the coalition chronicle - cobgrte.org
TRANSCRIPT

1
The Coalition Chronicle
Coalition for Baccalaureate and Graduate Respiratory Therapy Education July 31, 2015 Volume 4 (7)
Spotlight Article
DEPARTMENT OF CARDIORESPIRATORY CARE UNIVERSITY OF SOUTH ALABAMA
MOBILE, ALABAMA
Introduction
The Department of Cardiorespiratory Care (CRC) at the University of South Alabama is located
in Mobile, Alabama with clinical sites reaching into Florida and Mississippi. USA is a state
supported comprehensive university that offers a wide range of health professional degrees
including medicine, allied health, and nursing. The CRC program offers a 5-semester
undergraduate curriculum leading to a Bachelor of Science degree. In conjunction with the
College of Education, CRC also offers a Master of Science degree in Instructional Design and
Development for BS/RRTs interested in a career option in education. The undergraduate
curriculum uses a combination of different teaching and learning strategies: problem-based
learning, team-based learning, human simulation lab, and online testing. During the senior year,
a 3-semester research sequence provides students an opportunity to conduct scientific inquires.
In 2015, nine research abstracts were accepted for poster discussion or presentation at the AARC
International Congress.
Curriculum
The Cardiorespiratory Care (CRC) curriculum at the University of South Alabama provides the didactic,
laboratory, and clinical education needed to graduate with a Bachelor of Science degree in
Cardiorespiratory Sciences. The pre-professional component consists of 59 semester hours in the
freshman and sophomore years of college; the professional component calls for 62 semester hours which
are taken over the course of 5 consecutive semesters beginning in the junior year.

2
CRC Professional component:
Semester 1 (fall)
CRC 330 Assessment skills
CRC 331 Respiratory Anatomy and Physiology
CRC 334 Pharmacology
CRC 342 Intermittent Cardiorespiratory Care Practicum
Total semester hours: 14
Semester 2 (spring)
CRC 332 Intermittent and Diagnostic Cardiorespiratory Care
CRC 335 Intensive Cardiorespiratory Care
CRC 345 Intensive Cardiorespiratory Care Practicum
Total semester hours: 14
Semester 3 (summer)
CRC 415 Research Methodology
CRC 430 Neonatal/Pediatric Cardiorespiratory Care
CRC 431 Special Procedures
Total semester hours: 8
Semester 4 (fall)
CRC 435 Critical Care Concepts
CRC 440 Advanced Clinical I
CRC 447 Cardiorespiratory Care Management
CRC 450 Clinical Research I
Total semester hours: 13
Semester 5 (spring)
CRC 441 Advanced Clinical II
CRC 446 Cardiorespiratory Care Education
CRC 451 Clinical Research II
CRC 460 Advanced-Level Exam Review
Total semester hours: 13
3
Problem-based learning (PBL) is included in several courses of the CRC curriculum, and encourages
development of student knowledge and skills by working for an extended time to investigate and respond
to patient cases. The progressive disclosure of the case in a small-group setting is facilitated by the faculty
and the process engages students in critical thinking, while fostering patient assessment and decision-
making skills. The PBL courses incorporate small group discussions, enrichment lectures, and
laboratories.
Senior students in the CRC program complete research projects to gain insight and understanding of the
basics of the research process. A course in education provides learning in the foundational principles of
education, as well as practical application of teaching as students present lectures and workshops. The
course in critical care concepts is
designed to prepare the student to
work in the intensive care arena and
to succeed in obtaining the Adult
Critical Care Specialty Credential.
The management course provides a
broad view of the healthcare
environment while also drilling
down into challenges that the
respiratory care department
leadership face day-by-day. The
special procedures course provides
a close-up look at sub-acute care,
hyperbaric oxygen therapy, sleep,
open-heart surgery, and cardiac bypass with the perfusionist, bronchoscopy, non-invasive and invasive
cardiac diagnostic and therapeutic procedures (such as cardiac catheterization, echocardiography, nuclear
cardiology, and ambulatory monitoring), and hemodynamic monitoring.
Every semester in the CRC program includes a clinical component. Students obtain clinical experience in,
at least, four or five hospitals during their junior and senior years. The program has clinical affiliation
with 13 hospitals across the Gulf coast region in Alabama, the Florida panhandle, and Mississippi.
Students gain valuable clinical experience in neonatal and pediatric care during rotations in two children’s
hospitals in the area that house level III NICUs. In addition, working with the faculty in the outpatient
environment at a local pulmonary clinic for uninsured adults has enhanced student skill and experience in
performing patient assessment, gathering diagnostic evidence, and case management while giving back to
the community in a service-learning environment.
Use of simulations has become an excellent learning environment. The CRC program regularly works
with the state-of-the-art simulation lab that is shared with various health professions in the Patsy Capps
Covey College of Allied Health Professions and the College of Nursing. Along with simulations that are
designed for the CRC students, the department participates in several inter-professional education events
and simulations to increase the student exposure and experience working with a team of professionals.
Health Sciences building, housing the Pat Capps Covey College
of Allied Health and the College of Nursing

