thrombolytic reversal of acute human cerebral ischemic injury shown by diffusion/perfusion magnetic...
TRANSCRIPT
Thrombolytic Reversal of Acute HumanCerebral Ischemic Injury Shown by
Diffusion/Perfusion MagneticResonance Imaging
Chelsea S. Kidwell, MD,*† Jeffrey L. Saver, MD,*† James Mattiello, PhD,‡ Sidney Starkman, MD,*†§Fernando Vinuela, MD,*‡ Gary Duckwiler, MD,*‡ Y. Pierre Gobin, MD,*‡
Reza Jahan, MD,*‡ Paul Vespa, MD,*†\ Mary Kalafut, MD,*† and Jeffry R. Alger, PhD*‡
Diffusion magnetic resonance imaging provides an early marker of acute cerebral ischemic injury. Thrombolytic reversalof diffusion abnormalities has not previously been demonstrated in humans. Serial diffusion and perfusion imagingstudies were acquired in patients experiencing acute hemispheric cerebral ischemia treated with intra-arterial thrombo-lytic therapy within 6 hours of symptom onset. Seven patients met inclusion criteria of prethrombolysis and postthrom-bolysis magnetic resonance studies, presence of large artery anterior circulation occlusion at angiography, and achieve-ment of vessel recanalization. Mean diffusion-weighted imaging lesion volume at baseline was 23 cm3 (95% confidenceinterval [95% CI], 8–38 cm3) and decreased to 10 cm3 (95% CI, 3–17 cm3) 2.5 to 9.5 hours after thrombolysis. Meanapparent diffusion coefficient lesion volume decreased from 9 cm3 (95% CI, 2–16 cm3) at baseline to 1 cm3 (95% CI,0.4–2 cm3) early after thrombolysis. A secondary increase in diffusion volumes was seen in 3 of 6 patients at day 7. Inall 4 patients in whom perfusion imaging was obtained before and after treatment, complete resolution of the perfusiondeficit was shown. Diffusion magnetic resonance signatures of early tissue ischemic injury can be reversed in humans byprompt thrombolytic vessel recanalization. The ischemic penumbra includes not only the region of diffusion/perfusionmismatch, but also portions of the region of initial diffusion abnormality.
Kidwell CS, Saver JL, Mattiello J, Starkman S, Vinuela F, Duckwiler G, Gobin YP, Jahan R, Vespa P, Kalafut M,Alger JR. Thrombolytic reversal of acute human cerebral ischemic injury shown by diffusion/perfusion magnetic
resonance imaging. Ann Neurol 2000;47:462–469
Intravenous thrombolysis is of proven benefit for thetreatment of acute ischemic stroke within 3 hours ofsymptom onset,1 and intra-arterial thrombolytic ther-apy shows promise up to 6 hours after symptom on-set.2 Treatment of most patients, however, is limitedby the narrow time window recommended for initia-tion of therapy.3,4 There is a recognized need for ob-jective neuroimaging methods to identify the best can-didates for treatment and to monitor individual patientresponse to therapy.5,6 Imaging characterization of anexisting ischemic penumbra could extend the time win-dow available for treatment in some patients by allow-ing physicians to treat a “tissue clock” rather than a“ticking clock.”7
Diffusion/perfusion magnetic resonance imaging(MRI) is of established utility in evaluating patientswith acute brain ischemia.8–10 Diffusion-weighted im-
aging (DWI) detects decreases in the self-diffusion ofwater molecules, appearing as hyperintensity on DWIsequences associated with a reduced apparent diffusioncoefficient (ADC) value.9,11 These changes, seenwithin minutes of ischemia, are related, at least in part,to cellular energy failure and early cytotoxic edema.Perfusion-weighted imaging (PWI) provides a qualita-tive map of relative cerebral blood flow to identify re-gions of hypoperfusion.
ADC values typically decease sharply shortly afterstroke onset, remain low for at least 72 to 96 hours,then gradually increase, reaching or surpassing normallevels.12 Serial studies have shown that the typical nat-ural history of early acute ischemic diffusion lesion vol-umes is to grow over time.13,14 In various series, be-tween 62% and 88% of patients imaged initially under6 hours exhibited lesion growth on follow-up imaging,
From the *UCLA Stroke Center, and Departments of †Neurology,‡Radiological Sciences, §Emergency Medicine, and iNeurosurgery,UCLA Medical Center, Los Angeles, CA.
Received Sep 14, 1999, and in revised form Oct 20. Accepted forpublication Nov 23, 1999.
Address correspondence to Dr Kidwell, UCLA Stroke Center, 710Westwood Plaza, UCLA Medical Center, Los Angeles, CA 90095.
462 Copyright © 2000 by the American Neurological Association

with the percent change in lesion volume ranging from32% to 107%.13,15,16 It is speculated that this lesiongrowth may be the result of gradual failure of energy me-tabolism in the ischemic penumbra as it is recruited intothe infarct core if early reperfusion does not occur.13
Diffusion/perfusion MRI has been suggested as ameans to identify the ischemic penumbra.17 A preva-lent view posits that, in humans, the area of diffusionabnormality constitutes an already irreversible core in-farction field and that the penumbra is the regionshowing perfusion but not yet diffusion abnormality(diffusion/perfusion mismatch). However, animal stud-ies suggest that this model of the ischemic penumbramay underestimate the volume of tissue that is salvage-able early after ischemic onset. When reperfusion oc-curs within 2 to 3 hours in these animal models, theperfusion deficit resolves and is accompanied by partialreversal of the DWI and ADC abnormalities.18–22 Wehypothesized that in humans, as in animals, portions ofthe DWI and ADC lesions could be salvaged withearly reperfusion.
