study of twak shareer wsr to kitibha kustha
TRANSCRIPT
“Study of Twak Shareer w.s.r to Kitibha Kustha” By
Dr. Sapna Hiremath.
A dissertation submitted to the
RRR aaa jjj iii vvv GGG aaa nnn ddd hhh iii UUU nnn iii vvv eee rrr sss iii ttt yyy ooo fff HHH eee aaa lll ttt hhh SSS ccc iii eee nnn ccc eee sss ,,, KKK aaa rrr nnn aaa ttt aaa kkk aaa ,,, BBB aaa nnn ggg aaa lll ooo rrr eee .
In partial fulfillment of the requirements for the degree of
AYURVEDA VACHASPATHI - M.D (AYURVEDA)
In
RACHANA SHAREERA
Co-Guide Guide Dr. N.G. Mulimani Dr. J.K. Bhargava
MD (S.R.) M.S.A.M.
Post Graduate Department Of Rachana Shareera
N.K.J. Ayurvedic Medical College & PG Centre, Bidar.
2009.
RRR aaa jjj iii vvv GGG aaa nnn ddd hhh iii UUU nnn iii vvv eee rrr sss iii ttt yyy ooo fff HHH eee aaa lll ttt hhh SSS ccc iii eee nnn ccc eee sss ,,, KKK aaa rrr nnn aaa ttt aaa kkk aaa ,,, BBB aaa nnn ggg aaa lll ooo rrr eee .
Declaration by the candidate
I, here by declare that this dissertation/ thesis entitled
“Study of Twak Shareer w.s.r to Kitibha Kustha” Is a bonafide
and genuine research work carried out by me under the guidance
of Dr. J.K. Bhargava, M.S.A.M. Professor & H.O.D.
Department of Rachana Shareera.
Date:
Place: Bidar
Signature of the candidate Dr. Sapna Hiremath.
RRR aaa jjj iii vvv GGG aaa nnn ddd hhh iii UUU nnn iii vvv eee rrr sss iii ttt yyy ooo fff HHH eee aaa lll ttt hhh SSS ccc iii eee nnn ccc eee sss ,,, KKK aaa rrr nnn aaa ttt aaa kkk aaa ,,, BBB aaa nnn ggg aaa lll ooo rrr eee .
Copyright
Declaration by the candidate
I here by declare that the Rajiv Gandhi University of Health
Sciences, Karnataka shall declare the rights to preserve, use and
disseminate this dissertation/ thesis in print or electronic format for
academic/ research purpose.
Date:
Place: Bidar
© Rajiv Gandhi University of Health Sciences, Karnataka
Signature of the candidate Dr. Sapna Hiremath.
RRR aaa jjj iii vvv GGG aaa nnn ddd hhh iii UUU nnn iii vvv eee rrr sss iii ttt yyy ooo fff HHH eee aaa lll ttt hhh SSS ccc iii eee nnn ccc eee sss ,,, KKK aaa rrr nnn aaa ttt aaa kkk aaa ,,, BBB aaa nnn ggg aaa lll ooo rrr eee .
CERTIFICATE BY THE GUIDE
This is to certify that the dissertation entitled “Study of
Twak Shareer w.s.r to Kitibha Kustha” is a bonafide research
work done by Dr. Sapna Hiremath, in partial fulfillment of the
requirement for the degree of Ayurveda Vachaspathi - M.D.
(Ayurveda).
Date: Date: Place: Bidar Place: Bidar
Signature of the Guide Dr. J.K. Bhargava
M.S.A.M. Professor & H.O.D.,
Department of Rachana Shareera NKJ Ayurvedic Medical College & P G
Centre Bidar – 585403
Signature of the Co-Guide Dr. N.G. Mulimani
MD (SR). Professor,
Department of Shareera Rachana Bidar Institute of Medical Sciences
Bidar – 585403 Karnataka.
EEENNNDDDOOORRRSSSEEEMMMEEENNNTTT BBBYYY TTTHHHEEE HHHOOODDD,,, PPPRRRIIINNNCCCIIIPPPAAALLL/// HHHEEEAAADDD OOOFFF TTTHHHEEE IIINNNSSSTTTIIITTTUUUTTTIIIOOONNN
This is to certify that the dissertation entitled “Study of
Twak Shareer w.s.r to Kitibha Kustha” is a bonafide research
work done by Dr. Sapna Hiremath under the guidance of
Dr. J.K. Bhargava Prof. & H.O.D. department of Rachana
Shareera.
Date: Date: Place: Bidar. Place: Bidar.
Seal and signature of H.O.D. Dr .J.K.Bhargav M.S.A.M. Prof & H.O.D Dept. Of Post Graduate Studies In Rachana Shareera N.K.J. A.M.C. & PG Centre, Bidar – 585403 Karnataka.
Seal and signature of the Principal/Dean
Dr.K.V.L.N Acharyulu. M.D. (Basic principles)
N.K.J. A.M.C. & PG Centre, Bidar – 585403 Karnataka.
Abbreviations
ABBREVIATIONS
1. Cha. - Charaka samhita
2. Su. - Sushruta samhita
3. A.S. - Astanga sangraha
4. Su (Dalhana) - Dalhana tika on Sushruta samhita
5. A.H. - Astanga hridayam
6. Sha. Pra. - Sharangadhara Prathama kanda
7. Ayu. Sha. - Ayurveda Shareera rachana
8. B.P. Pu. - Bhavaprakasha Purvarda
9. M.Ni. - Madhava Nidana
10. Y.R. - Yogarathnakara
11. D.G. - Dravyaguna
12. Vi. - Vimanasthana
13. Sha - Shareera
14. Ni - Nidanasthana
15. Si. - Siddisthana
16. Chi. - Chikitsasthana
17. Ut. - Uttarasthana
ABSTRACT
Introduction:
Ayurveda describe the organization of the body in term of doshas, dhatus and
malas.Twacha is one among the updhatus which provide protective layer over the
body that protect from the heat, cold & external infection.
The union of sukra(spermatozoa) & sonita(ovum) while being cooked
(processed by heat) give rise to the formation of seven twaka (skin) just like formation
of cream when milk is boiled. Acharya sushrut and other Acharyas are described
twaka shareeram in detail.Acharya sushrut defined Twacha as upadhatu of mamsa
dhatu.Twacha is one among the panch jyanendriya,which carry sensation of touch.&
It covers external part as well as internal part of body.
Since antiquity human being often suffered from many type of diseases, out
of them skin disease is one of the major problem for the community, because there is
a change in the structural appearance of the skin & it make entire body ugly.
There are different theories among the Acharyas regarding the number of
layers.Acharyas Charak consider that Twacha is made up of six layers where other
Acharyas consider seven layers.In this layers of twacha ,different type of diseases
observe in different layers. Out of this, a very commonly seen “Kustha” disease is
found in one of the twacha.Kustha is a skin disease.
“Kitibha” is one among the type of Ksudra kustha which is common and chronic
disorder of twacha. Acharyas describe symptoms of kitibha like - red, with dry &
silvery white scale which may be obvious only after scrapping the surface, skin is not
sweating , resemble the scale of fish, producing sound (while scratching) rough,
itching course & black in colour.(AS.Ni 4/22.) Although twacha has been explained
in our classic, we get very vague and very less description about the disease related to
twacha sharer.And it is outermost protective layer of the body,so it becomes essential
to know the structural and anatomical changes occur in the Kitibha.Now a days
Kitibha disease largely spread in the human being. While diagnosing the patients of
Kitibha kustha ,there is difficulty regarding the identification of structural deformity
,hence need is felt to study the kitibha & twak sharer.
REVIEW OF LITERATURE 1) Description available regarding twak sharer in Ayurvedic classics. 2) Description of kitibha kustha.has been explained in Ayurvedic classics. 3) Description available in modern text book regarding skin. 4) Description of psoriasis available in modern text.
MATERIAL AND METHODS:
SOURCE OF DATA
1. Literary & conceptual study will be undertaken by data compilations from
Brihatrayis, Laghutrayis & other classical texts including journals, presented
papers, previous thesis work done & correlated, analysed with the knowledge
of contemporary science on the subject.
2. A special case proforma will be prepared with all the points of
KITIBHA.Observation of minimum 30 patients will be selected for study.
Structural abnormality will be observed with the help of Skin Biopsy.
Design of the study :
a) Clinically diagnosed 30 patients of kitibha
b) Clinically examination is carried out by skin biopsy.
c) Skin biopsy will be taken of each patient to assess the structural changes in the
twacha layers in case of kitibha & will be analysed statistically.
A) Inclusive criteria:
Diagnosed patients of kitibha
Patients having pratyatma lakashanas of kitibha
Patients of both the sex between middle age group will be selected.
B) Exclusive criteria:
Burn
Leprosy
Other skin diseases.
C) Assessment criteria:
Diagnosed patients of kitibha kustha are clinically examined for signs &
symptoms, structural abnormalities are observed in skin biopsy examination &
correlated with anatomical features.
Observations:
1) There is some controversy regarding number of Twacha. Some Acharyas have
told six types of Twacha while some have told seven types.
2) Acharya Charaka and Acharya Sushruta both have told different Vyadhis in
layers of Twacha. e.g.Sushruta told Kitibha in fourth layer.
3) Measurement of thickness of Twacha told by Sushruta is near about same
which is quoted in modern textbooks. The measurement of Dalhana doesn’t
matches with the modern measurement.
4) The symptoms of Kitibha and psoriasis show tremendous similarity with each
other.
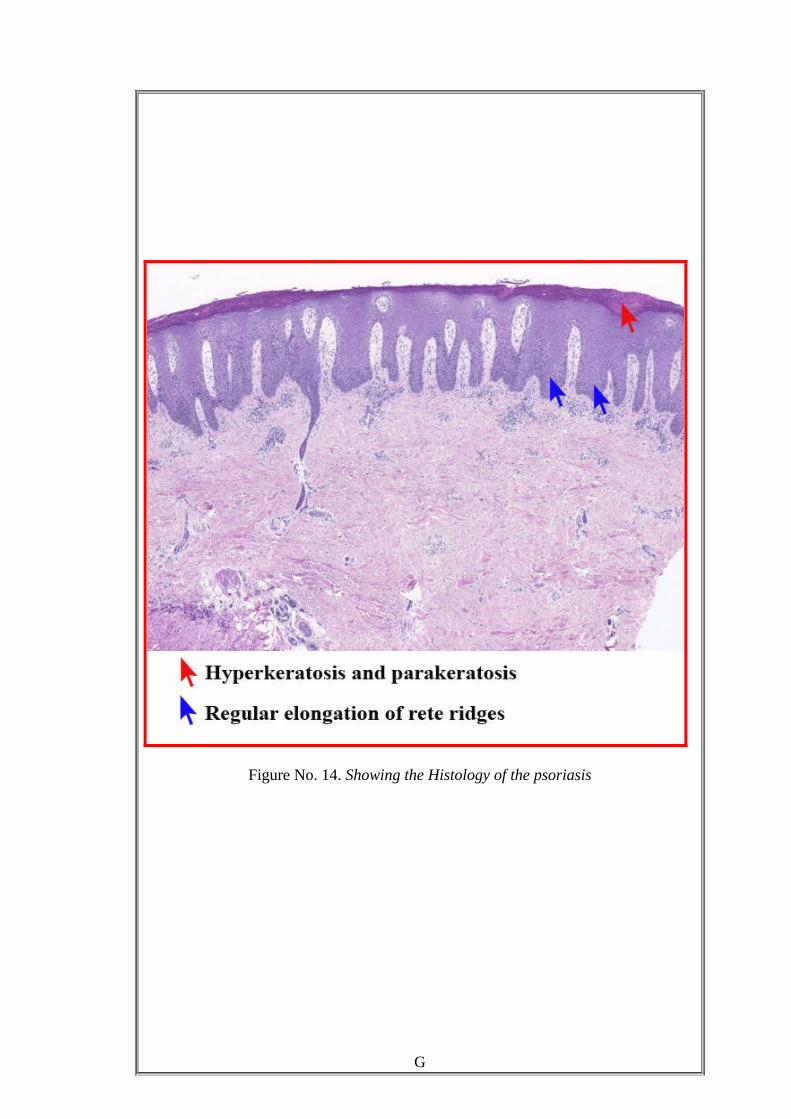
5) After histopathological study the aupitz sign and fish like appearance is seen
under microscope.
Discussion:
Kitibha Kushtha –Psoriasis:
• Klinna - Sticky in nature
• Mahavastum - Lesions are found all over the body.
• Khara Sparsha – Rough in touch
• Parusha – Hard in nature(crack).
• Vruttam – Round in shape.
• Ghana – Solid
• Sravi and Shyava – In chronic condition psoriatic patches on the skin are
exudative in nature and blackish discolouration.
The lakshanas of kitibha kustha mentioned by Charaka, Vagbhata and Sushruta
are described here in detail in comparison with psoriasis.
Key words:
Kitibha Kustha, Twacha Shareera, Twacha Varna, Psoriasis, parakerotosis,
Orthrokeratosis, Rete ridge, Auspitz sign. Silver scales, Epidermopoiesis,
“Study of Twak Shareer w.s.r to Kitibha Kustha” By
Dr. Sapna Hiremath.
A dissertation submitted to the
RRR aaa jjj iii vvv GGG aaa nnn ddd hhh iii UUU nnn iii vvv eee rrr sss iii ttt yyy ooo fff HHH eee aaa lll ttt hhh SSS ccc iii eee nnn ccc eee sss ,,, KKK aaa rrr nnn aaa ttt aaa kkk aaa ,,, BBB aaa nnn ggg aaa lll ooo rrr eee .
In partial fulfillment of the requirements for the degree of
AYURVEDA VACHASPATHI - M.D (AYURVEDA)
In
RACHANA SHAREERA
Co-Guide Guide Dr. N.G. Mulimani Dr. J.K. Bhargava
MD (S.R.) M.S.A.M.
Post Graduate Department Of Rachana Shareera
N.K.J. Ayurvedic Medical College & PG Centre, Bidar.
2009.
RRR aaa jjj iii vvv GGG aaa nnn ddd hhh iii UUU nnn iii vvv eee rrr sss iii ttt yyy ooo fff HHH eee aaa lll ttt hhh SSS ccc iii eee nnn ccc eee sss ,,, KKK aaa rrr nnn aaa ttt aaa kkk aaa ,,, BBB aaa nnn ggg aaa lll ooo rrr eee .
Declaration by the candidate
I, here by declare that this dissertation/ thesis entitled
“Study of Twak Shareer w.s.r to Kitibha Kustha” Is a bonafide
and genuine research work carried out by me under the guidance
of Dr. J.K. Bhargava, M.S.A.M. Professor & H.O.D.
Department of Rachana Shareera.
Date:
Place: Bidar
Signature of the candidate Dr. Sapna Hiremath.
RRR aaa jjj iii vvv GGG aaa nnn ddd hhh iii UUU nnn iii vvv eee rrr sss iii ttt yyy ooo fff HHH eee aaa lll ttt hhh SSS ccc iii eee nnn ccc eee sss ,,, KKK aaa rrr nnn aaa ttt aaa kkk aaa ,,, BBB aaa nnn ggg aaa lll ooo rrr eee .
Copyright
Declaration by the candidate
I here by declare that the Rajiv Gandhi University of Health
Sciences, Karnataka shall declare the rights to preserve, use and
disseminate this dissertation/ thesis in print or electronic format for
academic/ research purpose.
Date:
Place: Bidar
© Rajiv Gandhi University of Health Sciences, Karnataka
Signature of the candidate Dr. Sapna Hiremath.
RRR aaa jjj iii vvv GGG aaa nnn ddd hhh iii UUU nnn iii vvv eee rrr sss iii ttt yyy ooo fff HHH eee aaa lll ttt hhh SSS ccc iii eee nnn ccc eee sss ,,, KKK aaa rrr nnn aaa ttt aaa kkk aaa ,,, BBB aaa nnn ggg aaa lll ooo rrr eee .
CERTIFICATE BY THE GUIDE
This is to certify that the dissertation entitled “Study of
Twak Shareer w.s.r to Kitibha Kustha” is a bonafide research
work done by Dr. Sapna Hiremath, in partial fulfillment of the
requirement for the degree of Ayurveda Vachaspathi - M.D.
(Ayurveda).
Date: Date: Place: Bidar Place: Bidar
Signature of the Guide Dr. J.K. Bhargava
M.S.A.M. Professor & H.O.D.,
Department of Rachana Shareera NKJ Ayurvedic Medical College & P G
Centre Bidar – 585403
Signature of the Co-Guide Dr. N.G. Mulimani
MD (SR). Professor,
Department of Shareera Rachana Bidar Institute of Medical Sciences
Bidar – 585403 Karnataka.
EEENNNDDDOOORRRSSSEEEMMMEEENNNTTT BBBYYY TTTHHHEEE HHHOOODDD,,, PPPRRRIIINNNCCCIIIPPPAAALLL/// HHHEEEAAADDD OOOFFF TTTHHHEEE IIINNNSSSTTTIIITTTUUUTTTIIIOOONNN
This is to certify that the dissertation entitled “Study of
Twak Shareer w.s.r to Kitibha Kustha” is a bonafide research
work done by Dr. Sapna Hiremath under the guidance of
Dr. J.K. Bhargava Prof. & H.O.D. department of Rachana
Shareera.
Date: Date: Place: Bidar. Place: Bidar.
Seal and signature of H.O.D. Dr .J.K.Bhargav M.S.A.M. Prof & H.O.D Dept. Of Post Graduate Studies In Rachana Shareera N.K.J. A.M.C. & PG Centre, Bidar – 585403 Karnataka.
Seal and signature of the Principal/Dean
Dr.K.V.L.N Acharyulu. M.D. (Basic principles)
N.K.J. A.M.C. & PG Centre, Bidar – 585403 Karnataka.
Abbreviations
ABBREVIATIONS
1. Cha. - Charaka samhita
2. Su. - Sushruta samhita
3. A.S. - Astanga sangraha
4. Su (Dalhana) - Dalhana tika on Sushruta samhita
5. A.H. - Astanga hridayam
6. Sha. Pra. - Sharangadhara Prathama kanda
7. Ayu. Sha. - Ayurveda Shareera rachana
8. B.P. Pu. - Bhavaprakasha Purvarda
9. M.Ni. - Madhava Nidana
10. Y.R. - Yogarathnakara
11. D.G. - Dravyaguna
12. Vi. - Vimanasthana
13. Sha - Shareera
14. Ni - Nidanasthana
15. Si. - Siddisthana
16. Chi. - Chikitsasthana
17. Ut. - Uttarasthana
A
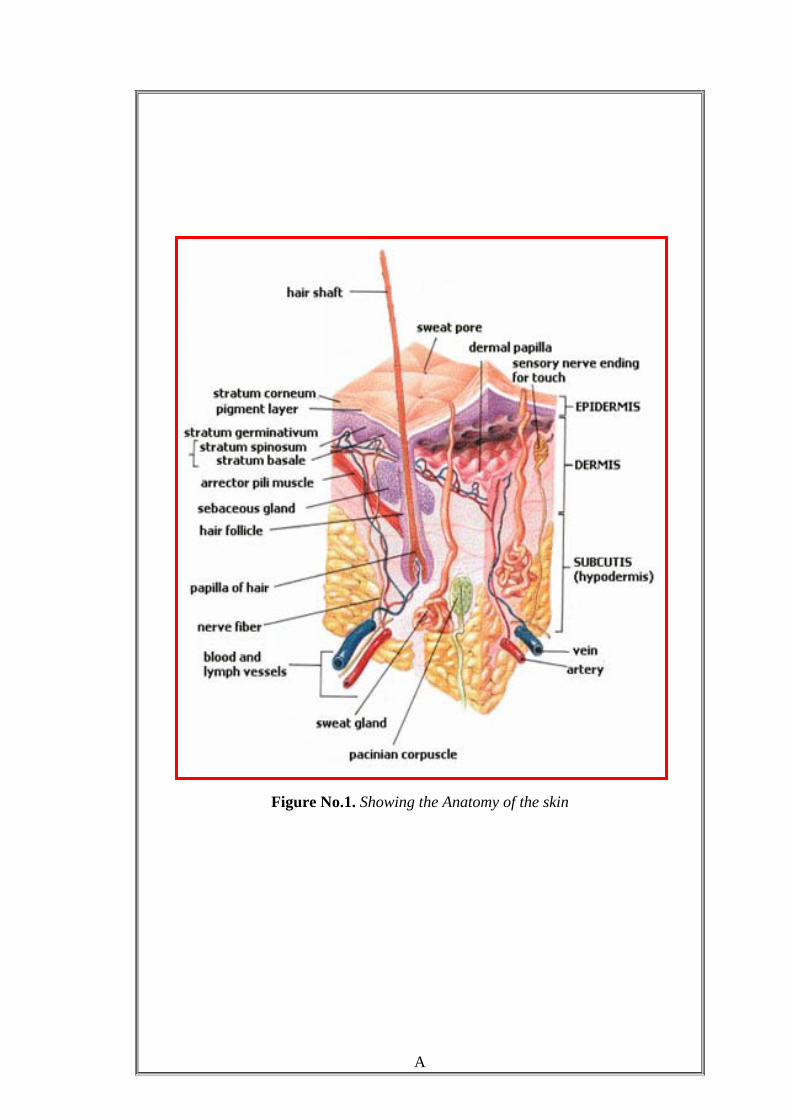
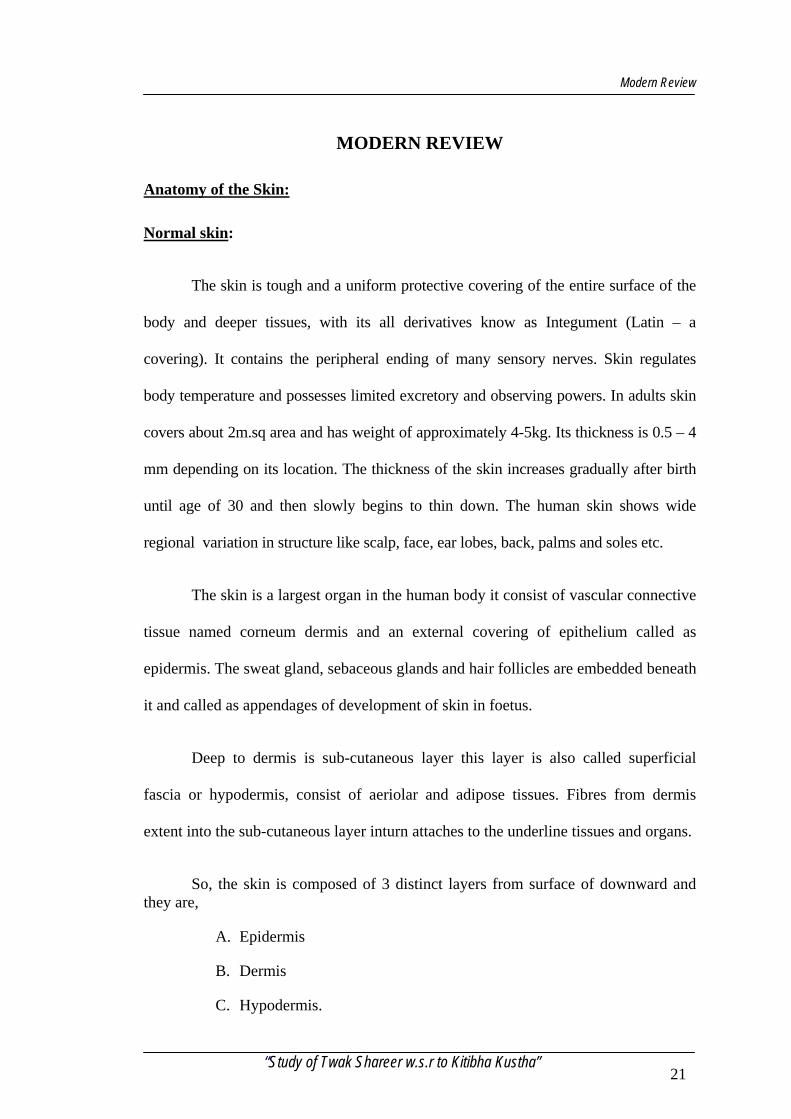
Figure No.1. Showing the Anatomy of the skin
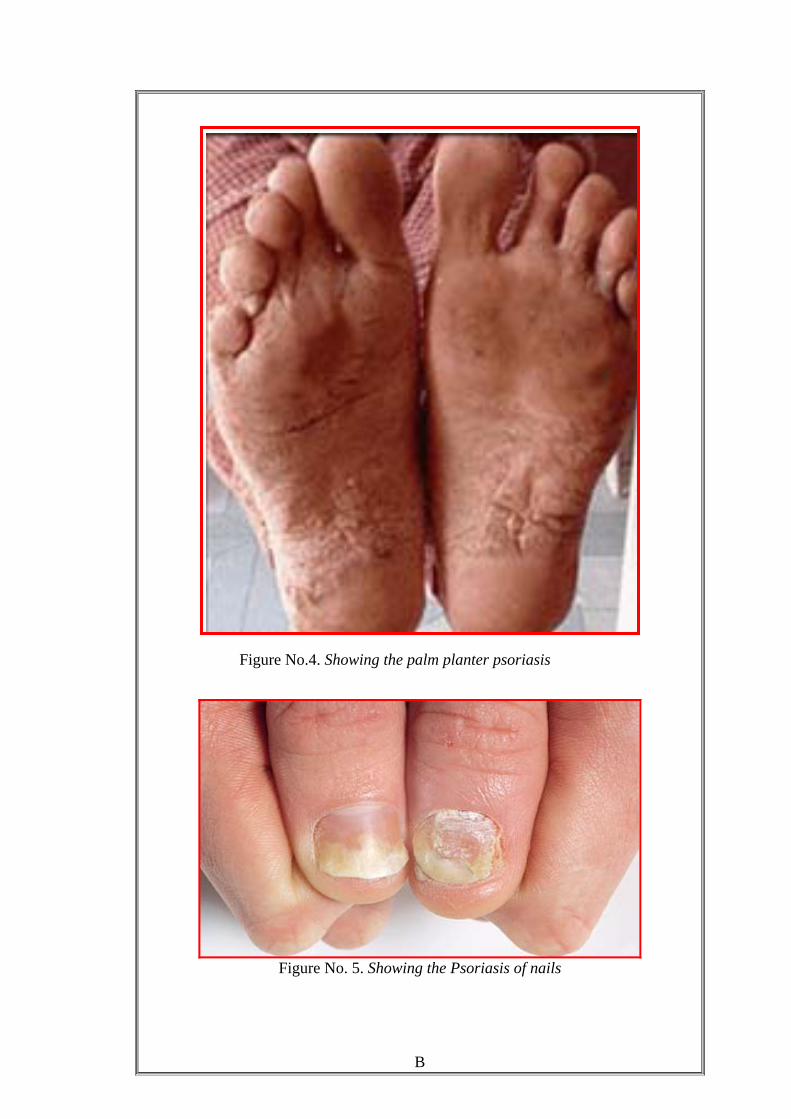
Figure No.4. Showing the palm planter psoriasis
B
Figure No. 5. Showing the Psoriasis of nails

Figure No. 6. Showing the Guttate psoriasis
C
Figure No. 7. Showing the psoriasis of the scalp
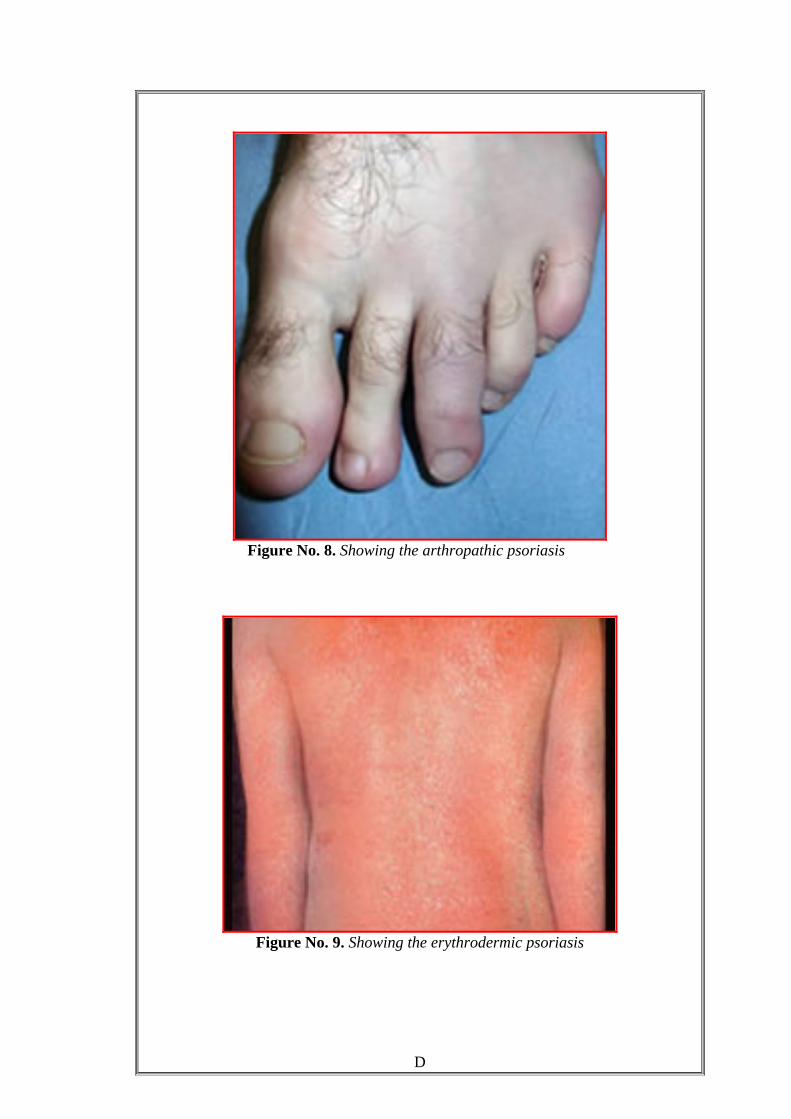
Figure No. 8. Showing the arthropathic psoriasis
Figure No. 9. Showing the erythrodermic psoriasis
D
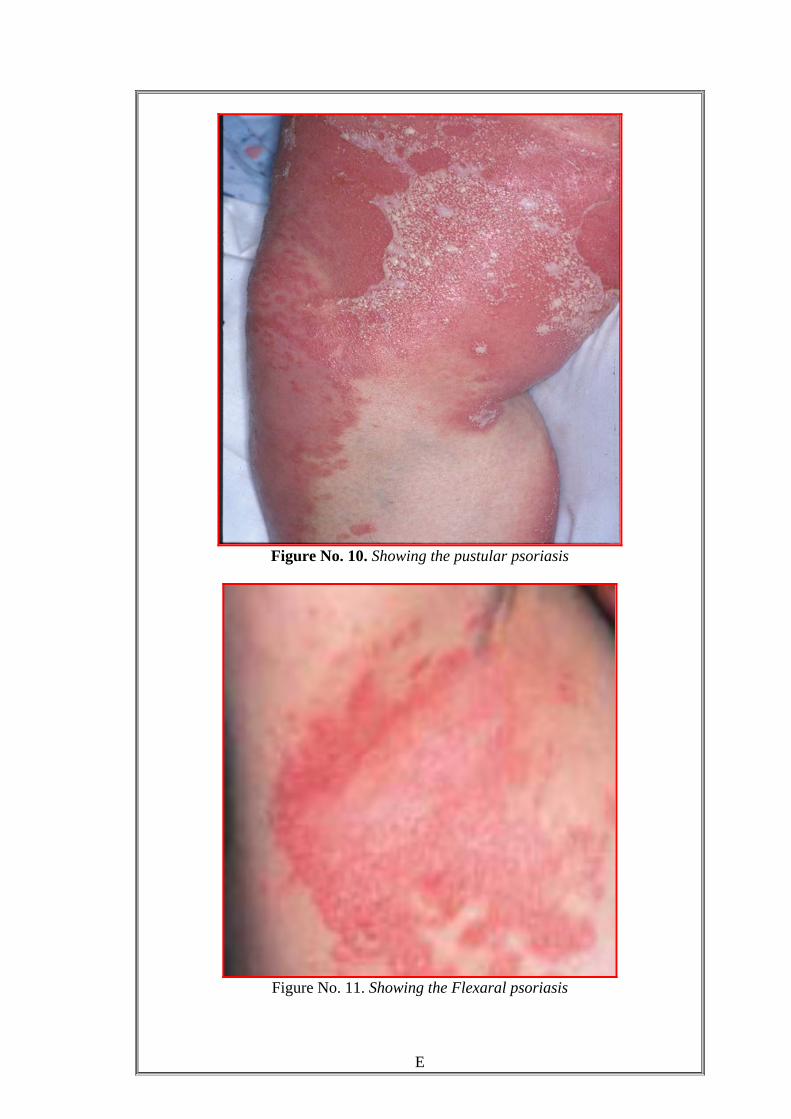
Figure No. 10. Showing the pustular psoriasis
Figure No. 11. Showing the Flexaral psoriasis
E
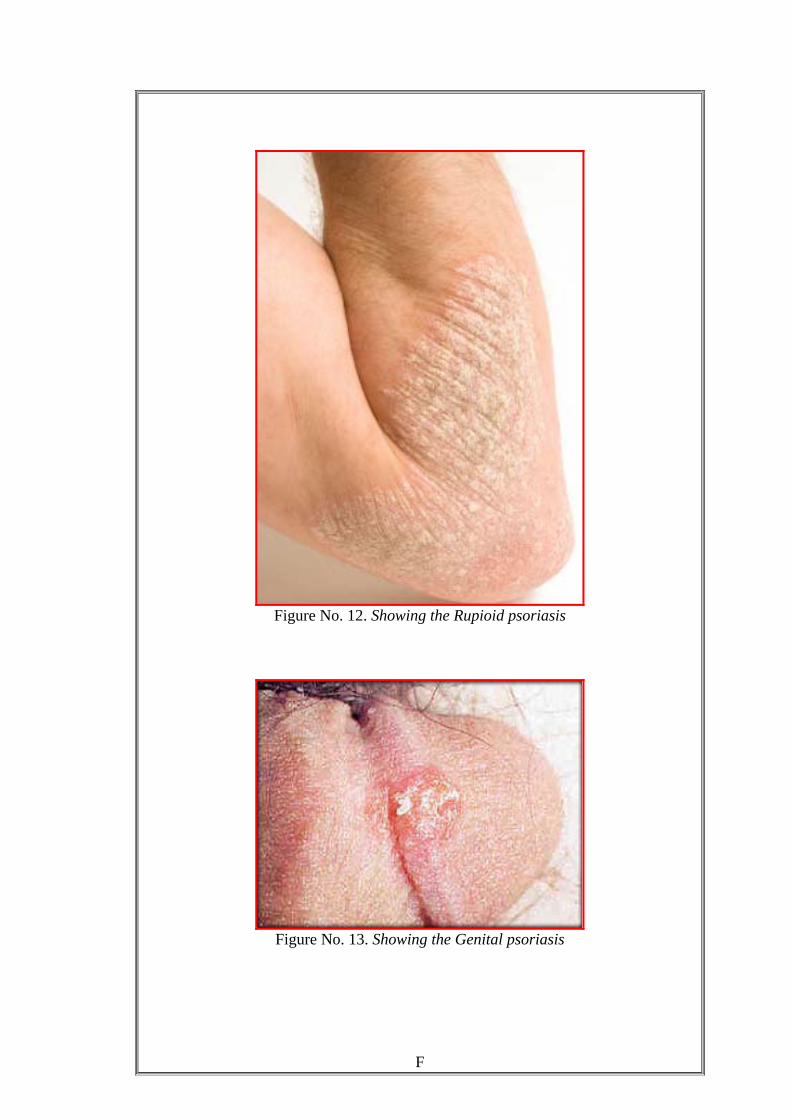
Figure No. 12. Showing the Rupioid psoriasis
F
Figure No. 13. Showing the Genital psoriasis
G
Figure No. 14. Showing the Histology of the psoriasis
ACKNOWLEDGEMENT
I offer my prayers to Revansiddeshwar, Shirdi Saibaba who gave me strength to overcome
all the difficulties during this Thesis work.
