the evidence base for public health
TRANSCRIPT

TISAJ
B
M
R
C
I
TllwDiItcbteome
FISdetN
ToA
A©
he Evidence Base for Public Healthnforming Policy at the Centers for Disease Control and Preventiontephen B. Thacker, MD, MSc, Robin M. Ikeda, MD, MPH, Karen E. Gieseker, PhD, MS,aron B. Mendelsohn, PhD, MPH, Sharon H. Saydah, PhD, MS, Cecilia W. Curry, PhD,
ean W. Yuan, MD, MPH
ackground: As part of a major re-examination of its organization, in 2004, the Centers for DiseaseControl and Prevention (CDC) assessed the evidence base for the effectiveness ofpopulation-based public health intervention programs.
ethods: For the leading causes of disease, injury, and disability, evidence was systematically reviewedfor modifiable risk factors and their attributable fractions, and for public health interven-tions and their preventable fractions.
esults: For 31 conditions, 194 modifiable risk factors were identified, and attributable fractions werefound for 65 (33.5%). For 137 (70.6%) of the risk factors, 702 population-based interventionswere found. Preventable fractions were found for 31 (4.4%) of the interventions.
onclusions: Despite considerable information about both modifiable risk factors and interventionsdesigned to reduce the risks of the major causes of disease, injury, and disability, theevidence base that describes the effectiveness of these interventions is limited. The CDC iscommitted to support research that will set priorities for program development andidentify effective public health interventions.(Am J Prev Med 2005;28(3):227–233) © 2005 American Journal of Preventive Medicine
abpcpm
dbpmrrpiomatmteoecpi
ntroduction
he 20th century was notable for dramatic improve-ments in public health credited largely to theinterplay of social changes and clinical and popu-
ation-based interventions.1 Further improvements in theength and quality of life in this century are achievableith effective public health programs. The Centers forisease Control and Prevention (CDC) has completed an
ntensive examination of its role and mission, the Futuresnitiative, which has resulted in a major reorganization ofhe agency to prepare for the challenges of the 21stentury.2 A key element of the CDC effort has alwayseen the determination of the effectiveness of interven-ions that prevent disease, injury, and disability, and theffect of public health programs on these conditions. Inther words, what works and what difference does itake? Just as clinicians have recognized the value of
vidence-based medicine, practitioners of public health
rom the Office of Workforce and Career Development (Thacker,keda, Gieseker, Mendelsohn, Saydah, Curry), Epidemic Intelligenceervice, Career Development Division (Gieseker, Mendelsohn, Say-ah), and Presidential Management Fellow Program, Office of Strat-gy and Innovation (Curry), Centers for Disease Control and Preven-ion, Atlanta, Georgia; and Mount Sinai School of Medicine (Yuan),ew York, New YorkAddress correspondence and reprint requests to: Stephen B.
hacker, MD, MSc, Director, Office of Workforce and Career Devel-
apment, MS E94, Centers for Disease Control and Prevention,tlanta GA 30333. E-mail: [email protected].
m J Prev Med 2005;28(3)2005 American Journal of Preventive Medicine • Published by
re realizing that their work should be based on theest available scientific evidence.3 Implementation ofopulation-based interventions with demonstrated effi-acy should increase the effectiveness of public healthrograms and provide an optimal return on the invest-ent of public resources.Most of the major causes of disease, injury, and
isability in the United States have risk factors that cane reduced or eliminated, and hundreds of availableopulation-based interventions are directed at theseodifiable risk factors (conditions without modifiable
isk factors such as ovarian cancer require more basicesearch). When a priority health problem is identified,ublic health practitioners try to identify specific, mod-
fiable risk factors for the problem to guide the devel-pment of appropriate interventions. Such risk factorsust be evaluated according to the degree that they are
ssociated with a specific condition. In other words, athe population level (local, state, or national), how
uch of a reduction in the health burden is estimatedo occur after introduction of an intervention? How-ver, the evidence base to document the effectivenessf these interventions in populations is limited. Thisvidence gap limits public health planning because oneannot estimate the likely impact of an interventionrogram without this evidence. Accurate estimates of
mpact provide those with the responsibility of resource
llocation a better science base for decision making.227.e10749-3797/05/$–see front matterElsevier Inc. doi:10.1016/j.amepre.2005.05.007

Thoee
ehTata
M
Uiytamtmcsficuautpmbdhgifrtatmpsf
2cpcrssflala
AwCtpttt
wtp
wie
R
Totwwtccipfihgsctrdd
woSrmeamapuf
htf
2
he likely effect of most public health interventions onealth outcomes in any given target population cannly be approximated. It is a significant problem thatstimates of these effects are rarely approached in anxplicit and rigorous way.The Futures Initiative prompted exploration of the
vidence base to assess the effectiveness of publicealth programs relevant to the mission of the CDC.his report evaluates the evidence base for the modifi-ble risk factors and interventions related to conditionshat result in a major burden on public heath and thatre addressed by programs funded by the CDC.
ethods
sing eight measures of burden of disease, injury, and disabilityn the United States (mortality, years of life lost before age 75ears, disability-adjusted life years, actual causes of death, hospi-alizations, hospital days, disability, and direct medical costs),pproximately 20 leading conditions were reviewed for eacheasure (Appendix 1). Some measures had �20 conditions; in
hese cases, all conditions were included. During review of theseeasures, we noted many related conditions and chose to
ombine some conditions (e.g., heart disease, hypertension, andtroke combined as cardiovascular disease). We defined “modi-able” as those behavioral and environmental risk factors thatould be changed by public health interventions (e.g., tobaccose or alcohol-impaired driving) but excluded risk factors suchs age, gender, race/ethnicity, education, or poverty. The attrib-table fraction is a measure of the amount of disease or injury
hat could be eliminated if a risk factor never occurred in a givenopulation.4 The preventable fraction, on the other hand, is aeasure of the proportion of a health problem that can actually
e avoided when a prevention strategy or intervention has beeneveloped and implemented.4 This analysis focuses on publicealth interventions that are directed at populations (geo-raphic, institutions, worksites, and so on) rather than clinicalnterventions that are directed at persons (e.g., standing ordersor vaccines rather than vaccine administration). Guidelines andecommendations were not included as interventions unlesshey were linked to an action such as legislation, regulation, orprogram that ensured compliance with them. For each condi-
ion, information was sought about modifiable risk factors,easures of attributable fraction or population attributable risk,
opulation-based interventions directed at both primary andecondary prevention of these conditions, and preventableractions.
The search included PubMed for entries dated 1966 to June004 in all languages by using the following search terms:ommunity, risk, attributable risk, modifiable attributable risk,reventable fraction, attributable fraction, preventive fraction,ommunity intervention, intervention, prevention, prevention/isk, public health, public health intervention, coupled with thepecific diseases and conditions listed in Table 2. We alsoearched the archives of the Morbidity and Mortality Weekly Reportrom January 1980 through July 2004, and the Cochrane Col-aboration website (www.cochrane.org/index0.htm), and wesked CDC programs to provide relevant published or unpub-ished research. Additionally, we reviewed the references from
rticles to identify other sources not evident in our initial search. o27.e2 American Journal of Preventive Medicine, Volume 28, Nu
rticles without information on risk factors or interventionsere excluded, as were articles covered by topics in the Guide toommunity Preventive Services for years prior to the publication of
he Guide chapter on a topic. When attributable fraction (AF),opulation attributable risk percent (AFp), or preventable frac-ion (PFp) were not calculated by the authors, we estimatedhese numbers, when possible, from information provided inhe articles by using the following standard formulas4:
AFp � Pe(RR � 1) ⁄ (1 � Pe[RR – 1]
here RR is the rate ratio Ie/Iu (incidence in the exposed tohe risk factor/incidence in the unexposed) and Pe is therevalence of the exposure.
PFp � (Ip � Ie) ⁄ Ip
here Ip is the incidence rate in the total population and Ies the incidence rate in the exposed persons in the populationxposed to the intervention.
esults
he search yielded 682 relevant publications for review;f those, 34 were systematic reviews. The assessment ofhe effectiveness of interventions in some topical areasere based on systematic reviews (e.g., lung cancer),hereas in other fields systematic reviews of interven-
ion effectiveness were less common (e.g., prostateancer). Based on review of the eight burden measureshosen, 41 conditions were identified with the greatestmpact on health. Based on input from the CDCrogram staff, we excluded four conditions (cysticbrosis, cerebral palsy, learning disability, and mentalealth) that were not addressed directly by CDC pro-rams. We also combined some categories to reflect thetructure of CDC programs, leaving a total of 31onditions for study (Table 1). Four of the 31 condi-ions—blindness, epilepsy, mental retardation, and pa-alysis—can be secondary complications of other con-itions under study (e.g., diabetes, vaccine-preventableiseases, and injuries).For the 31 conditions, 194 modifiable risk factors
ere identified (see Appendix 2 on the American Journalf Preventive Medicine website at www.ajpm-online.net).ome modifiable risk factors (e.g., tobacco use) wereisk factors for multiple conditions and were includedultiple times in the total (e.g., tobacco use appears
ight times). Modifiable risk factors were identified forll of the 31 conditions; 21 conditions had four or moreodifiable risk factors. For these 194 risk factors,
ttributable fraction or population attributable risk wasrovided or could be estimated for 65 (33.5%). Attrib-table risk could be calculated for at least one riskactor for 21 (67.7%) of the 31 conditions.
The search identified 703 population-based, publicealth interventions for 28 (90.3%) of the 31 condi-
ions. Population-based interventions were identifiedor 139 (71.6%) of the 194 risk factors. There were four
r more interventions for 75 risk factors (range: 0 tomber 3

