systemic mastocytosis associated with generalized osteopenia
TRANSCRIPT
25. Haggit, R. C., and Pitcock, J. A.: Familial juvenile polyposis of the colon. Cancer, 26:1232, 1970.
26. Sachatello, C. R., Hahn, I. S., and Carrington, C. B.: Juvenile gastrointestinal polyposis in a female infant: report of a case and review of the literatnre of a recently recognized syn- drome. Surgery, 75:107, 1974.
27. Soper, R. T., and Kent, T. H.: Fatal juvenile polyposis in in- fancy. Surgery, 69:693, 1971.
28. Velcek, F. T., Coopersmitb, I. S., Chen, C. K., Kassner, E. G., Klotz, D. M., and Kottmeier, P. K.: Familial juvenile adenomatous polyposis. J. Ped. Surg., 11:781, 1976.
29. Schwartz, A. M., and McCauley, R. G. K.: Juvenile gastroin- testinal polyposis. Radiology, 121:441, 1976.
-300, Tung-hua, L., Min-chang, C., and Hsien-chiu, T.: Malig- nant change of a juvenile polyp of colon: a case report. Chin. Med. J., 4:434, 1978.
31. Kaye, G. I., Fenoglio, C. N., Pascal, R. R., and Lane, N.: Com- parative electron microscopic features of normal, hyperplastic and adenomatous colonic epithelium. Gas- troenterology, 64:926, 1973.
MULTIPLE JUVENILE POLYPOS1S---LIPPER ET AL.
32. Hayashi, T., Yatani, R., Apostol,J., and Stemmermann, G. N.: Pathogenesis of hyperplastic polyps of the colon: a hypothe- sis based on uhrastructure and in vitro cell kinetics. Gas- troenterology, 66:347, 1974.
33. Estrada, R. G., and Spjut, H.J.: Hyperplastic polyps of the large bowel. Am. J. Surg. Pathol., 4:127, 1980.
34. Rijke, R. P. C., and Gart, R.: Epithelial cell kinetics in the de- scending colon of the rat. 1. The effect of ischemia-induced epithelial cell loss. Virchows Archiv. (Cell Pathol.), 31:15, 1979.
35. Price, A.B.: Benign lymphoid polyps and inflammatory polyps. In Morson, C. V. (Editor): The Pathogenesis of Co- Iorectal Cancer. Plfiladelphia, W. B. Saunders Company, 1978, pp. 33-37.
36. Enterline, H. T.: Pathology of the gastrointestinal tract: polyps and cancer of the large bowel. Curr. Top. Pathol., 63:97, 1976.
37. Williams, G. T., Arthur, J. F., Bussey, It. J. R., and Morson, B.C.: Metaplastic polyps and polyposis of the colorectum. Histopathology, 4:155, 1980.
Department of Pathology Long Island Jewish-ltillside Medical Center
New Hyde Park, New York 11042 (Dr. Lipper)
SYSTEMIC MASTOCYTOSIS ASSOCIATED W I T H GENERALIZED O S T E O P E N I A Histopathological Characterization of the Skeletal Lesion Using Undecalcified Bone f rom Two Patients
Michael D. Fallon, M.D.,* Michael P. Whyte, M.D.,~f and Steven L. Teitelbaum, M.D. +
Abstract
A h h o u g h mas t cell p ro l i f e r a t i on in t i le b o n e m a r r o w f r e q u e n t l y occurs in systemic mas- tocytosis a n d is o f t e n associated with r ad iog raph i ca l l y de tec tab le b o n e lesions, the pa tho log ic cor re la tes o f the skeletal a b n o r m a l i t i e s are poor ly cha rac te r i zed . We t h e r e f o r e e x a m i n e d t h r ee nondeca l c i f i ed t rans i l iac crest b iopsy s p e c i m e n s f r o m two pa t i en t s with systentic mastocytosis a n d d i f fuse o s t e o p e n i a with ve r t eb ra l c r u sh f rac tures . M a r r o w i n v o l v e m e n t i n c l u d e d u n u s u a l nmst cell aggrega tes , as r evea led by m e t a c h r o m a t i c s t a in ing , tha t m i m i c k e d g r a n u l o m a s . His-
Acceptedafor publication October 6, 1980.
Study supported in part by NIH training grant AM-07033, CRC grant RR-00036, NIH grant AM-11674, and a grant- in-aid from the Shriners Hospitals for Crippled Children (St. Louis Unit).
Presented in part at the First Annual Scientific Meeting of the American Society for Bone and ~ Mineral Research, Anaheim, California, June 11-12, 1979.
* Instructor in Pathology, Washington University School of Medicine. Chief Resident, Department of Pathology, The Jewish Hospital of St. Louis, St. Louis, Missouri.
t Assistant Professor of Medicine, Department of Medicine, Division of Bone and Mineral Metabolism, Washington University School of Medicine. Assistant Professor, Department of Medicine, The Jewish tlospital of St. Louis, St. Louis, Missouri.
