transanal one-stage endorectal pull-through for hirschsprung's disease: a multicenter study
TRANSCRIPT

B
(sti
M
gppfpat(np
R
(bpg
TtemadTifrr
tdpe(a
t
J
Transanal One-Stage Endorectal Pull-Through for Hirschsprung’sDisease: A Multicenter Study
By Essam A. Elhalaby, A. Hashish, M.M. Elbarbary, H.A. Soliman, M.K. Wishahy, A. Elkholy, S. Abdelhay,M. Elbehery, N. Halawa, T. Gobran, S. Shehata, N. Elkhouly, and A.F. Hamza
Tanta, Cairo, Ain Shams, Zagazig, and Alexandria, Egypt
msdt426(a1(fi
C
smaJr
I
ackground/Purpose: Transanal endorectal pull-throughTEPT) is the latest development in treatment of Hirsch-prung’s disease (HD). This prospective study was designedo evaluate the safety and efficacy of 1 stage TEPT techniquen the management of patients with HD.
ethods: One hundred forty-nine children (116 boys and 33irls) aged 8 days to 14 years underwent 1 stage TEPTrocedure over an 18-month period at 5 Egyptian academicediatric surgical centers and affiliated hospitals. Medianollow-up was 12 months (range, 3 to 21 months). Theseatients were evaluated with regard to age, sex, length of theganglionic segment, intraoperative details, and postopera-ive functional results or complications. An electromyogramEMG), endorectal ultrasound scan, and lower gastrointesti-al (GI) motility studies were reserved for patients withostoperative problems with bowel control.
esults: Mean operating time was 120.2 � 27.8 minutesrange, 60 to 210 minutes). The average length of resectedowel was 26.8 � 12.4 cm (range, 15 to 45 cm). Thirteenatients required laparotomy because of extension of agan-
lionic segment beyond the sigmoid colon in 9, tear in the t)pt ois-for
c-l
la-esalh a
gateas antiousughance
venissue diagnosis of HD were treated at 5 academic pediatric surgica
cTwpwwtd1
dc
DaUsd
S
B
ournal of Pediatric Surgery, Vol 39, No 3 (March), 2004: pp 345-351
esenteric vessels in 2, and difficulties in getting to theubmucosal plane in 2. Three deaths (2%) occurred 3 days, 4ays, and 4 weeks postoperatively, respectively. Postopera-ive complications included transient perianal excoriation in8 patients (30 were �3 months of age), enterocolitis (n �6), anastomotic stricture (n � 7), recurrent constipation (n �), hypoganglionosis at distal end of pulled through segmentn � 2), cuff abscess (n � 3), anastomotic leak (n � 1),dhesive bowel obstruction (n � 1), and rectal prolapse (n �). Complete anorectal continence was noted in 35 of 4283.3%) children older than 3 years, whereas soiling andrequent accidents still occur in 7, who showed a steadymprovement in their continence status.
onclusions: One-stage TEPT technique is both feasible andafe technique in properly selected children with rectosig-oid HD in all ages. The technique is easily learned and is
ssociated with excellent clinical results.Pediatr Surg 39:345-351. © 2004 Elsevier Inc. All rights
eserved.
NDEX WORDS: Hirschsprung’s disease, transanal pull-
hrough, one-stage repair.2002.ad a
onthose
onepull-fully
le for
ents’rativeding
RANSANAL ENDORECTAL pull-through (TEPTrepresents the latest development in the conce
he minimally invasive surgery for Hirschsprung’s dase (HD).1-9 Transanal mucosectomy was practicedany years in conventional10,11and during laparoscopissisted endorectal pull-through for HD.12 The noveescription of an entirely TEPT approach by Deorre-Mondragon and Ortega-Salgado in 19981 was rap
dly followed by similar promising early experiencrom various centers.2-9 However, most of these initieports reflect a single institution’s experience witelatively small number of patients.
This prospective study was undertaken to investihe safety and efficacy of 1-stage TEPT techniqueefinitive treatment for patients with HD in differeediatric age groups and to find out whether a prevxperience with the conventional endorectal pull-throEPT) technique has an impact on operative performnd outcome of TEPT approach.
