the role of the l-arginine-nitric oxide pathway in preeclampsia
TRANSCRIPT

http://tak.sagepub.com/Therapeutic Advances in Cardiovascular Disease
http://tak.sagepub.com/content/2/4/261The online version of this article can be found at:
DOI: 10.1177/1753944708092277
2008 2: 261Ther Adv Cardiovasc DisPatricio López-Jaramillo, William D. Arenas, Ronald G. García, Melvin Y. Rincon and Marcos López
Review: The role of the L-arginine-nitric oxide pathway in preeclampsia
Published by:
http://www.sagepublications.com
can be found at:Therapeutic Advances in Cardiovascular DiseaseAdditional services and information for
http://tak.sagepub.com/cgi/alertsEmail Alerts:
http://tak.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://tak.sagepub.com/content/2/4/261.refs.htmlCitations:
What is This?
- Aug 18, 2008Version of Record >>
at Katholieke Univ Leuven on March 26, 2014tak.sagepub.comDownloaded from at Katholieke Univ Leuven on March 26, 2014tak.sagepub.comDownloaded from

Therapeutic Advances in Cardiovascular Disease Review
Therapeutic Advances inCardiovascular Disease
(2008) 2(4) 261–275
DOI: 10.1177/1753944708092277
©SAGE Publications 2008Los Angeles, London,New Delhi and Singapore
The role of the L-arginine-nitric oxide pathwayin preeclampsiaPatricio López-Jaramillo, William D. Arenas, Ronald G. García, Melvin Y. Rincon and Marcos López
Abstract: Preeclampsia (PE) is a major cause of maternal and perinatal mortality, especially indeveloping countries. Its etiology involves multiple factors, but no specific cause has beenidentified. Evidence suggests that clinical manifestations are caused by endothelialdysfunction. Nitric oxide (NO), which is synthesized from L-arginine in endothelial cells by theendothelial nitric oxide synthase (eNOS), provides a tonic dilator tone and regulates theadhesion of white blood cells and platelet aggregation. Alterations in the L-arginine-NOpathway have been associated with the development of PE. Various studies, reportingdecreased, elevated or unchanged levels of nitrite (NO2) and nitrate (NO3), two end products ofNO metabolism, have been published. Our group contributed to those contradictory reportsdescribing cases of PE with both elevated and decreased levels of NO2 and NO3. Apparently,diminished levels of NO could be related to deficiencies in the ingestion of dietary calciumassociated to low levels of plasma ionic calcium, which is crucial to the eNOS’ activity. Also, lowlevels of NO could be associated with the presence of eNOS polymorphisms or the presence ofincreased levels of ADMA, the endogenous inhibitor of NO. High levels of NO associated to lowlevels of cGMP suggest a decreased bioactivity of NO, which is probably related to an increaseddegradation of NO caused by a high production of superoxide in states of infection andinflammation. The present article analyses and reviews the reported paradoxical roles of theL-arginine-NO pathway in PE and gives a possible explanation for these results.
Keywords: preeclampsia, endothelium, nitric oxide, inflammation, infection
IntroductionHypertensive pregnancy disorders are the maincause of maternal and perinatal morbidity andmortality. Preeclampsia (PE) is the most impor-tant among these pathologies [WHO, 2004;Walker, 2000] Preeclampsia, defined as the onsetof hypertension and proteinuria after 20 weeksof gestation in previously normotensive non-proteinuric pregnant women [Walker, 2000], isa multiorgan disease, affecting the liver, kid-neys, brain, and blood clotting system. Despiteits importance, the etiology of PE is not welldefined and multiple risk factors have beenidentified [Lopez-Jaramillo et al. 2001; Lopez-Jaramillo, 2000]. The impact of each of themvaries in different populations, with considerabledifferences between developed and developingcountries [Lopez-Jaramillo et al. 2005]. In LatinAmerica, the high frequency of risk factors,such as inappropriate nutrition, young mater-nal age, and inadequate prenatal care pro-grams, is reflected in the high incidence of
PE [WHO, 2004, 1987] and elevated maternal Correspondence to:Patricio López–JaramilloVILANO Group. ResearchInstitute, FundaciónCardiovascular deColombia, Floridablanca,Santander, Colombia andResearch Department,Medical School,Universidad de Santander(UDES), Bucaramanga,[email protected];[email protected]
William D. Arenas,Ronald G. García,Melvin Y. RinconVILANO Group. ResearchInstitute, FundaciónCardiovascular deColombia, Floridablanca,Santander, Colombia
Marcos LópezFree Radical ResearchCenter, Department ofBiophysics, MedicalCollege of Wisconsin,Milwaukee, WI, USA
mortality, which is 10–20 times higher thanin developed countries [WHO InternationalCollaborative Study of Hypertensive Disorders ofPregnancy, 1998].
Pregnancy is a physiological state in whichthere are important hemodynamic adaptationsthat are maintained by an increased peripheralvasodilation [Lopez-Jaramillo, 1996]. The vas-cular endothelial cells provide a tonic dilatortone, which is mainly maintained not only bythe production of NO, but also by prostacyclinand endothelium-derived hyperpolarizing factor(EDHF). Furthermore, these substances inhibitthe adhesion and migration of leukocytes andplatelets to the vascular wall [Sladek et al. 1997;Moncada et al. 1991].
Nitric oxide is synthesized from the amino acidL-arginine by a family of enzymes denominatedNO synthases (NOS). The endothelial NOS
http://tac.sagepub.com 261
at Katholieke Univ Leuven on March 26, 2014tak.sagepub.comDownloaded from

Therapeutic Advances in Cardiovascular Disease
(eNOS) is a NADPH and Ca2+ dependentenzyme [Moncada et al. 1991]. Moreover, wehave demonstrated the crucial role of extracel-lular calcium concentrations in the productionof endothelial NO and in the control of vas-cular tone [Lopez-Jaramillo et al. 1990]. NOacts as a potent vasodilator via the activation ofcGMP [Sladek et al. 1997] (Figure 1). eNOSis expressed in human placental syncytiotro-phoblasts and extravillous trophoblasts [Sladeket al. 1997]. NO is inactivated when react-ing with superoxide (O−
2 ) to form peroxynitrite(ONOO−) a potent oxidant responsible for thelipid peroxidation and the nitration of tyrosine.An increased production of O−
2 during pregnancyhas been reported, especially in case of infectionand/or inflammation. Moreover, O−
2 is producedby eNOS when there is a deficiency of tetrahydro-biopterin (BH4) [Ronson et al. 1999; Moncadaet al. 1991].
The aim of the present review was to evaluatethe role of the L-arginine-NO pathway in normalpregnancy, and to analyze the conflicting resultsreported in the literature about the role of NOin PE. We searched PubMed for articles pub-lished between 1990 and 2005. The keywordsused were ‘Preeclampsia,’ ‘nitric oxide,’ ‘nitrites/nitrates,’ ‘cyclic guanosine monophosphate,’ and
‘L-arginine.’ We also searched the bibliographiesof the articles retrieved for further relevantreferences. Reports, letters to the editor andpapers not specifically focused on this topic wereexcluded. Because of the large number of articlesidentified, the decision on which to include wasbased on personal judgment.
Hemodynamic changes in normal pregnancyNormal pregnancy is characterized by pro-found anatomical, physiological, and biochemicalchanges to support growth and development ofthe fetus [Heilmann, 1987; Taylor and Lind,1979; Chesley, 1972; Lund and Donovan, 1967].The hemodynamic changes observed duringpregnancy are: increased blood volume, heartrate, cardiac output, and a decreased periph-eral vascular resistance [Moutquin et al. 1985;Metcalfe and Ueland, 1974; Lees et al. 1967].This decrease in resistance is achieved by bothperipheral vasodilatation and reduction in bloodviscosity [Heilmann, 1987].
In normal pregnancy, plasma volume increasesto about 40% above pre-pregnancy levels at30-week gestation [Chesley, 1972; Lund andDonovan, 1967]. Furthermore, during gesta-tion red cell mass increases linearly to reach atterm, a level 25% higher than before pregnancy
Endothelialcell
Receptoragonist
Shearstress
Inhibits plateletahesion andaggregation Inhibits monocytes
adhesion andmigrationCa2+
Ca2+/Calmodulin - Bh4
NOS
NO
NO
L-Citruline
NO
SGC
cGMPGTP
Vasodilation
R R
Smoothmusclecell
L-Arginine + O2
Figure 1. Regulation of the production of NO in the vascular endothelium and antithrombotic, antiatherogenicand vasodilation actions. SGC: Soluble guanylate cyclase. GTP: Guanosine 5′-triphosphate. cGMP: Cyclicguanosine monophosphate.
262 http://tac.sagepub.com
at Katholieke Univ Leuven on March 26, 2014tak.sagepub.comDownloaded from
Review
[Taylor and Lind, 1979; Chesley, 1972; Lundand Donovan, 1967], besides cardiac output risesfrom 30 to 40% compared with nonpregnantresting stage [Lees et al. 1967]. The increase incardiac output occurs as early as the twelvethweek, probably as a result of afterload due toperipheral vasodilation [Metcalfe and Ueland,1974]. Despite these increases in cardiac outputand plasma volume, blood pressure falls duringnormal pregnancy [Moutquin et al. 1985]. Thereasons for the fall in peripheral vascular resis-tance have not been completely established buthave been associated with an increased produc-tion of prostacyclin and NO [Lopez-Jaramilloet al. 1995; Felix et al. 1991].
