stem cell strategies in burns care
TRANSCRIPT
b u r n s 3 3 ( 2 0 0 7 ) 2 8 2 – 2 9 1
Review
Stem cell strategies in burns care
A. Burd *, K. Ahmed, S. Lam, T. Ayyappan, L. Huang
Division of Plastic & Reconstructive Surgery, Department of Surgery, The Chinese University of Hong Kong,
Prince of Wales Hospital, Hong Kong, China
Contents
1. Introduction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 282
2. Stem cells and skin tissue engineering . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 283
3. Stem cells and wound healing modulation. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 285
4. Clinical challenge . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 285
5. Hypothesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 287
6. Cord blood . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 287
7. Stem cell fractions. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 288
8. Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 288
Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 289
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 289
a r t i c l e i n f o
Article history:
Accepted 15 August 2006
Keywords:
Stem cells
Marrow suppression
Burns
a b s t r a c t
The prospect of being able to replace damaged tissue by the process of regeneration would
dramatically and irrevocably change the impact, management and outcome of burns. The
current understanding of stem cell-based modulation and therapy together with their
potential developments do bring this prospect ever closer to a clinical reality. This paper
gives a background to stem cell strategies in burns care and identifies actual or prospective
applications which, collectively, will forever change burns care throughout the world.
# 2006 Elsevier Ltd and ISBI. All rights reserved.
avai lable at www.sc iencedi rec t .com
journal homepage: www.e lsevier .com/ locate /burns
1. Introduction
The last 30 years has seen a tremendous evolution in
conceptual strategies in the field of burns care. The three
‘R’’s, replace, reconstruct, regenerate have their clinical
application in transplantation, tissue engineering and now,
stem cells therapies [1]. When Rheinwald and Green described
the serial cultivation of strains of human epidermal kerati-
nocytes with the formation of keratinizing colonies from
single cells over 30 years ago [2], naive claims were made by
* Corresponding author. Tel.: +852 2632 2639; fax: +852 2632 4675.E-mail address: [email protected] (A. Burd).
0305-4179/$30.00 # 2006 Elsevier Ltd and ISBI. All rights reserved.doi:10.1016/j.burns.2006.08.031
some laboratory scientists that the burns care of the future
would be a simple matter of quick and easy cover after
the excision of burn wounds. Unfortunately this is far from
reality [3,4]. The next decade brought the concept of tissue
engineering.
When the term ‘tissue engineering’ was officially coined at
a National Science Foundation Workshop in the USA in 1988, it
was understood to mean ‘the application of principles and
methods of engineering and life sciences toward the funda-
mental understanding of structure–function relationships in

Table 1 – Potential plasticity of adult stem cells (adaptedfrom Rosenthal [22])
Location of stem cell Type of cells generated
Brain Neurons, oligodendrites, skeletal
muscle, blood cells
Bone marrow Endothelial cells, blood cells, cartilage,
bone, adipocytes, cardiac muscle,
skeletal muscle, neuronal cells, dermal
fibroblasts, oval cells, gastrointestinal
tract cells, thymus, pulmonary
epithelial cells
Skeletal muscle Skeletal muscle, bone, cartilage, fat,
smooth muscle
Myocardium Myocytes, endothelial cells
Skin Keratinocytes
Liver Liver cells
Tests and ovaries Gonads
Pancreatic ducts Islet cells
Adipose tissue Fat, muscle, cartilage, bone
b u r n s 3 3 ( 2 0 0 7 ) 2 8 2 – 2 9 1 283
normal and pathological mammalian tissues and the devel-
opment of biological substitutes to restore, maintain or
improve tissue function’. This concept has unfortunately led
to some serious misconceptions that have resulted in the early
promise of skin tissue engineering being slow to be realized in
clinical practice. The misconception was that skin is a tissue,
like cartilage, and would be relatively simple to address as a
tissue engineering challenge. Skin however is NOT a tissue but
an extremely complex organ that brings into conjunction cells
from three different embryological origins, ectoderm, meso-
derm and neural crest [5]. It serves multiple functions [6]. The
original futuristic claims of producing ‘off-the shelf’ skin
replacements have become far more restrained in their
expectation and now tissue engineering skin products are
being described as skin substitutes to aid healing and repair,
temporary skin replacements and occasionally aids to
regeneration [7–19].
How will the current era of stem cell exploration be
reviewed in retrospect? The ‘stem cell’ concept in burns care is
not new and it was Barrendon, working in Howard Green’s
Harvard Laboratory who introduced the concept of the clonal
differentiation of cultured keratinocytes identifying the
holoclone with the greatest proliferative capacity [20]. Can
holoclones be regarded as adult skin stem cells?
Stem cells can be variously classified. One way is to identify
the source and thus we can regard stem cells to be embryonic,
foetal or adult in nature. An alternative perspective is to look at
the stage of evolution of the stem cell line and describe the
cells as being totipotent, pluripotent and multipotent.
The totipotent cells contain all the complete genetic
information needed to manufacture all the cells of the body
as well as the placenta. These cells are present immediately
after fertilization of the egg and for three to four divisions
thereafter. As the cells become more specialized they are
described as pluripotent. The cells are extremely adaptable
and can develop into any cell type with the exception of
placenta. Further division of the pluripotent cells will give rise
to multipotent cells. These are far more specialized and can
only generate a limited number of cell types [21].
The true stem cell must satisfy certain criteria: it must be
clonogenic i.e. capable of unlimited self-renewal by symmetric
division; it must also be able to divide asymmetrically, with
one daughter cell resembling the mother (to perpetuate the
clone) but the other capable of giving rise to multiple types of
differentiated cells which indeed represent derivatives of all
three primitive embryonic germ layers.
It is this concept of ‘plasticity’ which makes the stem cell so
attractive to the tissue engineer and so one critical aspect of
stem cells will be the variable expression of plasticity related
to source. In Table 1 the potential plasticity of some adult stem
cells is detailed which does indicate the wide range of cells
that have thus far been generated from bone marrow cells [22].
It is evident, however, that this plasticity is limited in adult
stem cells, certainly compared to stem cells derived from the
inner cell mass of the early embryonic blastocyst (ES cells),
which can both proliferate indefinitely but also give rise to
virtually any type of cell [1].
Adult stem cells have been incorporated into tissue
engineered constructs used by reconstructive surgeons. A
recent review focused on the four components in developing
tissue substitutes: gene therapy, growth factors and pharma-
logical preparations, scaffolds and cells. It is this last
component, the cells, where increasing attention is focusing
on stem cells particularly in true tissue, as opposed to organ,
engineering. Bone, cartilage, tendon and muscle have all been
developed to some degree of success from adult stem cells.
