trans-inferior orbital rim anchorage and fascia roll multi-loop temporal anchorage in midface...
TRANSCRIPT
The transorbital fixation in malar elevation.
P. Albrecht.Plastic surgeonMarbella
Introduction:
A new paradigm recently appeared in the FACE lift field. Considering anatomy- especially the Furnas1 ligaments- and embryology, Thierry Besins2 promoted the three sectors concept, based on the pro-face, meso-face, and meta-face reality.Sector -1 (pro-face in embryology):nose, medial lip, chin, medial forehead, considered as fixed and tightly held by prominent bones and short and strong muscles.Sector-2 “Aging sector” (Meso-face) is the adipose and muscular area of the face, from the temporal area (with most of the eye-brow), to the mandibular .Sector-3 (Meta-cara) Furnas ligaments and fibrotic SMAS, from the preoricular area to the SCM muscle.
The technique consist in a subperiostial cheek dissection through a precanthal incision, a malar anchorage/suspensionwith a temporal fixation, an Orbicularis Oculii anchorage/suspension with a forehead fixation, a temporal lift, a ENDOTINE forehead lift, a lower neck and jaw lines lift respecting the Furnas ligaments.
De acuerdo con Hamra3, Besins promotes the idea that the Malar portion of the Orbicularis Oculii is the key of the full rejuvenation of the face through its tight continuity/imbrication with the malar fat .
Since its first presentation at the IMCAS 2002 congress in Paris, we have performed over 100 of those “vertical” face lifts. Due to a drastic malar elevation, this wonderful newparadigm has its learning curve, especially to achieve a
proper symmetry of both lateral canthuses, to avoid furtherectropion and a wavy aspect of the skin in the orbicular area. I had to retouch 5 ectropions and 3 assymetries.
Also the two first patients (operated together with T. Besins) reported discomfort due to the malar and orbicularis far temporal and forehead fixations with thick non absorbable threads (2/0 Gore-tex) which led us to remove them and to rethink the fixation points straight from the beginning.
We would like to present an alternative to far fixation which can be of interest in some cases, and that we have also used in lower lids reconstruction, after bad surprises.
But before we would like to expose what Our experience shows after 3 years of practice of that techinque:
- That the malar area, hardly moves up when the patient opens the mouth wide.
- Therefore the best vector to pull up the malar areais exactly perpendicular to nasolabial fold.
- The result of that techniques relies on the Orbicularis Ocullii proper suspension due to its elasticity and its tight relation to the malar fat.The vector should rather be vertical than oblique to avoid diastasis.
- Most of the far thread based suspensions will drop due to a “butter cutting like” thread effect. The forces applied on the soft tissues by the thread when the patient moves- especially when he opens the mouth- will just cut them or at least squash them.
- Most the far thread based suspensions will allow the soft tissues to move during the post-op and therefore prevent a good scar tissue to built up and stick them with periostium to the bone.
- That can be partly compensated during the early post-op phase with proper tight dressings and bandages to wait for scar tissue to build up.
- Nevertheless, even if a patient would be kept with a tight bandage during one month, without opening the mouth wide or smiling, to allow strong scar tissue to “stick” the lifted structures in an upper position, we can predict that they will always settle back where they are supposed to allowthe proper face dynamics
- This are the reasons why the R.A.R.E technique mainly relies on the use of non absorbable Gore Texthreads, especially for the Orbicularis Oculii which is the only anatomical structure that will keep holding the malar soft tissues.
- We prefer the close fixation points in any soft tissue suspension strategy. For that purpose we have developed the trans orbital rim points combinewith the Flowers4 zygoma ascending branch ones.
-We have successfully performed 98 procedures.
