solitary fibrous tumor of the soft tissue
TRANSCRIPT
ANATOMIC PATHOLOGY Original Article
Solitary Fibrous Tumor of the Soft Tissue An Immunohistochemical and Ultrastructural Study
TADASHI H A S E G A W A , M D , TAKANORI HIROSE, M D , KUNIHIKO SEKI, M D , PENG YANG, M D , A N D TOSHIAKI SANO, M D
Solitary fibrous tumor is a rare spindle cell neoplasm of adults that usually arises in the pleura, recently reported in other locations. The authors describe three cases of solitary fibrous tumors in adults that occurred as circumscribed masses in the somatic soft tissue, including the arm, back, and abdomen. Histologically, they were characterized by a proliferation of spindle cells separated by thick bands of collagen and prominent vascularity often showing a hemangiopericytoma-like pattern. The spindle cells, having low mitotic figures and little nuclear atypicality, exhibited a variety of growth patterns, including storiform,
Solitary fibrous tumor is a rare spindle cell neoplasm of adults that was first described by Klemperer and Rabin in 1931.' This tumor that usually arises in the pleura2"9 has subsequently been recognized in a variety of sites, including other serosal surfaces: the peritoneum and pericardium,10" 12 and nonserosal sites: the breast,13 thyroid,'4 lung,12'5 mediastinum,1216 orbit,1718 parotid gland,19 upper respiratory tract,20 and nasal cavity and paranasal sinuses.21 Recently, several cases of solitary fibrous tumor have been reported in somatic soft tissues unrelated to serosal surfaces.18'22'23
The tumors occurring at soft parts are poorly recognized and often confused with other neoplasms.
The CD34 antigen, originally expressed on the surface of human hematopoietic progenitor cells, has subsequently been detected in vascular endothelial cells and a diverse group of neoplasms, such as leukemias and vascular, nerve sheath, and smooth muscle neoplasms.24'25 CD34 immu-noreactivity has been found in other miscellaneous lesions, including hemangiopericytomas, epithelioid sarcomas, de-rmatofibrosarcoma protuberans, and solitary fibrous tumors of the pleura and other sites. This marker has been used as an adjuvant in the diagnosis of solitary fibrous tu-
From the First Department of Pathology. University ofTokushima School of Medicine, Tokushima. Japan.
Manuscript received January 10, 1996: revision accepted March 6, 1996.
Address reprint requests to Dr. Tadashi Hasegawa: First Department of Pathology, University ofTokushima School of Medicine, 3-18-15 Kuramoto-cho, Tokushima 770, Japan.
fascicular and herringbone, and nuclear palisading. Vimentin and CD34 immunoreactivities were observed in many spindle cells of all tumors. They had ultrastructural features of fibroblast and myofibroblast in two cases examined. Solitary fibrous tumors seem to represent distinct mesenchymal neoplasms that require us to identify their unusual location other than the pleura and be familiar with their histologic appearances for arriving at the correct diagnosis. (Key words: Solitary fibrous tumor; Soft tissue; CD34; Myofibroblast) Am J Clin Pathol 1996; 106:325-331.
m o r 13.18.19.23.26-28 j n t n j s r e p o r t w e p r e s e n t clinicopatho-logic, immunohistochemical, and ultrastructural features of solitary fibrous tumors of the soft tissue in three patients, and describe its differential diagnosis for distinction from other histologically similar tumors.
MATERIALS AND METHODS
The cases were collected from the files of the First Department of Pathology, University ofTokushima School of Medicine. Representative tissue samples obtained at surgery were fixed in 10% buffered formalin and embedded in paraffin. Sections of 4 |tm thickness were prepared both for staining with hematoxylin-and-eosin and for immunohistochemical examination.
