stapled transanal rectal resection for outlet obstruction: a prospective, multicenter trial
TRANSCRIPT
OriginalContributions
Stapled Transanal Rectal Resection forOutlet Obstruction: A Prospective,Multicenter TrialPaolo Boccasanta, M.D., E.B.S.Q.,1 Marco Venturi, M.D.,1 Angelo Stuto, M.D.,2
Corrado Bottini, M.D.,3 Angelo Caviglia, M.D.,4 Alfonso Carriero, M.D.,5
Domenico Mascagni, M.D.,6 Roberto Mauri, M.D.,7 Luigi Sofo, M.D.,8
Vincenzo Landolfi, M.D.9
1 Ospedale Maggiore di Milano I.R.C.C.S., University of Milan, Milan, Italy2 Pordenone General Hospital, Pordenone, Italy3 Gallarate General Hospital, Varese, Italy4 C. Forlanini General Hospital, Rome, Italy5 Pelvic Floor Center, Montecchio Emilia, Italy6 La Sapienza University of Rome, Rome, Italy7 Erba General Hospital, Como, Italy8 Catholic University of Rome, Rome, Italy9 Solofra General Hospital, Avellino, Italy
PURPOSE: This prospective, multicenter trial was designedto assess the safety and effectiveness of a novel technique inthe treatment of outlet obstruction caused by the combina-tion of intussusception and rectocele by using a double-transanal, 33-mm circular stapler. METHODS: From Januaryto October 2001, 90 patients with outlet obstruction wereoperated on and followed (mean, 16.3 ± 2.9 months) by thevalidated Constipation Scoring and Continence Grading Sys-tems, clinical examination, defecography, and anorectal ma-nometry. Anal ultrasound also was performed in 58 multipa-rous patients. RESULTS: Operative time and hospital staywere short (mean, 43.3 ± 8.7 minutes and 2.1 ± 0.8 days,
respectively), and postoperative pain was minimal. Themean time to resume normal activity was 10.2 ± 4.5 days.Complications were 17.8 percent fecal urgency, 8.9 percentincontinence to flatus, 5.5 percent urinary retention, 4.4percent bleeding, 3.3 percent anastomotic stenosis, and 1.1percent pneumonia. All constipation symptoms signifi-cantly improved (P < 0.001) without worsening of analcontinence. No patient complained of dyspareunia. At post-operative defecography, all patients had a double incisureof the lower rectal outline in the site of anastomosis, withthe disappearance of both intussusception and rectocele.Anal pressure was not significantly modified, whereas rectalcompliance was restored (P < 0.05). No lesions of analsphincters caused by the operation were found in multipa-rous patients. The outcome at one year was excellent in 48of 90 patients, good in 33, fairly good in 5, and poor in 4.CONCLUSIONS: This novel technique seems to be safe andeffective in the treatment of outlet obstruction caused bythe combination of intussusception and rectocele. Random-ized trials are required to confirm these findings. [Keywords: Transanal surgery; Outlet obstruction; Intussuscep-tion; Rectocele; Pelvic floor disease]
S ymptoms related to outlet obstruction syndrome(OOS) are frequent in patients referred to a colo-
proctologist. The patient (usually female) complainsof incomplete evacuation with painful effort, unsuc-cessful attempts with long periods spent in bathroom,
Supported by a grant from “Fondazione Camillo Corti per laricerca sulle malattie del colon,” Piazza Martini 9, I - 20137 Milano.
The Governing Council of the Italian Association of Coloproctol-ogy Units approved the study protocol. No financial contributionhas been received from any potentially concerned party during thepreparation of the trial.
Read at the meeting of The American Society of Colon and RectalSurgeons, New Orleans, Louisiana, June 21 to 26, 2003.
Correspondence to: Paolo Boccasanta, M.D., E.B.S.Q., via G.B.Morgagni, 39, 20129, Milan, Italy, e-mail: [email protected]
Dis Colon Rectum 2004; 47: 1285–1297DOI: 10.1007/s10350-004-0582-3© The American Society of Colon and Rectal SurgeonsPublished online: 12 August 2004
1285

use of perineal support and/or odd posture, insertionof fingers into the vagina and/or the anal canal, bleed-ing after defecation, and seems to be greatly understress for the impaired quality of life. Laxative and/orenema abuse is frequent and become less effectivewith time.
An uncoordinated inhibitory pattern, progressingfrom pubococcygeus to puborectalis muscle and/orexternal sphincter has been reported to cause OOS.1
In these patients, biofeedback can achieve the reac-tivation of the inhibition capacity of all muscles of thepelvic floor during defecation, avoiding surgery. Oth-erwise, OOS can depend on the intussusception ofthe rectal wall, extending into the anal canal, definedas internal prolapse2 and frequently combined withrectocele.3 These patients, usually multiparous fe-males with dystocia, may benefit from surgery.
There is little agreement on the best surgicalapproach for dealing with the problem. The intus-susception may be corrected by an abdominal lapa-rotomic,4 laparoscopic5 rectopexy, sigmoid re-section-rectopexy,6 or transanal Delorme’s excision.7
Various surgical techniques with a transanal,8–10
transperineal,11 or transvaginal12 approach have beenused for rectocele. Finally, both intussusceptionand rectocele can be corrected by a double-abdominal and vaginal13 approach. All these tech-niques have important limitations. Starting from theobservation that a stapled anopexy for hemorrhoids,or mucosal prolapse, may reduce the bulging of aconcomitant rectocele, a new technique, using asingle transanal circular stapler, combined with a per-ineal levatorplasty, has been proposed to correct bothmucosal prolapse and rectocele.14,15 However, peri-neal levatorplasty may frequently result in delayedhealing of the perineal wound and dyspareunia.16 Toovercome this, Antonio Longo, M.D., recently pro-posed the transanal use of two circular staplers: thefirst to anteriorly reduce the intussusception and thebulging of rectocele, correcting the anterior rectal wallmuscle defect, the second to posteriorly correct theintussusception. This study was to designed assess thesafety and effectiveness of this novel stapled transanalrectal resection (STARR) in a large series of patientsaffected by OOS caused by the combination of intus-susception and rectocele.
PATIENTS AND METHODS
From January to October 2001, of 156 patients withOOS, 90 (87 females; mean age, 57.6 (standard devia-
tion, 14.2) years) in whom a combination of intussus-ception and rectocele was found were selected andoperated on in nine colorectal surgical units withequal distribution of cases
Preoperative assessment was performed by the sur-geon and consisted of:● A questionnaire concerning pregnancies, episioto-
my, previous gynecologic, urologic, or anorectalsurgery. The validated Constipation Scoring Sys-tem17 and Continence Grading System18 and VisualAnalog Scale for pain (with a score from 0 = nopain to 10 = maximum pain) were used and fre-quency of rectal bleeding was recorded. The samequestionnaire for symptoms was used during thefollow-up.
● Clinical examination of the perineum, rectum, andvagina to evaluate the perineal descent, size andextension of rectocele, voluntary contraction ofboth external sphincter and puborectalis muscle,and presence of enterocele or genital prolapse.
