symptom management of affective and cognitive disturbance with a group of cancer survivors
TRANSCRIPT
Available online at www.sciencedirect.com
SNC
FC
170E©0d
Arc
Symptom Management of Affective andCognitive Disturbance With a Group of
Cancer Survivors
Graham J. McDougall, Heather Becker, Taylor W. Acee,Phillip W. Vaughan, and Carol L. Delville
ponsor's rolT00094731.rom The Uniorresponding0 Red River,-mail addres2011 Elsevi
883-9417/18oi:10.1016/j.
hives of Psyc
Cancer survivors 65 years of age and older experience treatment-inducedmemory impairments. However, clinicians do not intervene for these cogni-tive problems. This article describes the findings from a pilot study of amemory versus health training intervention and its adaptability for cancersurvivors for symptom management.Design and Methods: A convenience sample of older adults was enrolled ina longitudinal study of a memory and health training intervention and testedon five occasions for 2 years postintervention. The memory training wasdesigned to increase cognitive performance, reduce anxiety, decreasenegative attributions, promote health, and increase memory self-efficacy.In this analysis, we included change over time for the first four of the fivedata collection points. We calculated means and standard deviations onthe memory measures for cancer survivors in the intervention (n = 8) andcomparison (n = 14) groups. The analysis consisted of a mixed design ana-lysis of variance comparing the two intervention groups across four periodsfor 12 months.Results: The typical cancer survivor in the sample was a 74-year-old Cauca-sian female; 14% were minorities. Because of the small sample, some of theeffects were not statistically significant. Moderate to large effects wererevealed in everyday and verbal memory performance scores, memory self-efficacy, strategy use, and memory complaints. There were also moderateeffects for group-by-time interactions on the visual memory performancemeasure, the memory self-efficacy measure, the depression, the trait anxi-ety measure, and the complaints subscale. The memory intervention grouptended to improve more than the health training group, although this was notalways consistent. The results suggested that the participants benefitedfrom the memory training intervention.Implications: Clinicians are often at a loss on how to intervene with cancersurvivors who are experiencing cognitive problems following chemotherapytreatment. Evidenced-based interventions for this aspect of symptom man-agement are almost nonexistent. The Cognitive Behavioral Model of Every-
e: None. Trial Registration ClinicalTrials.gov NCT00094731 http://www.clinicaltrials.gov/ct/show/
versity of Texas at Austin, School of Nursing; and Texas State University.Author: Graham J. McDougall, PhD, MN, FAAN, The University of Texas at Austin School of Nursing,Austin, TX 78701.s: [email protected] Inc. All rights reserved.01-0005$34.00/0apnu.2010.05.004
hiatric Nursing, Vol. 25, No. 1 (February), 2011: pp 24–35 24

25AFFECTIVE AND COGNITIVE FUNCTION OF CANCER SURVIVORS
day Memory (CBMEM), derived from Self-Efficacy theory provides an evi-dence-based intervention for symptom management.© 2011 Elsevier Inc. All rights reserved.
THE PREVALENCE OF cognitive deficits isestimated to be 20%–30% among cancer
survivors who received chemotherapy (Tannock,Ahles, Ganz, & van Dam, 2004). More than 6.8million people in the United States are consideredat high-risk for memory impairments and mildcognitive impairment (MCI), both because theyare cancer survivors and because they are morethan 65 years of age (Office of Cancer Survivor-ship, National Cancer Institute, 2005, 2010).Estimates from 2006 indicate that 60% of allcancer survivors are 65 years or older. Anindividual is considered to be a cancer survivorfrom the time of a cancer diagnosis through thebalance of his or her life. Because two thirds ofadults diagnosed with cancer will be alive in 5years, the health and life of a person with a historyof cancer beyond the acute diagnosis and treatmentphase has become of interest to the medical andscientific community. Decreasing cognitive andfunctional ability may lead to a poorer quality oflife and may determine which adults will remainindependent and which will require care andformal services (Ahles et al., 2002; Beer et al.,2006; McDougall, Becker, & Arheart, 2006).Although the risk of developing cognitive impair-ment is 3.5 times higher in patients treated withhigh-dose chemotherapy, the neuropsychologicalside effects of cancer treatment have not beensufficiently treated.
Cancer survivors experience high levels ofdepression, stress, and anxiety associated with thefear that the cancer may return and uncertaintyabout how to interpret and appropriately handlesymptoms (Caplette-Gingras, & Savard, 2008;Segar, Katch, Roth, Garcia, Portner et al., 1998).Psychological needs are the most frequentlyreported and discussed in the literature. Somestudies have demonstrated that cancer survivorsexperience significantly higher levels of psycho-logical morbidity than healthy women (Fann,Thomas-Rich, Katon, Cowley, & Pepping et al.,2008). However, although much has been writtenabout psychological morbidity among patients withcancer, there are very few publications describing
interventions for helping cancer survivors, particu-larly older adult survivors with psychological andemotional issues (Badger, Segrin, Dorros, Meek, &Lopez, 2007; Perkins, Small, Balducci, Extermann,Robb et al., 2007).
COGNITIVE IMPAIRMENT ANDCANCER TREATMENT
Three meta-analyses and one systematic reviewprovide evidence for the cognitive impairmentsexperienced by cancer survivors who receivedchemotherapy. Matsuda et al. (2005) reviewed 10studies of MCI in patients with breast cancer whocompleted adjuvant chemotherapy. The identifiedcognitive symptoms included memory loss, lack ofattention, and concentration difficulties. Theauthors concluded that although the MCI symptomswere transient, they nevertheless took several yearsto disappear. Jansen, Miaskowski, Dodd, Dowling,and Kramer (2005) reviewed 16 studies thatincluded eight cognitive domains. This reviewincluded 996 patients who averaged 48 years ofage (SD = 7.54). Most (84%) of the patients werefemale; 56% of the sample were breast cancerstudies. Although all significant effect sizes were inthe negative direction, consistent with previousmeta-analyses, visual memory was the sole cogni-tive domain that had significant chemotherapy-induced impairment across all comparison types.Falleti, Sanfilippo, Maruff, Weih, and Phillips(2005) reviewed 6 studies that included sixcognitive domains. Their conclusions were thatcognitive impairment occurred in women who hadundergone adjuvant chemotherapy for breast cancerbut that the magnitude of this impairment dependedon the study design.
