taxane-induced nail changes: incidence, clinical presentation and outcome
TRANSCRIPT
Annals of Oncology 14: 333–337, 2003
Clinical case DOI: 10.1093/annonc/mdg050
© 2003 European Society for Medical Oncology
Taxane-induced nail changes: incidence, clinical presentation and outcomeA. M. Minisini1, A. Tosti2, A. F. Sobrero3, M. Mansutti4, B. M. Piraccini2, C. Sacco4 & F. Puglisi1*
*Correspondence to: Dr F. Puglisi, Clinica Oncologica, Policlinico Universitario, 33100 Udine, Italy. Tel: +39-0432-559304; Fax: +39-0432-559305; E-mail: [email protected]
1Clinical Oncology, University of Udine, Udine; 2Department of Dermatology, University of Bologna, Bologna; 3Clinical Oncology, San Martino Hospital, Genoa; 4Clinical Oncology, General Hospital, Udine, Italy
Received 5 June 2002; accepted 3 July 2002
The clinical characteristics of nail changes in seven patients receiving taxane-containing chemotherapy are
described. They include nail pigmentation, subungual hematoma, Beau’s lines and onycholysis and subungual
suppuration.
The incidence of such changes (ranging from 0% to 44%) is reviewed from a Medline search of the
literature.
Key words: chemotherapy, nail changes, side-effects, taxanes
Introduction
The taxanes, paclitaxel (P) (Taxol®; Bristol-Myers SquibbCompany; Princeton, NJ, USA) and docetaxel (D) (Taxotere®;Aventis Pharmaceuticals; Collegeville, PA, USA), were intro-duced in the late 1980s. Since then both drugs have proved to beeffective in the treatment of a variety of solid tumors includingbreast, ovarian, lung and bladder cancers [1, 2]. Taxanes exerttheir cytotoxic effect by reversibly binding the β-subunit oftubulin, thereby inducing tubulin polymerization and inhibitingmicrotubule depolymerization [3, 4]. A balance between poly-merization and depolymerization is needed for normal micro-tubule function. Taxanes disrupt this balance, leading to arrest atthe G2/M phase of the cell cycle.
P and D are administered intravenously and their pharmaco-kinetics show a large volume of distribution and a rapid elimin-ation from the plasma with a short terminal half-life of 5 and 12 h,respectively [5, 6]. Both compounds are metabolized by the liver,and require dose adjustment for patients with hepatic dysfunction[7]. They are usually administered every 3 weeks; however,weekly administration is also common. Taxanes have a predict-able toxicity profile on an every-3-week basis [8]. The standarddose of P according to this schedule is 175 mg/m2 (3-h infusion)with the most common side-effects including myelosuppression,neuropathy, alopecia, hypersensitivity reactions and myalgias/arthralgias.
In women with advanced breast cancer, D is usually admin-istered as a 1-h intravenous infusion at 75–100 mg/m2 every3 weeks. The dose-limiting toxicity is myelosuppression and a90–95% incidence of grade 3/4 neutropenia is reported in mostpublished series. Other side-effects include asthenia/fatigue,
alopecia, skin reaction, stomatitis, hypersensitivity reactions anda fluid-retention syndrome.
Recently, weekly schedules of taxanes have been proposed as apossible therapeutic alternative with the aim of minimizing theacute toxicity while enhancing dose density [9–12]. However, todate results are awaited from randomized trials comparing theclinical effect of every-3-week and weekly schedules. The weeklyadministration significantly alters the side-effect profile of theagents reducing the incidence and grade of myelosuppression.Neuropathy becomes the most common side-effect of P whenadministered at 80 mg/m2/week [11]. For weekly D the usual doseranges between 36 and 40 mg/m2 and fatigue/asthenia becomesthe dose-limiting toxicity [9].
Cutaneous toxicity has been reported with taxanes and includeserythema and desquamation, involving primarily the hands. Nailchanges are described in different series and case reports, but thereal incidence of this side-effect is probably underestimated. Inaddition, a wide clinical spectrum of nail disorders is possible andconstitutes the focus of this review.
