the microbiota and the gut-brain axis: insights from the temporal and spatial mucosal alterations...
TRANSCRIPT

Spatiotemporal maps reveal regional differences in the
effects on gut motility for Lactobacillus reuteri and
rhamnosus strains
R. Y. WU,* M. PASYK,* B. WANG,** P. FORSYTHE,*,�,§ J. BIENENSTOCK,*,� Y.-K. MAO,* P. SHARMA,*A. M. STANISZ* & W. A. KUNZE*,�,–
*McMaster Brain-Body Institute, St. Joseph’s Healthcare, Hamilton, ON, Canada
�Department of Medicine, McMaster University, Hamilton, ON, Canada
�Farncombe Family Digestive Health Research Institute, McMaster University, Hamilton, ON, Canada
§Firestone Institute for Respiratory Health, Hamilton, ON, Canada
–Department of Psychiatry and Behavioural Neurosciences, McMaster University, Hamilton, ON, Canada
**Centre for Simulation-Based Learning, Health Sciences Centre, McMaster University, Hamilton, ON, Canada
Abstract
Background Commensal bacteria such as probiotics
that are neuroactive acutely affect the amplitudes of
intestinal migrating motor complexes (MMCs). What
is lacking for an improved understanding of these
motility effects are region specific measurements of
velocity and frequency. We have combined intralu-
minal pressure recordings with spatiotemporal dia-
meter maps to analyze more completely effects of
different strains of beneficial bacteria on motility.
Methods Intraluminal peak pressure (PPr) was mea-
sured and video recordings made of mouse ex vivo
jejunum and colon segments before and after intra-
luminal applications of Lactobacillus rhamnosus
(JB-1) or Lactobacillus reuteri (DSM 17938). Migrating
motor complex frequency and velocity were calcu-
lated. Key Results JB-1 decreased jejunal frequencies
by 56% and 34% in colon. Jejunal velocities increased
171%, but decreased 31% in colon. Jejunal PPr
decreased by 55% and in colon by 21%. DSM 17938
increased jejunal frequencies 63% and in colon 75%;
jejunal velocity decreased 57%, but increased in colon
146%; jejunal PPr was reduced 26% and 12% in colon.
TRAM-34 decreased frequency by 71% and increased
velocity 200% for jejunum, but increased frequency
46% and velocity 50% for colon; PPr was decreased
59% for jejunum and 39% for colon. Conclusions &
Inferences The results show that probiotics and other
beneficial bacteria have strain and region-specific
actions on gut motility that can be successfully dis-
criminated using spatiotemporal mapping of diameter
changes. Effects are not necessarily the same in colon
and jejunum. Further research is needed on the
detailed effects of the strains on enteric neuron
currents for each gut region.
Keywords Lactobacilli, migrating motor complex,
motility, probiotics, spatiotemporal map.
INTRODUCTION
Ingestion of commensal and probiotic bacteria may
modulate gut motility to benefit the host. In general,
beneficial effects of ingestion may also include alter-
ations in the composition of the microbiome,1 changes
in rat enteric neuron function,2 alterations in mouse
brain neurochemistry and behavior,3,4 reduction in
blood pressure,5,6 increased anti-inflammatory and
immunoregulatory activity,7 and modulation of motil-
ity with reductions in either diarrhea or constipation.8
The cellular mechanisms through which these effects
are mediated are not clear. The influence of gastroin-
testinal commensals on motility is demonstrated from
studies of germfree mice 9,10 and those whose normal
bacterial community has been disrupted using
antibiotics.11–13
Address for Correspondence
Wolfgang A. Kunze, The McMaster Brain-Body Institute,T3306 Juravinski Innovation Tower, St Joseph’s Healthcare,50 Charlton Ave. East, Hamilton, ON L8N 4A6, Canada.Tel: +1 9055221155 ext. 35994; fax: +1 9055406593;e-mail: [email protected]: 21 September 2012Accepted for publication: 9 December 2012
Neurogastroenterol Motil (2013) 25, e205–e214 doi: 10.1111/nmo.12072
� 2013 Blackwell Publishing Ltd e205
Neurogastroenterology & Motility

Probiotics have been used therapeutically to help
treat motility disturbances in humans and experimen-
tal animals. Meta-analysis of the research literature
indicates that Lactobacillus species can be used to
treat diarrhea in adults or infants.14
Probiotic organisms decreased colon contraction
frequency and were used in double-blind controlled
studies to treat infectious (Lactobacillus reuteri DSM
1793815) or functional (Bifidobacterium lactis
HN01916) diarrhea in humans.15,16
DSM 17938 (DSM) gavage decreased rotavirus-in-
duced diarrhea in mice.17 It also reduced infantile colic
after 21 days oral administration18 in a randomized
double-blind controlled trial. Infantile colic is a well-
described common symptom in infants, but whether it
is due to spasm of smooth muscle in the colon or
jejunum is not known. It is plausible to suggest
beneficial effects in the reduction in pain might have
been due to decreased giant contractions of the small or
large bowel.19
Functional and slow transit constipation can occur
in infants or adulthood and is especially common in
the institutionalized elderly.20 Probiotics may be use-
ful in this condition. This would be particularly
important because few long-term effective treatments
for constipation exist, and those that are used often
have significant side effects.21 DSM supplementation
increased the frequency of bowel movements in
chronically constipated infants.22 Lactobacillus casei
Lcr35 was as effective as magnesium oxide in treating
children with chronic constipation,23 while Bifidobac-
terium breve decreased abdominal pain and fecal
incontinence while increasing defecation frequency
in chronically constipated children.24 In constipated
but otherwise healthy human adults, ingestion of
L. plantarum SN35N or SN13T strains increased
defecation frequency compared with control bacteria
(Lactococcus lactis A6 and Streptococcus thermo-
philes) in a randomized double-blind experimental
design.25 A mixture of Lactobacillus, Bifidobacterium,
and Streptococcus strains had a positive effect (reduced
diarrhea, constipation, and improved nutritional
status) on bowel movements among orthopedic reha-
bilitation in elderly (>80 years) patients.26
That microbiota can control or influence motility is
evident from the disruption of intestinal myoelectric
complexes of germfree rats.27 Conventionalization of
such animals with normal feces or even a single
bacterial strain restored adult type frequency of gut
motility complexes. It is not immediately obvious how
such studies add to the understanding of potential
therapeutic probiotic modulation of gut motility. Pro-
biotics do not need to colonize the gut to exert an effect
on the host and their action is transient requiring
regular repeated applications for the effect to be
maintained.28 Because of this, we have devised exper-
iments to study acute effects on motility, where the
bacteria are placed into the gut lumen,29 although
some investigators have added bacteria so that they
contact the serosa (intraperitoneal) rather than the
epithelial surface.30
To identify biomarkers for effective probiotics in a
mouse model for human diarrhea or constipation,31 it
would be desirable to differentiate between the effects
of different probiotic strains on gut contractions. The
motility effects of probiotics have been mainly mea-
sured using intraluminal pressure recordings from
ex vivo gut segments in modified Trendelenburg
preparations.2,29,32 In this way, the concentration of
bacteria or derived compounds can be controlled and
confounding influences of circulating hormones and
supra-intestinal autonomic reflexes are removed. Nine
day feeding of Lactobacillus rhamnosus (JB-1) to rats
decreased colon migrating motor complex (MMC)
amplitudes ex vivo,2 and this effect was reproduced
within 15 min of introducing the same bacterium into
the lumen of ex vivo segments of mouse jejunum.29
The dose responses obtained, suggest that, similar to
many therapeutic compounds, those produced by, or
emanating from JB-1, also have a dose dependent ‘drug-
like’ action on peristalsis.