4
Registered respiratory therapists with baccalaureate degrees in respiratory care or other disciplines who
have completed specific prerequisite courses can enroll in graduate school through the College of
Education and earn the Master of Science degree in Instructional Design & Development.
Faculty
William V. Wojciechowski MS, RRT, Associate Professor and program
Chair received his BS from the University of Dayton and his Master’s in
Education from the University of Illinois. Bill teaches our pulmonary
physiology and special procedures. He has been the program Chair since its
founding in 1979.
William Pruitt MBA, RRT, CPFT, AE-C, FAARC received his BA from
Georgia College, and his MBA from Brenau College. Bill serves as the
director of clinical education. He is responsible for our pulmonary function
preparation and his management background prepared him for his course in
management. He has been with the program since 1999.
Timothy Op’t Holt, EdD, RRT, AE-C, FAARC received his BS from
Michigan State University, a Master’s in Health Professions Education from
University of Illinois, and an EdD from Auburn University. Tim introduced
and integrated problem-based learning in the curriculum in 1999. He has been
with the program for 31 years.
David Chang, EdD, RRT received his BS from the University of Northern
Iowa, MEd. from Columbus State University Columbus Ga, and an EdD, from
Nova Southeastern University. David came to the program from Athens
Technical College in Athens, Ga, where he was the director of clinical
education. He has been instrumental in introducing team-based learning in our
curriculum, and helps prepare our students for the registry examinations. He has
been with the program since 2007.
5
Coincidentally, these four faculty members are graduates of the respiratory therapy program at
the University of Chicago. In 2014, the faculty worked in Dammam, Saudi Arabia to assist the
University of Dammam with teaching duties and in faculty preparation for problem-based
learning. The program director at the University of Dammam is an alumnus of the
Cardiorespiratory Care (CRC) program. He recognized the utility of PBL and wanted to
incorporate the technique in his program. Also, a program in Riyadh uses the CRC curriculum.
Jennifer McDaniel, BSRT, is an alumnus of our program and is our neonatal/pediatric
instructor, Jennifer serves as a full-time therapist in the neonatal intensive care at USA
Children’s and Women’s Hospital in Mobile, AL.
Our Students
Most of our students are from the southeast region of the United States, but we have hosted
students from Saudi Arabia, Hong Kong, India, Iran, Somalia, South Korea, Russia, and Kenya.
Summary
The Cardiorespiratory Care Program at the University of South Alabama was established in 1979
and has had over 300 graduates who are practicing all over the U.S. and world-wide. Our
baccalaureate curriculum incorporates traditional teaching as well as team-based and problem-
based learning, simulation, and hospital and clinic-based clinical experiences. All students
complete a research project and courses in education and management. Presently, the University
of South Alabama is the only baccalaureate respiratory therapy program in Alabama.
Action Required
As an AARC member you recently received an important message from AARC President, Frank
R. Salvatore, RRT, MBA, FAARC, urging you to send a message to your members of Congress
asking for their support for HR 2948 the Medicare Telehealth Parity Act. CoBGRTE
leadership encourages all respiratory therapy educators and students to respond to the AARC call
for action. AARC has made it easy by use of their Capitol Connection
http://capwiz.com/aarc/issues/?style=d. Read the bill using the AARC provided link:
https://www.govtrack.us/congress/bills/114/hr2948. Take action today – it is important!

6
Transfer Credits – A Holistic View
Robert Joyner, PhD, RRT, RRT-ACCS, FAARC
Associate Dean, Henson School of Science and Technology
Director, Respiratory Therapy Program
Salisbury University Salisbury, MD
Recently Dr. Ellen Becker (Rush University – Respiratory Care),
solicited opinions in the AARC Education Section listserv regarding
an article published in Inside Higher Ed discussing the challenges for
students transferring from a two-year community college to a four
year university.1 Essentially the article Dr. Becker referenced
summarizes the opinion of a Connecticut based Legislative Program
Review and Investigations Committee (PRI) who analyzed data
originating from the University of Connecticut on credit/course
transfers from a two-year community college to a four-year
university. The original analysis can be found here:
http://gatewayct.edu/Offices-Departments/Public-Affairs/Faculty-Staff-News/faculty-staff-
news/ost-transfer-credits-at-UConn-costs-Community-Coll. The Inside Higher Ed article was not
specifically written with Respiratory Care education in mind, but it certainly resonates with the
current initiative of the profession of Respiratory Care to move toward more baccalaureate
degree prepared respiratory care providers.
I applaud Dr. Becker for bringing transfer status as an issue to the educators of our profession.
The data analysis presented in the article only presents a limited understanding for those who
read it, and could be misleading to students who are looking to fast-track their degree
completion. I propose that the issue of transfer credits has at least two perspectives. The article
alludes to the idea that there should be a direct relationship between the two years spent in an
associate degree designed program and a four year baccalaureate program (I say this generically,
not Respiratory Care specifically). This idea can be very attractive to students, community
colleges and legislators who are looking for the fastest way to degree completion (i.e., think
reduction in costs) possible.
Another perspective would be that the institution being transferred into has autonomy over the
general education and program pre-requisites required to complete a degree from said institution.
In defense of this issue, university general education and major curricula are designed by the
faculty to provide a student with what they believe is the best education that their institution can
offer.
7
It is an unrealistic expectation of a student to move directly from one institution to the other
without the need for additional course work. Institutions have different ideologies regarding what
they believe is best for their students/graduates.
In regard to credit being transferred in to a four year institution, there are usually limits (in the
University System of Maryland that limit is approximately 74 credits), but as long as the number
of credits don't exceed those limits then the credits usually transfer (assuming a passing grade
from the transferring course). Students in Maryland community colleges have access to the
systems online articulation system: http://artsys.usmd.edu/ (All states should have something
similar, but likely do not.)
What can happen is that some of those credits don't have a direct course equivalence in the
institution accepting transfer credit. As a silly example -- If a student takes a 3 credit "Basic
Klingon" at a two year institution and the four year institution does not have an equivalent
course, the credits may transfer, but the course itself does not fulfill a required course at the four
year institution. The credit count would go toward the number of credits needed to graduate from
the four year institution, but would not fulfill a specific course requirement.
When potential transfer students ask questions about our program they generally have a desire to
graduate with a baccalaureate degree in Respiratory Care in the shortest time possible. We can
help with that, but they also need to buy into the idea that they are graduating with a degree from
Salisbury University (SU). SU is not unique from other educational institutions in that it has
certain expectations of all of their graduates (i.e., general education and degree requirements).
For our program curriculum issues for potential transfer/post-associate degree students arise
almost every time we discuss needs. Very commonly and because of SU's general education
requirements incoming students need an additional English, History, and Physical Education, but
more importantly they usually need a General Chemistry course or two, and a statistics course.
They complain and ask "what does that have to do with Respiratory Care" and I explain not only
are you seeking a degree in Respiratory Care, but you are seeking a degree from Salisbury
University and these are the general education and basic science courses every graduate from the
University and our program are required to take. It is at that point that they either embrace the
idea of getting a baccalaureate degree from SU or lose interest. What is usually not understood is
that it is these general education and basic sciences courses that are an important part of what
makes a SU grad desirable to employers. In no way am I saying that we have a perfect system,
we don’t; we just have our system.
I don't think we should move into the direction of creating two plus two programs unless they are
specifically designed and advertised that way. While I may be a relic among new growth, I
believe there is a “Je ne sais quoi” in seeking out the knowledge that can be provided by a
university education for its knowledge sake, and for continuing that quest for knowledge for a
life time.