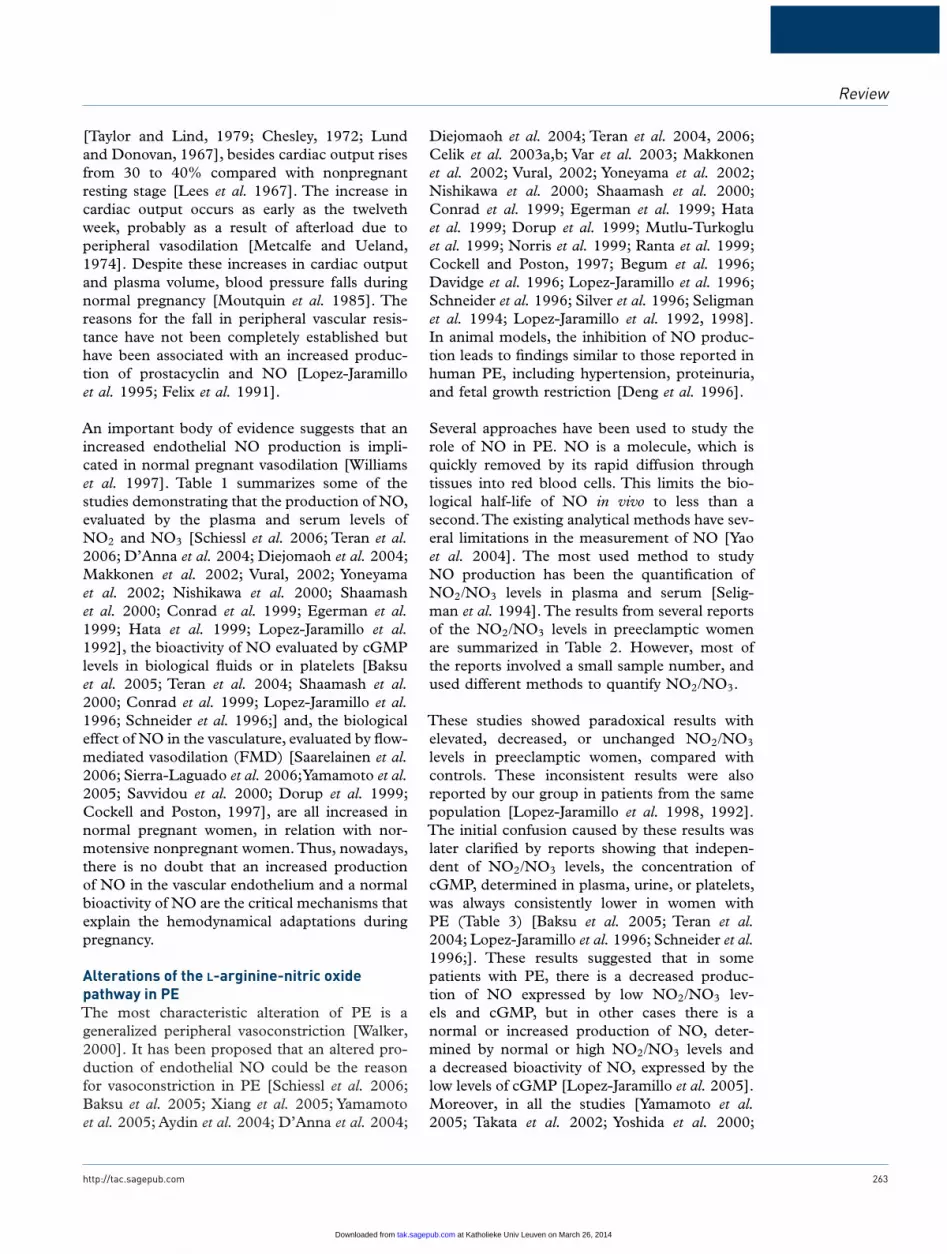
An important body of evidence suggests that anincreased endothelial NO production is impli-cated in normal pregnant vasodilation [Williamset al. 1997]. Table 1 summarizes some of thestudies demonstrating that the production of NO,evaluated by the plasma and serum levels ofNO2 and NO3 [Schiessl et al. 2006; Teran et al.2006; D’Anna et al. 2004; Diejomaoh et al. 2004;Makkonen et al. 2002; Vural, 2002; Yoneyamaet al. 2002; Nishikawa et al. 2000; Shaamashet al. 2000; Conrad et al. 1999; Egerman et al.1999; Hata et al. 1999; Lopez-Jaramillo et al.1992], the bioactivity of NO evaluated by cGMPlevels in biological fluids or in platelets [Baksuet al. 2005; Teran et al. 2004; Shaamash et al.2000; Conrad et al. 1999; Lopez-Jaramillo et al.1996; Schneider et al. 1996;] and, the biologicaleffect of NO in the vasculature, evaluated by flow-mediated vasodilation (FMD) [Saarelainen et al.2006; Sierra-Laguado et al. 2006;Yamamoto et al.2005; Savvidou et al. 2000; Dorup et al. 1999;Cockell and Poston, 1997], are all increased innormal pregnant women, in relation with nor-motensive nonpregnant women. Thus, nowadays,there is no doubt that an increased productionof NO in the vascular endothelium and a normalbioactivity of NO are the critical mechanisms thatexplain the hemodynamical adaptations duringpregnancy.
Alterations of the L-arginine-nitric oxidepathway in PEThe most characteristic alteration of PE is ageneralized peripheral vasoconstriction [Walker,2000]. It has been proposed that an altered pro-duction of endothelial NO could be the reasonfor vasoconstriction in PE [Schiessl et al. 2006;Baksu et al. 2005; Xiang et al. 2005; Yamamotoet al. 2005; Aydin et al. 2004; D’Anna et al. 2004;
Diejomaoh et al. 2004; Teran et al. 2004, 2006;Celik et al. 2003a,b; Var et al. 2003; Makkonenet al. 2002; Vural, 2002; Yoneyama et al. 2002;Nishikawa et al. 2000; Shaamash et al. 2000;Conrad et al. 1999; Egerman et al. 1999; Hataet al. 1999; Dorup et al. 1999; Mutlu-Turkogluet al. 1999; Norris et al. 1999; Ranta et al. 1999;Cockell and Poston, 1997; Begum et al. 1996;Davidge et al. 1996; Lopez-Jaramillo et al. 1996;Schneider et al. 1996; Silver et al. 1996; Seligmanet al. 1994; Lopez-Jaramillo et al. 1992, 1998].In animal models, the inhibition of NO produc-tion leads to findings similar to those reported inhuman PE, including hypertension, proteinuria,and fetal growth restriction [Deng et al. 1996].
Several approaches have been used to study therole of NO in PE. NO is a molecule, which isquickly removed by its rapid diffusion throughtissues into red blood cells. This limits the bio-logical half-life of NO in vivo to less than asecond.The existing analytical methods have sev-eral limitations in the measurement of NO [Yaoet al. 2004]. The most used method to studyNO production has been the quantification ofNO2/NO3 levels in plasma and serum [Selig-man et al. 1994]. The results from several reportsof the NO2/NO3 levels in preeclamptic womenare summarized in Table 2. However, most ofthe reports involved a small sample number, andused different methods to quantify NO2/NO3.
These studies showed paradoxical results withelevated, decreased, or unchanged NO2/NO3
levels in preeclamptic women, compared withcontrols. These inconsistent results were alsoreported by our group in patients from the samepopulation [Lopez-Jaramillo et al. 1998, 1992].The initial confusion caused by these results waslater clarified by reports showing that indepen-dent of NO2/NO3 levels, the concentration ofcGMP, determined in plasma, urine, or platelets,was always consistently lower in women withPE (Table 3) [Baksu et al. 2005; Teran et al.2004; Lopez-Jaramillo et al. 1996; Schneider et al.1996;]. These results suggested that in somepatients with PE, there is a decreased produc-tion of NO expressed by low NO2/NO3 lev-els and cGMP, but in other cases there is anormal or increased production of NO, deter-mined by normal or high NO2/NO3 levels anda decreased bioactivity of NO, expressed by thelow levels of cGMP [Lopez-Jaramillo et al. 2005].Moreover, in all the studies [Yamamoto et al.2005; Takata et al. 2002; Yoshida et al. 2000;
http://tac.sagepub.com 263
at Katholieke Univ Leuven on March 26, 2014tak.sagepub.comDownloaded from

Therapeutic Advances in Cardiovascular DiseaseTa
ble
1.Le
vels
ofm
etab
olite
sof
nitr
icox
ide,
cGM
P,a
ndFM
Din
nonp
regn
antw
omen
(NP
)and
norm
oten
sive
preg
nant
wom
en(N
TP).
Nitr
icox
ide
met
abol
ites
(NO
2/N
O3
leve
ls)
Aut
hor
NP
nN
TPn
pM
etho
dFl
uid/
Cel
l
Lope
z-Ja
ram
illo
[199
8]18
±4
uM10
25±
4uM
10<
0.05
Spec
trop
hoto
met
ric
Pla
sma
Hat
aet
al.[
1999
]1.
13±
0.22
uM10
0.48
±0.
17uM
10<
0.05
Fluo
rom
etri
cas
say
Pla
sma
Con
rad
etal
.[19
99]
36±
3uM
1534
±2
uM22
NS
Gri
ess
reac
tion
Pla
sma
Nis
hika
wa
etal
.[20
00]
24.7
2±
2.17
uM11
23.6
3±
1.87
uM16
NS
Spec
trop
hoto
met
ric
Seru
mSh
aam
ash
etal
.[20
00]
7.6
±1.
4um
ol/L
2120
.5±
6.7
umol
/L32
<0.
001
Gri
ess
reac
tion
Seru
mVu
ral[
2002
]54
.86
±11
.15
umol
/L20
62.6
3±
9.52
umol
/L20
<0.
05G
rish
am’s
met
hod
Pla
sma
Tera
net
al.[
2006
]19
.2±
1.3
uM30
23.4
±1.
9uM
600.