~; Associate Professor of Pathology, Department of Pathology, Division of Bone and Mineral Metabolism, Washington University School of Medicine. Associate Pathologist, Department of Pathology, The Jewish Hospital of St. Louis, St. Louis, Missouri.
HUMAN PATHOLOGY--VOLUME 12, NUMBER 9 September 1981 8 l 3

HUMAN PATIIOLOGY~VOLUME 12, NUMBER 9 September 1981
tomorphometric analysis of trabectflar bone revealed accelerated bone remodeling or "turn- over" characterized by osteoidosis, peritrabecular fibrosis, increased numbers of osteoblasts and osteoclasts, and an increase in osteoclastic resorbing surfaces.
Our observations and review of the literature suggest that with the recent development of techniques for assessing undecalcified bone biopsy specimens, mastocytosis will probably be shown to be a more common etiology in "osteoporosis" than previously recognized. Meta- chromatic staining of the biopsy specimen should be a routine procedure in the investigation of any patient who undergoes diagnostic bone biopsy.
"Mastocytosis" is a generic term used to describe the spectrum of disorders characterized by a prolif- eration of tissue mast cells. "Mastocytoma" and "ur- ticaria pigmentosa" generally refer to the unifocal and multifocal accumulation of dermal mast cells, respec- tively, whereas "systemic mastocytosis" denotes pro- liferation of mast cells in the viscera---especially liver, spleen, lymph nodes, gastrointestinal tract, and b o n e )
Approximately 70 per cent o f the patients with systemic mastocytosis develop radiographically de- tectable bone lesions. 2 The most common abnormality has been reported to be diffuse, poorly demarcated, sclerotic and lucent areas involving the axial skele- ton. 2'3 Circumscribed lesions, especially of tile skull and extremities, are also well documented. Although generalized osteopenia alone has been reported, it is believed to be a less common radiographic finding. ~'5
Because the histologic evaluation of bone in- volvement in systemic mastocytosis is generally lim- ited to bone marrow aspiration and not biopsy, tile pathologic correlates of the skeletal radiographic ab- normalities are poorly characterized. We report light and electron microscopic findings in undecalcified iliac crest bone in two women with diffuse osteopenia and compression fractures associated with systemic mastocytosis. Our observations and review of the lit- e ra ture suggest that generalized osteopenia and fracture may be a common presentation of systemic mastocytosis.
CASE REPORTS
Case 1
A 61 year old Caucasian spinster gave a history of increasing allergic symptoms and recurrent episodes of nausda, vomiting, and abdoufinal discomfort dur- ing adulthood. At age 50 she sustained the first of several vertebral compression fractures. Five years later her physician noted a faint hyperpigmented macular dematosis on her thorax and upper abdo- men. Circulating eosinophilia (~11 per cent) lind been unexplained for about 15 years. She was re- ferred to us at age 60 when an iliac crest bone biopsy specimen reported.ly showed "eosinophilic granulo- mas." No medicat ions had been taken for four months prior to study. Physical examination revealed a kyphotic woman without lymphadenopathy or or- ganomegaly. Numerous faint brownish macules were noted on her back, but they did not urticate (Darier's
814
sign negative). Laboratory studies confirmed the eosinophilia. A review of radiographs taken during tile decade before admission showed rapidly increas- ing generalized osteopenia and vertebral compression fractures but no discrete osteolytic or osteosclerotic areas suggestive of systemic mastocytosis. Biopsy of the area of dermatosis and small intestine revealed a modest increase in mast cells. Following a three day course of Declomycin hydrochloride (300 rag. twice daily) the patient underwent an iliac crest biopsy two days after her last dose of tetracycline (biopsy 2). Specimens from the iliac crest biopsy performed b~, her referring physician were available for review (biopsy 1).
Case 2
A 58 year old Caucasian woman fractured the neck of the left femur with minimal trauma at age 51. Subsequently she sustained multiple vertebral com- pression fractures. Asymptomatic dermatosis had developed about two years before study. One month before admission she bad sustained a spontaneous rib fracture. She denied allergic or gastrointestinal symptoms. Physical examination revealed a kyphotic woman with a profuse brown-red ntaculopapular rash, predominantly on the trunk, which did not ur- ticate. Routine laboratory studies were remarkable only because of a 5 per cent circulating eosinophilia value. Radiographic studies showed di f fuse os- teopenia with vertebral collapse. Skin biopsy findings were consistent with urticaria pigmentosa. Open wedge biopsy of the iliac crest was performed without prior tetracycline administration.
M E T H O D S
Light Microscopy Bone biopsy specimens were placed in buffered
formalin fixative, dehydrated in acetone, embedded in methyl methacrylate, cut into undecalcified sec- tions (5 /~m.) on a J u n g model K sledge micro- tome, and then ei ther were stained by one of tile following techniques--modified Masson trichrome, Goldner, toluidine blue, or Geimsa6--and examined by routine light microscopy, or were acid decalcified, stained with hematoxylin and eosin, and then exam- ined with polarized light microscopy. Fluorescent tetracycline labels were observed in undecalcified, unstained, 10 #m. sections. Tile following histomor-

SYSTEMIC MASTOCYTOSIS WITH GENERALIZED OSTEOPENIA--FALt,OX eT AL.
phometr ic parameters were quanti tated with either a Merz-Schenk integrating eyepiece or a linear reticule and then compared to data f rom 16 normal indi- viduals evaluated in our laboratory in a similar fash- ion: r
1. Total bone volume (%)--the percentage of marrow space occupied by trabecular bone tissue (mineralized and nonmineralized bone).