Anderson-Hanley, Sherman, Riggs, Agocha, andCompas (2003) evaluated 30 studies across sevencognitive domains. The study included patients (n =838) who were on average 49 years of age and 86weeks (SD = 124.1) from either a diagnosis ortreatment. Gender of the sample was not provided,although only 28% of the sample was composed ofbreast cancer studies. Large negative effects weremost pronounced in the three cognitive domains
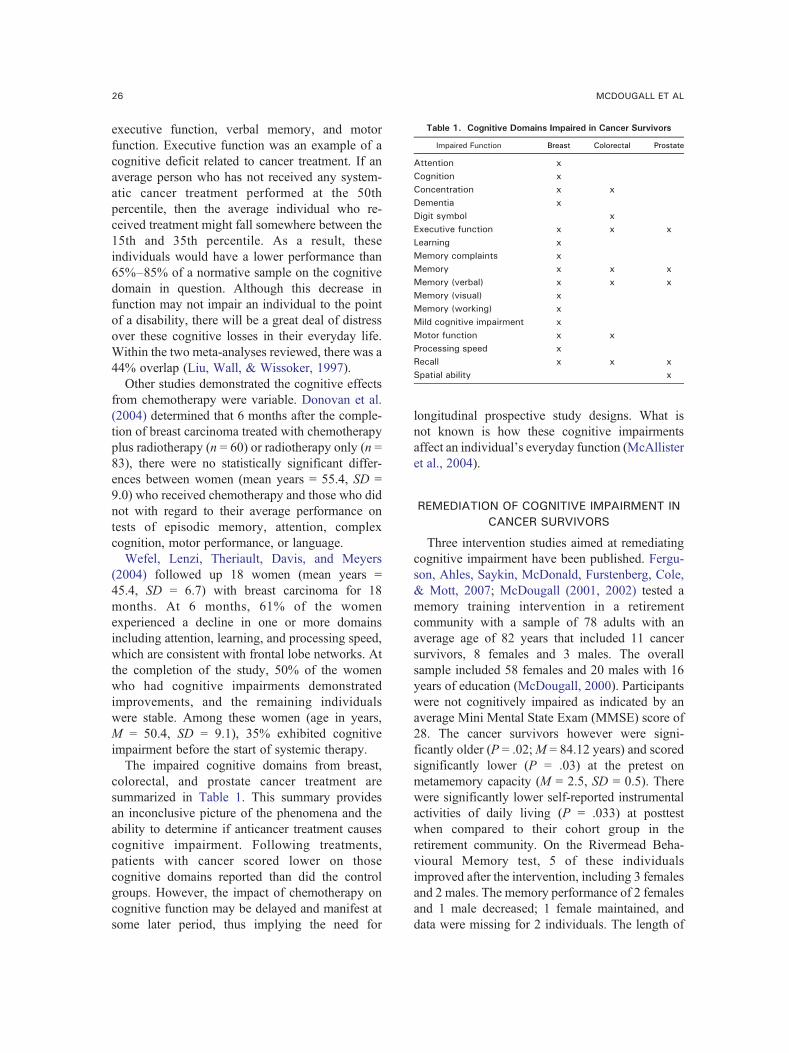
Table 1. Cognitive Domains Impaired in Cancer Survivors
Impaired Function Breast Colorectal Prostate
Attention xCognition xConcentration x xDementia xDigit symbol xExecutive function x x xLearning xMemory complaints xMemory x x xMemory (verbal) x x xMemory (visual) xMemory (working) xMild cognitive impairment xMotor function x xProcessing speed xRecall x x xSpatial ability x
26 MCDOUGALL ET AL
executive function, verbal memory, and motorfunction. Executive function was an example of acognitive deficit related to cancer treatment. If anaverage person who has not received any system-atic cancer treatment performed at the 50thpercentile, then the average individual who re-ceived treatment might fall somewhere between the15th and 35th percentile. As a result, theseindividuals would have a lower performance than65%–85% of a normative sample on the cognitivedomain in question. Although this decrease infunction may not impair an individual to the pointof a disability, there will be a great deal of distressover these cognitive losses in their everyday life.Within the two meta-analyses reviewed, there was a44% overlap (Liu, Wall, & Wissoker, 1997).
Other studies demonstrated the cognitive effectsfrom chemotherapy were variable. Donovan et al.(2004) determined that 6 months after the comple-tion of breast carcinoma treated with chemotherapyplus radiotherapy (n = 60) or radiotherapy only (n =83), there were no statistically significant differ-ences between women (mean years = 55.4, SD =9.0) who received chemotherapy and those who didnot with regard to their average performance ontests of episodic memory, attention, complexcognition, motor performance, or language.
Wefel, Lenzi, Theriault, Davis, and Meyers(2004) followed up 18 women (mean years =45.4, SD = 6.7) with breast carcinoma for 18months. At 6 months, 61% of the womenexperienced a decline in one or more domainsincluding attention, learning, and processing speed,which are consistent with frontal lobe networks. Atthe completion of the study, 50% of the womenwho had cognitive impairments demonstratedimprovements, and the remaining individualswere stable. Among these women (age in years,M = 50.4, SD = 9.1), 35% exhibited cognitiveimpairment before the start of systemic therapy.
The impaired cognitive domains from breast,colorectal, and prostate cancer treatment aresummarized in Table 1. This summary providesan inconclusive picture of the phenomena and theability to determine if anticancer treatment causescognitive impairment. Following treatments,patients with cancer scored lower on thosecognitive domains reported than did the controlgroups. However, the impact of chemotherapy oncognitive function may be delayed and manifest atsome later period, thus implying the need for
longitudinal prospective study designs. What isnot known is how these cognitive impairmentsaffect an individual's everyday function (McAllisteret al., 2004).
REMEDIATION OF COGNITIVE IMPAIRMENT INCANCER SURVIVORS
Three intervention studies aimed at remediatingcognitive impairment have been published. Fergu-son, Ahles, Saykin, McDonald, Furstenberg, Cole,& Mott, 2007; McDougall (2001, 2002) tested amemory training intervention in a retirementcommunity with a sample of 78 adults with anaverage age of 82 years that included 11 cancersurvivors, 8 females and 3 males. The overallsample included 58 females and 20 males with 16years of education (McDougall, 2000). Participantswere not cognitively impaired as indicated by anaverage Mini Mental State Exam (MMSE) score of28. The cancer survivors however were signi-ficantly older (P = .02;M = 84.12 years) and scoredsignificantly lower (P = .03) at the pretest onmetamemory capacity (M = 2.5, SD = 0.5). Therewere significantly lower self-reported instrumentalactivities of daily living (P = .033) at posttestwhen compared to their cohort group in theretirement community. On the Rivermead Beha-vioural Memory test, 5 of these individualsimproved after the intervention, including 3 femalesand 2 males. The memory performance of 2 femalesand 1 male decreased; 1 female maintained, anddata were missing for 2 individuals. The length of

27AFFECTIVE AND COGNITIVE FUNCTION OF CANCER SURVIVORS
time since the completion of active cancer treatmentwas unknown.
Recently, Ferguson et al. (2007) tested whether acognitive–behavioral intervention was effective inmanaging dysfunction in attention and self-reportedmemory problems following chemotherapy inbreast cancer survivors (BCS) with Stage I or IIbreast cancer (Ferguson & Ahles, 2003). In a quasi-experimental pre–post group design, 29 womenparticipated in four in-office monthly visits (30–50 minutes each) and three contacts between visits,for seven total contacts. The participants showedsignificant improvements over baseline in verbaland executive function, self-reported cognitivefunction. Limitations of this study included lackof a control group, an all-Caucasian sample, andvariable cancer diagnoses (Folstein, Folstein, &McHugh, 1975).
SENIORWISE STUDY
This paper reports the outcomes of a memory-training intervention originally developed forcommunity-residing older adults, with a group ofself-identified cancer survivors, and proposes anadaptation of the intervention for cancer survivors.The Cognitive Behavioral Model of EverydayMemory (CBMEM), a conceptual model derivedfrom Self-Efficacy theory, posits that mental frailtyand cognitive vulnerability are influenced bymodifiable risk factors such as health (physicaland emotional) and self-efficacy beliefs, whichinfluence the metamemory and memory perfor-mance relationship. The hypothesis tested in thelarger study was that at-risk older adults in theCBMEM-based memory training interventionwould show significantly better memory self-efficacy, metamemory, memory performance, andbetter function in the instrumental activities of dailyliving than the subjects in the health promotioncomparison condition at postclass (2 months afterbaseline), and these benefits would be maintainedover the remaining four assessment points: post-classroom (2 months), postbooster (6 months),postclassroom follow-up (14 months), and end ofstudy (26 months).