MATERIALS AND METHODS
One hundred forty-nine children (116 boys and 33 girls) with pro
fenters and affiliated hospitals between December 2000 and Juneheir ages ranged from 8 days to 14 years. All patients hell-defined transition zone at or distal to midsigmoid colonreoperative contrast enema. Patients with previous colostomy orith either an ill-defined or more proximally located transition zere treated by either single-or multiple-staged conventional
hrough approach. Likewise, infants who could not be successecompressed by rectal irrigation were considered not suitab-stage TEPT.A data chart was designed to collect the following data: (1) Pati
emographics including sex and age at diagnosis; (2) preopelinical data and diagnostic studies; (3) operative details inclu
From the Department of Pediatric Surgery, Tanta University, Tanta;epartment of Pediatric Surgery, Cairo University Specialized Pedi-tric Hospital, Cairo; the Department of Pediatric Surgery, Ain Shamsniversity, Cairo; Department of Pediatric Surgery, Zagazig Univer-
ity, Zagazig; and Department of Pediatric Surgery, Elshatby Chil-ren’s Hospital, Alexandria, Egypt.Presented at the 34th Annual Meeting of the American Pediatric
urgical Association, Fort Lauderdale, Florida, May 25-28, 2003.Address reprint requests to Essam A. Elhalaby, MD, 5 Elhayaa St,
org Elestad, Tanta, 31111, Egypt.© 2004 Elsevier Inc. All rights reserved.0022-3468/04/3903-0018$30.00/0
l doi:10.1016/j.jpedsurg.2003.11.038
345

pdtdaorfephareoSwT
S
papjveieattebTdmiclodrtiscu
epaaw3
ic
l5 tube and seromuscular cuff are prolapsed outside the anus.
346 ELHALABY ET AL
osition of patient, the level of starting the submucosal dissection,egree of difficulties in submucosal dissection and/or colon mobiliza-ion, length of the remaining cuff, iatrogenic injury of any structureuring surgery, length of the excised specimen, estimated blood lossnd blood transfusion, conversion to laparotomy and its cause, andperating time; (4) early postoperative course particularly time ategain of peristalsis, timing of first passage of stool, and starting of oraleeding; (5) postoperative complications such as significant perinealxcoriation, anastomotic leak, anorectal stricture, enterocolitis, anderineal or pelvic infection; (6) functional outcome as judged by bowelabits, recurrent abdominal distension, and anorectal continence status;nd (7) need for a secondary surgical procedure such as myectomy, oredo pull-through. Postoperative investigations including contrast en-ma, anorectal motility, and electromyogram (EMG) were performednly for patients with complications or problems with bowel control.pecial inquiry was made regarding type of pull-through technique,hich was practiced by each of the participating surgeons beforeEPT.
urgical Technique