03C
hem
iolu
min
isce
nce
Pla
sma
cGM
Ple
vels
Aut
hor
NP
nN
TPn
pM
etho
dFl
uid/
Cel
l
Lope
z-Ja
ram
illo
etal
.[1
996]
0.46
±0.
12nM
220.
94±
0.23
nM22
<0.
05Sp
ecifi
cra
dioi
mm
uno
assa
y(R
IA)
Pla
sma
18.4
±10
.3uM
2250
.1±
15.7
uM22
<0.
05R
IAU
rine
Con
rad
etal
.[19
99]
6.3
±0.
5nm
ol/L
156.
9±
0.7
nmol
/L22
NS
RIA
Pla
sma
843
±55
nmol
/24
h15
1311
±94
nmol
/24h
22<
0.05
RIA
Uri
neTe
ran
etal
.[20
04]
7.6
±0.
3fm
ol/1
05
plat
elet
s15
19.8
±2.
6fm
ol/1
05
plat
elet
s15
0.00
1En
zym
e-lin
ked
imm
unos
orbe
ntas
say
Intr
apla
tele
t
Yam
amot
oet
al.
[200
5]0.
746
±0.
381
pmol
/mL/
10(8
)cel
ls20
2.21
±1.
10pm
ol/m
L/10
(8)c
ells
20<
0.05
Enzy
me-
linke
dim
mun
osor
bent
assa
y
Intr
apla
tele
t
FMD
(%)
Aut
hor
NP
nN
TPn
p
Coc
kell
etal
.[19
97]
10.1
±7.
3%10
48.3
±8.
0%20
<0.
01D
orup
etal
.[19
99]
7.2
±2.
8%37
10.6
±4.
4a %29
<0.
001
Savv
idou
etal
.[20
00]
6.42
±2.
45%
198.
84±
3.2b
%15
70.
002
Yam
amot
oet
al.[
2005
]10
8.7
±3.
9%20
115.
1±
6.5%
200.
01Si
erra
-Lag
uado
etal
.[20
06]
15±
1%56
17±
1%13
6<
0.00
01Sa
arel
aine
net
al.[
2006
]9.
48±
4.05
%62
11.1
±5.
3a %22
<0.
004
aLa
stTr
imes
ter,
NS:
nons
igni
ficat
ive.
bbe
twee
n10
and
30w
eeks
.
264 http://tac.sagepub.com
at Katholieke Univ Leuven on March 26, 2014tak.sagepub.comDownloaded from

Review
Table 2. Levels of NO metabolites in biological fluids of preeclamptic women compared to women with normalpregnancy.
Similar levels
Author/Year Method n
Davidge et al. [1996] Spectrophotometric – Griess reaction 13Silver et al. [1996] Chemiluminescence 21Hata et al. [1999] Fluorometric assay 13Conrad et al. [1999] Griess reaction 15Egerman et al. [1999] Spectrophotometric 12Yanik et al. [2001] Spectrophotometer 38Diejomaoh et al. [2004] Liquid chromatography 34Schiessl et al. [2006] Griess reaction 13McCord et al. [2006] DAF-FM DA fluorescent dye 10
Decreased levels
Author/Year Method n
Lopez-Jaramillo et al. [1992] Spectrophotometric 9Begum et al. [1996] Griess reaction 12Mutlu-Türkoglu et al. [1999] Griess reaction 20Celik et al. [2003] Spectrophotometric 21Celik et al. [2003] Griess reaction 20Var et al. [2003] Griess reaction 19Aydinl et al. [2004] Colorimetric assay 34Xiang et al. [2005] Nitrate reductase method 11Teran et al. [2006] Chemioluminiscence 30
Increased levels
Author/Year Method n
Lopez-Jaramillo [1998] Spectrophotometric 10Ranta et al. [1999] Griess reaction 20Norris et al. [1999] Griess reaction 16Nishikawa et al. [2000] Spectrophotometric 17Shaamash et al. [2000] Griess reaction 31Makkonen et al. [2002] Colorimetric assay 20Yoneyama et al. [2002] Griess reaction 25Vural [2002] The Grisham’s method 19D’Anna et al. [2004] Chemiluminescence detection 30Pasaoglu et al. [2004] Spectrophotometric 40
n = Number of patients.
Cockell and Poston, 1997] that reported FMDin women with PE, there was a decreased vasodi-lating response to hyperemia (Table 3).
All these results reveal that PE is characterized bya decreased bioavailability of NO, which explainsthe peripheral vasoconstriction, the endothelialdysfunction, and the clinical manifestations ofthis disease. Furthermore, these results supportthe proposal of multicausality of the disease withdifferent mechanisms conducting alterations inthe activity of NO [Lopez-Jaramillo et al. 2001;Lopez-Jaramillo, 2000].
In the case of PE with low production ofNO (low NO2/NO3 levels) some alterations inthe L-arginine-NO pathway have been described(Figure 2):
1. Deficiency in the substrate L-arginine or inits transport [McCord et al. 2006; Neri et al.2000].
2. Deficiency in the cofactors needed for thenormal activity of eNOS, such as ionic cal-cium [Herrera et al. 2006; Steinert et al. 2002;Lopez-Jaramillo et al. 2001] and BH4 [Varet al. 2003; Toth, 2002].
http://tac.sagepub.com 265
at Katholieke Univ Leuven on March 26, 2014tak.sagepub.comDownloaded from

Therapeutic Advances in Cardiovascular Disease
Tabl
e3.
cGM
Ple
vels
,(FM
D)i
npr
eecl
ampt
icw
omen
(PE)
and
norm
oten
sive
preg
nant
wom
en(N
TP).
cGM
P
Aut
hor
PE
nN
TPn
pM
etho
dFl
uid/
Cel
l
Lope
z-Ja
ram
illo
etal
.[19
96]
0.48
±0.
10nM
220.
94±
0.23
nM22
<0.
05Sp
ecifi
cra
dioi
mm
unoa
ssay
(RIA
)
Pla
sma
Tera
net
al.[
2004
]11
.3±
1.8
fmol
/10
5 plat
elet
s15
19.8
±2.
6fm
ol/1
05
plat
elet
s15
0.05
Enzy
me-
linke
dim
mun
osor
bent
assa
y
Intr
apla
tele
t
Con
rad
etal
.[19
99]
7.2
±1.
0nm
ol/L
156.
9±
0.7
nmol
/L22
NS
RIA
Pla
sma
Bak
suet
al.[
2005
]3.
4±
1.2
nmol
/L43
4.5
±1.
3nm
ol/L
410.
002
RIA
Uri
ne
Schi
essl
etal
.[20
06]
9.02
±4.
47pm
ol/m
l13
6.82
±2.
57pm
ol/m
L49
0.07
2R
IAP
lasm
a51
8.13
±41
8.68
nmol
/L61
2.95
±44
0.63
nmol
/L0.
656
RIA
Uri
ne
FMD
Aut
hor
PE
nN
TPn
p
Coc
kell
etal
.[19
97]
1.2
±7.
2%6
19.2
±10
.6%
20<
0.01
Yosh
ida
[200
0]7.
9±
3.0%
1817
.4±
4.2%
58<
.001
Taka
taet
al.[
2002
]a2.
3±
3.7%
b25
5.0%
±3.
2%32
<0.
05Ya
mam
oto
etal
.[20
05]
106.
8%±
2.7%
1511
5.1%
±6.
5%20
0.04
9
aU
teri
near
tery
.bSe
vere
pree
clam
psia
.
266 http://tac.sagepub.com
at Katholieke Univ Leuven on March 26, 2014tak.sagepub.comDownloaded from

Review
Synthesis
PRMT
Protein
eNOS
NO
Citruline
eNOS
NOSpolymorphism
Proteolysis
Methil arginines
Asimmetricdimethilarginine
DDAH IDDAH II
L-Arginine
Calciumdeficience
BH4deficience
Figure 2. Different factors that can affect the production of NO in the vascular endothelium duringpregnancy. DDAH: Dimethylarginine dimethylaminohydrolase. PRMT: Protein arginine methyltransferase.BH4: tetrahydrobiopterin.
3. Accumulation of asymmetric dimethylarginine(ADMA), an endogenous inhibitor of eNOS[Slaghekke et al. 2006].
4. Presence of polymorphic alterations of theeNOS that results in a lower enzymatic activity[Serrano et al. 2004].
In the case of PE with normal or high productionof NO and normal or increased NO2/NO3 levelsbut with lower bioactivity of NO, an increaseddegradation of NO has been proposed. Due tothe high reactivity of NO with O−
2 to form perox-initrite, increased oxidative stress in PE has beenreported as the cause of the rapid degradation ofNO [Sharma et al. 2006; Myatt and Cui, 2004;Lowe, 2000; Sagol et al. 1999].
