the gladel multinational latin american prospective inception cohort of 1,214 patients with systemic...
TRANSCRIPT
The GLADEL Multinational Latin American ProspectiveInception Cohort of 1,214 Patients With Systemic
Lupus ErythematosusEthnic and Disease Heterogeneity Among ‘‘Hispanics’’
Bernardo A. Pons-Estel, MD, Luis J. Catoggio, MD, Mario H. Cardiel, MD, MSc,
Enrique R. Soriano, MD, Silvana Gentiletti, MD, Antonio R. Villa, MD, MSc, Isaac Abadi, MD,
Francisco Caeiro, MD, Alejandro Alvarellos, MD, and Donato Alarcon-Segovia, MD, PhD,
on behalf of the Grupo Latinoamericano de Estudio del Lupus (GLADEL)
Abstract: Clinical and laboratory manifestations and outcome of
systemic lupus erythematosus (SLE) may vary in different pop-
ulations. A prospective multinational inception cohort should prove
useful in identifying the influence of ethnicity on the clinical char-
acteristics of SLE. We therefore analyzed clinical, laboratory, and
prognostic variables in Latin American SLE patients with disease
of recent onset who were entered into a prospective cohort, and
compared these variables in the cohort’s 3 major ethnic groups.
Thirty-four centers from 9 Latin American countries participated by
randomly incorporating SLE patients within 2 years of diagnosis
into a standardized database. Participating centers were selected for
their expertise in diagnosing and managing SLE. We were then able
to evaluate prospectively socioeconomic variables, ethnicity, type
of medical care, clinical and laboratory features, disease activity,
damage, and mortality at each site. A coordinating center controlled
the quality of the information submitted.Of the 1,214 SLE patients included in the cohort, 537 were mes-
tizos, 507 were white, and 152 were African-Latin American (ALA).
(There were also small numbers of pure Amerindian and oriental
individuals.) Significant differences were found between them in
socioeconomic characteristics, type of care, and level of education
favoring whites. Mestizos and ALA were younger at onset. Delay to
diagnosis and disease duration was shorter in ALA. Fever was more
frequent in whites; discoid lesions in ALA; renal disease and
lymphopenia in mestizos and ALA. Although we found differences in
background variables between ethnic groups from different
countries, mestizos from 2 distant countries (Argentina and Mexico)
were clinically akin and showed similar differences to whites.
Mortality was associated with lower education, poor medical
coverage, and shorter follow-up. In an exploratory model nonwhite
ethnicity was associated with renal disease and lymphopenia,
damage, and cumulative American College of Rheumatology
criteria. These differences in clinical, prognostic, socioeconomic,
educational, and access to medical care features in Latin American
lupus patients of 3 major ethnic groups from 9 different countries
may have an impact on the patients’ disease. ‘‘Hispanics,’’ as they
have come to be generically termed on the basis of language, actually
constitute a markedly heterogeneous group of subjects.
(Medicine 2004;83:1–17)
INTRODUCTION
Systemic lupus erythematosus (SLE) is a complex auto-
immune disease that may result from the interplay of
genetic, hormonal, and environmental factors12. Although
its prognosis has improved remarkably in the past deca-
des22,23,30, it remains a potentially serious condition. Several
studies have shown that some sociodemographic character-
istics such as ethnicity, gender, age, income, education, and
access to health care are important variables associated with
the outcome of SLE21,29,35,43,44,56,63,68,72,75,80,82. Disease activity,
Abbreviations: ACR = American College of Rheumatology, ALA =
African-Latin American, SLE = systemic lupus erythematosus.
Medicine � Volume 83, Number 1, January 2004 1
From Servicio de Reumatologıa (BAP-E), Hospital Escuela Eva Peron,
Granadero Baigorria, Rosario, Argentina; Seccion Reumatologıa (LJC,
ERS), Servicio de Clınica Medica Hospital Italiano, Buenos Aires,
Argentina; Departamento de Inmunologıa y Reumatologıa (MHC, DA-S)
and Unidad de Epidemiologıa Clınica (ARV), Instituto Nacional de
Ciencias Medicas y Nutricion Salvador Zubiran, Mexico DF, Mexico;
Servicio de Reumatologıa (SG), Hospital Provincial de Rosario, Rosario,
Argentina; Servicio de Reumatologıa (IA), Centro Nacional de
Enfermedades Reumaticas, Hospital Universitario de Caracas, Caracas,
Venezuela; and Servicio de Reumatologıa (FC, AA), Hospital Privado,
Centro Medico de Cordoba, Cordoba, Argentina.
Supported in part by grants from the Pan American League of Associations
for Rheumatology (PANLAR).
Address reprint requests to: Bernardo A. Pons-Estel, MD, Avenida del
Huerto 1375, Piso 24, (2000) Rosario, Argentina. E-mail: baponsestel@
buenaventuraguarani.com.ar.
Copyright n 2004 by Lippincott Williams & Wilkins
ISSN: 0025-7974/04/8301-0001
DOI: 10.1097/01.md.0000104742.42401.e2
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

organ damage, infection, and treatment have also been identified
asfactorsinfluencingtheprognosis2,3,13,14,19,20,39,54,57,61,71,76,77,83.
The LUMINA study has compared clinical, socioeco-
nomic status, and disease-related variables in 3 ethnic groups
in clinical centers in the United States4–8,10,11,15,27,64,84. Im-
portant differences were detected in clinical and immuno-
genetic variables that could help identify associations with
clinical manifestations, disease activity, and physician’s global
scores. The epidemiology of SLE has been evaluated mainly
in North America2–11,21,27,29,48,54–56,64,76,77,81,84 and in some
European countries17,19,20,38–40,42,46, but little information is
available from Latin America1,16,22,23,26,36,37,41,47,49,51,52,65,79.
For obvious reasons, the Latin American studies make few
comparisons between ethnic groups, although some have
shown a poor prognosis and a high prevalence of infections in
African-Latin American (ALA) SLE patients, both of which
may relate to socioeconomic variables.
Several studies from the United States have included
Latin American patients, usually referring to them as
‘‘Hispanics’’5–7,9–11,27,39,60,64,81,84, a term that is mainly de-
rived from their language rather than their ethnic back-
ground, which can vary between and within Latin American
countries. Notwithstanding, the so-called Hispanics in the
United States have been shown to have more severe disease
and poorer outcomes than whites, often equating African
Americans, whose lupus tends to have poor prognosis11,64.
Interpreting and comparing those studies has also been
difficult due to the inclusion of diverse proportions of
hospital patients with varying degrees of disease duration.
Using a prospective cohort enables researchers to avoid
under-registry of information, evaluate characteristics both at
baseline and throughout the clinical course of the disease,
and ascertain the influence of diverse treatment strategies
and comorbid states. The incorporation of patients early after
diagnosis also minimizes the exclusion of early deaths, an
important variable in a chronic disease such as SLE.
These considerations were taken into account in the
development of the Grupo Latinoamericano de Estudio del
Lupus (GLADEL) cohort, started in 1997 as a multinational
inception prospective cohort in Latin American centers
having expertise in the diagnosis and management of SLE.
For this task we used a computer database available to all
groups and interconnected among them.
Herein we describe the cohort and the general char-
acteristics of the first 1,214 Latin American SLE patients
with recent-onset SLE incorporated into the predetermined
database and followed prospectively for a mean of 20
months. We analyze the potential differences by ethnic, na-
tional, and sociodemographic variables.
PATIENTS AND METHODSThe GLADEL study held an investigator meeting in
1997 in Mexico City. During 4 days, participants developed
a common protocol, consensus definitions, and selected out-
come measures, and received direct training in the database
software.
Center SelectionThe 34 centers participating in the GLADEL cohort
are distributed among 9 Latin American countries. To be
included, they had to meet the following criteria: have ex-
perience in SLE (referral centers with a lupus clinic, an
academic profile, and a rheumatology training program);
have a genuine interest in the research project; and have an
identified leader, as well as adequate human, technical, and
communication facilities.
Patient SelectionIn order to have a balanced representation of centers
in the initial cohort, each center was asked to incorporate a
minimum of 20 and a maximum of 30 randomly selected
patients. Randomization was done locally in each center. The
first patients were entered in October 1997, and to insure
their recent onset they could only be included if the diagnosis
of SLE had been made after 1 January 1996 by a rheu-
matologist or a qualified internist with experience in SLE.
Fulfillment of 4 American College of Rheumatology (ACR)
1982 SLE criteria73 at the time of diagnosis was not man-
datory. After incorporating the initial 30 patients, each group
continued to include 1 new randomly selected patient per
month diagnosed within the previous 2 years.
DatabaseAll groups started using ARTHROS 2.058 as a common
database for collection of information and moved on to the
new version ARTHROS 6.0. This is a user-friendly rheu-
matology database developed by Argentine rheumatologists
using a Windows platform. One of its many advantages is the
lack of language barriers: for example, data collected in
Spanish can be retrieved by an English-speaking investigator
since all characteristics are coded.
In order to obtain reliable information all investigators
were trained in a similar fashion. Patient data were collected
by a clinician trained in the program in small groups and
personalized sessions with 1 of the developers of the program.
At a coordinator center, strict control and supervision of the
data received was undertaken, with permanent communica-
tion with the submitting center for any queries arising.
Clinical InformationEach patient was interviewed and her or his clinical
chart information was validated. Investigators were asked to
establish precisely the dates of disease onset, diagnosis, and
fulfillment of ACR SLE criteria. They also were asked to
capture all relevant clinical and laboratory evaluations as
clinically indicated. Disease features were defined according
to ACR or other well-accepted criteria62. The clinical course
2 n 2004 Lippincott Williams & Wilkins
Pons-Estel et al Medicine � Volume 83, Number 1, January 2004
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

can be described as seen by both patient and physician at the
time of each visit (that is, same, better, worse). Disease
activity using both SLEDAI18 and MEX-SLEDAI34 were
measured in all patients at the time of entry and every
6 months thereafter. Systemic Lupus International Collabo-
rating Clinics/American College of Rheumatology (SLICC/
ACR) Damage Index for systemic lupus erythematosus31,32
was measured yearly. All researchers followed local
regulations according to their institutional review boards.
Definition of Demographic VariablesEthnic groups: An operational definition was neces-
sary. It was developed by consensus including an expert in
immunogenetics. These definitions were determined accord-
ing to the parents’ and all 4 grandparents’ self-reported
ethnicity5. Patients were questioned as to their place of birth,
as well as to that of their parents and grandparents. They
were thus classified as the following:
White: individuals with all white European ancestors;
Mestizo: individuals born in Latin America who had
both Amerindian and white ancestors;
African-Latin Americans (ALA): individuals born in
Latin America with at least 1 African ancestor irrespective of
whether other ancestors were white or Amerindian.
Pure Amerindians were those individuals who had all
autochthonous ancestors.
Final assignment of patients was the prerogative of the
clinician, who considered anthropomorphic characteristics
for this.
Socioeconomic status: Socioeconomic status was eval-
uated using the Graffar method33, a validated scale
previously used in Latin America78. The Graffar scale takes
into account 5 variables: parent’s occupation, parent’s level
of education, main source of income, housing, and neigh-
borhood quality. Each variable has 5 categories with in-
dependent and progressive scores. A final score classifies
subjects in 5 categories: high, medium-high, medium, me-
dium-low, and low.
Type of medical care was divided into the following
categories:
Institutional: patients treated primarily in public in-
stitutions. Partial coverage: patients who receive limited
support toward medical care expenses. Complete coverage:
patients who have all expenses paid for. Without coverage:
patients who have no economic support and have to pay for
all their expenses for medical care.
Private: patients cared for in private institutions or
practice. With coverage: patients with prepaid or insurance-
paid support. Without coverage: patients who pay for their
private care.
Education: we considered from 0 (illiterate) up to 20
years of formal education.
Laboratory StudiesStudies were done in the standard routine laboratory at
each center. Autoantibodies and complement tests were per-
formed at each center and the cutoff values were considered
valid. Standardization of immunologic tests between centers
is being incorporated but was not yet available at the time
of the current study.
Statistical AnalysisOverall comparisons of the clinical, sociodemographic,
and immunologic categorical variables among the major
ethnic groups (white, mestizo, ALA, and other) were
performed using cross tabulations, and their significance as-
sessed by means of the chi-square statistic. When a sig-
nificant result was found, bivariated comparisons were
performed to identify groups that were statistically different
by the Fisher exact test. A similar analysis was applied when
comparing the 3 selected ethnic groups: Argentine white,
Argentine mestizo, and Mexican mestizo.
For continuous variables (age at onset; age at diagnosis;
delay to diagnosis—defined as time between onset of disease
and diagnosis; disease duration; follow-up; positive results in
immunologic tests; and scores of SLEDAI, MEX-SLEDAI, and
SLICC) the comparison between ethnic groups was established
by Kruskal-Wallis test, and the comparison for 2 samples was
done using Mann-Whitney U test. Thus, ethnic group was
considered the main independent variable. To test the main
effect of this variable over clinical outcomes, we factorized it in
2 ways. In the first, we built 3 dummy variables taking the major
categories of the variable ethnic group: white vs. mestizo, white
vs. ALA, and white vs. other. In the second, we established the
comparison between 2 dummy variables: Argentine white vs.
Argentine mestizo, and Argentine white vs. Mexican mestizo.
The multivariate models were adjusted by gender (female vs.
male), education (<10 yr vs. �10 yr), medical coverage (partial
or no coverage vs. full medical coverage), age at SLE diagnosis
(>27 yr vs.�27 yr), delay to SLE diagnosis (�6 mo vs. <6 mo),
follow-up (�20 mo vs. <20 mo), number of hospitalizations
(�1 vs. 0), marital status (single vs. all others), socioeconomic
status (lower middle/lower vs. all others), and country
(Argentina vs. the rest). All these variables were entered into
the models to diminish differences in the heterogeneity in both
clinical and sociodemographic variables of our populations.
The criterion to stratify the continuous variables was based in
the median value. Clinical outcomes as dependent variables
were built and tested in the different multivariate models. We
showed selected models. All the multivariate analyses were
conducted by means of unconditional logistic regression to
derive the odds ratio as association measure adjusted by
multiple covariates. Multicollinearity was probed in all models
by means of the covariance matrix. All statistical analyses were
performed separately with SAS v. 870, and with SPSS/PC v.