After induction of anesthesia, the patient is placed supine with theelvis elevated at the end of the operating table with the lower limbsttached to an inverted U-shaped bar. The abdomen and perineum arerepared in the standard fashion. Two surgeons prefer the proneackknife position for assuming more direct access to mesentericessels. A bladder catheter is not routinely inserted. The anal canal isxposed with Scott anal retractor or with stay sutures. Submucosalnjection of epinephrine or saline is not routinely used. A circumfer-ntial row of 4-0 silk stay sutures is inserted approximately 0.5 to 1 cmbove the dentate line. The rectal mucosa is incised just distal to theraction sutures and lifted circumferentially using fine diathermy needleo develop the submucosal plane. Once the submucosal plane isstablished, the dissection can be easily continued proximally usinglunt dissection and cauterization of submucosal infiltrating vessels.he traction on mucosal tube facilitates proximal extension of mucosalissection until the level proximal to peritoneal reflection (approxi-ately 10 to 15 cm above the dentate line; Fig 1). Four stay sutures are
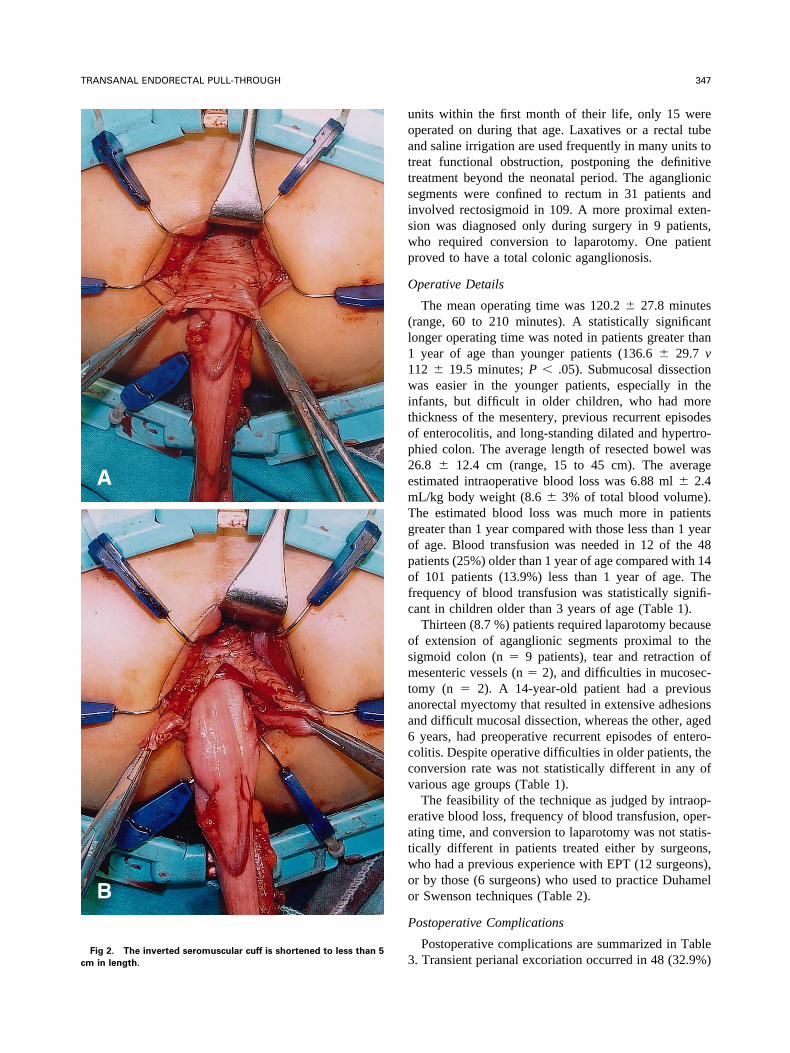
nserted to control the upper end of muscular cuff, which is incisedircumferentially allowing exposure of the full-thickness sigmoid co-on. Mobilization of the colon is continued as proximal to the grosslybvious or histologically confirmed transition zone as possible byividing the rectosigmoid vessels after cauterizing them. Ligatures arearely needed in infants. The long seromuscular cuff is inverted outsidehe anus and shortened to less than 5 cm in length before retuning it tots normal position (Fig 2A & B). After resection of the aganglionicegment, the normally innervated bowel is pulled through the muscularuff and anastomosed to the remaining mucosa above the dentate linesing 4-0 slowly absorbable suture material.Feeding was allowed the day after the procedure. First rectal digital
xamination was performed after 10 days. Routine anal dilations wereerformed in all neonates and young infants once or twice weekly fort least 3 weeks. The anal dilatation was performed in older children if
developing stricture was palpated. Follow-up was arranged onceeekly for 3 weeks followed by once monthly for 3 months then everymonths thereafter.Results are expressed as range and mean � SD. Statistical compar-
son was done with unpaired t and �2 tests, with P value less than .05onsidered significant.
RESULTS
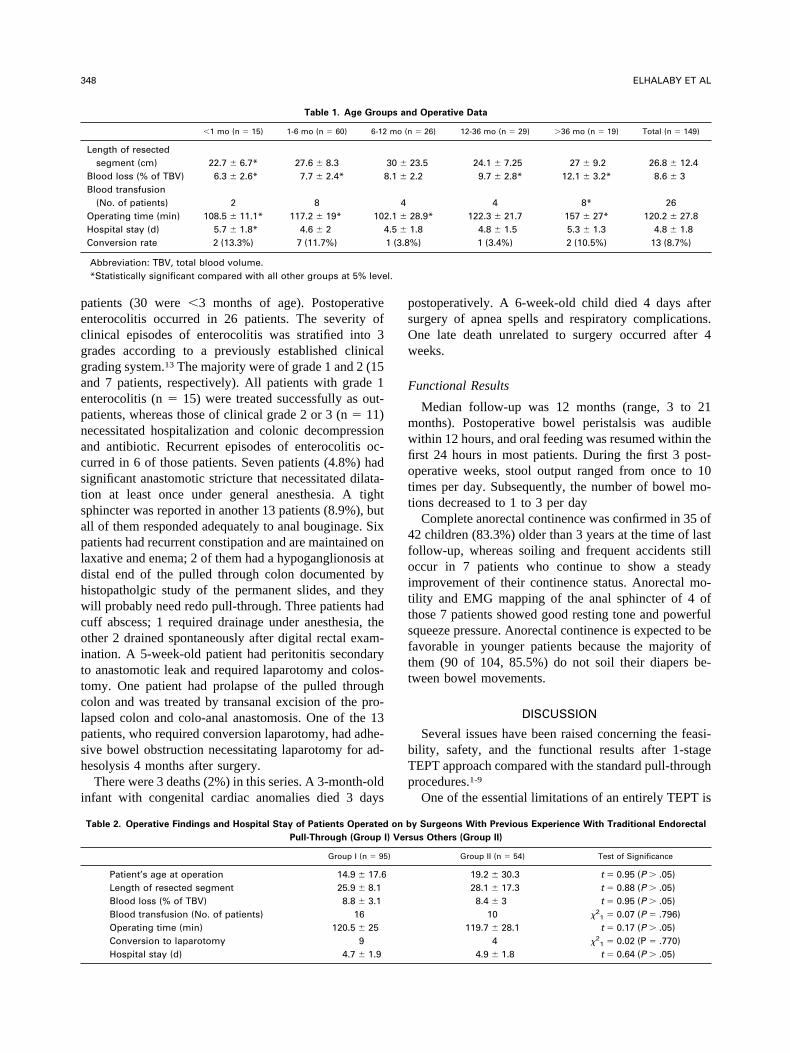
More than two thirds of patients (101, 67.8%) wereess than 1 year old at time of TEPT (Table 1). Although
8 (39%) patients were referred to pediatric surgicalFig 1. Transanal mucosectomy is completed. The long mucosal
uoattsiswp
O
(l11witop2emTgopofc
osmtaa6ccv
eatwoo
P
3cm in length.
