the effect of seizures on working memory and executive functioning performance
TRANSCRIPT

Epilepsy & Behavior 17 (2010) 412–419
Contents lists available at ScienceDirect
Epilepsy & Behavior
journal homepage: www.elsevier .com/locate /yebeh
The effect of seizures on working memory and executive functioning performance
Leah Chapman Black a,1, Bruce K. Schefft a,b,*, Steven R. Howe a, Jerzy P. Szaflarski a,b,c, Hwa-shain Yeh d,e,Michael D. Privitera b
a Department of Psychology, University of Cincinnati, Cincinnati, OH, USAb Department of Neurology, University of Cincinnati, Cincinnati, OH, USAc Department of Psychiatry and the Neuroscience Graduate Program, University of Cincinnati, Cincinnati, OH, USAd Department of Neurosurgery, University of Cincinnati, Cincinnati, OH, USAe University of Cincinnati Academic Health Center, Cincinnati, OH, USA
a r t i c l e i n f o a b s t r a c t
Article history:Received 15 October 2009Revised 28 December 2009Accepted 8 January 2010Available online 13 February 2010
Keywords:Temporal lobe epilepsyHigher cognitionPsychogenic nonepileptic seizureTemporal lobe epilepsySeizure load
1525-5050/$ - see front matter � 2010 Elsevier Inc. Adoi:10.1016/j.yebeh.2010.01.006
* Corresponding author. Address: Department oCincinnati, PO Box 210376, Cincinnati, OH 45221-037
E-mail address: [email protected] (B.K. Sche1 This work was part of the first author’s Master’s
author in the Department of Psychology, University of C
The aim of this study was to assess whether duration of seizure disorder and lifetime seizure load areassociated with deficits in higher cognitive functions in patients with temporal lobe epilepsy (TLE)(N = 207) or psychogenic nonepileptic seizures (PNES) (N = 216). Multivariate regression analysesrevealed that age at onset, duration, and group assignment were significant predictors of neuropsycho-logical performance (all P 6 0.02), with group having a moderating relationship. Univariate analysesrevealed different patterns of predictor effects on cognitive functioning within each diagnostic group.An impairment index was calculated for each individual, and univariate analyses revealed that age atTLE but not PNES onset was the only significant predictor of impairment (b = –0.005, P < 0.001). Theresults suggest that earlier age at seizure onset, longer duration, and higher lifetime seizure frequencyaffect cognitive functioning in both the TLE and PNES groups, but differently within each group. Theseresults have implications for early diagnosis and intervention in both groups.
� 2010 Elsevier Inc. All rights reserved.
1. Introduction
Working memory and executive functions are skills developedto deal with complexities in life and are necessary for effectiveand adaptive behaviors. According to Baddeley [1], working mem-ory constitutes a tripartite system: the central executive, the pho-nological loop, and the visuospatial sketch pad. Each componentworks to store and manipulate information in a temporary short-term memory system that is essential to human memory. Areasof the brain involved in working memory include the frontal lobesand select posterior brain regions [2]. Executive functions includethe control and organization of complex cognitive operations thatallow a person to plan strategies, solve problems, and modifybehaviors as a result of new information [3]. Working memoryand executive functions are integral aspects of higher cognition.
Epilepsy is ‘‘a disorder of the brain characterized by an enduringpredisposition to generate epileptic seizures and by the neurobio-logic, cognitive, psychological, and social consequences of this con-dition” [4]. Twenty-five percent of the people diagnosed with
ll rights reserved.
f Psychology, University of6, USA.fft).Thesis, chaired by the secondincinnati, Cincinnati, OH, USA.
epilepsy have medically intractable seizures [5]. For all patientswith epilepsy, but especially individuals with medication-refrac-tory seizures, research is needed on the mechanisms that underliethe cognitive deficits to design more effective interventions aimedat ameliorating these deficits.
Medically intractable epilepsy may negatively affect cognitionby disrupting cognitive processes through chronic and persistentseizures. Empirical work that focuses on the effects of seizureson cognition is relatively limited and has resulted in mixed find-ings [6–13]. Past research has found that epileptic seizures resultin poorer performance on psychometric tests compared withhealthy individuals, especially in cases of generalized tonic–clonicseizures [10,11]. Furthermore, deficits across a wide range of do-mains have been found in individuals with recurrent temporal lobeseizures [8,12,13]. Patients with mesial temporal lobe epilepsy(MTLE) and longer seizure duration display more severe cognitivedeficits than those with other epilepsies irrespective of seizure on-set laterality [7,12]. Within the MTLE population, earlier age at on-set and increased exposure to antiepileptic drugs (AEDs) are likelyto play a large role in the cognitive deficits seen in this population[12]. In addition, research suggests that as duration of epilepsy andnumber of complex partial seizures increase, there is a decline inexecutive function abilities on serial testing [14].
How temporal lobe seizures affect working memory perfor-mance is unclear. Research to date has not been conclusive, with

L.C. Black et al. / Epilepsy & Behavior 17 (2010) 412–419 413
some research suggesting that patients with medication-resistantMTLE and hippocampal sclerosis show no impairments on tasksthat target working memory [15] and others finding specific work-ing memory deficits that may rely on the functional integrity of thehippocampus [16].
Another group of individuals with paroxysmal events who alsoexperience cognitive deficits are patients experiencing psycho-genic nonepileptic seizures (PNES). PNES is the most common con-dition misdiagnosed as epilepsy and consists of events that appearto alter neurological function but lack EEG ictal changes during theclinical event(s) [17,18]. PNES has been attributed to both psycho-logical disorders [19,20] and organic brain dysfunction [21,22].Although PNES is different from TLE in many ways, there are alsomany commonalities between the groups that are important toinvestigate. Both TLE and PNES are unpredictable disorders thatare persistent and stressful and characterized by frequent, unpre-dictable, and unremitting seizures that have similar negative ef-fects on such things as quality of life and driving [23,24].Similarly, research has also shown that the more often seizuresare occurring, the more debilitating the disorder may be for theindividual [25]. In patients with PNES, previous research has docu-mented impaired neuropsychological performance on the Hal-stead–Reitan battery [20], below-average performance on theneuropsychological battery for epilepsy [22], and impaired verbalmemory performance [7]. It has been suggested that the overall le-vel of neuropsychological impairment in PNES is comparable tothat in epileptic seizures [26]. Thus, there is evidence that the PNESpopulation experiences cognitive impairments, similar to those ofthe population with epileptic seizures, but it is unclear if or howthe duration of PNES or seizure load affects higher cognitivefunctioning.
