cryopreserved arterial allograft reconstruction after excision of thoracic malignancies
TRANSCRIPT

Cryopreserved arterial allograft reconstruction forperipheral graft infectionYves Castier, MD,a Fady Francis, MD,a Pierre Cerceau, MD,a Mathieu Besnard, MD,a Jérome Albertin,MD,a Laurent Fouilhe, MD,a Olivier Cerceau, MD,a Pierre Albaladejo, MD,b and Guy Lesèche, MD,a
Clichy, France
Objective: This prospective, observational study evaluated the safety and efficacy of cryopreserved arterial allograftreconstruction in the management of major peripheral arterial graft infections.Methods: From April 1996 to May 2003, data from patients with major peripheral arterial graft infection who underwentgraft excision and cryopreserved arterial allograft reconstruction were prospectively collected. Arterial allografts wereharvested from multiple organ donors and cryopreserved at �80 °C. The patients were observed for survival, limbsalvage, persistence or recurrence of infection, and allograft patency. The results were calculated with the Kaplan-Meiermethod.Results: During the 7-year study period, 17 patients (14 men, 3 women; mean age, 68 years) with major peripheral graftinfection underwent graft excision and cryopreserved arterial allograft reconstruction. Eight patients (47%) had systemicsepsis, 5 (29%) had acute ischemia at the time of the allograft reconstruction, and 9 (53%) had experienced anastomoticrupture. Allograft reconstruction was performed as an emergency procedure in 7 patients (41%). There were noperioperative deaths or early amputations. Two patients had allograft ruptures in the groin during the early postoperativeperiod. The mean follow-up period was 34 months (range, 8 to 80 months). There was no persistent or recurrentinfection, and none of the patients received long-term (>3 months) antibiotic therapy. Reoperation for allograft revision,excision, or replacement was performed in 2 patients. The 18-month primary and secondary allograft patency rates were68% and 86%; the overall limb salvage rate was 82% at 2 years.Conclusion: Our experience with cryopreserved arterial allograft in the management of major peripheral bypass graftinfection suggests that this technique seems to be a useful option for treating one of the most dreaded vascular
complications. ( J Vasc Surg 2005;41:30-7.)Major peripheral arterial graft infection is an uncom-mon but severe and potentially devastating complication ofvascular surgery that is associated with significant mortalityand high amputation rates.1-3 The basic goal of therapy inpatients with lower-extremity graft infection is to eradicateinfection and maintain adequate perfusion. Radical excisionof infected perigraft tissue is the recommended treatmentto eradicate infection and is mandatory in cases of systemicsepsis, anastomotic disruption, or graft occlusion.4,5 Autol-ogous saphenous veins are considered the best arterialsubstitute for lower-extremity revascularization in infectedfields, but they are often unavailable or unsuitable in thesepatients.6
Having been faced with this dilemma and encouragedby good long-term results obtained with cryopreservedarterial allograft reconstructions in infected prostheticgrafts and mycotic aneurysms of the abdominal aorta,7,8 weinvestigated cryopreserved arterial allografts in the manage-ment of major peripheral arterial graft infection. This pro-spective observational study evaluated the safety and effi-
From the Service de Chirurgie Vasculaire et Thoracique,a and Serviced’anesthésie-réanimation,b Hôpital Beaujon, Assistance Publique Hopi-taux de Paris (AP-HP).
Competition of interest: none.Reprint requests: Guy Lesèche, MD, Service de Chirurgie Vasculaire et
Thoracique, Hôpital Beaujon (AP-HP), 100 Boulevard du GénéralLeclerc, 92110 Clichy, France (e-mail: [email protected]).
0741-5214/$30.00Copyright © 2005 by The Society for Vascular Surgery.
doi:10.1016/j.jvs.2004.09.02530
cacy of cryopreserved arterial allograft reconstruction in thelatter indication. The main variables studied were patientsurvival, freedom from persistent or recurrent infection,allograft patency, and avoidance of major amputation.
PATIENTS AND METHODS
From April 1996 to May 2003, data from patients withmajor peripheral bypass graft infection treated by graftexcision and cryopreserved arterial allograft reconstructionin the Department of Vascular and Thoracic Surgery at ourinstitution were prospectively collected. These data in-cluded demographics, atherosclerotic risk factors, originalprocedures, modes of presentation, surgical details, periop-erative morbidity, and bacteriologic findings.
The diagnosis of peripheral bypass graft infection wasmade by using clinical criteria, ultrasound scanning, com-puted tomographic scanning, and bacteriology tests. Indi-cations for graft excision were systemic sepsis, disruptedanastomosis (infected pseudoaneurysm or hemorrhage),graft occlusion, infection due to virulent gram-negativeorganisms, infection of the entire graft, or a combination ofthese criteria.
The decision to perform revascularization in patientswhose limbs were salvageable and whose vessels could bereconstructed was made on indication for initial peripheralbypass grafting, clinical presentation at the time of allograftreconstruction, and arteriographic findings. A cryopre-served arterial allograft was used after first considering
revascularization with autologous greater saphenous veins
JOURNAL OF VASCULAR SURGERYVolume 41, Number 1 Castier et al 31
(upper limb, superficial femoropopliteal and lesser saphe-nous veins were not considered). The patients initiallyunderwent treatment with broad-spectrum intravenous an-tibiotics.