347TRANSANAL ENDORECTAL PULL-THROUGH
nits within the first month of their life, only 15 wereperated on during that age. Laxatives or a rectal tubend saline irrigation are used frequently in many units toreat functional obstruction, postponing the definitivereatment beyond the neonatal period. The aganglionicegments were confined to rectum in 31 patients andnvolved rectosigmoid in 109. A more proximal exten-ion was diagnosed only during surgery in 9 patients,ho required conversion to laparotomy. One patientroved to have a total colonic aganglionosis.
perative Details
The mean operating time was 120.2 � 27.8 minutesrange, 60 to 210 minutes). A statistically significantonger operating time was noted in patients greater than
year of age than younger patients (136.6 � 29.7 v12 � 19.5 minutes; P � .05). Submucosal dissectionas easier in the younger patients, especially in the
nfants, but difficult in older children, who had morehickness of the mesentery, previous recurrent episodesf enterocolitis, and long-standing dilated and hypertro-hied colon. The average length of resected bowel was6.8 � 12.4 cm (range, 15 to 45 cm). The averagestimated intraoperative blood loss was 6.88 ml � 2.4L/kg body weight (8.6 � 3% of total blood volume).he estimated blood loss was much more in patientsreater than 1 year compared with those less than 1 yearf age. Blood transfusion was needed in 12 of the 48atients (25%) older than 1 year of age compared with 14f 101 patients (13.9%) less than 1 year of age. Therequency of blood transfusion was statistically signifi-ant in children older than 3 years of age (Table 1).
Thirteen (8.7 %) patients required laparotomy becausef extension of aganglionic segments proximal to theigmoid colon (n � 9 patients), tear and retraction ofesenteric vessels (n � 2), and difficulties in mucosec-
omy (n � 2). A 14-year-old patient had a previousnorectal myectomy that resulted in extensive adhesionsnd difficult mucosal dissection, whereas the other, agedyears, had preoperative recurrent episodes of entero-
olitis. Despite operative difficulties in older patients, theonversion rate was not statistically different in any ofarious age groups (Table 1).The feasibility of the technique as judged by intraop-
rative blood loss, frequency of blood transfusion, oper-ting time, and conversion to laparotomy was not statis-ically different in patients treated either by surgeons,ho had a previous experience with EPT (12 surgeons),r by those (6 surgeons) who used to practice Duhamelr Swenson techniques (Table 2).
ostoperative Complications
Postoperative complications are summarized in Table
. Transient perianal excoriation occurred in 48 (32.9%)Fig 2. The inverted seromuscular cuff is shortened to less than 5
pecggaepnacstsapldhwcoittclpsh
i
psOw
F
mwfiott
4foittsftt
bTp
l.