The preferred source of adult stem cells, however, remains
uncertain and the functional plasticity of adult stem cells
exists more of interest in scientific experimentation than in
clinical application [23,24].
2. Stem cells and skin tissue engineering
The skin is indeed a complex structure incorporating a
fusion of multiple cell types, integrated within a three-
dimensional matrix containing both fibrillar and non-
fibrillar elements. To synthesize such a complex structure
by identifying the component parts and to put them together
is neither practical nor realistic. It must be observed,
however, that this integrative strategy has been the major
one used in skin tissue engineering during its less productive
phase [19]. The great attraction of stem cells in the
construction of a complex tissue or organ is that the
component parts can be simplified at the initial stage and
a significantly greater proportion of the neogenerative
process can be driven by the intrinsic bioengineering
capacity of the cells and tissues. It is important to realize
that cells by themselves cannot generate organs and the
matrix provides a critical element in defining appropriate
differentiation and three-dimensional organization. Stem
cells are going to play an increasingly important role in
tissue engineering and they will be derived from a range of
sources as described above. Of particular interest is human
umbilical cord blood (HUCB). Considerable attention is now
being addressed to expanding the number of stem cells at
differing stages of maturity. Expansion factors of 10 to more
than 1000 have been claimed and one aspect of considerable
significance is that undifferentiated stem cells can be
expanded. Cell process engineering for expansion does rely
in three-dimensional matrices in bioreactors [25–27].

Fig. 1 – Biological concepts of skin tissue engineering.
b u r n s 3 3 ( 2 0 0 7 ) 2 8 2 – 2 9 1284
Cord blood and cells derived from the umbilical cord
have been used in a variety of tissue engineering projects.
Living patches of tissue have been fabricated from a
combination of synthetic polymers (PGA/P4HB) seeded with
fibroblasts harvested from umbilical cord tissue and
endothelial progenitor cells which were cultured in a
perfusion bioreactor. These patches have the potential of
being used in congenital cardiac conditions [28]. Attempts to
engineer microvessels using similar endothelial progenitor
cells and poly-glycolic acid–poly-L-lactic acid (PGA–PLLA)
scaffolds demonstrated a lack of vessel formation. However,
when the same cells were co-cultured with human smooth
muscle cells, microvessel formation was observed on the
porous (PGA–PLLA) scaffolds [29]. Skeletal myogenic differ-
entiation was observed in mesenchymal cells isolated from
HUCB [30].
Fig. 2 – The conceptual pr
The 21st century tissue engineer faces the challenges of
both possibility and practicality. Complex and costly products
will not find commercial applications. In the meantime the
biological complexity of the skin has been appreciated and it is
no longer viewed as a bilaminar tissue but a multidimensional
organ. The tissue engineer must ask how much of this
complex biological tissue is going to be constructed. Fig. 1
shows the ‘biological’ as opposed to the ‘engineering’ concepts
of the skin structure. The skin began in the embryonic stage as
a conjunction of cells which integrated their specialized
functions. The key cell of the epidermis is the keratinocyte
which produces keratin. It is the outer layer of keratin filled,
dead cells, the stratum corneum that is responsible for the
principle protective functions of the skin. The mesodermal
fibroblasts are principally involved in the formation and
maintenance of the dermis. The problem for the tissue
ocess of construction.

b u r n s 3 3 ( 2 0 0 7 ) 2 8 2 – 2 9 1 285
engineer is that the time scale for cellular matrix production is
too slow in clinical application. A preformed matrix is required
either as a permanent or temporary scaffold. The problem
with the permanent scaffold is biocompatibility and the problem
with the temporary scaffold is stability.
For the permanent replacement of lost skin it is necessary
to use a dermal analogue which is slowly replaced by an
autologous dermis. Such a product might be formed by an
immune modulated allogeneic or xenogenic dermis modified
with mesenchymal stem cells, either of marrow or adipocyte
origin. This layer would need to be seeded with a stem cell-
enriched keratinocyte formulation possibly including mela-
nocytes. The attachment is critical and will require a medium
such as hyaluronic acid which can support the cells whilst
promoting proliferation and attachment. These ex vivo
derived components would be combined for in vivo culture.
Such a process can be simply conveyed diagrammatically
(Fig. 2) but the practicality of such a construct presents
considerable challenges. The history of the evolution of skin
tissue engineering does suggest, however, that for permanent
skin replacement the body’s own ‘tissue engineering’ capacity
must be harnessed using stem cell technology with or without
synthesized matrix support. For tissue-engineered skin sub-
stitutes to provide temporary wound cover materials, science
and technology already show promise but the challenge is to
reduce costs. Again for products which are aimed at
modulating wound healing, living cells can be genetically
engineered to restore molecular balance to chronic wounds.
Again, knowledge and technology are available but the
challenge is to develop products that are safe, effective, easy
to use but also affordable. Another fascinating prospect is the
clinical application of human umbilical cord-derived stem
cells. Preliminary results suggest that these can be expanded
in culture and applied to burn wounds where they differ-
entiate into non-antigenic keratinocytes. This truly would
have a dramatic impact on burns care but of course further
indepth studies will be needed to explore the real clinical
potential of such an approach [31].
3. Stem cells and wound healing modulation
In this situation cells will be placed into a pathological
environment for example a chronic or non-healing burn
wound. They will undertake an assessment of the physiolo-
gical deficiencies in terms of matrix composition and cytokine
milieu and correct these by producing the appropriate wound
healing modulators. In a sense this means that the cells are
acting as an intelligent, interperative biofeedback control
mechanism that can autoregulate biological systems. Bone
marrow, peripheral blood and umbilical cord blood have all
been used in chronic wounds to modulate the healing
response. Whilst the early experience is limited, the prospects
are promising and some of the concerns about incorporating
stem cell-derived tissue, into the body are unwarranted [32].
Of particular interest is the effect of topical applications of
bone marrow-derived cells on chronic wounds. Although the
reports are few, the consistent theme is that a chronic wound
changes its nature to become an acute wound that heals or
becomes healthy and can be closed with a skin graft [33–35].
Laboratory studies looking at cutaneous healing in a chimeric
mouse model indicate that when marrow is transplanted it
can contribute to the reconstitution of the dermal fibroblast
population in the wound although local cutaneous cells
reconstitute the epidermis [36]. An in vitro study indicated
that collagen synthesis and levels of bFGF and VEGF were
much higher in bone marrow stromal cells than those in
dermal fibroblasts. This suggests the potential of topically
applied bone marrow cells to accelerate wound healing [37]. A
further study examined the effects of a bone marrow-
impregnated collagen matrix and found a significantly
increased angiogenic effect in an experimental mouse model.
This same group applied an autogenous bone marrow-
impregnated collagen matrix to a patient with a chronic leg
ulcer and observed a dramatic healing response [38].
