CRT relative to noadjuvant treatment. A global nonparametric test wasused to test the difference in median FOSS scores bypostoperative adjuvant therapy (none, adjuvant RT,or CRT).
RESULTS
Patients, Tumor, and HPV Characteristics. Therewere 214 patients with stage III or stage IV oropha-ryngeal squamous cell carcinoma (OPSCC) registeredin the respective centers’ TLM databases from Sep-tember 1996 to November of 2006. Ten living patientswere excluded because all had been followed up for
less than the required 2 years (mean follow up ¼ 11� 7.4 months). Thus, a total of 204 patients met entrycriteria for this study with known follow-up of at least2 years, or to death. There were 181 men and 23women, with a total median cohort age of 57 years.Mean (� SD) and median (minimum–maximum) fol-low-up intervals were 48 (� 27) months and 42 (1–132) months, respectively. In the entire populationduring the study period, 42 of 204 patients (20.5%)died, 19 patients (9.3%) from the disease under treat-ment, 19 patients (9.3%) of nonoropharyngeal cancer-
Table 2. Patient characteristics and prognostic variable
analysis (n ¼ 204).
Characteristic
No. of
patients
n (%)
Univariable
analysis
p value
Multivariable
analysis
HR (95% CI):
p value
Center of study
WUSM 89 (43.6)
Mayo–Scottsdale 62 (30.4)
Mayo–Jacksonville 53 (26.0)
Age, y
Mean (range) 58 (35–86) .32
Sex
Male 181 (89)
Female 23 (11) .84
Tumor subsite
Base of tongue 106 (52)
Tonsil and soft palate 98 (48) .11
T classification
T1 61 (30) .025* 2.30
(1.22–4.35)T2 74 (36)
p ¼ .010T3 45 (22)
T4 24 (12)
N classification
N0 15 (7.5) 006*
N1 39 (19)
N2 135 (66)
N3 15 (7.5)
AJCC stage
III 49 (24)
IV 155 (76) .34
HPV ISH (N ¼ 174)
Positive 126 (74) .013* 0.42
(0.21–0.84)
p ¼ .014
Negative 44 (26)
p16 staining (N ¼ 185)
Positive 167 (90) <.0001* 0.12
(0.059–0.025)
p < .0001
Negative 18 (10)
Histopathology (N ¼ 193)
Nonkeratinizing 127 (66)
Keratinizing 29 (15)
Hybrid 37 (19)
ECS (N ¼ 194)
Positive 125 (64)
Negative 69 (36) .23 1.91
(0.89–4.11)
p ¼ .098 (n.s.)
Abbreviations: HR, hazard ratio; CI, confidence interval; WUSM, Washington Univer-sity School of Medicine; AJCC, American Joint Committee on Cancer; HPV, humanpapillomavirus; ISH, in situ hybridization; ECS, extracapsular spread; n.s, notsignificant.*Significant at p < .05.
Table 1. Functional Outcome Swallowing Scale (FOSS).
Stage Symptoms
0 Normal function and asymptomatic
1 Normal function with episodic or daily symptoms
of dysphagia
2 Compensated abnormal function manifested by
considerable dietary modifications or prolonged
mealtime (without weight loss or aspiration)
3 Decompensated abnormal function with weight loss
of 10% of body weight over 6 months, attributed to
dysphagia or daily cough, gagging, or aspiration
during meals
4 Severely decompensated abnormal function with weight
loss of 10% of body weight over 6 months, attributed
to dysphagia or severe aspiration with
bronchopulmonary complications. Nonoral
feeding for most nutrition.
5 Nonoral feeding for all nutrition
1686 TLM for Advanced-Stage Oropharyngeal Cancer HEAD & NECK—DOI 10.1002/hed December 2011

related causes, and 4 patients (2%) of unknown cause.These 4 cases were counted as deaths of disease forthe DSS calculation.
Of the 204 patients in the study, p16-stainingdata were available for 185 patients (91%), with 167patients (90%) staining positive for p16 and 18patients (10%) negative. HPV ISH staining was avail-able for 174 patients (85%), with 126 patients (74%)staining positive and 44 negative (26%). Other demo-graphic, tumor, and pathologic characteristics are dis-played in Table 2.
Treatment and Hospital Stay. Summaries of treat-ment data are available in Tables 3 and 4. Seven of204 patients (3%) were completed as open proceduresthrough a small pharyngotomy created at the time ofthe simultaneous neck dissection, to remove minimalgross or suspected microscopic tumor residue, not ac-cessible transorally. Fifteen patients (7%) had micro-scopic positive margins reported on permanentpathologic analysis following the initial resection.From this group, 5 patients had negative margins fol-lowing reresection and 1 patient had positive micro-scopic margins despite 3 additional resections. Neckdissections were performed in 197 patients (96%), ip-silateral in 164 patients (80%), and bilateral in 33patients (16%). The decision for bilateral neck dissec-tion was based on the presence or risk of contralat-eral metastasis, the risk presumed higher whenprimary tumor was present at or near the midline.
The mean (median) hospital stay was 4.4 (4) days,with a minimum (min) of 0 and maximum (max) of 23days.
Adjuvant Therapy. Adjuvant RT was administeredto 150 patients (74% of total series), 117 (58%) receiv-ing adjuvant RT alone, whereas 33 patients (16%)received adjuvant CRT. Of 203 patients with RT sitedata available, 105 patients (52%) received plannedRT to the primary site, whereas 146 patients (72%)received planned RT to the neck. Because somepatients received RT at outside facilities, the dose andtype of RT administered were not available for allpatients. At Washington University (n ¼ 89), adju-vant RT was administrated to 81 patients (91%), fromwhich 50 patients (61.7%) received radiotherapyalone and 31 patients (34.8%) received concomitantCRT. Intensity-modulated radiation therapy (IMRT)was the radiation modality in 85% (n ¼ 69/81) ofthe patients. Planned RT of median dose 66 Gy (Min–Max: 44–70 Gy) was administered at the primary sitein 80 patients and ipsilateral neck in 81 patients.Only 2 patients received a dose of 70 Gy. The contra-lateral neck when treated received planned adjuvantRT in 74 of 81 patients (91%) at a median dose of 56Gy (Min–Max: 36–66 Gy).