348 ELHALABY ET AL
atients (30 were �3 months of age). Postoperativenterocolitis occurred in 26 patients. The severity oflinical episodes of enterocolitis was stratified into 3rades according to a previously established clinicalrading system.13 The majority were of grade 1 and 2 (15nd 7 patients, respectively). All patients with grade 1nterocolitis (n � 15) were treated successfully as out-atients, whereas those of clinical grade 2 or 3 (n � 11)ecessitated hospitalization and colonic decompressionnd antibiotic. Recurrent episodes of enterocolitis oc-urred in 6 of those patients. Seven patients (4.8%) hadignificant anastomotic stricture that necessitated dilata-ion at least once under general anesthesia. A tightphincter was reported in another 13 patients (8.9%), butll of them responded adequately to anal bouginage. Sixatients had recurrent constipation and are maintained onaxative and enema; 2 of them had a hypoganglionosis atistal end of the pulled through colon documented byistopatholgic study of the permanent slides, and theyill probably need redo pull-through. Three patients had
uff abscess; 1 required drainage under anesthesia, thether 2 drained spontaneously after digital rectal exam-nation. A 5-week-old patient had peritonitis secondaryo anastomotic leak and required laparotomy and colos-omy. One patient had prolapse of the pulled througholon and was treated by transanal excision of the pro-apsed colon and colo-anal anastomosis. One of the 13atients, who required conversion laparotomy, had adhe-ive bowel obstruction necessitating laparotomy for ad-esolysis 4 months after surgery.There were 3 deaths (2%) in this series. A 3-month-old
nfant with congenital cardiac anomalies died 3 days
Table 1. Age Grou
�1 mo (n � 15) 1-6 mo (n � 60) 6-12
Length of resectedsegment (cm) 22.7 � 6.7* 27.6 � 8.3
Blood loss (% of TBV) 6.3 � 2.6* 7.7 � 2.4* 8Blood transfusion
(No. of patients) 2 8Operating time (min) 108.5 � 11.1* 117.2 � 19* 102Hospital stay (d) 5.7 � 1.8* 4.6 � 2 4Conversion rate 2 (13.3%) 7 (11.7%)
Abbreviation: TBV, total blood volume.*Statistically significant compared with all other groups at 5% leve
Table 2. Operative Findings and Hospital Stay of Patients Operated
Pull-Through (Group I
Group I (n � 95
Patient’s age at operation 14.9 � 17.6Length of resected segment 25.9 � 8.1Blood loss (% of TBV) 8.8 � 3.1Blood transfusion (No. of patients) 16Operating time (min) 120.5 � 25Conversion to laparotomy 9Hospital stay (d) 4.7 � 1.9
ostoperatively. A 6-week-old child died 4 days afterurgery of apnea spells and respiratory complications.ne late death unrelated to surgery occurred after 4eeks.
unctional Results
Median follow-up was 12 months (range, 3 to 21onths). Postoperative bowel peristalsis was audibleithin 12 hours, and oral feeding was resumed within therst 24 hours in most patients. During the first 3 post-perative weeks, stool output ranged from once to 10imes per day. Subsequently, the number of bowel mo-ions decreased to 1 to 3 per day
Complete anorectal continence was confirmed in 35 of2 children (83.3%) older than 3 years at the time of lastollow-up, whereas soiling and frequent accidents stillccur in 7 patients who continue to show a steadymprovement of their continence status. Anorectal mo-ility and EMG mapping of the anal sphincter of 4 ofhose 7 patients showed good resting tone and powerfulqueeze pressure. Anorectal continence is expected to beavorable in younger patients because the majority ofhem (90 of 104, 85.5%) do not soil their diapers be-ween bowel movements.
