spermatids as gametes: indications and limitations
TRANSCRIPT

Spermatids as gametes: indications andlimitations
Jan Tesarik1'5, Mario Sousa2, Ermanno Greco3 andCarmen Mendoza4
'Laboratoire d'Eylau, 55 Rue Saint-Didier, 75116 Paris, France,laboratory of Cell Biology, Institute of Biomedical Sciences, Universityof Porto, 2 Largo Abel Salazar, Porto, Portugal, 3Centre of ReproductiveMedicine, European Hospital, Via Portuense 700, 00149 Rome, Italy and4Institute of Biotechnology, Faculty of Sciences, University of Granada,
Campus Universitario Fuentenueva, Granada, Spain5To whom correspondence should be addressed
The feasibility of achieving viable embryos, developing to term after transferinto the uterus, by fertilizing oocytes with spermatids has been demonstratedboth in animal studies and in preliminary human clinical trials. Here wereview the current clinical indications of spermatid conception and discussthe predictable success rates associated with each of these indications.Potential health hazards relating to the use of spermatids for conception areupdated taking into account the risk of abnormal or incomplete epigeneticmodifications of newly discovered human imprinted genes. We also add newexperimental data showing the occurrence of spermatids in patients lackingspermatozoa and demonstrating that round spermatids recovered frompatients with complete spermiogenesis failure (no elongated spermatids orspermatozoa ever detected in the patient's history) are often deficient in thefactor(s) responsible for oocyte activation. The possible consequences of thisdeficiency for the occurrence of abnormal fertilization patterns and for theimpairment of further preimplantation and post-implantation developmentare discussed. It is concluded that the development of diagnostic tests toassess the intrinsic quality of spermatids, with regard to their ability to actas gametes, is urgently needed as part of pre-treatment diagnosis beforeinfertile couples are included in a spermatid conception programme. Centreswishing to use spermatids in human assisted reproduction should also beprepared to offer adequate diagnostic methods to control genomic imprintingabnormalities in the progeny.Key words: fertilization/genomic imprinting/medical counselling/spermatid con-ception/spermiogenesis failure
Introduction
Spermatids are haploid cells of the spermatogenic line from which spermatozoaare subsequently formed through a series of morphological and molecular
Human Reproduction Volume 13 Supplement 3 1998 © European Society for Human Reproduction and Embryology 89
by guest on October 2, 2014
http://humrep.oxfordjournals.org/
Dow
nloaded from
J.Tesarik et al.
modifications collectively termed spermiogenesis. Since most of these modifica-tions were supposed to provide the male gamete with an ability to negotiate theoocyte vestments and to penetrate into ooplasm, it was postulated that spermatidsmight be used as gametes in patients with spermiogenesis block, provided thatthey are introduced into the oocyte by an appropriate micromanipulation technique(Edwards et al, 1994). The feasibility of this concept was indeed corroboratedboth by experiments with oocyte fertilization by round spermatids conducted inmice (Ogura et al, 1994; Kimura and Yanagimachi, 1995) and rabbits (Sofikitiset al, 1994, 1996a), resulting in births of normal young, and by preliminaryhuman clinical trials leading to pregnancies and births after uterine transfer ofembryos obtained by fertilizing oocytes with round (Tesarik et al., 1995, 1996;Tesarik and Mendoza, 1996a) and elongated spermatids (Fishel et al, 1995,1996). The first pregnancies and births in the mouse model were achieved byelectrofusing oocytes with whole round spermatids previously injected into theperivitelline space (Ogura et al, 1994). Subsequently, round spermatid nucleusinjection (ROSNI) into oocyte cytoplasm was demonstrated to be more efficientin the mouse (Kimura and Yanagimachi, 1995) and was also applied in humans(Yamanaka et al, 1997). Notwithstanding, most clinical studies have used intra-oocyte injection of whole spermatids, i.e. round spermatid injection (ROSI) andelongated spermatid injection (ELSI) as described by Tesarik and Mendoza(1996a). These data show clearly that viable embryos can be obtained byfertilizing oocytes with spermatids. Nevertheless, the significance of this findingfor the treatment of human infertility still remains to be evaluated.
The highly variable and unpredictable outcomes of human spermatid conceptionattempts, in terms of fertilization, implantation, fetal development and pregnancyloss (Hannay et al, 1995; Tesarik et al, 1995, 1996; Tesarik and Mendoza,1996a; Mansour et al, 1996; Araki et al, 1997; Yamanaka et al, 1997; Antinoriet al, 1997a; Amer et al, 1997), remain a major problem. Moreover, thecompleteness of the meiotic reduction in spermatids does not necessarily meanthat all epigenetic (nuclear and cytoplasmic) modifications have attained a degreecompatible with the behaviour of spermatids as fully developmentally competentgametes. This has led to some concern about the possible health hazards forchildren resulting from the use of spermatids for assisted reproduction (Tesarik,1996; Tesarik and Mendoza, 1996b).
In this study, we performed a critical analysis of the actual state of the art ofspermatid conception with particular reference to its practical application in thetreatment of human sterility. We also add some new experimental data suggestingthat the fertilization potential of spermatids is highly dependent on the type ofpathology underlying the spermatogenic defect. These findings are discussedwith regard to the attitudes to be taken by physicians and other health professionalswho may be confronted with the complex problem of spermatid conception intheir counselling, diagnostic and treatment practice.
Spermiogenesis block: what is it and how frequent is it?
Traditionally, spermatogenic block has been supposed to occur mainly at theentry of germ cells to the first meiotic division, i.e. at the primary spermatocyte
90
by guest on October 2, 2014
http://humrep.oxfordjournals.org/
Dow
nloaded from
Clinical use of spermatids
stage (maturation arrest). However, recent data have suggested that, in cases ofsevere spermatogenic disorder, some germ cells can escape the primary spermato-cyte arrest and continue further to be arrested at the spermatid stage. In most ofthese cases, a partial block at the primary spermatocyte stage does occur, asevidenced by accumulation of primary spermatocytes seen in tissue samplesrecovered by testicular biopsy. By meticulous examination of such samples,however, infrequent round or elongated spermatids can be identified.
The aetiological factors that can arrest spermatogenesis at the spermatid stageremain to be determined. In some cases, genetic abnormalities impairing thefunction of germ cells or of Sertoli cells can be at the cause. For instance, c-kitproto-oncogene, encoding a transmembrane receptor tyrosine-kinase (Yardenet al, 1987), appears to be involved in mouse spermatid elongation (Albanesiet al, 1996). In addition, the c-kit receptor and the corresponding ligand, forwhich different terms have been used (stem-cell factor, steel factor, mast-cellgrowth factor), play an important role in the partitioning of spermatogonial stemcells of the testis between the renewal, the apoptotic and the meiotic differentiationpathways (reviewed in Dym, 1994). Mutations in the W (white spotting) locusof the mouse, encoding the c-kit receptor (Chabot et al, 1988; Geissler et al,1988) or in the SI locus, encoding the c-kit ligand (Huang et al, 1990; Andersonet al, 1990), may thus be responsible for spermatogenesis problems both at pre-meiotic stages and at an early spermatid stage. An incomplete pre-meiotic block,leaving some germ cells to develop up to the spermatid stage, is a frequentobservation in human spermatogenic disorders. Similarly, mutations irv the genesencoding retinoic acid receptor a (Akmal et al, 1997) and retinoic X receptor(3 (Kastner et al, 1996) are likely to cause spermiogenesis arrest. In fact,transgenic mice carrying a mutation in the retinoid X receptor (3 gene showed ahighly abnormal Sertoli cell-germ cell interaction with abnormal spermatiddifferentiation (Kastner et al, 1996). A research into homologous human genesand their function in men with spermiogenesis arrest is warranted. In addition tothese genetic causes, a number of non-genetic factors, such as radio- andchemotherapy, long-term oestrogen therapy, nutritional factors, heat, infections,endocrinopathies, cryptorchidism and idiopathic aetiology, can also be involved inspermiogenic block (Creasy and Foster 1991; Martin-du-Pan and Campana, 1993).