Surgical technique. Bacteriology culture tests wereperformed on the perigraft fluid and the infected graft.Wounds were carefully excised to obtain macroscopicallynormal tissue. To make sure that all involved infected tissuewas completely resected, the anastomotic and perianasto-motic regions were dissected and exposed thoroughly dur-ing surgery.
Dissection of popliteal and tibial arteries was restrictedto the presenting aspect only, with no circumferential dis-section and without the use of arterial clamps (Esmarchbandage). The arterial allografts were implanted usingpolypropylene sutures for proximal and distal anastomoses.The allograft was tunneled using the previous pathway (insitu) or a new pathway, depending on the location of thesepsis. To allow close surveillance, the arterial allograft wasrouted subcutaneously when possible.
Once reconstruction had been completed, arteriogra-phy was routinely performed when the allograft extendedinto an infrageniculate outflow site, any technical errors orproblems were corrected immediately, and another radio-graph was taken to confirm a satisfactory situation. Allincisions were drained, and the skin was closed primarily inall cases. Fasciotomy was routinely performed in patientswho presented with acute limb ischemia.
Arterial allograft. Harvesting, preservation, andpreparation of allografts have been previously described.8,9
Arterial allografts (aortic bifurcation, iliac, femoral, andpopliteal arteries) were carefully harvested from brain-deadmultiple-organ donors. Informed consent was given by thedonor’s family, in accordance with French law. Bacteriol-ogy and virology tests were performed for all donors.
After harvesting, arterial allografts were flushed withheparinized saline solution to eliminate any residual intra-arterial blood and stored at 4 °C in M199 medium (GibcoLaboratories, Gaithersburg, Md) containing gentamicin(0.50 mg/mL) and amphotericin B (0.25 mg/mL). Thedelay before freezing did not exceed 18 hours in all cases.Allografts were permeated for 20 minutes at 4 °C in M199medium containing 12% dimethylsulfoxide and subse-quently frozen at �80 °C without rate-controlled freezing.Allografts were stored an average of 48 � 21.4 days.
Upon request from the vascular surgeon, the bag con-taining the artery was rapidly thawed by immersion in waterprewarmed to 37 °C. Once the ice had melted, allograftsunderwent successive washouts in heparinized saline solu-tion at room temperature. The final washout fluid wassampled for bacteriology culture.
Because of the few available allografts, matching bloodcompatibility between recipient and donor was not possiblein all cases. Cryopreserved arterial allografts were ABOcompatible with the recipient in 14 patients (82%) andmismatched in 3 patients. None of the patients received
immunosuppression therapy.Postoperative management and follow-up examination.Intravenous antibiotics were administered for 2 weeks, andculture-determined oral antibiotics were continued for 6weeks. After discharge, routine late follow-up included aclinical and duplex scanning examination at 1 month andevery 6 months thereafter. Late arteriography was per-formed depending on the results of duplex scanning. Pa-tients were routinely prescribed daily low-dose aspirin (100mg). For the purposes of this report, the status of allsurvivors was updated in April 2004. Patency, limb salvagerate, and survival were determined with the Kaplan-Meiermethod.
RESULTS
Patients and initial procedures. During the 7-yearstudy period, 17 patients (14 men, 3 women; mean age of68 years, range, 50 to 83 years) who had major peripheralgraft infection underwent graft excision and cryopreservedarterial allograft reconstruction. The baseline characteris-tics of the patients are shown in Table I. Systemic riskfactors for infection, including diabetes mellitus, malig-nancy, steroid use, and malnutrition were present in 7patients (41%).
The indications for initial peripheral bypass graftingwere critical leg ischemia in 10 (59%) patients, severeclaudication in 5 (29%), and popliteal aneurysm in 2 (12%).The types and indications of initial peripheral reconstruc-tions with infection are described in Table II. Prostheticfemoropopliteal bypass was the most frequently infectedreconstruction. Graft material was polytetrafluoroethylene(PTFE) in 10 patients, Dacron in 3, and autologous saphe-nous vein in 4.
The median time from placement of the bypass to the
Table I. Clinical characteristics of the 17 patients withperipheral graft infection
Clinical characteristics Value (%)
Age (y)Mean � SD 68 � 8.75Range 50-83
SexMale 14 (82)Female 3 (18)
Cigarette smoking 14 (82)Hypertension 12 (70)Dyslipidemia 5 (29)Coronary artery disease* 9 (53)Cerebrovascular event† 2 (12)Obesity 3 (18)Diabetes mellitus 4 (23)Malignancy 1 (6)Steroid use 1 (6)Malnutrition‡ 3 (18)
*Six patients had coronary artery bypass.†Cerebrovascular event was defined as a transient ischemic attack or stroke orprior carotid endarterectomy.‡Malnutrition was defined as recent weight loss of greater than 15% bodyweight, a body weight below ideal body weight by at least 15%, or both.
initial symptom of graft infection was 22 days (range, 10

JOURNAL OF VASCULAR SURGERYJanuary 200532 Castier et al
days to 52 months); this time was less than 30 days in 11(65%) of the 17 patients. The median time from graftplacement to definitive treatment of the graft infection was31 days (range, 10 days to 72 months). Six (35%) of these17 patients had been initially operated on in our center,whereas 11 (65%) were referred to us after a mean of 2.1 �1.3 operations (range, 1 to 5) had been performed else-where.
