surgical indications and procedures for resection of hepatic malignancies confined to segment vii
TRANSCRIPT

SURGICAL TECHNIQUE
Surgical Indications and Procedures for Resection of HepaticMalignancies Confined to Segment VII
Chetana Lim, MD,∗† Takeaki Ishizawa, MD, PhD,∗ Akinori Miyata, MD,∗ Yoshihiro Mise, MD,∗
Yoshihiro Sakamoto, MD, PhD,∗ Kiyoshi Hasegawa, MD, PhD,∗ Yasuhiko Sugawara, MD, PhD,∗
and Norihiro Kokudo, MD, PhD∗
Objective: To establish a strategy for surgical resection of hepatic malignan-cies confined to segment VII.Background: Various surgical procedures can be used to resect hepatic ma-lignancies in segment VII, the deepest region of the liver, by open and/or la-paroscopic approaches: nonanatomic wedge resection (WR), segmentectomyVII, right lateral sectionectomy (RLS), and right hepatectomy.Methods: WR and segmentectomy VII were applied as first-line surgical pro-cedures for colorectal liver metastasis (CRLM) and hepatocellular carcinoma(HCC), respectively. RLS and right hepatectomy were indicated only whentumor infiltration to the proximal Glissonian sheath was suspected. Operativeoutcomes were evaluated in 200 consecutive patients who underwent hepaticresection for HCC (n = 120) or CRLM (n = 80).Results: WR, segmentectomy VII, RLS, and right hepatectomy were per-formed in 104 (52.0%), 57 (28.5%), 22 (11.0%), and 17 (8.5%) patients,respectively. Local hepatectomy (WR and segmentectomy VII) led to shorteroperation times and lower blood loss volumes than did extensive hepatectomy(RLS and right hepatectomy). Thoracotomy was performed in half of the WRand two-thirds of the segmentectomy VII procedures. The availability of alaparoscopic approach was 40% (8 patients) after its application in October2012.Conclusions: Even for hepatic malignancies located in segment VII, WR andsegmentectomy should be prioritized over extensive hepatectomy to preservethe postoperative functional hepatic volume. Full mobilization of the right liverand a good surgical field provided by a large thoracoabdominal or abdominalincision or a laparoscopic approach are key factors for safe performance ofdeep hepatic transection.
Keywords: anatomical segmentectomy, colorectal liver metastasis, hepato-cellular carcinoma, right hepatectomy, right lateral sectionectomy, segmentVII, wedge resection
(Ann Surg 2015;00:1–9)
D espite recent advances in surgical hepatectomy techniques, re-section of hepatic malignancies located in Couinaud’s segment
VII remains one of the most challenging procedures. Segment VII islocated behind the plane defined by the vena cava and right hepatic
From the ∗Hepatobiliary Pancreatic Surgery Division, Department of Surgery,Graduate School of Medicine, The University of Tokyo, Tokyo, Japan; and†Department of Hepatobiliary Pancreatic Surgery and Liver Transplantation,Henri Mondor Hospital, Creteil, France.
Disclosure: The authors declare no conflicts of interest. This work was supportedby grants from the Takeda Science Foundation; the Kanae Foundation for thePromotion of Medical Science; the Ministry of Education, Culture, Sports,Science and Technology of Japan (No. 23689060); and the Ministry of Health,Labour and Welfare of Japan.
Reprints: Norihiro Kokudo, MD, PhD, Hepatobiliary Pancreatic Surgery Divi-sion, Department of Surgery, Graduate School of Medicine, The Univer-sity of Tokyo, 7-3-1 Hongo, Bunkyo-ku, Tokyo 113-8655, Japan. E-mail:[email protected].
Copyright C© 2015 Wolters Kluwer Health, Inc. All rights reserved.ISSN: 0003-4932/15/00000-0001DOI: 10.1097/SLA.0000000000001118
vein (RHV) in situ and is biologically adhered to the right diaphragmin the area without peritoneum (bare area).1 Thus, resection of seg-ment VII lesions usually requires full mobilization of the right liverfrom the diaphragm, right adrenal gland, and vena cava by dividing thethick short hepatic veins (inferior RHVs). The bifurcation of the seg-ment VII portal pedicle also lies deep within the hepatic parenchyma,which makes it difficult to identify the boundary of segment VII be-fore hepatic dissection using dye-staining techniques2 or a Glissonianapproach.3 During hepatic transection, the RHV tributaries should bedivided in the deepest aspects of the liver.
A variety of surgical procedures can be adopted to remove seg-ment VII hepatic malignancies with curative intent. Nonanatomic par-tial resection is the most commonly used procedure for treatment ofcolorectal liver metastasis (CRLM) located in segment VII, whereasanatomic resection [segmentectomy VII or right lateral sectionectomy(RLS)] has been recommended in the treatment of hepatocellular car-cinoma (HCC).2,4 Although right hepatectomy is usually too invasivefor resection of segment VII lesions because it leads to the sacrificeof large volumes of noncancerous hepatic parenchyma, this proce-dure can be indicated if tumor infiltration to the proximal Glissoniansheath is suspected. In addition, both laparoscopic procedures andopen hepatectomy have recently been used for resection of segmentVII hepatic malignancies.5,6
Considering the unique anatomy of segment VII and the varietyof surgical procedures that can be applied, a surgical strategy focusingon the treatment of segment VII lesions should be established. Theaim of this study was to evaluate the operative outcomes of a surgicalstrategy for the treatment of CRLM or HCC confined to segment VIIin 200 consecutive patients.