The goal of this study was to evaluate the effects of epilepsyduration and lifetime seizure load on working memory and execu-tive functions in individuals with TLE and PNES in a cross-sectionalstudy. Although studies have documented impaired performanceof individuals with TLE and PNES on tests of executive functionsand working memory, few have explored the effects of seizureduration on higher cognitive functions. Most studies have usedmodest sample sizes, and none have explored the role of lifetimenumber of seizures in neuropsychological performance. It washypothesized that patients with longer duration of epilepsy wouldexperience a decrease in working memory and executive functionsas compared with patients with PNES. Furthermore, it was ex-pected that the effect of seizures on working memory domainswould be influenced by the laterality of seizure onset (right vs leftvs bilateral TLE) and lifetime seizure load. In addition, in evaluationof the relationship between prospective lifetime seizure load andneuropsychological performance, it was expected that patientswith lower seizure loads would perform better on working mem-ory and executive functions than patients with higher lifetime sei-zure loads but would fare worse than patients with PNES.
2. Method
2.1. Sample
Participants were a convenience sample of individuals withconfirmed intractable TLE or PNES from the epilepsy monitoringunit at University Hospital in Cincinnati, OH, USA, who were seenbetween 1994 and 2005. Participants were drawn from a largersample of patients to whom a comprehensive neuropsychologicalbattery was administered. All individuals gave their informed con-sent prior to participating in the study. The study was approved bythe institutional review board at the University of Cincinnati. Thepresent study included patients with TLE and PNES. All subjects
met the following criteria: (1) age P 17 years; (2) minimum of8 years of education; (3) confirmed TLE (either unilateral or bilat-eral TLE) or confirmed PNES (patients with a mixed diagnosis suchas PNES and epilepsy were excluded); (4) no prior epilepsy sur-gery; (5) absence of significant neurological or psychiatric prob-lems (e.g., schizophrenia, Parkinson’s disease, bipolar disorder,posttraumatic stress disorder) other than depression or anxietydisorders as recorded in medical records or via self-report of diag-nosis by another physician; (6) Wechsler Adult Intelligence ScaleIII (WAIS-III) or Wechsler Adult Intelligence Scale—Revised(WAIS-R) Full Scale IQ P 70; and (7) completion of more than halfof the neuropsychological assessment data. Patients with PNESwere excluded if their interictal EEG showed epileptiform dis-charges or if they had a remote history of events that were not re-corded during prolonged video/EEG monitoring (PVEM).
2.2. Procedures
The diagnosis of temporal lobe epilepsy was based on review ofstereotypical seizure events recorded during PVEM and concor-dance of seizure semiology, neuroimaging, and EEG findings. Thefinal diagnosis was not established until the case was reviewedand discussed at a multidisciplinary epilepsy conference that in-cluded at least three epilepsy specialists, the neuropsychologist,and the neurosurgeon.
The diagnosis of PNES was made after habitual spells were re-corded during PVEM that were not associated with any EEG corre-lates; patients with brief stereotypical events without impairmentof consciousness were excluded because differentiating PNES fromfrontal lobe seizures may at times be difficult [27]. The final diag-nosis was established after video recordings of habitual spells andcorresponding EEGs were reviewed by epilepsy specialists.
Each patient’s chart was reviewed to determine seizure fre-quency. Some patients had been followed for variable amounts oftime in the outpatient clinics of the Cincinnati Epilepsy Centerwhere monthly seizure counts were documented in a database,whereas other patients were referred directly to the epilepsy mon-itoring unit by local neurologists. All available medical recordswere reviewed for as many years as possible to establish mean sei-zure frequency prior to admission. All seizure frequencies werebased on patient self-report as reported to the neurologists andneuropsychologist, and all seizure types were used in the calcula-tion with the exception of absence seizures and febrile seizures.Many individuals in the sample were experiencing more thanone seizure type (i.e., complex partial seizures, simple partial mo-tor seizures, simple partial motor seizures with secondary general-ization), so we chose to include in the lifetime seizure count focalseizures associated with changes in the level of consciousness (e.g.,complex partial seizures with/without secondary generalization)or simple partial motor seizures. The number of seizures through-out the patient’s life (lifetime seizure load) was calculated bydetermining the mean annual number of seizures for each individ-ual over the evaluable time and multiplying the annual estimate bythe number of years from diagnosis of epilepsy to date of neuro-psychological testing. This estimate also took into account periodsof seizure freedom and changes in seizure frequency whenavailable.
2.3. Measures
Neuropsychological measures used for this study were takenfrom a larger comprehensive exam administered to presurgicalcandidates on the EMU as well as individuals with PNES and in-cluded the following: the working memory deviation quotient(WMDQ), verbal/conceptual deviation quotient (VCDQ) and per-ceptual/constructional deviation quotient (PCDQ) of the WAIS-III
414 L.C. Black et al. / Epilepsy & Behavior 17 (2010) 412–419
[28] or WAIS-R [29], Trails A (TrailsA) and Trails B (TrailsB) [30],the Color/Word interference score on the Stroop Task (StroopCW)[31], the number of perseverative errors and number of categoriesachieved on the Wisconsin Card Sort Test (WCSTPer and WCSTCat)[32], and the number of words generated on a verbal fluency test(WordFlu) [33]. The aforementioned tests are commonly used neu-ropsychological measures of working memory and executive func-tioning [34].