Interestingly, spermatids can often be found in the ejaculate of patientssuffering from spermiogenesis arrest, and the actual presence or absence ofspermatids does not appear to be related to serum follicle stimulating hormone(FSH) concentrations (Mendoza and Tesarik, 1996). The massive release ofspermatids to the ejaculate is likely to result from an abnormal relationshipbetween spermatids and Sertoli cells in these patients. A similar detachment ofround spermatids, accompanied by spermiogenesis arrest, can be producedexperimentally in rats by testosterone withdrawal (O'Donnell et al, 1996).Testosterone has been shown to promote the adhesion of rat round spermatids toSertoli cells in an in-vitro co-culture (Cameron and Muffly, 1991; Cameron et al,1993), but a previous priming of the Sertoli cells with FSH appears to be requiredto render them 'binding competent' (Muffly et al, 1994). These observations
91
by guest on October 2, 2014
http://humrep.oxfordjournals.org/
Dow
nloaded from

J.Tesarik et al.
point out the possibility of several additional genetic aetiologies of humanspermiogenesis arrest. These include abnormalities of the FSH and testosteronereceptor and of steroid conversion pathways, in addition to the possible non-genetic aetiologies such as local deficiencies of Leydig cell distribution andfunction in the testis or abnormalities of testicular minivasculature leading tolocally reduced concentrations of FSH in certain parts of the testis.
The frequent finding of round spermatids in the ejaculate of patients with non-obstructive azoospermia prompted us to perform a prospective study comparingthe occurrence of round spermatids in the ejaculate and in the testicular biopsysamples obtained at the same day from patients undergoing a spermatid conceptionattempt. The patients were asked to produce a semen sample early on the day ofthe planned testicular biopsy. When no spermatids were found in this sample,another semen sample was requested 1-2 h later. Bilateral open testicular biopsywas then performed. Samples from at least three different locations in each testiswere taken. The biopsy was done even in those cases in which spermatids wereidentified in the ejaculate, for two reasons. Firstly, when round or early elongatingspermatids are the most differentiated spermatogenic cells seen to be present inthe ejaculate, there is still some hope of recovering a few late elongatedspermatids or spermatozoa from the testis (Amer et al, 1997). Secondly, thepercentage of viable spermatids recovered from the testis is usually superior ascompared with the ejaculate. The biopsy material was disintegrated mechanicallywith the use of microscope slides and inspected in the native state. Thereafter,the samples were fixed, and spermatids were identified by cytochemical visualiza-tion of acrosin using two different methods, a one-step staining with fluorescein-conjugated Pisum sativum agglutinin (Mendoza and Tesarik, 1996) and a two-step immunocytochemical method with 4D4 anti-proacrosin monoclonal antibody(Mendoza et al, 1996). We have previously confirmed by fluorescent in-situhybrization (FISH) the haploid status of cells of round spermatid size stainingpositive for acrosin with 4D4 monoclonal antibody (Mendoza et al, 1996). Thisantibody is also suitable for identification of those round spermatids that havenot yet developed a morphologically distinct acrosomal granule because it reactswith the protein core of the proacrosin molecule even in spermatocytes andGolgi-phase spermatids (Mendoza et al, 1996). Thus, this immunocytochemicalmethod has a higher sensitivity, and at least the same specificity, as the recentlysuggested method for round spermatid identification using an inverted microscope-associated computer-assisted image analysis system (Yamanaka et al, 1997). Itcan be expected to give similar results as transmission electron microscopy withwhich the Golgi phase of the acrosomal development can also be identified(Yamanaka et al, 1997).
This prospective study is still under way. Data available nowadays indicatethat only round spermatids, lacking any signs of elongation, are present in aboutone half of these men, whereas the other half either lack spermatids at all orpresent different stages of spermatid elongation. We use the term completespermiogenesis failure (Amer et al, 1997) for those cases in which no more
92
by guest on October 2, 2014
http://humrep.oxfordjournals.org/
Dow
nloaded from
Clinical use of spermatids
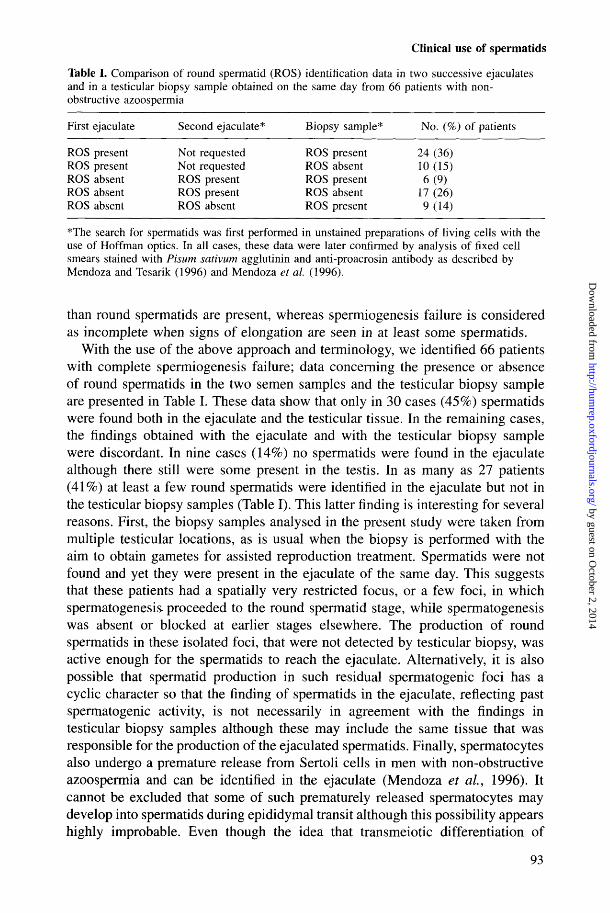
Table I. Comparison of round spermatid (ROS) identification data in two successive ejaculatesand in a testicular biopsy sample obtained on the same day from 66 patients with non-obstructive azoospermia
First ejaculate Second ejaculate* Biopsy sample* No. (%) of patients
ROS present Not requested ROS present 24 (36)ROS present Not requested ROS absent 10 (15)ROS absent ROS present ROS present 6 (9)ROS absent ROS present ROS absent 17 (26)ROS absent ROS absent ROS present 9 (14)
*The search for spermatids was first performed in unstained preparations of living cells with theuse of Hoffman optics. In all cases, these data were later confirmed by analysis of fixed cellsmears stained with Pisum sativum agglutinin and anti-proacrosin antibody as described byMendoza and Tesarik (1996) and Mendoza et al. (1996).
than round spermatids are present, whereas spermiogenesis failure is consideredas incomplete when signs of elongation are seen in at least some spermatids.
