textbook of pharmacology for dental and allied health
TRANSCRIPT
Textbook ofPharmacology for Dental and
Allied Health Sciences

Textbook ofPharmacology for Dentaland Allied Health Sciences
Padmaja UdaykumarProfessor and Head
Department of PharmacologyFr. Muller Medical College, Mangalore
KarnatakaIndia
JAYPEE BROTHERSMEDICAL PUBLISHERS (P) LTD.
New Delhi
SECOND EDITION
Published by
Jitendar P VijJaypee Brothers Medical Publishers (P) LtdB-3 EMCA House, 23/23B Ansari Road, Daryaganj, New Delhi 110 002, IndiaPhones: +91-11-23272143, +91-11-23272703, +91-11-23282021, +91-11-23245672, Rel: 32558559Fax: +91-11-23276490, +91-11-23245683e-mail: [email protected] Visit our website: www.jaypeebrothers.com
Branches 2/B, Akruti Society, Jodhpur Gam Road Satellite
Ahmedabad 380 015, Phones: +91-079-26926233, Rel: +91-079-32988717, Fax: +91-079-26927094e-mail: [email protected]
202 Batavia Chambers, 8 Kumara Krupa Road, Kumara Park EastBengaluru 560 001, Phones: +91-80-22285971, +91-80-22382956, Rel: +91-80-32714073Fax:+91-80-22281761, e-mail: [email protected]
282 IIIrd Floor, Khaleel Shirazi Estate, Fountain Plaza, Pantheon RoadChennai 600 008, Phones: +91-44-28193265, +91-44-28194897, Rel: +91-44-32972089Fax: +91-44-28193231, e-mail: [email protected]
4-2-1067/1-3, 1st Floor, Balaji Building, Ramkote Cross RoadHyderabad 500 095, Phones: +91-40-66610020, +91-40-24758498, Rel:+91-40-32940929Fax:+91-40-24758499, e-mail: [email protected]
No. 41/3098, B & B1, Kuruvi Building, St. Vincent RoadKochi 682 018, Kerala, Phones: 0484-4036109, +91-0484-2395739, +91-0484-2395740e-mail: [email protected]
1-A Indian Mirror Street, Wellington SquareKolkata 700 013, Phones: +91-33-22651926, +91-33-22276404, +91-33-22276415Rel: +91-33-32901926, Fax: +91-33-22656075, e-mail: [email protected]
106 Amit Industrial Estate, 61 Dr SS Rao Road, Near MGM Hospital, ParelMumbai 400 012, Phones: +91-22-24124863, +91-22-24104532, Rel: +91-22-32926896Fax: +91-22-24160828, e-mail: [email protected]
“KAMALPUSHPA” 38, Reshimbag, Opp. Mohota Science College, Umred RoadNagpur 440 009 (MS), Phones: Rel: 3245220, Fax: 0712-2704275, e-mail: [email protected]
Textbook of Pharmacology for Dental and Allied Health Sciences
© 2007, Padmaja Udaykumar
All rights reserved. No part of this publication should be reproduced, stored in a retrieval system, or transmitted in any formor by any means: electronic, mechanical, photocopying, recording, or otherwise, without the prior written permission of theauthor and the publisher.
This book has been published in good faith that the material provided by author is original. Every effort is made to ensureaccuracy of material, but the publisher, printer and author will not be held responsible for any inadvertent error(s). Incase of any dispute, all legal matters are to be settled under Delhi jurisdiction only.
First Edition: 2002Reprint: 2003, 2006Second Edition: 2007
ISBN 81-8448-149-7
Typeset at JPBMP typesetting unitPrinted at Paras Press

Dedicated toMy beloved mother
Mrs. Lalitha Narayan

It is a daunting challenge to a studious student of a subject to write a textbook. This is particularly soin case of pharmacology, a subject having tremendous potential for expansion.
Medicine is said to be the most dynamic amongst biological disciplines; pharmacology can be saidto be so amongst health science disciplines. It has stupendously grown in its own right and on its ownwicket. In addition, it has been quick in responding to advances in other disciplines. Ramification ofpharmacology into various other disciplines has resulted in mutual sharing of knowledge andimpetuous for further study. This has resulted in the continuing growth of both factual and conceptualknowledge-base, too rapid and huge to comprehend. These facts weigh on the mind of a studiousstudent.
A textbook for undergraduate students has to be clear, lucid, comprehensive and concise. Thisrequires a critical and shrewd sifting and sieving of the vast data, to pick-up those that are necessaryand relevant in a given context. Such a job demands grit, knowledge, ability and prudence. Dr (Mrs)Padmaja Udaykumar, a young pharmacologist has gratifyingly demonstrated these in her venture ofwriting a textbook in pharmacology for students of dental, physiotherapy and allied branches ofhealth sciences.
Most textbooks on this subject contain data and information that suit medical students. But manystudent-groups of other streams of health sciences require knowledgeability in the subject pharmacologyin a way that is meaningful and relevant to their respective field. Indeed pharmacology is one of thecore-subjects in these courses. This point in view, the author has made a commendable attempt in thisdirection.
Need for condensation of the vast data inevitably makes the text and approach more catalogic andless thematic. Yet there is enough factual data as well as sufficient thematic message synchronized, avery important point in a text for undergraduates.
Dr Padmaja Udaykumar has brought out a concise book in pharmacology with clear andcomprehensive coverage of the topics in a systematically organized manner and presented in a simple—‘easy to read and grasp’ style. This book though primarily meant for dental, physiotherapy andnursing students, it contains enough material to be useful even for medical students, particularly forquick revision.
Teacher, like parent, gets proud pleasure at the progress and deserving achievements of the nextgeneration. I did derive such pleasure while going through the text of this nice book by Dr PadmajaUdaykumar and say a few words about it.
Prof DR KulkarniHead of the Department of Medical Education
BM Patil Medical College, BijapurFormer Principal, DY Patil Medical College, Kollapur
Former President, Indian Association of Pharmacologists
Foreword

Pharmacology is a subject that has been rapidly growing. To keep pace with it, books inpharmacology need to be updated frequently. The book has been thoroughly revised withappropriate additions, deletions and tailored to the needs of a dental student. In responseto the feedback received, wherever applicable, the relevance of the topic to a dentist hasbeen highlighted. More figures, charts and tables have been added and the book is broughtout in multiple colours, all of which make it more student-friendly. Many universities haveintroduced ‘Compare and Contrast’, between related drugs in the question papers. There-fore a series of ‘Compare and Contrast’ have been given in all relevant chapters. Keeping inmind the burden on students, efforts have been made to include only the necessary thingsand prune the unwanted ones. A chapter on emergencies in dental practice has beenincluded as required by some universities.
The First edition of the book was titled ‘Short Textbook of Pharmacology for Dentaland Allied Health Sciences’ and has been renamed in the second edition as Textbook ofPharmacology for Dental and Allied Health Sciences.
I hope the book makes learning pharmacology a pleasurable experience.
Please send your feedback to [email protected].
Padmaja Udaykumar
Preface to the Second Edition


Pharmacology is a science that forms the basis for modern medicine. It is a rapidly changing field withnew drugs being constantly introduced. The knowledge of pharmacology is important for all thosewho deal with drugs apart from medical practitioners. But the depth could vary. The need was felt fora short textbook for Dental, Nursing, Physiotherapy and other health science students. Hence thisbook was brought out, keeping in mind the size of the book and information required.
General pharmacology has been discussed in detail as it forms the basis for understandingpharmacology. Similarly chemotherapy, particularly general chemotherapy, analgesics, anaestheticsand corticosteroids are dealt with in adequate depth. Mechanisms of action have been discussed inbrief. In each chapter, the prototype drug has been discussed in detail while the differing features ofothers are then mentioned. Simple figures have been used wherever necessary. Common druginteractions are given in the Appendices. Accepted abbreviations have been used. References forfurther reading are mentioned at the end of the text. The chapter on Dental Pharmacology is included.Adequate importance has been given to essential drugs.
I hope this book serves to make pharmacology easy for the students of Health Sciences.
Padmaja Udaykumar
Preface to the First Edition
I wish to express my sincere thanks to Prof. D.R. Kulkarni for writing Foreword to thisbook and for his valuable guidance.
I place on record my heartfelt gratitude to Dr. Lakshmikant Chatra, Professor of OralMedicine, Yenepoya Dental College, for his help and suggestions. I wish to thank Profes-sors of Pharmacology Prof. Nataraj K.V., Prof. Vijayaraghavan, Prof. Parvathi Bhat, Prof.K.S.Karanth, Prof. M.C. Alwar, Prof. Ahalya Devi, Prof. Vasanth Kumar, Prof. K.L. Bairy,Prof. Holla R., Prof. M.R.S.M.Pai, Prof. Venkatadri and Prof. Tara Shanbogue.
I also thank my colleagues Dr.Vijayalakshmi M., Dr. Princy, Dr. Prasannalakshmi,Dr. Manohar Revonkar and Miss Deepa for their support. I am extremely thankful to themanagement of Fr. Muller Medical College—Director Fr. Baptist Menezes, AdministratorsFr. Lawrence C D’Souza, Fr. Dennis D’Sa and Dean Dr. Sanjeev Rai for their encouragement.
I wish to thank Dr. Prasanna Kumar J. Asst. Professor in oral medicine for his help.
I owe a special note of thanks to my husband Prof. Udaykumar K. for his constantencouragement, valuable suggestions and support in this endeavor.
I thank Jaypee Brothers Medical Publishers, New Delhi for bringing out this colourfulbook.
Acknowledgements
SECTION 1
General Pharmacology
1. Introduction and Sources of Drugs ................................................................................................. 1
2. Routes of Drug Administration ....................................................................................................... 3
3. Pharmacokinetics ............................................................................................................................ 10
4. Pharmacodynamics ......................................................................................................................... 24
5. Adverse Drug Reactions and Drug Interactions, Drug Nomenclature and
Essential Drugs Concept ................................................................................................................ 36
SECTION 2
Autonomic Nervous System
6. Introduction to Autonomic Pharmacology ................................................................................... 42
7. Cholinergic System ......................................................................................................................... 46
8. Anticholinergic Drugs ..................................................................................................................... 56
9. Skeletal Muscle Relaxants ............................................................................................................. 60
10. Adrenergic System .......................................................................................................................... 66
11. Adrenergic Drugs (Sympathomimetics) ...................................................................................... 69
12. Adrenergic Antagonists .................................................................................................................. 76
SECTION 3
Drugs Acting on the Kidney
13. Diuretics and Antidiuretics ........................................................................................................... 82
SECTION 4
Cardiovascular System
14. Cardiac Glycosides and Treatment of Cardiac Failure ............................................................. 90
15. Calcium Channel Blockers ............................................................................................................. 96
16. Antiarrhythmic Drugs ..................................................................................................................... 99
17. Drugs Used in Angina Pectoris and Myocardial Infarction ...................................................104
18. Antihypertensive Drugs ............................................................................................................... 110
19. Plasma Expanders and Pharmacotherapy of Shock ................................................................120
Contents
Textbook of Pharmacology for Dental and Allied Health Sciencesxiv
SECTION 5
Central Nervous System
20. General Anaesthetics ....................................................................................................................122
21. Local Anaesthetics .........................................................................................................................130
22. Sedative Hypnotics .......................................................................................................................137
23. Alcohols ...........................................................................................................................................143
24. Antiepileptics .................................................................................................................................146
25. Drugs Used in Parkinsonism .......................................................................................................155
26. Opioid Analgesics .........................................................................................................................158
27. Nonsteroidal Anti-inflammatory Drugs (NSAIDs) ..................................................................172
28. Drugs Used in Rheumatoid Arthritis and Gout ........................................................................185
29. Drugs Used in Psychiatric Disorders .........................................................................................190
30. CNS StimulantS ..............................................................................................................................201
SECTION 6Autacoids
31. Autacoids
• Histamine ....................................................................................................................................... 203
• 5-Hydroxytryptamine ....................................................................................................................207
• Ergot Alkaloids ...............................................................................................................................208
• Eicosanoids .....................................................................................................................................210
• Other Autacoids .............................................................................................................................212
SECTION 7Respiratory System
32. Drugs Acting on Respiratory System
• Drugs Used in the Treatment of Bronchial Asthma ................................................................214
• Drugs Used in the Treatment of Cough .....................................................................................220
xvContents
SECTION 8Blood
33. Haematopoietic System
• Haematinics ...................................................................................................................................222
• Drugs Used in the Disorders of Coagulation ............................................................................226
• Hypolipidaemic Drugs .................................................................................................................235
SECTION 9Gastrointestinal Tract
34. Drugs Used in Gastrointestinal Disorders
• Drugs Used in Peptic Ulcer ..........................................................................................................237
• Prokinetic Agents ..........................................................................................................................243
• Emetics and Antiemetics ..............................................................................................................244
• Drugs for Constipation and Diarrhoea ......................................................................................247
SECTION 10Chemotherapy I
35. General Considerations ................................................................................................................252
36. Sulfonamides, Cotrimoxazole and Quinolones .......................................................................262
37. Beta-lactam Antibiotics .................................................................................................................267
38. Broad Spectrum Antibiotics .........................................................................................................276
39. Aminoglycosides ...........................................................................................................................280
40. Macrolides, Other Antibacterial Agents and
Chemotherapy of Urinary Tract Infections ...............................................................................284
SECTION 11Chemotherapy II
41. Chemotherapy of Tuberculosis and Leprosy ............................................................................291
42. Antifungal Drugs ...........................................................................................................................299
43. Antiviral Drugs ..............................................................................................................................305
44. Chemotherapy of Malaria ............................................................................................................312
45. Drugs Used in Amoebiasis, Leishmaniasis and Trypanosomiasis .......................................319
46. Anthelmintics .................................................................................................................................324
47. Cancer Chemotherapy ..................................................................................................................328
Textbook of Pharmacology for Dental and Allied Health Sciencesxvi
SECTION 12Hormones
48. Hypothalamus and Anterior Pituitary Hormones ....................................................................337
49. Thyroid Hormones and Antithyroid Drugs ...............................................................................342
50. Corticosteroids ................................................................................................................................347
51. Oestrogens, Progestins and Hormonal Contraceptives ...........................................................355
52. Androgens and Anabolic Steroids ..............................................................................................362
53. Insulin and Oral Hypoglycaemics ..............................................................................................364
54. Agents Affecting Bone Mineral Turnover .................................................................................372
SECTION 13Miscellaneous Drugs
55. Miscellaneous Drugs
• Immunopharmacology .................................................................................................................376
• Antiseptics and Disinfectants .....................................................................................................378
• Chelating Agents ...........................................................................................................................382
• Vitamins ..........................................................................................................................................383
• Gene Therapy ................................................................................................................................387
SECTION 14Dental Pharmacology
56 Dental Pharmacology ....................................................................................................................389
Appendix 1- Important Drug Interactions ........................................................................................405
Apendix 2-Prescription Writing ....................................................................................................... 408
Further Reading ................................................................................................................................ 411
Index ................................................................................................................................................. 413
1HISTORICAL ASPECTS
Pharmacology is the science that deals withthe study of drugs and their interaction withthe living systems.
The useful and toxic effects of many plantand animal products were known to man inancient times. The earliest writings on drugsare the Egyptian Medical Papyrus (1600 BC).The largest of them, Ebers Papyrus lists some800 preparations.
In early days there was a close relationshipbetween religion and treatment of diseases.The knowledge of the use of drugs oftenrested with the priest or holyman. Drugswere thought to be magical in their actions.
Several cultures like the Chinese, Greek,Indian, Roman, Persian, European and manyothers contributed a great deal to thedevelopment of medicine in early times. Thedrug prescriptions included preparationsfrom herbs, plants, animals and minerals. Inthe middle ages many herbal gardens werecultivated particularly by monasteries.
Though medicine developed simulta-neously in several countries, the spread ofknowledge was limited because of poorlydeveloped communication across the world.
India’s earliest pharmacological writingsare from the ‘Vedas’. An ancient Indianphysician Charaka and then, Sushruta andVagbhata, described many herbalpreparations included in ‘Ayurveda’(meaning ‘the science of life’). Indianspracticed vaccination as early as 550 BC.
Various other traditional systems ofmedicine were practiced in different parts ofthe world – like Homeopathy, Unani, Siddhasystem and Allopathy.
Allopathy means ‘the other suffering’. Thisword still being used for the modern systemof medicine, is a misnomer. Homoeopathymeaning ‘similar suffering’ was introducedby Hanneman. The principles of this systeminclude ‘like cures like’ and ‘dilution enhancesthe potency of drugs’.
Thus several systems of medicine wereintroduced, of which only a few survived.The basic reason for the failure of manysystems is that man’s concepts about diseaseswere incorrect and baseless in those days.By the end of the 17th century the importanceof experimentation, observation andscientific methods of study became clear.Francois Magendie and Claude Bernardpopularised the use of animal experimentsto understand the effects of drugs.Simultaneous development of other branchesof science viz, botany, zoology, chemistryand physiology helped in the betterunderstanding of pharmacology.
The last century has seen a rapid growthof the subject with several new drugs, newconcepts and techniques being introduced.We now know much more about receptorsand molecular mechanisms of action of manydrugs. Several diseases, which wereconsidered incurable and fatal, can now becompletely cured with just a few tablets.
Introduction andSources of Drugs
Section 1General Pharmacology

Textbook of Pharmacology for Dental and Allied Health Sciences2
DEFINITIONS
The word pharmacology is derived fromthe Greek word—Pharmacon meaning anactive principle and logos meaning a study(discourse).Drug (Drogue—a dry herb in French) is asubstance used in the diagnosis, preventionor treatment of a disease. WHO definition—“A drug is any substance or product that isused or intended to be used to modify orexplore physiological systems or pathologicalstates for the benefit of the recipient.”Pharmacodynamics is the study of the effectsof the drugs on the body and theirmechanisms of action, i.e. what the drug doesto the body.Pharmacokinetics is the study of the absorption,distribution, metabolism and excretion ofdrugs, i.e. what the body does to the drug(in Greek Kinesis = movement).Therapeutics deals with the use of drugs in theprevention and treatment of disease.Pharmacoeconomics deals with the cost, i.e.economic aspects of drugs used therapeutically.Pharmacogenomics is a branch of pharmaco-genetics which deals with the use of geneticinformation in selecting drugs for a person.Pharmacoepidemiology is the study of both theuseful and adverse effects of drugs on largenumbers of people. Pharmacovigilance is abranch of pharmacoepidemiology which dealswith the epidemiologic study of adverse drugeffects.Toxicology deals with the adverse effects ofdrugs and also the study of poisons, i.edetection, prevention and treatment of poiso-nings (Toxicon=poison in Greek).Chemotherapy is the use of chemicals for thetreatment of infections. The term now alsoincludes the use of chemical compounds totreat malignancies.Pharmacopoeia (in Greek Pharmacon = drug;poeia=to make) is the official publicationcontaining a list of drugs and medicinal
preparations approved for use, their formulaeand other information needed to prepare adrug; their physical properties, tests for theiridentity, purity and potency. Each countrymay follow its own pharmacopoeia to guideits physicians and pharmacists. We thus havethe Indian Pharmacopoeia (IP), the BritishPharmacopoeia (BP) and the United StatesPharmacopoeia (USP). The list is revised atregular periods to delete obsolete drugs andto include newly introduced ones.Pharmacy is the science of identification,compounding and dispensing of drugs. It alsoincludes collection, isolation, purification,synthesis and standardisation of medicinalsubstances.
SOURCES OF DRUGSThe sources of drugs could be natural orsynthetic.Natural sources Drugs can be obtained from:1. Plants, e.g. atropine, morphine, quinine,
and digoxin.2. Animals, e.g. insulin, heparin, gonad-
otrophins and antitoxic sera.3. Minerals, e.g. magnesium sulphate,
aluminium hydroxide, iron, sulphur andradioactive isotopes.
4. Microorganisms—antibacterial agents areobtained from some bacteria and fungi. Wethus have penicillin, cephalosporins,tetracyclines and other antibiotics.
5. Human—some drugs are obtained fromhuman beings, e.g. immunoglobulins fromblood, growth hormone from anteriorpituitary and chorionic gonadotrophinsfrom the urine of pregnant women.
Synthetic Most drugs used now are synthetic,e.g. quinolones, omeprazole, neostigmine,sulfonamides.
Many drugs are obtained by cell cultures, e.g.urokinase from cultured human kidney cells.Some are now produced by recombinant DNAtechnology, e.g. human insulin, tissue plasminogenactivator, haematopoietic growth factors likeerythropoietin and some others by hybridomatechnique eg. monoclonal antibiodies.
2Drugs may be administered by variousroutes. The choice of the route in a givenpatient depends on the properties of the drugand the patient’s requirements. A knowledgeof the advantages and disadvantages of thedifferent routes of administration is essential.The routes can be broadly divided into:• Enteral• Parenteral• Local.
ENTERAL ROUTE (ORAL INGESTION)Enteral route is the most commonly used,oldest and safest route of drug adminis-tration. The large surface area of thegastrointestinal tract, the mixing of itscontents and the differences in pH atdifferent parts of the gut facilitate effectiveabsorption of the drugs given orally.However, the acid and enzymes secreted inthe gut and the biochemical activity of thebacterial flora of the gut can destroy somedrugs before they are absorbed.
Advantages
1. Safest route2. Most convenient3. Most economical4. Drugs can be self-administered5. Non-invasive route.
Disadvantages
1. Onset of action is slower as absorptionneeds time.
2. Irritant and unpalatable drugs cannot beadministered.
3. Some drugs may not be absorbed due tocertain physical and chemical characte-ristics, e.g. streptomycin is not effectiveorally.
4. Irritation to the gastrointestinal tract maylead to vomiting.
5. There may be irregularities in absorption.6. Some drugs may be destroyed by gastric
juices, e.g. insulin.7. Oral preparations cannot be given to
unconscious and uncooperative patients.8. Some drugs may undergo extensive first
pass metabolism in the liver.To overcome some of the disadvantages,
irritants are given in capsules, while bitterdrugs are given as sugar coated tablets.Sometimes drugs are coated with substanceslike synthetic resins, gums, sugar, colouringand flavouring agents making them moreacceptable.
Enteric Coated TabletsSome tablets are coated with substances likecellulose-acetate, phthalate, gluten, etc. whichare not digested by the gastric acid but getdisintegrated in the alkaline juices of theintestine. This will:• prevent gastric irritation.• avoid destruction of the drug by the
stomach.• provide higher concentration of the drug
in the small intestine.
Routes of DrugAdministration
Textbook of Pharmacology for Dental and Allied Health Sciences4
• retard the absorption, and therebyprolong the duration of action.
But if the coating is inappropriate, thetablet may be expelled without beingabsorbed at all. Similarly controlled-releaseor sustained-release preparations aredesigned to prolong the rate of absorptionand thereby the duration of action of drugs.This is useful for short-acting drugs. In newercontrolled release formulations, the tablet iscoated with a semipermeable membranethrough which water enters and displaces thedrug out.
Advantages
• Frequency of administration may bereduced.
• Therapeutic concentration may bemaintained specially when nocturnalsymptoms are to be treated.
Disadvantages
• There may be ‘failure of the preparation’resulting in release of the entire amountof the drug in a short time, leading totoxicity.
• Enteric coated tablets are moreexpensive.
Certain precautions are to be taken duringoral administration of drugs—capsules andtablets should be swallowed with a glass ofwater with the patient in upright postureeither sitting or standing. This facilitatespassage of the tablet into the stomach andits rapid dissolution. It also minimiseschances of the drug getting into the larynxor behind the epiglottis. Recumbent patientshould not be given drugs orally as somedrugs may remain in the esophagus due tothe absence of gravitational force facilitatingthe passage of the drug into the stomach. Suchdrugs can damage the esophageal mucosa,e.g. iron salts, tetracyclines.
Though enteral route mainly includes oralingestion, sublingual and rectal adminis-tration may also be considered as enteralroute.
PARENTERAL ROUTE
Routes of administration other than theenteral (intestinal) route are known asparenteral routes. Here the drugs are directlydelivered into tissue fluids or blood.
Advantages
• Action is more rapid and predictable thanoral administration.
• These routes can be employed in anunconscious or uncooperative patient.
• Gastric irritants can be given parenterallyand therefore irritation to the gastroin-testinal tract can be avoided.
• It can be used in patients with vomitingor those unable to swallow.
• Digestion by the gastric and intestinaljuices and the first pass metabolism areavoided.Therefore, in emergencies parenteralroutes are very useful routes of drugadministration as the action is rapid andpredictable and are useful even inunconscious patients.
Disadvantages
• Asepsis must be maintained.• Injections may be painful.• More expensive, less safe and
inconvenient.• Injury to nerves and other tissues may
occur.
Parenteral routes include :
1. Injections2. Inhalation3. Transdermal route4. Transmucosal route.
Routes of Drug Administration 5
INJECTIONS
Intradermal
The drug is injected into the layers of theskin raising a bleb, (e.g. BCG vaccine, testsfor allergy) or by multiple punctures of theepidermis through a drop of the drug, e.g.smallpox vaccine. Only a small quantity canbe administered by this route and it may bepainful.
Subcutaneous (SC) Injection
Here the drug is deposited in the SC tissue,e.g. insulin, heparin. As this tissue is lessvascular, absorption is slow and largelyuniform making the drug long-acting. It isreliable and patients can be trained for self-administration. Absorption can be enhancedby the addition of the enzyme hyaluronidase.
Disadvantages
• As SC tissue is richly supplied by nerves,irritant drugs cannot be injected becausethey can cause severe pain.
• In shock, absorption is not dependablebecause of vasoconstriction.
• Repeated injections at the same site cancause lipoatrophy resulting in erraticabsorption.
Hypodermoclysis is the SC administration oflarge volumes of saline employed inpaediatric practice.Drugs can also be administered sub-cutaneously as:1. Dermojet In this method, a high velocity
jet of drug solution is projected from afine orifice using a gun. The solution getsdeposited in the SC tissue from where itis absorbed. As needle is not required,this method is painless. It is suitable forvaccines.
2. Pellet implantation Small pellets packedwith drugs are implanted subcutaneously.
The drug is slowly released for weeks ormonths to provide constant blood levels,e.g. testosterone, DOCA.
3. Sialistic implants The drug is packed insialistic tubes and implanted sub-cutaneously. The drug gets absorbed overmonths to provide constant blood levels,e.g. hormones and contraceptives. Theempty non-biodegradable implant has tobe removed.
Intramuscular (IM)
Aqueous solution of the drug is injected intoone of the large skeletal muscles—deltoid,triceps, gluteus or rectus femoris. Absorptioninto the plasma occurs by simple diffusion.Larger molecules enter through thelymphatic channels. As the muscles arevascular, absorption is rapid and quiteuniform. Drugs are absorbed faster from thedeltoid region than gluteal region especiallyin women. The volume of injection shouldnot exceed 10 ml. For infants, rectus femorisis used instead of gluteus because gluteus isnot well-developed till the child startswalking. If the drug is injected as an oilysolution or suspension, absorption is slowand steady.
Advantages
• Intramuscular route is reliable.• Absorption is rapid.• Soluble substances, mild irritants, depot
preparations, suspensions and colloids canbe injected by this route.
Disadvantages
• Intramuscular injection may be painful andmay even result in an abscess.
• Irritant solutions can damage the nerveif injected near a nerve. Nerve injuryshould be avoided.
Textbook of Pharmacology for Dental and Allied Health Sciences6
Intravenous (IV)
Here, the drug is injected into one of thesuperficial veins so that it directly reachesthe circulation and is immediately availablefor action.Drugs can be given IV as:1. A bolus—where an initial large dose is
given, e.g. heparin. The drug is dissolvedin a suitable amount of the vehicle andinjected slowly.
2. Slow injection—over 15-20 minutes, e.g.aminophylline.
3. Slow infusion—when constant plasmaconcentrations are required, e.g. oxytocinin labour or when large volumes have tobe given, e.g. dextrose, saline. Generallyabout one litre of solution is infused over3 to 4 hours. However, the patient'scondition and the drug factors like theonset and duration of action of the drugdictates the rate of infusion.
Advantages
• Most useful route in emergencies becausethe drug is immediately available foraction.
• Provides predictable blood concentrationswith 100% bioavailability.
• Large volumes of solutions can be given.• Irritants can be given by this route as they
get quickly diluted in blood.• Rapid dose adjustments are possible—if
unwanted effects occur, infusion can bestopped; if higher levels are required,infusion rate can be increased—speciallyfor short-acting drugs.
Disadvantages
• Once injected, the drug cannot bewithdrawn.
• Irritation of the veins may causethrombophlebitis.
• Extravasation of some drugs may causesevere irritation and sloughing.
• Only aqueous solutions can be given IVbut not suspensions, oily solutions anddepot preparations.
• Self medication is difficult.Intraperitoneal Peritoneum offers a largesurface area for absorption. Fluids areinjected intraperitoneally in infants. This routeis also used for peritoneal dialysis.Intrathecal Drugs can be injected into thesubarachnoid space for action on the CNS,e.g. spinal anaesthetics. Some antibiotics andcorticosteroids are also injected by this routeto produce high local concentrations. Strictaseptic precautions are a must.
Drugs are also given extradurally.Morphine can be given epidurally toproduce analgesia. Direct intraventricularadministration of drugs may be employed inbrain tumors.Intra-articular Drugs are injected directlyinto a joint for the treatment of arthritis andother diseases of the joints, e.g.hydrocortisone is injected into the affectedjoint in rheumatoid arthritis. Strict asepticprecautions are required.Intra-arterial Here drug is injected directlyinto the arteries. It is used only in thetreatment of(i) peripheral vascular diseases,
(ii) local malignancies(iii) diagnostic studies like angiograms.Intramedullary Injection into a bone marrow—now rarely used.
INHALATION
Volatile liquids and gases are given byinhalation, e.g. general anaesthetics. Inaddition, drugs can be administered as solidparticles, i.e. solutions of drugs can beatomised and the fine droplets are inhaledas aerosol, e.g. salbutamol. These inhaleddrugs and vapours may act on the pulmonaryepithelium and mucous membranes of the
Routes of Drug Administration 7
respiratory tract and are also absorbedthrough these membranes.
Advantages
• Almost instantaneous absorption of thedrug is achieved because of the largesurface area of the lungs.
• In pulmonary diseases, it serves almostas a local route as the drug is deliveredat the desired site making it moreeffective and less harmful.
• Hepatic first pass metabolism is avoided.• Blood levels of volatile anaesthetics can
be conveniently controlled as theirabsorption and excretion through thelungs are governed by the laws of gases.
Disadvantage
• Irritant gases may enhance pulmonarysecretions—should be avoided.This is an important route of entry ofcertain drugs of abuse.
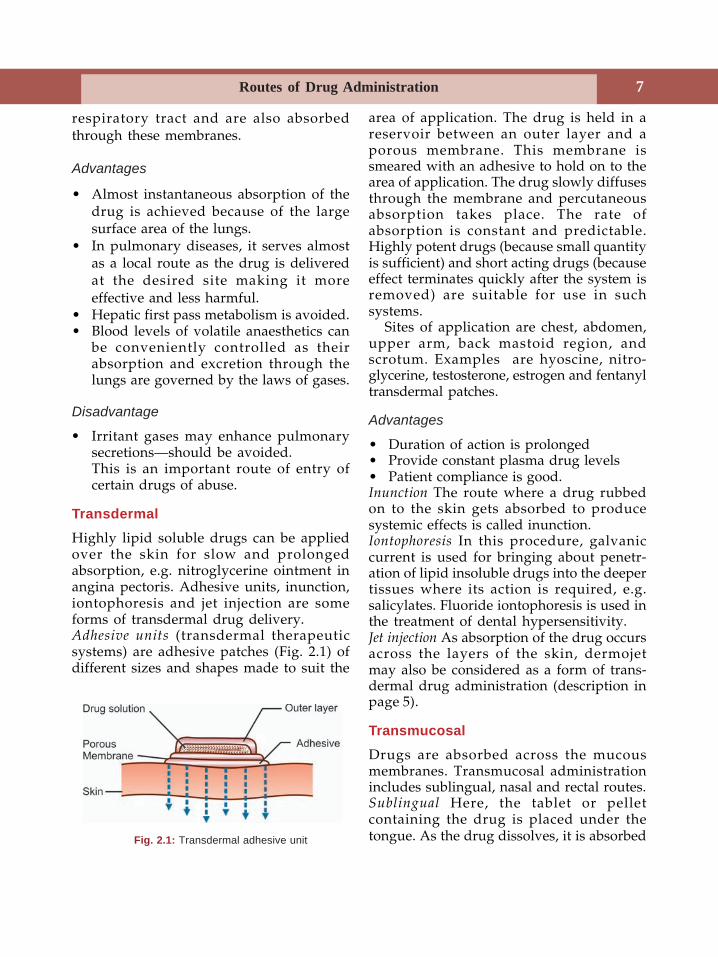
TransdermalHighly lipid soluble drugs can be appliedover the skin for slow and prolongedabsorption, e.g. nitroglycerine ointment inangina pectoris. Adhesive units, inunction,iontophoresis and jet injection are someforms of transdermal drug delivery.Adhesive units (transdermal therapeuticsystems) are adhesive patches (Fig. 2.1) ofdifferent sizes and shapes made to suit the
area of application. The drug is held in areservoir between an outer layer and aporous membrane. This membrane issmeared with an adhesive to hold on to thearea of application. The drug slowly diffusesthrough the membrane and percutaneousabsorption takes place. The rate ofabsorption is constant and predictable.Highly potent drugs (because small quantityis sufficient) and short acting drugs (becauseeffect terminates quickly after the system isremoved) are suitable for use in suchsystems.
Sites of application are chest, abdomen,upper arm, back mastoid region, andscrotum. Examples are hyoscine, nitro-glycerine, testosterone, estrogen and fentanyltransdermal patches.
Advantages
• Duration of action is prolonged• Provide constant plasma drug levels• Patient compliance is good.Inunction The route where a drug rubbedon to the skin gets absorbed to producesystemic effects is called inunction.Iontophoresis In this procedure, galvaniccurrent is used for bringing about penetr-ation of lipid insoluble drugs into the deepertissues where its action is required, e.g.salicylates. Fluoride iontophoresis is used inthe treatment of dental hypersensitivity.Jet injection As absorption of the drug occursacross the layers of the skin, dermojetmay also be considered as a form of trans-dermal drug administration (description inpage 5).
TransmucosalDrugs are absorbed across the mucousmembranes. Transmucosal administrationincludes sublingual, nasal and rectal routes.Sublingual Here, the tablet or pelletcontaining the drug is placed under thetongue. As the drug dissolves, it is absorbedFig. 2.1: Transdermal adhesive unit
Textbook of Pharmacology for Dental and Allied Health Sciences8
across the sublingual mucosa. The for-mulation should be lipid soluble, e.g.nitroglycerine, nifedipine, buprenorphine.
Advantages
• Absorption is rapid—within minutes thedrug reaches the circulation.
• First pass metabolism is avoided.• After the desired effect is obtained, the
drug can be spat out to avoid theunwanted effects.
Disadvantages
• Buccal ulceration can occur.• Lipid insoluble drugs cannot be given.Nasal Drugs can be administered throughnasal route either for systemic absorption orfor local effects.E.g.(a) for systemic absorption — oxytocin spray(b) for local effect—decongestant nasal
drops, e.g. oxymetazoline; budesonidenasal spray for allergic rhinitis.
Rectal Rectum has a rich blood supply anddrugs can cross the rectal mucosa to beabsorbed for systemic effects. Drugsabsorbed from the upper part of the rectumare carried by the superior haemorrhoidalveins to the portal circulation (can undergofirst pass metabolism), while that absorbedfrom the lower part of the rectum is carriedby the middle and inferior haemorrhoidalveins to the systemic circulation. Drugs likeindomethacin, chlorpromazine, diazepam andparaldehyde can be given rectally.
Some irritant drugs are given rectally assuppositories because they cannot be given orally.
Advantages
• Gastric irritation is avoided.• Can be administered by unskilled
persons.• Useful in geriatric patients; patients with
vomiting and those unable to swallow.
Disadvantages
• Irritation of the rectum can occur.• Absorption may be irregular and
unpredictable.
Drugs may also be given by rectal routeas enema.Enema is the administration of a drug in aliquid form into the rectum. Enema may beevacuant or retention enema.Evacuant enema In order to empty the bowel,about 600 ml of soap water is administeredper rectum. Water distends and thusstimulates the rectum while soap lubricates.Enema is given prior to surgeries, obstetricprocedures and radiological examination ofthe gut.Retention enema The drug is administered withabout 100 ml of fluids and is retained in therectum for local action, e.g. prednisoloneenema in ulcerative colitis.
TOPICAL
Drugs may be applied on the skin for localaction as ointment, cream, gel, powder, paste,etc. Drugs may also be applied on the mucousmembrane as in the eyes, ears and nose asointment, drops and sprays. Drugs may beadministered as suppository for rectum, bougiefor urethra and pessary and douche for vagina.Pessaries are oval shaped tablets to be placedin the vagina to provide high localconcentrations of the drug at the site, e.g.antifungal pessaries in vaginal candidiasis.
SPECIAL DRUG DELIVERY SYSTEMS
In order to improve drug delivery, toprolong the duration of action and therebyimprove patient compliance, special drugdelivery systems are being tried. Drugtargeting, i.e. to deliver drugs at the sitewhere it is required to act is also being aimedat, especially for anticancer drugs. Some such

Routes of Drug Administration 9
systems are ocuserts, progestaserts,transdermal adhesive units, prodrugs,osmotic pumps, computerised pumps andmethods using monoclonal antibodies andliposomes as carriers.Ocusert Ocusert systems are thin ellipticalunits that contain the drug in a reservoirwhich slowly releases the drug through amembrane by diffusion at a steady rate, e.g.pilocarpine ocusert used in glaucoma isplaced under the lid and can deliverpilocarpine for 7 days.Progestasert is inserted into the uterus whereit delivers progesterone constantly for overone year.Transdermal adhesive units See page 7.
Prodrug is an inactive form of a drug whichgets metabolised to the active derivative inthe body. A prodrug may overcome someof the disadvantages of the conventionalforms of drug administration, e.g. dopaminedoes not cross the BBB; levodopa, a prodrugcrosses the BBB and is then converted todopamine in the CNS. Prodrugs may also beused to achieve longer duration of action,e.g. Bacampicillin (a prodrug of ampicillin)is longer acting than ampicillin.Cyclophosphamide - an anticancer drug -gets converted to its active metabolitealdophosphamide in the liver. This allowsoral administration of cyclophosphamidewithout causing much gastrointestinaltoxicity. Zidovudine is taken up by virusinfected cells and gets activated in these cells.This results in selective toxicity to infectedcells. A prodrug may be more stable at gastric
pH, e.g. aspirin is converted to salicylic acidwhich is the active drug and aspirin is bettertolerated than salicylic acid.Osmotic pumps– are small tablet shaped unitscontaining the drug and an osmotic substancein two different chambers. The tablet iscoated with a semipermeable membrane inwhich a minute laser-drilled hole is made.When the tablet is swallowed and reachesthe gut, water enters into the tablet throughthe semipermeable membrane. The osmoticlayer swells and pushes the drug slowly outof the laser-drilled orifice. This allows slowand constant delivery of the drug over a longperiod of time. It is also calledGastrointestinal Therapeutic System (GITS).Some drugs available in this formulation areiron and prazosin.Computerised miniature pumps These areprogrammed to release drugs at a definiterate either continuously as in case of insulinor intermittently in pulses as in case ofGnRH.
Various methods of drug targeting aretried especially for anticancer drugs toreduce toxicity.Monoclonal antibodies against the tumorspecific antigens are used to deliveranticancer drugs to specific tumor cells.Liposomes are phospholipids suspendedin aqueous vehicles to form minute vesicles.Drugs encapsulated in liposomes are taken upmainly by the reticuloendothelial cells of theliver and are also concentrated in malignanttumors. Thus site-specific delivery of drugsmay be possible with the help of liposomes.
Textbook of Pharmacology for Dental and Allied Health Sciences10
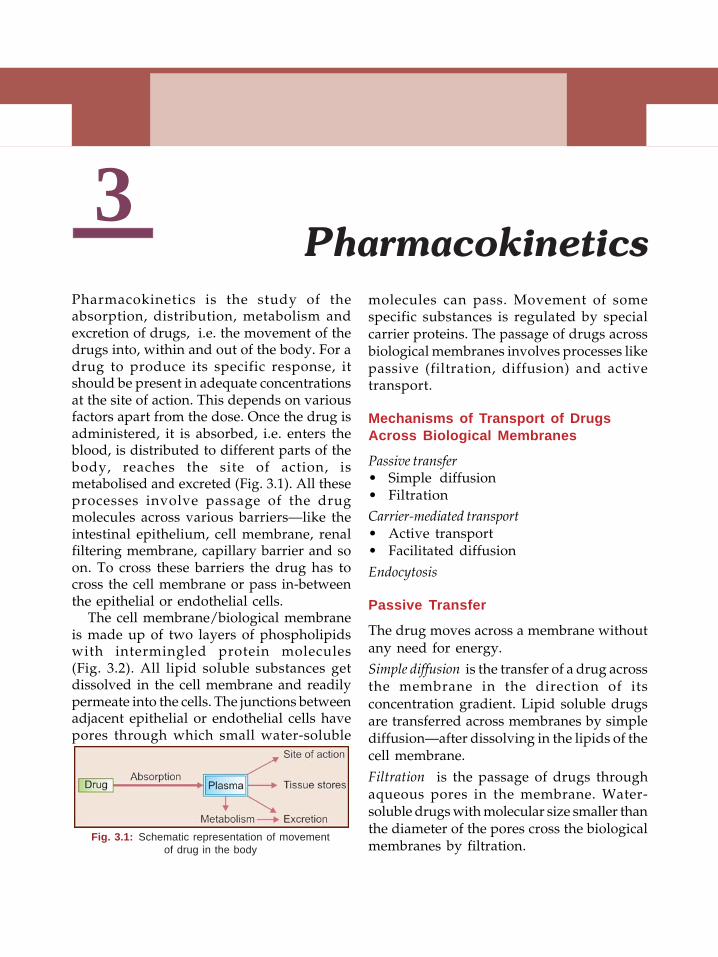
3Pharmacokinetics is the study of theabsorption, distribution, metabolism andexcretion of drugs, i.e. the movement of thedrugs into, within and out of the body. For adrug to produce its specific response, itshould be present in adequate concentrationsat the site of action. This depends on variousfactors apart from the dose. Once the drug isadministered, it is absorbed, i.e. enters theblood, is distributed to different parts of thebody, reaches the site of action, ismetabolised and excreted (Fig. 3.1). All theseprocesses involve passage of the drugmolecules across various barriers—like theintestinal epithelium, cell membrane, renalfiltering membrane, capillary barrier and soon. To cross these barriers the drug has tocross the cell membrane or pass in-betweenthe epithelial or endothelial cells.
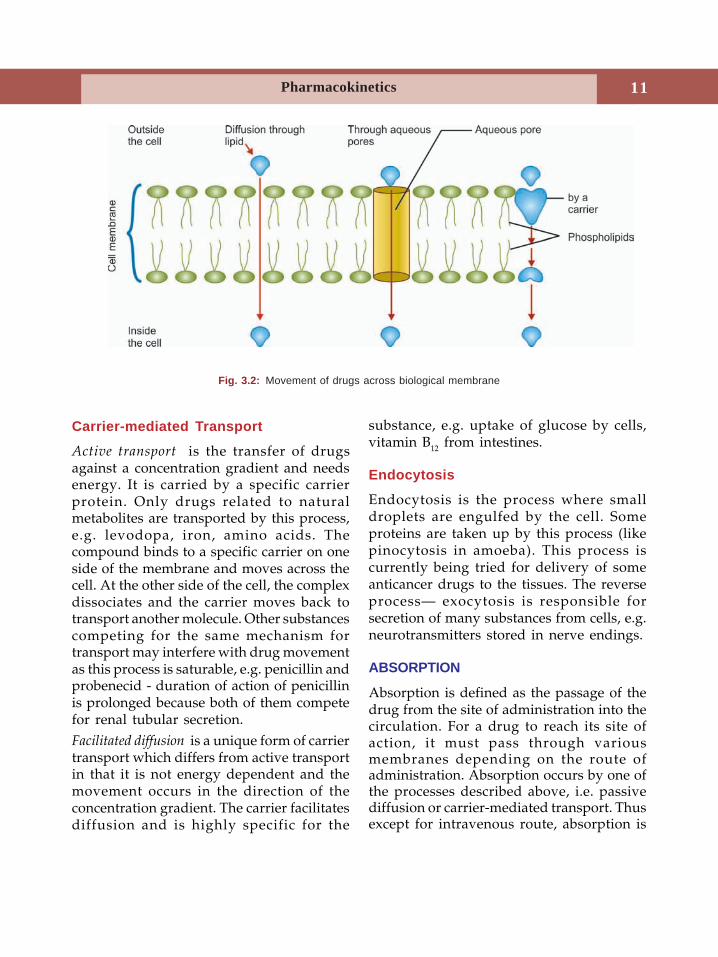
The cell membrane/biological membraneis made up of two layers of phospholipidswith intermingled protein molecules(Fig. 3.2). All lipid soluble substances getdissolved in the cell membrane and readilypermeate into the cells. The junctions betweenadjacent epithelial or endothelial cells havepores through which small water-soluble
molecules can pass. Movement of somespecific substances is regulated by specialcarrier proteins. The passage of drugs acrossbiological membranes involves processes likepassive (filtration, diffusion) and activetransport.
Mechanisms of Transport of DrugsAcross Biological Membranes
Passive transfer• Simple diffusion• FiltrationCarrier-mediated transport• Active transport• Facilitated diffusion
Endocytosis
Passive Transfer
The drug moves across a membrane withoutany need for energy.Simple diffusion is the transfer of a drug acrossthe membrane in the direction of itsconcentration gradient. Lipid soluble drugsare transferred across membranes by simplediffusion—after dissolving in the lipids of thecell membrane.
Filtration is the passage of drugs throughaqueous pores in the membrane. Water-soluble drugs with molecular size smaller thanthe diameter of the pores cross the biologicalmembranes by filtration.
Pharmacokinetics
Fig. 3.1: Schematic representation of movementof drug in the body
Pharmacokinetics 11
Carrier-mediated Transport
Active transport is the transfer of drugsagainst a concentration gradient and needsenergy. It is carried by a specific carrierprotein. Only drugs related to naturalmetabolites are transported by this process,e.g. levodopa, iron, amino acids. Thecompound binds to a specific carrier on oneside of the membrane and moves across thecell. At the other side of the cell, the complexdissociates and the carrier moves back totransport another molecule. Other substancescompeting for the same mechanism fortransport may interfere with drug movementas this process is saturable, e.g. penicillin andprobenecid - duration of action of penicillinis prolonged because both of them competefor renal tubular secretion.Facilitated diffusion is a unique form of carriertransport which differs from active transportin that it is not energy dependent and themovement occurs in the direction of theconcentration gradient. The carrier facilitatesdiffusion and is highly specific for the
substance, e.g. uptake of glucose by cells,vitamin B12 from intestines.
Endocytosis
Endocytosis is the process where smalldroplets are engulfed by the cell. Someproteins are taken up by this process (likepinocytosis in amoeba). This process iscurrently being tried for delivery of someanticancer drugs to the tissues. The reverseprocess— exocytosis is responsible forsecretion of many substances from cells, e.g.neurotransmitters stored in nerve endings.
ABSORPTION
Absorption is defined as the passage of thedrug from the site of administration into thecirculation. For a drug to reach its site ofaction, it must pass through variousmembranes depending on the route ofadministration. Absorption occurs by one ofthe processes described above, i.e. passivediffusion or carrier-mediated transport. Thusexcept for intravenous route, absorption is
Fig. 3.2: Movement of drugs across biological membrane
Textbook of Pharmacology for Dental and Allied Health Sciences12
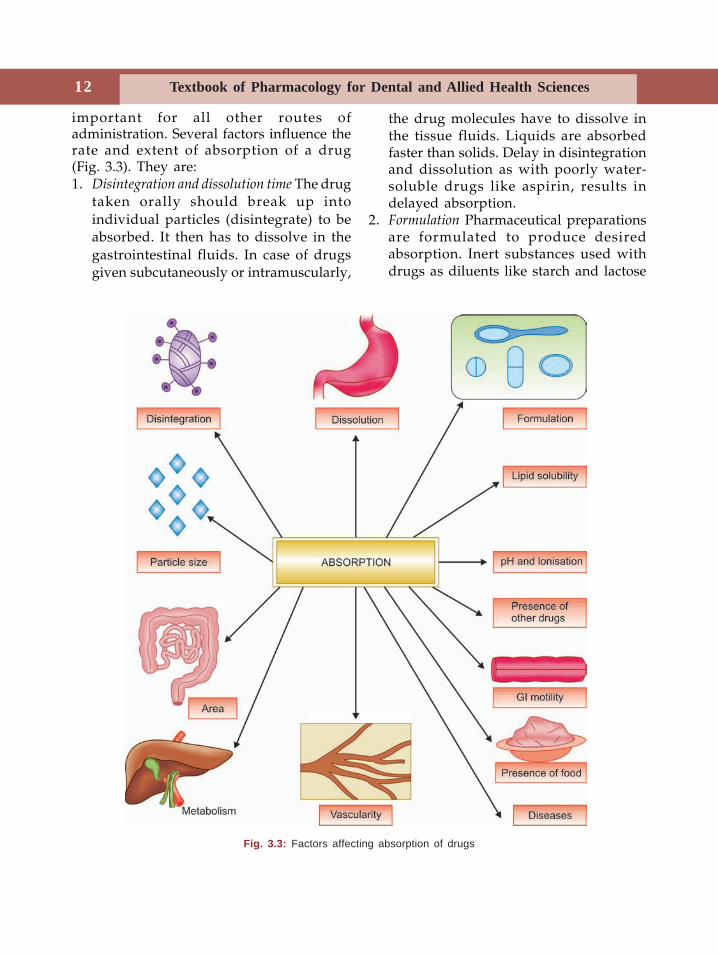
important for all other routes ofadministration. Several factors influence therate and extent of absorption of a drug(Fig. 3.3). They are:1. Disintegration and dissolution time The drug
taken orally should break up intoindividual particles (disintegrate) to beabsorbed. It then has to dissolve in thegastrointestinal fluids. In case of drugsgiven subcutaneously or intramuscularly,
the drug molecules have to dissolve inthe tissue fluids. Liquids are absorbedfaster than solids. Delay in disintegrationand dissolution as with poorly water-soluble drugs like aspirin, results indelayed absorption.
2. Formulation Pharmaceutical preparationsare formulated to produce desiredabsorption. Inert substances used withdrugs as diluents like starch and lactose
Fig. 3.3: Factors affecting absorption of drugs
Pharmacokinetics 13
may sometimes interfere with absorption.3. Particle size Small particle size is important
for better absorption of drugs. Drugs likecorticosteroids, griseofulvin, digoxin,aspirin and tolbutamide are betterabsorbed when given as small particles.On the other hand, when a drug has toact on the gut and its absorption is notdesired, then particle size should be keptlarge, e.g. anthelmintics like bepheniumhydroxynaphthoate.
4. Lipid solubility Lipid soluble drugs areabsorbed faster and better by dissolvingin the phospholipids of the cell membrane.
5. pH and ionisation Ionised drugs are poorlyabsorbed while unionised drugs are lipidsoluble and are well absorbed. Mostdrugs are weak electrolytes and exist inboth ionized and unionized forms. But thedegree of ionisation depends on the pH.Thus acidic drugs remain unionised in theacidic medium of the stomach and arerapidly absorbed from the stomach, e.g.aspirin, barbiturates. Basic drugs areunionised when they reach the alkalinemedium of the intestine from where theyare rapidly absorbed, e.g. pethidine,ephedrine.
Strong acids and bases are highlyionised and therefore poorly absorbed,e.g. heparin, streptomycin.
6. Area and vascularity of the absorbing surface
The larger the area of absorbing surfaceand more the vascularity—better is theabsorption. Thus most drugs are absorbedfrom the small intestine.
7. Gastrointestinal motilityGastric emptying time—if gastric
emptying is faster, the passage of the drugto the intestines is quicker and henceabsorption is faster.
Intestinal motility—when highlyincreased as in diarrhoeas, drugabsorption is reduced.
8. Presence of food delays gastric emptying,dilutes the drug and delays absorption.Drugs may form complexes with foodconstituents and such complexes arepoorly absorbed, e.g. tetracyclines chelatecalcium present in the food because ofwhich their bioavailability is decreased.Moreover, certain drugs like ampicillin,roxithromycin and rifampicin are wellabsorbed only on empty stomach.
9. Metabolism Some drugs may be degradedin the GI tract, e.g. nitroglycerine, insulin.Such drugs should be given in higherdoses or by alternative routes.
10. Diseases of the gut like malabsorption andachlorhydria result in reduced absorptionof drugs.
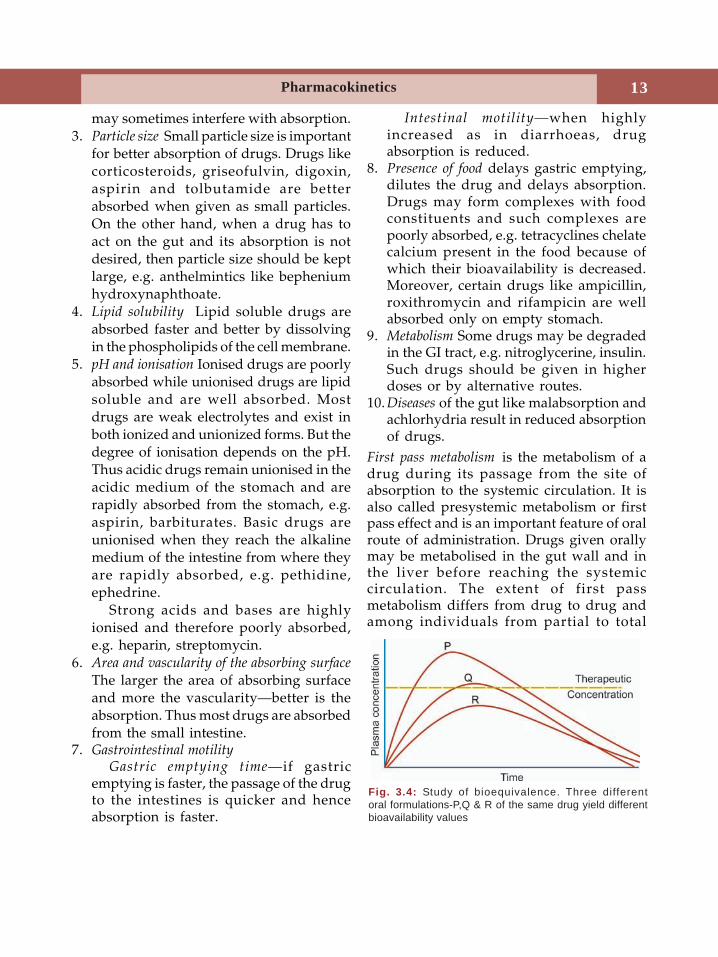
First pass metabolism is the metabolism of adrug during its passage from the site ofabsorption to the systemic circulation. It isalso called presystemic metabolism or firstpass effect and is an important feature of oralroute of administration. Drugs given orallymay be metabolised in the gut wall and inthe liver before reaching the systemiccirculation. The extent of first passmetabolism differs from drug to drug andamong individuals from partial to total
Fig. 3.4: Study of bioequivalence. Three differentoral formulations-P,Q & R of the same drug yield differentbioavailability values

Textbook of Pharmacology for Dental and Allied Health Sciences14
inactivation. When it is partial, it can becompensated by giving higher dose of theparticular drug, e.g. nitroglycerine,propranolol, salbutamol. But for drugs thatundergo complete first pass metabolism, theroute of administration has to be changed,e.g. isoprenaline, hydrocortisone, insulin.Bioavailability of many drugs is increased inpatients with liver disease due to reductionin hepatic metabolism.
First Pass Metabolism
• is metabolism of a drug during its firstpassage through gut wall and liver
• reduces bioavailability• extent of metabolism depends on the
drug and individuals• measures to compensate first pass
effect— dose has to be increased for somedrugs like propranolol— route has to be changed for someothers like hydrocortisone
• Examples: morphine, chlorpromazine,nitroglycerine, verapamil, testos-terone, insulin, lignocaine.
Bioavailability
Bioavailability is the fraction of the drug thatreaches the systemic circulation followingadministration by any route. Thus for a druggiven intravenously, the bioavailability is100%. On IM/SC injection, drugs are almostcompletely absorbed while by oral route,bioavailability may be low due to incompleteabsorption and first pass metabolism. Forexample bioavailability of chlortetracyclineis 30%, carbamazepine 70%, chloroquine80%, minocycline and diazepam 100%.Transdermal preparations are absorbedsystemically and may have 80-100%bioavailability. Infact all the ten factors whichinfluence the absorption of a drug also alter
the bioavailability. Large bioavailabilityvariations of a drug particularly when it isunpredictable can result in toxicity ortherapeutic failure as in case of halofantrine.
Bioequivalence
Comparison of bioavailability of differentformulations of the same drug is the studyof bioequivalence. Often oral formulationscontaining the same amount of a drug fromdifferent manufacturers may result indifferent plasma concentrations, i.e. there isno bioequivalence among them (Fig. 3.4.)Such differences occur with poorly soluble,slowly absorbed drugs mainly due todifferences in the rate of disintegration anddissolution. Variations in bioavailability(nonequivalence) can result in toxicity ortherapeutic failure in drugs that have lowsafety margin like digoxin and drugs thatneed precise dose adjustment likeanticoagulants and corticosteroids. For suchdrugs, in a given patient, the preparationsfrom a single manufacturer should be used.
DISTRIBUTION
After a drug reaches the systemic circulation,it gets distributed to other tissues. It shouldcross several barriers before reaching the siteof action. Like absorption, distribution alsoinvolves the same processes, i.e. filtration,diffusion and specialised transport. Variousfactors determine the rate and extent ofdistribution, viz lipid solubility, ionisation,blood flow and binding to plasma proteinsand cellular proteins. Unionised lipid solubledrugs are widely distributed throughout thebody.
Plasma Protein Binding
On reaching the circulation most drugs bindto plasma proteins; acidic drugs bind mainlyalbumin and basic drugs to alpha-acid
Pharmacokinetics 15
glycoprotein. The free or unbound fractionof the drug is the only form available foraction, metabolism and excretion while theprotein bound form serves as a reservoir. Theextent of protein binding varies with eachdrug, e.g. warfarin is 99% and morphine is35% protein bound while binding ofethosuximide and lithium is 0%, i.e. they aretotally free (Table 3.1).
Clinical Significance of Plasma Protein Binding
1. Only free fraction is available for action,metabolism and excretion. When the freedrug levels in the plasma fall, bound drugis released.
2. Protein binding serves as a store(reservoir) of the drug and the drug isreleased when free drug levels fall.
3. Protein binding prolongs the duration ofaction of the drug.
4. Many drugs may compete for the samebinding sites. Thus one drug maydisplace another from the binding sitesand result in displacement interactions,e.g. warfarin is 99% protein bound (i.e.free fraction is 1%). If another drug likeindomethacin reduces its binding to 95%,the free form then becomes 5% whichmeans, there is a 5-fold increase in freewarfarin levels which could result intoxicity. Fortunately the body largelycompensates by enhancing metabolismand excretion.
5. Chronic renal failure and chronic liverdisease result in hypoalbuminaemia withreduced protein binding of drugs. Highlyprotein bound drugs should be carefullyused in such patients.
Table 3.1: Some highly protein bound drugs
Warfarin Tolbutamide PhenytoinFrusemide Clofibrate SulfonamidesDiazepam Salicylates PhenylbutazoneIndomethacin
Tissue binding Some drugs get bound tocertain tissue constituents because of specialaffinity for them. Tissue binding delayselimination and thus prolongs the durationof action of the drug. For example, lipidsoluble drugs are bound to adipose tissue.Tissue binding also serves as a reservoir ofthe drug.
Tissue Binding drugs
Adipose tissue Thiopentone sodium,benzodiazepines
Muscles EmetineBone Tetracyclines, LeadRetina ChloroquineThyroid Iodine
Redistribution When some highly lipid solubledrugs are given intravenously or byinhalation, they get rapidly distributed intohighly perfused tissues like brain, heart andkidney. But soon they get redistributed intoless vascular tissues like the muscle and fatresulting in termination of the action of thesedrugs. The best example is the intravenousanaesthetic thiopental sodium which inducesanaesthesia in 10-20 seconds but the effectceases in 5-15 minutes due to redistribution.
Blood-brain barrier (BBB) The endothelial cellsof the brain capillaries lack intercellular poresand instead have tight junctions. Moreover,glial cells envelop the capillaries and togetherthese form the BBB. Only lipid soluble,unionised drugs can cross this BBB. Duringinflammation of the meninges, the barrierbecomes more permeable to drugs, e.g.penicillin readily penetrates duringmeningitis. The barrier is weak at some areaslike the CTZ, posterior pituitary and partsof hypothalamus and allows somecompounds to diffuse.Placental barrier Lipid soluble, unionised drugsreadily cross the placenta while lipidinsoluble drugs cross to a much lesser extent.
Textbook of Pharmacology for Dental and Allied Health Sciences16
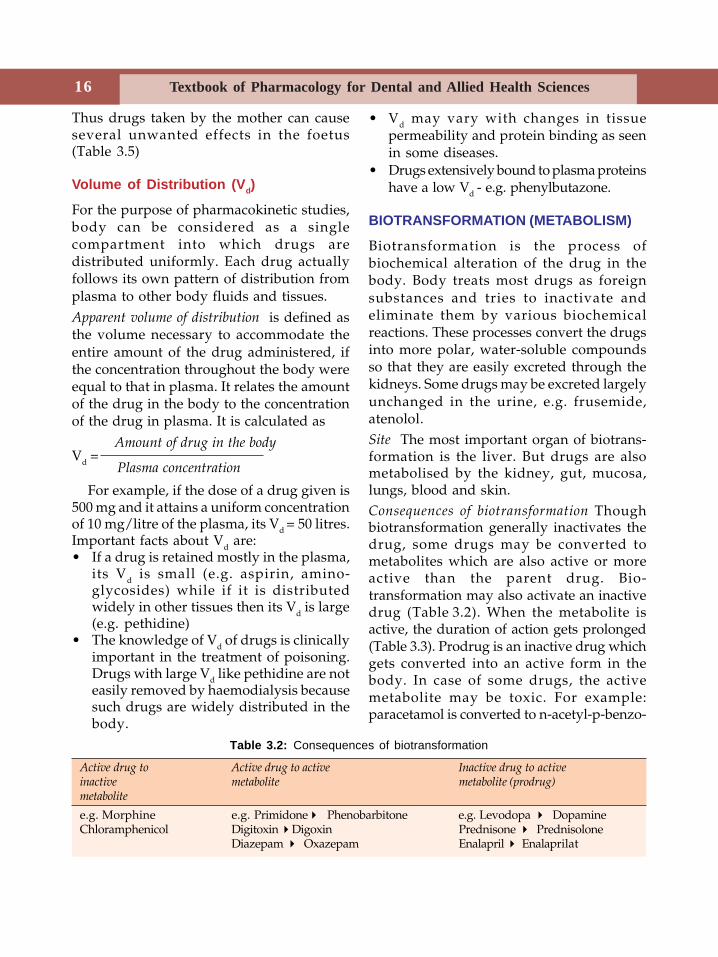
Table 3.2: Consequences of biotransformation
Active drug to Active drug to active Inactive drug to activeinactive metabolite metabolite (prodrug)metabolite
e.g. Morphine e.g. PrimidonePhenobarbitone e.g. Levodopa DopamineChloramphenicol Digitoxin Digoxin Prednisone Prednisolone
Diazepam Oxazepam Enalapril Enalaprilat
Thus drugs taken by the mother can causeseveral unwanted effects in the foetus(Table 3.5)
Volume of Distribution (Vd)
For the purpose of pharmacokinetic studies,body can be considered as a singlecompartment into which drugs aredistributed uniformly. Each drug actuallyfollows its own pattern of distribution fromplasma to other body fluids and tissues.Apparent volume of distribution is defined asthe volume necessary to accommodate theentire amount of the drug administered, ifthe concentration throughout the body wereequal to that in plasma. It relates the amountof the drug in the body to the concentrationof the drug in plasma. It is calculated as
Amount of drug in the bodyVd =
Plasma concentration
For example, if the dose of a drug given is500 mg and it attains a uniform concentrationof 10 mg/litre of the plasma, its Vd = 50 litres.Important facts about Vd are:• If a drug is retained mostly in the plasma,
its Vd is small (e.g. aspirin, amino-glycosides) while if it is distributedwidely in other tissues then its Vd is large(e.g. pethidine)
• The knowledge of Vd of drugs is clinicallyimportant in the treatment of poisoning.Drugs with large Vd like pethidine are noteasily removed by haemodialysis becausesuch drugs are widely distributed in thebody.
• Vd may vary with changes in tissuepermeability and protein binding as seenin some diseases.
• Drugs extensively bound to plasma proteinshave a low Vd - e.g. phenylbutazone.
BIOTRANSFORMATION (METABOLISM)
Biotransformation is the process ofbiochemical alteration of the drug in thebody. Body treats most drugs as foreignsubstances and tries to inactivate andeliminate them by various biochemicalreactions. These processes convert the drugsinto more polar, water-soluble compoundsso that they are easily excreted through thekidneys. Some drugs may be excreted largelyunchanged in the urine, e.g. frusemide,atenolol.Site The most important organ of biotrans-formation is the liver. But drugs are alsometabolised by the kidney, gut, mucosa,lungs, blood and skin.Consequences of biotransformation Thoughbiotransformation generally inactivates thedrug, some drugs may be converted tometabolites which are also active or moreactive than the parent drug. Bio-transformation may also activate an inactivedrug (Table 3.2). When the metabolite isactive, the duration of action gets prolonged(Table 3.3). Prodrug is an inactive drug whichgets converted into an active form in thebody. In case of some drugs, the activemetabolite may be toxic. For example:paracetamol is converted to n-acetyl-p-benzo-
Pharmacokinetics 17
quinoneimine which causes hepatotoxicity;cyclophosphamide is converted to acroleinwhich causes bladder toxicity.Enzymes in biotransformation The biotrans-formation reactions are catalysed by specificenzymes located either in the livermicrosomes (microsomal enzymes) or in thecytoplasm and mitochondria of the liver cellsand also in the plasma and other tissues (non-microsomal enzymes).
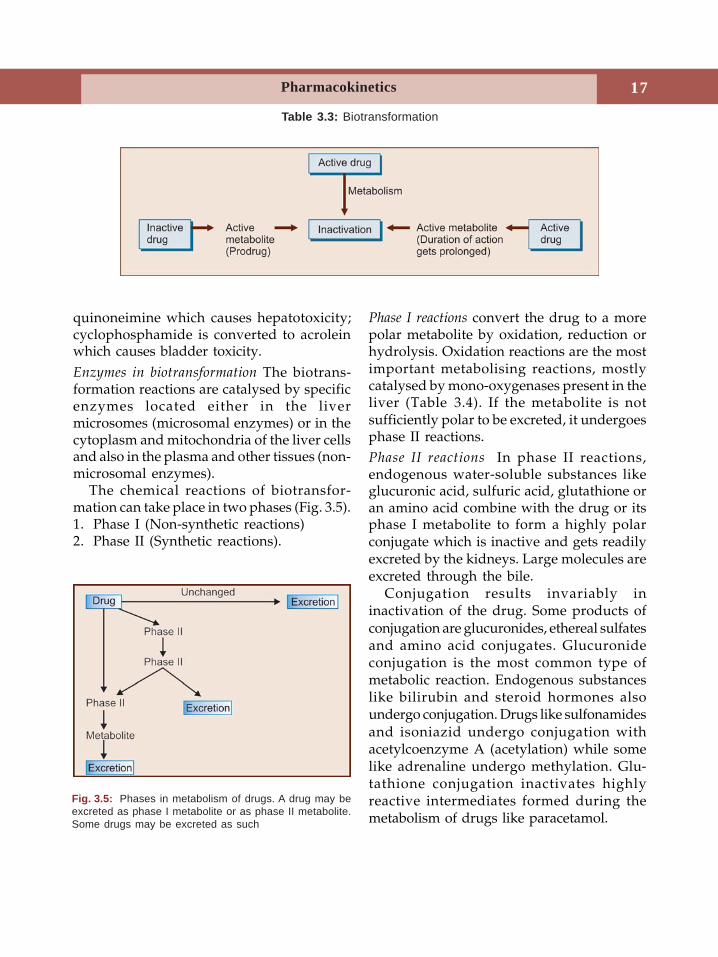
The chemical reactions of biotransfor-mation can take place in two phases (Fig. 3.5).1. Phase I (Non-synthetic reactions)2. Phase II (Synthetic reactions).
Phase I reactions convert the drug to a morepolar metabolite by oxidation, reduction orhydrolysis. Oxidation reactions are the mostimportant metabolising reactions, mostlycatalysed by mono-oxygenases present in theliver (Table 3.4). If the metabolite is notsufficiently polar to be excreted, it undergoesphase II reactions.Phase II reactions In phase II reactions,endogenous water-soluble substances likeglucuronic acid, sulfuric acid, glutathione oran amino acid combine with the drug or itsphase I metabolite to form a highly polarconjugate which is inactive and gets readilyexcreted by the kidneys. Large molecules areexcreted through the bile.
Conjugation results invariably ininactivation of the drug. Some products ofconjugation are glucuronides, ethereal sulfatesand amino acid conjugates. Glucuronideconjugation is the most common type ofmetabolic reaction. Endogenous substanceslike bilirubin and steroid hormones alsoundergo conjugation. Drugs like sulfonamidesand isoniazid undergo conjugation withacetylcoenzyme A (acetylation) while somelike adrenaline undergo methylation. Glu-tathione conjugation inactivates highlyreactive intermediates formed during themetabolism of drugs like paracetamol.
Fig. 3.5: Phases in metabolism of drugs. A drug may beexcreted as phase I metabolite or as phase II metabolite.Some drugs may be excreted as such
Table 3.3: Biotransformation
Textbook of Pharmacology for Dental and Allied Health Sciences18
ENZYME INDUCTION
Microsomal enzymes are located in themicrosomes that line the smooth endoplasmicreticulum of the liver cells. The synthesis ofthese enzymes, mainly cytochrome P450 canbe enhanced by certain drugs and enviro-nmental pollutants. This is called enzymeinduction and this process speeds up thebiotransformation of the inducing drug itselfand other drugs metabolised by themicrosomal enzymes, e.g. phenobarbitone,rifampicin, alcohol, cigarette smoke, DDT,griseofulvin, carbamazepine and phenytoinare some enzyme inducers.
Clinical relevance of microsomal enzymeinduction:1. Drug interactions
a. Therapeutic failure - By speeding upmetabolism, enzyme induction mayreduce the duration of action of someother drugs which can result intherapeutic failure, e.g. failure of oralcontraceptives in patients taking rifam-picin.
b. Toxicity - Enzyme induction may resultin toxicity due to production of higheramounts of the toxic intermediatemetabolites, e.g. a patient undergoingtreatment with rifampicin is likely todevelop hepatotoxicity with paraceta-mol because a higher amount of the
toxic intermediate metabolite ofparacetamol is formed due to enzymeinduction.
2. Tolerance to drugs may develop as in case ofcarbamazepine since it induces its ownmetabolism called autoinduction.
3. Result in disease—antiepileptics enhance thebreakdown of vitamin D resulting inosteomalacia on long-term adminis-tration.
4. Variable response In chronic smokers andalcoholics, enzyme induction may resultin failure to achieve the expected responseto some drugs metabolised by the sameenzymes.
5. Therapeutic application of enzyme inductionNeonates are deficient in both microsomaland non-microsomal enzymes. Hence theircapacity to conjugate bilirubin is low whichresults in jaundice. Administration ofphenobarbitone - an enzyme inducer,helps in rapid clearance of the jaundice inthem by enhancing bilirubin conjugation.
Enzyme inhibition Some drugs inhibitcytochrome P450 enzyme activity. Drugs likecimetidine and ketoconazole bind tocytochrome P450 and thus competitivelyinhibit the metabolism of endogenoussubstances like testosterone and other drugsgiven concurrently. Enzyme inhibition bydrugs is the basis of several drug interactions.
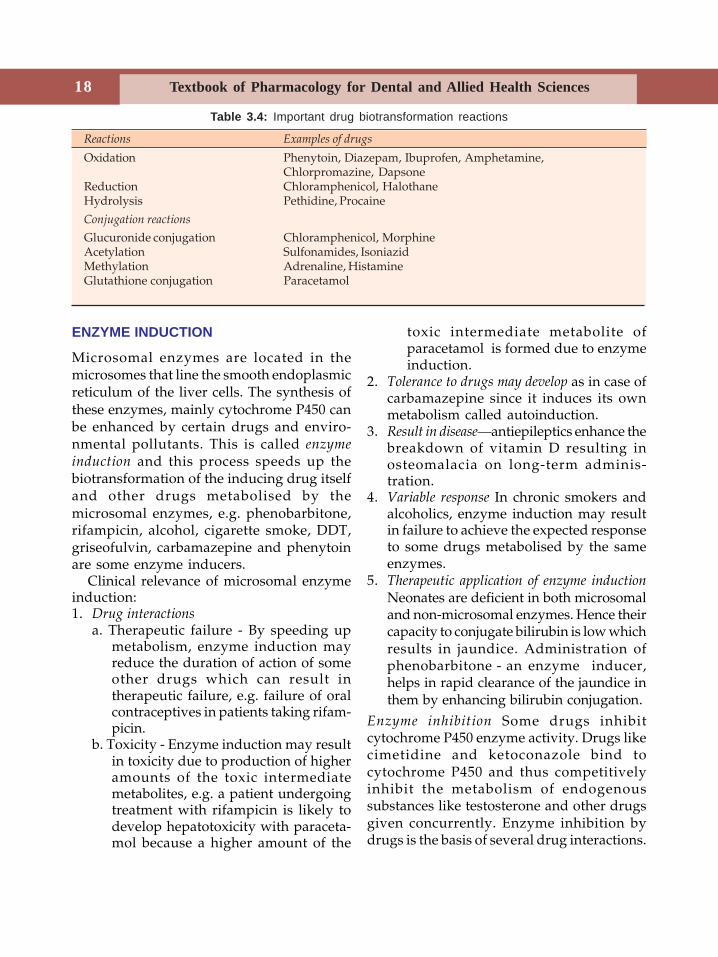
Table 3.4: Important drug biotransformation reactions
Reactions Examples of drugs
Oxidation Phenytoin, Diazepam, Ibuprofen, Amphetamine,Chlorpromazine, Dapsone
Reduction Chloramphenicol, HalothaneHydrolysis Pethidine, Procaine
Conjugation reactions
Glucuronide conjugation Chloramphenicol, MorphineAcetylation Sulfonamides, IsoniazidMethylation Adrenaline, HistamineGlutathione conjugation Paracetamol
Pharmacokinetics 19
Chloramphenicol, erythromycin, ketoco-nazole, cimetidine, ciprofloxacin andverapamil are some enzyme inhibitors.
Factors that Influence Biotransformation
Genetic variation results in altered metabolismof drugs, e.g. succinylcholine is metabolisedvery slowly in people with defectivepseudocholinesterase resulting in prolongedapnoea.Environmental pollutants like cigarette smokecause enzyme induction.Age At extremes of age, the activity ofmetabolic enzymes in the liver is low andhence there is increased risk of toxicity withdrugs.Diseases of the liver markedly affectmetabolism of drugs.
Drugs are excreted from the body afterbeing converted to water-soluble metaboliteswhile some are directly eliminated withoutmetabolism. The major organs of excretionare the kidneys, the intestine, the biliarysystem and the lungs. Drugs are alsoexcreted in small amounts in the saliva, sweatand milk.
EXCRETION
Renal Excretion
Kidney is the most important organ of drugexcretion. The three processes involved inthe elimination of drugs through kidneys areglomerular filtration, active tubular secretionand passive tubular reabsorption.Glomerular filtration The rate of filtrationthrough the glomerulus depends on GFR,concentration of free drug in the plasma andits molecular weight. Ionised drugs of lowmolecular weight (< 10,000) are easily filteredthrough the glomerular membrane.Active tubular secretion Cells of the proximaltubules actively secrete acids and bases bytwo transport systems. Thus acids like
penicillin, salicylic acid, probenecid,frusemide and bases like amphetamine andhistamine are so excreted. Drugs maycompete for the same transport systemresulting in prolongation of action of eachother, e.g. penicillin and probenecid.Passive tubular reabsorption Passive diffusionof drug molecules can occur in eitherdirection in the renal tubules depending onthe drug concentration, lipid solubility andpH. As highly lipid soluble drugs are largelyreabsorbed, their excretion is slow. Acidicdrugs get ionised in alkaline urine and areeasily excreted while bases are excretedfaster in acidic urine. This property is usefulin the treatment of poisoning. In poisoningwith acidic drugs like salicylates andbarbiturates, forced alkaline diuresis(Diuretic + sodium bicarbonate + IV fluids)is employed to hasten drug excretion.Similarly, elimination of basic drugs likequinine and amphetamine is enhanced byforced acid diuresis.
Faecal and Biliary Excretion
Unabsorbed portion of the orally adminis-tered drugs are eliminated through thefaeces. Liver transfers acids, bases andunionised molecules into bile by specific acidtransport processes. Large water-solubleconjugates are excreted in the bile. Somedrugs may get reabsorbed in the lowerportion of the gut and are carried back tothe liver. Such recycling is called enterohepaticcirculation and it prolongs the duration ofaction of the drug; examples are chloram-phenicol, tetracycline, oral contraceptives anderythromycin.
Pulmonary Excretion
The lungs are the main route of eliminationfor gases and volatile liquids viz. generalanaesthetics and alcohol. This also has legalimplications in medicolegal practice.
Textbook of Pharmacology for Dental and Allied Health Sciences20
Other Routes of Excretion
Small amounts of some drugs are eliminatedthrough the sweat and saliva. Excretion insaliva may result in a unique taste with somedrugs like phenytoin, clarithromycin;metallic taste with metronidazole,metoclopramide and disulfiram. Drugs likeiodide, rifampicin and heavy metals areexcreted through sweat.
The excretion of drugs in the milk is insmall amounts and is of no significance tothe mother. But, for the suckling infant, itmay be sometimes important especiallybecause of the infant’s immature metabolicand excretory mechanisms. Though mostdrugs can be taken by the mother withoutsignificant toxicity to the child, there are afew exceptions (Table 3.5).
CLINICAL PHARMACOKINETICS
The knowledge of pharmacokinetics isclinically useful for several purposesincluding selection and adjustment of thedosage regimen, and to obtain optimumeffects from a drug. The three mostimportant pharmacokinetic parameters arebioavailability (page 14), volume ofdistribution (page 16) and clearance.Clearance (CL) is the volume of plasma freedcompletely of the drug in unit time. It can becalculated by the ratio of the rate ofelimination to the plasma concentration.
Rate of eliminationThus, CL =
Plasma concentration
Clearance is expressed as ml/litre/unittime.
Clearance is the most important factordetermining drug concentration and shouldbe considered when any drug is intended forlong-term administration.
Drugs are metabolised/eliminated fromthe body by:
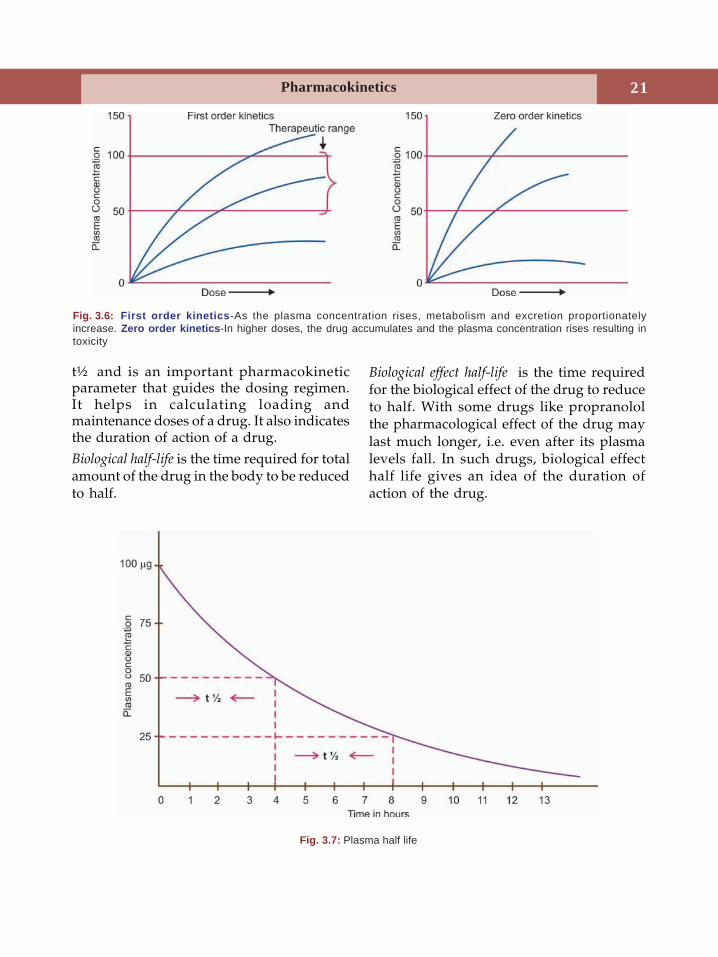
1. First-order kinetics In first order kinetics, aconstant fraction of the drug ismetabolised/eliminated per unittime. Most drugs follow first orderkinetics and the rate of metabolism/excretion is dependent on theirconcentration (exponential) in the body(Fig. 3.6). It also holds good forabsorption of drugs.
2. Zero order kinetics (Saturation kinetics) Herea constant amount of the drug present inthe body is metabolised/eliminated per unittime. The metabolic enzymes get saturatedand hence with increase in dose, the plasmadrug level increases disproportionatelyresulting in toxicity.
Some drugs like phenytoin and warfarinare eliminated by both processes, i.e. by firstorder initially and by zero order at higherconcentrations.Example of drugs that follow zero orderkinetics:• Alcohol• Phenytoin• Aspirin• Heparin• Phenylbutazone.
Plasma Half-life and SteadyState Concentration
Plasma half-life (t½) is the time taken for theplasma concentration of a drug to be reducedto half it’s value (Fig. 3.7). Four to five half-lives are required for the completeelimination of a drug. Each drug has its own
Table 3.5: Example of drugs that could be toxic tothe suckling infant when taken by the mother
Sulphasalazine DoxepinTheophylline AmiodaroneAnticancer drugs PrimidoneSalicylates EthosuximideChloramphenicol PhenobarbitoneNalidixic acid PhenothiazinesNitrofurantoin β-blockers
Pharmacokinetics 21
t½ and is an important pharmacokineticparameter that guides the dosing regimen.It helps in calculating loading andmaintenance doses of a drug. It also indicatesthe duration of action of a drug.
Biological half-life is the time required for totalamount of the drug in the body to be reducedto half.
Biological effect half-life is the time requiredfor the biological effect of the drug to reduceto half. With some drugs like propranololthe pharmacological effect of the drug maylast much longer, i.e. even after its plasmalevels fall. In such drugs, biological effecthalf life gives an idea of the duration ofaction of the drug.
Fig. 3.6: First order kinetics-As the plasma concentration rises, metabolism and excretion proportionatelyincrease. Zero order kinetics-In higher doses, the drug accumulates and the plasma concentration rises resulting intoxicity
Fig. 3.7: Plasma half life
Textbook of Pharmacology for Dental and Allied Health Sciences22
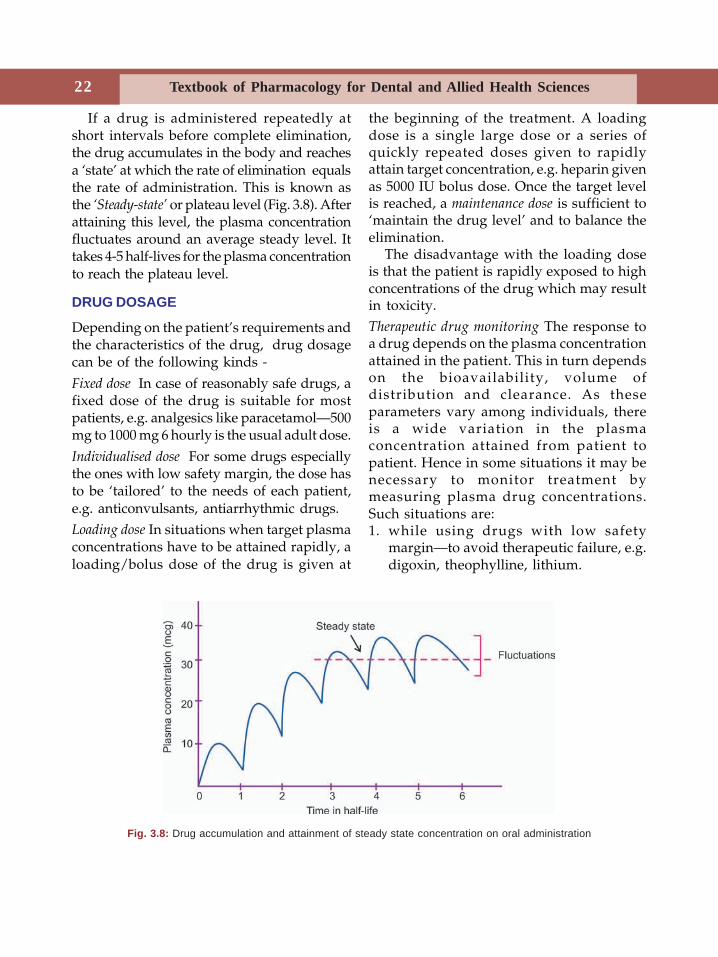
If a drug is administered repeatedly atshort intervals before complete elimination,the drug accumulates in the body and reachesa ‘state’ at which the rate of elimination equalsthe rate of administration. This is known asthe ‘Steady-state’ or plateau level (Fig. 3.8). Afterattaining this level, the plasma concentrationfluctuates around an average steady level. Ittakes 4-5 half-lives for the plasma concentrationto reach the plateau level.
DRUG DOSAGE
Depending on the patient’s requirements andthe characteristics of the drug, drug dosagecan be of the following kinds -
Fixed dose In case of reasonably safe drugs, afixed dose of the drug is suitable for mostpatients, e.g. analgesics like paracetamol—500mg to 1000 mg 6 hourly is the usual adult dose.
Individualised dose For some drugs especiallythe ones with low safety margin, the dose hasto be ‘tailored’ to the needs of each patient,e.g. anticonvulsants, antiarrhythmic drugs.Loading dose In situations when target plasmaconcentrations have to be attained rapidly, aloading/bolus dose of the drug is given at
the beginning of the treatment. A loadingdose is a single large dose or a series ofquickly repeated doses given to rapidlyattain target concentration, e.g. heparin givenas 5000 IU bolus dose. Once the target levelis reached, a maintenance dose is sufficient to‘maintain the drug level’ and to balance theelimination.
The disadvantage with the loading doseis that the patient is rapidly exposed to highconcentrations of the drug which may resultin toxicity.Therapeutic drug monitoring The response toa drug depends on the plasma concentrationattained in the patient. This in turn dependson the bioavailability, volume ofdistribution and clearance. As theseparameters vary among individuals, thereis a wide variation in the plasmaconcentration attained from patient topatient. Hence in some situations it may benecessary to monitor treatment bymeasuring plasma drug concentrations.Such situations are:1. while using drugs with low safety
margin—to avoid therapeutic failure, e.g.digoxin, theophylline, lithium.
Fig. 3.8: Drug accumulation and attainment of steady state concentration on oral administration
Pharmacokinetics 23
2. to reduce the risk of toxicity, e.g.aminoglycosides.
3. when there are no reliable methods toassess benefit, e.g. antidepressants.
4. to treat poisoning.5. when there is unexplainable therapeutic
failure—to check patient compliance.But, for drugs whose response can be
easily measured, e.g. blood pressure for anti-hypertensives and for ‘hit and run’drugs whose effects persist for a longtime even after the drug is eliminated,monitoring of plasma drug concentration isnot required.
Methods of Prolonging Drug Action(Table 3.6)In several situations it may be desirable touse long-acting drugs. But when such drugsare not available, the duration of action of theavailable drugs may be prolonged.
The duration of action of drugs can beprolonged by interfering with thepharmacokinetic processes, i.e. by1. slowing absorption.2. using a more plasma protein bound
derivative.3. inhibiting metabolism.4. delaying excretion.
Table 3.6: Methods of prolonging duration of action of drugs
Processes Methods Examples
AbsorptionOral Sustained release preparation, Iron, deriphylline
coating with resins, etc.Parenteral 1. Reducing solubility Procaine + Penicillin
— Oily suspension Depot progestins2. Altering particle size-given as Insulin zinc suspension
large crystals that are slowly absorbed3. Pellet implantation DOCA
— Sialistic capsules Testosterone4. Reduction in vascularity Adrenaline + lignocaine
of the absorbing surface (vasoconstrictor)5. Combining with protein Protamine + zinc + insulin6. Chemical alteration
— Esterification OestrogenTestosterone
Dermal Transdermal adhesive patches, ScopolamineOintments Nitroglycerin
Ocuserts (Transmucosal)—used in eye Pilocarpine
Distribution Choosing more protein bound Sulfonamides-likemember of the group sulfamethoxypyridazine
Metabolism Inhibiting the metabolising Physostigmine prolongsenzyme cholinesterase the action of acetylcholineBy inhibiting enzyme peptidase Cilastatin—prolongs thein renal tubular cells action of imipenem
Excretion Competition for same transport system Probenecid prolongs the— for renal tubular secretion action of penicillin and ampicillin
Textbook of Pharmacology for Dental and Allied Health Sciences24
4Pharmacodynamics is the study of actions ofthe drugs on the body and their mechanismsof action, i.e. to know what drugs do andhow they do it.
Drugs produce their effects by interactingwith the physiological systems of theorganisms. By such interaction, drugs merelymodify the rate of functions of the varioussystems. But they cannot bring aboutqualitative changes, i.e. they cannot changethe basic functions of any physiologicalsystem. Thus drugs act by:1. Stimulation2. Depression3. Irritation4. Replacement5. Anti-infective or cytotoxic action6. Modification of the immune status.Stimulation is the increase in activity of thespecialised cells, e.g. adrenaline stimulates theheart.Depression is the decrease in activity of thespecialised cells, e.g. quinidine depresses theheart; barbiturates depress the centralnervous system. Some drugs may stimulateone system and depress another, e.g.morphine depresses the CNS but stimulatesthe vagus.Irritation: This can occur on all types of tissuesin the body and may result in inflammation,corrosion and necrosis of cells.Replacement: Drugs may be used forreplacement when there is deficiency ofnatural substances like hormones, metabolites
or nutrients, e.g. insulin in diabetes mellitus,iron in anaemia, vitamin C in scurvy.Anti-infective and cytotoxic action: Drugs mayact by specifically destroying infectiveorganisms, e.g. penicillins, or by cytotoxiceffect on cancer cells, e.g. anticancer drugs.Modification of immune status: Vaccines andsera act by improving our immunity whileimmunosuppressants act by depressingimmunity, e.g. glucocorticoids.
MECHANISMS OF DRUG ACTION
Most drugs produce their effects by binding tospecific target proteins like receptors, enzymesand ion channels. Drugs may act on the cellmembrane, inside or outside the cell to producetheir effect. Drugs may act by one or morecomplex mechanisms of action. Some of themare yet to be understood. But the fundamentalmechanisms of drug action may be:• through receptors• through enzymes and pumps• through ion channels• by physical action• by chemical interaction• by altering metabolic processes.
Through Receptors
Drugs may act by interacting with specificreceptors in the body (see below).
Through Enzymes and Pumps
Drugs may act by inhibition of variousenzymes, thus altering the enzyme-mediated
Pharmacodynamics
Pharmacodynamics 25
reactions, e.g. allopurinol inhibits the enzymexanthine oxidase; acetazolamide inhibitscarbonic anhydrase, enalapril inhibitsangiotensin converting enzyme, aspirininhibits cyclo-oxygenase, neostigmine inhibitsacetylcholinesterase.
Membrane pumps like H+ K+ ATPase andNa+ K+ ATPase may be inhibited by drugslike omeprazole and digoxin respectively.
Through Ion Channels
Drugs may interfere with the movement ofions across specific channels, e.g. calciumchannel blockers, sodium channel blockers,potassium channel openers and GABA gatedchloride channel modulators.
Physical Action
The action of a drug could result from itsphysical properties like:
Adsorption – Activated charcoalin poisoning
Mass of the drug – Bulk laxatives likepsyllium, bran
Osmotic property – Osmotic diuretics -Mannitol
– Osmoticpurgatives-Magnesiumsulphate
Radioactivity – 131IRadio-opacity – Barium sulphate
contrast media.
Chemical Interaction
Drugs may act by chemical reaction.Antacids – neutralise gastric
acidsOxidising agents – like potassium
permanganate isgermicidal
Chelating agents – bind heavy metalsmaking themnontoxic.
Altering Metabolic Processes
Drugs like antimicrobials alter the metabolicpathway in the microorganisms resulting indestruction of the microorganism, e.g.sulfonamides interfere with bacterial folicacid synthesis.
RECEPTOR
The works of Langley and Ehrlich put forththe concept of a ‘receptor substance.’ In thelate 19th century, Langley noted that curarecould oppose contraction of skeletal musclescaused by nicotine but did not blockcontraction due to electrical stimulation. PaulEhrlich observed that some organic chemicalshad antiparasitic activity while others withslightly different structures did not have suchactivity. Clark put forward a theory toexplain the drug action based on the drug-receptor occupation.
Last three decades have seen an explosionin our knowledge of the receptors. Variousreceptors have been identified, isolated andextensively studied.Definition A receptor is a macromolecular siteon the cell with which an agonist binds tobring about a change.Affinity is the ability of a drug to bind to areceptor.Intrinsic activity or efficacy is the ability of adrug to elicit a response after binding to thereceptor.Agonist An agonist is a substance that binds tothe receptor and produces a response. It hasaffinity and intrinsic activity. E.g. adrenaline isan agonist at adrenergic receptors.Antagonist An antagonist is a substance thatbinds to the receptor and prevents the actionof the agonist on the receptor. It has affinity

Textbook of Pharmacology for Dental and Allied Health Sciences26
but no intrinsic activity. E.g. Tubocurarine isan antagonist at nicotinic receptors.Partial agonist binds to the receptor but haslow intrinsic activity. Pentazocine is a partialagonist at μ opioid receptors.Inverse agonist Some drugs, after binding tothe receptors produce actions opposite tothose produced by a pure agonist. They areknown as inverse agonists, e.g. Diazepamacting on benzodiazepine receptors producessedation, anxiolysis, muscle relaxation andcontrols convulsions, while inverse agonistsβ-carbolines bind to the same receptors tocause arousal, anxiety, increased muscle toneand convulsions.Ligand is a molecule which binds selectivelyto a specific receptor.Spare receptors Some experiments showed thathigh concentration of an agonist can stillproduce maximal response in presence of anirreversible antagonist and this was becauseof the presence of ‘spare’ or reserve receptors.Thus it is possible to stimulate themyocardium even when 90% of the cardiac βadrenergic receptors are blocked by anirreversible β blocker.Silent receptors are receptors to which anagonist binds but does not produce aresponse. Presence of such silent receptorsmay explain the phenomenon of tolerance.Site The receptors may be present in the cellmembrane, in the cytoplasm or on thenucleus.Nature of receptors Receptors are proteins.Synthesis and lifespan Receptor proteins aresynthesized by the cells. They have a definitelifespan after which the receptors aredegraded by the cell and new receptors aresynthesized.Functions of receptors The two functions ofreceptors are - • Recognition and binding of the ligand. • Propagation of the message.
For the above functions, the receptor hastwo functional domains (areas):
i. A ligand binding domain—the site to bindthe drug molecule.
ii. An effector domain—which undergoes achange to propagate the message.
Several theories have been proposed toexplain drug receptor interaction. Drug-receptor interaction has been considered tobe similar to ‘lock and key’ relationship wherethe drug specifically fits into the particularreceptor (lock) like a key. The rate theoryproposes that the magnitude of responsedepends on the rate of agonist–receptorassociation and dissociation. The rate ofreceptors binding is more initially but afterit reaches the peak there is a decrease.
The occupation theory suggests that themagnitude of drug response depends on theproportion of the receptors occupied by thedrug. Interaction of the agonist with thereceptor brings about changes in the receptorwhich in turn conveys the signal to theeffector system. The final response is broughtabout by the effector system through secondmessengers. The agonist itself is the firstmessenger. The entire process involves achain of events triggered by drug receptorinteraction.
Receptor Families
On stimulation of a receptor, the timerequired to elicit the response varies largelyfrom a fraction of a second in some receptorsto hours and days in others. This differenceis because of the variation in mechanismsinvolved in linking the receptor and theeffector systems (transduction mechanisms).Based on this, four types or super families ofreceptors are identified. They are bestunderstood with the help of Figure 4.1. Thereceptor types are:1. Ion channels (inotropic receptor)2. G-protein coupled receptors (metabo-
tropic receptor)
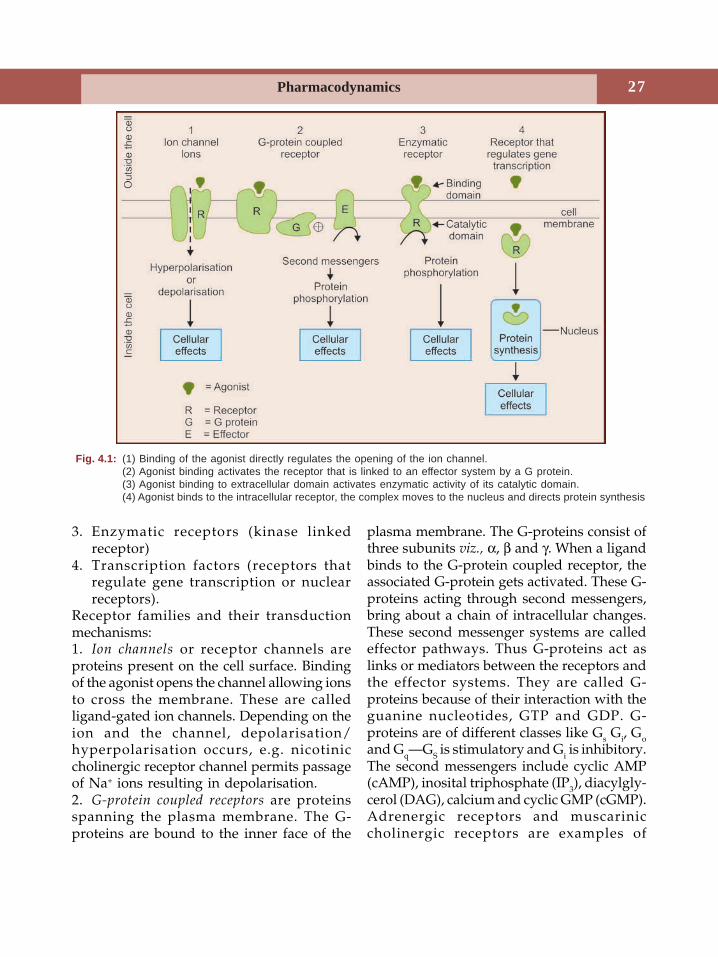
Pharmacodynamics 27
3. Enzymatic receptors (kinase linkedreceptor)
4. Transcription factors (receptors thatregulate gene transcription or nuclearreceptors).
Receptor families and their transductionmechanisms:1. Ion channels or receptor channels areproteins present on the cell surface. Bindingof the agonist opens the channel allowing ionsto cross the membrane. These are calledligand-gated ion channels. Depending on theion and the channel, depolarisation/hyperpolarisation occurs, e.g. nicotiniccholinergic receptor channel permits passageof Na+ ions resulting in depolarisation.2. G-protein coupled receptors are proteinsspanning the plasma membrane. The G-proteins are bound to the inner face of the
plasma membrane. The G-proteins consist ofthree subunits viz., α, β and γ. When a ligandbinds to the G-protein coupled receptor, theassociated G-protein gets activated. These G-proteins acting through second messengers,bring about a chain of intracellular changes.These second messenger systems are calledeffector pathways. Thus G-proteins act aslinks or mediators between the receptors andthe effector systems. They are called G-proteins because of their interaction with theguanine nucleotides, GTP and GDP. G-proteins are of different classes like Gs Gi, Goand Gq—GS is stimulatory and Gi is inhibitory.The second messengers include cyclic AMP(cAMP), inosital triphosphate (IP3), diacylgly-cerol (DAG), calcium and cyclic GMP (cGMP).Adrenergic receptors and muscariniccholinergic receptors are examples of
Fig. 4.1: (1) Binding of the agonist directly regulates the opening of the ion channel.(2) Agonist binding activates the receptor that is linked to an effector system by a G protein.(3) Agonist binding to extracellular domain activates enzymatic activity of its catalytic domain.(4) Agonist binds to the intracellular receptor, the complex moves to the nucleus and directs protein synthesis
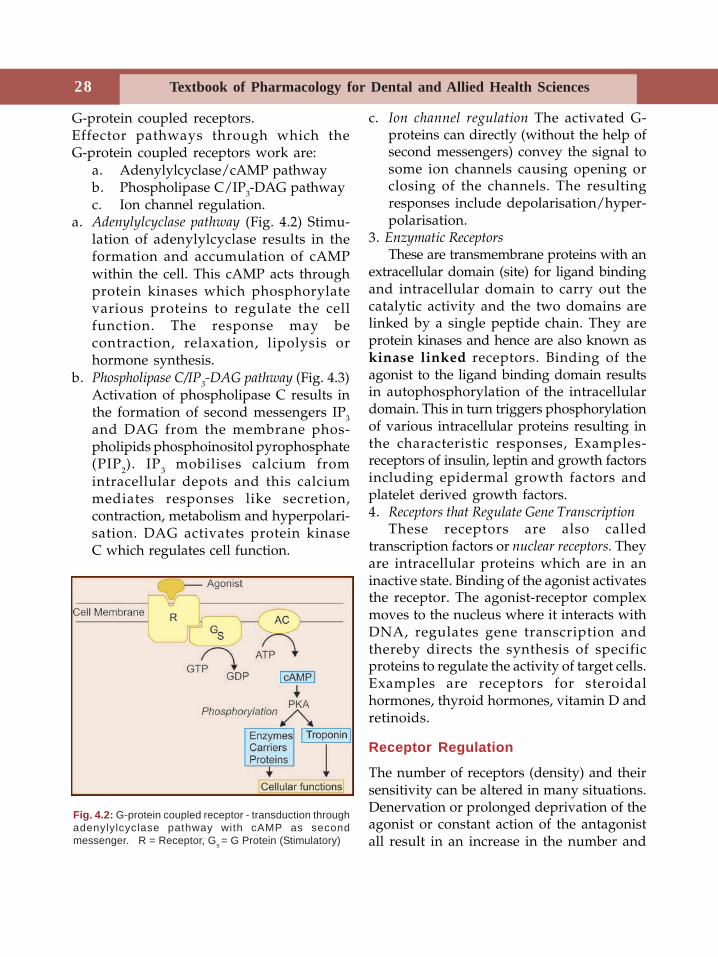
Textbook of Pharmacology for Dental and Allied Health Sciences28
G-protein coupled receptors.Effector pathways through which theG-protein coupled receptors work are:
a. Adenylylcyclase/cAMP pathwayb. Phospholipase C/IP3-DAG pathwayc. Ion channel regulation.
a. Adenylylcyclase pathway (Fig. 4.2) Stimu-lation of adenylylcyclase results in theformation and accumulation of cAMPwithin the cell. This cAMP acts throughprotein kinases which phosphorylatevarious proteins to regulate the cellfunction. The response may becontraction, relaxation, lipolysis orhormone synthesis.
b. Phospholipase C/IP3-DAG pathway (Fig. 4.3)
Activation of phospholipase C results inthe formation of second messengers IP3
and DAG from the membrane phos-pholipids phosphoinositol pyrophosphate(PIP2). IP3 mobilises calcium fromintracellular depots and this calciummediates responses like secretion,contraction, metabolism and hyperpolari-sation. DAG activates protein kinaseC which regulates cell function.
c. Ion channel regulation The activated G-proteins can directly (without the help ofsecond messengers) convey the signal tosome ion channels causing opening orclosing of the channels. The resultingresponses include depolarisation/hyper-polarisation.
3. Enzymatic ReceptorsThese are transmembrane proteins with an
extracellular domain (site) for ligand bindingand intracellular domain to carry out thecatalytic activity and the two domains arelinked by a single peptide chain. They areprotein kinases and hence are also known askinase linked receptors. Binding of theagonist to the ligand binding domain resultsin autophosphorylation of the intracellulardomain. This in turn triggers phosphorylationof various intracellular proteins resulting inthe characteristic responses, Examples-receptors of insulin, leptin and growth factorsincluding epidermal growth factors andplatelet derived growth factors.4. Receptors that Regulate Gene Transcription
These receptors are also calledtranscription factors or nuclear receptors. Theyare intracellular proteins which are in aninactive state. Binding of the agonist activatesthe receptor. The agonist-receptor complexmoves to the nucleus where it interacts withDNA, regulates gene transcription andthereby directs the synthesis of specificproteins to regulate the activity of target cells.Examples are receptors for steroidalhormones, thyroid hormones, vitamin D andretinoids.
Receptor Regulation
The number of receptors (density) and theirsensitivity can be altered in many situations.Denervation or prolonged deprivation of theagonist or constant action of the antagonistall result in an increase in the number and
Fig. 4.2: G-protein coupled receptor - transduction throughadenylylcyclase pathway with cAMP as secondmessenger. R = Receptor, Gs = G Protein (Stimulatory)
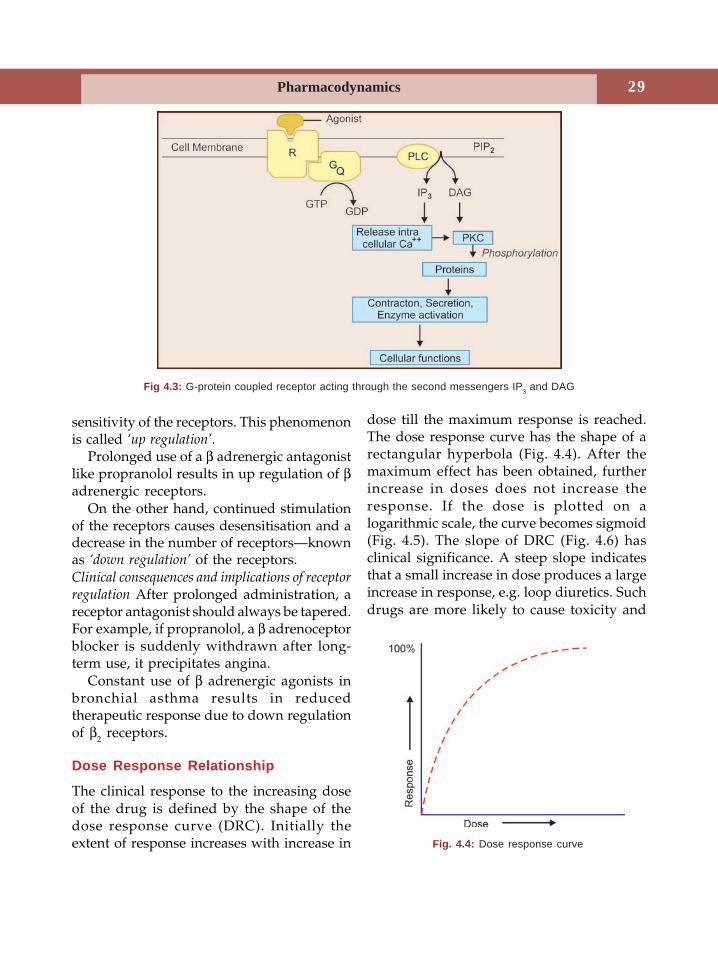
Pharmacodynamics 29
sensitivity of the receptors. This phenomenonis called ‘up regulation’.
Prolonged use of a β adrenergic antagonistlike propranolol results in up regulation of βadrenergic receptors.
On the other hand, continued stimulationof the receptors causes desensitisation and adecrease in the number of receptors—knownas ‘down regulation’ of the receptors.Clinical consequences and implications of receptorregulation After prolonged administration, areceptor antagonist should always be tapered.For example, if propranolol, a β adrenoceptorblocker is suddenly withdrawn after long-term use, it precipitates angina.
Constant use of β adrenergic agonists inbronchial asthma results in reducedtherapeutic response due to down regulationof β2 receptors.
Dose Response Relationship
The clinical response to the increasing doseof the drug is defined by the shape of thedose response curve (DRC). Initially theextent of response increases with increase in
dose till the maximum response is reached.The dose response curve has the shape of arectangular hyperbola (Fig. 4.4). After themaximum effect has been obtained, furtherincrease in doses does not increase theresponse. If the dose is plotted on alogarithmic scale, the curve becomes sigmoid(Fig. 4.5). The slope of DRC (Fig. 4.6) hasclinical significance. A steep slope indicatesthat a small increase in dose produces a largeincrease in response, e.g. loop diuretics. Suchdrugs are more likely to cause toxicity and
Fig 4.3: G-protein coupled receptor acting through the second messengers IP3 and DAG
Fig. 4.4: Dose response curve
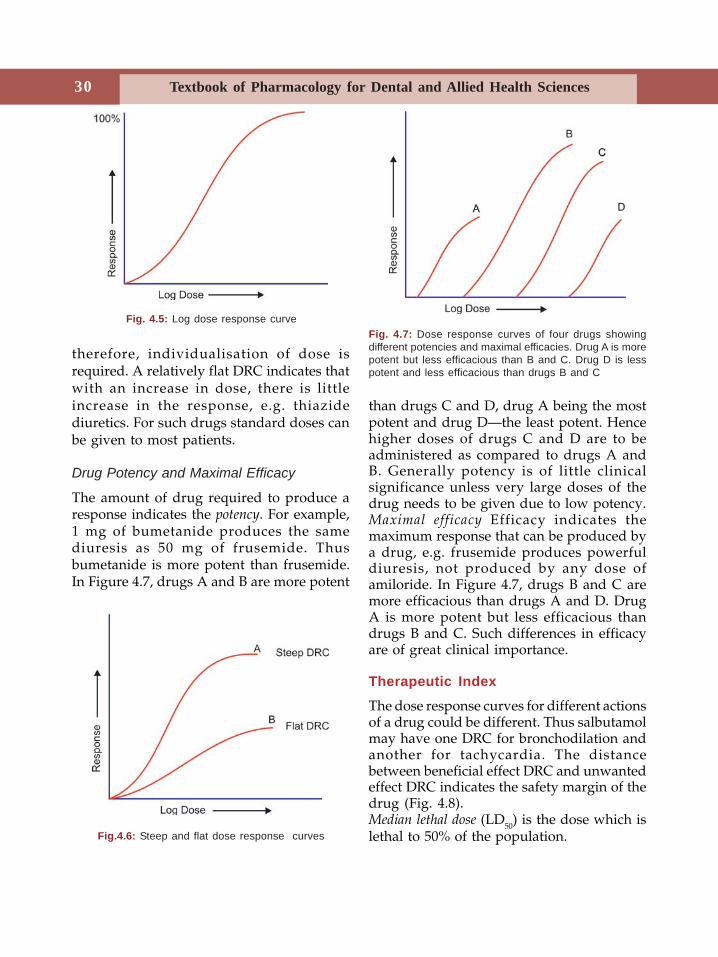
Textbook of Pharmacology for Dental and Allied Health Sciences30
therefore, individualisation of dose isrequired. A relatively flat DRC indicates thatwith an increase in dose, there is littleincrease in the response, e.g. thiazidediuretics. For such drugs standard doses canbe given to most patients.
Drug Potency and Maximal Efficacy
The amount of drug required to produce aresponse indicates the potency. For example,1 mg of bumetanide produces the samediuresis as 50 mg of frusemide. Thusbumetanide is more potent than frusemide.In Figure 4.7, drugs A and B are more potent
than drugs C and D, drug A being the mostpotent and drug D—the least potent. Hencehigher doses of drugs C and D are to beadministered as compared to drugs A andB. Generally potency is of little clinicalsignificance unless very large doses of thedrug needs to be given due to low potency.Maximal efficacy Efficacy indicates themaximum response that can be produced bya drug, e.g. frusemide produces powerfuldiuresis, not produced by any dose ofamiloride. In Figure 4.7, drugs B and C aremore efficacious than drugs A and D. DrugA is more potent but less efficacious thandrugs B and C. Such differences in efficacyare of great clinical importance.
Therapeutic Index
The dose response curves for different actionsof a drug could be different. Thus salbutamolmay have one DRC for bronchodilation andanother for tachycardia. The distancebetween beneficial effect DRC and unwantedeffect DRC indicates the safety margin of thedrug (Fig. 4.8).Median lethal dose (LD50) is the dose which islethal to 50% of the population.
Fig. 4.5: Log dose response curve
Fig.4.6: Steep and flat dose response curves
Fig. 4.7: Dose response curves of four drugs showingdifferent potencies and maximal efficacies. Drug A is morepotent but less efficacious than B and C. Drug D is lesspotent and less efficacious than drugs B and C
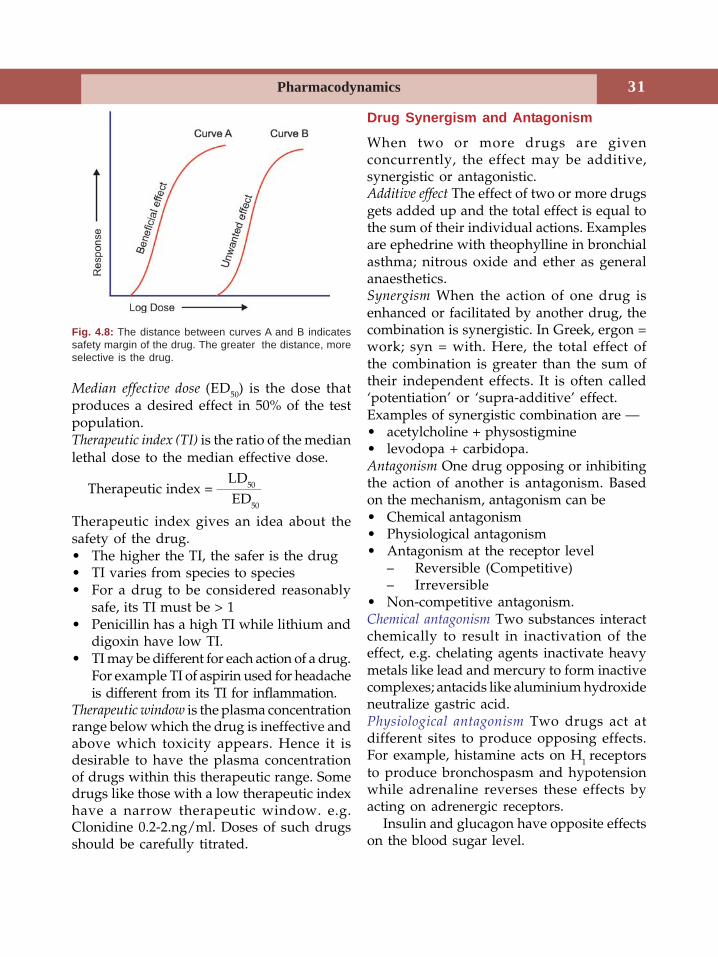
Pharmacodynamics 31
Median effective dose (ED50) is the dose thatproduces a desired effect in 50% of the testpopulation.Therapeutic index (TI) is the ratio of the medianlethal dose to the median effective dose.
LD50Therapeutic index = ___________
ED50
Therapeutic index gives an idea about thesafety of the drug.• The higher the TI, the safer is the drug• TI varies from species to species• For a drug to be considered reasonably
safe, its TI must be > 1• Penicillin has a high TI while lithium and
digoxin have low TI.• TI may be different for each action of a drug.
For example TI of aspirin used for headacheis different from its TI for inflammation.
Therapeutic window is the plasma concentrationrange below which the drug is ineffective andabove which toxicity appears. Hence it isdesirable to have the plasma concentrationof drugs within this therapeutic range. Somedrugs like those with a low therapeutic indexhave a narrow therapeutic window. e.g.Clonidine 0.2-2.ng/ml. Doses of such drugsshould be carefully titrated.
Drug Synergism and Antagonism
When two or more drugs are givenconcurrently, the effect may be additive,synergistic or antagonistic.Additive effect The effect of two or more drugsgets added up and the total effect is equal tothe sum of their individual actions. Examplesare ephedrine with theophylline in bronchialasthma; nitrous oxide and ether as generalanaesthetics.Synergism When the action of one drug isenhanced or facilitated by another drug, thecombination is synergistic. In Greek, ergon =work; syn = with. Here, the total effect ofthe combination is greater than the sum oftheir independent effects. It is often called‘potentiation’ or ‘supra-additive’ effect.Examples of synergistic combination are —• acetylcholine + physostigmine• levodopa + carbidopa.Antagonism One drug opposing or inhibitingthe action of another is antagonism. Basedon the mechanism, antagonism can be• Chemical antagonism• Physiological antagonism• Antagonism at the receptor level
– Reversible (Competitive)– Irreversible
• Non-competitive antagonism.Chemical antagonism Two substances interactchemically to result in inactivation of theeffect, e.g. chelating agents inactivate heavymetals like lead and mercury to form inactivecomplexes; antacids like aluminium hydroxideneutralize gastric acid.Physiological antagonism Two drugs act atdifferent sites to produce opposing effects.For example, histamine acts on H
1 receptorsto produce bronchospasm and hypotensionwhile adrenaline reverses these effects byacting on adrenergic receptors.
Insulin and glucagon have opposite effectson the blood sugar level.
Fig. 4.8: The distance between curves A and B indicatessafety margin of the drug. The greater the distance, moreselective is the drug.
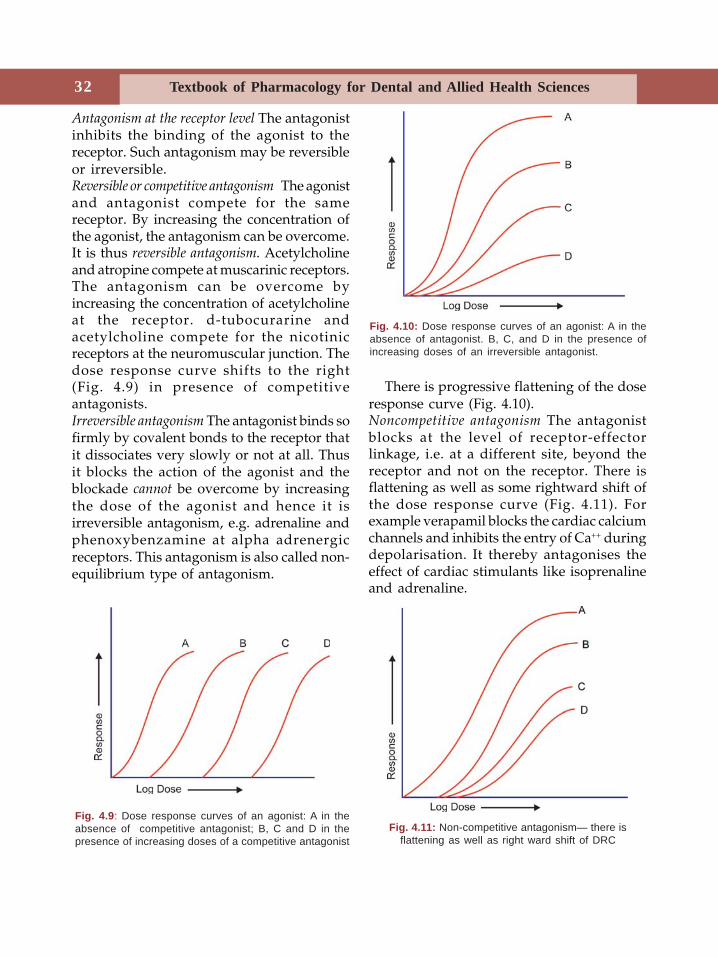
Textbook of Pharmacology for Dental and Allied Health Sciences32
Antagonism at the receptor level The antagonistinhibits the binding of the agonist to thereceptor. Such antagonism may be reversibleor irreversible.Reversible or competitive antagonism The agonistand antagonist compete for the samereceptor. By increasing the concentration ofthe agonist, the antagonism can be overcome.It is thus reversible antagonism. Acetylcholineand atropine compete at muscarinic receptors.The antagonism can be overcome byincreasing the concentration of acetylcholineat the receptor. d-tubocurarine andacetylcholine compete for the nicotinicreceptors at the neuromuscular junction. Thedose response curve shifts to the right(Fig. 4.9) in presence of competitiveantagonists.Irreversible antagonism The antagonist binds sofirmly by covalent bonds to the receptor thatit dissociates very slowly or not at all. Thusit blocks the action of the agonist and theblockade cannot be overcome by increasingthe dose of the agonist and hence it isirreversible antagonism, e.g. adrenaline andphenoxybenzamine at alpha adrenergicreceptors. This antagonism is also called non-equilibrium type of antagonism.
There is progressive flattening of the doseresponse curve (Fig. 4.10).Noncompetitive antagonism The antagonistblocks at the level of receptor-effectorlinkage, i.e. at a different site, beyond thereceptor and not on the receptor. There isflattening as well as some rightward shift ofthe dose response curve (Fig. 4.11). Forexample verapamil blocks the cardiac calciumchannels and inhibits the entry of Ca++ duringdepolarisation. It thereby antagonises theeffect of cardiac stimulants like isoprenalineand adrenaline.
Fig. 4.9: Dose response curves of an agonist: A in theabsence of competitive antagonist; B, C and D in thepresence of increasing doses of a competitive antagonist
Fig. 4.10: Dose response curves of an agonist: A in theabsence of antagonist. B, C, and D in the presence ofincreasing doses of an irreversible antagonist.
Fig. 4.11: Non-competitive antagonism— there isflattening as well as right ward shift of DRC

Pharmacodynamics 33
FACTORS THAT MODIFY THE EFFECTSOF DRUGS
The same dose of a drug can produce differentdegrees of response in different patients andeven in the same patient under differentsituations. Various factors modify theresponse to a drug. They are:1. Body weight The recommended dose is
calculated for medium built persons. Forthe obese and underweight persons, thedose has to be calculated individually.Though body surface area is a betterparameter for more accurate calculationof the dose, it is inconvenient and hencenot generally used.Formula
Body weight (kg)Dose= _____________________ × average adult dose
702. Age The pharmacokinetics of many drugs
change with age resulting in alteredresponse in extremes of age. In thenewborn, the liver and kidneys are notfully mature to handle the drugs, e.g.chloramphenicol can produce grey babysyndrome. The blood-brain barrier is notwell-formed and drugs can easily reachthe brain. The gastric acidity is low,intestinal motility is slow, skin is delicateand permeable to drugs applied topically.Hence calculation of the appropriate dosebased on the body weight is important toavoid toxicity. Also pharmacodynamicdifferences could exist, e.g. barbiturateswhich produce sedation in adults mayproduce excitation in children.Formula for calculation of dose for childrenYoung’s formula
Age (years)Child’s dose= ______________________ × Adult dose
Age + 12In the elderly, the capacity of the liver andkidney to handle the drug is reduced andthey are more susceptible to adverse
effects. Hence lower doses are recom-mended, e.g. elderly are at a higher riskof ototoxicity and nephrotoxicity bystreptomycin.
3. Sex The hormonal effects and smaller bodysize may influence drug response inwomen. Special care is necessary whileprescribing for pregnant and lactatingwomen and during menstruation.
4. Species and race Response to drugs mayvary with species and race. For example,rabbits are resistant to atropine. Suchvariation makes it difficult to extrapolatethe results of animal experiments. Blacksneed higher doses of atropine to producemydriasis.
5. Diet and environment Food interferes withthe absorption of many drugs. Forexample, tetracyclines form complexeswith calcium present in the food and arepoorly absorbed.
Polycyclic hydrocarbons present in thecigarette smoke may induce microsomalenzymes resulting in enhancedmetabolism of some drugs.
6. Route of administration Occasionally routeof administration may modify thepharmacodynamic response, e.g.magnesium sulfate given orally is apurgative. But given IV it causes CNSdepression and has anticonvulsant effects.Applied topically (poultice), it reduceslocal edema. Hypertonic magnesiumsulfate retention enema reducesintracranial tension.
7. Genetic factors Variations in an individual’sresponse to drugs could be geneticallymediated. Pharmacogenetics is concernedwith the genetically mediated variationsin drug responses. The differences inresponse is most commonly due tovariations in the amount of drugmetabolising enzymes since theproduction of these enzymes is geneticallycontrolled.
Textbook of Pharmacology for Dental and Allied Health Sciences34
Examples
a. Acetylation of drugs The rate of drugacetylation differs among individuals whomay be fast or slow acetylators, e.g. INH,sulfonamides and hydralazine areacetylated. Slow acetylators treated withhydralazine are more likely to developlupus erythematosus.
b. Atypical pseudocholinesterase Succinylcholineis metabolised by the enzyme pseudo-cholinesterase. Some people inherit anatypical pseudocholinesterase whichcannot quickly metabolise succinylcholine.When succinylcholine is given to suchpeople they develop a prolonged apnoeadue to persistant action of succinyl-choline.
c. G6PD deficiency Primaquine, sulphones and
quinolones can cause hemolysis in suchpeople.
d. Malignant hyperthermia Halothane andsuccinylcholine can trigger malignanthyperthermia in some geneticallypredisposed individuals. (page 124)
e. Hepatic porphyrias Some people lack anenzyme required for haeme synthesis, andthis results in accumulation of porphyrin-containing haeme precursors. Some drugslike barbiturates, griseofulvin andcarbamazepine induce the enzymerequired for porphyrin synthesis resultingin accumulation of porphyrins. In both theabove cases neurological, gastrointestinaland behavioural abnormalities can occurdue to excess porphyrins.
8. Dose It is fascinating that the response toa drug may be modified by the doseadministered. Generally as the dose isincreased, the magnitude of the responsealso increases proportionately till the‘maximum’ is reached. Further increasesin doses may with some drugs produceeffects opposite to their lower-dose effect,e.g. (i) in myasthenia gravis, neostigmine
enhances muscle power in therapeuticdoses, but in high doses it causes muscleparalysis, (ii) physiological doses ofvitamin D promotes calcification whilehypervitaminosis D leads to decalcifi-cation.
9. Diseases Presence of certain diseases caninfluence drug responses, e.g.• Malabsorption Drugs are poorly
absorbed.• Liver diseases Rate of drug metabolism
is reduced due to dysfunction ofhepatocytes. Also protein binding isreduced due to low serum albumin.
• Cardiac diseases In CCF, there is edemaof the gut mucosa and decreasedperfusion of liver and kidneys. Thesemay result in cumulation and toxicityof drugs like propranolol andlignocaine.
• Renal dysfunction Drugs mainlyexcreted through kidneys are likely toaccumulate and cause toxicity, e.g.Streptomycin, amphotericin B—dosesof such drugs need to be reduced.
10. Repeated dosing can result in • cumulation • tolerance • tachyphylaxis.
Cumulation Drugs like digoxin which areslowly eliminated may cumulate resulting intoxicity.Tolerance Tolerance is the requirement ofhigher doses of a drug to produce a givenresponse. Tolerance may be natural oracquired.• Natural tolerance The species/race showsless sensitivity to the drug, e.g. rabbits showtolerance to atropine; Black race are tolerantto mydriatics.• Acquired tolerance develops on repeatedadministration of a drug. The patient whowas initially responsive becomes tolerant, e.g.barbiturates, opioids and nitrites producetolerance.

Pharmacodynamics 35
Tolerance may develop to some actions ofthe drug and not to others, e.g. morphine—tolerance develops to analgesic and euphoriceffects of morphine but not to its constipatingand miotic effects. Barbiturates—tolerancedevelops to sedative but not antiepilepticeffects of barbiturates.Mechanisms The mechanisms of developmentof tolerance could be:Pharmacokinetic Changes in absorption,distribution, metabolism and excretion ofdrugs may result in reduced concentrationof the drug at the site of action and is alsoknown as dispositional tolerance, e.g.barbiturates induce microsomal enzymes andenhance their own metabolism.Pharmacodynamic Changes in the target tissue,may make it less responsive to the drug. It isalso called functional tolerance. It could bedue to down regulation of receptors as inopioids or due to compensatory mechanismsof the body, e.g. blunting of response to someantihypertensives due to salt and waterretention.Cross tolerance is the development of toleranceto pharmacologically related drugs, i.e. todrugs belonging to a particular group. Thuschronic alcoholics also show tolerance tobarbiturates and general anaesthetics.Tachyphylaxis is the rapid development oftolerance. When some drugs are administeredrepeatedly at short intervals, tolerancedevelops rapidly and is known astachyphylaxis or acute tolerance, e.g.ephedrine, amphetamine, tyramine and 5-hydroxytryptamine. This is thought to be dueto depletion of noradrenaline stores as theabove drugs act by displacing norad-
renaline from the sympathetic nerveendings. Other mechanisms involvedmay be slow dissociation of the drug fromthe receptor thereby blocking the receptor.Thus ephedrine given repeatedly inbronchial asthma may not give the desiredresponse.11. Psychological factor-The doctor-patient
relationship influences the response to adrug often to a large extent by acting onthe patient’s psychology. The patientsconfidence in the doctor may itself besufficient to relieve a suffering, particularlythe psychosomatic disorders. This can besubstantiated by the fact that large numberof patients respond to placebo. Placebo isthe inert dosage form with no specificbiological activity but only resembles theactual preparation in appearance (dummymedication). Placebo means ‘I shall bepleasing’ (in Latin).
Placebo medicines are used in -1. clinical trials as a control to compare and
assess whether the new compound issignificantly better than the placebo.
2. to benefit or please a patientpsychologically when he does notactually require an active drug as inmild psychosomatic disorders and inchronic incurable diseases.
In fact all forms of treatment includingphysiotherapy and surgery have someplacebo effect. Substances used as placeboinclude lactose, some vitamins, minerals anddistilled water injections.12. Presence of other drugs The concurrent use
of two or more drugs can influence theresponse of each other (see DrugInteractions Chapter No 5).
Textbook of Pharmacology for Dental and Allied Health Sciences36
Adverse Drug Reactions,Drug Interactions, Drug
Nomenclature and EssentialDrugs Concept
5
ADVERSE DRUG REACTIONS
All drugs can produce unwanted effects.WHO has defined an adverse drug reactionas “any response to a drug that is noxiousand unintended and that occurs at doses usedin man for prophylaxis, diagnosis ortherapy.”
All drugs can cause adverse effects. Somepatients are more likely to exhibit adverseeffects to drugs. Pharmacovigilance deals withthe epidemiologic study of adverse drugeffects.1. Side EffectsSide effects are unwanted effects of a drugthat are extension of pharmacological effectsand are seen with the therapeutic dose of thedrug. They are predictable, common and canoccur in all people, e.g. hypoglycaemia dueto insulin; hypokalaemia followingfrusemide.2. Toxic EffectsToxic effects are seen with higher doses ofthe drug and can be serious, e.g. morphinecauses respiratory depression in overdosage.3. IntoleranceDrug intolerance is the inability of a personto tolerate a drug and is unpredictable.Patients show exaggerated response to evensmall doses of the drug, e.g. vestibular
dysfunction after a single dose of strep-tomycin may be seen in some patients.Intolerance could also be qualitative, e.g.idiosyncrasy and allergic reactions.Idiosyncrasy is a genetically determinedabnormal reaction to a drug, e.g. primaquineand sulfonamides induce haemolysis inpatients with G6PD deficiency; some patientsshow excitement with barbiturates. Inaddition, some responses like chloram-phenicol-induced agranulocytosis, where nodefinite genetic background is known, arealso included under idiosyncrasy. In somecases the person may be highly sensitive evento low doses of a drug (e.g. a single dose ofquinine can produce cinchonism in some) orhighly insensitive even to high doses of thedrug.Allergic reactions to drugs are immuno-logically-mediated reactions which are notrelated to the therapeutic effects of thedrug. The drug or its metabolite acts as anantigen to induce antibody formation.Subsequent exposure to the drug mayresult in allergic reactions. Themanifestations of allergy are seen mainlyon the target organs viz. skin, respiratorytract, gastrointestinal tract, blood andblood vessels.
37Adverse Drug Reactions, Drug Interactions, Drug Nomenclature and Essential
Types of Allergic Reactions and theirMechanisms
Drugs can induce both types of allergicreactions viz humoral and cell-mediatedimmunity. Mechanisms involved in type I, IIand III are humoral while type IV is by cell-mediated immunity.
Type I (Anaphylactic) reaction The druginduces the synthesis of IgE antibodieswhich are fixed to the mast cells. Onsubsequent exposure, the antigen-antibodycomplexes cause degranulation of mast cellsreleasing the mediators of inflammation likehistamine, leukotrienes, prostaglandins andplatelet-activating factor. These areresponsible for the characteristic signs andsymptoms of anaphylaxis like bronchospasm,laryngeal edema and hypotension whichcould be fatal. Allergy develops withinminutes and is called immediatehypersensitivity reaction, e.g. penicillins.Skin tests may predict this type of reactions.Penicillins, cephalosporins, lignocaine,procaine, iron dextran and streptomycin aresome drugs known to cause anaphylaxis.Type II (Cytolytic) reactions The drug binds toa protein and together they act as antigensand induce the formation of antibodies. Theantigen antibody complexes activate thecomplement system resulting in cytolysiscausing thrombocytopenia, agranulocytosisand aplastic anaemia. Examples are carba-mazepine, phenytoin, sulphonamides andphenylbutazone. Mismatched bloodtransfusion reactions are also cytolyticreactions.Type III (Arthus) reactions The antigen bindsto circulating antibodies and the complexesare deposited on the vessel wall where itinitiates the inflammatory response resultingin vasculitis. Rashes, fever, arthralgia, lym-phadenopathy, serum sickness and Stevens-
Johnson syndrome are some of themanifestations of arthus type reactions.Serum sickness is characterized by fever,arthritis, nephritis, oedema and skin rashes.Penicillins, sulfonamides, phenytoin,streptomycin and heparin can cause serumsickness. Stevens-Johnson syndrome (SJS) ischaracterized by severe bullous erythemamultiformae particularly in the mucousmembranes with fever and malaise. ToxicEpidermal Necrolysis (TEN) is the mostserious form of drug allergy with cutaneousreactions that can be fatal. Aminopenicillins,sulphonamides, phenytoin, barbiturates,carbamazepine and phenylbutazone are thedrugs associated with SJS and TEN.
Type IV (Delayed hypersensitivity) reactions aremediated by T-lymphocytes and macro-phages. The antigen reacts with receptors onT-lymphocytes which produce lymphokinesleading to a local allergic reaction, e.g.contact dermatitis in nurses and doctorshandling penicillins and local anaesthetics.4. Iatrogenic Diseases (Physician Induced)These are drug induced diseases. Even afterthe drug is withdrawn, toxic effects canpersist, e.g. isoniazid induced hepatitis;chloroquine induced retinopathy. Drugs likechlorpromazine, haloperidol and otherphenothiazines and metoclopramide andreserpine can induce parkinsonism.5. Drug DependenceDrugs that influence the behaviour and moodare often misused to obtain pleasurableeffects. Repeated use of such drugs result independence. Several words like drug abuse,addiction and dependence are usedconfusingly. Drug dependence is a state ofcompulsive use of drugs in spite of theknowledge of the risks associated with itsuse. It is also referred to as drug addiction.Dependence could be ‘psychologic’ or‘physical’ dependence. Psychologic
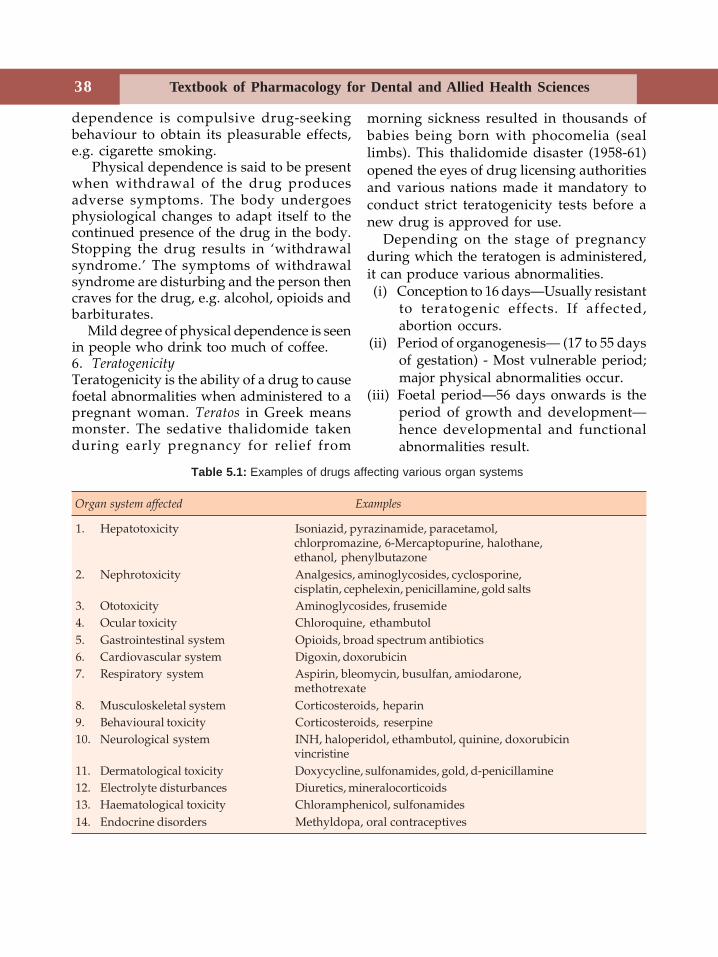
Textbook of Pharmacology for Dental and Allied Health Sciences38
dependence is compulsive drug-seekingbehaviour to obtain its pleasurable effects,e.g. cigarette smoking.
Physical dependence is said to be presentwhen withdrawal of the drug producesadverse symptoms. The body undergoesphysiological changes to adapt itself to thecontinued presence of the drug in the body.Stopping the drug results in ‘withdrawalsyndrome.’ The symptoms of withdrawalsyndrome are disturbing and the person thencraves for the drug, e.g. alcohol, opioids andbarbiturates.
Mild degree of physical dependence is seenin people who drink too much of coffee.6. TeratogenicityTeratogenicity is the ability of a drug to causefoetal abnormalities when administered to apregnant woman. Teratos in Greek meansmonster. The sedative thalidomide takenduring early pregnancy for relief from
morning sickness resulted in thousands ofbabies being born with phocomelia (seallimbs). This thalidomide disaster (1958-61)opened the eyes of drug licensing authoritiesand various nations made it mandatory toconduct strict teratogenicity tests before anew drug is approved for use.
Depending on the stage of pregnancyduring which the teratogen is administered,it can produce various abnormalities.(i) Conception to 16 days—Usually resistant
to teratogenic effects. If affected,abortion occurs.
(ii) Period of organogenesis— (17 to 55 daysof gestation) - Most vulnerable period;major physical abnormalities occur.
(iii) Foetal period—56 days onwards is theperiod of growth and development—hence developmental and functionalabnormalities result.
Table 5.1: Examples of drugs affecting various organ systems
Organ system affected Examples
1. Hepatotoxicity Isoniazid, pyrazinamide, paracetamol,chlorpromazine, 6-Mercaptopurine, halothane,ethanol, phenylbutazone
2. Nephrotoxicity Analgesics, aminoglycosides, cyclosporine,cisplatin, cephelexin, penicillamine, gold salts
3. Ototoxicity Aminoglycosides, frusemide4. Ocular toxicity Chloroquine, ethambutol5. Gastrointestinal system Opioids, broad spectrum antibiotics6. Cardiovascular system Digoxin, doxorubicin7. Respiratory system Aspirin, bleomycin, busulfan, amiodarone,
methotrexate8. Musculoskeletal system Corticosteroids, heparin9. Behavioural toxicity Corticosteroids, reserpine10. Neurological system INH, haloperidol, ethambutol, quinine, doxorubicin
vincristine11. Dermatological toxicity Doxycycline, sulfonamides, gold, d-penicillamine12. Electrolyte disturbances Diuretics, mineralocorticoids13. Haematological toxicity Chloramphenicol, sulfonamides14. Endocrine disorders Methyldopa, oral contraceptives

39Adverse Drug Reactions, Drug Interactions, Drug Nomenclature and Essential
Therefore, in general, drugs should beavoided during pregnancy specially in thefirst trimester. The type of malformationalso depends on the drug, e.g. thalidomidecauses phocomelia; tetracyclines causedeformed teeth; sodium valproate causesspina bifida-See Table 5.1 for the organsystems affected.7. Carcinogenicity and MutagenicitySome drugs can cause cancers and geneticabnormalities. For example anticancer drugscan themselves be carcinogenic; otherexamples are radioactive isotopes and somehormones.8. Other Adverse Drug ReactionsDrugs can also damage various organsystems.
DRUG INTERACTIONS
Definition Drug interaction is the alterationin the duration or magnitude of thepharmacological effects of one drug byanother drug.
When two or more drugs are givenconcurrently, the response may be greateror lesser than the sum of their individualeffects. Such responses may be beneficial orharmful. For example a combination of drugsis used in hypertension—hydralazine +propranolol for their beneficial interaction.But unwanted drug interactions may resultin severe toxicity. Such interactions can beavoided by adequate knowledge of theirmechanisms and by judicious use of drugs.Some important drug interactions arementioned in Appendix-1.Site Drug interactions can occur:
(i) In vitro in the syringe beforeadministration—mixing of drugs insyringes can cause chemical or physicalinteractions—such drug combinationsare incompatible in solution, e.g.penicillin and gentamicin should neverbe mixed in the same syringe.
(ii) In vivo, i.e. in the body afteradministration.
Pharmacological basis of drug interactions Thetwo major mechanisms of drug interactionsinclude pharmacokinetic and pharmaco-dynamic interactions.Pharmacokinetic mechanisms Alteration in theextent or duration of response may beproduced by influencing absorption,distribution, metabolism or excretion of onedrug by another.Absorption of drugs from the gut may beaffected by:
(i) Binding—Tetracyclines chelate iron andantacids resulting in reduced absorption.Cholestyramine is a bile acid bindingresin which also binds many drugs.
(ii) Altering gastric pH-Antacids raisegastric pH and interfere with theabsorption of drugs like iron andanticoagulants.
(iii) Altering GI motility. Atropine andmorphine slow gastric emptying anddelay the absorption of drugs.Purgatives reduce the absorption ofriboflavin.
Distribution Competition for plasma proteinor tissue binding results in displacementinteractions, e.g. warfarin is displaced byphenylbutazone from protein binding sites.Metabolism Enzyme induction and inhibitionof metabolism can both result in druginteractions (page 18), e.g. phenytoin,phenobarbitone, carbamazepine andrifampicin are enzyme inducers whilechloramphenicol and cimetidine are someenzyme inhibitors.Excretion When drugs compete for the samerenal tubular transport system, they prolongeach other’s duration of action, e.g. penicillinand probenecid.Pharmacodynamic mechanisms Drugs actingon the same receptors or physiologicalsystems result in additive, synergistic or
Textbook of Pharmacology for Dental and Allied Health Sciences40
antagonistic effects. Many clinicallyimportant drug interactions have this basis.Examples are-• Atropine opposes the effects of
physostigmine.• Naloxone antagonises morphine.• Antihypertensive effects of β blockers are
reduced by ephedrine or othervasoconstrictors present in cold remedies.
• Many diuretics produce hypokalaemiawhich potentiate digitalis toxicity.
• Organic nitrates (used in angina) act byincreasing cGMP activity. Sildenafilinhibits phosphodiesterase whichinactivates cGMP and thereby potentiatesthe effects of nitrates. Hence thecombination can cause severe hypotensionand even deaths have been reported.
• Aspirin inhibits platelet aggregation andenhances the risk of bleeding due to oralanticoagulants like warfarin.
• Many antihistamines produce sedationwhich may be enhanced by alcohol intake.
Drug Nomenclature
A drug can have three names.1. Chemical name2. Nonproprietary (generic) name3. Proprietary (brand) name.The chemical name gives the chemicaldescription of the drug, e.g. 3, (10, 11-dihydro-5H-dibenz (b,f) -azepin-5-yl)propyldimethylamine. This is lengthy,complex and unsuitable for prescribing.The nonproprietary name is given by an officialagency like WHO and is internationallyaccepted, i.e. the drug has the same genericname all over the world. It gives a clue tothe class of the drug, because they soundsimilar as they end with the same letters, e.g.propranolol, atenolol, esmolol, metoprolol—all are β-blockers and cimetidine, ranitidine,famotidine and roxatidine are all H2 receptor
blockers. It is convenient and the drug issometimes cheaper when prescribed bygeneric name. The nonproprietary name ofthe above example given under chemical nameis imipramine.Proprietary name is the brand name given bythe manufacturer. Hence each drug may havemany brand names, e.g. Crocin, Metacin,Pacemol, Calpol are different brand namesof paracetamol. The main advantage in usingbrand name is the consistency of the productespecially bioavailability. Hence, for drugswith low therapeutic index like digoxin andantiepileptics, prescribing the same brandname is beneficial.
Essential Drugs Concept
WHO has compiled a list of drugs that arerequired to meet the primary health careneeds of majority of the population and arecalled essential drugs. Essential drugs havebeen defined by WHO as those that satisfythe health care needs of majority of thepopulation and should therefore be availableat all times in adequate amounts and in theappropriate dosage forms. The original listhas undergone revisions and updating fromtime to time to meet the changing require-ments. Based on the WHO guidelines forselection of essential drugs and by referringits model list, each country puts forth itsnational list of essential drugs.• Adoption of the list has resulted in greater
coordination in health care development.• The list serves as a guideline for indenting
and stocking essential drugs.• The concept has also helped in the
development of national formularies.• A short list is compiled for community
health workers to aid in providing primaryhealth care.
• The use of Essential Drug List has alsoemphasised the need for drug research and
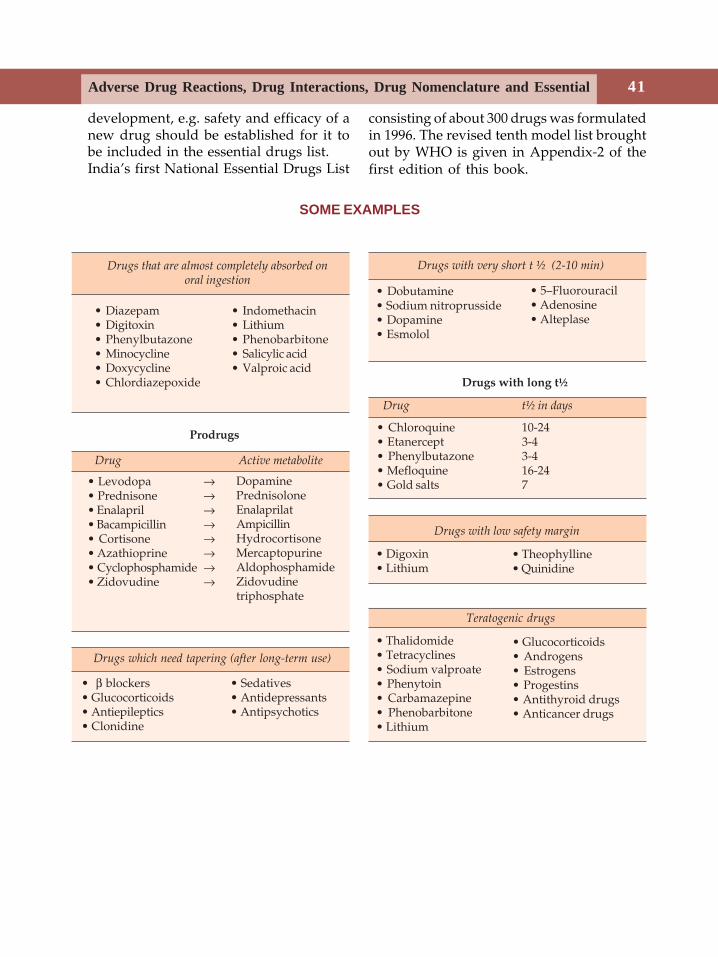
41Adverse Drug Reactions, Drug Interactions, Drug Nomenclature and Essential
SOME EXAMPLES
• Diazepam• Digitoxin• Phenylbutazone• Minocycline• Doxycycline• Chlordiazepoxide
• Indomethacin• Lithium• Phenobarbitone• Salicylic acid• Valproic acid
Drugs that are almost completely absorbed onoral ingestion
Prodrugs
• Levodopa →• Prednisone →• Enalapril →• Bacampicillin →• Cortisone →• Azathioprine →• Cyclophosphamide →• Zidovudine →
DopaminePrednisoloneEnalaprilatAmpicillinHydrocortisoneMercaptopurineAldophosphamideZidovudinetriphosphate
Drug Active metabolite
Drugs with very short t ½ (2-10 min)
Drugs which need tapering (after long-term use)
• β blockers• Glucocorticoids• Antiepileptics• Clonidine
• Sedatives• Antidepressants• Antipsychotics
Drugs with long t½
Drug t½ in days
• Chloroquine 10-24• Etanercept 3-4• Phenylbutazone 3-4• Mefloquine 16-24• Gold salts 7
Drugs with low safety margin
• Digoxin• Lithium
• Theophylline• Quinidine
Teratogenic drugs
• Thalidomide• Tetracyclines• Sodium valproate• Phenytoin• Carbamazepine• Phenobarbitone• Lithium
• Glucocorticoids• Androgens• Estrogens• Progestins• Antithyroid drugs• Anticancer drugs
• 5–Fluorouracil• Adenosine• Alteplase
• Dobutamine• Sodium nitroprusside• Dopamine• Esmolol
development, e.g. safety and efficacy of anew drug should be established for it tobe included in the essential drugs list.India’s first National Essential Drugs List
consisting of about 300 drugs was formulatedin 1996. The revised tenth model list broughtout by WHO is given in Appendix-2 of thefirst edition of this book.
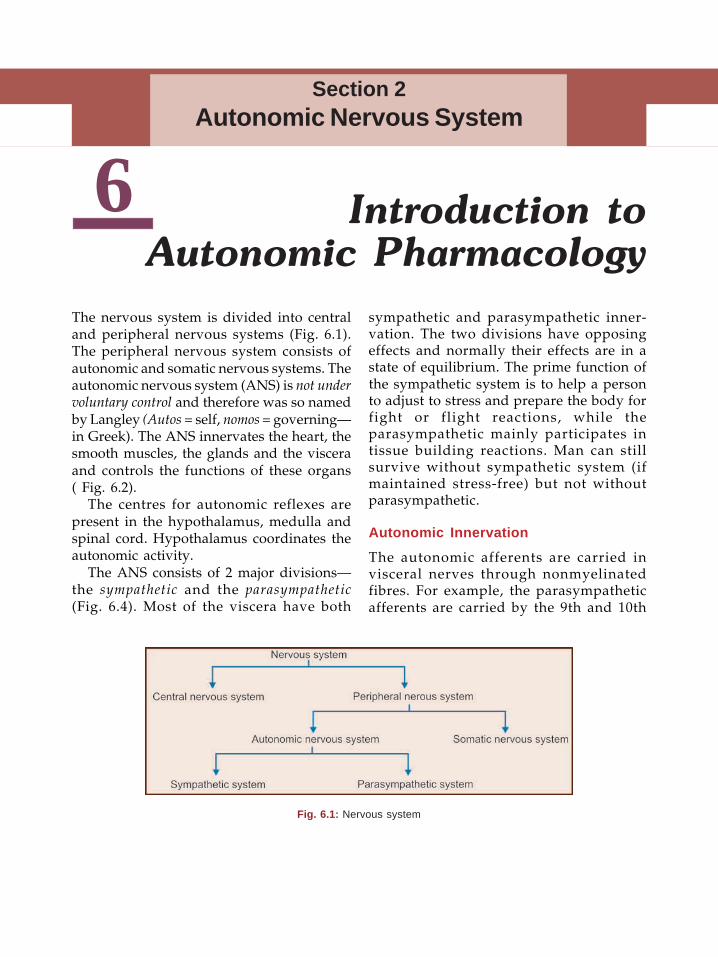
42 Textbook of Pharmacology for Dental and Allied Health Sciences
6The nervous system is divided into centraland peripheral nervous systems (Fig. 6.1).The peripheral nervous system consists ofautonomic and somatic nervous systems. Theautonomic nervous system (ANS) is not undervoluntary control and therefore was so namedby Langley (Autos = self, nomos = governing—in Greek). The ANS innervates the heart, thesmooth muscles, the glands and the visceraand controls the functions of these organs( Fig. 6.2).
The centres for autonomic reflexes arepresent in the hypothalamus, medulla andspinal cord. Hypothalamus coordinates theautonomic activity.
The ANS consists of 2 major divisions—the sympathetic and the parasympathetic(Fig. 6.4). Most of the viscera have both
sympathetic and parasympathetic inner-vation. The two divisions have opposingeffects and normally their effects are in astate of equilibrium. The prime function ofthe sympathetic system is to help a personto adjust to stress and prepare the body forfight or flight reactions, while theparasympathetic mainly participates intissue building reactions. Man can stillsurvive without sympathetic system (ifmaintained stress-free) but not withoutparasympathetic.
Autonomic Innervation
The autonomic afferents are carried invisceral nerves through nonmyelinatedfibres. For example, the parasympatheticafferents are carried by the 9th and 10th
Introduction toAutonomic Pharmacology
Section 2Autonomic Nervous System
Fig. 6.1: Nervous system
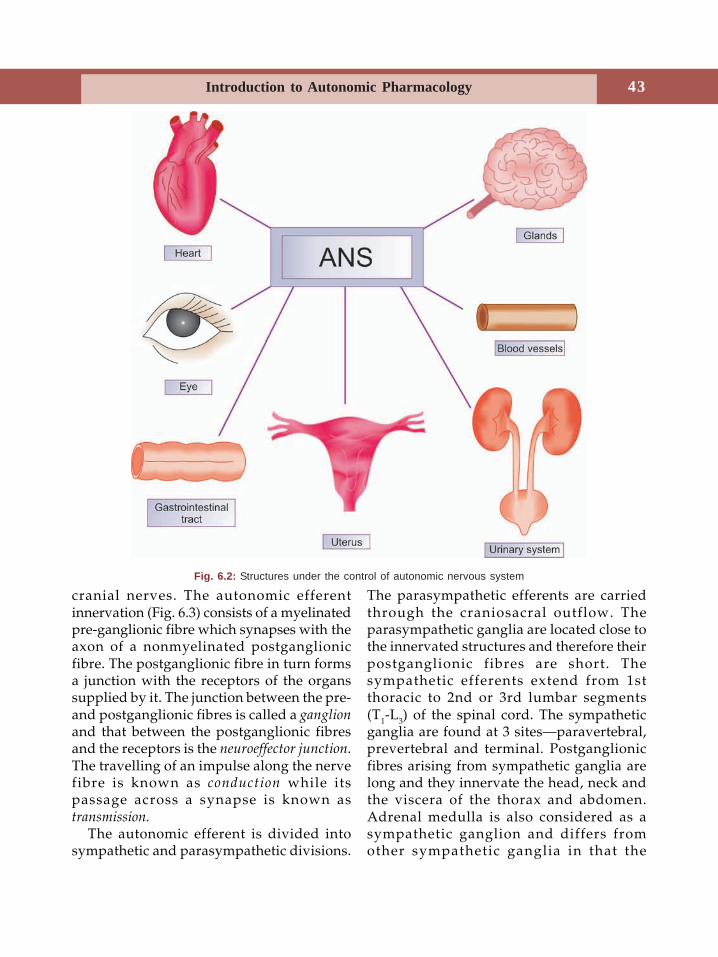
43Introduction to Autonomic Pharmacology
cranial nerves. The autonomic efferentinnervation (Fig. 6.3) consists of a myelinatedpre-ganglionic fibre which synapses with theaxon of a nonmyelinated postganglionicfibre. The postganglionic fibre in turn formsa junction with the receptors of the organssupplied by it. The junction between the pre-and postganglionic fibres is called a ganglionand that between the postganglionic fibresand the receptors is the neuroeffector junction.The travelling of an impulse along the nervefibre is known as conduction while itspassage across a synapse is known astransmission.
The autonomic efferent is divided intosympathetic and parasympathetic divisions.
The parasympathetic efferents are carriedthrough the craniosacral outflow. Theparasympathetic ganglia are located close tothe innervated structures and therefore theirpostganglionic fibres are short. Thesympathetic efferents extend from 1stthoracic to 2nd or 3rd lumbar segments(T1-L3) of the spinal cord. The sympatheticganglia are found at 3 sites—paravertebral,prevertebral and terminal. Postganglionicfibres arising from sympathetic ganglia arelong and they innervate the head, neck andthe viscera of the thorax and abdomen.Adrenal medulla is also considered as asympathetic ganglion and differs fromother sympathetic ganglia in that the
Fig. 6.2: Structures under the control of autonomic nervous system
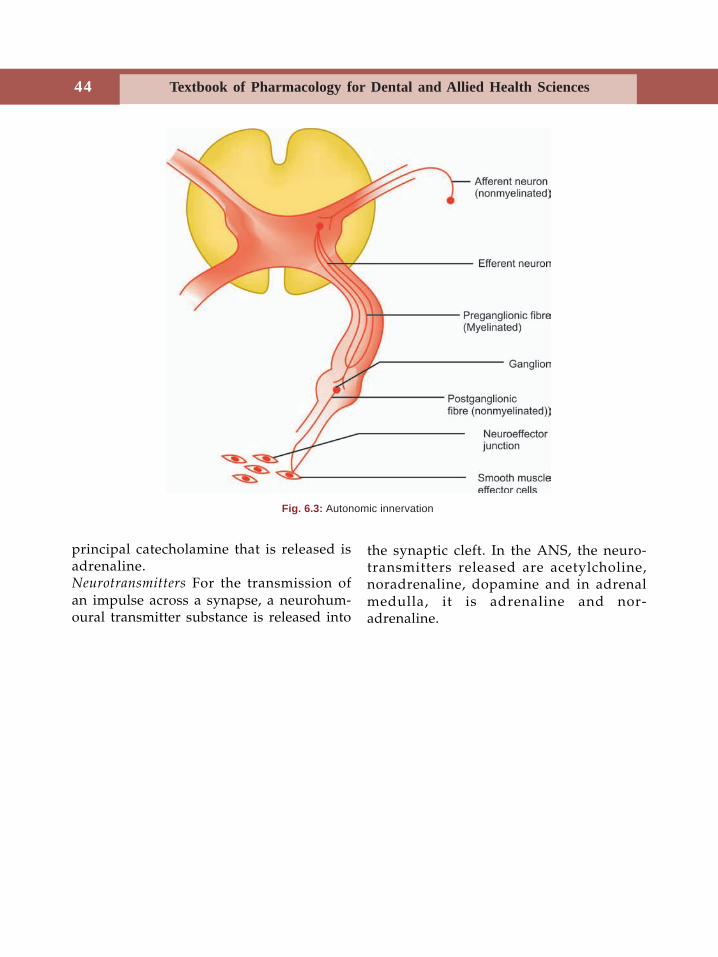
44 Textbook of Pharmacology for Dental and Allied Health Sciences
principal catecholamine that is released isadrenaline.Neurotransmitters For the transmission ofan impulse across a synapse, a neurohum-oural transmitter substance is released into
Fig. 6.3: Autonomic innervation
the synaptic cleft. In the ANS, the neuro-transmitters released are acetylcholine,noradrenaline, dopamine and in adrenalmedulla, it is adrenaline and nor-adrenaline.
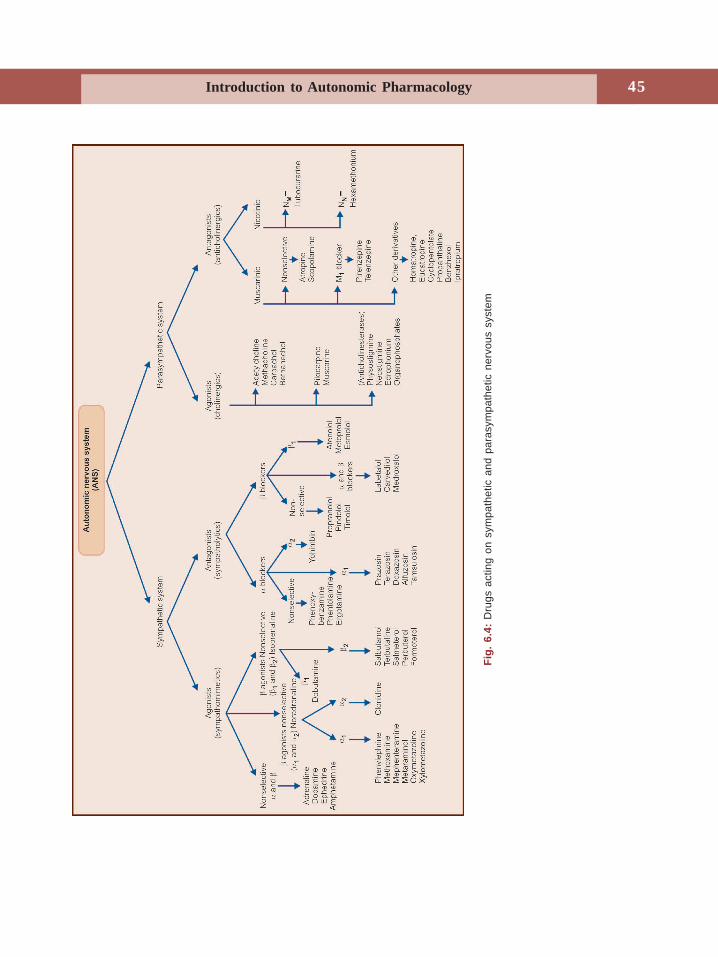
45Introduction to Autonomic Pharmacology
Fig.
6.4
: D
rugs
act
ing
on s
ympa
thet
ic a
nd p
aras
ympa
thet
ic n
ervo
us s
yste
m
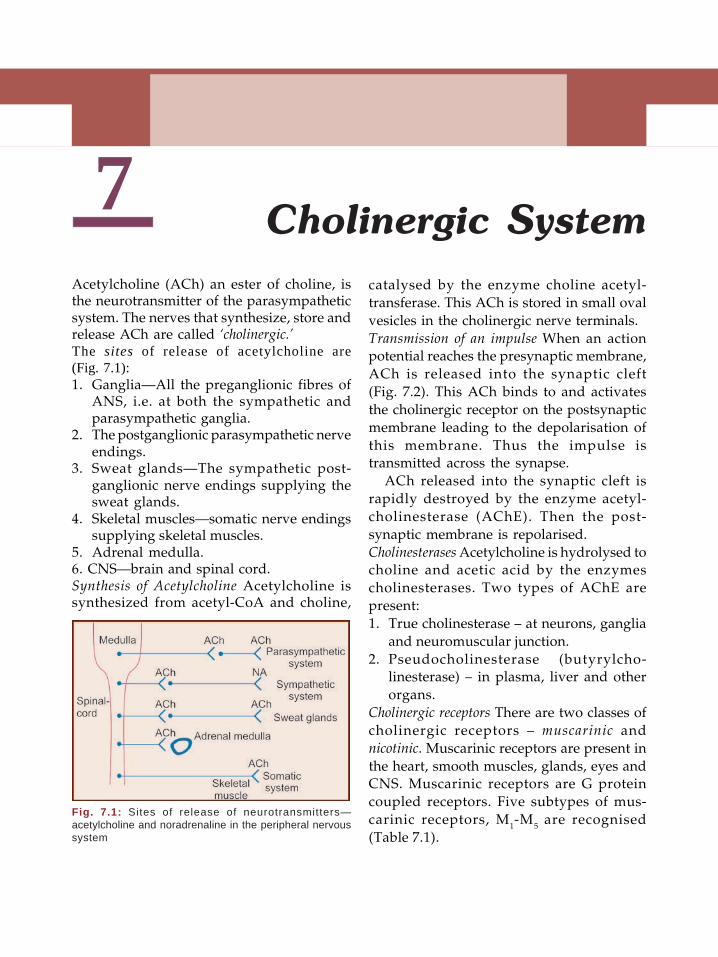
46 Textbook of Pharmacology for Dental and Allied Health Sciences
7Acetylcholine (ACh) an ester of choline, isthe neurotransmitter of the parasympatheticsystem. The nerves that synthesize, store andrelease ACh are called ‘cholinergic.’The sites of release of acetylcholine are(Fig. 7.1):1. Ganglia—All the preganglionic fibres of
ANS, i.e. at both the sympathetic andparasympathetic ganglia.
2. The postganglionic parasympathetic nerveendings.
3. Sweat glands—The sympathetic post-ganglionic nerve endings supplying thesweat glands.
4. Skeletal muscles—somatic nerve endingssupplying skeletal muscles.
5. Adrenal medulla.6. CNS—brain and spinal cord.Synthesis of Acetylcholine Acetylcholine issynthesized from acetyl-CoA and choline,
catalysed by the enzyme choline acetyl-transferase. This ACh is stored in small ovalvesicles in the cholinergic nerve terminals.Transmission of an impulse When an actionpotential reaches the presynaptic membrane,ACh is released into the synaptic cleft(Fig. 7.2). This ACh binds to and activatesthe cholinergic receptor on the postsynapticmembrane leading to the depolarisation ofthis membrane. Thus the impulse istransmitted across the synapse.
ACh released into the synaptic cleft israpidly destroyed by the enzyme acetyl-cholinesterase (AChE). Then the post-synaptic membrane is repolarised.Cholinesterases Acetylcholine is hydrolysed tocholine and acetic acid by the enzymescholinesterases. Two types of AChE arepresent:1. True cholinesterase – at neurons, ganglia
and neuromuscular junction.2. Pseudocholinesterase (butyrylcho-
linesterase) – in plasma, liver and otherorgans.
Cholinergic receptors There are two classes ofcholinergic receptors – muscarinic andnicotinic. Muscarinic receptors are present inthe heart, smooth muscles, glands, eyes andCNS. Muscarinic receptors are G proteincoupled receptors. Five subtypes of mus-carinic receptors, M1-M5 are recognised(Table 7.1).
Cholinergic System
Fig. 7.1: Sites of release of neurotransmitters—acetylcholine and noradrenaline in the peripheral nervoussystem
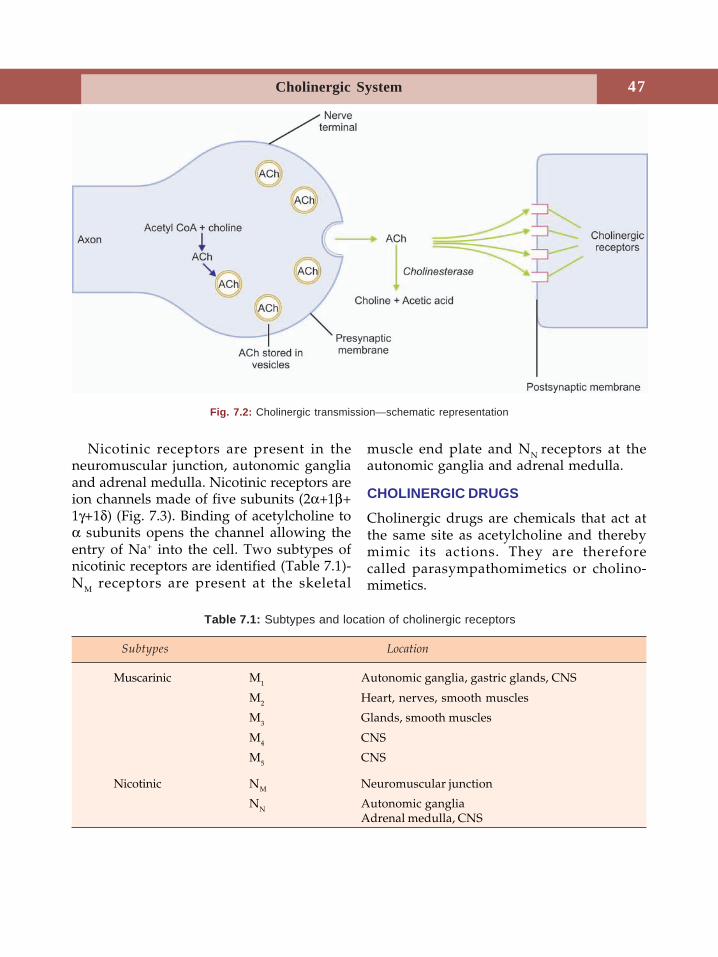
47Cholinergic System
Nicotinic receptors are present in theneuromuscular junction, autonomic gangliaand adrenal medulla. Nicotinic receptors areion channels made of five subunits (2α+1β+1γ+1δ) (Fig. 7.3). Binding of acetylcholine toα subunits opens the channel allowing theentry of Na+ into the cell. Two subtypes ofnicotinic receptors are identified (Table 7.1)-NM receptors are present at the skeletal
muscle end plate and NN receptors at theautonomic ganglia and adrenal medulla.
CHOLINERGIC DRUGS
Cholinergic drugs are chemicals that act atthe same site as acetylcholine and therebymimic its actions. They are thereforecalled parasympathomimetics or cholino-mimetics.
Fig. 7.2: Cholinergic transmission—schematic representation
Table 7.1: Subtypes and location of cholinergic receptors
Subtypes Location
Muscarinic M1 Autonomic ganglia, gastric glands, CNS
M2 Heart, nerves, smooth muscles
M3 Glands, smooth muscles
M4 CNS
M5 CNS
Nicotinic NM Neuromuscular junction
NN Autonomic gangliaAdrenal medulla, CNS
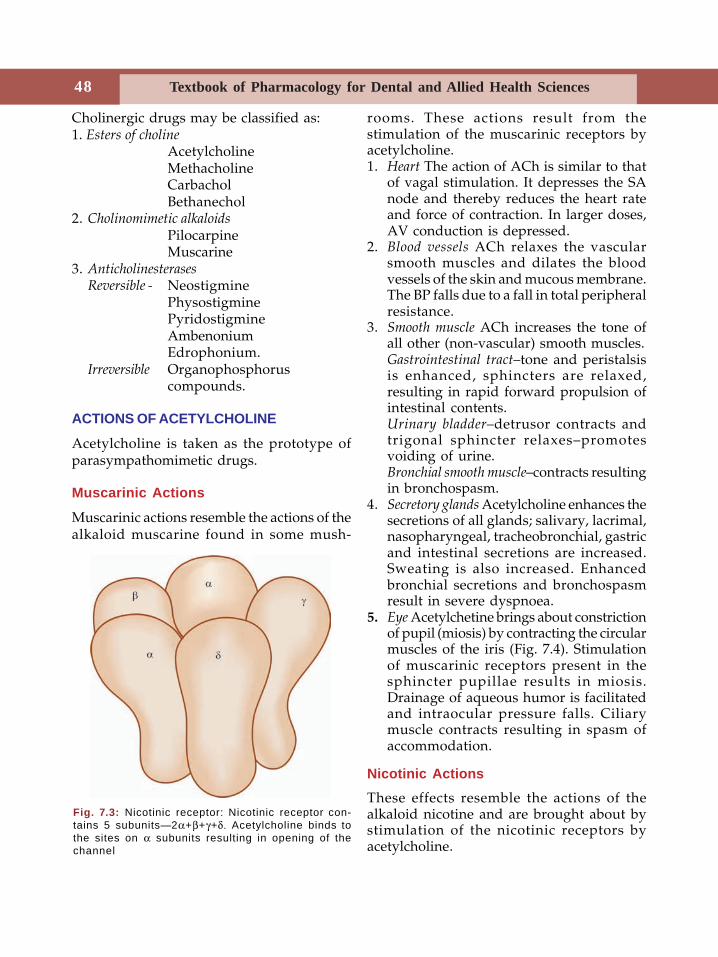
48 Textbook of Pharmacology for Dental and Allied Health Sciences
Cholinergic drugs may be classified as:1. Esters of choline
AcetylcholineMethacholineCarbacholBethanechol
2. Cholinomimetic alkaloidsPilocarpineMuscarine
3. AnticholinesterasesReversible - Neostigmine
PhysostigminePyridostigmineAmbenoniumEdrophonium.
Irreversible Organophosphoruscompounds.
ACTIONS OF ACETYLCHOLINE
Acetylcholine is taken as the prototype ofparasympathomimetic drugs.
Muscarinic Actions
Muscarinic actions resemble the actions of thealkaloid muscarine found in some mush-
rooms. These actions result from thestimulation of the muscarinic receptors byacetylcholine.1. Heart The action of ACh is similar to that
of vagal stimulation. It depresses the SAnode and thereby reduces the heart rateand force of contraction. In larger doses,AV conduction is depressed.
2. Blood vessels ACh relaxes the vascularsmooth muscles and dilates the bloodvessels of the skin and mucous membrane.The BP falls due to a fall in total peripheralresistance.
3. Smooth muscle ACh increases the tone ofall other (non-vascular) smooth muscles.Gastrointestinal tract–tone and peristalsisis enhanced, sphincters are relaxed,resulting in rapid forward propulsion ofintestinal contents.Urinary bladder–detrusor contracts andtrigonal sphincter relaxes–promotesvoiding of urine.Bronchial smooth muscle–contracts resultingin bronchospasm.
4. Secretory glands Acetylcholine enhances thesecretions of all glands; salivary, lacrimal,nasopharyngeal, tracheobronchial, gastricand intestinal secretions are increased.Sweating is also increased. Enhancedbronchial secretions and bronchospasmresult in severe dyspnoea.
5. Eye Acetylchetine brings about constrictionof pupil (miosis) by contracting the circularmuscles of the iris (Fig. 7.4). Stimulationof muscarinic receptors present in thesphincter pupillae results in miosis.Drainage of aqueous humor is facilitatedand intraocular pressure falls. Ciliarymuscle contracts resulting in spasm ofaccommodation.
Nicotinic ActionsThese effects resemble the actions of thealkaloid nicotine and are brought about bystimulation of the nicotinic receptors byacetylcholine.
Fig. 7.3: Nicotinic receptor: Nicotinic receptor con-tains 5 subunits—2α+β+γ+δ. Acetylcholine binds tothe sites on α subunits resulting in opening of thechannel