The intervention component of the CBMEMaddresses anxiety, depression, health, metamemory,and memory self-efficacy, which are known toinfluence memory performance (McDougall, 1998,1999, 2009). The memory improvement interven-tion, based on this model, has four components:
stress inoculation, health promotion, memory self-efficacy, and memory strategy training. The intentwas to transfer the learning from the classroom toeveryday experience. The emphasis was on everydaymemory and strategy use. In addition, participantslearn skill building through modeling techniques,observing performance, developing awareness andmastery coping, handling of controlled challenges,and becoming confident and realistic.
SELF-EFFICACY THEORY
Bandura (1997) postulated four principal sourcesof self-efficacy information. Each component of thetheory is proposed in the CBMEM intervention.First, enactive mastery experience is built into thecurriculum so that the exercises increase gentlyfrom less difficult to more difficult. As people beginto feel more competent and comfortable, they wereencouraged to take more risks. Principles of adultlearning were used throughout the program so thatno one is embarrassed or intimidated in front of thegroup, and all relevant experience was discussed.Next, vicarious experiences that alter efficacybeliefs through transmission of competencies andcomparison with the attainments of others wereoperationalized through the group format and groupsharing of the experiences. Third, verbal persuasionand allied social influences to reinforce that onepossesses certain capabilities were operationalizedthrough continual feedback on performance accom-plishments and encouragement for continued prog-ress. Finally, physiological and affective states werepracticed for twenty minutes at the beginning ofeach class with relaxation and stress inoculation.People tend to feel anxious in situations wherecompetence is questioned. Stress inoculation taughtand practiced in subsequent sessions assistedparticipants to deal with stressful cognitive situa-tions in everyday life. Participants were alsoreminded to practice relaxation techniques such astake a few deep breaths at stressful times to alleviatememory anxiety. Specific examples of self-efficacytheory operationalized to the memory trainingcurriculum are described.
During the eight-session classroom componentof the intervention, at least 30 minutes of practicewith memory strategies was allocated within eachclass to strengthen enactive mastery experience, thestrongest component of the self-efficacy theory. Inaddition, an enabling booster session was alsoprovided to enhance perceived self-efficacy and

28 MCDOUGALL ET AL
instrumental activities of daily living. Each memorytraining session began with a twenty-minuterelaxation exercise. The various topics includedmemory and health, memory functions andmechanisms, factors affecting memory for peopleof all ages, memory beliefs and aging, and use ofinternal and external memory strategies. Thememory training was based on self-efficacy theory,and therefore, the use of the female septuagenarianrole model was the intended role model for thatcondition and looked like the participants. She onlytaught the memory training classes. If she had tomiss a training session, the PI taught the class.However, this never occurred. On completion of thestudy, all participants received a copy of thememory improvement book written for older adultsentitled Improving Your Memory (Fogler &Stern, 1994).
Health Training
The curriculum goals for the health group wereto provide a meaningful educational offering, bothto fulfill the purpose of the comparison group and tohold the interest of the participants for 26 months,enough to guarantee their continued involvement inthe project over the period of the study. Consider-ation was given to the need for inclusion of healthtopics with an emphasis on successful aging. As weprogressed through the study, additional healthtopics were added and lectures built around them,as more topics appeared in the news and asparticipants expressed their interest in certainsubjects. We developed lectures that included 18topics covering a wide range of health concernsrelated to successful aging. The health interventionemphasized successful aging based on focusgroups. Topics included Exercise, Spirituality andHealth, Alternative Medicine, Weight Manage-ment, Getting the Most from Your Doctor Visit,Caring for the Caretaker, Healing Foods, DrugInteractions, Osteoporosis, Maintaining Relation-ships, Health Myths, Consumer Fraud, Nutrition,Leisure Activities, Writing Family Stories, HealthMonitoring Tests for Home Use, and Buying Drugsin Foreign Countries. The comparison groupreceived health promotion training.
The curriculum consisted of 18 different healthtopics, which varied by cohort group at differentsites (McDougall et al., 2010). Each health topic wasdelivered in PowerPoint format and received thesame information on the topic across cohort groups.
Handouts were also standardized so that when agroup was presented the health topic they received astandard set of handouts to enhance the content.Each group began with the Alternative Medicinetopic because of its widespread interest to a diversityof people and the media coverage of scientific trialsthat often appeared in the newspaper.
Booster Sessions
The four mandatory, 2-hour booster sessions,were offered weekly for 1 month, for bothexperimental and comparison subjects within 3months of the end of the initial training. They wereintegral to the training and provide a transitionalexperience between the theoretical and practicalconcerns of memory improvement. The goals of thebooster sessions were to boost learning, to enhanceretention and, to assist with transfer of memorystrategies to everyday life. The emphasis of thebooster sessions was on practical everyday memorystrategies needed for instrumental activities of dailyliving (IADL). Individuals were given opportuni-ties to practice strategies that can be incorporatedinto their everyday activities and routines.
The health training group received training innew areas of health promotion not previouslypresented in their earlier eight sessions.
A convenience sample of 267 participants drawnfrom a metropolitan area in Central Texas wasenrolled in the study over a 2-year period. Theirparticipation lasted for 26 months, and they weretested on five occasions during that period. Fromour health questionnaire, it appeared that 44individuals might have been cancer survivors. Toconfirm this self-reported information, we calledeach individual by telephone and asked fivequestions related to their diagnosis, treatment,recurrence, and termination of treatment. Fifteenindividuals did not have cancer, and another 7either dropped out before completing the study orwere not able to be contacted.
The final sample of confirmed cancer survivorsconsisted of 22 individuals. Of those individuals, 5had prostate cancer, 8 had breast cancer, 2 haduterine cancer, 1 had lymphoma and leukemia, 1had throat cancer, 1 had lung cancer, and 3 hadfacial and/or had basal cells on the nose. Of those,59% were female (n = 13) and 86% (n = 19) wereCaucasian, and there were 2 African Americans and1 Hispanic adult. The typical survivor had a mean

29AFFECTIVE AND COGNITIVE FUNCTION OF CANCER SURVIVORS
age of 73.86 years (SD = 4.82 years) with 16 yearsof education. In self-ranking their socioeconomicstatus, 4 individuals (18%) said they had enough forbills and things; 1 had enough for bills and outings(5%); 11 (50%) had enough for bills, things, andoutings; and 6 (27%) had enough not to worry.Length of time from active treatment was unknown.
MEASURES
Verbal memory was tested with the HopkinsVerbal Learning Test-Revised (HVLT-R), whichtests immediate recall, delayed recall, and recogni-tion memory (Brandt, 1991; Benedict, 1997). Test/Retest correlation was .66 for the Delayed RecallSubscale, which was used in these data analyses.
Visual memory was assessed with the BriefVisuospatial Memory Test—Revised (Benedict,1997; Benedict, Dobraski, & Goldstein, 1999).Test/Retest correlation was .72.