Manifestation and preoperative diagnosis. The clin-ical events in 17 patients with an infected peripheral graftare described in Table III. One false aneurysm developed atthe below-knee popliteal level and resulted in a neurologicdeficit due to tibial nerve compression. Because of arterialstatus, failed reoperations, or end-to-end bypasses, restora-tion of lower-limb arterial circulation was required to sal-vage the limb after removal of the infected patent graft inthe 12 patients without acute ischemia.
Graft infection was localized to the area of the proximalanastomosis in 4 patients (23%), to the area of the distalanastomosis in 4 (23%), and involved the entire graft in 7(41%). Two patients (12%) had isolated areas of infectionsinvolving a portion of a prosthetic graft distant from bothanastomotic sites. According to the classification of graftinfection from the Montefiore Medical Center,2 all thepatients in this series had major graft infections at the timeof presentation:
● 2 patients with group III (infections involved the body ofthe graft but not an anastomosis);
● 2 patients with group IV (infections surrounded anexposed anastomosis but bacteremia or anastomotic
Table II. Types and indications of peripheralreconstructions with infection in 17 patients
Reconstruction Material n Indication
Axillobifemoral Dacron 1 CLICrossover
femorofemoralPTFE 1 Claud
Iliofemoral PTFE 1 ClaudIliofemoral patch
angioplastyDacron 1 Claud
Iliofemoral patchangioplasty �femoropopliteal(AKPA)
Dacron 1 CLI
Iliopopliteal (AKPA) PTFE 1 CLIFemoropopliteal
(AKPA)PTFE 2 Claud
Femoropopliteal(BKPA)
PTFE 4 CLI (2)/FempopGSV 1 Aneur (2)
CLIFemorotibial* PTFE 1 CLI
GSV 3 CLI
BKPA, Below-knee popliteal artery; AKPA, above-knee popliteal artery;PTFE, polytetrafluoroethylene; GSV, greater saphenous vein; Ilio, externaliliac artery; CLI, critical limb ischemia; Claud, claudication; Fempop aneur,femoropopliteal aneurysm.*Site of proximal anastomosis was an aortofemoral graft in 1 patient.
bleeding had not occurred); and
● 13 patients with group V (infections involved a graft-to-artery anastomosis and were associated with septicemia,anastomotic bleeding, or both).
Because of acute bleeding in 2, a severe neurologic deficit in1, and severe acute ischemia in 4, allograft reconstructionwas performed as an emergency procedure in 7 patients(41%), whereas it was a planned procedure in 10 patients(59%).
Treatment. Bacteriology cultures were positive in allcases and are listed in Table IV. A single organism wasidentified in 10 (59%) cultures and multiple organisms in 7(41%). Infection was due to a variety of organisms, mostfrequently Staphylococcus aureus followed by Pseudomonasaeruginosa.
In 14 patients (82%), the greater saphenous veins werenot available either because they had already been used inother revascularizations or had been stripped. In 2 patients,the saphenous vein was present but was deliberately notused because of a discrepancy between the diameter of thevein and the external iliac artery. A unique greater saphe-nous vein was used in 1 patient for a femorofemoral cross-over in addition to allograft reconstruction. During thestudy period, 7 patients were treated with greater saphe-nous vein reconstruction for peripheral graft infection (3crossover, 1 iliofemoral, and 3 femoropopliteal bypasses).
At surgery, removal of the entire graft was felt to bemandatory in 100% of patients with infected prostheticgrafts and in 50% with infected saphenous grafts. In thelatter 2 patients, the distal end of the saphenous was pre-served as a “cuff” for a distal allograft anastomosis. Types ofarterial allograft reconstruction for all 17 patients are de-tailed in Table V.
The proximal anastomosis was located at the same levelin 7 patients (41%) and was different in 10 (59%). The distalanastomosis was located at the same level in 9 patients(53%) and was more distal in 8 (47%). Reconstruction wasperformed in situ in 6 patients (35%) and ex situ in 11(65%). Of the 3 patients with iliofemoral infection, theallograft was placed in situ in 2 cases and a crossover wasmade in 1. Subcutaneous routing was performed in 13
Table III. Clinical events of the 17 patients withinfected peripheral graft
Events n (%)
Sepsis (fever, leukocytosis, blood positive culture) 8 (47)Anastomotic rupture 9 (53)Hemorrhage 6Pseudoaneurysm* 3Acute ischemia 5 (29)
grade IIa 4grade IIb 1
Infected sinus tract 5 (29)Abscess adjacent to the graft 2 (11)Graft exposure 5 (29)
*Including 1 patient with tibial nerve compression and neurologic deficit.
patients (76%).

JOURNAL OF VASCULAR SURGERYVolume 41, Number 1 Castier et al 33
Additional procedures included fasciotomy in 4, localfibrinolysis of the tibial arteries during the procedure in 2,and surgical drainage of suppurative arthritis of the knee in1. No myoplasty was performed. The mean duration of theprocedures was 306 minutes (range, 200 to 440).
Early outcome (<3 months). There were no periop-erative deaths, no early occlusions of the allograft recon-struction, and no early amputation in this series. Fivepatients (29%) had complications that were not related tothe allograft: transient renal failure in 2, delirium tremens in1, neurologic postischemic sequelae of the limb in 2, andcongestive heart failure in 1.