Complications
Primary Tumor/TLM. There were no direct, treatment-related deaths in this cohort, although 1 patient sus-tained a myocardial infarction in the perioperative pe-riod, dying on postoperative day 17. Six patientsexperienced bleeding, 3 incidences of which occurred onpostoperative days 3, 6, and 27, and required a returnto the operating room. The airway was lost on 1 patientundergoing anesthetic induction for reresection ofa positive margin, necessitating an operativecricothyrotomy. One patient developed bilateral hypo-glossal nerve paresis, a documented, stretch-relatedcomplication of endoscopic approaches to the pharynx(eg, tonsillectomy). Eleven patients demonstrated post-operative velopharyngeal incompetence, although nonesevere enough to prevent oral intake or good speechintelligibility. Tracheotomy was performed at the time ofTLM or within 30 days of surgery in 36 patients (18%),and after 30 days in 1 patient.
Table 4. T and N classifications and
adjuvant treatment (n ¼ 203).
Classification
No adjuvant
n (%)
RT alone
n (%)
CRT
n (%) Total
T classification
T1 14 (23) 40 (66) 7 (11) 61
T2 14 (19) 46 (62) 14 (19) 74
T3 20 (42) 19 (42) 6 (16) 45
T4 5 (21) 12 (54) 6 (25) 23
N classification
N0 9 (60) 5 (33) 1 (7) 15
N1 16 (38) 20 (51) 3 (10) 39
N2 24 (18) 85 (63) 26 (19) 135
N3 4 (27) 7 (53) 3 (20) 14
Total 53 (26) 117 (58) 33 (17) 203
Abbreviations: RT, radiotherapy; CRT, chemoradiotherapy.
Table 3. Treatment and margins data analysis.
Treatment and
margin status
No. of
patients
n (%)
Univariable
analysis
p value
Multivariable
analysis HR
(95% CI):
p value
TLM for primary
resection
204 (100)
Neck dissection (N ¼ 204)
None 7 (3.5)
Unilateral 164 (80.5)
Bilateral 33 (16.0)
Margin status
Negative 189 (93)
Positive 15 (7) .030 2.6 (1.09–6.2)
p ¼ .032
Adjuvant treatment (N ¼ 203)
Yes 150 (74)
No 53 (26)
Type of adjuvant treatment
None 53 (26)
Radiation therapy
alone
117 (58) .047 0.48 (0.23–0.99)
P ¼ .046
CRT 33 (16) (n.s.)
Abbreviations: HR, hazard ratio; CI, confidence interval; CRT, chemoradiotherapy;n.s, not significant.
TLM for Advanced-Stage Oropharyngeal Cancer HEAD & NECK—DOI 10.1002/hed December 2011 1687
Neck Dissection and Medical Complications. Of the 230neck dissections performed, there were 5 spinal acces-sory nerve injuries, 3 each of neck infections andchyle leaks, 2 seromas, and 2 hematomas, 1 of whichwas treated conservatively, whereas another requiredsurgical intervention. There was 1 each of myocardialinfarction and perioperative pulmonary embolism.
Adjuvant Therapy. Six patients developed late radiation-induced esophageal stenosis, 2 trismus, 2 osteoradionec-rosis of the mandible, and 1 late radiation necrosis ofthe pharynx and parapharyngeal space, necessitatingfree flap reconstruction.
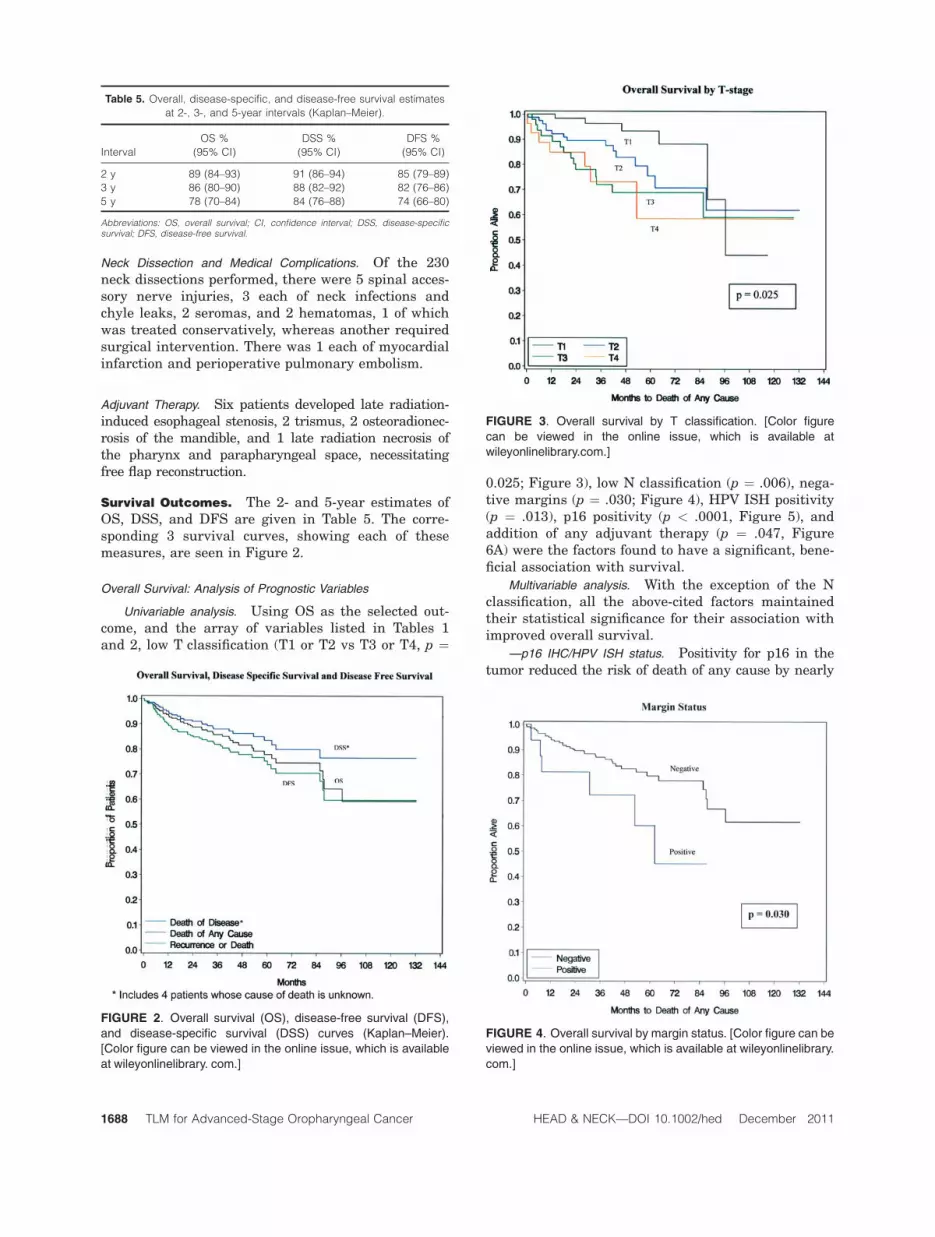
Survival Outcomes. The 2- and 5-year estimates ofOS, DSS, and DFS are given in Table 5. The corre-sponding 3 survival curves, showing each of thesemeasures, are seen in Figure 2.