2. Relative osteoid volume (%)--the percentage of trabecular bone tissue that is unmineralized, i.e., osteoid.
3. Total osteoid surface (%)~the percentage of t-rabecular bone surface covered by osteoid.
4. Osteoblastic osteoid surface (%)--the percentage of ("active") trabecular bone surface covered by osteoid that is lined by typical pluntp osteoblasts.
5. Mean osteoid seam width (/mt,)--the average width of the osteoid seams on the trabecular bone surface, a deci- mal value obtained by dividing the relative osteoid volume by tlte absolute linear extent of osteoid over tim trabecular surface.
6. Osteoclasts per sq. mm. of trabecular bone. 7. Osteoclastic resorbing surface (%)--the percentage
of trabecular bone surface with osteoclasts in apposition to resorption bays (Howship's lacunae).
8. Nonosteoclastic resorbing surface (%)--the per- centage of trabecular bone surface containing resorption bays not in apposition to osteodasts.
9. Fibrous tissue surface (%)~the percentage of trabecular bone surface covered by fibrous tissue.
Additionally, the n u m b e r and location o f mast cell "granulomas" were recorded. In areas o f marrow outside the granulomas, the identity o f tim cells in 10 groups o f 100 nucleated cells each were noted, and tim mean n u m b e r o f mast cells per 100 cells was calcu- lated.
Electron Microscopy
Electron microscopy o f material previously em- bedded in methyl methacrylate was pe r fo rmed as follows: Thick sections (50/tm.) were placed in xylene at 65 ~ C. for 24 to 48 bours to remove the plastic. Sections were then rehydra ted and decalcified in a 7 per cent versene--2 .5 per cent glutaraldehyde solu- tion and postfixed in osmium tetroxide. Following ser ia l a l coho l i c d e h y d r a t i o n , sec t ions w e r e re- embedded in Araldite, cut on a d iamond knife, and stained with uranyl acetate and lead citrate. 8
RESULTS
Routine Microscopy
In tile undecalcified bone biopsy specimens f rom each case, the mar row contained multiple nodules resembling granulomas, 0.15 to 0.45 mm. in diame-
Figure 1. Typical osseous change associated with'mast .cell granulomas. Plump osteoblasts (arrows) lind osteoid seams (white arrow- heads). Peritrabecular fibrosis (F) is associated with a nest of mast cells (square). Osteoclasts (black arrowheads) are associated with scalloped bone margins. Patient I, biopsy 2. InSet, Detail of area corresponding to square showing nest of mast cells adjacent to bone. (Modified Masson trichrome stain. Original magnification • 100. Inset, Toluidine blue stain. Original magnification x400.)