● Anoscopy to evaluate any concomitant anorectaldisease and colonoscopy to detect inflammatorybowel disease or cancer.Defecography was performed before and three
months after the operation using a previously de-scribed technique.19,20 The classifications of Wexner,for the extension of rectoanal intussusception in theanal canal,21 and Marti, for the size and shape of rec-tocele,22 were used. Retention of contrast after def-ecation also was considered.
Anorectal manometry was performed before andthree months after the operation, according to a pre-viously described technique,23 for the evaluation ofthe resting and squeeze pressures in the anal canaland the rectal sensitivity threshold volume. Rectalcompliance was calculated by taking the slope of thepressure/volume curve at the first sensation level.24
Anal ultrasound (AUS) was performed before and sixmonths after the operation to detect sphincterial le-sions in multiparous patients. Patients were examinedfrom the left-lateral position with a Bruel and Kjaerdiagnostic ultrasound system 3535 with a 10-Mhz ro-tating probe, and serial images were obtained onwithdrawal of the probe down the anal canal.25
Biofeedback was performed by a modified devicefor anorectal manometry (Sat Elite™, Rush, Milan,Italy). Before visual training, digital reeducation wasperformed to obtain the awareness of the muscu-lar activity. The training time was 20 minutes forfour sessions, twice per week, for a two-month pe-riod.
1286 BOCCASANTA ET AL Dis Colon Rectum, August 2004

Inclusion CriteriaPatients selected for surgery were those with: 1)
failure of medical therapy (1.5 liters/day of water,low-fiber diet, lactulose 10 g/day) and biofeedbackperformed for two months, with persistence of at leastthree of the following symptoms: feeling of incom-plete evacuation, painful effort, unsuccessful attemptswith long periods spent in bathroom, defecation withuse of perineal support and/or odd posture, digitalassistance, evacuation obtained only with use of en-emas, 2) at least two of the following findings at de-fecography: rectoanal intussusception � 10 mm ex-tending into the anal canal; rectocele deeper than 3cm on straining; entrapping barium contrast after def-ecation. The presence of hemorrhoids was not a con-traindication to the operation.
Exclusion CriteriaSixty-six patients (42.3 percent) were excluded
from the study: 27 with nonrelaxing puborectalismuscle at defecography and good results after reha-bilitative therapy, 14 with genital prolapse, or cysto-cele requiring associated transvaginal operations, 8with recurrent rectocele and/or enterocele, 8 with fe-cal incontinence (Continence Grading Scale score >8), 3 with mental disorders, 3 with general contrain-dications to surgery, 2 who declined postoperativeinvestigation, and 1 for whom there was incompleteinformation.
The ethical committee of the Italian Association ofColoproctology Units approved the study protocol.All patients gave informed, written consent. All surgi-cal teams had previous experience in conventionaloperations for rectocele, rectal prolapse, and stapledanopexy for hemorrhoids (at least 30 operations). Allpatients were operated on by the same surgical teamin each center, using the following technique withoutmodifications.
Surgical TechniquePreoperatively, a cleansing enema was given, and
the patient received a routine antibiotic prophylaxis(cefotaxime 2 g and metronidazole 500 mg intrave-nously), immediately after the induction of anesthe-sia. The operation was performed under general orcaudal anesthesia, with the patient in lithotomic po-sition. A circular stapler with a disposable circularanal dilator and a pursestring suture anoscope wereused (PPH-01™; Ethicon Endo-Surgery, Inc.,Pomezia, Italy). The anal verge was gently dilatedwith one and then two fingers for 60 seconds, four
radial stitches were applied to the perineal skin tobetter expose the anal verge, and the lubricated ob-turator of the dilator was introduced and left in for 60seconds. Finally, the lubricated anal dilator (CAD 33)was gently introduced into the anal canal and held byknotting stitches. The posterior rectal wall was pro-tected by a retractor, inserted in the lower hole on theCAD 33, and pushed along the anal canal (Fig. 1). Theanoscope (PSA 33) was introduced into the CAD 33and three separated one-half (180°) pursestrings withProlene™ 2-0 (Ethicon, Somerville, NJ), including mu-cosa, submucosa, and rectal muscle wall, were in-serted 1 to 2 cm above the hemorrhoidal apex toinclude the top of rectocele and internal rectal pro-lapse. The 33-mm circular stapler was opened and thehead placed above the three anterior one-half purse-strings. Before firing the stapler, the posterior vaginalwall was carefully checked with fingers and a vaginalvalve to prevent entrapment (Fig. 2). The stapler wasthen fired and gently withdrawn. A minimal mucosalbridge with a staple connecting the two edges of theanastomosis was sometimes found and cut with scis-sors. The anterior stapled line was reinforced using2-3 Vicryl™ 3-0 sutures (Ethicon) and inspected forbleeding (Fig. 3). The procedure was repeated in theposterior rectal wall, with the retractor inserted intothe upper hole of the dilator. Two or three separatedone-half (180°) pursestrings with Prolene™ 2-0 wereprepared above the hemorrhoid apex, including mu-cosa, submucosa, and rectal muscle wall, to reducethe posterior intussusception. The second stapler de-vice was then closed, fired, and withdrawn. The pos-terior stapled line was reinforced using 2 Vicryl™ 3-0sutures. Hemostatic stitches were occasionally re-quired (Figs. 4 and 5). All removed tissues were mea-sured and sent for histologic examination (Fig. 6).
Follow-UpPostoperative pain was assessed using a Visual
Analog Scale score. Paracetamol plus codeine, 500 mgeffervescent tablets, was used for postoperative paincontrol on patient’s demand. Patients were seen 1week, 2 weeks, and 1, 3, 6, and 12 months postop-eratively. The clinical controls consisted of compila-tion of the same questionnaire used preoperativelyand proctologic examination with proctoscopy. Clini-cal outcome was considered excellent when patientswere symptom-free, good with one to two episodesper month of laxative use without digital assistance,use of enema, or bleeding, fairly good with more thantwo episodes per month of laxative use, and poor if
1287STAPLED RECTAL RESECTION FOR OUTLET OBSTRUCTIONVol. 47, No. 8

unchanged. Defecography and anorectal manometrywere repeated three months after surgery. Six monthsafter the operation, 58 multiparous patients under-went AUS.
Statistical Analysis
The data consisting of repeated measures acrossmultiple time points during the period of observa-
tion were compared using the ANOVA test, andassociation of qualitative nonindependent valueswere verified by the McNemar test with Bonferronicorrection. Wilcoxon’s rank-sum test for paired datawas used to compare preoperative and postopera-tive manometric data. Differences were consideredsignificant at P < 0.05 (<0.002 with Bonferroni correc-tion).
Figure 1. After introduction ofthe anoscope PSA 33 intothe CAD 33, the posteriorwall was protected by aretractor, inserted in the CAD33 lower hole, and pushedalong the anal canal.
Figure 2. Three separatedone-half (180°) pursestringswith Prolene™ 2-0 includingmucosa, submucosa, rectalmuscle wall were insertedabove the hemorrhoidal apexto include the top of rectoceleand internal rectal prolapse.The 33-mm, circular stapler(PPH-01™) was opened andthe head was placed abovethe three anterior one-halfpursestrings. Before firing thestapler, the posterior vaginalwall was carefully checkedwith fingers and a vaginalvalve to prevent entrapment.
Figure 3. The stapler wasfired and gently withdrawn.The anterior stapled line wasstrengthened by using two tothree Vicryl™ 3-0 suturesand inspected for bleeding.