METHODS
Surgical IndicationsThe surgical indications and procedures for resection of seg-
ment VII lesions were determined on the basis of the tumor–vesselrelationships and hepatic functional reserve. In patients with HCC,anatomic resection of segment VII was prioritized over nonanatomicpartial resection, defined as wedge resection (WR) in this study, be-cause complete resection of cancer-bearing hepatic segments has theadvantage of reducing the risk of postoperative recurrence.4 In pa-tients with CRLM, WR was usually performed. For both kinds oftumors, RLS or right hepatectomy was considered when the tumorsinfiltrated the Glissonian sheath proximal to the bifurcation of thesegment VII branch (Fig. 1).
In terms of liver function, the acceptable ranges of resectedhepatic volumes were defined in detail on the basis of the indocya-nine green retention rate at 15 minutes (ICGR15).7 Simply stated, thiscriterion permitted right hepatectomy when the ICGR15 was less than10%, RLS when the ICGR15 was less than 20%, segmentectomy VIIwhen the ICGR15 was less than 30%, and WR or enucleation whenthe ICGR15 was 30% or more. If removal of segment VII lesionsrequired concomitant resection of the major hepatic veins, the hep-atic volume of the veno-occlusive area and its portal uptake function
Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
Annals of Surgery � Volume 00, Number 00, 2015 www.annalsofsurgery.com | 1

Lim et al Annals of Surgery � Volume 00, Number 00, 2015
FIGURE 1. Surgical strategy to resect hepatic malignanciesconfined to segment VII. The first-choice surgical procedureis segmentectomy VII for HCC and WR for CRLM. If tumorsinfiltrate the proximal Glissonian sheath, RLS or right hepatec-tomy (extensive hepatectomy) are considered. When patients’liver function does not permit extensive hepatectomy for tu-mors invading the Glissonian sheath, segmentectomy VII orLR is indicated, and the tumors are peeled off the Glissoniansheath (dotted arrows).
were estimated by preoperative computed tomography (CT) and intra-operative ICG fluorescence imaging.8,9 When the estimated volumeof the future remnant liver was insufficient for right hepatectomy,preoperative portal vein embolization was applied.10
Basic Surgical Techniques for Open HepatectomyA J-shaped incision was used for laparotomy. When necessary,
thoracotomy was added to obtain a sufficient view and working spacearound the vena cava. In patients with no suspicious lesions requir-ing removal from the left liver, thoracophrenolaparotomy was appliedusing an oblique incision along the eighth intercostal space with thepatient in the left lateral decubitus position (Figs. 2A, B). For segmen-tectomy VII or larger hepatectomy, the right liver was fully mobilizedto expose the root of the RHV by dissecting the right adrenal gland anddividing the retrocaval ligament.11,12 Intraoperative ultrasonographywas mandatory to identify special relationships between the intrahep-atic vascular anatomy and hepatic lesions to be removed. The hepaticparenchyma was transected mainly by the clamp–crush technique13
under inflow occlusion (15-minute clamping periods separated by5-min intervals). After hepatectomy, an abdominal drain was insertednear the cut surface of the liver and connected to a closed drainagesystem. A thoracic tube was placed on a suction pump with a pressureof −20 cm H2O when thoracotomy was performed. The postoperativemanagement strategy and follow-up are described elsewhere.14
Segmentectomy VIIThe boundary of segment VII was identified by injection of
blue indigo carmine dye (Daiichi Sankyo, Tokyo, Japan) into the por-tal branch toward segment VII under ultrasound guidance (Figs. 2C,D). Although segment VII is usually supplied by 1 major portalbranch,1 subsegments of segment VII could also be identified by in-jection of dye into the corresponding small portal branches (Fig. 2E).When direct puncture of the portal branch of segment VII was tech-nically difficult, the counter-staining technique15 (ie, staining of the
adjacent hepatic segments, namely segment VI and the dorsal regionsof segment VIII) was applied to identify segment VII (Fig. 2D). Hep-atic transection was started along the boundary of the stained regionson the liver surface and proceeded toward the root of the Glissoniansheath toward segment VII, exposing the RHV as a landmark of theintrahepatic segmental boundaries. After division of the Glissoniansheath of segment VII, parenchymal transection was continued to thecranial aspects along the RHV (Fig. 2F).
Right Lateral Sectionectomy (Resection of SegmentsVI and VII)
The boundary of the right lateral sector was identified by dis-section of the hepatic hilum to close the arterial and portal branchesthat feed this hepatic region. The Glissonian approach or dye-stainingtechnique could also be applied to identify the right lateral sector. Thefull length of the RHV should be exposed on the raw liver surfaceafter anatomically accurate RLS.