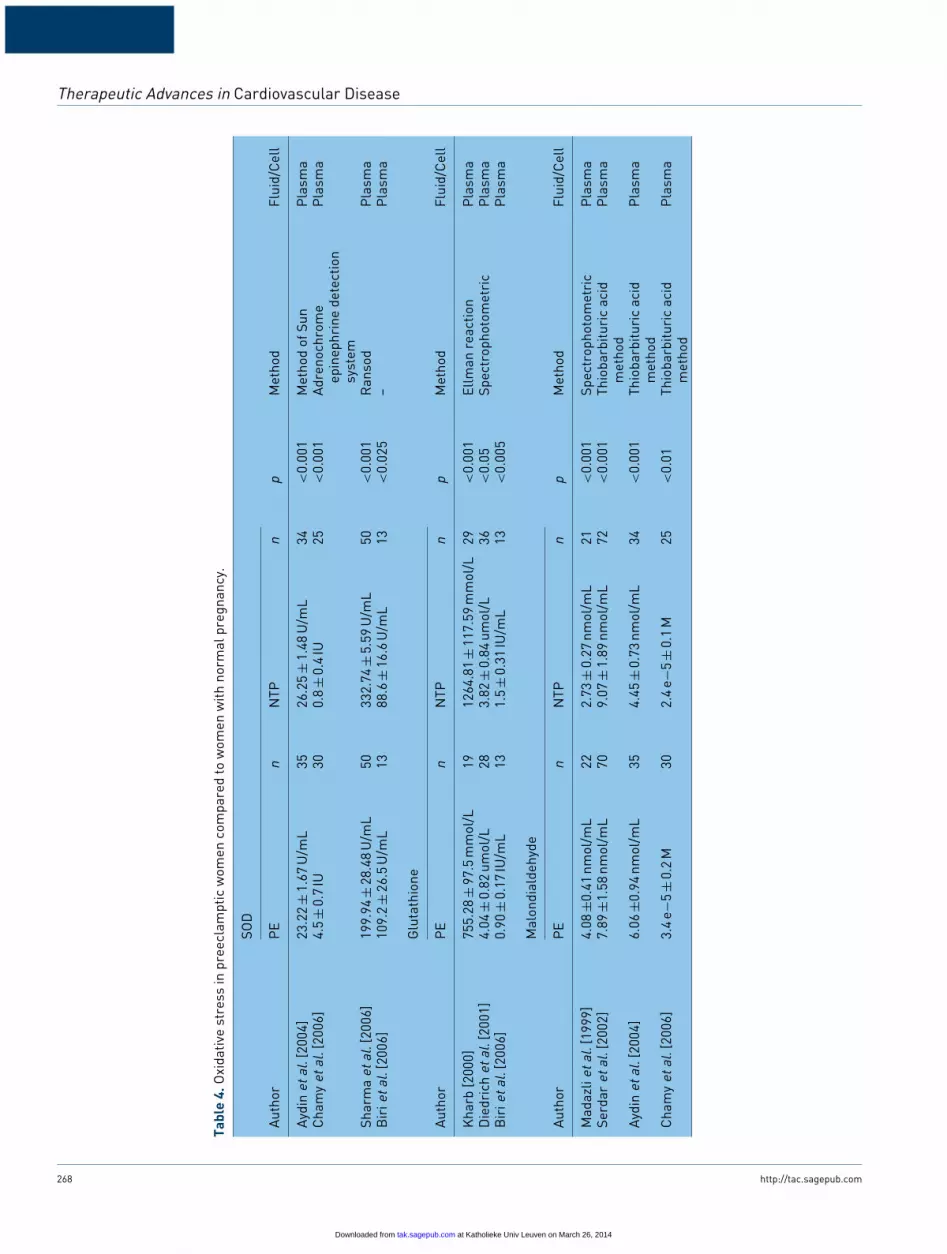
Table 4 summarizes the results of several stud-ies using different methods to evaluate thestate of oxidative stress in PE. It is clear that,regardless of the method used to quantify oxy-gen reactive species, most of the studies foundan increased superoxide production in preg-nant women with PE [Biri et al. 2007; Chamyet al. 2006; Sharma et al. 2006; Myatt and Cui,2004; Pasaoglu et al. 2004; Serdar et al. 2002;Diedrich et al. 2001; Yanik et al. 2001; Kharb,2000; Lowe, 2000; Sagol et al. 1999; Madazliet al. 1999]. Below are some of the causesdescribed to explain the reduced bioavailability
of NO and the increased state of oxidativestress in PE.
1. Presence of antibodies anti receptors AT1 ofangiotensin II [Dechend et al. 2000; Xia et al.2003].
2. Early abnormal placentation with placentalischemia and hypoxia [Gilbert et al. 2007].
3. Alterations in the metabolism of carbohy-drates and lipids associated to insulin resis-tance, overweight, and obesity [Joffe et al.1998].
4. Subclinical infections in the vagina, urinarytract system, and periodontal disease [Herreraet al. 2001, 2007; Trogstad et al. 2001; Hillet al. 1986].
A defective placentation has been proposedas the primary cause of preeclampsia [Gilbertet al. 2007]. An inadequate trophoblastic inva-sion of uterine spiral arteries results in placen-tal ischaemia, oxidative stress, inflammation, andalteration of maternal endothelial cell function[Sankaraligam et al. 2006]. It has been sug-gested that a reduced formation of NO couldbe responsible for the abnormal placental per-fusion in PE [Lowe et al. 2000]. However,there is accumulating evidence that supports thatpreeclamptic placenta has a normal capacity tosynthesize NO [Baylis et al. 1998]. Moreover, as
http://tac.sagepub.com 267
at Katholieke Univ Leuven on March 26, 2014tak.sagepub.comDownloaded from
Therapeutic Advances in Cardiovascular Disease
Tabl
e4.
Oxi
dativ
est
ress
inpr
eecl
ampt
icw
omen
com
pare
dto
wom
enw
ithno
rmal
preg
nanc
y.
SOD
Aut
hor
PE
nN
TPn
pM
etho
dFl
uid/
Cel
l
Ayd
inet
al.[
2004
]23
.22
±1.
67U
/mL
3526
.25
±1.
48U
/mL
34<
0.00
1M
etho
dof
Sun
Pla
sma
Cha
my
etal
.[20
06]
4.5
±0.
7IU
300.
8±
0.4
IU25
<0.
001
Adr
enoc
hrom
eep
inep
hrin
ede
tect
ion
syst
em
Pla
sma
Shar
ma
etal
.[20
06]
199.
94±
28.4
8U
/mL
5033
2.74
±5.
59U
/mL
50<
0.00
1R
anso
dP
lasm
aB
irie
tal.
[200
6]10
9.2
±26
.5U
/mL
1388
.6±
16.6
U/m
L13
<0.
025
–P
lasm
a
Glu
tath
ione
Aut
hor
PE
nN
TPn
pM
etho
dFl
uid/
Cel
l
Kha
rb[2
000]
755.
28±
97.5
mm
ol/L
1912
64.8
1±
117.
59m
mol
/L29
<0.
001
Ellm
anre
actio
nP
lasm
aD
iedr
ich
etal
.[20
01]
4.04
±0.
82um
ol/L
283.
82±
0.84
umol
/L36
<0.
05Sp
ectr
opho
tom
etri
cP
lasm
aB
irie
tal.
[200
6]0.
90±
0.17
IU/m
L13
1.5
±0.
31IU
/mL
13<
0.00
5P
lasm
a
Mal
ondi
alde
hyde
Aut
hor
PE
nN
TPn
pM
etho
dFl
uid/
Cel
l
Mad
azli
etal
.[19
99]
4.08
±0.4
1nm
ol/m
L22
2.73
±0.
27nm
ol/m
L21
<0.
001
Spec
trop
hoto
met
ric
Pla
sma
Serd
aret
al.[
2002
]7.
89±1
.58
nmol
/mL
709.
07±
1.89
nmol
/mL
72<
0.00
1Th
ioba
rbitu
ric
acid
met
hod
Pla
sma
Ayd
inet
al.[
2004
]6.
06±0
.94
nmol
/mL
354.
45±
0.73
nmol
/mL
34<
0.00
1Th
ioba
rbitu
ric
acid
met
hod
Pla
sma
Cha
my
etal
.[20
06]
3.4
e−5
±0.
2M
302.
4e−
5±
0.1
M25
<0.
01Th
ioba
rbitu
ric
acid
met
hod
Pla
sma
268 http://tac.sagepub.com
at Katholieke Univ Leuven on March 26, 2014tak.sagepub.comDownloaded from
Review
we previously mentioned, the concentration ofcGMP in placental circulation is lower thannormal [Kovasc et al. 1994], suggesting thatPE is a condition of normal placental pro-duction of NO, but with a reduced activityof this substance. One mechanism, by whichNO bioavailability is reduced in PE, could bethe increased production of oxygen free rad-icals, which scavenge this potent vasodilator[Sankaraligam et al. 2006]. Another pathwaythat might result in reduced NO bioavailabil-ity involves arginase, an enzyme that cataly-ses the conversion of L-arginine to L-ornithineand urea [Li et al. 2001]. There are two iso-forms of arginase (arginase I and II) that arelocated in the cytosol and mitochondria, respec-tively. Noris et al. [2004] found that arginaseII m RNA expression was more than 4-foldhigher in villous tissue of preeclamptic than innormal pregnant women. In addition, levels ofarginase II mRNA in villous tissue correlatedinversely with fetal L-arginine concentration, sug-gesting excess consumption of the substrate.Since L-arginine is also a substrate for NOS,arginase reciprocally regulates NOS [Berkowitzet al. 2003]. Higher than normal expressionof arginase II causes that less L-arginine beavailable for eNOS in trophoblast cells thanin the villous endothelium. A decrease in theL-arginine concentrations could result in uncou-pling of eNOS, thus increasing the generationof O−
2 [Kuzkaya et al. 2003]. This might resultin increased scavenging of NO by superoxide togenerate peroxynitrite [Xia et al. 1996]. Markersof oxidative stress are increased in placenta ofwomen with PE, and nitrotyrosine staining, amarker of peroxynitrite, has been found in thepreeclamptic placenta [Myatt et al. 1996; Manyet al. 2000]. The peroxynitrite is an anion thatinhibits mitochondrial electron transport, oxi-dizes proteins, initiates lipid peroxidation, nitratesaromatic amino acids, and decreases prosta-cyclin synthase expression, producing periph-eral vasoconstriction and increasing maternalblood pressure [Radi et al. 1991]. Peroxynitritealso activates pro-inflammatory transcription fac-tors such as NF-κB, which controls expres-sion of adhesion molecules and other inflam-matory factors [Li and Karin, 1999]. Thusperoxynitrite contributes to the establishmentof the generalized intravascular inflammatoryreaction that produces endothelial dysfunctionearly in pregnancy and predisposes women to ahigher risk of developing PE [Sankaraligam et al.2000].
