transformational improvement in quality care ... - bmc medicine
TRANSCRIPT

CORRESPONDENCE Open Access
Transformational improvement in qualitycare and health systems: the next decadeJeffrey Braithwaite1* , Charles Vincent2, Ezequiel Garcia-Elorrio3, Yuichi Imanaka4, Wendy Nicklin5,Sodzi Sodzi-Tettey6 and David W. Bates7
Abstract
Background: Healthcare is amongst the most complex of human systems. Coordinating activities and integratingnewer with older ways of treating patients while delivering high-quality, safe care, is challenging. Three landmarkreports in 2018 led by (1) the Lancet Global Health Commission, (2) a coalition of the World Health Organization,the Organisation for Economic Co-operation and Development and the World Bank, and (3) the National Academies ofSciences, Engineering and Medicine of the United States propose that health systems need to tackle care quality,create less harm and provide universal health coverage in all nations, but especially low- and middle-income countries.The objective of this study is to review these reports with the aim of advancing the discussion beyond a conceptualdiagnosis of quality gaps into identification of practical opportunities for transforming health systems by 2030.
Main body: We analysed the reports via text-mining techniques and content analyses to derive their key themes andconcepts. Initiatives to make progress include better measurement, using the capacities of information and communicationstechnologies, taking a systems view of change, supporting systems to be constantly improving, creating learning healthsystems and undergirding progress with effective research and evaluation. Our analysis suggests that the world needs tomove from 2018, the year of reports, to the 2020s, the decade of action. We propose three initiatives to support this move:first, developing a blueprint for change, modifiable to each country’s circumstances, to give effect to thereports’ recommendations; second, to make tangible steps to reduce inequities within and across healthsystems, including redistributing resources to areas of greatest need; and third, learning from what goes rightto complement current efforts focused on reducing things going wrong. We provide examples of targetedfunding which would have major benefits, reduce inequalities, promote universality and be better at learningfrom successes as well as failures.
Conclusion: The reports contain many recommendations, but lack an integrated, implementable, 10-yearaction plan for the next decade to give effect to their aims to improve care to the most vulnerable, savelives by providing high-quality healthcare and shift to measuring and ensuring better systems- and patient-level outcomes. This article signals what needs to be done to achieve these aims.
Keywords: Health systems, Patient safety, Quality of care, Universal health coverage, Low-, middle- and high-income countries
© The Author(s). 2020 Open Access This article is licensed under a Creative Commons Attribution 4.0 International License,which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you giveappropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate ifchanges were made. The images or other third party material in this article are included in the article's Creative Commonslicence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commonslicence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtainpermission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to thedata made available in this article, unless otherwise stated in a credit line to the data.
* Correspondence: [email protected] for Healthcare Resilience and Implementation Science, AustralianInstitute of Health Innovation, Macquarie University, Level 6, 75 Talavera road,North Ryde, NSW 2113, AustraliaFull list of author information is available at the end of the article
Braithwaite et al. BMC Medicine (2020) 18:340 https://doi.org/10.1186/s12916-020-01739-y

We need health systems that enable the provision ofhigher-quality and safer healthcare, reflect popula-tion needs, and facilitate better assessment andmanagement of population health. Three major re-ports in 2018 argue for such systems transformation[1–3]. Can it be achieved?
BackgroundThe organisation and provision of healthcare is changing.Looking back over the centuries, physicians and otherhealthcare professionals had rudimentary practices, pa-tients had modest expectations and there was no realhealth system as clinicians were independent providers.However, by the late twentieth century, healthcare hadevolved to become the most complex of human endeav-ours [4]. The range of patient types and conditions, proce-dures, tests, technologies available, drugs, specialistworkers and settings in which care was delivered, even inlow- and middle-income countries (LMICs) with modestresources, grew exponentially [5, 6]. This demanded ex-tensive supporting structures and coordination.Fast forward to the third decade of the twenty-first
century. We now have sophisticated information andtelecommunications technologies, genomics, precisionmedicine, artificial intelligence, advanced pharma andunrivalled devices to support care, all of which are add-ing more capacity to deliver better treatment and inter-ventions [7]. While LMICs have some access to these,they must do things less expensively—for example, byusing mobile technology and microgrids rather thanlarge computer systems. These new additions to the car-ing environment confer benefits to patients yet are im-measurably increasing systems complexity [8], andaccelerating the need to be even better at coordinationso all in the healthcare orchestra sing from the samesong sheet.
Major reports in 2018Three recent milestone contributions address the issueof quality of care primarily as it affects the developingworld yet with key messages for all health systems, de-veloping or mature [1–3]. They offer recommendationsfor how to create better delivery systems and improvecare quality. They each aspire, amongst all this complex-ity, to put care on an improvement gradient—to make itsafer, of higher quality, and more responsive to demandsacross time. They also suggest that systems are becom-ing tougher to manage and coordinate, and enhance-ment of care and care settings, from policy tomanagement to practice, is very hard to achieve. In thisarticle, we analyse these reports individually and as awhole, and, as Academicians of the International Acad-emy of Quality and Safety (IAQS) established by the
International Society for Quality in Health Care (ISQua),we aim to describe the commonalities and differencesand establish the platform from which we can improvecare internationally. We begin with a synthesis of themain thrust of the arguments in the three reports.The Lancet report (Box 1) makes a set of recommen-
dations for how national governments and funding part-ners can take the lead in creating better, more caring,less harmful systems. It argues that a core enabler forachieving these goals will be a research agenda to under-pin the key advances which need to be achieved (seeBox 1 for a summary).The WHO/OECD/World Bank report (Box 2) envis-
ages widespread enabling action by governments, healthsystems and citizens, patients and health workers. It sug-gests that these bodies and groups should be encouragedto collaborate and conspire to deliver improved careacross-the-board (see Box 2 for a summary).The National Academies’ report (Box 3) represents a
clarion call for more research, better measurement andconcerted international efforts. It suggests creating alearning health system which contrasts with today’s for-getting system, and encourages people to think in
Box 1: The Lancet Global Health Commission report:High-Quality Health Systems in the Sustainable GoalsEra: Time for a Revolution [3]
� Looks across low-, middle-, and high-income countries.
� Acknowledges patients in health systems in less wealthy
countries, and vulnerable populations, need priority
attention.
� Indicates that the lives of millions of people could be saved
or enhanced if high-quality health systems were in place.
� Contends that delivery systems need to contribute, measure
and report on what matters—effective care provided on the
front lines, meeting patients’ not just providers’ needs, and
supplying high-quality care to the maximum extent
achievable.
� Summarises what is needed—more resources in the right
places, better use of existing resources and providers taking
a systems perspective, adopting things known to deliver
better care, e.g. adherence to evidence based guidelines, use
of Information and Communications Technology (ICT)
known to improve decision-making and treatment, and scal-
ing up good practices regionally and nationally.
� Advances universal actions, chief of which are to: govern for
quality; redesign service delivery to optimise quality;
transform the health workforce; and stimulate population
demand for high-quality care.
Braithwaite et al. BMC Medicine (2020) 18:340 Page 2 of 17
systems terms rather than in silos or episodes (see Box 3for a summary).