The Rivermead Everyday Behavioural MemoryTest was used to assess everyday memory perfor-mance in 12 domains (Cockburn & Smith, 1989;Wilson, Cockburn, Baddeley, & Hiorns, 1989). Foreach subtest, two scores are produced, a pass/failscreening score and a standardized profile score(SPS) with a range from 0 to 24. The analysisreported here used the SPS scores and had alphareliabilities of .73 to .80.
The Direct Assessment of Functional Status(DAFS) is a performance-based measure thatcontains 85 items (Lowenstein et al., 1989, 1992).An adapted version of the DAFS was used in thisstudy with alpha reliabilites of .79 to .84. TheDAFS domains used were time orientation, com-munication abilities, transportation, financial skills,and shopping skills. A fifth domain, that is,medication knowledge, was added for the study.
Anxiety was measured with the State/TraitAnxiety measure had alpha reliabilities of .85 to.92 (Spielberger, Gorsuch, & Lushene, 1970).Alpha reliabilities were .85 and .89.
The Centers for Epidemiologic Studies Depres-sion Scale (CES-D) was used to measure depres-sion had alpha reliabilities of .78 to .87 (Radloff &Teri, 1986). Alpha reliability in this study was .78.
The Metamemory in Adulthood Questionnaire(MIA) measures seven aspects of memory knowl-edge had alpha reliabilities of .84 to .87 (Dixon,Hultsch & Hertzog, 1988). We used the Strategysubscale (18 items), which indicates how oftensomeone uses both internal (elaboration, rehearsal,
etc.) and external memory (lists, notes, etc.)strategies to facilitate their everyday memoryfunction. Alpha reliabilities were .78 and .77,respectively.
Memory complaints were measured with anenhanced version of the change subscale of theMIA (McDougall et al., 2006). The original changesubscale determines individuals' perception of theirmemory abilities as generally stable or subject tolong-term decline. Alpha reliability was .91.
The Memory Self-Efficacy Questionnaire(MSEQ) consists of 50 questions, 5 for each of 10everyday tasks: everyday objects, text details,shopping list, people's names, main points fromstory, digits, line drawings, animal names, tele-phone numbers, and objects (Berry, West, &Dennehey, 1989). Subjects make performancepredictions on self-efficacy level (yes or no) andon strength and confidence in each performanceprediction, from 10% to 100%. In this study, thetext details (B), digits (F), and line drawings (G)subscales were dropped to shorten the time requiredfor the test battery. Alpha reliabilities of the MSEQwere .95 to .96.
FINDINGS
We examined change over time for thoseindividuals who indicated they were cancer survi-vors on the background questionnaire that Senior-WISE participants completed when they entered thestudy. The analysis included only the first four ofthe five data collection points to maximize thesample size. Data used here were collected prior tothe classes, at the end of classes, at the end of thebooster session, and 6 months later. The analysisconsisted of a mixed design analysis of variancecomparing the two intervention groups across fourperiods for 12 months. Means and standarddeviations were calculated for survivors in theintervention (n = 8) and comparison (n = 14) groupsacross the four time points.
Table 2 shows the means and standard deviationsfor survivors in the intervention (n = 8) andcomparison (n = 14) groups across the four timepoints. The last two columns indicate the partialeta2 associated with change across time and thetime-by-group interaction effects. Because of thesmall sample size, some of the moderate effects(i.e., partial eta2 greater than .20) were notstatistically significant, yet they suggest thatmeaningful differences were occurring.
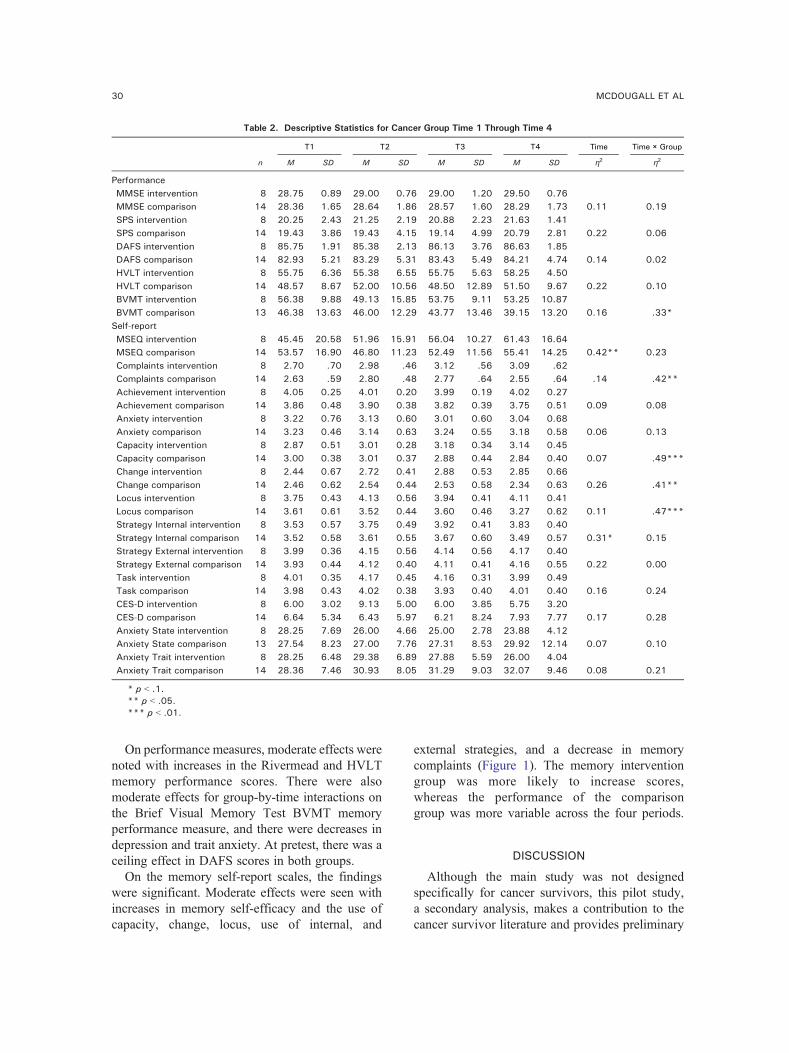
Table 2. Descriptive Statistics for Cancer Group Time 1 Through Time 4
n
T1 T2 T3 T4 Time Time × Group
M SD M SD M SD M SD η2 η2