49Cholinergic System
1. NMJ Acetylcholine brings aboutcontraction of skeletal muscles bystimulating NM receptors present in theneuromuscular junction. Large doses causepersistent depolarisation of skeletalmuscles resulting in paralysis.
2. Autonomic ganglia Acetylcholine stimulatesthe sympathetic and parasympatheticganglia and the adrenal medulla.
3. CNS Acetylcholine is a neurotransmitterat several sites in the CNS.
The important actions of acetylcholine aresummarised in Table 7.2.Uses Acetylcholine is destroyed in the gutwhen given orally. On intravenousadministration, it is rapidly metabolised bypseudocholinesterases in the plasma and bytrue cholinesterase at the site of action.Therefore it is not used therapeutically exceptoccasionally as 1% eyedrops to producemiosis during some eye surgeries.Esters of choline are effective orally; carbacholand bethanechol are resistant to bothcholinesterases and have a longer durationof action. Their muscarinic actions areprominent with a sustained effect on g.i.smooth muscles and urinary bladder.Methacholine is rarely used. Carbachol isused in glaucoma. Bethanechol may be usedin hypotonia of bladder and g.i. smoothmuscles and in some cases of postoperativeparalytic ileus and urinary retention; It mayalso be used in xerostomia as an alternativeto pilocarpine.
Adverse effects include diarrhoea, flushing,salivation, sweating, bradycardia, hypo-tension, syncope and bronchospasm.
CHOLINOMIMETIC ALKALOIDS
Pilocarpine is an alkaloid obtained from theleaves of Pilocarpus microphyllus. Like ACh itstimulates cholinergic receptors, but itsmuscarinic actions are prominent.
Its actions on the eye are important–whenapplied to the eye it causes miosis, spasm ofaccommodation and a fall in intraoculartension. It also increases sweat (diaphoretic)and salivary secretions (sialogogue).Adverse effects When used as eyedrops,burning sensation and painful spasm ofaccommodation, browache and cornealedema can occur. Long term use can causeretinal detachment.
Uses
1. Pilocarpine is used in glaucoma (seebelow). Pilocarpine ocusert is availableand can deliver pilocarpine constantly for7 days.
2. Pilocarpine is also used alternately withmydriatics like homatropine to break theadhesions between the iris and the lens.
3. It is used to counter dryness of mouth thatis seen following radiation of head andneck.
Glaucoma is an eye disease characterised byincreased intraocular pressure. Aqueoushumor is secreted by the ciliary body and itdrains through the canal of Schlemn. Rise inintraocular pressure (above 30 mm of Hg)can damage the optic nerve. If untreated,irreversible damage can occur - optic nervedegenerates leading to permanent blindness.Glaucoma is one of the common causes ofblindness. Hypertension, myopia and familyhistory of glaucoma are risk factors.Glaucoma is of two types :
Table 7.2: Actions of acetylcholine
CVS — ↓HR ↓BPNon-vascular — contraction, ↑gut peristalsis,
promotes urine voidingSmooth muscle — bronchospasmGlands — ↑secretionEye — miosis, spasm of
accommodation, ↓IOPNMJ — muscle contractionGanglia — stimulation
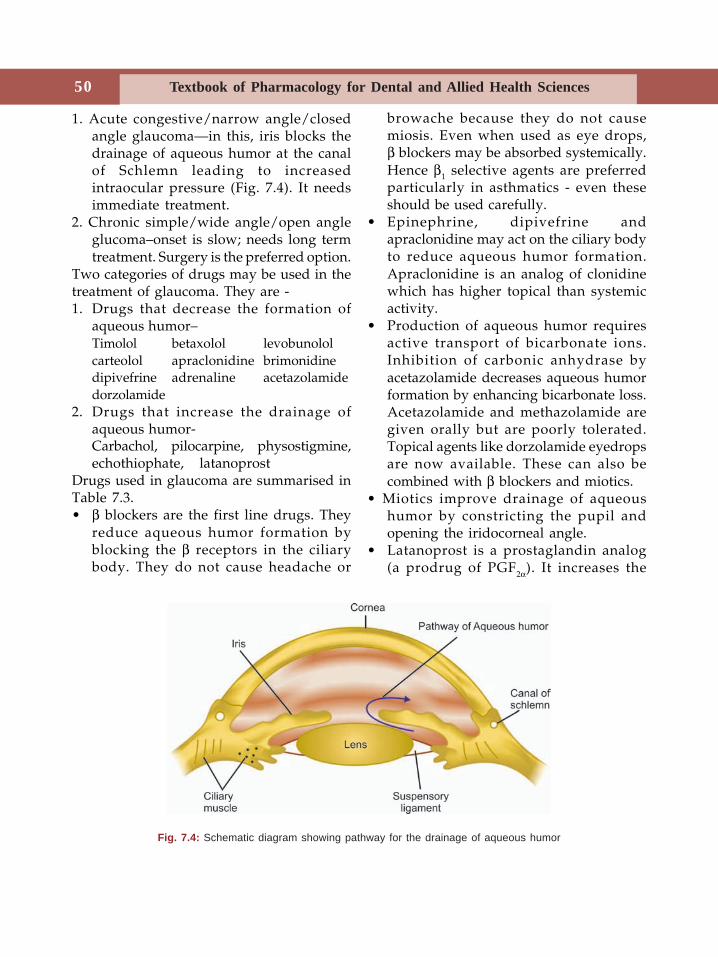
50 Textbook of Pharmacology for Dental and Allied Health Sciences
1. Acute congestive/narrow angle/closedangle glaucoma—in this, iris blocks thedrainage of aqueous humor at the canalof Schlemn leading to increasedintraocular pressure (Fig. 7.4). It needsimmediate treatment.
2. Chronic simple/wide angle/open angleglucoma–onset is slow; needs long termtreatment. Surgery is the preferred option.
Two categories of drugs may be used in thetreatment of glaucoma. They are -1. Drugs that decrease the formation of
aqueous humor–Timolol betaxolol levobunololcarteolol apraclonidine brimonidinedipivefrine adrenaline acetazolamidedorzolamide
2. Drugs that increase the drainage ofaqueous humor-Carbachol, pilocarpine, physostigmine,echothiophate, latanoprost
Drugs used in glaucoma are summarised inTable 7.3.• β blockers are the first line drugs. They
reduce aqueous humor formation byblocking the β receptors in the ciliarybody. They do not cause headache or
browache because they do not causemiosis. Even when used as eye drops,β blockers may be absorbed systemically.Hence β1 selective agents are preferredparticularly in asthmatics - even theseshould be used carefully.
• Epinephrine, dipivefrine andapraclonidine may act on the ciliary bodyto reduce aqueous humor formation.Apraclonidine is an analog of clonidinewhich has higher topical than systemicactivity.
• Production of aqueous humor requiresactive transport of bicarbonate ions.Inhibition of carbonic anhydrase byacetazolamide decreases aqueous humorformation by enhancing bicarbonate loss.Acetazolamide and methazolamide aregiven orally but are poorly tolerated.Topical agents like dorzolamide eyedropsare now available. These can also becombined with β blockers and miotics.
• Miotics improve drainage of aqueoushumor by constricting the pupil andopening the iridocorneal angle.
• Latanoprost is a prostaglandin analog(a prodrug of PGF2α). It increases the
Fig. 7.4: Schematic diagram showing pathway for the drainage of aqueous humor
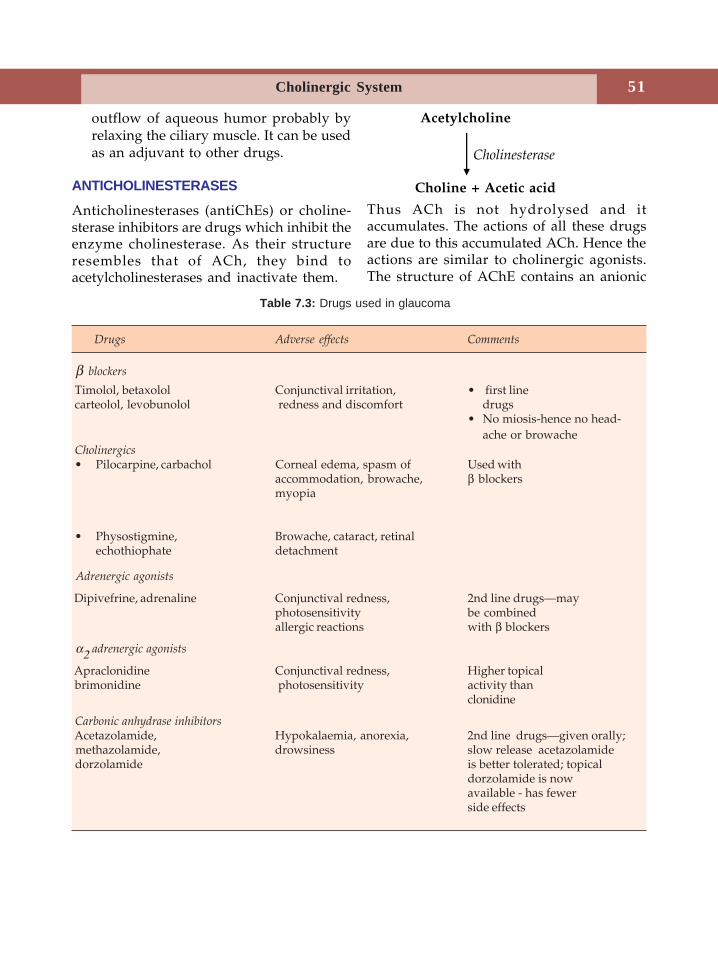
51Cholinergic System
outflow of aqueous humor probably byrelaxing the ciliary muscle. It can be usedas an adjuvant to other drugs.
ANTICHOLINESTERASES
Anticholinesterases (antiChEs) or choline-sterase inhibitors are drugs which inhibit theenzyme cholinesterase. As their structureresembles that of ACh, they bind toacetylcholinesterases and inactivate them.
Acetylcholine
Cholinesterase
Choline + Acetic acid
Thus ACh is not hydrolysed and itaccumulates. The actions of all these drugsare due to this accumulated ACh. Hence theactions are similar to cholinergic agonists.The structure of AChE contains an anionic
Table 7.3: Drugs used in glaucoma
Drugs Adverse effects Comments
β blockers
Timolol, betaxolol Conjunctival irritation, • first linecarteolol, levobunolol redness and discomfort drugs
• No miosis-hence no head-ache or browache
Cholinergics• Pilocarpine, carbachol Corneal edema, spasm of Used with
accommodation, browache, β blockersmyopia
• Physostigmine, Browache, cataract, retinalechothiophate detachment
Adrenergic agonists
Dipivefrine, adrenaline Conjunctival redness, 2nd line drugs—mayphotosensitivity be combinedallergic reactions with β blockers
α2 adrenergic agonists
Apraclonidine Conjunctival redness, Higher topical brimonidine photosensitivity activity than
clonidine
Carbonic anhydrase inhibitors Acetazolamide, Hypokalaemia, anorexia, 2nd line drugs—given orally; methazolamide, drowsiness slow release acetazolamide dorzolamide is better tolerated; topical
dorzolamide is nowavailable - has fewerside effects
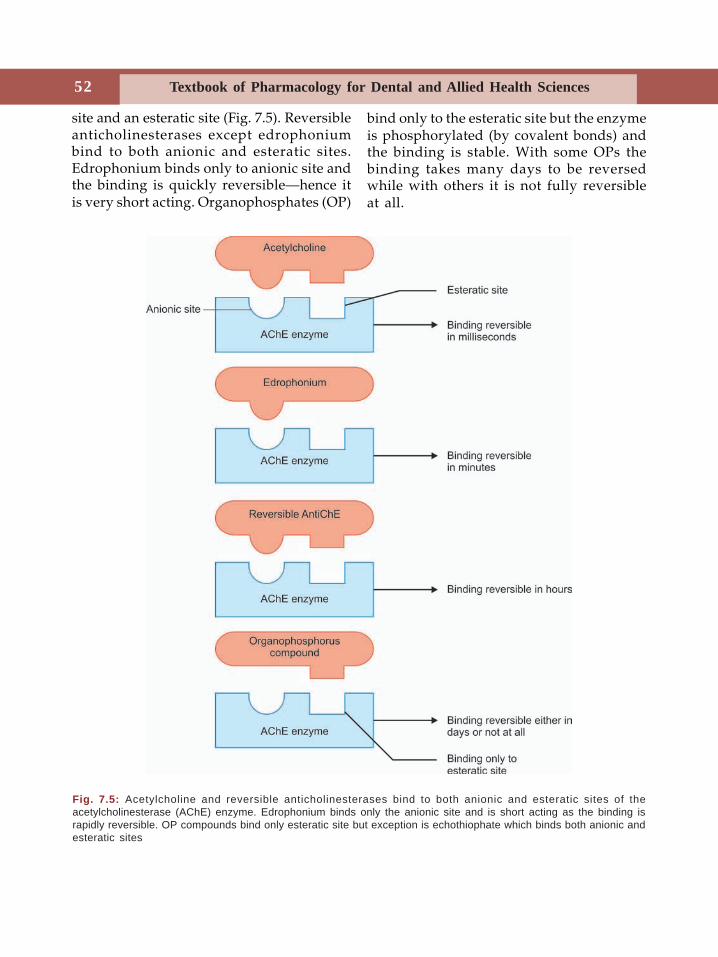
52 Textbook of Pharmacology for Dental and Allied Health Sciences
site and an esteratic site (Fig. 7.5). Reversibleanticholinesterases except edrophoniumbind to both anionic and esteratic sites.Edrophonium binds only to anionic site andthe binding is quickly reversible—hence itis very short acting. Organophosphates (OP)
bind only to the esteratic site but the enzymeis phosphorylated (by covalent bonds) andthe binding is stable. With some OPs thebinding takes many days to be reversedwhile with others it is not fully reversibleat all.
Fig. 7.5: Acetylcholine and reversible anticholinesterases bind to both anionic and esteratic sites of theacetylcholinesterase (AChE) enzyme. Edrophonium binds only the anionic site and is short acting as the binding israpidly reversible. OP compounds bind only esteratic site but exception is echothiophate which binds both anionic andesteratic sites
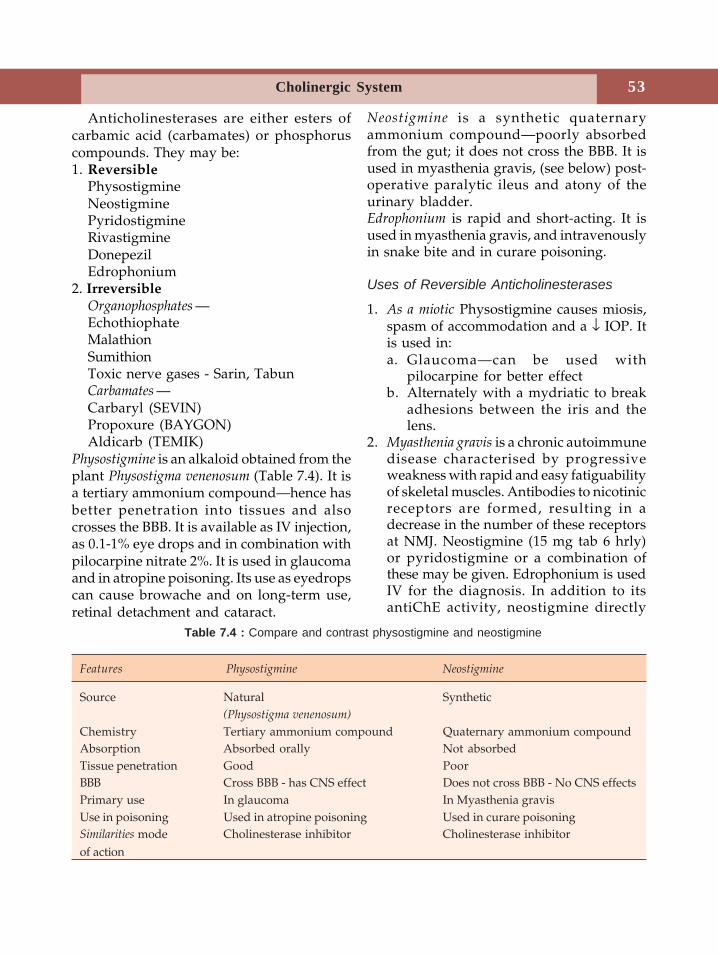
53Cholinergic System
Anticholinesterases are either esters ofcarbamic acid (carbamates) or phosphoruscompounds. They may be:1. Reversible
PhysostigmineNeostigminePyridostigmineRivastigmineDonepezilEdrophonium
2. IrreversibleOrganophosphates —EchothiophateMalathionSumithionToxic nerve gases - Sarin, TabunCarbamates —Carbaryl (SEVIN)Propoxure (BAYGON)Aldicarb (TEMIK)
Physostigmine is an alkaloid obtained from theplant Physostigma venenosum (Table 7.4). It isa tertiary ammonium compound—hence hasbetter penetration into tissues and alsocrosses the BBB. It is available as IV injection,as 0.1-1% eye drops and in combination withpilocarpine nitrate 2%. It is used in glaucomaand in atropine poisoning. Its use as eyedropscan cause browache and on long-term use,retinal detachment and cataract.
Neostigmine is a synthetic quaternaryammonium compound—poorly absorbedfrom the gut; it does not cross the BBB. It isused in myasthenia gravis, (see below) post-operative paralytic ileus and atony of theurinary bladder.Edrophonium is rapid and short-acting. It isused in myasthenia gravis, and intravenouslyin snake bite and in curare poisoning.
Uses of Reversible Anticholinesterases
1. As a miotic Physostigmine causes miosis,spasm of accommodation and a ↓ IOP. Itis used in:a. Glaucoma—can be used with
pilocarpine for better effectb. Alternately with a mydriatic to break
adhesions between the iris and thelens.
2. Myasthenia gravis is a chronic autoimmunedisease characterised by progressiveweakness with rapid and easy fatiguabilityof skeletal muscles. Antibodies to nicotinicreceptors are formed, resulting in adecrease in the number of these receptorsat NMJ. Neostigmine (15 mg tab 6 hrly)or pyridostigmine or a combination ofthese may be given. Edrophonium is usedIV for the diagnosis. In addition to itsantiChE activity, neostigmine directly
Table 7.4 : Compare and contrast physostigmine and neostigmine
Features Physostigmine Neostigmine
Source Natural Synthetic(Physostigma venenosum)
Chemistry Tertiary ammonium compound Quaternary ammonium compoundAbsorption Absorbed orally Not absorbedTissue penetration Good PoorBBB Cross BBB - has CNS effect Does not cross BBB - No CNS effectsPrimary use In glaucoma In Myasthenia gravisUse in poisoning Used in atropine poisoning Used in curare poisoningSimilarities mode Cholinesterase inhibitor Cholinesterase inhibitorof action
54 Textbook of Pharmacology for Dental and Allied Health Sciences
stimulates the nicotinic receptors andincreases the amount of ACh releasedduring each nerve impulse. AntiChEsenhance ACh levels at NMJ by preventingits destruction. They thus increase the forceof contraction and improve muscle powerby more frequent activation of the existingnicotinic receptors. In advanced diseaseantiChEs are not effective because theavailable nicotinic receptors are very few.
Factors like infection, surgery andstress can result in severe muscleweakness called-myasthenic crisis. Butsevere weakness may also result from anexcess dose of an anticholinesterase drug(flaccid paralysis due to more ofacetylcholine) called-cholinergic crisis.These two crises can be differentiated byadministering edrophonium 2 mgintravenously. The patient immediatelyimproves if it is myasthenic crisis but theweakness worsens if it is cholinergic crisis.Treatment of cholinergic crisis is withatropine while myasthenic crisis requiresa higher dose of or an alternativeanticholinergic drug.Other drugs used in myasthenia gravis are• Glucocorticoids–inhibit the production of
antibodies to the nicotinic receptors.These are used when anticholinesterasesalone are not adequate.
• Immunosuppressants–Azathioprine andcyclosporine can be used as alternativesto prednisolone in advanced myasthe-nia gravis. They inhibit the productionof antinicotinic receptor antibodies.
3. Poisoning due to anticholinergic drugsPhysostigmine is used in atropine poisoningand in toxicity due to other drugs withanticholinergic activity like phenothiazines,tricyclic antidepressants and antihis-tamines. Because physostigmine crosses theBBB, it reverses all the symptoms ofatropine poisoning including CNS effects.
4. Curare poisoning Skeletal muscle paralysiscaused by curare can be antagonisedby AntiChEs. Though edrophonium hasfast action, it is less effective thanneostigmine.
5. Postoperative paralytic ileus and urinaryretention Neostigmine may be useful.
6. Cobra bite Cobra venom, a neurotoxincauses skeletal muscle paralysis. Specifictreatment is antivenom. Intravenousedrophonium prevents respiratoryparalysis.
7. Alzheimer's disease - To overcome thedeficient cholinergic neurotransmission,rivastigmine and donepezil are tried inAlzheimer's disease. Tacrine is anotherreversible anticholinesterase tried in thisdisease but tacrine is not preferredbecause it causes hepatotoxicity.
Irreversible Anticholinesterases
Organophosphorus (OP) compounds arepowerful inhibitors of AChE enzyme;binding with the enzyme is stable–bycovalent bonds. They bind only the esteraticsite and the enzyme is phosphorylated.Effects are similar to that of cholinergicstimulation as ACh accumulates in the tissues.Organophosphates are highly lipid solubleand hence are absorbed from all routesincluding intact skin. This makes OPpoisoning possible even while insecticides areused for spraying.
Uses
Glaucoma—echothiophate eyedrops aresometimes used in glaucoma.
Organophosphorus Poisoning
Acute Toxicity
As organophosphates are used asagricultural and domestic insecticides,
55Cholinergic System
poisoning by them is quite common.Poisoning may be occupational—as whilespraying insecticides, accidental or suicidal.Symptoms result from muscarinic, nicotinicand central effects; vomiting, abdominalcramps, diarrhoea, miosis, sweating,increased salivary, tracheobronchial andgastric secretions and bronchospasm;hypotension, muscular twitchings,weakness, convulsions and coma. Death isdue to respiratory paralysis.
Treatment
1. If poisoning is through skin–removeclothing and wash the skin with soap andwater; if consumed by oral route–gastriclavage is given.
2. Maintain BP and patent airway.3. Drug of choice is atropine IV 2 mg every
10 minutes till pupil dilates. Maximumdose can be anything from 50 to 100 mgor more depending on the severity of thepoisoning. Treatment should be carefullymonitored because of the risk ofreappearance of symptoms due to delayedabsorption of the OP compounds.
4. Cholinesterase reactivators–pralidoxime,obidoxime, diacetylmonoxime. These oximecompounds combine with cholinesteraseorganophosphate complex, release thebinding and set free AChE enzyme. Thusthey reactivate the cholinesteraseenzyme. They should be given withinminutes after poisoning preferably
immediately, because the complexundergoes ‘ageing’ and the enzymecannot be released. The complex becomesmore stable by loss of a chemical groupand this is responsible for ‘ageing’.Cholinesterase reactivators are not usefulin poisoning due to carbamate com-pounds because these compounds do nothave a free site for the binding of oximes.Moreover, pralidoxime itself has weakanticholinesterase activity particularly athigher doses. In severe poisoning 1-2 gof IV pralidoxime given within fiveminutes of poisoning gives best results.But in practice it is rather uncommon fora patient to get such quick treatmentwithin minutes particularly in the ruralsetup and cholinesterase reactivators aretried upto a few hours (maximum 24hours) after poisoning.
Chronic Organophosphate Toxicity
Some OP compounds can produce neuro-toxicity (polyneuropathy) several days afterexposure to the compound. This toxicity cameto light when thousands of people developedparalysis in America after consuming"Jamaica ginger" which contained smallamounts of an OP compound (triortho-cresylphosphate). The symptoms includeweakness, fatigue, ataxia, sensorydisturbances, muscle twitching and in severecases flaccid paralysis - which may last forseveral years.
56 Textbook of Pharmacology for Dental and Allied Health Sciences
8Anticholinergic drugs are agents which blockthe effects of acetylcholine on cholinergicreceptors but conventionally antimuscarinicdrugs are referred to as anticholinergicdrugs. They are also called cholinergicblocking or parasympatholytic drugs. Drugsthat block the nicotinic receptors are ganglionblockers and neuromuscular blockers.
Anticholinergic drugs include atropine andrelated drugs—atropine is the prototype.
Atropine is obtained from the plant Atropa
belladonna. Atropine and scopolamine(hyoscine) are the belladonna alkaloids. Theycompete with acetylcholine for muscarinicreceptors and block these receptors—they aremuscarinic antagonists.
Classification
1. Natural alkaloids
Atropine, hyoscine (scopolamine)2. Semisynthetic derivatives
Homatropine, ipratropium bromide,tiotroprium bromide
3. Synthetic substitutes
• MydriaticsEucatropine, cyclopentolate, tropicamide
• Antispasmodic-antisecretory agentsPropantheline, dicyclomine,
oxyphenonium, glycopyrrolate,
telenzepine, tolterodine, propiverine
• Antiparkinsonian agentsBenzhexol, benztropine, trihexyphenidyl.
Actions
The actions of atropine and scopolamine aresimilar except that atropine is a CNSstimulant while scopolamine is a CNSdepressant and causes sedation.1. CVS—Atropine increases heart rate. In
large doses, vasodilation and hypo-tension occurs.
2. Secretions—Atropine reduces allsecretions except milk. Lacrimal, salivary,nasopharyngeal, tracheobronchial andgastric secretions are decreased.Decreased salivation results in dry mouthand difficulty in swallowing—it is anantisialogogue. Sweating is also reduced.
3. Smooth muscle• GIT – ↓ tone and motility and relieves
spasm →may result in constipation.• Biliary tract – smooth muscles are relaxed;
biliary spasm is relieved.• Bronchi – atropine causes broncho-
dilatation.• Urinary bladder – relaxes ureter and
urinary bladder and may cause urinaryretention particularly in the elderly menbecause they may be having prostatichypertrophy.
4. Eye—On local instillation, atropineproduces mydriasis by blocking themuscarinic receptors in the sphincterpupillae. The ciliary muscle is paralysedresulting in cycloplegia or paralysis ofaccommodation. Because of mydriasis,
Anticholinergic Drugs
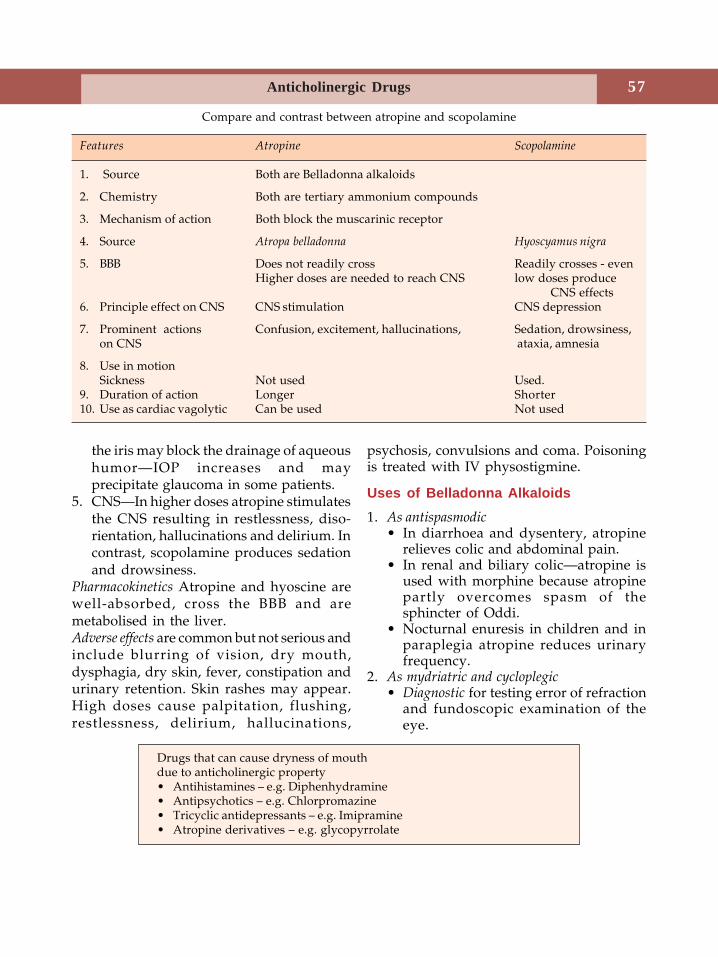
57Anticholinergic Drugs
the iris may block the drainage of aqueoushumor—IOP increases and mayprecipitate glaucoma in some patients.
5. CNS—In higher doses atropine stimulatesthe CNS resulting in restlessness, diso-rientation, hallucinations and delirium. Incontrast, scopolamine produces sedationand drowsiness.
Pharmacokinetics Atropine and hyoscine arewell-absorbed, cross the BBB and aremetabolised in the liver.Adverse effects are common but not serious andinclude blurring of vision, dry mouth,dysphagia, dry skin, fever, constipation andurinary retention. Skin rashes may appear.High doses cause palpitation, flushing,restlessness, delirium, hallucinations,
psychosis, convulsions and coma. Poisoningis treated with IV physostigmine.
Uses of Belladonna Alkaloids1. As antispasmodic
• In diarrhoea and dysentery, atropinerelieves colic and abdominal pain.
• In renal and biliary colic—atropine isused with morphine because atropinepartly overcomes spasm of thesphincter of Oddi.
• Nocturnal enuresis in children and inparaplegia atropine reduces urinaryfrequency.
2. As mydriatric and cycloplegic• Diagnostic for testing error of refraction
and fundoscopic examination of theeye.
Compare and contrast between atropine and scopolamine
Features Atropine Scopolamine
1. Source Both are Belladonna alkaloids
2. Chemistry Both are tertiary ammonium compounds
3. Mechanism of action Both block the muscarinic receptor
4. Source Atropa belladonna Hyoscyamus nigra
5. BBB Does not readily cross Readily crosses - evenHigher doses are needed to reach CNS low doses produce
CNS effects6. Principle effect on CNS CNS stimulation CNS depression
7. Prominent actions Confusion, excitement, hallucinations, Sedation, drowsiness,on CNS ataxia, amnesia
8. Use in motionSickness Not used Used.
9. Duration of action Longer Shorter10. Use as cardiac vagolytic Can be used Not used
Drugs that can cause dryness of mouthdue to anticholinergic property• Antihistamines – e.g. Diphenhydramine• Antipsychotics – e.g. Chlorpromazine• Tricyclic antidepressants – e.g. Imipramine• Atropine derivatives – e.g. glycopyrrolate
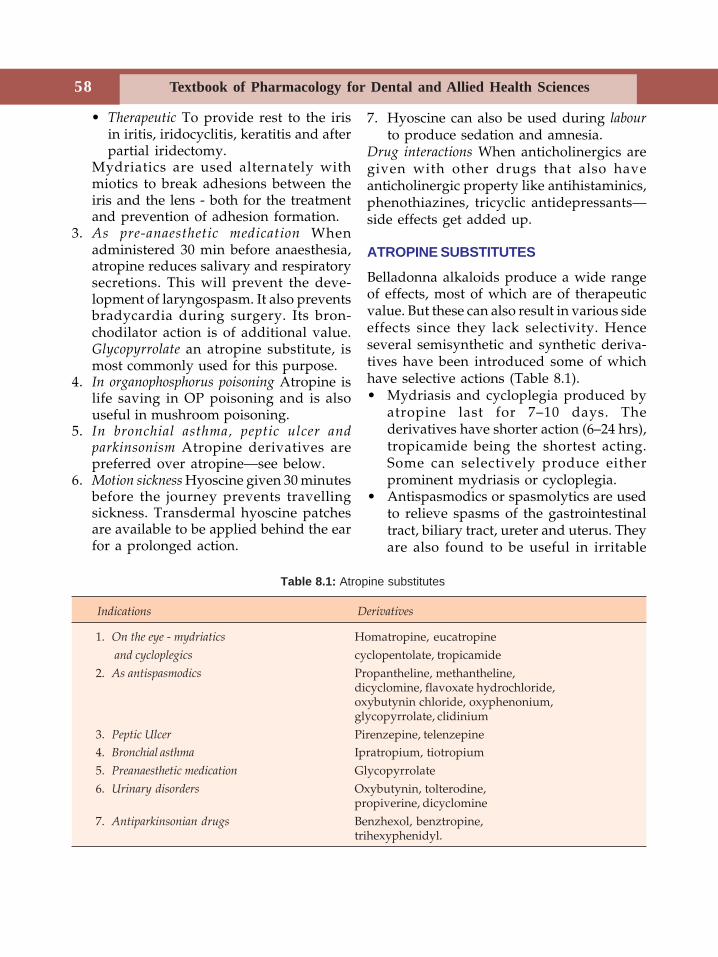
58 Textbook of Pharmacology for Dental and Allied Health Sciences
• Therapeutic To provide rest to the irisin iritis, iridocyclitis, keratitis and afterpartial iridectomy.
Mydriatics are used alternately withmiotics to break adhesions between theiris and the lens - both for the treatmentand prevention of adhesion formation.
3. As pre-anaesthetic medication Whenadministered 30 min before anaesthesia,atropine reduces salivary and respiratorysecretions. This will prevent the deve-lopment of laryngospasm. It also preventsbradycardia during surgery. Its bron-chodilator action is of additional value.Glycopyrrolate an atropine substitute, ismost commonly used for this purpose.
4. In organophosphorus poisoning Atropine islife saving in OP poisoning and is alsouseful in mushroom poisoning.
5. In bronchial asthma, peptic ulcer andparkinsonism Atropine derivatives arepreferred over atropine—see below.
6. Motion sickness Hyoscine given 30 minutesbefore the journey prevents travellingsickness. Transdermal hyoscine patchesare available to be applied behind the earfor a prolonged action.
7. Hyoscine can also be used during labourto produce sedation and amnesia.
Drug interactions When anticholinergics aregiven with other drugs that also haveanticholinergic property like antihistaminics,phenothiazines, tricyclic antidepressants—side effects get added up.
ATROPINE SUBSTITUTES
Belladonna alkaloids produce a wide rangeof effects, most of which are of therapeuticvalue. But these can also result in various sideeffects since they lack selectivity. Henceseveral semisynthetic and synthetic deriva-tives have been introduced some of whichhave selective actions (Table 8.1).• Mydriasis and cycloplegia produced by
atropine last for 7–10 days. Thederivatives have shorter action (6–24 hrs),tropicamide being the shortest acting.Some can selectively produce eitherprominent mydriasis or cycloplegia.
• Antispasmodics or spasmolytics are usedto relieve spasms of the gastrointestinaltract, biliary tract, ureter and uterus. Theyare also found to be useful in irritable
Table 8.1: Atropine substitutes
Indications Derivatives
1. On the eye - mydriatics Homatropine, eucatropine and cycloplegics cyclopentolate, tropicamide
2. As antispasmodics Propantheline, methantheline,dicyclomine, flavoxate hydrochloride,oxybutynin chloride, oxyphenonium,glycopyrrolate, clidinium
3. Peptic Ulcer Pirenzepine, telenzepine4. Bronchial asthma Ipratropium, tiotropium5. Preanaesthetic medication Glycopyrrolate6. Urinary disorders Oxybutynin, tolterodine,
propiverine, dicyclomine7. Antiparkinsonian drugs Benzhexol, benztropine,
trihexyphenidyl.

59Anticholinergic Drugs
bowel syndrome. Some of them inaddition, reduce gastrointestinal motility.
• Pirenzepine and telenzepine are selectiveM1 blockers which inhibit gastric secretionat doses that do not affect other functions.Pirenzepine also does not cross the BBB –hence has no CNS effects. They are triedin peptic ulcer.
• When used in bronchial asthma, atropinethickens the bronchial secretions andinterferes with the movement of cilia, thusfavouring formation of mucus plugs.Ipratropium bromide is a bronchodilatorthat does not affect mucociliary activity.When given as inhalation it acts only onthe airways and does not produce anysignificant systemic effects because it ispoorly absorbed.
• Glycopyrrolate is an antisialogogue(reduces salivary secretions). It is aquaternary amine – does not cross the BBB– therefore no effects on the CNS. It isgiven IM as preanaesthetic medication andin dental practice when it is necessary toreduce salivary secretions.
• Benztropine, benzhexol and trihexy-phenidyl are the derivatives used in druginduced parkinsonism.
• Urinary disorders – atropine substitutesare used to reduce urinary urgency andfrequency to relieve bladder spasm andimprove bladder capacity in urinarydisorders and following urologicsurgeries. They are also tried in nocturnalenuresis in children.
60 Textbook of Pharmacology for Dental and Allied Health Sciences
9Skeletal muscle relaxants (SMR) are drugsthat reduce the muscle tone either by actingperipherally at the neuromuscular junction(neuromuscular blockers) or centrally in thecerebrospinal axis or directly on thecontractile mechanism. They reduce thespasticity in a variety of neurologicalconditions and are also useful in surgeries.
CLASSIFICATION
Skeletal muscle relaxants may be classifiedas follows:1. Drugs acting peripherally at the NMJ
Competitive blockers(Nondepolarising agents)–
d-Tubocurarine,pancuronium,alcuronium,atracurium,mivacurium,rocuronium,doxacurium,pipecuronium,vecuronium,rapacuronium,gallamine
Depolarising blockers–Succinylcholine,decamethonium
2. Drugs acting centrally-Diazepam, baclofen,mephenesin,tizanidine.
3. Drugs acting directly on the muscle–Dantrolene.
PERIPHERALLY ACTING SKELETALMUSCLE RELAXANTSNeuromuscular Blockers (NMB)Competitive Blockers
Curare was used by the South AmericanIndians as an arrow poison for hunting wildanimals because curare paralysed theanimals. On extensive research, the activeprinciple from curare, tubocurarine wasidentified.
d-tubocurarine (d-Tc) is the dextro-rotatory quaternary ammonium alkaloidobtained from the plant Chondrodendrontomentosum and plants of the Strychnosspecies (l-tubocurarine is less potent). Severalsynthetic agents have been developed. Allthese are quaternary ammonium compoundsbecause of which they are not well absorbedand are quickly excreted.Mechanism of action Non-depolarisingblockers bind to nicotinic receptors on themotor end plate and block the actions ofacetylcholine by competitive blockade(Fig. 9.1). These compounds slowlydissociate from the receptors and trans-mission is gradually restored. Thus theaction of d-Tc is reversible.
TubocurarinePharmacological Actions
Skeletal muscle On parenteral adminis-tration, tubocurarine initially causes muscularweakness followed by flaccid paralysis.Small muscles of the eyes and fingers are
Skeletal MuscleRelaxants
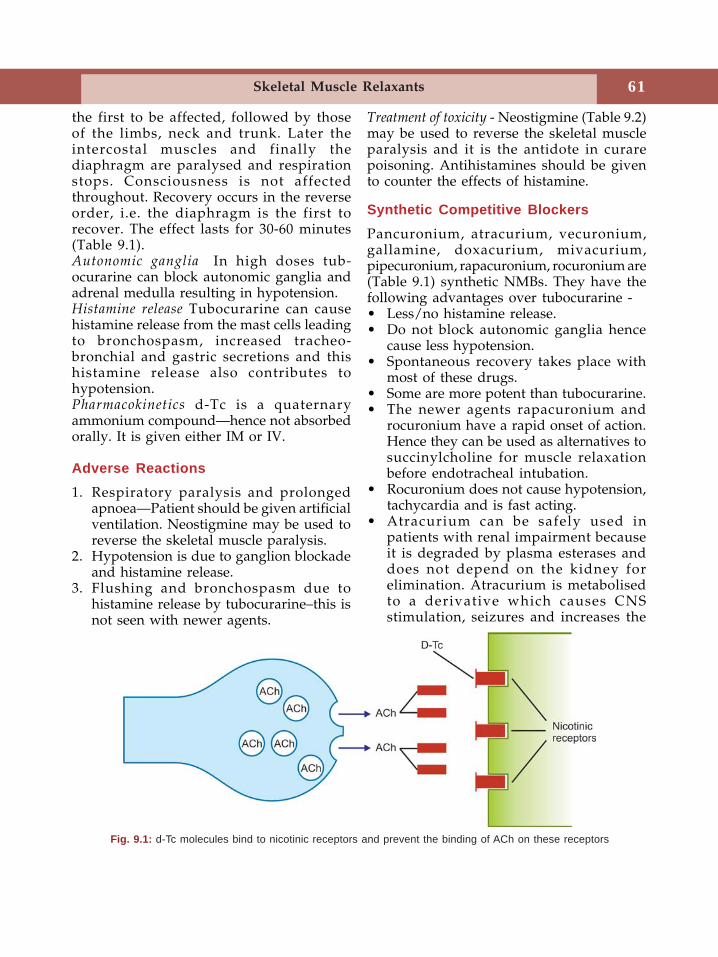
61Skeletal Muscle Relaxants
the first to be affected, followed by thoseof the limbs, neck and trunk. Later theintercostal muscles and finally thediaphragm are paralysed and respirationstops. Consciousness is not affectedthroughout. Recovery occurs in the reverseorder, i.e. the diaphragm is the first torecover. The effect lasts for 30-60 minutes(Table 9.1).Autonomic ganglia In high doses tub-ocurarine can block autonomic ganglia andadrenal medulla resulting in hypotension.Histamine release Tubocurarine can causehistamine release from the mast cells leadingto bronchospasm, increased tracheo-bronchial and gastric secretions and thishistamine release also contributes tohypotension.Pharmacokinetics d-Tc is a quaternaryammonium compound—hence not absorbedorally. It is given either IM or IV.
Adverse Reactions1. Respiratory paralysis and prolonged
apnoea—Patient should be given artificialventilation. Neostigmine may be used toreverse the skeletal muscle paralysis.
2. Hypotension is due to ganglion blockadeand histamine release.
3. Flushing and bronchospasm due tohistamine release by tubocurarine–this isnot seen with newer agents.
Treatment of toxicity - Neostigmine (Table 9.2)may be used to reverse the skeletal muscleparalysis and it is the antidote in curarepoisoning. Antihistamines should be givento counter the effects of histamine.
Synthetic Competitive BlockersPancuronium, atracurium, vecuronium,gallamine, doxacurium, mivacurium,pipecuronium, rapacuronium, rocuronium are(Table 9.1) synthetic NMBs. They have thefollowing advantages over tubocurarine -• Less/no histamine release.• Do not block autonomic ganglia hence
cause less hypotension.• Spontaneous recovery takes place with
most of these drugs.• Some are more potent than tubocurarine.• The newer agents rapacuronium and
rocuronium have a rapid onset of action.Hence they can be used as alternatives tosuccinylcholine for muscle relaxationbefore endotracheal intubation.
• Rocuronium does not cause hypotension,tachycardia and is fast acting.
• Atracurium can be safely used inpatients with renal impairment becauseit is degraded by plasma esterases anddoes not depend on the kidney forelimination. Atracurium is metabolisedto a derivative which causes CNSstimulation, seizures and increases the
Fig. 9.1: d-Tc molecules bind to nicotinic receptors and prevent the binding of ACh on these receptors
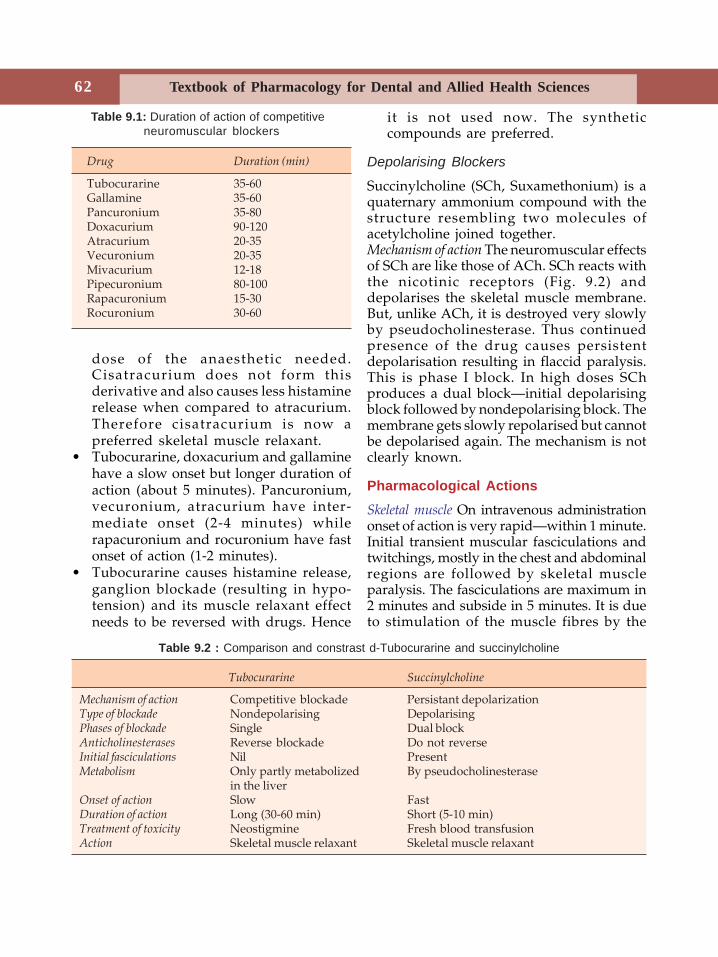
62 Textbook of Pharmacology for Dental and Allied Health Sciences
dose of the anaesthetic needed.Cisatracurium does not form thisderivative and also causes less histaminerelease when compared to atracurium.Therefore cisatracurium is now apreferred skeletal muscle relaxant.
• Tubocurarine, doxacurium and gallaminehave a slow onset but longer duration ofaction (about 5 minutes). Pancuronium,vecuronium, atracurium have inter-mediate onset (2-4 minutes) whilerapacuronium and rocuronium have fastonset of action (1-2 minutes).
• Tubocurarine causes histamine release,ganglion blockade (resulting in hypo-tension) and its muscle relaxant effectneeds to be reversed with drugs. Hence
it is not used now. The syntheticcompounds are preferred.
Depolarising Blockers
Succinylcholine (SCh, Suxamethonium) is aquaternary ammonium compound with thestructure resembling two molecules ofacetylcholine joined together.Mechanism of action The neuromuscular effectsof SCh are like those of ACh. SCh reacts withthe nicotinic receptors (Fig. 9.2) anddepolarises the skeletal muscle membrane.But, unlike ACh, it is destroyed very slowlyby pseudocholinesterase. Thus continuedpresence of the drug causes persistentdepolarisation resulting in flaccid paralysis.This is phase I block. In high doses SChproduces a dual block—initial depolarisingblock followed by nondepolarising block. Themembrane gets slowly repolarised but cannotbe depolarised again. The mechanism is notclearly known.
Pharmacological ActionsSkeletal muscle On intravenous administrationonset of action is very rapid—within 1 minute.Initial transient muscular fasciculations andtwitchings, mostly in the chest and abdominalregions are followed by skeletal muscleparalysis. The fasciculations are maximum in2 minutes and subside in 5 minutes. It is dueto stimulation of the muscle fibres by the
Table 9.1: Duration of action of competitiveneuromuscular blockers
Drug Duration (min)
Tubocurarine 35-60Gallamine 35-60Pancuronium 35-80Doxacurium 90-120Atracurium 20-35Vecuronium 20-35Mivacurium 12-18Pipecuronium 80-100Rapacuronium 15-30Rocuronium 30-60
Table 9.2 : Comparison and constrast d-Tubocurarine and succinylcholine
Tubocurarine Succinylcholine
Mechanism of action Competitive blockade Persistant depolarizationType of blockade Nondepolarising DepolarisingPhases of blockade Single Dual blockAnticholinesterases Reverse blockade Do not reverseInitial fasciculations Nil PresentMetabolism Only partly metabolized By pseudocholinesterase
in the liverOnset of action Slow FastDuration of action Long (30-60 min) Short (5-10 min)Treatment of toxicity Neostigmine Fresh blood transfusionAction Skeletal muscle relaxant Skeletal muscle relaxant
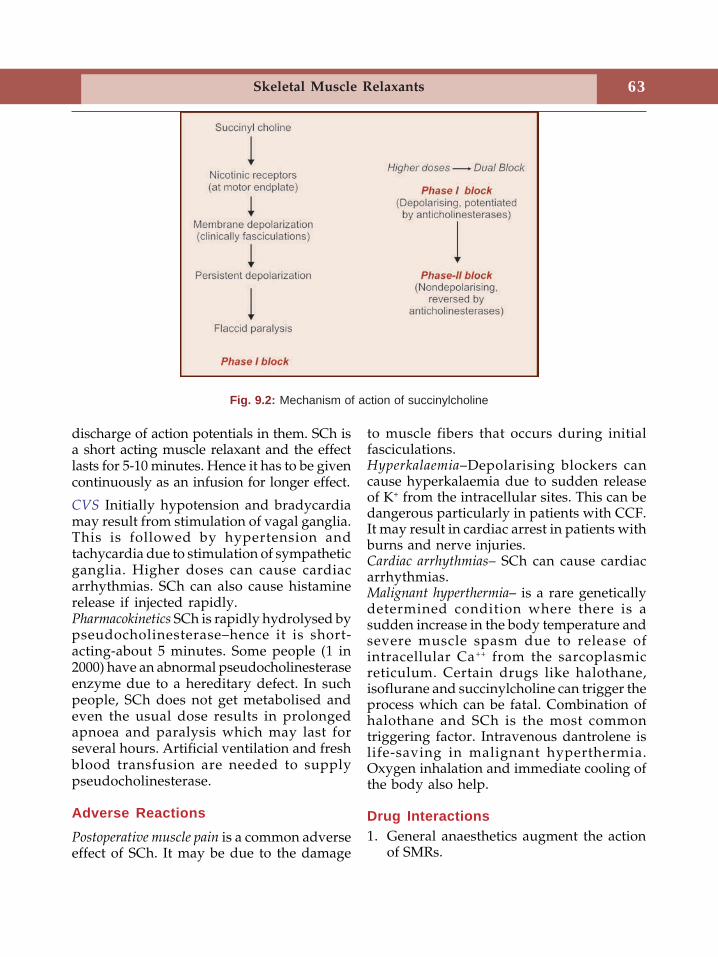
63Skeletal Muscle Relaxants
discharge of action potentials in them. SCh isa short acting muscle relaxant and the effectlasts for 5-10 minutes. Hence it has to be givencontinuously as an infusion for longer effect.
CVS Initially hypotension and bradycardiamay result from stimulation of vagal ganglia.This is followed by hypertension andtachycardia due to stimulation of sympatheticganglia. Higher doses can cause cardiacarrhythmias. SCh can also cause histaminerelease if injected rapidly.Pharmacokinetics SCh is rapidly hydrolysed bypseudocholinesterase–hence it is short-acting-about 5 minutes. Some people (1 in2000) have an abnormal pseudocholinesteraseenzyme due to a hereditary defect. In suchpeople, SCh does not get metabolised andeven the usual dose results in prolongedapnoea and paralysis which may last forseveral hours. Artificial ventilation and freshblood transfusion are needed to supplypseudocholinesterase.
Adverse ReactionsPostoperative muscle pain is a common adverseeffect of SCh. It may be due to the damage
to muscle fibers that occurs during initialfasciculations.Hyperkalaemia–Depolarising blockers cancause hyperkalaemia due to sudden releaseof K+ from the intracellular sites. This can bedangerous particularly in patients with CCF.It may result in cardiac arrest in patients withburns and nerve injuries.Cardiac arrhythmias– SCh can cause cardiacarrhythmias.Malignant hyperthermia– is a rare geneticallydetermined condition where there is asudden increase in the body temperature andsevere muscle spasm due to release ofintracellular Ca++ from the sarcoplasmicreticulum. Certain drugs like halothane,isoflurane and succinylcholine can trigger theprocess which can be fatal. Combination ofhalothane and SCh is the most commontriggering factor. Intravenous dantrolene islife-saving in malignant hyperthermia.Oxygen inhalation and immediate cooling ofthe body also help.
Drug Interactions1. General anaesthetics augment the action
of SMRs.
Fig. 9.2: Mechanism of action of succinylcholine
64 Textbook of Pharmacology for Dental and Allied Health Sciences
2. Anticholinesterases like neostigminereverse the action of competitive blockers.
3. Aminoglycosides and calcium channelblockers potentiate the action of SMRs.
Uses of Peripherally Acting SkeletalMuscle RelaxantsInappropriate use of peripherally acting SMRscan be fatal. Hence they should be given onlyby qualified anaesthetists or adequatelytrained doctors.1. Adjuvant to anaesthesia Adequate muscle
relaxation is essential during surgeries.Skeletal muscle relaxants are used asadjuvants to general anaesthesia. Shortacting SMRs like succinylcholine are usedduring endotracheal intubation. SMRs arealso useful in laryngoscopy, bronc-hoscopy, esophagoscopy and inorthopaedic procedures like reduction offractures and dislocations.
2. In electroconvulsive therapy SMRs protect thepatient from convulsions and traumaduring ECT.
3. In spastic disorders SMRs are used toovercome the spasm of tetanus, athetosisand status epilepticus.
CENTRALLY ACTING MUSCLE RELAXANTSThese drugs act on higher centres and causemuscle relaxation without loss of conscious-ness. They also have sedative properties.
Mechanism of ActionCentrally acting muscle relaxants depress thespinal polysynaptic reflexes. These reflexesmaintain the muscle tone. By depressing thesespinal reflexes, centrally acting musclerelaxants reduce the muscle tone.Diazepam has useful antispastic activity. It canbe used in relieving muscle spasm of almostany origin including local muscle trauma(see Page 140).Baclofen is an analog of the inhibitoryneurotransmitter GABA. It is a GABAB
agonist. It depresses the monosynaptic andpolysynaptic reflexes in the spinal cord. Itrelieves painful spasms including flexor andextensor spasms and may also improvebladder and bowel functions in patients withspinal lesions. Normal tendon reflexes arenot affected.
Baclofen is generally given orally. It shouldbe gradually withdrawn after prolonged usebecause abrupt withdrawal can cause anxiety,palpitations and hallucinations.
Side effects are drowsiness, weakness andataxia.Mephenesin is not preferred due to its sideeffects. A number of related drugs likecarisoprodol, methocarbamol, chlorzoxazone areused in acute muscle spasm caused by localtrauma. All of them also cause sedation.Tizanidine is a congener of clonidine. It is acentral α2 agonist like clonidine. It increasespresynaptic inhibition of motor neurons andreduces muscle spasms. Adverse effectsinclude drowsiness, weakness, hypotensionand dry mouth. Tizanidine is used in thetreatment of spasticity due to stroke, multiplesclerosis and amyotropic lateral sclerosis.
Other centrally acting spasmolytic agentsinclude riluzole, gabapentin and progabide.Riluzole has both presynaptic and post-synaptic effects. It inhibits glutamate releasein the CNS. It is well tolerated with minoradverse effects like nausea and diarrhoea. Itis used to reduce spasticity in amyotropiclateral sclerosis.
Uses of Centrally Acting MuscleRelaxants1. Musculoskeletal disorders like muscle strains,
sprains, myalgias, cervical rootsyndromes, herniated disc syndromes,low backache, dislocations, arthritis,fibrositis and bursitis all cause painfulmuscle spasms. Muscle relaxants are usedwith analgesics in these conditions.
2. Spastic neurological disorders like cerebralpalsy, multiple sclerosis, poliomyelitis,

65Skeletal Muscle Relaxants
hemiplegia and quadriplegia are treatedwith diazepam or baclofen.
3. Tetanus Diazepam is given IV.4. ECT Diazepam is given along with
peripherally acting SMRs.5. Orthopaedic procedures like fracture
reduction may be done afteradministering diazepam.
DIRECTLY ACTING MUSCLE RELAXANTSDantrolene directly affects the skeletal musclecontractile mechanism. It inhibits the musclecontraction by preventing the calcium releasefrom the sarcoplasmic reticulum.
Adverse effects include drowsiness,dizziness, fatigue, diarrhoea, muscleweakness and rarely hepatotoxicity. Liverfunction tests should be done to look forhepatotoxicity.Uses Dantrolene is used in spastic disorderslike hemiplegia, paraplegia, spinal injuries,multiple sclerosis and cerebral palsy.Dantrolene is the drug of choice in malignanthyperthermia which is due to excessiverelease of calcium from the sarcoplasmicreticulum. Dantrolene blocks the release ofCa++ from the sarcoplasmic reticulum andrelieves muscle spasm in malignanthyperthermia.
DRUGS USED IN THE TREATMENT OFLOCAL MUSCLE SPASMSeveral agents are used for the treatment oflocal muscle spasms which may result frominjury or strain. Cyclobenzaprine, metax-alone, carisoprodol, chlorzoxazone, mep-robamate and methocarbamol are some ofthem. They have the following commonfeatures-
• All these drugs act by depressing spinalpolysynaptic reflexes.
• Common adverse reactions includedrowsiness and dizziness.
• Cyclobenzaprine has anticholinergiceffects and can therefore cause drynessof mouth, drowsiness and dizziness.
• Many of them are available incombination with NSAIDs.
• NSAIDs are equally or more effective inrelieving muscle spasms.
Botulinum toxin is produced by the anaerobicbacterium Clostridium botulinum. The toxininhibits the release of acetylcholine at thecholinergic synapses resulting in flaccidparalysis of skeletal muscles.
Botulinum toxin is useful (local injection)in the treatment of dystonias, includingsports or writer’s cramps, muscle spasms,tremors, cerebral palsy and in rigidity seenin extrapyramidal disorders. It is commonlyused to relieve blepharospasm (spasm of theorbicularis oculi muscle of the eyes).Botulinum toxin is also gaining popularity incosmetic therapy to remove facial lines bylocal injection.Skeletal muscle relaxants in dentistry1. Spasm SMRs like mephenesin, diazepam
and others along with analgesics are usedto relieve the spasm of the masticatorymuscles. Such spasm can cause pain aroundtemporomandibular joint.
2. Dislocation–Sometimes in temporo-mandibular joint dislocation, just relaxingthe related muscles with SMRs may besufficient to set right the dislocation.
3. Fractures–SMRs may also be used toreduce fractures of the mandible.
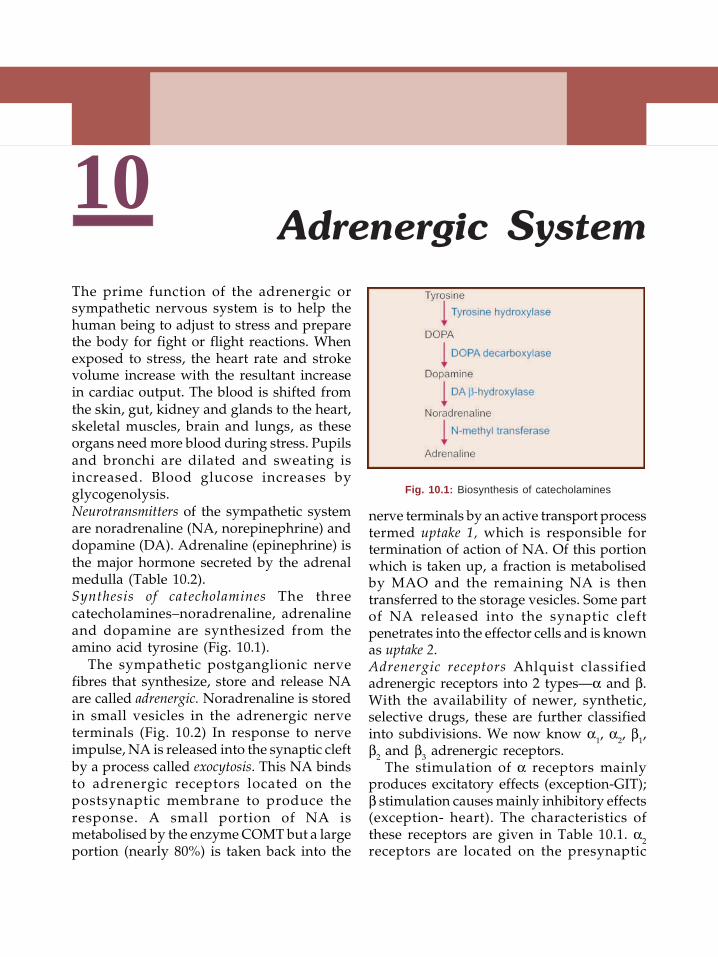
66 Textbook of Pharmacology for Dental and Allied Health Sciences
10The prime function of the adrenergic orsympathetic nervous system is to help thehuman being to adjust to stress and preparethe body for fight or flight reactions. Whenexposed to stress, the heart rate and strokevolume increase with the resultant increasein cardiac output. The blood is shifted fromthe skin, gut, kidney and glands to the heart,skeletal muscles, brain and lungs, as theseorgans need more blood during stress. Pupilsand bronchi are dilated and sweating isincreased. Blood glucose increases byglycogenolysis.Neurotransmitters of the sympathetic systemare noradrenaline (NA, norepinephrine) anddopamine (DA). Adrenaline (epinephrine) isthe major hormone secreted by the adrenalmedulla (Table 10.2).Synthesis of catecholamines The threecatecholamines–noradrenaline, adrenalineand dopamine are synthesized from theamino acid tyrosine (Fig. 10.1).
The sympathetic postganglionic nervefibres that synthesize, store and release NAare called adrenergic. Noradrenaline is storedin small vesicles in the adrenergic nerveterminals (Fig. 10.2) In response to nerveimpulse, NA is released into the synaptic cleftby a process called exocytosis. This NA bindsto adrenergic receptors located on thepostsynaptic membrane to produce theresponse. A small portion of NA ismetabolised by the enzyme COMT but a largeportion (nearly 80%) is taken back into the
nerve terminals by an active transport processtermed uptake 1, which is responsible fortermination of action of NA. Of this portionwhich is taken up, a fraction is metabolisedby MAO and the remaining NA is thentransferred to the storage vesicles. Some partof NA released into the synaptic cleftpenetrates into the effector cells and is knownas uptake 2.Adrenergic receptors Ahlquist classifiedadrenergic receptors into 2 types—α and β.With the availability of newer, synthetic,selective drugs, these are further classifiedinto subdivisions. We now know α1, α2, β1,β2 and β3 adrenergic receptors.
The stimulation of α receptors mainlyproduces excitatory effects (exception-GIT);β stimulation causes mainly inhibitory effects(exception- heart). The characteristics ofthese receptors are given in Table 10.1. α2receptors are located on the presynaptic
Adrenergic System
Fig. 10.1: Biosynthesis of catecholamines
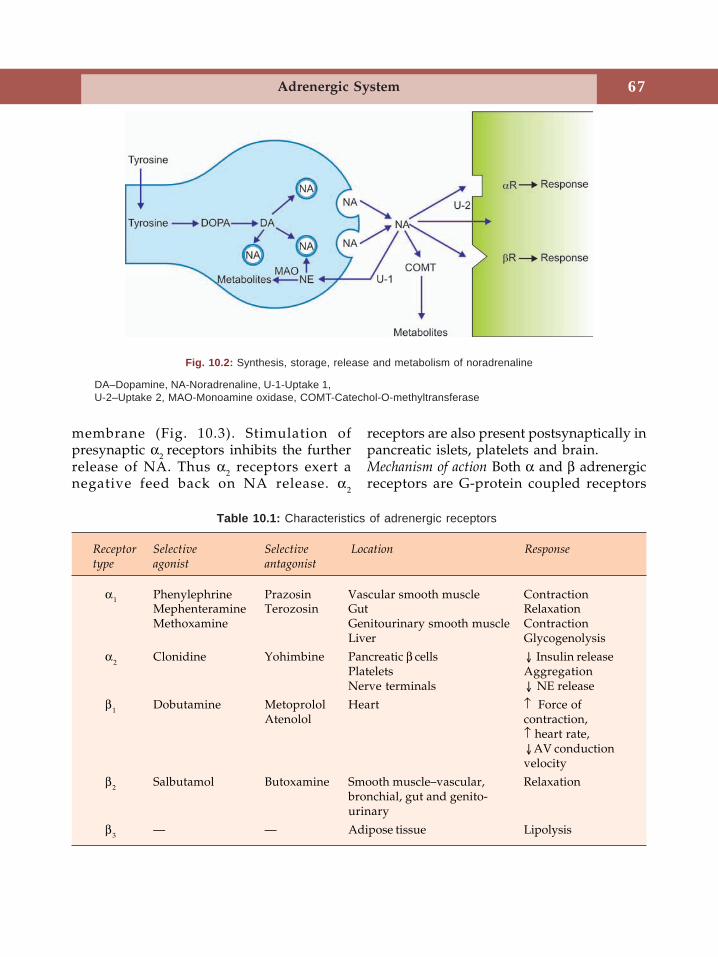
67Adrenergic System
membrane (Fig. 10.3). Stimulation ofpresynaptic α2 receptors inhibits the furtherrelease of NA. Thus α2 receptors exert anegative feed back on NA release. α2
receptors are also present postsynaptically inpancreatic islets, platelets and brain.Mechanism of action Both α and β adrenergicreceptors are G-protein coupled receptors
Fig. 10.2: Synthesis, storage, release and metabolism of noradrenaline
Table 10.1: Characteristics of adrenergic receptors
Receptor Selective Selective Location Responsetype agonist antagonist
α1 Phenylephrine Prazosin Vascular smooth muscle ContractionMephenteramine Terozosin Gut RelaxationMethoxamine Genitourinary smooth muscle Contraction
Liver Glycogenolysis
α2 Clonidine Yohimbine Pancreatic β cells Insulin releasePlatelets AggregationNerve terminals NE release
β1 Dobutamine Metoprolol Heart ↑ Force ofAtenolol contraction,
↑ heart rate,AV conductionvelocity
β2 Salbutamol Butoxamine Smooth muscle–vascular, Relaxationbronchial, gut and genito-urinary
β3 — — Adipose tissue Lipolysis
DA–Dopamine, NA-Noradrenaline, U-1-Uptake 1,U-2–Uptake 2, MAO-Monoamine oxidase, COMT-Catechol-O-methyltransferase
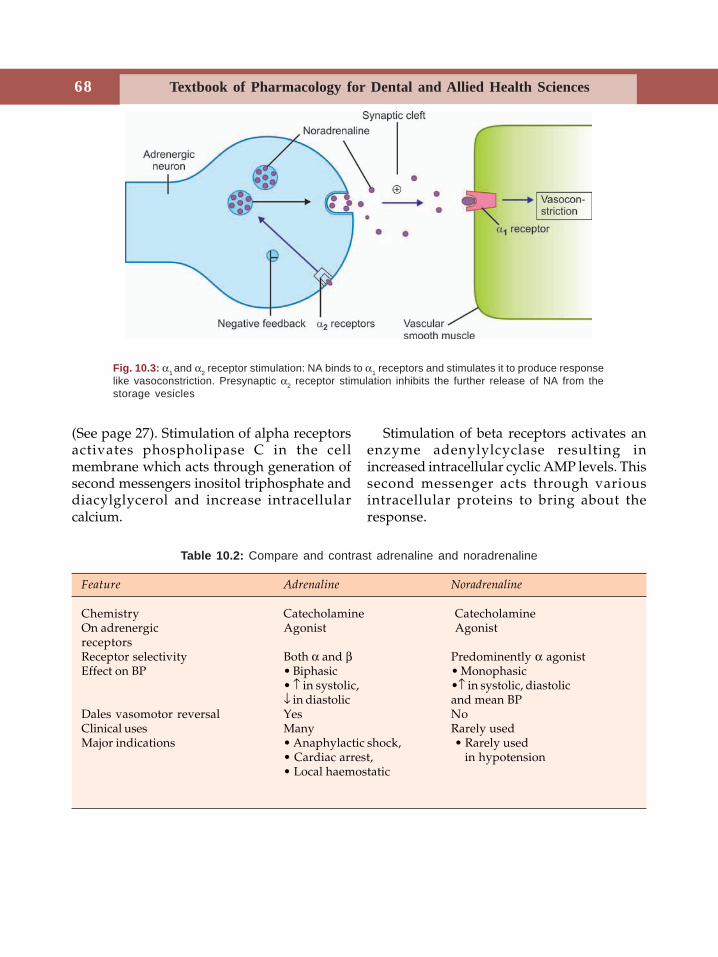
68 Textbook of Pharmacology for Dental and Allied Health Sciences
(See page 27). Stimulation of alpha receptorsactivates phospholipase C in the cellmembrane which acts through generation ofsecond messengers inositol triphosphate anddiacylglycerol and increase intracellularcalcium.
Stimulation of beta receptors activates anenzyme adenylylcyclase resulting inincreased intracellular cyclic AMP levels. Thissecond messenger acts through variousintracellular proteins to bring about theresponse.
Table 10.2: Compare and contrast adrenaline and noradrenaline
Feature Adrenaline Noradrenaline
Chemistry Catecholamine CatecholamineOn adrenergic Agonist AgonistreceptorsReceptor selectivity Both α and β Predominently α agonistEffect on BP • Biphasic • Monophasic
• ↑ in systolic, •↑ in systolic, diastolic↓ in diastolic and mean BP
Dales vasomotor reversal Yes NoClinical uses Many Rarely usedMajor indications • Anaphylactic shock, • Rarely used
• Cardiac arrest, in hypotension• Local haemostatic
Fig. 10.3: α1 and α2 receptor stimulation: NA binds to α1 receptors and stimulates it to produce responselike vasoconstriction. Presynaptic α2 receptor stimulation inhibits the further release of NA from thestorage vesicles
11Sympathomimetics are drugs whose actionsmimic that of sympathetic stimulation.Catecholamines and sympathomimetics oradrenergic drugs may be classified in variousways depending on the presence/absence ofcatechol nucleus, mode of action andtherapeutic indications as follows:
CLASSIFICATION
I. Chemical classification—based on the
presence/absence of catechol nucleus
1. Catecholamines
Noradrenaline (NA),Adrenaline,Dopamine (DA),Isoprenaline (Synthetic)
2. Non-catecholamines
Ephedrine,Amphetamine
II. Depending on the mode of action
1. Directly acting sympathomimetics(by interacting with adrenergicreceptors)Noradrenaline, adrenaline,
dopamine, isoprenaline
2. Indirectly acting sympathomimetics(by releasing NA from nerveterminals)Amphetamine, tyramine
3. Mixed action amines(both direct and indirect actions)Ephedrine, methoxamine
III. Therapeutic or clinical classification1. Vasopressors Noradrenaline,
dopamine, methoxamine,metaraminol
2. Cardiac stimulantsAdrenaline, dopamine,dobutamine,isoprenaline, ephedrine
3. CNS stimulantsAmphetamine,ephedrine
4. BronchodilatorsAdrenaline, isoprenaline,salbutamol, terbutaline,salmeterol, perbuterol,fenoterol, formoterol
5. Nasal decongestantsEphedrine,pseudoephedrine,phenylpropanolamine,phenylephrine,oxymetazoline,xylometazoline
6. Appetite suppressants(anorectics) Fenfluramine,
dexfenfluramine
7. Uterine relaxantsSalbutamol, terbutaline,isosxuprine, ritodrine
Actions
1. Cardiovascular SystemHeart Adrenaline is a powerful cardiacstimulant. Acting through β1 receptors, it
Adrenergic Drugs(Sympathomimetics)
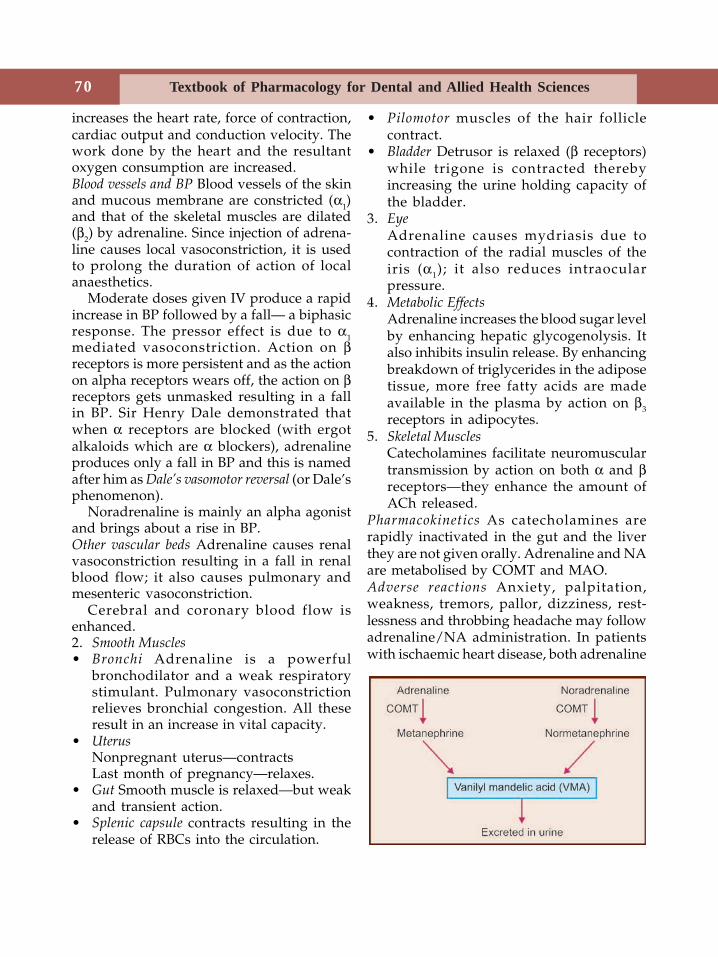
70 Textbook of Pharmacology for Dental and Allied Health Sciences
increases the heart rate, force of contraction,cardiac output and conduction velocity. Thework done by the heart and the resultantoxygen consumption are increased.Blood vessels and BP Blood vessels of the skinand mucous membrane are constricted (α1)and that of the skeletal muscles are dilated(β2) by adrenaline. Since injection of adrena-line causes local vasoconstriction, it is usedto prolong the duration of action of localanaesthetics.
Moderate doses given IV produce a rapidincrease in BP followed by a fall— a biphasicresponse. The pressor effect is due to α1mediated vasoconstriction. Action on βreceptors is more persistent and as the actionon alpha receptors wears off, the action on βreceptors gets unmasked resulting in a fallin BP. Sir Henry Dale demonstrated thatwhen α receptors are blocked (with ergotalkaloids which are α blockers), adrenalineproduces only a fall in BP and this is namedafter him as Dale’s vasomotor reversal (or Dale’sphenomenon).
Noradrenaline is mainly an alpha agonistand brings about a rise in BP.Other vascular beds Adrenaline causes renalvasoconstriction resulting in a fall in renalblood flow; it also causes pulmonary andmesenteric vasoconstriction.
Cerebral and coronary blood flow isenhanced.2. Smooth Muscles• Bronchi Adrenaline is a powerful
bronchodilator and a weak respiratorystimulant. Pulmonary vasoconstrictionrelieves bronchial congestion. All theseresult in an increase in vital capacity.
• UterusNonpregnant uterus—contractsLast month of pregnancy—relaxes.
• Gut Smooth muscle is relaxed—but weakand transient action.
• Splenic capsule contracts resulting in therelease of RBCs into the circulation.
• Pilomotor muscles of the hair folliclecontract.
• Bladder Detrusor is relaxed (β receptors)while trigone is contracted therebyincreasing the urine holding capacity ofthe bladder.
3. EyeAdrenaline causes mydriasis due tocontraction of the radial muscles of theiris (α1); it also reduces intraocularpressure.
4. Metabolic EffectsAdrenaline increases the blood sugar levelby enhancing hepatic glycogenolysis. Italso inhibits insulin release. By enhancingbreakdown of triglycerides in the adiposetissue, more free fatty acids are madeavailable in the plasma by action on β3receptors in adipocytes.
5. Skeletal MusclesCatecholamines facilitate neuromusculartransmission by action on both α and βreceptors—they enhance the amount ofACh released.
Pharmacokinetics As catecholamines arerapidly inactivated in the gut and the liverthey are not given orally. Adrenaline and NAare metabolised by COMT and MAO.Adverse reactions Anxiety, palpitation,weakness, tremors, pallor, dizziness, rest-lessness and throbbing headache may followadrenaline/NA administration. In patientswith ischaemic heart disease, both adrenaline

71Adrenergic Drugs (Sympathomimetics)
and NA can precipitate anginal pain. RapidIV injection can cause sudden sharp rise inBP which may precipitate arrhythmias,subarachnoid haemorrhage or hemiplegia.Preparations Adrenaline 1:1000, 1: 10,000 and1:1,00,000 solutions are available for injection.Adrenaline is given SC/IM; intracardiac inemergencies. Adrenaline aerosol forinhalation and 2% ophthalmic solution arealso available.
Uses of Adrenaline
1. Anaphylactic shock Adrenaline is the drugof choice (0.3-0.5 ml of 1:1000 solution). Itpromptly reverses hypotension, laryngealoedema and bronchospasm and is lifesaving in presence of anaphylactic shock.IM route is preferred as absorption by SCroute is not reliable in presence of shock.Dentists should be well versed with theuse of adrenaline for this purpose becauseanaphylaxis can occur following the useof any drug even in dental practice.
2. Cardiac arrest Sudden cardiac arrest (Table11.2) due to drowning, electrocution, etc.are treated with intracardiac adrenaline(into 4th or 5th intercostal space, 2-3inches from the sternum); before injecting,ensure that the tip of the needle is in theheart–when the piston is withdrawn,blood should enter the syringe.
3. Control of haemorrhage Cotton or gauzesoaked in adrenaline–1: 10,000 to 1 : 20,000concentration is used as a topicalhaemostatic to control bleeding. Bleedingstops due to vasoconstriction. Adrenalinepacks are used to control bleeding aftertooth extraction and in epistaxis.
4. With local anaesthetics (see page 130)Injected with LA, adrenaline producesvasoconstriction and reduces the rate ofabsorption of the LA. By this it prolongsthe action of the LA. It also reducessystemic toxicity of LA because as andwhen the LA is getting absorbed, it gets
metabolised. 1: 10,000 to 1: 2,00,000adrenaline is used for this purpose.
5. Acute bronchial asthma Adrenalineproduces bronchodilation. It may be givenSC/inhalation, but is not preferred as moreselective drugs are available (See page216).
6. Glaucoma (see page 49) Adrenaline ↓ IOPand can be used in glaucoma. But it hasthe disadvantages of being - (1) poorlyabsorbed, (2) short acting as it is quicklymetabolised in the eye. Dipivefrin is aprodrug which gets converted toadrenaline in the eye by the action ofcorneal esterases. Dipivefrin has goodpenetrability due to high lipid solubilityand it is used in glaucoma.
Contraindications
Adrenaline is contraindicated in patients withangina pectoris, hypertension and in patientson β blockers.Noradrenaline can be used in shock to increaseBP—but it is very rarely used.Isoprenaline (Isoproterenol, Isopropylarterenol) is a synthetic catecholamine withpredominantly β receptor stimulant actionand negligible α actions. It has cardiacstimulant and smooth muscle relaxantproperties. Due to vasodilation BP falls; it isa potent bronchodilator. Adverse effectsinclude palpitation, angina, headache andflushing.
Isoprenaline is used in heart block andshock for its cardiac stimulant actions. It canbe used in bronchial asthma (page 216).Dopamine is the precursor of NA. It acts ondopaminergic and adrenergic receptors. It isa central neurotransmitter. Low dosesstimulate vascular D1 receptors in renal,mesenteric and coronary beds causingvasodilatation in these vessels. Hence renalblood flow and GFR increase. Higher dosescause cardiac stimulation through β1 receptorsand in high doses α1 receptors are activated

72 Textbook of Pharmacology for Dental and Allied Health Sciences
resulting in vasoconstriction and increasedBP. Dopamine does not cross the BBB - henceit has no CNS effects. It is given IV (2-5 μg/Kg/min). It is short acting and the infusionrate can be adjusted to get the appropriateeffect by monitoring BP. Dopamine ismetabolised by COMT and MAO. Epinine(Ibopamine) is an ester of methyldopaminewhich acts like dopamine.Adverse effects Nausea, vomiting, palpitation,headache, angina, sudden rise in BP mayoccur.Uses Dopamine is used in the treatment ofshock—cardiogenic, hypovolaemic and septicshock for the following reasons:• Dopamine increases renal blood flow and
thereby GFR.• DA stimulates the heart-increases force of
contraction, cardiac output and B.P.Hence it is of special value when shock isassociated with renal dysfunction and lowcardiac output.
• Because DA is short acting, the responsecan be easily controlled by modifying theinfusion rate.
Dopexamine is a synthetic analog of dopamineacting on D1 D2 and β2 receptors. It is foundto have beneficial effects in CCF.Dobutamine a derivative of dopamine, is arelatively selective β1 agonist. Though it alsoactivates α1 receptors, in therapeutic dosesthe only dominant action is an increase in theforce of contraction of the heart without asignificant increase in the heart rate. Hencethe increase in myocardial oxygen demandis milder when compared to dopamine andis therefore more useful than dopamine incardiogenic shock. Dobutamine is used inpatients with CCF or acute myocardialinfarction or following cardiac surgery whenthere may be pump failure.Fenoldopam is a selective D1 agonist whichdilates coronary, renal and mesenteric
arteries. It is used as an IV infusion in severehypertension to rapidly reduce the BP.
NONCATECHOLAMINES
Noncatecholamines are devoid of catecholnucleus, they act both by direct stimulationof the adrenergic receptors and indirectly byreleasing NA. In contrast to catecholamines,they are effective orally (Table 11.1),relatively resistant to MAO and therefore arelonger-acting; they cross the blood-brainbarrier and have CNS effects.Ephedrine is an alkaloid obtained from theplants of the genus Ephedra. Ephedrine actsby direct stimulation of α and β receptorsand indirectly through release of NA.Repeated administration at short intervalsresult in tachyphylaxis. Ephedrine raises BPby peripheral vasoconstriction and byincreasing the cardiac output. Like adrenalineit relaxes smooth muscles; it is a CNSstimulant and produces insomnia,restlessness, anxiety, tremors and increasedmental activity.Adverse effects include gastric upset, insomnia,tremors and difficulty in micturition.Uses1. Bronchial asthma Ephedrine is useful in
mild chronic bronchial asthma (Seepage 218) but it is not preferred.
2. Nasal decongestion Ephedrine nasal dropsare used. Pseudoephedrine—an isomer ofephedrine is used orally for decongestion.It causes vasoconstriction in the skin andmucous membrane but its effects on theCNS and the heart are milder.
3. Mydriasis Ephedrine eyedrops are usedto produce mydriasis without cycloplegia.
4. Hypotension For prevention and treat-ment of hypotension during spinal an-aesthesia—IM ephedrine is used.
5. Narcolepsy is a condition with anirresistible desire and tendency to sleep.As ephedrine is a CNS stimulant, it isuseful in narcolepsy.
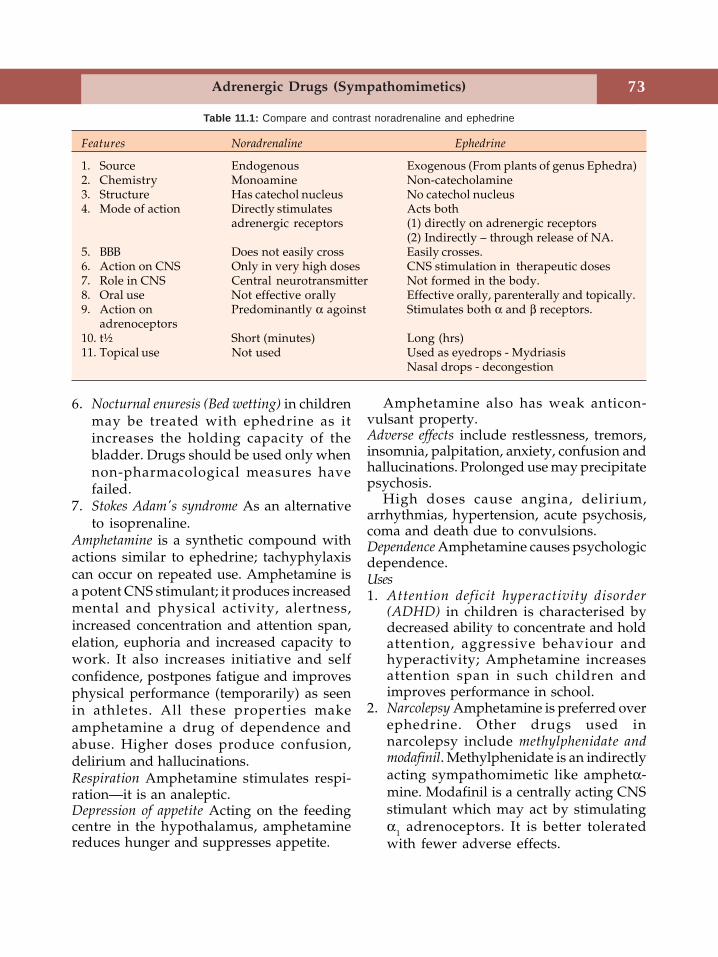
73Adrenergic Drugs (Sympathomimetics)
6. Nocturnal enuresis (Bed wetting) in childrenmay be treated with ephedrine as itincreases the holding capacity of thebladder. Drugs should be used only whennon-pharmacological measures havefailed.
7. Stokes Adam's syndrome As an alternativeto isoprenaline.
Amphetamine is a synthetic compound withactions similar to ephedrine; tachyphylaxiscan occur on repeated use. Amphetamine isa potent CNS stimulant; it produces increasedmental and physical activity, alertness,increased concentration and attention span,elation, euphoria and increased capacity towork. It also increases initiative and selfconfidence, postpones fatigue and improvesphysical performance (temporarily) as seenin athletes. All these properties makeamphetamine a drug of dependence andabuse. Higher doses produce confusion,delirium and hallucinations.Respiration Amphetamine stimulates respi-ration—it is an analeptic.Depression of appetite Acting on the feedingcentre in the hypothalamus, amphetaminereduces hunger and suppresses appetite.
Amphetamine also has weak anticon-vulsant property.Adverse effects include restlessness, tremors,insomnia, palpitation, anxiety, confusion andhallucinations. Prolonged use may precipitatepsychosis.
High doses cause angina, delirium,arrhythmias, hypertension, acute psychosis,coma and death due to convulsions.Dependence Amphetamine causes psychologicdependence.Uses1. Attention deficit hyperactivity disorder
(ADHD) in children is characterised bydecreased ability to concentrate and holdattention, aggressive behaviour andhyperactivity; Amphetamine increasesattention span in such children andimproves performance in school.
2. Narcolepsy Amphetamine is preferred overephedrine. Other drugs used innarcolepsy include methylphenidate andmodafinil. Methylphenidate is an indirectlyacting sympathomimetic like amphetα-mine. Modafinil is a centrally acting CNSstimulant which may act by stimulatingα1 adrenoceptors. It is better toleratedwith fewer adverse effects.
Features Noradrenaline Ephedrine
1. Source Endogenous Exogenous (From plants of genus Ephedra)2. Chemistry Monoamine Non-catecholamine3. Structure Has catechol nucleus No catechol nucleus4. Mode of action Directly stimulates Acts both
adrenergic receptors (1) directly on adrenergic receptors(2) Indirectly – through release of NA.
5. BBB Does not easily cross Easily crosses.6. Action on CNS Only in very high doses CNS stimulation in therapeutic doses7. Role in CNS Central neurotransmitter Not formed in the body.8. Oral use Not effective orally Effective orally, parenterally and topically.9. Action on Predominantly α agoinst Stimulates both α and β receptors.
adrenoceptors10. t½ Short (minutes) Long (hrs)11. Topical use Not used Used as eyedrops - Mydriasis
Nasal drops - decongestion
Table 11.1: Compare and contrast noradrenaline and ephedrine
74 Textbook of Pharmacology for Dental and Allied Health Sciences
3. Obesity Though appetite is suppressed,due to risk of dependence and other sideeffects, amphetamine should not be usedfor this purpose.
4. Epilepsy Amphetamine can be used asadjuvant and to counter the sedation dueto antiepileptics.
Methamphetamine has more prominent centralthan peripheral actions. Methylphenidate,phenmetrazin and pemoline are otheramphetamine-like drugs with actions andabuse potential similar to amphetamine.
VASOPRESSORS
These are α1 agonists and includemetaraminol, mephenteramine, pheny-lephrine and methoxamine. They increase theBP by increasing total peripheral resistance(TPR) or cardiac output (CO) or both. Theyare given parenterally with constantmonitoring of BP. Tachyphylaxis maydevelop.Uses Vasopressors are used to raise the BP inhypotension as seen in cardiogenic orneurogenic shock and during spinalanaesthesia.Metaraminol is an alpha stimulant and also actsindirectly by NA release. CO is increased. Itis also a nasal decongestant.Mephenteramine acts on both α and β receptorsto increase TPR and CO and thereby raisesBP. It is orally effective. Pressor effect isaccompanied by bradycardia.Phenylephrine is a selective α1 stimulant; it isalso a nasal decongestant. Reflex bradycardiais prominent. It produces mydriasis withoutcycloplegia.Methoxamine has actions similar tophenylephrine.
NASAL DECONGESTANTS
Nasal decongestants are α1 agonists. Theybring about vasoconstriction of the nasal
mucosa, resulting in its shrinkage and theydecrease the volume of the mucosa. Thus theyrelieve nasal congestion and decreaseresistance to airflow through the nose.Theyalso reduce nasal secretion. The nasaldecongestants thus provide symptomaticrelief in rhinitis due to allergy and upperrespiratory infections.Mechanism of action - Nasal decongestants actby stimulating the α1 receptors present in theblood vessels of the nasal mucosa.
They bring about vasoconstriction of thenasal mucosa resulting in its shrinkage. Thusthey relieve nasal congestion.
They may be used:1. Orally Ephedrine
Pseudoephedrine2. Topically (as nasal drops)
Oxymetazoline,XylometazolineNaphazoline,PhenylephrineMephenteramineMetaraminol
Adverse effects
When used orally ephedrine and pseudo-ephedrine can cause insomnia, tremors andirritability. On topical use, nasal irritation canoccur.
Most disadvantages result from long termuse - prolonged use of topical agents cancause-• atrophy of the nasal mucosa due to
intense vasoconstriction.• recongestion or 'after congestion' may
result when the drug is stopped (due tovasodilatation).
• loss of efficacy or tolerance due todesensitization of the receptors.
Nasal decongestants should be usedcarefully in patients with hypertension. Theuse of phenylpropanolamine is associatedwith an increased risk of haemorrhagicstroke and is therefore banned.
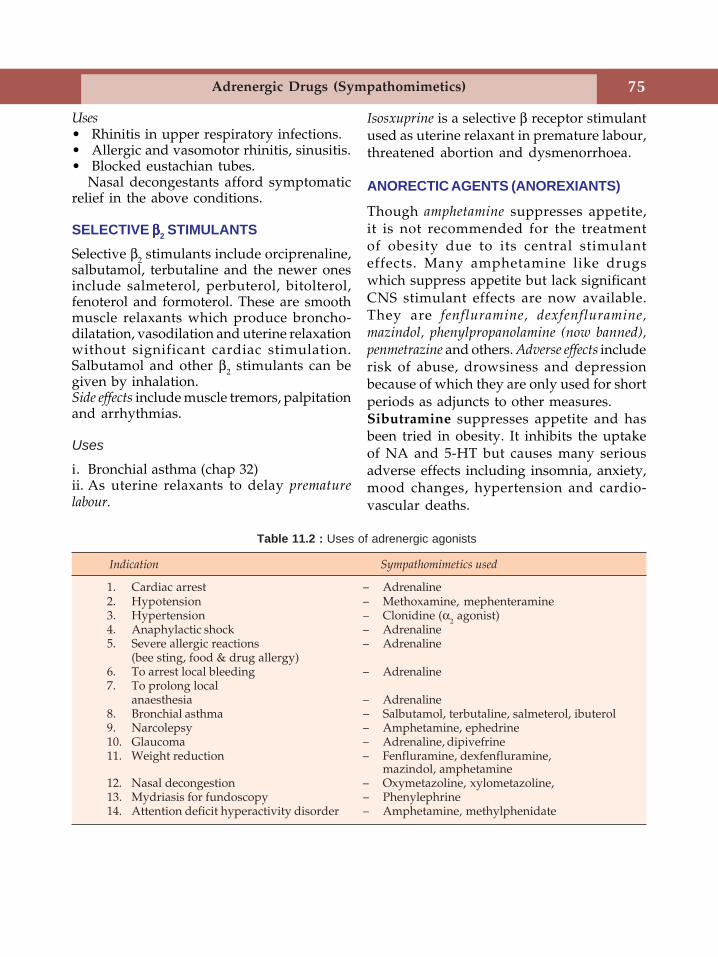
75Adrenergic Drugs (Sympathomimetics)
Uses• Rhinitis in upper respiratory infections.• Allergic and vasomotor rhinitis, sinusitis.• Blocked eustachian tubes.
Nasal decongestants afford symptomaticrelief in the above conditions.
SELECTIVE βββββ2 STIMULANTSSelective β2 stimulants include orciprenaline,salbutamol, terbutaline and the newer onesinclude salmeterol, perbuterol, bitolterol,fenoterol and formoterol. These are smoothmuscle relaxants which produce broncho-dilatation, vasodilation and uterine relaxationwithout significant cardiac stimulation.Salbutamol and other β2 stimulants can begiven by inhalation.Side effects include muscle tremors, palpitationand arrhythmias.
Uses
i. Bronchial asthma (chap 32)ii. As uterine relaxants to delay prematurelabour.
Table 11.2 : Uses of adrenergic agonists
Indication Sympathomimetics used
1. Cardiac arrest – Adrenaline2. Hypotension – Methoxamine, mephenteramine3. Hypertension – Clonidine (α2 agonist)4. Anaphylactic shock – Adrenaline5. Severe allergic reactions – Adrenaline
(bee sting, food & drug allergy)6. To arrest local bleeding – Adrenaline7. To prolong local
anaesthesia – Adrenaline8. Bronchial asthma – Salbutamol, terbutaline, salmeterol, ibuterol9. Narcolepsy – Amphetamine, ephedrine10. Glaucoma – Adrenaline, dipivefrine11. Weight reduction – Fenfluramine, dexfenfluramine,
mazindol, amphetamine12. Nasal decongestion – Oxymetazoline, xylometazoline,13. Mydriasis for fundoscopy – Phenylephrine14. Attention deficit hyperactivity disorder – Amphetamine, methylphenidate
Isosxuprine is a selective β receptor stimulantused as uterine relaxant in premature labour,threatened abortion and dysmenorrhoea.
ANORECTIC AGENTS (ANOREXIANTS)
Though amphetamine suppresses appetite,it is not recommended for the treatmentof obesity due to its central stimulanteffects. Many amphetamine like drugswhich suppress appetite but lack significantCNS stimulant effects are now available.They are fenfluramine, dexfenfluramine,mazindol, phenylpropanolamine (now banned),penmetrazine and others. Adverse effects includerisk of abuse, drowsiness and depressionbecause of which they are only used for shortperiods as adjuncts to other measures.Sibutramine suppresses appetite and hasbeen tried in obesity. It inhibits the uptakeof NA and 5-HT but causes many seriousadverse effects including insomnia, anxiety,mood changes, hypertension and cardio-vascular deaths.
76 Textbook of Pharmacology for Dental and Allied Health Sciences
12Adrenergic blockers bind to the adrenergicreceptors and prevent the action ofadrenergic drugs. They may block alpha orbeta receptors or both.
ALPHA ADRENERGIC BLOCKING AGENTS
Alpha receptor antagonists block theadrenergic responses mediated throughalpha adrenergic receptors. Some of themhave selectivity for α1 or α2 receptors.
Actions
The important effects of α receptorstimulation are α1 mediated vasoconstrictionand α2- (presynaptic) receptor mediatedinhibition of NA release. The result of alphablockade by α-antagonists (Fig 10.3, Page 68)are:
α1-blockade—inhibits vasoconstriction --leading to vasodilation and thereby ↓ BP.This fall in BP is opposed by the baroreceptorreflexes which tend to ↑ heart rate andcardiac output.
α2-blockade—enhances release of NAwhich stimulates β receptors (α are alreadyblocked) - β1 stimulation in heart results intachycardia and increased cardiac output.
Thus the predominant effects of non-selective α-blockade is hypotension withtachycardia. This is because α2 receptors areblocked and there is no increase in NArelease.
Selective α1-blockade—results in hypo-tension without significant tachycardia.
Selective α2-blockade—↑NA releaseresulting in hypertension.
α-blockade also results in miosis and nasalstuffiness. α-blockade in the bladder andprostate leads to decreased resistance to theflow of urine.Adverse effects of α-blockers—Posturalhypotension, palpitation, nasal stuffiness,miosis, impaired ejaculation and impotence.α blockers are classified as follows—1. Non-selective
a. Non-competitive blockerPhenoxybenzamine
b. Competitive blockersErgot alkaloids (ergotamine), tolazo-line, phentolamine, chlorpromazine
2. Selectivea. α
1-blockers
Prazosin, terazosin, doxazosin,tamsulosin, alfuzosin
b. α2-blocker
YohimbinePhenoxybenzamine binds covalently to alphareceptors causing irreversible blockade.Given IV, blood pressure gradually falls andis associated with tachycardia and increasedCO. The action lasts for 3-4 days. It alsoblocks histamine, 5-HT and cholinergicreceptors. Phenoxybenzamine can be usedorally in the treatment of pheochromocy -toma (Table 12.1).Ergot alkaloids (Page 208) Ergotamine,ergotoxine and their derivatives arecompetitive antagonists and the blockade is
Adrenergic Antagonists
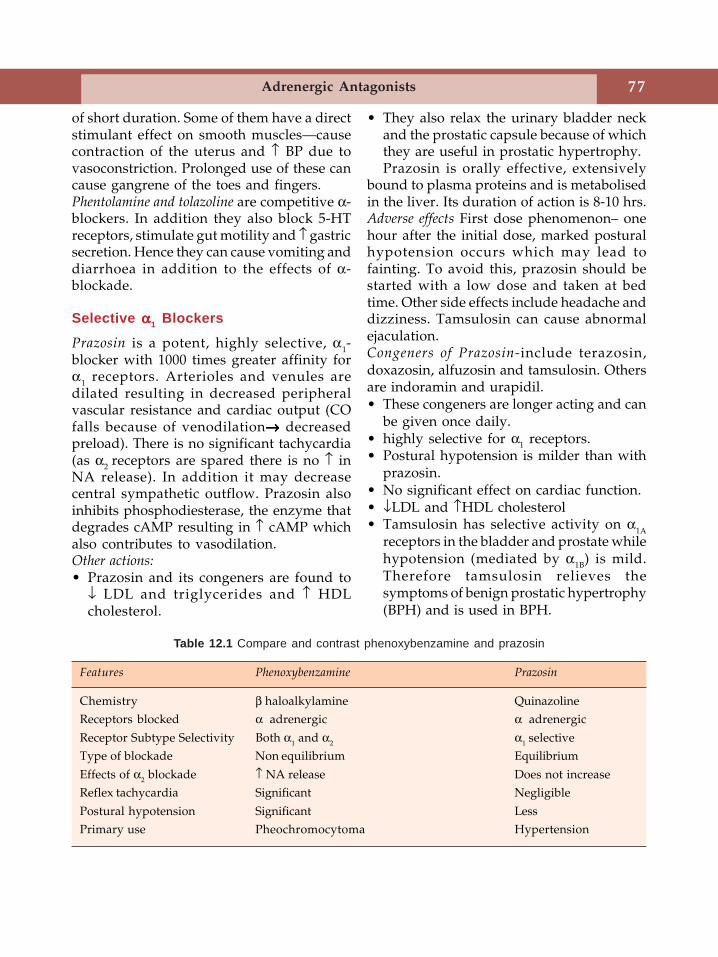
77Adrenergic Antagonists
of short duration. Some of them have a directstimulant effect on smooth muscles—causecontraction of the uterus and ↑ BP due tovasoconstriction. Prolonged use of these cancause gangrene of the toes and fingers.Phentolamine and tolazoline are competitive α-blockers. In addition they also block 5-HTreceptors, stimulate gut motility and ↑ gastricsecretion. Hence they can cause vomiting anddiarrhoea in addition to the effects of α-blockade.
Selective ααααα1 Blockers
Prazosin is a potent, highly selective, α1-blocker with 1000 times greater affinity forα1 receptors. Arterioles and venules aredilated resulting in decreased peripheralvascular resistance and cardiac output (COfalls because of venodilation→→→→→ decreasedpreload). There is no significant tachycardia(as α2 receptors are spared there is no ↑ inNA release). In addition it may decreasecentral sympathetic outflow. Prazosin alsoinhibits phosphodiesterase, the enzyme thatdegrades cAMP resulting in ↑ cAMP whichalso contributes to vasodilation.Other actions:• Prazosin and its congeners are found to
↓ LDL and triglycerides and ↑ HDLcholesterol.
• They also relax the urinary bladder neckand the prostatic capsule because of whichthey are useful in prostatic hypertrophy.Prazosin is orally effective, extensively
bound to plasma proteins and is metabolisedin the liver. Its duration of action is 8-10 hrs.Adverse effects First dose phenomenon– onehour after the initial dose, marked posturalhypotension occurs which may lead tofainting. To avoid this, prazosin should bestarted with a low dose and taken at bedtime. Other side effects include headache anddizziness. Tamsulosin can cause abnormalejaculation.Congeners of Prazosin-include terazosin,doxazosin, alfuzosin and tamsulosin. Othersare indoramin and urapidil.• These congeners are longer acting and can
be given once daily.• highly selective for α1 receptors.• Postural hypotension is milder than with
prazosin.• No significant effect on cardiac function.• ↓LDL and ↑HDL cholesterol• Tamsulosin has selective activity on α1A
receptors in the bladder and prostate whilehypotension (mediated by α1B) is mild.Therefore tamsulosin relieves thesymptoms of benign prostatic hypertrophy(BPH) and is used in BPH.
Table 12.1 Compare and contrast phenoxybenzamine and prazosin
Features Phenoxybenzamine Prazosin
Chemistry β haloalkylamine QuinazolineReceptors blocked α adrenergic α adrenergic
Receptor Subtype Selectivity Both α1 and α2 α1 selectiveType of blockade Non equilibrium Equilibrium
Effects of α2 blockade ↑ NA release Does not increaseReflex tachycardia Significant Negligible
Postural hypotension Significant LessPrimary use Pheochromocytoma Hypertension
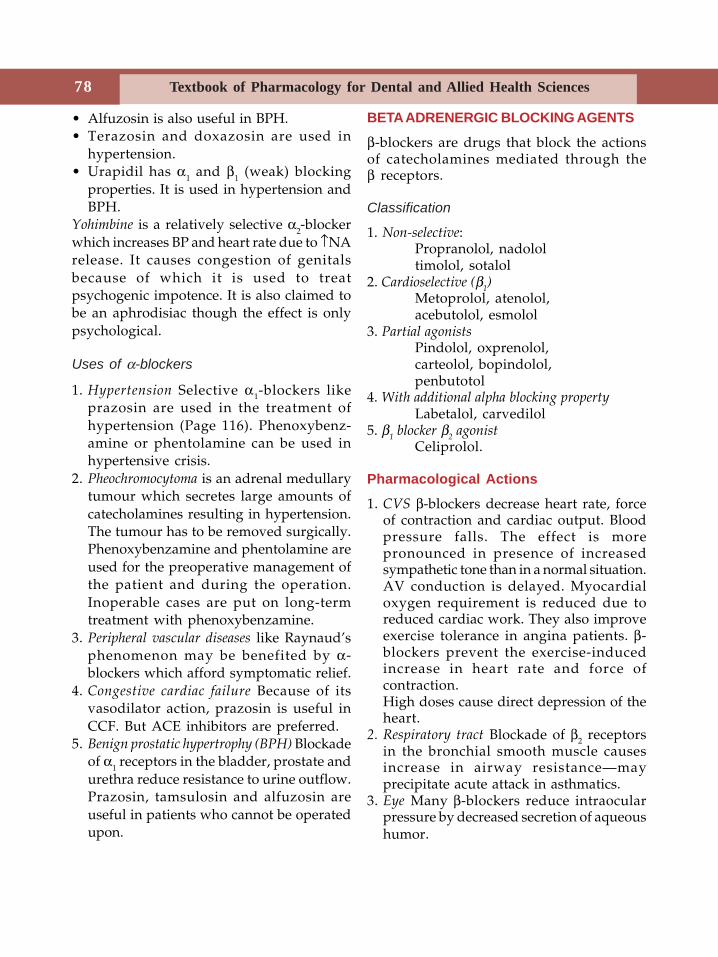
78 Textbook of Pharmacology for Dental and Allied Health Sciences
• Alfuzosin is also useful in BPH.• Terazosin and doxazosin are used in
hypertension.• Urapidil has α1 and β1 (weak) blocking
properties. It is used in hypertension andBPH.
Yohimbine is a relatively selective α2-blockerwhich increases BP and heart rate due to ↑NArelease. It causes congestion of genitalsbecause of which it is used to treatpsychogenic impotence. It is also claimed tobe an aphrodisiac though the effect is onlypsychological.
Uses of α-blockers
1. Hypertension Selective α1-blockers likeprazosin are used in the treatment ofhypertension (Page 116). Phenoxybenz-amine or phentolamine can be used inhypertensive crisis.
2. Pheochromocytoma is an adrenal medullarytumour which secretes large amounts ofcatecholamines resulting in hypertension.The tumour has to be removed surgically.Phenoxybenzamine and phentolamine areused for the preoperative management ofthe patient and during the operation.Inoperable cases are put on long-termtreatment with phenoxybenzamine.
3. Peripheral vascular diseases like Raynaud’sphenomenon may be benefited by α-blockers which afford symptomatic relief.
4. Congestive cardiac failure Because of itsvasodilator action, prazosin is useful inCCF. But ACE inhibitors are preferred.
5. Benign prostatic hypertrophy (BPH) Blockadeof α1 receptors in the bladder, prostate andurethra reduce resistance to urine outflow.Prazosin, tamsulosin and alfuzosin areuseful in patients who cannot be operatedupon.
BETA ADRENERGIC BLOCKING AGENTS
β-blockers are drugs that block the actionsof catecholamines mediated through theβ receptors.
Classification
1. Non-selective:Propranolol, nadololtimolol, sotalol
2. Cardioselective (β1)
Metoprolol, atenolol,acebutolol, esmolol
3. Partial agonistsPindolol, oxprenolol,carteolol, bopindolol,penbutotol
4. With additional alpha blocking propertyLabetalol, carvedilol
5. β1 blocker β
2 agonist
Celiprolol.
Pharmacological Actions
1. CVS β-blockers decrease heart rate, forceof contraction and cardiac output. Bloodpressure falls. The effect is morepronounced in presence of increasedsympathetic tone than in a normal situation.AV conduction is delayed. Myocardialoxygen requirement is reduced due toreduced cardiac work. They also improveexercise tolerance in angina patients. β-blockers prevent the exercise-inducedincrease in heart rate and force ofcontraction.High doses cause direct depression of theheart.
2. Respiratory tract Blockade of β2 receptorsin the bronchial smooth muscle causesincrease in airway resistance—mayprecipitate acute attack in asthmatics.
3. Eye Many β-blockers reduce intraocularpressure by decreased secretion of aqueoushumor.
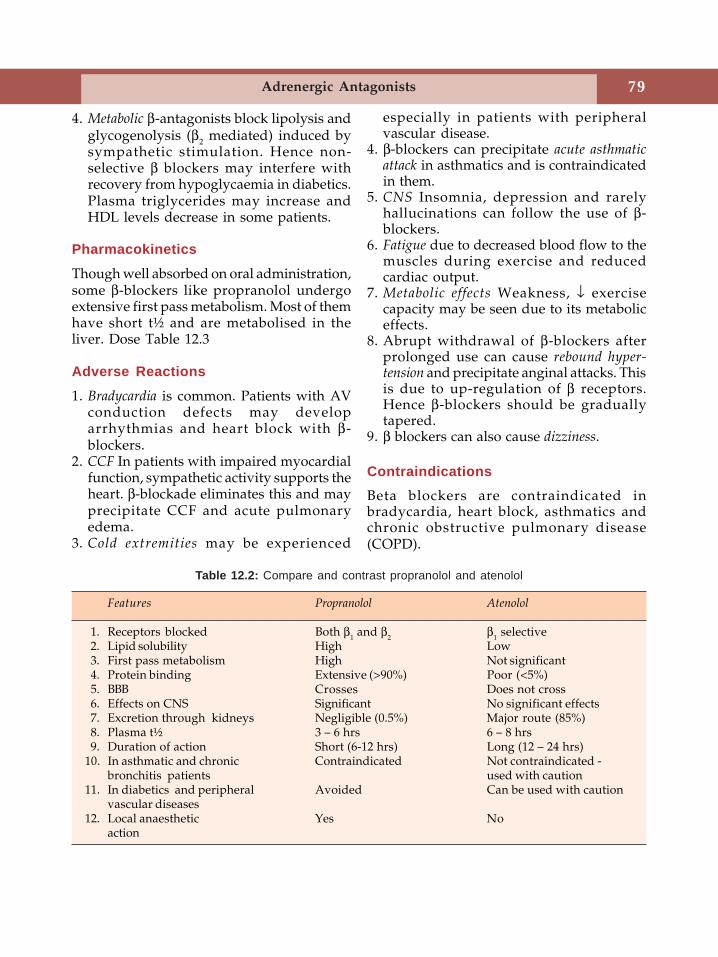
79Adrenergic Antagonists
4. Metabolic β-antagonists block lipolysis andglycogenolysis (β2 mediated) induced bysympathetic stimulation. Hence non-selective β blockers may interfere withrecovery from hypoglycaemia in diabetics.Plasma triglycerides may increase andHDL levels decrease in some patients.
Pharmacokinetics
Though well absorbed on oral administration,some β-blockers like propranolol undergoextensive first pass metabolism. Most of themhave short t½ and are metabolised in theliver. Dose Table 12.3
Adverse Reactions
1. Bradycardia is common. Patients with AVconduction defects may developarrhythmias and heart block with β-blockers.
2. CCF In patients with impaired myocardialfunction, sympathetic activity supports theheart. β-blockade eliminates this and mayprecipitate CCF and acute pulmonaryedema.
3. Cold extremities may be experienced
especially in patients with peripheralvascular disease.
4. β-blockers can precipitate acute asthmaticattack in asthmatics and is contraindicatedin them.
5. CNS Insomnia, depression and rarelyhallucinations can follow the use of β-blockers.
6. Fatigue due to decreased blood flow to themuscles during exercise and reducedcardiac output.
7. Metabolic effects Weakness, ↓ exercisecapacity may be seen due to its metaboliceffects.
8. Abrupt withdrawal of β-blockers afterprolonged use can cause rebound hyper-tension and precipitate anginal attacks. Thisis due to up-regulation of β receptors.Hence β-blockers should be graduallytapered.
9. β blockers can also cause dizziness.
ContraindicationsBeta blockers are contraindicated inbradycardia, heart block, asthmatics andchronic obstructive pulmonary disease(COPD).
Features Propranolol Atenolol
1. Receptors blocked Both β1 and β2 β1 selective2. Lipid solubility High Low3. First pass metabolism High Not significant4. Protein binding Extensive (>90%) Poor (<5%)5. BBB Crosses Does not cross6. Effects on CNS Significant No significant effects7. Excretion through kidneys Negligible (0.5%) Major route (85%)8. Plasma t½ 3 – 6 hrs 6 – 8 hrs9. Duration of action Short (6-12 hrs) Long (12 – 24 hrs)
10. In asthmatic and chronic Contraindicated Not contraindicated -bronchitis patients used with caution
11. In diabetics and peripheral Avoided Can be used with cautionvascular diseases
12. Local anaesthetic Yes Noaction
Table 12.2: Compare and contrast propranolol and atenolol
80 Textbook of Pharmacology for Dental and Allied Health Sciences
Some Important Drug Interactions
1. Propranolol + insulin—when diabetics oninsulin also receive propranolol:i. β-blockade masks tachycardia which is
the first warning signal of hypo-glycaemia.
ii. β-blockade delays the recovery fromhypoglycaemia by preventingglycogenolysis induced by sympatheticstimulation (acting through β2receptors). This may be avoided byusing a β1 selective blocker.
2. Propranolol + verapamil—Because boththese cause myocardiac depression,profound depression may result if both areused together. Hence the combinationshould be avoided.
3. β-blockers + catecholamines—in patientson nonselective β-blockers, blockade ofvascular β receptors results in up regulationof the receptors and intense vasocons-triction is possible from even small dosesof adrenaline that is used with LAs. Henceit is safer to use plain local anaesthesia insuch patients.
Cardioselective β-blockers e.g. Atenolol,metoprolol, esmolol.These drugs:• Selectively block β1 receptors; β2-blockade
is weak• Bronchospasm is less/negligible• Inhibition of glycogenolysis is lower—
hence safer in diabetics• Exercise performance is impaired to a
lesser degree• Lesser chances of peripheral vascular
disease.Partial agonists—Pindolol, oxprenolol.These have some sympathomimetic activitydue to their partial β-agonistic property. Asa result, bradycardia and myocardiacdepression are less marked. They aretherefore preferred in patients who are likelyto have severe bradycardia.
Some Individual βββββ-antagonists
Atenolol (see Table 12.2)
• Selective β1-blocker• Longer acting-given once daily• Less lipid soluble-does not cross BBB-
hence no CNS side effects• No side effects on lipid profile.
Hence very commonly used (25-100 mgdaily)
Esmolol
• Selective β1-blocker• Ultra short-acting– t½–8 minutes.• Used IV• Safer in critically ill patients and in
emergencies when immediate β-blockadeis needed.
Metoprolol
• Selective β1 blocker• Well absorbed but undergoes significant
first-pass metabolism• Given twice daily (50-200 mg)• Used in hypertension and angina pectoris
Acebutolol
• β1 selective with some partial agonisticeffects
• May be used in hypertension andarrhythmias.
Celiprolol
• β1 blocker and β2 agonistic effects• Safer in asthmatics• Used in hypertension.
Timolol
• Nonselective, short-acting• Used in glaucoma—as eyedrops.
Uses of βββββ-blockers1. Hypertension β-blockers are useful in the
treatment of mild to moderate hyper-
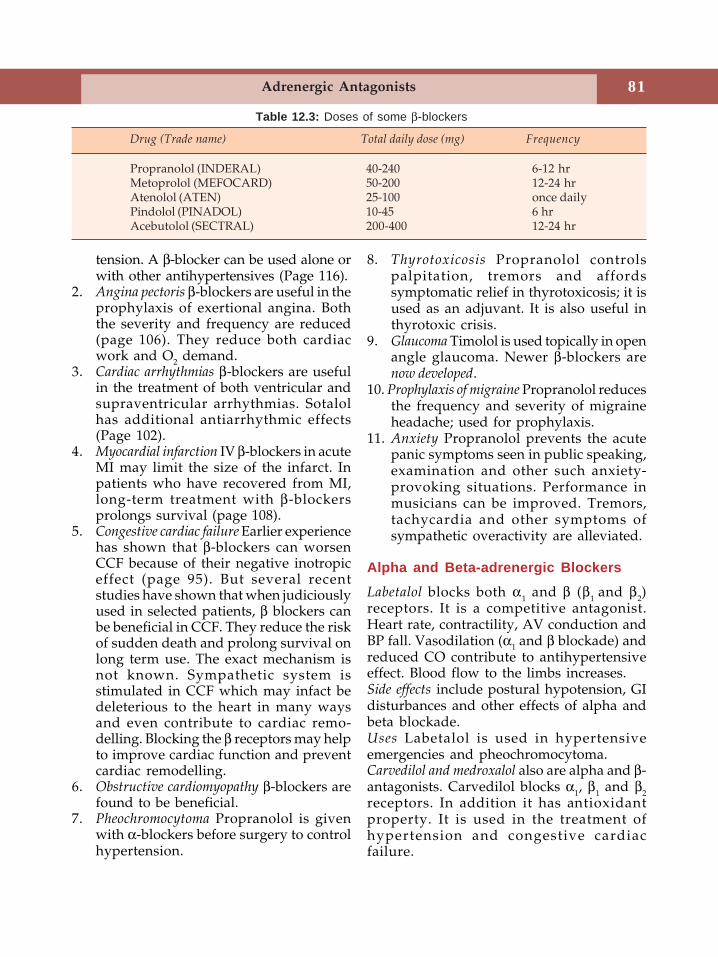
81Adrenergic Antagonists
tension. A β-blocker can be used alone orwith other antihypertensives (Page 116).
2. Angina pectoris β-blockers are useful in theprophylaxis of exertional angina. Boththe severity and frequency are reduced(page 106). They reduce both cardiacwork and O2 demand.
3. Cardiac arrhythmias β-blockers are usefulin the treatment of both ventricular andsupraventricular arrhythmias. Sotalolhas additional antiarrhythmic effects(Page 102).
4. Myocardial infarction IV β-blockers in acuteMI may limit the size of the infarct. Inpatients who have recovered from MI,long-term treatment with β-blockersprolongs survival (page 108).
5. Congestive cardiac failure Earlier experiencehas shown that β-blockers can worsenCCF because of their negative inotropiceffect (page 95). But several recentstudies have shown that when judiciouslyused in selected patients, β blockers canbe beneficial in CCF. They reduce the riskof sudden death and prolong survival onlong term use. The exact mechanism isnot known. Sympathetic system isstimulated in CCF which may infact bedeleterious to the heart in many waysand even contribute to cardiac remo-delling. Blocking the β receptors may helpto improve cardiac function and preventcardiac remodelling.
6. Obstructive cardiomyopathy β-blockers arefound to be beneficial.
7. Pheochromocytoma Propranolol is givenwith α-blockers before surgery to controlhypertension.
Table 12.3: Doses of some β-blockers
Drug (Trade name) Total daily dose (mg) Frequency
Propranolol (INDERAL) 40-240 6-12 hrMetoprolol (MEFOCARD) 50-200 12-24 hrAtenolol (ATEN) 25-100 once dailyPindolol (PINADOL) 10-45 6 hrAcebutolol (SECTRAL) 200-400 12-24 hr
8. Thyrotoxicosis Propranolol controlspalpitation, tremors and affordssymptomatic relief in thyrotoxicosis; it isused as an adjuvant. It is also useful inthyrotoxic crisis.
9. Glaucoma Timolol is used topically in openangle glaucoma. Newer β-blockers arenow developed.
10. Prophylaxis of migraine Propranolol reducesthe frequency and severity of migraineheadache; used for prophylaxis.
11. Anxiety Propranolol prevents the acutepanic symptoms seen in public speaking,examination and other such anxiety-provoking situations. Performance inmusicians can be improved. Tremors,tachycardia and other symptoms ofsympathetic overactivity are alleviated.
Alpha and Beta-adrenergic Blockers
Labetalol blocks both α1 and β (β1 and β2)receptors. It is a competitive antagonist.Heart rate, contractility, AV conduction andBP fall. Vasodilation (α1 and β blockade) andreduced CO contribute to antihypertensiveeffect. Blood flow to the limbs increases.Side effects include postural hypotension, GIdisturbances and other effects of alpha andbeta blockade.Uses Labetalol is used in hypertensiveemergencies and pheochromocytoma.Carvedilol and medroxalol also are alpha and β-antagonists. Carvedilol blocks α1, β1 and β2receptors. In addition it has antioxidantproperty. It is used in the treatment ofhypertension and congestive cardiacfailure.
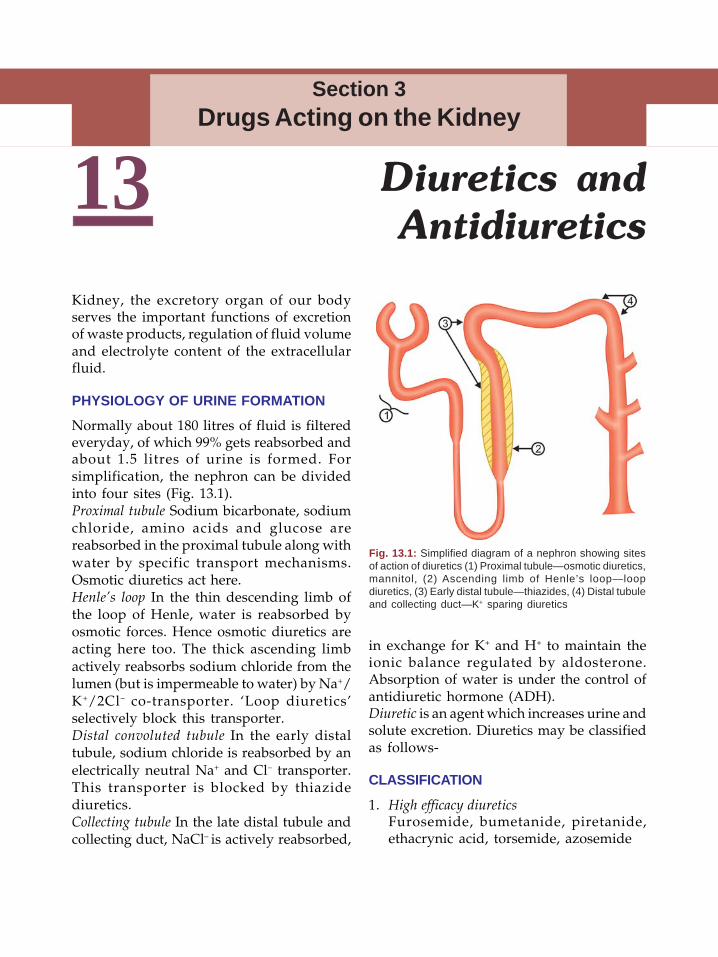
82 Textbook of Pharmacology for Dental and Allied Health Sciences
13Kidney, the excretory organ of our bodyserves the important functions of excretionof waste products, regulation of fluid volumeand electrolyte content of the extracellularfluid.
PHYSIOLOGY OF URINE FORMATION
Normally about 180 litres of fluid is filteredeveryday, of which 99% gets reabsorbed andabout 1.5 litres of urine is formed. Forsimplification, the nephron can be dividedinto four sites (Fig. 13.1).Proximal tubule Sodium bicarbonate, sodiumchloride, amino acids and glucose arereabsorbed in the proximal tubule along withwater by specific transport mechanisms.Osmotic diuretics act here.Henle’s loop In the thin descending limb ofthe loop of Henle, water is reabsorbed byosmotic forces. Hence osmotic diuretics areacting here too. The thick ascending limbactively reabsorbs sodium chloride from thelumen (but is impermeable to water) by Na+/K+/2Cl– co-transporter. ‘Loop diuretics’selectively block this transporter.Distal convoluted tubule In the early distaltubule, sodium chloride is reabsorbed by anelectrically neutral Na+ and Cl– transporter.This transporter is blocked by thiazidediuretics.Collecting tubule In the late distal tubule andcollecting duct, NaCl– is actively reabsorbed,
in exchange for K+ and H+ to maintain theionic balance regulated by aldosterone.Absorption of water is under the control ofantidiuretic hormone (ADH).Diuretic is an agent which increases urine andsolute excretion. Diuretics may be classifiedas follows-
CLASSIFICATION
1. High efficacy diureticsFurosemide, bumetanide, piretanide,ethacrynic acid, torsemide, azosemide
Diuretics andAntidiuretics
Section 3Drugs Acting on the Kidney
Fig. 13.1: Simplified diagram of a nephron showing sitesof action of diuretics (1) Proximal tubule—osmotic diuretics,mannitol, (2) Ascending limb of Henle’s loop—loopdiuretics, (3) Early distal tubule—thiazides, (4) Distal tubuleand collecting duct—K+ sparing diuretics
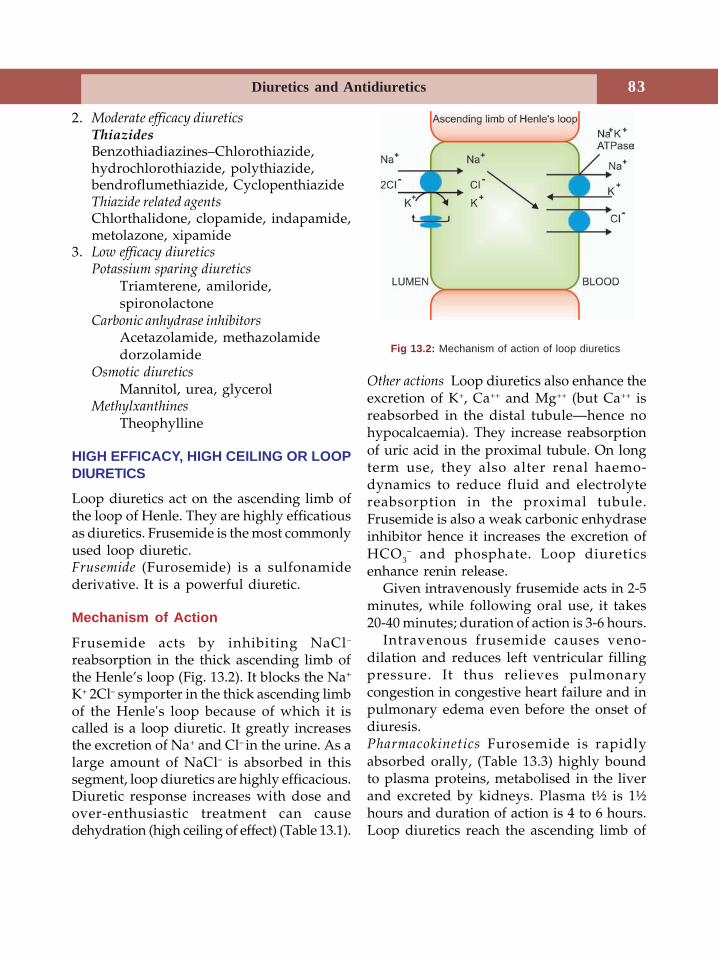
83Diuretics and Antidiuretics
2. Moderate efficacy diureticsThiazidesBenzothiadiazines–Chlorothiazide,hydrochlorothiazide, polythiazide,bendroflumethiazide, CyclopenthiazideThiazide related agentsChlorthalidone, clopamide, indapamide,metolazone, xipamide
3. Low efficacy diureticsPotassium sparing diuretics
Triamterene, amiloride,spironolactone
Carbonic anhydrase inhibitorsAcetazolamide, methazolamidedorzolamide
Osmotic diureticsMannitol, urea, glycerol
MethylxanthinesTheophylline
HIGH EFFICACY, HIGH CEILING OR LOOPDIURETICS
Loop diuretics act on the ascending limb ofthe loop of Henle. They are highly efficatiousas diuretics. Frusemide is the most commonlyused loop diuretic.Frusemide (Furosemide) is a sulfonamidederivative. It is a powerful diuretic.
Mechanism of Action
Frusemide acts by inhibiting NaCl–
reabsorption in the thick ascending limb ofthe Henle’s loop (Fig. 13.2). It blocks the Na+
K+ 2Cl– symporter in the thick ascending limbof the Henle's loop because of which it iscalled is a loop diuretic. It greatly increasesthe excretion of Na+ and Cl– in the urine. As alarge amount of NaCl– is absorbed in thissegment, loop diuretics are highly efficacious.Diuretic response increases with dose andover-enthusiastic treatment can causedehydration (high ceiling of effect) (Table 13.1).
Other actions Loop diuretics also enhance theexcretion of K+, Ca++ and Mg++ (but Ca++ isreabsorbed in the distal tubule—hence nohypocalcaemia). They increase reabsorptionof uric acid in the proximal tubule. On longterm use, they also alter renal haemo-dynamics to reduce fluid and electrolytereabsorption in the proximal tubule.Frusemide is also a weak carbonic enhydraseinhibitor hence it increases the excretion ofHCO3
– and phosphate. Loop diureticsenhance renin release.
Given intravenously frusemide acts in 2-5minutes, while following oral use, it takes20-40 minutes; duration of action is 3-6 hours.
Intravenous frusemide causes veno-dilation and reduces left ventricular fillingpressure. It thus relieves pulmonarycongestion in congestive heart failure and inpulmonary edema even before the onset ofdiuresis.Pharmacokinetics Furosemide is rapidlyabsorbed orally, (Table 13.3) highly boundto plasma proteins, metabolised in the liverand excreted by kidneys. Plasma t½ is 1½hours and duration of action is 4 to 6 hours.Loop diuretics reach the ascending limb of
Fig 13.2: Mechanism of action of loop diuretics
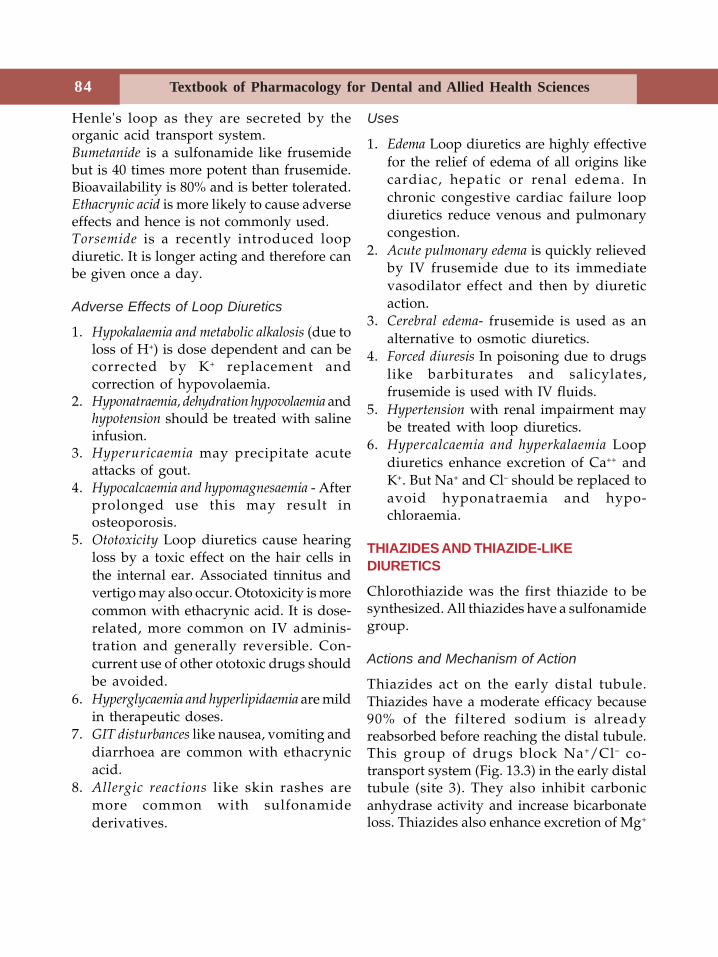
84 Textbook of Pharmacology for Dental and Allied Health Sciences
Henle's loop as they are secreted by theorganic acid transport system.Bumetanide is a sulfonamide like frusemidebut is 40 times more potent than frusemide.Bioavailability is 80% and is better tolerated.Ethacrynic acid is more likely to cause adverseeffects and hence is not commonly used.Torsemide is a recently introduced loopdiuretic. It is longer acting and therefore canbe given once a day.
Adverse Effects of Loop Diuretics
1. Hypokalaemia and metabolic alkalosis (due toloss of H+) is dose dependent and can becorrected by K+ replacement andcorrection of hypovolaemia.
2. Hyponatraemia, dehydration hypovolaemia andhypotension should be treated with salineinfusion.
3. Hyperuricaemia may precipitate acuteattacks of gout.
4. Hypocalcaemia and hypomagnesaemia - Afterprolonged use this may result inosteoporosis.
5. Ototoxicity Loop diuretics cause hearingloss by a toxic effect on the hair cells inthe internal ear. Associated tinnitus andvertigo may also occur. Ototoxicity is morecommon with ethacrynic acid. It is dose-related, more common on IV adminis-tration and generally reversible. Con-current use of other ototoxic drugs shouldbe avoided.
6. Hyperglycaemia and hyperlipidaemia are mildin therapeutic doses.
7. GIT disturbances like nausea, vomiting anddiarrhoea are common with ethacrynicacid.
8. Allergic reactions like skin rashes aremore common with sulfonamidederivatives.
Uses
1. Edema Loop diuretics are highly effectivefor the relief of edema of all origins likecardiac, hepatic or renal edema. Inchronic congestive cardiac failure loopdiuretics reduce venous and pulmonarycongestion.
2. Acute pulmonary edema is quickly relievedby IV frusemide due to its immediatevasodilator effect and then by diureticaction.
3. Cerebral edema- frusemide is used as analternative to osmotic diuretics.
4. Forced diuresis In poisoning due to drugslike barbiturates and salicylates,frusemide is used with IV fluids.
5. Hypertension with renal impairment maybe treated with loop diuretics.
6. Hypercalcaemia and hyperkalaemia Loopdiuretics enhance excretion of Ca++ andK+. But Na+ and Cl– should be replaced toavoid hyponatraemia and hypo-chloraemia.
THIAZIDES AND THIAZIDE-LIKEDIURETICS
Chlorothiazide was the first thiazide to besynthesized. All thiazides have a sulfonamidegroup.
Actions and Mechanism of Action
Thiazides act on the early distal tubule.Thiazides have a moderate efficacy because90% of the filtered sodium is alreadyreabsorbed before reaching the distal tubule.This group of drugs block Na+/Cl– co-transport system (Fig. 13.3) in the early distaltubule (site 3). They also inhibit carbonicanhydrase activity and increase bicarbonateloss. Thiazides also enhance excretion of Mg+
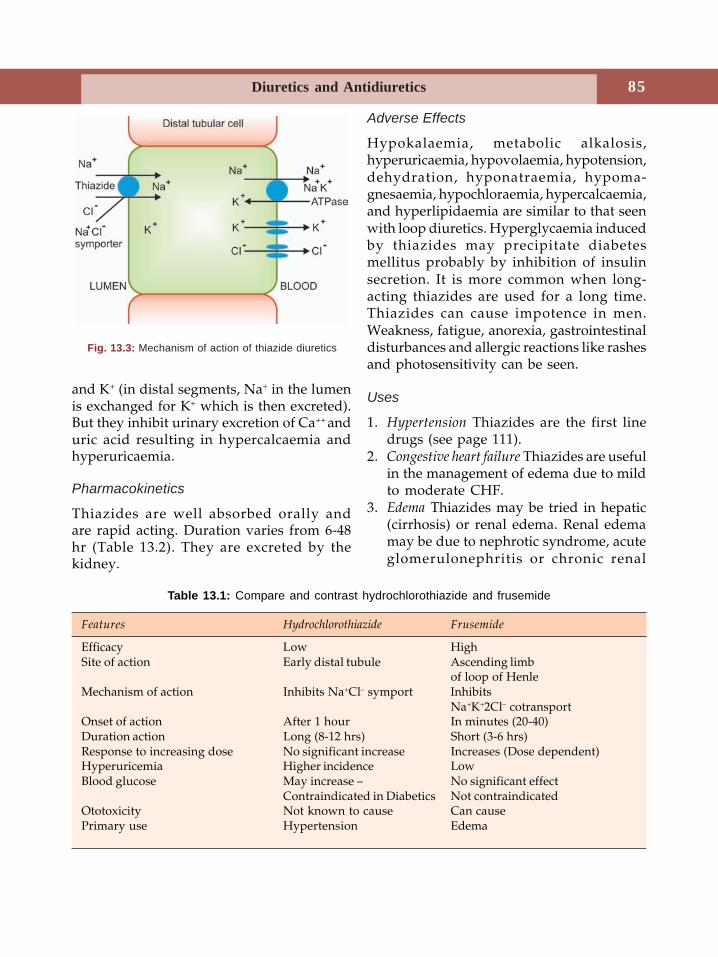
85Diuretics and Antidiuretics
Adverse Effects
Hypokalaemia, metabolic alkalosis,hyperuricaemia, hypovolaemia, hypotension,dehydration, hyponatraemia, hypoma-gnesaemia, hypochloraemia, hypercalcaemia,and hyperlipidaemia are similar to that seenwith loop diuretics. Hyperglycaemia inducedby thiazides may precipitate diabetesmellitus probably by inhibition of insulinsecretion. It is more common when long-acting thiazides are used for a long time.Thiazides can cause impotence in men.Weakness, fatigue, anorexia, gastrointestinaldisturbances and allergic reactions like rashesand photosensitivity can be seen.
Uses
1. Hypertension Thiazides are the first linedrugs (see page 111).
2. Congestive heart failure Thiazides are usefulin the management of edema due to mildto moderate CHF.
3. Edema Thiazides may be tried in hepatic(cirrhosis) or renal edema. Renal edemamay be due to nephrotic syndrome, acuteglomerulonephritis or chronic renal
Fig. 13.3: Mechanism of action of thiazide diuretics
and K+ (in distal segments, Na+ in the lumenis exchanged for K+ which is then excreted).But they inhibit urinary excretion of Ca++ anduric acid resulting in hypercalcaemia andhyperuricaemia.
Pharmacokinetics
Thiazides are well absorbed orally andare rapid acting. Duration varies from 6-48hr (Table 13.2). They are excreted by thekidney.
Table 13.1: Compare and contrast hydrochlorothiazide and frusemide
Features Hydrochlorothiazide Frusemide
Efficacy Low HighSite of action Early distal tubule Ascending limb
of loop of HenleMechanism of action Inhibits Na+Cl– symport Inhibits
Na+K+2Cl– cotransportOnset of action After 1 hour In minutes (20-40)Duration action Long (8-12 hrs) Short (3-6 hrs)Response to increasing dose No significant increase Increases (Dose dependent)Hyperuricemia Higher incidence LowBlood glucose May increase – No significant effect
Contraindicated in Diabetics Not contraindicatedOtotoxicity Not known to cause Can causePrimary use Hypertension Edema
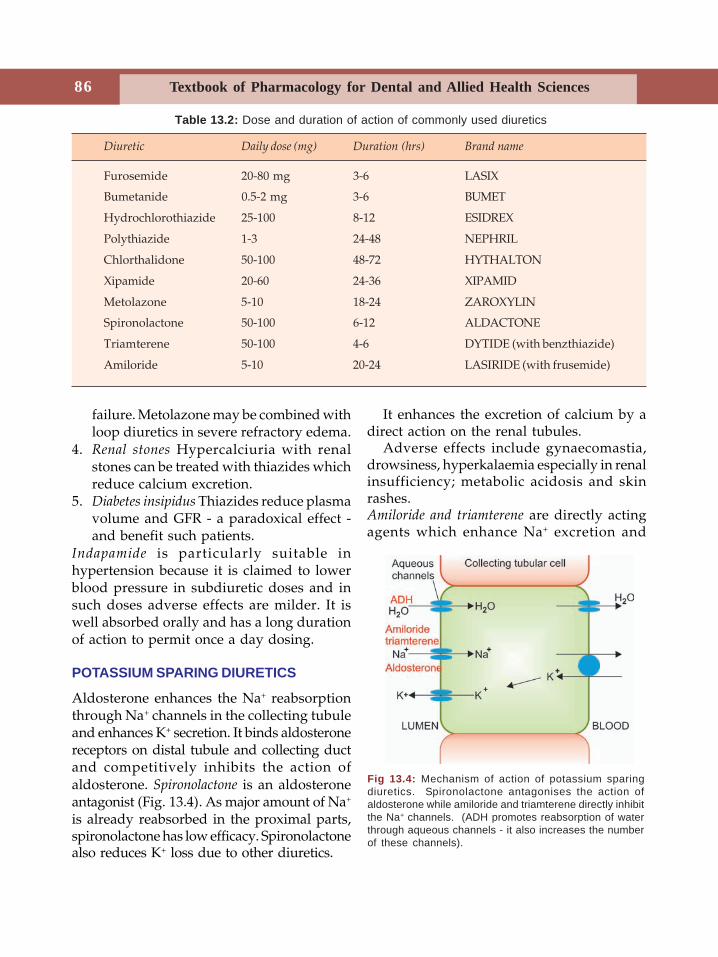
86 Textbook of Pharmacology for Dental and Allied Health Sciences
failure. Metolazone may be combined withloop diuretics in severe refractory edema.
4. Renal stones Hypercalciuria with renalstones can be treated with thiazides whichreduce calcium excretion.
5. Diabetes insipidus Thiazides reduce plasmavolume and GFR - a paradoxical effect -and benefit such patients.
Indapamide is particularly suitable inhypertension because it is claimed to lowerblood pressure in subdiuretic doses and insuch doses adverse effects are milder. It iswell absorbed orally and has a long durationof action to permit once a day dosing.
POTASSIUM SPARING DIURETICS
Aldosterone enhances the Na+ reabsorptionthrough Na+ channels in the collecting tubuleand enhances K+ secretion. It binds aldosteronereceptors on distal tubule and collecting ductand competitively inhibits the action ofaldosterone. Spironolactone is an aldosteroneantagonist (Fig. 13.4). As major amount of Na+
is already reabsorbed in the proximal parts,spironolactone has low efficacy. Spironolactonealso reduces K+ loss due to other diuretics.
It enhances the excretion of calcium by adirect action on the renal tubules.
Adverse effects include gynaecomastia,drowsiness, hyperkalaemia especially in renalinsufficiency; metabolic acidosis and skinrashes.Amiloride and triamterene are directly actingagents which enhance Na+ excretion and
Fig 13.4: Mechanism of action of potassium sparingdiuretics. Spironolactone antagonises the action ofaldosterone while amiloride and triamterene directly inhibitthe Na+ channels. (ADH promotes reabsorption of waterthrough aqueous channels - it also increases the numberof these channels).
Diuretic Daily dose (mg) Duration (hrs) Brand name
Furosemide 20-80 mg 3-6 LASIX
Bumetanide 0.5-2 mg 3-6 BUMET
Hydrochlorothiazide 25-100 8-12 ESIDREX
Polythiazide 1-3 24-48 NEPHRIL
Chlorthalidone 50-100 48-72 HYTHALTON
Xipamide 20-60 24-36 XIPAMID
Metolazone 5-10 18-24 ZAROXYLIN
Spironolactone 50-100 6-12 ALDACTONE
Triamterene 50-100 4-6 DYTIDE (with benzthiazide)
Amiloride 5-10 20-24 LASIRIDE (with frusemide)
Table 13.2: Dose and duration of action of commonly used diuretics
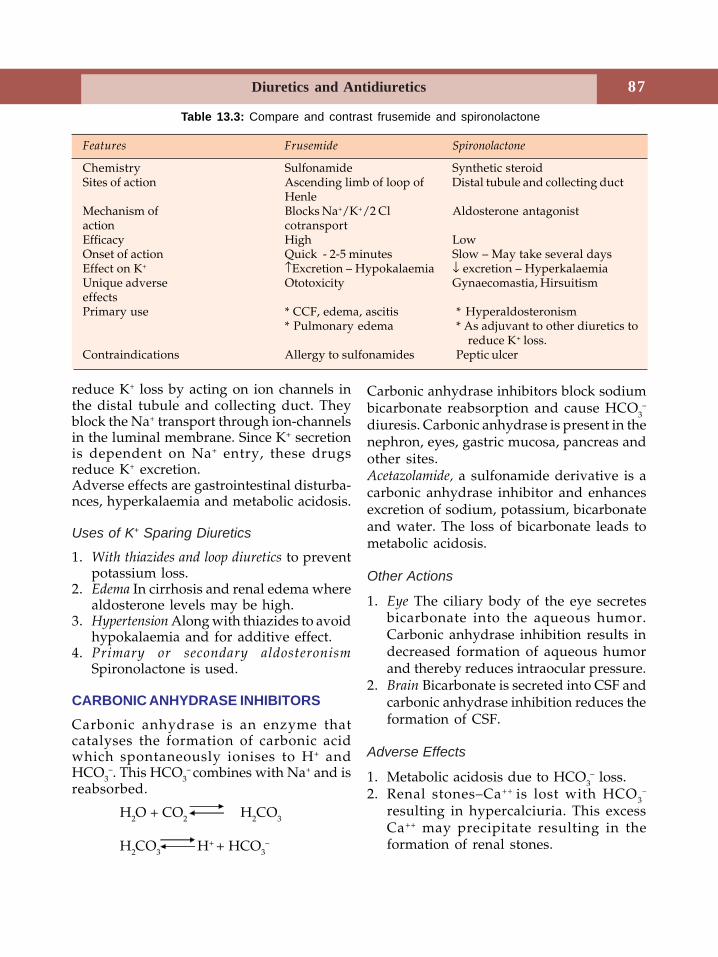
87Diuretics and Antidiuretics
reduce K+ loss by acting on ion channels inthe distal tubule and collecting duct. Theyblock the Na+ transport through ion-channelsin the luminal membrane. Since K+ secretionis dependent on Na+ entry, these drugsreduce K+ excretion.Adverse effects are gastrointestinal disturba-nces, hyperkalaemia and metabolic acidosis.
Uses of K+ Sparing Diuretics
1. With thiazides and loop diuretics to preventpotassium loss.
2. Edema In cirrhosis and renal edema wherealdosterone levels may be high.
3. Hypertension Along with thiazides to avoidhypokalaemia and for additive effect.
4. Primary or secondary aldosteronismSpironolactone is used.
CARBONIC ANHYDRASE INHIBITORSCarbonic anhydrase is an enzyme thatcatalyses the formation of carbonic acidwhich spontaneously ionises to H+ andHCO3
–. This HCO3– combines with Na+ and is
reabsorbed.
H2O + CO2 H2CO3
H2CO3 H+ + HCO3
–
Carbonic anhydrase inhibitors block sodiumbicarbonate reabsorption and cause HCO3
–
diuresis. Carbonic anhydrase is present in thenephron, eyes, gastric mucosa, pancreas andother sites.Acetazolamide, a sulfonamide derivative is acarbonic anhydrase inhibitor and enhancesexcretion of sodium, potassium, bicarbonateand water. The loss of bicarbonate leads tometabolic acidosis.
Other Actions
1. Eye The ciliary body of the eye secretesbicarbonate into the aqueous humor.Carbonic anhydrase inhibition results indecreased formation of aqueous humorand thereby reduces intraocular pressure.
2. Brain Bicarbonate is secreted into CSF andcarbonic anhydrase inhibition reduces theformation of CSF.
Adverse Effects
1. Metabolic acidosis due to HCO3– loss.
2. Renal stones–Ca++ is lost with HCO3–
resulting in hypercalciuria. This excessCa++ may precipitate resulting in theformation of renal stones.
Table 13.3: Compare and contrast frusemide and spironolactone
Features Frusemide Spironolactone
Chemistry Sulfonamide Synthetic steroidSites of action Ascending limb of loop of Distal tubule and collecting duct
HenleMechanism of Blocks Na+/K+/2 Cl Aldosterone antagonistaction cotransportEfficacy High LowOnset of action Quick - 2-5 minutes Slow – May take several daysEffect on K+ ↑Excretion – Hypokalaemia ↓ excretion – HyperkalaemiaUnique adverse Ototoxicity Gynaecomastia, HirsuitismeffectsPrimary use * CCF, edema, ascitis * Hyperaldosteronism
* Pulmonary edema * As adjuvant to other diuretics to reduce K+ loss.
Contraindications Allergy to sulfonamides Peptic ulcer
88 Textbook of Pharmacology for Dental and Allied Health Sciences
3. Hypokalaemia, drowsiness and allergicreactions can occur.
Uses
1. Glaucoma–(see page 49) Intraocularpressure is decreased by acetazolamide;it is given orally. Newer ones–methazo-lamide and dorzolamide are better toleratedand are available as eye drops.
2. Alkalinization of urine–as requiredin overdosage of acidic drugs. Also, uricacid and cysteine excretion can beenhanced as these are soluble in alkalineurine.
3. Metabolic alkalosis–acetazolamideenhances HCO3
– excretion.
4. Mountain sickness–In mountain climberswho rapidly ascend great heights, severepulmonary edema or cerebral edema mayoccur. Acetazolamide may relievesymptoms by reducing the formation andpH of CSF-it can also be used forprophylaxis.
5. Epilepsy–acetazolamide is used as anadjuvant as it increases the seizurethreshold.
OSMOTIC DIURETICS
Mannitol is a pharmacologically inertsubstance. When given IV (orally notabsorbed), mannitol gets filtered by theglomerulus but not reabsorbed. It causeswater to be retained in the proximal tubuleand descending limb of Henle’s loop byosmotic effect resulting in water diuresis.There is also some loss of sodium.
Adverse effects are dehydration, ECFvolume expansion, headache and allergicreactions.
Uses
1. To maintain urine volume and preventoliguria in conditions like massivehaemolysis and shock.
2. To reduce intracranial and intraocularpressure–following head injury andglaucoma respectively.
Glycerol is effective orally. It reducesintraocular and intracranial pressure.Methylxanthines like theophylline have milddiuretic effect.
Drug Interactions with Diuretics
1. Frusemide and ethacrynic acid are highlyprotein bound and may compete withdrugs like warfarin and clofibrate forprotein binding sites.
2. Other ototoxic drugs like aminoglycosidesshould not be used with loop diuretics toavoid enhanced toxicity.
3. Hypokalaemia induced by diureticsenhance digitalis toxicity.
4. NSAIDs blunt the effect of diuretics asthey cause salt and water retention toavoid enhanced toxicity.
5. Diuretics enhance lithium toxicity byreducing renal excretion of lithium.
6. Other drugs that cause hyperkalaemia(ACE inhibitors) and oral K+ supplementsshould be avoided with K+ sparingdiuretics because, given together they cancause severe hyperkalaemia.
DIURETICS AND DENTISTRY
1. When a patient is on concurrent medicationwith anticoagulants like warfarin anddiuretics like frusemideprofound anti-coagulant activity would be present. Minordental procedures including dentalextraction can cause severe bleeding.
2. When a patient is already receivingfrusemide or other loop diuretics, avoidusing aminoglycoside antibiotics as theototoxicity can get added up.
3. It is necessary to be cautious when it isrequired to give any of the NSAIDs to apatient who is already receiving diuretics
89Diuretics and Antidiuretics
because NSAIDs blunt the diuretic effect.However one or two doses of analgesicsdoes not matter much.
ANTIDIURETICS
Antidiuretics are drugs that reduce urinevolume. These include
1. Antidiuretic hormone (Vasopressin)2. Thiazide diuretics3. Miscellaneous
– Chlorpropamide– Carbamazepine.
Antidiuretic hormone (ADH) is secreted by theanterior pituitary along with oxytocin. It issynthesized in the supraoptic andparaventricular nuclei of the hypothalamus,transported along the hypothalamo-hypophyseal tract to the posterior pituitaryand is stored there.
ADH is released in response to two stimuli –dehydration and rise in plasma osmolarity.
Vasopressin Receptors
ADH acts on V1 and V2 receptors. V1 receptorsare present in vascular and other smoothmuscles, kidneys and anterior pituitary whileV2 receptors are present in collecting duct inthe kidneys. (See Fig 13.4).
Actions
ADH enhances water reabsorption by actingon the collecting duct. ADH activates the V2
receptors present on the cell membrane ofthe collecting duct and increases the waterpermeability of these cells. ADH causesvasoconstriction and raises BP mediated byV1 receptors. It also acts on other smoothmuscles to increase peristalsis in the gut andcontracts the uterus.
Vasopressin is given parenterally asinjection- SC/IM/IV.
Adverse Effects
When used intranasally ADH can cause nasalirritation, allergy, rhinitis and atrophy ofnasal mucosa. Other effects include nausea,abdominal cramps and backache (due tocontractions of the uterus).
Uses
1. Diabetes insipidus of pituitary origin–Desmopressin is the preparation used. Itshould be used life long.
2. Bleeding oesophageal varices–ADHconstricts mesenteric blood vessels (V1
receptors) and may help. Analogs likedesmopressin, terlipressin and lypressincan be used.
3. Before abdominal radiography—expelsgases from the bowel.
4. Haemophilia and Von Willebrand’sdisease - ADH may release factor VIII andprevent bleeding.
Vasopressin Analogs
Desmopressin is selective for V2 receptors andis longer acting. It is given as nasal spray.Terlipressin is longer acting while felypressinis short acting. Felypressin is used with localanaesthetics to prolong the duration of actionbecause of its vasoconstrictor properties.Lypressin is another analog used in place ofADH.
Miscellaneous
Thiazides Paradoxically thiazides reduce urinevolume in diabetes insipidus of bothpituitary and renal origin by an unknownmechanism.Chlorpropamide an oral hypoglycaemic,sensitizes the kidney to ADH action.Carbamazepine an antiepileptic, stimulates ADHsecretion.
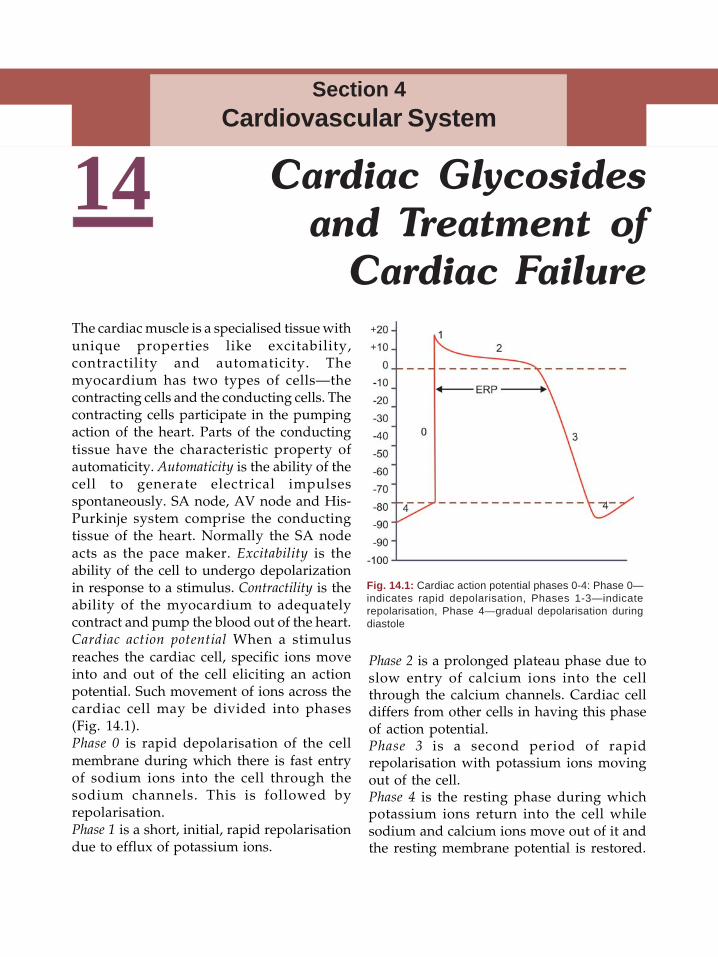
Textbook of Pharmacology for Dental and Allied Health Sciences90
14The cardiac muscle is a specialised tissue withunique properties like excitability,contractility and automaticity. Themyocardium has two types of cells—thecontracting cells and the conducting cells. Thecontracting cells participate in the pumpingaction of the heart. Parts of the conductingtissue have the characteristic property ofautomaticity. Automaticity is the ability of thecell to generate electrical impulsesspontaneously. SA node, AV node and His-Purkinje system comprise the conductingtissue of the heart. Normally the SA nodeacts as the pace maker. Excitability is theability of the cell to undergo depolarizationin response to a stimulus. Contractility is theability of the myocardium to adequatelycontract and pump the blood out of the heart.Cardiac action potential When a stimulusreaches the cardiac cell, specific ions moveinto and out of the cell eliciting an actionpotential. Such movement of ions across thecardiac cell may be divided into phases(Fig. 14.1).Phase 0 is rapid depolarisation of the cellmembrane during which there is fast entryof sodium ions into the cell through thesodium channels. This is followed byrepolarisation.Phase 1 is a short, initial, rapid repolarisationdue to efflux of potassium ions.
Phase 2 is a prolonged plateau phase due toslow entry of calcium ions into the cellthrough the calcium channels. Cardiac celldiffers from other cells in having this phaseof action potential.Phase 3 is a second period of rapidrepolarisation with potassium ions movingout of the cell.Phase 4 is the resting phase during whichpotassium ions return into the cell whilesodium and calcium ions move out of it andthe resting membrane potential is restored.
Cardiac Glycosidesand Treatment of
Cardiac Failure
Section 4Cardiovascular System
Fig. 14.1: Cardiac action potential phases 0-4: Phase 0—indicates rapid depolarisation, Phases 1-3—indicaterepolarisation, Phase 4—gradual depolarisation duringdiastole
91Cardiac Glycosides and Treatment of Cardiac Failure
During phases 1 and 2, the cell does notdepolarise in response to another impulse,i.e. it is in absolute refractory period. Butduring phases 3 and 4, the cell is in relativerefractory period and may depolarise inresponse to a powerful impulse.
The cardiac output is determined by heartrate and stroke volume. The stroke volumein turn depends on the preload, afterload andcontractility. Preload is the load on the heartdue to the volume of blood reaching the leftventricle. It depends on the venous return.Afterload is the resistance to the leftventricular ejection, i.e. the total peripheralresistance.Congestive cardiac failure (CCF) is one of thecommon causes of morbidity and mortality.In congestive cardiac failure, the heart isunable to provide adequate blood supply tomeet the body’s oxygen demand. Thepumping ability of the heart is reduced andthe cardiac output decreases. The ventriclesare not completely emptied resulting inincreased venous pressure in the pulmonaryand systemic circulation. This causespulmonary oedema, dyspnoea, liverenlargement and peripheral oedema. As acompensatory mechanism, there isstimulation of the sympathetic system, reninangiotensin system and release of atrialnatriuretic peptides which help inmaintaining the cardiac output. Atria,ventricles and vascular endothelium storenatriuretic peptides and release them involume overload. These peptides increaserenal excretion of salt and water and dilatevascular smooth muscles. The myocardiumalso undergoes structural alterations likeventricular hypertrophy and remodelling toadapt itself to the stressful situation. Thesecompensatory changes maintain the cardiacoutput for sometime.
Depending on the cardiac output, cardiacfailure may be of two types-low outputfailure and high output failure.
Low output failure could result fromischaemic heart disease, hypertension,valvular and congenital heart diseases. Highoutput failure results from anaemia,thyrotoxicosis, beriberi and certain congenitalheart diseases.
The drugs used in CCF include diuretics,vasodilators and cardiac glycosides. Thepharmacology of cardiac glycosides has beendiscussed first, followed by the role of otherdrugs in CCF.
CARDIAC GLYCOSIDESCardiac glycosides are obtained from theplants of the foxglove family. Though theseplants were known to Egyptians 3000 yearsago, they were irrationally used. WilliamWithering, an English physician firstdescribed the clinical effects of digitalis inCCF in 1785.Source Digitoxin is obtained from the leavesof Digitalis purpurea. From the leaves ofDigitalis lanata, digitoxin and digoxin arederived and the seeds of Strophanthus gratuscontain ouabain. They are all called cardiacglycosides but digoxin is the most commonlyused of them because of its favourablepharmacokinetic properties. The worddigitalis is used to mean cardiac glycosides.Chemistry The glycosides consist of an aglyconattached to sugars. The aglycon haspharmacodynamic activity while sugarsinfluence pharmacokinetic properties.
Pharmacological Actions1. Cardiac actions• Positive inotropic effect Cardiac glycosides
are cardiotonic drugs - they increase theforce of contraction of the heart - thestroke volume increases and thereby thecardiac output. The systole is shortenedand the diastole is prolonged whichallows more rest to the heart. Theventricles are more completely emptiedbecause of more forceful contractions.
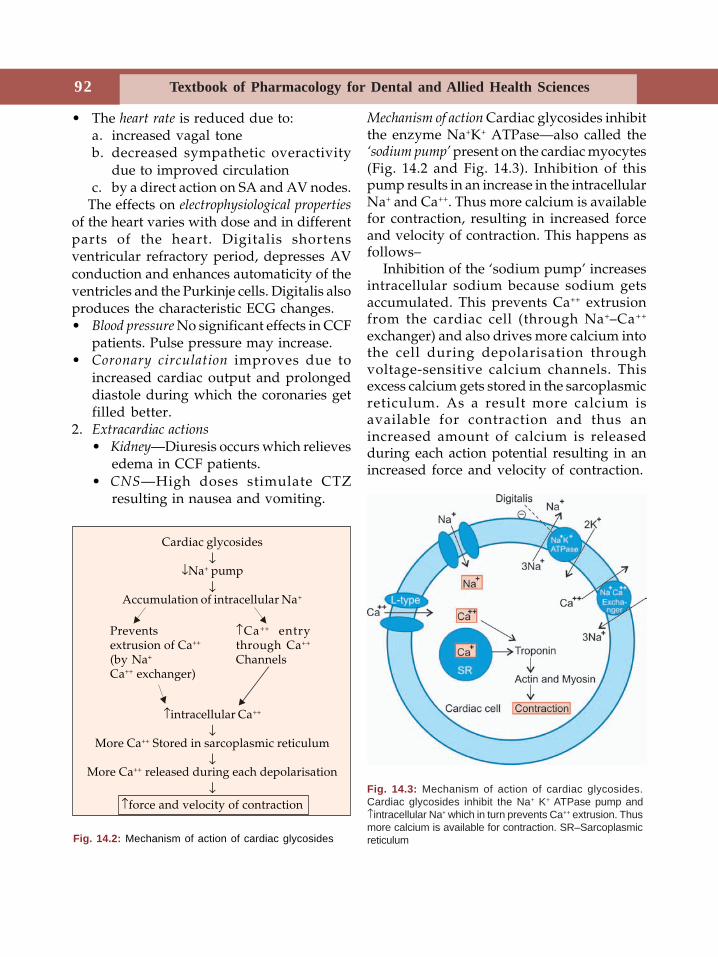
Textbook of Pharmacology for Dental and Allied Health Sciences92
• The heart rate is reduced due to:a. increased vagal toneb. decreased sympathetic overactivity
due to improved circulationc. by a direct action on SA and AV nodes.
The effects on electrophysiological propertiesof the heart varies with dose and in differentparts of the heart. Digitalis shortensventricular refractory period, depresses AVconduction and enhances automaticity of theventricles and the Purkinje cells. Digitalis alsoproduces the characteristic ECG changes.• Blood pressure No significant effects in CCF
patients. Pulse pressure may increase.• Coronary circulation improves due to
increased cardiac output and prolongeddiastole during which the coronaries getfilled better.
2. Extracardiac actions• Kidney—Diuresis occurs which relieves
edema in CCF patients.• CNS—High doses stimulate CTZ
resulting in nausea and vomiting.
Mechanism of action Cardiac glycosides inhibitthe enzyme Na+K+ ATPase—also called the‘sodium pump’ present on the cardiac myocytes(Fig. 14.2 and Fig. 14.3). Inhibition of thispump results in an increase in the intracellularNa+ and Ca++. Thus more calcium is availablefor contraction, resulting in increased forceand velocity of contraction. This happens asfollows–
Inhibition of the ‘sodium pump’ increasesintracellular sodium because sodium getsaccumulated. This prevents Ca++ extrusionfrom the cardiac cell (through Na+–Ca++
exchanger) and also drives more calcium intothe cell during depolarisation throughvoltage-sensitive calcium channels. Thisexcess calcium gets stored in the sarcoplasmicreticulum. As a result more calcium isavailable for contraction and thus anincreased amount of calcium is releasedduring each action potential resulting in anincreased force and velocity of contraction.
Fig. 14.2: Mechanism of action of cardiac glycosides
Cardiac glycosides↓
↓Na+ pump↓
Accumulation of intracellular Na+
↑intracellular Ca++
↓More Ca++ Stored in sarcoplasmic reticulum
↓More Ca++ released during each depolarisation
↓↑force and velocity of contraction
Preventsextrusion of Ca++
(by Na+
Ca++ exchanger)
↑Ca++ entrythrough Ca++
Channels
Fig. 14.3: Mechanism of action of cardiac glycosides.Cardiac glycosides inhibit the Na+ K+ ATPase pump and↑intracellular Na+ which in turn prevents Ca++ extrusion. Thusmore calcium is available for contraction. SR–Sarcoplasmicreticulum
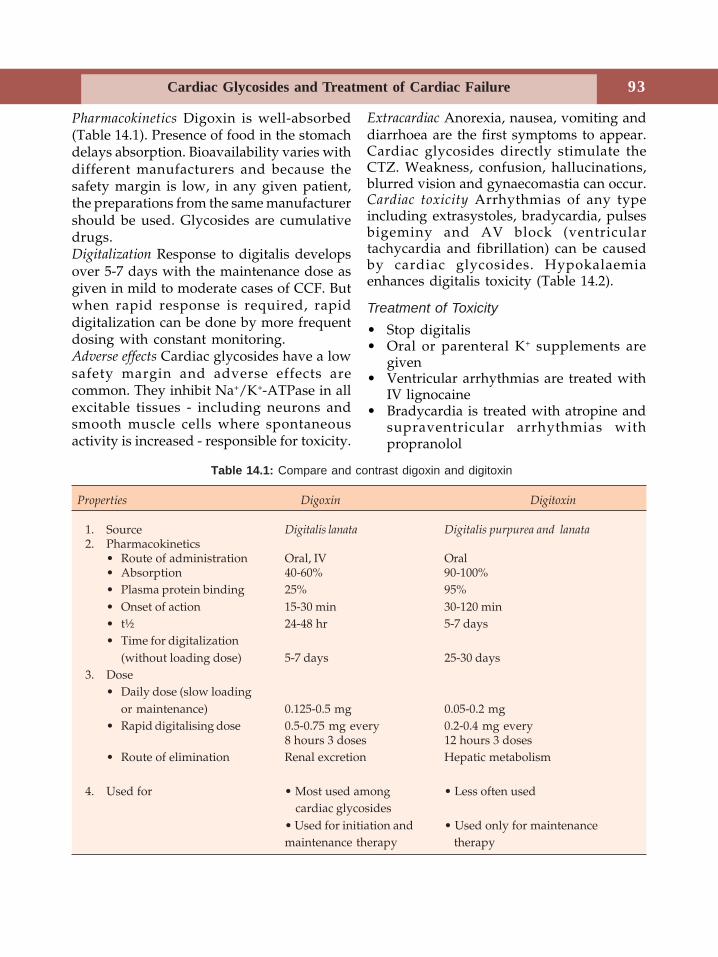
93Cardiac Glycosides and Treatment of Cardiac Failure
Extracardiac Anorexia, nausea, vomiting anddiarrhoea are the first symptoms to appear.Cardiac glycosides directly stimulate theCTZ. Weakness, confusion, hallucinations,blurred vision and gynaecomastia can occur.Cardiac toxicity Arrhythmias of any typeincluding extrasystoles, bradycardia, pulsesbigeminy and AV block (ventriculartachycardia and fibrillation) can be causedby cardiac glycosides. Hypokalaemiaenhances digitalis toxicity (Table 14.2).
Treatment of Toxicity• Stop digitalis• Oral or parenteral K+ supplements are
given• Ventricular arrhythmias are treated with
IV lignocaine• Bradycardia is treated with atropine and
supraventricular arrhythmias withpropranolol
Table 14.1: Compare and contrast digoxin and digitoxin
Properties Digoxin Digitoxin
1. Source Digitalis lanata Digitalis purpurea and lanata2. Pharmacokinetics
• Route of administration Oral, IV Oral• Absorption 40-60% 90-100%• Plasma protein binding 25% 95%• Onset of action 15-30 min 30-120 min• t½ 24-48 hr 5-7 days• Time for digitalization
(without loading dose) 5-7 days 25-30 days3. Dose
• Daily dose (slow loadingor maintenance) 0.125-0.5 mg 0.05-0.2 mg
• Rapid digitalising dose 0.5-0.75 mg every 0.2-0.4 mg every8 hours 3 doses 12 hours 3 doses
• Route of elimination Renal excretion Hepatic metabolism
4. Used for • Most used among • Less often used cardiac glycosides• Used for initiation and • Used only for maintenancemaintenance therapy therapy
Pharmacokinetics Digoxin is well-absorbed(Table 14.1). Presence of food in the stomachdelays absorption. Bioavailability varies withdifferent manufacturers and because thesafety margin is low, in any given patient,the preparations from the same manufacturershould be used. Glycosides are cumulativedrugs.Digitalization Response to digitalis developsover 5-7 days with the maintenance dose asgiven in mild to moderate cases of CCF. Butwhen rapid response is required, rapiddigitalization can be done by more frequentdosing with constant monitoring.Adverse effects Cardiac glycosides have a lowsafety margin and adverse effects arecommon. They inhibit Na+/K+-ATPase in allexcitable tissues - including neurons andsmooth muscle cells where spontaneousactivity is increased - responsible for toxicity.
Textbook of Pharmacology for Dental and Allied Health Sciences94
• In severe toxicity–antidigoxin immuno-therapy (antidigoxin antibodies) is nowavailable. It can be life saving in severedigoxin overdosage.
Uses
1. Congestive cardiac failure (see below)2. Cardiac arrhythmias
• Atrial fibrillation and atrial flutter—digoxin reduces the ventricular rate
• Paroxysmal supraventricular tachy-cardia (PSVT)—digoxin is an alter-native to verapamil.
Precautions and contraindications todigitalis therapy• Hypokalaemia—enhances toxicity• MI, thyrotoxicosis patients and elderly—
more prone to arrhythmias• Acid base imbalance—prone to toxicity.
Other Positive-inotropic DrugsPhosphodiesterase inhibitors–Amrinone(inamrinone) and milrinone-These drugs inhibitthe enzyme phosphodiesterase (whichdegrades cAMP) resulting in ↑cAMP levels.They increase the force of contraction andalso cause vasodilatation. But because of theadverse effects and increased mortality seenwith the use of these drugs, they aregenerally not preferred. However, they maybe used for short periods in severe heartfailure. Milrinone has shorter t½ and fewerside effects.
DRUGS USED IN CONGESTIVECARDIAC FAILURE
In congestive cardiac failure, the heart isunable to provide adequate blood supply tomeet the demand. The aim of treatment is toreduce morbidity and mortality by restoringcardiac output and relieving congestion.
The drugs used in CCF include:1. Diuretics2. Vasodilators3. Positive inotropic agents -
• Digitalis• β adrenergic agonists• Phosphodiesterase (PDE) inhibitors• Others
1. Diuretics High ceiling diuretics likefrusemide are used. They increase salt andwater excretion and reduce blood volume.By this they reduce preload and venouspressure, improve cardiac performanceand relieve oedema.
2. Vasodilators reduce the mortality in patientswith cardiac failure. Vasodilators may bearteriolar or venular dilators or both.• Arteriolar dilators (↓ after load) —
hydralazine-relax arterial smoothmuscles, thus reducing peripheralvascular resistance (↓ afterload). As aresult, the work load on the heart isreduced.
• Venodilators (↓ preload) — nitrates -reduce the venous return to the heart(↓ preload) thus reducing the stretchingof the ventricular walls and myocardialoxygen requirements.Organic nitrates: Nitroglycerine andisosorbide dinitrate are goodvasodilators with a rapid and shortaction. They can be used for shortperiods to decrease the ventricularfilling pressure in acute heart failure.Nitroglycerine can be used IV in acuteCCF. Nitrates may be given incombination with hydralazine.
Table 14.2: Drug interactions
Drugs that enhance digoxin toxicity
• Diuretics (due to hypokalaemia), calcium• Quinidine, verapamil, methyldopa–
↑digoxin levelsDrugs that reduce digoxin levels
• Antacids, neomycin, metoclopramide–↓ absorption
• Rifampicin, phenobarbitone–hasten meta-bolism due to enzyme induction

95Cardiac Glycosides and Treatment of Cardiac Failure
• Both arteriolar and venular dilators—ACE inhibitors, sodium nitroprusside,prazosin, calcium channel blockers -these reduce both preload andafterload.
Angiotensin converting enzyme inhibitors(ACE-I) (Page 111) like captopril, enalapril,lisinopril and ramipril act by -i. reduction of afterload Angiotensin II is a
powerful vasoconstrictor present in theplasma in high concentrations in cardiacfailure. ACE-I prevent the conversion ofangiotensin I to angiotensin II and therebyreduce the after load.
ii. reduction of preload Aldosterone causes saltand water retention and increases plasmavolume. ACE-I prevent the formation ofaldosterone (by reducing Ang-II) andthereby reduce the preload. They alsoprevent bradykinin degradation andincrease bradykinin levels which alsocauses vasodilatation.
iii. reversing compensatory changes AngiotensinII formed locally in the myocardium isresponsible for various undesirablecompensatory changes like ventricularhypertrophy and ventricular remodellingseen in CCF. ACE-I reverse these changes.
ACE inhibitors are the most preferred drugsin chronic congestive cardiac failure.Sodium nitroprusside is a powerful vasodilator.Since it dilates both arterioles and venules,it reduces both ventricular filling pressureand peripheral arterial resistance. It is givenIV, has a rapid (30-60 sec) and short action (3minutes). Hence it is useful in acute severeheart failure.Prazosin an α
1 antagonist, is a vasodilator. Itcan be used in acute heart failure for longerperiods than nitrates.Calcium channel blockers are not routinely used.Amlodipine or felodipine may be tried in
patients in whom other vasodilators arecontraindicated.3. Positive inotropic agentsDigitalis: Mild to moderate cases of lowoutput failure are treated with diuretics andvasodilators (ACE-inhibitors preferred).When patients are not controlled by these,they may be given digoxin. Digoxin improvescardiac performance in the dilated, failingheart. If there is associated atrial fibrillation,digoxin is the preferred drug in suchpatients.β adrenergic agonists: Dobutamine is a positiveinotropic agent. It stimulates the cardiac β1receptors and enhances the force ofcontraction of the cardiac muscle. It increasesthe cardiac output without significanttachycardia. It also produces somevasodilation by stimulating the β2 receptors.Dopamine may be used in patients withassociated renal impairment becausedopamine increases renal perfusion in additionto increased cardiac output.PDE Inhibitors: Amrinone or milrinone maybe used for short periods to enhance thecardiac output in severe heart failure.4. Othersβ Adrenergic blockers : Though β blockers arenegative inotropic agents, several recentstudies have shown that when used carefullyalong with other drugs, β blockers canimprove long-term survival (Page 80).
Cardiac Failure and Dentistry1. The antibiotic neomycin can reduce
digoxin absorption and could worsenCCF. Alternative antibiotic may be usedif its long-term use is required.
2. Use of NSAIDs especially long-term usecan cause salt and water retention andworsen CCF.
3. A knowledge of CCF is necessary as adentist has to be careful while carryingon surgical procedures in such patients.
96 Textbook of Pharmacology for Dental and Allied Health Sciences
15The discovery of the calcium channels in thecardiac cells helped in understanding themechanisms involved in smooth musclecontraction. Verapamil was the first agentfound to have calcium channel blockingproperties and now we have many more.
Dihydropyridines
Nifedipine NicardipineNimodipine NitrendipineNisoldipine FelodipineAmlodipine Isradipine
Others
Verapamil DiltiazemBepridil
The depolarisation of the cardiac andvascular smooth muscle cells depend on theentry of extracellular calcium into the cellthrough the calcium channels. Intracellularcalcium is also increased by receptor-mediated action – i.e. agonist induced calciumrelease. This calcium triggers the release ofintracellular calcium from the sarcoplasmicreticulum. All these calcium ions bring aboutcontraction of the cardiac and vascularsmooth muscle cells.
Calcium channel antagonists inhibit theentry of calcium by blocking the L-typeof calcium channels. (There are 3 types of
calcium channels - L, N and T types). Thisdecreases calcium current and calcium entryinto cardiac and vascular smooth muscle cellsresulting in the following effects—1. Vascular smooth muscle Relaxation of the
arteriolar smooth muscles results inreduced peripheral vascular resistanceand blood pressure. The effect on venousbeds is not significant. Reflex tachycardiamay occur with some CCBs likenifedipine. Dihydropyridine CCBs haveprominent effects on the blood vessels,i.e. they are vascular selective.
2. Heart CCBs depress myocardialcontractility, reduce heart rate and inhigher doses they slow AV conduction.They reduce cardiac work and therebymyocardial oxygen consumption.Verapamil, bepridil and diltiazem haveprominent cardiac effects.
3. Coronary circulation CCBs dilate thecoronary vessels, increasing the coronaryblood flow. Hence they are useful invariant angina.
4. Other effects
• Nimodipine is highly lipid soluble,crosses the BBB and relaxes thecerebral blood vessels.
• CCBs relax the uterus and may beuseful in premature labour.
Calcium ChannelBlockers
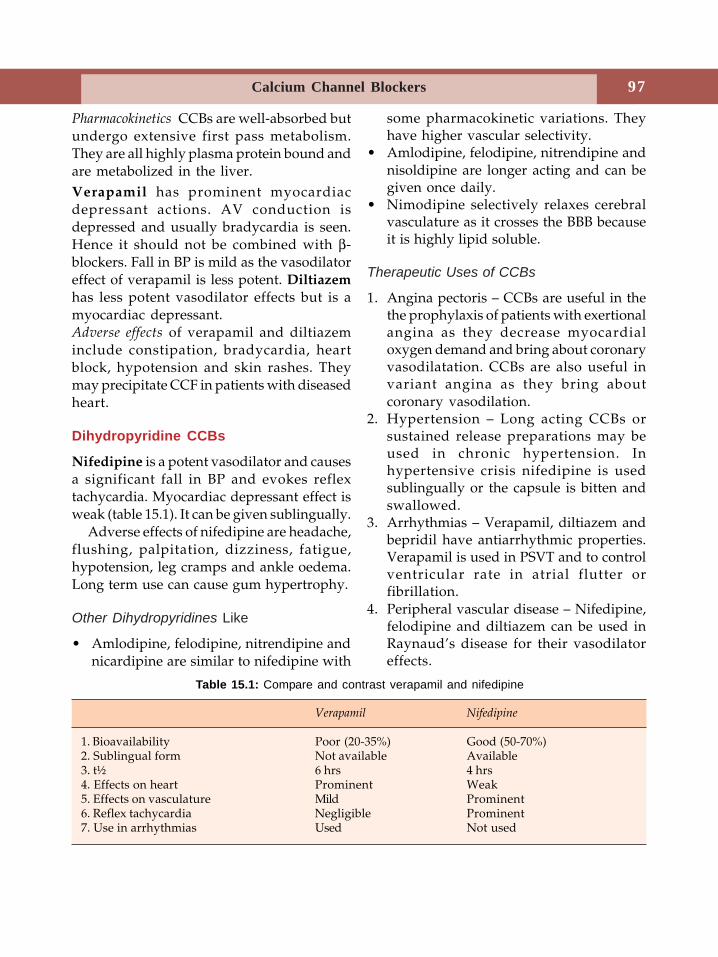
97Calcium Channel Blockers
Pharmacokinetics CCBs are well-absorbed butundergo extensive first pass metabolism.They are all highly plasma protein bound andare metabolized in the liver.Verapamil has prominent myocardiacdepressant actions. AV conduction isdepressed and usually bradycardia is seen.Hence it should not be combined with β-blockers. Fall in BP is mild as the vasodilatoreffect of verapamil is less potent. Diltiazemhas less potent vasodilator effects but is amyocardiac depressant.Adverse effects of verapamil and diltiazeminclude constipation, bradycardia, heartblock, hypotension and skin rashes. Theymay precipitate CCF in patients with diseasedheart.
Dihydropyridine CCBs
Nifedipine is a potent vasodilator and causesa significant fall in BP and evokes reflextachycardia. Myocardiac depressant effect isweak (table 15.1). It can be given sublingually.
Adverse effects of nifedipine are headache,flushing, palpitation, dizziness, fatigue,hypotension, leg cramps and ankle oedema.Long term use can cause gum hypertrophy.
Other Dihydropyridines Like
• Amlodipine, felodipine, nitrendipine andnicardipine are similar to nifedipine with
some pharmacokinetic variations. Theyhave higher vascular selectivity.
• Amlodipine, felodipine, nitrendipine andnisoldipine are longer acting and can begiven once daily.
• Nimodipine selectively relaxes cerebralvasculature as it crosses the BBB becauseit is highly lipid soluble.
Therapeutic Uses of CCBs
1. Angina pectoris – CCBs are useful in thethe prophylaxis of patients with exertionalangina as they decrease myocardialoxygen demand and bring about coronaryvasodilatation. CCBs are also useful invariant angina as they bring aboutcoronary vasodilation.
2. Hypertension – Long acting CCBs orsustained release preparations may beused in chronic hypertension. Inhypertensive crisis nifedipine is usedsublingually or the capsule is bitten andswallowed.
3. Arrhythmias – Verapamil, diltiazem andbepridil have antiarrhythmic properties.Verapamil is used in PSVT and to controlventricular rate in atrial flutter orfibrillation.
4. Peripheral vascular disease – Nifedipine,felodipine and diltiazem can be used inRaynaud’s disease for their vasodilatoreffects.
Verapamil Nifedipine
1. Bioavailability Poor (20-35%) Good (50-70%)2. Sublingual form Not available Available3. t½ 6 hrs 4 hrs4. Effects on heart Prominent Weak5. Effects on vasculature Mild Prominent6. Reflex tachycardia Negligible Prominent7. Use in arrhythmias Used Not used
Table 15.1: Compare and contrast verapamil and nifedipine
98 Textbook of Pharmacology for Dental and Allied Health Sciences
5. Other uses(i) Hypertrophic cardiomyopathy -
Verapamil can be beneficial due to itsnegative inotropic effects on the heart.
(ii) Migraine – Verapamil is useful in theprophylaxis of migraine
(iii) Subarachnoid haemorrhage –Vasospasm that follows subarachnoidhaemorrhage is believed to beresponsible for neurological defects.As nimodipine brings about cerebralvasodilatation, it is used to treatneurological deficits in patients withcerebral vasospasm.
(iv) Preterm labour – Nifedipine inhibitsuterine contractions and is found tobe useful in delaying labour inpremature uterine contractions.
Drug Interactions
• Verapamil and diltiazem should be avoidedin patients receiving beta-adrenergicblockers because the myocardiac dep-ressant effects get added up.
• Verapamil can precipitate digoxin toxicityby increasing digoxin levels (verapamilreduces digoxin excretion).
99Antiarrhythmic Drugs
16Arrhythmia is an abnormality of the rate,rhythm or site of origin of the cardiacimpulse or an abnormality in the impulseconduction. The word dysrhythmia is alsoused by some. Cardiac arrhythmias may bedue to abnormal generation or conductionof impulses. Factors like myocardial hypoxia,myocardial ischaemia, electrolyte distur-bances, trauma, drugs and autonomicinfluences can cause arrhythmias.
Arrhythmias may be tachyarrhythmias,bradyarrhythmias or digitalis-inducedarrhythmias. Based on the site of impulseorigin, they may be grouped as supra-ventricular (SA node, AV node, atria) orventricular arrhythmias (in ventricles).Ventricular arrhythmias are a common causeof death, particularly sudden death.
CLASSIFICATION
Based on the cardiac cycle, Vaughan Williamsclassified antiarrhythmics as follows:Class I. Sodium channel blockers
A. Prolong repolarization- Quinidine, procainamide,disopyramide, moricizine
B. Shorten repolarization- Lignocaine, mexiletine,phenytoin
C. Little effect on repolarization- Encainide, flecainide,propafenone
Class II. β-adrenergic blockers(reduce sympathetic tone)- Propranolol, acebutolol,esmolol, etc.
Class III. K+ channel blockers(Prolong repolarization)- Amiodarone, bretylium, sotalol,dofetilide, ibutilide
Class IV. Ca++ channel blockers(Prolong conduction andrefractoriness specially in SAand AV nodes)- Verapamil, diltiazem
Sodium Channel Blockers
Mechanism of action All drugs in Class I blockthe sodium channels and prevent the inwardmovement of Na+ ions. The sodium channelsexist in three states—resting, open andinactivated (refractory) state. Sodiumchannel blockers preferrentially bind Na+
channels in the open and inactivated stateand thus interfere with depolarisation.
Class IA drugs block Na+ channels anddepress phase-0 depolarisation. They alsoprolong repolarisation by blocking K+
channels. (Fig. 16.1)
Quinidine
Quinidine is the D-isomer of quinineobtained from the cinchona bark. By blockingNa+ channels, it depresses all cardiac
Antiarrhythmic Drugs
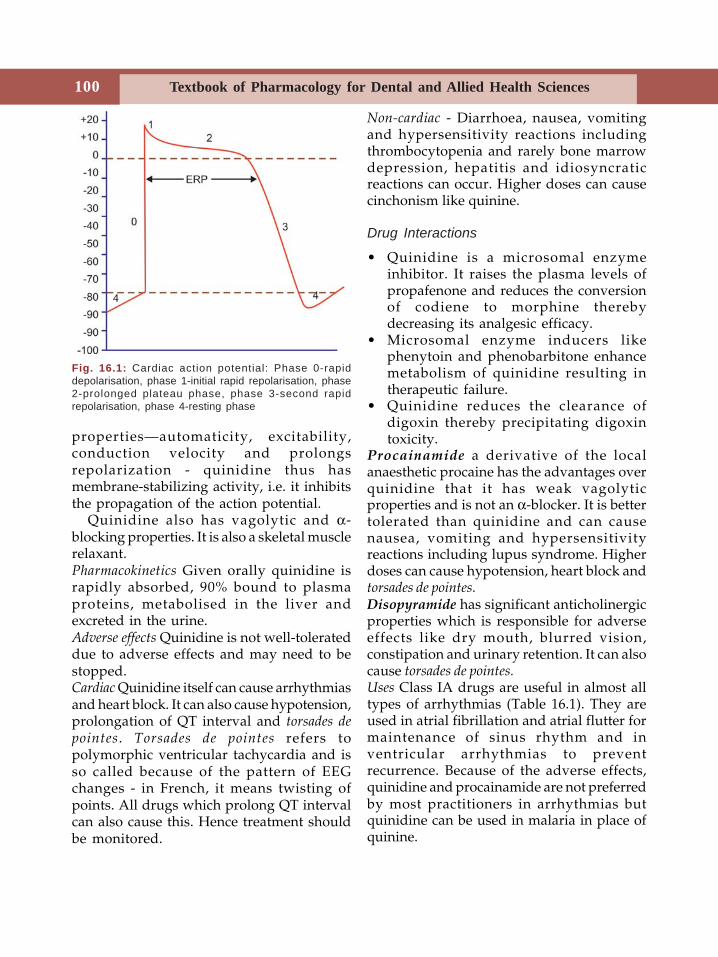
Textbook of Pharmacology for Dental and Allied Health Sciences100
properties—automaticity, excitability,conduction velocity and prolongsrepolarization - quinidine thus hasmembrane-stabilizing activity, i.e. it inhibitsthe propagation of the action potential.
Quinidine also has vagolytic and α-blocking properties. It is also a skeletal musclerelaxant.Pharmacokinetics Given orally quinidine israpidly absorbed, 90% bound to plasmaproteins, metabolised in the liver andexcreted in the urine.Adverse effects Quinidine is not well-tolerateddue to adverse effects and may need to bestopped.Cardiac Quinidine itself can cause arrhythmiasand heart block. It can also cause hypotension,prolongation of QT interval and torsades depointes. Torsades de pointes refers topolymorphic ventricular tachycardia and isso called because of the pattern of EEGchanges - in French, it means twisting ofpoints. All drugs which prolong QT intervalcan also cause this. Hence treatment shouldbe monitored.
Non-cardiac - Diarrhoea, nausea, vomitingand hypersensitivity reactions includingthrombocytopenia and rarely bone marrowdepression, hepatitis and idiosyncraticreactions can occur. Higher doses can causecinchonism like quinine.
Drug Interactions
• Quinidine is a microsomal enzymeinhibitor. It raises the plasma levels ofpropafenone and reduces the conversionof codiene to morphine therebydecreasing its analgesic efficacy.
• Microsomal enzyme inducers likephenytoin and phenobarbitone enhancemetabolism of quinidine resulting intherapeutic failure.
• Quinidine reduces the clearance ofdigoxin thereby precipitating digoxintoxicity.
Procainamide a derivative of the localanaesthetic procaine has the advantages overquinidine that it has weak vagolyticproperties and is not an α-blocker. It is bettertolerated than quinidine and can causenausea, vomiting and hypersensitivityreactions including lupus syndrome. Higherdoses can cause hypotension, heart block andtorsades de pointes.Disopyramide has significant anticholinergicproperties which is responsible for adverseeffects like dry mouth, blurred vision,constipation and urinary retention. It can alsocause torsades de pointes.Uses Class IA drugs are useful in almost alltypes of arrhythmias (Table 16.1). They areused in atrial fibrillation and atrial flutter formaintenance of sinus rhythm and inventricular arrhythmias to preventrecurrence. Because of the adverse effects,quinidine and procainamide are not preferredby most practitioners in arrhythmias butquinidine can be used in malaria in place ofquinine.
Fig. 16.1: Cardiac action potential: Phase 0-rapiddepolarisation, phase 1-initial rapid repolarisation, phase2-prolonged plateau phase, phase 3-second rapidrepolarisation, phase 4-resting phase
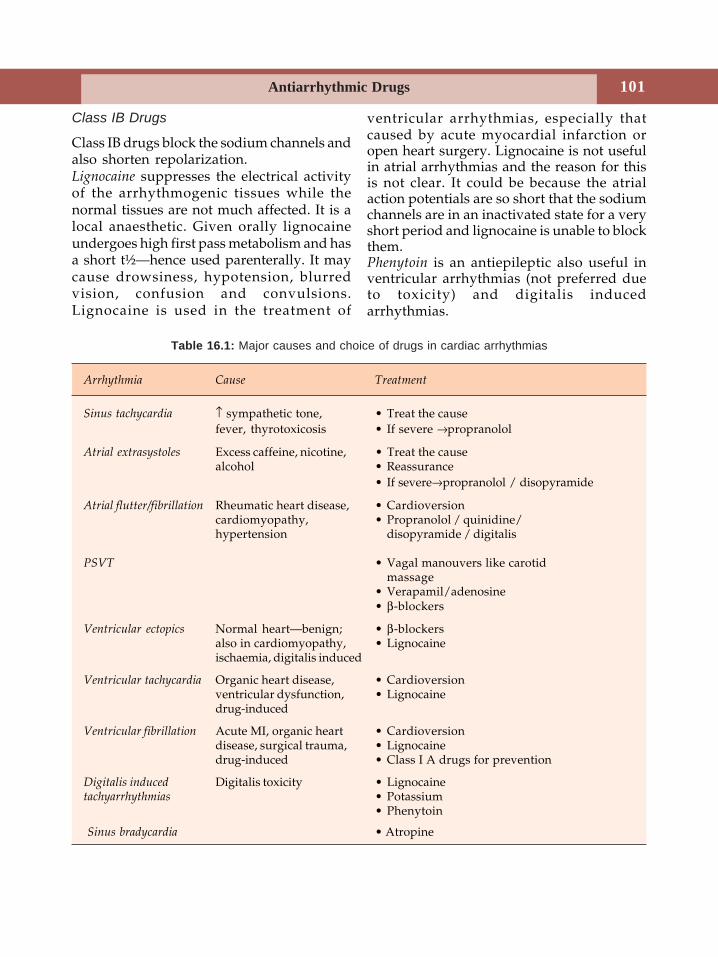
101Antiarrhythmic Drugs
Class IB Drugs
Class IB drugs block the sodium channels andalso shorten repolarization.Lignocaine suppresses the electrical activityof the arrhythmogenic tissues while thenormal tissues are not much affected. It is alocal anaesthetic. Given orally lignocaineundergoes high first pass metabolism and hasa short t½—hence used parenterally. It maycause drowsiness, hypotension, blurredvision, confusion and convulsions.Lignocaine is used in the treatment of
ventricular arrhythmias, especially thatcaused by acute myocardial infarction oropen heart surgery. Lignocaine is not usefulin atrial arrhythmias and the reason for thisis not clear. It could be because the atrialaction potentials are so short that the sodiumchannels are in an inactivated state for a veryshort period and lignocaine is unable to blockthem.Phenytoin is an antiepileptic also useful inventricular arrhythmias (not preferred dueto toxicity) and digitalis inducedarrhythmias.
Table 16.1: Major causes and choice of drugs in cardiac arrhythmias
Arrhythmia Cause Treatment
Sinus tachycardia ↑ sympathetic tone, • Treat the causefever, thyrotoxicosis • If severe →propranolol
Atrial extrasystoles Excess caffeine, nicotine, • Treat the causealcohol • Reassurance
• If severe→propranolol / disopyramide
Atrial flutter/fibrillation Rheumatic heart disease, • Cardioversioncardiomyopathy, • Propranolol / quinidine/hypertension disopyramide / digitalis
PSVT • Vagal manouvers like carotidmassage
• Verapamil/adenosine• β-blockers
Ventricular ectopics Normal heart—benign; • β-blockersalso in cardiomyopathy, • Lignocaineischaemia, digitalis induced
Ventricular tachycardia Organic heart disease, • Cardioversionventricular dysfunction, • Lignocainedrug-induced
Ventricular fibrillation Acute MI, organic heart • Cardioversiondisease, surgical trauma, • Lignocainedrug-induced • Class I A drugs for prevention
Digitalis induced Digitalis toxicity • Lignocainetachyarrhythmias • Potassium
• Phenytoin
Sinus bradycardia • Atropine

Textbook of Pharmacology for Dental and Allied Health Sciences102
Mexiletine can be used orally; causes doserelated neurologic adverse effects includingtremors and blurred vision. Nausea iscommon. It is used as an alternative tolignocaine in ventricular arrhythmias.
Class IC Drugs
Class IC drugs are the most potent sodiumchannel blockers. Because of the risk ofcardiac arrest, sudden death and otheradverse effects, they are not commonly used.They may be used in severe ventriculararrhythmias and to maintain sinus rhythm inatrial fibrillation.
Class II Drugs
β-blockers (Chapter 12) like propranolol exertantiarrhythmic effect due to blockade ofcardiac β receptors. They depress myocardialcontractility, automaticity and conductionvelocity. In higher doses they also havemembrane stabilising activity like class Idrugs.Propranolol and cardioselective β blockers likeatenolol and metoprolol are used in thetreatment and prevention of supraventriculararrhythmias especially those associated withexercise, emotion or hyperthyroidism.Esmolol given intravenously is rapid andshort-acting and can be used to treatarrhythmias during surgeries, followingmyocardial infarction and other emergencies.
Class III Drugs
These drugs prolong the action potentialduration and refractory period by blockingthe potassium channels.Amiodarone an analog of thyroid hormone isa powerful antiarrhythmic. It acts by multiplemechanisms.
– prolongs APD by blocking K+ channels.– blocks sodium channels.– blocks β adrenergic receptors.
Amiodarone can cause various adverseeffects like heart block, cardiac failure,hypotension, bluish discolouration of theskin, hypothyroidism, gastrointestinaldisturbances and hepatotoxicity. It can causepulmonary fibrosis that can be fatal.Amiodarone is used only in resistant casesof chronic ventricular arrhythmias and toprevent recurrence of atrial fibrillation andflutter.Bretylium is an adrenergic neurone blockerused in resistant ventricular arrhythmias.Sotalol a β-blocker also prolongs the actionpotential duration and is classified underclass III antiarrhythmic drugs and is oftenpreferred when a β-blocker is needed.
Class IV Drugs
Calcium channel blockers (Page 96) inhibitthe inward movement of calcium resultingin reduced contractility, automaticity and AVnodal conduction. Verapamil, diltiazem, andbepridil have prominent cardiac effects,because they block the calcium channels inthe cardiac cells in therapeutic doses.Verapamil is used to terminate paroxysmalsupraventricular tachycardia (PSVT). It is alsoused to control ventricular rate in atrialflutter or fibrillation because it depresses theAV nodal conduction. Diltiazam can be usedin place of verapamil.Dofetilide is a newly introduced and selectiveK+ channel blocker. It has no other actions asit is a pure K+ channel blocker and prolongsAPD. It is used orally in atrial fibrillation toconvert and to maintain sinus rhythm. Theonly adverse effect known is torsades de pointes
in 1% patients.Ibutilide is a K+ channel blocker used asintravenous infusion to quickly convert atrialflutter/fibrillation to sinus rhythm. It cancause torsades de pointes.