MethodTo understand more deeply the tenor and extent of thereports, we conducted an analysis of them using text-mining software provided by Leximancer 4.51, an auto-mated content analysis computer program [9, 10]. Lexi-mancer facilitates the interrogation of texts—words, andword segments—and creates a thesaurus of significantterms, known as textual concepts. The software allowsthe examination of the connectivity and relationship be-tween concepts in large text documents. Groups of themost highly connected concepts are referred to asthemes. Leximancer produces a ranked list of themesand a visual map of their connections, providing detailsof both the strength of a concept as it recurs within thetext and the extent of connections to other concepts.Leximancer’s automated interrogation of documents canbe applied to PDF and word processed documents. Es-sentially, the Leximancer program breaks down textualmaterial into its key categories (themes, concepts) inorder to visualise and quantify the text [10, 11].
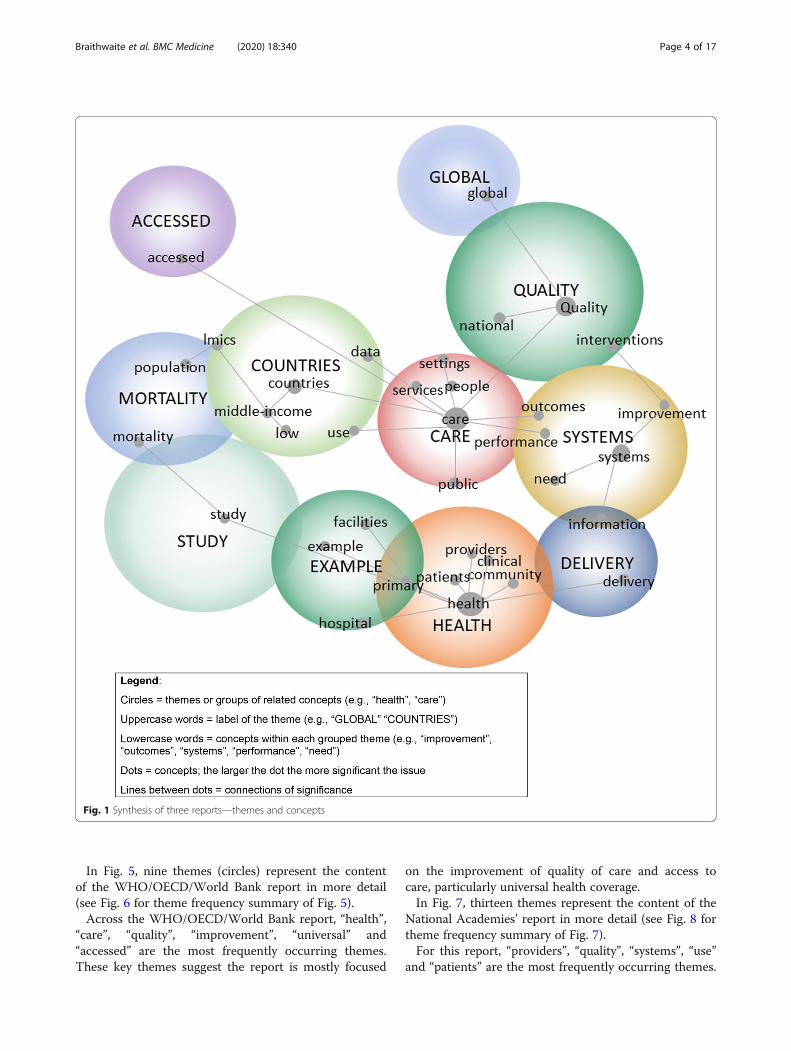
ResultsFigures 1, 3, 5 and 7 provide the Leximancer maps ofthemes and concepts, accompanied by the frequency oftheir highest recurring themes (Figs. 2, 4, 6 and 8).In the first visual diagram (Fig. 1), eleven themes
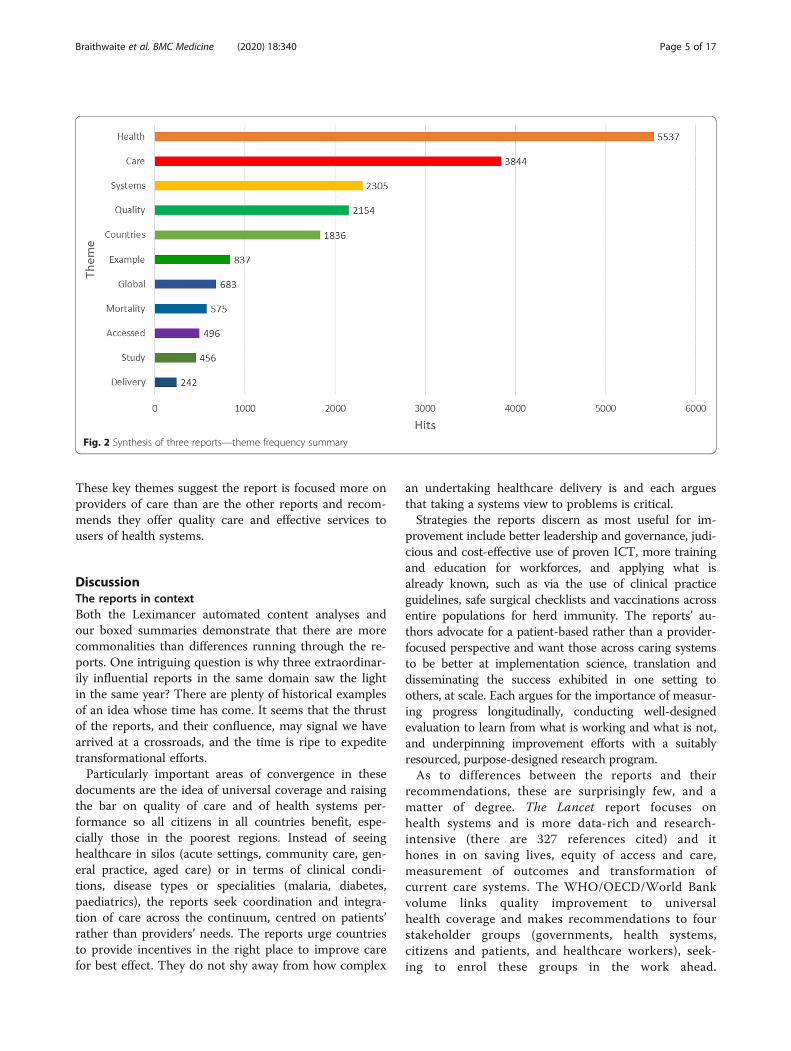
(circles) represent the content of the three reports inbroad outline (see Fig. 2 for theme frequency sum-mary of Fig. 1).Across the three reports, “health”, “care”, “systems”,
“Quality”, “countries” and “examples” are the most fre-quently occurring themes. These key themes suggest thereports are largely focused on the quality of care pro-vided by health systems within and across various coun-tries, with multiple examples provided. The graphicalrepresentation of Fig. 1 depicted in Fig. 2 shows thestrength of the recurrences (“hits”) of each theme.In Fig. 3, thirteen themes (circles) represent the con-
tent of the Lancet report in more detail (see Fig. 4 fortheme frequency summary of Fig. 3).Over the pages of the Lancet report, “health”, “sys-
tem”, “care”, “people”, “data” and “countries” are themost frequently occurring themes. These key themesshow how the report is mostly focused on people anddata in healthcare systems across all countries of theworld.