Right Hepatectomy (Resection of Segments V, VI,VII, and VIII)
The right hepatic arteries and portal veins were usually dis-sected and divided at the hepatic hilum before hepatic transection.When a tumor thrombus extended into the right portal vein, it couldbe peeled off from the venous wall through a venotomy on the por-tal vein (Fig. 3E).16 The hepatic parenchyma was transected along ademarcation between the right and left liver, with the middle hepaticvein exposed on the raw surfaces (Fig. 3F).
Laparoscopic Approach to Resectionof Segment VII Lesions
Since October 2012, laparoscopic procedures have been ap-plied to the resection of segment VII lesions. Totally laparoscopichepatectomy was applied only to WR of the peripheral aspect of seg-ment VII using transthoracic trocars; this was originally reported as a“lateral approach.”6 For anatomic resection of segment VII lesions, ahybrid technique was used (ie, laparoscopic mobilization of the rightliver followed by hepatic transection through a 10- to 14-cm midlineincision).17,18
Evaluation of Surgical OutcomesIn total, 2255 patients underwent liver resection for HCC
(n = 1633, 72%) or CRLM (n = 622, 28%) at the University ofTokyo Hospital from April 1993 to December 2013. Of these 2255patients, the surgical indications and postoperative outcomes wereevaluated in 200 consecutive patients who had undergone hepatic re-section for HCC (n = 120) or CRLM (n = 80) confined to segmentVII.
Postoperative mortality and morbidity were defined as allevents occurring at any time during the hospital stay according to theClavien–Dindo classification.19 Liver failure was defined as a peakpostoperative serum bilirubin level of more than 119.7 μmol/L.20
Bile leakage was defined according to the definition of the Interna-tional Study Group of Liver Surgery.21 Ascites was defined as asciticfluid drainage of more than 10 mL/kg body weight.14 Recurrence wasidentified during radiological assessments using CT and/or magneticresonance imaging.
Statistical AnalysisIn this study, WR and segmentectomy VII were defined as local
hepatectomy, whereas RLS and RH were defined as extensive hepa-tectomy. Continuous variables are expressed as median (range) andwere compared using the Mann–Whitney U test. Categorical variableswere analyzed by the Fisher exact test. Statistical significance was
Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
2 | www.annalsofsurgery.com C© 2015 Wolters Kluwer Health, Inc. All rights reserved.

Annals of Surgery � Volume 00, Number 00, 2015 Resection of Liver Malignancies in Segment VII
FIGURE 2. Surgical procedures of segmentectomy VII. A, J-shaped laparotomy with thoracotomy (arrow) or thoracophrenola-parotomy toward the eighth intercostal space (dotted arrow) is used for segmentectomy VII. B, The operation is performed bythoracophrenolaparotomy toward the eighth intercostal space. The caudal subsegment of segment VII is stained by the dye-injection technique. (C) Three-dimensional images based on preoperative CT in a patient with HCC (indicated in red on the left)located between the cranial (green, on the right) and caudal (purple) subsegments of segment VII. (D) Intraoperative view ofthis patient. The boundaries of segment VII are clearly delineated on the liver surface after injection of blue dye into the portalbranches toward the cranial and caudal subsegments of segment VII. (E) After completion of segmentectomy VII. The wall of theRHV (thick arrow) and stump of the segment VII Glissonian sheath (arrowhead) are identified on the raw surface of the liver.
Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
C© 2015 Wolters Kluwer Health, Inc. All rights reserved. www.annalsofsurgery.com | 3