103Antiarrhythmic Drugs
Drug Interactions
Verapamil displaces digoxin from tissuebinding sites and also reduces its renalclearance resulting in digoxin toxicity - doseof digoxin should be reduced.
Other Antiarrhythmics
Adenosine, atropine, digoxin and magnesiumsulphate also have antiarrhythmic propertiesbut are not included in Vaughan Willamsclassification.Adenosine is a purine nucleotide having rapidand short antiarrhythmic action. Given IV itsuppresses automaticity, AV conduction anddilates the coronaries. Adenosine is the drug
of choice for acute termination of paroxysmalsupraventricular tachycardias (PSVT).
Adverse effects are nausea, dyspnoea,flushing, dizziness and headache but are ofshort duration. Theophylline blocks ade-nosine receptors and inhibits the action ofadenosine.Atropine is used in sinus bradycardia. It actsby blocking M2 muscarinic receptors.Digitalis depresses AV conduction, reducesheart rate and increases the force ofcontraction of the myocardium. Digoxin isused in atrial fibrillation to control theventricular rate.Magnesium sulphate is used IV to treat digitalisinduced arrhythmias and torsades de pointes.
Textbook of Pharmacology for Dental and Allied Health Sciences104
17Angina pectoris is the chief symptom ofischaemic heart disease (IHD) characterisedby sudden, severe, substernal discomfort orpain which may radiate to the left shoulderand along the flexor surface of the left arm.Myocardial oxygen consumption depends onpreload (determined by venous return andstretching of the heart), afterload (deter-mined by peripheral arterial resistance) andheart rate. When the oxygen supply to themyocardium is insufficient for its needs,myocardial ischaemia develops. Pain is dueto accumulation of metabolites in the cardiacmuscle.
Two Forms of Angina are
1. Classical angina (stable angina, angina ofeffort, exertional angina) Pain is induced byexercise or emotion, both of which increasemyocardial oxygen demand. In suchpatients there is narrowing of thecoronary arteries due to atherosclerosisand therefore the coronaries cannot dilateto increase the blood supply duringexercise. Hence there is an imbalancebetween oxygen supply and demand.
2. Variant or Prinzmetal’s angina occurs at restand is caused by spasm of the coronaryartery.
Drugs are used to improve the balancebetween oxygen supply and demand eitherby increasing oxygen supply to the
myocardium (coronary dilation) or byreducing the oxygen demand (reducingpreload/afterload/heart rate or all of these).Drugs used in the treatment of angina are asfollows:
Classification
1. NitratesNitroglycerine, isosorbide dinitrate,isosorbide mononitrate, penta erythritoltetranitrate.
2. Calcium channel blockersVerapamil, diltiazem, amlodipine,nifedipine.
3. β-blockersPropranolol, atenolol, etc.
4. Potassium channel openersNicorandil
5. MiscellaneousDipyridamole, aspirin, trimetazidine
Nitrates
Mechanism of action Nitrates are vasodilators(Fig. 17.1). They are converted to nitric oxidewhich activates vascular guanylyl cyclasewhich in turn increases the synthesis ofcGMP. This cGMP catalyses the phosp-horylation of protein kinases causingrelaxation of the smooth muscles.Pharmacological actions Nitrates arepredominantly venodilators. Venodilationreduces venous return to the heart thereby
Drugs Used inAngina Pectoris and
Myocardial Infarction
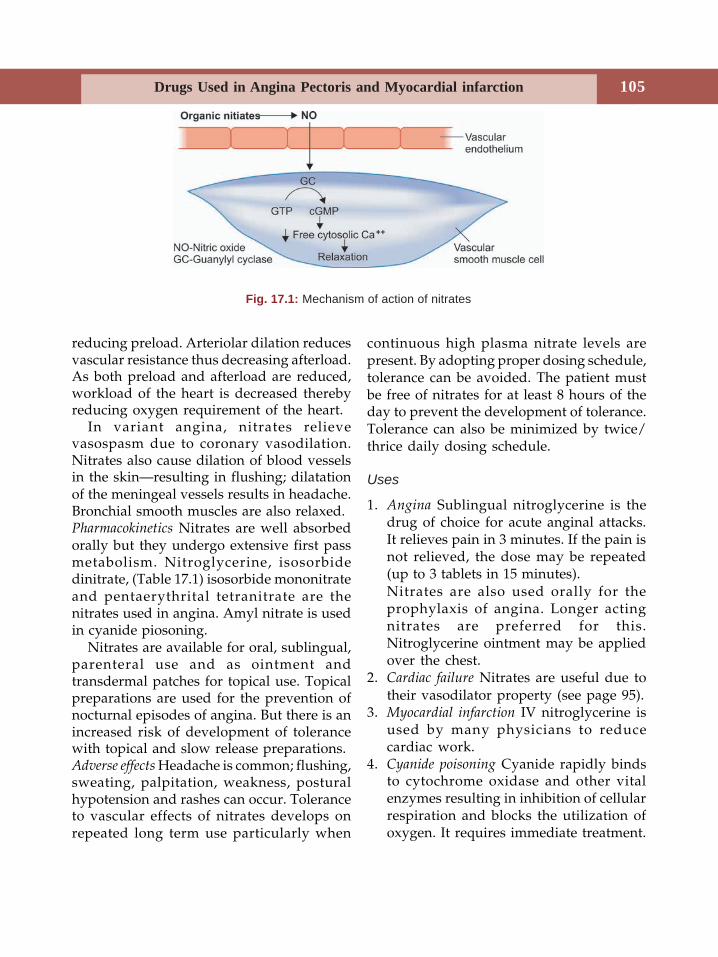
105Drugs Used in Angina Pectoris and Myocardial infarction
reducing preload. Arteriolar dilation reducesvascular resistance thus decreasing afterload.As both preload and afterload are reduced,workload of the heart is decreased therebyreducing oxygen requirement of the heart.
In variant angina, nitrates relievevasospasm due to coronary vasodilation.Nitrates also cause dilation of blood vesselsin the skin—resulting in flushing; dilatationof the meningeal vessels results in headache.Bronchial smooth muscles are also relaxed.Pharmacokinetics Nitrates are well absorbedorally but they undergo extensive first passmetabolism. Nitroglycerine, isosorbidedinitrate, (Table 17.1) isosorbide mononitrateand pentaerythrital tetranitrate are thenitrates used in angina. Amyl nitrate is usedin cyanide piosoning.
Nitrates are available for oral, sublingual,parenteral use and as ointment andtransdermal patches for topical use. Topicalpreparations are used for the prevention ofnocturnal episodes of angina. But there is anincreased risk of development of tolerancewith topical and slow release preparations.Adverse effects Headache is common; flushing,sweating, palpitation, weakness, posturalhypotension and rashes can occur. Toleranceto vascular effects of nitrates develops onrepeated long term use particularly when
continuous high plasma nitrate levels arepresent. By adopting proper dosing schedule,tolerance can be avoided. The patient mustbe free of nitrates for at least 8 hours of theday to prevent the development of tolerance.Tolerance can also be minimized by twice/thrice daily dosing schedule.
Uses
1. Angina Sublingual nitroglycerine is thedrug of choice for acute anginal attacks.It relieves pain in 3 minutes. If the pain isnot relieved, the dose may be repeated(up to 3 tablets in 15 minutes).Nitrates are also used orally for theprophylaxis of angina. Longer actingnitrates are preferred for this.Nitroglycerine ointment may be appliedover the chest.
2. Cardiac failure Nitrates are useful due totheir vasodilator property (see page 95).
3. Myocardial infarction IV nitroglycerine isused by many physicians to reducecardiac work.
4. Cyanide poisoning Cyanide rapidly bindsto cytochrome oxidase and other vitalenzymes resulting in inhibition of cellularrespiration and blocks the utilization ofoxygen. It requires immediate treatment.
Fig. 17.1: Mechanism of action of nitrates
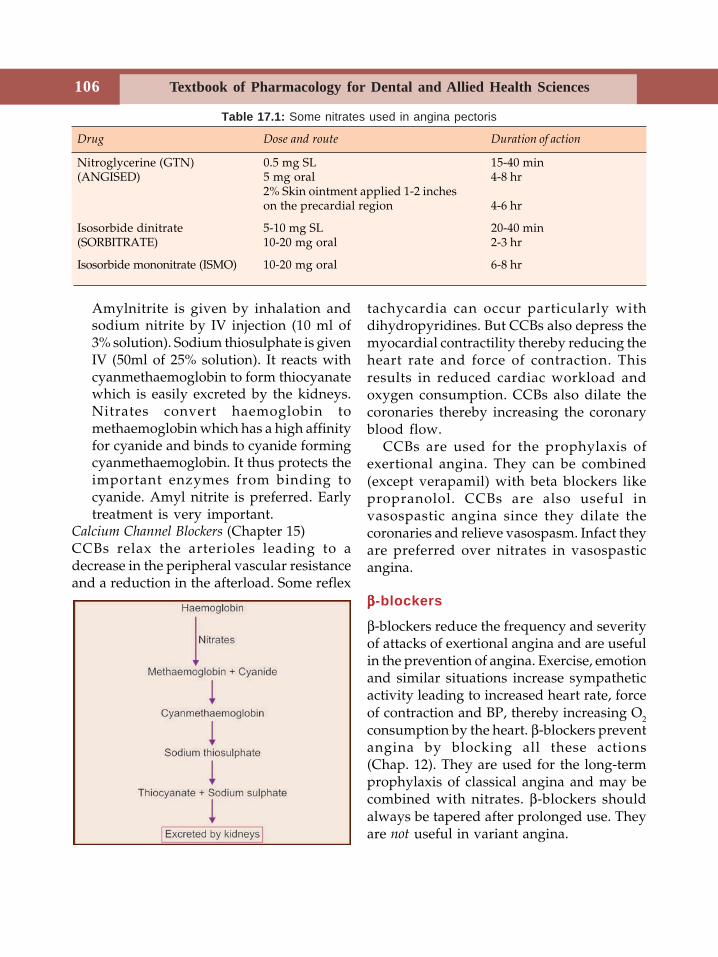
Textbook of Pharmacology for Dental and Allied Health Sciences106
Amylnitrite is given by inhalation andsodium nitrite by IV injection (10 ml of3% solution). Sodium thiosulphate is givenIV (50ml of 25% solution). It reacts withcyanmethaemoglobin to form thiocyanatewhich is easily excreted by the kidneys.Nitrates convert haemoglobin tomethaemoglobin which has a high affinityfor cyanide and binds to cyanide formingcyanmethaemoglobin. It thus protects theimportant enzymes from binding tocyanide. Amyl nitrite is preferred. Earlytreatment is very important.
Calcium Channel Blockers (Chapter 15)CCBs relax the arterioles leading to adecrease in the peripheral vascular resistanceand a reduction in the afterload. Some reflex
tachycardia can occur particularly withdihydropyridines. But CCBs also depress themyocardial contractility thereby reducing theheart rate and force of contraction. Thisresults in reduced cardiac workload andoxygen consumption. CCBs also dilate thecoronaries thereby increasing the coronaryblood flow.
CCBs are used for the prophylaxis ofexertional angina. They can be combined(except verapamil) with beta blockers likepropranolol. CCBs are also useful invasospastic angina since they dilate thecoronaries and relieve vasospasm. Infact theyare preferred over nitrates in vasospasticangina.
βββββ-blockers
β-blockers reduce the frequency and severityof attacks of exertional angina and are usefulin the prevention of angina. Exercise, emotionand similar situations increase sympatheticactivity leading to increased heart rate, forceof contraction and BP, thereby increasing O2
consumption by the heart. β-blockers preventangina by blocking all these actions(Chap. 12). They are used for the long-termprophylaxis of classical angina and may becombined with nitrates. β-blockers shouldalways be tapered after prolonged use. Theyare not useful in variant angina.
Table 17.1: Some nitrates used in angina pectoris
Drug Dose and route Duration of action
Nitroglycerine (GTN) 0.5 mg SL 15-40 min(ANGISED) 5 mg oral 4-8 hr
2% Skin ointment applied 1-2 incheson the precardial region 4-6 hr
Isosorbide dinitrate 5-10 mg SL 20-40 min(SORBITRATE) 10-20 mg oral 2-3 hr
Isosorbide mononitrate (ISMO) 10-20 mg oral 6-8 hr
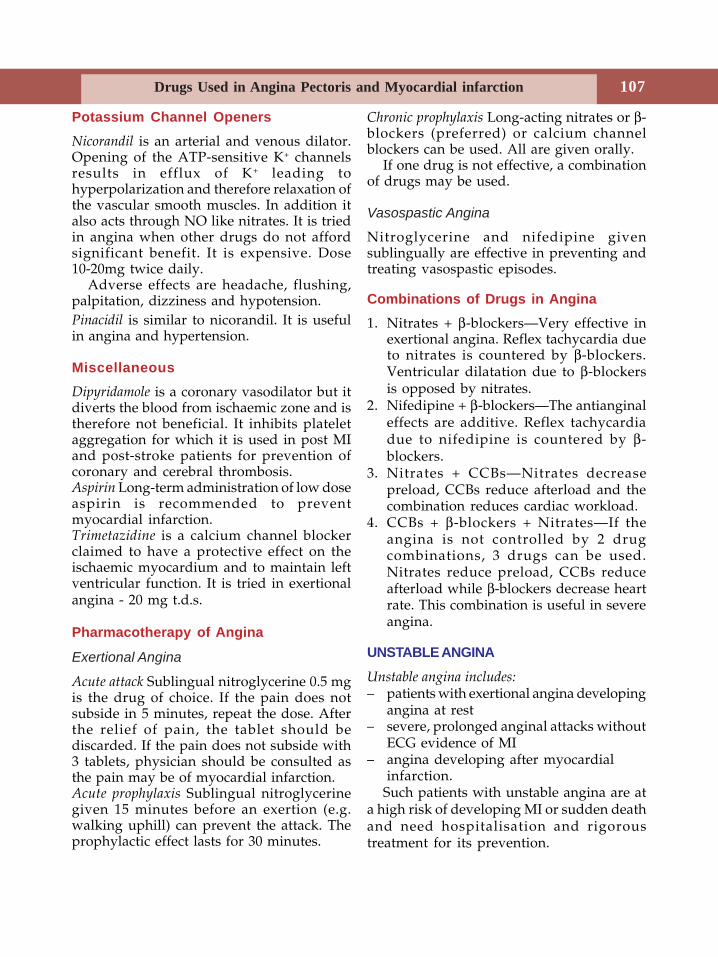
107Drugs Used in Angina Pectoris and Myocardial infarction
Potassium Channel OpenersNicorandil is an arterial and venous dilator.Opening of the ATP-sensitive K+ channelsresults in efflux of K+ leading tohyperpolarization and therefore relaxation ofthe vascular smooth muscles. In addition italso acts through NO like nitrates. It is triedin angina when other drugs do not affordsignificant benefit. It is expensive. Dose10-20mg twice daily.
Adverse effects are headache, flushing,palpitation, dizziness and hypotension.Pinacidil is similar to nicorandil. It is usefulin angina and hypertension.
MiscellaneousDipyridamole is a coronary vasodilator but itdiverts the blood from ischaemic zone and istherefore not beneficial. It inhibits plateletaggregation for which it is used in post MIand post-stroke patients for prevention ofcoronary and cerebral thrombosis.Aspirin Long-term administration of low doseaspirin is recommended to preventmyocardial infarction.Trimetazidine is a calcium channel blockerclaimed to have a protective effect on theischaemic myocardium and to maintain leftventricular function. It is tried in exertionalangina - 20 mg t.d.s.
Pharmacotherapy of Angina
Exertional Angina
Acute attack Sublingual nitroglycerine 0.5 mgis the drug of choice. If the pain does notsubside in 5 minutes, repeat the dose. Afterthe relief of pain, the tablet should bediscarded. If the pain does not subside with3 tablets, physician should be consulted asthe pain may be of myocardial infarction.Acute prophylaxis Sublingual nitroglycerinegiven 15 minutes before an exertion (e.g.walking uphill) can prevent the attack. Theprophylactic effect lasts for 30 minutes.
Chronic prophylaxis Long-acting nitrates or β-blockers (preferred) or calcium channelblockers can be used. All are given orally.
If one drug is not effective, a combinationof drugs may be used.
Vasospastic Angina
Nitroglycerine and nifedipine givensublingually are effective in preventing andtreating vasospastic episodes.
Combinations of Drugs in Angina1. Nitrates + β-blockers—Very effective in
exertional angina. Reflex tachycardia dueto nitrates is countered by β-blockers.Ventricular dilatation due to β-blockersis opposed by nitrates.
2. Nifedipine + β-blockers—The antianginaleffects are additive. Reflex tachycardiadue to nifedipine is countered by β-blockers.
3. Nitrates + CCBs—Nitrates decreasepreload, CCBs reduce afterload and thecombination reduces cardiac workload.
4. CCBs + β-blockers + Nitrates—If theangina is not controlled by 2 drugcombinations, 3 drugs can be used.Nitrates reduce preload, CCBs reduceafterload while β-blockers decrease heartrate. This combination is useful in severeangina.
UNSTABLE ANGINA
Unstable angina includes:– patients with exertional angina developing
angina at rest– severe, prolonged anginal attacks without
ECG evidence of MI– angina developing after myocardial
infarction.Such patients with unstable angina are at
a high risk of developing MI or sudden deathand need hospitalisation and rigoroustreatment for its prevention.
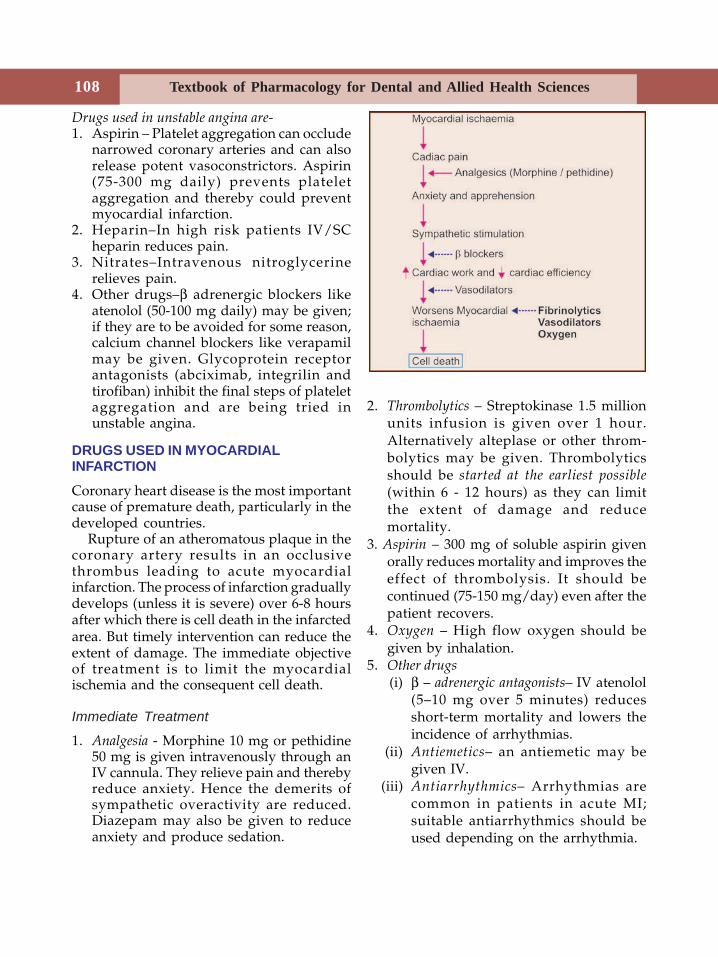
Textbook of Pharmacology for Dental and Allied Health Sciences108
Drugs used in unstable angina are-1. Aspirin – Platelet aggregation can occlude
narrowed coronary arteries and can alsorelease potent vasoconstrictors. Aspirin(75-300 mg daily) prevents plateletaggregation and thereby could preventmyocardial infarction.
2. Heparin–In high risk patients IV/SCheparin reduces pain.
3. Nitrates–Intravenous nitroglycerinerelieves pain.
4. Other drugs–β adrenergic blockers likeatenolol (50-100 mg daily) may be given;if they are to be avoided for some reason,calcium channel blockers like verapamilmay be given. Glycoprotein receptorantagonists (abciximab, integrilin andtirofiban) inhibit the final steps of plateletaggregation and are being tried inunstable angina.
DRUGS USED IN MYOCARDIALINFARCTION
Coronary heart disease is the most importantcause of premature death, particularly in thedeveloped countries.
Rupture of an atheromatous plaque in thecoronary artery results in an occlusivethrombus leading to acute myocardialinfarction. The process of infarction graduallydevelops (unless it is severe) over 6-8 hoursafter which there is cell death in the infarctedarea. But timely intervention can reduce theextent of damage. The immediate objectiveof treatment is to limit the myocardialischemia and the consequent cell death.
Immediate Treatment
1. Analgesia - Morphine 10 mg or pethidine50 mg is given intravenously through anIV cannula. They relieve pain and therebyreduce anxiety. Hence the demerits ofsympathetic overactivity are reduced.Diazepam may also be given to reduceanxiety and produce sedation.
2. Thrombolytics – Streptokinase 1.5 millionunits infusion is given over 1 hour.Alternatively alteplase or other throm-bolytics may be given. Thrombolyticsshould be started at the earliest possible(within 6 - 12 hours) as they can limitthe extent of damage and reducemortality.
3. Aspirin – 300 mg of soluble aspirin givenorally reduces mortality and improves theeffect of thrombolysis. It should becontinued (75-150 mg/day) even after thepatient recovers.
4. Oxygen – High flow oxygen should begiven by inhalation.
5. Other drugs (i) β – adrenergic antagonists– IV atenolol
(5–10 mg over 5 minutes) reducesshort-term mortality and lowers theincidence of arrhythmias.
(ii) Antiemetics– an antiemetic may begiven IV.
(iii) Antiarrhythmics– Arrhythmias arecommon in patients in acute MI;suitable antiarrhythmics should beused depending on the arrhythmia.

109Drugs Used in Angina Pectoris and Myocardial infarction
Long-term Treatment
Once the patient is stabilized, certaindrugs are recommended for prevention offurther ischaemic events. Long-termadministration of low dose aspirin, a β–adrenergic blocker and an ACE inhibitor areuseful in reducing long-term mortality. ACEinhibitors prevent ventricular remodellingand cardiac failure.
Risk Factor Management
• Smoking should be stopped. • Hyperlipidaemia if any should be
controlled. • Body weight should be reduced if needed. • Regular moderate exercises should be
advised. • Adequate control of diabetes and
hypertension if any.
Dental implications: A majority of dentalprocedures can evoke anxiety in the patient.This could precipitate an attack of angina orrarely even myocardial infarction. Utmostimportance is given to keep the patient stress-free. Adequate antianxiety agents, analgesicsand anaesthetics are used to avoid pain andanxiety. Patient is taken for the procedure asthe first case in the morning because waitingin anxiety could be harmful to such patients.Adrenaline is avoided in such patients. Thedentist should know to handle the emergencyif the need arises and then shift the patientto the physician’s care at the earliest. For anacute episode of angina, nitroglycerine 0.5mg is given sublingually immediately. Thepain should subside in 3-5 minutes (See Page107). If MI is suspected, injection pethidine50 mg should be given immediately evenbefore shifting the patient to the physician.
Textbook of Pharmacology for Dental and Allied Health Sciences110
18Hypertension is an elevation of systolic and/or diastolic BP above 140/90 mm of Hg. It isa common cardiovascular entity. Hyper-tension (HT) may be primary (essential)hypertension—where the cause is not knownor secondary—when it is secondary to otherconditions like renal, endocrine or vasculardisorders.
Based on the degree of severity,hypertension can be graded as:• Mild—diastole up to 104• Moderate—105-114• Severe— more than 115.
Blood pressure is determined by cardiacoutput (CO) and total peripheral vascularresistance (PVR). Blood pressure is controlledby baroreceptor reflexes acting throughautonomic nervous system along with therenin-angiotensin-aldosterone system.
Prolonged hypertension damages theblood vessels of the heart, brain and thekidneys and may result in severalcomplications like stroke, coronary arterydisease or renal failure. Hence hypertensionneeds to be treated even though as such itdoes not generally produce obvioustroublesome symptoms.
Antihypertensives act by influencing theBP regulatory systems viz. the autonomicsystem, renin-angiotensin system, calciumchannels or sodium and water balance(plasma volume).
Antihypertensives may be classified asfollows :
Antihypertensive Drugs
CLASSIFICATION
1. Diuretics
• Thiazides
Hydrochlorothiazide,chlorthalidone, indapamide
• Loop diuretics
Frusemide, bumetanide, torsemide• K+ Sparing diuretics
Spironolactone, amiloride, triamterene.
2. Angiotensin converting enzyme inhibitors
Captopril, enalapril, lisinopril,ramipril, perindopril, fosinopril,trandolapril, quinapril, benazepril.
3. Angiotensin II receptor antagonists
Losartan, candesartan, valsartan,eprosartan, irbesartan.
4. Sympatholytics
• Centrally acting drugs
Clonidine, methyldopa, guanabenz,guanfacine
• Ganglion blockers
Trimethaphan• Adrenergic neuron blockers
Guanithidine, reserpine• Adrenergic receptor blockers:
– α blockers
Prazosin, terazosin, doxazinphenoxybenzamine, Phentolamine
Antihypertensive Drugs 111
Diuretics (see Chap. 13) The antihypertensiveeffect of diuretics is mild—BP falls by 15-20mm of Hg over 2-4 weeks. Diuretics act asantihypertensives as follows.
Diuretics enhance the excretion of sodiumand water resulting in1. ↓ Plasma volume → ↓ cardiac output →
↓ BP2. ↓ Body sodium → relaxation of vascular
smooth muscles (due to Na+ depletion inthe vascular smooth muscle) - ↓ PVR →↓ BP.
Restriction of dietary salt intake willreduce the dose of the diuretic needed.Thiazides are the first-line antihypertensivesand are inexpensive. An initial dose of 12.5mg daily hydrochlorothiazide/chlorth-alidone is given. If the response is notadequate the dose may be increased to amaximum of 25 mg daily. They may becombined with a K+ sparing diuretic which isthe best way to avoid hypokalaemia-1.25 mgamiloride with 12.5 mg hydrochlo-rothiazide.Thiazides may be used in combination withother antihypertensives particularly withthose that cause salt and water retention asa side effect.Indapamide is particularly useful inhypertension because it lowers BP in
subdiuretic doses. Moreover it causes milderelectrolyte disturbances.Loop diuretics - Although loop diuretics likefrusemide are powerful diuretics, theirantihypertensive efficacy is low. They areused only in hypertension with chronic renalfailure or congestive heart failure.
Angiotensin Converting Enzyme (ACE)Inhibitors
Angiotensin II is a powerful vasoconstrictor.Aldosterone also raises the BP by increasingthe plasma volume (Fig. 18.2). ACE inhibitorsprevent the formation of angiotensin II and(indirectly) aldosterone. There is vaso-dilation and decrease in PVR resulting in afall in BP. As ACE also degrades bradykinin,ACE inhibitors raise the bradykinin levelswhich is a potent vasodilator. This alsocontributes to the fall in BP.
The blood flow to the kidneys, brain andheart increases due to selective vasodilationand thus maintains adequate blood supplyto these vital organs.Pharmacokinetics ACE inhibitors are generallywell-absorbed. Except captopril and lisinoprilall others are prodrugs. They differ in theirpotency and pharmacokinetic properties(Table 18.1) like bioavailability, distribution,plasma t1/2 and excretion. Most ACEinhibitors are excreted through the kidney→ dose should be reduced in renal dys-function.Adverse effects ACE inhibitors are well-tolerated. Adverse effects include:1. Persistent dry cough due to ↑ bradykinin
levels is more common in women. It mayrequire withdrawal of the ACE inhibitors.An angiotension II receptor antagonistmay be used in such patients (Page 114)
2. Hypotension–On initiation of therapy, ACEinhibitors may cause significant hypo-
– β blockersPropranolol, atenolol, esmolol,metoprolol.
– α and β blockersLabetalol, carvedilol
5. Ca++ channel blockersVerapamil, nifedipine, nicardipinenimodipine, amlodipine, felodipine.
6. Vasodilators• Arteriolar dilators
Hydralazine, minoxidil, diazoxide• Arteriolar and venular dilators
Sodium nitroprusside.
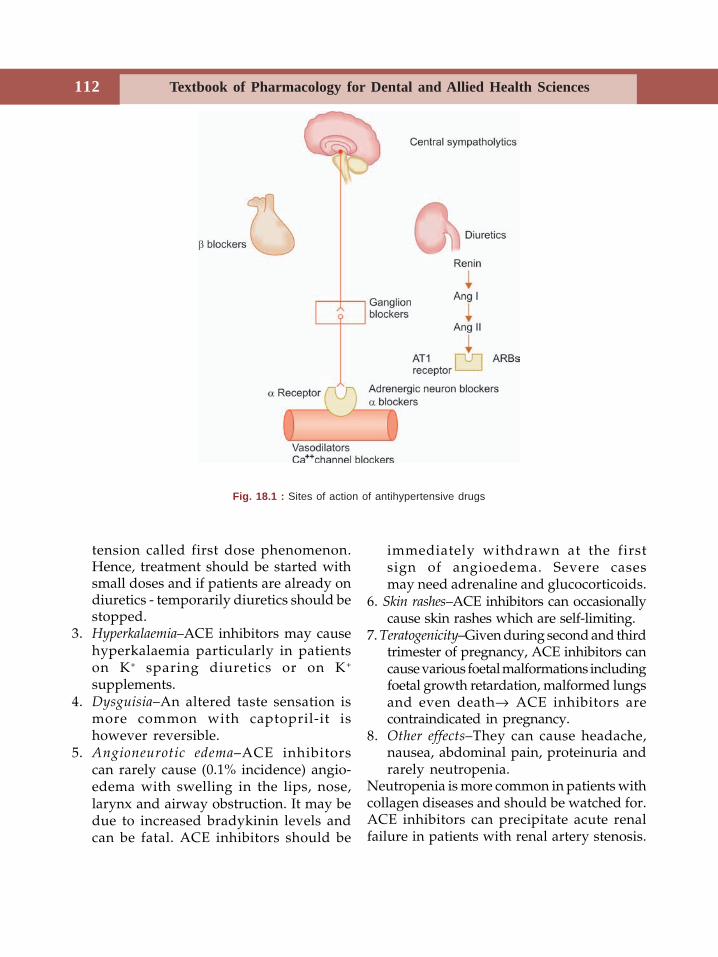
Textbook of Pharmacology for Dental and Allied Health Sciences112
tension called first dose phenomenon.Hence, treatment should be started withsmall doses and if patients are already ondiuretics - temporarily diuretics should bestopped.
3. Hyperkalaemia–ACE inhibitors may causehyperkalaemia particularly in patientson K+ sparing diuretics or on K+
supplements.4. Dysguisia–An altered taste sensation is
more common with captopril-it ishowever reversible.
5. Angioneurotic edema–ACE inhibitorscan rarely cause (0.1% incidence) angio-edema with swelling in the lips, nose,larynx and airway obstruction. It may bedue to increased bradykinin levels andcan be fatal. ACE inhibitors should be
immediately withdrawn at the firstsign of angioedema. Severe casesmay need adrenaline and glucocorticoids.
6. Skin rashes–ACE inhibitors can occasionallycause skin rashes which are self-limiting.
7. Teratogenicity–Given during second and thirdtrimester of pregnancy, ACE inhibitors cancause various foetal malformations includingfoetal growth retardation, malformed lungsand even death→ ACE inhibitors arecontraindicated in pregnancy.
8. Other effects–They can cause headache,nausea, abdominal pain, proteinuria andrarely neutropenia.
Neutropenia is more common in patients withcollagen diseases and should be watched for.ACE inhibitors can precipitate acute renalfailure in patients with renal artery stenosis.
Fig. 18.1 : Sites of action of antihypertensive drugs
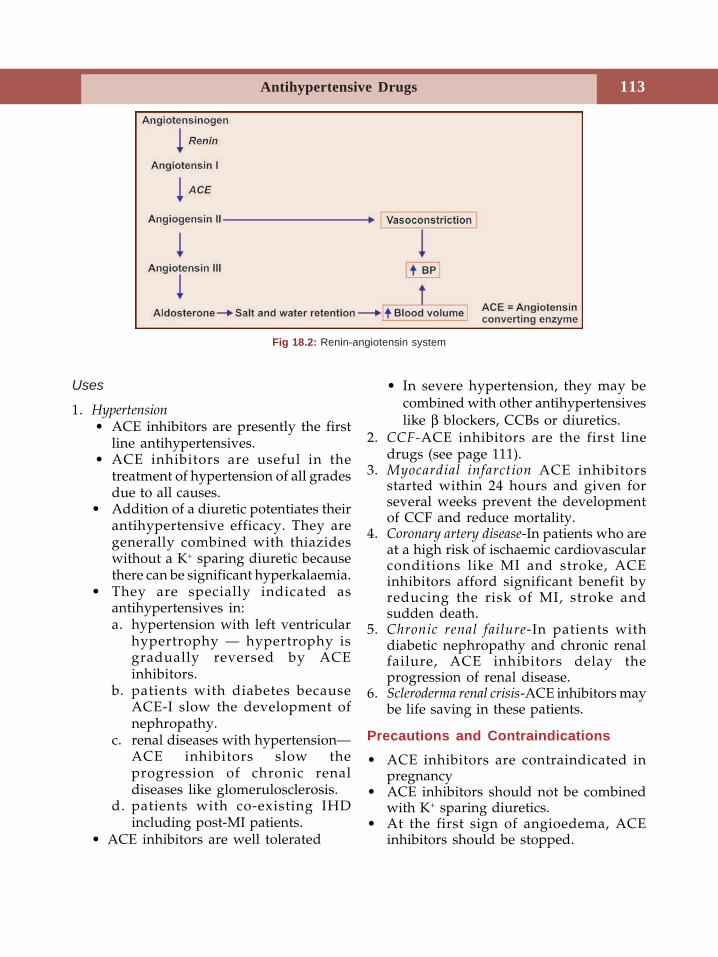
Antihypertensive Drugs 113
Uses
1. Hypertension • ACE inhibitors are presently the first
line antihypertensives. • ACE inhibitors are useful in the
treatment of hypertension of all gradesdue to all causes.
• Addition of a diuretic potentiates theirantihypertensive efficacy. They aregenerally combined with thiazideswithout a K+ sparing diuretic becausethere can be significant hyperkalaemia.
• They are specially indicated asantihypertensives in:a. hypertension with left ventricular
hypertrophy — hypertrophy isgradually reversed by ACEinhibitors.
b. patients with diabetes becauseACE-I slow the development ofnephropathy.
c. renal diseases with hypertension—ACE inhibitors slow theprogression of chronic renaldiseases like glomerulosclerosis.
d. patients with co-existing IHDincluding post-MI patients.
• ACE inhibitors are well tolerated
• In severe hypertension, they may becombined with other antihypertensiveslike β blockers, CCBs or diuretics.
2. CCF-ACE inhibitors are the first linedrugs (see page 111).
3. Myocardial infarction ACE inhibitorsstarted within 24 hours and given forseveral weeks prevent the developmentof CCF and reduce mortality.
4. Coronary artery disease-In patients who areat a high risk of ischaemic cardiovascularconditions like MI and stroke, ACEinhibitors afford significant benefit byreducing the risk of MI, stroke andsudden death.
5. Chronic renal failure-In patients withdiabetic nephropathy and chronic renalfailure, ACE inhibitors delay theprogression of renal disease.
6. Scleroderma renal crisis-ACE inhibitors maybe life saving in these patients.
Precautions and Contraindications• ACE inhibitors are contraindicated in
pregnancy• ACE inhibitors should not be combined
with K+ sparing diuretics.• At the first sign of angioedema, ACE
inhibitors should be stopped.
Fig 18.2: Renin-angiotensin system
Textbook of Pharmacology for Dental and Allied Health Sciences114
• They are contraindicated in patients withrenal artery stenosis as they can causerenal failure in them.
• ACE inhibitors may enhance plasma levelsof digoxin.
Angiotensin II Receptor Blockers (ARBs)
Losartan was the first orally effective AT1
receptor antagonist to be developed. Thereare 2 subtypes of angiotensin II receptors—AT1 and AT2. AT1 receptors are present invascular and myocardial tissue, brain, kidneyand adrenal glomerular cells. Losartan hashigh affinity for AT1 receptors whencompared to AT2 receptors. By blocking AT1
receptors, losartan blocks the effect ofangiotensin II. It thus relaxes vascular smoothmuscles, promotes salt and water excretionand reduces plasma volume.
The main advantage of ARBs over ACEinhibitors is that there is no increase inbradykinin levels and its associated adverseeffects like dry cough and angioedemabecause angiotensin converting enzyme is notinhibited.
Many other ARBs have now beensynthesized including candesartan,irbesartan, valsartan, telmisartan andeprosartan.
ARBs are all given orally. Theirbioavailability is generally <50%. They are
all extensively protein bound and excretedby kidneys.Adverse effects ARBs are well tolerated. Theycan cause hypotension and hyperkalaemia likeACE inhibitors. Angioedema is rare. ARBsare contraindicated in pregnancy because oftheir teratogenic potential.
Uses
1. Hypertension–ARBs are used in thetreatment of hypertension in similarindications as that of ACE inhibitors asalternatives to ACE inhibitors. They canbe considered as the first line drugs inhypertension. Losartan, candesartan andirbesartan are available in India. ARBs canbe usefully combined with diuretics(Table 18.2)
2. Cardiac failure–ARBs may be used asalternatives to ACE inhibitors in cardiacfailure. i.e., in patients who poorly tolerateACE inhibitors.
SYMPATHOLYTICS
I. Drugs Acting Centrally
Clonidine an imidazoline derivative is aselective α2 agonist. Stimulation of α2receptors in the CNS (in the vasomotor centreand hypothalamus), decreases centralsympathetic outflow, blocks the release ofnoradrenaline from the nerve terminalsleading to a fall in BP and bradycardia.
Table 18.1: Dose and duration of action of some commonly used ACE inhibitors
Drug Duration of action (in hrs) Daily dose in hypertension (mg)
Captopril 6-12 12.5-50 mg BD
Enalapril 24 2.5-20 mg OD
Lisinopril >24 5-40 mg OD
Ramipril 8-48 1.25-10 mg OD
Fosinopril 12-24 10-60 mgBenazepril 12-24 10-40 mgPerindopril 24 2-8 mg
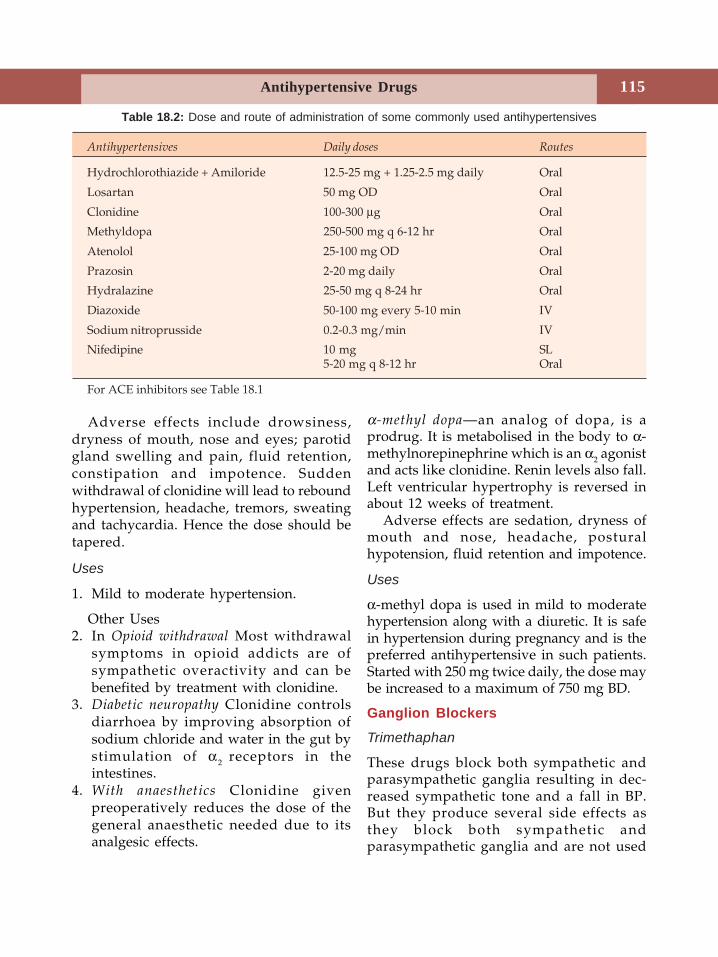
Antihypertensive Drugs 115
Adverse effects include drowsiness,dryness of mouth, nose and eyes; parotidgland swelling and pain, fluid retention,constipation and impotence. Suddenwithdrawal of clonidine will lead to reboundhypertension, headache, tremors, sweatingand tachycardia. Hence the dose should betapered.
Uses
1. Mild to moderate hypertension.
Other Uses2. In Opioid withdrawal Most withdrawal
symptoms in opioid addicts are ofsympathetic overactivity and can bebenefited by treatment with clonidine.
3. Diabetic neuropathy Clonidine controlsdiarrhoea by improving absorption ofsodium chloride and water in the gut bystimulation of α2 receptors in theintestines.
4. With anaesthetics Clonidine givenpreoperatively reduces the dose of thegeneral anaesthetic needed due to itsanalgesic effects.
α-methyl dopa—an analog of dopa, is aprodrug. It is metabolised in the body to α-methylnorepinephrine which is an α2 agonistand acts like clonidine. Renin levels also fall.Left ventricular hypertrophy is reversed inabout 12 weeks of treatment.
Adverse effects are sedation, dryness ofmouth and nose, headache, posturalhypotension, fluid retention and impotence.
Uses
α-methyl dopa is used in mild to moderatehypertension along with a diuretic. It is safein hypertension during pregnancy and is thepreferred antihypertensive in such patients.Started with 250 mg twice daily, the dose maybe increased to a maximum of 750 mg BD.
Ganglion Blockers
Trimethaphan
These drugs block both sympathetic andparasympathetic ganglia resulting in dec-reased sympathetic tone and a fall in BP.But they produce several side effects asthey block both sympathetic andparasympathetic ganglia and are not used
Antihypertensives Daily doses Routes
Hydrochlorothiazide + Amiloride 12.5-25 mg + 1.25-2.5 mg daily Oral
Losartan 50 mg OD Oral
Clonidine 100-300 μg Oral
Methyldopa 250-500 mg q 6-12 hr Oral
Atenolol 25-100 mg OD Oral
Prazosin 2-20 mg daily Oral
Hydralazine 25-50 mg q 8-24 hr Oral
Diazoxide 50-100 mg every 5-10 min IV
Sodium nitroprusside 0.2-0.3 mg/min IV
Nifedipine 10 mg SL5-20 mg q 8-12 hr Oral
For ACE inhibitors see Table 18.1
Table 18.2: Dose and route of administration of some commonly used antihypertensives

Textbook of Pharmacology for Dental and Allied Health Sciences116
now. Trimethaphan is the only ganglionblocker in use. It is used intravenously toproduce controlled hypotension duringcertain surgeries for its rapid and shortaction (15 minutes).
Adrenergic Neuron Blockers
Guanethidine depletes the stores ofnoradrenaline in the adrenergic neurons andalso blocks its release. Because of the adverseeffects like postural hypotension, diarrhoeaand sexual dysfunction, it is not used.Reserpine is an alkaloid obtained fromRauwolfia serpentina (Sarpagandhi) that growsin India. In the adrenergic neurons, it bindsto the vesicles that store monoamines likenoradrenaline, dopamine and 5-HT anddestroys these vesicles. It thus depletes thestores of these monoamines and reduces BP.Reserpine also has antipsychotic effects forwhich it is used in psychosis. Reserpine causesvarious side effects like drowsiness,depression, parkinsonism, postural hypo-tension, edema and sexual dysfunction.Though it is generally not preferred. It hasthe advantages of being inexpensive,effective, long acting (once daily dose) andgenerally well tolerated when given with adiuretic.
Adrenergic Receptor Blockers
β-blockers (see Chapter 12) are mildantihypertensives. Blockade of cardiac β1receptors results in decreased myocardialcontractility and cardiac output. Thus theyreduce the BP due to a fall in the cardiacoutput. They also lower plasma renin activityand have an additional central antihy-pertensive action.
β blockers are effective and well-toleratedand are of special value in patients who alsohave arrhythmias or angina. They may beused alone but are also suitable for
combination with other antihypertensivesparticularly with drugs that cause tachycardiaas their side effect (e.g. vasodilators). Theyare thus the first line antihypertensive drugsin mild to moderate hypertension. Atenololis the preferred β-blocker because of theadvantages like once a day dosing, absenceof CNS side effects and β1 selectivity.β-blockers should always be tapered whilewithdrawing.α-blockers (see Chapter 12) Nonselective αblockers like phenoxybenzamine andphentolamine are used in the treatment ofhypertension due to pheochromocytoma.Selective α1 blockers like prazosin, terazosinand doxazosin dilate both arterioles andvenules. Peripheral vascular resistance isdecreased leading to a fall in BP with onlymild tachycardia.
‘First dose phenomenon’ can be avoidedby starting with a low dose prazosin (0.5 mg)given at bed time. Dose is graduallyincreased. α1 blockers are used in mild tomoderate hypertension; they may becombined with diuretics and β-blockers.α and β-blockers Labetalol and carvedilol blockα1 and β receptors. It is used IV in thetreatment of hypertension in pheochro-mocytoma and in hypertensive emergencies.
Calcium Channel Blockers
Calcium channel blockers (see chap 15) areanother important group of antihyper-tensives. They dilate the arterioles resultingin reduced peripheral vascular resistance.Nifedipine produces some reflex tachycardiawhile this is not seen with verapamil anddiltiazem as they are cardiac depressants.Fluid retention is negligible unlike otherarteriolar dilators. Calcium channel blockerswere earlier considered first line antihyper-tensives and were extensively used. Butseveral recent large scale studies have shownthem to have many disadvantages. They are
Antihypertensive Drugs 117
not preferred in patients who also have leftventricular hypertrophy and previousmyocardial infarction. Short acting DHPsproduce frequent changes in BP andsympathetic activity and hence should beavoided in hypertension.
Use in Hypertension
• CCBs are well-tolerated, and effective.• CCBs are particularly effective in elderly
patients.• CCBs may be used as monotherapy or in
moderate to severe HT along with otherantihypertensives.
• It has now been shown that sublingualnifedipine does not actually achieveplasma concentration quicker than oralformulation. Thus in hypertensiveemergencies, short acting DHPs can beused parenterally.
• There is a growing concern that use ofCCBs, especially short acting ones, isassociated with increased mortality andrisk of sudden death.
• Sustained release preparations or longacting dihydropyridine CCBs may beused for smoother control of BP.
Vasodilators
Vasodilators relax the vascular smoothmuscles thus reducing BP due to decreasedperipheral vascular resistance. Salt and water
retention and reflex tachycardia are commonwith vasodilators.Hydralazine is a directly acting arteriolardilator. The fall in BP is associated withtachycardia, renin release and fluid retention.Coronary, cerebral and renal blood flow areincreased.
Hydralazine is metabolised by acetylationin the liver (like INH) and the rate ofacetylation is genetically determined - peoplemay be fast or slow acetylalors.Adverse effects are headache, dizziness,flushing, palpitation, nausea, hypotensionand salt and water retention. It mayprecipitate angina in some patients becauseof increased O2 demand due to reflextachycardia and decreased myocardial bloodsupply due to peripheral vasodilatation.Hypersensitivity reactions like serumsickness and lupus erythematosus (arthralgia,fever, pleuritis, pericarditis) may occur andis more common in slow acetylators.Uses Hydralazine is used with a β-blockerand/or a diuretic in moderate to severehypertension not controlled by the first linedrugs. It can be given in hypertension duringpregnancy (2nd and 3rd trimester).Minoxidil is a directly acting arteriolar dilatorused in severe hypertension not respondingto other drugs. It acts by opening K+ channelsin the smooth muscles. Opening of the K+
channels causes efflux of K+ resulting inhyperpolarisation and smooth musclerelaxation.Minoxidil is used along with a diuretic - as areserve drug in patients with severehypertension who do not respond to otherdrugs. Minoxidil stimulates the growth ofhair on prolonged use (hypertrichosis).Hence it is used topically (2% solution) inalopecia. Young men with relative alopecia aremore likely to respond. Minoxidil can causefluid retention, tachycardia and anginal
Textbook of Pharmacology for Dental and Allied Health Sciences118
episodes. Growth of hair on the face, arms,legs and back make it unacceptable in women.Diazoxide is related to thiazide diuretics andis a potent arteriolar dilator. It’s mechanismof action is like minoxidil. Diazoxide cancause hyperglycaemia because it inhibits theinsulin secretion from pancreas. Other sideeffects include salt and water retention,palpitation and myocardial ischaemia. It isused intravenously in hypertensive emer-gencies where monitoring of infusion is notpossible. Diazoxide has a long duration ofaction (24 hours) and is suitable in suchsituations.Sodium nitroprusside is a rapidly actingvasodilator and it relaxes both arterioles andvenules. Both peripheral resistance andcardiac output are reduced resulting in lowermyocardial oxygen consumption.
Nitroprusside acts through the release ofnitric oxide which activates guanylyl cyclase,resulting in the formation of cGMP whichrelaxes the vascular smooth muscles. On IVadministration, it is rapid (acts within 30seconds) and short-acting (duration 3 minutes)allowing titration of the dose. This makes itsuitable for use in hypertensive emergencieswith close monitoring. It decomposes on
exposure to light the infusion bottle and tubingshould therefore be covered with opaque foil.Adverse reactions are palpitation, sweating,weakness, nausea, vomiting and hypo-tension. In higher doses nitroprusside getsconverted to cyanide and thiocyanate whichcan result in toxicity. Symptoms of toxicityinclude nausea, anorexia, weakness, disor-ientation and psychosis. Administration ofsodium thiosulphate along with nitroprussideprevents the accumulation of cyanide.
Uses
1. Nitroprusside is the drug of choice inhypertensive emergencies.
2. It is used in situations where short-termreduction of myocardial work load isrequired as in myocardial infarction.
Drug Interactions
1. Sympathomimetics and tricyclicantidepressants can antagonise the effectsof sympatholytics.
2. Antihistamines add to sedation producedby clonidine and methyldopa.
3. NSAIDs tend to cause salt and waterretention and may blunt the effect ofantihypertensives.
Treatment of Hypertension
Mild hypertension Treatment is started withlow dose of a single drug—a thiazide diureticor a β-blocker. If the patient does notadequately respond in 3-4 weeks, an ACEinhibitor or a calcium channel blocker shouldbe tried. If BP is not controlled by one drug,another should be added.Moderate hypertension A combination of adiuretic with a sympatholytic may be given.If response is inadequate add a third drug.Severe hypertension may be associated withcardiac or renal disorder. A vasodilator witha diuretic and a β-blocker is useful.

Antihypertensive Drugs 119
Hypertensive emergencies Conditions likehypertensive encephalopathy and acutecardiac failure due to hypertension requireimmediate reduction of BP. Parenteral drugsare preferred. IV sodium nitroprusside underclose monitoring is the drug of choice (insome conditions BP should be loweredgradually to avoid ischaemia to vital organs).IV esmolol, diazoxide and sublingualnifedipine are alternatives. BP should beconstantly monitored because drugs likesodium nitroprusside can bring down BPsuddenly which results in hypoperfusion ofvital organs. As soon as possible switch overto oral drugs.Hypertension in pregnancy The drugs foundsafe are—methyldopa orally for maintenanceand hydralazine (parenteral) for reductionof BP in emergency. However they shouldbe used only after the first trimester. Cardio-selective β-blockers (atenolol) can also beused.Combination of antihypertensives When it is notpossible to achieve adequate control of BPwith a single drug, a combination may beused. Antihypertensives may also becombined to overcome the side effects of oneanother. This also allows use of lower dosesof each drug.
Sympatholytics and vasodilators causefluid retention which can be overcome byadding a diuretic.
Vasodilators like nifedipine andhydralazine evoke reflex tachycardia. Thiscan be countered by β-blockers, whilepropranolol may cause initial rise in PVRwhich is countered by vasodilators.
Combination of ACE inhibitors anddiuretics is synergistic.Non-pharmacological measures Low salt diet,weight reduction and transidental meditation-all go a long way in controlling the bloodpressure. Smoking and alcohol should begiven up. These measures also help in reducingthe dose of the antihypertensive needed.
Hypertension and Dentistry
A dentist may have to carry on surgeries andother procedures on a hypertensive patientand needs caution. It may not matter muchin minor procedures but in major procedures,good control of BP should be ensured before,during and after the procedure. BP ismaintained below 150/100 mm of Hg. Tocontrol postoperative bleeding ethamsylateis given. When local anaesthetic is required,for minor procedures plain lignocaine is usedand adrenaline avoided. Procedures are donein multiple sittings. For example if multipleteeth are to be pulled out, 1-2 teeth areextracted at a time. If the bleeding is more,botropase or gel foam application is used andnot adrenaline packs.
Textbook of Dental Pharmacology120
19
PLASMA EXPANDERS
Plasma expanders are high molecular weightsubstances which when infused IV exertosmotic pressure and remain in the body fora long time to increase the volume ofcirculating fluid.
An ideal plasma expander should exertoncotic pressure comparable to plasma, belong-acting, non-antigenic and pharma-cologically inert.
The plasma expanders used are dextrans,gelatin polymer, hydroxyethyl starches andpolyvinyl pyrrolidone - all colloidalcompounds. Human albumin obtained frompooled human plasma is also useful.Dextrans (Dextran 70 - mol. wt. 70,000 anddextran 40 - mol. wt. 40,000) arepolysaccharides obtained from sugar beet.Their osmotic pressure is similar to that ofplasma proteins. Dextran 70 effectivelyexpands the plasma volume and remains sofor 24 hours. It interferes with coagulation,blood grouping and cross matching.
Dextran 40 is faster but shorter acting. Itcan improve microcirculation in shock bypreventing rouleax formation of RBCs andhave an antisludging effect. It can clog renaltubules resulting in renal failure - though rareshould be watched for. Allergic reactions arecommon as dextrans are antigenic.
Dextrans have a long shelf-life (10 years)and can be easily sterilized. Dextrans are thecommonly used plasma expanders.Gelatin products have a mol. wt. of 30,000 anda duration of action of 12 hours. Gelatinpolymers can remain stable for almost 3 yearsat a pH of 7.2-7.3. They do not interfere withcoagulation, blood grouping and crossmatching. They can rarely cause urticaria,allergic reactions and bronchospasm.Hydroxyethyl starch (Hetastarch) maintainsblood volume for a long period. Allergicreactions are rare and it does not interferewith coagulation.Polyvinyl pyrrolidone (PVP) is a syntheticpolymer. It is not preferred due to variousdisadvantages like - it provokes histaminerelease and interferes with blood grouping.Human albumin is obtained from pooledhuman blood. It is given as 5% or 20%solution. It is nonantigenic, does not interferewith coagulation, blood grouping or crossmatching.
Human albumin is used in oedema, burns,hypovolaemic shock, hypoproteinaemia,acute liver failure and in dialysis.
Allergic reactions and fever can occurthough rarely.Uses of plasma expanders These are used asplasma substitutes in hypovolaemic shock,
Plasma Expanders andPharmacotherapy
of Shock

121Plasma Expanders and Pharmacotherapy of Shock
burns and in extensive fluid loss—as anemergency measure to restore plasmavolume.
PHARMACOTHERAPY OF SHOCK
Shock is acute circulatory failure withunderperfusion of tissues. Symptoms ofsympathetic overactivity are generally seen—like pallor, sweating, cold extremities andtachycardia. Shock may be:1. Hypovolaemic shock Decreased fluid volume
due to sudden loss of plasma or blood asin haemorrhage, burns or dehydration—results in hypovolaemic shock.Fluid andelectrolytes (See page 401) should bereplaced and BP monitored.
2. Septic shock is precipitated by severebacterial infection. It may be due torelease of bacterial toxins — should betreated with appropriate antibiotics apartfrom general measures.
3. Cardiogenic shock is due to failure of heartas a pump as in myocardial infarction. IVmorphine is the drug of choice to relievepain and anxiety (see page 108).
4. Anaphylactic shock Type I hypersensitivityreaction causing release of massiveamounts of histamine which is triggeredby antigen-antibody reaction. Adrenaline0.3–0.5 ml of 1:1000 solution givenintramuscularly is the drug of choice (seepage 71)
5. Neurogenic shock is due to venous poolingas following spinal anaesthesia,abdominal or testicular trauma.
Shock of any type needs immediatetreatment:
General Measures
a. The cause should be identified and treatedb. Maintain BP and plasma volumec. Correct the acid base and electrolyte
disturbancesd. Ensure adequate urine output.To restore the intravascular volume, thecomponent that is lost should ideally bereplaced-like plasma in burns and blood afterhaemorrhage. But in emergency, immediatevolume replacement is important. In suchsituations plasma expanders and intravenousfluids are used.
Textbook of Pharmacology for Dental and Allied Health Sciences122
20General Anaesthetics
Section 5Central Nervous System
General Anaesthetics are agents that bringabout reversible loss of sensation andconsciousness. Before 1846, alcohol, opium,packing a limb with ice and concussion, i.e.making the patient unconscious by a blowon the head were used to relieve surgicalpain. Dr Horace Wells a dentist, tried todemonstrate the effect of nitrous oxide as ananaesthetic in 1844 but was unsuccessful ashe removed the gas bag too early. Dr WilliamMorton who was present at thedemonstration, worked on it and in 1846demonstrated ether anaesthesia successfully.Since then several anaesthetics have beensynthesized over the decades.
Stages of General Anaesthesia
1. Stage of analgesia is from the beginning ofinhalation of the anaesthetic to loss ofconsciousness.
2. Stage of delirium This stage is from loss ofconsciousness to beginning of surgicalanaesthesia. It may be associated withexcitement—shouting, crying and violentbehaviour.
3. Stage of surgical anaesthesia This has 4planes. As anaesthesia passes to deeperplanes, respiratory depression is seen.There is gradual loss of reflexes andrelaxation of skeletal muscles.
4. Stage of medullary paralysis is seen only withoverdose. It is the stage of medullary
depression → cessation of breathing,circulatory failure and death may follow.
Ideal anaesthetic should be pleasant, non-irritating, provide adequate analgesia,immobility and muscle relaxation; should benon-inflammable and administration should beeasy and controllable and have a wide marginof safety. Induction and recovery should besmooth and should not affect cardiovascularfunctions. It should be inexpensive.
Mechanism of Action of General AnaestheticsThe exact mechanism of action of generalanaesthetics is not known. The most acceptedmechanisms of action are as follows.1. Inhaled and some intravenous
anaesthetics bind to specific sites onGABA receptor chloride channels andactivate these receptors. By this theyincrease the inhibitory neurotransmissionand depress the CNS.
2. Inhalational anaesthetics also enhance thesensitivity of glycine-gated chloridechannels to glycine. These glycinereceptors bring about inhibitoryneurotransmission in the brainstem.
3. Some anaesthetics like ketamine andnitrous oxide bind to and inhibit the N-methyl D – aspartate (NMDA) receptors.
4. Inhalational and intravenous agents act atmultiple sites in the nervous system anddepress the neuronal activity at manysites in the brain.
123General Anaesthetics
General anaesthetics are as follows-
CLASSIFICATION
I . InhalationalA. Gases
– Nitrous oxide, cyclopropaneB. Liquids
– Ether, halothane, enflurane,isoflurane, methoxyflurane,desflurane, sevoflurane
II. IntravenousA. Inducing agents
–Thiopentone sodium,methohexitone, propofol,etomidate
B. Dissociative anaesthesia– Ketamine
C. Neuroleptanalgesia– Fentanyl + droperidol
D. Benzodiazepines– Diazepam, lorazepam,midazolam
Inhalational anaesthetics are either gases orvolatile liquids. Given by inhalation they areabsorbed by the pulmonary circulation. Onattaining adequate concentration in the brain,they produce general anaesthesia.Pharmacokinetics Inhalational anaesthetics areadministered at a specific concentration.Since the brain is a highly perfused organ,steady state can be achieved quickly. Whenthe steady state is reached, the partialpressure of the anaesthetic in the lung andthe brain are equal and this makes it possibleto monitor the anaesthesia. But, foranaesthetics with high solubility in blood andtissues, rise in alveolar partial pressure (andthereby induction) is slower. Suchanaesthetics need to be administered athigher pressures.
Inhaled anaesthetics are largely eliminatedunchanged by the lungs. Agents which aresoluble in fat and tissues require longer time
for elimination and therefore recovery isslower.
Minimum alveolar concentration (MAC) isthe concentration that immobilizes 50% ofsubjects in response to a surgical skin incision.MAC is used to describe the potencies ofdifferent volatile anaesthetics.Nitrous oxide is a gas with a slightly sweetishodour. It produces light anaesthesia withoutsignificant depression of respiration orvasomotor centre (Table 20.1).
Advantages
1. Strong analgesic2. Induction is rapid and smooth3. It is non-irritating and non-inflammable4. Recovery is rapid5. Postoperative nausea is not significant6. Has little effect on respiration and
cardiovascular functions, hence ideal forcombination
7. It is non-toxic to liver, kidney and brainand is quickly removed from lungs.
Disadvantages
1. It is less potent and should be used withother agents.
2. Poor muscle relaxant.3. N2O displaces nitrogen from the air-filled
cavities and while doing so, it enters thecavities faster, i.e. even before nitrogenescapes. This results in expansion of suchcavities like in patients with pneumothoraxand air embolus. Hence N2O should beavoided in such patients.
4. Repeated use can depress the bonemarrow.
5. Long-term exposure (like in staff ofoperation theatre) to low doses can impairDNA synthesis which may result in foetalabnormalities on conception.
Status in anaesthesia Nitrous oxide is used asan adjuvant to other anaesthetics. It is usedalong with oxygen (30%).
Textbook of Pharmacology for Dental and Allied Health Sciences124
Ether is a colourless volatile liquid. It is highlyinflammable; vapours are irritating.
Advantages
1. Potent and reliable anaesthetic.2. Good analgesic.3. Effect on cardiovascular and respiratory
functions are not significant in therapeuticdoses; reflexes are well-maintained.
4. It is a bronchodilator.5. Provides full muscle relaxation in deep
anaesthesia.6. Does not sensitize the heart to adrenaline.7. Easy to administer as complicated
equipment is not necessary.8. Inexpensive.
Disadvantages
1. It is inflammable—hence diathermy iscontraindicated.
2. Highly soluble in body tissues—inductionis slow and unpleasant.
3. It is irritating and therefore enhancesrespiratory secretions. Premedicationwith atropine is essential—laryngealspasm may occur during induction.
4. Postoperative nausea and vomiting arefrequent.
5. Recovery is slow.Status in anaesthesia Ether is now notpreferred because of flammability andirritant property. But it is still used indeveloping countries like India because it ischeap, easy to administer (by open dropmethod) and relatively safe.
Halothane is a colourless volatile liquid witha sweet odour. It is non-irritant and non-inflammable.
Advantages
1. Potent, non-inflammable anaesthetic.
2. Induction is smooth and rapid—in 2-5 minsurgical anaesthesia can be produced.
3. Non-irritant—therefore does notaugment salivary or bronchial secretions.
4. Recovery is rapid (Table 20.2).5. Postoperative nausea and vomiting are of
low incidence.
Disadvantages
1. Neither a good analgesic nor a musclerelaxant.
2. Halothane is a direct myocardiacdepressant. Cardiac output and BP startfalling and heart rate may decrease. Itsensitizes the heart to the arrhythmogenicaction of adrenaline.
3. It also causes some respiratorydepression.
4. Severe hepatitis which may be fatal occursin 1: 50,000 patients. A metabolite may beresponsible for this toxicity.
5. Malignant hyperthermia—a geneticallydetermined reaction occurs rarely.Succinylcholine accentuates this effect ofhalothane. It is due to intracellular releaseof calcium from the sarcoplasmicreticulum which causes muscle contractionand increased heat production. It is treatedwith dantrolene.
6. Expensive when compared to ether.Status in anaesthesia Halothane is one of themost popular anaesthetics. Analgesics andmuscle relaxants are used as adjuvants. Non-flammability, non-irritant property, rapidinduction and recovery has made it animportant and preferred anaesthetic—mostwidely used.
Enflurane is similar to halothane except that:1. it is metabolised to a lesser extent than
halothane—therefore safer regarding theliver toxicity.
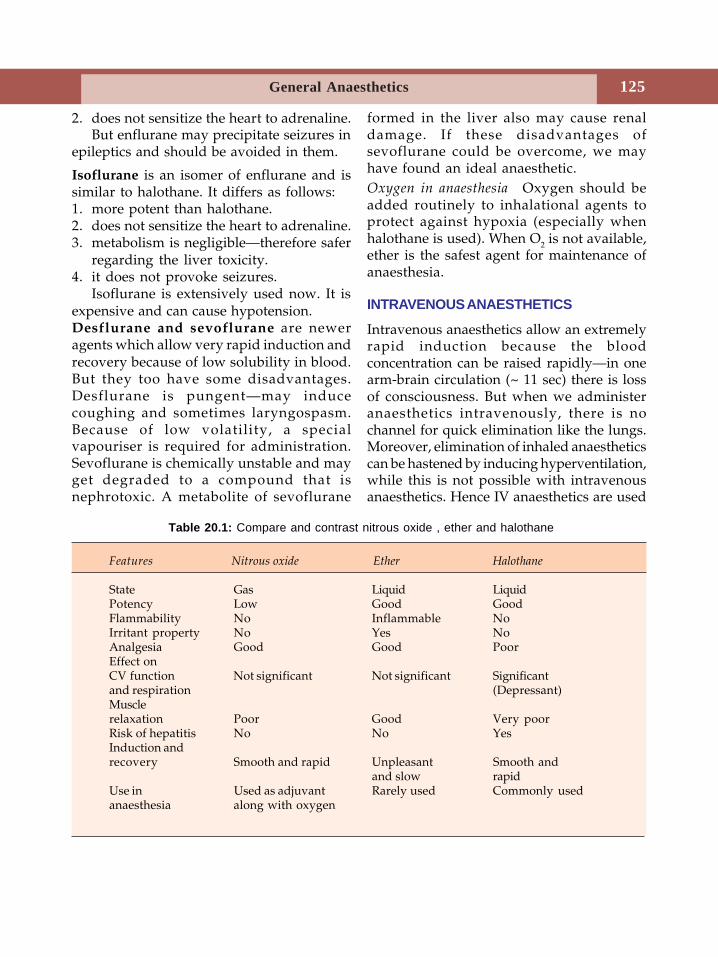
125General Anaesthetics
2. does not sensitize the heart to adrenaline.But enflurane may precipitate seizures in
epileptics and should be avoided in them.
Isoflurane is an isomer of enflurane and issimilar to halothane. It differs as follows:1. more potent than halothane.2. does not sensitize the heart to adrenaline.3. metabolism is negligible—therefore safer
regarding the liver toxicity.4. it does not provoke seizures.
Isoflurane is extensively used now. It isexpensive and can cause hypotension.Desflurane and sevoflurane are neweragents which allow very rapid induction andrecovery because of low solubility in blood.But they too have some disadvantages.Desflurane is pungent—may inducecoughing and sometimes laryngospasm.Because of low volatility, a specialvapouriser is required for administration.Sevoflurane is chemically unstable and mayget degraded to a compound that isnephrotoxic. A metabolite of sevoflurane
formed in the liver also may cause renaldamage. If these disadvantages ofsevoflurane could be overcome, we mayhave found an ideal anaesthetic.Oxygen in anaesthesia Oxygen should beadded routinely to inhalational agents toprotect against hypoxia (especially whenhalothane is used). When O2 is not available,ether is the safest agent for maintenance ofanaesthesia.
INTRAVENOUS ANAESTHETICS
Intravenous anaesthetics allow an extremelyrapid induction because the bloodconcentration can be raised rapidly—in onearm-brain circulation (~ 11 sec) there is lossof consciousness. But when we administeranaesthetics intravenously, there is nochannel for quick elimination like the lungs.Moreover, elimination of inhaled anaestheticscan be hastened by inducing hyperventilation,while this is not possible with intravenousanaesthetics. Hence IV anaesthetics are used
Table 20.1: Compare and contrast nitrous oxide , ether and halothane
Features Nitrous oxide Ether Halothane
State Gas Liquid LiquidPotency Low Good GoodFlammability No Inflammable NoIrritant property No Yes NoAnalgesia Good Good PoorEffect onCV function Not significant Not significant Significantand respiration (Depressant)Musclerelaxation Poor Good Very poorRisk of hepatitis No No YesInduction andrecovery Smooth and rapid Unpleasant Smooth and
and slow rapidUse in Used as adjuvant Rarely used Commonly usedanaesthesia along with oxygen
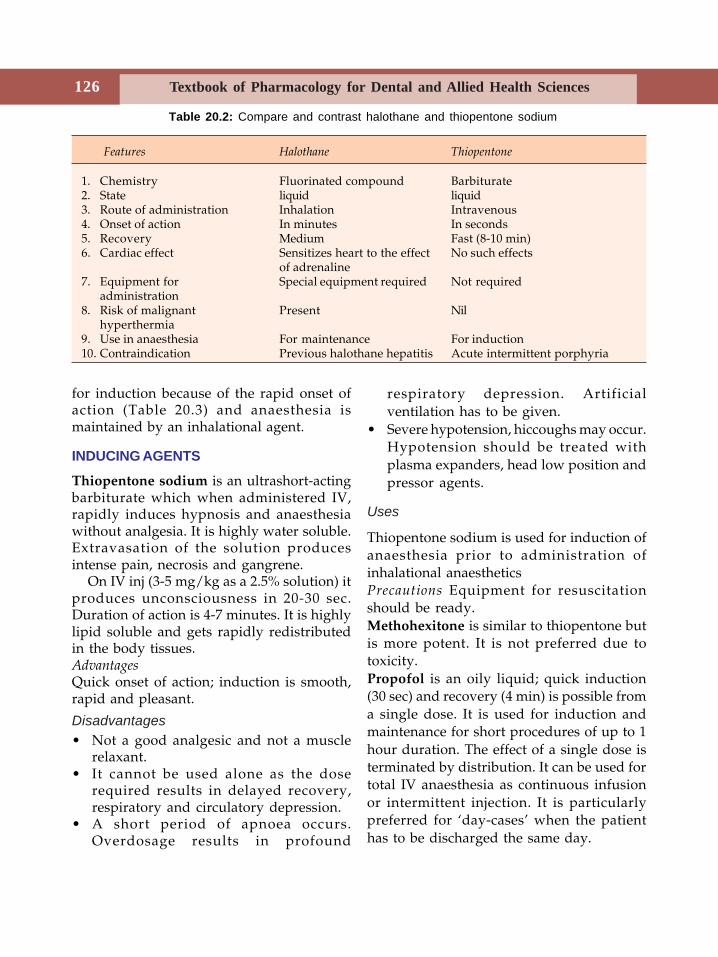
Textbook of Pharmacology for Dental and Allied Health Sciences126
for induction because of the rapid onset ofaction (Table 20.3) and anaesthesia ismaintained by an inhalational agent.
INDUCING AGENTS
Thiopentone sodium is an ultrashort-actingbarbiturate which when administered IV,rapidly induces hypnosis and anaesthesiawithout analgesia. It is highly water soluble.Extravasation of the solution producesintense pain, necrosis and gangrene.
On IV inj (3-5 mg/kg as a 2.5% solution) itproduces unconsciousness in 20-30 sec.Duration of action is 4-7 minutes. It is highlylipid soluble and gets rapidly redistributedin the body tissues.AdvantagesQuick onset of action; induction is smooth,rapid and pleasant.
Disadvantages• Not a good analgesic and not a muscle
relaxant.• It cannot be used alone as the dose
required results in delayed recovery,respiratory and circulatory depression.
• A short period of apnoea occurs.Overdosage results in profound
respiratory depression. Artificialventilation has to be given.
• Severe hypotension, hiccoughs may occur.Hypotension should be treated withplasma expanders, head low position andpressor agents.
Uses
Thiopentone sodium is used for induction ofanaesthesia prior to administration ofinhalational anaestheticsPrecautions Equipment for resuscitationshould be ready.Methohexitone is similar to thiopentone butis more potent. It is not preferred due totoxicity.Propofol is an oily liquid; quick induction(30 sec) and recovery (4 min) is possible froma single dose. It is used for induction andmaintenance for short procedures of up to 1hour duration. The effect of a single dose isterminated by distribution. It can be used fortotal IV anaesthesia as continuous infusionor intermittent injection. It is particularlypreferred for ‘day-cases’ when the patienthas to be discharged the same day.
Table 20.2: Compare and contrast halothane and thiopentone sodium
Features Halothane Thiopentone
1. Chemistry Fluorinated compound Barbiturate2. State liquid liquid3. Route of administration Inhalation Intravenous4. Onset of action In minutes In seconds5. Recovery Medium Fast (8-10 min)6. Cardiac effect Sensitizes heart to the effect No such effects
of adrenaline7. Equipment for Special equipment required Not required
administration8. Risk of malignant Present Nil
hyperthermia9. Use in anaesthesia For maintenance For induction10. Contraindication Previous halothane hepatitis Acute intermittent porphyria
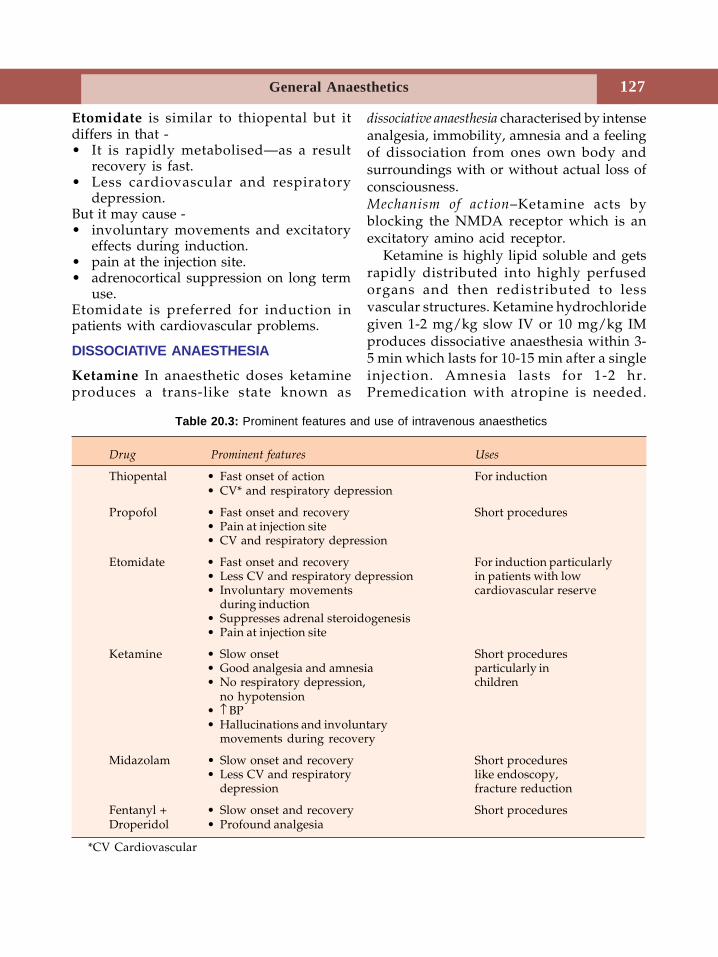
127General Anaesthetics
Etomidate is similar to thiopental but itdiffers in that -• It is rapidly metabolised—as a result
recovery is fast.• Less cardiovascular and respiratory
depression.But it may cause -• involuntary movements and excitatory
effects during induction.• pain at the injection site.• adrenocortical suppression on long term
use.Etomidate is preferred for induction inpatients with cardiovascular problems.
DISSOCIATIVE ANAESTHESIA
Ketamine In anaesthetic doses ketamineproduces a trans-like state known as
dissociative anaesthesia characterised by intenseanalgesia, immobility, amnesia and a feelingof dissociation from ones own body andsurroundings with or without actual loss ofconsciousness.Mechanism of action–Ketamine acts byblocking the NMDA receptor which is anexcitatory amino acid receptor.
Ketamine is highly lipid soluble and getsrapidly distributed into highly perfusedorgans and then redistributed to lessvascular structures. Ketamine hydrochloridegiven 1-2 mg/kg slow IV or 10 mg/kg IMproduces dissociative anaesthesia within 3-5 min which lasts for 10-15 min after a singleinjection. Amnesia lasts for 1-2 hr.Premedication with atropine is needed.
Table 20.3: Prominent features and use of intravenous anaesthetics
Drug Prominent features Uses
Thiopental • Fast onset of action For induction• CV* and respiratory depression
Propofol • Fast onset and recovery Short procedures• Pain at injection site• CV and respiratory depression
Etomidate • Fast onset and recovery For induction particularly• Less CV and respiratory depression in patients with low• Involuntary movements cardiovascular reserve
during induction• Suppresses adrenal steroidogenesis• Pain at injection site
Ketamine • Slow onset Short procedures• Good analgesia and amnesia particularly in• No respiratory depression, children
no hypotension• ↑ BP• Hallucinations and involuntary
movements during recovery
Midazolam • Slow onset and recovery Short procedures• Less CV and respiratory like endoscopy,
depression fracture reduction
Fentanyl + • Slow onset and recovery Short proceduresDroperidol • Profound analgesia
*CV Cardiovascular

Textbook of Pharmacology for Dental and Allied Health Sciences128
Return to ‘consciousness’ is gradual.Delirium with vivid dreams may beaccompanied. If diazepam is administeredpre- and postoperatively, delirium can beavoided. Heart rate, Cardiac output and BPare increased due to sympathetic stimulation.
Advantages
• Provides profound analgesia and amnesia;can be used as the sole agent for minorprocedures
• Respiration is not depressed, does notinduce hypotension
• Less likely to induce vomiting• Pharyngeal and laryngeal reflexes are only
slightly affected• It is of particular value in children and
poor-risk patients and also in asthmaticpatients since it does not inducebronchospasm.
Disadvantages
• Hallucinations and involuntary move-ments may occur during recovery if usedas a sole agent.
• May be dangerous in hypertensives as itraises the BP.
• Ketamine increases cerebral blood flowand intracranial pressure.
Contraindications Hypertension, CCF, cerebralhaemorrhage, increased intracranial tension,psychiatric disorders and pregnancy beforeterm.Precautions Pulse and BP should be closelymonitored; during recovery patients must beundisturbed and under observation.
NEUROLEPTANALGESIA
A combination of a neuroleptic (droperidol)with an analgesic (fentanyl) is used.Fentanyl is a short-acting (30-50 min) andpotent opioid analgesic (See Page 166).Droperidol is a rapidly acting, potentneuroleptic related to haloperidol.
When the combination is given IV, a stateof neuroleptanalgesia is produced. This ischaracterised by quiescence, psychicindifference and intense analgesia withoutloss of consciousness. It lasts for 30-40 min.Fentanyl 0.05 mg + droperidol 2.5 mg/ml – 4to 6 ml of the solution is infused IV over 10min. Patient is drowsy but cooperative.Respiratory depression is present. There is aslight fall in BP and HR (vagal stimulation).During recovery extra pyramidal symptomsmay be seen—due to droperidol. It isemployed for endoscopies, burn dressing,angiographies and other diagnostic and minorsurgical procedures.Neuroleptanaesthesia Addition of 65% N2O +35% O2 to the above combination producesneuroleptanaesthesia.
BENZODIAZEPINESBenzodiazepines like diazepam, lorazepamand midazolam are used to induce orsupplement anaesthesia. They cause sedation,amnesia and reduce anxiety which arebeneficial in such patients. BZDs may beemployed alone in procedures likeendoscopies, reduction of fractures, cardiaccatheterisation and cardioversion. IVmidazolam is particularly preferred as it isfaster and shorter-acting, more potent, doesnot cause significant respiratory andcardiovascular depression and does not causepain or irritation at the injection sites. BZDsare also used as preanaesthetic medication.Dentistry and general anaesthesia–Thoughseveral dental procedures require generalanaesthesia, they are usually administered byan anaesthetist.
PREANAESTHETIC MEDICATIONPrior to anaesthesia, certain drugs areadministered in order to make anaesthesiasafer and more pleasant and is known aspreanaesthetic medication. It is given in orderto:1. decrease anxiety

129General Anaesthetics
2. provide amnesia for the preoperativeperiod
3. relieve preoperative pain if present4. make anaesthesia safer5. reduce side effects of anaesthetics6. reduce gastric acidity.
To achieve the above purpose, more thanone drug is required. An informative,supportive, preoperative visit by theanaesthesiologist is very much essential.Sedative hypnotics Antianxiety agents likebenzodiazepines are used extensively aspreanaesthetic medication. They reduceanxiety and produce sedation. Diazepam 5-10 mg is given orally. It also producesamnesia. Barbiturates are not preferred dueto the disadvantages like respiratorydepression.Antihistamines have sedative, antiemetic andanticholinergic properties and are useful, e.g.promethazine.Antiemetics Metoclopromide, domperidoneor ondansetron may be used. Antihistamineswith antiemetic properties may also be used.Anticholinergic drugs Some irritant anaestheticslike ether increase the salivary andrespiratory secretions. The secretions fromthe oral cavity and trachea may creep intothe larynx inducing laryngospasm. They mayenter into the lungs causing aspirationpneumonia. This indicated the need for drugsthat reduce secretions. Fortunately we nowhave less irritant anaesthetics and secretionsare less of a problem. Atropine 0.6 mg IM orscopolamine 0.6 mg IM or glycopyrrolate —can be used.
They
• reduce the secretions• prevent bradycardia due to vagal
stimulation
• prevent laryngospasm which is due toexcessive secretions.
Scopolamine produces more sedation.Glycopyrrolate—as compared to atropine,glycopyrrolate is longer acting, is a betterantisialogogue and is less likely to causesignificant tachycardia. It also produces lesssedation than scopolamine.Drugs that reduce acidity General anaestheticsmay induce vomiting. This is associated withan increased risk of aspiration into therespiratory tract because normal protectiveairway reflexes are blunted by anaesthetics.Aspiration of the acidic gastric contents intothe lungs cause damage to the lungs. H2blockers like ranitidine decrease gastric acidsecretion and are given on the night beforesurgery. Decrease in gastric secretionsreduces the damage to lungs if aspirationoccurs while on anaesthesia.Gastrokinetic agents metoclopramide is adopamine antagonist that promotesgastrointestinal motility and increases thetone of oesophageal end of the stomach. This
speeds gastric emptying. The combination ofH2 blocker + metoclopramide provides bestprotection against aspiration.Opioids like morphine and pethidine reduceanxiety and apprehension, provide analgesiaand reduce the dose of the anaestheticrequired. But they depress respiration andmay cause hypotension, postoperativeconstipation, and urinary retention;precipitate asthma and delay recovery.
Balanced Anaesthesia
Since it is not possible to achieve idealanaesthesia with a single drug, multiple drugsare employed to attain this—preanaestheticmedication, IV anaesthetics for induction,inhalational agents for maintenance, oxygen,skeletal muscle relaxants and analgesics. Thisis termed balanced anaesthesia.
Textbook of Pharmacology for Dental and Allied Health Sciences130
21Local Anaesthetics
Local anaesthetics are drugs that block nerveconduction when applied locally to nervetissue in appropriate concentrations. Theiraction is completely reversible. They act onevery type of nerve fibre and can cause bothsensory and motor paralysis in theinnervated area. They act on axons, cell body,dendrites, synapses and other excitablemembranes that utilize sodium channels asthe primary means of action potentialgeneration.
Cocaine was the first agent to be isolatedby Niemann in 1860. In spite of its addictionpotential, cocaine was used for 30 years as asurface anaesthetic. In an effort made toimprove the properties of cocaine, procainewas synthesized in 1905. It ruled the fieldfor the next 50 years. In 1943, lignocaine wassynthesized and it continues to dominate thefield till today.
Classification of local anaesthetics (LAs)based on the route of administration andduration of action is as follows.
CLASSIFICATIONI. Injectable
1. Short-actingProcaine, chloroprocaine
2. Intermediate-actingLignocaine, prilocaine
3. Long-actingTetracaine (amethocaine),bupivacaine, dibucaine,ropivacaine, etidocaine.
II. Surface anaestheticsLignocaine, cocaine,tetracaine, benzocaine,oxethazaine.
Chemistry
Local anaesthetics are bases and consist of ahydrophilic amino group on one side and alipophilic aromatic residue on the other,joined by an intermediate chain through anester or amide linkage. Since ester links aremore prone to hydrolysis than amide links,generally esters have a shorter duration ofaction. Depending on the linkage, LAs canbe classified as:• Ester Linked
– Cocaine, procaine, tetracaine,benzocaine, chloroprocaine
• Amide Linked– Lignocaine (Lidocaine), mepivacaine,
bupivacaine, etidocaine, prilocaine,ropivacaine
Since local anaesthetics are weak bases andthe infected tissues have a low extracellularpH, LA ionise in such medium and a verylow fraction of non-ionised LA is availablefor diffusion into the cell. Therefore LAs aremuch less effective in infected tissues.
Mechanism of Action
Local anaesthetics prevent the generation andthe conduction of nerve impulses (Fig. 21.1).
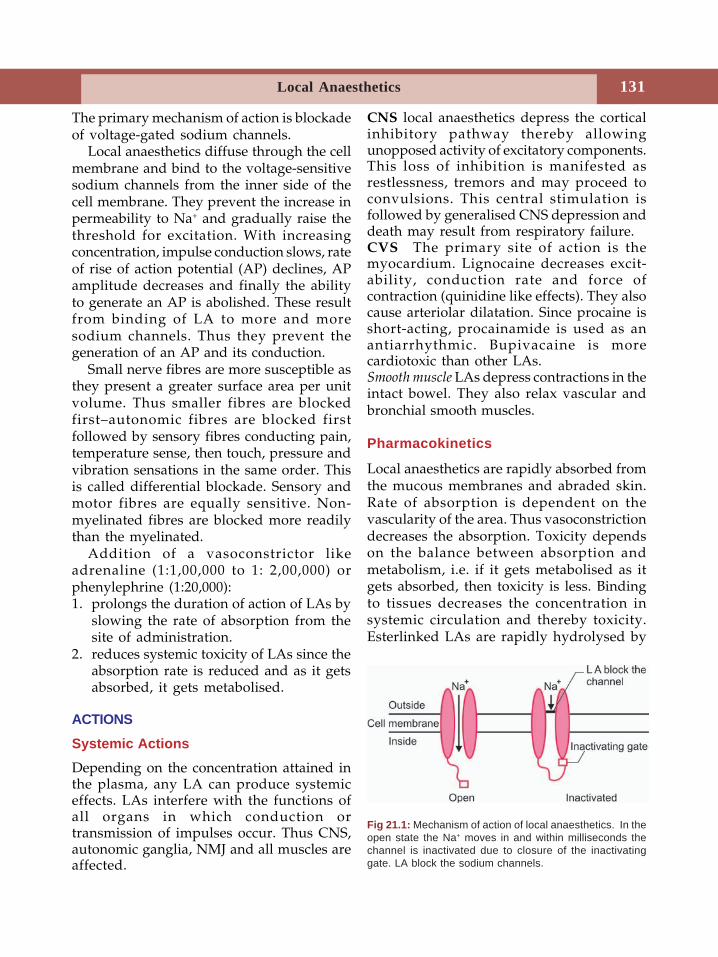
131Local Anaesthetics
The primary mechanism of action is blockadeof voltage-gated sodium channels.
Local anaesthetics diffuse through the cellmembrane and bind to the voltage-sensitivesodium channels from the inner side of thecell membrane. They prevent the increase inpermeability to Na+ and gradually raise thethreshold for excitation. With increasingconcentration, impulse conduction slows, rateof rise of action potential (AP) declines, APamplitude decreases and finally the abilityto generate an AP is abolished. These resultfrom binding of LA to more and moresodium channels. Thus they prevent thegeneration of an AP and its conduction.
Small nerve fibres are more susceptible asthey present a greater surface area per unitvolume. Thus smaller fibres are blockedfirst–autonomic fibres are blocked firstfollowed by sensory fibres conducting pain,temperature sense, then touch, pressure andvibration sensations in the same order. Thisis called differential blockade. Sensory andmotor fibres are equally sensitive. Non-myelinated fibres are blocked more readilythan the myelinated.
Addition of a vasoconstrictor likeadrenaline (1:1,00,000 to 1: 2,00,000) orphenylephrine (1:20,000):1. prolongs the duration of action of LAs by
slowing the rate of absorption from thesite of administration.
2. reduces systemic toxicity of LAs since theabsorption rate is reduced and as it getsabsorbed, it gets metabolised.
ACTIONS
Systemic ActionsDepending on the concentration attained inthe plasma, any LA can produce systemiceffects. LAs interfere with the functions ofall organs in which conduction ortransmission of impulses occur. Thus CNS,autonomic ganglia, NMJ and all muscles areaffected.
CNS local anaesthetics depress the corticalinhibitory pathway thereby allowingunopposed activity of excitatory components.This loss of inhibition is manifested asrestlessness, tremors and may proceed toconvulsions. This central stimulation isfollowed by generalised CNS depression anddeath may result from respiratory failure.CVS The primary site of action is themyocardium. Lignocaine decreases excit-ability, conduction rate and force ofcontraction (quinidine like effects). They alsocause arteriolar dilatation. Since procaine isshort-acting, procainamide is used as anantiarrhythmic. Bupivacaine is morecardiotoxic than other LAs.Smooth muscle LAs depress contractions in theintact bowel. They also relax vascular andbronchial smooth muscles.
Pharmacokinetics
Local anaesthetics are rapidly absorbed fromthe mucous membranes and abraded skin.Rate of absorption is dependent on thevascularity of the area. Thus vasoconstrictiondecreases the absorption. Toxicity dependson the balance between absorption andmetabolism, i.e. if it gets metabolised as itgets absorbed, then toxicity is less. Bindingto tissues decreases the concentration insystemic circulation and thereby toxicity.Esterlinked LAs are rapidly hydrolysed by
Fig 21.1: Mechanism of action of local anaesthetics. In theopen state the Na+ moves in and within milliseconds thechannel is inactivated due to closure of the inactivatinggate. LA block the sodium channels.

Textbook of Pharmacology for Dental and Allied Health Sciences132
plasma pseudocholinesterase and in the liver.Amide-linked LAs are metabolised by theliver microsomes by dealkylation andhydrolysis and are not effective orally (asantiarrhythmics). They undergo extensivefirst pass metabolism.
Adverse Effects (Table 21.1)
1. Hypersensitivity reactions– include skinrashes, dermatitis, asthma or rarelyanaphylaxis. These reactions are morecommon with ester type of drugs. Estertype LA are metabolised to PABAderivatives. These are responsible forallergic reactions while with amides, allergyis rare. Intradermal sensitivity test shouldbe done before using these drugs. Drugsneeded to manage such reactions shouldbe kept ready. Moreover, allergy is mostoften due to the preservative methyl-paraben. Preparations that do not containthis preservative are now available.
2. CNS–Dizziness, auditory and visualdisturbances, mental confusion, dis-orientation, anxiety, muscle tremors,convulsions and respiratory failure canresult from large doses. Intravenousdiazepam controls convulsions. Infact,these can be prevented by preanaestheticadministration of diazepam (1-2 mg/kg),especially if large doses are to be used.
3. CVS–Hypotension, bradycardia andarrhythmias may be encountered. Rarelycardiac arrest can occur.
4. Local irritation–can be seen with bupivacaine.Wound healing may be delayed.
Individual CompoundsA. Injectable (Table 21.2)
1. Lignocaine is the most widely used LA. Itis fast and long-acting. It is useful for alltypes of blocks. Maximum anaestheticeffect is seen in 2-5 minutes and lasts for30-45 minutes. In contrast to other LAs,lignocaine causes drowsiness and mentalclouding. Though it is a good cornealanaesthetic, it is not generally preferredbecause it causes irritation.Lignocaine (XYLOCAINE) is available as4% topical solution, 2% jelly, 5% ointment,1% and 2% injection, 5% for spinalanaesthesia and 10% spray. Thoughlignocaine can be used on the eye forsurface anaesthesia, it is not preferredbecause it causes some irritation.
2. Bupivacaine HCl–widely used. However,it can cause more cardiotoxicity thanothers. Injection 0.25-0.5% with orwithout adrenaline. Levobupivacainehydrochoride is a derivative ofbupivacaine that seems to be lessneurotoxic and less cardiotoxic thanbupivacaine.
3. Ropivacaine–is similar to bupivacaineexcept that it is less cardiotoxic.
4. Chloroprocaine HCl–potency is twice thatof procaine and its toxicity is lowerbecause of its more rapid metabolism.
5. Etidocaine HCl–its analgesic action lasts 2-3 times longer. It is used for epidural andall types of infiltration and regionalanaesthesia.
Table 21.1: Adverse effects of local anaesthetics
CNS : Dizziness, confusion, anxiety, tremors, occasionallyconvulsions and respiratory depression
CVS : Hypotension, bradycardia, arrhythmiasHypersensitivity : Rashes, dermatitis, asthma, rarely anaphylaxisreactions
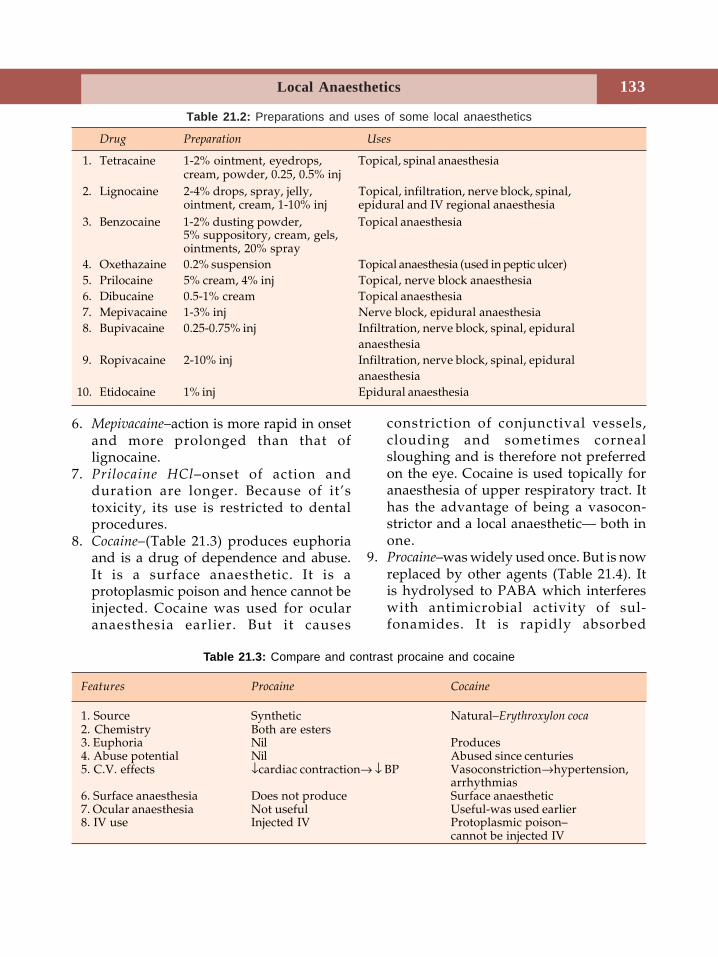
133Local Anaesthetics
6. Mepivacaine–action is more rapid in onsetand more prolonged than that oflignocaine.
7. Prilocaine HCl–onset of action andduration are longer. Because of it’stoxicity, its use is restricted to dentalprocedures.
8. Cocaine–(Table 21.3) produces euphoriaand is a drug of dependence and abuse.It is a surface anaesthetic. It is aprotoplasmic poison and hence cannot beinjected. Cocaine was used for ocularanaesthesia earlier. But it causes
constriction of conjunctival vessels,clouding and sometimes cornealsloughing and is therefore not preferredon the eye. Cocaine is used topically foranaesthesia of upper respiratory tract. Ithas the advantage of being a vasocon-strictor and a local anaesthetic— both inone.
9. Procaine–was widely used once. But is nowreplaced by other agents (Table 21.4). Itis hydrolysed to PABA which interfereswith antimicrobial activity of sul-fonamides. It is rapidly absorbed
Table 21.2: Preparations and uses of some local anaesthetics
Drug Preparation Uses
1. Tetracaine 1-2% ointment, eyedrops, Topical, spinal anaesthesiacream, powder, 0.25, 0.5% inj
2. Lignocaine 2-4% drops, spray, jelly, Topical, infiltration, nerve block, spinal,ointment, cream, 1-10% inj epidural and IV regional anaesthesia
3. Benzocaine 1-2% dusting powder, Topical anaesthesia5% suppository, cream, gels,ointments, 20% spray
4. Oxethazaine 0.2% suspension Topical anaesthesia (used in peptic ulcer)5. Prilocaine 5% cream, 4% inj Topical, nerve block anaesthesia6. Dibucaine 0.5-1% cream Topical anaesthesia7. Mepivacaine 1-3% inj Nerve block, epidural anaesthesia8. Bupivacaine 0.25-0.75% inj Infiltration, nerve block, spinal, epidural
anaesthesia9. Ropivacaine 2-10% inj Infiltration, nerve block, spinal, epidural
anaesthesia10. Etidocaine 1% inj Epidural anaesthesia
Table 21.3: Compare and contrast procaine and cocaine
Features Procaine Cocaine
1. Source Synthetic Natural–Erythroxylon coca2. Chemistry Both are esters3. Euphoria Nil Produces4. Abuse potential Nil Abused since centuries5. C.V. effects ↓cardiac contraction→ ↓ BP Vasoconstriction→hypertension,
arrhythmias6. Surface anaesthesia Does not produce Surface anaesthetic7. Ocular anaesthesia Not useful Useful-was used earlier8. IV use Injected IV Protoplasmic poison–
cannot be injected IV
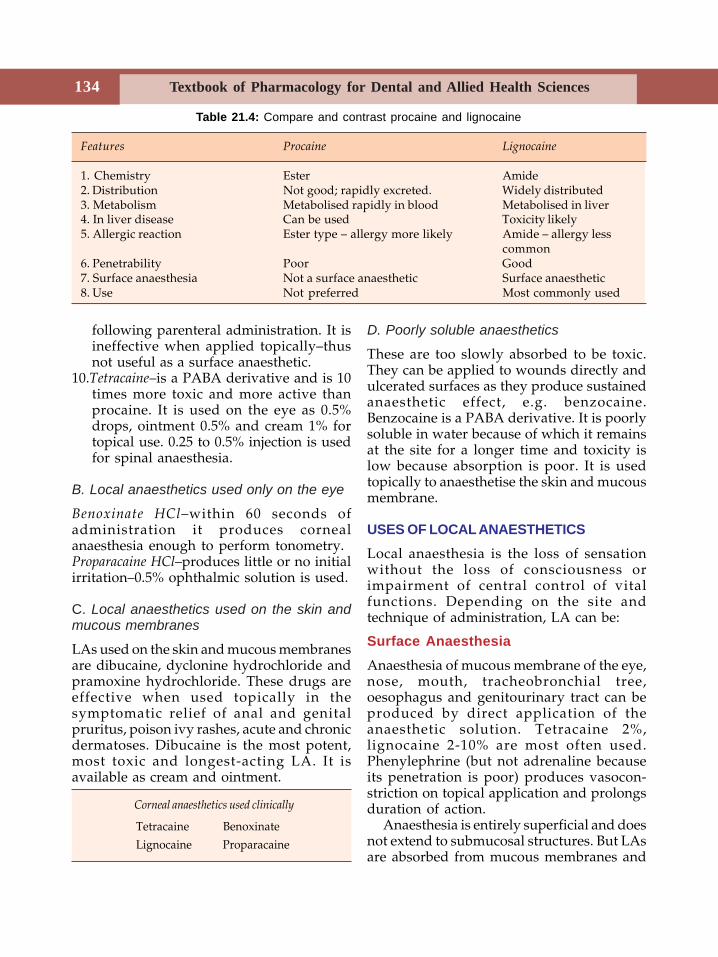
Textbook of Pharmacology for Dental and Allied Health Sciences134
following parenteral administration. It isineffective when applied topically–thusnot useful as a surface anaesthetic.
10.Tetracaine–is a PABA derivative and is 10times more toxic and more active thanprocaine. It is used on the eye as 0.5%drops, ointment 0.5% and cream 1% fortopical use. 0.25 to 0.5% injection is usedfor spinal anaesthesia.
B. Local anaesthetics used only on the eye
Benoxinate HCl–within 60 seconds ofadministration it produces cornealanaesthesia enough to perform tonometry.Proparacaine HCl–produces little or no initialirritation–0.5% ophthalmic solution is used.
C. Local anaesthetics used on the skin andmucous membranes
LAs used on the skin and mucous membranesare dibucaine, dyclonine hydrochloride andpramoxine hydrochloride. These drugs areeffective when used topically in thesymptomatic relief of anal and genitalpruritus, poison ivy rashes, acute and chronicdermatoses. Dibucaine is the most potent,most toxic and longest-acting LA. It isavailable as cream and ointment.
D. Poorly soluble anaesthetics
These are too slowly absorbed to be toxic.They can be applied to wounds directly andulcerated surfaces as they produce sustainedanaesthetic effect, e.g. benzocaine.Benzocaine is a PABA derivative. It is poorlysoluble in water because of which it remainsat the site for a longer time and toxicity islow because absorption is poor. It is usedtopically to anaesthetise the skin and mucousmembrane.
USES OF LOCAL ANAESTHETICSLocal anaesthesia is the loss of sensationwithout the loss of consciousness orimpairment of central control of vitalfunctions. Depending on the site andtechnique of administration, LA can be:
Surface AnaesthesiaAnaesthesia of mucous membrane of the eye,nose, mouth, tracheobronchial tree,oesophagus and genitourinary tract can beproduced by direct application of theanaesthetic solution. Tetracaine 2%,lignocaine 2-10% are most often used.Phenylephrine (but not adrenaline becauseits penetration is poor) produces vasocon-striction on topical application and prolongsduration of action.
Anaesthesia is entirely superficial and doesnot extend to submucosal structures. But LAsare absorbed from mucous membranes and
Table 21.4: Compare and contrast procaine and lignocaine
Features Procaine Lignocaine
1. Chemistry Ester Amide2. Distribution Not good; rapidly excreted. Widely distributed3. Metabolism Metabolised rapidly in blood Metabolised in liver4. In liver disease Can be used Toxicity likely5. Allergic reaction Ester type – allergy more likely Amide – allergy less
common6. Penetrability Poor Good7. Surface anaesthesia Not a surface anaesthetic Surface anaesthetic8. Use Not preferred Most commonly used
Corneal anaesthetics used clinically
Tetracaine BenoxinateLignocaine Proparacaine
135Local Anaesthetics
may result in systemic toxicity. Patient shouldbe cautioned to expectorate the excesssolution to avoid excess absorption. Localanaesthetics can also be used on abradedskin. Surface anaesthesia is useful.1. On the eye
(a) for tonometry, surgery(b) to remove foreign bodies from the
cornea and conjunctiva(c) for preoperative preparation
2. OthersNasal lesions, stomatitis, sore throat,tonsillectomy, endoscopies, intubation,gastric ulcer, burns and proctoscopy.An eutectic mixture containing 2.5% each oflignocaine and prilocaine at room temperaturehas a lower melting point than either of thedrugs. This is emulsified and applied as acream to anaesthetise the intact skin. Thecream should be applied on the skin underan occlusive dressing and can produceanaesthesia upto a depth of 5 mm. It can beused for procedures like venipuncture andskin graft harvesting.
Infiltration Anaesthesia
Injection of a local anaesthetic solutiondirectly into the tissue can be (i) superficial–only into the skin, or (ii) into deeperstructures including intra-abdominal organs.Duration can be doubled by adrenaline(1:2,00,000). Adrenaline should not be used(i) around end arteries to avoid necrosis, and(ii) intracutaneously to avoid sloughing.Drugs used are lignocaine, procaine,bupivacaine.Advantage By using infiltration anaesthesia,it is possible to provide anaesthesia withoutdisruption of normal bodily functions.Disadvantage In major surgeries–systemictoxicity due to local anaesthetic is likely aslarge amounts of the anaesthetic is requiredfor such procedures.Uses For minor procedures like incisions,drainage of an abscess, excision, etc.
Field BlockSubcutaneous injection of a LA solutionproximal to the site to be anaesthetised,interrupts nerve transmission in the regiondistal to the injection. Sites such as forearm,scalp, anterior abdominal wall and lowerextremity are used for field block. Knowledgeof the relevant neuroanatomy is essential.Advantage Lesser dose can be used to providea greater area of anaesthesia.
Nerve BlockInjection of a solution of a LA about/aroundindividual peripheral nerves or nerveplexuses produces larger areas of anaesthesiawith a smaller amount of the drug than theabove techniques. Anaesthesia starts a fewcentimeters distal to the injection.Nerve block anaesthesia is useful for:1. blocks of brachial plexus for procedures
on the arm (distal to deltoid).2. intercostal nerve blocks to anaesthetise
anterior abdominal wall.3. cervical plexus block for surgery of the
neck.4. sciatic and femoral nerve blocks for
surgeries distal to the knee.5. blocks of nerves at wrist and ankle.6. radial and ulnar nerve block at the elbow.7. sensory cranial nerves block.8. facial and lingual nerves block.9. inferior alveolar nerve block for extraction
of lower jaw teeth.Onset of action is within 3 minutes with
lignocaine. Duration depends on lipidsolubility and protein binding. Anaesthesialasts longer than by field block or infiltrationtechniques. Nerve blocks are done for toothextraction, operations on the eye, limbs andin neuralgias.
Spinal Anaesthesia (SA)Local anaesthetic solution is injected into thesubarachnoid space between L2-3 or L3-4

Textbook of Pharmacology for Dental and Allied Health Sciences136
below the lower end of the spinal cord. Thedrug acts on nerve roots. Lower abdomenand lower limbs are anaesthetised andparalysed. The level of anaesthesia can bealtered by the volume of injection, specificgravity of the solution and posture of thepatient. Generally a hyperbaric solution (in10% glucose) is injected. Isobaric andhypobaric solutions can also be given. Levelof sympathetic block produced is twosegments higher and motor paralysis twosegments lower than sensory or cutaneousanaesthesia. Duration depends on theconcentration, dose and the drug itself.Lignocaine, tetracaine, bupivacaine andropivacaine are used for spinal anaesthesia.
Advantages
Safer, affords good analgesia and musclerelaxation and there is no loss ofconsciousness. In cardiac, pulmonary andrenal diseases, SA may be preferred overgeneral anaesthesia whenever possible.
Uses
Surgical procedures on the lower limb, pelvis,lower abdomen, obstetric procedures,caesarean section and other operations aredone on spinal anaesthesia.
Complications of SA
1. Hypotension and bradycardia–sympatheticblockade results in venous pooling of theblood leading to decreased venous return,decreased cardiac output and hypo-tension.
2. Respiratory paralysis–hypotension andischaemia of the respiratory centre resultsin respiratory failure. Due to paralysis ofthe abdominal muscles, cough reflex is lesseffective resulting in stasis of respiratorysecretions leading to respiratory infections.
3. Headache due to seepage of CSF can betreated with analgesics.
4. Cauda equina syndrome is uncommon–control over bladder and bowel sphinctersis lost because of damage to nerve roots.
5. Sepsis–resulting in meningitis6. Nausea and vomiting–premedication can be
given to prevent this.
Epidural AnaesthesiaLA is injected into the spinal extradural space.It acts on nerve roots while small amountsdiffuse into subarachnoid space. It istechnically more difficult and comparativelylarger volumes of the anaesthetic are needed.After repeated injections tachyphylaxis maydevelop.
Advantages
1. Sensory blockade is 4-5 segments higherthan motor blockade. This difference isuseful for obstetric analgesia, as themother has painless labour and can stillcooperate in the process of labour and isconscious throughout.
2. As there is no risk of injecting intosubarachnoid space, there are no chancesof infection.
Intravenous Regional AnaesthesiaThis type of anaesthesia is useful for rapidanaesthetization of an extremity. A rubberbandage is used to force the blood out ofthe limb (veins) and a tourniquet is appliedto prevent the re-entry of the blood. A dilutesolution of the local anaesthetic is theninjected intravenously. It diffuses intoextravascular tissues. Onset of anaesthesia isin 2 minutes. Because of the pain producedby the tourniquet, this type of anaesthesiais used for procedures lasting less than onehour. About 25% of the drug enters into thesystemic circulation. This type of anaes-thesia is commonly used on the upper limbsthough it can also be used on the legs and thethighs.
137Sedative Hypnotics
22Sedative Hypnotics
Sedative is a drug that produces a calming orquietening effect and reduces excitement. Itmay induce drowsiness. Hypnotic is a drugthat induces sleep resembling natural sleep.Both sedation and hypnosis may beconsidered as different grades of CNSdepression.
All human beings need sleep. Insomnia issleeplessness. Approximately 1/3rd of ourlife is spent in sleep. Since centuries man hassought the help of drugs and other remediesfor insomnia.
Sleep can be classified into two typesdepending on the physiological characte-ristics -1. Non-rapid eye movement (NREM)-sleep2. Rapid eye movement sleep (REM).
Throughout the night, NREM and REMsleep cycles repeat alternately for briefperiods.
CLASSIFICATION
1. Benzodiazepines• Long-acting (24-48 hours)
DiazepamChlordiazepoxideClonazepamFlurazepamChlorazepateClobazam
• Short-acting (12-24 hours)TemazepamLorazepam
OxazepamNitrazepamAlprazolamHalazepam.
• Ultra short acting (< 6 hours)Triazolam,Midazolam
2. Newer agents ZolpidemZopicloneZaleplon
3. Barbiturates PhenobarbitoneMephobarbitoneSecobarbitonePentobarbitoneThiopentoneHexobarbitone
4. Miscellaneous ParaldehydeChloral hydrateGlutethimideMeprobamate
BENZODIAZEPINES (BZD)Chlordiazepoxide was the first BZD to beintroduced into clinical medicine in 1961 andsince then thousands of BZDs have beensynthesized of which about 35 are now inclinical use.Pharmacological actions The most importantactions of BZDs are on the CNS and include:1. Sedation and hypnosis2. Reduction in anxiety3. Muscle relaxation4. Anticonvulsant effects5. Amnesia.
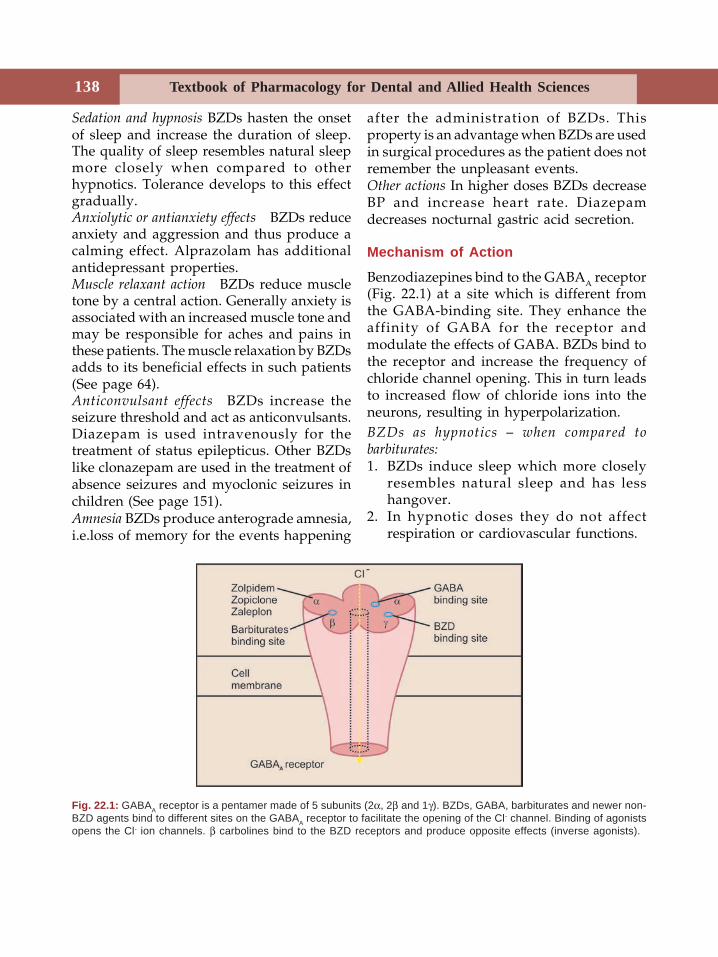
Textbook of Pharmacology for Dental and Allied Health Sciences138
Sedation and hypnosis BZDs hasten the onsetof sleep and increase the duration of sleep.The quality of sleep resembles natural sleepmore closely when compared to otherhypnotics. Tolerance develops to this effectgradually.Anxiolytic or antianxiety effects BZDs reduceanxiety and aggression and thus produce acalming effect. Alprazolam has additionalantidepressant properties.Muscle relaxant action BZDs reduce muscletone by a central action. Generally anxiety isassociated with an increased muscle tone andmay be responsible for aches and pains inthese patients. The muscle relaxation by BZDsadds to its beneficial effects in such patients(See page 64).Anticonvulsant effects BZDs increase theseizure threshold and act as anticonvulsants.Diazepam is used intravenously for thetreatment of status epilepticus. Other BZDslike clonazepam are used in the treatment ofabsence seizures and myoclonic seizures inchildren (See page 151).Amnesia BZDs produce anterograde amnesia,i.e.loss of memory for the events happening
after the administration of BZDs. Thisproperty is an advantage when BZDs are usedin surgical procedures as the patient does notremember the unpleasant events.Other actions In higher doses BZDs decreaseBP and increase heart rate. Diazepamdecreases nocturnal gastric acid secretion.
Mechanism of Action
Benzodiazepines bind to the GABAA receptor(Fig. 22.1) at a site which is different fromthe GABA-binding site. They enhance theaffinity of GABA for the receptor andmodulate the effects of GABA. BZDs bind tothe receptor and increase the frequency ofchloride channel opening. This in turn leadsto increased flow of chloride ions into theneurons, resulting in hyperpolarization.BZDs as hypnotics – when compared tobarbiturates:1. BZDs induce sleep which more closely
resembles natural sleep and has lesshangover.
2. In hypnotic doses they do not affectrespiration or cardiovascular functions.
Fig. 22.1: GABAA receptor is a pentamer made of 5 subunits (2α, 2β and 1γ). BZDs, GABA, barbiturates and newer non-BZD agents bind to different sites on the GABAA receptor to facilitate the opening of the Cl- channel. Binding of agonistsopens the Cl- ion channels. β carbolines bind to the BZD receptors and produce opposite effects (inverse agonists).
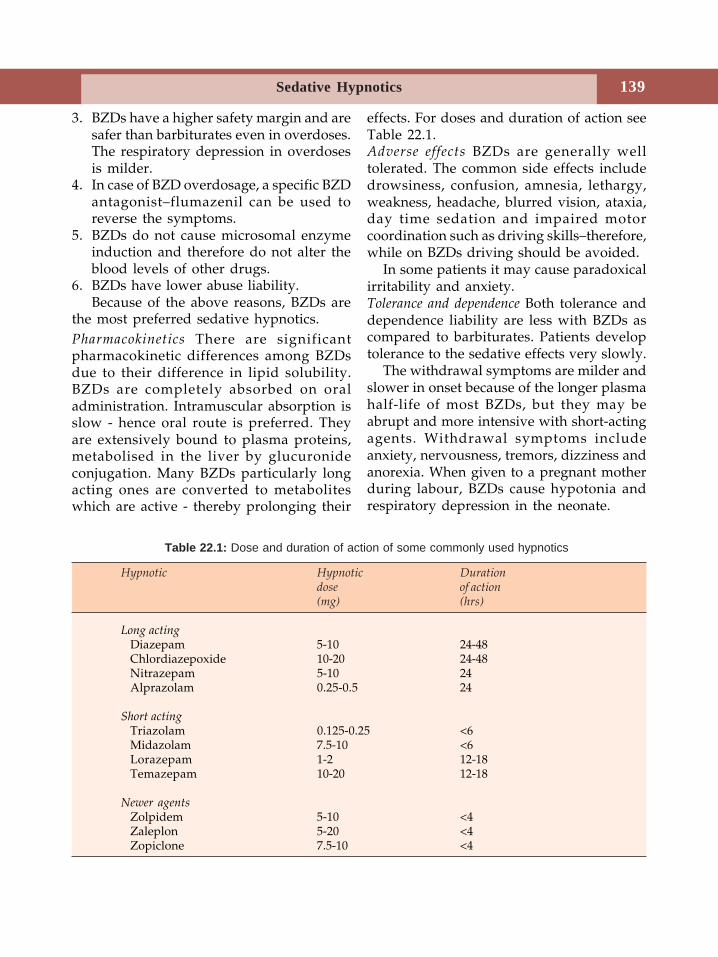
139Sedative Hypnotics
3. BZDs have a higher safety margin and aresafer than barbiturates even in overdoses.The respiratory depression in overdosesis milder.
4. In case of BZD overdosage, a specific BZDantagonist–flumazenil can be used toreverse the symptoms.
5. BZDs do not cause microsomal enzymeinduction and therefore do not alter theblood levels of other drugs.
6. BZDs have lower abuse liability.Because of the above reasons, BZDs are
the most preferred sedative hypnotics.Pharmacokinetics There are significantpharmacokinetic differences among BZDsdue to their difference in lipid solubility.BZDs are completely absorbed on oraladministration. Intramuscular absorption isslow - hence oral route is preferred. Theyare extensively bound to plasma proteins,metabolised in the liver by glucuronideconjugation. Many BZDs particularly longacting ones are converted to metaboliteswhich are active - thereby prolonging their
effects. For doses and duration of action seeTable 22.1.Adverse effects BZDs are generally welltolerated. The common side effects includedrowsiness, confusion, amnesia, lethargy,weakness, headache, blurred vision, ataxia,day time sedation and impaired motorcoordination such as driving skills–therefore,while on BZDs driving should be avoided.
In some patients it may cause paradoxicalirritability and anxiety.Tolerance and dependence Both tolerance anddependence liability are less with BZDs ascompared to barbiturates. Patients developtolerance to the sedative effects very slowly.
The withdrawal symptoms are milder andslower in onset because of the longer plasmahalf-life of most BZDs, but they may beabrupt and more intensive with short-actingagents. Withdrawal symptoms includeanxiety, nervousness, tremors, dizziness andanorexia. When given to a pregnant motherduring labour, BZDs cause hypotonia andrespiratory depression in the neonate.
Hypnotic Hypnotic Durationdose of action(mg) (hrs)
Long actingDiazepam 5-10 24-48Chlordiazepoxide 10-20 24-48Nitrazepam 5-10 24Alprazolam 0.25-0.5 24
Short actingTriazolam 0.125-0.25 <6Midazolam 7.5-10 <6Lorazepam 1-2 12-18Temazepam 10-20 12-18
Newer agentsZolpidem 5-10 <4Zaleplon 5-20 <4Zopiclone 7.5-10 <4
Table 22.1: Dose and duration of action of some commonly used hypnotics
Textbook of Pharmacology for Dental and Allied Health Sciences140
Acute overdosage–BZD overdosage inducessleep but the respiratory depression is mild.Hence BZDs are safe and the availability of aspecific antagonist- flumazenil- makes it saferto use BZDs because poisoning can be treated.
Uses of BZDs
1. Insomnia When drugs are to be used to treatinsomnia, BZDs are the agents of choice.Lorazepam, oxazepam, temazepam,nitrazepam or triazolam may be used.
2. In anxiety states BZDs are the mostcommonly used anxiolytics for thetreatment of anxiety states and anxietyneuroses (see Page 194). Any of the BZDsexcept the ultra short acting ones may beused.
3. As anticonvulsants IV diazepam is the drugof choice in the treatment of statusepilepticus. Clonazepam or clobazam areused as adjuncts with other anti-epilepticdrugs (Page 151).
4. Muscle relaxant BZDs are centrally actingmuscle relaxants used in chronic musclespasm and spasticity.
5. As preanaesthetic medication–for theirsedation and anxiolytic effects BZDs areuseful (Page 128).
6. During alcohol withdrawal–BZDs are usefulin patients during withdrawal of alcoholor other sedative-hypnotics.
BENZODIAZEPINE ANTAGONIST
Flumazenil is a BZD receptor antagonist whichcompetes with BZDs for the receptor. Givenintravenously flumazenil is rapid and shortacting. It may rarely induce seizures.
Uses
1. To reverse BZD sedation/anaesthesia2. In BZD overdosage.
NEWER AGENTS
Newer agents include zolpidem, zopicloneand zaleplon.• They are not BZDs but produce their
effects by binding to benzodiazepine siteon the GABAA receptors and facilitate theinhibitory actions of GABA.
• They are all rapid and short acting agentsand produce minimum hangover.
• Their actions are blocked by flumazenil.• They are used for short periods when
short acting hypnotics are needed.Zolpidem is a good hypnotic but has weakanticonvulsant and muscle relaxant effects.It is short acting (t½ - 2 hours) but the effectson sleep continue for a long time even afterstopping zolpidem.It is well absorbed from the gut andmetabolized in the liver. Dose should bereduced in hepatic dysfunction.Zaleplon is rapidly absorbed from the gut andhas a short t½ of about 1 hour. It ismetabolised in the liver. It has the advantagesthat no withdrawal symptoms are reportedafter stopping it and no tolerance develops.It has rapid onset and short duration ofaction. No side effects are reported.Zopiclone is another newly introducedhypnotic. Its actions resemble those of BZDs.
BARBITURATES
Barbiturates are derivatives of barbituric acidand were the largest group of hypnotics inclinical use until the 1960s.
Classification
Barbiturates can be classified based on theirduration of action as:• Long-acting
Phenobarbitone, Mephobarbitone
141Sedative Hypnotics
• Short-actingPentobarbitone, Butobarbitone
• Ultrashort-actingThiopentone, Hexobarbitone,Methohexitone
Mechanism of Action
Barbiturates bind to a specific site on theGABA receptor Cl– channel complex. Theyfacilitate inhibitory neurotransmission byopening chloride ion channels andhyperpolarise the neural membrane.
Pharmacological Actions
1. CNS Barbiturates cause depression of allexcitable tissues of which CNS is the mostsensitive.Sedation and hypnosis In hypnotic doses,barbiturates induce sleep and prolong theduration of sleep. The REM-NREM sleepcycle is altered with decreased duration ofREM and prolonged NREM sleep. Onwaking up there is hangover with headacheand residual sedation.
Barbiturates reduce anxiety, impair short-term memory and judgement. They canproduce euphoria and are drugs of addictionwhile some people may experience dys-phoria. Barbiturates produce hyperalgesia(increased sensitivity to pain). Thereforebarbiturates, when given as hypnotics for apatient in pain may be more troublesomethan being of any benefit.Anaesthesia In higher doses barbituratesproduce general anaesthesia. The ultrashort-acting barbiturates are used intravenously forthis effect.Anticonvulsant effects All barbiturates haveanticonvulsant actions. Phenobarbitone andmephobarbitone have specific anticonvulsantactivity in subhypnotic doses and are usedin the treatment of epilepsy.
2. Respiratory system Barbiturates depress therespiration. High doses bring about a directparalysis of the medullary respiratory centreand can be fatal.3. Cardiovascular system Hypnotic doses ofbarbiturates produce a slight reduction inblood pressure and heart rate as seen duringnatural sleep.
Toxic doses of barbiturates produce asignificant fall in BP due to direct decreasein myocardial contractility and vasomotorcentre depression.4. Skeletal muscles Higher doses of barbi-turates depress the excitability of theneuromuscular junction.
Pharmacokinetics
Barbiturates are well-absorbed and widelydistributed in the body. The highly lipidsoluble barbiturates like thiopentone have afast onset of action and duration is short dueto redistribution into adipose tissues.Barbiturates are metabolised in the liver.They are hepatic microsomal enzymeinducers. The metabolites are excreted inurine.
Adverse Reactions
Hangover–due to residual depression of theCNS may be accompanied by nausea,vomiting, vertigo and diarrhoea. Distortionsof mood, impaired judgement and fine motorskills may be evident. Barbiturates may causeexcitement and irritability in some patientsparticularly children.
Barbiturates cause respiratory depressionand in the presence of respiratory disorderseven the hypnotic doses of barbiturates cancause serious respiratory depression.Hypersensitivity reactions like skin rashes,swelling of the eyelids and lips and rarelyexfoliative dermatitis may be seen.
Textbook of Pharmacology for Dental and Allied Health Sciences142
Barbiturates are contraindicated inporphyrias because they increase porphyrinsynthesis.Tolerance and dependence On repeatedadministration, tolerance develops to theeffects of barbiturates.
Development of both psychological andphysical dependence to barbiturates makethem one of the drugs with abuse liability.Withdrawal symptoms include anxiety,restlessness, abdominal cramps, hallucin-ations, delirium and convulsions.Acute barbiturate poisoning The fatal dose ofphenobarbitone is 6-10 gm. Manifestationsinclude respiratory depression with slow andshallow breathing, hypotension, skineruptions, cardiovascular collapse and renalfailure.Treatment There is no specific antidote. Themeasures include:1. Gastric lavage followed by administration
of activated charcoal to prevent furtherabsorption of barbiturates.
2. General supportive measures likemaintenance of BP, patent airway,adequate ventilation and oxygenadministration.
3. Forced alkaline diuresis with sodiumbicarbonate, a diuretic and IV fluids willhasten the excretion of long-actingbarbiturates through the kidneys sincethey are acidic drugs.
4. Haemodialysis should be done especiallyif there is renal failure.
Uses Because of respiratory depression andabuse liability, barbiturates are generally notpreferred.1. Anaesthesia Thiopentone sodium is used
IV for the induction of general anaes-thesia.
2. Antiepileptic Phenobarbitone is used asan antiepileptic (page 149).
3. Neonatal jaundice Phenobarbitone is amicrosomal enzyme inducer and therebyenhances the production of glucuronyltransferase—the enzyme required formetabolism and excretion of bilirubin. Ittherefore helps in the clearance of jaundicein the neonates.
4. Sedation and hypnosis Benzodiazepines arepreferred to barbiturates as sedativehypnotics.
5. Preanesthetic medication Barbiturates wereused earlier for the sedative-hypnoticproperty, but are not preferred now.
MISCELLANEOUS
Chloral hydrate is used as an alternative toBZD. It has a bad taste and is an irritant-causes nausea and vomiting. It produceshypnosis without affecting respiratory andcardiovascular functions.Meprobamate has sedative and antianxietyproperties but is now not recommended. Itproduces respiratory depression, ataxia andis a drug of abuse.Paraldehyde is a colourless, transparent,pungent, inflammable liquid. It is an irritantand can dissolve plastic—cannot be given bya plastic syringe. It is a good hypnotic causinglittle hangover. It can be given rectally,intramuscularly or orally.
It also has anticonvulsant properties.
Uses
1. As anticonvulsant in status epilepticusparticularly in children; tetanus andeclampsia.
2. Hypnotic–rarely used.
143Alcohols
23Alcohols
ETHYL ALCOHOL (ETHANOL)
Ethyl alcohol is a monohydroxy alcoholmanufactured by fermentation of sugars. Itis a colourless, volatile, inflammable liquid.The ethanol content of various alcoholicbeverages ranges from 4-55%.
Actions
1. Local On topical application, ethanolevaporates quickly and has a cooling effect.It is an astringent–precipitates surfaceproteins and hardens the skin. 40-50% alcoholis rubefacient and counter irritant. Alcoholis also an antiseptic. At 70%, it has maximumantiseptic properties which decrease abovethat. It is not effective against spores.2. CNS Alcohol is a CNS depressant. Smalldoses cause euphoria, relief of anxiety andloss of social inhibitions. Moderate dosesimpair muscular coordination and visualacuity making driving dangerous. Withhigher doses mental clouding, impairedjudgement, drowsiness and loss of selfcontrol result. High doses cause stupor andcoma. Death is due to respiratory depression.
Alcohol may precipitate convulsions inepileptics. Tolerance develops on long-termuse.3. CVS The actions are dose dependent.Small doses cause cutaneous vasodilationresulting in flushing and feeling of warmth.Large doses cause hypotension due to
depression of myocardium and vasomotorcentre.4. GIT and liver Alcohol is an irritant–increases gastric secretion and producesvasodilation and warmth. It is an appetizer.Chronic alcoholism results in peptic ulcer.
Chronic consumption of moderateamounts of alcohol results in accumulationof fat in the liver, enlargement of the liver,followed by fatty degeneration and cirrhosis.
Alcohol induces microsomal enzymes.5. Other effects Though alcohol is called anaphrodisiac, this effect could be due to lossof inhibition. Low doses taken over a longtime increases HDL and lowers LDLcholesterol. Alcohol is a diuretic (↓ADHsecretion). It interferes with folatemetabolism and may cause megaloblasticanaemia. Though alcohol causes a feeling ofwarmth, heat loss is increased due tovasodilation and should not be used for‘warming up’ in cold surroundings. Foodvalue is 7 calories/gram.
Mechanism of Action
Ethanol acts by -1. inhibiting central neuronal nicotinic
acetylcholine receptors.2. inhibiting excitatory NMDA (N-methyl-D-
asparate receptors mediate excitatoryresponses in the CNS and kainate receptorfunctions.
Textbook of Pharmacology for Dental and Allied Health Sciences144
3. promoting the function of 5 HT3receptors.
4. ethanol also influences many ion channelsincluding K+ channels.
Pharmacokinetics
Alcohol is rapidly absorbed from the stomachand is metabolised in the liver by alcohol andaldehyde dehydrogenase.
Metabolism follows zero order kinetics–aconstant amount is metabolised per unit time,i.e. about 10 ml absolute alcohol ismetabolised per hour. It is excreted throughkidneys and lungs.
polyneuritis, anaemia and pellagra can occur.In pregnant women, alcohol is teratogenic.Even moderate drinking during pregnancycan produce ‘fetal alcohol syndrome’ withmanifestations like low IQ, microcephaly,growth retardation and facial anomalies inthe foetus. It can also cause stillbirths andabortions.
Chronic alcoholics have poor dentalhygiene resulting in a higher rate ofassociated dental ailments like periodontitis,gingivitis and dental plaque.
Treatment of alcohol dependenceDisulfiram
Disulfiram inhibits the enzyme aldehydedehydrogenase. If alcohol is consumed aftertaking disulfiram, acetaldehyde accumulatesand within few minutes it can produceflushing, throbbing headache, nausea,vomiting, sweating, hypotension andconfusion - called the antabuse reaction, due toaccumulation of acetaldehyde. The effect lastsfor 7-14 days after stopping disulfiram. The
Drug Interactions
1. Alcohol potentiates other CNSdepressants including hypnotics, opioidsand antipsychotics.
2. Sulfonylureas, metronidazole andgriseofulvin have disulfiram like effectson alcohol consumption.
3. Alcohol is an enzyme inducer.
Uses
1. Antiseptic–70% alcohol is applied topically.2. Bedsores–When rubbed onto the skin,
alcohol hardens the skin and prevents bed-sores.
3. Fever Alcoholic sponges are used forreduction of body temperature in fevers.
4. Appetite stimulant–About 50 ml of 6-10%alcohol given before meals is an appetitestimulant.
5. Neuralgias–In severe neuralgias liketrigeminal neuralgia, injection of alcoholaround the nerve causes permanent lossof transmission and relieves pain.
6. In methanol poisoning (See below)
Acute alcoholic intoxication causes severegastritis, hypotension, hypoglycaemia,respiratory depression, coma and death.Treatment measures include gastric lavage,airway maintenance, positive pressureventilation and maintenance of fluid andelectrolyte balance. Haemodialysis is neededin severe intoxication.Chronic alcoholism causes dependence.Wernicke’s encephalopathy, Korsakoff’spsychosis, tremors, cirrhosis of liver,hypertension and cardiomyopathy can occur.In addition, nutritional deficiencies such as

145Alcohols
reactions can sometimes be very severe andtherefore treatment should be given in ahospital.
Other drugs that cause antabuse reactionare metronidazole, chlorpropamide, tol-butamide, griseofulvin, cephalosporins andphenylbutazone.Contraindications Patients with liver disease,patients physically dependent on alcohol.Other drugs-Several drugs are being tried inthe pharmacotherapy of alcohol dependence.Orally effective opioid antagonistsnaltrexone and nalmefene reduce the urgeand craving to drink and are recommendedas adjuvants to other measures. They alsoreduce the chances of relapse of heavydrinking. Ondansetron, a 5HT3 antagonistantiemetic has been shown to reduce alcoholconsumption and is being evaluated for usein alcohol withdrawal. Benzodiazepinesreduce the symptoms of alcohol withdrawallike anxiety and insomnia. Clonidine an α2agonist also reduces symptoms of sympa-thetic overactivity like tremors andtachycardia. Acamprosate an antagonist ofNMDA receptor is also found to preventrelapse of heavy drinking.
METHYL ALCOHOL (METHANOL, WOODALCOHOL)
Methanol is used to denature ethyl alcohol.It is of no therapeutic value. Ingestion resultsin methanol poisoning. Methanol isconverted to formaldehyde - catalysed byalcohol dehydrogenase; formaldehyde isconverted to formic acid by the action ofaldehyde dehydrogenase. Toxic effects aredue to formic acid.
Manifestations of toxicity are vomiting,headache, vertigo, severe abdominal pain,
hypotension, delirium, acidosis and coma.Formic acid has affinity for optic nerve andcauses retinal damage resulting in blindness.There are reports of even 15 ml of methanolcausing blindness. Death is due to respiratoryfailure.
Treatment
1. Correction of acidosis As acidosis hastensretinal damage, immediate correction ofacidosis with IV sodium bicarbonateinfusion helps in preventing blindness.
2. Protect eyes Patient should be kept in a darkroom to protect the eyes.
3. Gastric lavage should be given.4. BP and ventilation should be maintained.5. Ethyl alcohol should be given imme-
diately. It competes with methanol foralcohol dehydrogenase, because of itshigher affinity for alcohol dehydro-genase. It thus slows the metabolism ofmethanol and prevents the formation oftoxic metabolites. A loading dose of 0.6g/Kg is followed by an infusion of 10 g/hour.
6. Antidote Fomepizole specifically inhibitsthe enzyme alcohol dehydrogenaseand thereby prevents the formation oftoxic metabolites—formaldehyde andformic acid. Fomepizole thus acts as anantidote in methanol poisoning. It has anadvantage over ethyl alcohol that it doesnot cause any intoxication by itself.
7. Haemodialysis should be started at theearliest possible.
Textbook of Pharmacology for Dental and Allied Health Sciences146
24Antiepileptics
Epilepsy is a common neurological abnor-mality that affects about 0.5-1% of thepopulation. Epilepsy is a chronic disordercharacterised by recurrent seizures oftenaccompanied by episodes of unconsciousnessand/or amnesia. It is a disorder of brainfunction.
Seizure indicates a transient alteration inbehaviour because of disordered firing ofgroups of brain neurons. Such discharges mayspread to other parts of the brain to differentextents. In most of the cases, the cause is notknown. It may be due to various reasonsincluding trauma during birth process, headinjury, childhood fevers, brain tumours,meningitis or drug induced.
Seizures have been classified into partialand generalised seizures.Partial seizures account for about 60% of allepilepsies and begin focally in the cortex, i.e.they involve focal brain regions. It is classifiedas simple partial in which there is noimpairment of consciousness and complexpartial seizures with impairment ofconsciousness. When reticular formation isaffected unconsciousness results.Simple partial seizures There is no impairmentof consciousness. The manifestation dependson the site in the cortex that is activated bythe seizure, e.g. if the motor cortexrepresenting the right thumb is involved,there is recurrent contractions of the right
thumb. If the sensory area representing theleft palm is involved, there is numbness orparaesthesia of the left palm. This type ofseizures lasts for 20-60 seconds.Complex partial seizures are the most commontypes of epilepsy.They are characterised bypurposeless movements like lipsmaking, handwringing or swallowing that lasts for 30 secto 2 minutes. Consciousness is impaired andmay be preceded by an aura.Partial with secondarily generalised seizuresSimple or complex partial seizure may evolveinto a generalised seizure.Generalised seizures Account for 40% of allepilepsies and is usually of genetic aetiology.Generalised seizures affect the whole brain.They may be:Absence seizures (petit mal) In this, there is asudden onset of impaired consciousnessassociated with staring. The person stops allon-going activities and the episode lasts fora brief period usually less than 30 sec.Myoclonic seizures involve a sudden, brief,shock like contraction of muscles. It may belimited to a part of the body or may affectthe whole body.Atonic seizures (Drop attacks) are characterisedby sudden loss of postural tone and the headmay drop for a few seconds or the personmay drop to the ground for no obviousreasons.Tonic-clonic seizures (Grand mal epilepsy) ischaracterised by sudden loss of consciousness
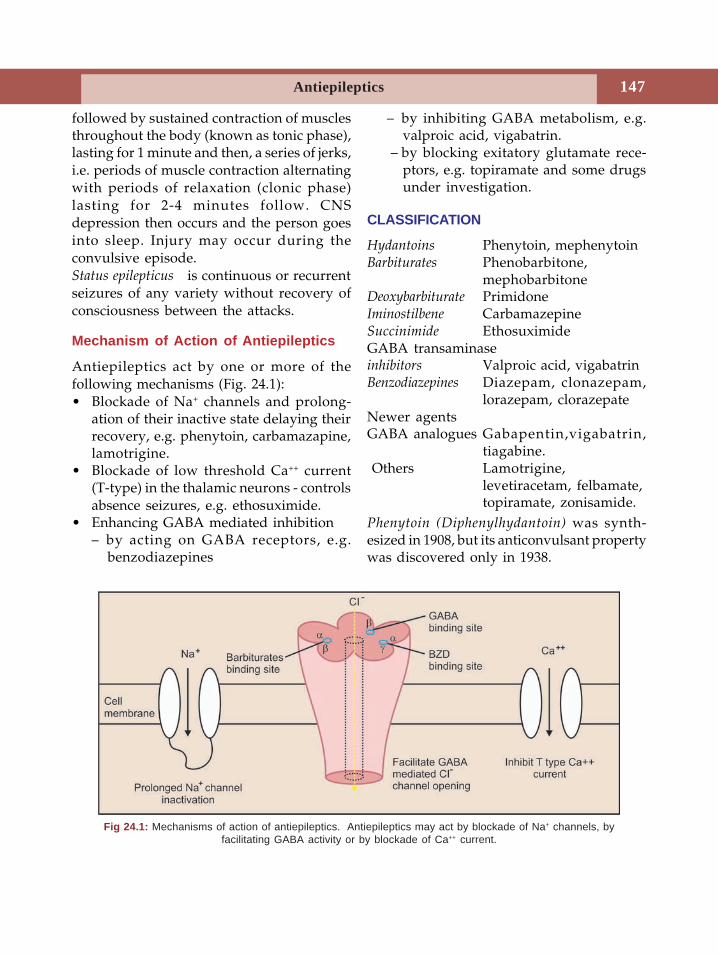
147Antiepileptics
followed by sustained contraction of musclesthroughout the body (known as tonic phase),lasting for 1 minute and then, a series of jerks,i.e. periods of muscle contraction alternatingwith periods of relaxation (clonic phase)lasting for 2-4 minutes follow. CNSdepression then occurs and the person goesinto sleep. Injury may occur during theconvulsive episode.Status epilepticus is continuous or recurrentseizures of any variety without recovery ofconsciousness between the attacks.
Mechanism of Action of Antiepileptics
Antiepileptics act by one or more of thefollowing mechanisms (Fig. 24.1):• Blockade of Na+ channels and prolong-
ation of their inactive state delaying theirrecovery, e.g. phenytoin, carbamazapine,lamotrigine.
• Blockade of low threshold Ca++ current(T-type) in the thalamic neurons - controlsabsence seizures, e.g. ethosuximide.
• Enhancing GABA mediated inhibition– by acting on GABA receptors, e.g.
benzodiazepines
– by inhibiting GABA metabolism, e.g.valproic acid, vigabatrin.
– by blocking exitatory glutamate rece-ptors, e.g. topiramate and some drugsunder investigation.
CLASSIFICATION
Hydantoins Phenytoin, mephenytoinBarbiturates Phenobarbitone,
mephobarbitoneDeoxybarbiturate PrimidoneIminostilbene CarbamazepineSuccinimide EthosuximideGABA transaminaseinhibitors Valproic acid, vigabatrinBenzodiazepines Diazepam, clonazepam,
lorazepam, clorazepateNewer agentsGABA analogues Gabapentin,vigabatrin,
tiagabine. Others Lamotrigine,
levetiracetam, felbamate,topiramate, zonisamide.
Phenytoin (Diphenylhydantoin) was synth-esized in 1908, but its anticonvulsant propertywas discovered only in 1938.
Fig 24.1: Mechanisms of action of antiepileptics. Antiepileptics may act by blockade of Na+ channels, byfacilitating GABA activity or by blockade of Ca++ current.
Textbook of Pharmacology for Dental and Allied Health Sciences148
Pharmacological Actions
CNS Phenytoin has good antiseizure activityand is one of the most effective drugs againstgeneralised tonic-clonic seizures and partialseizures. It brings about its effects withoutcausing general depression of the CNS.
Mechanism of Action
Phenytoin causes blockade of the voltagedependent sodium channels and stabilizes theneuronal membrane. It inhibits the generationof repetitive action potentials.
Voltage dependent Na+channels enter aninactive stage after each action potential.Phenytoin blocks the Na+ channels which arein an inactivated state and delay the recoveryof these channels from inactivation. Itdecreases the number of channels which areavailable for the generation of actionpotentials and it inhibits the membraneexcitability of these voltage-dependent Na+
channels. Phenytoin preferentially blockshigh frequency firing (neurons in normal statehave low frequency firing while in seizures,high-frequency firing occurs).
Pharmacokinetics
Phenytoin is poorly water-soluble–henceabsorption is slow. Phenytoin is 90% boundto plasma proteins. Valproic acid competeswith phenytoin for plasma protein bindingsites and may result in phenytoin toxicity. Itis metabolised in the liver initially by firstorder and later by zero order kinetics as thedose increases. Therefore monitoring ofplasma concentration is useful. Phenytoin isan enzyme inducer. Dose table 24.1.
Adverse Effects
Adverse effects depend on the dose,duration and route of administration.1. Nausea, vomiting, epigastric pain,
anorexia.
2. Nystagmus, diplopia, ataxia are common.3. Gingival hyperplasia–Long-term adminis-
tration of phenytoin can result in gingivalhyperplasia particularly in children withpoor oral hygiene. Maintaining good oralhygiene can prevent this. However, it isgenerally reversible though it takes 1-2years after the discontinuation ofphenytoin.
4. Peripheral neuropathy.5. Endocrine
i. Hirsutism, acne, coarsening of facialfeatures.
ii. Hyperglycaemia – as phenytoininhibits insulin release.
iii. ↓ release of ADH.iv. Osteomalacia, hypocalcaemia due to
altered metabolism of vitamin D andinhibition of intestinal absorption ofCa++. Phenytoin also reduces targettissue sensitivity to vitamin D.
6. Hypersensitivity–rashes, hepatic necrosis,lym-phadenopathy and neutropenia.Idiosyncratic reactions including hepaticnecrosis and systemic lupus erythe-matosis, have been reported.
7. Megaloblastic anaemia–because phenytoindecreases absorption and increasesexcretion of folates.
8. Teratogenicity–when taken by thepregnant lady, phenytoin produces foetalhydantoin syndrome characterised byhypoplastic phalanges, cleft palate, harelipand microcephaly in the offspring.
Toxic doses–cerebellar and vestibular effectsare prominent; drowsiness, delirium,confusion, hallucinations, altered behaviourand coma follow.
Uses
1. Generalised tonic-clonic seizures andpartial seizures (not useful in absenceseizures).
149Antiepileptics
2. Status epilepticus–phenytoin is used byslow IV injection.
3. Trigeminal neuralgia–as an alternative tocarbamazepine.
4. Cardiac arrhythmias–Phenytoin is usefulin digitalis induced arrhythmias (see page101).
Drug Interactions
• Phenytoin is an enzyme inducer. Givenwith phenobarbitone, both increase eachother's metabolism. Also phenobarbitonecompetitively inhibits phenytoinmetabolism.
• Carbamazepine and phenytoin enhanceeach other’s metabolism.
• Valproate displaces protein boundphenytoin and may result in phenytointoxicity.
• Cimetidine and chloramphenicol inhibitthe metabolism of phenytoin resulting intoxicity.
• Antacids ↓ absorption of phenytoin.Mephenytoin, ethatoin and phenacemideare congeners of phenytoin. Ethatoin canbe used as an alternative in patientsallergic to phenytoin. Adverse effects ofethatoin are milder. Phenacemide is usedin patients with refractory partial seizureswhen other drugs fail. It is a highly toxicdrug.
PHENOBARBITONE (See Chap 22)
Phenobarbitone was the first effectiveantiepileptic drug to be introduced in 1912.It still remains one of the widely used drugs.Antiepileptic actions Phenobarbitone hasspecific antiepileptic activity and raises theseizure threshold. Primidone which is rarelyused now is metabolised to phenobarbitone.Phenobarbitone is effective in tonic-clonicseizures and is ineffective in absence seizures.Though other barbiturates also have
anticonvulsant effects, the dose requiredproduces significant sedation.Mechanism of action Barbiturates enhance theinhibitory neurotransmission in the CNS byenhancing the activation of GABAA receptorsand thus facilitating the GABA-mediatedopening of chloride ion channels.Pharmacokinetics Oral absorption of pheno-barbitone is slow but complete. About 50%is bound to plasma proteins. It is a microsomalenzyme inducer and can result in many druginteractions.Adverse effects Sedation is the most commonside effect.Tolerance develops to some extentto sedation after prolonged use. Pheno-barbitone can also cause nystagmus, ataxia,megaloblastic anaemia and osteomalacia likephenytoin. Skin rashes and other hypersensi-tivity reactions can occur.Uses Phenobarbitone is still widely usedbecause of its efficacy and low cost. However,carbamazepine and phenytoin are oftenpreferred. Phenobarbitone can be used in:1. Generalised tonic-clonic seizures.2. Partial seizures.
CARBAMAZEPINE
Carbamazepine is a tricyclic compound closelyrelated to imipramine. It is one of the mostcommonly used antiepileptic drugs.
PHENYTOIN
• Blocks voltage dependent Na+ channels.• Preferably blocks high frequency firing that
is seen in seizures.• Blocks Na+ channels in an inactivated state
and delays their recovery.• Main adverse effects include vestibular
effects, G.I. disturbances; long term useresults in gum hyperplasia, hirsutism andmegaloblastc anaemia.
• It is teratogenic.• Used in partial and generalised tonic-
clonic seizures.
Textbook of Pharmacology for Dental and Allied Health Sciences150
Antiseizure activity Carbamazepine has goodanti-seizure activity. It’s mechanism of actionand antiepileptic actions are similar tophenytoin, i.e. it blocks sodium channels.
Carbamazepine is also useful in thetreatment of trigeminal neuralgia (severe painalong the distribution of the trigeminalnerve) and glossopharyngeal neuralgia. It isalso found to be beneficial in mood disorders.Carbamazepine has mild antidiuretic effects.Pharmacokinetics Absorption is slow anderratic; has a t½ of 10-30 hours. Carbamaze-pine is a powerful microsomal enzymeinducer. Therefore, after repeated adminis-tration, its t½ reduces to 15 hours due toautoinduction.Adverse effects Drowsiness, vertigo, ataxia,diplopia, blurring of vision, nausea, vomitingand dizziness are common. Driving istherefore dangerous for patients oncarbamazepine. It also causes water retentiondue to antidiuretic effects. Hypersensitivityreactions–like skin rashes may occur.Haematological toxicity includes leukopenia,thrombocytopenia and rarely agranulocytosisand aplastic anaemia. It is a teratogen. Itst½ reduces to 15 hrs due to autoinduction.
Uses
1. Generalised tonic-clonic seizures (grandmal epilepsy).
2. Simple and complex partial seizures–especially temporal lobe epilepsy.
3. Trigeminal neuralgia and glosso-pharyngeal neuralgia–carbamazepine isthe drug of choice for these neuralgias andhas to be given for several months.
4. Carbamazepine is also found to be usefulin chronic neuropathic pain and in tabeticpain.
5. Bipolar mood disorder–carbamazepine isused as an alternative to lithium as a moodstabilizer (see Page 200).
Oxcarbazepine– is similar to carbamazepine inaction and uses. It has the following
advantages over carbamazepine - fewerhypersensitivity reactions, milder inductionof microsomal enzymes - hence fewer druginteractions. It has been tried as an alternativeto carbamazepine in partial seizures.
ETHOSUXIMIDE
Ethosuximide is a succinimide. It raises theseizure threshold.Mechanism of action Ethosuximide reduces thelow threshold calcium currents (T-currents)in the thalamic neurons. These T currents arethought to be responsible for absenceseizures.Pharmacokinetics Absorption is complete onadministration of oral dosage forms. It ismetabolised in the liver.Adverse effects The most common adverseeffects are nausea, vomiting, epigastric pain,gastric irritation and anorexia. These can beavoided by starting with a low dose andgradually increasing it. CNS effects likedrowsiness, fatigue, lethargy, euphoria,dizziness, headache and hiccough are dose-related effects. Hypersensitivity reactions likerashes, urticaria, leukopenia, thrombo-cytopenia or pancytopenia have beenreported.Uses Ethosuximide is the drug of choice forabsence seizures.
VALPROIC ACID
Valproic acid (salt→sodium valproate) is avery effective antiepileptic drug useful inmany types of epilepsies including absenceseizures, partial and generalised tonic-clonicseizures.
Divalproex sodium is a combination ofvalproic acid and sodium valproate. Thecombination is said to have a betterbioavailability and is better tolerated.Mechanism of action Valproic acid acts bymultiple mechanisms.
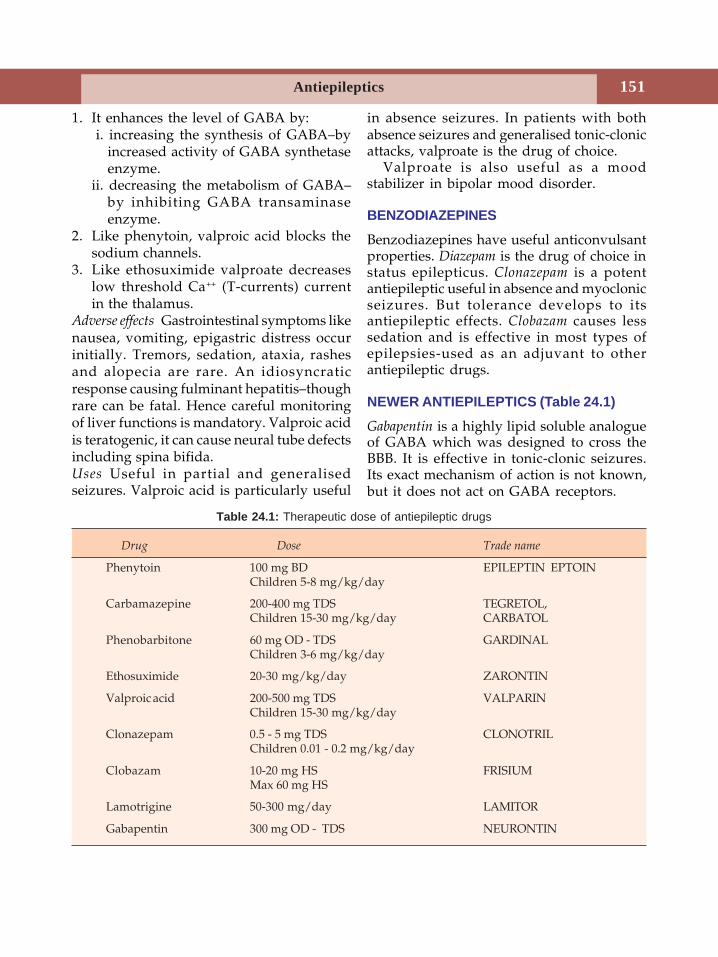
151Antiepileptics
1. It enhances the level of GABA by: i. increasing the synthesis of GABA–by
increased activity of GABA synthetaseenzyme.
ii. decreasing the metabolism of GABA–by inhibiting GABA transaminaseenzyme.
2. Like phenytoin, valproic acid blocks thesodium channels.
3. Like ethosuximide valproate decreaseslow threshold Ca++ (T-currents) currentin the thalamus.
Adverse effects Gastrointestinal symptoms likenausea, vomiting, epigastric distress occurinitially. Tremors, sedation, ataxia, rashesand alopecia are rare. An idiosyncraticresponse causing fulminant hepatitis–thoughrare can be fatal. Hence careful monitoringof liver functions is mandatory. Valproic acidis teratogenic, it can cause neural tube defectsincluding spina bifida.Uses Useful in partial and generalisedseizures. Valproic acid is particularly useful
in absence seizures. In patients with bothabsence seizures and generalised tonic-clonicattacks, valproate is the drug of choice.
Valproate is also useful as a moodstabilizer in bipolar mood disorder.
BENZODIAZEPINES
Benzodiazepines have useful anticonvulsantproperties. Diazepam is the drug of choice instatus epilepticus. Clonazepam is a potentantiepileptic useful in absence and myoclonicseizures. But tolerance develops to itsantiepileptic effects. Clobazam causes lesssedation and is effective in most types ofepilepsies-used as an adjuvant to otherantiepileptic drugs.
NEWER ANTIEPILEPTICS (Table 24.1)
Gabapentin is a highly lipid soluble analogueof GABA which was designed to cross theBBB. It is effective in tonic-clonic seizures.Its exact mechanism of action is not known,but it does not act on GABA receptors.
Table 24.1: Therapeutic dose of antiepileptic drugs
Drug Dose Trade name
Phenytoin 100 mg BD EPILEPTIN EPTOINChildren 5-8 mg/kg/day
Carbamazepine 200-400 mg TDS TEGRETOL,Children 15-30 mg/kg/day CARBATOL
Phenobarbitone 60 mg OD - TDS GARDINALChildren 3-6 mg/kg/day
Ethosuximide 20-30 mg/kg/day ZARONTIN
Valproic acid 200-500 mg TDS VALPARINChildren 15-30 mg/kg/day
Clonazepam 0.5 - 5 mg TDS CLONOTRILChildren 0.01 - 0.2 mg/kg/day
Clobazam 10-20 mg HS FRISIUMMax 60 mg HS
Lamotrigine 50-300 mg/day LAMITOR
Gabapentin 300 mg OD - TDS NEURONTIN
Textbook of Pharmacology for Dental and Allied Health Sciences152
Advantages Absorption of gabapentindepends on a carrier protein and does notincrease with increase in dose - hence it issafe. It is well tolerated. It does not influencethe plasma concentrations of otherantiepileptics.Adverse effects include ataxia, fatigue,drowsiness and dizziness. Tolerancedevelops to these effects in 1-2 weeks.Gabapentin is used in combination with otherantiepileptic drugs, as an add-on drug inpartial seizures. It is also used in migraine,neuropathic pain and in bipolar mooddisorder.Progabalin is a prodrug, which is more potentthan gabapentin.Lamotrigine has a broad spectrum ofantiepileptic activity. It inhibits the sodiumchannels and also inhibits the release of theexcitatory amino acids like glutamate. It iscompletely absorbed from the gut.Lamotrigine may cause skin rashes, nausea,ataxia and dizziness. It is used either aloneor with other drugs in partial andgeneralized seizures.Vigabatrin is a GABA analogue which acts byirreversibly inhibiting the enzyme GABAtransaminase thereby raising brain GABAlevels. It can cause depression in somepatients. Vigabatrin is useful in patients notresponding to other antiepileptics.
Levetiracetam is effective against partial andsecondarily generalized seizures. Itsmechanism of action is not known. It is notan enzyme inducer-no related druginteractions. Levetiracetam can be used as anadd-on drug in refractory partial seizures.Tiagabine a GABA analogue, inhibits thereuptake of GABA into neurons and therebyenhances extracellular GABA levels. It maycause drowsiness and dizziness. Tiagabinecan be used as an add-on drug for refractorypartial seizures.Topiramate a monosaccharide, acts by multiplemechanisms. It blocks the sodium channels,enhances GABAA receptor currents, blocksAMPA receptors (glutamate receptor). It iseffective in partial and generalized seizures.Topiramate can be used as add-on therapyin refractory epilepsy.Felbamate an analogue of meprobamate isfound to have good antiepileptic action. Itblocks the NMDA receptors in addition toweak sodium channel blocking effect. Butfelbamate can sometimes cause seriousadverse effects like aplastic anaemia andhepatitis because of which it is employedonly in refractory epilepsy.Zonisamide a sulfonamide derivative acts byinhibiting T type Ca++ currents and also byblocking Na+ channels. It is well toleratedand is indicated in refractory partialseizures.
TREATMENT OF EPILEPSIES
An attempt should be made to detect thecause. When drugs are found to benecessary, the goal of therapy is to keepthe patient free of seizures (Table 24.2)without interfering with normal dailyactivity. Treatment should be started witha single drug at a low dose; dosage isincreased gradually, preferably bymonitoring the drug levels in plasma.
Newer antiepileptics:• Gabapentin, vigabatrin, tiagabine,
lamotrigine, levetiracetam, topira-mate, felbamate, zonisamide.
• All are generally well tolerated exceptthat felbamate can rarely cause aplasticanaemia and hepatitis.
• Presently they are recommended asadd-on drugs in refractory partialseizures.
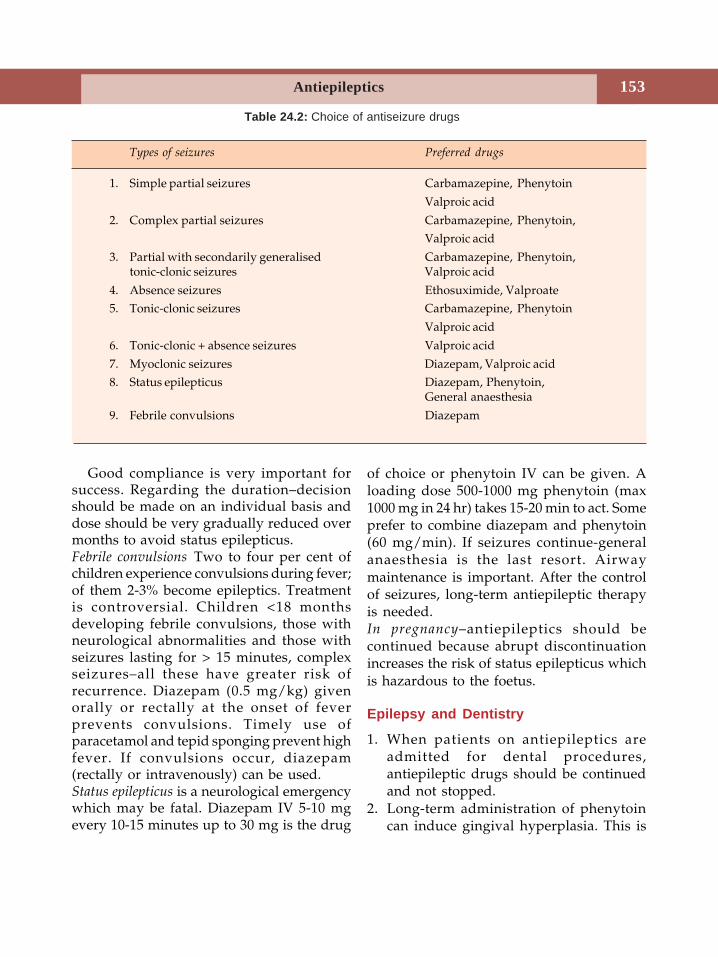
153Antiepileptics
Good compliance is very important forsuccess. Regarding the duration–decisionshould be made on an individual basis anddose should be very gradually reduced overmonths to avoid status epilepticus.Febrile convulsions Two to four per cent ofchildren experience convulsions during fever;of them 2-3% become epileptics. Treatmentis controversial. Children <18 monthsdeveloping febrile convulsions, those withneurological abnormalities and those withseizures lasting for > 15 minutes, complexseizures–all these have greater risk ofrecurrence. Diazepam (0.5 mg/kg) givenorally or rectally at the onset of feverprevents convulsions. Timely use ofparacetamol and tepid sponging prevent highfever. If convulsions occur, diazepam(rectally or intravenously) can be used.Status epilepticus is a neurological emergencywhich may be fatal. Diazepam IV 5-10 mgevery 10-15 minutes up to 30 mg is the drug
Types of seizures Preferred drugs
1. Simple partial seizures Carbamazepine, Phenytoin
Valproic acid
2. Complex partial seizures Carbamazepine, Phenytoin,Valproic acid
3. Partial with secondarily generalised Carbamazepine, Phenytoin,tonic-clonic seizures Valproic acid
4. Absence seizures Ethosuximide, Valproate5. Tonic-clonic seizures Carbamazepine, Phenytoin
Valproic acid
6. Tonic-clonic + absence seizures Valproic acid
7. Myoclonic seizures Diazepam, Valproic acid8. Status epilepticus Diazepam, Phenytoin,
General anaesthesia
9. Febrile convulsions Diazepam
Table 24.2: Choice of antiseizure drugs
of choice or phenytoin IV can be given. Aloading dose 500-1000 mg phenytoin (max1000 mg in 24 hr) takes 15-20 min to act. Someprefer to combine diazepam and phenytoin(60 mg/min). If seizures continue-generalanaesthesia is the last resort. Airwaymaintenance is important. After the controlof seizures, long-term antiepileptic therapyis needed.In pregnancy–antiepileptics should becontinued because abrupt discontinuationincreases the risk of status epilepticus whichis hazardous to the foetus.
Epilepsy and Dentistry
1. When patients on antiepileptics areadmitted for dental procedures,antiepileptic drugs should be continuedand not stopped.
2. Long-term administration of phenytoincan induce gingival hyperplasia. This is

Textbook of Pharmacology for Dental and Allied Health Sciences154
more common in children with poor oralhygiene. It is thought to be an exaggerateddrug induced response of gingival tissuesto the oral plaque.
3. Though uncommon, some patients mighthave convulsions while undergoing adental procedure (See page 400). Theprocedure should be immediately stopped.All instruments and dentures should beremoved from the oral cavity. Gentlepassive restraints should be used to preventphysical injury. A padded tonguedepressor should be placed in the mouth
to protect the tongue from getting bitten.The head should be turned to a side sothat the tongue does not obstruct theairway. If the convulsions continue,diazepam 10 mg may be given intravenouslyover 1-2 minutes. Physicians' help shouldbe sought at the earliest possible.
4. Long-term administration of someantiepileptics like sodium valproate canincrease the bleeding tendency. Appro-priate precautions should be taken tocontrol bleeding during dental pro-cedures.
25 Drugs Used inParkinsonism
Parkinsonism is a chronic, progressive, motordisorder characterised by rigidity, tremorsand bradykinesia. Other symptoms includeexcessive salivation, abnormalities of postureand gait, seborrhoea and mood changes. Itwas described by James Parkinson in 1817and is therefore named after him.
The incidence is about 1 per cent ofpopulation above 65 years of age. It is usuallyidiopathic in origin but can also be druginduced. In idiopathic parkinsonism, there isdegeneration of nigrostriatal neurons in thebasal ganglia resulting in dopaminedeficiency. The balance between inhibitorydopaminergic neurons and excitatorycholinergic neurons is disturbed.
Antiparkinsonian drugs can only help toalleviate the symptoms and improve thequality of life. The two strategies in thetreatment are-(i) to enhance dopamine activity(ii) to depress cholinergic overactivity.
Often combination of drugs are used toinfluence both functions.
CLASSIFICATION
Drugs used in parkinsonism can be classifiedas -1. Drugs that increase dopamine levels
i. DA precursorLevodopa
ii. Drugs that release dopamineAmantadine
iii. Dopaminergic agonistsBromocryptineLisurideRopinirolePramipexole
iv. Inhibit dopamine metabolism• MAO inhibitors
Selegiline• COMT inhibitors
TolcaponeEntacapone
2. Drugs influencing cholinergic systemi. Central anticholinergics
BenztropineBenzhexolBiperidineTrihexyphenidyl
ii. AntihistaminesDiphenhydramineOrphenadrinePromethazine
DOPAMINE PRECURSOR
Levodopa
Though parkinsonism is due to dopaminedeficiency, dopamine is of no therapeuticvalue because it does not cross the blood-brain barrier. Levodopa is a prodrug whichis converted to dopamine in the body. Itcrosses the BBB and is taken up by thesurviving nigrostriatal neurons.
Textbook of Pharmacology for Dental and Allied Health Sciences156
Dopadecarboxylase
Levodopa _________________________→ DopamineAntiparkinsonian effect On administration oflevodopa, there is an overall improvementin the patient as all the symptoms subside.Other actions Large amounts of levodopa areconverted to dopamine in the peripherywhich brings about other actions.• CTZ—Dopamine stimulates the CTZ to
induce vomiting.• CVS— It causes postural hypotension,
tachycardia and arrhythmias. Dopamineis a catecholamine.
• Endocrine—Dopamine suppresses theprolactin secretion.
Pharmacokinetics
Levodopa is rapidly absorbed from the smallintestine. Presence of food delays absorption.Some amino acids in the food compete withlevodopa for absorption and transport to thebrain. It undergoes first pass metabolism inthe gut and the liver. Its t½ is 1-2 hours.
Adverse Reactions
As 95% of levodopa is converted to dopaminein the periphery, several adverse effects areexpected. Nausea, vomiting, anorexia,postural hypotension, palpitation andoccasionally arrhythmias can occur. Tolerancedevelops to these effects after some time.These peripheral effects can be prevented byconcurrent administration of domperidonewhich is a peripheral dopamine antagonist.Behavioural effects like anxiety, depression,hallucinations and sometimes psychosis canoccur.Abnormal involuntary movements like facial tics,grimacing, choreoathetoid movements of thelimbs may develop after a few months of useand require reduction in the dose of levodopa.
Fluctuation in response to levodopa can occurafter 2-5 years of use—known as ‘on-off’phenomenon—where the patient swingsalternately from periods of good responseto severe disabling disease.Uses Levodopa is the most effective drug inidiopathic parkinsonism but is not useful indrug induced parkinsonism.Drug interactions
1. Pyridoxine enhances peripheral decarbo-xylation of levodopa and thus reduces itsavailability to the CNS.
2. Phenothiazines and metoclopramide areDA antagonists. They reverse the effectsof levodopa.
Carbidopa and Benserazide
Carbidopa and benserazide are peripheraldopa decarboxylase inhibitors. Whencarbidopa or benserazide are given withlevodopa, they prevent the formation ofdopamine in the periphery. They do not crossthe BBB and hence allow levodopa to reachthe CNS. The combination is synergistic andtherefore levodopa is always given withcarbidopa/benserazide.Advantages of the combination1. Dose of L-dopa can be reduced by 75%.2. Response to L-dopa appears earlier.3. Side effects like vomiting and tachycardia
are largely reduced.4. Pyridoxine does not interfere with
treatment.
DRUGS THAT RELEASE DOPAMINE
Amantadine is an antiviral drug. It enhancesthe release of DA in the brain and diminishesthe re-uptake of DA. The response starts earlyand its adverse effects are minor. Large dosesproduce insomnia, dizziness, vomiting,postural hypotension, hallucinations andankle oedema.

