training with computer-supported motor imagery in post-stroke rehabilitation
TRANSCRIPT

Training with Computer-Supported Motor Imagery in Post-Stroke Rehabilitation
A GAGGIOLI MS F MORGANTI PhD R WALKER BA A MENEGHINI MD M ALCANIZ PhD JA LOZANO PhD J MONTESA PhD JA GIL PhD
and G RIVA PhD
ABSTRACT
Converging lines of evidence suggest that motor imagery (the mental simulation of a motoract within working memory) is associated with subliminal activation of the motor systemThis observation has led to the hypothesis that cortical activation during motor imagery mayaffect the acquisition of specific motor skills and help the recovery of motor function In thispaper we describe a clinical protocol in which we use interactive tools to stimulate motor im-agery in hemiplegic stroke patients thereby helping them to recover lost motor function Theprotocol consists of an inpatient and an outpatient phase combining physical and mentalpractice In the inpatient phase patients are trained in a laboratory setting using a custom-made interactive workbench (VR Mirror) After discharge patients use a portable device toguide mental and physical practice in a home setting The proposed strategy is based on thehypotheses that (a) combined physical and mental practice can make a cost-effective contri-bution to the rehabilitation of stroke patients (b) effective mental practice is not possiblewithout some form of support from a therapist (as in our inpatient phase) or from technology(as in the outpatient phase) (c) the inclusion of an outpatient phase will allow the patient topractice more often than would otherwise be possible therefore increasing the speed andoreffectiveness of learning and (d) the use of interactive technology will reduce the patientrsquosneed for skilled support therefore improving the cost-effectiveness of training
327
CYBERPSYCHOLOGY amp BEHAVIORVolume 7 Number 3 2004copy Mary Ann Liebert Inc
INTRODUCTION
HEMIPLEGIA is total paralysis of the arm leg andtrunk on one side of the body The paralysis
presents a weakness that may be associated withabnormal muscle tone (eg rigidity or spasticity)The most common cause is stroke which occurswhen a rupture or blood clot reduces blood flow to
a specific area of the brain killing cells and disrupt-ing the abilities or functions they control Hemiple-gia can be caused by damage to a variety ofstructures including primary sensorimotor areassupplementary motor premotor and parietal cor-tices basal ganglia andor the thalamus1 Strokesaffect some 700000 individuals every year in theUnited States alone in 2003 Americans paid about
Applied Technology for Neuro-Psychology Lab Istituto Auxologico Italiano Milan Italy
13658C04PGS 61504 236 PM Page 327
$51 billion for stroke-related medical costs anddisability2
Traditional rehabilitation after stroke focuses onpassive (non-specific) movement or on compensa-tory training of the non-paretic arm3 Recently sev-eral researchers have proposed the use of mentalpractice as a therapeutic tool to promote motorrecovery in stroke patients with upper-limb disabil-ity45 Mental practice also called symbolic re-hearsal or motor rehearsal is a training techniquein which the patients repeatedly ldquorehearserdquo amotor act in working memory4 without producingany overt motor output6 In the first section of thispaper we describe the rationale for using mentalpractice in neurological rehabilitation focusing onthe conditions under which it is believed to be mosteffective We then describe a clinical protocol inwhich we use interactive tools to help hemiplegicstroke patients to use mental practice during theirrehabilitation The authors intend that this protocolwill serve as the basis for a small-scale pilot trialdesigned as a feasibility study for a larger-scalerandomized clinical trial The protocol describedbelow and an earlier version of the protocol de-scribed elsewere7 have been developed as part of I-Learning a project in the EU-funded FET ISTProgram
MENTAL PRACTICE AND MOTOR IMAGERY IN
NEUROLOGICAL REHABILITATION
ldquoMotor imageryrdquo can be defined as the mentalsimulation of a motor act in working memory withno gross muscular activation ldquoMotor imageryrdquoshould be distinguished from ldquovisual imageryrdquo invisual imagery subjects imagine the environmentin which they are moving in motor imagery theyimagine the kinesthetic sensations associated withmovement8 To avoid confusion sport psycholo-gists often refer to kinesthetic imagery
Scientific investigation of motor imagery datesback to 1885 when the Viennese psychologistStricker collected empirical evidence that overtand covert motor behaviors involve the same pro-cessing resources9 Over the past 30 years many re-searchers have used subjective behavioral andphysiological methods to investigate this hypothe-sis further10 These studies have provided converg-ing evidence that imagining a motor act is acognitive task that engages parts of the executivemotor system in particular the supplementarymotor area the cerebellum as well as the premotorcingulated superior inferior parietal sensorimotor
and primary motor cortices Drawing on thesefindings investigators have suggested that trainingwith motor imagery (mental practice) could be ef-fective in learning new motor skills or in promotingmotor recovery after damage to the central nervoussystem Pascual-Leone et al11 for example usedTMS to compare changes in the functional organi-zation of the brain after mental and after physicalrehearsal of a one-handed piano exercise The ex-periment showed not only that mental and physi-cal rehearsal over a five day period producedequivalent improvements in performance but thatthese were marked by equivalent increases in thesize of the contralateral cortical output map for thelong finger flexor and extensor muscles Thoughmental practice took five days to produce the sameimprovement that physical practice produced inthree the investigators showed that a single physi-cal training session was enough to bring the mentalpractice group to the same level as subjects whohad trained physically
Jackson et al4 have recently created a modelcomparing the potential therapeutic effects of men-tal practice with other forms of training The modelassumes that practice involves declarative knowl-edge non-conscious processes and physical execu-tion In their model declarative knowledge is theexplicit knowledge that subjects need before prac-ticing a motor task (ie a knowledge of the se-quence of movements to be performed) skills thatare not directly accessible to verbal descriptionsuch as the timing of motor responses to cues or theco-articulation of small segments of movementand the rapid sequential activation or inhibitionof different muscle groups are regulated by non-conscious processes physical execution is the mus-culoskeletal activity necessary to carry out theintended action
According to Jackson et al4 these different levelsof processing interact in different ways in differentforms of training Physical practice involves allthree levels of processing in mental practice on theother hand learning depends crucially on theinteraction between declarative knowledge andnon-conscious processes in physical practice it ispossible to learn a motor task implicitly in mentalpractice subjects have a good declarative knowl-edge of the different components of the task beforethey start practicing The similarity between thecircuitry involved in imagining and executingmovements suggests however that the neuronalnetwork implicated in the non-conscious aspects ofa task can be primed as effectively through mentalas through physical practice In addition the modelpredicts that internally driven images promoting
328 GAGGIOLI ET AL
13658C04PGS 61504 236 PM Page 328
kinesthetic ldquosensationsrdquo of movement could behighly effective in activating the non-consciousprocesses involved in motor training According toJackson and his colleagues this would explain whykinesthetic imagery is more effective than purelyvisual imagery According to their model mentalpractice with motor imagery can be conceptualizedas a means to access the otherwise non-consciouslearning processes involved in a task They recog-nize however that the absence of direct feedbackfrom physical execution makes mental practice onits own a less effective training method than physi-cal practice
SUPPORTING MENTAL PRACTICE WITH INTERACTIVE TECHNOLOGY
THE I-LEARNING REHABILITATION PROTOCOL
Clinical studies have shown that the rehabilita-tion of hemiplegic and hemiparetic patients can bemade more effective by combining physical prac-tice with mental rehearsal51213 However for manypatients with damage to the CNS mental simula-tion of movements can be difficult even when therelevant neural circuitry has been spared14 Thegoal of the I-learning rehabilitation protocol is thusto use interactive technology to assist patients increating motor imagery which they can then useduring ldquomental practicerdquo The treatment consists ofan inpatient phase and an outpatient phase
Inpatient phase
The rehabilitation program starts 15 days afterhospitalization The intervention consists of onedaily session (in the morning) 5 days a week for 4consecutive weeks In each session the patient sitsat a table in front of the apparatus To ensure com-fort the patientrsquos ankles are in neutral dorsiflexionthe knees and hips are placed at 90deg the shouldersin 0deg flexion the elbows in 60deg flexion the wristsare neither extended nor flexed The apparatusused by the patients consists of a movement track-ing system and a custom-designed interactiveworkbench that we call the virtual reality (VR) mir-ror (Fig 1) The idea of the VR mirror is inspired byprevious work with stroke patients by Stevens et alin which mirror images of movement by a healthylimb (created by a physical mirror) were effectivelyused to stimulate motor imagery of movement bythe paretic limb5 In the I-Learning protocol the VRmirror displays a 3D electronic image of the move-ment performed by the patientrsquos healthy limb Thisis viewed from an ego-centric perspective that fa-cilitates the generation of kinesthetic motor im-agery by the patient
Each session of inpatient treatment consists offour consecutive sub-phases pre-training physicaltraining with the unimpaired limb imagery train-ing and VR mirror training The training focuseson elbow flexionextension pronationsupinationof the forearm wrist flexionextension openclo-sure of the hand and fine finger movements Dur-ing the pre-training phase the patient receives
COMPUTER-SUPPORTED MOTOR IMAGERY IN POST-STROKE REHABILITATION 329
FIG 1 The VR mirror interactive workbench
13658C04PGS 61504 236 PM Page 329