2Hfptittldcedl(
ivcaahvf
vp
D
Obpfifimsitadttrert
Td
ABKLPC
ellitu
Ti
M
4
a ood a
5). Some interventions addressed multiple conditions.owever, no such interventions were found for risk
actors related to three conditions (9.7%) (arthritis,rostate cancer, and hearing loss). Preventable frac-ions could be estimated for 28 (4.0%) of the 703nterventions; these interventions were related to 9 ofhe 31 conditions. The evidence base for the preven-ion of alcohol-related, motor-vehicle–crash deaths il-ustrates how findings were organized for the 31 con-itions. In this example, the fractions of motor-vehicle–rash deaths attributable to alcohol use has beenstimated to be 41%, and 7% of these alcohol-relatedeaths could be prevented by states lowering the legal
imits for drinking while driving from 0.10% to 0.08%Table 2).5–8
Many interventions were beneficial, but others hadnsufficient evidence to assess effectiveness.9 One inter-ention was found to be harmful.10,11 If the fouronditions noted above to be secondary complicationsre excluded from the analysis, the number of modifi-ble risk factors decrease to 177, of which 53 (29.9%)ave an attributable fraction. Population-based inter-entions were identified for 124 (70.1%) of the risk
able 1. Conditions of high priority at Centers for Disease Cisability, and cost (n � 31)
lzheimer’s disease Chronic lunirth defects Asthmaidney disease (chronic) Chronic oiver disease (chronic) CVD/circularegnancy (high risk)/perinatal conditions Cardiovascancer DisabilitiesBreast ArthritisCervical Blindness/Colorectal Hearing imLung Mental retProstate ParalysisSkin Diseases of t
Epilepsy
Endocrine aDiabetes m
able 2. Risk of death in motor vehicle crashes attributed tonterventions
ortality Risk factorAttributablfraction
2,8155 total; 17,4195 alcoholrelated
Alcohol use 41%a
Includes 1498 alcohol-impaired pedestrians killed by drivers with bl
actors. This reduced list of conditions had 451 inter- m
entions; 19 (4.2%) had sufficient data to calculatereventable fractions.
iscussion
ur findings suggest that the availability of evidence-ased, public health research is limited. In particular,reventable fractions—a measure of the expected ef-ect of these interventions—are calculable for approx-mately 5% of the interventions directed toward modi-able risk factors. Although many of these practicesay be effective, the evidence to support them is
parse. Our findings underscore the need for researchnto the effectiveness of specific population-based in-erventions and for systematic reviews of all the avail-ble evidence for all population-based interventionsesigned to prevent conditions of public health impor-ance. Rigorously obtained data on preventable frac-ion are essential for rational decision making, and forecommending what works and what provides the larg-st return on investment. The well-documented expe-ience in clinical medicine suggests that many interven-ions will not prove to be effective, and some actually
l and Prevention based on burden of morbidity, mortality,
ase Infectious diseaseDiarrheal diseases
ctive pulmonary disease HIV/AIDS/STDsPneumonia and influenza
disease Sepsis/nosocomial infectionsTuberculosisVaccine preventable diseases
l impairments Injuries, unintentionalments Motor vehicle crashesion Poisoning
Injuries, intentionalrvous system Suicide/self-inflicted injury
Homicide/interpersonalviolence
etabolic disorderss
hol and preventable fraction from selected effective
Intervention Preventable fraction
Lower blood alcohol limit(0.10–0.08) laws
7% of alcohol-related, 3% oftotal deaths (1228 lives);15,183 injuries7
Sobriety check-points 20% of alcohol-related, 8%of total deaths (3500lives); 50,000 injuries7
Mass media campaigns 10% to 13% of alcohol-related, 4% to 5% of totaldeaths (1700–2300 lives);30,000 injuries8
lcohol concentrations �0.08.6
ontro
g dise
bstrutoryular
visuapair
ardat
he ne
nd m
alco
e
ight be harmful, underscores the need for such
Am J Prev Med 2005;28(3) 227.e3

dap
ttitiptinpM“tspossimnatlstrri
mrnaiHlaaolrtvh
finaphwt
drTiumpfiwotamptpgaErmeocoreopvftrpfmneisbavac
tHbTimmope
2
ata.12 Success depends on making these data available,nd recognizing that they are an integral part of theolicy and planning process.Several reasons can explain the paucity of informa-
ion about preventable fractions. First, the literature onhe development and evaluation of population-basednterventions is limited. This finding is consistent withhat of investigators in the Cochrane Collaboration whodentified �200 systematic reviews in the field of healthromotion and public health.13 In contrast, there arehousands of clinical reviews. Second, population-basednterventions for many public health conditions stilleed to be conceptualized, developed, and, most im-ortant, evaluated for their effectiveness and cost.any existing public health interventions are based on
best practices” as determined by expert opinion ratherhan systematically collected and analyzed data. Third,ome interventions become established public healthractice without the benefit of rigorous evaluation,ften because of the dearth of appropriate data, andometimes because solutions appear obvious (e.g., re-tricting access to chemical or radiologic waste sites). Asnterventions are developed and evaluated for efficacy,
ore information is needed about both the effective-ess of these interventions in various populations andssociated preventable fraction calculations. In addi-ion to the relatively young state of the field, there isittle funding for population-based effectiveness re-earch in public health compared with basic and pa-ient-oriented clinical research. This situation mighteflect, in part, the analytic challenges of this kind ofesearch or the absence of societal commitment tonvest resources in such research.
Another explanation for the small number of esti-ates of attributable and preventable fractions is a
esult of our study design. Our review was systematic,ot exhaustive. In particular, we limited our data aboutttributable fraction and population attributable risk tonformation contained within the papers we reviewed.
owever, we tried to be quite flexible by doing calcu-ations if the data were available in the manuscript andccepting any estimates of attributable risk or prevent-ble fraction provided by the authors. If we exploredther data sources, we might have been able to calcu-
ate attributable fractions or population attributableisks for more risk factors. We are less convinced thathe estimates of preventable fraction for the 703 inter-entions we identified are readily available, even if wead conducted a more extensive literature search.Other limitations to this study might affect our
ndings. First, the complexities that underlie effective-ess of specific interventions are often understated,nd only the basic elements of attributable risk andreventable fraction are emphasized. Second, we reliedeavily on published reviews and individual studies,hich might have resulted in ascertainment bias, al-
hough we identified and reviewed some unpublished i
27.e4 American Journal of Preventive Medicine, Volume 28, Nu
ata provided by CDC programs and some unpublishedeviews from the Guide for Community Preventive Services.his might account for the inability to identify some
nterventions and to estimate attributable fraction, pop-lation attributable risk, and preventable fraction forost risk factors and interventions. At the same time,
ublished literature tends to be biased toward positivendings, so we most likely under-represented studiesith no effect or a negative effect. Our review identifiednly one intervention with a negative preventable frac-ion. Third, several decisions described in the methodsffected our findings. We required risk factors to beodifiable by public health interventions; hence, im-
ortant social measures such as poverty and educa-ional status were not included. The focus on CDClanning needs omitted the impact on health of otherovernment agencies such as the Centers for Medicarend Medicaid Services and the U.S. Department ofducation, except as they related directly to CDC. Theequirement that interventions be linked to specificodifiable risk factors excluded from our review gen-
ral categories of risk such as “occupation.” The focusn population-based interventions excluded effectivelinical interventions such as immunization and antibi-tic therapy. Similarly, we did not count guidelines orecommendations in isolation, which undervalues theirffectiveness but also recognizes that the promulgationf a recommendation does not, in itself, ensure com-liance. Fourth, the cumulative effect of multiple inter-entions (e.g., mass media campaigns and legislation)or the same condition is not additive,14 which suggestshat we have evidence for an even smaller effectiveeduction of burden than by adding together thereventable fractions that are available. Fifth, the ef-ects of interventions (e.g., smoking cessation) on co-
orbid conditions (e.g., heart disease and cancer) haveot been described in most settings,15 which mightnhance or reduce the overall impact of effectiventervention programs. Finally, since most interventiontudies are conducted in defined populations—limitedy age, gender, geography, race/ethnicity, social class,nd so on—extrapolation of the effect of application ofarious interventions on a national level is problematicnd will only be a small part of the broader political andultural changes that will affect health.
Several organizations conduct systematic reviews onopics of clinical16,17 and public health18 importance.owever, important differences exist between evidence-ased medicine and evidence-based public health.19
he population-based orientation in public health typ-cally limits the use of randomized trials, obtains results
ore slowly, and often relies on group consensus toake decisions regarding the use of results rather than
n individual decisions. The difference that mightrovide the greatest challenge is that the volume ofvidence in clinical medicine is much larger than that
n public health. The Task Force for Community Pre-mber 3

vtanCcwpfwv
thPvmeiqhtre(
pitsfvifirbnaseBmtctbpt
destDitt
hcsdatapkdoimocshaa
geifpppbmerbcofTfaaaterap
Nt
R
entive Services reviews systematically the evidence forhe effectiveness of population-based interventions,nd had approved 162 systematic reviews at the begin-ing of 2004; 90 had been published in the Guide toommunity Preventive Services (P. Briss, CDC, personalommunication, 2004). From these 162 reviews, thereas not sufficient evidence to conclude for or against aarticular intervention for 85, highlighting the needor evaluation research at several levels. Interventionsere recommended for 75 interventions and two inter-entions were not recommended.
The Community Guide has established the standard forhe synthesis of evidence for the effectiveness of publicealth interventions much like the Guide to Clinicalreventive Services is the standard for preventive inter-entions in clinical practice.20 However, while the Com-unity Guide provides the best available evidence on theffectiveness of an increasing number of public healthnterventions, it does not address the critical policyuestion of how large an impact will an interventionave on an outcome of interest in a county, a state, or
he nation. If a community were to invest limitedesources, decision makers want to know what return toxpect on their investment in terms of health burdeni.e., what is the preventable fraction?).
What is the research agenda for evidence-basedublic health? First, basic research is needed to address
nadequacies in the measurement of health burden ando identify gaps in attributable risk data. Second, re-earch must be conducted on those modifiable riskactors and conditions to identify evidence-based inter-entions. In particular, research should be conductedn different populations to assess the external validity ofndings on specific interventions and to identify theirelative effectiveness in various populations. Evidence-ased research in public health rarely addresses theeeds of populations with special needs, whether theyre defined by age, race/ethnicity, gender, refugeetatus, socioeconomic status, or disability; therefore,fforts are especially needed in these populations (P.riss, CDC, personal communication, 2004). Third,ethodologic research should assess the effect of mul-
iple interventions on a single condition and the out-ome of a particular intervention on comorbid condi-ions. Finally, cost-effectiveness, cost utility, and cost-enefit of these interventions should be assessed torovide guidance to those setting policy at all levels ofhe public health system.
In addition, evaluation research requires study of theissemination and implementation of interventions. Forxample, research regarding effective methods to dis-eminate research findings or to expand the implemen-ation of effective intervention programs is needed.eveloping systems to monitor the use of effective
nterventions and those that are unproven or ineffec-ive would be helpful to assess the status of implemen-
ation and dissemination efforts.As we undertake such research, however, publicealth practitioners should confront methodologicomplexities more aggressively. Observational and qua-i-experimental studies are more practical than ran-omized trials in public health for logistical, financial,nd methodologic reasons.19 Additionally, the limita-ions of randomized trials in terms of external validityre also a concern.21 Large, simple trials have beenroposed as an alternative approach in public health,eeping both exclusion criteria and measurements andata collection to a minimum.22 At the same time,ther endeavors are essential to maintaining scientific
ntegrity, transparency in the application of researchethods and findings, and flexibility in the application
f new knowledge. To address these methodologichallenges, more investigators need to be trained andupported in the diverse disciplines relevant to publicealth, including, but not limited to the followingreas: epidemiology, laboratory sciences, behavioralnd social sciences, economics, and decision science.
This report discusses conditions that are having thereatest effect on health in the United States, and uncov-rs serious deficiencies in what we know about what worksn public health. These deficiencies demonstrate thaturther delay in investing in an evidence base for effectiveublic health practice is not defensible. The CDC and itsartners need the best science to deliver preventionrograms efficiently and effectively. We must approachoth research and program with the question, “Howuch difference is this investment in time, thought,
nergy, and money likely to make on health status?” As aesult of a recent strategic planning effort, the CDC iseing reorganized to address many of these researchhallenges more effectively and more efficiently.2 Newffices devoted to strategy and innovation and to work-orce and career development have been established.hese offices, along with the newly created CDC Office
or Public Health Research within the recently expandednd reorganized Office of the Chief Science Officer, willssist the agency identifying specific research and associ-ted workforce needs. To achieve the specific health goalshat will drive future prevention programs, the CDC mustnsure that significant resources are directed toward aesearch agenda that supports both internal researchersnd external partners to strengthen the science base inublic health.
o financial conflict of interest was reported by the author ofhis paper.
eferences1. Centers for Disease Control and Prevention. Achievements in public
health, 1990–1999: changes in the public health system. MMWR MorbMortal Wkly Rep 1999;48:1141–7.
2. Centers for Disease Control and Prevention. Future initiatives. Available at:www.cdc.gov/futures. Accessed November 3 2004.
Am J Prev Med 2005;28(3) 227.e5