With the use of the above approach and terminology, we identified 66 patientswith complete spermiogenesis failure; data concerning the presence or absenceof round spermatids in the two semen samples and the testicular biopsy sampleare presented in Table I. These data show that only in 30 cases (45%) spermatidswere found both in the ejaculate and the testicular tissue. In the remaining cases,the findings obtained with the ejaculate and with the testicular biopsy samplewere discordant. In nine cases (14%) no spermatids were found in the ejaculatealthough there still were some present in the testis. In as many as 27 patients(41%) at least a few round spermatids were identified in the ejaculate but not inthe testicular biopsy samples (Table I). This latter finding is interesting for severalreasons. First, the biopsy samples analysed in the present study were taken frommultiple testicular locations, as is usual when the biopsy is performed with theaim to obtain gametes for assisted reproduction treatment. Spermatids were notfound and yet they were present in the ejaculate of the same day. This suggeststhat these patients had a spatially very restricted focus, or a few foci, in whichspermatogenesis proceeded to the round spermatid stage, while spermatogenesiswas absent or blocked at earlier stages elsewhere. The production of roundspermatids in these isolated foci, that were not detected by testicular biopsy, wasactive enough for the spermatids to reach the ejaculate. Alternatively, it is alsopossible that spermatid production in such residual spermatogenic foci has acyclic character so that the finding of spermatids in the ejaculate, reflecting pastspermatogenic activity, is not necessarily in agreement with the findings intesticular biopsy samples although these may include the same tissue that wasresponsible for the production of the ejaculated spermatids. Finally, spermatocytesalso undergo a premature release from Sertoli cells in men with non-obstructiveazoospermia and can be identified in the ejaculate (Mendoza et al, 1996). Itcannot be excluded that some of such prematurely released spermatocytes maydevelop into spermatids during epididymal transit although this possibility appearshighly improbable. Even though the idea that transmeiotic differentiation of
93
by guest on October 2, 2014
http://humrep.oxfordjournals.org/
Dow
nloaded from
J.Tesarik et al.
human spermatogenic cells may occur without Sertoli cell support is weaklycompatible with the traditional view of spermatogenesis control, Sertoli cell-independent differentiation of bovine secondary spermatocytes into spermatidscapable of fertilizing oocytes with subsequent development to the blastocyststage has been achieved in vitro, in the absence of any additional cellular support(Goto et al, 1996). If spermatids are found both in the ejaculate and in atesticular biopsy sample, the latter can be expected to be of higher biologicalquality because of the likely oxidative damage having occurred as spermatidsaged during the epididymal transit.
In spite of the frequent failure of spermatid recovery from testicular biopsysamples, we still believe that testicular biopsy is worth doing in any ROSIattempt. When compared with ejaculated spermatids, testicular spermatids usuallyhave a better viability, and their fertilizing ability may still be increased by in-vitro culture which is much more problematic for the more aged ejaculatedspermatids. In most patients, ejaculated spermatids are also more frequently proneto apoptosis in comparison with testicular spermatids (J.Tesarik, unpublishedobservation). Cryopreservation of testicular tissue may avoid the need for repeatedbiopsy for future ROSI attempts.
Irrespective of the underlying biological mechanism, these data show that thefinding of round spermatids is a frequent situation in cases in which spermatozoafail to be found. It is thus important to perform a deeper analysis of these casesin order to establish additional criteria for prediction of success rates and healthhazards of the use of spermatids obtained in these particular situations for assistedreproduction. On the other hand, numerous primary spermatocytes are usuallypresent in those cases in which only very few spermatids can be obtained. If in-vitro culture methods supporting the development of primary spermatocytes intospermatids are available, the treatment of such cases would obviously be renderedmuch easier.
Factors affecting success and failure of spermatid conception
Complete and incomplete spermiogenesis failure
We have recently used the term complete spermiogenesis failure for those casesin which the round spermatid is the latest stage of spermatogenesis ever detectedin the patient's history (Amer et al, 1997). Spermatid conception was attemptedin 59 such cases, but ongoing clinical pregnancies were only achieved in twoout of three cases in which late elongated spermatids were unexpectedly recoveredby testicular biopsy and injected into oocytes (Amer et al, 1997). Hence, thespermiogenesis failure was in fact incomplete in these successful treatment cycleswhich thus bore much resemblance to the successful spermatid conception cyclesdescribed previously by ourselves (Tesarik et al, 1995, 1996; Tesarik andMendoza, 1996a) and others (Fishel et al, 1995; Araki et al, 1997). A similardifference in ROSNI success rates between patients with complete and incomplete
94
by guest on October 2, 2014
http://humrep.oxfordjournals.org/
Dow
nloaded from
Clinical use of spermatids
spermiogenesis failure has been reported recently by Vanderzwalmen et al.(1997). These clinical data are in agreement with a previous experimental studyshowing that the reproductive capacity of round spermatids selected from animalswith primary testicular damage was lower than that of round spermatids recoveredfrom healthy animals (Sofikitis et al, 1996b).
Notwithstanding, our fertilization and cleavage rates obtained in patients withcomplete spermiogenesis failure (Amer et al, 1997) were not dissimilar to thosewe reported previously for cases in which spermiogenesis failure was incomplete(Tesarik and Mendoza, 1996a). Moreover, four biochemical pregnancies wereestablished with round spermatids from patients with complete spermiogenesisfailure; of these, however, none developed into a clinical pregnancy (Amer et al,1997). This means that the factors responsible for the failure of spermatidconception in cases of complete spermiogenesis failure act mainly around thetime of implantation and in the early post-implantation period rather than atfertilization and during early preimplantation development. These factors, largelyunknown for the time being, may be related to genetic anomalies or to variouscytological, biochemical and cell-signalling disorders most of which may impacton embryonic gene dosage and activity and can thus be characterized asepigenetic factors.
Genetic anomalies
Several genes have been suggested as causative factors in human spermatogenicdisorders. Three candidate genes, YRRM1 and YRRM2 (Y-specific genes withRNA recognition motif) (Ma et al, 1993) and DAZ (deleted in azoospermia)(Reijo et al, 1995), have been characterized. They all map to the long arm ofthe human Y chromosome, to a region called AZF (azoospermia factor) becausethe association of major deletions (detectable in karyotype) in this region withsevere spermatogenic disorders suggested that it contained one or several loci(AZF loci) responsible for spermatogenesis (Tiepolo and Zuffardi, 1976). Itcannot be excluded that other yet unidentified genes can be localized in this Y-chromosome region. In addition, an autosomal homologue of DAZ, called DAZLA(DAZ-like autosomal) has been discovered on the human chromosome 3 (Yenet al, 1996). Tiny deletions (microdeletions) or mutations in the AZF region,which are not detectable in the karyotype but can be revealed by polymerasechain reaction, have been shown to be associated with some cases of azoospermiaor severe oligoasthenoteratozoospermia (for recent reviews, see Qureshi et al,1996; Pryor et al, 1997).
A complex interplay between different genes involved in spermatogenesis issupposed to control individual stages of this process. The polygenic control ofhuman spermatogenesis may explain why deletions of the same size andchromosomal location can be associated with different gravity of the spermatog-enic disorder in different patients. It is not known in what proportion ofazoospermic patients with Y-chromosome microdeletions spermatids can berecovered for assisted reproduction. No analysis of the Y chromosome integrity,
95
by guest on October 2, 2014
http://humrep.oxfordjournals.org/
Dow
nloaded from

J.Tesarik et al.
beyond routine karyotype examination, has been performed in any of thespermatid-injection treatment cycles yet reported in the literature. However, ifsuch microdeletions were present in the spermatids used for treatment, this wouldbe unlikely to jeopardize the fertilization performance of these spermatids orsubsequent embryonic and fetal development. In fact, this kind of geneticabnormality, though affecting sperm differentiation and function, does not appearto affect embryo viability and can be transmitted to progeny when fertilizationis assisted by appropriate micromanipulation techniques (Mulhall et al, 1997).Consequently, if the failure of embryonic or fetal development after fertilizingoocytes with spermatids is due to genetic factors, the gene(s) responsible fordevelopmental failure are unlikely to be identical with the known genes responsiblefor spermatogenic failure and still remain to be identified. Alternatively, thefactors responsible for developmental failure in these cases may be of epigeneticrather than genetic origin.