The limitation of these approaches is that intralu-
minal pressure recordings sample a restricted informa-
tion set. They cannot measure parameters such as
MMC propagation velocity, or frequency when several
MMCs occur simultaneously. Neither do they readily
distinguish between MMCs and stationary contrac-
tions.33 Spatiotemporal maps constructed from video
movies of the contracting gut can overcome these
limitations because they do not record information
from a single locus. This allows spatial and temporal
patterns to be measured simultaneously.
For the present experiments, we have used ex vivo
segments of small and large mouse intestine to study
the effects of introducing intraluminal probiotic
bacteria on motility. We used DSM, a probiotic
strain with therapeutic effects in children and adults,
and JB-1 whose effects on rodent myenteric intestinal
primary afferent neurons have been previously stud-
ied.2 Lactobacillus salivarius and L. reuteri PTA
6475 were used as comparators and controls. Spatio-
temporal maps of motility were constructed from
video recordings before, during and after luminal
application of the bacteria, revealing motor patterns
which are not readily detected using other
methods.33
R. Y. Wu et al. Neurogastroenterology and Motility
� 2013 Blackwell Publishing Ltde206

METHODS
We used adult male Swiss Webster mice (20–30 g) from CharlesRiver Laboratories (Wilmington, MA, USA; http:// http://www.criver.com). The mice were killed by cervical dislocation,in line with McMaster guidelines for the use and care of animals.All ensuing procedures were ex vivo.
Organ bath motility recordings
Four or more centimeter long jejunal or distal colon segmentswere excised and the contents emptied by flushing the segmentwith Krebs saline under a 2 hPa gravity pressure head. Eachsegment was mounted in a 20-mL organ bath chamber andsubmerged in oxygenated Krebs (Fig. 1A). Oral and anal ends werecannulated, and the lumen was gravity perfused with carbogen-gassed Krebs using several Mariotte bottles.34 The intraluminalcompartment was perfused at 0.5 mL min)1 with room temper-ature buffer (19–22 �C) according to the precedent set by previousex vivo gut segment preparations29,32,35,36 for which MMC can berecorded without rundown for at least 2 h. Pilot experiments haveshown that raising the temperature to 34 �C decreases theduration for which steady-state MMCs could be recorded withoutrundown to 30 min; presumably because a higher mucosalmetabolic demand and the lack of a blood supply.
The organ chamber (serosal compartment) was perfused withprewarmed (34 �C), carbogen-gassed, Krebs solution at a rate of5 mL min)1). Oxygenated Krebs buffer was of the followingcomposition (mmol L)1): 118 NaCl, 4.8 KCl, 25 NaHCO3, 1.0NaH2PO4, 1.2 MgSO4, 11.1 glucose, and 2.5 CaCl2 bubbled withcarbogen gas (95% O2 and 5% CO2).At the beginning of theexperiment, intraluminal pressure was adjusted to 3 hPa byadjusting the heights of inflow and outflow tubes and therecordings were made at this filling pressure. Bacteria wereapplied by switching the oral luminal inflow from Krebs to Krebsplus 8.0 log cfu mL)129 bacteria by closing and opening theappropriate stopcocks, as illustrated in Fig. 1A.
Intraluminal pressure changes were measured at the midpointof the longitudinal axis of the gut segment using a Krebs-filled0.58-mm external diameter non-distensible polyethylene tube asdescribed in.32. The tube emerged from the anal and was attachedto a COBE pressure transducer (Sorin Biomedical Inc., Irvine, CA,USA). The pressure signal was amplified, digitized, stored on a PCcomputer, and analyzed off-line using PClamp 9 software (Molec-ular Devices; Sunnyvale, CA, USA).32 Peak phasic intraluminalpressure increases (PPr) were identified and measured as describedin.29
Images were recorded using a video camcorder (JVC EverioHard Disk Camcorder Model GZ-MG155U) which was placed10 cm above a gut segment (Fig. 1A). Recording was started insynchrony with the pressure recording using an 8–12 cm field of
CarbogenCarbogen
Stop cock
Pressure sensor connected to amplifier & recording system
Krebsinflow
Krebs outlfow
Krebs+ bacteria Krebs
Camera
Lumen
Perspex organ bath
Inflow tubeOutflow tube
Oral
Anal
Optical slice
2 hPa
30 s 0.4 cm
10 mm
30 s
A
B
C
D
Figure 1 Experimental setup for video and
pressure recordings. (A) Canulated intestinal
segment was maintained in preheated oxygen-
ated Krebs solution and additives are adminis-
tered through Mariotte inflow tubes. A pressure
sensor placed at the midpoint tracked the
intraluminal pressure, while a camera placed
atop captured videos of the intestinal move-
ment; (B) The spatiotemporal map was produced
via our StMap plugin which converts gut
diameter into black and white hues for repre-
sentation. Oral to anal black lines represent
contractions, lighter areas are relaxations. The
dotted line indicates the position of pressure
sensor; (C) Diameter changes at the dotted line;
(D) Pressure changes recorded at the dotted line.
Volume 25, Number 3, March 2013 Spatiotemporal maps: probiotic effects on motility
� 2013 Blackwell Publishing Ltd e207
view for the duration of the experiment. The camera output wasin raw video format (MOD) at 30 frames per second (fps). Ten-minute long video clips were excised from the MOD file usingvideo editing software (Avidemux version 2.5.0; http://www.avid-emux.org). The clips were then converted into the MOV formatusing a video converter (Zune converter version 1.1; http://ffmpeg.mplayerhq.hu). The final video clips were resampled to aresolution of 384 · 256 pixels and 25 fps.