Two patients had allograft ruptures in the groin onpostoperative days 20 and 45. The previously infectedgroin in these two patients had been re-exposed and nomyoplasty had been performed during allograft reconstruc-tion. Healing was delayed and skin necrosis occurred, re-sulting in arterial allograft exposure and subsequent rup-ture. Both patients underwent emergency surgery with anuneventful recovery.
The first patient had undergone a femorofemoral and adistal extension to peroneal artery allograft reconstruction.Infection of the initial arterial graft was due to S. aureus,and the patient was treated with an oral antistaphylococcusregimen (oxacillin) at the time of rupture. After the proxi-mal end of the distal extension ruptured, the distal exten-sion of the allograft was reimplanted in the profunda fem-oral artery and a myoplasty was performed.
The second patient had undergone a complex allograftreconstruction associating an iliofemoral and a femoro-femoral crossover plus femoropopliteal revascularization.Infection of the initial arterial graft was due to S. aureusassociated with P. aeruginosa, and the patient was treatedwith an oral antibiotics regimen (pristinamycin and cipro-floxacin) at the time of rupture. After the proximal end ofthe femorofemoral crossover ruptured, the femorofemoralcrossover was ligated and a prosthetic (PTFE) axillofemoralwas performed as an inflow conduit for the femoropoplitealallograft. At the time of reoperation, there were no clinicalor biological signs of persistent infection and bacteriologycultures from surgery were negative in both cases. The twoallografts that ruptured had been stored for a period of 27and 53 days.
Blood transfusion was required in 10 patients (59%)
Table IV. Bacteriology of peripheral graft infections in 17
Single orga
No. of patients (%) 10 (59Organisms (No.) Staphylococcus aure
Staphylococcus epid
with a mean of 4.8 red blood cell units (range, 2 to 10
units) per patient. Mean duration of hospitalization was 24� 12.6 days.
Late outcome. All patients were available for follow-up (mean, 34 months; range, 8 to 80 months). Six patientsdied during late follow-up in postoperative months 8, 9,18, 22, 30, and 52, none for treatment-related reasons.Causes of later deaths were myocardial infarction in 4,prostate cancer in 1, and pulmonary embolism in 1. Thecumulative survival rate was 88% at 1 year and 74% at 2years.
Four allografts thrombosed during follow-up at 6, 7,12, and 20 months. The 3 patients whose grafts occluded at7, 12, and 20 months did not undergo surgery because of avery poor runoff. Two of them had occlusion of a femo-rotibial extension with a patent femorofemoral crossoverand required below-knee amputation. The third patienthad a thrombosed femoropopliteal reconstruction that re-sulted in critical limb ischemia. The fourth patient under-went successful thrombectomy at 6 months (which was stillpatent at 23 months).
Aneurysmal deterioration of the cryopreserved allograft
ents
Multiple organisms
7 (41)) Staphylococcus aureus (4)is (2) Pseudomonas aeruginosa (6)
Proteus mirabilis (1)Bacteroides fragilis (1)Enterobacter cloacae (1)Enterobacter faecalis (1)Morganella morganii (1)
Table V. Types of arterial allograft reconstructions withinfection in 17 patients
Reconstruction n
Subclavian-brachial � axillofemoral* 1Crossover femorofemoral 1Crossover femorofemoral � iliofemoral �
femoropopliteal (BKPA)1
Crossover femorofemoral � femorotibial 2Iliofemoral 1Iliofemoral � femoropopliteal (AKPA) 1Iliofemoral � femorotibial 2Common iliac-popliteal (BKPA) 1Iliotibial 1Femoropopliteal (BKPA) 1Femorotibial† 5
BKPA, below-knee popliteal artery; AKPA, above-knee popliteal artery;Ilio, external iliac artery.*A femoral allograft conduit was used to perform the axillohumeral bypass,an ilio-femoropopliteal allograft conduit was used to perform the axil-lofemoral, and great saphenous vein was used for the femorofemoral cross-over.†Site of proximal anastomosis was an aorto-femoral graft in one case.
pati
nism
)us (8ermid
occurred twice in 1 patent, graft requiring 2 segmental

with
JOURNAL OF VASCULAR SURGERYJanuary 200534 Castier et al
replacements with PTFE at 24 and 36 months. This patientdied of myocardial infarction 16 months after the lastprocedure with a patent allograft.