Epigenetic disorders
Nuclear proteins
The development of spermatids into spermatozoa is marked by salient changesin the composition of nuclear proteins, histones being progressively removedand replaced with protamines, basic proteins rich in S-S bonds responsible fornuclear condensation, whereas an inverse protamine-histone transition occurs inthe male nucleus after fertilization (reviewed in Perreault, 1990). A questionarises about what happens when an early spermatid nucleus, with DNA stillassociated with histones, is exposed to oocyte cytoplasmic factors regulating theS-S bond reduction, protamine-histone transition and the male pronucleardevelopment (Tesarik and Kopecny, 1989a) without the previous passage throughthe protamine-associated configuration. It has already been proven that the timingof hamster sperm nuclear decondensation and male pronucleus formation isrelated to sperm nuclear disulphide bond content (Naish et al, 1987). A relativelyrapid (<10 h) appearance of pronuclei has been reported after human ROSI(Tesarik and Mendoza, 1996a) and ROSNI (Yamanaka et al, 1997). Recent workin an anuran amphibian, Rana catesbeiana, has suggested that a complete removalof sperm-specific histone variants is not necessary for the sperm nucleusremodelling into somatic chromatin that takes place after fertilization (Itoh et al.,1997). Moreover, unlike most mammalian species in which virtually all nuclearhistones are replaced with protamines during spermiogenesis (Meistrich, 1989),~10% of the DNA of mature human spermatozoa remains bound to histones(Tanphaichitr et al, 1978; Gatewood et al, 1987; Choudhary et al, 1995). It isthus possible that a complete removal of spermatid histones does not necessarilyoccur during the development of the male pronucleus after human ROSI.However, the unusual respective dosage of histones of the male and of the femaleorigin, along with the presence of a variable amount of protamines, may alterthe normal sequence of early post-fertilization chromatin functions, including the
96
by guest on October 2, 2014
http://humrep.oxfordjournals.org/
Dow
nloaded from
Clinical use of spermatids
early transcriptional activity detected in human pronuclear zygotes (Tesarikand Kopecny, 1989b, 1990). Such irregularities may be responsible for theabnormalities in the pronuclear development observed after human ROSI, suchas the persistence of a very small dense nucleus or a prolonged appearance of asingle syngamic nucleus after previous development of two normal-sized pronuclei(Tesarik and Mendoza, 1996a).
Centriole
Spermatids possess a pair of centrioles, proximal and distal, of which the latterdisappears in late elongated (Sd2) spermatids (De Kretser and Kerr, 1988).Consequently, the mature sperm cell has only one centriole, associated with amicrotubule-organizing centre (MTOC); this sperm-derived MTOC is responsiblefor the organization of zygote microtubules including those of the mitotic spindlesemployed in the forthcoming cleavage divisions (Sathanthan et al, 1991; Palermo,et al, 1994; Simerly et al, 1995). It is not known whether the spermatid's distalcentriole is also associated with an MTOC that can become active within theoocyte cytoplasm. If so, this might lead to the creation of multipolar mitoticspindles and thus cause an irregular distribution of chromosomes at anaphaseresulting in numerical chromosomal abnormalities. An abnormal function of thesperm centriole is one of the mechanisms suspected to be involved in thedevelopment of chromosome abnormalities after intracytoplasmic sperm injection(ICSI) (Tesarik, 1995), and this concern is even more substantiated in the caseof the use of spermatids. The examination of the karyotype of all babies resultingfrom spermatid conception is thus strongly recommended.
Oocyte-activating factor
As in other mammalian species, sperm-induced activation of human oocytes atfertilization is mediated by a special form of Ca2+ signal, consisting of a seriesof repetitive sharp and short increases (spikes) of intracellular free Ca2+
concentration ([Ca2+]j) referred to as Ca2+ spiking or Ca2+ oscillations (Tayloret al, 1993; Tesarik and Sousa, 1994). The sperm-induced Ca2+ oscillations alsodevelop after ICSI (Tesarik and Sousa, 1994; Tesarik et al, 1994) and aresupposed to be dependent on the action of an oocyte-activating factor containedin the cytoplasm of the injected spermatozoon. A recently characterized protein,termed oscillin (Parrington et al, 1996), is a candidate for this function. Eventhough an increase in [Ca2+]j is regularly produced by the ICSI procedure itself,and this artificial [Ca2+]j increase has been shown to potentiate the action of theoocyte-activating factor (Tesarik and Sousa, 1995), Ca2+ oscillations do notdevelop in the absence of sperm (Tesarik and Testart, 1994; Tesarik et al, 1994;Tesarik and Sousa, 1995). Because Ca2+ oscillations are believed to be requiredfor normal oocyte activation in mammals (reviewed in Swann and Ozil, 1994),it is important to know whether the oocyte-activating factor is already present inspermatids and whether it has reached its full biological activity by this stage.
97
by guest on October 2, 2014
http://humrep.oxfordjournals.org/
Dow
nloaded from

12345
87885
23100
J.Tesarik et al.
Table II. The ability of round spermatids from patients with complete spermiogenesis failure tosupport Ca2+ oscillations in oocytes
No. of oocytes
Patient Injected Oscillating at 30-60 min Oscillating at 1-2 h
1*0001
*This oocyte was one of the two that oscillated at the 30-60 min observation interval.
To answer this question, surnumerary human oocytes, donated by consentingpatients, were injected with different stages of spermatogenic cells or withpolymorphonuclear leukocytes, and the subsequent Ca2+ response was evaluatedby confocal microscopy (Sousa et al, 1996a). Data obtained showed that Ca2+
oscillations, similar to those following the injection of a mature spermatozoon,developed after the injection of a round spermatid but not after the injection ofa primary or secondary spermatocyte or of a polymorphonuclear leukocyte (Sousaet al, 1996a). Hence, electrical stimulation is not required for normal activationof spermatid-injected human oocytes (Tesarik et al., 1995), similarly as forcynomolgus monkey oocytes (Ogura et al, 1997), whereas it is important foroptimal oocyte activation after ROSI and ROSNI in the mouse (Kimura andYanagimachi, 1995) and rabbit (Sofikitis et al, 1996a).
However, the above results were obtained with spermatids from men whoproduced apparently normal mature spermatozoa. Here we performed additionalexperiments in which we used the same materials and methods (Sousa et al,1996a) to assess the function of the oocyte-activating factor of spermatids frompatients with complete spermiogenesis failure, in whom spermatids did notdevelop beyond the Sa stage according to the classification of de Kretser andKerr (1988). Briefly, oocytes were injected with spermatids without performingthe vigorous ooplasmic aspiration, thus avoiding a rapid oocyte activation, andsubsequently loaded with the Ca2+ indicator fluo-3. The oocytes were challengedwith 10 |oM ionophore A23187 to boost activation and examined in a confocallaser scanning microscope for the subsequent development of Ca2+ oscillations.Results of these experiments are shown in Table II. When [Ca2+]j was monitored30-60 min after the ionophore challenge, only six out of 36 oocytes injected(17%) showed Ca2+ oscillations, and only two oocytes (6%) oscillated whenexamined 2-3 h after ionophore treatment (Table II). This contrasted with ourprevious data on the occurrence of Ca2+ oscillations after injection of spermatidsfrom men capable of completing spermiogenesis, showing the development ofCa2+ oscillations in 13 out of 17 oocytes (76%) injected with round spermatids(Sousa et al, 1996a), as well as with the duration of the Ca2+-oscillation periodin human oocytes injected with mature spermatozoa, which was superior to 2 h(Tesarik and Sousa, 1994; Tesarik et al, 1994; Sousa et al, 1996b). The existence
98
by guest on October 2, 2014
http://humrep.oxfordjournals.org/
Dow
nloaded from

Clinical use of spermatids
of these differences suggests that, in spite of the presence of oocyte-activatingfactor in round spermatids from men with normal spermatogenesis, this factormay be deficient in many round spermatids recovered from men with completespermiogenesis failure.