I bow my head on the feet of His Holiness Sri Sri Sri Shivkumar Swamiji the President of
C S S, Bidar, for his endless service to society.
I express my sincere gratitude to most honourable and esteemed teacher, guide and
co-guide Dr. J.K. Bhargav and Dr. N G Mulimani respectively for their unforgettable parental
affection and patience cooperation to give suggestions at every step in accomplishing the present
work.
I am very much thankful to Prof. K. V. L. N. Acharyulu, Principal, for his untiring
encouragement and providing me an opportunity to join this reputed institution.
It is a privilege for me to express my sense of indebtedness to my savant teachers
Dr. S B Kottur, Prof. P G Bhatt, Dr. P V Savnur and for their inspiring support.
My most respects to Dr.Ashwini wagmare , Dr.Shelly Divyadarshan , Dr.Sanjeev kumar
Joteppa, Dr.Anup Bosgikar for their valuable suggestions.
I feel great pleasure to thanks to my classmates Dr.Santosh Dixit. Dr.Anita Murki,
Dr.Shankerling, Dr. Raghavendra, for their patience cooperation
It is a privilege for me to express my thanks to all my junior friends
Dr. Geetha Dolle, Dr.Satyamma, Dr. Rajshekhar Tokre, Dr. Vivek, Dr.Shivsharanayya,
Dr.Akkamahadevi, Dr. Suharini Sulgunte.
On this occasion with a great reverence I offer my gratitude to my Husband Dr.
Brahmanand Swamy, and my son Master Atharva.
I feel great pleasure in expressing my pranamas at the lotus feet of my mother-in-law
Smt.Shakunatala and father-in-law Sri. K. V. Swamy, my mother Smt. Sarala and father
Sri V.N. Hiremath and Amma Bhagwan who have cooperated during of this work
May Lord Dhanwantari bless all with hitayu and sukhayu who helped me directly and
indirectly in completing this work.
I sincerely thank all my patients for their support in completing this work successfully.
Dr. Sapana. V. Hiremath
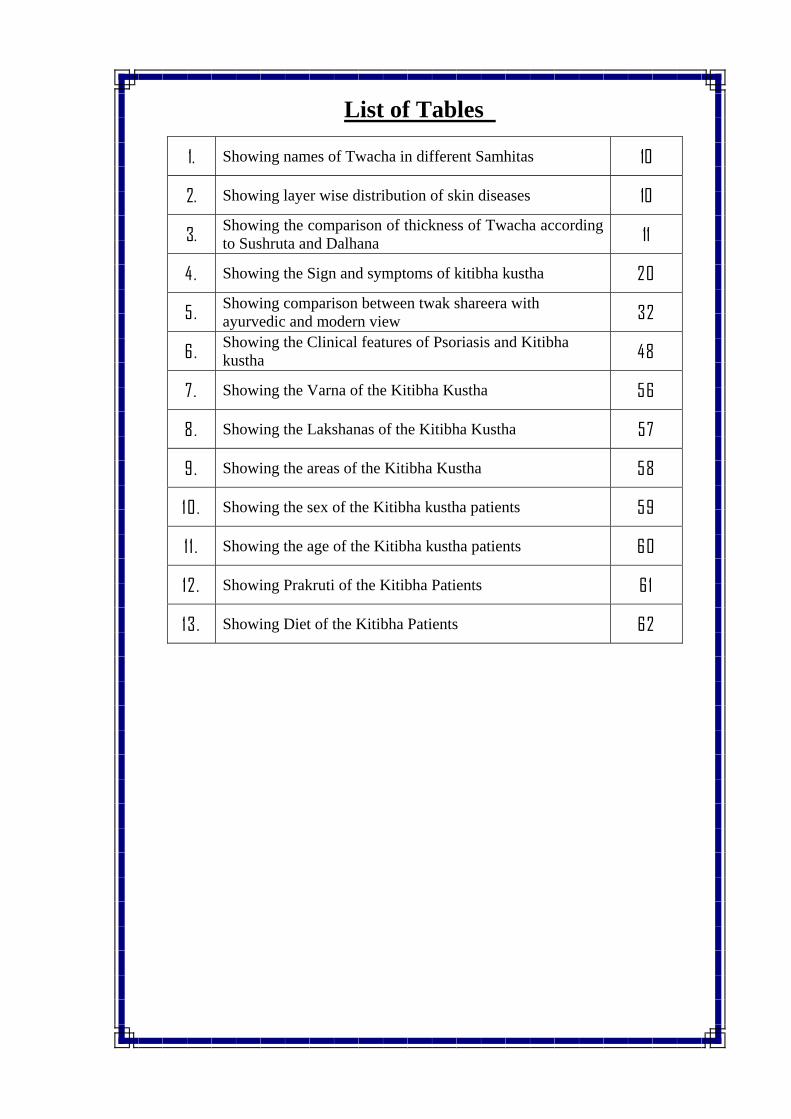
List of Tables
1. Showing names of Twacha in different Samhitas 10
2. Showing layer wise distribution of skin diseases 10
3. Showing the comparison of thickness of Twacha according to Sushruta and Dalhana 11
4 . Showing the Sign and symptoms of kitibha kustha 20
5. Showing comparison between twak shareera with ayurvedic and modern view 32
6. Showing the Clinical features of Psoriasis and Kitibha kustha 48
7. Showing the Varna of the Kitibha Kustha 56
8. Showing the Lakshanas of the Kitibha Kustha 57
9. Showing the areas of the Kitibha Kustha 58
10. Showing the sex of the Kitibha kustha patients 59
1 1 . Showing the age of the Kitibha kustha patients 60
12. Showing Prakruti of the Kitibha Patients 61
13. Showing Diet of the Kitibha Patients 62
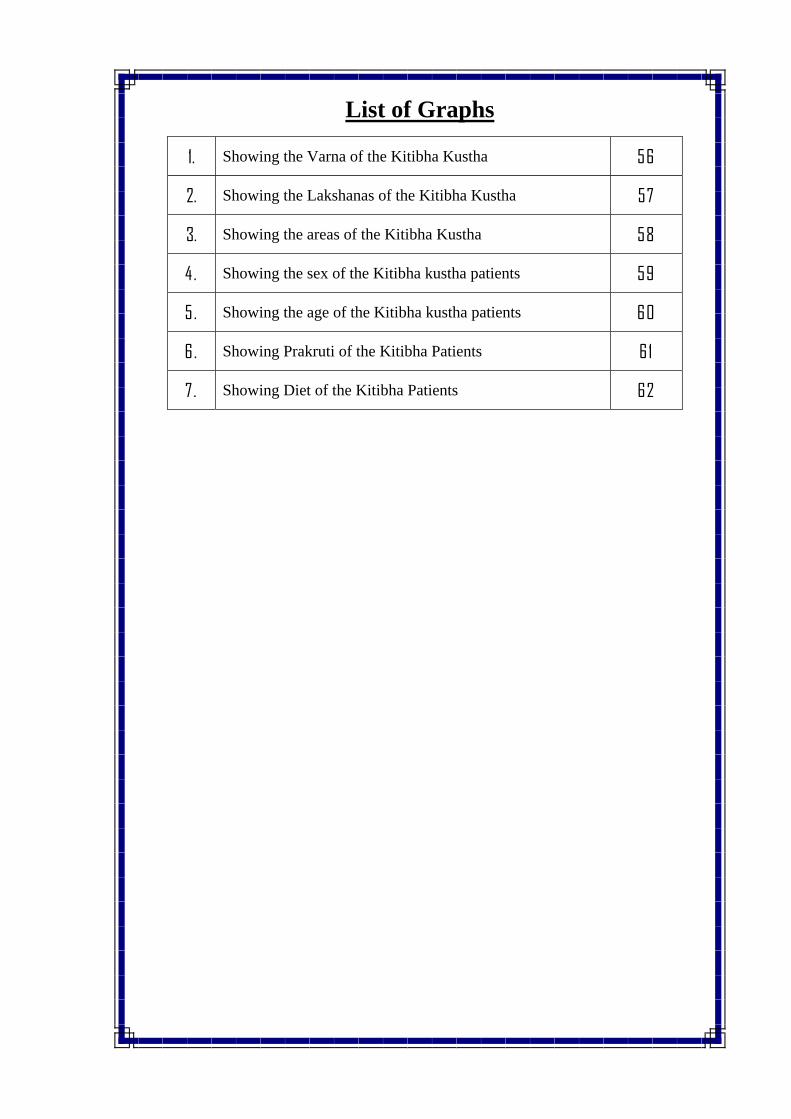
List of Graphs
1. Showing the Varna of the Kitibha Kustha 56
2. Showing the Lakshanas of the Kitibha Kustha 57
3. Showing the areas of the Kitibha Kustha 58
4. Showing the sex of the Kitibha kustha patients 59
5. Showing the age of the Kitibha kustha patients 60
6. Showing Prakruti of the Kitibha Patients 61
7 . Showing Diet of the Kitibha Patients 62
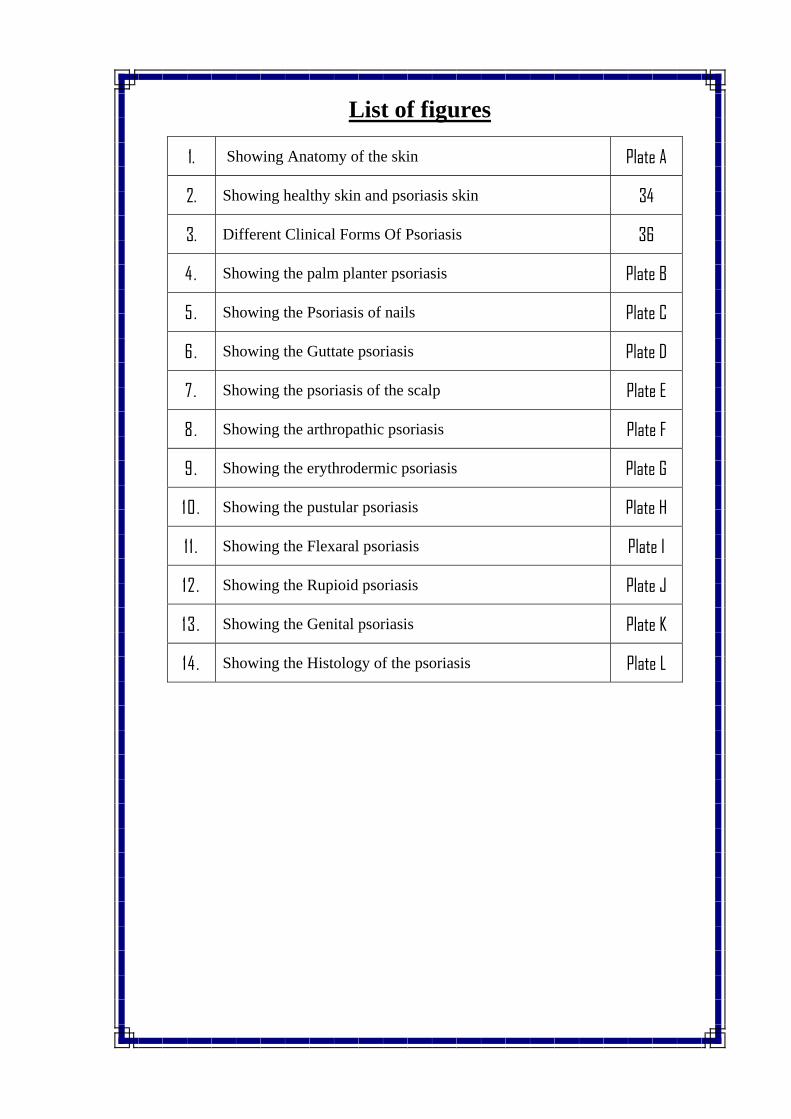
List of figures
1. Showing Anatomy of the skin Plate A
2. Showing healthy skin and psoriasis skin 34
3. Different Clinical Forms Of Psoriasis 36
4. Showing the palm planter psoriasis Plate B
5. Showing the Psoriasis of nails Plate C
6. Showing the Guttate psoriasis Plate D
7 . Showing the psoriasis of the scalp Plate E
8. Showing the arthropathic psoriasis Plate F
9. Showing the erythrodermic psoriasis Plate G
10. Showing the pustular psoriasis Plate H
1 1 . Showing the Flexaral psoriasis Plate I
12 . Showing the Rupioid psoriasis Plate J
13. Showing the Genital psoriasis Plate K
14 . Showing the Histology of the psoriasis Plate L
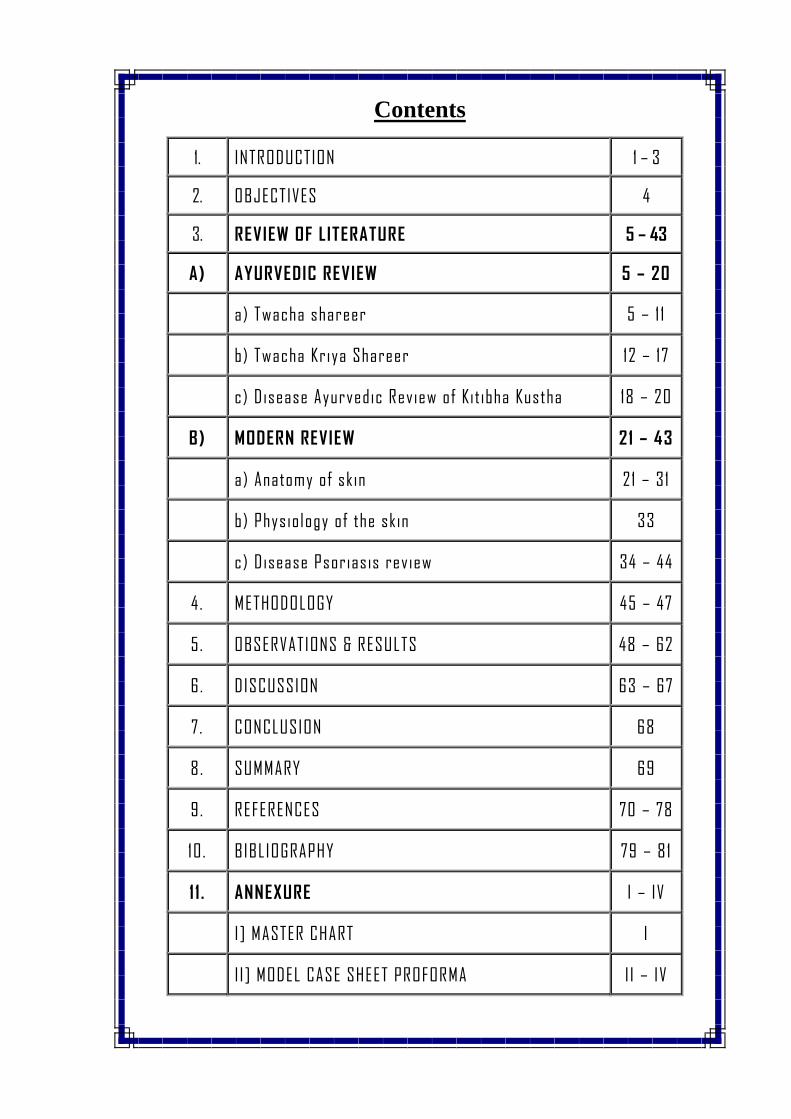
Contents
1. INTRODUCTION 1 – 3
2. OBJECTIVES 4
3. REVIEW OF LITERATURE 5 – 43
A) AYURVEDIC REVIEW 5 – 20
a) Twacha shareer 5 – 1 1
b) Twacha Kriya Shareer 12 – 17
c) Disease Ayurvedic Review of Kit ibha Kustha 18 – 20
B) MODERN REVIEW 21 – 43
a) Anatomy of skin 21 – 31
b) Physiology of the skin 33
c) Disease Psoriasis review 34 – 44
4 . METHODOLOGY 45 – 47
5. OBSERVATIONS & RESULTS 48 – 62
6. DISCUSSION 63 – 67
7 . CONCLUSION 68
8. SUMMARY 69
9. REFERENCES 70 – 78
10. BIBLIOGRAPHY 79 – 81
1 1 . ANNEXURE I – IV
I] MASTER CHART I
I I] MODEL CASE SHEET PROFORMA I I – IV
Introduction
INTRODUCTION
Ayurveda is an ancient pathy which was uniquely practiced before five
thousand years. Its origin is being linked to Atharvaveda and it makes a holistic
approach towards life.
Ayurveda follows laws of nature and propounds number applied doctrines for
the understanding of life, health and diseases. Many of these doctrines are valid even
in today’s running life and may throw a new light on several undissolved issues
regarding science of medicine and solve many uncertainties.
In Ayurvedic classics like Charaka Samhita, Sushruta Samhita etc. a huge
knowledge regarding Shareer. Nidana and Chikitsa are available. For an expert
Vaidya to treat a disease thorough knowledge about the disease and Shareer of its
related part is very mandatory.
One who knows Shareer (i.e. anatomy and physiology of human body) in
detail, only he can know and understand Ayurveda which can bring happiness to the
universe1.
For any successful Vaidya or Shalya Chikitsaka thorough knowledge of
Shareer is very essential for diagnosis and treatment or to perform surgical
procedures.
So, are who wants to have undoubtful knowledge of Shalyatantra, he should
go for dissection and study each and every macro and micro structure of human
body2. But these are many structures in the human body which can not be visualized
by naked eyes. It is possible to explain these minute structures only in this modern era
with the help of advanced technology which has given us ZOOM view. Although in
ancient classics some description of such minute structures is available. It was
possible for Acharyas with the help of “Gnyanachakshu” and “Tapaschakshu”.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 1
Introduction
It is not possible to see minute structures in the body with the help of naked
eyes. They each are visualized only with the help of Gnyanachakshu and
Tapaschakshu3.
In Ayurveidc texts knowledge of Ayurveda is classified in eight main
branches.
Kaya (Medicine), Bala (Pediatrics), Grahachikitsa. Urdhwanga
(Ophthalmology & ENT), Shalya (Surgery), Danshtra (Toxicology). Jara
(Rejuvenation) and Vrisha (Virilification) are the eight branches of Ayurveda4.
The knowledge of these eight branches is present in various texts like
Brihatrayi, Laghutrayi and other textbooks. The authors of these texts have given
special contributed of to a particular branch. So they are considered master of that
branch.
Acharya Sushruta is master in Shareer (Anatomy), Acharya Charaka is master
in Chikitsa (Medicine), Acharya Madhava is famous for Nidana (Diagnosis) and
Acharya Vagbhata is famous for basic principles of Ayurveda described in
Sootrasthana5.
In Sushruta Samhita, Acharya Sushruta has described the structures of human
body in detail. He studied the human body by the technique of human body
preservation and dissection which is very much different from today’s method
Acharya Sushruta was the first to dissect human body.
In Shareersthana of Sushruta Samhita, detail knowledge of human body is
present. In Garbhavyakarana adhyaya, a detail description of Twacha Shareer is
present which will be studied in further topics. Also relation of Tamra Twacha and
Kitibha kustha will be studied.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 2
Introduction
SELECTION OF TOPIC:
Today there is a cosmetic era. People are getting more and more
consciousness about healthy skin. Especially females are seeking more attention
towards healthy skin to be top in the fastest growing field of fashion.
So, to fulfill people’s demand and giving them healthy skin. We must study
the anatomy and physiology of skin and its variation from one person to another
because every individual have different nature of skin depending upon his Prakruti
and many other factors. After studying the nature of one’s skin. We will be in a
position to advice do’s and don’ts or treatment to that person accordingly.
But before doing this, the basic thing is to study normal anatomy and
physiology of skin. So the subject is selected.
There is another reason for doing extensive study of Kitibha which can be
compared to Psoriasis according to modern science.
Today about 30% people are getting affected with skin diseases especially in
tropics. Tinea Virsicolor, Eczema, Dermatitis. Leukoderma is some of the common
skin problems people are facing. Out of this psoriasis is a disease occurring in skin
which is as common as uneasily curable.
It is mainly associated with scales on palm sole, scalp and hands which are
having itchy nature. Due to this complaint (itching), one may loose his concentration
from his routine work and may land up in awkward situation affecting his civil life.
So, the second part of this thesis will be to study kitibha according to
Ayurveda. Psoriasis according to modern science and compare these diseases
according to their symptoms.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 3
Aims and Objectives
AIMS AND OBJECTIVES
1) To make comprehensive literary study on twak shareer.
2) Comparative study of twak sharer with modern and ayurvedic view.
3) To give appropriate & elaborate description on kitibha & its relation with the
4th layer of skin.
4) To study regarding kitibha kustha with modern correlation.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 4
Ayurvedic Review
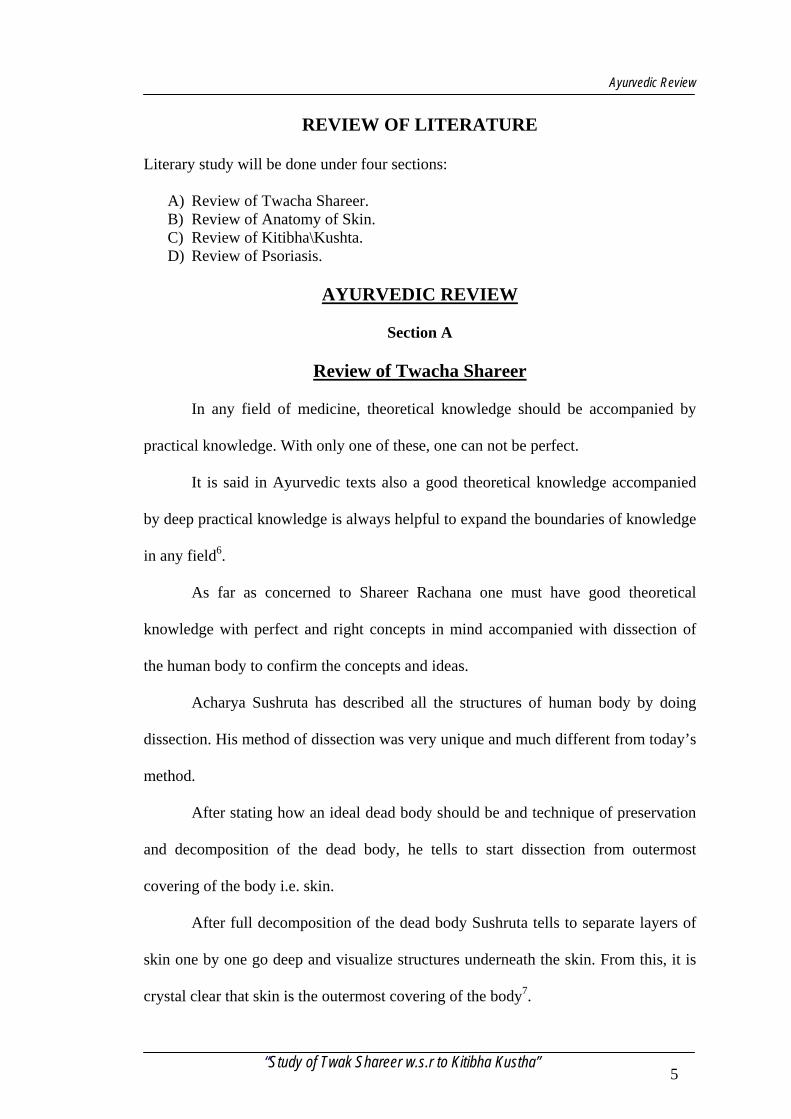
REVIEW OF LITERATURE
Literary study will be done under four sections:
A) Review of Twacha Shareer. B) Review of Anatomy of Skin. C) Review of Kitibha\Kushta. D) Review of Psoriasis.
AYURVEDIC REVIEW
Section A
Review of Twacha Shareer
In any field of medicine, theoretical knowledge should be accompanied by
practical knowledge. With only one of these, one can not be perfect.
It is said in Ayurvedic texts also a good theoretical knowledge accompanied
by deep practical knowledge is always helpful to expand the boundaries of knowledge
in any field6.
As far as concerned to Shareer Rachana one must have good theoretical
knowledge with perfect and right concepts in mind accompanied with dissection of
the human body to confirm the concepts and ideas.
Acharya Sushruta has described all the structures of human body by doing
dissection. His method of dissection was very unique and much different from today’s
method.
After stating how an ideal dead body should be and technique of preservation
and decomposition of the dead body, he tells to start dissection from outermost
covering of the body i.e. skin.
After full decomposition of the dead body Sushruta tells to separate layers of
skin one by one go deep and visualize structures underneath the skin. From this, it is
crystal clear that skin is the outermost covering of the body7.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 5
Ayurvedic Review
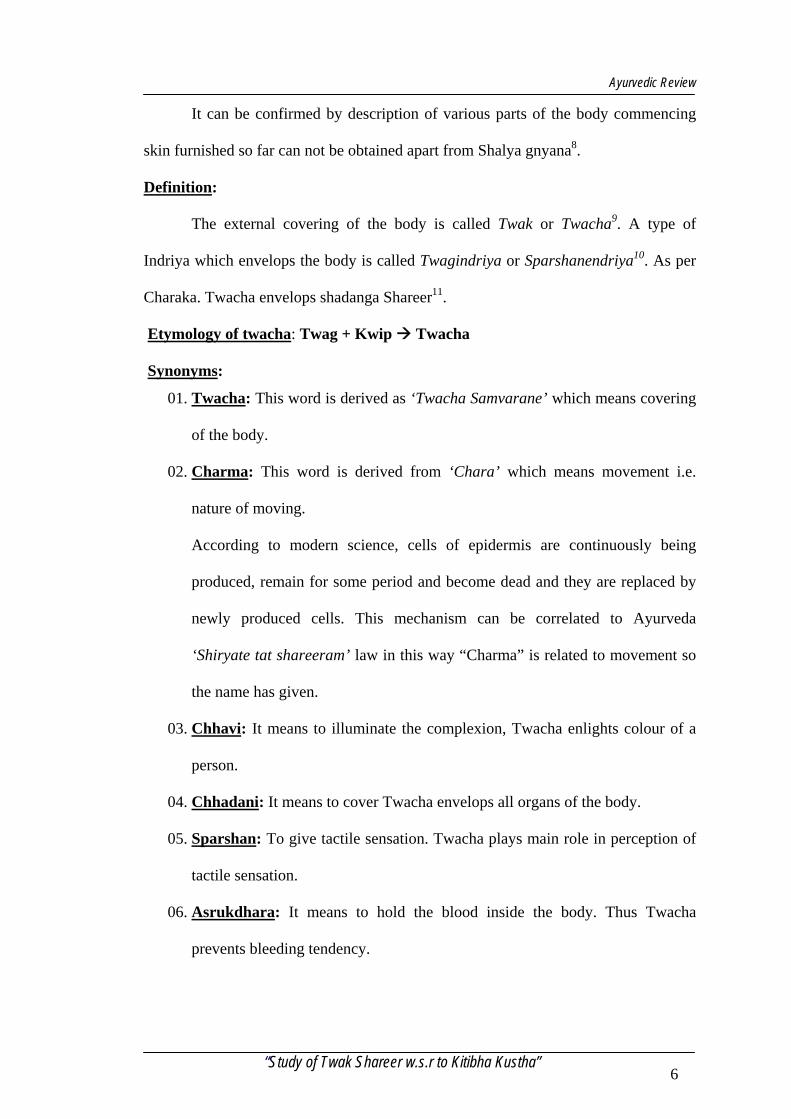
It can be confirmed by description of various parts of the body commencing
skin furnished so far can not be obtained apart from Shalya gnyana8.
Definition:
The external covering of the body is called Twak or Twacha9. A type of
Indriya which envelops the body is called Twagindriya or Sparshanendriya10. As per
Charaka. Twacha envelops shadanga Shareer11.
Etymology of twacha: Twag + Kwip Twacha
Synonyms:
01. Twacha: This word is derived as ‘Twacha Samvarane’ which means covering
of the body.
02. Charma: This word is derived from ‘Chara’ which means movement i.e.
nature of moving.
According to modern science, cells of epidermis are continuously being
produced, remain for some period and become dead and they are replaced by
newly produced cells. This mechanism can be correlated to Ayurveda
‘Shiryate tat shareeram’ law in this way “Charma” is related to movement so
the name has given.
03. Chhavi: It means to illuminate the complexion, Twacha enlights colour of a
person.
04. Chhadani: It means to cover Twacha envelops all organs of the body.
05. Sparshan: To give tactile sensation. Twacha plays main role in perception of
tactile sensation.
06. Asrukdhara: It means to hold the blood inside the body. Thus Twacha
prevents bleeding tendency.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 6
Ayurvedic Review
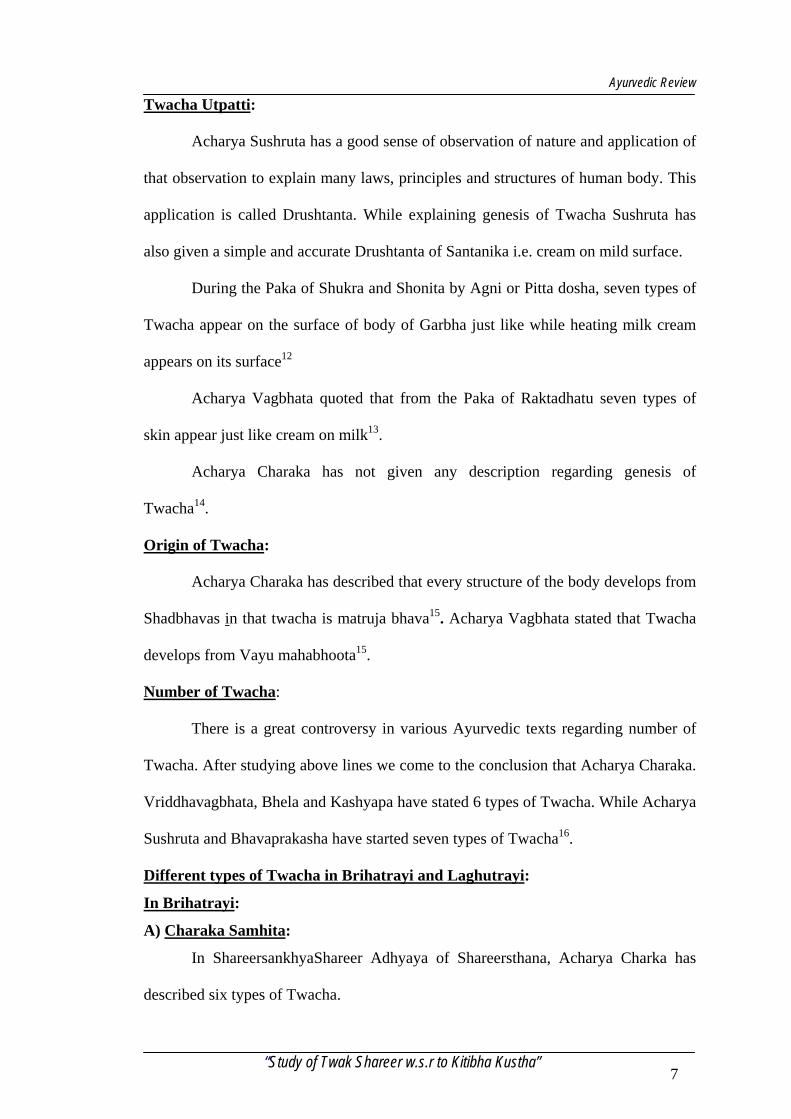
Twacha Utpatti:
Acharya Sushruta has a good sense of observation of nature and application of
that observation to explain many laws, principles and structures of human body. This
application is called Drushtanta. While explaining genesis of Twacha Sushruta has
also given a simple and accurate Drushtanta of Santanika i.e. cream on mild surface.
During the Paka of Shukra and Shonita by Agni or Pitta dosha, seven types of
Twacha appear on the surface of body of Garbha just like while heating milk cream
appears on its surface12
Acharya Vagbhata quoted that from the Paka of Raktadhatu seven types of
skin appear just like cream on milk13.