3. Results
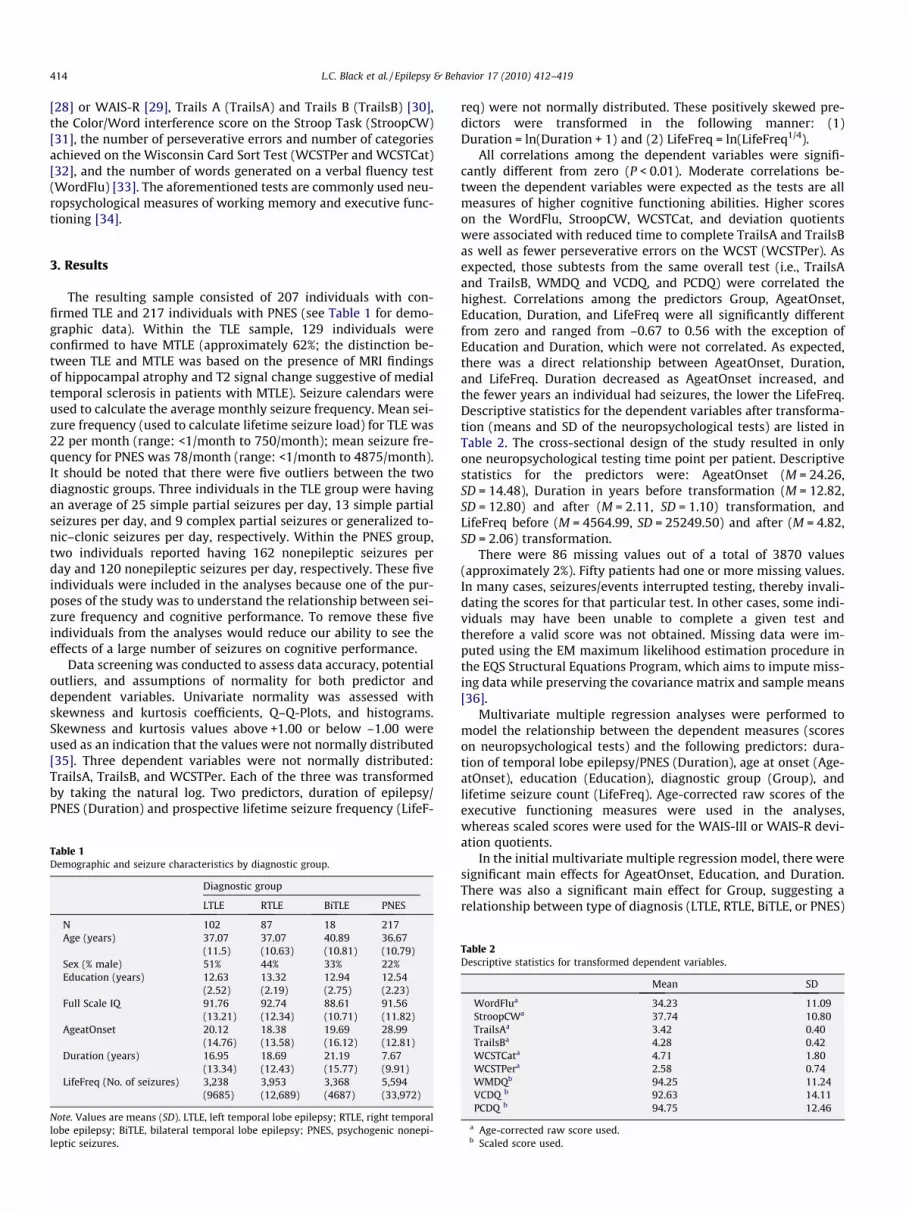
The resulting sample consisted of 207 individuals with con-firmed TLE and 217 individuals with PNES (see Table 1 for demo-graphic data). Within the TLE sample, 129 individuals wereconfirmed to have MTLE (approximately 62%; the distinction be-tween TLE and MTLE was based on the presence of MRI findingsof hippocampal atrophy and T2 signal change suggestive of medialtemporal sclerosis in patients with MTLE). Seizure calendars wereused to calculate the average monthly seizure frequency. Mean sei-zure frequency (used to calculate lifetime seizure load) for TLE was22 per month (range: <1/month to 750/month); mean seizure fre-quency for PNES was 78/month (range: <1/month to 4875/month).It should be noted that there were five outliers between the twodiagnostic groups. Three individuals in the TLE group were havingan average of 25 simple partial seizures per day, 13 simple partialseizures per day, and 9 complex partial seizures or generalized to-nic–clonic seizures per day, respectively. Within the PNES group,two individuals reported having 162 nonepileptic seizures perday and 120 nonepileptic seizures per day, respectively. These fiveindividuals were included in the analyses because one of the pur-poses of the study was to understand the relationship between sei-zure frequency and cognitive performance. To remove these fiveindividuals from the analyses would reduce our ability to see theeffects of a large number of seizures on cognitive performance.
Data screening was conducted to assess data accuracy, potentialoutliers, and assumptions of normality for both predictor anddependent variables. Univariate normality was assessed withskewness and kurtosis coefficients, Q–Q-Plots, and histograms.Skewness and kurtosis values above +1.00 or below –1.00 wereused as an indication that the values were not normally distributed[35]. Three dependent variables were not normally distributed:TrailsA, TrailsB, and WCSTPer. Each of the three was transformedby taking the natural log. Two predictors, duration of epilepsy/PNES (Duration) and prospective lifetime seizure frequency (LifeF-
Table 1Demographic and seizure characteristics by diagnostic group.
Diagnostic group
LTLE RTLE BiTLE PNES
N 102 87 18 217Age (years) 37.07 37.07 40.89 36.67
(11.5) (10.63) (10.81) (10.79)Sex (% male) 51% 44% 33% 22%Education (years) 12.63 13.32 12.94 12.54
(2.52) (2.19) (2.75) (2.23)Full Scale IQ 91.76 92.74 88.61 91.56
(13.21) (12.34) (10.71) (11.82)AgeatOnset 20.12 18.38 19.69 28.99
(14.76) (13.58) (16.12) (12.81)Duration (years) 16.95 18.69 21.19 7.67
(13.34) (12.43) (15.77) (9.91)LifeFreq (No. of seizures) 3,238 3,953 3,368 5,594
(9685) (12,689) (4687) (33,972)
Note. Values are means (SD). LTLE, left temporal lobe epilepsy; RTLE, right temporallobe epilepsy; BiTLE, bilateral temporal lobe epilepsy; PNES, psychogenic nonepi-leptic seizures.
req) were not normally distributed. These positively skewed pre-dictors were transformed in the following manner: (1)Duration = ln(Duration + 1) and (2) LifeFreq = ln(LifeFreq1/4).
All correlations among the dependent variables were signifi-cantly different from zero (P < 0.01). Moderate correlations be-tween the dependent variables were expected as the tests are allmeasures of higher cognitive functioning abilities. Higher scoreson the WordFlu, StroopCW, WCSTCat, and deviation quotientswere associated with reduced time to complete TrailsA and TrailsBas well as fewer perseverative errors on the WCST (WCSTPer). Asexpected, those subtests from the same overall test (i.e., TrailsAand TrailsB, WMDQ and VCDQ, and PCDQ) were correlated thehighest. Correlations among the predictors Group, AgeatOnset,Education, Duration, and LifeFreq were all significantly differentfrom zero and ranged from –0.67 to 0.56 with the exception ofEducation and Duration, which were not correlated. As expected,there was a direct relationship between AgeatOnset, Duration,and LifeFreq. Duration decreased as AgeatOnset increased, andthe fewer years an individual had seizures, the lower the LifeFreq.Descriptive statistics for the dependent variables after transforma-tion (means and SD of the neuropsychological tests) are listed inTable 2. The cross-sectional design of the study resulted in onlyone neuropsychological testing time point per patient. Descriptivestatistics for the predictors were: AgeatOnset (M = 24.26,SD = 14.48), Duration in years before transformation (M = 12.82,SD = 12.80) and after (M = 2.11, SD = 1.10) transformation, andLifeFreq before (M = 4564.99, SD = 25249.50) and after (M = 4.82,SD = 2.06) transformation.