instructions which explain how the treatmentworks encouraging the patient to relax and reduc-ing fear and performance anxiety The instructionsare accompanied by relaxing music In the nextphysical training phase the therapist shows the pa-tient how to perform the movement with the unaf-fected arm The movement is accompanied byrhythmic auditory cues designed to stabilize thespeed of the movement (guaranteeing that the pa-tient performs the same movement each time)3 andto provide the patient with an attentional goal(matching the sound with the movement) a strat-egy known to facilitate motor learning15 When thepatient then performs the task the system tracksher arm identifying ldquokey framesrdquo and creating a3D model of the movement Next in the imagerytraining phase the patient is asked to create a men-tal image (kinesthetic imagery) of the impaired armperforming the movement as viewed from an in-ternal perspective When the patient starts to imag-ine the movement she presses a button (using herhealthy hand) pressing it again when she has fin-ished This allows the therapist to measure the timeshe takes to imagine each movement This is thepatientrsquos Response Time (RT) Basic research hasshown that response times for physical and imag-ined movements are subject to common laws andprinciples616 comparing a patientrsquos RTs whileimagining and physically performing the samemovements allows the therapist to statistically as-sess the quality of the patientrsquos motor imagery
After the patient has completed the mental re-hearsal exercise she is instructed to watch the dis-
play on the VR mirror (VR mirror training phase)The 3D model created earlier is used to generate amirror image of the movement originally per-formed by the unimpaired arm As the movementis displayed it is accompanied by the same rhyth-mic auditory cues used in the physical trainingphase This multimodal sensorial stimulation hastwo advantages the image of the reflected limbprovides the patient with direct perceptual cuessuggesting how the impaired limb could completea smooth well-controlled movement meanwhileauditory cueing synchronized with key frameshelps the patient to memorize the rhythmical struc-ture of the movement3
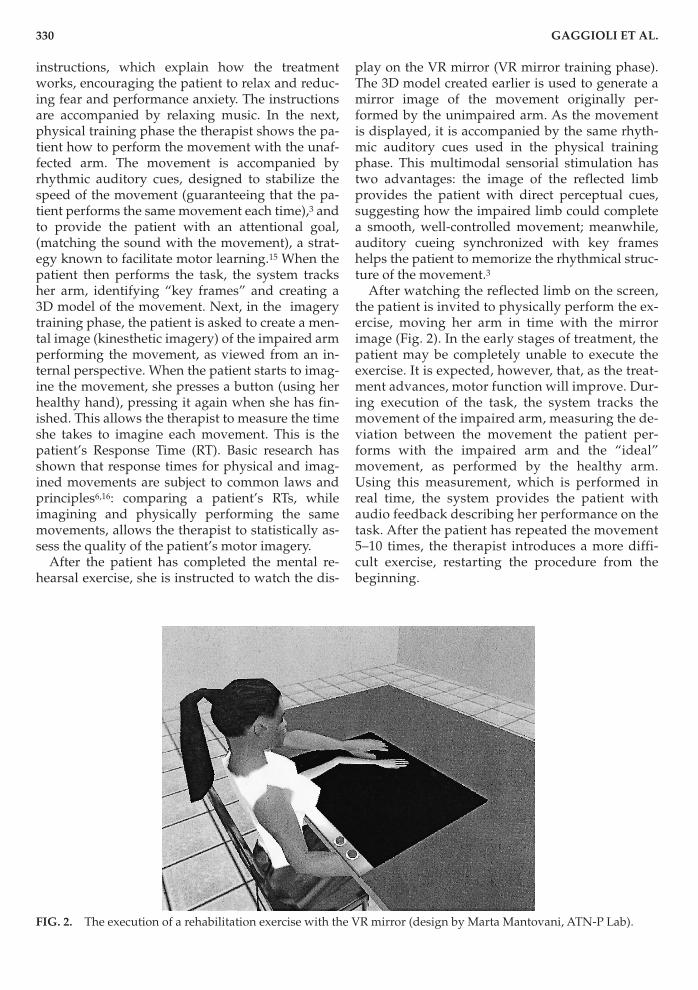
After watching the reflected limb on the screenthe patient is invited to physically perform the ex-ercise moving her arm in time with the mirrorimage (Fig 2) In the early stages of treatment thepatient may be completely unable to execute theexercise It is expected however that as the treat-ment advances motor function will improve Dur-ing execution of the task the system tracks themovement of the impaired arm measuring the de-viation between the movement the patient per-forms with the impaired arm and the ldquoidealrdquomovement as performed by the healthy armUsing this measurement which is performed inreal time the system provides the patient withaudio feedback describing her performance on thetask After the patient has repeated the movement5ndash10 times the therapist introduces a more diffi-cult exercise restarting the procedure from thebeginning
330 GAGGIOLI ET AL
FIG 2 The execution of a rehabilitation exercise with the VR mirror (design by Marta Mantovani ATN-P Lab)
13658C04PGS 61504 236 PM Page 330
Outpatient phase home-based rehabilitation
Home-based rehabilitation has the advantagethat stroke patients can practice skills and developcompensatory strategies in the environment wherethey normally live The benefits of this approachmost frequently citied in the literature includefocus on long-term outcomes a reduction of therisks associated with inpatient care respect for pa-tient preferences and savings in the direct cost oftreatment1718 It is nonetheless necessary to providepatients with specialized equipment to support therehabilitation process19 In the I-learning outpatientprogram the equipment provided is a Home Porta-ble Device (a portable computer or a PDA) withmultimedia capabilities The device provides pa-tients with instructions and visual cues allowingthem to mentally rehearse and physically practicethe motor tasks prescribed by the training protocolthe same device monitors their performance
At the beginning of each home-based rehabilita-tion session the Home Portable Device displays asequence of computer-generated movies picturingthe movement to be learned performed at differentspeeds using both the left and the right arm andviewed from different angles as prescribed inStevens and Stoykovrsquos protocol5 The movementsdisplayed on the screen are accompanied by rhyth-mic auditory cues After viewing the movies thepatient is instructed to take a first-person perspec-tive and to imagine performing the task with theimpaired arm At the start and on completion of thetask the patient uses her healthy hand to press akey on the HPD Once this mental practice has beencompleted the patient is asked to physically per-form the movement with the impaired arm
The patient performs this sequence of exerciseson a daily basis for the first two weeks after dis-charge from hospital three times a week startingfrom the 21st day after discharge and two times aweek from the fourth week after discharge onWhen she returns to hospital for follow-up (at 3and 6 months after discharge) the therapist con-nects the portable device to a desktop computerand downloads the data recorded during the exer-cises This includes (a) mental performance datathe response times recorded by the patient duringmental practicemdashby comparing RTs for mentalpractice with data recorded during physical exer-cise the therapist can assess the quality of the pa-tientrsquos motor imagery and (b) compliance datadata describing the dates and times of sessions al-lows the therapist to assess how far the patient hascomplied with the schedule specified in the treat-ment protocol
Assessment
Assessmentmdashbased on behavioral and clinicalindicators of physical competencymdashwill be carriedout before the intervention immediately after dis-charge from the hospital at 3 months and at 6months after discharge from the hospital
DISCUSSION
The rehabilitation technique described in thispaper combines mental and physical practice usinginteractive technology to provide the patient withvisual and auditory cues that draw her attention tothe underlying dynamic structure of a movementfacilitating the generation of mental imagery Theprotocol integrates inpatient treatmentmdashusingnovel apparatusmdashwith outpatient treatment As faras concerns the inpatient phase the solution wehave developed has at least four advantages Firstthe combination of audio and visual cues providedby the VR mirror greatly facilitates the patientrsquos taskin generating the kind of motor imagery requiredfor effective mental rehearsal second the use of amirror metaphor eliminates the need for pre-pro-grammed computer exercises a well-known short-coming of traditional computer-based rehabilitationexercises third the use of an external displayavoids the need for the patient to wear cumbersomeor invasive equipment (such as a Head MountedDisplay or shutter glasses) and last but not leastarm-tracking makes it possible to record the dy-namic features of a movement allowing objectivereal-time comparison between the movement of theimpaired limb and the ldquoideal performancerdquo as re-corded with the healthy limb As a result the com-puterized system provides the therapist with acontinuous flow of feedback about the patientrsquos per-formance making it possible to adjust the treatmentaccordingly The same data is used to provide per-formance feedback to the patient a key requirementfor effective motor learning2021
As far as concerns the outpatient phase the useof a Home Portable Device to support mental prac-tice makes it possible to increase the duration fre-quency and intensity of the therapy provided topatients In the longer term it may become possibleto connect these devices to the Internet allowing atherapist to remotely monitor a patientrsquos progress
The strategy presented in this paper is justifiedby four key hypotheses (a) combined physical andmental practice can make a cost-effective contribu-tion to the rehabilitation of stroke patients (b) ef-fective mental practice is not possible without
COMPUTER-SUPPORTED MOTOR IMAGERY IN POST-STROKE REHABILITATION 331
13658C04PGS 61504 236 PM Page 331
some form of support from a therapist (as in ourinpatient phase) or from technology (as in the out-patient phase) (c) the inclusion of an outpatientphase will allow the patient to practice more oftenthan would otherwise be possible therefore in-creasing the speed andor effectiveness of learn-ing and (d) the use of interactive technology willreduce the patientrsquos need for skilled supporttherefore improving the cost-effectiveness of train-ing If clinical trials show these hypotheses to becorrect the protocol described in this paper couldmake a useful contribution to improving the effec-tiveness and reducing the duration and cost ofpost-stroke rehabilitation
ACKNOWLEDGMENTS
The present work was supported by the Com-mission of the European Communities (CEC) inparticular by the IST programme (Project I-Learn-ing IST 2001ndash38861) and by the Italian Ministryof University and Research FIRB grant (ProjectNeuroTIV)
REFERENCES
1 Johnson SH Sprehn G amp Saykin AJ (2002) Intactmotor imagery in chronic upper limb hemiplegicsevidence for activity-independent action representa-tions Journal of Cognitive Neuroscience 14841ndash852
2 American Heart Association (2003) Stroke facts 20033 Whitall J McCombe Waller S Silver KH et al
(2000) Repetitive bilateral arm training with rhyth-mic auditory cueing improves motor function inchronic hemiparetic stroke Stroke 312390ndash2395
4 Jackson PL Lafleur MF Malouin F et al (2001)Potential role of mental practice using motor im-agery in neurologic rehabilitation Archives of PhysicalMedicine and Rehabilitation 821133ndash1141
5 Stevens JA amp Stoykov ME (2003) Using motorimagery in the rehabilitation of hemiparesis Archivesof Physical Medicine and Rehabilitation 841090ndash1092
6 Decety J amp Jeannerod M (1995) Mentally simu-lated movements in virtual reality does Fittsrsquos lawhold in motor imagery Behav Brain Res 72127ndash134
7 Morganti F Gaggioli A Castelnuovo G et al(2003) The use of technology-supported mental im-agery in neurological rehabilitation a research proto-col CyberPsychology amp Behavior 6421ndash427
8 Jeannerod M (1994) The representing brain neuralcorrelates of motor intention and imagery Brain andBehavioral Sciences 17187ndash245
9 Sirigu A amp Duhamel JR (2001) Motor and visualimagery as two complementary but neurally disso-ciable mental processes Journal of Cognitive Neuro-science 13910ndash919
10 Annett J (1995) Motor imagery perception or ac-tion Neuropsychologia 331395ndash1417