1
1
1
1
1
1
1
1
1
1
2
2
A
M
11111111112
Y
D
11
11
C
2
3. Brownson RC, Gurney JG, Land G. Evidence-based decision making inpublic health. J Public Health Management Pract 1999;5:86–97.
4. Last JM. A dictionary of epidemiology. New York: Oxford University Press,2001.
5. National Highway Traffic Safety Administration. Traffic safety facts 2002.Washington DC: National Center for Statistics and Analysis, U.S. Depart-ment of Transportation, 2004 (report DOT H5809620).
6. Evans L. Traffic safety. Bloomfield Hills MI: Science Serving Society, 2004.7. Shults RA, Elder RW, Sleet DA, et al. Reviews of evidence regarding
interventions to reduce alcohol-impaired driving. Am J Prev Med2001;21:66–88.
8. Elder RW, Shults RA, Sleet DA, et al. Effectiveness of mass media campaignsfor reducing drinking and driving and alcohol-involved crashes: a system-atic review. Am J Prev Med 2004;27:57–65.
9. Task Force for Community Preventive Services. The guide to communitypreventive services: what works to promote health? New York: OxfordUniversity Press, 2005.
0. Fergusson DM, Horwood LJ, Beautrais AL, et al. A controlled field trial ofa poisoning prevention method. Pediatrics 1982;69:515–20.
1. Vernberg K, Culver-Dickinson P, Spyker DA. The deterrent effect ofpoison-warning stickers. Am J Dis Child 1984:139:1018–20.
2. Chalmers I, Enkin M, Keirse MJN, eds. Effective care in pregnancy and
27.e6 American Journal of Preventive Medicine, Volume 28, Nu
3. Doyle J, Waters E, Yach D, et al. Global priority setting for Cochranesystematic reviews of health promotion and public health research. JEpidemiol Community Health 2005;59:193–7.
4. Rowe AK, Powell KE, Flanders WD. Why population attributable factionscan sum to more than one. Am J Prev Med 2004;26:243–9.
5. McElduff P, Attia J, Ewald B, et al. Estimating the contribution of individualrisk factors to disease in a person with more than one risk factor. J ClinEpidemiol 2002;55:588–92.
6. U.S. Preventive Services Task Force. Guide to clinical preventive services:report of the U.S. Preventive Services Task Force. 2nd ed. Baltimore:William & Wilkins, 1996.
7. Cochrane Collaboration. Cochrane Collaboration handbook. Available at:www.cochrane.co.uk. Accessed March 2004.
8. Zaza S, Lawrence RS, Mahan CS, et al. Scope and organization of theGuide to Community Preventive Services. Am J Prev Med 2000;18(suppl1):27–34.
9. Brownson RC, Baker EA, Leet TL, et al. Evidence-based public health. NewYork: Oxford University Press, 2003.
0. McGinnis JM, Foege W. Guide to Community Preventive Services: harness-ing the science. Am J Prev Med 2000;18:1–2.
1. Rothwell PM. External validity of randomized controlled trials: “To whomdo the results of this trial apply?” Lancet 2005;365:82–93.
childbirth. Oxford: Oxford University Press, 1989.22. Yusuf S, Collins R, Peto R. Why do we need some large, simple randomized
trials? Stat Med 1984:3:409–22.
ppendix 1. Leading Causes of Public Health Burden Using Alternative Measures of Burden
ortality (top 20) (2001)1 YPLL before age 75 (top 20) (2001)1
1. Heart disease 1. Malignant neoplasms2. Malignant neoplasms 2. Heart disease3. Cerebrovascular disease 3. Unintentional injuries4. Chronic lower respiratory disease 4. Perinatal period5. Unintentional injuries 5. Suicide6. Diabetes mellitus 6. Homicide7. Influenza and pneumonia 7. Congenital anomalies8. Alzheimer’s disease 8. Cerebrovascular disease9. Nephritis 9. Diabetes mellitus0. Septicemia 10. Chronic lower respiratory disease1. Suicide 11. HIV2. Liver disease 12. Liver disease3. Homicide 13. Influenza and pneumonia4. Hypertension 14. Septicemia5. Pneumonitis 15. Nephritis6. Parkinson’s disease 16. Viral hepatitis7. Aortic aneurysm 17. Benign neoplasms8. HIV 18. Hypertension9. Atherosclerosis 19. Aortic aneurysm0. Perinatal period 20. Pneumonitis
PLL, years of potential life lost.
ALYs (top 13) (1996)2 Actual causes of death (top 9) (2000)3
1. Ischemic heart disease 1. Tobacco2. Cerebrovascular disease 2. Poor diet and physical inactivity3. Motor vehicle crashes 3. Alcohol consumption4. Unipolar major depression 4. Microbial agents5. Lung trachea or bronchial cancer 5. Toxic agents6. COPD 6. Motor vehicle7. Alcohol use 7. Firearms8. HIV 8. Sexual behavior9. Diabetes mellitus 9. Illicit drug use0. Osteoarthritis1. Dementia and other degenerative and
hereditary CNS disorders2. Congenital abnormalities3. Homicide and violence
NS, central nervous system; COPD, chronic obstructive pulmonary disease; DALYs, disability-adjusted life years.
mber 3

H
11111111
D
11111111112
R
ospital discharge (top 17) (1999)4 Hospital days (top 17) (1999)4
1. Heart disease 1. Heart disease2. Females with deliveries 2. Psychoses3. Pneumonia 3. Females with deliveries4. Psychoses 4. Malignant neoplasms5. Malignant neoplasms 5. Pneumonia6. Fractures, all sites 6. Fractures, all sites7. Cerebrovascular disease 7. Cerebrovascular disease8. Diabetes mellitus 8. Diabetes mellitus9. Chronic bronchitis 9. Septicemia0. Asthma 10. Chronic bronchitis1. Volume depletion 11. Osteoarthrosis and allied disorders2. Osteoarthrosis and allied disorders 12. Volume depletion3. Benign neoplasms 13. Cellulitis and abscess4. Cellulitis and abscess 14. Asthma5. Cholelithiasis 15. Cholelithiasis6. Septicemia 16. Benign neoplasms7. Intervertebral disc disorder 17. Intervertebral disc disorder
isability (top 20) (1999)5 Costly conditions (top 15) (2000)6
1. Arthritis or rheumatism 1. Heart disease2. Back or spine problem 2. Cancer3. Heart trouble/hardening of the arteries 3. Trauma4. Lung or respiratory problem 4. Mental disorder5. Deafness or hearing problem 5. Pulmonary conditions6. Limb/extremity stiffness 6. Diabetes7. Mental or emotional problem 7. Hypertension8. Diabetes 8. Cerebrovascular disease9. Blindness or vision problem 9. Osteoarthritis0. Stroke 10. Pneumonia1. Broken bone/fracture 11. Back problems2. Mental retardation 12. Kidney disease3. Cancer 13. Endocrine disorders4. High blood pressure 14. Skin disorders5. Head or spinal cord injury 15. Infectious diseases6. Learning disability7. Alzheimer’s disease/senility/dementia8. Kidney problems9. Paralysis0. Missing limbs
eferences for Appendix 11. National Center for Health Statistics Vital Statistics
System. Hyattsville MD: Department of Healthand Human Services, National Center for HealthStatistics. Available at: www.cdc.gov/ncipc/wisqars/.Accessed December 2003.
2. McKenna MT, Michaud CM, Murray CJL, Marks JS.Assessing the burden of disease in the U.S. using disabil-ity-adjusted life years. Am J Prev Med 2005;28:415–23.
3. Mokdad AH, Marks JS, Stroup DF, Gerberding JL.Actual causes of death in the United States, 2000. JAMA2004;291:1238–45.
4. National Center for Health Statistics. National Hospital
Discharge Survey: 1999 annual summary with detaileddiagnosis and procedure data. Vital and Health Statis-tics;13(151). Hyattsville MD: Department of Health andHuman Services, National Center for Health Statistics,2001. Available at: www.cdc.gov/nchs/data/series/sr_13/sr13_151.pdf. Accessed January 2004.
5. Centers for Disease Control and Prevention. Prevalenceof disabilities and associated health conditions amongadults—United States, 1999. MMWR Morb Mortal WklyRep 2001;50:120–5.
6. Cohen J, Krauss N. Spending and service use amongpeople with the fifteen most costly medical conditions.
Health Aff 1997;22:129–38.Am J Prev Med 2005;28(3) 227.e7

