chronicity of stroke: survivors recovery of life
TRANSCRIPT
CHRONICITY OF STROKE
SURVIVORS RECOVERY OF LIFE
MSC MEDICAL ANTHROPOLOGY AND SOCIOLOGY
Author: Michaela Hubmann
Student Number: 10601295
Supervisor: Dr Kristine Krause
2nd Reader: Dr Anja Hiddinga
Submission Date: 22/07/2014

1
ABSTRACT
For centuries the biomedical acute-chronic disease classification has dominated the
everyday public discourse of illness, as well as the representation of the health transition.
This thesis aims to understand how this binary shapes stroke survivors’ experiences with
their after-care provision; and to what extent survivors’ chronicity, their resistance
tactics as well as the institutionalised care and therapy provision strategies are
constituted by the acute-chronic distinction. The survivors illness experiences are
fundamentally shaped by structural factors; hence the chronicity of stroke is as much a
technical, economic and political fact as it is a medical one. Rather than investigating
chronicity from a biomedical perspective, the Chronicity of Life itself, with its constant
mundane and major disruptions, has to be taken as the point of departure in order to
understand stroke survivors navigation tactics which they employ on the way towards
their personal recovery.
2
TABLE OF CONTENTS
Abstract ............................................................................................................................................................... 1
Acknowledgement .......................................................................................................................................................... 4
Chapter 1: Introduction ............................................................................................................................................... 5
Chapter 2: Context .......................................................................................................................................................... 9
2.1 Medical Definitions and Treatment Options .............................................................................................. 9
2.2 Principles and Efficacy of Stroke Rehabilitation .................................................................................... 10
2.3 Critique on the current Rehabilitation Approach .................................................................................. 11
2.4 Acute Landscape ................................................................................................................................................. 12
2.5 Sub-Acute or Rehabilitation Landscape .................................................................................................... 13
2.6 Chronic Landscape ............................................................................................................................................. 14
2.7 Long-Term Care in Context ............................................................................................................................. 14
2.8 Summary ................................................................................................................................................................ 16
Chapter 3: Theoretical Framework........................................................................................................ 18
3.1 Chronicity of Life ................................................................................................................................................. 18
3.2 Fluid Concepts of Acute and Chronic: The Dichotomy ........................................................................ 19
3.3 Anthropological Critique on Chronicity .................................................................................................... 20
3.4 (Counter) Concept of Recovery ..................................................................................................................... 21
3.5 Tactics, Strategies and Social Navigation .................................................................................................. 23
3.5.1 Social Navigation ......................................................................................................................................... 24
3.6 Summary ................................................................................................................................................................ 25
Chapter 4: Methodology ............................................................................................................................. 26
4.1 Methods, Data Analysis, Ethical Considerations and Limitations ................................................... 26
4.2 Difficulty of doing Research at ‘Home’: a Back and Forth Journey ................................................. 28
4.3 Issues with Gendered Encounters and Loneliness ............................................................................... 28
4.4 Summary ................................................................................................................................................................ 29
Chapter 5: Chronicity of the Built and Material Environment ..................................................... 30
5.1 Location and Architecture ............................................................................................................................... 30
5.2 Chronicity of Spatial Design: Ground Floors ........................................................................................... 31
5.3 Chronicity of Spatial Design: The Floors ................................................................................................... 32
5.4 Spatial Chronicity versus Spatial Temporality ....................................................................................... 33
5.5 Summary ................................................................................................................................................................ 34
3
Chapter 6: Chronicity of Politics of Time and Timing...................................................................... 36
6.1 Chronopolitics of Daily Routines .................................................................................................................. 36
6.1.1 Strategies of Silencing ............................................................................................................................... 38
6.2 Chronopolitics of Boredom and Social Isolation .................................................................................... 39
6.3 Chronopolitics of Therapy and Care Provision ...................................................................................... 40
6.3.1 Waiting times ............................................................................................................................................... 41
6.3.2 Compressed Therapy Agenda versus (Non) Vital Rhythm ........................................................ 42
6.4 Summary ................................................................................................................................................................ 45
Chapter 7: Chronicity of Life - The Continuum of Recovery .......................................................... 47
7.1 Acuteness of Recovery ...................................................................................................................................... 47
7.2 Continuum of Disruption ................................................................................................................................. 49
7.3 Chronicity of Life: Towards a Recovery of Existence ........................................................................... 51
7.4 Summary ................................................................................................................................................................ 54
Chapter 8: Conclusion ................................................................................................................................. 56
Bibliography ................................................................................................................................................... 60
Appendix .......................................................................................................................................................... 64
4
ACKNOWLEDGEMENT
This thesis would not have been possible without the help of very many people.
I am profoundly grateful to my supervisor, Dr Kristine Krause, who wisely guided me
through the ever changing turns and directions of my research, and who comforted me
with constructive, yet sensible, criticism throughout. I could not have wished for a more
supportive and ever present supervisor, where emergency Skype meetings took place on
weekends and late evenings.
My grateful thanks is extended to the two Cordaan Institutions which opened up their
doors and whose medical and managerial professionals patiently answered my many
questions. I felt very welcomed in both institutions.
I owe my deepest gratitude to my informants, who not only shared their life stories with
me, but also allowed me to observe their every move. We laughed, we cried, we cooked
and went on outings together.
This year would not have been possible without the emotional and financial support of
my family. Without you I would not be where I am. My thanks is extended to my proof
reading team, Nicole and Mark. You rock.
Finally, my love goes out to Jonathan, who had to put up with my many selves during the
writing process. I could not have done it without you. Nakupenda wewe.
5
CHAPTER 1: INTRODUCTION
This thesis contributes to the understanding of how the acute-chronic binary impacts
upon the stroke survivors illness and after-care provision experiences, and to what extent
this dichotomy constitute survivors’ chronicity1. The after-care landscape in Amsterdam
is divided into acute, sub-acute (rehabilitation), and chronic phases, whereby this
research focused on the latter two2. The care division is based upon the acute – chronic
dichotomy: the former is equivalent to curable and hence marked by temporariness.
Chronic in contrast is understood to be incurable, ongoing, with persistent and re-
occurring symptoms (Smith-Morris 2010: 21). Time, timing and temporariness therefore
are essential markers of the aforementioned divide. Speaking more globally, the stroke
(after) care landscape can be understood as being constructed by temporal modes of
socially organised timescapes: e.g. speed, rhythmicity, duration, length or continuity
(Ferzacca 2010). Furthermore, those who are the powerful employ the politics of time and
timing - which I refer to as chronopolitics - by way of regulating daily routines (ibid). As
will become apparent throughout this thesis, these human timescapes and the employed
chronopolitics are inherently political and used as form of social control (ibid). By its very
nature then, the acute-chronic binary not only dominates the biomedical discourse
(including biomedical practices and public health policy making), it also functions as
social navigator for it produces specific care provision strategies as well as stroke
survivors’ resistance tactics. This thesis therefore attempts to find answers on how this
dichotomy influences, if not produces, the chronicity of stroke survivors’ lived reality3, by
means of asking the following questions: How does the acute-chronic binary constitute the
experience of chronicity by way of determining the care landscape, and does the binary in
turn function as navigator through which the post-stroke experience is determined? How
does the binary influence long-term health care policies? How in turn do these policies
constitute the chronicity of stroke? How does this binary influence the institutional care and
therapy strategies and which tactics do stroke survivors’ employ in order to cope with such?
How is this dichotomy reflected in the built environment, and how is time experienced by
both acute and chronic stroke survivors? Throughout this thesis it becomes clear that this
1Chronicity refers to the state of being chronic or lasting for a long time (Ferzacca 2010), and the term was
introduced into the academic literature as ever more acute diseases are transformed into chronic. 2The sub-acute phase I investigated in a rehabilitation institution and the chronic phase in a nursing
home. 3Stroke is understood to be an acute and chronic condition.
6
binary influences the care landscape: by indexing healthcare resources; through
organising the medical, therapeutic and care practices; by means of determining the
chronopolitics of institutionalised daily routines, and via co-producing the built set up of
institutions. This in turn co-produces stroke survivors’ chronic identities.
Chronicity of stroke is marked by punctuated experiences of acute sickness
episodes (Eristroff 1993), as for instance survivors, when suffering another stroke or
acute flare-ups of their co-morbidities, are being temporally transmuted into acute
patients, whilst at the same time continuing to suffer from their ongoing chronic post-
stroke disabilities. Hence, stroke survivor, and chronic patients in general, experience not
one disruptive event (e.g. the initial stroke onset), they encounter disruption on a
continuum throughout their life-spans. It is the Chronicity of Life of a patient which should
concern researchers, and not so much the singular occurring disruptions. The
anthropological literature on the post-stroke experience, however, has largely focused on
the latter, by stressing upon biographical disruption (Bury 1981), fateful moments
(Giddens 1993) and significant events (Charmaz 1993). This thesis, then, contributes to
the knowledge on the chronicity of life by way of asking: How is the continuum of
disruption experienced by stroke survivors? How do past disruptions influence the lived
reality in the present, and how is their future informed by those? To what extent do
institutional practices constitute disruptions throughout the post-stroke recovery process,
and which tactics and navigators are used to combat those?
In order to promote a holistic rehabilitation provision, the focus has to shift from
a sole clinical (bodily) rehabilitation to a more holistic recovery concept, which ideally
should include the chronicity of a stroke patient’s life. Current post-stroke therapies
unfortunately are primarily focused on rehabilitating survivor back to their productive
potentials. However, as will be demonstrated throughout this thesis, post-stroke recovery
entails much more than the temporal rehabilitation of physical and cognitive symptoms
and disabilities. Rather, stroke rehabilitation is a life-long process, encompassing a stroke
survivor’s social, relational, and emotional environment, ultimately leading towards their
personal recovery. The concept of recovery not only encompasses these factors, wider
structural factors are furthermore included, as for instance, the acute-chronic binary
indexes the survivors access to rehabilitative resources. Those termed ‘hopeful’ to recover,
consequently, receive intensive therapeutic regimen, whereas less is invested in ‘hopeless’
7
cases, for their recovery is deemed to be unlikely. For those already termed chronic,
investment in rehabilitative therapy is minimal to non-existent. For this research,
therefore, it was of utmost interest to investigate to what extent such a holistic recovery
approach is incorporated into current rehabilitation provision. As has been demonstrated
throughout this thesis, such a holistic concept of recovery is entirely absent in the current
stroke rehabilitation provision. Subsequently stroke survivor and their wider social
network are left to their own devices when dealing with the aftermaths of the emotional
and relational impacts of the chronicity of stroke. In summary then, the chronicity of
stroke
[i]s no longer defined by the natural course of disease but by the availability of
biotechnical strategies to address them, hence chronicity of an illness
experience is not a medical fact, but a technological, political and economic one
(Smith-Morris 2010:21).
Carolyn Smith-Morris’s precise summary constitutes the red threat throughout this thesis
as the following chapters explore in more in-depth.
Chapter 2 places this research into context, by way of analysing the medical
definition, its treatments, its rehabilitation options and their shortcomings. It becomes
clear that the technical, political and economic facts not only determine all stages of
investigation, the stroke care landscape and the long-term health care policies are also
affected by those.
Chapter 3 provides an overview of the theoretical building blocks which informed
this research throughout: the acute-chronic binary with its resulting biomedical construct
of Chronicity; the counter concept of Chronicity of Life, which takes the human lifespan,
with its continuous disruptions. The Concept of (Personal) Recovery promotes a holistic
approach when helping survivor to recover their lives. Through analysing of strategies,
tactics and social navigation, the lived reality of my informants is further stressed upon.
Chapter 4 engages with the employed methodology, its ethics, data analysis and
limitations. Furthermore, the encountered difficulties of urban ethnography, as well as
how being a friend can cause sociability issues.
8
The next three ethnographic chapters draw upon how the acute-chronic divide
constructed my informants’ chronic identities, whereby chapter 5 and 6 demonstrate how
this binary was replicated in the built and material environment, as well as in the
institutional usage of time and timing. The chronicity of life, in contrast, is paid attention
to in Chapter 7.
Chapter 5 explores how the aforementioned divide was reflected in the
architecture and the interior design in both institutions. The modern, well-lit and
equipped rehabilitation institution fostered a quick recovery, whereas the old, dark and
scarcely equipped nursing environment co-produced chronic identities. As such the built
environment functioned as the social navigator in the production of care and therapeutic
strategies which my informants combated with certain tactics of resistance.
Chapter 6 demonstrates how this binary is replicated in the institutionalised usage
of time and timing, where chronopolitics were used as a powerful tool to regulate daily
routines. The almost hectic days in the rehabilitation setting contrasted sharply to the
endless unstructured days in the nursing home, which fostered boredom and social
isolation. Tactics and social navigators functioned as coping mechanisms in order to
combat the imposed chronopolitics in one way or the other.
Chapter 7 takes the alternative concept of Chronicity of Life as the point of
departure to highlight that the continuous disrupted pre- and post-stroke life span
informed my informants’ illness experiences. The different stages during which my
informants encountered these disruptions were informed by migration, discrimination or
divorces, and continued to be co-produced by structural factors which are promoted by
the acute-chronic binary.
This leads to the conclusion that the chronicity of my informants’ stroke illness
experience was informed by powerful technological, political and economic forces.

9
CHAPTER 2: CONTEXT
In order to be able to understand my interlocutors’ illness experience, stroke, as a medical
condition, has to be defined, its treatment options investigated and the rehabilitation
process reflected upon. The biomedical understanding of acute and chronic punctuated
every stage of the post-stroke experience, as the long-term health care policies and the
stroke after-care landscape in Amsterdam are constructed by the aforementioned binary
distinction. In this chapter I summarise the biomedical knowledge of stroke and its
rehabilitation. This biomedical knowledge is one of multiplicity, where different medical
(therapeutic) disciplines cater for different stroke symptoms. By critically reflecting upon
this knowledge, I will draw upon the boundaries of the stroke biomedical and clinical
rehabilitative knowledge and treatment options. I further explore the stroke care
landscape in Amsterdam, as well as the long-term healthcare policy reforms.
2.1 MEDICAL DEFINITIONS AND TREATMENT OPTIONS
A stroke occurs when the blood flow to the brain is cut off - either by a clot (Ischemic
stroke) or the breaking of a blood vessel (Hemorrhagic stroke) - causing damage to the
part of the brain that is deprived of blood (WebMD 2005-2014). The best treatment for
an Ischemic Stroke available to date is called Thrombolysis4, and for Hemmorhagic Stroke
it is interventional radiology. The former is treated with clot-dissolving drugs which are
directly injected in the affected blood vessel, the latter with non-invasive interventional
radiology via inserting a balloon in order to widen or to close off blood vessels in the brain
(ibid). Speed is essential, as the quicker the corrections are being done, the less brain
damage occurs. Partial skull removal constitutes another possible treatment option for
patients who suffer a severe stroke (regardless of the type), to provide their brain enough
time and space to recover and reduce swelling5, which might take only a week or several
months (ibid).
It is generally believed that hemorrhagic stroke survivors have better neurological
and functional prognoses than the ones who suffered an Ischemic stroke (Paolucci 2003:
4This form of acute treatment is only affective within the four hour time window from the onset of the
stroke. 5The majority of stroke mortalities are due the extensive brain swelling which occurs after a severe stroke
(WebMD 2005-2014). The removed skull is stored under the skin of the patient’s abdomen.
10
2861). However, these results are to be read with caution as many other factors (e.g. age,
the location where the stroke occurs, and the initial disability level) 6 determine the
recovery outcome (ibid)7. Spontaneous neurological recovery peaks within the first 1-3
months and may continue slowly for several months. Functional recovery, however, can
continue for some time after the neurological recovery is complete (Teasell et al 2013a:
30). Post-stroke symptoms are many and vary from one individual to the next: from
emotional and cognitive, to physical disabilities, and the extent of the stroke disability
determines and navigates a survivor through the rehabilitation process.
2.2 PRINCIPLES AND EFFICACY OF STROKE REHABILITATION
Studies have shown that rehabilitation in the sub-acute phase can dramatically improve
functional performances (Teasell et al 2013a: 18). The two most powerful predictors of
functional recovery, which also determine appropriate stroke rehabilitation
programmes, are the initial stroke severity and the patient’s age (ibid). Patients who
suffered a moderate to severe stroke are frequently admitted to stroke-specific
rehabilitation units, where they receive at least three hours of physically demanding
activities. Survivors need to be ‘fit’ enough to tolerate such intense programmes (Teasell
et al 2013b: 14). In Amsterdam such patients are mostly placed at READE8. Stroke
survivors with severe disabilities, limited physical endurance and/or limited attention
spans receive after-care in lower intensity inpatient programmes 9 , with treatments
spanning from three to five days a week, for up to three hours a day (ibid). Finally, mild
stroke patients are rehabilitated in an outpatient setting (ibid). However, this
categorisation is problematic, as not everyone with a ‘mild’ stroke can be catered for in
such an outpatient setting. I will focus upon the problematic further below.