11 Pascual-Leone A Nguyet D Cohen LG et al(1995) Modulation of muscle responses evoked bytranscranial magnetic stimulation during the acqui-sition of new fine motor skills Journal of Neurophysi-ology 741037ndash1045
12 Page SJ Levine P Sisto S et al (2001) A random-ized efficacy and feasibility study of imagery in acutestroke Clinical Rehabilitation 15233ndash240
13 Page SJ Levine P Sisto SA et al (2001) Mentalpractice combined with physical practice for upper-limb motor deficit in subacute stroke Physical Ther-apy 811455ndash1462
14 Goldenberg G (1989) The ability of patients withbrain damage to generate mental visual imagesBrain 112305ndash325
15 Locke EA amp Bryan JF (1966) Cognitive aspects ofpsychomotor performance The effects of perfor-mance goals on level of performance J Appl Psychol50286ndash291
16 Decety J Jeannerod M amp Prablanc C (1989) Thetiming of mentally represented actions Behav BrainRes 3435ndash42
17 Anderson C Rubenach S Mhurchu CN et al(2000) Home or hospital for stroke rehabilitation re-sults of a randomized controlled trial I Health out-comes at 6 months Stroke 311024ndash1031
18 Disler PB amp Wade DT (2003) Should all stroke re-habilitation be home based Am J Phys Med Rehabil82733ndash735
19 NINDS (2003) Post-stroke rehabilitation fact sheet[Online] Available wwwnindsnihgovhealth andmedicalpubspoststrokerehabhtm
20 Salmoni AW (1980) The effect of precision ofknowledge of results on the performance of a simpleline drawing task for children and adults Res Q ExercSport 51572ndash575
21 Salmoni AW Schmidt RA amp Walter CB (1984)Knowledge of results and motor learning a reviewand critical reappraisal Psychological Bulletin 95355ndash386
Address reprint requests toAndrea Gaggioli MS
Applied Technology for Neuro-Psychology LabIstituto Auxologico Italiano
Via Pelizza da Volpedo 4120149 Milan Italy
E-mail andreagaggioliauxologicoit
332 GAGGIOLI ET AL
13658C04PGS 61504 236 PM Page 332

$51 billion for stroke-related medical costs anddisability2
Traditional rehabilitation after stroke focuses onpassive (non-specific) movement or on compensa-tory training of the non-paretic arm3 Recently sev-eral researchers have proposed the use of mentalpractice as a therapeutic tool to promote motorrecovery in stroke patients with upper-limb disabil-ity45 Mental practice also called symbolic re-hearsal or motor rehearsal is a training techniquein which the patients repeatedly ldquorehearserdquo amotor act in working memory4 without producingany overt motor output6 In the first section of thispaper we describe the rationale for using mentalpractice in neurological rehabilitation focusing onthe conditions under which it is believed to be mosteffective We then describe a clinical protocol inwhich we use interactive tools to help hemiplegicstroke patients to use mental practice during theirrehabilitation The authors intend that this protocolwill serve as the basis for a small-scale pilot trialdesigned as a feasibility study for a larger-scalerandomized clinical trial The protocol describedbelow and an earlier version of the protocol de-scribed elsewere7 have been developed as part of I-Learning a project in the EU-funded FET ISTProgram
MENTAL PRACTICE AND MOTOR IMAGERY IN
NEUROLOGICAL REHABILITATION
ldquoMotor imageryrdquo can be defined as the mentalsimulation of a motor act in working memory withno gross muscular activation ldquoMotor imageryrdquoshould be distinguished from ldquovisual imageryrdquo invisual imagery subjects imagine the environmentin which they are moving in motor imagery theyimagine the kinesthetic sensations associated withmovement8 To avoid confusion sport psycholo-gists often refer to kinesthetic imagery
Scientific investigation of motor imagery datesback to 1885 when the Viennese psychologistStricker collected empirical evidence that overtand covert motor behaviors involve the same pro-cessing resources9 Over the past 30 years many re-searchers have used subjective behavioral andphysiological methods to investigate this hypothe-sis further10 These studies have provided converg-ing evidence that imagining a motor act is acognitive task that engages parts of the executivemotor system in particular the supplementarymotor area the cerebellum as well as the premotorcingulated superior inferior parietal sensorimotor
and primary motor cortices Drawing on thesefindings investigators have suggested that trainingwith motor imagery (mental practice) could be ef-fective in learning new motor skills or in promotingmotor recovery after damage to the central nervoussystem Pascual-Leone et al11 for example usedTMS to compare changes in the functional organi-zation of the brain after mental and after physicalrehearsal of a one-handed piano exercise The ex-periment showed not only that mental and physi-cal rehearsal over a five day period producedequivalent improvements in performance but thatthese were marked by equivalent increases in thesize of the contralateral cortical output map for thelong finger flexor and extensor muscles Thoughmental practice took five days to produce the sameimprovement that physical practice produced inthree the investigators showed that a single physi-cal training session was enough to bring the mentalpractice group to the same level as subjects whohad trained physically
Jackson et al4 have recently created a modelcomparing the potential therapeutic effects of men-tal practice with other forms of training The modelassumes that practice involves declarative knowl-edge non-conscious processes and physical execu-tion In their model declarative knowledge is theexplicit knowledge that subjects need before prac-ticing a motor task (ie a knowledge of the se-quence of movements to be performed) skills thatare not directly accessible to verbal descriptionsuch as the timing of motor responses to cues or theco-articulation of small segments of movementand the rapid sequential activation or inhibitionof different muscle groups are regulated by non-conscious processes physical execution is the mus-culoskeletal activity necessary to carry out theintended action
According to Jackson et al4 these different levelsof processing interact in different ways in differentforms of training Physical practice involves allthree levels of processing in mental practice on theother hand learning depends crucially on theinteraction between declarative knowledge andnon-conscious processes in physical practice it ispossible to learn a motor task implicitly in mentalpractice subjects have a good declarative knowl-edge of the different components of the task beforethey start practicing The similarity between thecircuitry involved in imagining and executingmovements suggests however that the neuronalnetwork implicated in the non-conscious aspects ofa task can be primed as effectively through mentalas through physical practice In addition the modelpredicts that internally driven images promoting
328 GAGGIOLI ET AL
13658C04PGS 61504 236 PM Page 328
kinesthetic ldquosensationsrdquo of movement could behighly effective in activating the non-consciousprocesses involved in motor training According toJackson and his colleagues this would explain whykinesthetic imagery is more effective than purelyvisual imagery According to their model mentalpractice with motor imagery can be conceptualizedas a means to access the otherwise non-consciouslearning processes involved in a task They recog-nize however that the absence of direct feedbackfrom physical execution makes mental practice onits own a less effective training method than physi-cal practice
SUPPORTING MENTAL PRACTICE WITH INTERACTIVE TECHNOLOGY
THE I-LEARNING REHABILITATION PROTOCOL
Clinical studies have shown that the rehabilita-tion of hemiplegic and hemiparetic patients can bemade more effective by combining physical prac-tice with mental rehearsal51213 However for manypatients with damage to the CNS mental simula-tion of movements can be difficult even when therelevant neural circuitry has been spared14 Thegoal of the I-learning rehabilitation protocol is thusto use interactive technology to assist patients increating motor imagery which they can then useduring ldquomental practicerdquo The treatment consists ofan inpatient phase and an outpatient phase
Inpatient phase
The rehabilitation program starts 15 days afterhospitalization The intervention consists of onedaily session (in the morning) 5 days a week for 4consecutive weeks In each session the patient sitsat a table in front of the apparatus To ensure com-fort the patientrsquos ankles are in neutral dorsiflexionthe knees and hips are placed at 90deg the shouldersin 0deg flexion the elbows in 60deg flexion the wristsare neither extended nor flexed The apparatusused by the patients consists of a movement track-ing system and a custom-designed interactiveworkbench that we call the virtual reality (VR) mir-ror (Fig 1) The idea of the VR mirror is inspired byprevious work with stroke patients by Stevens et alin which mirror images of movement by a healthylimb (created by a physical mirror) were effectivelyused to stimulate motor imagery of movement bythe paretic limb5 In the I-Learning protocol the VRmirror displays a 3D electronic image of the move-ment performed by the patientrsquos healthy limb Thisis viewed from an ego-centric perspective that fa-cilitates the generation of kinesthetic motor im-agery by the patient
Each session of inpatient treatment consists offour consecutive sub-phases pre-training physicaltraining with the unimpaired limb imagery train-ing and VR mirror training The training focuseson elbow flexionextension pronationsupinationof the forearm wrist flexionextension openclo-sure of the hand and fine finger movements Dur-ing the pre-training phase the patient receives
COMPUTER-SUPPORTED MOTOR IMAGERY IN POST-STROKE REHABILITATION 329
FIG 1 The VR mirror interactive workbench
13658C04PGS 61504 236 PM Page 329
instructions which explain how the treatmentworks encouraging the patient to relax and reduc-ing fear and performance anxiety The instructionsare accompanied by relaxing music In the nextphysical training phase the therapist shows the pa-tient how to perform the movement with the unaf-fected arm The movement is accompanied byrhythmic auditory cues designed to stabilize thespeed of the movement (guaranteeing that the pa-tient performs the same movement each time)3 andto provide the patient with an attentional goal(matching the sound with the movement) a strat-egy known to facilitate motor learning15 When thepatient then performs the task the system tracksher arm identifying ldquokey framesrdquo and creating a3D model of the movement Next in the imagerytraining phase the patient is asked to create a men-tal image (kinesthetic imagery) of the impaired armperforming the movement as viewed from an in-ternal perspective When the patient starts to imag-ine the movement she presses a button (using herhealthy hand) pressing it again when she has fin-ished This allows the therapist to measure the timeshe takes to imagine each movement This is thepatientrsquos Response Time (RT) Basic research hasshown that response times for physical and imag-ined movements are subject to common laws andprinciples616 comparing a patientrsquos RTs whileimagining and physically performing the samemovements allows the therapist to statistically as-sess the quality of the patientrsquos motor imagery