In our own experience we applied autologous bone marrow
to a chronic unhealed burn wound, a donor site that had
repeatedly failed to heal and a chronic wound at the extremity
of latissimus dorsi free muscle flap where the graft was being
traumatized by footwear as well as non-burns related leg
ulcers. The burn wound changed from being chronic and non-
healing to re-epithelializing and was closed with a graft. The
donor site that had failed to heal and also had repeatedly failed
to take a graft, healed with no grafting necessary. The chronic
heel wound and leg ulcers became more vascular and were
definitively closed with skin grafts. Another recent report
describes the use of allogenic bone marrow mesenchymal
stem cells for the treatment of a patient with deep skin burns
[39].
4. Clinical challenge
Bone marrow suppression has documented association with
major burns either as a result of toxicity by silver sulphadia-
zine [40] or as a result of sepsis [41,42]. The relation of
mesenchymal stem cell activity and burn wound healing is,
however, a newer concept that has received little attention.
The following case illustrates a number of dilemmas in
contemporary burn management.
A 53-year-old man presented with 94% BSA burns which
were of mixed depth. The proposed strategy was to treat the
wounds conservatively with the expectation that the majority
were capable of healing within 3–4 weeks as judged by the
depth of burn. By the end of the fourth week the face had
healed and other areas of the trunk and limbs were showing
signs of punctate re-epithelialization. At this stage the patient
began to become progressively anaemic with no evidence of
blood loss and the progress of healing appeared to have halted.
The patient was treated with blood transfusions and oxan-
drolone and the potential for restimulating wound healing by
topical preparations were considered. Our evolving hypoth-
esis is that mesenchymal stem cells (MSC) are biological
catalysts that catalyse a change in profile from a chronic to an
acute wound. We considered the increasing urgency of
intervention in our patient and also the availability of ethically
approved stem cell sources. We discounted allogenic marrow
in view of the donor supply and time needed for MSC
expansion and sought our institutional ethical committee
approval for the use of human umbilical cord blood. This has,
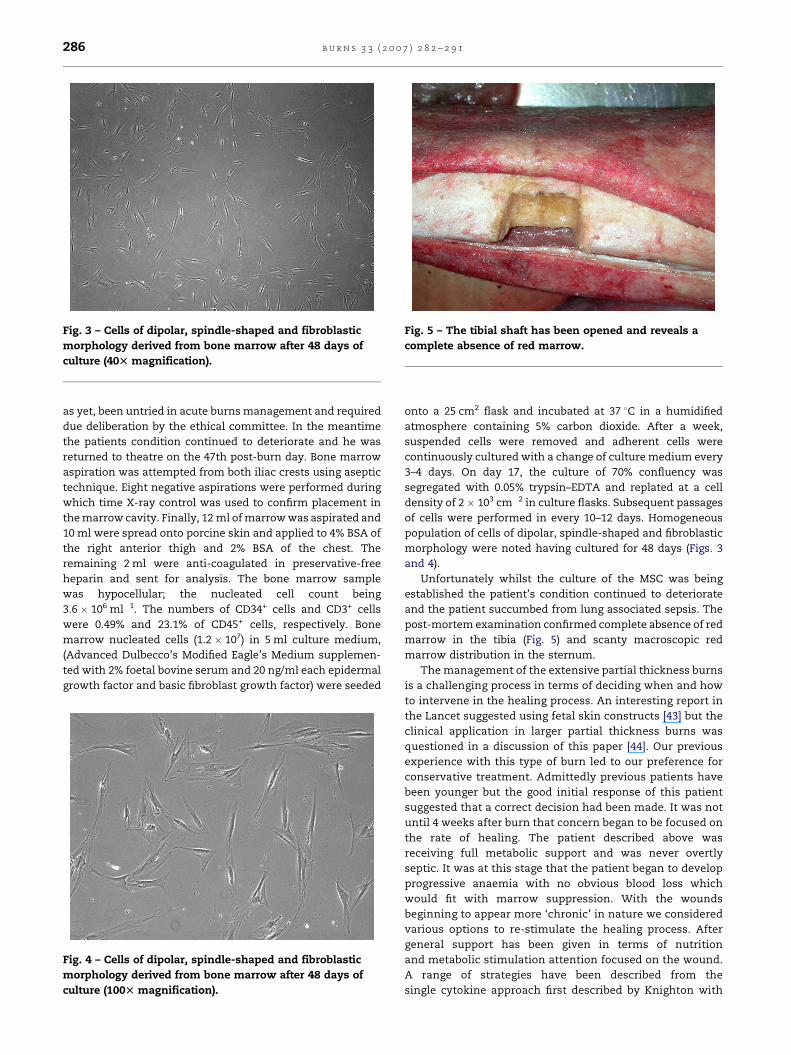
Fig. 3 – Cells of dipolar, spindle-shaped and fibroblastic
morphology derived from bone marrow after 48 days of
culture (40T magnification).
Fig. 5 – The tibial shaft has been opened and reveals a
complete absence of red marrow.
b u r n s 3 3 ( 2 0 0 7 ) 2 8 2 – 2 9 1286
as yet, been untried in acute burns management and required
due deliberation by the ethical committee. In the meantime
the patients condition continued to deteriorate and he was
returned to theatre on the 47th post-burn day. Bone marrow
aspiration was attempted from both iliac crests using aseptic
technique. Eight negative aspirations were performed during
which time X-ray control was used to confirm placement in
the marrow cavity. Finally, 12 ml of marrow was aspirated and
10 ml were spread onto porcine skin and applied to 4% BSA of
the right anterior thigh and 2% BSA of the chest. The
remaining 2 ml were anti-coagulated in preservative-free
heparin and sent for analysis. The bone marrow sample
was hypocellular; the nucleated cell count being
3.6 � 106 ml�1. The numbers of CD34+ cells and CD3+ cells
were 0.49% and 23.1% of CD45+ cells, respectively. Bone
marrow nucleated cells (1.2 � 107) in 5 ml culture medium,
(Advanced Dulbecco’s Modified Eagle’s Medium supplemen-
ted with 2% foetal bovine serum and 20 ng/ml each epidermal
growth factor and basic fibroblast growth factor) were seeded
Fig. 4 – Cells of dipolar, spindle-shaped and fibroblastic
morphology derived from bone marrow after 48 days of
culture (100T magnification).
onto a 25 cm2 flask and incubated at 37 8C in a humidified
atmosphere containing 5% carbon dioxide. After a week,
suspended cells were removed and adherent cells were
continuously cultured with a change of culture medium every
3–4 days. On day 17, the culture of 70% confluency was
segregated with 0.05% trypsin–EDTA and replated at a cell
density of 2 � 103 cm�2 in culture flasks. Subsequent passages
of cells were performed in every 10–12 days. Homogeneous
population of cells of dipolar, spindle-shaped and fibroblastic
morphology were noted having cultured for 48 days (Figs. 3
and 4).