1288 BOCCASANTA ET AL Dis Colon Rectum, August 2004

RESULTS
Preoperative Data
Clinical examination and proctoscopy. Of 90 pa-tients, 58 were multiparous, with a mean of 2.1 ± 2parity, and 57 patients (65.5 percent) had a previousepisiotomy. Previous urogynecologic and proctologicoperations and Constipation and Continence scores
are reported in Tables 1 and 2, respectively. Table 3shows the incidence of preoperative symptoms. Atproctologic examination and proctoscopy, 90 patientshad mucosal prolapse, 87 rectocele, 28 hemorrhoids,and 1 rectal polyp.
Colonoscopy. All patients were submitted to colo-noscopy, and none had inflammatory bowel diseaseor cancer.
Figure 4. The procedure wasrepeated in the posteriorrectal wall with the retractorinserted into the upper holeof the dilator. Two or threeseparated one-half (180°)pursestrings with Prolene™2-0 were prepared above thehemorrhoidal apex, includingmucosa, submucosa, andrectal muscle wall to reduceposterior intussusception.The second stapler devicewas then closed, fired, andwithdrawn. The posteriorstapled line was reinforcedusing two Vicryl™ 3-0sutures. Hemostatic stitcheswere occasionally required.
Figure 5. At the end of theoperation, two suture lineswere created on the inferiorrectal wall.
1289STAPLED RECTAL RESECTION FOR OUTLET OBSTRUCTIONVol. 47, No. 8
Defecography. Preoperatively, a rectoanal intussus-ception � 10 mm, extending into the anal canal wasfound in all patients, with a Wexner stage of 1 in 76patients and 2 in 14 patients; a rectocele was found in87 patients (35 with Marti Type 2 and 52 with Type 3).Entrapping contrast was demonstrated in 79 patients(87.8 percent).
Anorectal manometry. Of 90 patients, 19 had in-creased rectal compliance (>8 ml/mmHg) and 16 hadreduced mean anal resting (<50 mmHg) and squeeze(<160 mmHg) pressures.
Anal ultrasound. Of 58 multiparous patients, 10had a right anterolateral defect of anal sphincters: 8external and 2 both external and internal (<20 percentof the circumference).
Operative Data
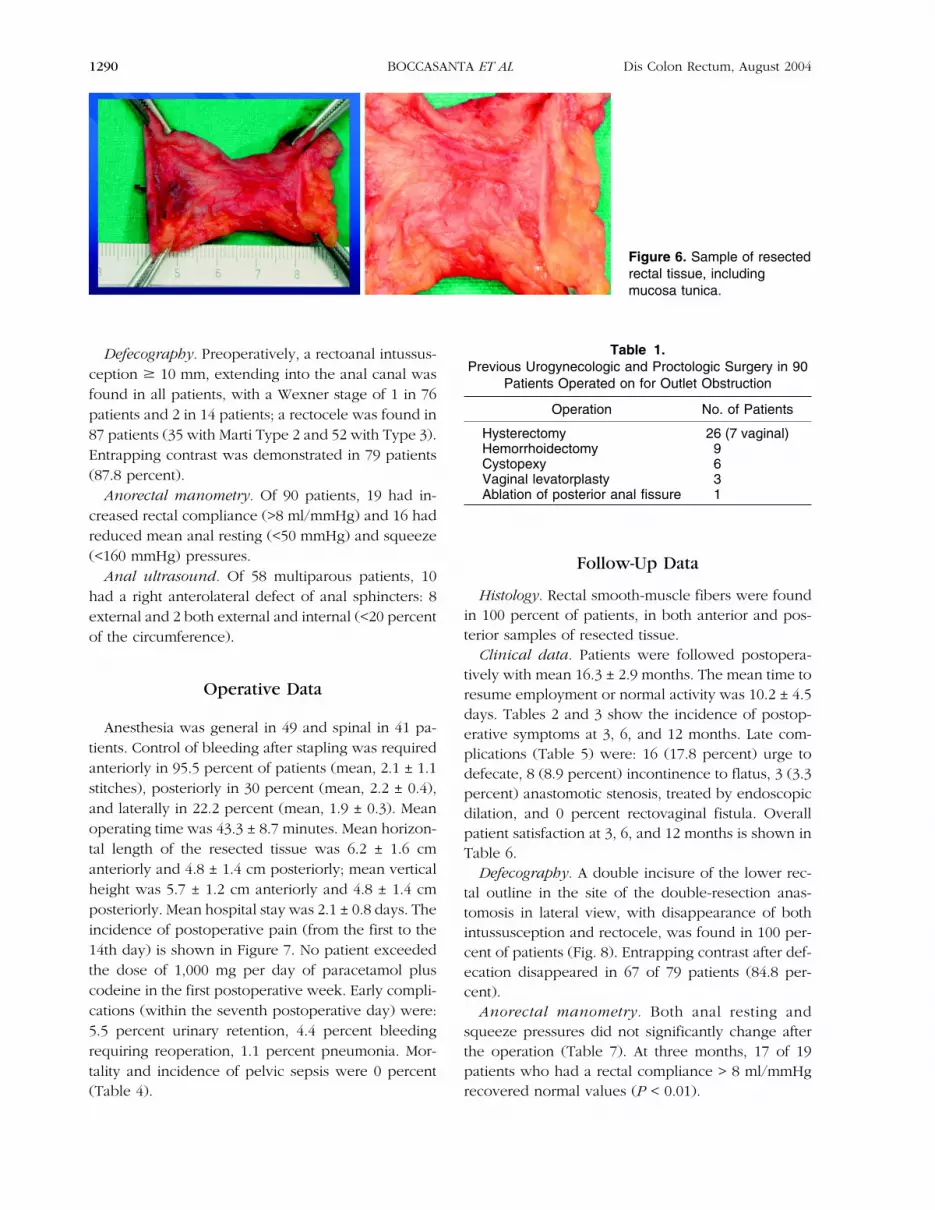
Anesthesia was general in 49 and spinal in 41 pa-tients. Control of bleeding after stapling was requiredanteriorly in 95.5 percent of patients (mean, 2.1 ± 1.1stitches), posteriorly in 30 percent (mean, 2.2 ± 0.4),and laterally in 22.2 percent (mean, 1.9 ± 0.3). Meanoperating time was 43.3 ± 8.7 minutes. Mean horizon-tal length of the resected tissue was 6.2 ± 1.6 cmanteriorly and 4.8 ± 1.4 cm posteriorly; mean verticalheight was 5.7 ± 1.2 cm anteriorly and 4.8 ± 1.4 cmposteriorly. Mean hospital stay was 2.1 ± 0.8 days. Theincidence of postoperative pain (from the first to the14th day) is shown in Figure 7. No patient exceededthe dose of 1,000 mg per day of paracetamol pluscodeine in the first postoperative week. Early compli-cations (within the seventh postoperative day) were:5.5 percent urinary retention, 4.4 percent bleedingrequiring reoperation, 1.1 percent pneumonia. Mor-tality and incidence of pelvic sepsis were 0 percent(Table 4).
Follow-Up Data
Histology. Rectal smooth-muscle fibers were foundin 100 percent of patients, in both anterior and pos-terior samples of resected tissue.