8
While I am in no way disrespectful of the degree seeking student that is out for the degree solely
for the opportunities it may bring, I am in awe of the student whose desire is to advance their
knowledge because they believe it will result in improved care for their patients.
We should teach students to understand the difference in these two strategies and find resources
to support both.
Another Perspective on Transfer Credit
Ellen Becker, PhD, RRT-NPS, RPFT, AE-C, FAARC
Professor, Respiratory Care
Rush University, Chicago, IL
Here is another perspective on the article1 and a challenge for advocacy
in our educational leadership roles. Dr. Joyner accurately described how
transfer credits work in our current educational system and why the
number of credits that transfer into various baccalaureate degree bridge
programs may differ. Within the current structure, it is important for
prospective respiratory care students to have realistic expectations when
transferring with an associate degree into a baccalaureate degree
program.
I would like to see a more effective process for transferring credits
within systems acknowledging the path will not be easy, nor quick. As
respiratory care leaders, we are positioned to advocate for change. First the landscape, federal
and state governments are putting less money into education systems and more costs are being
shifted to students. Today’s student graduates with more college debt than in the past. High debt
loads may deter individuals who would normally be willing to pursue advanced degrees, but who
simply cannot take on more debt. I am especially concerned about bright, driven individuals
from underprivileged backgrounds. They have to be concerned not only about debt, but also with
the amount of time they spend in school and away from wage-earning and caregiving
responsibilities. In order to have a diverse respiratory therapist workforce at all levels, education
needs to be accessible to all – or at least have unnecessary roadblocks removed.
Is it possible for systems to streamline the transfer process while maintaining their individual
missions? Partly yes, however this process will take effort from both the associate degree and
baccalaureate degree programs. For example, almost a decade ago the Wisconsin Technical
College System forced all of its associate degree respiratory care programs to have the same
curriculum to facilitate transfer credit if a resident needed to relocate within the state. As Dr.
Joyner noted above for the Maryland system, students can access an online resource to evaluate
in advance the credits that will transfer. If a student is aware that statistics and chemistry are
9
required for an advanced degree, the student may choose some of these courses as electives or
consider substituting higher-level courses in the present curriculum that will have a greater
likelihood of transferring toward an upper level degree. Thus, assuring that students who are
entering the profession are informed about their current entry-level program requirements and
the implications for transfer to advanced degree programs is essential.
To facilitate the AARC’s goal of having 80% of respiratory therapists holding or in the process
of earning a baccalaureate degree by 2020, faculty from associate, baccalaureate, and graduate
degree programs have to work together to help students maximize opportunities for credit
transfer. This responsibility will take a partnership across all levels of respiratory care.
REFERENCE
1. Smith AA. Two-year transfers are finding not all of their credits go with them. Inside Higher Ed.
2015, June 8 https://www.insidehighered.com/news/2015/06/08/two-year-transfers-are-finding-not-
all-their-credits-go-them Accessed 07/23/2015.
Role Model for Professionalism
Tom Barnes, EdD, RRT, FAARC
Professor Emeritus of Cardiopulmonary Sciences
Northeastern University, Boston
Respiratory therapy faculty members have a responsibility to serve as a
role model for professionalism. It starts by assuring that all faculty
members, full-time, part-time, adjuncts, clinical instructors and clinical
preceptors are active members of their professional associations: AARC,
CoBGRTE and NBRC. It was recently reported in the 2014 AARC
Human Resources Study that 172,921 RTs have been given a license by
state agencies to deliver respiratory care (150 were estimated by a
representative of the Alaska Society for Respiratory), and the NBRC
reported that they had in July of 2014, 136,807 credentialed therapists in their database.1 Given
the large workforce there should be over 100,000 respiratory therapists that are active members
of their professional associations. Member support is needed to support the AARC’s legislative
effort to include RTs in the Medicare Telehealth Parity Act under consideration in Congress, and
to support important educational activities and programs. The NBRC needs more active
members to support their continuing competency program. CoBGRTE needs membership
support to help establish baccalaureate and graduate RT education as a standard for entry into the
profession. Faculty members can educate their students and colleagues on the importance of
becoming a member of their professional associations by example and by taking the time to
explain why it is important to the profession and to the individual’s career. When faculty