Unfortunately whilst the culture of the MSC was being
established the patient’s condition continued to deteriorate
and the patient succumbed from lung associated sepsis. The
post-mortem examination confirmed complete absence of red
marrow in the tibia (Fig. 5) and scanty macroscopic red
marrow distribution in the sternum.
The management of the extensive partial thickness burns
is a challenging process in terms of deciding when and how
to intervene in the healing process. An interesting report in
the Lancet suggested using fetal skin constructs [43] but the
clinical application in larger partial thickness burns was
questioned in a discussion of this paper [44]. Our previous
experience with this type of burn led to our preference for
conservative treatment. Admittedly previous patients have
been younger but the good initial response of this patient
suggested that a correct decision had been made. It was not
until 4 weeks after burn that concern began to be focused on
the rate of healing. The patient described above was
receiving full metabolic support and was never overtly
septic. It was at this stage that the patient began to develop
progressive anaemia with no obvious blood loss which
would fit with marrow suppression. With the wounds
beginning to appear more ‘chronic’ in nature we considered
various options to re-stimulate the healing process. After
general support has been given in terms of nutrition
and metabolic stimulation attention focused on the wound.
A range of strategies have been described from the
single cytokine approach first described by Knighton with
b u r n s 3 3 ( 2 0 0 7 ) 2 8 2 – 2 9 1 287
autologous—platelet derived growth factor (PDGF) [45] to the
use of cells within a morphological construct that can
develop targeted cytokine responses [46]. Our previous
experience with chronic wound healing stimulation
involved autologous bone marrow application. Autologous
bone marrow is a rich source of adult mesenchymal stem
cells which are multipotent besides containing a host of
healing factors. By virtue of being an autologous transfer the
question of immune related problems and ethical issues are
non-existent (graft versus host reaction is a potential
concern if human umbilical cord blood is used). Another
potential advantage of applying the cells directly without
subjecting them to expansion in the laboratory is saving
time. There has been a report published describing the
beneficial effects of applying allogenic fibroblast-like bone
marrow mesenchymal stem cells onto the surface of a deep
thermal burn [39]. In that case the chronic non-healing burn
wound changed in appearance with more angiogenesis and
the patient was healed with autologous skin grafts.
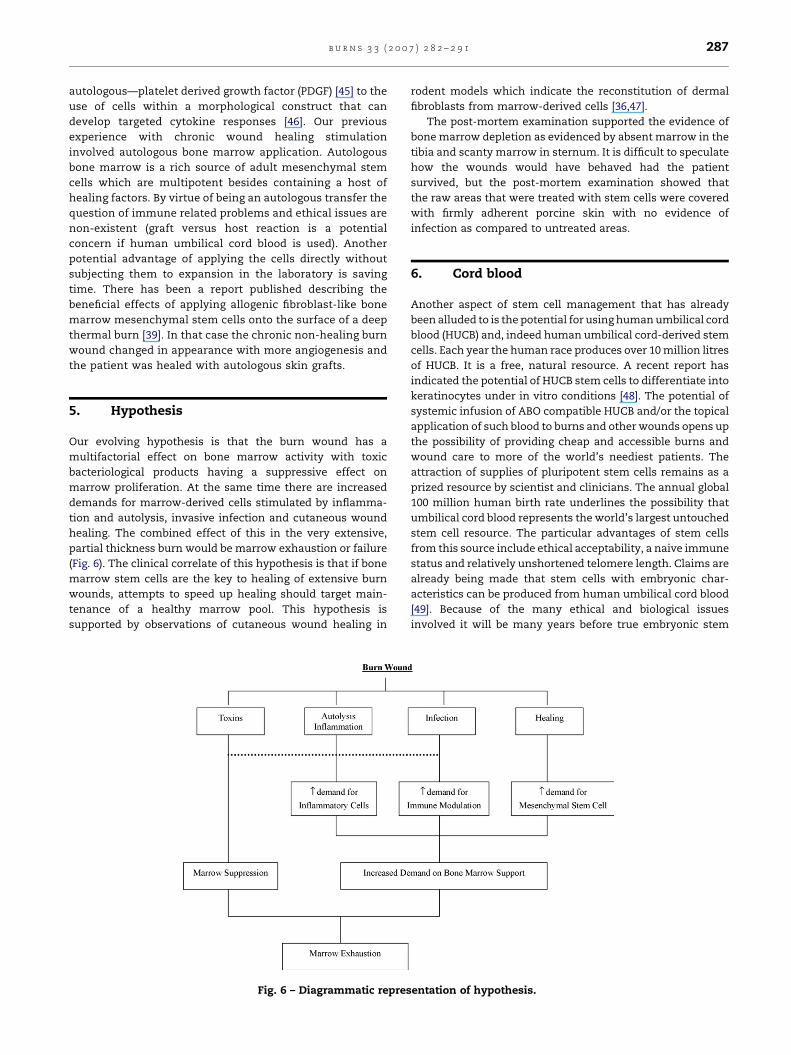
5. Hypothesis
Our evolving hypothesis is that the burn wound has a
multifactorial effect on bone marrow activity with toxic
bacteriological products having a suppressive effect on
marrow proliferation. At the same time there are increased
demands for marrow-derived cells stimulated by inflamma-
tion and autolysis, invasive infection and cutaneous wound
healing. The combined effect of this in the very extensive,
partial thickness burn would be marrow exhaustion or failure
(Fig. 6). The clinical correlate of this hypothesis is that if bone
marrow stem cells are the key to healing of extensive burn
wounds, attempts to speed up healing should target main-
tenance of a healthy marrow pool. This hypothesis is
supported by observations of cutaneous wound healing in
Fig. 6 – Diagrammatic repres
rodent models which indicate the reconstitution of dermal
fibroblasts from marrow-derived cells [36,47].
The post-mortem examination supported the evidence of
bone marrow depletion as evidenced by absent marrow in the
tibia and scanty marrow in sternum. It is difficult to speculate
how the wounds would have behaved had the patient
survived, but the post-mortem examination showed that
the raw areas that were treated with stem cells were covered
with firmly adherent porcine skin with no evidence of
infection as compared to untreated areas.