Patients and MethodsEligibility and Inclusion CriteriaPatients with symptoms of acute hemispheric ischemic strokepresenting to University of California, Los Angeles (UCLA)Medical Center were screened for this prospective study. In-clusion criteria included the following: symptom duration ofless than 6 hours, no contraindications to MRI or thrombol-ysis, absence of hemorrhage on head computed tomographicscan, and presence of a large artery occlusion in the anteriorcirculation with partial or complete vessel recanalizationachieved after thrombolysis. The study was approved by theUCLA Institutional Review Board and informed consent wasobtained in all patients.
Eligible patients were treated with combined intravenous/intra-arterial tissue plasminogen activator if treatment wasinitiated within 3 hours of the time the patient was lastknown well, or only intra-arterial urokinase if treatment wasinitiated within greater than 3 and less than 6 hours of thetime the patient was last known well or if a contraindicationto intravenous therapy was present in patients treated in lessthan 3 hours. Combined intravenous/intra-arterial tissueplasminogen activator was administered intravenously at adose of 0.6 mg/kg, 10% bolus over 1 minute, the remainderinfused over 30 minutes, followed by a 10 mg/hr intra-arterial infusion until recanalization was achieved or a max-imum intra-arterial dose of 20 mg was reached.23 Urokinasewas infused at the site of the clot at the time of angiographyuntil recanalization was achieved or a maximum of1,000,000 units was reached. Gentle mechanical clot disrup-tion was also performed at the time of intra-arterial throm-bolytic infusion.
Clinical outcome was assessed by using the National In-stitutes of Health Stroke Scale (NIHSS) at baseline, early af-ter thrombolysis at the time of the repeat MRI scan, and atdays 1, 3, 7, and 90. The Barthel Index, Modified Rankin
Scale, and Glasgow Outcome Scale were assessed at baseline(premorbid) and day 90.
MRI MethodsMRI scans were performed on a 1.5-T Siemens Vision Sys-tem (Iselin, NJ) equipped with echo-planar imaging data-acquisition capability. Baseline MRI scans included axial T1-weighted, T2-weighted (T2-W), and DWI sequences in allpatients (;7 minutes of scanning time) and, when patientstatus and the urgent clinical setting allowed, also includedaxial PWIs, and extracranial and intracranial magnetic reso-nance angiography. Follow-up MRI scans were obtainedearly after recanalization (target, 3 hours) and at day 7 andincluded axial T1-weighted, T2-W, DWI, and PWI se-quences.
DWIs were acquired by using 18 slices with 7-mm slicethickness and no interslice gap, field-of-view of 240 mm.Two levels of diffusion sensitization (b-values 5 0 and 1,000sec/mm2), the latter applied in each of the three principalgradient directions (x, y, and z), were used to calculate theADC. Perfusion MRI was performed by using the bolus pas-sage of contrast method (0.1 mmol/kg dose via power injec-tor) with gradient-echo echo-planar imaging.
Data AnalysisBased on the techniques described by Ostergaard and col-leagues,24–26 a Research System Inc IDL computer programwas developed that allowed for routine analysis of the perfu-sion data. From the deconvolution of an “arterial input func-tion” and the tissue concentration curves, the “residue func-tion” was determined. Images showing when the residuefunction maximized were calculated to show delayed contrastdelivery.
MRI volume measures were performed jointly by two in-vestigators (C.S.K. and J.M.) blinded to the clinical data,using an open consensus method without initial independentratings. DWI, T2-W, and PWI lesion volumes were firstidentified by visual inspection for regions of abnormality,then measured by outlining regions of interest by hand. Day7 infarct volumes were calculated by using the larger lesionfrom T2-W or DWI sequences. Regions having abnormal(low) ADC signal intensities were identified by using an au-tomated thresholding image analysis procedure, where re-gions having an ADC of less than 550 mm2/sec were iden-tified. This threshold, approximately 40% less than normalvalues, was chosen because previous studies of animals sug-gested this is the level reached after prolonged periods ofcomplete ischemia.27
Statistical analyses were performed by using JMP software(SAS Inc, Cary, NC). Changes in lesion volumes andNIHSS scores were analyzed by using the Wilcoxon signedrank test.
ResultsBetween January 1998 and February 1999, 8 patientsunderwent pretreatment MRI scanning before intra-arterial thrombolysis. Seven patients met full study in-clusion criteria, including achievement of partial orcomplete vessel recanalization after intra-arterial throm-bolysis (Table). In 1 patient with occlusion of the in-
Kidwell et al: MRI of Thrombolytic Reversal of Ischemia 463
tracranial internal carotid artery bifurcation (carotid“T” occlusion), recanalization was not achieved andfollow-up MRI scanning was not obtained because ofrapid clinical deterioration with eventual fatal outcome.
