summary of top risks (ranked by current residual risk score)
TRANSCRIPT
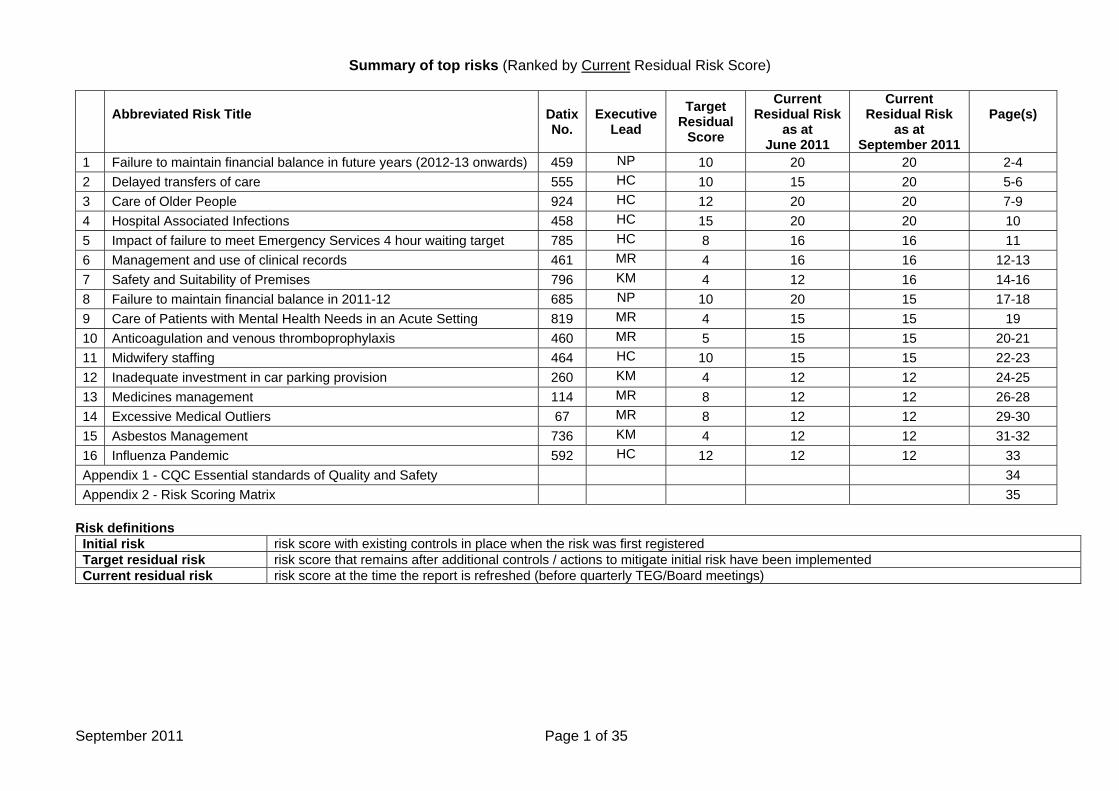
Summary of top risks (Ranked by Current Residual Risk Score)
Abbreviated Risk Title Datix No.
Executive
Lead Target
Residual Score
Current Residual Risk
as at June 2011
Current Residual Risk
as at September 2011
Page(s)
1 Failure to maintain financial balance in future years (2012-13 onwards) 459 NP 10 20 20 2-4 2 Delayed transfers of care 555 HC 10 15 20 5-6 3 Care of Older People 924 HC 12 20 20 7-9 4 Hospital Associated Infections 458 HC 15 20 20 10 5 Impact of failure to meet Emergency Services 4 hour waiting target 785 HC 8 16 16 11 6 Management and use of clinical records 461 MR 4 16 16 12-13 7 Safety and Suitability of Premises 796 KM 4 12 16 14-16 8 Failure to maintain financial balance in 2011-12 685 NP 10 20 15 17-18 9 Care of Patients with Mental Health Needs in an Acute Setting 819 MR 4 15 15 19 10 Anticoagulation and venous thromboprophylaxis 460 MR 5 15 15 20-21 11 Midwifery staffing 464 HC 10 15 15 22-23 12 Inadequate investment in car parking provision 260 KM 4 12 12 24-25 13 Medicines management 114 MR 8 12 12 26-28 14 Excessive Medical Outliers 67 MR 8 12 12 29-30 15 Asbestos Management 736 KM 4 12 12 31-32 16 Influenza Pandemic 592 HC 12 12 12 33 Appendix 1 - CQC Essential standards of Quality and Safety 34 Appendix 2 - Risk Scoring Matrix 35
Risk definitions Initial risk risk score with existing controls in place when the risk was first registered Target residual risk risk score that remains after additional controls / actions to mitigate initial risk have been implemented Current residual risk risk score at the time the report is refreshed (before quarterly TEG/Board meetings)
September 2011 Page 1 of 35
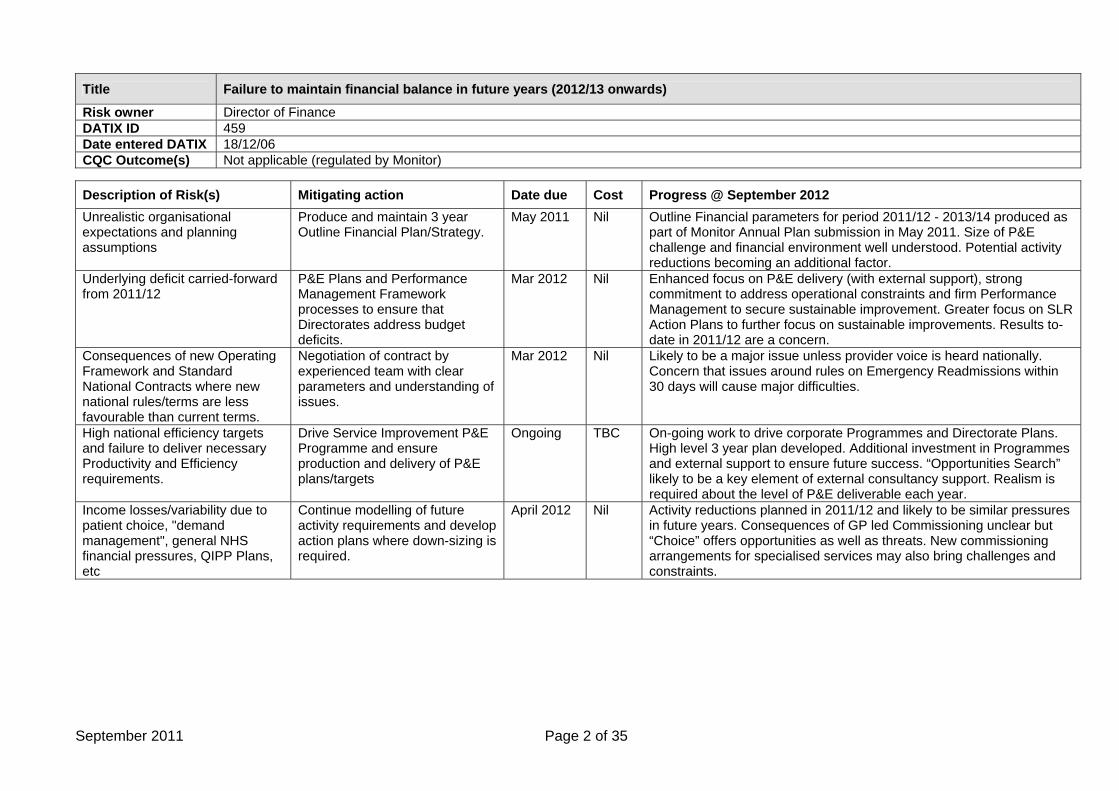
Title Failure to maintain financial balance in future years (2012/13 onwards)
Risk owner Director of Finance DATIX ID 459 Date entered DATIX 18/12/06 CQC Outcome(s) Not applicable (regulated by Monitor)
Description of Risk(s) Mitigating action Date due Cost Progress @ September 2012 Unrealistic organisational expectations and planning assumptions
Produce and maintain 3 year Outline Financial Plan/Strategy.
May 2011
Nil Outline Financial parameters for period 2011/12 - 2013/14 produced as part of Monitor Annual Plan submission in May 2011. Size of P&E challenge and financial environment well understood. Potential activity reductions becoming an additional factor.
Underlying deficit carried-forward from 2011/12
P&E Plans and Performance Management Framework processes to ensure that Directorates address budget deficits.
Mar 2012 Nil Enhanced focus on P&E delivery (with external support), strong commitment to address operational constraints and firm Performance Management to secure sustainable improvement. Greater focus on SLR Action Plans to further focus on sustainable improvements. Results to-date in 2011/12 are a concern.
Consequences of new Operating Framework and Standard National Contracts where new national rules/terms are less favourable than current terms.
Negotiation of contract by experienced team with clear parameters and understanding of issues.
Mar 2012 Nil Likely to be a major issue unless provider voice is heard nationally. Concern that issues around rules on Emergency Readmissions within 30 days will cause major difficulties.
High national efficiency targets and failure to deliver necessary Productivity and Efficiency requirements.
Drive Service Improvement P&E Programme and ensure production and delivery of P&E plans/targets
Ongoing
TBC On-going work to drive corporate Programmes and Directorate Plans. High level 3 year plan developed. Additional investment in Programmes and external support to ensure future success. “Opportunities Search” likely to be a key element of external consultancy support. Realism is required about the level of P&E deliverable each year.
Income losses/variability due to patient choice, "demand management", general NHS financial pressures, QIPP Plans, etc
Continue modelling of future activity requirements and develop action plans where down-sizing is required.
April 2012 Nil Activity reductions planned in 2011/12 and likely to be similar pressures in future years. Consequences of GP led Commissioning unclear but “Choice” offers opportunities as well as threats. New commissioning arrangements for specialised services may also bring challenges and constraints.
September 2011 Page 2 of 35
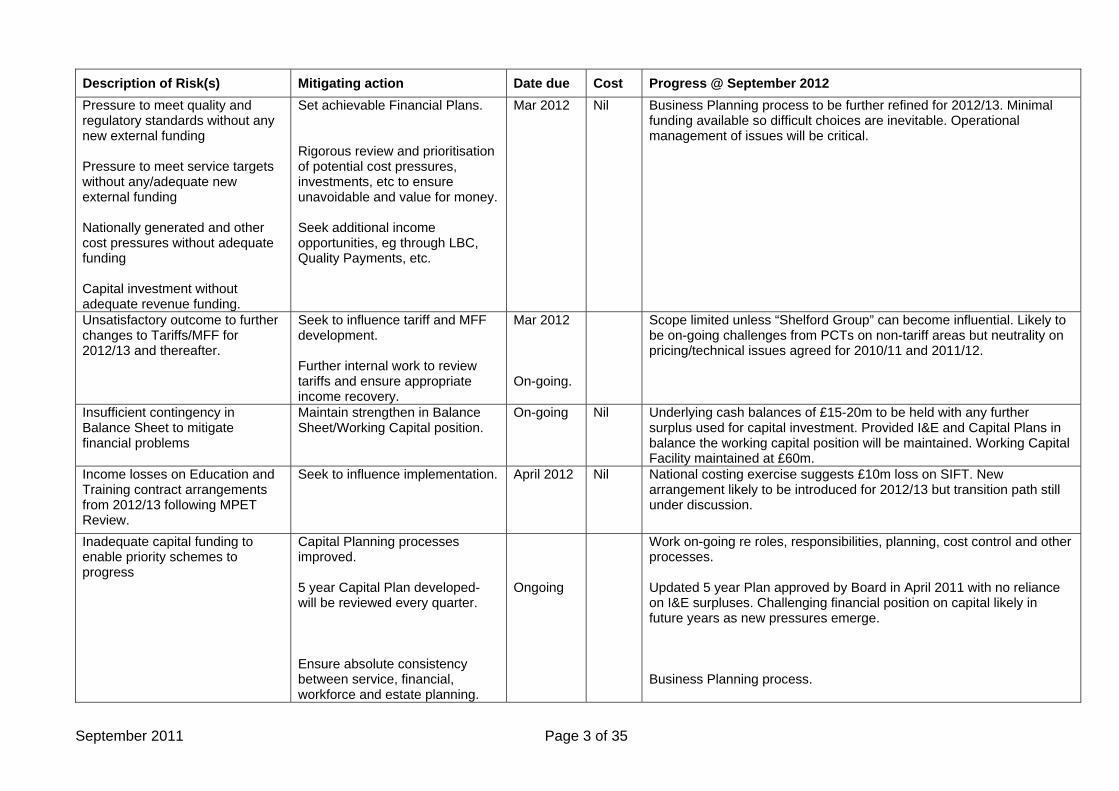
Description of Risk(s) Mitigating action Date due Cost Progress @ September 2012 Pressure to meet quality and regulatory standards without any new external funding Pressure to meet service targets without any/adequate new external funding Nationally generated and other cost pressures without adequate funding Capital investment without adequate revenue funding.
Set achievable Financial Plans. Rigorous review and prioritisation of potential cost pressures, investments, etc to ensure unavoidable and value for money. Seek additional income opportunities, eg through LBC, Quality Payments, etc.
Mar 2012 Nil Business Planning process to be further refined for 2012/13. Minimal funding available so difficult choices are inevitable. Operational management of issues will be critical.
Unsatisfactory outcome to further changes to Tariffs/MFF for 2012/13 and thereafter.
Seek to influence tariff and MFF development. Further internal work to review tariffs and ensure appropriate income recovery.
Mar 2012 On-going.
Scope limited unless “Shelford Group” can become influential. Likely to be on-going challenges from PCTs on non-tariff areas but neutrality on pricing/technical issues agreed for 2010/11 and 2011/12.
Insufficient contingency in Balance Sheet to mitigate financial problems
Maintain strengthen in Balance Sheet/Working Capital position.
On-going
Nil Underlying cash balances of £15-20m to be held with any further surplus used for capital investment. Provided I&E and Capital Plans in balance the working capital position will be maintained. Working Capital Facility maintained at £60m.
Income losses on Education and Training contract arrangements from 2012/13 following MPET Review.
Seek to influence implementation.
April 2012
Nil
National costing exercise suggests £10m loss on SIFT. New arrangement likely to be introduced for 2012/13 but transition path still under discussion.
Inadequate capital funding to enable priority schemes to progress
Capital Planning processes improved. 5 year Capital Plan developed- will be reviewed every quarter. Ensure absolute consistency between service, financial, workforce and estate planning.
Ongoing
Work on-going re roles, responsibilities, planning, cost control and other processes. Updated 5 year Plan approved by Board in April 2011 with no reliance on I&E surpluses. Challenging financial position on capital likely in future years as new pressures emerge. Business Planning process.
September 2011 Page 3 of 35
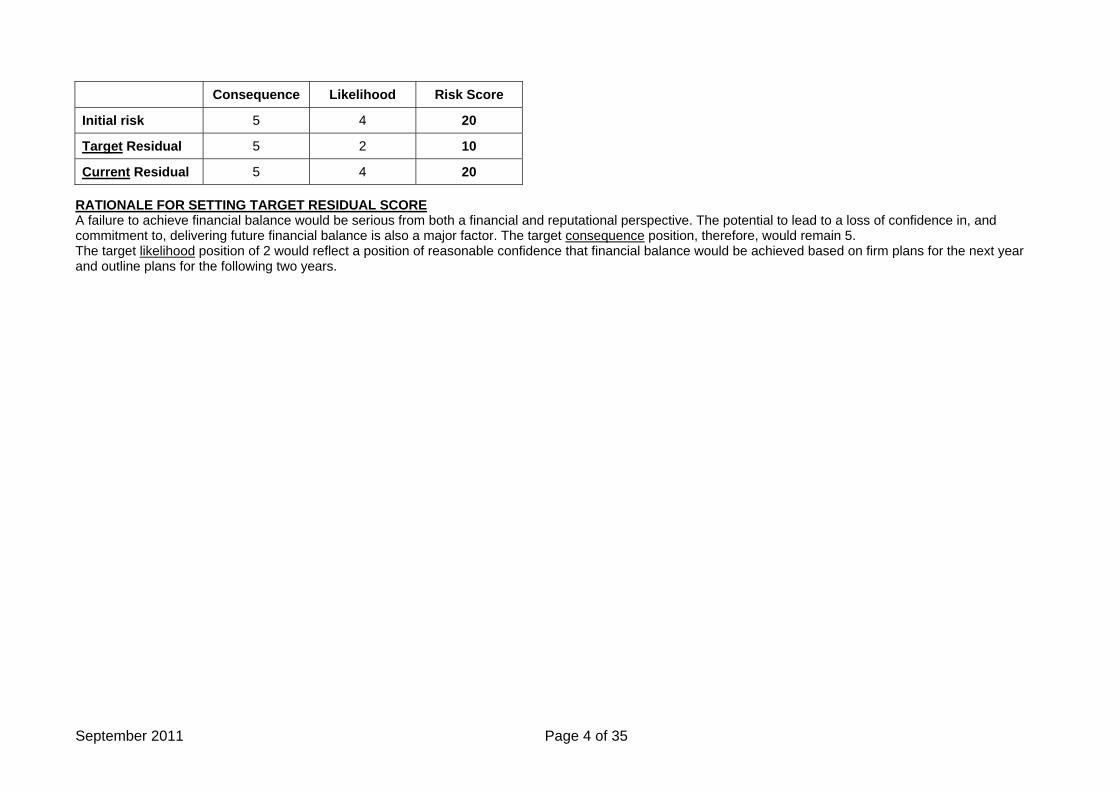
Consequence Likelihood Risk Score
Initial risk 5 4 20
Target Residual 5 2 10
Current Residual 5 4 20 RATIONALE FOR SETTING TARGET RESIDUAL SCORE A failure to achieve financial balance would be serious from both a financial and reputational perspective. The potential to lead to a loss of confidence in, and commitment to, delivering future financial balance is also a major factor. The target consequence position, therefore, would remain 5. The target likelihood position of 2 would reflect a position of reasonable confidence that financial balance would be achieved based on firm plans for the next year and outline plans for the following two years.