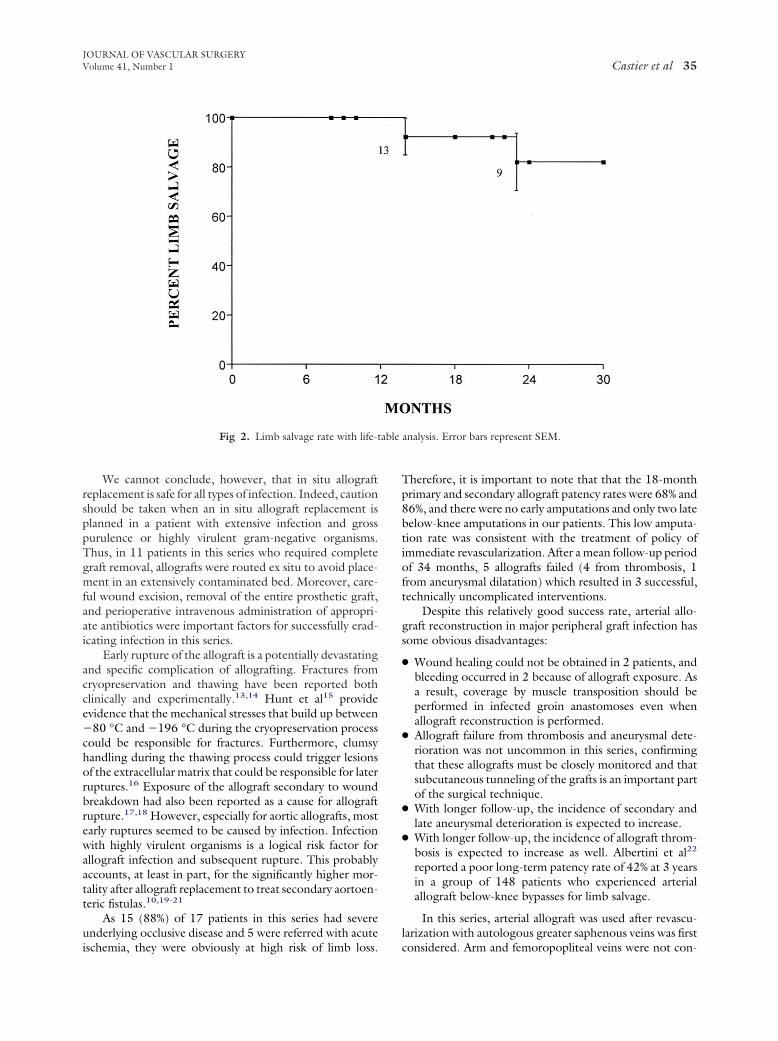
There was no persistent or recurrent infection, andnone of the patients received long-term (�3 months) orindefinite antibiotic therapy. The 18-month primary andsecondary allograft patency rates were 68% and 86% (Fig 1).The overall limb salvage rate was 82% at 2 years (Fig 2).
DISCUSSION
Our experience with cryopreserved arterial allografts inthe management of major peripheral bypass infections sug-gests that this technique is a useful option for treating one ofthe most dreaded vascular complications. Although the num-ber of cases reported is small, this is the largest surgical seriesdealing with cryopreserved arterial allograft in the manage-ment of peripheral bypass infection described in the literature.Most patients in this series represent the most desperately illpatients presenting with peripheral bypass infection. Eightpatients (47%) had systemic sepsis, 5 (29%) had acute ischemiaat the time of allograft reconstruction, and 9 (53%) hadexperienced anastomotic rupture. In addition, multiple or-ganisms were present in 41%, including virulent P. aeruginosain 35%. Despite these difficulties, there were no perioperativedeaths or early amputations in this series.
The optimal management of major peripheral graftinfection is still controversial. Total graft excision is gener-ally required if any of the following conditions exist: (1)signs of systemic sepsis, (2) anastomotic disruption, (3) thepresence of virulent gram-negative organisms on culture,(4) involvement of the entire graft, or (5) associated graftthrombosis. All the patients in this series presented one ormore preoperative conditions and required total graft exci-sion. However at surgery, the distal part of the vein was
Fig 1. Primary and secondary patency rates
judged to be uninfected in 2 patients who had an infected
saphenous graft, and it was successfully preserved as a“cuff” for allograft anastomosis. All the patients in thisseries required arterial reconstruction to preserve limb via-bility, whereas none had available or suitable saphenousveins to perform a complete lower-limb arterial reconstruc-tion.
We embarked on a cryopreserved allograft replacementprogram because
● We were dissatisfied with the more conventional treat-ments in terms of mortality, reinfection, and amputationrates.
● Cryopreserved arterial allograft reconstruction is highlyapplicable in the management of serious graft infection,even for emergency use.8
● The results of experimental studies and clinical resultssuggest that arterial allografts have a good resistance toinfection.8,10-12
● Arterial allografts harvested from brain-dead donors areavailable as part of an active, local, multiorgan transplant-retrieval program.
None of the patients in this series experienced persis-tent or recurrent infection. Although two allograft rupturesoccurred in 2 patients in the early postoperative period, wefeel that these ruptures were due to allograft exposurerather than to infection because no objective clinical orbiological signs of persistent or recurrent infection werefound during reoperation and bacteriology cultures fromsurgery were negative.
Although another concern could be whether a longerfollow-up period will reveal recurrent infection, the meanfollow-up period of 34 months, with all allografts observedfor at least 8 months, is reassuring. Furthermore, no rein-fections occurred in the 2 patients who required implanta-
life-table analysis. Error bars represent SEM.
tion of a new prosthetic graft.
able
JOURNAL OF VASCULAR SURGERYVolume 41, Number 1 Castier et al 35
We cannot conclude, however, that in situ allograftreplacement is safe for all types of infection. Indeed, cautionshould be taken when an in situ allograft replacement isplanned in a patient with extensive infection and grosspurulence or highly virulent gram-negative organisms.Thus, in 11 patients in this series who required completegraft removal, allografts were routed ex situ to avoid place-ment in an extensively contaminated bed. Moreover, care-ful wound excision, removal of the entire prosthetic graft,and perioperative intravenous administration of appropri-ate antibiotics were important factors for successfully erad-icating infection in this series.