Lim et al Annals of Surgery � Volume 00, Number 00, 2015
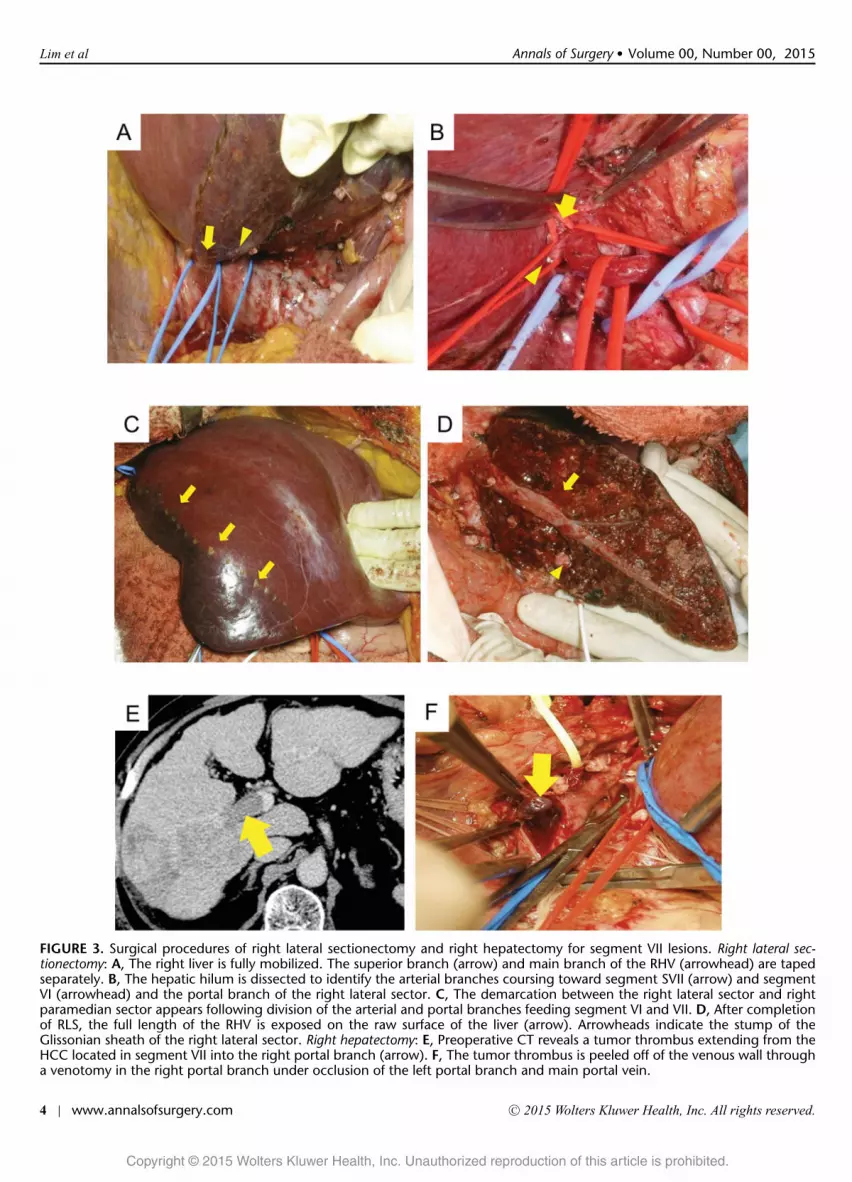
FIGURE 3. Surgical procedures of right lateral sectionectomy and right hepatectomy for segment VII lesions. Right lateral sec-tionectomy: A, The right liver is fully mobilized. The superior branch (arrow) and main branch of the RHV (arrowhead) are tapedseparately. B, The hepatic hilum is dissected to identify the arterial branches coursing toward segment SVII (arrow) and segmentVI (arrowhead) and the portal branch of the right lateral sector. C, The demarcation between the right lateral sector and rightparamedian sector appears following division of the arterial and portal branches feeding segment VI and VII. D, After completionof RLS, the full length of the RHV is exposed on the raw surface of the liver (arrow). Arrowheads indicate the stump of theGlissonian sheath of the right lateral sector. Right hepatectomy: E, Preoperative CT reveals a tumor thrombus extending from theHCC located in segment VII into the right portal branch (arrow). F, The tumor thrombus is peeled off of the venous wall througha venotomy in the right portal branch under occlusion of the left portal branch and main portal vein.
Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
4 | www.annalsofsurgery.com C© 2015 Wolters Kluwer Health, Inc. All rights reserved.

Annals of Surgery � Volume 00, Number 00, 2015 Resection of Liver Malignancies in Segment VII
FIGURE 4. Laparoscopic approach for resection of segment VII lesion. Pure laparoscopic WR of segment VII lesion: A, The hepatictransection line is determined using contrast-enhanced intraoperative ultrasonography for confirmation of a metastatic tumorlocated in segment VII. B, The hepatic parenchyma is transected using transthoracic trocars for a bipolar forceps manipulatedby the surgeon’s left hand and a laparoscope. Hybrid technique for RLS: C, Trocar placement (small circles indicate 5-mm trocars,and large circle indicates 12-mm trocar) for laparoscopic mobilization of the right liver and midline incision (dotted arrow)for subsequent open hepatic transection. D, Laparoscopic mobilization of the right liver in a patient with HCC in segment VII(arrow). Because tumor infiltration to the retroperitoneum is suspected, Gerota’s fascia is dissected during dissection of the dorsalaspect of the right liver. E, Completion of mobilization of the right liver. The diaphragm (arrowhead) and inferior RHV (arrow)are demonstrated. F, Mobilization of the right liver through a midline incision. G, The demarcation line is delineated followingdivision of the arterial and portal branches toward the right lateral sector. H, The RHV is exposed on the raw surface of the liverafter RLS.
defined by a P < 0.05. Calculations were performed using statisticalsoftware (StatView, version 5; SAS Institute Inc, Cary, NC).
RESULTSSurgical Indications
WR, segmentectomy VII, RLS, and right hepatectomy wereperformed in 104 (52.0%), 57 (28.5%), 22 (11.0%), and 17 (8.5%)
of the 200 patients with HCC or CRLM confined to segmentVII, respectively (Table 1). Among local hepatectomy procedures(WR and segmentectomy VII), segmentectomy VII was indicatedmore frequently in patients with HCC, a larger tumor diame-ter, or a higher tumor number and in those undergoing hepatec-tomy for the first time. Dye-staining technique enabled identifica-tion of segmental boundaries in all the 57 patients who underwentsegmentectomy VII.
Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
C© 2015 Wolters Kluwer Health, Inc. All rights reserved. www.annalsofsurgery.com | 5

Lim et al Annals of Surgery � Volume 00, Number 00, 2015
TAB
LE1.