10.069, and the data then compared.
n 2004 Lippincott Williams & Wilkins 3
Medicine � Volume 83, Number 1, January 2004 Lupus in Latin America: GLADEL Inception Cohort
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
RESULTS
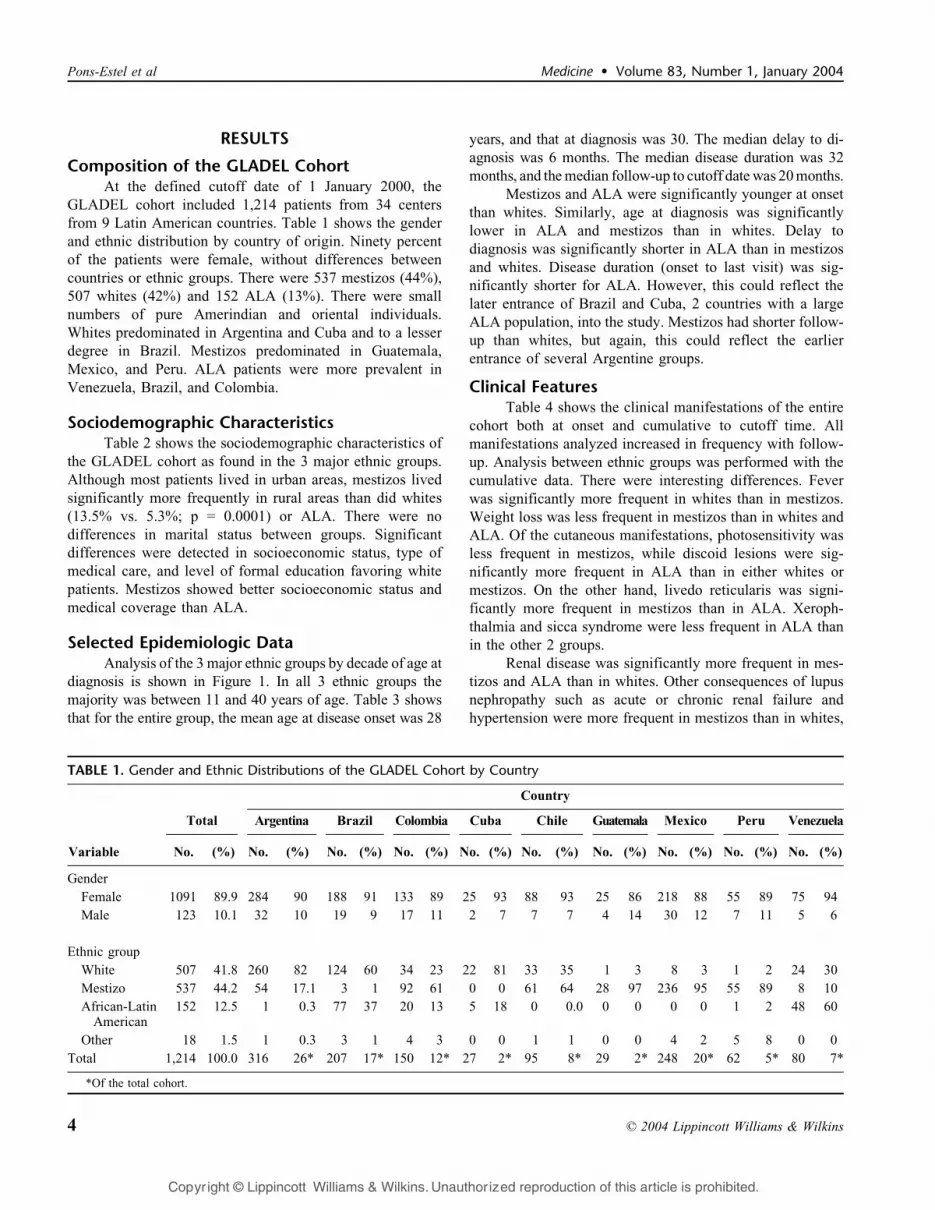
Composition of the GLADEL CohortAt the defined cutoff date of 1 January 2000, the
GLADEL cohort included 1,214 patients from 34 centers
from 9 Latin American countries. Table 1 shows the gender
and ethnic distribution by country of origin. Ninety percent
of the patients were female, without differences between
countries or ethnic groups. There were 537 mestizos (44%),
507 whites (42%) and 152 ALA (13%). There were small
numbers of pure Amerindian and oriental individuals.
Whites predominated in Argentina and Cuba and to a lesser
degree in Brazil. Mestizos predominated in Guatemala,
Mexico, and Peru. ALA patients were more prevalent in
Venezuela, Brazil, and Colombia.
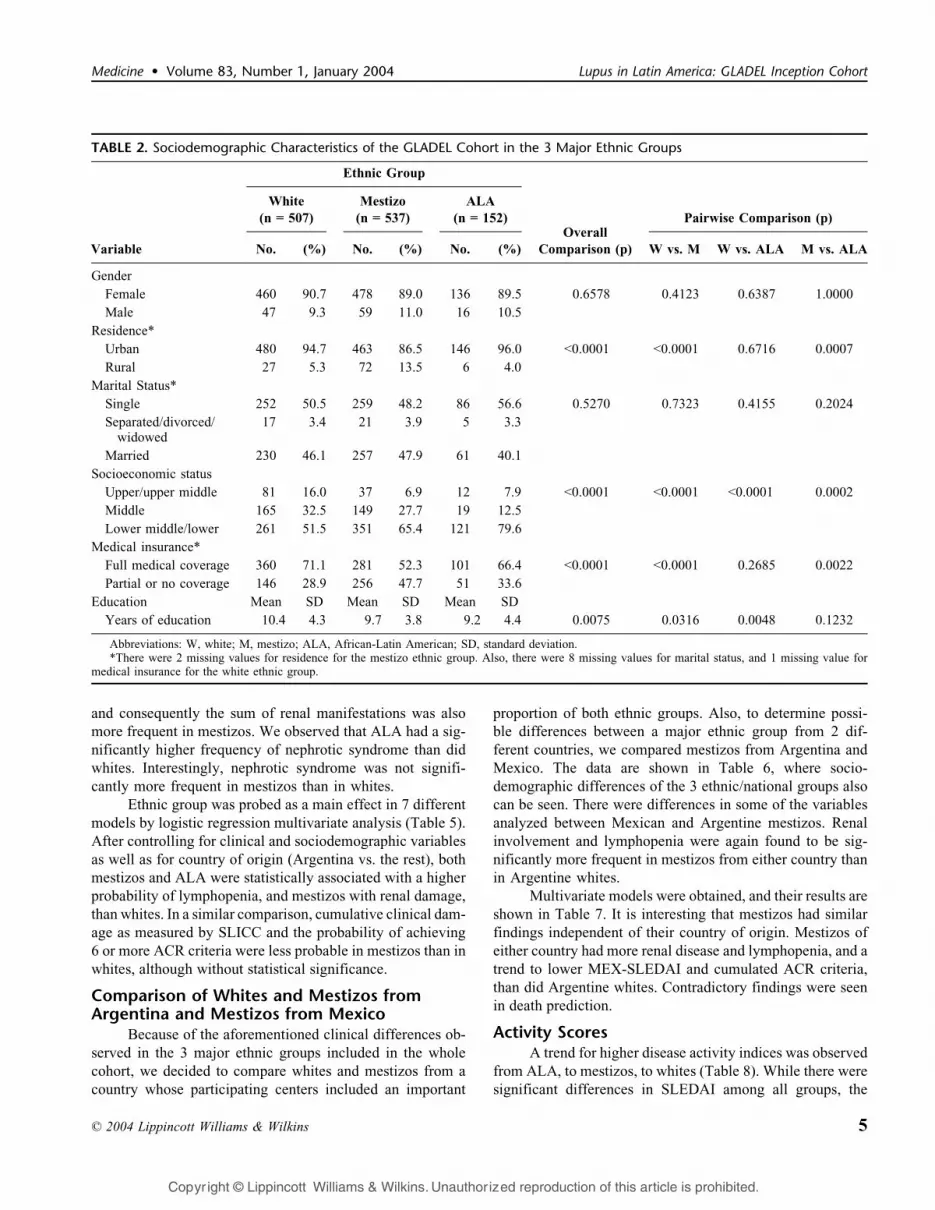
Sociodemographic CharacteristicsTable 2 shows the sociodemographic characteristics of
the GLADEL cohort as found in the 3 major ethnic groups.
Although most patients lived in urban areas, mestizos lived
significantly more frequently in rural areas than did whites
(13.5% vs. 5.3%; p = 0.0001) or ALA. There were no
differences in marital status between groups. Significant
differences were detected in socioeconomic status, type of
medical care, and level of formal education favoring white
patients. Mestizos showed better socioeconomic status and
medical coverage than ALA.
Selected Epidemiologic DataAnalysis of the 3 major ethnic groups by decade of age at
diagnosis is shown in Figure 1. In all 3 ethnic groups the
majority was between 11 and 40 years of age. Table 3 shows
that for the entire group, the mean age at disease onset was 28
years, and that at diagnosis was 30. The median delay to di-
agnosis was 6 months. The median disease duration was 32
months, and the median follow-up to cutoff date was 20 months.
Mestizos and ALA were significantly younger at onset
than whites. Similarly, age at diagnosis was significantly
lower in ALA and mestizos than in whites. Delay to
diagnosis was significantly shorter in ALA than in mestizos
and whites. Disease duration (onset to last visit) was sig-
nificantly shorter for ALA. However, this could reflect the
later entrance of Brazil and Cuba, 2 countries with a large
ALA population, into the study. Mestizos had shorter follow-
up than whites, but again, this could reflect the earlier
entrance of several Argentine groups.
Clinical FeaturesTable 4 shows the clinical manifestations of the entire
cohort both at onset and cumulative to cutoff time. All
manifestations analyzed increased in frequency with follow-
up. Analysis between ethnic groups was performed with the
cumulative data. There were interesting differences. Fever
was significantly more frequent in whites than in mestizos.
Weight loss was less frequent in mestizos than in whites and
ALA. Of the cutaneous manifestations, photosensitivity was
less frequent in mestizos, while discoid lesions were sig-
nificantly more frequent in ALA than in either whites or
mestizos. On the other hand, livedo reticularis was signi-
ficantly more frequent in mestizos than in ALA. Xeroph-
thalmia and sicca syndrome were less frequent in ALA than
in the other 2 groups.
Renal disease was significantly more frequent in mes-
tizos and ALA than in whites. Other consequences of lupus
nephropathy such as acute or chronic renal failure and
hypertension were more frequent in mestizos than in whites,
TABLE 1. Gender and Ethnic Distributions of the GLADEL Cohort by Country
Variable
Country
Total Argentina Brazil Colombia Cuba Chile Guatemala Mexico Peru Venezuela
No. (%) No. (%) No. (%) No. (%) No. (%) No. (%) No. (%) No. (%) No. (%) No. (%)
Gender
Female 1091 89.9 284 90 188 91 133 89 25 93 88 93 25 86 218 88 55 89 75 94
Male 123 10.1 32 10 19 9 17 11 2 7 7 7 4 14 30 12 7 11 5 6
Ethnic group
White 507 41.8 260 82 124 60 34 23 22 81 33 35 1 3 8 3 1 2 24 30
Mestizo 537 44.2 54 17.1 3 1 92 61 0 0 61 64 28 97 236 95 55 89 8 10
African-LatinAmerican
152 12.5 1 0.3 77 37 20 13 5 18 0 0.0 0 0 0 0 1 2 48 60
Other 18 1.5 1 0.3 3 1 4 3 0 0 1 1 0 0 4 2 5 8 0 0
Total 1,214 100.0 316 26* 207 17* 150 12* 27 2* 95 8* 29 2* 248 20* 62 5* 80 7*
*Of the total cohort.
4 n 2004 Lippincott Williams & Wilkins
Pons-Estel et al Medicine � Volume 83, Number 1, January 2004
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
and consequently the sum of renal manifestations was also
more frequent in mestizos. We observed that ALA had a sig-
nificantly higher frequency of nephrotic syndrome than did
whites. Interestingly, nephrotic syndrome was not signifi-
cantly more frequent in mestizos than in whites.
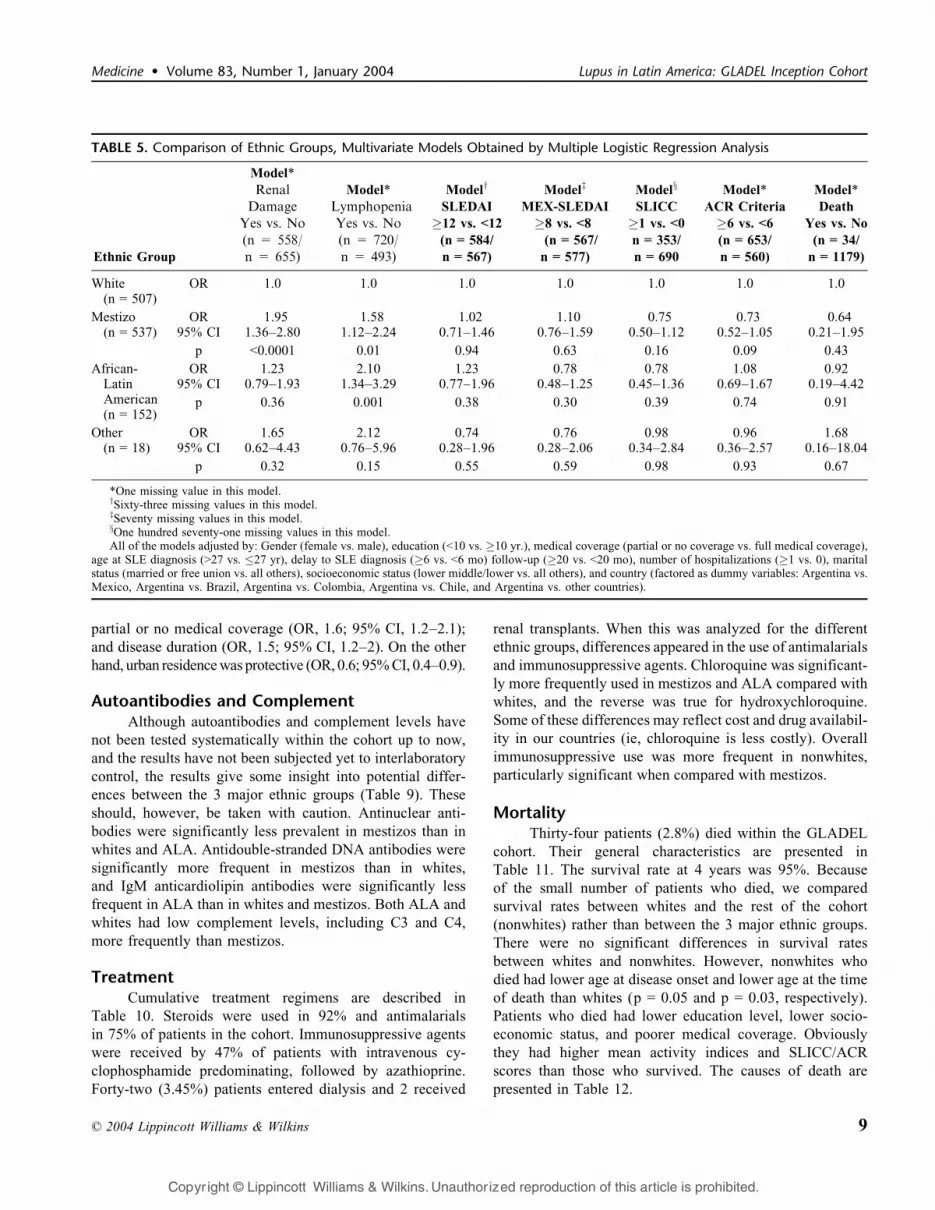
Ethnic group was probed as a main effect in 7 different
models by logistic regression multivariate analysis (Table 5).
After controlling for clinical and sociodemographic variables
as well as for country of origin (Argentina vs. the rest), both
mestizos and ALA were statistically associated with a higher
probability of lymphopenia, and mestizos with renal damage,
than whites. In a similar comparison, cumulative clinical dam-
age as measured by SLICC and the probability of achieving
6 or more ACR criteria were less probable in mestizos than in
whites, although without statistical significance.