Effective stroke rehabilitation programmes are interdisciplinary. A rehabilitation
team consists of physio-, logo-, ergotherapists, psychologists, geriatrists, general
6Socio-structural factors, such as the proximity of the nearest stroke unit, is undoubtedly another aspect of recovery. 7The medical director of the institution I conducted research in confirmed that according to her experience, Ischemic stroke recovery starts within the first 24 hours of initial onset, with stagnation later on. In contrast, hemorrhagic stroke recovery might take several weeks to kick off. However, once the recovery process starts, these patients have a more drastic recovery curve and better recovery outlook. 8READE provides a wide range of rehabilitation options for all types of injuries and more than 7000 clients are rehabilitated annually, ranging from children to the elderly. READE is located in West-Amsterdam (Reade 2014). 9The sub-acute institution I conducted my research with offered such low intensity programmes.
11
practitioners and dieticians, in order to provide the best possible treatment options for
patients (WebMD 2005-2014). Physiotherapists focus on problems with movement,
balance and coordination; ergotherapists on the activities of daily living (ADL), such as
eating, bathing, dressing or writing; logotherapists on relearning language skills and
swallowing impairments; psychologists with a patient's emotions and the dietician is
concerned with their diet (ibid). A stroke survivor’s body, therefore, is divided in
accordance to the different therapeutic practices, which in turn contribute to the
multiplicity of stroke and its enactments (Mol 2002: 55).
Interdisciplinary meetings are held shortly after a stroke survivors admission to
plan and coordinate their therapy regimen (ibid: 116). Such meetings therefore function
as point of departure, from where the different therapy pathways are mapped out, by way
of establishing rehabilitation plans and goals (ibid). If a patient no longer continues to
improve, the team plans their discharge. This rehabilitation approach has been criticised
by various disciplines to overly emphasise on the physical-, and to ignore non-physical,
hence social and also cultural needs (Peoples & Satink et al. 2011). It is argued that stroke
is never a linear physical condition, but rather co-produced by socio-cultural, economic,
environmental and political factors (Mol 2002, von Peter 2013).
2.3 CRITIQUE ON THE CURRENT REHABILITATION APPROACH
As explored above, the re-establishment or re-organisation of physical ability and of the
ADL(s) are the main focus in the stroke recovery. The emphasis is thereby solely given
upon the patient who has to overcome the physical, practical and cognitive challenges
post-stroke. Hence the patient is required to carry out the therapeutic work, whereby a
positive attitude and motivation is closely tied to the recovery potential (Becker &
Kaufman 1995: 169). Ellis-Hill (2000) states that
although the emotional and social difficulties experienced by stroke survivors
have long been recognised, these issues are rarely taken into account in the
clinical rehabilitation process” (ibid: 725).
This was also a major issue for my informants, especially for those already considered to
be in the chronic phase, for their need for support be it psychological or social, is even
greater. Though Becker & Kaufman (1995) questioned the implantation of the
rehabilitation policies in current health care systems, they did so by addressing this in
12
relation to the continuing rehabilitation for old people in the community setting (1995:
170). Ongoing rehabilitation, however, is also of utmost importance for institutionalised
chronic stroke survivors, as rehabilitation would not only contribute towards their
overall wellbeing, but it may also prevent co-morbidities. Unfortunately the reality is
somewhat different: as chronic stroke survivors’ recovery is highly unlikely, they are
termed incurable and unworthy of continuous rehabilitation. Funding for therapy
treatment (through the established ZZPs 10 ) is therefore limited, if available at all.
However, my informants confirmed that therapies contributed to their well-being, as for
instance, a stiff body can relax whilst on the cycling machine. As can be seen from this
short summary, the acute - chronic dichotomy greatly influences the rehabilitation
provision, as stroke or any other illness, is conceptualised as temporally bounded
(Manderson & Smith-Morris 2010). Rehabilitation should rather be based upon a
patient’s lifespan, which is marked by a multiplicity of social, somatic and bodily
disruptions continuously impacting upon their post-stroke self. Yet, the acute-chronic
dichotomy informs the well-developed stroke after-care landscape in Amsterdam and
throughout the Netherlands, as it is divided into acute, sub-acute and chronic.
2.4 ACUTE LANDSCAPE
As mentioned above, acute stroke care requires a vast range of specialised diagnostic
equipment and knowledge. Not all hospitals throughout the Netherlands have the
technical apparatus and the medical expertise to effectively treat stroke survivors. The
focus is laid upon special Stroke Chains (CVA Zorgketens), where regional health care
providers11 deliver coherent stroke care (Kennisnetwerk CVA NL n.d.). The hospitals are
specialised on the newest and most advanced stroke diagnostic treatment options, and
employ highly experienced medical personnel. Five Stroke Chains 12 are located in
Amsterdam and my informants were mostly treated within the South East cluster, where
sufferers are admitted to the AMC13 for acute and emergency treatment, and to Cordaan
Berkenstede and READE for sub-acute care. Depending on their condition, a stroke
survivor might stay in the hospital for one week up to six months. Since time matters,
10For an explanation of the ZZPs as assessment tool please refer to the next section which deals with the
long-term health care policies. 11Such as hospitals, rehabilitation institutions, nursing homes, homecare and general practitioners. 12Amsterdam Noord, West, Zuid, Oost, Zuid-Oost (Kennisnetwerk CVA NL n.d.). 13AMC stands for Academisch Medisch Centrum and it is a University Medical Centre (Academisch Medisch
Centrum 2013).
13
physical distance to such specialised hospitals might affect the rural population’s acute
stroke care.
2.5 SUB-ACUTE OR REHABILITATION LANDSCAPE
In the rehabilitation/sub-acute phase there is a vast array of rehabilitation options
available to a survivor. Which option is best is dependent on the medical assessment14
shortly before stroke survivors are discharged from hospital, where the package of the
intensity of needed care (ZZP15) is established.
Mild strokes survivor are usually discharged into the community, where the
regional stroke chain provides ambulant therapy in a survivor’s home; in a local hospital’s
rehabilitation unit; or in private physiotherapy centres. Depending upon their ZZP, stroke
survivors might also be eligible for formal homecare services, or the possibility to attend
day care centres16. Those who suffered from moderate strokes are best managed in a
comprehensive, well-staffed and intensive rehabilitation unit (Teasell et al 2013b: 14),
such as READE. The duration of their stay is dependent on their progress. My informants
reported to have been admitted to READE from three weeks up to eight months. Severe
stroke survivors or the elderly are the least likely to achieve functional independence
regardless of treatment, and are therefore transferred to a less intensive rehabilitation
programme (ibid), e.g. Berkenstede. The duration of their stay is again dependent upon
their recovery progress, however the mean average time is around eight weeks.
Arguably the acute-chronic dichotomy determines this phase and its institutions,
as moderate stroke survivors are the most ‘hopeful’ cases to achieve the best clinical
recovery. Through intensive rehabilitation it is hoped to rehabilitate them to the point
where they can be discharged into their informal care network, and at some point become
productive citizens again. In contrast, clinical recovery of severe stroke survivors is
deemed unlikely and not worth the costs. However, some flexibility is given where there
is a glimmer of hope for even the slightest improvement, severe stroke survivors are at
times upgraded and transferred to intensive rehabilitation programmes. One of my
14The assessment also includes a meeting with the patient’s therapy team, his/her family and social or
community workers in order to establish a comprehensive stroke-after care plan. 15ZZP assessment procedures are explored in more detail further below. 16Survivors are able to socialise, receive therapies, train their brain and participate in group activities in
such day care centres.
14
informants experienced such upgrading, as it was hoped that due to his young age he
might profit more from the intense programme offered at READE, which unfortunately
turned out to be not the case. It can be argued that the post-stroke body functions as the
social navigator, as its post-stroke disabilities specify which rehabilitation programme a
stroke survivor is admitted to (Vigh 2009).
2.6 CHRONIC LANDSCAPE17
When there is no more clinical recovery to be gained a stroke survivor is deemed to be
chronic. They are either discharged to the community and into informal care, or admitted
to care and nursing homes, assisted living environments or into sheltered housing18 .
There are seventy-six care and nursing homes spread throughout Amsterdam
(Zoorgkaart 2014). Most of my informants lived in South-East Amsterdam prior the
stroke onset, and this was taken into consideration when deciding on a care or nursing
home19. However, it is not always possible to cater for the wishes of the survivors and
their families, as sometimes the first choice institution cannot provide the necessary
medical care.
2.7 LONG-TERM CARE (LTC) IN CONTEXT
The Dutch Welfare State (DWS) can be understood as a hybrid between types of
corporatism (Esping-Andersen 1990) and social-democracy (van Orschot 2002: 52-60)20.
A universal 'people's insurances' covers all Dutch citizens, and insurance and assistance
benefits are comprehensive and relatively generous (ibid). The Dutch long-term care
(LTC) scheme was introduced in 1968 through a national compulsory social insurance
system, which was created by the AWBZ21 (da Roit 2012: 228). The LTC and elderly care
was marked by a high percentage of institutionalisation in the 70s and 80s, which was
17For more detailed information on the long term care system please refer to the following section. 18For more information regarding the assessment criteria’s please see below. 19Medical professionals, therapists, the patients’ family and the stroke survivor discuss the possible routes.
However, the decision is also very much dependent upon the stroke survivors ZZP which will be discussed
below. 20In corporatist welfare states, social benefits are granted via status. The state is the major provider of welfare and the market has a marginal role. In contrast, means testing benefits are the main characteristics of the social-democracy welfare state where social insurance plans are moderate. Rather the state interferes in the market system by subsidizing private welfare schemes (van Orschot 2002: 52-60). 21 AWBZ stands for Exceptional Medical Expenses Act through which the long-term care market is governed. Contribution is deducted from all people in employment or on benefits. The AWBZ is concerned with the provision of the best possible care, nursing and support for people who are termed incurable (NZA 2012: 43).

15
informed by solidarity and collectiveness (da Roit 2010: 22). The 1980s22, however, saw
a shift towards personal responsibility (van Orschot 2002: 52-60), which was
characterised by an introduction of risk differentiation, activation, privatisation and
decentralisation (ibid). Due to the democratic nature of the DWS, the expenditure for
long-term care (AWBZ)23 has risen from 14 billion in 2000, to 24,6 billion in 2011 (NZa
2012: 43). Therefore, in 2009 the payment system for long-term care was reformed, with
2015 as the actual implementation year (ibid), whereby 2014 functioned as ‘transition’
year in order to give institutions and municipalities the chance to adjust. Before the
reforms, long-term care institutions were paid on the basis on the intake of patients,
hence upon their capacity. Since 2009, however, payments are based on the intensity and
complexity of the care provided (The Health Systems and Policy Monitor 2014), which is
divided into several care intensity packages (Zorgzwaartepakketten or ZZP) 24 :: 10
packages for the nursing and caring sector (where stroke long term care falls under), 13
for the mental care sector, and 29 for the care for disabled people. The Dutch Health Care
Authority (NZa) provides the budget for the ZZPs, which varies from €55 per day to €300
per day (ibid). In order to be eligible for LTC, people undergo a ‘Care Needs Assessment’25,
where the intensity of needed care is assessed (the so called ‘indicatie’) (NZA 2012: 44).
The ZZP system is of crucial importance for this thesis, as a stroke survivors’
condition is assessed before being discharged from the hospital26. This is done by a team
of medical professionals and social workers. If a stroke survivor is cared for in a
specialised stroke chain, then professionals from the other institutions also attend the
meeting. The completed assessment protocols are sent to CIZ, who open up a ZZP from
this report. Professionals thus play a major role in assessing needs and formulating care
plans, as through their judgement, or discretionary power, an individual’s access to
resources is determined (Da Roit 2012: 234). My professional informants admitted to
often stretching their assessment roles in order to provide the best possible care plans
22This was due to the global oil and economic crisis in the late 1970s. This shift took also place in Northern European countries, where the enhancement of community care was favoured over institutionalisation (da Roit 2012: 230). 23 The goal of the AWBZ is to provide collective cover for healthcare risks which cannot be insured
individually, and which private insurance companies are reluctant to cover (ibid). 24The funding system used for the care intensity packages mean that healthcare providers are paid on the
basis of health care actually provided and no longer on the basis of the size of their organisation. 25Assessment is done by the Centre for Needs Assessment (CIZ). 26The disabling nature of their condition, the level of care needed, or whether or not one is eligible for a
scoot mobile is being assessed.
16
for stroke survivors. It therefore can be argued that they employed discretionary power
as a tactic in order to poach in the terrain of the new health policies (de Certeau 1984). If,
however, a stroke survivor is assessed with an indication of ZZP 4/5 or below, his/her
care requirements are deemed to be relatively ‘light’ and to be cared for in their own
home environment from 2015 onwards (NZa 2012: 13). My institutionalised informants
were indicated with a ZZP 3-4, all of them were gravely disabled and they needed to rely
on 24/7 care. Henceforth their care requirements were far from ‘light’. They were aware
of the policy changes and expressed concerns of having to leave the nursing home once
the changes are implemented.
Taking the above into consideration, it can be argued that the professionals, as well
as the ZZP system, function as social navigator through which a stroke survivor’s care
pathway27 is decided upon. For an in-depth exploration how the LTC reforms impact
upon the long-term health care employment market, its educational standardisation, and
how these reforms impact upon the home care provision system, please refer to Appendix
A.
2.8 SUMMARY
The post-stroke illness experience is marked by the biomedical acute –chronic distinction
with its linear temporalities of diagnosis, treatment and recovery. This was not only
reflected in the stroke treatment, where time is of utmost importance to ensure the best
recovery outcome. Such an understanding also determined the rehabilitation process,
which is focused on making a patient physically fit and productive, hence ‘normal’, as soon
as possible. The stroke care landscapes as well as the LTC policies are furthermore
determined by this dichotomy. Through the ZZPs a stroke survivor’s care pathway is
established, whereby the medical professionals, through their discretionary power,
function as crucial navigators. However, as this assessment very much relies on
interpersonal contact and practices it is prone for abuse, e.g. favouritism or
discrimination. Yet, it is the discretionary power, through which the professionals
tactically use the available resources in order to carve out the best care plan for a stroke
survivor. Care workers too are victims of the chronicity of the long-term care policies,
as their qualifications are not standardised, and their wages are the lowest in the LTC
27Whether someone is institutionalised or well enough to be cared for at home.
17
sector. Therefore, the chronicity of stroke is as much constructed by medical facts, as it is
determined by socio-structural and political factors, which the following theory chapter
further stresses upon.
18
CHAPTER 3: THEORETICAL FRAMEWORK
In order to understand the after-care experience of stroke survivors, the
distinction of ‘acute’ and ‘chronic’ has to be put into context by way of relating it to current
anthropological and biomedical explanations. What follows is an exploration of the
biomedically understanding of chronicity - which is informed by a linear and temporal
timeline, such as diagnosis, treatment and recovery - highlighting the duration of illness.
Alternative approaches to chronicity, however, stress upon the chronicity of life, which
draws upon continuous disruptions, punctuating not only the lifespans of the chronic ill
but also of the healthy. This chapter also highlights the tactics and navigation strategies
which the ‘weak’ employ in order to ‘poach’ in the terrain of the powerful in order to find
their way towards their personal recovery.
3.1 CHRONICITY OF LIFE
With the increased academic attention towards chronic conditions 28 the
establishment of ‘chronicity’ took hold, in order to describe the state of being chronic. In
relation to illness, Ferzacca (2010) defines chronic states as unending and repetitive
illness episodes, which frequently re-occur, and with symptoms persisting beyond the
expected (ibid: 158). Chronic diseases are unending due to the un-availability of disease
modifying treatments and an individual’s recovery is therefore unlikely. However,
chronicity not only highlights the duration of health, it also draws upon the human
lifespan in general (Smith-Morris 2010: 37). As such the human lifespan can be regarded
as fragmented as it is continuously punctuated by mundane disruption of everyday life29,
and major disruptions such as the sudden onset of stroke (ibid).
However, the investigation of chronicity with its disruptive nature, contributed to
an overuse of the social science concepts of biographical disruption (Bury 1982), fateful
moment (Giddens 1991), or significant event (Charmaz 1991), hence feeding into the
biomedical fragmentation of acute and chronic self. Anthropologists such as Gay Becker
(1998) and Smith-Morris (2010), as well as other health researchers like von Peter
(2013) argue to break with such fragmentation. In so doing, rather than investigating
28Chronic conditions are not only disease related; they are also related to global structural inequalities. 29People encounter disruption throughout their lifespan, e.g. childbirth; divorce of parents, unemployment, migration, marriage, but also in their everyday lives through stress for instance.
19
chronicity as a circumscribed state, the chronicity of life, with its continuous and constant
disruption, is stressed (Smith-Morris 2010: 37). Henceforth, illness events should be
placed in an individual’s continuous biographical flow, which is marked not by a pre-, or
a post illness self, but rather human encountering of multiple selves along the way30 (von
Peter 2013).