Back
grou
ndC
hara
cter
istic
san
dTu
mor
-Rel
ated
Fact
ors
Loc
alH
epat
ecto
my
(n=
161)
Ext
ensi
veH
epat
ecto
my
(n=
39)
Ove
rall
WR
(n=
104,
65%
)
Segm
ente
ctom
yV
II(n
=57
,35
%)
P(W
Rvs
Segm
ente
ctom
yV
II)
Ove
rall
RL
S(n
=22
,57%
)
Rig
htH
epat
ecto
my
(n=
17,4
4%)
P(L
ocal
vsE
xten
sive
)
Age
,yr
66(2
9–84
)65
(29–
84)
67(3
7–83
)0.
486
65(3
1–78
)63
(31–
78)
69(3
5–78
)0.
803
Sex
,mal
e,n
(%)
112
(70)
69(6
6)43
(75)
0.23
029
(74)
16(7
3)13
(77)
0.55
6IC
GR
15(%
)10
.5(0
.0–7
5.4)
10.8
(2.0
–75.
4)10
.4(0
.0–7
2.3)
0.86
09.
7(2
.9–2
1.9)
8.8
(2.9
–21.
9)11
.8(4
.0–1
7.9)
0.07
5L
C,∗
pres
ent,
n(%
)39
(25)
17(1
6)22
(39)
0.00
26
(15)
2(9
)4
(24)
0.22
9R
epea
ted
hepa
tect
omy,
n(%
)54
(33)
47(4
5)7
(12)
<0.
001
2(5
)1
(5)
1(6
)<
0.00
1Pa
thol
ogy,
HC
C/C
RL
M,n
(%)
92(5
7)/6
9(4
3)50
(48)
/64
(62)
52(9
1)/5
(9)
<0.
001
28(7
2)/1
1(2
8)14
(64)
/8(3
6)14
(82)
/3(1
8)0.
094
Num
ber
oftu
mor
s,≥2
,n(%
)43
(27)
36(3
5)7
(12)
0.00
211
(28)
5(2
3)6
(35)
0.85
0M
axim
altu
mor
diam
eter
,∗m
m27
(2–9
0)24
.5(2
–90)
30(4
–90)
0.01
955
(12–
145)
55(1
2–95
)55
(26–
145)
<0.
001
∗ Bas
edon
path
olog
ical
exam
inat
ion.
Right hepatectomy was indicated in 17 patients (HCC, n = 14;CRLM, n = 3) because of suspicion of tumor infiltration to the Glisso-nian sheath. Preoperative portal vein embolization was performed in6 patients. Microscopically, vascular infiltration to the right proximalGlissonian sheath was revealed in 9 patients. When the backgroundcharacteristics and tumor-related factors of the patients who under-went extensive hepatectomy (RLS or right hepatectomy) were com-pared with those of the patients who underwent local hepatectomy,the maximal tumor diameter was significantly larger in the formergroup (Table 1).
Intraoperative FindingsTable 2 summarizes the intraoperative and postoperative out-
comes. Local hepatectomy (WR and segmentectomy VII) led to morefavorable outcomes than did extensive hepatectomy in terms of theoperation time, amount of blood loss, and requirement for blood trans-fusion. Segmentectomy was associated with wider surgical marginsduring hepatectomy for HCC than was WR. Thoracotomy was per-formed in half of the patients who underwent WR, two thirds of thepatients who underwent segmentectomy VII, and half of the patientswho underwent extensive hepatectomy. A laparoscopic approach wasapplied mainly for local hepatectomy procedures, and its proportionwas 40% (8 patients; 2 purely laparoscopic WRs and 6 hepatectomiesby the hybrid technique) among 20 patients who underwent hepatec-tomy for segment VII lesions after the use of a laparoscopic approachsince October 2012. Among the 20 patients in whom a laparoscopicapproach was applied, the operation time and blood loss volume were424 (202–525) minutes and 900 (600–1270) mL, respectively.
Postoperative OutcomesNo in-hospital deaths occurred after any hepatectomy proce-
dures. The morbidity rate (Clavien–Dindo grade III or higher) shownno statistically significant differences between patients who under-went WR (9%) and those who underwent segmentectomy VII (14%)or between the local hepatectomy group (11%) and the extensivehepatectomy group (5%) (Table 2). Postoperative biliary fistulas oc-curred with an incidence of 6% after nonanatomic resection (WR)and after anatomic resection (segmentectomy VII, RLS, or right hep-atectomy). The incidence of pleural effusion tended to be higher inpatients who underwent hepatectomy with thoracotomy (11%) thanin those who underwent hepatectomy without thoracotomy (4%, P =0.101). Recurrence occurred in 63 patients (32%) within 1 year afterhepatectomy for HCC (n = 39) or CRLM (n = 24). The 1-year recur-rence rate was similar between the WR and segmentectomy groups,but it was significantly higher in the extensive hepatectomy group(46%) than in the local hepatectomy group (28%, P = 0.028).
DISCUSSIONIn this series, minor hepatectomy (WR or segmentectomy VII)
was performed in approximately 80% of patients with HCC or CRLMconfined to segment VII, leading to more favorable operative out-comes with respect to the operation time and blood loss volume than inpatients who underwent extensive hepatectomy (RLS or right hepate-ctomy). Extensive hepatectomy was also safely indicated when tumorinfiltration to the Glissonian sheath proximal to segment VII was sus-pected. The 1-year recurrence rate after local hepatectomy (28%) waslower than that after extensive hepatectomy (46%), although tumor-related factors were quite different between the 2 groups. These resultssuggest that segmentectomy or smaller resection should be consid-ered as the first-line surgical procedure unless tumor infiltration tothe proximal portal pedicles is suspected on the basis of preoperativeimaging results or intraoperative examination findings.