Video recordings were analyzed using in-house image processingsoftware (StMap) developed as a plug-in for NIH ImageJ (version1.43c; NIH, Bethesda, MD, USA). The software converts the image(Fig. 1B) in each frame of the video into a black-and-whitesilhouette (Fig. 1C) and generates a spatiotemporal map using anedge detection routine. The routine first measures the diameter ateach position along the gut and then represents the physicaldiameter at each position as a hue value (ranges from 0 to 255,black–white). As gut diameter decreases during contractions, thehue value is reduced toward 0 and will be shown as darker values.As the software reads through each 10-min clip, it generates aspatiotemporal map – a pattern of alternating bands of light anddark hues that contains three sets of information: position along thegut, time, and gut diameter. Using these variables, the spatiotem-poral map becomes a motility ‘fingerprint’ whose sensitivity couldbe critically important in defining the detailed and perhaps nuancedeffects that specific bacterial strains could have on motility.
As the StMap measures the diameter changes at each position,StMap can be interpreted as a stacking of numerous 2D diametersvs time graphs. In fact, for a spatiotemporal map, if the location ofthe pressure transducer were identified (dotted line in Fig. 1B) andwere shown as a gray scale vs time graph (Fig. 1C), this graphwould be in register with the simultaneously recorded pressure vs
time recording at that locus (Fig. 1D). The diameter of the gut ateach point was plotted as a color as previously described byRoberts et al.36; and, for ease of visualization, 3D maps wereproduced by adding a z-axis that plotted the diameter (Fig 2A).
Motility parameters were measured from the spatiotemporalmap using the StMap plugin. Neurogenic, anally propagating,
migrating motor complexes MCs of the type described in Wanget al.29 generated thick dark bands that slant diagonally from leftto right. The propagation velocity (mm s)1) was measured fromthe slope of each band or trough in the each 3D map; the twomeasures are equivalent. For each treatment, slopes of 10–15successive MMCs were averaged to calculate the propagationvelocity. Migrating motor complex frequency (mHz) was calcu-lated by counting the number of MMCs during a 10-min segment.
Bacteria and drugs
JB-1 bacteria were taken from in-house stock (see Bravo et al.4)DSM18 and L. reuteri PTA 6475 (PTA 6475) were donated byBioGaia AB, Stockholm, Sweden. L. salivarius was a gift from theAlimentary Pharmabiotic Centre, University College Cork.37
Cell numbers were determined optically,38 and viability wasalways checked by ability to grow after plating on growth mediumagar plates. All other methods are as reported previously.2,38 Cellsfrom frozen stocks were thawed and centrifuged at 500 g for15 min, and the pellet was suspended in equal volume of Krebsbuffer. Then, the suspension was washed by centrifugation at thesame speed, and the cells were removed and resuspended in Krebsat the original concentration. Just prior to use, bacteria werediluted to a working concentration of 8 log cfu mL)1 in fresh Krebsbuffer.
Krebs containing bacteria were fed to the intraluminal com-partment while ion channel modulating drugs added to the Krebsbuffer perfusing the serosal compartment. The time required forthe drug solution to flow from the tap to the recording chamberwas 30 s. The intermediate conductance calcium-dependentpotassium (IKCa) ion channel blocker 1-[(2-chlorophenyl) diphe-nylmethyl]- 1H-pyrazole (TRAM-34) (Tocris Bioscience, Ellisville,MO, USA; http://www.tocris.com) distributed by Cedarlane Lab-oratories Ltd., Burlington, ON, Canada) was dissolved with puredimethyl sulphoxide (DMSO) to make 10-mmol L)1 stock solu-tions, and these were diluted in oxygenated Krebs to makeworking concentrations 30 min before use.
Statistics
Statistics were calculated using GraphPad Prism 5.0 (GraphPadSoftware, San Diego, CA, USA). Descriptive statistics are given asmeans ± SD, but in concentration-response plots, sampling errorsare displayed using SEM; the sample size is denoted by n. Thestatistically discernible difference for tests of significance was setat P = 0.05; all tests were paired t-test and two tailed.
RESULTS
Segments from 77 mice showed propagating MMC and
recordings were made from 43 jejunal and 34 distal
colonic segments taken from these animals. Migrating
motor complexes propagated in the oral to anal direc-
tion spanning from 50% to 100% of the ex vivo
segment. These contractions were in register with the
pressure pulses recorded by the intraluminal probe
when both were measured at the same locus (Fig. 1B).
Similar to Roberts et al.36 we also observed rare colonic
retrograde moving contractions, stationary or mixing
motility patterns or motor complexes that only prop-
agated for short distances (<50%); these were excluded
Krebs
Krebs + TTX
A
B
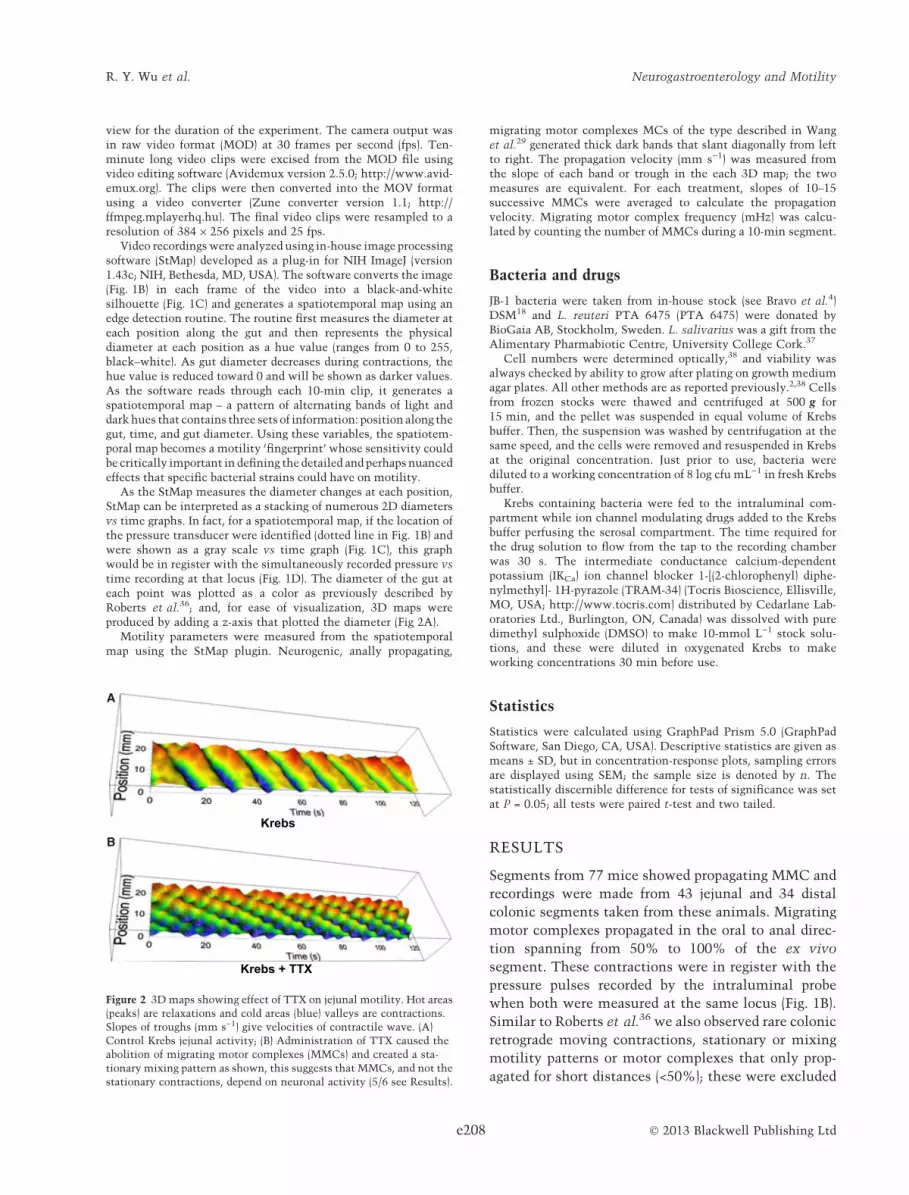
Figure 2 3D maps showing effect of TTX on jejunal motility. Hot areas
(peaks) are relaxations and cold areas (blue) valleys are contractions.