After the patient has completed the mental re-hearsal exercise she is instructed to watch the dis-
play on the VR mirror (VR mirror training phase)The 3D model created earlier is used to generate amirror image of the movement originally per-formed by the unimpaired arm As the movementis displayed it is accompanied by the same rhyth-mic auditory cues used in the physical trainingphase This multimodal sensorial stimulation hastwo advantages the image of the reflected limbprovides the patient with direct perceptual cuessuggesting how the impaired limb could completea smooth well-controlled movement meanwhileauditory cueing synchronized with key frameshelps the patient to memorize the rhythmical struc-ture of the movement3
After watching the reflected limb on the screenthe patient is invited to physically perform the ex-ercise moving her arm in time with the mirrorimage (Fig 2) In the early stages of treatment thepatient may be completely unable to execute theexercise It is expected however that as the treat-ment advances motor function will improve Dur-ing execution of the task the system tracks themovement of the impaired arm measuring the de-viation between the movement the patient per-forms with the impaired arm and the ldquoidealrdquomovement as performed by the healthy armUsing this measurement which is performed inreal time the system provides the patient withaudio feedback describing her performance on thetask After the patient has repeated the movement5ndash10 times the therapist introduces a more diffi-cult exercise restarting the procedure from thebeginning
330 GAGGIOLI ET AL
FIG 2 The execution of a rehabilitation exercise with the VR mirror (design by Marta Mantovani ATN-P Lab)
13658C04PGS 61504 236 PM Page 330
Outpatient phase home-based rehabilitation
Home-based rehabilitation has the advantagethat stroke patients can practice skills and developcompensatory strategies in the environment wherethey normally live The benefits of this approachmost frequently citied in the literature includefocus on long-term outcomes a reduction of therisks associated with inpatient care respect for pa-tient preferences and savings in the direct cost oftreatment1718 It is nonetheless necessary to providepatients with specialized equipment to support therehabilitation process19 In the I-learning outpatientprogram the equipment provided is a Home Porta-ble Device (a portable computer or a PDA) withmultimedia capabilities The device provides pa-tients with instructions and visual cues allowingthem to mentally rehearse and physically practicethe motor tasks prescribed by the training protocolthe same device monitors their performance
At the beginning of each home-based rehabilita-tion session the Home Portable Device displays asequence of computer-generated movies picturingthe movement to be learned performed at differentspeeds using both the left and the right arm andviewed from different angles as prescribed inStevens and Stoykovrsquos protocol5 The movementsdisplayed on the screen are accompanied by rhyth-mic auditory cues After viewing the movies thepatient is instructed to take a first-person perspec-tive and to imagine performing the task with theimpaired arm At the start and on completion of thetask the patient uses her healthy hand to press akey on the HPD Once this mental practice has beencompleted the patient is asked to physically per-form the movement with the impaired arm
The patient performs this sequence of exerciseson a daily basis for the first two weeks after dis-charge from hospital three times a week startingfrom the 21st day after discharge and two times aweek from the fourth week after discharge onWhen she returns to hospital for follow-up (at 3and 6 months after discharge) the therapist con-nects the portable device to a desktop computerand downloads the data recorded during the exer-cises This includes (a) mental performance datathe response times recorded by the patient duringmental practicemdashby comparing RTs for mentalpractice with data recorded during physical exer-cise the therapist can assess the quality of the pa-tientrsquos motor imagery and (b) compliance datadata describing the dates and times of sessions al-lows the therapist to assess how far the patient hascomplied with the schedule specified in the treat-ment protocol
Assessment
Assessmentmdashbased on behavioral and clinicalindicators of physical competencymdashwill be carriedout before the intervention immediately after dis-charge from the hospital at 3 months and at 6months after discharge from the hospital
DISCUSSION
The rehabilitation technique described in thispaper combines mental and physical practice usinginteractive technology to provide the patient withvisual and auditory cues that draw her attention tothe underlying dynamic structure of a movementfacilitating the generation of mental imagery Theprotocol integrates inpatient treatmentmdashusingnovel apparatusmdashwith outpatient treatment As faras concerns the inpatient phase the solution wehave developed has at least four advantages Firstthe combination of audio and visual cues providedby the VR mirror greatly facilitates the patientrsquos taskin generating the kind of motor imagery requiredfor effective mental rehearsal second the use of amirror metaphor eliminates the need for pre-pro-grammed computer exercises a well-known short-coming of traditional computer-based rehabilitationexercises third the use of an external displayavoids the need for the patient to wear cumbersomeor invasive equipment (such as a Head MountedDisplay or shutter glasses) and last but not leastarm-tracking makes it possible to record the dy-namic features of a movement allowing objectivereal-time comparison between the movement of theimpaired limb and the ldquoideal performancerdquo as re-corded with the healthy limb As a result the com-puterized system provides the therapist with acontinuous flow of feedback about the patientrsquos per-formance making it possible to adjust the treatmentaccordingly The same data is used to provide per-formance feedback to the patient a key requirementfor effective motor learning2021
As far as concerns the outpatient phase the useof a Home Portable Device to support mental prac-tice makes it possible to increase the duration fre-quency and intensity of the therapy provided topatients In the longer term it may become possibleto connect these devices to the Internet allowing atherapist to remotely monitor a patientrsquos progress
The strategy presented in this paper is justifiedby four key hypotheses (a) combined physical andmental practice can make a cost-effective contribu-tion to the rehabilitation of stroke patients (b) ef-fective mental practice is not possible without
COMPUTER-SUPPORTED MOTOR IMAGERY IN POST-STROKE REHABILITATION 331
13658C04PGS 61504 236 PM Page 331
some form of support from a therapist (as in ourinpatient phase) or from technology (as in the out-patient phase) (c) the inclusion of an outpatientphase will allow the patient to practice more oftenthan would otherwise be possible therefore in-creasing the speed andor effectiveness of learn-ing and (d) the use of interactive technology willreduce the patientrsquos need for skilled supporttherefore improving the cost-effectiveness of train-ing If clinical trials show these hypotheses to becorrect the protocol described in this paper couldmake a useful contribution to improving the effec-tiveness and reducing the duration and cost ofpost-stroke rehabilitation
ACKNOWLEDGMENTS
The present work was supported by the Com-mission of the European Communities (CEC) inparticular by the IST programme (Project I-Learn-ing IST 2001ndash38861) and by the Italian Ministryof University and Research FIRB grant (ProjectNeuroTIV)
REFERENCES
1 Johnson SH Sprehn G amp Saykin AJ (2002) Intactmotor imagery in chronic upper limb hemiplegicsevidence for activity-independent action representa-tions Journal of Cognitive Neuroscience 14841ndash852
2 American Heart Association (2003) Stroke facts 20033 Whitall J McCombe Waller S Silver KH et al
(2000) Repetitive bilateral arm training with rhyth-mic auditory cueing improves motor function inchronic hemiparetic stroke Stroke 312390ndash2395
4 Jackson PL Lafleur MF Malouin F et al (2001)Potential role of mental practice using motor im-agery in neurologic rehabilitation Archives of PhysicalMedicine and Rehabilitation 821133ndash1141
5 Stevens JA amp Stoykov ME (2003) Using motorimagery in the rehabilitation of hemiparesis Archivesof Physical Medicine and Rehabilitation 841090ndash1092
6 Decety J amp Jeannerod M (1995) Mentally simu-lated movements in virtual reality does Fittsrsquos lawhold in motor imagery Behav Brain Res 72127ndash134
7 Morganti F Gaggioli A Castelnuovo G et al(2003) The use of technology-supported mental im-agery in neurological rehabilitation a research proto-col CyberPsychology amp Behavior 6421ndash427
8 Jeannerod M (1994) The representing brain neuralcorrelates of motor intention and imagery Brain andBehavioral Sciences 17187ndash245
9 Sirigu A amp Duhamel JR (2001) Motor and visualimagery as two complementary but neurally disso-ciable mental processes Journal of Cognitive Neuro-science 13910ndash919
10 Annett J (1995) Motor imagery perception or ac-tion Neuropsychologia 331395ndash1417
11 Pascual-Leone A Nguyet D Cohen LG et al(1995) Modulation of muscle responses evoked bytranscranial magnetic stimulation during the acqui-sition of new fine motor skills Journal of Neurophysi-ology 741037ndash1045
12 Page SJ Levine P Sisto S et al (2001) A random-ized efficacy and feasibility study of imagery in acutestroke Clinical Rehabilitation 15233ndash240
13 Page SJ Levine P Sisto SA et al (2001) Mentalpractice combined with physical practice for upper-limb motor deficit in subacute stroke Physical Ther-apy 811455ndash1462
14 Goldenberg G (1989) The ability of patients withbrain damage to generate mental visual imagesBrain 112305ndash325
15 Locke EA amp Bryan JF (1966) Cognitive aspects ofpsychomotor performance The effects of perfor-mance goals on level of performance J Appl Psychol50286ndash291
16 Decety J Jeannerod M amp Prablanc C (1989) Thetiming of mentally represented actions Behav BrainRes 3435ndash42