Acharya Charaka has not given any description regarding genesis of
Twacha14.
Origin of Twacha:
Acharya Charaka has described that every structure of the body develops from
Shadbhavas in that twacha is matruja bhava15. Acharya Vagbhata stated that Twacha
develops from Vayu mahabhoota15.
Number of Twacha:
There is a great controversy in various Ayurvedic texts regarding number of
Twacha. After studying above lines we come to the conclusion that Acharya Charaka.
Vriddhavagbhata, Bhela and Kashyapa have stated 6 types of Twacha. While Acharya
Sushruta and Bhavaprakasha have started seven types of Twacha16.
Different types of Twacha in Brihatrayi and Laghutrayi:
In Brihatrayi:
A) Charaka Samhita:
In ShareersankhyaShareer Adhyaya of Shareersthana, Acharya Charka has
described six types of Twacha.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 7
Ayurvedic Review
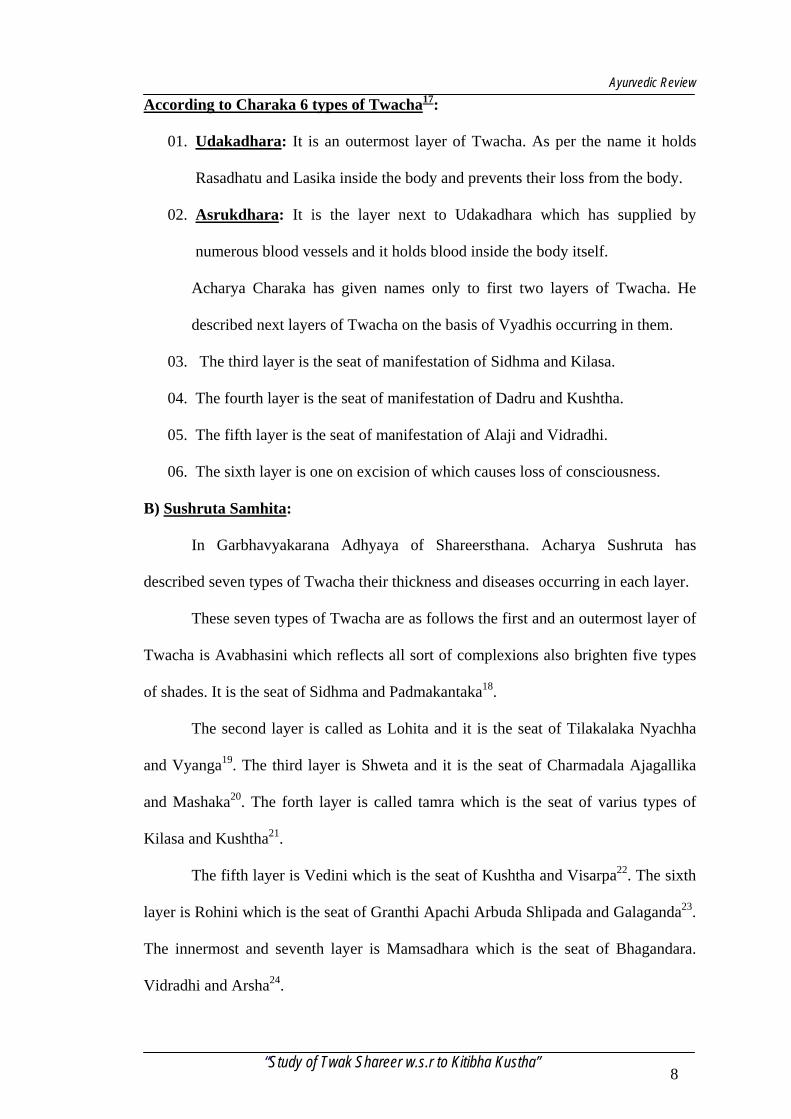
According to Charaka 6 types of Twacha17:
01. Udakadhara: It is an outermost layer of Twacha. As per the name it holds
Rasadhatu and Lasika inside the body and prevents their loss from the body.
02. Asrukdhara: It is the layer next to Udakadhara which has supplied by
numerous blood vessels and it holds blood inside the body itself.
Acharya Charaka has given names only to first two layers of Twacha. He
described next layers of Twacha on the basis of Vyadhis occurring in them.
03. The third layer is the seat of manifestation of Sidhma and Kilasa.
04. The fourth layer is the seat of manifestation of Dadru and Kushtha.
05. The fifth layer is the seat of manifestation of Alaji and Vidradhi.
06. The sixth layer is one on excision of which causes loss of consciousness.
B) Sushruta Samhita:
In Garbhavyakarana Adhyaya of Shareersthana. Acharya Sushruta has
described seven types of Twacha their thickness and diseases occurring in each layer.
These seven types of Twacha are as follows the first and an outermost layer of
Twacha is Avabhasini which reflects all sort of complexions also brighten five types
of shades. It is the seat of Sidhma and Padmakantaka18.
The second layer is called as Lohita and it is the seat of Tilakalaka Nyachha
and Vyanga19. The third layer is Shweta and it is the seat of Charmadala Ajagallika
and Mashaka20. The forth layer is called tamra which is the seat of varius types of
Kilasa and Kushtha21.
The fifth layer is Vedini which is the seat of Kushtha and Visarpa22. The sixth
layer is Rohini which is the seat of Granthi Apachi Arbuda Shlipada and Galaganda23.
The innermost and seventh layer is Mamsadhara which is the seat of Bhagandara.
Vidradhi and Arsha24.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 8
Ayurvedic Review
C) Astanga Sangraha:
In Anga Vibhaga Shareer Adhyaya of Shareersthana. Vriddha Vagbhata has
described seven layers of Twacha.
Acharya Vagbhata has given description of Twacha more or less similar to
Charaka. According to him.
01. First layer is Udakadhara.
02. Second layer is Asrukdhara.
03. Third layer is the seat of Sidhma and Kilasa.
04. Fourth layer is the seat of all types of Kushtha.
05. Fifth layer is the seat of Alaji and Vidradhi.
06. Sixth layer is Pranadhara25.
D) Ashtanga Hridaya:
Acharya Vagbhata has not given any details of twacha except the genesis of
Twacha.
In Laghutrayi:
E) Sharangadhara Samhita:
In Kaladikakhyana Adhyaya of Prathama Khanda Sharangadhara described
seven Twachas.
According to Sharangadhara:
01. First layer is Avabhasini seat of Sidhma.
02. Second is Lohita seat of Tilakalaka.
03. Third is Shweta seat of Charmadala.
04. Fourth is Tamara seat of Kilasa and Shwitra.
05. Fifth is Vedini seat of all Kushtha.
06. Sixth is Rohini seat of Granthi ganda and Apachi.
07. Seventh is Sthoola the seat of Vidradhi and it is thick equal to two Vrihi26.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 9
Ayurvedic Review
F) Madhava Nidana:
There is no description regarding Twacha in Madhavanidana.
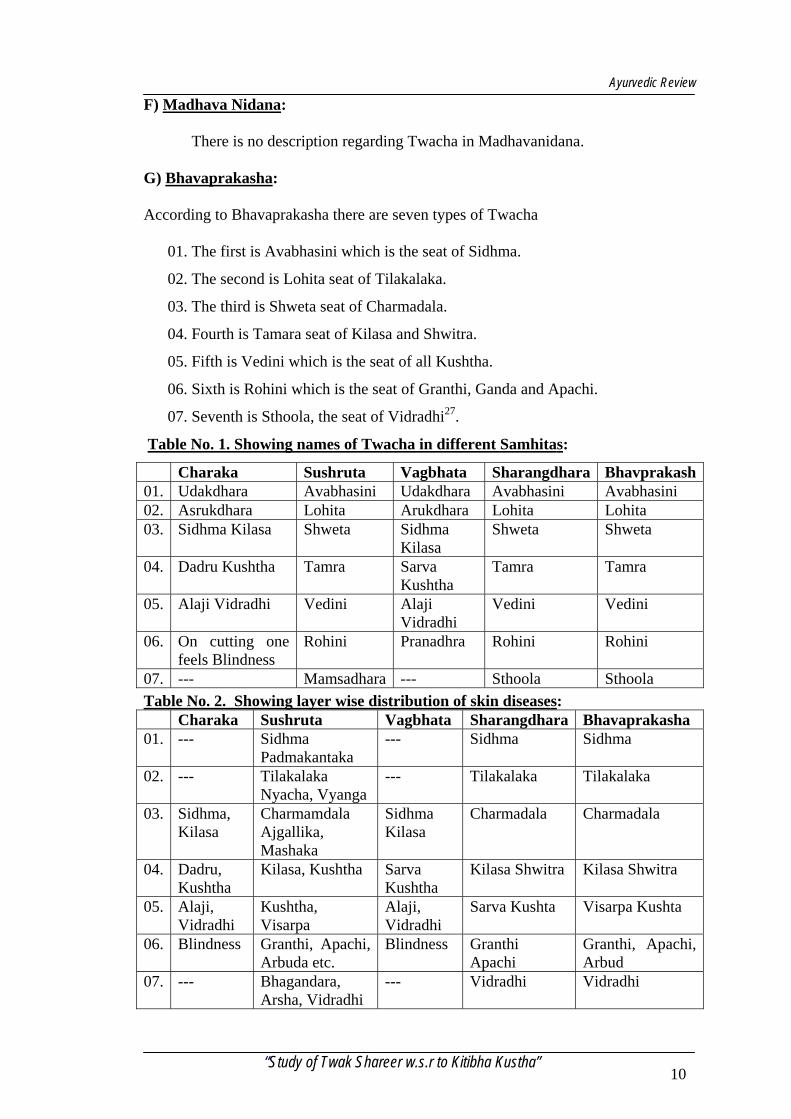
G) Bhavaprakasha:
According to Bhavaprakasha there are seven types of Twacha
01. The first is Avabhasini which is the seat of Sidhma.
02. The second is Lohita seat of Tilakalaka.
03. The third is Shweta seat of Charmadala.
04. Fourth is Tamara seat of Kilasa and Shwitra.
05. Fifth is Vedini which is the seat of all Kushtha.
06. Sixth is Rohini which is the seat of Granthi, Ganda and Apachi.
07. Seventh is Sthoola, the seat of Vidradhi27.
Table No. 1. Showing names of Twacha in different Samhitas:
Charaka Sushruta Vagbhata Sharangdhara Bhavprakash01. Udakdhara Avabhasini Udakdhara Avabhasini Avabhasini 02. Asrukdhara Lohita Arukdhara Lohita Lohita 03. Sidhma Kilasa Shweta Sidhma
Kilasa Shweta Shweta
04. Dadru Kushtha Tamra Sarva Kushtha
Tamra Tamra
05. Alaji Vidradhi Vedini Alaji Vidradhi
Vedini Vedini
06. On cutting one feels Blindness
Rohini Pranadhra Rohini Rohini
07. --- Mamsadhara --- Sthoola Sthoola
Table No. 2. Showing layer wise distribution of skin diseases: Charaka Sushruta Vagbhata Sharangdhara Bhavaprakasha 01. --- Sidhma
Padmakantaka --- Sidhma Sidhma
02. --- Tilakalaka Nyacha, Vyanga
--- Tilakalaka Tilakalaka
03. Sidhma, Kilasa
Charmamdala Ajgallika, Mashaka
Sidhma Kilasa
Charmadala Charmadala
04. Dadru, Kushtha
Kilasa, Kushtha Sarva Kushtha
Kilasa Shwitra Kilasa Shwitra
05. Alaji, Vidradhi
Kushtha, Visarpa
Alaji, Vidradhi
Sarva Kushta Visarpa Kushta
06. Blindness Granthi, Apachi, Arbuda etc.
Blindness Granthi Apachi
Granthi, Apachi, Arbud
07. --- Bhagandara, Arsha, Vidradhi
--- Vidradhi Vidradhi
“Study of Twak Shareer w.s.r to Kitibha Kustha” 10
Ayurvedic Review
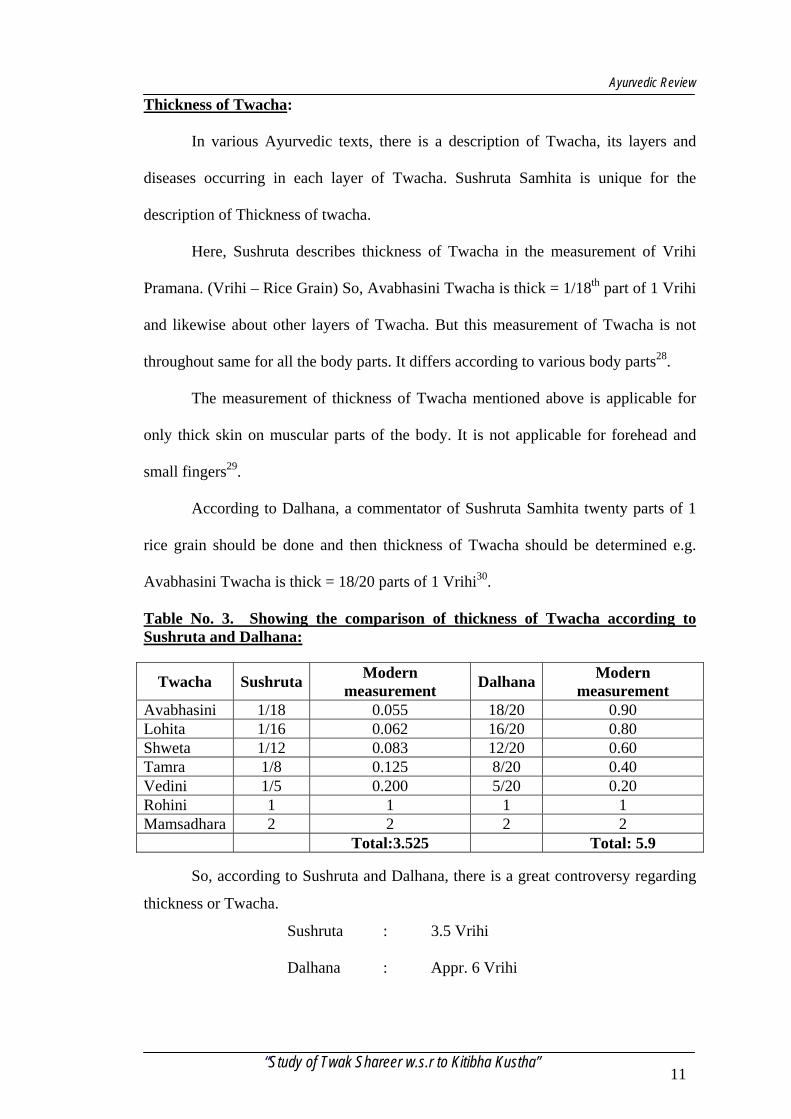
Thickness of Twacha:
In various Ayurvedic texts, there is a description of Twacha, its layers and
diseases occurring in each layer of Twacha. Sushruta Samhita is unique for the
description of Thickness of twacha.
Here, Sushruta describes thickness of Twacha in the measurement of Vrihi
Pramana. (Vrihi – Rice Grain) So, Avabhasini Twacha is thick = 1/18th part of 1 Vrihi
and likewise about other layers of Twacha. But this measurement of Twacha is not
throughout same for all the body parts. It differs according to various body parts28.
The measurement of thickness of Twacha mentioned above is applicable for
only thick skin on muscular parts of the body. It is not applicable for forehead and
small fingers29.
According to Dalhana, a commentator of Sushruta Samhita twenty parts of 1
rice grain should be done and then thickness of Twacha should be determined e.g.
Avabhasini Twacha is thick = 18/20 parts of 1 Vrihi30.
Table No. 3. Showing the comparison of thickness of Twacha according to Sushruta and Dalhana:
Twacha Sushruta Modern measurement Dalhana Modern
measurement Avabhasini 1/18 0.055 18/20 0.90 Lohita 1/16 0.062 16/20 0.80 Shweta 1/12 0.083 12/20 0.60 Tamra 1/8 0.125 8/20 0.40 Vedini 1/5 0.200 5/20 0.20 Rohini 1 1 1 1 Mamsadhara 2 2 2 2
Total:3.525 Total: 5.9
So, according to Sushruta and Dalhana, there is a great controversy regarding
thickness or Twacha.
Sushruta : 3.5 Vrihi
Dalhana : Appr. 6 Vrihi
“Study of Twak Shareer w.s.r to Kitibha Kustha” 11
Ayurvedic Review
If practically observed and thickness of 1 vrihi is measured it becomes average
1mm. So, the thickness of twacha told by Sushruta and Dalhana expressed in modern
measured will be:
Sushruta : 3.5 mm
Dalhana : Appr. 6 mm
If we want to compare this measurement with modern measurement (skin
thickness = 1.5 to 4 mm), then Sushruta seems to be perfect and more accurate in
telling thickness of skin. Because according to Dalhana, it becomes 6mm which is
highly impossible.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 12
Ayurvedic Review
TWACHA KRIYA SHAREERA
Twacha & Tridosha relation:
01. Vata Dosha:
While describing abodes of Doshas, Vagbhata says Twacha is one of the
abode of Vatadosha. Out of 5 types or Vata, especially Prana and Udana are directly
related to Twacha. Pranavayu is responsible for the tactile sensation. Twacha is able
to perceive sensations like cold, heat, roughness, smoothness with the help of
Pranavayu itself31.
The other type of Vata i.e. Udana Vayu produces varna and if it gets vitiated
then there is discolouration of skin32.
2. Pitta Dosha:
Besides Vatadosha. Twacha is an abode of Pittadosha also Nabhi, Amashaya,
Sweda, Lasika, Rakta, Rasa, Druk(Drushti) and Sparshana (Twacha) are the abodes of
Pitta. Out of five types of Pitta. Bhrajaka Pitta is mainly related to Twacha33.
Bhrajaka Pitta is situated in the skin and its main function is Bhrajana of
Twacha34 (i.e. to maintain the Teja of Twacha).
The Pitta in the skin is known as Bhrajaka pitta, which is responsible for
absorption of drugs externally in the form of massage, bath, dipping, paste etc. and
also illuminates various shades of complexion35.
3. Kapha Dosha:
One of the Gunas of Kapha is Snigdha due to this Guna of Kapha oily nature
of Twacha is maintained. If Kshaya of Kapha dhatu happens, then Snigdha guna
decreases and due to this Twacha becomes dry and cracky in nature.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 13
Ayurvedic Review
Twacha & Saptadhatu relation:
There is a very close relation between Saptadatus and Twacha.
01. Rasa : Twacha is a huge structure and it requires nourishment
of Rasadhatu for its well beings.
02. Rakta : Raktadhatu is present in raktavahi Dhamnis. Twacha is
richly supplied by Raktadhatu and also called as
Asrukdhara.
03. Mamsa : Twacha is theMoolasthana of Mamsavaha Srotasa. Vasa
and shat Twacha are generated from the mamsa itself.
So that mamsa dhatu and Twacha are intimately related
to each other.
04. Meda : The mala of meda dhatu is Sweda and Sweda is
expelled out of the body through Twacha and in this
way these two are related.
05. Asthi : The kitta of Asthi are Kesha and Loma which emerge
out from Twacha.
06. Majja : Mala of Majja is Sneha of Netra. Purisha and Twacha.
Twacha & Mala Relation:
Twacha is mainly related to Sweda. Twacha is having innumerable
Bahirmukha srotamsi through which Sweda is excreted out f the body. Thus Twacha
acts as biggest Malayana of body. Decrease in amount of Sweda causes hair loss, loss
of sensation and cracks in the skin36.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 14
Ayurvedic Review
Twacha & Panchamahabhoota Relation:
Each and every structure of the body is having Panchabhautik constitution
even on the cell level also.
Twacha is also having Panchabhautik nature.
Element Structure Parthiva Kesha, Loma Aapya Rasa, Lasiak Tejas Kanti, Varna Vayviya Sparsha, Samvedna Akashiya Lomakoopa, Sweda Vahi Nalika
Twacha & Upadhatu Relation: Every Dhatu have its own Upadhatu Vasa and Shat – Twacha are Upadhatu of
Mamsadhatu37.
Twacha & Srotasa Relation:
Twacha is closely related to Swedavaha Srotasa and mamsavaha Srotasa.
01. Swedawaha Srotasa:
Meda and Lomakoopa are the roots of Swedavaha Srotasa out of which
Lomakoopa are present in the skin in the form of numerous openings. Also twacha
acts as a medium for evaporation of Sweda outside the body38.
02. Mamsavaha Srotasa:
According to Sushruta and Charaka, Snayu and Twacha are the roots of
mamsavaha Srotasa39.
Twacha and Varna Relation:
Varna of a person is expressed in the Twacha. It is determined during foetal
life. In Charaka Shareera the varna of a foetal is determined in sixth month of
intrauterine life40.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 15
Ayurvedic Review
This Varna is of four types:
Teja element is the main factor for the complexion. When at the time of
conception. It is predominantly associated with Aapa element, it makes Gaura Varna.
If Prithvi dhatu is predominant, then it produces Shyma (black) Varna. Predominance
of Prithvi and Akasha with it produces Krishna Shyama (black sky) Varna. While
predominance of Aapa and Aakasha element produces. Gaura Shyama (Fair Sky)
complexion41.
Some Acharyas say that diet taken by a pregnant woman determines
complexion of the foetus. But Charaka has described three types of Varna.
Tejas element in combination with Udaka and Antariksha produces Avadata
(fair) Varna with Prithvi and vayu produces Krushna (black) Varna and with the same
amount of all elements produces Shyama (Blackish) Varna42. On the other hand.
Charka describes four types of Varna in Indriyasthana. These are Krishna (black)
Shyama (Blackish), Shyamavadata and Avadata43 (fair).
Twacha & Prakriti Relation:
01. Vata Prakruti: Persons having Vata prakruti have Ruksha, Khara. Twacha
and is of Sheeta Sparsha. It is blackish in colour and almost having no sweat
or less sweat.
02. Pitta Prakruti: Persons of Pitta Prakruti have fair or yellowish Twacha
having Ushana Sparsha and there is profuse sweating from the skin with bad
odour.
03. Kapha Prakruti: People having Kapha Prakruti have soft, while (Gaura) and
oily skin.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 16
Ayurvedic Review
Twacha & Sara Relation:
Sara is considered to be the cream part of the respective Dhatu. Each Dhatu has its sara
and in the person having sarata of particular Dhatu, there are all good characters of that Dhatu.
In case of Twacha, Rasasara is considered as Twaksara. As Rasadhatu is spread all over the
Twacha. Rasasara is considered as Twaksara44. Twaksara person have a fresh, lustrous, smooth
skin with deep routed and tender hair45. According to Charaka, Twaksara person is having
unctuous smooth, soft, clear, fine, less numerous, deep routed and tender hair46.
Twacha & Rogamarga Relation:
There are three types of Rogamarga these are Shakha, Marma, Asthi, Sandhi and
Koshtha. Twacha is included in Shakha marga alongwith Rakta and other dhatus. These come
in Bahya Rogamarga47.
Twacha as a Gnyanendriya:
Human body is made up of Pancha Gnyanendriya and Panch Karmendriya. Ear, Skin,
Eyes, Tongue and Nose are five sense organs according to Ayurveda48. These organs are the
abodes of their respective Indriyas49. Twacha is one of Gnyanednriyas which is Vayaviya in
nature50.
The Indriya, which is responsible for reception of touch sense is Sparshnendriya and
Twacha is its abode (i.e. Adhishthana)51
The important property of Vayu is Sparsha and its reception through Sparshanendriya
to enable all the movements in the body to bring lightness to body and to create impulses in
body52.
In all Indriyas, Sparshanendriya is an entity that occupies all other Indtriyas, Mana is
also intimately related to Twacha as it is also all encompassing as well as Twacha occupies the
whole body53.
Prithvi, Jala, Teja and Vayu are characterized by Kharatva (roughness), dravatva
(Liquidity), Chalatva (mobility) and Apratighata (Unobstructibility) respectively. All these
attributes are perceived by tactile sense organ. Touch together with its absence is perceived by
tactile sense organ54.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 17
Ayurvedic Review
DISEASE REVIEW:
Kitibha:
The disorder kustha is said to occur in the 4th and 5th layer of skin (su.sha.4/4).
Nidana of kitibha:
There is no specific reference regarding the etiological factor for kitibha
kustha, at the same time no particular aetiology has been depicted for any of the
different varieties of kustha specifically. The general causes have been described
which becomes aetiological factors for the formation of kustha.
For example – taking diet against the regimen given in the literatures specially
eating guru and virudha and asatmya ahara, eating during indigestion after
consumption of liquid substances or post vomiting period, after exercise, after coitus
etc, eating non-veg with milk etc , entering extreme heat, causing sudden vomiting
with holding vomiting ( Su. Ni 5/4)
Further it is stated that the effect of karma like murder of a Brahmin, lady,
pious person, abducting other women etc causes kustha (Su. Ni 5/30)
It is stated that kustha occurs even after the rebirth of person afflicted with
disease in the previous life. (Su. Ni 5/31)
In susrutha chikitsa 9/9 the similar aetiology has been given in nutshell.
Charaka 7/48, M.N. 49/1-5, B.P 54, given the similar opinion regarding the aetiology
of kustha in genera.
This general description of aetiology in respect to kustha is applicable too
either of the 18 kusthas and this applies to kitibha kustha too.
Samprapti:
The vitiated doshas, influence the dhatus in general and rakta in particularly
the above said factors vitiated pitta, rakta and sleshma along with vayu which is
“Study of Twak Shareer w.s.r to Kitibha Kustha” 18
Ayurvedic Review
vitiated and increased, move along tiryak sirah and erupt in bahya marga and exhibit
their present. The lodging of vitiated and increased doshas caused circumscribed
lesion on the skin. Then this doshas get localized increase and if neglected enter the
other dhatu. Su.Ni.5./5, cha. Chi9-10, M.Ni.49/6 BP 54/6.
Astanga hrudaya states, the aggravated doshas enters the channels and vitiates
the twacha, lasika , raktas and muscles and discolouration of skin noted ( A.S.Ni 14/3-
5, A.H.Ni 14/2-3)
Purvarupa:
In general their will be roughness of skin horripilation (Roma harsha) itching
(kandu), excessive sweating or no sweating at all, sometimes anesthesia of the part,
blackish discolouration seen as a premonitory symptom of kusthas ( Su.Ni. 5/4)
Charaka further says burning sensation, instantaneous appearance of ulcer,
excessive pain, all explanation of patches etc as the premonitory symptoms (Cha.Chi.
7/11-12)
The kusthas are said to occur due to Vata, Pita and also due to formation of
krimi or bacteria. However, dosha predominance is supreme in manifestation of this
disease (Su.Ni.5/6).
Roga lakshana:
As far as aetiology, pathology and premonitory symptomatology is concerned,
all the acharyas have given the general description of kustha only. However the
symptomatology has been specified by all the authors as far as the separate varieties
are concerned.
The symptoms of kitibha are circumscribed, eruption, discharge, thick skin,
itching, glossy or blackish in colour, cloudy in colour (Su.Ni 5/13)
Ca.Ci 7/21, M.Ni 49/17, B.P 54/25, Y.R.Ni 20/20,
“Study of Twak Shareer w.s.r to Kitibha Kustha” 19
Ayurvedic Review
Agree with the susrutha’s opinion along with addition of parusha, sparsha.
Astanga sangraha adds to above symptoms cryptation on scratching (A.S.Ni 14/22)
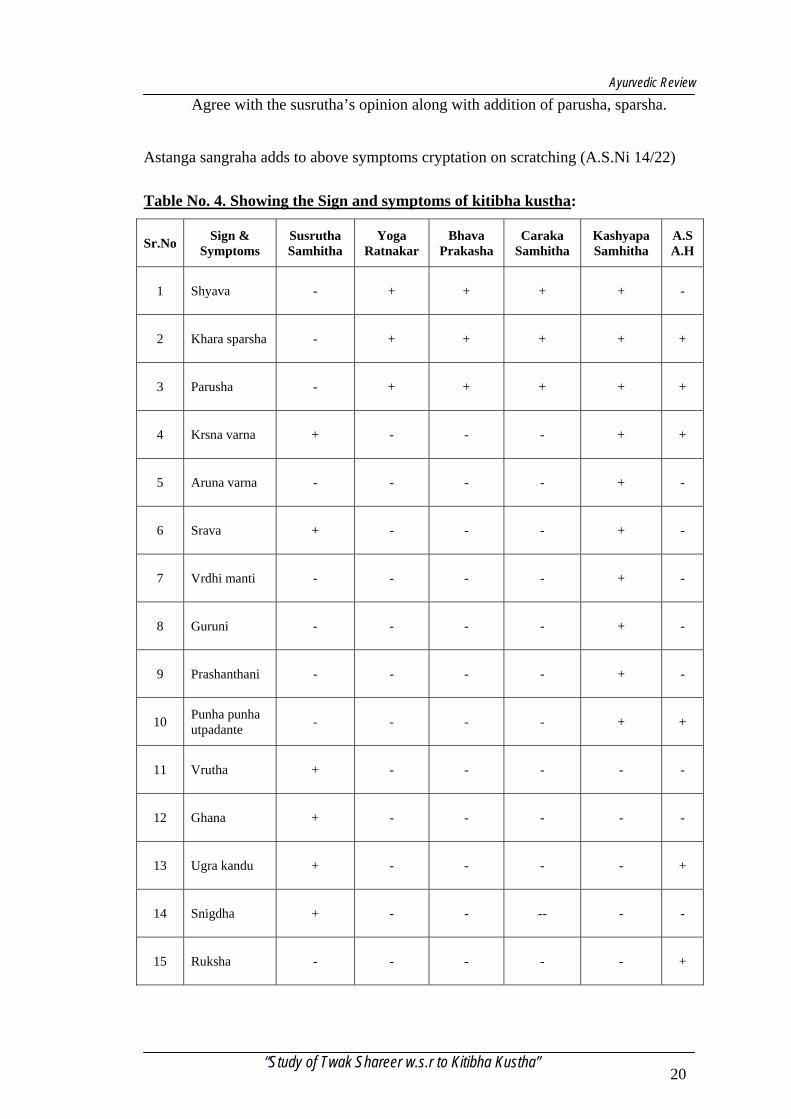
Table No. 4. Showing the Sign and symptoms of kitibha kustha:
Sr.No Sign & Symptoms
Susrutha Samhitha
Yoga Ratnakar
Bhava Prakasha
Caraka Samhitha
Kashyapa Samhitha
A.S A.H
1 Shyava - + + + + -
2 Khara sparsha - + + + + +
3 Parusha - + + + + +
4 Krsna varna + - - - + +
5 Aruna varna - - - - + -
6 Srava + - - - + -
7 Vrdhi manti - - - - + -
8 Guruni - - - - + -
9 Prashanthani - - - - + -
10 Punha punha utpadante - - - - + +
11 Vrutha + - - - - -
12 Ghana + - - - - -
13 Ugra kandu + - - - - +
14 Snigdha + - - -- - -
15 Ruksha - - - - - +
“Study of Twak Shareer w.s.r to Kitibha Kustha” 20
Modern Review
MODERN REVIEW
Anatomy of the Skin:
Normal skin:
The skin is tough and a uniform protective covering of the entire surface of the
body and deeper tissues, with its all derivatives know as Integument (Latin – a
covering). It contains the peripheral ending of many sensory nerves. Skin regulates
body temperature and possesses limited excretory and observing powers. In adults skin
covers about 2m.sq area and has weight of approximately 4-5kg. Its thickness is 0.5 – 4
mm depending on its location. The thickness of the skin increases gradually after birth
until age of 30 and then slowly begins to thin down. The human skin shows wide
regional variation in structure like scalp, face, ear lobes, back, palms and soles etc.
The skin is a largest organ in the human body it consist of vascular connective
tissue named corneum dermis and an external covering of epithelium called as
epidermis. The sweat gland, sebaceous glands and hair follicles are embedded beneath
it and called as appendages of development of skin in foetus.
Deep to dermis is sub-cutaneous layer this layer is also called superficial
fascia or hypodermis, consist of aeriolar and adipose tissues. Fibres from dermis
extent into the sub-cutaneous layer inturn attaches to the underline tissues and organs.
So, the skin is composed of 3 distinct layers from surface of downward and they are,
A. Epidermis
B. Dermis
C. Hypodermis.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 21
Modern Review
Embryological formation of skin:
A. Epidermis - Surface ectoderm, melanoblast (dendritic cells) from neural crest.
B. Dermis - Mesenchyme derived from dermatomes of Somites.
C. Nails - Ectoderm of each digital tip, later migrates to dorsal surface.
D. Hair - Surface ectoderm, which is modified to form hair follicles.
E. Sebaceous glands – Arise as diverticula’s from hair follicles.
F. Sweat glands - Develop as down growth from the epidermis later canalized.
Epidermis:
The epidermis is formed by non-vascular stratified epithelium. It varies in
thickness from 0.04 mm on the eyelid to 1.6 mm on the palms with an average
thickness of less than 0.17mm (1/200th of an inch) in most areas except for those areas
chronically exposed to pressure and friction but it may exist to an extent at birth.
The most superficial layers of cells from the horny zone (Stratum chorneum)
which may be separated by maceration from deeper stratum turned as germinative
zone. There is network of linear furrows of variable size divide the surface into
number of polygonal or lozenge shaped areas. These furrows are conspicuous
opposite the flexures of joint. The lines are fine but very distinct upon the palmer
surface of hands, fingers and soles of the feet. The lines of the tips of finger and
thumbs from distinct pattern.
The deeper surface of epidermis is accurately molded upon the papillary layer
of corneum which prevent the epithelium from being stripped off. The surface of the
“Study of Twak Shareer w.s.r to Kitibha Kustha” 22
Modern Review
skin by sharing stresses it is metabolically active, stratified squamous, cornifying
epithelium i.e. populated 4 types of cell. Keratinocytes is for the most part and
Melanocytes, langerhans cell and marked cells in decreasing sparsity.
Epidermis:
The stratified, squamous, cornifying epithelium that is populated by 4 types of cells.
a. Keratinocytes
b. Melanocytes
c. Langerhan cells
d. Merkel cells
A. Keratinocytes:
90% of epidermal cells are Keratinocytes they produce a protein called
keratin. These substances helps waterproof and protect the skin and underlying tissues
from light, heat, microbes, many chemicals. Anchoring junctions, desmosomes held
Keratinocytes to one another.