815
- �9 �9 ~ -, .
~..:-~ .- .- ,_ ' ,~* ~.~'~ . .. . . . . , , , _ . , : ;
i + ~ ~ : d + ~+ " , " ~ ~ " +~'dl t '~ " " ' ~ +: , 'o~. - ~ : ,~ " ' d k :: '" " " : ' " . - ~ a " ", . . . . r ~ , " ~ . , . - - r I~ : +
r . :
r ~ O ' + _ ~ ' ~ - ; - ~II , ~ _ ; . . ~ . v . . . . . +:+ + +_
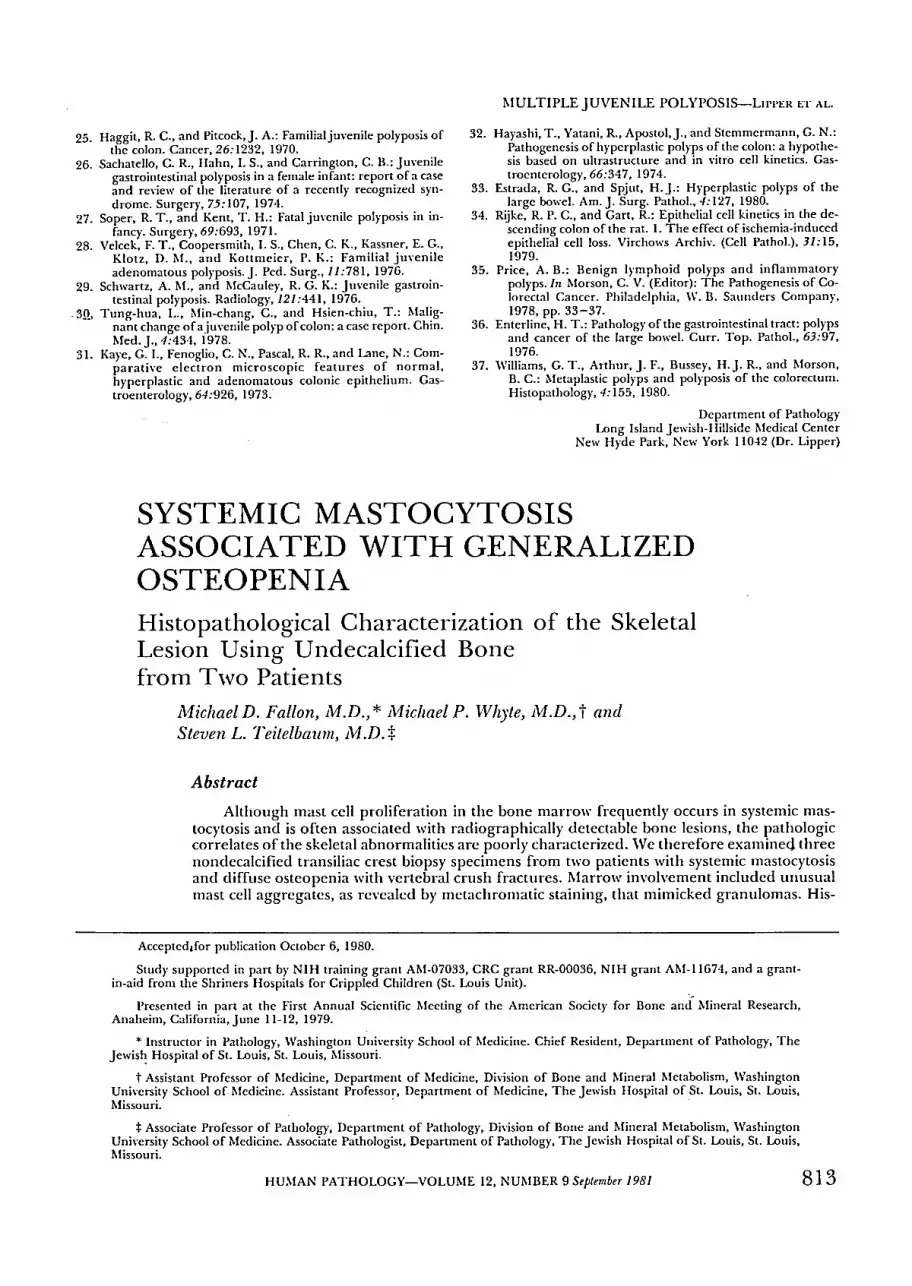
Figure 2. A perivascular mast cell gra,mloma. Spindle shaped and oval mast cells with (lark staining cytoplasmic granules (arrows). Eosinophils are present, but the granules are faint. Patient 1, biopsy 2. (Geimsa stain. Original magnification x250.)
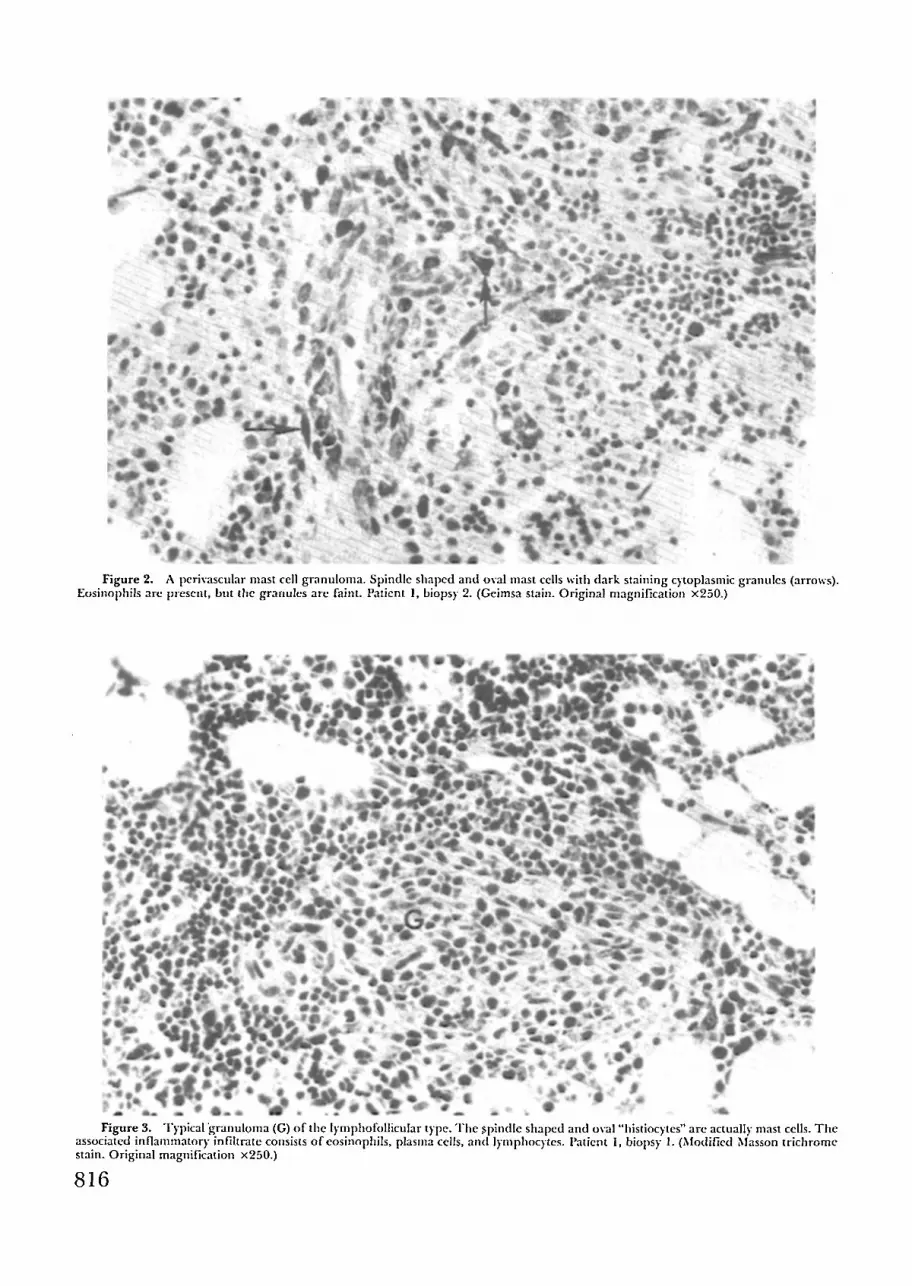
Figure 3. Typical granuloma (G) of tile lymphofollicular type, Tile ~l)indle shaped and oval "histiocytes" are actually mast cells. Tile associated inflammatory infihrate consists of eosinophils, plasma cells, and lymphocytes. Patient 1, biopsy 1. (Modified Masson trichrome stain. Original magnification x250.}
8 1 6

TABLE 1.
SYSTEMIC MASTOCYTOSIS WITH GENERALIZED OSTEOPENIA--FALLO,~ ET AL.
MAST CELL " G R A N U L O M A S ' : N U M B E R A N D L O C A T I O N IN ILIAC CREST B O N E FROM TWO W O M E N W I T H SYSTEMIC MASTOCYTOSIS
Subject
Tota l No. Mast Cell Mast Cel ls
Total Area T y p e Mast Cell Granu lomas Observed '~'~~ Granu lomas per 100 Counted (sq. mm.) Perivascular Follicular Perisinusoidal Peritrabecular per sq. mm. Marrow Cel l s
Case 1 Biopsy 1 Biopsy 2
Case 2
27.32 4 7 2 5 0.66 25.8 -+ 8.6 23.41 2 1 0 7 0.43 27.8 -+ 6.4
24.07 3 0 3 6 0.50 36.3 -+ 5.5
- . * M e a n -+ S.E.M. Nortnal, 0-107
ter, consis t ing o f collections o f oval and spindle shaped mast cells, eosinophils, lymphocytes , and plasma cells (Figs. 1, 2). The granulomatous appear- ance o f these nodules was due to the presence o f ag- gregated epitheloid and spindle shaped cells resem- bling histiocytes and fibroblasts, respectively. However, these cells contained metachromatically staining cyto- plasmic granules typical o f mast cells. These "granu- lomas" were distributed in four histological patterns (Table 1): 9a~