17 Anderson C Rubenach S Mhurchu CN et al(2000) Home or hospital for stroke rehabilitation re-sults of a randomized controlled trial I Health out-comes at 6 months Stroke 311024ndash1031
18 Disler PB amp Wade DT (2003) Should all stroke re-habilitation be home based Am J Phys Med Rehabil82733ndash735
19 NINDS (2003) Post-stroke rehabilitation fact sheet[Online] Available wwwnindsnihgovhealth andmedicalpubspoststrokerehabhtm
20 Salmoni AW (1980) The effect of precision ofknowledge of results on the performance of a simpleline drawing task for children and adults Res Q ExercSport 51572ndash575
21 Salmoni AW Schmidt RA amp Walter CB (1984)Knowledge of results and motor learning a reviewand critical reappraisal Psychological Bulletin 95355ndash386
Address reprint requests toAndrea Gaggioli MS
Applied Technology for Neuro-Psychology LabIstituto Auxologico Italiano
Via Pelizza da Volpedo 4120149 Milan Italy
E-mail andreagaggioliauxologicoit
332 GAGGIOLI ET AL
13658C04PGS 61504 236 PM Page 332

kinesthetic ldquosensationsrdquo of movement could behighly effective in activating the non-consciousprocesses involved in motor training According toJackson and his colleagues this would explain whykinesthetic imagery is more effective than purelyvisual imagery According to their model mentalpractice with motor imagery can be conceptualizedas a means to access the otherwise non-consciouslearning processes involved in a task They recog-nize however that the absence of direct feedbackfrom physical execution makes mental practice onits own a less effective training method than physi-cal practice
SUPPORTING MENTAL PRACTICE WITH INTERACTIVE TECHNOLOGY
THE I-LEARNING REHABILITATION PROTOCOL
Clinical studies have shown that the rehabilita-tion of hemiplegic and hemiparetic patients can bemade more effective by combining physical prac-tice with mental rehearsal51213 However for manypatients with damage to the CNS mental simula-tion of movements can be difficult even when therelevant neural circuitry has been spared14 Thegoal of the I-learning rehabilitation protocol is thusto use interactive technology to assist patients increating motor imagery which they can then useduring ldquomental practicerdquo The treatment consists ofan inpatient phase and an outpatient phase
Inpatient phase
The rehabilitation program starts 15 days afterhospitalization The intervention consists of onedaily session (in the morning) 5 days a week for 4consecutive weeks In each session the patient sitsat a table in front of the apparatus To ensure com-fort the patientrsquos ankles are in neutral dorsiflexionthe knees and hips are placed at 90deg the shouldersin 0deg flexion the elbows in 60deg flexion the wristsare neither extended nor flexed The apparatusused by the patients consists of a movement track-ing system and a custom-designed interactiveworkbench that we call the virtual reality (VR) mir-ror (Fig 1) The idea of the VR mirror is inspired byprevious work with stroke patients by Stevens et alin which mirror images of movement by a healthylimb (created by a physical mirror) were effectivelyused to stimulate motor imagery of movement bythe paretic limb5 In the I-Learning protocol the VRmirror displays a 3D electronic image of the move-ment performed by the patientrsquos healthy limb Thisis viewed from an ego-centric perspective that fa-cilitates the generation of kinesthetic motor im-agery by the patient
Each session of inpatient treatment consists offour consecutive sub-phases pre-training physicaltraining with the unimpaired limb imagery train-ing and VR mirror training The training focuseson elbow flexionextension pronationsupinationof the forearm wrist flexionextension openclo-sure of the hand and fine finger movements Dur-ing the pre-training phase the patient receives
COMPUTER-SUPPORTED MOTOR IMAGERY IN POST-STROKE REHABILITATION 329
FIG 1 The VR mirror interactive workbench
13658C04PGS 61504 236 PM Page 329
instructions which explain how the treatmentworks encouraging the patient to relax and reduc-ing fear and performance anxiety The instructionsare accompanied by relaxing music In the nextphysical training phase the therapist shows the pa-tient how to perform the movement with the unaf-fected arm The movement is accompanied byrhythmic auditory cues designed to stabilize thespeed of the movement (guaranteeing that the pa-tient performs the same movement each time)3 andto provide the patient with an attentional goal(matching the sound with the movement) a strat-egy known to facilitate motor learning15 When thepatient then performs the task the system tracksher arm identifying ldquokey framesrdquo and creating a3D model of the movement Next in the imagerytraining phase the patient is asked to create a men-tal image (kinesthetic imagery) of the impaired armperforming the movement as viewed from an in-ternal perspective When the patient starts to imag-ine the movement she presses a button (using herhealthy hand) pressing it again when she has fin-ished This allows the therapist to measure the timeshe takes to imagine each movement This is thepatientrsquos Response Time (RT) Basic research hasshown that response times for physical and imag-ined movements are subject to common laws andprinciples616 comparing a patientrsquos RTs whileimagining and physically performing the samemovements allows the therapist to statistically as-sess the quality of the patientrsquos motor imagery
After the patient has completed the mental re-hearsal exercise she is instructed to watch the dis-
play on the VR mirror (VR mirror training phase)The 3D model created earlier is used to generate amirror image of the movement originally per-formed by the unimpaired arm As the movementis displayed it is accompanied by the same rhyth-mic auditory cues used in the physical trainingphase This multimodal sensorial stimulation hastwo advantages the image of the reflected limbprovides the patient with direct perceptual cuessuggesting how the impaired limb could completea smooth well-controlled movement meanwhileauditory cueing synchronized with key frameshelps the patient to memorize the rhythmical struc-ture of the movement3
After watching the reflected limb on the screenthe patient is invited to physically perform the ex-ercise moving her arm in time with the mirrorimage (Fig 2) In the early stages of treatment thepatient may be completely unable to execute theexercise It is expected however that as the treat-ment advances motor function will improve Dur-ing execution of the task the system tracks themovement of the impaired arm measuring the de-viation between the movement the patient per-forms with the impaired arm and the ldquoidealrdquomovement as performed by the healthy armUsing this measurement which is performed inreal time the system provides the patient withaudio feedback describing her performance on thetask After the patient has repeated the movement5ndash10 times the therapist introduces a more diffi-cult exercise restarting the procedure from thebeginning
330 GAGGIOLI ET AL
FIG 2 The execution of a rehabilitation exercise with the VR mirror (design by Marta Mantovani ATN-P Lab)
13658C04PGS 61504 236 PM Page 330
Outpatient phase home-based rehabilitation
Home-based rehabilitation has the advantagethat stroke patients can practice skills and developcompensatory strategies in the environment wherethey normally live The benefits of this approachmost frequently citied in the literature includefocus on long-term outcomes a reduction of therisks associated with inpatient care respect for pa-tient preferences and savings in the direct cost oftreatment1718 It is nonetheless necessary to providepatients with specialized equipment to support therehabilitation process19 In the I-learning outpatientprogram the equipment provided is a Home Porta-ble Device (a portable computer or a PDA) withmultimedia capabilities The device provides pa-tients with instructions and visual cues allowingthem to mentally rehearse and physically practicethe motor tasks prescribed by the training protocolthe same device monitors their performance
At the beginning of each home-based rehabilita-tion session the Home Portable Device displays asequence of computer-generated movies picturingthe movement to be learned performed at differentspeeds using both the left and the right arm andviewed from different angles as prescribed inStevens and Stoykovrsquos protocol5 The movementsdisplayed on the screen are accompanied by rhyth-mic auditory cues After viewing the movies thepatient is instructed to take a first-person perspec-tive and to imagine performing the task with theimpaired arm At the start and on completion of thetask the patient uses her healthy hand to press akey on the HPD Once this mental practice has beencompleted the patient is asked to physically per-form the movement with the impaired arm
The patient performs this sequence of exerciseson a daily basis for the first two weeks after dis-charge from hospital three times a week startingfrom the 21st day after discharge and two times aweek from the fourth week after discharge onWhen she returns to hospital for follow-up (at 3and 6 months after discharge) the therapist con-nects the portable device to a desktop computerand downloads the data recorded during the exer-cises This includes (a) mental performance datathe response times recorded by the patient duringmental practicemdashby comparing RTs for mentalpractice with data recorded during physical exer-cise the therapist can assess the quality of the pa-tientrsquos motor imagery and (b) compliance datadata describing the dates and times of sessions al-lows the therapist to assess how far the patient hascomplied with the schedule specified in the treat-ment protocol
Assessment
Assessmentmdashbased on behavioral and clinicalindicators of physical competencymdashwill be carriedout before the intervention immediately after dis-charge from the hospital at 3 months and at 6months after discharge from the hospital
DISCUSSION
The rehabilitation technique described in thispaper combines mental and physical practice usinginteractive technology to provide the patient withvisual and auditory cues that draw her attention tothe underlying dynamic structure of a movementfacilitating the generation of mental imagery Theprotocol integrates inpatient treatmentmdashusingnovel apparatusmdashwith outpatient treatment As faras concerns the inpatient phase the solution wehave developed has at least four advantages Firstthe combination of audio and visual cues providedby the VR mirror greatly facilitates the patientrsquos taskin generating the kind of motor imagery requiredfor effective mental rehearsal second the use of amirror metaphor eliminates the need for pre-pro-grammed computer exercises a well-known short-coming of traditional computer-based rehabilitationexercises third the use of an external displayavoids the need for the patient to wear cumbersomeor invasive equipment (such as a Head MountedDisplay or shutter glasses) and last but not leastarm-tracking makes it possible to record the dy-namic features of a movement allowing objectivereal-time comparison between the movement of theimpaired limb and the ldquoideal performancerdquo as re-corded with the healthy limb As a result the com-puterized system provides the therapist with acontinuous flow of feedback about the patientrsquos per-formance making it possible to adjust the treatmentaccordingly The same data is used to provide per-formance feedback to the patient a key requirementfor effective motor learning2021