Overall Survival: Analysis of Prognostic Variables
Univariable analysis. Using OS as the selected out-come, and the array of variables listed in Tables 1and 2, low T classification (T1 or T2 vs T3 or T4, p ¼
0.025; Figure 3), low N classification (p ¼ .006), nega-tive margins (p ¼ .030; Figure 4), HPV ISH positivity(p ¼ .013), p16 positivity (p < .0001, Figure 5), andaddition of any adjuvant therapy (p ¼ .047, Figure6A) were the factors found to have a significant, bene-ficial association with survival.
Multivariable analysis. With the exception of the Nclassification, all the above-cited factors maintainedtheir statistical significance for their association withimproved overall survival.
—p16 IHC/HPV ISH status. Positivity for p16 in thetumor reduced the risk of death of any cause by nearly
Table 5. Overall, disease-specific, and disease-free survival estimates
at 2-, 3-, and 5-year intervals (Kaplan–Meier).
Interval
OS %
(95% CI)
DSS %
(95% CI)
DFS %
(95% CI)
2 y 89 (84–93) 91 (86–94) 85 (79–89)
3 y 86 (80–90) 88 (82–92) 82 (76–86)
5 y 78 (70–84) 84 (76–88) 74 (66–80)
Abbreviations: OS, overall survival; CI, confidence interval; DSS, disease-specificsurvival; DFS, disease-free survival.
FIGURE 2. Overall survival (OS), disease-free survival (DFS),
and disease-specific survival (DSS) curves (Kaplan–Meier).
[Color figure can be viewed in the online issue, which is available
at wileyonlinelibrary. com.]
FIGURE 3. Overall survival by T classification. [Color figure
can be viewed in the online issue, which is available at
wileyonlinelibrary.com.]
FIGURE 4. Overall survival by margin status. [Color figure can be
viewed in the online issue, which is available at wileyonlinelibrary.
com.]
1688 TLM for Advanced-Stage Oropharyngeal Cancer HEAD & NECK—DOI 10.1002/hed December 2011

90% (HR ^ 0.11–0.12) relative to patients having nega-tive staining. Presence of HPV ISH positivity reducedthe risk of death by 60% to 70% (HR ^ 0.3–0.4) rela-tive to patients who are HPV ISH negative.
—T classification. Having a tumor of T classifica-tion 3 or 4 versus 1 or 2 approximately doubled therisk of death (HR 2.0–2.3).
—Margins. After the first resection, 189 patients(93%) were rendered margin negative at the primarysite. Positive margins after surgery raised the risk ofdeath by 2.5- to 3.0-fold (HR 2.5–3.1) relative topatients with negative margins. Of interest, althoughthe margin negative group had fewer T3 and T4 casesthan the margin positive group (34% vs 50%), this dif-ference was not statistically significant (p ¼ .25, Fish-ers exact test). Furthermore, there were nosignificant differences between the 2 margin statusgroups in p16 status (p ¼ .18, Fisher exact test) oradministration of adjuvant therapy (p ¼ .42, Fisherexact test). The close matching of these 2 groups andthe sustained, independent significant effect of mar-gin status point to the critical beneficial role of thesurgical component of treatment at the primary site,independent of adjuvant therapy.
—Adjuvant therapies. Adjuvant radiotherapy wasadministered in 150 of 203 patients (74%). Of these 150patients, 33 also received chemotherapy. Receiving RTreduced the risk of death by �50% (HR 0.33–0.48) rela-tive to receiving no adjuvant treatment. There was nostatistical evidence from our study that adding chemo-therapy to the adjuvant radiation treatment reduced therisk of death. The frequency of recurrence was similar inpatients receiving adjuvant RT alone (11%) or in combi-nation with chemotherapy (9%) (n.s., Table 6).
In a separate analysis of the ‘‘high risk’’ patientswith ECS or positive margins, the 2 CRT and RT-alone
adjuvant groups are closely matched, with exactly thesame proportion of p16 positive patients (90% each, 0.99,Fisher exact test) and no significant differences in T-clas-sification distribution (p ¼ .13, Fisher exact test) ormean age (54 vs 57 years, p ¼ .06, Fisher exact test). The5-year Kaplan–Meier OS estimate for the CRT high-riskgroup (n ¼ 33) and the RT-alone high-risk group (n ¼111) were 82% and 79%, respectively (n.s., log-rank)
Extracapsular Spread. Table 1 indicates that 63% ofpatients (n ¼ 125/197) undergoing neck dissection hadECS identified in lymph nodes, but this finding wasnot statistically associated with the survival status.This confirms the result seen in the single-center St.Louis study.20
Disease-Free Survival: Analysis of Prognostic Variables
Univariable analysis. Using DFS as the outcome ofinterest during the study period, the following factorsFIGURE 5. Overall survival by p16 staining. [Color figure can
be viewed in the online issue, which is available at
wileyonlinelibrary.com.]