Comparison of Whites and Mestizos fromArgentina and Mestizos from Mexico
Because of the aforementioned clinical differences ob-
served in the 3 major ethnic groups included in the whole
cohort, we decided to compare whites and mestizos from a
country whose participating centers included an important
proportion of both ethnic groups. Also, to determine possi-
ble differences between a major ethnic group from 2 dif-
ferent countries, we compared mestizos from Argentina and
Mexico. The data are shown in Table 6, where socio-
demographic differences of the 3 ethnic/national groups also
can be seen. There were differences in some of the variables
analyzed between Mexican and Argentine mestizos. Renal
involvement and lymphopenia were again found to be sig-
nificantly more frequent in mestizos from either country than
in Argentine whites.
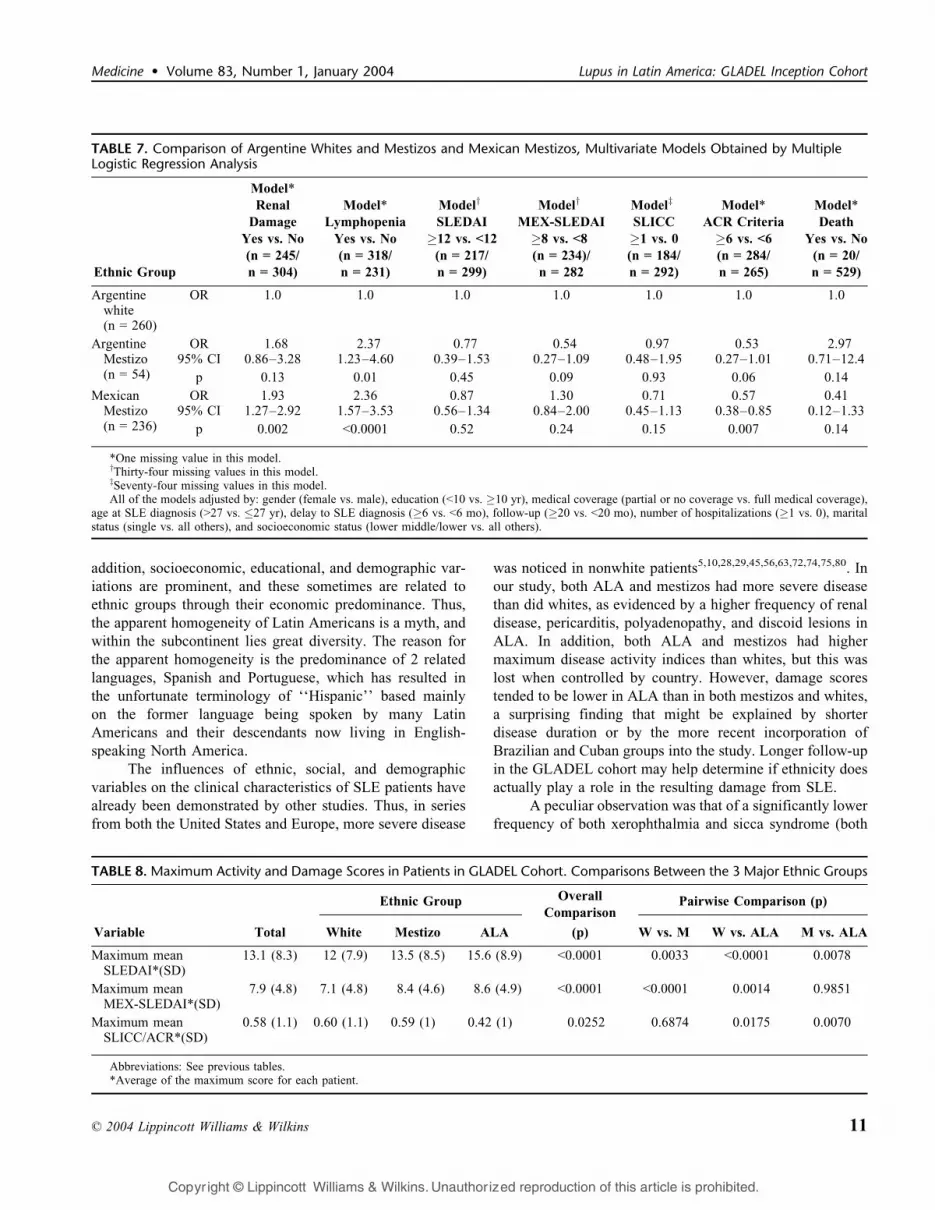
Multivariate models were obtained, and their results are
shown in Table 7. It is interesting that mestizos had similar
findings independent of their country of origin. Mestizos of
either country had more renal disease and lymphopenia, and a
trend to lower MEX-SLEDAI and cumulated ACR criteria,
than did Argentine whites. Contradictory findings were seen
in death prediction.
Activity ScoresA trend for higher disease activity indices was observed
from ALA, to mestizos, to whites (Table 8). While there were
significant differences in SLEDAI among all groups, the
TABLE 2. Sociodemographic Characteristics of the GLADEL Cohort in the 3 Major Ethnic Groups
Ethnic Group
Overall
Comparison (p)
White
(n = 507)
Mestizo
(n = 537)
ALA
(n = 152) Pairwise Comparison (p)
Variable No. (%) No. (%) No. (%) W vs. M W vs. ALA M vs. ALA
Gender
Female 460 90.7 478 89.0 136 89.5 0.6578 0.4123 0.6387 1.0000
Male 47 9.3 59 11.0 16 10.5
Residence*
Urban 480 94.7 463 86.5 146 96.0 <0.0001 <0.0001 0.6716 0.0007
Rural 27 5.3 72 13.5 6 4.0
Marital Status*
Single 252 50.5 259 48.2 86 56.6 0.5270 0.7323 0.4155 0.2024
Separated/divorced/widowed
17 3.4 21 3.9 5 3.3
Married 230 46.1 257 47.9 61 40.1
Socioeconomic status
Upper/upper middle 81 16.0 37 6.9 12 7.9 <0.0001 <0.0001 <0.0001 0.0002
Middle 165 32.5 149 27.7 19 12.5
Lower middle/lower 261 51.5 351 65.4 121 79.6
Medical insurance*
Full medical coverage 360 71.1 281 52.3 101 66.4 <0.0001 <0.0001 0.2685 0.0022
Partial or no coverage 146 28.9 256 47.7 51 33.6
Education Mean SD Mean SD Mean SD
Years of education 10.4 4.3 9.7 3.8 9.2 4.4 0.0075 0.0316 0.0048 0.1232
Abbreviations: W, white; M, mestizo; ALA, African-Latin American; SD, standard deviation.*There were 2 missing values for residence for the mestizo ethnic group. Also, there were 8 missing values for marital status, and 1 missing value for
medical insurance for the white ethnic group.
n 2004 Lippincott Williams & Wilkins 5
Medicine � Volume 83, Number 1, January 2004 Lupus in Latin America: GLADEL Inception Cohort
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

MEX-SLEDAI did not reach significance between mestizo
and ALA patients. Stepwise multiple logistic regression anal-
ysis produced a large predictive model for disease activity,
defined as a score higher than 12 in SLEDAI and 8 in MEX-
SLEDAI. Results were similar with both indices, and there-
fore we present only the SLEDAI data. Variables associated
with higher disease activity were formal education of less
than 10 years odds ratio [OR], 1.5; 95% confidence interval
[CI], 1.1–1.9); partial or no medical coverage (OR, 1.4;
95% CI, 1.1–1.8), age older than 27 years (OR, 1.6; 95%
CI, 1.2–2.1), time of follow-up �20 months (OR, 1.6; 95%
CI, 1.2–2.2), delay to diagnosis �6 months (OR, 0.6; 95% CI,
0.5–0.8), and disease duration �32 months (OR, 0.7; 95% CI,
0.5–0.9) (data not shown).
FIGURE 1. Age distribution of patients at diagnosis in the 3 major ethnic groups.
TABLE 3. Selected Epidemiologic Data of the GLADEL Cohort in the 3 Major Ethnic Groups
Ethnic Group
Total
(n = 1,214)
White
(n = 507)
Mestizo
(n = 537)
ALA
(n = 152)Overall W vs. W vs. M vs.
Variable Mean SD Mean SD Mean SD Mean SD Comparison (p) M ALA ALA
Age atonset (yr)
28 12 29.5 12.2 28.1 12.3 26.2 10.6 0.0077 0.0219 0.0058 0.2018
Age atdiagnosis (yr)
30 12 31.1 12.5 29.9 12.5 26.9 10.8 0.0010 0.0488 0.0003 0.0157
Median Range Median Range Median Range Median Range
Delay todiagnosis (mo)
6 0.4–490 6.0 0.4–301 6.9 0.4–490 3.8 0.4–84 <0.0001 0.6872 <.0001 <.0001
Diseaseduration (mo)
32 0.9–534 34.2 0.9–333 30.9 1.5–534 27.2 2.4–111 0.0002 0.0851 <.0001 0.0041
Follow-up (mo) 19.9 0.0–162 22.3 0.0–53 17.8 0.0–162 19.9 0.0–52 0.0299 0.0112 0.1379 0.5341
Abbreviations: See previous table.
Pairwise Comparison
6 n 2004 Lippincott Williams & Wilkins
Pons-Estel et al Medicine � Volume 83, Number 1, January 2004
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
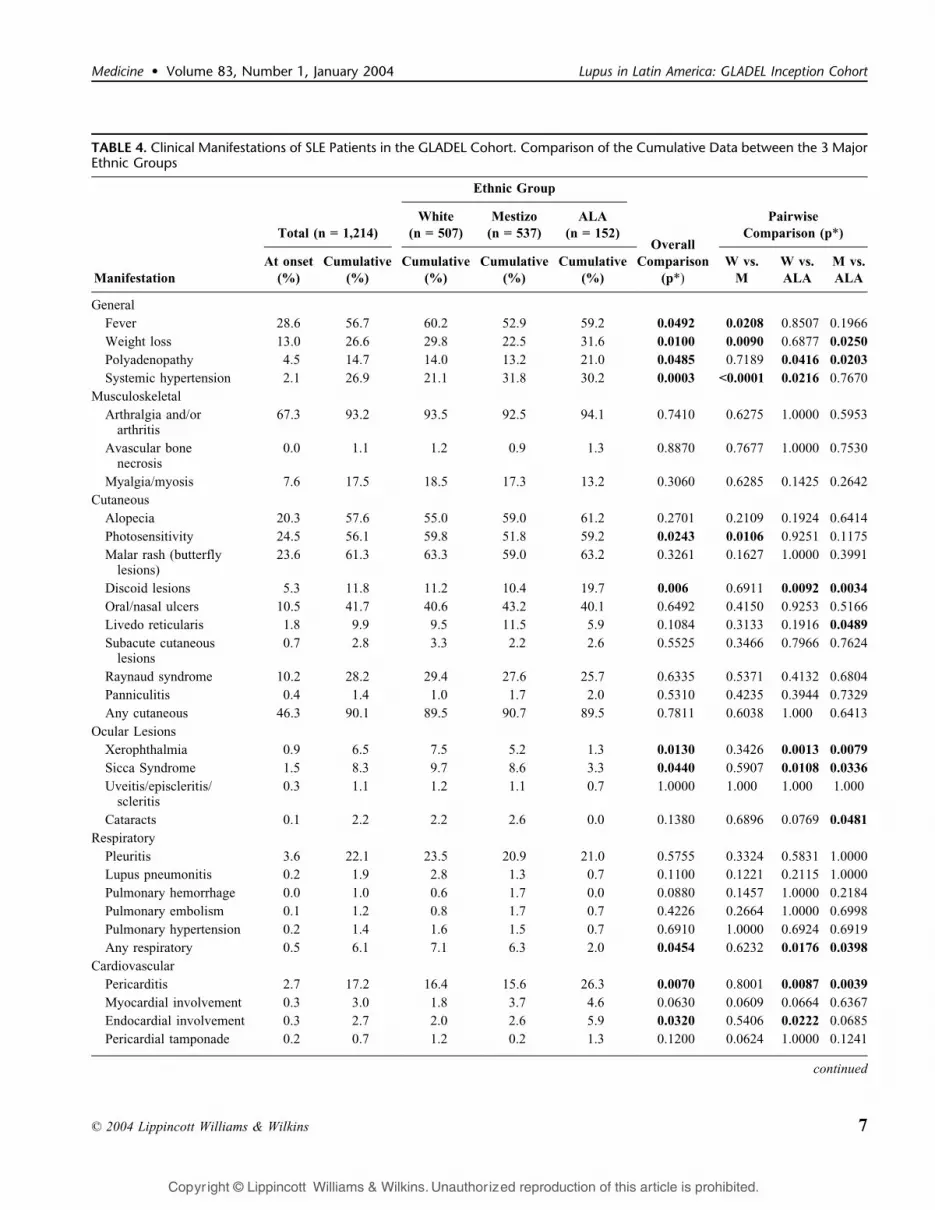
TABLE 4. Clinical Manifestations of SLE Patients in the GLADEL Cohort. Comparison of the Cumulative Data between the 3 MajorEthnic Groups
Ethnic Group
Total (n = 1,214)
White
(n = 507)
Mestizo
(n = 537)
ALA
(n = 152)Overall
Pairwise
Comparison (p*)
Manifestation
At onset
(%)
Cumulative
(%)
Cumulative
(%)
Cumulative
(%)
Cumulative
(%)
Comparison
(p*)W vs.
M
W vs.
ALA
M vs.