PerformanceMMSE intervention 8 28.75 0.89 29.00 0.76 29.00 1.20 29.50 0.76MMSE comparison 14 28.36 1.65 28.64 1.86 28.57 1.60 28.29 1.73 0.11 0.19SPS intervention 8 20.25 2.43 21.25 2.19 20.88 2.23 21.63 1.41SPS comparison 14 19.43 3.86 19.43 4.15 19.14 4.99 20.79 2.81 0.22 0.06DAFS intervention 8 85.75 1.91 85.38 2.13 86.13 3.76 86.63 1.85DAFS comparison 14 82.93 5.21 83.29 5.31 83.43 5.49 84.21 4.74 0.14 0.02HVLT intervention 8 55.75 6.36 55.38 6.55 55.75 5.63 58.25 4.50HVLT comparison 14 48.57 8.67 52.00 10.56 48.50 12.89 51.50 9.67 0.22 0.10BVMT intervention 8 56.38 9.88 49.13 15.85 53.75 9.11 53.25 10.87BVMT comparison 13 46.38 13.63 46.00 12.29 43.77 13.46 39.15 13.20 0.16 .33*
Self-reportMSEQ intervention 8 45.45 20.58 51.96 15.91 56.04 10.27 61.43 16.64MSEQ comparison 14 53.57 16.90 46.80 11.23 52.49 11.56 55.41 14.25 0.42** 0.23Complaints intervention 8 2.70 .70 2.98 .46 3.12 .56 3.09 .62Complaints comparison 14 2.63 .59 2.80 .48 2.77 .64 2.55 .64 .14 .42**Achievement intervention 8 4.05 0.25 4.01 0.20 3.99 0.19 4.02 0.27Achievement comparison 14 3.86 0.48 3.90 0.38 3.82 0.39 3.75 0.51 0.09 0.08Anxiety intervention 8 3.22 0.76 3.13 0.60 3.01 0.60 3.04 0.68Anxiety comparison 14 3.23 0.46 3.14 0.63 3.24 0.55 3.18 0.58 0.06 0.13Capacity intervention 8 2.87 0.51 3.01 0.28 3.18 0.34 3.14 0.45Capacity comparison 14 3.00 0.38 3.01 0.37 2.88 0.44 2.84 0.40 0.07 .49***Change intervention 8 2.44 0.67 2.72 0.41 2.88 0.53 2.85 0.66Change comparison 14 2.46 0.62 2.54 0.44 2.53 0.58 2.34 0.63 0.26 .41**Locus intervention 8 3.75 0.43 4.13 0.56 3.94 0.41 4.11 0.41Locus comparison 14 3.61 0.61 3.52 0.44 3.60 0.46 3.27 0.62 0.11 .47***Strategy Internal intervention 8 3.53 0.57 3.75 0.49 3.92 0.41 3.83 0.40Strategy Internal comparison 14 3.52 0.58 3.61 0.55 3.67 0.60 3.49 0.57 0.31* 0.15Strategy External intervention 8 3.99 0.36 4.15 0.56 4.14 0.56 4.17 0.40Strategy External comparison 14 3.93 0.44 4.12 0.40 4.11 0.41 4.16 0.55 0.22 0.00Task intervention 8 4.01 0.35 4.17 0.45 4.16 0.31 3.99 0.49Task comparison 14 3.98 0.43 4.02 0.38 3.93 0.40 4.01 0.40 0.16 0.24CES-D intervention 8 6.00 3.02 9.13 5.00 6.00 3.85 5.75 3.20CES-D comparison 14 6.64 5.34 6.43 5.97 6.21 8.24 7.93 7.77 0.17 0.28Anxiety State intervention 8 28.25 7.69 26.00 4.66 25.00 2.78 23.88 4.12Anxiety State comparison 13 27.54 8.23 27.00 7.76 27.31 8.53 29.92 12.14 0.07 0.10Anxiety Trait intervention 8 28.25 6.48 29.38 6.89 27.88 5.59 26.00 4.04Anxiety Trait comparison 14 28.36 7.46 30.93 8.05 31.29 9.03 32.07 9.46 0.08 0.21
* p b .1.** p b .05.*** p b .01.
30 MCDOUGALL ET AL
On performance measures, moderate effects werenoted with increases in the Rivermead and HVLTmemory performance scores. There were alsomoderate effects for group-by-time interactions onthe Brief Visual Memory Test BVMT memoryperformance measure, and there were decreases indepression and trait anxiety. At pretest, there was aceiling effect in DAFS scores in both groups.
On the memory self-report scales, the findingswere significant. Moderate effects were seen withincreases in memory self-efficacy and the use ofcapacity, change, locus, use of internal, and
external strategies, and a decrease in memorycomplaints (Figure 1). The memory interventiongroup was more likely to increase scores,whereas the performance of the comparisongroup was more variable across the four periods.
DISCUSSION
Although the main study was not designedspecifically for cancer survivors, this pilot study,a secondary analysis, makes a contribution to thecancer survivor literature and provides preliminary
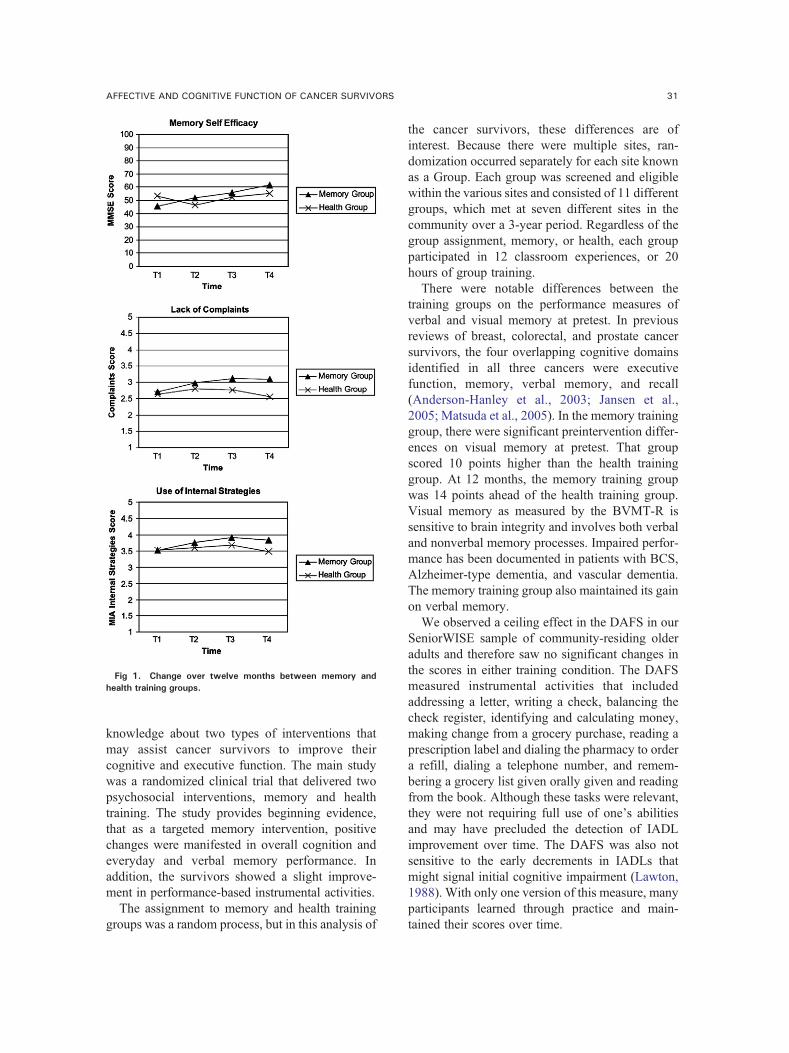
Fig 1. Change over twelve months between memory andhealth training groups.
31AFFECTIVE AND COGNITIVE FUNCTION OF CANCER SURVIVORS
knowledge about two types of interventions thatmay assist cancer survivors to improve theircognitive and executive function. The main studywas a randomized clinical trial that delivered twopsychosocial interventions, memory and healthtraining. The study provides beginning evidence,that as a targeted memory intervention, positivechanges were manifested in overall cognition andeveryday and verbal memory performance. Inaddition, the survivors showed a slight improve-ment in performance-based instrumental activities.