There were 86 missing values out of a total of 3870 values(approximately 2%). Fifty patients had one or more missing values.In many cases, seizures/events interrupted testing, thereby invali-dating the scores for that particular test. In other cases, some indi-viduals may have been unable to complete a given test andtherefore a valid score was not obtained. Missing data were im-puted using the EM maximum likelihood estimation procedure inthe EQS Structural Equations Program, which aims to impute miss-ing data while preserving the covariance matrix and sample means[36].
Multivariate multiple regression analyses were performed tomodel the relationship between the dependent measures (scoreson neuropsychological tests) and the following predictors: dura-tion of temporal lobe epilepsy/PNES (Duration), age at onset (Age-atOnset), education (Education), diagnostic group (Group), andlifetime seizure count (LifeFreq). Age-corrected raw scores of theexecutive functioning measures were used in the analyses,whereas scaled scores were used for the WAIS-III or WAIS-R devi-ation quotients.
In the initial multivariate multiple regression model, there weresignificant main effects for AgeatOnset, Education, and Duration.There was also a significant main effect for Group, suggesting arelationship between type of diagnosis (LTLE, RTLE, BiTLE, or PNES)
Table 2Descriptive statistics for transformed dependent variables.
Mean SD
WordFlua 34.23 11.09StroopCWa 37.74 10.80TrailsAa 3.42 0.40TrailsBa 4.28 0.42WCSTCata 4.71 1.80WCSTPera 2.58 0.74WMDQb 94.25 11.24VCDQ b 92.63 14.11PCDQ b 94.75 12.46
a Age-corrected raw score used.b Scaled score used.

L.C. Black et al. / Epilepsy & Behavior 17 (2010) 412–419 415
and performance. Education accounted for 33% of the variance inthe model. As education plays an integral part in performance onmany neuropsychological tests, especially IQ tests [37], it was ex-cluded from further analysis to allow focus on more clinically rel-evant predictors. The omnibus test of whether all of the R2 valueswere zero was significant, Wilk’s K = 0.53, F(45, 1837) = 6.14,P < 0.0001, indicating a significant relationship between the groupof dependent variables and the set of predictor variables. Theresulting model (summarized in Table 3), which excluded Educa-tion, showed a main effect of AgeatOnset, Group, and Duration.The omnibus test of whether all of the R2 values were zero withoutEducation in the model was significant: Wilk’s K = 0.76,F(36, 1542) = 3.18, P < 0.0001. As AgeatOnset and Duration in-creased, scores on many of the neuropsychological tests worsened.
Additional analyses, not reported here, showed no significantmultivariate differences among the three TLE groups. Therefore, toevaluate the effect of TLE versus PNES, further analyses were donecollapsing LTLE, RTLE, and BiTLE into one TLE group. Moderated uni-variate regression analyses were conducted in which three addi-tional predictors were added to each model shown in Table 3, thethree being centered interaction terms created by multiplying thedummy variable for Group (coded 0 for TLE and 1 for PNES) withthe deviation of each of the three continuous predictors from theirrespective means. If the incremental change in R2 that resulted fromthese three added predictors was significant, it was evidence that theregressive relationship varied as a function of group. Six of thenine univariate models showed significant evidence of moderation:WordFlu (R2 = 0.032), F(6, 417) = 2.27, P = 0.036; StroopCW (R2 =0.037), F(6, 417) = 2.64, P = 0.016; WCSTCat (R2 = 0.035),F(6, 417) = 2.53, P = 0.021; VCDQ (R2 = 0.082), F(6, 417) = 6.20,P < 0.001; TrailsA (R2 = 0.049), F(6, 417) = 3.55, P = 0.002; and TrailsB
Table 3Multivariate and univariate regression model results for dependent and predictor variable
Multivariate results
Total model Group AgeatO
Wilks’ K 0.76 0.90 0.89F 3.18 1.68 5.67df 36,1542 27,1195 9,409P <0.001a 0.02a 0.00a
Power 0.99 1.00
b Weight
Intercept Group (relative to PNES)
LTLE RTLE BiTLE
WordFlu 36.39 –3.31a –0.17 –0.74StroopCW 40.40 3.36a 4.92a –1.09WCSTCat 5.41 0.28 0.09 0.23WCSTPer 2.54 –0.06 –0.01 0.05WMDQ 92.15 1.62 2.77 –0.74VCDQ 83.14 –1.62 2.31 –1.48PCDQ 89.25 3.30a 2.33 –2.25TrailsA 3.11 –0.15 –0.07 0.19TrailsB 3.87 –0.01 –0.02 0.16
Univariate results
R2 F
WordFlu 0.03 1.93StroopCW 0.05 3.54WCSTCat 0.01 0.83WCSTPer 0.01 0.43WMDQ 0.02 1.72VCDQ 0.07 5.21PCDQ 0.02 1.71TrailsA 0.06 4.4TrailsB 0.06 4.74
a P < 0.05.
(R2 = 0.077), F(6, 417) = 5.78, P < 0.001. PCDQ (R2 = 0.029) withF(6, 417) = 2.09, P = 0.053, approached significance.
To understand the nature of the moderated models, we con-ducted separate regressions for the PNES and TLE groups. Tables4 and 5 summarize the models for the PNES and TLE groups,respectively. Within the PNES sample, the independent variablesof AgeatOnset, Duration, and LifeFreq accounted for significant var-iation in one or more of the following dependent variables: WCST-Cat, PCDQ, TrailsA, and TrailsB (see Table 4 for univariate values forthe PNES group). Within the TLE sample, the independent variablesof AgeatOnset and LifeFreq accounted for significant variation inone or more of the following dependent variables: StroopCW,VCDQ, TrailsA, and TrailsB (see Table 5 for univariate values forthe TLE group). On the StroopCW, increased number of lifetime sei-zures resulted in fewer word colors correctly identified in the TLEgroup (b = –2.98) than in the PNES group (b = –1.70). On the WCST-Cat, as age at disorder onset became earlier in the PNES group, thenumber of categories achieved improved (b = –0.04), whereas theopposite was true in the TLE group (b = 0.02). On the VCDQ, laterage at disorder onset resulted in better performance in the TLEgroup (b = 0.41) than in the PNES group (b = 0.15). On the PCDQ,the longer the individual had the disorder, the better his or her per-formance was in the PNES group (b = 0.96), but the worse his or herperformance was in the TLE group (b = –0.25). On TrailsA, in-creased number of lifetime seizures resulted in longer latenciesin both the PNES (b = 0.09) and TLE (b = 0.11) groups. On TrailsB,increased number of lifetime seizures resulted in longer latenciesin both the PNES (b = 0.13) and TLE (b = 0.10) groups. Also onTrailsB, the earlier the disorder onset, the longer the latency tocomplete the trail in the PNES group (b = 0.01) but to a lesser ex-tent in the TLE group (b = 0.003).