ALA
General
Fever 28.6 56.7 60.2 52.9 59.2 0.0492 0.0208 0.8507 0.1966
Weight loss 13.0 26.6 29.8 22.5 31.6 0.0100 0.0090 0.6877 0.0250
Polyadenopathy 4.5 14.7 14.0 13.2 21.0 0.0485 0.7189 0.0416 0.0203
Systemic hypertension 2.1 26.9 21.1 31.8 30.2 0.0003 <0.0001 0.0216 0.7670
Musculoskeletal
Arthralgia and/orarthritis
67.3 93.2 93.5 92.5 94.1 0.7410 0.6275 1.0000 0.5953
Avascular bonenecrosis
0.0 1.1 1.2 0.9 1.3 0.8870 0.7677 1.0000 0.7530
Myalgia/myosis 7.6 17.5 18.5 17.3 13.2 0.3060 0.6285 0.1425 0.2642
Cutaneous
Alopecia 20.3 57.6 55.0 59.0 61.2 0.2701 0.2109 0.1924 0.6414
Photosensitivity 24.5 56.1 59.8 51.8 59.2 0.0243 0.0106 0.9251 0.1175
Malar rash (butterflylesions)
23.6 61.3 63.3 59.0 63.2 0.3261 0.1627 1.0000 0.3991
Discoid lesions 5.3 11.8 11.2 10.4 19.7 0.006 0.6911 0.0092 0.0034
Oral/nasal ulcers 10.5 41.7 40.6 43.2 40.1 0.6492 0.4150 0.9253 0.5166
Livedo reticularis 1.8 9.9 9.5 11.5 5.9 0.1084 0.3133 0.1916 0.0489
Subacute cutaneouslesions
0.7 2.8 3.3 2.2 2.6 0.5525 0.3466 0.7966 0.7624
Raynaud syndrome 10.2 28.2 29.4 27.6 25.7 0.6335 0.5371 0.4132 0.6804
Panniculitis 0.4 1.4 1.0 1.7 2.0 0.5310 0.4235 0.3944 0.7329
Any cutaneous 46.3 90.1 89.5 90.7 89.5 0.7811 0.6038 1.000 0.6413
Ocular Lesions
Xerophthalmia 0.9 6.5 7.5 5.2 1.3 0.0130 0.3426 0.0013 0.0079
Sicca Syndrome 1.5 8.3 9.7 8.6 3.3 0.0440 0.5907 0.0108 0.0336
Uveitis/episcleritis/scleritis
0.3 1.1 1.2 1.1 0.7 1.0000 1.000 1.000 1.000
Cataracts 0.1 2.2 2.2 2.6 0.0 0.1380 0.6896 0.0769 0.0481
Respiratory
Pleuritis 3.6 22.1 23.5 20.9 21.0 0.5755 0.3324 0.5831 1.0000
Lupus pneumonitis 0.2 1.9 2.8 1.3 0.7 0.1100 0.1221 0.2115 1.0000
Pulmonary hemorrhage 0.0 1.0 0.6 1.7 0.0 0.0880 0.1457 1.0000 0.2184
Pulmonary embolism 0.1 1.2 0.8 1.7 0.7 0.4226 0.2664 1.0000 0.6998
Pulmonary hypertension 0.2 1.4 1.6 1.5 0.7 0.6910 1.0000 0.6924 0.6919
Any respiratory 0.5 6.1 7.1 6.3 2.0 0.0454 0.6232 0.0176 0.0398
Cardiovascular
Pericarditis 2.7 17.2 16.4 15.6 26.3 0.0070 0.8001 0.0087 0.0039
Myocardial involvement 0.3 3.0 1.8 3.7 4.6 0.0630 0.0609 0.0664 0.6367
Endocardial involvement 0.3 2.7 2.0 2.6 5.9 0.0320 0.5406 0.0222 0.0685
Pericardial tamponade 0.2 0.7 1.2 0.2 1.3 0.1200 0.0624 1.0000 0.1241
continued
n 2004 Lippincott Williams & Wilkins 7
Medicine � Volume 83, Number 1, January 2004 Lupus in Latin America: GLADEL Inception Cohort
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
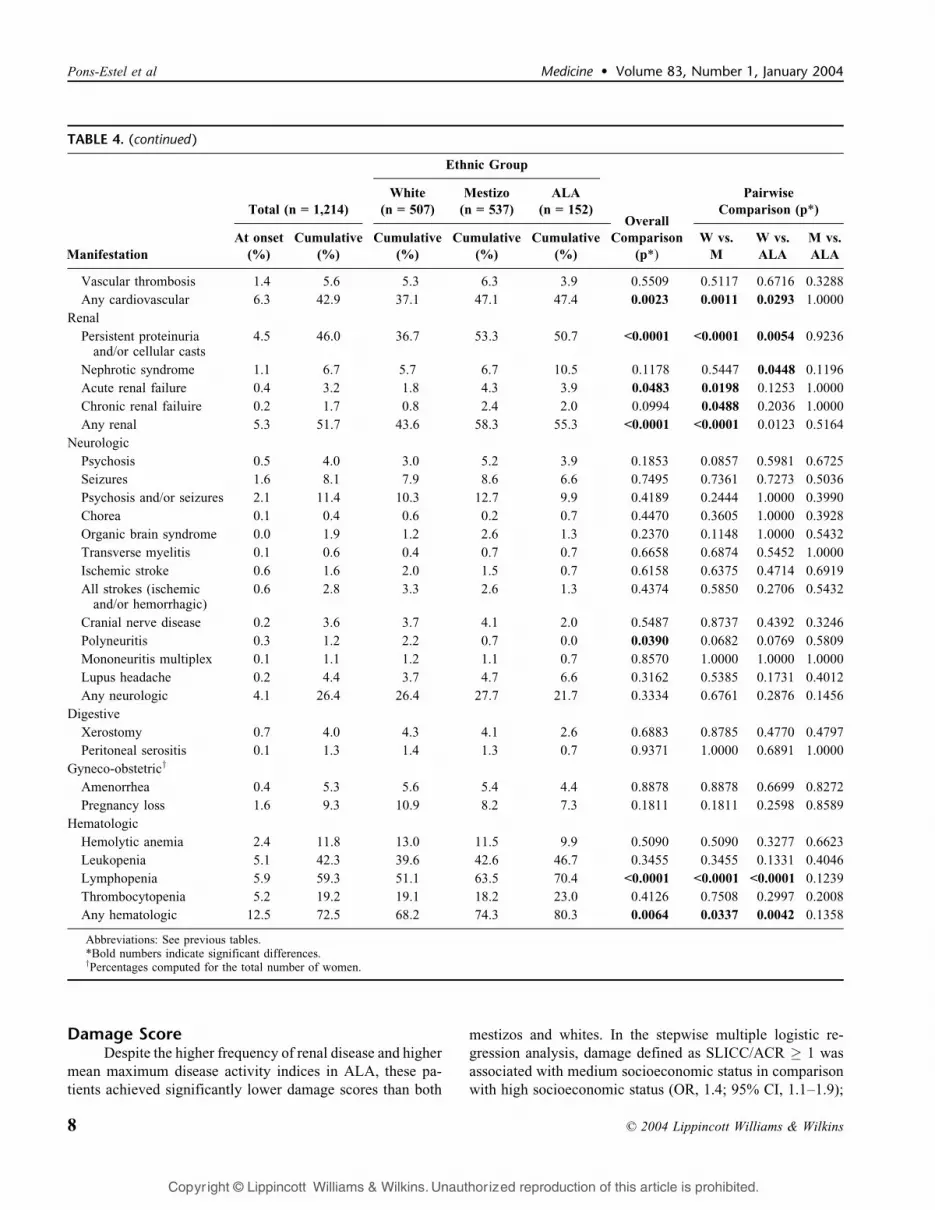
Damage ScoreDespite the higher frequency of renal disease and higher
mean maximum disease activity indices in ALA, these pa-
tients achieved significantly lower damage scores than both
mestizos and whites. In the stepwise multiple logistic re-
gression analysis, damage defined as SLICC/ACR � 1 was
associated with medium socioeconomic status in comparison
with high socioeconomic status (OR, 1.4; 95% CI, 1.1–1.9);
TABLE 4. (continued )
Ethnic Group
Total (n = 1,214)
White
(n = 507)
Mestizo
(n = 537)
ALA
(n = 152)Overall
Pairwise
Comparison (p*)
Manifestation
At onset
(%)
Cumulative
(%)
Cumulative
(%)
Cumulative
(%)
Cumulative
(%)
Comparison
(p*)
W vs.
M
W vs.
ALA
M vs.
ALA
Vascular thrombosis 1.4 5.6 5.3 6.3 3.9 0.5509 0.5117 0.6716 0.3288
Any cardiovascular 6.3 42.9 37.1 47.1 47.4 0.0023 0.0011 0.0293 1.0000
Renal
Persistent proteinuriaand/or cellular casts
4.5 46.0 36.7 53.3 50.7 <0.0001 <0.0001 0.0054 0.9236
Nephrotic syndrome 1.1 6.7 5.7 6.7 10.5 0.1178 0.5447 0.0448 0.1196
Acute renal failure 0.4 3.2 1.8 4.3 3.9 0.0483 0.0198 0.1253 1.0000
Chronic renal failuire 0.2 1.7 0.8 2.4 2.0 0.0994 0.0488 0.2036 1.0000
Any renal 5.3 51.7 43.6 58.3 55.3 <0.0001 <0.0001 0.0123 0.5164
Neurologic
Psychosis 0.5 4.0 3.0 5.2 3.9 0.1853 0.0857 0.5981 0.6725
Seizures 1.6 8.1 7.9 8.6 6.6 0.7495 0.7361 0.7273 0.5036
Psychosis and/or seizures 2.1 11.4 10.3 12.7 9.9 0.4189 0.2444 1.0000 0.3990
Chorea 0.1 0.4 0.6 0.2 0.7 0.4470 0.3605 1.0000 0.3928
Organic brain syndrome 0.0 1.9 1.2 2.6 1.3 0.2370 0.1148 1.0000 0.5432
Transverse myelitis 0.1 0.6 0.4 0.7 0.7 0.6658 0.6874 0.5452 1.0000
Ischemic stroke 0.6 1.6 2.0 1.5 0.7 0.6158 0.6375 0.4714 0.6919
All strokes (ischemicand/or hemorrhagic)
0.6 2.8 3.3 2.6 1.3 0.4374 0.5850 0.2706 0.5432
Cranial nerve disease 0.2 3.6 3.7 4.1 2.0 0.5487 0.8737 0.4392 0.3246
Polyneuritis 0.3 1.2 2.2 0.7 0.0 0.0390 0.0682 0.0769 0.5809
Mononeuritis multiplex 0.1 1.1 1.2 1.1 0.7 0.8570 1.0000 1.0000 1.0000
Lupus headache 0.2 4.4 3.7 4.7 6.6 0.3162 0.5385 0.1731 0.4012
Any neurologic 4.1 26.4 26.4 27.7 21.7 0.3334 0.6761 0.2876 0.1456
Digestive
Xerostomy 0.7 4.0 4.3 4.1 2.6 0.6883 0.8785 0.4770 0.4797
Peritoneal serositis 0.1 1.3 1.4 1.3 0.7 0.9371 1.0000 0.6891 1.0000
Gyneco-obstetricy
Amenorrhea 0.4 5.3 5.6 5.4 4.4 0.8878 0.8878 0.6699 0.8272
Pregnancy loss 1.6 9.3 10.9 8.2 7.3 0.1811 0.1811 0.2598 0.8589
Hematologic
Hemolytic anemia 2.4 11.8 13.0 11.5 9.9 0.5090 0.5090 0.3277 0.6623
Leukopenia 5.1 42.3 39.6 42.6 46.7 0.3455 0.3455 0.1331 0.4046
Lymphopenia 5.9 59.3 51.1 63.5 70.4 <0.0001 <0.0001 <0.0001 0.1239
Thrombocytopenia 5.2 19.2 19.1 18.2 23.0 0.4126 0.7508 0.2997 0.2008
Any hematologic 12.5 72.5 68.2 74.3 80.3 0.0064 0.0337 0.0042 0.1358
Abbreviations: See previous tables.*Bold numbers indicate significant differences.yPercentages computed for the total number of women.
8 n 2004 Lippincott Williams & Wilkins
Pons-Estel et al Medicine � Volume 83, Number 1, January 2004
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
partial or no medical coverage (OR, 1.6; 95% CI, 1.2–2.1);
and disease duration (OR, 1.5; 95% CI, 1.2–2). On the other
hand, urban residence was protective (OR, 0.6; 95% CI, 0.4–0.9).
Autoantibodies and ComplementAlthough autoantibodies and complement levels have
not been tested systematically within the cohort up to now,
and the results have not been subjected yet to interlaboratory
control, the results give some insight into potential differ-
ences between the 3 major ethnic groups (Table 9). These
should, however, be taken with caution. Antinuclear anti-
bodies were significantly less prevalent in mestizos than in
whites and ALA. Antidouble-stranded DNA antibodies were
significantly more frequent in mestizos than in whites,
and IgM anticardiolipin antibodies were significantly less
frequent in ALA than in whites and mestizos. Both ALA and
whites had low complement levels, including C3 and C4,
more frequently than mestizos.
TreatmentCumulative treatment regimens are described in
Table 10. Steroids were used in 92% and antimalarials
in 75% of patients in the cohort. Immunosuppressive agents
were received by 47% of patients with intravenous cy-
clophosphamide predominating, followed by azathioprine.
Forty-two (3.45%) patients entered dialysis and 2 received
renal transplants. When this was analyzed for the different
ethnic groups, differences appeared in the use of antimalarials
and immunosuppressive agents. Chloroquine was significant-
ly more frequently used in mestizos and ALA compared with
whites, and the reverse was true for hydroxychloroquine.
Some of these differences may reflect cost and drug availabil-
ity in our countries (ie, chloroquine is less costly). Overall
immunosuppressive use was more frequent in nonwhites,
particularly significant when compared with mestizos.
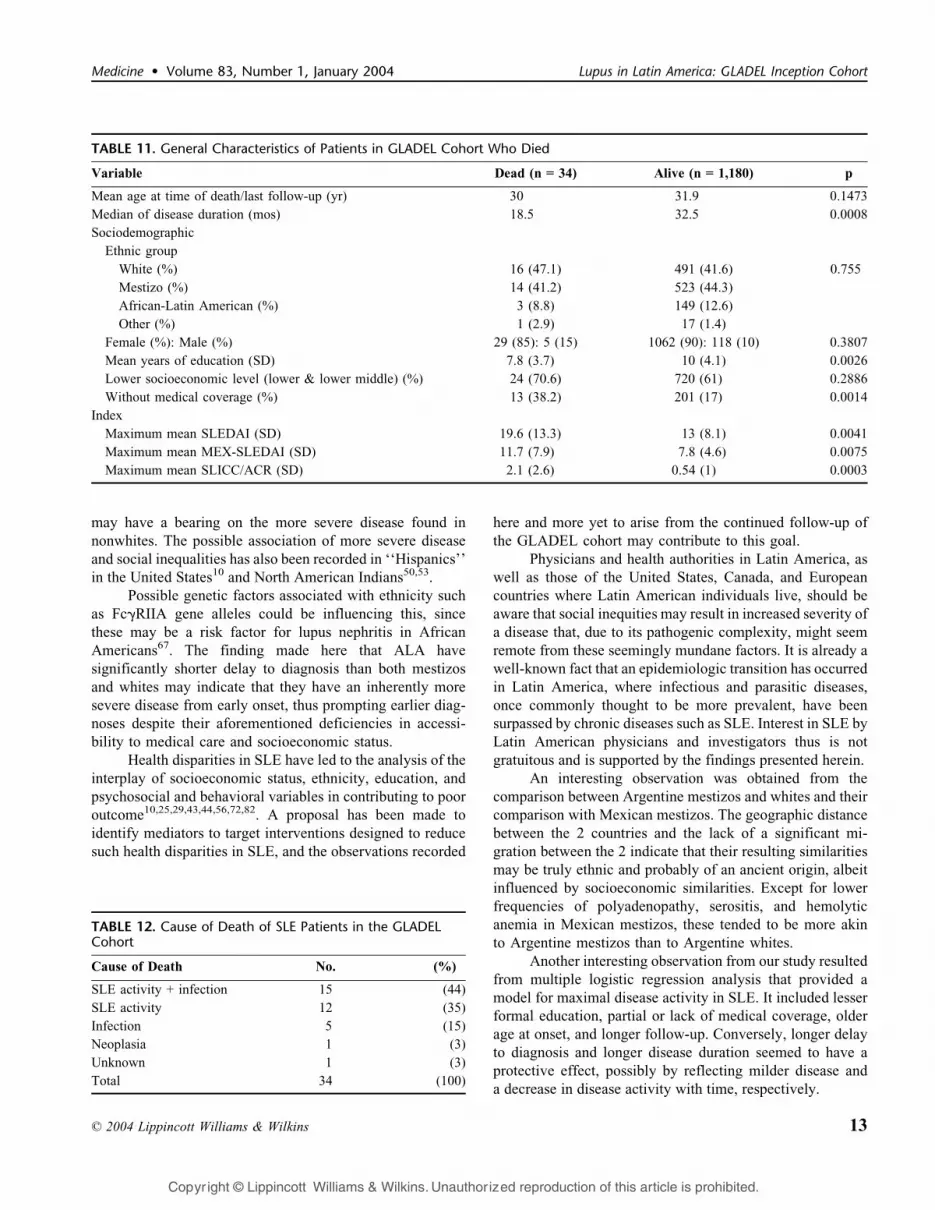
MortalityThirty-four patients (2.8%) died within the GLADEL
cohort. Their general characteristics are presented in
Table 11. The survival rate at 4 years was 95%. Because
of the small number of patients who died, we compared
survival rates between whites and the rest of the cohort
(nonwhites) rather than between the 3 major ethnic groups.