6. Cord blood
Another aspect of stem cell management that has already
been alluded to is the potential for using human umbilical cord
blood (HUCB) and, indeed human umbilical cord-derived stem
cells. Each year the human race produces over 10 million litres
of HUCB. It is a free, natural resource. A recent report has
indicated the potential of HUCB stem cells to differentiate into
keratinocytes under in vitro conditions [48]. The potential of
systemic infusion of ABO compatible HUCB and/or the topical
application of such blood to burns and other wounds opens up
the possibility of providing cheap and accessible burns and
wound care to more of the world’s neediest patients. The
attraction of supplies of pluripotent stem cells remains as a
prized resource by scientist and clinicians. The annual global
100 million human birth rate underlines the possibility that
umbilical cord blood represents the world’s largest untouched
stem cell resource. The particular advantages of stem cells
from this source include ethical acceptability, a naive immune
status and relatively unshortened telomere length. Claims are
already being made that stem cells with embryonic char-
acteristics can be produced from human umbilical cord blood
[49]. Because of the many ethical and biological issues
involved it will be many years before true embryonic stem
entation of hypothesis.

b u r n s 3 3 ( 2 0 0 7 ) 2 8 2 – 2 9 1288
cells reach the clinic. Research in this field has not been helped
by the highly publicized claims of scientific fraud by some high
profile researchers [50]. Cord blood on the other hand, is being
used for an increasing number of clinical and experimental
applications which highlighted the reduced incidence of graft
versus host reaction when the haemopoietic fraction is used
as an allogenic transplant [51].
A point of note is the difference between transplantation
and transfusion. In the context of using the stem cell
component to be a permanent replacement for the host stem
cell source as in haematological malignancies, then the use of
the term transplant is appropriate. The concept is of a
procedure with a long term, if not life long, implication for
safety and efficacy. Transfusion is another matter where the
time scale of interaction is shorter. When considering HUCB as
an adjunct therapy for a critically ill patient it would be more
appropriate to regard it as a transfusion and not demand such
strict compatibility criteria.
The response and interaction of stem cells and target cell
differentiation is a focus of particular interest to the Burn
Surgeon. The review by Heng et al. discusses strategies for
directing keratinocyte stem cell lineage in vitro using selective
purification and proliferation [52]. A three-step process is
described with the first-step being to induce commitment of
the (non-epidermal) stem cell into keratinocyte progenitors.
These progenitors have to then be selected and purified and
finally this purified population of committed keratinocyte
progenitors has to be expanded by proliferation and allowed to
differentiate. A recent article in Burns has re-affirmed this
potential strategy in resurfacing burns [48].
Various strategies are discussed for committing stem cells
to the keratinocyte lineage including induction with exogen-
ous cytokines, growth factors, chemicals and extracellular
matrix. It is becoming obvious that stem cell biology is very
complex if such strategies are to be adopted to direct stem cell
differentiation and maintain it.
It is evident, however, that there are going to be consider-
able challenges in the development of reliable protocols that
can confidently preclude risks of teratoma formation and
other, as yet unforeseen complications.
Nevertheless we do see cord blood as a biological wound
healing modulator. It is of interest to note that amniotic
membranes have been used as biological dressings for wounds
but concerns about risks of disease transmission have
severely limited this practice in many parts of the world
[53]. Similarly the question of potential risk of disease
transmission when using cord blood may also be raised.
However, there are already well-defined screening processes
to reduce and/or elimate such risks as applied in routine blood
banking. Another consideration is that this use of cord blood is
temporary and the relative lack of immunogenicity will limit
adverse effects.
7. Stem cell fractions
As the range and nature of the stem cell composition from
various sources becomes more clear, it may be possible to
apply more selective fractions onto both chronic and acute
wounds to modulate the biological healing mechanisms.
Fractionation of cells is conventionally performed using
FicollTM gradient centrifugation, although more and more
advanced cell filtration devices are being developed. By the
conventional method, a cell fraction of mononuclear cells
(MNCs), which contains the significant number of stem/
progenitor cells, will be isolated. The reduction rates of RBCs,
platelets (75–85%) and granulocytes (80%) were significant,
which may be minimally effective for the preparation of stem
cells [54]. Stem cells, however, constitute only a small fraction
(less than 1%) of all MNCs in the BM, and an even smaller
percentage of cells in the peripheral blood and cord blood.
Both hematopoietic stem cells (HSCs) and mesenchymal stem
cells (MSCs) have been isolated from all the three sources.
Although the exact relationship between HSCs and MSCs is yet
unclear, was reported that purified HSC fraction is not limited
to forming blood cells, but may also function as multipotent
progenitors for non-hematopoietic cells, for example, to
generate liver, etc. [55]. Conversely, MSCs play very important
roles in the maintenance, proliferation and differentiation of
HSCs. There has been some debate about the ease of isolation
of MSC from the different fractions. Wexler identified adult
bone marrow as the richest source compared to umbilical cord
and adult peripheral blood [56]. Kern again observed better
rates of isolation of MSC from bone marrow (100%) compared
to cord blood (63%) but interestingly also reported 100%
success rate in isolated MSC’s from adipose tissue isolated
from cosmetic liposuction [57]. The isolation of MSC from
adult peripheral blood can be enhanced by prior treatment
with granulocyte colony stimulating factor (G-CSF) [58]. The
significance of the MSC fractions is already a major research
area issue. The heterogenicity of the fractions isolated from
human umbilical cord blood is demonstrated by differential
gene expression profiling [59,60]. Experimental studies in
animals also indicate a wide variety of conditions that can be
treated, delayed or otherwise modulated by IV administration
of human umbilical cord MSC fractions. These conditions
include prostate cancer [61], type 1 [62] and type 2 [63] diabetes,
Parkinson’s disease [64], Alzheimer’s disease [65] and amyo-
trophic lateral sclerosis [66].
It would certainly be a mistake to underestimate the
complexity of stem cell biology and the clinical applications.
Nevertheless research and developments in this field will
undoubtedly have far reaching effects on burns practice
throughout the world.
8. Summary
We are moving into a new and exciting era of burns care where
perhaps we are going to exercise more humility in the face of
the enormous complexity of biological processes than
acknowledged by our purely science oriented colleagues.