As far as concerns the outpatient phase the useof a Home Portable Device to support mental prac-tice makes it possible to increase the duration fre-quency and intensity of the therapy provided topatients In the longer term it may become possibleto connect these devices to the Internet allowing atherapist to remotely monitor a patientrsquos progress
The strategy presented in this paper is justifiedby four key hypotheses (a) combined physical andmental practice can make a cost-effective contribu-tion to the rehabilitation of stroke patients (b) ef-fective mental practice is not possible without
COMPUTER-SUPPORTED MOTOR IMAGERY IN POST-STROKE REHABILITATION 331
13658C04PGS 61504 236 PM Page 331
some form of support from a therapist (as in ourinpatient phase) or from technology (as in the out-patient phase) (c) the inclusion of an outpatientphase will allow the patient to practice more oftenthan would otherwise be possible therefore in-creasing the speed andor effectiveness of learn-ing and (d) the use of interactive technology willreduce the patientrsquos need for skilled supporttherefore improving the cost-effectiveness of train-ing If clinical trials show these hypotheses to becorrect the protocol described in this paper couldmake a useful contribution to improving the effec-tiveness and reducing the duration and cost ofpost-stroke rehabilitation
ACKNOWLEDGMENTS
The present work was supported by the Com-mission of the European Communities (CEC) inparticular by the IST programme (Project I-Learn-ing IST 2001ndash38861) and by the Italian Ministryof University and Research FIRB grant (ProjectNeuroTIV)
REFERENCES
1 Johnson SH Sprehn G amp Saykin AJ (2002) Intactmotor imagery in chronic upper limb hemiplegicsevidence for activity-independent action representa-tions Journal of Cognitive Neuroscience 14841ndash852
2 American Heart Association (2003) Stroke facts 20033 Whitall J McCombe Waller S Silver KH et al
(2000) Repetitive bilateral arm training with rhyth-mic auditory cueing improves motor function inchronic hemiparetic stroke Stroke 312390ndash2395
4 Jackson PL Lafleur MF Malouin F et al (2001)Potential role of mental practice using motor im-agery in neurologic rehabilitation Archives of PhysicalMedicine and Rehabilitation 821133ndash1141
5 Stevens JA amp Stoykov ME (2003) Using motorimagery in the rehabilitation of hemiparesis Archivesof Physical Medicine and Rehabilitation 841090ndash1092
6 Decety J amp Jeannerod M (1995) Mentally simu-lated movements in virtual reality does Fittsrsquos lawhold in motor imagery Behav Brain Res 72127ndash134
7 Morganti F Gaggioli A Castelnuovo G et al(2003) The use of technology-supported mental im-agery in neurological rehabilitation a research proto-col CyberPsychology amp Behavior 6421ndash427
8 Jeannerod M (1994) The representing brain neuralcorrelates of motor intention and imagery Brain andBehavioral Sciences 17187ndash245
9 Sirigu A amp Duhamel JR (2001) Motor and visualimagery as two complementary but neurally disso-ciable mental processes Journal of Cognitive Neuro-science 13910ndash919
10 Annett J (1995) Motor imagery perception or ac-tion Neuropsychologia 331395ndash1417
11 Pascual-Leone A Nguyet D Cohen LG et al(1995) Modulation of muscle responses evoked bytranscranial magnetic stimulation during the acqui-sition of new fine motor skills Journal of Neurophysi-ology 741037ndash1045
12 Page SJ Levine P Sisto S et al (2001) A random-ized efficacy and feasibility study of imagery in acutestroke Clinical Rehabilitation 15233ndash240
13 Page SJ Levine P Sisto SA et al (2001) Mentalpractice combined with physical practice for upper-limb motor deficit in subacute stroke Physical Ther-apy 811455ndash1462
14 Goldenberg G (1989) The ability of patients withbrain damage to generate mental visual imagesBrain 112305ndash325
15 Locke EA amp Bryan JF (1966) Cognitive aspects ofpsychomotor performance The effects of perfor-mance goals on level of performance J Appl Psychol50286ndash291
16 Decety J Jeannerod M amp Prablanc C (1989) Thetiming of mentally represented actions Behav BrainRes 3435ndash42
17 Anderson C Rubenach S Mhurchu CN et al(2000) Home or hospital for stroke rehabilitation re-sults of a randomized controlled trial I Health out-comes at 6 months Stroke 311024ndash1031
18 Disler PB amp Wade DT (2003) Should all stroke re-habilitation be home based Am J Phys Med Rehabil82733ndash735
19 NINDS (2003) Post-stroke rehabilitation fact sheet[Online] Available wwwnindsnihgovhealth andmedicalpubspoststrokerehabhtm
20 Salmoni AW (1980) The effect of precision ofknowledge of results on the performance of a simpleline drawing task for children and adults Res Q ExercSport 51572ndash575
21 Salmoni AW Schmidt RA amp Walter CB (1984)Knowledge of results and motor learning a reviewand critical reappraisal Psychological Bulletin 95355ndash386
Address reprint requests toAndrea Gaggioli MS
Applied Technology for Neuro-Psychology LabIstituto Auxologico Italiano
Via Pelizza da Volpedo 4120149 Milan Italy
E-mail andreagaggioliauxologicoit
332 GAGGIOLI ET AL
13658C04PGS 61504 236 PM Page 332
instructions which explain how the treatmentworks encouraging the patient to relax and reduc-ing fear and performance anxiety The instructionsare accompanied by relaxing music In the nextphysical training phase the therapist shows the pa-tient how to perform the movement with the unaf-fected arm The movement is accompanied byrhythmic auditory cues designed to stabilize thespeed of the movement (guaranteeing that the pa-tient performs the same movement each time)3 andto provide the patient with an attentional goal(matching the sound with the movement) a strat-egy known to facilitate motor learning15 When thepatient then performs the task the system tracksher arm identifying ldquokey framesrdquo and creating a3D model of the movement Next in the imagerytraining phase the patient is asked to create a men-tal image (kinesthetic imagery) of the impaired armperforming the movement as viewed from an in-ternal perspective When the patient starts to imag-ine the movement she presses a button (using herhealthy hand) pressing it again when she has fin-ished This allows the therapist to measure the timeshe takes to imagine each movement This is thepatientrsquos Response Time (RT) Basic research hasshown that response times for physical and imag-ined movements are subject to common laws andprinciples616 comparing a patientrsquos RTs whileimagining and physically performing the samemovements allows the therapist to statistically as-sess the quality of the patientrsquos motor imagery
After the patient has completed the mental re-hearsal exercise she is instructed to watch the dis-
play on the VR mirror (VR mirror training phase)The 3D model created earlier is used to generate amirror image of the movement originally per-formed by the unimpaired arm As the movementis displayed it is accompanied by the same rhyth-mic auditory cues used in the physical trainingphase This multimodal sensorial stimulation hastwo advantages the image of the reflected limbprovides the patient with direct perceptual cuessuggesting how the impaired limb could completea smooth well-controlled movement meanwhileauditory cueing synchronized with key frameshelps the patient to memorize the rhythmical struc-ture of the movement3
After watching the reflected limb on the screenthe patient is invited to physically perform the ex-ercise moving her arm in time with the mirrorimage (Fig 2) In the early stages of treatment thepatient may be completely unable to execute theexercise It is expected however that as the treat-ment advances motor function will improve Dur-ing execution of the task the system tracks themovement of the impaired arm measuring the de-viation between the movement the patient per-forms with the impaired arm and the ldquoidealrdquomovement as performed by the healthy armUsing this measurement which is performed inreal time the system provides the patient withaudio feedback describing her performance on thetask After the patient has repeated the movement5ndash10 times the therapist introduces a more diffi-cult exercise restarting the procedure from thebeginning
330 GAGGIOLI ET AL
FIG 2 The execution of a rehabilitation exercise with the VR mirror (design by Marta Mantovani ATN-P Lab)
13658C04PGS 61504 236 PM Page 330
Outpatient phase home-based rehabilitation
Home-based rehabilitation has the advantagethat stroke patients can practice skills and developcompensatory strategies in the environment wherethey normally live The benefits of this approachmost frequently citied in the literature includefocus on long-term outcomes a reduction of therisks associated with inpatient care respect for pa-tient preferences and savings in the direct cost oftreatment1718 It is nonetheless necessary to providepatients with specialized equipment to support therehabilitation process19 In the I-learning outpatientprogram the equipment provided is a Home Porta-ble Device (a portable computer or a PDA) withmultimedia capabilities The device provides pa-tients with instructions and visual cues allowingthem to mentally rehearse and physically practicethe motor tasks prescribed by the training protocolthe same device monitors their performance
At the beginning of each home-based rehabilita-tion session the Home Portable Device displays asequence of computer-generated movies picturingthe movement to be learned performed at differentspeeds using both the left and the right arm andviewed from different angles as prescribed inStevens and Stoykovrsquos protocol5 The movementsdisplayed on the screen are accompanied by rhyth-mic auditory cues After viewing the movies thepatient is instructed to take a first-person perspec-tive and to imagine performing the task with theimpaired arm At the start and on completion of thetask the patient uses her healthy hand to press akey on the HPD Once this mental practice has beencompleted the patient is asked to physically per-form the movement with the impaired arm