These data may explain why the fertilization rates reported after ROSI inpatients with severe disorders of spermiogenesis is lower than for ICSI withmature spermatozoa (Tesarik et al, 1995; Tesarik and Mendoza, 1996a; Fishelet al, 1997), although at least one study (Yamanaka et al, 1997) reports fairlyhigh oocyte activation rates after ROSNI in patients with complete spermiogenesisfailure. The reason of these differences is not known. Moreover, the suboptimalactivity of the oocyte-activating factor in patients' spermatids may have develop-mental consequences reaching far beyond fertilization and can also be responsiblefor the low implantation rate and the high early-abortion rate after transfer ofspermatid-derived embryos that were observed in cases of complete spermiogen-esis failure (Amer et al, 1997). It is now clear that the quality of Ca2+ signalsgenerated in freshly fertilized oocytes influences developmental processes farbeyond the reactivation of the zygote's cell cycle and the pronuclear development.In the mouse model, transient [Ca2+]i increases were shown to regulate embryonicgrowth and differentiation throughout preimplantation development (Stacheckiand Armant, 1996), and the form of Ca2+ signals in mouse zygotes andearly embryos was related to the progression of embryonic cell division anddifferentiation during both preimplantation and early postimplantation develop-ment (Bos-Mikich et al, 1997). Similarly, human preimplantation embryos wereshown to generate Ca2+ signals that appeared to be related to the blastomere cellcycle and viability (Sousa et al, 1996b). It is thus possible that the quality ofthe initial fertilization-induced Ca2+ signal may affect the forthcoming Ca2+
signalling events controlling further development of human embryos. Furtherimprovement of ROSI success rates in patients with complete spermiogenesisfailure will thus depend on our ability to mimick the normal pattern of fertilization-associated and embryonic Ca2+ signals in the absence or relative insufficiencyof the oocyte-activating factor in the patients' spermatids.
Potential health hazards
Health hazards relating to the use of spermatids in human assisted reproductionhave been largely discussed previously (Tesarik, 1996; Tesarik and Mendoza,1996b). Besides the risk of transmission of infertility genes, which does notappear to be higher than for ICSI with mature spermatozoa in cases of severespermatogenic defects, the risk of genomic imprinting abnormalities represent amajor concern (Tesarik and Mendoza, 1996b). This concern is based on theuncertainty of whether the process of genomic imprinting, taking place duringan unknown period of gametogenesis, is actually completed in immaturespermatogenic cells, although minor abnormalities may be repaired after fertiliza-tion (Howlett and Reik, 1991). In addition to the three imprinted genes known
99
by guest on October 2, 2014
http://humrep.oxfordjournals.org/
Dow
nloaded from
J.Tesarik et al.
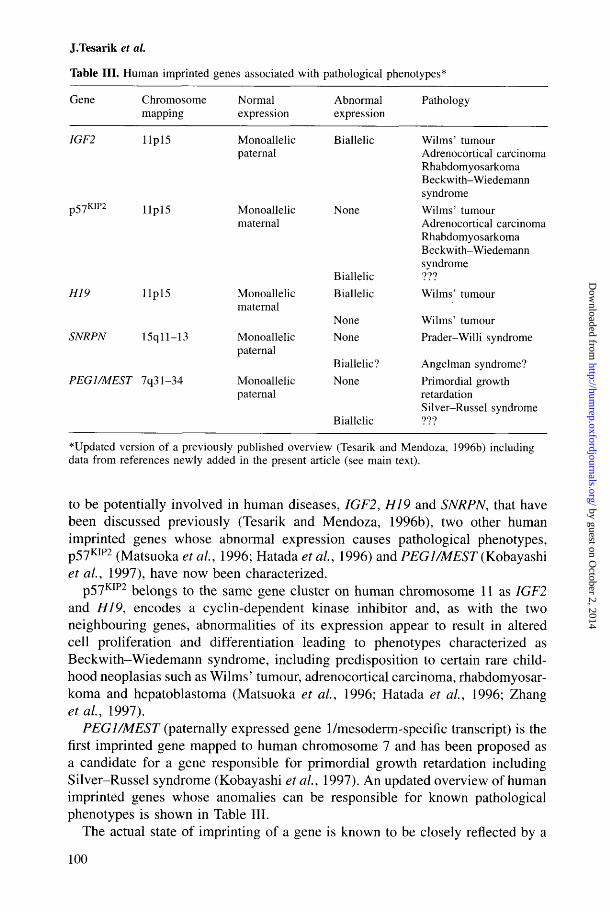
Table III. Human imprinted genes associated with pathological phenotypes*
Gene
1GF2
p57K I P 2
H19
SNRPN
PEG1/MEST
Chromosomemapping
Ilpl5
Ilpl5
Ilpl5
15qll-13
7q31-34
Normalexpression
Monoallelicpaternal
Monoallelicmaternal
Monoallelicmaternal
Monoallelicpaternal
Monoallelicpaternal
Abnormalexpression
Biallelic
None
Biallelic
Biallelic
None
None
Biallelic?None
Biallelic
Pathology
Wilms' tumourAdrenocortical carcinomaRhabdomyosarkomaBeckwith-Wiedemannsyndrome
Wilms' tumourAdrenocortical carcinomaRhabdomyosarkomaBeckwith-Wiedemannsyndrome???
Wilms' tumour
Wilms' tumour
Prader-Willi syndrome
Angelman syndrome?Primordial growthretardationSilver-Russel syndrome777
* Updated version of a previously published overview (Tesarik and Mendoza, 1996b) includingdata from references newly added in the present article (see main text).
to be potentially involved in human diseases, IGF2, H19 and SNRPN, that havebeen discussed previously (Tesarik and Mendoza, 1996b), two other humanimprinted genes whose abnormal expression causes pathological phenotypes,p57KIP2 (Matsuoka et al, 1996; Hatada et al, 1996) and PEG1/MEST (Kobayashiet al, 1997), have now been characterized.
p57KIP2 belongs to the same gene cluster on human chromosome 11 as IGF2and HI9, encodes a cyclin-dependent kinase inhibitor and, as with the twoneighbouring genes, abnormalities of its expression appear to result in alteredcell proliferation and differentiation leading to phenotypes characterized asBeckwith-Wiedemann syndrome, including predisposition to certain rare child-hood neoplasias such as Wilms' tumour, adrenocortical carcinoma, rhabdomyosar-koma and hepatoblastoma (Matsuoka et al, 1996; Hatada et al, 1996; Zhangetal, 1997).
PEG1/MEST (paternally expressed gene 1/mesoderm-specific transcript) is thefirst imprinted gene mapped to human chromosome 7 and has been proposed asa candidate for a gene responsible for primordial growth retardation includingSilver-Russel syndrome (Kobayashi etal, 1997). An updated overview of humanimprinted genes whose anomalies can be responsible for known pathologicalphenotypes is shown in Table III.
The actual state of imprinting of a gene is known to be closely reflected by a
100
by guest on October 2, 2014
http://humrep.oxfordjournals.org/
Dow
nloaded from
Clinical use of spermatids
specific pattern of DNA methylation, concerning CpG dinucleotides, in the geneitself or its promoter (Brandeis et al, 1993). However, all methylated CpG sitesare not involved in genomic imprinting. Even though the specific sites involvedin imprinting are not yet known for all human imprinted genes, knowledge inthis field is emerging rapidly (Jinno et al, 1996). Once the specific methylatedsites are definitely identified, it will be possible to check the imprinting statusof the respective genes by evaluating their methylation pattern by analysis of thesize of DNA fragments after digestion with methylation-sensitive restrictionenzymes. Methods for the distinction of monoallelic versus biallelic geneexpression, using reverse transcription followed by polymerase chain reaction,are also known and can be used to check the parent-specific allele repression ofimprinted genes, although the expression studies also have not yet been fullyconclusive (Szabo and Mann, 1995a,b), and much remains to be done. Hopefully,these methods will be available in the near future to analyse the five imprintedhuman genes (Table III) in lymphocytes of children resulting from spermatidconception. We believe that the availability of this screening should be ensuredin any future spermatid-conception clinical programme because the eventualdetection of imprinting abnormalities can call attention to children at a higherrisk of disease, to whom a special clinical surveillance is to be offered in orderto ensure early diagnosis to propose efficient treatment in case of a developingpathology.