Box 2: WHO/OECD/World Bank report, DeliveringQuality Health Services: A Global Imperative forUniversal Health Coverage [2]
� Argues for universal health coverage (UHC) for every health
system such that all citizens have access to the range of
quality health services they need as affordably as possible.
� Laments the low quality of care and poor adherence to
clinical practice guidelines, even in high-income countries;
and notes that it is far worse in low-income countries.
� Observes that there is lots of variation in outcomes across
health systems, and therefore much scope to improve; for
instance, screening, prevention, immunisation and
community support vary across countries and are sometimes
at such poor levels that large numbers in the population
suffer.
� Expresses concern that sub-optimal clinical practices are
common across the spectrum of public, private, primary and
acute care in many countries.
� Articulates the need for a highly trained workforce, excellent
service provision from facilities, safe and effective use of
technology, drugs, and devices, better use of health
information systems, and financing mechanisms that
incentivise quality care and continuous improvement.
� Specifies a range of interventions to improve care and
supports the scale up of successful interventions.
Box 3: The National Academies of Sciences,Engineering and Medicine report: Crossing the GlobalQuality Chasm: Improving Health Care Worldwide [1]
� Sounds alarm at the harm healthcare creates, the current
state of caring systems, the scale of the problems and the
poor performance of many health systems in not delivering
high-quality care, especially to LMICs.
� Sees core needs for much better monitoring and evaluation
systems, customer satisfaction surveys, research and
evaluation.
� Indicates that part of the solution rests in training people to
be better at systems thinking and factoring in the
complexity of the system.
� Argues in favour of patient centred thinking and wants to
focus on optimising the patient journey.
� Asks for reformers not to forget that much care that takes
place in informal settings by family and friends, outside of
the formal structures and delivery systems.
� Articulates a problem not covered by other systems reports
sufficiently well, namely corruption and its deleterious
impact on healthcare.
� Argues for embedding quality within UHC and implores
everyone everywhere to establish a culture of continuous
improvement.
Braithwaite et al. BMC Medicine (2020) 18:340 Page 3 of 17
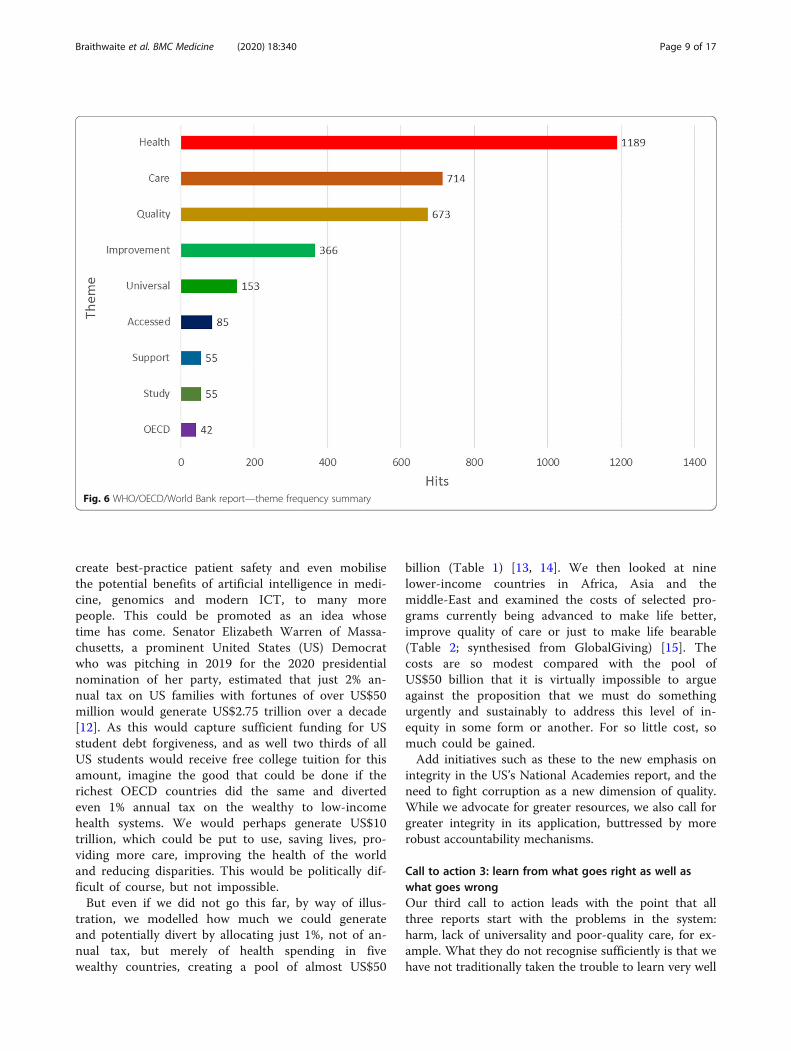
In Fig. 5, nine themes (circles) represent the contentof the WHO/OECD/World Bank report in more detail(see Fig. 6 for theme frequency summary of Fig. 5).Across the WHO/OECD/World Bank report, “health”,
“care”, “quality”, “improvement”, “universal” and“accessed” are the most frequently occurring themes.These key themes suggest the report is mostly focused
on the improvement of quality of care and access tocare, particularly universal health coverage.In Fig. 7, thirteen themes represent the content of the
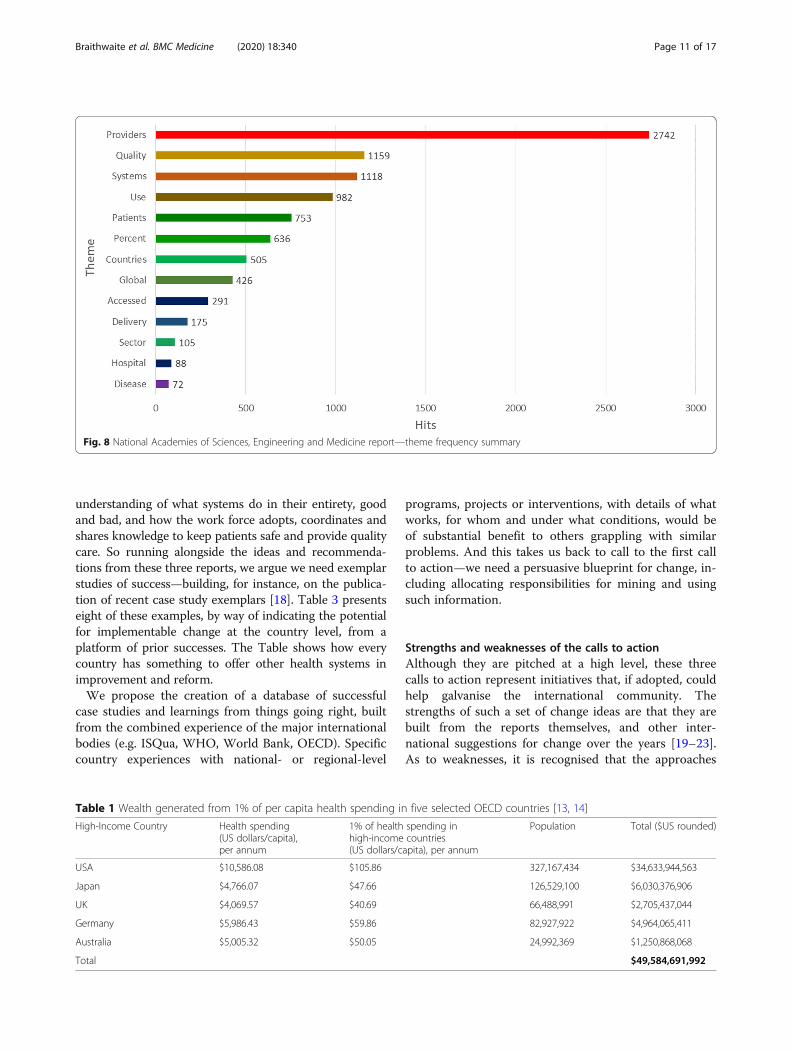
National Academies’ report in more detail (see Fig. 8 fortheme frequency summary of Fig. 7).For this report, “providers”, “quality”, “systems”, “use”
and “patients” are the most frequently occurring themes.