1. Peritrabecular--the most frequently observed pattern---consisted of nodules of mast cells with little as- sociated inflammatory infiltrate (Fig. 1, inset).
2. Perivascular--vasocentric "granulomas" (Fig. 2). 3. Lymphofollicular~mast cell granulomas associated
with a centrally or peripherally placed lymphoid follicle (Fig. 3).
4. Perisinusoidal---crescent shaped "granulomas" lin- ing sinusoidal spaces (the least frequently observed pat- tern).
T h e marrow also contained numerous scattered solitary oval and spindle shaped mast cells as well as aggregates o f four to five mast cells. Mast cells com- posed 26 to 36 per cent o f the nucleated marrow cells (Table 1). Other marrow elements were qualitatively and quantitatively normal.
Both cortical and trabecular bone showed evi- d e n c e sugges t ive o f acce le ra t ed bone t u r n o v e r characterized by elevated values for the histomor- phometr ic parameters o f bone format ion and re- sorption (Table 2; Fig. 1). Many trabeculae were lined by osteoid seams (resulting in increased relative os- teoid volume and total osteoid surface values). In both patients osteoid seams were always less than three lamellae wide and the mean osteoid seam width
was less than 7 #m.---cvidence against a mineraliza- tion defect, n Excessive osteoid lined by osteoblasts (osteoblastic osteoid surface) suggested an increase in the number o f bone forming units, while the presence o f a prominent nucleolus and perinuclear clear zone in the osteoblasts suggested increased cellular activity. Peritrabecular fibrosis--a frequently seen but non- diagnostic feature o f increased bone turnover- -was present in all three biopsy specimens. With special stains some of the spindle shaped cells in the fibrous tissue were found to be mast ceils (Fig. 4). Cortical and trabecular bone contained irregular scalloped margins, and osteoclasts were readily apparent (Table 2). Peritrabecular granulomas were associated with both large excavated resorption bays and areas of new bone formation (Fig. I, inset). Individual mast cells were found adjacent to osteoclasts as well as osteo- blasts. When viewed by polarized light, all bone was lamellar. Fluorescence microscopy o f the second biopsy specimen from case 1 showed an increased surface extent of discrete linear tetracycline labels, confirming the impression o f increased bone synthe- sis and excluding a mineralization defect.