The upregulation of arginase II in PE, provides apotential rational for L-arginine supplementation.A preclinical study performed in rats, showedthat L-arginine attenuates the hypertension pro-duced in response to a chronic reduction inuterine perfusion pressure in the pregnant rat,suggesting that L-arginine supplementation maybe beneficial in attenuating the hypertension inPE [Alexander et al. 2004]. In humans, adminis-tration of L-arginine improves uterine-placentalcirculation [Neri et al. 1996], lowers maternalblood pressure [Facchinetti et al. 1999], andreduces platelet aggregation [Neri et al. 1998].However, few studies have evaluated the effectsof L-arginine supplementation on clinical out-comes of women with PE. Staff et al. [2004]evaluated the effects of oral administration of12 g of L-arginine or placebo on preeclampticwomen with gestational length ranging from 28to 36 weeks. They found no significant effectson diastolic blood pressure values, time of deliv-ery, or mean birth weight between the groups.However, this study was limited by the smallsample size (15 subjects in each group) andthe short-term treatment (two days). Recently,Facchineti et al. [Facchinetti et al. 2007] in astudy with a larger sample size demonstrated thatthe daily intravenous administration of L-arginine(20 g/500 ml), for five days followed by 4 g/dayorally administered for two weeks, prolongedpregnancy and reduced blood pressure in womenwith gestational hypertension in comparison withplacebo. Despite these promising results, theeffectiveness of L-arginine in preventing thedevelopment of PE remains to be determined.
Because oxidative stress has been proposed asa key factor involved in the development ofendothelial dysfunction and PE, supplementa-tion with antioxidants, like vitamin C and E,during pregnancy has also been proposed as apossible strategy to prevent or delay the onsetof PE. Recently, a systematic review performedby Rumbold et al. [2007] involving seven tri-als with 6082 women, found that supplementingwomen with any antioxidant during pregnancycompared with control or placebo was associatedwith a reduced risk of developing preeclamp-sia (RR 0.61; 95% CI 0.50–0.75) or having asmall-for-gestational-age infant (RR 0.64; 95%CI 0.47–0.87). However, the reviewers mentionthat these results should be interpreted with cau-tion, and results of larger studies are neededbefore antioxidants can be recommended forclinical practice.
http://tac.sagepub.com 269
at Katholieke Univ Leuven on March 26, 2014tak.sagepub.comDownloaded from

Therapeutic Advances in Cardiovascular Disease
In addition to an increased oxidative stress, it hasbeen suggested that placenta-derived circulatingfactors may induce endothelial dysfunction lead-ing to preeclampsia [Maynard et al. 2003]. Ithas been demonstrated that high levels of cir-culating sFlt1 (soluble fms-like tyrosine kinase)of placental origin, bind to and neutralize theproangiogenic actions of vascular endothelialgrowth factor (VEGF) and placental growth fac-tor (PIGF). Thus, by preventing the binding ofVEFG to Flt1 receptor in cytotrophoblast cells,the excessive production of sFlt1 in placental tro-phoblast could be responsible for the defectivecytotrophoblast differentiation and abnormal pla-centation of PE [Noris et al. 2005]. High concen-trations of sFlt1 along with decreased free VEGFare observed before the onset of clinical symp-toms in women with PE [Levine et al. 2004].VEGF also induces endothelial cell productionof vasodilatory NO and prostacyclin [Brockelsbyet al. 1999], and may be important in the reg-ulation of vascular tone. It has been suggestedthat the induction of hypertension by placenta-derived sFlt1could be related with the impair-ment of VEGF-dependent activation of eNOS[Maynard et al. 2003]. Recently, it has beenfound that Endoglina (sEng) or CD105, a cell-surface coreceptor for transforming growth factor(TGF)-β1 and TGF-β3 isoforms, is also elevatedin the sera of preeclamptic women. The concen-tration of this molecule correlates with the diseaseseverity and diminishes after delivery [Venkateshaet al. 2006]. sEng impairs binding of TGF-b1 toits receptors and downstream signaling includingeffects on activation of eNOS and vasodilation,suggesting that sEng leads to dysregulated TGF-b signaling in the vasculature, contributing tothe endothelial dysfunction characteristic of PE[Venkatesha et al. 2006].
Besides the placental factors already explained,there are environmental factors such as insulinresistance and subclinical infections that couldalso contribute to an increased inflammatoryresponse early in pregnancy, and consequently tothe development of endothelial dysfunction andPE. Recently, in two nested case-control stud-ies that involved an important sample of womenwith PE [Garcia et al. 2007; Sierra-Laguadoet al. 2007] we reported increased levels ofC-reactive protein (CRP), leukocytes count andinsulin resistance using the homeostatic modelassessment (HOMA); risk factors that precedethe development of the clinical manifestationsof PE. These alterations were evident as early
as in the first trimester of gestation. Moreover,both, high CRP and increased HOMA were asso-ciated with a decreased FMD; which suggeststhat inflammation associated to infection and/orinsulin resistance might also be an importantcause of the endothelial dysfunction that precedesthe development of PE.
Implications in the management of PESince huge differences in the PE incidence andmortality are observed between developed anddeveloping countries, the understanding of thedifferent mechanisms that result in an alterationin the L-arginine-NO pathway and endothelialdysfunction is highly important because of itsimplications in the preventive and therapeuticalapproaches. For instance, the maternal mortal-ity by PE in UK is about 10/100,000 deliveriesand in Colombia is about 176/100,000 deliver-ies [Lopez-Jaramillo, 2000; WHO InternationalCollaborative Study of Hypertensive Disordersof Pregnancy, 1998]. These enormous differ-ences are probably related with the quality ofprenatal care, and with the demonstration thatin developing countries the nutritional deficien-cies and the subclinical chronic infections inpregnant women have a higher prevalence thanin developed countries [Lopez-Jaramillo et al.2005]. This situation has been already solved indeveloped countries where the major risk fac-tors for the PE are genetic and immunologi-cal alterations [Lopez-Jaramillo et al. 2005]. Insupport of this proposal, we have demonstratedthat ADMA, in our population, has no respon-sibility in the development of PE [Maas et al.2004; Lopez-Jaramillo et al. 1996]. However, indeveloped countries, it is an important factorthat inhibits the endothelial production of NO[Savvidou et al. 2003; Ellis et al. 2001; Holdenet al. 1998; Fickling et al. 1993]. This contradic-tory situation may be related with the fact thatthe high incidence of infection dilutes the role ofADMA in our population [Lopez-Jaramillo et al.2005]. Preventive interventions to decrease therisk of PE, such as supplementation with calcium[Lopez-Jaramillo, 1996; Lopez-Jaramillo et al.1997, 1995, 1990, 1989], conjugated linoleic acid[Herrera et al. 2005], early diagnosis, and treat-ment of infections [Herrera et al. 2001], seemto be more determining in clinical trials con-ducted in developing countries. It is possible thatby improving the prenatal care system in undevel-oped countries, the prevalence of PE comes to besimilar to that observed in developed countries.Therefore, to demonstrate this proposal, an
270 http://tac.sagepub.com
at Katholieke Univ Leuven on March 26, 2014tak.sagepub.comDownloaded from

Review
international collaborative study comparing thesimilarities and differences in the incidence ofthe risk factors for PE between developed andundeveloped countries is necessary. Moreover,such a study will provide further insights aboutthe role of the L-arginine-NO pathway in theetiology of PE.
ConclusionsDuring pregnancy the adaptative hemodynamicchanges are mediated by a higher productionof NO and bioactivity of the L-arginine-NOpathway. To guarantee the correct production ofNO, different factors such as nutrition, infections,genetic alteration, metabolism, placentation, andmaybe ethnical aspects must be considered. Analteration in the NO production or its activityis associated with the development of PE. Boththe understanding of the etiology of PE and therole played by the differences in the environ-mental factors between developed and developingcountries, should be a research priority.
AcknowledgmentWe would like to thank Jean Noël Guillemot forhis contribution to the correction of the Englishstyle.
The authors would like to acknowledge Colcien-cias for the financial support to the VILANOGroup (Grant N. 6566-04-18061). MelvinRincón received a young investigator grant forColciencias.
Conflict of interest statementNone declared.
ReferencesAlexander, B.T., Llinas, M.T., Kruckeberg, W.C. andGranger, J.P. (2004) L-Arginine attenuateshypertension in pregnant rats with reduced uterineperfusion pressure. Hypertension 43: 832–836.
Aydin, S., Benian, A., Madazli, R., Uludag, S.,Uzun, H. and Kaya, S. (2004) Plasmamalondialdehyde, superoxide dismutase, sE-selectin,fibronectin, endothelin-1 and nitric oxide levels inwomen with preeclampsia. Eur J Obstet GynecolReprod Biol 113: 21–25.
Baksu, B., Davas, I., Baksu, A., Akyol, A. andGulbaba, G. (2005) Plasma nitric oxide, endothelin-1and urinary nitric oxide and cyclic guanosinemonophosphate levels in hypertensive pregnantwomen. Int J Gynaecol Obstet 90: 112–117.
Baylis, C., Beinder, E., Suto, T. and August, P. (1998)Recent insights into the roles of nitric oxide andrenin-angiotensin in the pathophysiology ofpreeclamptic pregnancy. Semin Nephrol 18: 208–230.
Begum, S.,Yamasaki, M. and Mochizuki, M. (1996)Urinary levels of nitric oxide metabolites in normalpregnancy and preeclampsia. J Obstet Gynaecol Res22: 551–559.
Berkowitz, D.E., White, R., Li, D., Minhas, K.M.,Cernetich, A., Kim, S. et al. Arginase reciprocallyregulates nitric oxide synthase activity andcontributes to endothelial dysfunction in aging bloodvessels. Circulation 108: 2000–2006.