Clinical data. Patients were followed postopera-tively with mean 16.3 ± 2.9 months. The mean time toresume employment or normal activity was 10.2 ± 4.5days. Tables 2 and 3 show the incidence of postop-erative symptoms at 3, 6, and 12 months. Late com-plications (Table 5) were: 16 (17.8 percent) urge todefecate, 8 (8.9 percent) incontinence to flatus, 3 (3.3percent) anastomotic stenosis, treated by endoscopicdilation, and 0 percent rectovaginal fistula. Overallpatient satisfaction at 3, 6, and 12 months is shown inTable 6.
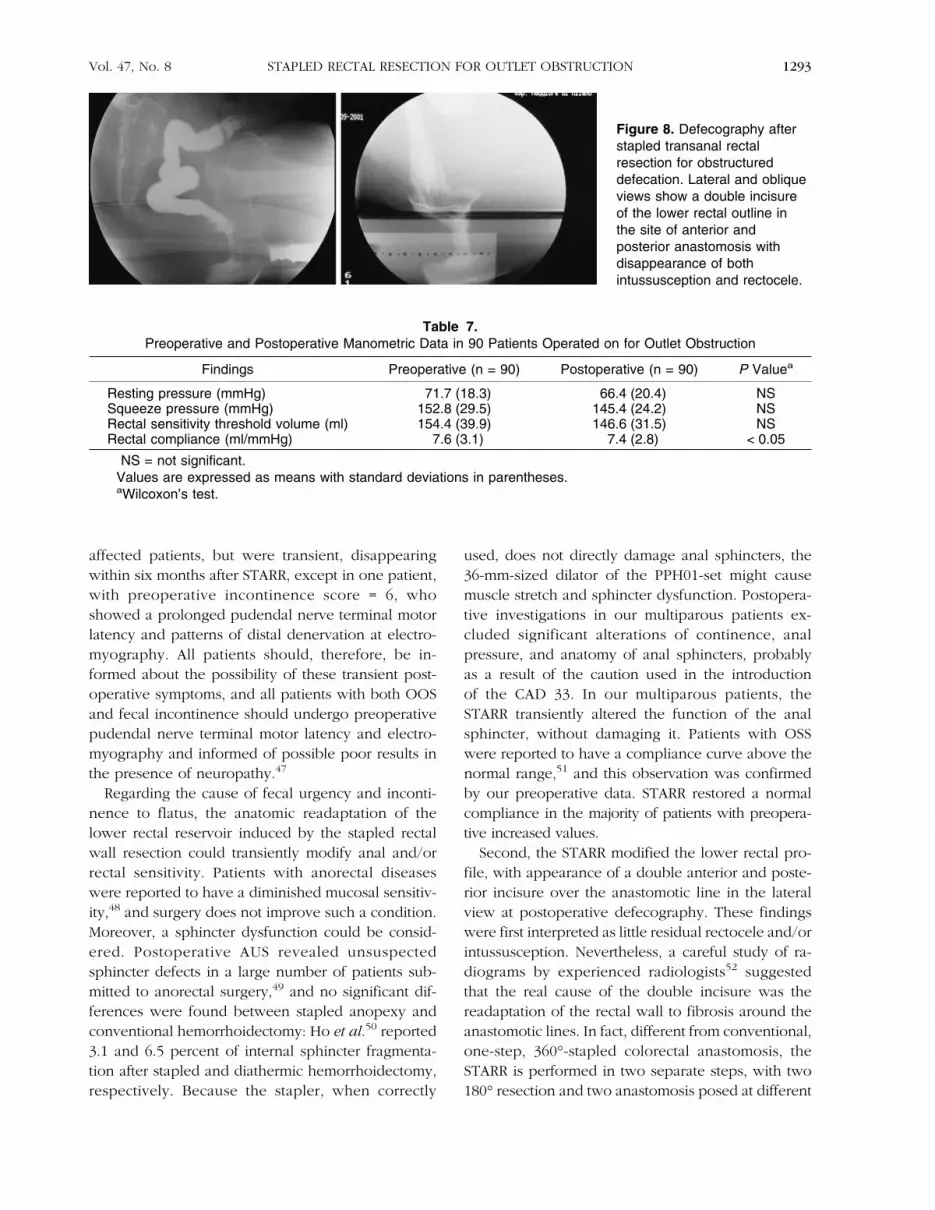
Defecography. A double incisure of the lower rec-tal outline in the site of the double-resection anas-tomosis in lateral view, with disappearance of bothintussusception and rectocele, was found in 100 per-cent of patients (Fig. 8). Entrapping contrast after def-ecation disappeared in 67 of 79 patients (84.8 per-cent).
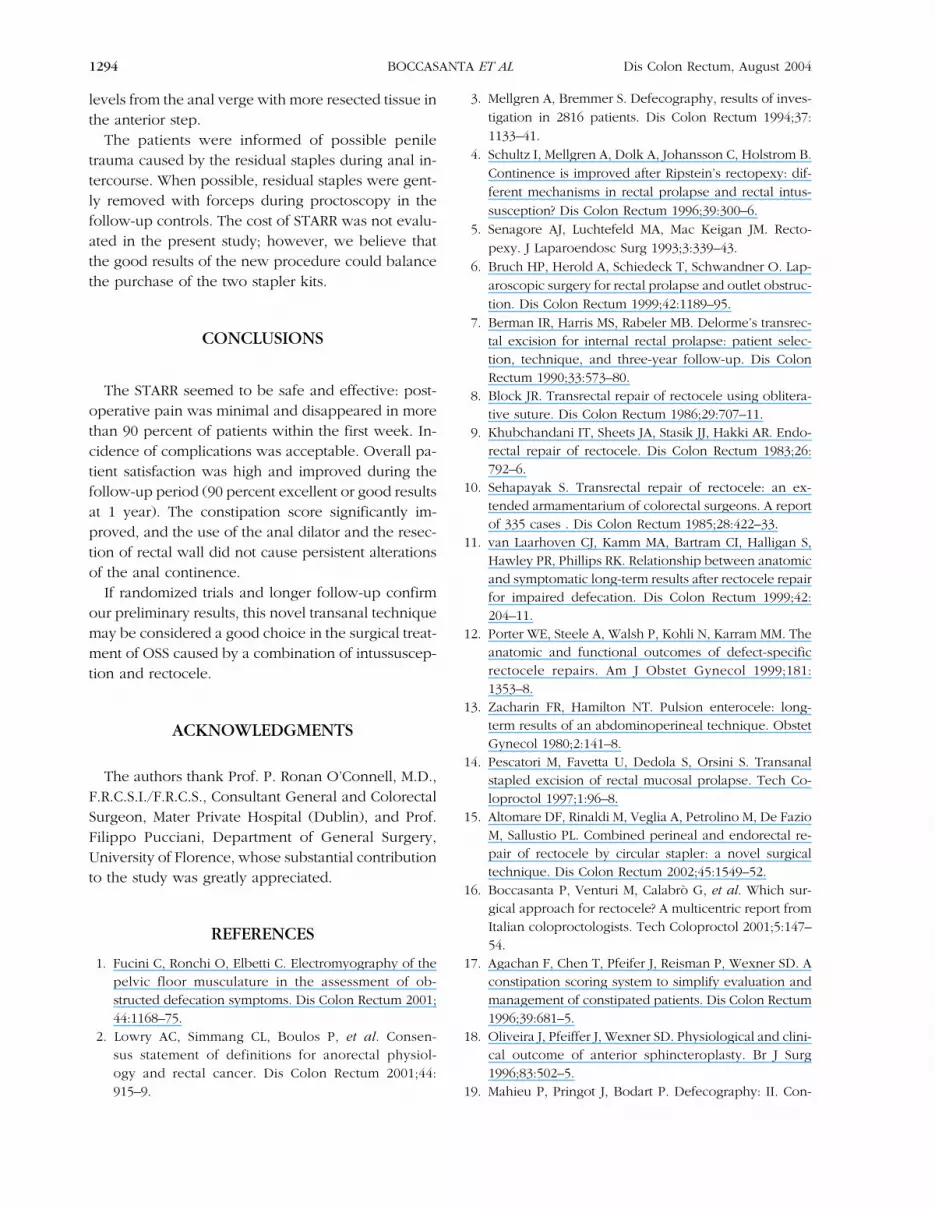
Anorectal manometry. Both anal resting andsqueeze pressures did not significantly change afterthe operation (Table 7). At three months, 17 of 19patients who had a rectal compliance > 8 ml/mmHgrecovered normal values (P < 0.01).