The biomedical interpretation of chronicity, in contrast, is not informed by the
continuum of disruption, but rather by a linear timeline. As such, “time is not a neutral
concept within biomedicine, it is rather powerfully used in diagnosis, treatment and the
labelling of illness process” (Foucault 1977, cited in Ferzacca 2010: 158). The diagnosis
process is defined and determined by temporal factors such as treatment and recovery,
where the sick are labelled as ‘acute’ or ‘chronic’. Hence a heterogeneous group is made
homogeneous (Hacking 2006, cited in van Peter 2013: 51). This in turn not only impacts
upon a survivor’s understanding of self, it also impacts upon their access to rehabilitation
options. A further exploration of the biomedical acute – chronic dichotomy is therefore
necessary in order to understand chronicity.
3.2 FLUID CONCEPTS OF ACUTE AND CHRONIC: THE DICHOTOMY
Since centuries the biomedical and public discourse of the transition from health to illness
was dominated by the acute–chronic dichotomy31 (Manderson & Smith-Morris 2010: 3).
The concept of acute, however, fails to distinguish between benign, terminal and fatal
conditions. In the past, the aforementioned dichotomy was a useful instrument in order
to convey the implications of a biomedical diagnosis to the lay public (ibid), where the
acuteness of a diagnosis almost always corresponded to a fatal outcome. This however
changed with the introduction of new technologies, interventions and pharmaceuticals,
and former acute, infectious or incurable diseases have become chronic and controllable
(ibid). HIV is a good example for this fluidity of disease, which shifted from being an acute
and terminal illness, to a lifelong manageable disease (Russell & Seeley et al. 2007), hence,
both the acute and chronic stage is experienced fluidly. Stroke survivors similarly
experience their disease: from a potentially fatal initial onset to a life marked by co-
30One is not only his/her illness self, he/she is a parent, a child, sibling, friend and colleague, hence labelling a particular habitus ‘chronic’ becomes futile (von Peters 2013: 52). 31Other related dichotomies are: IDs :: NCDs; curable :: incurable; visible :: invisibility; dramatic onset ::
insidious.
20
morbidities and post-stroke disabling conditions, which in turn are punctuated by acute
illness episodes. Time and temporality is essential for the creation of the acute-chronic
dichotomy, as it is one of temporality and linearity. Throughout this thesis it will become
clear that stroke illness patterns and hence illness experiences vary enormously. This
binary has fostered the establishment of chronicity, which in turn was criticised by social
and health scientists.
3.3 ANTHROPOLOGICAL CRITIQUE ON CHRONICITY
As much as we are unable to define acute as distinct and confined states of illness, the
same holds true for chronicity as it is a punctuated experience where sufferers encounter
a constant flux between acute and chronic sickness episodes (Eristoff 1993). Sue Eristroff
(1993) was one of the first anthropologists to recognise that
chronicity and disabilities are constructed by: the temporal persistence of self and
other-perceived dysfunction, continual contact with powerful others who diagnose
and treat, gradual but forceful redefinition of identity by kin and close associates
who observe, are affected by, or share debility; and accompanying loss of roles and
identities that are other than illness related (ibid: 259).
This not only recognises that chronic diseases are defined by the identity of the sufferer,
but they are also constructed by social relations and by wider socio-cultural factors.
Dennis Wiedman (2010) also acknowledges this when writing about the theory of
chronicity in relation to the global pandemic of metabolic syndrome (Mets). Wiedman
(2010) argues that socio-cultural factors, rather than genetic and biological ones have to
be employed in order to explain chronic conditions. She further argues that chronic
metabolic disorders 32 reflect the physical body’s response to the ‘chronicities of
modernity’, e.g. the shift in food and lifestyle practices due to global capitalism (ibid: 38-
39). Henceforth, the control of chronic conditions often require stringent medical, care
and drug regimen, through which a sufferers life is transformed from being active and
productive, to one of daily chronicity marked by dependency, control and routines.
Wiedman’s (2010) theory of modernity can be transferred to the Dutch LTC policies,
which determine the after-care landscape, and as such index stroke survivors’
accessibilities to health-care and rehabilitation resources. In this respect, LTC policies
32Diabetes mellitus is the most common metabolic disorder (Wiedman 2010).
21
are co-responsible for the establishment of chronic conditions. This is particularly the
case when survivors are institutionalised, where life is marked by immobility, which in
turn fosters the establishment of co-morbidities, hence reinforce chronicity. Taking the
above into account it becomes clear that “[…..][c]hronicity of an illness experience is not
a medical fact, but a technological, political and economic one” (Smith-Morris 2010:21).
In order to capture these facts, throughout this thesis I will demonstrate how
stroke survivors experienced their health status in relation to their participation in social
and economic life: e.g. Emiel’s drive to re-establish his business; Dominik’s engagement
with a traditional healer in hope to regain his mobility in order to take up his study of
medicine again; or Mr Osei’s social navigators, whom he employed in order to be able to
re-establish a meaningful life as a lone parent outside the nursing home. Therefore,
instead of concentrating on the temporariness of acute and chronic illnesses, von Peter
(2013) argues that the focus should rather be laid upon a person’s healthy and productive
facets. This should foster resilience and self-management, the development of a sick
person’s independence and their self-determination (ibid: 49). It is further understood
that “health and illness exist on a continuum and during the recovery process a person’s
own diversity is respected and encouraged” (ibid). Unfortunately I have seen little
evidence that this approach is adopted in the post-stroke recovery process, rather the sole
focus is laid upon the clinical, hence bodily recovery.
3.4 (COUNTER) CONCEPT OF RECOVERY
For this thesis the concept of recovery is of particular interest, as it describes the
continuous journey throughout a sufferer's lifespan post-stroke. This concept is a widely
used one in mental health literature, as well as practically applied in mental health
services (Slade & Amering et al. 2014). There are two forms of recovery recognised: the
clinical recovery with its focus on changing people through treatment in order to ‘fit in’,
to become ‘normal’ and ‘independent’ again (ibid). Personal recovery is the second form
which focuses on living a satisfying, hopeful and contributing life even with limitations
caused by illness. Anthony (1993) defines personal recovery as
a deeply personal, unique process of changing one's attitudes, values,
feelings, goals, skills and roles. It is a way of living a satisfying, hopeful, and
contributing life even with limitations caused by the illness. Recovery
22
involves the development of new meaning and purpose in one's life as one
grows beyond the catastrophic effects of [….] illness (cited in Slade & Amering
et al. 2008: 130)
From this point of view, recovery can be understood to be a way of living life rather than
a state to be accomplished, and it is as much a process as it is an outcome. Although this
model might evoke criticism for solely laying the responsibility of recovery in the
individual’s hands, hence shifting attention away from possible structural factors,
through the empowering mode promoted by this concept, these structural factors might
as well be made explicit. In this perspective personal recovery can also be termed as social
recovery (Slade & Amering et al. 2014), as it is about “recovering a life”: the right to
participate in all facets of civic and economic life as an equal citizen (ibid: 14). As much as
chronicity fosters exclusion (e.g. by isolating stroke survivors in nursing homes), personal
and social recovery fosters inclusion by reducing or eliminating social barriers.
Furthermore, the concept of recovery also stresses upon the lifelong identity work, in
which the chronicities of daily adjustment, improvements and rebuilding punctuate the
lives of the sick and the healthy (Smith Morris 2010: 36). Hence “[co]ntinuity is not an
illusion [….], the illusion is in our labelling of lifetime illness episodes as distinct from an
otherwise disease free life (ibid: 35). Chronic identities, therefore, are neither pre-
existing nor given, they are rather performed through mundane enactments and
composed of relationships with other bodies or material objects (von Peters 2013: 55).
As such the chronic body is in
(a) state of permanent flux, simultaneously transforming and being
transformed, thus [the chronic body] is far from being a simply passive,
representative container…. Identities are acted out in relation to various
sites and places, including their material constraints and surrounding
objects. Consequently the material world must therefore also be included if
we want to fully comprehend the nature of ‘chronic’ beings (ibid: 54-55).
Von Peter (2013) stresses upon the importance of how people relate to their
environment through practices, tactics, strategies and social navigations. These are
important themes throughout this thesis, as stroke survivors tactically navigated their
23
way through the stroke care landscape and resisted the institutionalised care provision
strategies.
3.5 TACTICS, STRATEGIES AND SOCIAL NAVIGATION
In order to analyse everyday practices, many authors refer to Michel de Certeau’s (1984)
distinction between ‘strategies’ and ‘tactics’ 33 . De Certeau (1984) argues that the
powerless or ‘weak’ people adopt a bricolage of tactics in order to create space for
themselves in environments which are defined by institutional or other people’s
strategies which often function as forms of social control (ibid: 30 - 42). Social control
always generates some form of resistance, and according to de Certeau (1984), the ‘weak’
employ certain tactics in order to ‘poach’ in the terrain of the powerful. This poaching
theory is especially interesting when investigating chronic ill people’s tactics for gaining
access to resources such as sickness or disability allowances, equipment, or the possibility
for re-training. By employing poaching tactics therefore, the ‘weak’ convert their
powerlessness into strategies through which they gain some control back over their lives.
Poaching tactics are ever more important for the institutionalised chronic sick, as
by tactically employing strategies they try to regain some control over their lives by, for
instance, combating the institutionalised time regimen. The politics of time and timing
functions as a form of social control through which the institutionalised daily routines are
structured (Ferzacca 2010: 157). Ferzacca (2010) calls this form of social control
‘chronopolitics’. My informants tactically used me in order to resist and advance their
situation by way of asking for yet another cup of coffee, by using me to ‘escape’ the
boredom on the ward, or by ‘employing’ me to prepare their dinner. Hence, the ‘weak’,
with their employed tactics of resistance, situational transform into the powerful and in
charge of their lives (ibid). De Certeau (1984) therefore might be criticised for
essentializing the weak, as the concepts of strategies and tactics can lead to the
polarisation of humans (e.g. weak and powerful). Rather, his concept should be employed
in order to describe subject positions and how humans act, as both strategies and tactics
are constructed by the practices of everyday life.
33These practices are always reproduced and negotiated in a given society or community (Styhre 2004), e.g.
the reproduction of therapeutic and care practices and how they are influenced by health care policies.
24
De Certeau’s (1984) theory of tactics, strategies and poaching, is useful for this
thesis as all of my informants tried to carve out a niche for themselves within an
institutionalised setting, where they encountered (powerful) strategies not only through
health and health care policies, but also through the care personnel. My informants also
employed such tactics when navigating their way through the stroke care and after-care
landscape, a process which Vigh34 (2009) calls social navigation.
3.5.1 SOCIAL NAVIGATION
Social navigation, as Vigh (2006) argues, “is primary a question of evaluating the
movement of the social environment, one’s own possibilities for moving through it, and
its effects on ones planned and actual movement” (ibid: 13). Social navigation, therefore,
is always related to human tactics, strategies and every day (poaching) practices. In
relation to my thesis, the stroke survivor’s illness experiences are intertwined with
complex social (powerful) forces, such as the care landscape, long-term care policies, and
professional and/or informal care providers. As such, both, the individuals experience
and the social forces, are in continuous motion, hence ever changing and dependent upon
each other (van der Sijpt 2014: 2). Thus stroke survivors’ decision making does not
happen in a vacuum but is rather a result of the constant involvement of social others.
However, this social navigation is also influenced by the post-stroke body, as its
symptoms function as navigator for medical assessments, for the establishment of care-
packages (ZZPs), and the choice of rehabilitation institutions. A stroke survivors’ body
therefore “both directs and demands navigation” (van der Sijpt 2014: 11), hence “the
bodily navigation […..] is always dialectically related to social navigation” (ibid).
Vigh (2009) further understands social navigation to be attuned to the way
humans move in relation to their future. In this manner, navigation is related to
movement through both the “socially immediate and the socially imagined” (Vigh 2009:
425). The imagined nature of social navigation, therefore, is constructed by concerns,
problems and anxieties which individuals encounter in the present, as well as by future
dreams and aspiration, where people “move towards positions they perceive as being
better than their current location and the possibilities within them (ibid: 432). In this
34 Vigh (2006) highlights this by drawing upon the processes of mobilization of urban youth during Guinea
Bissau’s civil war.

25
respect an individual’s horizon changes, which affects “both our vistas (points of views)
and our attainable social positions” (ibid: 426). The imagined social navigation of stroke
survivors’ is informed by their immediate concerns of bodily recovery in the sub-acute
phase and in the chronic phase by their desire for a better life outside the nursing home.
3.6 SUMMARY
I aimed to demonstrate that acute and chronic illnesses are not temporary bounded
illness states; but rather in constant motion where illness episodes are experienced in a
continuum. When investigating chronicity it is important to examine the whole lifespan
of a diseased, and not just the duration of health, which biomedically is understood to be
linear and temporal. Therefore, the chronicity of life has to be taken as point of departure
when investigating chronic states of being, as the human lifespan is constantly and
continuous disordered, not just by re-occurring illness episodes, but also by wider socio-
economic and cultural disruptive factors. The post-stroke recovery and rehabilitation
process, consequently, has to take these factors into account. Recovery not only
constitutes the clinical rehabilitation, it includes to an even greater degree the personal
recovery of stroke survivors which promotes a way of living a dignified and meaningful
live, even with ones acquired post-stroke disabilities. Yet such a personal recovery
approach is not promoted in nursing homes, where many of the gravely disabled stroke
survivors spend the rest of their lives. Instead the politics of time and timing function as
an instrument of social control, hence supressing any efforts of personal recovery. In
order to better their lives, residents employ certain poaching tactics to carve out a niche
for them to make space for the recovering process of their lives. The chapters to come will
demonstrate this in more detail by way of drawing upon how my informants’ resisted the
chronicity of built environment and the politics of time and timing. The next chapter,
however, draws upon the employed methods, the difficulty of conducting urban
ethnography and on issues regarding friendship and loneliness.
26
CHAPTER 4: METHODOLOGY
This thesis is based on ten weeks of qualitative ethnographic research conducted in
south-east Amsterdam (SEA), in two of the Cordaans’ 35 institutions (a rehabilitation
institution and a nursing home), and with one Ghanaian stroke survivor living in another
independent living establishment. With the latter participant and the ones in the nursing
home and I was able to conduct research for eight consecutive weeks, one day per week.
In the rehabilitation institution my research spanned over three consecutive weeks, four
days per week. Research participants in the rehabilitation institution comprised of one
stroke survivor of non-Dutch, and two of Dutch origin. In the nursing home I was able to
recruit four participants of non-Dutch, and one of Dutch origin36. Care and managerial
personnel, as well as external health care experts also participated in this study. What
follows is a reflection on the methods, analysis, ethics and limitations of my research. I
then explore the problematic of doing research in an urban environment, and how being
a friend can cause sociability issues.
4.1 METHODS, DATA ANALYSIS, ETHICAL CONSIDERATIONS AND LIMITATIONS
On the first day in each research setting, care personnel, team or location managers and
the medical director introduced me to potential informants; they explained the purpose
of my research and asked for informed consent. In addition I informed my interlocutors
about the anonymity and voluntarily aspect of their participation and their possibility of
withdrawal. All agreed to participate and with all I could converse in English. The main
method of information extraction was by conducting informal and semi-structured in-
depth interviews. Though I prepared questions, I let my informants decide where to take
the interview, hence to “develop their own account of the issues important to them”
(Green & Thurgood 2011: 94). Through this method, interesting, though sometimes
unrelated topics, emerged. Expert Interviews were semi-structured in nature, whereby I
paid attention not to disturb the flow of the interview. I also joined lunch breaks with
various professionals: in the nurse room, with cleaners in the canteen, and with medical
35Cordaan is a health and elderly care organisation, which has rehabilitation centres, nursing and elderly
homes spread throughout Amsterdam. 36Please note that I used first names for those informants I had a particular close research relationship. All
names have been changed to protect the identity of my informants. For further demographic
information please refer to Appendix B.
27
doctors and therapists. At these occasions I was able to observe the interaction between
them, and I could ask questions about my informants in order to obtain a holistic picture
of their condition and their family situation. Professionals in turn could ask me questions
and we shared jokes and food, hence rapport was established in an informal manner.
Triangulation of methods was crucial during the fieldwork. Not only did I
frequently talk to all of my informants, I also applied participant observation to notice
their behaviour, their practices and interaction with each other, and with the care
personnel. Henceforth, I could gain useful insights in the running of these two institutions.
Depending on the given situation, I employed two methods of data collection: note taking
and tape recording, and every evening I transcribed the recorded interviews and
digitalised the notes. For the analysis of my data I used various theories and techniques,
such as open coding and mind mapping in order to find broad themes, whereby sub-
themes emerged through the writing out of ethnographies. Hence my theory is based on
the data I collected, which I analysed by using practice and chronicity theories.
Participant’s consent and confidentiality are core principles which informed my
research throughout (Green &Thurgood 2009:62). I tried to protect my informant’s
privacy, integrity and autonomy at all times by providing an informed consent form at the
first encounter, and I talked them through their rights, responsibilities, benefits and risks.