Fig. 1 Synthesis of three reports—themes and concepts
Braithwaite et al. BMC Medicine (2020) 18:340 Page 4 of 17
These key themes suggest the report is focused more onproviders of care than are the other reports and recom-mends they offer quality care and effective services tousers of health systems.
DiscussionThe reports in contextBoth the Leximancer automated content analyses andour boxed summaries demonstrate that there are morecommonalities than differences running through the re-ports. One intriguing question is why three extraordinar-ily influential reports in the same domain saw the lightin the same year? There are plenty of historical examplesof an idea whose time has come. It seems that the thrustof the reports, and their confluence, may signal we havearrived at a crossroads, and the time is ripe to expeditetransformational efforts.Particularly important areas of convergence in these
documents are the idea of universal coverage and raisingthe bar on quality of care and of health systems per-formance so all citizens in all countries benefit, espe-cially those in the poorest regions. Instead of seeinghealthcare in silos (acute settings, community care, gen-eral practice, aged care) or in terms of clinical condi-tions, disease types or specialities (malaria, diabetes,paediatrics), the reports seek coordination and integra-tion of care across the continuum, centred on patients’rather than providers’ needs. The reports urge countriesto provide incentives in the right place to improve carefor best effect. They do not shy away from how complex
an undertaking healthcare delivery is and each arguesthat taking a systems view to problems is critical.Strategies the reports discern as most useful for im-
provement include better leadership and governance, judi-cious and cost-effective use of proven ICT, more trainingand education for workforces, and applying what isalready known, such as via the use of clinical practiceguidelines, safe surgical checklists and vaccinations acrossentire populations for herd immunity. The reports’ au-thors advocate for a patient-based rather than a provider-focused perspective and want those across caring systemsto be better at implementation science, translation anddisseminating the success exhibited in one setting toothers, at scale. Each argues for the importance of measur-ing progress longitudinally, conducting well-designedevaluation to learn from what is working and what is not,and underpinning improvement efforts with a suitablyresourced, purpose-designed research program.As to differences between the reports and their
recommendations, these are surprisingly few, and amatter of degree. The Lancet report focuses onhealth systems and is more data-rich and research-intensive (there are 327 references cited) and ithones in on saving lives, equity of access and care,measurement of outcomes and transformation ofcurrent care systems. The WHO/OECD/World Bankvolume links quality improvement to universalhealth coverage and makes recommendations to fourstakeholder groups (governments, health systems,citizens and patients, and healthcare workers), seek-ing to enrol these groups in the work ahead.
Fig. 2 Synthesis of three reports—theme frequency summary
Braithwaite et al. BMC Medicine (2020) 18:340 Page 5 of 17

Authors of Crossing the Global Quality Chasm arefocused on the six dimensions of quality (safety; ef-fectiveness; person-centredness; accessibility, timeli-ness, affordability; efficiency; and equity), and take asystems perspective on change, establishing agreedprinciples for systems redesign and seeking to har-ness digital progress across countries. They alsomount strong arguments for change proponents to
focus on informal care and carers, and to reducecorruption.They all note that poor-quality care remains an
entrenched, wicked problem. All-in-all, collectively, theauthors of the three volumes challenge those presidingover every health system to lift their game and do betterfor the benefit over the medium to long term of billionsof people.
Fig. 3 Lancet report—themes and concepts
Braithwaite et al. BMC Medicine (2020) 18:340 Page 6 of 17

Calling for international actionHow can we move from 2018, the publication year ofthe reports, to 2020 and beyond, as the decade of action?Going beyond the extensive learnings within these docu-ments, we argue for three calls to action.
Call to action 1: establish a 10-year blueprint for changeThe combined recommendations of the reports willdoubtless shape the work of the international commu-nity over at least the next 10 years. Yet a very real con-cern we have is that too often with almost allauthoritative reports on health systems reform, whethernational, regional or global, much effort is expended onconducting the studies and formulating the recommen-dations and then the study task force membership dis-solves and individuals go back to their normal activities.Less attention is later given to how recommendationsmight be implemented, translated into learning andadoption strategies, and for political and policy impetusfor change to match the importance of the recommen-dations. We hesitate to call for yet another report todocument how to put the recommendations into action;however, we need a blueprint for change and a plan tomeasure progress. This would articulate, as everythingcannot be done simultaneously, the optimal stages to befollowed in addressing all the change suggested by thereports, who should do what and with what levels of ac-countability, and how the interactions between stake-holders will play out. We also need a much clearer idea
of how the international community and individualhealth systems might design rigorous evaluation studiesto assess progress and feed that progress back to stake-holders in the system responsible for the improvements.Overall, we must find better ways to document how todisseminate best-practice models, and to achieve im-provement at scale, and incorporate these in the blue-print for 2030.