September 2011 Page 4 of 35
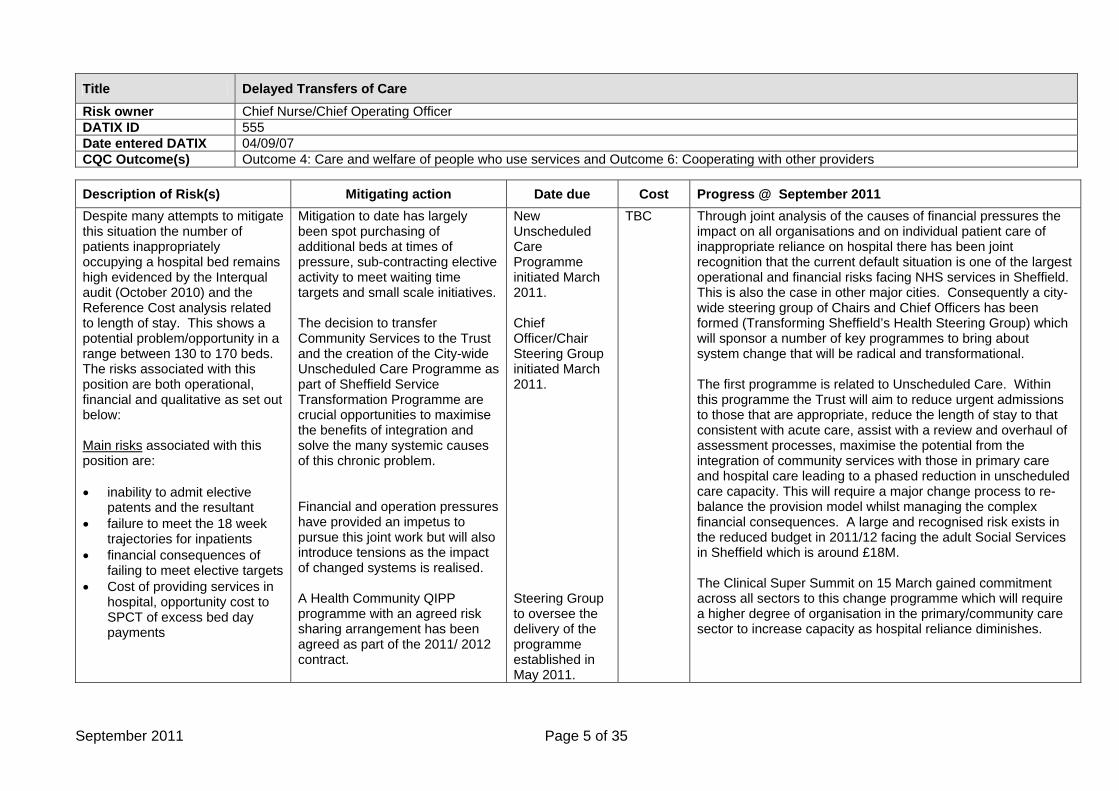
Title Delayed Transfers of Care Risk owner Chief Nurse/Chief Operating Officer DATIX ID 555 Date entered DATIX 04/09/07 CQC Outcome(s) Outcome 4: Care and welfare of people who use services and Outcome 6: Cooperating with other providers
Description of Risk(s) Mitigating action Date due Cost Progress @ September 2011 Despite many attempts to mitigate this situation the number of patients inappropriately occupying a hospital bed remains high evidenced by the Interqual audit (October 2010) and the Reference Cost analysis related to length of stay. This shows a potential problem/opportunity in a range between 130 to 170 beds. The risks associated with this position are both operational, financial and qualitative as set out below: Main risks associated with this position are: • inability to admit elective
patents and the resultant • failure to meet the 18 week
trajectories for inpatients • financial consequences of
failing to meet elective targets • Cost of providing services in
hospital, opportunity cost to SPCT of excess bed day payments
Mitigation to date has largely been spot purchasing of additional beds at times of pressure, sub-contracting elective activity to meet waiting time targets and small scale initiatives. The decision to transfer Community Services to the Trust and the creation of the City-wide Unscheduled Care Programme as part of Sheffield Service Transformation Programme are crucial opportunities to maximise the benefits of integration and solve the many systemic causes of this chronic problem. Financial and operation pressures have provided an impetus to pursue this joint work but will also introduce tensions as the impact of changed systems is realised. A Health Community QIPP programme with an agreed risk sharing arrangement has been agreed as part of the 2011/ 2012 contract.
New Unscheduled Care Programme initiated March 2011. Chief Officer/Chair Steering Group initiated March 2011. Steering Group to oversee the delivery of the programme established in May 2011.
TBC Through joint analysis of the causes of financial pressures the impact on all organisations and on individual patient care of inappropriate reliance on hospital there has been joint recognition that the current default situation is one of the largest operational and financial risks facing NHS services in Sheffield. This is also the case in other major cities. Consequently a city-wide steering group of Chairs and Chief Officers has been formed (Transforming Sheffield’s Health Steering Group) which will sponsor a number of key programmes to bring about system change that will be radical and transformational. The first programme is related to Unscheduled Care. Within this programme the Trust will aim to reduce urgent admissions to those that are appropriate, reduce the length of stay to that consistent with acute care, assist with a review and overhaul of assessment processes, maximise the potential from the integration of community services with those in primary care and hospital care leading to a phased reduction in unscheduled care capacity. This will require a major change process to re-balance the provision model whilst managing the complex financial consequences. A large and recognised risk exists in the reduced budget in 2011/12 facing the adult Social Services in Sheffield which is around £18M. The Clinical Super Summit on 15 March gained commitment across all sectors to this change programme which will require a higher degree of organisation in the primary/community care sector to increase capacity as hospital reliance diminishes.
September 2011 Page 5 of 35
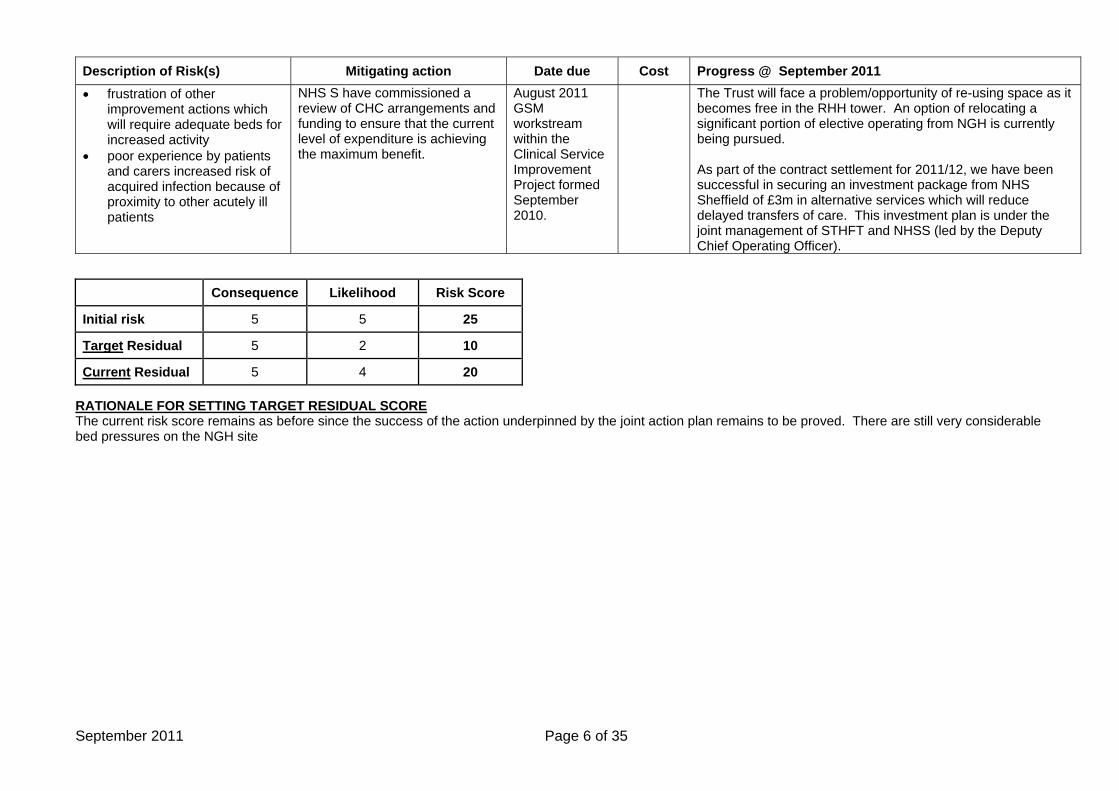
Description of Risk(s) Mitigating action Date due Cost Progress @ September 2011 • frustration of other
improvement actions which will require adequate beds for increased activity
• poor experience by patients and carers increased risk of acquired infection because of proximity to other acutely ill patients
NHS S have commissioned a review of CHC arrangements and funding to ensure that the current level of expenditure is achieving the maximum benefit.
August 2011 GSM workstream within the Clinical Service Improvement Project formed September 2010.
The Trust will face a problem/opportunity of re-using space as it becomes free in the RHH tower. An option of relocating a significant portion of elective operating from NGH is currently being pursued. As part of the contract settlement for 2011/12, we have been successful in securing an investment package from NHS Sheffield of £3m in alternative services which will reduce delayed transfers of care. This investment plan is under the joint management of STHFT and NHSS (led by the Deputy Chief Operating Officer).
Consequence Likelihood Risk Score
Initial risk 5 5 25
Target Residual 5 2 10
Current Residual 5 4 20 RATIONALE FOR SETTING TARGET RESIDUAL SCORE The current risk score remains as before since the success of the action underpinned by the joint action plan remains to be proved. There are still very considerable bed pressures on the NGH site
September 2011 Page 6 of 35
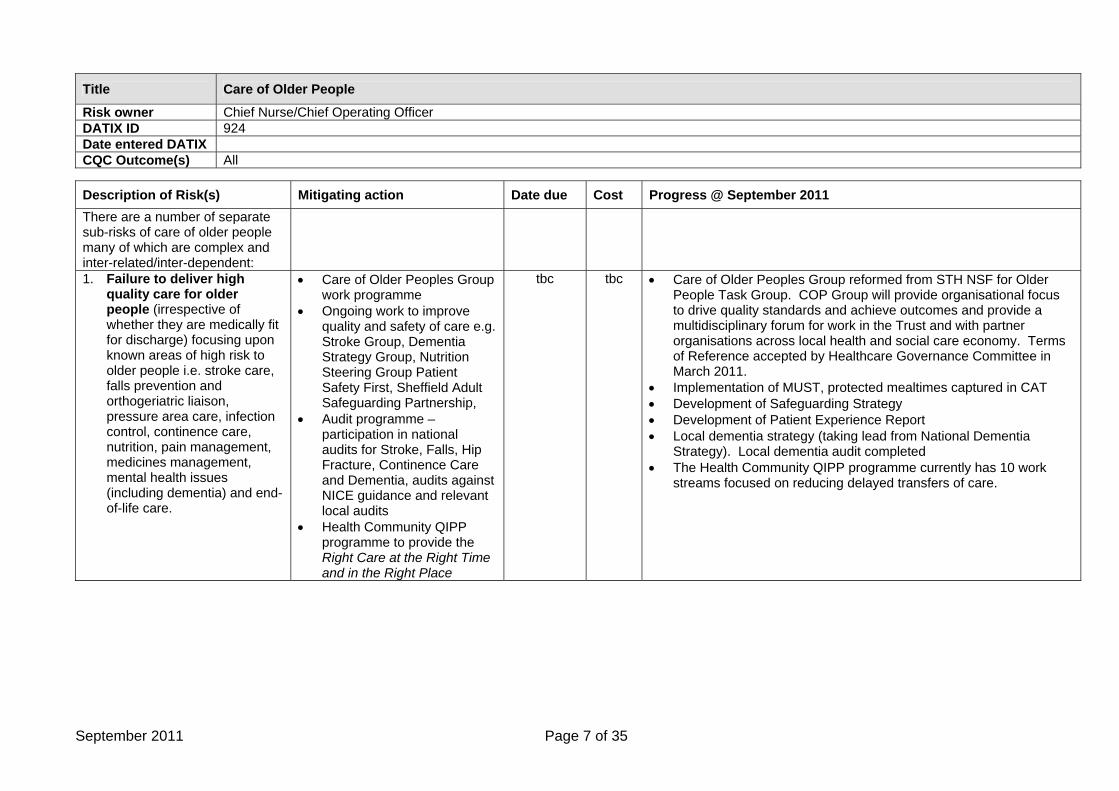
Title Care of Older People
Risk owner Chief Nurse/Chief Operating Officer DATIX ID 924 Date entered DATIX CQC Outcome(s) All
Description of Risk(s) Mitigating action Date due Cost Progress @ September 2011 There are a number of separate sub-risks of care of older people many of which are complex and inter-related/inter-dependent:
1. Failure to deliver high quality care for older people (irrespective of whether they are medically fit for discharge) focusing upon known areas of high risk to older people i.e. stroke care, falls prevention and orthogeriatric liaison, pressure area care, infection control, continence care, nutrition, pain management, medicines management, mental health issues (including dementia) and end-of-life care.
• Care of Older Peoples Group work programme
• Ongoing work to improve quality and safety of care e.g. Stroke Group, Dementia Strategy Group, Nutrition Steering Group Patient Safety First, Sheffield Adult Safeguarding Partnership,
• Audit programme – participation in national audits for Stroke, Falls, Hip Fracture, Continence Care and Dementia, audits against NICE guidance and relevant local audits
• Health Community QIPP programme to provide the Right Care at the Right Time and in the Right Place
tbc tbc • Care of Older Peoples Group reformed from STH NSF for Older People Task Group. COP Group will provide organisational focus to drive quality standards and achieve outcomes and provide a multidisciplinary forum for work in the Trust and with partner organisations across local health and social care economy. Terms of Reference accepted by Healthcare Governance Committee in March 2011.
• Implementation of MUST, protected mealtimes captured in CAT • Development of Safeguarding Strategy • Development of Patient Experience Report • Local dementia strategy (taking lead from National Dementia
Strategy). Local dementia audit completed • The Health Community QIPP programme currently has 10 work
streams focused on reducing delayed transfers of care.
September 2011 Page 7 of 35
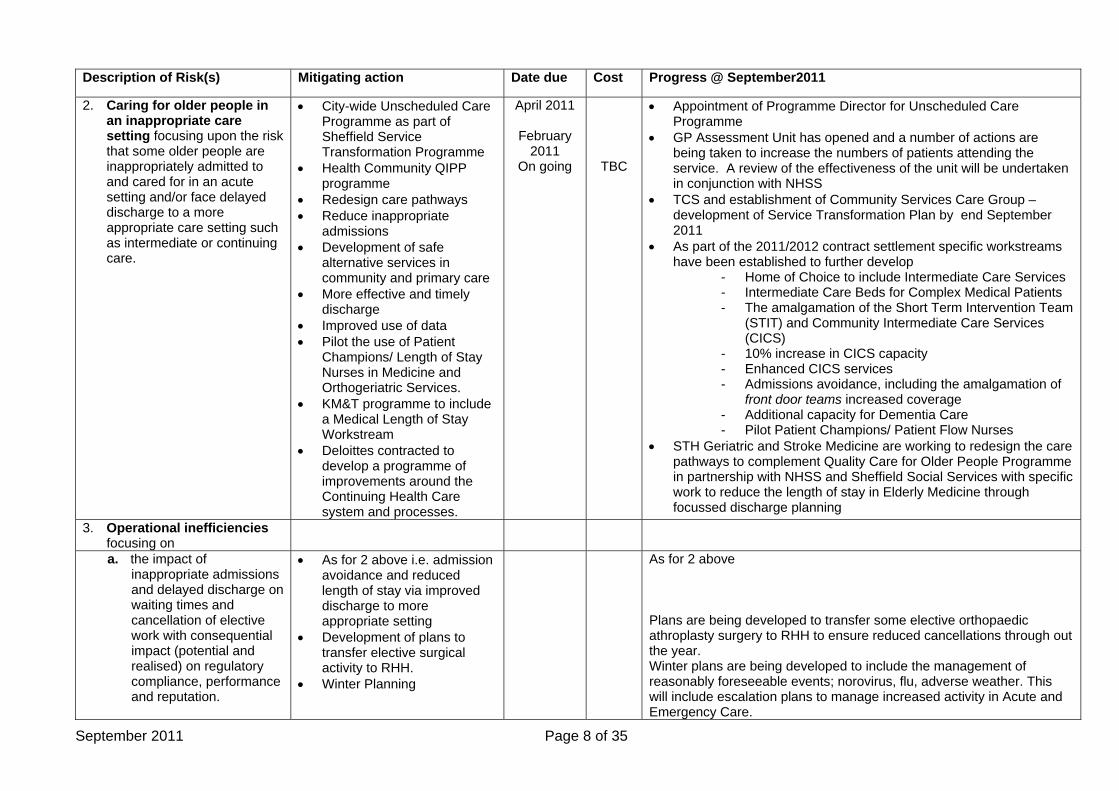
Description of Risk(s) Mitigating action Date due Cost Progress @ September2011
2. Caring for older people in an inappropriate care setting focusing upon the risk that some older people are inappropriately admitted to and cared for in an acute setting and/or face delayed discharge to a more appropriate care setting such as intermediate or continuing care.
• City-wide Unscheduled Care Programme as part of Sheffield Service Transformation Programme
• Health Community QIPP programme
• Redesign care pathways • Reduce inappropriate
admissions • Development of safe
alternative services in community and primary care
• More effective and timely discharge
• Improved use of data • Pilot the use of Patient
Champions/ Length of Stay Nurses in Medicine and Orthogeriatric Services.
• KM&T programme to include a Medical Length of Stay Workstream
• Deloittes contracted to develop a programme of improvements around the Continuing Health Care system and processes.
April 2011
February 2011
On going
TBC
• Appointment of Programme Director for Unscheduled Care Programme
• GP Assessment Unit has opened and a number of actions are being taken to increase the numbers of patients attending the service. A review of the effectiveness of the unit will be undertaken in conjunction with NHSS
• TCS and establishment of Community Services Care Group – development of Service Transformation Plan by end September 2011
• As part of the 2011/2012 contract settlement specific workstreams have been established to further develop
- Home of Choice to include Intermediate Care Services - Intermediate Care Beds for Complex Medical Patients - The amalgamation of the Short Term Intervention Team
(STIT) and Community Intermediate Care Services (CICS)
- 10% increase in CICS capacity - Enhanced CICS services - Admissions avoidance, including the amalgamation of
front door teams increased coverage - Additional capacity for Dementia Care - Pilot Patient Champions/ Patient Flow Nurses
• STH Geriatric and Stroke Medicine are working to redesign the care pathways to complement Quality Care for Older People Programme in partnership with NHSS and Sheffield Social Services with specific work to reduce the length of stay in Elderly Medicine through focussed discharge planning
3. Operational inefficiencies focusing on
a. the impact of inappropriate admissions and delayed discharge on waiting times and cancellation of elective work with consequential impact (potential and realised) on regulatory compliance, performance and reputation.