FIGURE 6. (A) Overall survival (OS) by use and type of adju-
vant therapy. (B) Disease-free survival (DFS) by use and type
of adjuvant therapy. [Color figure can be viewed in the online
issue, which is available at wileyonlinelibrary.com.]
TLM for Advanced-Stage Oropharyngeal Cancer HEAD & NECK—DOI 10.1002/hed December 2011 1689

were found to be significant: age >75 years (n ¼ 19, p¼ .0023), high N classification (p ¼ .048), positivemargins (p ¼ .029), histologic tumor typing (p <.0001), HPV ISH positivity (p ¼ .0055), p16 positivity(p < .0001), and the use of adjuvant therapy (p ¼.0088).
Multivariable analysis. The following predictors werefound to be significant using DFS as the outcome ofinterest: T classification, HPV ISH positivity, p16 posi-tivity, and adjuvant treatment.
—T classification. The risk of death or recurrenceincreased by about 2.5-fold in patients with T3 or T4tumors relative to those with T1 or T2 disease (HR ¼2.46; confidence interval [CI] 1.05–5.53).
—Adjuvant treatment. Patients with adjuvant RT hada reduction of 62% in the risk of recurrence or deathrelative to those with no adjuvant therapy (HR ¼ 0.38;CI 0.20–0.73). Addition of chemotherapy to adjuvant RThad no further risk reduction (see Figure 6B).
—p16/HPV ISH positivity. p16-positive patients havea reduction of 83% (HR ¼ 0.17; CI 0.088–0.34) in therisk of recurrence or death than p16-negativepatients, even after taking into account the effect ofadjuvant treatment. HPV-positive patients had areduction of 64% in risk relative to HPV-negativepatients (HR ¼ 0.36; CI 0.20–0.68).
Locoregional Control Rate and Patterns of
Failure. Twenty-six patients (12.7%) had disease re-currence at any site and, of these, recurrenceoccurred at more than 1 site in 4 patients. Sevenpatients (3.4%) had recurrence at the primary site, 7patients (3.4%) had recurrence in the neck, both loca-tions occurring at median intervals of 10 months fromsurgery, for an overall locoregional control rate of93.2%. Of the 7 local recurrences, only 1 had knownpositive margins, and 3 received radiotherapy, 2 tothe primary and 1 to the neck. Twelve patients (5.9%)developed distant metastasis, at a median (mini-mum–maximum) interval of 14 (2–62) months fromsurgery. Of the 7 neck recurrences, 2 of 3 patientswho did receive adjuvant therapy (all including theneck) died of disease. Three of 4 patients who did notreceive adjuvant therapy died of disease.
Table 7 summarizes these findings, showing recur-rences by T and N classification. Distant metastasis
was exclusively observed in N-positive patients. Localrecurrences were only slightly more common in T3 orT4 tumors (4/7) than in T1or T2 tumors (3/7).
Swallowing Function. FOSS scores at last follow-upwere available for 203 patients. Eighty-seven percent ofthese patients had FOSS stages from 0 to 2, which rep-resents either normal swallowing, or up to compen-sated, mild dysphagia, without weight loss oraspiration. The impact of postoperative adjuvant ther-apy on swallowing was evaluated for 202 patients(incomplete adjuvant treatment data, n ¼ 1). Signifi-cant differences in median FOSS score existed betweentreatment categories (p ¼ .0022), ie, between patientswith no adjuvant treatment and adjuvant RT alone (p¼ .012), and between patients with no adjuvant treat-ment and CRT (p ¼ .0006). The proportion of patientswith FOSS score 0 to 2 was highest in those receivingno adjuvant treatment (90%), followed by group withadjuvant RT alone (88%) and was least in patientstreated with CRT (78.7%). Conversely, the proportion ofpatients with FOSS score 3 to 5 was highest in patientsreceiving CRT (21%), followed by those treated with RTalone (12%) and least in patients with no adjuvanttherapy (9.6%). The odds of poor swallowing were 2.5-fold higher in patients receiving CRT than in thosewith no adjuvant treatment; however, the small num-ber with FOSS scores 3 to 5 group limits significance(C.I. 0.73, 8.8) (see Figure 7 and Table 8).
Gastrostomy rates as a swallowing measurewere available in a subset of patients (WashingtonUniversity in St. Louis, n ¼ 89). Thirty-nine of 89patients (43.8%) had a gastrostomy tube placed atsome point during their overall treatment for can-cer. Seventy patients (83%), however, progressedthrough a 1-month perioperative period before ini-tiation of adjuvant therapy, without a G-tube. The
Table 6. Distribution of site of recurrences by type of postoperative adjuvant therapy (n ¼ 203 patients), 26 patients with recurrence.*
Site of
recurrence
No adjuvant
therapy (n ¼ 53)
Adjuvant RT (n ¼ 117) by site of RT delivery CRT (n ¼33)
Total
Primary
alone (n ¼ 4)
Neck alone
(n ¼ 45)
Primary þ neck
(n ¼ 68)
RT to
primary þ neck
Local 5 2 1 0 0 8
Regional 6 0 1 2 2 11
Distant 4 1 3 3 1 12
Total 15 3 5 5 3 31
Abbreviations: RT, radiotherapy; CRT, chemoradiotherapy.*12 patients received no adjuvant therapy, 12 adjuvant RT, and 2 CRT.
Table 7. Site of recurrence by T and N classifications.
T classification Local Regional Distant
T1 and T2N0* 0 0 0
T1 and T2Nþ* 3 5 8
T3 and T4N0** 1 2 0
T3 and T4Nþ** 4 4 4
Total number of patients: *T1 and T2 ¼ 135; **T3 and T4 ¼ 69.