Another ethical consideration revolved around the emotional consequences of
interviews, especially for those informants who were severe disabled (ibid: 62). I aimed
to make the interview experience a positive one for my informants, where research
questions reflected their concerns and opinions. Finally, in order to protect my
informants from the emotional pain of losing a friend, I was very clear about the limited
nature of this research and of the interpersonal relationship.
The short-levity of this study, my research focus on stroke, and the language
barrier only permitted a small sample of respondents. All of my informants had a very
good command of English, and though most of them suffered from aphasia, all could
express themselves clear enough to me. As the majority of my participants were male, this
gendered focus undoubtedly shaped, but also limited the outcome of this research. As a
white, middle aged woman, not the building up of rapport was the issue, but rather the
emotional and sexual deprivation which my informants’ experienced. Hence, at times I
was in need to discontinue with the interview due to the sexual intimations I encountered,
28
but also because it emotionally affected my informants. Furthermore, due to timely
constraints of this research I was not able to include family-members and partners and
neither could I observe their visits. To partly overcome this issue, I obtained third hand
knowledge about my informants’ family situation by way of talking to the care personnel,
who knew the families very well.
4.2 DIFFICULTY OF DOING RESEARCH AT ‘HOME’: A BACK AND FORTH JOURNEY
As I conducted my fieldwork in SEA I consider it to be a research at ‘home’. Although I am
Austrian by origin, since one year I call Amsterdam my home with work, study and social
commitments to fulfil. My lifestyle did not change during fieldwork, in contrast, it just
added another layer to my already busy daily schedule. A fieldworker’s persona,
according to Carputo (2000), is “made up of partial identities that abruptly shift according
to changes in context (e.g. at work or in the field)” (ibid: 27). Furthermore she argues that
conducting research at home is not one of ‘leaving for the field’, it is rather a constant
coming and going to and from the field (ibid). As such a ‘total’ immersion into the field is
difficult to achieve (Amit 2000: 6; Carputo 2000: 28), which during the first months of
research contributed to a sense of not being able to carry out ‘proper research’, and of
‘just scratching the surface’. This was especially due to the fact that I was in need to move
house and to adhere to work commitment37.
4.3 ISSUES WITH GENDERED ENCOUNTERS AND LONELINESS
Charmaz (1991) argues that social isolation can be directly translated into loneliness
which can contribute to a ‘superficial’ sociability, where institutionalised chronic sick or
the elderly seek contact with whomever possible (ibid: 97). Tillman-Healy (2003) further
argues that friendship and fieldwork are similar as both involve being in the world and to
both entrée must be gained (ibid: 732). Furthermore, conversations, every day
involvements, compassion, giving and vulnerability - which mark friendships - are also
the cornerstones for data gathering (e.g. participant observations and formal/informal
interviews) (ibid). It was not difficult to establish a trustful, though temporary, friendship
with my interlocutors after a short period. I did so by taking them out for walks or to
37Effective days to conduct fieldwork in the first month were from Monday to Wednesday.

29
outings (e.g. lunch or to the church), by preparing and cooking dinner for, and with them,
or simply by spending time with my informants.
However, establishing a friendship relationship, especially with institutionalised
and lonely male participants, also bears the risk to develop romantic and sexual feelings
towards the (female) researcher. This was also acknowledged by Shuttleworth (2000),
who argues that disabled men are hoping for the development of a sexual relationship by
first establishing a friendship with a woman (ibid: 266). As most of my informants were
male, the topics of emotional relationships and sexuality were a constant companion
throughout the research period38. This was also difficult for me as a researcher, as to how
to react to sexual intimations and to the praising of affections. Hammersley & Atkinson
(1998: 118-119) argue that women fieldworker are thought to be vulnerable to sexual
imitations, especially when conducting fieldwork in an institutionalised setting. This was
particular the case with the one male informant who lived in that independent living
environment, and who was fairly mobile. He constantly tried to touch and kiss me, at
times aggressively. I tried to keep distance, by reminding him about the purpose of my
presence. Unfortunately, I needed to discontinue the research with him, as he could not
accept the social boundaries of a researcher-informant relationship.
4.4 SUMMARY
The lessons learned from this research experience are many. First, and most importantly,
when conducting research with institutionalised participants, their social isolation and
loneliness can contribute to a rather complicated research situation. Second, as stated
above, if the research period is short, an institutional setting might be best. Third, I now
appreciate the fact that one day in the field is not the best way to extract results. Despite
of all the difficulties encountered, this research grounded me as an ethnographer, which
hopefully is reflected in the following ethnographic chapters. The next chapter explores
how chronicity of my informants’ illness experience is co-produced by the built and
material environment.
38All of my informants in the chronic phase expressed their concerns about possible future emotional
relationships and about their sexual (unmet) needs. I have seen little evidence that issues surrounding
emotional relationships and sexuality are dealt with in the latter stages of the sub-acute phase and even
less so in the chronic phase which, due to the lack of privacy in such homes, might be difficult to establish.
The psychologist in the rehabilitation institution confirmed that this is an area of unmet needs.
30
CHAPTER 5: CHRONICITY OF THE BUILT AND MATERIAL ENVIRONMENT
This chapter investigates how my informants’ chronic identities were composed in
relation to the built environment and its resulting practices (von Peter 2013). The spatial
set-up of both institutions replicated the acute – chronic divide, as the rehabilitation
institution was designed much like a hospital environment, with the purpose of
temporarily hosting stroke survivors, until they are well enough to be discharged. The
spatial set-up of the nursing home, in contrast, conveyed the characteristics of chronicity,
where a stable and long-term living environment was promoted. This division was
apparent in the institutions architecture, their spatial segregation, the availability of
communal spaces, and the set-up of the rooms. What becomes clear is that the chronicity
of the built environment fosters exclusion, as chronic sick are “the other to able-bodied
people” (Maynard 2010: 208) and ‘hidden’ and isolated in such homes. This in turn
prevents residents to recover a meaningful and contributing life.
5.1 LOCATION AND ARCHITECTURE
Both institutions were located in South-East Amsterdam: the nursing home in Gein and
the rehabilitation establishment in Diemen. The latter was located near a main road,
easily accessible from the city centre, and hence conveying an urban feeling. As this
institution was built in the mid-90s, its architecture was modern, with three to four high
rise buildings39 constructed in a circular compound set-up. The buildings were suffused
with light and the ground floor was openly built, transmitting the impression of lightness
and space, with views onto the water. Every building accommodated several so-called
‘towers’, where different pathological needs were catered for. The tower I conducted my
research in was called ‘Blumentor’ where mainly neurological rehabilitation clients were
treated. I was based on the first and second floor, whereby the first floor mainly saw
passing through stroke patients. Long stay and chronic (stroke) patients, were located on
the second floor.
The nursing home in contrast was located in a residential suburb and the
architecture replicated the 70s style: a long-drawn-out and contorted four storey
building, where the interior was not well lit and the ground floor conveyed a rather
39 Please refer to Appendix C for pictures.
31
cramped impression. The first and second floor accommodated residents who needed
24/7 care; the third and fourth floor promoted an independent living environment. The
architecture as well as the location of both buildings replicated the acute – chronic divide
as the temporality of recovery was promoted by the rehabilitation institutions' modern
and spacious set-up, as well as the close proximity to the city centre. Chronicity in contrast
was co-produced by the rather old, dark and contorted interior architecture of the
nursing home and the quiet residential surrounding. A further in-depth exploration of
each institutions spatial design will draw upon the importance of the divide in regards to
the co-production of my informants’ chronic identities.
5.2 CHRONICITY OF SPATIAL DESIGN: GROUND FLOORS
The ground floor in both institutions functioned as the ‘productive’ and socialising space,
where therapy and training rooms, a hairdresser, the computer rooms, a restaurant, a
shop and a café were located. The difference however was produced by the spatial design:
As mentioned above, the ground floor of the rehabilitation institution was suffused with
light as it was open planned, where the main corridor was lined with comfortable
couches, inviting clients and their visitors to rest and socialise. However, the small café
was the favourite socialising spot for clients and professionals alike. The ground floor in
the nursing home, in contrast, was rather dark and narrow, and henceforth residents
preferred to socialise in the outdoor smoking and adjusted non-smoking area, where they
could enjoy the sun and observe the hustle and bustle.
Thus, residents in both establishments appreciated one material environment
over the other (Pols 2005). The ‘acute’ and the ‘chronic’ identities of my informants were
furthermore co-produced by the spatial design of the ground floor. Chronicity in the
nursing home was further produced by the scarcity of funding, as there was only a rather
smallish therapy area available, with only two physiotherapists, one logo-, and one
ergotherapist in charge for more than one hundred residents. This contrasted sharply to
the dozens of therapists, the many therapy rooms, and the well-equipped gym in the
rehabilitation institution. The acute-chronic dichotomy therefore was indexing the access
to rehabilitative resources, as investment in such a nursing home was deemed to be
unnecessary. The availability of funds was also reflected in the spatial design of the floors
in both institutions.

32
5.3 CHRONICITY OF SPATIAL DESIGN: THE FLOORS
The first and second floor40 of the rehabilitation institution presented a similar set up:
single rooms41 for clients, one nurse room, one dining and one living room. The dining
and the living room presented the communal spaces on the floors, most of the socialising,
however, happened in the former. In each dining room there was a large kitchenette42
located, which made the room more homely. Clients and their relatives, as well as the care
personnel regularly used the kitchen to warm up or cook food. The interaction in these
social spaces differed quite dramatically between those two floors: clients dominated the
dynamic on the first floor, as jokes and laughter were a constant companion during meal
times, and the enjoyment of eating and spending time together was quite traceable, which
in turn contributed to a strong group solidarity. On the second floor, in contrast, the
nurses dominated the dynamic of that dining room, due to the connected nursing room,
and due to the need of having to keep a watchful eye on the residents during mealtimes.
Henceforth, the social interaction between the clients was a passive and quiet one, as most
of them were severely cognitive and bodily impaired. It can be argued that the more active
and able-bodied residents on the first floor, as well as the care personnel on the second
floor functioned as social navigators through which the lived reality on the floor was co-
produced (Vigh 2009). This contrasted starkly to the lived reality in the nursing home,
where not only the care personnel, but also the built and material environment co-
produced the chronic identities of the residents.
Every floor in the nursing home consisted of thirty-two apartments, two nursing
rooms, administration offices, and a doctor’s office on the second floor. The first floor
accommodated a communal area and an enormous terrace, which sometimes functioned
as entertainment area, where during mild afternoons and evenings activities such as
Bingo were organised. I conducted my research on the second floor which did not offer a
communal space for residents. This was palpable in the atmosphere: everyone kept to
themselves and if they were not mobile enough to move around, they stayed all day in
40And I believe this is also the case for the floors in all the other towers. 41The rooms were small but comfortable and equipped with a single bed, a bed side table, a sofa chair, a
small coffee table and a big wardrobe. The shape of the room was rectangular. 42It was well equipped with stove, oven, micro-wave, grill, and with two fridges where clients and nurses
could store their food.
33
their apartment. In this respect it can be argued that the spatial design of the second floor
disabled the resident’s sociability (Pols 2005). The chronicity of the built environment
(Wiedman 2010), as well as its accompanied strategies (Segrott & Doel 2004),
contributed towards the resident’s immersion of illness, their isolation and loneliness.
Hence, the chronicity of the built environment hindered my informants from regaining
their lives by way of developing new meanings and purpose despite their gravely disabled
bodies (Slade & Amering et al. 2014). How the strategies of the built environment
produced the chronic identities of my informants comes in particular to the fore when
comparing the spatial design of the apartments with the room set-up in the rehabilitation
institution.
5.4 SPATIAL CHRONICITY VERSUS SPATIAL TEMPORALITY
All apartments in the nursing home were equipped with a private disabled bathroom, a
kitchenette and a living/sleeping room with an adjustable single bed, a dining table, a
night table and a few chairs for visitors. Therefore, the apartments were designed to
function as residential homes, providing a dignified and comfortable living environment,
with the advantage of a 24/7 care provision service. However, as most of the residents
were immobile, gravely disabled and hence dependent upon the care personnel, the
apartment doors were kept open during the day. For the more mobile residents the
institutionalised care strategies contributed to a rather unsatisfactory and uncomfortable
living situation, as they often felt observed with an accompanied feeling of loss of their
privacy. For complete immobile residents, on the other hand, the open doors were the
only way to be part of the daily life on the ward. They therefore appreciated daily life in a
passive and observing way, whereby their appreciation was co-produced by the
restrictions of the built environment and social others (Pols 2005). Henceforth, the
chronic ‘being’ of residents were composed in relation with the care personnel
observational strategies, but also by the spatial set-up of the apartments (von Peter
2013). However, the state of being chronic is not a static one, as for instance, mobile
informants tactically escaped the observational nature of the care practices by way of
leaving their apartment, and also the nursing home for some time.
It was not so much the room door, but rather the unlockable bathroom door which
contributed to the clients’ loss of privacy in the rehabilitation institution. The room set-
up resembled the ones of (private) hospital rooms: they were small but comfortable and
34
equipped with a single bed, a bed side table, a sofa chair, a small coffee table and a big
wardrobe. Clients shared a disabled bathroom with their neighbour, whereby the two
bathroom sliding doors leading to each room were not lockable. It therefore frequently
happened that nurses came into the room from the bathroom without knocking. This was
in particular problematic for long stay clients on the second floor. My informants’ reduced
the time in their rooms as much as they could, by socialising in the dining room, in the
ground floor café or by checking their emails in the computer room. Even those who were
not as mobile tactically escaped by quietly spending their days in the dining room with
other immobile residents.
In this way it can be concluded that the apartment and room set up in both
institutions resembled the acute – chronic divide, as the spatial design of the apartment
in the nursing home fostered chronicity and the residents’ immersion of illness by way of
sustaining social isolation and boredom. The rather hospital like set-up of the rooms in
the rehabilitation institution, in contrast, resembled the biomedical understanding of
acute, for the unlockable bathroom doors can be regarded as a sign of temporality, where
the lack of privacy was the price clients needed to pay for being rehabilitated back to
‘normality’.
5.5 SUMMARY
The spatial set up of both establishments replicated the acute-chronic dichotomy: on the
first floor of the rehabilitation institution a palpable optimistic atmosphere was
prevalent, where clients and care personnel were optimistic about the recovery process.
In contrast, on the second floor, and more so, in the nursing home, a rather passive and
negative atmosphere was prevalent. The optimism for recovery was replaced by the
chronicity of everyday life, which was constituted by the mundane and unstructured days,
resulting in boredom and social isolation. The acute-chronic divide was furthermore set
in stone in the actual architecture, and in the interior design in both institutions: due to
sufficient funding, a quick recovery was fostered by the modern, well-lit recovery
rehabilitation environment, as well as by the well-equipped therapy and training units.
Scarce funding, in contrast, contributed to an old and not well-lit nursing home
environment, where the lack of therapeutic and care resources contributed to the
residents worsening of their life quality, as well as to the establishment of their chronic
identities. Consequently, the built environment, as well as the availability of funds, not

35
only constituted the economic, environmental and political facts of chronicity, both
factors also functioned as the social navigator in the production of care and therapeutic
strategies which my informants combated with certain tactics of resistance. The chronic
identities of my informants were also co-produced by the politics of time and timing.

36
CHAPTER 6: CHRONICITY OF POLITICS OF TIME AND TIMING
This chapter explores how the acute – chronic dichotomy is reflected in the use and the
experience of time. Those who are the powerful, employ a politics of time and timing -
which Ferzacca (2010) terms ‘chronopolitics’ - by way of regulating daily routines (ibid:
157). Chronopolitics was used in both institutions as a means of social control, for the
daily institutionalised routines were marked by either a heavily structured routine in the
rehabilitation institution, or by the non-structured daily rhythm in the nursing home. As
such my informants found themselves at the mercy of the daily routines, as well as the
chronopolitics of the therapy and care provision. Chronopolitics therefore was co-
responsible for my informants’ chronicity. What follows is an exploration of how my
informants experienced the politics of time and timing, and which tactics they employed
in order to cope with such.
6.1 CHRONOPOLITICS OF DAILY ROUTINES
Daily routines in each institution were structured around core assemblages of
morning/evening hygiene, medical regimen, meal and resting times. The major difference
however can be found in the way how these core routines were implemented and
executed. Life on the first floor in the rehabilitation institution was organised around
therapies, with three therapy sessions43 scheduled in the morning and three therapy
units organised in the afternoon. The therapy schedule in turn was organised around the
institutional core routines: breakfast from nine-thirty to ten-thirty; lunch44 at twelve-
thirty and resting times45 after lunch until three in the afternoon. From three onwards
there were group activities, therapy sessions or doctor meetings on the agenda. Dinner
was arranged at six in the evening, after which the residents had free time. The routines
on the second floor differed in regards to the therapy schedule, as chronic residents
received therapies only occasionally. Their days therefore were rather unstructured, with
meal and resting times as the only fixed anchor points (Charmaz 1991: 244).