• As for 2 above i.e. admission avoidance and reduced length of stay via improved discharge to more appropriate setting
• Development of plans to transfer elective surgical activity to RHH.
• Winter Planning
As for 2 above Plans are being developed to transfer some elective orthopaedic athroplasty surgery to RHH to ensure reduced cancellations through out the year. Winter plans are being developed to include the management of reasonably foreseeable events; norovirus, flu, adverse weather. This will include escalation plans to manage increased activity in Acute and Emergency Care.
September 2011 Page 8 of 35
Description of Risk(s) Mitigating action Date due Cost Progress @ September 2011
b. the higher cost of
providing care inappropriately in an acute setting compared to intermediate or continuing care
• As for 2 above i.e. admission avoidance and reduced length of stay via improved discharge to more appropriate setting
As for 2 above
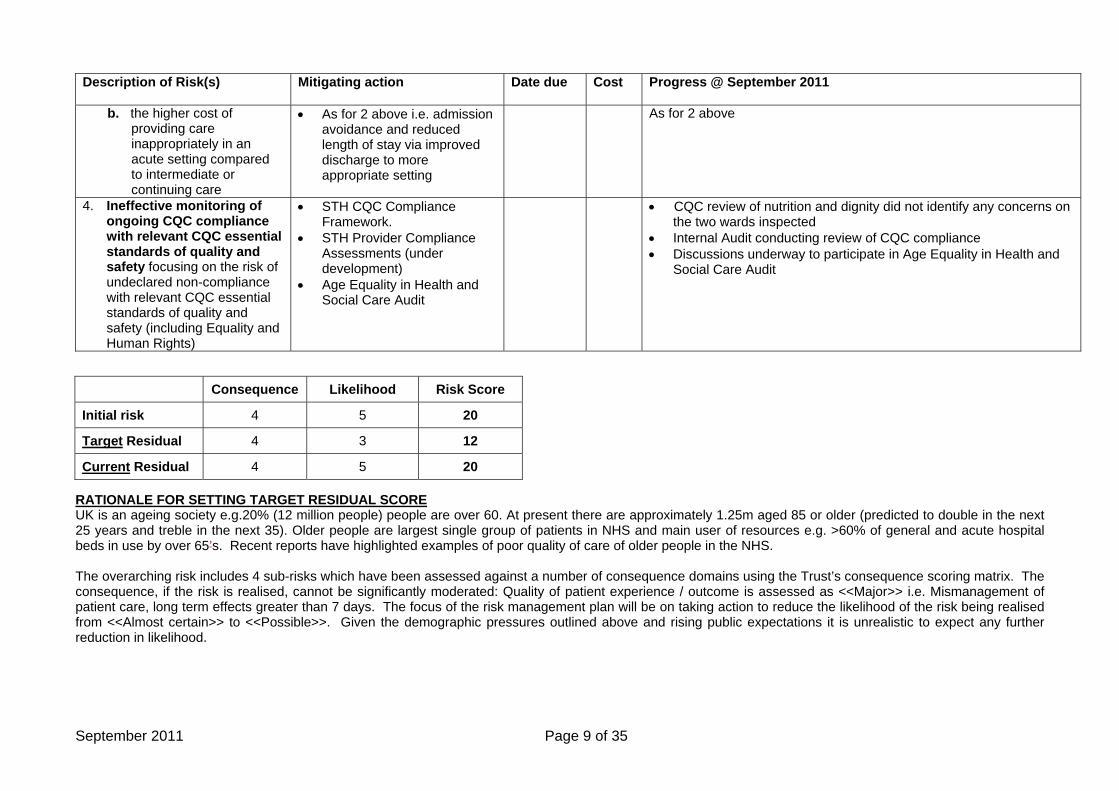
4. Ineffective monitoring of ongoing CQC compliance with relevant CQC essential standards of quality and safety focusing on the risk of undeclared non-compliance with relevant CQC essential standards of quality and safety (including Equality and Human Rights)
• STH CQC Compliance Framework.
• STH Provider Compliance Assessments (under development)
• Age Equality in Health and Social Care Audit
• CQC review of nutrition and dignity did not identify any concerns on the two wards inspected
• Internal Audit conducting review of CQC compliance • Discussions underway to participate in Age Equality in Health and
Social Care Audit
Consequence Likelihood Risk Score
Initial risk 4 5 20
Target Residual 4 3 12
Current Residual 4 5 20 RATIONALE FOR SETTING TARGET RESIDUAL SCORE UK is an ageing society e.g.20% (12 million people) people are over 60. At present there are approximately 1.25m aged 85 or older (predicted to double in the next 25 years and treble in the next 35). Older people are largest single group of patients in NHS and main user of resources e.g. >60% of general and acute hospital beds in use by over 65’s. Recent reports have highlighted examples of poor quality of care of older people in the NHS. The overarching risk includes 4 sub-risks which have been assessed against a number of consequence domains using the Trust’s consequence scoring matrix. The consequence, if the risk is realised, cannot be significantly moderated: Quality of patient experience / outcome is assessed as <<Major>> i.e. Mismanagement of patient care, long term effects greater than 7 days. The focus of the risk management plan will be on taking action to reduce the likelihood of the risk being realised from <<Almost certain>> to <<Possible>>. Given the demographic pressures outlined above and rising public expectations it is unrealistic to expect any further reduction in likelihood.
September 2011 Page 9 of 35
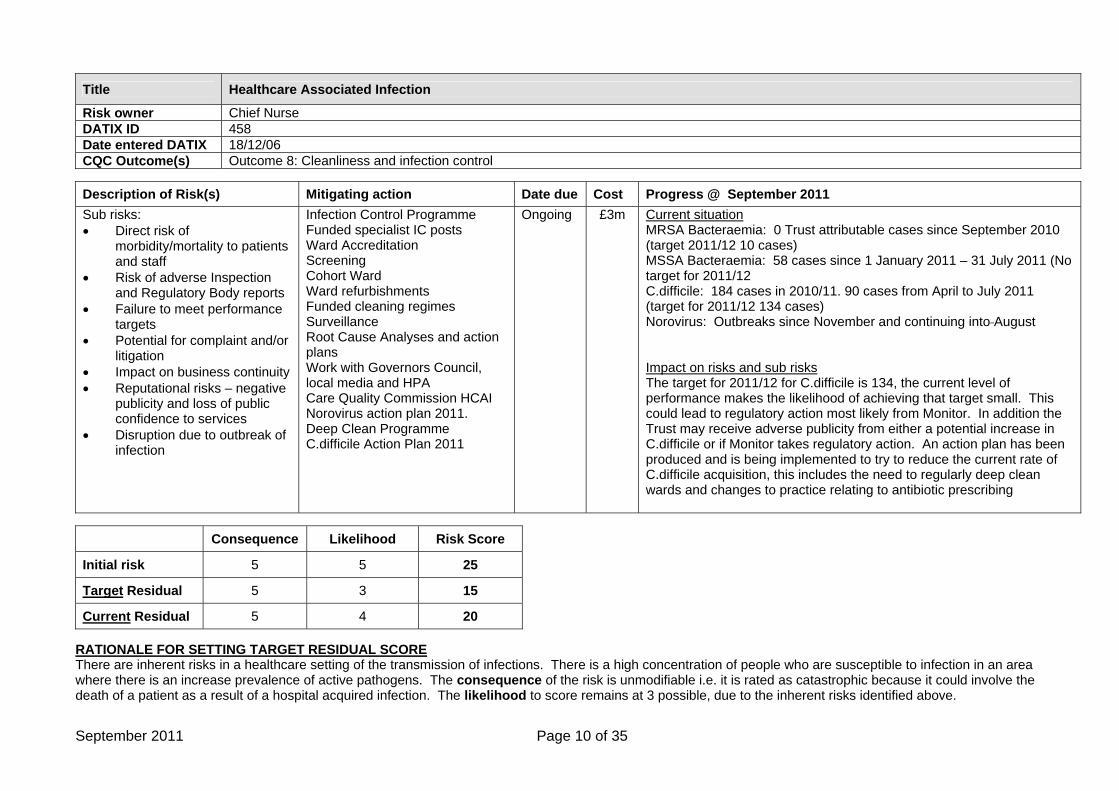
Title Healthcare Associated Infection
Risk owner Chief Nurse DATIX ID 458 Date entered DATIX 18/12/06 CQC Outcome(s) Outcome 8: Cleanliness and infection control
Description of Risk(s) Mitigating action Date due Cost Progress @ September 2011 Sub risks: • Direct risk of
morbidity/mortality to patients and staff
• Risk of adverse Inspection and Regulatory Body reports
• Failure to meet performance targets
• Potential for complaint and/or litigation
• Impact on business continuity • Reputational risks – negative
publicity and loss of public confidence to services
• Disruption due to outbreak of infection
Infection Control Programme Funded specialist IC posts Ward Accreditation Screening Cohort Ward Ward refurbishments Funded cleaning regimes Surveillance Root Cause Analyses and action plans Work with Governors Council, local media and HPA Care Quality Commission HCAI Norovirus action plan 2011. Deep Clean Programme C.difficile Action Plan 2011
Ongoing
£3m
Current situation MRSA Bacteraemia: 0 Trust attributable cases since September 2010 (target 2011/12 10 cases) MSSA Bacteraemia: 58 cases since 1 January 2011 – 31 July 2011 (No target for 2011/12 C.difficile: 184 cases in 2010/11. 90 cases from April to July 2011 (target for 2011/12 134 cases) Norovirus: Outbreaks since November and continuing into August Impact on risks and sub risks The target for 2011/12 for C.difficile is 134, the current level of performance makes the likelihood of achieving that target small. This could lead to regulatory action most likely from Monitor. In addition the Trust may receive adverse publicity from either a potential increase in C.difficile or if Monitor takes regulatory action. An action plan has been produced and is being implemented to try to reduce the current rate of C.difficile acquisition, this includes the need to regularly deep clean wards and changes to practice relating to antibiotic prescribing
Consequence Likelihood Risk Score
Initial risk 5 5 25
Target Residual 5 3 15
Current Residual 5 4 20 RATIONALE FOR SETTING TARGET RESIDUAL SCORE There are inherent risks in a healthcare setting of the transmission of infections. There is a high concentration of people who are susceptible to infection in an area where there is an increase prevalence of active pathogens. The consequence of the risk is unmodifiable i.e. it is rated as catastrophic because it could involve the death of a patient as a result of a hospital acquired infection. The likelihood to score remains at 3 possible, due to the inherent risks identified above.
September 2011 Page 10 of 35
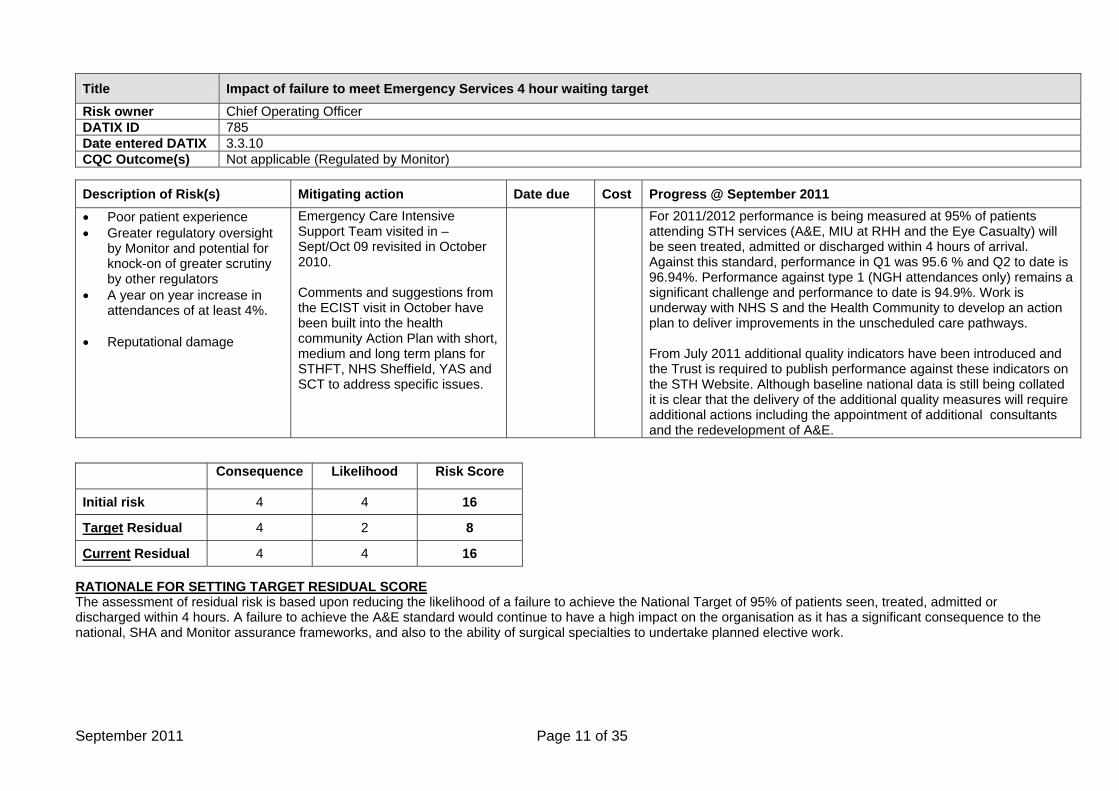
Title Impact of failure to meet Emergency Services 4 hour waiting target Risk owner Chief Operating Officer DATIX ID 785 Date entered DATIX 3.3.10 CQC Outcome(s) Not applicable (Regulated by Monitor)
Description of Risk(s) Mitigating action Date due Cost Progress @ September 2011 • Poor patient experience • Greater regulatory oversight
by Monitor and potential for knock-on of greater scrutiny by other regulators
• A year on year increase in attendances of at least 4%.
• Reputational damage
Emergency Care Intensive Support Team visited in – Sept/Oct 09 revisited in October 2010. Comments and suggestions from the ECIST visit in October have been built into the health community Action Plan with short, medium and long term plans for STHFT, NHS Sheffield, YAS and SCT to address specific issues.
For 2011/2012 performance is being measured at 95% of patients attending STH services (A&E, MIU at RHH and the Eye Casualty) will be seen treated, admitted or discharged within 4 hours of arrival. Against this standard, performance in Q1 was 95.6 % and Q2 to date is 96.94%. Performance against type 1 (NGH attendances only) remains a significant challenge and performance to date is 94.9%. Work is underway with NHS S and the Health Community to develop an action plan to deliver improvements in the unscheduled care pathways. From July 2011 additional quality indicators have been introduced and the Trust is required to publish performance against these indicators on the STH Website. Although baseline national data is still being collated it is clear that the delivery of the additional quality measures will require additional actions including the appointment of additional consultants and the redevelopment of A&E.
Consequence Likelihood Risk Score
Initial risk 4 4 16
Target Residual 4 2 8
Current Residual 4 4 16 RATIONALE FOR SETTING TARGET RESIDUAL SCORE The assessment of residual risk is based upon reducing the likelihood of a failure to achieve the National Target of 95% of patients seen, treated, admitted or discharged within 4 hours. A failure to achieve the A&E standard would continue to have a high impact on the organisation as it has a significant consequence to the national, SHA and Monitor assurance frameworks, and also to the ability of surgical specialties to undertake planned elective work.
September 2011 Page 11 of 35
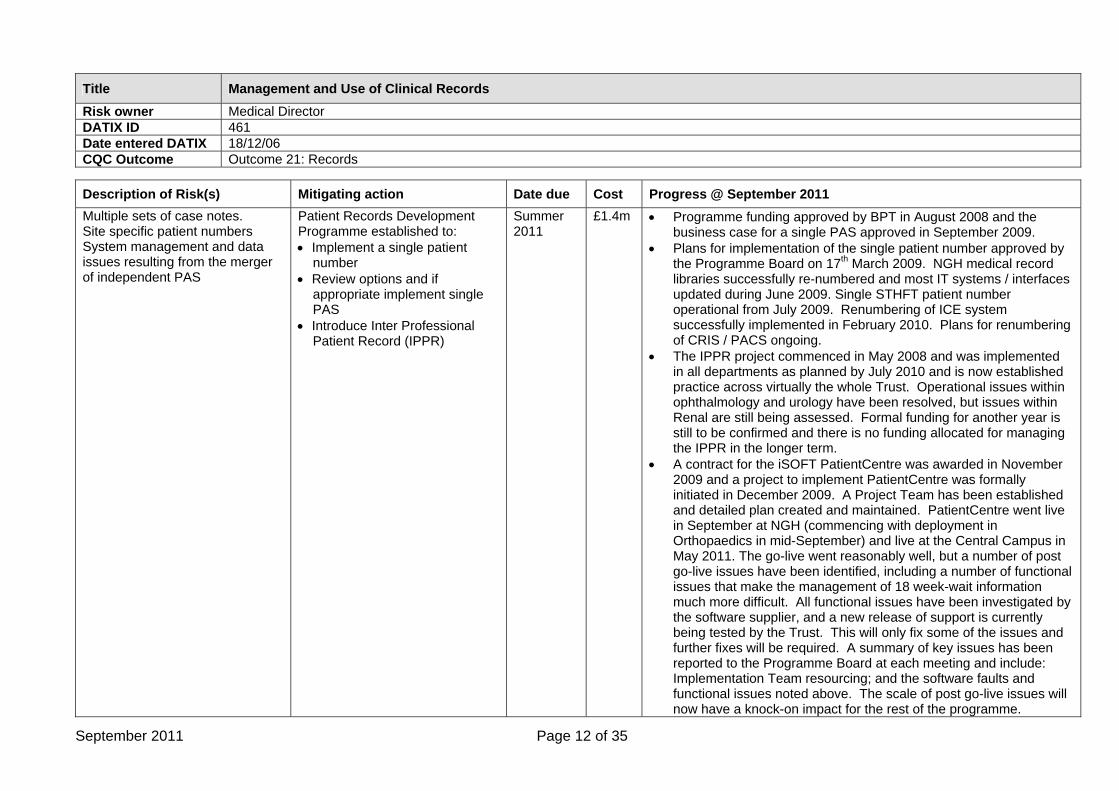
Title Management and Use of Clinical Records Risk owner Medical Director DATIX ID 461 Date entered DATIX 18/12/06 CQC Outcome Outcome 21: Records
Description of Risk(s) Mitigating action Date due Cost Progress @ September 2011 Multiple sets of case notes. Site specific patient numbers System management and data issues resulting from the merger of independent PAS
Patient Records Development Programme established to: • Implement a single patient
number • Review options and if
appropriate implement single PAS
• Introduce Inter Professional Patient Record (IPPR)
Summer 2011
£1.4m • Programme funding approved by BPT in August 2008 and the business case for a single PAS approved in September 2009.