Immunohistochemical staining was accomplished by the labelled streptavidin biotin (LSAB) method with an LSAB kit (Dako, Carpinteria, CA). The primary antibodies that were used in this study were as follows: vimentin (clone V10, 1:10, Dako); cytokeratin (clone CAM5.2, prediluted, Becton Dickinson, San Jose, CA); cytokeratin (clone AE1/AE3, 1: 50, Dako); desmin (clone D33, 1: 50, Dako); epithelial membrane antigen (1: 50, Dako); alpha-smooth muscle actin (clone 1A4, 1: 1000, Biomakor, Kiryat Weizmann, Israel); CD34 (clone My 10, 1: 25, Becton Dickinson); type IV collagen (1: 50, Dako); factor VIII-RAG (1: 50, Dako); S100 protein (1: 4000, Takahashi and colleagues29); and K.i-67 (clone MIB1, 1: 100, Immunotech, Cedex, France). The tissue sections with MIB1 antibody were preheated by a
325
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/106/3/325/1756902 by guest on 29 M
arch 2022
326 ANATOMIC PATHOLOGY Original Article
TABLE 1. SUMMARY OF CLINICAL FINDINGS
Patient No. Age (years) Sex Anatomic Site Size (cm) Clinical Presentation Treatment Follow-up
1 85 F Right upper arm 4 X 3 . 5 X 2 10-year history of painless mass Excision NED, 4.5 years 2 50 M Left back 4 X 3 X 2 2-year history of painless mass Excision NED, 6 months 3 50 F Abdomen 3 X 2 . 5 X 2 5-year history of painless mass Excision Recent case
NED = no evidence of disease.
microwave oven in 10 mM citrate buffer, pH 6.0 for 10 minutes at 90 °C.
Tissues for electron microscopic studies were fixed in 3% glutaraldehyde and processed in the usual manner. Thin sections stained with uranyl acetate and lead citrate were examined with an electron microscope.
RESULTS
Clinical and Radiographic Findings
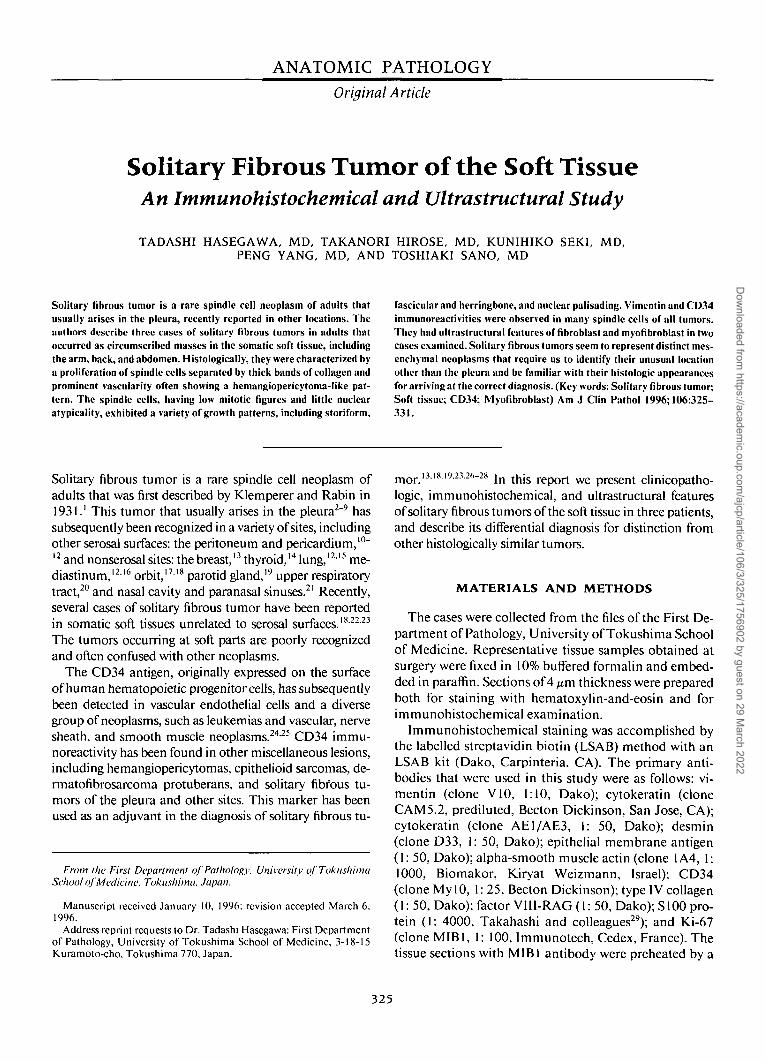
The clinical findings are summarized in Table 1. The patients were 50, 50, and 85 years of age. All three presented with a 2- to 10-year history of painless mass. The masses were located in the arm, back, and abdomen. There was no relevant medical or family history, and laboratory findings were within normal limits on these patients. Computed tomography available in cases 1 and 3 showed well-defined, noncalcified homogeneous density or mass in the subcutis. Magnetic resonance imaging in case 1 showed a well-circumscribed, subcutaneous soft
FIG. 1. Sagital T1 -weighted magnetic resonance imaging after gadolinium injection in case 1 showing a well-circumscribed mass with inho-mogeneous signal enhancement in the subcutis adjacent to the triceps.