Patient characteristics are provided in the Table.Mean intervals from the time the patient was lastknown well to key protocol events were as follows:computed tomographic scan, 2 hours 14 minutes; base-line MRI, 2 hours 37 minutes; start of intra-arterialdrug infusion, 4 hours 19 minutes; and completion ofintra-arterial drug infusion (recanalization), 5 hours 43minutes. The Thrombolysis in Myocardial Infarction(TIMI) grade after thrombolysis was II in 5 patientsand III in 2 patients.28 Early follow-up MRI studieswere performed a mean of 5.5 hours after recanaliza-tion (range, 2.5–9.5 hours).
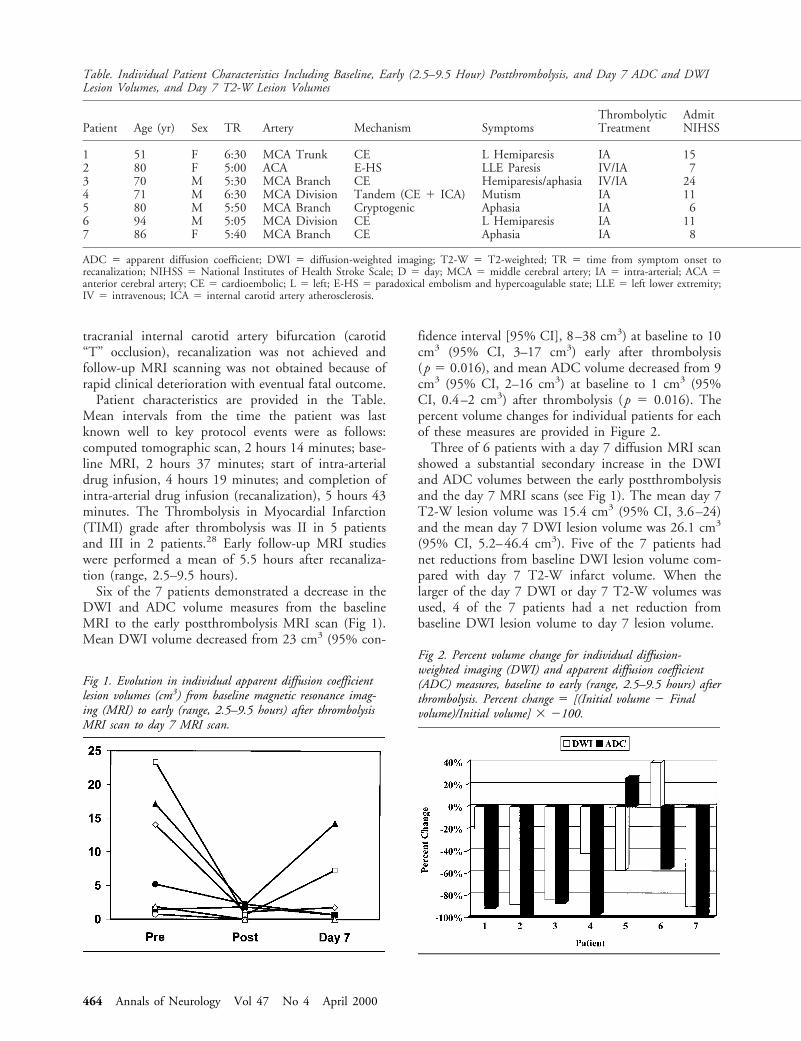
Six of the 7 patients demonstrated a decrease in theDWI and ADC volume measures from the baselineMRI to the early postthrombolysis MRI scan (Fig 1).Mean DWI volume decreased from 23 cm3 (95% con-
fidence interval [95% CI], 8–38 cm3) at baseline to 10cm3 (95% CI, 3–17 cm3) early after thrombolysis(p 5 0.016), and mean ADC volume decreased from 9cm3 (95% CI, 2–16 cm3) at baseline to 1 cm3 (95%CI, 0.4–2 cm3) after thrombolysis (p 5 0.016). Thepercent volume changes for individual patients for eachof these measures are provided in Figure 2.
Three of 6 patients with a day 7 diffusion MRI scanshowed a substantial secondary increase in the DWIand ADC volumes between the early postthrombolysisand the day 7 MRI scans (see Fig 1). The mean day 7T2-W lesion volume was 15.4 cm3 (95% CI, 3.6–24)and the mean day 7 DWI lesion volume was 26.1 cm3
(95% CI, 5.2–46.4 cm3). Five of the 7 patients hadnet reductions from baseline DWI lesion volume com-pared with day 7 T2-W infarct volume. When thelarger of the day 7 DWI or day 7 T2-W volumes wasused, 4 of the 7 patients had a net reduction frombaseline DWI lesion volume to day 7 lesion volume.