• Plans for implementation of the single patient number approved by the Programme Board on 17th March 2009. NGH medical record libraries successfully re-numbered and most IT systems / interfaces updated during June 2009. Single STHFT patient number operational from July 2009. Renumbering of ICE system successfully implemented in February 2010. Plans for renumbering of CRIS / PACS ongoing.
• The IPPR project commenced in May 2008 and was implemented in all departments as planned by July 2010 and is now established practice across virtually the whole Trust. Operational issues within ophthalmology and urology have been resolved, but issues within Renal are still being assessed. Formal funding for another year is still to be confirmed and there is no funding allocated for managing the IPPR in the longer term.
• A contract for the iSOFT PatientCentre was awarded in November 2009 and a project to implement PatientCentre was formally initiated in December 2009. A Project Team has been established and detailed plan created and maintained. PatientCentre went live in September at NGH (commencing with deployment in Orthopaedics in mid-September) and live at the Central Campus in May 2011. The go-live went reasonably well, but a number of post go-live issues have been identified, including a number of functional issues that make the management of 18 week-wait information much more difficult. All functional issues have been investigated by the software supplier, and a new release of support is currently being tested by the Trust. This will only fix some of the issues and further fixes will be required. A summary of key issues has been reported to the Programme Board at each meeting and include: Implementation Team resourcing; and the software faults and functional issues noted above. The scale of post go-live issues will now have a knock-on impact for the rest of the programme.
September 2011 Page 12 of 35
Description of Risk(s) Mitigating action Date due Cost Progress @ September 2011
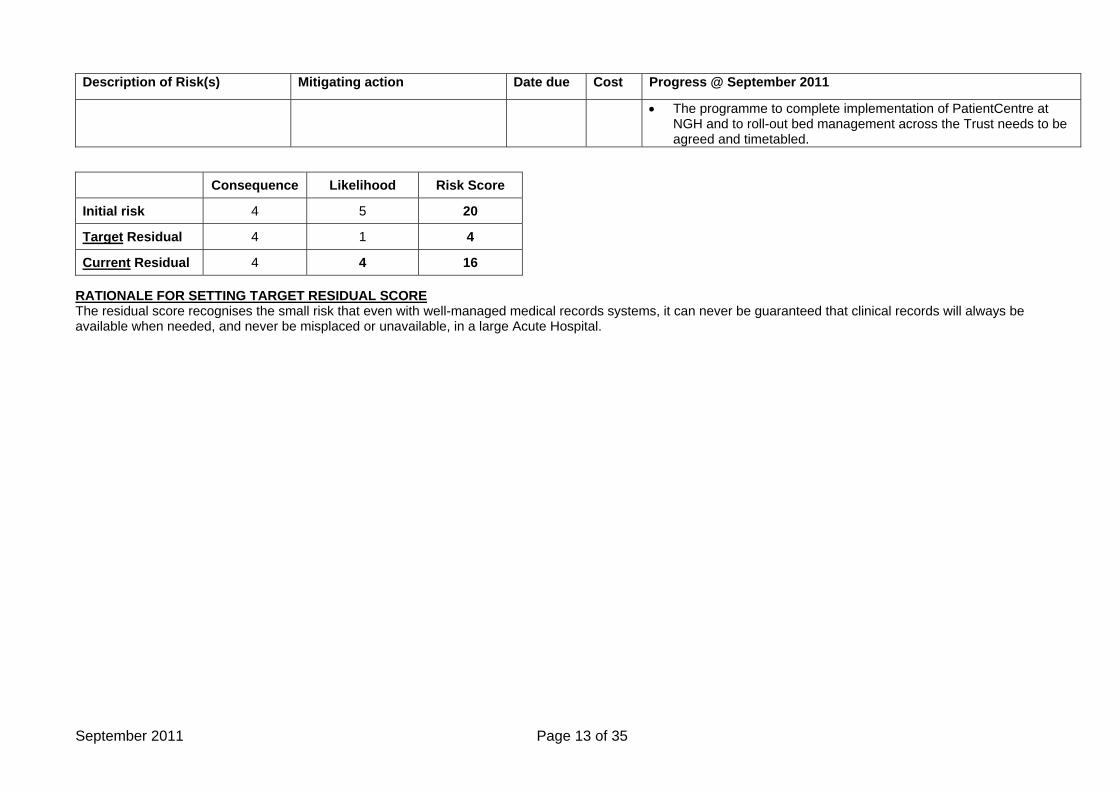
• The programme to complete implementation of PatientCentre at NGH and to roll-out bed management across the Trust needs to be agreed and timetabled.
Consequence Likelihood Risk Score
Initial risk 4 5 20
Target Residual 4 1 4
Current Residual 4 4 16 RATIONALE FOR SETTING TARGET RESIDUAL SCORE The residual score recognises the small risk that even with well-managed medical records systems, it can never be guaranteed that clinical records will always be available when needed, and never be misplaced or unavailable, in a large Acute Hospital.
September 2011 Page 13 of 35
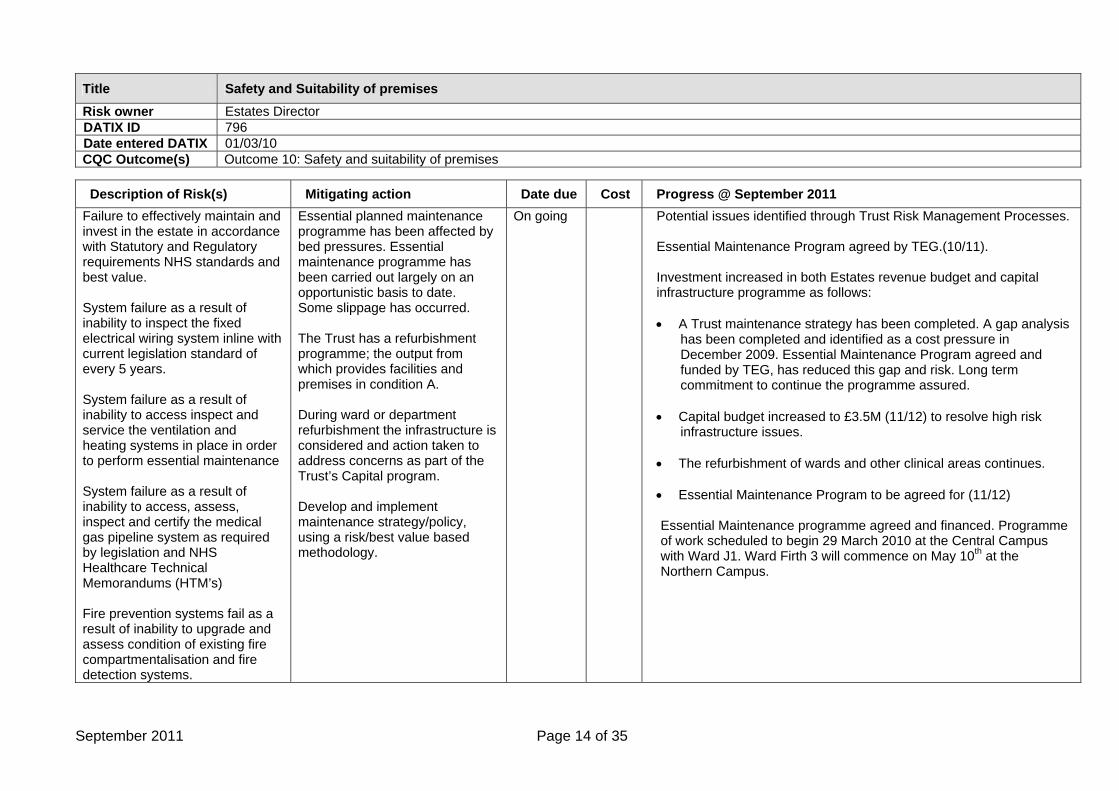
Title Safety and Suitability of premises Risk owner Estates Director DATIX ID 796 Date entered DATIX 01/03/10 CQC Outcome(s) Outcome 10: Safety and suitability of premises
Description of Risk(s) Mitigating action Date due Cost Progress @ September 2011 Failure to effectively maintain and invest in the estate in accordance with Statutory and Regulatory requirements NHS standards and best value. System failure as a result of inability to inspect the fixed electrical wiring system inline with current legislation standard of every 5 years. System failure as a result of inability to access inspect and service the ventilation and heating systems in place in order to perform essential maintenance System failure as a result of inability to access, assess, inspect and certify the medical gas pipeline system as required by legislation and NHS Healthcare Technical Memorandums (HTM’s) Fire prevention systems fail as a result of inability to upgrade and assess condition of existing fire compartmentalisation and fire detection systems.
Essential planned maintenance programme has been affected by bed pressures. Essential maintenance programme has been carried out largely on an opportunistic basis to date. Some slippage has occurred.
The Trust has a refurbishment programme; the output from which provides facilities and premises in condition A. During ward or department refurbishment the infrastructure is considered and action taken to address concerns as part of the Trust’s Capital program.
Develop and implement maintenance strategy/policy, using a risk/best value based methodology.
On going
Potential issues identified through Trust Risk Management Processes. Essential Maintenance Program agreed by TEG.(10/11). Investment increased in both Estates revenue budget and capital infrastructure programme as follows: • A Trust maintenance strategy has been completed. A gap analysis
has been completed and identified as a cost pressure in December 2009. Essential Maintenance Program agreed and funded by TEG, has reduced this gap and risk. Long term commitment to continue the programme assured.
• Capital budget increased to £3.5M (11/12) to resolve high risk
infrastructure issues. • The refurbishment of wards and other clinical areas continues.
• Essential Maintenance Program to be agreed for (11/12) Essential Maintenance programme agreed and financed. Programme of work scheduled to begin 29 March 2010 at the Central Campus with Ward J1. Ward Firth 3 will commence on May 10th at the Northern Campus.
September 2011 Page 14 of 35
Description of Risk(s) Mitigating action Date due Cost Progress @ September 2011
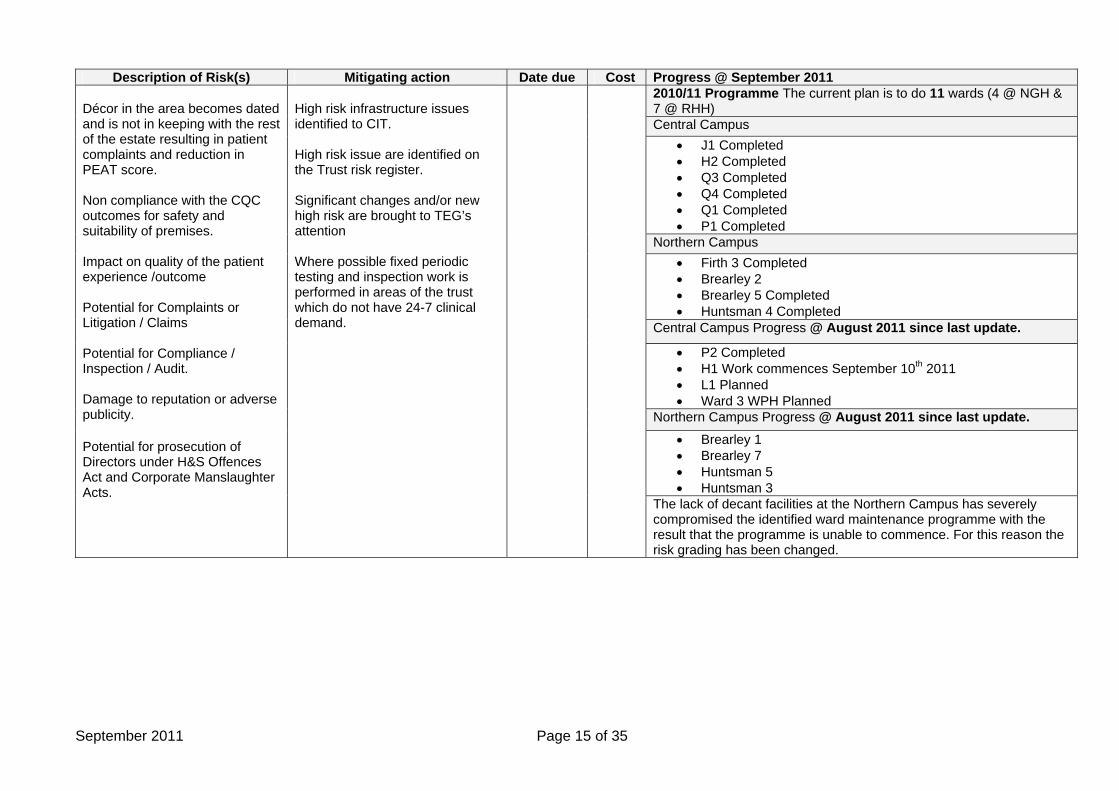
2010/11 Programme The current plan is to do 11 wards (4 @ NGH & 7 @ RHH) Central Campus
• J1 Completed • H2 Completed • Q3 Completed • Q4 Completed • Q1 Completed • P1 Completed
Northern Campus • Firth 3 Completed • Brearley 2 • Brearley 5 Completed • Huntsman 4 Completed
Central Campus Progress @ August 2011 since last update.
• P2 Completed • H1 Work commences September 10th 2011 • L1 Planned • Ward 3 WPH Planned
Northern Campus Progress @ August 2011 since last update. • Brearley 1 • Brearley 7 • Huntsman 5 • Huntsman 3
Décor in the area becomes dated and is not in keeping with the rest of the estate resulting in patient complaints and reduction in PEAT score. Non compliance with the CQC outcomes for safety and suitability of premises. Impact on quality of the patient experience /outcome Potential for Complaints or Litigation / Claims Potential for Compliance / Inspection / Audit. Damage to reputation or adverse publicity. Potential for prosecution of Directors under H&S Offences Act and Corporate Manslaughter Acts.
High risk infrastructure issues identified to CIT. High risk issue are identified on the Trust risk register. Significant changes and/or new high risk are brought to TEG’s attention Where possible fixed periodic testing and inspection work is performed in areas of the trust which do not have 24-7 clinical demand.
The lack of decant facilities at the Northern Campus has severely compromised the identified ward maintenance programme with the result that the programme is unable to commence. For this reason the risk grading has been changed.
September 2011 Page 15 of 35
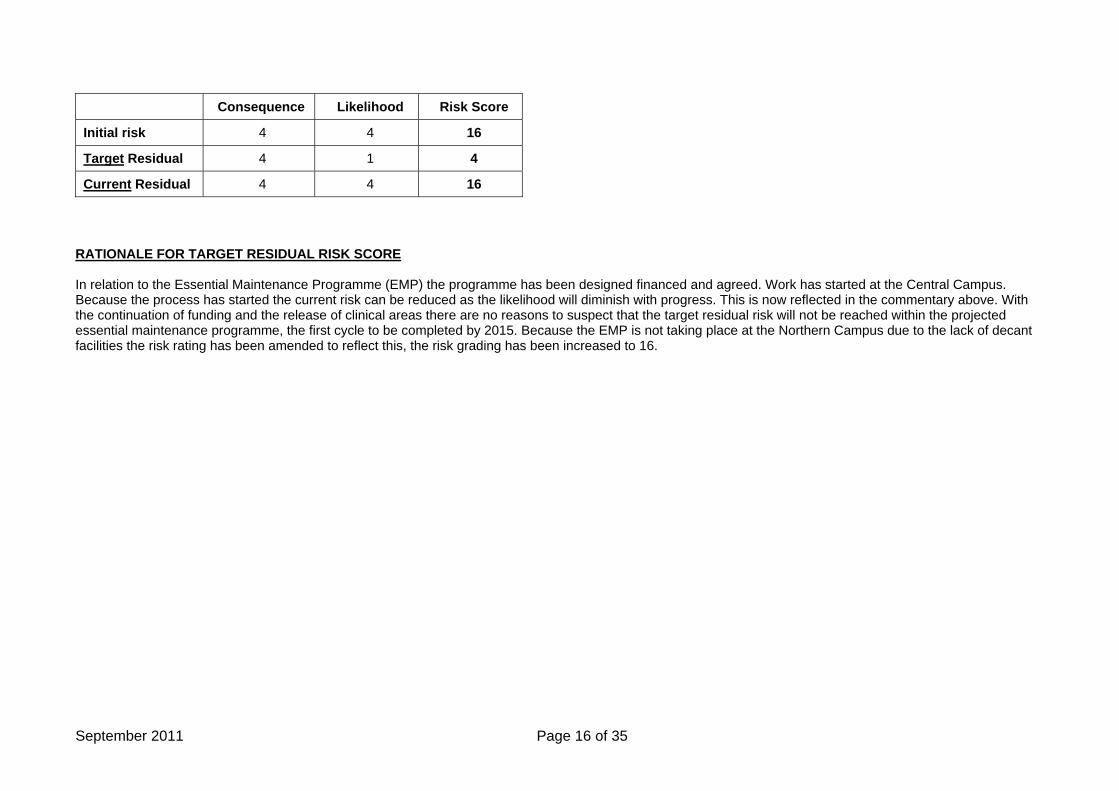
Consequence Likelihood Risk Score
Initial risk 4 4 16
Target Residual 4 1 4
Current Residual 4 4 16 RATIONALE FOR TARGET RESIDUAL RISK SCORE In relation to the Essential Maintenance Programme (EMP) the programme has been designed financed and agreed. Work has started at the Central Campus. Because the process has started the current risk can be reduced as the likelihood will diminish with progress. This is now reflected in the commentary above. With the continuation of funding and the release of clinical areas there are no reasons to suspect that the target residual risk will not be reached within the projected essential maintenance programme, the first cycle to be completed by 2015. Because the EMP is not taking place at the Northern Campus due to the lack of decant facilities the risk rating has been amended to reflect this, the risk grading has been increased to 16.