tissue mass closely attached to the triceps. The tumor had intermediate signal intensity on Tl-weighted images and high signal intensity on T2-weighted images. A minimal increase in signal intensity was present on gadolin-ium-DTPA-enhanced Tl-weighted images (Fig. 1). The masses were treated by excision, with no evidence of tumor invasion of adjacent soft tissue at the time of surgery. Except for the recent case 3, two patients have no evidence of disease or recurrence of symptoms from 6 months to 4.5 years following surgery.
Pathologic Findings
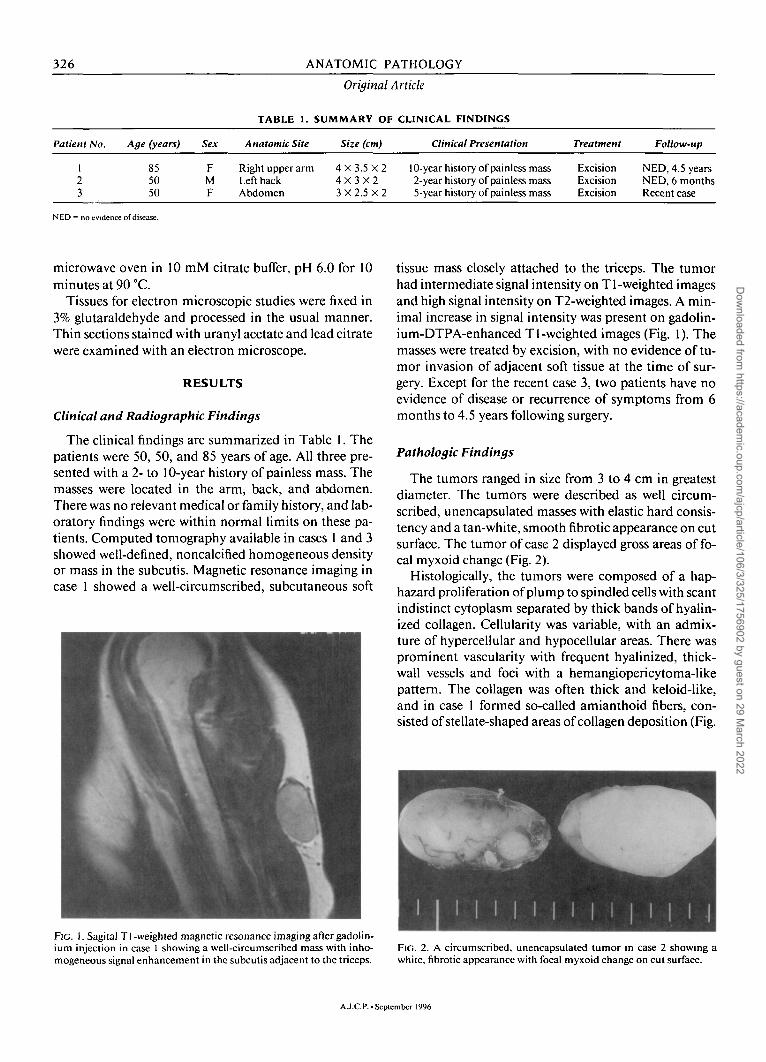
The tumors ranged in size from 3 to 4 cm in greatest diameter. The tumors were described as well circumscribed, unencapsulated masses with elastic hard consistency and a tan-white, smooth fibrotic appearance on cut surface. The tumor of case 2 displayed gross areas of focal myxoid change (Fig. 2).