DISCUSSION
Several issues have been raised concerning the feasi-ility, safety, and the functional results after 1-stageEPT approach compared with the standard pull-throughrocedures.1-9
One of the essential limitations of an entirely TEPT is
d Operative Data
� 26) 12-36 mo (n � 29) �36 mo (n � 19) Total (n � 149)
23.5 24.1 � 7.25 27 � 9.2 26.8 � 12.42.2 9.7 � 2.8* 12.1 � 3.2* 8.6 � 3
4 8* 2628.9* 122.3 � 21.7 157 � 27* 120.2 � 27.81.8 4.8 � 1.5 5.3 � 1.3 4.8 � 1.8%) 1 (3.4%) 2 (10.5%) 13 (8.7%)
y Surgeons With Previous Experience With Traditional Endorectal
sus Others (Group II)
Group II (n � 54) Test of Significance
19.2 � 30.3 t � 0.95 (P � .05)28.1 � 17.3 t � 0.88 (P � .05)8.4 � 3 t � 0.95 (P � .05)
10 �21 � 0.07 (P � .796)
119.7 � 28.1 t � 0.17 (P � .05)4 �2
1 � 0.02 (P � .770)4.9 � 1.8 t � 0.64 (P � .05)
ps an
mo (n
30 �
.1 �
4.1 �
.5 �
1 (3.8
on b
) Ver
)

tytdfiuactzcltcmbonbtiv
Epecplbdpeoowen
tmcm
ccssemmatspat
lgttobllamm
adsbibpig
pdcsor
349TRANSANAL ENDORECTAL PULL-THROUGH
he proximal extension of the aganglionic segment be-ond the sigmoid colon. Cadaveric dissection showedhat the lower one third of the descending colon could beissected and pulled out of the anus because of its loosexation to the retroperitoneum.8 A long segment ornclear transition zone should not be considered anbsolute contraindication for TEPT approach. The pro-edure can be started transanally, switching to an addi-ional laparotomy if a histologically proven transitionone cannot be reached from below.7 Even cases of totalolonic aganglionosis can be treated with conversion toaparotomy and a straight EPT after completing theransanal mucosectomy. Because of the possibility ofonversion to laparotomy, the supine position is recom-ended rather than the prone position, which is preferred
y some surgeons with the assumption of better controln mesenteric vessels.1 Conversion to laparotomy shouldot be considered a failure of TEPT technique, and theasic principles of treatment of HD, which entails resec-ion of the aganglionic segment and bringing a normallynnervated bowel down to the anus, should never beiolated at the expense of avoiding laparotomy.The remaining seromuscular cuff after conventional
PT or TEPT has been accused for the development ofostoperative obstructive symptoms, constipation, andnterocolitis in some patients.14 Albanese et al3 left aonsiderable long cuff, but they cut it posteriorly. Werefer to continue mucosectomy for a relatively longength to be sure that intraabdominal part of rectum haseen reached, to avoid injury to the ureter and or vaseferens, which are at risk if dissection started beloweritoneal reflection, and because it is both technicallyasy and fast to continue mucosectomy more proximallynce the correct plane is established. The TEPT approachffers an excellent exposure and control of the cuff,hich is inverted outside the anus and shortened to the
xactly needed length before returning it back to itsormal position.One of the crucial critiques for the TEPT approach is
he significant stretching of the anal sphincters duringucosectomy with its potential impact on postoperative
ontinence status particularly in older children with7,15
Table 3. Postoperative Comp
Postoperative Complications �12 mo (n � 98) �12
Perianal excoriation 38Enterocolitis 20Anastomotic stricture 4Recurrent constipation 4Cuff abscess 0Adhesive obstruction 1Rectal prolapse 1Anastomotic leak 1
*Statistically significant at 5% level.
arked hypertrophy and dilatation of the colon. The t
urrent study showed that a transient soiling and in-reased frequency of bowel motions does occur in aignificant number of patients probably because of thetretch effect. However, this proved to be a transientffect, and bowel movements became normal in theajority of cases within a period from 2 weeks to 3onths. Parents should be informed about this squeal
head of time to alleviate their potential anxiety duringhis period. The postoperative EMG mapping of analphincters proved to be within normal range in thoseatients. Similarly, van Leeuwen et al15 reported thatnorectal manometric studies were similar in both pa-ients undergone TEPT or conventional EPT.