Table. Individual Patient Characteristics Including Baseline, Early (2.5–9.5 Hour) Postthrombolysis, and Day 7 ADC and DWILesion Volumes, and Day 7 T2-W Lesion Volumes
Patient Age (yr) Sex TR Artery Mechanism SymptomsThrombolyticTreatment
AdmitNIHSS
1 51 F 6:30 MCA Trunk CE L Hemiparesis IA 152 80 F 5:00 ACA E-HS LLE Paresis IV/IA 73 70 M 5:30 MCA Branch CE Hemiparesis/aphasia IV/IA 244 71 M 6:30 MCA Division Tandem (CE 1 ICA) Mutism IA 115 80 M 5:50 MCA Branch Cryptogenic Aphasia IA 66 94 M 5:05 MCA Division CE L Hemiparesis IA 117 86 F 5:40 MCA Branch CE Aphasia IA 8
ADC 5 apparent diffusion coefficient; DWI 5 diffusion-weighted imaging; T2-W 5 T2-weighted; TR 5 time from symptom onset torecanalization; NIHSS 5 National Institutes of Health Stroke Scale; D 5 day; MCA 5 middle cerebral artery; IA 5 intra-arterial; ACA 5anterior cerebral artery; CE 5 cardioembolic; L 5 left; E-HS 5 paradoxical embolism and hypercoagulable state; LLE 5 left lower extremity;IV 5 intravenous; ICA 5 internal carotid artery atherosclerosis.
Fig 1. Evolution in individual apparent diffusion coefficientlesion volumes (cm3) from baseline magnetic resonance imag-ing (MRI) to early (range, 2.5–9.5 hours) after thrombolysisMRI scan to day 7 MRI scan.
Fig 2. Percent volume change for individual diffusion-weighted imaging (DWI) and apparent diffusion coefficient(ADC) measures, baseline to early (range, 2.5–9.5 hours) afterthrombolysis. Percent change 5 [(Initial volume 2 Finalvolume)/Initial volume] 3 2100.
464 Annals of Neurology Vol 47 No 4 April 2000

Five patients had baseline perfusion studies. Of these5, all had a significant diffusion/perfusion mismatchwith perfusion volume exceeding diffusion volume by amean of 79% (range, 57–94%). Four of these patientshad a follow-up perfusion study (2 patients at 3 hoursafter recanalization and 2 patients at day 7). In all 4,there was complete resolution of the initial perfusiondeficit.
All 7 patients improved clinically after thrombolysis.Mean NIHSS decreased from 12 points at baseline to8 points early after arterial recanalization (p 5 0.06) to4 points on day 7 (p , 0.016) to 2 points on day 90(p , 0.03). Mean day 90 outcome measures were asfollows: Modified Rankin, 1.3; Barthel Index, 92; andGlasgow Outcome Scale, 1.3.
Two patient examples are shown in Figures 3 and 4.
DiscussionThis study is the first report of reversibility of bothdiffusion and perfusion MRI abnormalities afterthrombolytic therapy in human ischemic stroke pa-tients. Although preliminary, this finding provides im-portant insights into the imaging characterization ofthe ischemic penumbra. The results suggest that diffu-sion MRI lesions do not invariably represent irrevers-ible injury, and that the ischemic penumbra includesnot only the areas of diffusion/perfusion mismatch butalso portions within the diffusion abnormality itself.
There have been occasional previous case reports ofspontaneous reversal of ischemic diffusion abnormali-ties.29,30 These scattered observations provide furtherevidence that diffusion abnormalities do not necessarilyrepresent irreversible injury. However, no previous re-port has so uniformly shown reversal of diffusion lesions,nor linked reversal to thrombolytic therapy. Two groupshave reported results of serial diffusion-weighted andperfusion-weighted imaging in patients undergoing in-travenous thrombolysis, and our findings are in accordwith and extend their results. Jansen and colleagues31
found inhibition of lesion growth in patients experi-encing reperfusion compared with patients with persis-tent perfusion deficits. Marks and colleagues32 foundregions of higher ADC within the initial ischemic field
on follow-up imaging in patients undergoing reperfu-sion within 36 hours of onset compared with non-reperfusers. However, in these intravenous thrombolysisstudies, baseline pre-recanalization MRI scans were notobtained in one cohort, and the timing of initial MRIscans relative to recanalization was not specified in theother. Our study uniquely obtained pre-recanalizationand post-recanalization diffusion and perfusion MRIscans in all patients, and synchronized early post-treatment MRI scans to recanalization time, providing asnapshot of postthrombolysis pathophysiology obtainedat a uniform time point across different patients.
Findings from our study, based on small sample sizeand without matched controls, must be considered pre-liminary. However, a recent large-scale clinical trialsuggested a beneficial effect of intra-arterial thrombol-ysis on clinical end points.2 Our study provides phys-iological insights into the mechanism by which intra-arterial thrombolysis may confer benefit in selectpatients. The finding that recanalization achieved byintra-arterial thrombolysis leads not only to salvage ofregions of diffusion/perfusion mismatch, but also dra-matic reduction in the region of diffusion abnormality,delineates an anatomical mechanism by which intra-arterial therapy can improve clinical outcome.