Method:
Pre-op marking or drawing:
Pre-op marking for malar suspension should be done with patient standing and focusing on the safe John Little pointalso described in the R.A.R.E technique down the lateral cantus when the line crosses the nose base level. The vertical vector at that point only gives a limited ascending opportunity, leaving to the Orbicularis Oculii
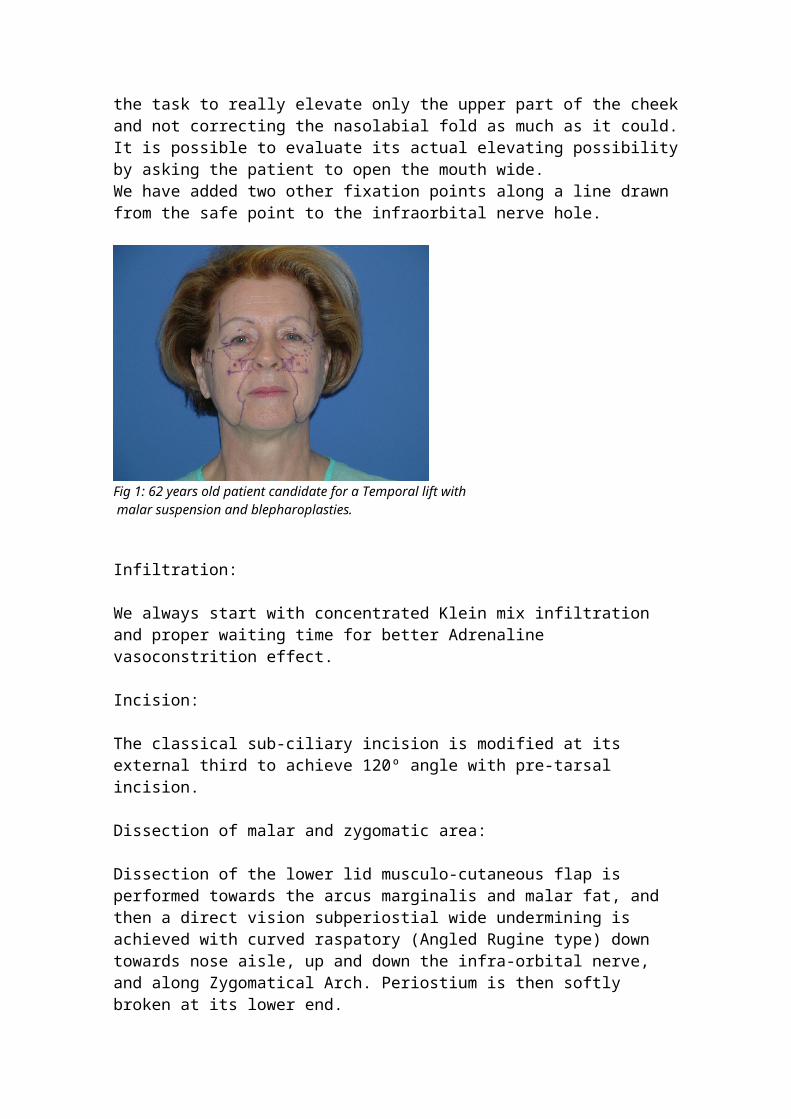
the task to really elevate only the upper part of the cheekand not correcting the nasolabial fold as much as it could.It is possible to evaluate its actual elevating possibilityby asking the patient to open the mouth wide.We have added two other fixation points along a line drawn from the safe point to the infraorbital nerve hole.
Fig 1: 62 years old patient candidate for a Temporal lift with malar suspension and blepharoplasties.
Infiltration:
We always start with concentrated Klein mix infiltration and proper waiting time for better Adrenaline vasoconstrition effect.
Incision:
The classical sub-ciliary incision is modified at its external third to achieve 120º angle with pre-tarsal incision.
Dissection of malar and zygomatic area:
Dissection of the lower lid musculo-cutaneous flap is performed towards the arcus marginalis and malar fat, and then a direct vision subperiostial wide undermining is achieved with curved raspatory (Angled Rugine type) down towards nose aisle, up and down the infra-orbital nerve, and along Zygomatical Arch. Periostium is then softly broken at its lower end.