The potential advantage of local hepatectomy lies in the factthat it can preserve a larger functional volume of the hepatic remnant
Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
6 | www.annalsofsurgery.com C© 2015 Wolters Kluwer Health, Inc. All rights reserved.

Annals of Surgery � Volume 00, Number 00, 2015 Resection of Liver Malignancies in Segment VII
TAB
LE2.
Intr
aop
erat
ive
Fact
ors
and
Post
oper
ativ
eO
utco
mes
Loc
alH
epat
ecto
my
(n=
161)
Ext
ensi
veH
epat
ecto
my
(n=
39)
Ove
rall
WR
(n=
104,
65%
)Se
gmen
tect
omy
VII
(n=
57,3
5%)
P(W
Rvs
Segm
ente
ctom
yV
II)
Ove
rall
RL
S(n
=22
,57%
)
Rig
htH
epat
ecto
my
(n=
17,4
4%)
P(L
ocal
vsE
xten
sive
)
Intr
aope
rativ
efa
ctor
sT
hora
coto
my,
n(%
)95
(59)
53(5
1)42
(74)
0.00
519
(49)
12(5
5)7
(41)
0.24
4O
bliq
uein
cisi
on21
(13)
7(7
)14
(25)
1(3
)1
(5)
0J-
shap
edin
cisi
on74
(46)
46(4
4)28
(49)
18(4
6)11
(50)
7(4
1)L
apar
osco
pic
appr
oach
,n(%
)7
(4)
5(5
)2
(4)
0.70
01
(3)
1(5
)0
0.61
0
Ope
rativ
eti
me,
min
367
(105
–979
)37
5(1
05–9
79)
360
(172
–684
)0.
760
445
(50–
1020
)38
5(5
0–58
9)49
6(2
66–1
020)
0.01
4B
lood
loss
,mL
648
(10–
4255
)60
2(1
0–42
55)
710
(125
–348
0)0.
610
880
(130
–842
0)81
0(1
30–1
500)
980
(200
–842
0)0.
001
Blo
odtr
ansf
usio
n,n
(%)
15(9
)10
(10)
5(9
)0.
831
10(2
6)3
(14)
7(4
1)0.
006
Sur
gica
lmar
gins
,mm
Tota
l3
(0–2
5)1
(0–1
5)4
(0–2
5)0.
018
1.5
(0–3
0)52
(0–2
2)1
(0–3
0)0.
152
HC
C3
(0–2
5)1
(0–1
5)5
(0–2
5)1
(0–2
2)2
(0–2
2)0
(0–2
1)C
RL
M2
(0–1
1)2
(0–1
1)1
(1–3
)4
(1–3
0)2
(1–5
)5
(1–3
0)Po
sitiv
esu
rgic
alm
argi
ns6
(3.7
)4
(3.8
)2
(3.5
)0.
257
2(5
.1)
1(4
.5)
1(5
.9)
0.56
9Po
stop
erat
ive
outc
omes
Hos
pita
lsta
y,d
16(0
–52)
16(0
–51)
16(9
–52)
0.73
416
(7–6
0)15
(7–3
1)16
(7–6
0)0.
440
Mor
bidi
ty,n
(%)
Bil
iary
fist
ula
9(6
)6
(6)
3(5
)0.
894
3(8
)1
(5)
2(1
2)0.
620
Ble
edin
g1
(1)
01
(2)
0.17
50
00
0.62
2A
scit
es8
(5)
4(4
)4
(7)
0.37
64
(10)
04
(24)
0.21
2P
leur
alef
fusi
on12
(8)
5(5
)7
(12)
0.08
43
(8)
2(9
)1
(6)
0.96
0C
lavi
en-D
indo
grad
e≥
III
17(1
1)9
(9)
8(1
4)0.
288
2(5
)2
(9)
0(0
)0.
299
Rec
urre
nce
wit
hin
1y
afte
rsu
rger
y,n
(%)
45(2
8)32
(31)
13(2
3)0.
282
18(4
6)6
(27)
12(7
0.6)
0.02
8
Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
C© 2015 Wolters Kluwer Health, Inc. All rights reserved. www.annalsofsurgery.com | 7

Lim et al Annals of Surgery � Volume 00, Number 00, 2015
than can RLS or right hepatectomy, leading to better recovery of post-operative hepatic function and a greater chance of successful repeatedhepatectomy for future intrahepatic recurrence of HCC22 or CRLM.23
Among surgical procedures for local hepatectomy, anatomic resec-tion of segment VII should be prioritized over WR in the treatmentof HCC in patients with preserved liver function. This is becauseanatomic resection has advantages over WR with respect to eradicat-ing intrahepatic metastases that have spread along the portal systems24
and reducing the risk of postoperative recurrence.4 The oncologicalbenefit of anatomic resection in the treatment of CRLM has not beensupported.25 However, segmentectomy may also have a role in hepate-ctomy for CRLM when segment VII tumors are not clearly identifiedduring surgery because of the effect of previous hepatectomy or pre-operative chemotherapy,26 especially in laparoscopic resection fordeeply located tumors.