Call to action 2: buy more equitable, high-quality care forthe greatest numberSecond, collectively the reports plead for everycountry to move along an improvement gradient; im-plementation is proposed as a country-level responsi-bility but with a global commitment, supported byinternational bodies such as the UN’s agencies, theWHO and OECD. So, let us take the word “global”,which each of the three contributions uses emblemat-ically and often, seriously. Say we wanted to do thevery best we can for the 7.7 billion people in theworld, taking what these reports have said to heart,and as a broad framework for change. What is that“very best we can”? It will need to be something thatwould galvanise the international community and seekto create sufficient leverage for major step-changes inthe healthiness of the world.It seems to us that if we wanted to buy the greatest
amount of high-quality care we could, do the mostgood for the most people and maximise reductions inharm, we would find ways to genuinely divert tangible
Fig. 4 Lancet report—theme frequency summary
Braithwaite et al. BMC Medicine (2020) 18:340 Page 7 of 17

allocations of money to low- and middle-incomehealth systems. That single action (as hard as it mightbe to accomplish, as it would mean generating ortransferring substantial amounts of funding from thebudgets of wealthy countries to less wealthy popula-tions) would reduce inequalities and buy more healthgain for more people at the least cost than
continuously increasing the spending of GDP on richhealth systems already consuming between 10 and17% of national income such as the USA, Japan,France and Canada. If we did this, at a stroke wewould provide more life-saving, life-enhancing initia-tives and could share the advantages of higher-qualitycare, institute training in continuous improvement,
Fig. 5 WHO/OECD/World Bank report—themes and concepts
Braithwaite et al. BMC Medicine (2020) 18:340 Page 8 of 17
create best-practice patient safety and even mobilisethe potential benefits of artificial intelligence in medi-cine, genomics and modern ICT, to many morepeople. This could be promoted as an idea whosetime has come. Senator Elizabeth Warren of Massa-chusetts, a prominent United States (US) Democratwho was pitching in 2019 for the 2020 presidentialnomination of her party, estimated that just 2% an-nual tax on US families with fortunes of over US$50million would generate US$2.75 trillion over a decade[12]. As this would capture sufficient funding for USstudent debt forgiveness, and as well two thirds of allUS students would receive free college tuition for thisamount, imagine the good that could be done if therichest OECD countries did the same and divertedeven 1% annual tax on the wealthy to low-incomehealth systems. We would perhaps generate US$10trillion, which could be put to use, saving lives, pro-viding more care, improving the health of the worldand reducing disparities. This would be politically dif-ficult of course, but not impossible.But even if we did not go this far, by way of illus-
tration, we modelled how much we could generateand potentially divert by allocating just 1%, not of an-nual tax, but merely of health spending in fivewealthy countries, creating a pool of almost US$50
billion (Table 1) [13, 14]. We then looked at ninelower-income countries in Africa, Asia and themiddle-East and examined the costs of selected pro-grams currently being advanced to make life better,improve quality of care or just to make life bearable(Table 2; synthesised from GlobalGiving) [15]. Thecosts are so modest compared with the pool ofUS$50 billion that it is virtually impossible to argueagainst the proposition that we must do somethingurgently and sustainably to address this level of in-equity in some form or another. For so little cost, somuch could be gained.Add initiatives such as these to the new emphasis on
integrity in the US’s National Academies report, and theneed to fight corruption as a new dimension of quality.While we advocate for greater resources, we also call forgreater integrity in its application, buttressed by morerobust accountability mechanisms.
Call to action 3: learn from what goes right as well aswhat goes wrongOur third call to action leads with the point that allthree reports start with the problems in the system:harm, lack of universality and poor-quality care, for ex-ample. What they do not recognise sufficiently is that wehave not traditionally taken the trouble to learn very well
Fig. 6 WHO/OECD/World Bank report—theme frequency summary
Braithwaite et al. BMC Medicine (2020) 18:340 Page 9 of 17

from things going right and to develop ways of support-ing this. This perspective, coming from scholars of resili-ent healthcare and Safety-II, asks not why do things gowrong, but in systems as complex as healthcare (and, aswe have seen, in LMIC systems, as resource-deprived),how come so much goes right? Why do some providers,teams and microsystems deal capably with everydaychallenges, producing good care despite other providers,
teams and microsystems in the same system producingworse outcomes—yet they all face the same constraints?What workarounds are developed by staff to overcomesystem deficiencies? Lack of resources, poor support sys-tems and less than optimal ICT are all perennial problemsevery system—even wealthy ones—faces. Traditionally,change agents and quality and safety advocates have beenmore interested in stamping out harm than extending
Fig. 7 National Academies of Sciences, Engineering and Medicine report: Crossing the Global Quality Chasm: Improving Health CareWorldwide—themes and concepts
Braithwaite et al. BMC Medicine (2020) 18:340 Page 10 of 17
understanding of what systems do in their entirety, goodand bad, and how the work force adopts, coordinates andshares knowledge to keep patients safe and provide qualitycare. So running alongside the ideas and recommenda-tions from these three reports, we argue we need exemplarstudies of success—building, for instance, on the publica-tion of recent case study exemplars [18]. Table 3 presentseight of these examples, by way of indicating the potentialfor implementable change at the country level, from aplatform of prior successes. The Table shows how everycountry has something to offer other health systems inimprovement and reform.We propose the creation of a database of successful
case studies and learnings from things going right, builtfrom the combined experience of the major internationalbodies (e.g. ISQua, WHO, World Bank, OECD). Specificcountry experiences with national- or regional-level
programs, projects or interventions, with details of whatworks, for whom and under what conditions, would beof substantial benefit to others grappling with similarproblems. And this takes us back to call to the first callto action—we need a persuasive blueprint for change, in-cluding allocating responsibilities for mining and usingsuch information.
Strengths and weaknesses of the calls to actionAlthough they are pitched at a high level, these threecalls to action represent initiatives that, if adopted, couldhelp galvanise the international community. Thestrengths of such a set of change ideas are that they arebuilt from the reports themselves, and other inter-national suggestions for change over the years [19–23].As to weaknesses, it is recognised that the approaches
Table 1 Wealth generated from 1% of per capita health spending in five selected OECD countries [13, 14]
High-Income Country Health spending(US dollars/capita),per annum
1% of health spending inhigh-income countries(US dollars/capita), per annum
Population Total ($US rounded)
USA $10,586.08 $105.86 327,167,434 $34,633,944,563
Japan $4,766.07 $47.66 126,529,100 $6,030,376,906
UK $4,069.57 $40.69 66,488,991 $2,705,437,044
Germany $5,986.43 $59.86 82,927,922 $4,964,065,411
Australia $5,005.32 $50.05 24,992,369 $1,250,868,068
Total $49,584,691,992
Fig. 8 National Academies of Sciences, Engineering and Medicine report—theme frequency summary
Braithwaite et al. BMC Medicine (2020) 18:340 Page 11 of 17

we are suggesting may not receive sufficient attention inthe present pandemic era. The current pandemic itselfraises serious questions about health system resilienceand the quality of Covid-19 and routine non-Covid-19care. The Covid-19 pandemic amplifies the need forhealth system strengthening to address gnawing qualityof care gaps that have intensified in the wake of theglobal crisis. Regarding the second call, rather than waitfor resources to be released from the benevolence of richcountries, the Covid-19 pandemic teaches that it is timefor resource-constrained countries to reprioritize healthresource allocation. Ghana, for example, has
demonstrated this through activation of local manufac-turing of personal protective equipment.That being said, development of a blueprint for action
with a clear picture of what healthcare in 2030 shouldlook like is possible; the funding required for call to ac-tion 2, despite the good it could bring to the world, maynot be given priority by wealthy health systems; and callto action 3, more thoroughly understanding health sys-tems from a systems standpoint and learning fromthings going right is increasingly receiving attention[24–28], yet has not yet become a mainstream idea.While these recommendations are for the long term,
Table 2 Life-sustaining or quality-of-care-enhancing programs in nine selected lower-income countries [15–17]
Low-incomeCountry [14]
Types of initiatives Cost ($US) of program
Afghanistan Training midwives in Afghanistan. $50,000 (e.g. $600 contributes to thedevelopment of three training modules to train100 midwives each)As a preventative approach to the high maternal and infant mortality rates in
Afghanistan, this initiative funds midwifery training to improve equity and accessto essential women’s healthcare in rural areas.
Burundi Providing healthcare to 1000s in Bujumbura slum. $20,000 (e.g. $300 funds a 3-day trauma healingworkshop for gender-based violence survivors)
Funds healthcare support, trauma healing workshops and AIDS testing to theNtaseka Clinic, for more than 5000 people per annum. Patients include survivorsof gender-based violence and abuse, people who are HIV positive, and the gen-eral population.