Would it be true to say that one stem cell is worth 10n
individually characterized and engineered proteins? Currently
the challenge is to define the optimum source, processing and
method of application of stem cells as well as defining their
role. The clinical application of embryonic stem cells is likely
to beset with numerous ethical but also safety concerns. Fetal
tissue, likewise, will be associated with ethical issues. The
reality of widespread applications of stem cells devoid of
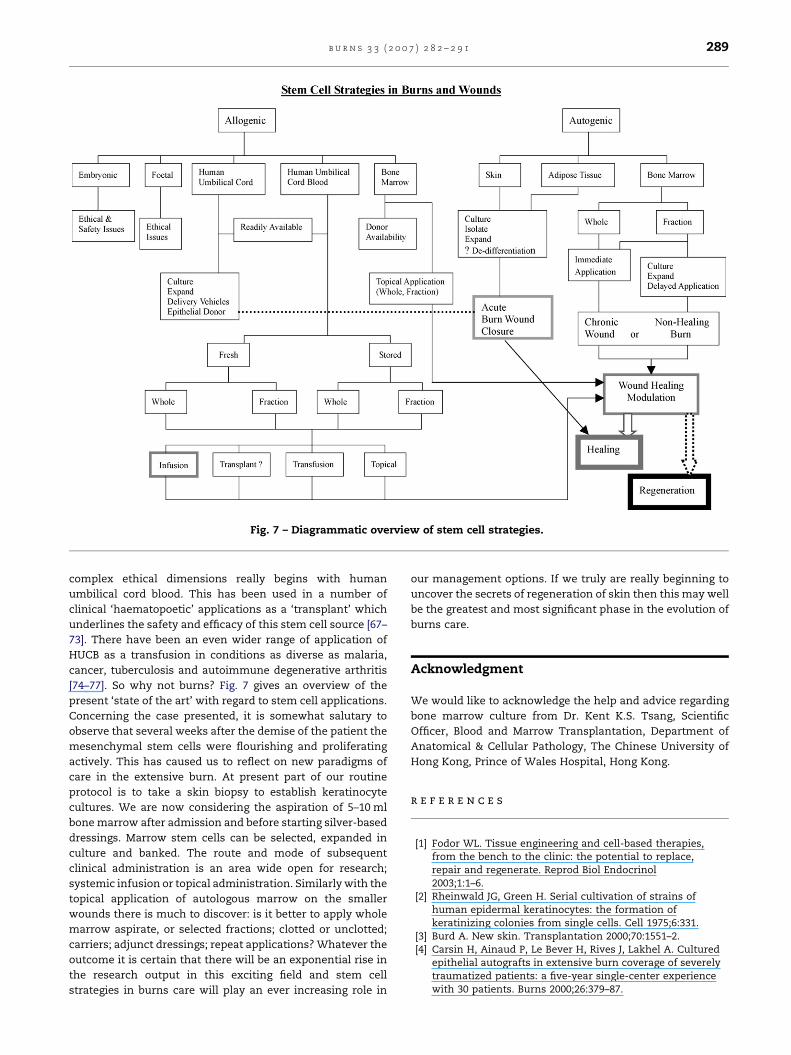
Fig. 7 – Diagrammatic overview of stem cell strategies.
b u r n s 3 3 ( 2 0 0 7 ) 2 8 2 – 2 9 1 289
complex ethical dimensions really begins with human
umbilical cord blood. This has been used in a number of
clinical ‘haematopoetic’ applications as a ‘transplant’ which
underlines the safety and efficacy of this stem cell source [67–
73]. There have been an even wider range of application of
HUCB as a transfusion in conditions as diverse as malaria,
cancer, tuberculosis and autoimmune degenerative arthritis
[74–77]. So why not burns? Fig. 7 gives an overview of the
present ‘state of the art’ with regard to stem cell applications.
Concerning the case presented, it is somewhat salutary to
observe that several weeks after the demise of the patient the
mesenchymal stem cells were flourishing and proliferating
actively. This has caused us to reflect on new paradigms of
care in the extensive burn. At present part of our routine
protocol is to take a skin biopsy to establish keratinocyte
cultures. We are now considering the aspiration of 5–10 ml
bone marrow after admission and before starting silver-based
dressings. Marrow stem cells can be selected, expanded in
culture and banked. The route and mode of subsequent
clinical administration is an area wide open for research;
systemic infusion or topical administration. Similarly with the
topical application of autologous marrow on the smaller
wounds there is much to discover: is it better to apply whole
marrow aspirate, or selected fractions; clotted or unclotted;
carriers; adjunct dressings; repeat applications? Whatever the
outcome it is certain that there will be an exponential rise in
the research output in this exciting field and stem cell
strategies in burns care will play an ever increasing role in
our management options. If we truly are really beginning to
uncover the secrets of regeneration of skin then this may well
be the greatest and most significant phase in the evolution of
burns care.
Acknowledgment
We would like to acknowledge the help and advice regarding
bone marrow culture from Dr. Kent K.S. Tsang, Scientific
Officer, Blood and Marrow Transplantation, Department of
Anatomical & Cellular Pathology, The Chinese University of
Hong Kong, Prince of Wales Hospital, Hong Kong.
r e f e r e n c e s
[1] Fodor WL. Tissue engineering and cell-based therapies,from the bench to the clinic: the potential to replace,repair and regenerate. Reprod Biol Endocrinol2003;1:1–6.
[2] Rheinwald JG, Green H. Serial cultivation of strains ofhuman epidermal keratinocytes: the formation ofkeratinizing colonies from single cells. Cell 1975;6:331.
[3] Burd A. New skin. Transplantation 2000;70:1551–2.[4] Carsin H, Ainaud P, Le Bever H, Rives J, Lakhel A. Cultured
epithelial autografts in extensive burn coverage of severelytraumatized patients: a five-year single-center experiencewith 30 patients. Burns 2000;26:379–87.
b u r n s 3 3 ( 2 0 0 7 ) 2 8 2 – 2 9 1290
[5] McGrath JA, Eady RAJ, Pope FM. Anatomy and organizationof human skin. In: Burns T, Breathnach S, Cox N, Griffiths C,editors. 7th ed., Rook’s textbook of dermatology, vol. 1, 7thed. UK: Blackwell Publishing; 2004. p. 3.1–3.84.
[6] Archer CB. Functions of the skin. In: Burns T, Breathnach S,Cox N, Griffiths C, editors. 7th ed., Rook’s textbook ofdermatology, vol. 1, 7th ed. UK: Blackwell Publishing; 2004.
p. 4.1–4.12.[7] Berthod F, Damour O. In vitro reconstructed skin models for
wound coverage in deep burns. Brit J Dermatol1997;136:809–16.
[8] Cooper ML, Spielvogel RL. Artificial skin for wound healing.Clin Dermatol 1994;12:183–91.
[9] Hansbrough JF, Cooper ML. Methods of skin coverage:achieving temporary and permanent coverage. Crit CareRep 1990;2:50–62.
[10] Sefton MV, Woodhouse KA. Tissue engineering. J CutanMed Surg 1998;3(Suppl. 1):18–23.
[11] Cooper ML, Hansbrough JF, Spielvogel RL, Cohen R. In vivooptimization of a living dermal substitute employingcultured human fibroblasts on a biodegradable polyglycolicacid or polyglactin mesh. Biomats 1991;12:243–8.
[12] Falanga V, Margolis D, Alvarez O, Auletta M. Rapid healingof venous ulcers and lack of clinical rejection with anallogeneic cultured human skin equivalent. Arch Dermatol1998;134:293–300.