The patient performs this sequence of exerciseson a daily basis for the first two weeks after dis-charge from hospital three times a week startingfrom the 21st day after discharge and two times aweek from the fourth week after discharge onWhen she returns to hospital for follow-up (at 3and 6 months after discharge) the therapist con-nects the portable device to a desktop computerand downloads the data recorded during the exer-cises This includes (a) mental performance datathe response times recorded by the patient duringmental practicemdashby comparing RTs for mentalpractice with data recorded during physical exer-cise the therapist can assess the quality of the pa-tientrsquos motor imagery and (b) compliance datadata describing the dates and times of sessions al-lows the therapist to assess how far the patient hascomplied with the schedule specified in the treat-ment protocol
Assessment
Assessmentmdashbased on behavioral and clinicalindicators of physical competencymdashwill be carriedout before the intervention immediately after dis-charge from the hospital at 3 months and at 6months after discharge from the hospital
DISCUSSION
The rehabilitation technique described in thispaper combines mental and physical practice usinginteractive technology to provide the patient withvisual and auditory cues that draw her attention tothe underlying dynamic structure of a movementfacilitating the generation of mental imagery Theprotocol integrates inpatient treatmentmdashusingnovel apparatusmdashwith outpatient treatment As faras concerns the inpatient phase the solution wehave developed has at least four advantages Firstthe combination of audio and visual cues providedby the VR mirror greatly facilitates the patientrsquos taskin generating the kind of motor imagery requiredfor effective mental rehearsal second the use of amirror metaphor eliminates the need for pre-pro-grammed computer exercises a well-known short-coming of traditional computer-based rehabilitationexercises third the use of an external displayavoids the need for the patient to wear cumbersomeor invasive equipment (such as a Head MountedDisplay or shutter glasses) and last but not leastarm-tracking makes it possible to record the dy-namic features of a movement allowing objectivereal-time comparison between the movement of theimpaired limb and the ldquoideal performancerdquo as re-corded with the healthy limb As a result the com-puterized system provides the therapist with acontinuous flow of feedback about the patientrsquos per-formance making it possible to adjust the treatmentaccordingly The same data is used to provide per-formance feedback to the patient a key requirementfor effective motor learning2021
As far as concerns the outpatient phase the useof a Home Portable Device to support mental prac-tice makes it possible to increase the duration fre-quency and intensity of the therapy provided topatients In the longer term it may become possibleto connect these devices to the Internet allowing atherapist to remotely monitor a patientrsquos progress
The strategy presented in this paper is justifiedby four key hypotheses (a) combined physical andmental practice can make a cost-effective contribu-tion to the rehabilitation of stroke patients (b) ef-fective mental practice is not possible without
COMPUTER-SUPPORTED MOTOR IMAGERY IN POST-STROKE REHABILITATION 331
13658C04PGS 61504 236 PM Page 331
some form of support from a therapist (as in ourinpatient phase) or from technology (as in the out-patient phase) (c) the inclusion of an outpatientphase will allow the patient to practice more oftenthan would otherwise be possible therefore in-creasing the speed andor effectiveness of learn-ing and (d) the use of interactive technology willreduce the patientrsquos need for skilled supporttherefore improving the cost-effectiveness of train-ing If clinical trials show these hypotheses to becorrect the protocol described in this paper couldmake a useful contribution to improving the effec-tiveness and reducing the duration and cost ofpost-stroke rehabilitation
ACKNOWLEDGMENTS
The present work was supported by the Com-mission of the European Communities (CEC) inparticular by the IST programme (Project I-Learn-ing IST 2001ndash38861) and by the Italian Ministryof University and Research FIRB grant (ProjectNeuroTIV)
REFERENCES
1 Johnson SH Sprehn G amp Saykin AJ (2002) Intactmotor imagery in chronic upper limb hemiplegicsevidence for activity-independent action representa-tions Journal of Cognitive Neuroscience 14841ndash852
2 American Heart Association (2003) Stroke facts 20033 Whitall J McCombe Waller S Silver KH et al
(2000) Repetitive bilateral arm training with rhyth-mic auditory cueing improves motor function inchronic hemiparetic stroke Stroke 312390ndash2395
4 Jackson PL Lafleur MF Malouin F et al (2001)Potential role of mental practice using motor im-agery in neurologic rehabilitation Archives of PhysicalMedicine and Rehabilitation 821133ndash1141
5 Stevens JA amp Stoykov ME (2003) Using motorimagery in the rehabilitation of hemiparesis Archivesof Physical Medicine and Rehabilitation 841090ndash1092
6 Decety J amp Jeannerod M (1995) Mentally simu-lated movements in virtual reality does Fittsrsquos lawhold in motor imagery Behav Brain Res 72127ndash134
7 Morganti F Gaggioli A Castelnuovo G et al(2003) The use of technology-supported mental im-agery in neurological rehabilitation a research proto-col CyberPsychology amp Behavior 6421ndash427
8 Jeannerod M (1994) The representing brain neuralcorrelates of motor intention and imagery Brain andBehavioral Sciences 17187ndash245
9 Sirigu A amp Duhamel JR (2001) Motor and visualimagery as two complementary but neurally disso-ciable mental processes Journal of Cognitive Neuro-science 13910ndash919
10 Annett J (1995) Motor imagery perception or ac-tion Neuropsychologia 331395ndash1417
11 Pascual-Leone A Nguyet D Cohen LG et al(1995) Modulation of muscle responses evoked bytranscranial magnetic stimulation during the acqui-sition of new fine motor skills Journal of Neurophysi-ology 741037ndash1045
12 Page SJ Levine P Sisto S et al (2001) A random-ized efficacy and feasibility study of imagery in acutestroke Clinical Rehabilitation 15233ndash240
13 Page SJ Levine P Sisto SA et al (2001) Mentalpractice combined with physical practice for upper-limb motor deficit in subacute stroke Physical Ther-apy 811455ndash1462
14 Goldenberg G (1989) The ability of patients withbrain damage to generate mental visual imagesBrain 112305ndash325
15 Locke EA amp Bryan JF (1966) Cognitive aspects ofpsychomotor performance The effects of perfor-mance goals on level of performance J Appl Psychol50286ndash291
16 Decety J Jeannerod M amp Prablanc C (1989) Thetiming of mentally represented actions Behav BrainRes 3435ndash42
17 Anderson C Rubenach S Mhurchu CN et al(2000) Home or hospital for stroke rehabilitation re-sults of a randomized controlled trial I Health out-comes at 6 months Stroke 311024ndash1031
18 Disler PB amp Wade DT (2003) Should all stroke re-habilitation be home based Am J Phys Med Rehabil82733ndash735
19 NINDS (2003) Post-stroke rehabilitation fact sheet[Online] Available wwwnindsnihgovhealth andmedicalpubspoststrokerehabhtm
20 Salmoni AW (1980) The effect of precision ofknowledge of results on the performance of a simpleline drawing task for children and adults Res Q ExercSport 51572ndash575
21 Salmoni AW Schmidt RA amp Walter CB (1984)Knowledge of results and motor learning a reviewand critical reappraisal Psychological Bulletin 95355ndash386
Address reprint requests toAndrea Gaggioli MS
Applied Technology for Neuro-Psychology LabIstituto Auxologico Italiano
Via Pelizza da Volpedo 4120149 Milan Italy
E-mail andreagaggioliauxologicoit
332 GAGGIOLI ET AL
13658C04PGS 61504 236 PM Page 332

Outpatient phase home-based rehabilitation
Home-based rehabilitation has the advantagethat stroke patients can practice skills and developcompensatory strategies in the environment wherethey normally live The benefits of this approachmost frequently citied in the literature includefocus on long-term outcomes a reduction of therisks associated with inpatient care respect for pa-tient preferences and savings in the direct cost oftreatment1718 It is nonetheless necessary to providepatients with specialized equipment to support therehabilitation process19 In the I-learning outpatientprogram the equipment provided is a Home Porta-ble Device (a portable computer or a PDA) withmultimedia capabilities The device provides pa-tients with instructions and visual cues allowingthem to mentally rehearse and physically practicethe motor tasks prescribed by the training protocolthe same device monitors their performance
At the beginning of each home-based rehabilita-tion session the Home Portable Device displays asequence of computer-generated movies picturingthe movement to be learned performed at differentspeeds using both the left and the right arm andviewed from different angles as prescribed inStevens and Stoykovrsquos protocol5 The movementsdisplayed on the screen are accompanied by rhyth-mic auditory cues After viewing the movies thepatient is instructed to take a first-person perspec-tive and to imagine performing the task with theimpaired arm At the start and on completion of thetask the patient uses her healthy hand to press akey on the HPD Once this mental practice has beencompleted the patient is asked to physically per-form the movement with the impaired arm
The patient performs this sequence of exerciseson a daily basis for the first two weeks after dis-charge from hospital three times a week startingfrom the 21st day after discharge and two times aweek from the fourth week after discharge onWhen she returns to hospital for follow-up (at 3and 6 months after discharge) the therapist con-nects the portable device to a desktop computerand downloads the data recorded during the exer-cises This includes (a) mental performance datathe response times recorded by the patient duringmental practicemdashby comparing RTs for mentalpractice with data recorded during physical exer-cise the therapist can assess the quality of the pa-tientrsquos motor imagery and (b) compliance datadata describing the dates and times of sessions al-lows the therapist to assess how far the patient hascomplied with the schedule specified in the treat-ment protocol
Assessment
Assessmentmdashbased on behavioral and clinicalindicators of physical competencymdashwill be carriedout before the intervention immediately after dis-charge from the hospital at 3 months and at 6months after discharge from the hospital
DISCUSSION