Ac
C
D
A
I
2
ppendix 2. Modifiable risk factors (194) and population-based interventions (703) found for 31 high-priorityonditions related to programs at the Centers for Disease Control and Prevention, 2003
ONDITION RISK FACTOR INTERVENTION
iabetes mellitus1. Overweight/obesity 1. Lifestyle interventions2. Diet 2. Community-wide informational campaigns3. Lack of physical activity 3. Point-of-decision prompts
4. Mass media campaigns5. Classroom-based health education focused
on providing information6. School-based physical education7. Individually adapted health behavior
change programs8. Social support interventions in community
settings9. College-based health education and
physical education10. Classroom-based health education focused
on reducing TV viewing and video gameplaying
11. Family-based social support12. Creation of enhanced access to places for
PA combined with informational outreachactivities
rthritis1. Repeated injury
njury: Motor vehicle crashes1. Lack of visibility of motorcyclist
not wearing reflective clothing1. Wear reflective or fluorescent clothing
2. Lack of visibility of motorcyclistnot wearing non-dark or whitehelmet
2. Wear non-dark or white helmet
3. Lack of visibility of motorcyclistnot using headlights in daytime
3. Use headlights in daytime
4. Lack of regular vehicleinspections
4. Vehicle inspections every 6 months
5. Lack of tire inflation 5. Child safety seat laws6. Driver sleepiness 6. Distribution and education programs7. Lack of seatbelt use 7. Community-wide information and
enforcement programs8. Lack of child seat use 8. Incentive and education programs9. Alcohol impaired driving 9. Education-only programs
10. Motorcycle rider not wearinghelmet
10. Safety belt laws
11. Young children riding in frontseat
11. Primary enforcement laws
12. Enhanced enforcement13. 0.08% BAC laws14. Minimum legal drinking age laws at age
21 years15. Sobriety checkpoint16. Random breath tests17. Selective breath tests18. Lower BAC for young and inexperienced
drivers19. Intervention training for servers of
alcoholic beverages (under certainconditions)
20. Mass media campaigns (under certainconditions)
21. Administrative license suspensionmandatory substance abuse assessmentand treatment for persons convicted ofDUI
27.e8 American Journal of Preventive Medicine, Volume 28, Number 3

C
I
I
I
ONDITION RISK FACTOR INTERVENTION
22. Child endangerment laws that apply topersons who drive while intoxicated with achild in vehicle
23. Repealing motorcycle helmet lawsnjury: Poisoning
1. No CO alarms 1. CO alarm ordinance2. CO exhaust from confined
spaces2. Community multiphase program
3. Nonfunctioning CO alarms 3. State air quality standards for indoor icerinks
4. Access to mediation by children 4. CO alarm ordinance/distribution5. Use of contaminated drug
(OTC drug with unintendedingredient)
5. Poison Prevention Packaging Act
6. Misuse of drug 6. FDA-mandated recall7. Use of drug with unintended
effects7. State regulations
8. Use of deliberatelycontaminated mediation
8. Voluntary recall
9. Use of illegally importedmaterials
njury: Suicide and self-inflicted injury
1. One or more adverse childhoodexperiences
1. Crisis centers and hotlines
2. Child maltreatment 2. School-based programs3. Access to guns 3. Physical education programs4. Access to means 4. Bans on specified firearms or ammunition5. Lack of provider knowledge 5. Firearm acquisition restrictions6. Exposure to suicide 6. Waiting period for firearm acquisitions7. Substance abuse 7. Firearm registration and licensing of
firearm owners8. Previous attempted suicide 8. “Shall issue” concealed weapons carry laws9. Substance abuse, lack of
family/peer support9. Child access prevention (CAP) laws
10. Lack of access to health services 10. Zero tolerance of firearms in schools11. Societal beliefs regarding
acceptability of suicide11. Combinations of firearm laws
12. Social isolation 12. Alter composition of domestic gas13. Community disintegration14. Stressful life events 13. Change packaging of carbamozine15. Mental illness, anxiety 14. General suicide education16. Depression 15. Screening programs17. Other types of violence (e.g.,
physical fighting)16. Peer support programs
18. Expressions of suicidal thoughts 17. Restriction of access to lethal means19. Family discord 18. Intervention after a suicide.20. Arguments with
boyfriend/girlfriend19. Various multifaceted intervention
programs21. School-related problems 20. Community gate-keeper training22. Hopelessness 21. Multifaceted program23. Contact with juvenile justice
system24. Contagion (media exposure)25. Violence between intimate
partnersnjury: Homicide and
interpersonal violence1. History of abuse 1. Early childhood home visitation to
prevent violence against child(maltreatment, abuse, or neglect)
2. Community/family instability 2. Early childhood home visitation toprevent intimate partner violence
Am J Prev Med 2005;28(3) 227.e9
C
K
C
C
2
ONDITION RISK FACTOR INTERVENTION
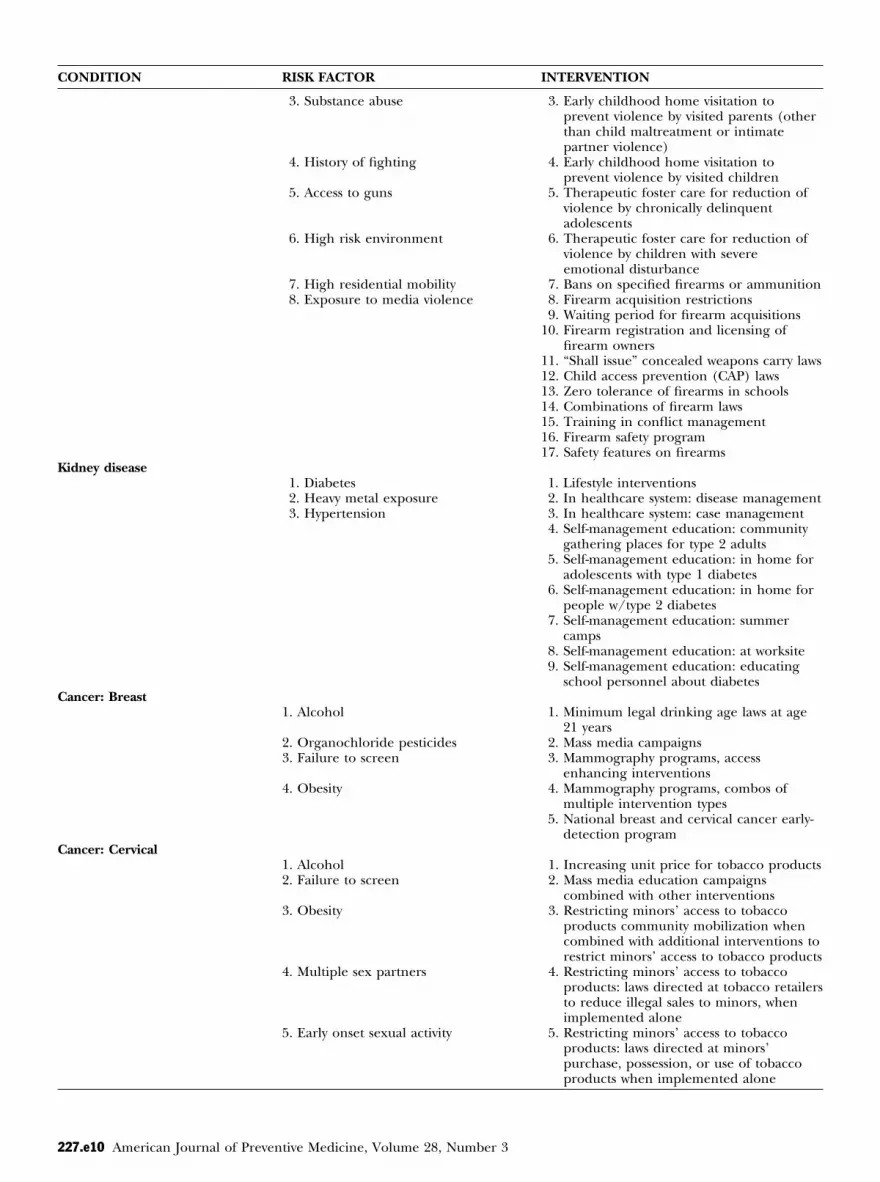
3. Substance abuse 3. Early childhood home visitation toprevent violence by visited parents (otherthan child maltreatment or intimatepartner violence)
4. History of fighting 4. Early childhood home visitation toprevent violence by visited children
5. Access to guns 5. Therapeutic foster care for reduction ofviolence by chronically delinquentadolescents
6. High risk environment 6. Therapeutic foster care for reduction ofviolence by children with severeemotional disturbance
7. High residential mobility 7. Bans on specified firearms or ammunition8. Exposure to media violence 8. Firearm acquisition restrictions
9. Waiting period for firearm acquisitions10. Firearm registration and licensing of
firearm owners11. “Shall issue” concealed weapons carry laws12. Child access prevention (CAP) laws13. Zero tolerance of firearms in schools14. Combinations of firearm laws15. Training in conflict management16. Firearm safety program17. Safety features on firearms
idney disease1. Diabetes 1. Lifestyle interventions2. Heavy metal exposure 2. In healthcare system: disease management3. Hypertension 3. In healthcare system: case management
4. Self-management education: communitygathering places for type 2 adults
5. Self-management education: in home foradolescents with type 1 diabetes
6. Self-management education: in home forpeople w/type 2 diabetes
7. Self-management education: summercamps
8. Self-management education: at worksite9. Self-management education: educating
school personnel about diabetesancer: Breast
1. Alcohol 1. Minimum legal drinking age laws at age21 years
2. Organochloride pesticides 2. Mass media campaigns3. Failure to screen 3. Mammography programs, access
enhancing interventions4. Obesity 4. Mammography programs, combos of
multiple intervention types5. National breast and cervical cancer early-
detection programancer: Cervical
1. Alcohol 1. Increasing unit price for tobacco products2. Failure to screen 2. Mass media education campaigns
combined with other interventions3. Obesity 3. Restricting minors’ access to tobacco
products community mobilization whencombined with additional interventions torestrict minors’ access to tobacco products
4. Multiple sex partners 4. Restricting minors’ access to tobaccoproducts: laws directed at tobacco retailersto reduce illegal sales to minors, whenimplemented alone
5. Early onset sexual activity 5. Restricting minors’ access to tobaccoproducts: laws directed at minors’purchase, possession, or use of tobaccoproducts when implemented alone
27.e10 American Journal of Preventive Medicine, Volume 28, Number 3

C
C
ONDITION RISK FACTOR INTERVENTION
6. Smoking 6. Active enforcement of sales laws directedat retailers, when implemented alone
7. Retailer education with reinforcement,when implemented alone
8. Retailer education without reinforcement,when implemented alone
9. Community education regarding minors’access to tobacco products, whenimplemented alone
10. Increasing unit price for tobacco products11. Mass media education campaigns
combined with other interventions12. Healthcare provider reminder systems13. Healthcare provider reminder systems
with provider education, with or withoutclient education
14. Reducing client out-of-pocket costs foreffective cessation therapies
15. Multicomponent interventions thatinclude client telephone support
16. Mass media education–cessation series17. Mass media education–cessation contests18. Healthcare provider education alone19. Healthcare provider feedback alone20. Smoking bans and restrictions21. Community education to reduce exposure
to environmental tobacco smoke in home22. Screening programs23. National breast and cervical cancer early
detection program24. School-based sex education25. Community-based sex education26. Minimum legal drinking age laws at age
21 years27. Mass media campaigns
ancer: Colorectal1. Diet 1. Increasing unit price for tobacco products2. Smoking 2. Mass media education campaigns
combined with other interventions3. Failure to screen 3. Restricting minors’ access to tobacco
products community mobilization whencombined with additional interventions torestrict minors’ access to tobacco products
4. Obesity 4. Restricting minors’ access to tobaccoproducts: laws directed at tobacco retailersto reduce illegal sales to minors, whenimplemented alone
5. Physical inactivity 5. Restricting minors’ access to tobaccoproducts: laws directed at minors’purchase, possession, or use of tobaccoproducts when implemented alone
6. Active enforcement of sales laws directedat retailers, when implemented alone
7. Retailer education with reinforcement,when implemented alone
8. Retailer education without reinforcement,when implemented alone
9. Community education regarding minors’access to tobacco products, whenimplemented alone
10. Increasing unit price for tobacco products11. Mass media education campaigns
combined with other interventions12. Healthcare provider reminder systems
Am J Prev Med 2005;28(3) 227.e11