With regard to the technical aspects of hepatectomy for seg-ment VII lesions, full mobilization of the right liver to identify theconfluence of the RHV into the vena cava is the key step in assur-ing control of venous bleeding during transection of the deep hepaticparenchyma. During mobilization of the right liver, care must be takento avoid bleeding from the right inferior phrenic vein,27 retrocaval lig-ament, and right adrenal gland.11,12 Thoracophrenolaparotomy by aJ-shaped incision28–30 or oblique incision31–33 provides the best surgi-cal field and working space for hepatic mobilization and parenchymaltransection during resection of segment VII lesions, although the useof thoracotomy may increase the risk of postoperative pulmonarycomplications such as pleural effusion and pneumonia. To ensure thecompletion of anatomically accurate segmentectomy or bisegmentec-tomy for segment VII lesions, the boundary of the hepatic segment(s)must be identified by injecting blue dye into the corresponding portalvein (dye-injection technique),2 as mainly performed in the presentseries, or by closing the corresponding portal pedicle to visualize theischemic regions of the liver surfaces (Glissonian approach).3 Afteridentification of the hepatic segment(s) to be removed, the hepaticparenchyma should be transected with the RHV exposed on the rawsurface as a landmark of the segmental boundary. This procedure isimportant for both complete removal of tumor-bearing hepatic seg-ments and avoidance of unexpected injury to the RHV tributaries,which may lead to uncontrollable bleeding.
Although hepatectomy for segment VII lesions provides favor-able operative outcomes, the creation of a large incision that can beused even for small lesions in segment VII remains a clinical prob-lem that may decrease patients’ quality of life after surgery and delayinitiation of adjuvant chemotherapy. As recently reported,17,18 thehybrid laparoscopic approach (ie, laparoscopic hepatic mobilizationfollowed by open hepatic transection through a small incision) maybe useful to reduce the need for creation of a transverse incision andperformance of thoracotomy in patients undergoing hepatectomy forsegment VII lesions. Totally laparoscopic hepatectomy has the poten-tial to enhance the short-term outcomes after resection of segment VIIlesions,6 although further technical advances in identification of theboundaries of the hepatic segments34 and control of venous bleedingduring hepatic transection are needed before active application of thetotally laparoscopic approach to segmentectomy VII and RLS.
CONCLUSIONSThe first-line surgical procedure for segment VII lesions is WR
for CRLM and segmentectomy for HCC because such minor hep-atectomy procedures preserve the postoperative functional hepaticremnant to the greatest extent possible. Although segmentectomy VIIand WR for deeply located lesions in segment VII sometimes requirecomplicated surgical procedures, easy application of major hepatec-tomy with an aim to simply facilitate hepatic transection should beavoided.
ACKNOWLEDGMENTSThe authors thank Drs J. Kaneko and T. Aoki, the members of
this study group, for their significant contributions.
REFERENCES1. Couinaud C. Surgical Anatomy of the Liver Revisited. Ed. Paris, France; 1989.2. Makuuchi M, Hasegawa H, Yamazaki S. Ultrasonically guided subsegmentec-
tomy. Surg Gynecol Obstet. 1985;161:346–350.3. Takasaki K. Glissonean pedicle transection method for hepatic resection: a new
concept of liver segmentation. J Hepatobiliary Pancreat Surg. 1998;5:286–2914. Hasegawa K, Kokudo N, Imamura H, et al. Prognostic impact of anatomic
resection for hepatocellular carcinoma. Ann Surg. 2005;242:252–259.5. Buell JF, Cherqui D, Geller DA, et al. The international position on laparo-
scopic liver surgery: the Louisville Statement, 2008. Ann Surg. 2009;250:825–830.
6. Ishizawa T, Gumbs AA, Kokudo N, et al. Laparoscopic segmentectomy of theliver: from segment I to VIII. Ann Surg. 2012;256:959–964.
7. Makuuchi M, Kosuge T, Takayama T, et al. Surgery for small liver cancers.Semin Surg Oncol. 1993;9:298–304.
8. Mise Y, Hasegawa K, Satou S, et al. Venous reconstruction based on vir-tual liver resection to avoid congestion in the liver remnant. Br J Surg.2011;98:1742–1751.
9. Kawaguchi Y, Ishizawa T, Miyata Y, et al. Portal uptake function in veno-occlusive regions evaluated by real-time fluorescent imaging using indocyaninegreen. J Hepatol. 2012;58:247–253.
10. Makuuchi M, Thai BL, Takayasu K, et al. Preoperative portal embolization toincrease safety of major hepatectomy for hilar bile duct carcinoma: a prelimi-nary report. Surgery. 1990;107:521–527.
11. Makuuchi M, Yamamoto J, Takayama T, et al. Extrahepatic division of theright hepatic vein in hepatectomy. Hepatogastroenterology. 1991;38:176–179.