s.
nset (years) Duration LifeFreq (No. of seizures)
0.92 0.973.82 1.299,409 9,4090.00a 0.240.99 0.63
AgeatOnset (years) Duration LifeFreq (No. of seizures)
0.01 –0.64 –0.05–0.01 –2.09a 0.03–0.01 –0.21 –0.010.0001 0.06 –0.020.10 0.42 –0.440.30a 1.90 –0.380.11 –0.19 0.450.004a 0.10a 0.010.01a 0.12a 0.005
df P
6417 0.086417 0.0026417 0.556417 0.866417 0.126417 <0.0001a
6417 0.126417 <0.0001a
6417 <0.0001a

Table 4b weights and univariate regression model results for PNES dependent and predictorvariables.
b Weight
Intercept AgeatOnset(years)
Duration LifeFreq (No.of seizures)
WordFlu 38.24 –0.09 0.20 –0.68StroopCW 39.97 –0.02 0.04 –1.70WCSTCat 6.32 –0.04a –0.04 –0.23VCDQ 86.34 0.15 –0.15 2.07PCDQ 89.91 0.03 0.96a –0.61TrailsA 3.12 0.005 –0.002 0.09a
TrailsB 3.78 0.01a –0.01 0.13a
Univariate results
R2 F df P
WordFlu 0.10 0.67 3213 0.57StroopCW 0.03 1.97 3213 0.12WCSTCat 0.06 4.35 3213 0.01a
VCDQ 0.02 1.42 3213 0.24PCDQ 0.03 1.79 3213 0.15TrailsA 0.04 2.94 3213 0.03a
TrailsB 0.09 7.31 3213 <0.001a
a P < 0.05.
Table 5b weights and univariate regression model results for the dependent and predictorvariables.
b Weight
Intercept AgeatOnset(years)
Duration LifeFreq (No. ofseizures)
WordFlu 34.50 0.08 –0.29 –0.61StroopCW 47.10 –0.04 –0.01 –2.98a
WCSTCat 4.22 0.02 0.08 –0.11VCDQ 82.65 0.41a –0.51 1.55PCDQ 94.14 0.13 –0.25 0.11TrailsA 2.96 0.004 0.02 0.11a
TrailsB 3.89 0.003 0.02 0.10a
Univariate results
R2 F df P
WordFlu 0.03 1.94 3203 0.12StroopCW 0.04 2.84 3203 0.04a
WCSTCat 0.03 2.37 3203 0.07VCDQ 0.14 10.86 3203 <0.001a
PCDQ 0.03 1.81 3203 0.15TrailsA 0.06 3.94 3203 0.0a
TrailsB 0.05 3.37 3203 0.02a
a P < 0.05.
416 L.C. Black et al. / Epilepsy & Behavior 17 (2010) 412–419
A robust regression analysis was calculated to identify the mostinfluential data points and these points were weighted accordinglyto make all data points of equal importance. Comparing the resultsfrom the robust regression analysis with those from the univariateanalyses did not reveal significant changes in the unstandardized bweights.
Relative performance across the domains of working memoryand executive functions was analyzed by creating an impairmentindex to gauge the overall working memory and executive func-tioning level in each patient. The index was the proportion of testscores that fell outside normal limits (1.5 SD below the mean)[38,39] and represents the level of cognitive morbidity on an indi-vidual basis. The greater the impairment index, the more impairedthe individual was on neuropsychological testing as a whole. Uni-variate analyses were conducted with the impairment index as thedependent variable. The model was significant at the P < 0.001 le-vel in the overall sample. AgeatOnset was the only significant pre-dictor of impairment. When looked at individually, the model was
significant in the TLE group, but not in the PNES group. Again, Age-atOnset was the only significant predictor of impairment (b = –0.005, P < 0.001), with earlier AgeatOnset resulting in more neuro-psychological impairments. All analyses were a priori, plannedcomparisons and derived from the main hypotheses; therefore nocorrections were needed.
4. Discussion
The results of previous studies regarding the effects of seizureson higher cognitive functioning have been mixed [14–16]. The goalof the present study was to explore the impact of seizure durationand lifetime seizure load on working memory and executive func-tioning performance of individuals with TLE or PNES. Our findingsdisagree with the hypothesis that patients with longer duration ofepilepsy would experience decreases in working memory andexecutive functioning performance when compared with patientswith PNES. Instead, the closely related predictor of age at seizureonset emerged as the strongest predictor in both groups. The find-ings suggest that group (PNES vs TLE) has a moderating relation-ship on neuropsychological performance. Individuals diagnosedwith PNES were negatively affected by age at seizure onset andlifetime seizure load, but positively affected by duration of PNES.Age at seizure onset and lifetime seizure load were the significantpredictors of cognitive functioning in the TLE group regardless ofseizure lateralization. Furthermore, the results supported thehypothesis that lifetime seizure load is a significant predictor ofperformance on tests of higher cognition in both diagnostic groups.Although we found that lifetime seizure load was a significant pre-dictor, it should be noted that there were five outliers between thetwo diagnostic groups. These five individuals were not excludedfrom the study because the purpose of the study was to test thehypothesis that lifetime seizure load may be related to the degreeof cognitive dysfunction. To remove these patients from analysiswas to risk changing the accurate detection of that relationship.AgeatOnset was the strongest overall predictor of working memoryand executive function, accounting for 11% of the variance in theoverall model. In the PNES group, AgeatOnset remained a consis-tent predictor of neuropsychological performance, but the effectof prospective lifetime seizure frequency became significant aswell. This suggests that the earlier the onset of events and the morefrequently the events occur, the more influence PNES will have onhigher cognitive functioning.
The follow-up univariate analyses in the PNES group imply thatTrailsA and TrailsB were affected negatively by one or both of thepredictors. One relationship in the PNES group was difficult to ex-plain. As AgeatOnset increased, the number of categories achievedon the WCST decreased. It is possible that the planning abilities ofindividuals with PNES are affected by the disorder, even later inlife.