C
C
2
ONDITION RISK FACTOR INTERVENTION
13. Healthcare provider reminder systemswith provider education, with or withoutclient education
14. Reducing client out-of-pocket costs foreffective cessation therapies
15. Multicomponent interventions thatinclude client telephone support
16. Mass media education–cessation series17. Mass media education–cessation contests18. Healthcare provider education alone19. Healthcare provider feedback alone20. Smoking bans and restrictions21. Community education to reduce exposure
to environmental tobacco smoke in home22. Community-wide informational campaigns23. Point-of-decision prompts24. Mass media campaigns25. Classroom-based health education focused
on providing information26. School-based physical education27. Individually adapted health behavior
change programs28. Social support interventions in community
settings29. College-based health education and
physical education30. Classroom-based health education focused
on reducing TV viewing and video gameplaying
31. Family-based social support32. Creation of enhanced access to places for
PA combined with informational outreachactivities
ancer: Lung1. Environmental tobacco smoke 1. Increasing unit price for tobacco products2. Tobacco 2. Mass media education campaigns
combined with other interventions3. Diet 3. Restricting minors’ access to tobacco
products community mobilization whencombined with additional interventions torestrict minors’ access to tobacco products
4. Indoor radon 4. Restricting minors’ access to tobaccoproducts: laws directed at tobacco retailersto reduce illegal sales to minors, whenimplemented alone
5. Indoor and outdoor airpollution
5. Restricting minors’ access to tobaccoproducts: laws directed at minors’purchase, possession, or use of tobaccoproducts when implemented alone
6. Active enforcement of sales laws directedat retailers, when implemented alone
7. Retailer education with reinforcement,when implemented alone
8. Retailer education without reinforcement,when implemented alone
9. Community education regarding minors’access to tobacco products, whenimplemented alone
10. Increasing unit price for tobacco products11. Mass media education campaigns
combined with other interventions12. Healthcare provider reminder systems13. Healthcare provider reminder systems
with provider education, with or withoutclient education
27.e12 American Journal of Preventive Medicine, Volume 28, Number 3
C
C
C
A
C
ONDITION RISK FACTOR INTERVENTION
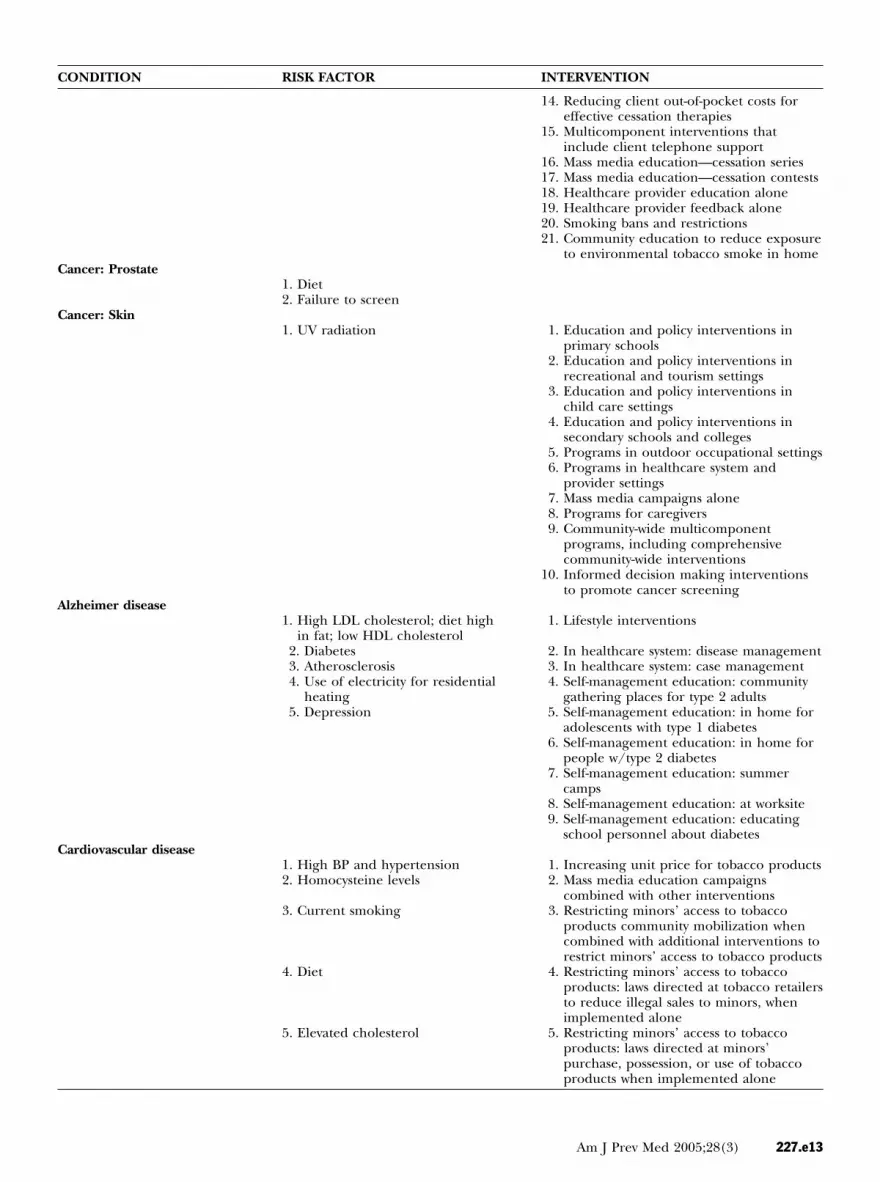
14. Reducing client out-of-pocket costs foreffective cessation therapies
15. Multicomponent interventions thatinclude client telephone support
16. Mass media education—cessation series17. Mass media education—cessation contests18. Healthcare provider education alone19. Healthcare provider feedback alone20. Smoking bans and restrictions21. Community education to reduce exposure
to environmental tobacco smoke in homeancer: Prostate
1. Diet2. Failure to screen
ancer: Skin1. UV radiation 1. Education and policy interventions in
primary schools2. Education and policy interventions in
recreational and tourism settings3. Education and policy interventions in
child care settings4. Education and policy interventions in
secondary schools and colleges5. Programs in outdoor occupational settings6. Programs in healthcare system and
provider settings7. Mass media campaigns alone8. Programs for caregivers9. Community-wide multicomponent
programs, including comprehensivecommunity-wide interventions
10. Informed decision making interventionsto promote cancer screening
lzheimer disease1. High LDL cholesterol; diet high
in fat; low HDL cholesterol1. Lifestyle interventions
2. Diabetes 2. In healthcare system: disease management3. Atherosclerosis 3. In healthcare system: case management4. Use of electricity for residential
heating4. Self-management education: community
gathering places for type 2 adults5. Depression 5. Self-management education: in home for
adolescents with type 1 diabetes6. Self-management education: in home for
people w/type 2 diabetes7. Self-management education: summer
camps8. Self-management education: at worksite9. Self-management education: educating
school personnel about diabetesardiovascular disease
1. High BP and hypertension 1. Increasing unit price for tobacco products2. Homocysteine levels 2. Mass media education campaigns
combined with other interventions3. Current smoking 3. Restricting minors’ access to tobacco
products community mobilization whencombined with additional interventions torestrict minors’ access to tobacco products
4. Diet 4. Restricting minors’ access to tobaccoproducts: laws directed at tobacco retailersto reduce illegal sales to minors, whenimplemented alone
5. Elevated cholesterol 5. Restricting minors’ access to tobaccoproducts: laws directed at minors’purchase, possession, or use of tobaccoproducts when implemented alone
Am J Prev Med 2005;28(3) 227.e13