[13] Boyce ST. Skin substitutes from cultured cells and collagen-GAG polymers. Med Biol Eng Comput 1998;36:791–800.
[14] Kearney JN. Clinical evaluation of skin substitutes. Burns2001;27:545–51.
[15] Burke JF. Observations on the development and clinical useof artificial skin—an attempt to employ regeneration ratherthan scar formation in wound healing. Jpn J Surg1987;17:431–8.
[16] Wainwright D, Madden M, Luterman A. Clinical evaluationof an a cellular allograft dermal matrix in full-thicknessburns. Burn Care Rehabil 1996;17:124–36.
[17] Boyce ST. Design principles for composition and perfor-mance of cultured skin substitutes. Burns 2001;27:523–33.
[18] Navarro FA, Stoner ML, Lee HB, Park CS, Wood FM, OrgillDP. Melanocyte repopulation in full-thickness woundsusing a cell spray apparatus. J Burn Care Rehabil2001;22:41–6.
[19] Metcalfe AD, Ferguson MWJ. Harnessing wound healingand regeneration for tissue engineering. Biochem Soc Trans2005;33:413–7.
[20] Barrandon Y, Green H. Three clonal types of keratinocytewith different capacities for multiplication. Proc Natl AcadSci 1987;84:2302–6.
[21] http://serendip.brynmawr.edu/bb/neuro/neuro04/web2/abruce.html; [accessed 29.12.2005].
[22] Rosenthal N. Prometheus’s vulture and the stem-cellpromise. N Engl J Med 2003;349:267–74.
[23] Hedrick MH, Daniels EJ. The use of adult stem cells inregenerative medicine. Clin Plast Surg 2003;30:499–505.
[24] Quesenberry PJ, Dooner G, Colvin G, Abedi M. Stem cellbiology and the plasticity polemic. Exp Hematol2005;33:389–94.
[25] Takagi M. Cell processing engineering for ex vivo expansionof hematopoietic cells. J Biosci Bioeng 2005;99:189–96.
[26] Curran JM, Chen R, Hunt JA. The guidance of humanmesenchymal stem cell differentiation in vitro bycontrolled modifications to the cell substrate. Biomaterials2006;27:4783–93.
[27] Chen X, Xu HB, Wan C, McCaigue M, Li G. Bioreactorexpansion of human adult bone marrow-derivedmesenchymal stem cells (MSCs). Stem Cells 2006, [Epubahead of print].
[28] Schmidt D, Mol A, Neuenschwander S, Breymann C, GossiM, Zund G, et al. Living patches engineered from humanumbilical cord derived fibroblasts and endothelialprogenitor cells. Eur J Cardiothor Surg 2005;27:795–800.
[29] Wu X, Rabkin-Aikawa E, Guleserian KJ, Perry TE, Masuda Y,Sutherland FWH, et al. Tissue-engineered microvessels onthree-dimensional biodegradable scaffolds using humanendothelial progenitor cells. Am J Physiol Heart Circ Physiol2004;287:480–7.
[30] Gang EJ, Jeong JA, Hong SH, Hwang SH, Kim SW, Yang IH,et al. Skeletal myogenic differentiation of mesenchymalstem cells isolated from human umbilical cord blood. StemCells 2004;22:617–24.
[31] Press Release: New applications for cord lining stemcells—diabetes and wound healing. http://www.newswiretoday.com/news/4701/; [accessed on12.06.2006].
[32] Valbonesi M, Giannini G, Migliori F, Dalla Costa R, DejanaAM. Cord blood (CB) stem cells for wound repair.Preliminary report of 2 cases. Transfus Apher Sci2004;30:153–6.
[33] Badiavas EV, Falanga V. Treatment of chronic wounds withbone marrow-derived cells. Arch Dermatol 2003;139:510–6.
[34] Humpert PM, Bartsch U, Konrade I, Hammes HP, Morcos M,Kasper M, et al. Locally applied mononuclear bone marrowcells restore angiogenesis and promote wound healing in atype 2 diabetic patient. Exp Clin Endocrinol Diabetes2005;113:538–40.
[35] Ayyappan T, Chadha A, Shaikh MF, Naik N, Desai I, Kadam.et al. Topically applied autologous bone marrow in healingof chronic non-healing raw areas—a pilot study. Indian JBurns 2004;12:42–7.
[36] Fathke C, Wilson L, Hutter J, Kapoor V, Smith A, Hocking A,et al. Contribution of bone marrow-derived cells to skin:collagen deposition and wound repair. Stem Cells2004;22:812–22.
[37] Han SK, Yoon TH, Lee DG, Lee MA, Kim WK. Potential ofhuman bone marrow stromal cells to accelerate woundhealing in vitro. Ann Plast Surg 2005;55:414–9.
[38] Ichioka S, Kouraba S, Sekiya N, Ohura N, Nakatsuka T. Bonemarrow-impregnated collagen matrix for wound healing:experimental evaluation in a microcirculatory model ofangiogenesis, and clinical experience. Brit J Plast Surg2005;58:1124–30.
[39] Rasulov MF, Vasilchenkov AV, Onishchenko NA,Krasheninnikov ME, Kravchenko VI, Gorshenin TL, et al.First experience of the use bone marrow mesenchymalstem cells for the treatment of a patient with deep skinburns. Bull Exp Boil Med 2005;139:141–4.
[40] Gamelli RL, Paxton TP, O’Reilly M. Bone marrow toxicity bysilver sulfadiazine. Surg Gynecol Obstet 1993;177:115–20.
[41] Gamelli RL, He LK, Liu H. Recombinant human granulocytecolony-stimulating factor treatment improves macrophagesuppression of granulocyte and macrophage growth afterburn and burn wound infection. J Trauma 1995;39:1141–7.
[42] Shoup M, Weisenberger JM, Wang JL, Pyle JM, Gamelli RL,Shankar R. Mechanisms of neutropenia involving myeloidmaturation arrest in burn sepsis. Ann Surg 1998;228:112–22.
[43] Hohlfeld J, de Buys Roessingh A, Hirt-Burri N, Chaubert P,Gerber S, Scaletta C, et al. Tissue engineered fetal skinconstructs for paediatric burns. Lancet 2005;366:840–2.
[44] Norbury WB, Jeschke MG, Herndon DN. Tissue engineeredfetal skin constructs for pediatric burns. Crit Care2005;9:533–4.
[45] Knighton DR, Ciresi KF, Fiegel VD, Austin LL, Butler EL.Classification and treatment of chronic non-healingwounds. Successful treatment with autologous platelet-
b u r n s 3 3 ( 2 0 0 7 ) 2 8 2 – 2 9 1 291
derived wound healing factors (PDWHF). Ann Surg1986;204:322–30.
[46] Shen JT, Falanga V. Innovative therapies in wound healing.J Cutan Med Surg 2003;7:217–24.