Chad Life skills and peer education for Chadian Youth. $33,913 (e.g. $200 supports one communityoutreach even in N’Djamena)
Funds quality programs to the Chadian youth; the programs which are peer-based, disseminate information about the risks of drugs, alcohol, and transmissionof HIV/AIDS.
Ethiopia Simple surgery to restore sight to Ethiopians. $6000 (e.g. $12 funds the cost to conduct twoeye surgeries to reverse the effects of blindingtrachoma)Funds simple eye surgeries in Ethiopia, including remote Ethiopia, for those
suffering from trachoma. The hope is to eradicate the eye disease.
Liberia Restoring healthcare to women and girls in Liberia. $100,000 (e.g. $1500 pays all clinic operatingcosts in Liberia for a month)
Funds community-based preventative care and an acute care clinic in Kakata towomen and girls in Margibi County, Liberia. The clinic provides emergency careand has over 200,000 patients.
Malawi End mother to child transmission of HIV in Malawi. $5000 (e.g. $25 can pay for 1500 text messagesto support and educate adolescents on HIV andsafe sex)This is the largest country program, and the first that employs and recruit’s HIV
positive men as Expert Clients. There are over 270 Expert Clients in 98 clinics whosupport and educate other men in the area about HIV.
Nepal Rescue children suffering from severe malnutrition. $50,000 (e.g. $10 gives medicine to one childwhile they are restored to health at a NutritionalRehabilitation Home)“Fifty percent of Nepali children under five-years-old are malnourished … Malnu-
trition is the main cause of death for as many as 50,000 Nepali children each year.”This program funds Nutritional Rehabilitation homes to restore the health of childand educate parents of the risks.
Tanzania Make motherhood safe for Tanzanian women. $400,000 (e.g. $1000 funds a C-section andrecovery)
Funds the construction, equipment and training of staff for a new maternityhospital in Dar es Salaam, Tanzania. There will be 22 facilities and a 200-bed hos-pital to improve maternal health and assist with decreasing the high maternalmortality rate in Tanzania.
Uganda Stop Ugandan women and children dying at childbirth. $36,000 (e.g. $4200 will buy one portableultrasound scanning (Clarius) machine from theUSA.)Funds maternal health and welfare in Uganda and increases the quality of care for
women in childbirth through effective equipment, training of midwives, socialworkers and radiographers and supporting outreach programs.
[Source: GlobalGiving [15]]
Braithwaite et al. BMC Medicine (2020) 18:340 Page 12 of 17

Table
3Eigh
texam
ples
ofcoun
try-levelreform
orim
provem
ent[7]
Cou
ntry
Keyindicators
Initiative
Successfeatures
Outcomes
Argen
tina
Popu
latio
n:44,494,502
Implemen
tation
ofvariou
squa
lity
andsafety
initiative
sinclud
ingthe
Categ
orisingAutho
rizationProg
ram,
NationalP
rogram
ofQuality
Assurance
ofHealth
care,and
the
NationalP
rogram
ofEpidem
iology
andHospitalInfectio
nCon
trol
•Financingby
World
Bank
andnatio
naland
provincialgo
vernmen
ts•Unificationof
licen
cing
rules
GDPpe
rcapita,PPP:
$20,567.30
•Externalqu
ality
andpatient
safety
evaluatio
ns•Redu
ctionof
treatm
entvariability
Life
expe
ctancy
atbirth(bothsexes):
76.7years
•Con
tributionfro
mspecialised
scientific
societies
•Health
care
coverage
forpreg
nancy,
childbirth,po
stpartum
care
andpaed
iatric
care
•Pay-for-pe
rform
ance
strategy
Expend
iture
onhealth
asaprop
ortio
nof
GDP:7.5%
•Training
initiatives
onqu
ality
andpatient
safety
•Health
care
coverage
foradolescentsand
wom
en
Estim
ated
ineq
uity,G
iniInd
ex:40.6%
Brazil
Popu
latio
n:209,469,333
Laun
chof
Proq
ualis—aweb
site
featuringrelevant
andcurren
tpu
blications
abou
tQuality
Improvem
ent(QI)initiatives,social
med
iaplatform
s,andQItoo
lsand
strategies
•Organisationof
web
site
anded
itorialp
olicy
allowingforeasy
retrievalo
finform
ation
•Provisionof
relevant
andreliableQI
inform
ationto
consum
ers
GDPpe
rcapita,PPP:
$16,068.02
•Standardised
term
inolog
yviaaglossary
ofterm
s•Increasedaccess
toQIinformationforhe
alth
profession
alsandmanagers
Life
expe
ctancy
atbirth(bothsexes):
75.7years
•Pu
blications
specify
therelevanceto
the
Brazilian
context
•Im
proved
access
totoolsandstrategies
tosupp
ortQIfor
health
profession
als
Expend
iture
onhealth
asaprop
ortio
nof
GDP:11.8%
•Allmaterialsarefre
eto
access
•Inform
ationaccessibleon
tabletsandmob
ileph
ones
•Increasedcommun
icationthroug
hsocial
med
iaplatform
sEstim
ated
ineq
uity,G
iniInd
ex:53.3%
India
Popu
latio
n:1.35
billion
Introd
uction
ofUnive
rsal
Hea
lth
Cov
erag
ethroug
hapu
blic-private
partne
rshipmod
el
•Supp
ortfro
mprivatehe
althcare
providers
andinsurancecompanies
•Moreaccessible,affo
rdable,safeand
approp
riate
health
services
GDPpe
rcapita,PPP:$7761.60
•Morethan
50%
ofIndia’spo
pulatio
ncovered
byhe
alth
insurance
Life
expe
ctancy
atbirth(bothsexes):
68.8years
•Financialp
rotectionto
families
livingbe
low
thepo
vertyline
Expend
iture
onhealth
asaprop
ortio
nof
GDP:3.7%
Estim
ated
ineq
uity,G
iniInd
ex:35.7
Jordan
Popu
latio
n:9,956,011
Form
ationof
theHea
lthCare
AccreditationCou
ncil—
anatio
nal
healthcare
accred
itatio
nagen
cy
•Start-up
fund
ingfro
mUSA
ID•Develop
men
tof
internationalaccep
ted
standards
•Em
ployee
training
thou
ghconsultatio
nand
educationde
partmen
tsGDPpe
rcapita,PPP:$9347.94
•Develop
men
tof
health
profession
als’
capacity
toim
provequ
ality
andpatient
safety
Life
expe
ctancy
atbirth(bothsexes):
74.5years
•App
licationof
atotalq
ualitymanagem
ent
philosoph
yto
encouragesustainablechange
•Increaseduseof
family
planning
metho
dsby
clients
Expend
iture
onhealth
asaprop
ortio
nof
GDP:5.5%
•Moreeffectivemanagem
entof
certain
cond
ition
s,e.g.