Biri, A., Bozkurt, N., Gunaydin, G., Korucuoglu, U.,Durak, I. and Kavutcu, M. (2007) Antioxidantenzyme activities and lipid peroxidation inpreeclampsia. Int J Gynaecol Obstet 96: 196–197.
Brockelsby, J., Hayman, R., Ahmed, A., Warren, A.,Johnson, I. and Baker, P. (1999) VEGF via VEGFreceptor-1 (Flt-1) mimics preeclamptic plasma ininhibiting uterine blood vessel relaxation inpregnancy: implications in the pathogenesis ofpreeclampsia. Lab Invest 79: 1101–1111.
Celik, O., Hascalik, S. and Turkoz,Y. (2003) cFN andNO levels as indexes of endothelial damage inpre-eclampsia. Int J Gynaecol Obstet 81: 51–52.
Celik, O., Hascalik, S., Turkoz,Y., Hascalik, M. andGokdeniz, R. (2003) Cerebrospinal fluid nitric oxidelevel changes in preeclampsia. Eur J Obstet GynecolReprod Biol 111: 141–145.
Chamy, V.M., Lepe, J., Catalan, A., Retamal, D.,Escobar, J.A. and Madrid, E.M. (2006) Oxidativestress is closely related to clinical severity ofpre-eclampsia. Biol Res 39: 229–236.
Chesley, L.C. (1972) Plasma and red cell volumesduring pregnancy. Am J Obstet Gynecol 112:440–450.
Cockell, A.P. and Poston, L. (1997) Flow-mediatedvasodilatation is enhanced in normal pregnancy butreduced in preeclampsia. Hypertension 30: 247–251.
Conrad, K.P., Kerchner, L.J. and Mosher, M.D.(1999) Plasma and 24-h NO(x) and cGMP duringnormal pregnancy and preeclampsia in women on areduced NO(x) diet. Am J Physiol 277: F48–F57.
D’Anna, R., Baviera, G., Corrado, F., Crisafulli, A.,Ientile, R., Buemi, M. et al. (2004) Neurokinin B andnitric oxide plasma levels in pre-eclampsia andisolated intrauterine growth restriction. BJOG 111:1046–1050.
Davidge, S.T., Stranko, C.P. and Roberts, J.M.(1996) Urine but not plasma nitric oxide metabolitesare decreased in women with preeclampsia. Am JObstet Gynecol 174: 1008–1013.
Dechend, R., Homuth, V., Wallukat, G., Kreuzer, J.,Park, J.K., Theuer, J. et al. AT(1) receptor agonisticantibodies from preeclamptic patients cause vascularcells to express tissue factor. Circulation 101:2382–2387.
Deng, A., Engels, K. and Baylis, C. (1996) Impact ofnitric oxide deficiency on blood pressure andglomerular hemodynamic adaptations to pregnancy inthe rat. Kidney Int 50: 1132–1138.
http://tac.sagepub.com 271
at Katholieke Univ Leuven on March 26, 2014tak.sagepub.comDownloaded from

Therapeutic Advances in Cardiovascular Disease
Diedrich, F., Renner, A., Rath, W., Kuhn, W. andWieland, E. (2001) Lipid hydroperoxides and freeradical scavenging enzyme activities in preeclampsiaand HELLP (hemolysis, elevated liver enzymes, andlow platelet count) syndrome: no evidence forcirculating primary products of lipid peroxidation.Am J Obstet Gynecol 185: 166–172.
Diejomaoh, F.M., Omu, A.E., Al Busiri, N., Taher, S.,Al Othman, S., Fatinikun, T. et al. (2004)Nitric oxideproduction is not altered in preeclampsia. ArchGynecol Obstet 269: 237–243.
Dorup, I., Skajaa, K. and Sorensen, K.E. (1999)Normal pregnancy is associated with enhancedendothelium-dependent flow-mediated vasodilation.Am J Physiol 276: H821–H825.
Egerman, R.S., Andersen, R.N., Manejwala, F.M.and Sibai, B.M. (1999) Neuropeptide Y and nitritelevels in preeclamptic and normotensive gravidwomen. Am J Obstet Gynecol 181: 921–923.
Ellis, J., Wennerholm, U.B., Bengtsson, A., Lilja, H.,Pettersson, A., Sultan, B. et al. (2001) Levels ofdimethylarginines and cytokines in mild and severepreeclampsia. Acta Obstet Gynecol Scand 80:602–608.
Facchinetti, F., Longo, M., Piccinini, F., Neri, I. andVolpe, A. (1999) L-Arginine infusion reduces bloodpressure in preeclamptic women through nitric oxiderelease. J Soc Gynecol Invest 6: 202–207.
Facchinetti, F., Saade, G.R., Neri, I., Pizzi, C.,Longo, M. and Volpe, A. (2007) L-argininesupplementation in patients with gestationalhypertension: a pilot study. Hypertens Preg 26:121–130.
Felix, C., Lopez, A., Delgado, F., Amores, E.,Narvaez, M. and Lopez-Jaramillo, P. (1991) Vascularprostacyclin production in Andean women withpregnancy-induced hypertension. Braz J Med Biol Res24: 59–62.
Fickling, S.A., Williams, D., Vallance, P., Nussey, S.S.and Whitley, G.S. (1993) Plasma concentrations ofendogenous inhibitor of nitric oxide synthesis innormal pregnancy and pre-eclampsia. Lancet 342:242–243.
Garcia, R.G., Celedon, J., Sierra-Laguado, J.,Alarcon, M.A., Luengas, C., Silva, F. et al. (2007)Raised C-reactive protein and impairedflow-mediated vasodilation precede the developmentof preeclampsia. Am J Hypertens 20: 98–103.
Gilbert, J.S., Ryan, M.J., La Marca, B.B., Sedeek,M.H., Murphy, S.R. and Granger, J.P. (2007)Pathophysiology of hypertension during preeclampsia:linking placental ischemia with endothelialdysfunction. Am J Physiol Heart Circ Physiol 294:H541–H550.
Hata,T., Hashimoto, M., Kanenishi, K., Akiyama, M.,Yanagihara, T. and Masumura, S. (1999) Maternalcirculating nitrite levels are decreased in bothnormal normotensive pregnancies and pregnancieswith preeclampsia. Gynecol Obstet Invest 48:93–97.
Heilmann, L. (1987) Blood rheology and pregnancy.Baillieres Clin Haematol 1: 777–799.
Herrera, J.A., Arevalo-Herrera, M.,Shahabuddin, A.K., Ersheng, G., Herrera, S.,Garcia, R.G. et al. (2006) Calcium and conjugatedlinoleic acid reduces pregnancy-induced hypertensionand decreases intracellular calcium in lymphocytes.Am J Hypertens 19: 381–387.
Herrera, J.A., Chaudhuri, G. and Lopez-Jaramillo, P.(2001) Is infection a major risk factor forpreeclampsia? Med Hypotheses 57: 393–397.
Herrera, J.A., Parra, B., Herrera, E., Botero, J.E.,Arce, R.M., Contreras, A. et al. (2007) Periodontaldisease severity is related to high levels of C-reactiveprotein in pre-eclampsia. J Hypertens 25: 1459–1464.
Herrera, J.A., Shahabuddin, A.K., Ersheng, G.,Wei,Y., Garcia, R.G. and Lopez-Jaramillo, P. (2005)Calcium plus linoleic acid therapy forpregnancy-induced hypertension. Int J GynaecolObstet 91: 221–227.
Hill, J.A., Devoe, L.D. and Bryans Jr, C.I. (1986)Frequency of asymptomatic bacteriuria inpreeclampsia. Obstet Gynecol 67: 529–532.
Holden, D.P., Fickling, S.A., Whitley, G.S. andNussey, S.S. (1998) Plasma concentrations ofasymmetric dimethylarginine, a natural inhibitor ofnitric oxide synthase, in normal pregnancy andpreeclampsia. Am J Obstet Gynecol 178: 551–556.
Joffe, G.M., Esterlitz, J.R., Levine, R.J.,Clemens, J.D., Ewell, M.G., Sibai, B.M. et al. (1998)The relationship between abnormal glucose toleranceand hypertensive disorders of pregnancy in healthynulliparous women. Calcium for PreeclampsiaPrevention (CPEP) Study Group. Am J ObstetGynecol 179: 1032–1037.
Kharb, S. (2000) Low whole blood glutathione levelsin pregnancies complicated by preeclampsia anddiabetes. Clin Chim Acta 294: 179–183.
Kovasc, A.G., Makary, A., Peto, J. and Steinmetz, G.(1994) Deficiency of cGMP level in placentalcirculation in pregnancy-induced hypertensivedisorders: possibility of decreasedendothelium-derived relaxing factor. Hypertens Pregn13: 163–169.
Kuzkaya, N., Weissmann, N., Harrison, D.G. andDikalov, S. (2003) Interactions of peroxynitrite,tetrahydrobiopterin, ascorbic acid, and thiols:implications for uncoupling endothelial nitric-oxidesynthase. J Biol Chem 278: 22546–22554.
Lees, M.M., Taylor, S.H., Scott, D.B. and Kerr, M.G.(1974) A study of cardiac output at rest throughoutpregnancy. J Obstet Gynaecol Br Commonw 74:319–328.
Levine, R.J., Maynard, S.E., Quian, C., Lim, K.H.,England, L.J.,Yu, K.F. et al. (2004) Circulatingangiogenic factors and the risk of preeclampsia.N Engl J Med 350: 672–683.
Li, H., Meininger, C.J., Hawker Jr, J.R., Haynes, T.E.,Kepka-Lenhart, D., Mistry, S.K. et al. (2001)
272 http://tac.sagepub.com
at Katholieke Univ Leuven on March 26, 2014tak.sagepub.comDownloaded from

Review
Regulatory role of arginase I and II in nitric oxide,polyamine, and proline syntheses in endothelial cells.Am J Physiol Endocrinol Metab 280: E75–82.