Electron Microscopy
Although the majority o f the patients' mast cells were spindle shaped, they showed ul t ras t ructura l features similar to both normal mast cells and those observed in other tissues in mastocytosis (Fig. 5). n The cytoplasm contained variable numbers of round to oval, electron dense granules with either a fine or coarse g r a n u l a r i n t e r n a l s t r uc tu r e . However , a lamellar or scroll-like internal structure, seen in nor- mal mast cell granules, was not observed. The sur-
TABLE 2. H I S T O M O R P H O M E T R I C ANALYSIS OF ILIAC CREST B O N E FROM T W O W O M E N W I T H SYSTEMIC MASTOCYTOSIS*
Surface
Fibrous Total Relative Total Osteoblastlc Mean Osteoid Osteoclasts Non-osteoclastic Osteoclastic Tissue Bone Osteoid Osteold Osteold Seam Width per sq. ram. Resorbing Resorbing Surface
Volume (%) Volume (%) Surface (%) Surface (%) (#m.) Trabecular Bone Surface (%) Surface (%) (%)
Controls i 1.3-37.2 0.0-3. i 0.0-24.5 0.0-3.7 0-24 0-0.38 0-4.60 0-0.54 0.0 Case 1
Biopsy 1 9.3t 3.9t 26.8 4.4t 6.9 0.4It 2.75 0.45 21.8t Biopsy 2 9.2t 9.0t 43.4t 6.4t 4.8 0.5It 3.47 0.99t 44.0t
Case 2 4.7t 4.1 t 26.6t 3. ! 6.6 0.27 0.62 0.31 4.0t
* The normal range (mean -+ 2 S.D.) fo? each histomorphometric parameter (16 control subjects) is given at the top of each column. t Abnormal result.
817

• p • q p � 9 .~ . - ~ " v �9 , i . - , u m r j - �9 m
. , ~ . , t ~ , 0 �9 o . . . " d .1~ ~ ' m , ~, = ~ ~ ~ / " w . "
~ . B.W, , _j # � 9 ~ ~ ~ �9 *el- f tl~ , Q ~r 0 I1�9 m qk.
-qD ~ ' ,~.. , o �9 �9 �9 ,J . . . . . _ . l t l l " - ~"~-" 'Ilk ~ " qb , , . ~, �9 "@ qk ~ " . .
"-- . . . . . . w ~I~." i.m - " ,m~ , o ~ ~,- �9
. _ ~" 7 l " h 0
1 r ~ ~- l~a~ " " ~,
e~,- "" " 1;.,.~'~-~4 �9 " 4 ~ . - ~ ~ .
, . . . . ~;~, , , ,
F i g u r e 4. P e r i t r a b e c u l a r f ibros is (F). T h e s p i n d l e s h a p e d cel ls w i t h d a r k c y t o p l a s m i c g r a n n i e s a r e m a s t cel ls (a r rows) . O s t e o b l a s t s ( a r r o w h e a d s ) a r e fomad a d j a c e n t to t he b o n e (B). Pa t i en t 2. ( T o l u i d i n e b l u e s ta in . O r i g i n a l m a g n i f i c a t i o n •
F i g u r e 5. E l e c t r o n m i c r o g r a p h o f s p i n d l e s h a p e d m a s t cell. N o t e e l e c t r o n d e n s e g r a n u l e s (G), m i t o c h o n c l r i a (M), a n d f i l a m e n t o u s c y t o p l a s m (ar rows) . G r a n u l e s l ack t i l e sc ro l l - l ike o r l a m e l l a r i n t e r n a l s t r t l c t u r e . Pa t i en t 1, b iopsy 2. ( U r a n y l a c e t a t e a n d l ead c i t r a t e s ta in . O r i g i n a l m a g n i f i c a t i o n • 13,000.)
8 1 8

S Y S T E M I C M A S T O C Y T O S I S W I T H G E N E R A L I Z E D OSTEOPENIA--F ,xHx) .~ E'r AL.
r o u n d i n g cytoplasm was f i l amentous . A b u n d a n t numbers of mitrochondria and ribosomes were also present.