Case reports
Case 1
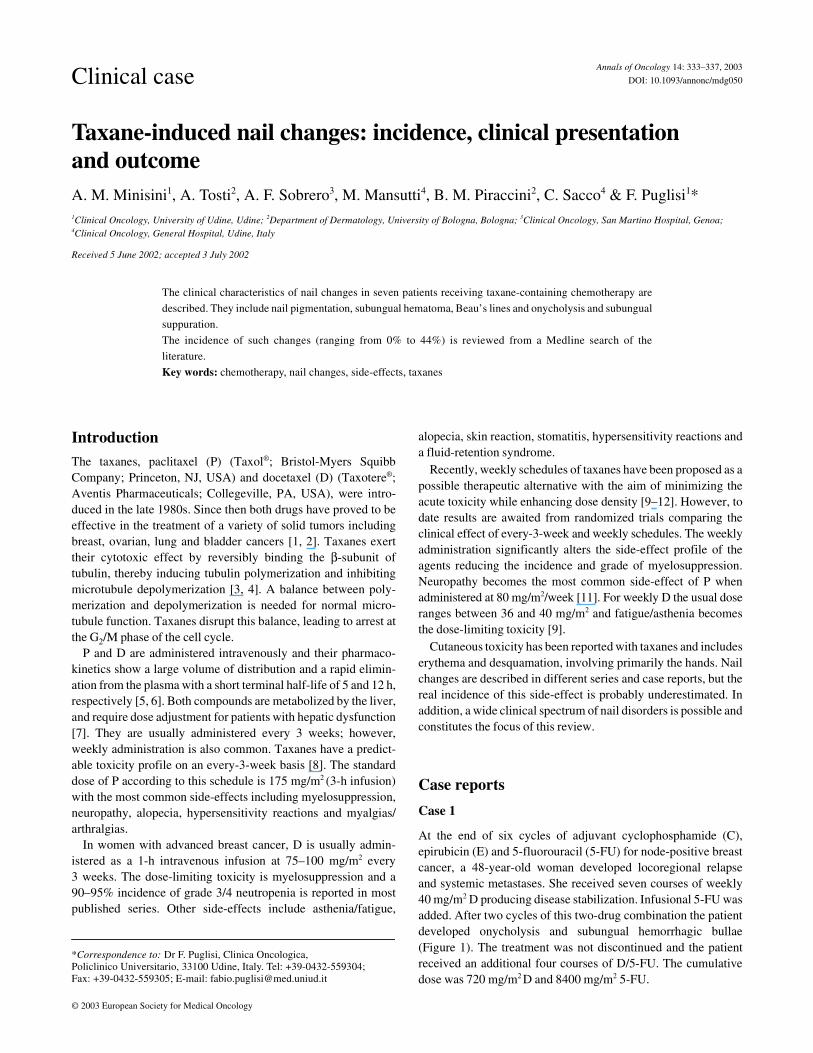
At the end of six cycles of adjuvant cyclophosphamide (C),epirubicin (E) and 5-fluorouracil (5-FU) for node-positive breastcancer, a 48-year-old woman developed locoregional relapseand systemic metastases. She received seven courses of weekly40 mg/m2 D producing disease stabilization. Infusional 5-FU wasadded. After two cycles of this two-drug combination the patientdeveloped onycholysis and subungual hemorrhagic bullae(Figure 1). The treatment was not discontinued and the patientreceived an additional four courses of D/5-FU. The cumulativedose was 720 mg/m2 D and 8400 mg/m2 5-FU.
334
Nail suppuration with right arm lymphedema occurred about1 month after the discontinuation of D. A microbiological testshowed the presence of Enterobacter cloacae and Staphylo-coccus aureus; the patient was treated with ciprofloxacin 500 mgb.i.d. and fluconazole with complete recovery 1 month later.
Case 2
After three lines of palliative hormonal treatments and four linesof chemotherapy for advanced breast cancer, a 55-year-oldwomen was treated with D 35 mg/m2/week. After 12 courses ofweekly D she presented Beau’s lines and onycholysis with sup-puration of fingers and toenails. Microbiological culture demon-strated the presence of infection by Staphyolococcus warnerii,which was treated with ciprofloxacin 500 mg b.i.d. with fullrecovery.