There were no significant differences in survival rates
between whites and nonwhites. However, nonwhites who
died had lower age at disease onset and lower age at the time
of death than whites (p = 0.05 and p = 0.03, respectively).
Patients who died had lower education level, lower socio-
economic status, and poorer medical coverage. Obviously
they had higher mean activity indices and SLICC/ACR
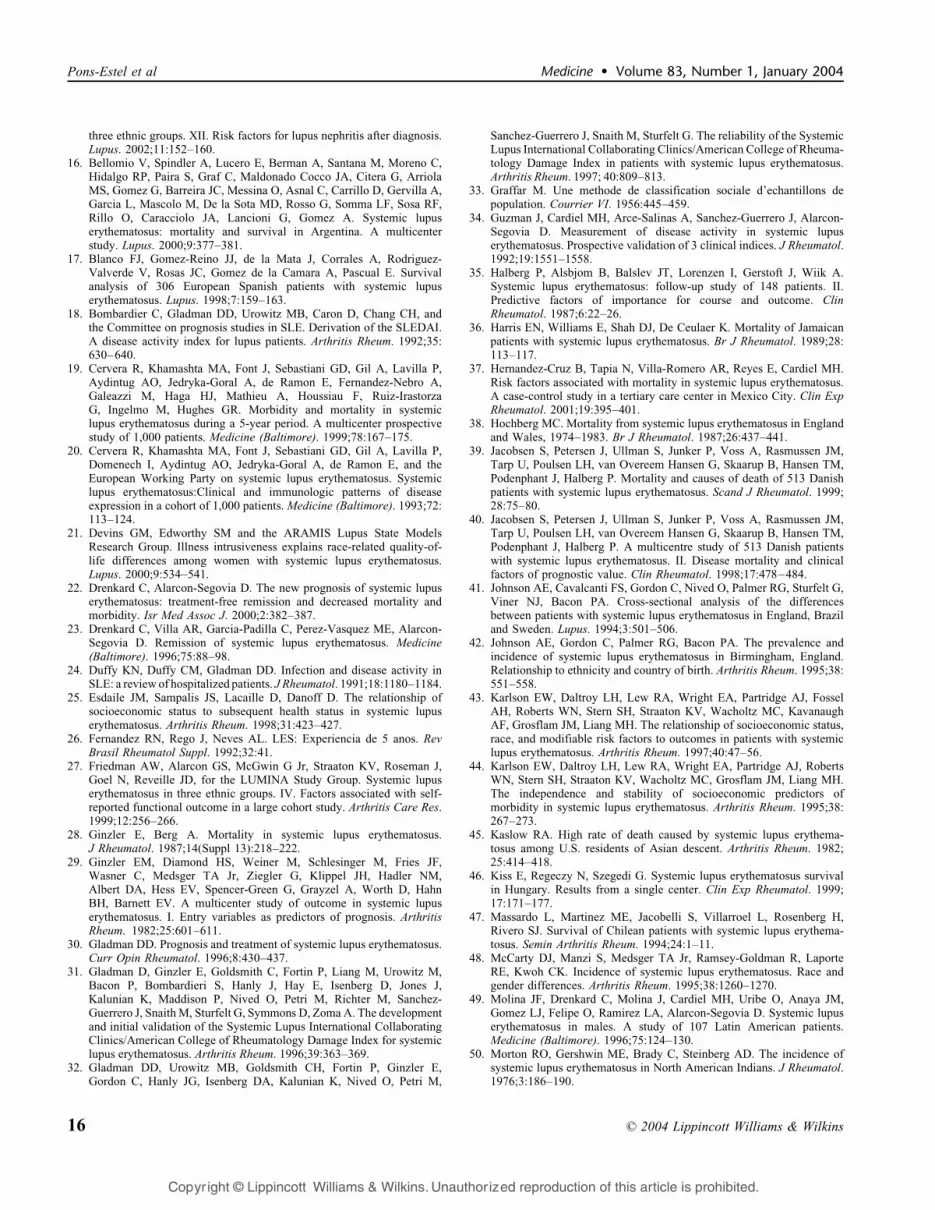
scores than those who survived. The causes of death are
presented in Table 12.
TABLE 5. Comparison of Ethnic Groups, Multivariate Models Obtained by Multiple Logistic Regression Analysis
Ethnic Group
Model*
RenalDamage
Yes vs. No
(n = 558/n = 655)
Model*
LymphopeniaYes vs. No
(n = 720/n = 493)
Modely
SLEDAI
�12 vs. <12
(n = 584/
n = 567)
Modelz
MEX-SLEDAI
�8 vs. <8
(n = 567/
n = 577)
Modelx
SLICC
�1 vs. <0
n = 353/
n = 690
Model*
ACR Criteria
�6 vs. <6
(n = 653/
n = 560)
Model*
Death
Yes vs. No
(n = 34/
n = 1179)
White(n = 507)
OR 1.0 1.0 1.0 1.0 1.0 1.0 1.0
Mestizo(n = 537)
OR 1.95 1.58 1.02 1.10 0.75 0.73 0.6495% CI 1.36–2.80 1.12–2.24 0.71–1.46 0.76–1.59 0.50–1.12 0.52–1.05 0.21–1.95
p <0.0001 0.01 0.94 0.63 0.16 0.09 0.43
African-LatinAmerican(n = 152)
OR 1.23 2.10 1.23 0.78 0.78 1.08 0.9295% CI 0.79–1.93 1.34–3.29 0.77–1.96 0.48–1.25 0.45–1.36 0.69–1.67 0.19–4.42
p 0.36 0.001 0.38 0.30 0.39 0.74 0.91
Other(n = 18)
OR 1.65 2.12 0.74 0.76 0.98 0.96 1.6895% CI 0.62–4.43 0.76–5.96 0.28–1.96 0.28–2.06 0.34–2.84 0.36–2.57 0.16–18.04
p 0.32 0.15 0.55 0.59 0.98 0.93 0.67
*One missing value in this model.ySixty-three missing values in this model.zSeventy missing values in this model.xOne hundred seventy-one missing values in this model.All of the models adjusted by: Gender (female vs. male), education (<10 vs. �10 yr.), medical coverage (partial or no coverage vs. full medical coverage),
age at SLE diagnosis (>27 vs. �27 yr), delay to SLE diagnosis (�6 vs. <6 mo) follow-up (�20 vs. <20 mo), number of hospitalizations (�1 vs. 0), maritalstatus (married or free union vs. all others), socioeconomic status (lower middle/lower vs. all others), and country (factored as dummy variables: Argentina vs.Mexico, Argentina vs. Brazil, Argentina vs. Colombia, Argentina vs. Chile, and Argentina vs. other countries).
n 2004 Lippincott Williams & Wilkins 9
Medicine � Volume 83, Number 1, January 2004 Lupus in Latin America: GLADEL Inception Cohort
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Mortality could be predicted in a stepwise logistic
regression model by the following: education (<10 yr vs.
�10 yr; OR, 3.2; 95% CI, 1.3–7.6), SLICC score (�1 vs. 0;
OR, 2.8; 95% CI, 1.2–6.4), time of follow-up (�20 mo vs.
<20 mo; OR, 0.26; 95% CI, 0.10–0.65), marital status (single
vs. others; OR, 2.4; 95% CI, 1.0–5.7), medical coverage
(partial or no coverage vs. full medical coverage; OR, 2.7;
95% CI, 1.1–6.5), and country (Argentina vs. the rest; OR,
3.0; 95% CI, 1.3–7.1).
DISCUSSIONWe describe the GLADEL cohort, a multicenter, mul-
tinational, prospective inception cohort of Latin American
SLE patients seen in their countries of origin and treated by
their local physicians. Both the size and origin of this cohort
make it unique. An effort was made to keep equilibrium so
no single group with a large number of patients would
predominate and introduce a bias. Data were entered into a
user-friendly database that requires no writing and crosses
language barriers, thus allowing participation of Portuguese-
speaking groups. Throughout the study, a supervising group
conducted quality control of the data entered, facilitated by
built-in characteristics of the database that detect contra-
dictions. In addition, individuals coordinating the cohort were
in regular communication and had periodic meetings to set
policies and define variables and terms. The ultimate size of
the cohort will now be predetermined in order to have patient
representation from each country according to its population.
Latin America is a large subcontinent rich in the
variety of racial admixtures between and within countries. In
TABLE 6. Comparison of Sociodemographic Characteristics and Clinical Manufestations of SLE Between White and Mestizos fromArgentina and Mestizos from Mexico
Ethnic Group
Argentine
White
(n = 260)
Argentine
Mestizo
(n = 54)
Mexican
Mestizo
(n = 236) Overall
Comparison AW vs. AW vs. AM vs.
Variable (%) (%) (%) (p*) AM MM MM
GenderFemale 90.0 88.9 87.3 0.6280 0.8056 0.3945 1.000
Male 10.0 11.1 12.7
Socioeconomic statusUpper/upper middle 11.5 0.0 8.0 <0.0001 <0.0001 <0.0001 0.0149
Middle 44.6 11.1 19.5
Lower middle/lower 43.9 88.9 72.5
Medical insuranceFull medical coverage 54.1 33.3 47.0 0.0154 0.0069 0.1266 0.0708
Partial or no coverage 45.9 66.7 53.0
EducationYears of education
(mean, SD)10.8 (4.1) 8.9 (3.2) 9.1 (3.6) <0.0001 0.0017 <0.0001 0.9386
Clinical manifestationFever 62.7 57.4 46.6 0.0014 0.5385 0.0004 0.1735
Polyadenopathy 17.7 22.2 10.6 0.0226 0.4433 0.0288 0.0388
Photosensitivity 53.8 33.3 52.5 0.0201 0.0070 0.7875 0.0153
Oral/nasal ulcers 39.2 29.6 50.0 0.0064 0.2178 0.0186 0.0097
Livedo reticularis 7.7 14.8 14.8 0.0273 0.1135 0.0145 1.0000
Sicca syndrome 13.8 11.1 6.8 0.0329 0.8259 0.0122 0.2643
Persistent proteinuria/cell cast
35.8 51.8 53.0 <0.0001 0.0317 0.0001 0.8813
Psychosis 1.5 7.4 5.9 0.0108 0.0322 0.0140 0.7537
Hemolytic anemia 15.8 18.5 6.8 0.0018 0.6849 0.0018 0.0141
Lymphopenia 48.1 64.8 66.9 <0.0001 0.0356 <0.0001 0.7520
Abbreviations: AW, Argentine white; AM, Argentine mestizo; MM, Mexican mestizo.*Bold numbers indicate significant differences of clinical manifestaions.
Pairwise Comparison (p*)
10 n 2004 Lippincott Williams & Wilkins
Pons-Estel et al Medicine � Volume 83, Number 1, January 2004
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
addition, socioeconomic, educational, and demographic var-
iations are prominent, and these sometimes are related to
ethnic groups through their economic predominance. Thus,
the apparent homogeneity of Latin Americans is a myth, and
within the subcontinent lies great diversity. The reason for
the apparent homogeneity is the predominance of 2 related
languages, Spanish and Portuguese, which has resulted in
the unfortunate terminology of ‘‘Hispanic’’ based mainly
on the former language being spoken by many Latin
Americans and their descendants now living in English-
speaking North America.
The influences of ethnic, social, and demographic
variables on the clinical characteristics of SLE patients have
already been demonstrated by other studies. Thus, in series
from both the United States and Europe, more severe disease
was noticed in nonwhite patients5,10,28,29,45,56,63,72,74,75,80. In
our study, both ALA and mestizos had more severe disease
than did whites, as evidenced by a higher frequency of renal
disease, pericarditis, polyadenopathy, and discoid lesions in
ALA. In addition, both ALA and mestizos had higher
maximum disease activity indices than whites, but this was
lost when controlled by country. However, damage scores
tended to be lower in ALA than in both mestizos and whites,
a surprising finding that might be explained by shorter
disease duration or by the more recent incorporation of
Brazilian and Cuban groups into the study. Longer follow-up
in the GLADEL cohort may help determine if ethnicity does
actually play a role in the resulting damage from SLE.
A peculiar observation was that of a significantly lower
frequency of both xerophthalmia and sicca syndrome (both
TABLE 7. Comparison of Argentine Whites and Mestizos and Mexican Mestizos, Multivariate Models Obtained by MultipleLogistic Regression Analysis
Ethnic Group
Model*
Renal
Damage
Yes vs. No
(n = 245/
n = 304)
Model*
Lymphopenia
Yes vs. No
(n = 318/
n = 231)
Modely
SLEDAI
�12 vs. <12
(n = 217/
n = 299)
Modely
MEX-SLEDAI
�8 vs. <8
(n = 234)/
n = 282
Modelz
SLICC
�1 vs. 0
(n = 184/
n = 292)
Model*
ACR Criteria
�6 vs. <6
(n = 284/
n = 265)
Model*
Death
Yes vs. No
(n = 20/
n = 529)
Argentinewhite(n = 260)
OR 1.0 1.0 1.0 1.0 1.0 1.0 1.0
ArgentineMestizo(n = 54)
OR 1.68 2.37 0.77 0.54 0.97 0.53 2.9795% CI 0.86–3.28 1.23–4.60 0.39–1.53 0.27–1.09 0.48–1.95 0.27–1.01 0.71–12.4
p 0.13 0.01 0.45 0.09 0.93 0.06 0.14
MexicanMestizo(n = 236)
OR 1.93 2.36 0.87 1.30 0.71 0.57 0.4195% CI 1.27–2.92 1.57–3.53 0.56–1.34 0.84–2.00 0.45–1.13 0.38–0.85 0.12–1.33
p 0.002 <0.0001 0.52 0.24 0.15 0.007 0.14
*One missing value in this model.yThirty-four missing values in this model.zSeventy-four missing values in this model.All of the models adjusted by: gender (female vs. male), education (<10 vs. �10 yr), medical coverage (partial or no coverage vs. full medical coverage),
age at SLE diagnosis (>27 vs. �27 yr), delay to SLE diagnosis (�6 vs. <6 mo), follow-up (�20 vs. <20 mo), number of hospitalizations (�1 vs. 0), maritalstatus (single vs. all others), and socioeconomic status (lower middle/lower vs. all others).