C
A
2
ONDITION RISK FACTOR INTERVENTION
6. Increased BMI/obesity 6. Active enforcement of sales laws directedat retailers, when implemented alone
7. Physical inactivity 7. Retailer education with reinforcement,when implemented alone
8. Smoking, obesity or overweight,poor diet, lack of exercise, andalcohol (as a group)
8. Retailer education without reinforcement,when implemented alone
9. Diabetes 9. Community education regarding minors’access to tobacco products, whenimplemented alone
10. Increasing unit price for tobacco products11. Mass media education campaigns
combined with other interventions12. Healthcare provider reminder systems13. Healthcare provider reminder systems
with provider education, with or withoutclient education
14. Reducing client out-of-pocket costs foreffective cessation therapies
15. Multicomponent interventions thatinclude client telephone support
16. Mass media education–cessation series17. Mass media education–cessation contests18. Healthcare provider education alone19. Healthcare provider feedback alone20. Smoking bans and restrictions21. Community education to reduce exposure
to environmental tobacco smoke in home22. Lifestyle interventions23. In healthcare system: case management24. In healthcare system: disease management25. Self-management education: community
gathering places for type 2 adults26. Self-management education: in home for
adolescents with type 1 diabetes27. Self-management education: in home for
people w/type 2 diabetes28. Self-management education: summer
camps29. Self-management education: at worksite30. Self-management education: educating
school personnel about diabetes31. Point-of-decision prompts32. Mass media campaigns33. Classroom-based health education focused
on providing information34. School-based physical education35. Individually adapted health behavior
change programs36. Social support interventions in community
settings37. College-based health education and
physical education38. Classroom-based health education focused
on reducing TV viewing and video gameplaying
39. Family-based social support40. Creation of enhanced access to places for
PA combined with informational outreachactivities
41. Community-wide informational campaignssthma
1. Pet-related allergies 1. Increasing unit price for tobacco products2. Exposure to environmental
tobacco smoke2. Mass media education campaigns
combined with other interventions
27.e14 American Journal of Preventive Medicine, Volume 28, Number 3
C
B
B
ONDITION RISK FACTOR INTERVENTION
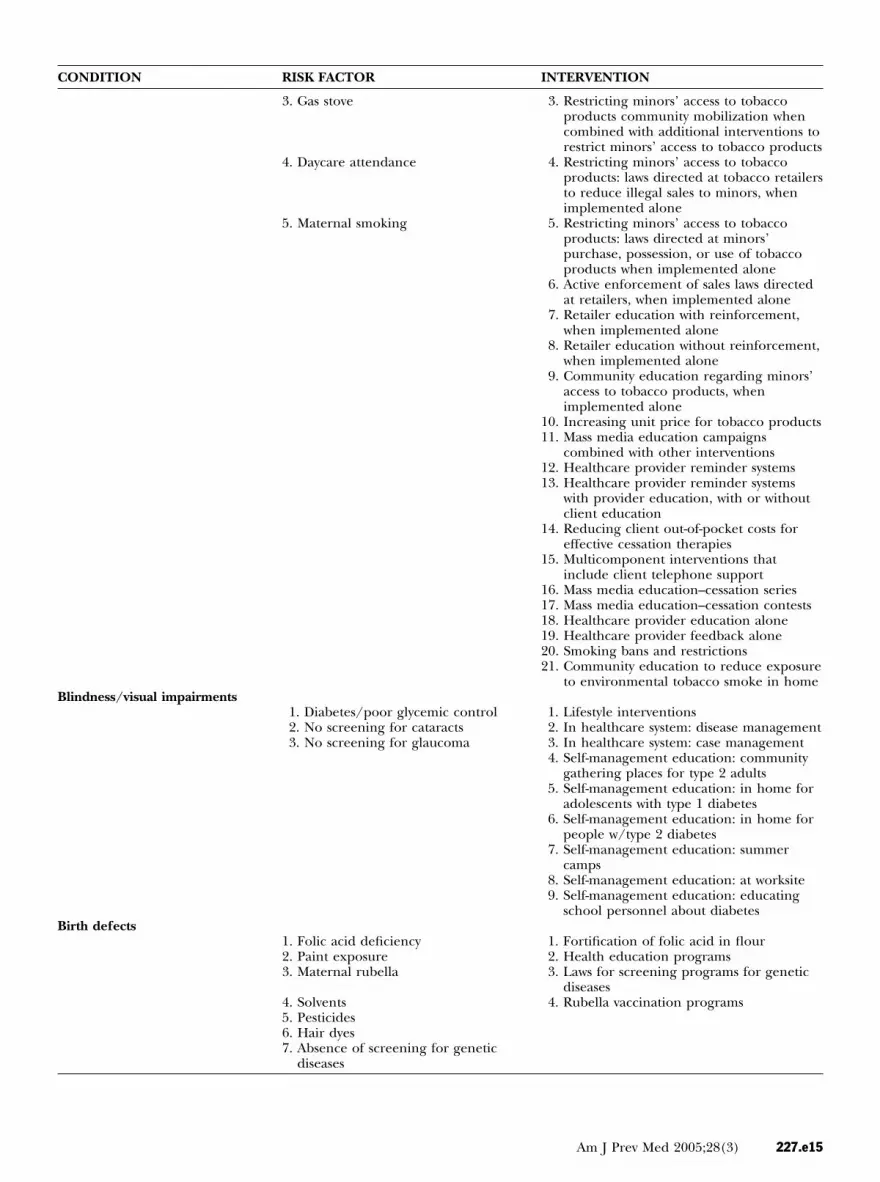
3. Gas stove 3. Restricting minors’ access to tobaccoproducts community mobilization whencombined with additional interventions torestrict minors’ access to tobacco products
4. Daycare attendance 4. Restricting minors’ access to tobaccoproducts: laws directed at tobacco retailersto reduce illegal sales to minors, whenimplemented alone
5. Maternal smoking 5. Restricting minors’ access to tobaccoproducts: laws directed at minors’purchase, possession, or use of tobaccoproducts when implemented alone
6. Active enforcement of sales laws directedat retailers, when implemented alone
7. Retailer education with reinforcement,when implemented alone
8. Retailer education without reinforcement,when implemented alone
9. Community education regarding minors’access to tobacco products, whenimplemented alone
10. Increasing unit price for tobacco products11. Mass media education campaigns
combined with other interventions12. Healthcare provider reminder systems13. Healthcare provider reminder systems
with provider education, with or withoutclient education
14. Reducing client out-of-pocket costs foreffective cessation therapies
15. Multicomponent interventions thatinclude client telephone support
16. Mass media education–cessation series17. Mass media education–cessation contests18. Healthcare provider education alone19. Healthcare provider feedback alone20. Smoking bans and restrictions21. Community education to reduce exposure
to environmental tobacco smoke in homelindness/visual impairments
1. Diabetes/poor glycemic control 1. Lifestyle interventions2. No screening for cataracts 2. In healthcare system: disease management3. No screening for glaucoma 3. In healthcare system: case management
4. Self-management education: communitygathering places for type 2 adults
5. Self-management education: in home foradolescents with type 1 diabetes
6. Self-management education: in home forpeople w/type 2 diabetes
7. Self-management education: summercamps
8. Self-management education: at worksite9. Self-management education: educating
school personnel about diabetesirth defects
1. Folic acid deficiency 1. Fortification of folic acid in flour2. Paint exposure 2. Health education programs3. Maternal rubella 3. Laws for screening programs for genetic
diseases4. Solvents 4. Rubella vaccination programs5. Pesticides6. Hair dyes7. Absence of screening for genetic
diseases
Am J Prev Med 2005;28(3) 227.e15

C
C
P
2
ONDITION RISK FACTOR INTERVENTION
hronic obstructivepulmonary disease (COPD)
1. Smoking 1. Increasing unit price for tobaccoproducts
2. Mass media education campaignscombined with other interventions
3. Restricting minors’ access to tobaccoproducts community mobilization whencombined with additional interventionsto restrict minors’ access to tobaccoproducts
4. Restricting minors’ access to tobaccoproducts: laws directed at tobaccoretailers to reduce illegal sales to minors,when implemented alone
5. Restricting minors’ access to tobaccoproducts: laws directed at minors’purchase, possession, or use of tobaccoproducts when implemented alone
6. Active enforcement of sales laws directedat retailers, when implemented alone
7. Retailer education with reinforcement,when implemented alone
8. Retailer education withoutreinforcement, when implemented alone
9. Community education regarding minors’access to tobacco products, whenimplemented alone
10. Increasing unit price for tobaccoproducts
11. Mass media education campaignscombined with other interventions
12. Healthcare provider reminder systems13. Healthcare provider reminder systems
with provider education, with or withoutclient education
14. Reducing client out-of-pocket costs foreffective cessation therapies
15. Multicomponent interventions thatinclude client telephone support
16. Mass media education–cessation series17. Mass media education–cessation contests18. Healthcare provider education alone19. Healthcare provider feedback alone20. Smoking bans and restrictions21. Community education to reduce
exposure to environmental tobaccosmoke in home
aralysis1. Cardiovascular disease 1. Increasing unit price for tobacco products2. Lack of immunizations 2. Mass media education campaigns
combined with other interventions3. Birth defects 3. Restricting minors’ access to tobacco
products community mobilization whencombined with additional interventionsto restrict minors’ access to tobaccoproducts
4. Injuries 4. Restricting minors’ access to tobaccoproducts: laws directed at tobaccoretailers to reduce illegal sales to minors,when implemented alone
5. Restricting minors’ access to tobaccoproducts: laws directed at minors’purchase, possession, or use of tobaccoproducts when implemented alone
27.e16 American Journal of Preventive Medicine, Volume 28, Number 3
C
ONDITION RISK FACTOR INTERVENTION6. Active enforcement of sales laws directedat retailers, when implemented alone
7. Retailer education with reinforcement,when implemented alone
8. Retailer education withoutreinforcement, when implemented alone
9. Community education regarding minors’access to tobacco products, whenimplemented alone
10. Increasing unit price for tobaccoproducts
11. Mass media education campaignscombined with other interventions
12. Healthcare provider reminder systems13. Healthcare provider reminder systems
with provider education, with or withoutclient education
14. Reducing client out-of-pocket costs foreffective cessation therapies
15. Multicomponent interventions thatinclude client telephone support
16. Mass media education–cessation series17. Mass media education–cessation contests18. Healthcare provider education alone19. Healthcare provider feedback alone20. Smoking bans and restrictions21. Community education to reduce
exposure to environmental tobaccosmoke in home
22. Lifestyle interventions23. In healthcare system: disease
management24. Self-management education: community
gathering places for type II adults25. Self-management education: in home for
adolescents with type 1 diabetes26. Self-management education: in home for
people w/type II diabetes27. Self-management education: summer
camps28. Self-management education: at worksite29. Self-management education: educating
school personnel about diabetes30. Community-wide informational
campaigns31. Point-of-decision prompts32. Mass media campaigns33. Classroom-based health education
focused on providing information34. School-based physical education35. Individually adapted health behavior
change programs36. Social support interventions in
community settings37. College-based health education and
physical education38. Classroom-based health education
focused on reducing TV viewing andvideo game playing
39. Family-based social support40. Creation of enhanced access to places
for PA combined with informationaloutreach activities
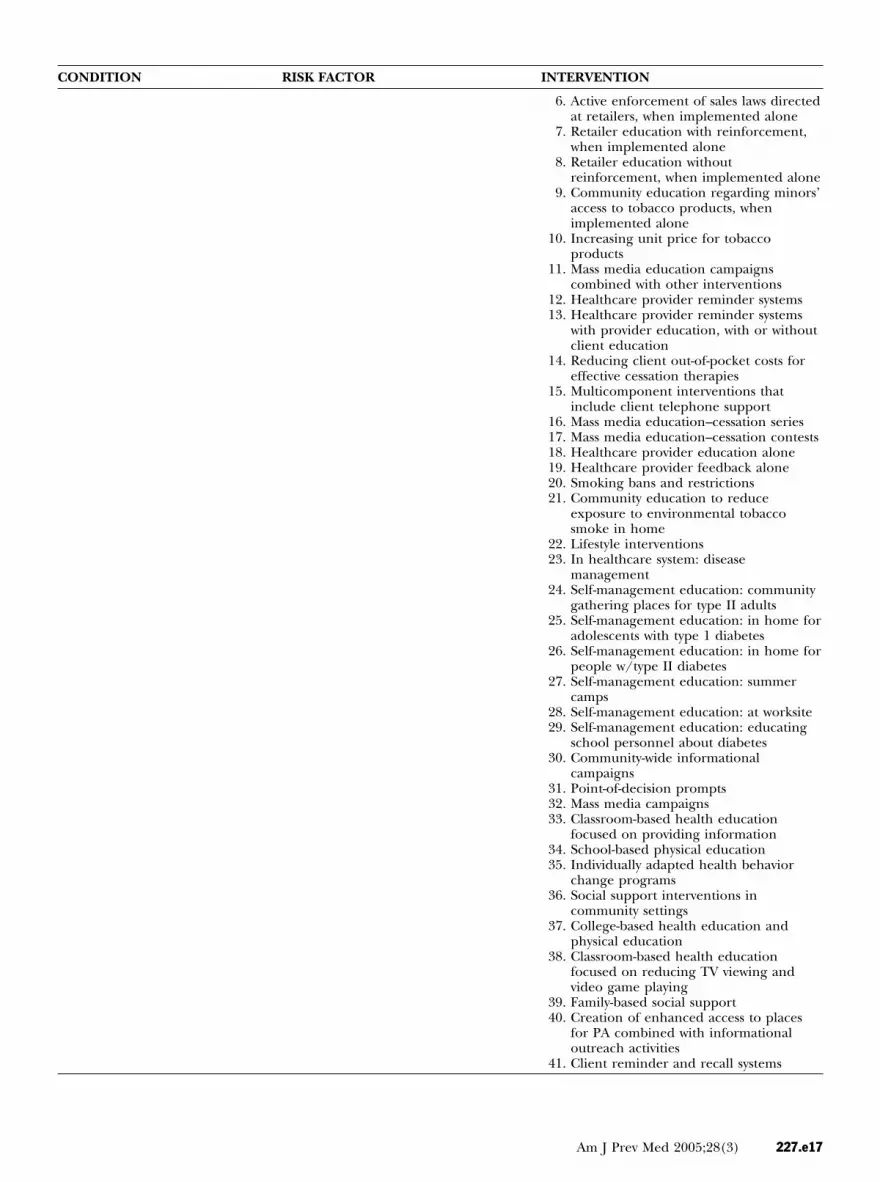
41. Client reminder and recall systems
Am J Prev Med 2005;28(3) 227.e17