1690 TLM for Advanced-Stage Oropharyngeal Cancer HEAD & NECK—DOI 10.1002/hed December 2011

highest rate of G-tubes was 33.7%, seen at 3months postoperatively, which is simultaneous withthe delivery of adjuvant therapy. The prevalence ofpatients with G-tubes over time was 18.8% at 1year, 9.3% at 2 years, 3.4% at 3 years, 4.7% at 4years, and 3.8% at 5 years from surgery.
DISCUSSION
Although use of the most common head and neck can-cer carcinogen, tobacco, has been falling in the UnitedStates,25 the overall incidence of upper aerodigestivetract malignancies has remained stable. The majorfactor contributing to this observation is a rising inci-dence of oropharyngeal cancer, to the point where itis now one of the most common primary head andneck sites seen at cancer treatment centers.1,26 HPVhas been implicated as a causative agent in head andneck cancer, especially in the oropharynx.2 Disease ofthis ilk strikes at a younger age than has historicallybeen the typical age for head and neck cancer toappear, and a growing number of studies have dem-onstrated that HPV-associated tumors carry a veryfavorable prognosis.13,27 This is in the context ofusing a variety of intense treatment protocols hith-erto used on tumors not apparently of viral origin,which carried a more guarded if not grim prognosis.
Chemoradiation was once thought to be a way ofpreserving organs,28,29 but this outcome has now beenshown to fall off markedly in addition to low survivalrates in patients, 5 years from treatment.30 In oropha-
ryngeal cancer, the impact of current CRT regimens onsurvival, a fundamental outcome, and on organ preser-vation has never been tested against the surgicalapproaches and, in particular, the contemporary mini-mally invasive techniques such as TLM in a random-ized controlled trial. Despite this lack of proof, anddifferences in the pathophysiology of oropharyngealcancer from more broadly investigated laryngeal can-cer, chemoradiation has been promoted as the treat-ment of choice for the oropharynx,6,31–36 apparentlybased on its (now somewhat disappointing) perform-ance in the larynx. Thus, to date, the emphasis and in-sistence on nonsurgical treatment for oropharyngealcancer, practiced at many major cancer centers,appears to be based on a scientifically invalid premise,ie, the untested assumption that surgery results in in-ferior functional outcomes and probably survival aswell. To compound this problem and as many headand neck oncologists know from their practices, it hasbeen confirmed by mature cooperative group analysesthat CRT treatment protocols carry high rates ofacute37,38 and late, prolonged ‘‘toxicities,’’ or sideeffects of treatment, the most common of which isswallowing dysfunction, which carries its own mortal-ity independent of disease.11
These facts invite scrutiny of a new wave of treat-ment methods that confer excellent oncologic progno-sis but with reduced treatment-related functional lossand cost for patients, especially those with an a pri-ori, biologically driven good prognosis.39
Surgery, in general, has made rapid strides towardminimally invasive techniques in most disciplines. In thehead and neck, we have seen such approaches for theaerodigestive tract, thyroid, parathyroid, and skullbase.17 In the oropharynx, smaller TLM studies encom-passing the full range of, but with predominantly earlierT classifications and limited follow-up, have been pub-lished.19 Most oropharyngeal cancers, however, presentat an advanced overall stage. A recent single-centerstudy has shown promising results for stage III andstage IV oropharyngeal SCC treated with TLM � adju-vant therapy.20 For this reason we undertook to presentthe current, expanded multicenter study in which theprimary treatment for advanced-stage oropharyngealmalignancy was TLM þ neck dissection, with or withoutadjuvant therapy, as indicated by ‘‘high-risk’’ pathologicor clinical features.
Table 8. Distribution of FOSS scores (0–5) by types of adjuvant therapy
in multicenter series (n ¼ 202 patients).
FOSS score
No adjuvant
therapy (%)
Adjuvant
RT (%)
CRT
(%) Total
0–2 47 (90.0) 103 (88) 26 (78.7) 176
3–5 5 (9.6) 14 (12) 7 (21.0) 26
Total 52 117 33 202
Abbreviations: FOSS, Functional Outcome Swallowing Scale; RT, radiotherapy;CRT, chemoradiotherapy.*p value for differences in FOSS scores between patients with no adjuvant treatmentand adjuvant treatment ¼ .012; no adjuvant treatment versus CRT ¼ .0006.
FIGURE 7. Distribution of FOSS (Functional Outcome Swallow-
ing Scale) scores among cancer patients with stages III and IV
oropharyngeal cancer treated with transoral laser microsurgery
(TLM) as the primary treatment modality.
TLM for Advanced-Stage Oropharyngeal Cancer HEAD & NECK—DOI 10.1002/hed December 2011 1691

In contrast to chemoradiation protocols, patient eli-gibility for TLM is broad and is not necessarily con-strained by age, hematologic, biochemical, renal,cardiopulmonary, or performance status criteria. Con-traindications to TLM include inadequate endoscopicaccess (which is rare for the oropharynx) or projectedunresectability because of a probable positive margin.Examples of this are lateral extension of tonsil tumorsthrough the infratemporal fossa to invade the greatvessels or ventral extension of tongue base tumors intothe anterior floor of mouth. TLM is still an appropriateapproach for patients who require microvascular freeflap reconstruction because of great vessel exposure orthe size of the wound in that inset of the flap can beaccomplished endoscopically. Thus it is not theadvanced T or N classification of disease but thepatient’s anatomy and/or tumor extent that may limitthe use of TLM as a primary treatment.
Survival Outcomes. With 204 patients in this seriesfollowed for a minimum of 2 years and an average of4 years, we believe that the current multicenter studyprovides definitive evidence for the efficacy of TLM asthe primary treatment approach for advanced oropha-ryngeal cancer. Our study demonstrates 2- and 5-yearOS estimates of 89% and 78%, DSS estimates of 91%and 84%, and DFS estimates of 85% and 74%, respec-tively (Table 5). These results compare favorably withstudies using chemoradiation approaches, some inwhich nonsurgical treatment methods were used de-spite the tumors being designated as resectable.Although some of these studies may differ fromours in proportions of T classification or reporting ofpositivity for HPV biomarkers, those that are compa-rable reveal very similar oncologic outcomes. A recentCRT study (n ¼ 71) by Huang containing 32% T3 andT4 cases, reported an overall survival of 83% at 3 years,a locoregional control rate of 90% (salvage surgeryincluded), but a gastrostomy tube rate of 35%.34 In thecurrent study (n ¼ 204) with 34% T3 and T4 tumors,the overall survival was 86% at 3 years, locoregionalcontrol was 93%, and a long term G-tube rate wasapproximately 4% in the single-center, St. Louis subset(n¼ 89, St. Louis).