Figure 6. Sample of resectedrectal tissue, includingmucosa tunica.
Table 1.Previous Urogynecologic and Proctologic Surgery in 90
Patients Operated on for Outlet Obstruction
Operation No. of Patients
Hysterectomy 26 (7 vaginal)Hemorrhoidectomy 9Cystopexy 6Vaginal levatorplasty 3Ablation of posterior anal fissure 1
1290 BOCCASANTA ET AL Dis Colon Rectum, August 2004
Anal ultrasound. The STARR did not modify thepreoperative findings in multiparous patients.
DISCUSSION
The treatment of OOS is a widely debated topic.The first problem is to identify the right indicationsfor surgery. The association between intussuscep-
tion, rectocele, and functional disorders (irritablebowel syndrome, pudendal neuropathy, or mus-cle pelvic floor disfunction) is frequent and it oftenis difficult to establish the real cause of com-plaints.26
Table 2.Preoperative and Postoperative Symptom Scores in 90 Patients Operated on for Outlet Obstruction
Signs and Symptoms Preoperative 3 Months 6 Months 12 Months
Constipation Scoring System (17)Frequency 1.52 (0.05) 0.71 (0.05) 0.58 (0.05) 0.57 (0.05)Difficulty 1.54 (0.06) 0.62 (0.05) 0.52 (0.06) 0.51 (0.05)Completeness 2.98 (0.02) 0.74 (0.05) 0.66 (0.07) 0.62 (0.05)Pain 1.01 (0.03) 0.57 (0.05) 0.47 (0.05) 0.45 (0.05)Time 1.57 (0.05) 0.43 (0.05) 0.25 (0.04) 0.24 (0.04)Assistance 1.53 (0.05) 0.11 (0.03) 0.09 (0.03) 0.09 (0.03)Failure 1.30 (0.05) 0.57 (0.05) 0.48 (0.05) 0.47 (0.05)History 1.57 (0.05) 1.57 (0.05) 1.57 (0.05) 1.57 (0.05)
Mean total score 13.02 (0.04) 5.23 (0.05) 4.62 (0.05) 4.52 (0.05)Continence Grading Scale (18)
Mean total score 0.24 (0.14) 0.78 (0.29) 0.39 (0.19) 0.39 (0.19)
Values are expressed as means with standard errors of the means in parentheses.ANOVA test for repeated measures was used. Regarding the Constipation Scoring System, all comparisons vs.
preoperative data were statistically significant (P < 0.001); no significance was found in the Continence Grading Scale(P = not significant).
Table 3.Preoperative and Postoperative Symptoms in 90 Patients Operated on for Outlet Obstruction
Signs and Symptoms Preoperative 3 Months 6 Months 12 Months
Feeling of incomplete evacuation 89 (98.9) 22 (24.4) 19 (21.1) 17 (18.9)Assistance 79 (87.8) 5 (5.6) 4 (4.4) 4 (4.4)Painful evacuation effort 57 (63.3) 23 (25.6) 19 (21.1) 18 (20)Laxatives (>2 episode/month) 47 (52.2) 12 (13.3) 9 (10) 9 (10)Enema 40 (44.4) 4 (4.4) 2 (2.2) 2 (2.2)Abdominal pain 26 (28.8) 15 (16.7) 12 (13.3) 11 (12.2)Bleeding (>1 episode/week) 16 (17.8) 4 (4.4) 2 (2.2) 2 (2.2)
Values are expressed as number of patients with percentages in parentheses.McNemar test, with Bonferroni correction, was used. All comparisons vs. preoperative data were statistically sig-
nificant (P < 0.001).
Table 4.Earlya Complications in 90 Patients Operated on for
Outlet Obstruction
Urinary Retention 5 (5.6)Bleedingb 4 (4.4)Pneumonia 1 (1.1)Pelvic sepsis 0Mortality 0
Values are expressed as number of patients with per-centages in parentheses.
aWithin the seventh postoperative day.bRequiring readmission.
Figure 7. Postoperative pain pattern in 90 patients oper-ated on for outlet obstruction.
1291STAPLED RECTAL RESECTION FOR OUTLET OBSTRUCTIONVol. 47, No. 8
To avoid unnecessary and potentially dangerousoperations, some authors (and we agree with them)suggested trying conservative treatments in all pa-tients with OSS27: 38.5 and 30.8 percent of patientswith large rectoanal intussusception had an im-provement of symptoms only with diet and bio-feedback, respectively.28 In the present study, weused strict selection criteria and all patients with non-relaxing puborectalis muscle at defecography, fecalincontinence, enterocele, recurrent rectocele, con-comitant genital prolapse, or cystocele were ex-cluded. Nevertheless, the possibility to perform aSTARR after a failed biofeedback, or in associationwith gynecologic or urologic operations, could not beexcluded.
Regarding the choice of the surgical technique, athorough review of the literature does not yield de-finitive guidelines. No randomized trial has clearly es-tablished the best approach, and in most cases thetraining and experience of the surgeon seems to bedecisive.
All the traditional operations have important limi-tations. Briefly, transvaginal and perineal approachesdo not correct the intussusception (and its symp-toms). Rectopexy increases defecation difficulties andconsequently should be avoided.29–32 Sigmoid resec-tion-rectopexy requires long operating time (laparos-copy) and hospital stay (laparotomy).6 The learningcurve and surgical risks related to colonic resection in
a functional disease may be taken into account.33 De-lorme’s transrectal excision is not easy to perform;complication rate and incidence of failure are high(>20 percent),34 particularly in patients with descend-ing perineum.35 The combined approach of Zacha-rin’s procedure36 is subjected to high complicationrate, related to laparotomy, rectopexy, and levator-plasty.37 The association of single stapler and perineallevatorplasty had a high incidence of delayed healingof the perineal wound and dyspareunia, whereas thecombination of endoanal and perineal approach in-creased the risk of postoperative sepsis, caused byfecal contamination, with a fatal case of pelvic gan-grene.16
The STARR corrects both intussusception and rec-tocele with a unique approach, avoiding the perineallevatorplasty and its complications. We had no mor-tality, local or pelvic sepsis, or rectovaginal fistula;however, the risk of major complications should notbe excluded, because STARR provides a resection ofthe mucosa, submucosa, and rectal muscle wall.Moreover, all procedures involving the anorectaljunction can cause pelvic and retroperitoneal sepsis,whose origin remains uncertain.38–46
The STARR requires training and experience,both in transanal conventional surgery and stapleruse, however, when correctly indicated and ap-plied, it seems to give many benefits: it is technicallyeasier than the over-described techniques, opera-tive time and hospital stay are short, postopera-tive pain and bleeding are minimal, and time to re-turn to work is fast. The effectiveness of STARRis demonstrated by the significant improvement ofall constipation symptoms. Medium-term follow-upsuggests that early postoperative benefits are main-tained.