Practical recommendations
Quality assurance
It is important to stress that, many times in cases of non-obstructive azoospermia,spermatids are far from being predominant cells in patients' ejaculate andtesticular biopsy samples, even when methods for preparation of spermatid-enriched fractions are used. Thus, the recognition of living round spermatidsfrom other round cells requires considerable skill. This skill can be best acquiredby a person who is involved not only in spermatid injection trials but also in thediagnostic procedures aimed at the identification of individual stages of germcells in patients' samples. In this way, the student of spermatid morphology isfirst confronted with a relatively easy task of identifying germ cells with the useof cytological stains and more-or-less specific markers. The recently describedmethods for identification of round spermatids by a selective staining of acrosincontained in the developing acrosome with the use of fluorescein-labelled Pisumsativum agglutinin (Mendoza and Tesarik, 1996) or a more specific methodvisualizing proacrosin with the use of a monoclonal antibody (Mendoza et al,1996) are examples of this approach. The latter method can be successfullycombined with the detection of haploid cells by FISH (Mendoza et al, 1996)and is also suitable for the identification of spermatocytes and Golgi-phase roundspermatids (stage 1) that still do not possess a distinct acrosomal vesicle. Among
101
by guest on October 2, 2014
http://humrep.oxfordjournals.org/
Dow
nloaded from
J.Tesarik et al.
the positively reacting cells, the distinction between spermatocytes and spermatidscan then be made on the basis of cell size (Mendoza et al., 1996). This backgroundknowledge is very useful for passing to the much more difficult task which is toidentify round spermatids in fresh, unstained cell preparations (Tesarik andMendoza, 1996a). The identification of elongated spermatids is easier as comparedto round spermatids. However, individual stages of elongated spermatid develop-ment should be distinguished, at least on the basis of classical histology, and themorphology of the spermatids used for injection should be described in thegreatest detail possible to avoid confusion of data interpretation when clinicalresults obtained with different patients are compared (Tesarik, 1997).
The injection of spermatids also requires additional skill as compared withICSI (Tesarik and Mendoza, 1996a) and should be learned with animal models(mouse or hamster oocytes) before going to human application. The timing ofpronuclear development after fertilization with spermatids is often different fromICSI and requires more frequent inspection of the injected oocytes. The specialfeatures of spermatid-derived zygote development, particularly the frequentdevelopment of a large syngamy nucleus (Tesarik and Mendoza, 1996a), havealso to be taken into account.
Spermatid and spermatocyte cryopreservation: an obligatory step in cases oftesticular sperm recovery failure
The failure of sperm recovery from testicular biopsy samples on the day ofplanned ICSI treatment is a relatively frequent complication. In many such cases,spermatids or spermatocytes can be identified. Moreover, it appears that it is justthis situation of unexpected sperm absence which predicts better results ofspermatid conception as compared to cases in which no spermatozoa have everbeen detected (see above). However, if previous informed consent applicable tothis situation has not been obtained, the use of spermatids in the present treatmentcycle is impossible. Because the couple may demand a spermatid conceptionattempt at a later date, and in order to avoid the need for a new surgicalintervention on that occasion, we recommend cryopreserving all the testicularbiopsy samples for eventual future use. In fact, a human pregnancy has beenachieved after fertilizing oocytes with frozen-thawed round spermatids (Antinorietal, 1997b).
Furthermore, many testicular biopsy samples lack both spermatozoa andspermatids but contain relatively high numbers of primary spermatocytes.Although the technique of fertilization with primary spermatocytes has not yetbeen developed, it is likely to emerge in the near future, possibly making use oftransmeiotic in-vitro development of primary spermatocytes into spermatids orof injection of primary spermatocytes into germinal vesicle oocytes allowingboth the male and the female nucleus to undergo simultaneous reduction divisionswithin the oocyte. Because a rapid degradation of spermatogenesis, progressingfrom maturation arrest to Sertoli cell-only syndrome, is not an uncommon finding,cryopreservation of testicular tissue containing primary spermatocytes is highly
102
by guest on October 2, 2014
http://humrep.oxfordjournals.org/
Dow
nloaded from

Clinical use of spermatids
recommendable to preserve the individual's reproductive potential for the timeat which an adequate assisted reproduction method will be available.
Medical counselling
When discussing the predictable success rates of spermatid conception withconcerned couples, it is absolutely necessary to avoid drawing general conclusionsfrom the small series of cases yet published. Nevertheless, it seems that prognosisis better when at least a small number of mature spermatozoa has been identifiedby previous patient's examinations (in the ejaculate or in a testicular biopsysample). If spermatozoa have never been found in the patient's history, theprognosis of spermatid conception is poor and is often further compromised bythe wife's age. As an example, in our consultation, we inform patients that, withthe actual state of the art, the predictable take-home-baby rate for a spermatidconception attempt is 5-10% in cases with past sperm production in which thewife's age is <35 years. This prediction drops to 1-5% in cases of suspectedcomplete spermiogenesis failure and when the wife's age approaches 40 years.Such a realistic estimation, accompanied by a detailed explanation of the potentialhealth hazards the method can create (see above), makes part of pre-treatmentcounselling sessions after which couples decide whether they wish to enter thespermatid conception programme.
In all cases, it has to be recalled to the couples that there is a rapid increaseof knowledge in the field so that success rates are likely to improve in the nearfuture. This will be possible partly because of a progress in diagnostic methods,thus avoiding the treatment of those couples in which successful conception isimpossible due to genetic or epigenetic factors that cannot be therapeuticallyovercome, partly because of improvements of the laboratory techniques used forthe introduction of male germ cells into oocytes and subsequent oocyte activation.However, the time for which couples can wait is limited by the wife's age.Unfortunately, couples in whom we are urged to rush because of the wife's ageare often those in which the poor quality of oocytes is an additional adversefactor. No straightforward lead can be formulated as to how to manage thesesituations whose solution depends on the free decision of each couple, based oncomplete information about the actual and predictable future state of the art, theprobable success rate, motivation of both partners and their social background.
Acknowledgements
We are most grateful to Professor Claudio Sunkel, CCEP, University of Porto for providing theconfocal imaging facilitities and to Eng. A.Almeida Foundation for librarian financial support.
References
Akmal, K.A., Dufour, J.M. and Kim, K.H. (1997) Retinoic acid receptor a gene expression in therat testis: potential role during the prophase of meiosis and in the transition from round toelongating spermatids. Biol. Reprod., 56, 549-556.
103
by guest on October 2, 2014
http://humrep.oxfordjournals.org/
Dow
nloaded from
J.Tesarik et al.
Albanesi, C , Geremia, R., Giorgio, M. et al. (1996) A cell- and developmental stage-specificpromoter drives the expression of a truncated c-kit protein during mouse spermatid elongation.Development, 122, 1291-1302.
Amer, M., Soliman, E., El-Sadek, M. et al. (1997) Is complete spermiogenesis failure a goodindication for spermatid conception? Lancet, 350, 116.
Anderson, D.M., Lyman, S.D., Baird, A. et al. (1990) Molecular cloning of mast cell growthfactor, a hematopoietin that is active in both membrane bound and soluble forms. Cell, 63,235-243.
Antinori, S., Versaci, C, Dani, G. et al. (1997a) Fertilization with human testicular spermatids:four successful pregnancies. Hum. Reprod., 12, 286-291.
Antinori, S., Versaci, C, Dani, G. et al. (1997b) Successful fertilization and pregnancy afterinjection of frozen-thawed round spermatids into human oocytes. Hum. Reprod., 12, 554-556.
Araki, Y., Motoyama, M., Yoshida, A. et al. (1997) Intracytoplasmic injection with late spermatids:a successful procedure in achieving childbirth for couples in which the male partner suffersfrom azoospermia due to deficient spermatogenesis. Fertil. Steril, 67, 559-561.
Bos-Mikich, A., Whittingham, D.G. and Jones, K.T. (1997) Meiotic and mitotic Ca2+ oscillationsaffect cell composition in resulting blastocysts. Dev. Biol, 182, 172-179.
Brandeis, M., Kafri, T., Ariel, M. et al. (1993) The ontogeny of allele-specific methylationassociated with imprinted genes in the mouse. EMBO J., 12, 3669-3677.
Cameron, D.F. and Muffly, K.E. (1991) Hormonal regulation of spermatid binding. J. Cell ScL,100, 623-633.