diabetes
•Im
proved
leadership
commitm
ent,em
ployee
involvem
entandteam
work
Estim
ated
ineq
uity,G
iniInd
ex:33.7
•Increasedconsum
ersatisfaction
Braithwaite et al. BMC Medicine (2020) 18:340 Page 13 of 17

Table
3Eigh
texam
ples
ofcoun
try-levelreform
orim
provem
ent[7](Con
tinued)
Cou
ntry
Keyindicators
Initiative
Successfeatures
Outcomes
•Influen
cedtheMinistryof
Health
toincrease
itsQualityDep
artm
entbu
dget
and
person
nel
Rwanda
Popu
latio
n:12,301,939
Establishm
entof
Com
mun
ity-
based
health
insuranc
e•Nationw
ideinitiative
•90%
coverage
ofpo
pulatio
n
•Strong
andsustaine
dpo
liticalcommitm
ent
GDPpe
rcapita,PPP:$2253.52
•Im
proved
access
tohe
alth
services
•Financialinvestm
entfro
mthego
vernmen
tLife
expe
ctancy
atbirth(bothsexes):
67.5years
•Im
provem
entsin
healthcare
utilisatio
n
•Legislativesupp
ort
•Con
sensus
from
thepo
pulatio
nthat
healthcare
access
shou
ldbe
equitableand
affordable
•Redu
ctionof
financialcatastroph
eand
impo
verishm
entdu
eto
out-of-pocketcosts
Expend
iture
onhealth
asaprop
ortio
nof
GDP:6.8%
•Introd
uctio
nof
astratificationsystem
based
onindividu
alassets
•Im
provem
entof
health
indicators,e.g.
redu
cedmaternalm
ortalityandun
der5
years’de
aths
Estim
ated
ineq
uity,G
iniInd
ex:43.7
Spain
Popu
latio
n:46,723,749
Advanc
emen
tof
theSp
anish
Nationa
lTransplant
Organ
ization
(ONT)
•Existin
glegal,organisatio
naland
technical
framew
orks
•Increase
inthenu
mbe
rof
patientsreceiving
transplants
GDPpe
rcapita,PPP:$40,854.58
•Coo
rdinationof
dono
ractivities
atthe
natio
nal,region
alandho
spitallevel
•Increasedorgando
natio
nrates
Life
expe
ctancy
atbirth(bothsexes):
83.3years
•Highe
stde
ceased
donatio
nratesforalarge
coun
try
•Em
ploymen
tof
transplant
coordinatorsto
facilitateiden
tificationandreferralof
possibledo
nors
•Don
ationratesabovethat
oftheEurope
anUnion
orUSA
Expe
nditu
reon
health
asaprop
ortio
nof
GDP:9.0%
•Training
ofprofession
alsin
orgando
natio
n
•Develop
men
tof
apo
sitivepu
blicattitud
etowards
orgando
natio
nthou
ghmassmed
iaandan
open
commun
ications
policy
Estim
ated
ineq
uity,G
iniInd
ex:36.2%
•Hospitalreimbu
rsem
entsfordo
natio
nsand
transplantationactivities
Taiwan
Popu
latio
n:23,508,428
Adop
tion
ofhe
alth
inform
ation
tech
nology,e.g.
USB-based
elec-
tron
icpe
rson
alhe
alth
record
system
,MyH
ealth
Bank
web
site,rep
lacemen
tof
pape
r-basedID
cardswith
smart
card,and
clou
d-basedsystem
s
•Sing
le-payer
system
•Cost-effectiven
ess,e.g.
redu
ctionin
adminis-
trativecosts
•Develop
men
tof
securitymechanism
sto
protectconsum
ers’privacyandinform
ation
GDPpe
rcapita,PPP:$47,800
•Moreefficient,streamlined
processes
Life
expe
ctancy
atbirth(bothsexes):
80.1years
•Im
proved
quality
ofinform
ation
•Im
proved
med
icationsafety
Expe
nditu
reon
health
asaprop
ortio
nof
GDP:6.2%
•Enhanced
collabo
ratio
nandinform
ation
transfer
betw
eenproviders
Estim
ated
ineq
uity,G
iniInd
ex:33.8%
•Unifiedpu
bliche
alth
andclinicalmed
icine
inform
ationsystem
s
•Engage
men
tof
consum
ersin
theirow
ncare
•Redu
ctionof
fraud
•Con
tinuity
ofcare
Braithwaite et al. BMC Medicine (2020) 18:340 Page 14 of 17

Table
3Eigh
texam
ples
ofcoun
try-levelreform
orim
provem
ent[7](Con
tinued)
Cou
ntry
Keyindicators
Initiative
Successfeatures
Outcomes
WestAfrica
(Guine
a,Libe
riaandSierra
Leon
e)
Totalp
opulation:24,883,449
Applicationof
qua
lity
improve
men
teffortsin
Ebola-
effected
coun
tries
•Em
phasison
recovery
processes
•Kn
owledg
esharingbe
tween
GDPpe
rcapita,PPP:$1846.67*
•System
aticpo
st-disasterne
edsassessmen
ts•Ebola-affected
coun
tries
Lifeexpectancy
atbirth(bothsexes):
58.61*
•Focuson
infectionpreven
tionandcontrol,
andhe
alth
workerprotectio
n•‘Globalp
oolo
fkno
wledg
e’
•Dem
onstratio
nof
amod
elto
combatEbola
with
applicationto
othe
rinfectious
diseases
Expend
iture
onhealth
asaprop
ortio
nof
GDP:10.54%
*•Com
mun
ityinpu
t
•Clearlyarticulated
vision
forun
iversalh
ealth
coverage
•Strong
leadership
andgu
idance
Estim
ated
ineq
uity,G
iniInd
ex:33.6*
*Dataaverag
edacross
Guine
a,Libe
riaan
dSierra
Leon
eAllda
taarefrom
theWorld
Health
Organ
izationan
dWorld
Bank
.Availableda
taused
asat
Aug
ust20
19GDPgrossdo
mestic
prod
uct,PPPPu
rcha
sing
Power
Parity
Braithwaite et al. BMC Medicine (2020) 18:340 Page 15 of 17

determination and a willingness to begin, even during apandemic, are essential. Who has the courage to takethe lead?
ConclusionIf we actioned these calls to arms over the decade of the2020s, and move the reports’ proposals into the realworld with a template for change which synthesises andincorporates their recommendations, we might find our-selves on a path to progress in a strategic rather thanpiecemeal or fragmented way. And the potential benefitsto humankind, of putting our money where our mouthis, galvanising the world’s expertise into an actionableplan, buying better care for less fortunate populationsand more thoroughly understanding the whole caringenterprise, building on past success? These would beenormous.
AbbreviationsC-section: Caesarean section; GDP: Gross domestic product; HIV: Humanimmunodeficiency viruses; IAQS: International Academy of Quality andSafety; ICT: Information and Communications Technology; ID: Identitydocument; ISQua: International Society for Quality in Health Care;LMICs: Low- and middle-income countries; OECD: The Organisation forEconomic Co-operation and Development; ONT: National TransplantOrganization; PPP: Purchasing power parity; QI: Quality improvement;UHC: Universal health coverage; UN: United Nations; US: United States;USAID: United States Agency for International Development; USB-based: Universal serial bus based; WHO: World Health Organization
AcknowledgementsWe would like to thank and acknowledge research assistants Ms. MeaganWarwick, Ms. Kristiana Ludlow, Ms. Chiara Pomare, Dr. Kathryn Gibbons andMs. Kelly Nguyen for their editorial and research assistance.