C
2
ONDITION RISK FACTOR INTERVENTION
42. Multicomponent interventions thatinclude education
43. Vaccination requirements for child careand school and college attendance
44. Community-wide education only; mail,radio, TV, newspaper, posters
45. Clinic-based education only46. Client or family incentives47. Client-held medical records48. Reducing out-of-pocket expenses49. Expanding access in healthcare settings
as part of a multicomponentintervention
50. Vaccination programs in women, infants,and children (WIC) settings
51. Vaccination programs in schools52. Home visits53. Expanding access in healthcare settings,
when used alone54. Vaccination programs in child care
center55. Provider reminder and recall systems56. Assessment plus feedback for vaccination
providers57. Standing orders for adults58. Standing orders for children59. Provider education only60. Nurse-initiated vaccine protocols for
pneumococcal vaccine61. Fortification of folic acid in flour62. Health education programs63. Laws for screening programs for genetic
diseases64. Rubella vaccination programs65. Wear reflective or fluorescent clothing66. Wear non-dark or white helmet67. Use headlights in daytime68. Vehicle inspections every 6 months69. Child safety seat laws70. Distribution and education programs71. Community-wide information and
enforcement programs72. Incentive and education programs73. Education-only programs74. Safety belt laws75. Primary enforcement laws76. Enhanced enforcement77. 0.08% BAC laws78. Minimum legal drinking age laws at age
21 years79. Sobriety checkpoint80. Random breath tests81. Selective breath tests82. Lower BAC for young and inexperienced
drivers83. Intervention training for servers of
alcoholic beverages (under certainconditions)
84. Mass media campaigns (under certainconditions)
85. Administrative license suspensionmandatory substance abuse assessmentand treatment for persons convicted ofDUI
27.e18 American Journal of Preventive Medicine, Volume 28, Number 3

C
E
ONDITION RISK FACTOR INTERVENTION
86. Child endangerment laws that apply topersons who drive while intoxicated witha child in vehicle
87. Repealing motorcycle helmet laws88. CO alarm ordinance89. Community multiphase program90. State air quality standards for indoor ice
rinks91. CO alarm ordinance/distribution92. Poison Prevention Packaging Act93. FDA-mandated recall94. State regulations95. Voluntary recall96. Crisis centers and hotlines97. School-based programs98. Physical education programs99. Bans on specified firearms or
ammunition100. Firearm acquisition restrictions101. Waiting period for firearm acquisitions102. Firearm registration and licensing of
firearm owners103. “Shall issue” concealed weapons carry
laws104. Child access prevention (CAP) laws105. Zero tolerance of firearms in schools106. Combinations of firearm laws107. Alter composition of domestic gas108. Change packaging of carbamozine109. General suicide education110. Screening programs111. Peer support programs112. Restriction of access to lethal means113. Intervention after a suicide114. Various multifaceted intervention
programs115. Community gate-keeper training116. Multifaceted program117. Early childhood home visitation to
prevent violence against child(maltreatment, abuse, or neglect)
118. Early childhood home visitation toprevent intimate partner violence
119. Early childhood home visitation toprevent violence by visited parents(other than child maltreatment orintimate partner violence)
120. Early childhood home visitation toprevent violence by visited children
121. Therapeutic foster care for reduction ofviolence by chronically delinquentadolescents
122. Therapeutic foster care for reduction ofviolence by children with severeemotional disturbance
123. Community smoke detector program124. Smoke alarm/fire safety prevention
programs125. In healthcare system: case management
pilepsy1. Cerebrovascular disease 1. Increasing unit price for tobacco
products2. Trauma 2. Mass media education campaigns
combined with other interventions
Am J Prev Med 2005;28(3) 227.e19

C
2
ONDITION RISK FACTOR INTERVENTION
3. Restricting minors’ access to tobaccoproducts community mobilization whencombined with additional interventions torestrict minors’ access to tobacco products
4. Restricting minors’ access to tobaccoproducts: laws directed at tobacco retailersto reduce illegal sales to minors, whenimplemented alone
5. Restricting minors’ access to tobaccoproducts: laws directed at minors’purchase, possession, or use of tobaccoproducts when implemented alone
6. Active enforcement of sales laws directedat retailers, when implemented alone
7. Retailer education with reinforcement,when implemented alone
8. Retailer education without reinforcement,when implemented alone
9. Community education regarding minors’access to tobacco products, whenimplemented alone
10. Increasing unit price for tobacco products11. Mass media education campaigns
combined with other interventions12. Healthcare provider reminder systems13. Healthcare provider reminder systems
with provider education, with or withoutclient education
14. Reducing client out-of-pocket costs foreffective cessation therapies
15. Multicomponent interventions thatinclude client telephone support
16. Mass media education–cessation series17. Mass media education–cessation contests18. Healthcare provider education alone19. Healthcare provider feedback alone20. Smoking bans and restrictions21. Community education to reduce exposure
to environmental tobacco smoke in home22. Lifestyle interventions23. In healthcare system: disease management24. Self-management education: community
gathering places for type 2 adults25. Self-management education: in home for
adolescents with type 1 diabetes26. Self-management education: in home for
people w/type 2 diabetes27. Self-management education: summer
camps28. Self-management education: at worksite29. Self-management education: educating
school personnel about diabetes30. Community-wide informational campaigns31. Point-of-decision prompts32. Mass media campaigns33. Classroom-based health education focused
on providing information34. School-based physical education35. Individually adapted health behavior
change programs36. Social support interventions in community
settings37. College-based health education and
physical education
27.e20 American Journal of Preventive Medicine, Volume 28, Number 3

C
H
M
ONDITION RISK FACTOR INTERVENTION
38. Classroom-based health education focusedon reducing TV viewing and video gameplaying
39. Family-based social support40. Creation of enhanced access to places for
PA combined with information outreachactivities
41. Crisis centers and hotlines42. School-based programs43. Physical education programs44. Bans on specified firearms or ammunition45. Firearm acquisition restrictions46. Waiting period for firearm acquisitions47. Firearm registration and licensing of
firearm owners48. “Shall issue” concealed weapons carry laws49. Child access prevention (CAP) laws50. Zero tolerance of firearms in schools51. Combinations of firearm laws52. Alter composition of domestic gas53. Change packaging of carbamozine54. General suicide education55. Screening programs56. Peer support programs57. Restriction of access to lethal means58. Intervention after a suicide.59. Various multifaceted intervention
programs60. Community gate-keeper training61. Multifaceted program62. Early childhood home visitation to
prevent violence against child(maltreatment, abuse, or neglect)
63. Early childhood home visitation toprevent intimate partner violence
64. Early childhood home visitation toprevent violence by visited parents (otherthan child maltreatment or intimatepartner violence)
65. Early childhood home visitation toprevent violence by visited children
66. Therapeutic foster care for reduction ofviolence by chronically delinquentadolescents
67. Therapeutic foster care for reduction ofviolence by children with severeemotional disturbance
68. In healthcare system: case managementearing impairments
1. Noiseental retardation
1. Lack of screening 1. Screening for PKU2. Maternal alcohol 2. Screening for lead3. Lack of folic acid 3. Fortification of flour with folic acid4. Motor vehicle crash 4. Wear reflective or fluorescent clothing5. Drop/abuse 5. Wear non-dark or white helmet6. Other trauma 6. Use headlights in daytime7. Lack of immunization 7. Vehicle inspections every 6 months8. Poisoning 8. Child safety seat laws
9. Distribution and education programs10. Community-wide information and
enforcement programs11. Incentive and education programs12. Education-only programs13. Safety belt laws
Am J Prev Med 2005;28(3) 227.e21

C
2
ONDITION RISK FACTOR INTERVENTION
14. Primary enforcement laws15. Enhanced enforcement16. Minimum legal drinking age laws at age
21 years17. Mass media campaigns (under certain
conditions)18. Repealing motorcycle helmet laws19. Early childhood home visitation to
prevent violence against child(maltreatment, abuse, or neglect)
20. Early childhood home visitation toprevent intimate partner violence
21. Early childhood home visitation toprevent violence by visited parents (otherthan child maltreatment or intimatepartner violence)
22. Early childhood home visitation toprevent violence by visited children
23. Therapeutic foster care for reduction ofviolence by chronically delinquentadolescents
24. Therapeutic foster care for reduction ofviolence by children with severeemotional disturbance
25. Client reminder and recall systems26. Multicomponent interventions that
include education27. Vaccination requirements for child care
and school and college attendance28. Community-wide education only; mail,
radio, TV, newspaper, posters29. Clinic-based education only30. Client or family incentives31. Client-held medical records32. Reducing out-of-pocket expenses33. Expanding access in healthcare settings as
part of a multicomponent intervention34. Vaccination programs in women, infants,
and children (WIC) settings35. Vaccination programs in schools36. Home visits37. Expanding access in healthcare settings,
when used alone38. Vaccination programs in child care center39. Provider reminder and recall systems40. Assessment plus feedback for vaccination
providers41. Standing orders for adults42. Standing orders for children43. Provider education only44. Nurse-initiated vaccine protocols for
pneumococcal vaccine45. CO alarm ordinance46. Community multiphase program47. State air quality standards for indoor ice
rinks48. CO alarm ordinance/distribution49. Poison Prevention Packaging Act50. FDA-mandated recall51. State regulations52. Voluntary recall
27.e22 American Journal of Preventive Medicine, Volume 28, Number 3