Epidermal Keratinocytes undergoes characteristic changes as they are
progressively moved upward from basal of epidermis to the chornified layer. Four
interrelated cellular layer i.e. basal, spinosum, granular, chornified can be recognized
as successive stage of differentiation of germinal Keratinocytes to chornified
keratinocyte.
Epidermal chornification is a form of cellular differentiation that results in the
formation of the outermost dead layer of skin.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 23
Modern Review
B. Melanocytes:
Melanocytes are dendritic cells Melanocytes are pigment producing cells of
neuro ectodermal origin. This cell synthesized melanin from tyrosin, a pigment
responsible for skin colour and essential for protection from UV light. Amount of the
melanin in Keratinocytes determines the skin colour. Facial differences in colour are
the result of metabolically active Melanocytes.
Melanocytes appear microscopically as clear cells in and immediately beneath
the basal layer of epidermis. The nucleus of a Melanocytes is smaller and more deeply
basophilic then that of Keratinocytes.
The ratio of Melanocytes to Keratinocytes in the basal layer of epidermis
varies from 1:4 to 1:10 depending on the region of body ex:- Melanocytes are more
abundant in the skin of chicks then in that of abdomen.
There are two classes of integumentary melanin. Eumelanin produced in
ellipsoidal melanosomes (Eumelanosomes) account for the brown and black colours
of both skin and hair. Pheomelanin, produced in perikal melanosomes
(pheomelanosome) account for the lighter colour of hair, ranging from yellow to
reddish brown.
It is the amount of melanin in Keratinocytes that determines the degree of
pigmentation of skin and hair. The principle function of melanin is to protect the skin
from the harmful effect of sunshine by scattering and observing ultraviolet.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 24
Modern Review
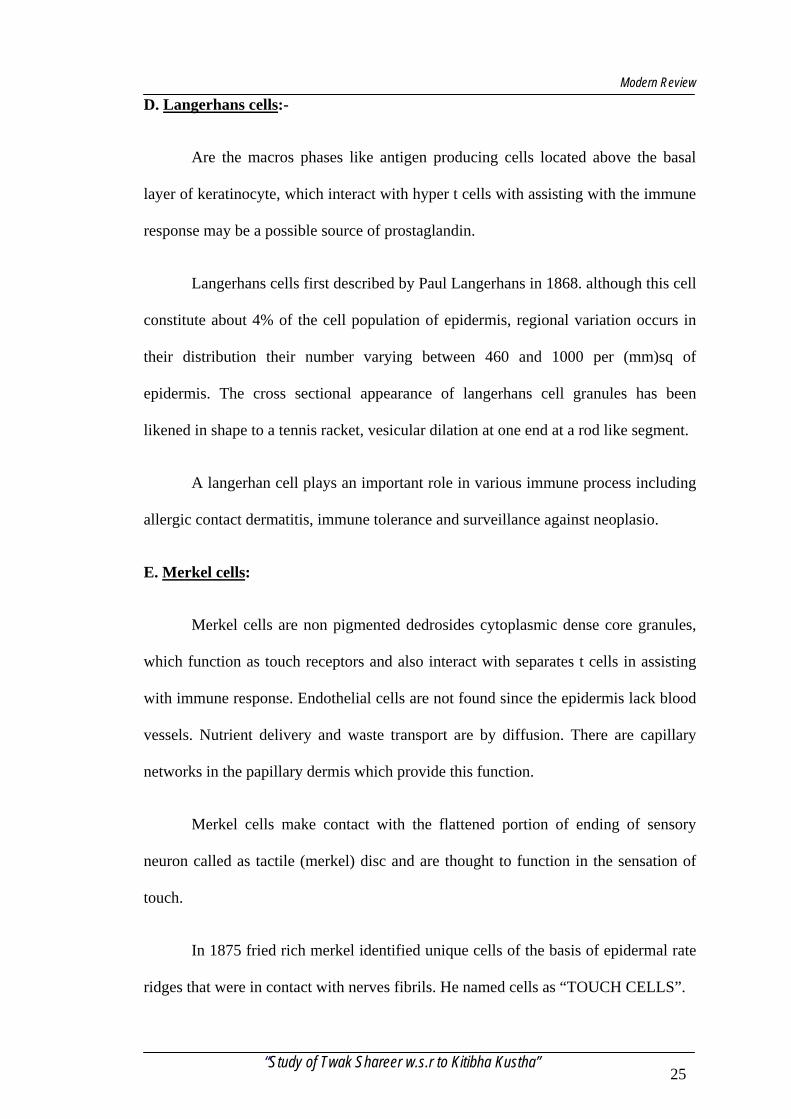
D. Langerhans cells:-
Are the macros phases like antigen producing cells located above the basal
layer of keratinocyte, which interact with hyper t cells with assisting with the immune
response may be a possible source of prostaglandin.
Langerhans cells first described by Paul Langerhans in 1868. although this cell
constitute about 4% of the cell population of epidermis, regional variation occurs in
their distribution their number varying between 460 and 1000 per (mm)sq of
epidermis. The cross sectional appearance of langerhans cell granules has been
likened in shape to a tennis racket, vesicular dilation at one end at a rod like segment.
A langerhan cell plays an important role in various immune process including
allergic contact dermatitis, immune tolerance and surveillance against neoplasio.
E. Merkel cells:
Merkel cells are non pigmented dedrosides cytoplasmic dense core granules,
which function as touch receptors and also interact with separates t cells in assisting
with immune response. Endothelial cells are not found since the epidermis lack blood
vessels. Nutrient delivery and waste transport are by diffusion. There are capillary
networks in the papillary dermis which provide this function.
Merkel cells make contact with the flattened portion of ending of sensory
neuron called as tactile (merkel) disc and are thought to function in the sensation of
touch.
In 1875 fried rich merkel identified unique cells of the basis of epidermal rate
ridges that were in contact with nerves fibrils. He named cells as “TOUCH CELLS”.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 25
Modern Review
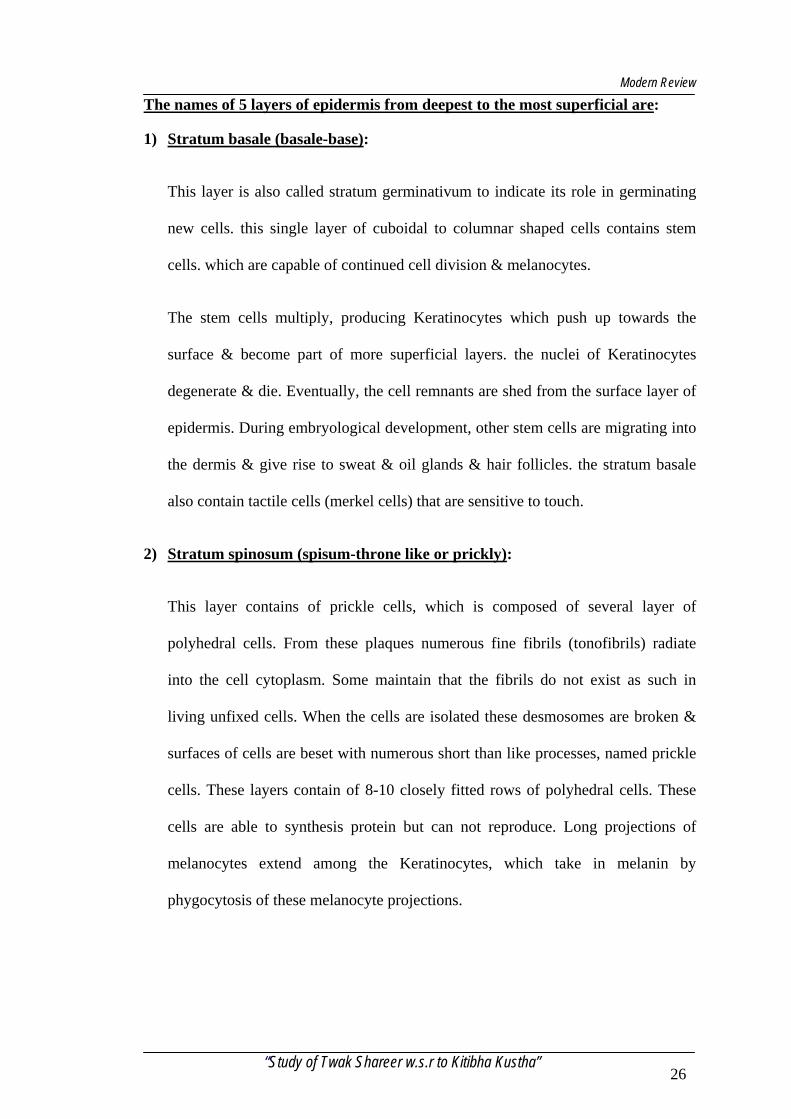
The names of 5 layers of epidermis from deepest to the most superficial are:
1) Stratum basale (basale-base):
This layer is also called stratum germinativum to indicate its role in germinating
new cells. this single layer of cuboidal to columnar shaped cells contains stem
cells. which are capable of continued cell division & melanocytes.
The stem cells multiply, producing Keratinocytes which push up towards the
surface & become part of more superficial layers. the nuclei of Keratinocytes
degenerate & die. Eventually, the cell remnants are shed from the surface layer of
epidermis. During embryological development, other stem cells are migrating into
the dermis & give rise to sweat & oil glands & hair follicles. the stratum basale
also contain tactile cells (merkel cells) that are sensitive to touch.
2) Stratum spinosum (spisum-throne like or prickly):
This layer contains of prickle cells, which is composed of several layer of
polyhedral cells. From these plaques numerous fine fibrils (tonofibrils) radiate
into the cell cytoplasm. Some maintain that the fibrils do not exist as such in
living unfixed cells. When the cells are isolated these desmosomes are broken &
surfaces of cells are beset with numerous short than like processes, named prickle
cells. These layers contain of 8-10 closely fitted rows of polyhedral cells. These
cells are able to synthesis protein but can not reproduce. Long projections of
melanocytes extend among the Keratinocytes, which take in melanin by
phygocytosis of these melanocyte projections.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 26
Modern Review
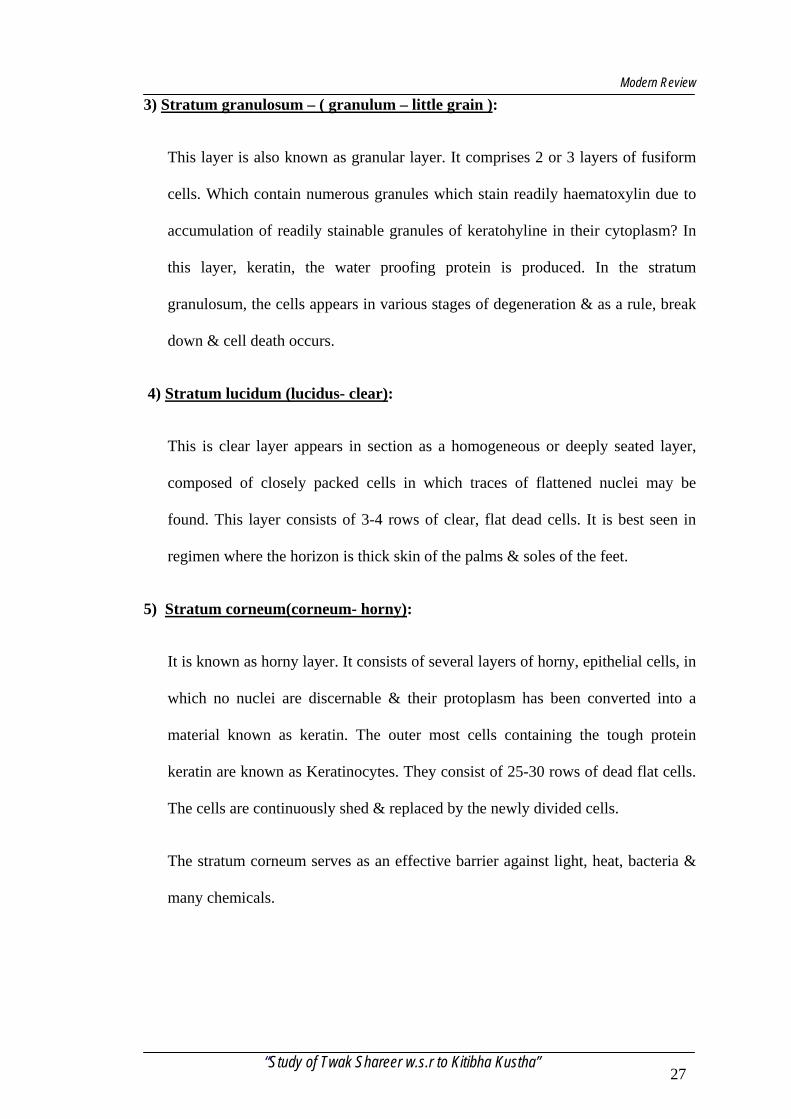
3) Stratum granulosum – ( granulum – little grain ):
This layer is also known as granular layer. It comprises 2 or 3 layers of fusiform
cells. Which contain numerous granules which stain readily haematoxylin due to
accumulation of readily stainable granules of keratohyline in their cytoplasm? In
this layer, keratin, the water proofing protein is produced. In the stratum
granulosum, the cells appears in various stages of degeneration & as a rule, break
down & cell death occurs.
4) Stratum lucidum (lucidus- clear):
This is clear layer appears in section as a homogeneous or deeply seated layer,
composed of closely packed cells in which traces of flattened nuclei may be
found. This layer consists of 3-4 rows of clear, flat dead cells. It is best seen in
regimen where the horizon is thick skin of the palms & soles of the feet.
5) Stratum corneum(corneum- horny):
It is known as horny layer. It consists of several layers of horny, epithelial cells, in
which no nuclei are discernable & their protoplasm has been converted into a
material known as keratin. The outer most cells containing the tough protein
keratin are known as Keratinocytes. They consist of 25-30 rows of dead flat cells.
The cells are continuously shed & replaced by the newly divided cells.
The stratum corneum serves as an effective barrier against light, heat, bacteria &
many chemicals.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 27
Modern Review
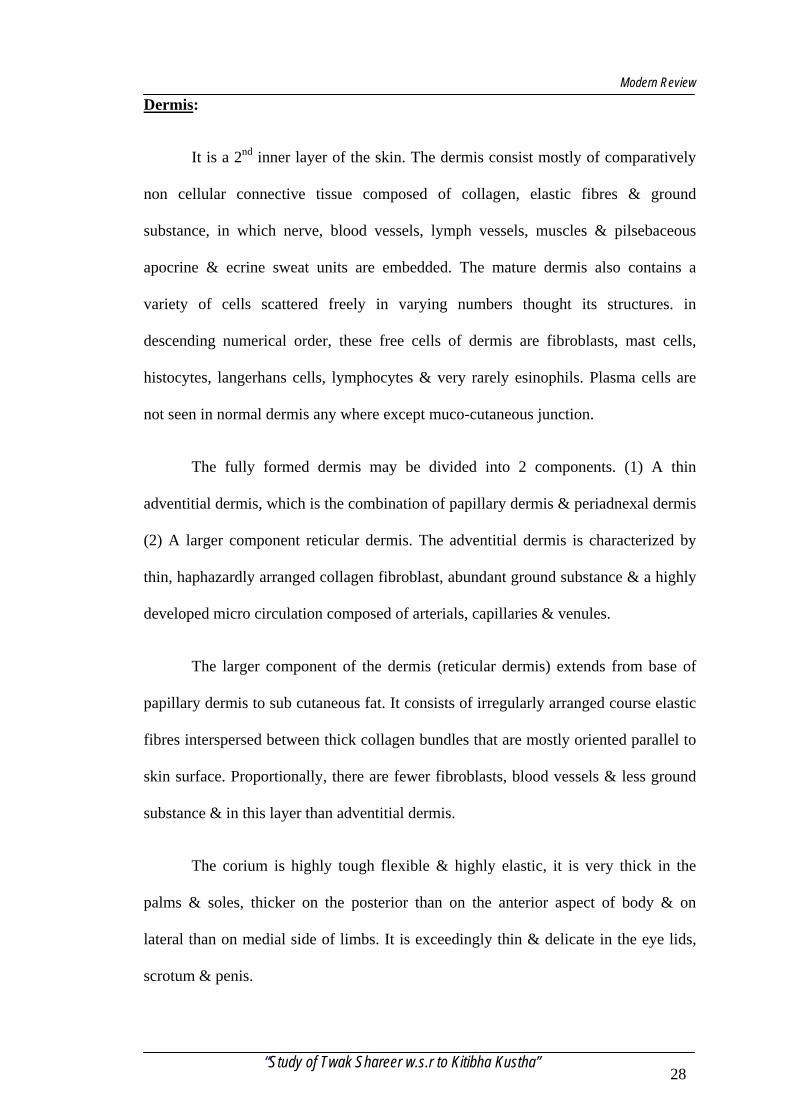
Dermis:
It is a 2nd inner layer of the skin. The dermis consist mostly of comparatively
non cellular connective tissue composed of collagen, elastic fibres & ground
substance, in which nerve, blood vessels, lymph vessels, muscles & pilsebaceous
apocrine & ecrine sweat units are embedded. The mature dermis also contains a
variety of cells scattered freely in varying numbers thought its structures. in
descending numerical order, these free cells of dermis are fibroblasts, mast cells,
histocytes, langerhans cells, lymphocytes & very rarely esinophils. Plasma cells are
not seen in normal dermis any where except muco-cutaneous junction.
The fully formed dermis may be divided into 2 components. (1) A thin
adventitial dermis, which is the combination of papillary dermis & periadnexal dermis
(2) A larger component reticular dermis. The adventitial dermis is characterized by
thin, haphazardly arranged collagen fibroblast, abundant ground substance & a highly
developed micro circulation composed of arterials, capillaries & venules.
The larger component of the dermis (reticular dermis) extends from base of
papillary dermis to sub cutaneous fat. It consists of irregularly arranged course elastic
fibres interspersed between thick collagen bundles that are mostly oriented parallel to
skin surface. Proportionally, there are fewer fibroblasts, blood vessels & less ground
substance & in this layer than adventitial dermis.
The corium is highly tough flexible & highly elastic, it is very thick in the
palms & soles, thicker on the posterior than on the anterior aspect of body & on
lateral than on medial side of limbs. It is exceedingly thin & delicate in the eye lids,
scrotum & penis.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 28
Modern Review
Structural anatomy:
The corium consists of felted connected tissue with a varying number of
elastic fibres, numerous blood vessels, lymphatic vessels & nerves. The connective
tissue is arranged in 2 layers, deeper (reticular) & superficial(papillary) layer.
Unstirred muscular fibres are found in superficial layers wherever hairs are
present; they are also present in subcutaneous aeriolar tissue of scrotum, penis, labia
majora & nipples.
It is derived from the mesoderm & its thickness is varying from 2-4 mm.
dermis is vascularised & innervated. It is composed of connective tissue containing
collagenous & elastic fibres, which provides strength & elasticity to the dermis.
A] Papillary layer:
The papillary layer consist of numerous highly sensitive & vascular eminences
, termed papillae which rise perpendicularly .The papillae are minute conical
projections , having round or blunted extremities ,which may be surfaces of
epidermis. On the general surface of the body & especially in parts endowed with
slight sensibility, they are few in number & exceedingly minute. But upon the palmer
surfaces of hands & fingers & plantar surfaces of feet & toes, they are larger &
closely aggregated together & arranged in parallel curved lines forming elevated
ridges seen on the epidermis.
Each ridge contains 2 rows of papillae & between the rows the ducts of sweat
gland pass outwards to open on the summits of the ridges. Each papillae consist of
very small & closely interlacing bundles of finely fibrillated tissue, with a few elastic
“Study of Twak Shareer w.s.r to Kitibha Kustha” 29
Modern Review
fibres, within this tissue there is a capillary loop & in some papillae especially in
palms of hands & fingers. There are tactile corpuscles.
Papillary layer has many small, elongated projections called rete peges, also
contains loops of capillaries & these projects into epidermis. Size & arrangement of
dermal papillae from ridge which are external surface of epidermis & provide
attachment of epidermis to dermis & its collagen fibres. In some dermal papillae are
present meissner’s corpuscles, the nerve ending sensitive to light touch.
B] Reticular layer:
It consist of strong inter lacing bands, composed cheaply of white fibrous
tissue & containing some yellow elastic fibres, which vary in number in different
parts. In the deeper part the fasciculi are course & large intervals left by their
interlacement are occupied by adipose tissue & sweat glands. below reticular layer,
there is subcutaneous areolar tissue which except in a few situations contains fat. The
connective tissue bands in reticular layer lie for the main part in parallel bundles so
that if conical object is stabbed through skin & then withdrawn it leaves a linear
wound since the fibres are forced apart with much rupture. The directions taken by the
parallel bundles vary in different part of the body & constitute what are termed the”
cleavage lines”, which heal with formation of scar tissue, where as the incision across
these lines, owing to retraction of the several fibres lead to the formation of the broad
scar.
The cleavage lines are arranged longitudinally in the skin of the limbs & more
or less horizontally in the trunk & neck. With increasing age the yellow elastic fibres
atrophy and the skin loses much of its elasticity and become wrinkled. If the skin
becomes much stretched (as by rapidly growing tumours, fat deposition or pregnancy)
“Study of Twak Shareer w.s.r to Kitibha Kustha” 30
Modern Review
the fibres in reticular layer may undergo partial rupture, followed by scar formation;
these areas may show on the surface as white streaks. These are commonly seen in the
anterior wall of abdominal wall after pregnancy and known as linear gravidarum.
In many regions the skin is separated from deep fascia or other structures by
loose areolar tissue and where the skin is freely movable over the deeper structures.
Elsewhere, however, the skin may be firmly anchored to structures like the
periosteum over” subcutaneous” parts of bones or to the deep fascia in regions related
to movements of underlying joints. In joints there are permanent creases known as
“flexure lines”; they are particularly evident on the palm of the hand and flexor
surfaces of the digits, where they are arranged in relation to the movements of the
digits.
The remaining reticular layer is made of dense irregular, collagenous tissue,
which allows strength & flexibility in every direction. The primary cell of this layer is
fibroblast, which produce the key structure of extra cellular matrix protein namely
collagen & elastin. These cells produce the key adhesive proteins used to attach
epidermal cells to the basement membrane & are used for epidermal cell migration &
replication. The fibronectin is a key fibroblast derived signal protein for the
orchestration of the healing ground substance or matrix. This is made of
polysaccharide protein complexes known as GAG or hyaluronic acid, which is semi
fluid that allows cells & connective tissue orientation, provide nutrients diffusion to
the cells & also provides scaffolding for cell migration. The space between interfacing
connective tissue fibres are occupied by adipose tissue, blood vessels, sweat glands,
nerves & hair follicles. It is attached to the underlined structure by the subcutaneous
layer of tissue.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 31
Modern Review
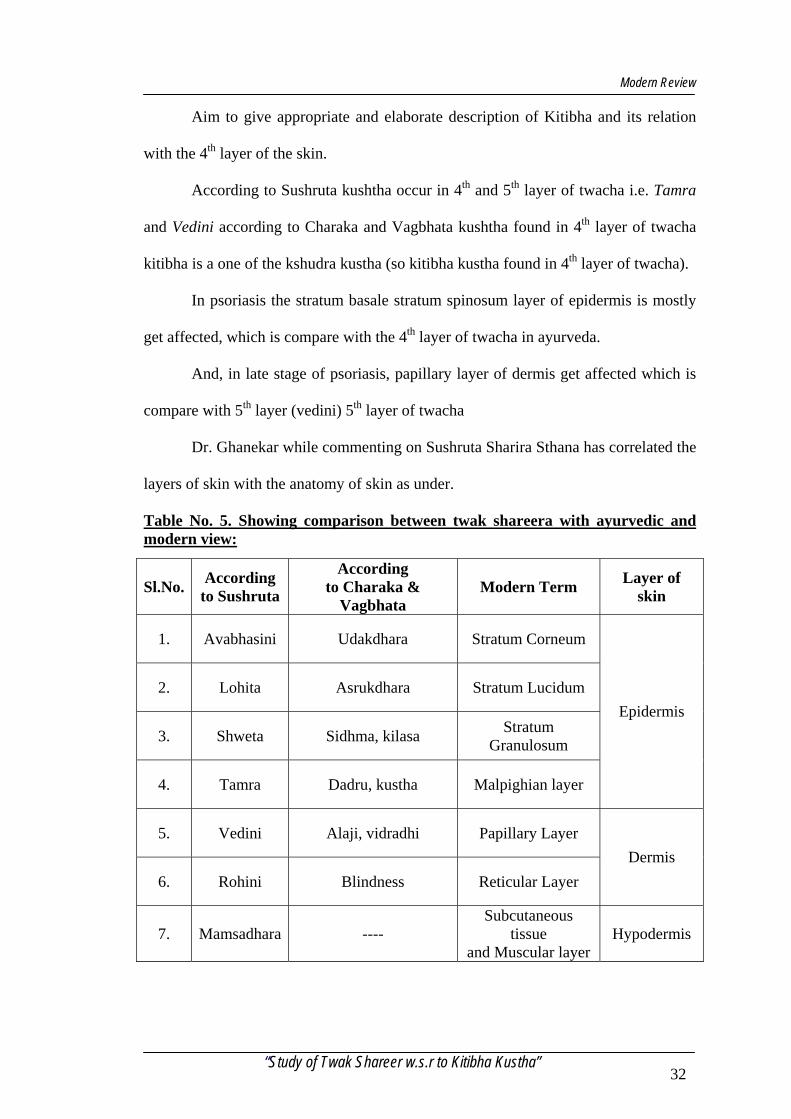
Aim to give appropriate and elaborate description of Kitibha and its relation
with the 4th layer of the skin.
According to Sushruta kushtha occur in 4th and 5th layer of twacha i.e. Tamra
and Vedini according to Charaka and Vagbhata kushtha found in 4th layer of twacha
kitibha is a one of the kshudra kustha (so kitibha kustha found in 4th layer of twacha).
In psoriasis the stratum basale stratum spinosum layer of epidermis is mostly
get affected, which is compare with the 4th layer of twacha in ayurveda.
And, in late stage of psoriasis, papillary layer of dermis get affected which is
compare with 5th layer (vedini) 5th layer of twacha
Dr. Ghanekar while commenting on Sushruta Sharira Sthana has correlated the
layers of skin with the anatomy of skin as under.
Table No. 5. Showing comparison between twak shareera with ayurvedic and modern view:
Sl.No. According to Sushruta
According to Charaka &
Vagbhata Modern Term Layer of
skin
1. Avabhasini Udakdhara Stratum Corneum
2. Lohita Asrukdhara Stratum Lucidum
3. Shweta Sidhma, kilasa Stratum Granulosum
4. Tamra Dadru, kustha Malpighian layer
Epidermis
5. Vedini Alaji, vidradhi Papillary Layer
6. Rohini Blindness Reticular Layer Dermis
7. Mamsadhara ---- Subcutaneous
tissue and Muscular layer
Hypodermis
“Study of Twak Shareer w.s.r to Kitibha Kustha” 32
Modern Review
PHYSIOLOGY OF THE SKIN The skin is a metabolically active organ with vital functions including the
protection and homeostasis of the body.
a. Regulation of body temperature:
Skin does the evaporation of sweat and converts the high temperature into
lower elevated body temperatures or to the normal. Changes in the flow of
blood to the skin also help the regulation of body temperature.
b. Protection:
The skin is considered under the Integumentary system. It provides a physical
barrier that protects the underlying tissues from physical abrasion, bacterial
invasion, and dehydration and UV radiation.
c. Sensation:
The skin contains abundant nerve endings and receptor that detect stimuli
related to temperatures, touch, pressures and pain.
d. Immunity:
Sweat of the epidermal cells is important components of the skin immune
system, which tends off foreign invaders.
e. Excretion:
Sweat is the vehicle for loss of a small quantity of ions and several organic
compounds along with removal of heat and some part of water.
f. Blood Reservoir:
The dermis is a house of extensive networks of blood vessels that carry 8 to
10% of the total blood flow in a resting adult. In moderate exercise this flow
increase, which helps to dissipate the heat from the body. While during the
exercise skin’s blood vessels constrict so this allows more blood to circulate
through contracting muscles.
g. Synthesis of Vitamin – D:
Synthesis of vitamin D begins with activation of a precursor molecule in the skin by
ultraviolet rays in the sunlight. Enzymes in the liver kidneys then modify this
molecule and produces calcitrol, the most active from of vitamin D.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 33
Modern Review
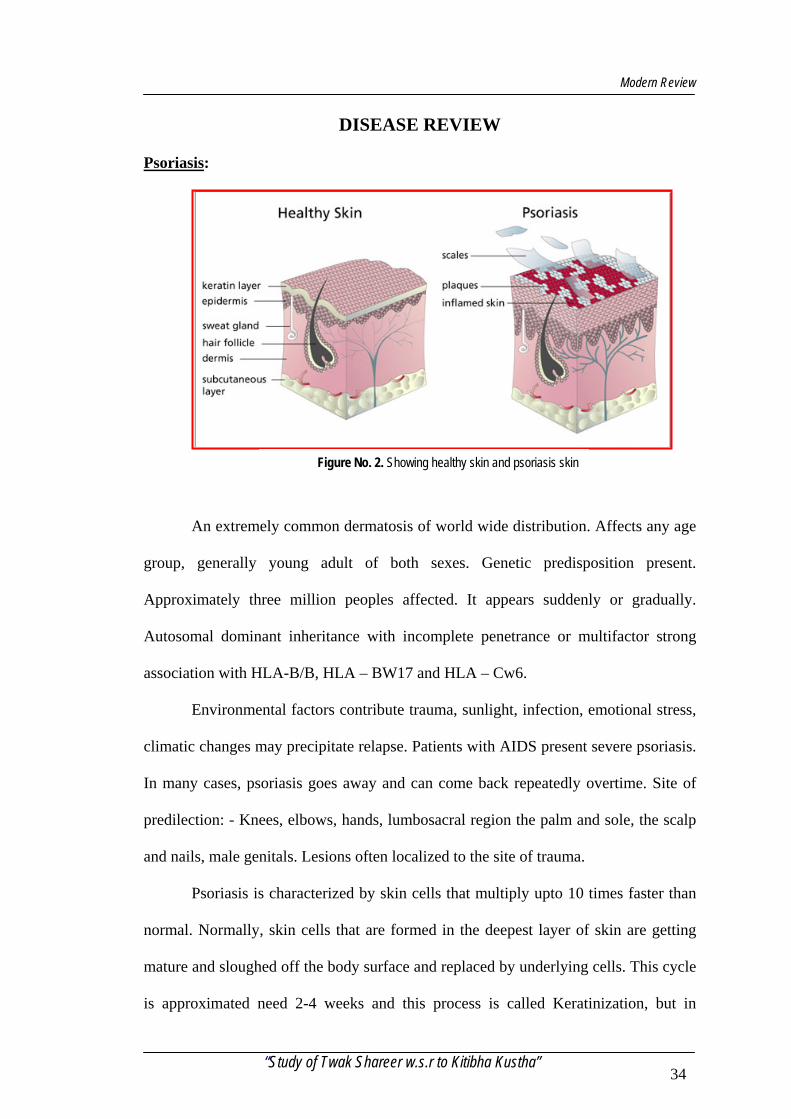
DISEASE REVIEW
Psoriasis:
Figure No. 2. Showing healthy skin and psoriasis skin
An extremely common dermatosis of world wide distribution. Affects any age
group, generally young adult of both sexes. Genetic predisposition present.
Approximately three million peoples affected. It appears suddenly or gradually.
Autosomal dominant inheritance with incomplete penetrance or multifactor strong
association with HLA-B/B, HLA – BW17 and HLA – Cw6.
Environmental factors contribute trauma, sunlight, infection, emotional stress,
climatic changes may precipitate relapse. Patients with AIDS present severe psoriasis.
In many cases, psoriasis goes away and can come back repeatedly overtime. Site of
predilection: - Knees, elbows, hands, lumbosacral region the palm and sole, the scalp
and nails, male genitals. Lesions often localized to the site of trauma.
Psoriasis is characterized by skin cells that multiply upto 10 times faster than
normal. Normally, skin cells that are formed in the deepest layer of skin are getting
mature and sloughed off the body surface and replaced by underlying cells. This cycle
is approximated need 2-4 weeks and this process is called Keratinization, but in
“Study of Twak Shareer w.s.r to Kitibha Kustha” 34
Modern Review
psoriasis, the immune system is mistakenly activated, resulting in an abnormally rapid
skin cell cycle. This mean the cells move from deepest layer of skin to the surface in
about 4 to 7 days. Since they migrate so quickly, they do not have time to properly
mature. So immature cells are sloughs off which looks silvery, white dry scaly in
nature.
Causes of psoriasis:
The cause disease of the immune system, when immune system is accidentally
activated (natural protection against bacteria, virus and other foreign invaders) which
resulting in an acceleration of normal skin cell of psoriasis is unclear. Psoriasis is now
recognized as an inflammatory cycle. This in term causes an accumulation of skin
cells on the surface of the skin. Heredity, environmental, diet and psychological
factors may also play a role.
Classical Psoriasis:
Asymptomatic or often itchy, red scaly papules and plaques of varying in size
and configuration and sharp delineation distributed on the extensors of the body,
flexors sometimes involved. Lesions covered with varying amount of loosely attached
silvery white scales overlying an adherent translucent membranous scale. Removal
latter reveals punctuate bleeding spot (from the elongated capillary looks in dermal
papillae) the characteristic Auspitz Sign.
Course unpredictable and variable; spontaneous remission and relapses of
characteristic feature most of (patients worsen in winter, some in summer).