Two more issues were identified from the presentstudy. First, there was a remarkable incidence of urgeto defecate and incontinence to flatus, with no signifi-cant increase in the Continence Score. These symp-toms represented a significant problem for most of the
Table 5.Late Complications in 90 Patients Operated on for Outlet Obstruction
1 Month 3 Months 6 Months 12 Months
Urge to defecate 16 (17.8) 9 (10) 1 (1.1) 1 (1.1)Incontinence to flatus 8 (8.9) 6 (6.7) 1 (1.1) 1 (1.1)Stenosis 2 (2.2) 3 (3.3) 3 (3.3) 3 (3.3)Rectovaginal Fistula 0 0 0 0Dyspareunia 0 0 0 0
Values are expressed as number of patients with percentages in parentheses.
Table 6.Overall Patient Satisfaction in 90 Patients Operated on
for Outlet Obstruction
1Month
3Months
6Months
12Months
Excellent 32 (35.5) 39 (43.3) 47 (52.2) 48 (53.3)Good 42 (46.7) 39 (43.3) 34 (37.8) 33 (36.7)Fairly good 11 (12.2) 7 (7.8) 5 (5.6) 5 (5.6)Poor 5 (5.6) 5 (5.6) 4 (4.4) 4 (4.4)
Values are expressed as number of patients with per-centages in parentheses.
1292 BOCCASANTA ET AL Dis Colon Rectum, August 2004
affected patients, but were transient, disappearingwithin six months after STARR, except in one patient,with preoperative incontinence score = 6, whoshowed a prolonged pudendal nerve terminal motorlatency and patterns of distal denervation at electro-myography. All patients should, therefore, be in-formed about the possibility of these transient post-operative symptoms, and all patients with both OOSand fecal incontinence should undergo preoperativepudendal nerve terminal motor latency and electro-myography and informed of possible poor results inthe presence of neuropathy.47
Regarding the cause of fecal urgency and inconti-nence to flatus, the anatomic readaptation of thelower rectal reservoir induced by the stapled rectalwall resection could transiently modify anal and/orrectal sensitivity. Patients with anorectal diseaseswere reported to have a diminished mucosal sensitiv-ity,48 and surgery does not improve such a condition.Moreover, a sphincter dysfunction could be consid-ered. Postoperative AUS revealed unsuspectedsphincter defects in a large number of patients sub-mitted to anorectal surgery,49 and no significant dif-ferences were found between stapled anopexy andconventional hemorrhoidectomy: Ho et al.50 reported3.1 and 6.5 percent of internal sphincter fragmenta-tion after stapled and diathermic hemorrhoidectomy,respectively. Because the stapler, when correctly
used, does not directly damage anal sphincters, the36-mm-sized dilator of the PPH01-set might causemuscle stretch and sphincter dysfunction. Postopera-tive investigations in our multiparous patients ex-cluded significant alterations of continence, analpressure, and anatomy of anal sphincters, probablyas a result of the caution used in the introductionof the CAD 33. In our multiparous patients, theSTARR transiently altered the function of the analsphincter, without damaging it. Patients with OSSwere reported to have a compliance curve above thenormal range,51 and this observation was confirmedby our preoperative data. STARR restored a normalcompliance in the majority of patients with preopera-tive increased values.
Second, the STARR modified the lower rectal pro-file, with appearance of a double anterior and poste-rior incisure over the anastomotic line in the lateralview at postoperative defecography. These findingswere first interpreted as little residual rectocele and/orintussusception. Nevertheless, a careful study of ra-diograms by experienced radiologists52 suggestedthat the real cause of the double incisure was thereadaptation of the rectal wall to fibrosis around theanastomotic lines. In fact, different from conventional,one-step, 360°-stapled colorectal anastomosis, theSTARR is performed in two separate steps, with two180° resection and two anastomosis posed at different
Figure 8. Defecography afterstapled transanal rectalresection for obstructureddefecation. Lateral and obliqueviews show a double incisureof the lower rectal outline inthe site of anterior andposterior anastomosis withdisappearance of bothintussusception and rectocele.
Table 7.Preoperative and Postoperative Manometric Data in 90 Patients Operated on for Outlet Obstruction
Findings Preoperative (n = 90) Postoperative (n = 90) P Valuea
Resting pressure (mmHg) 71.7 (18.3) 66.4 (20.4) NSSqueeze pressure (mmHg) 152.8 (29.5) 145.4 (24.2) NSRectal sensitivity threshold volume (ml) 154.4 (39.9) 146.6 (31.5) NSRectal compliance (ml/mmHg) 7.6 (3.1) 7.4 (2.8) < 0.05
NS = not significant.Values are expressed as means with standard deviations in parentheses.aWilcoxon’s test.
1293STAPLED RECTAL RESECTION FOR OUTLET OBSTRUCTIONVol. 47, No. 8
levels from the anal verge with more resected tissue inthe anterior step.
The patients were informed of possible peniletrauma caused by the residual staples during anal in-tercourse. When possible, residual staples were gent-ly removed with forceps during proctoscopy in thefollow-up controls. The cost of STARR was not evalu-ated in the present study; however, we believe thatthe good results of the new procedure could balancethe purchase of the two stapler kits.
CONCLUSIONS
The STARR seemed to be safe and effective: post-operative pain was minimal and disappeared in morethan 90 percent of patients within the first week. In-cidence of complications was acceptable. Overall pa-tient satisfaction was high and improved during thefollow-up period (90 percent excellent or good resultsat 1 year). The constipation score significantly im-proved, and the use of the anal dilator and the resec-tion of rectal wall did not cause persistent alterationsof the anal continence.
If randomized trials and longer follow-up confirmour preliminary results, this novel transanal techniquemay be considered a good choice in the surgical treat-ment of OSS caused by a combination of intussuscep-tion and rectocele.
ACKNOWLEDGMENTS
The authors thank Prof. P. Ronan O’Connell, M.D.,F.R.C.S.I./F.R.C.S., Consultant General and ColorectalSurgeon, Mater Private Hospital (Dublin), and Prof.Filippo Pucciani, Department of General Surgery,University of Florence, whose substantial contributionto the study was greatly appreciated.
REFERENCES
1. Fucini C, Ronchi O, Elbetti C. Electromyography of thepelvic floor musculature in the assessment of ob-structed defecation symptoms. Dis Colon Rectum 2001;44:1168–75.