The assignment to memory and health traininggroups was a random process, but in this analysis of
the cancer survivors, these differences are ofinterest. Because there were multiple sites, ran-domization occurred separately for each site knownas a Group. Each group was screened and eligiblewithin the various sites and consisted of 11 differentgroups, which met at seven different sites in thecommunity over a 3-year period. Regardless of thegroup assignment, memory, or health, each groupparticipated in 12 classroom experiences, or 20hours of group training.
There were notable differences between thetraining groups on the performance measures ofverbal and visual memory at pretest. In previousreviews of breast, colorectal, and prostate cancersurvivors, the four overlapping cognitive domainsidentified in all three cancers were executivefunction, memory, verbal memory, and recall(Anderson-Hanley et al., 2003; Jansen et al.,2005; Matsuda et al., 2005). In the memory traininggroup, there were significant preintervention differ-ences on visual memory at pretest. That groupscored 10 points higher than the health traininggroup. At 12 months, the memory training groupwas 14 points ahead of the health training group.Visual memory as measured by the BVMT-R issensitive to brain integrity and involves both verbaland nonverbal memory processes. Impaired perfor-mance has been documented in patients with BCS,Alzheimer-type dementia, and vascular dementia.The memory training group also maintained its gainon verbal memory.
We observed a ceiling effect in the DAFS in ourSeniorWISE sample of community-residing olderadults and therefore saw no significant changes inthe scores in either training condition. The DAFSmeasured instrumental activities that includedaddressing a letter, writing a check, balancing thecheck register, identifying and calculating money,making change from a grocery purchase, reading aprescription label and dialing the pharmacy to ordera refill, dialing a telephone number, and remem-bering a grocery list given orally given and readingfrom the book. Although these tasks were relevant,they were not requiring full use of one's abilitiesand may have precluded the detection of IADLimprovement over time. The DAFS was also notsensitive to the early decrements in IADLs thatmight signal initial cognitive impairment (Lawton,1988). With only one version of this measure, manyparticipants learned through practice and main-tained their scores over time.

32 MCDOUGALL ET AL
In this pilot study, the cancer survivors signifi-cantly improved the subjective aspects of theircognitive function, such as increased confidence,greater capacity, and reduced memory complaints,and improved their control beliefs that theirmemory difficulties were able to be managed. Forexample, on memory self-efficacy, the interventiongroup at pretest scored significantly lower than thehealth training group—an 8-point difference.However, at 12 months, the memory traininggroup was ahead of the comparison group by 6points. Although this was not a significantdifference, the changes over time in the memorytraining group were significant. This gain of 16points represented a notable positive change in thecancer survivors' confidence about their everydaymemory performance.
Participants' self-reported knowledge of memoryvis-à-vis the MIA subscales was a positive outcomeof the intervention. The participants maintainedthese gains at 15 months. Following the inter-vention, the cancer survivors reported using morememory strategies, a compensatory mechanism thatfacilitates the adaption of the individual to thecognitive limitations and losses. Of the two types ofmemory strategies, it was the internal ones thatwere reported being utilized significantly moreoften. Findings from memory research indicate thatolder adults do not use effective acquisitionstrategies and have limited repertoires of alternativememory strategies.
In previous studies, findings pertaining to theassociation between memory strategy use andmemory performance have been equivocal (Devolder& Pressley, 1992; Intons-Peterson & Fournier,1986). Other cognitive aging researchers determinedthere were no differences in strategy use as a functionof causal beliefs for recall, recognition, and appoint-ment-keeping tasks (prospective memory). Theyconcluded that for the older adults despite thedifferences in effort expenditure as a function ofcausal beliefs even, there were no differences instrategy use reported. They concluded that the olderadults were less strategic and believed that theirability was a more important influence on theirperformance than was their use of strategies, whichwas the opposite view of the younger participants.Although the findings were not significant, therewere noticeable differences in anxiety and depressionscores at 14 months. The memory training group ofcancer survivors had lower scores on both measures.
The cancer survivors who represented approx-imately 10% of the sample had many cancerdiagnoses. Further, the generalizability of thefindings is limited due to the convenience samplerecruited for the main study. Nevertheless, thememory training intervention provided participantswith the confidence, knowledge, skills, andsupport necessary to deal with their memoryproblems and consequently their everyday func-tioning. Competing explanations for the changesmay be best addressed by looking at thedemographic characteristics of the two groups.We acknowledge that other differences besidestheir being in the intervention versus healthcomparison group could account for the differ-ences in responses—which is another argument forreplication with a larger sample.
In the Ferguson et al. (2007) intervention, theBCS received 25% of the dose (3 vs. 12 hours)delivered in the SeniorWISE study; however, thetwo samples were substantially divergent in age,gender, and comorbidities. When compared withMcDougall's 2001 study, that study provides amore comprehensive picture of how an interventionmight contribute to the cognitive difficultiesexperienced by cancer survivors (Gonzalez, Fer-rante, Van Durme, Pal, & Roetzheim, 2001).
ESSENTIAL COMPONENTS OR FEATURES OFMODIFIED INTERVENTION
To adapt the content of SeniorWISE for a groupof cancer survivors, we recommend these topics.In Class 1, emphasize Stress and Relaxation anddiscuss the effects of chemo brain and fatigue(i.e., symptoms) on concentration and memoryand ways to cope (Berger & Walker, 2001; Boweret al., 2000; Castellon et al., 2004). Emphasiswould be placed on the importance of beingorganized and on the insidious nature of self-criticism, such as using terms like chemo brain.Further, there is a discussion of the effects ofstress on the body and memory by introducingseveral relaxation techniques and practicing theseat the beginning of each lesson to enhancelearning. Next, define the parts of memory,encoding, recognition, and recall and discussreasons for forgetting. Finally, describe howmemory works, how we put information intoand retrieve it from long-term memory. Provideexercises illustrating the use of cues in memory.

33AFFECTIVE AND COGNITIVE FUNCTION OF CANCER SURVIVORS
In Class 2, the focus would emphasize Memoryand Attributions. Begin with stress inoculation andrelaxation. Next, introduce false beliefs concerningmemory and discuss findings that refute thesebeliefs and changes in memory due to medication-impaired states.
Provide instruction on how to encode informa-tion into long-term memory. Then, offer exercisesillustrating the difficulty of performing dividedattention chores, the ways in which people groupinformation for encoding. Finally, discuss factorsaffecting memory, such as alcohol consumption,grief, medications, and stress. Introduce strategiesto enhance memory function.
In Class 3, the topic would highlight Memoryand Chemo Brain. Begin with stress inoculationand relaxation. Compare the changes in memorythat come with aging to those resulting fromanticancer therapy and ways to protect memory.Next, illustrate the effect of medications andchemotherapy on memory, including nutraceuticalsand vitamins. Finally, illustrate factors affectingmemory in greater depth, including depression andillnesses, and steps to take to forestall depression.Provide exercises on the effects of medications onmemory. Discuss the seven sins of memory.Provide strategies for overcoming negative infor-mation about memory. Provide exercises thatillustrate active observation.
In Class 4, focus primarily on Memory Reme-diation Techniques. Begin with stress inoculationand relaxation, with specific emphasis on thecognitive problems associated with anticancertreatment. Emphasize strategies such as association,elaboration, visualization, and active observationand the best ways to use these techniques ineveryday situations. Next, introduce strategies forremembering more than one thing at a time. Followwith new technologies for memory training.Provide exercises to practice strategies in acontrolled setting.