Case 3
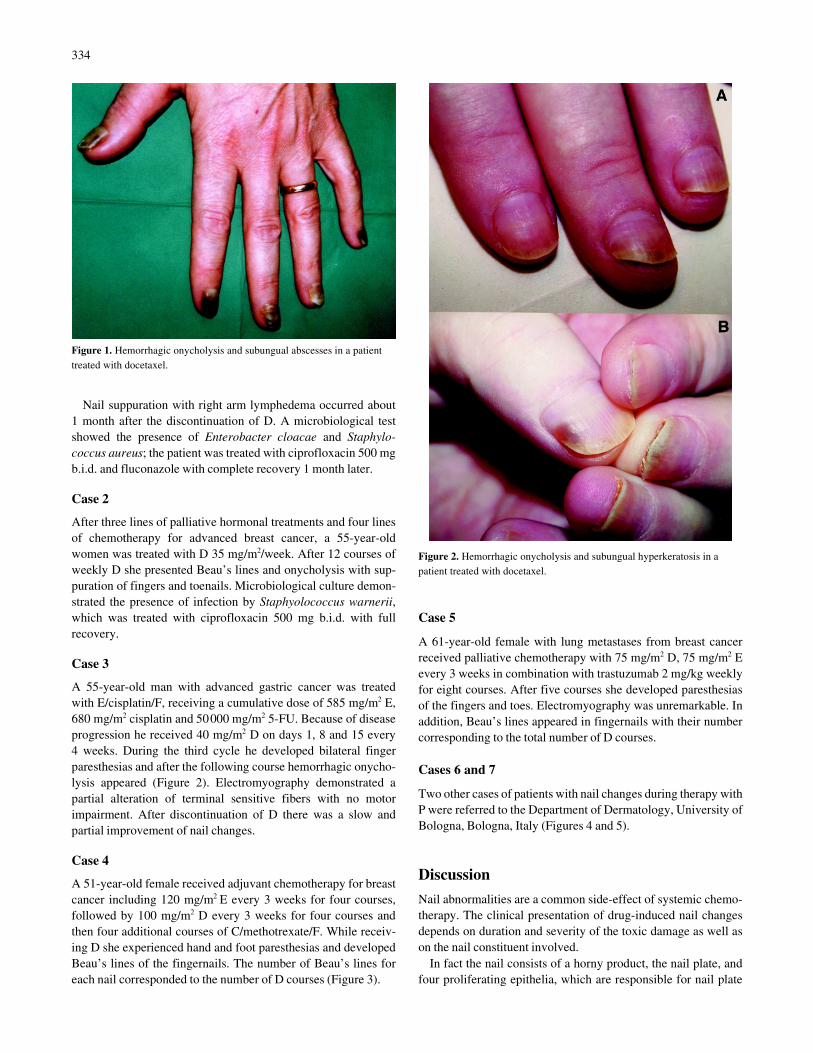
A 55-year-old man with advanced gastric cancer was treatedwith E/cisplatin/F, receiving a cumulative dose of 585 mg/m2 E,680 mg/m2 cisplatin and 50000 mg/m2 5-FU. Because of diseaseprogression he received 40 mg/m2 D on days 1, 8 and 15 every4 weeks. During the third cycle he developed bilateral fingerparesthesias and after the following course hemorrhagic onycho-lysis appeared (Figure 2). Electromyography demonstrated apartial alteration of terminal sensitive fibers with no motorimpairment. After discontinuation of D there was a slow andpartial improvement of nail changes.
Case 4
A 51-year-old female received adjuvant chemotherapy for breastcancer including 120 mg/m2 E every 3 weeks for four courses,followed by 100 mg/m2 D every 3 weeks for four courses andthen four additional courses of C/methotrexate/F. While receiv-ing D she experienced hand and foot paresthesias and developedBeau’s lines of the fingernails. The number of Beau’s lines foreach nail corresponded to the number of D courses (Figure 3).
Case 5
A 61-year-old female with lung metastases from breast cancerreceived palliative chemotherapy with 75 mg/m2 D, 75 mg/m2 Eevery 3 weeks in combination with trastuzumab 2 mg/kg weeklyfor eight courses. After five courses she developed paresthesiasof the fingers and toes. Electromyography was unremarkable. Inaddition, Beau’s lines appeared in fingernails with their numbercorresponding to the total number of D courses.
Cases 6 and 7
Two other cases of patients with nail changes during therapy withP were referred to the Department of Dermatology, University ofBologna, Bologna, Italy (Figures 4 and 5).
Discussion
Nail abnormalities are a common side-effect of systemic chemo-therapy. The clinical presentation of drug-induced nail changesdepends on duration and severity of the toxic damage as well ason the nail constituent involved.
In fact the nail consists of a horny product, the nail plate, andfour proliferating epithelia, which are responsible for nail plate
Figure 1. Hemorrhagic onycholysis and subungual abscesses in a patient treated with docetaxel.