2. Lowry AC, Simmang CL, Boulos P, et al. Consen-sus statement of definitions for anorectal physiol-ogy and rectal cancer. Dis Colon Rectum 2001;44:915–9.
3. Mellgren A, Bremmer S. Defecography, results of inves-tigation in 2816 patients. Dis Colon Rectum 1994;37:1133–41.
4. Schultz I, Mellgren A, Dolk A, Johansson C, Holstrom B.Continence is improved after Ripstein’s rectopexy: dif-ferent mechanisms in rectal prolapse and rectal intus-susception? Dis Colon Rectum 1996;39:300–6.
5. Senagore AJ, Luchtefeld MA, Mac Keigan JM. Recto-pexy. J Laparoendosc Surg 1993;3:339–43.
6. Bruch HP, Herold A, Schiedeck T, Schwandner O. Lap-aroscopic surgery for rectal prolapse and outlet obstruc-tion. Dis Colon Rectum 1999;42:1189–95.
7. Berman IR, Harris MS, Rabeler MB. Delorme’s transrec-tal excision for internal rectal prolapse: patient selec-tion, technique, and three-year follow-up. Dis ColonRectum 1990;33:573–80.
8. Block JR. Transrectal repair of rectocele using oblitera-tive suture. Dis Colon Rectum 1986;29:707–11.
9. Khubchandani IT, Sheets JA, Stasik JJ, Hakki AR. Endo-rectal repair of rectocele. Dis Colon Rectum 1983;26:792–6.
10. Sehapayak S. Transrectal repair of rectocele: an ex-tended armamentarium of colorectal surgeons. A reportof 335 cases . Dis Colon Rectum 1985;28:422–33.
11. van Laarhoven CJ, Kamm MA, Bartram CI, Halligan S,Hawley PR, Phillips RK. Relationship between anatomicand symptomatic long-term results after rectocele repairfor impaired defecation. Dis Colon Rectum 1999;42:204–11.
12. Porter WE, Steele A, Walsh P, Kohli N, Karram MM. Theanatomic and functional outcomes of defect-specificrectocele repairs. Am J Obstet Gynecol 1999;181:1353–8.
13. Zacharin FR, Hamilton NT. Pulsion enterocele: long-term results of an abdominoperineal technique. ObstetGynecol 1980;2:141–8.
14. Pescatori M, Favetta U, Dedola S, Orsini S. Transanalstapled excision of rectal mucosal prolapse. Tech Co-loproctol 1997;1:96–8.
15. Altomare DF, Rinaldi M, Veglia A, Petrolino M, De FazioM, Sallustio PL. Combined perineal and endorectal re-pair of rectocele by circular stapler: a novel surgicaltechnique. Dis Colon Rectum 2002;45:1549–52.
16. Boccasanta P, Venturi M, Calabro G, et al. Which sur-gical approach for rectocele? A multicentric report fromItalian coloproctologists. Tech Coloproctol 2001;5:147–54.
17. Agachan F, Chen T, Pfeifer J, Reisman P, Wexner SD. Aconstipation scoring system to simplify evaluation andmanagement of constipated patients. Dis Colon Rectum1996;39:681–5.
18. Oliveira J, Pfeiffer J, Wexner SD. Physiological and clini-cal outcome of anterior sphincteroplasty. Br J Surg1996;83:502–5.
19. Mahieu P, Pringot J, Bodart P. Defecography: II. Con-
1294 BOCCASANTA ET AL Dis Colon Rectum, August 2004

tribution to the diagnosis of defecation disorders. Gas-trointest Radiol 1984;9:253–61.
20. Costalat G, Garrigues JM, Drawed F, Noel P, Veyrac M,Vernhet J. Rectopexie antero-posterieure pour troublesde la statique rectale: resultats cliniques et ra-diologiques. Interet de la rectographie dinamique nu-merisee. A propos de trente cas. Ann Chir 1989;43:733–43.
21. Lau CW, Heymen S, Alabaz O, Iroatulam AJ, WexnerSD. Prognostic significance of rectocele, intussuscep-tion, and abnormal perineal descent in biofeedbacktreatment for constipated patients with paradoxical pu-borectalis contraction . Dis Colon Rectum 2000;43:478–82.
22. Marti MC, Deleaval J, Roche B. Rectoceles: value ofvideodefecography in selection of treatment policy.Colorect Dis 1999;1:324–9.
23. Basilisco G, Velio P, Bianchi PA. Oesophageal manom-etry in the evaluation of megacolon with onset in adultlife. Gut 1997;40:188–91.
24. Sorensen M, Rasmussen OO, Tetzschner T, ChristiansenJ. Physiological variation in rectal compliance. Br J Surg1992;79:1106–8.
25. Frudinger A, Bartram CI, Halligan S, Kamm M. Exami-nation techniques for endosonography of the anal ca-nal. Abdom Imaging 1998;23:301–3.
26. Rotholtz NA, Efron JE, Weiss EG, Nogueras JJ, WexnerSD. Anal manometric predictors of significant rectocelein constipated patients. Tech Coloproctol 2002;6:73–7.
27. Choi JS, Hwang YH, Salum MR, et al. Outcome andmanagement of patients with large rectoanal intussus-ception. Am J Gastroenterol 2001;96:740–4.
28. Mimura T, Roy AJ, Storrie JB, Kamm MA. Treatment ofimpaired defecation associated with rectocele by be-havioral retraining (biofeedback). Dis Colon Rectum2000;43:1267–72.
29. Holmstrom B, Broden G, Dolk A. Results of the Ripsteinoperation in the treatment of rectal prolapse and inter-nal rectal procidentia. Dis Colon Rectum 1986;29:845–8.
30. Keighley MR, Fielding JW, Alexander-Williams J. Resultsof Marlex mesh abdominal rectopexy for rectal pro-lapse in 100 consecutive patients. Br J Surg 1983;70:229–32.
31. Orrom WJ, Bartolo DC, Miller R, Mortensen NJ, Roe AM.Rectopexy is ineffective treatment of obstructed defeca-tion. Dis Colon Rectum 1991;34:41–6.
32. Duthie GS, Bartolo DC. Abdominal rectopexy for rectalprolapse: a comparison of technique. Br J Surg 1992;79:107–13.
33. Boccasanta P, Rosati R, Venturi M, et al. Surgical treat-ment of complete rectal prolapse: results of abdominaland perineal procedures. J Laparoendosc Adv SurgTech 1999;9:235–8.
34. Lieberman H, Hughes C, Dippolito A. Evaluation andoutcome of the Delorme procedure in the treatment of
rectal outlet obstruction. Dis Colon Rectum 2000;43:188–92.
35. Sielezneff I, Malouf A, Cesari J, Brunet C, Sarles JC,Sastre B. Selection criteria for internal rectal prolapserepair by Delorme’s transrectal excision. Dis Colon Rec-tum 1999;42:367–73.
36. Kuah SE, Lee KW, Houghton CR, Korda AR. The man-agement of pulsion rectocele with the Zacharin ab-dominoperineal technique (and mesh sacrocolpopexy).ANZ J Obstet Gynaecol 2000;40:303–7.
37. Brieger GM, Kordan AR, Houghton CR. Abdominoperi-neal repair of pulsion rectocele. J Obstet Gynaecol Res1996;22:151–6.