Slopes of troughs (mm s)1) give velocities of contractile wave. (A)
Control Krebs jejunal activity; (B) Administration of TTX caused the
abolition of migrating motor complexes (MMCs) and created a sta-
tionary mixing pattern as shown, this suggests that MMCs, and not the
stationary contractions, depend on neuronal activity (5/6 see Results).
R. Y. Wu et al. Neurogastroenterology and Motility
� 2013 Blackwell Publishing Ltde208

from analysis as they did not represent full MMCs nor
a repeatable and stable pattern.36 In no case (n = 8) did
application of TRAM-34 (serosally) or JB-1 (intralumi-
nally) convert these irregular patterns to conventional
MMCs as described by Roberts et al.36 Migrating
motor complex frequencies ranged for 8–14 mHz
which is comparable with Powell et al. 39 who reported
a MMC frequency of 8 mHz (1.5-min interevent inter-
val) in a similar ex vivo mouse gut preparation. Four
jejunal segments did not display anally propagating
MMCs but exhibited multiple stationary contractions
similar to those described by Gwynne et al.33 although
only when Krebs buffer was in the lumen. To test
whether stationary contractions are generated by the
enteric nervous system, we added 0.6 lmol L)1 TTX to
the Krebs buffer perfusing the serosal surface for six
jejunal segments. In 5/6 experiments, propulsive
MMCs were abolished and stationary, mixing-type
contractions developed (Fig. 2), suggesting that, in
mouse jejunum, MMCs, but not stationary contrac-
tions, are dependent on neural activity. Adding log
8 cfu mL)1 JB-1 to the lumen (n = 5) did not change the
stationary contractions nor convert them to propagat-
ing ones. The stationary contractions were not exam-
ined further.
To demonstrate the strain specificity of the motor
effects of specific bacteria, we tested additional bacte-
ria or candidate probiotics. Log 8 cfu mL)1 of the
bacteria were applied to the lumen for 30 min. The
anti-inflammatory probiotic bacteria L. salivarius,
which was without effect in a clinical trial in IBS,37
was also ineffective in previous jejunal motility exper-
iments.29 Another L. reuteri, PTA 6475 with potent
anti-inflammatory activity40 was also tested. In all, we
tested five jejunal and five colonic segments for each of
these bacterial strains. Neither L. salivarius nor PTA
6475 had any effect on MMC amplitudes, frequencies
or velocities (data not shown).
Intraluminal JB-1 and DSM modulated motility. The
onset latencies of the observed motor effects ranged
from 10 to 20 min and plateaued at 20–30 min, and the
effects were not reversible with 20 min Krebs
washout.29
Nine jejunal and seven colonic segments were
exposed to intraluminal JB-1 (Fig. 3): MMC frequencies
decreased (Krebs vs JB-1) from 41 ± 18 to 18 ± 8 mHz
(56%) (P = 0.004) for jejunum and from 14 ± 4.5 to
9.3 ± 5.0 mHz (34%) (P = 0.02) for colon. Migrating
motor complex velocities for jejunum increased from
1.7 ± 0.9 to 4.6 ± 1.8 mm s)1 (171%) (P = 0.004), but
decreased from 1.6 ± 0.5 to 1.1 ± 0.4 mm s)1 for colon
(31%) (P = 0.02). Jejunal PPr decreased from 17 ± 4.1 to
7.6 ± 4.4 hPa (55%) (P = 0.004), and also decreased
from 42 ± 4.1 to 33 ± 6.5 hPa (21%) (P = 0.03) for
colon.
Ten jejunal and seven colonic segments were
exposed to DSM (Fig. 4). Migrating motor complex
frequencies decreased from 51 ± 16 to 19 ± 16 mHz
(63%) (P = 0.008) for jejunum, but increased from
8.0 ± 4.7 to 14 ± 7.9 (75%) (P = 0.02) for colon. DSM
decreased jejunal MMC velocity from 2.0 ± 0.81 to
Krebs
JB-1
0
20
40
60
80
100Fr
eque
ncy
(mH
z)
Krebs
JB-1
0
2
4
6
8
10
Vel
ocity
(mm
s–1
)
PP
r (hP
a)
Krebs
JB-1
–10
0
10
20
30Fr
eque
ncy
(mH
z)
Krebs
JB1
0
5
10
15
20
25
Krebs
JB1
0.0
0.5
1.0
1.5
2.0
2.5
Vel
ocity
(mm
s–1
)
PP
r (hP
a)
Krebs
JB-1
0
20
40
60
Colon
** ** **
* * *
Krebs
Krebs + JB-1
JejunumA
B
C D E
F G H
Figure 3 Effects of JB1 on intestinal motility. (A) 3D map taken from
jejunal recording; (B) The administration of JB1 altered the frequency
and conduction velocity of the migrating motor complexes (MMCs);
(C–H) Summaries of before and after experiments. (C–E) For jejunum
JB1 reduced MMC frequency, increased MMC velocity, and reduced
MC peak pressure. (F–H) for colon JB-1 reduced MMC frequency (F),
reduced MMC velocity (G), and the MMC peak pressure (PPr) (H).