We believe, based on these valid comparisons,that TLM as the primary treatment approach offers asurgical alternative for treatment of the primary tu-mor that potentially avoids the acute and chronicthreat to upper aerodigestive tract function posed byhigh-dose radiotherapy targeted at the pharynx, oftensensitized to an even greater functional impact byconcurrent chemotherapy.
Prognostic Factors. Study of a set of predictors inthese data provides valuable information regarding a va-riety of independent prognostic variables, confirms theconcept of a highly favorable prognosis group (p16-posi-tive stainers), and guides treatment recommendations
for the future. The most powerful prognostic effect in ourstudy population was the presence of HPV biomarkers inthe tumor. The 3- and 5-year survival rates for p16-posi-tive patients were 92% and 86%, respectively, whereasfor p16-negative patients the rates were 52% and 30%,respectively. p16-positive patients also seem to obviatethe high risk traditionally thought to exist for the pres-ence of a high N classification. This finding has beenreported recently in other surgical p16-positive oropha-ryngeal SCC patient series.14 Furthermore, ECS frommetastatic nodes, despite a prevalence of 64%, did notachieve prognostic significance in either the univariableor multivariable analyses for OS. Taken together, p16positivity conferred an excellent outcome, independent ofthe hitherto widely reported risk factors of high N classi-fication and ECS. These facts promote consideration byscientific societies of a new staging system for oropharyn-geal cancer, stratified by p16, much as we currently strat-ify thyroid cancer stages by age. We propose this findingis critical since it hypothesizes that ECS-positivepatients, the majority, are not at high risk and may qual-ify for deintensified adjuvant treatment. This is possiblysupported by our other finding that chemotherapy wasnot associated with significant survival benefit inpatients hitherto considered high risk. The discussion ofdeintensified therapy has also been espoused in nonsur-gical series of advanced oropharyngeal cancer,26 andalthough a prospective trial would be desirable, it is diffi-cult to accomplish over a reasonable time asan equivalency study design, to prove the hypothesis.
The fact that we detected a high prevalence ofp16 positivity, higher than that seen in most nonsur-gical studies, may be explained by the availability ofwhole surgical specimens to the study pathologist,e.g., one recent non-surgical retrospective study usingarchived material showed a 50% (215/433) prevalence.It should be noted that there are no known anecdotalor evidence-based clinical criteria for identification ofp16-positive tumors, versus p16-negative, that wereor could have been used in this series for patientselection. The discrepancy we observed between thepositivity rates of p16 (90%) and HPV (74%) is attrib-uted to the more moderate sensitivity of HPV ISH. Inprevious studies, approximately 15% to 20% of p16-positive oropharyngeal SCCs have been found to beHPV ISH negative.8,40,41
The negative impact of high T classification onprognosis is expected and is frequently seen in otherstudies, both surgical and nonsurgical. The fact thatwe had a lower T3 and T4 prevalence than is oftenseen in some nonsurgical studies of advanced oropha-ryngeal disease may be attributable to staging ‘‘creep’’created by clinical staging versus the pathologic stag-ing available from surgical specimens.42 This conceptis especially pertinent when staging base of tonguetumors by imaging/scanning, since lingual tonsillartissue may be difficult to distinguish on CT or MRIfrom tumor, and may be erroneously included in tu-mor measurements. Some T3/T4 tumors were
1692 TLM for Advanced-Stage Oropharyngeal Cancer HEAD & NECK—DOI 10.1002/hed December 2011

deliberately selected out from our presenting popula-tion, however, based on unresectability.
Positive margins as a significant negative prognosti-cator is another expected result, and motivates the TLMsurgeon to pursue a microscopically negative margin ifat all possible, even to the extent of returning patients tosurgery for reresection. The finding also underscores thecritical importance of the surgical component of ourpatients’ excellent local control.
The benefit of adjuvant radiotherapy in high (espe-cially Nþ) classification or histopathologically high-risk disease is a well-established practice.43,44 How-ever, a recent analysis recommended CRT rather thanRT alone for ‘‘high risk’’ necks (ie, N2 or greater andthe presence of ECS).37 Neither of these variables wasnegatively prognostic in this study, nor was the ab-sence of chemotherapy for adjuvant treatment. Rather,any adjunctive therapy was associated with an inde-pendent survival benefit on our patient group (T classi-fication and margin status were controlled for). Thismay suggest that the high tumor volume in cases withadvanced T classification is associated with residualmicroscopic disease after surgery, in which the poten-tial for death is significantly reduced by RT. A similareffect was also detected in an earlier TLM seriesstudying a variety of primary sites.45 However, thisdoes not constitute level I evidence for treatment deci-sion making because of the retrospective nature of ouradjuvant therapy analyses e.g. some patients may nothave received adjuvant therapy for high comorbidityreasons. The survival advantage of using adjuvant RTafter TLM raises the question, ‘‘Why use 2 modalitiesrather than RT or CRT alone?’’ We believe the equiva-lent or better survival and local control rates seen inour data over recent CRT studies8 justifies ourapproach. TLM with adjuvant RT also seems to allowbetter long-term function because of lower than ‘‘defin-itive’’ (or no) RT doses to the pharynx and infrequentor no use of chemotherapy.