Figure 2. Hemorrhagic onycholysis and subungual hyperkeratosis in a patient treated with docetaxel.

335
production and growth correction. These include the nail matrix,the nail bed, the proximal nail fold and the hyponychium.
The nail matrix epithelium is formed by highly proliferatingcells that differentiate and keratinize to produce the nail plate.The epithelium contains numerous melanocytes that are normally
quiescent. The nail matrix epithelium is very susceptible to toxicnoxae. An acute damage of the matrix, as it may occur during sys-temic chemotherapy, results in a defective nail plate production.The most typical changes are Beau’s lines and onychomadesis(which are signs of an arrest in the epithelial proliferation) orleukonychia, which indicates an abnormal keratinization. Toxic-ity to the matrix epithelium often results in melanocyte activationwith nail plate pigmentation and melanonychia.
The nail bed epithelium is a very thin epithelium that is mainlyresponsible for the adhesion of the nail plate to the underlyingstructures. An acute toxic damage to the nail bed causes nail platedetachment with onycholysis.
The proximal nail fold and the hyponychium contribute tomaintain correct nail growth and protect the nail matrix from theenvironment. A toxic damage to the proximal nail fold results inparonychia with subsequent nail matrix exposure and damage.
Taxane probably cause nail changes more commonly thanother drugs.
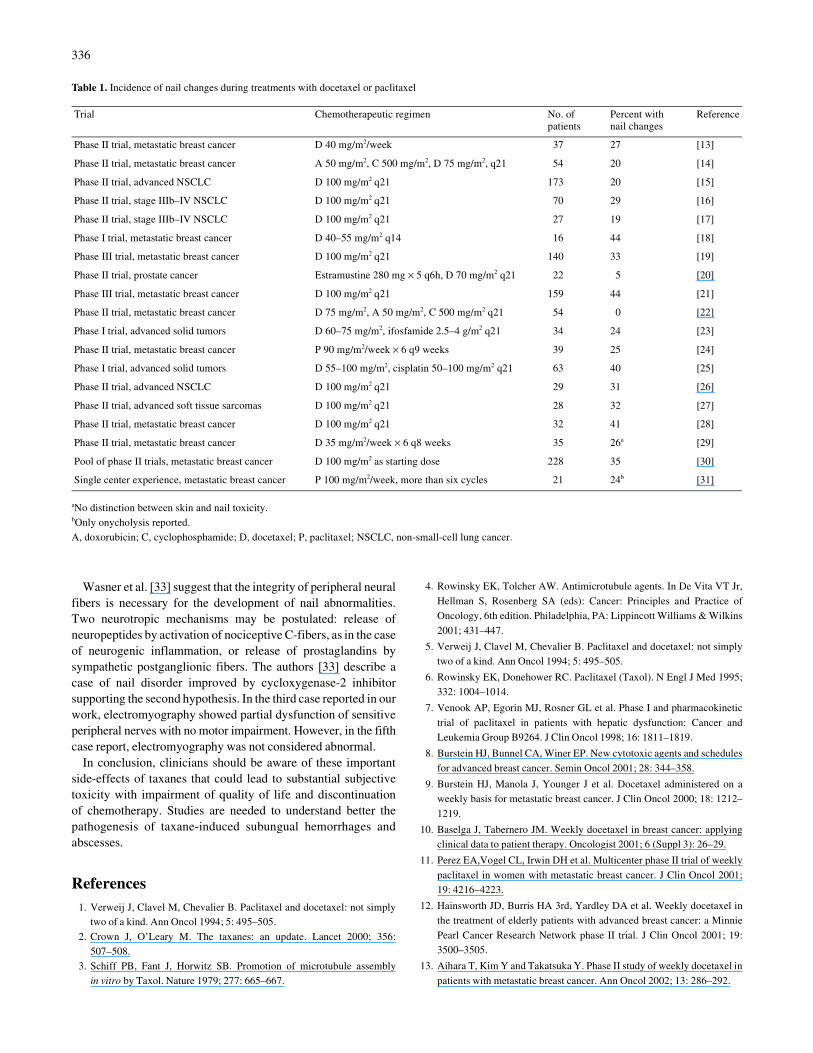
A Medline search of the literature using the terms ‘nail’,‘docetaxel’ and ‘paclitaxel’ indicated an incidence of nail toxic-ity ranging from 0% to 44% (Table 1). The majority of studiesciting nail changes among drug induced toxicity are related toD use [13–23, 25–30] whereas only two trials describe naildisease as part of P-related side-effects [24, 31].