Volume 25, Number 3, March 2013 Spatiotemporal maps: probiotic effects on motility
� 2013 Blackwell Publishing Ltd e209

0.86 ± 1.5 mm s)1 (57%) (P = 0.04), but increased
velocity in colon from 1.3 ± 0.9 to 3.2 ± 1.6 mm s)1
(146%) (P = 0.02). PPr decreased from 12 ± 0.7 to
8.9 ± 3.0 (26%) (P = 0.08) hPa for jejunum and 42 ± 12
to 37 ± 6 hPa for colon (12%) (P = 0.1).
We have previously shown that heat-killed JB-1 had
no effect on mouse jejunum MMC PPr or frequency.29
However, we did not measure velocity in these exper-
iments and thus cannot exclude the possibility that
heat-killed bacteria somehow altered velocity without
affecting the other parameters. We thus used heat-
killed JB-1 (n = 5) and DSM (n = 5) to exclude this
possibility. Migrating motor complex frequencies
(mHz), velocities (mm s)1), and PPr (hPa) Krebs vs
heat-killed JB-1 were 41 ± 10 vs 45 ± 13 (P = 0.5),
1.5 ± 0.7 vs 1.3 ± 0.6 (P = 0.7), and 15 ± 4 vs 18 ± 4
(P = 0.3). The same parameters when DSM were
applied to the jejunum were as follows: 44 ± 5 vs
44 ± 8 (P = 0.9), 1.7 ± 0.5 vs 1.9 ± 0.6 (P = 0.7), and
15 ± 2 vs 16 ± 4 (P = 0.03).
TRAM-34 was added to the Krebs buffer perfusing
the serosal surface of eight jejunal and ten colonic
segments (Fig. 5). TRAM-34 changed rat jejunal pat-
terns of intraluminal pressure waves so that they were
less evenly spaced than for Krebs controls. The
contractions appeared to occur more in clusters with
longer intervals between clusters.41 Consistent with
these former observations, we found that intervals
between clustered jejunal MMC lengthened (Fig. 5A,B)
so that the average frequency of MMCs decreased from
34 ± 24 to 10 ± 6 mHz (71%) (P = 0.008). For colon the
MMC pattern remained the same after adding TRAM-
34, but there was an increase in frequency from
5.9 ± 4.3 to 8.6 ± 3.1 (46%) (P = 0.03). MMC velocity
was increased from 1.5 ± 0.7 to 4.5 ± 3.6 (200%)
(P = 0.04) for jejunum, and from 1.0 ± 0.3
to 1.5 ± 0.04 mm s)1 (50%) (P = 0.03) for colon.
**
** *
* *
*
Jejunum
Colon
Krebs
TRAM-340
20
40
60
80
100
Krebs
TRAM-340
5
10
15
Krebs
TRAM-340
5
10
15
20
25
Freq
uenc
y (m
Hz)
Krebs
TRAM-340
5
10
15
20
Krebs
TRAM-340.0
0.5
1.0
1.5
2.0
2.5
Vel
ocity
(mm
s–1
)
PP
r (hP
a)
Freq
uenc
y (m
Hz)
Vel
ocity
(mm
s–1
)
PP
r (hP
a)
Krebs
TRAM-340
20
40
60
80
A B C
D E F
Figure 5 Effects of TRAM-34 on intestinal motility. (A–C) TRAM-34
decreased jejunal migrating motor complex (MMC) frequency, in-
creased MMC velocity, and decreased intraluminal peak pressure (PPr).
(D–F) Colonic MMC frequency and velocity were increased by TRAM-
34, but PPr decreased.
Krebs
DSM0
20
40
60
80
Freq
uenc
y (m
Hz)
**
Krebs
DSM0
1
2
3
4
Vel
ocity
(mm
s–1
)
**
PP
r (hP
a)
Freq
uenc
y (m
Hz)
Vel
ocity
(mm
s–1
)
PP
r (hP
a)
Krebs
DSM0
5
10
15 ns
Jejunum
Krebs
DSM0
10
20
30 *
Krebs
DSM
0
2
4
6
8 *
Krebs
DSM0
20
40
60
80 nsKrebs + L. reuteri DSM 17938
Krebs
Colon
A B C
F
D
E
G H
Figure 4 Effects of DSM on intestinal motility. (A–C) DSM reduced
jejunal migrating motor complex (MMC) frequency, velocity, but not
MMC peak pressure (PPr). (D–E) Representative 3D maps representing
colon motility before (D) and 20 min after (E) adding DSM to lumen.
(F–H) DSM increased colon MMC frequency and conduction velocity
with no effect on PPr.
R. Y. Wu et al. Neurogastroenterology and Motility
� 2013 Blackwell Publishing Ltde210

TRAM-34 reduced PPr for jejunum and colon, the
respective reductions being from 14 ± 5.5 to 5.8 ± 2.4
(59%) (P = 0.02) and from 54 ± 7.9 to 33 ± 8.3 hPa
(39%) (P = 0.002).
DISCUSSION
Evidence is accumulating that certain probiotic strains
have acute actions in vivo5 and ex vivo,29 on the host’s
autonomic reflexes. These effects can occur within
minutes suggesting that the inter-kingdom signaling
responsible for them would not rely on colonization,
alteration in the microbiome composition or other
longer term adjustments.
Our experiments utilized established ex vivo mouse
jejunal29 or colon 36,39 perfusion models for which
MMCs have been shown to be generated by the enteric
nervous system because they are abolished by silencing
the neurons using TTX.29,32,36 We applied the bacteria
intraluminally, a technique that has been used for
probiotics5 or 5-HT,42 and used the methods of intra-
luminal pressure recording and spatiotemporal map-
ping36,43–45 to measure MMC parameters as previously
described.46 The use of these substantiated techniques
to compare probiotics strains in colon vs jejunal
segments has not previously been attempted.