Patients will ill define erythematous and a warm lesion indicates unstable form
could progress on to erythroderma. Lesion with pronounced mound. Like scales in
seen in rupioid psoriasis.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 35
Modern Review
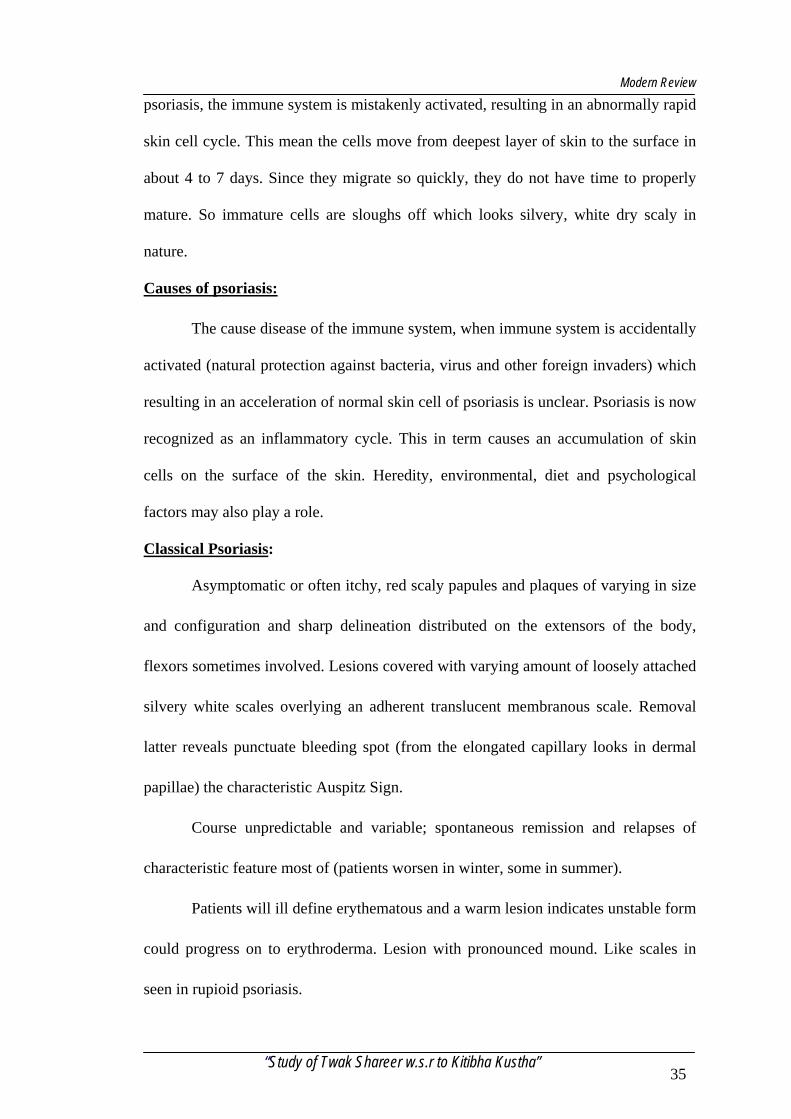
Basic pathogentic mechanism of the disease will understand. Chief cutaneous
manifestations result from hyperplasia of the epidermis. Epidermopoiesis is more
rapid and transit time of epidermal cells diminished; immature nucleated epidermal
cells present in the stratum corneum (Parakeratosis).
Figure No. 3. Different Clinical Forms of Psoriasis
Types of psoriasis:
1. Plaque psoriasis (psoriasis vulgaris):
Most commonly seen 80% of psoriasis is plaque psoriasis appears as dry,
scaly, inflamed patches of the skin. Silvery in colour, silvery white scales are
slough out on rubbing the area, affected area found all over the body.
2. Palm planter psoriasis:
Varied manifestations well defined red plaques with thick scales or
hyperkeratosis fissured, erythematous, ill defined plaques on the heels or other
parts of soles and palms often bilaterally symmetrical.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 36
Modern Review
3. Guttate psoriasis:
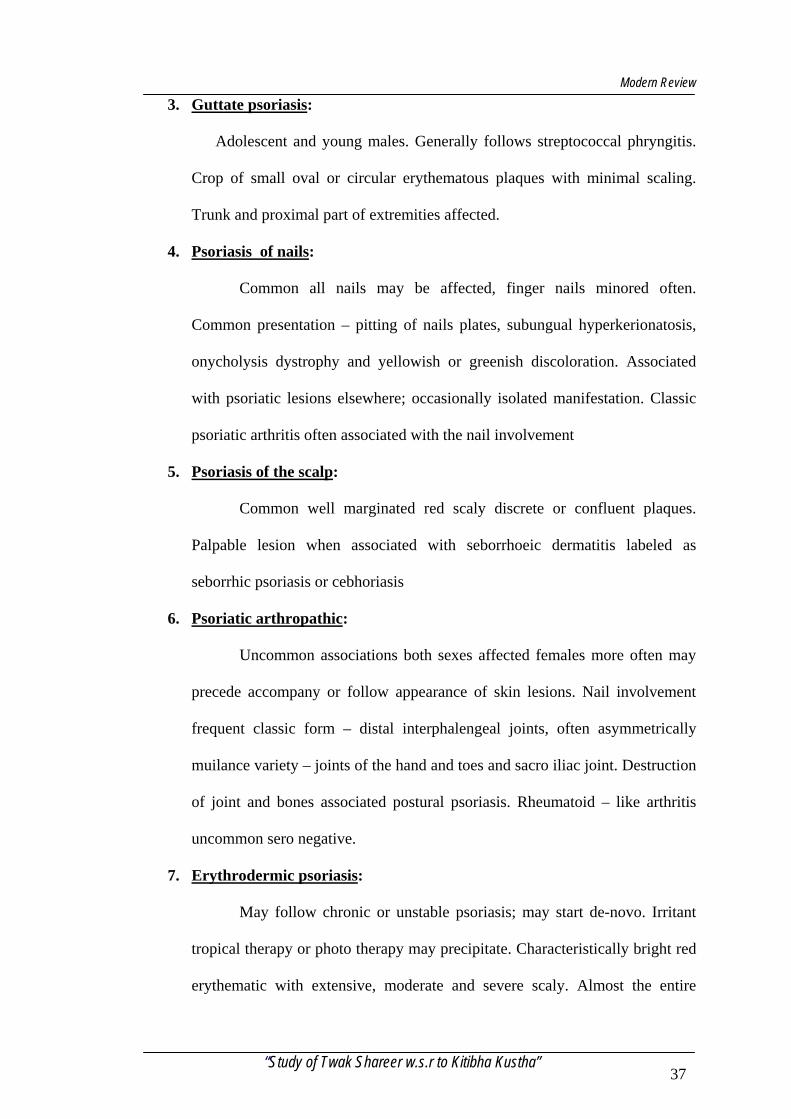
Adolescent and young males. Generally follows streptococcal phryngitis.
Crop of small oval or circular erythematous plaques with minimal scaling.
Trunk and proximal part of extremities affected.
4. Psoriasis of nails:
Common all nails may be affected, finger nails minored often.
Common presentation – pitting of nails plates, subungual hyperkerionatosis,
onycholysis dystrophy and yellowish or greenish discoloration. Associated
with psoriatic lesions elsewhere; occasionally isolated manifestation. Classic
psoriatic arthritis often associated with the nail involvement
5. Psoriasis of the scalp:
Common well marginated red scaly discrete or confluent plaques.
Palpable lesion when associated with seborrhoeic dermatitis labeled as
seborrhic psoriasis or cebhoriasis
6. Psoriatic arthropathic:
Uncommon associations both sexes affected females more often may
precede accompany or follow appearance of skin lesions. Nail involvement
frequent classic form – distal interphalengeal joints, often asymmetrically
muilance variety – joints of the hand and toes and sacro iliac joint. Destruction
of joint and bones associated postural psoriasis. Rheumatoid – like arthritis
uncommon sero negative.
7. Erythrodermic psoriasis:
May follow chronic or unstable psoriasis; may start de-novo. Irritant
tropical therapy or photo therapy may precipitate. Characteristically bright red
erythematic with extensive, moderate and severe scaly. Almost the entire
“Study of Twak Shareer w.s.r to Kitibha Kustha” 37
Modern Review
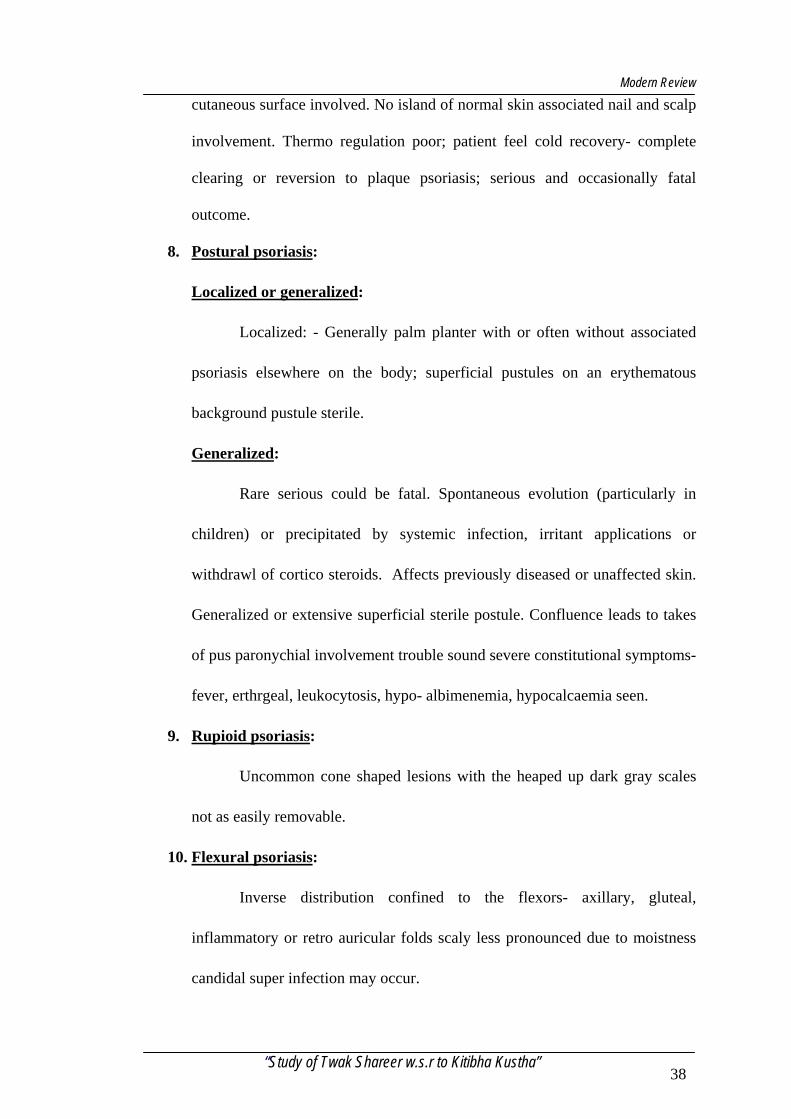
cutaneous surface involved. No island of normal skin associated nail and scalp
involvement. Thermo regulation poor; patient feel cold recovery- complete
clearing or reversion to plaque psoriasis; serious and occasionally fatal
outcome.
8. Postural psoriasis:
Localized or generalized:
Localized: - Generally palm planter with or often without associated
psoriasis elsewhere on the body; superficial pustules on an erythematous
background pustule sterile.
Generalized:
Rare serious could be fatal. Spontaneous evolution (particularly in
children) or precipitated by systemic infection, irritant applications or
withdrawl of cortico steroids. Affects previously diseased or unaffected skin.
Generalized or extensive superficial sterile postule. Confluence leads to takes
of pus paronychial involvement trouble sound severe constitutional symptoms-
fever, erthrgeal, leukocytosis, hypo- albimenemia, hypocalcaemia seen.
9. Rupioid psoriasis:
Uncommon cone shaped lesions with the heaped up dark gray scales
not as easily removable.
10. Flexural psoriasis:
Inverse distribution confined to the flexors- axillary, gluteal,
inflammatory or retro auricular folds scaly less pronounced due to moistness
candidal super infection may occur.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 38
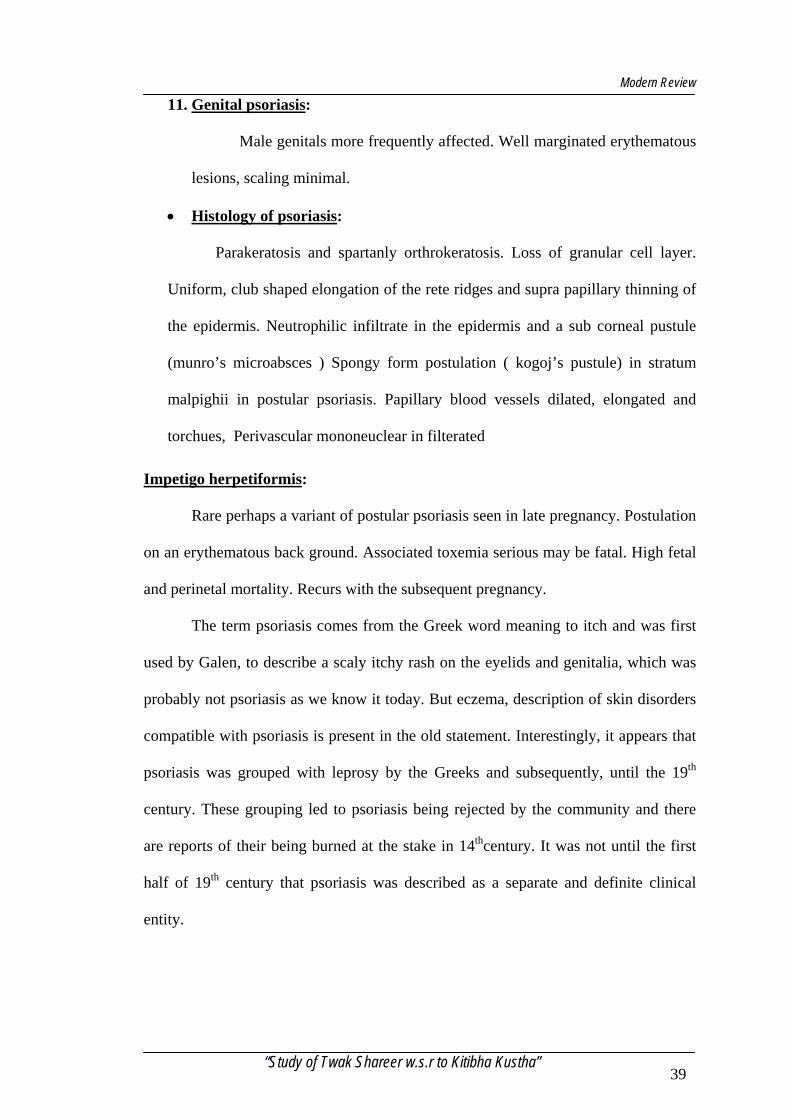
Modern Review
11. Genital psoriasis:
Male genitals more frequently affected. Well marginated erythematous
lesions, scaling minimal.
• Histology of psoriasis:
Parakeratosis and spartanly orthrokeratosis. Loss of granular cell layer.
Uniform, club shaped elongation of the rete ridges and supra papillary thinning of
the epidermis. Neutrophilic infiltrate in the epidermis and a sub corneal pustule
(munro’s microabsces ) Spongy form postulation ( kogoj’s pustule) in stratum
malpighii in postular psoriasis. Papillary blood vessels dilated, elongated and
torchues, Perivascular mononeuclear in filterated
Impetigo herpetiformis:
Rare perhaps a variant of postular psoriasis seen in late pregnancy. Postulation
on an erythematous back ground. Associated toxemia serious may be fatal. High fetal
and perinetal mortality. Recurs with the subsequent pregnancy.
The term psoriasis comes from the Greek word meaning to itch and was first
used by Galen, to describe a scaly itchy rash on the eyelids and genitalia, which was
probably not psoriasis as we know it today. But eczema, description of skin disorders
compatible with psoriasis is present in the old statement. Interestingly, it appears that
psoriasis was grouped with leprosy by the Greeks and subsequently, until the 19th
century. These grouping led to psoriasis being rejected by the community and there
are reports of their being burned at the stake in 14thcentury. It was not until the first
half of 19th century that psoriasis was described as a separate and definite clinical
entity.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 39
Modern Review
Morphology of the Lesion:
The typical psoriatic lesion is a raised red scaly patch with a sharply
demarcated edge between clinically involved skin and the plaque. The size of this
lesions are varies from a few millimeters to several centimeters and are may be large
confluent areas of psoriasis the trunk or limbs on rare occasions this may be extend to
involved all the skin .
If the scale is thick the plaque has a grayish white colour. However to, if the
scale is not too thick the patch so psoriasis has a predominantly red colour. If the
plaque is excoriated with a wooden spatula (Grattage) The red patch develops a white
flaky surface as the scale in psoriasis is loosely bound. These are a useful sign in
distinguishing psoriasis from other dermatosis. Another useful sign is removed of all
the scale by more vigorous excoriation with the spatula, and then a red glistening
surface with capillary bleeding points appears. Occasionally when the scaling the
plaque is very thick deep fissures develop which can be painful.
Rare forms of psoriasis are the so called rupioid lesions. These are thicker than
common plaque psoriasis and have a conical shape. They have a yellowish brown
colour and are most frequently seen on the feet, the appearance is produced by the
thicker and more adherent scale, which becomes heaped.
Age of Onset:
Psoriasis may begin at any age. However it is rare before the age of 5yrs. The
average age of onset has been found to be in the 20”s in most large studies 10% of
patients have an onset before 10yrs, 35% before 20yrs and 58% before 30yrs of age.
However, average age of onset is not the same in the different clinical patterns of
psoriasis this may be due to different genetic and or environmental factors which
determines the clinical expression of the disease, and age of onset is one of them.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 40
Modern Review
Symptoms:
In the majority of the patients psoriasis gives rise to very few physical
symptoms. It is likely to lead to many more psycho social problems because of
appearance of the rash.
Itching:
A Small proposition of patients, approximately 5-10% will complain of
irritation. Only in a minority of these does the irritation become severe enough to
warrant specific anti itch therapy. If the itch is severe then active treatment to clear
psoriasis is the best approach.
Pain:
Psoriasis will cause pain if the skin splits and fissures develop. Fissures are
most commonly seen in flexural and intertriginous psoriasis, thick plaque psoriasis
over joints and in severe psoriasis on palms and soles
Scaling:
Patient often complains bitterly of the excessive scaling of the skin when there
is scale involvement this give rise to dandruff on the cloth. When there is extensive
involvement of the skin, patients produced a sure of scale when they take their cloths
off, and they will find it too embarrassing to go to hotels or stay with friends. Some
get over this problem by taking a small vacuum cleaner or dust pan and brush with
them
Loss of mobility:
Confluent psoriasis over joint may lead to lack of mobility as psoriasis is not
as piably as normal as normal skin. This may be severe problem when the hands are
involved
“Study of Twak Shareer w.s.r to Kitibha Kustha” 41
Modern Review
Skin patches:
- Dry and rough in touch.
- Usually round and covered with silvery scales.
- Raised patches of skin are hard in nature.
- Accompanied by red border
- In chronic condition patches are exudative and sticky in nature with
blackish discolouration.
Shivering:
This occurs in erythrodermic psoriasis patient a great deal of heat in this form
of the disease because of the increased blood flow through the skin.
Constitutional upset:
Fever and malaise occur with generalized postural psoriasis.
Psychosocial aspect:
In the majority of the patient the appearance of the rash is the only side effect
which effect the rash on the (patient) usually depends on the personality of the
individual many patients with severe disease appear to cope well, while other minimal
involvement find it difficult to accept the disability. Obviously the rash is visible i.e.
on the hand or face then this may lead to greater problems.
In the majority of patients in psoriasis there will be some withdrawl from
social contact. Apart from the appearance there is a still widely held belief by the non
sufferers that psoriasis is a contagious disorder and therefore sufferer should be
avoided. This in addition to the appearance of the rash lead to isolation. The age of
onset of psoriasis is important in degree of harm it may cause socially. The adolescent
will have more problems adjusting then the mature adult in a family situation.
Psoriasis is also been shown, not surprisingly, to have an effect on sexual behavior,
“Study of Twak Shareer w.s.r to Kitibha Kustha” 42
Modern Review
the effect being greater upon women the majority of patients will not include in
sporting activity, particularly swimming. For this reason will not take holydays in the
sun and sea.
Psoriasis may also lead to problem with employment if there is involvement of
the hands and the face occupations involving coming into contact with public will be
difficult in this situation. The two psychological disorders which are increased in
psoriasis are – depression and obsesstinal status.
These would appear to be direct result of the physical disability in the subject
which possible pre disposition to this status.
Natural history of prognosis:
Psoriasis runs a variable course, and it is not possible to predict if and when
spontaneous resolution may occur, if the disease will remain static, or whatever it will
become more extensive. However the various clinical patterns of psoriasis tend to
have difficult prognosis.
Plaque psoriasis, which begins in childhood and adolescence, then to have a
poorer prognosis that late onset disease and it, is more likely to be persistent. Other
poor prognostic signs are extents of disease and appearance of new lesions. When the
rash is very wide spread remission are less likely to in sue. If the patients find the
involvement is gradually increasing the remission is unlikely in the near future. In
long term follow up studies of patients with plaque psoriasis the incidence of
spontaneous remission has been found to be approximately 40%.
Guttate psoriasis usually has a good prognosis and 955 of patient the irruption
will disappear within 3-4 months of onset. Occasionally the guttate psoriasis may
convert into plaque disease and prognosis is that of the later which is unpredictable
and variable. Patients who have had one attacks of guttate psoriasis are likely to
“Study of Twak Shareer w.s.r to Kitibha Kustha” 43
Modern Review
develop further episodes if they have infections with the streptococcus or certain
viruses.
Guttate psoriasis may occur in individuals who have no previous lesions are
those who have plaque disease. In the later the guttate lesions clear after 3-4 months,
but plaque disease in variably persist.
The prognosis in erythrodermic psoriasis tends to be poor. Patients with this
form of the disease need active treatment often with symptomatic drugs. The natural
history of the disease modifies by treatment. The majority of patients often the active
phase may revert to extensive chronic plaque disease, which again usually requires
long term active systemic therapy. Erythrodermic phase are likely to reoccur, unless
there is an identifiable curse which can be prevented or patients are maintained on
indefinite systemic therapy.
Generalized postular psoriasis has a risk death the acute episode of postulation
may last many week but it is now modified with therapy ones the postular phase has
subsided the condition usually revet to the chronic plaque state. However further
bouts of acute postular psoriasis associated with acrodermatitis continue tend to have
a bad prognosis.
Localized postular psoriasis on the palms and soles tends to be very persistent
over a 10 yrs period only approximately 25% patients are likely to achieve a
diminution. The disease however is not commonly seen in the elderly, so presumably
spontaneous remission does occur but only after 20-30yrs.
Acrodermatitis continua (postular involvement around the nails and on the nail
bed) have a poor prognosis in the elderly. The condition is very persistent and not
responsive to treatment usually gradually progresses to wide spread plaque disease
with a tendency to generalized postular psoriasis.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 44
Materials and Methods
MATERIAL AND METHODS
Study design:
The study of twak shareera with special reference to kitibha kustha has been
designed as follows
1) Literary study.
2) Clinical study.
3) Histopathalogical study.
1) Literary study: All the information regarding “Twacha” collected from
Brihattrayi, Laghutrayi and other classics of Ayurveda. Definition of Twacha its
etymology genesis and synonyms are complied form different texts. Compilation of
number names and Vyadhis occurring to the layers of Twacha is done and their
comparative study is done. Comparative study of thickness f Twacha told by Sushruta
and Dalhana is done.
Also relation of Twacha with other factors like Doshas, Dhatus, Malas,
Upadhatu, Srotasa, Varna, Prakruti, Sara and Gnyanendriya is studied.
In case of modern aspect of “Twacha” all the information regarding anatomy
of skin is complied from textbooks of anatomy. Study of embryology of skin. Its
layers, functions and glands is done.
Also study of kitibha Vyadhi form all the Samhitas is done. The causative
factors of Katibha, its symptoms dosha Pradhanya and classification is studies.
Compilation of information regarding psoriasis is done form the textbooks of
dermatology. This compilation includes study of causative factors, pathogenesis
symptoms. Clinical features and investigations.
Finally, the correlation of Kitibha and psoriasis is done on the basis of
symptoms and results of histopathological investigations.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 45
Materials and Methods
2) Clinical Study:
This study is done at various skin clinics under the guidance of
Dermatologists. Already diagnosed 30 patients of psoriasis were examined for the
clinical study of the disease. The morphology of scales, nature of symptoms area of
predilection was studied.
The patients were convinced for the biopsy of skin to rule out whether the
stratum most alone gets affected in this disease. So only seven patients skin biopsy
has been in the study. Those biopsy reports have been enclosed in this thesis.
Photographs of patients are taken to show the morphology of scales. Also
scraping of scales is done and they are processed with KOH to rule out the auspitz
sign is seen.
3) Histopathological study:
The histopathological study can be done in two steps i.e. skin biopsy and skin
scrapping.
A) Skin biopsy:
There are different methods of skin biopsy like shave biopsy, scalpel biopsy,
punch biopsy and scissor biopsy etc. But we did skin biopsy by punch skin biopsy
method because it is most commonly used and get full thickness of skin sample in
small area. And even also need only one or two stitches needed to close the wound.
This is helpful for cosmetic purpose. In other types of biopsy we can not get full
thickness of skin and even need more stitches to close the wound.
Procedure: The skin in cleansed and local anaesthesia is administered. A
small cylindrical punch is screwed into the region through the full thickness of the
skin and plug of tissue is removed.
B) Skin Scrapping:
It is done by scraping the scales with sterile blade and they are collected in a
clear bulb and can be examined under the microscope.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 46
Materials and Methods
Laboratory experiment:
It includes 2 methods
1) KOH mount (without heating)
2) KOH Preparation (with heating). This experiment is done by KOH
preparation.
First one drop of KOH (Potassium Hydroxide with calcoflour white) is placed
on a clear glass slide. Then collected specimen of scales is immersed in drop of KOH.
Cover slip is kept on the specimen. KOH mixture is heated by passing the slide
through a Bunsen burner flame several times. Preparation is examined under 10X and
40X. auspitz sign and whitish silvery scale appearance is observed.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 47
Discussions
DISCUSSION
Twacha is the external covering of the body. It is also called “sparshanendriya
or twagndriya” which envelops the body. It plays a great role in perception of
sensations like touch, pain, heat, cold.
The organ genesis of twacha occur during paka of Shukra and Shonita by
Agni, seven types of Twacha gets formed on the surface of Garbha just like while
heating milk cream is formed on its surface. Twacha is a Matruja Bhava and it is
having predominance of Vayu mahabhoota and sparsha Vishishta guna.
There is some controversy regarding number of Twacha in various texts.
Acharya Sushruta tells seven types of Twacha while Charaka and Vagbhata tell six
types. Also regarding Vyadhis occurring in different layers there is variation in
opinion of Acahryas e.g. Sushruta tells Kitibha occur in fourth and fifth layer of
twacha while Charaka and Vagbhata tells it in fourth layer.
Thickness of Twacha told by Sushruta and Dalhana is having great difference.
Sushruta seems to be more accurate in telling thickness of Twacha which is more or
less same to the thickness quoted in modern textbooks of Anatomy.
Considering relation of Doshas with Twacha, Vata dosha especially Prana and
Udana have close relation with Twacha. Pranavayu is responsible for the perception
of touch sensation. Udanavayu produces Varna and if its gets vitiated then there will
be discolouration of the skin. If pitta dosha is considered. Bhrajaka Pitta is situated in
Twacha which maintains Teja of Twacha. It is responsible for absorption of drugs
externally in the form of massage, oils, paste etc. kapha dosha is having Snigdha
guna. If Snigdha guna decreases then Twacha will be dry and cracky in nature.
Considering relation of dhatus with Twacha. Rasa dhatu is present in Twacha
and it gives nourishment to it for its well being. Twacha is supplied by numerous
“Study of Twak Shareer w.s.r to Kitibha Kustha” 63
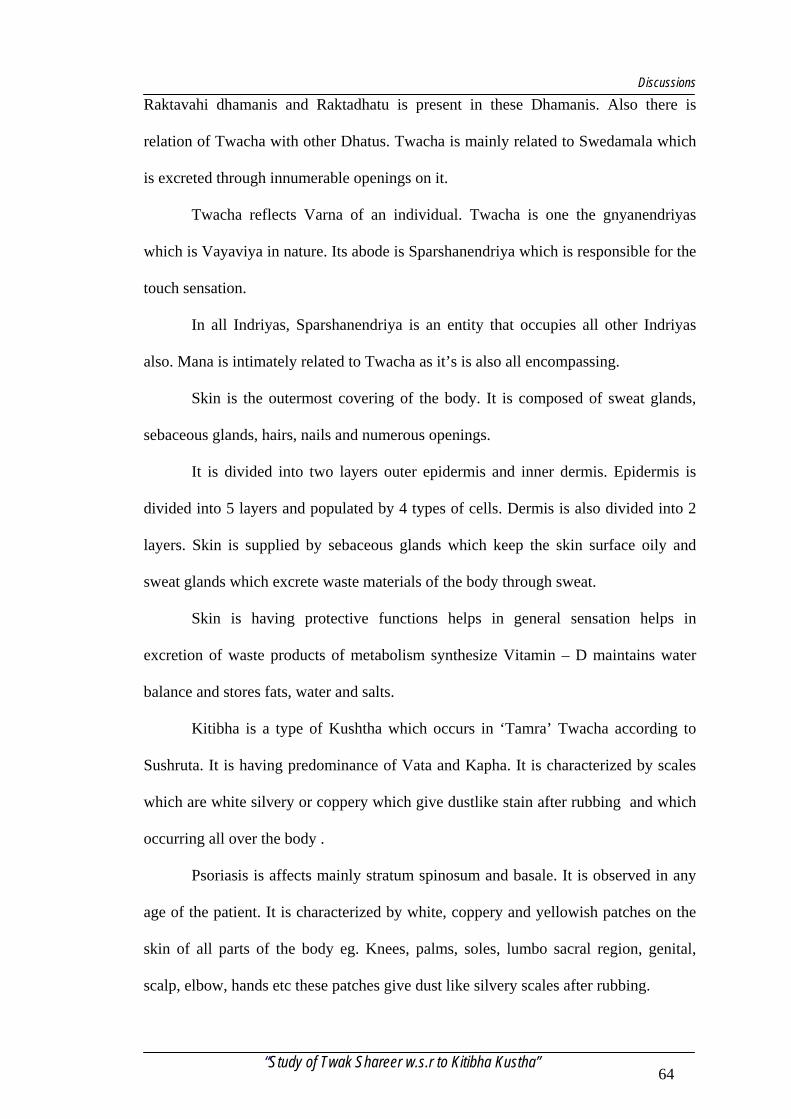
Discussions
Raktavahi dhamanis and Raktadhatu is present in these Dhamanis. Also there is
relation of Twacha with other Dhatus. Twacha is mainly related to Swedamala which
is excreted through innumerable openings on it.
Twacha reflects Varna of an individual. Twacha is one the gnyanendriyas
which is Vayaviya in nature. Its abode is Sparshanendriya which is responsible for the
touch sensation.
In all Indriyas, Sparshanendriya is an entity that occupies all other Indriyas
also. Mana is intimately related to Twacha as it’s is also all encompassing.
Skin is the outermost covering of the body. It is composed of sweat glands,
sebaceous glands, hairs, nails and numerous openings.
It is divided into two layers outer epidermis and inner dermis. Epidermis is
divided into 5 layers and populated by 4 types of cells. Dermis is also divided into 2
layers. Skin is supplied by sebaceous glands which keep the skin surface oily and
sweat glands which excrete waste materials of the body through sweat.
Skin is having protective functions helps in general sensation helps in
excretion of waste products of metabolism synthesize Vitamin – D maintains water
balance and stores fats, water and salts.
Kitibha is a type of Kushtha which occurs in ‘Tamra’ Twacha according to
Sushruta. It is having predominance of Vata and Kapha. It is characterized by scales
which are white silvery or coppery which give dustlike stain after rubbing and which
occurring all over the body .
Psoriasis is affects mainly stratum spinosum and basale. It is observed in any
age of the patient. It is characterized by white, coppery and yellowish patches on the
skin of all parts of the body eg. Knees, palms, soles, lumbo sacral region, genital,
scalp, elbow, hands etc these patches give dust like silvery scales after rubbing.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 64
Discussions
Discussion on observation:
Age:
Out of 30 patients 15 patients are of the 30 – 40 age group and Vata and Kapha
prakruti persons this may be the cause for the psoriasis occur in this age group.
Diet:
It is observed that out of 30 patients 18 patients are mixed diet and consuming more
non-vegetarian food is one among the cause for formation of psoriasis or Kitibha
kustha
Prakruti:
Out of 30 patients 15 patients are assessed as Kaphaja Prakruti persons and these
persons are prone to suffer from psoriasis.
Site of Psoriasis:
It is observed out of 30 patients the psoriasis found 8 patients in hands, 8 patients in scalp,
6 patients in lumbo sacral region, 4 patients in elbow joints, 2 patients in knees and 2 patients in
genitals and hands are prone appear psoriasis.
Sex:
Out of 30 patients 18 patients are males and 12 patients are females, so it shows that
males are more affected than the females.
Varna:
Among 30 patients shweta varna is observed in 18 patients tamra varna
observed in 5 patients and the pita varna is observed 07 patients and 03 - 03
shweta-tamra and pita-shweta varna.
Psoriasis and Kitibha Kustha:
It is difficult to say what psoriasis is in terms of Ayurveda. There is no disease
in Ayurveda which can exactly be correlated with Psoriasis. Many research workers
have tried to attribute psoriasis with one or other type of Kushtha. All the workers
“Study of Twak Shareer w.s.r to Kitibha Kustha” 65
Discussions
included psoriasis under Kshudra Kushtha, but while on co-relation with specific type
they differed. Some correlated it with Kitibha and others with Sidhma or Eka
Kushtha. Here, Kitibha Kushtha sign and symptoms are correlated as psoriasis
because the description & characteristic features of it are co-inciding with description
of psoriasis than any other type of Kushtha. In Kitibha the lesions are Klinna, Khara
sparsha, Parusha, Kandu, Ruksha, Vrutta and Ghana. But is psoriasis the lesions are
dry, rough in touch, round, hard in nature, crack on rubbing, psoriasis the lesion are
distributed all over the body. Description & characteristic features of Kitibha
Kushtha very closely match the description of psoriasis.