DISCUSSION
In systemic'mastocytosis, needle aspiration o f bone marrow tins often shown increased numbers o f mast cells, consti tuting 2 to nearly 100 per cent o f the nucleated marrow cells. 3 However, despite the prev-
a lence o f skeletal abnormalities noted radiographi- cally, the histopathologic changes in bone are not well characterized. This may be due in part to technical limitations imposed by routine decalcification o f bone specimens, a process that can destroy mast cell mor- p h o l o g y and obscu re the d e l i n e a t i o n b e t w e e n mineralized and unmineralized bone matrix. In both our patients undecalcified iliac crest biopsy specimens revealed excessive numbdrs of mast cells compared to normal cells and unusual nmrrow "granulomas" con- sisting in large part o f spindle shaped mast cells, and bistologic evidence o f accelerated bone turnover with peritrabecular fibrosis. This informat ion enabled us to establish a diagnosis of systemic mastocytosis. Sub- sequently our review of the literature suggested that there could be considerable confusion regarding the clinical significance o f our findings.
In 1956 Stark and coworkers 13 were the first to report the lfistopathologic features of a radiographi- cally discernible bone lesion in mastocytosis. The i r patient lind a de rmopa thy consistent with urticaria p igmentosa and diffuse skeletal abnormali t ies on radiographic study. Affected ribs contained multiple small rarefied loci visible on x-ray examination. His- topathologic s tudy o f a rib biopsy specimen revealed granulomas and evidence o f osteoid deposition and active bone resorption. Most of the cells in the gran- ulomas were unusua l slender, spindle shaped, or stellate mast cells. Stark proposed the term "mast cell g ranuloma" to describe these unusual nodula r le- sions. Because o f the distinctive granulomatous ap- pea r a nc e o f these mast cell agg rega t e s , we have cont inued to use the term "mast cell g ranuloma" as originally suggested by Stark. ~3 In 1968 Barer et al. ~a described the bone biopsy findings in two patients whose radiographically discernible abnormalities re- sembled those o f dissenfinated metastatic disease. Mast cell granulomas similar to those repor ted by Stark et al. were Jaoted in one patient on sternal mar- row aspiration and in another on cure t tement o f a lyric focus in the ilium. Despite these two reports showing mast cell granulomas in the skeletal lesions o f patients with "urticaria pigmentosa," most reports concerning systemic mastocytosis describe marrow infiltration by typical mast cells either without bone abnormalities or, more commonly, with marrow fi- brosis and trabecular sclerosis? 5-~r According to the
. older literature, spindle shziped mast cell granulomas would not appear to be a common abnormali ty in systemic mastocytosis.
Recen t ly ev idence has been p u b l i s h e d tha t
suggests that mast cell granulomas, and indeed sys- temic mastocytosis , may be more c o m m o n than realized previously. In 1972 Rywlin et al. 9 described an "eosinophilic fibrohistiocytic lesion of bone mar- row" in five patients who were being investigated for unexplained eosinophilia. In all five patients bone marrow aspirations from the posterior iliac spine or s t e rnum revealed lesions consist ing o f fibrohistio- cytes, numerous eosinophils, some plasnm ceils, and "occasional"-mast cells. Because the lesions occasion- ally regressed after medications were stopped, the marrow lesions were a t t r ibuted to probable d r u g hypersensitivity. However, in 1978 te Velde et al. I~ reported seven patients with generalized osteopenia in whom bone marrow biopsy revealed nodular infil- trates consisting of elongated mast ceils, eosinophils, plasma cells, and varying numbers of lymphocytes. Only one showed urticaria pigmentosa; the other six had no abnormalities to suggest mastocytosis. These authors believed that the lesions observed were the same as those described by Rywlin and that the true nature o f the "fibrohistocytes" (mast cells) noted by Rywlin had been obscured by technical factors. Te Velde considered that his patients had a new form o f mastocellular disease, because their review of the lit- erature failed to include the observations of Stark et al? 3 and Barer et al. 14 Since visceral involvement without cutaneous lesions has been reported in sys- temic mastocytosis," we suggest that te Velde's pa- tients, and probably those o f Rywlin et al., had a form of systemic mastocytosis. In turn, it would appear that generalized osteopenia alone nmy be a common pre- sentation in mastocytosis. T h e lytic foci and diffuse o s t e o p e n i a associa ted with mastocytos is may be media ted by the chemical products o f mast cells. Heparin in particular is a potent in vitro bone re- sorbing agent, ~s and osteopenia has resulted from long term heparin therapy? s Fur thermore , there is ev idence tha t mast cells may play a role in the pathogenesis o f senile osteoporosis3 ~ However, os- teosclerotic loci in systemic mastocytosis are common, and on histologic examination these sites show ap- pos i t i ona l new bone f o r m a t i o n and t h i c k e n e d trabeculae3 ~ As in our patients, active bone forfl'mtion was evident but was apparent ly overcome by a con- comitant acceleration o f bone resorption, which re- sulted in a decreased skeletal mass.
With the recent development of teclmiques for closed lilac crest biopsy and histopathologic assess- ment o f undecalcified bone specimens, mastocytosis will probably be shown to be a more common etiology for diffuse "osteoporosis" than recognized previously. Me t a c h r o ma t i c s ta in ing o f tffe biopsy spec imen should be a routine procedure in the investigation o f any patient who undergoes bone biopsy in investiga- tion o f metabolic bone disease.