September 2011 Page 16 of 35
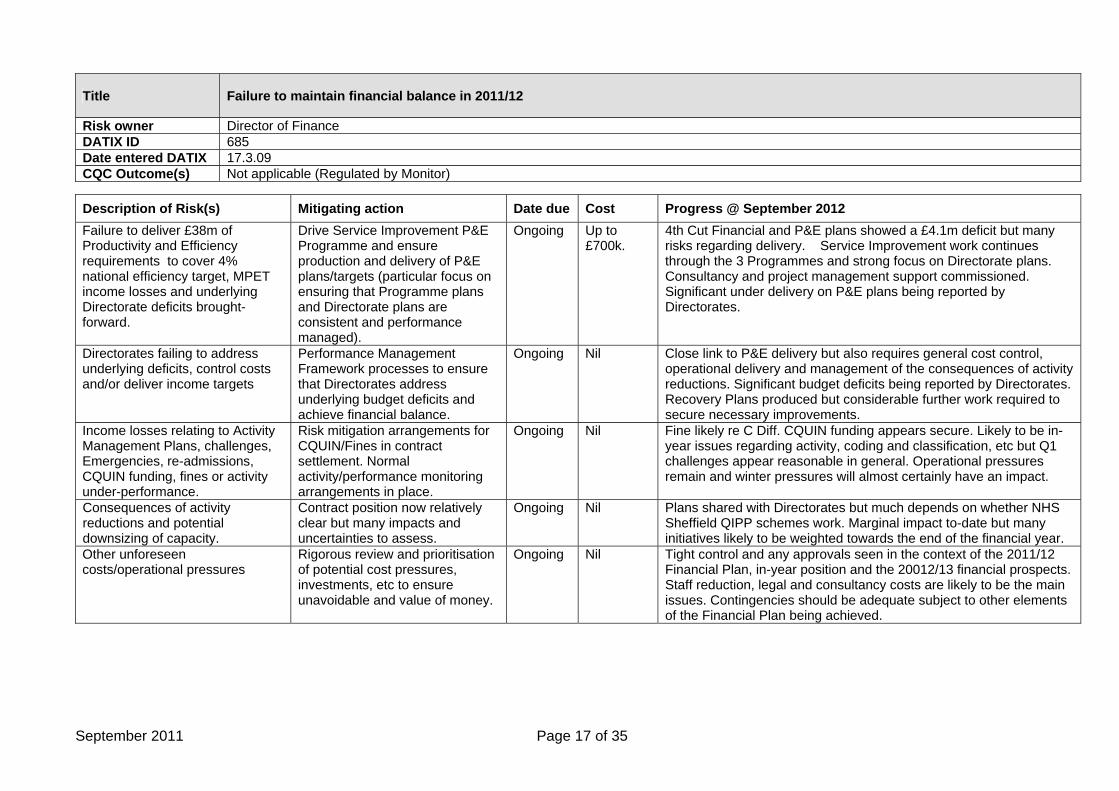
Title Failure to maintain financial balance in 2011/12
Risk owner Director of Finance DATIX ID 685 Date entered DATIX 17.3.09 CQC Outcome(s) Not applicable (Regulated by Monitor)
Description of Risk(s) Mitigating action Date due Cost Progress @ September 2012 Failure to deliver £38m of Productivity and Efficiency requirements to cover 4% national efficiency target, MPET income losses and underlying Directorate deficits brought-forward.
Drive Service Improvement P&E Programme and ensure production and delivery of P&E plans/targets (particular focus on ensuring that Programme plans and Directorate plans are consistent and performance managed).
Ongoing Up to £700k.
4th Cut Financial and P&E plans showed a £4.1m deficit but many risks regarding delivery. Service Improvement work continues through the 3 Programmes and strong focus on Directorate plans. Consultancy and project management support commissioned. Significant under delivery on P&E plans being reported by Directorates.
Directorates failing to address underlying deficits, control costs and/or deliver income targets
Performance Management Framework processes to ensure that Directorates address underlying budget deficits and achieve financial balance.
Ongoing Nil Close link to P&E delivery but also requires general cost control, operational delivery and management of the consequences of activity reductions. Significant budget deficits being reported by Directorates. Recovery Plans produced but considerable further work required to secure necessary improvements.
Income losses relating to Activity Management Plans, challenges, Emergencies, re-admissions, CQUIN funding, fines or activity under-performance.
Risk mitigation arrangements for CQUIN/Fines in contract settlement. Normal activity/performance monitoring arrangements in place.
Ongoing Nil Fine likely re C Diff. CQUIN funding appears secure. Likely to be in-year issues regarding activity, coding and classification, etc but Q1 challenges appear reasonable in general. Operational pressures remain and winter pressures will almost certainly have an impact.
Consequences of activity reductions and potential downsizing of capacity.
Contract position now relatively clear but many impacts and uncertainties to assess.
Ongoing Nil Plans shared with Directorates but much depends on whether NHS Sheffield QIPP schemes work. Marginal impact to-date but many initiatives likely to be weighted towards the end of the financial year.
Other unforeseen costs/operational pressures
Rigorous review and prioritisation of potential cost pressures, investments, etc to ensure unavoidable and value of money.
Ongoing Nil Tight control and any approvals seen in the context of the 2011/12 Financial Plan, in-year position and the 20012/13 financial prospects. Staff reduction, legal and consultancy costs are likely to be the main issues. Contingencies should be adequate subject to other elements of the Financial Plan being achieved.
September 2011 Page 17 of 35
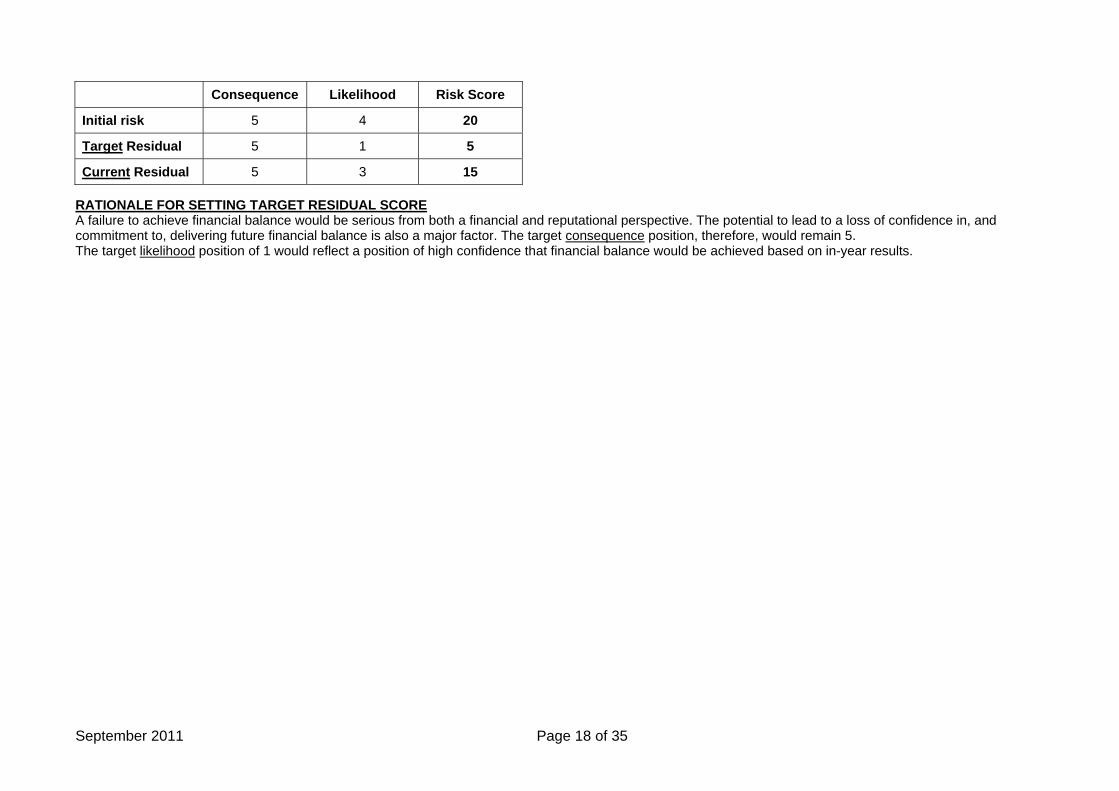
Consequence Likelihood Risk Score
Initial risk 5 4 20
Target Residual 5 1 5
Current Residual 5 3 15 RATIONALE FOR SETTING TARGET RESIDUAL SCORE A failure to achieve financial balance would be serious from both a financial and reputational perspective. The potential to lead to a loss of confidence in, and commitment to, delivering future financial balance is also a major factor. The target consequence position, therefore, would remain 5. The target likelihood position of 1 would reflect a position of high confidence that financial balance would be achieved based on in-year results.
September 2011 Page 18 of 35
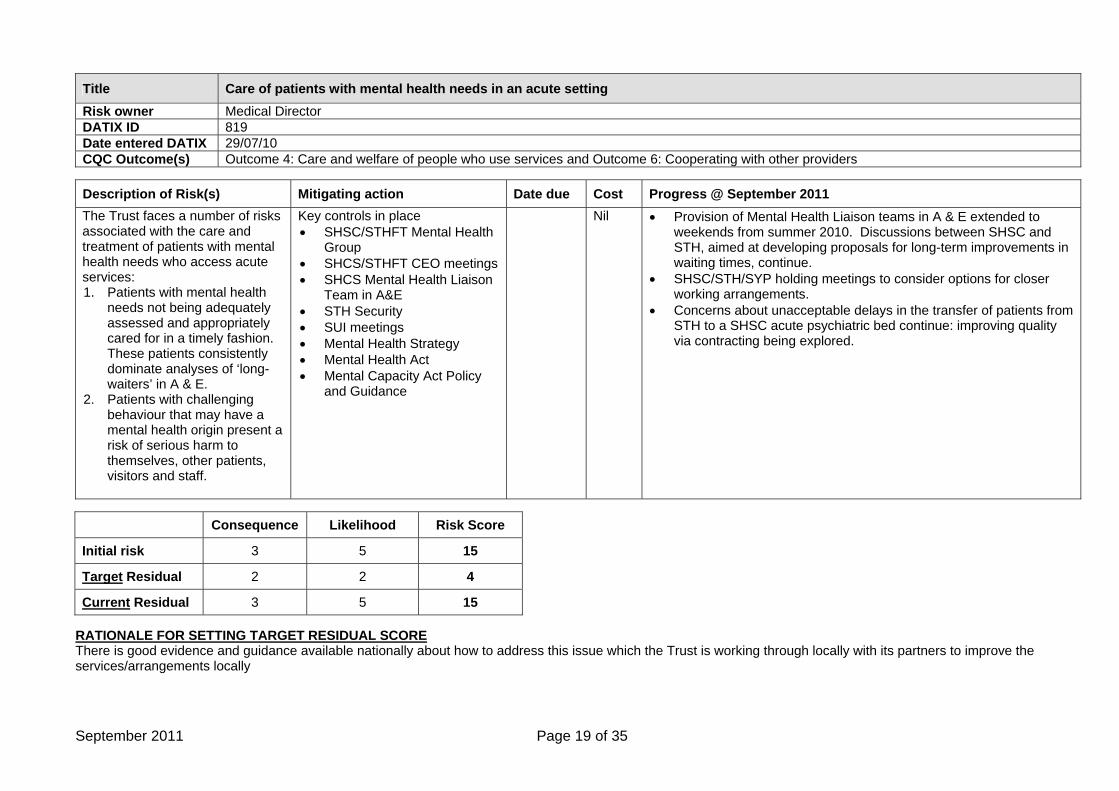
Title Care of patients with mental health needs in an acute setting Risk owner Medical Director DATIX ID 819 Date entered DATIX 29/07/10 CQC Outcome(s) Outcome 4: Care and welfare of people who use services and Outcome 6: Cooperating with other providers
Description of Risk(s) Mitigating action Date due Cost Progress @ September 2011 The Trust faces a number of risks associated with the care and treatment of patients with mental health needs who access acute services: 1. Patients with mental health
needs not being adequately assessed and appropriately cared for in a timely fashion. These patients consistently dominate analyses of ‘long-waiters’ in A & E.
2. Patients with challenging behaviour that may have a mental health origin present a risk of serious harm to themselves, other patients, visitors and staff.
Key controls in place • SHSC/STHFT Mental Health
Group • SHCS/STHFT CEO meetings • SHCS Mental Health Liaison
Team in A&E • STH Security • SUI meetings • Mental Health Strategy • Mental Health Act • Mental Capacity Act Policy
and Guidance
Nil • Provision of Mental Health Liaison teams in A & E extended to weekends from summer 2010. Discussions between SHSC and STH, aimed at developing proposals for long-term improvements in waiting times, continue.
• SHSC/STH/SYP holding meetings to consider options for closer working arrangements.
• Concerns about unacceptable delays in the transfer of patients from STH to a SHSC acute psychiatric bed continue: improving quality via contracting being explored.
Consequence Likelihood Risk Score
Initial risk 3 5 15
Target Residual 2 2 4
Current Residual 3 5 15 RATIONALE FOR SETTING TARGET RESIDUAL SCORE There is good evidence and guidance available nationally about how to address this issue which the Trust is working through locally with its partners to improve the services/arrangements locally
September 2011 Page 19 of 35
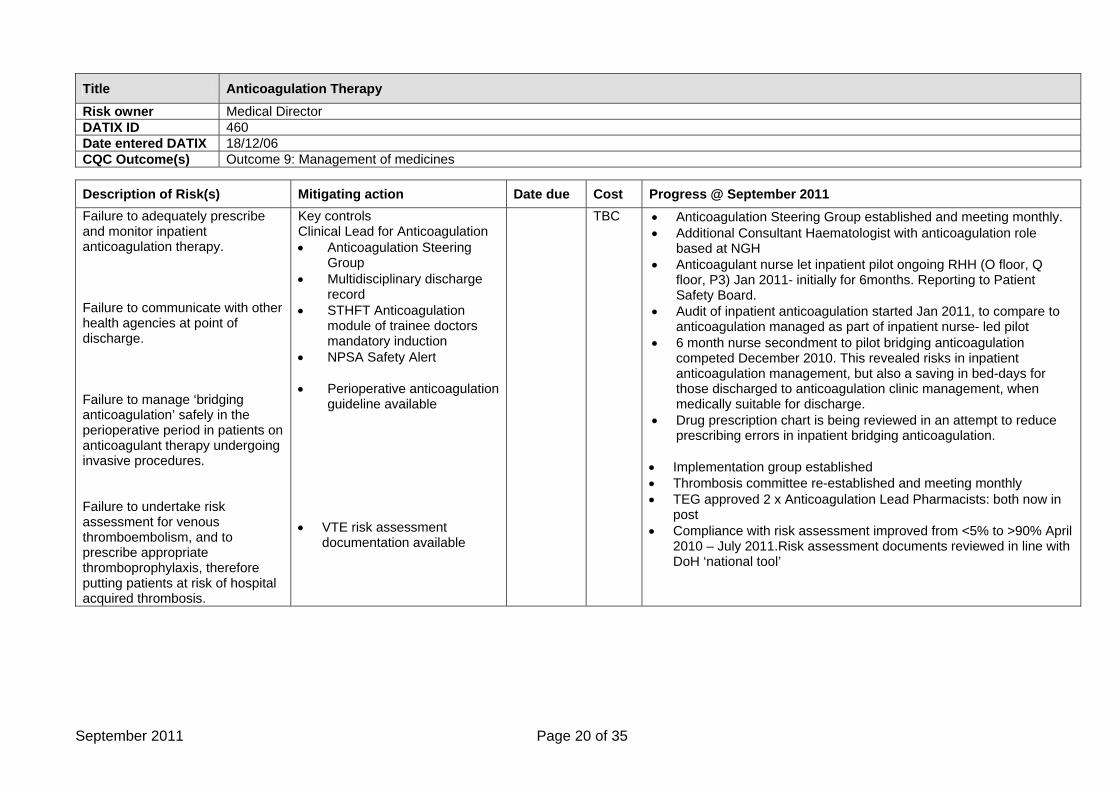
Title Anticoagulation Therapy Risk owner Medical Director DATIX ID 460 Date entered DATIX 18/12/06 CQC Outcome(s) Outcome 9: Management of medicines
Description of Risk(s) Mitigating action Date due Cost Progress @ September 2011 Failure to adequately prescribe and monitor inpatient anticoagulation therapy. Failure to communicate with other health agencies at point of discharge. Failure to manage ‘bridging anticoagulation’ safely in the perioperative period in patients on anticoagulant therapy undergoing invasive procedures. Failure to undertake risk assessment for venous thromboembolism, and to prescribe appropriate thromboprophylaxis, therefore putting patients at risk of hospital acquired thrombosis.
Key controls Clinical Lead for Anticoagulation • Anticoagulation Steering
Group • Multidisciplinary discharge
record • STHFT Anticoagulation
module of trainee doctors mandatory induction
• NPSA Safety Alert • Perioperative anticoagulation
guideline available • VTE risk assessment
documentation available
TBC
• Anticoagulation Steering Group established and meeting monthly. • Additional Consultant Haematologist with anticoagulation role
based at NGH • Anticoagulant nurse let inpatient pilot ongoing RHH (O floor, Q
floor, P3) Jan 2011- initially for 6months. Reporting to Patient Safety Board.
• Audit of inpatient anticoagulation started Jan 2011, to compare to anticoagulation managed as part of inpatient nurse- led pilot
• 6 month nurse secondment to pilot bridging anticoagulation competed December 2010. This revealed risks in inpatient anticoagulation management, but also a saving in bed-days for those discharged to anticoagulation clinic management, when medically suitable for discharge.
• Drug prescription chart is being reviewed in an attempt to reduce prescribing errors in inpatient bridging anticoagulation.
• Implementation group established • Thrombosis committee re-established and meeting monthly • TEG approved 2 x Anticoagulation Lead Pharmacists: both now in
post • Compliance with risk assessment improved from <5% to >90% April
2010 – July 2011.Risk assessment documents reviewed in line with DoH ‘national tool’
September 2011 Page 20 of 35
Description of Risk(s) Mitigating action Date due Cost Progress @ September 2011 Action
• Anticoagulation Pharmacists in Assessment Units
• Participation in Patient Safety First Campaign
Aug 2010 ongoing
£100k TBC
• Patient Safety First Campaign – Anticoagulation workstream
underway
Consequence Likelihood Risk Score
Initial risk 5 3 15
Target Residual 5 1 5
Current Residual 5 3 15 RATIONALE FOR SETTING TARGET RESIDUAL SCORE The prescription and monitoring of anticoagulation is recognised as a high risk process in all healthcare systems. It is anticipated that current developments at STH will significantly reduce this risk, and audit systems are being established to track the success of ongoing initiatives.