In addition, several case reports in the literature relate to aD- and/or P-induced onycopathy [31–46].
Nail abnormalities related to taxanes include nail pigmen-tation, splinter hemorrhage and subungual hematoma, Beau’slines, acute paronychia and onycholysis.
Nail abnormalities occurring during taxane treatments are inmost cases not serious but hemorrhagic onycholysis and sub-ungual abscesses can occur producing important morbidity. Thelatter side-effects are quite exclusive of taxane therapy and cancause potentially severe complications since patients may becomeneutropenic during chemotherapy, enhancing the risk of sepsis.
Possible explanations for subungual hematoma and hemor-rhagic onycholysis are the taxane-induced thrombocytopenia andvascular abnormalities.
Figure 3. Beau’s lines affecting all fingernails. The presence of multiple lines in each nail indicates repetitive exposure to the drug.
Figure 4. Diffuse fingernail orange discoloration due to hemorrhagic suffusion of the nail bed and toenail onycholysis with subungual suppuration of the left great toenail in a patient treated with paclitaxel.
Figure 5. Hemorrhagic onycholysis. Development of the nail lesions was associated with intense pain.
336
Wasner et al. [33] suggest that the integrity of peripheral neuralfibers is necessary for the development of nail abnormalities.Two neurotropic mechanisms may be postulated: release ofneuropeptides by activation of nociceptive C-fibers, as in the caseof neurogenic inflammation, or release of prostaglandins bysympathetic postganglionic fibers. The authors [33] describe acase of nail disorder improved by cycloxygenase-2 inhibitorsupporting the second hypothesis. In the third case reported in ourwork, electromyography showed partial dysfunction of sensitiveperipheral nerves with no motor impairment. However, in the fifthcase report, electromyography was not considered abnormal.
In conclusion, clinicians should be aware of these importantside-effects of taxanes that could lead to substantial subjectivetoxicity with impairment of quality of life and discontinuationof chemotherapy. Studies are needed to understand better thepathogenesis of taxane-induced subungual hemorrhages andabscesses.
References1. Verweij J, Clavel M, Chevalier B. Paclitaxel and docetaxel: not simply
two of a kind. Ann Oncol 1994; 5: 495–505.
2. Crown J, O’Leary M. The taxanes: an update. Lancet 2000; 356:507–508.
3. Schiff PB, Fant J, Horwitz SB. Promotion of microtubule assemblyin vitro by Taxol. Nature 1979; 277: 665–667.
4. Rowinsky EK, Tolcher AW. Antimicrotubule agents. In De Vita VT Jr,
Hellman S, Rosenberg SA (eds): Cancer: Principles and Practice ofOncology, 6th edition. Philadelphia, PA: Lippincott Williams & Wilkins
2001; 431–447.
5. Verweij J, Clavel M, Chevalier B. Paclitaxel and docetaxel: not simplytwo of a kind. Ann Oncol 1994; 5: 495–505.
6. Rowinsky EK, Donehower RC. Paclitaxel (Taxol). N Engl J Med 1995;332: 1004–1014.
7. Venook AP, Egorin MJ, Rosner GL et al. Phase I and pharmacokinetic
trial of paclitaxel in patients with hepatic dysfunction: Cancer andLeukemia Group B9264. J Clin Oncol 1998; 16: 1811–1819.
8. Burstein HJ, Bunnel CA, Winer EP. New cytotoxic agents and schedules
for advanced breast cancer. Semin Oncol 2001; 28: 344–358.
9. Burstein HJ, Manola J, Younger J et al. Docetaxel administered on aweekly basis for metastatic breast cancer. J Clin Oncol 2000; 18: 1212–
1219.
10. Baselga J, Tabernero JM. Weekly docetaxel in breast cancer: applyingclinical data to patient therapy. Oncologist 2001; 6 (Suppl 3): 26–29.
11. Perez EA,Vogel CL, Irwin DH et al. Multicenter phase II trial of weekly
paclitaxel in women with metastatic breast cancer. J Clin Oncol 2001;19: 4216–4223.
12. Hainsworth JD, Burris HA 3rd, Yardley DA et al. Weekly docetaxel inthe treatment of elderly patients with advanced breast cancer: a Minnie
Pearl Cancer Research Network phase II trial. J Clin Oncol 2001; 19:3500–3505.