10
members are active regionally and nationally in professional associations it sends a clear
message to their students and colleagues on the importance of leadership and support to help
respiratory therapists assume a wider scope of practice, more recognition and higher wages.
Respiratory department managers/directors have a responsibility to only hire applicants that are
AARC and NBRC active members since this is a fundamental sign of professionalism. If
applicants support baccalaureate and graduate respiratory therapy education during employment
interviews they should be asked about their active CoBGRTE membership. I challenge you to
aim for 100% AARC, 100% NBRC and 100% CoBGRTE active or student membership among
your colleagues, new hires and students in your BSRT or graduate RT program. Settle for
nothing less than 100% and insist that everyone is on board with their professional association
memberships. No one should be allowed to instruct your students or work in your respiratory
department unless they serve as a model for professionalism by being a member and active with
three key professional associations: AARC, NBRC and CoBGRTE. Ask your students, new hires
and colleagues to prepare three, five and 10 year goals for professional service and help them to
understand where they can help advance respiratory care. The bottom line are the patients that
will benefit from a more professional and educated workforce.
REFERENCE
1. Shaw R, Benavente J. 2014 AARC Human Resource Survey of Respiratory Therapists.
AARC, 2014, Irving, Texas.
Report on Round Table Discussion Dinner in Phoenix
The following discussion leaders have provided a summary of the discussion at their tables at the Yard
House Restaurant in Phoenix on July 14. Save the date for the next round table discussion dinner that will
be held in Tampa at the historic Columbia Restaurant on Monday November 9, 7:00 to 9:30 PM.
Advanced Practice Respiratory Therapists – José D Rojas, PhD, RRT
This discussion group included individuals from education and clinical practice. We had lively
discussions about the role of respiratory therapists in the ever-evolving health care system. Given
the Association of American Medical Colleges' predicted shortage of primary and specialty care
physicians in the United States by 2025, and the void for access to health care for patients with
chronic respiratory conditions that this will create, the group agreed that this projected void
could be filled by respiratory therapists trained in advanced practice. Several in the group knew
of respiratory therapists serving in advanced practice roles in physician's practices. We
acknowledged that the use of physician extenders to provide better access to health care is not a
new concept. Nurse practitioners and physician assistants scope of practice has been in primary
care and specialty care areas and these clinicians provide services in multiple settings including
physician practices and hospitals. The educational programs for both of these physician extender

11
roles are two-year master’s degree programs that include didactic and clinical training. The
group agreed that one limitation to respiratory therapists providing advanced practice was that of
reimbursement; however, we are optimistic for the future of our profession and the possibility of
advanced practice with
reintroduction of H.R.
2948-The Medicare
Health Parity Act. The
group would encourage
our profession to
advocate for this
legislation as a crucial
step in providing for
the reimbursement of
chronic care
management services.
As we continued in our
discussion, the group
was asked for
suggestions on how to identify both the number and scope of practice of therapists currently
providing advanced practice in either physician's offices or hospital settings. The rationale being
that this data is essential for guiding the development of specific areas of advanced practice. This
information will be essential in preparing a specimen curriculum for advanced practice graduate
programs in respiratory therapy. Several at the table commented that the AARC's advancement
of the Pulmonary Disease Educator Course was also useful in defining roles in advanced
practice. As we closed the evening, the group was reminded of the CoBGRTE APRT committee
and its goal to prepare a specimen curriculum for advanced practice graduate programs in
respiratory therapy. They were encouraged to contact committee chair José Rojas, PhD, RRT
<[email protected]> if they were interested in participating or if they could provide contact
information for therapists currently providing advanced practice.
New BSRT Programs – Gregg Marshall, PhD, RRT, RPSGT
Our table was filled with lively discussion as we enjoyed meeting each other from all across the US and
learning our commonalities and connections from the various universities and institutions.
The question posed to the group was this: “What are the barriers to beginning new BSRT Programs
throughout the country in order to raise the number of BSRT graduates each year?” A summary of the
comments follows:
1) Lack of university funding: everyone agreed that higher education is being stretched financially and
university administrators are seeking those degree opportunities that will yield a large, successful
graduating cohort.