Authors’ contributionsJB, CV and DWB conceptualised the manuscript. All authors were part of theanalysis, drafting and finalisation of the manuscript. The authors read andapproved the final manuscript.
FundingJB is Professor of Health Systems Research and Founding Director of theAustralian Institute of Health Innovation at Macquarie University, Sydney, Australia.This work was supported by the Australian Institute of Health Innovation whichreceives 80% of its core funding from category one, peer-reviewed grants, chiefly,the National Health and Medical Research Council (NHMRC) and Australian Re-search Council (ARC) funding which includes the NHMRC Partnership Grant forHealth Systems Sustainability (ID: 9100002).
Availability of data and materialsThe datasets used and/or analysed during the current study are availablefrom the corresponding author on reasonable request.
Ethics approval and consent to participateNot applicable.
Consent for publicationNot applicable.
Competing interestsNone to declare.
Author details1Centre for Healthcare Resilience and Implementation Science, AustralianInstitute of Health Innovation, Macquarie University, Level 6, 75 Talavera road,North Ryde, NSW 2113, Australia. 2Department of Experimental Psychology,
University of Oxford, Oxford OX2 6GG, UK. 3Institute for Clinical Effectivenessand Health Policy (IECS), Viamonte 2146 – 3 Piso, C1056ABH Ciudad de,Buenos Aires, Argentina. 4Graduate School of Medicine and Faculty ofMedicine, Yoshida-Konoe-cho, Sakyo-ku, Kyoto University, Kyoto 606-8501,Japan. 5International Society for Quality in Health Care (ISQua), HuguenotHouse, Dublin D02 NY63, Ireland. 6Institute for Healthcare Improvement,Boston, MA 02109, USA. 7Harvard Medical School, Boston, MA 02115, USA.
Received: 6 May 2020 Accepted: 6 August 2020
References1. National Academics of Sciences, Engineering and Medicine. Crossing the
global quality chasm: improving health care worldwide. Washington, DC:The National Academies Press; 2018.
2. World Health Organization, Organisation for Economic Co-Operation andDevelopment, and The World Bank. Delivering quality health services: aglobal imperative for Universal Health Coverage. Washington, DC: WHO,OECD, World Bank; 2018.
3. Kruk ME, Gage AD, Arsenault C, Jordan K, Leslie HH, Roder-DeWan S, et al.High-quality health systems in the sustainable development goals era: timefor revolution. Lancet Glob Health Comm High Qual Health Syst SDG Era.2018;6:PE1196–E252.
4. Le Fanu R. The rise and fall of modern medicine. New York: IngramPublishing Services; 2012.
5. Riley D, Hao JJ, Kiene H, Kienle G, Mittelman M, Plotnikoff GA. Globaladvances in health and medicine. Glob Adv Health Med. 2012;1(1):5–6.
6. Mills A. Health care systems in low- and middle-income countries. N Engl JMed. 2014;370(6):552–7.
7. Braithwaite J, Mannion R, Matsuyama Y, Shekelle P, Whittaker S, Al-Adawi S,editors. Healthcare systems: future predictions for global care. Boca Raton:CRC Press; 2018.
8. Braithwaite J, Churruca K, Ellis LA, Long J, Clay-Williams R, Damen N, et al.Complexity science in healthcare – aspirations, approaches, applications andaccomplishments: a white paper. Sydney: Australian Institute of HealthInnovation, Macquarie University; 2017.
9. Watson M, Smith A, Watter S. Leximancer concept mapping of patient casestudies. In: Khosla R, Howlett RJ, Jain LC, editors. Knowledge-basedintelligent information and engineering systems, vol. 3683. Berlin,Heidelberg: Springer; 2005.
10. Lamprell G, Braithwaite J. Mainstreaming gender and promoting intersectionalityin Papua New Guinea’s health policy: a triangulated analysis applying data-mining and content analytic techniques. Int J Equity Health. 2017;16:65.
11. Nunez-Mir GC, Iannone BV III, Pijanowski BC, Kong N, Fei S. Automatedcontent analysis: addressing the big literature challenge in ecology andevolution. Methods Ecol Evol. 2016;7:1262–72.
12. Qui L. Fact-checking Elizabeth Warren on the campaign trail. New York:New York Times; 2019.
13. Organisation for Economic Co-Operation and Development. Healthspending (indicator). 2018. https://data.oecd.org/healthres/health-spending.htm. Accessed 7 July 2020.
14. The World Bank. Population, total. 2018. https://data.worldbank.org/indicator/sp.pop.totl. Accessed 7 July 2020.
15. Global Giving. Health - explore projects. 2019. https://www.globalgiving.org/search/?size=10&nextPage=1&sortField=sortorder&selectedThemes=health&loadAllResults=true. Accessed 7 July 2020.
16. The World Bank. World Bank country and lending groups. 2019. https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups. Accessed 7 July 2020.
17. The World Bank. Current health expenditure (% of GDP). 2019. https://data.worldbank.org/indicator/SH.XPD.CHEX.GD.ZS?locations=XM. Accessed7 July 2020.
18. Braithwaite J, Mannion R, Matsuyama Y, Shekelle P, Whittaker S, Al-Adawi S,editors. Health systems improvement across the globe: success stories from60 countries. Boca Raton: CRC Press; 2018.
19. Braithwaite J, Mannion R, Matsuyama Y, Shekelle PG, Whittaker S, Al-AdawiS, et al. The future of health systems to 2030: a roadmap for global progressand sustainability. Int J Qual Health Care. 2018;30(10):823–31.
20. Clements BJ, Coady D, Gupta S, editors. The economics of public healthcare reform in advanced and emerging economies. Washington DC:International Monetary Fund; 2012.
Braithwaite et al. BMC Medicine (2020) 18:340 Page 16 of 17
21. Ranade W. Markets and health care: a comparative analysis. Oxon:Routledge; 2018.
22. World Health Organization. Strategizing national health in the 21st century: ahandbook. WHO. 2016. https://www.who.int/publications/i/item/strategizing-national-health-in-the-21st-century-a-handbook. Accessed 7 July 2020.
23. de Looper M, Lafortune G. Measuring disparities in health status and inaccess and use of health care in OECD countries. OECD health workingpapers, no. 43. Paris: OECD Publishing; 2009. https://doi.org/10.1787/225748084267. Accessed 7 July 2020.
24. Hollnagel E, Braithwaite J, Wears RL, editors. Resilient health care. Farnham:Ashgate Publishing; 2013.
25. Wears RL, Hollnagel E, Braithwaite J. Editors. Resilient health care volume. 2:the resilience of everyday clinical work. Farnham: Ashgate Publishing; 2015.
26. Braithwaite J, Wears RL, Hollnagel E, editors. Resilient health care volume 3:reconciling work-as-imagined and work-as-done. Abingdon: Taylor & Francis; 2017.
27. Hollnagel E, Braithwaite J, Wears RL. Resilient health care volume 4: deliveringresilient health care. Abingdon: Routledge: Taylor & Francis Group; 2018.
28. Braithwaite J, Hollnagel E, Hunte GS. Resilient health care volume 5: workingacross boundaries. Boca Raton: Routledge: Taylor & Francis Group; 2019.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations.
Braithwaite et al. BMC Medicine (2020) 18:340 Page 17 of 17