13. Aihara T, Kim Y and Takatsuka Y. Phase II study of weekly docetaxel in
patients with metastatic breast cancer. Ann Oncol 2002; 13: 286–292.
Table 1. Incidence of nail changes during treatments with docetaxel or paclitaxel
aNo distinction between skin and nail toxicity.bOnly onycholysis reported. A, doxorubicin; C, cyclophosphamide; D, docetaxel; P, paclitaxel; NSCLC, non-small-cell lung cancer.
Trial Chemotherapeutic regimen No. of patients
Percent with nail changes
Reference
Phase II trial, metastatic breast cancer D 40 mg/m2/week 37 27 [13]
Phase II trial, metastatic breast cancer A 50 mg/m2, C 500 mg/m2, D 75 mg/m2, q21 54 20 [14]
Phase II trial, advanced NSCLC D 100 mg/m2 q21 173 20 [15]
Phase II trial, stage IIIb–IV NSCLC D 100 mg/m2 q21 70 29 [16]
Phase II trial, stage IIIb–IV NSCLC D 100 mg/m2 q21 27 19 [17]
Phase I trial, metastatic breast cancer D 40–55 mg/m2 q14 16 44 [18]
Phase III trial, metastatic breast cancer D 100 mg/m2 q21 140 33 [19]
Phase II trial, prostate cancer Estramustine 280 mg × 5 q6h, D 70 mg/m2 q21 22 5 [20]
Phase III trial, metastatic breast cancer D 100 mg/m2 q21 159 44 [21]
Phase II trial, metastatic breast cancer D 75 mg/m2, A 50 mg/m2, C 500 mg/m2 q21 54 0 [22]
Phase I trial, advanced solid tumors D 60–75 mg/m2, ifosfamide 2.5–4 g/m2 q21 34 24 [23]
Phase II trial, metastatic breast cancer P 90 mg/m2/week × 6 q9 weeks 39 25 [24]
Phase I trial, advanced solid tumors D 55–100 mg/m2, cisplatin 50–100 mg/m2 q21 63 40 [25]
Phase II trial, advanced NSCLC D 100 mg/m2 q21 29 31 [26]
Phase II trial, advanced soft tissue sarcomas D 100 mg/m2 q21 28 32 [27]
Phase II trial, metastatic breast cancer D 100 mg/m2 q21 32 41 [28]
Phase II trial, metastatic breast cancer D 35 mg/m2/week × 6 q8 weeks 35 26a [29]
Pool of phase II trials, metastatic breast cancer D 100 mg/m2 as starting dose 228 35 [30]
Single center experience, metastatic breast cancer P 100 mg/m2/week, more than six cycles 21 24b [31]

337
14. Nabholtz JM, Mackey JR, Smyle M et al. Phase II study of docetaxel,doxorubicin, and cyclophosphamide as first-line chemotherapy for meta-static breast cancer. J Clin Oncol 2001; 19: 314–321.
15. Mattson K, Bosquee L, Dabouis G et al. Phase II study of docetaxel inthe treatment of patients with advanced non-small cell lung cancer inroutinely daily practice. Lung Cancer 2000; 29: 205–216.
16. Robinet G, Thomas P, Pérol M et al. Phase II study of docetaxel ininoperable advanced non small cell lung cancer. Bull Cancer 2000; 87:253–258.
17. Robinet G, Thomas P, Pérol M et al. Efficacy of docetaxel in non-smallcell lung cancer in patients previously treated with platinum-containingchemotherapy. Rev Mal Respir 2000; 17: 83–89.
18. Shin E, Ihitobi M, Hiraoia M et al. Phase I study of docetaxel adminis-tered by bi-weekly infusion to patients with metastatic breast cancer.Anticancer Res 2000; 20: 4721–4726.
19. Sjöström J, Blomqvist C, Mouridsen H et al. Docetaxel compared withsequential methotrexate and 5-fluorouracil in patients with advancedbreast cancer after anthracycline failure: a randomised phase III studywith crossover on progression by the Scandinavian Breast Group. EurJ Cancer 1999; 35: 1194–1201.
20. Wah Sinibaldi VJ, Caducci M, Laufer M, Eisenberg M. Preliminaryevaluation of short course of estramustine phosphate and docetaxel(Taxotere) in the treatment of hormone-refractory prostate cancer. SeminOncol 1999; 26 (Suppl 17): 45–48.