Cameron, D.F., Muffly, K.E. and Nazian, S.J. (1993) Testosterone stimulates spermatid binding tobinding competent Sertoli cells in vitro. Endocr. J., 1, 61-65.
Chabot, B., Stephenson, D.A., Chapman, V.M. et al. (1988) The protooncogene c-kit encoding atransmembrane tyrosine kinase receptor maps to the mouse W locus. Nature, 335, 88-89.
Choudhary, S.K., Wykes, S.M., Mohamed, A.K. et al. (1995) A haploid expressed gene clusterexists as a single chromatin domain in human sperm. J. Biol. Chem., 270, 8755-8762.
Creasy, D.M. and Foster, M.D. (1991) Male reproductive system. In Haschek, W.M. and Rousseaux,C.G. (eds), Handbook of Toxicologic Pathology. Academic Press, New York,
de Kretser, D.M. and Kerr, J.B. (1988) The cytology of the testis. In Knobil, E. and Neill, J. (eds),The Physiology of Reproduction. Raven Press, New York, USA, pp. 837-932.
Dym, M. (1994) Spermatogonial stem cells of the testis. Proc. Natl. Acad. Sci. USA, 91,11287-11289.Edwards, R.G., Tarin, J.J., Dean, N. et al. (1994) Are spermatid injections into human oocytes
now mandatory? Hum. Reprod., 9, 2217-2219.Fishel, S., Aslam, I. and Tesarik, J. (1996) Spermatid conception: a stage too early, or a time too
soon? Hum. Reprod., 11, 1371-1375.Fishel, S., Green, S., Bishop, M. et al. (1995) Pregnancy after intracytoplasmic injection of
spermatid. Lancet, 345, 1641-1642.Fishel, S., Green, S., Hunter, A. et al. (1997) Human fertilization with round and elongated
spermatids. Hum. Reprod., 12, 336-340.Gatewood, J.M., Cook, G.R., Balhorn, R. et al. (1987) Sequence-specific packaging of DNA in
human sperm chromatin. Science, 236, 962-964.Geissler, E.N., Ryan, M.A. and Housman, D.E. (1988) The dominant White Spotting (HO locus of
the mouse encodes the c-kit protooncogene. Cell, 55, 185-192.Goto, K., Kinoshita, A., Nakanishi, Y. and Ogawa, K. (1996) Blastocyst formation following
intracytoplasmic injection of in-vitro derived spermatids into bovine oocytes. Hum. Reprod., 11,824-829.
Hannay, T. (1995) New Japanese IVF method finally made available in Japan. Nature Med., 1,289-290.
Hatada, I., Inazawa, J., Abe, T. et al. (1996) Genomic imprinting of human p57A7P2 and its reducedexpression in Wilms' tumors. Hum. Mol. Genet., 5, 783-788.
Howlett, S.H. and Reik, W. (1991) Methylation levels of maternal and paternal genomes duringpreimplantation development. Development, 113, 119-127.
Huang, E., Nocka, K., Beier, D.R. et al. (1990) The hematopoietic growth factor KL is encodedby the 5/ locus and is the ligand of the c-kit receptor, the gene product of the W locus. Cell, 63,225-233.
104
by guest on October 2, 2014
http://humrep.oxfordjournals.org/
Dow
nloaded from
Clinical use of spermatids
Itoh, T., Ausio, J. and Katagiri, C. (1997) Histone HI variants as sperm-specific nuclear proteinsof Rana catesbeiana, and their role in maintaining a unique condensed state of sperm chromatin.Mol. Reprod. Dev., 47, 181-190.
Jinno, Y., Senkogu, K., Nakao, M. et al. (1996) Mouse/human sequence divergence in a regionwith a paternal-specific methylation imprint at the human HI9 locus. Hum. Mol. Genet., 5,1155-1161.
Kastner, P., Mark, M., Leid, M. et al. (1996) Abnormal spermatogenesis in RXR(3 mutant mice.Genes Dev., 10, 80-92.
Kimura, Y. and Yanagimachi, R. (1995) Mouse oocytes injected with testicular spermatozoa andround spermatids can develop into normal offspring. Development, 121, 2397-2405.
Kobayashi, S., Kohda, T., Miyoshi, N. et al. (1997) Human PEG1/MEST, an imprinted gene onchromosome 7. Hum. Mol. Genet., 6, 781-786.
Ma, K., Inglis, J.D., Sharkey, A. et al. (1993) A Y chromosome gene family with RNA-bindingprotein homology: candidates for the azoospermia factor AZF controlling human spermatogenesis.Cell, 75, 1287-1295.
Mansour, R.T., Aboulghar, M.A., Serour, et al. (1996) Pregnancy and delivery after intracytoplasmicinjection of spermatids into human oocytes. Middle East Fertil. Soc. J., 1, 223-225.
Martin-du-Pan, R.C. and Campana, A. (1993) Physiopathology of spermatogenic arrest. Fertil.Steril, 60, 937-946
Matsuoka, S., Thompson, J.S., Edwards, M.C. et al. (1996) Imprinting of the gene coding a humancyclin-dependent kinase inhibitor, p57KIP2, on chromosome Ilpl5. Proc. Natl. Acad. Sci. USA,93, 3026-3030.
Meistrich, M.L. (1989) Histone and basic nuclear protein transitions in mammalian spermatogenesis.In Hnilica, C.S., Stein, G.S. and Stein, J.L. (eds), Histones and Other Basic Nuclear Proteins.CRC Press, Boca Raton, FL, USA, pp. 165-182.
Mendoza, C. and Tesarik, J. (1996) The occurrence and identification of round spermatids in theejaculate of men with nonobstructive azoospermia. Fertil. Steril., 66, 826-829.
Mendoza, C, Benkhalifa, M., Cohen-Bacrie, P. et al. (1996) Combined use of proacrosinimmunocytochemistry and autosomal DNA in situ hybridization for evaluation of humanejaculated germ cells. Zygote, 4, 279-283.
Muffiy, K.E., Nazian, S.J. and Cameron, D.F. (1994) Effects of follicle-stimulating hormone onthe junction-related Sertoli cell cytoskeleton and daily sperm production in testosterone-treatedhypophysectomized rats. Biol. Reprod., 51, 158-166.
Mulhall, J.P., Reijo, R., Alagappan, R. et al. (1997) Azoospermic men with deletion of the DAZgene cluster are capable of completing spermatogenesis: fertilization, normal embryonicdevelopment and pregnancy occur when retrieved testicular spermatozoa are used forintracytoplasmic sperm injection. Hum. Reprod., 12, 503-508.
Naish, S.J., Perreault, S.D., Foehner, A.L. and Zirkin, B.R. (1987) DNA synthesis in the fertilizinghamster sperm nucleus: sperm template availability and egg cytoplasmic control. Biol. Reprod.,36, 245-253. -
O'Donnell, L., McLachlan, R.I., Wreford, N.G. et al. (1996) Testosterone withdrawal promotesstage-specific detachment of round spermatids from the rat seminiferous epithelium. Biol.Reprod, 55, 895-901.
Ogura, A., Matsuda, J., Suzuki, O. et al. (1997) Cryopreservation of mammalian spermatids.J.Reprod. Dev., 43, Suppl., 103-104.
Ogura, A., Matsuda, J. and Yanagimachi, R. (1994) Birth of normal young after electrofusion ofmouse oocytes with round spermatids. Proc. Natl. Acad. Sci. USA, 91, 7460-7462.
Palermo, G., Munne, S. and Cohen, J. (1994) The human zygotes inherits its mitotic potentialfrom the male gamete. Hum. Reprod., 9, 1220-1225.
Parrington, J., Swann, K., Shevchenko, V.I. et al. (1996) Calcium oscillations in mammalian eggstriggered by a soluble sperm protein. Nature, 379, 364-368.