September 2011 Page 21 of 35
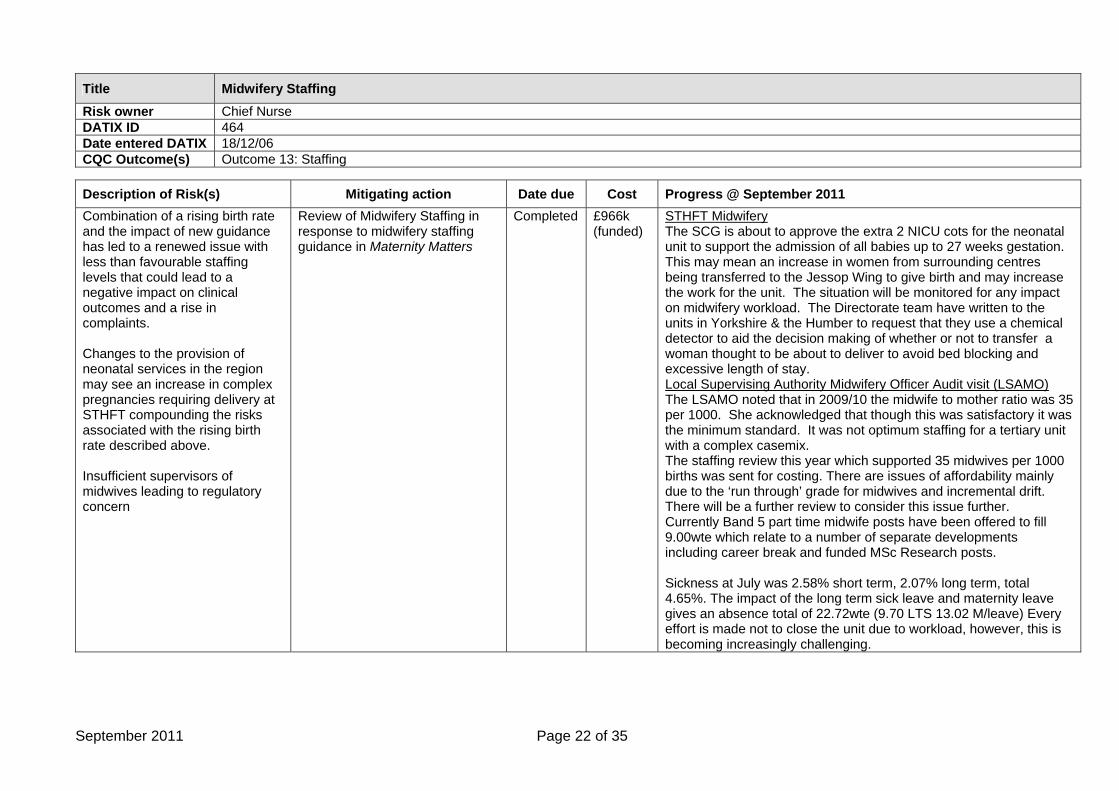
Title Midwifery Staffing Risk owner Chief Nurse DATIX ID 464 Date entered DATIX 18/12/06 CQC Outcome(s) Outcome 13: Staffing
Description of Risk(s) Mitigating action Date due Cost Progress @ September 2011 Combination of a rising birth rate and the impact of new guidance has led to a renewed issue with less than favourable staffing levels that could lead to a negative impact on clinical outcomes and a rise in complaints. Changes to the provision of neonatal services in the region may see an increase in complex pregnancies requiring delivery at STHFT compounding the risks associated with the rising birth rate described above. Insufficient supervisors of midwives leading to regulatory concern
Review of Midwifery Staffing in response to midwifery staffing guidance in Maternity Matters
Completed £966k (funded)
STHFT Midwifery The SCG is about to approve the extra 2 NICU cots for the neonatal unit to support the admission of all babies up to 27 weeks gestation. This may mean an increase in women from surrounding centres being transferred to the Jessop Wing to give birth and may increase the work for the unit. The situation will be monitored for any impact on midwifery workload. The Directorate team have written to the units in Yorkshire & the Humber to request that they use a chemical detector to aid the decision making of whether or not to transfer a woman thought to be about to deliver to avoid bed blocking and excessive length of stay. Local Supervising Authority Midwifery Officer Audit visit (LSAMO) The LSAMO noted that in 2009/10 the midwife to mother ratio was 35 per 1000. She acknowledged that though this was satisfactory it was the minimum standard. It was not optimum staffing for a tertiary unit with a complex casemix. The staffing review this year which supported 35 midwives per 1000 births was sent for costing. There are issues of affordability mainly due to the ‘run through’ grade for midwives and incremental drift. There will be a further review to consider this issue further. Currently Band 5 part time midwife posts have been offered to fill 9.00wte which relate to a number of separate developments including career break and funded MSc Research posts. Sickness at July was 2.58% short term, 2.07% long term, total 4.65%. The impact of the long term sick leave and maternity leave gives an absence total of 22.72wte (9.70 LTS 13.02 M/leave) Every effort is made not to close the unit due to workload, however, this is becoming increasingly challenging.
September 2011 Page 22 of 35
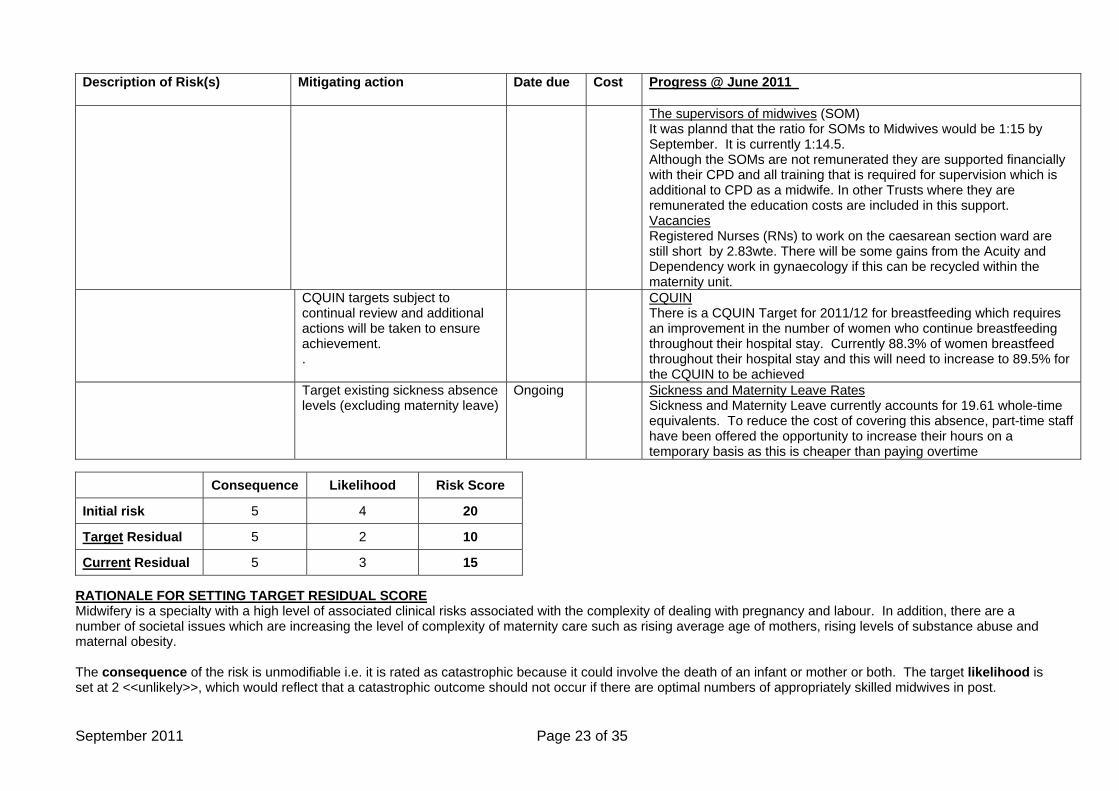
Description of Risk(s) Mitigating action Date due Cost Progress @ June 2011
The supervisors of midwives (SOM) It was plannd that the ratio for SOMs to Midwives would be 1:15 by September. It is currently 1:14.5. Although the SOMs are not remunerated they are supported financially with their CPD and all training that is required for supervision which is additional to CPD as a midwife. In other Trusts where they are remunerated the education costs are included in this support. Vacancies Registered Nurses (RNs) to work on the caesarean section ward are still short by 2.83wte. There will be some gains from the Acuity and Dependency work in gynaecology if this can be recycled within the maternity unit.
CQUIN targets subject to continual review and additional actions will be taken to ensure achievement. .
CQUIN There is a CQUIN Target for 2011/12 for breastfeeding which requires an improvement in the number of women who continue breastfeeding throughout their hospital stay. Currently 88.3% of women breastfeed throughout their hospital stay and this will need to increase to 89.5% for the CQUIN to be achieved
Target existing sickness absence levels (excluding maternity leave)
Ongoing Sickness and Maternity Leave Rates Sickness and Maternity Leave currently accounts for 19.61 whole-time equivalents. To reduce the cost of covering this absence, part-time staff have been offered the opportunity to increase their hours on a temporary basis as this is cheaper than paying overtime
Consequence Likelihood Risk Score
Initial risk 5 4 20
Target Residual 5 2 10
Current Residual 5 3 15 RATIONALE FOR SETTING TARGET RESIDUAL SCORE Midwifery is a specialty with a high level of associated clinical risks associated with the complexity of dealing with pregnancy and labour. In addition, there are a number of societal issues which are increasing the level of complexity of maternity care such as rising average age of mothers, rising levels of substance abuse and maternal obesity. The consequence of the risk is unmodifiable i.e. it is rated as catastrophic because it could involve the death of an infant or mother or both. The target likelihood is set at 2 <<unlikely>>, which would reflect that a catastrophic outcome should not occur if there are optimal numbers of appropriately skilled midwives in post.
September 2011 Page 23 of 35
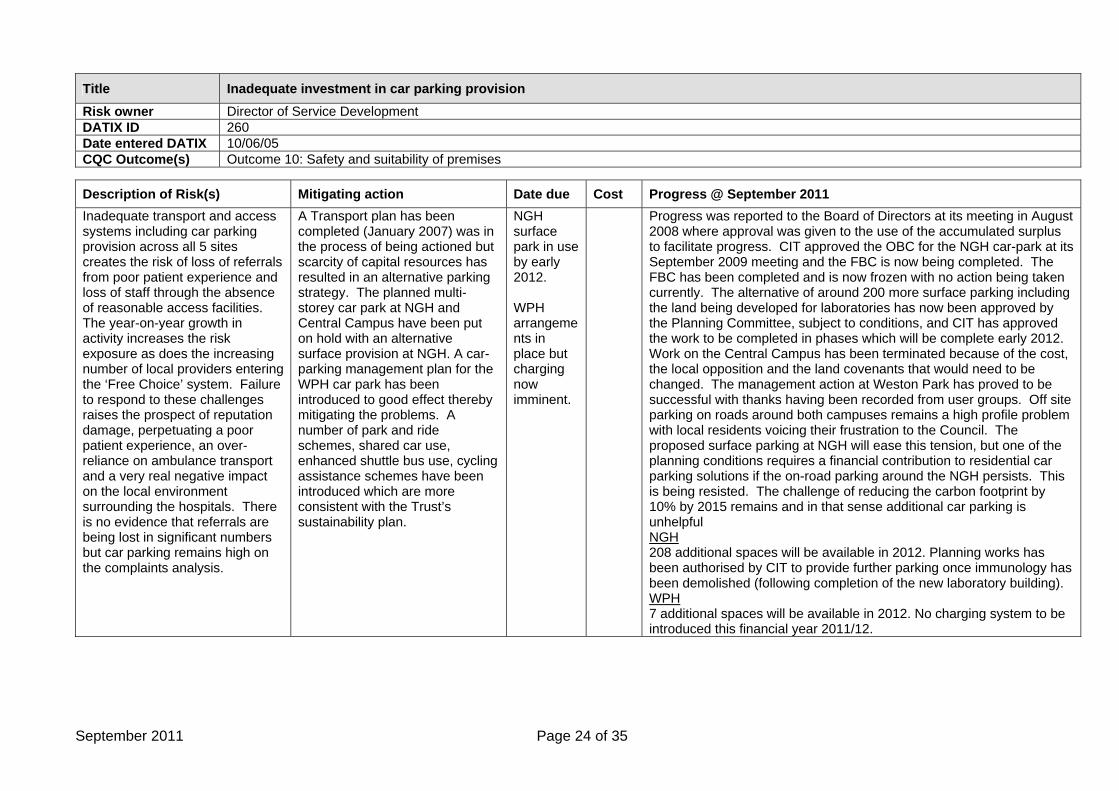
Title Inadequate investment in car parking provision Risk owner Director of Service Development DATIX ID 260 Date entered DATIX 10/06/05 CQC Outcome(s) Outcome 10: Safety and suitability of premises
Description of Risk(s) Mitigating action Date due Cost Progress @ September 2011 Inadequate transport and access systems including car parking provision across all 5 sites creates the risk of loss of referrals from poor patient experience and loss of staff through the absence of reasonable access facilities. The year-on-year growth in activity increases the risk exposure as does the increasing number of local providers entering the ‘Free Choice’ system. Failure to respond to these challenges raises the prospect of reputation damage, perpetuating a poor patient experience, an over-reliance on ambulance transport and a very real negative impact on the local environment surrounding the hospitals. There is no evidence that referrals are being lost in significant numbers but car parking remains high on the complaints analysis.
A Transport plan has been completed (January 2007) was in the process of being actioned but scarcity of capital resources has resulted in an alternative parking strategy. The planned multi-storey car park at NGH and Central Campus have been put on hold with an alternative surface provision at NGH. A car-parking management plan for the WPH car park has been introduced to good effect thereby mitigating the problems. A number of park and ride schemes, shared car use, enhanced shuttle bus use, cycling assistance schemes have been introduced which are more consistent with the Trust’s sustainability plan.
NGH surface park in use by early 2012. WPH arrangements in place but charging now imminent.
Progress was reported to the Board of Directors at its meeting in August 2008 where approval was given to the use of the accumulated surplus to facilitate progress. CIT approved the OBC for the NGH car-park at its September 2009 meeting and the FBC is now being completed. The FBC has been completed and is now frozen with no action being taken currently. The alternative of around 200 more surface parking including the land being developed for laboratories has now been approved by the Planning Committee, subject to conditions, and CIT has approved the work to be completed in phases which will be complete early 2012. Work on the Central Campus has been terminated because of the cost, the local opposition and the land covenants that would need to be changed. The management action at Weston Park has proved to be successful with thanks having been recorded from user groups. Off site parking on roads around both campuses remains a high profile problem with local residents voicing their frustration to the Council. The proposed surface parking at NGH will ease this tension, but one of the planning conditions requires a financial contribution to residential car parking solutions if the on-road parking around the NGH persists. This is being resisted. The challenge of reducing the carbon footprint by 10% by 2015 remains and in that sense additional car parking is unhelpful NGH 208 additional spaces will be available in 2012. Planning works has been authorised by CIT to provide further parking once immunology has been demolished (following completion of the new laboratory building). WPH 7 additional spaces will be available in 2012. No charging system to be introduced this financial year 2011/12.
September 2011 Page 24 of 35
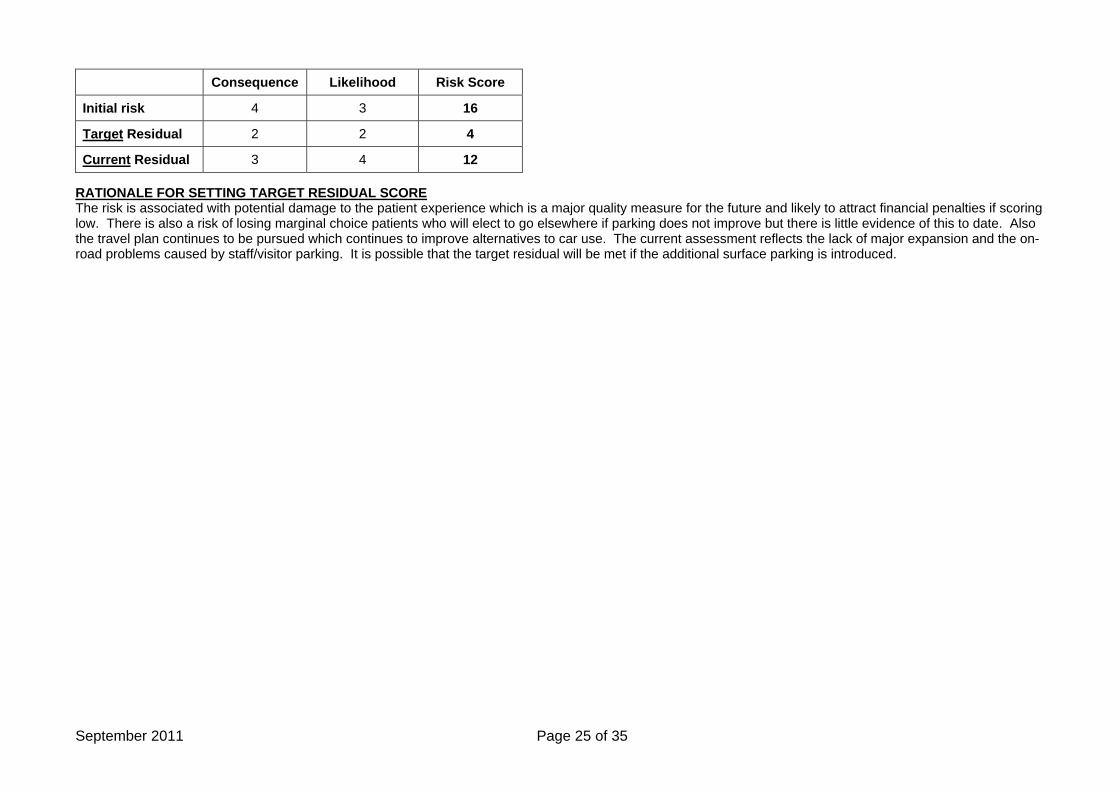
Consequence Likelihood Risk Score
Initial risk 4 3 16
Target Residual 2 2 4
Current Residual 3 4 12 RATIONALE FOR SETTING TARGET RESIDUAL SCORE The risk is associated with potential damage to the patient experience which is a major quality measure for the future and likely to attract financial penalties if scoring low. There is also a risk of losing marginal choice patients who will elect to go elsewhere if parking does not improve but there is little evidence of this to date. Also the travel plan continues to be pursued which continues to improve alternatives to car use. The current assessment reflects the lack of major expansion and the on-road problems caused by staff/visitor parking. It is possible that the target residual will be met if the additional surface parking is introduced.