We found that a late secondary drop in the ADCoccurred in approximately one-half the patients. Thisdelayed growth of the ADC volume generally compro-mised some, but not all, of the region of ADC abnor-mality initially reversed by recanalization. These find-ings are the first demonstration of a late secondarydrop in the ADC in humans after successful recanali-zation, a phenomenon only recently described in ani-mal reperfusion models.33,34 Potential mechanisms ofthis late secondary ADC decline include reperfusion in-jury,35 possibly related to inflammation or oxygen freeradicals, ongoing excitotoxic injury emanating from thecore infarct zone, and apoptosis. It is important for cli-nicians to be aware that some tissue that appears ini-tially to be salvaged on early MRI scan when ADCnormalizes may nonetheless proceed to late tissue in-farction. In future studies, this MRI-delineated process
PostNIHSS
D 7NIHSS
Pre-DWIVol (cm3)
Post-DWIVol (cm3)
D 7 DWI,Vol (cm3)
Pre-ADCVol (cm3)
Post-ADCVol (cm3)
D 7 ADCVol (cm3)
D 7 T2-WVol (cm3)
11 5 21.8 17.5 35.1 14.0 1.1 1.8 25.13 0 9.5 1.2 No data 0.7 0.0 No data 0.3
17 13 55.8 9.2 69.1 17.1 2.2 14.3 18.011 9 47.0 27.3 34.7 23.3 0.6 1.9 34.66 1 9.4 4.0 3.2 1.5 1.8 0.7 3.65 1 8.6 12.2 13.7 5.2 2.2 0.7 25.24 0 8.9 0.9 0.8 1.8 0.0 0.04 1.0
Kidwell et al: MRI of Thrombolytic Reversal of Ischemia 465
466 Annals of Neurology Vol 47 No 4 April 2000
of secondary injury may be an appropriate distinct tar-get for neuroprotective therapy.
Our findings may have important implications foracute stroke management in the future, because earlyassessment of the extent and reversibility of ischemia isneeded to guide appropriate acute interventions. Previ-ous studies have shown that the typical natural historyof diffusion lesions in untreated patients is to growover the first few days after symptom onset, especiallyin patients imaged early after symptom onset with largeartery occlusions.13,15,16,36 Our demonstration that thisgrowth can be arrested or even partially reversed with
thrombolytic treatment illustrates that MRI offers amethod to monitor treatment response in individualpatients. It has been suggested that MRI screening mayimprove selection of the most appropriate candidatesfor treatment and possibly extend the therapeutic win-dow beyond a rigid time frame in select patients. How-ever, our results suggest that the use of DWI alone oreven the presence of diffusion/perfusion mismatch maynot provide the optimal data with which to makethrombolytic treatment decisions. Future studies thatanalyze the combined data from perfusion measuresand ADC values may delineate more specific MRI sig-
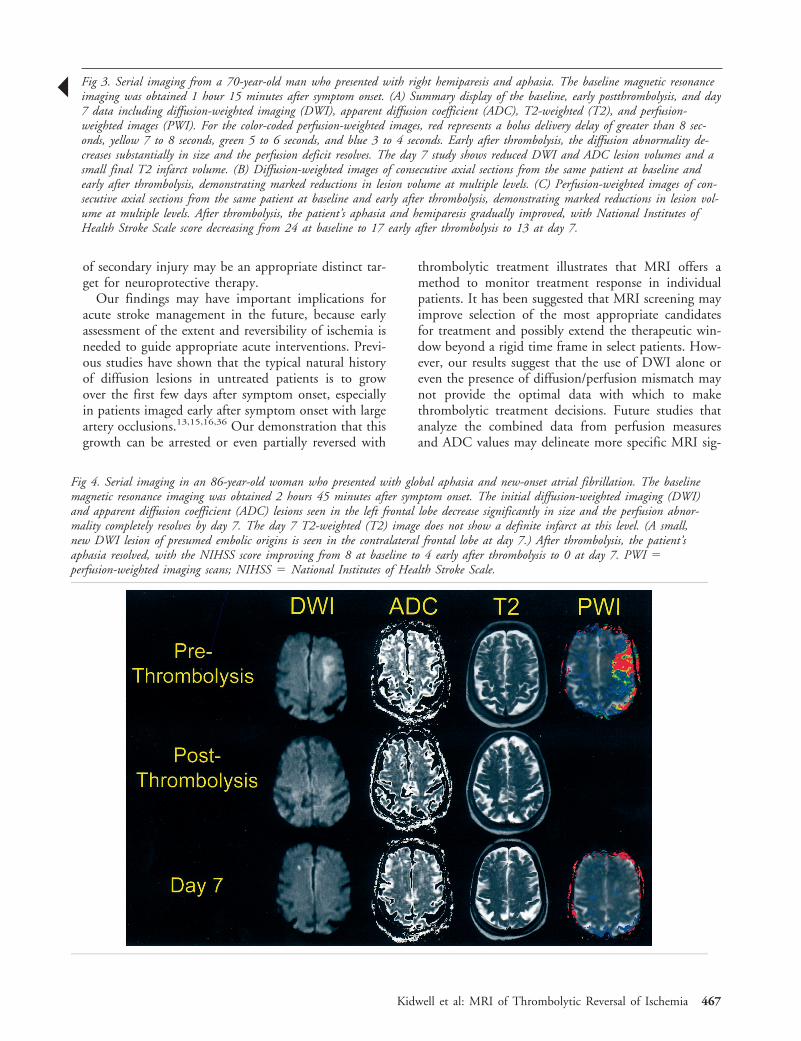
Fig 4. Serial imaging in an 86-year-old woman who presented with global aphasia and new-onset atrial fibrillation. The baselinemagnetic resonance imaging was obtained 2 hours 45 minutes after symptom onset. The initial diffusion-weighted imaging (DWI)and apparent diffusion coefficient (ADC) lesions seen in the left frontal lobe decrease significantly in size and the perfusion abnor-mality completely resolves by day 7. The day 7 T2-weighted (T2) image does not show a definite infarct at this level. (A small,new DWI lesion of presumed embolic origins is seen in the contralateral frontal lobe at day 7.) After thrombolysis, the patient’saphasia resolved, with the NIHSS score improving from 8 at baseline to 4 early after thrombolysis to 0 at day 7. PWI 5perfusion-weighted imaging scans; NIHSS 5 National Institutes of Health Stroke Scale.