43Each therapy session lasted for thirty minutes. 44Lunch and dinner was served in the dining room on each floor. During lunch I was able to observe my
informants interaction with each other. 45 Resting times were considered as important, especially for stroke patients. The medical director
confirmed that in order to guarantee the best recovery outcome the brain has to be given ‘out times’ with
no sensational input: “Sometimes I tell clients that they have to close their eyes for a few minutes in order
for them to be able to focus and concentrate again”.
37
Although the core assemblages of daily routines were of course a constant in the
nursing home, its implementation was much more flexible. This was mainly due to the
fact that lunch was the only meal per day which the institution provided. Henceforth, the
provision of food for breakfast and dinner was the residents (or their families) own
responsibility, and eating times were aligned to the residents schedule. However, as most
of them were unable to cater for themselves, they were dependent upon the carer for
these meals too. Therefore, usually breakfast took place at around nine-thirty, lunch at
twelve-thirty and dinner at six in the evening. However, due to chronic understaffing,
breakfast and dinner time schedules shifted regularly for up to two hours, which not only
left the residents hungry, it also affected their medical regimen. It can be reasoned that
the acute – chronic dichotomy was mirrored in the core assemblages of both institutions:
sufficient financial funding guaranteed a smooth running of the daily routine in the
rehabilitation institution, whereas insufficient funds, constituted the chronicity of
understaffing in the nursing home, which in turn contributed to a rather irregular core
routine.
In the nursing home certain institutional strategies were employed in order to reduce
the pressure upon the chronic exhausted care personnel, and to make the daily routine
run smoothly. For instance time regulations for the evening hygiene should prevent
residents to fall asleep too early and as a consequence have a restless night. However, Mr
Kaanu perceived those strategies rather as a control technique:
They always want to have the last word. If it’s my wish (to brush his teeth at
18:00) they should listen to me. Everything you ask they don’t do, they have
a different opinion. I hate to be dependent!
In a way the carers strategies disempowered Mr Kaanu, as he lost agency upon his
decision making. He resisted, however, by way of ‘using’ visitors (e.g. me) for his purpose,
e.g. to brush his teeth at the time he thought was appropriate. Not only did Mr Kaanu use
tactics in order to resist the chronopolitics of daily routines, it was also the care personnel
themselves who resisted the LTC policies by way of employing tactics to cope with the
chronicities of understaffing. Silencing residents was another cope mechanism employed
by the care personnel.
38
6.1.1 STRATEGIES OF SILENCING
Thomas once told me that it is best to shut his mouth, as “carers always have the last word.
It’s better to shut up and let carers talk over you”. Henceforth, his chronic identity was co-
produced through the interaction with the dominant care personnel (Pols 2005), which
Mr Osei’s case further illustrates
One afternoon I witnessed a major argument between a Surinamese carer
and Mr Osei, regarding his laundry. At first Mr Osei argued and tried to
explain his opinion to the carer. She tried, in turn, to make him understand
why it was necessary to have his clothes labelled. The argument went on for
at least 20 minutes. This situation became very heated and the carer ever
more dominating. At some point, Mr Osei just kept silent. I could see in his
facial expression and body language how much he disagreed with what she
said, how much he wanted to defend himself. When the carer eventually left
the room, he started to cry. He tearfully told me “They want to force their
will upon me, they treat me like a child. I will never let them rule over me!”
(Notes, 22/04/2013)
In order to not give up his authority, Mr Osei, and all the other informants, employed
certain tactics of resistance to enhance their quality of life in one way or the other. For
instance when Mr Osei encountered the above incident he involved me in order to
strengthen his argument
Tell her what you have seen last time, that she (his social worker) took two
bags of my clothes downstairs and till now (two weeks later) I did not
receive them back. Tell her! Tell her!!
His body language was emphasising on the importance of getting me involved as he was
facing and aggressively pointing towards me when he was talking to the carer. Whereas
when he spoke to the carer he was often just staring at the floor. Thus, he tactically used
me in order to make him heard.
Taking the above into consideration it can be argued that the employed
institutionalised chronopolitics fostered a hectic and dynamic therapeutic rhythm on the
first floor in the rehabilitation institution, where patients were encouraged to work on
39
their health, with the aim to re-establish their ‘normal’ self (Ferzacca 2010: 160-162).
This therapeutic rhythm in turn conforms to the concept of clinical rehabilitation, where
a patients recovery is enhanced, hence “[resting and therapy] time is invested to re-
establish a [patients] capitalist productivity” (ibid). In contrast on the second floor, and
even more so in the nursing home, chronopolitics were responsible for the irregular and
unstructured daily routines. As such, the politics of time and timing contributed to the
residents’ disempowerment, with a loss of autonomy and an immersion of illness as an
outcome. Furthermore, the lack of funds and the non-availability of therapies or
structured activities, fostered the chronicity of social isolation and boredom in the
nursing home.
6.2 CHRONOPOLITICS OF BOREDOM AND SOCIAL ISOLATION
The most frequently mentioned reason for the experiencing of boredom was an
unstructured daily routine, which was coupled with a lack of variety. Mr Kaanu for
instance mentioned that “I only sit in my chair all day, staring out the window and do
nothing… I wanna go out”46. This was also confirmed by Dominik who complained that
only the therapies offer some distraction but
then nothing. I only see this place, this people, this environment and nothing else.
I have to stay in this one [wheel chair] all-day. It is very, very tiring.
I saw residents sleeping in their wheelchair, when awake staring at a wall or out of the
window, and for many the television programmes were the only other alternative to
combat boredom. As such all these factors informed and navigated my informants lived
experiences by way of restricting their daily routines which was also reflected in the
futility of day care activities as Emiel confirmed
Today it was nothing to do at day care. I was sitting in my chair all day and
waited till it was time to go. Here day activities are not purposeful. We don’t
create or do something purposeful.
The consequences of boredom, of the unstructured daily routines and activities caused
Emiel, and many other residents, to develop depression and suicidal thoughts. Despite
of all the difficulties encountered, my chronic informants employed certain tactics in
order to better their quality of life. For instance, in order to bring some variety in his life,
46As mentioned in the methodology section, I took my informants ‘out for a walks’ in order break up their
boredom.
40
Emiel stationed himself near the main entrance where he could observe the coming and
going, and where he had the chance to interact with strangers. He employed this tactic
to “feel that I am not dead, that I am still alive”, and to temporarily navigate himself out
of the imposed social isolation and to gain some control back over his practices of
sociability. Mr Osei escaped the chronicity of boredom by way of attending day care
activities three times a week, which were organised by the Ghanaian organisation
Akwaaba47. This he did by driving the short distance from and to the organisation with
his scoot mobile. He was also frequently visited by a bible group, his social worker and
his friends. Hence, his own mobility and his social network functioned as navigators out
of boredom and social isolation.
In this respect it can be concluded that the politics of time and timing functioned
as a form of social control, as chronopolitics were employed in order to organise the daily
routines in both institutions (Ferzacca 2010). These chronopolitics in turn are informed
by the acute – chronic distinction, as the hectic therapeutic rhythm of the rehabilitation
institutions reflected the temporality of clinical recovery. The unending nature of
chronicity, in contrast, determined the daily routines in the chronic institution, where
days were perceived as endless and repetitive, causing boredom and social isolation.
The acute and the chronic ‘being’ of stroke survivors thus were composed of relationships
with other, more powerful social actors (e.g. the care personnel). These powerful others
played an important part in the co-production of the residents’ daily reality, their
navigation through the daily routines, and of their active or passive sociability (von Peter
2013: 54, Vigh 2009, Pols 2005). As such stroke survivors’ identities were constantly
changing in accordance to different situations (ibid), which the next section further
illustrates.
6.3 CHRONOPOLITICS OF THERAPY AND CARE PROVISION
In both institutions chronopolitics not only regulated the daily routine, the politics of time
and timing was also responsible for prolonged waiting times, for the institutional
compressed therapy agenda, and the (non) vital rhythm (Ferzacca 2010: 160). As such
these human timescapes, with its temporal modes of length and rhythmicity, functioned
as a form of social control in both establishments (ibid).
47Akwaaba provides home care and day care services for mentally and physically disabled Ghanaians.
41
6.3.1 WAITING TIMES
In the rehabilitation institution waiting time was induced by the rather unscheduled
therapy agenda as only a few therapies were planned and agreed in advanced, leading to
prolonged waiting times which Mr Olm confirmed
B: The planning for physiotherapy is for four times a week, and ergo three times
a week. At the moment I am not quite sure [when the therapies take place] as I
am waiting for the agenda. But what really is sure for the moment is that I have
two times this week physiotherapy, but may be more. I am waiting for the
agenda
M: The agenda will be given to you every Monday?
B: No sometimes in the morning they say ‘well physiotherapy is at ten or at
eleven. And every morning you can hear when the physiotherapy or the ergo
therapy is, but not for the whole week. I am just waiting. I just wait all the time.
The politics of time and timing, therefore “[is] experienced as instruments of power in the
context of therapy” (Ferzacca 2010: 157). According to the institutionalised logic it was
assumed that there was no need to inform Mr Olm, or all the other residents for that
matter, about the daily changing of the therapy agendas, as clients were expected to be
flexible, adherent, compliant, and focused upon their therapeutic regimen. In this respect
chronopolitics fostered chronicity, as whilst waiting for the daily therapy schedule, clients
were restricted in their movements and hence transmuted into chronic beings (von Peter
2013). Mr Olm filled these prolonged waiting periods by watching movies which he stored
on his laptop, or by reading the newspapers. In a way he tactically used the imposed
waiting time for his advantage as the otherwise hectic daily schedule would have not
allowed him to have those enjoyable and relaxing moments.
In the nursing home waiting time had a much more serious impact upon my
informants’ quality of life, as it affected their physical, psychological and emotional well-
being. Waiting times for care personnel could span from twenty minutes up to six hours
or longer. For instance, Mr Kaanu and Mr Osei needed to wait for the carers in order to be
brought to the toilet, causing Mr Osei to lie in his own excrements for hours.
42
However, despite of feeling really bad, he was grateful when the nurse eventually put him
under the shower and made up his bed. Although he had such a dreadful experience, he
was also aware that the nurse was alone during the weekend. In a sense his judgement
and knowledge about why he needed to go through such an appalling situation gave him
agency to cope with the whole situation. Both, Mr Osei and Mr Kaanu, experienced
institutionalised strategies, which not only affected them, those strategies also affected
the nurse, who was the sole care provider on duty for thirty-two residents.
Waiting time in both institutions, therefore, was as much a construct of the politics
of time and timing, as it was socio-politically produced. This in turn co-produced my
informants’ chronic identities. Institutionalised chronopolitics played also an important
part in the construction of the therapeutic and vital rhythm in each institution.
6.3.2 COMPRESSED THERAPY AGENDA VERSUS (NON) VITAL RHYTHM
The timescapes of compressed therapeutic rhythms in the rehabilitation institution, and
the non-existence of vital rhythms in the nursing home, were important navigators in the
illness experience of my informants. The former experienced through compressed
therapy sessions of thirty minutes and the tight therapy schedule of the professionals; the
latter through the irregularity of the medical regimen. The tensed therapy agenda in the
rehabilitation institution impacted upon the (felt) quality of the provided therapies, as
exercises were often dismissed or discontinued, due to the tight therapy schedule of the
professionals. This was especially the case with severe cognitive impaired or freshly
admitted clients. Mr Suso’s case study will illustrate my observations further.
Mr Suso, suffered two strokes, whereby the second left him severely cognitive and
bodily impaired: right side brain damage causing a total paralysis of his left body side;
severe aphasia, the loss of rationality and emotions, as well as no disease recognition. His
short term memory was affected and he suffered from apnoea syndrome, causing
constant tiredness as his breathing regularly stopped for a few seconds. Full recovery was
unlikely, in contrary; his prognosis was rather bleak with the likelihood of becoming a
nursing case for the rest of his life. His therapy focused on ADL training, on aphasia
therapy, and on the strengthening of his healthy body side. I was
43
able to observe the whole therapy range and the time issue was especially prevalent
during the Ergo-, and Logotherapy.
Ergotherapy:
During therapy sessions, I experienced the ergo-therapist as a very calm, quiet and
positive person. T-shirt training48 was one of the exercises where the-therapist needed
to explain every step of the T-shirt dressing procedure for several times so that his brain
could memories these steps. This was at times difficult as his condition also caused him
to lose control of his actions, resulting in frantic and aggressive bodily movements, which
needed to be physically stopped by the therapist. What also contributed to Mr Suso’s
frustration was the shortness of the therapy session, as when he finally managed to take
off his shirt, it was already over. It may have been advisable to adjust the therapy duration
according to Mr Suso’s physical and cognitive needs, e.g. by extending the therapy
duration to one hour. However, the tight agenda of the therapists made a more flexible
approach impossible.
Logotherapy:
The Logotherapist usually picked Mr Suso up from his room (in his wheelchair) and
brought him downstairs to the therapy room (which itself took up several minutes of the
therapy time). One time she came late and shortly after the therapy started she needed to
pick up the phone for several times. This not only interrupted the flow of the therapy, it
also caused loss of time. When the therapy finally continued, only twenty minutes were
left, and the time pressure was palpable throughout the therapy session. A sense of being
rushed, and an atmosphere of restlessness was traceable throughout all the other
logotherapies.
These two short extracts bring the inequality of time and timing to the fore: on the
one hand residents needed to endure long waiting times and uncertainty regarding the
therapy schedule. On the other hand, the therapy sessions were often felt to be too short
and not productive or demanding enough. Time and timing, therefore, not only shaped
48T-shirt training is part of the ADL training, where the basics of grooming, dressing and toileting are re-
learned.
44
the medical and therapeutic perception of patients, it also shaped the practices
of the medical professionals (Ferzacca 2010: 157), which was especially apparent in the
nursing home.
A regular time schedule for the administering of medication is of utmost
importance in order to successfully manage stroke survivors’ co-morbidities and other
bodily symptoms. Hence a strict time schedule ideally should function not only as an
important therapeutic tool, but also should represent a vital institutional rhythm
(Ferzacca 2010: 160). Unfortunately, such a vital institutional rhythm was non-existent
in the nursing home, rather it frequently happened that drugs were not administered on
time, the wrong amount of pills were handed out, or none were in stock. This caused
bodily, emotional and psychological discomfort, especially for the residents who were
diabetic, a condition which requires as stringent adherence to the medical regimen
(Ferzacca 2010). The administration of insulin has to take place shortly before the
consumption of food, and regular eating times are therefore essential (ibid). However,
this strict regimen most often could not be followed due the busy routine on the ward.
As a result Emiel experienced distress when he was first admitted to the nursing
home. During the day he administered the insulin by himself, but in the evening when
already in bed, he had no access to the insulin which was stored in the kitchenette.
Therefore he was dependent on the nurses for the last insulin injection at night, and the
first in the morning. This was at times problematic as the care personnel could not attend
him every day at the same time. However, as the time span for the night insulin has to be
exactly calculated, it is vital to have the last injection administered on time 49 . This
irregularity prevented Emiel to establish a vital rhythm of regular eating and drug
consumption (Ferzacca: 160). In this regard, he experienced the chronopolitics of medical
regimen. Emiel solved this problem by taking the insulin injector with him to bed, stored
in a bag which he attached to the over bed hoist handle. In this bag he also stored his
phone and other important items, such as a spare set of medication. He therefore
employed a creative tactic of resistance, through which he not only overcame the
institutionalised timescapes and strategies, he also combated the strategies of the built
environment with its spatial segregation between kitchenette and bed (Segrott & Doll
49A too short time span can result in excess insulin, which in turn causes hypoglycemia. Hypoglycemia is
caused by low blood sugar, which results an inadequate supply of glucose to the brain (Ferzacca 2010).
45
2004). It has to be acknowledged that chronic understaffing50 made it impossible for the
carer workers to adhere to this strict medical regimen. Henceforth, the carers, as much as
the residents, were the victims of the political and economic facts of chronicity.
In essence, the politics of time and timing was responsible for the tight therapy
agenda in the rehabilitation institution, and likewise for the erratic drug distribution and
administration in the nursing home. Therefore, time in this perspective, can be regarded
as disruptive source of self-management, as time was manipulated by the professionals
to meet the institutional daily (tight) schedule and to smoothen the care provision
practices (Ferzacca 2010: 170).
6.4 SUMMARY
Throughout this chapter I aimed to demonstrate how the acute – chronic dichotomy is
replicated in the institutionalised usage of time and timing. As such I referred to the
term of chronopolitics, which according to Ferzacca (2010) is used by the powerful to
regulate daily routines in institutionalised settings. The daily routines in the
rehabilitation and nursing establishment were similar in their core structure, e.g. resting
and mealtimes, but differed significantly in their execution. The completely different
ways of implementation, however, replicated the acute-chronic divide as the daily routine
in the rehabilitation institution had fixed timings at its core, with a busy therapy schedule
organised around this core structure. This contributed to rather busy, hectic and
‘productive’ days, which were aimed to rehabilitate stroke survivors’ back to fit and
‘normal’ citizens. In the nursing home, in contrast, the characteristics of chronicity
were also apparent in the daily routine. The core daily routines were handled in a much
more flexible way, where residents often needed to wait for the care personnel in order
to receive their meals, or to have their personal and medical needs attended. The
different implementation modes have to be ascribed on how the acute-chronic divide
indexes health care resources, as the well-staffed rehabilitation institution stands in stark
contrast to the chronic understaffed nursing home, which in turn contributed to the
chronopolitics of care provision strategies: to the silencing of residents; to the
unstructured days; and to the chronic boredom and social isolation. My informants
combated the chronopolitics of the institutions therapy and care practices by way of
50As explained in Appendix A.