September 2011 Page 25 of 35
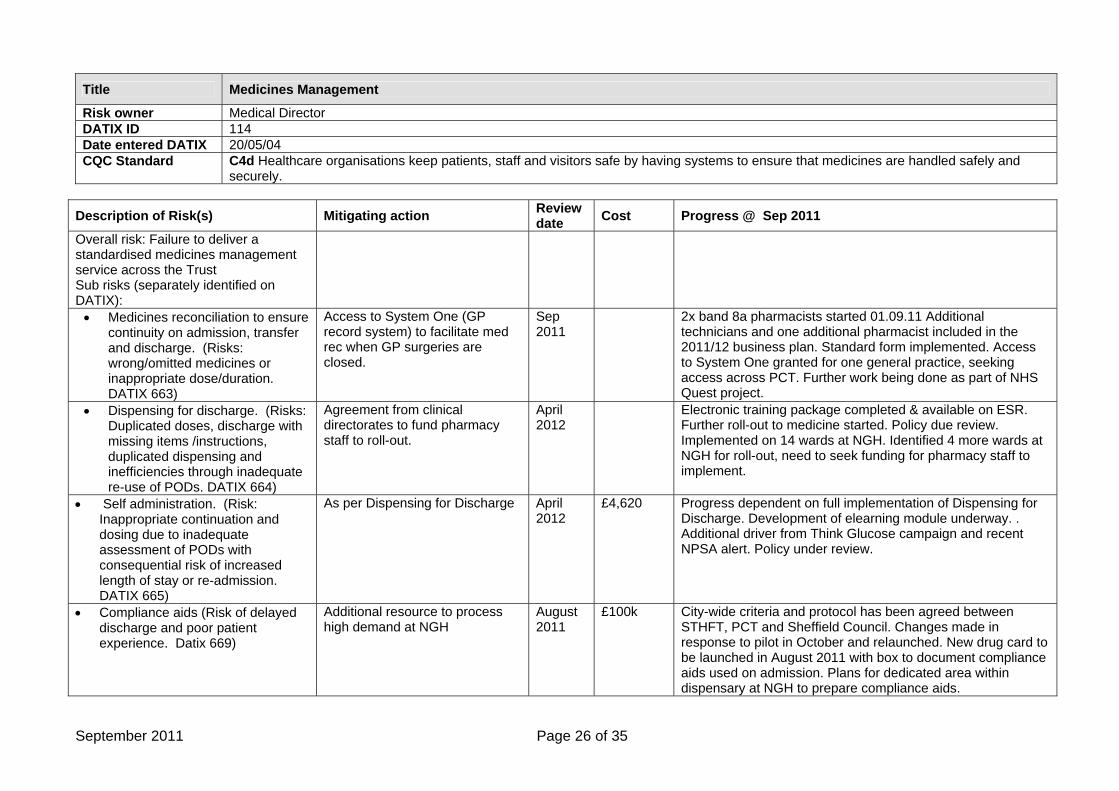
Title Medicines Management
Risk owner Medical Director DATIX ID 114 Date entered DATIX 20/05/04 CQC Standard C4d Healthcare organisations keep patients, staff and visitors safe by having systems to ensure that medicines are handled safely and
securely.
Description of Risk(s) Mitigating action Review date Cost Progress @ Sep 2011
Overall risk: Failure to deliver a standardised medicines management service across the Trust Sub risks (separately identified on DATIX):
• Medicines reconciliation to ensure continuity on admission, transfer and discharge. (Risks: wrong/omitted medicines or inappropriate dose/duration. DATIX 663)
Access to System One (GP record system) to facilitate med rec when GP surgeries are closed.
Sep 2011
2x band 8a pharmacists started 01.09.11 Additional technicians and one additional pharmacist included in the 2011/12 business plan. Standard form implemented. Access to System One granted for one general practice, seeking access across PCT. Further work being done as part of NHS Quest project.
• Dispensing for discharge. (Risks: Duplicated doses, discharge with missing items /instructions, duplicated dispensing and inefficiencies through inadequate re-use of PODs. DATIX 664)
Agreement from clinical directorates to fund pharmacy staff to roll-out.
April 2012
Electronic training package completed & available on ESR. Further roll-out to medicine started. Policy due review. Implemented on 14 wards at NGH. Identified 4 more wards at NGH for roll-out, need to seek funding for pharmacy staff to implement.
• Self administration. (Risk: Inappropriate continuation and dosing due to inadequate assessment of PODs with consequential risk of increased length of stay or re-admission. DATIX 665)
As per Dispensing for Discharge April 2012
£4,620 Progress dependent on full implementation of Dispensing for Discharge. Development of elearning module underway. . Additional driver from Think Glucose campaign and recent NPSA alert. Policy under review.
• Compliance aids (Risk of delayed discharge and poor patient experience. Datix 669)
Additional resource to process high demand at NGH
August 2011
£100k
City-wide criteria and protocol has been agreed between STHFT, PCT and Sheffield Council. Changes made in response to pilot in October and relaunched. New drug card to be launched in August 2011 with box to document compliance aids used on admission. Plans for dedicated area within dispensary at NGH to prepare compliance aids.
September 2011 Page 26 of 35
Description of Risk(s) Mitigating action Review
date Cost Progress @ Sep 2011
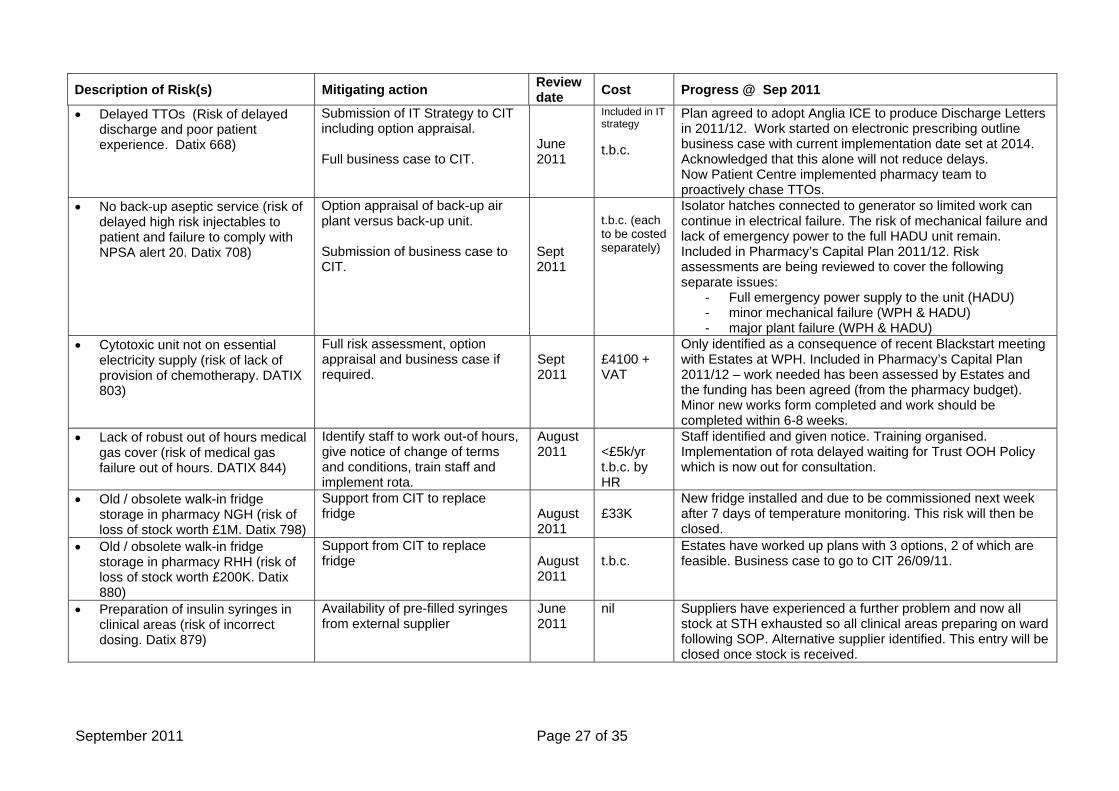
• Delayed TTOs (Risk of delayed discharge and poor patient experience. Datix 668)
Submission of IT Strategy to CIT including option appraisal. Full business case to CIT.
June 2011
Included in IT strategy t.b.c.
Plan agreed to adopt Anglia ICE to produce Discharge Letters in 2011/12. Work started on electronic prescribing outline business case with current implementation date set at 2014. Acknowledged that this alone will not reduce delays. Now Patient Centre implemented pharmacy team to proactively chase TTOs.
• No back-up aseptic service (risk of delayed high risk injectables to patient and failure to comply with NPSA alert 20. Datix 708)
Option appraisal of back-up air plant versus back-up unit. Submission of business case to CIT.
Sept 2011
t.b.c. (each to be costed separately)
Isolator hatches connected to generator so limited work can continue in electrical failure. The risk of mechanical failure and lack of emergency power to the full HADU unit remain. Included in Pharmacy’s Capital Plan 2011/12. Risk assessments are being reviewed to cover the following separate issues:
- Full emergency power supply to the unit (HADU) - minor mechanical failure (WPH & HADU) - major plant failure (WPH & HADU)
• Cytotoxic unit not on essential electricity supply (risk of lack of provision of chemotherapy. DATIX 803)
Full risk assessment, option appraisal and business case if required.
Sept 2011
£4100 + VAT
Only identified as a consequence of recent Blackstart meeting with Estates at WPH. Included in Pharmacy’s Capital Plan 2011/12 – work needed has been assessed by Estates and the funding has been agreed (from the pharmacy budget). Minor new works form completed and work should be completed within 6-8 weeks.
• Lack of robust out of hours medical gas cover (risk of medical gas failure out of hours. DATIX 844)
Identify staff to work out-of hours, give notice of change of terms and conditions, train staff and implement rota.
August 2011
<£5k/yr t.b.c. by HR
Staff identified and given notice. Training organised. Implementation of rota delayed waiting for Trust OOH Policy which is now out for consultation.
• Old / obsolete walk-in fridge storage in pharmacy NGH (risk of loss of stock worth £1M. Datix 798)
Support from CIT to replace fridge
August 2011
£33K
New fridge installed and due to be commissioned next week after 7 days of temperature monitoring. This risk will then be closed.
• Old / obsolete walk-in fridge storage in pharmacy RHH (risk of loss of stock worth £200K. Datix 880)
Support from CIT to replace fridge
August 2011
t.b.c.
Estates have worked up plans with 3 options, 2 of which are feasible. Business case to go to CIT 26/09/11.
• Preparation of insulin syringes in clinical areas (risk of incorrect dosing. Datix 879)
Availability of pre-filled syringes from external supplier
June 2011
nil Suppliers have experienced a further problem and now all stock at STH exhausted so all clinical areas preparing on ward following SOP. Alternative supplier identified. This entry will be closed once stock is received.
September 2011 Page 27 of 35
Description of Risk(s) Mitigating action Review
date Cost Progress @ Sep 2011
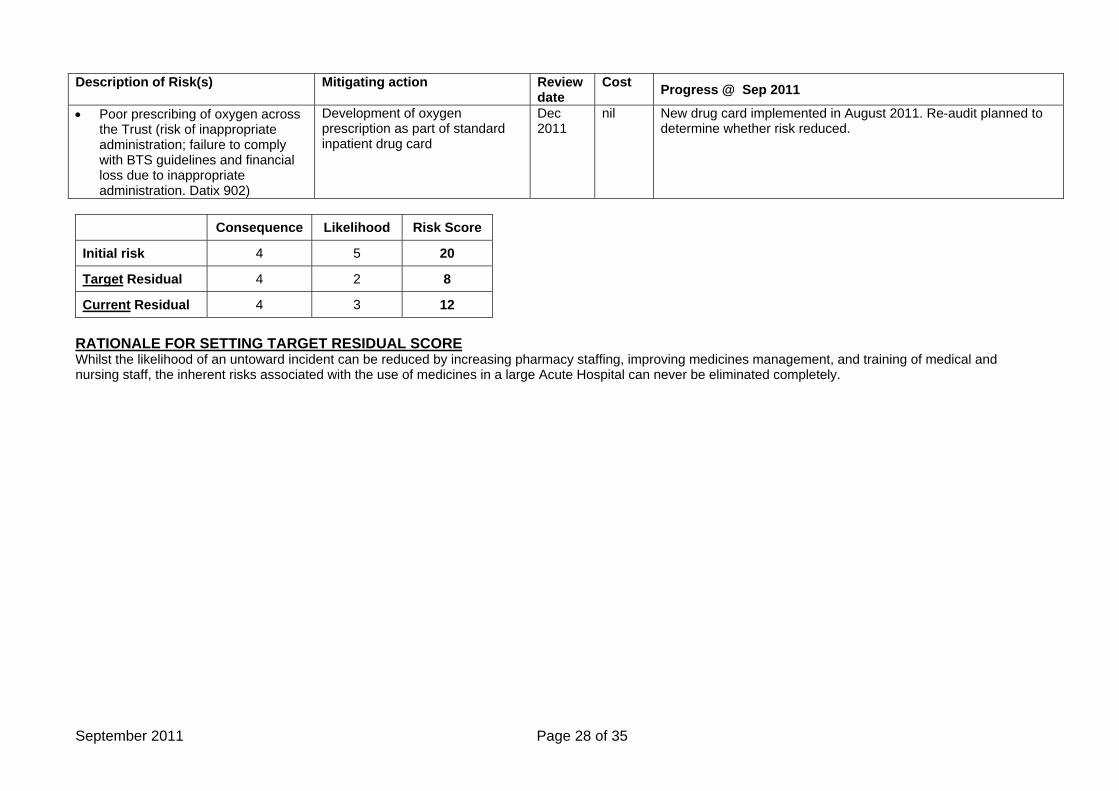
• Poor prescribing of oxygen across the Trust (risk of inappropriate administration; failure to comply with BTS guidelines and financial loss due to inappropriate administration. Datix 902)
Development of oxygen prescription as part of standard inpatient drug card
Dec 2011
nil New drug card implemented in August 2011. Re-audit planned to determine whether risk reduced.
Consequence Likelihood Risk Score
Initial risk 4 5 20
Target Residual 4 2 8
Current Residual 4 3 12 RATIONALE FOR SETTING TARGET RESIDUAL SCORE Whilst the likelihood of an untoward incident can be reduced by increasing pharmacy staffing, improving medicines management, and training of medical and nursing staff, the inherent risks associated with the use of medicines in a large Acute Hospital can never be eliminated completely.
September 2011 Page 28 of 35
Title Excessive Medical Outliers
Risk owner Medical Director DATIX ID 67 Date entered DATIX Re-entered 17/02/10 CQC Outcome(s) Outcome 4: Care and welfare of people who use services
Description of Risk(s) Mitigating action Date due Cost Progress @ September 2011 Clinical risk – compromised
quality of care and safety for outlying patients
Poorer outcome and quality of patient experience
Increased length of stay and consequent impact on costs
Impact on activity and targets from cancellation of elective admissions
For excessive medical outliers: bed management cohorting outliers on wards ward based working when
necessary increased weekend
Consultant discharge rounds in all medical specialties
commencing 12th April 2010, outlying medical patients will be cared for by subspecialty team appropriate to their presenting complaint.
active monitoring by Medical Director and Chief Operating Officer
NA
NA NA
The number of medical outliers has again fallen over the last two months, averaging 28. Delayed transfers of care remain a significant problem, and remain up to 60-100/week, although initiatives to address this issue continue across the Trust and in liaison with appropriate external agencies. The third MAU and appointment of Acute Physicians were delivered as planned in December 2009. Indications are that new triage arrangements are successfully allocating patients to the most appropriate specialty early in their admission. The surgical assessment unit opened at the NGH campus in October 2010. An escalation plan for the management of medical outliers has been agreed with Medical Specialties, and requires that ward-based working replaces ‘keep your own patients’ when outlier numbers exceed 50 for three consecutive days, or when there is a sudden and unexpected increase in outliers on a single day. The Stroke pathway is now embedded at the central campus, and audit data continue to demonstrate that 90% of stroke patients spend >90% of their admission in dedicated stroke facilities. To mitigate against the impact of Norovirus, a Norovirus escalation policy has been agreed, and entails the establishment of a dedicated cohorting ward on Robert Hadfield 2 when a threshold number of Norovirus cases is reached. The norovirus policy and the flu policy are currently being reviewed as part of winter planning. The ‘Hospital at Night’ programme was extended to the Northern General Campus as planned in August 2011. Data on the impact of this initiative on the triaging of patients, targeting of appropriately-trained staff to sick patients, and efficiency of patient management will be available via audit data over the coming months. Plans are being made to extend this initiative to weekend hours, though a target introduction date has not yet been agreed.
September 2011 Page 29 of 35
Consequence Likelihood Risk Score
Initial risk 4 4 16
Target Residual 4 2 8
Current Residual 4 3 12 RATIONALE FOR SETTING TARGET RESIDUAL SCORE It is never possible to guarantee that no medical patients will need to outlie to non-medical wards. Some risk will therefore always remain, even if outlying of medical patients occurs only rarely
September 2011 Page 30 of 35
Title Asbestos Management Risk owner Estates Director DATIX ID 736 Date entered DATIX 27 August 2009 CQC Outcome(s) Outcome 10: Safety and suitability of premises
Description of Risk(s) Mitigating action Date due Cost Progress @ September 2011 • Lack of funding to be able to
Decontaminate/remove identified sources of Asbestos Containing Materials (ACM’s) from the Estate at various locations.
• Assigned funding may not be used due to restrictions on spending of monies identified as capital on cleaning up existing infrastructure of Estate.
• Areas of the Estate cannot be used to their full potential because of the certain exposure to ACM’s
• Essential plant is not being maintained inline with PPM strategy
• In the case of a need for emergency access to an area identified as containing ACM’s delays would be caused by the need to ensure appropriate safety precautions are in place
• Decontamination / Removal of ACM’s is done as part of a capital project following the relevant survey
• Areas are prioritised based on amount and type of asbestos and frequency of access required
• Permit to enter system in place with agreed use of PPE and RPE
Competent contractor appointed to identify and prioritise areas which need action
• Costing for removal of ACM’s obtained and provided to Healthcare Governance Department
2016 603K • Risk identified, assessed and entered onto Datix August 2009. • September 2009 Health and Safety Executive visit Trust and
examine management arrangements for asbestos. Trust faces possibility of Improvement notice if suitable and sufficient action plan not developed within short timescale.
• Action plan completed and submitted to HSE in time to prevent enforcement action; content of action plan agreed with Patient Healthcare Governance department.
• Top ten priorities identified; costing obtained for containment and abatement of asbestos containing materials and paper provided to Trust Executive Group November 2009.