CONCLUSIONS
Deficits in cognitive function have been docu-mented before and after adjuvant therapy and maybe related to affect or stress as much as neurologicalfactors. How this information will be interpreted topatients is frustrating to clinicians. An interventionmay be intended to improve memory skill orcapacity, memory function in day-to-day living, orparticipant perception of or efficacy for memory
functions, or all of the above. The concerns aboutcognitive difficulties and perceived impairments indaily living related to cognitive deficits, such asdiminished memory skills, are primary concerns ofsurvivors and are components of symptom man-agement (Greiner, Snowdon, & Schmitt, 1996).
Complaints of cognitive impairment followingbreast cancer treatment are well known and havebeen frequently studied, although questions stillexist regarding the prevalence of genuine organicimpairment versus, for example, subjective com-plaints that are not demonstrated on cognitivetesting, sequelae of depression and/or fatigue thatare not related to chemotherapy, or natural age-related deterioration. Regardless of the source ofpatient complaints, interventions that might im-prove cognitive functioning have clear potential toremediate the cognitive losses for that subset ofpatients affected.
IMPLICATIONS
In the booklet, Life After Cancer Treatment(National Institutes of Health, 2004; No. 04-2424),Chapter 3 (Your Mind and Your Feelings afterCancer Treatment) provides tips for improvingmemory and concentration and validates theexperience of many cancer survivors. However,evidenced-based interventions for this aspect ofsymptom management are almost nonexistent.Clinicians are often at a loss on how to withsurvivors intervene for cognitive problems expe-rienced posttreatment. Adult cancer survivorsexperiencing memory problems want to improvetheir everyday memory in specific domains thatare of concern, such as remembering faces andnames, dates and telephone numbers, householdobjects, recent and past events, meetings andappointments, information and facts, and direc-tions. Whether cognitive stimulation or memoryinterventions will alleviate the cognitive difficul-ties experienced by cancer survivors remainsunknown. Based on the inadequate sample sizein this pilot study, we were unable to determine ifthe changes noted were clinically significant. Theresults suggest that cancer survivors can benefitfrom a memory training intervention, whichseemed to have specific impacts on self-reportedmemory measures and visual memory. The Cog-nitive Behavioral Model of Everyday Memory(CBMEM), derived from Self-Efficacy theory

34 MCDOUGALL ET AL
provides one type of evidence-based interventionfor symptom management.
ACKNOWLEDGMENT
Support for this research was provided by NIAGrant R01 AG15384. The findings have beenpresented at the 9th National Conference on CancerNursing Research in 2007 in Hollywood, CA; the4th Annual Conference of the American Psychoso-cial Oncology Society in 2007 in Austin, TX; andthe National Academies Keck Futures Initiative—Future of the Human Healthspan: Demography,Evolution, Medicine, & Bioengineering in 2007 inIrvine, CA.
REFERENCES
Ahles, T. A., Saykin, A. J., Furstenberg, C. T., Cole, B., Mott, L.A, Skalla, K., Whedon, M. B., Bivens, S., Mitchell, T.,Greenberg, E. R., & Silberfarb, P. M. (2002). Neurop-sychologic impact of standard-dose systemic chemother-apy in long-term survivors of breast cancer andlymphoma. Journal of Clinical Oncology, 15(2),485–493.
Anderson-Hanley, C., Sherman, M. L., Riggs, R., Agocha, V. B.,& Compas, B. E. (2003). Neuropsychological effects oftreatments for adults with cancer: A meta-analysis andreview of the literature. Journal of the InternationalNeuropsychological Society, 9(7), 967–982.
Badger, T., Segrin, C., Dorros, S. M., Meek, P., & Lopez, A. M.(2007). Depression and anxiety in women with breastcancer and their partners. Nursing Research, 56(1),44–53.
Bandura, A. (1997). Self-efficacy: The exercise of control. NewYork: W. H. Freeman and Company.
Beer, T. M., Bland, L. B., Bussiere, J. R., Neiss, M. B.,Wersinger, E. M., Garzotto, M., Ryan, C. W., &Janowsky, J. S. (2006). Testosterone loss and estradioladministration modify memory in men. Journal Urology,175(1), 130–135.
Benedict, R. H. B. (1997). Brief Visuospatial Memory Test—Revised: Professional manual. Odessa, FL: Psycholog-ical Assessment Resources, Inc.
Benedict, R. H. B., Dobraski, M., & Goldstein, M. Z. (1999). Apreliminary study of the association between changes inmood and in a mixed geriatric sample. Journal ofGerontology: Psychological Sciences, 54B(2), P94–P99.
Berger, A. M., & Walker, S. N. (2001). An explanatory model offatigue in women receiving adjuvant breast cancerchemotherapy. Nursing Research, 50(1), 42–52.
Berry, J. M., West, R. L., & Dennehey, D. M. (1989). Reliabilityand validity of the Memory Self-Efficacy Questionnaire.Developmental Psychology, 25(5), 701–713.
Bower, J. E., Ganz, P. A., Desmond, K. A., Rowland, J. H.,Meyerowitz, B. E., & Belin, T. R. (2000). Fatigue inbreast cancer survivors: Occurrence, correlates, andimpact on quality of life. Journal of Clinical Oncology,18(4), 743–753.
Brandt, J. (1991). The Hopkins Verbal Learning Test: Develop-ment of a new memory test with six equivalent forms.The Clinical Neuropsychologist, 5, 125–142.
Caplette-Gingras, A., & Savard, J. (2008). Depression in womenwith metastatic breast cancer: a review of the literature.Palliative Support Care, 6(4), 377–387.
Castellon, S. A., Ganz, P. A., Bower, J. E., Petersen, L.,Abraham, L., & Greendale, G. A. (2004). Neurocognitiveperformance in breast cancer survivors exposed toadjuvant chemotherapy and tamoxifen. Journal ofClinical and Experimental Neuropsychology, 26(7),955–969.
Cockburn, J., & Smith, P. T. (1989). The Rivermead BehaviouralMemory Test. Supplement 3: Elderly people. Bury St.Edmunds, Suffolk: Thames Valley Test Company.
Devolder, P. A., & Pressley, M. (1992). Causal attributions andstrategy use in relation to memory performance differ-ences in younger and older adults. Applied CognitivePsychology, 6, 629–642.
Dixon, R. A., Hultsch, D. F., & Hertzog, C. (1988). TheMetamemory in Adulthood (MIA) questionnaire.Psychopharmacology Bulletin, 24(4), 671–688.
Donovan, K. A., Small, B. J., Andrykowski, M. A., Schmitt, F.A, Munster, P., & Jacobsen, P. B. (2004). Cognitivefunctioning after adjuvant chemotherapy and/or radio-therapy for early-stage breast carcinoma. Cancer, 104(11), 2499–2507.
Falleti, M. G., Sanfilippo, A., Maruff, P., Weih, L., &Phillips, K. A. (2005). The nature and severity ofcognitive impairment associated with adjuvant chemother-apy in women with breast cancer: A meta-analysis of thecurrent literature. Brain and Cognition, 59(1), 60–70.
Fann, J. R., Thomas-Rich, A. M., Katon, W. J., Cowley, D.,Pepping,M.,McGregor, B.A.,&Gralow, J. (2008).Majordepression after breast cancer: a review of epidemiologyand treatment. General Hospital Psychiatry, 30(2),112–126.