12
2) Lack of recognition of the value of the BS degree by industry: the group felt that industry must lead
the way in valuing the BS degree by offering either pay differences for terminal degrees or providing
career ladders to provide incentive for continued education. Also, the group felt that industry must
“make a place for the BSRT” in the function of the department through clear job description/degree-
related positions.
3) Lack of
recognition of
BS for
insurance
reimbursement:
there was lively
discussion
regarding the
role of
insurance
reimbursement
that recognized
a profession
with a BS
degree.
Comments
were made
about current
legislation before Congress (ie: H.R. 2948 expanding opportunities for Medicare beneficiaries who
suffer from pulmonary disease by 1) covering respiratory services when furnished via an interactive
telecommunications system, 2) including an individual’s home as a telehealth site, and 3) naming
respiratory therapists as qualified telehealth professionals.)
4) Proprietary competition with the proliferation of programs in one city with poor pass rates and
poor representatives of the profession to industry: discussion by two dinner guests from
California was quite intense as they painted the picture of the poor quality of graduates from
proprietary programs and frustration with CoARC for granting program status to so many
programs within the same geographic region. This glut of programs dilutes the applicant pool
to a stronger, more demanding BSRT program possibility.
13
AARC – CoBGRTE Goal Alignment – Jennifer Anderson, EdD, RRT
Jamy Chulak, Lynda Goodfellow, Tim Op’t Holt, Marc Mays, Warren Guiste, Lisa Trujillo, and
Jennifer Anderson attended the AARC Roundtable discussion table. The CoBGRTE members at
the roundtable
were a mix of
educators, a
manager, and a
student. Many
members at the
table currently
serve on the
AARC board of
directors or in
the House of
Delegates. The
table had a
wonderful
discussion about
the two
organizations.
Below you will find a few topics that were discussed:
The role of CoBGRTE is unique to that of other partners within the “tripartite”
Why can’t CoBGRTE be better partners and have a seat at the table?
CoBGRTE and AARC goals are aligned more than ever, how can our focus and work
compliment the work to advance the profession?
In summary, CoBGRTE membership includes some of the most talented educators in respiratory
therapy education who are also AARC members. CoBGRTE members are committed to assisting
the AARC in moving the profession forward to Bachelor’s entry education and RRT entry for
licensure. The AARC and CoBGRTE have many commonalities and therefore it is important for
the AARC and CoBGRTE to work together.

14
CAAHEP – ARC-RT – Tom Barnes, EdD, RRT, FAARC, David Shelledy, PhD, RRT,
FAARC
At the Round Table Discussion Dinner our table discussed the proposed Accreditation Review
Committee for Respiratory Therapy (ARC-RT), a new committee on accreditation (CoA) to be
developed under the
auspices of the
Commission on
Accreditation of
Allied Health
Education Programs
(CAAHEP) and
CoBGRTE. The
rationale for ARC-
RT is to improve the
quality of
respiratory therapist
educational
programs by
developing and
implementing a
collegial and collaborative, peer-review accreditation system and associated standards with a
focus on outcomes evaluation. Features of this new accreditation system should include: 1)
programs must award the BS or MS degree in respiratory care (or equivalent degree title); 2) use
of RRT examination performance as a primary outcome measure (instead of CRT pass rate); 3)
emphasis on the AARC approved competencies developed from the second AARC 2015 and
Beyond Conference; 4) strong representation of BSRT and MSRT entry to practice programs and
faculty as members of the ARC-RT; 5) a philosophy of consultation and support of accredited
programs; 6) direct communication with the program leadership at the college level; 7) use of
100% digital records during self-studies and site visits; 8) site visits limited to one day; 8)
support for direct entry (i.e. first professional) master’s degree programs and the development of
advanced practice respiratory therapist (APRT) master’s and doctoral degree (professional)
programs; 9) advance respiratory care education in a manner consistent with current and future
needs of the profession; and 10) decrease the number of hours required by faculty members to
maintain accreditation standards. The timelines for CAAHEP approval of the ARC-RT and the
development of standards, guidelines, policies, and methods for feedback of the community of
interest were discussed.

15
Direct-Entry Master’s Programs – DeDe Gardner, MHSP, RRT-NPS, FAARC
The Direct-Entry Master’s Program group answered a few questions:
1. Define Direct-Entry Master’s Program
2. Identify the skills, expectations of a prospective student
3. Identify the barriers associated with a Direct-Entry Master’s Program
4. Describe the benefits of a Direct-Entry Master’s program workforce.
The Direct-Entry Master’s Program group defined this type of program as one for students who have a
bachelor’s degree in any subject and interest in pursuing a degree in health care. The Direct-Entry
Master’s Programs are direct path to care for patients. The program provides the competencies to be an
advanced level
respiratory therapist at
the Registered
Respiratory Therapist
level with added skills
such as clinical
education, leadership
and research.
The Direct-Entry
Master’s Program
prospective students
should have critical
thinking skills and the
ability to
communicate well for
engaging in team care.
These prospective
students should have a high Science and Math GPA (greater than a 3.0); Letters of recommendation from
the math and science teachers that speak to the student’s abilities to critically think and communicate;
possibly have a high GRE score; and an understanding of respiratory therapy as a profession.
The group identified barriers to the Direct-Entry Master’s Program include the entry level to practice in
most states is the associate degree with a certified respiratory therapist (CRT) credential. The current
workforce does not recognize the importance of a Direct-Entry Master’s program and therefore the pay
scales are usually based on a credential unless a career ladder is in place which would allow for the
education level to come into play.
The benefits of Direct-Entry Master’s Program graduates would provide a unique workforce that would
be ready to move into the department leadership as team leaders; assist with quality improvement plans
and other types of clinical research and provide preceptors/clinical educators for students in the hospital
setting. This unique workforce overtime would be able to step in to a junior faculty position or research
and development positions. The career ladder could be wide open for these graduates.