Data on neuropsychological functioning of patients with PNES issuggestive of significant underlying organic brain dysfunction,which is in agreement with our results. Although one of the earlieststudies comparing patients with PNES and epilepsy on neuropsy-chological measures found no differences between groups on mul-tiple measures after adjusting for the differences in educationalachievements [40], numerous subsequent studies identified signif-icant neurocognitive differences between the groups (for a detailedreview of the literature see [41]). Subsequent studies, for instanceby Kent et al. [7], showed that increased seizure duration nega-tively impacted memory in TLE and in PNES. Fargo et al. showedthat despite the lack of epileptic focus, verbal paraphasic errorson confrontation naming were as common in PNES as in nondom-inant TLE [42]. Recent research has also shown that patients withPNES perform as poorly as or worse than patients with epilepsy

L.C. Black et al. / Epilepsy & Behavior 17 (2010) 412–419 417
on most neuropsychological measures [26]. This suggests that psy-chological factors may contribute substantially to cognitive dys-function in PNES. Several other studies have found evidence thatindividuals with PNES show significant impairment on many neu-ropsychological measures, underscoring the importance of theinterplay between psychological health and cognitive performance[20,43,44]. Furthermore, there is evidence that high stress leads toelevated glucocorticoid levels in the brain, with the hippocampusbeing especially vulnerable. Studies have shown hippocampal atro-phy in high stress-related psychiatric disorders including posttrau-matic stress disorder, dissociative disorders, and severe depression[45]. Therefore, patients with PNES may be at risk for cognitiveimpairment as a result of exposure to prolonged periods of stressand, resultant from it, intermittent or prolonged glucocorticoidsurges with a long-term consequence of cognitive dysfunction;prolonged seizures may reflect prolonged stress-related experi-ences which have a cumulative effect over time. The results ofthe currently available studies raise a question regarding the etiol-ogy of PNES: Are the abnormal results of neuropsychological test-ing a mere consequence of the psychopathology and theexperienced events or is there an underlying brain pathology(functional and not necessarily anatomical) that precedes theemergence of PNES with its presence leading to abnormal responseto external events that eventually result in this condition?
The fact that age at event onset and prospective lifetime seizureload had a significant negative effect on neuropsychological perfor-mance in individuals in the PNES group may also be explained bypoor health perceptions. Research looking at health-related qualityof life (HRQOL) suggests that individuals with PNES have a poorerview of their own HRQOL than individuals with epilepsy and individ-uals with depression [46]. There is also a large discrepancy betweensubjective measures of cognitive functioning and objective neuro-psychological testing in individuals with PNES, with persons withPNES endorsing greater perceived memory disturbance comparedwith those with epilepsy, which has been related to negative moodstate [26]. These negative views of life and inaccurate views of func-tioning may be related to greater psychological stress, which, in turn,fosters poorer cognitive performance [7]. Other researchers suggestthat the unique patterns seen on neuropsychological tests are a re-sult of psychological factors rather than organic brain disorder [44].
Results of the current study underscore the importance of earlyaccurate diagnosis and treatment of individuals with PNES. Typi-cally, diagnosis of PNES is delayed on average by about 7 years[23], which leads to inappropriate and potentially dangerous useof antiepileptic drugs in a majority of the patients with PNES[47]. Research needs to be undertaken to verify the expectationthat early diagnosis and psychological treatment may reduce thedisease burden, including cognitive decline, in this population.
In the TLE group, AgeatOnset was the only significant predictorin the overall multivariate model. Contrary to our hypothesis, therewere no significant differences between the three groups of pa-tients with TLE (left, right, or bilateral). At the univariate level,the predictors AgeatOnset and LifeFreq affected different neuro-psychological tests than in the PNES group, with the exception ofTrailsA and TrailsB. Of note, the TLE group was affected more onthese neuropsychological variables by each predictor as more betaweights were much larger than those of the PNES group. Also ofinterest, only the TLE group showed significantly greater impair-ment indices explained by AgeatOnset. This finding reveals thatAgeatOnset has a greater impact on cognitive dysfunction in theTLE group than in the PNES group. It is also interesting to note thatalthough overall neuropsychological performance was impaired inthe PNES group, the TLE group had a greater proportion oftests P1.5 SD below the normative sample, suggestive of an over-all greater impact of epilepsy vis-à-vis PNES on cognitive function-ing. The results obtained in the TLE group underscore the roles that
age at seizure onset and lifetime seizure load have in the develop-ment of higher cognitive functioning abilities and are consistentwith work done by Hermann and colleagues [38,48]. Duration ofTLE was found to detrimentally impact speed of psychomotor pro-cessing, novel problem solving, working memory, and fluency [38].In some cases, the deficits seen in the aforementioned domainswere as large as the deficits in memory that have been reportedfor years. Additionally, similar deficits have been accompanied bybrain abnormalities evidenced by increased total cerebrospinalfluid and decreased total gray and white matter volumes as shownby MRI [48], suggestive of a modest effect of duration of epilepsyon higher cognitive functioning.
There is evidence that working memory tasks activate temporallobe structures in addition to frontal lobe structures. A magnetoen-cephalography (MEG) study by Campo et al. [49] found activationof medial temporal lobe structures during a spatial working mem-ory task, with the majority of the activation located in the righttemporal structures including the hippocampal gyrus, parahippo-campal gyrus, subiculum, and entorhinal cortex in healthy adults.A recent fMRI study using a verbal memory recognition task founddifferent activation patterns in patients with epilepsy vis-à-vishealthy controls, suggestive of compensatory (but possibly ineffec-tive) verbal memory mechanisms in patients with epilepsy [50].The current findings suggest that the longer and more often theseintegral structures are impacted by seizures, the more likely dam-age or disturbance is to occur.
4.1. Strengths and limitations
Strengths of the current study include the large number of sub-jects, allowing for the multivariable comparisons. In addition, theeffect of lifelong number of seizures on neuropsychological perfor-mance has not been previously investigated. The fact that the num-ber of lifelong seizures was found to be a significant predictor ofneuropsychological functioning in the PNES group highlights theimportance of considering seizure load in the evaluation of cogni-tive functioning. This is one predictor of neuropsychological per-formance in PNES that would appear amenable to interventionand change. As preliminary data suggest that level of psychologicalstress and number of seizures in PNES may be altered by psycho-logical intervention [51], not only seizure freedom but also de-crease in seizure frequency should be considered potentialtherapeutic targets in these patients.
A potential limitation of this study is that, of the patients withconfirmed TLE enrolled, only 62% of the group were diagnosed withdefinitive MTLE through MRI confirmation of medial temporal scle-rosis. This may have reduced the likelihood of finding significantdeficits in the cognitive domains included. Many past studies usinga pure sample of MTLE have found significant executive functiondeficits [14,16,52]. Follow-up research could focus on MTLE specif-ically and look at the impact of lifetime seizure load and seizureduration on executive function performance, with the expectationthat there would be relatively robust effects of these variables.