Drugs Used in Parkinsonism 157
Amantadine is used in mild cases ofparkinsonism. It can also be used along withlevodopa as an adjunct.
DOPAMINE RECEPTOR AGONISTS
Bromocriptine and pergolide are ergotderivatives having dopamine agonisticactivity at D2 receptors. Bromocriptine is alsoa partial agonist while pergolide is an agonistat D1 receptors. The newer agents ropiniroleand pramipexole are selective D2 agonists,are better tolerated, quickly attain therapeuticlevels and adverse effects are milder exceptthat they may cause some sleep disorders.
Dopamine agonists are all longer actingbecause of which they are useful in thetreatment of ‘on-off’ phenomenon.
Adverse effects include nausea, vomiting,hallucinations and skin eruptions. Ergotderivatives can cause postural hypotensionor hypertension initially and first dosephenomenon–sudden cardiovascular collapse.DA agonists are used:1. in the treatment of ‘on-off’ phenomenon2. as alternatives in the initial treatment of
parkinsonism (particularly newer agents).Lisuride is similar to bromocriptine.
DRUGS THAT INHIBIT DA METABOLISM
MAO Inhibitor
Selegiline (Deprenyl) is a selective MAO-Binhibitor. MAO-B is present in DA containingregions of the CNS. Selegiline prolongs theaction of levodopa by preventing itsdegradation. Selegiline may delay theprogression of parkinsonism.Adverse effects include nausea, posturalhypotension, confusion and hallucinations.Uses Mild cases of parkinsonism are startedon selegiline. It is also used as an adjunct tolevodopa.
COMT Inhibitors
Tolcapone and entacapone inhibit the peripheralmetabolism of levodopa thereby increasingits bioavailability. Tolcapone crosses the BBBand enhances the availability of levodopain the brain.
Adverse effects are nausea, orthostatichypotension, confusion and hallucinations.Tolcapone can also cause hepatotoxicity.
COMT inhibitors are used as add-ondrugs in parkinsonism.
ANTICHOLINERGICS
The cholinergic overactivity is overcome byanticholinergics. Tremors, seborrhoea andsialorrhoea are reduced more than rigidity.Atropine derivatives like benzhexol,benztropine, trihexyphenidyl are used.Antihistamines owe their beneficial effectsin parkinsonism to their anticholinergicproperties. Atropine-like side effects suchas dry mouth, constipation, urinaryretention and blurred vision may beencountered.Uses Anticholinergics are used as (i) adjunctto levodopa, (ii) drugs of choice in drug-induced parkinsonism.Drug induced parkinsonism Drugs likereserpine, metoclopramide and pheno-thiazines can induce parkinsonism. Reserpinedepletes catecholamine stores, whilemetoclopramide and phenothiazines aredopamine antagonists.Treatment Withdrawal of the drug usuallyreverses the symptoms. When drugs areneeded, one of the anticholinergics areeffective. Levodopa or other dopamineagonists are not effective because DAreceptors are blocked by drugs likemetoclopramide and phenothiazines.
Textbook of Pharmacology for Dental and Allied Health Sciences158
26Opioid Analgesics
Pain or algesia is an unpleasant subjectivesensation. It cannot be easily defined. Pain isa warning signal and indicates that there isan impairment of structural and functionalintegrity of the body. It is the most importantsymptom that brings the patient to the doctorand demands immediate relief. Prompt reliefof pain instills enormous confidence in thepatient regarding the doctor's treatingability.
Pain arising from the skin andintegumental structures, muscles, bones andjoints is known as somatic pain. It is usuallycaused by inflammation and is well-definedor sharp pain.
Pain arising from the viscera is vague, dull-aching type, difficult to pinpoint to a site andis known as visceral pain. It may beaccompanied by autonomic responses likesweating, nausea and hypotension. It may bedue to spasm, ischaemia or inflammation.
When pain is referred to a cutaneous areawhich receives nerve supply from the samespinal segment as that of the affected viscera,it is known as referred pain, e.g. cardiac painreferred to the left arm.
Pain consists of 2 components - the original‘sensation’ and the ‘reaction’ to it. The originalsensation is carried by the afferent nervefibres and is the same in all. The reactioncomponent differs widely from one person toanother. Perception of pain is increased in
presence of anxiety. A person who is alreadyin stress can poorly tolerate pain.
Pain may be acute or chronic. Acute painmay result from wounds, irritants, burns orfrom ischaemia. The cause is usually welldefined. In chronic pain the origin may notbe well defined. Example: Pain due toarthritis, cancers and neuropathic pain.
Analgesic
Analgesic is a drug which relieves painwithout loss of consciousness. Analgesicsonly afford symptomatic relief from painwithout affecting the cause.Analgesics are of 2 classes.
• Opioid or morphine type of analgesics• Non-opioid or aspirin type of analgesics.
OPIOID ANALGESICS
Opioid analgesics are one of the oldestremedies for relief of pain.
Opium is the dark brown gummy exudateobtained from the poppy capsule (Papaversomniferum). On incising the unripe seedcapsule, a milky juice emerges which turnsbrown on drying and this is crude opium.The word opium is derived from Greek inwhich ‘opos’ means juice. Opium has been inuse since 4000 BC. It was used both formedicinal and recreational purposes. By 18thcentury, opium smoking had become quite
159Opioid Analgesics
popular in Europe. It was Serturner whoisolated a pure opium alkaloid in 1806. Henamed it Morphine after Morpheus, the GreekGod of dreams. As the research progressed,opium was found to contain 20 alkaloids. Byaround 19th century, the pure opiumalkaloids were available for therapeutic use- but because they were equally abused,efforts were made to isolate their analgesicproperty, i.e. to obtain an opioid that is onlyan analgesic and has no euphoric effects. Inthe process, various agonists, antagonists andpartial agonists were synthesized. ‘Opioid’ isthe term used for drugs with morphine-likeactions. They were earlier called narcoticanalgesics.
CLASSIFICATION
Based on receptor occupation1. Agonists
Natural opium alkaloidsMorphine, codeine
Synthetic opioidsPethidine, methadone
2. AntagonistsNaloxone, naltrexone
3. Mixed agonist-antagonistsPentazocine, nalbuphine,butorphanol, buprenorphine, nalorphine
Chemically the opium alkaloids can begrouped into:1. The Phenanthrene group
Morphine, codeine, thebaine2. The Benzylisoquinoline group
Papaverine, noscapine, narcine.
Opioids can also be classified depending ontheir source as1. Natural opium alkaloids
Morphine, codeine, noscapine2. Semisynthetic derivatives
Heroin, oxymorphone, pholcodeine3. Synthetic opioids
Pethidine, fentanyl, diphenoxylate,loperamide, dextropropoxyphene,methadone, tramadol, ethoheptazine.
Morphine
Morphine is the most important alkaloid ofopium. Many new opioids with actions similarto morphine have been synthesized. But noneof them are superior to morphine as ananalgesic. Morphine is discussed as theprototype of the group.
Mechanism of Action
Morphine and other opioids produce theireffects by acting on specific opioid receptors.(Fig. 26.1) These receptors are abundant inthe CNS and other tissues. The opioidreceptors are mu (μ), kappa (k) and delta (δ). Itis found that there are 3 families ofendogenous opioid peptides released in thebody is response to pain viz the enkephalins,the endorphins and the dynorphins. Thisindicates that we have a natural system inthe body that releases various opioidpeptides in response to pain. These opioidpeptides act on opioid receptors and relievepain. Most pharmacological effects of opioidsincluding analgesia, sedation, euphoria,respiratory depression, miosis andconstipation are mediated through μreceptors. ‘Endomorphins’ are endogenousligands for μ receptors but other endogenouspeptides also bind to μ receptors. Dynorphinsare endogenous ligands for k receptors whileenkephalins bind δ receptors. Varioussubtypes of these receptors are now known.A fourth type of opioid receptor was recentlyidentified. It is called nociceptin (N) /orphanin FQ receptor.
All opioid receptors are G-protein-coupledreceptors. Stimulation of these receptorsinhibits adenylyl cyclase resulting indecreased intracellular cAMP formation. Theyalso facilitate the opening of K+ channelsleading to hyperpolarisation and inhibit theentry of calcium into the cell. In addition tothis they inhibit the opening of calcium
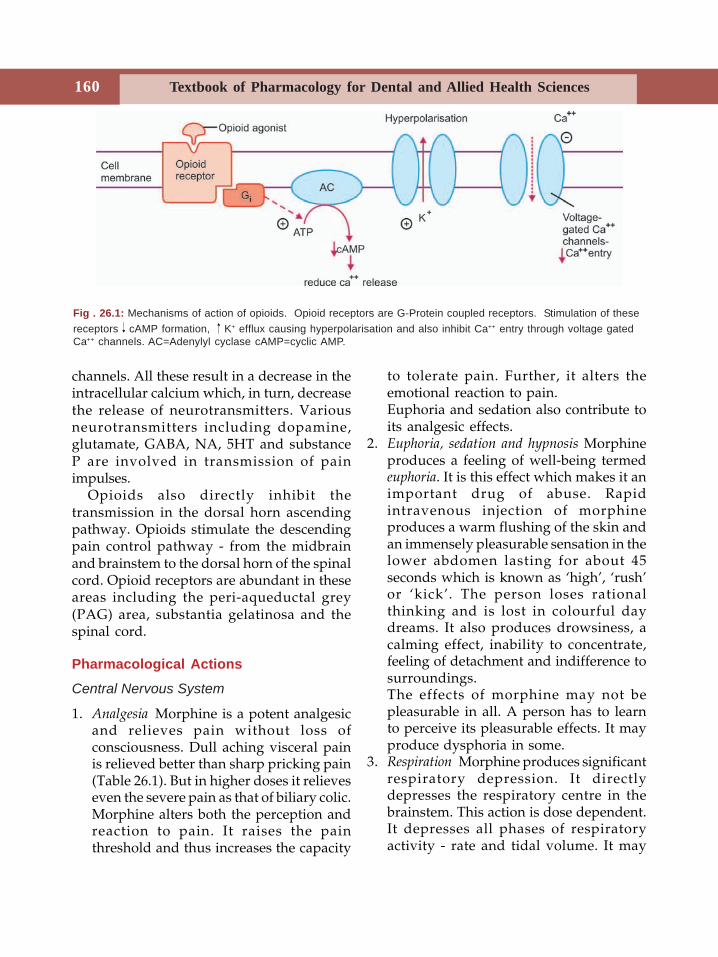
Textbook of Pharmacology for Dental and Allied Health Sciences160
channels. All these result in a decrease in theintracellular calcium which, in turn, decreasethe release of neurotransmitters. Variousneurotransmitters including dopamine,glutamate, GABA, NA, 5HT and substanceP are involved in transmission of painimpulses.
Opioids also directly inhibit thetransmission in the dorsal horn ascendingpathway. Opioids stimulate the descendingpain control pathway - from the midbrainand brainstem to the dorsal horn of the spinalcord. Opioid receptors are abundant in theseareas including the peri-aqueductal grey(PAG) area, substantia gelatinosa and thespinal cord.
Pharmacological Actions
Central Nervous System
1. Analgesia Morphine is a potent analgesicand relieves pain without loss ofconsciousness. Dull aching visceral painis relieved better than sharp pricking pain(Table 26.1). But in higher doses it relieveseven the severe pain as that of biliary colic.Morphine alters both the perception andreaction to pain. It raises the painthreshold and thus increases the capacity
to tolerate pain. Further, it alters theemotional reaction to pain.Euphoria and sedation also contribute toits analgesic effects.
2. Euphoria, sedation and hypnosis Morphineproduces a feeling of well-being termedeuphoria. It is this effect which makes it animportant drug of abuse. Rapidintravenous injection of morphineproduces a warm flushing of the skin andan immensely pleasurable sensation in thelower abdomen lasting for about 45seconds which is known as ‘high’, ‘rush’or ‘kick’. The person loses rationalthinking and is lost in colourful daydreams. It also produces drowsiness, acalming effect, inability to concentrate,feeling of detachment and indifference tosurroundings.The effects of morphine may not bepleasurable in all. A person has to learnto perceive its pleasurable effects. It mayproduce dysphoria in some.
3. Respiration Morphine produces significantrespiratory depression. It directlydepresses the respiratory centre in thebrainstem. This action is dose dependent.It depresses all phases of respiratoryactivity - rate and tidal volume. It may
Fig . 26.1: Mechanisms of action of opioids. Opioid receptors are G-Protein coupled receptors. Stimulation of thesereceptors cAMP formation, K+ efflux causing hyperpolarisation and also inhibit Ca++ entry through voltage gatedCa++ channels. AC=Adenylyl cyclase cAMP=cyclic AMP.
161Opioid Analgesics
also alter the rhythm to produce irregularand periodic breathing. Death frommorphine poisoning is almost always dueto respiratory arrest.Morphine suppresses neurogenic (ori-ginating in RAS), chemical (hyper-capnoeic) and hypoxic drive in the order.The respiratory centre is insensitive toincreased plasma CO2 concentration. Withtoxic doses, breathing is maintained byhypoxic drive.Sedation and indifference to surroundingsadd to the depression.
4. Cough centre It directly depresses thecough centre and thereby suppressescough.
5. Nausea and emesis Morphine directlystimulates the CTZ in the medulla causingnausea and vomiting. In higher doses itdepresses the vomiting centre and hencethere is no vomiting in poisoning.Therefore, emetics should not even betried in morphine poisoning.
6. Pupils Morphine produces miosisresulting in a characteristic pinpoint pupilin high doses. This is due to stimulationof (EW) nucleus of the third cranial nerve.Thus by a central effect it produces miosis.Hence morphine used as eyedrops doesnot produce miosis.
7. Vagus Morphine stimulates vagal centrecausing bradycardia.
8. Heat regulation Opioids shift theequilibrium point of heat-regulatingcentre so that body temperature fallsslightly.
9. Excitatory effect In high doses opioidsproduce convulsions. They may increasethe excitability of the spinal cord.
Cardiovascular System
In therapeutic doses, morphine produceshypotension by:
• direct peripheral vasodilatation• inhibition of baroreceptor reflexes
In higher doses it causes depression of thevasomotor centre and histamine release bothcontributing to a fall in BP. Posturalhypotension and fainting may occur.
GIT
Opioids decrease the motility of the gut.Stomach Gastric motility is decreasedresulting in increased gastric emptying time.Oesophageal reflux may increase. Gastric acidsecretion is reduced. Opioids increase thetone of the antrum and first part of theduodenum which also contribute to delayedemptying by almost 12 hours and this canretard the absorption of orally given drugs.Intestines Morphine diminishes all intestinalsecretions, delays digestion of food in thesmall intestine; resting tone is increased.There can be spasms of the intestine. Thetone of the sphincters is increased leading tospasm. The intestinal motility (propulsive) ismarkedly diminished. The resulting delay inthe passage of the intestinal contents in thelarge intestine, together with reducedsecretions and inattention to the sensorystimuli for defecation reflex - all contributeto produce marked constipation. The effectsof morphine on the gut are by stimulation ofμ and δ receptors in the gut.
Other Smooth Muscles
Biliary tract Morphine causes spasm of thesphincter of Oddi. Intrabiliary pressure risesand may cause biliary colic. Atropine partlyantagonises this while opioid antagonistsrelieve it.Urinary bladder and ureter Tone and amplitudeof contractions of the ureter is increased;tone of external sphincter and volume of thebladder are increased. Opioids inhibit
Textbook of Pharmacology for Dental and Allied Health Sciences162
urinary voiding reflex. All these result inurinary retention especially in the elderlymale with prostatic hypertrophy.Uterus No significant effect. May prolonglabour in high doses.Bronchi Morphine causes release of histaminefrom the mast cells leading to broncho-constriction. This can be dangerous inasthmatics.
Neuroendocrine Effects
Morphine acts in the hypothalamus to inhibitthe release of gonadotrophin-releasinghormone and CRF, thus decreasing bloodlevels of FSH, LH, ACTH and β-endorphins.Tolerance develops after long-term use.These effects are reversible on cessation oftherapy.
Pharmacokinetics
Given orally, absorption of morphine is slowand incomplete. Morphine undergoesextensive first pass metabolism. Bioa-vailability is 20 to 40%. Some opioids are alsogiven as rectal suppositories while highlylipid soluble opioids are available astransdermal preparation. Dose - Table 26.3.
Given subcutaneously, onset of action isin 15-20 min, peak effect - in 1 hr, durationof action is - 3-5 hr. Morphine is metabolisedin the liver by glucuronide conjugation. Theactive metabolite morphine-6-glucuronide, ismore potent than morphine and is excretedthrough the kidneys. Morphine undergoesenterohepatic circulation.
Adverse Effects
Morphine can produce a wide range ofadverse effects like nausea, vomiting,dizziness, mental clouding, respiratorydepression, constipation, dysphoria, urinaryretention and hypotension.
Allergic reactions including skin rashes,pruritus and wheal at the site of injection ofmorphine may be seen. Morphine is ahistamine liberator and this action isresponsible for the allergic effects. Rarelyintravenous injection can cause anaphylaxisdue to the same reason. It is a drug ofdependence.
Tolerance
Repeated administration of morphine resultsin the development of tolerance to some ofits effects including respiratory depression,analgesia, sedation and euphoriant effectsand other CNS depressant effects. Consti-pation and miosis show no tolerance. Thoughlethal dose of morphine is about 250 mg,addicts can tolerate morphine in grams.Patients in pain can also tolerate a higher doseof morphine. Cross-tolerance is seen amongdifferent opioids.
Tolerance is mainly pharmacodynamic,where the cells adapt to the effect of opioids -at the receptor level, though pharmacokineticmechanisms like increased metabolism alsocontribute. An addict needs progressivelyhigher doses to get his ‘kick’ or ‘rush’.
Dependence
Opium has been a drug of addiction for manycenturies. Its ability to produce euphoriamakes it a drug of addiction. Opioids produceboth psychological and physical dependence.Sudden cessation of opioids or adminis-tration of opioid antagonists producesignificant withdrawal symptoms in suchdependent individuals. Manifestations arelacrimation, sweating, yawning, anxiety,apprehension, restlessness, rhinorrhoea andtremors - seen 8-12 hr after the last dose. Theperson craves for the drug. As the syndromeprogresses, fever, insomnia, abdominal colic,
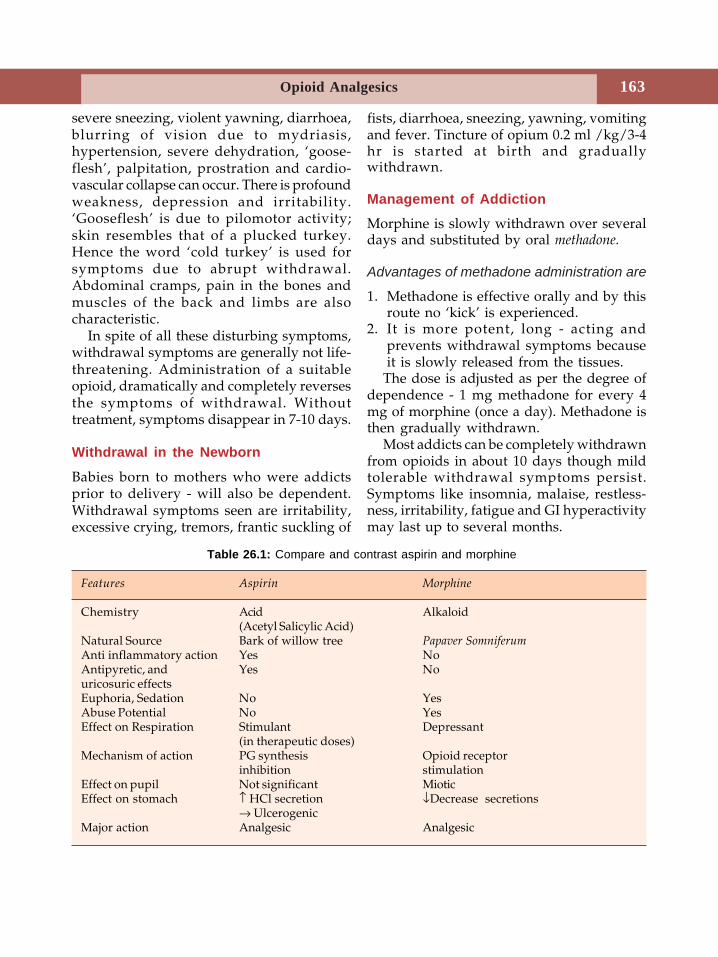
163Opioid Analgesics
severe sneezing, violent yawning, diarrhoea,blurring of vision due to mydriasis,hypertension, severe dehydration, ‘goose-flesh’, palpitation, prostration and cardio-vascular collapse can occur. There is profoundweakness, depression and irritability.‘Gooseflesh’ is due to pilomotor activity;skin resembles that of a plucked turkey.Hence the word ‘cold turkey’ is used forsymptoms due to abrupt withdrawal.Abdominal cramps, pain in the bones andmuscles of the back and limbs are alsocharacteristic.
In spite of all these disturbing symptoms,withdrawal symptoms are generally not life-threatening. Administration of a suitableopioid, dramatically and completely reversesthe symptoms of withdrawal. Withouttreatment, symptoms disappear in 7-10 days.
Withdrawal in the Newborn
Babies born to mothers who were addictsprior to delivery - will also be dependent.Withdrawal symptoms seen are irritability,excessive crying, tremors, frantic suckling of
fists, diarrhoea, sneezing, yawning, vomitingand fever. Tincture of opium 0.2 ml /kg/3-4hr is started at birth and graduallywithdrawn.
Management of Addiction
Morphine is slowly withdrawn over severaldays and substituted by oral methadone.
Advantages of methadone administration are
1. Methadone is effective orally and by thisroute no ‘kick’ is experienced.
2. It is more potent, long - acting andprevents withdrawal symptoms becauseit is slowly released from the tissues.
The dose is adjusted as per the degree ofdependence - 1 mg methadone for every 4mg of morphine (once a day). Methadone isthen gradually withdrawn.
Most addicts can be completely withdrawnfrom opioids in about 10 days though mildtolerable withdrawal symptoms persist.Symptoms like insomnia, malaise, restless-ness, irritability, fatigue and GI hyperactivitymay last up to several months.
Table 26.1: Compare and contrast aspirin and morphine
Features Aspirin Morphine
Chemistry Acid Alkaloid(Acetyl Salicylic Acid)
Natural Source Bark of willow tree Papaver SomniferumAnti inflammatory action Yes NoAntipyretic, and Yes Nouricosuric effectsEuphoria, Sedation No YesAbuse Potential No YesEffect on Respiration Stimulant Depressant
(in therapeutic doses)Mechanism of action PG synthesis Opioid receptor
inhibition stimulationEffect on pupil Not significant MioticEffect on stomach ↑ HCl secretion ↓Decrease secretions
→ UlcerogenicMajor action Analgesic Analgesic
Textbook of Pharmacology for Dental and Allied Health Sciences164
Clonidine a central α2 agonist can suppresssome of the autonomic withdrawal symp-toms like anxiety, nausea, vomiting anddiarrhoea. It is given for 7 - 10 days andwithdrawn over 3 - 4 days. Night timesedation with a hypnotic like diazepam ishelpful.
Acute Morphine Poisoning
Acute morphine poisoning may be accidental,suicidal or homicidal. Lethal dose in non -addicts is about 250 mg but addicts cantolerate grams of morphine. Signs andsymptoms include respiratory depressionwith shallow breathing, pin point pupils,hypotension, shock, cyanosis, flaccidity,stupor, hypothermia, coma and death due torespiratory failure and pulmonary oedema.
Treatment
1. Positive pressure respiration.2. Maintenance of BP.3. Gastric lavage with potassium per-
manganate to remove unabsorbed drug.4. Specific antidote is naloxone - 0.4 - 0.8 mg
IV repeated every 10-15 min.
Precautions and Contraindications
1. Avoid opioids in patients with respiratoryinsufficiency - COPD.
2. An attack of bronchial asthma can beprecipitated by morphine.
3. In extremes of age - more susceptible torespiratory depression.
4. Head injury - morphine is contraindicatedin head injury because:(i) morphine increases CSF pressure by
retaining CO2 and thereby increasesthe intracranial tension.
(ii) causes marked respiratory depression.
(iii) vomiting, miosis and mental cloudingseen with morphine interfere withdiagnosis and assessment of progressin head injuries.
5. In hypovolaemic shock, morphine furtherdecreases the BP.
6. Opioids potentiate CNS depressants.7. Undiagnosed acute abdomen - Morphine
relieves pain and may interfere with thediagnosis. It induces vomiting and itsspasmogenic effect may add to itsdrawbacks. Hence it can be administeredonly after the diagnosis is established - ifnecessary.
Other Opioids
Heroin or diamorphine or diacetyl morphine isconverted to morphine in the body. It hashigher lipid solubility because of whicheuphoric effects are faster and greaterresulting in higher abuse potential. It has astrong smell of vinegar. Though it can beused as an analgesic, it is banned in mostcountries.Levorphanol is similar to morphine but it islonger acting.Codeine is a naturally occurring opiumalkaloid. Codeine depresses the cough centrein subanalgesic doses. It is effective orallyand is well-absorbed.
It is less potent (one-sixth) than morphineas an analgesic (60 mg codeine = 10 mgmorphine).
It produces less respiratory depression andis less constipating. Codeine has less addictionliability and tolerance is uncommon.
Hence codeine is used as an antitussive. Itis well-absorbed when given orally com-pared to morphine. Duration of action is 4-6hours. 10 to 30 mg is the antitussive dose.About 10% of codeine is converted tomorphine. Constipation is the most commonside effect.
165Opioid Analgesics
Uses Codeine is a commonly used antitussive.It is also available in combination withparacetamol for analgesia. It is to be given atbed time (CODOPLUS - Codeine 30 mg +Paracetamol 500 mg).
Papaverine is devoid of opioid and analgesicactivity.Noscapine is a naturally occurring opiumalkaloid. In therapeutic doses, it has nosignificant actions on the CNS except forantitussive effects. Hence it has nodisadvantages of opioids. In large doses itmay cause bronchoconstriction due to therelease of histamine. Dose: 15-30 mg, 3-4times a day. Noscapine is highly effectiveand safe. The only adverse effect is nausea.It is used as a cough suppressant.
Several other centrally acting antitussiveshave been synthesized including,pholcodeine, and dextromethorphan.Pholcodeine though structurally related toopioids, has no other opioid-like actions. Itis as effective as codeine as an antitussive;has a long half-life and therefore can be givenonce a day.Dextromethorphan has no analgesic oraddictive properties. It acts centrally toelevate the threshold for coughing for whichit is as effective as codeine. Toxicity is verylow; extremely high doses cause CNSdepression. Antitussive dose: 10 - 30 mg, 3 -4 times a day.Tramadol is a recently developed syntheticcodeine analog. It is an effective analgesic butits mechanism of action is not clear. It is aweak opioid agonist. In addition it inhibitsthe reuptake of noradrenaline and serotoninin the CNS.
Adverse effects include drowsiness,dryness of mouth, sedation and nausea.Respiratory depression is mild. It is a drugof dependence. It may precipitate seizures.
It should be avoided in patients on MAOinhibitors because tramadol inhibitsserotonin uptake.
Tramadol is used in acute and chronic pain,like postoperative pain and neuralgias.
Pethidine (Meperidine)
Pethidine is a phenylpiperidine derivative ofmorphine. Many of its actions resemble thatof morphine Table 26.2. When compared tomorphine:• pethidine is 1 10 th as potent as morphine
(100 mg pethidine = 10 mg morphine).However, efficacy as an analgesic is equalto morphine
• the onset of action is more rapid andduration of action is shorter
• it produces corneal anaesthesia• it is not a good antitussive• it is less constipating• in some patients, it may cause dysphoria• it also has anticholinergic effects which
can cause dry mouth, and blurring ofvision.
• in toxic doses, pethidine sometimesproduces CNS stimulation with tremors,restlessness and convulsions instead ofsedation. This is because of the toxicmetabolite - norpethidine.
Adverse effects are similar to morphine exceptthat constipation and urinary retention areless common.
Uses
Dose 25-100 mg IM/SC is the analgesic dose.In pain Pethidine is used as an analgesic invisceral pain and also for other indicationsof morphine. Because of its better oralefficacy and less spasmogenic effect,pethidine is preferred to morphine.During labour Given during labour, pethidineproduces less respiratory depression in the
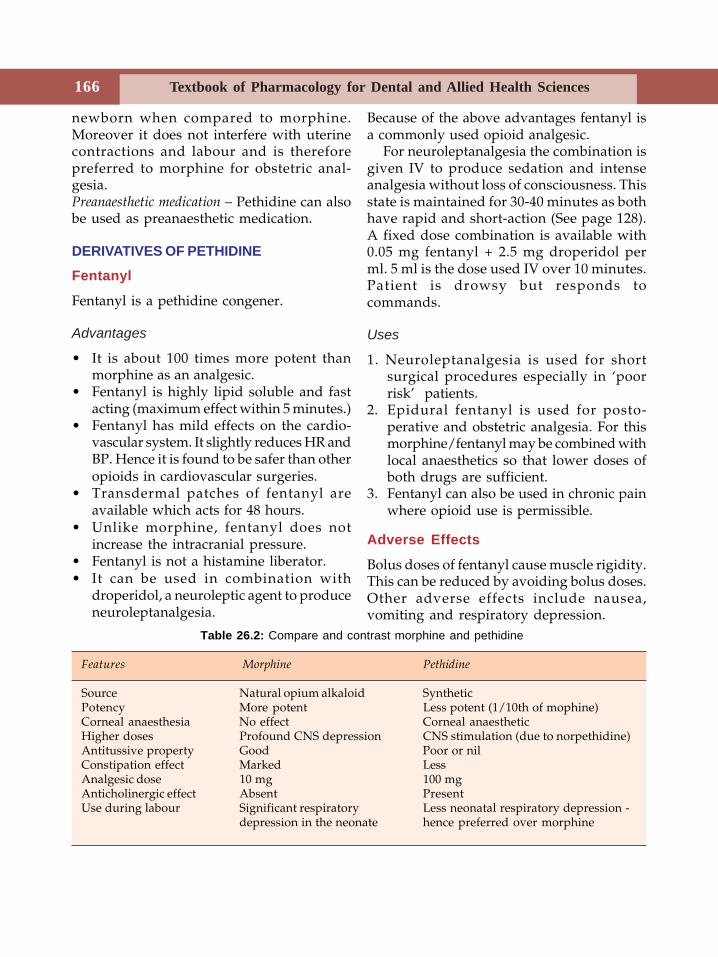
Textbook of Pharmacology for Dental and Allied Health Sciences166
newborn when compared to morphine.Moreover it does not interfere with uterinecontractions and labour and is thereforepreferred to morphine for obstetric anal-gesia.Preanaesthetic medication – Pethidine can alsobe used as preanaesthetic medication.
DERIVATIVES OF PETHIDINE
Fentanyl
Fentanyl is a pethidine congener.
Advantages
• It is about 100 times more potent thanmorphine as an analgesic.
• Fentanyl is highly lipid soluble and fastacting (maximum effect within 5 minutes.)
• Fentanyl has mild effects on the cardio-vascular system. It slightly reduces HR andBP. Hence it is found to be safer than otheropioids in cardiovascular surgeries.
• Transdermal patches of fentanyl areavailable which acts for 48 hours.
• Unlike morphine, fentanyl does notincrease the intracranial pressure.
• Fentanyl is not a histamine liberator.• It can be used in combination with
droperidol, a neuroleptic agent to produceneuroleptanalgesia.
Because of the above advantages fentanyl isa commonly used opioid analgesic.
For neuroleptanalgesia the combination isgiven IV to produce sedation and intenseanalgesia without loss of consciousness. Thisstate is maintained for 30-40 minutes as bothhave rapid and short-action (See page 128).A fixed dose combination is available with0.05 mg fentanyl + 2.5 mg droperidol perml. 5 ml is the dose used IV over 10 minutes.Patient is drowsy but responds tocommands.
Uses
1. Neuroleptanalgesia is used for shortsurgical procedures especially in ‘poorrisk’ patients.
2. Epidural fentanyl is used for posto-perative and obstetric analgesia. For thismorphine/fentanyl may be combined withlocal anaesthetics so that lower doses ofboth drugs are sufficient.
3. Fentanyl can also be used in chronic painwhere opioid use is permissible.
Adverse Effects
Bolus doses of fentanyl cause muscle rigidity.This can be reduced by avoiding bolus doses.Other adverse effects include nausea,vomiting and respiratory depression.
Table 26.2: Compare and contrast morphine and pethidine
Features Morphine Pethidine
Source Natural opium alkaloid SyntheticPotency More potent Less potent (1/10th of mophine)Corneal anaesthesia No effect Corneal anaestheticHigher doses Profound CNS depression CNS stimulation (due to norpethidine)Antitussive property Good Poor or nilConstipation effect Marked LessAnalgesic dose 10 mg 100 mgAnticholinergic effect Absent PresentUse during labour Significant respiratory Less neonatal respiratory depression -
depression in the neonate hence preferred over morphine
167Opioid Analgesics
Congeners of fentanyl are sufentanil, alfentaniland remifentanil. Alfentanil and remifentanilare faster acting (act within one minute) andrecovery is rapid. They are used for shortsurgical procedures.
Methadone
Methadone a synthetic opioid, has actionssimilar to morphine. Its outstanding featuresare:• It is an effective analgesic• It is effective by oral route• It has a long duration of action ( t½ 24 -
36 hours) and therefore effectivelysuppresses withdrawal symptoms inaddicts.
Methadone is about 90% bound to plasmaproteins; it is firmly bound to proteins invarious tissues, including brain. Afterrepeated administration, it graduallyaccumulates in tissues. When administrationis discontinued, the drug is slowly releasedfrom these binding sites. This probablyaccounts for its milder withdrawal symptoms.As euphoric effects are less intense, abusepotential is less. Tolerance develops moreslowly. Even in addicts, withdrawal symp-toms are gradual in onset, less intense, butprolonged.Preparation 10 mg inj, (2 mg/5 ml syrup) Dose- 10 mg oral or IM.
Uses
1. Substitution therapy In opioid dependence,1 mg oral methadone is given for every 4mg morphine.
2. Opioid maintenance: Gradually increasingdoses of methadone is given orally toproduce a high degree of tolerance. Suchsubjects do not experience the pleasurableeffects of IV morphine, i.e. opioids are notpleasurable in them and they give up thehabit.
3. Methadone can also be used as an analgesic.
LAAM (L - alpha - acetyl - methadol) is aderivative of methadone. L- alpha- acetyl-methadol is found to have longer durationof action than methadone so that it can begiven three times a week. It is used to preventwithdrawal symptoms in addicts.
Dextropropoxyphene
Dextropropoxyphene is a congener ofmethadone. It binds to the opioid receptorsand produces effects similar to morphine. Itis less constipating, longer acting and hasgood oral efficacy. But dextropropoxypheneis an irritant when given parenterally. Largedoses cause CNS stimulation. It also has abusepotential.
Uses
Used in mild to moderate pain. It is marketedin combination with aspirin.Dextropropoxyphene 32 mg+aspirin 600 mg.
Ethoheptazine
Ethoheptazine is related to pethidine and hasmild analgesic effects with low addictionpotential. It is used orally are combinationwith NSAIDs for relief of pain.
Uses of Morphine and Its Congeners
Dose Morphine 10 to 20 mg IM/SC; 20 mgtablets of ethylmorphine are now availablefor oral use.1. Analgesic Morphine is one of the most
potent analgesics available. It affordssymptomatic relief of pain without affectingthe underlying disease. It is an excellentanalgesic for severely painful conditionssuch as acute myocardial infarction,fractures, burns, pulmonary embolism,terminal stages of cancer, acute peri-carditis, spontaneous pneumothorax and

Textbook of Pharmacology for Dental and Allied Health Sciences168
postoperative pain. In excruciating pain,morphine can be given IV.In myocardial infarction, morphine relievespain and thereby apprehension. As a resultreflex sympathetic stimulation is reducedand shock is minimized.• Morphine is given with atropine to
relieve renal and biliary colic. Atropinerelieves spasm of the sphincter of oddi.Morphine relieves pain in biliary colicbut may cause spasm of the sphincterof Oddi which in turn raises intra-biliary pressure. Hence atropine isgiven to relieve the spasm of thesphincter of Oddi.
• Since opiate receptors are present inthe spinal cord, epidural morphine canbe used to produce epidural analgesia.Such analgesia is segmental indistribution and there is nointerference with motor function orautonomic changes and no systemicadverse effects. Small doses ofmorphine can produce profoundanalgesia for 12-24 hours.
• Obstetric analgesia Pethidine is preferredto morphine for this condition.
• Opioids can be liberally given tocontrol pain of terminal illness likecancers.
• But opioids should not be freely usedin case of other chronic pain due totheir addiction liability.
Various alternative routes ofadministration are tried for opioids - inorder to reduce their systemic effects andprovide longer duration of analgesiaparticularly for patients with chronic pain.Morphine and other opioids are beingtried as intraspinal infusion, rectal,transmucosal, transdermal administrationand by inhalation. In patient controlledanalgesia (PCA) with opioids, the patientsdecide their own need for the analgesic.By the press of a button, a specific dose
of the opioid is pushed through anintravenous device. Careful monitoring isneeded to avoid over-dosage.
2. As preanaesthetic medication Morphine andpethidine are commonly used aspreanaesthetic medication. They reduceanxiety, provide analgesia, allowsmoother induction and reduce the doseof the anaesthetic required. But they havecertain disadvantages:• Opioids depress respiration• Morphine precipitates bronchospasm
and is dangerous in patients with poorrespiratory reserve
• They cause vasomotor depression• They may induce vomiting• They may interfere with pupillary
response to anaesthesia because theycause miosis.
• Postoperative urinary retention andconstipation may be troublesome.
3. Acute left ventricular failure Morphine isused to alleviate the dyspnoea of LVF andpulmonary oedema in which the responseto IV morphine may be dramatic. Themechanism is not clear. The relief may bedue to:
(i) alteration in the patient’s reaction toimpaired respiratory function.
(ii) reduction in the work of the heartdue to decreased fear and appre-hension. Reduced anxiety decreasessympathetic stimulation which inturn decreases cardiac work.
(iii) cardiovascular effects like decreasedPVR leading to shifting of blood frompulmonary to peripheral circulation,thereby reducing cardiac workload.
Morphine is contraindicated in bronchialasthma and pulmonary oedema due torespiratory irritants.4. Diarrhoea Opioids are effective for the
symptomatic treatment of diarrhoea.
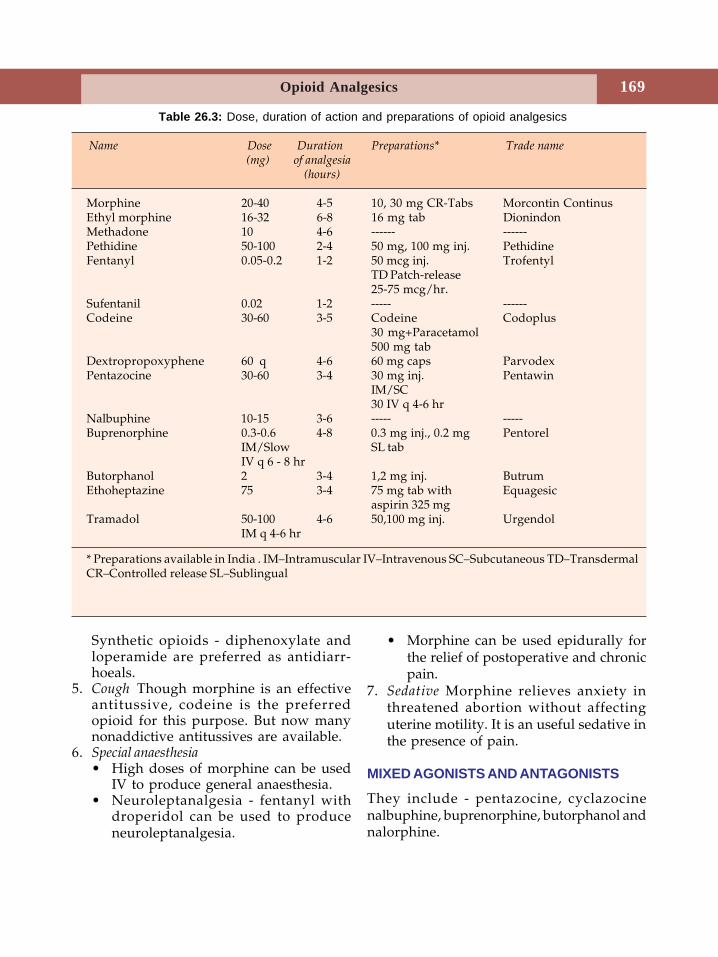
169Opioid Analgesics
Synthetic opioids - diphenoxylate andloperamide are preferred as antidiarr-hoeals.
5. Cough Though morphine is an effectiveantitussive, codeine is the preferredopioid for this purpose. But now manynonaddictive antitussives are available.
6. Special anaesthesia• High doses of morphine can be used
IV to produce general anaesthesia.• Neuroleptanalgesia - fentanyl with
droperidol can be used to produceneuroleptanalgesia.
• Morphine can be used epidurally forthe relief of postoperative and chronicpain.
7. Sedative Morphine relieves anxiety inthreatened abortion without affectinguterine motility. It is an useful sedative inthe presence of pain.
MIXED AGONISTS AND ANTAGONISTS
They include - pentazocine, cyclazocinenalbuphine, buprenorphine, butorphanol andnalorphine.
Table 26.3: Dose, duration of action and preparations of opioid analgesics
Name Dose Duration Preparations* Trade name(mg) of analgesia
(hours)
Morphine 20-40 4-5 10, 30 mg CR-Tabs Morcontin ContinusEthyl morphine 16-32 6-8 16 mg tab DionindonMethadone 10 4-6 ------ ------Pethidine 50-100 2-4 50 mg, 100 mg inj. PethidineFentanyl 0.05-0.2 1-2 50 mcg inj. Trofentyl
TD Patch-release25-75 mcg/hr.
Sufentanil 0.02 1-2 ----- ------Codeine 30-60 3-5 Codeine Codoplus
30 mg+Paracetamol500 mg tab
Dextropropoxyphene 60 q 4-6 60 mg caps ParvodexPentazocine 30-60 3-4 30 mg inj. Pentawin
IM/SC30 IV q 4-6 hr
Nalbuphine 10-15 3-6 ----- -----Buprenorphine 0.3-0.6 4-8 0.3 mg inj., 0.2 mg Pentorel
IM/Slow SL tabIV q 6 - 8 hr
Butorphanol 2 3-4 1,2 mg inj. ButrumEthoheptazine 75 3-4 75 mg tab with Equagesic
aspirin 325 mgTramadol 50-100 4-6 50,100 mg inj. Urgendol
IM q 4-6 hr
* Preparations available in India . IM–Intramuscular IV–Intravenous SC–Subcutaneous TD–TransdermalCR–Controlled release SL–Sublingual
Textbook of Pharmacology for Dental and Allied Health Sciences170
Pentazocine
In an attempt to develop an analgesic withless addiction liability and low adverseeffects, pentazocine was developed. Penta-zocine it is a k receptor agonist.• CNS effects of pentazocine are similar to
morphine. 20 mg pentazocine = 10 mgmorphine. Euphoria is seen only in lowdoses. With higher doses - above 60 mgdysphoria can occur due to k receptorstimulation.
• Sedation and respiratory depression areless marked.
• It has weak antagonistic properties at μreceptors.
• Tolerance and dependence develop onrepeated use.
• CVS - In contrast to morphine, pentazocineincreases BP and heart rate and therebyincreases cardiac work. It is therefore notsuitable in MI.
• Biliary spasm and constipation are lesssevere.
Preparations Pentazocine can be given bothorally and parenterally. It undergoes firstpass metabolism.Dose 50-100 mg oral; 30-60 mg IM(FORTWIN).Adverse effects Sedation, sweating, dizziness,nausea, dysphoria with anxiety, nightmaresand hallucinations which are unpleasant areseen above 60 mg. As it is an irritant, IMinjection can be painful and cause sterileabscesses.
Uses
Pentazocine is a commonly used opioidanalgesic especially in postoperative andchronic pain - abuse liability is less thanmorphine.Cyclazocine is similar to pentazocine.
Nalbuphine
Nalbuphine is an agonist - antagonist - morepotent than pentazocine. It is a goodanalgesic. Though it produces respiratorydepression like morphine, it has a ceilingeffect at 30 mg, i.e. an increase in dose beyond30 mg does not increase respiratorydepression further. Higher doses producedysphoria.Uses As analgesic - 10-20 mg IM.
Buprenorphine
Buprenorphine is a highly lipid solublesynthetic thebaine congener. It is a partial μagonist, 25 times as potent as morphine.Though onset of action is slow, duration ofanalgesia is long. Other CNS effects aresimilar to morphine while respiratorydepression is less marked. Patients exhibitlower degree of tolerance and dependenceliability. Withdrawal syndrome appears lateand is mild.Dose 0.3-0.6 mg SC, IM or sublingual (oralnot available).Uses Chronic pain like in terminal cancerpatients. Buprenorphine can also be used asa maintenance drug in opioid addicts as thewithdrawal symptoms are mild.Butorphanol is similar to pentazocine.
Nalorphine
Nalorphine is also an agonist - antagonist.At low doses, it is a good analgesic. But withincrease in dose there is no increase inanalgesia.It causes dysphoria (k agonist) andrespiratory depression even in low doses.Hence it cannot be used as an analgesic. Athigh doses it acts as an antagonist andcounters all the actions of opioids.Uses Nalorphine may be used in acute opioidpoisoning. It can also be used for thediagnosis of opioid addiction.
171Opioid Analgesics
Newer Agonist-Antagonists
Meptazinol
Meptazinol is a short acting agonist -antagonist with additional anticholinergiceffects. It produces short duration analgesiawith less respiratory depression and istherefore suitable for obstetric analgesia.
Dezocine
Dezocine is a partial agonist at μ receptors.Its analgesic actions are similar to morphinebut respiratory depression does not increasewith an increase in dose (ceiling effect).
OPIOID ANTAGONISTS
Naloxone
Naloxone acts as a competitive antagonist toall types of opioid receptors. It is a pureantagonist. In normal individuals, it does notproduce any significant actions. But in opiumaddicts, given IV, it promptly antagonises allthe actions of morphine including respiratorydepression and sedation and precipitateswithdrawal syndrome. It also blocks theaction of endogenous opioid peptides -endorphins, enkephalins and dynorphins. Itblocks the analgesia produced by placebo andacupuncture. This suggests that endogenousopioid peptides are responsible for analgesiaby these techniques.
Given orally it undergoes first passmetabolism and is metabolised by the liver.Hence it is given intravenously. Duration ofaction is 3-4 hours.Dose 0.4 mg IV.
Uses
1. Naloxone is the drug of choice formorphine overdosage.
2. It is also used to reverse neonatal asphyxiadue to opioids used in labour.
3. Naloxone can also be used for thediagnosis of opioid dependence - itprecipitates withdrawal symptoms.
4. Hypotension seen during shock could bedue to endogenous opioids releasedduring such stress. Naloxone has beenfound to be beneficial in reversinghypotension.
Naltrexone
Naltrexone is another pure opioid antagonist.It is• more potent than naloxone• orally effective• has a longer duration of action of 1-2 days.
Uses
1. Naltrexone is used for ‘opioid blockade’therapy in post addicts (50-100 mg/ dayorally) so that even if the addicts take anopioid, they do not experience thepleasurable effects and therefore lose thecraving.
2. Alcohol craving is also reduced bynaltrexone and is used to prevent relapseof heavy drinking (See page 145).
Nalmefene
Nalmefene is orally effective and longeracting. It has better bioavailability and is nothepatotoxic. It is used in opioid overdosage.
Textbook of Pharmacology for Dental and Allied Health Sciences172
27 Nonsteroidal Anti-inflammatory Drugs
(NSAIDs)
Nonsteroidal anti-inflammatory drugs areaspirin-type or non-opioid analgesics. Inaddition, they have anti-inflammatory ,antipyretic and uricosuric properties -without addiction liability.
The medicinal effects of the bark of theWillow tree have been known since centuries.The active principle ‘salicin’ was isolated fromthe Willow bark. This salicin is converted toglucose and salicylic acid in the body. In 1875,sodium salicylate was first used in thetreatment of rheumatic fever. After its anti-inflammatory and uricosuric properties wereestablished, efforts were made to synthesizederivatives which were less expensive. Nowthey have replaced the natural ones in themarket.
CLASSIFICATION
A. Nonselective COX Inhibitors
1. Salicylic acid derivativesAspirin, sodium salicylatediflunisal
2. Para-aminophenol derivativesParacetamol
3. Pyrazolone derivativesPhenylbutazoneazapropazone
4. Indole acetic acid derivativesIndomethacin, sulindac
5. Arylacetic acid derivativesDiclofenac, ketorolac, tolmetin
6. Propionic acid derivativesIbuprofen, fenoprofen,carprofen, naproxen,ketoprofen, flurbiprofenoxaprozin
7. Anthranilic acids (Fenamates)Flufenamic acidmefenamic acidenfenamic acidmeclofenamic acid
8. OxicamsPiroxicam, tenoxicammeloxicam
9. AlkanonesNabumetone
B. Selective COX-2 Inhibitors
Nimesulide, celecoxib,rofecoxib, valdecoxib, etodolac
MECHANISM OF ACTIONDuring inflammation, arachidonic acidliberated from membrane phospholipids isconverted to prostaglandins (PGs), catalysedby the enzyme cyclo-oxygenase (COX). Theseprostaglandins produce hyperalgesia - theysensitize the nerve endings to pain causedby other mediators of inflammation likebradykinin and histamine.
Nonsteroidal Anti-inflammatory Drugs (NSAIDs) 173
NSAIDs inhibit the PG synthesis byinhibiting the enzyme cyclo-oxygenase.
Aspirin is an irreversible inhibitor of COX(by acetylation) while the others arereversible competitive COX inhibitors. Thereare two forms of cyclo-oxygenase viz., COX-1 and COX-2 (see page 210). COX-1 is foundin most of the normal cells (constitutive) andis involved in maintaining tissue homeostasis.COX-2 is induced in the inflammatory cellsby cytokines and other mediators ofinflammation. This COX-2 catalyses thesynthesis of prostanoids which are themediators of inflammation. Most NSAIDsinhibit both COX-1 and COX-2 while somenewer agents like celecoxib and rofecoxibselectively inhibit only COX-2.
SALICYLATES
Salicylates are salts of salicylic acid, e.g.methyl salicylate, sodium salicylate, acetylsalicylic acid (aspirin). Aspirin is taken as theprototype.
Pharmacological Actions
1. AnalgesiaAspirin is a good analgesic and relieves painof inflammatory origin. This is because PGsare formed during inflammation and theysensitize the tissues to pain and aspirininhibits PG synthesis and thereby acts as ananalgesic. Pain originating from theintegumental structures like muscles, bones,joints, and pain in connective tissues is
relieved. But in vague visceral pain, aspirinis relatively ineffective.
The pain is relieved without euphoria andhypnosis. Hence there is no development oftolerance and dependence. But aspirin is aweak analgesic when compared to morphine.(Table 27.3)2. Antipyretic actionIn presence of fever, salicylates bring downthe temperature to normal level. But, innormal individuals, there is no change intemperature.
In fever, pyrogen - a protein, circulates inthe body and this increases the synthesis ofPGs in the hypothalamus, thereby raising itstemperature set point. The thermostaticmechanism in the hypothalamus is thusdisturbed. Aspirin inhibits PG synthesis inthe hypothalamus and resets the thermostatat the normal level bringing down thetemperature.
Enhanced sweating and cutaneous vasodi-latation promote heat loss and assist in theantipyretic action.3. Anti-inflammatory actionAt higher doses of 4-6 gm/day, aspirin actsas an anti-inflammatory agent. Signs ofinflammation like tenderness, swelling,erythema and pain are all reduced orsuppressed. But, the progression of thedisease in rheumatoid arthritis, rheumaticfever or osteoarthritis is not affected.
Once again the mechanism involved is PGsynthesis inhibition-PGs present ininflammatory tissues are responsible foroedema, erythema and pain. In addition,aspirin also interferes with the formation ofchemical mediators of the kallikrein system.As a result, it decreases the adherence ofgranulocyte to the damaged vasculature,stabilizes lysosomes and decreases themigration of the polymorphonuclearleukocytes and macrophages into the site ofinflammation.
Textbook of Pharmacology for Dental and Allied Health Sciences174
4. RespirationIn therapeutic doses of 4-6 gm/day -salicylates increase consumption of oxygenby skeletal muscles. As a result there isincreased CO2 production. This increasedCO2 stimulates respiratory centre. Salicylatesalso directly stimulate the medullaryrespiratory centre. Both these actions increasethe rate and depth of respiration. Theseeffects are dose dependent.
As a result of this stimulation ofrespiration, plasma CO2 is washed outleading to respiratory alkalosis. With toxicdoses, the respiratory centre is depressedleading to respiratory failure.5. Acid-base and electrolyte balanceIn anti-inflammatory doses, salicylatesproduce significant respiratory stimulation -CO2 is washed out resulting in respiratoryalkalosis; pH becomes alkaline. This iscompensated by increased excretion ofHCO3
– in urine accompanied by Na+, K+ andwater. pH then returns to normal. This stageis known as compensated respiratoryalkalosis.
With toxic doses, salicylates depress therespiratory centre directly. As a result, CO2
accumulates because more CO2 is producedthan is exhaled. Thus plasma CO2 rises andpH decreases. Since the concentration ofHCO3
– is already low due to enhanced renalexcretion, the change results inuncompensated respiratory acidosis. This issuperimposed by metabolic acidosis causedby accumulation of acids.
Toxic doses also depress vasomotor centre.This vasomotor depression impairs renalfunction resulting in accumulation of strongacids of metabolic origin like lactic, pyruvicand acetoacetic acids.
The above effects are accompanied bydehydration due to:• water lost in urine with HCO3
–, Na+ andK+
• increased sweating• water lost during hyperventilation.
Thus there is severe dehydration withacidosis.
6. Metabolic effectsSalicylates enhance the cellular metabolismdue to uncoupling of oxidativephosphorylation. More of O2 is used andmore CO2 is produced, especially in skeletalmuscles, leading to increased heatproduction.
In toxic doses, hyperpyrexia, increasedprotein catabolism with resultantaminoaciduria and negative nitrogen balanceare seen. Enhanced utilization of glucose leadsto mild hypoglycaemia. But in toxic doses,hyperglycaemia occurs due to centralsympathetic stimulation which increasesadrenaline levels.7. Gastrointestinal tractAspirin is a gastric irritant. Irritation of thegastric mucosa leads to epigastric distress,nausea and vomiting. Aspirin also stimulatesthe CTZ to produce vomiting.
Erosive gastritis, mucosal congestion,gastric ulceration and GI bleeding resultingin malaena and occasionally haematemesiscan occur particularly in higher doses.
Mechanism of Action
(i) In the acidic pH of the stomach, salicylatesremain unionised. These drug particlesadhere to the mucosa producing irritation.These particles also promote local backdiffusion of acid.
(ii) Aspirin decreases prostaglandin syn-thesis. PGs inhibit gastric acid secretion,increase mucus production and act ascytoprotectives in gastric mucosa. Thisdefense mechanism is lost due to PGinhibition.The above actions make aspirin ulcero-
genic. In addition, it decreases platelet
Nonsteroidal Anti-inflammatory Drugs (NSAIDs) 175
aggregation which also increases thetendency to bleed.
With soluble aspirin, gastric irritation isless. The selective COX-2 inhibitors cause lessgastric irritation.8. CVSIn therapeutic doses no significantcardiovascular effects are seen. In toxic dosesit depresses the VMC and thus depresses thecirculation.9. Immunological effectsIn higher doses, salicylates suppress severalantigen-antibody reactions includinginhibition of antibody production, Ag-Abaggregation and antigen induced release ofhistamine. These effects might also contributeto the beneficial effects in rheumatic fever.10. Uric acid excretionUric acid is excreted by secretion from thedistal tubules. In a dose of 1-2 gm/day,aspirin increases plasma urate levels by urateretention because it interferes with uratesecretion by the distal tubules.
Large doses of > 5 gm/day increase urateexcretion because it inhibits reabsorption ofurate by proximal tubule causing uricosuria.But, its uricosuric effect cannot be usedtherapeutically because high doses arerequired and such doses result in prominentadverse effects.11. BloodEven in small doses aspirin irreversiblyinhibits platelet cyclooxygenase and therebyTXA2 synthesis by the platelets. It thereforeinterferes with platelet aggregation andprolongs the bleeding time. Even a singledose can irreversibly inhibit TXA2 synthesiswhich is for the life of the platelets (8-11days).As platelets cannot synthesize proteins whichmeans COX cannot be regenerated, freshplatelets have to be formed to restore TXA2activity. Moreover aspirin inhibits plateletCOX in the portal circulation itself andtherefore even small doses (40 mg daily) of
aspirin is adequate for its antiplateletaggregatory effect.12. Local effects Salicylic acid when applied locally is akeratolytic. It also has mild antiseptic andfungistatic properties. Salicylic acid is also anirritant for the broken skin.
Pharmacokinetics
Salicylates being acidic drugs are absorbedfrom the stomach and the upper smallintestine. But aspirin as such is poorly soluble,hence not well-absorbed. When administeredas microfine particles, absorption increases.Thus particle size, pH of the GIT, solubilityof the preparation and presence of food inthe stomach influence the absorption.
Salicylic acid and methylsalicylate areabsorbed from the intact skin. They areextensively bound to plasma proteins.Aspirin is deacetylated in the liver, plasmaand other tissues to release salicylic acidwhich is the active form. Plasma t½ of aspirinis 3-5 hours. Elimination is dose dependent.It follows first order kinetics in small dosesand zero order kinetics in higher doses.Therefore in anti-inflammatory doses, t½increases to 12 hr. Salicylates are excreted inurine.
Adverse Effects
Analgesic doses are generally well toleratedbut anti-inflammatory doses are usuallyassociated with adverse effects especiallywhen used over a long period.• GI tract Nausea, epigastric distress,
vomiting, erosive gastritis, peptic ulcer,increased occult blood loss in stools arecommon.
• Allergic reactions are not common and maybe manifested as rashes, urticaria, photosensitivity, rhinorrhoea, angio-oedemaand asthma especially in those with ahistory of allergies.
Textbook of Pharmacology for Dental and Allied Health Sciences176
As aspirin inhibits only cyclo-oxygenasepathway, arachidonic acid is available forconversion by lipoxygenase pathway intoleukotrienes. Leukotrienes are powerfulbronchoconstrictors. Hence aspirin canprecipitate bronchial asthma in someindividuals. Of the currently availableNSAIDs, diclofenac and indomethacininhibit the synthesis of both PGs and LTs.
• Haemolysis: Salicylates can causehaemolysis in patients with G6PDdeficiency.
• Nephrotoxicity: Almost all NSAIDs cancause nephrotoxicity after long-term use.Salt and water retention and impairedrenal function can occur.
• Hepatotoxicity can also occur when highdoses of NSAIDs are used over a longperiod. Plasma levels of liver enzymes areraised.
• Reye’s syndrome seen in children is a formof hepatic encephalopathy which may befatal. It develops a few days after a viralinfection especially influenza and varicella.An increased incidence of this syndromehas been noted when aspirin is used totreat fever. Hence aspirin iscontraindicated in children with viralfever.
• Pregnancy and infancy Aspirin when takenat term delays the onset of labour due toinhibition of PG synthesis (PGs play animportant role in the initiation of labour).Premature closure of ductus arteriosusmay occur in the foetus resulting in portalhypertension. It can also increasepostpartum bleeding due to inhibition ofplatelet aggregation.
• Salicylism Higher doses given for a longtime as in treatment of rheumatoidarthritis may cause chronic salicylateintoxication termed ‘Salicylism’. Thesyndrome is characterised by headache,vertigo, dizziness, tinnitus, vomiting,
mental confusion, diarrhoea, sweating,difficulty in hearing, thirst anddehydration. These symptoms arereversible on withdrawal of salicylates.
Acute salicylate intoxication Poisoning may beaccidental or suicidal. It is more common inchildren, 15-30 grams is the fatal dose of aspirin.
Symptoms and Signs
Dehydration, hyperpyrexia, GI irritation,vomiting, sometimes haematemesis, acid-baseimbalance, restlessness, delirium,hallucinations, metabolic acidosis, tremors,convulsions, coma and death due torespiratory failure and CV collapse.
Treatment is Symptomatic and Includes:
1. Gastric lavage to eliminate unabsorbeddrugs.
2. IV fluids to correct acid-base imbalanceand dehydration.
3. Temperature is brought down by externalcooling with alcohol or cold watersponges.
4. If haemorrhagic complications are seen,blood transfusion and vitamin K areneeded.
5. The IV fluids should contain Na+, K+,HCO3
– and glucose (to treat hypokalaemiaand acidosis). Blood pH should bemonitored.
6. In severe cases, forced alkaline diuresiswith sodium bicarbonate and a diureticlike frusemide is given along with IVfluids. Sodium bicarbonate ionizessalicylates making them water soluble andenhances their excretion through kidneys.
Precautions and Contraindications
Peptic ulcer, liver diseases, bleedingtendencies and viral fever in childrencontraindicate the use of aspirin/salicylates
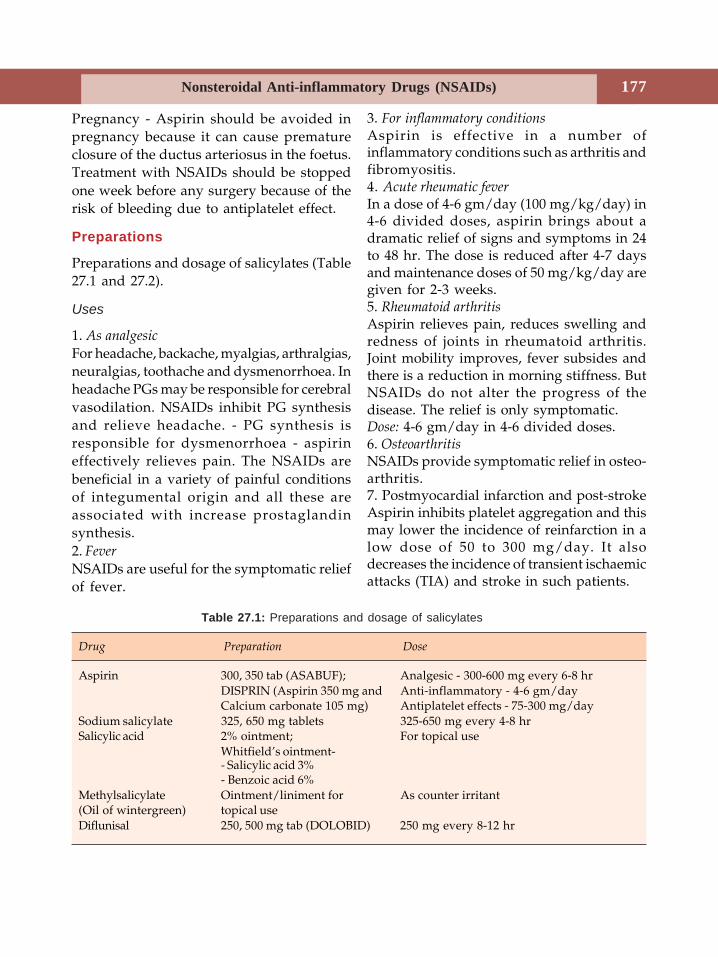
Nonsteroidal Anti-inflammatory Drugs (NSAIDs) 177
Pregnancy - Aspirin should be avoided inpregnancy because it can cause prematureclosure of the ductus arteriosus in the foetus.Treatment with NSAIDs should be stoppedone week before any surgery because of therisk of bleeding due to antiplatelet effect.
Preparations
Preparations and dosage of salicylates (Table27.1 and 27.2).
Uses
1. As analgesic
For headache, backache, myalgias, arthralgias,neuralgias, toothache and dysmenorrhoea. Inheadache PGs may be responsible for cerebralvasodilation. NSAIDs inhibit PG synthesisand relieve headache. - PG synthesis isresponsible for dysmenorrhoea - aspirineffectively relieves pain. The NSAIDs arebeneficial in a variety of painful conditionsof integumental origin and all these areassociated with increase prostaglandinsynthesis.2. Fever
NSAIDs are useful for the symptomatic reliefof fever.
3. For inflammatory conditionsAspirin is effective in a number ofinflammatory conditions such as arthritis andfibromyositis.4. Acute rheumatic feverIn a dose of 4-6 gm/day (100 mg/kg/day) in4-6 divided doses, aspirin brings about adramatic relief of signs and symptoms in 24to 48 hr. The dose is reduced after 4-7 daysand maintenance doses of 50 mg/kg/day aregiven for 2-3 weeks.5. Rheumatoid arthritisAspirin relieves pain, reduces swelling andredness of joints in rheumatoid arthritis.Joint mobility improves, fever subsides andthere is a reduction in morning stiffness. ButNSAIDs do not alter the progress of thedisease. The relief is only symptomatic.Dose: 4-6 gm/day in 4-6 divided doses.6. OsteoarthritisNSAIDs provide symptomatic relief in osteo-arthritis.7. Postmyocardial infarction and post-strokeAspirin inhibits platelet aggregation and thismay lower the incidence of reinfarction in alow dose of 50 to 300 mg/day. It alsodecreases the incidence of transient ischaemicattacks (TIA) and stroke in such patients.
Table 27.1: Preparations and dosage of salicylates
Drug Preparation Dose
Aspirin 300, 350 tab (ASABUF); Analgesic - 300-600 mg every 6-8 hrDISPRIN (Aspirin 350 mg and Anti-inflammatory - 4-6 gm/dayCalcium carbonate 105 mg) Antiplatelet effects - 75-300 mg/day
Sodium salicylate 325, 650 mg tablets 325-650 mg every 4-8 hrSalicylic acid 2% ointment; For topical use
Whitfield’s ointment-- Salicylic acid 3%- Benzoic acid 6%
Methylsalicylate Ointment/liniment for As counter irritant(Oil of wintergreen) topical useDiflunisal 250, 500 mg tab (DOLOBID) 250 mg every 8-12 hr
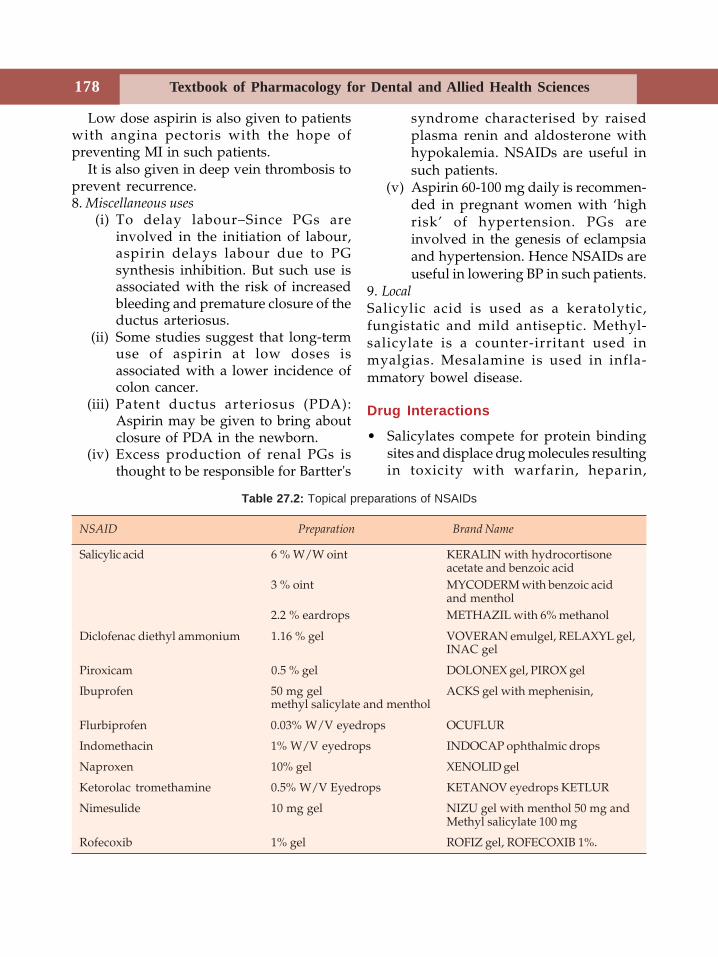
Textbook of Pharmacology for Dental and Allied Health Sciences178
Low dose aspirin is also given to patientswith angina pectoris with the hope ofpreventing MI in such patients.
It is also given in deep vein thrombosis toprevent recurrence.8. Miscellaneous uses
(i) To delay labour–Since PGs areinvolved in the initiation of labour,aspirin delays labour due to PGsynthesis inhibition. But such use isassociated with the risk of increasedbleeding and premature closure of theductus arteriosus.
(ii) Some studies suggest that long-termuse of aspirin at low doses isassociated with a lower incidence ofcolon cancer.
(iii) Patent ductus arteriosus (PDA):Aspirin may be given to bring aboutclosure of PDA in the newborn.
(iv) Excess production of renal PGs isthought to be responsible for Bartter's
syndrome characterised by raisedplasma renin and aldosterone withhypokalemia. NSAIDs are useful insuch patients.
(v) Aspirin 60-100 mg daily is recommen-ded in pregnant women with ‘highrisk’ of hypertension. PGs areinvolved in the genesis of eclampsiaand hypertension. Hence NSAIDs areuseful in lowering BP in such patients.
9. Local Salicylic acid is used as a keratolytic,fungistatic and mild antiseptic. Methyl-salicylate is a counter-irritant used inmyalgias. Mesalamine is used in infla-mmatory bowel disease.
Drug Interactions
• Salicylates compete for protein bindingsites and displace drug molecules resultingin toxicity with warfarin, heparin,
Table 27.2: Topical preparations of NSAIDs
NSAID Preparation Brand Name
Salicylic acid 6 % W/W oint KERALIN with hydrocortisoneacetate and benzoic acid
3 % oint MYCODERM with benzoic acidand menthol
2.2 % eardrops METHAZIL with 6% methanol
Diclofenac diethyl ammonium 1.16 % gel VOVERAN emulgel, RELAXYL gel,INAC gel
Piroxicam 0.5 % gel DOLONEX gel, PIROX gel
Ibuprofen 50 mg gel ACKS gel with mephenisin,methyl salicylate and menthol
Flurbiprofen 0.03% W/V eyedrops OCUFLUR
Indomethacin 1% W/V eyedrops INDOCAP ophthalmic drops
Naproxen 10% gel XENOLID gel
Ketorolac tromethamine 0.5% W/V Eyedrops KETANOV eyedrops KETLUR
Nimesulide 10 mg gel NIZU gel with menthol 50 mg andMethyl salicylate 100 mg
Rofecoxib 1% gel ROFIZ gel, ROFECOXIB 1%.

Nonsteroidal Anti-inflammatory Drugs (NSAIDs) 179
naproxen, phenytoin and sulfonylureas.Inhibition of platelet aggregation mayincrease the risk of bleeding with oralanticoagulants.
• In low doses salicylates can counter theuricosuric actions of probenecid bydecreasing uric acid excretion.
Diflunisal
Diflunisal is a difluorophenyl derivative ofsalicylic acid. Diflunisal is 3-4 times morepotent than aspirin as an anti-inflammatoryagent but is a poor antipyretic due to poorpenetration into CNS. Gastrointestinal andantiplatelet effects are less intense thanaspirin. Side effects are fewer.
Uses Osteoarthritis, strain and sprains initialdose 500-1000 mg followed by 250 bd/tid.
PARA-AMINOPHENOL DERIVATIVES
Paracetamol (acetaminophen)
Phenacetin was the first drug used in thisgroup. But, due to severe adverse effects itis now banned.
Paracetamol, a metabolite of phenacetin isfound to be safer and effective.
Actions
Paracetamol has analgesic, good antipyreticand weak anti-inflammatory properties. Dueto weak PG inhibitory activity in theperiphery, it has poor anti-inflammatoryactions.
Paracetamol is active on cyclo-oxygenasein the brain which accounts for its antipyreticaction. In the presence of peroxides whichare present at the site of inflammation,paracetamol has a poor ability to inhibitcyclo-oxygenase. It does not stimulaterespiration, has no actions on acid-basebalance, cellular metabolism, cardiovascular
system and platelet function; it is not auricosuric agent and gastric irritation is mild.
Pharmacokinetics
Paracetamol is well-absorbed orally and 30%protein bound; it is metabolised by thehepatic microsomal enzymes: by glucuronideconjugation (60%) and glutathione conju-gation (20%).
Adverse Effects
In antipyretic doses, paracetamol is safe andwell-tolerated. Nausea and rashes may occur.But when large doses are taken, acuteparacetamol poisoning results. Children aremore susceptible because their ability toconjugate by glucuronidation is poor. 10-15grams in adults cause serious toxicity.Symptoms are - nausea, vomiting, anorexiaand abdominal pain during first 24 hours.Paracetamol is hepatotoxic and causes severehepatic damage. Manifestations are seenwithin 2-4 days and include increased serumtransaminases, jaundice, liver tenderness andprolonged prothrombin time which mayprogress to liver failure in some patients.Hepatic lesions are reversible when promptlytreated.
Nephrotoxicity may result in acute renalfailure in some.
Mechanism
A small portion of paracetamol is metabolisedto a highly reactive intermediate - N-acetyl-benzoquinone-imine which is detoxifiedgenerally by conjugation with glutathione.But when large doses of paracetamol aretaken, hepatic glutathione is depleted and thetoxic metabolite binds to sulphydryl groupsin hepatic proteins resulting in hepaticnecrosis.
Textbook of Pharmacology for Dental and Allied Health Sciences180
Chronic alcoholics and infants are moreprone to hepatotoxicity.
Treatment
Stomach wash is given. Activated charcoalprevents further absorption. Antidote is-N-acetylcysteine (150 mg/kg IV infusion over15 min repeated as required; oral loadingdose - 140 mg/kg followed by 70 mg/kgevery 4 hr - 17 doses) - more effective whengiven early. N-acetylcysteine partlyreplenishes the glutathione stores of the liverand prevents binding of toxic metabolites tothe cellular constituents.
Uses
• Paracetamol is used as an analgesic inpainful conditions like toothache,headache and myalgia
• As an antipyretic• Chronic pulpitis, periodontal abscess,
post-extraction - paracetamol is used withibuprofen.
PYRAZOLONE DERIVATIVES
Phenylbutazone
Phenylbutazone has good anti-inflammatoryactivity, is more potent, but has pooreranalgesic and antipyretic effects. It is auricosuric agent.
Phenylbutazone causes retention of Na+
and water. Thus after 1-2 weeks of useoedema results. It can also precipitatecongestive cardiac failure.
Pharmacokinetics
Phenylbutazone is completely absorbedorally; IM injection is not recommendedbecause its absorption is slow as it binds tolocal tissue proteins and also causes localtissue damage. It is 98% bound to plasmaproteins; t½ is 60 hr.
Dose 100-200 mg, BD. Small doses may begiven 3-4 times a day to avoid gastricirritation.
Adverse Effects
• Phenylbutazone is more toxic than aspirinand is poorly tolerated - dyspepsia,epigastric distress, nausea and vomitingare common. Peptic ulceration anddiarrhoea may occur. Oedema is a limitingfactor and may precipitate CCF.
• Hypersensitivity reactions like rashes,serum sickness, stomatitis, hepatitis,nephritis, dermatitis and jaundice canoccur. Phenylbutazone may cause serioushaematological complications such as bonemarrow depression, aplastic anaemia,agranulocytosis and thrombocytopenia.
• It may inhibit iodine uptake by thyroid,resulting in hypothyroidism and goitre onlong-term use.
• CNS effects like insomnia, vertigo, opticneuritis, blurring of vision and convulsionsmay be encountered.
Because of its toxicity, phenylbutazone iswithdrawn from the market in many westerncountries.
Uses
1. Rheumatoid arthritis2. Ankylosing spondylitis3. Osteoarthritis4. Gout - phenylbutazone produces satis-
factory relief from pain and inflammationin acute attacks
5. Other musculoskeletal disorders.Azapropazone is structurally related tophenylbutazone but is less likely to causeagranulocytosis; t½ is 12-16 hours.Metamizol is a potent analgesic andantipyretic, but poor anti-inflammatory agentand has no uricosuric properties (ANALGIN,NOVALGIN) Dose: 500 mg 3-4 times a day.
Nonsteroidal Anti-inflammatory Drugs (NSAIDs) 181
It offers no advantages over aspirin. Notrecommended in children upto 6 years.Propiphenazone is similar to metamizol.Dose 300-600 mg 3-4 times a day (SARIDON).
INDOLE ACETIC ACID DERIVATIVES
Indomethacin is a potent anti-inflammatoryagent, antipyretic and good analgesic. It iswell-absorbed, 90% bound to plasmaproteins; t½ - 4-6 hr.Dose 25-50 mg b.d-t.d.s.Adverse effects are high; gastrointestinalirritation with nausea, GI bleeding, vomiting,diarrhoea and peptic ulcers can occur.CNS effects include headache, dizziness,ataxia, confusion, hallucinations, depressionand psychosis.
Hypersensitivity reactions like skin rashes,leukopenia, and asthma in aspirin sensitiveindividuals. It can also cause bleeding dueto decreased platelet aggregation andoedema due to salt and water retention.Drug interactions Indomethacin blunts thediuretic action of furosemide and theantihypertensive action of thiazides,furosemide, β-blockers and ACE inhibitorsby causing salt and water retention.
Uses (Table 27.3)
• Rheumatoid arthritis• Gout• Ankylosing spondylitis• Psoriatic arthritis• For closure of patent ductus arteriosus.Sulindac has weaker analgesic, antipyretic andanti-inflammatory actions but is less toxic.Does not antagonize the diuretic andantihypertensive actions of thiazides. It maybe used as an alternative drug forinflammatory conditions.
ARYLACETIC ACID DERIVATIVES
Diclofenac is an analgesic, antipyretic and anti-inflammatory agent. Its tissue penetrability
is good and attains good concentration insynovial fluid which is maintained for a longtime. Adverse effects are mild.Dose 50 mg bd-tds. Gel is available for topicalapplication (INAC GEL). Ophthalmic prepar-ation is available for use in postoperative pain.
Uses
1. Treatment of chronic inflammatoryconditions like rheumatoid arthritis andosteoarthritis.
2. Acute musculoskeletal pain, painful dentallesions.
3. Postoperatively for relief of pain andinflammation.
Ketorolac is another PG synthesis inhibitorhaving good analgesic and anti-inflammatoryproperties. It is used for its analgesicproperties to relieve postoperative pain. It ismostly used parenterally though it can alsobe given orally.
PROPIONIC ACID DERIVATIVESIbuprofen is better tolerated than aspirin.Analgesic, antipyretic and anti-inflammatoryefficacy is slightly lower than aspirin. It is99% bound to plasma proteins.Adverse effects are milder when compared toother NSAIDs and the incidence is low.Nausea, vomiting, gastric discomfort, CNSeffects, hypersensitivity reactions, fluidretention are all similar but less severe thanphenylbutazone or indomethacin.Dose Ibuprofen - 400-800 mg TDS (BRUFEN)ibuprofen + paracetamol (COMBIFLAM)
Uses
1. As an analgesic in painful conditions.2. In fever.3. Soft tissue injuries, fractures, following
tooth extraction, to relieve postoperativepain, dysmenorrhoea and osteoarthritis.
4. Gout.5. Surgical removal of impacted tooth-a
combination of ibuprofen with a skeletalmuscle relaxant like chlorzoxazone isrecommended.
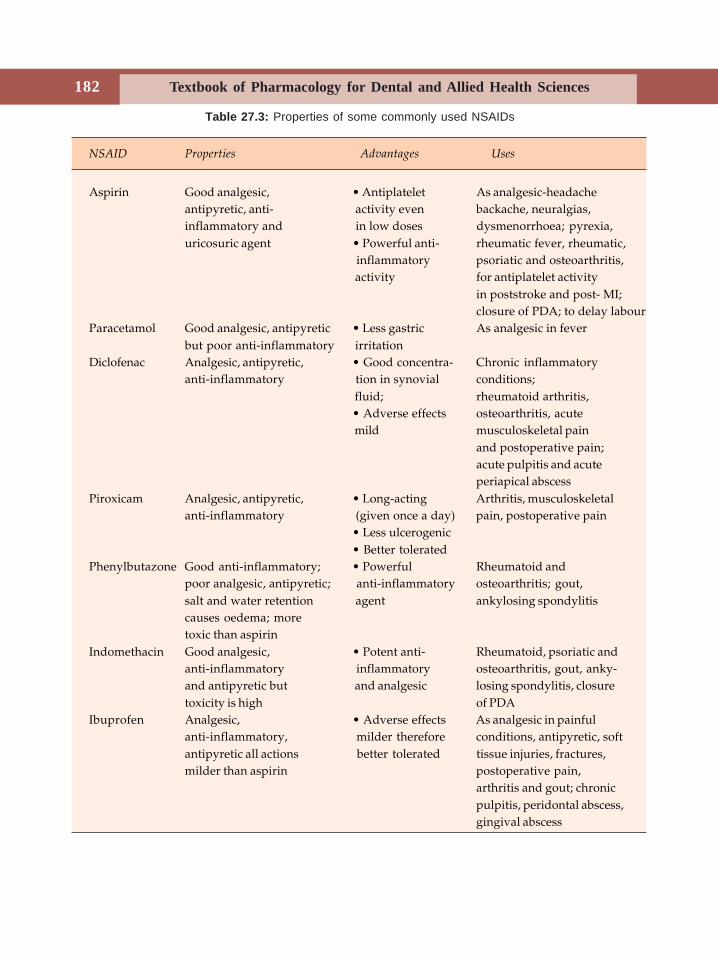
Textbook of Pharmacology for Dental and Allied Health Sciences182
Table 27.3: Properties of some commonly used NSAIDs
NSAID Properties Advantages Uses
Aspirin Good analgesic, • Antiplatelet As analgesic-headacheantipyretic, anti- activity even backache, neuralgias,inflammatory and in low doses dysmenorrhoea; pyrexia,uricosuric agent • Powerful anti- rheumatic fever, rheumatic,
inflammatory psoriatic and osteoarthritis, activity for antiplatelet activity
in poststroke and post- MI;closure of PDA; to delay labour
Paracetamol Good analgesic, antipyretic • Less gastric As analgesic in feverbut poor anti-inflammatory irritation
Diclofenac Analgesic, antipyretic, • Good concentra- Chronic inflammatoryanti-inflammatory tion in synovial conditions;
fluid; rheumatoid arthritis,• Adverse effects osteoarthritis, acute mild musculoskeletal pain
and postoperative pain;acute pulpitis and acuteperiapical abscess
Piroxicam Analgesic, antipyretic, • Long-acting Arthritis, musculoskeletalanti-inflammatory (given once a day) pain, postoperative pain
• Less ulcerogenic• Better tolerated
Phenylbutazone Good anti-inflammatory; • Powerful Rheumatoid andpoor analgesic, antipyretic; anti-inflammatory osteoarthritis; gout,salt and water retention agent ankylosing spondylitiscauses oedema; moretoxic than aspirin
Indomethacin Good analgesic, • Potent anti- Rheumatoid, psoriatic andanti-inflammatory inflammatory osteoarthritis, gout, anky-and antipyretic but and analgesic losing spondylitis, closuretoxicity is high of PDA
Ibuprofen Analgesic, • Adverse effects As analgesic in painfulanti-inflammatory, milder therefore conditions, antipyretic, softantipyretic all actions better tolerated tissue injuries, fractures,milder than aspirin postoperative pain,
arthritis and gout; chronicpulpitis, peridontal abscess,gingival abscess

Nonsteroidal Anti-inflammatory Drugs (NSAIDs) 183
ANTHRANILIC ACID DERIVATIVES
Fenamates are analgesic, antipyretic, anti-inflammatory drugs with less efficacy, andare more toxic; contraindicated in children.They should not be used for more than oneweek. They are not generally preferred.Adverse effects GI side effects are similar toaspirin but GI bleeding is less. Diarrhoea iscommon.Uses Analgesic in myalgias, dysmenorrhoea,(250-500 mg TDS).
OXICAMS
Piroxicam is an oxicam derivative. It is long-acting, has good anti-inflammatory, analgesicand antipyretic activity. No clinicallysignificant drug interactions are seen; bettertolerated as it is less ulcerogenic. It is areversible COX inhibitor. Dose 20 mg OD. Itis long-acting. Piroxicam is used for rheu-matoid arthritis, osteoarthritis, ankylosingspondylitis, acute musculoskeletal pain andpostoperative pain and painful dental lesions.Meloxicam is similar to piroxicam but in lowerdoses it causes less gastric irritation thanpiroxicam. It is therefore better tolerated.Dose 7.5-15 mg once daily.
Many other oxicams are being developedwith the idea of obtaining one which isnonulcerogenic. But most of them areprodrugs of piroxicam and in lower dosessome of them are selective COX-2 inhibitors.
ALKANONES
Nabumetone is an anti-inflammatory agentwith significant efficacy in rheumatoidarthritis and osteoarthritis. It shows arelatively low incidence of side effects, it iscomparatively less ulcerogenic. It is a prodrugand also selectively inhibits COX-2 - bothaccount for the low ulcerogenic potential.
It is used in rheumatoid and osteoarthritis.
SELECTIVE COX-2 INHIBITORS
Celecoxib, rofecoxib and valdecoxib are diarylsubstituted compounds. They are highlyselective COX-2 inhibitors. They have goodanti-inflammatory, analgesic and antipyreticproperties but do not affect plateletaggregation (Table 27.4).
They are better tolerated because of mildergastric irritation (due to COX-2 selectivity) -but more long term studies are needed.
Disadvantages
The coxibs can cause hypertension andoedema which can be troublesome in patientswith cardiovascular problems. Studies haveshown that use of coxibs can increase the riskof myocardial infarction and stroke. The exactcause is not known but could be because ofinhibition of PGI2 production withoutinhibiting TXA2. This results in a pro-thrombotic effect leading to myocardialinfarction and stroke. Because they arederivatives of sulphonamides, allergicreactions including Stevens–Johnsonsyndrome have been reported. Hence mostcoxibs have been with-drawn from themarket. Celecoxib has been approved for usein osteoarthritis and rheumatoid arthritis inthe lowest effective dose and for the shortestperiod possible.
Dose:
Celecoxib - anti-inflammatory - 100-200 mgonce or twice daily.
Rofecoxib - 12.5-25 mg daily.Valdecoxib-20 mg twice daily.
Other coxibs include etoricoxib, lumira-coxib and paracoxib. They have propertiessimilar to other coxibs.Nimesulide a sulfonamide compound is asulfonanilide derivative. It is a weak inhibitorof PG synthesis with a higher affinity forCOX-2 than COX-1. It inhibits leukocytefunction, prevents the release of mediatorsand in addition has antihistaminic and
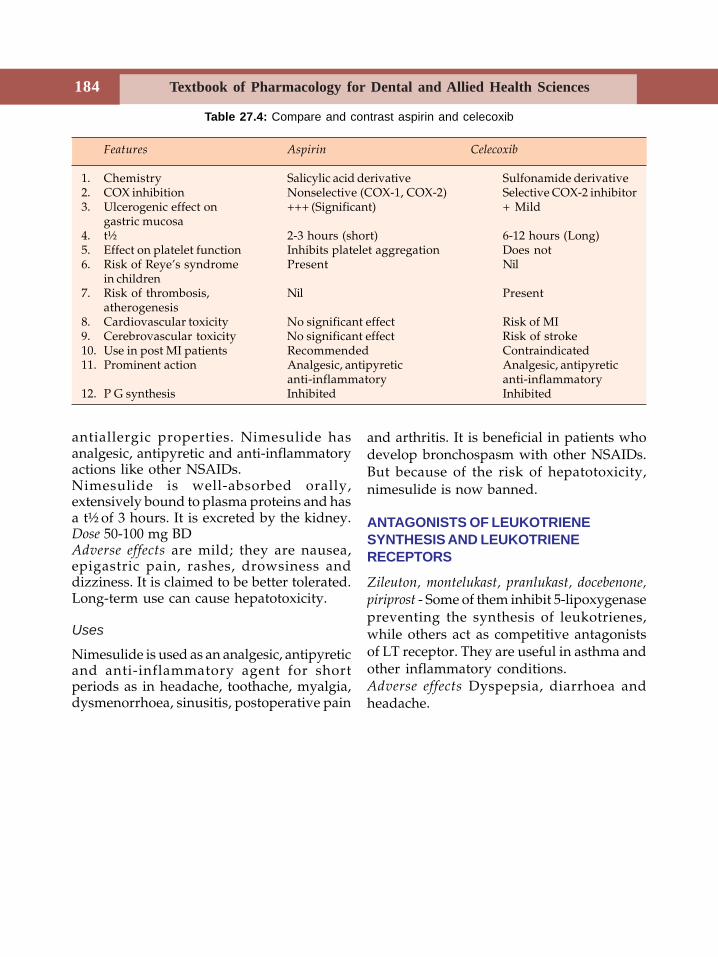
Textbook of Pharmacology for Dental and Allied Health Sciences184
antiallergic properties. Nimesulide hasanalgesic, antipyretic and anti-inflammatoryactions like other NSAIDs.Nimesulide is well-absorbed orally,extensively bound to plasma proteins and hasa t½ of 3 hours. It is excreted by the kidney.Dose 50-100 mg BDAdverse effects are mild; they are nausea,epigastric pain, rashes, drowsiness anddizziness. It is claimed to be better tolerated.Long-term use can cause hepatotoxicity.
Uses
Nimesulide is used as an analgesic, antipyreticand anti-inflammatory agent for shortperiods as in headache, toothache, myalgia,dysmenorrhoea, sinusitis, postoperative pain
and arthritis. It is beneficial in patients whodevelop bronchospasm with other NSAIDs.But because of the risk of hepatotoxicity,nimesulide is now banned.
ANTAGONISTS OF LEUKOTRIENESYNTHESIS AND LEUKOTRIENERECEPTORS
Zileuton, montelukast, pranlukast, docebenone,piriprost - Some of them inhibit 5-lipoxygenasepreventing the synthesis of leukotrienes,while others act as competitive antagonistsof LT receptor. They are useful in asthma andother inflammatory conditions.Adverse effects Dyspepsia, diarrhoea andheadache.
Features Aspirin Celecoxib
1. Chemistry Salicylic acid derivative Sulfonamide derivative2. COX inhibition Nonselective (COX-1, COX-2) Selective COX-2 inhibitor3. Ulcerogenic effect on +++ (Significant) + Mild
gastric mucosa4. t½ 2-3 hours (short) 6-12 hours (Long)5. Effect on platelet function Inhibits platelet aggregation Does not6. Risk of Reye’s syndrome Present Nil
in children7. Risk of thrombosis, Nil Present
atherogenesis8. Cardiovascular toxicity No significant effect Risk of MI9. Cerebrovascular toxicity No significant effect Risk of stroke10. Use in post MI patients Recommended Contraindicated11. Prominent action Analgesic, antipyretic Analgesic, antipyretic
anti-inflammatory anti-inflammatory12. P G synthesis Inhibited Inhibited
Table 27.4: Compare and contrast aspirin and celecoxib
185Drugs Used in Rheumatoid Arthritis and Gout
28 Drugs Usedin Rheumatoid
Arthritis and Gout
RHEUMATOID ARTHRITIS
Rheumatoid arthritis (RA) is a chronic,progressive, autoimmune, inflammatorydisease, mainly affecting the joints and theperiarticular tissues. The antigen-antibodycomplexes trigger the pathological process.Mediators of inflammation released in thejoints initiate the inflammatory process. Theearliest lesion is vasculitis, followed bysynovial oedema and infiltration withinflammatory cells. There is local synthesisof prostaglandins and leukotrienes.Prostaglandins cause vasodilation and pain.The inflammatory cells release lysosomalenzymes which cause damage to bones andcartilage.Drugs used in the treatment of rheumatoid arthritis1. NSAIDs2. Disease modifying agents
Gold, d-penicillamine, chloroquine andhydroxychloroquine, sulphasalazine, TNFblocking drugs
3. ImmunosuppressantsMethotrexate, cyclophosphamide,azathioprine, leflunomide
4. AdjuvantsGlucocorticoids
Nonsteroidal anti-inflammatory drugs are thefirst line drugs in RA. NSAIDs affordsymptomatic relief but do not modify thecourse of the disease.
Disease modifying drugs (DMDs) are also calleddisease modifying anti-rheumatic drugs(DMARDs). These are the second line drugsand are reserved for patients withprogressive disease who do not obtainsatisfactory relief from NSAIDs. They arecapable of arresting the progress of thedisease and inducing remission in thesepatients. The effects of these drugs may take6 weeks to 6 months to become evident andare therefore called slow-acting anti-rheumatic drugs (SAARDs).Gold salts were introduced for the treatmentof RA in 1920s. They are considered to bethe most effective agents for arresting thedisease process.
On treatment, a gradual reduction of thesigns and symptoms are seen. It brings abouta decrease in the rheumatoid factor andimmunoglobulins.Mechanism of action is not exactly known - butgold depresses cell-mediated immunity(CMI). Gold salts concentrate in tissues richin mononuclear phagocytes, selectivelyaccumulate in the lysosomes of synovial cellsand other macrophages in the inflamedsynovium. They alter the structure andfunctions of the macrophages, depress theirmigration and phagocytic activity. They alsoinhibit lysosomal enzyme activity. Thus goldsalts depress CMI.
Textbook of Pharmacology for Dental and Allied Health Sciences186
Preparations Aurothiomalate sodium andauronofin are given orally. Aurothioglucoseis given parenterally.Adverse effects Treatment with gold isassociated with several adverse effects andonly 60% of patients remain on treatment atthe end of 2 years.Adverse effects include:1. On skin and mucous membrane Dermatitis,
pruritus, stomatitis, pharyngitis, glossitis,gastritis, colitis and vaginitis. A grey bluepigmentation on exposed parts of the skinmay be seen.
2. Renal toxicity Haematuria, glomerulo-nephritis.
3. Nervous system Encephalitis, peripheralneuritis.
4. Liver Hepatitis, cholestatic jaundice.5. Blood Thrombocytopenia, leukopenia,
agranulocytosis, aplastic anaemia.6. CVS Postural hypotension.7. Lungs Pulmonary fibrosis.Contraindications Kidney, liver and skindiseases; pregnancy and blood dyscrasias.
Uses
1. Rheumatoid arthritis–gold is used in activearthritis that progresses despite anadequate course of NSAIDs, rest andphysiotherapy. In most patients gold saltsarrest the progression of the disease,improve grip strength, reduce morningstiffness and prevent involvement ofunaffected joints.Gold is also beneficial in:
2. Juvenile rheumatoid arthritis3. Psoriatic arthritis4. Pemphigus5. Lupus erythematosus.d-penicillamine is an analog of the amino acidcysteine and a metabolite of penicillin. It is achelating agent that chelates copper. Itsactions and toxicities are similar to gold butis less effective than gold. Hence it is not
preferred. It is used as an alternative to goldin early, mild and non-erosive disease.Adverse effects include drug fever, skin rashes,proteinuria, leucopenia, thrombocytopenia,aplastic anaemia, a variety of autoimmunediseases including lupus erythematosus,thyroiditis and haemolytic anaemia. Anorexia,nausea, vomiting, loss of taste perception andalopecia may also be seen.Chloroquine and hydroxychloroquine Theseantimalarial drugs are found to be useful inmild non-erosive rheumatoid arthritis. Theyinduce remission in 50% of patients. They areless effective but are better tolerated than gold.
Mechanism of action is not exactlyunderstood but they are known to depresscell-mediated immunity.Toxicity Chloroquine and hydroxy-chloroquine accumulate in tissues leading totoxicity. The most significant side effect isthe retinal damage on long-term use. Thistoxicity is less common and reversible withhydroxychloroquine which is thereforepreferred over chloroquine in rheumatoidarthritis. Every 3 months eyes should betested. Other adverse effects includemyopathy, neuropathy and irritable bowelsyndrome.Sulphasalazine is a compound of sulpha-pyridine and 5-amino salicylic acid. Inthe colon, sulphasalazine is split by thebacterial action and sulphapyridine getsabsorbed. This has anti-inflammatory actionsthough the mechanism is not known. Adverseeffects include gastrointestinal upset and skinrashes.
TNF Blocking Agents
Cytokines, particularly tumour necrosisfactor (TNF) play an important role in theprocess of inflammation. TNF produced bymacrophages and activated T cells, actsthrough TNF receptors to stimulate the

187Drugs Used in Rheumatoid Arthritis and Gout
release of other cytokines. TNF blockingdrugs are found to be useful in rheumatoidarthritis.Infliximab is a monoclonal antibody whichspecifically binds to human TNF. When givenin combination with methotrexate, it slowsthe progression of rheumatoid arthritis.Adverse effects of the combination includeincreased susceptibility to upper respiratoryinfections, nausea, headache, cough, sinusitisand skin rashes.Etanercept is a recombinant fusion protein thatbinds to TNF molecules. It is found to slowthe progression of the disease in rheumatoidarthritis patients. It is also found to be usefulin psoriatic and juvenile arthritis. Etanerceptis also given with methotrexate and thecombination has a higher efficacy. It cancause pain, itching and allergic reactions atthe site of injection.Immunosuppressants are reserved for patientswith seriously crippling disease withreversible lesions after conventional therapyhas failed. Among the immunosuppressants,methotrexate (see page 330) is the besttolerated. Weekly regimens of low oral dosesare given.Leflunomide is a prodrug. The activemetabolite inhibits autoimmune T cellproliferation and production of auto-antibodies by B cells. Leflunomide is orallyeffective, and has a long t½ of 5-40 days.Adverse effects include diarrhoea and raisedhepatic enzymes.
Leflunomide is used with methotrexate inrheumatoid arthritis patients who do notrespond to methotrexate alone.
Corticosteroids
Glucocorticoids (chap-55) have anti-inflammatory and immunosuppressantactivity. They produce prompt and dramaticrelief of symptoms but do not arrest the
progress of the disease. However, long-termuse of these drugs leads to several adverseeffects. Moreover, on withdrawal of gluco-corticoids, there may be an exacerbation ofthe disease. Therefore glucocorticoids areused as adjuvants. They may be used to treatexacerbations. Low dose long-term treatmentwith prednisolone is used in some patients(5-10 mg/day).
Intra-articular corticosteroids are helpfulto relieve pain in severely inflamed joints.
Diet and Inflammation
Clinical studies have shown that whenpatients of rheumatoid arthritis are given adiet rich in unsaturated fatty acids (such asmarine fish), there is a decrease in morningstiffness, pain and swelling of the joints.Unsaturated fatty acids compete witharachidonic acid for uptake and metabolism.Many products of arachidonic acid meta-bolism are mediators of inflammation.Adequate consumption of marine fish shouldbe recommended. For people who do not eatfish, eicosapentaenoic acid 1-4 gm/day maybe given as tablets. It serves as an adjuvant.
Relevance in Dentistry
1. Treatment with gold can cause glossitis.2. Gold, d-penicillamine, immunosupp-
ressants and glucocorticoids depressimmunity. Treatment of dental infectionrequires powerful antibiotics in suchpatients.
PHARMACOTHERAPY OF GOUT
Gout is a familial metabolic disorder chara-cterised by recurrent episodes of acutearthritis due to deposits of monosodium uratein the joints and cartilage. There is aninherent abnormality of purine metabolismresulting in over production of uric acid—amajor end product of purine metabolism. As

Textbook of Pharmacology for Dental and Allied Health Sciences188
uric acid is poorly water soluble, it getsprecipitated—especially at low pH and isdeposited in the cartilages of joints and ears,subcutaneous tissues, bursae and sometimesin kidneys. An acute attack of gout occurs asan inflammatory reaction to crystals ofsodium urate deposited in the joint tissue.There is infiltration of granulocytes whichphagocytize the urate crystals and release aglycoprotein that causes joint destruction.The joint becomes red, swollen, tender andextremely painful.
Secondary hyperuricaemia may be druginduced or may occur in lymphomas andleukaemias. Gout may also be due todecreased excretion of uric acid.
Strategies in the treatment of gout is eitherto decrease the biosynthesis of uric acid orenhance the excretion of uric acid.
Drugs Used in Gout
In acute gout:Colchicine, NSAIDs.
In chronic gout:Uric acid synthesis inhibitor
AllopurinolUricosuric drugs
Probenecid, sulphinpyrazone,benzbromarone.
Colchicine is an alkaloid of Colchicumautumnale. It is a unique anti-inflammatoryagent effective only against gouty arthritis.It is not an analgesic.Actions In gout, colchicine is highly effectivein acute attacks and it dramatically relievespain within a few hours. It increases gutmotility by neurogenic stimulation.Mechanism of action Colchicine inhibits themigration of granulocytes into the inflamedarea and the release of glycoprotein by them.Colchicine binds to micro-tubules and arrestscell division in metaphase.Pharmacokinetics Colchicine is rapidlyabsorbed orally, metabolised in the liver andundergoes enterohepatic circulation.
Adverse effects are dose related. Nausea,vomiting, diarrhoea and abdominal pain arethe earliest side effects and may be avoidedby giving colchicine intravenously. Anaemia,leukopenia and alopecia may be seen. In highdoses haemorrhagic gastroenteritis,nephrotoxicity, CNS depression, muscularparalysis and respiratory failure can occur.
Uses
1. Acute gout—colchicine 1 mg orally initiallyfollowed by 0.5 mg every 2-3 hoursrelieves pain and swelling within 12 hours.But diarrhoea limits its use.
2. Prophylaxis—Colchicine may also be usedfor the prophylaxis of recurrent episodesof gouty arthritis.
NSAIDs afford symptomatic relief in thetreatment of gout. Indomethacin is the mostcommonly used agent in acute gout.Piroxicam, naproxen and other newerNSAIDs are also used. They relieve an acuteattack in 12-24 hours and are better toleratedthan colchicine. But NSAIDs are notrecommended for long-term use due to theirtoxicity.Allopurinol is an analog of hypoxanthine andinhibits the biosynthesis of uric acid.Mechanism of action Purine nucleotides aredegraded to hypoxanthine. Uric acid isproduced as shown in Figure 28.1.Allopurinol and its metabolite alloxanthineboth inhibit the enzyme xanthine oxidase andthereby prevent the synthesis of uric acid. Theplasma concentration of uric acid is reduced.Pharmacokinetics Allopurinol is 80% absorbedorally; t½ of allopurinol is 2-3 hr; t½ ofalloxanthine is 24 hours.Adverse effects are mild. Hypersensitivityreactions include fever and rashes.Gastrointestinal irritation, headache, nauseaand dizziness may occur.
Attacks of acute gouty arthritis may be seenfrequently during the initial months oftreatment with allopurinol.
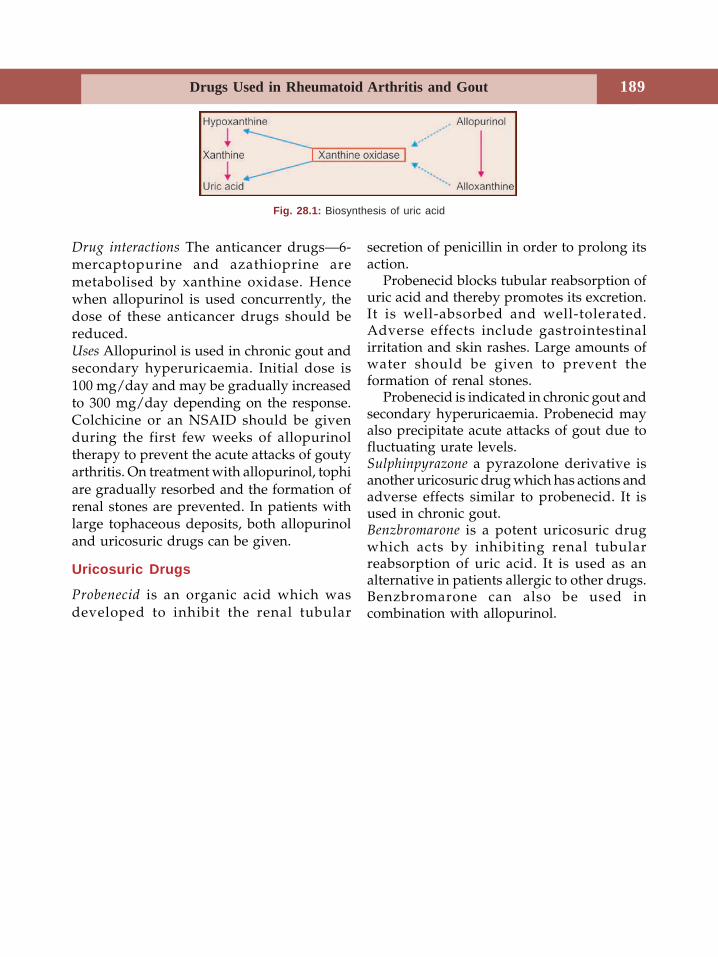
189Drugs Used in Rheumatoid Arthritis and Gout
Drug interactions The anticancer drugs—6-mercaptopurine and azathioprine aremetabolised by xanthine oxidase. Hencewhen allopurinol is used concurrently, thedose of these anticancer drugs should bereduced.Uses Allopurinol is used in chronic gout andsecondary hyperuricaemia. Initial dose is100 mg/day and may be gradually increasedto 300 mg/day depending on the response.Colchicine or an NSAID should be givenduring the first few weeks of allopurinoltherapy to prevent the acute attacks of goutyarthritis. On treatment with allopurinol, tophiare gradually resorbed and the formation ofrenal stones are prevented. In patients withlarge tophaceous deposits, both allopurinoland uricosuric drugs can be given.
Uricosuric Drugs
Probenecid is an organic acid which wasdeveloped to inhibit the renal tubular
secretion of penicillin in order to prolong itsaction.
Probenecid blocks tubular reabsorption ofuric acid and thereby promotes its excretion.It is well-absorbed and well-tolerated.Adverse effects include gastrointestinalirritation and skin rashes. Large amounts ofwater should be given to prevent theformation of renal stones.
Probenecid is indicated in chronic gout andsecondary hyperuricaemia. Probenecid mayalso precipitate acute attacks of gout due tofluctuating urate levels.Sulphinpyrazone a pyrazolone derivative isanother uricosuric drug which has actions andadverse effects similar to probenecid. It isused in chronic gout.Benzbromarone is a potent uricosuric drugwhich acts by inhibiting renal tubularreabsorption of uric acid. It is used as analternative in patients allergic to other drugs.Benzbromarone can also be used incombination with allopurinol.
Fig. 28.1: Biosynthesis of uric acid
Textbook of Pharmacology for Dental and Allied Health Sciences190
29 Drugs Used inPsychiatric Disorders
ANTIPSYCHOTICS
Since ages man has sought the help of drugsto modify behaviour, mood and emotion.Psychoactive drugs were used both forrecreational purposes and for the treatmentof mental illnesses (Psyche = mind).
In 1931 Sen and Bose showed that Rawolfiaserpentina is useful in the treatment ofinsanity. Electroconvulsive therapy (ECT)was introduced in 1937 for the treatment ofdepression. In 1950 chlorpromazine wassynthesized in France and its usefulness inpsychiatric patients was demonstrated in1952. During the second half of the twentiethcentury, extensive research has been carriedout in psychopharmacology and we now haveseveral useful drugs in this branch ofpharmacology.Psychiatric conditions are broadly dividedinto psychoses, neuroses and personalitydisorders.Psychoses are the more severe psychiatricdisorders of the three and involve a markedimpairment of behaviour, inability to thinkcoherently, and to comprehend reality.Patients have no ‘insight’ into theseabnormalities.Psychoses could be due to:(i) An organic cause, i.e. there is a definable
toxic, metabolic or pathological change–as following head injury.
(ii) Functional or idiopathic disorders–wherethere is no definable cause like inschizophrenia, paranoia and affectivedisorders.
Schizophrenia (split mind) affects about 1% ofpopulation, starts at an early age and is highlyincapacitating. It has a strong heriditarytendency and is characterised by delusions,hallucinations, irrational conclusions,interpretations and withdrawal from socialcontacts. Symptoms are grouped as positiveand negative.Positive symptoms includedelusions, hallucinations and disorders ofthought while negative symptoms include poorconcentration, social withdrawal, poverty ofspeech and lack of initiative and energy.Negative symptoms generally indicate poorprognosis and these symptoms do notrespond to antipsychotic drugs. Patients withchronic schizophrenia have progressiveshrinkage of the brain.
The pathology is not exactly understood butavailable evidence suggest overactivity of theneurotransmitters—mainly dopamine andprobably others including glutamate and 5-HT.Neuroses are the milder forms of psychiatricdisorders and include anxiety, moodchanges, panic disorders, obsessions,irrational fears and reactive depression asseen following tragedies.Personality disorders include paranoid,schizoid, histrionic, avoidant, antisocial andobsessive compulsive personality types.
Drugs Used in Psychiatric Disorders 191
Drugs used in psychiatric illnesses may be groupedas:1. Antipsychotics or neuroleptics – used in
psychoses.2. Antidepressant drugs – used in affective
disorders.3. Antianxiety drugsPsychotropic drugs are drugs used in mentalillnesses - they are drugs capable of affectingthe mind, emotions and behaviour.Neuroleptic is a drug that reduces initiative,brings about emotional quietening and inducesdrowsiness. Tranquilliser is a drug that bringsabout tranquillity by calming, soothing andquietening effects. This is the older terminology.Neuroleptics or antipsychotics were called‘major tranquillisers’ and antianxiety drugs werecalled ‘minor tranquillisers’. These terminologiesare no longer used.
ANTIPSYCHOTICS (NEUROLEPTICS)Classification1. Classical/typical neuroleptics
a. Phenothiazines–Chlorpromazine, triflupromazine,thioridazine, mesoridazine,trifluoperazine, fluphenazine.
b. Butyrophenones–Haloperidol, droperidol,trifluperidol, penfluridol.
c. Thioxanthenes–Thiothixene, chlorprothixene,flupenthixol
2. Atypical neuroleptics–Clozapine, olanzapine,risperidone, quetiapine,ziprasidone, amisulpride,remoxipride.
3. Miscellaneous–Reserpine, loxapine,pimozide.
Chlorpromazine (CPZ)Mechanism of action– Typical neuroleptics actby blocking the dopamine D2 receptors in the
CNS (Fig. 29.1). Since dopaminergicoveractivity, mainly in the limbic area, isthought to be responsible for schizophrenia,DA receptor blockade helps. Some of themlike phenothiazines also block D1, D3, and D4receptors. (There are 5 subtypes of dopaminereceptors D1 to D5). Dopamine receptorblockade also is responsible for the classicalside effects of these agents.
Pharmacological Actions
CNS Behavioural effects–in normal subjectsCPZ reduces motor activity, producesdrowsiness and indifference to surroundings.In psychotic agitated patients, it reducesaggression, initiative and motor activity,relieves anxiety and brings about emotionalquietening and drowsiness. It normalises thesleep disturbances characteristic of psychoses.Other CNS Actions1. Cortex CPZ lowers seizure threshold and
can precipitate convulsions in untreatedepileptics.
2. Hypothalamus CPZ decreases gonado-trophin secretion and may result inamenorrhoea in women. It increases thesecretion of prolactin resulting ingalactorrhoea and gynaecomastia.
3. Basal ganglia CPZ acts as a dopamineantagonist and therefore results inextrapyramidal motor symptoms (druginduced parkinsonism).
4. Brainstem Vasomotor reflexes aredepressed leading to a fall in BP.
5. CTZ Neuroleptics block the dopamine(DA) receptors in the CTZ and therebyact as antiemetics.
Autonomic nervous system The actions on theANS are complex. CPZ is an alpha blocker.The alpha blocking potency varies with eachneuroleptic. CPZ also has anticholinergicproperties which leads to side effects likedryness of mouth, blurred vision, reducedsweating, decreased gastric motility,
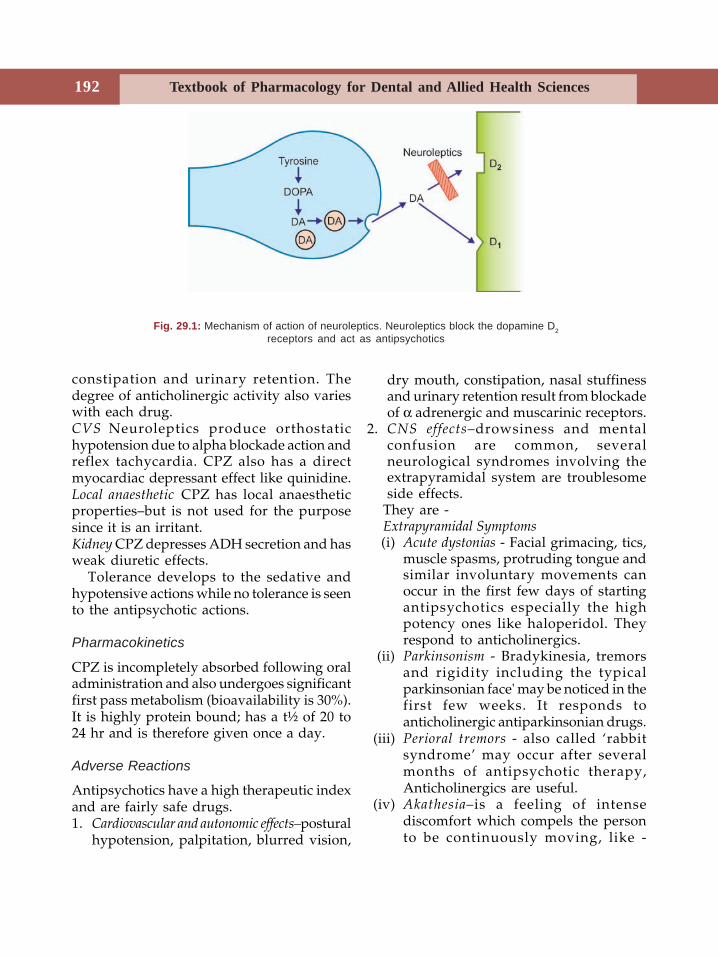
Textbook of Pharmacology for Dental and Allied Health Sciences192
Fig. 29.1: Mechanism of action of neuroleptics. Neuroleptics block the dopamine D2receptors and act as antipsychotics
constipation and urinary retention. Thedegree of anticholinergic activity also varieswith each drug.CVS Neuroleptics produce orthostatichypotension due to alpha blockade action andreflex tachycardia. CPZ also has a directmyocardiac depressant effect like quinidine.Local anaesthetic CPZ has local anaestheticproperties–but is not used for the purposesince it is an irritant.Kidney CPZ depresses ADH secretion and hasweak diuretic effects.
Tolerance develops to the sedative andhypotensive actions while no tolerance is seento the antipsychotic actions.
Pharmacokinetics
CPZ is incompletely absorbed following oraladministration and also undergoes significantfirst pass metabolism (bioavailability is 30%).It is highly protein bound; has a t½ of 20 to24 hr and is therefore given once a day.
Adverse Reactions
Antipsychotics have a high therapeutic indexand are fairly safe drugs.1. Cardiovascular and autonomic effects–postural
hypotension, palpitation, blurred vision,
dry mouth, constipation, nasal stuffinessand urinary retention result from blockadeof α adrenergic and muscarinic receptors.
2. CNS effects–drowsiness and mentalconfusion are common, severalneurological syndromes involving theextrapyramidal system are troublesomeside effects.
They are -Extrapyramidal Symptoms(i) Acute dystonias - Facial grimacing, tics,
muscle spasms, protruding tongue andsimilar involuntary movements canoccur in the first few days of startingantipsychotics especially the highpotency ones like haloperidol. Theyrespond to anticholinergics.
(ii) Parkinsonism - Bradykinesia, tremorsand rigidity including the typicalparkinsonian face' may be noticed in thefirst few weeks. It responds toanticholinergic antiparkinsonian drugs.
(iii) Perioral tremors - also called ‘rabbitsyndrome’ may occur after severalmonths of antipsychotic therapy,Anticholinergics are useful.
(iv) Akathesia–is a feeling of intensediscomfort which compels the personto be continuously moving, like -
Drugs Used in Psychiatric Disorders 193
constant walking. It necessitates areduction in antipsychotic dosage andtreatment with propranolol or otherantianxiety drugs.
(v) Tardive dyskinesia–appears after monthsor years of therapy and is characterisedby involuntary movements of the face,tongue, eyelids, trunk and limbs. It canbe disabling. Atypical antipsychoticslike clozapine may be beneficial in suchpatients.
(vi) Malignant neuroleptic syndrome ischaracterised by immobility, tremorsand fever with autonomic effects likefluctuating blood pressure and heartrate. It can be fatal and requiresimmediate stopping of the neuroleptic.Dantrolene and bromocriptine may beuseful.
3. Endocrine disturbances–gynaecomastia,amenorrhoea and galactorrhoea due toDA receptor blockade.
4. Hypersensitivity reactions–jaundice,agranulocytosis and skin rashes.
Drug Interactions
Neuroleptics enhance the sedative effects ofCNS depressants, alpha blockers and ofanticholinergic drugs. When combined withthese groups of drugs, the effects may beadditive.
Neuroleptics antagonise the actions ofdopamine agonists and levodopa.
Uses
Neuroleptics are given orally. (Table 29.1).In acute psychosis they may be givenintramuscularly and response is seen in 24 hrwhile in chronic psychosis it takes 2-3 weeksof treatment to demonstrate the beginningof obvious response.1. Psychiatric conditions Psychoses including
schizophrenia and organic brain
syndromes like delirium and dementia allrespond to antipsychotics.
2. Nausea, vomiting CPZ is a good antiemeticand is used in vomiting due to radiationsickness and drug induced vomiting.
3. Hiccough CPZ can control intractablehiccough though the mechanism of actionis not known.
4. Other neuropsychiatric syndromes Neuro-leptics are useful in the treatment ofseveral syndromes with psychiatricfeatures like psychoses associated withchronic alcoholism, Huntington’s diseaseand Gilles de La Tourette’s syndrome.
Haloperidol is a potent antipsychotic withactions similar to chlorpromazine. It differsfrom chlorpromazine in that it has lesserincidence of autonomic side effects and istherefore preferred in older patients.
Haloperidol is useful in acute schizo-phrenia, and is the drug of choice in Gillesde la Tourette’s syndrome and Huntington'sdisease.
Atypical Antipsychotics
The newer atypical antipsychotics likeclozapine and others have the advantages of1. Causing fewer side effects like less
sedation2. Being effective in suppressing both
positive and negative symptoms ofschizophrenia
3. Effective in resistant cases of psychoses.Clozapine is an effective antipsychotic. Itblocks the dopamine D
1 and D4 receptors buthas low affinity for D2 receptors. Hence ithas very low incidence of extrapyramidal sideeffects (EPS). Clozapine also blocks 5-HT2, αadrenergic and muscarinic receptors.Clozapine has the following advantages overconventional antipsychotics:1. Very low incidence of EPS2. Sedation is low.
Textbook of Pharmacology for Dental and Allied Health Sciences194
3. No endocrine side effects no galac-torrhoea and gynaecomastia.
4. It is effective in patients not respondingto conventional antipsychotics.
Adverse effects: The most importantdisadvantage with clozapine is that it maycause agranulocytosis in some patients, whichcan be fatal. Hence its use should be restrictedto patients not responding to otherconventional drugs. Moreover, regular WBCcounts are a must.Clozapine can also cause sedation, weightgain and hypotension.Olanzapine is similar to clozapine in actionsand advantages except that, olanzapine doesnot cause agranulocytosis.Quetiapine is an effective antipsychotic,similar in actions to clozapine. Drowsinessand postural hypotension are seen.Risperidone blocks serotonin (5HT2A) anddopamine (D2) receptors. It is effective againstboth positive and negative symptoms ofschizophrenia.
Advantages
1. At low doses no EPS dysfunction.2. Low sedation.Ziprasidone is an effective antipsychotic withactions and mechanism of action similar torisperidone.Amisulpride is a potent D2 and D3 antagonist.Its actions and advantages are similar torisperidone.Riserpine acts by depleting monoamines, i.e.NA and DA. It causes serious side effectsincluding depression because of which it isnow not preferred as an antipsychotic.
ANTIANXIETY DRUGS (ANXIOLYTICS)
Anxiety is tension or apprehension which isa normal response to certain situations in life.It is a universal human emotion. But when itbecomes excessive and disproportionate tothe situation, it becomes disabling and needstreatment.Antianxiety Drugs IncludeBenzodiazepines
Diazepam, chlordiazepoxide,lorazepam, alprazolam.
5-HT agonist-antagonistsBuspirone, gepirone, ipsapirone.
β-blockersPropranolol.
OthersMeprobamate, hydroxyzine.
Benzodiazepines (Chap 22) have goodantianxiety actions and are the mostcommonly used drugs for anxiety. They areCNS depressants. Alprazolam in addition hasantidepressant properties.Buspirone is an azapirone with good anxiolyticproperties. It is a selective 5-HT1A partialagonist. 5-HT1A receptors are inhibitoryautoreceptors and binding of buspironeinhibits the release of 5HT. Buspirone is alsoa weak D2 antagonist. It is useful in mild tomoderate anxiety. Antianxiety effect
Table 29.1: Therapeutic dosage of commonly used antipsychotics
Drug Antipsychotic
dose in mg/day
Chlorpromazine 100-800Triflupromazine 50-200Thioridazine 100-400Trifluoperazine 2-20Fluphenazine 1-10Haloperidol 2-20Trifluperidol 1-8Flupenthixol 3-15Loxapine 20-100Clozapine 50-300Olanzapine 2.5-10Risperidone 2-12Pimozide 2-6Sertindol 4-24
Drugs Used in Psychiatric Disorders 195
develops slowly over 2 weeks. Unlikediazepam, it is not a muscle relaxant, not ananticonvulsant, does not produce significantsedation, tolerance or dependence and is notuseful in panic attacks.
Buspirone is rapidly absorbed andmetabolised in the liver.Dose 5-15 mg OD or TDS.Side effects are mild including headache,dizziness, nausea and rarely restlessness.Uses Buspirone is used in mild to moderateanxiety and is particularly beneficial whensedation is to be avoided. Ipsapirone andgepirone are similar to buspirone.β-blockers (Chap 12) In patients withprominent autonomic symptoms of anxietylike tremors, palpitation and hypertension,propranolol may be useful. β-blockers arealso useful in anxiety inducing states likepublic speaking and stage performance.They can be used as adjuvants tobenzodiazepines.
OthersMeprobamate has anxiolytic property but is notpreferred now as it is less effective andcauses high sedation.Hydroxyzine is an antihistaminic withanxiolytic actions. But due to high sedationit is not preferred.
ANTIDEPRESSANTS
Affective disorders are a group of psychosesassociated with changes of mood, i.e.depression and mania.Depression is a common psychiatric disorderbut the aetiology of it is not clear.Depression could be1. Unipolar
• Reactive• Endogenous
2. Bipolar mood disorder or manicdepressive illness.
Reactive depression is due to stressful anddistressing circumstances in life.
Endogenous depression is major depression andresults from a biochemical abnormality in thebrain. Deficiency of monoamine (NA, 5HT)activity in the CNS is thought to beresponsible for endogenous depression.Symptoms are• Emotional symptoms - sadness, misery,
hopelessness, low self esteem, loss ofinterest and suicidal thoughts.
• Biological symptoms - fatigue, apathy, lossof libido, loss of appetite, lack ofconcentration and sleep disturbances.
Bipolar depression is characterised by alternatemania and depression. It is less common andis associated with a hereditary tendency.Mania can be considered opposite ofdepression with elation, over-enthusiasm,over-confidence, often associated withirritation and aggression.
Drugs Used in Affective Disorders are
Classification
1. Tricyclic antidepressants (TCA)–Imipramine, desipramine,clomipramine, amitriptyline,nortriptyline, doxepin
2. Selective serotonin reuptake inhibitors (SSRI)–Fluoxetine, fluoxamine, paroxetine,citalopram, sertraline,
3. Monoamine oxidase (MAO) inhibitors –Phenelzine, tranylcypromine,isocarboxazid, moclobemide.
4. Atypical antidepressantsTrazodone, nefazodone,venlafaxine, bupropion, mianserine,mirtazapine, reboxetine.
Tricyclic Antidepressants
Pharmacological Actions
1. CNS In normal subjects, TCA causedizziness, drowsiness, confusion anddifficulty in thinking. In depressed
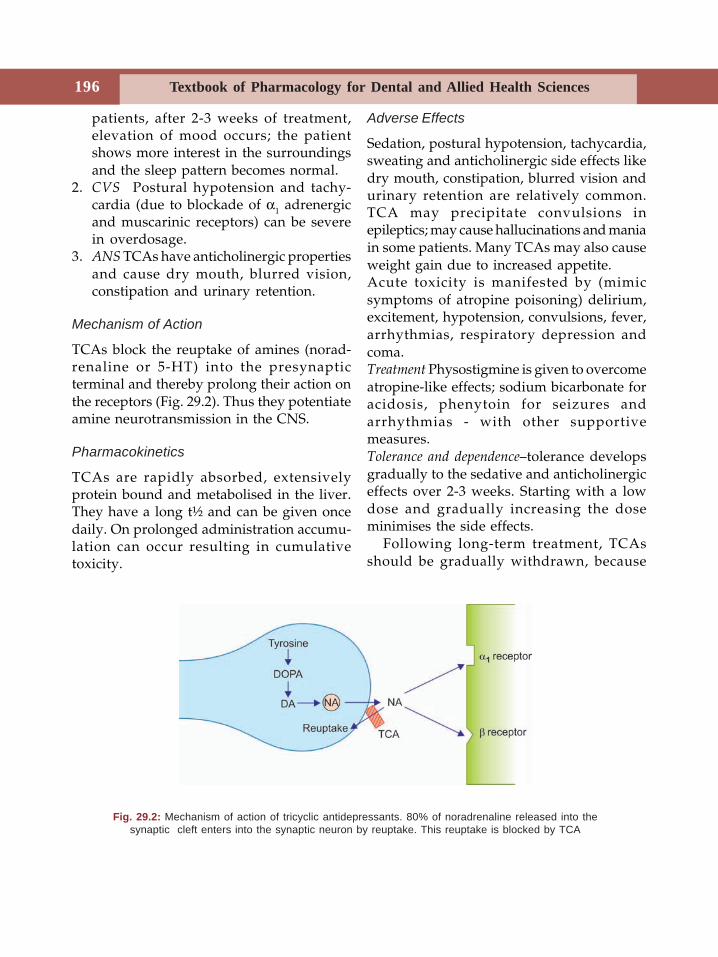
Textbook of Pharmacology for Dental and Allied Health Sciences196
patients, after 2-3 weeks of treatment,elevation of mood occurs; the patientshows more interest in the surroundingsand the sleep pattern becomes normal.
2. CVS Postural hypotension and tachy-cardia (due to blockade of α1 adrenergicand muscarinic receptors) can be severein overdosage.
3. ANS TCAs have anticholinergic propertiesand cause dry mouth, blurred vision,constipation and urinary retention.
Mechanism of Action
TCAs block the reuptake of amines (norad-renaline or 5-HT) into the presynapticterminal and thereby prolong their action onthe receptors (Fig. 29.2). Thus they potentiateamine neurotransmission in the CNS.
Pharmacokinetics
TCAs are rapidly absorbed, extensivelyprotein bound and metabolised in the liver.They have a long t½ and can be given oncedaily. On prolonged administration accumu-lation can occur resulting in cumulativetoxicity.
Adverse Effects
Sedation, postural hypotension, tachycardia,sweating and anticholinergic side effects likedry mouth, constipation, blurred vision andurinary retention are relatively common.TCA may precipitate convulsions inepileptics; may cause hallucinations and maniain some patients. Many TCAs may also causeweight gain due to increased appetite.Acute toxicity is manifested by (mimicsymptoms of atropine poisoning) delirium,excitement, hypotension, convulsions, fever,arrhythmias, respiratory depression andcoma.Treatment Physostigmine is given to overcomeatropine-like effects; sodium bicarbonate foracidosis, phenytoin for seizures andarrhythmias - with other supportivemeasures.Tolerance and dependence–tolerance developsgradually to the sedative and anticholinergiceffects over 2-3 weeks. Starting with a lowdose and gradually increasing the doseminimises the side effects.
Following long-term treatment, TCAsshould be gradually withdrawn, because
Fig. 29.2: Mechanism of action of tricyclic antidepressants. 80% of noradrenaline released into thesynaptic cleft enters into the synaptic neuron by reuptake. This reuptake is blocked by TCA
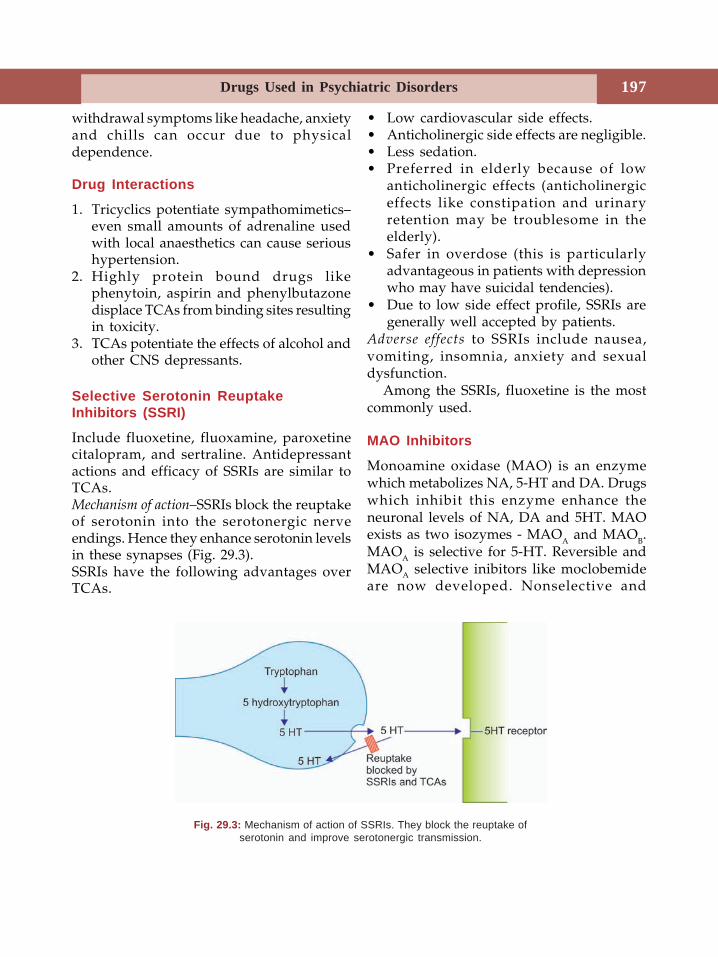
Drugs Used in Psychiatric Disorders 197
withdrawal symptoms like headache, anxietyand chills can occur due to physicaldependence.
Drug Interactions
1. Tricyclics potentiate sympathomimetics–even small amounts of adrenaline usedwith local anaesthetics can cause serioushypertension.
2. Highly protein bound drugs likephenytoin, aspirin and phenylbutazonedisplace TCAs from binding sites resultingin toxicity.
3. TCAs potentiate the effects of alcohol andother CNS depressants.
Selective Serotonin ReuptakeInhibitors (SSRI)
Include fluoxetine, fluoxamine, paroxetinecitalopram, and sertraline. Antidepressantactions and efficacy of SSRIs are similar toTCAs.Mechanism of action–SSRIs block the reuptakeof serotonin into the serotonergic nerveendings. Hence they enhance serotonin levelsin these synapses (Fig. 29.3).SSRIs have the following advantages overTCAs.
• Low cardiovascular side effects.• Anticholinergic side effects are negligible.• Less sedation.• Preferred in elderly because of low
anticholinergic effects (anticholinergiceffects like constipation and urinaryretention may be troublesome in theelderly).
• Safer in overdose (this is particularlyadvantageous in patients with depressionwho may have suicidal tendencies).
• Due to low side effect profile, SSRIs aregenerally well accepted by patients.
Adverse effects to SSRIs include nausea,vomiting, insomnia, anxiety and sexualdysfunction.
Among the SSRIs, fluoxetine is the mostcommonly used.
MAO Inhibitors
Monoamine oxidase (MAO) is an enzymewhich metabolizes NA, 5-HT and DA. Drugswhich inhibit this enzyme enhance theneuronal levels of NA, DA and 5HT. MAOexists as two isozymes - MAOA and MAOB.MAOA is selective for 5-HT. Reversible andMAOA selective inibitors like moclobemideare now developed. Nonselective and
Fig. 29.3: Mechanism of action of SSRIs. They block the reuptake ofserotonin and improve serotonergic transmission.
Textbook of Pharmacology for Dental and Allied Health Sciences198
irreversible MAO inhibitors- phenelzine andtranylcypromine are associated with severalside effects and risk of many food-druginteractions.Tranylcypromine and Phenelzine:• Irreversibly inhibit the enzyme MAO and
enhance neuronal levels of noradrenaline,dopamine and 5-HT.
• Antidepressant actions develop slowlyover weeks of treatment.
• Most of them are long acting and require1-2 weeks for recovery of MAO activityafter stopping the drug.
• Side effects are hypotension, weight gain,restlessness, insomnia (due to CNSstimulation), anticholinergic effects andrarely liver dysfunction.
• They interact with many drugs and food.• Patients on MAO inhibitors taking
tyramine containing foods like cheese,beer, wine, yeast, buttermilk and fish–develop severe hypertension and isknown as ‘cheese reaction.’ Tyramine isnormally metabolised by MAO in the gutwall. On inhibition of MAO by drugs,tyramine escapes metabolism anddisplaces NA from nerve endings leadingto hypertension.
• Similar interaction with SSRIs can resultin severe hypertension (serotoninsyndrome).
• Because of the side effects and druginteractions, MAO inhibitors are not thepreferred antidepressants.
Moclobemide is a reversible, competitive,selective MAOA inhibitor. It is short actingand MAO activity recovers within 1-2 daysafter stopping the drug. It is found to be aneffective antidepressant and has theadvantages that it is not a sedative, does notproduce cardiovascular and anticholinergicside effects. Hence it is well tolerated. Nosignificant drug interactions are seen.
Adverse effects include nausea, insomnia,headache and dizziness.
Moclobemide is used in mild to moderatedepression as an alternative to TCA.
Atypical Antidepressants
Atypical antidepressants include trazodone,bupropion, mianserin, nefazodone andmirtazapine.
Advantages
• Fewer side effects–particularly sedationand anticholinergic effects
• Safer in overdose• Effective in patients not responding to
TCA.Trazodone is a weak serotonin reuptakeinhibitor. It is short acting (t ½ - 6 hr) andlacks anticholinergic activity. It is welltolerated and safe in overdosage. It can causepostural hypotension and priapism due to itsα1 blocking effects.Nefazodone blocks serotonin reuptake and isan effective antidepressant. It is welltolerated-causes sedation and mild posturalhypotension. Nefazodone is used in theprophylaxis of recurrent depression.Venlafaxine is considered by some as atypialantidepressant because it inhibits thereuptake of noradrenaline in addition to 5HT (Serotonin and noradrenaline reuptakeinhibitor - SNRI). It is thought to be fasteracting and may be useful in patients notresponding to other antidepressants.Mirtazapine blocks 5HT2, 5HT3 and α2
receptors and enhances the release of NA and5HT. It is faster acting - action starts by oneweek of treatment. It causes sedation butother side effects are negligible.Bupropion is a weak DA reuptake inhibitorand has CNS stimulant effects. It is used indepression with anxiety. Bupropion is alsoused to help stop smoking (along withnicotine patch).
Drugs Used in Psychiatric Disorders 199
Mianserin acts by blocking presynaptic α2receptors but toxicity including blooddyscrasias, seizures and liver damage haslimited its use.
Uses of Antidepressants
1. Endogenous depression Antidepressants areused over a long period. The responseappears after 2-3 weeks of treatment. Thechoice of drug depends on the side effectsand patient factors like age. In severedepression with suicidal tendencies,electroconvulsive therapy (ECT) is given.
2. Panic attacks, Post-traumatic stress disordersand other anxiety disorders–all respondto antidepressants (acute episodes ofanxiety are known as panic attacks).
3. Obsessive compulsive disorders SSRIs andclomipramine are effective.
4. Nocturnal enuresis in children may betreated with antidepressants only whenother measures fail and drugs areindicated.
5. Psychosomatic disorders Newer antide-pressants are tried in fibromyalgia,irritable bowel syndrome, chronic fatigue,tics, migraine and sleep apnoea.
6. Other indications Attention deficithyperactivity disorder, chronic pain andchronic alcoholism–may result indepression–antidepressants are tried.
MOOD STABILIZERSMood stabilzers control the mood swingsthat are seen in bipolar mood disorders.Mood stablizers include–LithiumSodium valproateCarbamazepineLamotrigineGabapentinLithium has been used for several decadesbut several antiepileptics like carbamazepine,valproic acid and gabapentin are now beingtried.
Lithium is a monovalent cation. Onprophylactic use in bipolar mood disorder(manic-depressive illness), lithium acts as amood stabilizer. It prevents swings of moodand thus reduces both the depressive andmanic phases of the illness. Given in acutemania, it gradually suppresses the episodeover weeks.Mechanism of action of lithium is complex andnot fully understood. It is thought thatlithium blocks the formation of inositol fromIP3 and thereby inhibits the regeneration ofphosphotidyl inositol (PI) Depletion ofmembrane phosphotidyl inositol results ininhibition of receptor mediated effectsthrough IP3 and DAG. This is the acceptedmechanism of action.Pharmacokinetics Lithium is a small ion andmimics the role of sodium in excitable tissues.Given orally it is well-absorbed. It is filteredat the glomerulus but reabsorbed likesodium. Steady state concentration is reachedin 5-6 days. Lithium is secreted in sweat,saliva and breast milk. Since safety margin isnarrow, plasma lithium concentration needs tobe monitored (0.5-1 mEq/lit is the therapeuticplasma concentration). 3-5 mEq/lit can causefatal toxicity.Adverse effects Lithium is a drug of lowtherapeutic index and side effects arecommon. Nausea, vomiting, mild diarrhoea,thirst and polyuria occur initially in mostpatients. Weight gain can also occur. As theplasma concentration rises, hypothyroidism,CNS effects like coarse tremors, drowsiness,giddiness, confusion, ataxia, blurred visionand nystagmus are seen. In severeoverdosage, delirium, muscle twitchings,convulsions, arrhythmias and renal failuredevelop.
Precautions
1. Minimum effective dose should be used.2. Patients should always use the same
formulation.
Textbook of Pharmacology for Dental and Allied Health Sciences200
3. Patients should be made aware of the firstsymptom of toxicity.
4. Lithium is contraindicated in pregnancy.
Drug Interactions
1. Diuretics enhance sodium loss and lithiumabsorption from the kidney. Thisincreases plasma lithium levels resultingin toxicity.
2. NSAIDs reduce lithium elimination andenhance toxicity.
Uses
1. Prophylaxis of bipolar mood disorder–episodes of mania and depression andtheir severity are reduced.
2. Acute mania – since the response to lithiumis slow, neuroleptics are preferred.
3. Depression – Lithium is tried along withother antidepressants as an add-on drugin the treatment of severe recurrentdepression.
4. Other uses – Lithium is tried in recurrentneuropsychiatric disorders, childhoodmood disorders, hyperthyroidism andinappropriate ADH secretion syndrome.
Other Mood Stabilizers
Because of difficulty in using lithium, otherdrugs are being tried. The antiepilepticscarbamazepine, sodium valproate andgabapentin are found to be useful, less toxicalternatives (see Chap 24).Carbamazepine is found to be effective inpreventing the relapses of bipolor mooddisorder and in the treatment of acutemania. It can be combined with lithium forbetter therapeutic effects but lithium canenhance the toxicity of carbamazepine.Sodium valproate can be tried alone in mild tomoderate cases or along with lithium inrefractory cases.Lamotrigine, gabapentin and other newerantiepileptics are being tried in theprophylaxis of bipolar mood disorder asalternatives to lithium.
200CNS Stimulants
30CNS Stimulants
Drugs that have a predominantly stimulanteffect on the CNS may be broadly dividedinto:1. Respiratory stimulants
Doxapram, nikethamide2. Psychomotor stimulants
Amphetamine, cocainemethylxanthines
3. ConvulsantsLeptazol, strychnine.
Respiratory stimulants are also called analeptics.These drugs stimulate respiration and aresometimes used to treat respiratory failure.Though they may bring about temporaryimprovement in respiration, the mortality isnot reduced. They have a low safety marginand may produce convulsions.Doxapram appears to act mainly on thebrainstem and spinal cord and increase theactivity of respiratory and vasomotorcentres.Adverse effects are nausea, cough,restlessness, hypertension, tachycardia,arrhythmias and convulsions.
Uses
1. Doxapram is occasionally used IV as ananaleptic in acute respiratory failure.
2. Apnoea in premature infants notresponding to theophylline.
Nikethamide is not used because of the risk ofconvulsions.
Psychomotor stimulants Amphetamine anddextroamphetamine are sympathomimeticdrugs (Chapter 11).Cocaine is a CNS stimulant, produces euphoriaand is a drug of abuse (Page 133).Methylxanthines Caffeine, theophylline andtheobromine are the naturally occurringxanthine alkaloids. The beverages—coffeecontains caffeine; tea contains theophyllineand caffeine; cocoa has caffeine andtheobromine.
Actions
CNS Caffeine and theophylline are CNSstimulants. They bring about an increase inmental alertness, a reduction of fatigue,produce a sense of well being and improvemotor activity and performance with a clearerflow of thought. Caffeine stimulates therespiratory centre. Higher doses produceirritability, nervousness, restlessness,insomnia, excitement and headache. Highdoses can result in convulsions.CVS Methylxanthines increase the force ofcontraction of the myocardium and increasethe heart rate and therefore increase thecardiac output. But, they also produceperipheral vasodilatation which tends todecrease the BP. The changes in BP aretherefore not consistent. Caffeine causesvasoconstriction of cerebral blood vessels.

Textbook of Pharmacology for Dental and Allied Health Sciences202
Kidneys The xanthines have a diuretic effectand thereby increase the urine output.Smooth muscle Xanthines cause relaxation ofsmooth muscles especially the bronchialsmooth muscle (Page 218).Skeletal muscle Xanthines enhance the powerof muscle contraction and thereby increasethe capacity to do muscular work by both acentral stimulant effect and the peripheralactions.GI tract Xanthines increase the secretion ofacid and pepsin in the stomach and are gastricirritants.Adverse effects include nervousness, insomnia,tremors, tachycardia, hypotension, arrhy-thmias, headache, gastritis, nausea, vomiting,epigastric pain and diuresis. High dosesproduce convulsions. Tolerance developsafter sometime. Habituation to caffeine iscommon.
Uses
(i) Headache Because of the effect of caffeineon cerebral blood vessels, it is combined
with ergotamine for the relief of migraineheadache. Caffeine is also combined withaspirin/paracetamol for the treatment ofheadache.
(ii) Bronchial asthma Theophylline is used inthe treatment of bronchial asthma.
NOOTROPICS
Nootropics are drugs that improve memoryand cognition. They are also called cognitionenhancers.Piracetam – described as a ‘nootropic agent’is thought to protect cerebral cortex fromhypoxia and improve learning and memory.In higher doses it also inhibits plateletaggregation. Adverse effects include inso-mnia, weight-gain, nervousness, depressionand gastrointestinal disturbances.Piracetam has been tried in dementia,myoclonus, stroke and other cerebrovascularaccidents; alcoholism, behavioural disordersand learning problems in children and invertigo. The beneficial effects in all these arenot proved.
31Autacoids
Section 6Autacoids
Autacoids are substances formed in varioustissues, have complex physiologic andpathologic actions and act locally at the siteof synthesis. They have a brief action andare destroyed locally. Hence they are called‘local hormones’ and differ from truehormones which are produced by specificcells and reach their target tissues throughcirculation. The word autacoid is derivedfrom Greek: autos = self akos = remedy.
Autacoids Include (Fig. 31.1)
Histamine, 5-hydroxytryptamineAngiotensin, kinins,Prostaglandins, leukotrienes,platelet activating factor.
HISTAMINE
Histamine or tissue amine (Histos = tissue) isa biogenic amine formed in many tissues. Itis also found in the venoms of bees, waspsand other stinging secretions.
Synthesis, Storage, Distribution andDegradation
In humans, histamine is formed by thedecarboxylation of the amino acid histidine.Large amounts are found in the lungs, skinand intestines. It is stored in the granules ofthe mast cells and basophils in an inactiveform. Non-mast cell histamine found in brain,
serves as a neurotransmitter. Degranulationof the mast cells release histamine which isquickly degraded by deamination andmethylation.
Mechanism of Action
Histamine produces its effects by acting onthe histamine receptors. Three subtypes areknown.• H1—present in lungs, gut, blood vessels,
nerve endings and brain.• H2—stomach (gastric glands), heart, blood
vessels and brain.• H3—CNS.
Actions
1. CVS Histamine dilates small blood vesselsresulting in hypotension accompanied by reflextachycardia. Cerebral blood vessels dilatewhich causes severe throbbing headache.Triple response Intradermal injection of his-tamine elicits triple response comprising of:
(i) red spot at the site (flush) - due to localcapillary dilation.
(ii) flare - redness surrounding the ‘flush’due to arteriolar dilatation.
(iii) wheal - local oedema due to the escapeof fluid from the capillaries.
This response is accompanied by pain anditching.2. Smooth muscle Histamine causes contr-action of the nonvascular smooth muscles.
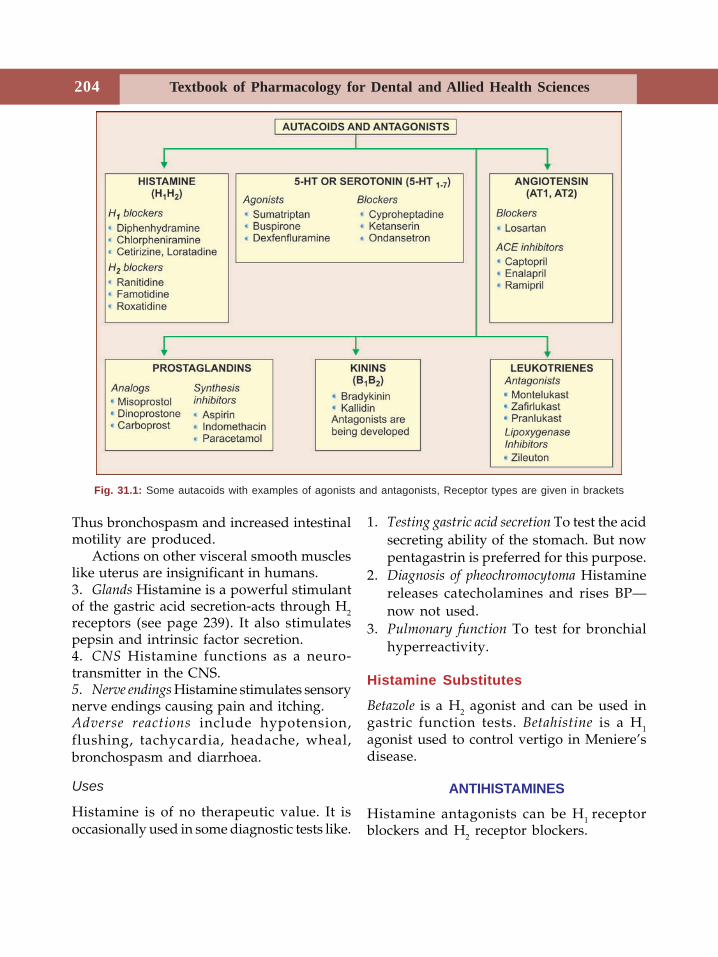
Textbook of Pharmacology for Dental and Allied Health Sciences204
Thus bronchospasm and increased intestinalmotility are produced.
Actions on other visceral smooth muscleslike uterus are insignificant in humans.3. Glands Histamine is a powerful stimulantof the gastric acid secretion-acts through H2receptors (see page 239). It also stimulatespepsin and intrinsic factor secretion.4. CNS Histamine functions as a neuro-transmitter in the CNS.5. Nerve endings Histamine stimulates sensorynerve endings causing pain and itching.Adverse reactions include hypotension,flushing, tachycardia, headache, wheal,bronchospasm and diarrhoea.
Uses
Histamine is of no therapeutic value. It isoccasionally used in some diagnostic tests like.
1. Testing gastric acid secretion To test the acidsecreting ability of the stomach. But nowpentagastrin is preferred for this purpose.
2. Diagnosis of pheochromocytoma Histaminereleases catecholamines and rises BP—now not used.
3. Pulmonary function To test for bronchialhyperreactivity.
Histamine Substitutes
Betazole is a H2 agonist and can be used ingastric function tests. Betahistine is a H1agonist used to control vertigo in Meniere’sdisease.
ANTIHISTAMINES
Histamine antagonists can be H1 receptorblockers and H2 receptor blockers.
Fig. 31.1: Some autacoids with examples of agonists and antagonists, Receptor types are given in brackets
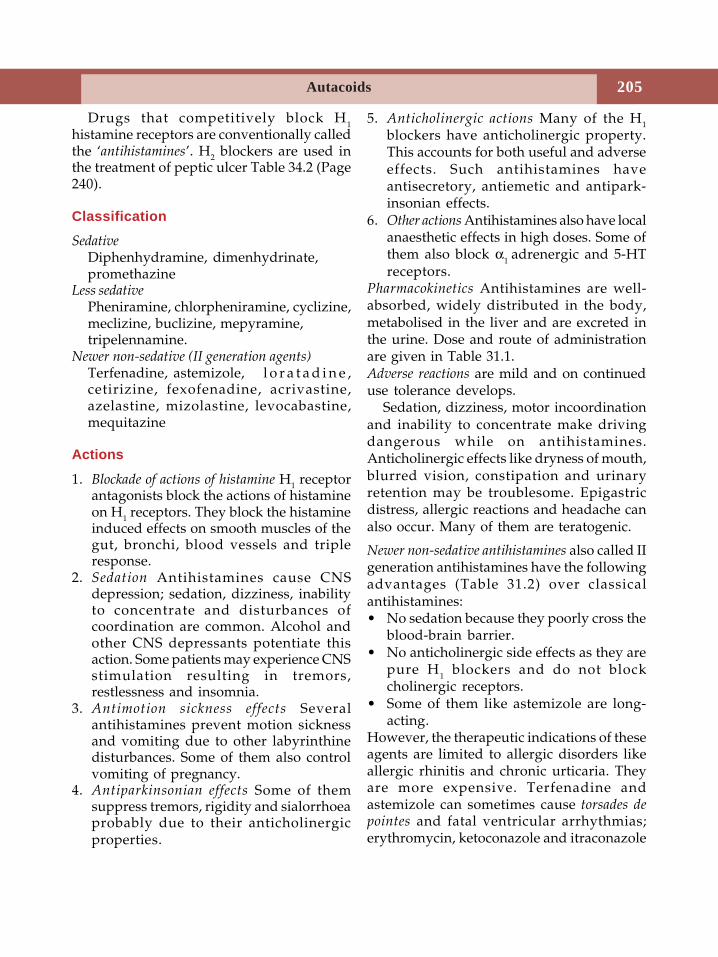
Autacoids 205
Drugs that competitively block H1histamine receptors are conventionally calledthe ‘antihistamines’. H2 blockers are used inthe treatment of peptic ulcer Table 34.2 (Page240).
Classification
SedativeDiphenhydramine, dimenhydrinate,promethazine
Less sedativePheniramine, chlorpheniramine, cyclizine,meclizine, buclizine, mepyramine,tripelennamine.
Newer non-sedative (II generation agents)Terfenadine, astemizole, l o r a t a d i n e ,cetirizine, fexofenadine, acrivastine,azelastine, mizolastine, levocabastine,mequitazine
Actions
1. Blockade of actions of histamine H1 receptorantagonists block the actions of histamineon H1 receptors. They block the histamineinduced effects on smooth muscles of thegut, bronchi, blood vessels and tripleresponse.
2. Sedation Antihistamines cause CNSdepression; sedation, dizziness, inabilityto concentrate and disturbances ofcoordination are common. Alcohol andother CNS depressants potentiate thisaction. Some patients may experience CNSstimulation resulting in tremors,restlessness and insomnia.
3. Antimotion sickness effects Severalantihistamines prevent motion sicknessand vomiting due to other labyrinthinedisturbances. Some of them also controlvomiting of pregnancy.
4. Antiparkinsonian effects Some of themsuppress tremors, rigidity and sialorrhoeaprobably due to their anticholinergicproperties.
5. Anticholinergic actions Many of the H1
blockers have anticholinergic property.This accounts for both useful and adverseeffects. Such antihistamines haveantisecretory, antiemetic and antipark-insonian effects.
6. Other actions Antihistamines also have localanaesthetic effects in high doses. Some ofthem also block α1 adrenergic and 5-HTreceptors.
Pharmacokinetics Antihistamines are well-absorbed, widely distributed in the body,metabolised in the liver and are excreted inthe urine. Dose and route of administrationare given in Table 31.1.Adverse reactions are mild and on continueduse tolerance develops.
Sedation, dizziness, motor incoordinationand inability to concentrate make drivingdangerous while on antihistamines.Anticholinergic effects like dryness of mouth,blurred vision, constipation and urinaryretention may be troublesome. Epigastricdistress, allergic reactions and headache canalso occur. Many of them are teratogenic.
Newer non-sedative antihistamines also called IIgeneration antihistamines have the followingadvantages (Table 31.2) over classicalantihistamines:• No sedation because they poorly cross the
blood-brain barrier.• No anticholinergic side effects as they are
pure H1 blockers and do not blockcholinergic receptors.
• Some of them like astemizole are long-acting.
However, the therapeutic indications of theseagents are limited to allergic disorders likeallergic rhinitis and chronic urticaria. Theyare more expensive. Terfenadine andastemizole can sometimes cause torsades depointes and fatal ventricular arrhythmias;erythromycin, ketoconazole and itraconazole
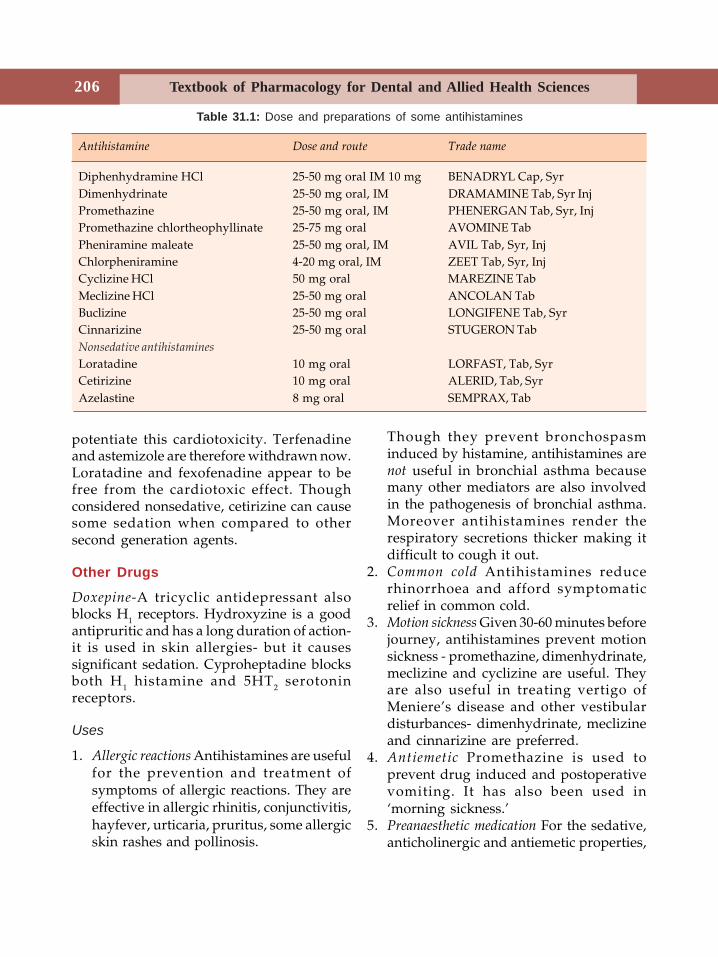
Textbook of Pharmacology for Dental and Allied Health Sciences206
potentiate this cardiotoxicity. Terfenadineand astemizole are therefore withdrawn now.Loratadine and fexofenadine appear to befree from the cardiotoxic effect. Thoughconsidered nonsedative, cetirizine can causesome sedation when compared to othersecond generation agents.
Other Drugs
Doxepine-A tricyclic antidepressant alsoblocks H1 receptors. Hydroxyzine is a goodantipruritic and has a long duration of action-it is used in skin allergies- but it causessignificant sedation. Cyproheptadine blocksboth H1 histamine and 5HT2 serotoninreceptors.
Uses
1. Allergic reactions Antihistamines are usefulfor the prevention and treatment ofsymptoms of allergic reactions. They areeffective in allergic rhinitis, conjunctivitis,hayfever, urticaria, pruritus, some allergicskin rashes and pollinosis.
Though they prevent bronchospasminduced by histamine, antihistamines arenot useful in bronchial asthma becausemany other mediators are also involvedin the pathogenesis of bronchial asthma.Moreover antihistamines render therespiratory secretions thicker making itdifficult to cough it out.
2. Common cold Antihistamines reducerhinorrhoea and afford symptomaticrelief in common cold.
3. Motion sickness Given 30-60 minutes beforejourney, antihistamines prevent motionsickness - promethazine, dimenhydrinate,meclizine and cyclizine are useful. Theyare also useful in treating vertigo ofMeniere’s disease and other vestibulardisturbances- dimenhydrinate, meclizineand cinnarizine are preferred.
4. Antiemetic Promethazine is used toprevent drug induced and postoperativevomiting. It has also been used in‘morning sickness.’
5. Preanaesthetic medication For the sedative,anticholinergic and antiemetic properties,
Table 31.1: Dose and preparations of some antihistamines
Antihistamine Dose and route Trade name
Diphenhydramine HCl 25-50 mg oral IM 10 mg BENADRYL Cap, SyrDimenhydrinate 25-50 mg oral, IM DRAMAMINE Tab, Syr InjPromethazine 25-50 mg oral, IM PHENERGAN Tab, Syr, InjPromethazine chlortheophyllinate 25-75 mg oral AVOMINE TabPheniramine maleate 25-50 mg oral, IM AVIL Tab, Syr, InjChlorpheniramine 4-20 mg oral, IM ZEET Tab, Syr, InjCyclizine HCl 50 mg oral MAREZINE TabMeclizine HCl 25-50 mg oral ANCOLAN TabBuclizine 25-50 mg oral LONGIFENE Tab, SyrCinnarizine 25-50 mg oral STUGERON TabNonsedative antihistamines
Loratadine 10 mg oral LORFAST, Tab, SyrCetirizine 10 mg oral ALERID, Tab, SyrAzelastine 8 mg oral SEMPRAX, Tab
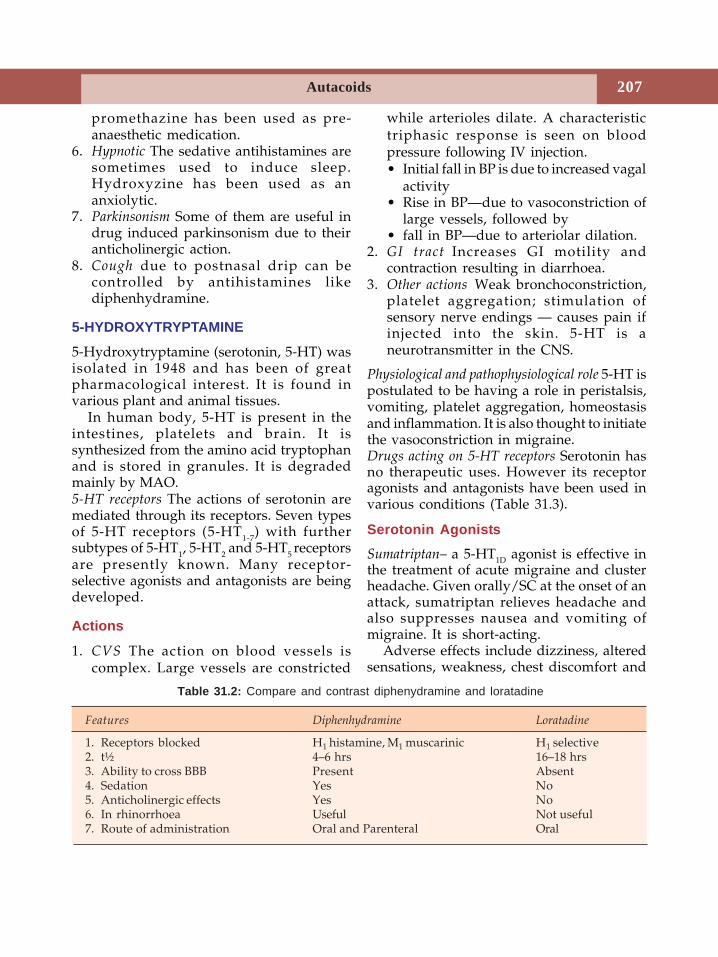
Autacoids 207
promethazine has been used as pre-anaesthetic medication.
6. Hypnotic The sedative antihistamines aresometimes used to induce sleep.Hydroxyzine has been used as ananxiolytic.
7. Parkinsonism Some of them are useful indrug induced parkinsonism due to theiranticholinergic action.
8. Cough due to postnasal drip can becontrolled by antihistamines likediphenhydramine.
5-HYDROXYTRYPTAMINE
5-Hydroxytryptamine (serotonin, 5-HT) wasisolated in 1948 and has been of greatpharmacological interest. It is found invarious plant and animal tissues.
In human body, 5-HT is present in theintestines, platelets and brain. It issynthesized from the amino acid tryptophanand is stored in granules. It is degradedmainly by MAO.5-HT receptors The actions of serotonin aremediated through its receptors. Seven typesof 5-HT receptors (5-HT1-7) with furthersubtypes of 5-HT1, 5-HT2 and 5-HT5 receptorsare presently known. Many receptor-selective agonists and antagonists are beingdeveloped.
Actions
1. CVS The action on blood vessels iscomplex. Large vessels are constricted
while arterioles dilate. A characteristictriphasic response is seen on bloodpressure following IV injection.• Initial fall in BP is due to increased vagal
activity• Rise in BP—due to vasoconstriction of
large vessels, followed by• fall in BP—due to arteriolar dilation.
2. GI tract Increases GI motility andcontraction resulting in diarrhoea.
3. Other actions Weak bronchoconstriction,platelet aggregation; stimulation ofsensory nerve endings — causes pain ifinjected into the skin. 5-HT is aneurotransmitter in the CNS.
Physiological and pathophysiological role 5-HT ispostulated to be having a role in peristalsis,vomiting, platelet aggregation, homeostasisand inflammation. It is also thought to initiatethe vasoconstriction in migraine.Drugs acting on 5-HT receptors Serotonin hasno therapeutic uses. However its receptoragonists and antagonists have been used invarious conditions (Table 31.3).
Serotonin Agonists
Sumatriptan– a 5-HT1D agonist is effective inthe treatment of acute migraine and clusterheadache. Given orally/SC at the onset of anattack, sumatriptan relieves headache andalso suppresses nausea and vomiting ofmigraine. It is short-acting.
Adverse effects include dizziness, alteredsensations, weakness, chest discomfort and
Table 31.2: Compare and contrast diphenydramine and loratadine
Features Diphenhydramine Loratadine
1. Receptors blocked H1 histamine, M1 muscarinic H1 selective2. t½ 4–6 hrs 16–18 hrs3. Ability to cross BBB Present Absent4. Sedation Yes No5. Anticholinergic effects Yes No6. In rhinorrhoea Useful Not useful7. Route of administration Oral and Parenteral Oral
Textbook of Pharmacology for Dental and Allied Health Sciences208
neck pain. It is contraindicated in coronaryartery disease.
Other Agonists
• Buspirone (Page 194) is a 5-HT1A agonist-antagonist used as an antianxiety agent.
• Dexfenfluramine (Page 75) is used as anappetite suppressant.
Serotonin Antagonists
• Cyproheptadine blocks 5-HT2, H1 histamineand cholinergic receptors. It increasesappetite and is used to promote weightgain especially in children. It is also usedin carcinoid tumours.
• Ketanserin blocks 5-HT2 receptors andantagonises vasoconstriction and plateletaggregation promoted by 5-HT. It is usedin hypertension.
• Ondansetron is a 5-HT3 antagonist (seepage 245) used in the prevention andtreatment of vomiting.
Many other drugs including someantihistamines also block serotonin receptors.
Ergot Alkaloids
Ergot alkaloids are produced by Clavicepspurpurea, a fungus that infects rye, millet andother grains. Consumption of such grainsresults in ‘ergotism’ manifested as gangreneof the hands and feet, hallucinations andother CNS effects. Barger and Dale isolatedergot alkaloids in 1906.
Natural ergot alkaloids includeergometrine, ergotamine and ergotoxine. Thesemisynthetic derivatives are also available.
Actions
Ergot alkaloids have agonist, partial agonistand antagonistic actions at 5-HT and alphaadrenergic receptors and agonistic actions atCNS dopamine receptors. Thus their actions
are complex. Some of them are powerfulhallucinogens, e.g. lysergic acid diethylamide(LSD). They cause stimulation of smoothmuscles—some stimulate mainly vascularsmooth muscles and others mainly uterinesmooth muscles. The vasoconstrictor effectis responsible for gangrene.Adverse effects like nausea, vomiting anddiarrhoea are common. Prolonged use resultsin gangrene due to persistent vasospasm.
Uses
1. Migraine2. Postpartum haemorrhage—ergometrine is
used for prevention and treatment
Drugs Used in the Treatment of Migraine
Migraine is a common disorder characterisedby severe, throbbing, unilateral, headacheoften associated with nausea, vomiting andfatigue lasting for several hours. In theclassical migraine, a brief ‘aura’ of visualdisturbances occurs prior to the headache.An attack is triggered by factors like stress,anxiety, excitement, food (like chocolate andcheese) and hormonal changes. Thesetriggering factors stimulate the release ofvasoactive substances from nerve endingswhich are responsible for the events thatfollow. However the exact pathophysiologyis not understood and several hypotheseshave been put forward.
Drugs Used in Acute Attacks
Drugs should be taken at the initiation ofattack.• Aspirin, paracetamol or other NSAIDs are
effective.• Metoclopramide can be combined with
aspirin as it is an antiemetic and alsospeeds up absorption of aspirin.
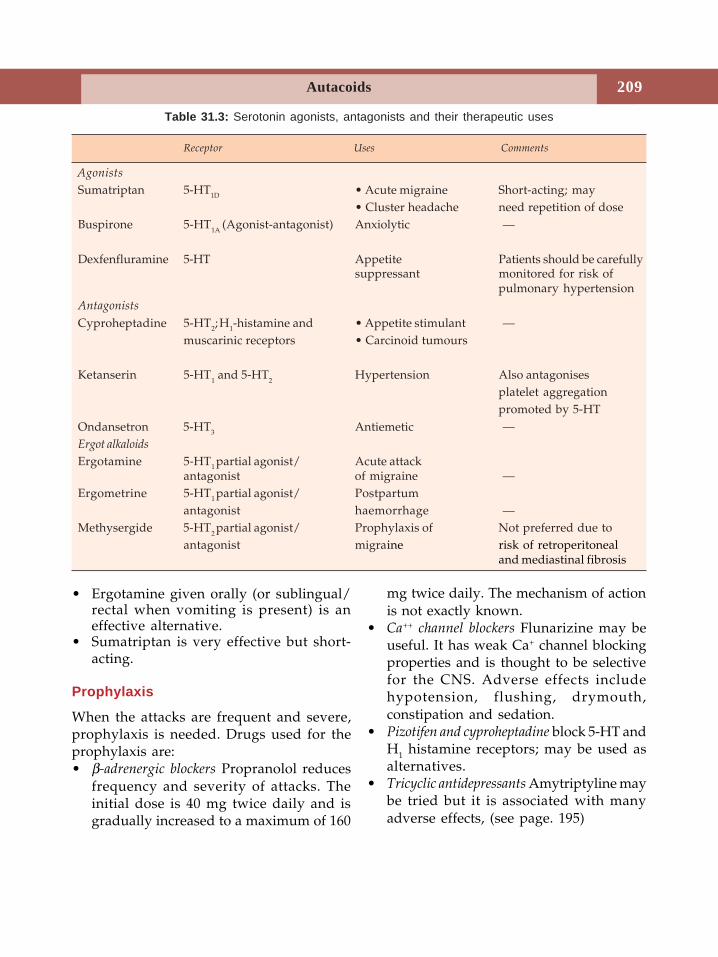
Autacoids 209
• Ergotamine given orally (or sublingual/rectal when vomiting is present) is aneffective alternative.
• Sumatriptan is very effective but short-acting.
Prophylaxis
When the attacks are frequent and severe,prophylaxis is needed. Drugs used for theprophylaxis are:• β-adrenergic blockers Propranolol reduces
frequency and severity of attacks. Theinitial dose is 40 mg twice daily and isgradually increased to a maximum of 160
mg twice daily. The mechanism of actionis not exactly known.
• Ca++ channel blockers Flunarizine may beuseful. It has weak Ca+ channel blockingproperties and is thought to be selectivefor the CNS. Adverse effects includehypotension, flushing, drymouth,constipation and sedation.
• Pizotifen and cyproheptadine block 5-HT andH1 histamine receptors; may be used asalternatives.
• Tricyclic antidepressants Amytriptyline maybe tried but it is associated with manyadverse effects, (see page. 195)
Table 31.3: Serotonin agonists, antagonists and their therapeutic uses
Receptor Uses Comments
Agonists
Sumatriptan 5-HT1D • Acute migraine Short-acting; may• Cluster headache need repetition of dose
Buspirone 5-HT1A (Agonist-antagonist) Anxiolytic —
Dexfenfluramine 5-HT Appetite Patients should be carefullysuppressant monitored for risk of
pulmonary hypertensionAntagonists
Cyproheptadine 5-HT2; H1-histamine and • Appetite stimulant —muscarinic receptors • Carcinoid tumours
Ketanserin 5-HT1 and 5-HT2 Hypertension Also antagonisesplatelet aggregationpromoted by 5-HT
Ondansetron 5-HT3 Antiemetic —Ergot alkaloids
Ergotamine 5-HT1 partial agonist/ Acute attackantagonist of migraine —
Ergometrine 5-HT1 partial agonist/ Postpartumantagonist haemorrhage —
Methysergide 5-HT2 partial agonist/ Prophylaxis of Not preferred due toantagonist migraine risk of retroperitoneal
and mediastinal fibrosis
Textbook of Pharmacology for Dental and Allied Health Sciences210
• Methysergide blocks 5-HT receptors butdue to adverse effects like retroperitonealfibrosis, it is not preferred.
EICOSANOIDS
Eicosanoids are 20-carbon (eicosa referringto the 20-carbon atoms) unsaturated fattyacids derived mainly from arachidonic acidin the cell walls. The principal eicosanoidsare the prostaglandins (PG), the throm-boxanes (TX), and the leukotrienes (LT).
Biosynthesis
Eicosanoids are synthesized locallyin most tissues from arachidonic acid.The pathway for synthesis is shown inFigure. 31.2.
The cyclo-oxygenase (COX) pathwaygenerates PGs and TXs while lipoxygenase(LOX) pathway generates LTs. There are 2cyclo-oxygenase isozymes viz. COX-1 andCOX-2. COX-1 is present in almost all cellsand prostanoids (PGs and TXs) obtainedfrom COX-1 mainly take part inphysiological functions. COX-2 is inducedby inflammation in the inflammatory cellsand the prostanoids produced by COX-2 are
involved in inflammatory and pathologicalchanges. All products of COX pathway aremetabolised by oxidation and excreted inurine.
PROSTAGLANDINS AND THROMBOXANES
In 1930s it was found that human semencontains a substance that contracts uterinesmooth muscle. As this substance wasthought to originate in the prostate, theycalled it ‘Prostaglandin’ but it was laterfound to be produced in many tissues.
Prostanoid receptors
The prostanoids bring about their effects byacting on prostanoid receptors, which are G-protein coupled receptors. There are fiveclasses of prostanoid receptors. They are-• DP (for PGD2)• EP (for PGE2)• FP (for PGF2α)• IP (for PGI2)• TP (for TXA2)
Actions
The prostanoids act on many tissues to bringabout the following effects.1. CVS Prostacyclin causes vasodilation
while TXA2 causes vasoconstriction. PGE2and PGF2α are weak cardiac stimulants.
2. GIT Most PGs and TXs stimulategastrointestinal smooth muscle resultingin colic and watery diarrhoea. PGE2inhibits gastric acid secretion and enhancesmucous production. Thus they have aprotective effect on gastric mucosa.
3. Airways PGE2 and PGI2 relax bronchialsmooth muscles while TXA2 and PGF2αcontract them. They may have a role inthe pathophysiology of bronchial asthma.
4. Platelets TXA2 induces platelet aggregationwhile PGI2 inhibits platelet aggregation.
5. Uterus PGE2 and PGF2α contract humanuterus which is more sensitive to PGsFig. 31.2: Biosynthesis of eicosanoids
Autacoids 211
during pregnancy. They also soften thecervix. Thus PGs may be involved in theinitiation and progression of labour. PGsare produced by foetal tissues duringlabour. PGs present in the semen mayfacilitate movement of sperms andfertilization by coordinating themovement of the uterus. They also play arole in dysmenorrhoea and menorrhagia.
6. Kidneys PGE2 and PGI2 cause renalvasodilation and have a diuretic effect.
7. CNS PGs increase body temperature whenadministered into cerebral ventricles.They also induce sleep.
8. Nerves PGs sensitize sensory nerveendings to pain and on intradermalinjection cause pain. They have a role inthe genesis of inflammation.
9. Bone PGs stimulate bone resorption andformation-increase bone turnover.
10. Some PGs lower intraocular pressure.Adverse effects depend on the type of PG, doseand route. Diarrhoea, nausea, vomiting,
fever, hypotension and pain due to uterinecontractions are common.
PG analogs used therapeuticallyMisoprostol PGE1Gemeprost PGE1Rioprostil PGE1Alprostadil PGE1Enprostil PGE2Dinoprostone PGE2Carboprost 15-Methyl PGF2αLatanoprost PGF2αDinoprost PGF2α
Epoprostenol PGI2
Uses
1. Gynaecological and obstetricala. Abortion For I and II trimester
abortion and ripening of cervix duringabortion, PGE2 and PGF2α are used.They are also used with mifepristoneto ensure complete expulsion of theproducts of conception.
b. Facilitation of labour As alternative tooxytocics in patients with renal failure.
c. Cervical priming Intravaginal PGE2 isused.
d. Postpartum haemorrhage IntramuscularPGF2α is used as an alternative toergometrine.
2. GastrointestinalPeptic ulcer PGE1 (misoprostol) and PGE2
(enprostil) are used for the prevention ofpeptic ulcer in patients on high doseNSAIDs.
3. Cardiovascular
a. Patent ductus arteriosus Patency of foetalductus arteriosus depends on local PGsynthesis. In neonates with somecongenital heart diseases, patency ofthe ductus arteriosus is maintainedwith PGs until surgery is done.
b. To prevent platelet aggregation duringhaemodialysis.
Prostaglandins
• 20-carbon unsaturated fatty acidssynthesized from arachidonic acidthrough cyclo-oxygenase pathway
• Prostacycline (PGI2) causes vasodilationwhile TXA2 causes vasoconstriction
• PGs contract g.i. and bronchial (TXA2,PGE2) smooth muscles. TXA2 inducesplatelet aggregation (PGI2 inhibits);PGE2 and PGF2α contract uterus. PGsstimulate bone turnover and sensitizethe nerve endings to pain
• Uses Abortion, facilitation of labour,cervical priming, to control post-partumhaemorrhage, to maintain the patencyof ductus arteriosus, for prevention ofplatelet aggregation, open angleglaucoma and peptic ulcer.
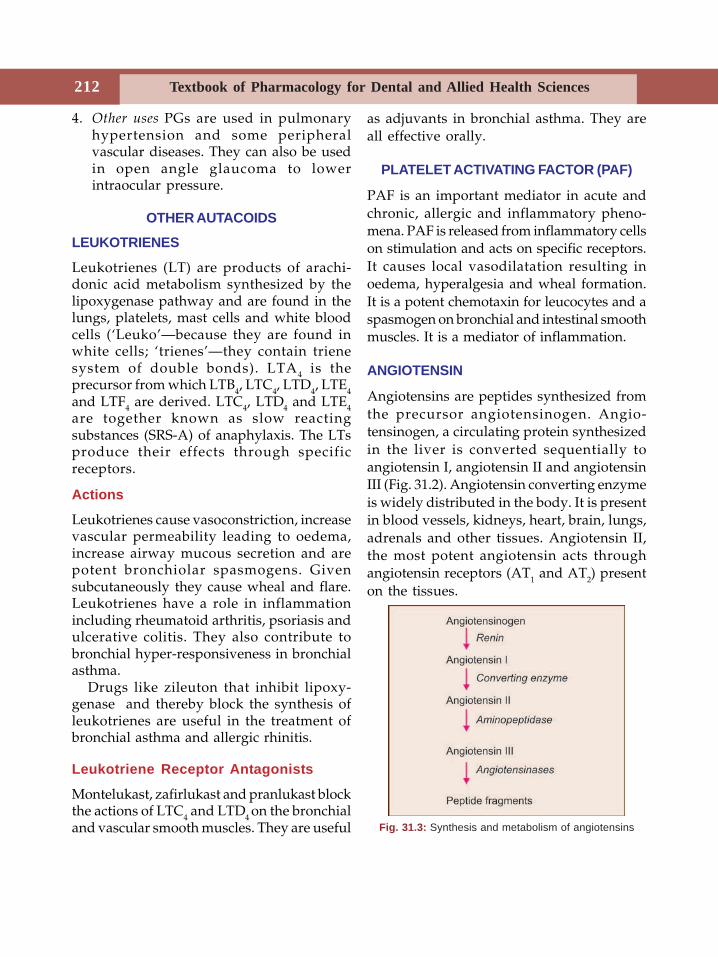
Textbook of Pharmacology for Dental and Allied Health Sciences212
4. Other uses PGs are used in pulmonaryhypertension and some peripheralvascular diseases. They can also be usedin open angle glaucoma to lowerintraocular pressure.
OTHER AUTACOIDS
LEUKOTRIENES
Leukotrienes (LT) are products of arachi-donic acid metabolism synthesized by thelipoxygenase pathway and are found in thelungs, platelets, mast cells and white bloodcells (‘Leuko’—because they are found inwhite cells; ‘trienes’—they contain trienesystem of double bonds). LTA4 is theprecursor from which LTB4, LTC4, LTD4, LTE4and LTF4 are derived. LTC4, LTD4 and LTE4are together known as slow reactingsubstances (SRS-A) of anaphylaxis. The LTsproduce their effects through specificreceptors.
Actions
Leukotrienes cause vasoconstriction, increasevascular permeability leading to oedema,increase airway mucous secretion and arepotent bronchiolar spasmogens. Givensubcutaneously they cause wheal and flare.Leukotrienes have a role in inflammationincluding rheumatoid arthritis, psoriasis andulcerative colitis. They also contribute tobronchial hyper-responsiveness in bronchialasthma.
Drugs like zileuton that inhibit lipoxy-genase and thereby block the synthesis ofleukotrienes are useful in the treatment ofbronchial asthma and allergic rhinitis.
Leukotriene Receptor Antagonists
Montelukast, zafirlukast and pranlukast blockthe actions of LTC4 and LTD4 on the bronchialand vascular smooth muscles. They are useful
as adjuvants in bronchial asthma. They areall effective orally.
PLATELET ACTIVATING FACTOR (PAF)
PAF is an important mediator in acute andchronic, allergic and inflammatory pheno-mena. PAF is released from inflammatory cellson stimulation and acts on specific receptors.It causes local vasodilatation resulting inoedema, hyperalgesia and wheal formation.It is a potent chemotaxin for leucocytes and aspasmogen on bronchial and intestinal smoothmuscles. It is a mediator of inflammation.
ANGIOTENSIN
Angiotensins are peptides synthesized fromthe precursor angiotensinogen. Angio-tensinogen, a circulating protein synthesizedin the liver is converted sequentially toangiotensin I, angiotensin II and angiotensinIII (Fig. 31.2). Angiotensin converting enzymeis widely distributed in the body. It is presentin blood vessels, kidneys, heart, brain, lungs,adrenals and other tissues. Angiotensin II,the most potent angiotensin acts throughangiotensin receptors (AT1 and AT2) presenton the tissues.
Fig. 31.3: Synthesis and metabolism of angiotensins

Autacoids 213
Actions
Angiotensin II causes vasoconstrictionresulting in increased blood pressure. Itstimulates the synthesis of aldosterone bythe adrenal cortex, increases sodium reabs-orption by the kidneys and increases thesecretion of vasopressin. Angiotensin II alsopromotes the growth of vascular and cardiacmuscle cells and may play a role in thedevelopment of cardiac hypertrophy as inhypertension. By these actions, renin-angiotensin system regulates the fluid andelectrolyte balance as well as bloodpressure.
Inhibitors of ACE and blockers ofangiotensin II receptors are now used inthe treatment of hypertension, congestiveheart failure and other conditions that are dueto excess of angiotensin II activity (seeSection 4).
KININS
Kinins are vasodilator peptides formed fromthe precursor kininogen by the action of theenzymes called kallikreins. Kallikreins arepresent in the plasma, kidneys, pancreas,intestines, salivary glands and other tissues.Bradykinin is the chief kinin.
Kinins are rapidly degraded by kininaseII which is same as ACE and has a very shortt½ (< 15 seconds).
Actions
Kinins are potent vasodilators and cause abrief fall in BP. They stimulate contractionof other smooth muscles — thus they inducebronchospasm in asthmatics, slow contr-action of intestines (Brady= slow) and uterus.Kinins mediate inflammation, and stimulatethe pain nerve endings. Kinins produce theiractions by acting through B1 and B2receptors.
Drugs affecting the kallikrein-kininsystem—B1 and B2 antagonists are now beingdeveloped.
CYTOKINES
Cytokines are also considered as autacoids.They are peptides released from theinflammatory cells. They are classified into 5families.• Interleukins• Colony stimulating factors• Chemokines• Growth factor and tumour necrosis factors• Interferons
Cytokines stimulate specific receptors tobring about their effects. IL-1 and TNF - αare involved in inflammation - they are pro-inflammatory cytokines while IL-4, IL-10 andIL-13 inhibit inflammatory activity - they areanti-inflammatory cytokines. The interferonsα and β have antiviral activity whileinterferon γ has immunoregulatory activityand is used in multiple sclerosis.
Textbook of Pharmacology for Dental and Allied Health Sciences214
32 Drugs Acting onRespiratory System
Section 7Respiratory System
DRUGS USED IN THE TREATMENT OFBRONCHIAL ASTHMA
Bronchial asthma is characterised bydyspnoea and wheeze due to increasedresistance to the flow of air through thebronchi. Bronchospasm, mucosal congestionand oedema result in increased resistance.The tracheobronchial smooth muscle ishyper-responsive to various stimuli likedust, allergens, cold air, infection anddrugs. These trigger-factors trigger anacute attack.Antigen-antibody interaction on the surfaceof mast cells cause (Fig. 32.1):(i) degranulation of mast cells releasing
stored mediators of inflammation(ii) synthesis of other inflammatory
mediators which are responsible forbronchospasm, mucosal congestion andoedema.
Inflammation is the primary pathology.Clinically 2 types of asthma are identified.(a) Extrinsic asthma Starts at an early age,
occurs in episodes; the patient has afamily history of allergies.
(b) Intrinsic asthma Starts in the middle ageand assumes chronic form. There is nofamily history of allergies.
Drugs used in the bronchial asthma may be groupedas follows.
CLASSIFICATION
1. Bronchodilatorsa. Sympathomimetics
i. Selective β2 agonistsShort acting-
– Salbutamol, terbutaline.Longer acting -– Salmeterol, fenoterol, formoterol,
pirbuterol, Ibuterolii. Nonselective agents
– Adrenaline, isoprenaline,ephedrine.
b. Methylxanthines -Theophylline, aminophylline.
c. Anticholinergics -Ipratropium bromide, atropine.
2. Anti-inflammatory agentsa. Systemic - Glucocorticoids
Hydrocortisone, Prednisolone.b. Inhalational -
Beclomethasone, Budesonide,Flunisolide, Triamcinolone
3. Mast cell stabilizers -Disodium cromoglycate, Nedocromil,Ketotifen.
4. Leukotriene receptor antagonists -Montelukast, zafirlukast.
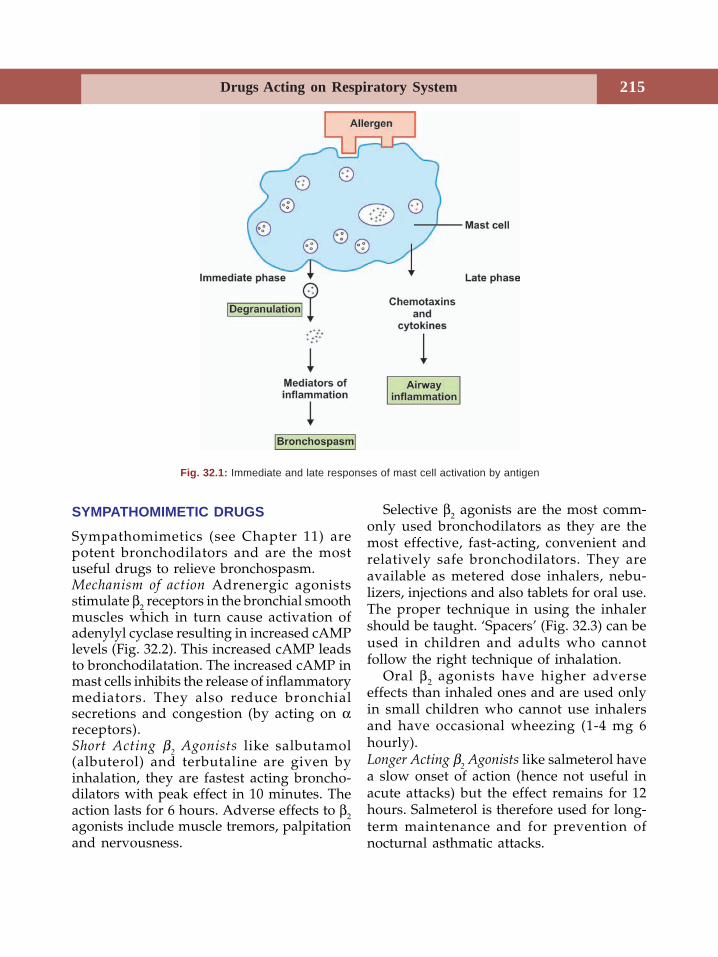
Drugs Acting on Respiratory System 215
SYMPATHOMIMETIC DRUGS
Sympathomimetics (see Chapter 11) arepotent bronchodilators and are the mostuseful drugs to relieve bronchospasm.Mechanism of action Adrenergic agonistsstimulate β2 receptors in the bronchial smoothmuscles which in turn cause activation ofadenylyl cyclase resulting in increased cAMPlevels (Fig. 32.2). This increased cAMP leadsto bronchodilatation. The increased cAMP inmast cells inhibits the release of inflammatorymediators. They also reduce bronchialsecretions and congestion (by acting on αreceptors).Short Acting β
2 Agonists like salbutamol
(albuterol) and terbutaline are given byinhalation, they are fastest acting broncho-dilators with peak effect in 10 minutes. Theaction lasts for 6 hours. Adverse effects to β2agonists include muscle tremors, palpitationand nervousness.
Selective β2 agonists are the most comm-only used bronchodilators as they are themost effective, fast-acting, convenient andrelatively safe bronchodilators. They areavailable as metered dose inhalers, nebu-lizers, injections and also tablets for oral use.The proper technique in using the inhalershould be taught. ‘Spacers’ (Fig. 32.3) can beused in children and adults who cannotfollow the right technique of inhalation.
Oral β2 agonists have higher adverseeffects than inhaled ones and are used onlyin small children who cannot use inhalersand have occasional wheezing (1-4 mg 6hourly).Longer Acting β
2 Agonists like salmeterol have
a slow onset of action (hence not useful inacute attacks) but the effect remains for 12hours. Salmeterol is therefore used for long-term maintenance and for prevention ofnocturnal asthmatic attacks.
Fig. 32.1: Immediate and late responses of mast cell activation by antigen
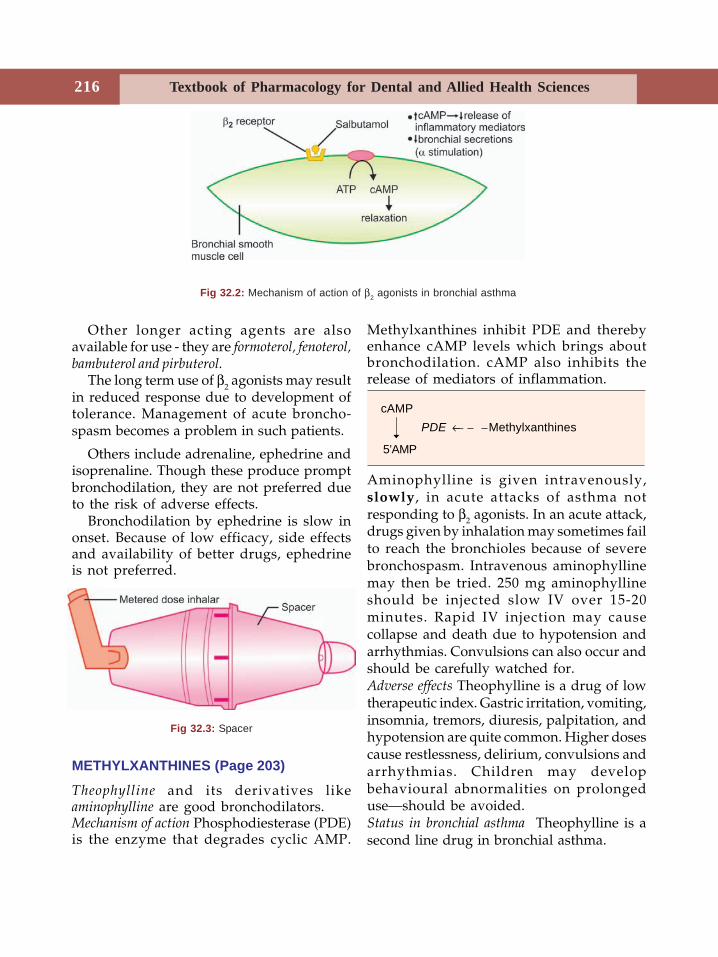
Textbook of Pharmacology for Dental and Allied Health Sciences216
Other longer acting agents are alsoavailable for use - they are formoterol, fenoterol,bambuterol and pirbuterol.
The long term use of β2 agonists may resultin reduced response due to development oftolerance. Management of acute broncho-spasm becomes a problem in such patients.
Others include adrenaline, ephedrine andisoprenaline. Though these produce promptbronchodilation, they are not preferred dueto the risk of adverse effects.
Bronchodilation by ephedrine is slow inonset. Because of low efficacy, side effectsand availability of better drugs, ephedrineis not preferred.
Fig 32.2: Mechanism of action of β2 agonists in bronchial asthma
Fig 32.3: Spacer
Methylxanthines inhibit PDE and therebyenhance cAMP levels which brings aboutbronchodilation. cAMP also inhibits therelease of mediators of inflammation.
Aminophylline is given intravenously,slowly, in acute attacks of asthma notresponding to β2 agonists. In an acute attack,drugs given by inhalation may sometimes failto reach the bronchioles because of severebronchospasm. Intravenous aminophyllinemay then be tried. 250 mg aminophyllineshould be injected slow IV over 15-20minutes. Rapid IV injection may causecollapse and death due to hypotension andarrhythmias. Convulsions can also occur andshould be carefully watched for.Adverse effects Theophylline is a drug of lowtherapeutic index. Gastric irritation, vomiting,insomnia, tremors, diuresis, palpitation, andhypotension are quite common. Higher dosescause restlessness, delirium, convulsions andarrhythmias. Children may developbehavioural abnormalities on prolongeduse—should be avoided.Status in bronchial asthma Theophylline is asecond line drug in bronchial asthma.
cAMP PDE ← Methylxanthines
5’AMP
METHYLXANTHINES (Page 203)
Theophylline and its derivatives likeaminophylline are good bronchodilators.Mechanism of action Phosphodiesterase (PDE)is the enzyme that degrades cyclic AMP.