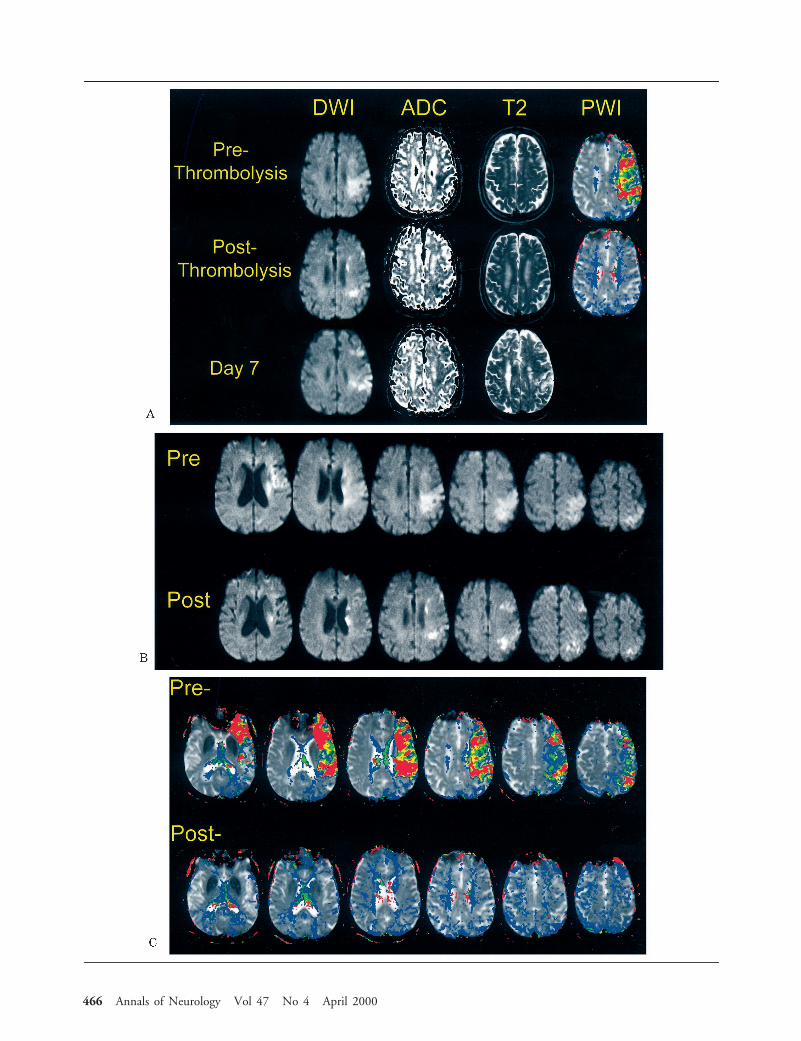
Fig 3. Serial imaging from a 70-year-old man who presented with right hemiparesis and aphasia. The baseline magnetic resonanceimaging was obtained 1 hour 15 minutes after symptom onset. (A) Summary display of the baseline, early postthrombolysis, and day7 data including diffusion-weighted imaging (DWI), apparent diffusion coefficient (ADC), T2-weighted (T2), and perfusion-weighted images (PWI). For the color-coded perfusion-weighted images, red represents a bolus delivery delay of greater than 8 sec-onds, yellow 7 to 8 seconds, green 5 to 6 seconds, and blue 3 to 4 seconds. Early after thrombolysis, the diffusion abnormality de-creases substantially in size and the perfusion deficit resolves. The day 7 study shows reduced DWI and ADC lesion volumes and asmall final T2 infarct volume. (B) Diffusion-weighted images of consecutive axial sections from the same patient at baseline andearly after thrombolysis, demonstrating marked reductions in lesion volume at multiple levels. (C) Perfusion-weighted images of con-secutive axial sections from the same patient at baseline and early after thrombolysis, demonstrating marked reductions in lesion vol-ume at multiple levels. After thrombolysis, the patient’s aphasia and hemiparesis gradually improved, with National Institutes ofHealth Stroke Scale score decreasing from 24 at baseline to 17 early after thrombolysis to 13 at day 7.
Š
Kidwell et al: MRI of Thrombolytic Reversal of Ischemia 467

natures that will predict tissue response after vesselrecanalization.
Our data provide support for the use of diffusion/perfusion MRI as a clinically meaningful ancillary orauxiliary outcome measure for clinical trials of acutestroke therapy. A reliable auxiliary outcome measurefor therapeutic interventions in acute human strokewould allow more rapid and inexpensive trials usingsmaller numbers of patients to show effect.37–40 Previ-ous studies showed that initial DWI and PWI lesionvolumes correlate well with final infarct volume andclinical outcome.16,41–43 It has not previously beenwell demonstrated that changes induced by a therapyon MRI auxiliary measures correlate well with changesin clinically meaningful end points, a critical require-ment for an auxiliary outcome measure. In our smallcohort, beneficial effects on MRI lesion volume corre-lated moderately well with improved clinical outcomeson standard rating measures of deficit, disability, andhandicap.