12. Ishizawa T, Kokudo N, Makuuchi M. Right hepatectomy for hepatocellularcarcinoma: is the anterior approach superior to the conventional approach?Ann Surg. 2008;247:390–391; author reply 391–392.
13. Takayama T, Makuuchi M, Kubota K, et al. Randomized comparison of ultra-sonic vs clamp transection of the liver. Arch Surg. 2001;136:922–928.
14. Ishizawa T, Hasegawa K, Kokudo N, et al. Risk factors and managementof ascites after liver resection to treat hepatocellular carcinoma. Arch Surg.2009;144:46–51.
15. Takayama T, Makuuchi M, Watanabe K, et al. A new method for map-ping hepatic subsegment: counterstaining identification technique. Surgery.1991;109:226–229.
16. Inoue Y, Hasegawa K, Ishizawa T, et al. Is there any difference in survivalaccording to the portal tumor thrombectomy method in patients with hepato-cellular carcinoma? Surgery. 2009;145:9–19.
17. Nitta H, Sasaki A, Fujita T, et al. Laparoscopy-assisted major liver re-sections employing a hanging technique: the original procedure. Ann Surg.2010;251:450–453.
18. Soyama A, Takatsuki M, Adachi T, et al. A hybrid method of laparoscopic-assisted open liver resection through a short upper midline laparotomy can beapplied for all types of hepatectomies. Surg Endosc. 2014;28:203–211.
19. Dindo D, Demartines N, Clavien PA. Classification of surgical complications:a new proposal with evaluation in a cohort of 6336 patients and results of asurvey. Ann Surg. 2004;240:205–213.
20. Mullen JT, Ribero D, Reddy SK, et al. Hepatic insufficiency and mortality in1,059 noncirrhotic patients undergoing major hepatectomy. J Am Coll Surg.2007;204:854–862; discussion 862–864.
21. Koch M, Garden OJ, Padbury R, et al. Bile leakage after hepatobiliary andpancreatic surgery: a definition and grading of severity by the InternationalStudy Group of Liver Surgery. Surgery. 2011;149:680–688.
22. Ishizawa T, Hasegawa K, Aoki T, et al. Neither multiple tumors nor por-tal hypertension are surgical contraindications for hepatocellular carcinoma.Gastroenterology. 2008;134:1908–1916.
23. Saiura A, Yamamoto J, Hasegawa K, et al. Liver resection for multiple colorec-tal liver metastases with surgery up-front approach: bi-institutional analysis of736 consecutive cases. World J Surg. 2012;36:2171–2178.
24. Nakashima T, Kojiro M. Pathologic characteristics of hepatocellular carci-noma. Semin Liver Dis. 1986;6:259–266.
25. Kokudo N, Tada K, Seki M, et al. Anatomical major resection versusnonanatomical limited resection for liver metastases from colorectal carci-noma. Am J Surg. 2001;181:153–159.
Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
8 | www.annalsofsurgery.com C© 2015 Wolters Kluwer Health, Inc. All rights reserved.

Annals of Surgery � Volume 00, Number 00, 2015 Resection of Liver Malignancies in Segment VII
26. Spatz J, Holl G, Sciuk J, et al. Neoadjuvant chemotherapy affects stagingof colorectal liver metastasis—a comparison of PET, CT and intraoperativeultrasound. Int J Colorectal Dis. 2010;26:165–171.
27. Torzilli G, Montorsi M, Palmisano A, et al. Right inferior phrenic vein indi-cating the right hepatic vein confluence into the inferior vena cava. Am J Surg.2006;192:690–694.
28. Kise Y, Takayama T, Yamamoto J, et al. Comparison between thora-coabdominal and abdominal approaches in occurrence of pleural effu-sion after liver cancer surgery. Hepatogastroenterology. 1997;44:1397–1400.
29. Tsugita M, Takasaki K, Ohtsubo T, et al. Right side hepatic resection underright thoracoabdominal incision with special reference to a highly anatomicalsystematized method. Int Surg. 1995;80:242–246.
30. Xia F, Poon RT, Fan ST, et al. Thoracoabdominal approach for right-sided
hepatic resection for hepatocellular carcinoma. J Am Coll Surg. 2003;196:418–427.
31. Ko S, Nakajima Y, Kanehiro H, et al. Transthoracic transdiaphragmatic ap-proach for hepatectomy of Couinaud’s segments VII and VIII. World J Surg.1997;21:86–90.
32. Shimada M, Matsumata T, Taketomi A, et al. A new approach for liver surgery.Transdiaphragmatic hepatectomy for cirrhotic patients with hepatocellular car-cinoma. Arch Surg. 1995;130:157–160.
33. Takenaka K, Fujiwara Y, Gion T, et al. A thoracoabdominal hepatectomy and atransdiaphragmatic hepatectomy for patients with cirrhosis and hepatocellularcarcinoma. Arch Surg. 1998;133:80–83.
34. Ishizawa T, Zuker NB, Kokudo N, et al. Positive and negative staining ofhepatic segments by use of fluorescent imaging techniques during laparoscopichepatectomy. Arch Surg. 2012;147:393–394.
Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
C© 2015 Wolters Kluwer Health, Inc. All rights reserved. www.annalsofsurgery.com | 9