16
Virtual Ventilator: the advantages of immersive simulation, the
convenience of a web-based computer application
Craig D. Smallwood, BS, RRT
Research Associate
Boston Children's Hospital
Harvard Medical School
Boston, MA
The virtual ventilator is a cutting edge training tool offering state of the art digital simulation
training for respiratory clinicians. The ventilator offers a comprehensive representation of a
mechanical ventilation bedside experience including patient appearance, physiologic monitor,
pulmonary mechanics and more. “Blurring the lines between computer simulation and bedside
experience”
Unlike many other online
training tools, the virtual
ventilator requires users to
use patient assessment
skills including
auscultation, blood gas
interpretation, chest X-ray
interpretation, waveform
analysis (including
capnography) and more.
Treating the patient is
very close to the dynamic
bedside experience; you’ll
not only have to choose
appropriate ventilator
settings but also administer aerosolized medication and perform other physical interventions
such as needle decompression.
The application is structured in three areas to offer fundamental information to those new to
mechanical ventilation through use of the knowledge guide, identification and treatment of
specific isolated conditions and the tactics required to treat them (hypocarbia, hypoxia, airway
obstruction, pneumothorax) and lastly, a complete case simulation using patient data and
following the time course of a patients response to mechanical ventilation.
The knowledge guide offers users fundamental information about mechanical ventilation
through the use of written content, display of important graphics on the ventilator and
explanations of important ventilation concepts. A total of 11 tactics that require identification of
17
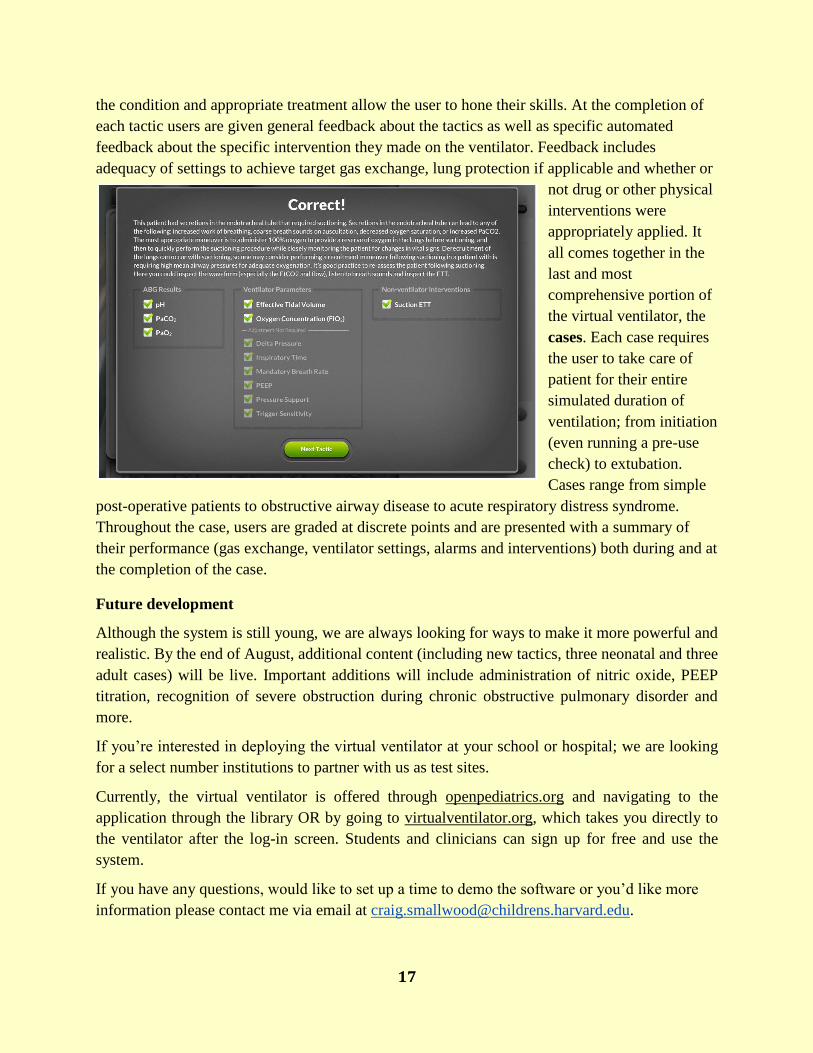
the condition and appropriate treatment allow the user to hone their skills. At the completion of
each tactic users are given general feedback about the tactics as well as specific automated
feedback about the specific intervention they made on the ventilator. Feedback includes
adequacy of settings to achieve target gas exchange, lung protection if applicable and whether or
not drug or other physical
interventions were
appropriately applied. It
all comes together in the
last and most
comprehensive portion of
the virtual ventilator, the
cases. Each case requires
the user to take care of
patient for their entire
simulated duration of
ventilation; from initiation
(even running a pre-use
check) to extubation.
Cases range from simple
post-operative patients to obstructive airway disease to acute respiratory distress syndrome.
Throughout the case, users are graded at discrete points and are presented with a summary of
their performance (gas exchange, ventilator settings, alarms and interventions) both during and at
the completion of the case.
Future development
Although the system is still young, we are always looking for ways to make it more powerful and
realistic. By the end of August, additional content (including new tactics, three neonatal and three
adult cases) will be live. Important additions will include administration of nitric oxide, PEEP
titration, recognition of severe obstruction during chronic obstructive pulmonary disorder and
more.
If you’re interested in deploying the virtual ventilator at your school or hospital; we are looking
for a select number institutions to partner with us as test sites.
Currently, the virtual ventilator is offered through openpediatrics.org and navigating to the
application through the library OR by going to virtualventilator.org, which takes you directly to
the ventilator after the log-in screen. Students and clinicians can sign up for free and use the
system.
If you have any questions, would like to set up a time to demo the software or you’d like more
information please contact me via email at [email protected].