Another critical issue is related to the relatively distalevel of rectoanal anastomosis in many patients under-oing TEPT technique. A low anastomosis at or distal tohe dentate line may damage the delicate nerve endingshat play a part of anorectal continence.7 The routine usef Scott anal retractor offers excellent exposure at theeginning of mucosectomy, which should be started ateast 1 cm proximal to the dentate line. Patients withower anastomosis at or distal to the dentate line weressociated with higher frequency of transient soiling forore prolonged periods than in those with more proxi-ally located anastomosis.The limited operative field and exposure is considereddisadvantage of TEPT approach. There is a potential
ifficulty in controlling the bleeding from retracted ves-els during mobilization of the colon. All vessels shoulde cauterized carefully or ligated before cutting. Twist-ng of the pulled through colon is another potential riskecause of the limited exposure. A rectal tube should beassed before starting the anastomosis if a colonic twists suspected. Ruling out this possibility by laparoscopy isenerally unnecessary.Enterocolitis has been considered one of the main
roblems in patients with HD both before and afterefinitive treatment.13-16 Liu et al4 reported a signifi-antly higher rate of enterocolitis after transanal muco-ectomy. Their results cannot be confirmed in our studyr in several other reported series1-3,7 van Leeuwen et al15
eported a relatively a high incidence of post–pull-
ns in 146 Surviving Patients
� 48) No of patients (% of total 146) �21 (P Value)
48 (32.9%) 3.92 (.048)*26 (17.8%) 0.89 (.347)7 (4.8%) 0.03 (.870)6 (4%) 0.18 (.975)3 (2%) 0.36 (.551)1 (0.7%) 0.13 (.671)1 (0.7%) 0.13 (.671)1 (0.7%) 0.13 (.671)
licatio
mo (n
106323000
hrough enterocolitis after both conventional and

tlscroapptde
wp12r
gisit
fTb
asifctTeowam
PSaUo
r1
S3
p
t
fa
o3
td
s
i
vps
350 ELHALABY ET AL
ransanal approaches (53% versus 56%). The relativeow incidence of enterocolitis after TEPT in the currenteries may be related in part to the short seromuscularuff, the low coloanal anastomosis, and our policy ofoutine postoperative anal dilatation particularity in ne-nates and infants. There is a general tendency to reservenal dilation or bouginage to cases with existing orotential risk of stricture formation.2 We believe thatostoperative routine anorectal bouginage is an effectiveool to prevent the occurrence of anal stricture and toecrease both the frequency as well as the severity ofnterocolitis particularly in neonates and young infants.
The mortality rate in our series (2%) is comparableith other series. De la Torre and Ortega-Salgado6 re-orted 1 death of 10 patients treated by TEPT. Likewise,of the 9 patients in the early series of Langer et al2 died.5 months after surgery. The deaths were not directlyelated to the technique in either our series or in others.
Normal bowel function is the ultimate goal after sur-ery for HD. Complete anorectal continence was notedn 83.3% of children older than 3 years as well as ateady improvement in continence status of the remain-ng. We agree with Langer et al2 that there is no reason
o believe that long-term problems will be any more (REFEREN
nsufflation facilitates endorectal mucosectomy in transanal endorectal
pd
s
ms
pd
at
tc
md1
ac
Discuss
app
requent than in patients undergoing conventional EPT.he incidence of recurrent constipation certainly shoulde less because of constant low anastomosis.The current study substantiates the previously reported
dvantages of TEPT such as early postoperative feeding,ignificantly shorter hospital stay, no visible scars, min-mal intraabdominal dissection, lower risk of adhesionormation, and lower cost, without an increased risk ofomplications.1-7 A previous experience with the tradi-ional EPT is not mandatory to accomplish TEPT safely.he technique can be quickly learned regardless of previousxperience. It should not be considered a sophistication ofrdinary treatment of HD but appears to be a simplificationithout loss of safety. We believe that 1-stage TEPT
pproach is qualified to be the new gold standard foranagement of the majority of patients with HD.
ACKNOWLEDGMENT
The authors thank Richard Azizkhan, MD, Professor & Chief ofediatric Surgery, Cincinnati Children’s Hospital for Sponsoring theubmission of the Abstract and for Reviewing the Manuscript. Theuthors thank Gamalat M. Aly, PhD, Professor of Public Health, Tantaniversity for her help in statistical analysis, and appreciate the effortf all other members of Egyptian Pediatric Surgical Association
EPSA) and their residents, who actively participated in this study.CES
1. De la Torre-Mondragon L, Ortega-Salgado JA: Transanal endo-ectal pull-through for Hirschsprung’s disease. J Pediatr Surg 33:1283-286, 19982. Langer JC, Minkes RK, Mazziotti MV, et al: Transanal one-stage