21. Chan S, Friedrichs K, Noel D et al. Prospective randomized trial ofdocetaxel versus doxorubicin in patients with metastatic breast cancer.J Clin Oncol 1999; 17: 2341–2354.
22. Nabholtz JM, Mackey J, Smyle M, Tonkin K. Taxane-based three-drugcombination in metastatic and adjuvant treatment of breast cancer. SeminOncol 1998; 25 (Suppl 12): 27–31.
23. Pronk LC, Schrijvers D, Schellens JHM et al. Phase I study on docetaxeland ifosfamide in patients with advanced solid tumours. Br J Cancer1998; 77: 153–158.
24. Lüftner D, Flath B, Akrivakis C et al. Dose-intensified weekly paclitaxelinduces multiple nail disorders. Ann Oncol 1998; 9: 1139–1141.
25. Pronk LC, Schellens JHM, Planting AST et al. Phase I and pharmaco-logic study of docetaxel and cisplatin in patients with advanced solidtumors. J Clin Oncol 1997; 15: 1071–1079.
26. Saarinen A, Jekunen A, Halme M et al. A phase II trial of docetaxelin advanced non-small cell lung cancer. Anticancer Drugs 1996; 7:890–892.
27. Van Hoesel QGCM, Verweij J, Catimel G et al. Phase II study withdocetaxel (Taxotere®) in advanced soft tissue sarcomas of the adult. AnnOncol 1994; 5: 539–542.
28. Ten Bokkel Huinink WW, Prove AM, Piccart M et al. A phase II trial of
docetaxel (Taxotere®) in second line treatment with chemotherapy for
advanced breast cancer. Ann Oncol 1994; 5: 527–532.
29. Stemmler HJ, Gutschow K, Sommer H et al. Weekly docetaxel
(Taxotere®) in patients with metastatic breast cancer. Ann Oncol 2001;
12: 1393–1398.
30. Trudeau ME. Docetaxel (Taxotere): an overview of first-line mono-
therapy. Semin Oncol 1995; 22 (6 Suppl 13): 17–21.
31. Hussain S, Anderson DN, Salvatti ME et al. Onycholysis as a compli-
cation of systemic chemotherapy. Report of five cases associated with
prolonged weekly paclitaxel therapy and review of the literature. Cancer
2000; 88: 2367–2371.
32. Pavithran K, Doval DC. Nail changes due to docetaxel. Br J Dermatol
2002; 146: 709–710.
33. Wasner G, Hilpert F, Baron R, Pfisterer J. Nail changes secondary to
docetaxel. Lancet 2001; 357: 910.
34. Vanhooteghem O, Richert B, Vindevoghel A et al. Subungual abscess: a
new ungual side-effect related to docetaxel therapy. Br J Dermatol 2000;
143: 462–464.
35. Almagro M, Del Pozo J, Garcia-Silva J et al. Nail alterations secondary
to paclitaxel therapy. Eur J Dermatol 2000; 10: 146–147.
36. Flory SM, Solimando DA Jr, Webster CJ et al. Onycholysis associated
with weekly administration of paclitaxel. Ann Pharmacother 1999; 33:
584–586.
39. Correia O, Azevedo C, Pinto Ferreira E et al. Nail changes secondary to
docetaxel (Taxotere). Dermatology 1999; 198: 288–290.
40. Auvinet M, Dahan S, Dingremont C et al. Yellow nails. Rev Méd Interne
1998; 19: 353–354.
41. Obermair A, Binder M, Barrada M et al. Onycholysis in patients treated
with docetaxel. Ann Oncol 1998; 9: 230–231.
42. Jacob CI, Patten SF. Nail bed dyschromia secondary to docetaxel
therapy. Arch Dermatol 1998; 134: 1167–1168.
43. Vanhooteghem O, André J, Vindevoghel A et al. Docetaxel-induced
subungual hemorrhage. Dermatology 1997; 194: 419–420.
44. Llombart-Cussac A, Pivot X, Spielman M. Docetaxel chemotherapy
induces transverse superficial loss of the nail plate. Arch Dermatol 1997;
133: 1466–1467.
45. Slee PHTJ. Nail changes after chemotherapy. N Engl J Med 1997; 337:
168.
46. Link CJ Jr, Sarosy GA, Kohn EC et al. Cutaneous manifestations of
Taxol therapy. Invest New Drugs 1995; 13: 261–263.