18
Congratulations Class of 2015
The University of Arkansas for Medical Sciences BS Degree Class of 2015
Long Island University BS Degree Class of 2015

19
Long Island University Scholars
The Long Island University Respiratory Care program has had its
second consecutive NBRC/AMP scholar with Ms. Christina Rocks
(class of 2015) winning both the 2014 William W. Burgin Jr. MD
and the Robert M. Lawrence MD Education Recognition Award
for her paper on The Peri-operative Respiratory Care of the LVAD
Patient. Christina has just heard that her paper has been accepted for
publication through the Journal of Lung, Pulmonary & Respiratory
Research: http://medcraveonline.com/JLPRR/. She presented this
paper to the New Jersey Society for Respiratory Care's Shore
Conference in October 2014. In 2013, Ms. Katherine Meza (Class
of 2014) won the Robert M. Lawrence Education Recognition
Award at the AARC 2013 International Congress. The Long Island
University Respiratory Care Program received another consecutive award for “Distinguished
Credentialing Success” at the 2015 AARC Summer Forum in Phoenix.
CHI Health Midland University Baccalaureate Class of 2015
L to R, Andrea Hall, Essam Al-Yami, Jannae Takemoto

20
CoBGRTE Board Meets in Phoenix
The Board of Directors met in Phoenix following the AARC Summer Forum. Dr. Ellen Becker,
Chair of the AARC Education Section, visited the meeting to report on activities on current and
future activities. She mentioned the importance of introducing students to AARC membership
and encouraged
faculty
members to
help them
become
members while
in school and
when they
graduate. Dr.
Becker
emphasized the
importance of
becoming a
member of the AARC Education Section thereby helping to assure that the Section qualifies for a
seat on the AARC Board of Directors. She encouraged everyone to submit nominations for the
AARC Education Section “Practitioner of the Year Award.” She shared information on the
AARC’s Strategic Plan that includes a goal of 80% of respiratory therapists in the workforce
either holding or working on a baccalaureate degree by 2020.
The Executive Committee members reported to the Board on a
meeting of the CoBGRTE and AARC Executive Committees and
AARC professional staff members that was held immediately prior
to the CoBGRTE Board meeting. The joint session provided a
forum to report activities occurring in both associations.
Opportunities to move forward together to develop both
baccalaureate and graduate education while “grandfathering” the
associate degree programs to assure an adequate workforce were
discussed. The leadership of AARC President, Frank Salvatore, in
arranging the joint meeting was greatly appreciated by all in
attendance. President Salvatore stated that the AARC was
supporting baccalaureate education and that it was an important
part of their Strategic Plan. Tom Kallstrom, AARC Executive
Director offered to provide information for The Coalition
Chronicle on the Strategic Plan and President Salvatore’s goals. Tom Barnes, CoBGRTE
President offered to work with BSRT and MSRT program directors to assist with, AARC

21
membership (see article on pages 9-10). All in attendance of the combined Executive
Committees meeting agreed that the meeting led to positive communication.
Also, joining the Board of Directors meeting was Grace Richards, Marketing Manager, for Jones
and Bartlett Publishers. The Board thanked Ms. Richards for the support that J&B has provided
as a CoBGRTE sponsor since 2013. Plans were discussed for a J&B sponsored program in
Tampa, preceding the 2015 AARC Congress on how to use software that accompanies J&B
textbooks to enhance the learning experience.
CoBGRTE President, Dr. Tom Barnes, reported a healthy
growth of membership including a 25% increase in
institutional members that now total 61 and represent most
universities offering baccalaureate and graduate degrees to
RT students. In 2015, the Membership Committee has
encouraged academic health science centers, major
clinical affiliates, and respiratory care state societies
interested in supporting baccalaureate and graduate RT
education to become institutional members of CoBGRTE.
Dr. Barnes reviewed continued work on the
recommendations of the CoBGRTE Accreditation Task
Force White Paper on Accreditation published in 2014. He
reported that on July 1, 2015 CoBGRTE became an
Associate Organizational Member of the Commission for
Accreditation of Allied Health Education Programs
(CAAHEP). Dr. Barnes reviewed a major revision of the
CoBGRTE Bylaws prepared by the Executive Committee.
Changes include an addition of a Medical Advisor to the Board of Directors, three new members
on the Executive Committee, President-Elect, Past President, and separation of the
Secretary/Treasurer into two positions of Treasurer and Secretary. The revised Bylaws also
establish an Institutional Member Council with the Chair of the Council serving on the Board of
Directors. Active members of CoBGRTE will vote on the revised Bylaws in September as part of
the Election of three new directors to the Board. The remainder of the Board meeting was
dedicated to a review and action on minutes from past Board and Executive Committee
meetings, and other committee reports.
22
Why I’m a CoBGRTE Member
Paul G. Eberle, PhD, RRT
Professor & Department Chair / Respiratory Therapy
Dr. Ezekiel R. Dumke College of Health Professions
Weber State University
Ogden, Utah
Three reasons why I’m a CoBGRTE member:
“As we transition into increasing professional responsibilities as life-
support experts, we find ourselves creatively learning how to help our
patients as advocates, educators, collaborators, and disease consultants to
pathologies that affect their health. In these roles, it is important to
develop knowledgeable, competent, and capable practitioners with
competencies that advance our expertise as a health provider. I am a
member of CoBGRTE because the association advocates for advancing
educational pathways for professional growth, is actively engaged in
supporting programs with resources and mentors to improve outcomes, and has prepared a
vision for future development.”
Professional positions posted at http://www.cobgrte.org/professionalpositions.html
Bellarmine University
University of Texas Health Science Center at San Antonio
Nova Southeastern University
Indiana University Health
Georgia State University
Highline College
Northern Kentucky University
Salisbury University
University of Texas Medical Branch Galveston
Cincinnati Children’s Hospital
University of Dammam
University of North Carolina at Charlotte
Wexner Medical Center