One limitation to widespread use of physiologicalMRI scanning to guide early decision making in acutestroke is that diffusion/perfusion MRI is not currentlyavailable in many small community hospitals. How-ever, MRI with echo-planar imaging capability is al-ready widely used in large hospitals and academicstroke centers, where intra-arterial thrombolysis islikely to be most extensively offered, and is rapidly dis-seminating into the community. Although our seriessuggests that it is feasible to obtain pretreatment MRIscans in acute stroke patients, it is important to em-phasize that this is a labor-intensive task that requires awell-coordinated stroke team and rapid MRI scanningavailability.
In conclusion, we have demonstrated reversibility ofischemic lesions visualized with diffusion/perfusionMRI in patients treated with intra-arterial thromboly-sis. These preliminary findings indicate that the MRIdefinition of the ischemic penumbra must be refinedto include both regions of diffusion/perfusion mis-match and regions of the diffusion abnormality itself.Studies that include larger numbers of patients under-going thrombolytic therapy may allow more precise de-lineation of MRI signatures of irreversible injury and ofsalvageability.
This study was supported in part by a grant from the AmericanHeart Association (Grant-in-Aid Program 9650621N to J.R.A.) andby a fellowship grant from the National Stroke Association (C.S.K.).
References1. NINDS rt-PA Stroke Group. Tissue plasminogen activator for
acute ischemic stroke. N Engl J Med 1995;333:1581–15872. Furlan AJ, Higashida R, Wechsler L, et al. Intra-arterial
prourokinase for acute ischemic stroke. The PROACT II study:a randomized controlled trial. JAMA 1999;282:2003–2011
3. Chiu D, Krieger D, Villar-Cordova C, et al. Intravenous tissueplasminogen activator for acute ischemic stroke: feasibility,safety, and efficacy in the first year of clinical practice. Stroke1998;29:18–22
4. O’Connor RE, McGraw P, Edelsohn L. Thrombolytic therapyfor acute ischemic stroke: why the majority of patients remainineligible for treatment. Ann Emerg Med 1999;33:9–14
5. Caplan LR, Mohr JP, Kistler JP, Koroshetz W. Should throm-bolytic therapy be the first-line treatment for acute ischemicstroke? Thrombolysis—not a panacea for ischemic stroke.N Engl J Med 1997;337:1309–1310
6. Fisher M. Characterizing the target of acute stroke therapy.Stroke 1997;28:866–872
7. Koroshetz WJ, Gonzalez G. Diffusion-weighted MRI: an ECGfor “brain attack”? Ann Neurol 1997;41:565–566
8. Warach S, Gaa J, Siewert B, et al. Acute human stroke studiedby whole brain echo planar diffusion-weighted magnetic reso-nance imaging. Ann Neurol 1995;37:231–241
9. Baird AE, Warach S. Magnetic resonance imaging of acutestroke. J Cereb Blood Flow Metab 1998;18:583–609
10. Lutsep HL, Albers GW, DeCrespigny A, et al. Clinical utilityof diffusion-weighted magnetic resonance imaging in the assess-ment of ischemic stroke. Ann Neurol 1997;41:574–580
11. Moseley ME, Kucharczyk J, Mintorovitch J, et al. Diffusion-weighted MR imaging of acute stroke: correlation with T2-weighted and magnetic susceptibility-enhanced MR imaging incats. AJNR 1990;11:423–429
12. Schlaug G, Siewert B, Benfield A, et al. Time course of theapparent diffusion coefficient (ADC) abnormality in humanstroke. Neurology 1997;49:113–119
13. Baird AE, Benfield A, Schlaug G, et al. Enlargement of humancerebral ischemic lesion volumes measured by diffusion-weighted magnetic resonance imaging. Ann Neurol 1997;41:581–589
14. Albers GW, Lansberg MG, O’Brien MW, et al. Evolution ofcerebral infarct volume assessed by diffusion-weighted MRI:implication for clinical stroke trials. Neurology 1999;52:A453(Abstract)
15. Barber PA, Darby DG, Desmond PM, et al. Prediction ofstroke outcome with echoplanar perfusion- and diffusion-weighted MRI. Neurology 1998;51:418–426
16. Tong DC, Yenari MA, Albers GW, et al. Correlation ofperfusion- and diffusion-weighted MRI with NIHSS score inacute (,6.5 hour) ischemic stroke. Neurology 1998;50:864–870
17. Fisher M, Garcia JH. Evolving stroke and the ischemic penum-bra. Neurology 1996;47:884–888
18. Dijkhuizen RM, Berkelbach van der Sprenkel JW, TullekenKA, Nicolay K. Regional assessment of tissue oxygenation andthe temporal evolution of hemodynamic parameters and waterdiffusion during acute focal ischemia in rat brain. Brain Res1997;750:161–170
19. Mintorovitch J, Moseley ME, Chileuitt L, et al. Comparison ofdiffusion- and T2-weighted MRI for the early detection of ce-rebral ischemia and reperfusion in rats. Magn Reson Med 1991;18:39–50