• Decision made to centralise all asbestos records on MICAD system Asbestos consultancy commissioned to transfer and format the information.
• Paper provided to HCGC March 2010 with current issues and areas of concern identified.
• April 2010 funding provided for 2010/11 financial year to address priority areas of concern.
• 2010 funding used removing asbestos containing materials from top 2 priority areas identified in paper to March Healthcare Governance Committee.
• Asbestos Surveys continue on properties which Sheffield Teaching Hospitals NHS Foundation Trust have identified as Duty Holder. Priority established using Risk Management Principles and HSG 264
• Asbestos Consultancy out to tender. Returns mid-June 2010 • The asbestos contract has been awarded to the Broadland Group
Ltd following the success tender process. Broadland Group is a local company from Chesterfield and has been awarded the contract with effect from November 1st 2010. The contract will run for 5 years.
September 2011 Page 31 of 35
Description of Risk(s) Mitigating action Date due Cost Progress @ September 2011
• Priority areas for asbestos abatement work have been identified and prioritised for the 2011/12 financial year and subject to funding being made available again will be progressed.
• These and other high risk areas will be re-inspected during the 2011/12 year, proactive air monitoring will be taken and the effectiveness of the current control measures assessed.
• MiCAD Lite and the Trust Intranet Property Register have been updated to reflect the current information held by the Trust relating to asbestos management. The Asbestos Register and Asbestos Management plan will continue to be updated on an ongoing basis.
• Situation continues to be monitored areas known or suspected to contain ACM’s are assessed prior to access. All areas which are part of the essential maintenance program have a refurbishment and demolition asbestos survey prior to commencement of work.
• The introduction of HSG 264 as a replacement to MDHS 100 now requires that any area which is having an asbestos survey must be vacated prior to the work starting. This can cause delays and reduces timescales in the EMP if not effectively managed.
• Paper prepared for the HCGC March 2011 with current issues and areas of concern identified.
• Orders have been placed to have asbestos removed from a number of locations at the NC.
• Priority areas have been identified and funding secured for removal of asbestos a the CC.
• Areas of the NC not yet surveyed have been identified and a program of inspections identified.
Consequence Likelihood Risk Score
Initial risk 4 5 20
Target Residual 4 1 4
Current Residual 4 3 12 RATIONALE FOR SETTING TARGET RESIDUAL SCORE Progress has been made against the original assessment with the migration of information onto one database the continual assessment of areas of the Trust during capital schemes and planned asbestos surveys. The results of these surveys will be available to all staff and to contractors. Funding has been provided for the 2010/11 financial to address those areas of concern identified in TEG & HCGC reports. With the continuation of funding for the 2011/12 year and onwards there are no reasons to suspect that the target will not be reached within the projected six year asbestos management plan.
September 2011 Page 32 of 35
2011 Page 33 of 35
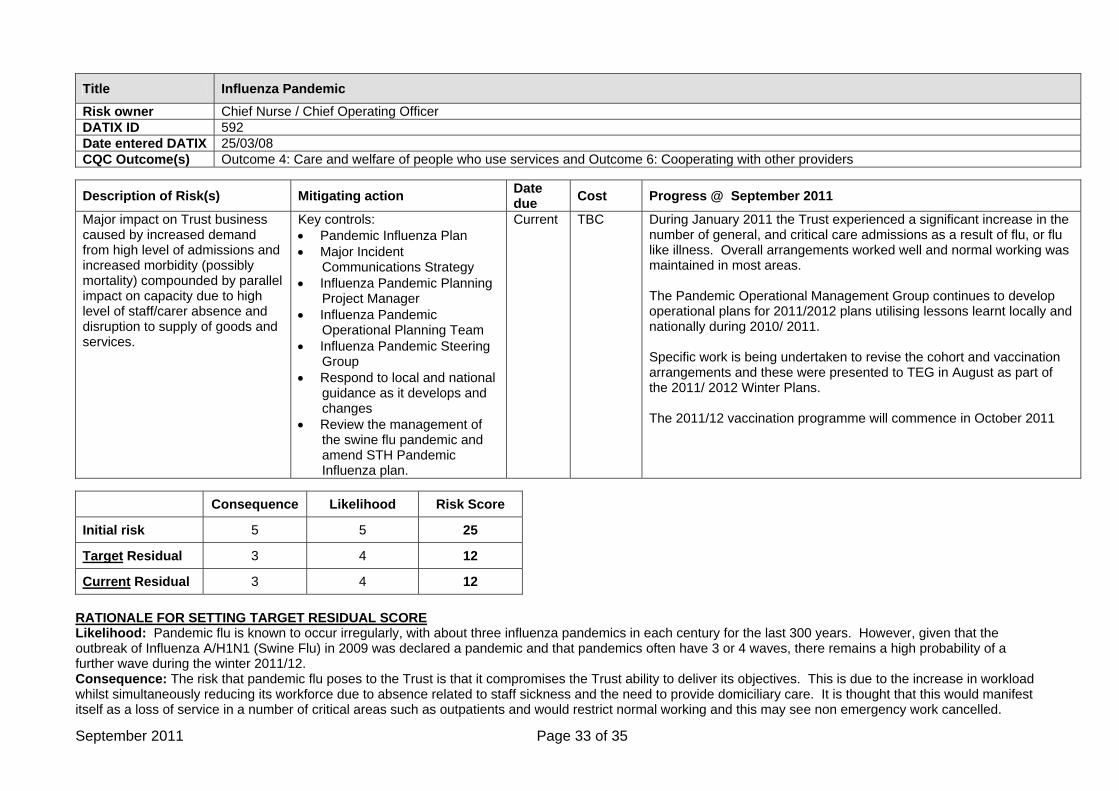
Title Influenza Pandemic Risk owner Chief Nurse / Chief Operating Officer DATIX ID 592 Date entered DATIX 25/03/08 CQC Outcome(s) Outcome 4: Care and welfare of people who use services and Outcome 6: Cooperating with other providers
Description of Risk(s) Mitigating action Date due Cost Progress @ September 2011
Major impact on Trust business caused by increased demand from high level of admissions and increased morbidity (possibly mortality) compounded by parallel impact on capacity due to high level of staff/carer absence and disruption to supply of goods and services.
Key controls: • Pandemic Influenza Plan • Major Incident
Communications Strategy • Influenza Pandemic Planning
Project Manager • Influenza Pandemic
Operational Planning Team • Influenza Pandemic Steering
Group • Respond to local and national
guidance as it develops and changes
• Review the management of the swine flu pandemic and amend STH Pandemic Influenza plan.
Current TBC During January 2011 the Trust experienced a significant increase in the number of general, and critical care admissions as a result of flu, or flu like illness. Overall arrangements worked well and normal working was maintained in most areas. The Pandemic Operational Management Group continues to develop operational plans for 2011/2012 plans utilising lessons learnt locally and nationally during 2010/ 2011. Specific work is being undertaken to revise the cohort and vaccination arrangements and these were presented to TEG in August as part of the 2011/ 2012 Winter Plans. The 2011/12 vaccination programme will commence in October 2011
Consequence Likelihood Risk Score
Initial risk 5 5 25
Target Residual 3 4 12
Current Residual 3 4 12 RATIONALE FOR SETTING TARGET RESIDUAL SCORE Likelihood: Pandemic flu is known to occur irregularly, with about three influenza pandemics in each century for the last 300 years. However, given that the outbreak of Influenza A/H1N1 (Swine Flu) in 2009 was declared a pandemic and that pandemics often have 3 or 4 waves, there remains a high probability of a further wave during the winter 2011/12. Consequence: The risk that pandemic flu poses to the Trust is that it compromises the Trust ability to deliver its objectives. This is due to the increase in workload whilst simultaneously reducing its workforce due to absence related to staff sickness and the need to provide domiciliary care. It is thought that this would manifest itself as a loss of service in a number of critical areas such as outpatients and would restrict normal working and this may see non emergency work cancelled.
September
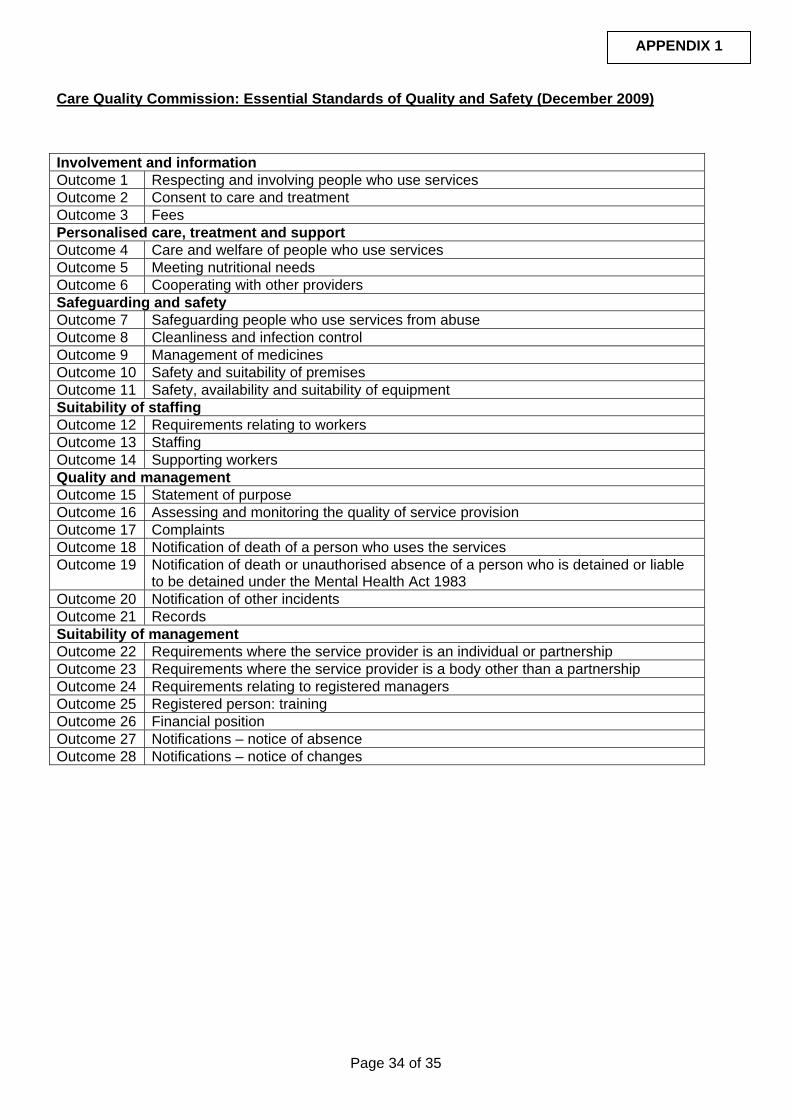
Care Quality Commission: Essential Standards of Quality and Safety (December 2009)
Involvement and information Outcome 1 Respecting and involving people who use services Outcome 2 Consent to care and treatment Outcome 3 Fees Personalised care, treatment and support Outcome 4 Care and welfare of people who use services Outcome 5 Meeting nutritional needs Outcome 6 Cooperating with other providers Safeguarding and safety Outcome 7 Safeguarding people who use services from abuse Outcome 8 Cleanliness and infection control Outcome 9 Management of medicines Outcome 10 Safety and suitability of premises Outcome 11 Safety, availability and suitability of equipment Suitability of staffing Outcome 12 Requirements relating to workers Outcome 13 Staffing Outcome 14 Supporting workers Quality and management Outcome 15 Statement of purpose Outcome 16 Assessing and monitoring the quality of service provision Outcome 17 Complaints Outcome 18 Notification of death of a person who uses the services Outcome 19 Notification of death or unauthorised absence of a person who is detained or liable
to be detained under the Mental Health Act 1983 Outcome 20 Notification of other incidents Outcome 21 Records Suitability of management Outcome 22 Requirements where the service provider is an individual or partnership Outcome 23 Requirements where the service provider is a body other than a partnership Outcome 24 Requirements relating to registered managers Outcome 25 Registered person: training Outcome 26 Financial position Outcome 27 Notifications – notice of absence Outcome 28 Notifications – notice of changes
APPENDIX 1
Page 34 of 35
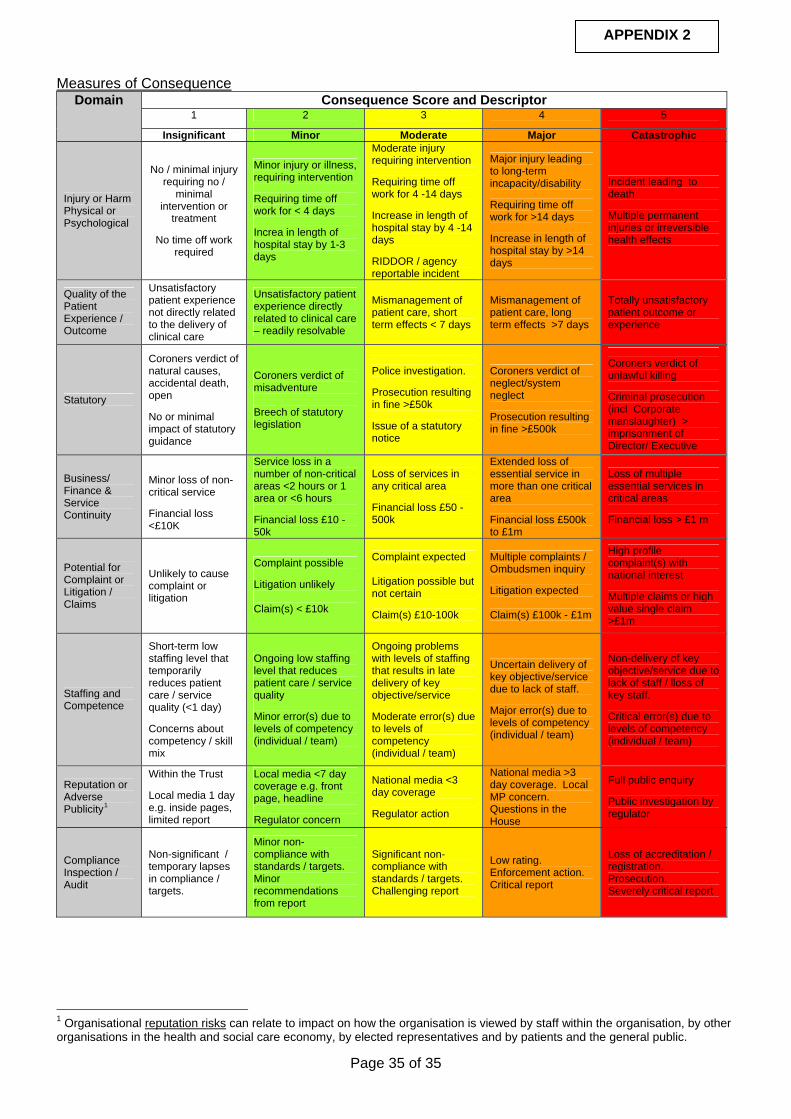
APPENDIX 2
Measures of ConsequenceConsequence Score and Descriptor
1 2 3 4 5 Domain
Insignificant Minor Moderate Major Catastrophic
Injury or Harm Physical or Psychological
No / minimal injury requiring no /
minimal intervention or
treatment
No time off work required
Minor injury or illness, requiring intervention Requiring time off work for < 4 days Increa in length of hospital stay by 1-3 days
Moderate injury requiring intervention Requiring time off work for 4 -14 days Increase in length of hospital stay by 4 -14 days RIDDOR / agency reportable incident
Major injury leading to long-term incapacity/disability Requiring time off work for >14 days Increase in length of hospital stay by >14 days
Incident leading to death Multiple permanent injuries or irreversible health effects
Quality of the Patient Experience / Outcome
Unsatisfactory patient experience not directly related to the delivery of clinical care
Unsatisfactory patient experience directly related to clinical care – readily resolvable
Mismanagement of patient care, short term effects < 7 days
Mismanagement of patient care, long term effects >7 days
Totally unsatisfactory patient outcome or experience
Statutory
Coroners verdict of natural causes, accidental death, open No or minimal impact of statutory guidance
Coroners verdict of misadventure Breech of statutory legislation
Police investigation. Prosecution resulting in fine >£50k Issue of a statutory notice
Coroners verdict of neglect/system neglect Prosecution resulting in fine >£500k
Coroners verdict of unlawful killing Criminal prosecution (incl Corporate manslaughter) > imprisonment of Director/ Executive
Business/ Finance & Service Continuity
Minor loss of non-critical service Financial loss <£10K
Service loss in a number of non-critical areas <2 hours or 1 area or <6 hours Financial loss £10 -50k
Loss of services in any critical area Financial loss £50 -500k
Extended loss of essential service in more than one critical area Financial loss £500k to £1m
Loss of multiple essential services in critical areas Financial loss > £1 m
Potential for Complaint or Litigation / Claims
Unlikely to cause complaint or litigation
Complaint possible Litigation unlikely Claim(s) < £10k
Complaint expected Litigation possible but not certain Claim(s) £10-100k
Multiple complaints / Ombudsmen inquiry Litigation expected Claim(s) £100k - £1m
High profile complaint(s) with national interest Multiple claims or high value single claim >£1m
Staffing and Competence
Short-term low staffing level that temporarily reduces patient care / service quality (<1 day) Concerns about competency / skill mix
Ongoing low staffing level that reduces patient care / service quality Minor error(s) due to levels of competency (individual / team)
Ongoing problems with levels of staffing that results in late delivery of key objective/service Moderate error(s) due to levels of competency (individual / team)
Uncertain delivery of key objective/service due to lack of staff. Major error(s) due to levels of competency (individual / team)
Non-delivery of key objective/service due to lack of staff / lloss of key staff. Critical error(s) due to levels of competency (individual / team)
Reputation or Adverse Publicity1
Within the Trust Local media 1 day e.g. inside pages, limited report
Local media <7 day coverage e.g. front page, headline Regulator concern
National media <3 day coverage Regulator action
National media >3 day coverage. Local MP concern. Questions in the House
Full public enquiry Public investigation by regulator
Compliance Inspection / Audit
Non-significant / temporary lapses in compliance / targets.
Minor non-compliance with standards / targets. Minor recommendations from report
Significant non-compliance with standards / targets. Challenging report
Low rating. Enforcement action. Critical report
Loss of accreditation / registration. Prosecution. Severely critical report
1 Organisational reputation risks can relate to impact on how the organisation is viewed by staff within the organisation, by other organisations in the health and social care economy, by elected representatives and by patients and the general public.
Page 35 of 35