oave procedure for infants with Hirschsprung’s disease. J Pediatr Surg4:148-152, 19993. Albenese CT, Jennings RW, Smith B, et al: Perineal one-stage
ull-through for Hirschsprung’s disease. J Pediatr Surg 34:377-380, 19994. Liu DC, Rodriguez J, Loe WA Jr: Transanal mucosectomy in the
reatment of Hirschsprung’s disease. J Pediatr Surg 35:235-238, 20005. Langer JC, Seifert M, Minkes RK: One-Stage Soave pull-through
or Hirschsprung’s disease: A comparison of the transanal and openpproaches. J Pediatr Surg 35:820-822, 2000
6. De la Torre-Mondragon L, Ortega-Salgado JA: Transanal versuspen endorectal pull-through for Hirschsprung’s disease. J Pediatr Surg5:1630-1632, 20007. Hollwarth ME, Rivosecchi M, Schleef J, et al: The role of
ransanal endorectal pull-through in the treatment of Hirschsprung’sisease—A multicenter experience. Pediatr Surg Int 18:344-348, 2002
8. Teeraratkul S: Transanal one-stage endorectal pull-through for Hirsch-prung’s disease in infants and children. J Pediatr Surg 38:184-187, 2003
9. Ergun O, Celik A, Dokumcu Z, et al: Submucosal pressure-air
ull-through procedure in patients with Hirschsprung’s disease. J Pe-iatr Surg 38:188-190, 200310. Boley SJ: New modification of the surgical treatment of Hirsch-
prung’s disease. Surgery 56:1015-1017, 196411. Saltzman DA, Telander MJ, Brennom WS, et al: Transanalucosectomy: A modification of the Soave procedure for Hirsch-
prung’s disease. J Pediatr Surg 31:1272-1275, 199612. Georgeson KE, Fuenfer MM, Hardin WD: Primary laparoscopic
ull-through for Hirschsprung’s Disease in infants and children. J Pe-iatr Surg 30:1017-1022, 199513. Elhalaby EA, Coran AG, Blane CE, et al: Enterocolitis associ-
ted with Hirschsprung’s disease: A clinical-radiological characteriza-ion based on 168 patients. J Pediatr Surg 30:76-83, 1995
14. Gao Y, Li G, Zhang X, et al: Primary transanal rectosigmodec-omy for Hirschsprung’s disease: Preliminary results in the initial 33ases. J Pediatr Surg 36:1816-1819, 2001
15. van Leeuwen K, Geiger JD, Barnett JL, et al: Stooling andanometric findings after primary pull-throughs in Hirschsprung’s
isease: Perineal versus abdominal approaches. J Pediatr Surg 37:1321-325, 200216. Elhalaby EA, Teitelbaum DH, Coran AG, et al: Enterocolitis
ssociated with Hirschsprung’s disease: A clinical histopathological
orrelative study. J Pediatr Surg 30:1023-1027, 1995ion
W. Holcomb (Kansas City Ks): I enjoyed your paperery much. Would you expand on the older group ofatients in this study, for instance, those over a month oro of age? Did those patients have a colostomy initially
nd then have this procedure, or were all of these primaryrocedures without colostomies, even in the olderatients?E. Elhalaby (response): Thank you for your question.

Acseeteerc
mp
dhs
p
Stvtaepwee
ceisdy2
351TRANSANAL ENDORECTAL PULL-THROUGH
ll of them had no colostomy as a part of the inclusionriteria. Most of older age groups had a relatively shortegment, and they were maintained on suppositories andnemata, none of them had a previous surgery beforexcept one who had myectomy. In his file, it was men-ioned as just biopsy, but actually, it was rather anxtensive myectomy. The patient was maintained onnemata for 14 years by his mother who is a nurse. Heequired conversion to laparotomy, as the transanal mu-osectomy was very difficult in his case.
W. Holcomb: So, in your mind, the rectum and sig-oid colon were not markedly dilated even in these older
atients?E. Elhalaby (response): Some of them had a markedly
ilated colon. When we see the patient like that, we keepim on enemata until we have a reasonable decompres-ion of the colon before going to surgery.
A. Coran (Ann Arbor, MI): That’s a nice series, and it
arallels the paper that was presented to the American surgical by Jack Langer, which was also a multiinstitu-ional study in the United States with 141 patients andery similar results. My question really revolves aroundhe incidence you state here of enterocolitis. In thebstract it says 6 patients of these 149 patients hadnterocolitis. As you well know, having studied theroblem in our institution a few years ago when youere there, that’s a very, very low of incidence of
nterocolitis in any series. What is your definition ofnterocolitis, and why is it so low?
E. Elhalaby (response): Recurrent attacks of entero-olitis occurred in 6 patients, another 20 have only 1pisode of postoperative enterocolitis. So we have totalncidence of 26 of the 149 patients. The definition andeverity of enterocolitis was made according to the stan-ard 3 clinical grades, which has been published by us 10ears ago. Almost 22 of the 26 patients had grade 1 and. So, I think the 17% incidence of enterocolitis in this
eries is comparable with many other series.