Perreault, S.D. (1990) Regulation of sperm nuclear reactivation during fertilisation. In Cummins,J. and Roldan, E.R.S. (eds), Fertilisation in Mammals. Serono Symposia, Norwell, MA, USA,pp. 285-296.
Pryor, J.L., Kent-First, M., Muallem, A. et al. (1997) Microdeletions in the Y chromosome ofinfertile men. N. Engl. J. Med, 336, 534-539.
105
by guest on October 2, 2014
http://humrep.oxfordjournals.org/
Dow
nloaded from
J.Tesarik et al.
Qureshi, S.J., Ross, A.R., Ma, K. et al. (1996) Polymerase chain reaction screening for Ychromosome microdeletions: a first step towards the diagnosis of genetically determinedspermatogenic failure in men. Mol. Hum. Reprod., 2, 775-779.
Reijo, R., Lee, T.-Y., Salo, P. et al. (1995) Diverse spermatogenic defects in humans caused by Ychromosome deletions encompassing a novel RNA-binding protein gene. Nature Genet., 10,383-392.
Sathananthan, A.H., Kola, I., Osborne, J. et al. (1991) Centrioles in the beginning of humandevelopment. Proc. Natl. Acad. Sci. USA, 88, 4806^810.
Simerly, C , Wu, G.J., Zoran, S. et al. (1995) The paternal inheritance of the centrosome, the cell'smicrotubule-organizing center, in humans and the implication for infertility. Nature Med., 1,47-52.
Sofikitis, N.V., Miyagawa, I., Agapitos, E. et al. (1994) Reproductive capacity of the nucleus ofthe male gamete after completion of meiosis. /. Assis. Reprod. Genet., 11, 335-341.
Sofikitis, N.V., Toda, T., Miyagawa, I. et al. (1996a) Beneficial effects of electrical stimulationbefore round spermatid nuclei injections into rabbit oocytes on fertilization and subsequentembryonic development. Fertil. Steril, 65, 176-185.
Sofikitis, N.V., Miyagawa, I., Andrighetti, S. et al. (1996b) Detrimental effect of left varicoceleon the reproductive capacity of the early haploid male gamete. J. Uroi, 156, 267-270.
Sousa, M., Barros, A. and Tesarik, J. (1996b) Developmental changes in calcium dynamics, proteinkinase C distribution and endoplasmic reticulum organization in human preimplantation embryos.Mol. Hum. Reprod., 2, 967-977.
Sousa, M., Mendoza, C , Barros, A. and Tesarik, J. (1996a) Calcium responses of human oocytesafter intracytoplasmic injection of leukocytes, spermatocytes and round spermatids. Mol. Hum.Reprod., 2, 853-857.
Stachecki, J.J. and Armant, D.R. (1996) Transient release of calcium from inositol 1,4,5—trisphosphate-specific stores regulates mouse preimplantation development. Development, 122,2485-2496.
Swann, K. and Ozil, J.P. (1994) The dynamics of the calcium signal that triggers mammalian eggactivation. Int. Rev. Cytol., 152, 182-222.
Szabo, P.E. and Mann J.R. (1995a) Biallelic expression of imprinted genes in the mouse germline: implications for erasure, establishment, and mechanism of genomic imprinting. Genes Dev.,9, 1857-1868.
Szabo, P.E. and Mann J.R. (1995b) Allele-specific expression and total expression levels ofimprinted genes during early mouse development: implications for imprinting mechanisms.Genes Dev., 9, 3097-3108.
Tanphaichitr, N., Sobhon, P., Taluppech, N. and Chalermisarachai, P. (1978) Basic nuclear proteinsin testicular cells and ejaculated spermatozoa in man. Exp.Cell Res., 117, 347-356.
Taylor, C.T., Lawrence, Y.M., Kingsland, C. et al. (1993) Oscillations in intracellular free calciuminduced by spermatozoa in human oocytes at fertilization. Hum. Reprod., 8, 2174-2179.
Tesarik, J. (1995) Sex chromosome abnormalities after intracytoplasmic sperm injection. Lancet,346, 1096.
Tesarik, J. (1996) Fertilization of oocytes by injecting spermatozoa, spermatids and spermatocytes.Rev. Reprod., 1, 149-152.
Tesarik, J. (1997) Sperm or spermatid conception? Fertil. Steril., 68, 214-216.Tesarik, J. and Kopecny, V. (1989a) Developmental control of the human male pronucleus by
ooplasmic factors. Hum. Reprod., 4, 962-968.Tesarik, J. and Kopecny, V. (1989b) Nucleic acid synthesis and development of human male
pronucleus. J. Reprod. Fertil., 86, 549-558.Tesarik, J. and Kopecny, V. (1990) Assembly of the nucleolar precursor bodies in human male
pronuclei is correlated with an early RNA synthetic activity. Exp. Cell Res., 191, 153-156.Tesarik, J. and Mendoza, C. (1996a) Spermatid injection into human oocytes. I. Laboratory
techniques and special features of zygote development. Hum. Reprod., 11, 772-779.Tesarik, J. and Mendoza, C. (1996b) Genomic imprinting abnormalities: a new potential risk of
assisted reproduction. Mol. Hum. Reprod., 2, 295-298.Tesarik, J. and Sousa, M. (1994) Comparison of Ca2+ responses in human oocytes fertilized by
subzonal insemination and by intracytoplasmic sperm injection. Fertil. Steril., 62, 1197-1204.
106
by guest on October 2, 2014
http://humrep.oxfordjournals.org/
Dow
nloaded from
Clinical use of spermatids
Tesarik, J. and Sousa M. (1995) Key elements of a highly efficient intracytoplasmic sperm injectiontechnique: Ca2+ fluxes and oocyte cytoplasmic dislocation. Fertil. Steril, 64, 770-776.
Tesarik, J. and Testart, J. (1994) Treatment of sperm-injected human oocytes with Ca2+ ionophoresupports the development of Ca2+ oscillations. Biol. Reprod., 51, 385-391.
Tesarik, J., Mendoza, C. and Testart, J. (1995) Viable embryos from injection of round spermatidsinto oocytes. N. Engl. J. Med., 333, 525.
Tesarik. J., Rolet, R, Brami, C. et al. (1996) Spermatid injection into human oocytes. II. Clinicalapplication in the treatment of infertility due to non-obstructive azoospermia. Hum. Reprod., 11,780-783.
Tesarik, J., Sousa, M. and Testart, J. (1994) Human oocyte activation after intracytoplasmic sperminjection. Hum. Reprod., 9, 511-518.
Tiepolo, L. and Zuffardi, O. (1976) Localization of factors controlling spermatogenesis in thenonfluorescent portion of the human Y chromosome long arm. Hum. Genet., 34, 119-124.
Vanderzwalmen, P., Zech, H., Birkenfeld, A. et al. (1997) Intracytoplasmic injection of spermatidsretrieved from testicular tissue: influence of testicular pathology, type of selected spermatidsand oocyte activation. Hum. Reprod., 12, 1203-1213.
Yamanaka, K., Sofikitis, N.V., Miyagawa, I. et al. (1997) Ooplasmic round spermatid nuclearinjection procedures as an experimental treatment for nonobstructive azoospermia. J. Assist.Reprod. Genet., 14, 55-62.
Yarden, Y, Kuang, W.-J., Yang-Feng, T. et al. (1987) Human proto-oncogene c-kit: a new cellsurface receptor tyrosine kinase for an unidentified ligand. EMBO J., 6, 3341-3351.
Yen, P.H., Chai, N.N. and Salido, B.C. (1996) The human autosomal gene DAZLA: testis specificityand a candidate for male infertility. Hum. Mol. Genet., 5, 2013-2017.
Zhang, P., Liegeois, N.J., Wong, C. et al. (1997) Altered cell differentiation and proliferation inmice lacking p57KIP2 indicates a role in Beckwith-Wiedemann syndrome. Nature, 387, 151-158.
107
by guest on October 2, 2014
http://humrep.oxfordjournals.org/
Dow
nloaded from