Drugs Acting on Respiratory System 217
1. Chronic asthma Oral theophylline can beused to control mild to moderate asthma.Etophylline + 80% theophylline (Deri-phylline) injections (IM) are used torelieve acute attacks. When used over along-term, plasma levels should bemonitored.
2. Acute severe asthma (status asthmaticus)
Intravenous aminophylline is tried whensympathomimetics fail to relieve broncho-spasm—but is found to be less effective.
ANTICHOLINERGICS
Anticholinergics (See chap. 8) relax bronchialsmooth muscles but response is slower thansympathomimetics. Ipratropium bromide isgiven by inhalation and its actions are largelyconfined to the respiratory tract. It is moreeffective in chronic bronchitis includingchronic obstructive pulmonary disease(COPD). It is safe and well-tolerated. Unlikeatropine it does not dry up the secretions andhence does not inhibit mucociliary motility.Infact it may increase mucociliary clearance.
Uses
1. As an adjunct to β2 agonists particularlyin severe acute episodes.
2. As a bronchodilator in some cases ofchronic bronchitis and COPD.
ANTI-INFLAMMATORY DRUGS
Glucocorticoids Since inflammation is theprimary pathology in bronchial asthma,antiinflammatory agents afford significantbenefit (See chap. 54).Mechanism of action Steroids are notbronchodilators. They suppress theinflammatory response to antigen-antibodyreaction and thereby reduce mucosal oedemaand hyperirritability. They bind to steroid
receptors in the cytoplasm, drug receptorcomplex moves to the nucleus, binds to DNAand induces the synthesis of specific mRNA.This in turn results in the synthesis of specificproteins to bring about the following effects(Fig. 54.2, Page 349)1. they decrease the formation of cytokines.2. ↓ PG synthesis.3. inhibit the production of leukotrienes and
platelet activating factor.4. reduce the influx of eosinophils into the
lungs and thus reduce the release ofmediators from them.
5. ↓ synthesis of interleukins.6. restore response to β2 agonist -(if tolerance
has developed)-by upregulating β2
receptors.Glucocorticoids may be given systemically
in acute episodes. Oral prednisolone iscommonly used (dose 30-60 mg/day).Theonset of response requires about 12 hours.Chronic asthma requires prophylaxis withinhaled steroids.Inhaled steroids The use of inhalational steroidslargely minimizes the adverse effects ofsteroids because of the small dose required,but they are not effective in acute attacks andare only of prophylactic value. They preventepisodes of acute asthma, reduce bronchialhyperreactivity and effectively controlsymptoms. The effect gradually developsafter 1 week of treatment.Side effects of inhaled steroids includehoarseness of voice - (by a direct effect onvocal cords), sore throat and oropharyngealcandidiasis. Rinsing the mouth and throatwith water after each use can reduce theincidence of candidiasis and sore throat. HPAaxis suppression is generally not seen in therecommended doses. But, the drug that isswallowed may be systemically absorbed.Large doses given for a long time mayoccasionally result in systemic effects of
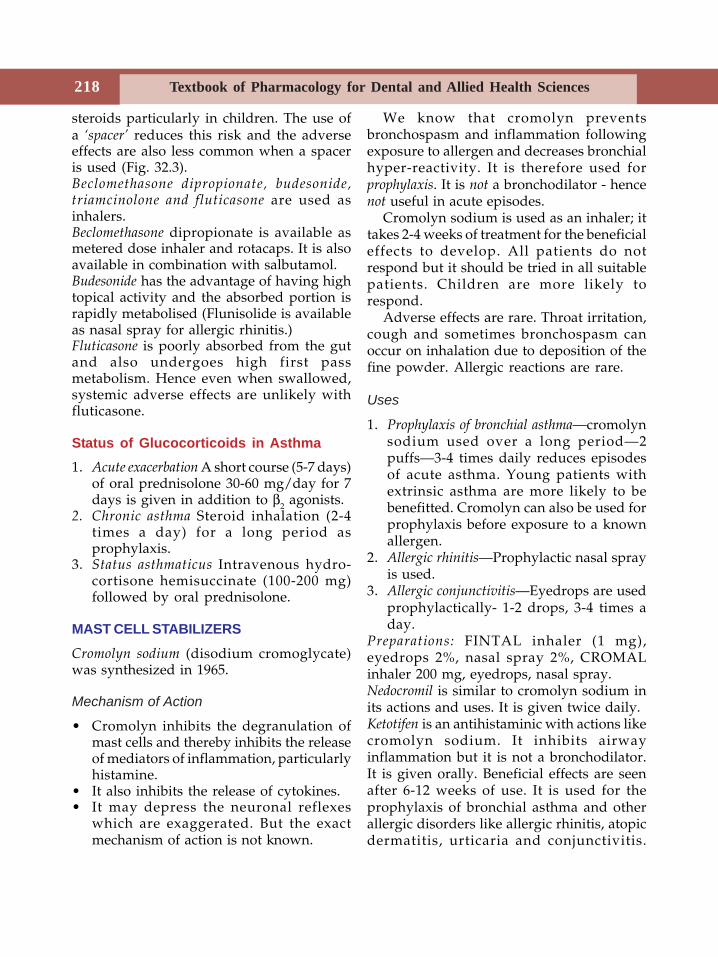
Textbook of Pharmacology for Dental and Allied Health Sciences218
steroids particularly in children. The use ofa ‘spacer’ reduces this risk and the adverseeffects are also less common when a spaceris used (Fig. 32.3).Beclomethasone dipropionate, budesonide,triamcinolone and fluticasone are used asinhalers.Beclomethasone dipropionate is available asmetered dose inhaler and rotacaps. It is alsoavailable in combination with salbutamol.Budesonide has the advantage of having hightopical activity and the absorbed portion israpidly metabolised (Flunisolide is availableas nasal spray for allergic rhinitis.)Fluticasone is poorly absorbed from the gutand also undergoes high first passmetabolism. Hence even when swallowed,systemic adverse effects are unlikely withfluticasone.
Status of Glucocorticoids in Asthma1. Acute exacerbation A short course (5-7 days)
of oral prednisolone 30-60 mg/day for 7days is given in addition to β2 agonists.
2. Chronic asthma Steroid inhalation (2-4times a day) for a long period asprophylaxis.
3. Status asthmaticus Intravenous hydro-cortisone hemisuccinate (100-200 mg)followed by oral prednisolone.
MAST CELL STABILIZERS
Cromolyn sodium (disodium cromoglycate)was synthesized in 1965.
Mechanism of Action
• Cromolyn inhibits the degranulation ofmast cells and thereby inhibits the releaseof mediators of inflammation, particularlyhistamine.
• It also inhibits the release of cytokines.• It may depress the neuronal reflexes
which are exaggerated. But the exactmechanism of action is not known.
We know that cromolyn preventsbronchospasm and inflammation followingexposure to allergen and decreases bronchialhyper-reactivity. It is therefore used forprophylaxis. It is not a bronchodilator - hencenot useful in acute episodes.
Cromolyn sodium is used as an inhaler; ittakes 2-4 weeks of treatment for the beneficialeffects to develop. All patients do notrespond but it should be tried in all suitablepatients. Children are more likely torespond.
Adverse effects are rare. Throat irritation,cough and sometimes bronchospasm canoccur on inhalation due to deposition of thefine powder. Allergic reactions are rare.
Uses
1. Prophylaxis of bronchial asthma—cromolynsodium used over a long period—2puffs—3-4 times daily reduces episodesof acute asthma. Young patients withextrinsic asthma are more likely to bebenefitted. Cromolyn can also be used forprophylaxis before exposure to a knownallergen.
2. Allergic rhinitis—Prophylactic nasal sprayis used.
3. Allergic conjunctivitis—Eyedrops are usedprophylactically- 1-2 drops, 3-4 times aday.
Preparations: FINTAL inhaler (1 mg),eyedrops 2%, nasal spray 2%, CROMALinhaler 200 mg, eyedrops, nasal spray.Nedocromil is similar to cromolyn sodium inits actions and uses. It is given twice daily.Ketotifen is an antihistaminic with actions likecromolyn sodium. It inhibits airwayinflammation but it is not a bronchodilator.It is given orally. Beneficial effects are seenafter 6-12 weeks of use. It is used for theprophylaxis of bronchial asthma and otherallergic disorders like allergic rhinitis, atopicdermatitis, urticaria and conjunctivitis.
Drugs Acting on Respiratory System 219
Drowsiness and dry mouth are common sideeffects. It can also cause dizziness and weightgain.
LEUKOTRIENE RECEPTOR ANTAGONISTS
Leukotrienes are one of the importantmediators of inflammation. They bring aboutbronchospasm, mucosal oedema, increase theinflux of inflammatory cells and mucousproduction, by their actions on leukotrienereceptors. Zafirlukast, montelukast andpranlukast are highly selective andcompetitive antagonists of leukotrienereceptors. They block the effects ofleukotrienes and thereby reduce mucosaloedema and relieve bronchospasm. Theydecrease the response to allergens. Theyinhibit exercise-induced and aspirin - inducedbronchospasm. Adverse effects are rare -headache, rashes and gastrointestinaldisturbances.Montelukast and zafirlukast can be used inthe prophylaxis of mild to moderate asthmaas alternatives or as add-on drugs. They alsoreduce the dose of the steroid required.Bronchodilator effect is additive with β2agonists. Their place in asthma is yet to beclearly known.Zileuton inhibits leukotriene synthesis byinhibiting the enzyme lipoxygenase. But itcauses a rise in liver enzymes. Hence notpreferred.
Treatment of Asthma
Mild asthma–Rapidly acting, inhaled β2stimulants like salbutamol.Moderate asthma– Regular prophylaxis withcromoglycate. If the patient does not respondto cromolyn—inhaled steroids are given forprophylaxis. Acute episodes are managedwith inhaled β2 agonists.Severe asthmaa. Regular inhaled steroidsb. Inhaled β2 agonists 3-4 times a day
c. Oral steroids may be consideredd. Additional inhaled ipratropium bromide
or oral theophylline may be given.Acute severe asthma or status asthmaticus is anacute exacerbation. It is a medical emergency;may be triggered by an acute respiratoryinfection, abrupt withdrawal of steroids afterprolonged use, by drugs, allergens oremotional stress.
Treatment
1. Nebulization of β2 agonist andipratropium alternately—every 30minutes. Additional salbutamol 0.4 mgIM/SC may be given. Severe tachycardiashould be watched for.
2. Hydrocortisone hemisuccinate IV 100 mgstat followed by 100 mg every 8 hoursinfusion followed by a course of oralprednisolone.
3. Oxygen inhalation.4. Antibiotics - if infection is present.5. IV fluids to correct dehydration and
acidosis.6. Aminophylline 250 mg slow IV over 15-
20 minutes has been used by somephysicians should be given carefully—watching for adverse effects but is nownot preferred.
7. Artificial ventilation may be required inextreme cases.
Bronchial Asthma and Dentistry
1. A small amount of water or dentalmaterials used in dental procedures mayaspirate into the respiratory passageand trigger an acute attack of bronchialasthma. Salbutamol inhalation shouldbe given immediately. The dentalprocedure may be continued after thepatient recovers.
2. Analgesics (NSAIDs) prescribed for reliefof pain may trigger acute episodes of
Textbook of Pharmacology for Dental and Allied Health Sciences220
asthma. This should be kept in mind.Depending on the severity of asthma andthe dose of the NSAID required,appropriate drug should be prescribed.If the patient has severe asthma andrequires an antiinflammatory drug for hisdental problem prednisolone should beconsidered.
3. If the patient has been receiving steroidinhalation for prophylaxis of bronchialasthma for a long period, the oralmicroflora could be altered. Thispredisposes the oral mucosa to infectionwith microorganisms like candida andcertain bacteria. Appropriate care shouldbe taken.
DRUGS USED IN THE TREATMENT OFCOUGHCough is a protective reflex that removes theirritant matter and secretions from therespiratory tract. It could be due to infection,allergy, pleural diseases and malignancy.Since it is a protective mechanism, unduesuppression of cough can cause more harmthan benefit. In some conditions, as in dryannoying cough, it may serve no usefulpurpose. In such situations, antitussives orcough suppressants may be used.Antitussives only provide symptomatic reliefand do not alter the cause.
Antitussives1. Central cough suppressants
Codeine, pholcodeine, noscapine,dextromethorphan, antihistamines,benzonatate.
2. Pharyngeal demulcentsLozenges, cough drops, linctuses
3. ExpectorantsPotassium iodide, Guaiphenesin, ammonium chloride, ipecacuanha
Central Cough SuppressantsCentral cough suppressants act by inhibitingcough centre in the medulla.
Codeine is a good antitussive with lessaddiction liability. However, nausea,constipation and drowsiness are common.Dose 10-15 mg every 6 hours (See page 164).Noscapine is a natural opium alkaloid whichis a potent antitussive. No other CNS effectsare prominent in therapeutic doses (See page164). Nausea is the only occasional sideeffect. Dose 15-30 mg every 6 hours.
Dextromethorphan and pholcodeine are syntheticopioid derivatives with antitussive actionslike codeine but with lesser side effects.Pholcodeine is longer-acting - given twicedaily.
Benzonatate is chemically related to the localanaesthetic procaine. It acts on the coughreceptors in the lungs and also has a centraleffect. It is given orally - 100 mg thrice daily.
Antihistamines are useful in cough due toallergy except that due to bronchial asthma.They thicken the secretions which may bedifficult to cough out. An antihistamine isgenerally one of the components of coughsyrups. Their sedative property may be ofadditional value in suppressing cough.
Other centrally acting antitussives includecarbetapentane, chlophedianol andcaramiphen. More extensive studies arerequired to prove their efficacy.
Pharyngeal Demulcents
Pharyngeal demulcents (demulcere = tocaress soothingly - in LATIN) increase theflow of saliva which produces a soothingeffect on the pharyngeal mucosa and reduceafferent impulses arising from the irritatedmucosa. Dry cough due to irritation of thepharyngeal mucosa is relieved. Candy sugaror a few drops of lemon also serve thispurpose.

Drugs Acting on Respiratory System 221
Expectorants
Expectorants (Latin - expectorare = to drivefrom the chest) increase the production ofrespiratory tract secretions which cover theirritated mucosa. As the secretions becomethin and less viscid, they can be easilycoughed out. Expectorants may increase thesecretions directly or reflexly.• Direct stimulants Volatile oils like
eucalyptus oil; creosotes, alcohol, cidarwood oil - when administered byinhalation with steam can increaserespiratory secretions.
• Reflex expectorants are given orally, theyare gastric irritants and reflexly increaserespiratory secretions.
Potassium iodide acts both directly andreflexly.Ipecacuanha is an emetic. In sub-emetic dosesit is used as an expectorant.
Bronchodilators
Bronchodilators like salbutamol andterbutaline relieve cough that results frombronchospasm.
The antitussive preparations generally havea combination of a central cough suppressant,an expectorant, an antihistaminic andsometimes a bronchodilator and a mucolyticagent.
Mucolytics
Normally the respiratory mucous is watery.The glycoproteins in the mucous are linkedby disulphide bonds to form polymersmaking it slimy. In respiratory diseases, theglycoproteins form larger polymers with
plasma proteins present in the exudate andthe secretions become thick and viscid.Mucolytics liquefy the sputum making it lessviscid so that it can be easily expectorated.The following are mucolytics -Bromhexine, a semisynthetic compoundrelated to vasicine (an alkaloid from the plantAdhatoda vasica) is a good mucolytic. Itdepolymerises the mucopolysaccharides inthe mucus. It is given orally (8-16 mg thricedaily). Side effects are minor - may causerhinorrhoea.Ambroxol is a metabolite of bromhexine withactions similar to it. Ambroxol may be givenorally or by inhalation. It can be used as analternative to bromhexine.Acetylcysteine opens disulfide bonds inmucoproteins of the sputum reducing itsviscosity. It is given by aerosol. Side effectsare common and hence not preferred.Carbocysteine Carbocysteine is similar toacetylcysteine and is used orally.Pancreatic dornase Deoxyribonucleoprotein isa major component of the purulentrespiratory tract secretions. Pancreaticdornase is a deoxyribonuclease obtainedfrom the beef pancreas. It breaks thedeoxyribonucleic acid (DNA) into smallerparts thus making the secretions thin and lessviscid. It is administered by inhalation.
Pancreatic dornase can cause allergicreactions.Steam inhalation offers an effective andinexpensive alternative to drugs. It humidifiesthe sputum as well as respiratory mucosa.This helps in reducing the irritation and foreasier expectoration of the sputum. Inpresence of dehydration, just rehydrating thepatient is found to be beneficial.
Textbook of Pharmacology for Dental and Allied Health Sciences222
33Haematopoietic System
HAEMATINICS
Haematinics are compounds required in theformation of blood and are employed in thetreatment of anaemias. Haematinics includeiron, vitamin B12 and folic acid. Haema-topoietic growth factors are also discussedhere.
Iron
Iron, vitamin B12 and folic acid are essentialfor normal erythropoiesis.
Iron is essential for haemoglobinproduction. Total body iron is about 2.5 to 5grams, two-thirds of which is present inhaemoglobin. Each molecule of haemoglobinhas 4 iron containing residues. It is alsopresent in myoglobin, the cytochromes andother enzymes.
Distribution of Iron in the Body
Haemoglobin 66%Ferritin, haemosiderin 25%Myoglobin (in muscles) 03%Enzymes (cytochromes, etc.) 06%
Daily Requirement of Iron
Adult male 0.5-1 mgAdult female 1-2 mgPregnancy and lactation 3-5 mg
Dietary sources of iron Food items that are richin iron are liver, egg yolk, meat, fish, chicken,spinach, dry fruits, wheat and apple.
Absorption
The average Indian diet provides about 10-20 mg of iron. 10 percent of this iron isabsorbed. Dietary iron may be present ashaeme or as inorganic iron. It is mostlyabsorbed from the upper gut in the ferrousform. During deficiency, absorption is better.Haeme iron is better absorbed than inorganiciron.
Factors that Influence Iron Absorption
Ascorbic acid, amino acids, meat, ↑gastric,acidity – Increase absorption.Antacids, phosphates, phytates, tetracyclinespresence of food in the stomach–Decreaseabsorption.
Transport and DistributionIron is transported with the help of aglycoprotein transferrin and stored as ferritinand haemosiderin, in liver, spleen and bonemarrow.
ExcretionDaily 0.5-1 mg of iron is excreted. A largepart is lost in shedding of intestinal mucosalcells and small amounts in the bile,desquamated skin and urine. In females, ironis also lost in menstruation.
Preparations of Iron
Iron is generally given orally–but can begiven parenterally.
Section 8Blood
223Haematopoietic System
Oral Iron Preparations
1. Ferrous sulphate–200 mg tab2. Ferrous fumarate–200 mg tab3. Ferrous gluconate–300 mg tab4. Ferrous succinate–100 mg5. Iron calcium complex–5% iron6. Ferric ammonium citrate–45 mg.
• Ferrous salts are better absorbed thanferric salts and are cheaper.
• The last three preparations given aboveare claimed to be better tolerated butare more expensive.
• Expensive preparations of iron withvitamins, liver extract, amino acids,etc. are available but offer no obviousbenefits.
• Dose Ferrous sulphate 200 mg - 3-4tablets daily. The elemental ironcontent of different salts varies.
Adverse Effects of Oral Iron
Epigastric pain, nausea, vomiting, gastritis,metallic taste, constipation (due to astringenteffect) or diarrhoea (irritant effect) are theusual adverse effects. Liquid preparations ofiron cause staining of the teeth.
Parenteral Iron
Intramuscular injection of iron is given deepIM in the gluteal region using ‘Z’ techniqueto avoid staining of the skin. Intravenousiron is given slowly over 5-10 minutes or asinfusion after a test dose.
Indications
1. When oral iron is not tolerated2. Failure of absorption–as in malabsorption,
chronic bowel disease3. Noncompliance4. Severe deficiency with bleeding.
Preparations
1. Iron dextran has 50 mg elemental iron/ml(2 ml ampoule) - it is the only preparationthat can be given intravenously. It can alsobe given IM.
2. Iron-sorbitol - citric acid complex –contains50 mg elemental iron/ml; given only IM.This preparation should not be given IVbecause it quickly saturates the transferrinstores. As a result free iron levels in theplasma rises and can cause toxicity.
Dose is to be calculated using a formula.Iron requirement=4.4×body weight ×Hb deficit (mg) (kg) (g/dl)This also includes iron needed forreplenishment of stores.
Adverse Effects
Local Pain at the site of injection, pigmentationof the skin and sterile abscess.Systemic Fever, headache, joints pain,palpitation, difficulty in breathing, lymphnode enlargement and rarely anaphylaxis.Acute iron poisoning is common in infantsand children in whom about 10 tablets (1-2g) can be lethal. Manifestations includevomiting, abdominal pain, haematemesis,bloody diarrhoea, shock, drowsiness,cyanosis, acidosis, dehydration, cardio-vascular collapse and coma. Immediatediagnosis and treatment are important asdeath may occur in 6-12 hr.
Treatment
• Gastric lavage with sodium bicarbonatesolution.
• Desferrioxamine is the antidote. It isinstilled into the stomach after lavage, toprevent iron absorption; injected IV/IM.
• Correction of acidosis and shock.
Textbook of Pharmacology for Dental and Allied Health Sciences224
Indications for Iron
Iron deficiency anaemia–both for theprophylaxis and treatment. The cause for irondeficiency should be identified. Treatmentshould be continued depending on theresponse for 3-6 months to replenish ironstores. Prophylactically iron is given inconditions with increased iron requirementas in pregnancy, infancy and professionalblood donors.
VITAMIN B12 AND FOLIC ACID
Vitamin B12 and folic acid are water solublevitamins, belonging to the B-complex group.They are essential for normal DNA synthesis.Their deficiency leads to impaired DNAsynthesis and abnormal maturation of RBCsand other rapidly dividing cells. This resultsin megaloblastic anaemia, characterised bythe presence of red cell precursors in theblood and bone marrow. Vitamin B12 andfolic acid are therefore called maturationfactors. Other manifestations of deficiencyinclude glossitis, stomatitis and mala-bsorption; neurological manifestations canalso result.
Vitamin B12
Vitamin B12 (Cyanocobalamin) is synthesizedby microorganisms. Liver, fish, egg yolk,meat, cheese and pulses are the dietarysources of B12.
Vitamin B12 or extrinsic factor is absorbedwith the help of intrinsic factor, a protein
secreted by the stomach. It is carried in theplasma by B12–binding proteins calledtranscobalamin and is stored in the liver.
Functions
Vitamin B12 and folic acid act as coenzymesfor several vital metabolic reactions and areessential for DNA synthesis.Daily requirement– (Table 33.1).
Deficiency
B12 deficiency may be due to:1. Addisonian pernicious anaemia Thomas
Addison first described cases of anaemianot responding to iron. There is deficiencyof intrinsic factor due to destruction ofparietal cells resulting in failure of B12absorption.
2. Other causes Gastrectomy, chronicgastritis, malabsorption and fishtapeworm infestation (fish tapewormconsumes B12).
Preparations
• Cyanocobalamin–100 μg/ml injection maybe given IM or deep SC - hypersensitivityreactions can occur.
• Hydroxocobalamin–100, 500, 1000 μg/mlinjection-has longer lasting effect buthydroxocobalamin administration canresult in the formation of antibodies.
• Multivitamin preparations containvariable amounts of vitamin B12 with orwithout intrinsic factor for oral use.
Table 33.1: Daily requirement of vitamin B12 and folic acid
Adults Pregnancy and lactation
Vitamin B12 1-3 μg 3-5 μgFolic acid 50-100 μg 200-400 μg
As 50% of ingested drug is lost, double the amount is recommended for daily dietary intake
225Haematopoietic System
Uses
1. B12
deficiency Prophylaxis and treatment ofmegaloblastic anaemia due to B12
deficiency of any cause. If B12 deficiencyis due to lack of intrinsic factor, it is givenIM or SC. Pernicious anaemia needs lifelong treatment with B12. Oral folic acidshould be added because B12 induced briskhaemopoiesis may also increase thedemand for folic acid. Prophylactic doseof vitamin B12 is 3-10 μg daily.
2. B12
neuropathies like subacute combineddegeneration respond to vitamin B12.
Folic Acid
Folic acid is pteroylglutamic acid. It was firstisolated from spinach and therefore namedas folic acid (from leaf).Dietary source Green vegetables, liver, yeast,egg, milk and some fruits. Prolonged cookingwith spices destroys folic acid.Absorption takes place in the duodenum andjejunum and is transported in the blood byactive and passive transport, widelydistributed in the body and is stored in theliver.Functions Folic acid is converted todihydrofolic acid and then to tetrahydrofolicacid which serves as a coenzyme for manyvital (one-carbon transfer) reactionsnecessary for DNA synthesis.Deficiency Folate deficiency may be due todietary folate deficiency, malabsorption andother diseases of the small intestine or druginduced. Phenytoin, phenobarbitone, oralcontraceptives, methotrexate and trime-thoprim can induce folate deficiency.Increased requirement as in growingchildren, pregnancy and lactation can alsocause deficiency. Manifestations includemegaloblastic anaemia, glossitis, diarrhoeaand weakness.
Uses
1. Megaloblastic anaemia due to folate as wellas B12 deficiency–folic acid 2-5 mg/day isgiven orally along with vitamin B12. In folicacid deficiency due to malabsorptionsyndromes, folic acid is given IM.
2. Prophylactically in pregnancy, lactation,infancy and other situations withincreased requirement of folic acid - 500μg daily orally.
Folinic acid (citrovorum factor, leucovorin)is N-formyl tetrahydrofolic acid and is theactive coenzyme form which overcomesmethotrexate toxicity (Page 330).
HAEMATOPOIETIC GROWTH FACTORS
Haematopoietic growth factors are hormonesthat regulate erythropoiesis. Many of theseglycoproteins have now been produced forclinical use by recombinant DNA technology.Frequent blood counts are needed to monitortherapy with these growth factors.Haemotopoietic Growth Factors Include:• Erythropoietin• Myeloid growth factors
GM-CSFG-CSFM-CSF
• Megakaryocyte growth factorsThrombopoietinInterleukin-II
Erythropoietin is produced by the kidney inresponse to hypoxia and anaemia. It binds toerythropoietin receptors on red cellprogenitors and stimulates red cellproduction.
It can cause hypertension, thrombosis andallergic reactions. Parenteral iron may beneeded to prevent iron deficiency that isprecipitated by rapid erythropoiesis.Uses - Erythropoietin is useful in the treatmentof anaemia seen in chronic renal failure, bonemarrow disorders, malignancies, chronic
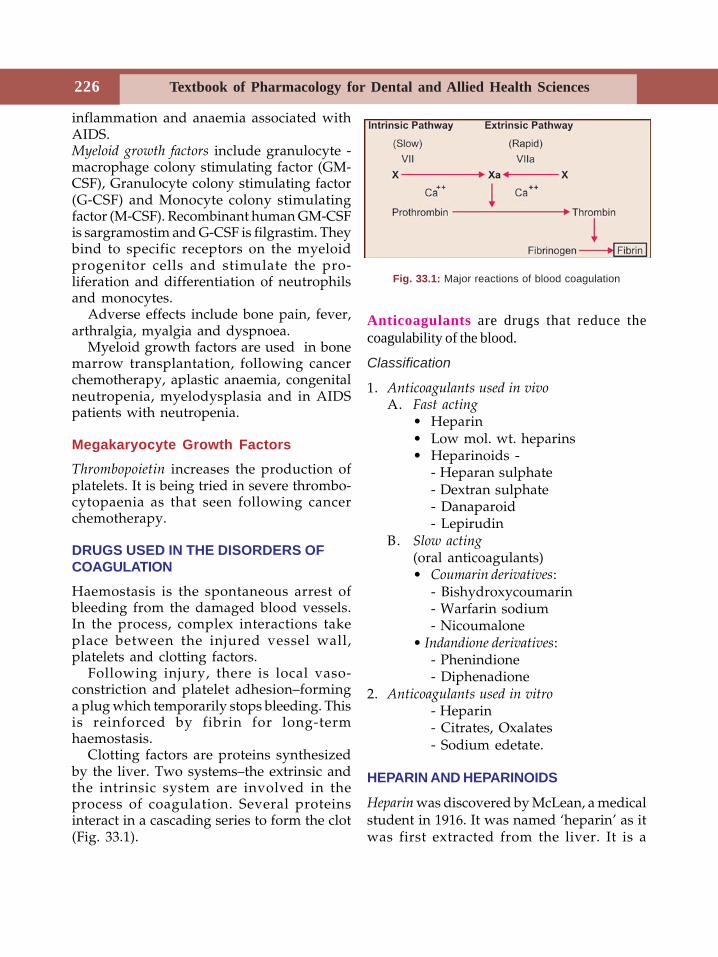
Textbook of Pharmacology for Dental and Allied Health Sciences226
inflammation and anaemia associated withAIDS.Myeloid growth factors include granulocyte -macrophage colony stimulating factor (GM-CSF), Granulocyte colony stimulating factor(G-CSF) and Monocyte colony stimulatingfactor (M-CSF). Recombinant human GM-CSFis sargramostim and G-CSF is filgrastim. Theybind to specific receptors on the myeloidprogenitor cells and stimulate the pro-liferation and differentiation of neutrophilsand monocytes.
Adverse effects include bone pain, fever,arthralgia, myalgia and dyspnoea.
Myeloid growth factors are used in bonemarrow transplantation, following cancerchemotherapy, aplastic anaemia, congenitalneutropenia, myelodysplasia and in AIDSpatients with neutropenia.
Megakaryocyte Growth Factors
Thrombopoietin increases the production ofplatelets. It is being tried in severe thrombo-cytopaenia as that seen following cancerchemotherapy.
DRUGS USED IN THE DISORDERS OFCOAGULATION
Haemostasis is the spontaneous arrest ofbleeding from the damaged blood vessels.In the process, complex interactions takeplace between the injured vessel wall,platelets and clotting factors.
Following injury, there is local vaso-constriction and platelet adhesion–forminga plug which temporarily stops bleeding. Thisis reinforced by fibrin for long-termhaemostasis.
Clotting factors are proteins synthesizedby the liver. Two systems–the extrinsic andthe intrinsic system are involved in theprocess of coagulation. Several proteinsinteract in a cascading series to form the clot(Fig. 33.1).
Fig. 33.1: Major reactions of blood coagulation
Anticoagulants are drugs that reduce thecoagulability of the blood.
Classification
1. Anticoagulants used in vivoA. Fast acting
• Heparin• Low mol. wt. heparins• Heparinoids -
- Heparan sulphate- Dextran sulphate- Danaparoid- Lepirudin
B. Slow acting(oral anticoagulants)• Coumarin derivatives:
- Bishydroxycoumarin- Warfarin sodium- Nicoumalone
• Indandione derivatives:- Phenindione- Diphenadione
2. Anticoagulants used in vitro- Heparin- Citrates, Oxalates- Sodium edetate.
HEPARIN AND HEPARINOIDS
Heparin was discovered by McLean, a medicalstudent in 1916. It was named ‘heparin’ as itwas first extracted from the liver. It is a
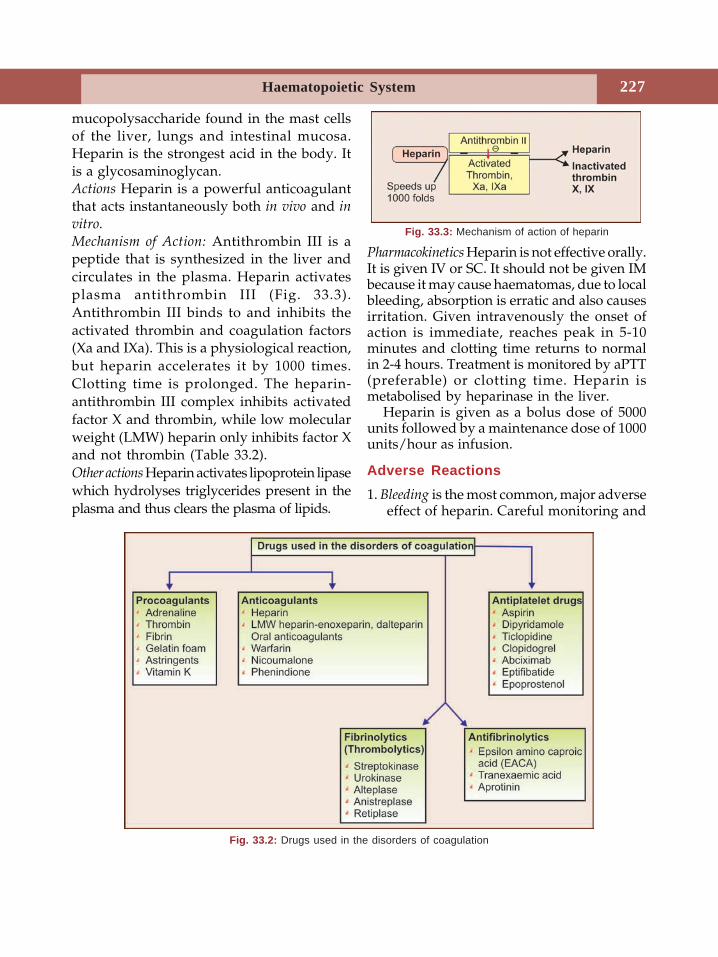
227Haematopoietic System
mucopolysaccharide found in the mast cellsof the liver, lungs and intestinal mucosa.Heparin is the strongest acid in the body. Itis a glycosaminoglycan.Actions Heparin is a powerful anticoagulantthat acts instantaneously both in vivo and invitro.
Mechanism of Action: Antithrombin III is apeptide that is synthesized in the liver andcirculates in the plasma. Heparin activatesplasma antithrombin III (Fig. 33.3).Antithrombin III binds to and inhibits theactivated thrombin and coagulation factors(Xa and IXa). This is a physiological reaction,but heparin accelerates it by 1000 times.Clotting time is prolonged. The heparin-antithrombin III complex inhibits activatedfactor X and thrombin, while low molecularweight (LMW) heparin only inhibits factor Xand not thrombin (Table 33.2).Other actions Heparin activates lipoprotein lipasewhich hydrolyses triglycerides present in theplasma and thus clears the plasma of lipids.
Pharmacokinetics Heparin is not effective orally.It is given IV or SC. It should not be given IMbecause it may cause haematomas, due to localbleeding, absorption is erratic and also causesirritation. Given intravenously the onset ofaction is immediate, reaches peak in 5-10minutes and clotting time returns to normalin 2-4 hours. Treatment is monitored by aPTT(preferable) or clotting time. Heparin ismetabolised by heparinase in the liver.
Heparin is given as a bolus dose of 5000units followed by a maintenance dose of 1000units/hour as infusion.
Adverse Reactions1. Bleeding is the most common, major adverse
effect of heparin. Careful monitoring and
Fig. 33.2: Drugs used in the disorders of coagulation
Fig. 33.3: Mechanism of action of heparin
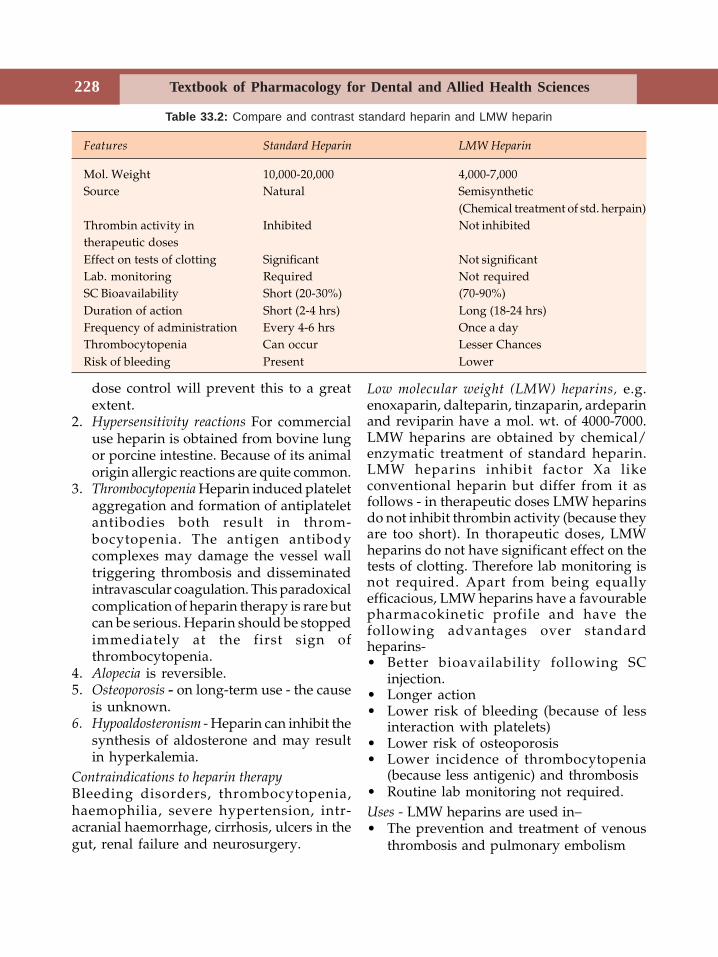
Textbook of Pharmacology for Dental and Allied Health Sciences228
dose control will prevent this to a greatextent.
2. Hypersensitivity reactions For commercialuse heparin is obtained from bovine lungor porcine intestine. Because of its animalorigin allergic reactions are quite common.
3. Thrombocytopenia Heparin induced plateletaggregation and formation of antiplateletantibodies both result in throm-bocytopenia. The antigen antibodycomplexes may damage the vessel walltriggering thrombosis and disseminatedintravascular coagulation. This paradoxicalcomplication of heparin therapy is rare butcan be serious. Heparin should be stoppedimmediately at the first sign ofthrombocytopenia.
4. Alopecia is reversible.5. Osteoporosis - on long-term use - the cause
is unknown.6. Hypoaldosteronism - Heparin can inhibit the
synthesis of aldosterone and may resultin hyperkalemia.
Contraindications to heparin therapyBleeding disorders, thrombocytopenia,haemophilia, severe hypertension, intr-acranial haemorrhage, cirrhosis, ulcers in thegut, renal failure and neurosurgery.
Low molecular weight (LMW) heparins, e.g.enoxaparin, dalteparin, tinzaparin, ardeparinand reviparin have a mol. wt. of 4000-7000.LMW heparins are obtained by chemical/enzymatic treatment of standard heparin.LMW heparins inhibit factor Xa likeconventional heparin but differ from it asfollows - in therapeutic doses LMW heparinsdo not inhibit thrombin activity (because theyare too short). In thorapeutic doses, LMWheparins do not have significant effect on thetests of clotting. Therefore lab monitoring isnot required. Apart from being equallyefficacious, LMW heparins have a favourablepharmacokinetic profile and have thefollowing advantages over standardheparins-• Better bioavailability following SC
injection.• Longer action• Lower risk of bleeding (because of less
interaction with platelets)• Lower risk of osteoporosis• Lower incidence of thrombocytopenia
(because less antigenic) and thrombosis• Routine lab monitoring not required.Uses - LMW heparins are used in–• The prevention and treatment of venous
thrombosis and pulmonary embolism
Table 33.2: Compare and contrast standard heparin and LMW heparin
Features Standard Heparin LMW Heparin
Mol. Weight 10,000-20,000 4,000-7,000Source Natural Semisynthetic
(Chemical treatment of std. herpain)Thrombin activity in Inhibited Not inhibitedtherapeutic dosesEffect on tests of clotting Significant Not significantLab. monitoring Required Not requiredSC Bioavailability Short (20-30%) (70-90%)Duration of action Short (2-4 hrs) Long (18-24 hrs)Frequency of administration Every 4-6 hrs Once a dayThrombocytopenia Can occur Lesser ChancesRisk of bleeding Present Lower

229Haematopoietic System
• In unstable angina• To maintain the patency of tubes in
dialysis patients.Heparin antagonist Mild heparin overdosagecan be treated by just stopping heparinbecause heparin is short acting. In severeheparin overdose, an antagonist may beneeded to arrest its anticoagulant effects.Protamine sulphate is a protein obtained fromthe sperm of certain fish. Given intra-venously, it neutralises heparin (1 mg forevery 100 units of heparin). In the absence ofheparin, protamine sulphate can itself act asa weak anticoagulant. Hence overdoseshould be avoided. Protamine sulphate is astrongly basic protein which binds with thestrongly acidic groups of heparin forming astable complex which is devoid ofanticoagulant activity–this is the pharma-cological basis for using protamine sulphatein heparin overdosage.
Whole blood transfusion may be needed.
Heparinoids
Heparan sulfate present in some tissues issimilar to heparin. It is believed to beresponsible for antithrombotic activity on thevascular endothelium.Hirudin is the anticoagulant found in thesalivary glands of leeches. It is a powerfulthrombin inhibitor. Lepirudin is produced byrecombinant DNA technology and can beused in patients allergic to heparin but it hasno antagonist yet.Danaparoid is a mixture of heparinoids andacts by inhibiting factor Xa. It does notprolong aPTT and is longer acting. It is usedsubcutaneously in the treatment of deep veinthrombosis and in other conditions as analternative to heparin.
ORAL ANTICOAGULANTS
Cattle that were fed on spoiled sweet cloverhay, developed a haemorrhagic disease in
North America in 1924. This turned out to bedue to bishydroxycoumarin, an anticoagulantin the spoiled sweet clover. Many relatedcompounds were then developed and are alsobeing used as rat poison.Mechanism of action Warfarin and itscongeners act as anticoagulants only in vivobecause they act by interfering with thesynthesis of vitamin K dependent clottingfactors in the liver. They block the γcarboxylation of glutamate residues inprothrombin, factors VII, IX and X. γcarboxylation is necessary for these factorsto participate in coagulation.
The onset of action is slow; anticoagulanteffect develops over 1-3 days because oralanticoagulants do not destroy the alreadycirculating clotting factors. Prothrombin time(PT) is measured to monitor the treatment.It takes 5-7 days for PT to return to normalafter stopping oral anticoagulants.Pharmacokinetics Warfarin is completelyabsorbed orally and is 99% bound to plasmaproteins.
Adverse Effects
1. Haemorrhage is the main hazard. Bleedingin the intestines or brain can be trou-blesome. Minor episodes of epistaxis andbleeding gums are common.Treatment–depends on the severity:a. Stop the anticoagulant.b. Fresh blood transfusion is given to
supply clotting factors.c. Antidote The specific antidote is vitamin
K1 oxide. It allows synthesis of clotting
factors. But even on IV administration,the response to vitamin K1 oxide needsseveral hours. Hence in emergency,fresh whole blood is necessary to counterthe effects of oral anticoagulants.
2. Other adverse effects include allergicreactions, gastrointestinal disturbancesand teratogenicity.
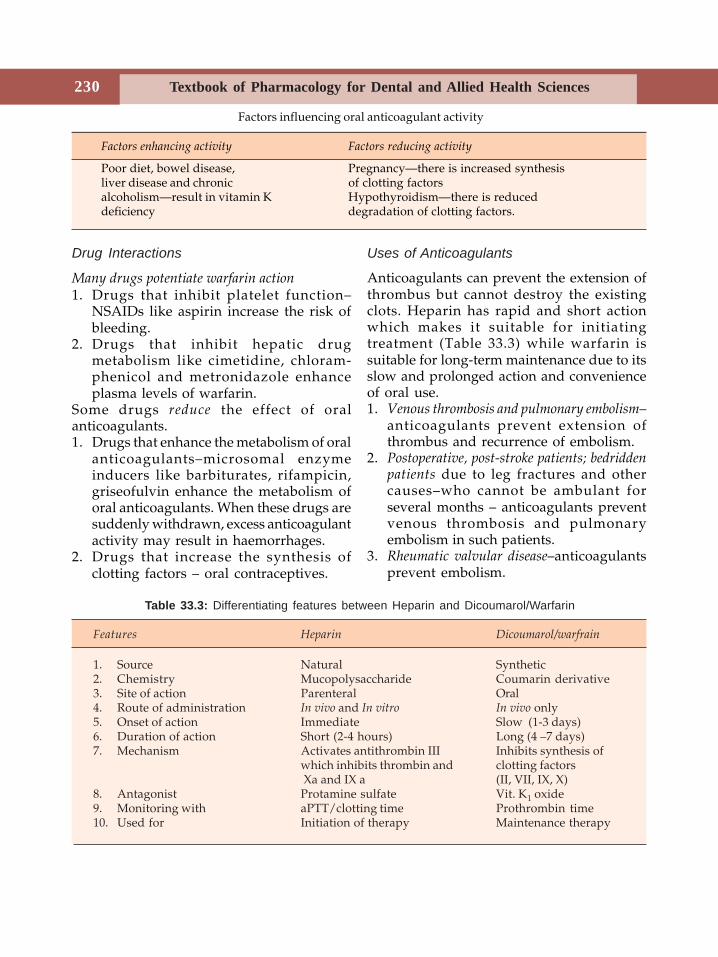
Textbook of Pharmacology for Dental and Allied Health Sciences230
Drug Interactions
Many drugs potentiate warfarin action1. Drugs that inhibit platelet function–
NSAIDs like aspirin increase the risk ofbleeding.
2. Drugs that inhibit hepatic drugmetabolism like cimetidine, chloram-phenicol and metronidazole enhanceplasma levels of warfarin.
Some drugs reduce the effect of oralanticoagulants.1. Drugs that enhance the metabolism of oral
anticoagulants–microsomal enzymeinducers like barbiturates, rifampicin,griseofulvin enhance the metabolism oforal anticoagulants. When these drugs aresuddenly withdrawn, excess anticoagulantactivity may result in haemorrhages.
2. Drugs that increase the synthesis ofclotting factors – oral contraceptives.
Uses of Anticoagulants
Anticoagulants can prevent the extension ofthrombus but cannot destroy the existingclots. Heparin has rapid and short actionwhich makes it suitable for initiatingtreatment (Table 33.3) while warfarin issuitable for long-term maintenance due to itsslow and prolonged action and convenienceof oral use.1. Venous thrombosis and pulmonary embolism–
anticoagulants prevent extension ofthrombus and recurrence of embolism.
2. Postoperative, post-stroke patients; bedriddenpatients due to leg fractures and othercauses–who cannot be ambulant forseveral months – anticoagulants preventvenous thrombosis and pulmonaryembolism in such patients.
3. Rheumatic valvular disease–anticoagulantsprevent embolism.
Factors influencing oral anticoagulant activity
Factors enhancing activity Factors reducing activity
Poor diet, bowel disease, Pregnancy—there is increased synthesisliver disease and chronic of clotting factorsalcoholism—result in vitamin K Hypothyroidism—there is reduceddeficiency degradation of clotting factors.
Table 33.3: Differentiating features between Heparin and Dicoumarol/Warfarin
Features Heparin Dicoumarol/warfrain
1. Source Natural Synthetic2. Chemistry Mucopolysaccharide Coumarin derivative3. Site of action Parenteral Oral4. Route of administration In vivo and In vitro In vivo only5. Onset of action Immediate Slow (1-3 days)6. Duration of action Short (2-4 hours) Long (4 –7 days)7. Mechanism Activates antithrombin III Inhibits synthesis of
which inhibits thrombin and clotting factors Xa and IX a (II, VII, IX, X)
8. Antagonist Protamine sulfate Vit. K1 oxide9. Monitoring with aPTT/clotting time Prothrombin time10. Used for Initiation of therapy Maintenance therapy
231Haematopoietic System
4. Unstable angina–heparin reduces the riskof myocardial infarction in patients withunstable angina.
5. Vascular surgery, artificial heart valves andhaemodialysis–anticoagulants preventthromboembolism.
Contraindications to anticoagulant therapy• Bleeding disorders including throm-
bocytopenia• Severe hypertension• Malignancies• Bacterial endocarditis• Liver and kidney diseases.• Recent surgery (in the last 10-15 days)• History of cerebrovascular accident
THROMBOLYTICS (FIBRINOLYTICS)Thrombolytics lyse the clot or thrombi byactivating the natural fibrinolytic system.
Plasminogen circulates in the plasma andalso some of it is bound to fibrin. Tissueplasminogen activator (tPA) activatesplasminogen which is converted to plasmin.Plasmin degrades fibrin thereby dissolvingthe clot. Thrombolytic agents are streptokinase,urokinase, alteplase and reteplase. All areexpensive drugs.Streptokinase obtained from β-haemolyticstreptococci activates plasminogen. Anti-streptococcal antibodies present in the blooddue to previous streptococcal infectionsinactivate a large amount of streptokinase.
Streptokinase is antigenic and can causeallergy. The antibodies formed may persistfor five years. Hence if thrombolytics arerequired during that period, others like tPAor urokinase should be used. Streptokinasealso causes hypotension.
Anistreplase
Anistreplase (Anisoylated plasminogenstreptokinase activator complex) is a form ofstreptokinase which is long acting and canbe injected in a single IV bolus. Hence it ismore convenient to use.
Urokinase
Urokinase is an enzyme prepared fromcultures of human kidney cells (it was firstisolated from human urine–hence the name).It activates plasminogen. It is more expensivethan streptokinase.
Tissue Plasminogen Activator
Tissue plasminogen activator (tPA) pre-ferentially activates plasminogen that isbound to fibrin (clot) which means circulatingplasminogen is largely spared.
Alteplase, Duteplase
Alteplase, duteplase are tPA produced byrecombinant DNA technology. They are veryexpensive.
Reteplase
Reteplase is modified human tPA obtainedby genetic engineering .It is claimed to havethe following advantages over tPA• faster reperfusion• bleeding tendency is negligible.
Tenecteplase
Tenecteplase is longer acting and can begiven as an IV bolus injection. Its ability tobind fibrin is better than that of alteplase.
Adverse Effects of Thrombolytics
Bleeding is the major toxicity of allthrombolytics. Hypotension and fever canoccur. Allergic reactions are common withstreptokinase.
Textbook of Pharmacology for Dental and Allied Health Sciences232
Uses
1. Acute myocardial infarction–Intravenousthrombolytics given immediately reducethe mortality rate in acute MI. They shouldbe given within 12 hours but preferablyimmediately because early treatmentlargely reduces mortality.
2. Deep vein thrombosis and largepulmonary emboli are also treated withfibrinolytics.
Contraindications to thrombolytic therapy• Recent surgery, injury, gastrointestinal
bleeding, stroke.• Severe hypertension.• Bleeding disorders.
ANTIFIBRINOLYTICS
Antifibrinolytics inhibit plasminogenactivation and thus prevent fibrinolysis.Epsilon aminocaproic acid (EACA) and itsanalogue tranexaemic acid are antifibrinolytics.They bind to plasminogen and plasmin andprevent the binding of fibrin to theseproteins. Aprotinin is another fibrinolyticdrug which acts by inhibiting proteolyticenzymes. Antifibrinolytics are used inoverdose of fibrinolytics and to reducebleeding after prostatic surgery and somepatients undergoing cardiac surgeries orafter tooth extraction in haemophiliacs–butthe beneficial effect is uncertain.
ANTIPLATELET DRUGS
Platelets form the initial haemostatic plug atthe site of vascular injury and are alsoinvolved in the formation of atherosclerosis.By inhibiting the platelet function, throm-bosis and atherosclerotic vascular disease canbe largely prevented.Antiplatelet drugs or drugs interfering withplatelet function include -
1. PG synthesis inhibitors -Aspirin
2. Phosphodiesterase inhibitor -Dipyridamol
3. ADP antagonists -TiclopidineClopidogrel
4. Glycoprotein IIb/IIIa receptor antagonists -AbciximabEptifibatideTirofiban
5. Others- PGI2Aspirin (see chap 27) Thromboxane A2promotes platelet aggregation. Aspirininactivates cyclo-oxygenase (COX) andthereby inhibits the synthesis of throm-boxane A2 even in low doses (75 mg/day).The COX inhibition is irreversible and theeffect lasts for 7 to 10 days–till fresh plateletsare formed. Aspirin is the most commonlyused antiplatelet drug.Dipyridamole is a phosphodiesterase inhibitorwhich interferes with platelet function byincreasing platelet cyclic AMP levels. It is usedalong with aspirin for the prophylaxis ofthromboemboli in patients with prostheticheart valves.
ADP Antagonists
Ticlopidine ADP binds to receptors onplatelets to bring about platelet aggregation.Ticlopidine is a prodrug. Its active metaboliteblocks ADP receptors and prevents plateletaggregation. Onset of action is slow(7-11 days) and the antiplatelet effect remainsfor some days even after stopping the drug.Dose: 250 mg twice daily. Adverse effectsinclude dyspepsia, diarrhoea, bleeding andleukopenia. It is used in patients who cannottolerate aspirin.Clopidogrel has structural similarity toticlopidine with similar mechanism of action.Like ticlopidine it is a prodrug and the active
233Haematopoietic System
metabolite blocks ADP receptors. Its actionsare additive with aspirin as the mechanismsare different. Toxicity is milder with lesserincidence of leukopenia and throm-bocytopenia.
Clopidogrel is used as an alternative whenaspirin cannot be used. It can also be usedwith aspirin for additive effects.Glycoprotein IIb/IIIA receptor antagonists
Fibrinogen and von Willebrand factor bindto glycoprotein IIb/IIIA receptors on theplatelets and mediate platelet aggregation byplatelet agonists like thrombin, collagen andTXA2. Drugs that block these receptors inhibitplatelet aggregation induced by all plateletagonists.Abciximab is a monoclonal antibody whichbinds GP IIb/IIIA receptors and inhibitsplatelet aggregation. It can cause bleeding andallergic reactions. It is used in patientsundergoing coronary angioplasty.Eptifibatide and tirofiban are peptides given asIV infusion. They are short acting and aretried in unstable angina and myocardialinfarction.
Others
Epoprostenol (PGI2) can be used duringhaemodialysis to prevent platelet aggregationas an alternative to heparin.
Uses of Antiplatelet Drugs
1. Myocardial infarction Aspirin with throm-bolytics improves survival in acute MI.Long-term treatment with aspirin reducesreinfarction in post MI patients.
2. Unstable angina and stable angina pectoris-Aspirin reduces the risk of acute MI.Clopidogrel may be added to aspirin inunstable angina.
3. In patients with prosthetic heart valves,valvular heart disease, coronary artery by-
pass surgery–long-term use of low doseaspirin is recommended.
4. Cerebral thrombosis and TIA In patients withtransient ischaemic attacks aspirin reducesthe incidence of stroke and mortality. Incerebral thrombosis aspirin preventsrecurrence.
5. Atrial fibrillation If oral anticoagulants cannot be given, aspirin is useful.
COAGULANTS
Coagulants are drugs that promotecoagulation (procoagulants) and controlbleeding. They are also called haemostatics.
They may be used locally or systemically.Local haemostatics are called styptics. Physicalmethods like local application of pressure,tourniquet or ice can control bleeding.Styptics are local haemostatics that are usedon bleeding sites like tooth socket andwounds.They are:1. Adrenaline Sterile cotton soaked in 1:10,000
solution of adrenaline is commonly usedin tooth sockets and as nasal packs forepistaxis. Adrenaline arrests bleeding byvasoconstriction.
2. Thrombin powder is dusted over thebleeding surface following skin grafting.It is obtained from bovine plasma.
3. Fibrin obtained from human plasma isavailable as sheets. It is used for coveringor packing bleeding surfaces.
4. Gelatin foam is porous spongy gelatin usedwith thrombin to control bleeding fromwounds. It gets completely absorbed in 4to 6 weeks and can be left in place aftersuturing of the wound.
5. Thromboplastin powder is used in surgeryas a styptic.
6. Astringents like tannic acid are used onbleeding gums.
Textbook of Pharmacology for Dental and Allied Health Sciences234
Coagulants Used Systemically are
• Vitamin K• Fibrinogen• Specific deficient factor–factors, II, VII,
VIII, IX, X• Ethamsylate
Vitamin K
Vitamin K is a fat-soluble vitamin essentialfor the biosynthesis of clotting factors. Thereare three compounds:• Vitamin K1– present in food from plant
source• Vitamin K2– produced in the gut by
bacteria.• Vitamin K3– a synthetic compound used
therapeutically.Actions Vitamin K is essential for thebiosynthesis of clotting factors–prothrombinand factors VII, IX and X by the liver.Human requirement-Not clearly known-recommended intake in adults is 50-70 mg/dayDeficiency—Vitamin K deficiency results fromliver diseases, malabsorption, long-termantibiotic therapy and rarely by dietarydeficiency. It is manifested as bleedingtendencies.
Adverse reactions are seen on parenteraladministration of vitamin K–allergicreactions and jaundice can occur.
Uses
1. Vitamin K deficiency2. Newborn babies lack intestinal flora and
have low levels of prothrombin and otherclotting factors. Routine administration ofvitamin K–1 mg IM prevents haemo-rrhagic disease of the newborn.
3. Oral anticoagulant toxicity.
OTHER COAGULANTS
• Fresh plasma or whole blood is useful inmost coagulation disorders as it containsall the clotting factors.
• Concentrated plasma fractions likefibrinogen, factors VIII, II, VII, IX and Xare available for the treatment of specificdeficiencies.
• Snake venom Some venoms like Russelsviper venom stimulate thrombokinase andpromote coagulation.
• Ethamsylate is used orally to arrestbleeding. The exact mode of action is notknown but it is thought that it acts byinhibiting the synthesis of prostacycline(PGI2) and correct the abnormal plateletfunction. It may also stabilize the wall ofthe capillaries and reduce capillarybleeding. Ethamsylate is given orally tocontrol bleeding in–1. Dental extraction and other procedures
in patients with coagulation disorders.2. Menorrhagia3. Post-partum haemorrhage.4. Haematemesis and malena
Dentistry and Drugs Affecting Coagulation
Most dental procedures including minor oneslike scaling and tooth extraction involvessome amount of bleeding. In patients withnormal haemostasis, this is not much of aproblem as bleeding stops by itself. However,even minor dental procedures may result incontinuous bleeding from the site in thefollowing patients–• Patients receiving drugs that inhibit
coagulation.• Thrombocytopenic purpura• Vitamin C deficiency• Haemophiliacs• Long-term glucocorticoid therapy.
For management of bleeding-See page 399
235Haematopoietic System
HYPOLIPIDAEMIC DRUGS
Lipids and proteins form complexes calledlipoproteins and circulate in the bloodvessels. There are four types of lipoproteins-• Low density lipoproteins (LDL)• High density lipoproteins (HDL)• Very low density lipoproteins (VLDL)• Chylomicrons.LDL is the primary carrier of cholesterolwhile VLDL carry triglycerides. Hyperli-poproteinaemias (HPL) are conditions inwhich the concentration of cholesterol ortriglyceride (TG) carrying lipoproteins in theplasma is elevated above normal (Table 33.4)Increase in lipoproteins can hasten thedevelopment of atherosclerosis and is a riskfactor for myocardial infarction. Therefore,along with reduction of body weight and lowcholesterol diet, significant hyperlip-oproteinaemias should be treated withhypolipidaemic drugs. It should be noted thatHDL is known to have antiatherogeniceffects. Low levels of HDL can increase therisk of atherosclerosis. It is thereforedesirable to have higher HDL levels with lowLDL and TG levels.
HYPOLIPIDAEMICS
1. HMG CoA reductase inhibitors —LovastatinSimvastatinPravastatinAtorvastatin
2. Fibric acids —GemfibrozilClofibrateFenofibrateBezafibrateCiprofibrate
3. Bile acid binding resins—CholestyramineColestipol
4. Antioxidant —Probucol
5. Miscellaneous —Nicotinic acidNeomycinGugulipid
HMG CoA Reductase Inhibitors (Statins)Hydroxymethylglutaryl-CoA (HMG-CoA) isthe rate-controlling enzyme in the bio-synthesis of cholesterol. Lovastatin and itscongeners are competitive inhibitors of theenzyme HMG-CoA. They lower plasma LDLcholesterol and triglycerides. The con-centration of HDL-cholesterol (the protectivelipoprotein) increases by 10%.Pharmacokinetics Statins are well absorbedwhen given orally but may undergo extensivefirst pass metabolism in the liver. Foodenhances their absorption. Simvastatin is aprodrug converted to its active metabolitein the liver.Adverse effects include GI disturbances,headache, insomnia, rashes, and rarely angio-oedema. Statins can rarely cause muscletenderness and myopathy with inflammationof the skeletal muscles causing muscle painand weakness.
Uses
1. Several large scale studies have shownstatins to be useful in lowering morbidityand mortality in patients with coronaryheart disease. Hence they are used inpatients with MI, angina, stroke andtransient ischemic attacks to lowercholesterol levels.
2. HMG CoA reductase inhibitors are thefirst line drugs for hyperlipidaemias(Table 33.5) both for familial andsecondary hyperlipidaemias as in diabetesmellitus.
Fibric Acids (Fibrates)Fibric acids enhance activity of the enzymelipoprotein lipase which degrades VLDLresulting in lowering of triglycerides. Theyalso increase HDL levels.
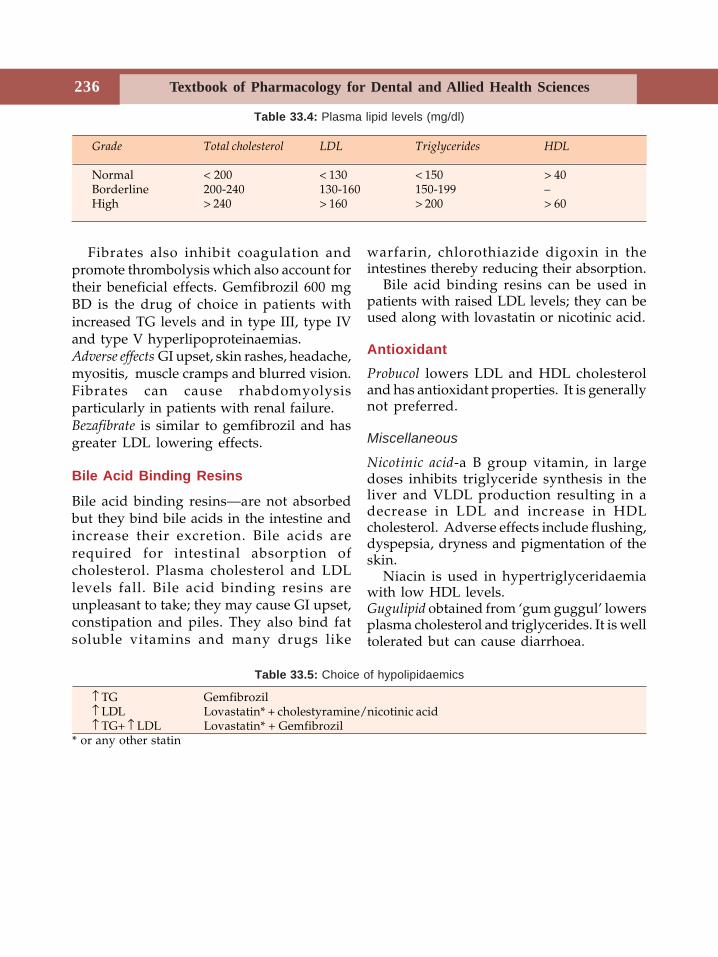
Textbook of Pharmacology for Dental and Allied Health Sciences236
Fibrates also inhibit coagulation andpromote thrombolysis which also account fortheir beneficial effects. Gemfibrozil 600 mgBD is the drug of choice in patients withincreased TG levels and in type III, type IVand type V hyperlipoproteinaemias.Adverse effects GI upset, skin rashes, headache,myositis, muscle cramps and blurred vision.Fibrates can cause rhabdomyolysisparticularly in patients with renal failure.Bezafibrate is similar to gemfibrozil and hasgreater LDL lowering effects.
Bile Acid Binding Resins
Bile acid binding resins—are not absorbedbut they bind bile acids in the intestine andincrease their excretion. Bile acids arerequired for intestinal absorption ofcholesterol. Plasma cholesterol and LDLlevels fall. Bile acid binding resins areunpleasant to take; they may cause GI upset,constipation and piles. They also bind fatsoluble vitamins and many drugs like
warfarin, chlorothiazide digoxin in theintestines thereby reducing their absorption.
Bile acid binding resins can be used inpatients with raised LDL levels; they can beused along with lovastatin or nicotinic acid.
AntioxidantProbucol lowers LDL and HDL cholesteroland has antioxidant properties. It is generallynot preferred.
Miscellaneous
Nicotinic acid-a B group vitamin, in largedoses inhibits triglyceride synthesis in theliver and VLDL production resulting in adecrease in LDL and increase in HDLcholesterol. Adverse effects include flushing,dyspepsia, dryness and pigmentation of theskin.
Niacin is used in hypertriglyceridaemiawith low HDL levels.Gugulipid obtained from ‘gum guggul’ lowersplasma cholesterol and triglycerides. It is welltolerated but can cause diarrhoea.
Table 33.4: Plasma lipid levels (mg/dl)
Grade Total cholesterol LDL Triglycerides HDL
Normal < 200 < 130 < 150 > 40Borderline 200-240 130-160 150-199 –High > 240 > 160 > 200 > 60
Table 33.5: Choice of hypolipidaemics
↑ TG Gemfibrozil↑ LDL Lovastatin* + cholestyramine/nicotinic acid↑ TG+ ↑ LDL Lovastatin* + Gemfibrozil
* or any other statin
34Drugs Used in
Gastrointestinal DisordersDRUGS USED IN PEPTIC ULCER
Acid-peptic disease is common in the presentdays that are full of tension and anxiety.Peptic ulcer is thought to result from animbalance between acid-pepsin secretion andmucosal defense factors. The stomachsecretes about 2.5 litres of gastric juice daily.The chief cells secrete pepsinogen while theparietal cells secrete HCl and intrinsic factor.
Gastric acid secretion is regulated by threepathways–vagus (through acetylcholine),gastrin and local release of histamine–eachacting through its own receptors (Fig. 34.1).These activate H+ K+ ATPase (proton pump)on the parietal cells resulting in the secretionof H+ into the gastric lumen where it combines
with Cl– (drawn from plasma) and HCl issecreted. Acetylcholine and gastrin act bothdirectly on the parietal cells and indirectly byreleasing histamine from the enterochromaffincells. Histamine acts through H2 receptors onparietal cells while acetylcholine through M1
muscarinic and gastrin through G receptors.The factors that protect the mucosa are its
ability to secrete mucous, bicarbonate andprostaglandins. The mucous and bicarbonateform a layer which protects the gastricmucosa from gastric acid. Prostaglandins(PGE2&I2) stimulate the secretion of mucusand bicarbonate, bring about vasodilation andalso inhibit acid secretion. They act on the PGreceptors present on the parietal cell.
Section 9Gastrointestinal Tract
1. Drugs that neutralise gastric acid - Antacids - Magnesium hydroxide, aluminiumhydroxide, calcium carbonate, sodiumbicarbonate
2. Drugs that reduce gastric acid secretiona. H2 receptor blockers - Cimetidine, ranitidine, famotidine, roxati-
dine, nizatidineb. Proton pump inhibitors - Omeprazole, lansoprazole, esomeprazole,
pantoprazole, rabeprazolec. Muscarinic antagonists - Pirenzepine, telenzepine
3. Ulcer protectives - Sucralfate, bismuth compounds4. Other drugs - Carbenoxolone, cisapride, prostaglandins.
CLASSIFICATION
Drugs used in peptic ulcer may be classified as follows:
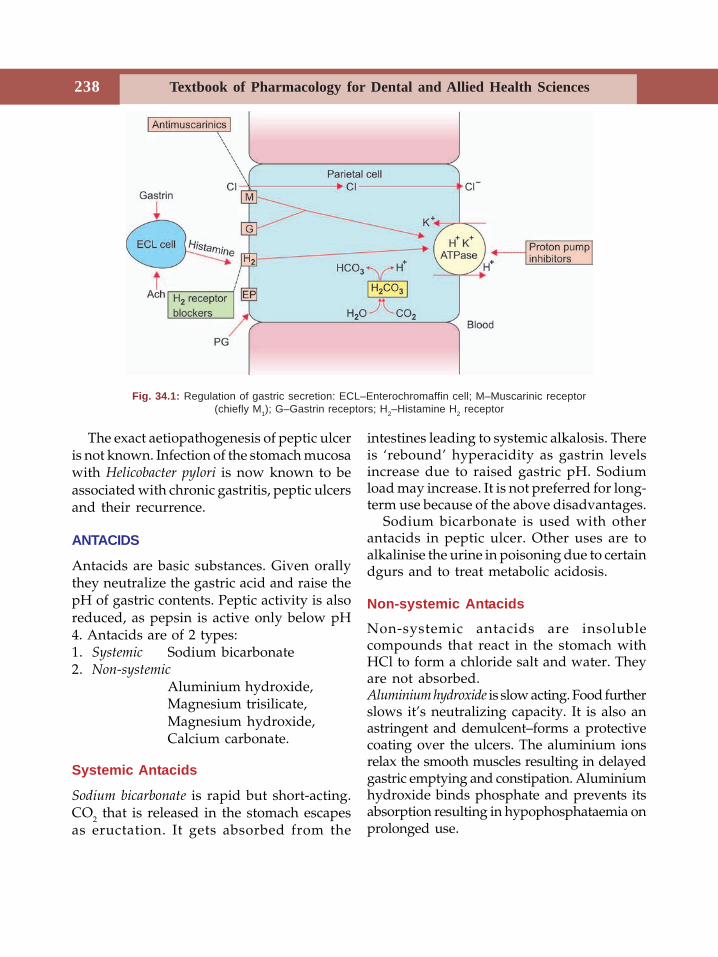
Textbook of Pharmacology for Dental and Allied Health Sciences238
The exact aetiopathogenesis of peptic ulceris not known. Infection of the stomach mucosawith Helicobacter pylori is now known to beassociated with chronic gastritis, peptic ulcersand their recurrence.
ANTACIDS
Antacids are basic substances. Given orallythey neutralize the gastric acid and raise thepH of gastric contents. Peptic activity is alsoreduced, as pepsin is active only below pH4. Antacids are of 2 types:1. Systemic Sodium bicarbonate2. Non-systemic
Aluminium hydroxide,Magnesium trisilicate,Magnesium hydroxide,Calcium carbonate.
Systemic Antacids
Sodium bicarbonate is rapid but short-acting.CO2 that is released in the stomach escapesas eructation. It gets absorbed from the
intestines leading to systemic alkalosis. Thereis ‘rebound’ hyperacidity as gastrin levelsincrease due to raised gastric pH. Sodiumload may increase. It is not preferred for long-term use because of the above disadvantages.
Sodium bicarbonate is used with otherantacids in peptic ulcer. Other uses are toalkalinise the urine in poisoning due to certaindgurs and to treat metabolic acidosis.
Non-systemic Antacids
Non-systemic antacids are insolublecompounds that react in the stomach withHCl to form a chloride salt and water. Theyare not absorbed.Aluminium hydroxide is slow acting. Food furtherslows it’s neutralizing capacity. It is also anastringent and demulcent–forms a protectivecoating over the ulcers. The aluminium ionsrelax the smooth muscles resulting in delayedgastric emptying and constipation. Aluminiumhydroxide binds phosphate and prevents itsabsorption resulting in hypophosphataemia onprolonged use.
Fig. 34.1: Regulation of gastric secretion: ECL–Enterochromaffin cell; M–Muscarinic receptor(chiefly M1); G–Gastrin receptors; H2–Histamine H2 receptor
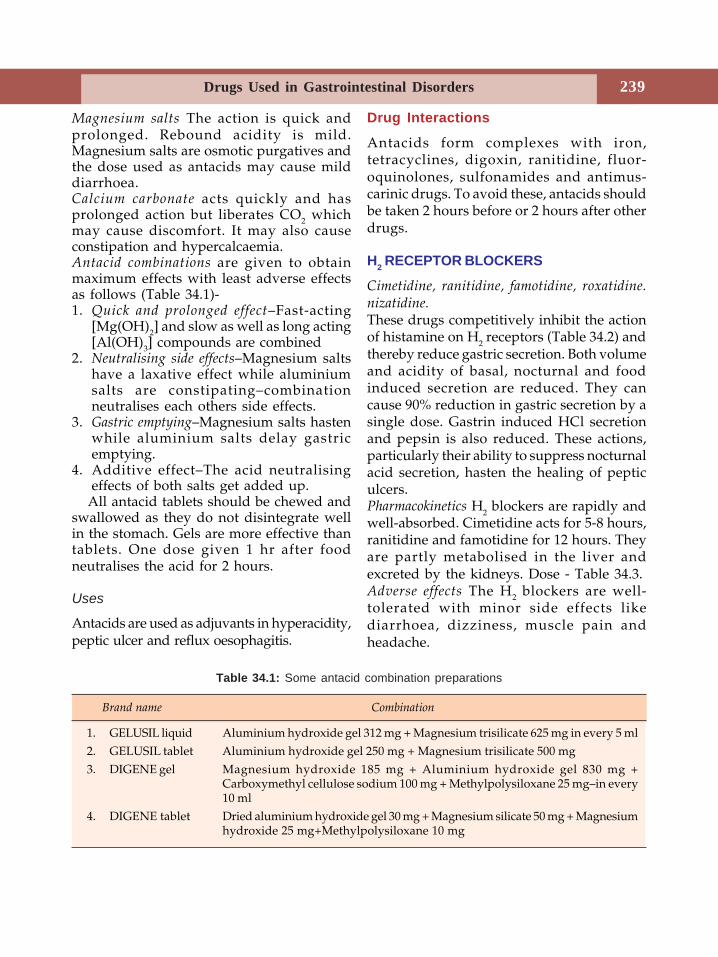
239Drugs Used in Gastrointestinal Disorders
Magnesium salts The action is quick andprolonged. Rebound acidity is mild.Magnesium salts are osmotic purgatives andthe dose used as antacids may cause milddiarrhoea.Calcium carbonate acts quickly and hasprolonged action but liberates CO2 whichmay cause discomfort. It may also causeconstipation and hypercalcaemia.Antacid combinations are given to obtainmaximum effects with least adverse effectsas follows (Table 34.1)-1. Quick and prolonged effect–Fast-acting
[Mg(OH)2] and slow as well as long acting[Al(OH)3] compounds are combined
2. Neutralising side effects–Magnesium saltshave a laxative effect while aluminiumsalts are constipating–combinationneutralises each others side effects.
3. Gastric emptying–Magnesium salts hastenwhile aluminium salts delay gastricemptying.
4. Additive effect–The acid neutralisingeffects of both salts get added up.
All antacid tablets should be chewed andswallowed as they do not disintegrate wellin the stomach. Gels are more effective thantablets. One dose given 1 hr after foodneutralises the acid for 2 hours.
Uses
Antacids are used as adjuvants in hyperacidity,peptic ulcer and reflux oesophagitis.
Drug Interactions
Antacids form complexes with iron,tetracyclines, digoxin, ranitidine, fluor-oquinolones, sulfonamides and antimus-carinic drugs. To avoid these, antacids shouldbe taken 2 hours before or 2 hours after otherdrugs.
H2 RECEPTOR BLOCKERS
Cimetidine, ranitidine, famotidine, roxatidine.nizatidine.These drugs competitively inhibit the actionof histamine on H2 receptors (Table 34.2) andthereby reduce gastric secretion. Both volumeand acidity of basal, nocturnal and foodinduced secretion are reduced. They cancause 90% reduction in gastric secretion by asingle dose. Gastrin induced HCl secretionand pepsin is also reduced. These actions,particularly their ability to suppress nocturnalacid secretion, hasten the healing of pepticulcers.Pharmacokinetics H2 blockers are rapidly andwell-absorbed. Cimetidine acts for 5-8 hours,ranitidine and famotidine for 12 hours. Theyare partly metabolised in the liver andexcreted by the kidneys. Dose - Table 34.3.Adverse effects The H2 blockers are well-tolerated with minor side effects likediarrhoea, dizziness, muscle pain andheadache.
Brand name Combination
1. GELUSIL liquid Aluminium hydroxide gel 312 mg + Magnesium trisilicate 625 mg in every 5 ml2. GELUSIL tablet Aluminium hydroxide gel 250 mg + Magnesium trisilicate 500 mg3. DIGENE gel Magnesium hydroxide 185 mg + Aluminium hydroxide gel 830 mg +
Carboxymethyl cellulose sodium 100 mg + Methylpolysiloxane 25 mg–in every10 ml
4. DIGENE tablet Dried aluminium hydroxide gel 30 mg + Magnesium silicate 50 mg + Magnesiumhydroxide 25 mg+Methylpolysiloxane 10 mg
Table 34.1: Some antacid combination preparations
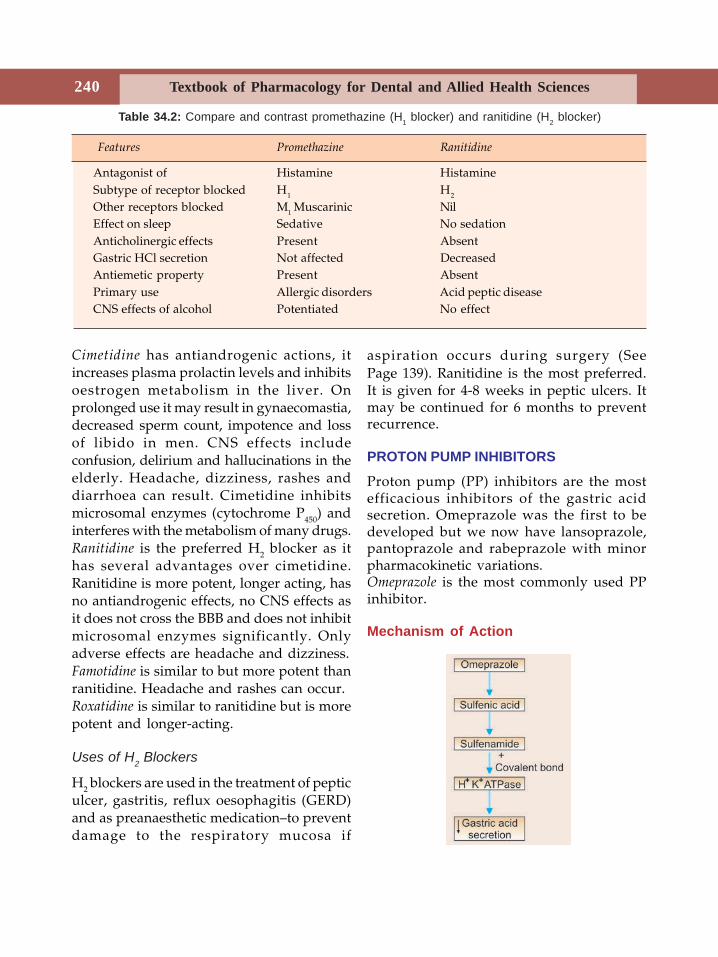
Textbook of Pharmacology for Dental and Allied Health Sciences240
Cimetidine has antiandrogenic actions, itincreases plasma prolactin levels and inhibitsoestrogen metabolism in the liver. Onprolonged use it may result in gynaecomastia,decreased sperm count, impotence and lossof libido in men. CNS effects includeconfusion, delirium and hallucinations in theelderly. Headache, dizziness, rashes anddiarrhoea can result. Cimetidine inhibitsmicrosomal enzymes (cytochrome P450) andinterferes with the metabolism of many drugs.Ranitidine is the preferred H2 blocker as ithas several advantages over cimetidine.Ranitidine is more potent, longer acting, hasno antiandrogenic effects, no CNS effects asit does not cross the BBB and does not inhibitmicrosomal enzymes significantly. Onlyadverse effects are headache and dizziness.Famotidine is similar to but more potent thanranitidine. Headache and rashes can occur.Roxatidine is similar to ranitidine but is morepotent and longer-acting.
Uses of H2 Blockers
H2 blockers are used in the treatment of pepticulcer, gastritis, reflux oesophagitis (GERD)and as preanaesthetic medication–to preventdamage to the respiratory mucosa if
aspiration occurs during surgery (SeePage 139). Ranitidine is the most preferred.It is given for 4-8 weeks in peptic ulcers. Itmay be continued for 6 months to preventrecurrence.
PROTON PUMP INHIBITORS
Proton pump (PP) inhibitors are the mostefficacious inhibitors of the gastric acidsecretion. Omeprazole was the first to bedeveloped but we now have lansoprazole,pantoprazole and rabeprazole with minorpharmacokinetic variations.Omeprazole is the most commonly used PPinhibitor.
Mechanism of Action
Table 34.2: Compare and contrast promethazine (H1 blocker) and ranitidine (H2 blocker)
Features Promethazine Ranitidine
Antagonist of Histamine HistamineSubtype of receptor blocked H1 H2
Other receptors blocked M1 Muscarinic NilEffect on sleep Sedative No sedationAnticholinergic effects Present AbsentGastric HCl secretion Not affected DecreasedAntiemetic property Present AbsentPrimary use Allergic disorders Acid peptic diseaseCNS effects of alcohol Potentiated No effect
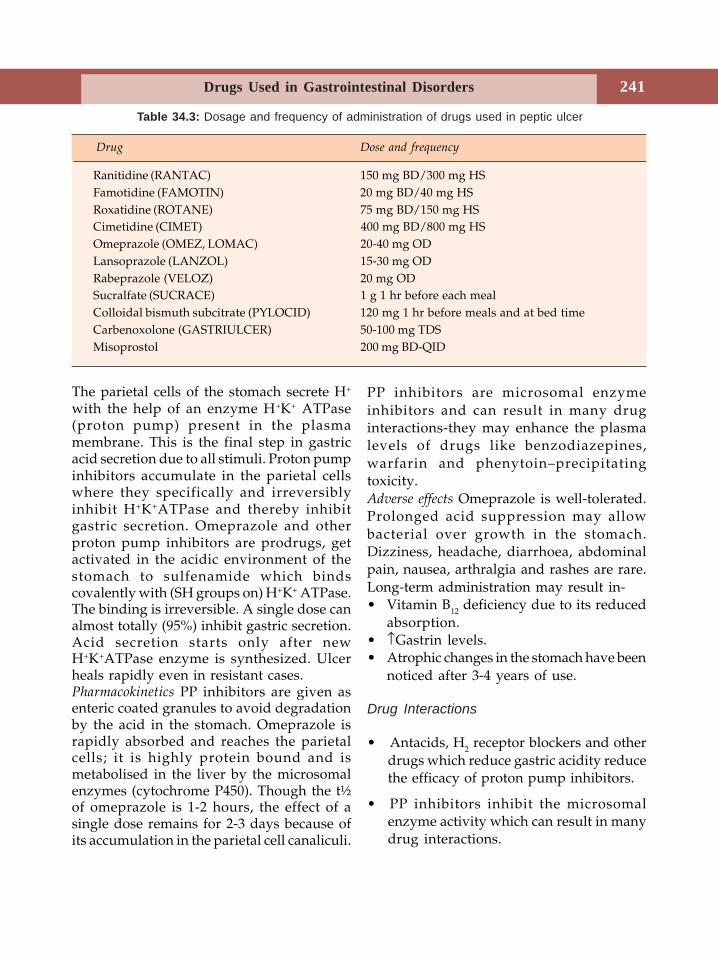
241Drugs Used in Gastrointestinal Disorders
The parietal cells of the stomach secrete H+
with the help of an enzyme H+K+ ATPase(proton pump) present in the plasmamembrane. This is the final step in gastricacid secretion due to all stimuli. Proton pumpinhibitors accumulate in the parietal cellswhere they specifically and irreversiblyinhibit H+K+ATPase and thereby inhibitgastric secretion. Omeprazole and otherproton pump inhibitors are prodrugs, getactivated in the acidic environment of thestomach to sulfenamide which bindscovalently with (SH groups on) H+K+ ATPase.The binding is irreversible. A single dose canalmost totally (95%) inhibit gastric secretion.Acid secretion starts only after newH+K+ATPase enzyme is synthesized. Ulcerheals rapidly even in resistant cases.Pharmacokinetics PP inhibitors are given asenteric coated granules to avoid degradationby the acid in the stomach. Omeprazole israpidly absorbed and reaches the parietalcells; it is highly protein bound and ismetabolised in the liver by the microsomalenzymes (cytochrome P450). Though the t½of omeprazole is 1-2 hours, the effect of asingle dose remains for 2-3 days because ofits accumulation in the parietal cell canaliculi.
PP inhibitors are microsomal enzymeinhibitors and can result in many druginteractions-they may enhance the plasmalevels of drugs like benzodiazepines,warfarin and phenytoin–precipitatingtoxicity.Adverse effects Omeprazole is well-tolerated.Prolonged acid suppression may allowbacterial over growth in the stomach.Dizziness, headache, diarrhoea, abdominalpain, nausea, arthralgia and rashes are rare.Long-term administration may result in-• Vitamin B12 deficiency due to its reduced
absorption.• ↑Gastrin levels.• Atrophic changes in the stomach have been
noticed after 3-4 years of use.
Drug Interactions
• Antacids, H2 receptor blockers and otherdrugs which reduce gastric acidity reducethe efficacy of proton pump inhibitors.
• PP inhibitors inhibit the microsomalenzyme activity which can result in manydrug interactions.
Table 34.3: Dosage and frequency of administration of drugs used in peptic ulcer
Drug Dose and frequency
Ranitidine (RANTAC) 150 mg BD/300 mg HSFamotidine (FAMOTIN) 20 mg BD/40 mg HSRoxatidine (ROTANE) 75 mg BD/150 mg HSCimetidine (CIMET) 400 mg BD/800 mg HSOmeprazole (OMEZ, LOMAC) 20-40 mg ODLansoprazole (LANZOL) 15-30 mg ODRabeprazole (VELOZ) 20 mg ODSucralfate (SUCRACE) 1 g 1 hr before each mealColloidal bismuth subcitrate (PYLOCID) 120 mg 1 hr before meals and at bed timeCarbenoxolone (GASTRIULCER) 50-100 mg TDSMisoprostol 200 mg BD-QID
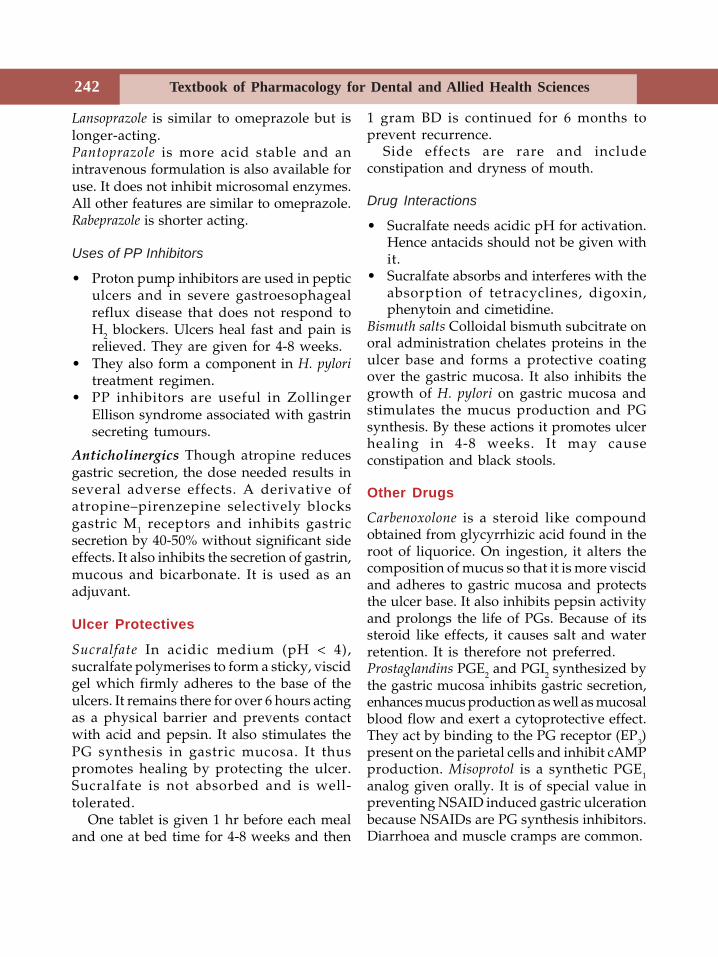
Textbook of Pharmacology for Dental and Allied Health Sciences242
Lansoprazole is similar to omeprazole but islonger-acting.Pantoprazole is more acid stable and anintravenous formulation is also available foruse. It does not inhibit microsomal enzymes.All other features are similar to omeprazole.Rabeprazole is shorter acting.
Uses of PP Inhibitors
• Proton pump inhibitors are used in pepticulcers and in severe gastroesophagealreflux disease that does not respond toH2 blockers. Ulcers heal fast and pain isrelieved. They are given for 4-8 weeks.
• They also form a component in H. pyloritreatment regimen.
• PP inhibitors are useful in ZollingerEllison syndrome associated with gastrinsecreting tumours.
Anticholinergics Though atropine reducesgastric secretion, the dose needed results inseveral adverse effects. A derivative ofatropine–pirenzepine selectively blocksgastric M1 receptors and inhibits gastricsecretion by 40-50% without significant sideeffects. It also inhibits the secretion of gastrin,mucous and bicarbonate. It is used as anadjuvant.
Ulcer Protectives
Sucralfate In acidic medium (pH < 4),sucralfate polymerises to form a sticky, viscidgel which firmly adheres to the base of theulcers. It remains there for over 6 hours actingas a physical barrier and prevents contactwith acid and pepsin. It also stimulates thePG synthesis in gastric mucosa. It thuspromotes healing by protecting the ulcer.Sucralfate is not absorbed and is well-tolerated.
One tablet is given 1 hr before each mealand one at bed time for 4-8 weeks and then
1 gram BD is continued for 6 months toprevent recurrence.
Side effects are rare and includeconstipation and dryness of mouth.
Drug Interactions
• Sucralfate needs acidic pH for activation.Hence antacids should not be given withit.
• Sucralfate absorbs and interferes with theabsorption of tetracyclines, digoxin,phenytoin and cimetidine.
Bismuth salts Colloidal bismuth subcitrate onoral administration chelates proteins in theulcer base and forms a protective coatingover the gastric mucosa. It also inhibits thegrowth of H. pylori on gastric mucosa andstimulates the mucus production and PGsynthesis. By these actions it promotes ulcerhealing in 4-8 weeks. It may causeconstipation and black stools.
Other Drugs
Carbenoxolone is a steroid like compoundobtained from glycyrrhizic acid found in theroot of liquorice. On ingestion, it alters thecomposition of mucus so that it is more viscidand adheres to gastric mucosa and protectsthe ulcer base. It also inhibits pepsin activityand prolongs the life of PGs. Because of itssteroid like effects, it causes salt and waterretention. It is therefore not preferred.Prostaglandins PGE2 and PGI2 synthesized bythe gastric mucosa inhibits gastric secretion,enhances mucus production as well as mucosalblood flow and exert a cytoprotective effect.They act by binding to the PG receptor (EP3)present on the parietal cells and inhibit cAMPproduction. Misoprotol is a synthetic PGE1analog given orally. It is of special value inpreventing NSAID induced gastric ulcerationbecause NSAIDs are PG synthesis inhibitors.Diarrhoea and muscle cramps are common.
243Drugs Used in Gastrointestinal Disorders
Treatment of H. pylori Infection
The gram-negative bacterium H. pylori isadapted to living in the stomach. Infectionwith H. pylori is associated with gastro-duodenal disease including gastritis and pepticulcer. It is also thought to be responsible forrecurrence of peptic ulcer disease and isconsidered as a major risk factor for stomachcancer. Eradication of H. pylori along withdrugs that reduce acid secretion has shownto reduce the relapse rate.
Various combination regimens are triedwith clarithromycin, amoxicillin ortetracycline; metronidazole and omeprazoleor a H2 receptor blocker for 1-2 weeks. Useof a PP inhibitor in the regimen improves theefficacy of the antibiotics in eradicating H.Pylori by raising gastric pH and enhancingantibiotic stability - activity of amoxicillin andclarithromycin are pH dependent. Someregimens are:1. Clarithromycin 250 mg BD + metro-
nidazole 400 mg BD + omeprazole 20 mgBD–for one week.
2. Clarithromycin 500 mg TDS/amoxicillin750 mg TDS + omeprazole 20 mg BD–fortwo weeks.
Relevance in Dentistry
Many drugs used by dentists particularlyNSAIDs, can cause gastric irritation ofvarying degree. Dentists should be carefulin using NSAIDs and other gastric irritantdrugs including some antibiotics likedoxycycline, ciprofloxacin, etc. in patientssuffering from acid peptic disease. Thoughprophylactic ranitidine/omeprazole has beencommonly prescribed with ulcerogenic drugs,routine use of such drugs is not reco-mmended.
PROKINETIC AGENTS
Drugs that enhance gastroduodenal motilityand hasten gastric emptying are called
prokinetic agents. Metoclopramide, domper-idone and cisapride are some prokineticagents.
Metoclopramide
Actions
GIT–Metoclopramide promotes forwardmovement of contents of the upper GI tract.It raises lower esophageal sphincter pressure,speeds up gastric emptying, prevents refluxesophagitis and also slightly enhancesintestinal peristalsis.CNS– Metoclopramide acts as an antiemeticby its actions on CTZ and by speeding upgastric emptying.
Mechanism of Action
Prokinetics act:(i) by blocking D2 dopamine receptors.
Antiemetic action is due to blockade ofD2 receptors in the CTZ.
(ii) by enhancing acetylcholine release fromthe cholinergic neurons in the gut.
Adverse effects are sedation, dystonia anddiarrhoea; gynaecomastia, galactorrhoea andparkinsonism (extrapyramidal symptoms) canoccur on long-term use.
Uses
1. Reflux oesophagitis–‘heart burn’ due toreflux of acid into the oesophagus isbenefited by prokinetic agents.
2. As antiemetics – in postoperative periodand vomiting due to anticancer drugs.
3. As preanaesthetic medication to promotegastric emptying before induction ofgeneral anaesthesia in emergency.
4. In endoscopy–to assist passage of tubesinto the duodenum.
Domperidone is a D2 dopamine receptor blockerlike metoclopramide. It does not cross theblood-brain barrier and hence extrapyramidal
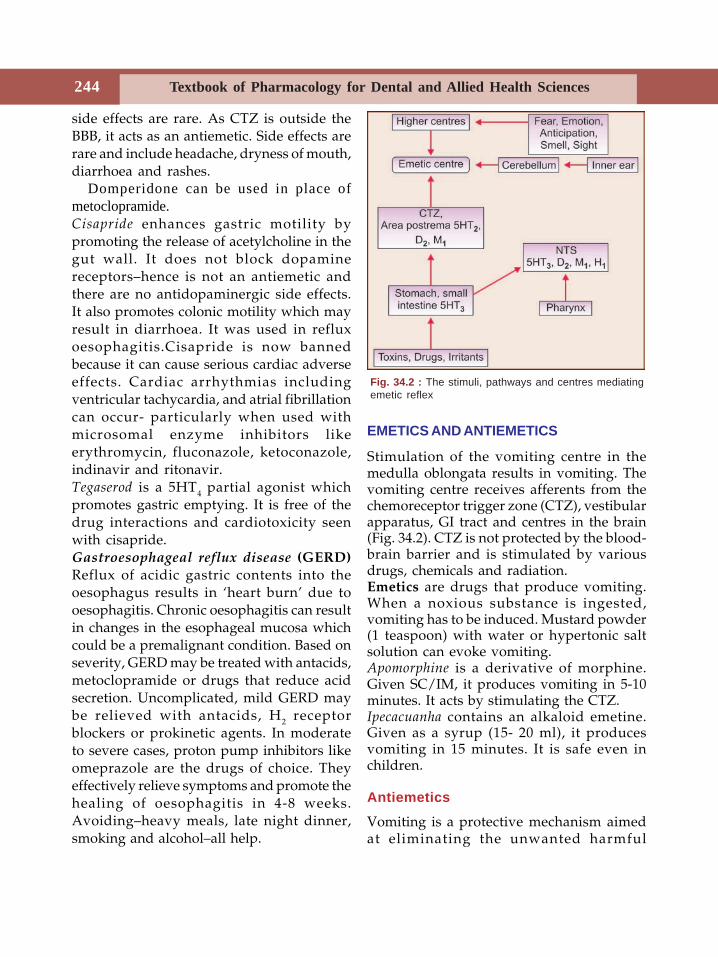
Textbook of Pharmacology for Dental and Allied Health Sciences244
side effects are rare. As CTZ is outside theBBB, it acts as an antiemetic. Side effects arerare and include headache, dryness of mouth,diarrhoea and rashes.
Domperidone can be used in place ofmetoclopramide.Cisapride enhances gastric motility bypromoting the release of acetylcholine in thegut wall. It does not block dopaminereceptors–hence is not an antiemetic andthere are no antidopaminergic side effects.It also promotes colonic motility which mayresult in diarrhoea. It was used in refluxoesophagitis.Cisapride is now bannedbecause it can cause serious cardiac adverseeffects. Cardiac arrhythmias includingventricular tachycardia, and atrial fibrillationcan occur- particularly when used withmicrosomal enzyme inhibitors likeerythromycin, fluconazole, ketoconazole,indinavir and ritonavir.Tegaserod is a 5HT4 partial agonist whichpromotes gastric emptying. It is free of thedrug interactions and cardiotoxicity seenwith cisapride.Gastroesophageal reflux disease (GERD)Reflux of acidic gastric contents into theoesophagus results in ‘heart burn’ due tooesophagitis. Chronic oesophagitis can resultin changes in the esophageal mucosa whichcould be a premalignant condition. Based onseverity, GERD may be treated with antacids,metoclopramide or drugs that reduce acidsecretion. Uncomplicated, mild GERD maybe relieved with antacids, H2 receptorblockers or prokinetic agents. In moderateto severe cases, proton pump inhibitors likeomeprazole are the drugs of choice. Theyeffectively relieve symptoms and promote thehealing of oesophagitis in 4-8 weeks.Avoiding–heavy meals, late night dinner,smoking and alcohol–all help.
EMETICS AND ANTIEMETICS
Stimulation of the vomiting centre in themedulla oblongata results in vomiting. Thevomiting centre receives afferents from thechemoreceptor trigger zone (CTZ), vestibularapparatus, GI tract and centres in the brain(Fig. 34.2). CTZ is not protected by the blood-brain barrier and is stimulated by variousdrugs, chemicals and radiation.Emetics are drugs that produce vomiting.When a noxious substance is ingested,vomiting has to be induced. Mustard powder(1 teaspoon) with water or hypertonic saltsolution can evoke vomiting.Apomorphine is a derivative of morphine.Given SC/IM, it produces vomiting in 5-10minutes. It acts by stimulating the CTZ.Ipecacuanha contains an alkaloid emetine.Given as a syrup (15- 20 ml), it producesvomiting in 15 minutes. It is safe even inchildren.
Antiemetics
Vomiting is a protective mechanism aimedat eliminating the unwanted harmful
Fig. 34.2 : The stimuli, pathways and centres mediatingemetic reflex
245Drugs Used in Gastrointestinal Disorders
material from the stomach. But in somesituations, vomiting may not serve anyuseful purpose and may only betroublesome. It can cause dehydration,weakness and electrolyte imbalance. In suchcircumstances, vomiting needs to besuppressed with drugs.
CLASSIFICATION
1. Dopamine D2 antagonists–prokinetics -
Metoclopramide, domperidone2. 5HT
3 antagonistsOndansetron, granisetrondolasetron, tropisetron
3. AntimuscarinicsHyoscinecyclizinepromethazinediphenhydramine.
4. NeurolepticsChlorpromazine,prochlorperazine, haloperidol
5. Other agentsCisapride, corticosteroids.
Dopamine D2 Antagonists
Metoclopramide and domperidone (page 243)act centrally by blocking dopamine D2receptors in the CTZ. They enhance the toneof the lower oesophageal sphincter and alsoenhance gastric peristalsis. They are used innausea and vomiting due to gastrointestinaldisorders, migraine, in postoperative periodand vomiting due to cytotoxic drugs andradiotherapy.
5-HT3 Antagonists
Ondansetron 5-hydroxytryptamine released inthe gut is an important transmitter of emesis.It is believed that anticancer drugs inducethe release of 5-HT in the gut which initiatesemetic reflex through 5-HT3 receptors present
in the gut, NTS and area postrema.Ondansetron blocks 5-HT3 receptors in theGI tract, CTZ and nucleus tractus solitariusand prevents vomiting. It is a powerfulantiemetic and can be given orally orintravenously (4-8 mg).
Granisetron is more potent than ondansetronas an antiemetic. Though granisetron,dolasetron and tropisetron have longer t½, theirbiological effect half-life remains the sameand they can all be given once daily.
5HT3 antagonists are well absorbed fromthe gut and are metabolised by the liver.They can be given both orally, IM and IV.
All 5HT3 antagonists are well toleratedwith minor adverse effects like headache andconstipation.
Uses
5HT3 antagonists are used to controlvomiting induced by anticancer drugs orradiotherapy. They are also useful inpostoperative vomiting and other druginduced vomiting (Table 34.4).
Antimuscarinics
Hyoscine (see Chap. 8) is a labyrinthinesedative very effective in motion sickness.Motion sickness or travelling sickness is due
H1 anti-histamines{
5-HT3 antagonists
• Block 5-HT3 receptors in the gut, CTZand NTS.
• Efficient antiemetics.• Some are effective both orally and
parenterally.• Largely safe – no sedation or other
CNS/autonomic side effects.• Adverse effects negligible – headache,
gastrointestinal disturbances.• Drugs of choice in postoperative and
anticancer drug-induced vomiting.

Textbook of Pharmacology for Dental and Allied Health Sciences246
to over stimulation of the vestibularapparatus along with psychological andenvironmental factors. Hyoscine also relaxesthe gastrointestinal smooth muscle. Taken 30minutes before journey, hyoscine (0.4-0.6 mgoral) acts for 6 hours and the dose should berepeated if the journey is longer than that. Atransdermal patch delivers hyoscineconstantly over 3 days and is to be appliedbehind the ear. Sedation and dry mouth arecommon side effects.Dicyclomine is used to control vomiting inmorning sickness and motion sickness (Table34.3).H
1 antihistamines (see Chap. 31) like
promethazine, diphenhydramine, cyclizineand cinnarizine have anticholinergicproperties. Antihistamines block H1 receptorsin the area postrema as well as muscarinicreceptors in the CNS. They probably also acton the GI tract. Some of them are useful inmotion sickness and postoperative vomiting.Neuroleptics (Chap. 29) also block D2-receptors in the CTZ and are useful invomiting due to most causes except motionsickness. Sedation and extrapyramidalsymptoms are the common side effects.Prochlorperazine is mainly used as anantiemetic in vomiting and is also effectivein vertigo associated with vomiting.
Other Antiemetics
Corticosteroids are used in combination withother antiemetics like ondansetron ormetoclopramide. Corticosteroids controldelayed vomiting following anticancer drugtherapy.Pyridoxine is used in the prevention ofvomiting in pregnancy without any knownpharmacological basisSedative hypnotics–Barbiturates andbenzodiazepines may raise the threshold forvomiting by depressing the CNS. Theiranxiolytic and sedative properties also help.Sedative hypnotics are used as adjuvants toother antiemetics in treating anticancer drug-induced vomiting.Cannabinoids–Dronabinol, a cannabinoid hasantiemetic properties. It may act by thestimulation of the cannabinoid receptors(CB1) in the vomiting centre. It also increasesappetite. Dronabinol can cause behaviouralabnormalities and dependence. It can be usedas an alternative in the prevention ofvomiting when other drugs are ineffective.
Antiemetic Combinations
Severe retching and vomiting like thatinduced by anticancer drugs are treated witha combination of antiemetics including
Table 34.4: Preferred drugs for vomiting due to various causes
Conditions Drugs
Motion sickness Hyoscine, Cyclizine, Promethazine, Cinnarizine
Vomiting due to cytotoxic drugs 1. Ondansetron + Dexamethasone
2. Metoclopramide + dexamethasone + diphenhydramine+ lorazepam
Vomiting due to other drugs Chlorpromazine, Metoclopramide
Postoperative vomiting Ondansetron, Metoclopramide
Vomiting in pregnancy Dicyclomine, Pyridoxine, Cyclizine, Meclizine,Metoclopramide

247Drugs Used in Gastrointestinal Disorders
ondansetron, metoclopramide, glucocorti-coids and sedative-hypnotics.
Later cycles of anticancer drug regimenscan cause ‘anticipatory’ vomiting i.e.vomitingat the sight/thought of receiving anticancerdrugs. This can be avoided by usingappropriate antiemetics from the initial cyclesof anticancer therapy.
DRUGS USED IN THE TREATMENTOF CONSTIPATION
Purgatives are drugs that promote defecation.They are also called laxatives or cathartics.Laxatives have milder action while catharticsor purgatives are more powerful evacuants.Purgatives may be classified as-
CLASSIFICATION
1. Bulk laxativesBran, plantago seeds, agar, methyl-cellulose, ispaghula husk
2. Faecal softenersDocusate sodium, liquid paraffin(emollients)
3. Osmotic purgativesMagnesium sulphate, Magnesiumhydroxide, Sodium phosphate,Sodium sulphate, Magnesium citrate,Lactulose, Sorbitol, Polyethyleneglycol
4. Stimulant purgativesPhenolphthalein, bisacodyl, castor oil,Anthraquinones - cascara sagrada,senna
Bulk laxatives include indigestible vegetablefibre and hydrophilic colloids that increasethe volume and lower the viscosity ofintestinal contents forming a large, soft, solidstool. Dietary fibre consists of cell walls andother parts of fruits and vegetables that areunabsorbable. Adding fibre to the diet is asafe and natural way of treating constipationin persons on low-fibre diet.
Bran is the residue left when flour is madefrom cereals and contains 40% fibre–but isunpalatable and can cause flatulence.Ispaghula and plantago seeds contain naturalmucilage which absorbs water to form agelatinous mass and are more palatable thanbran. Methylcellulose is a semisyntheticderivative of cellulose. Adequate waterintake should be stressed.
Faecal Softeners
Docusate sodium (dioctyl sodium sulpho-succinate) softens faeces by lowering thesurface tension of the intestinal contentswhich allows more water to be retained inthe faeces.Liquid paraffin is a chemically inert mineraloil that is not digested. It lubricates andsoftens faeces. It is unpalatable; aspirationmay cause lipoid pneumonia; small amountsabsorbed in intestines may cause paraf-finomas; it may leak out of the anus causingdiscomfort. Long-term use can result indeficiency of fat - soluble vitamins due toimpaired absorption. Hence not preferred.
Osmotic Purgatives
Osmotic purgatives are solutes that are notabsorbed in the intestine, osmotically retainwater and increase the bulk of intestinalcontents. They increase peristalsis to evacuatea fluid stool. They produce soft liquid stoolsin 1-3 hours. Osmotic purgatives include• nonabsorbable salts (saline purgatives)• nonabsorbable sugars - Lactulose• polyethylene glycolNonabsorbable salts Magnesium hydroxide,magnesium sulphate, sodium potassiumtartrate (Rochelle’s salt), sodium sulphate andphosphate are some inorganic salts used asosmotic or saline purgatives. They are used toprepare the bowel before surgery and infood poisoning.
Textbook of Pharmacology for Dental and Allied Health Sciences248
Nonabsorbable sugars Lactulose is a syntheticdisaccharide that is not absorbed, holdswater and acts as an osmotic purgative.Flatulence and cramps may be accompanied.In the colon, lactulose is fermented to lacticand acetic acids which inhibit the growth ofcolonic ammonia - producing bacteria. It alsoinhibits the absorption of ammonia bylowering pH and lowers blood ammonialevels. It is used in hepatic coma for this effect(hepatic coma is worsened by ammonia).Sorbitol is similar to lactulosePolyethylene glycol (PEG) is a nonabsorbablesugar. Balanced isotonic solution containingPEG with sodium sulphate, sodium chloride,sodium bicarbonate and potassium chlorideis given orally. The solution is balanced insuch a way that it avoids electrolyteimbalance or fluid shift into the gut. Largevolumes are rapidly ingested→ 3-4 litres over2 hours - for cleaning the bowel. PEG powdermay be taken with water for chronicconstipation. It has the advantage that thereis no associated flatulence or abdominalcramps.
Stimulant Purgatives
Stimulant purgatives increase intestinalmotility and increase secretion of water andelectrolytes by the mucosa. They may causeabdominal cramps.
When anthraquinones like cascara sagradaand senna (source: plants) are given orally,active anthraquinones are liberated in theintestines and stimulate the myenteric plexesin the colon. Evacuation takes 6-8 hr. Long-term use causes melanotic pigmentation ofthe colon.Phenolphthalein an indicator, acts on the colonafter 6 to 8 hours to produce soft, semiliquidstools with some gripping. It undergoesenterohepatic circulation which prolongs itsactions. Allergic reactions including pink
coloured skin erruptions, other severe formsof allergy and risk of cardiac toxicity and coliclimit it’s use.Bisacodyl related to phenolphthalein isconverted to active metabolite in theintestines. It can be given orally (5 mg) butusually is used as rectal suppositories (10 mg)which results in defecation in 15-30 minutes.It is safe except that prolonged use may causelocal inflammation.Castor oil is hydrolysed in the upper smallintestine to ricinoleic acid, a local irritant thatincreases intestinal motility. It is a powerfuland one of the oldest purgatives. Stool issemiliquid and is accompanied by gripping.It is not preferred.Enema Enema produces defecation bysoftening stools and distending the bowel.Evacuant enema is used to prepare the gutfor surgery, endoscopy and radiologicalexamination (see Page 8).Use of laxatives in constipation Fibre rich diet,adequate fluid intake and physical activityare the best measures to prevent and treatconstipation in the otherwise normal subjects.If these measures are inadequate, a laxativemay be given (Table 34.5).Drug induced constipation Drugs likeanticholinergics, NSAIDs, opioids, clonidine,iron, calcium channel blockers; antihistaminesand tricyclic antidepressants (due toanticholinergic effect) can cause constipation.When withdrawal of the causative agent isnot possible, a laxative may be used.Laxative abuse Habitual use of laxatives,especially stimulant laxatives may lead tovarious gastrointestinal disturbances likeirritable bowel syndrome, loss of electrolytes,loss of calcium in the stool andmalabsorption. Misconceptions regardingbowel habits should be cleared. The patientshould be convinced that normal bowelhabits may vary between 3 motions daily and2 motions per week.
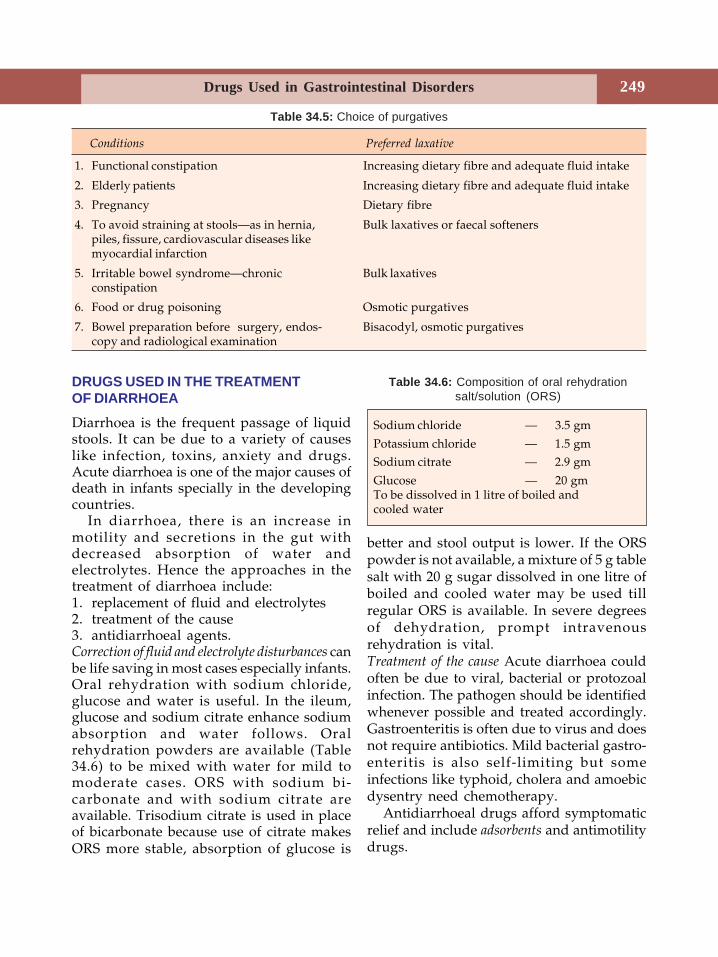
249Drugs Used in Gastrointestinal Disorders
DRUGS USED IN THE TREATMENTOF DIARRHOEA
Diarrhoea is the frequent passage of liquidstools. It can be due to a variety of causeslike infection, toxins, anxiety and drugs.Acute diarrhoea is one of the major causes ofdeath in infants specially in the developingcountries.
In diarrhoea, there is an increase inmotility and secretions in the gut withdecreased absorption of water andelectrolytes. Hence the approaches in thetreatment of diarrhoea include:1. replacement of fluid and electrolytes2. treatment of the cause3. antidiarrhoeal agents.Correction of fluid and electrolyte disturbances canbe life saving in most cases especially infants.Oral rehydration with sodium chloride,glucose and water is useful. In the ileum,glucose and sodium citrate enhance sodiumabsorption and water follows. Oralrehydration powders are available (Table34.6) to be mixed with water for mild tomoderate cases. ORS with sodium bi-carbonate and with sodium citrate areavailable. Trisodium citrate is used in placeof bicarbonate because use of citrate makesORS more stable, absorption of glucose is
better and stool output is lower. If the ORSpowder is not available, a mixture of 5 g tablesalt with 20 g sugar dissolved in one litre ofboiled and cooled water may be used tillregular ORS is available. In severe degreesof dehydration, prompt intravenousrehydration is vital.Treatment of the cause Acute diarrhoea couldoften be due to viral, bacterial or protozoalinfection. The pathogen should be identifiedwhenever possible and treated accordingly.Gastroenteritis is often due to virus and doesnot require antibiotics. Mild bacterial gastro-enteritis is also self-limiting but someinfections like typhoid, cholera and amoebicdysentry need chemotherapy.
Antidiarrhoeal drugs afford symptomaticrelief and include adsorbents and antimotilitydrugs.
Conditions Preferred laxative
1. Functional constipation Increasing dietary fibre and adequate fluid intake
2. Elderly patients Increasing dietary fibre and adequate fluid intake
3. Pregnancy Dietary fibre
4. To avoid straining at stools—as in hernia, Bulk laxatives or faecal softenerspiles, fissure, cardiovascular diseases likemyocardial infarction
5. Irritable bowel syndrome—chronic Bulk laxativesconstipation
6. Food or drug poisoning Osmotic purgatives
7. Bowel preparation before surgery, endos- Bisacodyl, osmotic purgativescopy and radiological examination
Table 34.5: Choice of purgatives
Table 34.6: Composition of oral rehydrationsalt/solution (ORS)
Sodium chloride — 3.5 gm
Potassium chloride — 1.5 gmSodium citrate — 2.9 gm
Glucose — 20 gmTo be dissolved in 1 litre of boiled andcooled water
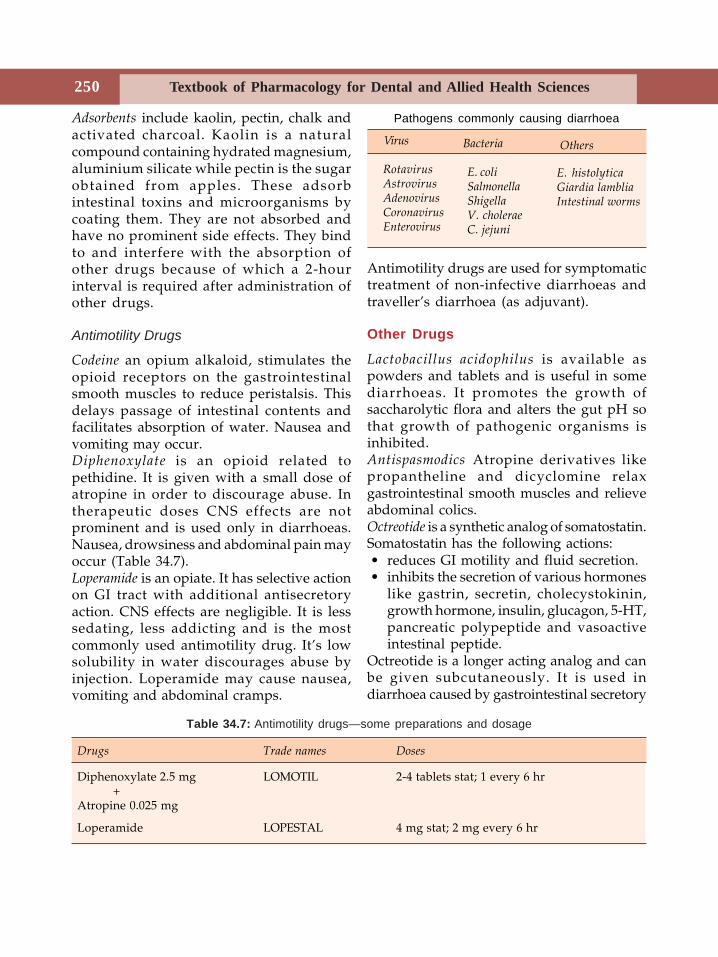
Textbook of Pharmacology for Dental and Allied Health Sciences250
Adsorbents include kaolin, pectin, chalk andactivated charcoal. Kaolin is a naturalcompound containing hydrated magnesium,aluminium silicate while pectin is the sugarobtained from apples. These adsorbintestinal toxins and microorganisms bycoating them. They are not absorbed andhave no prominent side effects. They bindto and interfere with the absorption ofother drugs because of which a 2-hourinterval is required after administration ofother drugs.
Antimotility Drugs
Codeine an opium alkaloid, stimulates theopioid receptors on the gastrointestinalsmooth muscles to reduce peristalsis. Thisdelays passage of intestinal contents andfacilitates absorption of water. Nausea andvomiting may occur.Diphenoxylate is an opioid related topethidine. It is given with a small dose ofatropine in order to discourage abuse. Intherapeutic doses CNS effects are notprominent and is used only in diarrhoeas.Nausea, drowsiness and abdominal pain mayoccur (Table 34.7).Loperamide is an opiate. It has selective actionon GI tract with additional antisecretoryaction. CNS effects are negligible. It is lesssedating, less addicting and is the mostcommonly used antimotility drug. It’s lowsolubility in water discourages abuse byinjection. Loperamide may cause nausea,vomiting and abdominal cramps.
Antimotility drugs are used for symptomatictreatment of non-infective diarrhoeas andtraveller’s diarrhoea (as adjuvant).
Other Drugs
Lactobacillus acidophilus is available aspowders and tablets and is useful in somediarrhoeas. It promotes the growth ofsaccharolytic flora and alters the gut pH sothat growth of pathogenic organisms isinhibited.Antispasmodics Atropine derivatives likepropantheline and dicyclomine relaxgastrointestinal smooth muscles and relieveabdominal colics.Octreotide is a synthetic analog of somatostatin.Somatostatin has the following actions: • reduces GI motility and fluid secretion. • inhibits the secretion of various hormones
like gastrin, secretin, cholecystokinin,growth hormone, insulin, glucagon, 5-HT,pancreatic polypeptide and vasoactiveintestinal peptide.
Octreotide is a longer acting analog and canbe given subcutaneously. It is used indiarrhoea caused by gastrointestinal secretory
Pathogens commonly causing diarrhoea
Bacteria
E. coliSalmonellaShigellaV. choleraeC. jejuni
Virus
RotavirusAstrovirusAdenovirusCoronavirusEnterovirus
Others
E. histolyticaGiardia lambliaIntestinal worms
Drugs Trade names Doses
Diphenoxylate 2.5 mg LOMOTIL 2-4 tablets stat; 1 every 6 hr+
Atropine 0.025 mg
Loperamide LOPESTAL 4 mg stat; 2 mg every 6 hr
Table 34.7: Antimotility drugs—some preparations and dosage

251Drugs Used in Gastrointestinal Disorders
tumours and in diarrhoea due to vagotomy,dumping syndrome and AIDS.
Traveller’s diarrhoea
Infection is the most common cause oftraveller’s diarrhoea and should be treatedwith suitable antimicrobials like doxycyclineor ciprofloxacin. Oral rehydration salts andloperamide may also be used.
IRRITABLE BOWEL SYNDROME
Irritable bowel syndrome (IBS) is a commoncondition characterised by abnormal bowelfunctions with no specific organic cause.
Diarrhoea or constipation with abdominalpain are seen. Causes could be stress, lack ofdietary fibre, food allergy or emotionaldisturbances. When constipation isprominent, soluble dietary fiber likeispaghula is recommended and loperamideis preferred for diarrhoea. Benzodiazepinesare given for the treatment of anxiety andother appropriate measures are takendepending on the symptoms and probablecause.
Newer drugs like alosetron and tegaserodwhich act on 5-HT receptors have beenfound to be useful in IBS.
Textbook of Pharmacology for Dental and Allied Health Sciences252
35 GeneralConsiderations
INTRODUCTION
Chemotherapy can be defined as the use ofchemicals in infectious diseases to destroymicroorganisms without damaging the hosttissues. Antibiotics are substances producedby microorganisms which suppress thegrowth of or destroy other microorganisms.
Pasteur and Joubert were the first toidentify that microorganisms could destroyother microorganisms. Paul Ehrlich ‘The fatherof Modern Chemotherapy’ coined the term‘chemotherapy’. He showed that certain dyescan destroy microbes and demonstrated thatmethylene blue can be used in malaria. Healso synthesised some arsenical compoundsfor the treatment of syphilis and sleepingsickness. Domagk in 1936 demonstrated thatprontosil, a sulfonamide dye is effective insome infections. The production of penicillinfor clinical use in 1941 marked the beginningof the ‘golden era’ of antibiotics. In the last60 years, several powerful antibiotics andtheir semisynthetic derivatives have beenproduced.
Many infectious diseases which wereearlier incurable can now be treated withjust a few doses of antimicrobial drugs.Thus the development of antimicrobialdrugs is one of the important advances ofmodern medicine. Infact antimicrobials areone of the most commonly prescribed drugsbut are often the most over used ormisused drugs.
CLASSIFICATION
Based on their mechanisms of action, anti-microbials are classified (Fig. 35.1) as follows.
Drugs that:
1. Inhibit cell wall synthesis-Penicillins, cephalosporins, vancomycin,bacitracin, cycloserine.
2. Damage cell membranes--causing leakage of cell contents -Polymyxins, colistin, amphotericin B,nystatin.
3. Bind to ribosomes and inhibit proteinsynthesis -Chloramphenicol, tetracyclines, erythro-mycin, aminoglycosides, clindamycin,linezolid, streptogramins.
4. Inhibit DNA gyrase-Fluoroquinolones like ciprofloxacin,norfloxacin
5. Inhibit DNA function-(DNA dependent RNA polymerase)Rifampicin
6. Interfere with metabolic steps--Antimetabolite action- sulfonamides,sulfones, trimethoprim, pyrimethamine
Antimicrobials may also be Classified as-
1. Bacteriostatic - agents that suppress thegrowth of bacteria.For example, Sulfonamides, tetracyclines,linezolid chloramphenicol, clindamycin.
Section 10Chemotherapy I
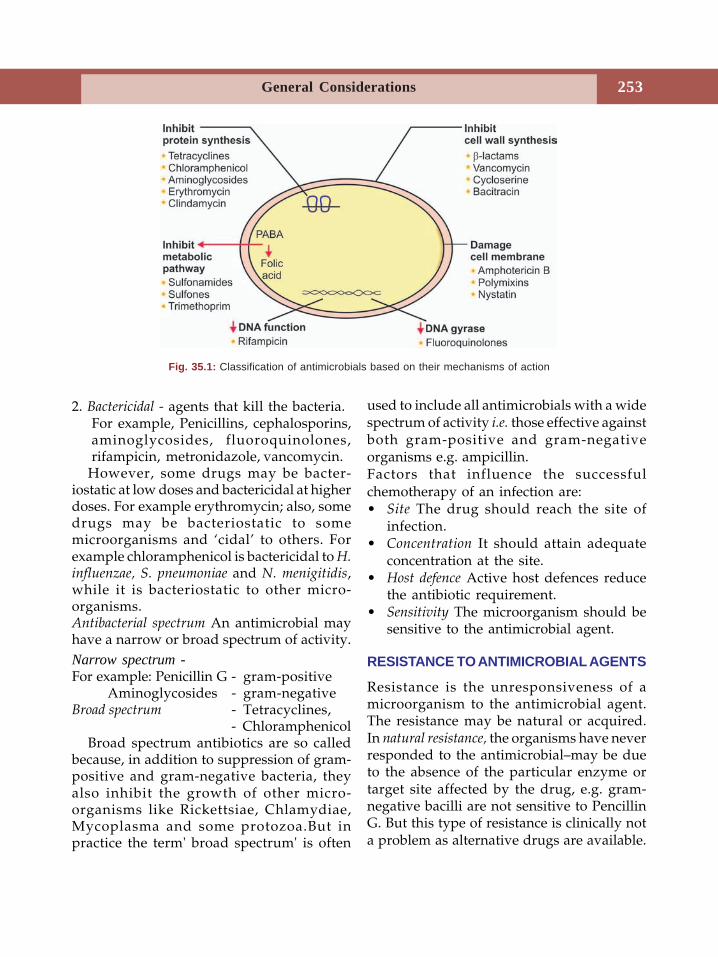
252
General Considerations 253
2. Bactericidal - agents that kill the bacteria.For example, Penicillins, cephalosporins,aminoglycosides, fluoroquinolones,rifampicin, metronidazole, vancomycin.
However, some drugs may be bacter-iostatic at low doses and bactericidal at higherdoses. For example erythromycin; also, somedrugs may be bacteriostatic to somemicroorganisms and ‘cidal’ to others. Forexample chloramphenicol is bactericidal to H.influenzae, S. pneumoniae and N. menigitidis,while it is bacteriostatic to other micro-organisms.Antibacterial spectrum An antimicrobial mayhave a narrow or broad spectrum of activity.Narrow spectrum -For example: Penicillin G - gram-positive
Aminoglycosides - gram-negativeBroad spectrum - Tetracyclines,
- ChloramphenicolBroad spectrum antibiotics are so called
because, in addition to suppression of gram-positive and gram-negative bacteria, theyalso inhibit the growth of other micro-organisms like Rickettsiae, Chlamydiae,Mycoplasma and some protozoa.But inpractice the term' broad spectrum' is often
used to include all antimicrobials with a widespectrum of activity i.e. those effective againstboth gram-positive and gram-negativeorganisms e.g. ampicillin.Factors that influence the successfulchemotherapy of an infection are:• Site The drug should reach the site of
infection.• Concentration It should attain adequate
concentration at the site.• Host defence Active host defences reduce
the antibiotic requirement.• Sensitivity The microorganism should be
sensitive to the antimicrobial agent.
RESISTANCE TO ANTIMICROBIAL AGENTS
Resistance is the unresponsiveness of amicroorganism to the antimicrobial agent.The resistance may be natural or acquired.In natural resistance, the organisms have neverresponded to the antimicrobial–may be dueto the absence of the particular enzyme ortarget site affected by the drug, e.g. gram-negative bacilli are not sensitive to PencillinG. But this type of resistance is clinically nota problem as alternative drugs are available.
Fig. 35.1: Classification of antimicrobials based on their mechanisms of action
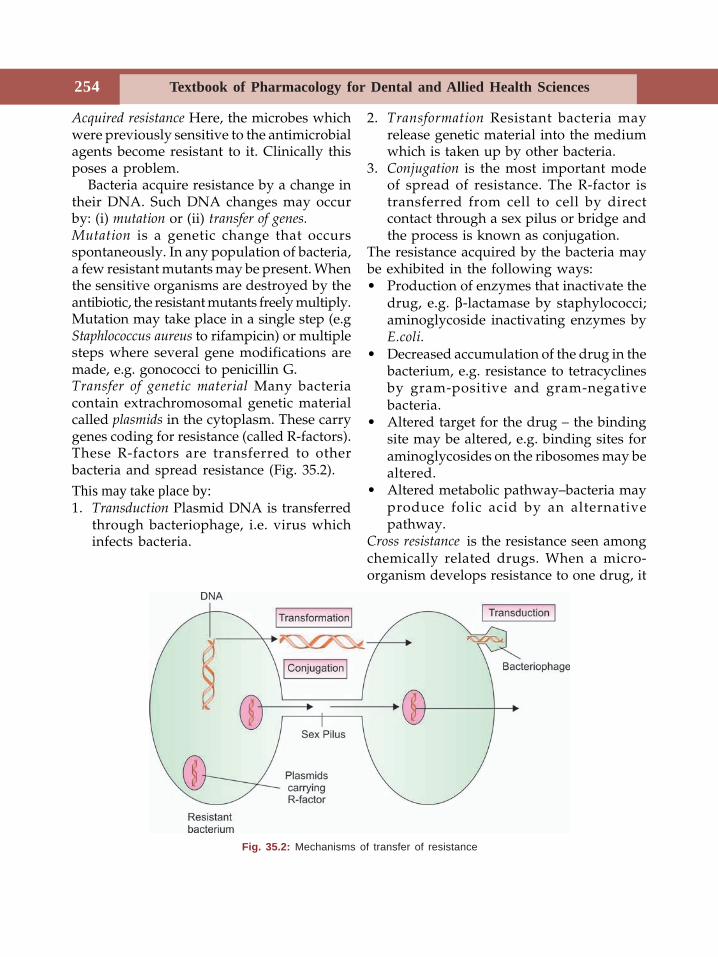
Textbook of Pharmacology for Dental and Allied Health Sciences254
Acquired resistance Here, the microbes whichwere previously sensitive to the antimicrobialagents become resistant to it. Clinically thisposes a problem.
Bacteria acquire resistance by a change intheir DNA. Such DNA changes may occurby: (i) mutation or (ii) transfer of genes.Mutation is a genetic change that occursspontaneously. In any population of bacteria,a few resistant mutants may be present. Whenthe sensitive organisms are destroyed by theantibiotic, the resistant mutants freely multiply.Mutation may take place in a single step (e.gStaphlococcus aureus to rifampicin) or multiplesteps where several gene modifications aremade, e.g. gonococci to penicillin G.Transfer of genetic material Many bacteriacontain extrachromosomal genetic materialcalled plasmids in the cytoplasm. These carrygenes coding for resistance (called R-factors).These R-factors are transferred to otherbacteria and spread resistance (Fig. 35.2).This may take place by:1. Transduction Plasmid DNA is transferred
through bacteriophage, i.e. virus whichinfects bacteria.
2. Transformation Resistant bacteria mayrelease genetic material into the mediumwhich is taken up by other bacteria.
3. Conjugation is the most important modeof spread of resistance. The R-factor istransferred from cell to cell by directcontact through a sex pilus or bridge andthe process is known as conjugation.
The resistance acquired by the bacteria maybe exhibited in the following ways:• Production of enzymes that inactivate the
drug, e.g. β-lactamase by staphylococci;aminoglycoside inactivating enzymes byE.coli.
• Decreased accumulation of the drug in thebacterium, e.g. resistance to tetracyclinesby gram-positive and gram-negativebacteria.
• Altered target for the drug – the bindingsite may be altered, e.g. binding sites foraminoglycosides on the ribosomes may bealtered.
• Altered metabolic pathway–bacteria mayproduce folic acid by an alternativepathway.
Cross resistance is the resistance seen amongchemically related drugs. When a micro-organism develops resistance to one drug, it
Fig. 35.2: Mechanisms of transfer of resistance
254
General Considerations 255
is also resistant to other drugs of the samegroup, even when not exposed to it, e.g.resistance to one tetracycline meansresistance to all other tetracyclines.
Prevention of Resistance toAntimicrobials
Development of resistance to drugs can beavoided to some extent by the followingmeasures:• antibiotics should be used only when
necessary• selection of the appropriate antibiotic is
absolutely important• correct dose and duration of treatment
should be followed• combination of drugs should be used as
in tuberculosis to delay the developmentof resistance.
Selection of an Antibacterial Agent
Antibiotics are used in 2 ways:1. Empiric therapy The antibiotic must cover
all the likely pathogens. A combinationor a broad spectrum agent may be used.This therapy should be employed only insome specific situations.
2. Definitive therapy When the organism isidentified, specific antibacterial agentsshould be given.
Various factors should be considered inselection of an antibiotic like, the patientfactors, the microbe factors, the propertiesof the drug and the clinical assessment. Siteof infection is the prime factor that guidesthe choice of the drug and its route ofadministration. Age of the patient, hostdefence status, renal and hepatic functionsshould be considered. Whenever possible,bacteriological culture report should guidethe drug selection. When not available,empirical therapy should be started to coverall the likely organisms. Infact for most dental
infections, selection of an antibiotic isempirical. For acute dental infections theantibiotic should have a spectrum thatincludes streptococcal species and anaerobicbacteria. When samples can be taken withoutcontamination or when empiric therapy fails,antibiotic selection should be based onculture report. Drug toxicity and cost shouldbe borne in mind. With proper clinicaljudgement–considering the above factors,most infections can be successfully treated(Table 35.1).
DOSE OF THE ANTIMICROBIALS
The dose of the antimicrobial should beadequate enough for the drug to attain plasmaconcentrations above the minimum inhibitoryconcentration (MIC). MIC is the lowestconcentration of the antimicrobial agent thatprevents visible growth of the microorganismafter 18 to 24 hours of incubation. Thebactericidal effect with many drugs is dose-dependent i.e. higher the concentration,greater is the bactericidal effect, e.g.aminoglycosides.Postantibiotic effect - Some antibiotics have apostantibiotic effect i.e., they continue tosuppress the bacterial multiplication evenafter their plasma concentration falls belowthe MIC. Aminoglycosides and fluoro-quinolones have such effect against gram-negative bacteria.
COMBINATION OF ANTIMICROBIALS
Use of a combination of antimicrobials mayhave synergistic, antagonistic or indiffe-rent (no change) effects. Hence appropriatedrugs should be used for combination.
Two bactericidal drugs given together (e.g:Penicillin + aminoglycosides) are generallysynergistic.
Combination of a bacteriostatic with abactericidal drug is not useful becausebacteriostatic drugs inhibit the multiplication
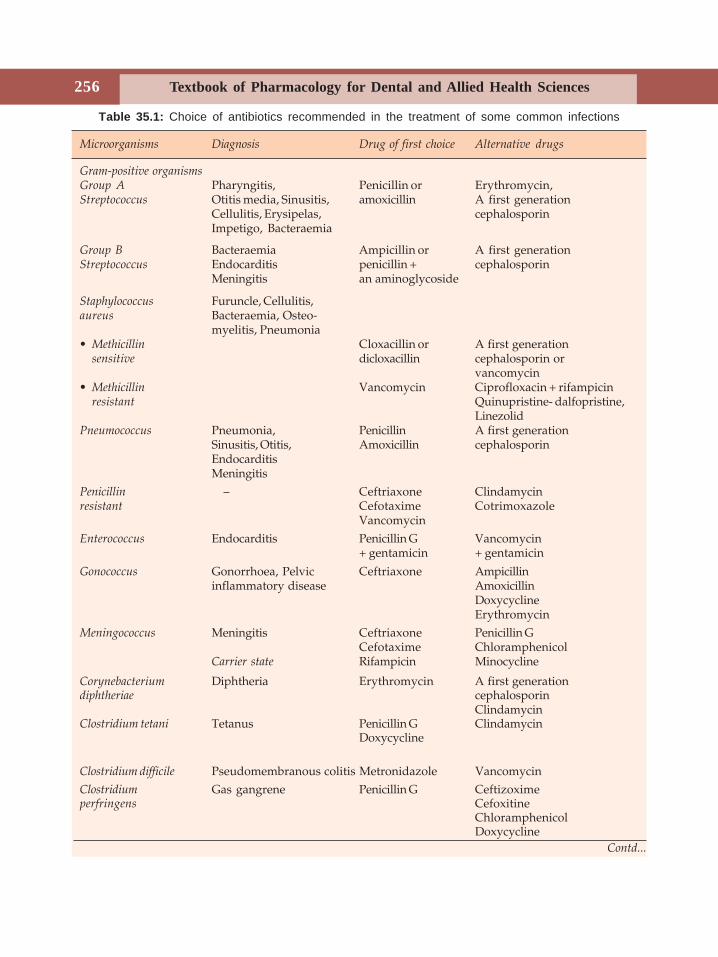
Textbook of Pharmacology for Dental and Allied Health Sciences256
Contd...
Table 35.1: Choice of antibiotics recommended in the treatment of some common infections
Microorganisms Diagnosis Drug of first choice Alternative drugs
Gram-positive organismsGroup A Pharyngitis, Penicillin or Erythromycin,Streptococcus Otitis media, Sinusitis, amoxicillin A first generation
Cellulitis, Erysipelas, cephalosporinImpetigo, Bacteraemia
Group B Bacteraemia Ampicillin or A first generationStreptococcus Endocarditis penicillin + cephalosporin
Meningitis an aminoglycoside
Staphylococcus Furuncle, Cellulitis,aureus Bacteraemia, Osteo-
myelitis, Pneumonia• Methicillin Cloxacillin or A first generation
sensitive dicloxacillin cephalosporin orvancomycin
• Methicillin Vancomycin Ciprofloxacin + rifampicinresistant Quinupristine- dalfopristine,
LinezolidPneumococcus Pneumonia, Penicillin A first generation
Sinusitis, Otitis, Amoxicillin cephalosporinEndocarditisMeningitis
Penicillin – Ceftriaxone Clindamycinresistant Cefotaxime Cotrimoxazole
VancomycinEnterococcus Endocarditis Penicillin G Vancomycin
+ gentamicin + gentamicin
Gonococcus Gonorrhoea, Pelvic Ceftriaxone Ampicillininflammatory disease Amoxicillin
DoxycyclineErythromycin
Meningococcus Meningitis Ceftriaxone Penicillin GCefotaxime Chloramphenicol
Carrier state Rifampicin Minocycline
Corynebacterium Diphtheria Erythromycin A first generationdiphtheriae cephalosporin
ClindamycinClostridium tetani Tetanus Penicillin G Clindamycin
Doxycycline
Clostridium difficile Pseudomembranous colitis Metronidazole VancomycinClostridium Gas gangrene Penicillin G Ceftizoximeperfringens Cefoxitine
ChloramphenicolDoxycycline
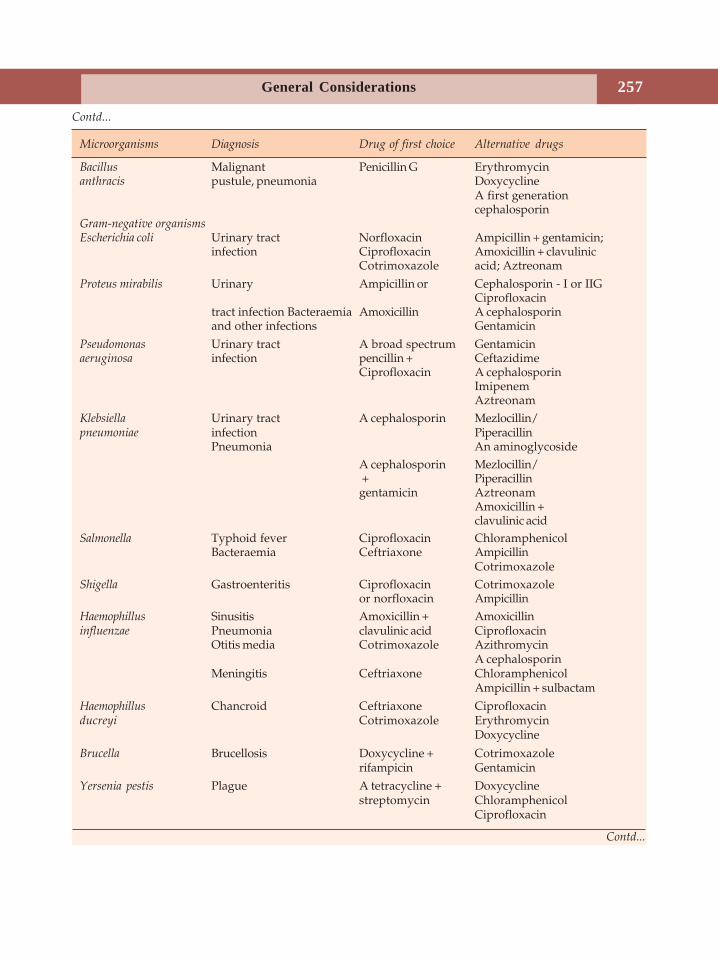
256
General Considerations 257
Contd...
Contd...
Microorganisms Diagnosis Drug of first choice Alternative drugs
Bacillus Malignant Penicillin G Erythromycinanthracis pustule, pneumonia Doxycycline
A first generationcephalosporin
Gram-negative organismsEscherichia coli Urinary tract Norfloxacin Ampicillin + gentamicin;
infection Ciprofloxacin Amoxicillin + clavulinicCotrimoxazole acid; Aztreonam
Proteus mirabilis Urinary Ampicillin or Cephalosporin - I or IIGCiprofloxacin
tract infection Bacteraemia Amoxicillin A cephalosporinand other infections Gentamicin
Pseudomonas Urinary tract A broad spectrum Gentamicinaeruginosa infection pencillin + Ceftazidime
Ciprofloxacin A cephalosporinImipenemAztreonam
Klebsiella Urinary tract A cephalosporin Mezlocillin/pneumoniae infection Piperacillin
Pneumonia An aminoglycosideA cephalosporin Mezlocillin/ + Piperacillingentamicin Aztreonam
Amoxicillin +clavulinic acid
Salmonella Typhoid fever Ciprofloxacin ChloramphenicolBacteraemia Ceftriaxone Ampicillin
CotrimoxazoleShigella Gastroenteritis Ciprofloxacin Cotrimoxazole
or norfloxacin AmpicillinHaemophillus Sinusitis Amoxicillin + Amoxicillininfluenzae Pneumonia clavulinic acid Ciprofloxacin
Otitis media Cotrimoxazole AzithromycinA cephalosporin
Meningitis Ceftriaxone ChloramphenicolAmpicillin + sulbactam
Haemophillus Chancroid Ceftriaxone Ciprofloxacinducreyi Cotrimoxazole Erythromycin
Doxycycline
Brucella Brucellosis Doxycycline + Cotrimoxazolerifampicin Gentamicin
Yersenia pestis Plague A tetracycline + Doxycyclinestreptomycin Chloramphenicol
Ciprofloxacin
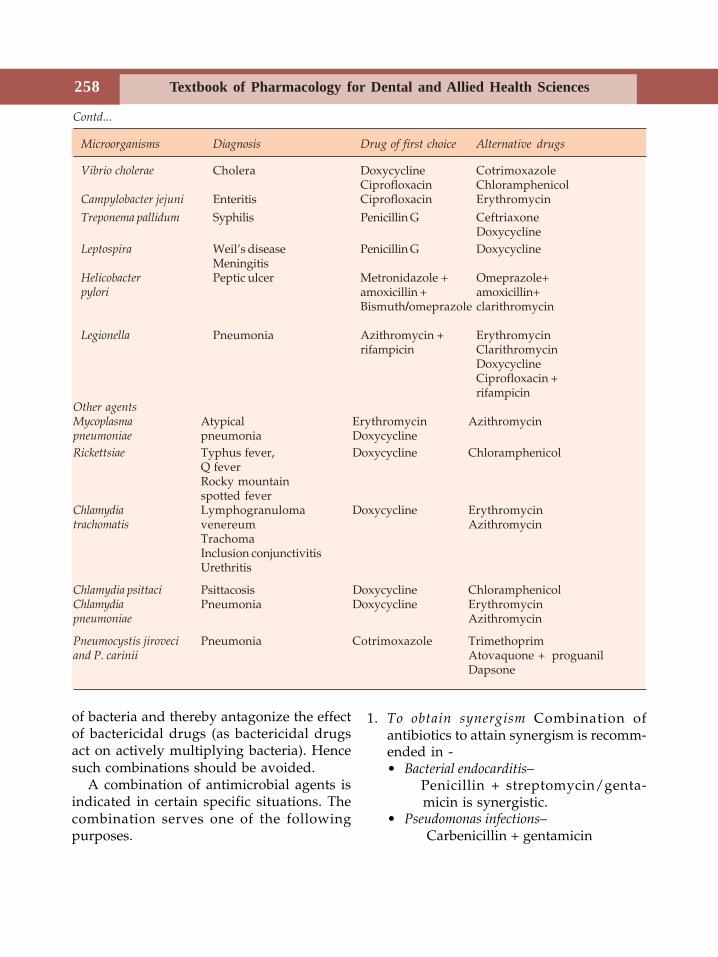
Textbook of Pharmacology for Dental and Allied Health Sciences258
Contd...
of bacteria and thereby antagonize the effectof bactericidal drugs (as bactericidal drugsact on actively multiplying bacteria). Hencesuch combinations should be avoided.
A combination of antimicrobial agents isindicated in certain specific situations. Thecombination serves one of the followingpurposes.
1. To obtain synergism Combination ofantibiotics to attain synergism is recomm-ended in -• Bacterial endocarditis–
Penicillin + streptomycin/genta-micin is synergistic.
• Pseudomonas infections– Carbenicillin + gentamicin
Microorganisms Diagnosis Drug of first choice Alternative drugs
Vibrio cholerae Cholera Doxycycline CotrimoxazoleCiprofloxacin Chloramphenicol
Campylobacter jejuni Enteritis Ciprofloxacin ErythromycinTreponema pallidum Syphilis Penicillin G Ceftriaxone
DoxycyclineLeptospira Weil’s disease Penicillin G Doxycycline
MeningitisHelicobacter Peptic ulcer Metronidazole + Omeprazole+pylori amoxicillin + amoxicillin+
Bismuth/omeprazole clarithromycin
Legionella Pneumonia Azithromycin + Erythromycinrifampicin Clarithromycin
DoxycyclineCiprofloxacin +rifampicin
Other agentsMycoplasma Atypical Erythromycin Azithromycinpneumoniae pneumonia DoxycyclineRickettsiae Typhus fever, Doxycycline Chloramphenicol
Q feverRocky mountainspotted fever
Chlamydia Lymphogranuloma Doxycycline Erythromycintrachomatis venereum Azithromycin
TrachomaInclusion conjunctivitisUrethritis
Chlamydia psittaci Psittacosis Doxycycline ChloramphenicolChlamydia Pneumonia Doxycycline Erythromycinpneumoniae Azithromycin
Pneumocystis jiroveci Pneumonia Cotrimoxazole Trimethoprimand P. carinii Atovaquone + proguanil
Dapsone
258
General Considerations 259
• Pneumocystis carinii pneumonia–Trimethoprim + sulfamethoxazole
• β-lactamase producing organisms likeH. influenzae -
Amoxicillin + clavulinic acid• Tuberculosis – INH + rifampicin.
2. Treatment of mixed infections Orodental,intra-abdominal infections, brainabscesses, genitourinary infections andtraumatic wound infections are oftenmixed infections. Aerobic and anaerobicorganisms may be involved. Two or moreantimicrobials can be used depending onthe culture and sensitivity report. Dentistsgenerally use a combination of apenicillin/cephalosporin/macrolide withmetronidazole.
3. Initial treatment of severe infections Drugscovering both gram-positive and gram-negative pathogens may be used initiallytill the culture report is available, e.g.penicillin + aminoglycoside; cephalosporin+ aminoglycoside. If anaerobes are likelyto be present, metronidazole may beadded. Samples for culture shouldhowever be taken before starting theantibiotics.
4. To prevent the emergence of resistance In thetreatment of tuberculosis and leprosy,combination of drugs is used to preventthe development of resistance.
5. To reduce the adverse effects The dosesneeded may be lower when a combinationis used. This may reduce the incidence andseverity of adverse effects, e.g. Ampho-tericin B + flucytosine in cryptococcalmeningitis.
Disadvantages of Antimicrobial Combination
1. Risk of toxicity from each agent–especiallyif toxicity is overlapping–may get addedup e.g. many antitubercular drugs arehepatotoxic.Toxicity of one drug may be enhanced byanother e.g.,
Vancomycin + aminoglycoside →→→→→ moresevere renal toxicity
2. Selection of resistant strains–The fewresistant mutants that remain maymultiply unchecked.
3. Emergence of organisms resistant tomultiple drugs.
4. Increased cost of therapy.
CHEMOPROPHYLAXIS
Chemoprophylaxis is the use of antimicrobialagents to prevent infection.In dentistry– Prophylactic use of antibioticsmay not be required in routine dentaltreatment if the patient's immune function isnormal. Certain dental procedures, includingdeep scaling, tooth extraction, periodontalprocedures, oral and maxillofacial surgeriescan produce transient bacteremia. In patientsat special risk including those with depressedimmunity, insertion of prosthesis, implantsand prolonged surgeries would requireantibiotic prophylaxis (Table 35.2). In generalchemoprophylaxis is recommended in thefollowing situations:1. To protect healthy persons
• Penicillin G is given for prevention ofgonorrhoea or syphilis in patients aftercontact with infected persons -postexposure prophylaxis.
• For preventing meningococcal infectionin healthy children during anepidemic–rifampicin or sulfonamidesmay be used.
• Malaria- In healthy individuals visitingan endemic area.
2. To prevent infection in high risk patients• In neutropenic patients- like patients
receiving anticancer drugs, immuno-suppressive agents and patients withAIDS, a penicillin or fluoroquinolonesor cotrimoxazole may reduce theincidence of bacterial infection.
• In patients with valvular heart diseasesprosthetic heart valves, and previous
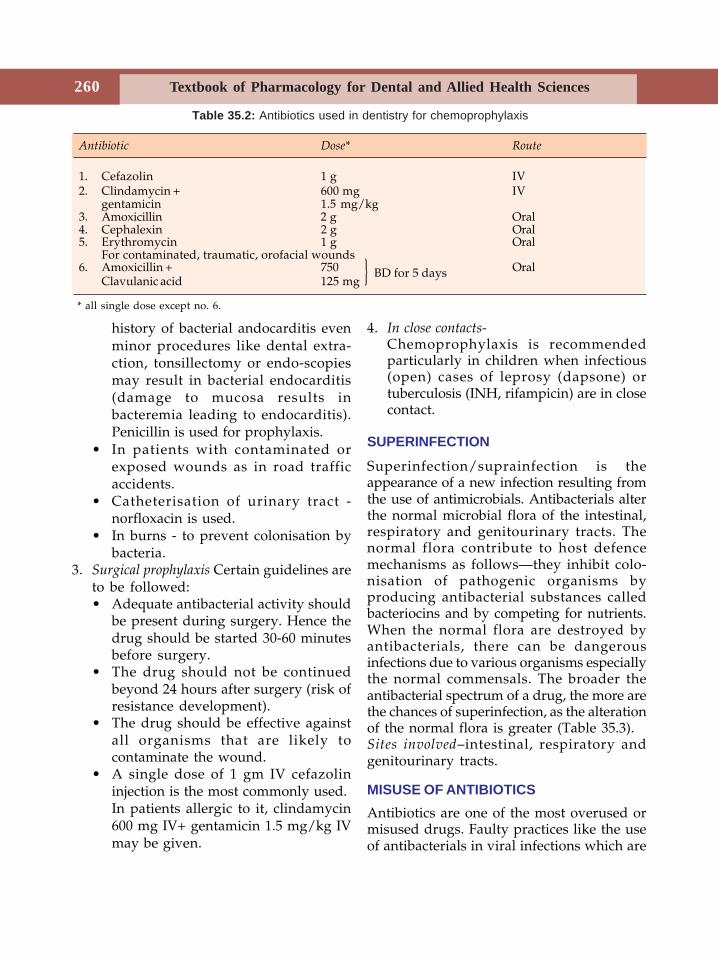
Textbook of Pharmacology for Dental and Allied Health Sciences260
history of bacterial andocarditis evenminor procedures like dental extra-ction, tonsillectomy or endo-scopiesmay result in bacterial endocarditis(damage to mucosa results inbacteremia leading to endocarditis).Penicillin is used for prophylaxis.
• In patients with contaminated orexposed wounds as in road trafficaccidents.
• Catheterisation of urinary tract -norfloxacin is used.
• In burns - to prevent colonisation bybacteria.
3. Surgical prophylaxis Certain guidelines areto be followed:• Adequate antibacterial activity should
be present during surgery. Hence thedrug should be started 30-60 minutesbefore surgery.
• The drug should not be continuedbeyond 24 hours after surgery (risk ofresistance development).
• The drug should be effective againstall organisms that are likely tocontaminate the wound.
• A single dose of 1 gm IV cefazolininjection is the most commonly used.In patients allergic to it, clindamycin600 mg IV+ gentamicin 1.5 mg/kg IVmay be given.
4. In close contacts-Chemoprophylaxis is recommendedparticularly in children when infectious(open) cases of leprosy (dapsone) ortuberculosis (INH, rifampicin) are in closecontact.
SUPERINFECTION
Superinfection/suprainfection is theappearance of a new infection resulting fromthe use of antimicrobials. Antibacterials alterthe normal microbial flora of the intestinal,respiratory and genitourinary tracts. Thenormal flora contribute to host defencemechanisms as follows—they inhibit colo-nisation of pathogenic organisms byproducing antibacterial substances calledbacteriocins and by competing for nutrients.When the normal flora are destroyed byantibacterials, there can be dangerousinfections due to various organisms especiallythe normal commensals. The broader theantibacterial spectrum of a drug, the more arethe chances of superinfection, as the alterationof the normal flora is greater (Table 35.3).Sites involved–intestinal, respiratory andgenitourinary tracts.
MISUSE OF ANTIBIOTICSAntibiotics are one of the most overused ormisused drugs. Faulty practices like the useof antibacterials in viral infections which are
Table 35.2: Antibiotics used in dentistry for chemoprophylaxis
Antibiotic Dose* Route
1. Cefazolin 1 g IV2. Clindamycin + 600 mg IV
gentamicin 1.5 mg/kg3. Amoxicillin 2 g Oral4. Cephalexin 2 g Oral5. Erythromycin 1 g Oral
For contaminated, traumatic, orofacial wounds6. Amoxicillin + 750 Oral
Clavulanic acid 125 mg
* all single dose except no. 6.
BD for 5 days}
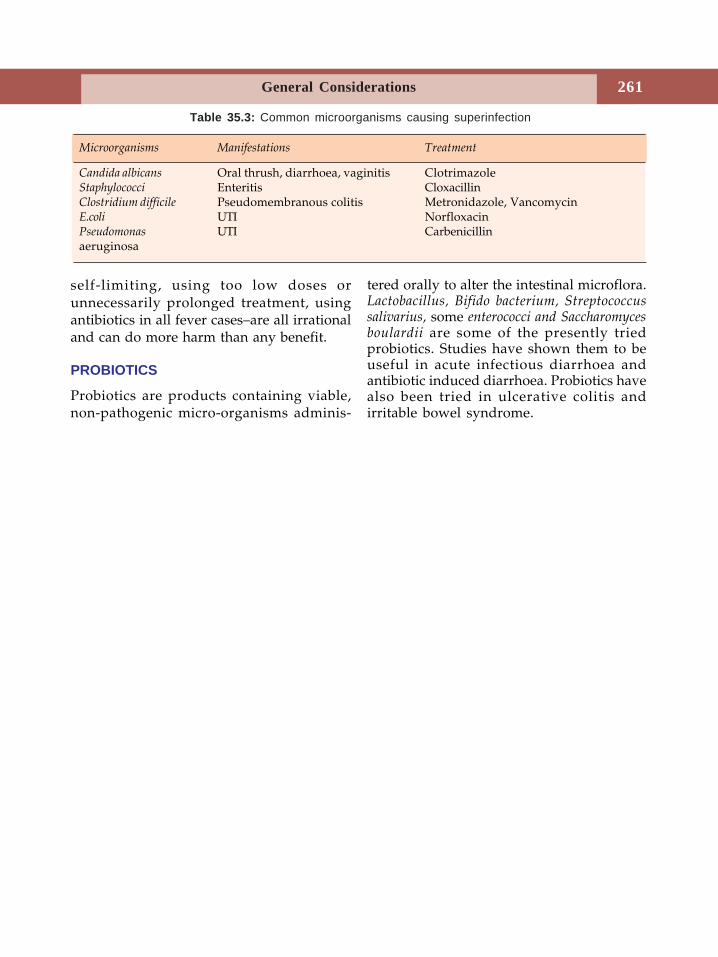
260
General Considerations 261
self-limiting, using too low doses orunnecessarily prolonged treatment, usingantibiotics in all fever cases–are all irrationaland can do more harm than any benefit.
PROBIOTICS
Probiotics are products containing viable,non-pathogenic micro-organisms adminis-
tered orally to alter the intestinal microflora.Lactobacillus, Bifido bacterium, Streptococcussalivarius, some enterococci and Saccharomycesboulardii are some of the presently triedprobiotics. Studies have shown them to beuseful in acute infectious diarrhoea andantibiotic induced diarrhoea. Probiotics havealso been tried in ulcerative colitis andirritable bowel syndrome.
Table 35.3: Common microorganisms causing superinfection
Microorganisms Manifestations Treatment
Candida albicans Oral thrush, diarrhoea, vaginitis ClotrimazoleStaphylococci Enteritis CloxacillinClostridium difficile Pseudomembranous colitis Metronidazole, VancomycinE.coli UTI NorfloxacinPseudomonas UTI Carbenicillinaeruginosa
Textbook of Pharmacology for Dental and Allied Health Sciences262
36 Sulfonamides,Cotrimoxazole
and Quinolones
SULFONAMIDES
Sulfonamides were the first effectiveantibacterial agents to be used systemicallyin man. They are synthetic agents that containa sulfonamide group.Antibacterial spectrum Sulfonamides inhibitgram-positive and some gram-negativebacteria, nocardia, chlamydiae, Plasmodiumfalciparum and Toxoplasma gondii.
Mechanism of Action
PABA↓ Folic acid synthetase ←←←←← SulfonamidesDihydrofolic Acid
Bacteria synthesize their own folic acid fromp-amino benzoic acid (PABA) with the helpof the enzyme folic acid synthetase.Sulfonamides are structurally similar toPABA and competitively inhibit the enzymefolic acid synthetase. This results in folic aciddeficiency and injury to the bacterial cell.
Human cells are not affected becausethey require preformed folic acid suppliedfrom the diet and cannot synthesize folicacid by themselves. Sulfonamides arebacteriostatic.
Presence of pus, blood and tissuebreakdown products make sulfonamidesineffective as these are rich in PABA.
Resistance Bacteria acquire resistance tosulfonamides by:1. Mutations–resulting in over production of
PABA.2. Using alternative metabolic pathway for
folic acid synthesis.3. Low permeability to sulfonamides.
Classification
1. Short-actingSulfisoxazole, sulfadiazine
2. Intermediate-actingSulfamethoxazole
3. Long-actingSulfamethoxypyridazine,Sulfadoxine
4. Poorly absorbedSulfasalazine
5. TopicalSulfacetamide, mefenideSilver sulfadiazine.
Pharmacokinetics Sulfonamides are well-absorbed, extensively bound to plasmaproteins and are well distributed to alltissues. They are metabolized in the liver byacetylation.
Adverse Effects
1. Renal irritation, haematuria, albuminuriaand crystalluria–due to precipitation of the
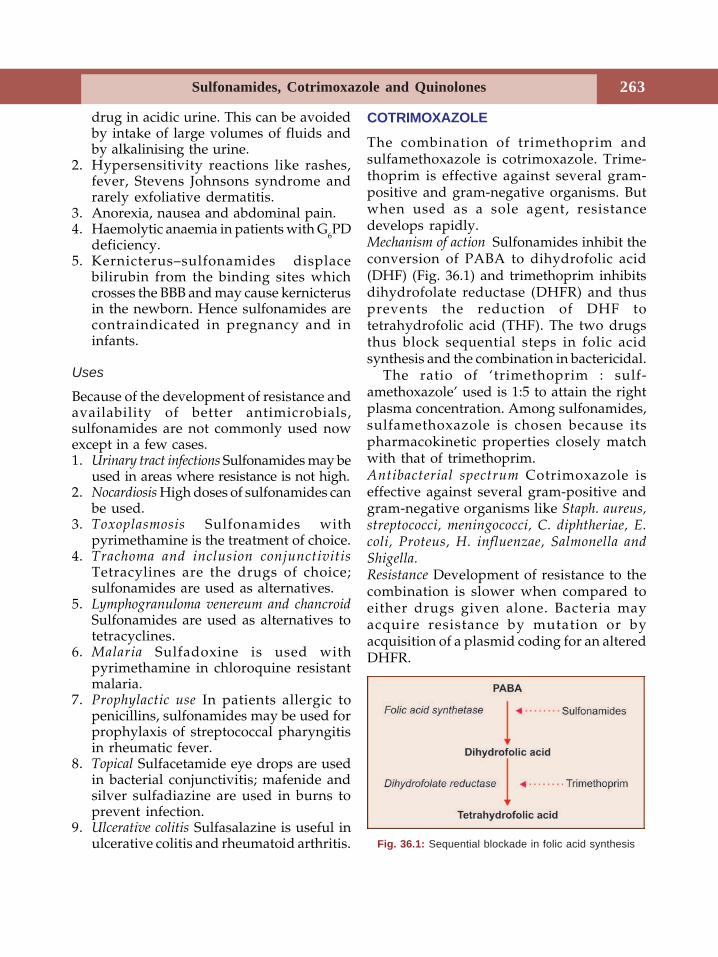
Sulfonamides, Cotrimoxazole and Quinolones 263
drug in acidic urine. This can be avoidedby intake of large volumes of fluids andby alkalinising the urine.
2. Hypersensitivity reactions like rashes,fever, Stevens Johnsons syndrome andrarely exfoliative dermatitis.
3. Anorexia, nausea and abdominal pain.4. Haemolytic anaemia in patients with G6PD
deficiency.5. Kernicterus–sulfonamides displace
bilirubin from the binding sites whichcrosses the BBB and may cause kernicterusin the newborn. Hence sulfonamides arecontraindicated in pregnancy and ininfants.
Uses
Because of the development of resistance andavailability of better antimicrobials,sulfonamides are not commonly used nowexcept in a few cases.1. Urinary tract infections Sulfonamides may be
used in areas where resistance is not high.2. Nocardiosis High doses of sulfonamides can
be used.3. Toxoplasmosis Sulfonamides with
pyrimethamine is the treatment of choice.4. Trachoma and inclusion conjunctivitis
Tetracylines are the drugs of choice;sulfonamides are used as alternatives.
5. Lymphogranuloma venereum and chancroidSulfonamides are used as alternatives totetracyclines.
6. Malaria Sulfadoxine is used withpyrimethamine in chloroquine resistantmalaria.
7. Prophylactic use In patients allergic topenicillins, sulfonamides may be used forprophylaxis of streptococcal pharyngitisin rheumatic fever.
8. Topical Sulfacetamide eye drops are usedin bacterial conjunctivitis; mafenide andsilver sulfadiazine are used in burns toprevent infection.
9. Ulcerative colitis Sulfasalazine is useful inulcerative colitis and rheumatoid arthritis.
COTRIMOXAZOLE
The combination of trimethoprim andsulfamethoxazole is cotrimoxazole. Trime-thoprim is effective against several gram-positive and gram-negative organisms. Butwhen used as a sole agent, resistancedevelops rapidly.Mechanism of action Sulfonamides inhibit theconversion of PABA to dihydrofolic acid(DHF) (Fig. 36.1) and trimethoprim inhibitsdihydrofolate reductase (DHFR) and thusprevents the reduction of DHF totetrahydrofolic acid (THF). The two drugsthus block sequential steps in folic acidsynthesis and the combination in bactericidal.
The ratio of ‘trimethoprim : sulf-amethoxazole’ used is 1:5 to attain the rightplasma concentration. Among sulfonamides,sulfamethoxazole is chosen because itspharmacokinetic properties closely matchwith that of trimethoprim.Antibacterial spectrum Cotrimoxazole iseffective against several gram-positive andgram-negative organisms like Staph. aureus,streptococci, meningococci, C. diphtheriae, E.coli, Proteus, H. influenzae, Salmonella andShigella.Resistance Development of resistance to thecombination is slower when compared toeither drugs given alone. Bacteria mayacquire resistance by mutation or byacquisition of a plasmid coding for an alteredDHFR.
Fig. 36.1: Sequential blockade in folic acid synthesis
Textbook of Pharmacology for Dental and Allied Health Sciences264
Adverse Effects
• Nausea, vomiting, headache, glossitis,stomatitis and allergic skin rashes arerelatively common. In fact all the adverseeffects to sulphonamides can also be seenwith cotrimoxazole because it containssulfamethoxazole.
• In patients with folate deficiency,cotrimoxazole may precipitate megalo-blastic anaemia.
• Haematological reactions like anaemiaand granulocytopenia are rare.
• AIDS patients are more prone to adverseeffects to cotrimoxazole.
• Patients with renal disease may developuraemia.
Preparations
Trimethoprim Sulfamethoxazole (SEPTRAN, CIPLIN)
80 mg 400 mg160 mg 800 mg–double strength (DS)
Uses
1. Urinary tract infection Uncomplicated acuteUTI is treated for 7-10 days (DS, twice aday) with cotrimoxazole.Chronic and recurrent UTI–small dosesare given for prophylaxis.Bacterial prostatitis–Trimethoprim attainshigh concentration in prostatic fluid.
2. Respiratory tract infections Upper andlower respiratory infections includingbronchitis, sinusitis and otitis mediarespond.
3. Bacterial gastroenteritis due to Shigella andE. coli respond to cotrimoxazole.
4. Typhoid Cotrimoxazole is used as analternative to fluoroquinolones.
5. Pneumocystis carinii infection (nowidentified as Pneumocystis jiroveci)Cotrimoxazole is used for prophylaxis andhigh doses for treatment of Pneumocystiscarinii pneumonia in neutropenic and
AIDS patients. It also protects againstinfection with other gram-negativebacteria.
6. Chancroid Cotrimoxazole (DS, BD for 7days) is the drug of choice.
7. Orodental infections–Cotrimoxazole may beused the treatment of mild infections asan alternative to penicillin.
QUINOLONESThe quinolones are a group of syntheticantimicrobial agents. Nalidixic acid is theolder agent in the group. Oxalinic acid andcinoxacin are other quinolones.
Nalidixic AcidNalidixic acid is bactericidal against variousgram-negative organisms like E. coli, Shigella,Proteus and Klebsiella. Its mechanism of actionis same as that of fluoroquinolones (seebelow). Nalidixic acid is well absorbedorally. However, the plasma concentrationof the drug is inadequate to have systemiceffects but it attains high concentrations inthe urine.Adverse effects Haemolytic anaemia, allergicreactions and CNS effects like headache,myalgia and drowsiness may be encoun-tered.
Uses
Nalidixic acid is used in uncomplicated UTIand diarrhoea due to E.coli, Shigella andProteus (GRAMONEG 0.5-1g 3-4 times a day).Oxalinic acid and cinoxacin have properties anduses similar to nalidixic acid.
FLUOROQUINOLONESThe quinolones were fluorinated to obtaincompounds with a wider spectrum of activity,fewer side effects, lesser chance of resistanceand better tissue penetration when comparedto quinolones. The fluoroqui-nolones (FQs)include norfloxacin, ciprofloxacin, pefloxacin,