Another limitation of the present study was that other aspectsof the TLE and PNES populations were not controlled for, such aslevel of depression, past history of mild to moderate head injury,and substance abuse. Although major depression can affect cogni-tive performance, controlling for this factor in a population thattends to have an increased incidence of depression [53] would re-duce the generalizability of these findings. Similarly, excludingindividuals who had experienced a mild to moderate head injuryat any point in their lives would also reduce generalizability. Eachindividual was asked about previous head injuries and those withserious injuries as defined by prior brain surgery, abnormal imag-ing due to a head injury, loss of consciousness, or depressed skullfracture were excluded from the study, but those who had a con-

418 L.C. Black et al. / Epilepsy & Behavior 17 (2010) 412–419
cussion without loss of consciousness remained in the sample.Substance abuse information was gathered on all individuals viaself-report, but was outside of the scope of the present study.Although the importance of taking depression, past head injury,and substance abuse into account in this population was recog-nized, the purpose of this study was to sample both patient popu-lations as they typically present to epilepsy centers.
A third limitation of the present study was the calculation oflifetime seizure load. Even though the calculations incorporatedall of the available information from patient reports and previousmedical records, the resulting numbers were only estimates. Giventhe reliance on patient report to calculate this number, the result-ing values may not be as accurate as some individuals over- orunderestimate their seizure frequency, as evidenced by the fiveoutliers within the diagnostic groups. On the other hand, the onlymethod for gaining this information is through patient report, andpatient report is the method used in the great majority of random-ized controlled trials of epilepsy treatments. Until a more accurateway of calculating seizure frequency is identified, future studiescould use more accurate variables such as number of failed medi-cations, duration, and age at first seizure.
A final limitation of this study concerns the design. While thecross-sectional design allows for a large sampling of individuals,it limits our ability to fully understand the changes in neuropsy-chological test performance over time. Future research involvinglongitudinal designs may provide a more complete understandingof the effects of TLE and PNES on cognition. Results of the currentstudy underscore the importance of early accurate diagnosis andtreatment of individuals with PNES. Given that some aspects ofhigher cognitive functioning performance were negatively affectedby higher lifetime seizure counts, it would appear important tofind a treatment (either psychological or pharmacological) thatcan minimize the number of seizures experienced overall. Withinthe TLE group, age at onset is uncontrollable, but providing individ-uals with strategies to help overcome their weaknesses in highercognitive functioning may be beneficial for the future. Additionally,minimizing the number of seizures experienced by individualswith TLE would also be important in reducing the chance of furthercognitive decreases. Overall, the results of the study broadenknowledge of factors that affect higher cognitive functions in TLEand PNES, but they also highlight the importance of not assumingall cognitive functions are impaired. It is important for clinicians torecognize that certain variables such as age at onset and seizureload operate differently on different aspects of cognitive function-ing within different diagnostic groups.
Acknowledgments
This study was supported in part by funds from the Pamela andCharles L. Shor Foundation for Epilepsy Research awarded to thesecond author. Dr. Szaflarski is currently supported by NIH K23NS052468.
References
[1] Baddeley A. The fractionation of working memory. Proc Natl Acad Sci USA1996;93:13468–72.
[2] Stuss DT, Levine B. Adult clinical neuropsychology: lessons from studies of thefrontal lobes. Annu Rev Psychol 2002;53:401–33.
[3] Salthouse TA. Relations between cognitive abilities and measures of executivefunctioning. Neuropsychology 2005;19:532–45.
[4] Fisher RS, van Emde Boas W, Blume W, et al. Epileptic seizures and epilepsy:definitions proposed by the International League Against Epilepsy (ILAE) andthe International Bureau for Epilepsy (IBE). Epilepsia 2005;46:470–2.
[5] Epilepsy Foundation. Treatment effectiveness. 2005. Retrieved on: January 15,2007 from http://www.epilepsyfoundation.org/answerplace/Medical/treatment/medications/effectiveness.cfm.
[6] Hermann B, Seidenberg M. Neuropsychology and temporal lobe epilepsy. CNSSpectr 2002;7:343–8.
[7] Kent GP, Schefft BK, Szaflarski JP, Howe SR, Yeh HS, Privitera MD. The effects ofduration of intractable epilepsy on memory function. Epilepsy Behav2006;9:469–77.
[8] Hermann BP, Wyler AR, Richey ET, Rea JM. Memory function and verballearning ability in patients with complex partial seizures of temporal lobeorigin. Epilepsia 1987;28:547–54.
[9] Testa SM, Schefft BK, Privatera MD, Yeh HS. Warrington’s recognition memoryfor faces: interpretive strategy and diagnostic utility in temporal lobe epilepsy.Epilepsy Behav 2004;5:236–43.
[10] Kløve H, Matthews CG. Psychometric and adaptive abilities in epilepsy anddifferential etiology. Epilepsy Behav 2003;4:366–70.
[11] Dodrill CB. Neuropsychological effects of seizures. Epilepsy Behav2004;5:S21–4.
[12] Hermann BP, Seidenberg M, Schoenfeld J, Davies K. Neuropsychologicalcharacteristics of the syndrome of mesial temporal lobe epilepsy. ArchNeurol 1997;54:369–75.
[13] Schefft BK, Testa SM, Dulay MF, Privitera MD, Yeh HS. Preoperative assessmentof confrontation naming ability and interictal paraphasia production inunilateral temporal lobe epilepsy. Epilepsy Behav 2003;4:161–8.
[14] Thompson PJ, Duncan JS. Cognitive decline in severe intractable epilepsy.Epilepsia 2005;46:1780–7.
[15] Cowey CM, Green S. The hippocampus: a ‘‘working memory” structure? Theeffect of hippocampal sclerosis on working memory. Memory 1996;4:19–30.
[16] Abrahams S, Morris RG, Polkey CE, et al. Hippocampal involvement in spatialand working memory: a structural MRI analysis of patients with unilateralmesial temporal lobe sclerosis. Brain Cogn 1999;41:39–65.
[17] Benbadis SR. The problem of psychogenic symptoms: is the psychiatriccommunity in denial? Epilepsy Behav 2005;6:9–14.
[18] Alper K, Devinsky O, Perrine K, et al. Dissociation in epilepsy and conversionnonepileptic seizures. Epilepsia 1997;38:991–7.