Our results (Table 1) clearly show that such dis-
crimination was indeed possible for the Lactobacillus
strains tested and TRAM-34 in terms of the effect on
motor behavior of both small and large intestine. In
this regard, we had the surprising result that DSM and
JB-1 acted differently on the small compared with the
large intestine. There is at present no theory of enteric
neurophysiology that might explain such region-
specific differences, highlighting the scantiness of
basic research data in this area. The finding that
L. salivarius which was ineffective in vivo in an IBS
clinical trial, was also without effect on MMCs in
jejunum29 and in the present experiments on frequen-
cies or velocity in the colon, support the specificity of
the results. In addition, heat-killed JB-1 had no effect on
jejunal MMC velocity, extending the previous findings
that killed JB-1 do not alter PPr or frequency.29 Our
findings may have important clinical ramifications as
the motor disturbances of small or large intestines could
give rise to different clinical signs and symptoms which
then may require region-specific treatments.
TRAM-34 is an IKCa channel blocker with a high
degree of specificity for this channel.47 The blocker is
thought to selectively act on intrinsic primary afferent
neurons-IPANs (AH cells), increasing their excitability
by reducing the postspike slow afterhyperpolarization
(sAHP), as only these neurons functionally express
IKCa channels when there is no inflammation.32,48,49
In healthy guinea pig distal colon 10 lmol L)1
TRAM-34 applied serosally reduced pellet velocity.50,51
Conversely, in guinea pig jejunum 1 lmol L)1 TRAM-
34 was reported to not alter the number or velocity of
long distance propagating contractions.52 In rat colon,
there was no change in MMC frequency for 3 lmol L)1
TRAM-34,32 and in mouse jejunum with 5 lmol L)1
TRAM-34 there was a non-significant trend for reduc-
tion in MMC frequency of 4.9–4.1 mHz.29 In vivo rat
jejunum TRAM-34 1 mg kg)1 clustered MMCs inter-
vals so that MMCs within each cluster may have
increased in frequency, but there appeared to be longer
intervals between the clusters.41Thus, there is at
present no current consensus on species-specific
effects of TRAM-34 on propagated propulsive contrac-
tions in small vs large intestine.
JB-1 has previously been studied in terms of action
on the gut’s neuromuscular machinery. We have
shown that when myenteric neurons have been
silenced by adding TTX to the superfusate, small and
large intestinal MMCs vanish and the bacterium does
not modulate remaining neurally independent contrac-
tile activity in either rat or mouse.29,32 Furthermore,
intraluminal application decreased the amplitude of
anally propagated MMCs. Repeated daily ingestion or
acute epithelial application of JB-1 reduced the magni-
tude and duration of the IPAN sAHP. The sAHP is
generated by IKCa channel opening and TRAM-34
similarly decreases IPAN sAHP. Arguing by anal-
ogy,29,32 we proposed that JB-1 exerted its effects on
IPAN excitability, and therefore motility, by reducing
IKCa channel opening and thus the sAHP.
The present results (Table 1) for JB-1 and DSM and
TRAM-34 demonstrate that a decrease in the IKCa
channel opening is insufficient to explain all the
temporal changes evoked in jejunal and colonic
Table 1 Summary table for the effects of JB1, DSM, and TRAM-34 on
jejunum and colon › indicates an increase, fl a decrease, and s no
change in MMC parameters measured
Jejunum Colon
JB-1
Frequency fl flVelocity › flPeak pressure fl fl
DSM
Frequency fl ›Velocity fl ›Peak pressure s s
TRAM-34
Frequency fl ›Velocity › ›Peak pressure fl fl
Volume 25, Number 3, March 2013 Spatiotemporal maps: probiotic effects on motility
� 2013 Blackwell Publishing Ltd e211

MMCs. Somatic ion channels other than IKCa, or
synaptic transmission between IPANs or from IPANs
to inter-or motor neurons might also be modulated by
the probiotics to achieve the overall motor effects. It is
also possible, but less likely, as they do not innervate
the mucosa, that inter-or motor neurons might have
their firing patterns altered by the bacteria.
As IPANs are thought to transmit to excitatory
motor neurons by a fast neurotransmission53 and
inhibitory in the neurons predominantly via slow
transmission,52,54 it has been postulated that the
timing of muscle contractile patterns depends on a
complex interaction between these neural subcircuits
and sensory feedback from contracting muscle fibers.52
In this schema, the degree of suppression of the IPAN
sAHP (TRAM-34 dose) may be critical in determining
final form and timing of the overall motor pattern.55
DSM has been shown to be effective in well-
conducted trials in human infantile colic18 and also
on functional gastric disturbances, thought to be due to
disordered gastric motility.56 Our results suggest that
in terms of infantile colic the beneficial effects of the
probiotic may be due to effects on jejunum as much as
the colon as jejunal MMC frequency and velocity were
decreased in our model (Table 1). In this respect, the
use of the mouse colon as a surrogate for human
pharmacologic effectiveness of bioactive molecules is
strongly supported by other data.31 Thus, the demon-
stration that another L. reuteri (PTA 6475), with strong
anti-inflammatory activity had no effects on either
small or large intestinal segments predicts that it
would have little to no effect in infantile colic.
Furthermore, DSM has been used clinically to help
treat pediatric functional constipation.22 In our system,
DSM increased both colonic MMC frequency and
velocity (Table 1), an outcome which is again in
register with the idea that the recording of mouse
colon MMCs can be used to screen for positive effects
of candidate bacteria or products. We tentatively
predict that based on the effects of DSM on adult
mouse colon, DSM might have therapeutic potential in
slow transit constipation in elderly adults.
In conclusion, we have presented a model system
that can effectively differentiate between Lactobacil-
lus strains in terms of several key parameters of mouse
gut MMCs, and between the actions they have on the
small vs large intestine. This approach may help to
screen and identify potential therapeutic effects of
currently used or newly identified probiotic strains,
and help in correlating the specific effects of such
bacteria on the enteric nervous system with their
actions on gut motility.
FUNDING
This study was supported by a grant from the Natural Sciencesand Engineering Council of Canada (371955-2009), the GugliettiFamily Foundation, and an unrestricted grant from BioGaia AB.
DISCLOSURE
No competing interests declared.
AUTHOR CONTRIBUTIONS
WAK and RYW designed the research and wrote the manuscriptand PF helped with the design; MP, BW, YM, PS, and AMSperformed the experiments; RYW and MP analyzed the data; JBcontributed to drafting and editing the manuscript. All authorsapproved the manuscript for publication. Experiments wereconducted in the McMaster Brain-Body Institute at St Joseph’sHealthcare Hamilton.
REFERENCES
1 Riboulet-Bisson E, Sturme MH, Jeff-ery IB et al. Effect of Lactobacillussalivarius bacteriocin Abp118 on themouse and pig intestinal microbiota.PLoS ONE 2012; 7: e31113.