Li, N. and Karin, M. (1999) Is NF-kappaB thesensor of oxidative stress? FASEB J 13: 1137–1143.
Lopez-Jaramillo, P. (1996) Prevention ofpreeclampsia with calcium supplementation and itsrelation with the L-arginine:nitric oxide pathway. BrazJ Med Biol Res 29: 731–741.
López-Jaramillo, P. (2000) Calcium, nitric oxide andpreclampsia. Sem Perinatol 24: 33–36.
Lopez-Jaramillo, P., Casas, J.P. and Serrano, N.(2001) Preeclampsia: from epidemiologicalobservations to molecular mechanisms. Braz J MedBiol Res 34: 1227–1235.
Lopez-Jaramillo, P., Delgado, F., Jacome, P.,Teran, E., Ruano, C. and Rivera, J. (1997) Calciumsupplementation and the risk of preeclampsia inEcuadorian pregnant teenagers. Obstet Gynecol 90:162–167.
Lopez-Jaramillo, P., García, R. and Silva, F. (2005)Asymetric Dimethylarginine (ADMA):patophysiological reality or biological curiosity. InHernandez-Hernandez, R., Armas-Hernandez, M.(ed.), Current advances in hypertension, EditorialMonduzzi: Bologna, pp. 57–62.
Lopez-Jaramillo, P., Garcia, R.G. and Lopez, M.(2005) Preventing pregnancy-induced hypertension:are there regional differences for this global problem?J Hypertens 23: 1121–1129.
Lopez-Jaramillo, P., Gonzalez, M.C., Palmer, R.M.and Moncada, S. (1990) The crucial role ofphysiological Ca2+ concentrations in the productionof endothelial nitric oxide and the control of vasculartone. Br J Pharmacol 101: 489–493.
Lopez-Jaramillo, P., Narvaez, M., Calle, A., Rivera, J.,Jacome, P., Ruano, C. et al. (1996) Cyclic guanosine3’,5’ monophosphate concentrations in pre-eclampsia:effects of hydralazine. Br J Obstet Gynaecol 103:33–38.
Lopez-Jaramillo, P., Narvaez, M., Felix, C. andLopez, A. (1990) Dietary calcium supplementationand prevention of pregnancy hypertension. Lancet335: 293.
Lopez-Jaramillo, P., Narvaez, M., Felix, C., Sosa, C.,Calle, A., Nava, E. et al. (1992) Decreased nitricoxide synthesis in Andean Ecuadorian women withpregnancy-induced hypertension. Biology of nitricoxide, Portland Press: London, p. 376.
Lopez-Jaramillo, P., Narvaez, M., Weigel, R.M.and Yepez, R. (1989) Calcium supplementationreduces the risk of pregnancy-induced hypertensionin an Andes population. Br J Obstet Gynaecol 96:648–655.
Lopez-Jaramillo, P., Teran, E. and Moncada, S.(1995) Calcium supplementation preventspregnancy-induced hypertension by increasing theproduction of vascular nitric oxide. Med Hypotheses45: 68–72.
López-Jaramillo, P.,Teran, E., Ringgvist, A., Moya,W.,Rivera, J. and Berrazueta, J.R. (1998) Oxidisedlow-density lipoproteins and nitric oxide duringnormal pregnancy and preeclampsia. InMoncada, S.,Toda, N., Maeda, H., Higgs, E.A. (ed.),Biology of nitric oxide, Part 6. Portland Press:London, p. 322.
Lowe, D.T. (2000) Nitric oxide dysfunction in thepathophysiology of preeclampsia. Nitric Oxide 4:441–458.
Lund, C.J. and Donovan, J.C. (1967) Blood volumeduring pregnancy. Significance of plasma and red cellvolumes. Am J Obstet Gynecol 98: 394–403.
Maas, R., Boger, R.H., Schwedhelm, E., Casas, J.P.,Lopez-Jaramillo, P., Serrano, N. et al. (2004) Plasmaconcentrations of asymmetric dimethylarginine(ADMA) in Colombian women with pre-eclampsia.JAMA 291: 823–824.
Madazli, R., Benian, A., Gumustas, K., Uzun, H.,Ocak, V. and Aksu, F. (1999) Lipid peroxidation andantioxidants in preeclampsia. Eur J Obstet GynecolReprod Biol 85: 205–208.
Makkonen, N., Heinonen, S., Hongisto, T.,Penttila, I. and Kirkinen, P. (2002) Normalization ofvasoactive changes in preeclampsia precedes clinicalrecovery. Hypertens Pregnancy 21: 51–64.
Many, A., Hubel, C.A., Fisher, S.J., Roberts, J.M.and Zhou,Y. (2000) Invasive cytotrophoblastsmanifest evidence of oxidative stress in preeclampsia.Am J Pathol 156: 321–331.
Maynard, S.E., Min, J.Y., Merchan, J., Lim, K.H.,Li, J., Mondal, S. et al. (2003) Excess placentalsoluble fms-like tyrosine kinase 1 (sFlt1) maycontribute to endothelial dysfunction, hypertension,and proteinuria in preeclampsia. J Clin Invest 111:649–658.
McCord, N., Ayuk, P., McMahon, M., Boyd, R.C.,Sargent, I. and Redman, C. (2006) System y+arginine transport and NO production in peripheralblood mononuclear cells in pregnancy andpreeclampsia. Hypertension 47: 109–115.
Metcalfe, J. and Ueland, K. (1974) Maternalcardiovascular adjustments to pregnancy. ProgCardiovasc Dis 16: 363–374.
Moncada, S., Higgs, Hodson, H.F., Knowles, R.G.,López-Jaramillo, P., McCall, T. et al. (1991) TheL-arginine: nitric oxide pathway. Journal ofCardiovascular Pharmacology 17: s1–s9.
Moutquin, J.M., Rainville, C., Giroux, L.,Raynauld, P., Amyot, G., Bilodeau, R. et al. (1985)A prospective study of blood pressure in pregnancy:prediction of preeclampsia. Am J Obstet Gynecol 151:191–196.
Mutlu-Turkoglu, U., Aykac-Toker, G.,Ibrahimoglu, L., Ademoglu, E. and Uysal, M. (1999)Plasma nitric oxide metabolites and lipid peroxidelevels in preeclamptic pregnant women before andafter delivery. Gynecol Obstet Invest 48:247–250.
http://tac.sagepub.com 273
at Katholieke Univ Leuven on March 26, 2014tak.sagepub.comDownloaded from

Therapeutic Advances in Cardiovascular Disease
Myatt, L. and Cui, X. (2004) Oxidative stress in theplacenta. Histochem Cell Biol 122: 369–382.
Myatt, L., Rosenfield, R.B., Eis, A.L.W.,Brockman, D.E., Greer, I. and Lyall, F. (1996)Nitrotyrosine residues in placenta. Evidence ofperoxynitrite formation and action. Hypertension 28:488–493.
Neri, I., Marietta, M., Piccinini, F., Volpe, A. andFacchinetti, F. (1998) The L-arginine-nitric oxidesystem regulates platelet aggregation in pregnancy.J Soc Gynecol Invest 5: 192–196.
Neri, I., Mazza, V., Galassi, M.C., Volpe, A. andFacchinetti, F. (1996) Effects of L-arginineon utero-placental circulation in growth-retarded fetuses. Acta Obstet Gynecol Scand 75:208–212.
Neri, I., Piccinini, F., Marietta, M., Facchinetti, F.and Volpe, A. (2000) Platelet responsiveness toL-arginine in hypertensive disorders of pregnancy.Hypertens Pregnancy 19: 323–330.
Nishikawa, S., Miyamoto, A.,Yamamoto, H.,Ohshika, H. and Kudo R. (2000) The relationshipbetween serum nitrate and endothelin-1concentrations in preeclampsia. Life Sci 67:1447–1454.
Noris, M., Perico, N. and Remuzzi, G. (2005)Mechanisms of disease: pre-eclampsia. Nat Clin PractNephrol 1: 98–114.
Noris, M., Todeschini, M., Cassis, P., Pasta, F.,Cappellini, A., Bonazzola, S. et al. (2004) L-argininedepletion in preeclampsia orients nitric oxide synthasetoward oxidant species. Hypertension 43: 614–622.
Norris, L.A., Higgins, J.R., Darling, M.R., Walshe, J.J.and Bonnar, J. (1999) Nitric oxide in theuteroplacental, fetoplacental, and peripheralcirculations in preeclampsia. Obstet Gynecol 93:958–963.
Pasaoglu, H., Bulduk, G., Ogus, E., Pasaoglu, A. andOnalan, G. (2004) Nitric oxide, lipid peroxides, anduric acid levels in pre-eclampsia and eclampsia.Tohoku J Exp Med 202: 87–92.
Radi, R., Beckman, J.S., Bush, K.M. andFreeman, B.A. (1991) Peroxynitrite-inducedmembrane lipid peroxidation: the cytotoxic potentialof superoxide and nitric oxide. Arch Biochem Biophys288: 481–487.
Ranta, V., Viinikka, L., Halmesmaki, E. andYlikorkala, O. (1999) Nitric oxide production withpreeclampsia. Obstet Gynecol 93: 442–445.
Ronson, R.S., Nakamura, M. and Vinten-Johansen, J.(1999) The cardiovascular effects and implications ofperoxynitrite. Cardiovasc Res 44: 47–59.
Rumbold, A., Duley, L., Crowther, C. andHaslam, R. (2007) Antioxidants for preventingpre-eclampsia (Cochrane Review). In TheCochrane Library, Issue 4, Update Software: Oxford.