46
usefully filling the imposed waiting time, or by creatively inventing tactics in order to gain
some control, and to re-establish some form of vital rhythm in their lives. It can be
argued that my informants’ chronicity was determined by the economic and political
facts of the chronopolitics, which in turn was responsible for the experience of the
continuum of disruption of my informants’ post-stroke life-span. Having looked at how
the built environment and the politics of time and timing replicates the biomedical
understanding of chronicity, I now want to turn to the alternative concept of chronicity:
Chronicity of Life.

47
CHAPTER 7: CHRONICITY OF LIFE - THE CONTINUUM OF RECOVERY
Smith-Morris (2010) argues that in order to understand the experience of chronically ill,
not their punctuated duration of health has to be investigated, but rather their whole life-
span with its continuous disruption (ibid: 25). My informants’ life-spans’ were
punctuated by such disruptions, of which the onset of stroke was just another, though
major one. Their post-stroke lives continued to be disrupted, not only by the occasional
flare ups of their co-morbidities which often transmuted them back into an acute state of
being. It was also the institutions therapeutic and care provision strategies, as well as the
effects of the built environment, which contributed to my interlocutors’ continuum of
disruptions. This chapter therefore investigates the chronicity of my informants’ lives by
way of drawing upon the different stages in which they encountered disruptions: during
the acuteness of recovery process which was marked by uncertainty and fear to remain
permanently disabled. During the continuous punctuation of everyday life through
mundane and major disruptions which not only shaped their rehabilitation experience,
such punctuation also shaped the recovering process of their lives in general. These
disruptions therefore informed their past, their decision making in the present, and
guided their navigation towards the recovering of their lives (Vigh 2009).
7.1 ACUTENESS OF RECOVERY
Time was a major disruptive factor in my informants’ post-stroke life, and an especially
pressing one in the rehabilitation phase. For recovery goals and progress are closely
monitored in a certain time frame, which were regulated by specific medical standards.
In the rehabilitation institution, importance is laid upon clinical recovery that is to make
the client fit, productive and ‘normal’ as soon as possible (Slade & Amering et al. 2014).
Time, in this perspective, was used as a powerful tool for social control (Ferzacca 2010),
and the resulting time pressure contributed to my informants fear to continue their life
span as disabled persons. Henceforth, all worked very hard to prevent this to happen.
Maarten, for instance, mentioned that in order to get better quicker, one needs to adhere
to the rules of the house (e.g. resting times), and to strictly follow the therapy regimen.
If you listen to what they tell you, you have a good start. You shouldn’t try it
yourself. They give you tips how to walk best and they have experience so
you better do what they say. For instance, sometimes you have to bend
48
forward on the stairs, but then you fall down. And she [physiotherapist]
explained to me what to do and how to do it. And then it works. If I do something
I want to know why, and how.
Maarten embodied, what (Ferzacca 2010) and (Kitson & Dow et al. 2013) describe as self-
management practice, and Becker & Kaufman (1995) termed therapy regimen. As such a
patient is expected to be actively involved in the therapies, and to be willing to work on
behavioural and environmental adjustments (ibid). Maarten learned to implement his
post-stroke restrictions into his everyday life, by way of practicing how to climb the stairs.
Mr Suso, in contrast, was very negative about the time structure of this institution which
he then attributed to his progress:
I thought I will start the gym here… but nothing. In the first two weeks [since
admission] they did do nothing. This is too long! The others they are home by
now. What must I do here? What? Sleeping only? I don't see any improvements.
They don’t do nothing.
By comparing himself to other residents who already ‘left’, the feeling of ‘failure’ and one
of ‘staying behind’ was dominating his mood (Pols 2005: 205). Furthermore, he compared
his somewhat ‘abnormal’ body to the ones of his fellow residents which appeared to him
as ‘normal’ (Manderson 2010: 104). By employing the tactic of comparison, henceforth,
he performed and enacted his chronic identity (von Peter 2013: 14). In a way then, Mr
Suso embodied the discourse of clinical recovery (ibid) which in the case of stroke, is
determined by the politics of time and timely progress (Ferzacca 2010). His time
perception also contributed in the objectifying of his body, where, according to Doolittle
(1991), the shock of sudden immobility and paralysis left him “suspended in a passive
objectified body” (citied in Ellis-Hill 2000: 237). As such Mr Suso viewed his paralysed
arm in a passive and objectified manner.
My arm is terrible and sometimes I want to get rid of it [emphasised with cut off
motion]. I am tired of it as it is heavy and painful. I need to do exercises. Need to
do it five to six times a day and it will start coming back to normal. It takes too
long. The doctor said that in three to five months after stroke the hand shall be
back [to normal].
49
It becomes clear that the discourse of clinical recovery not only impacted upon Mr Susos’
perception of time and his understanding of normality, it also caused him to negatively
view and objectify his paralysed arm, which Charmaz (1991) terms ‘conceptional
packaging’. She argues that people treat their illness in the way they think and categories
about it (ibid: 67-68). Mr Suso wanted to cut off his paralysed and ‘abnormal’ arm because
he felt that time is running out for him to get better and to become ‘normal’ again. The
fear of continuing with life as disabled and dependent was imprinted in his actions,
practices and discourse. Mr Suso’s and Maarten’s acute rehabilitation experience was
marked by disruptions which were mainly caused by the chronopolitics of clinical
recovery, which also determined Maarten’s past experience.
7.2 CONTINUUM OF DISRUPTION
Maarten’s drive to get better was partly determined by his disturbing encounter with the
emergency services at the AMC, where he was first admitted after he suffered the initial
onset of his stroke. This incidence made him question the whole medical apparatus. Yet,
Maarten’s experience illustrates the continuous disruption which humans encounter
throughout their life spans.
Maarten suffered his initial onset in late February, which after running of several
standard tests by the neurologist on duty, appeared to be a TIA51. After several hours in
the neurological emergency unit, where his condition improved remarkable, Maarten was
sent home. However, during the night his symptom worsened and when he was rushed
back to the AMC the next morning, it was too late for the specialised Thrombolysis
treatment. The medical director of the rehabilitation institution acknowledged that if
patients improve on such dramatic scale, and if there are no clear signs of a clot on the x-
ray images, then a TIA is the common diagnosis. Maarten, however, was unfortunately
very unlucky as the clot was ‘hiding’, and according to the medical director, the worsening
of his condition could have happened in the hospital (during the night) as well. It can be
argued that Maarten encountered not the biomedical linear diagnosis process (e.g.
diagnosis, treatment and recovery), his experience was rather informed by the continuum
of disruption, as after his discharge from the hospital his symptoms worsened instead of
vanishing (Ferzacca 2010). This disruptive event led Maarten to develop a rather negative
perception of his time in the hospital
51TIA stands for Transient Ischaemic Attack or mini stroke.
50
I went to the hospital and they did several tests on me. They did scans and I had
a 'film', you know the rotating machine (MRI). They saw nothing. But if there is a
bleeding you first see that...so it was a stroke. So if they had taken precautions
straight away they could have avoided it…. Everybody saw [that I can’t walk
properly] except the doctor. All the treatments [at AMC] are very good, no
complains about that…..The nurses are very good. It was just one person... When
I got home it started to get worse. And then I was all night on the sofa…. and in the
morning I went back to the hospital but it was too late by then.
Maarten blamed the neurologist for the worsening of his condition. Hence feeding into the
biomedical discourse that doctors are omniscient, always in charge and aware of what is
best for their patients (Pols 2002). He also lost trust in the power of biomedicine, as the
neurologist failed not only to cure him, but to establish the correct diagnosis in the first
place (Good & Delvecchio-Good 1993:90). The temporality of the biomedical diagnostic
system, as well as the neurologist henceforth functioned as the navigator for the
establishment of Maarten’s chronic identity (Vigh 2009).
This disruption continued to influence upon his experience in the present, as he
was working extremely hard during therapies, and whilst exercising independently, in
order to be able to continue with his many hobbies in the future. In order to do so the aim
was to gain some movements back in his paralysed right arm and hand. He was also
extremely keen to be able to walk the stairs in his house, so that he was not required to
sleep on that sofa on the ground floor, which certainly brought back the memories of this
significant disruptive night, which he associated with life threatening fears, dependency
and disabilities. Maarten therefore not only suffered one significant or disruptive event,
which informed his post-stroke illness experience, rather, past disruptive events mingled
with disruptive events in the present, in turn informed his future which, at this stage,
was focused upon the bodily recovery. This contrasted the chronicity of life of my ‘chronic’
informants, as due to the non-improvement of their bodily symptoms, their recovery was
rather navigated by the aim to re-establish a dignified and purposeful life.

51
7.3 CHRONICITY OF LIFE: TOWARDS A RECOVERY OF EXISTENCE
Chronicity not only highlights the duration of health, it also draws upon chronic structural
factors (e.g. discrimination, racism, or lack of access to health and rehabilitation
resource), and the human lifespan in general (Ferzacca 2010: 158, Smith-Morris 2010:
37). It is therefore important to employ such a holistic analytical lens when wanting to
understand how past disruptive events informed the lived reality of my informants’ in the
nursing home, which in turn fostered their desire to establish a satisfying and meaningful
life outside this institution. As such, all of my informants worked hard towards the
recovery of their lives, which included the acceptance, and hence, successful
incorporation of their post-stroke disabilities which the following three accounts further
demonstrate.
Mr Osei
Mr Osei’s life-span was informed by migration to and from Ghana. He first migrated to
Nigeria in the 70s due to the economic crisis in Ghana in order to work as a lorry driver,
and a few years later he was repatriated. In 1991 he migrated to Europe, where he sought
unsuccessfully for asylum in East Germany, later in Belgium until when in 1992 he finally
arrived in Amsterdam. He married twice, had two daughters but lost both wives. For
the purpose of papers he paid a Surinamese woman in Amsterdam to get married. As soon
as he received the papers some four years later, he immediately filed the divorce, after
which he moved to the UK for the purpose of work. In 2008 his stroke onset occurred
when he was working for a cleaning company in Manchester, UK, where he also was
hospitalised and later institutionalised. He was transferred back to Amsterdam in 2012,
where he first was admitted to a nursing home in Haarlem, but soon was transferred to
the current nursing home. He then spent seven months with his daughters in Ghana,
where he also received herbal treatment, which however proved unsuccessful. His family
relationships were marked by jealousy and greed of his relative wealth; going back to
Ghana for good, therefore, was not an option.
His past experience influenced his present ones in the nursing home, for the
marriage with the Surinamese woman has shaped his perception of Surinamese people
in general. He called them ‘money eating’, as according to him, they spend their money
only on daily life expenditure. The (Surinamese) care personnel were unaware of his
52
capability to understand the Surinamese language when they shouted abusive words at
him during bathing times. This in turn made him aggressive towards them which resulted
in a general worsening of his situation.
In order to escape the care personnel abusive behaviour, and the disempowering
institutionalised strategies in general, Mr Osei employed certain tactics and navigators so
to be able to establish a new and independent life outside the nursing home. For instance
with help of his social worker from Akwaaba he applied for social housing. His social
worker, therefore, not only helped him navigate his way through the bureaucratic social
housing landscape, she also helped to apply for permanent visas for his daughters. The
social worker furthermore functioned as social navigator between Mr Osei, the carers and
the nursing home management. Mr Osei’s journey towards personal recovery, henceforth,
was driven by his desperate wish to live a dignified life, and to take up his role as lone
parent again.
Dominik
Migration from Togo to the Netherlands equally disrupted Dominik’s lifespan. Ever since
he arrived some seventeen years ago, he faced discrimination and racism. As his medical
degree was not recognised at a Dutch University he obtained a diploma as a
pharmaceutical representative, which did not lead him to a job position. Instead he
needed to support himself through ‘dirty’ and low paid jobs. His past experiences caused
him to develop adverse feelings towards Dutch employment policies
They push you just to get 'any' job. They ask you to do things which are not for
your level (of education). For instance, if you finish your study and if you want to
find a job, they force you to do everything, otherwise they stop paying (job seeker
allowance). I was looking everywhere for a job. In Holland they are the bushman
from Europe!
Yet, he never stopped hoping and working towards his aim to become a plastic surgeon,
which was also the main drive for his personal recovery. Dominik suffered the initial
stroke onset some nine months ago (August 2013), which left him severely cognitive
and bodily impaired, namely wheelchair bound and his left arm paralysed. Although he
53
was well aware of the medical implications of his condition 52 , his hope for personal
recovery included traditional healing through which he anticipated to regain his mobility.
Dominik, therefore, employed hope as a navigating tool in the management and
construction of his future personal recovery goals. In this respect Dominik also hoped to
be able to form an emotional and sexual relationship, leading to the establishment of a
family.
The chronicity of my migrant informants’ lives’ was informed by socio-economic
and political facts, which can partly explain their employed disease practices in the
present. These facts also informed their future as they were well aware on how to ‘exploit’
the Dutch welfare state (DWS) by way of applying for disability allowances or pension.
Hence they poached in the terrain of the powerful DWS. The biographies of my Dutch
interlocutors were equally marked by many twists and changes.
Emiel
Emiel encountered many disruptions in his life: from the early death of his maternal
mother to the re-marriage of his father, with the result that his step mother emotionally
abandoned him. He was married twice, whereby his first wife prohibited him to see his
children after their divorce. This was a major emotional drawback which caused him to
start to drink heavily for almost two years. At this time, only his work kept him ‘alive’,
which he spoke very fondly of. Soon after he stopped his excessive drinking habit, he
established his own successful tax return office some twenty years ago, and he also re-
married and became a father of a daughter. The stroke undoubtedly was the biggest
disruption in his lifespan as
I lost everything. The first thing I had to put away was the car. Then I lost my
office and then I lost my freedom to go do some things.
Emiel’s previous work experience was also the main ambition for his personal recovery,
as he planned to re-establish his tax office. Unfortunately his wife and the medical
professionals discouraged him in this endeavour, as according to them, Emiel would not
be able to cope with a demanding business. In a way, his wife and the medical
professionals co-produced Emiels chronic identity by way of redefining his former
52 To stay invalid for the rest of his life.
54
successful business self into an incapable chronic one (Eristroff 1993: 259). As such it was
expected that he should come to terms and accept his ‘new’ chronic identity, which Emiel
did not:
They say that I have to accept it [his stroke disabilities and dependency]. I will
never accept it as otherwise you don't fight anymore. You have to fight to come
through that, otherwise you better be dead. But I fight on. I want to have my
own life again. I am too young to do nothing anymore. I can go on for 30 years
perhaps.
Henceforth, the ones who advised Emiel against his future plans (e.g. his wife and the
medical professionals), as well as his own non-acceptance of his situation, functioned as
social navigator through which Emiel moved towards a fulfilled life (Vigh 2009). His
personal recovery, therefore, involved the development of new meaning and purpose in
his life, which also entailed the establishment of a meaningful emotional relationship,
either with his wife or with a new partner.
7.4 SUMMARY
My informants’ lifespans were punctuated with continuous mundane or major
disruptions, which all can be considered to be fateful moments53 at the time they occur.
Stroke was just another one, which of course was always a life changing experience. My
informants employed different tactics, and they went through different stages when
attempting to recover their lives: the acuteness of their rehabilitation experience which
was marked by the temporariness of clinical recovery. A continuum of disruption was
then experienced which was mainly connected to the acuteness of their recovery. The
chronicity of life in contrast determined the future determination of my informants in the
nursing home. Nevertheless, all of my informants’ chronicity of stroke was a lifelong
process of daily adjustments, improvements, and identity work (Smith-Morris 2010, von
Peter 2013). Therefore, rehabilitation and recovery efforts, as well as the LTC policies,
might be advised to let go of the temporariness of clinical recovery. Rather, stroke
rehabilitation should be based upon survivors’ lifespan, holistically including the social,
53Giddens (1991) termed fateful moments to be “phases at which things are wrenched out of joint, where a
given state of affairs is suddenly altered by a few key events (ibid: 113).

55
relational, somatic symptoms and disruptions, which are partly co-produced by
structural factors.
56
CHAPTER 8: CONCLUSION
This study set out to explore how the acute-chronic binary produced chronicity, and how
the latter was influencing my informants’ stroke illness and after care provision
experience. Stroke can be regarded to be acute at the initial onset, and chronic ever after
as its post-stroke disabilities are unending. Health-care and rehabilitation resources, as
well as stroke survivors’ access to such are divided accordingly. Throughout this thesis I
demonstrated that the acute-chronic distinction determines the Dutch LTC policies, the
built and material environment of care institutions, and the employed institutional time
regimen. All these factors in turn constitute the institutionalised care and therapy
provision strategies which not only co-produced survivors’ chronic identities, they also
shaped the poaching and resistance tactics of stroke survivors’ when attempting to create
space in the terrain of the powerful. This they did by strategically employing social
navigators, who helped to navigate stroke survivors’ ways towards their personal
recovery.