2 Kunze WA, Mao YK, Wang B et al.Lactobacillus reuteri enhances excit-ability of colonic AH neurons byinhibiting calcium-dependent potas-sium channel opening. J Cell Mol
Med 2009; 13: 2261–70.3 Forsythe P, Kunze WA. Voices from
within: gut microbes and the CNS.Cell Mol Life Sci 2012. [Epub aheadof print]. doi: 10.1007/s00018-012-1028-z.
4 Bravo JA, Forsythe P, Chew MV et al.Ingestion of Lactobacillus strainregulates emotional behavior and cen-tral GABA receptor expression in amouse via the vagus nerve. Proc Natl
AcadSciUSA2011;108:16050–5.5 Tanida M, Yamano T, Maeda K,
Okumura N, Fukushima Y, Nagai K.Effects of intraduodenal injection ofLactobacillus johnsonii La1 on renalsympathetic nerve activity and bloodpressure in urethane-anesthetizedrats. Neurosci Lett 2005; 389: 109–14.
6 Jauhiainen T, Vapaatalo H, Poussa T,KyronpaloS, Rasmussen M, KorpelaR.Lactobacillus helveticus fermentedmilk lowers blood pressure in hyper-tensive subjects in 24-h ambulatory
bloodpressuremeasurement[ast].AmJHypertens2005;18:1600–5.
7 Quigley EM. Probiotics in the man-agement of colonic disorders. CurrGastroenterol Rep 2007; 9: 434–40.
8 MoayyediP,FordA,TalleyNet al.Theefficacyofprobioticsinthetreatmentofirritable bowel syndrome: a systematicreview.Gut2010;59:325–32.
9 Caenepeel P, Janssens J, Vantrappen G,Eyssen H, Coremans G. Interdigestivemyoelectric complex in germ-free rats.DigDisSci1989;34:1180–4.
10 Husebye E, Hellstrom PM, MidtvedtT. Intestinal microflora stimulatesmyoelectric activity of rat smallintestine by promoting cyclic initia-tion and aboral propagation of
R. Y. Wu et al. Neurogastroenterology and Motility
� 2013 Blackwell Publishing Ltde212

migrating myoelectric complex. DigDis Sci 1994; 39: 946–56.
11 Barbara G, Stanghellini V, Brandi Get al. Interactions between commen-sal bacteria and gut sensorimotorfunction in health and disease. Am J
Gastroenterol 2005; 100: 2560–8.12 Abraham BP, Sellin JH. Drug-induced
diarrhea. In: Guandalini S, Vaziri H,eds. Diarrhea. Chpt. 23 in ClinicalGastroenterology, New York: HumanaPress, 2011: 393–423.
13 Verdu E, Bercik P, Collins S. Effect ofprobiotics on gastrointestinal func-tion: evidence from animal models.Therap Adv Gastroenterol 2009; 2:31–5.
14 Ritchie ML, Romanuk TN. A meta-analysis of probiotic efficacy for gas-trointestinal diseases. PLoS ONE
2012; 7: e34938.15 Francavilla R, Lionetti E, Castellane-
ta S et al. Randomised clinical trial:Lactobacillus reuteri DSM 17938 vs.placebo in children with acute diar-rhoea – a double-blind study. Aliment
Pharmacol Ther 2012; 36: 363–9.16 Waller PA, Gopal PK, Leyer GJ et al.
Dose-response effect of Bifidobacte-
rium lactis HN019 on whole guttransit time and functional gastroin-testinal symptoms in adults. Scand J
Gastroenterol 2011; 46: 1057–64.17 Preidis GA, Saulnier DM, Blutt SE
et al. Host response to probioticsdetermined by nutritional status ofrotavirus-infected neonatal mice. J
Pediatr Gastroenterol Nutr 2012; 55:299–307.
18 Savino F, Cordisco L, Tarasco V et al.
Lactobacillus reuteri DSM 17938 ininfantile colic: a randomized, double-blind, placebo-controlled trial. Pedi-
atrics 2010; 126: e526–33.19 Sarna S. Colonic Motility: From
Bench Side to Bedside. San Rafael(CA): Morgan & Claypool LifeSciences, 2010.
20 Gallegos-Orozco JF, Foxx-OrensteinAE, Sterler SM, Stoa JM. Chronicconstipation in the elderly. Am
J Gastroenterol 2012; 107: 18–25.21 Tack J, Muller-Lissner S, Stanghellini
V et al. Diagnosis and treatment ofchronic constipation – a Europeanperspective. NeurogastroenterolMotil 2011; 23: 697–710.
22 Coccorullo P, Strisciuglio C, Marti-nelli M, Miele E, Greco L, Staiano A.Lactobacillus reuteri (DSM 17938) ininfants with functional chronicconstipation: a double-blind, ran-
domized, placebo-controlled study.J Pediatr 2010; 157: 598–602.
23 Bu LN, Chang MH, Ni YH, Chen HL,Cheng CC. Lactobacillus caseirhamnosus Lcr35 in children withchronic constipation. Pediatr Int:
Official J Japan Pediatr Soc 2007; 49:485–90.
24 Tabbers MM, de Milliano I, Rose-boom MG, Benninga MA. Is Bifido-
bacterium breve effective in thetreatment of childhood constipation?Results from a pilot study Nutr J
2011; 10: 19–24.25 Higashikawa F, Noda M, Awaya T,
Nomura K, Oku H, Sugiyama M.Improvement of constipation andliver function by plant-derived lacticacid bacteria: a double-blind, ran-domized trial. Nutrition 2010; 26:367–74.
26 Zaharoni H, Rimon E, Vardi H, FrigerM, Bolotin A, Shahar DR. Probioticsimprove bowel movements in hospi-talized elderly patients – thePROAGE study. J Nutr Health Aging
2011; 15: 215–20.27 Husebye E, Hellstrom PM, Sundler F,
Chen J, Midtvedt T. Influence ofmicrobial species on small intestinalmyoelectric activity and transit ingerm-free rats. Am J Physiol Gastro-
intest Liver Physiol 2001; 280: G368–80.
28 Bourlioux P, Koletzko B, Guarner F,Braesco V. The intestine and itsmicroflora are partners for the pro-tection of the host: report on theDanone Symposium ‘‘The IntelligentIntestine,’’ held in Paris, June 14,2002. Am J Clin Nutr 2003; 78: 675–83.
29 Wang B, Mao YK, Diorio C et al.
Luminal administration ex vivo of alive Lactobacillus species moderatesmouse jejunal motility within min-utes. FASEB J 2010; 24: 4078–88.