23
24
CoBGRTE Institutional Members
Indiana Respiratory Therapy Consortium
Georgia State University
Weber State University
Boise State University
Bellarmine University
Rush University
Salisbury University
University of Toledo
The Ohio State University
State University of New York Upstate Medical University
Northeastern University
University of Texas Medical Branch - Galveston
Wheeling Jesuit University
Texas State University
University of South Alabama
Long Island University
University of North Carolina – Charlotte
Louisiana State University Health Science Center – New Orleans
Midwestern State University
Jefferson College of Health Sciences
Youngstown State University
Rutgers University - North
Nova Southeastern University
Loma Linda University
University of Arkansas for Medical Sciences
State University of New York at Stony Brook
University of Texas Health Science Center – San Antonio
University of Hartford
University of Cincinnati

25
CoBGRTE Institutional Members – Continued
University of Kansas Medical Center
College of Southern Nevada
Highline College
University of Akron
Oregon Institute of Technology
Georgia Regents University
St. Alexius Medical Center-University of Mary
Valencia College
Kettering College of Medical Arts
Shenandoah University
Middle Georgia State College
York College of Pennsylvania
University of Alabama at Birmingham
Respiratory Care Board of California
Texas Southern University
St. Catherine University
Armstrong State University
Cincinnati Children’s Hospital Medical Center
East Tennessee State University
University of Virginia Medical Center
University of Dammam
Seattle Central College
Florida Southwestern State College
Utah Society for Respiratory Care
Intermountain Healthcare
Southern Connecticut State University
Washington Adventist University
Rutgers University - South
Northern Kentucky University

26
CoBGRTE Institutional Members – Continued
Boston Children’s Hospital
California Society for Respiratory Care
Respiratory Care Society of Washington
If you haven’t already decided to become a CoBGRTE member after visiting www.cobgrte.org, the following are 10 reasons why you should join the coalition.
Ten Reasons Why You Should Become a CoBGRTE Member
1. Award scholarships to baccalaureate and graduate respiratory therapy students.
2. Assist in the development of ASRT to BSRT Bridge Programs.
3. Collectively work towards the day when all respiratory therapists enter the profession with a
baccalaureate or graduate degree in respiratory care.
4. Support a national association, representing the 55 colleges/universities awarding baccalaureate
and graduate degrees in respiratory care, to move forward the recommendations of the third 2015
conference.
5. Help start new baccalaureate and graduate RT programs thus leading to a higher quality of
respiratory therapist entering the workforce.
6. Work to change the image of the RT profession from technical-vocational-associate degree
education to professional education at the baccalaureate and graduate degree level.
7. Join colleagues to collectively develop standards for baccalaureate and graduate respiratory
therapist education.
8. Develop public relations programs to make potential students aware of baccalaureate and graduate
respiratory therapist programs.
9. Help to publicize, among department directors/managers, the differences between respiratory
therapists with associate, baccalaureate and graduate degrees.
10. Help to support maintaining a roster and web site for all baccalaureate and graduate respiratory
therapist programs.
Become a CoBGRTE member by completing the application on the Membership
Page: http://www.cobgrte.org/membership.html
Reminder: CoBGRTE Institutional Members receive free postings for open faculty member positions or hospital RT department staff and leadership positions at: http://www.cobgrte.org/professionalpositions.html

27
Editorial Board
Tom Barnes, EdD, RRT, FAARC - Editor in Chief Northeastern University
Boston, Massachusetts
Will Beachey, PhD, RRT, FAARC CHI St. Alexius Health/University of Mary
Bismarck, North Dakota
Paul Eberle, PhD, RRT, FAARC Weber State University
Ogden Utah
Christy Kane, PhD, RRT-NPS Bellarmine University
Louisville, Kentucky
Gregg Marshall, PhD, RRT, RPSGT, RST Texas State University
San Marcos, Texas
Jon Nilsestuen, PhD, RRT, FAARC University of Texas Medical Branch
Galveston, Texas
Timothy Op’t Holt, EdD, RRT, AE-C, FAARC University of South Alabama
Mobile, Alabama
“Dedicated to Improving Respiratory Therapy Education”
www.cobgrte.org
©Copyright 2015 Coalition for Baccalaureate and Graduate Respiratory Therapy Education
Follow Us