ACKNOWLEDGMENTS
We are grateful to Michele Bergfeld for some of tile histomorphometric measurements and to Jane Wodicker and Frances Ledbetter for expert secretarial help.
819

I I U M A N I ' A T I I O I . O G Y - - V O L U M E 12, N U M B E R 9 September 1981
R E F E R E N C E S
I. Szweda, J .A. , Abraham, J. P., Fine, G., Nixon, R. K., and Rupe, C. E.: Systemic mast cell disease. A review and report of three cases. Am. J. Med., 32:227-239, 1962.
2. Poppel, M. H., Gruber, W. F., Silber, R., Ilolder, A. K., and Christman, R. O.: The roentgen manifestations of urticaria p igmentosa (mastocytosis). Am. J . Roentgenol . , 82:239-248, 1959.
3. Sagher, F., and Evan-Paz, Z.: Mastocytosis anti the Mast Cell. Chicago, Year Book Medical Publishers, 1967.
4. Hirsou, C.: Urticaria pigmentosa with disseminated mas- tocytosis controlled with chlorambucil. Proc. R. Soc. Med., 58:697, 1965.
5. Ires, D. R., and Thompson, D. M.: Urticaria pigmentosa with spinal osteoporosis. Proc. R. Soc. Med., 66:175-176, 1973.
6. Whyte, M.P., Teitelbaum, S.L., Murphy, W.A., Bergfeld, M. A., and Avioli, L. V.: Adult hypophosphatasia, clinical, laboratory and genetic investigation of a large kindred with review of the literature. Medicine, 58:329-346, 1979.
7. Hruska, K. A., Teitelbaum, S. L., Kopelman, R., Richardson, C. A., Miller, P., Debnam,J., Martin, K., and Slatopolsky, E.: The predictability of the histologic features of uremic bone disease by non-invasive technique. Metabol. Bone Dis. Rel. Res., 1:39-44, 1978.
8. tl)'att, M.: Principles and Techniques of Electron Microscopy. Vol. 1: Biological Applications. New York, Van Nostrand Reinhold Company, 1970.
9. Rywlin, A. M., Iloffman, E. P., and Ortega, R. S.: Eosiuophilic fihrohistiocytic lesion of bone marrow: a distinctive new morphologic finding, probably related to drug Iwpersen- sitivity. Blood, 40:464-472, 1972.
10. te Velde, J., Vismans, F . J .F .E . , Leenheers-Binnendijk, L., Vos, C . J . , Smeenk, D., and Bijvoet, O . L . M . : T h e eosinophilic fibrohistiocytic lesion of the bone marrow. A
mastocellular lesion in bone disease. Virchows Arch. (Pathol. Anat.), 377:277-285, 1978.
11. Ellis, H.A., and Peart, K.M.: Quantitative observations on mineralized and non-mineralized bone in the iliac crest. J. Clin. Path., 25:277-286, 1972.
12. Spjut, l l .J . , Dorfman, It. D., Bechner, R. E., and Ackerman, L. V.: Tumors of Bone and Cartilage. Washington, D.C., Armed Forces Institute of Pathology, 1971, pp. 244-248.
13. Stark, E., Van Buskirk, F. W., and Daly, J. F.: Radiologic and pathologic bone changes associated with urticaria pigmen- tosa. Arch. Pathoh, 62:143-148, 1956.
14. Barer, M., Peterson, L. F. A., Dahlin, D. C., Winkelmann, R. K., and Steward, J. R.: Mastocytnsis with osseous lesions resembling metastatic malignant lesions in bone. J. Bone Joint Surg., 50A: 142-152, 1968.
15. Bendel, W. L., and Race, G. J.: Urticaria pigmentosa with bone involvement. J. Bone Joint Surg., 45A:1043-1056, 1963.
16. Havard,C. W. tt., and Scott, R. B.: Urticaria pigmentosa with visceral and skeletal lesions. Quart. J. Med., 28:459-,t69, 1959.
17. Sagher, F., Cohen, C., and Schorr, S.: Concomitant bone changes in urticaria pigmentosa. J. Invest. Dermatol., 18:425-.t32, 1952.
18. Goldhabcr, P.: }teparin enhancement of factors stimulating bone resorption in tissue culture. Science, 147:407-409, 1965.
19. Griffith, G. C., Nichols, G., Asher, J. D., and Flanagan, B:: tteparin osteoporosis. J.A.M.A., 193:91-94, 1965.
20. Frame, B., and Nixon, R. K.: Bone-marrow mast cells in os- teoporosis of aging. N. Engl. J. Med., 279:626-630, 1968.
21. Sagher, F., Liban, E., Ungar, H., and Schorr, S.: Urticaria plgmentosa with bone involvement. Mast cell aggregates in bone and myelosclerosis found at autopsy in a case dying of monocytic leukemia. J. Invest. Dernmtol., 27 :355-368 , 1956.
Department of Pathology The Jewish Hospital of St. Lotfis
216 South Kingshighway St. Ixmis, Missouri 63110 (Dr. Fallon)
820