Sulfonamides, Cotrimoxazole and Quinolones 265
ofloxacin, lomefloxacin and sparfloxacin—manymore are being added. The newer agentsinclude trovafloxacin, gatifloxacin, moxifloxacin,and clinafloxacin.
Mechanism of ActionFluoroquinolones are bactericidal. Theyinhibit the bacterial enzyme DNA gyrase(topoisomerase II) which is required for DNAreplication and transcription.
During DNA replication there is positivesupercoiling of the DNA. This is correctedby the enzyme DNA gyrase by introducingnegative supercoils and therefore this enzymeis necessary for DNA replication. Byinhibiting the enzyme DNA gyrase,fluoroquinolones inhibit DNA replication.Resistance is comparatively not very frequentdue to the unique mechanism of action.Resistance is due to mutations in the targetenzyme or a change in the permeability ofthe organism. Several strains of E.coli,Staphylococci, Pseudomonas and Serratia havenow developed resistance.Antibacterial spectrum Gram-negativeorganisms like gonococci, meningococci, H.influenzae, E. coli, Salmonella, Shigella,enterobacteria; H. pylorii and gram-positiveorganisms like staphylococci; chlamydiae,mycoplasma and myobacterium are susceptible.Some of the newer fluoroquinolones areeffective against some anaerobic organismsand Streptococcus pneumoniae.Pharmacokinetics On oral administration,fluoroquinolones are well-absorbed andwidely distributed. Food and antacidsinterfere with absorption; Pefloxacin andofloxacin cross the BBB. All FQs aremetabolised by hepatic microsomal enzymesand FQs are microsomal enzyme inhibitors –can result in related drug interactions. Thesedrugs are excreted by the kidneys. Hencedose should be reduced in renal failure.Plasma t½ varies from 3 hrs (norfloxacin), 10hrs (pefloxacin) to 18-20 hrs (sparfloxacingiven once daily) (Table 36.1).
Adverse reactions Fluoroquinolones are well-tolerated. Nausea, vomiting, abdominaldiscomfort, diarrhoea and rashes may beseen. Tendinitis with associated risk oftendon rupture has been reported.Fluoroquinolones damage the growingcartilage resulting in arthropathy and aretherefore contraindicated upto 18 years ofage. CNS effects include headache anddizziness. In patients receiving NSAIDs andother epileptogenic drugs like theophylline,fluoroquinolones can sometimes precipitateseizures. Grepafloxacin was found to causecardiac arrhythemias due to which it hasalready been withdrawn from the market.
Uses1. Urinary tract infections Very effective in UTI
even when caused by multi-drug resistantbacteria—norfloxacin is generally used (400mg—BD for 5-10 days).
2. Typhoid Ciprofloxacin is the drug ofchoice (500 mg BD—10 days)— it alsoeradicates carrier state.
3. Diarrhoea due to Shigella, E.coli andCampylobacter respond.
4. Gonorrhoea Single dose 250 mg cipro-floxacin is curative. Ciprofloxacin is usedfor 3 days.
5. Chancroid As an alternative to cotri-moxazole-ciprofloxacin is used for 3
Fig. 36.2: Schematic diagram of DNA
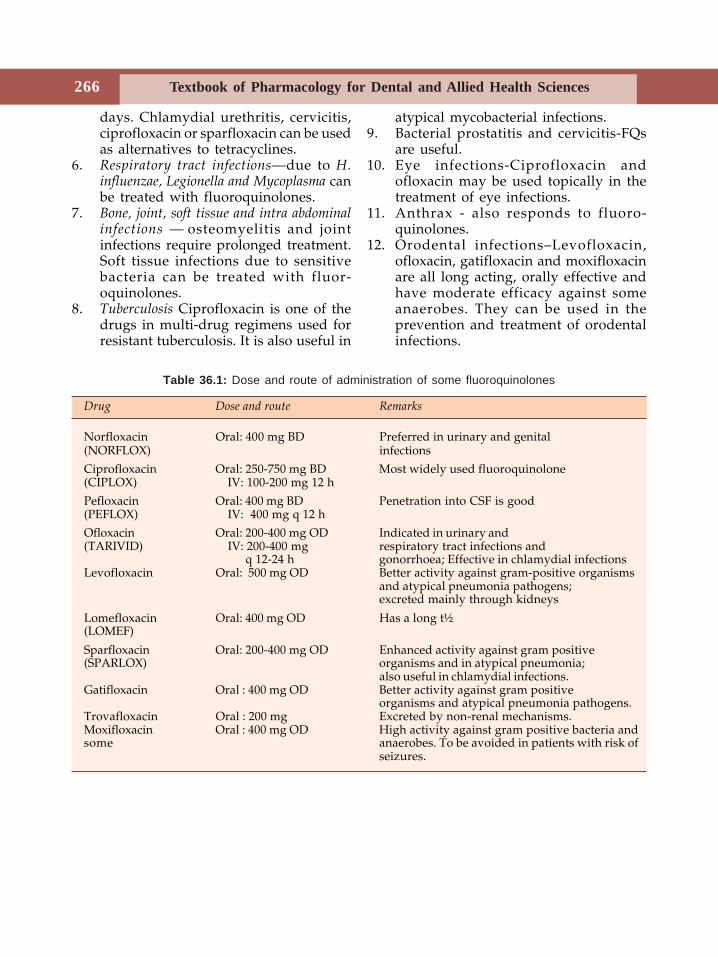
Textbook of Pharmacology for Dental and Allied Health Sciences266
days. Chlamydial urethritis, cervicitis,ciprofloxacin or sparfloxacin can be usedas alternatives to tetracyclines.
6. Respiratory tract infections—due to H.influenzae, Legionella and Mycoplasma canbe treated with fluoroquinolones.
7. Bone, joint, soft tissue and intra abdominalinfections — osteomyelitis and jointinfections require prolonged treatment.Soft tissue infections due to sensitivebacteria can be treated with fluor-oquinolones.
8. Tuberculosis Ciprofloxacin is one of thedrugs in multi-drug regimens used forresistant tuberculosis. It is also useful in
atypical mycobacterial infections.9. Bacterial prostatitis and cervicitis-FQs
are useful.10. Eye infections-Ciprofloxacin and
ofloxacin may be used topically in thetreatment of eye infections.
11. Anthrax - also responds to fluoro-quinolones.
12. Orodental infections–Levofloxacin,ofloxacin, gatifloxacin and moxifloxacinare all long acting, orally effective andhave moderate efficacy against someanaerobes. They can be used in theprevention and treatment of orodentalinfections.
Table 36.1: Dose and route of administration of some fluoroquinolones
Drug Dose and route Remarks
Norfloxacin Oral: 400 mg BD Preferred in urinary and genital(NORFLOX) infections
Ciprofloxacin Oral: 250-750 mg BD Most widely used fluoroquinolone(CIPLOX) IV: 100-200 mg 12 h
Pefloxacin Oral: 400 mg BD Penetration into CSF is good(PEFLOX) IV: 400 mg q 12 h
Ofloxacin Oral: 200-400 mg OD Indicated in urinary and(TARIVID) IV: 200-400 mg respiratory tract infections and
q 12-24 h gonorrhoea; Effective in chlamydial infectionsLevofloxacin Oral: 500 mg OD Better activity against gram-positive organisms
and atypical pneumonia pathogens;excreted mainly through kidneys
Lomefloxacin Oral: 400 mg OD Has a long t½(LOMEF)
Sparfloxacin Oral: 200-400 mg OD Enhanced activity against gram positive(SPARLOX) organisms and in atypical pneumonia;
also useful in chlamydial infections.Gatifloxacin Oral : 400 mg OD Better activity against gram positive
organisms and atypical pneumonia pathogens.Trovafloxacin Oral : 200 mg Excreted by non-renal mechanisms.Moxifloxacin Oral : 400 mg OD High activity against gram positive bacteria andsome anaerobes. To be avoided in patients with risk of
seizures.
Beta-lactam Antibiotics 267
37Beta-lactamAntibiotics
The β-lactam antibiotics have a β-lactam ring.Penicillins, cephalosporins, monobactams andcarbapenems are β-lactam antibiotics.
PENICILLINS
Sir Alexander Fleming discovered penicillinin 1928. Penicillins are one of the mostimportant groups of antibiotics. Penicillin isnow obtained from the fungus Penicillium
chrysogenum.
Mechanism of Action
The β-lactam antibiotics act by inhibiting thecell wall synthesis in the bacteria.
The rigid cell wall of the bacteria protectsit from lysis. Peptidoglycan—a complexpolymer, is an important component of thecell wall. It consists of glycan chains whichare cross-linked by peptide chains. Thesynthesis of this peptidoglycan requiresenzymes called transpeptidases. β-lactamantibiotics inhibit these transpeptidases andthus inhibit the synthesis of thepeptidoglycan, resulting in the formation ofcell wall deficient bacteria. Such bacteriaundergo lysis. Thus penicillins arebactericidal.
Classification
A. Natural— Penicillin GB. Semisynthetic
1. Acid resistant—Penicillin V2. Penicillinase resistant—
Methicillin, Oxacillin,Cloxacillin, Nafcillin
3. Aminopenicillins—Ampicillin, Bacampicillin,Amoxicillin
4. Antipseudomonal penicillins• Carboxypenicillins—
Carbenicillin, Ticarcillin• Ureidopenicillins—
Azlocillin, Mezlocillin,Piperacillin.
NATURAL PENICILLINS
Penicillin G (Benzyl Penicillin)
Antibacterial spectrum Penicillin G (PnG) has anarrow antibacterial spectrum (Table 37.2)and is effective against gram-positive cocciand bacilli and a few gram-negative cocci.Thus streptococci, pneumococci, gonococci,meningococci, B. anthracis, C. diphtheriae,clostridia, listeria and spirochetes are highlysensitive.Resistance Many organisms like staphylococciproduce a penicillinase which is a beta-
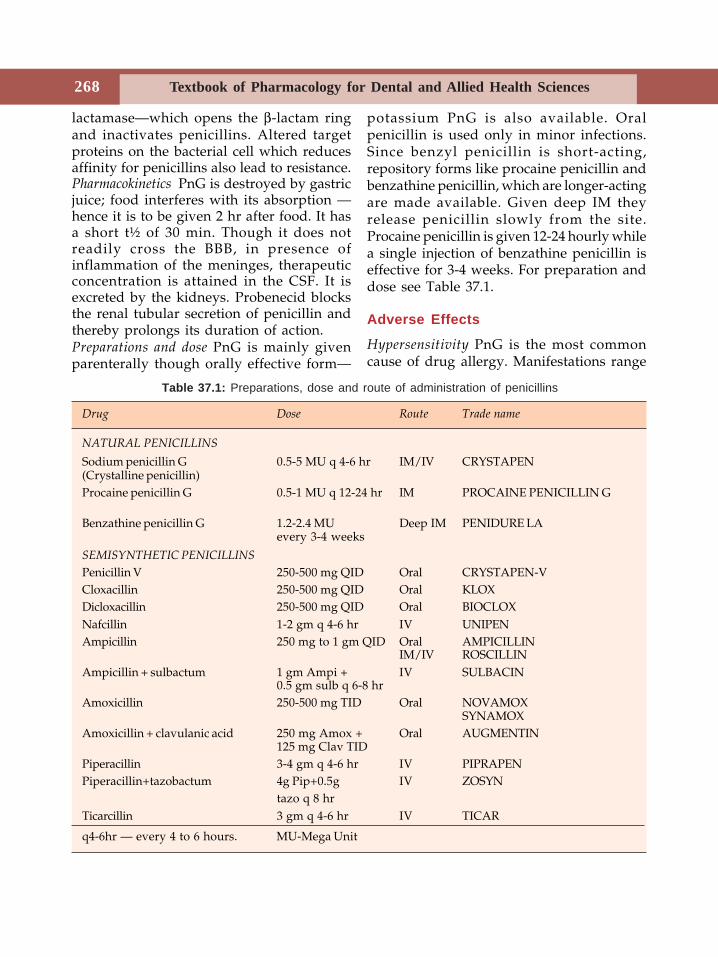
Textbook of Pharmacology for Dental and Allied Health Sciences268
lactamase—which opens the β-lactam ringand inactivates penicillins. Altered targetproteins on the bacterial cell which reducesaffinity for penicillins also lead to resistance.Pharmacokinetics PnG is destroyed by gastricjuice; food interferes with its absorption —hence it is to be given 2 hr after food. It hasa short t½ of 30 min. Though it does notreadily cross the BBB, in presence ofinflammation of the meninges, therapeuticconcentration is attained in the CSF. It isexcreted by the kidneys. Probenecid blocksthe renal tubular secretion of penicillin andthereby prolongs its duration of action.Preparations and dose PnG is mainly givenparenterally though orally effective form—
potassium PnG is also available. Oralpenicillin is used only in minor infections.Since benzyl penicillin is short-acting,repository forms like procaine penicillin andbenzathine penicillin, which are longer-actingare made available. Given deep IM theyrelease penicillin slowly from the site.Procaine penicillin is given 12-24 hourly whilea single injection of benzathine penicillin iseffective for 3-4 weeks. For preparation anddose see Table 37.1.
Adverse Effects
Hypersensitivity PnG is the most commoncause of drug allergy. Manifestations range
Table 37.1: Preparations, dose and route of administration of penicillins
Drug Dose Route Trade name
NATURAL PENICILLINS
Sodium penicillin G 0.5-5 MU q 4-6 hr IM/IV CRYSTAPEN(Crystalline penicillin)Procaine penicillin G 0.5-1 MU q 12-24 hr IM PROCAINE PENICILLIN G
Benzathine penicillin G 1.2-2.4 MU Deep IM PENIDURE LAevery 3-4 weeks
SEMISYNTHETIC PENICILLINS
Penicillin V 250-500 mg QID Oral CRYSTAPEN-VCloxacillin 250-500 mg QID Oral KLOXDicloxacillin 250-500 mg QID Oral BIOCLOXNafcillin 1-2 gm q 4-6 hr IV UNIPENAmpicillin 250 mg to 1 gm QID Oral AMPICILLIN
IM/IV ROSCILLINAmpicillin + sulbactum 1 gm Ampi + IV SULBACIN
0.5 gm sulb q 6-8 hrAmoxicillin 250-500 mg TID Oral NOVAMOX
SYNAMOXAmoxicillin + clavulanic acid 250 mg Amox + Oral AUGMENTIN
125 mg Clav TIDPiperacillin 3-4 gm q 4-6 hr IV PIPRAPENPiperacillin+tazobactum 4g Pip+0.5g IV ZOSYN
tazo q 8 hrTicarcillin 3 gm q 4-6 hr IV TICAR
q4-6hr — every 4 to 6 hours. MU-Mega Unit
Beta-lactam Antibiotics 269
from skin rashes, urticaria, fever,bronchospasm, serum sickness and rarelyexfoliative dermatitis and anaphylaxis.Though all forms of penicillins can causeallergy, anaphylaxis is more commonfollowing parenteral than oral preparations.The highest incidence is with procainepenicillin where allergy is most often due tothe procaine component. There is cross-sensitivity among different penicillins.Topical penicillins are highly sensitizing andtheir use is banned.
History of allergy to penicillins should betaken before prescribing; incidence of allergyis higher among atopic individuals. A scratchtest or intradermal sensitivity test with 2-10units should be done. Even if this is negative,it does not completely rule out allergy.Penicillin should be given cautiously and asyringe loaded with adrenaline to treatanaphylaxis should be kept ready.
Other Adverse Effects
Local Pain at the site of injection,thrombophlebitis on IV injection.CNS Large doses of PnG may produceconfusion, muscle twitchings, convulsionsand coma.Suprainfections are rare due to its narrowspectrum of activity.Jarisch-Herxheimer reaction When penicillin isinjected in a patient with syphilis, there issudden destruction of spirochetes and releaseof its lytic products. This triggers a reactionwith fever, myalgia, shivering, exacerbationof syphilitic lesions and vascular collapse.
Uses
Penicillin G is the antibiotic of choice forseveral infections unless the patient is allergicto it.(A) Orodental infections—Penicillin G iseffective against a variety of aerobic and
anaerobic microorganisms and therefore veryuseful in most orodental infections. Howeverthe disadvantages of parenteral adminis-tration and hypersensitivity reactions havelimited its use. Procaine Penicillin can be usedIM.(B) Other infections1. Pneumococcal infections For infections like
pneumonia, meningitis and osteomyelitisdue to penicillin-sensitive pneumococci,PnG is the drug of choice.
2. Streptococcal infections Pharyngitis, sinusitis,pneumonia, meningitis and endocarditisare all treated with penicillin. Infectiveendocarditis due to Strep. viridans istreated with high dose PnG ± anaminoglycoside.
3. Meningococcal infections PnG is the drugof choice for all meningococcal infections.
4. Staphylococcal infections Since moststaphylococci produce penicillinase, apenicillinase resistant penicillin should beused.
5. Syphilis is treated with procaine penicillinfor 10 days or with benzathine penicillin.
6. Diphtheria Antitoxin is the only effectivetreatment. PnG eliminates carrier state -PP6 given for 10-12 days.
7. Anaerobic infections Pulmonary, per-iodontal and brain abscesses due toanaerobes respond to PnG.
8. Actinomycosis PnG is the drug of choicefor all forms of actinomycosis. 12 to 20MU should be given for 6 weeks.
9. Tetanus and gas gangrene Antitoxin is thetreatment for tetanus—but PnG hasadjuvant value.Gas gangrene— PnG is the drug of choice.
10. Other infections PnG is the agent of choicefor infections like anthrax, trench mouth,rat bite fever and listeria infections.
11. Prophylactic uses:• Rheumatic fever Benzathine penicillin 1.2
MU every month prevents colonisationby streptococci and thereby decreases
Textbook of Pharmacology for Dental and Allied Health Sciences270
the recurrences of rheumatic fever. Itis to be continued for several years.
• Gonorrhoea and syphilis Sexual contactsare effectively protected against thesediseases when treated with penicillinwithin 12 hours of exposure.
• Valvular heart diseases—25% cases ofbacterial endocarditis are seenfollowing dental extractions. Patientswith valvular heart diseases under-going dental extractions, endoscopiesand other minor surgical proceduresthat may cause bacteraemia should begiven penicillin prophylaxis.
Disadvantages of natural penicillins are:1. they are not effective orally.2. have a narrow spectrum of activity.3. are susceptible to β lactamase.4. can cause hypersensitivity.
To overcome the above disadvantages,semisynthetic penicillins have been intro-duced.
SEMISYNTHETIC PENICILLINS
Acid resistant penicillins Penicillin V(Phenoxymethyl penicillin) is acid stable andcan be given orally. It is used only in mildstreptococcal pharyngitis, sinusitis and trenchmouth.Dose 250-500 mg 6 hourly.Penicillinase resistant penicillins are resistantto hydrolysis by penicillinase produced bybacteria. However, against other micro-organisms—they are less effective than PnG.Methicillin is destroyed by gastric juice—hence given parenterally. Cloxacillin is givenorally. Nafcillin is highly resistant topenicillinase and also has useful activityagainst nonpenicillinase producing org-anisms. It requires parenteral administrationbecause of its unreliable absorption from thegut.
Uses
Penicillinase resistant penicillins are the drugsof choice for infections with penicillinaseproducing staphylococci. Methicillin resistantstrains have now emerged and are treatedwith vancomycin.
Extended Spectrum Penicillins
Aminopenicillins These agents cover a widerantibacterial spectrum including many gram-negative bacilli. They are orally effective butare sensitive to betalactamases.Antibacterial spectrum Both gram-positive andgram-negative organisms including stre-ptococci, meningococci, pneumococci, H.influenzae, E. coli, Proteus, Salmonella, Shigellaand Klebsiella are sensitive. Many strains arenow resistant.Ampicillin is well-absorbed orally; foodinterferes with absorption. It is excretedmainly through kidneys.Adverse effects Diarrhoea due to irritation ofthe gut by the unabsorbed drug is the mostcommon adverse effect with ampicillin. Skinrashes are also fairly frequent.
Uses
1. Respiratory tract infections like bronchitis,sinusitis and otitis media respond toampicillin.
2. Urinary tract infections Though ampicillinwas the drug of choice earlier, manyorganisms have now become resistant.
3. Meningitis Ampicillin is given with acephalosporin.
4. Typhoid Ampicillin is an alternative tociprofloxacin.
5. Septicaemia due to gram-negative organisms.Intravenous ampicillin may be used, withan aminoglycoside.
6. Dental infections–Ampicillin is useful in thetreatment of most orodental infections.However, diarrhoea has limited its use.
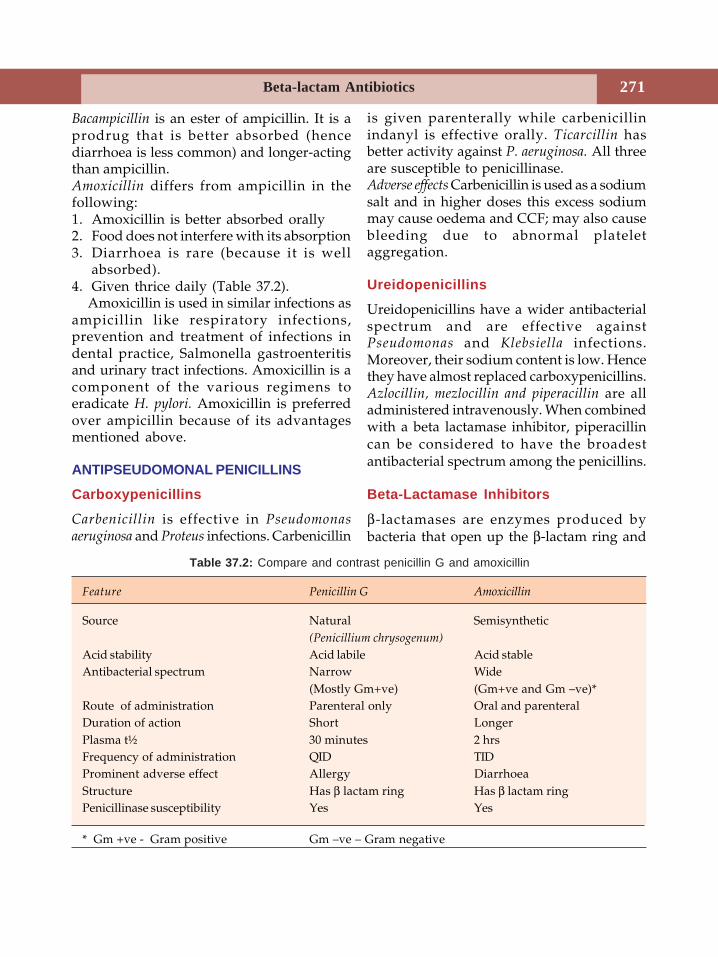
Beta-lactam Antibiotics 271
Bacampicillin is an ester of ampicillin. It is aprodrug that is better absorbed (hencediarrhoea is less common) and longer-actingthan ampicillin.Amoxicillin differs from ampicillin in thefollowing:1. Amoxicillin is better absorbed orally2. Food does not interfere with its absorption3. Diarrhoea is rare (because it is well
absorbed).4. Given thrice daily (Table 37.2).
Amoxicillin is used in similar infections asampicillin like respiratory infections,prevention and treatment of infections indental practice, Salmonella gastroenteritisand urinary tract infections. Amoxicillin is acomponent of the various regimens toeradicate H. pylori. Amoxicillin is preferredover ampicillin because of its advantagesmentioned above.
ANTIPSEUDOMONAL PENICILLINS
Carboxypenicillins
Carbenicillin is effective in Pseudomonasaeruginosa and Proteus infections. Carbenicillin
is given parenterally while carbenicillinindanyl is effective orally. Ticarcillin hasbetter activity against P. aeruginosa. All threeare susceptible to penicillinase.Adverse effects Carbenicillin is used as a sodiumsalt and in higher doses this excess sodiummay cause oedema and CCF; may also causebleeding due to abnormal plateletaggregation.
Ureidopenicillins
Ureidopenicillins have a wider antibacterialspectrum and are effective againstPseudomonas and Klebsiella infections.Moreover, their sodium content is low. Hencethey have almost replaced carboxypenicillins.Azlocillin, mezlocillin and piperacillin are alladministered intravenously. When combinedwith a beta lactamase inhibitor, piperacillincan be considered to have the broadestantibacterial spectrum among the penicillins.
Beta-Lactamase Inhibitors
β-lactamases are enzymes produced bybacteria that open up the β-lactam ring and
Table 37.2: Compare and contrast penicillin G and amoxicillin
Feature Penicillin G Amoxicillin
Source Natural Semisynthetic(Penicillium chrysogenum)
Acid stability Acid labile Acid stableAntibacterial spectrum Narrow Wide
(Mostly Gm+ve) (Gm+ve and Gm –ve)*Route of administration Parenteral only Oral and parenteralDuration of action Short LongerPlasma t½ 30 minutes 2 hrsFrequency of administration QID TIDProminent adverse effect Allergy DiarrhoeaStructure Has β lactam ring Has β lactam ringPenicillinase susceptibility Yes Yes
* Gm +ve - Gram positive Gm –ve – Gram negative
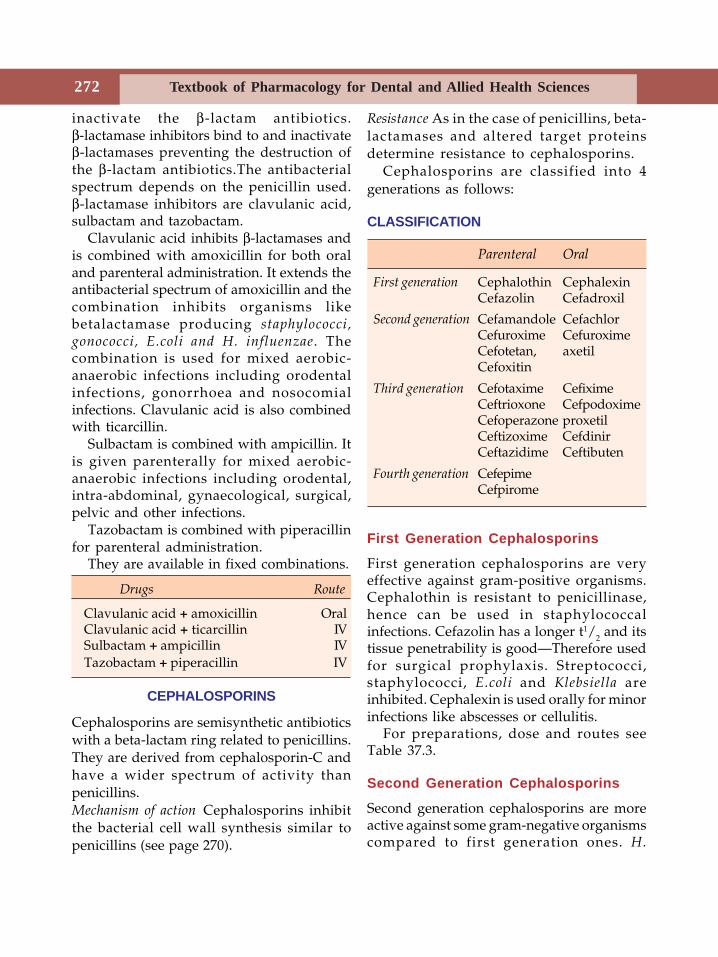
Textbook of Pharmacology for Dental and Allied Health Sciences272
inactivate the β-lactam antibiotics.β-lactamase inhibitors bind to and inactivateβ-lactamases preventing the destruction ofthe β-lactam antibiotics.The antibacterialspectrum depends on the penicillin used.β-lactamase inhibitors are clavulanic acid,sulbactam and tazobactam.
Clavulanic acid inhibits β-lactamases andis combined with amoxicillin for both oraland parenteral administration. It extends theantibacterial spectrum of amoxicillin and thecombination inhibits organisms likebetalactamase producing staphylococci,gonococci, E.coli and H. influenzae. Thecombination is used for mixed aerobic-anaerobic infections including orodentalinfections, gonorrhoea and nosocomialinfections. Clavulanic acid is also combinedwith ticarcillin.
Sulbactam is combined with ampicillin. Itis given parenterally for mixed aerobic-anaerobic infections including orodental,intra-abdominal, gynaecological, surgical,pelvic and other infections.
Tazobactam is combined with piperacillinfor parenteral administration.
They are available in fixed combinations.
Drugs Route
Clavulanic acid + amoxicillin OralClavulanic acid + ticarcillin IVSulbactam + ampicillin IVTazobactam + piperacillin IV
CEPHALOSPORINS
Cephalosporins are semisynthetic antibioticswith a beta-lactam ring related to penicillins.They are derived from cephalosporin-C andhave a wider spectrum of activity thanpenicillins.Mechanism of action Cephalosporins inhibitthe bacterial cell wall synthesis similar topenicillins (see page 270).
Resistance As in the case of penicillins, beta-lactamases and altered target proteinsdetermine resistance to cephalosporins.
Cephalosporins are classified into 4generations as follows:
CLASSIFICATION
Parenteral Oral
First generation Cephalothin CephalexinCefazolin Cefadroxil
Second generation Cefamandole CefachlorCefuroxime CefuroximeCefotetan, axetilCefoxitin
Third generation Cefotaxime CefiximeCeftrioxone CefpodoximeCefoperazone proxetilCeftizoxime CefdinirCeftazidime Ceftibuten
Fourth generation CefepimeCefpirome
First Generation Cephalosporins
First generation cephalosporins are veryeffective against gram-positive organisms.Cephalothin is resistant to penicillinase,hence can be used in staphylococcalinfections. Cefazolin has a longer t1/2 and itstissue penetrability is good—Therefore usedfor surgical prophylaxis. Streptococci,staphylococci, E.coli and Klebsiella areinhibited. Cephalexin is used orally for minorinfections like abscesses or cellulitis.
For preparations, dose and routes seeTable 37.3.
Second Generation Cephalosporins
Second generation cephalosporins are moreactive against some gram-negative organismscompared to first generation ones. H.
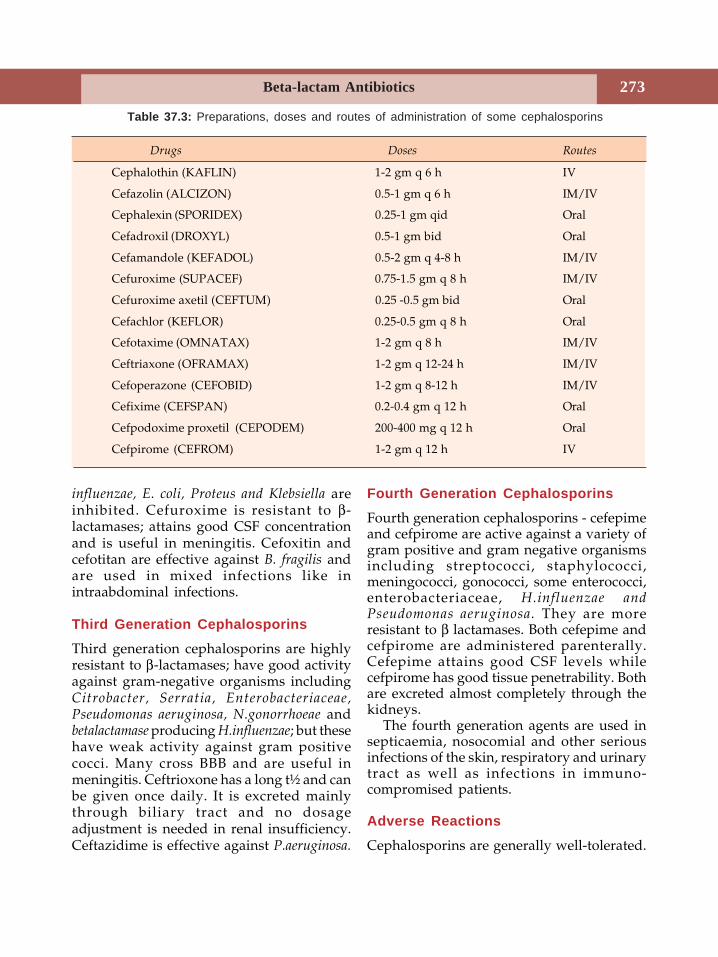
Beta-lactam Antibiotics 273
influenzae, E. coli, Proteus and Klebsiella areinhibited. Cefuroxime is resistant to β-lactamases; attains good CSF concentrationand is useful in meningitis. Cefoxitin andcefotitan are effective against B. fragilis andare used in mixed infections like inintraabdominal infections.
Third Generation Cephalosporins
Third generation cephalosporins are highlyresistant to β-lactamases; have good activityagainst gram-negative organisms includingCitrobacter, Serratia, Enterobacteriaceae,Pseudomonas aeruginosa, N.gonorrhoeae andbetalactamase producing H.influenzae; but thesehave weak activity against gram positivecocci. Many cross BBB and are useful inmeningitis. Ceftrioxone has a long t½ and canbe given once daily. It is excreted mainlythrough biliary tract and no dosageadjustment is needed in renal insufficiency.Ceftazidime is effective against P.aeruginosa.
Fourth Generation Cephalosporins
Fourth generation cephalosporins - cefepimeand cefpirome are active against a variety ofgram positive and gram negative organismsincluding streptococci, staphylococci,meningococci, gonococci, some enterococci,enterobacteriaceae, H.influenzae andPseudomonas aeruginosa. They are moreresistant to β lactamases. Both cefepime andcefpirome are administered parenterally.Cefepime attains good CSF levels whilecefpirome has good tissue penetrability. Bothare excreted almost completely through thekidneys.
The fourth generation agents are used insepticaemia, nosocomial and other seriousinfections of the skin, respiratory and urinarytract as well as infections in immuno-compromised patients.
Adverse Reactions
Cephalosporins are generally well-tolerated.
Table 37.3: Preparations, doses and routes of administration of some cephalosporins
Drugs Doses Routes
Cephalothin (KAFLIN) 1-2 gm q 6 h IV
Cefazolin (ALCIZON) 0.5-1 gm q 6 h IM/IV
Cephalexin (SPORIDEX) 0.25-1 gm qid Oral
Cefadroxil (DROXYL) 0.5-1 gm bid Oral
Cefamandole (KEFADOL) 0.5-2 gm q 4-8 h IM/IV
Cefuroxime (SUPACEF) 0.75-1.5 gm q 8 h IM/IV
Cefuroxime axetil (CEFTUM) 0.25 -0.5 gm bid Oral
Cefachlor (KEFLOR) 0.25-0.5 gm q 8 h Oral
Cefotaxime (OMNATAX) 1-2 gm q 8 h IM/IV
Ceftriaxone (OFRAMAX) 1-2 gm q 12-24 h IM/IV
Cefoperazone (CEFOBID) 1-2 gm q 8-12 h IM/IV
Cefixime (CEFSPAN) 0.2-0.4 gm q 12 h Oral
Cefpodoxime proxetil (CEPODEM) 200-400 mg q 12 h Oral
Cefpirome (CEFROM) 1-2 gm q 12 h IV
Textbook of Pharmacology for Dental and Allied Health Sciences274
1. Hypersensitivity reactions like skin rashes,fever, serum sickness and rarelyanaphylaxis are seen. 20% of patientsallergic to penicillin show cross-reactivityto cephalosporins. There are no reliableskin tests for testing allergy.
2. Nephrotoxicity Mild nephrotoxicity isnoted with some cephalosporins.Combination with other nephrotoxicdrugs should be avoided.
3. Diarrhoea can result from some of thecephalosporins.
4. Bleeding is due to hypoprothrombinaemiawhich is more common in malnourishedpatients.
5. Low WBC count may be seen thoughrarely.
6. Pain at the injection site may occur.7. Disulfiram-like reaction with alcohol is
reported with some cephalosporins.
Uses of Cephalosporins
1. Gram-negative infections Urinary,respiratory and soft tissue infections dueto gram-negative organisms respond–athird generation agent is used.
2. Surgical prophylaxis Cefazolin is preferreddue to its longer t1/2 and better tissuepenetrability for surgical prophylaxisincluding dental surgeries.
3. Gonorrhoea Ceftriaxone (single dose 250mg) is the drug of choice.
4. Meningitis due to H. influenzae,N. meningitidis and S. pneumoniae—thirdgeneration agents are useful - cefotaximeor ceftrioxone may be used. Pseudomonasmeningitis - ceftazidime + an amino-glycoside→→→→→ very effective.
5. Mixed aerobic-anaerobic infections–commonfollowing pelvic surgeries–a thirdgeneration agent is used.
6. Typhoid-As an alternative to ciprofloxacin.7. Nosocomial infections can be treated with
third generation cephalosporins.
8. Orodental infections–Orally effectivecephalosporins like cephalexin, cefaclor,cefuroxime axetil are used for thetreatment of orodental infections. Thelatter two also have good activity againstanaerobes which make them the preferredcephalosporins in dentistry. Cefazolin andcefotaxime are used for surgicalprophylaxis in dental surgeries.
CARBAPENEMS
Carbapenems contain a β-lactam ring fusedwith a five-membered penem ring. Carba-penems include imipenem, meropenem andertapenem.Antibacterial spectrum – Carbapenems have awide antibacterial spectrum and inhibitvarious gram-positive, gram-negativeorganisms and anaerobes includingstreptococci, staphylococci, enterococci, Listeria,enterobacteriaceae, Pseudomonas and B.fragilis.
Mechanism of Action
Carbapenems inhibit bacterial cell wallsynthesis similar to penicillins (see page 270).Imipenem-is not absorbed orally and isadministered intravenously (250-500 mgevery 6-8 hours); it has good tissuepenetrability. Imipenem is inactivated quicklyby a dehydropeptidase in the renal tubules.Hence it is always combined with cilastatin,an inhibitor of dehydropeptidase in order toprolong its plasma half life.Adverse effects to imipenem include nausea,vomiting, diarrhoea and allergic reactionsespecially in patients allergic to otherβ-lactam antibiotics. High doses canoccasionally cause seizures.
Uses
Imipenem-cilastatin is used in UTI,respiratory, skin, bone, soft tissue, intra-

Beta-lactam Antibiotics 275
abdominal and gynaecological infections dueto susceptible microorganisms. It is parti-cularly useful in enterobacter, penicillin-resistant pneumococci and other nosocomialinfections resistant to other antibiotics. It isused with an aminoglycoside in pseu-domonas infections.Meropenem has the following advantages overimipenem-• It is not destroyed by renal dipeptidase
and therefore does not require to becombined with cilastatin.
• Risk of seizures less than with imipenem.Indications of meropenem are similar toimipenem.Ertapenem is similar to meropenem except thatit is not useful against P. aeruginosa.
MONOBACTAMSMonobactams are monocyclic beta-lactams,i.e they contain a single ring–the beta-lactamring.Aztreonam is the monobactam available. It isactive against gram - negative bacilli includingPseudomonas aeruginosa but is not effectiveagainst gram-positive organisms andanaerobes. Aztreonam acts by inhibiting cellwall synthesis like penicillins. It is givenparenterally (IM/IV 1-2 G every 6-8 hrs).
Aztreonam can be used in patients allergicto penicillins because there is no crossallergenicity with other β-lactams. The onlyreported adverse effects are occasional skinrashes. Aztreonam is used in pseudomonasinfections especially nosocomial and in othergram-negative infections.
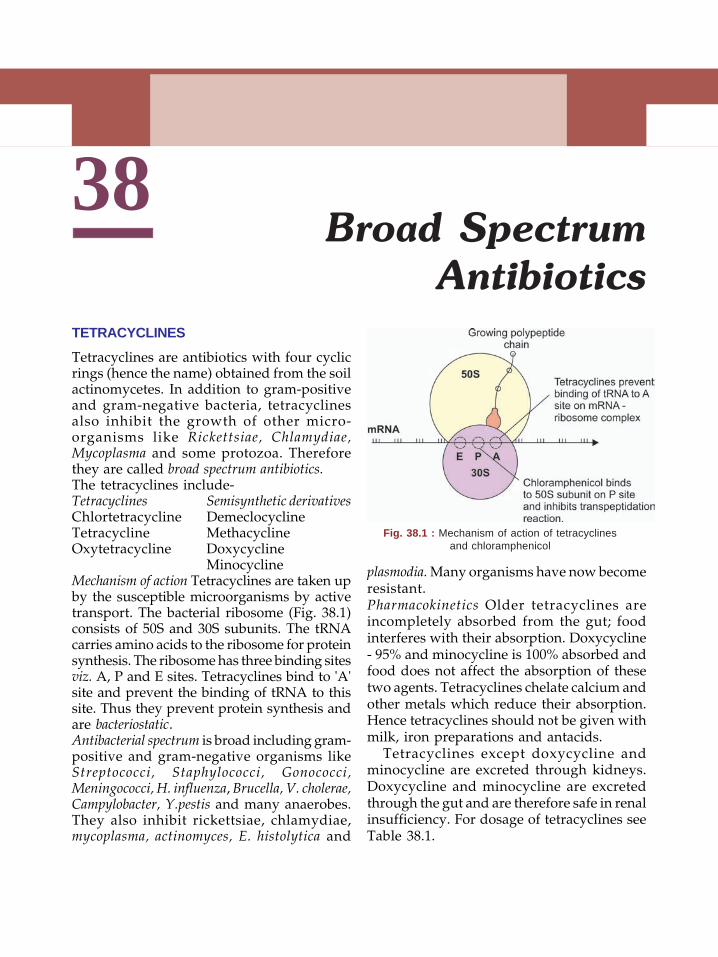
Textbook of Pharmacology for Dental and Allied Health Sciences276
38Broad Spectrum
AntibioticsTETRACYCLINES
Tetracyclines are antibiotics with four cyclicrings (hence the name) obtained from the soilactinomycetes. In addition to gram-positiveand gram-negative bacteria, tetracyclinesalso inhibit the growth of other micro-organisms like Rickettsiae, Chlamydiae,Mycoplasma and some protozoa. Thereforethey are called broad spectrum antibiotics.The tetracyclines include-Tetracyclines Semisynthetic derivativesChlortetracycline DemeclocyclineTetracycline MethacyclineOxytetracycline Doxycycline
MinocyclineMechanism of action Tetracyclines are taken upby the susceptible microorganisms by activetransport. The bacterial ribosome (Fig. 38.1)consists of 50S and 30S subunits. The tRNAcarries amino acids to the ribosome for proteinsynthesis. The ribosome has three binding sitesviz. A, P and E sites. Tetracyclines bind to 'A'site and prevent the binding of tRNA to thissite. Thus they prevent protein synthesis andare bacteriostatic.Antibacterial spectrum is broad including gram-positive and gram-negative organisms likeStreptococci, Staphylococci, Gonococci,Meningococci, H. influenza, Brucella, V. cholerae,Campylobacter, Y.pestis and many anaerobes.They also inhibit rickettsiae, chlamydiae,mycoplasma, actinomyces, E. histolytica and
plasmodia. Many organisms have now becomeresistant.Pharmacokinetics Older tetracyclines areincompletely absorbed from the gut; foodinterferes with their absorption. Doxycycline- 95% and minocycline is 100% absorbed andfood does not affect the absorption of thesetwo agents. Tetracyclines chelate calcium andother metals which reduce their absorption.Hence tetracyclines should not be given withmilk, iron preparations and antacids.
Tetracyclines except doxycycline andminocycline are excreted through kidneys.Doxycycline and minocycline are excretedthrough the gut and are therefore safe in renalinsufficiency. For dosage of tetracyclines seeTable 38.1.
Fig. 38.1 : Mechanism of action of tetracyclinesand chloramphenicol
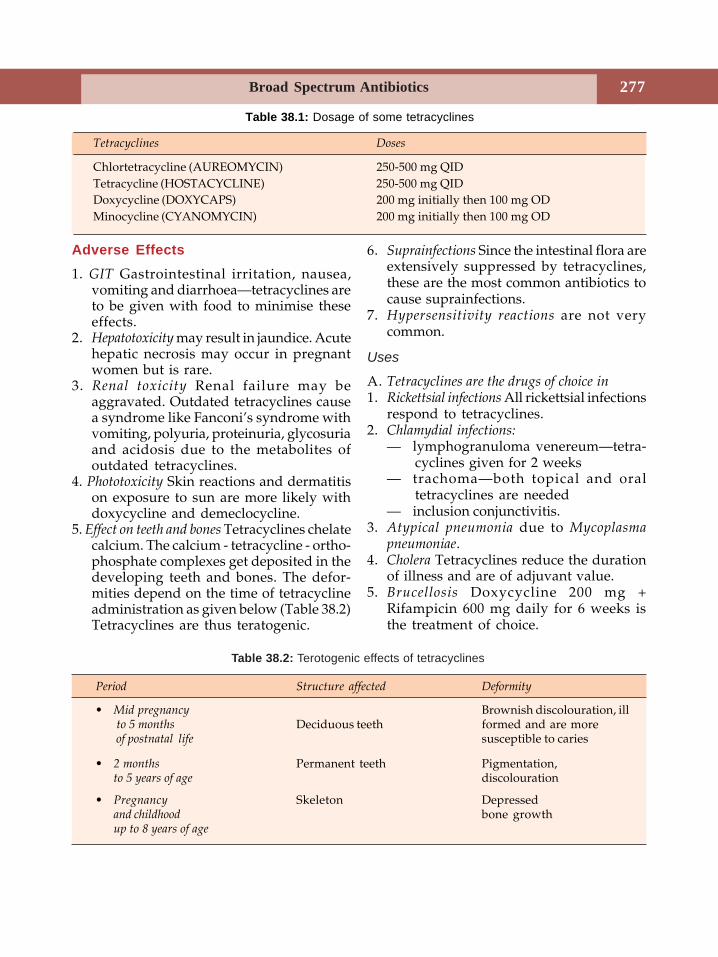
Broad Spectrum Antibiotics 277
Adverse Effects1. GIT Gastrointestinal irritation, nausea,
vomiting and diarrhoea—tetracyclines areto be given with food to minimise theseeffects.
2. Hepatotoxicity may result in jaundice. Acutehepatic necrosis may occur in pregnantwomen but is rare.
3. Renal toxicity Renal failure may beaggravated. Outdated tetracyclines causea syndrome like Fanconi’s syndrome withvomiting, polyuria, proteinuria, glycosuriaand acidosis due to the metabolites ofoutdated tetracyclines.
4. Phototoxicity Skin reactions and dermatitison exposure to sun are more likely withdoxycycline and demeclocycline.
5. Effect on teeth and bones Tetracyclines chelatecalcium. The calcium - tetracycline - ortho-phosphate complexes get deposited in thedeveloping teeth and bones. The defor-mities depend on the time of tetracyclineadministration as given below (Table 38.2)Tetracyclines are thus teratogenic.
6. Suprainfections Since the intestinal flora areextensively suppressed by tetracyclines,these are the most common antibiotics tocause suprainfections.
7. Hypersensitivity reactions are not verycommon.
Uses
A. Tetracyclines are the drugs of choice in1. Rickettsial infections All rickettsial infections
respond to tetracyclines.2. Chlamydial infections:
— lymphogranuloma venereum—tetra-cyclines given for 2 weeks
— trachoma—both topical and oraltetracyclines are needed
— inclusion conjunctivitis.3. Atypical pneumonia due to Mycoplasma
pneumoniae.4. Cholera Tetracyclines reduce the duration
of illness and are of adjuvant value.5. Brucellosis Doxycycline 200 mg +
Rifampicin 600 mg daily for 6 weeks isthe treatment of choice.
Period Structure affected Deformity
• Mid pregnancy Brownish discolouration, ill to 5 months Deciduous teeth formed and are more of postnatal life susceptible to caries
• 2 months Permanent teeth Pigmentation,to 5 years of age discolouration
• Pregnancy Skeleton Depressedand childhood bone growthup to 8 years of age
Table 38.1: Dosage of some tetracyclines
Tetracyclines Doses
Chlortetracycline (AUREOMYCIN) 250-500 mg QIDTetracycline (HOSTACYCLINE) 250-500 mg QIDDoxycycline (DOXYCAPS) 200 mg initially then 100 mg ODMinocycline (CYANOMYCIN) 200 mg initially then 100 mg OD
Table 38.2: Terotogenic effects of tetracyclines
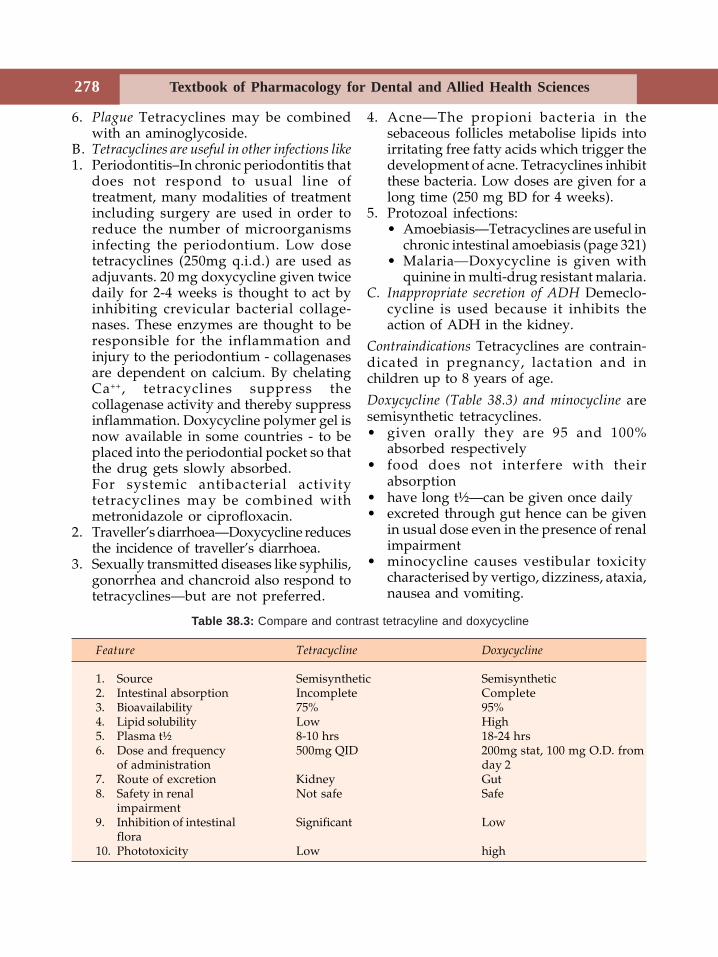
Textbook of Pharmacology for Dental and Allied Health Sciences278
6. Plague Tetracyclines may be combinedwith an aminoglycoside.
B. Tetracyclines are useful in other infections like1. Periodontitis–In chronic periodontitis that
does not respond to usual line oftreatment, many modalities of treatmentincluding surgery are used in order toreduce the number of microorganismsinfecting the periodontium. Low dosetetracyclines (250mg q.i.d.) are used asadjuvants. 20 mg doxycycline given twicedaily for 2-4 weeks is thought to act byinhibiting crevicular bacterial collage-nases. These enzymes are thought to beresponsible for the inflammation andinjury to the periodontium - collagenasesare dependent on calcium. By chelatingCa++, tetracyclines suppress thecollagenase activity and thereby suppressinflammation. Doxycycline polymer gel isnow available in some countries - to beplaced into the periodontial pocket so thatthe drug gets slowly absorbed.For systemic antibacterial activitytetracyclines may be combined withmetronidazole or ciprofloxacin.
2. Traveller’s diarrhoea—Doxycycline reducesthe incidence of traveller’s diarrhoea.
3. Sexually transmitted diseases like syphilis,gonorrhea and chancroid also respond totetracyclines—but are not preferred.
4. Acne—The propioni bacteria in thesebaceous follicles metabolise lipids intoirritating free fatty acids which trigger thedevelopment of acne. Tetracyclines inhibitthese bacteria. Low doses are given for along time (250 mg BD for 4 weeks).
5. Protozoal infections:• Amoebiasis—Tetracyclines are useful in
chronic intestinal amoebiasis (page 321)• Malaria—Doxycycline is given with
quinine in multi-drug resistant malaria.C. Inappropriate secretion of ADH Demeclo-
cycline is used because it inhibits theaction of ADH in the kidney.
Contraindications Tetracyclines are contrain-dicated in pregnancy, lactation and inchildren up to 8 years of age.
Doxycycline (Table 38.3) and minocycline aresemisynthetic tetracyclines.• given orally they are 95 and 100%
absorbed respectively• food does not interfere with their
absorption• have long t½—can be given once daily• excreted through gut hence can be given
in usual dose even in the presence of renalimpairment
• minocycline causes vestibular toxicitycharacterised by vertigo, dizziness, ataxia,nausea and vomiting.
Feature Tetracycline Doxycycline
1. Source Semisynthetic Semisynthetic2. Intestinal absorption Incomplete Complete3. Bioavailability 75% 95%4. Lipid solubility Low High5. Plasma t½ 8-10 hrs 18-24 hrs6. Dose and frequency 500mg QID 200mg stat, 100 mg O.D. from
of administration day 27. Route of excretion Kidney Gut8. Safety in renal Not safe Safe
impairment9. Inhibition of intestinal Significant Low
flora10. Phototoxicity Low high
Table 38.3: Compare and contrast tetracyline and doxycycline
Broad Spectrum Antibiotics 279
CHLORAMPHENICOLChloramphenicol is a broad spectrumantibiotic first obtained from Streptomycesvenezuelae in 1947.Mechanism of action Chloramphenicol isbacteriostatic but to some organisms it isbactericidal. It binds to 50S ribosomal subunitand inhibits protein synthesis - by inhibitingtranspeptidation reaction (Fig. 38.1).Antibacterial spectrum is broad and includesgram-negative organisms, some gram-positive organisms, anaerobic bacteria,Rickettsiae, Chlamydiae and Mycoplasma.Thus H. influenzae, Salmonella, Shigella,Bordatella, Brucella, gonococci, mening-ococci, streptococci, staphylococci, Clostri-dium, E.coli and Klebsiella—are inhibitedapart from Rickettsiae, Chlamydiae andMycoplasma.Resistance is plasmid mediated and may bedue to:1. Inactivating enzymes2. ↓ permeability of the microorganisms3. Ribosomal insensitivity.Pharmacokinetics Chloramphenicol is rapidlyabsorbed from the gut; penetration into tissuesis excellent; attains high concentration in CSF.It is metabolised in the liver by conjugation.
Adverse Reactions1. Gastrointestinal disturbances Nausea,
vomiting, diarrhoea.2. Bone marrow depression Chloramphenicol
may cause bone marrow depression intwo ways:(i) dose dependent anaemia, leukopenia
and thrombocytopenia due toinhibition of protein synthesis. It isreversible.
(ii) idiosyncratic response—resulting inaplastic anaemia which may be fatal.It may be due to a toxic metabolite.Incidence is 1 in 30,000 patients andoccurs in genetically predisposedindividuals. This toxicity has limitedthe use of chloramphenicol.
3. Gray baby syndrome Newborn babies givenhigh doses of chloramphenicol maydevelop vomiting, refusal of feeds,hypotonia, hypothermia, abdominaldistension, metabolic acidosis and ashengray cyanosis—described as gray babysyndrome. It may be fatal. As thenewborn cannot metabolize (due toinadequate hepatic glucuronidation) andexcrete chloramphenicol adequately,toxicity results.
4. Hypersensitivity reactions like rashes andfever are uncommon.
5. Superinfection can occur.
Drug Interactions
Chloramphenicol inhibits hepatic microsomalenzymes and thereby prolongs the half-lifeof drugs metabolised by this system. This mayresult in enhanced toxicity of some drugs likephenytoin, tolbutamide and dicumarol.
Uses
Because of the risk of bone marrow toxicityand availability of safer drugs, chloram-phenicol is not generally preferred either indentistry or general medicine. Theindications are:1. Typhoid fever Very effective in typhoid;
given for 14 days (500 mg QID till feversubsides then 250 mg QID up to 14th day).
2. Bacterial meningitis In meningococcal andH. influenzae meningitis—chloramphenicolis an alternative to penicillin.
3. Anaerobic infections Chloramphenicol +penicillin + an aminoglycoside can be usedin severe anaerobic infections as analternative to metronidazole andclindamycin.
4. Rickettsial infections As an alternative whentetracyclines are contraindicated.
5. Eye infections Chloramphenicol is usedtopically because of the good penetrationinto aqueous humour.
Textbook of Pharmacology for Dental and Allied Health Sciences280
39Aminoglycosides
Aminoglycosides are antibiotics with aminosugars in glycosidic linkages. They arederived from the soil actinomycetes of thegenus streptomyces (streptomycin, kana-mycin, tobramycin, neomycin) and the genusmicromonospora (gentamicin and netilmicin)- hence the difference in spelling. Amikacinand netilmicin are semisynthetic products.
Common Properties of Aminoglycosides
1. Aminoglycosides are not absorbed orally(as they ionize in solution) therefore theyare given parenterally.
2. They remain extracellularly and pene-tration into CSF is very poor.
3. They are excreted unchanged by thekidneys.
4. They are all bactericidal.5. They act by inhibiting bacterial protein
synthesis.6. They are mainly effective against gram-
negative organisms.7. They produce variable degrees of
ototoxicity and nephrotoxicity as adverseeffects.
Antibacterial spectrum Aminoglycosides havea narrow spectrum and are effective mainlyagainst aerobic gram-negative bacilli like E.coli, Proteus, Pseudomonas, Brucella, Salmonella,Shigella and Klebsiella.Mechanism of action Aminoglycosides, beingwater-soluble penetrate the bacterial cellmembrane through aqueous pores and from
there they are taken up by an active transportprocess. Inside the cell, (Fig. 39.1) amino-glycosides bind to 30S ribosomes and inhibitbacterial protein synthesis - block initiationof protein synthesis, cause termination ofprotein synthesis and cause addition ofincorrect amino acids resulting in thesynthesis of abnormal proteins. Amino-glycosides are bactericidal. Higher theconcentration, greater is the bactericidaleffect. A residual bactericidal effect—postantibiotic effect—remains even after theplasma levels of aminoglycosides fall. Hence,even though they have a short t½, they canbe given once a day (Table 39.1).Resistance to aminoglycosides is acquired by1. Aminoglycoside inactivating enzymes.2. Low affinity of ribosomes - acquired by
mutation.3. Decrease in permeability to the antibiotic.There is partial cross-resistance amongvarious aminoglycosides.
Pharmacokinetics
Aminoglycosides are not absorbed from thegut but when instilled into body cavities orapplied over large wounds, they may getrapidly absorbed. Following IM injectionpeak levels are seen in 60 minutes. They arenot bound to plasma proteins and do notenter cells or cross barriers - mostly remainin the vasculature. In patients with severe
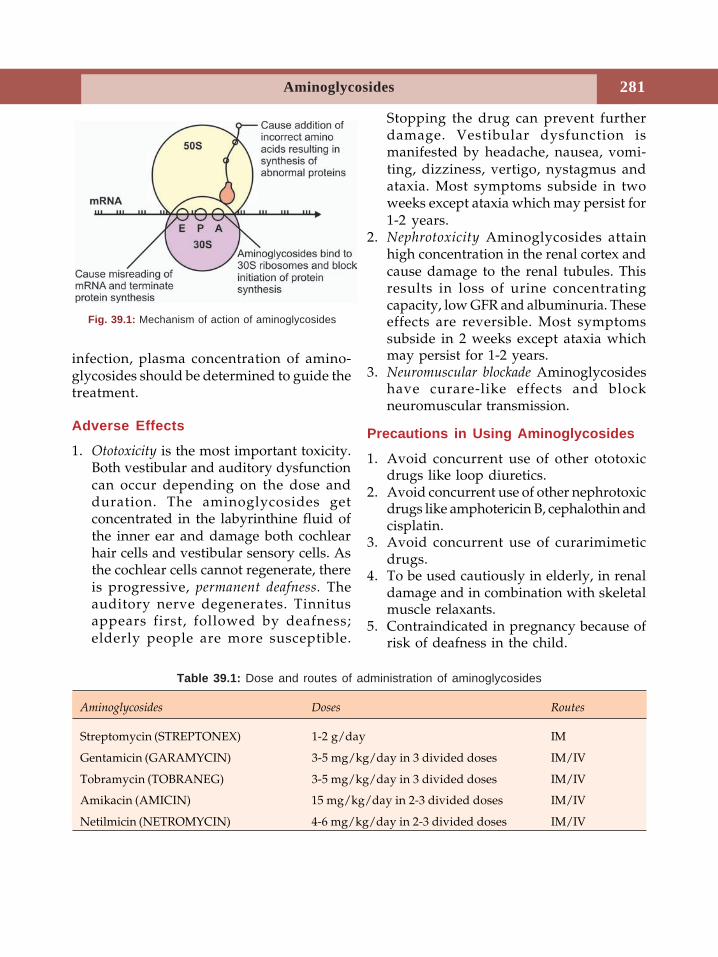
Aminoglycosides 281
infection, plasma concentration of amino-glycosides should be determined to guide thetreatment.
Adverse Effects
1. Ototoxicity is the most important toxicity.Both vestibular and auditory dysfunctioncan occur depending on the dose andduration. The aminoglycosides getconcentrated in the labyrinthine fluid ofthe inner ear and damage both cochlearhair cells and vestibular sensory cells. Asthe cochlear cells cannot regenerate, thereis progressive, permanent deafness. Theauditory nerve degenerates. Tinnitusappears first, followed by deafness;elderly people are more susceptible.
Stopping the drug can prevent furtherdamage. Vestibular dysfunction ismanifested by headache, nausea, vomi-ting, dizziness, vertigo, nystagmus andataxia. Most symptoms subside in twoweeks except ataxia which may persist for1-2 years.
2. Nephrotoxicity Aminoglycosides attainhigh concentration in the renal cortex andcause damage to the renal tubules. Thisresults in loss of urine concentratingcapacity, low GFR and albuminuria. Theseeffects are reversible. Most symptomssubside in 2 weeks except ataxia whichmay persist for 1-2 years.
3. Neuromuscular blockade Aminoglycosideshave curare-like effects and blockneuromuscular transmission.
Precautions in Using Aminoglycosides
1. Avoid concurrent use of other ototoxicdrugs like loop diuretics.
2. Avoid concurrent use of other nephrotoxicdrugs like amphotericin B, cephalothin andcisplatin.
3. Avoid concurrent use of curarimimeticdrugs.
4. To be used cautiously in elderly, in renaldamage and in combination with skeletalmuscle relaxants.
5. Contraindicated in pregnancy because ofrisk of deafness in the child.
Fig. 39.1: Mechanism of action of aminoglycosides
Aminoglycosides Doses Routes
Streptomycin (STREPTONEX) 1-2 g/day IM
Gentamicin (GARAMYCIN) 3-5 mg/kg/day in 3 divided doses IM/IV
Tobramycin (TOBRANEG) 3-5 mg/kg/day in 3 divided doses IM/IV
Amikacin (AMICIN) 15 mg/kg/day in 2-3 divided doses IM/IV
Netilmicin (NETROMYCIN) 4-6 mg/kg/day in 2-3 divided doses IM/IV
Table 39.1: Dose and routes of administration of aminoglycosides
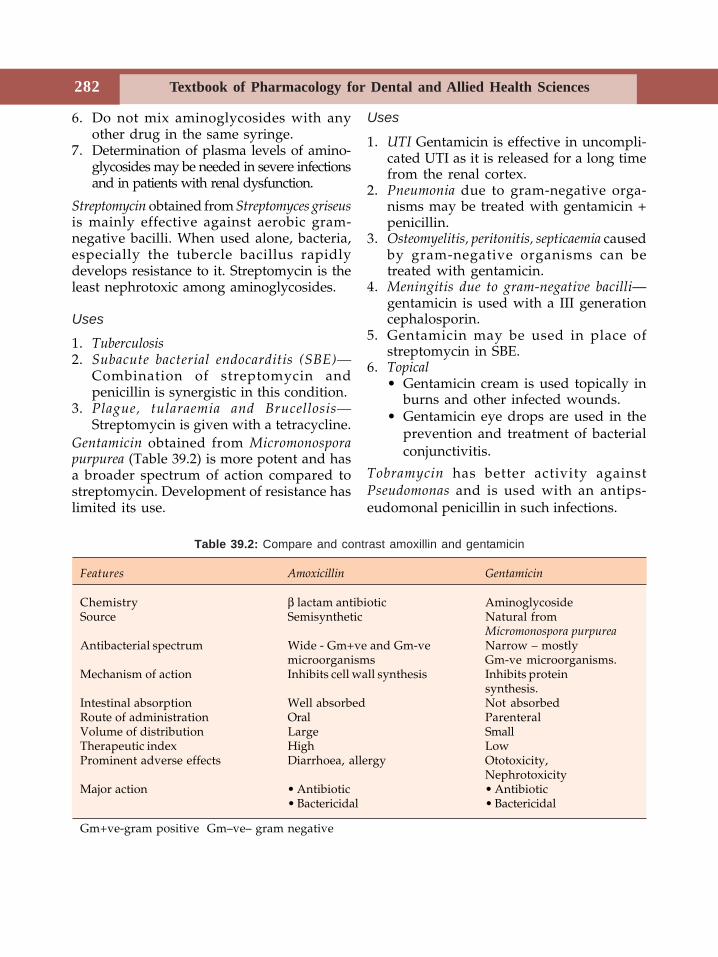
Textbook of Pharmacology for Dental and Allied Health Sciences282
6. Do not mix aminoglycosides with anyother drug in the same syringe.
7. Determination of plasma levels of amino-glycosides may be needed in severe infectionsand in patients with renal dysfunction.
Streptomycin obtained from Streptomyces griseusis mainly effective against aerobic gram-negative bacilli. When used alone, bacteria,especially the tubercle bacillus rapidlydevelops resistance to it. Streptomycin is theleast nephrotoxic among aminoglycosides.
Uses
1. Tuberculosis2. Subacute bacterial endocarditis (SBE)—
Combination of streptomycin andpenicillin is synergistic in this condition.
3. Plague, tularaemia and Brucellosis—Streptomycin is given with a tetracycline.
Gentamicin obtained from Micromonosporapurpurea (Table 39.2) is more potent and hasa broader spectrum of action compared tostreptomycin. Development of resistance haslimited its use.
Uses
1. UTI Gentamicin is effective in uncompli-cated UTI as it is released for a long timefrom the renal cortex.
2. Pneumonia due to gram-negative orga-nisms may be treated with gentamicin +penicillin.
3. Osteomyelitis, peritonitis, septicaemia causedby gram-negative organisms can betreated with gentamicin.
4. Meningitis due to gram-negative bacilli—gentamicin is used with a III generationcephalosporin.
5. Gentamicin may be used in place ofstreptomycin in SBE.
6. Topical• Gentamicin cream is used topically in
burns and other infected wounds.• Gentamicin eye drops are used in the
prevention and treatment of bacterialconjunctivitis.
Tobramycin has better activity againstPseudomonas and is used with an antips-eudomonal penicillin in such infections.
Features Amoxicillin Gentamicin
Chemistry β lactam antibiotic AminoglycosideSource Semisynthetic Natural from
Micromonospora purpureaAntibacterial spectrum Wide - Gm+ve and Gm-ve Narrow – mostly
microorganisms Gm-ve microorganisms.Mechanism of action Inhibits cell wall synthesis Inhibits protein
synthesis.Intestinal absorption Well absorbed Not absorbedRoute of administration Oral ParenteralVolume of distribution Large SmallTherapeutic index High LowProminent adverse effects Diarrhoea, allergy Ototoxicity,
NephrotoxicityMajor action • Antibiotic • Antibiotic
• Bactericidal • Bactericidal
Gm+ve-gram positive Gm–ve– gram negative
Table 39.2: Compare and contrast amoxillin and gentamicin
Aminoglycosides 283
Neomycin has a wide antibacterial spectrum.As it is highly ototoxic, it is not givensystemically. It is used topically asointments, creams and powder.Adverse effects Neomycin can causeskin rashes on topical use. Oral use cancause diarrhoea, steatorrhoea andmalabsorption due to damage to theintestinal villi. Superinfection with Candida
can also occur.
Uses
1. Neomycin is used topically in skininfections, burns, ulcers and wounds; eyeand ear infections.
2. Orally—neomycin is not absorbed whengiven orally. It is used to prepare thebowel for surgery, i.e. for preoperativegut sterilization.
3. Hepatic coma—ammonia produced bycolonic bacteria is absorbed andconverted to urea by the liver. In severehepatic failure, as liver is unable tohandle this NH3, blood NH3 levels riseresulting in encephalopathy. Asneomycin inhibits intestinal flora, NH3
production falls. Neomycin is givenorally for this purpose.
Antibiotics that inhibit protein synthesis bind to
ribosomes
50S 30S
Erythromycin TetracyclinesChloramphenicol AminoglycosidesClindamycinStreptograminsLinezolid
Kanamycin Due to its toxicity, its use islimited to multi-drug resistant tuberculosis.Amikacin has widest antibacterial spectrumamong the aminoglycosides. It is resistantto aminoglycoside inactivating enzymes.
Uses
1. Nosocomial infections due to gram-negative organisms
2. Tuberculosis—Amikacin is useful inmultidrug resistant tuberculosis incombination with other drugs. It is alsoused in infections due to atypicalmycobacteria in patients with AIDS.
Netilmicin Like amikacin, netilmicin isresistant to aminoglycoside inactivatingenzymes. It is used in serious infections dueto gram-negative bacilli.Sisomicin has actions, toxicity and usessimilar to gentamicin.
Textbook of Pharmacology for Dental and Allied Health Sciences284
40 Macrolides, OtherAntibacterial Agents
and Chemotherapy ofUrinary Tract Infections
Macrolides are antibiotics with a macrocycliclactone ring to which sugars are attached.Erythomycin and its semisynthetic deri-vatives roxithromycin, clarithromycin andazithromycin are macrolides.
ERYTHROMYCIN
Erythromycin is obtained from Streptomyceserythreus.Antibacterial spectrum Erythromycin has anarrow spectrum and is effective againstaerobic gram-positive bacteria and a fewgram-negative organisms.
Streptococci, pneumococci, staphylococci,gonococci, C. diphtheriae, C. jejuni, Mycoplasma,Chlamydiae and some atypical mycobacteriaare sensitive.
Mechanism of Action
Erythromycin is bacteriostatic at low andcidal at high concentrations. It binds to 50Sribosomes (Fig. 40.1) and inhibits bacterialprotein synthesis. Chloramphenicol andclindamycin also bind to 50 S ribosomesand the three may inhibit each othersactivity. Hence the combination should beavoided.
Resistance Resistance to macrolides is acquiredthrough plasmids. The mechanism involvedmay be:• Low permeability of the bacteria to the
antibiotic• Production of inactivating enzymes• Low affinity of ribosomes to macrolides.Pharmacokinetics Erythromycin is destroyedby gastric acid and is therefore given asenteric coated tablets. Good concentration isattained in most fluids except brain and CSF.It is mainly excreted through bile; doseadjustment is not needed in renal failure. Fordose and duration of treatment withmacrolide antibiotics see Table 40.1.
Adverse Effects
1. Hepatitis with cholestatic jaundice startsafter 2-3 weeks of treatment and is morecommon with the estolate salt. Thesymptoms—nausea, vomiting and abdo-minal cramps, mimic acute cholecystitisand may be wrongly treated. These arefollowed by jaundice and fever. It maybe an allergic response to the estolate salt.The patient recovers on stopping the drug.
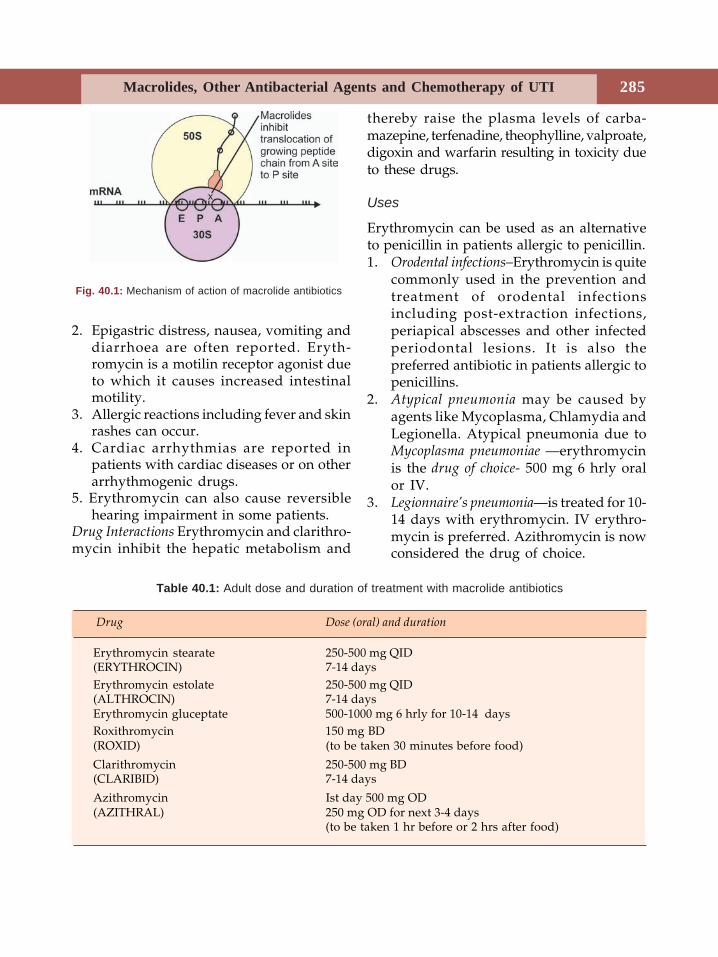
Macrolides, Other Antibacterial Agents and Chemotherapy of UTI 285
2. Epigastric distress, nausea, vomiting anddiarrhoea are often reported. Eryth-romycin is a motilin receptor agonist dueto which it causes increased intestinalmotility.
3. Allergic reactions including fever and skinrashes can occur.
4. Cardiac arrhythmias are reported inpatients with cardiac diseases or on otherarrhythmogenic drugs.
5. Erythromycin can also cause reversiblehearing impairment in some patients.
Drug Interactions Erythromycin and clarithro-mycin inhibit the hepatic metabolism and
thereby raise the plasma levels of carba-mazepine, terfenadine, theophylline, valproate,digoxin and warfarin resulting in toxicity dueto these drugs.
Uses
Erythromycin can be used as an alternativeto penicillin in patients allergic to penicillin.1. Orodental infections–Erythromycin is quite
commonly used in the prevention andtreatment of orodental infectionsincluding post-extraction infections,periapical abscesses and other infectedperiodontal lesions. It is also thepreferred antibiotic in patients allergic topenicillins.
2. Atypical pneumonia may be caused byagents like Mycoplasma, Chlamydia andLegionella. Atypical pneumonia due toMycoplasma pneumoniae —erythromycinis the drug of choice- 500 mg 6 hrly oralor IV.
3. Legionnaire’s pneumonia—is treated for 10-14 days with erythromycin. IV erythro-mycin is preferred. Azithromycin is nowconsidered the drug of choice.
Fig. 40.1: Mechanism of action of macrolide antibiotics
Table 40.1: Adult dose and duration of treatment with macrolide antibiotics
Drug Dose (oral) and duration
Erythromycin stearate 250-500 mg QID(ERYTHROCIN) 7-14 daysErythromycin estolate 250-500 mg QID(ALTHROCIN) 7-14 daysErythromycin gluceptate 500-1000 mg 6 hrly for 10-14 daysRoxithromycin 150 mg BD(ROXID) (to be taken 30 minutes before food)
Clarithromycin 250-500 mg BD(CLARIBID) 7-14 days
Azithromycin Ist day 500 mg OD(AZITHRAL) 250 mg OD for next 3-4 days
(to be taken 1 hr before or 2 hrs after food)
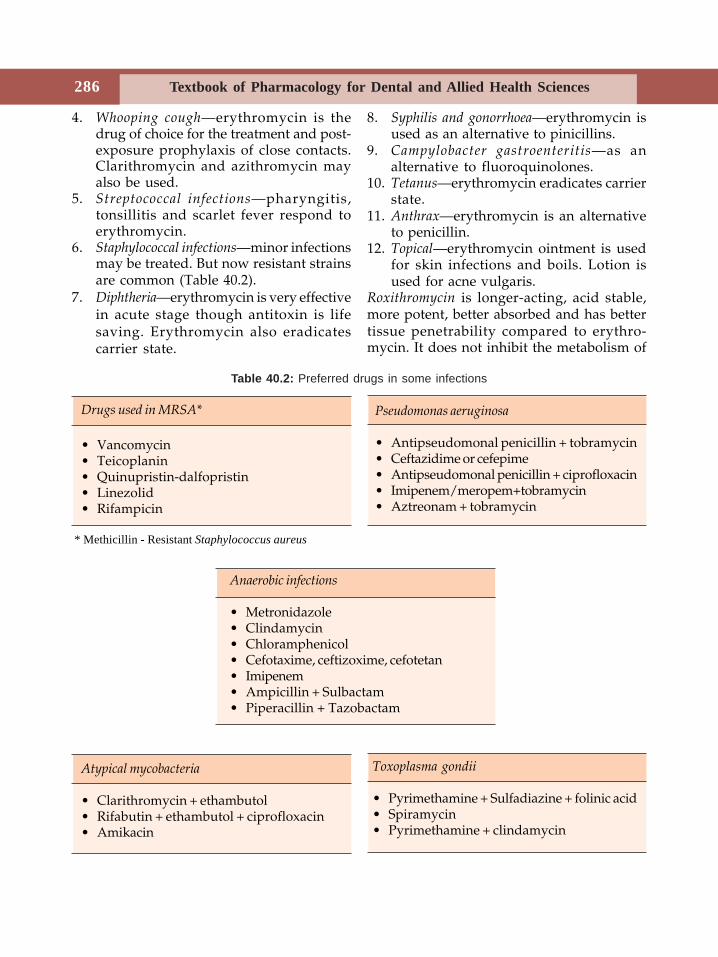
Textbook of Pharmacology for Dental and Allied Health Sciences286
4. Whooping cough—erythromycin is thedrug of choice for the treatment and post-exposure prophylaxis of close contacts.Clarithromycin and azithromycin mayalso be used.
5. Streptococcal infections—pharyngitis,tonsillitis and scarlet fever respond toerythromycin.
6. Staphylococcal infections—minor infectionsmay be treated. But now resistant strainsare common (Table 40.2).
7. Diphtheria—erythromycin is very effectivein acute stage though antitoxin is lifesaving. Erythromycin also eradicatescarrier state.
8. Syphilis and gonorrhoea—erythromycin isused as an alternative to pinicillins.
9. Campylobacter gastroenteritis—as analternative to fluoroquinolones.
10. Tetanus—erythromycin eradicates carrierstate.
11. Anthrax—erythromycin is an alternativeto penicillin.
12. Topical—erythromycin ointment is usedfor skin infections and boils. Lotion isused for acne vulgaris.
Roxithromycin is longer-acting, acid stable,more potent, better absorbed and has bettertissue penetrability compared to erythro-mycin. It does not inhibit the metabolism of
Pseudomonas aeruginosa
• Antipseudomonal penicillin + tobramycin• Ceftazidime or cefepime• Antipseudomonal penicillin + ciprofloxacin• Imipenem/meropem+tobramycin• Aztreonam + tobramycin
* Methicillin - Resistant Staphylococcus aureus
Drugs used in MRSA*
• Vancomycin• Teicoplanin• Quinupristin-dalfopristin• Linezolid• Rifampicin
Atypical mycobacteria
• Clarithromycin + ethambutol• Rifabutin + ethambutol + ciprofloxacin• Amikacin
Toxoplasma gondii
• Pyrimethamine + Sulfadiazine + folinic acid• Spiramycin• Pyrimethamine + clindamycin
Table 40.2: Preferred drugs in some infections
Anaerobic infections
• Metronidazole• Clindamycin• Chloramphenicol• Cefotaxime, ceftizoxime, cefotetan• Imipenem• Ampicillin + Sulbactam• Piperacillin + Tazobactam
Macrolides, Other Antibacterial Agents and Chemotherapy of UTI 287
other drugs—hence drug interactions areavoided. It should be taken 30 min beforefood.
It can be used as an alternative toerythromycin but is more expensive.Roxithromycin is quite a popular antibioticbecause of its advantages over erythromycin.It is used in orodental infections apart fromother indications of erythromycin.Clarithromycin Compared to erythromycin,clarithromycin is longer-acting, acid stableand better absorbed; it is more effectiveagainst atypical mycobacteria, H. pylori andsome protozoa. Clarithromycin is structurallysimilar to erythromycin and therefore itsdrug interactions are also similar toerythromycin.Clarithromycin is used:1. As a component of triple regimen for H.
pylori infections in peptic ulcer patients.2. Atypical mycobacterial infections.
Though clarithromycin is effective in otherindications of erythromycin, its higher costmakes it less preferable.Azithromycin an azalide, is a derivative oferythromycin with activity similar toclarithromycin. It is acid stable, rapidlyabsorbed, has better tissue penetrability, islonger acting and better tolerated thanerythromycin. It is given as a single loadingdose of 500 mg followed by 250 mg for thenext 4 days. Azithromycin is free of druginteractions as it does not suppress hepaticmetabolism of other drugs.
It is used in the prophylaxis and treatmentof atypical mycobacterial infections in AIDSpatients. Like erythromycin it can also beused in respiratory, genital and skininfections and in pneumonias.
KETOLIDES are modified macrolides thatare similar to newer macrolides except thatthey are effective against macrolide - resistantpneumococci. Telithromycin is a ketolide.
MISCELLANEOUS ANTIBIOTICS
Spectinomycin is related to aminoglycosidesand is effective against gram-negativebacteria. It is used only in gonorrhoea (2 gmIM) in patients allergic to penicillin andquinolones.
Lincosamides
Lincomycin and clindamycin are (Table 40.3)lincosamides. Lincomycin is no longer usedclinically.Clindamycin is a congener of lincomycin. Itbinds to 50S ribosomal subunit andsuppresses protein synthesis. Streptococci,staphylococci, pneumococci and manyanaerobes are inhibited by clindamycin.Clindamycin is well-absorbed on oraladministration. It attains good concentrationin the bone and many other tissues. It ismetabolised in the liver.Adverse effects include diarrhoea due topseudomembranous colitis, skin rashes andneuromuscular blockade. Intravenous use cancause thrombophlebitis.Uses Anaerobic infections—abdominal, pelvic,bone and joints infections due to anaerobesare treated with clindamycin. It may becombined with an aminoglycoside or acephalosporin.
Clindamycin is also useful in Pneumocystiscarinii pneumonia and toxoplasmosis in AIDSpatients.
GLYCOPEPTIDES
Vancomycin and teicoplanin are glycopeptides.(Table 40.2) Vancomycin produced byStreptococcus orientalis is active against gram-positive bacteria particularly staphylococciincluding those resistant to methicillin. It actsby inhibiting cell wall synthesis and isbactericidal. Vancomycin is not absorbedorally—given IV. It is widely distributed andexcreted through kidneys.
Textbook of Pharmacology for Dental and Allied Health Sciences288
Adverse effects are skin rashes, pain at the siteof injection, thrombophlebitis, ototoxicity andnephrotoxicity. Concurrent use of otherototoxic and nephrotoxic drugs should beavoided; dose should be adjusted in renaldysfunction.
Uses
1. Pseudomembranous colitis—oral vanco-mycin is used.
2. Methicillin resistant staphylococci—vancomycin is given IV for seriousinfections like osteomyelitis, endocarditisand soft-tissue abscesses.
3. Enterococcal endocarditis—as an alter-native to penicillin.
4. Penicillin resistant pneumococcal in-fections—vancomycin is recommendedwith a cephalosporin.
Teicoplanin has mechanism of action andantibacterial spectrum similar to vancomycin,but teicoplanin can be safely given intra-muscularly. It is also less toxic. Occasionallycauses allergic reactions. It is used inosteomyelitis and endocarditis due tomethicillin resistant staphylococci andenterococci. TARGOCID 200-400 mg/day.
POLYPEPTIDE ANTIBIOTICS
Polymyxin and Colistin are too toxic to be givensystemically. They are used topically.Polymyxin obtained from Bacillus polymyxa
and colistin from Bacillus colistinus areeffective against gram-negative bacteria.Mechanism of action Polymyxin and colistinalter the permeability of the cell membraneresulting in leakage of the cell contents. Theyare bactericidal.
Polypeptide antibiotics are not absorbedorally; applied topically, they may rarelycause skin rashes.
Uses
1. Used topically for skin infections, ear andeye infections.
2. Oral colistin is used in children fordiarrhoea due to gram-negative bacilli.
OTHER ANTIMICROBIAL AGENTS
Bacitracin produced by Bacillus subtilis iseffective against gram-positive bacteria. Itinhibits the cell wall synthesis and isbactericidal. It is too toxic to be givensystemically, not absorbed orally and istherefore used only for topical application—in skin infections, surgical wounds, ulcers andocular infections (NEOSPORIN powder isbacitracin + neomycin).Sodium Fusidate (Fusidic acid) obtained fromFusidium coccineum is effective against gram-positive organisms particularly staphylococci.It is bactericidal. It is mainly used topicallyas a 2% ointment (FUCIDIN). It may be givenorally for resistant staphylococcal infections.Mupirocin or pseudomonic acid is obtainedfrom Pseudomonas fluorescens. It is bactericidalagainst gram-positive and some gram-negative organisms including methicillinresistant Staphylococcus aureus. Mupirocin actsby inhibiting the enzyme tRNA synthetase.It is used as a 2% ointment (BACTROBAN)for minor skin infections particularly due tostaphylococci and streptococci. It is also usedintranasally as spray to eradicate stap-hylococcal carrier state.Fosfomycin is an analog of phosphoenolpyruvate. Fosfomycin is effective against bothgram-positive and gram-negative organisms.It acts by inhibiting the enzyme endo-pyruvate transferase. This enzyme is requiredfor the first step in bacterial cell wallsynthesis. Thus it inhibits bacterial cell wallsynthesis. The salt used is fosfomycintetrametol which is available for both oral
Macrolides, Other Antibacterial Agents and Chemotherapy of UTI 289
and parenteral use. It is excreted by thekidneys and attains high concentration in theurine. Fosfomycin is approved for use inuncomplicated lower UTI in women - single3G dose is effective.Cycloserine obtained from Streptomycesorchidaceus inhibits many gram-positive andgram-negative organisms includingM. tuberculosis. It acts by inhibiting proteinsynthesis and is used as a second line drugin tuberculosis (see page 294).
Newer Agents
Streptogramins quinupristin and dalfopristinare obtained from Streptomyces pristinaspiralis.A combination of quinupristin and dalfopristinin the ratio 30:70 is bactericidal against gram-positive cocci including methicillin-resistantstaphylococci.Mechanism of action Streptogramins bind to50S ribosomal subunit and inhibit proteinsynthesis.
Given intravenously, streptogramins arerapidly metabolised and excreted largelythrough faeces. Hence adjustment of dose isnot required in renal insufficiency. Adverseeffects include arthralgia, myalgia, nausea,vomiting, diarrhoea and pain at the site ofinjection. The combination is usedintravenously in the treatment of infectionsdue to streptococci, methicillin-resistantstaphylococci and enterococci. Strepto-gramins are not effective orally as they arerapidly metabolised in the liver - undergoextensive first pass metabolism.
Oxazolidinones
Linezolid is an oxazolidinone effectiveagainst gram-positive bacteria includingmethicillin resistant staphylococci andgram-positive anaerobic organisms. It actsby inhibiting protein synthesis on bindingto 50S ribosomes. Adverse effects include
nausea, diarrhoea, dizziness and throm-bocytopenia. It can be given orally or IV.Linezolid is useful in the treatment ofnosocomial infections resistant to otherdrugs.
Nitroimidazoles
Nitroimidazoles include metronidazole,tinidazole, secnidazole, ornidazole andsatranidazole. They are very effective in thetreatment of anaerobic microorganisms apartfrom amoebiasis. They are discussed underantiamoebic drugs (see page 321).
CHEMOTHERAPY OF URINARY TRACTINFECTION
Infection of the urinary tract is quite commonand may be acute or chronic. Urinaryantiseptics are drugs which exert antibacterialactivity only in the urinary tract (and nosystemic activity). They include nitro-furantoin and methenamine mandelate.Nitrofurantoin is bacteriostatic, but at higherconcentrations it may be bactericidal. It is asynthetic compound, effective against manygram-positive and gram-negative bacteria.Mechanism of action is not known.It israpidly and completely absorbed from thegut. It attains high concentration in urine andis used in acute UTI, long-term suppressionof chronic UTI (single dose 100 mg at bedtime) and for prophylaxis of UTI. It may causenausea,vomiting, diarrhoea and allergicreactions. Development of resistance is rare.Dose 50 - 100 mg 6 hrly (FURADANTIN).Methenamine mandelate—a salt of mandelicacid and methenamine, releases formal-dehyde in acidic urine below pH 5.5.Formaldehyde is bactericidal and resistancedoes not develop to it.High doses can cause nausea, epigastricdistress, haematuria and painful micturition.
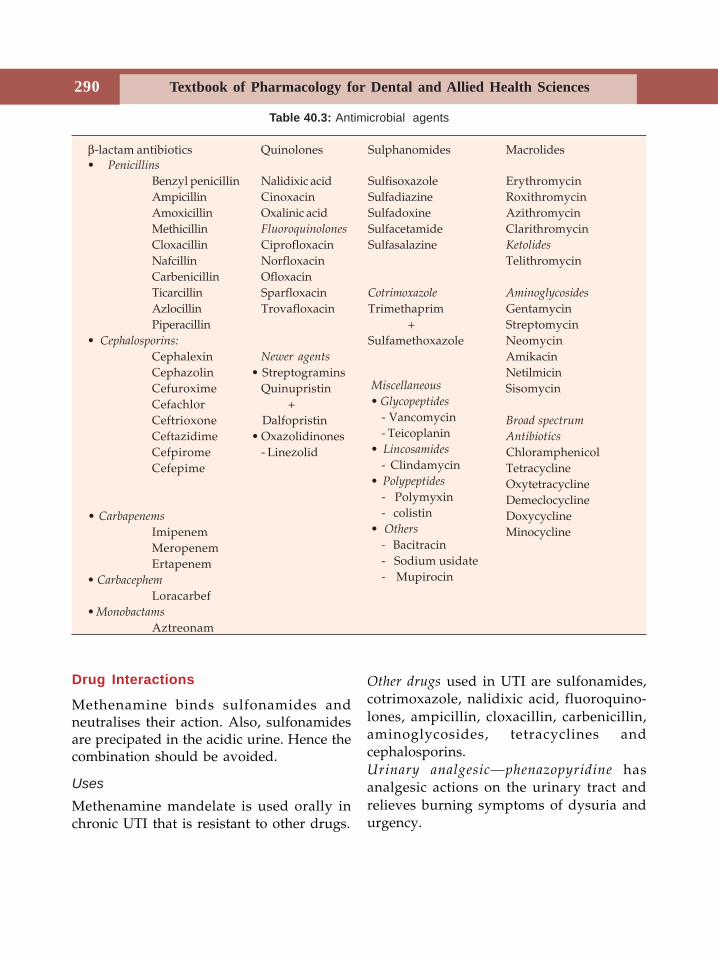
Textbook of Pharmacology for Dental and Allied Health Sciences290
β-lactam antibiotics Quinolones Sulphanomides Macrolides• Penicillins
Benzyl penicillin Nalidixic acid Sulfisoxazole ErythromycinAmpicillin Cinoxacin Sulfadiazine RoxithromycinAmoxicillin Oxalinic acid Sulfadoxine AzithromycinMethicillin Fluoroquinolones Sulfacetamide ClarithromycinCloxacillin Ciprofloxacin Sulfasalazine Ketolides
Nafcillin Norfloxacin TelithromycinCarbenicillin OfloxacinTicarcillin Sparfloxacin Cotrimoxazole Aminoglycosides
Azlocillin Trovafloxacin Trimethaprim GentamycinPiperacillin + Streptomycin
• Cephalosporins: Sulfamethoxazole NeomycinCephalexin Newer agents AmikacinCephazolin • Streptogramins NetilmicinCefuroxime Quinupristin SisomycinCefachlor +Ceftrioxone Dalfopristin Broad spectrum
Ceftazidime • Oxazolidinones Antibiotics
Cefpirome - Linezolid ChloramphenicolCefepime Tetracycline
OxytetracyclineDemeclocycline
• Carbapenems DoxycyclineImipenem MinocyclineMeropenemErtapenem
• Carbacephem
Loracarbef• Monobactams
Aztreonam
Miscellaneous
• Glycopeptides
- Vancomycin- Teicoplanin
• Lincosamides
- Clindamycin• Polypeptides
- Polymyxin- colistin
• Others
- Bacitracin- Sodium usidate- Mupirocin
Drug Interactions
Methenamine binds sulfonamides andneutralises their action. Also, sulfonamidesare precipated in the acidic urine. Hence thecombination should be avoided.
UsesMethenamine mandelate is used orally inchronic UTI that is resistant to other drugs.
Other drugs used in UTI are sulfonamides,cotrimoxazole, nalidixic acid, fluoroquino-lones, ampicillin, cloxacillin, carbenicillin,aminoglycosides, tetracyclines andcephalosporins.Urinary analgesic—phenazopyridine hasanalgesic actions on the urinary tract andrelieves burning symptoms of dysuria andurgency.
Table 40.3: Antimicrobial agents
41 Chemotherapy ofTuberculosis and
Leprosy
Tuberculosis is a chronic granulomatousdisease caused by Mycobacterium tuberculosis.In developing countries, it is a major publichealth problem; 5 lakh people die in Indiaevery year due to this disease. After thespread of AIDS, the problem has becomemore complex, as tuberculosis andMycobacterium avium complex (MAC)infections are more common and rapidlyprogress in these patients.
Drugs Used in Tuberculosis
• First line drugs Isoniazid, rifampicin,pyrazinamide, ethambutol, streptomycin.
• Second line drugs Ethionamide, thia-cetazone, para aminosalicylic acid (PAS),amikacin, ciprofloxacin, capreomycin,cycloserine, rifabutin, kanamycin.
Based on antitubercular activity, drugs maybe grouped as:• Tuberculocidal agents–Isoniazid, rifam-
picin, streptomycin, pyrazinamide,capreomycin, kanamycin, ciprofloxacin.
• Tuberculostatic agents–Ethambutol, ethio-namide, thiacetazone, cycloserine PAS.
First Line Drugs
IsoniazidIsoniazid (INH) is the most effective andcheapest primary antitubercular drug. It is
tuberculocidal for rapidly multiplying bacillibut static for resting bacilli. INH destroys:(i) intracellular bacilli as it penetrates into
the cells, i.e. tubercle bacilli inmacrophages, and
(ii) bacilli multiplying in the walls of thecavities. Thus it is effective against bothintra and extracellular organisms(Fig. 41.1, Table 41.2). If used alone,mycobacteria develop resistance to it.Hence it should be used in combinationwith other drugs.
Mechanism of action INH inhibits the synthesisof mycolic acids which are the importantcomponents of the mycobacterial cell wall.
INH enters the mycobacteria where it isconverted to an active metabolite. Thismetabolitie binds the enzymes necessary formycolic acid synthesis. Thus the synthesis ofmycolic acid is inhibited.
Pharmacokinetics INH is completely absorbedorally, penetrates all tissues, tubercularcavities, necrotic tissues and CSF. It ismetabolised by acetylation. Patients can befast or slow acetylators depending on thegenetic inheritance - slow acetylators respondbetter. The t½ in slow acetylators is 3-5 hourswhile in fast acetylators it is 1 hour. Peripheralneuropathy is more common in slowacetylators while hepatotoxicity is morelikely in fast acetylators. Metabolites of INHare excreted in urine.
Section 11Chemotherapy II
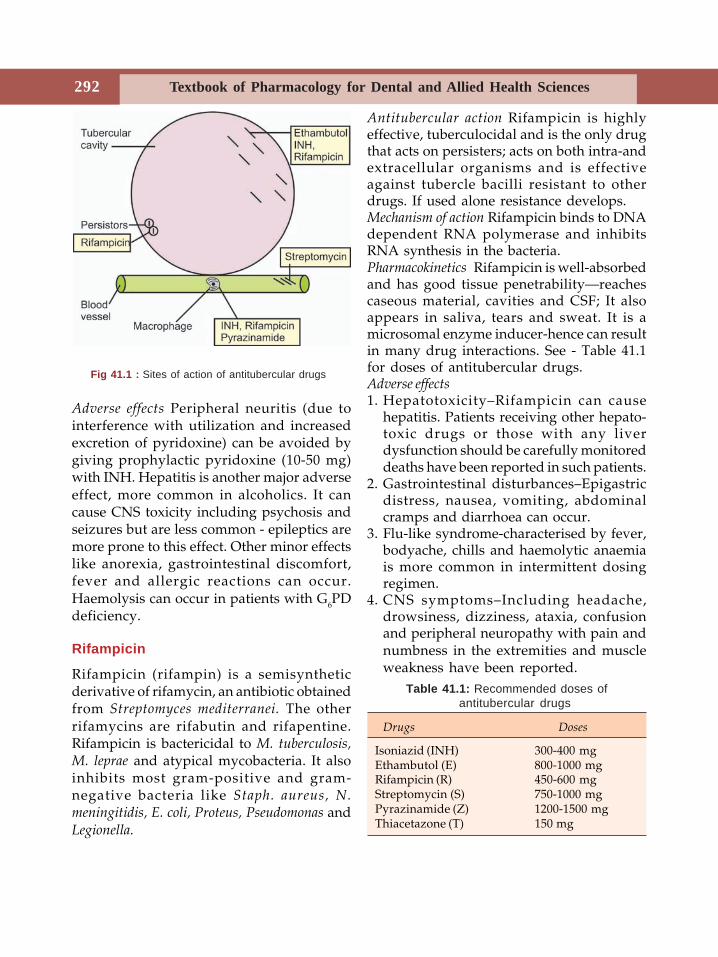
Textbook of Pharmacology for Dental and Allied Health Sciences292
Adverse effects Peripheral neuritis (due tointerference with utilization and increasedexcretion of pyridoxine) can be avoided bygiving prophylactic pyridoxine (10-50 mg)with INH. Hepatitis is another major adverseeffect, more common in alcoholics. It cancause CNS toxicity including psychosis andseizures but are less common - epileptics aremore prone to this effect. Other minor effectslike anorexia, gastrointestinal discomfort,fever and allergic reactions can occur.Haemolysis can occur in patients with G6PDdeficiency.
Rifampicin
Rifampicin (rifampin) is a semisyntheticderivative of rifamycin, an antibiotic obtainedfrom Streptomyces mediterranei. The otherrifamycins are rifabutin and rifapentine.Rifampicin is bactericidal to M. tuberculosis,M. leprae and atypical mycobacteria. It alsoinhibits most gram-positive and gram-negative bacteria like Staph. aureus, N.meningitidis, E. coli, Proteus, Pseudomonas andLegionella.
Antitubercular action Rifampicin is highlyeffective, tuberculocidal and is the only drugthat acts on persisters; acts on both intra-andextracellular organisms and is effectiveagainst tubercle bacilli resistant to otherdrugs. If used alone resistance develops.Mechanism of action Rifampicin binds to DNAdependent RNA polymerase and inhibitsRNA synthesis in the bacteria.Pharmacokinetics Rifampicin is well-absorbedand has good tissue penetrability—reachescaseous material, cavities and CSF; It alsoappears in saliva, tears and sweat. It is amicrosomal enzyme inducer-hence can resultin many drug interactions. See - Table 41.1for doses of antitubercular drugs.Adverse effects1. Hepatotoxicity–Rifampicin can cause
hepatitis. Patients receiving other hepato-toxic drugs or those with any liverdysfunction should be carefully monitoreddeaths have been reported in such patients.
2. Gastrointestinal disturbances–Epigastricdistress, nausea, vomiting, abdominalcramps and diarrhoea can occur.
3. Flu-like syndrome-characterised by fever,bodyache, chills and haemolytic anaemiais more common in intermittent dosingregimen.
4. CNS symptoms–Including headache,drowsiness, dizziness, ataxia, confusionand peripheral neuropathy with pain andnumbness in the extremities and muscleweakness have been reported.
Fig 41.1 : Sites of action of antitubercular drugs
Table 41.1: Recommended doses ofantitubercular drugs
Drugs Doses
Isoniazid (INH) 300-400 mgEthambutol (E) 800-1000 mgRifampicin (R) 450-600 mgStreptomycin (S) 750-1000 mgPyrazinamide (Z) 1200-1500 mgThiacetazone (T) 150 mg
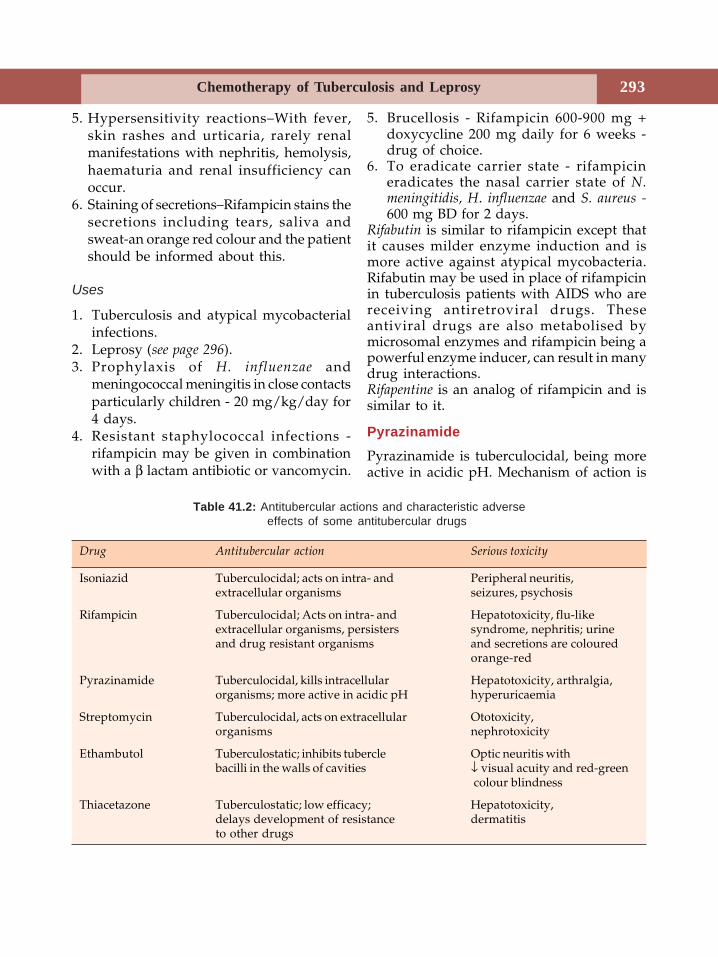
Chemotherapy of Tuberculosis and Leprosy 293
5. Hypersensitivity reactions–With fever,skin rashes and urticaria, rarely renalmanifestations with nephritis, hemolysis,haematuria and renal insufficiency canoccur.
6. Staining of secretions–Rifampicin stains thesecretions including tears, saliva andsweat-an orange red colour and the patientshould be informed about this.
Uses
1. Tuberculosis and atypical mycobacterialinfections.
2. Leprosy (see page 296).3. Prophylaxis of H. influenzae and
meningococcal meningitis in close contactsparticularly children - 20 mg/kg/day for4 days.
4. Resistant staphylococcal infections -rifampicin may be given in combinationwith a β lactam antibiotic or vancomycin.
5. Brucellosis - Rifampicin 600-900 mg +doxycycline 200 mg daily for 6 weeks -drug of choice.
6. To eradicate carrier state - rifampicineradicates the nasal carrier state of N.meningitidis, H. influenzae and S. aureus -600 mg BD for 2 days.
Rifabutin is similar to rifampicin except thatit causes milder enzyme induction and ismore active against atypical mycobacteria.Rifabutin may be used in place of rifampicinin tuberculosis patients with AIDS who arereceiving antiretroviral drugs. Theseantiviral drugs are also metabolised bymicrosomal enzymes and rifampicin being apowerful enzyme inducer, can result in manydrug interactions.Rifapentine is an analog of rifampicin and issimilar to it.
PyrazinamidePyrazinamide is tuberculocidal, being moreactive in acidic pH. Mechanism of action is
Table 41.2: Antitubercular actions and characteristic adverseeffects of some antitubercular drugs
Drug Antitubercular action Serious toxicity
Isoniazid Tuberculocidal; acts on intra- and Peripheral neuritis,extracellular organisms seizures, psychosis
Rifampicin Tuberculocidal; Acts on intra- and Hepatotoxicity, flu-likeextracellular organisms, persisters syndrome, nephritis; urineand drug resistant organisms and secretions are coloured
orange-red
Pyrazinamide Tuberculocidal, kills intracellular Hepatotoxicity, arthralgia,organisms; more active in acidic pH hyperuricaemia
Streptomycin Tuberculocidal, acts on extracellular Ototoxicity,organisms nephrotoxicity
Ethambutol Tuberculostatic; inhibits tubercle Optic neuritis withbacilli in the walls of cavities ↓ visual acuity and red-green
colour blindness
Thiacetazone Tuberculostatic; low efficacy; Hepatotoxicity,delays development of resistance dermatitisto other drugs
Textbook of Pharmacology for Dental and Allied Health Sciences294
not known. It is effective against intracellularbacilli. If used alone resistance develops. Itis well-absorbed (achieves good con-centration in CSF). Hepatotoxicity is the mostcommon adverse effect. Hyperuricaemia(due to ↓ excretion of uric acid may result ingouty arthritis), arthralgia, anorexia, vomit-ing and rashes may be seen.
Streptomycin
Streptomycin (page 282) is tuberculocidal,acts only against extracellular organisms dueto poor penetrating power. It has to be givenIM. When used alone resistance develops.Because of these disadvantages and itstoxicity (ototoxicity and nephrotoxicity),streptomycin is the least preferred of the firstline drugs.
Second Line Drugs
Ethambutol is tuberculostatic and acts on fastmultiplying bacilli in the cavities. It is alsoeffective against atypical mycobacteria. Itinhibits the incorporation of mycolic acidsinto the mycobacterial cell wall.
Optic neuritis resulting in ↓ visual acuityand inability to differentiate red from greenis an important adverse effect which needswithdrawal of the drug. Colour vision shouldbe monitored during treatment. Ethambutolis to be avoided in children because theirability to differentiate red from green cannotbe reliably tested. Other adverse effectsinclude nausea, anorexia, headache, fever andallergic reactions.Thiacetazone is tuberculostatic with lowefficacy; it delays the development ofresistance to other drugs and its low costmakes it a suitable drug in combinationregimens. Hepatotoxicity, dermatitis, allergicreactions and GI side effects may occur.
Ethionamide This tuberculostatic drug iseffective against both intra- and extracellular
organisms. It is also effective in atypicalmycobacteria.
Anorexia, nausea, vomiting and metallictaste in the mouth are the most commonadverse effects. It can also cause hepatitis,skin rashes and peripheral neuritis (needsprophylactic pyridoxine).
Ethionamide is a secondary agent usedonly when primary drugs are ineffective.
Para-aminosalicylic acid (PAS) related tosulfonamides is tuberculostatic. Gastro-intestinal effects like nausea, anorexia,epigastric pain and diarrhoea make it apoorly tolerated drug. Allergic reactions andhepatitis are also seen. It is rarely used.
Other Second Line Drugs
Amikacin, kanamycin and capreomycin aresecond line drugs that need parenteraladministration. They are ototoxic andnephrotoxic and are used only in resistantcases. Amikacin is also effective againstatypical mycobacteria.Cycloserine is an antibiotic that inhibits cell wallsynthesis, is tuberculostatic and is also effectiveagainst some gram-positive organisms. Itcauses CNS toxicity including headache,tremors, psychosis and sometimes seizures.It is used only in resistant tuberculosis.Fluoroquinolones Ciprofloxacin, ofloxacin andsparfloxacin inhibit tubercle bacilli andatypical mycobacteria. They are useful inmulti-drug resistant tuberculosis incombination with other drugs.
Treatment of Tuberculosis
Tuberculosis is one of the most difficultinfections to cure. The properties of themycobacteria like slow division, deve-lopment of resistance, ability to remain aspersisters for years and intracellular locationof the bacilli have enhanced the problem.

Chemotherapy of Tuberculosis and Leprosy 295
Moreover, the caseous material makes itdifficult for the drugs to reach. The need forlong-term treatment, drug toxicity, cost andthereby poor patient compliance have alladded to further complicate the problem. Butwith the availability of effective drugs, mostpatients can now be treated as outpatients.
The aim of treatment is to kill the dividingbacilli thus making the patient sputumnegative and to destroy the persisters inorder to prevent relapse and ensure completecure.A combination of drugs is used intuberculosis to -
1. delay the development of resistance2. reduce toxicity3. shorten the course of treatment.
Majority of cases are sensitive to first linedrugs. Initial treatment should be intensiveand include drugs that have maximum effect.Good patient compliance and cost of therapyshould also be considered.Chemotherapy is given in two phases-• First phase - initial, intensive phase of 1-3
months duration aimed at killing as manybacilli as possible.
• Second phase - continuation phase todestroy the dormant or persisters-duration 6-9 months.
Short-term Regimens
1. INH + R + Z + E/S daily for 2 monthsfollowed by INH + R daily for 4 months.
2. INH + R + Z daily for 2 months followedby INH + R daily for 7 months.
Advantages
Short-term therapy has rapid response, lowerfailure rates, lesser chances of resistance andbetter patient compliance.
Conventional Regimen
• INH + S + T daily for 2 months• INH + T daily for 10 months
Failure rates are high and compliance ispoor.Though many effective antitubercular drugsare available, the success of chemotherapydepends on regular intake of appropriatedrugs by the patients. Directly ObservedTreatment, Short course chemotherapy(DOTS) is a strategy that is found to beeffective and is recommended throughout theworld. In India, it is implemented by theRevised National Tuberculosis ControlProgramme (RNTCP) which was launched in1997. It involves providing most effectivemedicine and confirming that it is taken - ahealth worker ensures that the drug is takenby the patient. Patients are grouped into 3categories for treatment (Table 41.3).Resistant tuberculosis If sputum remainspositive even after 6 months of treatment,organisms are likely to be resistant. Suchpatients should be treated with 4-5 drugs, ofwhich 3 are first line drugs and treatment iscontinued for at least 1 year after the sputumbecomes negative. Fluoroquinolones andamikacin may be considered for multidrugresistant strains.Role of glucocorticoids As steroids depress hostdefense mechanisms, they should be usedonly in conditions like tubercular meningitis,miliary tuberculosis, pleural effusion, renaltuberculosis and rapidly progressingpulmonary tuberculosis. Steroids suppressinflammatory reaction which can lead toextensive fibrosis and damage.Chemoprophylaxis is given only in:(i) Contacts of open cases especially
children(ii) Patients with old inactive disease who
have not been adequately treated. INHis used daily (5 mg/kg) for 6-12 months.
(iii) HIV infected patients exposed to multidrug resistant tuberculosis rifampicinand pyrazinamide are given daily for 2months.
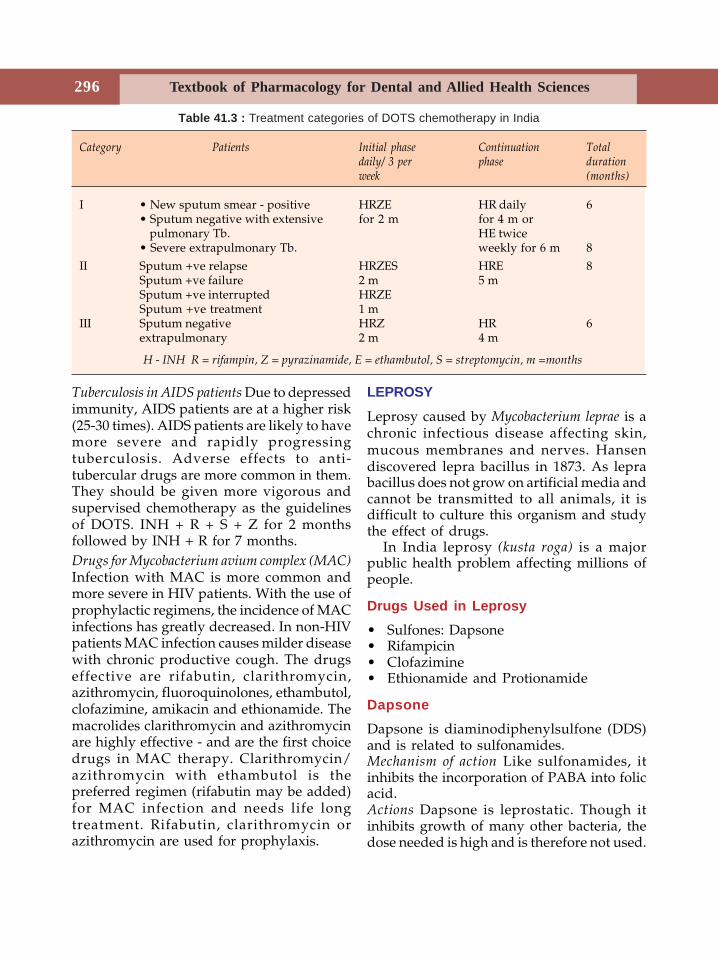
Textbook of Pharmacology for Dental and Allied Health Sciences296
Tuberculosis in AIDS patients Due to depressedimmunity, AIDS patients are at a higher risk(25-30 times). AIDS patients are likely to havemore severe and rapidly progressingtuberculosis. Adverse effects to anti-tubercular drugs are more common in them.They should be given more vigorous andsupervised chemotherapy as the guidelinesof DOTS. INH + R + S + Z for 2 monthsfollowed by INH + R for 7 months.Drugs for Mycobacterium avium complex (MAC)Infection with MAC is more common andmore severe in HIV patients. With the use ofprophylactic regimens, the incidence of MACinfections has greatly decreased. In non-HIVpatients MAC infection causes milder diseasewith chronic productive cough. The drugseffective are rifabutin, clarithromycin,azithromycin, fluoroquinolones, ethambutol,clofazimine, amikacin and ethionamide. Themacrolides clarithromycin and azithromycinare highly effective - and are the first choicedrugs in MAC therapy. Clarithromycin/azithromycin with ethambutol is thepreferred regimen (rifabutin may be added)for MAC infection and needs life longtreatment. Rifabutin, clarithromycin orazithromycin are used for prophylaxis.
LEPROSY
Leprosy caused by Mycobacterium leprae is achronic infectious disease affecting skin,mucous membranes and nerves. Hansendiscovered lepra bacillus in 1873. As leprabacillus does not grow on artificial media andcannot be transmitted to all animals, it isdifficult to culture this organism and studythe effect of drugs.
In India leprosy (kusta roga) is a majorpublic health problem affecting millions ofpeople.
Drugs Used in Leprosy• Sulfones: Dapsone• Rifampicin• Clofazimine• Ethionamide and Protionamide
DapsoneDapsone is diaminodiphenylsulfone (DDS)and is related to sulfonamides.Mechanism of action Like sulfonamides, itinhibits the incorporation of PABA into folicacid.Actions Dapsone is leprostatic. Though itinhibits growth of many other bacteria, thedose needed is high and is therefore not used.
Table 41.3 : Treatment categories of DOTS chemotherapy in India
Category Patients Initial phase Continuation Totaldaily/ 3 per phase durationweek (months)
I • New sputum smear - positive HRZE HR daily 6• Sputum negative with extensive for 2 m for 4 m or pulmonary Tb. HE twice• Severe extrapulmonary Tb. weekly for 6 m 8
II Sputum +ve relapse HRZES HRE 8Sputum +ve failure 2 m 5 mSputum +ve interrupted HRZESputum +ve treatment 1 m
III Sputum negative HRZ HR 6extrapulmonary 2 m 4 m
H - INH R = rifampin, Z = pyrazinamide, E = ethambutol, S = streptomycin, m =months
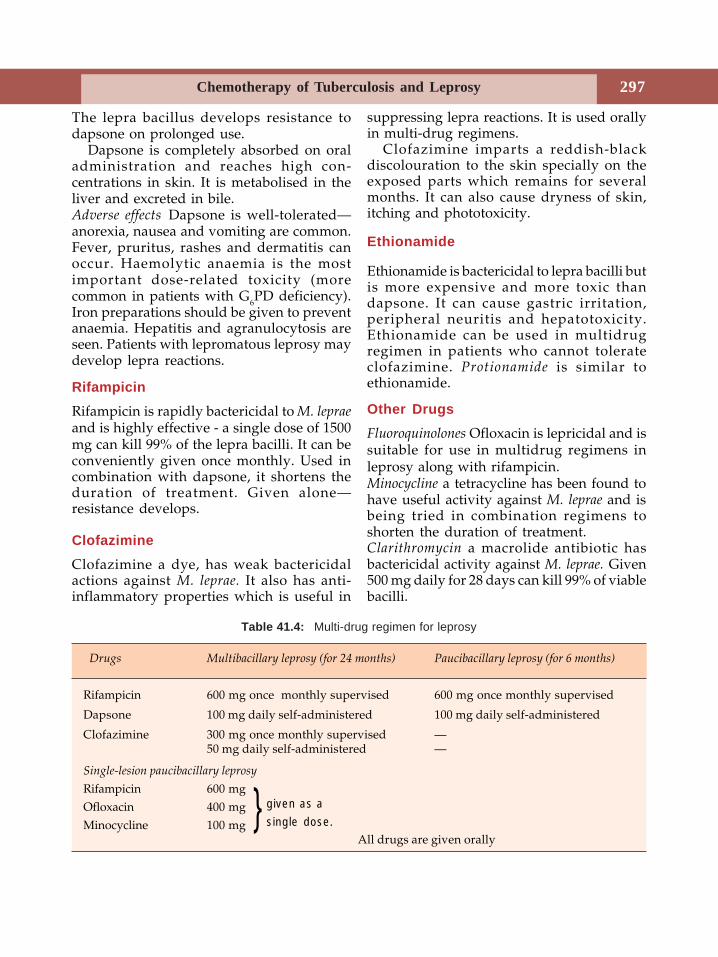
Chemotherapy of Tuberculosis and Leprosy 297
The lepra bacillus develops resistance todapsone on prolonged use.
Dapsone is completely absorbed on oraladministration and reaches high con-centrations in skin. It is metabolised in theliver and excreted in bile.Adverse effects Dapsone is well-tolerated—anorexia, nausea and vomiting are common.Fever, pruritus, rashes and dermatitis canoccur. Haemolytic anaemia is the mostimportant dose-related toxicity (morecommon in patients with G6PD deficiency).Iron preparations should be given to preventanaemia. Hepatitis and agranulocytosis areseen. Patients with lepromatous leprosy maydevelop lepra reactions.
RifampicinRifampicin is rapidly bactericidal to M. lepraeand is highly effective - a single dose of 1500mg can kill 99% of the lepra bacilli. It can beconveniently given once monthly. Used incombination with dapsone, it shortens theduration of treatment. Given alone—resistance develops.
ClofazimineClofazimine a dye, has weak bactericidalactions against M. leprae. It also has anti-inflammatory properties which is useful in
suppressing lepra reactions. It is used orallyin multi-drug regimens.
Clofazimine imparts a reddish-blackdiscolouration to the skin specially on theexposed parts which remains for severalmonths. It can also cause dryness of skin,itching and phototoxicity.
Ethionamide
Ethionamide is bactericidal to lepra bacilli butis more expensive and more toxic thandapsone. It can cause gastric irritation,peripheral neuritis and hepatotoxicity.Ethionamide can be used in multidrugregimen in patients who cannot tolerateclofazimine. Protionamide is similar toethionamide.
Other DrugsFluoroquinolones Ofloxacin is lepricidal and issuitable for use in multidrug regimens inleprosy along with rifampicin.Minocycline a tetracycline has been found tohave useful activity against M. leprae and isbeing tried in combination regimens toshorten the duration of treatment.Clarithromycin a macrolide antibiotic hasbactericidal activity against M. leprae. Given500 mg daily for 28 days can kill 99% of viablebacilli.
Drugs Multibacillary leprosy (for 24 months) Paucibacillary leprosy (for 6 months)
Rifampicin 600 mg once monthly supervised 600 mg once monthly supervised
Dapsone 100 mg daily self-administered 100 mg daily self-administered
Clofazimine 300 mg once monthly supervised —50 mg daily self-administered —
Single-lesion paucibacillary leprosy
Rifampicin 600 mgOfloxacin 400 mgMinocycline 100 mg
All drugs are given orally
Table 41.4: Multi-drug regimen for leprosy
} given as asingle dose.

Textbook of Pharmacology for Dental and Allied Health Sciences298
Treatment of Leprosy
For the sake of treatment, leprosy is dividedinto paucibacillary (non-infectious) andmultibacillary (infectious) leprosy. (Table41.4). Several atlernative and short termregimens including drugs like ofloxacin,minocycline and clarithromycin are underevaluation.
WHO has recommended a combination ofdrugs in leprosy in order to:1. eliminate persisters2. prevent drug resistance3. reduce the duration of therapy.
Lepra reactions are the acute exacerbationsthat occur in leprosy. They are triggered byacute infections, stress, anxiety and treatmentwith dapsone.
Type I reactions seen in tuberculoidleprosy are cell mediated, delayed hyper-sensitivity reactions to the antigens of M.leprae. Cutaneous ulcerations occur andexisting lesions show more erythema; nervesmay be painful and tender. They are treated
with corticosteroids or clofazimine while inmild cases aspirin suffices.
Type II reactions are seen in lepromatousleprosy (are known as erythema nodosumleprosum or ENL). New lesions appear andthe existing lesions become worse. Fever,lymphadenitis, myositis. and neuralgia mayoccur. It is a hypersensitivity reaction to theantigens of M. leprae - an arthus type reaction.
Type II reactions can be treated withclofazimine which is effective due to its anti-inflammatory properties. Chloroquine,corticosteroids or thalidomide are alsoeffective. Aspirin is effective in mild cases.Dapsone should be continued throughout.Chemoprophylaxis Only about 1% of contactsdevelop clinical disease. Dapsone 100 mgdaily and rifampicin 600 mg once a monthfor 6 months or till the contact case becomesnoninfectious are recommended for childcontacts. Acedapsone is found to beadvantageous for chemoprophylaxisas a single IM injection every 10 weeks.All contacts should be examined every 6months.
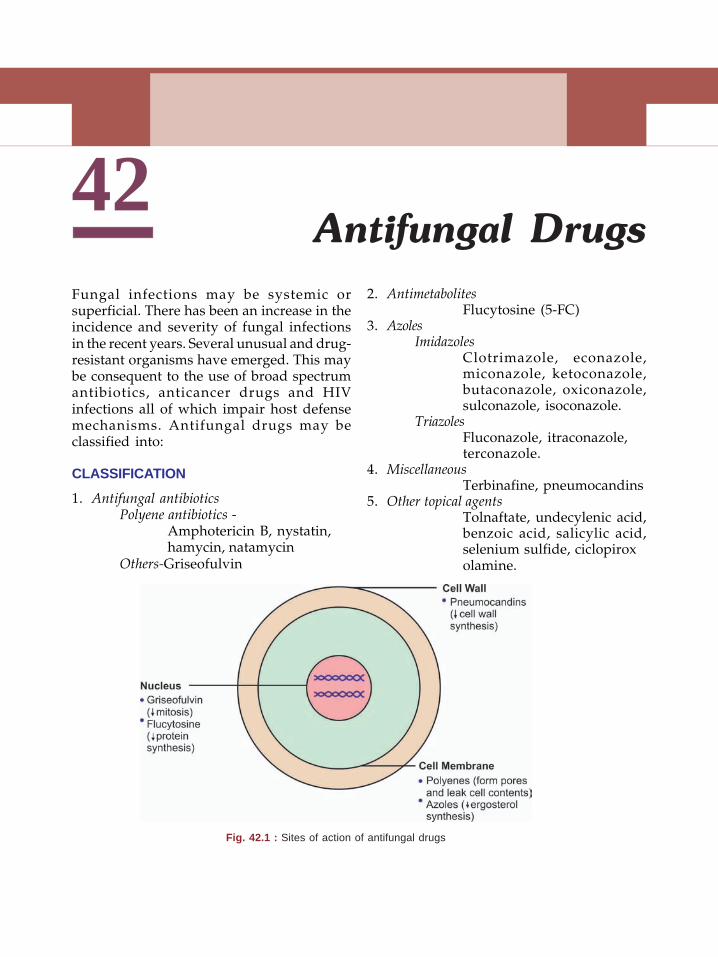
42Antifungal Drugs
Fungal infections may be systemic orsuperficial. There has been an increase in theincidence and severity of fungal infectionsin the recent years. Several unusual and drug-resistant organisms have emerged. This maybe consequent to the use of broad spectrumantibiotics, anticancer drugs and HIVinfections all of which impair host defensemechanisms. Antifungal drugs may beclassified into:
CLASSIFICATION
1. Antifungal antibioticsPolyene antibiotics -
Amphotericin B, nystatin,hamycin, natamycin
Others-Griseofulvin
2. AntimetabolitesFlucytosine (5-FC)
3. AzolesImidazoles
Clotrimazole, econazole,miconazole, ketoconazole,butaconazole, oxiconazole,sulconazole, isoconazole.
TriazolesFluconazole, itraconazole,terconazole.
4. MiscellaneousTerbinafine, pneumocandins
5. Other topical agentsTolnaftate, undecylenic acid,benzoic acid, salicylic acid,selenium sulfide, ciclopiroxolamine.
Fig. 42.1 : Sites of action of antifungal drugs
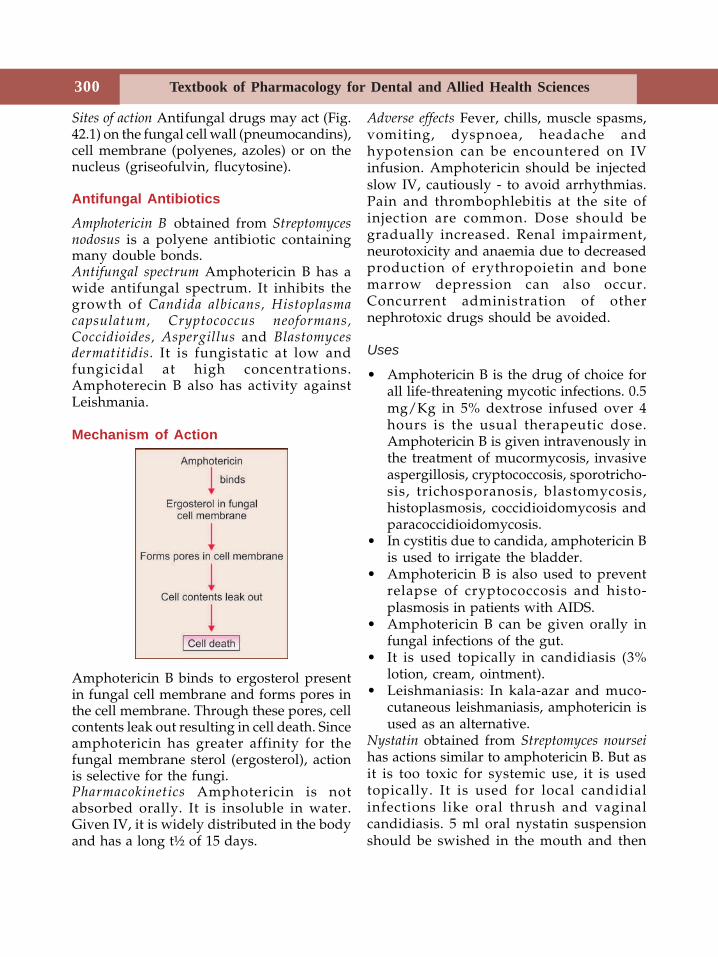
Textbook of Pharmacology for Dental and Allied Health Sciences300
Sites of action Antifungal drugs may act (Fig.42.1) on the fungal cell wall (pneumocandins),cell membrane (polyenes, azoles) or on thenucleus (griseofulvin, flucytosine).
Antifungal Antibiotics
Amphotericin B obtained from Streptomycesnodosus is a polyene antibiotic containingmany double bonds.Antifungal spectrum Amphotericin B has awide antifungal spectrum. It inhibits thegrowth of Candida albicans, Histoplasmacapsulatum, Cryptococcus neoformans,Coccidioides, Aspergillus and Blastomycesdermatitidis. It is fungistatic at low andfungicidal at high concentrations.Amphoterecin B also has activity againstLeishmania.
Mechanism of Action
Amphotericin B binds to ergosterol presentin fungal cell membrane and forms pores inthe cell membrane. Through these pores, cellcontents leak out resulting in cell death. Sinceamphotericin has greater affinity for thefungal membrane sterol (ergosterol), actionis selective for the fungi.Pharmacokinetics Amphotericin is notabsorbed orally. It is insoluble in water.Given IV, it is widely distributed in the bodyand has a long t½ of 15 days.
Adverse effects Fever, chills, muscle spasms,vomiting, dyspnoea, headache andhypotension can be encountered on IVinfusion. Amphotericin should be injectedslow IV, cautiously - to avoid arrhythmias.Pain and thrombophlebitis at the site ofinjection are common. Dose should begradually increased. Renal impairment,neurotoxicity and anaemia due to decreasedproduction of erythropoietin and bonemarrow depression can also occur.Concurrent administration of othernephrotoxic drugs should be avoided.
Uses
• Amphotericin B is the drug of choice forall life-threatening mycotic infections. 0.5mg/Kg in 5% dextrose infused over 4hours is the usual therapeutic dose.Amphotericin B is given intravenously inthe treatment of mucormycosis, invasiveaspergillosis, cryptococcosis, sporotricho-sis, trichosporanosis, blastomycosis,histoplasmosis, coccidioidomycosis andparacoccidioidomycosis.
• In cystitis due to candida, amphotericin Bis used to irrigate the bladder.
• Amphotericin B is also used to preventrelapse of cryptococcosis and histo-plasmosis in patients with AIDS.
• Amphotericin B can be given orally infungal infections of the gut.
• It is used topically in candidiasis (3%lotion, cream, ointment).
• Leishmaniasis: In kala-azar and muco-cutaneous leishmaniasis, amphotericin isused as an alternative.
Nystatin obtained from Streptomyces nourseihas actions similar to amphotericin B. But asit is too toxic for systemic use, it is usedtopically. It is used for local candidialinfections like oral thrush and vaginalcandidiasis. 5 ml oral nystatin suspensionshould be swished in the mouth and then
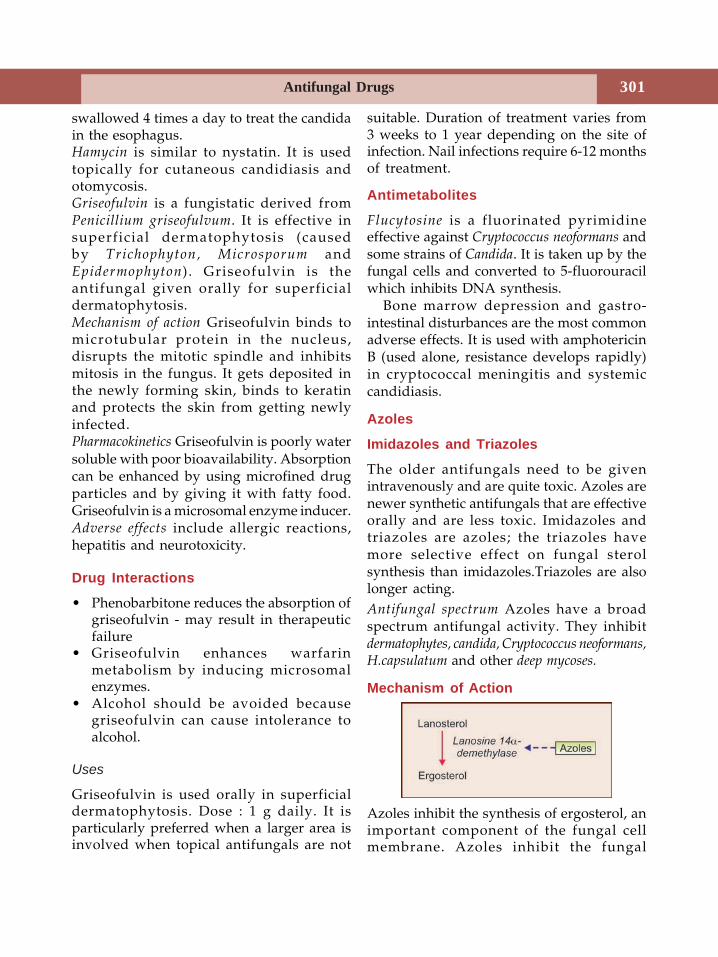
Antifungal Drugs 301
swallowed 4 times a day to treat the candidain the esophagus.Hamycin is similar to nystatin. It is usedtopically for cutaneous candidiasis andotomycosis.Griseofulvin is a fungistatic derived fromPenicillium griseofulvum. It is effective insuperficial dermatophytosis (causedby Trichophyton, Microsporum andEpidermophyton) . Griseofulvin is theantifungal given orally for superficialdermatophytosis.Mechanism of action Griseofulvin binds tomicrotubular protein in the nucleus,disrupts the mitotic spindle and inhibitsmitosis in the fungus. It gets deposited inthe newly forming skin, binds to keratinand protects the skin from getting newlyinfected.Pharmacokinetics Griseofulvin is poorly watersoluble with poor bioavailability. Absorptioncan be enhanced by using microfined drugparticles and by giving it with fatty food.Griseofulvin is a microsomal enzyme inducer.Adverse effects include allergic reactions,hepatitis and neurotoxicity.
Drug Interactions
• Phenobarbitone reduces the absorption ofgriseofulvin - may result in therapeuticfailure
• Griseofulvin enhances warfarinmetabolism by inducing microsomalenzymes.
• Alcohol should be avoided becausegriseofulvin can cause intolerance toalcohol.
Uses
Griseofulvin is used orally in superficialdermatophytosis. Dose : 1 g daily. It isparticularly preferred when a larger area isinvolved when topical antifungals are not
suitable. Duration of treatment varies from3 weeks to 1 year depending on the site ofinfection. Nail infections require 6-12 monthsof treatment.
Antimetabolites
Flucytosine is a fluorinated pyrimidineeffective against Cryptococcus neoformans andsome strains of Candida. It is taken up by thefungal cells and converted to 5-fluorouracilwhich inhibits DNA synthesis.
Bone marrow depression and gastro-intestinal disturbances are the most commonadverse effects. It is used with amphotericinB (used alone, resistance develops rapidly)in cryptococcal meningitis and systemiccandidiasis.
Azoles
Imidazoles and Triazoles
The older antifungals need to be givenintravenously and are quite toxic. Azoles arenewer synthetic antifungals that are effectiveorally and are less toxic. Imidazoles andtriazoles are azoles; the triazoles havemore selective effect on fungal sterolsynthesis than imidazoles.Triazoles are alsolonger acting.Antifungal spectrum Azoles have a broadspectrum antifungal activity. They inhibitdermatophytes, candida, Cryptococcus neoformans,H.capsulatum and other deep mycoses.
Mechanism of Action
Azoles inhibit the synthesis of ergosterol, animportant component of the fungal cellmembrane. Azoles inhibit the fungal
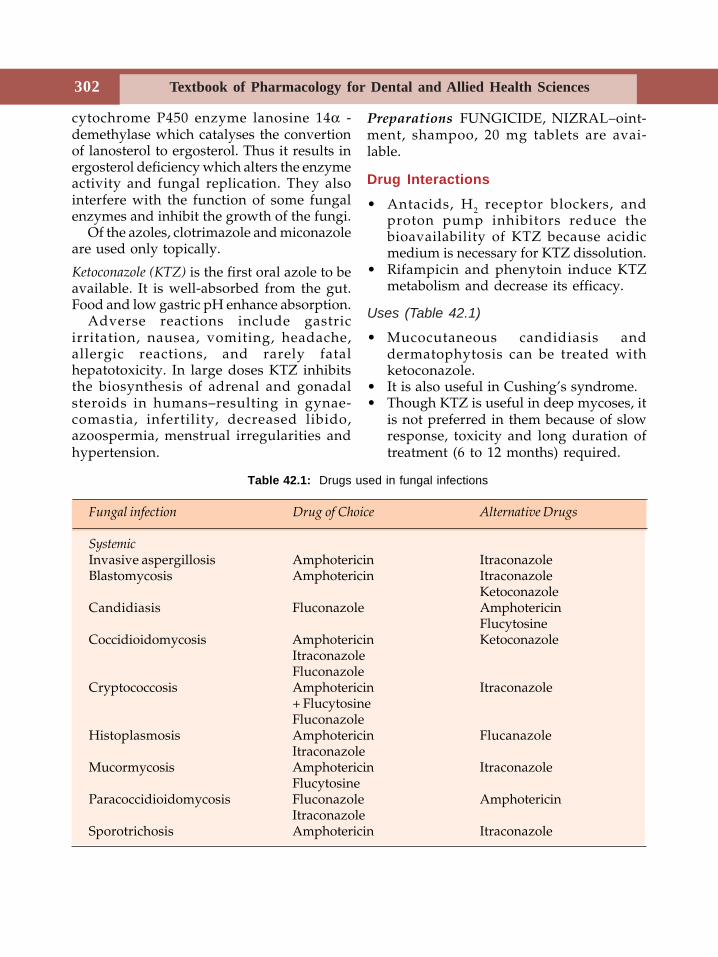
Textbook of Pharmacology for Dental and Allied Health Sciences302
cytochrome P450 enzyme lanosine 14α -demethylase which catalyses the convertionof lanosterol to ergosterol. Thus it results inergosterol deficiency which alters the enzymeactivity and fungal replication. They alsointerfere with the function of some fungalenzymes and inhibit the growth of the fungi.
Of the azoles, clotrimazole and miconazoleare used only topically.
Ketoconazole (KTZ) is the first oral azole to beavailable. It is well-absorbed from the gut.Food and low gastric pH enhance absorption.
Adverse reactions include gastricirritation, nausea, vomiting, headache,allergic reactions, and rarely fatalhepatotoxicity. In large doses KTZ inhibitsthe biosynthesis of adrenal and gonadalsteroids in humans–resulting in gynae-comastia, infertility, decreased libido,azoospermia, menstrual irregularities andhypertension.
Preparations FUNGICIDE, NIZRAL–oint-ment, shampoo, 20 mg tablets are avai-lable.
Drug Interactions
• Antacids, H2 receptor blockers, andproton pump inhibitors reduce thebioavailability of KTZ because acidicmedium is necessary for KTZ dissolution.
• Rifampicin and phenytoin induce KTZmetabolism and decrease its efficacy.
Uses (Table 42.1)
• Mucocutaneous candidiasis anddermatophytosis can be treated withketoconazole.
• It is also useful in Cushing’s syndrome.• Though KTZ is useful in deep mycoses, it
is not preferred in them because of slowresponse, toxicity and long duration oftreatment (6 to 12 months) required.
Table 42.1: Drugs used in fungal infections
Fungal infection Drug of Choice Alternative Drugs
SystemicInvasive aspergillosis Amphotericin ItraconazoleBlastomycosis Amphotericin Itraconazole
KetoconazoleCandidiasis Fluconazole Amphotericin
FlucytosineCoccidioidomycosis Amphotericin Ketoconazole
ItraconazoleFluconazole
Cryptococcosis Amphotericin Itraconazole+ FlucytosineFluconazole
Histoplasmosis Amphotericin FlucanazoleItraconazole
Mucormycosis Amphotericin ItraconazoleFlucytosine
Paracoccidioidomycosis Fluconazole AmphotericinItraconazole
Sporotrichosis Amphotericin Itraconazole
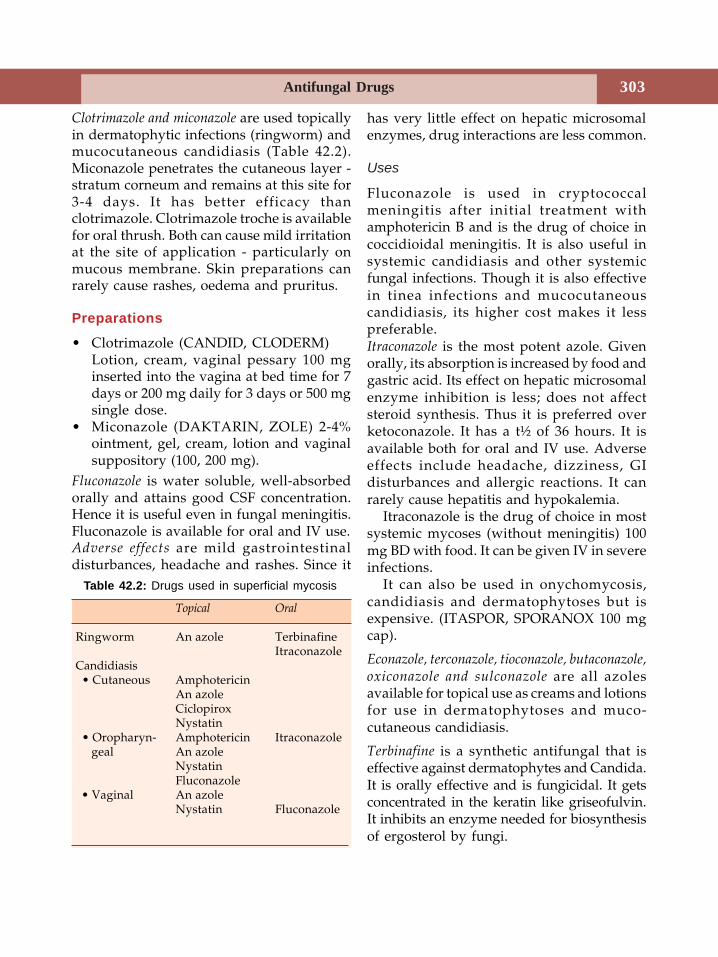
Antifungal Drugs 303
Clotrimazole and miconazole are used topicallyin dermatophytic infections (ringworm) andmucocutaneous candidiasis (Table 42.2).Miconazole penetrates the cutaneous layer -stratum corneum and remains at this site for3-4 days. It has better efficacy thanclotrimazole. Clotrimazole troche is availablefor oral thrush. Both can cause mild irritationat the site of application - particularly onmucous membrane. Skin preparations canrarely cause rashes, oedema and pruritus.
Preparations
• Clotrimazole (CANDID, CLODERM)Lotion, cream, vaginal pessary 100 mginserted into the vagina at bed time for 7days or 200 mg daily for 3 days or 500 mgsingle dose.
• Miconazole (DAKTARIN, ZOLE) 2-4%ointment, gel, cream, lotion and vaginalsuppository (100, 200 mg).
Fluconazole is water soluble, well-absorbedorally and attains good CSF concentration.Hence it is useful even in fungal meningitis.Fluconazole is available for oral and IV use.Adverse effects are mild gastrointestinaldisturbances, headache and rashes. Since it
has very little effect on hepatic microsomalenzymes, drug interactions are less common.
Uses
Fluconazole is used in cryptococcalmeningitis after initial treatment withamphotericin B and is the drug of choice incoccidioidal meningitis. It is also useful insystemic candidiasis and other systemicfungal infections. Though it is also effectivein tinea infections and mucocutaneouscandidiasis, its higher cost makes it lesspreferable.Itraconazole is the most potent azole. Givenorally, its absorption is increased by food andgastric acid. Its effect on hepatic microsomalenzyme inhibition is less; does not affectsteroid synthesis. Thus it is preferred overketoconazole. It has a t½ of 36 hours. It isavailable both for oral and IV use. Adverseeffects include headache, dizziness, GIdisturbances and allergic reactions. It canrarely cause hepatitis and hypokalemia.
Itraconazole is the drug of choice in mostsystemic mycoses (without meningitis) 100mg BD with food. It can be given IV in severeinfections.
It can also be used in onychomycosis,candidiasis and dermatophytoses but isexpensive. (ITASPOR, SPORANOX 100 mgcap).
Econazole, terconazole, tioconazole, butaconazole,oxiconazole and sulconazole are all azolesavailable for topical use as creams and lotionsfor use in dermatophytoses and muco-cutaneous candidiasis.
Terbinafine is a synthetic antifungal that iseffective against dermatophytes and Candida.It is orally effective and is fungicidal. It getsconcentrated in the keratin like griseofulvin.It inhibits an enzyme needed for biosynthesisof ergosterol by fungi.
Table 42.2: Drugs used in superficial mycosis
Topical Oral
Ringworm An azole TerbinafineItraconazole
Candidiasis • Cutaneous Amphotericin
An azoleCiclopiroxNystatin
• Oropharyn- Amphotericin Itraconazole geal An azole
NystatinFluconazole
• Vaginal An azoleNystatin Fluconazole