Kitibha Kushtha –Psoriasis:
• Klinna - Sticky in nature
• Mahavastum - Lesions are found all over the body.
• Khara Sparsha – Rough in touch
• Parusha – Hard in nature(crack).
• Vruttam – Round in shape.
• Ghana – Solid
• Sravi and Shyava – In chronic condition psoriatic patches on the skin are
exudative in nature and blackish discolouration.
• Punha punha utpadaute – psoriasis goes away and can come back repeatedly
overtime.
The lakshanas of kitibha kustha mentioned by Charaka are described here in detail
in comparison with psoriasis.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 66
Discussions
Mahavastum:
It means that lesions are found all over the body or coverer large area of the body.
Charaka says that the Sapta Dravya lesions are produced where the Doshas settle191.
It indicates that the uninvolved skin is also abnormal. It has been postulated &
supported by some experimental evidence that the uninvolved normal appearing skin
of psoriatic subjects is abnormal. Using the nude mice model to study psoriatic skin
removed form a psoriatic host, it was found that clinically involved psoriatic
epidermis maintained its high level of plasminogen activator activity & increased
labeling index when grafted on nude mice (Fraki et al, 1983). Moreover epidermis
from clinically uninvolved normal appearing psoriatic skin develops a significant
increase in plasminogen activator activity to the level of involved epidermis after
grafting & this is accompanied by a high thymidine-labeling index. Normal control
skin maintains it slow level of plasminogen activator & normal labeling index after
grafting to the nude mice. The data suggest that skin from psoriatic patients can
manifest marker of psoriasis, independent of psoriasis Thus the Clinical features of
psoriasis and Kitibha Kushta are almost similar. Mainly the plaque psoriasis can be
readily correlated to that of Kitibha Kushtha.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 67
summary
SUMMARY
01. It is conceptual observation study entitled study of twak shareer w.s.r. kitibha
kustha.
02. Kitibha kustha is a disease is mentioned as the one of the Asthamagadha and
this disease is very well correlated to skin disease (psoriasis).
03. In this study it was observed that the Kitibha kustha is mainly seen in between
age group of 30 to 40 years (50%) and it is more common in males (60%) and
may be because of more intake of mixed diet has also shown its role in the
causation of the disease.
04. Regarding kustha bedha out of 30 cases 15 patients are pertaining to kaphaja
kustha and 05 patients are vataja and 04 patients are pittaja, 03 patients are
vata kaphaja and 03 patients are pitta kaphaja.
05. About the site of psoriasis out of 30 patients 08 patients in hand, 08 patients in
scalp and remaining patients psoriasis found in lumbo sacral and genitals.
06. Out of 30 patients silvery scales found in almost all the cases.
07. Vedana, daha is found in limited patients.
08. On the basis of sign and symptoms and histo-pathalogical findings kitibha
kustha can be correlated to psoriasis.
09. The thickness of the skin as told by Acharya Sushruta in our classics is almost
similar to explanation of the modern authors.
10. Further, study is needed with large sample in multi-centres then only the clear
conclusion can be drawn.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 69
References
REFERENCES
1. zÉUÏUÇ xÉuÉïjÉÉ xÉuÉï xÉuÉïSÉ uÉåS rÉÉå ÍpÉwÉMçü |
AÉrÉÑuÉåïSÇ xÉ MüÉixlrÉåïlÉ uÉåS sÉÉåMüxÉÑZÉmÉëSqÉç ||
cÉ.zÉÉ. 6/19
2. iÉxqÉÉÍ³É xÉÇzÉrÉÇ ¥ÉÉlÉÇ Wû§ÉÉï zÉÉsrÉxrÉ uÉɧNèûiÉÉ |
zÉÉåbÉÌrÉiuÉÉ qÉ×iÉÇ xÉqrÉaSì¹urÉÉåXèûaÉÌuÉÌlÉzcÉrÉÈ ||
xÉÑ.zÉÉ. 5/51
3. lÉ zÉYrɶɤÉÑwÉÉ Sì¹ÒÇ SåWåû xÉÔ¤qÉiÉqÉÉå ÌuÉpÉÑÈ |
SØzrÉiÉå ¥ÉÉlÉcɤÉÑÍpÉïxiÉmɶɤÉÑÍpÉËUuÉ cÉ || xÉÑ.zÉÉ.
5/62
4. MüÉrÉoÉÉsÉaÉëWûÉåkuÉÉï¬èaÉzÉsrÉSÇ·íÉeÉUÉuÉ×wÉÉlÉç |
A.Wû.xÉÑ. 1/5
5. ÌlÉSÉlÉ qÉÉkÉuÉÈ ´Éå¸ xÉÔ§ÉxjÉÉlÉå iÉÑ uÉÉapÉOûÈ |
zÉÉUÏUå xÉÑ´ÉÑiÉÈ ´Éå¸È cÉUMüxiÉÑ ÍcÉÌMüÎixÉiÉå || qÉÉ.lÉÏ.
1/4
6. mÉëirɤÉiÉÉå ÌWû rÉSèSØ¹Ç zÉÉZÉSØ¹Ç cÉ rÉSèpÉuÉåiÉç |
xÉqÉÉxÉiÉxiÉSÒpÉrÉ pÉÔrÉÉå ¥ÉÉlÉÌuÉuÉkÉïlÉqÉç || xÉÑ.zÉÉ.
5/60
7. iÉxqÉÉiÉç xÉqÉxiÉaÉɧÉÇ......... zÉlÉæÈ
zÉlÉæUuÉbÉwÉïrÉÇxiÉuÉaÉÉSÏlÉç xÉuÉÌlÉuÉ | xÉÑ.zÉÉ. 5/61
8. iuÉMçümÉrÉïiÉxrÉ SåWûxrÉ rÉÉåÅrÉqÉXèûaÉÌuÉÌlÉzcÉrÉÈ |
zÉsrÉ¥ÉÉlÉÉSØiÉå lÉæwÉ uÉhrÉïiÉåÅXèûaÉåwÉÑ MåüzÉÑÍcÉiÉç
|| xÉÑ.zÉÉ. 5/58
“Study of Twak Shareer w.s.r to Kitibha Kustha” 70
References
9. xÉuÉï zÉUÏUxrÉ oÉÉWûrÉÇ AÉuÉUhÉÇ iuÉÌWûÌiÉ EcrÉiÉå |
xÉÑ.zÉÉ.2/5(bÉÉlÉåMüU OûÏMüÉ)
10. CÇÌSìrÉÇ xÉuÉïzÉUÏUuÉÌiÉï xmÉzÉïlÉåÇÌSìrÉÇ
iuÉÌaÉÇÌSìrÉÍqÉirÉÍpÉkÉÏrÉiÉå|xÉÑ.zÉÉ.2/11(bÉÉlÉåMüU
OûÏMüÉ)
11. zÉUÏUå wÉOèû iuÉcÉÈ..........LiÉÉÈ wÉQûQèûaÉÇ
zÉUÏUqÉuÉiÉsrÉ ÌiɸÎliÉ | cÉ.zÉÉ. 7/4
12. iÉxrÉ ZÉsuÉåuÉÇ mÉëuÉרÉxrÉ
zÉÑ¢üzÉÉåÍhÉiÉxrÉÉÍpÉmÉcrÉqÉÉlÉxrÉ
¤ÉÏUxrÉåuÉ xÉliÉÉÌlÉMüÉÈ xÉmiÉ iuÉcÉÉå pÉuÉÎliÉ | xÉÑ.zÉÉ.
4/3
13. iɧÉÉxÉ×eÉÈ mÉcrÉqÉÉlÉxrÉ ¤ÉÏUxrÉåuÉ xÉliÉÉÌlÉMüÉÈ
wÉOû iuÉcÉÉå pÉuÉÎliÉ | A.xÉÇ.zÉÉ. 5/16....... iÉ§É xÉmiÉ
iuÉcÉÉåÅxÉ×eÉÈ ||8||
mÉcrÉqÉÉlÉÉimÉëeÉÉrÉliÉå ¤ÉÏUÉixÉliÉÉÌlÉMüÉ CuÉ ||9||
A.WØû.zÉÉ. 3/8-9
14. ¤ÉÏUxrÉ mÉcrÉqÉÉlÉxrÉ rÉjÉÉ xÉliÉÉÌlÉMüÉ pÉuÉåiÉç |
mÉcrÉqÉÉlÉxrÉ zÉç¢üxÉÉ UeÉxÉzcÉ iÉjÉÉ iuÉcÉå ||
pÉÉ.mÉë.mÉÔ.ZÉÇ. 3/279
15. qÉÉiÉ×eÉzcÉÉrÉÇ aÉpÉïÈ............ iɱjÉÉ iuÉMçü cÉ
sÉÉåÌWûiÉÇ cÉ qÉÉÇxÉ cÉ............. YmÉÉuÉWûlÉÇ cÉåÌiÉ
qÉÉiÉ×eÉÉÌlÉ | cÉ.zÉÉ. 3/6
uÉÉiÉÉixmÉzÉïiuÉaÉÑcNèûuÉÉxÉÉ........... | A.WØû.zÉÉ. 3/3
16. xÉmiÉ iuÉcÉÉå pÉuÉÎliÉ | xÉÑ.zÉÉ. 4/3
CÌiÉ wÉOèû iuÉcÉÉ | cÉ.zÉÉ. 7/4
iÉ§É xÉmiÉ iuÉcÉÉåÅxÉ×eÉÈ | A.WØû.zÉÉ. 3/8
wÉOèû iuÉcÉÉå pÉuÉÎliÉ | A.xÉÇ.zÉÉ. 5/16
17. zÉUÏUå wÉOèû iuÉcÉÈ iɱjÉÉ ESMükÉUÉ iuÉqoÉÉWûrÉÉ,
̲iÉÏrÉÉ iuÉxÉ×akÉUÉ, iÉ×iÉÏrÉÉ ÍxÉkqÉÌMüsÉÉxÉ
“Study of Twak Shareer w.s.r to Kitibha Kustha” 71
References
xÉÇpÉuÉÉÍkɸÉlÉÉ, cÉiÉÑjÉÏï SSìÓMÑü¸xÉÇpÉuÉÉÍkɸÉlÉÉ,
mÉÇcÉqÉÏ iuÉsÉeÉÏÌuÉSìÍkÉxÉÇpÉuÉÍkɸÉlÉÉ, wÉ¸Ï iÉÑ rÉxrÉÉÇ
ÍNû³ÉÉrÉÉÇ iÉÉqrÉÉirÉÇkÉ CuÉ cÉ iÉqÉÈ mÉëÌuÉzÉÌiÉ.... |
cÉ.zÉÉ. 7/4
18. iÉÉxÉÉÇ mÉëjÉqÉÉÅuÉpÉÉÍxÉlÉÏ lÉÉqÉ, rÉÉ
xÉuÉïuÉhÉÉïlÉuÉpÉÉxÉrÉÌiÉ, mÉÇcÉÌuÉkÉÉÇ cÉ NûÉrÉÉÇ
mÉëMüÉzÉrÉÌiÉ, xÉÉoÉëÏWåûU¹ÉSzÉpÉÉaÉmÉëqÉÉhÉÉ
ÍxÉkqÉmÉ©MÇüOûMüÉÍkɸÉlÉÉ | xÉÑ.zÉÉ. 4/3
19. ̲iÉÏrÉÉ sÉÉåÌWûiÉÉ lÉÉqÉ wÉÉåQûzÉpÉÉaÉ mÉëqÉÉhÉÉ
ÌiÉsÉMüÉsÉMülrÉcNûurÉXûaÉÉÍkɸÉlÉÉ |
xÉÑ.zÉÉ. 4/3
20. iÉ×iÉÏrÉÉ µÉåiÉÉ lÉÉqÉ ²ÉSzÉpÉÉaÉmÉëqÉÉhÉÉ
cÉqÉïSsÉÉeÉaÉssÉÏMüqÉwÉMüÉÍkɸÉlÉÉ | xÉÑ.zÉÉ. 4/3
21. cÉiÉÑjÉÏï iÉÉqÉëÉ lÉÉqÉ A¹pÉÉaÉ mÉëqÉÉhÉÉ ÌuÉÌuÉkÉÉÌMüsÉÉxÉMÑü¸ÉÍkɸÉlÉÉ | xÉÑ.zÉÉ. 4/3
22. mÉÇcÉqÉÏ uÉåÌSlÉÏ lÉÉqÉ mÉÇcÉpÉÉaÉmÉëqÉÉhÉÉ
MÑü¸ÌuÉxÉmÉÉïÍkɸÉlÉÉ | xÉÑ.zÉÉ. 4/3
23. wÉ¸Ï UÉåÌWûhÉÏ lÉÉqÉ oÉëÏÌWûmÉëqÉÉhÉÉ aÉëljrÉmÉcrÉoÉÑïSzÉsÉÏmÉSaÉsÉaÉhQûÉÍkɸÉlÉÉ | xÉÑ.zÉÉ. 4/3
24. xÉmiÉqÉÏ qÉÉÇxÉkÉUÉ lÉÉqÉ oÉëÏWûÏSìrÉ mÉëqÉÉhÉÉ
pÉaÉlSUÌuÉSìkrÉzÉÉåïÅÍkɸÉlÉÉ | xÉÑ.zÉÉ. 4/3
25. iÉÉxÉÉqÉÑSMükÉUÉ cÉ±É | ̲iÉÏrÉÉÅxÉ×akÉUÉ | iÉ×iÉÏrÉÉ
ÍxÉkqÉÉÌMüsÉÉxÉÉÍkɸÉlÉÉ | cÉiÉÑjÉÏï xÉuÉïMÑü¸ÉÍkɸÉlÉÉ |
mÉÇcÉqÉÏ mÉÑlÉUsÉÎeÉÌuÉSìkrÉÍkɸÉlÉÉ | wÉ¸Ï iÉÑ
mÉëÉhÉkÉUÉ...A.xÉÇ.zÉÉ. 5/17
26. ¥ÉårÉÉuÉpÉÉÍxÉlÉÏ mÉÔuÉï ÍxÉkqÉÉxjÉÉlÉÇ cÉ xÉÉ qÉiÉÉ |
̲iÉÏrÉÉ sÉÉåÌWûiÉÉ ¥ÉårÉÉ ÌiÉsÉMüÉsÉMüeÉlqÉpÉÑÈ ||
µÉåiÉÉ iÉ×iÉÏrÉÉ xÉÇZrÉÉiÉÉ xjÉÉlÉÇ cÉqÉïSsÉxrÉ xÉÉ |
iÉÉqÉëÉ cÉiÉÑjÉÏï ÌuÉ¥ÉårÉÉ ÌMüsÉÉxÉÍ´uɧÉpÉÑÍqÉMüÉ ||
mÉÇcÉqÉÏ uÉåSlÉÏ ZrÉÉiÉÉ xÉuÉïMÑü¸ÉåSèpÉuÉxiÉiÉÈ |
ÌuÉZrÉÉiÉÉ UÉåÌWûhÉÏ wÉ¸Ï aÉëÎljÉaÉhQûÉmÉcÉÏ ÎxjÉÌiÉÈ ||
“Study of Twak Shareer w.s.r to Kitibha Kustha” 72
References
xjÉÔsÉÉ iuÉMçü xÉmiÉqÉÏ ZrÉÉiÉÉ ÌuÉSìkrÉÉSå ÎxjÉÌiÉzcÉ xÉÉ ||
CÌiÉ xÉmiÉ iuÉcÉÈ mÉëÉå£üÉ xjÉÔsÉÉ oÉëÏÌWû²rÉqÉɧÉrÉÉ ||
mÉë.ZÉÇ. 5/19-22
“Study of Twak Shareer w.s.r to Kitibha Kustha” 73
References
27. mÉÔuÉÉïuÉpÉÉÍxÉlÉÏ iÉÉxÉÉÇ ÍxÉkqÉxjÉÉlÉÇ cÉ xÉÉ xqÉ×iÉÉ |
̲iÉÏrÉÉ sÉÉåÌWûiÉÉ ¥ÉårÉÉ ÌiÉsÉMüÉsÉMüelqÉpÉÑÈ ||
iÉ×iÉÏrÉÉ iÉÑ puÉåcNûuÉåiÉÉ xjÉÉlÉÇ cÉqÉïSsÉxrÉ cÉ |
iÉÉqÉëÉ cÉiÉÑjÉÏï ÌuÉ¥ÉårÉÉ ÌMüsÉÉxÉÍ´uɧÉpÉÑÍqÉMüÉ ||
mÉÇcÉqÉÏ uÉåÌSlÉÏ lÉqlÉÉ mÉÇcÉpÉÉaÉmÉëqÉÉÍhÉMüÉ |
ÌuÉxÉmÉïMÑü¸ÉÍkɸÉlÉÉ ¥ÉårÉÉ wÉ¸Ï iÉÑ UÉåÌWûhÉÏ ||
ÌuÉZrÉÉiÉÉ UÉåÌWûhÉÏ wÉ¸Ï aÉëÎljÉaÉhQûÉmÉcÉÏÎxjÉiÉÏÈ |
oÉëÏWûÏqÉɧÉmÉëqÉÉhÉÉ xÉÉ UÉåÌWûhÉÏ aÉëljrÉÉmÉcÉÏ |
aÉsÉaÉhQûqÉÉsÉÉoÉÔSïzsÉÏmÉSÉlÉÉqÉÍkɸÉlÉqÉ ||
xjÉÔsÉÉ iuÉMüxÉmiÉqÉÏ ZrÉÉiÉÉ ÌuÉSìkrÉÉSåÈÎxjÉÌiÉzcÉ xÉÉ || mÉÔ.ZÉÇ.3/280-284(aÉpÉï mÉëMüUhÉ)
28. mÉëjÉqÉÉÅAÉuÉpÉÉÍxÉlÉÏ lÉÉqÉ ....
oÉëÏWåûU¹ÉSzÉpÉÉaÉmÉëqÉÉhÉÉ |
̲iÉÏrÉÉ sÉÉåÌWûiÉÉ lÉÉqÉ ....
uÉëÏÌWûwÉÉåQûwÉpÉÉaÉmÉëqÉÉhÉÉ |
iÉ×iÉÏrÉÉ µÉåiÉÉ lÉÉqÉÉ .... uÉëÏÌWû²ÉSzÉpÉÉaÉmÉëqÉÉhÉÉ |
cÉiÉÑjÉÏï iÉÉqÉëÉ lÉÉqÉ .... A¹pÉÉaÉmÉëqÉÉhÉÉ |
mÉÇcÉqÉÏ uÉåÌSlÉÏ lÉÉqÉ .... mÉÇcÉpÉÉaÉmÉëqÉÉhÉ |
wÉ¸Ï UÉåÌWûhÉÏ lÉÉqÉ .... uÉëÏWûÏmÉëqÉÉhÉÉ |
xÉmiÉqÉÏ qÉÉÇxÉkÉUÉ lÉÉqÉ .... uÉëÏWûϲrÉmÉëqÉÉhÉÉ |
xÉÑ.zÉÉ. 4/3
29. rÉSåiÉiÉç mÉëqÉÉhÉÇ ÌlÉÌSï¹Ç iÉlqÉÉÇxÉsÉåwuÉuÉMüÉzÉåwÉÑ,
lÉ sÉsÉÉiÉå xÉÔ¤qÉÉXèûaÉÑsrÉÉÌSwÉÑ....|
xÉÑ.zÉÉ. 4/3
30. uÉëÏÌWûU§É rÉuÉÈ, mÉëirÉåMÇü uÉëÏÌWûÌuÉxiÉÉUxrÉ
ÌuÉÇzÉÌiÉpÉÉïaÉÉÈ mÉËUMüsmÉlÉÏrÉÉÈ iÉå cÉɹÉSzÉpÉÉaÉÉ
AuÉpÉÉxÍÉlrÉÉÈ mÉëqÉÉhÉqÉç, LuÉÇ uɤrÉqÉhÉåwuÉÌmÉ
ÌuÉzÉÌiÉpÉÉaÉåwÉÑ wÉÉåQûwÉmÉëpÉ×iÉrÉÉå pÉÉaÉÉ
oÉÉåSèkÉurÉÉÈ || QûsWûhÉ OûÏMüÉ
“Study of Twak Shareer w.s.r to Kitibha Kustha” 74
References
31. mÉYuÉÉzÉrÉMüOûÏxÉÎYjÉ´ÉÉå§ÉÎxjÉxmÉzÉïlÉåÌSìrÉqÉç |
xjÉÉlÉÇ uÉÉiÉxrÉ iɧÉÉÌmÉ mÉYuÉkÉÉlÉÇ ÌuÉzÉåwÉiÉÈ ||
A.WØû.xÉÑ. 12/1
32. EUÈ xjÉÉlÉqÉÑSÉlÉxrÉ lÉÉxÉÉlÉÉÍpÉaÉsÉÉÇzcÉUåiÉç |
uÉÉMçümÉëuÉ×̨ÉmÉërɦÉÉåeÉÉïoÉsÉuÉhÉïxqÉ×ÌiÉÌ¢ürÉÈ ||
A.WØû.xÉÔ.12/5-6
33. SØMçü xmÉzÉïlÉÇ cÉ ÌmɨÉxrÉ lÉÉÍpÉU§É ÌuÉzÉåwÉiÉÈ | A.WØû.xÉÑ. 12/2
34. iuÉMçüxjÉÇ pÉëeÉMÇü pÉëeÉlÉÉiÉç iuÉcÉÈ | A.WØû.xÉÔ. 12/14
35. rɨÉÑ iuÉÍcÉ ÌmɨÉÇ iÉÎxqÉlÉç pÉëÉeÉMüÉåÅÎalÉËUÌiÉ xÉÇ¥ÉÉ
xÉÉåÅprÉÇaÉmÉËUwÉåMüÉuÉaÉÉWûÉsÉåmÉÉÌSlÉÉÇ Ì¢ürÉÉ
SìurÉÉhÉÉÇmÉ£üÉÇ NûÉrÉÉÇlÉÉ cÉ mÉëMüÉzÉMüÈ | xÉÑ.xÉÔ.
21/10
36. xuÉåS¤ÉrÉå UÉåqÉcrÉÑÌiÉÈ xiÉokÉUÉåqÉiÉÉ xTÔüOûlÉÇ iuÉcÉÈ
| A.WØû.xÉÔ. 11/22
37. UxÉÉiÉç xiÉlrÉÇ iÉiÉÉå U£üqÉxÉ×eÉÈ MühQûUÉÈ ÍxÉUÉÈ |
qÉÉÇxÉɲxÉÉ iuÉcÉÈ wÉOèû cÉ qÉåSxÉÈ xlÉÉrÉÑxÉÇpÉuÉÈ ||
cÉ.ÍcÉ. 14/17
38. xuÉåSuÉWûÉlÉÉÇ x§ÉÉåiÉxÉÉÇ qÉåSÉå qÉÔsÉÇ sÉÉåqÉMÑümÉÉzcÉ | cÉ.ÍcÉ. 5/8
39. qÉÉÇxÉuÉWåû ²å iÉrÉÉåqÉÔïsÉ, xlÉÉrÉÔ iuÉcÉÈ U£üuÉWûÉzcÉ
kÉqÉlrÉÈ | xÉÑ.zÉÉ. 9/12
qÉÉÇxÉuÉWûÉlÉÉ x§ÉÉåiÉxÉÉÇ xlÉÉrÉÑqÉÔïsÉÇ iuÉMçü cÉ |
cÉ.ÌuÉ. 5/10
40. wɸå qÉÉÍxÉ aÉpÉïxrÉ oÉsÉuÉhÉÉåïmÉcÉrÉÉå
pÉuÉirÉÍkÉMüqÉlrÉåprÉÉå qÉÉxÉåprÉÈ
iÉxqÉɨÉSÉ aÉÍpÉïhÉÏ oÉsÉuÉhÉïWûÉÌlÉqÉÉmɱiÉå ÌuÉzÉåwÉhÉ
| cÉ.zÉÉ. 4/22
“Study of Twak Shareer w.s.r to Kitibha Kustha” 75
References
41. iÉ§É iÉåeÉÉåkÉÉiÉÑÈ xÉuÉïuÉhÉÉïlÉÉ mÉëpÉuÉÈ xÉ rÉSÉ
aÉpÉïAÉåimɨÉÉuÉlkÉÉiÉÑ mÉërÉÉå pÉuÉÌiÉ iÉSÉ aÉpÉÉï
aÉÉæUÇ MüUÉåÌiÉ mÉ×ÍjÉuÉÏkÉÉiÉÑ mÉëÉrÉÈ ¢ÑüwhÉÇÈ
mÉ×ÍjÉurÉÉMüÉzÉkÉÉiÉÑ mÉëÉrÉÈ M×üwhÉzrÉÉqÉÇ,
iÉÉårÉÉMüÉzÉkÉÉiÉÑmÉërÉÉå aÉÉæUzrÉÉqÉqÉç |
rÉÉSØauÉhÉïqÉÉWûÉUqÉÑmÉxÉåuÉiÉå aÉÍpÉïhÉÏ
iÉÉSØauÉhÉïmÉëxÉuÉÉ pÉuÉiÉÏirÉåMåü pÉÉwÉliÉå | xÉÑ.zÉÉ.
2/36
42. AÌmÉ iÉÑ iÉåeÉÉåkÉÉiÉÑUmrÉÑSMüÉliÉËU¤ÉkÉÉiÉÑÈ
mÉërÉÉåÅuÉSÉiÉ uÉhÉïMüUÉå pÉuÉÌiÉ,
mÉ×ÍjÉuÉÏuÉÉrÉÑkÉÉiÉÑ mÉërÉÈ M×üwhÉ uÉhÉïMüUÈ,
xÉqÉxÉuÉïkÉÉiÉÑmÉërÉÈ, zrÉÉqÉuÉhÉïMüUÈ | cÉ.zÉÉ. 8/15
43. iɱjÉÉ–M×üwhÉ zrÉÉqÉÈ, zrÉÉqÉuÉSÉiÉÈ, AuÉSÉiɶÉåÌiÉ
mÉëM×üÌiÉuÉhÉÉïÈ zÉUÏUxrÉ pÉuÉÎliÉ | cÉ.CÇ. 1/8
44. iuÉYxÉÉUÇ UxÉxÉÉUÇ .... iuÉMçü zÉoSålÉ iuÉMüxjÉÉå
UxÉÉåÅÍpÉÌWûiÉÈ | xÉÑ.xÉÔ. 35/16
(QûsWûhÉ OûÏMüÉ)
45. xÉÑmÉëxɳÉqÉ×SÒsuÉaÉëÉåqÉÉhÉÇ iuÉMçüxÉÉUÇ ÌuɱÉiÉç |
xÉÑ.xÉÔ. 35/16 46. iÉ§É ÎxlÉakÉzsɤhÉ
qÉ×SÕmÉëxɳÉxÉѤqÉÉsmÉaÉÇpÉÏUxÉÑMÑüqÉÉUsÉÉåqÉÉ
xÉmÉëpÉåuÉ cÉ iuÉMçü iuÉMüxÉÉUÉhÉÉqÉç | cÉ.ÌuÉ. 8/102
47. §ÉrÉÉå UÉåaÉqÉÉaÉÉï CÌiÉ – zÉÉZÉÉ, qÉqÉÉïÎxjÉxÉlkÉrÉÈ
MüÉå¸zcÉ |
iÉ§É zÉÉZÉÉ U£üÉSrÉÉå kÉÉiÉuÉxiuÉMçü cÉ xÉ oÉÉWûrÉÉå
UÉåaÉqÉÉaÉïÈ .... | cÉ.xÉÑ. 11/48
48. iɱjÉÉ
´ÉÉå§ÉiuÉMçücɤÉÑÎeÉïuWûÉbÉëÉhÉÉuÉÉabÉxiÉÉåmÉxjÉ
mÉÉrÉÑmÉÉSqÉlÉÉÇxÉÏÌiÉ, iÉ§É mÉÔuÉÉïÍhÉ mÉÇcÉ
oÉÑÎkSÇÌSìrÉÉÍhÉ, CiÉUÉÍhÉ mÉÇcÉ MüqÉåïÌSìrÉÉÍhÉ .... |
“Study of Twak Shareer w.s.r to Kitibha Kustha” 76
References
xÉÑ.zÉÉ. 1/3
iÉ§É cɤÉÑÈ ´ÉÉå§ÉÇ bÉëhÉÇ UxÉlÉÇ xmÉzÉïlÉÍqÉÌiÉ
mÉÇcÉåÌSìrÉÉÍhÉ || cÉ.xÉÔ. 8/8
49. mÉÇcÉåÇÌSìrÉÉÍkɸÉlÉÉÌlÉ – AͤÉhÉÏ MühÉÉåï lÉÉÍxÉMåü ÎeÉuWûÉ iuÉMçü cÉåÌiÉ | cÉ.xÉÔ. 8/10
50. iuÉMçü xmÉzÉïlÉåÇÌSìrÉqÉç | A.WØû.xÉÔ. 12/1
iuÉÌaÉÇÌSìrÉqÉ mÉÇcÉ¥ÉÉlÉåÇÌSìrÉåwuÉåMüqÉç, iuÉMçü CSÇ
uÉÉrÉuÉÏrÉÍqÉÇÌSìrÉqÉç | xÉÑ.zÉÉ. 1/11
51. xmÉzÉïirÉlÉålÉåÌiÉ xmÉzÉïlÉqÉç | cÉ.xÉÔ. 8/8 52. uÉÉrÉurÉÉxiÉÑ xmÉzÉÉïÈ xmÉzÉïlÉåÇÌSìrÉÇ
xÉuÉïcÉå¹ÉxÉqÉÑWû xÉuÉïzÉUÏUxmÉlSlÉÇ sÉbÉÑiÉÉ cÉ |
xÉÑ. zÉÉ. 1/20
53. iɧÉæMÇü
xmÉzÉïlÉåÇÌSìrÉÉÍqÉÎlSìrÉÉhÉÉÍqÉÎlSìrÉurÉÉmÉMÇü, cÉåiÉÈ
xÉqÉuÉÉÌrÉ, xmÉzÉïlÉurÉÉmiÉåurÉÉïmÉMüqÉÌmÉ cÉåiÉ,
iÉxqÉÉiÉç xÉuÉåïÌSìrÉÉhÉÉÇ urÉÉmÉMüxmÉzÉïM×üiÉÉå rÉÉå
pÉÉuÉÌuÉzÉåwÉÈ .... | cÉ.xÉÔ. 11/38
54. ZÉUSìuÉcÉsÉÉåwhÉiuÉ pÉÔeÉsÉÉÌlÉsÉiÉåeÉxÉÉqÉç |
AÉMüÉzÉxrÉÉmÉëÌiÉkÉÉiÉÉå SØ¹Ç ÍsÉQèûaÉÇ rÉjÉÉ¢üqÉqÉç ||
sɤÉhÉÇ xÉuÉïqÉåiÉiÉç xmÉzÉïlÉåÇÌSìrÉaÉÉåcÉUqÉç |
xmÉzÉïlÉåÇÌSìrÉÌuÉ¥ÉårÉÈ xmÉzÉÉåï ÌWû xÉÌuÉmÉrÉïrÉÈ ||
cÉ.zÉÉ. 1/29,30
“Study of Twak Shareer w.s.r to Kitibha Kustha” 77
Bibliography
BIBLIOGRAPHY
1) Prof. Srikanth murthy K.R. sushrut samhita (sharer 4/4) chaukambha,
Varanasi,U.P. vol-1,2nd edition 2004,pp 289 on 50 pg.
2) Prof. Srikanth murthy K.R. sushrut samhita (sharer 4/4) chaukambha,
Varanasi,U.P. vol-1,2nd edition 2004,pp 289 on 51 pg.
3) Prof. Srikanth murthy , Astanga Samgraha of Vagbhata ,(sharer 5/16)
chaukhamba orientalia 5th edition U.P. vol-II, 2nd edition 2005.pp 622 on 62
pg.
4) Sharma P.V.Agnivesa charak samhita (nidan 5/14)) redacted by charaka and
Dridabala,chaukamba surabharati prakashan, Varanasi,U.P, vol-1,4th edition
2003, pp 544 on 277pg.
5) Prof.Srikanth murthy K.R. Madhav nidanas (rog viniscaya)of madhavkar
(chi.49/18) chaukambha orientalia,varanasi ,U.P. ,5th edition , 2003.,,pp 329
on 161 pg.
6) Clinical Anatomy – Richard S.Snell 7th edition 2003.pp 1012, pg 5 to 7
7) Principal of anatomy and physiology by Tortora Grabowski 10th edition
2003.pp 1104 pg 140.
8) A.P.I. Text book of medicine by G.S. SAINANI.1999 .pp 1367 pg 1198.
9) Ashtanga Hridaya: Commentary by Arundatta (Sarvangasundari) and
Hemadri (Ayurveda Rasayana), Chaukhamba Orientalia, Varanasi, 1982.
10) Ashtanga Sangraha: By Vagbhata with commentary of Indu, Atreya
Prakashna, Pune, 1980.
11) A Sanskrit – English Dictionary: By Monier and Williams, First edition,
1993.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 79
Bibliography
12) Bhavaprakasha Samhita: Acharya Ramanath Dwivedi, chaukhamba
Publication, 1st Edition.
13) Charaka Samhita: Poorvardha & Uttarardha, Chaukhamba Bharti Academy.
14) Charaka Samhita Ayurveda Dipika Tika: By Chakrapanidatta, Nirnaysagar
Press, Bombay.
15) Parishadya Shabdarth Sharir: By Ayurvedacharya P. Damodar Sharma
Gaud.
16) Sushruta Samhita: Kaviraj Ambikadatta Shastri, A.M.Ss. Chaukhamba
Sanskrit Sansthan.