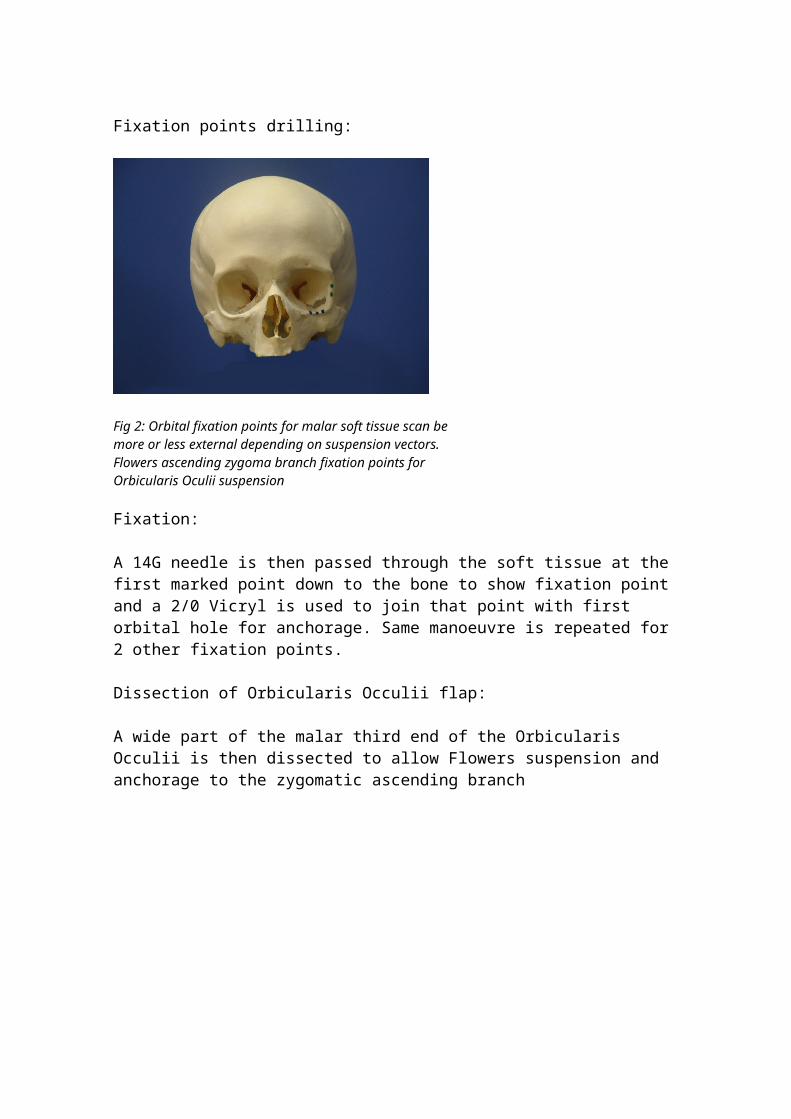
Fixation points drilling:
Fig 2: Orbital fixation points for malar soft tissue scan be more or less external depending on suspension vectors. Flowers ascending zygoma branch fixation points for Orbicularis Oculii suspension
Fixation:
A 14G needle is then passed through the soft tissue at the first marked point down to the bone to show fixation point and a 2/0 Vicryl is used to join that point with first orbital hole for anchorage. Same manoeuvre is repeated for 2 other fixation points.
Dissection of Orbicularis Occulii flap:
A wide part of the malar third end of the Orbicularis Occulii is then dissected to allow Flowers suspension and anchorage to the zygomatic ascending branch
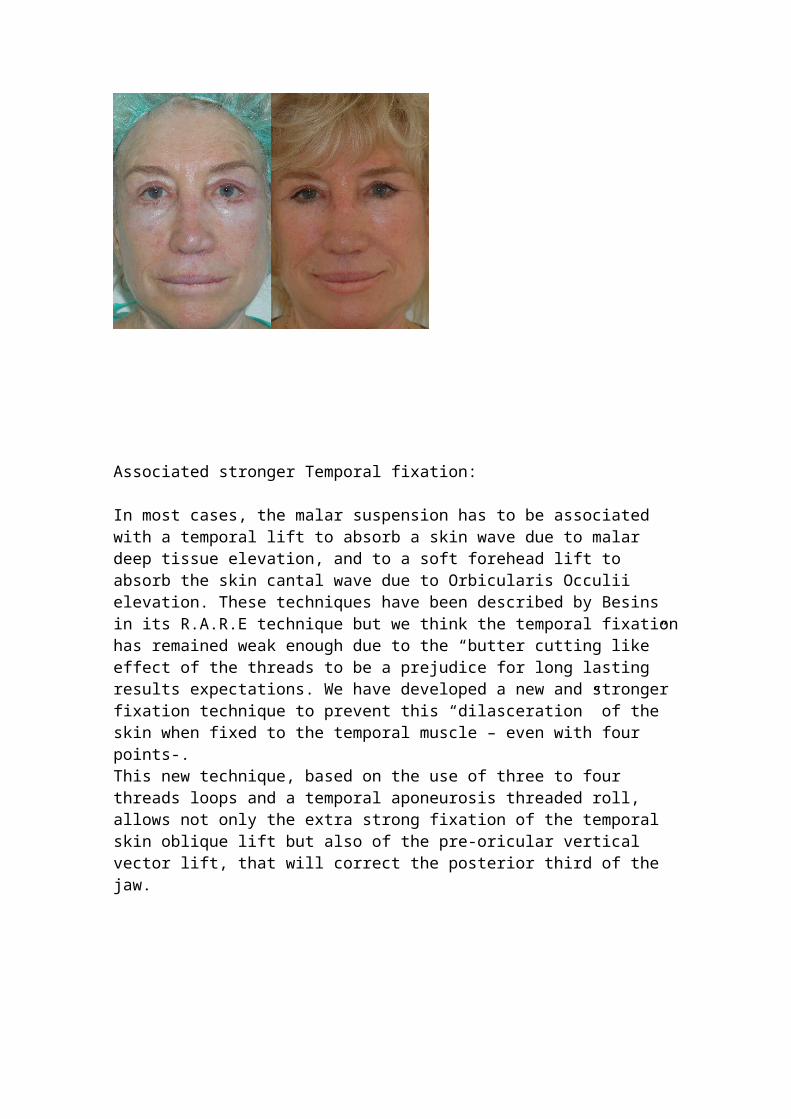
Associated stronger Temporal fixation:
In most cases, the malar suspension has to be associated with a temporal lift to absorb a skin wave due to malar deep tissue elevation, and to a soft forehead lift to absorb the skin cantal wave due to Orbicularis Occulii elevation. These techniques have been described by Besins in its R.A.R.E technique but we think the temporal fixationhas remained weak enough due to the “butter cutting like” effect of the threads to be a prejudice for long lasting results expectations. We have developed a new and stronger fixation technique to prevent this “dilasceration” of the skin when fixed to the temporal muscle – even with four points-.This new technique, based on the use of three to four threads loops and a temporal aponeurosis threaded roll, allows not only the extra strong fixation of the temporal skin oblique lift but also of the pre-oricular vertical vector lift, that will correct the posterior third of the jaw.
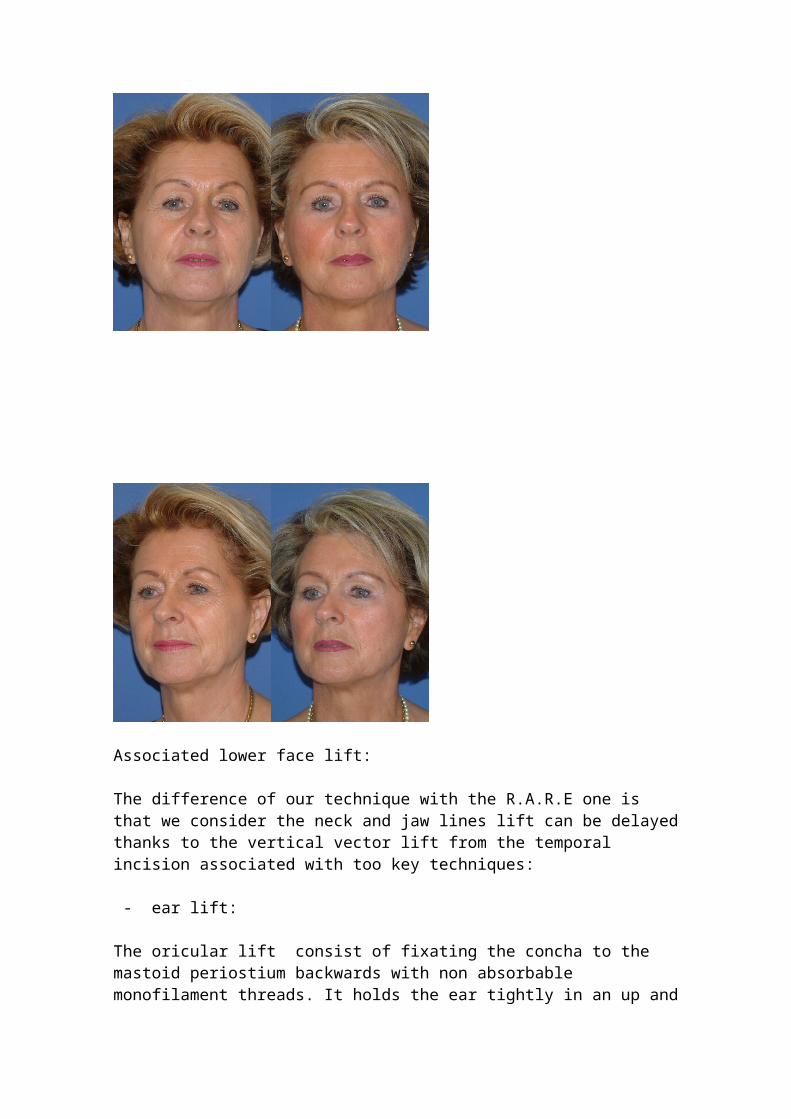
Associated lower face lift:
The difference of our technique with the R.A.R.E one is that we consider the neck and jaw lines lift can be delayedthanks to the vertical vector lift from the temporal incision associated with too key techniques:
- ear lift:
The oricular lift consist of fixating the concha to the mastoid periostium backwards with non absorbable monofilament threads. It holds the ear tightly in an up and
vertical position, prevents any further rotation that wouldreduce the mouth commissure -ear lobe distance. It also makes totally disappear the pre-oricular folds.
- wide submental fat removal:
Prior to the malar lift, it is convenient to alleviate the submental skin from its supra and retro platysmal fat, achieving a perfect definition of the jaw lines up to theirtwo third.The Timothy Martin submaxilar gland upper third removal is also a good complement.
Discussion:
Before performing any face lift, our point of view is that we should consider the “dynamic face” in addition to the anatomical and embryological realities to have a prognosis of our results and a precise idea of what can be achieved without mistakes.
That led us to consider the following:
First: Most of the patients drawings are made in a verticalposition and the procedures are performed in an horizontal position.Second: The before-after pictures are obviously static and shown with the mouth closed. It does not give any idea of the dynamics, like the smiling, turning the head from rightto left, moving the chin up and down.Third: if we would cut a vertical or horizontal thin strip of the skin and pull on both sides, we would have an elastic characteristic in young people, and a cord characteristic in elder people .
1 Furnas D.: The retaining ligament of the cheek, Plast Rec Surg, 83, Jan 89: 11-162 Besins T. : The R.A.R.E technique, Plast Aesthetic Surgery Journal, august 20043 Hamra Sam T. : Composite Rhytidectomy. QMP Inc, St Louis, MISSOURI 19934 Flower.R : The malar correction, Aesth. Surg. Journal. 2001