In order to analyse my informants’ post-stroke experience I have employed
several theoretical concepts. As mentioned above, the Acute-Chronic Distinction
provided the overarching framework through which the other theoretical building blocks
developed. This study unravelled how the chronic identities of my informants were
promoted by this binary, as when there is no more clinical and bodily improvement to be
gained all of them were banished, hidden and isolated in nursing homes. I attempted
to deconstruct the biomedical understanding of Chronicity – that is one of linearity and
temporariness – by way of employing the alternative concept of Chronicity of Life, which
rather is concerned with a human lifespan's continuum of disruption. Mundane and
major everyday disruptions not only affect a sick persons’ lifespan, such
disturbances interrupt all human lives as they are partly constructed by wider socio-
economic and cultural factors. Migration, discrimination and divorces, as well as the
onset of their stroke and the resulting institutionalised therapy and care provision
strategies were some of the disruptive events my informants encountered throughout
their lifespans. These disruptions therefore informed their experience and actions in the
present, which in turn navigated and informed their future outlook. As such, the
concept of Chronicity of Life not only critically investigates the biomedical understanding
of chronicity, but this alternative interpretation also questions the widespread
57
anthropological and sociological conceptualisation of the (biographical) disruptive
nature of chronic illnesses (see for example Bury 1981, Giddens 1991, Charmaz 1991,
Becker & Kaufman 1995, Ellis-Hill 2013). Henceforth, I follow Smith-Morris &
Manderson’s (2010) line of reasoning that instead of narrowly focusing on the
temporality of illness disruptions, pragmatic health solutions have to be developed which
holistically encompass the social, somatic and emotional facets of a chronic sick person.
The Personal Recovery Model with its focus upon lifelong identity work might function as
starting point.
Current recovery therapies for stroke survivors are primarily aimed to clinically
rehabilitate the post-stroke body back to ‘normal.’ The acuteness of diagnosis plays a
fundamental role for the post-stroke outcome, as through an effective acute treatment,
the potential life threatening disease is transmuted into a chronic one. The
recovery prognosis, however, is as much dependent on socio-economic factors (e.g.
proximity of specialised stroke unit), as it is on medical (e.g. extent of bleeding into the
brain) and technical (newest diagnostic machinery) ones. Furthermore, the impacts of
post-stroke symptoms and disabilities are never just confined to the body but are spread
upon the wider social environment of a survivor. My informants reported a lack of
support in social, emotional, interpersonal and sexual matters, and this often caused
additional distress which several studies acknowledged (Becker & Kaufman 1995,
Ellis –Hill 2000, Pols 2002). The concept of recovery includes the aforementioned
factors in the ongoing rehabilitation process of stroke survivors’ lives. Unfortunately I
have seen little evidence that such a holistic approach was implemented in the
rehabilitation institution, and even less so in the nursing home. Rather, the chronic
identities of my informants were solidified by both, the chronicity of the built and material
environment, as well as the institutionalised chronopolitics of daily routines. By its very
nature, the acute – chronic distinction fostered chronicity through informing LTC policies,
which in turn were responsible for the chronic understaffing in the nursing home, thus
shaping the institutionalised therapy and care provision strategies. In order to cope
with these strategies my informants employed poaching tactics and social navigators:
they used their mobility to not only escape the institutionalised chronopolitics of daily
routines but also tried to regain some form of control over their sociability by engaging
with strangers, social workers and friends. In this way they used these tactics to combat
the imposed social isolation. Furthermore, my informants used social others in order to

58
resist the politics of time and timing in the nursing home. The chronopolitics of the
rehabilitation institution was responsible for both a hectic daily schedule but also for
prolonged waiting times. My informants usefully filled the imposed waiting times by
enjoying some relaxing and private moments. In a sense then, the LTC policies and the
institutionalised care and therapy provision strategies were the social navigators through
which not only the chronicity of my informants lived reality were constructed, but these
factors also impacted upon the daily work reality of the care personnel.
In summation then, this research attempted to highlight how the acute-chronic
dichotomy influences, if not determines, the post-stroke experience throughout every
stage in the after-care process, as it is mirrored in the LTC policies and its funding
procedures. These policies in turn not only govern the stroke after-care landscape, they
also index the access to health-care and rehabilitation resources. The acute-chronic divide
is furthermore reflected in the built and material environment of care institutions, the
institutionalised chronopolitics, the long-term care employment and the long-term care
educational standardisation. The aforementioned division therefore is reflected in macro
forces (e.g. LTC policies), which in turn constitute the chronicity of stroke.
Several limitations were encountered during this research. Due to the short-levity
of this study, only a small sample of participants could be recruited. As a result, this
research might be criticised for ” its lack of impact on policy-making and practice, its
limited payoff in the everyday worlds of politics and work” (Atkinson & Hammersley
2007: 17). However, the results of this research certainly contribute to the provision of
impulses and ideas on how to promote a holistic post-stroke recovery process, where
instead of focusing on the temporariness of clinical recovery, the survivors’ social,
relational and emotional environments, as well as wider structural factors, have to be
taken into consideration. The focus on institutionalised stroke survivor is certainly
another limitation, as the post-stroke after care experience in a survivors’ home setting
might be a very different one. Further research in the home care setting is needed in order
to address this limitation.
This study identified further implications for future research. First, it is of utmost
importance to investigate how stroke survivors are navigating their way through the care
landscape. Do stroke survivors and their families have agency to decide on a possible care
59
pathway? If not, who are the key players in the decision making? Although this research
addressed some of these questions, there is an extensive knowledge gap apparent.
Second, how the Dutch LTC policy reforms impacted upon a stroke survivor’s after-care
experience was already transparent during my research. However, further research is
needed to investigate the reforms impact in the years to come. How will care and nursing
homes deal with the even more tightening annual budgets, and in which way will this impact
upon the care provision, and hence the lived reality of residents? My interlocutors informed
me that since I have completed my research in the nursing home, the situation has
worsened, as the management were in need to dismiss more care personnel.
Unfortunately this prolongs waiting times even more before the care personnel can
attend the resident’s needs. This might be countered by incorporating residents’ informal
networks into the institutional daily routine. Third, further research has to be carried out
in the home care provision sector, as ever more responsibility is shifted to the formal and
informal home care sector. Are appropriate adjustments being made in order to cater for
the ‘in-between’ stroke survivor with an indication of ZZP 3-4/5? If so, how? Are home care
providers better equipped to cater for those in-between survivors, through for instance the
re-direction of funds? How does the informal network cope with the additional burden,
especially considering the lack of emotional and relational counselling provision?
This list is not an exhaustive one, rather it might function as a starting point in
order to scrutinise the boundaries which the acute-chronic distinction still imposes upon
our chronic diseased society. The boundaries between the (sub)‘acute’ and ‘chronic’
stroke illness classifications are not so much induced by the natural course of the disease
itself, but rather by the accessibility of health-care and rehabilitation resources. As such
the chronicity of the stroke illness experience is informed by powerful technological,
political and economic forces.
60
BIBLIOGRAPHY
AMIT-TALAI, V., 2000. Constructing the Field: Ethnographic Fieldwork in the Contemporary World (eds.). London etc.: Routledge.
ATKINSON, P. and HAMMERSLEY, M., 2007. Ethnography: Principles in Practice. (3rd
edn.). London: Routledge.
BECKER, G., 1998. Disrupted Lives: How People Create Meaning in a Chaotic World. Berkley and Los Angeles: University of California Press.
BECKER, G. and KAUFMAN, S.R., 1995. Managing an Uncertain Illness Trajectory in Old Age: Patients' and Physicians' Views of Stroke. Medical Anthropology Quarterly, 9(2), pp. 165-187.
BURY, M., 1982. Chronic Illness as Biographical Disruption. Sociology of Health & Illness, 4(2), pp. 167-182.
CAPUTO, V., 2000. At 'home' and 'away': Reconfiguring the field for late twentieth-century anthropology. In: A. VERED, ed, Constructing the Field: Ethnographic Fieldwork in the Contemporary World. pp. 19-31.
CHARMAZ, K., 1991. Good Days, Bad Days: The Self in Chronic Illness and Time. New Brunswick, NJ: Rutgers University Press.
DA ROIT, B., 2012. The Netherlands: The Struggle Between Universalism and Cost Containment. HEALTH & SOCIAL CARE IN THE COMMUNITY, 20(3), pp. 228-237.
DA ROIT, B. and LE BIHAN, B., 2010. Similar and Yet So Different: Cash‐for‐ Care in Six European Countries’ Long‐ Term Care Policies. Milbank Quarterly, 88(3), pp. 286-309.
DE CERTEAU, M., 1984. Practices of Everyday Life. Berkley, CA: University of California Press.
Dutch Healthcare Authority, 2013. From Fact to Focus: Annual Statement of the Dutch Healthcare System 2013. Utrecht: Dutch Healthcare Authority (NZa).
Dutch Healthcare Authority, 2012. Seperating Fact from Fiction: Annual Statement of The Dutch Healthcare System 2012. Utrecht: Dutch Health Care Authority (NZa).
ELLIS-HILL, C., PAYNE, S. and WARD, C., 2000. Self-body Split: Issues of Identity in Physical Recovery Following a Stroke. Disability and Rehabilitation, 22(16), pp. 725.
ESPING-ANDERSEN, G., 1990. The Three Worlds of Welfare Capitalism. Cambridge: Polity Press.
ESTROFF, S.E., 1993. Identity, Disability, and Schizophrenia: The Problem of Chronicity. In: LINDENBAUM, S. and LOCK, M.(eds.). Knowledge, Power and Practice. pp. 247-286.
61
FERZACCA, S., 2010. Chronic Illness and the Assemblages of Time in Multisited Encounters. In: MANDERSON, L. & SMITH-MORRIS, C., (eds.). Chronic Conditions, Fluid States: Chronicity and the Anthropology of Illness. United States of America: Rutgers, The State University, pp. 157-174.
GIDDENS, A., 1991. Modernity and Self-Identity: Self and Society in the Late Modern Age. Cambridge: Polity.
GOOD, B.J. and DELVECCHIO GOOD, M., 1993. "Learning Medicine": The Constructing of Medical Knowledge at Harvard Medical School. In: LINDENBAUM, S. and LOCK, M. (eds.). Knowledge, Power and Practice. pp. 81-107.
GRAY, A., 2003. Research Practice for Cultural Studies: Ethnographic Methods and Lived Cultures. London: Sage Publications.
GREEN, J. and THOROGOOD, N., 2011. Qualitative Methods for Health Research. London: Sage.
GREEN, J. and THOROGOOD, N., 2009 [2004]. Qualitative Methods for Health Research. Los Angeles, London, New Delhi, Singapore, Washington DC: SAGE Publications.
HAMMERSLEY, M. and ATKINSON, P., 1995. Ethnography: Principles in Practice (eds.). London: Routledge.
KITSON, A.L., DOW, C., CALABRESE, J.D., LOCOCK, L. and ATHLIN, ÅM., 2013. Stroke Survivors’ Experiences of the Fundamentals of Care: A Qualitative Analysis. International Journal of Nursing Studies, 50(3), pp. 392-403.
MANDERSON, L., 2010. "Half a Woman": Embodied Disruptions and Ideas of Gender Among Australian Women. In: MANDERSON, L. & SMITH-MORRIS, C., (eds.). Chronic Conditions, Fluid States: Chronicity and the Anthropology of Illness. pp. 96-112.
MANDERSON, L. & SMITH-MORRIS, C., (eds.). 2010. Chronic Conditions, Fluid States: Chronicity and the Anthropology of Illness. New York: Rutgers, The State University.
MAYNARD, R., 2010. Disability and Dysappearance: Negotiating Physical and Social Risk with Cystic Fibrosis. In: MANDERSON, L. & SMITH-MORRIS, C., (eds.). Chronic Conditions, Fluid States: Chronicity and the Anthropology of Illness. United States of America: Rutgers, The State University, pp. 195-211.
MOL, A., 2002. The Body Multiple: Ontology in Medical Practice. Durham, NC, etc.: Duke University Press.
ORGANSIATION FOR ECONOMIC CO-OPERATION AND DEVELOPMENT (OECD), 2011. Help Wanted? Providing and Paying for Long-Term Care. OECD Publishing: Paris.
62
PAOLUCCI, S., ANTONUCCI, G., GRASSO, M.G., BRAGONI, M., COIRO, P., DE ANGELIS, D., FUSCO, F.R., MORELLI, D., VENTURIERO, V., TROISI, E. and PRATESI, L., 2003. Functional Outcome of Ischemic and Hemorrhagic Stroke Patients after Inpatient Rehabilitation: a matched comparison. Stroke: Journal of the American Heart Association, 34(12), pp. 2861-2865.
PEOPLES, H., SATINK, T. and STEULTJENS, E., 2011. Stroke Survivors' Experiences of Rehabilitation: A Systematic Review of Qualitative Studies. Scand J Occup Ther, 18(3), pp. 163-171.
POLS, J., 2005. Enacting Appreciations: Beyond the Patient Perspective. Health Care Analysis, 13(3), pp. 203-221.
RUSSELL, S., SEELEY, J., EZATI, E., WAMAI, N., WERE, W. and BUNNELL, R., 2007. Coming Back From the Dead: Living with HIV as a Chronic Condition in Rural Africa. Health Policy and Planning, 22(5), pp. 344-347.
SEGROTT, J. and DOEL, M.A., 2004. Disturbing Geography: Obsessive‐Compulsive Disorder as Spatial Practice. Social & Cultural Geography, 5(4), pp. 597-614.
SHUTTLEWORTH, R., 2000. The Search for Sexual Intimacy for Men with Cerebral Palsy. Sexuality and Disability, 18(4), pp. 263-282.
SLADE, M., AMERING, M., FARKAS, M., HAMILTON, B., O'HAGAN, M., PANTHER, G., PERKINS, R., SHEPHERD, G., TSE, S. and WHITLEY, R., 2014. Uses and Abuses of Recovery: Implementing Recovery-Oriented Practices in Mental Health Systems. World Psychiatry, 13(1), pp. 12-20.
SMITH-MORRIS, C., 2010. The Chronicity of Life, the Acuteness of Diagnosis. In: MANDERSON, L. & SMITH-MORRIS, C., (eds.). Chronic Conditions, Fluid States: Chronicity and the Anthropology of Illness. pp. 21-37.
STYHRE, A., 2004. The (Re)embodied Organization: Four Perspectives on the Body in Organizations. Human Resource Development International, 7(1), pp. 101-116.
TEASELL, R., HUSSEIN, N. and FOLEY, N., 2013. Background Concepts in Stroke Rehabilitation. www.ebrsr.com (edn.) London, Ontario, Canada: Evidence-Based Review of Stroke Rehabilitation.
TEASELL, R., HUSSEIN, N. and FOLEY, N., 2013. Clinical Consequences of Stroke. www.ebrsr.com (edn.) Evidence-Based Review of Stroke Rehabilitation: Evidence-Based Review of Stroke Rehabilitation.
TEASELL, R., HUSSEIN, N. and FOLEY, N., 2013. Managing the Stroke Rehabilitation Triage Process. www.ebrsr.com (edn). London, Ontario, Canada: Evidence-Based Review of Stroke Rehabilitation.
TILLMANN-HEALY, L., 2003. Friendship as Method. Qualitative Inquiry, 9(5), pp. 729-749.
63
VAN DER SIJPT, E., 2014. Complexities and Contingencies Conceptualised: Towards a Model of Reproductive Navigation. Sociology of Health & Illness, 36(2), pp. 278-290.
VAN OORSCHOT, W., 2006. The Dutch Welfare State: Recent Trends and Challenges in Historical Perspective. European Journal of Social Security, 8(1), pp. 57-76.
VIGH, H., 2009. Motion Squared. A Second Look at the Concept of Social Navigation. ANTHROPOLOGICAL THEORY, 9(4), pp. 419-438.
VIGH, H., 2006. Navigating Terrains of War. Youth and Soldiering in Guinea-Bissau. New York: Berghahn.
VON PETER, S., 2013. ‘Chronic’ identities in mental illness. Anthropology & Medicine, 20(1), pp. 48-58.
WIEDMAN, D., 2010. Globalizing the Chronicities of Modernity: Diabetes and the Metabolic Syndrome. In: MANDERSON, LENORE & SMITH-MORRIS, CAROLYN, ed, Chronic Conditions, Fluid States: Chronicity and the Anthropology of Illness. pp. 38-53.
Websites
Academisch Medisch Centrum (2013). CVA-zorgketen in het AMC. Available at:
https://www.amc.nl/web/Zorg/Patient/Afspraak-op-de-polikliniek/Polikliniek-
Neurologie/Patienteninformatie/CVAzorgketen-in-het-AMC-1.htm. [25/04/2014].