17) Sushruta Samhita: Ayurveda Rahasya Deepika Commentary by Dr. B.G.
Ghanekar, 13th edition, 1998, publication Meherehand Laxmandas, New
Delhi.
18) Suhruta Samhita: Dalhana Nibandha Sangraha Commentary, published by
krishnadas Academy.
19) Sharangdhara samhitha: Acharya Yadavji Trikamji, Chaukhamba
Publication.
20) Shabdakalpadrooma: Raja Radhakant dev, Naga Prakashana, Delhi.
1) A Textbook of Dermatology: Moschella and Hurley, 2nd edition part (1) and
(2).
2) Clinical oriented Anatomy: By Richard L. Drake, Wayne Vogal, Adam
W.M. Michell, Published by Churchill Livingstone, Edinburgh, London, 1st
Edition 2005.
3) Gray’s Anatomy: By Henry Gray edited by Peter Williams and others.
Published by Churchill Livingstone Edinburgh, London, 37th edition.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 80
Bibliography
4) Histopathology of skin: Water F. Leaver.
5) Human Embryology : BY I.B. Singh published by Rajiv Beri, for
Macmillan India Limited, New Delhi 7th Edition 2003.
6) Illustrated Synopsis of Dermatology and STD: by Neena Khanna,
PEEPEE Publications, 1st edition.
7) Medical laboratory Technique : Ramnik Sood, Jaypee Publicaitons.
8) Principles of Anatomy and Physiology :By G.J. Tortora and S.R.
Grabowski, published by Harper Collins College publishers, New Yord, 8th
edition, 1996.
9) Practice of Dermatology : P.N. Bhel, 7th edition CBS publications.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 81
Conclusion
CONCLUSION
From the observations based on literary and histopathological study and
discussion the following conclusions can be drawn.
1) According to Acharya Sushruta there are seven types of Twacha and out of
these seven Twacha. Kitibha occurs in fourth and fifth layer of Twacha i.e.
Tamra and Vedini.
2) Sushruta seems to be more accurate in telling thickness of Twacha. His
measurement of thickness of all the layers of Twacha expressed in modern
units is very much similar to the thickness of skin given in modern textbooks
of Anatomy.
3) Kitibha vyadhi a type of Kushtha and psoriasis a type of skin disease have
most of the same symptoms which are correlated on the basis of literary,
histopathalogical and clinical study of both Ayurveda and modern science.
4) Kitibha is mostly correlated with the plaque type of psoriasis.
5) The present study is carried out on 30 patients so which is a small sample. The
patients selected were having different types of psoriasis/kusthas. Here
suggestion is given for the further study to conduct on large number of
patients concentrating on particular types of psoriasis in multi-centres, after
which as clear conclusion can be drawn.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 68
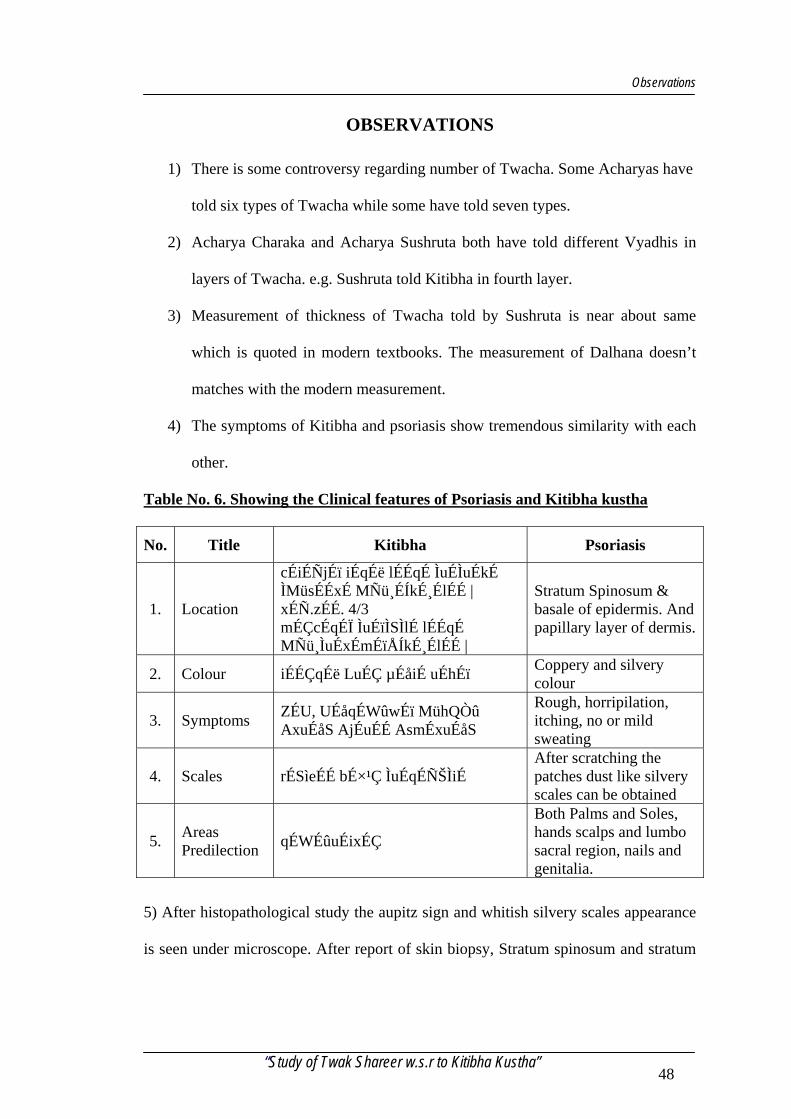
Observations
OBSERVATIONS
1) There is some controversy regarding number of Twacha. Some Acharyas have
told six types of Twacha while some have told seven types.
2) Acharya Charaka and Acharya Sushruta both have told different Vyadhis in
layers of Twacha. e.g. Sushruta told Kitibha in fourth layer.
3) Measurement of thickness of Twacha told by Sushruta is near about same
which is quoted in modern textbooks. The measurement of Dalhana doesn’t
matches with the modern measurement.
4) The symptoms of Kitibha and psoriasis show tremendous similarity with each
other.
Table No. 6. Showing the Clinical features of Psoriasis and Kitibha kustha
No. Title Kitibha Psoriasis
1. Location
cÉiÉÑjÉï iÉqÉë lÉÉqÉ ÌuÉÌuÉkÉ ÌMüsÉÉxÉ MÑü¸ÉÍkɸÉlÉÉ | xÉÑ.zÉÉ. 4/3 mÉÇcÉqÉÏ ÌuÉïÌSÌlÉ lÉÉqÉ MÑü¸ÌuÉxÉmÉïÅÍkɸÉlÉÉ |
Stratum Spinosum & basale of epidermis. And papillary layer of dermis.
2. Colour iÉÉÇqÉë LuÉÇ µÉåiÉ uÉhÉï Coppery and silvery colour
3. Symptoms ZÉU, UÉåqÉWûwÉï MühQÒû AxuÉåS AjÉuÉÉ AsmÉxuÉåS
Rough, horripilation, itching, no or mild sweating
4. Scales rÉSìeÉÉ bÉ×¹Ç ÌuÉqÉÑŠÌiÉ After scratching the patches dust like silvery scales can be obtained
5. Areas Predilection qÉWÉûuÉixÉÇ
Both Palms and Soles, hands scalps and lumbo sacral region, nails and genitalia.
5) After histopathological study the aupitz sign and whitish silvery scales appearance
is seen under microscope. After report of skin biopsy, Stratum spinosum and stratum
“Study of Twak Shareer w.s.r to Kitibha Kustha” 48
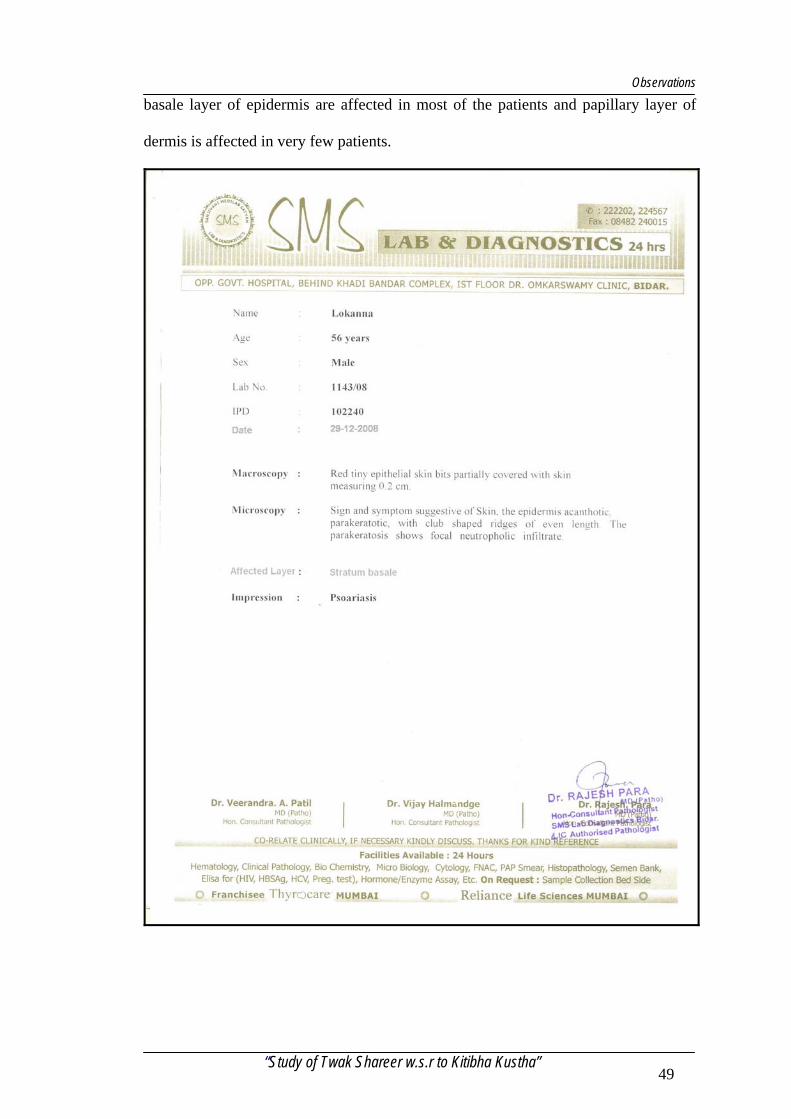
Observations
basale layer of epidermis are affected in most of the patients and papillary layer of
dermis is affected in very few patients.
“Study of Twak Shareer w.s.r to Kitibha Kustha” 49
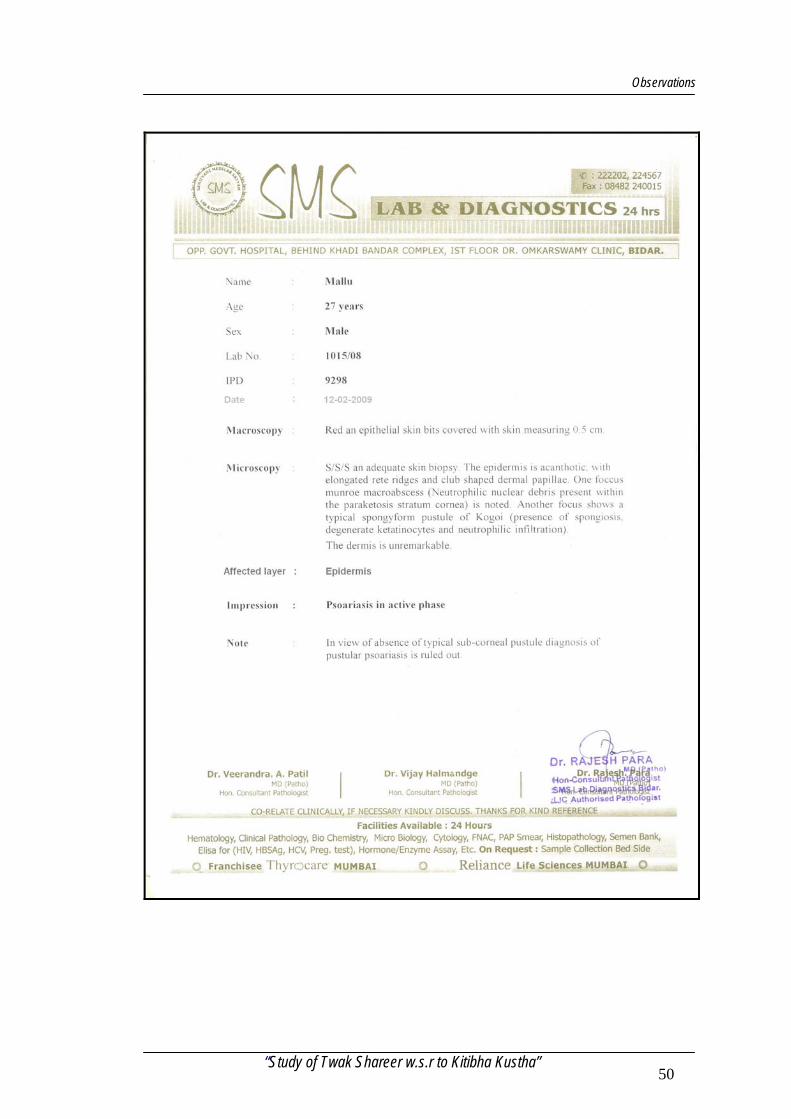
Observations
“Study of Twak Shareer w.s.r to Kitibha Kustha” 50
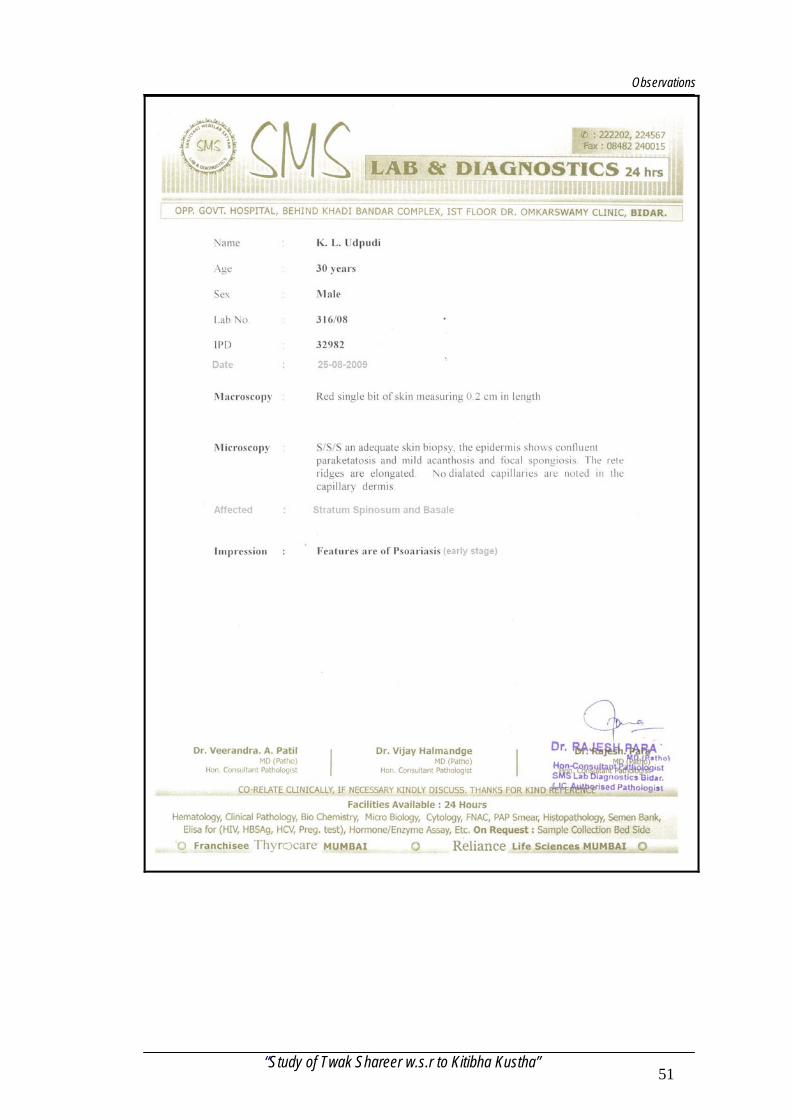
Observations
“Study of Twak Shareer w.s.r to Kitibha Kustha” 51
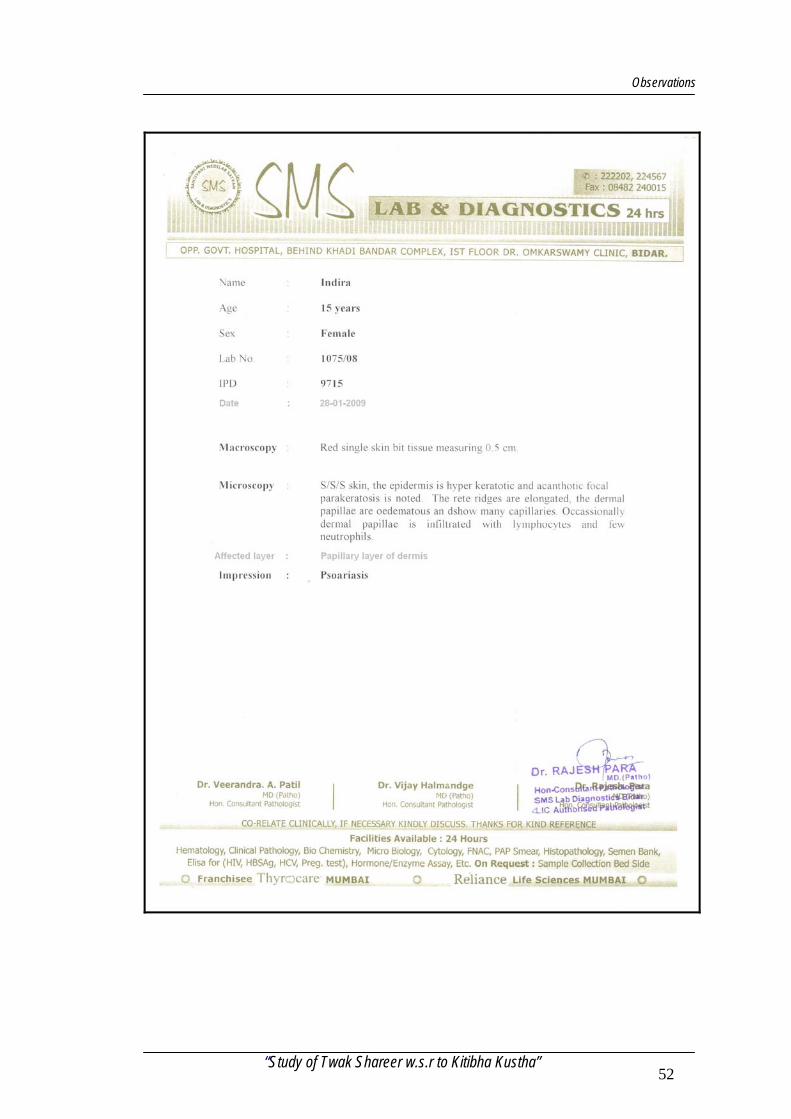
Observations
“Study of Twak Shareer w.s.r to Kitibha Kustha” 52
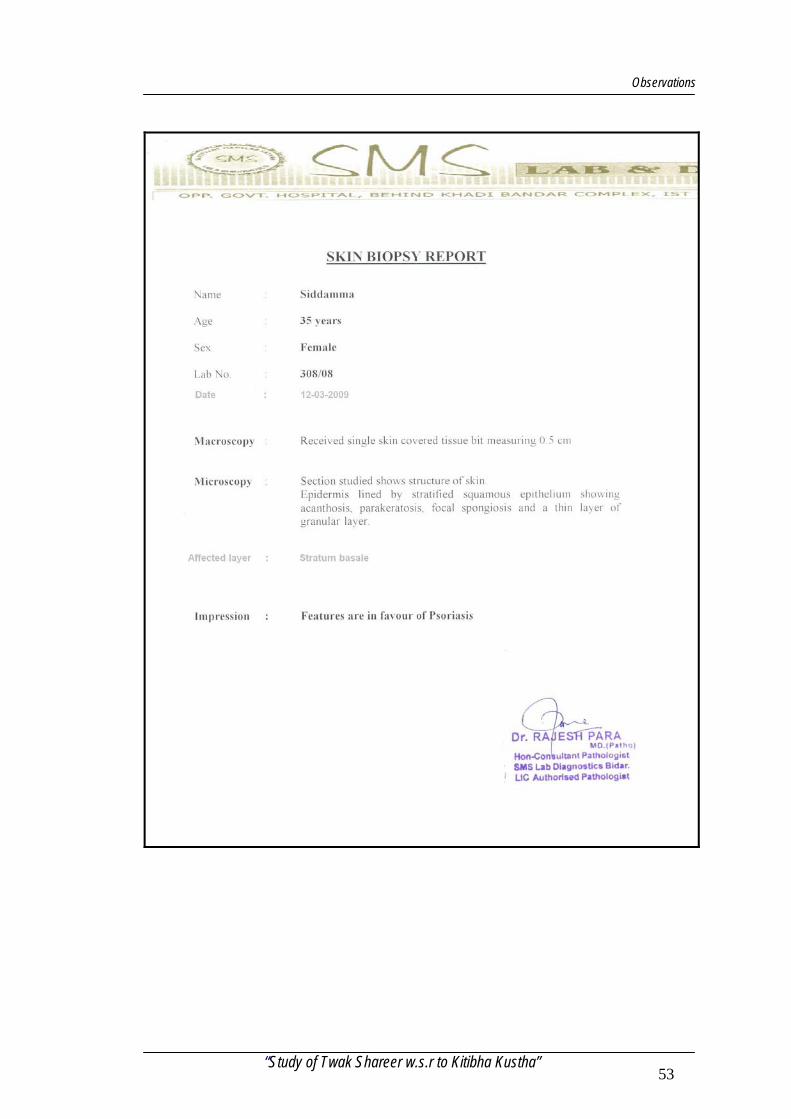
Observations
“Study of Twak Shareer w.s.r to Kitibha Kustha” 53
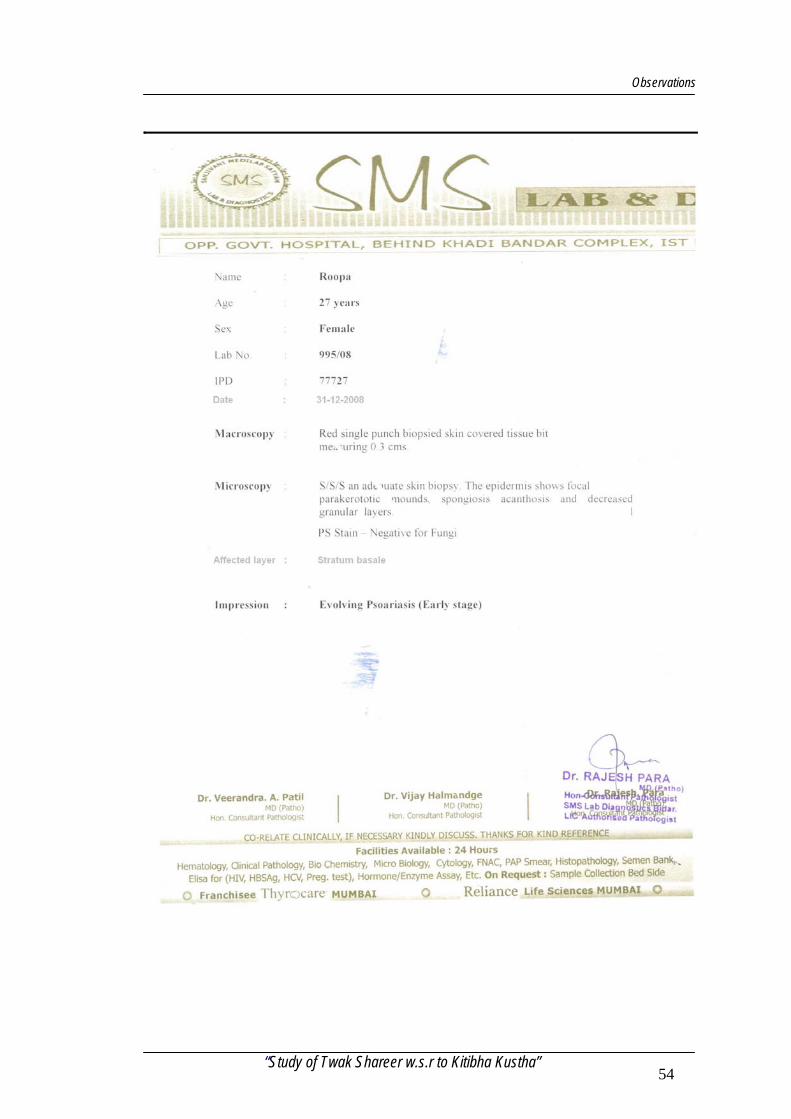
Observations
“Study of Twak Shareer w.s.r to Kitibha Kustha” 54
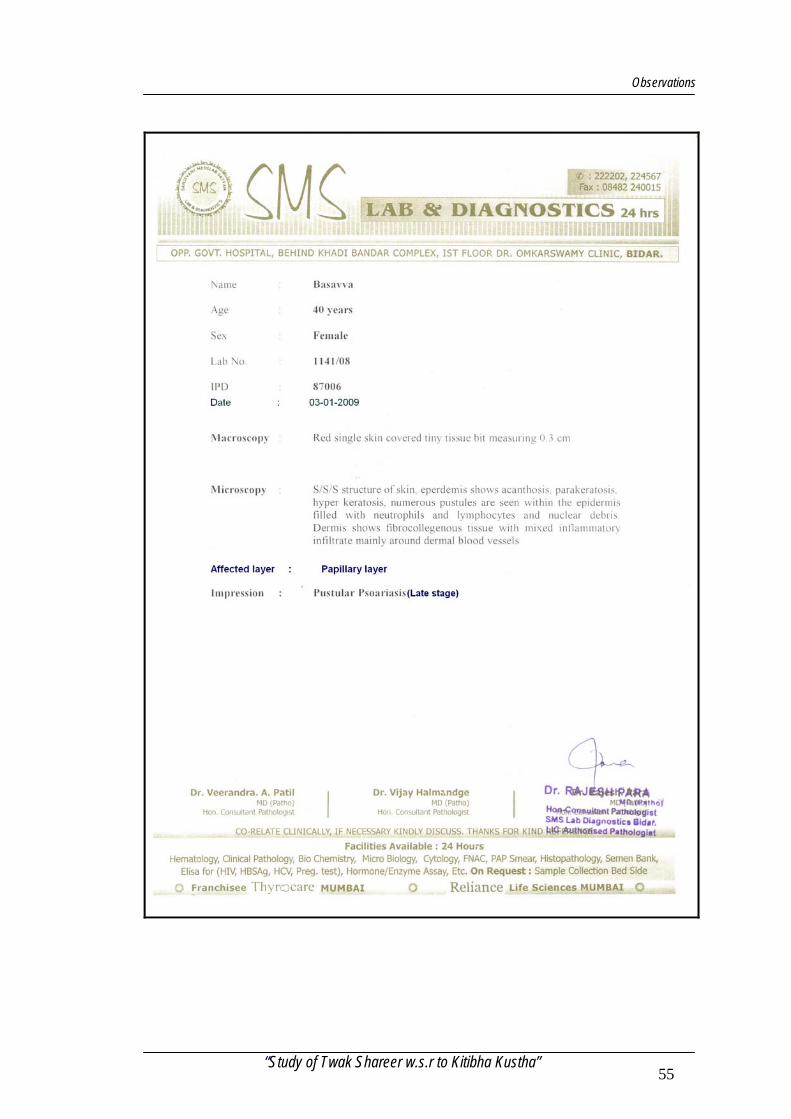
Observations
“Study of Twak Shareer w.s.r to Kitibha Kustha” 55
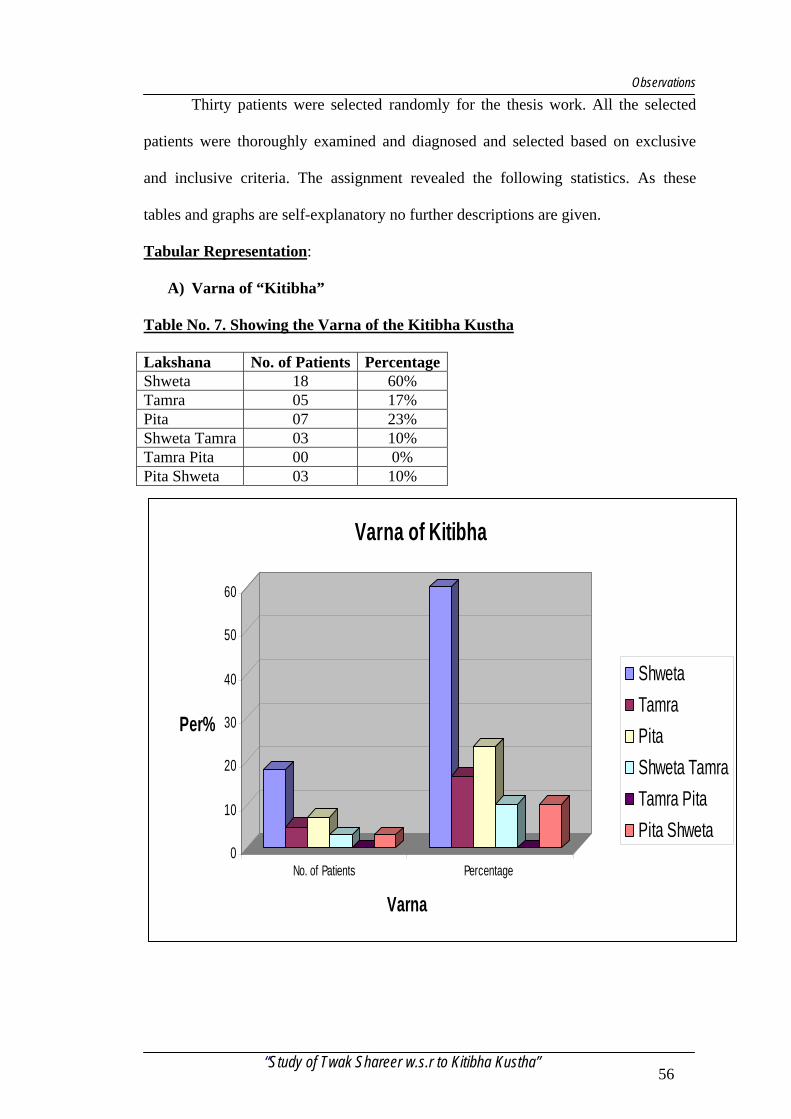
Observations
Thirty patients were selected randomly for the thesis work. All the selected
patients were thoroughly examined and diagnosed and selected based on exclusive
and inclusive criteria. The assignment revealed the following statistics. As these
tables and graphs are self-explanatory no further descriptions are given.