Fourth: As long as more likely elder people undergo facelifts, their skin characteristics are closer to those of cords than to those of elastics.Fith: Therefore, when we want to perform a face lift, our long lasting results can not be better than those obtained if we would lift the skin when the patient opens wide the mouth (fore the malar lift), lift the chin up, turns the head on the right and on the left (for the neck lift).Sixth: We have measured the before and after distances fromthe mouth commisure to the ear lobe and to the lower edge of the tragus in most available publications about face lifts. They have been reduced in 94 % of the cases between 5mm for the tragus to 1,5 cm for the ear lobe.Seven: We think that the concha can be considered as a “fixed point” compared to the surrounding soft tissue as Furnas has described it. Nevertheless we have observed thatin many cases there was a slight clockwise rotation of the left ears and anticlockwise of the right ones. Eight: We can than improve the natural aspect of the face lift results by just fixing the concha as backwards as possible prior to skin resection and stiching. In many cases of young patients, this simple manoeuvre will be sufficient to tighten the skin of the jaw and eliminate thepre-oricular folds, if combined with a temporal lift with vertical vector.Nine: In most cases, the definition of the jaw lines relieson the removal of the submental and jaw fat, together with a portion of the submaxilar gland as Timothy Martin has described.
Technique:
Conclusion:
The face lift is a static procedure that works against a dynamic condition of the face.An excess tightening always leads to a static face with less expressions

The natural tendancy of individuals to have mimics will lead to a midterm or long term loosening of the skin that has been tightened.If we want our patients to move properly after a facelift we cannot excise more skin that the one we have left after the patient had been asked to move in the above described way.