20. Hossmann KA, Fischer M, Bockhorst K, Hoehn-Berlage M.NMR imaging of the apparent diffusion coefficient (ADC) forthe evaluation of metabolic suppression and recovery after pro-longed cerebral ischemia. J Cereb Blood Flow Metab 1994;14:723–731
21. Hasegawa Y, Fisher M, Latour LL, et al. MRI diffusion map-ping of reversible and irreversible ischemic injury in focal brainischemia. Neurology 1994;44:1484–1490
22. Minematsu K, Li L, Sotak CH, et al. Reversible focal ischemicinjury demonstrated by diffusion-weighted magnetic resonanceimaging in rats. Stroke 1992;23:1304–1310
468 Annals of Neurology Vol 47 No 4 April 2000

23. Lewandowski CA, Frankel M, Tomsick TA, et al. Combinedintravenous and intra-arterial r-TPA versus intra-arterial therapyof acute ischemic stroke: Emergency Management of Stroke(EMS) Bridging Trial. Stroke 1999;30:2598–2605
24. Ostergaard L, Weisskoff RM, Chesler DA, et al. High resolu-tion measurement of cerebral blood flow using intravasculartracer bolus passages. Part I: mathematical approach and statis-tical analysis. Magn Reson Med 1996;36:715–725
25. Ostergaard L, Sorensen AG, Kwong KK, et al. High resolutionmeasurement of cerebral blood flow using intravascular tracerbolus passages. Part II: experimental comparison and prelimi-nary results. Magn Reson Med 1996;36:726–736
26. Ostergaard L, Johannsen P, Høst-Poulsen P, et al. Cerebralblood flow measurements by magnetic resonance imaging bolustracking: comparison with [(15)O]H2O positron emission to-mography in humans. J Cereb Blood Flow Metab 1998;18:935–940
27. Pierpaoli C, Alger JR, Righini A, et al. High temporal resolu-tion diffusion MRI of global cerebral ischemia and reperfusion.J Cereb Blood Flow Metab 1996;16:892–905
28. TIMI study group. The Thrombolysis in Myocardial Infarction(TIMI) trial: phase I findings: TIMI study group. N EnglJ Med 1985;312:932–936
29. Kidwell CS, Alger JR, Di Salle F, et al. Diffusion MRI in pa-tients with transient ischemic attacks. Stroke 1999;30:1174–1180
30. Marks MP, de Crespigny A, Lentz D, et al. Acute and chronicstroke: navigated spin-echo diffusion-weighted MR imaging.Radiology 1996;199:403–408
31. Jansen O, Schellinger P, Fiebach J, et al. Early recanalisation inacute ischaemic stroke saves tissue at risk defined by MRI. Lan-cet 1999;353:2036–2037 (Letter)
32. Marks MP, Tong DC, Beaulieu C, et al. Evaluation of earlyreperfusion and i.v. tPA therapy using diffusion- and perfusion-weighted MRI. Neurology 1999;52:1792–1798
33. Li F, Han SS, Tatlisumak T, et al. Reversal of acute apparentdiffusion coefficient abnormalities and delayed neuronal deathfollowing transient focal cerebral ischemia in rats. Ann Neurol1999;46:333–342
34. Dijkhuizen RM, Knollema S, van der Worp HB, et al. Dynam-ics of cerebral tissue injury and perfusion after temporaryhypoxia-ischemia in the rat: evidence for region-specific sensi-tivity and delayed damage. Stroke 1998;29:695–704
35. Hallenbeck JM, Dutka AJ. Background review and current con-cepts of reperfusion injury. Arch Neurol 1990;47:1245–1254
36. Rordorf G, Koroshetz WJ, Copen WA, et al. Regional ischemiaand ischemic injury in patients with acute middle cerebral ar-tery stroke as defined by early diffusion-weighted andperfusion-weighted MRI. Stroke 1998;29:939–943
37. Saver JL, Johnston KC, Homer D, et al. Infarct volume as asurrogate or auxiliary outcome measure in ischemic stroke clin-ical trials. Stroke 1999;30:293–298
38. Brass LM. Trial design issues: endpoints and sample size. Ce-rebrovasc Dis 1995;5:3–11
39. Temple RJ. A regulatory authority’s opinion about surrogateendpoints. In: Nimmo WS, Tucker GT, eds. Clinical measure-ment in drug evaluation. New York: John Wiley, 1995
40. Prentice RL. Surrogate endpoints in clinical trials: definitionand operational criteria. Stat Med 1989;8:431–440
41. Warach S, Dashe JF, Edelman RR. Clinical outcome in ische-mic stroke predicted by early diffusion-weighted and perfusionmagnetic resonance imaging: a preliminary analysis. J CerebBlood Flow Metab 1996;16:53–59
42. Lovblad KO, Baird AE, Schlaug G, et al. Ischemic lesion vol-umes in acute stroke by diffusion-weighted magnetic resonanceimaging correlate with clinical outcome. Ann Neurol 1997;42:164–170
43. Barber PA, Darby DG, Desmond PM, et al. Prediction ofstroke outcome with echoplanar perfusion- and diffusion-weighted MRI. Neurology 1998;51:418–426
Kidwell et al: MRI of Thrombolytic Reversal of Ischemia 469