30 Massi M, Ioan P, Budriesi R et al.
Effects of probiotic bacteria on gas-trointestinal motility in guinea-pigisolated tissue. World J Gastroenterol
2006; 12: 5987–94.31 Keating C, Martinez V, Ewart L et al.
The validation of an in vitro colonicmotility assay as a biomarker forgastrointestinal adverse drug reac-tions. Toxicol Appl Pharmacol 2010;245: 299–309.
32 Wang B, Mao YK, Diorio C et al.
Lactobacillus reuteri ingestion andIK(Ca) channel blockade have similareffects on rat colon motility and
myenteric neurones. Neurogastroen-terol Motil 2010; 22: 98–107.
33 Gwynne RM, Thomas EA, Goh SM,Sjovall H, Bornstein JC. Segmentationinduced by intraluminal fatty acid inisolated guinea-pig duodenum andjejunum. J Physiol 2004; 556: 557–69.
34 McCarthy EL. Mariotte’s bottle.Science 1934; 80: 100.
35 Huizinga JD, Ambrous K, Der-Sila-phet T. Co-operation between neuraland myogenic mechanisms in thecontrol of distension-induced peri-stalsis in the mouse small intestine.J Physiol 1998; 506: 843–56.
36 Roberts RR, Murphy JF, Young HM,Bornstein JC. Development of colonicmotility in the neonatal mouse-stud-ies using spatiotemporal maps. Am JPhysiol Gastrointest Liver Physiol
2007; 292: G930–8.37 O’Mahony L, McCarthy J, Kelly P
et al. Lactobacillus and Bifidobacte-rium in irritable bowel syndrome:symptom responses and relationshipto cytokine profiles. Gastroenterol-
ogy 2005; 128: 541–51.38 Kamiya T, Wang L, Forsythe P et al.
Inhibitory effects of Lactobacillus
reuteri on visceral pain induced bycolorectal distension in Sprague-Dawley rats. Gut 2006; 55: 191–6.
39 Powell AK, Fida R, Bywater RA.Motility in the isolated mouse colon:migrating motor complexes, myo-electric complexes and pressurewaves. Neurogastroenterol Motil
2003; 15: 257–66.40 Liu Y, Fatheree NY, Mangalat N,
Rhoads JM. Human-derived probioticLactobacillus reuteri strains differ-entially reduce intestinal inflamma-tion. Am J Physiol Gastrointest Liver
Physiol 2010; 299: G1087–96.41 Ferens D, Baell J, Lessene G, Smith
JE, Furness JB. Effects of modulatorsof Ca(2 + )-activated, intermediate-conductance potassium channels onmotility of the rat small intestine, invivo. Neurogastroenterol Motil 2007;19: 383–9.
42 Bulbring E, Lin RC. The effect ofintraluminal application of5-hydroxytryptamine and 5-hydroxy-tryptophan on peristalsis; the localproduction of 5-HT and its release inrelation to intraluminal pressure andpropulsive activity. J Physiol 1958;140: 381–407.
43 Hennig GW, Costa M, Chen BN,Brookes SJ. Quantitative analysis ofperistalsis in the guinea-pig small
Volume 25, Number 3, March 2013 Spatiotemporal maps: probiotic effects on motility
� 2013 Blackwell Publishing Ltd e213

intestine using spatio-temporalmaps. J Physiol 1999; 517(Pt 2): 575–90.
44 Bercik P, Bouley L, Dutoit P, BlumA, Kucera P. Quantitative analysisof intestinal motor patterns: spatio-temporal organization of nonneuralpacemaker sites in the rat ileum.Gastroenterology 2000; 119: 386–94.
45 Seerden TC, Lammers WJ, De WinterBY, De Man JG, Pelckmans PA. Spa-tiotemporal electrical and motilitymapping of distension-induced prop-agating oscillations in the murinesmall intestine. Am J Physiol Gas-
trointest Liver Physiol 2005; 289:G1043–51.
46 Lammers WJ, Cheng LK. Simulationand analysis of spatio-temporal mapsof gastrointestinal motility. Biomed
Eng Online 2008; 7: 2.47 Wulff H, Miller MJ, Hansel W,
Grissmer S, Cahalan MD, ChandyKG. Design of a potent and selectiveinhibitor of the intermediate-conductance Ca2 + -activated K+channel, IKCa1: a potential immu-nosuppressant. Proc Natl Acad Sci
USA 2000; 97: 8151–6.
48 Nurgali K, Nguyen TV, MatsuyamaH, Thacker M, Robbins HL, FurnessJB. Phenotypic changes of morpho-logically identified guinea-pig myen-teric neurons following intestinalinflammation. J Physiol 2007; 583:593–609.
49 Neylon CB, Nurgali K, Hunne B et al.Intermediate-conductance calcium-activated potassium channels in en-teric neurones of the mouse: phar-macological, molecular andimmunochemical evidence for theirrole in mediating the slow afterhy-perpolarization. J Neurochem 2004;90: 1414–22.
50 Hoffman J, McKnight N, Sharkey K,Mawe GM. The relationship betweeninflammation-induced neuronalexcitability and disrupted motoractivity in the guinea pig distal colon.Neurogastroenterol Motil 2011; 23:673–e279.
51 Strong DS, Sharkey KA, Mawe GM.Relationship between AH neuronexcitability and peristalsis in normalversus inflamed guinea pig distal co-lon. Neurogastroenterol Motil 2006;18: 695: A95.
52 Chambers JD, Bornstein JC, ThomasEA. Multiple neural oscillators andmuscle feedback are required for theintestinal fed state motor program.PLoS ONE 2011; 6: e19597.
53 Stebbing MJ, Bornstein JC. Electro-physiological mapping of fast excit-atory synaptic inputs tomorphologically and chemicallycharacterized myenteric neurons ofguinea-pig small intestine. Neurosci-
ence 1996; 73: 1017–28.54 Kunze WA, Furness JB, Bornstein JC.
Simultaneous intracellular recordingsfrom enteric neurons reveal thatmyenteric AH neurons transmit viaslow excitatory postsynaptic poten-tials. Neuroscience 1993; 55: 685–94.
55 Gwynne RM, Bornstein JC. Mecha-nisms underlying nutrient-inducedsegmentation in isolated guinea pigsmall intestine. Am J Physiol Gas-
trointest Liver Physiol 2007; 292:G1162–72.
56 Indrio F, Riezzo G, Raimondi F et al.
Lactobacillus reuteri accelerates gas-tric emptying and improves regurgi-tation in infants. Eur J Clin Invest
2011; 41: 417–22.
R. Y. Wu et al. Neurogastroenterology and Motility
� 2013 Blackwell Publishing Ltde214