[19] Roy A, Barris M. Psychiatric concepts in psychogenic nonepileptic seizures. In:Rowan AJ, Gates JR, editors. Non-epileptic seizures. Boston: Butterworth–Heinemann; 1993. p. 143–51.
[20] Kalogjera-Sackellares D, Sackellares JC. Intellectual and neuropsychologicalfeatures of patients with psychogenic pseudoseizures. Psychiatry Res1999;86:73–84.
[21] Lelliott PT, Fenwick P. Cerebral pathology in pseudoseizures. Acta NeurolScand 1991;83:129–32.
[22] Wilkus RJ, Dodrill CB, Thompson PM. Intensive EEG monitoring andpsychological studies of patients with pseudoepileptic seizures. Epilepsia1984;25:100–7.
[23] Szaflarski JP, Hughes C, Szaflarski M, et al. Quality of life in psychogenicnonepileptic seizures. Epilepsia 2003;44:236–42.
[24] Jacoby A, Gamble C, Doughty J, Marson A, Chadwick D. Quality of life outcomesof immediate or delayed treatment of early epilepsy or single seizures.Neurology 2007;68:1188–96.
[25] Bautista RED, Glen ET. Seizure severity is associated with quality of lifeindependent of seizure frequency. Epilepsy Behav 2009;16:325–9.
[26] Fargo JD, Schefft BK, Szaflarski JP, et al. Accuracy of self-reportedneuropsychological functioning in individuals with epileptic or psychogenicnonepileptic seizures. Epilepsy Behav 2004;5:143–50.
[27] Szaflarski JP, Ficker DM, Cahill WT, Privitera MD. Four-year incidence ofpsychogenic nonepileptic seizures in adults in Hamilton County. Neurology2000;55:1561–3.
[28] Wechsler D. Wechsler adult intelligence scale. 3rd. San Antonio: PsychologicalCorp.; 1997.
[29] Wechsler D. Wechsler adult intelligence scale—revised. San Antonio:Psychological Corp.; 1981.
[30] Reitan R, Wolfson D. The Halstead–Reitan neuropsychological test battery:theory and clinical interpretation. Tucson, AZ: Neuropsychology Press; 1993.
[31] Golden CJ. Stroop color and word test. Chicago: Stoeling Co.; 1978.[32] Heaton RK, Chelune GJ, Talley JL, Kay GG, Curtis G. Wisconsin card sorting test
(WCST) manual revised and expanded. Odessa, FL: Psychological AssessmentResources; 1993.
[33] Benton AL, Hamsher K, Rey GJ, Sivan AB. Multilingual aphasia examination. 3rded. Iowa City, IA: AJA Associates; 1994.
[34] Lezak MD, Howieson DB, Loring DW, Hannay HJ, Fischer JS.Neuropsychological assessment. 4th ed. New York: Oxford Univ. Press; 2004.
[35] Mertler CA, Vennatta R. Advanced and multivariate statistical methods:practical application and interpretation. 2nd ed. Los Angeles: Pyrczak; 2002.
[36] Multivariate Software Inc. EQS structural equations program manual. Encino,CA: Multivariate Software; 1995.
[37] Heaton RK, Ryan L, Grant I. Demographic influences and use ofdemographically corrected norms in neuropsychological assessment. In:Grant I, Adams KM, editors. Neuropsychological assessment ofneuropsychiatric and neuromedical disorders. New York: Oxford Univ. Press;2009. p. 127–55.
[38] Oyegbile TO, Dow C, Jones J, et al. The nature and course of neuropsychologicalmorbidity in chronic temporal lobe epilepsy. Neurology 2004;62:1736–42.
[39] Marques CM, Caboclo LO, da Silva TI, et al. Cognitive decline in temporal lobeepilepsy due to unilateral hippocampal sclerosis. Epilepsy Behav 2007;10:477–85.
[40] Wilkus RJ, Dodrill CB. Factors affecting the outcome of MMPI andneuropsychological assessments of psychogenic and epileptic seizurepatients. Epilepsia 1989;30:339–47.
[41] Swanson SJ, Springer JA, Benbadis SR, Morris, GL. Cognitive and psychologicalfunctioning in patients with non-epileptic seizures. In: Rowan AJ, Gates JR,

L.C. Black et al. / Epilepsy & Behavior 17 (2010) 412–419 419
editors. Non-epileptic seizures. 2nd ed. Boston: Butterworth–Heinemann;2000. p. 123–37.
[42] Fargo JD, Dulay MF, Schefft BK, Privitera MD, Yeh HS. Confrontation naming inindividuals with temporal lobe epilepsy: a quantitative analysis of paraphasicerror subtypes. Neuropsychology 2005;19:603–11.
[43] Binder LM, Kindermann SS, Heaton RK, Salinsky MC. Neuropsychologicimpairment in patients with nonepileptic seizures. Arch Clin Neuropsychol1998;13:513–22.
[44] Brown MC, Levin BE, Ramsay RE, Katz DA, Duchowny MS. Characteristics ofpatients with nonepileptic seizures. J Epilepsy 1991;4:225–9.
[45] Vermetten E, Schmahl C, Lindner S, Loewenstein RJ, Bremner JD. Hippocampaland amygdalar volumes in dissociative identity disorder. Am J Psychiatry2006;163:630–6.
[46] Szaflarski JP, Szaflarski M. Seizure disorders, depression, and health-relatedquality of life. Epilepsy Behav 2004;5:50–7.
[47] Reuber M, Elger CE. Psychogenic nonepileptic seizures: review and update.Epilepsy Behav 2003;4:205–16.
[48] Oyegbile TO, Bhattacharya A, Seidenberg M, Hermann BP. Quantitative MRIbiomarkers of cognitive morbidity in temporal lobe epilepsy. Epilepsia2006;47:143–52.
[49] Campo P, Maestu F, Capilla A, Fernandez S, Fernandez A, Ortiz T. Activity inhuman medial temporal lobe associated with encoding process in spatialworking memory revealed by magnetoencephalography. Eur J Neurosci2005;21:1741–8.
[50] Eliassen JC, Holland SK, Szaflarski JP. Compensatory brain activation forrecognition memory in patients with medication-resistant epilepsy. EpilepsyBehav 2008;13:463–9.
[51] Kalogjera-Sackellares D. Psychodynamics and psychotherapy ofpseudoseizures. New York: Crown House; 2004.
[52] Giovagnoli AR. Relation of sorting impairment to hippocampal damage intemporal lobe epilepsy. Neuropsychologia 2001;39:140–50.
[53] Hermann BP, Seidenberg M, Bell B. Psychiatric comorbidity in chronicepilepsy: identification, consequences, and treatment of major depression.Epilepsia 2000;41(Suppl. 2):S31–41.