C
P
ONDITION RISK FACTOR INTERVENTION
erinatal conditionspregnancy
1. Maternal hepatitis B 1. Increasing unit price for tobacco products2. Maternal HIV� 2. Mass media education campaigns
combined with other interventions3. Group B streptococcal 3. Restricting minors’ access to tobacco
products community mobilization whencombined with additional interventions torestrict minors’ access to tobacco products
4. Teen pregnancy 4. Restricting minors’ access to tobaccoproducts: laws directed at tobacco retailersto reduce illegal sales to minors, whenimplemented alone
5. Maternal smoking 5. Restricting minors’ access to tobaccoproducts: laws directed at minors’purchase, possession, or use of tobaccoproducts when implemented alone
6. High blood pressure 6. Active enforcement of sales laws directedat retailers, when implemented alone
7. Pre-eclampsia 7. Retailer education with reinforcement,when implemented alone
8. Alcohol exposed pregnancy 8. Retailer education without reinforcement,when implemented alone
9. Gestational diabetes 9. Community education regarding minors’access to tobacco products, whenimplemented alone
10. Diabetes 10. Increasing unit price for tobacco products11. Multiparity births 11. Mass media education campaigns
combined with other interventions12. Healthcare provider reminder systems13. Healthcare provider reminder systems
with provider education, with or withoutclient education
14. Reducing client out-of-pocket costs foreffective cessation therapies
15. Multicomponent interventions thatinclude client telephone support
16. Mass media education–cessation series17. Mass media education–cessation contests18. Healthcare provider education alone19. Healthcare provider feedback alone20. Smoking bans and restrictions21. Community education to reduce exposure
to environmental tobacco smoke in home22. 0.08% BAC laws23. Minimum legal drinking age laws at age
21 years24. Sex education25. Skill enhancement26. Access to contraception27. Lifestyle interventions28. In healthcare system: disease management29. In healthcare system: case management30. Self-management education: community
gathering places for type 2 adults31. Self-management education: in home for
adolescents with type 1 diabetes32. Self-management education: in home for
people w/type 2 diabetes33. Self-management education: summer
camps34. Self-management education: at worksite35. Self-management education: educating
school personnel about diabetes36. School-based vaccinations for hepatitis B
Am J Prev Med 2005;28(3) 227.e23

C
D
P
2
ONDITION RISK FACTOR INTERVENTION
37. Vaccination programs in WIC settings38. Prenatal HIV testing and counseling
iarrheal Diseases1. Poor hygiene/hand washing 1. FDA’s egg safety program2. Contaminated food 2. HACCP rules and regulations3. Consumption of high-risk foods
(runny eggs, raw shell fish, etc.)3. USDA food and safety inspections
4. Contaminated drinking water 4. Restaurant inspections5. Poor food-handling practices 5. Food safety education6. Daycare exposure 6. Beaches environmental assessment closure
and health program7. International travel 7. Ban of animal sales8. Male homosexual activity 8. Water regulations9. Drug use
10. Contaminatedsurface/recreational water
11. Contact with animalsneumonia/Influenza
1. Smoking 1. Increasing unit price for tobacco products2. Healthcare setting 2. Mass media education campaigns
combined with other interventions3. Daycare attendance 3. Restricting minors’ access to tobacco
products community mobilization whencombined with additional interventions torestrict minors’ access to tobacco products
4. Lack of vaccination in high-riskpopulations
4. Restricting minors’ access to tobaccoproducts: laws directed at tobacco retailersto reduce illegal sales to minors, whenimplemented alone
5. Restricting minors’ access to tobaccoproducts: laws directed at minors’purchase, possession, or use of tobaccoproducts when implemented alone
6. Active enforcement of sales laws directedat retailers, when implemented alone
7. Retailer education with reinforcement,when implemented alone
8. Retailer education without reinforcement,when implemented alone
9. Community education regarding minors’access to tobacco products, whenimplemented alone
10. Increasing unit price for tobacco products11. Mass media education campaigns
combined with other interventions12. Healthcare provider reminder systems13. Healthcare provider reminder systems
with provider education, with or withoutclient education
14. Reducing client out-of-pocket costs foreffective cessation therapies
15. Multicomponent interventions thatinclude client telephone support
16. Mass media education–cessation series17. Mass media education–cessation contests18. Healthcare provider education alone19. Healthcare provider feedback alone20. Smoking bans and restrictions21. Community education to reduce exposure
to environmental tobacco smoke in home22. Nosocomial infection control23. Client reminder and recall systems24. Multicomponent interventions that
include education
27.e24 American Journal of Preventive Medicine, Volume 28, Number 3

C
N
T
ONDITION RISK FACTOR INTERVENTION
25. Vaccination requirements for child careand school attendance
26. Community-wide education only27. Clinic-based education only28. Client or family incentives29. Client-held medical records30. Reducing out-of-pocket expenses31. Expanding access in healthcare settings as
part of a multicomponent intervention32. Vaccination programs in women, infants,
and children (WIC) settings33. Vaccination programs in schools34. Home visits35. Expanding access in healthcare settings,
when used alone36. Vaccination programs in child care center37. Provider reminder and recall systems38. Assessment plus feedback for vaccination
providers39. Standing orders for adults40. Standing orders for children41. Provider education only42. Sterilization/disinfection and
maintenance of equip43. Air handling44. Personnel restrictions
osocomial bloodstreaminfections and sepsis
1. Catheters 1. Infection control practices2. Transported out of PICU 2. Pneumococcal vaccination programs3. Longer ICU stay 3. Voluntary recall of product with provider
notification4. Artificial fingernails (sepsis
only)4. Industry standards of a voluntary
accreditation body5. Mechanical ventilation 5. FDA alert and recall6. No vaccination in high-risk
patients6. Medial Devices Act of 1990
7. Absence of nosocomialinfection control practices
7. Recall, design change, and more stringentindustry standards
8. Person to person transmission 8. Personnel restrictions9. Environmental contamination 9. Closing hospitals or wards
10. Contaminatedequipment/devices
10. Quarantine country
11. Host risk12. Contaminated formula13. Asymptomatic carriage in HCW14. Contaminated products15. Infected HCWs16. Exposure to infected HCW/
patientsuberculosis
1. Exposure to persons with TB 1. Directly observed therapy2. Air 2. Delivery of cues or reminders to take
medicine3. Correctional facilities 3. Improving social acceptance4. Foreign-born persons 4. Increased support5. Healthcare workers 5. Peer counseling and contingency
contracting6. Environmental control (ventilation, UV
radiation, negative pressure rooms, airdisinfection)
7. TB laws requiring health care providersand workers to report confirmed orsuspected cases
Am J Prev Med 2005;28(3) 227.e25

C
V
H
C4
2
ONDITION RISK FACTOR INTERVENTION
8. TB laws of time limits to report confirmedor suspected cases of 2 days
9. TB laws: states should have authority toimpose a penalty for willful failure toreport TB cases
10. TB laws: restricting activities of a personwith TB
11. TB laws on duty to report no adherentcases
12. TB screening13. Periodic tuberculin skin test
accine-preventable diseases1. Lack of vaccination 1. Client reminder and recall systems
2. Multicomponent interventions thatinclude education
3. Vaccination requirements for child careand school and college attendance
4. Community-wide education only; mail,radio, TV, newspaper, posters
5. Clinic-based education only6. Client or family incentives7. Client-held medical records8. Reducing out-of-pocket expenses9. Expanding access in healthcare settings as
part of a multicomponent intervention10. Vaccination programs in women, infants,
and children (WIC) settings11. Vaccination programs in schools12. Home visits13. Expanding access in healthcare settings,
when used alone14. Vaccination programs in child care center15. Provider reminder and recall systems16. Assessment plus feedback for vaccination
providers17. Standing orders for adults18. Standing orders for children19. Provider education only20. Nurse-initiated vaccine protocols for
pneumococcal vaccineIV/STDs
1. Chronic hemodialysis patients 1. Infection control practices2. Injection drug use 2. Needle exchange3. Transplants 3. Safe needle use education4. Transfusions 4. Blood and tissue testing5. Unprotected sex 5. HIV counseling and testing6. Vertical transmission 6. Partner notification7. Exposure to blood and body
fluids7. School-based education programs
8. Prenatal HIV counseling and testing9. FDA testing of condoms
10. School-based vaccination programs frohepatitis B
hronic liver disease–hepatitis B and C0% of liver disease is from hepatitis C; of that, 60% of risk is from intravenous drug use, 20% from sexual activity, and 10%from hospital-acquired infection.
1. Chronic hemodialysis patients 1. Serologic testing2. Transfusions 2. STD interventions3. Correctional facility 3. Immunization programs in Federal
Bureau of Prisons4. Vertical transmission 4. Hand hygiene5. Lack of immunization 5. Infection control practices6. Lack of infection control 6. Donor screening7. Binge drinking 7. Screening for hepatitis B in pregnant
women
27.e26 American Journal of Preventive Medicine, Volume 28, Number 3

C
BphlpN
ONDITION RISK FACTOR INTERVENTION
8. Excessive drinking 8. Client reminder and recall systems9. Organ recipient 9. Multicomponent interventions that
include education10. Consumption of kava-
containing products10. Vaccination requirements for child care
and school attendance11. Exposure to chemicals 11. Community-wide education only
12. Clinic-based education only13. Client or family incentives14. Client-held medical records15. Reducing out-of-pocket expenses16. Expanding access in healthcare settings as
part of a multicomponent intervention17. Vaccination programs in women, infants,
and children (WIC) settings18. Vaccination programs in schools19. Home visits20. Expanding access in healthcare settings,
when used alone21. Vaccination programs in child care center22. Provider reminder and recall systems23. Assessment plus feedback for vaccination
providers24. Standing orders for adults25. Standing orders for children26. Mass media campaigns (under certain
conditions)27. Minimum legal drinking age laws at age
21 years
AC, blood alcohol content; BEACH, Beaches Environmental Assessment Closure and Health Program; BMI, body mass index; BP, bloodressure; CO, carbon monoxide; DOT, directly observed therapy; DUI, driving under influence; FDA, Food and Drug Administration; HACCP,azard analysis and critical control points; HCW, healthcare worker; HDL, high-density lipoprotein; ICU, intensive care unit; LDL, low-density
ipoprotein; MVC, caudal part of medial vestibular nucleus; OTC, over-the-counter; PA, physical activity; PICU, pediatric intensive care unit; PKU,henylketonuria; STD, sexually transmitted disease; TB, tuberculosis; USDA, U.S. Department of Agriculture; WIC, Special Supplementalutrition Program for Women, Infants, and Children.
Am J Prev Med 2005;28(3) 227.e27