Functional Recovery: Swallowing Outcomes. Asexpected, we observed reduction in swallowing functionas adjuvant treatment intensified. By obviating chemo-sensitized radiation, often dosed to 70-Gy, the humanpharynx will function better. Even modest reductions indose to 60–66 Gy will probably preserve swallowingphysiology, and certainly when reduced to 40–45 Gy,which come through to the pharynx from adjacent neckradiation. Ideally, for long-term functional preservation,no radiation is the best option, as accomplished in nearlyhalf our patients to the pharynx and in 25% overall. De-spite 75% of patients receiving adjuvant RT, adequateoral intake was maintained in almost 90% of subjects.This increment over long-term swallowing dysfunctionrates (43%), reported from Cooperative Group chemora-diation studies,11 is noteworthy for patients and thehealthcare system in general. Our study is limited interms of such comparisons, however, because of the ab-
sence of RT dose detail and G-tube data for the entirecohort (n ¼ 204). The long-term G-tube rate of 3.4%experienced at one of the study’s sites (n ¼ 89) reinforcesthis finding, a major step toward functional organ pres-ervation in the management of advanced oropharyngealcancer.
CONCLUSIONS
We conclude that TLM is a highly effective primarytreatment option for management of advanced-stageoropharyngeal cancer, especially in the presence ofHPV-positive biomarkers. TLM surgery is associatedwith acceptably low complication rates and high,early functional recovery rates; moreover, it achievessuperior survival or local control outcomes when usedin conjunction with adjuvant therapy. Although anyform of adjuvant therapy was associated with signifi-cant survival benefit, the addition of chemotherapy toRT was not associated with significantly better onco-logic outcomes than RT alone, and 83% of this treatedpopulation was therefore not exposed to risks of che-motoxicity. Based on these data, we will continue torecommend the TLM approach to our patients withcancer with advanced-stage OPSCC when they meetselection criteria.
Acknowledgments. The authors gratefullyacknowledge the contribution of Parul Sinha, MBBS,MS, in preparation of the manuscript.
REFERENCES
1. Shiboski CH, Schmidt BL, Jordan RC. Tongue and tonsil carci-noma increasing trends in the U.S. population ages 20–44 years.Cancer 2005;103:1843–1849.
2. Gillison ML, Koch WM, Capone RB, et al. Evidence for a causalassociation between human papillomavirus and a subset of headand neck cancers. J Natl Cancer Inst 2000;92:709–720.
3. Forastiere AA, Trotti A. Radiotherapy and concurrent chemo-therapy: a strategy that improves locoregional control and sur-vival in oropharyngeal cancer. J Natl Cancer Inst 1999;91:2065–2066.
4. Finnegan V, Parsons JT, Greene BD, Sharma V. Neoadjuvantchemotherapy followed by concurrent hyperfractionated radia-tion therapy and sensitizing chemotherapy for locally advanced(T3–T4) oropharyngeal squamous cell carcinoma. Head Neck2009;31:167–174.
5. Denis F, Garaud P, Bardet E, et al. Final results of the 94-01French Head and Neck Oncology and Radiotherapy Grouprandomized trial comparing radiotherapy alone with concomitantradiochemotherapy in advanced stage oropharynx carcinoma. JClin Oncol 2004;22:69–76.
6. Calais G, Alfonsi M, Bardet E, et al. Randomized trial of radia-tion therapy versus concomitant chemotherapy and radiationtherapy for advanced-stage oropharynx carcinoma. J Natl Can-cer Inst 1999;91:2081–2086.
7. Zafereo ME, Hanasono MM, Rosenthal DI, et al. The role of sal-vage surgery in patients with recurrent squamous cell carci-noma of the oropharynx. Cancer 2009:15; 115:5723–5733.
8. Ang KK, Harris J, Wheeler R, et al. Human papillomavirus andsurvival of patients with oropharyngeal cancer. N Engl J Med2010;363:24–35.
9. Forastiere AA, Goepfert H, Maor M, et al. Concurrent chemo-therapy and radiotherapy for organ preservation in advanced la-ryngeal cancer. N Engl J Med 2003;349: 2091–2098.
TLM for Advanced-Stage Oropharyngeal Cancer HEAD & NECK—DOI 10.1002/hed December 2011 1693

10. Garden AS, Harris J, Trotti A, et al. Long-term results of con-comitant boost radiation plus concurrent cisplatin for advancedhead and neck carcinomas: a phase II trial of the radiation ther-apy oncology group (RTOG 99-14). Int J Radiation Oncology BiolPhys 2008;71:1351–1355.
11. Machtay M, Moughan J, Trotti A, et al. Factors associated withsevere late toxicity after concurrent chemoradiation for locallyadvanced head and neck cancer: an RTOG analysis. J Clin Oncol2008;26:3582–3589.
12. Seikaly H, Rieger J, Wolfaardt J, Moysa G, Harris MD, NareshJ. Functional outcomes after primary oropharyngeal cancerresection and reconstruction with the radial forearm free flap.Laryngoscope 2003;113:897–904.
13. Licitra L, Perrone F, Bossi P, et al. High-risk human papilloma-virus affects prognosis in patients with surgically treated oro-pharyngeal squamous cell carcinoma. J Clin Oncol 2006;24:5630–5636.
14. Fischer CA, Zlobec I, Green E, et al. Is the improved prognosisof p16 positive oropharyngeal squamous cell carcinoma depend-ent of the treatment modality? Int J Cancer 2010;126: 1256–1262.
15. Steiner W, Fierek O, Ambrosch P, Hommerich CP, Kron M.Transoral laser microsurgery for squamous cell carcinoma of thebase of tongue. Arch Otolaryngol Head Neck Surg 2003;129:36–43.
16. Vaughn CW, Strong MS, Shapshay SM. Modern technology incancer therapy: status of carbon dioxide laser. Otolaryngol ClinNorth Am 1980;13:459–465.
17. Steiner W, Ambrosch P, Knappe MV. Endoscopic laser surgery ofthe upper aerodigestive tract: with special emphasis on cancersurgery. New York: Thieme Medical Publishers; 2001.
18. Hinni ML, Salassa JR, Grant DG, et al. Transoral laser micro-surgery for advanced laryngeal cancer. Arch Otolaryngol HeadNeck Surg 2007;133:1198–1204.
19. Grant DG, Salassa JR, Hinni ML, Pearson BW, Perry WC. Carci-noma of the tongue base treated by transoral laser microsurgery,Part I: untreated tumors, a prospective analysis of oncologic andfunctional outcomes. Laryngoscope 2006:116:2150–2155.