TABLE 8. Maximum Activity and Damage Scores in Patients in GLADEL Cohort. Comparisons Between the 3 Major Ethnic Groups
Ethnic Group Overall
ComparisonPairwise Comparison (p)
Variable Total White Mestizo ALA (p) W vs. M W vs. ALA M vs. ALA
Maximum meanSLEDAI*(SD)
13.1 (8.3) 12 (7.9) 13.5 (8.5) 15.6 (8.9) <0.0001 0.0033 <0.0001 0.0078
Maximum meanMEX-SLEDAI*(SD)
7.9 (4.8) 7.1 (4.8) 8.4 (4.6) 8.6 (4.9) <0.0001 <0.0001 0.0014 0.9851
Maximum meanSLICC/ACR*(SD)
0.58 (1.1) 0.60 (1.1) 0.59 (1) 0.42 (1) 0.0252 0.6874 0.0175 0.0070
Abbreviations: See previous tables.*Average of the maximum score for each patient.
n 2004 Lippincott Williams & Wilkins 11
Medicine � Volume 83, Number 1, January 2004 Lupus in Latin America: GLADEL Inception Cohort
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
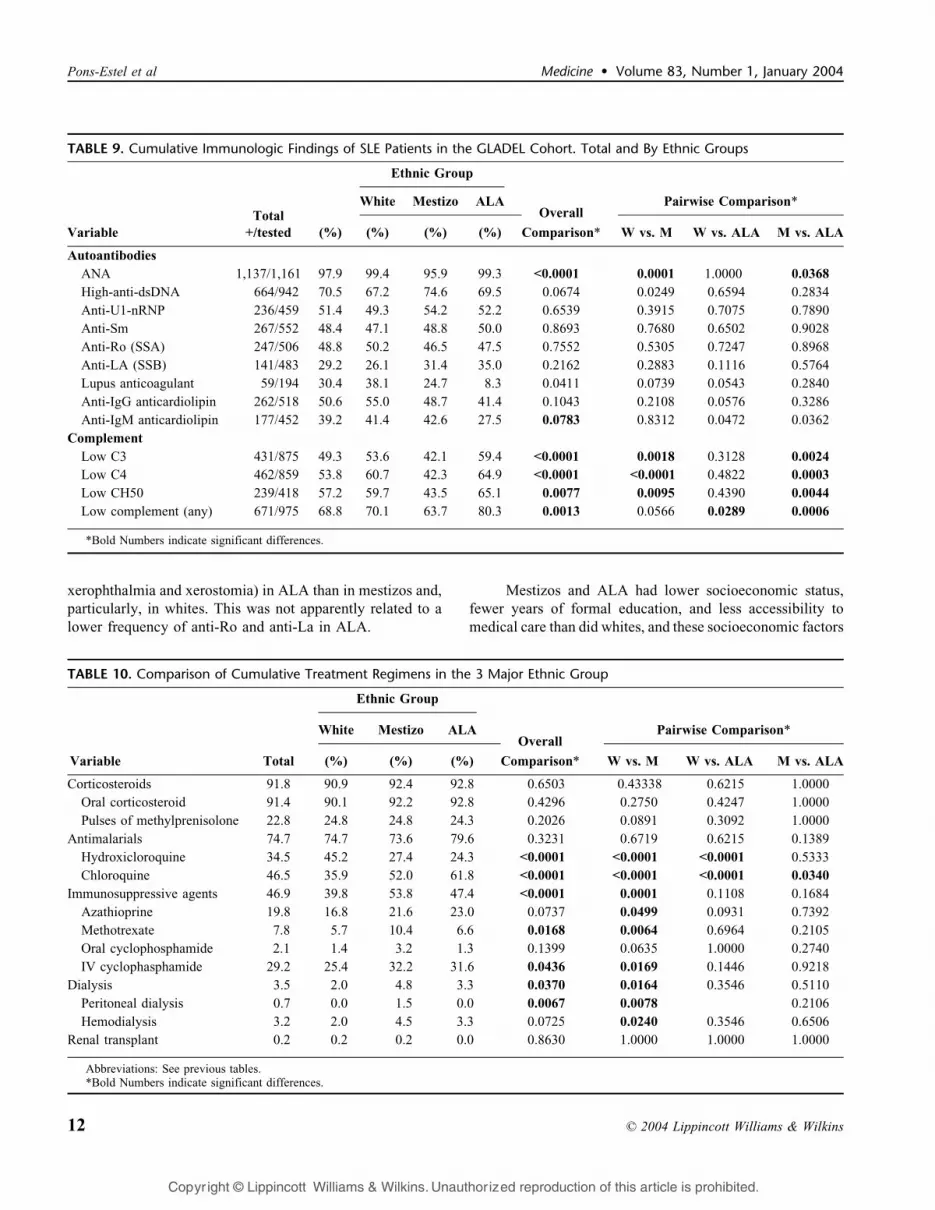
xerophthalmia and xerostomia) in ALA than in mestizos and,
particularly, in whites. This was not apparently related to a
lower frequency of anti-Ro and anti-La in ALA.
Mestizos and ALA had lower socioeconomic status,
fewer years of formal education, and less accessibility to
medical care than did whites, and these socioeconomic factors
TABLE 9. Cumulative Immunologic Findings of SLE Patients in the GLADEL Cohort. Total and By Ethnic Groups
Variable
Total
+/tested
Ethnic Group
White Mestizo ALAOverall
Pairwise Comparison*
(%) (%) (%) (%) Comparison* W vs. M W vs. ALA M vs. ALA
Autoantibodies
ANA 1,137/1,161 97.9 99.4 95.9 99.3 <0.0001 0.0001 1.0000 0.0368
High-anti-dsDNA 664/942 70.5 67.2 74.6 69.5 0.0674 0.0249 0.6594 0.2834
Anti-U1-nRNP 236/459 51.4 49.3 54.2 52.2 0.6539 0.3915 0.7075 0.7890
Anti-Sm 267/552 48.4 47.1 48.8 50.0 0.8693 0.7680 0.6502 0.9028
Anti-Ro (SSA) 247/506 48.8 50.2 46.5 47.5 0.7552 0.5305 0.7247 0.8968
Anti-LA (SSB) 141/483 29.2 26.1 31.4 35.0 0.2162 0.2883 0.1116 0.5764
Lupus anticoagulant 59/194 30.4 38.1 24.7 8.3 0.0411 0.0739 0.0543 0.2840
Anti-IgG anticardiolipin 262/518 50.6 55.0 48.7 41.4 0.1043 0.2108 0.0576 0.3286
Anti-IgM anticardiolipin 177/452 39.2 41.4 42.6 27.5 0.0783 0.8312 0.0472 0.0362
Complement
Low C3 431/875 49.3 53.6 42.1 59.4 <0.0001 0.0018 0.3128 0.0024
Low C4 462/859 53.8 60.7 42.3 64.9 <0.0001 <0.0001 0.4822 0.0003
Low CH50 239/418 57.2 59.7 43.5 65.1 0.0077 0.0095 0.4390 0.0044
Low complement (any) 671/975 68.8 70.1 63.7 80.3 0.0013 0.0566 0.0289 0.0006
*Bold Numbers indicate significant differences.
TABLE 10. Comparison of Cumulative Treatment Regimens in the 3 Major Ethnic Group
Variable Total
Ethnic Group
White Mestizo ALAOverall
Pairwise Comparison*
(%) (%) (%) Comparison* W vs. M W vs. ALA M vs. ALA
Corticosteroids 91.8 90.9 92.4 92.8 0.6503 0.43338 0.6215 1.0000
Oral corticosteroid 91.4 90.1 92.2 92.8 0.4296 0.2750 0.4247 1.0000
Pulses of methylprenisolone 22.8 24.8 24.8 24.3 0.2026 0.0891 0.3092 1.0000
Antimalarials 74.7 74.7 73.6 79.6 0.3231 0.6719 0.6215 0.1389
Hydroxicloroquine 34.5 45.2 27.4 24.3 <0.0001 <0.0001 <0.0001 0.5333
Chloroquine 46.5 35.9 52.0 61.8 <0.0001 <0.0001 <0.0001 0.0340
Immunosuppressive agents 46.9 39.8 53.8 47.4 <0.0001 0.0001 0.1108 0.1684
Azathioprine 19.8 16.8 21.6 23.0 0.0737 0.0499 0.0931 0.7392
Methotrexate 7.8 5.7 10.4 6.6 0.0168 0.0064 0.6964 0.2105
Oral cyclophosphamide 2.1 1.4 3.2 1.3 0.1399 0.0635 1.0000 0.2740
IV cyclophasphamide 29.2 25.4 32.2 31.6 0.0436 0.0169 0.1446 0.9218
Dialysis 3.5 2.0 4.8 3.3 0.0370 0.0164 0.3546 0.5110
Peritoneal dialysis 0.7 0.0 1.5 0.0 0.0067 0.0078 0.2106
Hemodialysis 3.2 2.0 4.5 3.3 0.0725 0.0240 0.3546 0.6506
Renal transplant 0.2 0.2 0.2 0.0 0.8630 1.0000 1.0000 1.0000
Abbreviations: See previous tables.*Bold Numbers indicate significant differences.
12 n 2004 Lippincott Williams & Wilkins
Pons-Estel et al Medicine � Volume 83, Number 1, January 2004
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
may have a bearing on the more severe disease found in
nonwhites. The possible association of more severe disease
and social inequalities has also been recorded in ‘‘Hispanics’’
in the United States10 and North American Indians50,53.
Possible genetic factors associated with ethnicity such
as FcgRIIA gene alleles could be influencing this, since
these may be a risk factor for lupus nephritis in African
Americans67. The finding made here that ALA have
significantly shorter delay to diagnosis than both mestizos
and whites may indicate that they have an inherently more
severe disease from early onset, thus prompting earlier diag-
noses despite their aforementioned deficiencies in accessi-
bility to medical care and socioeconomic status.
Health disparities in SLE have led to the analysis of the
interplay of socioeconomic status, ethnicity, education, and
psychosocial and behavioral variables in contributing to poor
outcome10,25,29,43,44,56,72,82. A proposal has been made to
identify mediators to target interventions designed to reduce
such health disparities in SLE, and the observations recorded
here and more yet to arise from the continued follow-up of
the GLADEL cohort may contribute to this goal.
Physicians and health authorities in Latin America, as
well as those of the United States, Canada, and European
countries where Latin American individuals live, should be
aware that social inequities may result in increased severity of
a disease that, due to its pathogenic complexity, might seem
remote from these seemingly mundane factors. It is already a
well-known fact that an epidemiologic transition has occurred
in Latin America, where infectious and parasitic diseases,
once commonly thought to be more prevalent, have been
surpassed by chronic diseases such as SLE. Interest in SLE by
Latin American physicians and investigators thus is not
gratuitous and is supported by the findings presented herein.
An interesting observation was obtained from the
comparison between Argentine mestizos and whites and their
comparison with Mexican mestizos. The geographic distance
between the 2 countries and the lack of a significant mi-
gration between the 2 indicate that their resulting similarities
may be truly ethnic and probably of an ancient origin, albeit
influenced by socioeconomic similarities. Except for lower
frequencies of polyadenopathy, serositis, and hemolytic
anemia in Mexican mestizos, these tended to be more akin
to Argentine mestizos than to Argentine whites.
Another interesting observation from our study resulted
from multiple logistic regression analysis that provided a
model for maximal disease activity in SLE. It included lesser
formal education, partial or lack of medical coverage, older
age at onset, and longer follow-up. Conversely, longer delay
to diagnosis and longer disease duration seemed to have a
protective effect, possibly by reflecting milder disease and
a decrease in disease activity with time, respectively.
TABLE 11. General Characteristics of Patients in GLADEL Cohort Who Died
Variable Dead (n = 34) Alive (n = 1,180) p
Mean age at time of death/last follow-up (yr) 30 31.9 0.1473
Median of disease duration (mos) 18.5 32.5 0.0008
Sociodemographic
Ethnic group
White (%) 16 (47.1) 491 (41.6) 0.755
Mestizo (%) 14 (41.2) 523 (44.3)
African-Latin American (%) 3 (8.8) 149 (12.6)
Other (%) 1 (2.9) 17 (1.4)
Female (%): Male (%) 29 (85): 5 (15) 1062 (90): 118 (10) 0.3807
Mean years of education (SD) 7.8 (3.7) 10 (4.1) 0.0026
Lower socioeconomic level (lower & lower middle) (%) 24 (70.6) 720 (61) 0.2886
Without medical coverage (%) 13 (38.2) 201 (17) 0.0014
Index
Maximum mean SLEDAI (SD) 19.6 (13.3) 13 (8.1) 0.0041
Maximum mean MEX-SLEDAI (SD) 11.7 (7.9) 7.8 (4.6) 0.0075
Maximum mean SLICC/ACR (SD) 2.1 (2.6) 0.54 (1) 0.0003
TABLE 12. Cause of Death of SLE Patients in the GLADELCohort
Cause of Death No. (%)
SLE activity + infection 15 (44)
SLE activity 12 (35)
Infection 5 (15)
Neoplasia 1 (3)
Unknown 1 (3)
Total 34 (100)
n 2004 Lippincott Williams & Wilkins 13
Medicine � Volume 83, Number 1, January 2004 Lupus in Latin America: GLADEL Inception Cohort
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Although our cohort is still young, it is thought pro-
voking that patients who died within the GLADEL cohort
had both poorer education and poorer medical coverage than
those who are still alive. As in other series2,3,24,57,66,76,77,82,
infection was an important cause of death of lupus patients in
the GLADEL cohort. A bimodal mortality pattern has been
shown in systemic lupus erythematosus76. Our inception
cohort has a median follow-up of 32 months. This was a
limiting factor for reporting events that occur later in the
disease course (second peak of mortality) such as cardio-
vascular mortality. The study of this would be among the
objectives of continued follow-up of this cohort. In addition,
SLE is a paradigm of complex disease where predisposing
disease-modifying and pharmacodynamic-influencing genes
interplay with environmental and hormonal factors to cause
an extraordinary heterogeneity12. Continued analysis of a
cohort with the characteristics described herein, ideally with
the concurrent study of participating genes, may help us to
dissect and, in time, understand the role of each in its
diversity. A recent observation of the association with SLE
of allele A of the SNP PD-1.3 of the PD-1 gene in the 2q37.3
chromosome region in Europeans, less frequent in Mexicans
and practically absent in African-Americans, suggests it to
be a recent mutation affecting mostly Europeans and, to a
lesser extent, populations admixed with them59. Analyses of
European populations and their admixtures within the Latin
American subcontinent as included in the GLADEL cohort
for associations with this and other genetic markers may help
determine the role of the various lupus-predisposing genes in
the clinical spectrum of SLE.
Our analysis of 3 major ethnic groups in this Latin
American lupus cohort gives us further insight into the role
of ethnicity and the associated social inequalities on the
clinical manifestations and outcomes of lupus. We also see
clearly that, at least as pertaining to SLE, ‘‘Hispanics’’ is not
a homogenous group.
The differences between Hispanic whites, mestizos,
and ALA are well recognized in patients living in Latin
America. However the differences should be of particular
relevance for Latin American patients living in North
America or Europe, where most of these patients would be
grouped together as Hispanics. The differences found in the
GLADEL cohort should be helpful for diagnosis and treat-
ment of these patients, since their clinical behavior may
be different. When a physician encounters a ‘‘Hispanic’’
patient with SLE, further efforts to characterize his or her
country of origin and ethnic background should provide
useful information.
ACKNOWLEDGMENTS
The authors express their gratitude to Daniel Wojdyla
for assistance in handling the database and statistical analysis
of the GLADEL cohort and to Daniel Villalba and Leonardo
Grasso for assistance with the software ARTHROS 6.0.