Early rupture of the allograft is a potentially devastatingand specific complication of allografting. Fractures fromcryopreservation and thawing have been reported bothclinically and experimentally.13,14 Hunt et al15 provideevidence that the mechanical stresses that build up between�80 °C and �196 °C during the cryopreservation processcould be responsible for fractures. Furthermore, clumsyhandling during the thawing process could trigger lesionsof the extracellular matrix that could be responsible for laterruptures.16 Exposure of the allograft secondary to woundbreakdown had also been reported as a cause for allograftrupture.17,18 However, especially for aortic allografts, mostearly ruptures seemed to be caused by infection. Infectionwith highly virulent organisms is a logical risk factor forallograft infection and subsequent rupture. This probablyaccounts, at least in part, for the significantly higher mor-tality after allograft replacement to treat secondary aortoen-teric fistulas.10,19-21
As 15 (88%) of 17 patients in this series had severeunderlying occlusive disease and 5 were referred with acute
Fig 2. Limb salvage rate with life-t
ischemia, they were obviously at high risk of limb loss.
Therefore, it is important to note that that the 18-monthprimary and secondary allograft patency rates were 68% and86%, and there were no early amputations and only two latebelow-knee amputations in our patients. This low amputa-tion rate was consistent with the treatment of policy ofimmediate revascularization. After a mean follow-up periodof 34 months, 5 allografts failed (4 from thrombosis, 1from aneurysmal dilatation) which resulted in 3 successful,technically uncomplicated interventions.
Despite this relatively good success rate, arterial allo-graft reconstruction in major peripheral graft infection hassome obvious disadvantages:
● Wound healing could not be obtained in 2 patients, andbleeding occurred in 2 because of allograft exposure. Asa result, coverage by muscle transposition should beperformed in infected groin anastomoses even whenallograft reconstruction is performed.
● Allograft failure from thrombosis and aneurysmal dete-rioration was not uncommon in this series, confirmingthat these allografts must be closely monitored and thatsubcutaneous tunneling of the grafts is an important partof the surgical technique.
● With longer follow-up, the incidence of secondary andlate aneurysmal deterioration is expected to increase.
● With longer follow-up, the incidence of allograft throm-bosis is expected to increase as well. Albertini et al22
reported a poor long-term patency rate of 42% at 3 yearsin a group of 148 patients who experienced arterialallograft below-knee bypasses for limb salvage.
In this series, arterial allograft was used after revascu-larization with autologous greater saphenous veins was first
analysis. Error bars represent SEM.
considered. Arm and femoropopliteal veins were not con-

JOURNAL OF VASCULAR SURGERYJanuary 200536 Castier et al
sidered. However, autologous reconstruction is anothervery relevant option for revascularization in infected fields.Very good revascularization results have been obtainedwith femoropopliteal or arm veins for aortic or peripheralinfection and critical limb ischemia.23-26
Harvesting and preparing these two types of conduitsare technically demanding (with the need to perform an-gioscopy in the case of an arm vein) and time-consumingprocedures. Furthermore, harvesting the femoropoplitealvein in the absence of the greater saphenous vein may leadto venous sequelae. Reconstruction with femoropoplitealor arm veins often necessitates a specialized two-team ap-proach to expedite the operation and to splice the compos-ite vein using venovenostomy to create a vein conduit ofsufficient length to allow the performance of the lower-extremity revascularization. Finally, in our opinion, thisapproach may be difficult in sick and infected patients whoneed urgent treatment.
Few series reported vascular allograft reconstructionafter excision of an infected peripheral bypass graft. After insitu fresh venous allograft reconstruction in 5 patients withpatent peripheral prosthetic graft infection, Snyder et al27
reported complete resolution of infection in all cases. Morerecently, Fujitani et al6 reported the use of cryopreservedhomograft veins to eradicate infection and achieve limbsalvage in all 6 patients with infected peripheral prostheticgrafts with a limited follow-up of 9.5 months.
Patency rates reported by many investigators with cryo-preserved venous allografts for limb salvage were low, how-
Table VI. Documented cases of management of peripherreported in the literature.*
Reference NLocation of infected
graft Material
Partiaor totagraft
remova
Bracale et al32
(1999)2 Axillofemoral PTFE
DacronTotal/2
Locati et al133
(2000)2 Axillobifemoral PTFE Partial/
Desgranges etal34 (1998)
5 2 Femoropopliteal1 Femorofemoral2 Iliofemoral
SVProstheticProsthetic
Partial/Total/1Total/2
Wagstaff et al17
(1996)4 1 Iliofemoral
1 Femorotibial1 Femoropopliteal1 Crossover
DacronAVPTFEDacron
At leasttotalgraftremov
Nevelsteen etal21 (1998)
3 3 Femorodistal Prosthetic Total
Lavigne et al16
(2003)4 3 Femoropopliteal
1 FemorofemoralProsthetic Total
Locati et al35
(2000)1 Femorotibial PTFE Total
SV, Saphenous vein; PTFE, polytetrafluoroethylene; AV, arm vein.*Axillobifemoral or bilateral axillofemoral following removal infected aortic†Mean follow-up of the indicated series that included patients treated for pthe dagger.
ever28,29 The largest experience was reported by Farber et
al,30 who performed 240 infrainguinal revascularizationsfor limb salvage and achieved a primary patency rate of 30%at 1 year and 18% at 2 years. Our experience was verysimilar, causing us to abandon this conduit for distal revas-cularization.9,31
We found 21 documented cases of arterial allograftreconstruction after excision of an infected peripheral by-pass graft reported in the English literature.16,17,21,32-35
The location of the infected grafts and the outcome of these21 cases are presented in Table VI. Reported results weregood, with no reinfection, one perioperative death, andone early amputation, but it is difficult to draw any conclu-sion from a group of small series or case reports.