[47] Yamaguchi Y, Kubo T, Murakami T, Takahashi M,Hakamata Y, Kobayashi E, et al. Bone marrow cellsdifferentiate into wound myofibroblasts and accelerate thehealing of wounds with exposed bones when combinedwith an occlusive dressing. Brit J Dermatol 2005;152:616–22.
[48] Kamolz LP, Kolbus A, Wick N, Mazal PR, Eisenbock B, BurjakS, et al. Cultured human epithelium: human umbilical cordblood stem cells differentiate into keratinocytes under invitro conditions. Burns 2006;32:16–9.
[49] McGuckin CP, Forraz N, Baradez MO, Navran S, Zhao J,Urban R, et al. Production of stem cells with embryoniccharacteristics from human umbilical cord blood. CellProlif 2005;38:245–55.
[50] Jones N, Cyranoski D. Investigation says Hwang lied. News[doi:10.1038/news051219-17].
[51] Lewis ID. Clinical and experimental uses of umbilical cordblood. Intern Med J 2002;32:601–9.
[52] Heng BC, Cao T, Liu H, Phan TT. Directing stem cells intothe keratinocyte lineage in vitro. Exp Dermatol2005;14:1–16.
[53] Gajiwala K, Gajiwala AL. Evaluation of lyophilized, gamma-irradiated amnion as a biological dressing. Cell Tissue Bank2004;5:73–80.
[54] Aoki M, Yasutake M, Murohara T. Derivation of functionalendothelial progenitor cells from human umbilical cordblood mononuclear cells isolated by a novel cell filtrationdevice. Stem Cells 2004;22:994–1002.
[55] Lagasse E, Connors H, Al-Dhalimy M, Reitsma M, Dohse M,Osborne L, et al. Purified hematopoietic stem cells candifferentiate into hepatocytes in vivo. Nat Med 2000;6:1229–34.
[56] Wexler SA, Donaldson C, Denning-Kendall P, Rice C,Bradley B, Hows JM. Adult bone marrow is a rich source ofhuman mesenchymal ‘stem’ cells but umbilical cord andmobilized adult blood are not. Brit J Haematol 2003;121:368–74.
[57] Kern S, Eichler H, Stoeve J, Kluter H, Bieback K.Comparative analysis of mesenchymal stem cells frombone marrow, umbilical cord blood, or adipose tissue. StemCells 2006;24:1294–301.
[58] Kassis I, Zangi L, Rivkin R, Levdansky L, Samuel S, Marx G,et al. Isolation of mesenchymal stem cells from G-CSF-mobilized human peripheral blood using fibrin microbeads.Bone Marrow Transplant 2006;37:967–76.
[59] Jeong JA, Hong SH, Gang EJ, Ahn C, Hwang SH, Yang IH,et al. Differential gene expression profiling of humanumbilical cord blood-derived mesenchymal stem cells byDNA microarray. Stem Cells 2005;23:584–93.
[60] Lu FZ, Fujino M, Kitazawa Y, Uyama T, Hara Y, FuneshimaN, et al. Characterization and gene transfer inmesenchymal stem cells derived from human umbilical-cord blood. J Lab Clin Med 2005;146:271–8.
[61] Ende N, Chen R, Reddi AS. Administration of humanumbilical cord blood cells delays the onset of prostatecancer and increases the lifespan of the TRAMP mouse.Cancer Lett 2006;231:123–8.
[62] Ende N, Chen R, Reddi AS. Effect of human umbilical cordblood cells on glycemia and insulitis in type 1 diabetic mice.Biochem Biophys Res Commun 2004;325:665–9.
[63] Ende N, Chen R, Reddi AS. Transplantation of humanumbilical cord blood cells improves glycemia andglomerular hypertrophy in type 2 diabetic mice. BiochemBiophys Res Commun 2004;321:168–71.
[64] Ende N, Chen R. Parkinson’s disease mice and humanumbilical cord blood. J Med 2002;33:173–80.
[65] Ende N, Chen R, Ende-Harris D. Human umbilical cordblood cells ameliorate Alzheimer’s disease in transgenicmice. J Med 2001;32:241–7.
[66] Chen R, Ende N. The potential for the use of mononuclearcells from human umbilical cord blood in the treatment ofamyotrophic lateral sclerosis in SOD1 mice. J Med2000;31:21–30.
[67] Gluckman E, Broxmeyer HA, Auerbach AD, et al.Hematopoietic reconstitution in a patient with Fanconi’sanemia by means of umbilical-cord blood from an HLA-identical sibling. N Engl J Med 1989;321:1174–8.
[68] Gluckman E, Rocha V, Boyer-Chammard A, et al. Outcomeof cord-blood transplantation from related and unrelateddonors. Eurocord Transplant Group and the EuropeanBlood and Marrow Transplantation Group. N Engl J Med1997;337:373–81.
[69] Kurtzberg J, Laughlin M, Graham ML, et al. Placental bloodas a source of hematopoietic stem cells for transplantationinto unrelated recipients. N Engl J Med 1996;335:157–66.
[70] Laughlin MJ, Eapen M, Rubinstein P, et al. Outcomes aftertransplantation of cord blood or bone marrow fromunrelated donors in adults with leukemia. N Engl J Med2004;351:2265–75.
[71] Gluckman E, et al. Factors associated with outcomes ofunrelated cord blood transplant: guidelines for donorchoice. Exp Hematol 2004;32:397–407.
[72] Rubinstein P, Carrier C, Scaradavou A, et al. Outcomesamong 562 recipients of placental-blood transplants fromunrelated donors. N Engl J Med 1998;339:1565–77.
[73] Laughlin MJ, Barker J, Bambach B, et al. Hematopoieticengraftment and survival in adult recipients of umbilicalcord blood from unrelated donors. N Engl J Med2001;344:1815–22.
[74] Bhattacharya N, Mukherijee K, Chettri MK, Banerjee T,Mani U, Bhattacharya S. A study report of 174 units ofplacental umbilical cord whole blood transfusion in 62patients as a rich source of fetal hemoglobin supply indifferent indications of blood transfusion. Clin Exp ObstetGynecol 2001;28:47–52.
[75] Bhattacharya N. A study of placental umbilical cord wholeblood transfusion in 72 patients with anemia andemaciation in the background of cancer. Eur J GynaecolOncol 2006;27:155–61.
[76] Bhattacharya N. A preliminary study of placental umbilicalcord whole blood transfusion in under resourced patientswith malaria in the background of anaemia. Malar J2006;5:20.
[77] Bhattacharya N. Placental umbilical cord whole bloodtransfusion: a safe and genuine blood substitute forpatients of the under-resourced world at emergency. J AmColl Surg 2005;200:557–63.