38. Roos P. Haemorrhoid surgery revised. Lancet 2000;355:1648.
39. Molloy RG, Kingsmore D. Life-threatening pelvic sepsisafter stapled haemorrhoidectomy. Lancet 2000;355:810.
40. Herold A, Kirsh JJ. Pain after stapled haemorrhoidec-tomy. Lancet 2000;356:2187.
41. Kriss BD, Porter JA, Slezak AF. Retroperitoneal air afterhemorrhoidectomy: report of a case. Dis Colon Rectum1990;33:971–3.
42. Murphy KJ. Tetanus after rubber-band ligation of haem-orrhoids. BMJ 1978;1:1590–1.
43. O’Hara VS. Fatal clostridial infection following hemor-rhoidal banding. Dis Colon Rectum 1980;23:570–1.
44. Scarpa FJ, Hillis W, Sabetta JR. Pelvis cellulitis: is a life-threatening complication of hemorrhoidal banding .Surgery 1988;103:383–5.
45. Barwell J, Watkins RM, Lloyd-Davies E, Wilkins DC.Life-threatening retroperitoneal sepsis after hemorrhoidinjection sclerotherapy. Dis Colon Rectum 1999;42:421–3.
46. Maw A, Eu KW, Seow-Chen F. Retroperitoneal sepsiscomplicating stapled hemorrhoidectomy. Dis ColonRectum 2002;45:826–8.
47. Felt-Bersma RJ, Cuesta MA, Koorevaar M, et al. Analendosonography: relationship with anal manometryand neurophysiologic tests. Dis Colon Rectum 1992;35:944–9.
48. Felt-Bersma RJ, Poen AC, Cuesta MA, Meuwissen SG.Anal sensitivity test: what does it measure and do weneed it ? Cause or derivative of anorectal complaints.Dis Colon Rectum 1997;40:811–6.
49. Felt-Bersma RJ, van Baren R, Koorevaar M, Strijers RL,Cuesta MA. Unsuspected sphincter defects shown byanal endosonography after anorectal surgery. A pro-spective study. Dis Colon Rectum 1995;38:249–53.
50. Ho YH, Cheong WK, Tsang C, et al. Stapled hemorrhoidectomy—cost and effectiveness. Randomized, con-trolled trial including incontinence scoring, anorectalmanometry and endoanal ultrasound assessment at upto three months. Dis Colon Rectum 2000;43:1666–75.
51. Gosselink MJ, Hop WC, Schouten WR. Rectal compli-ance in females with obstructed defecation. Dis ColonRectum 2001;44:971–7.
1295STAPLED RECTAL RESECTION FOR OUTLET OBSTRUCTIONVol. 47, No. 8

52. Piloni V, Pomerri F, Platania E, et al. The NationalWorkshop on Defecography: anorectal deformities witha functional origin (prolapse, intussusception, recto-cele). Radiol Med 1994;87:789–95.
Invited Commentary
To the Editor—This article personally causes meimmense problems. The presentation is immaculate.The description and drawings of the operation areclear and easy to follow. Every conceivable angle hasbeen considered (even to the extent of advising pa-tients of the possibility of trauma to a partner’s penisfrom residual staples!). This is a prospective, multi-center study, conducted with the highest rigor. Ap-propriate preoperative steps have been taken. We aretold that all patients have been carefully evaluatedand screened preoperatively and all have failed ap-propriate medical therapy, including biofeedback. Aperhaps surprisingly large number of patients havebeen recruited during an impressively short time; butthen, this is a multicenter study. The tightest statisticaltests have been used with the most rigorous correc-tions to account for multiple statistical comparisons.Follow-up, although not long, is at least for one year.In not one single category of 15 identifiers of symp-tom resolution (Tables 2 and 3) has there been evena hint of loss of efficacy with time, a remarkable find-ing in any study, and all the more notable in a studyin which the authors acknowledge psychologic fac-tors and hence a placebo effect declining with timemight be expected. There has been no loss of dataand no industry support at all; although it is not clearwhere the centralized database was kept or who werethe data managers and data clerks who achieved thisincomparable result.
And yet I am far from persuaded. The authors areaware of the likely high level of skepticism that willmeet this report. This skepticism arises because rec-toceles and internal intussusception may both be seenin normal, asymptomatic women.1 Abdominal recto-pexy to fix internal intussusception was abandoned atSt. Mark’s Hospital after analysis showed no real ben-efit.2 For those of us who consider patients withobstructive defecation to have a problem in bowelfunction rather than in bowel structure, a surgicalapproach makes as much sense as removing partof a lung to treat asthma or chopping off an arm totreat high blood pressure. What a gulf there is be-tween us!
REFERENCES
1. Shorvon PJ, McHugh S, Diamant NE, Somers S, Steven-son GW. Defaecography in normal volunteers: resultsand implications. Gut 1989;30:1737–49.
2. McCue JL, Thomson JP. Rectopexy for internal rectalintussusception. Br J Surg 1990;77:632–4.
Robin K. S. Phillips, M.S.Harrow, United Kingdom
The Authors Reply
To the Editor—We greatly appreciated the com-ment of R.K.S. Phillips for both compliments and con-structive criticisms. Our article required long prepara-tion and a lot of thought before deciding to submit itto DCR. We were conscious of the limitations of thework, particularly the absence of a control group.Nevertheless, not one of the traditional transanal op-eration for outlet obstruction was comparable toSTARR, because none provides a resection of the rec-tal wall, and the clinical and functional results ofSTARR were so encouraging to be known. A secondlimitation was the relatively short follow-up period,even if the actual results at more than two years afterthe operation do not differ from those reported at oneyear.
The centralized database of the work were keptby the Epidemiology Unit of Ospedale MaggiorePoliclinico di Milano I.R.C.C.S., directed by M. B. Ce-sana, M.D., who was responsible for the managementof data (and declined the offer to be cited in thework).
We agree that there is difficulty in correlating symp-toms to the anatomic findings and in deciding to op-erate on patients with functional bowel disorders(rectoanal intussusception must be considered a func-tional or an organic disease?).
We recommend using very strict selection criteriafor STARR, trying conservative treatment before theoperation, avoiding surgery for patients with puden-dal neuropathy, nonrelaxing puborectalis muscle, andsphincterial defects, very carefully controlling hemo-stasis during the operation, and always using prophy-lactic antibiotics.
Finally, on behalf of SIUCP (Italian United Societyof Coloproctology), we would be honored to inviteProf. Phillips or one of his coworkers for a demon-
1296 BOCCASANTA ET AL Dis Colon Rectum, August 2004

stration of the STARR technique and a meeting withthe operated patients in one of our Colorectal SIUCPcenters.
Paolo Boccasanta, M.D.Marco Venturi, M.D.
Milan, Italy
Angelo Stuto, M.D.Pordenone, Italy
Corrado Bottini, M.D.Varese, Italy
Angelo Caviglia, M.D.Domenico Mascagni, M.D.
Luigi Sofo, M.D.Rome, Italy
Alfonso Carriero, M.D.Montecchio Emilia, Italy
Roberto Mauri, M.D.Como, Italy
Vincenzo Landolfi, M.D.Avellino, Italy
1297STAPLED RECTAL RESECTION FOR OUTLET OBSTRUCTIONVol. 47, No. 8