Tabular Representation:
A) Varna of “Kitibha”
Table No. 7. Showing the Varna of the Kitibha Kustha
Lakshana No. of Patients Percentage Shweta 18 60% Tamra 05 17% Pita 07 23% Shweta Tamra 03 10% Tamra Pita 00 0% Pita Shweta 03 10%
0
10
20
30
40
50
60
Per%
No. of Patients Percentage
Varna
Varna of Kitibha
ShwetaTamraPitaShweta TamraTamra PitaPita Shweta
“Study of Twak Shareer w.s.r to Kitibha Kustha” 56
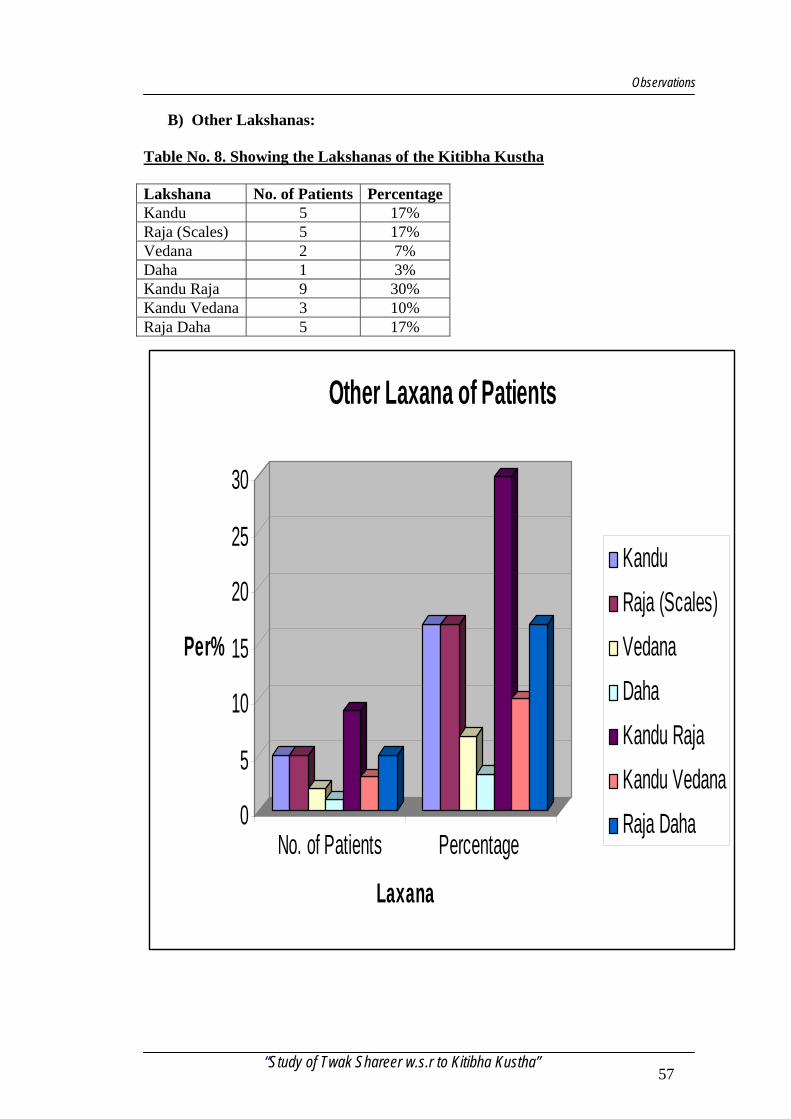
Observations
B) Other Lakshanas:
Table No. 8. Showing the Lakshanas of the Kitibha Kustha
Lakshana No. of Patients Percentage Kandu 5 17% Raja (Scales) 5 17% Vedana 2 7% Daha 1 3% Kandu Raja 9 30% Kandu Vedana 3 10% Raja Daha 5 17%
0
5
10
15
20
25
30
Per%
No. of Patients Percentage
Laxana
Other Laxana of Patients
KanduRaja (Scales)VedanaDahaKandu RajaKandu VedanaRaja Daha
“Study of Twak Shareer w.s.r to Kitibha Kustha” 57
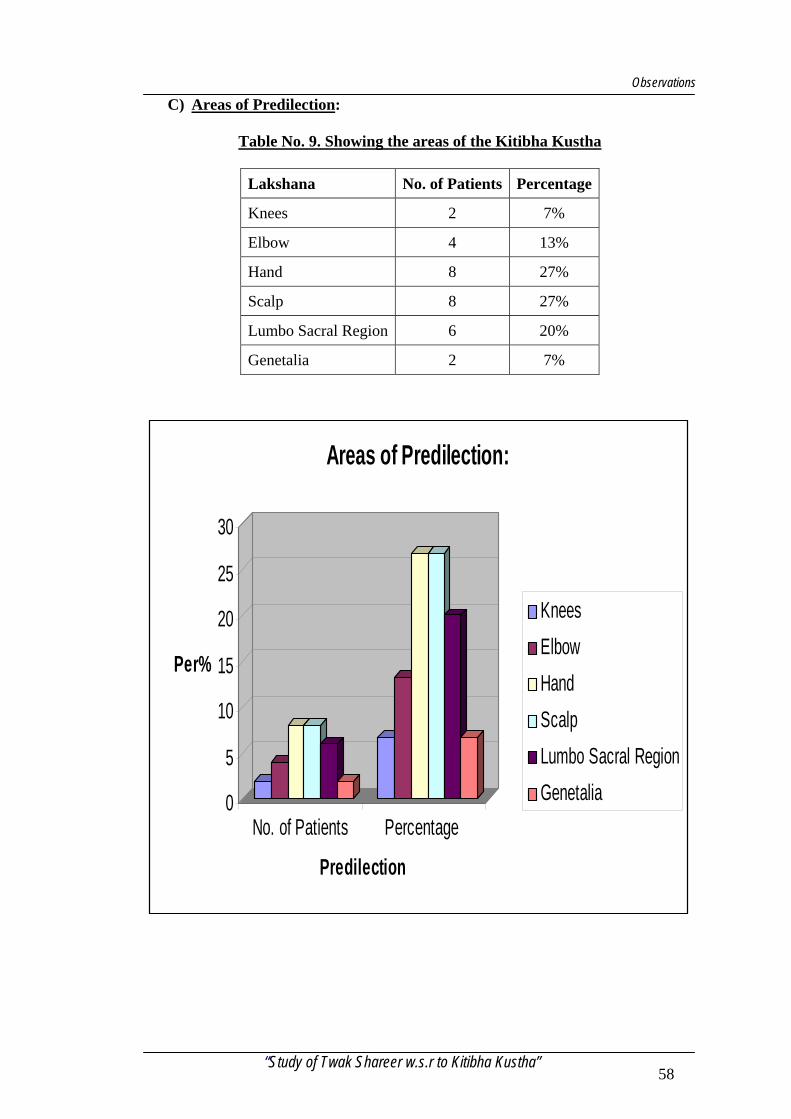
Observations
C) Areas of Predilection:
Table No. 9. Showing the areas of the Kitibha Kustha
Lakshana No. of Patients Percentage
Knees 2 7%
Elbow 4 13%
Hand 8 27%
Scalp 8 27%
Lumbo Sacral Region 6 20%
Genetalia 2 7%
0
5
10
15
20
25
30
Per%
No. of Patients Percentage
Predilection
Areas of Predilection:
KneesElbowHandScalpLumbo Sacral RegionGenetalia
“Study of Twak Shareer w.s.r to Kitibha Kustha” 58
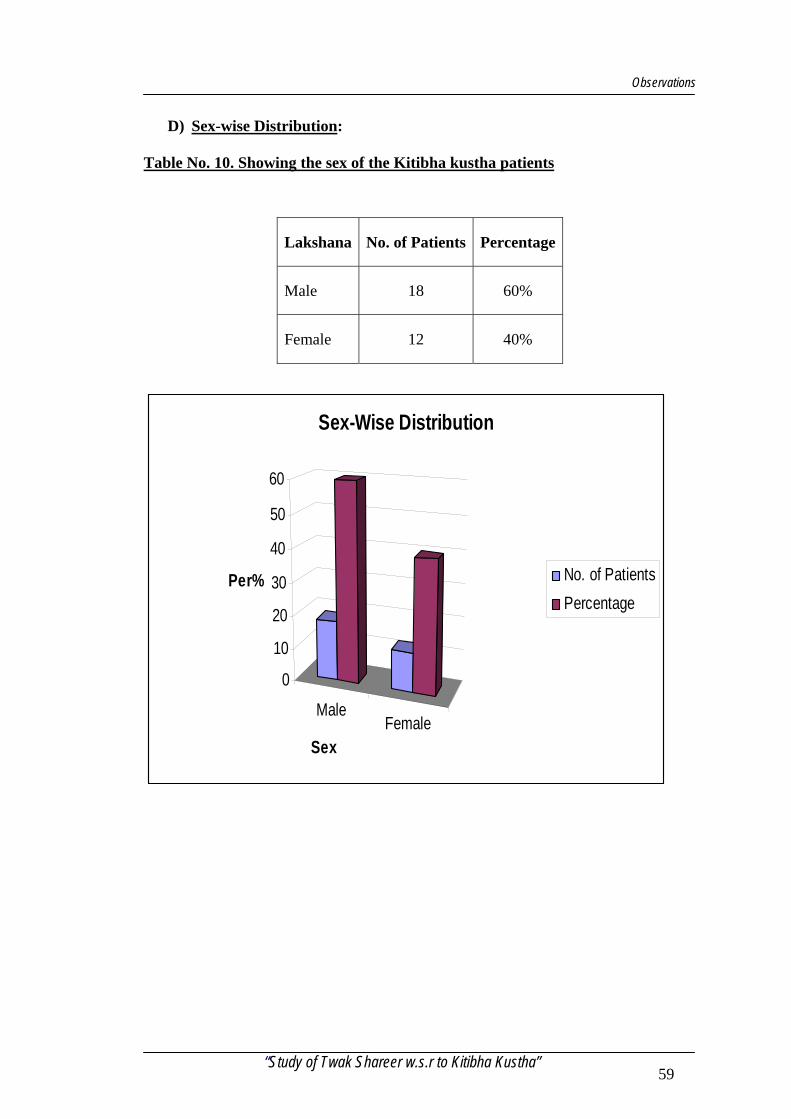
Observations
D) Sex-wise Distribution:
Table No. 10. Showing the sex of the Kitibha kustha patients
Lakshana No. of Patients Percentage
Male 18 60%
Female 12 40%
MaleFemale
0
10
20
30
40
50
60
Per%
Sex
Sex-Wise Distribution
No. of PatientsPercentage
“Study of Twak Shareer w.s.r to Kitibha Kustha” 59
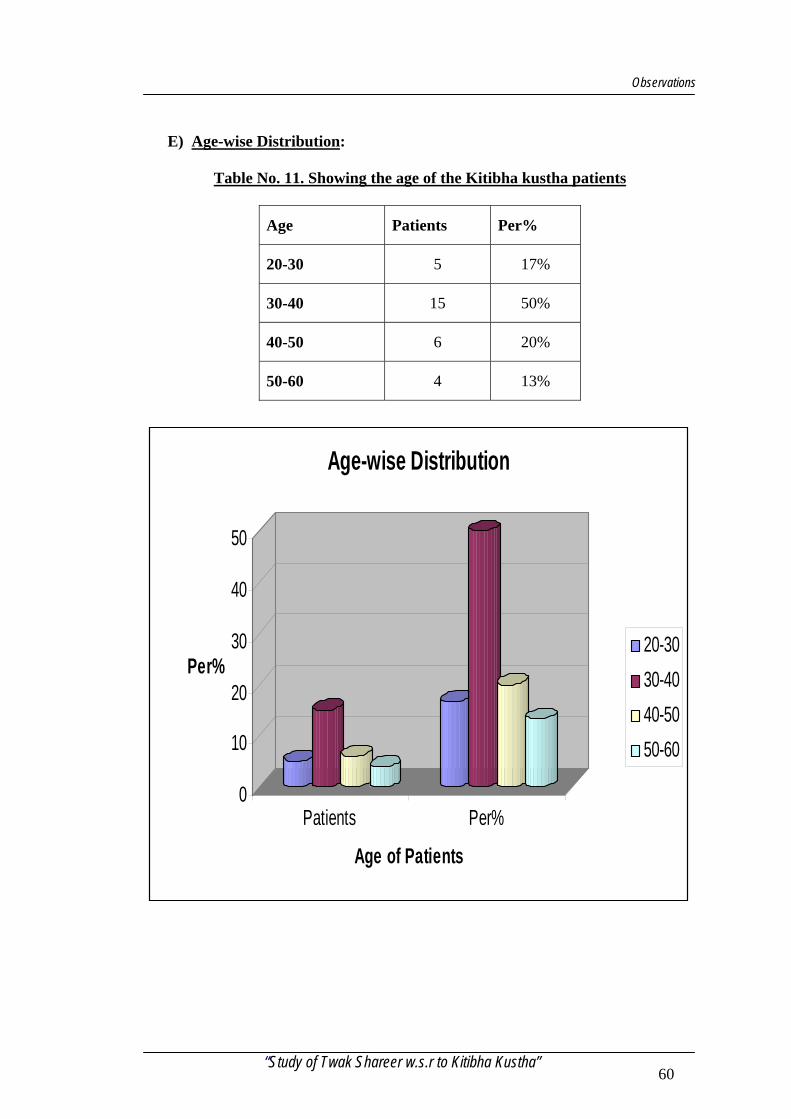
Observations
E) Age-wise Distribution:
Table No. 11. Showing the age of the Kitibha kustha patients
Age Patients Per%
20-30 5 17%
30-40 15 50%
40-50 6 20%
50-60 4 13%
0
10
20
30
40
50
Per%
Patients Per%
Age of Patients
Age-wise Distribution
20-3030-4040-5050-60
“Study of Twak Shareer w.s.r to Kitibha Kustha” 60
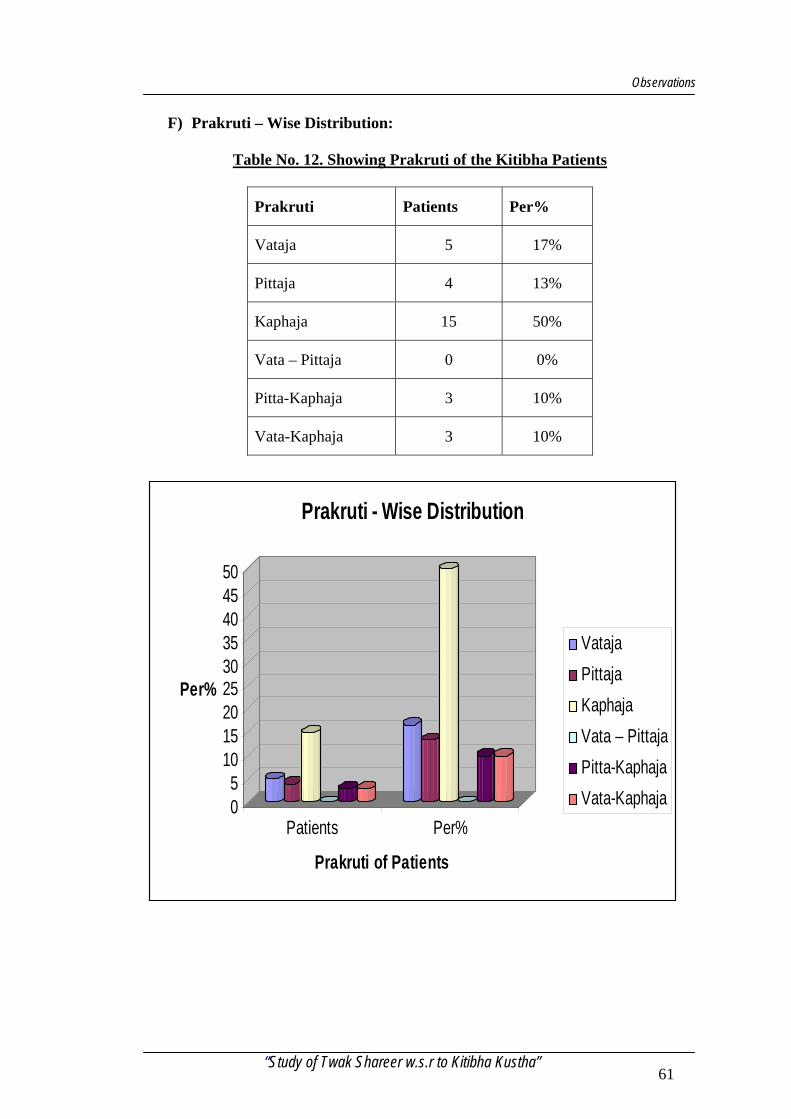
Observations
F) Prakruti – Wise Distribution:
Table No. 12. Showing Prakruti of the Kitibha Patients
Prakruti Patients Per%
Vataja 5 17%
Pittaja 4 13%
Kaphaja 15 50%
Vata – Pittaja 0 0%
Pitta-Kaphaja 3 10%
Vata-Kaphaja 3 10%
05
101520253035404550
Per%
Patients Per%
Prakruti of Patients
Prakruti - Wise Distribution
VatajaPittajaKaphajaVata – PittajaPitta-KaphajaVata-Kaphaja
“Study of Twak Shareer w.s.r to Kitibha Kustha” 61
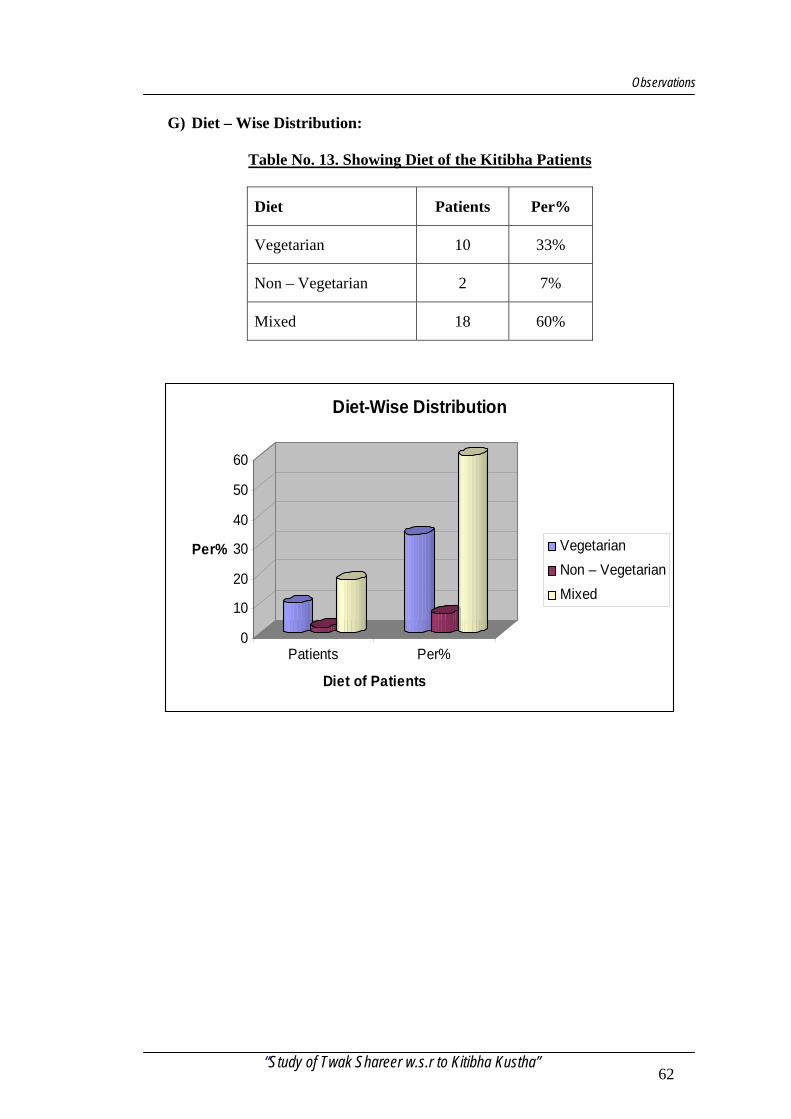
Observations
G) Diet – Wise Distribution:
Table No. 13. Showing Diet of the Kitibha Patients
Diet Patients Per%
Vegetarian 10 33%
Non – Vegetarian 2 7%
Mixed 18 60%
0
10
20
30
40
50
60
Per%
Patients Per%
Diet of Patients
Diet-Wise Distribution
VegetarianNon – VegetarianMixed
“Study of Twak Shareer w.s.r to Kitibha Kustha” 62
Case Sheet
DEPARTMENT OF P.G. STUDIES IN RACHANA SHAREER
N.K.J AYURVEDIC MEDICALCOLLEGE & PG CENTRE, BIDAR. RESEARCH CASE SHEET TITLE: STUDY OF TWAK SHAREER W.S.R. TO KITIBHA KUSTHA. Research scholar: Dr.Sapana Hiremath Co-guide:Dr.N.J. Mulimani. Guide: Dr.J.K.Bhargava. PRILIMINARY DATA: Name: Age : Sex : Religion: Occupation: Address: D.O.A.: D.O.D.: OPD/Ward/Bed: Diagnosis: Result : HISTORICAL DATA: PRADHAN VEDANA (Chief complaint): VEDANA VRITTANT (H/O Present illness): POORVA VYADHI VRITTANT (Past history): VIYAKTIKA VRITTANT (Personal history): KOUTUMBIKA VRITTANT (Family history):
I
Case Sheet SYSTEMIC EXAMINATION
1) Respiratory system: 2) C.V.S. :
B.P. 3) Abdomen: 4) C.N.S.: 5) Urinary system:
GENERAL EXAMINATION A)ASHTAVIDHA PAREEKSHA Nadi: Shabda: Mala: Sparsha: Mutra: Druk; Jiwha: Aakruti: B)DASHAVIDHA PAREEKSHA Prakritaha: Sarataha : Samharana: Satwataha : Aharshakti: Vyayamshakti: Vayaha : Pramana : Vikrititaha pariksha: Hetu (causative factor) Poorva roopa (premonitory factor) Roopa (symptoms) C)LOCAL EXAMINATION Inspection: Palpation : Percussion : Auscultation:
II
Case Sheet SAMPRAPTI
A) Udbhava sthana: B) Dosha : C) Agni : D) Sanchara : E) Adhishtana(dhatus involved) Rasa: Mamsa: Rakta: Ambu(lasika): F)Vyaktasthana INVESTIGATION Skin Biopsy Blood: TLC,DLC,ESR,Hb%,FBS,PPBS,CT,BT. Urine: Routine Microscopic Vyavacheda nidana(Differential Diagnosis): Vyadhi vinischay(Diagnosis): RESULT: Signature of the PG scholar Signature of co-guide Signature of guide
III
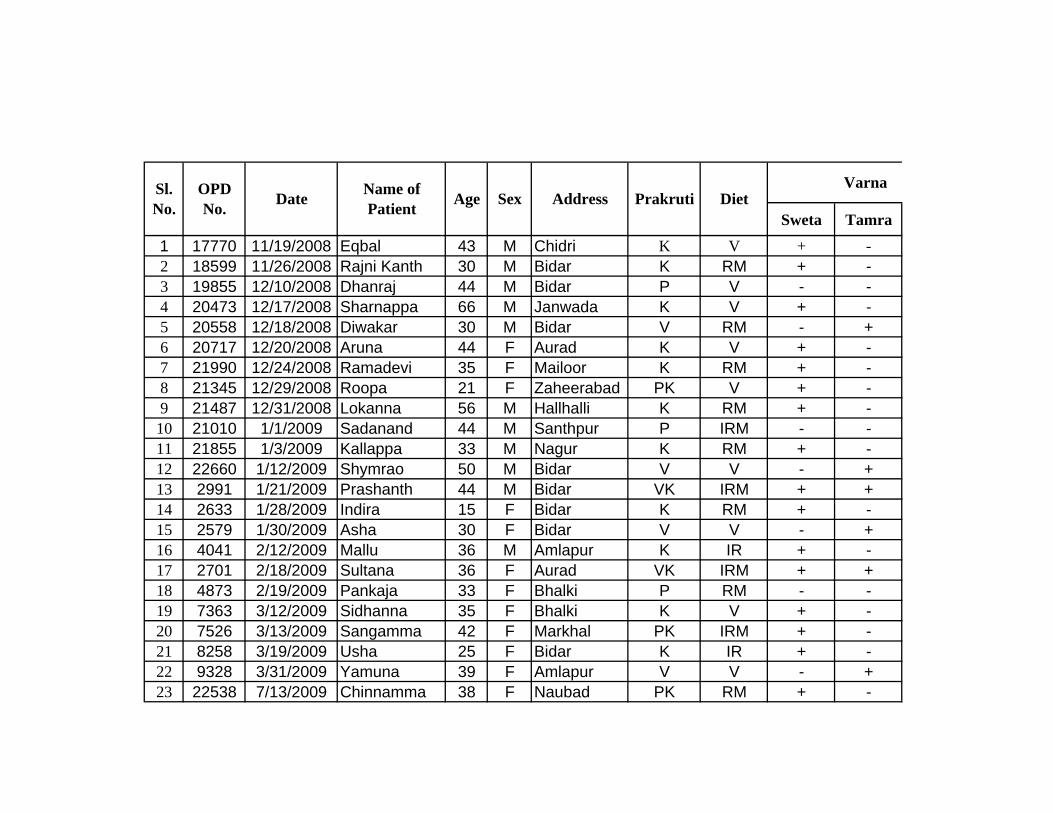
Sl.No.
OPD No. Date Name of
Patient Age Sex Address Prakruti DietVarna
Sweta Tamra
1 17770 11/19/2008 Eqbal 43 M Chidri K V + -2 18599 11/26/2008 Rajni Kanth 30 M Bidar K RM + -3 19855 12/10/2008 Dhanraj 44 M Bidar P V - -4 20473 12/17/2008 Sharnappa 66 M Janwada K V + -5 20558 12/18/2008 Diwakar 30 M Bidar V RM - +6 20717 12/20/2008 Aruna 44 F Aurad K V + -7 21990 12/24/2008 Ramadevi 35 F Mailoor K RM + -8 21345 12/29/2008 Roopa 21 F Zaheerabad PK V + -9 21487 12/31/2008 Lokanna 56 M Hallhalli K RM + -10 21010 1/1/2009 Sadanand 44 M Santhpur P IRM - -11 21855 1/3/2009 Kallappa 33 M Nagur K RM + -12 22660 1/12/2009 Shymrao 50 M Bidar V V - +13 2991 1/21/2009 Prashanth 44 M Bidar VK IRM + +14 2633 1/28/2009 Indira 15 F Bidar K RM + -15 2579 1/30/2009 Asha 30 F Bidar V V - +16 4041 2/12/2009 Mallu 36 M Amlapur K IR + -17 2701 2/18/2009 Sultana 36 F Aurad VK IRM + +18 4873 2/19/2009 Pankaja 33 F Bhalki P RM - -19 7363 3/12/2009 Sidhanna 35 F Bhalki K V + -20 7526 3/13/2009 Sangamma 42 F Markhal PK IRM + -21 8258 3/19/2009 Usha 25 F Bidar K IR + -22 9328 3/31/2009 Yamuna 39 F Amlapur V V - +23 22538 7/13/2009 Chinnamma 38 F Naubad PK RM + -
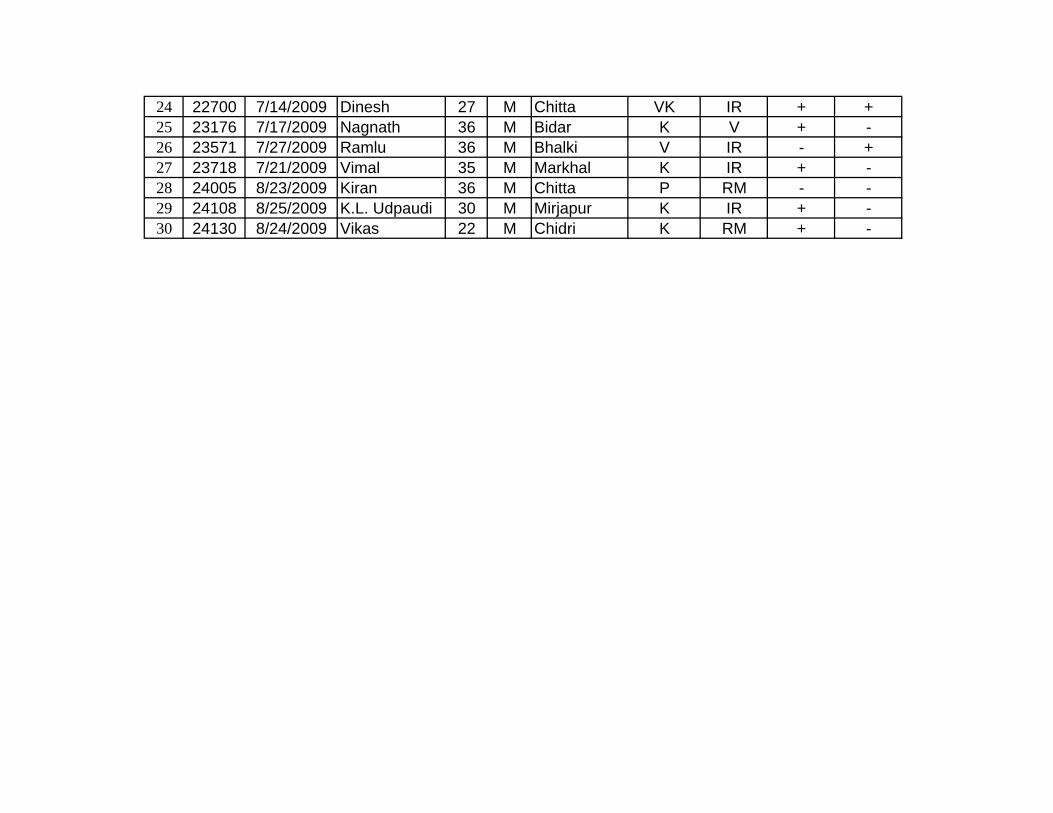
24 22700 7/14/2009 Dinesh 27 M Chitta VK IR + +25 23176 7/17/2009 Nagnath 36 M Bidar K V + -26 23571 7/27/2009 Ramlu 36 M Bhalki V IR - +27 23718 7/21/2009 Vimal 35 M Markhal K IR + -28 24005 8/23/2009 Kiran 36 M Chitta P RM - -29 24108 8/25/2009 K.L. Udpaudi 30 M Mirjapur K IR + -30 24130 8/24/2009 Vikas 22 M Chidri K RM + -
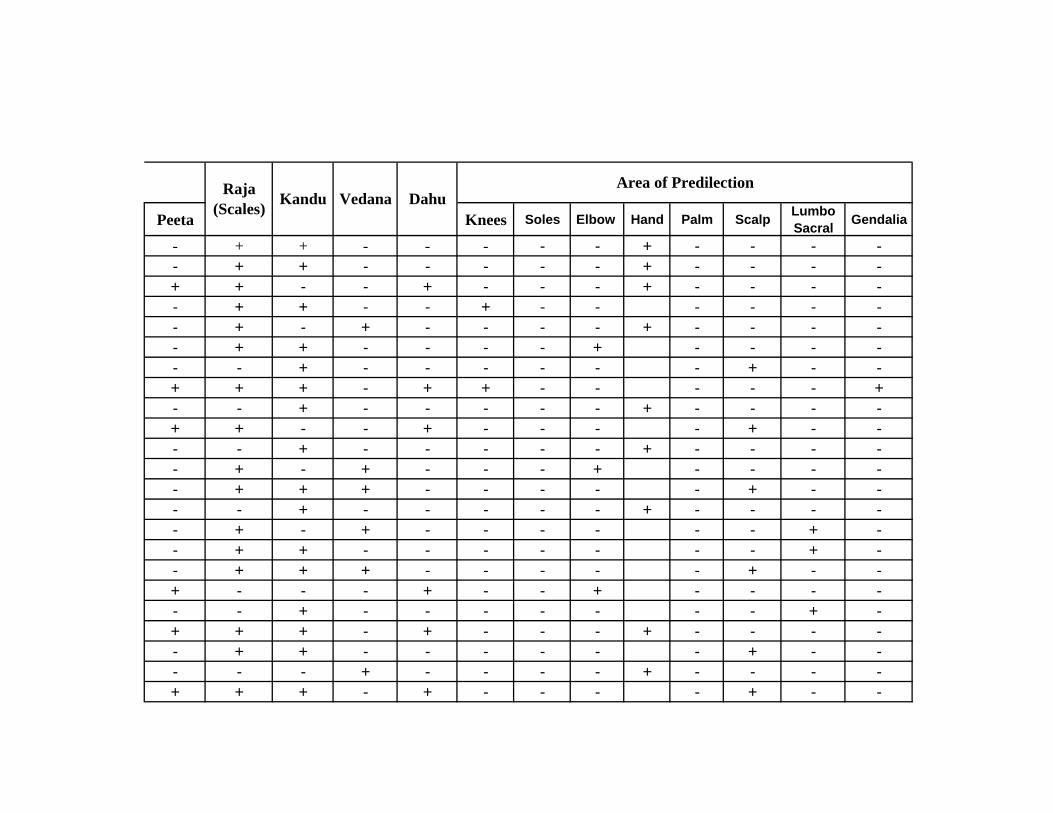
Raja (Scales) Kandu Vedana Dahu
Area of Predilection
Peeta Knees Soles Elbow Hand Palm Scalp Lumbo Sacral Gendalia
- + + - - - - - + - - - -- + + - - - - - + - - - -+ + - - + - - - + - - - -- + + - - + - - - - - -- + - + - - - - + - - - -- + + - - - - + - - - -- - + - - - - - - + - -+ + + - + + - - - - - +- - + - - - - - + - - - -+ + - - + - - - - + - -- - + - - - - - + - - - -- + - + - - - + - - - -- + + + - - - - - + - -- - + - - - - - + - - - -- + - + - - - - - - + -- + + - - - - - - - + -- + + + - - - - - + - -+ - - - + - - + - - - -- - + - - - - - - - + -+ + + - + - - - + - - - -- + + - - - - - - + - -- - - + - - - - + - - - -+ + + - + - - - - + - -
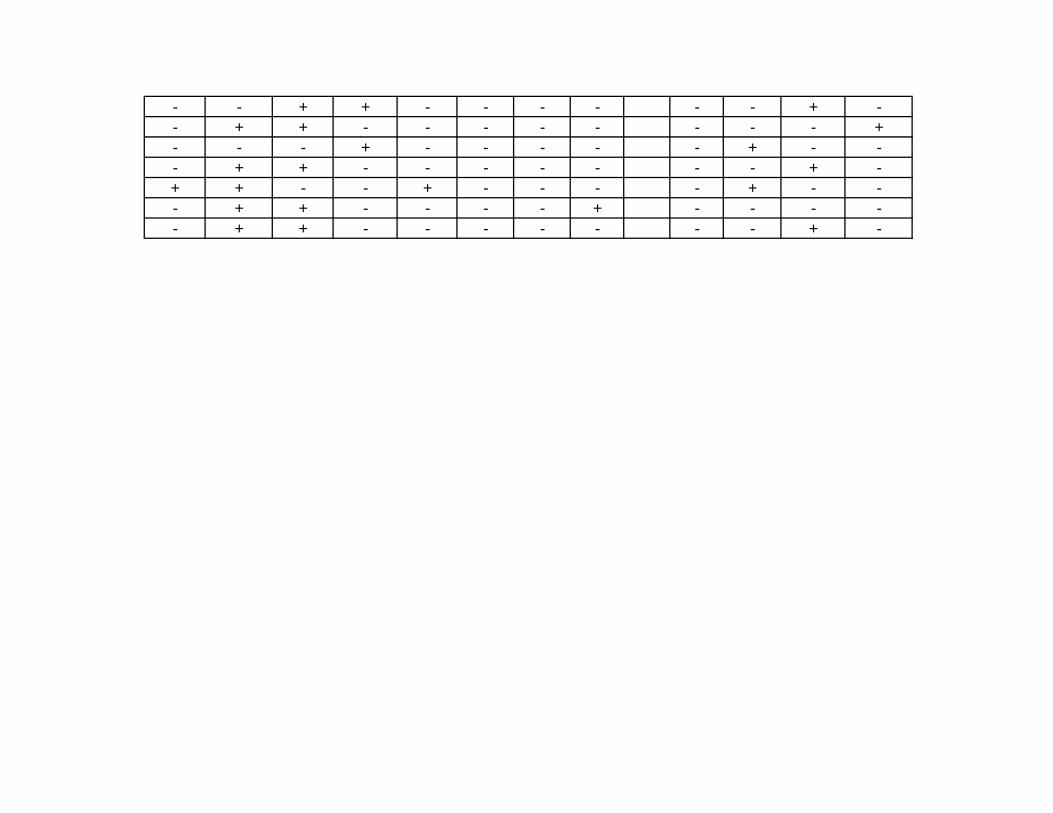
- - + + - - - - - - + -- + + - - - - - - - - +- - - + - - - - - + - -- + + - - - - - - - + -+ + - - + - - - - + - -- + + - - - - + - - - -- + + - - - - - - - + -