Textbook of Pharmacology for Dental and Allied Health Sciences304
Adverse effects are rare – gastrointestinaldisturbances, rashes and headache can occur.Terbinafine is used in dermatophytosis,pityriasis, onychomycosis and candidiasis. Itis particularly preferred in onychomycosis -250 mg OD for 12 weeks - where it is superiorto azoles and griseofulvin.
Dose 250 mg once daily; (SEBIFIN) 1% creamis also available.
Pneumocandins or Echinocandins
Pneumocandins inhibit the formation of thefungal cell wall. They inhibit the synthesis ofan important component of the fungal cellwall - a glucose polymer as a result of whichthe fungal cell lysis occurs.
Echinocandins include caspofungin, micafunginand amorolfine. Caspofungin has activity incandidiasis, aspergillosis and in Pneumocystiscarinii infections. Micofungin is effective againstcandida and aspergillus while amorolfine is usefulin fungal infections of the nail.
Other Topical Antifungal AgentsApart from nystatin, clotrimazole,miconazole and terbinafine, some drugs likesalicylic acid, benzoic acid, tolnaftate andcyclopirox olamine are used topically fordermatophytosis and pityriasis versicolor.
Selenium sulfide is useful in tinea versicolorcaused by Malassezia furfur, and also indandruff. SELSUN is 2.5% suspension ofselenium sulfide in a shampoo base. It is irritantto the eyes and the odour is unpleasant.
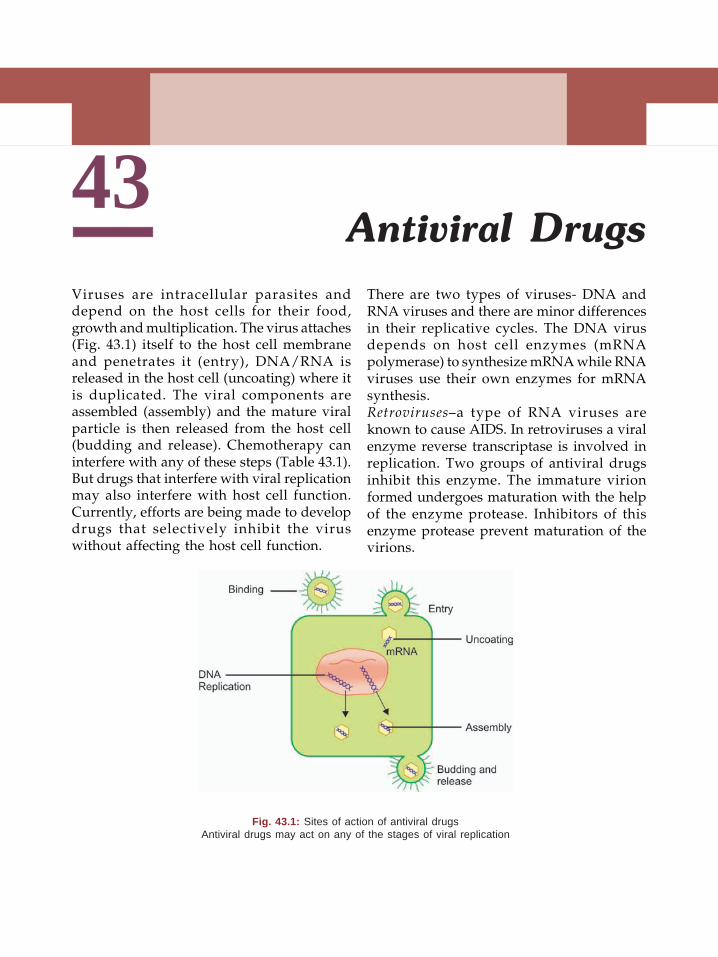
43Antiviral Drugs
Viruses are intracellular parasites anddepend on the host cells for their food,growth and multiplication. The virus attaches(Fig. 43.1) itself to the host cell membraneand penetrates it (entry), DNA/RNA isreleased in the host cell (uncoating) where itis duplicated. The viral components areassembled (assembly) and the mature viralparticle is then released from the host cell(budding and release). Chemotherapy caninterfere with any of these steps (Table 43.1).But drugs that interfere with viral replicationmay also interfere with host cell function.Currently, efforts are being made to developdrugs that selectively inhibit the viruswithout affecting the host cell function.
There are two types of viruses- DNA andRNA viruses and there are minor differencesin their replicative cycles. The DNA virusdepends on host cell enzymes (mRNApolymerase) to synthesize mRNA while RNAviruses use their own enzymes for mRNAsynthesis.Retroviruses–a type of RNA viruses areknown to cause AIDS. In retroviruses a viralenzyme reverse transcriptase is involved inreplication. Two groups of antiviral drugsinhibit this enzyme. The immature virionformed undergoes maturation with the helpof the enzyme protease. Inhibitors of thisenzyme protease prevent maturation of thevirions.
Fig. 43.1: Sites of action of antiviral drugsAntiviral drugs may act on any of the stages of viral replication
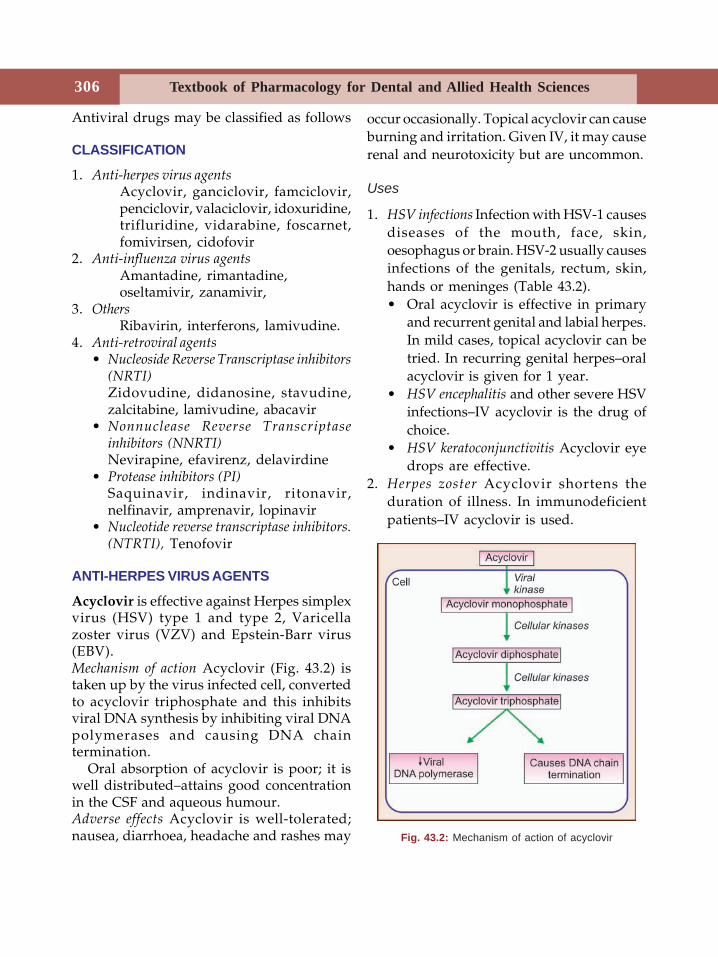
Textbook of Pharmacology for Dental and Allied Health Sciences306
Antiviral drugs may be classified as follows
CLASSIFICATION
1. Anti-herpes virus agentsAcyclovir, ganciclovir, famciclovir,penciclovir, valaciclovir, idoxuridine,trifluridine, vidarabine, foscarnet,fomivirsen, cidofovir
2. Anti-influenza virus agentsAmantadine, rimantadine,oseltamivir, zanamivir,
3. OthersRibavirin, interferons, lamivudine.
4. Anti-retroviral agents• Nucleoside Reverse Transcriptase inhibitors
(NRTI)Zidovudine, didanosine, stavudine,zalcitabine, lamivudine, abacavir
• Nonnuclease Reverse Transcriptaseinhibitors (NNRTI)Nevirapine, efavirenz, delavirdine
• Protease inhibitors (PI)Saquinavir, indinavir, ritonavir,nelfinavir, amprenavir, lopinavir
• Nucleotide reverse transcriptase inhibitors.(NTRTI), Tenofovir
ANTI-HERPES VIRUS AGENTS
Acyclovir is effective against Herpes simplexvirus (HSV) type 1 and type 2, Varicellazoster virus (VZV) and Epstein-Barr virus(EBV).Mechanism of action Acyclovir (Fig. 43.2) istaken up by the virus infected cell, convertedto acyclovir triphosphate and this inhibitsviral DNA synthesis by inhibiting viral DNApolymerases and causing DNA chaintermination.
Oral absorption of acyclovir is poor; it iswell distributed–attains good concentrationin the CSF and aqueous humour.Adverse effects Acyclovir is well-tolerated;nausea, diarrhoea, headache and rashes may
occur occasionally. Topical acyclovir can causeburning and irritation. Given IV, it may causerenal and neurotoxicity but are uncommon.
Uses
1. HSV infections Infection with HSV-1 causesdiseases of the mouth, face, skin,oesophagus or brain. HSV-2 usually causesinfections of the genitals, rectum, skin,hands or meninges (Table 43.2).• Oral acyclovir is effective in primary
and recurrent genital and labial herpes.In mild cases, topical acyclovir can betried. In recurring genital herpes–oralacyclovir is given for 1 year.
• HSV encephalitis and other severe HSVinfections–IV acyclovir is the drug ofchoice.
• HSV keratoconjunctivitis Acyclovir eyedrops are effective.
2. Herpes zoster Acyclovir shortens theduration of illness. In immunodeficientpatients–IV acyclovir is used.
Fig. 43.2: Mechanism of action of acyclovir
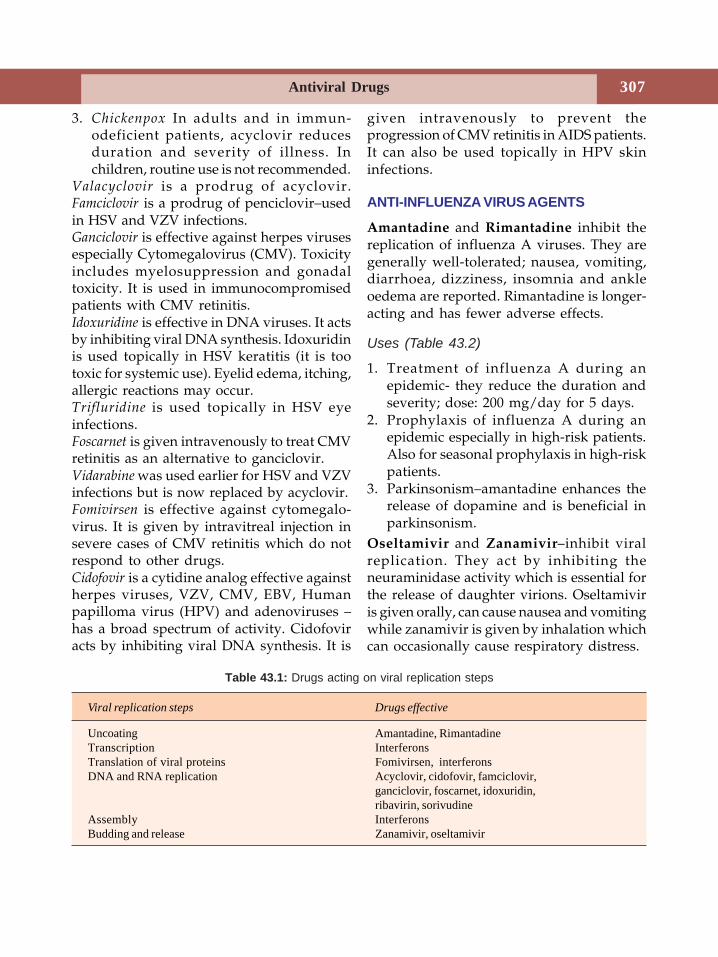
Antiviral Drugs 307
3. Chickenpox In adults and in immun-odeficient patients, acyclovir reducesduration and severity of illness. Inchildren, routine use is not recommended.
Valacyclovir is a prodrug of acyclovir.Famciclovir is a prodrug of penciclovir–usedin HSV and VZV infections.Ganciclovir is effective against herpes virusesespecially Cytomegalovirus (CMV). Toxicityincludes myelosuppression and gonadaltoxicity. It is used in immunocompromisedpatients with CMV retinitis.Idoxuridine is effective in DNA viruses. It actsby inhibiting viral DNA synthesis. Idoxuridinis used topically in HSV keratitis (it is tootoxic for systemic use). Eyelid edema, itching,allergic reactions may occur.Trifluridine is used topically in HSV eyeinfections.Foscarnet is given intravenously to treat CMVretinitis as an alternative to ganciclovir.Vidarabine was used earlier for HSV and VZVinfections but is now replaced by acyclovir.Fomivirsen is effective against cytomegalo-virus. It is given by intravitreal injection insevere cases of CMV retinitis which do notrespond to other drugs.Cidofovir is a cytidine analog effective againstherpes viruses, VZV, CMV, EBV, Humanpapilloma virus (HPV) and adenoviruses –has a broad spectrum of activity. Cidofoviracts by inhibiting viral DNA synthesis. It is
given intravenously to prevent theprogression of CMV retinitis in AIDS patients.It can also be used topically in HPV skininfections.
ANTI-INFLUENZA VIRUS AGENTS
Amantadine and Rimantadine inhibit thereplication of influenza A viruses. They aregenerally well-tolerated; nausea, vomiting,diarrhoea, dizziness, insomnia and ankleoedema are reported. Rimantadine is longer-acting and has fewer adverse effects.
Uses (Table 43.2)
1. Treatment of influenza A during anepidemic- they reduce the duration andseverity; dose: 200 mg/day for 5 days.
2. Prophylaxis of influenza A during anepidemic especially in high-risk patients.Also for seasonal prophylaxis in high-riskpatients.
3. Parkinsonism–amantadine enhances therelease of dopamine and is beneficial inparkinsonism.
Oseltamivir and Zanamivir–inhibit viralreplication. They act by inhibiting theneuraminidase activity which is essential forthe release of daughter virions. Oseltamiviris given orally, can cause nausea and vomitingwhile zanamivir is given by inhalation whichcan occasionally cause respiratory distress.
Viral replication steps Drugs effective
Uncoating Amantadine, RimantadineTranscription InterferonsTranslation of viral proteins Fomivirsen, interferonsDNA and RNA replication Acyclovir, cidofovir, famciclovir,
ganciclovir, foscarnet, idoxuridin,ribavirin, sorivudine
Assembly InterferonsBudding and release Zanamivir, oseltamivir
Table 43.1: Drugs acting on viral replication steps
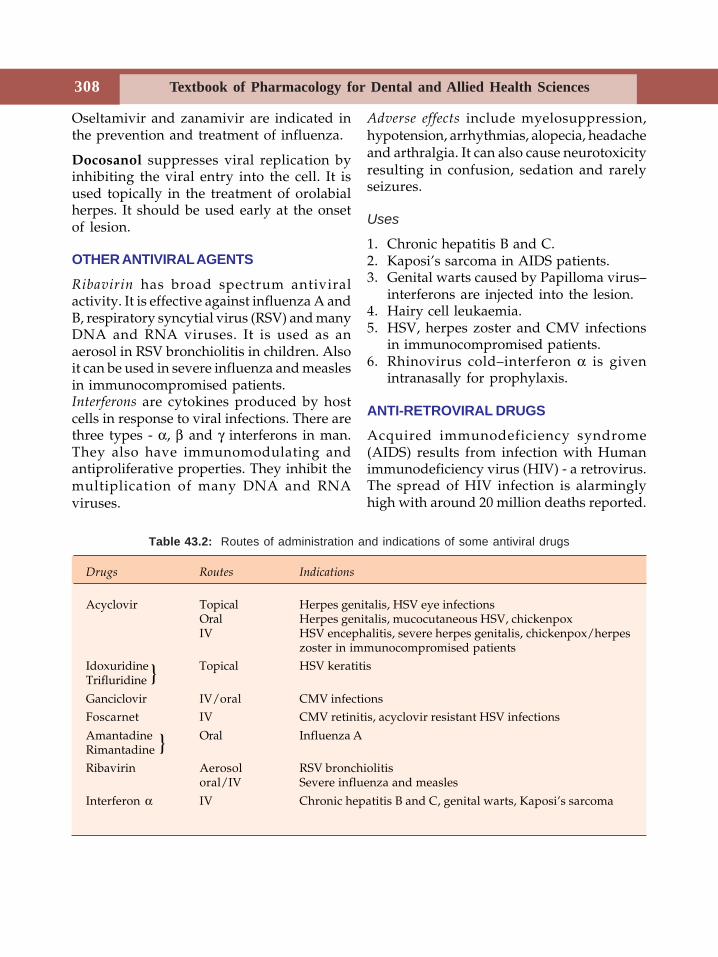
Textbook of Pharmacology for Dental and Allied Health Sciences308
Oseltamivir and zanamivir are indicated inthe prevention and treatment of influenza.
Docosanol suppresses viral replication byinhibiting the viral entry into the cell. It isused topically in the treatment of orolabialherpes. It should be used early at the onsetof lesion.
OTHER ANTIVIRAL AGENTS
Ribavirin has broad spectrum antiviralactivity. It is effective against influenza A andB, respiratory syncytial virus (RSV) and manyDNA and RNA viruses. It is used as anaerosol in RSV bronchiolitis in children. Alsoit can be used in severe influenza and measlesin immunocompromised patients.Interferons are cytokines produced by hostcells in response to viral infections. There arethree types - α, β and γ interferons in man.They also have immunomodulating andantiproliferative properties. They inhibit themultiplication of many DNA and RNAviruses.
Adverse effects include myelosuppression,hypotension, arrhythmias, alopecia, headacheand arthralgia. It can also cause neurotoxicityresulting in confusion, sedation and rarelyseizures.
Uses
1. Chronic hepatitis B and C.2. Kaposi’s sarcoma in AIDS patients.3. Genital warts caused by Papilloma virus–
interferons are injected into the lesion.4. Hairy cell leukaemia.5. HSV, herpes zoster and CMV infections
in immunocompromised patients.6. Rhinovirus cold–interferon α is given
intranasally for prophylaxis.
ANTI-RETROVIRAL DRUGS
Acquired immunodeficiency syndrome(AIDS) results from infection with Humanimmunodeficiency virus (HIV) - a retrovirus.The spread of HIV infection is alarminglyhigh with around 20 million deaths reported.
Table 43.2: Routes of administration and indications of some antiviral drugs
Drugs Routes Indications
Acyclovir Topical Herpes genitalis, HSV eye infectionsOral Herpes genitalis, mucocutaneous HSV, chickenpoxIV HSV encephalitis, severe herpes genitalis, chickenpox/herpes
zoster in immunocompromised patientsIdoxuridine Topical HSV keratitisTrifluridine
Ganciclovir IV/oral CMV infectionsFoscarnet IV CMV retinitis, acyclovir resistant HSV infections
Amantadine Oral Influenza ARimantadineRibavirin Aerosol RSV bronchiolitis
oral/IV Severe influenza and measles
Interferon α IV Chronic hepatitis B and C, genital warts, Kaposi’s sarcoma
}
}
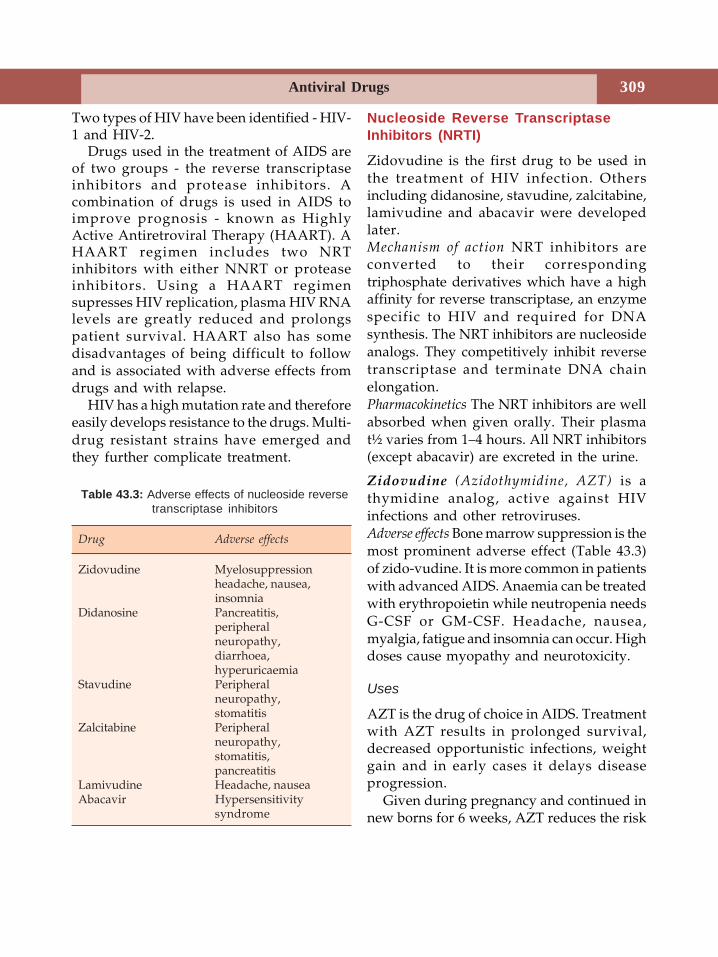
Antiviral Drugs 309
Two types of HIV have been identified - HIV-1 and HIV-2.
Drugs used in the treatment of AIDS areof two groups - the reverse transcriptaseinhibitors and protease inhibitors. Acombination of drugs is used in AIDS toimprove prognosis - known as HighlyActive Antiretroviral Therapy (HAART). AHAART regimen includes two NRTinhibitors with either NNRT or proteaseinhibitors. Using a HAART regimensupresses HIV replication, plasma HIV RNAlevels are greatly reduced and prolongspatient survival. HAART also has somedisadvantages of being difficult to followand is associated with adverse effects fromdrugs and with relapse.
HIV has a high mutation rate and thereforeeasily develops resistance to the drugs. Multi-drug resistant strains have emerged andthey further complicate treatment.
Nucleoside Reverse TranscriptaseInhibitors (NRTI)
Zidovudine is the first drug to be used inthe treatment of HIV infection. Othersincluding didanosine, stavudine, zalcitabine,lamivudine and abacavir were developedlater.Mechanism of action NRT inhibitors areconverted to their correspondingtriphosphate derivatives which have a highaffinity for reverse transcriptase, an enzymespecific to HIV and required for DNAsynthesis. The NRT inhibitors are nucleosideanalogs. They competitively inhibit reversetranscriptase and terminate DNA chainelongation.Pharmacokinetics The NRT inhibitors are wellabsorbed when given orally. Their plasmat½ varies from 1–4 hours. All NRT inhibitors(except abacavir) are excreted in the urine.
Zidovudine (Azidothymidine, AZT) is athymidine analog, active against HIVinfections and other retroviruses.Adverse effects Bone marrow suppression is themost prominent adverse effect (Table 43.3)of zido-vudine. It is more common in patientswith advanced AIDS. Anaemia can be treatedwith erythropoietin while neutropenia needsG-CSF or GM-CSF. Headache, nausea,myalgia, fatigue and insomnia can occur. Highdoses cause myopathy and neurotoxicity.
Uses
AZT is the drug of choice in AIDS. Treatmentwith AZT results in prolonged survival,decreased opportunistic infections, weightgain and in early cases it delays diseaseprogression.
Given during pregnancy and continued innew borns for 6 weeks, AZT reduces the risk
Table 43.3: Adverse effects of nucleoside reversetranscriptase inhibitors
Drug Adverse effects
Zidovudine Myelosuppressionheadache, nausea,insomnia
Didanosine Pancreatitis,peripheralneuropathy,diarrhoea,hyperuricaemia
Stavudine Peripheralneuropathy,stomatitis
Zalcitabine Peripheralneuropathy,stomatitis,pancreatitis
Lamivudine Headache, nauseaAbacavir Hypersensitivity
syndrome
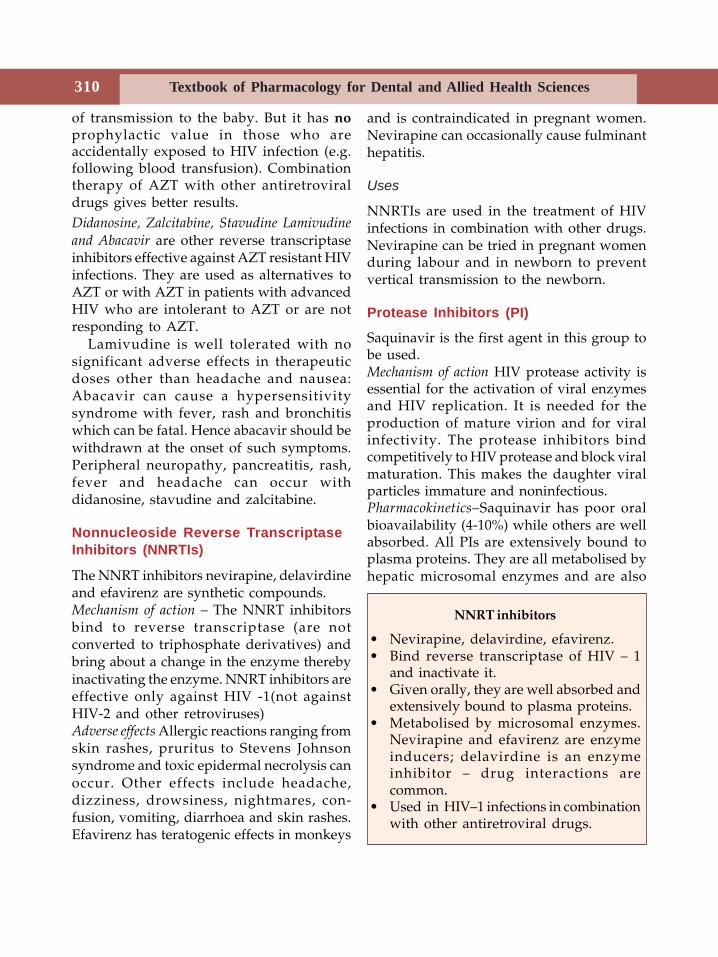
Textbook of Pharmacology for Dental and Allied Health Sciences310
of transmission to the baby. But it has noprophylactic value in those who areaccidentally exposed to HIV infection (e.g.following blood transfusion). Combinationtherapy of AZT with other antiretroviraldrugs gives better results.Didanosine, Zalcitabine, Stavudine Lamivudine
and Abacavir are other reverse transcriptaseinhibitors effective against AZT resistant HIVinfections. They are used as alternatives toAZT or with AZT in patients with advancedHIV who are intolerant to AZT or are notresponding to AZT.
Lamivudine is well tolerated with nosignificant adverse effects in therapeuticdoses other than headache and nausea:Abacavir can cause a hypersensitivitysyndrome with fever, rash and bronchitiswhich can be fatal. Hence abacavir should bewithdrawn at the onset of such symptoms.Peripheral neuropathy, pancreatitis, rash,fever and headache can occur withdidanosine, stavudine and zalcitabine.
Nonnucleoside Reverse TranscriptaseInhibitors (NNRTIs)
The NNRT inhibitors nevirapine, delavirdineand efavirenz are synthetic compounds.Mechanism of action – The NNRT inhibitorsbind to reverse transcriptase (are notconverted to triphosphate derivatives) andbring about a change in the enzyme therebyinactivating the enzyme. NNRT inhibitors areeffective only against HIV -1(not againstHIV-2 and other retroviruses)Adverse effects Allergic reactions ranging fromskin rashes, pruritus to Stevens Johnsonsyndrome and toxic epidermal necrolysis canoccur. Other effects include headache,dizziness, drowsiness, nightmares, con-fusion, vomiting, diarrhoea and skin rashes.Efavirenz has teratogenic effects in monkeys
and is contraindicated in pregnant women.Nevirapine can occasionally cause fulminanthepatitis.
Uses
NNRTIs are used in the treatment of HIVinfections in combination with other drugs.Nevirapine can be tried in pregnant womenduring labour and in newborn to preventvertical transmission to the newborn.
Protease Inhibitors (PI)
Saquinavir is the first agent in this group tobe used.Mechanism of action HIV protease activity isessential for the activation of viral enzymesand HIV replication. It is needed for theproduction of mature virion and for viralinfectivity. The protease inhibitors bindcompetitively to HIV protease and block viralmaturation. This makes the daughter viralparticles immature and noninfectious.Pharmacokinetics–Saquinavir has poor oralbioavailability (4-10%) while others are wellabsorbed. All PIs are extensively bound toplasma proteins. They are all metabolised byhepatic microsomal enzymes and are also
NNRT inhibitors
• Nevirapine, delavirdine, efavirenz.• Bind reverse transcriptase of HIV – 1
and inactivate it.• Given orally, they are well absorbed and
extensively bound to plasma proteins.• Metabolised by microsomal enzymes.
Nevirapine and efavirenz are enzymeinducers; delavirdine is an enzymeinhibitor – drug interactions arecommon.
• Used in HIV–1 infections in combinationwith other antiretroviral drugs.
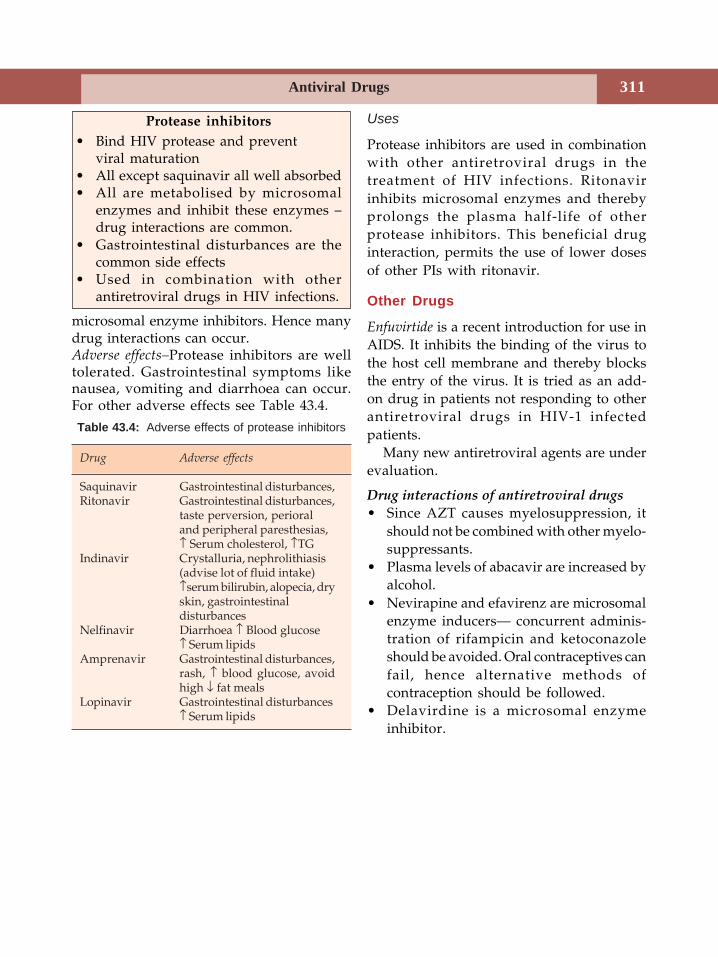
Antiviral Drugs 311
microsomal enzyme inhibitors. Hence manydrug interactions can occur.Adverse effects–Protease inhibitors are welltolerated. Gastrointestinal symptoms likenausea, vomiting and diarrhoea can occur.For other adverse effects see Table 43.4.
Uses
Protease inhibitors are used in combinationwith other antiretroviral drugs in thetreatment of HIV infections. Ritonavirinhibits microsomal enzymes and therebyprolongs the plasma half-life of otherprotease inhibitors. This beneficial druginteraction, permits the use of lower dosesof other PIs with ritonavir.
Other Drugs
Enfuvirtide is a recent introduction for use inAIDS. It inhibits the binding of the virus tothe host cell membrane and thereby blocksthe entry of the virus. It is tried as an add-on drug in patients not responding to otherantiretroviral drugs in HIV-1 infectedpatients.
Many new antiretroviral agents are underevaluation.
Drug interactions of antiretroviral drugs• Since AZT causes myelosuppression, it
should not be combined with other myelo-suppressants.
• Plasma levels of abacavir are increased byalcohol.
• Nevirapine and efavirenz are microsomalenzyme inducers— concurrent adminis-tration of rifampicin and ketoconazoleshould be avoided. Oral contraceptives canfail, hence alternative methods ofcontraception should be followed.
• Delavirdine is a microsomal enzymeinhibitor.
Protease inhibitors• Bind HIV protease and prevent
viral maturation• All except saquinavir all well absorbed• All are metabolised by microsomal
enzymes and inhibit these enzymes –drug interactions are common.
• Gastrointestinal disturbances are thecommon side effects
• Used in combination with otherantiretroviral drugs in HIV infections.
Table 43.4: Adverse effects of protease inhibitors
Drug Adverse effects
Saquinavir Gastrointestinal disturbances,Ritonavir Gastrointestinal disturbances,
taste perversion, perioraland peripheral paresthesias,↑ Serum cholesterol, ↑TG
Indinavir Crystalluria, nephrolithiasis(advise lot of fluid intake)↑serum bilirubin, alopecia, dryskin, gastrointestinaldisturbances
Nelfinavir Diarrhoea ↑ Blood glucose↑ Serum lipids
Amprenavir Gastrointestinal disturbances,rash, ↑ blood glucose, avoidhigh ↓ fat meals
Lopinavir Gastrointestinal disturbances↑ Serum lipids
Textbook of Pharmacology for Dental and Allied Health Sciences312
44 Chemotherapy ofMalaria
Malaria is caused by protozoa of the genusPlasmodium, transmitted through the bite ofa female Anopheles mosquito. It is a majorpublic health problem in most of thedeveloping countries including India. Everyyear about 200-500 million cases of malariaoccur throughout the world with about 2million deaths.Life cycle of the malaria parasite. The bite of aninfected female anopheles mosquitointroduces sporozoites into the blood streamof man (Fig 44.1). These sporozoites enterthe liver cells where they develop andmultiply and the cells rupture to releasemerozoites (pre-erythrocytic stage). Themerozoites enter red blood cells to developand mature (erythrocytic stage/erythrocyticschizogony) and the RBCs rupture releasingmerozoites which invade fresh RBCs andcontinue to multiply. The rupture of RBCsreleases the products of the parasite whichinduce chills and fever. In P. vivax and P. ovalespecies, some sporozoites in the liver cellsenter a dormant stage (hypnozoites orsleeping forms) which can multiply later(even after several months) resulting inrelapse (exoerythrocytic stage). Somemerozoites entering the RBCs, differentiateinto male and female sexual forms orgametocytes. These forms enter the mosquitowhen they suck the blood and undergo sexualcycle in the mosquito.
The 4 species of the malarial parasite include:• P. falciparum–causes most severe form of
malaria (malignant tertian) which can befatal. But relapses do not occur because ithas no exoerythrocytic stage in its lifecycle.
• P. vivax causes less severe malaria (benigntertian) with a low mortality rate. Relapsescan occur because of the exoerythrocyticforms or hypnozoites.
• P.ovale is mostly seen in Africa, causesmilder type similar to P.vivax - butrelapses can occur.
• P. malariae is also of milder type similarto P.vivax (benign quartan) with noexoerythrocytic cycle.
Chemical Classification
4-aminoquinolinesChloroquine, amodiaquine
8 – aminoquinolinesPrimaquine, bulaquine
Quinoline methanolsQuinine, quinidine, mefloquine
AcridineMepacrine
Folate antagonistsProguanil, sulfadoxine, pyrimethamine
Phenanthrene methanolHalofantrine, atovaquone
Sesquiterpine lactonesArtesunate, artemether, arteether
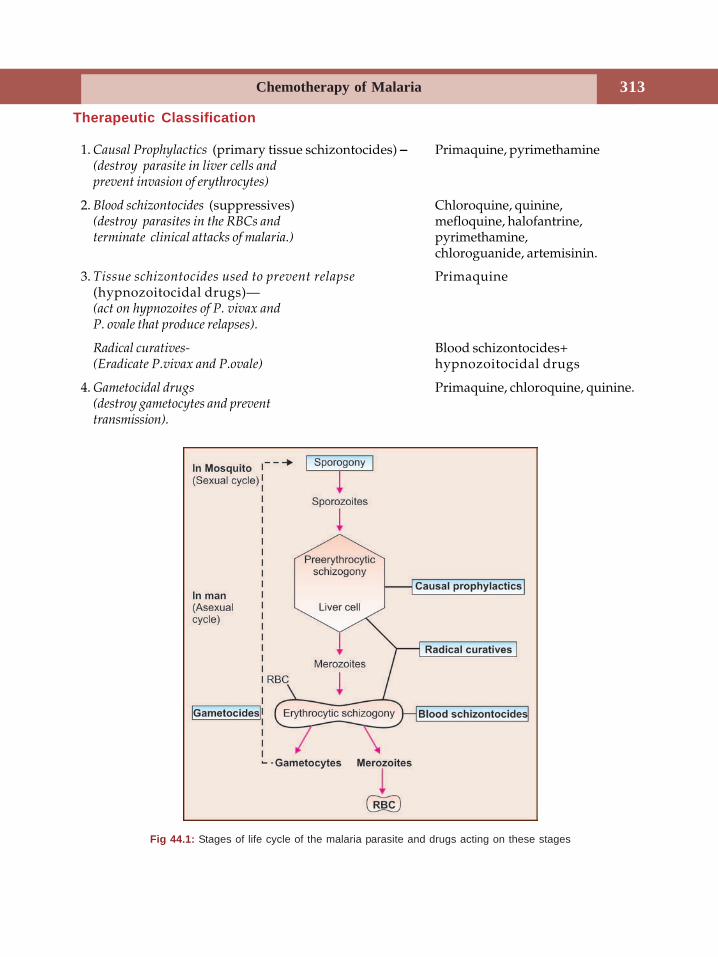
Chemotherapy of Malaria 313
Fig 44.1: Stages of life cycle of the malaria parasite and drugs acting on these stages
Therapeutic Classification
1. Causal Prophylactics (primary tissue schizontocides) −−−−− Primaquine, pyrimethamine(destroy parasite in liver cells andprevent invasion of erythrocytes)
2. Blood schizontocides (suppressives) Chloroquine, quinine,(destroy parasites in the RBCs and mefloquine, halofantrine,terminate clinical attacks of malaria.) pyrimethamine,
chloroguanide, artemisinin.
3. Tissue schizontocides used to prevent relapse Primaquine(hypnozoitocidal drugs)—(act on hypnozoites of P. vivax andP. ovale that produce relapses).
Radical curatives- Blood schizontocides+(Eradicate P.vivax and P.ovale) hypnozoitocidal drugs
4. Gametocidal drugs Primaquine, chloroquine, quinine.(destroy gametocytes and preventtransmission).
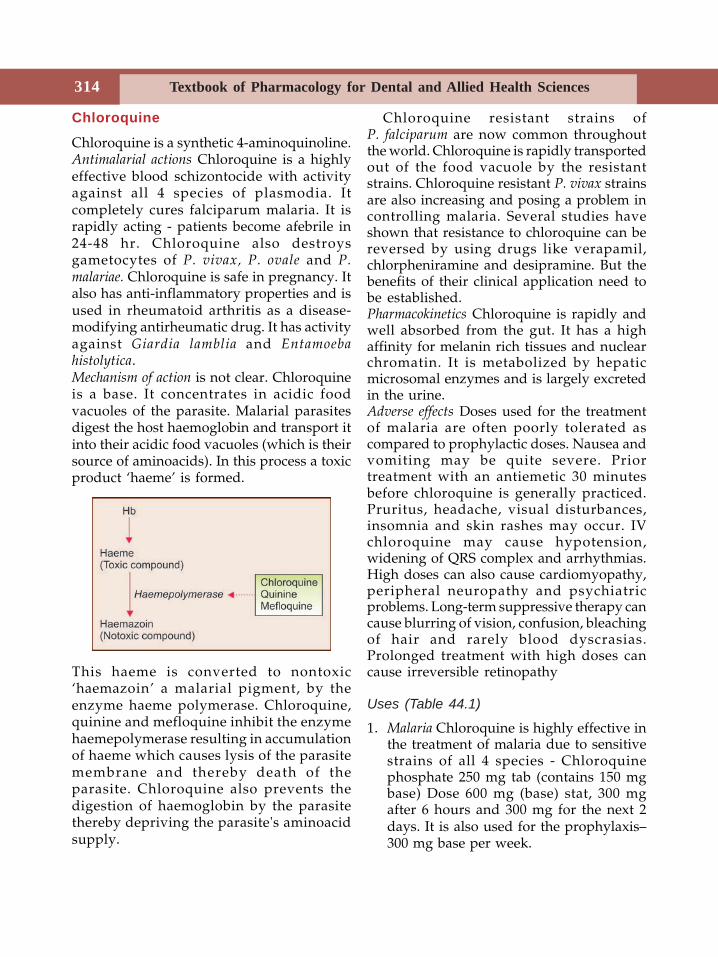
Textbook of Pharmacology for Dental and Allied Health Sciences314
Chloroquine
Chloroquine is a synthetic 4-aminoquinoline.Antimalarial actions Chloroquine is a highlyeffective blood schizontocide with activityagainst all 4 species of plasmodia. Itcompletely cures falciparum malaria. It israpidly acting - patients become afebrile in24-48 hr. Chloroquine also destroysgametocytes of P. vivax, P. ovale and P.malariae. Chloroquine is safe in pregnancy. Italso has anti-inflammatory properties and isused in rheumatoid arthritis as a disease-modifying antirheumatic drug. It has activityagainst Giardia lamblia and Entamoebahistolytica.Mechanism of action is not clear. Chloroquineis a base. It concentrates in acidic foodvacuoles of the parasite. Malarial parasitesdigest the host haemoglobin and transport itinto their acidic food vacuoles (which is theirsource of aminoacids). In this process a toxicproduct ‘haeme’ is formed.
This haeme is converted to nontoxic‘haemazoin’ a malarial pigment, by theenzyme haeme polymerase. Chloroquine,quinine and mefloquine inhibit the enzymehaemepolymerase resulting in accumulationof haeme which causes lysis of the parasitemembrane and thereby death of theparasite. Chloroquine also prevents thedigestion of haemoglobin by the parasitethereby depriving the parasite's aminoacidsupply.
Chloroquine resistant strains ofP. falciparum are now common throughoutthe world. Chloroquine is rapidly transportedout of the food vacuole by the resistantstrains. Chloroquine resistant P. vivax strainsare also increasing and posing a problem incontrolling malaria. Several studies haveshown that resistance to chloroquine can bereversed by using drugs like verapamil,chlorpheniramine and desipramine. But thebenefits of their clinical application need tobe established.Pharmacokinetics Chloroquine is rapidly andwell absorbed from the gut. It has a highaffinity for melanin rich tissues and nuclearchromatin. It is metabolized by hepaticmicrosomal enzymes and is largely excretedin the urine.Adverse effects Doses used for the treatmentof malaria are often poorly tolerated ascompared to prophylactic doses. Nausea andvomiting may be quite severe. Priortreatment with an antiemetic 30 minutesbefore chloroquine is generally practiced.Pruritus, headache, visual disturbances,insomnia and skin rashes may occur. IVchloroquine may cause hypotension,widening of QRS complex and arrhythmias.High doses can also cause cardiomyopathy,peripheral neuropathy and psychiatricproblems. Long-term suppressive therapy cancause blurring of vision, confusion, bleachingof hair and rarely blood dyscrasias.Prolonged treatment with high doses cancause irreversible retinopathy
Uses (Table 44.1)
1. Malaria Chloroquine is highly effective inthe treatment of malaria due to sensitivestrains of all 4 species - Chloroquinephosphate 250 mg tab (contains 150 mgbase) Dose 600 mg (base) stat, 300 mgafter 6 hours and 300 mg for the next 2days. It is also used for the prophylaxis–300 mg base per week.
Chemotherapy of Malaria 315
2. Extraintestinalamoebiasis (Page 321)
3. Rheumatoid arthritis4. Photogenic reactions5. Lepra reactions
(Page 298)
Precautions and Contraindications
• Chloroquine should be avoided or usedcarefully in patients with myopathy andhepatic, gastrointestinal or neurologicaldisorders.
• Concurrent use of gold or d-penicillaminewith chloroquine can cause more severedermatitis.
• Chloroquine, quinine and mefloquineshould not be given concurrently becausethey compete for accumulation in theparasite and may result in therapeuticfailure. Also, chloroquine + mefloquine→→→→→increased risk of seizures.
• Chloroquine + halofantrine →→→→→ increasedrisk of arrhythmias. Hence a gap of at least12 hours should be given if patientshave to be switched over from chloro-quine to quinine/mefloquine/halof-antrine.
• Chloroquine should be avoided in patientswith retinal diseases. When chloroquineis given in high doses for a long time,regular neurological and eye examinationshould be done.
Quinine
Quinine is an alkaloid obtained from the barkof the cinchona tree. It destroys erythrocyticforms of the parasite similar to chloroquineand is useful as a suppressive. It is alsogametocidal for three species of the malarialparasite except for P. falciparum. Mechanismof action is unknown. It may act likechloroquine by inhibiting the enzyme haemepolymerase.
Other Actions
• Quinine also has mild analgesic andantipyretic activity.
• Like quinidine it is also a myocardiacdepressant. IV administration can causesignificant hypotension.
• It acts as local anaesthetic and has skeletalmuscle relaxant properties.
• Quinine stimulates the uterus and is anabortifacient.
Pharmacokinetics Quinine is well absorbedorally, widely distributed in the body,metabolized in the liver and excreted in theurine.
Adverse Effects are high
• Quinine is highly bitter and is a gastricirritant-causes nausea, vomiting andepigastric pain-hence poorly tolerated.
• Hypoglycaemia can be quite profound toresult in coma. Hypoglycaemia may bebecause - i. quinine stimulates the insulinrelease. ii. parasite consumes glucose.
• Cinchonism with ringing in the ears,headache, nausea, visual disturbances andvertigo may be encountered.
• In more severe poisoning, hypoglycaemia,fever, delirium, confusion, hypotension,cardiac arrhythmias and coma maydevelop. Death is due to respiratoryarrest.
• Black water fever - quinine can precipitateacute haemolytic anaemia with renalfailure, haemoglobinuria and fever, whichcan be fatal. Fortunately this complicationis uncommon.
Uses
• Quinine is used in the treatment ofresistant falciparum malaria and cerebralmalaria. Dose - Table 44.1.
• Nocturnal muscle cramps.
Effectivebecause of antiinflammatoryproperty.
}
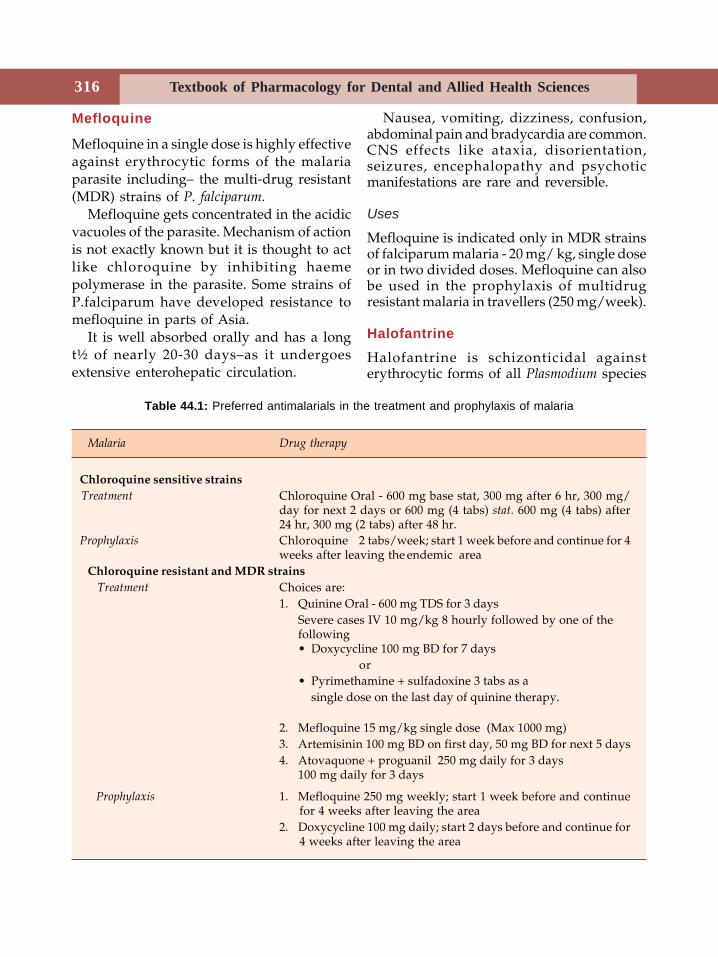
Textbook of Pharmacology for Dental and Allied Health Sciences316
Mefloquine
Mefloquine in a single dose is highly effectiveagainst erythrocytic forms of the malariaparasite including– the multi-drug resistant(MDR) strains of P. falciparum.
Mefloquine gets concentrated in the acidicvacuoles of the parasite. Mechanism of actionis not exactly known but it is thought to actlike chloroquine by inhibiting haemepolymerase in the parasite. Some strains ofP.falciparum have developed resistance tomefloquine in parts of Asia.
It is well absorbed orally and has a longt½ of nearly 20-30 days–as it undergoesextensive enterohepatic circulation.
Nausea, vomiting, dizziness, confusion,abdominal pain and bradycardia are common.CNS effects like ataxia, disorientation,seizures, encephalopathy and psychoticmanifestations are rare and reversible.
Uses
Mefloquine is indicated only in MDR strainsof falciparum malaria - 20 mg/ kg, single doseor in two divided doses. Mefloquine can alsobe used in the prophylaxis of multidrugresistant malaria in travellers (250 mg/week).
HalofantrineHalofantrine is schizonticidal againsterythrocytic forms of all Plasmodium species
Table 44.1: Preferred antimalarials in the treatment and prophylaxis of malaria
Malaria Drug therapy
Chloroquine sensitive strains Treatment Chloroquine Oral - 600 mg base stat, 300 mg after 6 hr, 300 mg/
day for next 2 days or 600 mg (4 tabs) stat. 600 mg (4 tabs) after24 hr, 300 mg (2 tabs) after 48 hr.
Prophylaxis Chloroquine 2 tabs/week; start 1 week before and continue for 4weeks after leaving the endemic area
Chloroquine resistant and MDR strains Treatment Choices are:
1. Quinine Oral - 600 mg TDS for 3 daysSevere cases IV 10 mg/kg 8 hourly followed by one of thefollowing• Doxycycline 100 mg BD for 7 days
or• Pyrimethamine + sulfadoxine 3 tabs as a
single dose on the last day of quinine therapy.
2. Mefloquine 15 mg/kg single dose (Max 1000 mg)3. Artemisinin 100 mg BD on first day, 50 mg BD for next 5 days4. Atovaquone + proguanil 250 mg daily for 3 days
100 mg daily for 3 days
Prophylaxis 1. Mefloquine 250 mg weekly; start 1 week before and continuefor 4 weeks after leaving the area
2. Doxycycline 100 mg daily; start 2 days before and continue for4 weeks after leaving the area
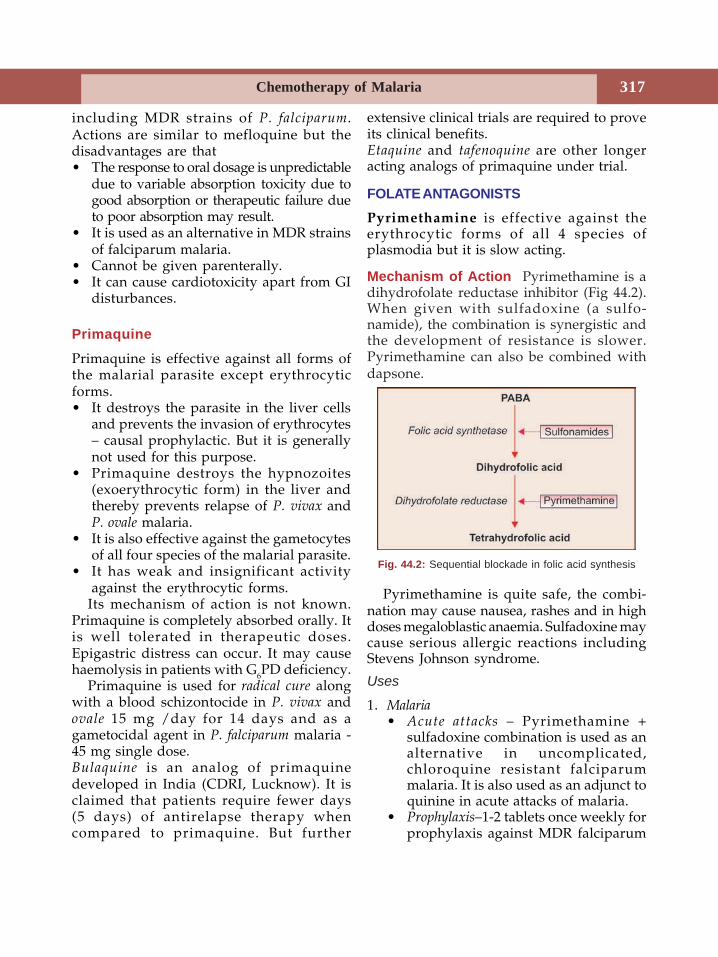
Chemotherapy of Malaria 317
including MDR strains of P. falciparum.Actions are similar to mefloquine but thedisadvantages are that• The response to oral dosage is unpredictable
due to variable absorption toxicity due togood absorption or therapeutic failure dueto poor absorption may result.
• It is used as an alternative in MDR strainsof falciparum malaria.
• Cannot be given parenterally.• It can cause cardiotoxicity apart from GI
disturbances.
Primaquine
Primaquine is effective against all forms ofthe malarial parasite except erythrocyticforms.• It destroys the parasite in the liver cells
and prevents the invasion of erythrocytes– causal prophylactic. But it is generallynot used for this purpose.
• Primaquine destroys the hypnozoites(exoerythrocytic form) in the liver andthereby prevents relapse of P. vivax andP. ovale malaria.
• It is also effective against the gametocytesof all four species of the malarial parasite.
• It has weak and insignificant activityagainst the erythrocytic forms.
Its mechanism of action is not known.Primaquine is completely absorbed orally. Itis well tolerated in therapeutic doses.Epigastric distress can occur. It may causehaemolysis in patients with G6PD deficiency.
Primaquine is used for radical cure alongwith a blood schizontocide in P. vivax andovale 15 mg /day for 14 days and as agametocidal agent in P. falciparum malaria -45 mg single dose.Bulaquine is an analog of primaquinedeveloped in India (CDRI, Lucknow). It isclaimed that patients require fewer days(5 days) of antirelapse therapy whencompared to primaquine. But further
extensive clinical trials are required to proveits clinical benefits.Etaquine and tafenoquine are other longeracting analogs of primaquine under trial.
FOLATE ANTAGONISTSPyrimethamine is effective against theerythrocytic forms of all 4 species ofplasmodia but it is slow acting.
Mechanism of Action Pyrimethamine is adihydrofolate reductase inhibitor (Fig 44.2).When given with sulfadoxine (a sulfo-namide), the combination is synergistic andthe development of resistance is slower.Pyrimethamine can also be combined withdapsone.
Pyrimethamine is quite safe, the combi-nation may cause nausea, rashes and in highdoses megaloblastic anaemia. Sulfadoxine maycause serious allergic reactions includingStevens Johnson syndrome.
Uses
1. Malaria• Acute attacks – Pyrimethamine +
sulfadoxine combination is used as analternative in uncomplicated,chloroquine resistant falciparummalaria. It is also used as an adjunct toquinine in acute attacks of malaria.
• Prophylaxis–1-2 tablets once weekly forprophylaxis against MDR falciparum
Fig. 44.2: Sequential blockade in folic acid synthesis
Textbook of Pharmacology for Dental and Allied Health Sciences318
malaria–when a person is visiting anendemic area.
2. Toxoplasmosis–Pyrimethamine + sulfa-doxine combination is the treatment ofchoice for Toxoplasma gondi infection.Pyrimethamine is given as 200 mg bolusdose followed by 50 mg daily for 4 to 6weeks along with sulfadoxine 4 g/day.Leucovorin (folinic acid) should be given10 mg daily to prevent severe folatedeficiency.
Chloroguanide (Proguanil) is a schizontocidewith causal prophylactic activity against thepre-erythrocytic forms of the malariaparasite. It is used -• with atovaquane in the treatment of MDR
falciparum malaria.• for causal prophylaxis of falciparum
malaria• as an alternative to pyrimethamine-
sulfadoxine for prophylaxis of MDRfalciparum malaria.
Atovaquone – is a naphthaquinone, effectiveagainst the erythrocytic forms of plasmodia.When combined with proguanil, the activityis synergistic and development of resistanceis less common.Mechanism of action– Atovaquone inhibits themitochondrial electron transport andcollapses the mitochondrial membrane in themalarial parasite. Proguanil potentiates thisaction.
Atovaquone is also effective againstT. gondii and P. carinii (P.jiroveci) infections.
Adverse effects include vomiting,headache and abdominal pain. It iscontraindicated in pregnancy.Uses Atovaquone + Proguanil can be used inthe treatment of chloroquine resistant andmulti drug–resistant falciparum malariaAtovaquone 250 mg + proguanil 100 mg dailyfor three days. Atovaquone may also be usedin P. carinii infection as an alternative tocotrimoxazole.
Artimisinin and Derivatives
Artemisinin is a sesquiterpine lactone obtainedfrom the plant Artemisia annua which has beenused in chinese traditional medicine‘Quinghaosu’ for almost 2000 years.Mechanism of action–Artemisinin interactswith heme resulting in the generation of freeradicals that bind to the membrane proteinand damages the parasite membrane.
Artemisinin is a potent, rapidly acting,blood schizontocide effective against all the4 plasmodial species, including MDR P.falciparum. It is also effective againstgametocytes. It is useful in cerebral malaria.No resistant strains are known so far.Recrudescence (the disease becomes activeagain after a period of remission) is commondue to its short t½. Combining withmefloquine avoids this. It has been shownthat it can be safely used in pregnancy.
Artesunate (oral, IM, IV, rectal) andartemether (IM, oral) artemisinin(oral) andarteether (IM) are the compounds used .Arteether is longer acting - given 150 mg (IM)for 3 days.
Artemisinin and derivatives are the besttolerated antimalarials–mild GI symptoms,fever, itching and bradycardia are reported.Uses Acute attacks of MDR falciparum malariaand cerebral malaria. Artemisinin can be usedeven in pregnancy.Dose Artemisinin - Orally 100 mg BD on firstday, 50 mg BD for the next 4 days and inmore severe cases, artesunate IV 120 mg onthe first day, 60 mg daily for the next 4 days;mefloquine (25 mg/kg)is given on the secondday.
Newer Antimalarials Lumefantrine andpyronaridine were synthesized in China.Both are effective against erythrocytic formsof the malaria parasite. Both have poor oralbioavailability. Lumefantrine is combinedwith artemisinin/mefloquine in the treatmentof MDR falciparum malaria.
45 Drugs Used inAmoebiasis,
Leishmaniasis andTrypanosomiasis
ANTIAMOEBIC DRUGS
Amoebiasis caused by the protozoanEntamoeba histolytia is a tropical diseasecommon in developing countries. It spreadsby faecal contamination of food and water.Though it primarily affects colon, otherorgans like liver, lungs and brain are thesecondary sites. Acute amoebiasis ischaracterised by bloody mucoid stools andabdominal pain. Chronic amoebiasismanifests as anorexia, abdominal pain,intermittent diarrhoea and constipation. Cystpassers or carriers are symptom free.
Classification
1. Drugs effective in both intestinal andextraintestinal amoebiasis
Metronidazole, Tinidazole,Secnidazole, Ornidazole,Satranidazole, EmetineDehydroemetine.
2. Drugs effective only in intestinal amoebiasis(Luminal amoebicides)Diloxanide furoate, Quiniodochlor,Iodoquinol, Tetracylines.
3. Drugs effective only in extraintestinalamoebiasis
Chloroquine
Metronidazole
Metronidazole a nitroimidazole, is a powerfulamoebicide. Apart from this it also inhibitsTrichomonas vaginalis, Giardia lamblia andBalantidium coli. Anaerobic bacteria are alsosensitive.Mechanism of action Metronidazole is aprodrug. Susceptible microorganisms reducethe nitro group of metronidazole by anitroreductase and convert it to a cytotoxicderivative which binds to DNA and inhibitsprotein synthesis.Aerobic bacteria lack thisnitroreductase and are therefore notsusceptible to metronidazole.Pharmacokinetics Metronidazole is well-absorbed and reaches adequate conc-entrations in the CSF; has a plasma t½ - 8 hr.It is metabolised in the liver by oxidation andglucuronide conjugation.Adverse effects Gastrointestinal effects likenausea, anorexia, abdominal pain andmetallic taste in the mouth are the mostfrequent. Headache, stomatitis, glossitis,furry tongue; dizziness, insomnia, ataxia,vertigo and rarely peripheral neuropathy canoccur. Pruritus, urticaria and skin rashes canalso occur. High doses can cause convulsions.

Textbook of Pharmacology for Dental and Allied Health Sciences320
Hence metronidazole should be cautiouslyused in patients with neurological diseasesand severe hepatic dysfunction. It iscontraindicated in pregnancy. Intravenousinjection can cause thrombophlebitis. This canbe avoided by adequate dilution of the drugsolution.
Drug Interactions
• Metronidazole can produce a disulfiram -like reaction in patients taking alcohol.Hence patients should be advised to avoidalcohol while on metronidazole.
• Drugs like cimetidine which aremicrosomal enzyme inhibitors, enhanceplasma levels of metronidazole resultingin toxicity.
Preparations
Metronidazole is available as 200, 400 mgtablets; 200 mg /5 ml suspension; 500 mg /100 ml inj and 1% gel and ointment.
Uses
1. Anaerobic infections(a) Ordental infections–Metronidozole andit congeners are one of the mostcommonly used antimicrobial agents indentistry because anaerobes are animportant component of the oral flora.Hence most acute odontogenic infectionsare caused by a combination of aerobicand anaerobic bacteria. Metronidazole isthe drug of choice for most odontogenicinfections especially those not controlledby penicillins. Odontogenic infections likeacute periapical abscess, periodontitis,acute ulcerative gingivitis, pericoronitisand other oral infections and salivary glandinfections are treated with metronidazole(200-400 mg TDS) in combination with anantibiotic effective against aerobes like apenicillin or a macrolide. Clindamycin
being effective against gram-positive andanaerobic bacteria is an alternative.(b) Anaerobic infections at other sites-Intra-abdominal infections, brainabscesses, genitourinary infections areoften mixed infections with aerobes andanaerobes. Metro-nidazole is used incombination with other antimicrobials.Metronidazole is given intravenously forserious anaerobic infections. It is alsouseful for surgical prophylaxis ofabdominal and pelvic infections.
2. Amoebiasis–Metronidazole is the drug ofchoice in all forms of amoebiasis in thedose of 400-800 mg TDS for 7-10 days.But it does not eradicate the cysts.
3. Trichomonas vaginitis–Metronidazole 200mg TDS for 7 days is the drug of choice.
4. Giardiasis–Metronidazole given 200 mgTDS for 7 days is the treatment of choice.
5. H. pylori infections in peptic ulcer patientscan be treated with a combination ofmetronidazole, clarithromycin andomeprazole/ranitidine.
6. Pseudomembranous colitis due to Clostridiumdifficile–responds to metronidazole.
7. Dracunculosis Metronidazole facilitatesextraction of the guinea worm.
8. Topical preparations - like gel and ointmentare used in skin infections and acne.
Tinidazole is longer-acting and is bettertolerated than metronidazole due to fewerside effects. It can be given 2 g once daily for3 days in amoebiasis and as a single dose formost other indications of metronidazole.Secnidazole is longer-acting (t½ 18-30 hrs) andcan be given as a single 2 g dose for mostindications of metronidazole.Ornidazole–is similar to tinidazole and islonger acting.Satranidazole – More potent and longer actingthan metronidazole. It is claimed to be bettertolerated particularly because it does notcause nausea or metallic taste.

Drugs Used in Amoebiasis, Leishmaniasis and Trypanosomiasis 321
Emetine and Dehydroemetine
Emetine and dehydroemetine derived fromIpecac (Brazil root) directly affect thetrophozoites but not the cysts. As oralabsorption is improper, they are givenparenterally. They can be used only in severeamoebiasis but are not preferred due totoxicity. Adverse effects include pain at theinjection site, thrombophlebitis, nausea,vomiting, diarrhoea and cardiotoxicity.
Diloxanide Furoate
Diloxanide furoate is directly amoebicidal.Flatulence, nausea and occasionallyabdominal cramps and rashes can occur. It isused alone in asymptomatic cyst passers, mildintestinal amoebiasis and along with anitroimidazole–for the cure of amoebiasis,because diloxanide eradicates cysts. It isgiven orally–500 mg TDS for 10 days. It isalso available in combination withmetronidazole (DYRADE-M).
Chloroquine
Chloroquine attains high concentration inthe liver, is directly toxic againsttrophozoites and is therefore useful inhepatic amoebiasis. As chloroquine iscompletely absorbed from the smallintestines, it is not effective againstamoebae in the colon. It is used (300 mg/day for 2-3 weeks) as an alternative tometronidazole in hepatic amoebiasis. Aluminal amoebicide should also be given.
Iodoquinol and Quiniodochlor
Iodoquinol and quiniodochlor (8-hydro-xyquinolines) are directly acting luminalamoebicides. They were used for eradicationof cysts but are not preferred now due totheir toxicity like subacute myelo-opticneuropathy.
Tetracylines The older tetracylines are notwell-absorbed and large amounts reach thecolon–hence these are useful in intestinalamoebiasis. They inhibit the intestinal floraand break the symbiosis between them andthe amoebae. Tetracyclines are used asadjuvants in chronic cases.
Treatment of Different Forms ofAmoebiasis
1. Acute intestinal amoebiasis–one of thefollowing can be given.• Metronidazole 400-800 mg TDS for 5-
7 days (METROGYL, FLAGYL)or
• Metronidazole 2.4 g OD for 3 daysor
• Tinidazole 2 g OD for 3 days (TINIBA)or
• Secnidazole 2 g single dose (SECZOL,SECNIL)
This should be followed by diloxanidefuroate 500 mg TDS for 10 days to eradicatethe cysts.2. Chronic amoebiasis Diloxanide furoate 500
mg TDS for 10 days or tetracycline 250mg qid for 10 days.
3. Hepatic amoebiasis requires intensivetreatment for the complete eradication ofthe parasite from the liver in order to avoidrelapses. A course of metronidazole ortinidazole are the first line drugs. In additionchloroquine may be given to ensurecomplete destruction of the liver forms. Acourse of diloxanide furoate should followin order to eradicate the cysts.
TREATMENT OF PNEUMOCYSTOSISPneumocystis carinii is a micro-organismhaving features of both protozoa and fungithough now considered by most to be afungus. Recent studies have shown thatpneumocystosis in human beings is causedby Pneumocystis jiroveci while P.carinii causespneumocystosis in animals.
Textbook of Pharmacology for Dental and Allied Health Sciences322
It is now known to cause opportunisticinfections particularly pneumonia in patientswith AIDS which can often be fatal.Drugs used in the treatment of pneumo-cystosis include• Cotrimoxazole - high oral dose of
Trimethoprim 20 mg/kg + sulphame-thoxazole 100 mg/kg daily.
• Pentamidine - 4 mg/kg daily for 14 daysparenterally.
• Atovaquone - as an alternative tocotrimoxazole.
LEISHMANIASIS
Leishmaniasis is caused by protozoa of thegenus Leishmania. Kala-azar or visceralleishmaniasis is caused by Leishmania donovani;oriental sore by L. tropica and mucocutaneousleishmaniasis by L. braziliensis. The infectionis transmitted by the bite of the femalesandfly phlebotomus. It is endemic in Bihar.Drugs used in leishmaniasis include:Antimony compounds Sodium stibogluconate
Meglumine antimonateDiamidines PentamidineOther drugs Amphotericin B, Ketoconazle,
Allopurinol, Paramomycin
Antimony Compounds
Sodium stibogluconate, a pentavalentantimonial is the most effective drug in kala-azar. It is also effective in mucocutaneous andcutaneous leishmaniasis. It is given as a 4%solution in the dose of 10-20 mg/kg IM(gluteal region) or IV for 20 days. Mechanismof action is unknown.
Adverse effects include a metallic taste inthe mouth, nausea, vomiting, diarrhoea,headache, myalgia, arthralgia, pain at theinjection site, bradycardia, skin rashes,haematuria and jaundice. Some cases ofsudden death due to shock have occurred.ECG should be monitored as arrhythmias canoccur during the later days of therapy.
Though sodium stibogluconate is quiteeffective, resistance has been encountered inendemic areas like Bihar.Meglumine antimonate and ethyl stibamine canalso be used in all forms of leishmaniasis.Pentamidine is an aromatic diamidine effectiveagainst Leishmania donovani, trypanosomes,Pneumocystis carinii and some fungi. Givenintramuscularly the drug is rapidly absorbedbut very little reaches the CNS. Dose 4 mg/kg deep IM/slow IV on alternate days for 5-25 weeks.
Adverse effects Pentamidine liberateshistamine which is responsible for vomiting,diarrhoea, flushing, pruritis, rashes,tachycardia and hypotension apart from painat the injection site. Other effects includehepatotoxicity, renal impairment, ECGchanges and in some patients diabetesmellitus may be precipitated.
Uses
1. Leishmaniasis Pentamidine can be used invisceral leishmaniasis as an alternative tosodium stibogluconate.
2. Trypanosomiasis Pentamidine can be usedas an alternative to suramin or along withsuramin in trypanosomiasis. It can also beused for chemoprophylaxis against Africantrypanosomiasis.
3. Pneumocystosis Pentamidine is analternative in Pneumocystis jiroveciinfections in patients unable to toleratecotrimoxazole.
Other Drugs
Amphotericin B (page 300) has been tried inleishmaniasis in the endemic areas whereantimonials may be ineffective.Ketoconazole inhibits ergosterol synthesis inthe leishmania and is effective in cutaneousleishmaniasis.

Drugs Used in Amoebiasis, Leishmaniasis and Trypanosomiasis 323
Allopurinol (page 188) In leishmania,allopurinol is converted to a metabolitewhich inhibits protein synthesis. It may beused along with antimonials.Dose: 300 mg 3-4 times a day for 2-4 weeks.Paramomycin (aminosidine) is an amoebicidaldrug which is also found to be effective inleishmaniasis. It is useful in all forms ofleishmaniasis. It can be used alone or incombination with antimonials.
TRYPANOSOMIASIS
Trypanosomiasis is caused by protozoa of thegenus Trypanosoma. African trypanosomiasisor sleeping sickness is caused by T. gambienseand T. rhodesiense while South Americantrypanosomiasis is caused by T. Cruzi. Drugsused in trypanosomiasis are suramin,pentamidine, melarsoprol, eflornithine,nifurtimox and benznidazole. Suramin sodium
is the drug of choice for early stage oftrypanosomiasis but it does not cross the BBBand therefore cannot be used in later stagesof the disease. It is also useful for theprophylaxis but pentamidine is preferable.Suramin is given IV; it is extensively boundto plasma proteins and may be traced fornearly 3 months in the plasma. Suramin isalso effective in eradicating adult forms ofOnchocerca volvulus.
Toxicity is high; vomiting, shock and lossof consciousness may follow IV injections.Rash, neuropathies, haemolytic anaemia andagranulocytosis may also occur.Melarsoprol is the preferred drug in laterstages of trypanosomiasis which is associatedwith encephalitis and meningitis.Eflornithine is used as an alternative in CNStrypanosomiasis. Nifurtimox and benznida-zole are useful in Chaga’s disease (Americantrypanosomiasis).
Textbook of Pharmacology for Dental and Allied Health Sciences324
46Anthelmintics
Worm infestations are more common in thedeveloping countries. It is seen in peoplewith poor hygiene. Anthelmintics aredeworming agents. A vermicidal kills while avermifuge promotes expulsion of worms.
BenzimidazolesBenzimidazoles include thiabendazole,mebendazole and albendazole. Thiaben-dazole the first agent of this group wasdiscovered in 1961 but now the newer ones,mebendazole and albendazole are morecommonly used due to lesser toxicity.
MebendazoleMebendazole a broad spectrum anthelminticcures roundworm, hookworm, pinworm andstrongyloides infestations. The eggs andlarvae are also destroyed. The dead parasitesare slowly expelled from the gut over severaldays.Mechanism of action Benzimidazoles bind toβ-tubulin with high affinity and inhibitglucose uptake in the parasite.Pharmacokinetics Mebendazole is poorlyabsorbed from the gut and also undergoesfirst pass metabolism - bioavailabilityaround 20%. Fatty food enhancesabsorption. Mebendazole is extensivelybound to plasma proteins and is metabolisedby the liver.Mebendazole is given orally 100 mg twice aday for 3 days.
Adverse effects Mebendazole is well-tolerated;nausea, abdominal pain and diarrhoea areseen in heavy infestations. Large doses mayrarely cause headache, dizziness, loss of hairand granulocytopenia. It may rarely provokeabnormal migration of the roundwormswhich may come out through the mouth ornose.Uses Mebendazole is used in the treatmentof roundworm, hookworm, pinworm,tapeworm, trichuriasis and hydatid disease.It is of special value in multiple worminfestations. (Table 46.1)
Albendazole
Albendazole is a congener of mebendazolewith actions and mechanism of action similarto mebendazole but it has several advantagesover it.
Advantages over Mebendazole
• Albendazole is better tolerated• Effective in single dose• Superior to mebendazole in hook worm
and thread worm infections, hydatiddisease and neurocysticercosis
• Albendazole also has some activity againstTrichomonas vaginalis, Giardia lamblia andWuchareria.bancrofti.
• The active metabolite of albendazoleachieves a higher concentration (100 timesmore) than mebendazole.
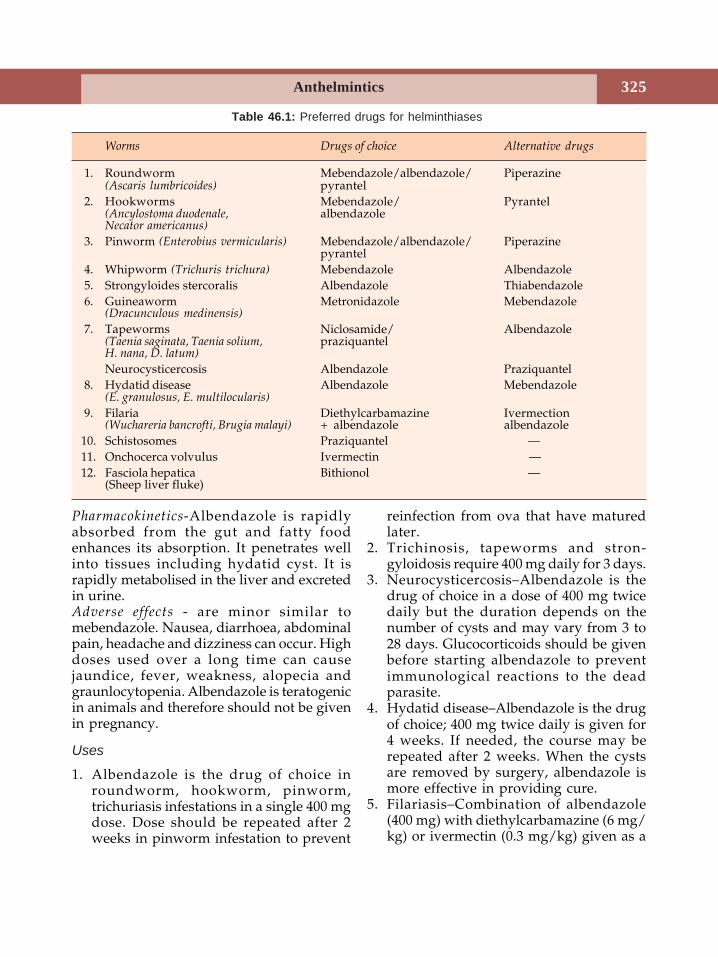
Anthelmintics 325
Pharmacokinetics-Albendazole is rapidlyabsorbed from the gut and fatty foodenhances its absorption. It penetrates wellinto tissues including hydatid cyst. It israpidly metabolised in the liver and excretedin urine.Adverse effects - are minor similar tomebendazole. Nausea, diarrhoea, abdominalpain, headache and dizziness can occur. Highdoses used over a long time can causejaundice, fever, weakness, alopecia andgraunlocytopenia. Albendazole is teratogenicin animals and therefore should not be givenin pregnancy.
Uses
1. Albendazole is the drug of choice inroundworm, hookworm, pinworm,trichuriasis infestations in a single 400 mgdose. Dose should be repeated after 2weeks in pinworm infestation to prevent
reinfection from ova that have maturedlater.
2. Trichinosis, tapeworms and stron-gyloidosis require 400 mg daily for 3 days.
3. Neurocysticercosis–Albendazole is thedrug of choice in a dose of 400 mg twicedaily but the duration depends on thenumber of cysts and may vary from 3 to28 days. Glucocorticoids should be givenbefore starting albendazole to preventimmunological reactions to the deadparasite.
4. Hydatid disease–Albendazole is the drugof choice; 400 mg twice daily is given for4 weeks. If needed, the course may berepeated after 2 weeks. When the cystsare removed by surgery, albendazole ismore effective in providing cure.
5. Filariasis–Combination of albendazole(400 mg) with diethylcarbamazine (6 mg/kg) or ivermectin (0.3 mg/kg) given as a
Table 46.1: Preferred drugs for helminthiases
Worms Drugs of choice Alternative drugs
1. Roundworm Mebendazole/albendazole/ Piperazine(Ascaris lumbricoides) pyrantel
2. Hookworms Mebendazole/ Pyrantel(Ancylostoma duodenale, albendazoleNecator americanus)
3. Pinworm (Enterobius vermicularis) Mebendazole/albendazole/ Piperazinepyrantel
4. Whipworm (Trichuris trichura) Mebendazole Albendazole5. Strongyloides stercoralis Albendazole Thiabendazole6. Guineaworm Metronidazole Mebendazole
(Dracunculous medinensis)
7. Tapeworms Niclosamide/ Albendazole(Taenia saginata, Taenia solium, praziquantelH. nana, D. latum)
Neurocysticercosis Albendazole Praziquantel8. Hydatid disease Albendazole Mebendazole
(E. granulosus, E. multilocularis)
9. Filaria Diethylcarbamazine Ivermection(Wuchareria bancrofti, Brugia malayi) + albendazole albendazole
10. Schistosomes Praziquantel —11. Onchocerca volvulus Ivermectin —12. Fasciola hepatica Bithionol —
(Sheep liver fluke)
Textbook of Pharmacology for Dental and Allied Health Sciences326
single dose is found to be effective in W.bancrofti in suppressing microfilariae forone year. This also prevents the spreadof filariasis and may be continued once ayear for 5-6 years.
ThiabendazoleThiabendazole a benzimidazole, acts likemebendazole. But due to frequent sideeffects, it is not preferred. Dizziness,anorexia, vomiting, diarrhoea, drowsiness,paraesthesia, bradycardia, hypotension,convulsions and liver damage can occur. It isused as an alternative to albendazole instrongyloidosis and cutaneous larva migrans.
Pyrantel PamoatePyrantel pamoate is effective againstroundworm, hookworm and pinworms. Itstimulates the nicotinic cholinergic receptorin the worm leading to persistentdepolarisation and spastic paralysis(depolarising neuromuscular blocker). Theparalysed worms are expelled.
It is well-tolerated; occasional abdominalpain, headache, rashes, weakness anddizziness may occur. Dose: 10-15 mg/kgsingle dose.Uses Pyrantel pamoate is used in thetreatment of roundworm, hookworm andpinworm infestations.Oxantel pamoate an analog of pyrantelpamoate is effective in the treatment oftrichuriasis infection.
Piperazine CitratePiperazine citrate is effective in roundwormand pinworm infestations. It competitivelyblocks the actions of acetylcholine andthereby contractions in the worms. Flaccidparalysis results and the worms are expelled.
Adverse effects are mild–gastrointestinalsymptoms, headache and dizziness are seenoccasionally. Piperazine citrate is indicatedfor roundworm and pinworm infestations.It is also safe in pregnancy.
LevamisoleLevamisole is effective against roundwormsand hookworms and can be used as analternative drug in these infestations. It iswell-tolerated and is effective in a single dose.It is also an immunomodulator.
Niclosamide
Niclosamide is effective against mosttapeworms. The segments of the deadtapeworms are partly digested and in caseof T. solium, the ova released from thesesegments may develop into larvae and reachvarious organs resulting in visceralcysticercosis. Purge may be given 2 hoursafter niclosamide to wash off the worms andavoid cysticercosis. The scolex detected in thestool ensures eradication.
Niclosamide is well-tolerated. Abdominaldiscomfort and rarely pruritus and rashesmay occur.Uses Niclosamide is the drug of choice ininfestations by tapeworms like T. solium,T. saginata, H. nana and D. latum. It is also analternative drug in intestinal fluke infestation.
PraziquantelPraziquantel is effective against schistosomesof all species, most other trematodes andcestodes including cysticercosis. It is effectiveas a single oral dose in most infestations. Itincreases cell membrane permeability tocalcium resulting in contraction followed byparalysis and the worms are expelled.Adverse effects are mild and include GIdisturbances, headache, dizziness, drow-siness, rashes and myalgia.
Uses
1. Schistosomiasis Praziquantel is the drug ofchoice in all forms of schistosomiasis.
2. Tapeworms Single dose (10 mg/kg) ofpraziquantel is effective in all tapeworminfestations. In T. solium it has the
Anthelmintics 327
advantage that it kills the larvae andtherefore visceral cysticercosis is avoided.
3. Neurocysticercosis Praziquantel is analternative to albendazole.
Diethylcarbamazine
Diethylcarbamazine (DEC) is the drug ofchoice in filariasis. It immobilizes themicrofilariae resulting in their displacementin the tissues and also alters their surfacestructure making them more susceptible tothe host defense mechanisms. Microfilariaerapidly disappear from the blood exceptthose present in hydrocele and nodules.Adverse effects are mild; anorexia, nausea,vomiting, dizziness and headache; allergicreactions with itching, rashes and fever dueto release of antigens from the dying wormsmay occur. Antihistamines are given withDEC to minimize these reactions. DEC canbe given during pregnancy.
Uses
• Filariasis DEC is the drug of choice (2 mg/kg TDS for 21 days). In 7 days patientsare rendered non-infective to mosquitoesas microfilariae rapidly disappear. Butadult worms may need repeated courses.
• Tropical eosinophilia (2 mg/kg TDS for 7days). Symptoms rapidly disappear.
Ivermectin
Ivermectin is a semisynthetic analog ofavermectin B obtained from streptomycesavermitilis. Ivermectin is effective againstmany nematodes, arthropods and filariae thatinfect animals and human beings. Ivermectinis very effective against the microfilaria ofOnchocerca volvulus. It is microfilaricidal andalso blocks the release of microfilariae fromthe uterus of adult worms. There is a rapiddecrease in the microfilarial count in the skinand eyes.
Ivermectin is believed to act by paralysingthe worms by binding to GABA–gatedchloride channels and enhancing GABAactivity.Ivermectin is as effective as DEC against W.bancrofti and B.malayi. It is also effectiveagainst Strongyloidis stercoralis, Ascarislumbricoides, and cutaneous larva migrans.Adverse effects–Ivermectin is well tolerated.Apart from nausea and vomiting, allergicreactions can result due to hypersensitivityto the dying microfilarial proteins (mazottireaction).Ivermectin should not be used with otherdrugs that influence GABA activity (e.g.benzodiazepines, valproic acid) in patientswith meningitis and sleeping sickness as theseconditions impair the blood brain barrier.
Uses
1. Ivermectin is the preferred drug in thetreatment of onchocerciasis.
2. Ivermectin is also useful in the treatmentof lymphatic filariasis.
3. A single dose of 400 mg/kg ivermectinwith 400 mg albendazole is given once ayear for mass chemotherapy of lymphaticfilariasis.
4. Strongyloidiasis – A single dose of 200mg/kg is curative in strongyloidiasis.However the dose is to be repeated onthe second day.
5. Ivermectin is also useful in cutaneous larvamigrans, ascariasis and in scabies.
Metrifonate is a prodrug that is convertedto dichlorovas–an organophosphorus insec-ticide. Metrifonate is used as an alternativeto praziquantel in the treatment ofSchistosoma haematobium infections.Oxamniquine is effective against S.mansoniand is used as an alternative to praziquantelin the treatment of S. mansoni infections.Bithionol is the drug of choice in thetreatment of Fasciola hepatica infections.
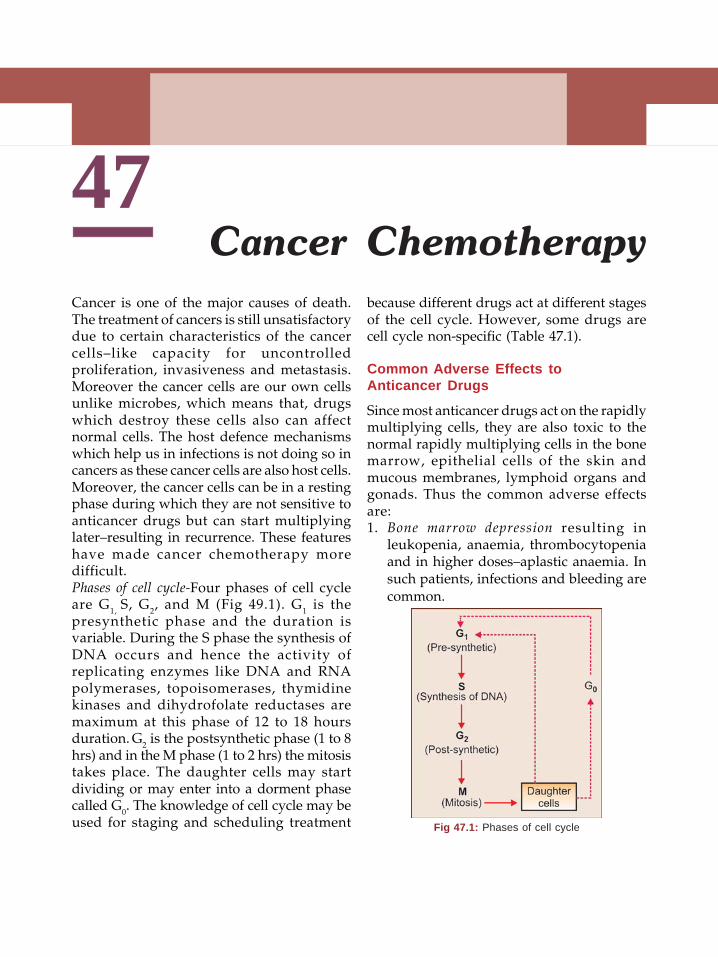
Textbook of Pharmacology for Dental and Allied Health Sciences328
47Cancer is one of the major causes of death.The treatment of cancers is still unsatisfactorydue to certain characteristics of the cancercells–like capacity for uncontrolledproliferation, invasiveness and metastasis.Moreover the cancer cells are our own cellsunlike microbes, which means that, drugswhich destroy these cells also can affectnormal cells. The host defence mechanismswhich help us in infections is not doing so incancers as these cancer cells are also host cells.Moreover, the cancer cells can be in a restingphase during which they are not sensitive toanticancer drugs but can start multiplyinglater–resulting in recurrence. These featureshave made cancer chemotherapy moredifficult.Phases of cell cycle-Four phases of cell cycleare G1, S, G2, and M (Fig 49.1). G1 is thepresynthetic phase and the duration isvariable. During the S phase the synthesis ofDNA occurs and hence the activity ofreplicating enzymes like DNA and RNApolymerases, topoisomerases, thymidinekinases and dihydrofolate reductases aremaximum at this phase of 12 to 18 hoursduration. G2 is the postsynthetic phase (1 to 8hrs) and in the M phase (1 to 2 hrs) the mitosistakes place. The daughter cells may startdividing or may enter into a dorment phasecalled G0. The knowledge of cell cycle may beused for staging and scheduling treatment
because different drugs act at different stagesof the cell cycle. However, some drugs arecell cycle non-specific (Table 47.1).
Common Adverse Effects toAnticancer Drugs
Since most anticancer drugs act on the rapidlymultiplying cells, they are also toxic to thenormal rapidly multiplying cells in the bonemarrow, epithelial cells of the skin andmucous membranes, lymphoid organs andgonads. Thus the common adverse effectsare:1. Bone marrow depression resulting in
leukopenia, anaemia, thrombocytopeniaand in higher doses–aplastic anaemia. Insuch patients, infections and bleeding arecommon.
Cancer Chemotherapy
Fig 47.1: Phases of cell cycle
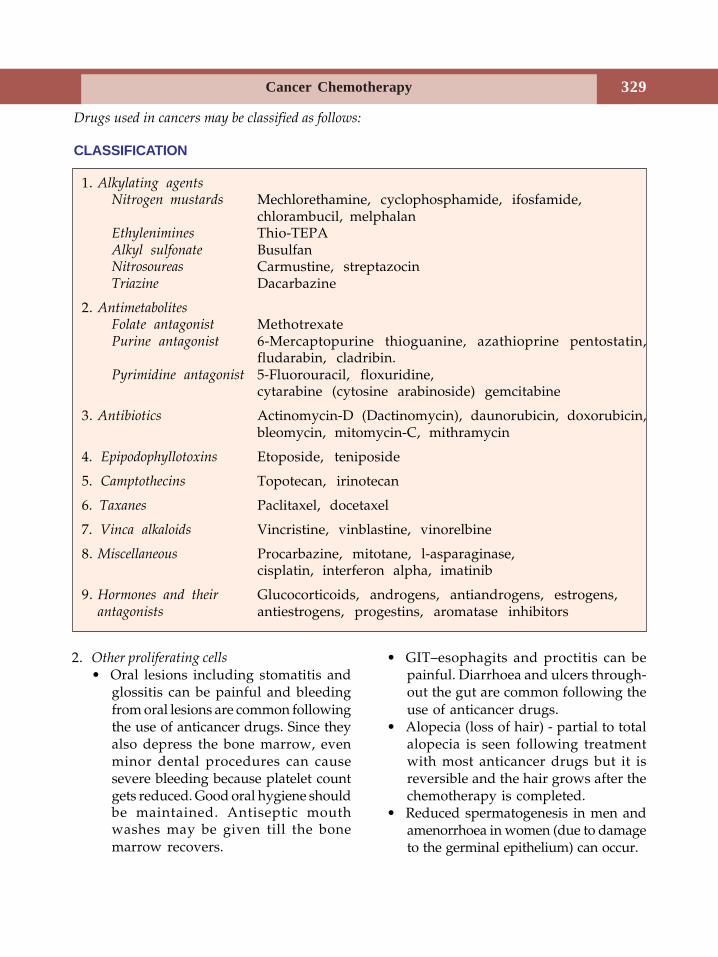
Cancer Chemotherapy 329
2. Other proliferating cells• Oral lesions including stomatitis and
glossitis can be painful and bleedingfrom oral lesions are common followingthe use of anticancer drugs. Since theyalso depress the bone marrow, evenminor dental procedures can causesevere bleeding because platelet countgets reduced. Good oral hygiene shouldbe maintained. Antiseptic mouthwashes may be given till the bonemarrow recovers.
• GIT–esophagits and proctitis can bepainful. Diarrhoea and ulcers through-out the gut are common following theuse of anticancer drugs.
• Alopecia (loss of hair) - partial to totalalopecia is seen following treatmentwith most anticancer drugs but it isreversible and the hair grows after thechemotherapy is completed.
• Reduced spermatogenesis in men andamenorrhoea in women (due to damageto the germinal epithelium) can occur.
Drugs used in cancers may be classified as follows:
CLASSIFICATION
1. Alkylating agentsNitrogen mustards Mechlorethamine, cyclophosphamide, ifosfamide,
chlorambucil, melphalanEthylenimines Thio-TEPAAlkyl sulfonate BusulfanNitrosoureas Carmustine, streptazocinTriazine Dacarbazine
2. AntimetabolitesFolate antagonist MethotrexatePurine antagonist 6-Mercaptopurine thioguanine, azathioprine pentostatin,
fludarabin, cladribin.Pyrimidine antagonist 5-Fluorouracil, floxuridine,
cytarabine (cytosine arabinoside) gemcitabine
3. Antibiotics Actinomycin-D (Dactinomycin), daunorubicin, doxorubicin,bleomycin, mitomycin-C, mithramycin
4. Epipodophyllotoxins Etoposide, teniposide
5. Camptothecins Topotecan, irinotecan
6. Taxanes Paclitaxel, docetaxel
7. Vinca alkaloids Vincristine, vinblastine, vinorelbine
8. Miscellaneous Procarbazine, mitotane, l-asparaginase,cisplatin, interferon alpha, imatinib
9. Hormones and their Glucocorticoids, androgens, antiandrogens, estrogens,antagonists antiestrogens, progestins, aromatase inhibitors
Textbook of Pharmacology for Dental and Allied Health Sciences330
3. Immediate adverse effects Nausea andvomiting are very common with mostcytotoxic drugs. They result from thestimulation of the vomiting centre andCTZ and starts about 4 to 6 hours aftertreatment and may continue for 1 to 2days. Prior treatment with powerfulantiemetics is required.
4. Teratogenicity All cytotoxic drugs areteratogenic and are therefore contra-indicated in pregnancy.
5. Carcinogenicity Cytotoxic drugs them-selves may cause secondary cancers, e.g.leukaemias are common after treatmentof Hodgkin’s lymphoma.
Apart from the above, the adverse effectsunique to some drugs are discussed underindividual drugs listed in Table 47.2.
ALKYLATING AGENTS
Actions Alkylating agents exert cytotoxic,immunosuppressant and radiomimetic effects(similar to radiotherapy).Mechanism of action These drugs form highlyreactive derivatives which transfer alkylgroups to various cellular constituents andbind them with covalent bonds. Thus suchconstituents are not available for normalmetabolic reactions. Moreover, alkylationof DNA results in breakage of the DNAstrand.
Mechlorethamine is given IV as it is a highlyirritant compound. It is used in Hodgkin’s(MOPP regime) and other lymphomas.Cyclophosphamide is converted to its activemetabolite aldophosphamide in the body. Itcan be given orally. Cyclophosphamidecauses cystitis due to a metabolite acrolein.This can be prevented by giving IV Mesna,
irrigating the bladder with acetylcysteine,and by taking in large amounts of fluids.Mesna (sodium-2 mercaptoethane sul-phonate) and acetylcysteine contain SHgroups which bind the toxic metabolites andinactivate them.
Cyclophosphamide is used in Hodgkin’slymphoma, leukaemias in children and as animmunosuppressive agent.Ifosfamide has actions and toxicities similar tocyclophosphamide except that it is longeracting.Chlorambucil (LEUKERAN) is very effectiveagainst lymphoid series. It is the drug ofchoice in chronic lymphocytic leukaemia.Melphalan is given orally in multiple myelomaIts actions and toxicities are similar to othernitrogen mustards.Busulfan (MYLERAN) has selective activityagainst cells of the myeloid series and is thedrug of choice in chronic myeloid leukaemia.Nitrosoureas Carmustine is effective inmeningeal leukaemias and brain tumoursbecause it crosses the blood-brain barrier. Itis also used in lymphomas and malignantmelanoma. Streptozocin is an antibiotic. It isused in pancreatic islet cell tumours.Dacarbazine is useful in malignant melanoma.
ANTIMETABOLITES
Folate Antagonist
Methotrexate is a folic acid antagonist. It bindsto dihydrofolate reductase (DHFR) andprevents the formation of tetrahydrofolate
Cell cycle specific drugs
S phase-Antimetabolites,Doxorubicin,Epipodophyllotoxins,Vinca alkaloids.
G2 and M Phases -
Bleomycin
M phase - Taxanes,Vinca alkaloids.
Cell cycle non specific drugs
Alkylating agentsAnticancer antibioticsCisplatinProcarbazine
Table 47.1: Cell cycle specific and non-specific drugs
Cancer Chemotherapy 331
(THF). This THF is a coenzyme essential inseveral reactions in protein synthesis. Thedeficiency results in inhibition of proteinsynthesis. Thus rapidly multiplying cells arethe most affected.
Actions Cytotoxic actions–methotrexatemainly affects the bone marrow, skin andgastrointestinal mucosa and other rapidlydividing cells.
It also has immunosuppressant and someanti-inflammatory properties.
Methotrexate toxicity can be largelyprevented by administering folinic acid. Thisfolinic acid (also called leucovorin orcitrovorum factor) gets converted to a formof THF that can be utilised by the cells.
Uses Methotrexate is curative in choriocarci-noma and is useful in acute leukaemias, breastcancer and soft tissue sarcomas. It is also usedin rheumatoid arthritis and psoriasis.
Purine Antagonists
6 Mercaptopurine, thioguanine, azathioprine,fludarabine, pentostatin and cladribine arepurine antagonists.Mechanism of action Purine antagonists enterthe cells and get converted to activemetabolites (triphosphates in mostcompounds) which are incorporated intoDNA. They cause breakages in DNA strandsand inhibit protein synthesis.Mercaptopurine (6-MP) undergoes extensivefirst pass metabolism. It is metabolised byxanthine oxidase. Adverse effects includebone marrow depression, anorexia, nausea,vomiting, stomatitis, jaundice and dermatitis.Drug interaction 6-Mercaptopurine ismetabolised by xanthine oxidase. Allopurinolinhibits xanthine oxidase and thus prolongsthe action of 6-MP.
Table 47.2: Specific adverse effects of some anticancer drugs
Drugs Specific adverse effects Other prominent adverse effects
Cyclo- Cystitis, stomatitis Bone marrow depression, alopecia,phosphamide vomiting, amenorrhoea, teratogenicity
Busulfan Pulmonary fibrosis, stomatitis Bone marrow depression, alopecia,vomiting, amenorrhoea, teratogenicity
Cisplatin Ototoxicity Renal dysfunction
Bleomycin Pulmonary fibrosis, Stomatitis, alopeciaoedema of hands
Daunorubicin Cardiotoxicity, red coloured urine Bone marrow depression, alopecia
Doxorubicin Cardiotoxicity Bone marrow depression, alopeciaMithramycin Hepatotoxicity Thrombocytopenia(Plicamycin)
Vincristine Neurotoxicity, Peripheral neuritis Muscle weakness, alopeciamental depression
Asparaginase Pancreatitis, hepatotoxicity, Allergic reactionsMitotane Dermatitis, mental depression Diarrhoea
Textbook of Pharmacology for Dental and Allied Health Sciences332
Uses 6-MP is used in acute leukaemias inchildren, choriocarcinoma and some solidtumours.Thioguanine is effective orally and is used inacute leukemias particularly acutegranulocytic leukaemia.Fludarabine is converted to an activetriphosphate derivative which inhibits DNAsynthesis. It is also incorporated into DNAand causes breakage and termination of theDNA chain. Adverse effects include nausea,vomiting, anorexia, bone marrow depression,and neurotoxicity.Fludarabine is used in the treatment ofchronic lymphocytic leukaemia (CLL) andHodgkin’s lymphomas.Pentostatin obtained from Streptomycesantibioticus inhibits the enzyme adenosinedeaminase and inhibits DNA synthesis.
Pentostatin can cause nausea, vomiting,diarrhoea, skin rashes and bone marrowsuppression.
Pentostatin is used intravenously in thetreatment of hairy cell leukaemia and otherchronic leukaemias and non-Hodgkin’slymphomas.Cladribine is the drug of choice in hairly cellleukaemia. It is also useful in CLL, AML andsome lymphomas. Cladribine causes mild
bone marrow suppression, nausea, vomiting,weakness and skin rashes.
PYRIMIDINE ANTAGONISTS
Pyrimidine antagonists are converted toactive metabolites which resemble naturalnucleotides. They compete with naturalnucleotides, are incorporated into DNA inplace of natural nucleotides and inhibit DNAsynthesis.5-Fluorouracil is a pyrimidine analog. Itinhibits the enzyme thymidylate synthetasedue to which it inhibits the synthesis ofthymine and thereby inhibits DNA synthesis.It is used in carcinoma of the stomach, colon,rectum, breast and ovaries.Cytosine arabinoside or cytarabine is the mosteffective agent in acute myelocytic leukaemia.It causes nausea, vomiting and bone marrowdepression.
Cytarabine is useful in acute leukaemiasparticularly myeloid leukaemia and inrelapsed cases of acute lymphocytic leukaemia.Gemcitabine is a recently developed analogof cytarabine with mechanism of actionsimilar to cytarabine. Adverse effects are
Mechanism of action of purine antagonists
Purine Antagonists• Purine antagonists get incorporated
into DNA and inhibit proteinsynthesis.
• Mercaptopurine, thioguanine areused in acute leukaemias, fludarabineand pentostatin in CLL and non-Hodgkin’s lymphomas; cladribin is thedrug of choice in hairy cell leukaemia.
• Purine antagonists share the commonadverse effects of anticancer drugs.Fludarabine and pentostatincombination can cause fatal lungtoxicity.
Cancer Chemotherapy 333
milder with flu-like syndrome and mild bonemarrow depression. It is used in pancreatic,lung, cervical, ovarian and breast cancers.
ANTIBIOTICS
Actinomycin D (Dactinomycin) acts byinhibiting DNA-dependent RNA synthesis.It is one of the most potent anticancer drugsand is used in Wilms’ tumour, rhabdo-myosarcoma, choriocarcinoma and some softtissue sarcomas.Daunorubicin and doxorubicin are anth-racyclines. They act by inhibiting DNAsynthesis. Cardiotoxicity with hypotension,arrhythmias and CCF, is unique to both thesedrugs. They also cause vomiting, stomatitis,alopecia and bone marrow depression.
Daunorubicin is used in acute leukaemiaswhile doxorubicin is useful in solid tumoursand in acute leukaemias.Epirubicin and mitoxantrone are analogs ofdoxorubicin which are less cardiotoxic.Mitomycin C is converted to an alkylatingagent in the body. It is used in cancers of thestomach, lungs and cervix.Bleomycin is obtained from Streptomyces
verticillus. It binds with iron and forms freeradicals and causes breakage in DNA strand.It has the advantage of the unique mechanismof action and is less toxic to the bonemarrow–this is advantageous in combinationregimens.
Bleomycin is used in solid tumours–testicular tumours, squamous cell carcinomaof the head, neck and oesophagus.
It’s most serious toxicity includespulmonary fibrosis and cutaneous toxicity butdoes not cause significant bone marrowdepression.Mithramycin (Plicamycin) is highly toxic, usedin disseminated testicular tumours and insevere hypercalcaemia due to bone cancers.It reduces plasma calcium levels by its actionon the osteoclasts.
EPIPODOPHYLLOTOXINS
Etoposide and teniposide are plant extractsobtained from the mandrake plant. They bindto topoisomerase II as well as DNA resultingin DNA strand breakages. They are used intesticular and lung cancers.
TAXANES
Paclitaxel was obtained from the bark of thewestern yew tree. It binds to β-tubulin ofmicrotubules and arrests mitosis. Paclitaxelis given intravenously; it is metabolised bythe liver microsomal enzymes. Adverseeffects include myelosuppression, myalgiaand peripheral neuropathy. Docetaxel is morepotent and orally effective.Taxanes are useful in breast cancers andovarian cancers. They are also found to beeffective in the cancers of the head and neck,oesophagus and lungs.
Drugs which cause least/nobone marrow depression
• Hormones• Vincristine• Bleomycin• L-asparaginase• Cisplatin
Curable cancers
• Hodgkin’s disease• Choriocarcinoma• Burkitt’s lymphoma• Testicular tumours• Wilms’ tumour• Acute leukaemias in children• Ewing’s sarcoma
Tumours resistant to treatment
• Carcinoma colon• Carcinoma rectum• Melanomas• Pancreatic tumours• Renal cancers• Some lung cancers

Textbook of Pharmacology for Dental and Allied Health Sciences334
CAMPTOTHECINS
Camptothecin the first anticancer agent inthis group was found to be too toxic. Itsanalogs, topotican and irinotecan are less toxicand useful. They inhibit topoisomerase Iresulting in DNA strand breakages leadingto cell death. They act on the S phase of thecell cycle. Both are given intravenously.
Toxicity is milder and includes diarrhoeaand reversible bone marrow suppression,nausea, weakness and skin rash. Irinotecaninhibits the enzyme acetylcholinesteraseresulting in accumulation of acetylcholinecausing excessive salivation, abdominalcramps, miosis, bradycardia and sweatingwhich respond to treatment with atropine.
VINCA ALKALOIDS
Vincristine and vinblastine are obtained fromVinca rosea, the periwinkle plant. They bindto microtubules in the mitotic apparatus andarrest cell division in metaphase. They arespindle poisons. The alkaloids differ intoxicity.Vincristine (Oncovin) is neurotoxic while bonemarrow depression is less. It is used inleukaemias, Hodgkin’s lymphoma, Wilms’tumour and brain tumour.Vinblastine causes bone marrow depression,alopecia and vomiting. It is used withbleomycin and cisplatin (VBC) in testiculartumours; it is also useful in Hodgkin’slymphoma.Vinorelbine is a semisynthetic vinca alkaloidused intravenously in lung cancers. It cancause granulocytopenia, nausea, vomiting andparaesthesias.
MISCELLANEOUS
Procarbazine is effective orally in Hodgkin’slymphoma (MOPP regime component). Itdamages DNA. This may make itcarcinogenic.
Cisplatin gets converted to its active form inthe cell, inhibits DNA synthesis and causescytotoxicity. It causes ototoxicity, nephro-toxicity, peripheral neuropathy, nausea,vomiting and anaemia. Anaphylactoidreactions can follow its use. It is relativelyless toxic to bone marrow. Cisplatin is usedin ovarian and testicular tumours and cancersof the head and neck.Carboplatin is a less toxic derivative ofcisplatin and is better tolerated than cisplatinas adverse effects are milder but it causesmyelosuppression.Oxaliplatin is effective in advanced colorectalcancer and in other cancers like ovarian andcervical cancers.L-asparaginase The amino acid asparagine issynthesized by normal cells but malignantcells are unable to synthesize asparagine anddepend on the host for the supply. As-paraginase is an enzyme that convertsasparagine to aspartic acid and deprives themalignant cells of asparagine suppliesresulting in inhibition of protein synthesis.It is used in acute leukaemias. It causesnausea, vomiting and CNS depression. Bonemarrow suppression is mild.Imatinib is a recent introduction in cancerchemotherapy. It acts by inhibiting someselective tyrosine kinases which areconsidered to be involved in the pathogenesisof chronic myeloid leukaemia.
Imatinib is almost completely absorbedwhen given orally. It can cause skin rashesand elevated serum transaminases. Imatinibis used in chronic myeloid leukaemia.
HORMONES IN CANCERCHEMOTHERAPY
Glucocorticoids Due to their lympholyticaction, glucocorticoids are used in acuteleukaemias and lymphomas. Rapid clinicalimprovement is seen but duration can vary

Cancer Chemotherapy 335
from 2 weeks to 9 months. They are used forinitiation of therapy due to their rapid action.Glucocorticoids are also of value in thefollowing:1. with radiation therapy to reduce
radiation oedema2. in intracranial tumours to reduce cerebral
oedema3. for symptomatic relief in critically ill
patients.Prednisolone or dexamethasone arecommonly used.Oestrogens are useful in (i) prostatic carcinomaas it is an androgen dependent tumour, (ii)breast cancer in males and in postmenopausalwomen–oestrogens are used in advancedcases where surgery or radiotherapy cannotbe employed.Progestins are useful in the palliativemanagement of endometrial carcinoma.Androgens are used in the palliative treatmentof breast cancer in postmenopausal womenalong with oophorectomy.
Hormone Antagonists
Aromatase inhibitors The enzyme aromatasecatalyzes the convertion of androgens tooestrogens. Inhibitors of aromatase havebeen found to be effective in breast cancers.Formestane, exemestane, anastrozole,vorozole and letrozole are the aromataseinhibitors used.Aminoglutethemide and trilastane inhibit theconvertion of cholesterol to pregnenolone(the first step in corticosteroid synthesis) andthereby inhibit the synthesis of adreno-corticoids. Aminoglutethemide is useful inadvanced breast cancers when cancer cellscontain oestrogen receptors.Antioestrogens Tamoxifen is an oestrogenreceptor antagonist used in estrogen receptorcontaining breast cancer (page 356).
GnRH analogs Long-term administration ofleuprolide, goserelin and buserelin are usefulin prostatic and breast cancers. They may becombined with tamoxifen in breast cancers.Antiandrogen Flutamide is used in prostaticcancer.
RADIOACTIVE ISOTOPES
Some radioactive isotopes can be used in thetreatment of certain specific cancers.Radiophosphorus P32 is used in polycythemiavera. It is taken up by the bone where it emitsβ rays and has a half-life of about 14 days.Strontium chloride emits β rays and has alonger t½ in the bony metastases. It is usedto alleviate pain in painful bony metastases.Radio active iodine I131 is used in the treatmentof thyroid cancers (See Page 344).
OTHER AGENTS
Several agents are used to beneficiallyinfluence the patients’ response to treatmentand to overcome some adverse effects. Thesehave also been termed biological responsemodifiers. They are as follows:1. Haematopoietic growth factors like
erythropoietin and myeloid growthfactors like GM-CSF, G-CSF, M-CSF andthrombopoietin (see Page 225) are usedto treat bone marrow suppression.
2. Interferons (see Page 308) like interferonα are used in hairy cell leukaemia, Kaposi’ssarcoma and condylomata acuminata.
3. Monoclonal antibodies are immu-noglobulins that react specifically withantigens present on the cancer cells.Allergic reactions are common.Trastuzumab also enhances host immuneresponses and is useful in breast cancers.Rituximab attaches to antigens on the Bcells causing lysis of these cells. It is usedin B cell lymphomas.
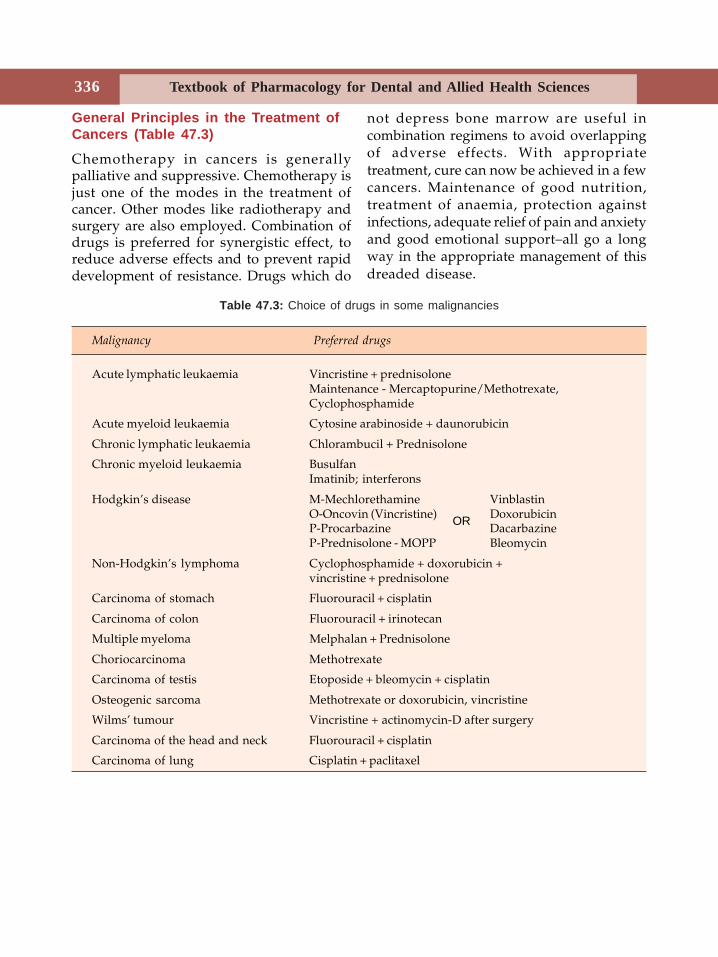
Textbook of Pharmacology for Dental and Allied Health Sciences336
General Principles in the Treatment ofCancers (Table 47.3)
Chemotherapy in cancers is generallypalliative and suppressive. Chemotherapy isjust one of the modes in the treatment ofcancer. Other modes like radiotherapy andsurgery are also employed. Combination ofdrugs is preferred for synergistic effect, toreduce adverse effects and to prevent rapiddevelopment of resistance. Drugs which do
not depress bone marrow are useful incombination regimens to avoid overlappingof adverse effects. With appropriatetreatment, cure can now be achieved in a fewcancers. Maintenance of good nutrition,treatment of anaemia, protection againstinfections, adequate relief of pain and anxietyand good emotional support–all go a longway in the appropriate management of thisdreaded disease.
Table 47.3: Choice of drugs in some malignancies
Malignancy Preferred drugs
Acute lymphatic leukaemia Vincristine + prednisoloneMaintenance - Mercaptopurine/Methotrexate,Cyclophosphamide
Acute myeloid leukaemia Cytosine arabinoside + daunorubicin
Chronic lymphatic leukaemia Chlorambucil + Prednisolone
Chronic myeloid leukaemia BusulfanImatinib; interferons
Hodgkin’s disease M-Mechlorethamine VinblastinO-Oncovin (Vincristine) DoxorubicinP-Procarbazine DacarbazineP-Prednisolone - MOPP Bleomycin
Non-Hodgkin’s lymphoma Cyclophosphamide + doxorubicin +vincristine + prednisolone
Carcinoma of stomach Fluorouracil + cisplatin
Carcinoma of colon Fluorouracil + irinotecan
Multiple myeloma Melphalan + Prednisolone
Choriocarcinoma Methotrexate
Carcinoma of testis Etoposide + bleomycin + cisplatin
Osteogenic sarcoma Methotrexate or doxorubicin, vincristine
Wilms’ tumour Vincristine + actinomycin-D after surgery
Carcinoma of the head and neck Fluorouracil + cisplatin
Carcinoma of lung Cisplatin + paclitaxel
OR
Hypothalamus and Anterior Pituitary Hormones 337
48
The pituitary gland, under the influence ofthe hypothalamus secretes many hormoneswhich either control the secretion of otherglands or directly act on the target tissues.These are peptides and act by binding tospecific receptors present on the target cells(Table 48.1).
Hypothalamic HormonesGrowth hormone releasing hormone (GHRH),(sermorelin) stimulates anterior pituitary tosecrete growth hormone. Sermorelin (Table48.2) is an analog of GHRH used in diagnostictests of growth hormone deficiency (Table48.3).Somatostatin is growth hormone release-inhibiting hormone present in thehypothalamus, parts of the CNS, pancreasand in gastrointestinal tract. It inhibits thesecretion of growth hormone, TSH, prolactin,insulin, glucagon and gastro the intestinalsecretions. But it is very short-acting.Octreotide is the synthetic analog ofsomatostatin which is longer-acting anduseful in acromegaly, some hormonesecreting tumours and in bleedingoesophageal varices.Thyrotrophin releasing hormone (TRH) secretedby the hypothalamus stimulates the releaseof TSH from the anterior pituitary. Protirelin
is a synthetic analog of TSH used in thediagnosis of thyroid disorders.Corticotrophin releasing factor (CRF) releasesACTH and β-endorphins from the anteriorpituitary. It is used in diagnostic tests inCushing’s disease.Gonadotrophin-releasing hormone (GnRH, LHRH,Gonadorelin)–secreted in a pulsatile manner,regulates the secretion of gonadotrophins–FSH and LH. It is used in diagnostic tests inhypogonadism. Therapeutically pulsatileadministration is used in infertility anddelayed puberty. Continuous administrationinhibits gonadotrophin secretion and is usedin prostatic cancers. GnRH analogue leuprolideis more potent and is used forpharmacological orchiectomy/oophorectomyin prostatic cancer and some gynaecologicalconditions like uterine fibroids andendometriosis.
ANTERIOR PITUITARY HORMONES
Growth hormone (GH) a peptide, stimulatesthe growth of all organs except brain and eye.It increases the uptake of amino acids by thetissues, promotes protein synthesis andpositive nitrogen balance. It causes lipolysisand reduces glucose uptake by skeletalmuscles. It brings about linear growth. These
Hypothalamus andAnterior Pituitary
Hormones
Section 12Hormones
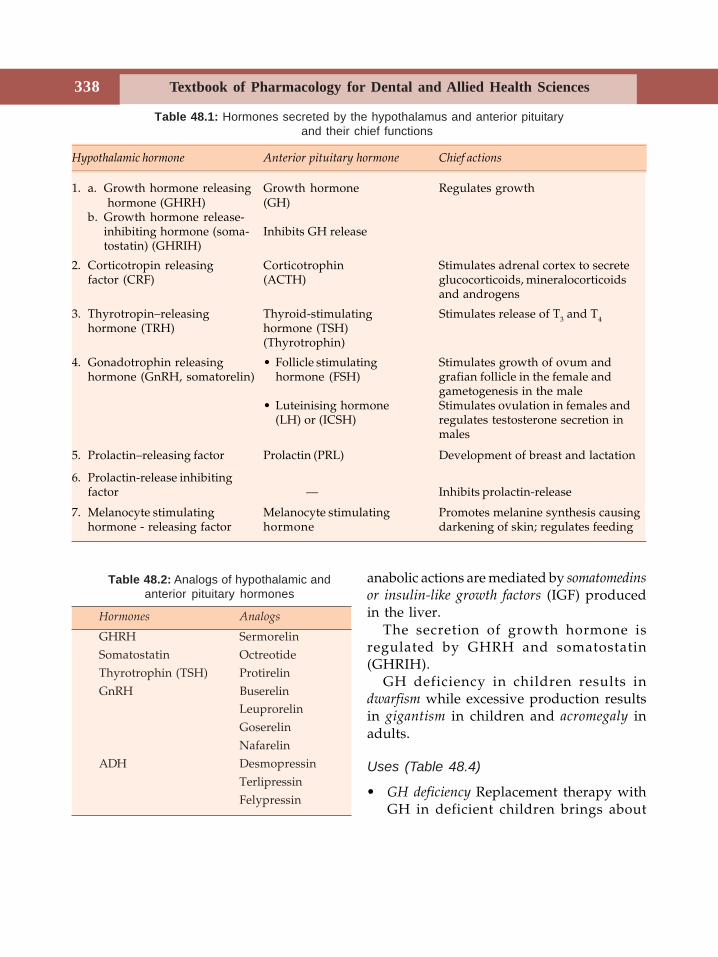
Textbook of Pharmacology for Dental and Allied Health Sciences338
anabolic actions are mediated by somatomedinsor insulin-like growth factors (IGF) producedin the liver.
The secretion of growth hormone isregulated by GHRH and somatostatin(GHRIH).
GH deficiency in children results indwarfism while excessive production resultsin gigantism in children and acromegaly inadults.
Uses (Table 48.4)
• GH deficiency Replacement therapy withGH in deficient children brings about
Table 48.1: Hormones secreted by the hypothalamus and anterior pituitaryand their chief functions
Hypothalamic hormone Anterior pituitary hormone Chief actions
1. a. Growth hormone releasing Growth hormone Regulates growth hormone (GHRH) (GH)
b. Growth hormone release-inhibiting hormone (soma- Inhibits GH releasetostatin) (GHRIH)
2. Corticotropin releasing Corticotrophin Stimulates adrenal cortex to secretefactor (CRF) (ACTH) glucocorticoids, mineralocorticoids
and androgens
3. Thyrotropin–releasing Thyroid-stimulating Stimulates release of T3 and T4hormone (TRH) hormone (TSH)
(Thyrotrophin)
4. Gonadotrophin releasing • Follicle stimulating Stimulates growth of ovum andhormone (GnRH, somatorelin) hormone (FSH) grafian follicle in the female and
gametogenesis in the male• Luteinising hormone Stimulates ovulation in females and
(LH) or (ICSH) regulates testosterone secretion inmales
5. Prolactin–releasing factor Prolactin (PRL) Development of breast and lactation
6. Prolactin-release inhibitingfactor — Inhibits prolactin-release
7. Melanocyte stimulating Melanocyte stimulating Promotes melanine synthesis causinghormone - releasing factor hormone darkening of skin; regulates feeding
Table 48.2: Analogs of hypothalamic andanterior pituitary hormones
Hormones Analogs
GHRH SermorelinSomatostatin OctreotideThyrotrophin (TSH) ProtirelinGnRH Buserelin
LeuprorelinGoserelinNafarelin
ADH DesmopressinTerlipressinFelypressin
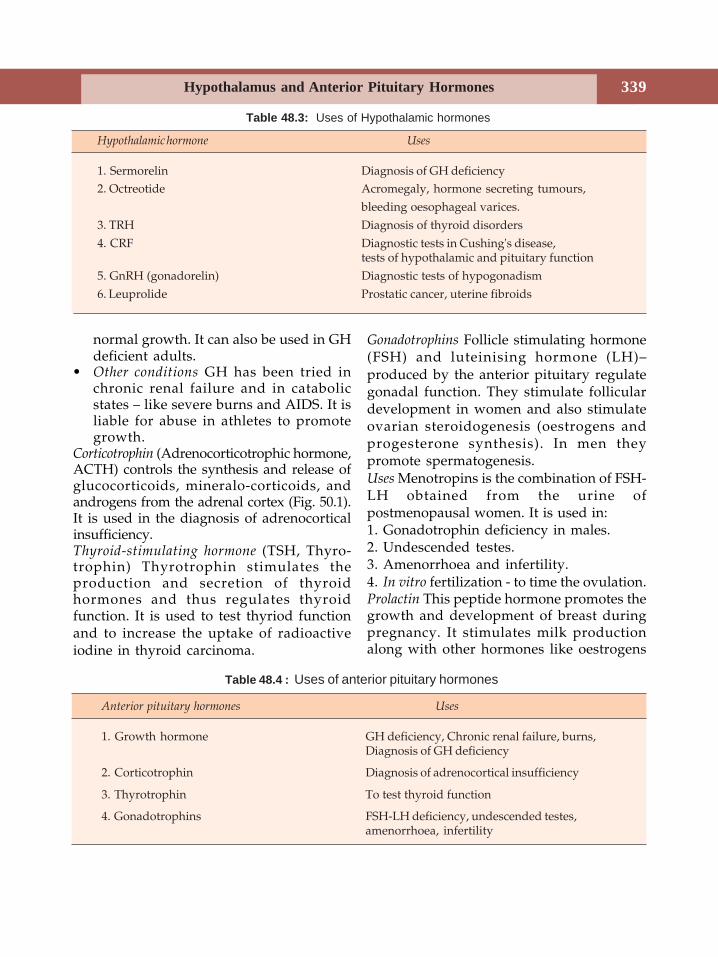
Hypothalamus and Anterior Pituitary Hormones 339
normal growth. It can also be used in GHdeficient adults.
• Other conditions GH has been tried inchronic renal failure and in catabolicstates – like severe burns and AIDS. It isliable for abuse in athletes to promotegrowth.
Corticotrophin (Adrenocorticotrophic hormone,ACTH) controls the synthesis and release ofglucocorticoids, mineralo-corticoids, andandrogens from the adrenal cortex (Fig. 50.1).It is used in the diagnosis of adrenocorticalinsufficiency.Thyroid-stimulating hormone (TSH, Thyro-trophin) Thyrotrophin stimulates theproduction and secretion of thyroidhormones and thus regulates thyroidfunction. It is used to test thyriod functionand to increase the uptake of radioactiveiodine in thyroid carcinoma.
Gonadotrophins Follicle stimulating hormone(FSH) and luteinising hormone (LH)–produced by the anterior pituitary regulategonadal function. They stimulate folliculardevelopment in women and also stimulateovarian steroidogenesis (oestrogens andprogesterone synthesis). In men theypromote spermatogenesis.Uses Menotropins is the combination of FSH-LH obtained from the urine ofpostmenopausal women. It is used in:1. Gonadotrophin deficiency in males.2. Undescended testes.3. Amenorrhoea and infertility.4. In vitro fertilization - to time the ovulation.Prolactin This peptide hormone promotes thegrowth and development of breast duringpregnancy. It stimulates milk productionalong with other hormones like oestrogens
Table 48.3: Uses of Hypothalamic hormones
Hypothalamic hormone Uses
1. Sermorelin Diagnosis of GH deficiency2. Octreotide Acromegaly, hormone secreting tumours,
bleeding oesophageal varices.3. TRH Diagnosis of thyroid disorders4. CRF Diagnostic tests in Cushing's disease,
tests of hypothalamic and pituitary function5. GnRH (gonadorelin) Diagnostic tests of hypogonadism6. Leuprolide Prostatic cancer, uterine fibroids
Table 48.4 : Uses of anterior pituitary hormones
Anterior pituitary hormones Uses
1. Growth hormone GH deficiency, Chronic renal failure, burns,Diagnosis of GH deficiency
2. Corticotrophin Diagnosis of adrenocortical insufficiency
3. Thyrotrophin To test thyroid function
4. Gonadotrophins FSH-LH deficiency, undescended testes,amenorrhoea, infertility
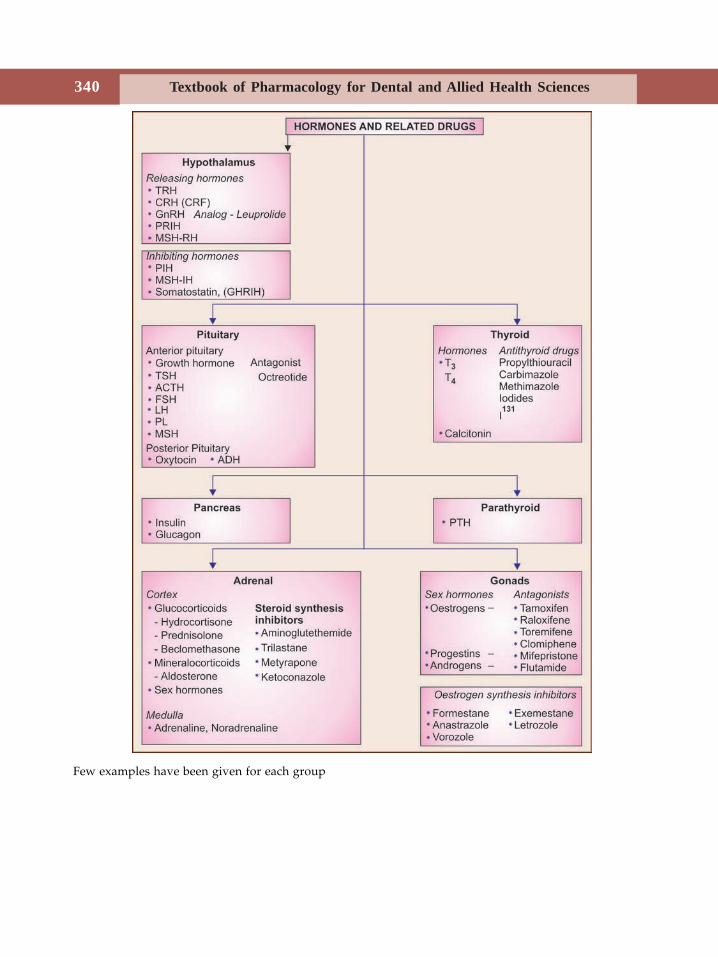
Textbook of Pharmacology for Dental and Allied Health Sciences340
Few examples have been given for each group

Hypothalamus and Anterior Pituitary Hormones 341
and progestins. Deficiency results in lactationfailure while excess prolactin results ingalactorrhoea.Regulation of secretion–suckling is the principalstimulus for prolactin secretion. Sucklingstimulates the release of prolactin-releasingfactor from hypothalamus. Oestrogens anddopamine antagonists also stimulateprolactin-release. Prolactin is not usedclinically.
Dopamine agonists like bromocriptineinhibit prolactin-release.Bromocriptine is an ergot derivative withdopamine agonistic properties.Bromocriptine is used1. To suppress lactation and breast
engorgement after delivery (like in still
birth) and following abortion. Bromo-criptine stimulates the dopamine receptorsin the pituitary to inhibit the release ofprolactin.
2. In galactorrhoea–due to excess prolactin.3. Prolactin secreting tumours or
prolactinomas.4. Parkinsonism–bromocriptine is used with
levodopa.5. Acromegaly–In normal subjects, dopamine
agonists stimulate the release of growthhormone by the pituitary but in patientswith acromegaly, they suppress growthhormone release by a paradoxical effect.Bromocriptine is therefore used inacromegaly. It also reduces prolactinrelease.
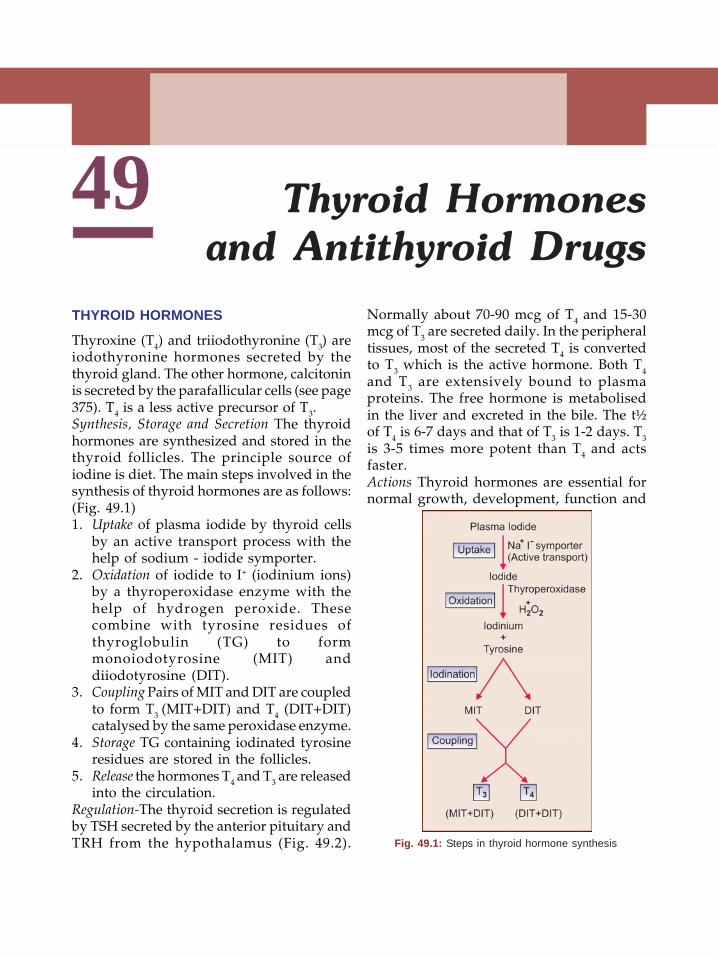
Textbook of Pharmacology for Dental and Allied Health Sciences342
49THYROID HORMONES
Thyroxine (T4) and triiodothyronine (T3) areiodothyronine hormones secreted by thethyroid gland. The other hormone, calcitoninis secreted by the parafallicular cells (see page375). T4 is a less active precursor of T3.Synthesis, Storage and Secretion The thyroidhormones are synthesized and stored in thethyroid follicles. The principle source ofiodine is diet. The main steps involved in thesynthesis of thyroid hormones are as follows:(Fig. 49.1)1. Uptake of plasma iodide by thyroid cells
by an active transport process with thehelp of sodium - iodide symporter.
2. Oxidation of iodide to I+ (iodinium ions)by a thyroperoxidase enzyme with thehelp of hydrogen peroxide. Thesecombine with tyrosine residues ofthyroglobulin (TG) to formmonoiodotyrosine (MIT) anddiiodotyrosine (DIT).
3. Coupling Pairs of MIT and DIT are coupledto form T3 (MIT+DIT) and T4 (DIT+DIT)catalysed by the same peroxidase enzyme.
4. Storage TG containing iodinated tyrosineresidues are stored in the follicles.
5. Release the hormones T4 and T3 are releasedinto the circulation.
Regulation-The thyroid secretion is regulatedby TSH secreted by the anterior pituitary andTRH from the hypothalamus (Fig. 49.2).
Normally about 70-90 mcg of T4 and 15-30mcg of T3 are secreted daily. In the peripheraltissues, most of the secreted T4 is convertedto T3 which is the active hormone. Both T4and T3 are extensively bound to plasmaproteins. The free hormone is metabolisedin the liver and excreted in the bile. The t½of T4 is 6-7 days and that of T3 is 1-2 days. T3is 3-5 times more potent than T4 and actsfaster.Actions Thyroid hormones are essential fornormal growth, development, function and
Thyroid Hormonesand Antithyroid Drugs
Fig. 49.1: Steps in thyroid hormone synthesis
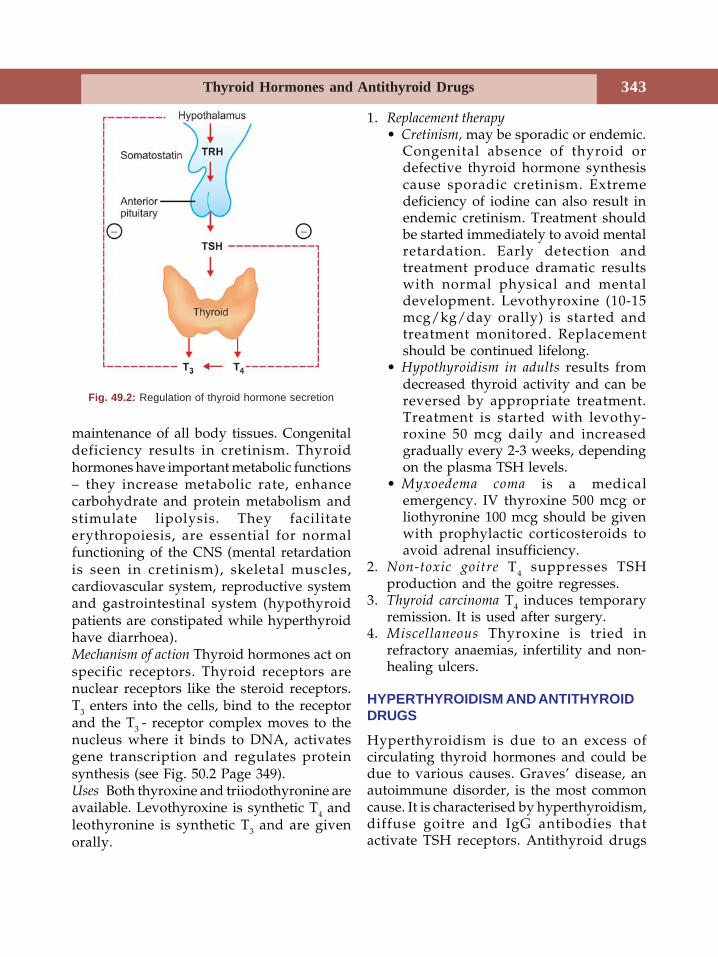
Thyroid Hormones and Antithyroid Drugs 343
maintenance of all body tissues. Congenitaldeficiency results in cretinism. Thyroidhormones have important metabolic functions– they increase metabolic rate, enhancecarbohydrate and protein metabolism andstimulate lipolysis. They facilitateerythropoiesis, are essential for normalfunctioning of the CNS (mental retardationis seen in cretinism), skeletal muscles,cardiovascular system, reproductive systemand gastrointestinal system (hypothyroidpatients are constipated while hyperthyroidhave diarrhoea).Mechanism of action Thyroid hormones act onspecific receptors. Thyroid receptors arenuclear receptors like the steroid receptors.T3 enters into the cells, bind to the receptorand the T3 - receptor complex moves to thenucleus where it binds to DNA, activatesgene transcription and regulates proteinsynthesis (see Fig. 50.2 Page 349).Uses Both thyroxine and triiodothyronine areavailable. Levothyroxine is synthetic T4 andleothyronine is synthetic T3 and are givenorally.
1. Replacement therapy• Cretinism, may be sporadic or endemic.
Congenital absence of thyroid ordefective thyroid hormone synthesiscause sporadic cretinism. Extremedeficiency of iodine can also result inendemic cretinism. Treatment shouldbe started immediately to avoid mentalretardation. Early detection andtreatment produce dramatic resultswith normal physical and mentaldevelopment. Levothyroxine (10-15mcg/kg/day orally) is started andtreatment monitored. Replacementshould be continued lifelong.
• Hypothyroidism in adults results fromdecreased thyroid activity and can bereversed by appropriate treatment.Treatment is started with levothy-roxine 50 mcg daily and increasedgradually every 2-3 weeks, dependingon the plasma TSH levels.
• Myxoedema coma is a medicalemergency. IV thyroxine 500 mcg orliothyronine 100 mcg should be givenwith prophylactic corticosteroids toavoid adrenal insufficiency.
2. Non-toxic goitre T4 suppresses TSHproduction and the goitre regresses.
3. Thyroid carcinoma T4 induces temporaryremission. It is used after surgery.
4. Miscellaneous Thyroxine is tried inrefractory anaemias, infertility and non-healing ulcers.
HYPERTHYROIDISM AND ANTITHYROIDDRUGS
Hyperthyroidism is due to an excess ofcirculating thyroid hormones and could bedue to various causes. Graves’ disease, anautoimmune disorder, is the most commoncause. It is characterised by hyperthyroidism,diffuse goitre and IgG antibodies thatactivate TSH receptors. Antithyroid drugs
Fig. 49.2: Regulation of thyroid hormone secretion
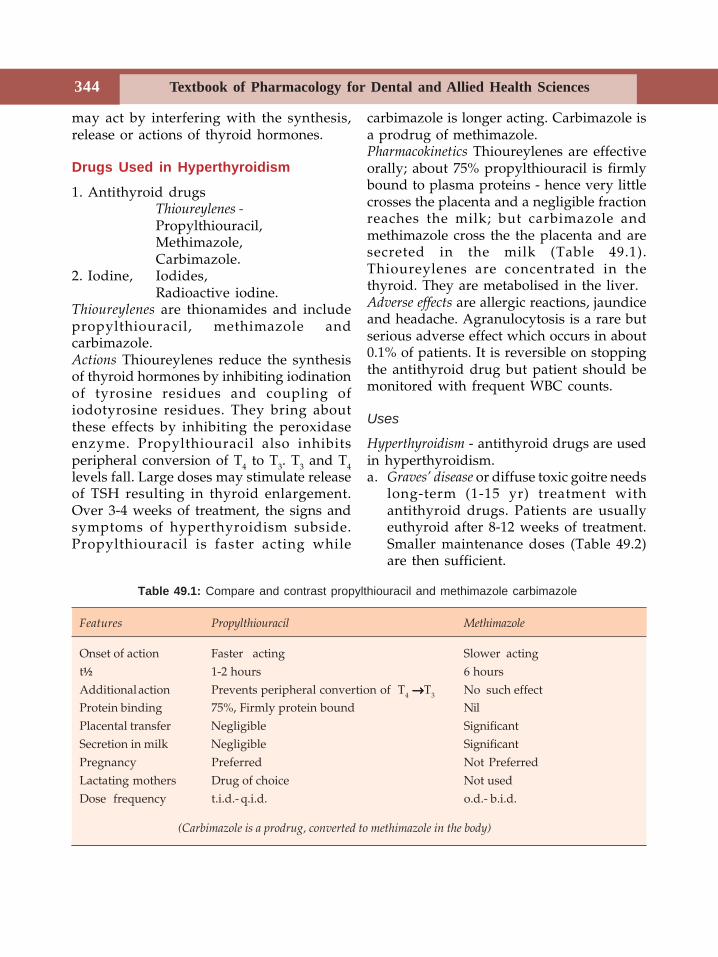
Textbook of Pharmacology for Dental and Allied Health Sciences344
may act by interfering with the synthesis,release or actions of thyroid hormones.
Drugs Used in Hyperthyroidism
1. Antithyroid drugsThioureylenes -Propylthiouracil,Methimazole,Carbimazole.
2. Iodine, Iodides,Radioactive iodine.
Thioureylenes are thionamides and includepropylthiouracil, methimazole andcarbimazole.Actions Thioureylenes reduce the synthesisof thyroid hormones by inhibiting iodinationof tyrosine residues and coupling ofiodotyrosine residues. They bring aboutthese effects by inhibiting the peroxidaseenzyme. Propylthiouracil also inhibitsperipheral conversion of T4 to T3. T3 and T4levels fall. Large doses may stimulate releaseof TSH resulting in thyroid enlargement.Over 3-4 weeks of treatment, the signs andsymptoms of hyperthyroidism subside.Propylthiouracil is faster acting while
carbimazole is longer acting. Carbimazole isa prodrug of methimazole.Pharmacokinetics Thioureylenes are effectiveorally; about 75% propylthiouracil is firmlybound to plasma proteins - hence very littlecrosses the placenta and a negligible fractionreaches the milk; but carbimazole andmethimazole cross the the placenta and aresecreted in the milk (Table 49.1).Thioureylenes are concentrated in thethyroid. They are metabolised in the liver.Adverse effects are allergic reactions, jaundiceand headache. Agranulocytosis is a rare butserious adverse effect which occurs in about0.1% of patients. It is reversible on stoppingthe antithyroid drug but patient should bemonitored with frequent WBC counts.
Uses
Hyperthyroidism - antithyroid drugs are usedin hyperthyroidism.a. Graves’ disease or diffuse toxic goitre needs
long-term (1-15 yr) treatment withantithyroid drugs. Patients are usuallyeuthyroid after 8-12 weeks of treatment.Smaller maintenance doses (Table 49.2)are then sufficient.
Features Propylthiouracil Methimazole
Onset of action Faster acting Slower actingt½ 1-2 hours 6 hoursAdditional action Prevents peripheral convertion of T4 →→→→→T3 No such effectProtein binding 75%, Firmly protein bound NilPlacental transfer Negligible SignificantSecretion in milk Negligible SignificantPregnancy Preferred Not PreferredLactating mothers Drug of choice Not usedDose frequency t.i.d.- q.i.d. o.d.- b.i.d.
(Carbimazole is a prodrug, converted to methimazole in the body)
Table 49.1: Compare and contrast propylthiouracil and methimazole carbimazole
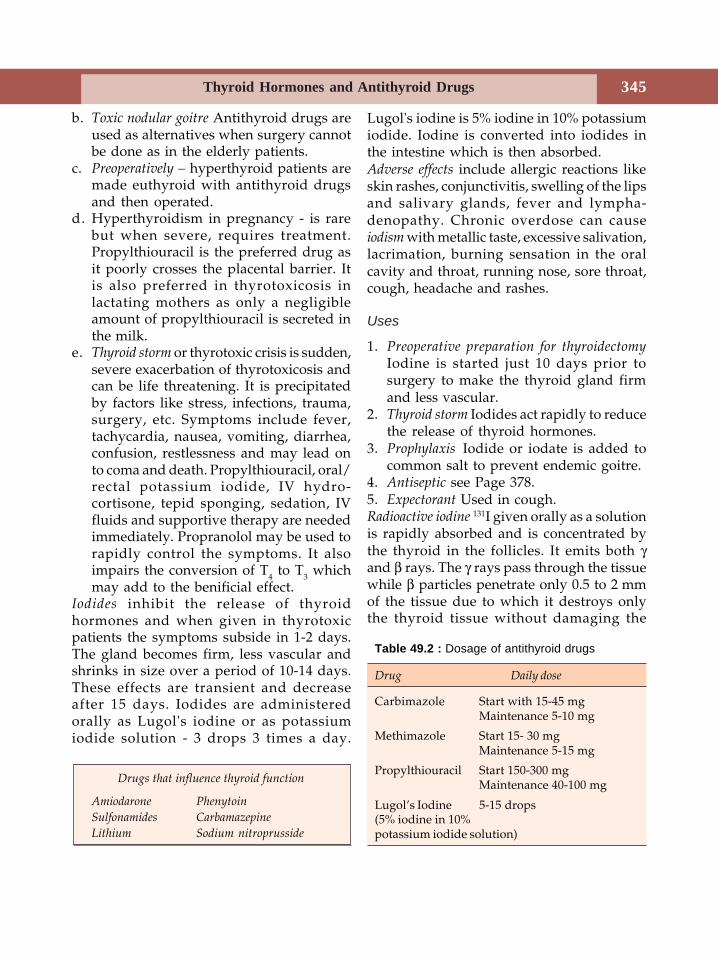
Thyroid Hormones and Antithyroid Drugs 345
b. Toxic nodular goitre Antithyroid drugs areused as alternatives when surgery cannotbe done as in the elderly patients.
c. Preoperatively – hyperthyroid patients aremade euthyroid with antithyroid drugsand then operated.
d. Hyperthyroidism in pregnancy - is rarebut when severe, requires treatment.Propylthiouracil is the preferred drug asit poorly crosses the placental barrier. Itis also preferred in thyrotoxicosis inlactating mothers as only a negligibleamount of propylthiouracil is secreted inthe milk.
e. Thyroid storm or thyrotoxic crisis is sudden,severe exacerbation of thyrotoxicosis andcan be life threatening. It is precipitatedby factors like stress, infections, trauma,surgery, etc. Symptoms include fever,tachycardia, nausea, vomiting, diarrhea,confusion, restlessness and may lead onto coma and death. Propylthiouracil, oral/rectal potassium iodide, IV hydro-cortisone, tepid sponging, sedation, IVfluids and supportive therapy are neededimmediately. Propranolol may be used torapidly control the symptoms. It alsoimpairs the conversion of T4 to T3 whichmay add to the benificial effect.
Iodides inhibit the release of thyroidhormones and when given in thyrotoxicpatients the symptoms subside in 1-2 days.The gland becomes firm, less vascular andshrinks in size over a period of 10-14 days.These effects are transient and decreaseafter 15 days. Iodides are administeredorally as Lugol's iodine or as potassiumiodide solution - 3 drops 3 times a day.
Lugol's iodine is 5% iodine in 10% potassiumiodide. Iodine is converted into iodides inthe intestine which is then absorbed.Adverse effects include allergic reactions likeskin rashes, conjunctivitis, swelling of the lipsand salivary glands, fever and lympha-denopathy. Chronic overdose can causeiodism with metallic taste, excessive salivation,lacrimation, burning sensation in the oralcavity and throat, running nose, sore throat,cough, headache and rashes.
Uses
1. Preoperative preparation for thyroidectomyIodine is started just 10 days prior tosurgery to make the thyroid gland firmand less vascular.
2. Thyroid storm Iodides act rapidly to reducethe release of thyroid hormones.
3. Prophylaxis Iodide or iodate is added tocommon salt to prevent endemic goitre.
4. Antiseptic see Page 378.5. Expectorant Used in cough.Radioactive iodine 131I given orally as a solutionis rapidly absorbed and is concentrated bythe thyroid in the follicles. It emits both γand β rays. The γ rays pass through the tissuewhile β particles penetrate only 0.5 to 2 mmof the tissue due to which it destroys onlythe thyroid tissue without damaging the
Drugs that influence thyroid function
Amiodarone Phenytoin
Sulfonamides Carbamazepine
Lithium Sodium nitroprusside
Table 49.2 : Dosage of antithyroid drugs
Drug Daily dose
Carbimazole Start with 15-45 mgMaintenance 5-10 mg
Methimazole Start 15- 30 mgMaintenance 5-15 mg
Propylthiouracil Start 150-300 mgMaintenance 40-100 mg
Lugol’s Iodine 5-15 drops(5% iodine in 10%potassium iodide solution)
Textbook of Pharmacology for Dental and Allied Health Sciences346
surrounding structures. Iodides also inhibitthe synthesis of thyroid hormone for 1-2 days(known as Wolff-Chaikoff effect). 131I has ahalf-life of 8 days but the radioactivity ispresent upto 2 months. It is given as a singledose; clinically the effect is seen after 1-2months.
Radioactive Iodine (3–10 m curie) is usedin the treatment of hyperthyroidism and inthyroid carcinoma. Small dose is used fordiagnostic purpose in thyroid function tests.
Advantages of 131I over thyroidectomy arethat
(i) administration is simple,(ii) convenient;
(iii) surgery and its associated risks can beavoided.
(iv) less expensive when compared tosurgery.
The disadvantages are:(i) the long time (3 months) taken for
maximum response(ii) the risk of hypothyroidism which may
develop after a few months or years.
The patient should be followed upfor the symptoms of hypo-thyroidism and replacement therapywith thyroid hormones should bepromptly given.
β-adrenergic blockers Many of the symptomsof hyperthyroidism are of sympathetic over-activity as there is increased tissue sensitivityto catecholamines in hyperthyroidism. βadrenergic blockers like propranolol relievesymptoms like palpitation, tremors,nervousness, sweating and myopathy. Theyonly afford symptomatic relief and are usedas adjuvants in hyperthyroidism andthyrotoxic crisis.Ionic inhibitors interfere with theconcentration of iodine by the thyroid gland.Thiocyanate and perchlorate inhibit theorganification of iodine but are not used nowdue to the adverse effects. Food items likecabbage; cigarette smoking and drugs likesodium nitroprusside, increase theconcentration of thiocyanate in the blood andmay result in hypothyroidism.
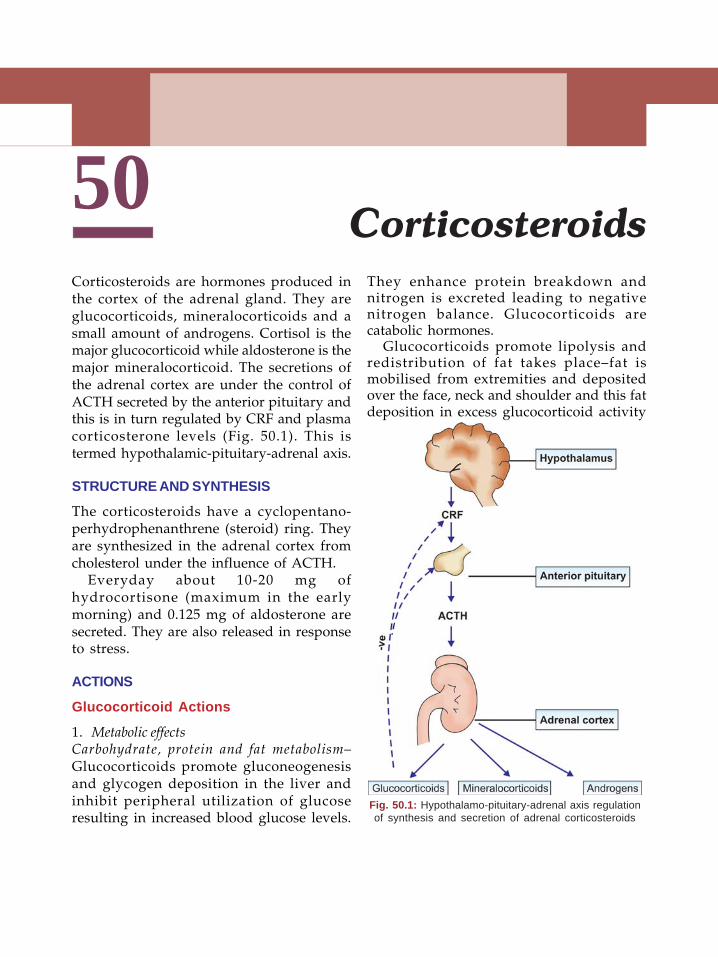
347Corticosteroids
50Corticosteroids are hormones produced inthe cortex of the adrenal gland. They areglucocorticoids, mineralocorticoids and asmall amount of androgens. Cortisol is themajor glucocorticoid while aldosterone is themajor mineralocorticoid. The secretions ofthe adrenal cortex are under the control ofACTH secreted by the anterior pituitary andthis is in turn regulated by CRF and plasmacorticosterone levels (Fig. 50.1). This istermed hypothalamic-pituitary-adrenal axis.
STRUCTURE AND SYNTHESIS
The corticosteroids have a cyclopentano-perhydrophenanthrene (steroid) ring. Theyare synthesized in the adrenal cortex fromcholesterol under the influence of ACTH.
Everyday about 10-20 mg ofhydrocortisone (maximum in the earlymorning) and 0.125 mg of aldosterone aresecreted. They are also released in responseto stress.
ACTIONS
Glucocorticoid Actions
1. Metabolic effectsCarbohydrate, protein and fat metabolism–Glucocorticoids promote gluconeogenesisand glycogen deposition in the liver andinhibit peripheral utilization of glucoseresulting in increased blood glucose levels.
They enhance protein breakdown andnitrogen is excreted leading to negativenitrogen balance. Glucocorticoids arecatabolic hormones.
Glucocorticoids promote lipolysis andredistribution of fat takes place–fat ismobilised from extremities and depositedover the face, neck and shoulder and this fatdeposition in excess glucocorticoid activity
Corticosteroids
Fig. 50.1: Hypothalamo-pituitary-adrenal axis regulationof synthesis and secretion of adrenal corticosteroids
Textbook of Pharmacology for Dental and Allied Health Sciences348
is described as ‘moon face’, ‘fish mouth’ and‘buffalo hump’.2. Anti-inflammatory and immunosuppressiveeffects Glucocorticoids suppress thedevelopment of inflammatory response to alltypes of stimuli like chemical, mechanical andimmunological stimuli. They inhibit bothearly and late manifestations of infla-mmation. Inhibition of late response likecapillary proliferation, collagen deposition,fibroblastic activity and scar formation maydelay wound healing. They inhibit migrationand depress the function of the leucocytesand macrophages and inhibit the release ofchemical mediators. The ability of these cellsto respond to antigens is decreased.Glucocorticoids - even a single dose bringabout a decrease in the number of WBCs -lymphocytes, monocytes, eosinophils andbasophils decline. In addition glucocorticoidsalso induce the synthesis of a protein -lipocortin, which inhibits phospholipase A2
thereby decreasing the production ofprostaglandins and leukotrienes.
Glucocorticoids thus suppress cell-mediated immunity, prevent manifestationsof allergy and prevent homograft rejection.Large doses also inhibit antibody production.3. Other actions
• Glucocorticoids reduce capillarypermeability, thereby reducing fluidexudation and maintain the tone ofarterioles. They have a positiveinotropic effect on the heart. Prolongeduse can cause hypertension.
• They are essential for normal muscularactivity.
• They are required for normalfunctioning of the central nervoussystem. Deficiency results in apathyand depression while large dosesresult in restlessness, anxiety andsometimes psychosis.
• GIT–Glucocorticoids enhance thesecretion of gastric acid and pepsin inthe stomach.
• Calcium metabolism–Glucocorticoidsinhibit absorption and enhance therenal excretion of calcium–theyantagonise the effect of vitamin D oncalcium absorption. Bone resorptiontakes place.
• Formed elements of blood–glucocorticoids have a lympholyticeffect which is very prominent inlymphomas; but they increase thenumber of platelets and RBCs.
• They are essential for maintainingnormal GFR.
4. Mineralocorticoid action Glucocorticoidsalso have a weak mineralocorticoid action–cause some salt and water retention andpotassium excretion. Some syntheticglucocorticoids are devoid of this activity.
Mechanism of Action
Corticosteroids enter the cells by simplediffusion, bind to specific receptors in thecytoplasm (Fig. 50.2) and activate them. Thedrug- receptor complex is then transportedinto the nucleus where it binds to specific siteson DNA and induce the synthesis of specificmRNA. By this they regulate the synthesisof new proteins that bring about the hormoneeffects.
PHARMACOKINETICS
Most glucocorticoids are well-absorbedorally. Hydrocortisone undergoes high firstpass metabolism. It is 95% bound to plasmaproteins–corticosteroid binding globulin(CBG) or transcortin. Glucocorticoids aremetabolised in the liver by oxidation andreduction followed by conjugation.Metabolites are excreted by the kidneys. The
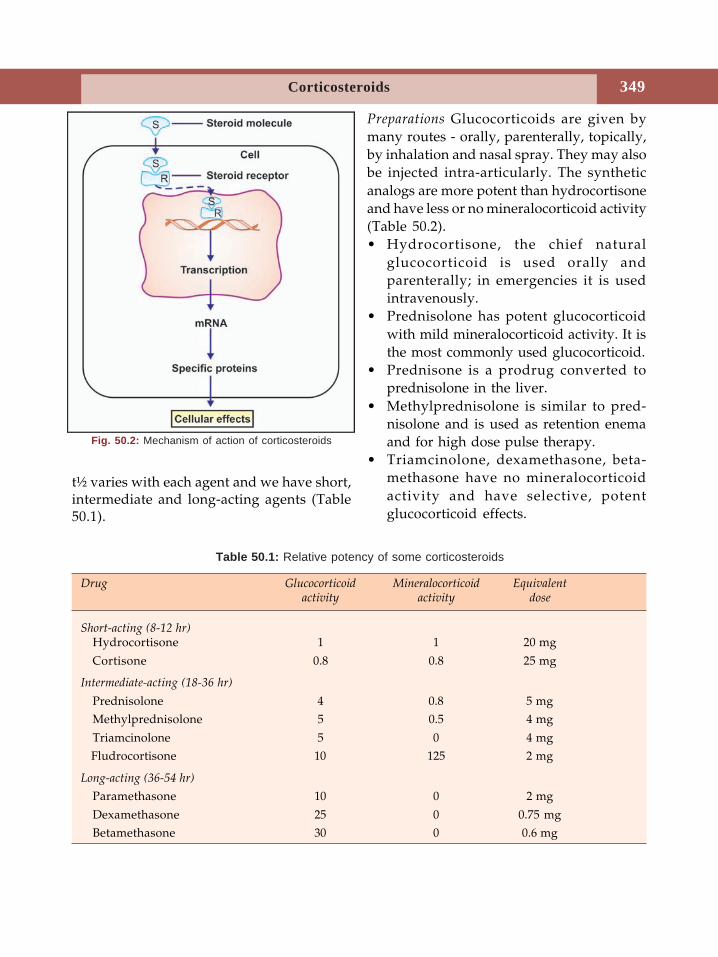
349Corticosteroids
t½ varies with each agent and we have short,intermediate and long-acting agents (Table50.1).
Preparations Glucocorticoids are given bymany routes - orally, parenterally, topically,by inhalation and nasal spray. They may alsobe injected intra-articularly. The syntheticanalogs are more potent than hydrocortisoneand have less or no mineralocorticoid activity(Table 50.2).• Hydrocortisone, the chief natural
glucocorticoid is used orally andparenterally; in emergencies it is usedintravenously.
• Prednisolone has potent glucocorticoidwith mild mineralocorticoid activity. It isthe most commonly used glucocorticoid.
• Prednisone is a prodrug converted toprednisolone in the liver.
• Methylprednisolone is similar to pred-nisolone and is used as retention enemaand for high dose pulse therapy.
• Triamcinolone, dexamethasone, beta-methasone have no mineralocorticoidactivity and have selective, potentglucocorticoid effects.
Table 50.1: Relative potency of some corticosteroids
Drug Glucocorticoid Mineralocorticoid Equivalentactivity activity dose
Short-acting (8-12 hr)Hydrocortisone 1 1 20 mg
Cortisone 0.8 0.8 25 mg
Intermediate-acting (18-36 hr)
Prednisolone 4 0.8 5 mgMethylprednisolone 5 0.5 4 mg
Triamcinolone 5 0 4 mg Fludrocortisone 10 125 2 mg
Long-acting (36-54 hr)
Paramethasone 10 0 2 mg
Dexamethasone 25 0 0.75 mgBetamethasone 30 0 0.6 mg
Fig. 50.2: Mechanism of action of corticosteroids
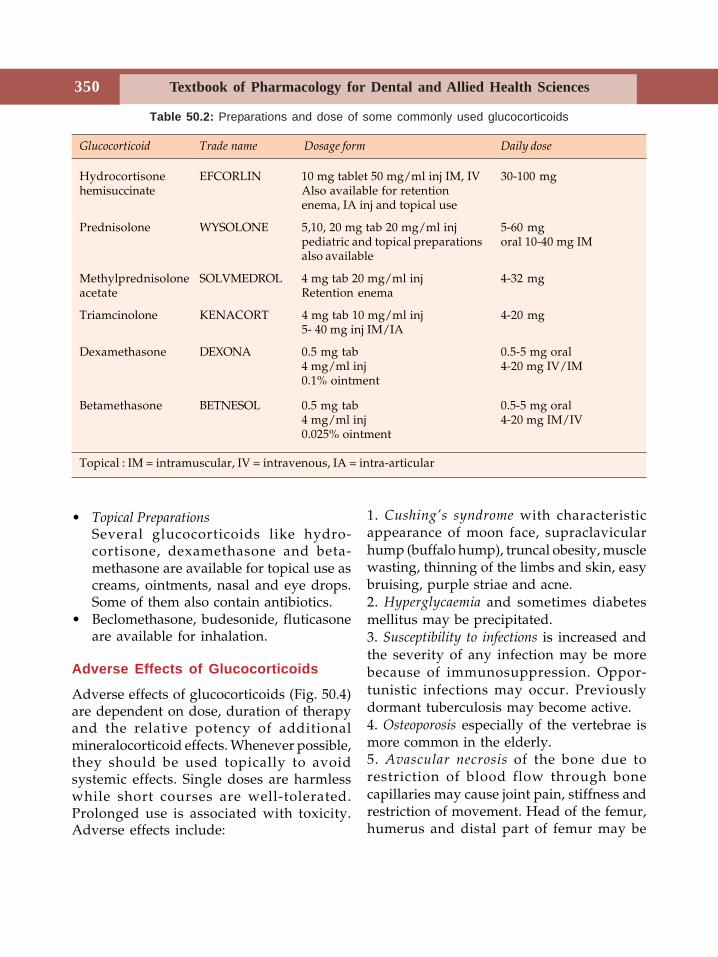
Textbook of Pharmacology for Dental and Allied Health Sciences350
• Topical PreparationsSeveral glucocorticoids like hydro-cortisone, dexamethasone and beta-methasone are available for topical use ascreams, ointments, nasal and eye drops.Some of them also contain antibiotics.
• Beclomethasone, budesonide, fluticasoneare available for inhalation.
Adverse Effects of Glucocorticoids
Adverse effects of glucocorticoids (Fig. 50.4)are dependent on dose, duration of therapyand the relative potency of additionalmineralocorticoid effects. Whenever possible,they should be used topically to avoidsystemic effects. Single doses are harmlesswhile short courses are well-tolerated.Prolonged use is associated with toxicity.Adverse effects include:
1. Cushing’s syndrome with characteristicappearance of moon face, supraclavicularhump (buffalo hump), truncal obesity, musclewasting, thinning of the limbs and skin, easybruising, purple striae and acne.2. Hyperglycaemia and sometimes diabetesmellitus may be precipitated.3. Susceptibility to infections is increased andthe severity of any infection may be morebecause of immunosuppression. Oppor-tunistic infections may occur. Previouslydormant tuberculosis may become active.4. Osteoporosis especially of the vertebrae ismore common in the elderly.5. Avascular necrosis of the bone due torestriction of blood flow through bonecapillaries may cause joint pain, stiffness andrestriction of movement. Head of the femur,humerus and distal part of femur may be
Table 50.2: Preparations and dose of some commonly used glucocorticoids
Glucocorticoid Trade name Dosage form Daily dose
Hydrocortisone EFCORLIN 10 mg tablet 50 mg/ml inj IM, IV 30-100 mghemisuccinate Also available for retention
enema, IA inj and topical use
Prednisolone WYSOLONE 5,10, 20 mg tab 20 mg/ml inj 5-60 mgpediatric and topical preparations oral 10-40 mg IMalso available
Methylprednisolone SOLVMEDROL 4 mg tab 20 mg/ml inj 4-32 mgacetate Retention enema
Triamcinolone KENACORT 4 mg tab 10 mg/ml inj 4-20 mg5- 40 mg inj IM/IA
Dexamethasone DEXONA 0.5 mg tab 0.5-5 mg oral4 mg/ml inj 4-20 mg IV/IM0.1% ointment
Betamethasone BETNESOL 0.5 mg tab 0.5-5 mg oral4 mg/ml inj 4-20 mg IM/IV0.025% ointment
Topical : IM = intramuscular, IV = intravenous, IA = intra-articular
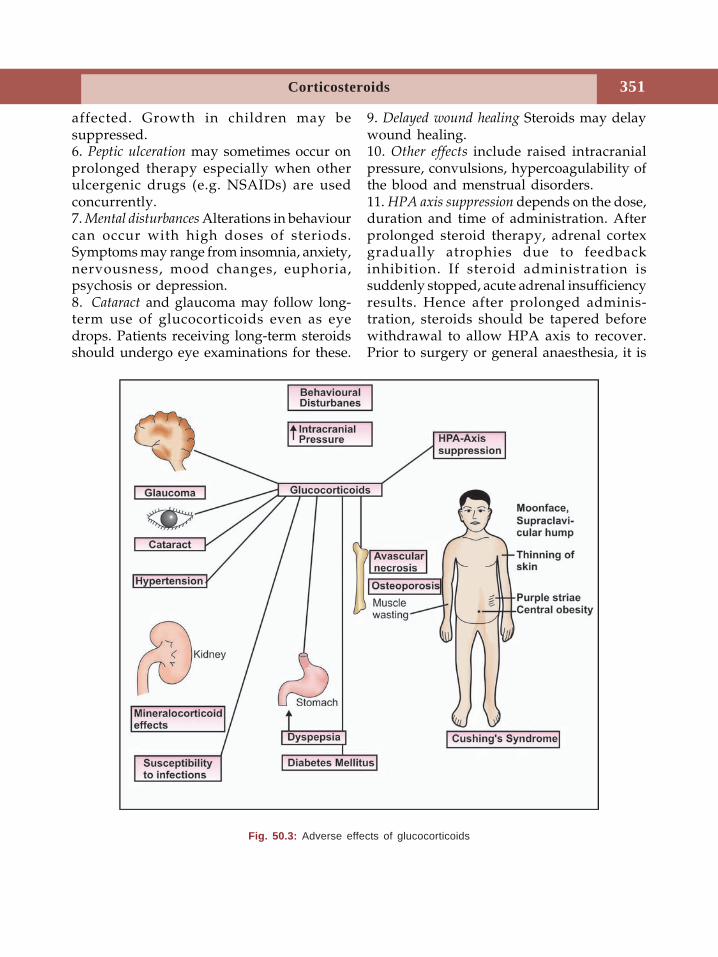
351Corticosteroids
affected. Growth in children may besuppressed.6. Peptic ulceration may sometimes occur onprolonged therapy especially when otherulcergenic drugs (e.g. NSAIDs) are usedconcurrently.7. Mental disturbances Alterations in behaviourcan occur with high doses of steriods.Symptoms may range from insomnia, anxiety,nervousness, mood changes, euphoria,psychosis or depression.8. Cataract and glaucoma may follow long-term use of glucocorticoids even as eyedrops. Patients receiving long-term steroidsshould undergo eye examinations for these.
9. Delayed wound healing Steroids may delaywound healing.10. Other effects include raised intracranialpressure, convulsions, hypercoagulability ofthe blood and menstrual disorders.11. HPA axis suppression depends on the dose,duration and time of administration. Afterprolonged steroid therapy, adrenal cortexgradually atrophies due to feedbackinhibition. If steroid administration issuddenly stopped, acute adrenal insufficiencyresults. Hence after prolonged adminis-tration, steroids should be tapered beforewithdrawal to allow HPA axis to recover.Prior to surgery or general anaesthesia, it is
Fig. 50.3: Adverse effects of glucocorticoids
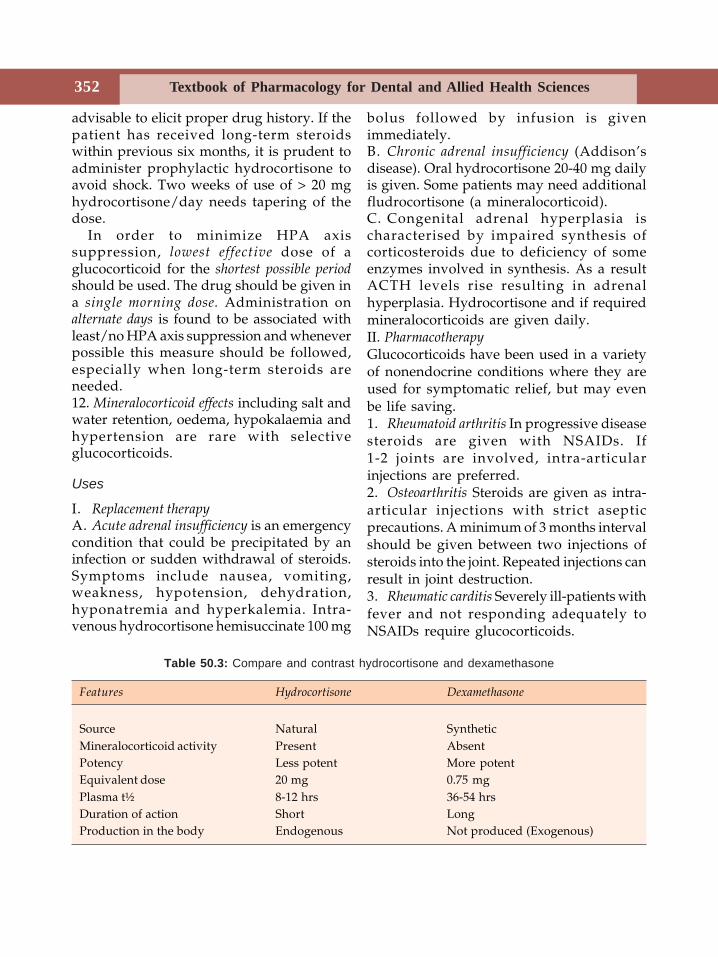
Textbook of Pharmacology for Dental and Allied Health Sciences352
advisable to elicit proper drug history. If thepatient has received long-term steroidswithin previous six months, it is prudent toadminister prophylactic hydrocortisone toavoid shock. Two weeks of use of > 20 mghydrocortisone/day needs tapering of thedose.
In order to minimize HPA axissuppression, lowest effective dose of aglucocorticoid for the shortest possible periodshould be used. The drug should be given ina single morning dose. Administration onalternate days is found to be associated withleast/no HPA axis suppression and wheneverpossible this measure should be followed,especially when long-term steroids areneeded.12. Mineralocorticoid effects including salt andwater retention, oedema, hypokalaemia andhypertension are rare with selectiveglucocorticoids.
Uses
I. Replacement therapyA. Acute adrenal insufficiency is an emergencycondition that could be precipitated by aninfection or sudden withdrawal of steroids.Symptoms include nausea, vomiting,weakness, hypotension, dehydration,hyponatremia and hyperkalemia. Intra-venous hydrocortisone hemisuccinate 100 mg
bolus followed by infusion is givenimmediately.B. Chronic adrenal insufficiency (Addison’sdisease). Oral hydrocortisone 20-40 mg dailyis given. Some patients may need additionalfludrocortisone (a mineralocorticoid).C. Congenital adrenal hyperplasia ischaracterised by impaired synthesis ofcorticosteroids due to deficiency of someenzymes involved in synthesis. As a resultACTH levels rise resulting in adrenalhyperplasia. Hydrocortisone and if requiredmineralocorticoids are given daily.II. PharmacotherapyGlucocorticoids have been used in a varietyof nonendocrine conditions where they areused for symptomatic relief, but may evenbe life saving.1. Rheumatoid arthritis In progressive diseasesteroids are given with NSAIDs. If1-2 joints are involved, intra-articularinjections are preferred.2. Osteoarthritis Steroids are given as intra-articular injections with strict asepticprecautions. A minimum of 3 months intervalshould be given between two injections ofsteroids into the joint. Repeated injections canresult in joint destruction.3. Rheumatic carditis Severely ill-patients withfever and not responding adequately toNSAIDs require glucocorticoids.
Table 50.3: Compare and contrast hydrocortisone and dexamethasone
Features Hydrocortisone Dexamethasone
Source Natural SyntheticMineralocorticoid activity Present AbsentPotency Less potent More potentEquivalent dose 20 mg 0.75 mgPlasma t½ 8-12 hrs 36-54 hrsDuration of action Short LongProduction in the body Endogenous Not produced (Exogenous)
353Corticosteroids
4. Acute gout When treatment with NSAIDshave not been successful, prednisolone is usedas an adjuvant.5. Allergic diseases like angioneurotic edema,hay fever, serum sickness, contact dermatitis,urticaria, drug reactions and anaphylaxis–steroids are indicated. Steroids are slowacting and in less severe cases, antihistaminesshould be preferred.6. Bronchial asthma
• Acute exacerbations – a short courseof prednisolone
• Status asthmaticus – intravenoushydrocortisone hemisuccinate 100-200mg repeated after 8 hrs 40-60 mg perday.
• Chronic asthma–Inhalational steroidsare used and in more severe cases lowdose oral prednisolone is indicated.COPD– exacerbation may be treatedwith short course of prednisolone.
7. Collagen diseases like polyarthritis nodosa,lupus erythematosus, polymyositis, Wegener’sgranulomatosis and other rheumatoiddisorders respond to glucocorticoids. Gluco-corticoids are the first-line drugs. Predni-solone is given for 6 weeks and tapered overanother 6 weeks.8. Eye diseases Allergic conjunctivitis, uveitis,optic neuritis and other inflammatoryconditions are treated with steroid eyedrops. Long-term steriods administration canincrease IOP which should be monitored. Inocular infections, steroids are contra-indicated.9. Renal diseases like nephrotic syndrome aretreated with steroids. Glucocorticoids arethe first line drugs.10. Skin diseases Atopic dermatitis, seborrhoeicdermatitis, inflammatory dermatoses andother local skin conditions are treated withtopical steroids. Systemic steroids are lifesaving in pemphigus.
11. Gastrointestinal diseases Mild inflammatorybowel diseases like ulcerative colitis aretreated with steroid retention enema whilesevere cases need oral prednisolone.12. Liver diseases Steroids are useful inconditions like autoimmune chronic activehepatitis and alcoholic hepatitis.13. Haematologic disorders like purpura andhaemolytic anaemia having immunologicalaetiology respond to steroids.14. Cerebral oedema Large doses of dexa-methasone reduces cerebral oedema occurringin some malignancies.15. Malignancies Because of their lympholyticeffects, steroids are used in the treatment ofacute lymphocytic leukaemia and lymphomas.Steroids are also used for rapid symptomaticrelief in other malignancies like breast cancer.16. Lung diseases Apart from bronchialasthma, steroids are used in other diseaseslike aspiration pneumonia and prevention ofinfant respiratory distress syndrome.17. Organ transplantation For prevention andtreatment of graft rejection, high doses ofprednisolone are started at the time ofsurgery with immunosuppressive agents.18. Others - Glucocorticoids are useful in
• Sarcoidosis to induce remission.• Pneumocystis carinii pneumonia is
common in patients with AIDS -Glucocorticoids reduce the risk ofrespiratory failure and decreasemortality.
1. Peptic ulcer2. Hypertension3. Infections4. Diabetes mellitus5. Ocular infections
particularly viralinfections
6. Osteoporosis7. Psychoses8. Epilepsy9. CCF10. Glaucoma11. Renal failure
Table 50.4: Contraindications toglucocorticoid therapy
Steroids should be used with caution in:

Textbook of Pharmacology for Dental and Allied Health Sciences354
• In haemolytic anaemia glucocorticoidsreduce the autoimmune destruction oferythrocytes.
Contraindications–see table 50.4.
MINERALOCORTICOIDS
The most important natural mineralocorticoidis aldosterone synthesized in zonaglomerulosa of the adrenal cortex. Smallamounts of desoxycorticosterone is alsoreleased.Actions Mineralocorticoids promote sodiumand water retention by distal renal tubuleswith loss of potassium.Adverse effects include weight gain, oedema,hypertension and hypokalaemia.Fludrocortisone has predominantlymineralocorticoid properties and is used forreplacement therapy in aldosteronedeficiency as in Addison’s disease. Althoughaldosterone is the principal naturalmineralocorticoid, it is not used therap-eutically since it is not effective orally.
INHIBITORS OF ADRENAL STEROIDSSYNTHESIS
Metyrapone, trilastane, aminoglutethimide andketoconazole These drugs inhibit the synthesisof adrenal steroids by inhibiting certainenzymes involved in steroid synthesis. Theyare used in Cushing’s syndrome and someprostatic and breast cancers.
Steroids and Dentistry
Glucocorticoids are one of the most widelyused drugs. When a patient on gluco-corticoids, especially on long-term steroidsrequires a dental procedure, adequateprecautions are to be taken.(a) Patients on steroids are more susceptibleto infections. Antibiotic coverage may beneeded depending on the procedure(b) If the patient is on steroids, it shouldbe continued because if steroids aresuddenly stopped, the patient may go intoacute adrenal insufficiency (due to HPA axissuppression) particularly following majorprocedures. Infact patients on long-termglucocorticoids may require an additionaldose of the steroid to manage the stress.(c) Long-term administration of glucocor-ticoids may delay wound healing.(d) If a patient on glucocorticoids, undergoesa dental procedure and requires NSAIDs foranalgesia, care should be taken to usethe ones which do not produce muchgastric irritation - paracetamol (400-600 mg)or ibuprofen may be given. Both NSAIDs andglucocorticoids can produce gastric irritationand when given together it can be severe.(e) Therapeutic use of steroids in dentalprocedures is not very common. Severeinflammation may rarely require steroids inaddition to NSAIDs.
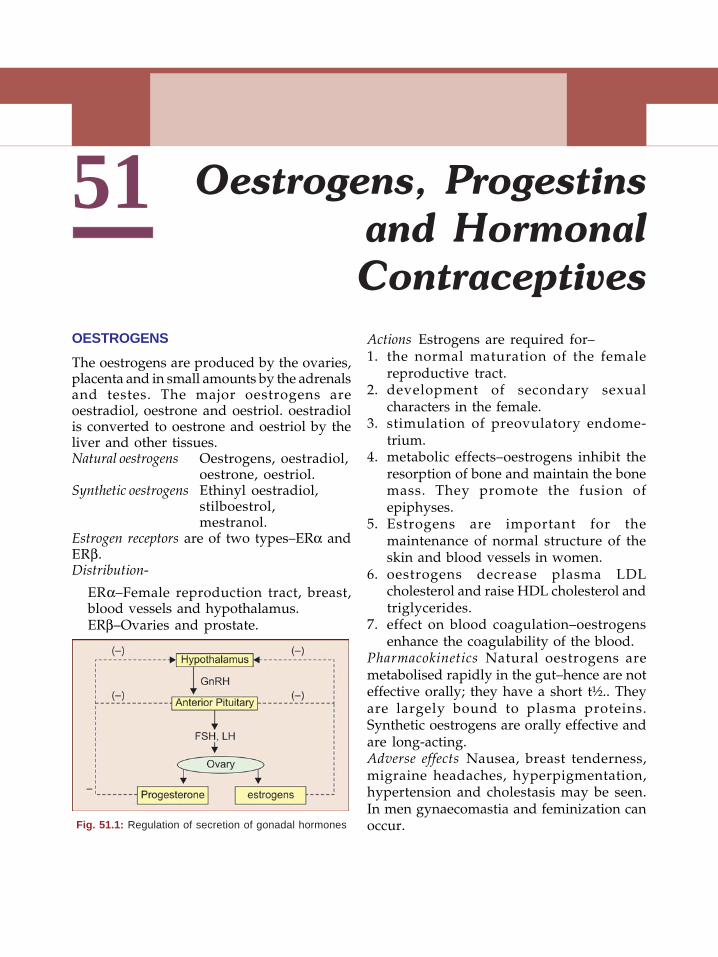
51
OESTROGENS
The oestrogens are produced by the ovaries,placenta and in small amounts by the adrenalsand testes. The major oestrogens areoestradiol, oestrone and oestriol. oestradiolis converted to oestrone and oestriol by theliver and other tissues.Natural oestrogens Oestrogens, oestradiol,
oestrone, oestriol.Synthetic oestrogens Ethinyl oestradiol,
stilboestrol,mestranol.
Estrogen receptors are of two types–ERα andERβ.Distribution-
ERα–Female reproduction tract, breast,blood vessels and hypothalamus.ERβ–Ovaries and prostate.
Actions Estrogens are required for–1. the normal maturation of the female
reproductive tract.2. development of secondary sexual
characters in the female.3. stimulation of preovulatory endome-
trium.4. metabolic effects–oestrogens inhibit the
resorption of bone and maintain the bonemass. They promote the fusion ofepiphyses.
5. Estrogens are important for themaintenance of normal structure of theskin and blood vessels in women.
6. oestrogens decrease plasma LDLcholesterol and raise HDL cholesterol andtriglycerides.
7. effect on blood coagulation–oestrogensenhance the coagulability of the blood.
Pharmacokinetics Natural oestrogens aremetabolised rapidly in the gut–hence are noteffective orally; they have a short t½.. Theyare largely bound to plasma proteins.Synthetic oestrogens are orally effective andare long-acting.Adverse effects Nausea, breast tenderness,migraine headaches, hyperpigmentation,hypertension and cholestasis may be seen.In men gynaecomastia and feminization canoccur.
Oestrogens, Progestinsand HormonalContraceptives
Fig. 51.1: Regulation of secretion of gonadal hormones
Textbook of Pharmacology for Dental and Allied Health Sciences356
Cancers Increased incidence of endometrialand breast cancers are reported on long-termoestrogen therapy.Teratogenic—When given to a pregnant ladyoestrogens may cause:• In female child–increased risk of vaginal
and cervical cancers• In male child–genital abnormalities.
Uses
1. Replacement therapy(a) In primary hypogonadism–Oestrogen
started at 11-13 years of agestimulates the development ofsecondary sexual characters andmenstruation.
(b) Postmenopausal syndrome-Due todecreased oestrogen production atmenopause, hot flushes, anxiety,fatigue, sweating, muscle and jointspain are common (Post menopausalsyndrome). Other longer-lastingchanges including osteoporosis,genital atrophy, skin changes,increased risk of cardiovasculardisease and psychological distur-bances may be seen. Oestrogens givenin low doses as hormone replacementtherapy (HRT) are highly effective inreversing most of the changes.
2. Senile vaginitis is common in elderlywomen due to reduced oestrogensynthesis by the ovary–ostrogen cream isused topically.
3. Osteoporosis In postmenopausal osteo-porosis, oestrogens restore calciumbalance and need to be given for a longtime.
4. Oral contraceptives Oestrogens are used(See Page 375) with progestins.
5. Dysmenorrhoea oestrogens combined withprogestins suppress ovulation and suchanovulatory cycles are painless.Oestrogens are used only in severedysmenorrhoea.
6. Dysfunctional uterine bleeding oestrogensare used as adjuvants to progesterone.
7. Carcinoma prostate is an androgendependent tumour. Oestrogensantagonise the action of androgens,suppress androgen production and areuseful for palliative therapy.
Contraindications Oestrogen dependenttumours, liver disease, thromboembolicdisorders.
Selective oestrogen receptormodulators (SERMs) and anti-oestrogens.
Tamoxifen
Tamoxifen was earlier considered to be anoestrogen antagonist. But now it isunderstood that it acts as an agonist,antagonist or partial agonist depending onthe site. Raloxifene and toremifene have actionssimilar to tamoxifen and are all termedselective oestrogen receptor modulators(SERMs). SERMs have tissue-selectiveoestrogenic activities. i.e.,• they act as agonists at bone, lipid, brain
and liver.• antagonists at breast, pituitary and
endometrium;• partial agonist at genitourinary
epithelium, in bone remodeling andcholesterol metabolism.
Tamoxifen By its tissue selective activity onthe oestrogen receptor, tamoxifen:• inhibits the proliferation of tumour cells
in the breast.• stimulates the proliferation of the
endometrium.• reduces bone resorption.• decreases total cholesterol
Side effects include hot flushes, nausea,vomiting, vaginal dryness, cataract and skinrashes. Tamoxifen increases the risk ofendometrial cancer and thromboembolism
357Oestrogens, Progestins and Hormonal Contraceptives
Uses Breast cancer–Tamoxifen is used in thepalliation of advanced breast cancer inpostmenopausal women with oestrogenreceptor positive tumours.Raloxifene acts as an oestrogen receptoragonist in the bone. In women withpostmenopausal osteoporosis, raloxifene hasantiresorptive effects on the bone. It reducesbone loss and may even help to gain bonemass. Raloxifene also lowers LDL. It acts asan oestrogen antagonist in the breast due towhich it reduces the incidence of breastcancer. Raloxifene does not stimulate theuterine endometrial proliferation.Adverse effects include hot flushes, leg crampsand an increased risk of deep vein thrombosisand pulmonary embolism.Raloxifene is indicated for the prevention ofpostmenopausal osteoporosis.Toremifene has actions similar to tamoxifenand is indicated in the treatment of metastaticbreast cancer in postmenopausal women.
Clomiphene Citrate
Clomiphene citrate binds to the oestrogenreceptors and acts as a competitive inhibitorof endogenous oestrogens. Like tamoxifen,it is also a partial agonist. Clomipheneopposes the negative feedback of endoge-nous oestrogens on the hypothalamo-pituitary axis resulting in increased gona-dotrophin secretion and thereby inducesovulation.Side effects include ovarian hyperstimulationresulting in multiple pregnancy, ovariancysts, hot flushes, headache and skin rashes.
Uses
1. Infertility Clomiphene citrate is used ininfertility due to ovarian disorders. It isgiven orally, 50 mg daily for 5 daysstarting from 5th day of the cycle; courseis repeated till ovulation occurs
2. In vitro fertilization Clomiphene inducedovulation is also useful in in vitrofertilization.
Oestrogen Synthesis Inhibitors
Aromatase inhibitors like formestane,exemestane, anastrozole, letrozole andvorazole block the production of oestrogensand are used in the treatment of breastcancer.
PROGESTINS
Progesterone is the natural progestinsynthesized in the ovary and placenta. It isalso synthesized by the testis and adrenalswhere it acts as a precursor of various steroidhormones (see under corticosteroids).
Progestins
Natural Progesterone
Synthetic Medroxyprogesterone acetateAllylestrenolMegestrolLevonorgestrelNorethisterone acetateLynestrenolNorgestimate
Actions
1. Uterus The secretory changes in theendometrium like increased tortuosity ofthe glands are due to progesterone. Inpregnancy, decidual changes in theendometrium take place under theinfluence of progesterone. Progesteroneis very important for the maintenance ofpregnancy (Progestin= favours pregnancy).
2. Cervix The watery cervical secretions arechanged to a viscid scanty secretion byprogesterone.
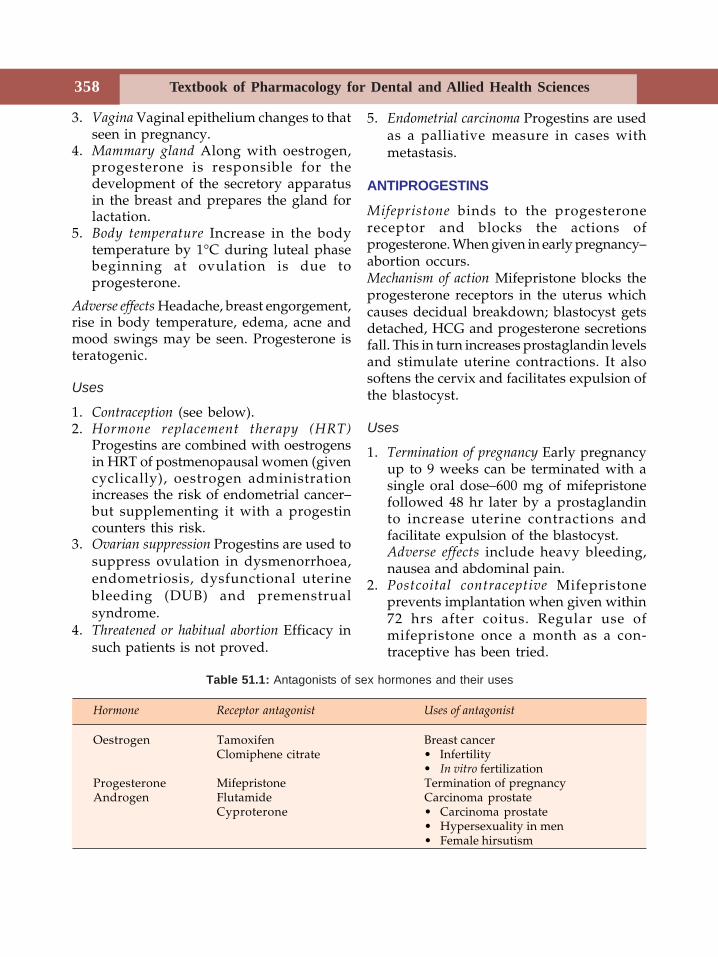
Textbook of Pharmacology for Dental and Allied Health Sciences358
3. Vagina Vaginal epithelium changes to thatseen in pregnancy.
4. Mammary gland Along with oestrogen,progesterone is responsible for thedevelopment of the secretory apparatusin the breast and prepares the gland forlactation.
5. Body temperature Increase in the bodytemperature by 1°C during luteal phasebeginning at ovulation is due toprogesterone.
Adverse effects Headache, breast engorgement,rise in body temperature, edema, acne andmood swings may be seen. Progesterone isteratogenic.
Uses
1. Contraception (see below).2. Hormone replacement therapy (HRT)
Progestins are combined with oestrogensin HRT of postmenopausal women (givencyclically), oestrogen administrationincreases the risk of endometrial cancer–but supplementing it with a progestincounters this risk.
3. Ovarian suppression Progestins are used tosuppress ovulation in dysmenorrhoea,endometriosis, dysfunctional uterinebleeding (DUB) and premenstrualsyndrome.
4. Threatened or habitual abortion Efficacy insuch patients is not proved.
5. Endometrial carcinoma Progestins are usedas a palliative measure in cases withmetastasis.
ANTIPROGESTINS
Mifepristone binds to the progesteronereceptor and blocks the actions ofprogesterone. When given in early pregnancy–abortion occurs.Mechanism of action Mifepristone blocks theprogesterone receptors in the uterus whichcauses decidual breakdown; blastocyst getsdetached, HCG and progesterone secretionsfall. This in turn increases prostaglandin levelsand stimulate uterine contractions. It alsosoftens the cervix and facilitates expulsion ofthe blastocyst.
Uses
1. Termination of pregnancy Early pregnancyup to 9 weeks can be terminated with asingle oral dose–600 mg of mifepristonefollowed 48 hr later by a prostaglandinto increase uterine contractions andfacilitate expulsion of the blastocyst.Adverse effects include heavy bleeding,nausea and abdominal pain.
2. Postcoital contraceptive Mifepristoneprevents implantation when given within72 hrs after coitus. Regular use ofmifepristone once a month as a con-traceptive has been tried.
Table 51.1: Antagonists of sex hormones and their uses
Hormone Receptor antagonist Uses of antagonist
Oestrogen Tamoxifen Breast cancerClomiphene citrate • Infertility
• In vitro fertilizationProgesterone Mifepristone Termination of pregnancyAndrogen Flutamide Carcinoma prostate
Cyproterone • Carcinoma prostate• Hypersexuality in men• Female hirsutism
359Oestrogens, Progestins and Hormonal Contraceptives
HORMONAL CONTRACEPTIVES
Millions of women around the world usehormonal contraceptives making them oneof the most widely prescribed drugs. Whenproperly used, they are the most effectivespacing methods of contraception. Hormonalcontraceptives have greatly contributed tothe control of population throughout theworld.
Oral pills Depot preparations
• Combined-pill • Injectables• Mini-pill • Subcutaneous
implants• Postcoital pill • Transdermal
patches• Vaginal rings
Oral Pill
1. Combined pill contains low doses of anoestrogen and a progestin. They are highlyefficacious (success rate 98%). Ethinylo-estradiol or mestranol (in the dose of 30-50mcg) are the oestrogens used. Newerprogestins like desogestrel and norgestimatecause least side effects. The pill is started onthe 5th day of the menstrual cycle, taken dailyfor 21 days followed by a gap of 7 daysduring which bleeding occurs. This ismonophasic regimen.
Oral contraceptives are also available asbiphasic or triphasic preparations (Table 51.2).This reduces the amount of hormones neededand more closely mimics menstrual cycle.
If a woman misses a pill, she should take 2pills the next day and continue the course. Ifmore than 2 pills are missed, then that courseshould be withdrawn, should follow analternative method of contraception for thatparticular cycle and restart the course on the5th day of the next menstrual cycle. If thewoman has conceived, the pregnancy shouldbe terminated because these hormones are
teratogenic. However, recent studies havefound low doses of the hormones to be nonteratogenic.2. Mini-pill A low dose progestin is takendaily without a gap. Oestrogen and itsaccompanied long-term adverse effects arealso eliminated. But efficacy is lower,menstrual cycles may be irregular and istherefore not popular.3. Postcoital contraceptives Postcoital pills actby preventing implantation. The earlier theyare given the better. High dose of anoestrogen was used earlier. Combination ofoestrogen and progestins is now preferreddue to lower doses needed and lesser sideeffects reported. The pill should be startedwithin 72 hours of coitus and has an efficacyof 90-98%.Benefits of combined pills
1. Effective and convenient method ofcontraception.
2. Reduced risk of ovarian cancers (ovarianstimulation by gonadotropins)
3 Reduced risk of endometrial cancers(progesterone antagonises the endo-metrial proliferation induced byoestrogens)
4. Reduced incidence of pelvic inflammatorydisease and ectopic pregnancy.
5. Menstrual benefits—less menstrual bloodloss, less iron-deficiency; premenstrualtension and dysmenorrhoea are lessintense.They are advocated as an emergency
method in situations following rape orcontraceptive failure.Depot preparations are given as:1. Progestin injections
a. Intramuscular injections at 3-6 monthsintervals, e.g. depot medroxyprogesteroneacetate (DMPA 150-400 mg) or Nore-thisterone enanthate (NET EN 200 mg).
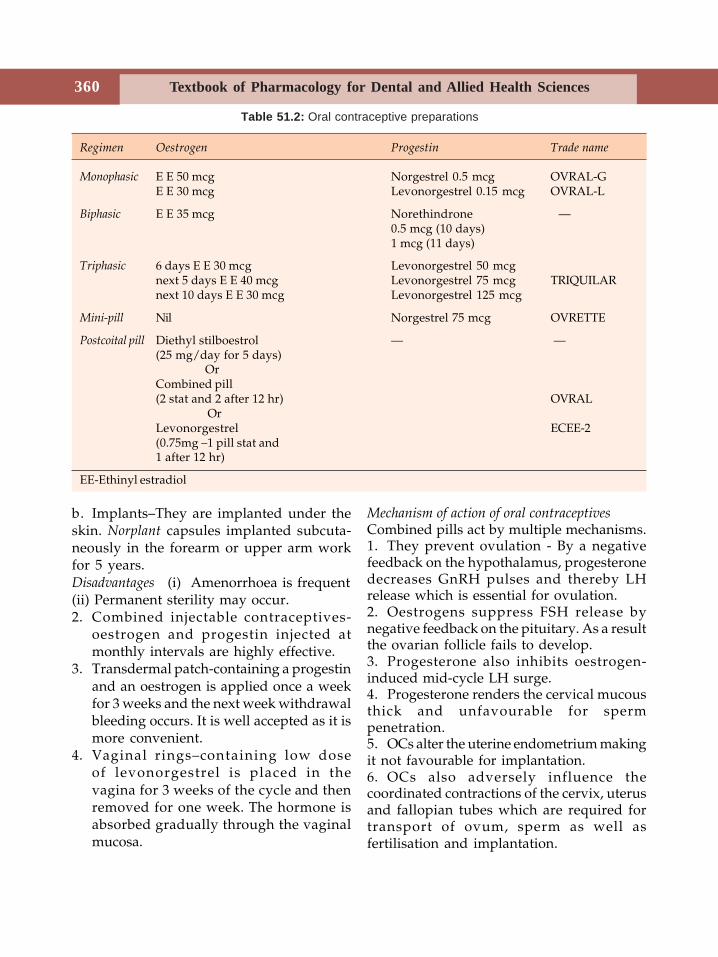
Textbook of Pharmacology for Dental and Allied Health Sciences360
b. Implants–They are implanted under theskin. Norplant capsules implanted subcuta-neously in the forearm or upper arm workfor 5 years.Disadvantages (i) Amenorrhoea is frequent(ii) Permanent sterility may occur.2. Combined injectable contraceptives-
oestrogen and progestin injected atmonthly intervals are highly effective.
3. Transdermal patch-containing a progestinand an oestrogen is applied once a weekfor 3 weeks and the next week withdrawalbleeding occurs. It is well accepted as it ismore convenient.
4. Vaginal rings–containing low doseof levonorgestrel is placed in thevagina for 3 weeks of the cycle and thenremoved for one week. The hormone isabsorbed gradually through the vaginalmucosa.
Mechanism of action of oral contraceptivesCombined pills act by multiple mechanisms.1. They prevent ovulation - By a negativefeedback on the hypothalamus, progesteronedecreases GnRH pulses and thereby LHrelease which is essential for ovulation.2. Oestrogens suppress FSH release bynegative feedback on the pituitary. As a resultthe ovarian follicle fails to develop.3. Progesterone also inhibits oestrogen-induced mid-cycle LH surge.4. Progesterone renders the cervical mucousthick and unfavourable for spermpenetration.5. OCs alter the uterine endometrium makingit not favourable for implantation.6. OCs also adversely influence thecoordinated contractions of the cervix, uterusand fallopian tubes which are required fortransport of ovum, sperm as well asfertilisation and implantation.
Table 51.2: Oral contraceptive preparations
Regimen Oestrogen Progestin Trade name
Monophasic E E 50 mcg Norgestrel 0.5 mcg OVRAL-GE E 30 mcg Levonorgestrel 0.15 mcg OVRAL-L
Biphasic E E 35 mcg Norethindrone —0.5 mcg (10 days)1 mcg (11 days)
Triphasic 6 days E E 30 mcg Levonorgestrel 50 mcgnext 5 days E E 40 mcg Levonorgestrel 75 mcg TRIQUILARnext 10 days E E 30 mcg Levonorgestrel 125 mcg
Mini-pill Nil Norgestrel 75 mcg OVRETTE
Postcoital pill Diethyl stilboestrol — —(25 mg/day for 5 days)
OrCombined pill(2 stat and 2 after 12 hr) OVRAL
OrLevonorgestrel ECEE-2(0.75mg –1 pill stat and1 after 12 hr)
EE-Ethinyl estradiol
361Oestrogens, Progestins and Hormonal Contraceptives
Adverse Effects
• Headache, migraine headache in somewomen, nausea, vomiting, oedema, breasttenderness, amenorrhoea and irregularmenstrual cycles may be commonly seen.• Weight gain, acne, mood swings andhirsutism may occur.More severe side effects include -• Cardiovascular effects - in women above35 years, OCs may increase the risk of MIand venous thromboembolism. OCs may alsoincrease the coagulability of blood. But thenewer low-dose preparations are found tobe safer when used in healthy women withno other risk factors for MI or throm-boembolism.• Hypertension-The high dose preparationsmay precipitate hypertension in some women.But the newer low dose preparations aresafer.• Cancers OCs may increase the incidenceof cervical, breast and other cancers–but therisk is not significant.• Cholestatic jaundice and gallstones Incidencemay be higher in high dose preparations.• Glucose tolerance OCs may impair glucosetolerance-but the newer low dosepreparations do not carry such risk.Contraindications to combined pill:• Thromboembolic and cerebrovascular
disease• breast cancers• liver disease• OCs should be used with caution in
diabetes, hypertension, convulsivedisorders, oedema and CCF.
Centchroman is a nonsteroidal oralcontraceptive developed by CDRI, Lucknow.It has antioestrogenic and antiprogestogenicactivity and may act by preventingimplantation. Onset of action is quick (< 60minutes) and duration of action is 7 days.Dosage (SAHELI, CENTRON) 30 mg twicea week for 3 months followed by once a weektill contraception is desired (The tablet shouldbe continued without withdrawing formenstruation). Success rate claimed is 97-99%and is devoid of the side effects of hormonalcontraceptives. It is well tolerated.
Drugs Acting on the Uterus
Uterine Stimulants (Ecbolics)
Drugs which stimulate the uterine contractionsare oxytocin, ergometrine and prostaglandins.They are used in obstetrics. Oxytocin is usedfor induction of labour; ergometrine is usedto prevent and control postpartum bleeding.Prostaglandins–PGE2 and PGF2α are used toinduce mid trimester abortion and for cervicalpriming.
Uterine Relaxants (Tocolytics)
Tocolytics are drugs that reduce uterinemotility. Beta adrenergic agonists likesalbutamol, terbutaline and isoxuprine andother drugs like ethyl alcohol, calciumchannel blockers, aspirin and magnesiumsulphate have tocolytic properties. They areused to delay premature labour, in threatenedabortion to inhibit uterine contractions andin dysmenorrhoea.
Textbook of Pharmacology for Dental and Allied Health Sciences362
52Androgens are produced chiefly in the testesand small amounts in the adrenal cortex. Inthe females, small amounts of androgens areproduced in the ovary and adrenal cortex.Testosterone is the most important naturalandrogen. In the adult male, 8-10 mg oftestosterone is produced daily. Secretion isregulated by gonadotrophins and GnRH.Physiological actions In the male, testosteroneis essential for the development of secondarysexual characters and sex organs. It isnecessary for normal spermatogenesis andis important for maintaining sexual functionin men. Testosterone promotes bone growth,enhances the muscle mass, protein synthesisand positive nitrogen balance—has anabolicactions.Mechanism of action is similar to other steroids.Androgens bind to androgen receptors onthe target cells, the complex moves to thenucleus where it stimulates protein synthesis.Adverse effects Masculinization and acne infemales, hepatotoxicity, increased libido andprecocious puberty can occur in young boys.With large doses, salt and water retention,suppression of spermatogenesis resulting ininfertility can be seen. Feminizing effects likegynaecomastia in men can occur as someandrogens are converted to oestrogens.
Androgens andAnabolic Steroids
Uses
1. Testicular failure Androgen replacementtherapy in primary and secondarytesticular failure.
2. Other uses Androgens may be used insenile osteoporosis and carcinoma of thebreast in premenopausal women.
ANABOLIC STEROIDS
Anabolic steroids are synthetic androgenswith higher anabolic and low androgenicactivity. These are believed to enhanceprotein synthesis and increase muscle mass.But with higher doses, the relative anabolicactivity is lost. Methandienone, nandrolone,oxandrolone and stanozolol are someanabolic steroids available at present. Adverseeffects are similar to those caused byandrogens.
Uses
1. Catabolic states Anabolic steroids maybenefit patients following surgery, trauma,prolonged illness and debilitating conditions.Given during convalescence, the negativenitrogen balance is corrected, appetiteimproves and there is a feeling of well being.2. Senile osteoporosis seen in elderly malesrespond by formation of new bone tissue.
Androgens and Anabolic Steroids 363
3. Growth stimulation in children Anabolicsteroids promote linear growth in prepubertalboys. They may be used only for shortperiods—but actual benefit on final height isnot established.4. Other uses Anabolic steroids are tried inchronic renal failure to reduce nitrogen loadon the kidneys. They may benefit inrefractory anaemias with bone marrowfailure.Abuse in athletes Anabolic steroids enjoy areputation for improving athleticperformance. When combined with adequateexercise, the muscle mass increases. But thedose used by athletes is very high and isassociated with serious adverse effects liketesticular atrophy, sterility andgynaecomastia in men and virilizing effectsin women; increased aggressiveness,psychotic symptoms and increased risk ofcoronary heart disease in both sexes.Moreover, there is no evidence that athleticperformance improves. Hence the use ofanabolic steroids by athletes has been bannedand is medically not recommended.
ANTIANDROGENS
Cyproterone acetate—a derivative ofprogesterone competitively binds toandrogen receptors and thus blocks theactions of androgens. It also has proge-stational activity. Cyproterone is used totreat severe hypersexuality in males, incarcinoma prostate and in female hirsuitism.Flutamide is a potent competitive antagonistat androgen receptors. It is used with GnRH/leuprolide in the treatment of carcinomaprostate.Danazol–has weak androgenic, anabolic andprogestational activity. It suppressesgonadotrophin secretion from the pituitary.
It is used in endometriosis in women andprecautious puberty in boys.Finasteride inhibits the enzyme 5-alphareductase and thus inhibits the convertion oftestosterone to its active metabolite dihy-drotestosterone which acts mainly in the maleurogenital tract. Finasteride is used in benignprostatic hypertrophy to reduce the prostatesize.
DRUGS USED IN MALE SEXUALIMPOTENCE
Sexual impotence is the inability of a man tohave satisfactory sexual intercourse due toinability to have and maintain an erection.Very often it is psychological while in somecases there could be an organic cause. Severaldrugs have been tried including testosterone,yohimbine, papaverine and antidepressants.The recent introduction—Sildenafil (Viagra)has been a success in a large percentage ofthem.
Sildenafil (Viagra)
Sildenafil is the first agent to be effectiveorally for the treatment of erectiledysfunction. Sildenafil inhibits the enzymephosphodiesterase in the penis and thusprolongs the life of cyclic GMP. This causesrelaxation of smooth muscle in the corpuscavernosum and vasodilation—bothresulting in cavernosal engorgement andpenile erection.
Sildenafil is given orally (50-100 mg) 1 hourbefore sexual activity.Adverse effects and precautions Due tovasodilation—headache, dizziness and nasalstuffiness can occur. It potentiates thehypotensive action of nitrates and iscontraindicated in patients on nitrates and inpatients with coronary artery disease. Elderlymen above 60 years need less dose (25 mg).
Textbook of Pharmacology for Dental and Allied Health Sciences364
53Diabetes mellitus is a chronic metabolic disordercharacterised by hyperglycaemia and alteredmetabolism of carbohydrates, lipids andproteins. It is a common condition affecting1-2% of population with a strong hereditarytendency.Diabetes mellitus can be of 2 types.Type I Insulin dependent diabetes mellitus(IDDM) is an autoimmune disorder whereantibodies destroy the β cells of the islets ofLangerhans. It usually occurs in the youngchildren and adolescents (hence calledjuvenile onset diabetes mellitus).Type II Non-insulin dependent diabetesmellitus (NIDDM) is of maturity onset. Mostpatients are obese. There is both reducedsensitivity of tissues to insulin and impairedregulation of insulin secretion.
Prolonged hyperglycaemia results invarious complications including prematureatherosclerosis, retinopathy, nephropathyand gangrene of the limbs. This is thought tobe due to reduced blood supply to thesestructures - because of thickening of thecapillary walls. Hence, it is necessary tomaintain normal blood glucose levels thoughdiabetes mellitus as such does not causesignificant troublesome symptoms. Treatmenthelps to prevent or delay the onset ofcomplications of diabetes.
INSULIN
In 1921 Banting and Best first obtainedinsulin in the form of pancreatic extract. In
Insulin and OralHypoglycaemics
1922 the extract containing insulin was firstused on a 14 years old boy suffering fromsevere diabetes mellitus with excellentresponse. Insulin was then purified in a fewyears.Chemistry, synthesis and secretion Naturalinsulin is a polypeptide synthesized from theprecursor proinsulin. It has two peptidechains - A chain (21 amino acids) and B chain(30 amino acids) linked by disulphidebridges. Human insulin differs from bovineinsulin by 3 amino acids and from porcineinsulin by 1 amino acid. Hence porcine insulinis closer to human insulin.
Insulin is stored in granules in the β isletcells of the pancreas. Normal pancreasreleases about 20-40 units of insulineveryday. The secretion is regulated byfactors like food, hormones and autonomicnervous system. Blood glucose concentrationis the main factor. The islets of Langerhansare composed of 4 types of cells–β cellssecrete insulin, α (A) cells glucagon, δ (D)cells somatostatin and P cells secretepancreatic polypeptide.
Insulin is metabolised in the liver, kidneyand muscle.
Actions of Insulin
1. Carbohydrate metabolism Insulin stimulatesthe uptake and metabolism of glucose in theperipheral tissues especially skeletal musclesand adipose tissue. It inhibits glucose
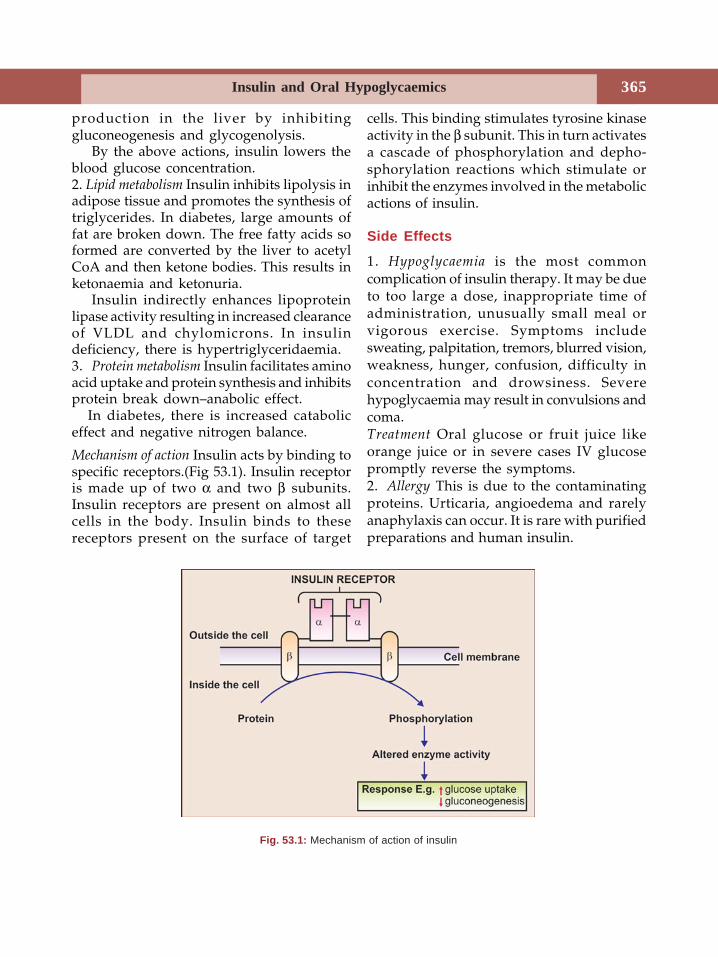
Insulin and Oral Hypoglycaemics 365
production in the liver by inhibitinggluconeogenesis and glycogenolysis.
By the above actions, insulin lowers theblood glucose concentration.2. Lipid metabolism Insulin inhibits lipolysis inadipose tissue and promotes the synthesis oftriglycerides. In diabetes, large amounts offat are broken down. The free fatty acids soformed are converted by the liver to acetylCoA and then ketone bodies. This results inketonaemia and ketonuria.
Insulin indirectly enhances lipoproteinlipase activity resulting in increased clearanceof VLDL and chylomicrons. In insulindeficiency, there is hypertriglyceridaemia.3. Protein metabolism Insulin facilitates aminoacid uptake and protein synthesis and inhibitsprotein break down–anabolic effect.
In diabetes, there is increased cataboliceffect and negative nitrogen balance.
Mechanism of action Insulin acts by binding tospecific receptors.(Fig 53.1). Insulin receptoris made up of two α and two β subunits.Insulin receptors are present on almost allcells in the body. Insulin binds to thesereceptors present on the surface of target
cells. This binding stimulates tyrosine kinaseactivity in the β subunit. This in turn activatesa cascade of phosphorylation and depho-sphorylation reactions which stimulate orinhibit the enzymes involved in the metabolicactions of insulin.
Side Effects
1. Hypoglycaemia is the most commoncomplication of insulin therapy. It may be dueto too large a dose, inappropriate time ofadministration, unusually small meal orvigorous exercise. Symptoms includesweating, palpitation, tremors, blurred vision,weakness, hunger, confusion, difficulty inconcentration and drowsiness. Severehypoglycaemia may result in convulsions andcoma.Treatment Oral glucose or fruit juice likeorange juice or in severe cases IV glucosepromptly reverse the symptoms.2. Allergy This is due to the contaminatingproteins. Urticaria, angioedema and rarelyanaphylaxis can occur. It is rare with purifiedpreparations and human insulin.
Fig. 53.1: Mechanism of action of insulin
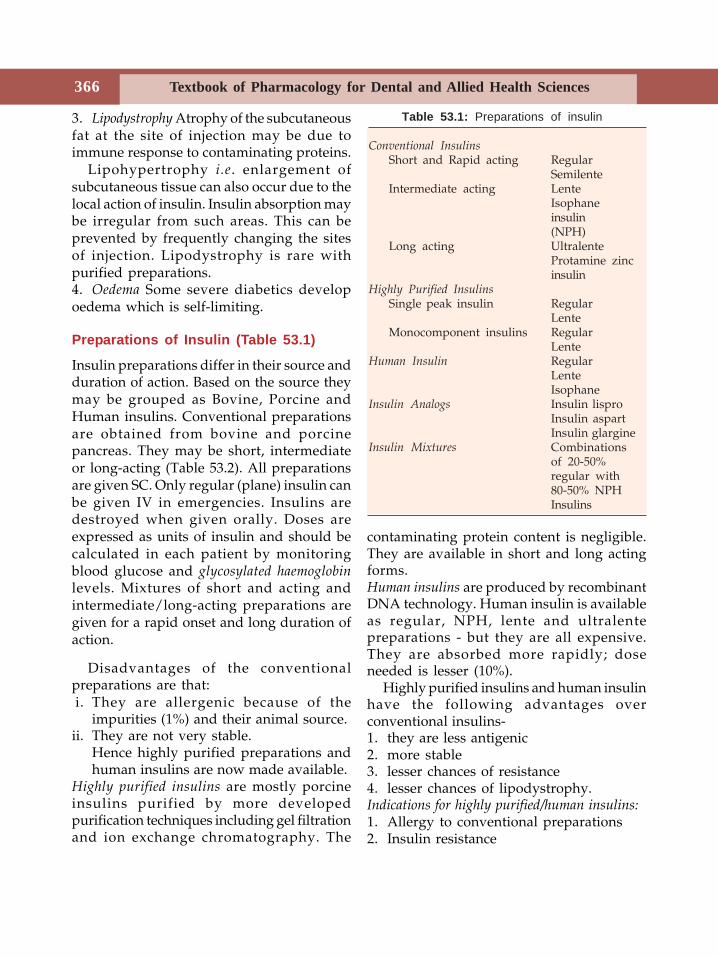
Textbook of Pharmacology for Dental and Allied Health Sciences366
Table 53.1: Preparations of insulin
Conventional InsulinsShort and Rapid acting Regular
SemilenteIntermediate acting Lente
Isophaneinsulin(NPH)
Long acting UltralenteProtamine zincinsulin
Highly Purified InsulinsSingle peak insulin Regular
LenteMonocomponent insulins Regular
LenteHuman Insulin Regular
LenteIsophane
Insulin Analogs Insulin lisproInsulin aspartInsulin glargine
Insulin Mixtures Combinationsof 20-50%regular with80-50% NPHInsulins
3. Lipodystrophy Atrophy of the subcutaneousfat at the site of injection may be due toimmune response to contaminating proteins.
Lipohypertrophy i.e. enlargement ofsubcutaneous tissue can also occur due to thelocal action of insulin. Insulin absorption maybe irregular from such areas. This can beprevented by frequently changing the sitesof injection. Lipodystrophy is rare withpurified preparations.4. Oedema Some severe diabetics developoedema which is self-limiting.
Preparations of Insulin (Table 53.1)
Insulin preparations differ in their source andduration of action. Based on the source theymay be grouped as Bovine, Porcine andHuman insulins. Conventional preparationsare obtained from bovine and porcinepancreas. They may be short, intermediateor long-acting (Table 53.2). All preparationsare given SC. Only regular (plane) insulin canbe given IV in emergencies. Insulins aredestroyed when given orally. Doses areexpressed as units of insulin and should becalculated in each patient by monitoringblood glucose and glycosylated haemoglobinlevels. Mixtures of short and acting andintermediate/long-acting preparations aregiven for a rapid onset and long duration ofaction.
Disadvantages of the conventionalpreparations are that:i. They are allergenic because of the
impurities (1%) and their animal source.ii. They are not very stable.
Hence highly purified preparations andhuman insulins are now made available.
Highly purified insulins are mostly porcineinsulins purified by more developedpurification techniques including gel filtrationand ion exchange chromatography. The
contaminating protein content is negligible.They are available in short and long actingforms.Human insulins are produced by recombinantDNA technology. Human insulin is availableas regular, NPH, lente and ultralentepreparations - but they are all expensive.They are absorbed more rapidly; doseneeded is lesser (10%).
Highly purified insulins and human insulinhave the following advantages overconventional insulins-1. they are less antigenic2. more stable3. lesser chances of resistance4. lesser chances of lipodystrophy.Indications for highly purified/human insulins:1. Allergy to conventional preparations2. Insulin resistance
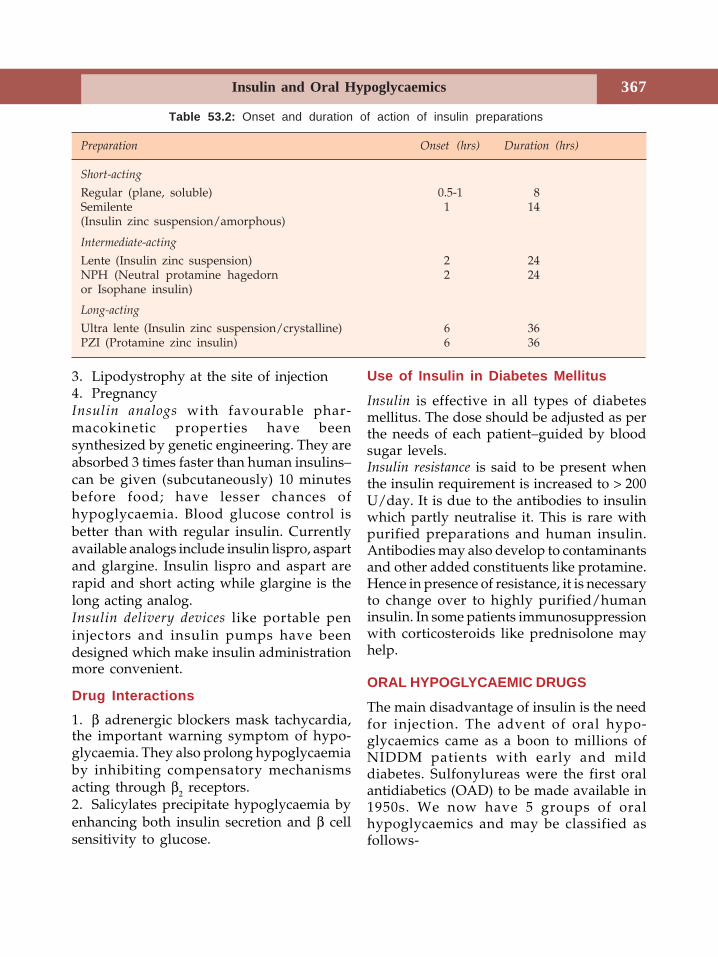
Insulin and Oral Hypoglycaemics 367
3. Lipodystrophy at the site of injection4. PregnancyInsulin analogs with favourable phar-macokinetic properties have beensynthesized by genetic engineering. They areabsorbed 3 times faster than human insulins–can be given (subcutaneously) 10 minutesbefore food; have lesser chances ofhypoglycaemia. Blood glucose control isbetter than with regular insulin. Currentlyavailable analogs include insulin lispro, aspartand glargine. Insulin lispro and aspart arerapid and short acting while glargine is thelong acting analog.Insulin delivery devices like portable peninjectors and insulin pumps have beendesigned which make insulin administrationmore convenient.
Drug Interactions1. β adrenergic blockers mask tachycardia,the important warning symptom of hypo-glycaemia. They also prolong hypoglycaemiaby inhibiting compensatory mechanismsacting through β2 receptors.2. Salicylates precipitate hypoglycaemia byenhancing both insulin secretion and β cellsensitivity to glucose.
Table 53.2: Onset and duration of action of insulin preparations
Preparation Onset (hrs) Duration (hrs)
Short-acting
Regular (plane, soluble) 0.5-1 8Semilente 1 14(Insulin zinc suspension/amorphous)
Intermediate-acting
Lente (Insulin zinc suspension) 2 24NPH (Neutral protamine hagedorn 2 24or Isophane insulin)
Long-acting
Ultra lente (Insulin zinc suspension/crystalline) 6 36PZI (Protamine zinc insulin) 6 36
Use of Insulin in Diabetes Mellitus
Insulin is effective in all types of diabetesmellitus. The dose should be adjusted as perthe needs of each patient–guided by bloodsugar levels.Insulin resistance is said to be present whenthe insulin requirement is increased to > 200U/day. It is due to the antibodies to insulinwhich partly neutralise it. This is rare withpurified preparations and human insulin.Antibodies may also develop to contaminantsand other added constituents like protamine.Hence in presence of resistance, it is necessaryto change over to highly purified/humaninsulin. In some patients immunosuppressionwith corticosteroids like prednisolone mayhelp.
ORAL HYPOGLYCAEMIC DRUGS
The main disadvantage of insulin is the needfor injection. The advent of oral hypo-glycaemics came as a boon to millions ofNIDDM patients with early and milddiabetes. Sulfonylureas were the first oralantidiabetics (OAD) to be made available in1950s. We now have 5 groups of oralhypoglycaemics and may be classified asfollows-
Textbook of Pharmacology for Dental and Allied Health Sciences368
CLASSIFICATION
1. SulfonylureasI generation
Tolbutamide,chlorpropamideacetohexamide, tolazamide
II generationGlibenclamide, glipizide,gliclazide, glimepiride
2. BiguanidesPhenformin, metformin
3. MeglitinidesRepaglinide, nateglinide
4. ThiazolidinedionesTroglitazone, rosiglitazone,pioglitazone
5. Alpha glucosidase inhibitorsAcarbose, miglitol
Sulfonylureas
A sulfonamide derivative used for itsantibacterial effects in typhoid patients producedhypoglycaemia. This observation led to thedevelopment of sulfonylureas.Mechanism of action Sulfonylureas reduce theblood glucose level by:1. stimulating the release of insulin from the
pancreatic β cells.2. increasing the sensitivity of peripheral
tissues to insulin.3. increasing the number of insulin receptors.4. suppressing hepatic gluconeogenesis.
Sulfonylureas bind to receptors onpancreatic β cells, and block the ATP -sensitive K+ channels. This reduced K+
conductance causes depolarization and Ca++
influx leading to increased insulin secretion.Thus some functional β cells are essential forthe action of sulfonyl ureas.
First Generation Agents
Tolbutamide is short acting and is thereforeassociated with lesser risk of hypoglycaemia- hence it is safer in the elderly diabetics.
Chlorpropamide is long acting (t½ 32 hrs) andcan cause prolonged hypoglycaemiaparticularly in the elderly. Tolazamide has aslow onset of action. Use of first generationagents can result in several drug interactions.
Second Generation AgentsSecond generation agents are more potent,have fewer side effects and drug interactions.But they can cause hypoglycaemia becauseof which they should be used cautiouslyparticularly in the elderly. They are allcontraindicated in renal and hepaticimpairment.Glibenclamide (Gliburide) is a commonly usedsulfonylurea. It is longer acting – can be givenonce a day. It can cause hypoglycaemia andrarely flushing after alcohol consumption.Glipizide has a short t½; food delays itsabsorption, it is less likely to causehypoglycaemia.Glimepiride is longer acting and can be givenas a single morning dose.
Pharmacokinetics Sulfonylureas are well-absorbed orally, extensively bound to plasmaproteins, metabolised in the liver and someare excreted in the urine. Hence they shouldbe avoided in patients with renal or liverdysfunction. Dose - Table 53.3.Adverse effects Second generation agents havefewer adverse effects. Hypoglycaemia is themost common adverse effect, least withtolbutamide due to its short t½ and lowpotency.
Nausea, vomiting, jaundice, and allergicreactions can occur (Table 53.4). Patients onsulfonylureas may have an increase in therate of cardiovascular death. However thisis still controversial and sulfonylureascontinue to be used.
Drug InteractionsI. Drugs that augment hypoglycaemic effect.
• NSAIDs, warfarin, sulfonamides –displace sulfonylureas from proteinbinding sites.
Insulin and Oral Hypoglycaemics 369
• Alcohol, chloramphenicol, cimetidine–inhibit metabolism
II. Drugs that decrease the action of sulfonylureas• Diuretics and corticosteroids – ↑blood
glucose levels.
BiguanidesBiguanides lower blood glucose level byinsulin-like effects on the tissues. Mechanismof action is not clear. They• Suppress hepatic gluconeogenesis.• Inhibit glucose absorption from the
intestines.• Stimulate peripheral uptake of glucose in
tissues in the presence of insulin.Phenformin is not used therapeutically as
it causes lactic acidosis. Metformin is saferwith lower incidence of lactic acidosis. It doesnot cause hypoglycaemia since it is aneuglycaemic agent.Adverse effects Nausea, diarrhoea, and metallictaste are self-limiting. Rarely lactic acidosiscan occur. Anorexia is advantageous as ithelps in reducing body weight. Long-termuse may interfere with vitamin B12
absorption.
Meglitinides
Repaglinide and nateglinide are insulinsecretogogues. Like sulphonylureas, megli-tinides enhance the release of insulin byblocking the ATP dependent K+ channels inthe pancreatic β cells.Both repaglinide and nateglinide are rapidlyabsorbed from the gut; repaglinide has a t½of 1 hour. Both drugs can cause hyper-sensitivity reactions and hypoglycaemia – butthe incidence is relatively lower withnateglinide. Gastrointestinal disturbancesare common with repaglinide.
Meglitinides can be used in type 2 diabetesmellitus either alone or with biguanides.
Thiazolidinediones (TZDs)
Thiazolidinediones or glitazones are agonistsat the PPAR γ receptors (gamma subtype ofperoxisome – proliferator activated receptors.)TZDs activate the PPARγ receptors and inducethe synthesis of genes which enhance insulinaction.• TZDs increase insulin–mediated glucose
transport into muscle and adipose tissue.• reduce hepatic gluconeogenesis• once a day administration• low potential for hypoglycaemia• ↑ HDL cholesterol• no clinically significant drug interactions
known so far.
Disadvantages• 6-12 weeks of treatment is required to
establish maximum therapeutic effect.• May cause weight gain and anaemia.• May cause oedema and precipitate or
worsen CCF.• Liver function should be monitored
regularly.• Troglitazone causes severe hepatotoxicity
and therefore is not used now.Uses-TZDs are used as adjuvants tosulfonylureas or biguanides in Type IIdiabetes mellitus. Though they can also beused as monotherapy in mild cases of type IIdiabetes, further studies are needed to provetheir long term benefits.
Biguanides
• Have insulin-like effects• Do not cause hypoglycaemia• Weight reduction—due to anorexia• Nausea, diarrhoea, metallic taste are
transient• Preferred in obese diabetics either
alone or with sulfonylureas• Contraindicated in renal, hepatic and
cardiac diseases
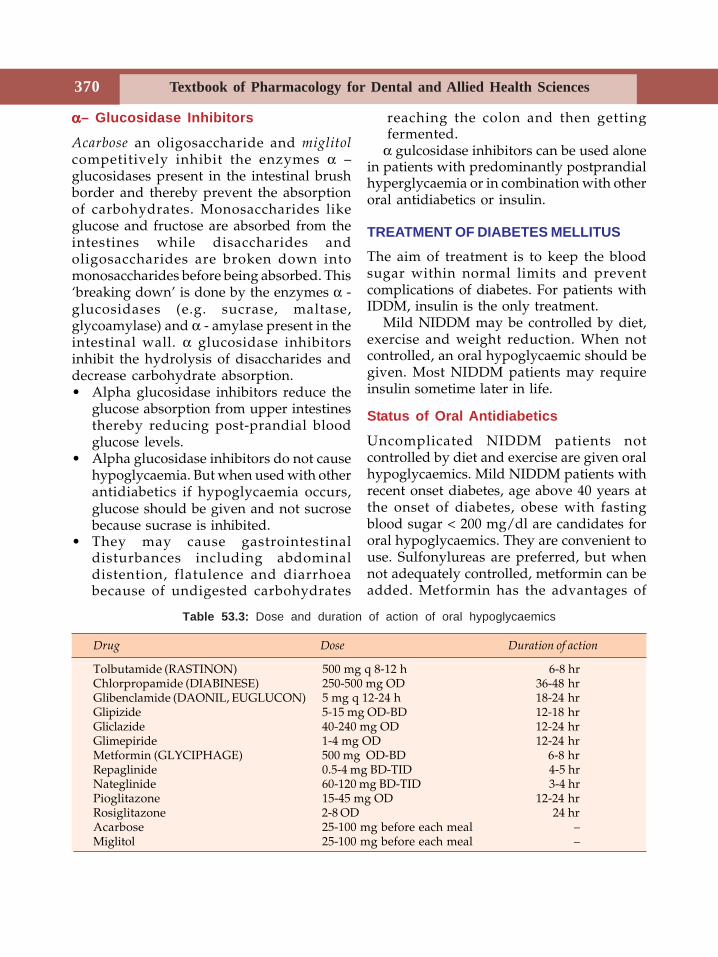
Textbook of Pharmacology for Dental and Allied Health Sciences370
ααααα– Glucosidase Inhibitors
Acarbose an oligosaccharide and miglitolcompetitively inhibit the enzymes α –glucosidases present in the intestinal brushborder and thereby prevent the absorptionof carbohydrates. Monosaccharides likeglucose and fructose are absorbed from theintestines while disaccharides andoligosaccharides are broken down intomonosaccharides before being absorbed. This‘breaking down’ is done by the enzymes α -glucosidases (e.g. sucrase, maltase,glycoamylase) and α - amylase present in theintestinal wall. α glucosidase inhibitorsinhibit the hydrolysis of disaccharides anddecrease carbohydrate absorption.• Alpha glucosidase inhibitors reduce the
glucose absorption from upper intestinesthereby reducing post-prandial bloodglucose levels.
• Alpha glucosidase inhibitors do not causehypoglycaemia. But when used with otherantidiabetics if hypoglycaemia occurs,glucose should be given and not sucrosebecause sucrase is inhibited.
• They may cause gastrointestinaldisturbances including abdominaldistention, flatulence and diarrhoeabecause of undigested carbohydrates
reaching the colon and then gettingfermented.
α gulcosidase inhibitors can be used alonein patients with predominantly postprandialhyperglycaemia or in combination with otheroral antidiabetics or insulin.
TREATMENT OF DIABETES MELLITUS
The aim of treatment is to keep the bloodsugar within normal limits and preventcomplications of diabetes. For patients withIDDM, insulin is the only treatment.
Mild NIDDM may be controlled by diet,exercise and weight reduction. When notcontrolled, an oral hypoglycaemic should begiven. Most NIDDM patients may requireinsulin sometime later in life.
Status of Oral Antidiabetics
Uncomplicated NIDDM patients notcontrolled by diet and exercise are given oralhypoglycaemics. Mild NIDDM patients withrecent onset diabetes, age above 40 years atthe onset of diabetes, obese with fastingblood sugar < 200 mg/dl are candidates fororal hypoglycaemics. They are convenient touse. Sulfonylureas are preferred, but whennot adequately controlled, metformin can beadded. Metformin has the advantages of
Table 53.3: Dose and duration of action of oral hypoglycaemics
Drug Dose Duration of action
Tolbutamide (RASTINON) 500 mg q 8-12 h 6-8 hrChlorpropamide (DIABINESE) 250-500 mg OD 36-48 hrGlibenclamide (DAONIL, EUGLUCON) 5 mg q 12-24 h 18-24 hrGlipizide 5-15 mg OD-BD 12-18 hrGliclazide 40-240 mg OD 12-24 hrGlimepiride 1-4 mg OD 12-24 hrMetformin (GLYCIPHAGE) 500 mg OD-BD 6-8 hrRepaglinide 0.5-4 mg BD-TID 4-5 hrNateglinide 60-120 mg BD-TID 3-4 hrPioglitazone 15-45 mg OD 12-24 hrRosiglitazone 2-8 OD 24 hrAcarbose 25-100 mg before each meal –Miglitol 25-100 mg before each meal –
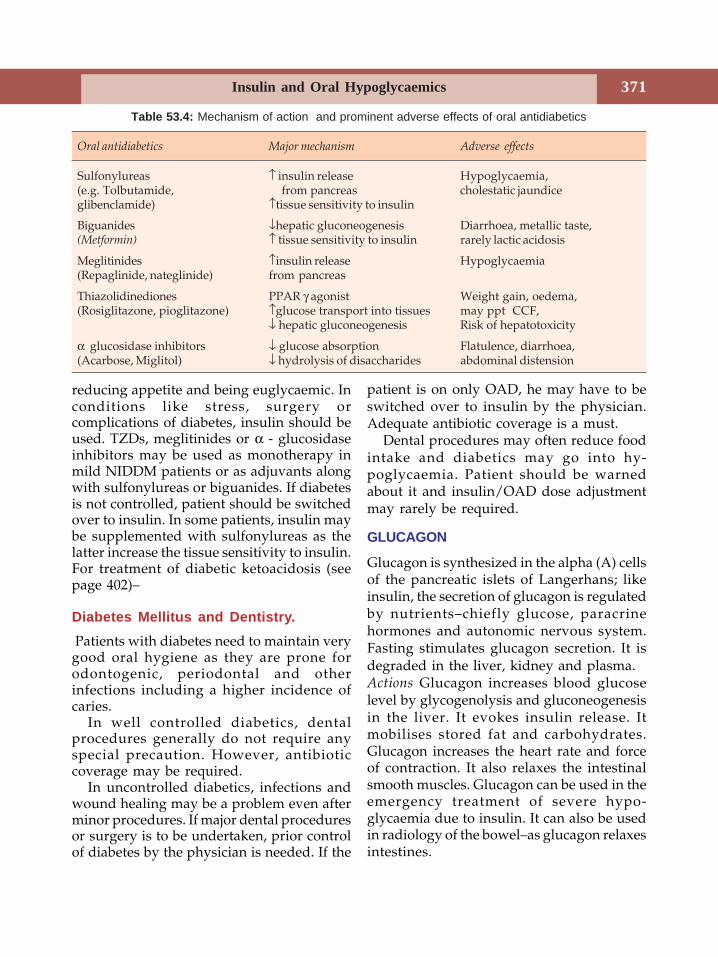
Insulin and Oral Hypoglycaemics 371
reducing appetite and being euglycaemic. Inconditions like stress, surgery orcomplications of diabetes, insulin should beused. TZDs, meglitinides or α - glucosidaseinhibitors may be used as monotherapy inmild NIDDM patients or as adjuvants alongwith sulfonylureas or biguanides. If diabetesis not controlled, patient should be switchedover to insulin. In some patients, insulin maybe supplemented with sulfonylureas as thelatter increase the tissue sensitivity to insulin.For treatment of diabetic ketoacidosis (seepage 402)–
Diabetes Mellitus and Dentistry. Patients with diabetes need to maintain verygood oral hygiene as they are prone forodontogenic, periodontal and otherinfections including a higher incidence ofcaries.
In well controlled diabetics, dentalprocedures generally do not require anyspecial precaution. However, antibioticcoverage may be required.
In uncontrolled diabetics, infections andwound healing may be a problem even afterminor procedures. If major dental proceduresor surgery is to be undertaken, prior controlof diabetes by the physician is needed. If the
patient is on only OAD, he may have to beswitched over to insulin by the physician.Adequate antibiotic coverage is a must.
Dental procedures may often reduce foodintake and diabetics may go into hy-poglycaemia. Patient should be warnedabout it and insulin/OAD dose adjustmentmay rarely be required.
GLUCAGON
Glucagon is synthesized in the alpha (A) cellsof the pancreatic islets of Langerhans; likeinsulin, the secretion of glucagon is regulatedby nutrients–chiefly glucose, paracrinehormones and autonomic nervous system.Fasting stimulates glucagon secretion. It isdegraded in the liver, kidney and plasma.Actions Glucagon increases blood glucoselevel by glycogenolysis and gluconeogenesisin the liver. It evokes insulin release. Itmobilises stored fat and carbohydrates.Glucagon increases the heart rate and forceof contraction. It also relaxes the intestinalsmooth muscles. Glucagon can be used in theemergency treatment of severe hypo-glycaemia due to insulin. It can also be usedin radiology of the bowel–as glucagon relaxesintestines.
Table 53.4: Mechanism of action and prominent adverse effects of oral antidiabetics
Oral antidiabetics Major mechanism Adverse effects
Sulfonylureas ↑ insulin release Hypoglycaemia,(e.g. Tolbutamide, from pancreas cholestatic jaundiceglibenclamide) ↑tissue sensitivity to insulin
Biguanides ↓hepatic gluconeogenesis Diarrhoea, metallic taste,(Metformin) ↑ tissue sensitivity to insulin rarely lactic acidosis
Meglitinides ↑insulin release Hypoglycaemia(Repaglinide, nateglinide) from pancreas
Thiazolidinediones PPAR γ agonist Weight gain, oedema,(Rosiglitazone, pioglitazone) ↑glucose transport into tissues may ppt CCF,
↓ hepatic gluconeogenesis Risk of hepatotoxicity
α glucosidase inhibitors ↓ glucose absorption Flatulence, diarrhoea,(Acarbose, Miglitol) ↓ hydrolysis of disaccharides abdominal distension
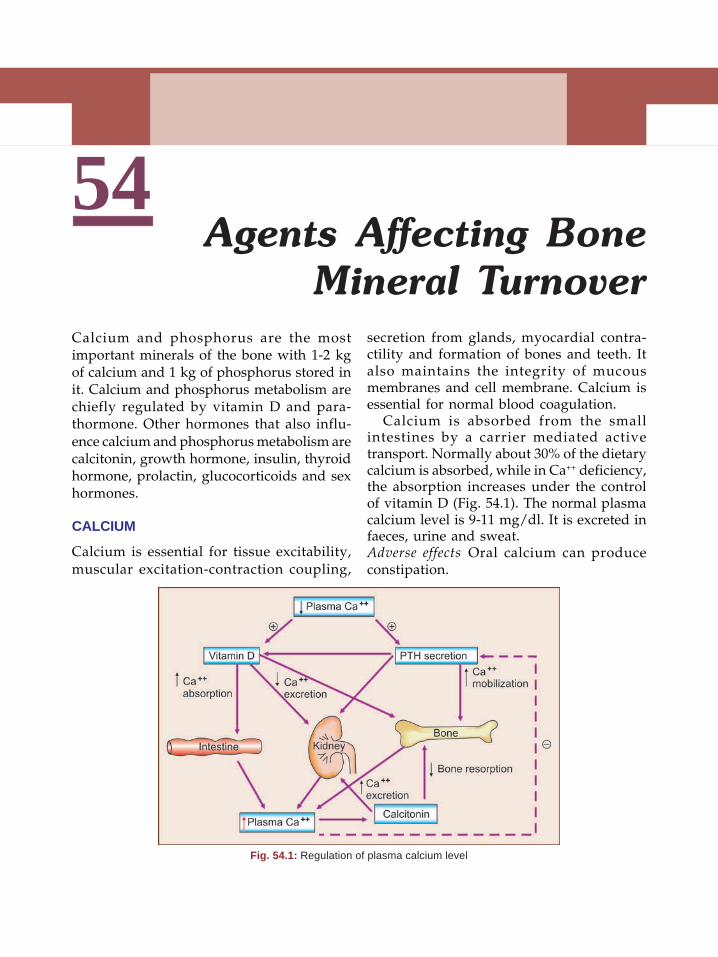
Textbook of Pharmacology for Dental and Allied Health Sciences372
54
Calcium and phosphorus are the mostimportant minerals of the bone with 1-2 kgof calcium and 1 kg of phosphorus stored init. Calcium and phosphorus metabolism arechiefly regulated by vitamin D and para-thormone. Other hormones that also influ-ence calcium and phosphorus metabolism arecalcitonin, growth hormone, insulin, thyroidhormone, prolactin, glucocorticoids and sexhormones.
CALCIUM
Calcium is essential for tissue excitability,muscular excitation-contraction coupling,
Agents Affecting BoneMineral Turnover
secretion from glands, myocardial contra-ctility and formation of bones and teeth. Italso maintains the integrity of mucousmembranes and cell membrane. Calcium isessential for normal blood coagulation.
Calcium is absorbed from the smallintestines by a carrier mediated activetransport. Normally about 30% of the dietarycalcium is absorbed, while in Ca++ deficiency,the absorption increases under the controlof vitamin D (Fig. 54.1). The normal plasmacalcium level is 9-11 mg/dl. It is excreted infaeces, urine and sweat.Adverse effects Oral calcium can produceconstipation.
Fig. 54.1: Regulation of plasma calcium level
373Agents Affecting Bone Mineral Turnover
Uses
1. To prevent and treat calcium deficiency.Calcium supplements are given orally inchildren, pregnant and lactating womenand in postmenopausal osteoporosis toprevent calcium deficiency.Tetany: 5-10 ml IV calcium gluconatefollowed by 50-100 ml slow IV infusionpromptly reverses the muscular spasm.The injection produces a sense of warmth.This is followed by oral calcium 1.5 gdaily for several weeks.
2. Vitamin D deficiency rickets—calcium isgiven along with vitamin D.
3. As an antacid—calcium carbonate is usedorally.
4. For placebo effect—IV calcium is used inweakness, pruritus and some dermatoses.The feeling of warmth produced by theinjection could afford psychologicalbenefit.
PHOSPHATE
Phosphates play a vital role in variousenzymatic reactions, are important for thestructure and function of the cells and areimportant constituents of teeth and bones.Phosphorus is absorbed by the small intestineand excreted through kidneys under theinfluence of parathormone.
Hypophosphataemia results in muscleweakness and abnormal bone mineralization.
PARATHYROID HORMONE(Parathormone, PTH)
Parathormone is a peptide secreted by theparathyroid gland. Secretion of PTH isregulated by plasma Ca++ concentration—lowplasma Ca++ stimulates PTH release, whilehigh levels inhibit secretion. Parathormonemaintains plasma calcium concentration bymobilising calcium from the bone, promotingreabsorption of Ca++ from the kidneys andby stimulating the synthesis of calcitriol
which in turn enhances calcium absorptionfrom the intestines. PTH also promotesphosphate excretion.
Hypoparathyroidism is characterised bylow plasma calcium levels with its associatedmanifestations. Hyperparathyroidism whichis most commonly due to parathyroid tumourproduces hypercalcaemia and deformities ofthe bone.
PTH is not therapeutically used. It is usedfor the diagnosis of pseudohypoparathy-roidism.
VITAMIN D
Vitamin D a fat-soluble vitamin, is aprehormone produced in the skin from 7-dehydrocholesterol under the influence ofultraviolet rays. It is converted to activemetabolites in the body which regulate plasmacalcium levels and various functions of thecells.
Hormones that influence bone metabolism• Vitamin D• Oestrogens• Parathormone• Glucocorticoids
Source
• Diet - as ergocalciferol (vitamin D2) fromplants.• Fish, liver, fish liver oils - (cod, shark liveroil); milk.• Cholecalciferol (vitamin D3) is synthesizedin the skin from 7-dehydrocholesterol.
Cholecalciferol (vitamin D3) is convertedto 25-OHD3 (calcifediol) in the liver(Fig. 54.2) which is in turn converted to1,25-dihydroxy-cholecalciferol (calcitriol) inthe kidneys. Calcitriol is the active form ofvitamin D while calcifediol is the mainmetabolite in circulation. Convertion ofcalcifediol to calcitriol is influenced by PTHand plasma phosphate concentration.
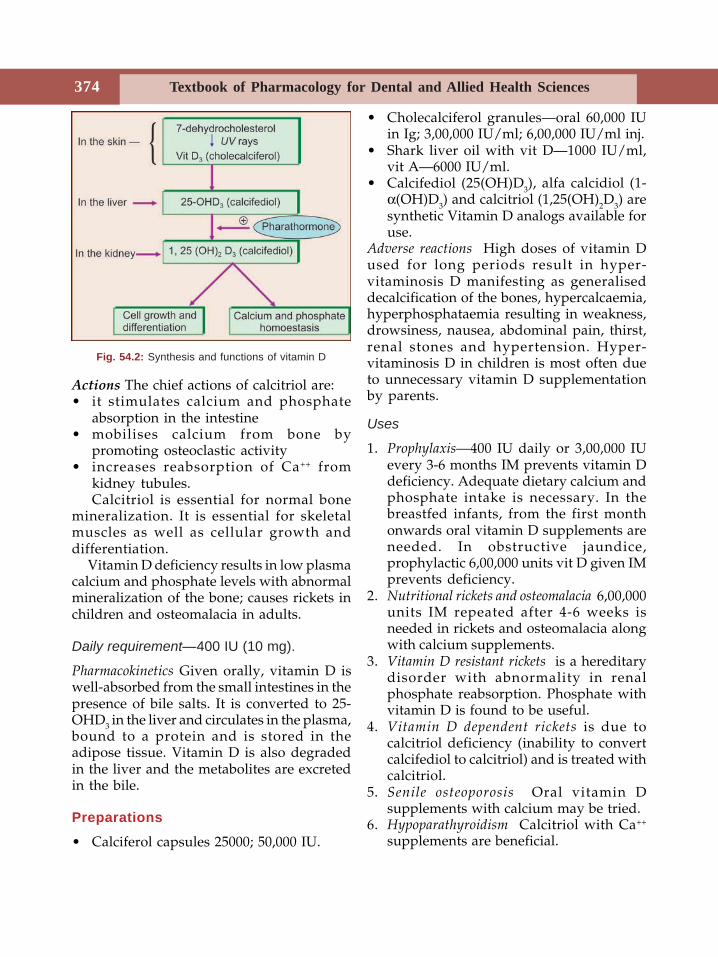
Textbook of Pharmacology for Dental and Allied Health Sciences374
Actions The chief actions of calcitriol are:• it stimulates calcium and phosphate
absorption in the intestine• mobilises calcium from bone by
promoting osteoclastic activity• increases reabsorption of Ca++ from
kidney tubules.Calcitriol is essential for normal bone
mineralization. It is essential for skeletalmuscles as well as cellular growth anddifferentiation.
Vitamin D deficiency results in low plasmacalcium and phosphate levels with abnormalmineralization of the bone; causes rickets inchildren and osteomalacia in adults.
Daily requirement—400 IU (10 mg).
Pharmacokinetics Given orally, vitamin D iswell-absorbed from the small intestines in thepresence of bile salts. It is converted to 25-OHD3 in the liver and circulates in the plasma,bound to a protein and is stored in theadipose tissue. Vitamin D is also degradedin the liver and the metabolites are excretedin the bile.
Preparations
• Calciferol capsules 25000; 50,000 IU.
• Cholecalciferol granules—oral 60,000 IUin Ig; 3,00,000 IU/ml; 6,00,000 IU/ml inj.
• Shark liver oil with vit D—1000 IU/ml,vit A—6000 IU/ml.
• Calcifediol (25(OH)D3), alfa calcidiol (1-α(OH)D3) and calcitriol (1,25(OH)2D3) aresynthetic Vitamin D analogs available foruse.
Adverse reactions High doses of vitamin Dused for long periods result in hyper-vitaminosis D manifesting as generaliseddecalcification of the bones, hypercalcaemia,hyperphosphataemia resulting in weakness,drowsiness, nausea, abdominal pain, thirst,renal stones and hypertension. Hyper-vitaminosis D in children is most often dueto unnecessary vitamin D supplementationby parents.
Uses
1. Prophylaxis—400 IU daily or 3,00,000 IUevery 3-6 months IM prevents vitamin Ddeficiency. Adequate dietary calcium andphosphate intake is necessary. In thebreastfed infants, from the first monthonwards oral vitamin D supplements areneeded. In obstructive jaundice,prophylactic 6,00,000 units vit D given IMprevents deficiency.
2. Nutritional rickets and osteomalacia 6,00,000units IM repeated after 4-6 weeks isneeded in rickets and osteomalacia alongwith calcium supplements.
3. Vitamin D resistant rickets is a hereditarydisorder with abnormality in renalphosphate reabsorption. Phosphate withvitamin D is found to be useful.
4. Vitamin D dependent rickets is due tocalcitriol deficiency (inability to convertcalcifediol to calcitriol) and is treated withcalcitriol.
5. Senile osteoporosis Oral vitamin Dsupplements with calcium may be tried.
6. Hypoparathyroidism Calcitriol with Ca++
supplements are beneficial.
Fig. 54.2: Synthesis and functions of vitamin D
375Agents Affecting Bone Mineral Turnover
CALCITONIN
Calcitonin is a peptide hormone secreted bythe parafollicular ‘C’ cells of the thyroidgland. Secretion is regulated by plasma Ca++
concentration—high plasma Ca++ stimulatescalcitonin release.Actions The chief effects of calcitonin are tolower serum calcium and phosphate by itsactions on the bone and kidney. It inhibitsosteoclastic bone resorption and in thekidney, it reduces both calcium andphosphate reabsorption.
In general the effects are opposite to thatof PTH. Calcitonin is used to controlhypercalcaemia, Paget’s disease, metastaticbone cancer and osteoporosis and to increasebone mineral density.Other hormones that regulate bone turnover areglucocorticoids and oestrogens. Gluco-corticoids antagonise vitamin D stimulatedintestinal calcium absorption and enhancerenal Ca++ excretion. Oestrogens reduce boneresorption by PTH and also enhance calcitriollevels. Oestrogen receptors are found inbone which suggests that they may also havea direct effect on bone remodeling.
DRUGS USED IN THE DISORDERS OFBONEDrugs used in disorders of bone are:• Bisphosphonates -
Alendronate etidronatePamidronate residronate
• Raloxifene (selective oestrogen receptormodulator)
• Vitamin DBisphosphonates-are analogs of pyrophosphate;they inhibit bone resorption. Bisphos-phonates get incorporated into bone matrix,are imbibed by osteoclasts and thenincapicitate the osteoclasts resulting inreduced bone resorption. They also slow theformation and dissolution of hydroxyapatitecrystals.
Fever, oesophagitis, gastritis and hypo-calcaemia can occur. Long-term use can lead
to osteomalacia due to inhibition of bonemineralisation.Uses Bisphosphonates are used in Paget’sdisease of the bone, hypercalcaemia and istried in postmenopausal osteoporosis.1. Paget's disease - Bisphosphonates relieve
pain and induce remission.2. Hypercalcaemia - Some malignancies are
associated with hypercalcaemia. Intra-venous pamidronate is useful in reducingplasma Ca++ levels.
3. Osteoporosis - Alendronate and residro-nate are tried with calcium and vitamin Dfor the prevention of postmenopausalosteoporosis.
Raloxifene is a SERM useful in women for theprevention of postmenopausal osteoporosis.Agents used in the prevention and treatmentof osteoporosisDrugs may be used either to prevent boneresorption or promote bone formation or acombination of both in the prevention andtreatment of osteoporosis. These agentsreduce the risk of fractures in patients withosteoporosis.
I. Drugs that Prevent Bone Resorption
• Calcium (↑ BMD*)• Vitamin D ( ↑ absorption of calcium)• Oestrogen (prevents osteoporosis)• Raloxifene – a SERM (↑ BMD)• Calcitonin (prevents bone resorption,
↑ BMD)• Bisphosphonates - ↓bone resorption,
(↑ BMD)BMD – Bone mineral density.
II. Drugs that Promote Bone Formation
• Fluoride (in small doses ↑ osteoblasticactivity - ↑ bone mass - but generally notpreferred).
• Testosterone (in hypogonadal men)• Anabolic steroids (in postmenopausal
women).• PTH analogs (are being tried).
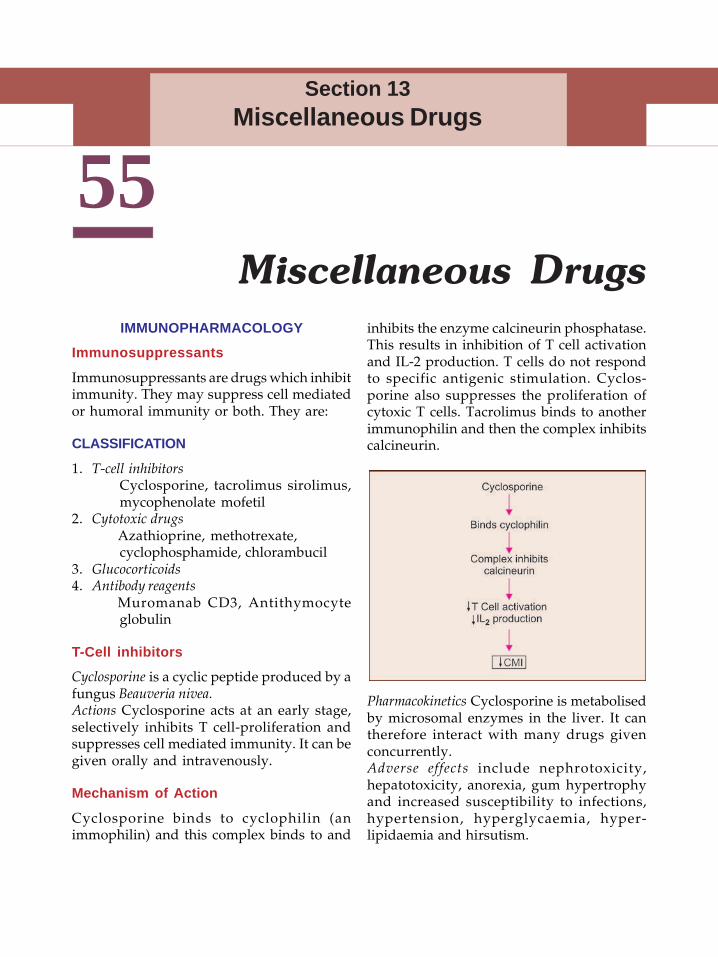
Textbook of Pharmacology for Dental and Allied Health Sciences376
55IMMUNOPHARMACOLOGY
Immunosuppressants
Immunosuppressants are drugs which inhibitimmunity. They may suppress cell mediatedor humoral immunity or both. They are:
CLASSIFICATION
1. T-cell inhibitorsCyclosporine, tacrolimus sirolimus,mycophenolate mofetil
2. Cytotoxic drugsAzathioprine, methotrexate,cyclophosphamide, chlorambucil
3. Glucocorticoids4. Antibody reagents
Muromanab CD3, Antithymocyteglobulin
T-Cell inhibitors
Cyclosporine is a cyclic peptide produced by afungus Beauveria nivea.Actions Cyclosporine acts at an early stage,selectively inhibits T cell-proliferation andsuppresses cell mediated immunity. It can begiven orally and intravenously.
Mechanism of Action
Cyclosporine binds to cyclophilin (animmophilin) and this complex binds to and
Miscellaneous Drugsinhibits the enzyme calcineurin phosphatase.This results in inhibition of T cell activationand IL-2 production. T cells do not respondto specific antigenic stimulation. Cyclos-porine also suppresses the proliferation ofcytoxic T cells. Tacrolimus binds to anotherimmunophilin and then the complex inhibitscalcineurin.
Section 13Miscellaneous Drugs
Pharmacokinetics Cyclosporine is metabolisedby microsomal enzymes in the liver. It cantherefore interact with many drugs givenconcurrently.Adverse effects include nephrotoxicity,hepatotoxicity, anorexia, gum hypertrophyand increased susceptibility to infections,hypertension, hyperglycaemia, hyper-lipidaemia and hirsutism.
377
Uses
• In organ transplantation Cyclosporine isvery effective for the prophylaxis andtreatment of graft rejection in organtransplantation surgeries–like kidney,liver, bone marrow and other transplants.
• Autoimmune disorders Cyclosporine is alsouseful in some autoimmune disorders likerheumatoid arthritis as an alternative inpatients who do not respond tomethotrexate. Cyclosporin is also tried insevere psoriasis, atopic dermatitis,inflammatory bowel disease andnephrotic syndrome.
Tacrolimus is a macrolide antibiotic obtainedfrom Streptomyces tsukubaensis. Its mechanismof action is similar to cyclosporine.Tacrolimus can be given both orally andparenterally but absorption from the gut isincomplete. It is extensively bound to plasmaproteins.
Adverse effects include nephrotoxicity,gastrointestinal disturbances, hypertension,hyperglycaemia, tremors and seizures.
Sirolimus obtained from Streptomyceshygroscopicus acts by inhibiting calcineurin likecyclosporine. Sirolimus may be used incombination with other drugs for theprophylaxis of organ transplant rejection andin psoriasis and uveoretinitis.
Toxicity includes hyperlipidaemia,gastrointestinal disturbances and anincreased risk of infections and lymphomas.
Mycophenolate mofetil a prodrug, isconverted to mycophenolic acid, whichinhibits guanine nucleotide synthesis andinhibits the proliferation and functions oflymphocytes.Mycophenolate mofetil is indicated as anadjunct to other immunosuppressive drugsin the prophylaxis of transplant rejection.
CYTOTOXIC DRUGS
Cytotoxic drugs like azathioprine, cyclo-phosphamide and methotrexate inhibit cellmediated immunity (while cyclophosphamidepredominantly suppresses humoral immunity).They are used in the prevention of graftrejection and in autoimmune disorders.
GlucocorticoidsGlucocorticoids have potent immuno-suppressant activity and are used in theprevention of organ transplant rejection andin autoimmune disorders.
Antibody ReagentsMuromonab CD3 is a monoclonal antibodyto CD3 antigens on T lymphocytes. Onintravenous administration, T cells disappearfrom the circulation within minutes. It is usedwith other immunosuppressants in organtransplantation. Fever, chills and pulmonaryoedema may occur.Antithymocyte globulin (ATG) binds to Tlymphocytes and depletes them therebysuppressing immune response. It is used inthe management of organ transplantation.Infliximab is a monoclonal antibody andetanercept is a protein that blocks TNFα. Theyare useful in rheumatoid arthritis and Crohn’sdisease.
IMMUNOSTIMULANTSImmunostimulating and immunomodulatingagents are drugs that modulate the immuneresponse and can be used to increase theimmune responsiveness of patients withimmunodeficiency as in AIDS, chronic illnessand cancers. This is yet a developing field ofpharmacology. The drugs currently used forthis purpose are BCG and levamisole. BCGhas been tried in cancers. Levamisole usedin helminthiasis is also found to enhance cell-mediated immunity in humans. It has beentried in some cancers.
Miscellaneous Drugs

Textbook of Pharmacology for Dental and Allied Health Sciences378
Interferons are cytokines with antiviral andimmunomodulatory properties. Recombinantinterferons α, β and γ are available for clinicaluse. They bind to specific receptors and bringabout immune activation and increase hostdefences. There is an increase in the numberand activity of cytotoxic and helper T cellsand killer cells (See Page 308)
Interferons α, and β are mainly used forantiviral effects while interferon γ for itsimmunomodulating actions.
Interferons are indicated in severaltumours including malignant melanoma,hairy cell leukaemia lymphomas, kasposi’ssarcoma, condylomata acuminata and in viralinfections.
ANTISEPTICS AND DISINFECTANTS
Disinfection is destruction of all pathogenicorganisms but not spores. If spores are alsokilled, it is called sterilization. A disinfectant isused on inanimate objects.Antiseptic is an agent that destroys micro-organisms and can be used on living tissues.The term germicide can be used for either drugs.Germicides are widely used in domesticproducts like soaps, tooth pastes and after-shave lotions.Mechanism of actionGermicides may act by the following mecha-nisms–1. Oxidation of bacterial protoplasm2. Denaturation of bacterial proteins3. Detergent like action4. Competition with essential substrates for
the important enzymes in the bacterial cell.An ideal germicide should have a wide
antibacterial spectrum, should be chemicallystable, should have rapid action, non-irritating to the tissues, not interfere withwound healing activity even in presence ofpus, exudates and tissue degradationproducts; it should not be absorbed intosystemic circulation.
CLASSIFICATION
1. Acids Boric acid, Benzoic acid.2. Alcohols Ethanol, Isopropyl alcohol3. Aldehydes Formaldehyde,
Glutaraldehyde.4. Surfactants Soaps, Benzalkonium,
Cetrimide,Cetylpyridinium chloride,Dequalinium chloride.
5. Phenol Phenol, Cresol, Resorcinal,derivatives Chlorhexidine,
Chloroxylenol,Hexachlorophene.
6. Halogens Iodine, Iodophores,Chlorine, Chloramines.
7. Oxidizing Hydrogen peroxide,agents Potassium permanganate,
Benzoyl peroxide.8. Dyes Gentian violet, Methylene
blue, Brilliant green,Acriflavin, Proflavine.
9. Metallic salts Mercurial compounds,Silver nitrate, Zinc comp-ounds.
Factors that influence the activity of germicidalagents
1. Concentration of the drug and duration ofcontact In general, higher the concen-tration of the antiseptic, greater is itseffect. But alcohol is an exception to thisand at 70% concentration maximumantiseptic effect is seen.
2. Susceptibility of the organism Spores andviruses are resistant to many antiseptics.
3. Temperature A rise in temperature willincrease antiseptic activity.
Acids
Boric acid and sodium borate (borax) have weakbacteriostatic and fungistatic activity.Aqueous solutions of boric acid are used forirrigating eyes, bladder, vagina and largewounds.
379
Benzoic acid is an antibacterial (below pH 5)and antifungal agent used as a preservativein laboratory.Salicylic acid has bacteriostatic, fungicidal andkeratolytic properties. It is used as a dustingpowder or 2% ointment for seborrhoeicdermatitis, warts and corns.
AlcoholsEthyl alcohol is employed as an antiseptic at60-90% concentration. The antiseptic activitydecreases above 90%. It rapidly denaturesthe bacterial proteins (page 143).
Disadvantages1. It has poor activity against spores, some
viruses and fungi2. Irritant—causes burning when applied on
open wounds3. Alcohols are flammable—should be
allowed to evaporate before using cauteryor laser surgery.
Uses Ethyl alcohol is used to clean the skinbefore injections and surgeries.Isopropyl alcohol is more potent and more toxicthan ethanol. It is used in 68-72%concentration as skin antiseptic.
AldehydesFormaldehyde is a gas at room temperatureused for fumigation; the 40% aqueous solutionis noncorrosive and has a broad antimicrobialspectrum. It has a pungent odour and is anirritant—highly irritating to respiratorymucous membranes and eyes. Formaldehydeis also a carcinogen and OSHA has setstandards to limit exposure of health careworkers to formaldehyde.Mechanism of action Aldehydes act byalkylation of chemical groups in proteins andnucleic acids.Uses Formaldehyde gas is used for fumigationand for sterilizing instruments which cannotbe moistened with solution. Formaldehyde40% solution (100% formalin) in water is used
for disinfection of surgical instruments andgloves; embalming and preservation oftissues. Fibre optic endoscopies, respiratorytherapy equipment, haemodialysers anddental hand pieces which cannot withstandhigh temperatures of stearn sterilisation aredisinfected with formaldehyde.Automatic circulating baths are used whichincrease penetration of aldehyde solution intothe instruments and decrease operatorexposure to the chemical. It’s rapidity ofaction increases by making a solution in 70%propanol.Glutaraldehyde is a dialdehyde used as a 2%solution. It is bactericidal, sporicidal,fungicidal and viricidal. pH should bebetween 7.4 and 8.5. It is less irritant thanformaldehyde; has greater sporicidal activity;does not damage lenses and cementingmaterial in endoscopes. Glutaraldehyde issuperior to formaldehyde for sterilisingrubber, plastic and metal appliances. Two percent solution is used for local application inidiopathic hyperhidrosis of palms and soles.
SurfactantsSurfactants are chemicals that lower thesurface tension of solutions and are termeddetergents. They may be anionic, cationic,ampholytic surfactants or polysorbates.Anionic surfactants e.g. soaps.• They dissociate in aqueous solutions to
form a large and complex anion whichlowers the surface tension.
• Effective for gram-positive and acid fastorganisms.
• Microorganisms are enmeshed in thelather and washed away on rinsing.
• Anionic surfactants have a narrowspectrum; precipitate in hard water; causedrying of the skin.
Preparations1. Potassium hydroxide or sodium
hydroxide + vegetable oil.2. Sodium lauryl sulphate-is effective in hard
water.
Miscellaneous Drugs
Textbook of Pharmacology for Dental and Allied Health Sciences380
Cationic surfactants-e.g. Benzalkonium chloride,Cetrimide, Cetylpyridinium chloride, Dequa-linium chloride. Cationic surfactants dissociateinto large cations.They are:• active against gram-positive and gram-
negative organisms (less active againstspores, viruses and fungi)
• most effective in neutral solution• non-irritating and safe• incompatible with anionic surfactants• absorbed by cotton and rubber• one of the most commonly used
germicidal agents.Benzalkonium chloride (ZEPHlRAN) has anaromatic odour and is soluble in water.• 1: 1000 solution for cleansing skin• 1:2000 for mucous membranes and
denuded skin• 1:20,000 for irrigation of the bladder and
urethra• It is also used for (1: 1000-4000) storing
sterilised surgical instruments. But instru-ments should be thoroughly washedbefore use.
Cetrimide (CETAVLON) 1% solution is usedlike above. It is also used as a cream. It isvery effective for cleaning wounds. Incombination with chlorhexidine it is the mostpopular antiseptic. SAVLON is cetrimide 3%+chlorhexidine.Dequalinium chloride is used in gum paints andlozenges.Cetylpyridinium chloride is used inmouthwashes and lozenges.
Phenol Derivatives
Phenol is one of the oldest antisepticsintroduced by Lord Lister in 1867. It isbactericidal and fungicidal but has pooraction against spores and viruses. It acts bydenaturing the bacterial proteins. It also hasa mild local anaesthetic action. Phenol rapidlypenetrates even intact skin and mucousmembrane. It is a protoplasmic poison.
Phenol is extremely irritant to exposedtissues (corrosive)-when swallowed, it burnsbuccal, oesophageal and gastric mucousmembrane.Uses Phenol is used to disinfect urine, faeces,sputum of patients and is sometimes used asantipruritic because of its local anaestheticaction.Cresol is methylphenol, which is as toxic asphenol but is more active. It is used as adisinfectant for utensils and excreta.Lysol is cresol with soap solution. It has higherantiseptic activity and is an useful disinfectantfor hospital and domestic use.Chloroxylenol (DETTOL) is a less toxicchlorinated phenol, effective against gram-positive and gram-negative organisms.Surgical dettol contains 1.4% of chloroxylenolfor skin; 6.25% for instruments and 1 to 3%in antiseptic cream.Hexachlorophene This chlorinated phenol actsby inhibiting bacterial enzymes and causinglysis. It is effective mainly against gram-positive organisms and has weak actionagainst gram-negative organisms. It isodourless and non-irritating to use on skin.It is used in soaps for surgical scrubbing, forcleaning the skin in obstetrics, carbuncles andseborrhoeic dermatitis. It may cause allergicreactions. It also reduces body odour bypreventing bacterial decomposition oforganic material and therefore is used as adeodorant. In USA, hexachlorophene wasused to wash newborn babies which resultedin brain damage in such babies and thereforeuse of > 3% hexachlorophene is banned.Chlorhexidine (HIBITANE) is effective againstgram-positive, gram-negative organisms andfungi. It is rapid acting and non-irritating.SAVLON is chlorhexidine + cetrimide.
Halogens
Iodine is one of the oldest antiseptics. It has abroad spectrum of activity, is a powerfulbactericidal, sporicidal, fungicidal and
381
viricidal agent. The activity is inhibited byorganic material but enhanced by alcohol.Disadvantages It is irritating, painful, stainsthe area, and may delay wound healing.Rashes, fever and generalised skin eruptionsmay develop in some patients who aresensitive to iodine. Prolonged systemic usecauses iodism.
Uses of iodine
1. Tincture iodine (I2 in KI + alcohol)-used toclean skin before surgery. Iodine crystalsare used to sterilize water for soakingvegetables and cleaning before use.
2. Mandl’s paint (Compound Iodide paint)is,used in the treatment of tonsillitis andpharyngitis. ‘
3. Iodine ointment-as fungicide in ringworm.Iodides have no antibacterial action.
lodophors Iodophors are soluble complexes ofiodine with surfactants like detergents. Thedetergents serve as carriers and slowlyrelease iodine, e.g. Povidone iodine (BETADINE)-5% solution; Piodine-10% solution.Advantages Iodophors are non-irritating, non-staining, water-soluble, less toxic and non-sensitizing to the skin.Uses Used for preoperative scrubbing, skinpreparation, disinfection of instruments, aslocal antiseptic in boils, furunculosis, burns,ulcers, ringworm and in oral/vaginalmoniliasis.Chlorine is a potent germicide and isbactericidal against several gram-positive and gram-negative organisms in avery low concentration (0.1 PPM in 30seconds). It also destroys protozoa andviruses. The’antibacterial activity of chlorineis reduced in presence of organic matter sincethey bind chlorine and therefore need higherconcentration of free chlorine. Chloraminesare compounds that release chlorine slowly.1. Chlorinated lime (bleaching powder) is
obtained by the action of chlorine on lime.It is used for disinfection of water inswimming pools and water for drinking.
2. Chloramine is an organic chloride. Thefreshly prepared solution is used formouthwash, for irrigating the bladderand urethra.
3. Eusol is a solution of chlorinated lime withboric acid.
Oxidizing AgentsHydrogen peroxide is a colourless and odourlessliquid. It liberates nascent oxygen whenapplied to tissues and then oxidizes bacteriaand necrotic tissue. On application, there iseffervescence and this helps in removingtissue debris, ear wax, etc. Hydrogenperoxide has poor penetrability and theaction is of short duration. On keeping, itloses its potency. It is also a deodorant.Uses Hydrogen peroxide is used for cleansingwounds, abscesses and for irrigation. Indentistry, it is used to clean septic socketsand root canals and also as a mouthwash anddeodorant gargle. It is used as ear dropswhile removing ear wax.Potassium permanganate is an oxidizing agentand an astringent. The purple crystals arewater-soluble. It acts by liberating oxygenwhich oxidizes bacterial protoplasm. Organicmatter reduces its activity and the solutiongets decolourised. It promotes rusting;concentrated solution is caustic and causesburns and blistering.
Uses
• 1:4000-1: 10000 solution of potassiumpermanganate is used for gargling,irrigating cavities, urethra and wounds.
• For stomach wash in alkaloidal poisoning(except atropine and cocaine because theseare not efficiently oxidized).
• 1% solution in mycotic infections likeathletes foot.
• 5% solution as a styptic.• Topically to oxidise venom in case of
snake and scorpion bite.• To purify well water.• To disinfect vegetables and fruits.
Miscellaneous Drugs

Textbook of Pharmacology for Dental and Allied Health Sciences382
Dyes
Gentian violet (aniline dye, crystal violet or
medicinal gentian violet) is effective againstgram-positive organisms and fungi. Stainingis the only disadvantage. It is a non-irritantand potent antiseptic. 0.5-1% solution is usedtopically on furunculosis, burns, boils, chroniculcers, infected eczema, thrush, ringwormand mycotic infections of the skin and mucousmembranes.Brilliant green Actions are similar to gentianviolet. Used as a 0.5-1% solution in thetreatment of burns, impetigo and infectedwounds like gentian violet.Methylene blue is used systemically in cyanidepoisoning as it converts methaemoglobin tohaemoglobin.Acriflavine and proflavine are acridine dyesactive against gram-positive bacteria andgonococci (proflavine is better). They arenon-irritant; efficacy is unaffected by organicmatter but is increased in alkaline medium;1: 1000 solution is used in infected woundsand burns, 2% pessary in vaginitis andcervicitis.Triple dye lotion contains gentian violet 0.25%+ brilliant green 0.25% + acriflavine orproflavine 0.1 %-it is used in burns dressing.
Metals
Silver compounds have antiseptic, astringentand caustic properties. Silver nitrate killsmicrobes rapidly and the action is prolongeddue to slow release of silver ions from silverproteinate that is formed by an interactionwith tissue proteins. The reduced silver getsdeposited and stains the tissues black.Silver nitrate is used for the prophylaxis ofophthalmia neonatorum.Silver sulfadiazine is active against Pseudomonas
and is used in burn wounds.
Colloidal silver compounds slowly release silver.They are non-corrosive, non-irritant, non-astringent and have better penetrability usedas nasal and eyedrops.Zinc salts like zinc oxide has astringent andmild antiseptic properties. It is used as anointment or lotion in eczema, impetigo andpsoriasis.Mercury compounds act by inhibitingsulphydryl enzymes of bacteria. They arebacteriostatic and are poor antiseptics-notcommonly used.
CHELATING AGENTS
Heavy metals bind to and inactivate thefunctional groups (ligands) of essential tissueenzymes. By this they interfere with normalcell functions which require these ligands.Heavy metals cannot be metabolised in thebody.
Chelating agents or heavy metal anta-gonists bind the heavy metal ions and makethem non-toxic. The chemical complex formedis called chelate (Chele = claw; in Greek). Theprocess of complex formation is chelation.The complex so formed is water-soluble andis eliminated by the kidneys.
The clinically useful chelating agents areCaNa2 EDTA, dimercaprol, d-penicillamineand desferrioxamine. Chelating agents aremore effective in preventing the utilizationof ligands than in reactivating them—hence,the earlier they are given, the better.Calcium disodium edetate (CaNa
2 EDTA)
chelates several divalent and trivalent metalslike zinc, manganese, iron and lead. It is usedin the treatment of lead poisoning. Givenparenterally, lead deposits in the bone aremobilised, chelated and excreted throughkidneys.Adverse effects include nephrotoxicity, fatigue,fever, myalgia and dermatitis.
CaNa2EDTA is mainly used in leadpoisoning. It can also be used in zinc,

383
manganese and iron poisoning. Sodiumedetate is used in severe hypercalcaemia.Dimercaprol is a colourless, oily liquiddeveloped by the British during World warII as an antidote to lewisite—an arsenical wargas. Hence it is also known as British Anti-lewisite or BAL. Dimercaprol chelatesarsenic, mercury, lead and other heavymetals. It is given IM; appropriate plasmaconcentrations should be maintained.Adverse effects are dose related and includehypertension, tachycardia, vomiting, swe-ating, burning sensation in the lips and mouthand headache.
Dimercaprol is used in arsenic andmercury poisoning; also used in leadpoisoning with CaNa2 EDTA.
Unithiol
Unithiol is a water soluble analog ofdimercaprol that can be given both orally andparenterally. It enhances the excretion ofmercury, arsenic and lead. Adverse effectsare mild and include allergic reactions.Unithiol may be used in mercury, lead andarsenic poisoning.
Succimer
Succimer is another water soluble analog ofdimercaprol. It protects against acute arsenicpoisoning and it is also effective in lead andmercury poisoning. It can be given both orallyand intravenously. Succimer is used in thetreatment of chronic lead poisoning and inmercury and arsenic poising. Anorexia,nausea, vomiting, diarrhoea and skin rashescan occur.d-Penicillamine is prepared by degradationof penicillin but has no antibacterial activity.It chelates copper, mercury, zinc and lead. Itis orally effective.Toxicity Patients allergic to penicillin maydevelop anaphylaxis; dermatitis may occur
in some. On long-term use renal, haemato-logical, dermatological and other toxicitiescan occur.
Uses
1. Treatment of copper, mercury and leadpoisoning.2. Wilson’s disease (hepatolenticulardegeneration)—copper is deposited in theliver and brain causing degeneration.3. Rheumatoid arthritis (Page 186).4. Cystinuria—promotes excretion ofcysteine by forming soluble complexesand prevents formation of cysteine stones.Desferrioxamine isolated from Streptomycespilosus, chelates iron. It has a high affinity foriron, forms stable complexes and removesiron from haemosiderin and ferritin. It doesnot chelate the iron in haemoglobin andcytochromes. It is given parenterally(Page 223).Toxicity Allergic reactions range from rashesto anaphylaxis (rare), diarrhoea, musclecramps and blurred vision.
Uses
1. Acute iron poisoning—desferrioxamine isthe drug of choice.
2. Chronic iron poisoning—as in thalas-saemia patients who receive repeatedblood transfusion.
Deferiprone chelates iron and is orally effective.It is used in thalassemia major to chelate ironas an alternative to desferrioxamine.
VITAMINS
Vitamins are organic compounds essential fornormal metabolism in the body. They aresupplied by the diet. A balanced diet suppliesadequate amounts of vitamins to fulfill thedaily requirement. The requirement isincreased during periods of rapid growth,
Miscellaneous Drugs

Textbook of Pharmacology for Dental and Allied Health Sciences384
pregnancy and lactation. Vitamin deficienciesresult in characteristic signs and symptoms.
Vitamins are grouped into fat-soluble andwater-soluble vitamins (Table 55.1).
FAT-SOLUBLE VITAMINS
Vitamin A
Vitamin A is present in the diet as retinol,dehydroretinol or as carotenoids. Caro-tenoids are pigments present in green yellowvegetables and fruits and is converted in thebody to retinol.Source Green leafy vegetables, carrots,mango, papaya, eggs, milk, butter, cheese,liver and fish liver oils. Maximum content isin Halibut liver oil - 9,00,000 mg/100 gm.Physiological functions Vitamin A has animportant role in dark adaptation. It isessential for the synthesis of rhodopsin, thephotosensitive pigment of rods. Vitamin Ais also essential for maintenance of theintegrity of epithelial cells, for growth andcell-mediated immunity.Signs and symptoms of deficiency Xerophthalmia(dryness of eyes), Bitot’s spots in theconjunctiva, night blindness, diarrhoea, dryand rough skin are seen in early stages. Inthe later stages, keratomalacia, perforationof the cornea, necrosis and blindness canoccur.Daily requirement–3000-5000 IU/day.
Uses
In the prophylaxis and treatment of vitaminA deficiency.1. Prophylaxis–3000-5000 IU/day in presence
of increased requirement.2. Treatment–50,000-1,00,000 IU intramus-
cularly or orally for 1-3 days followed byoral supplementation.
3. Acne–Retinoic acid or synthetic analogsof vitamin A like tretinoin or isotretinoinare used.
Hypervitaminosis A Since vitamin A is a fat-soluble vitamin, it accumulates in the bodyon prolonged administration. The symptomsare dry skin (hyperkeratosis), anorexia,fever, alopecia, anaemia, oedema, headache,skin ulcers and tenderness over the bones.Vitamin D See Page 373 Vitamin K See Page 234Vitamin EVitamin E or Alpha tocopherol is present inwheat germ oil, rice germ oil and soya beanoil.Physiological role Vitamin E acts as anantioxidant. It prevents the damage due tofree radicals in normal metabolic reactions.Vitamin E is essential for normal structureand function of the nervous system. It is alsorequired to maintain the integrity of thebiological membranes. Vitamin E deficiencyin animals results in reproductive andhaemopoietic system abnormalities, dege-nerative changes in the spinal cord and heart.Daily requirement is 10-15 mg.Uses Clinically vitamin E deficiency in humanbeings is not known. It has been tried in G-6-PD deficiency, sterility, menopausalsyndrome and other conditions with nodefinite evidence of obvious benefit.
WATER-SOLUBLE VITAMINS
Vitamin B-complex
B-complex group of vitamins includesthiamine, riboflavin, nicotinic acid, pyrido-xine, pantothenic acid, biotin and cyano-cobalamin.
Thiamine (Vitamin B1, Aneurine)
Sources Pulses, outer layers of cereals, ricepolishings, peas, nuts, green vegetables, eggand meat.Physiological role Thiamine is converted tothiamine pyrophosphate which acts as acoenzyme in carbohydrate metabolism.
385
Daily requirement 1-2 mg.
Symptoms of deficiency Thiamine deficiencyproduces Beriberi.Dry beriberi is characterised by peripheralneuritis and muscular atrophy.Wet beriberi The characteristic features aredependent oedema and high output cardiacfailure. Wernicke’s encephalopathy andKorsakoff’s psychosis are also thought to bedue to thiamine deficiency.
Uses
1. Prophylactically in presence of increaseddemand as in pregnancy, lactation andinfants.
2. Beriberi–50 mg daily parenterally. Oncethe patient recovers, maintenance dose of10 mg/day is given orally.
3. Chronic alcoholics–50 mg daily.4. Empirical use–thiamine is tried in several
neurological and cardiovascular disordersand morning sickness.
Riboflavin (Vitamin B2)
Sources Milk, egg, liver, meat, grains andgreen leafy vegetables.Physiological function Flavin mononucleotide(FMN) and flavin adenine dinucleotide(FAD) containing the active form ofriboflavin are coenzymes in variousoxidation-reduction reactions.Symptoms of deficiency Angular stomatitis,glossitis, seborrhoeic keratosis of the nose,ulcers in the mouth, dry skin, burningsensation in the plantar surface of the feet,vascularization of the cornea and alopecia.Uses Riboflavin is used for the prevention andtreatment (2-10 mg) of riboflavin deficiency.
Nicotinic Acid and Nicotinamide(Vitamin B3)
Nicotinic acid and nicotinamide are togetherknown as niacin.Sources Rice polishings, liver, fish, milk, eggs,nuts and pulses.
Physiological functions Nicotinic acid isconverted to nicotinamide. Nicotinamideadenine dinucleotide (NAD) and it’sphosphate (NADP) are coenzymes involvedin several oxidation-reduction reactions.
Nicotinic acid is also a lipid-loweringagent.Symptoms of deficiency Niacin deficiencyresults in Pellagra characterised bydermatitis, diarrhoea and dementia. Othersymptoms include: pigmentation of the skin,stomatitis, glossitis, headache, insomnia,hallucinations, confusion and megaloblasticanaemia. Chronic alcoholics, people living onmaize as the staple diet, patients withmalabsorption and cirrhosis developpellagra.
Uses
1. Prophylaxis and treatment of pellagra (50-500 mg).
2. Nicotinic acid is used in hyperlipo-proteinaemia (see Page 236).
Pyridoxine (Vitamin B6)
Sources Cereals, legumes, liver, milk, meatand eggs.Physiological functions Pyridoxal phosphate isa coenzyme involved in the synthesis ofseveral amino acids, biogenic amines andother compounds like GABA.Symptoms of deficiency Glossitis, peripheralneuritis, anaemia, dermatitis and low seizurethreshold due to decreased GABA levels inthe brain.
Uses
1. Prophylaxis and treatment of pyridoxinedeficiency.
2. INH induced peripheral neuritis–pyridoxine is used both for prophylaxisand treatment.
3. Convulsions in infants due to pyridoxinedeficiency.
Miscellaneous Drugs
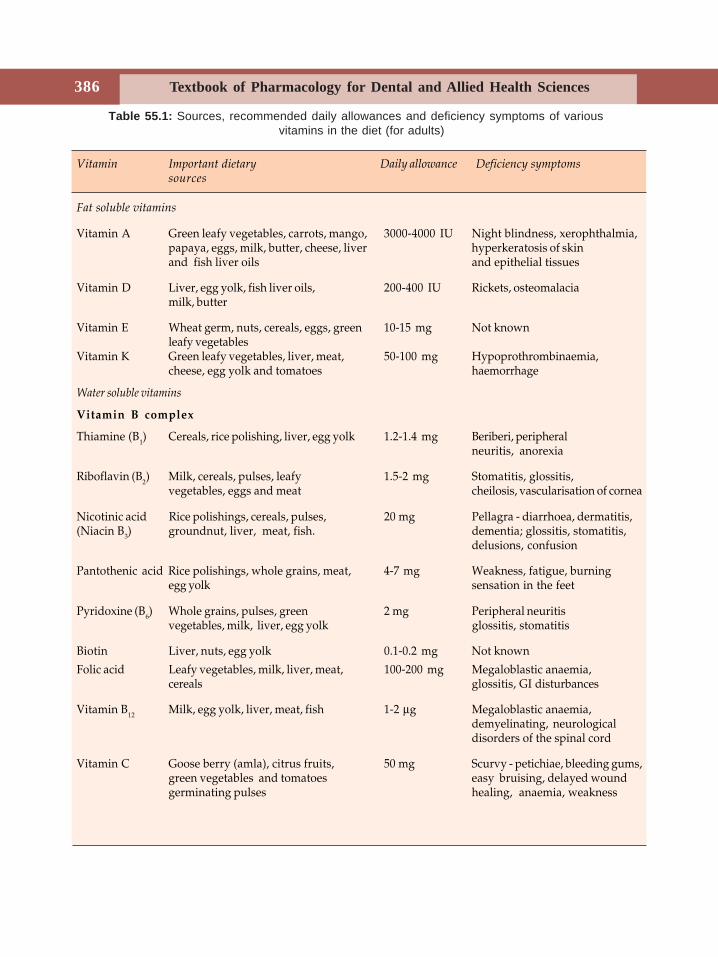
Textbook of Pharmacology for Dental and Allied Health Sciences386
Table 55.1: Sources, recommended daily allowances and deficiency symptoms of various vitamins in the diet (for adults)
Vitamin Important dietary Daily allowance Deficiency symptomssources
Fat soluble vitamins
Vitamin A Green leafy vegetables, carrots, mango, 3000-4000 IU Night blindness, xerophthalmia,papaya, eggs, milk, butter, cheese, liver hyperkeratosis of skinand fish liver oils and epithelial tissues
Vitamin D Liver, egg yolk, fish liver oils, 200-400 IU Rickets, osteomalaciamilk, butter
Vitamin E Wheat germ, nuts, cereals, eggs, green 10-15 mg Not knownleafy vegetables
Vitamin K Green leafy vegetables, liver, meat, 50-100 mg Hypoprothrombinaemia,cheese, egg yolk and tomatoes haemorrhage
Water soluble vitamins
Vitamin B complex
Thiamine (B1) Cereals, rice polishing, liver, egg yolk 1.2-1.4 mg Beriberi, peripheralneuritis, anorexia
Riboflavin (B2) Milk, cereals, pulses, leafy 1.5-2 mg Stomatitis, glossitis,vegetables, eggs and meat cheilosis, vascularisation of cornea
Nicotinic acid Rice polishings, cereals, pulses, 20 mg Pellagra - diarrhoea, dermatitis,(Niacin B3) groundnut, liver, meat, fish. dementia; glossitis, stomatitis,
delusions, confusion
Pantothenic acid Rice polishings, whole grains, meat, 4-7 mg Weakness, fatigue, burningegg yolk sensation in the feet
Pyridoxine (B6) Whole grains, pulses, green 2 mg Peripheral neuritisvegetables, milk, liver, egg yolk glossitis, stomatitis
Biotin Liver, nuts, egg yolk 0.1-0.2 mg Not known
Folic acid Leafy vegetables, milk, liver, meat, 100-200 mg Megaloblastic anaemia,cereals glossitis, GI disturbances
Vitamin B12 Milk, egg yolk, liver, meat, fish 1-2 μg Megaloblastic anaemia,demyelinating, neurologicaldisorders of the spinal cord
Vitamin C Goose berry (amla), citrus fruits, 50 mg Scurvy - petichiae, bleeding gums,green vegetables and tomatoes easy bruising, delayed woundgerminating pulses healing, anaemia, weakness

387
4. ‘Morning sickness’ in pregnancy–pyridoxine may reduce vomiting by anunknown mechanism.
Pantothenic Acid
Sources Wheat, cereals, milk, peanuts, liver,egg yolk and vegetables.Physiological role Pantothenic acid is convertedto coenzyme A which is involved in severalmetabolic reactions. Pantothenic aciddeficiency in human beings is not known.Experimentally induced deficiency results infatigue and paraesthesia. Calcium panto-thenate is a component of multivitaminpreparations.
Biotin
Biotin is an organic acid found in liver, nuts,egg yolk and other foods. Biotin deficiencyin humans is not known. Experimentallyinduced deficiency results in dermatitis,anorexia, alopecia and glossitis. Biotin is acoenzyme in several metabolic reactions. Itis present in many multi-vitaminpreparations. Avidin, a protein present in eggwhite prevents the absorption of biotin.
VITAMIN B12, FOLIC ACID (see Page 225)
VITAMIN C (ASCORBIC ACID)
Sources Citrous fruits, tomatoes, goose berry,green vegetables and potatoes are rich invitamin C.Physiological role Ascorbic acid is involved inseveral metabolic reactions includingoxidation reduction reactions and in cellularrespiration. It is essential for the integrity ofconnective tissue, for the development ofcartilage, bone and teeth and for woundhealing.Symptoms of deficiency Vitamin C deficiencyresults in scurvy characterised by connectivetissue defects resulting in haemorrhages in
subcutaneous tissues, petechiae, ecchymoses,impaired wound healing, tender bleedinggums, deformed teeth, brittle bones, anaemiaand growth retardation.
Uses1. Prevention of vitamin C deficiency–50-100
mg daily.2. Scurvy–500-1000 mg daily.3. Common cold–large doses (0.5-1.5 gm) of
vitamin C has been tried as prophylacticagainst common cold with controversialbenefits.
4. To acidify urine.
GENE THERAPY
Gene therapy is the replacement of defectivegene by the insertion of a normal, functionalgene. It is the genetic modification of cellsfor the prevention or treatment of a disease.Gene transfer may be done to replace amissing or defective gene or provide extra-copies of a normally expressed gene. Genetherapy is aimed at genetically correcting thedefect in the affected part of the body. Unlikeall other drugs which only alter the rate ofnormal cell functions, gene therapy canconfer new functions to the cell.
Vectors
Gene transfer requires the use of vectors todeliver the DNA material. An ideal vectorshould be safe and effective in inserting thetherapeutic gene into the target cells.Physical, chemical and biological vectors havebeen tried. • Physical vectors - DNA is complexed with
substances like lipids and administered. • Chemical vectors - Liposomes are used to
carry genes into the cells. • Biological vectors - The most important
biological vectors are viral vectors.Viruses invade cells and use the metabolic
Miscellaneous Drugs

Textbook of Pharmacology for Dental and Allied Health Sciences388
processes of these host cell for replication.This property of viruses helps to deliverthe gene — adenoviruses and retrovirusesare used for this purpose.
Therapeutic Applications ofGene Therapy
Gene therapy is at present a developingarea. Though originally it was seen as aremedy for inherited single gene defects,gene therapy has now been found to beuseful in several acquired disorders. Theprincipal applications are in single genedefects like thalassaemia, cystic fibrosis andhaemoglobinopathies and in the treatment ofcancer, cardiovascular diseases, atheros-clerosis, immunodeficiency disorders–particularly AIDS; anaemia, Alzheimer’sdisease and many infectious diseases.Some examples are-1. Growth hormone deficiency - Growth
hormone gene is transferred to myoblastsand these are implanted in patients.
2. Familial hypercholesterolaemia - LDL receptorgene is introduced into liver cells.
3. Cancer-a. introducing the gene which makes the
malignant cells sensitive to drugs.b. inactivating the expression of oncogenes.c. introducing genes that attaches to
cancer cells and make them susceptibleto host defense cells.
d. introducing genes to healthy cells toprotect them from cytotoxic drugs.
4. HIV infectionsa. Introducing genes coding for CD4 cells
that could inactivate HIV beforeentering the cell itself.
b. Introducing genes that enhanceimmunity against HIV.
5. Diabetes mellitus - Introducing insulingene into the liver which can produce insulin.
6. Coronary atherosclerosis - Prevention ofrestenosis and ischaemia in coronaryvessels by genes which inhibits thegrowth of vascular endothelial cells.
Dental Pharmacology 389
56DENTIFRICES
Dentifrices are therapeutic aids meant forcleaning the teeth with the help of atoothbrush. They are available in the formof powders, liquids and paste, e.g.toothpastes and tooth powders. Though theprime purpose of a dentifrice is to assist thebrush in cleaning the teeth, addition of certainsubstances like fluoride and antiseptics canafford additional benefits. The ingredientsare:
1. Abrasive Agents
Dental abrasives are fine powderedsubstances which assist the scouring actionof the toothbrush. They are inorganic saltsof low solubility, e.g. prepared chalk, calciumphosphate, calcium and magnesiumcarbonates; magnesium oxide, ferric oxide,charcoal, silicates, powder pumice, kaolinand stannic oxide. The abrasive powdershould be fine to avoid scratching of the teethsurfaces. Abrasives are also available aspastes. Generally powders are morepowerful abrasives than pastes.
Uses
1. Polishing the teeth and fillings.2. Cleaning the teeth.3. In toothpastes and tooth powders.
Dental Pharmacology
2. Detergents
Detergents are cleansing agents which act by:(i) lowering surface tension, i.e. they
possess emulsifying properties.(ii) dissolving fatty substances and mucus
plaques.(iii) foaming—on scrubbing the teeth,
detergents foam and act as lubricants.(iv) loosening the debris adhering to the
teeth.(v) some of them also liberate oxygen and
have antiseptic properties.Thus detergents act as deodorants, e.g.
sodium lauryl sulphate and soaps. Sodiumlauryl sulphate–a pale yellow powder iseffective in both acid and alkaline mediumand in hard water. It is also used as a skincleanser and in medicated shampoo.
3. Antiseptics
The small amount of antiseptics used indentifrices may not be sufficient to affordadequate antiseptic action. Antiseptics usedin dentistry are thymol, menthol, eugenol,benzoic acid, boric acid, myrrh, calcium andmagnesium peroxide. Thymol is a powerfulantiseptic and a deodorant used inmouthwashes and gargles. Eugenol has theodour of clove and is also a local anaestheticcommonly used for dental filling.
Section 14Dental Pharmacology
Textbook of Pharmacology for Dental and Allied Health Sciences390
4. Sweetening Agents
Sweetening agents are substances used toimpart a sweet taste to a pharmaceuticalpreparation. They are used to make the useof dentifrice more pleasant and acceptable.Saccharine sodium is commonly used in toothpowders and is intensely sweet. It is anartificial sugar 500 times sweeter than sugarand can be used as a dilute(1%) solution.Saccharine has no caloric value and isexcreted unchanged with in 24 hours. It isstable and nontoxic. Saccharine is less likelyto encourage the development of caries whencompared to other carbohydrates. Itenhances the palatability. Though sucrose canalso be used, it causes fermentation and istherefore not preferred.
5. Colouring Agents
Colouring agents are used to make thepreparation more attractive for commercialpurpose. Bright colours like cherry red, blueand green are used. Liquor rubri imparts redcolour while methylene blue gives bluecolour and chlorophyll is employed for greencolour. Most colours used commercially aresynthetically produced, though some of themmay also be obtained from natural sourceslike plants, animals or minerals. Onlypremitted colour can be used in dentifrices.
6. Flavouring Agents
Flavouring agents are substances used toimpart a pleasant smell and taste to thepreparation so that it is more palatable.Though natural flavouring agents areavailable, synthetic flavours are preferredbecause of their easy availablity. Generallyfruity and spicy flavours are preferred.Peppermint, lemon, mint and pineapple aresome natural flavours; synthetic flavoursinclude alcohols, aldehydes, esters and fattyacids.
7. Other Agents
Other agents used in dentifrices include(i) binding agents like mucilage of
tragacanth, gum acacia and bentonite;They help to bind the liquid and solidphases together in a paste.
(ii) humectants like glycerine and sorbitolprevent drying up of the paste.
(iii) Antacids like sodium bicarbonate-neutralize acidity in the oral cavity.
A good dentifrice should be pleasant intaste, odour and consistency; should notdamage the gums or the teeth.
OBTUNDENTSObtundents are agents that diminish dentinesensitivity. They are used to make theexcavation painless. Obtundents act by oneof the following mechanisms.1. Paralysing the sensory nerves, e.g. phenol,
menthol, thymol, clove oil, camphor,benzyl alcohol
2. Precipitating proteins Astringents like silvernitrate, zinc oxide and zinc chloride.
3. Destruction of nervous tissue, e.g. Absolutealcohol (Table 56.1).
But, the disadvantages with the use ofobtundents are: pulp may shrink and irritantsmay stimulate the formation of secondarydentine. After the advent of local anaesthetics,the use of obtundents has declined.
ANTISEPTICS
Antiseptics used in dentistry are phenol,cresol, chloroxylenol, hexachlorophene,chlorhexidine, sodium hypochlorite, iodineand iodophors and oxidising agents likehydrogen peroxide, and sodium perborate;alcohol and benzalkonium chloride. Fordetails see page 378.
MUMMIFYING AGENTS
Agents used to harden and dry the tissuesof the pulp are called mummifying agents.
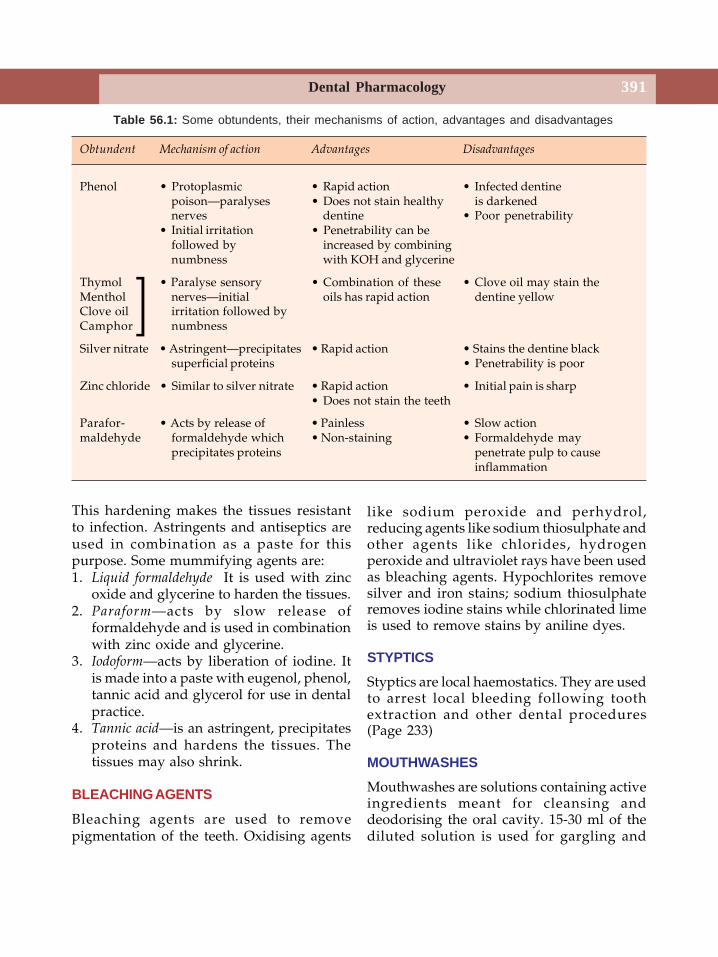
Dental Pharmacology 391
This hardening makes the tissues resistantto infection. Astringents and antiseptics areused in combination as a paste for thispurpose. Some mummifying agents are:1. Liquid formaldehyde It is used with zinc
oxide and glycerine to harden the tissues.2. Paraform—acts by slow release of
formaldehyde and is used in combinationwith zinc oxide and glycerine.
3. Iodoform—acts by liberation of iodine. Itis made into a paste with eugenol, phenol,tannic acid and glycerol for use in dentalpractice.
4. Tannic acid—is an astringent, precipitatesproteins and hardens the tissues. Thetissues may also shrink.
BLEACHING AGENTS
Bleaching agents are used to removepigmentation of the teeth. Oxidising agents
like sodium peroxide and perhydrol,reducing agents like sodium thiosulphate andother agents like chlorides, hydrogenperoxide and ultraviolet rays have been usedas bleaching agents. Hypochlorites removesilver and iron stains; sodium thiosulphateremoves iodine stains while chlorinated limeis used to remove stains by aniline dyes.
STYPTICS
Styptics are local haemostatics. They are usedto arrest local bleeding following toothextraction and other dental procedures(Page 233)
MOUTHWASHES
Mouthwashes are solutions containing activeingredients meant for cleansing anddeodorising the oral cavity. 15-30 ml of thediluted solution is used for gargling and
Table 56.1: Some obtundents, their mechanisms of action, advantages and disadvantages
Obtundent Mechanism of action Advantages Disadvantages
Phenol • Protoplasmic • Rapid action • Infected dentinepoison—paralyses • Does not stain healthy is darkenednerves dentine • Poor penetrability
• Initial irritation • Penetrability can befollowed by increased by combiningnumbness with KOH and glycerine
Thymol • Paralyse sensory • Combination of these • Clove oil may stain theMenthol nerves—initial oils has rapid action dentine yellowClove oil irritation followed byCamphor numbness
Silver nitrate • Astringent—precipitates • Rapid action • Stains the dentine blacksuperficial proteins • Penetrability is poor
Zinc chloride • Similar to silver nitrate • Rapid action • Initial pain is sharp• Does not stain the teeth
Parafor- • Acts by release of • Painless • Slow actionmaldehyde formaldehyde which • Non-staining • Formaldehyde may
precipitates proteins penetrate pulp to causeinflammation
]
Textbook of Pharmacology for Dental and Allied Health Sciences392
rinsing the mouth. Mouthwashes containastringents, antiseptics and/or obtundents,flavouring and sweetening agents. Prolongeduse of concentrated solutions result instaining.
Types of Mouthwashes
1. Antiseptic and astringent mouthwash—for soreness under dentures. They hardenthe mucous membrane.
2. Obtundent mouthwash—for sensitive orallesions.
3. Detergent mouthwash—for cleansing anddeodourising action.
Uses
1. Soreness under dentures.2. Sensitive oral lesions.3. Postoperative and other bedridden
patients for deodourising the oral cavityand to maintain oral hygiene;mouthwashes are refreshing.
4. In halitosis.5. Stomatitis.6. Surgical impaction—after removal of
impacted tooth.Chlorhexidine (CHLORHEX REXIDINE)
and Povidine iodine (BETADINE) are somecommonly used mouthwashes.
ASTRINGENTS
Astringents are agents which precipitatesuperficial proteins when applied to the skinor mucous membrane. They form aprotective coating and harden the surface.Astringents check minor haemorrhages—arrest capillary oozing as they promoteclotting and precipitate proteins on thebleeding surface. Astringents are thereforeused as obtundents, styptics andmummifying agents.
Types of Astringents
1. Vegetable astringents—tannic acid, gall.2. Metallic astringents—salts of zinc, copper,
iron, aluminium and silver; also alum.3. Miscellaneous—alcohol, dilute acids.Uses Astringents are used as mouthwashes,paints, lotions and dentifrices in aphthousulcers, stomatitis, gingivitis and as localhaemostatics.
DISCLOSING AGENTSDental plaques are relatively invisible.Certain agents (dyes) and iodine containingsolutions may be used to make the supra-gingival plaques visible and such agents arecalled disclosing agents.
Dyes used as disclosing agents are asfollows.
1. Erythrosin
Erythrosin tablets are dissolved into asolutions or chewed to dissolve in the mouth.It stains the plaque area red but also maystain soft tissues. It is the most widely useddisclosing agent.
2. Fluorescein Dye
On application, fluorescein dye stains theplaque yellow. It does not stain the softtissues. But special light is required to seethe stained plaque. It is more expensive.
3. Two-tone Dyes
A solution containing a combination of twodyes is used. Mature plaques are stained blue,while new plaques are stained red.
Advantages
• Dyes used as disclosing agents help todifferentiate mature and immatureplaques.
• They do not stain the gingival tissues.
Dental Pharmacology 393
4. Iodine Containing Solutions
Iodine containing solutions have been usedas disclosing agents but have thedisadvantage of causing a high incidence ofallergic reactions. They also have anunacceptable taste. Hence iodine solutionsare not preferred.
Methods of application To stain the plaque,solutions of disclosing agents may be usedas follows:
(i) Painting the teeth with a cotton swab(ii) Rinsing the mouth
(iii) As tablets/wafers to be cheweddissolving it in the saliva. The mouthshould then be rinsed with water.
SIALOGOGUES AND ANTISIALOGOGUESSialogogoues are agents which enhancesalivary secretions. Pilocarpine is generallyused as a sialogogue though other drugs likebethanechol, and anticholinesterases likeneostigmine also reduce salivary secretionsCevimeline a newly introduced drugenhances salivary secretion by directlystimulating the muscarinic receptors. It is usedto treat dry mouth in patients with Sjögren'ssyndrome.
(i) Sialogogues are used to treat acutesymptoms of sialoadenitis that may beseen in sialolithiasis. Surgical excisionis required in most cases.
(ii) Xerostomia-often follows radio-therapyof the head and neck. It may betroublesome because it causes difficultyin speaking and swallowing. It may betreated with pilocarpine.
(iii) Sjögren’s syndrome-cevimeline is used.
AntisialogogueAn antisialogogue is a substance that reducessalivary secretion. Propantheline bromide anatropine substitute is commonly used for thispurpose though atropine and many otheranticholinergic drugs also decrease salivarysecretion.
Uses1. Sialocele–An antisialogogue is used to
suppress glandular function duringhealing or to encourage spontaneousresolution of the sialocele. Propanthelenebromide (Pro-banthine) is given in thedose of 15 mg orally 4 times a day half anhour before food.
2. Post surgical–An antisialogogue is usedfor a short period following surgeries ofthe salivary glands and salivary ducts.Temporary reduction in the flow of salivais thought to be helpful in faster woundhealing.
3. In post-traumatic parotid fistulas andsialoceles.
4. Trauma to the salivary gland and salivaryducts.
ANTICARIES DRUGS
Caries is a degenerative condition charac-terised by decay of hard and soft parts ofthe teeth.
Fermentation of carbohydrates in the oralcavity results in the production of acids likelactic acid. These acids convert the insolublecalcium salts of the teeth into soluble salts(decalcification) which are easily removed.The oral flora produce proteolytic enzymeswhich digest the organic enamel matrix. Thusboth organic and inorganic matter of theteeth are destroyed. As the processcontinues, the pulp is penetrated and theinfection may gain access into the systemiccirculation.Fluorides Fluorine, a halogen, is the mostelectronegative of all elements and istherefore highly reactive. The efficacy offluoride in the prophylaxis of dental carieshas been well-established.Mechanism of action Fluorides alter thephysicochemical properties of the teeth asfollows:1. Fluorides inhibit bacterial enzymes which
produce acids and therefore preventdecalcification of the teeth.

Textbook of Pharmacology for Dental and Allied Health Sciences394
2. Fluorides convert the hydroxyapatite ofenamel and dentine to fluorapatite whichis more resistant to destruction by acids.Thus fluorides make the outer layers ofenamel harder and more resistant todemineralization.
3. Fluorides also stimulate remineralizationof the enamel.
Fluoridation of water supplies Fluoridation ofdrinking water is the most effective measurein preventing dental caries—if consumedprior to eruption of the permanent teeth.Several large-scale studies have establishedthe beneficial effects of optimum fluoridationof communal water supplies in preventingcaries. The optimum level of fluoride is 0.5-1ppm and is found to be safe and effective.More than 1-2 ppm result in toxicity—causedental fluorosis.
When communal water fluoridation isimpracticable, table salt can be fluorinated.Topical fluoride Topical use of high doses offluorides effectively prevents caries, It maybe used as:Fluoride dentifrices Several commercialpreparations containing fluoride salts areavailable. Sodium fluoride, sodiummonofluorophosphate or stannous fluoride arethe salts used in such dentifrices. Mouth shouldbe thoroughly rinsed and dentifrice should notbe swallowed; children should be speciallywarned—to avoid fluorosis. Used twice a dayregularly, they effectively prevent caries.Fluoride mouthrinses 0.2% sodium fluoridesolution containing 900 ppm of fluoride,retained in the mouth for one minute—to beused twice a week is effective in preventingcaries.Topical application by a dentist of 2% sodiumfluoride or 8% stannous fluoride once a weekfor 4 weeks also prevents caries but isexpensive. Special precaution should be takento avoid swallowing. Topical application isthe most effective if done just as the teetherupt.
Fluoride Toxicity
Chronic toxicity results in mottling of theenamel, brownish-black discolouration of theteeth, joints pain and stiffness, osteosclerosisof the spine and pelvis. Crippling fluorosis ischaracterised by thickening of the cortex oflong bones and bony exostoses specially inthe vertebrae.Acute toxicity could result from accidental orsuicidal overdose often due to ingestion offluoride-containing rat poisons. 2.5-5 gm isthe lethal dose in adults. Manifestationsinclude nausea, vomiting, diarrhoea,hypotension, hypocalcaemia, hypoma-gnesaemia, cardiac arrhythmias and acidosis.
Treatment
• Vomiting should be induced and gastriclavage should be given with fluidscontaining calcium.
• Cardiac arrhythmias should be treated.• Correction of acid base imbalance.• Alkaline diuresis to enhance fluoride
excretion.Prevention of caries Caries can be largelyprevented by the following measures:1. Resistance of the host can be increased by
fluoride therapy.2. Oral flora to be controlled by antiplaque
agents.3. Soluble carbohydrates present in ice-
creams, sweets, chocolates, etc.—thesubstrate for bacterial growth—should beavoided.
4. ‘In-between’ eating habits should bereduced.
5. Public should be educated regarding theproper use of toothbrush, dentifrices andprevention of caries.
DRUGS USED IN DENTAL PLAQUE
Plaque is the soft, non-mineralised bacterialdeposit formed on inadequately cleaned

Dental Pharmacology 395
teeth. Proteins in saliva adhere to the surfaceof the enamel. Microorganisms from oralcavity colonise on these to from a plaque. Asin caries, poor oral hygiene and carbohydraterich food encourage plaque formation whena plaque gets mineralised, it is called a dentalcalculus or tartar.Treatment All plaque should be removed asquickly as possible. The virulentmicroorganisms of the plaque flora likeStreptococcus mutans and Streptococcus sobrinusare associated with the pathogenesis of cariesand many periodontal diseases. Theseorganisms should be controlled either by asuitable antibacterial agent or altering toothsurface to prevent the bacterial attachmentto the plaque. Scaling is done to remove theplaque.
Antibacterial Agents
Though penicillins, erythromycin andtetracyclines are effective in controllingplaque, antibiotics which are not absorbedfrom the oral mucosa should be preferred.Vancomycin, kanamycin, bacitracin andpolymyxin-B are used as topical mouthrinsesor gels. Controlled delivery systemscontaining tetracyclines for intra pocketinsertion, effectively suppresses periodontalpathogens. However, long-term use ofantibiotics should be avoided because of therisk of toxicity.
Other agents that can be used in plaquecontrol are:1. Bis-biguanides Chlorhexidine (page 380) isthe most effective anti-plaque andantigingivitis agent. Chlorhexidine gluconate0.12–0.2% solution is used twice daily forrinsing–15 ml solution is retained for 30seconds in the month and then spat out. Forthe next 30 minutes, eating, drinking andrinsing the mouth should be avoided.Chlorhexidine binds to oral tissues and isslowly released for about 12 hours.
Mechanism of action–Chlorhexidine isbacteriastatic in low concentrations butbactericidal at higher concentrations.Chlorhexidine binds to the bacterial cell walland interferes with the uptake of sugars bythe bacteria. Higher doses cause precipitationof intracellular proteins leading to cell death.Long-term use of chlorhexidine can causeyellowish brown staining of the teeth,mucosal soreness, desquamation andoccasionally altered taste sensation. How-ever, systemic side effects are unlikely sincechlorhexidine is used topically. Alexidine canalso be used.
Uses
a. Bisbiguanides are used as mouthrinses,gels and in dentifrices for the control ofplaque and gingivitis.
b. Chlorhexidine mouth wash is also usedto disinfect the oral cavity before dentalprocedures.
c. Ulcerative gingivitis.d. Following oral surgery and denture
insertion.e. Prophylactically in immunocompromised
patients like those with leukaemia, AIDSand agranulocytosis.
2. Fluorides Stannous fluoride mouth rinsesor gels are effective in plaque control andmake the gums healthier. Fluorides inhibitenzymatic reactions involved in glycolysis.3. Oxygenating agents like hydrogen peroxide(page 381) and sodium perborate. Thesecompounds act by liberating nascent oxygen.4. Halogens Halogen releasing compoundslike chlorophors and iodophors are used inmany antiseptic mouthwashes. Chlorinedioxide and povidone iodine have beenwidely used—but these are not popularbecause of their unpleasant taste.
Textbook of Pharmacology for Dental and Allied Health Sciences396
5. Other compounds• Other antiseptics like phenol and its
derivatives hexylresorcinol andthymol are used in many anti-plaquemouthrinses. But their properties likedisagreeable taste, rapid discolourationand poor solubility make them lesspreferred.
• A combination of oils including thymol(0.06%, eucalyptus oil (0.09%),menthol (0.04) and methyl salicyte(0.06%) in an alcohol based vehicle isfound to be useful in inhibiting plaque.These oils act by inhibiting bacterialenzymes and alcohol acts on thebacterial cell wall. The combination isuseful in reducing plaque and gingivitis.
• Detergents like sodium lauryl sulphatehave also been used in severalmouthrinses.
• Nonionic bisphenols–Triclosan is agermicidal used in toothpaste and inother dental preparations. It has a wideantibacterial spectrum including manygram positive and gram negativebacteria. It causes leakage in thebacterial cell membrane leading tobacterial cell lysis. It is retained in thedental plaque for 8 hours. Triclosan alsoinhibits gingivitis. When triclosan isincorporated in a polyvinyl copolymerits antibacterial activity improves.Therefore triclosan is used along withthe copolymer in toothpaste and isfound to be useful in controlling plaqueand calculus formation.
DENTAL DESENSITISING AGENTS
Dentin hypersensitivity is a common problemaffecting millions of people all over the world.Pain could be evoked by mechanical, chemicalor thermal stimuli, i.e. the patient experiencespain while eating hot and cold, sweet or sourfood or even while brushing the teeth. The
hypersensitivity is due either to loss of enamelor exposure of the root surface. Loss ofenamel may follow mechanical wear orchemical erosion due to acidic food. The rootsurface gets exposed due to gingivalrecession as seen in old age, incorrecttoothbrushing habits or chronic periodontaldiseases.
An ideal desensitising agent should be non-irritant, non-toxic, painless, rapid acting, easyto use and have a long-lasting effect. Atpresent no such single agent is available.Hence multi-modal approach could beemployed depending on the severity.
Dental Desensitising Agents are
1. Agents occluding dentinal tubules: Potassiumnitrate, Potassium oxalate, Calciumhydroxide, Fluorides, Sodium citrate,Formaldehyde
2. Agents precipitating proteins:a. Astringents
Silver nitrate, Zinc chlorideb. Precipitating tubule proteins
causing occlusionStrontium chloride, Formaldehyde
3. Tubule sealants: 4-Methacryloxyethyltrimellitate
4. Physical methods: Restorations—Glassionomer cements, composites; Lasersealing of the tubule
1. Agents Occluding Dentinal Tubules
Five per cent potassium nitrate used daily iseffective in 4 weeks as a desensitising agent.It acts by occluding the dentinal tubulesthrough crystallisation. Used as a toothpastetwice a day, potassium nitrate is a populardesensitising agent.
SENQUEL, SENQUEL AD, THERMOSEAL, Potassium nitrate 5%.Calcium hydroxide supplies calcium ions whichhasten remineralisation of the exposed
Dental Pharmacology 397
dentin. But it has to be applied by a dentistand may require repeated application as theeffect is short lived.Fluorides High doses of fluorides used asdentifrices act by hardening the dentinsurface and is claimed to be effective in 3-4weeks. Fluoride iontophoresis (using 2%NaF) may be employed to occlude thedentinal tubule. The procedure is immediatelyeffective but is expensive and may requirerepetition.
2. Agents Precipitating Proteins
Astringents—Silvernitrate and zinc chloride actby precipitating proteins and were usedearlier. But they cause permanent staining ofthe teeth, are toxic to the gingiva and pulpand are therefore not preferred.
Strontium chloride and formaldehyde act byprecipitating proteins within the tubulesoccluding them. They have been used in theform of dentifrices in the past.
3. Tubule Sealants
The newer agents including 4–methacry-loxyethyl trimellitate have been tried asdesensitizers.
4. Physical Methods
Restorations to cover the dentinal tubulesusing glass ionomer and composites are foundto be effective in patients with eroded gingiva.A combination of glass ionomer and compositeresins is more beneficial when compared toeither agents used alone. In patients withgingival loss, soft tissue grafts cover theexposed dentin to relieve the sensitivity.
EMERGENCIES IN DENTAL PRACTICE
A dentist can come across several lifethreatening emergencies in dental practicealthough not frequently. Several factors havecontributed to an increase in the rate of theseemergencies like –
1. A rise in geriatric population and aconsequent increase in the number ofelderly patients seeking dental therapy.
2. the tendency for longer dental appoint-ments.
3. an increase in the use of drugs in denti-stry.
Dentists therefore, must be equipped withadequate knowledge for appropriatemanagement of such situations, because theycan be life threatening. Treatment andprevention of some of the commonemergencies that may be encountered indental practice are discussed below.
1. Anaphylaxis
Anaphylaxis: is an immediate type ofhypersensitivity reaction and can occurfollowing the use of drugs, and allergens.Anaphylaxis is more common followingparenteral administration of drugs. Thoughit can be induced by any or all drugs, somedrugs like lignocaine, penicillins, cepha-losporin and sulfonamides are more likelyto induce anaphylaxis. Antigen – antibodycomplexes bind to the mast cells leading tothe degranulation of these mast cells. Thisresults in the release of massive amounts ofhistamine and other inflammatory mediatorswhich are responsible for the symptoms ofanaphylaxis. Symptoms usually occur withinminutes of exposure to the offending agent.Signs and symptoms include—• Cutaneous – itching at the site of injection
and/or generalized itching, swelling ofsubcutaneous tissues, eyelids, lips andtongue.
• Respiratory–wheezing due to bronchos-pasm, cough and laryngeal oedema.
• Cardiovascular – hypotension resulting indizziness and in more severe cases loss ofconsciousness.

Textbook of Pharmacology for Dental and Allied Health Sciences398
When severe, it can be rapidly fatal. Hence,every medical and dental practitioner mustknow to manage anaphylaxis.Treatment – should be immediate.• Intramuscular injection of adrenaline 0.5ml
of 1:1000 solution is life saving. The dosemay be repeated every 10 minutes ifrequired. If hypotension is not significant,adrenaline may be injected subcutane-ously. If anaphylaxis is very severe, 0.5ml adrenaline may even be givenintravenously slowly. Dose may berepeated if needed after 5 to 10 minutes.
• The patient should be put in recliningposition.
• Arrangement should be made to transferthe patient to the nearest emergency ward.
• High flow oxygen should be given.• Vital signs should be carefully monitored.• Cardiopulmonary resuscitation may be
done if required.• Intravenous hydrocortisone hemisuc-
cinate 100-200 mg will be needed insevere cases particularly in asthmatics.
• An antihistamine like chlorpheniramine 20mg IM or diphenhydramine 50 mg IM maybe given as an adjuvant. Antihistaminesshould be continued orally for 2 to 3 days.
• Intravenous fluids should be started.Vasopressors like dopamine may be givenif needed.
2. Uncontrolled Bleeding
Most dental procedures cause some bleeding.It is mostly minor and local application ofmild pressure for 10-20 seconds wouldgenerally arrest bleeding. If bleedingcontinues, a cotton swab dipped in 1%adrenaline solution may be used as a pack.Ice pack for a few minutes may also be tried.Gel foam may be used in more severebleeding.
Uncontrolled bleeding following dentalprocedures may be seen in one of thefollowing-
1. Patients on antiplatelet drugs or those withthrombocytopenia due to any cause.
2. Patients on anticoagulant therapy3. Haemophiliacs4. Vitamin C deficiency5. Long-term glucocorticoid therapy
They should be controlled as follows:• Reduction in the platelet count or
impaired platelet function due to antiplateletdrugs can result in severe bleeding.Appropriate measures should be taken tocorrect the above before taking the patientfor surgery or other dental proceduresassociated with bleeding. If the patient is ondrugs that inhibit platelet aggregation,consult the physician 1-2 weeks before anelective surgery and under his guidance suchdrugs may be withdrawn temporarily.Duration of antiplatelet effects of clinicallyused drugs like ticlopidine and clopidogrelis around 7 to 10 days. Therefore these drugsshould be withdrawn about 7-8 days beforethe procedure and prothrombin time shouldbe brought down to 1½ to 2 times the controlvalue. The antiplatelet drugs should berestarted after adequate healing hasoccurred. Even minor bleeding includingpetichiae and ecchymoses should be watchedfor.
• If thrombocytopenia is due to anyother cause, platelet transfusion may berequired before any surgical procedure isundertaken in consultation with a physician.
• If the patient is on anticoagulants, theymay be temporarily withdrawn or the dosereduced in consultation with a physician.
• Drugs with antiplatelet effects likeNSAIDs should be used carefully.
• Vitamin C deficiency as such may resultin bleeding from the gums and may enhancebleeding from dental procedures and alsoimpair wound healing. Local application ofadrenaline pack or pressure may be neededfollowing minor dental procedures. Majordental procedures should be done after thecorrection of vitamin C deficiency.
Dental Pharmacology 399
• Glucocorticoid therapy—Patients onlong-term glucocorticoid therapy may bleedmore and wound healing may be impaired.Wounds are also more susceptible toinfections. Adequate local haemostaticmeasures should be taken.
• Haemophiliacs—are deficient incoagulation factor VIII and are thereforelikely to bleed more even from minor dentalprocedures. Factor VIII should besupplemented before the dental procedureand adequate local haemostatic measuresshould be taken.
3. Unconsciousness:
Patients with no response to stimuli needimmediate attention.
Unconsciousness in dental practice may bedue to one of the following causes-a. Vasovagal attack/syncope/faintingVasovagal attack is the transient loss ofconsciousness due to a painful or anemotional stimulus. Pathophysiologyinvolves an autonomic imbalance. In responseto the stimulus, the vagus is stimulated whichin turn results in bradycardia, reducedcardiac output and hypotension accompaniedby peripheral vasodilation. Hypotensionreduces the blood supply to the brain leadingto cerebral hypoxia which in turn results inunconsciousness. However, the patientrecovers in 1-2 minutes because thesympathetic system gets activated andreverses the symptoms.
Treatment:
• Loosen tight clothing to facilitate brea-thing.
• Elevate feet to increase venous return.• Give cold compress to promote peripheral
vasoconstriction and increase venousreturn.
• Oxygen inhalation may be given.
b. Hypoglycaemia – is to be expected inpatients with diabetes mellitus. Signs andsymptoms include sweating, tachycardia,tremors, blurred vision, weakness,hunger, confusion and drowsinessleading on to unconsciousness. In mildhypoglycaemia, oral administration ofsugar or sugar containing fruit juices aresufficient to overcome the symptoms. Inunconscious patients, 50 ml of 50%dextrose is given intravenously – usuallypatient recovers within a few minutes.
c. Seizures – see below.d. Arrhythmias – may be
• Bradyarrhythmias-transient loss ofconsciousness with slow irregular heartrate of <40 beats/minute.
• Tachyarrhythmias-Heart rate >150/minute may be associated with fatigue,breathlessness and syncope
e. Cardiac arrest is stoppage of the heart,also called cardiac standstill. If revivedon time the heart may recover.
Clinical features – Loss of consciousness– Absence of pulses– Gasping or absence of
breathing.Management• Maintain airway – turn the patient’s head
to a side, use mouth gag.• Raise the foot end.• Mouth to mouth respiration to be given-
take 4 quick, deep breaths and then exhaleinto the patient’s mouth. This has to berepeated 12 times per minute.
• As an alternative, bag mask may be usedwith 100% oxygen.
• External cardiac massage to be given at60 chest compressions per minute.
• 0.5ml of 1:1000 solution of adrenalineshould be injected intravenously or inmore severe cases intracardiac adrenalineinjection may be needed.
Textbook of Pharmacology for Dental and Allied Health Sciences400
• Medical assistance should be taken at theearliest possible.
4. Seizures
Patients can develop symptoms ranging frombrief lapses of awareness to generalizedconvulsions usually lasting for less than 5minutes.(i) If tonic clonic seizures start during a dental
procedure:• Remove instruments or dentures if
any from the oral cavity.• Place a gag or a padded tongue
depressor in the mouth between theteeth.
• Turn the head to a side this keeps theairway clear and prevents the tonguefrom falling back.
• If seizures continue, 10 mg diazepamshould be given intravenously.
• Whenever possible dental proceduremay be postponed.
• If the patient continues to haveseizures despite treatment, physicianshould be called and managed asstatus epilepticus. ( see page 153)
(ii) Absence seizures—There is suddenimpairment of consciousness associatedwith starring. The patient stops all on-going activities but recovers within afew seconds. The episode lasts for abrief period, generally less than 30seconds. It only requires reassurance.Patient should be advised to see aphysician later.
(iii) Atonic seizures—also called dropattacks are characterised by sudden lossof postural tone and the head may dropfor a few seconds or the person maydrop to the ground for no obviousreasons. The patient recovers usuallywithin a few seconds and only requiresreassurance particularly if the patient isalready on treatment by a physician.
5. Ischemic Heart Disease
Ischemic heart diseases include angina andmyocardial infarction.Angina pectoris is the principle symptom ofischemic heart disease and is characterisedby sudden severe substernal pain ordiscomfort which may radiate to the leftshoulder or medial aspect of the left arm. Itis precipitated by stress and anxiety. Mostdental procedures are painful and may evokesome anxiety. Therefore during a dentalprocedure, IHD patients may experience anepisode of exertional angina or very rarelydevelop myocardial infarction.1. IHD patients should be taken up for early
appointments in the morning and notmade to wait.
2. Patients with known IHD should be askedto carry their rescue medication i.enitroglycerine tablets for sublingual useto the dental clinic. In patients withmoderate to severe angina, prophylacticnitroglycerine ( 0.5mg tab sublingually)may be used 5 minutes before starting thedental procedure.
3. If a patient gets an acute episode of anginaduring a dental procedure.• Stop the dental procedure for a few
minutes• Administer tab nitroglycerine 0.5mg
sublingually. It relieves pain in 2-5minutes.
• Monitor pulse and BP.• If pain is not relieved in 8-10 minutes,
nitroglycerine dose may be repeated.(maximum of 3 tablets in 15-20 minutes).Even then, if the pain does not sub-side,there are chances that the patientmay be going into myocardialinfarction. Immediate medical attentionshould be sought.
Myocardial Infarction
Signs and symptoms – Severe substernal pain,radiating to the left shoulder, with nausea,

Dental Pharmacology 401
vomiting, palpitation, and sweating, patientappears pale and apprehensive. Patientshould be shifted to emergency care at theearliest possible. While such arrangementsare being done, injection pethidine 50 mg ormorphine 10 mg should given intramuscularly.Patient should be made to swallow a tabletof aspirin 300 mg. Oxygen inhalation shouldbe given if possible. For treatment see page108.
6. Shock
Treatment of shock is discussed in page 121.Intravenous fluids are given in almost all thedifferent types of shock. Therefore aknowledge of the different IV fluids availableis important.
Intravenous Fluids
Intravenous fluids are sterile solutions meantfor intravenous administration. The contentand quantity of solute varies. Intravenousfluids are used for replacement of fluid,electrolytes and nutrition. There aredifferent types of IV fluids to be givendepending on the patient’s requirements.
Types of IV Solutions
Intravenous solutions are of 3 typesdepending on osmolality - isotonic, hypotonicor hypertonic. Fluids having an osmolalitynearly equal to that of extracellular fluid(ECF) or if the electrolyte content (cations +anions) is nearly equal to 310 mEq/L – theyare considered isotonic.
Isotonic-electrolyte content = 310 mEq/LHypotonic-electrolyte content < 250 mEq/LHypertonic-electrolyte content > 375mEq/L(Plasma osmolality is nearly equal to 300m mol / L. Osmolality of 10% dextrose is505 m mol / L.)
Isotonic Fluids As isotonic fluids have anosmolality nearly equal to that of ECF, they
do not alter the size of RBCs (neither shrinknor swell). One litre of isotonic solutionexpands ECF by 1 litre. But it quickly diffusesinto the ECF compartment and thereforearound 3 litres of isotonic fluid is needed toreplenish volume of one litre of lost blood.However patients with hypertension andcardiac failure need careful monitoring toavoid fluid overload. Isotonic solutionsinclude normal saline and lactated ringersolution.Normal saline solution – 0.9 % sodium chlorideIt is used in hyponatraemia. It should beavoided in heart failure, pulmonary oedemaand renal impairment.Lactated ringer solution contains potassium,calcium and sodium chloride. It is used tocorrect dehydration, hyponatraemia and toreplace gastrointestinal fluids. Many othersimilar solutions are available with minorchanges in the electrolyte content.
Hypotonic fluids Hypotonic fluids replacecellular fluid because they are hypotonic ascompared to plasma. Half normal saline(0.45% sodium chloride solution) is thecommonly used hypotonic solution but otherelectrolyte solutions are also available.Hypotonic sodium solution is used inhypernatraemia and other hyperosmolarconditions. Overdosage can result inintravascular fluid depletion, hypotension,cellular edema and later cell damage.
Hypertonic fluids Five percent dextrose innormal saline or lactated ringer’s solution orin hypotonic solution has osmolality morethan ECF 45 to 50%. Dextrose solution maybe administered in hypoglycaemia or tosupplement calories. Since these solutions arestrongly hypertonic, they should be injectedinto central veins for rapid dilution.Hypertonic saline solutions draw water fromthe cells and the cells shrink. They should beinjected slowly and carefully to avoid ECFvolume overload.

Textbook of Pharmacology for Dental and Allied Health Sciences402
7. Diabetic Ketoacidosis
May be precipitated by infection, stress ortrauma. It is more common in patients withinsulin – dependent diabetes mellitus.Diabetic ketoacidosis is a medical emergencyand can be life threatening. Insulin deficiencyresults in severe hyperglycaemia (600 -800mg/dl) and excessive production ofketone bodies.
Clinical features include metabolicacidosis, dehydration with loss of sodiumand potassium in the urine causing electrolyteimbalance, impaired consciousness andhyperventilation – may proceed to coma.Diabetic ketoacidosis should be suspectedwhen the patient has IDDM, diabetes isuncontrolled, patient is under stress, or hasinfection and develops the above signs andsymptoms.
Treatment
• Correction of hyperglycaemia –intravenous regular (plane) insulin 0.1U/kgbolus followed by 0.1 U/kg/hour bycontinuous IV infusion till the patientrecovers. Once the patient has fullyrecovered, insulin should be administeredsubcutaneously 30 minutes before stoppingthe infusion.• Correction of dehydration – Fluid andelectrolyte replacement are important.Normal saline infusion 1 litre in the first hourand then 1 litre over the next 4 hours andthen the quantity can be titrated based onthe severity of dehydration.• Correction of acidosis – Sodiumbicarbonate may be needed in some patientswith severe acidosis.• Potassium – Rapid correction ofhyperglycaemia may result in the movementof potassium into the cells resulting inhypokalemia. 10-20 mEq/hour potassiumchloride is added to the drip. When serum
phosphate is also low, potassium biphosphatemay be given to supplement both potassiumand phosphorus.Hyperglycemic, hyperosmolar, nonketotic, coma –Severe hyperglycaemia and glycosuria resultin severe dehydration and increased plasmaosmolarity leading to coma and has a highmortality rate. The treatment is similar toketoacidosis with correction of fluid andelectrolyte balance and plane insulin.
8. Acute Addisonian CrisisAcute Addisonian crisis is an emergencycondition that could be precipitated by aninfection or sudden withdrawal of steroidsafter long-term administration. Proper drughistory is therefore very important. If thepatient has been on glucocorticoids like(prednisolone) for more than 2 weeks, itshould be continued. The dentist shouldmake sure that the patient receives his doseof glucocorticoid on the day of dentalprocedure particularly if it is a majorprocedure. Symptoms include nausea,vomiting, weakness, hypotension,dehydration, hyponatraemia and hyper-kalaemia. Intravenous hydrocortisonehemisuccinate 100 mg bolus followed byinfusion 100 mg every 4-6 hours is givenimmediately. The dose may be repeateddepending on the patient’s condition. Oncethe patient recovers, switch over to oralpreparations. Immediate correction of fluidand electrolyte balance is important. Whenacute adrenal insufficiency is not confirmed,dexamethasone (4mg IV) should be used inplace of hydrocortisone becausedexamethasone does not interfere in theestimation of hydrocortisone levels fordiagnosis.
9. TetanyTetany is due to hypocalcaemia (Page 373):Other features of hypocalcaemia includemuscle cramps, paraesthesias, laryngospasm

Dental Pharmacology 403
and in more severe cases – convulsions. Slowintravenous injection of 5-20ml of 10% calciumgluconate relieves tetany. Care should betaken to inject calcium slowly because rapidintravenous injection of calcium can causecardiac arrhythmias which can be fatal.
10. Status AsthmaticsAn acute attack of bronchial asthma may beprecipitated by dental procedures them-
selves, the stress or anxiety due to them orthe drugs and materials used in suchprocedures. A known asthmatic patientshould be told to attend the clinic withbronchodilator inhaler which the patient hasbeen taking - preferably salbutamol. An acuteattack should be treated with 1-2 puffs of 100-200 μg salbutamol (Page 215).
Acute severe asthma or status asthmaticsneeds immediate treatment (See Page 219).
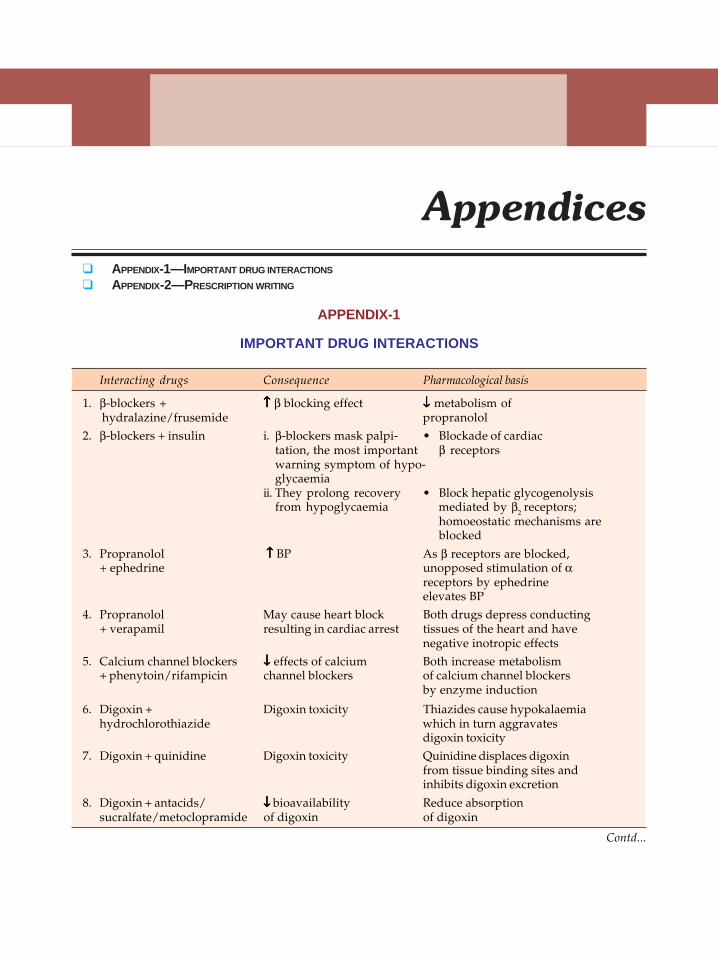
Appendices 405
APPENDIX-1
IMPORTANT DRUG INTERACTIONS
Interacting drugs Consequence Pharmacological basis
1. β-blockers + ↑↑↑↑↑ β blocking effect ↓↓↓↓↓ metabolism of hydralazine/frusemide propranolol
2. β-blockers + insulin i. β-blockers mask palpi- • Blockade of cardiactation, the most important β receptorswarning symptom of hypo-glycaemia
ii. They prolong recovery • Block hepatic glycogenolysisfrom hypoglycaemia mediated by β2 receptors;
homoeostatic mechanisms areblocked
3. Propranolol ↑↑↑↑↑ BP As β receptors are blocked,+ ephedrine unopposed stimulation of α
receptors by ephedrineelevates BP
4. Propranolol May cause heart block Both drugs depress conducting+ verapamil resulting in cardiac arrest tissues of the heart and have
negative inotropic effects5. Calcium channel blockers ↓↓↓↓↓ effects of calcium Both increase metabolism
+ phenytoin/rifampicin channel blockers of calcium channel blockersby enzyme induction
6. Digoxin + Digoxin toxicity Thiazides cause hypokalaemiahydrochlorothiazide which in turn aggravates
digoxin toxicity7. Digoxin + quinidine Digoxin toxicity Quinidine displaces digoxin
from tissue binding sites andinhibits digoxin excretion
8. Digoxin + antacids/ ↓↓↓↓↓ bioavailability Reduce absorptionsucralfate/metoclopramide of digoxin of digoxin
Contd...
Appendices
APPENDIX-1—IMPORTANT DRUG INTERACTIONS
APPENDIX-2—PRESCRIPTION WRITING
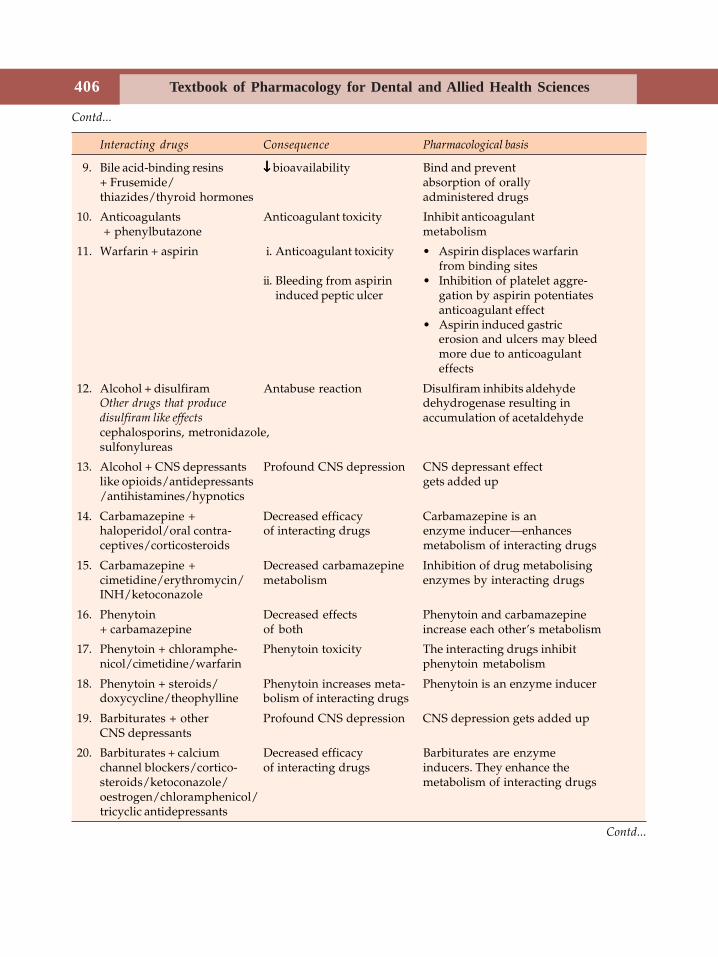
Textbook of Pharmacology for Dental and Allied Health Sciences406
Contd...
Interacting drugs Consequence Pharmacological basis
9. Bile acid-binding resins ↓↓↓↓↓ bioavailability Bind and prevent+ Frusemide/ absorption of orallythiazides/thyroid hormones administered drugs
10. Anticoagulants Anticoagulant toxicity Inhibit anticoagulant + phenylbutazone metabolism
11. Warfarin + aspirin i. Anticoagulant toxicity • Aspirin displaces warfarinfrom binding sites
ii. Bleeding from aspirin • Inhibition of platelet aggre-induced peptic ulcer gation by aspirin potentiates
anticoagulant effect• Aspirin induced gastric
erosion and ulcers may bleedmore due to anticoagulanteffects
12. Alcohol + disulfiram Antabuse reaction Disulfiram inhibits aldehydeOther drugs that produce dehydrogenase resulting indisulfiram like effects accumulation of acetaldehydecephalosporins, metronidazole,sulfonylureas
13. Alcohol + CNS depressants Profound CNS depression CNS depressant effectlike opioids/antidepressants gets added up/antihistamines/hypnotics
14. Carbamazepine + Decreased efficacy Carbamazepine is anhaloperidol/oral contra- of interacting drugs enzyme inducer—enhancesceptives/corticosteroids metabolism of interacting drugs
15. Carbamazepine + Decreased carbamazepine Inhibition of drug metabolisingcimetidine/erythromycin/ metabolism enzymes by interacting drugsINH/ketoconazole
16. Phenytoin Decreased effects Phenytoin and carbamazepine+ carbamazepine of both increase each other’s metabolism
17. Phenytoin + chloramphe- Phenytoin toxicity The interacting drugs inhibitnicol/cimetidine/warfarin phenytoin metabolism
18. Phenytoin + steroids/ Phenytoin increases meta- Phenytoin is an enzyme inducerdoxycycline/theophylline bolism of interacting drugs
19. Barbiturates + other Profound CNS depression CNS depression gets added upCNS depressants
20. Barbiturates + calcium Decreased efficacy Barbiturates are enzymechannel blockers/cortico- of interacting drugs inducers. They enhance thesteroids/ketoconazole/ metabolism of interacting drugsoestrogen/chloramphenicol/tricyclic antidepressants
Contd...
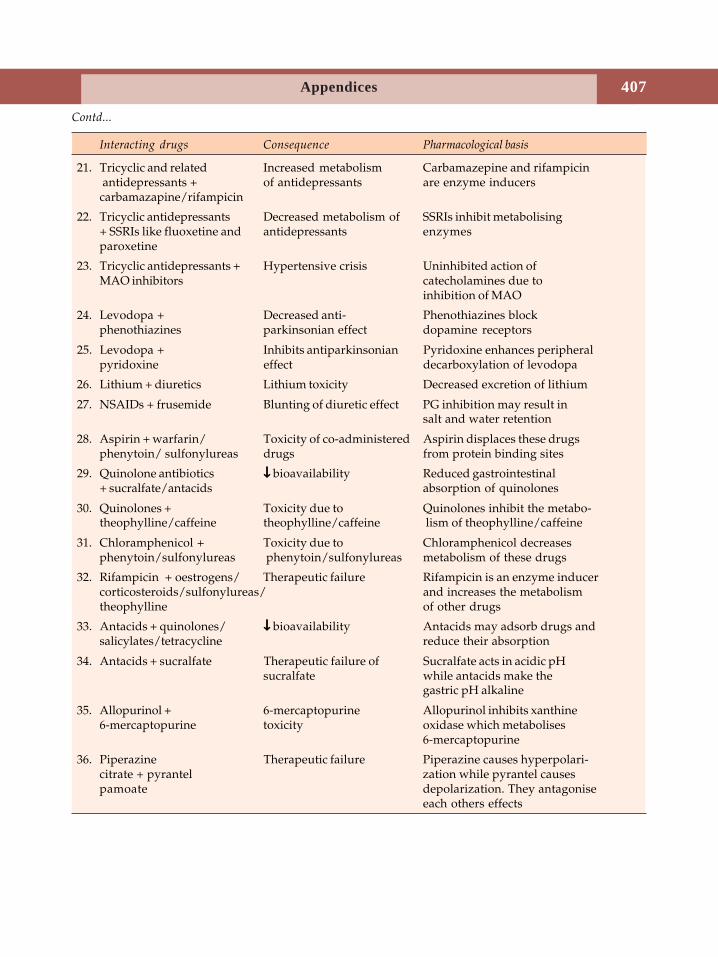
Appendices 407
Contd...
Interacting drugs Consequence Pharmacological basis
21. Tricyclic and related Increased metabolism Carbamazepine and rifampicin antidepressants + of antidepressants are enzyme inducerscarbamazapine/rifampicin
22. Tricyclic antidepressants Decreased metabolism of SSRIs inhibit metabolising+ SSRIs like fluoxetine and antidepressants enzymesparoxetine
23. Tricyclic antidepressants + Hypertensive crisis Uninhibited action ofMAO inhibitors catecholamines due to
inhibition of MAO
24. Levodopa + Decreased anti- Phenothiazines blockphenothiazines parkinsonian effect dopamine receptors
25. Levodopa + Inhibits antiparkinsonian Pyridoxine enhances peripheralpyridoxine effect decarboxylation of levodopa
26. Lithium + diuretics Lithium toxicity Decreased excretion of lithium
27. NSAIDs + frusemide Blunting of diuretic effect PG inhibition may result insalt and water retention
28. Aspirin + warfarin/ Toxicity of co-administered Aspirin displaces these drugsphenytoin/ sulfonylureas drugs from protein binding sites
29. Quinolone antibiotics ↓↓↓↓↓ bioavailability Reduced gastrointestinal+ sucralfate/antacids absorption of quinolones
30. Quinolones + Toxicity due to Quinolones inhibit the metabo-theophylline/caffeine theophylline/caffeine lism of theophylline/caffeine
31. Chloramphenicol + Toxicity due to Chloramphenicol decreasesphenytoin/sulfonylureas phenytoin/sulfonylureas metabolism of these drugs
32. Rifampicin + oestrogens/ Therapeutic failure Rifampicin is an enzyme inducercorticosteroids/sulfonylureas/ and increases the metabolismtheophylline of other drugs
33. Antacids + quinolones/ ↓↓↓↓↓ bioavailability Antacids may adsorb drugs andsalicylates/tetracycline reduce their absorption
34. Antacids + sucralfate Therapeutic failure of Sucralfate acts in acidic pHsucralfate while antacids make the
gastric pH alkaline
35. Allopurinol + 6-mercaptopurine Allopurinol inhibits xanthine6-mercaptopurine toxicity oxidase which metabolises
6-mercaptopurine
36. Piperazine Therapeutic failure Piperazine causes hyperpolari-citrate + pyrantel zation while pyrantel causespamoate depolarization. They antagonise
each others effects
Textbook of Pharmacology for Dental and Allied Health Sciences408
APPENDIX-2
PRESCRIPTION WRITING
The Prescription is a written order by a physician to the pharmacist to prepare and/or dispensespecific medication for a specific patient. A specific pattern should be followed in writingprescriptions, in order to avoid errors and to safeguard the interests of the patient. Moreover the factthat it is a medicolegal document makes it all the more important to be accurate and precise.
The following points should be remembered in writing a prescription:1. The writing should be legible.2. Indelible ink should be used in writing.3. Abbreviations should be avoided.4. In writing quantities—decimals should be avoided; when inevitable, zero should be used—
0.1 for .1.5. Less than 1 gm—should be written as milligrams, e.g. 200 mg and not 0.2 g. No abbreviation
should be used for micrograms and units.6. Blank space should be avoided between direction and the signature of the doctor. If blank
space is present, it should be striked off to avoid misuse of the space to obtain drugs illegally.
PARTS OF THE PRESCRIPTION1. Date of writing the prescription.2. Address of the prescriber—preferrably prescriptions are written on the letter pad with doctor’s
name and address printed at the top.3. Name, age, sex and address of the patient.4. Superscription—the symbol meaning ‘take thou’ is also considered as an invocation to the
Greek gods of healing—Jupitor and Horus.5. Drug name and strength. This is the body of the prescription—also called inscription.
Abbreviations should never be used.6. Directions to the pharmacist (subscription)—consists of instructions for compounding if any
and the quantity to be supplied.7. Directions to the patient—should be clear and should indicate the quantity, frequency, time,
route of administration and other information relevant to the preparation. If a drug is meantonly for external application or needs to be shaken well or mixed before using—suchinstructions should be mentioned.
8. Signature of the prescriber—the prescriber should sign along with registration number.
TYPES OF PRESCRIPTIONS
1. Precompounded prescription orders for a drug manufactured by a pharmaceutical company, has atrade name and is available for use.
2. Compounded or extemporaneous prescription the physician directs the pharmacist to compound apreparation. The ingredients, their quantity and the form of preparation (like mixture, powder orointment) is chosen by the physician and instructed accordingly.
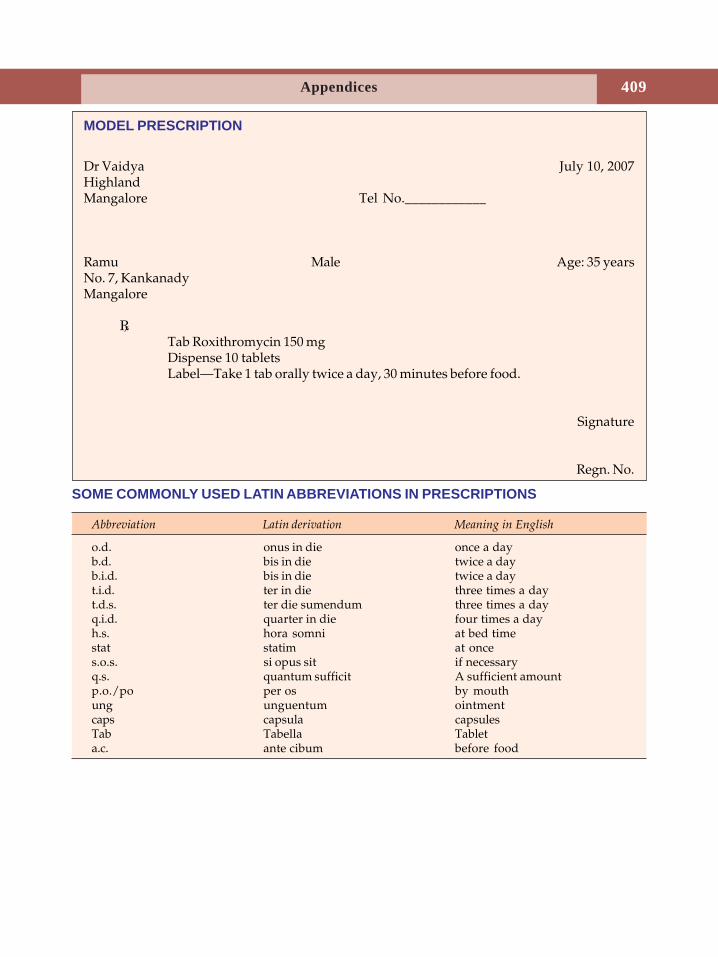
Appendices 409
MODEL PRESCRIPTION
Dr Vaidya July 10, 2007HighlandMangalore Tel No.____________
Ramu Male Age: 35 yearsNo. 7, KankanadyMangalore
Tab Roxithromycin 150 mgDispense 10 tabletsLabel—Take 1 tab orally twice a day, 30 minutes before food.
Signature
Regn. No.
SOME COMMONLY USED LATIN ABBREVIATIONS IN PRESCRIPTIONS
Abbreviation Latin derivation Meaning in English
o.d. onus in die once a dayb.d. bis in die twice a dayb.i.d. bis in die twice a dayt.i.d. ter in die three times a dayt.d.s. ter die sumendum three times a dayq.i.d. quarter in die four times a dayh.s. hora somni at bed timestat statim at onces.o.s. si opus sit if necessaryq.s. quantum sufficit A sufficient amountp.o./po per os by mouthung unguentum ointmentcaps capsula capsulesTab Tabella Tableta.c. ante cibum before food

411Dental Pharmacology
1. Katzung BG: Basic and Clinical Pharmacology (9th edn.) Mc Graw Hill International Edition2004.
2. Satoskar RS, Bhandarkar SD, Ainapure SS: Pharmacology and Pharmacotherapeutics. Revisedeighteenth edition 2005.
3. Tripathi KD: Essentials of Medical Pharmacology (5th edn.) Jaypee Brothers: New Delhi,2003.
4. Barar FSK: Essentials of Pharmacotherapeutics (3rd edn.) S. Chand & Company Ltd. NewDelhi, 2000.
5. Lawrence DR, Bennet PN, Brown MJ: Clinical Pharmacology (9th edn). ChruchillLivingstone: London, 2002.
6. Rang HP, Dale MM, Ritter JM: Pharmacology (5th edn.) Churchill Livingstone: NewYork, 2003.
7. Hardman JG, Limbird LE et al: Goodman and Gilman's: The Pharmacological Basis of
Therapeutics (10th edn.) MC Graw Hill: New York, 2001.8. Craig CR; Robert E. Stitzel Modern Pharmocology with Clinical Applications (6th edn).
Little Brown: Boston, 2003.9. Park K. Park's: Text book of Preventive and Social Medicine (17th edn.) M/s Bharanidas
Bhanot, Jabalpur, 2002.10. Page CP, Curtis MJ et al: Integrated Pharmacology (2nd edn) Mosby, London 2002.11. Martindale: The complete Drug Reference 33rd edn.) Pharmaceutical Press, 2002.12. Mary J. Mycek, Richard A. Harvey, Pamela C. Champe, Bruce D. Fisher, Lippincott's
illustrated Reviews (2nd edn.) Lippincot-Raven Publishers, 1992.13. Harrison's Principles of Internal Medicine 14th edition, Mc Graw Hill: 1998, International
edition.14. Robert E. Rakel, Conn's Current therapy 2000 W.B. Saunders Company, Pennsylvania.
Further Reading
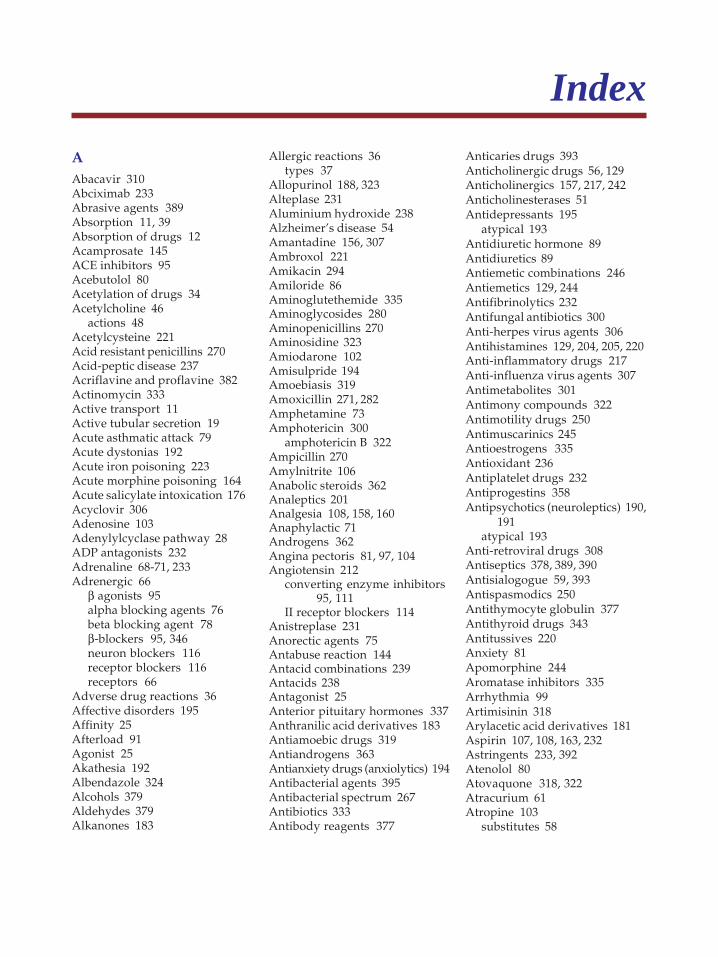
IndexAAbacavir 310Abciximab 233Abrasive agents 389Absorption 11, 39Absorption of drugs 12Acamprosate 145ACE inhibitors 95Acebutolol 80Acetylation of drugs 34Acetylcholine 46
actions 48Acetylcysteine 221Acid resistant penicillins 270Acid-peptic disease 237Acriflavine and proflavine 382Actinomycin 333Active transport 11Active tubular secretion 19Acute asthmatic attack 79Acute dystonias 192Acute iron poisoning 223Acute morphine poisoning 164Acute salicylate intoxication 176Acyclovir 306Adenosine 103Adenylylcyclase pathway 28ADP antagonists 232Adrenaline 68-71, 233Adrenergic 66
β agonists 95alpha blocking agents 76beta blocking agent 78β-blockers 95, 346neuron blockers 116receptor blockers 116receptors 66
Adverse drug reactions 36Affective disorders 195Affinity 25Afterload 91Agonist 25Akathesia 192Albendazole 324Alcohols 379Aldehydes 379Alkanones 183
Allergic reactions 36types 37
Allopurinol 188, 323Alteplase 231Aluminium hydroxide 238Alzheimer’s disease 54Amantadine 156, 307Ambroxol 221Amikacin 294Amiloride 86Aminoglutethemide 335Aminoglycosides 280Aminopenicillins 270Aminosidine 323Amiodarone 102Amisulpride 194Amoebiasis 319Amoxicillin 271, 282Amphetamine 73Amphotericin 300
amphotericin B 322Ampicillin 270Amylnitrite 106Anabolic steroids 362Analeptics 201Analgesia 108, 158, 160Anaphylactic 71Androgens 362Angina pectoris 81, 97, 104Angiotensin 212
converting enzyme inhibitors95, 111
II receptor blockers 114Anistreplase 231Anorectic agents 75Antabuse reaction 144Antacid combinations 239Antacids 238Antagonist 25Anterior pituitary hormones 337Anthranilic acid derivatives 183Antiamoebic drugs 319Antiandrogens 363Antianxiety drugs (anxiolytics) 194Antibacterial agents 395Antibacterial spectrum 267Antibiotics 333Antibody reagents 377
Anticaries drugs 393Anticholinergic drugs 56, 129Anticholinergics 157, 217, 242Anticholinesterases 51Antidepressants 195
atypical 193Antidiuretic hormone 89Antidiuretics 89Antiemetic combinations 246Antiemetics 129, 244Antifibrinolytics 232Antifungal antibiotics 300Anti-herpes virus agents 306Antihistamines 129, 204, 205, 220Anti-inflammatory drugs 217Anti-influenza virus agents 307Antimetabolites 301Antimony compounds 322Antimotility drugs 250Antimuscarinics 245Antioestrogens 335Antioxidant 236Antiplatelet drugs 232Antiprogestins 358Antipsychotics (neuroleptics) 190,
191atypical 193
Anti-retroviral drugs 308Antiseptics 378, 389, 390Antisialogogue 59, 393Antispasmodics 250Antithymocyte globulin 377Antithyroid drugs 343Antitussives 220Anxiety 81Apomorphine 244Aromatase inhibitors 335Arrhythmia 99Artimisinin 318Arylacetic acid derivatives 181Aspirin 107, 108, 163, 232Astringents 233, 392Atenolol 80Atovaquone 318, 322Atracurium 61Atropine 103
substitutes 58
414 Textbook of Pharmacology for Dental and Allied Health Sciences
Attention deficit hyperactivitydisorder 73
Autacoids 203Automaticity 90Autonomic ganglia 61Autonomic innervation 42Autonomic nervous system 45Azithromycin 287Azoles 301
BBacampicillin 271Bacitracin 288Baclofen 64Bactericidal agents 253Bacteriostatic agents 252Balanced anaesthesia 129Barbiturates 140Beclomethasone 218Bed wetting 73Belladonna alkaloids 57Benoxinate HCl 134Benserazide 156Benzalkonium chloride 380Benzbromarone 189Benzimidazoles 324Benznidazole 323Benzodiazepines 128, 137, 145,
151, 194antagonist 140
Benzoic acid 379Benzonatate 220Benztropine 59Benzyl penicillin 267Betazole 204Biguanides 369Bile acid binding resins 236Bioavailability 14Bioequivalence 14Biological half-life 21Biological response modifiers 335Biosynthesis of catecholamines 66Biotransformation 16, 17Bisacodyl 248Bis-biguanides 395Bismuth salts 242Bisphosphonates 375Bithionol 327Bleaching agents 391Bleomycin 333
Blockers 116α 116β 106, 116, 195competitive 60depolarising 62ganglion 115neuromuscular 60selective α1 76, 77synthetic competitive 61
Blood-brain barrier 15Boric acid 378Botulinum toxin 65Bradycardia 79Bran 247Bretylium 102Brilliant green 382Bromhexine 221Bromocriptine 157, 341Bronchial asthma 214Bronchodilators 221Budesonide 218Bupivacaine 132Buprenorphine 170Bupropion 198Buspirone 194
CCa++ channel blockers 209Calcitonin 375Calcium 372
carbonate 239channel blockers 95, 106, 116disodium edetate 382
Camptothecins 334Cancer 330Cannabinoids 246Capreomycin 294Carbamazepine 89, 149, 200Carbapenems 274Carbenoxolone 242Carbidopa 156Carbocysteine 221Carbonic anhydrase inhibitors 87Carboplatin 334Carboxypenicillins 271Carcinogenicity 39Cardiac action potential 90Cardiac arrest 71Cardiac arrhythmias 63, 81Cardiac failure and dentistry 95Cardiac glycosides 91
Cardioselective β-blockers 80Carvedilol 81Castor oil 248Catecholamines 70Celiprolol 80Centchroman 361Central cough suppressants 220Centrally acting muscle relaxants
64Cephalosporins 272, 273Cetrimide 380Cetylpyridinium chloride 380Cevimeline 393Chelating agents 382Chemoprophylaxis 259Chemotherapy 2, 252, 334Chloramine 381Chloramphenicol 279Chlorhexidine 380Chlorinated lime 381Chlorine 381Chloroguanide 318Chloroprocaine 132Chloroquine 186, 314, 321Chlorothiazide 84Chloroxylenol 380Chlorpromazine 191Chlorpropamide 89, 368Cholinergic drugs 47Cholinesterases 46Cholinomimetic alkaloids 49Cidofovir 307Cimetidine 240Cisapride 244Cisplatin 334Cladribine 332Clarithromycin 287, 297Clearance 20Clindamycin 287Clinical pharmacokinetics 20Clofazimine 297Clomiphene 357Clonidine 114, 145, 164Clopidogrel 232Clotrimazole 303Clozapine 193Coagulants 233Cocaine 130, 133, 201Codeine 164, 220, 250Colchicine 188Cold extremities 79
415Index
Colloidal silver compounds 382Colouring agents 390Combination of antimicrobials 255Combined pill 359Computerised miniature pumps 9COMT inhibitors 157Congeners of fentanyl 167Congestive cardiac failure 81, 91Conjugation 254Contractility 90Control of haemorrhage 71Corticosteroids 187, 246, 347, 349
actions 347glucocorticoid actions 347mechanism of action 348
adverse effects 350pharmacokinetics 348structure and synthesis 347
Corticotrophin 339releasing factor 337
Cotrimoxazole 263, 322Cough 220Cresol 380Cromolyn sodium 218Cross resistance 254Cross tolerance 35Cumulation 34Cyanide poisoning 105Cyclophosphamide 9Cycloserine 289, 294Cyclosporine 376Cyproheptadine 209Cyproterone acetate 363Cytarabine 332Cytokines 213Cytosine arabinoside 332Cytotoxic drugs 377
DDale’s phenomenon 70Dale’s vasomotor reversal 70Danaparoid 229Dantrolene 65Dapsone 296Daunorubicin 333Deferiprone 383Definitive therapy 255Dehydroemetine 321Dental desensitising agents 396Dental plaque 394Dentifrices 389
Depression 24, 195Dequalinium chloride 380Desferrioxamine 383Desflurane 125Desmopressin 89Detergents 389Dextrans 120Dextromethorphan 165, 220Dezocine 171Diabetes mellitus 364
treatment 370Diabetic neuropathy 115Diarrhoea 249Diazoxide 118Dicyclomine 246Didanosine 310Diethylcarbamazine 327Differential blockade 131Diffusion 10Diflunisal 179Digitalis 95Digitalization 93Digitoxin 91Digoxin 93Dihydropyridines 96, 97Diloxanide furoate 321Diltiazem 97, 98Dimercaprol 383Diphenoxylate 250Dipivefrin 71Dipyridamole 107Disclosing agents 392Disease modifying drugs 185Disinfection 378Disopyramide 100Dissociative anaesthesia 127Dissolution time 12Distribution 14, 39Disulfiram 144Diuretics 94, 111Diuretics and dentistry 88Dobutamine 72Docosanol 308Dofetilide 102Domperidone 243Dopamine 71, 72
D2 antagonists 245precursor 155receptor agonists 157
Dopexamine 72Dose of the antimicrobials 255
Dose response relationship 29Down regulation 29Doxapram 201Doxepine 206Doxorubicin 333Doxycycline 278d-penicillamine 186, 383Drop attacks 146Droperidol 128Drug 2
delivery system 8dependence 37dosage 22induced constipation 248interactions 18, 39nomenclature 40potency 30synergism and antagonism 31used in glaucoma 51
Duteplase 231Dyes 382Dysguisia 112
EEchinocandins 304Econazole 303Edrophonium 53Eflornithine 323Eicosanoids 210Emergencies in dental practice 397
acute addisonian crisis 402anaphylaxis 397diabetic ketoacidosis 402ischemic heart disease 400seizures 400shock 401status asthmatics 403tetany 402unconsciousness 399uncontrolled bleeding 398
Emetics 244Emetine 321Empiric therapy 255Endocytosis 11Enema 8, 248Enflurane 124Entacapone 157Enteral route 3Enteric coated tablet 3Enterohepatic circulation 19Enzyme induction 18
416 Textbook of Pharmacology for Dental and Allied Health Sciences
Enzyme inhibition 18Ephedrine 72Epidural anaesthesia 136Epilepsy 74, 146Epipodophyllotoxins 333Epirubicin 333Epoprostenol 233Eptifibatide 233Ergot alkaloids 76, 208Erythema nodosum leprosum 298Erythromycin 284Erythropoietin 225Erythrosin 392Esmolol 80Essential drugs concept 40Esters of choline 49Etanercept 187Ethambutol 294Ethamsylate 234Ether 124Ethionamide 294, 297Ethoheptazine 167Ethosuximide 150Ethyl alcohol (ethanol) 143, 379Ethyl stibamine 322Etidocaine 132Etomidate 127Etoposide 333Euphoria 160Eusol 381Excitability 90Excretion 19, 39Exocytosis 66Expectorants 221
FFaecal softeners 247Famciclovir 307Famotidine 240Felbamate 152Felypressin 89Fenamates 183Fenoldopam 72Fentanyl 128, 166Fibric acid (fibrates) 235Fibrin 233Field block 135Filtration 10First dose phenomenon 116First pass metabolism 13, 14First-order kinetics 20
Flavouring agents 390Fluconazole 303Flucytosine 301Fludarabine 332Flumazenil 140Flunarizine 209Fluorescein dye 392Fluoridation of drinking water 394Fluoride 393, 395
dentifrices 394mouthrinses 394toxicity 394
Fluoroquinolones 264, 294, 2975-fluorouracil 332Fluticasone 218Foetal hydantoin syndrome 148Folate antagonists 317Folic acid 224, 225Folinic acid 225Fomivirsen 307Formaldehyde 379Formulation 12Foscarnet 307Fosfomycin 288Frusemide 83, 85, 87Fungal infections 299
GGabapentin 151Ganciclovir 307Ganglion 43
blockers 115Gastric emptying time 13Gastroesophageal reflux disease
244Gastrokinetic agents 129Gelatin foam 233Gelatin products 120Gene therapy 387General anaesthetics 122Gentamicin 282Gentian violet 382Germicide 378Glaucoma 49, 71, 81Glibenclamide (gliburide) 368Glimepiride 368Glomerular filtration 19Glucagon 54Glucocorticoids 217, 295, 334, 347,
348, 354, 371, 377α-glucosidase inhibitors 370
Glutaraldehyde 379Glycerol 88Glycopeptides 287Glycoprotein 233Glycopyrrolate 59, 129GnRH analogs 335Gold salts 185Gonadorelin 337Gonadotrophin-releasing
hormone 337Gonadotrophins 339Gout 187G-protein coupled receptors 27Grand mal epilepsy 146Granisetron 245Gray baby syndrome 279Griseofulvin 301Growth hormone releasing
hormone 337Guanethidine 116
HH1 antihistamines 246H2 receptor blockers 239Haematinics 222Haematopoietic growth factors
225, 335Haemostasis 226Halofantrine 316Halogens 380, 395Haloperidol 193Halothane 124Hamycin 301Henle’s loop 82Heparan sulfate 229Heparin 108, 226
antagonist 229Heparinoids 229Heroin or diamorphine 164Hexachlorophene 380Hirudin 229Histamine 203HMG CoA reductase inhibitors
235Hormonal contraceptives 359Hormone antagonists 335Hormones and related drugs 340Hormones in cancer 3345-HT3 antagonists 245Human albumin 120Hydralazine 117
417Index
Hydrochlorothiazide 85Hydrogen peroxide 381Hydroxychloroquine 186Hydroxyethyl starch 1205-hydroxytryptamine 207Hydroxyzine 195Hyoscine 245Hyperkalaemia 63Hypertension 78, 110Hypertension and dentistry 119Hypertensive emergencies 119Hyperthyroidism 343Hypodermoclysis 5Hypolipidaemic drugs 235Hypothalamic hormones 337
IIbuprofen 181Ibutilide 102Idiosyncrasy 36Idoxuridine 307Imatinib 334Imidazoles 301Immunostimulants 377Immunosuppressants 54, 187, 376Implants 360Important drug interactions 405Indapamide 86Indole acetic acid derivatives 181Indomethacin 181Inducing agents 126Infiltration anaesthesia 135Infliximab 187, 377Inhalation 6
transdermal 7transmucosal 7
Inhalational anaesthetics 123Inhaled steroids 217Inhibitors of adrenal steroids 354Injections
intradermal 5intramuscular 5intravenous 6subcutaneous 5
Insulinactions 364drug interactions 367preparations 366side effects 365use in diabetes mellitus 367
Interferons 308, 335, 378
Intolerance 36Intravenous anaesthetics 125Intravenous fluids 401Intravenous regional anaesthesia
136Intrinsic activity 25Inverse agonist 26Iodides 345Iodine 380Iodine containing solutions 393Iodophors 381Iodoquinol 321Ion channels 27
regulation 28Ionic inhibitors 346Ipecacuanha 221, 244Iron 222Irreversible antagonism 32Irreversible anticholinesterases 54Irritable bowel syndrome 251Irritation 24Isoflurane 125Isoniazid 291Isoprenaline 71Itraconazole 303Ivermectin 327
KK+ sparing diuretics 87Kanamycin 283, 294Ketamine 127Ketoconazole 302, 322Ketolides 287Ketotifen 218Kinase linked 28Kinins 213
LLabetalol 81Lactobacillus acidophilus 250Lamivudine 310Lamotrigine 152Lansoprazole 242L-asparaginase 334Laxative abuse 248Laxatives 247Leflunomide 187Leishmaniasis 322Lepirudin 229Lepra reactions 298Leprosy 296
Leukotriene receptors 184antagonists 219
Leukotrienes 212Levamisole 326Levetiracetam 152Levodopa 155Levorphanol 164Ligand 26Lignocaine 101, 132Lincomycin 287Lincosamides 287Linezolid 289Liposomes 9Liquid paraffin 247Lithium 199Local anaesthetics 130Local hormones 203Loop diuretics 83, 84, 111Loperamide 250Losartan 114Lumefantrine 318Lysol 380
MMacrolides 284Magnesium
salts 239sulphate 103
Malaria 311Malignant hyperthermia 63Malignant neuroleptic syndrome
193Mannitol 88MAO inhibitor 157, 197Mast cell stabilizers 218Mebendazole 324Mechanisms of drug action 24Median effective dose 31Median lethal dose 30Medroxalol 81Mefloquine 316Megakaryocyte growth factors
226Meglitinides 369Meglumine antimonate 322Melarsoprol 323Mephenteramine 74Mepivacaine 133Meprobamate 142, 195Meptazinol 171Mercury compounds 382
418 Textbook of Pharmacology for Dental and Allied Health Sciences
Metabolism 39Metals 382Metaraminol 74Methadone 163, 167Methamphetamine 74Methanol 145Methenamine mandelate 289Methods of prolonging drug
action 23Methohexitone 126Methoxamine 74Methyl alcohol 145α-methyl dopa 115Methylene blue 382Methylphenidate 73Methylxanthines 201, 216Methysergide 210Metoclopramide 243, 245Metoprolol 80Metrifonate 327Metronidazole 319Mexiletine 102Mianserin 199Miconazole 303Mifepristone 358Migraine 208
prophylaxis 81Mineralocorticoids 354Mini-pill 359Minocycline 278, 297Minoxidil 117Mirtazapine 198Misoprotol 242Misuse of antibiotics 260Mithramycin (plicamycin) 333Mitoxantrone 333Mixed agonists and antagonists
169Moclobemide 198Modafinil 73Monobactams 275Monoclonal antibodies 9, 335Montelukast 219Mood stabilizers 199Morphine 159, 163Mouthwashes 391Mucolytics 221Mummifying agents 390Mupirocin 288Muromonab CD3 377Musculoskeletal disorders 64
Mutagenicity 39Mutation 254Myasthenia gravis 53Mycophenolate mofetil 377Mydriasis 72Myeloid growth factors 226Myocardial infarction 81, 400
NNabumetone 183Nalbuphine 170Nalmefene 145, 171Nalorphine 170, 171Naltrexone 145, 171Narcolepsy 72, 73Nasal decongestants 74Nedocromil 218Nefazodone 198Neomycin 283Neostigmine 53Nerve block 135Nervous system 42Netilmicin 283Neuroeffector junction 43Neuroleptanalgesia 128Neuroleptics 193, 246Neurotransmitters 44, 66Neutropenia 112Newer antiepileptics 151, 152Newer non-sedative antihista
mines 205Niclosamide 326Nicorandil 107Nifedipine 97, 116Nifurtimox 323Nikethamide 201Nimesulide 183Nimodipine 96Nitrates 104, 108Nitrofurantoin 289Nitroglycerine 105Nitroimidazoles 289Nitrous oxide 123Nocturnal enuresis 73Nonabsorbable salts 247Nonabsorbable sugars 248Noncatecholamines 72Noncompetitive antagonism 32Nonnucleoside reverse tran
scriptase inhibitors 310
Nonsteroidal anti-inflammatorydrugs 172, 185Non-systemic antacids 238Nootropics 202Noradrenaline 68, 71Noscapine 165Nucleoside reverse transcriptaseinhibitors 309Nystatin 300
OObesity 74Obstructive cardiomyopathy 81Obtundents 390Octreotide 250, 337Ocusert systems 9Oestrogen synthesis inhibitors 357Oestrogens 355Olanzapine 194Ondansetron 145, 245Opioid 129
analgesics 158antagonists 171withdrawal 115
Opium 162Oral anticoagulants 229Oral antidiabetics 370Oral hypoglycaemic drugs 367Oral pill 359Organic nitrates 94Organophosphate toxicity 55Organophosphorus 54Organophosphorus poisoning 54Ornidazole 320Oseltamivir 307Osmotic diuretics 88Osmotic pumps 9Osmotic purgatives 247Oxaliplatin 334Oxamniquine 327Oxantel pamoate 326Oxazolidinones 289Oxicams 183Oxidizing agents 381Oxygenating agents 395
PPaclitaxel 333Pain or algesia 158Pantoprazole 242Papaverine 165
419Index
Para-aminophenol derivatives179
Para-aminosalicyclic acid 294Paracetamol (acetaminophen) 179Paraldehyde 142Paramomycin 323Parathyroid hormone 373Parenteral iron 223Parenteral route 4Parkinsonism 155, 192Partial agonists 80PDE inhibitors 95Pellet implantation 5Penicillins 267
antipseudomonal 271beta-lactamase inhibitors 271extended spectrum 270natural 267semisynthetic 270
Pentamidine 322, 323Pentazocine 170Pentostatin 332Pergolide 157Perioral tremors 192Personality disorders 190Pethidine (meperidine) 165Petit mal 146Pharmacodynamics 2Pharmacoepidemiology 2Pharmacokinetics 2, 10Pharmacopoeia 2Pharmacotherapy of shock 121Pharmacovigilance 36Pharyngeal demulcents 220Phenazopyridine 290Phenelzine 198Phenobarbitone 149Phenol derivatives 380Phenolphthalein 248Phenoxybenzamine 76, 77Phentolamine 77Phenylbutazone 180Phenylephrine 74Phenytoin 101, 148Phenytoin (diphenylhydantoin)
147Pheochromocytoma 78, 81Pholcodeine 165, 220Phosphate 373Physostigmine 53Pilocarpine 49
Pinacidil 107Piperazine citrate 326Piracetam 202Pirenzepine 59Piroxicam 183Pizotifen 209Placental barrier 15Plasma expanders 120Plasma half-life 20Plasma lipid levels 236Plasma protein binding 14Plasmids 254Platelet activating factor 212Pneumocandins 304Pneumocystis carinii 321Polyethylene glycol 248Polymyxin and colistin 288Polypeptide antibiotics 288Polyvinyl pyrrolidone 120Positive-inotropic drugs 94, 95Postoperative muscle pain 63Potassium iodide 221Potassium permanganate 381Potassium sparing diuretics 86Pranlukast 219Praziquantel 326Prazosin 77, 95Preanaesthetic medication 128Preload 91Prescription writing 408Prilocaine 133Primaquine 317Probenecid 189Probiotics 261Probucol 236Procainamide 100Procaine 133Procarbazine 334Prodrug 9Progestins 357Prokinetic agents 243Prolactin 339Promethazine 206Proparacaine HCl 134Propionic acid derivatives 181Propiphenazone 181Propofol 126Propranolol 102Prostaglandins 210, 211, 242Prostanoid receptors 210Protamine sulphate 229
Protease inhibitors 310Proton pump inhibitors 240Proximal tubule 82Pseudocholinesterase 34Psychomotor stimulants 201Psychoses 190Psychotropic drugs 191Purgatives 247Purine antagonists 331, 332Pyrantel pamoate 326Pyrazinamide 293Pyrazolone derivatives 180Pyridoxine 246Pyrimethamine 317Pyrimidine antagonists 332Pyronaridine 318
QQuetiapine 194Quinidine 99Quinine 315Quiniodochlor 321Quinolones 264
RRabbit syndrome 192Radio active iodine I131 335, 345Radioactive isotopes 335Radiophosphorus 335Raloxifene 357, 373Ranitidine 240Rauwolfia serpentina 116, 190Receptor 25
cholinergic 46enzymatic 28families 26regulation 28nuclear 28silent 26spare 26
Redistribution 15Referred pain 158Renin-angiotensin system 113Replacement 24Resistance to antimicrobial agents
253Reteplase 231Retroviruses 305Reversible antagonism 32Revised National Tuberculosis
Control programme 295
420 Textbook of Pharmacology for Dental and Allied Health Sciences
Reye’s syndrome 176Rheumatoid arthritis 185Ribavirin 308Rifabutin 293Rifampicin 292, 297Rifapentine 293Riluzole 64Rimantadine 307Riserpine 194Risperidone 194Rituximab 335Ropivacaine 132Roxatidine 240
SSalicylates 173Salicylic acid 379Saline purgatives 247Saquinavir 310Satranidazole 320Schizophrenia 190Secnidazole 320Sedation and hypnosis 160Sedative 137Sedative hypnotics 129Seizure 146Selective cox-2 inhibitors 183Selective oestrogen receptor
modulators 356Selective serotonin reuptake in
hibitors 197Selective β2 stimulants 75Selegiline (deprenyl) 157Selenium sulfide 304Serotonin agonists 207Serotonin antagonists 208Sevoflurane 125Sialistic implants 5Sialogogues 393Sibutramine 75Side effects 36Sildenafil (viagra) 363Silver compounds 382Silver sulfadiazine 382Sirolimus 377Skeletal muscle 60Skeletal muscle relaxants in
dentistry 65Smooth muscles 70Snake venom 234Sodium bicarbonate 238
Sodium borate (borax) 378Sodium channel blockers 99Sodium fusidate 288Sodium nitroprusside 95, 118Sodium pump 92Sodium stibogluconate 322Sodium valproate 200Somatostatin 337Sources of drugs 2Spastic neurological disorders 64Spectinomycin 287Spinal anaesthesia 135Spironolactone 86, 87Split mind 190Statins 235Status epilepticus 147Stavudine 310Steady-state 22Steam inhalation 221Stimulant purgatives 248Stimulation 24Stokes Adam’s syndrome 73Streptogramins 289Streptomycin 294Strontium chloride 335Styptics 391Succimer 383Succinylcholine 62Sucralfate 242Sulfonamides 262Sulfonylureas 368Sulphasalazine 186Sulphinpyrazone 189Sumatriptan 207Superinfection 260Suramin 323Surface anaesthesia 134Surfactants
anionic 379cationic 380
Sweetening agents 390Sympatholytics 114Sympathomimetics 69, 215Systemic antacids 238
TTachyphylaxis 35Tacrolimus 377Tamoxifen 335, 356Tardive dyskinesia 193Taxanes 333
T-cell inhibitors 376Teicoplanin 288Telenzepine 59Telithromycin 287Tenecteplase 231Teniposide 333Teratogenicity 38, 112Terbinafine 303Terlipressin 89Tetracaine 134Tetracyclines 276, 278Theophylline 216Therapeutic index 30, 31Therapeutic window 31Therapeutics 2Thiabendazole 326Thiacetazone 294Thiazides 83, 89Thiazolidinediones 369Thioguanine 332Thiopentone sodium 126Thioureylenes 344Thrombin powder 233Thrombolytics (fibrinolytics) 108,
231Thromboplastin powder 233Thromboxanes 210Thyroid hormones 342Thyroid-stimulating hormone 339Thyrotoxicosis 81Thyrotrophin releasing hormone
337Thyroxine 342Ticlopidine 232Timolol 80Tinidazole 320Tirofiban 233Tissue binding 15Tissue plasminogen activator 231Tizanidine 64TNF blocking agents 186Tobramycin 282Tolazoline 77Tolbutamide 368Tolcapone 157Tolerance 34Tonic-clonic seizures 146Topical fluoride 394Topical preparations of NSAIDs
178Topical route 8
421Index
Topiramate 152Torsades de pointes 100, 103, 205Toxic effects 36Toxicity 18Toxicology 2Toxoplasmosis 318Tramadol 165Tranquilliser 191Transdermal patch 360Transduction 254Transformation 254Transmission 43Tranylcypromine 198Trastuzumab 335Traveller’s diarrhoea 251Trazodone 198Triamterene 86Triazoles 301Tricyclic antidepressants 195, 196,
209Trifluridine 307Triiodothyronine 342Trilastane 335Trimetazidine 107Trimethaphan 115Triple dye lotion 382Trypanosomiasis 323Tuberculosis 291Tubocurarine 60, 62Two-tone dyes 392
UUlcer protectives 242Unithiol 383
Unstable angina 107Up regulation 29Ureidopenicillins 271Uricosuric drugs 189Urine formation 82Urokinase 231Uses of iodine 381Uterine relaxants (tocolytics) 361Uterine stimulants (ecbolics) 361
VVaginal rings 360Valacyclovir 307Valproic acid 150Vancomycin 287Vascular smooth muscle 96Vasodilators 94, 117Vasopressin analogs 89Vasopressin receptors 89Vasopressors 74Vectors 387Venlafaxine 198Verapamil 97, 98, 102Vidarabine 307Vigabatrin 152Vinca alkaloids 334Viruses 305Vitamins 383
fat-solublevitamin A 384vitamin D 373vitamin K 234
water-soluble 384
biotin 387folic acid 387nicotinamide 385nicotinic acid 385pantothenic acid 387pyridoxine (vitamin B6) 385riboflavin (vitamin B2) 385thiamine (vitamin B1, aneu
rine) 384vitamin B12 224, 387vitamin B-complex 384vitamin C 387
Volume of distribution 16
WWood alcohol 145
YYohimbine 78
ZZafirlukast 219Zalcitabine 310Zaleplon 140Zanamivir 307Zero order kinetics 20Zidovudine 309Zinc salts 382Ziprasidone 194Zolpidem 140Zonisamide 152Zopiclone 140