The heterogeneity of patients, the numerous therapeu-tic strategies, and the general diagnosis of peripheral graftinfection make comparisons between series very difficult.Nevertheless, we think that the outcome of the midtermfollow-up in our series for mortality, limb salvage, andfreedom from reinfection compare favorably to other seriesusing more conventional methods.1-3,36 To compare dif-ferent series of peripheral bypass infections, a system isneeded to stratify these patients using standards similar tothose that have been developed in other areas of vascularsurgery.37,38
Conclusion. Although this study presents a small se-ries of patients with limited follow-up, reconstruction witha cryopreserved arterial allograft seemed to be a usefuloption for treating one of the most dreaded vascular com-plications. When major peripheral graft infection occurs in
pass infection with cryopreserved arterial allograft
erioperativemortality
Earlyamputation
Lateamputation
Secondaryinfection
Meanfollow-up(months)
0 0 0 0 13.5
0 0 0 0 21
/5 (20%) 1 0 0 20 (18†)
0 0 2 0 24.5 (7†)
0 0 0 0 24.5 (30†)
0 0 1 0 18 (22†)
0 0 0 0 18
hetic graft were excluded.tic aortic graft infection, number of patients in each series is indicated after
al by
ll
lP
2
2 1
3
al
prostrosthe
patients with severe underlying occlusive disease and autol-

JOURNAL OF VASCULAR SURGERYVolume 41, Number 1 Castier et al 37
ogous conduits are unavailable or unsuitable, the highoperative mortality, reinfection, and amputation rates are ofmajor concern and may be reduced with the use of theseallografts.
REFERENCES
1. Kikta MJ, Goodson SF, Bishara RA, Meyer JP, Schuler JJ, Flanigan DP.Mortality and limb loss with infected infrainguinal bypass grafts. J VascSurg 1987;5(4):566-71.
2. Samson RH, Veith FJ, Janko GS, Gupta SK, Scher LA. A modifiedclassification and approach to the management of infections involvingperipheral arterial prosthetic grafts. J Vasc Surg 1988;8(2):147-53.
3. Mertens RA, O’Hara PJ, Hertzer NR, Krajewski LP, Beven EG. Surgi-cal management of infrainguinal arterial prosthetic graft infections:review of a thirty-five-year experience. J Vasc Surg 1995;21(5):782-90.
4. Calligaro KD, Veith FJ, Schwartz ML, Dougherty MJ, DeLaurentisDA. Differences in early versus late extracavitary arterial graft infections.J Vasc Surg 1995;22(6):680-5.
5. Calligaro KD, Veith FJ, Valladares JA, McKay J, Schindler N, Dough-erty MJ. Prosthetic patch remnants to treat infected arterial grafts. JVasc Surg 2000;31(2):245-52.
6. Fujitani RM, Bassiouny HS, Gewertz BL, Glagov S, Zarins CK. Cryo-preserved saphenous vein allogenic homografts: an alternative conduitin lower extremity arterial reconstruction in infected fields. J Vasc Surg1992;15(3):519-26.
7. Kieffer E, Bahnini A, Koskas F, Ruotolo C, Le Blevec D, Plissonnier D.In situ allograft replacement of infected infrarenal aortic prostheticgrafts: results in forty-three patients. J Vasc Surg 1993;17(2):349-55.
8. Leseche G, Castier Y, Petit MD, Bertrand P, Kitzis M, Mussot S, et al.Long-term results of cryopreserved arterial allograft reconstruction ininfected prosthetic grafts and mycotic aneurysms of the abdominalaorta. J Vasc Surg 2001;34(4):616-22.
9. Castier Y, Leseche G, Palombi T, Petit MD, Cerceau O. Early experi-ence with cryopreserved arterial allografts in below-knee revasculariza-tion for limb salvage. Am J Surg 1999;177(3):197-202.
10. Kieffer E, Gomes D, Chiche L, Fleron MH, Koskas F, Bahnini A.Allograft replacement for infrarenal aortic graft infection: early and lateresults in 179 patients. J Vasc Surg 2004;39(5):1009-17.
11. Knosalla C, Goeau-Brissonniere O, Leflon V, Bruneval P, Eugene M,Pechere JC, et al. Treatment of vascular graft infection by in situreplacement with cryopreserved aortic allografts: an experimental study.J Vasc Surg 1998;27(4):689-98.
12. Camiade C, Goldschmidt P, Koskas F, Ricco JB, Jarraya M, Gerota J, etal. Optimization of the resistance of arterial allografts to infection:comparative study with synthetic prostheses. Ann Vasc Surg 2001;15(2):186-96.
13. Lehalle B, Geschier C, Fieve G, Stoltz JF. Early rupture and degenera-tion of cryopreserved arterial allografts. J Vasc Surg 1997;25(4):751-2.
14. Wassenaar C, Wijsmuller EG, Van Herwerden LA, Aghai Z, Van TrichtCL, Bos E. Cracks in cryopreserved aortic allografts and rapid thawing.Ann Thorac Surg 1995;60(2 Suppl):S165-7.
15. Hunt CJ, Song YC, Bateson EA, Pegg DE. Fractures in cryopreservedarteries. Cryobiology 1994;31(5):506-15.
16. Lavigne JP, Postal A, Kolh P, Limet R. Prosthetic vascular infectioncomplicated or not by aortoenteric fistula: comparison of treatmentwith and without cryopreserved allograft (homograft). Eur J VascEndovasc Surg 2003;25(5):416-23.