Ferguson, R. J., & Ahles, T. A. (2003). Low neuropsychologicperformance among adult cancer survivors treated withchemotherapy. Current Neurology and NeuroscienceReports, 3(3), 215–222.
Ferguson, R. J., Ahles, T. A., Saykin, A. J., McDonald, B. C.,Furstenberg, C. F., Cole, B. F., & Mott, L. A. (2007).Cognitive–Behavioral management of chemotherapy-related cognitive change. Psychooncology, 16(8),772–777.
Fogler, J., & Stern, L. (1994). Teaching memory improvement toadults (Rev ed). Baltimore, MD: John Hopkins Univer-sity Press.
Folstein, M. F., Folstein, S. E., & McHugh, P. R. (1975). Mini-mental state: A practical method for grading the cognitivestate of patients for the clinician. Journal of PsychiatricResearch, 2, 189–198.
Gonzalez, E. C., Ferrante, J. M., Van Durme, D. J., Pal, N., &Roetzheim, R. G. (2001). Comorbid illness and the earlydetection of cancer. Southern Medical Journal, 94(9),913–920.
Greiner, P. A., Snowdon, D. A., & Schmitt, F. A. (1996). Theloss of independence in activities of daily living: The roleof low normal cognitive function in elderly nuns.American Journal Public Health, 86(1), 62–66.
35AFFECTIVE AND COGNITIVE FUNCTION OF CANCER SURVIVORS
Intons-Peterson, M. J., & Fournier, J. (1986). External andinternal memory aids: When and how often do we usethem. Journal of Experimental Psychology General, 115(3), 267–280.
Jansen, C. E., Miaskowski, C., Dodd, M., Dowling, G., &Kramer, J. (2005). A meta analysis of studies of theeffects of cancer chemotherapy on various domains ofcognitive function. Cancer, 104(10), 2222–2233.
Lawton, M. P. (1988). Scales to measure competence ineveryday activities. Psychopharmacology Bulletin, 24(4), 609–614.
Liu, K., Wall, S., & Wissoker, D. (1997). Disability andMedicare costs of elderly persons. The Milbank Quar-terly, 75(4), 461–493.
Lowenstein, D., Amigo, E., Duara, R., Guterman, A., Hurwitz,D, Berkowitz, N., Wilkie, F., Weinberg, G., Black, B.,Gittelman, B., & Eisdorfer, C. (1989). A new scale forthe assessment of functional status in Alzheimer'sdisease and related disorders. Journal of Gerontology:Psychological Sciences, 44(4), P114–P121.
Lowenstein, D. A., Ardila, A., Rosselli, M., Hayden, S., Duara,R, Berkowitz, N., Linn-Fuentes, P., Mintzer, J., Norville,M, & Eisdorfer, C. (1992). A comparative analysis offunctional status among Spanish- and English-speakingpatients with dementia. Journal of Gerontology:Psychological Sciences, 47(6), P389–P394.
Matsuda, T., Takayama, T., Tashiro, M., Nakamura, Y., Ohashi,Y, & Shimozuma, K. (2005). Mild cognitive impairmentafter adjuvant chemotherapy in breast cancer patients—Evaluation of appropriate research design and method-ology to measure symptoms. Breast Cancer, 12(4),279–287.
McAllister, T. W., Ahles, T. A., Saykin, A. J., Ferguson, R. J.,McDonald, B. C., Lewis, L. D., & Flashman, L. A.(2004). Cognitive effects of cytotoxic cancer chemother-apy: Predisposing risk factors and potential treatments.Current Psychiatry Reports, 6(5), 364–371.
McDougall, G. J. (1998). Increasing memory self-efficacy andmemory strategy use in Hispanic elders. ClinicalGerontologist, 19(2), 57–76.
McDougall, G. J. (1999). Cognitive interventions among olderadults. Annual Review of Nursing Research, 17,219–240.
McDougall, G. J. (2000). Memory improvement in assisted livingelders. Issues in Mental Health Nursing, 21(2), 217–233.
McDougall, G. J. (2001). Memory improvement program forelderly cancer survivors. Geriatric Nursing, 22(4),185–190.
McDougall, G. J. (2002). Memory improvement in octogenar-ians. Applied Nursing Research, 15(1), 2–10.
McDougall, G. J. (2009). A Framework for cognitive interven-tions targeting everyday memory performance and
memory self-efficacy. Family & Community Health(Supplement 1): Advancing Healthy Aging, 32(1S),S15–S26.
McDougall Jr, G. J., Becker, H., Acee, T. W., Vaughan, P. W.,Pituch, K., & Delville, C. (2010). Health-trainingintervention for community-dwelling elderly in theSeniorWISE Study. Archives Psychiatric Nursing, 24(2), 125–136.
McDougall, G. J., Becker, H., & Arheart, K. L. (2006). Olderadults in the SeniorWISE study at-risk for mild cognitiveimpairment. Archives of Psychiatric Nursing, 20(3),126–134.
National Institutes of Health. (2004). Life after cancer treatment(No. 04-2424). Bethesda, MD: U. S. GovernementPrinting Office.
National Cancer Institute. (2005). Lifetime risk (percent) of beingdiagnosed with cancer by site, race, and sex (DevCansoftware, version 6.0). Rockville, MD: Author. Retrievedfrom http://srab.cancer.gov/devcan/.
Office of Cancer Survivorship. (2010). Estimated U.S. CancerPrevalence. National Cancer Institute http://cancercontrol.cancer.gov/ocs/prevalence/prevalence.html#survivor.
Perkins, E. A., Small, B. J., Balducci, L., Extermann, M.,Robb, C., & Haley, W. E. (2007). Individual differencesin well-being in older breast cancer survivors. CriticalReview Oncology and Hematology, 62(1), 74–83.
Radloff, L. S., & Teri, L. (1986). Use of the center forepidemiological studies-depression scale with olderadults. Clinical Gerontologist, 5(1/2), 119–136.
Segar,M. L., Katch,V. L., Roth, R. S., Garcia,A.W., Portner, T. L.,Glickman, S. G., Haslanger, S., & Wilkins, E. G.(1998). The effect of aerobic exercise on self-esteem anddepressive and anxiety symptoms among breast cancersurvivors. Oncology Nursing Forum, 25(1), 107–113.
Spielberger, C. D., Gorsuch, R. L., & Lushene, R. E. (1970).Manual for the State-Trait Anxiety Inventory (Self-Evaluation Questionnaire). Palo Alto, CA: ConsultingPsychologists Press.
Tannock, I. F., Ahles, T. A., Ganz, P. A., & van Dam, F. S.(2004). Cognitive impairment associated with chemo-therapy for cancer: Report of a workshop. Journal ofClinical Oncology, 22(11), 2233–2239.
Wefel, J. S., Lenzi, R., Theriault, R. L., Davis, R. N., & Meyers,C. (2004). The cognitive sequelae of standard-doseadjuvant chemotherapy in women with breast carcinoma:Results of a prospective, randomized, longitudinal trial.Cancer, 100(11), 2292–2299.
Wilson, B., Cockburn, J., Baddeley, A., & Hiorns, R. (1989).The development and validation of a test battery fordetecting and monitoring everyday memory problems.Journal of Clinical and Experimental Neuropsychology,11(6), 855–870.