Saarelainen, H., Laitinen, T., Raitakari, O.T.,Juonala, M., Heiskanen, N., Lyyra-Laitinen, T. et al.
(2006) Pregnancy-related hyperlipidemia andendothelial function in healthy women. Circ J 70:768–772.
Sagol, S., Ozkinay, E. and Ozsener, S. (1999)Impaired antioxidant activity in women withpre-eclampsia. Int J Gynaecol Obstet 64:121–127.
Sankaraligam, S., Arenas, I.A., Lalu, M.M. andDavidge, S.T. (2006) Preeclampsia: currentunderstanding of the molecular basis of vasculardysfunction. Expert Rev Mol Med 8: 1–20.
Savvidou, M.D., Hingorani, A.D., Tsikas, D.,Frolich, J.C., Vallance, P. and Nicolaides, K.H.(2003) Endothelial dysfunction and raised plasmaconcentrations of asymmetric dimethylarginine inpregnant women who subsequently developpre-eclampsia. Lancet 361: 1511–1517.
Savvidou, M.D., Kametas, N.A., Donald, A.E. andNicolaides, K.H. (2000) Non-invasive assessment ofendothelial function in normal pregnancy. UltrasoundObstet Gynecol 15: 502–507.
Schiessl, B., Strasburger, C., Bidlingmaier, M.,Mylonas, I., Jeschke, U., Kainer, F. et al. (2006)Plasma- and urine concentrations of nitrite/nitrateand cyclic Guanosinemonophosphate in intrauterinegrowth restricted and preeclamptic pregnancies. ArchGynecol Obstet 274: 150–154.
Schneider, F., Lutun, P., Baldauf, J.J., Quirin, L.,Dreyfus, M., Ritter, J. et al. (1996) Plasma cyclicGMP concentrations and their relationship withchanges of blood pressure levels in pre-eclampsia.Acta Obstet Gynecol Scand 75: 40–44.
Seligman, S.P., Buyon, J.P., Clancy, R.M.,Young, B.K. and Abramson, S.B. (1994) The role ofnitric oxide in the pathogenesis of preeclampsia.Am J Obstet Gynecol 171: 944–948.
Serdar, Z., Gur, E., Develioglu, O., Colakogullari, M.and Dirican, M. (2002) Placental and decidual lipidperoxidation and antioxidant defenses inpreeclampsia. Lipid peroxidation in preeclampsia.Pathophysiology 9: 21–25.
Serrano, N.C., Casas, J.P., Diaz, L.A., Paez, C.,Mesa, C.M., Cifuentes, R. et al. (2004) EndothelialNO synthase genotype and risk of preeclampsia: amulticenter case-control study. Hypertension 44:702–707.
Shaamash, A.H., Elsnosy, E.D., Makhlouf, A.M.,Zakhari, M.M., Ibrahim, O.A. and EL dien, H.M.(2000) Maternal and fetal serum nitric oxide (NO)concentrations in normal pregnancy, pre-eclampsiaand eclampsia. Int J Gynaecol Obstet 68: 207–214.
Sharma, J.B., Sharma, A., Bahadur, A., Vimala, N.,Satyam, A. and Mittal, S. (2006) Oxidative stressmarkers and antioxidant levels in normal pregnancyand pre-eclampsia. Int J Gynaecol Obstet 94: 23–27.
Sierra-Laguado, J., Garcia, R.G. andLopez-Jaramillo, P. (2006) Flow-mediated dilatationof the brachial artery in pregnancy. Int J GynaecolObstet 93: 60–61.
274 http://tac.sagepub.com
at Katholieke Univ Leuven on March 26, 2014tak.sagepub.comDownloaded from

Review
Sierra-Laguado, J., Garcia, R.G., Celedon, J.,Arenas-Mantilla, M., Pradilla, L.P., Camacho, P.A.et al. (2007) Determination of insulin resistance usingthe homeostatic model assessment (HOMA)and its relation with the risk of developingpregnancy-induced hypertension. Am J Hypertens20: 437–442.
Silver, R.K., Kupferminc, M.J., Russell, T.L.,Adler, L., Mullen, T.A. and Caplan, M.S. (1996)Evaluation of nitric oxide as a mediator ofsevere preeclampsia. Am J Obstet Gynecol 175:1013–1017.
Sladek, S.M., Magness, R.R. and Conrad, K.P.(1997) Nitric oxide and pregnancy. Am J Physiol 272:R441–R463.
Slaghekke, F., Dekker, G. and Jeffries, B. (2006)Endogenous inhibitors of nitric oxide andpreeclampsia: a review. J Matern Fetal Neonatal Med19: 447–452.
Staff, A.C., Berge, L., Haugen, G., Lorentzen, B.,Mikkelsen, B. and Henriksen, T. (2004) Diettarysupplementation with L-arginine or placebo inwomen with pre-eclampsia. Acta Obstet Gynecol Scand83: 103–107.
Steinert, J.R., Wyatt, A.W., Poston, L., Jacob, R. andMann, G.E. (2002) Preeclampsia is associated withaltered Ca2+ regulation and NO production inhuman fetal venous endothelial cells. FASEB J 16:721–723.
Takata, M., Nakatsuka, M. and Kudo, T. (2002)Differential blood flow in uterine, ophthalmic, andbrachial arteries of preeclamptic women. ObstetGynecol 100: 931–939.
Taylor, D.J. and Lind, T. (1979) Red cell mass duringand after normal pregnancy. Br J Obstet Gynaecol 86:364–370.
Teran, E., Escudero, C. and Moya, W. (2006)Abnormal release of nitric oxide from nitrosoproteinin preeclampsia. Int J Gynaecol Obstet 92: 260–261.
Teran, E., Escudero, C., Vivero, S., Enriquez, A. andCalle, A. (2004) Intraplatelet cyclicguanosine-3′,5′-monophosphate levels duringpregnancy and preeclampsia. Hypertens Pregnancy 23:303–308.
Toth, M. (2002) Role of tetrahydrobiopterin in theregulation of activity of human placental nitric oxidesynthase in normal and pre-eclamptic pregnancies.Orv Hetil 143: 391–398.
Trogstad, L.I., Eskild, A., Bruu, A.L., Jeansson, S.and Jenum, P.A. (2001) Is preeclampsia aninfectious disease? Acta Obstet Gynecol Scand 80:1036–1038.
Var, A.,Yildirim,Y., Onur, E., Kuscu, N.K.,Uyanik, B.S., Goktalay, K. et al. (2003) Endothelialdysfunction in preeclampsia. Increased homocysteineand decreased nitric oxide levels. Gynecol Obstet Invest56: 221–224.
Venkatesha, S., Toporsian, M., Lam, C., Hanai, J.,Mammoto, T., Kim,Y.M. et al. (2006) Soluble
endoglin contributes to the pathogenesis ofpreeclampsia. Nat Med 12: 642–649.
Vural, P. (2002) Nitric oxide/endothelin-1 inpreeclampsia. Clin Chim Acta 317: 65–70.
Walker, J.J. (2000) Pre-eclampsia. Lancet 356:1260–1265.
Williams, D.J., Vallance, P.J., Neild, G.H.,Spencer, J.A. and Imms, F.J. (1997) Nitricoxide-mediated vasodilation in human pregnancy.Am J Physiol 272: H748–H752.
World Health Organization (2004) Maternal mortalityin 2000: estimates developed by WHO, UNICEF andUNFPA.
World Health Organization InternationalCollaborative Study of Hypertensive Disorders ofPregnancy (1988) Geographic variation in theincidence of hypertension in pregnancy. Am J ObstetGynecol 158: 80–83.
World Health Organization. (1987) Technical ReportsSeries. The hypertensive disorders of pregnancy,Geneve.
Xia,Y., Dawson, V.L., Dawson, T.M., Snyder, S.H.amd Zweier, J.L. (1996) Nitric oxide synthasegenerates superoxide and nitric oxide inarginine-depleted cells leading toperoxynitritemediated cellular injury. Proc Natl AcadSci USA 93: 6770–6774.
Xia,Y., Wen, H., Bobst, S., Day, M.C. andKellems, R.E. (2003) Maternal autoantibodies frompreeclamptic patients activate angiotensin receptorson human trophoblast cells. J Soc Gynecol Investig10: 82–93.
Xiang, W., Chen, H., Xu, X., Zhang, M. and Jiang,R. (2005) Expression of endothelial nitric oxidesynthase traffic inducer in the placentas of womenwith pre-eclampsia. Int J Gynaecol Obstet 89:103–107.
Yamamoto, T., Suzuki,Y., Kojima, K. andSuzumori, K. (2005) Reduced flow-mediatedvasodilation is not due to a decrease in production ofnitric oxide in preeclampsia. Am J Obstet Gynecol192: 558–563.
Yanik, F.F., Amanvermez, R., Kocak, I.,Yanik, A. andCelik, C. (2001) Serum nitric oxide and glutathionelevels in preeclamptic and normotensive womenduring labor. Gynecol Obstet Invest 51: 110–115.
Visit SAGE journals onlinehttp://online.sagepub.com
Yao, D., Vlessidis, A.G. and Evmiridis, N.P. (2004)Determination of nitric oxide in biological samples.Microchimica Acta 147: 1–20.
Yoneyama,Y., Suzuki, S., Sawa, R., Miura, A.,Doi, D., Otsubo,Y. et al. (2002) Plasma nitric oxidelevels and the expression of P-selectin on plateletsin preeclampsia. Am J Obstet Gynecol 187:676–680.
Yoshida, A., Nakao, S., Kobayashi, M. andKobayashi, H. (2000) Flow-mediated vasodilationand plasma fibronectin levels in preeclampsia.Hypertension 36: 400–404.
http://tac.sagepub.com 275
at Katholieke Univ Leuven on March 26, 2014tak.sagepub.comDownloaded from