17. Wagstaff SA, Grigg MJ. Arterial homografts—a possible solution to aninfective dilemma. Cardiovasc Surg 1996;4(6):796-800.
18. Siat J, Hirsch JJ, Fieve G. [Exposed infra-inguinal bypass: conservativetreatment or in situ replacement]. J Mal Vasc 1996;21(Suppl A):158-61.
19. Noel AA, Gloviczki P, Cherry KJ Jr, Safi H, Goldstone J, Morasch MD,et al. Abdominal aortic reconstruction in infected fields: early results of
the United States cryopreserved aortic allograft registry. J Vasc Surg2002;35(5):847-52.
20. Verhelst R, Lacroix V, Vraux H, Lavigne JP, Vandamme H, Limet R, etal. Use of cryopreserved arterial homografts for management of infectedprosthetic grafts: a multicentric study. Ann Vasc Surg 2000;14(6):602-7.
21. Nevelsteen A, Feryn T, Lacroix H, Suy R, Goffin Y. Experience withcryopreserved arterial allografts in the treatment of prosthetic graftinfections. Cardiovasc Surg 1998;6(4):378-83.
22. Albertini JN, Barral X, Branchereau A, Favre JP, Guidicelli H, MagneJL, et al. Long-term results of arterial allograft below-knee bypass graftsfor limb salvage: a retrospective multicenter study. J Vasc Surg 2000;31(3):426-35.
23. Clagett GP, Valentine RJ, Hagino RT. Autogenous aortoiliac/femoralreconstruction from superficial femoral-popliteal veins: feasibility anddurability. J Vasc Surg 1997;25(2):255-66.
24. Gibbons CP, Ferguson CJ, Fligelstone LJ, Edwards K. Experience withfemoro-popliteal vein as a conduit for vascular reconstruction in in-fected fields. Eur J Vasc Endovasc Surg 2003;25(5):424-31.
25. Faries PL, Arora S, Pomposelli FB Jr, Pulling MC, Smakowski P, RohanDI, et al. The use of arm vein in lower-extremity revascularization:results of 520 procedures performed in eight years. J Vasc Surg 2000;31:50-9.
26. Calligaro KD, Veith FJ, Dougherty MJ, DeLaurentis DA. Managementand outcome of infrapopliteal arterial graft infections with distal graftinvolvement. Am J Surg 1996;172(2):178-80.
27. Snyder SO, Wheeler JR, Gregory RT, Gayle RG, Zirkle PK. Freshlyharvested cadaveric venous homografts as arterial conduits in infectedfields. Surgery 1987;101(3):283-91.
28. Martin RS 3rd, Edwards WH, Mulherin JL Jr, Edwards WH Jr, JenkinsJM, Hoff SJ. Cryopreserved saphenous vein allografts for below-kneelower extremity revascularization. Ann Surg 1994;219(6):664-70.
29. Carpenter JP, Tomaszewski JE. Immunosuppression for human saphe-nous vein allograft bypass surgery: a prospective randomized trial. J VascSurg 1997;26(1):32-42.
30. Farber A, Major K, Wagner WH, Cohen JL, Cossman DV, LauterbachSR, et al. Cryopreserved saphenous vein allografts in infrainguinalrevascularization: analysis of 240 grafts. J Vasc Surg 2003;38(1):15-21.
31. Leseche G, Penna C, Bouttier S, Joubert S, Andreassian B. Femorodis-tal bypass using cryopreserved venous allografts for limb salvage. AnnVasc Surg 1997;11(3):230-6.
32. Bracale GC, Porcellini M, Bernardo B, Bauleo A, Capasso R. Arterialhomografts in the management of infected axillofemoral prostheticgrafts. J Cardiovasc Surg (Torino) 1999;40(2):271-4.
33. Locati P, Socrate AM, Costantini E, Maggiolo F. Management ofinfected peripheral bypass by selective partial graft removal and arterialhomograft insertion. Two case reports. J Cardiovasc Surg (Torino)2000;41(2):311-5.
34. Desgranges P, Beaujan F, Brunet S, Cavillon A, Qvarfordt P, MelliereD, et al. Cryopreserved arterial allografts used for the treatment ofinfected vascular grafts. Ann Vasc Surg 1998;12(6):583-8.
35. Locati P, Socrate AM, Costantini E. Surgical repair of infected periph-eral graft and abdominal aortic aneurysm using arterial homograft. AnnVasc Surg 2000;14(2):176-80.
36. Cherry KJ Jr, Roland CF, Pairolero PC, Hallett JW Jr, Meland NB,Naessens JM, et al. Infected femorodistal bypass: is graft removalmandatory? J Vasc Surg 1992;15(2):295-303.
37. Chaikof EL, Blankensteijn JD, Harris PL, White GH, Zarins CK,Bernhard VM, et al. Reporting standards for endovascular aortic aneu-rysm repair. J Vasc Surg 2002;35(5):1048-60.
38. Sidawy AN, Gray R, Besarab A, Henry M, Ascher E, Silva M Jr, et al.Recommended standards for reports dealing with arteriovenous hemo-dialysis accesses. J Vasc Surg 2002;35(3):603-10.
Submitted Jun 30, 2004; accepted Sep 27, 2004.