20. Rich JT, Milov S, Lewis JS Jr, Thorstad WL, Adkins D,Haughey BH. Transoral laser microsurgery (TLM) � adjuvanttherapy for advanced stage oropharyngeal cancer: outcomes andprognostic factors. Laryngoscope 2009;119: 1709–1719.
21. Klussmann JP, Gultekin E, Weissenborn SJ, et al. Expression ofp16 protein identifies a distinct entity of tonsillar carcinomasassociated with human papillomavirus. Am J Pathol2003;162:747–753.
22. El-Mofty SK, Patil S. Human papillomavirus (HPV)-related oro-pharyngeal nonkeratinizing squamous cell carcinoma: character-ization of a distinct phenotype. Oral Surg Oral Med Oral PatholOral Radiol Endod 2006;101: 339–345.
23. Chernock RD, El-Mofty SK, Thorstad WL, Parvin CA, Lewis JSJr. HPV-related nonkeratinizing squamous cell carcinoma of theoropharynx: utility of microscopic features in predicting patientoutcome. Head and Neck Pathol 2009;3:186–194.
24. Salassa JR. A functional outcome swallowing scale for stagingoropharyngeal dysphagia. Dig Dis 1999;17:230–234.
25. Centers for Disease Control and Prevention (CDC). Tobaccouse: United States, 1900–1999. MMWR, Morb Mortal Wkly Rep1999;48:986–993.
26. Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CACancer J Clin 2008;58:71–96.
27. Fakhry C, Westra WH, Li S, et al. Improved survival of patientswith human papillomavirus-positive head and neck squamouscell carcinoma in a prospective clinical trial. J Natl Cancer Inst2008;100:261–269.
28. Wolf GT, et al. Induction chemotherapy plus radiation comparedwith surgery plus radiation in patients with advanced laryngeal
cancer: the Department of Veterans Affairs Laryngeal CancerStudy Group. N Engl J Med 1991;324:1685–1690.
29. Forastiere AA, Goepfert H, Maor M, et al. Concurrent chemo-therapy and radiotherapy for organ preservation in advanced la-ryngeal cancer. N Engl J Med 2003; 349:2091–2098.
30. Forastiere AA, Maor M, Weber RS. Long-term results of Inter-group RTOG 91-11: a phase III trial to preserve the larynx:induction cisplatin/5-FU and radiation therapy versus concur-rent cisplatin and radiation therapy versus radiation therapy. JClin Oncol ASCO Annual Meeting Proceedings (Post-MeetingEdition) 2006; 24 (Suppl 18):5517.
31. Nguyen NP, Vos P, Smith HJ, et al. Concurrent chemoradiationfor locally advanced oropharyngeal cancer. Am J Otolaryngol2007;28:3–8.
32. Urba SG, Moon J, Giri S, et al. Organ preservation for advancedresectable cancer of the base of tongue and hypopharynx: asouthwest oncology group trial. J Clin Oncol 2005;23:88–95.
33. Worden FP, Kumar B, Lee JS, et al. Chemoselection as a strat-egy for organ preservation in advanced oropharynx cancer:response and survival positively associated with HPV16 copynumber. J Clin Oncol 2008;26:1–11.
34. Huang K, Xia P, Chuang C, et al. Intensity-modulated chemora-diation for treatment of stage III and IV oropharyngeal carci-noma the University of California–San Francisco experience.Cancer 2008;113:497–507.
35. Cmelak AJ, Li S, Goldwasser MA, et al. Phase II trialof chemoradiation for organ preservation in resectable stage IIIor IV squamous cell carcinomas of the larynx or oropharynx;results of Eastern Cooperative Oncology Group Study E2399. JClin Oncol 2007;25:3971–3977.
36. Duvvuri U, Myers JN, Contemporary management of oropha-ryngeal cancer: anatomy and physiology of the oropharynx. CurrProbl Surg 2009;46:119–184.
37. Cooper JS, Pajak TF, Forastiere A, et al. Postoperative concur-rent radiotherapy and chemotherapy for high-risk squamous-cellcarcinoma of the head and neck. N Engl J Med 2004;350:1937–1944.
38. Greven K, White D, Brown J, et al. Swallowing dysfunction is acommon sequel after chemoradiation for oropharynx carcinoma.Am J Clin Oncol 2008;31:209–212.
39. Wolf GT. Tradition, teamwork, and tailored treatment surgicaloncology in the genomic era. Arch Otolaryngol Head Neck Surg2009;135:337–341.
40. Lewis JS Jr, Thorstad WL, Chernock RD, et al. p16 positive oro-pharyngeal squamous cell carcinoma: an entity with a favorableprognosis regardless of tumor HPV status. Am J Surg Pathol2010;34:1088–1096.
41. Smeets SJ, Hesselink AT, Speel EJ, et al. A novel algorithm forreliable detection of human papillomavirus in paraffin embeddedhead and neck cancer specimen. Int J Cancer 2007;121:2465–2472.
42. Walvekar RR, Li RJ, Gooding WE, et al. Role of surgery in lim-ited (T1-2, N0-1) cancers of the oropharynx. Laryngoscope2008;118:2129–2134.
43. Cooper JS, Pajak TF, Forastiere A, et al. Precisely defining high-risk operable head and neck tumors based on RTOG #85-03 and#88-24: targets for postoperative radiochemotherapy? HeadNeck 1998;20:588–594.
44. Bernier J, Cooper JS, Pajak TF, et al. Defining risk levels inlocally advanced head and neck cancers: a comparative analysisof concurrent postoperative radiation plus chemotherapy trialsof the EORTC (#22931) and RTOG (#9501). Head Neck2005;27:843–850.
45. Pradier O, Christiansen H, Schmidberger H, et al. Adjuvantradiotherapy after transoral laser microsurgery for advancedsquamous carcinoma of the head and neck. Int J Radiat OncolBiol Phys 2005;63:1368–1377.
1694 TLM for Advanced-Stage Oropharyngeal Cancer HEAD & NECK—DOI 10.1002/hed December 2011