The rehabilitation technique described in thispaper combines mental and physical practice usinginteractive technology to provide the patient withvisual and auditory cues that draw her attention tothe underlying dynamic structure of a movementfacilitating the generation of mental imagery Theprotocol integrates inpatient treatmentmdashusingnovel apparatusmdashwith outpatient treatment As faras concerns the inpatient phase the solution wehave developed has at least four advantages Firstthe combination of audio and visual cues providedby the VR mirror greatly facilitates the patientrsquos taskin generating the kind of motor imagery requiredfor effective mental rehearsal second the use of amirror metaphor eliminates the need for pre-pro-grammed computer exercises a well-known short-coming of traditional computer-based rehabilitationexercises third the use of an external displayavoids the need for the patient to wear cumbersomeor invasive equipment (such as a Head MountedDisplay or shutter glasses) and last but not leastarm-tracking makes it possible to record the dy-namic features of a movement allowing objectivereal-time comparison between the movement of theimpaired limb and the ldquoideal performancerdquo as re-corded with the healthy limb As a result the com-puterized system provides the therapist with acontinuous flow of feedback about the patientrsquos per-formance making it possible to adjust the treatmentaccordingly The same data is used to provide per-formance feedback to the patient a key requirementfor effective motor learning2021
As far as concerns the outpatient phase the useof a Home Portable Device to support mental prac-tice makes it possible to increase the duration fre-quency and intensity of the therapy provided topatients In the longer term it may become possibleto connect these devices to the Internet allowing atherapist to remotely monitor a patientrsquos progress
The strategy presented in this paper is justifiedby four key hypotheses (a) combined physical andmental practice can make a cost-effective contribu-tion to the rehabilitation of stroke patients (b) ef-fective mental practice is not possible without
COMPUTER-SUPPORTED MOTOR IMAGERY IN POST-STROKE REHABILITATION 331
13658C04PGS 61504 236 PM Page 331
some form of support from a therapist (as in ourinpatient phase) or from technology (as in the out-patient phase) (c) the inclusion of an outpatientphase will allow the patient to practice more oftenthan would otherwise be possible therefore in-creasing the speed andor effectiveness of learn-ing and (d) the use of interactive technology willreduce the patientrsquos need for skilled supporttherefore improving the cost-effectiveness of train-ing If clinical trials show these hypotheses to becorrect the protocol described in this paper couldmake a useful contribution to improving the effec-tiveness and reducing the duration and cost ofpost-stroke rehabilitation
ACKNOWLEDGMENTS
The present work was supported by the Com-mission of the European Communities (CEC) inparticular by the IST programme (Project I-Learn-ing IST 2001ndash38861) and by the Italian Ministryof University and Research FIRB grant (ProjectNeuroTIV)
REFERENCES
1 Johnson SH Sprehn G amp Saykin AJ (2002) Intactmotor imagery in chronic upper limb hemiplegicsevidence for activity-independent action representa-tions Journal of Cognitive Neuroscience 14841ndash852
2 American Heart Association (2003) Stroke facts 20033 Whitall J McCombe Waller S Silver KH et al
(2000) Repetitive bilateral arm training with rhyth-mic auditory cueing improves motor function inchronic hemiparetic stroke Stroke 312390ndash2395
4 Jackson PL Lafleur MF Malouin F et al (2001)Potential role of mental practice using motor im-agery in neurologic rehabilitation Archives of PhysicalMedicine and Rehabilitation 821133ndash1141
5 Stevens JA amp Stoykov ME (2003) Using motorimagery in the rehabilitation of hemiparesis Archivesof Physical Medicine and Rehabilitation 841090ndash1092
6 Decety J amp Jeannerod M (1995) Mentally simu-lated movements in virtual reality does Fittsrsquos lawhold in motor imagery Behav Brain Res 72127ndash134
7 Morganti F Gaggioli A Castelnuovo G et al(2003) The use of technology-supported mental im-agery in neurological rehabilitation a research proto-col CyberPsychology amp Behavior 6421ndash427
8 Jeannerod M (1994) The representing brain neuralcorrelates of motor intention and imagery Brain andBehavioral Sciences 17187ndash245
9 Sirigu A amp Duhamel JR (2001) Motor and visualimagery as two complementary but neurally disso-ciable mental processes Journal of Cognitive Neuro-science 13910ndash919
10 Annett J (1995) Motor imagery perception or ac-tion Neuropsychologia 331395ndash1417
11 Pascual-Leone A Nguyet D Cohen LG et al(1995) Modulation of muscle responses evoked bytranscranial magnetic stimulation during the acqui-sition of new fine motor skills Journal of Neurophysi-ology 741037ndash1045
12 Page SJ Levine P Sisto S et al (2001) A random-ized efficacy and feasibility study of imagery in acutestroke Clinical Rehabilitation 15233ndash240
13 Page SJ Levine P Sisto SA et al (2001) Mentalpractice combined with physical practice for upper-limb motor deficit in subacute stroke Physical Ther-apy 811455ndash1462
14 Goldenberg G (1989) The ability of patients withbrain damage to generate mental visual imagesBrain 112305ndash325
15 Locke EA amp Bryan JF (1966) Cognitive aspects ofpsychomotor performance The effects of perfor-mance goals on level of performance J Appl Psychol50286ndash291
16 Decety J Jeannerod M amp Prablanc C (1989) Thetiming of mentally represented actions Behav BrainRes 3435ndash42
17 Anderson C Rubenach S Mhurchu CN et al(2000) Home or hospital for stroke rehabilitation re-sults of a randomized controlled trial I Health out-comes at 6 months Stroke 311024ndash1031
18 Disler PB amp Wade DT (2003) Should all stroke re-habilitation be home based Am J Phys Med Rehabil82733ndash735
19 NINDS (2003) Post-stroke rehabilitation fact sheet[Online] Available wwwnindsnihgovhealth andmedicalpubspoststrokerehabhtm
20 Salmoni AW (1980) The effect of precision ofknowledge of results on the performance of a simpleline drawing task for children and adults Res Q ExercSport 51572ndash575
21 Salmoni AW Schmidt RA amp Walter CB (1984)Knowledge of results and motor learning a reviewand critical reappraisal Psychological Bulletin 95355ndash386
Address reprint requests toAndrea Gaggioli MS
Applied Technology for Neuro-Psychology LabIstituto Auxologico Italiano
Via Pelizza da Volpedo 4120149 Milan Italy
E-mail andreagaggioliauxologicoit
332 GAGGIOLI ET AL
13658C04PGS 61504 236 PM Page 332
some form of support from a therapist (as in ourinpatient phase) or from technology (as in the out-patient phase) (c) the inclusion of an outpatientphase will allow the patient to practice more oftenthan would otherwise be possible therefore in-creasing the speed andor effectiveness of learn-ing and (d) the use of interactive technology willreduce the patientrsquos need for skilled supporttherefore improving the cost-effectiveness of train-ing If clinical trials show these hypotheses to becorrect the protocol described in this paper couldmake a useful contribution to improving the effec-tiveness and reducing the duration and cost ofpost-stroke rehabilitation
ACKNOWLEDGMENTS
The present work was supported by the Com-mission of the European Communities (CEC) inparticular by the IST programme (Project I-Learn-ing IST 2001ndash38861) and by the Italian Ministryof University and Research FIRB grant (ProjectNeuroTIV)
REFERENCES
1 Johnson SH Sprehn G amp Saykin AJ (2002) Intactmotor imagery in chronic upper limb hemiplegicsevidence for activity-independent action representa-tions Journal of Cognitive Neuroscience 14841ndash852
2 American Heart Association (2003) Stroke facts 20033 Whitall J McCombe Waller S Silver KH et al
(2000) Repetitive bilateral arm training with rhyth-mic auditory cueing improves motor function inchronic hemiparetic stroke Stroke 312390ndash2395
4 Jackson PL Lafleur MF Malouin F et al (2001)Potential role of mental practice using motor im-agery in neurologic rehabilitation Archives of PhysicalMedicine and Rehabilitation 821133ndash1141
5 Stevens JA amp Stoykov ME (2003) Using motorimagery in the rehabilitation of hemiparesis Archivesof Physical Medicine and Rehabilitation 841090ndash1092
6 Decety J amp Jeannerod M (1995) Mentally simu-lated movements in virtual reality does Fittsrsquos lawhold in motor imagery Behav Brain Res 72127ndash134
7 Morganti F Gaggioli A Castelnuovo G et al(2003) The use of technology-supported mental im-agery in neurological rehabilitation a research proto-col CyberPsychology amp Behavior 6421ndash427
8 Jeannerod M (1994) The representing brain neuralcorrelates of motor intention and imagery Brain andBehavioral Sciences 17187ndash245
9 Sirigu A amp Duhamel JR (2001) Motor and visualimagery as two complementary but neurally disso-ciable mental processes Journal of Cognitive Neuro-science 13910ndash919
10 Annett J (1995) Motor imagery perception or ac-tion Neuropsychologia 331395ndash1417
11 Pascual-Leone A Nguyet D Cohen LG et al(1995) Modulation of muscle responses evoked bytranscranial magnetic stimulation during the acqui-sition of new fine motor skills Journal of Neurophysi-ology 741037ndash1045
12 Page SJ Levine P Sisto S et al (2001) A random-ized efficacy and feasibility study of imagery in acutestroke Clinical Rehabilitation 15233ndash240
13 Page SJ Levine P Sisto SA et al (2001) Mentalpractice combined with physical practice for upper-limb motor deficit in subacute stroke Physical Ther-apy 811455ndash1462
14 Goldenberg G (1989) The ability of patients withbrain damage to generate mental visual imagesBrain 112305ndash325
15 Locke EA amp Bryan JF (1966) Cognitive aspects ofpsychomotor performance The effects of perfor-mance goals on level of performance J Appl Psychol50286ndash291
16 Decety J Jeannerod M amp Prablanc C (1989) Thetiming of mentally represented actions Behav BrainRes 3435ndash42
17 Anderson C Rubenach S Mhurchu CN et al(2000) Home or hospital for stroke rehabilitation re-sults of a randomized controlled trial I Health out-comes at 6 months Stroke 311024ndash1031
18 Disler PB amp Wade DT (2003) Should all stroke re-habilitation be home based Am J Phys Med Rehabil82733ndash735
19 NINDS (2003) Post-stroke rehabilitation fact sheet[Online] Available wwwnindsnihgovhealth andmedicalpubspoststrokerehabhtm
20 Salmoni AW (1980) The effect of precision ofknowledge of results on the performance of a simpleline drawing task for children and adults Res Q ExercSport 51572ndash575
21 Salmoni AW Schmidt RA amp Walter CB (1984)Knowledge of results and motor learning a reviewand critical reappraisal Psychological Bulletin 95355ndash386
Address reprint requests toAndrea Gaggioli MS
Applied Technology for Neuro-Psychology LabIstituto Auxologico Italiano
Via Pelizza da Volpedo 4120149 Milan Italy
E-mail andreagaggioliauxologicoit
332 GAGGIOLI ET AL
13658C04PGS 61504 236 PM Page 332