Kennisnetwerk CVA NL (n.d.). Noord Holland. Available at:
http://www.kennisnetwerkcva.nl/noord-holland [25/04/2014].
Mezzo (n.d.) Mantelzorg. Available at: http://www.mezzo.nl/mantelzorg. [25/04/2014].
READE Revalidatie en Reumatologie (2014). Van mogelijkheden naar maximaal
resultaat. Available at: http://reade.nl/home. [28/05/2014].
The Health Systems and Policy Monitor (2014). Health Systems in Transition (HiT)
profile of Netherlands. Available at:
http://hspm.org/countries/netherlands25062012/livighit.aspx?Section=3.6%20P
ayment%20mechanisms&Type=Section [10/05/2014].
WebMD (2005-2014). Stroke Health Center. Available at:
http://www.webmd.com/stroke/default.htm [10/05/2014].
Zoorgkaart (2014). Zoek, vind & waardeer 127.985 zorgaanbieders. Available at:
http://www.zorgkaartnederland.nl/verpleeghuis-en-verzorgingshuis.
[25/04/2014].
64
APPENDIX
Appendix A
Chronicity of LTC reforms
As mentioned in the context chapter, the LTC policies are undergoing constant reforms.
Hence these policies not only impact upon the stroke survivors’ after-care experience,
such reforms, and policies in general, are also impacting on the long-term care
employment market, on the long-term care education system and on the home care
provision system.
Chronicity of Long-Term Care Work
The ZZP payment system provides an annual lump sum to institutions, and an
‘expenditure ceiling’ is set (NZa 2012: 23). This should urge nursing and elderly homes to
cut costs wherever possible, which is mainly done on two fronts: by a stricter intake, of
patients with indicated ZZP 4 and above, and by reducing care personnel whilst at the
same time increasing the remaining personnel’s working hours on the same salary band.
It has been reported that wages in the LTC are generally low, where care workers earn
just slightly more than low-skilled workers in general (OECD 2011: 169).
In both of my fieldwork sites those changes took hold, but it was in the nursing home
which saw the greatest impact. Not only did the reforms influence the quality of care, as
for instance in the afternoon shifts there were only two care professionals (one nurse and
one LTC worker) for 32 residents, the cuts were also partly responsible for higher rates
of mortality as one of the para-medical staff confirmed: ”It is terrible what happens here,
only two carers for the afternoon shift and only one during the night shift. No wonder that
bad things happen. People die here”. She referred to a Ghanaian resident who suffocated
on his vomitus the previous week. Sander, the team-manager of the second floor
confirmed that the under-staffing causes major problem as
…when 5 people ring the bell and only 1 comes through then the 2 [carers] will
be busy with that one person… at the end of the day you have like 4 or 5 more
persons who need to pee…. and that is the reality of the elderly healthcare…
65
An additional problem was that the average mean age of the care personnel was 45 – 50.
You have seen my staff. The average age is 54..it is like being a builder [working
on a construction site], and their bodies are racked after 30 years of lifting
people… they got lift up people who are heavy, they got to roll and bend them over
hundreds times.….I could use some young legs who are not tired after 4 hours of
running
This was also acknowledged in the OECD report (2011: 171) where care work can often
lead to early retirement due to stress and burnout. Furthermore, due to their demanding
and burdensome job, the carers in this nursing home were frequently on sick leave and
some even needed to discontinue their employment.
In this respect, LTC policies are the political facts of chronicity, as not only do they
affect the care provision in nursing homes with resulting increase of mortality rates, these
policies are also co-responsible for the chronicity of understaffing. And this, in turn, leads
to a chronic sick, and chronic frustrated care personnel. In a sense then, as much as
chronic conditions are perceived to be unending, recovery deemed to be unlikely and
hence not worth of investment (Ferzacca 2010: 158), so are (chronic) nursing institutions
and their care personnel regarded as not worth of (educational) investment.
CHRONICITY OF LOW-LEVEL EDUCATION
My informants frequently raised their concerns regarding the low-level qualifications of
care workers. It has been widely acknowledged that LTC workers hold low-level
qualifications as the standardisation of care worker qualifications is often lacking (OECD
2011: 163). In the Netherlands, between 17 and 60 per cent of the LTC employees do not
have relevant LTC-related qualification (ibid). Furthermore, elderly and long-term care,
especially in Amsterdam, is marked by migration flows mainly from Suriname or African
countries. Most of the migrants, especially the ones who migrated in the 70s and 80s
either did not obtain high quality nursing education, or they were ‘de-skilled’, e.g.
downgraded to a lower level (mostly to level 1-2) (da Roit 2010; OECD 2011: 175).
In the past care workers qualifications were sufficient for elderly and LTC. However,
as the population grows older and the medical conditions more complex (due to co-
morbidities), the call for better educated care workers was prevalent in both of my
66
fieldwork settings. Britt54 for instance reasoned that not only medical know-how should
be taught but also efficient case management.
[LTC workers] are trained in this particular field only; they poorly or don’t
perform a lot of the things which they have learnt a long time ago…This is why
they make mistakes. I mean it is a tricky business the elderly healthcare, and
the [educational] level [of the care workers] are the lowest of healthcare
compared to a hospital.
Although they receive in-house training, their second nature care practises are often hard
to change as Sander, the team manager of the nursing homes second floor confirmed
[T]here is more complicated care with more demanding inspections. So all adds
on…. [Care workers] want to keep some sort of tradition of things they are safe
with [e.g. care practices]. It is not possible to make changes all of the sudden
…..you got to provide them with time… I mean, yes there are loads of things going
wrong. So I can do two things [as a manager]: only bitch about everyone, or I
give them respect on how they go with me in this transformation. Point by point
we gonna make the changes towards a better care [with less staff].
Although Sander and his colleagues provide in-house training for care workers, his
reasoning points to a much wider problematic, namely, the lack of the LTC educational
standardisation. One of the effects of the long term policies is the prevalence of low-level
education, which in turn negatively impacts upon the care provision practices, not only in
care and nursing homes, but also on the home care provision55.
Chronicity of Homecare (reforms)
The Dutch home-care system is embedded in the LTC scheme, and home-care (HC) was
initially developed as a less costly substitute for residential care56 (Da Roit 2012). The
1990s and early 2000s saw an increase of HC due to the rise of the aging population, which
in turn contributed to an escalation of the HC systems expenditure (ibid: 230).
Henceforth, the call for cost-containment was voiced, which saw a transfer from AWBZ-
54 Britt works as a quality nurse in the rehabilitation institution. 55 Please refer to Appendix A for a detailed explanation of the formal home care setting. 56 The HC system was introduced in 1968 with the establishment of the AWBZ (da Roit 2012: 228).
67
financed home care to one which is financed by the municipalities 57 , under which
entitlement of specific types of care is not guaranteed (da Roit 2012: 234). Cost
containment was further achieved by way of introducing consumer-directed (or cash-for-
care) schemes, such as ‘Personal budget’ ((Persoonsgebonden budget (PGB)) and co-
payments. The former is based on a persons need for care and care is either purchased
from professional organisations or via live-in care modes (ibid: 233). The latter can be
regarded as an indirect way to restrict access to care services (ibid: 233). High-income
earners are to solve their care problems via the private care market. Low-income earners,
though still entitled to social assistance, are expected to be cared for within their informal
care network58 (ibid).
It is especially the latter development which was of major concern for my
professional informants, as to how to care for stroke survivors who are ‘in-between’59,
which is also acknowledged by the DHC Authority (NZa):
[T]here are possibilities for saving money via this outpatient health care [but]
there are also inherent risks [involved]. The plans are difficult to implement for
people with a more serious care requirement (ZZP 3-4)[…] A therapeutic social
climate and/or a safe or protected home environment may indeed be essential
for these clients in particular [and] additional measures are needed to safeguard
the quality of the health care for these clients (NZa 2012:13).
Hence, the DHCA acknowledges the chronicity of the reforms and the accompanying
structural factors, which also inform the establishment of ‘indicaties’. The eligibility for
formal, high quality HC provision is dependent on such assessments. Anneke, a nurse
working at the Stroke Advise Centre, reasoned that indications are easy to establish for
57 Shifting provisions from the AWBZ to the municipalities meant moving entitlements from a social insurance and individual rights-based scheme to a support system based on subsidiarity: within the municipalities, citizens themselves, independently or through their social networks, should arrange the support that they need (da Roit 2012: 234). 58Informal care in the Netherlands, in cooperates family members who provide 24/7 care, and the so-called ‘Mantelzorg’ tradition, where friends and family members are coming and going. Everyone does small tasks, and keep the sick person company. This informal Mantelzorg system is always connected with the formal homecare system (Mezzo n.d.). In order to compensate for the informal carers as annual allowance of €250,- can be claimed. 59In-between are those who are not well enough to be sufficiently independent (e.g. ZZP 1-4) and not ‘disabled’ enough (ZZP 4-5) to be admitted to nursing homes.
68
physical or psychological disabled people. For the ones with brain damage, however, it is
far more complex and difficult.
You have also classes but brain damage is not a class: neither physical nor
psychological disabled. But it’s more in the middle. That’s why it’s very, very
difficult to get good indication for people who have brain damage [such as
stroke survivors]. This is also the reason why some of the district nurses,
including the ones working for Cordaan, try to establish a system without
indications, as it costs a lot of afford and trial to get good indications. But now
the nurses already work without indications.
It can be argued, that the post-stroke body functions as the social navigator, as its post-
stroke disabilities specify the indications; which in turn determine the eligibility for
formal HC. It also can be argued that the district nurses employ resistance tactics (de
Certeau 1984) in order to bring about changes within the system.
Conclusion
The LTC reforms have wide reaching implications, not only for the stroke survivors, but
also for medical professionals, their employment situation and on the standardisation of
long-term care education. The reforms not only contributed to a chronic exhausted care
personnel in the nursing home, these reforms were also co-responsible for higher
mortality rates. The home care provision will be equally affected, as due to the new ZZP
assessment criteria’s, stroke survivor with severe disabilities and an indication of 4/5
have to be catered in the informal care setting. My professional informants’ voiced
concerns that these ‘in-between’ survivors, as well as their families, will suffer the most
from the policy changes. Hence the chronicity of the stroke illness experience is enhanced
by political and economic factors.
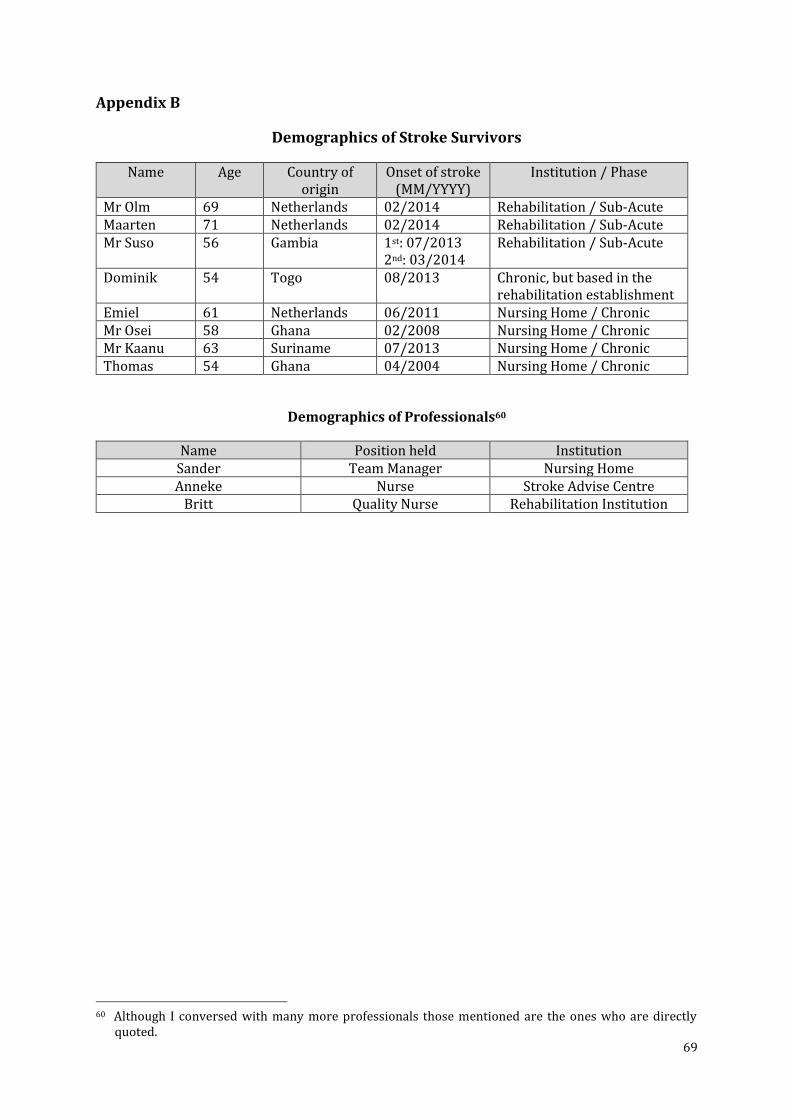
69
Appendix B
Demographics of Stroke Survivors
Name Age Country of origin
Onset of stroke (MM/YYYY)
Institution / Phase
Mr Olm 69 Netherlands 02/2014 Rehabilitation / Sub-Acute Maarten 71 Netherlands 02/2014 Rehabilitation / Sub-Acute Mr Suso 56 Gambia 1st: 07/2013
2nd: 03/2014 Rehabilitation / Sub-Acute
Dominik 54 Togo 08/2013 Chronic, but based in the rehabilitation establishment
Emiel 61 Netherlands 06/2011 Nursing Home / Chronic Mr Osei 58 Ghana 02/2008 Nursing Home / Chronic Mr Kaanu 63 Suriname 07/2013 Nursing Home / Chronic Thomas 54 Ghana 04/2004 Nursing Home / Chronic
Demographics of Professionals60
Name Position held Institution Sander Team Manager Nursing Home Anneke Nurse Stroke Advise Centre
Britt Quality Nurse Rehabilitation Institution
60 Although I conversed with many more professionals those mentioned are the ones who are directly
quoted.
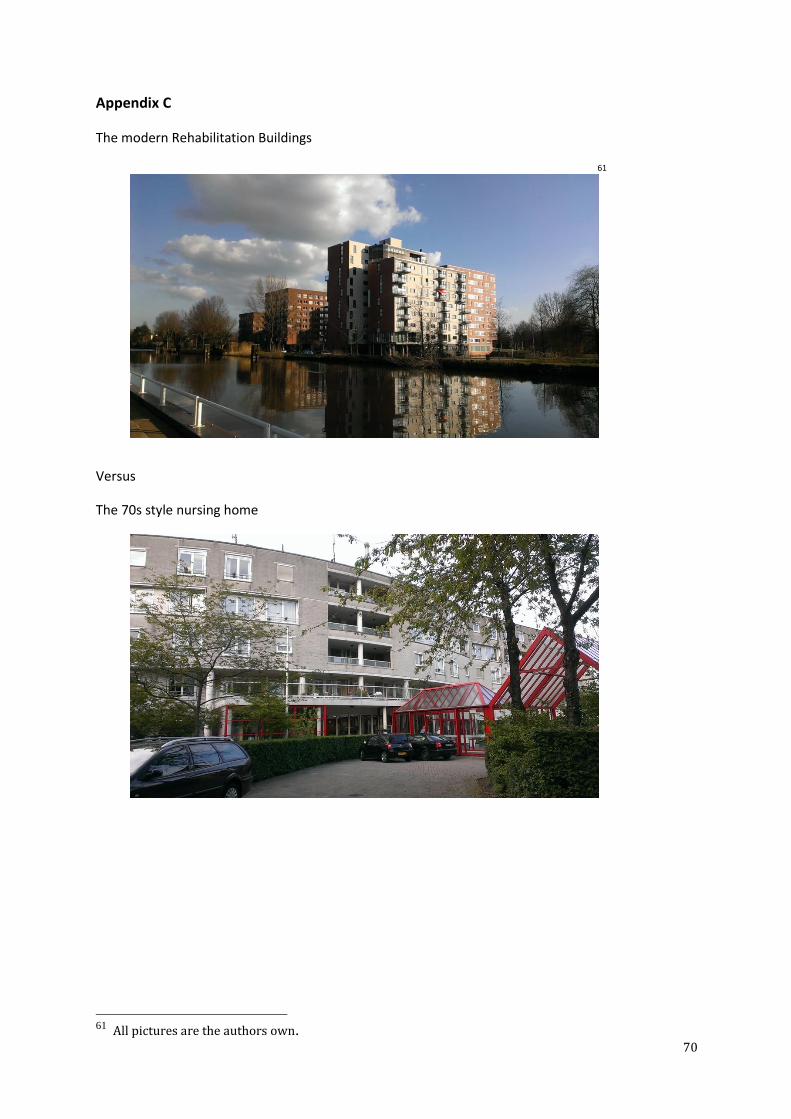
70
Appendix C
The modern Rehabilitation Buildings
61
Versus
The 70s style nursing home
61 All pictures are the authors own.