APPENDIX: GLADEL CO-AUTHORS
Coordinators: Bernardo A. Pons-Estel and Donato
Alarcon-Segovia. The following participants are members of
Grupo Latinoamericano de Estudio del Lupus (GLADEL)
and have incorporated at least 20 patients into the database.
ARGENTINA: Patricia M. Imamura, Seccion Reuma-
tologıa, Servicio de Clınica Medica Hospital Italiano,
Buenos Aires; Jorge A. Manni, Sebastian Grimaudo, and
Judith Sarano, Departamento de Inmunologıa, Instituto de
Investigaciones Medicas ‘‘Alfredo Lanari’’, Buenos Aires;
Jose A. Maldonado-Cocco, Maria S. Arriola, and Graciela
Gomez, Servicio de Reumatologıa, Instituto de Rehabilita-
cion Psicofısica, Buenos Aires; Mercedes A. Garcıa, Ana
Ines Marcos, and Juan Carlos Marcos, Servicio de Reuma-
tologıa, Hospital Interzonal General de Agudos General San
Martın, La Plata; Hugo R. Scherbarth, Pilar C. Marino, and
Estela L. Motta, Servicio de Reumatologıa, Hospital
Interzonal General de Agudos ‘‘Dr. Oscar Alende’’ Mar
del Plata; Cristina Drenkard, Susana Gamron, and Carlos M.
Onetti, Servicio de Reumatologıa, UHMI1, Hospital Nacio-
nal de Clınicas, Cordoba; Veronica Saurit, Servicio de
Reumatologıa, Hospital Privado, Centro Medico de Cordoba,
Cordoba; Norberto Quagliatto, Alberto A. Gentiletti, and
Daniel Machado, Servicio de Reumatologıa, Hospital
Provincial de Rosario, Rosario; Marcelo Abdala and Simon
Palatnik, Servicio de Reumatologıa, Hospital Provincial del
Centenario, Rosario; Guillermo Berbotto and Carlos A.
Battagliotti, Servicio de Reumatologıa Hospital Escuela Eva
Peron, Granadero Baigorria, Rosario, Argentina.
BRAZIL: Emilia Sato, Elaine M. C. Sella, and
Alexandre W. S. Souza, Disciplina de Reumatologıa, Uni-
versidade Federal da Sao Paulo (UNIFESP), Sao Paulo; Lilian
T. Lavras Costallat, Manoel Barros Bertolo, and Ibsen Bellini
Coimbra, Divisao de Reumatologıa, Faculdade de Ciencias
Medicas, Universidade Estadual da Campinas, Campinas;
Eduardo Ferreira Borba Neto and Eloisa Bonfa, Divisao de
Reumatologıa, Faculdade da Medicina, Universidade da Sao
Paulo, Sao Paulo; Joao Carlos Tavares Brenol, Ricardo
Xavier, and Joao Marasca, Servico de Reumatologıa, Hospital
da Clinicas da Porto Alegre, Universidade Federal do Rio
Grande do Sul; Fernando de Souza Cavalcanti, Angela Luzia
Branco Duarte, and Claudia Diniz Lopes Marques, Disciplina
de Reumatologıa, Centro de Ciencias da Saude, Universidade
Federal da Pernambuco, Pernambuco; Nilzio Antonio Da
Silva, Ana Carolina de O. e Silva, and Tatiana Ferracine
Pacheco, Servico da Reumatologıa, Faculdade de Medicina,
Universidade Federal de Goias, Goiania.
COLOMBIA: Jose Fernando Molina-Restrepo, Servi-
cio de Reumatologıa, Hospital Pablo Tobon Uribe, and Javier
Molina-Lopez, Seccion de Reumatologıa, Universidad de
14 n 2004 Lippincott Williams & Wilkins
Pons-Estel et al Medicine � Volume 83, Number 1, January 2004
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Antioquia, Hospital Universitario San Vicente de Paul,
Medellın; Antonio Iglesias-Gamarra, Facultad de Medicina,
Universidad Nacional de Colombia, and Antonio Iglesias-
Rodrıguez, Servicio de Reumatologıa, Hospital San Juan de
Dios, Facultad de Medicina, Universidad Nacional, Bogota;
Eduardo Egea-Bermejo, Departamento de Inmunologıa,
Universidad del Norte, Barranquilla; Oscar Uribe-Uribe, Luis
A. Ramırez, and Oscar Felipe, Seccion de Reumatologıa,
Universidad de Antioquia, Hospital Universitario San Vicente
de Paul, Medellın; Renato A. Guzman-Moreno and Jose F.
Restrepo-Suarez, Departamento de Medicina Interna e Inmuno-
Reumatologıa, Clınica Saludcoop 104 y Hospital San Juan
de Dios, Facultad de Medicina, Universidad Nacional de
Colombia, Bogota.
CUBA: Marlene Guibert-Toledano, Gil Alberto Reyes-
Llerena, and Alfredo Hernandez-Martınez, Servicio de
Reumatologıa, Centro de Investigaciones Medico Quirurg-
icas (CIMEQ), La Habana.
CHILE: Loreto Massardo, Nestor Gareca, and Sergio
Jacobelli, Departamento de Inmunologıa Clınica y Reuma-
tologıa, Escuela de Medicina, Pontificia Universidad Cato-
lica de Chile, Santiago; Oscar J. Neira, Leonardo R. Guzman,
and Marıa A. Alvarado, Seccion Reumatologıa, Hospital
del Salvador, Facultad de Medicina, Universidad de Chile,
Santiago.
GUATEMALA: Abraham Garcıa-Kutzbach, Ivette
Castro-Ampie, and Cesar Garcia, Servicio de Reumatologıa,
Hospital Universitario Esperanza, Ciudad de Guatemala.
MEXICO: Virginia Pascual-Ramos, Departamento de
Inmunologıa y Reumatologıa, Instituto Nacional de Ciencias
Medicas y Nutricion Salvador Zubiran, Mexico DF; Leonor
A. Barile-Fabris and Juan Manuel Miranda-Limon, Departa-
mento de Reumatologıa, Hospital de Especialidades, Centro
Medico Nacional La Raza, Instituto Mexicano de Seguro
Social, Mexico DF; Mary-Carmen Amigo and Luis H.
Silveira, Departamento de Reumatologıa y Departamento de
Bioquımica, Instituto Nacional de Cardiologıa Ignacio
Chavez, Mexico DF; Ignacio Garcıa De La Torre, Gerardo
Orozco-Barocio, and Magali L. Estrada-Contreras, Departa-
mento de Inmunologıa y Reumatologıa, Hospital General de
Occidente de la Secretarıa de Salud, Guadalajara, Jalisco;
Maria Josefina Sauza del Pozo, Laura E. Aranda Baca, and
Adelfia Urenda Quezada, Servicio de Reumatologıa, Insti-
tuto Mexicano de Seguro Social, Hospital de Especialidades
No 25, Monterrey, NL; Guillermo F. Huerta-Yanez, Servicio
de Reumatologıa, Hospital de Especialidades Miguel Hidal-
go, Aguascalientes.
PERU: Eduardo M. Acevedo-Vasquez, Jose Luis Alfaro-
Lozano, and Jorge M. Cucho-Venegas, Servicio de Reumato-
logıa, Hospital Nacional Guillermo Almenara Irigoyen,
ESSALUD, Lima; Maria Ines Segami, Cesar A. Ugarte, and
Felipe E. Becerra, Servicio de Reumatologıa, Hospital
Nacional Edgardo Rebagliatti Martins, ESSALUD, Lima.
VENEZUELA: Rosa Chacon-Dıaz and Soham Al Snih
Al Snih, Servicio de Reumatologıa, Centro Nacional de
Enfermedades Reumaticas, Hospital Universitario de Cara-
cas, Caracas; Maria H. Esteva-Spinetti and Jorge Vivas,
Unidad de Reumatologıa, Hospital Central de San Cristobal,
San Cristobal.
REFERENCES
1. Abadi I, Gonzalez N. Epidemiologia del lupus eritematoso sistemico enVenezuela. In: Sanchez A, Diaz M, Rondon F, eds. Lupus EritematosoSistemico. Sindrome Clinico e Inmunologico. Bogota: Ediciones ActaMedica Colombiana. 1990:17–22.
2. Abu-Shakra M, Urowitz MB, Gladman DD, Gough J. Mortality studiesin systemic lupus erythematosus. Results from a single center. I. Causesof death. J Rheumatol. 1995;22:1259–1264.
3. Abu-Shakra M, Urowitz MB, Gladman DD, Gough J. Mortality studiesin systemic lupus erythematosus. Results from a single center. II.Predictor variables for mortality. J Rheumatol. 1995;22:1265–1270.
4. Alarcon GS, Cianfrini L, Bradley LA, Sanchez ML, Brooks K,Friedman AW, Baethge BA, Fessler BJ, Bastian HM, Roseman JM,McGwin G Jr, Reveille JD. Systemic lupus erythematosus in threeethnic groups. X. Measuring cognitive impairment with the cognitivesymptoms inventory. Arthritis Rheum. 2002;47:310–319.
5. Alarcon GS, Friedman AW, Straaton KV, Moulds JM, Lisse J, BastianHM, McGwin G Jr, Bartolucci AA, Roseman JM, Reveille JD. Systemiclupus erythematosus in three ethnic groups. III. A comparison ofcharacteristics early in the natural history of the LUMINA cohort.Lupus. 1999;8:197–209.
6. Alarcon GS, McGwin G Jr, Bartolucci AA, Roseman J, Lisse J, FesslerBJ, Bastian HM, Friedman AW, Reveille JD. Systemic lupuserythematosus in three ethnic groups. IX. Differences in damageaccrual. Arthritis Rheum. 2001;44:2797–2806.
7. Alarcon GS, McGwin G Jr, Bastian HM, Roseman J, Lisse J, Fessler BJ,Friedman AW, Reveille JD, for the LUMINA study group. Systemiclupus erythematosus in three ethnic groups. VIII. Predictors of earlymortality in the LUMINA cohort. Arthritis Care Res. 2001;45:191–202.
8. Alarcon GS, McGwin G Jr, Brooks K, Roseman JM, Fessler BJ,Sanchez ML, Bastian HM, Friedman AW, Baethge BA, Reveille JD.Systemic lupus erythematosus in three ethnic groups. XI. Sources ofdiscrepancy in perception of disease activity: a comparison of phy-sician and patient visual analog scale scores. Arthritis Rheum. 2002;47:408–413.
9. Alarcon GS, McGwin G Jr, Petri M, Reveille JD, Ramsey-Goldman R,Kimberly RP. Baseline characteristics of a multiethnic lupus cohort:PROFILE. Lupus. 2002;11:95–101.
10. Alarcon GS, Rodriguez JL, Benavides G Jr, Brooks K, Kurusz H,Reveille JD. Systemic lupus erythematosus in three ethnic groups. V.Acculturation, health-related attitudes and behaviors, and diseaseactivity in Hispanic patients from the LUMINA cohort. Arthritis CareRes. 1999;12:267–276.
11. Alarcon GS, Roseman J, Bartolucci AA, Friedman AW, Moulds JM,Goel N, Straaton KV, Reveille JD. Systemic lupus erythematosus inthree ethnic groups. II. Features predictive of disease activity early in itscourse. Arthritis Rheum. 1998;41:1173–1180.
12. Alarcon-Segovia D, Alarcon-Riquelme ME. Etiopathogenesis ofsystemic lupus erythematosus: A tale of three troikas. Systemic lupuserythematosus. In: Lahita RG, ed. Systemic Lupus Erythematosus. NewYork: Academic Press. 1999:55–65.
13. Barr SG, Zonana-Nacach A, Magder LS, Petri M. Patterns of diseaseactivity in systemic lupus erythematosus. Arthritis Rheum. 1999;42:2682–2688.
14. Bastian HM, Mikhail I, Straaton KV, Friedman AW, Lisse JR, Burst N,Reveille JD, Alarcon GS, for the LUMINA study group. Factorsassociated with early death in African-American and Hispanic patientswith SLE [abstract]. Arthritis Rheum. 1997;40(Suppl 9):S160.
15. Bastian HM, Roseman JM, McGwin G Jr, Alarcon GS, Friedman AW,Fessler BJ, Baethge BA, Reveille JD. Systemic lupus erythematosus in
n 2004 Lippincott Williams & Wilkins 15
Medicine � Volume 83, Number 1, January 2004 Lupus in Latin America: GLADEL Inception Cohort
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
three ethnic groups. XII. Risk factors for lupus nephritis after diagnosis.Lupus. 2002;11:152–160.
16. Bellomio V, Spindler A, Lucero E, Berman A, Santana M, Moreno C,Hidalgo RP, Paira S, Graf C, Maldonado Cocco JA, Citera G, ArriolaMS, Gomez G, Barreira JC, Messina O, Asnal C, Carrillo D, Gervilla A,Garcia L, Mascolo M, De la Sota MD, Rosso G, Somma LF, Sosa RF,Rillo O, Caracciolo JA, Lancioni G, Gomez A. Systemic lupuserythematosus: mortality and survival in Argentina. A multicenterstudy. Lupus. 2000;9:377–381.
17. Blanco FJ, Gomez-Reino JJ, de la Mata J, Corrales A, Rodriguez-Valverde V, Rosas JC, Gomez de la Camara A, Pascual E. Survivalanalysis of 306 European Spanish patients with systemic lupuserythematosus. Lupus. 1998;7:159–163.
18. Bombardier C, Gladman DD, Urowitz MB, Caron D, Chang CH, andthe Committee on prognosis studies in SLE. Derivation of the SLEDAI.A disease activity index for lupus patients. Arthritis Rheum. 1992;35:630–640.
19. Cervera R, Khamashta MA, Font J, Sebastiani GD, Gil A, Lavilla P,Aydintug AO, Jedryka-Goral A, de Ramon E, Fernandez-Nebro A,Galeazzi M, Haga HJ, Mathieu A, Houssiau F, Ruiz-IrastorzaG, Ingelmo M, Hughes GR. Morbidity and mortality in systemiclupus erythematosus during a 5-year period. A multicenter prospectivestudy of 1,000 patients. Medicine (Baltimore). 1999;78:167–175.
20. Cervera R, Khamashta MA, Font J, Sebastiani GD, Gil A, Lavilla P,Domenech I, Aydintug AO, Jedryka-Goral A, de Ramon E, and theEuropean Working Party on systemic lupus erythematosus. Systemiclupus erythematosus:Clinical and immunologic patterns of diseaseexpression in a cohort of 1,000 patients. Medicine (Baltimore). 1993;72:113–124.
21. Devins GM, Edworthy SM and the ARAMIS Lupus State ModelsResearch Group. Illness intrusiveness explains race-related quality-of-life differences among women with systemic lupus erythematosus.Lupus. 2000;9:534–541.
22. Drenkard C, Alarcon-Segovia D. The new prognosis of systemic lupuserythematosus: treatment-free remission and decreased mortality andmorbidity. Isr Med Assoc J. 2000;2:382–387.
23. Drenkard C, Villa AR, Garcia-Padilla C, Perez-Vasquez ME, Alarcon-Segovia D. Remission of systemic lupus erythematosus. Medicine(Baltimore). 1996;75:88–98.
24. Duffy KN, Duffy CM, Gladman DD. Infection and disease activity inSLE: a review of hospitalized patients. J Rheumatol. 1991;18:1180–1184.
25. Esdaile JM, Sampalis JS, Lacaille D, Danoff D. The relationship ofsocioeconomic status to subsequent health status in systemic lupuserythematosus. Arthritis Rheum. 1998;31:423–427.
26. Fernandez RN, Rego J, Neves AL. LES: Experiencia de 5 anos. RevBrasil Rheumatol Suppl. 1992;32:41.
27. Friedman AW, Alarcon GS, McGwin G Jr, Straaton KV, Roseman J,Goel N, Reveille JD, for the LUMINA Study Group. Systemic lupuserythematosus in three ethnic groups. IV. Factors associated with self-reported functional outcome in a large cohort study. Arthritis Care Res.1999;12:256–266.
28. Ginzler E, Berg A. Mortality in systemic lupus erythematosus.J Rheumatol. 1987;14(Suppl 13):218–222.
29. Ginzler EM, Diamond HS, Weiner M, Schlesinger M, Fries JF,Wasner C, Medsger TA Jr, Ziegler G, Klippel JH, Hadler NM,Albert DA, Hess EV, Spencer-Green G, Grayzel A, Worth D, HahnBH, Barnett EV. A multicenter study of outcome in systemic lupuserythematosus. I. Entry variables as predictors of prognosis. ArthritisRheum. 1982;25:601–611.
30. Gladman DD. Prognosis and treatment of systemic lupus erythematosus.Curr Opin Rheumatol. 1996;8:430–437.
31. Gladman D, Ginzler E, Goldsmith C, Fortin P, Liang M, Urowitz M,Bacon P, Bombardieri S, Hanly J, Hay E, Isenberg D, Jones J,Kalunian K, Maddison P, Nived O, Petri M, Richter M, Sanchez-Guerrero J, Snaith M, Sturfelt G, Symmons D, Zoma A. The developmentand initial validation of the Systemic Lupus International CollaboratingClinics/American College of Rheumatology Damage Index for systemiclupus erythematosus. Arthritis Rheum. 1996;39:363–369.
32. Gladman DD, Urowitz MB, Goldsmith CH, Fortin P, Ginzler E,Gordon C, Hanly JG, Isenberg DA, Kalunian K, Nived O, Petri M,
Sanchez-Guerrero J, Snaith M, Sturfelt G. The reliability of the SystemicLupus International Collaborating Clinics/American College of Rheuma-tology Damage Index in patients with systemic lupus erythematosus.Arthritis Rheum. 1997; 40:809–813.
33. Graffar M. Une methode de classification sociale d’echantillons depopulation. Courrier VI. 1956:445–459.
34. Guzman J, Cardiel MH, Arce-Salinas A, Sanchez-Guerrero J, Alarcon-Segovia D. Measurement of disease activity in systemic lupuserythematosus. Prospective validation of 3 clinical indices. J Rheumatol.1992;19:1551–1558.
35. Halberg P, Alsbjom B, Balslev JT, Lorenzen I, Gerstoft J, Wiik A.Systemic lupus erythematosus: follow-up study of 148 patients. II.Predictive factors of importance for course and outcome. ClinRheumatol. 1987;6:22–26.
36. Harris EN, Williams E, Shah DJ, De Ceulaer K. Mortality of Jamaicanpatients with systemic lupus erythematosus. Br J Rheumatol. 1989;28:113–117.
37. Hernandez-Cruz B, Tapia N, Villa-Romero AR, Reyes E, Cardiel MH.Risk factors associated with mortality in systemic lupus erythematosus.A case-control study in a tertiary care center in Mexico City. Clin ExpRheumatol. 2001;19:395–401.
38. Hochberg MC. Mortality from systemic lupus erythematosus in Englandand Wales, 1974–1983. Br J Rheumatol. 1987;26:437–441.
39. Jacobsen S, Petersen J, Ullman S, Junker P, Voss A, Rasmussen JM,Tarp U, Poulsen LH, van Overeem Hansen G, Skaarup B, Hansen TM,Podenphant J, Halberg P. Mortality and causes of death of 513 Danishpatients with systemic lupus erythematosus. Scand J Rheumatol. 1999;28:75–80.
40. Jacobsen S, Petersen J, Ullman S, Junker P, Voss A, Rasmussen JM,Tarp U, Poulsen LH, van Overeem Hansen G, Skaarup B, Hansen TM,Podenphant J, Halberg P. A multicentre study of 513 Danish patientswith systemic lupus erythematosus. II. Disease mortality and clinicalfactors of prognostic value. Clin Rheumatol. 1998;17:478–484.
41. Johnson AE, Cavalcanti FS, Gordon C, Nived O, Palmer RG, Sturfelt G,Viner NJ, Bacon PA. Cross-sectional analysis of the differencesbetween patients with systemic lupus erythematosus in England, Braziland Sweden. Lupus. 1994;3:501–506.
42. Johnson AE, Gordon C, Palmer RG, Bacon PA. The prevalence andincidence of systemic lupus erythematosus in Birmingham, England.Relationship to ethnicity and country of birth. Arthritis Rheum. 1995;38:551–558.
43. Karlson EW, Daltroy LH, Lew RA, Wright EA, Partridge AJ, FosselAH, Roberts WN, Stern SH, Straaton KV, Wacholtz MC, KavanaughAF, Grosflam JM, Liang MH. The relationship of socioeconomic status,race, and modifiable risk factors to outcomes in patients with systemiclupus erythematosus. Arthritis Rheum. 1997;40:47–56.
44. Karlson EW, Daltroy LH, Lew RA, Wright EA, Partridge AJ, RobertsWN, Stern SH, Straaton KV, Wacholtz MC, Grosflam JM, Liang MH.The independence and stability of socioeconomic predictors ofmorbidity in systemic lupus erythematosus. Arthritis Rheum. 1995;38:267–273.
45. Kaslow RA. High rate of death caused by systemic lupus erythema-tosus among U.S. residents of Asian descent. Arthritis Rheum. 1982;25:414–418.
46. Kiss E, Regeczy N, Szegedi G. Systemic lupus erythematosus survivalin Hungary. Results from a single center. Clin Exp Rheumatol. 1999;17:171–177.
47. Massardo L, Martinez ME, Jacobelli S, Villarroel L, Rosenberg H,Rivero SJ. Survival of Chilean patients with systemic lupus erythema-tosus. Semin Arthritis Rheum. 1994;24:1–11.
48. McCarty DJ, Manzi S, Medsger TA Jr, Ramsey-Goldman R, LaporteRE, Kwoh CK. Incidence of systemic lupus erythematosus. Race andgender differences. Arthritis Rheum. 1995;38:1260–1270.
49. Molina JF, Drenkard C, Molina J, Cardiel MH, Uribe O, Anaya JM,Gomez LJ, Felipe O, Ramirez LA, Alarcon-Segovia D. Systemic lupuserythematosus in males. A study of 107 Latin American patients.Medicine (Baltimore). 1996;75:124–130.
50. Morton RO, Gershwin ME, Brady C, Steinberg AD. The incidence ofsystemic lupus erythematosus in North American Indians. J Rheumatol.1976;3:186–190.
16 n 2004 Lippincott Williams & Wilkins
Pons-Estel et al Medicine � Volume 83, Number 1, January 2004
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
51. Nossent JC. Course and prognostic value of Systemic Lupus Ery-thematosus Disease Activity Index in black Caribbean patients. SeminArthritis Rheum. 1993;23:16–21.
52. Nossent JC. SLICC/ACR damage index in Afro-Caribbean patients withsystemic lupus erythematosus: changes in and relationship to diseaseactivity, corticosteroid therapy and prognosis. J Rheumatol. 1998;25:654–659.
53. Peschken CA, Esdaile JM. Systemic lupus erythematosus in NorthAmerican Indians: a population based study. J Rheumatol. 2000;27:1884–1891.
54. Petri M. Hopkins Lupus Cohort 1999 update. Rheum Dis Clin North Am.2000;26:199–213.
55. Petri M, Genovese M, Engle E, Hochberg M. Definition, incidence andclinical description of flare in systemic lupus erythematosus. A pros-pective cohort study. Arthritis Rheum. 1991;34:937–944.
56. Petri M, Perez-Gutthann S, Longenecker JC, Hochberg M. Morbidity ofsystemic lupus erythematosus: role of race and socioeconomic status.Am J Med. 1991;91:345–353.
57. Pistiner M, Wallace DJ, Nessim S, Metzger AL, Klinenberg JR. Lupuserythematosus in the 1980s: a survey of 570 patients. Semin ArthritisRheum. 1991;21:55–64.
58. Pons-Estel B, Villalba D, Alvarellos A, Caeiro F, Catoggio LJ, SorianoER. ARTHROS 2.0: A rheumatology database [abstract]. Ann RheumDis. 1999;58:153.
59. Prokunina L, Castillejo-Lopez C, Oberg F, Gunnarsson I, Berg L,Magnusson V, Brookes AJ, Tentler D, Kristjansdottir H, Grondal G, BolstadAI, Svenungsson E, Lundberg I, Sturfelt G, Jonssen A, Truedsson L, Lima G,Alcocer-Varela J, Jonsson R, Gyllensten UB, Harley JB, Alarcon-SegoviaD, Steinsson K, Alarcon-Riquelme ME. A regulatory polymorphism inPDCD1 is associated with susceptibility to systemic lupus erythematosusin humans. Nat Genet. 2002;32:666–669.
60. Quintero-Del-Rio AI, Bacino D, Kelly J, Aberle T, Harley JB. Familialsystemic lupus erythematosus: a comparison of clinical manifestationsand antibody presentation in three ethnic groups. Cell Mol Biol (Noisy-le-grand). 2001;47:1223–1227.
61. Rahman P, Gladman DD, Urowitz MB, Hallett D, Tam LS. Earlydamage as measured by the SLICC/ACR damage index is a predictor ofmortality in systemic lupus erythematosus. Lupus. 2001;10:93–96.
62. Ramos Niembro F. Lupus eritematoso generalizado. In: Ramos NiembroF, ed. Enfermedades Reumaticas. Criterios y Diagnostico. Mexico:McGraw-Hill Interamericana; 1999:79–137.
63. Reveille JD, Bartolucci A, Alarcon GS. Prognosis in systemic lupuserythematosus. Negative impact of increasing age at onset, black race,and thrombocytopenia, as well as causes of death. Arthritis Rheum.1990;33:37–48.
64. Reveille JD, Moulds JM, Ahn C, Friedman AW, Baethge B, Roseman J,Straaton KV, Alarcon GS. Systemic lupus erythematosus in threegroups. I. The effects of HLA Class II, C4, and CR1 alleles, socio-economic factors, and ethnicity at disease onset. Arthritis Rheum. 1998;41:1161–1172.
65. Rojas-Serrano J, Cardiel MH. Lupus patients in an emergency unit.Causes of consultation, hospitalization and outcome. A cohort study.Lupus. 2000;9:601–606.
66. Rosner S, Ginzler EM, Diamond HS, Weiner M, Schlesinger M, Fries JF,Wasner C, Medsger TA Jr, Ziegler G, Klippel JH, Hadler NM, Albert DA,Hess EV, Spencer-Green G, Grayzel A, Worth D, Hahn BH, Barnett EV.A multicenter study of outcome in systemic lupus erythematosus. II.Causes of death. Arthritis Rheum. 1982;25:612–617.
67. Salmon JE, Millard S, Schachter LA, Arnett FC, Ginzler EM, GourleyMF, Ramsey-Goldman R, Peterson MG, Kimberly RP. Fc gamma RIIAalleles are heritable risk factors for lupus nephritis in African Amer-icans. J Clin Invest. 1996;97:1348–1354.
68. Seleznick MJ, Fries JF. Varibles associated with decreased survival insystemic lupus erythematosus. Semin Arthritis Rheum. 1991;21:73–80.
69. SPSS/PC v 10.0. Chicago: SPSS Inc, 2000.70. Stokes M, Davis C, Koch G. Categorical data analysis using the SAS
System. 2nd ed. Cary, NC: SAS Institute Inc, 2000.71. Stoll T, Sutcliffe N, Klaghofer R, Isenberg DA. Do present damage and
health perception in patients with systemic lupus erythematosus predictextent of future damage? A prospective study. Ann Rheum Dis. 2000;59:832–835.
72. Studensky S, Allen NB, Caldwell DS, Rice JR, Polisson RP. Survival insystemic lupus erythematosus. A multivariate analysis of demographicfactors. Arthritis Rheum. 1987;30:1326–1332.
73. Tan EM, Cohen AS, Fries JF, Masi AT, McShane DJ, Rothfield NF,Schaller JG, Talal N, Winchester RJ. The 1982 revised criteria for theclassification of systemic lupus erythematosus. Arthritis Rheum. 1982;25:1271–1277.
74. Thumboo J, Uramoto K, O’Fallon WM, Fong KY, Boey ML, Feng PH,Thio ST, Gabriel SE, Chng HH, Howe HS, Koh ET, Koh WH, LeongKH, Leong KP. A comparative study of the clinical manifestations ofsystemic lupus erythematosus in Caucasians in Rochester, Minnesota,and Chinese in Singapore, from 1980 to 1992. Arthritis Rheum. 2001;45:494–500.
75. Trager J, Ward M. Mortality and causes of death in systemic lupuserythematosus. Curr Opin Rheumatol. 2001;13:345–351.
76. Urowitz MB, Bookman AA, Koehler BE, Gordon DA, Smythe HA,Ogryzlo MA. The bimodal mortality pattern of systemic lupus ery-thematosus. Am J Med. 1976;60:221–225.
77. Urowitz MB, Gladman DD, Abu-Shakra M, Farewell VT. Mortalitystudies in systemic lupus erythematosus: results from a single center.III. Improved survival over 24 years. J Rheumatol. 1997;24:1061–1065.
78. Valenzuela Yuraidini J, Diaz Andrade E, Klagges Valenzuela B.Clasificacion social y estado nutritivo. Empleo de un nuevo metodo declasificacion social. Cuadernos Medico Sociales. XVIII (1), 1976.
79. Vila LM, Mayor AM, Valentin AH, Garcia-Soberal M, Vila S. Clinicaland immunological manifestations in 134 Puerto Rican patients withsystemic lupus erythematosus. Lupus. 1999;8:279–286.
80. Walsh SJ, Algert C, Gregorio DI, Reisine ST, Rothfield NF. Divergentracial trends in mortality from systemic lupus erythematosus. J Rheum-atol. 1995;22:1663–1668.
81. Walsh SJ, DeChello LM. Geographical variation in mortality fromsystemic lupus erytematosus in the United States. Lupus. 2001;10:637–646.
82. Ward MM, Pyun E, Studenski S. Long-term survival in systemic lupuserythematosus: patient characteristics associated with poorer outcomes.Arthritis Rheum. 1995;38:274–283.
83. Ward MM, Pyun E, Studenski S. Causes of death in systemic lupuserythematosus. Long-term follow-up of an inception cohort. ArthritisRheum. 1995;38:1492–1499.
84. Zonana-Nacach A, Roseman JM, McGwin G Jr, Friedman AW,Baethge BA, Reveille JD, Alarcon GS, for the LUMINA Study Group.Systemic lupus erythematosus in three ethnic groups. VI. Factorsassociated with fatigue within 5 years of criteria diagnosis. Lupus. 2000;9:101–109.
n 2004 Lippincott Williams & Wilkins 17
Medicine � Volume 83, Number 1, January 2004 Lupus in Latin America: GLADEL Inception Cohort
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.