Histologically, the tumors were composed of a haphazard proliferation of plump to spindled cells with scant indistinct cytoplasm separated by thick bands of hyalin-ized collagen. Cellularity was variable, with an admixture of hypercellular and hypocellular areas. There was prominent vascularity with frequent hyalinized, thick-wall vessels and foci with a hemangiopericytoma-like pattern. The collagen was often thick and keloid-like, and in case 1 formed so-called amianthoid fibers, consisted of stellate-shaped areas of collagen deposition (Fig.
FIG. 2. A circumscribed, unencapsulated tumor in case 2 showing a white, fibrotic appearance with focal myxoid change on cut surface.
A.J.C.P. •September 1996
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/106/3/325/1756902 by guest on 29 M
arch 2022
HASEGAWA ET AL. 327
Solitary Fibrous
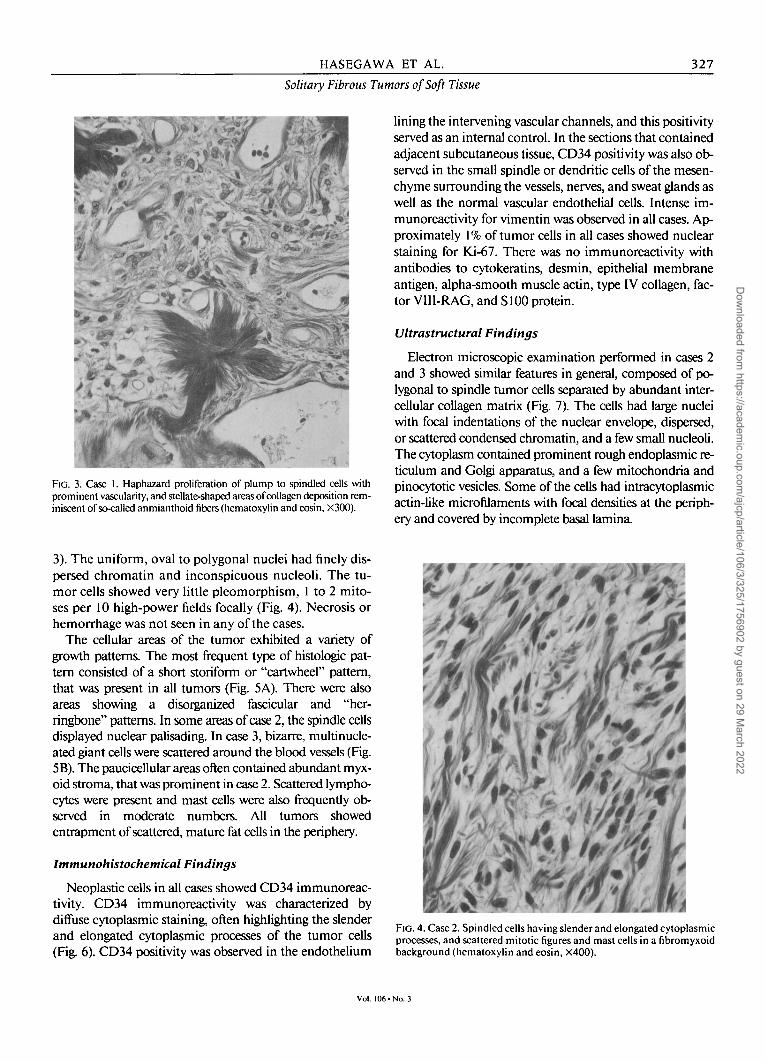
FIG. 3. Case 1. Haphazard proliferation of plump to spindled cells with prominent vascularity, and stellate-shaped areas of collagen deposition reminiscent of so-called anmianthoid fibers (hematoxylin and eosin, X300).
3). The uniform, oval to polygonal nuclei had finely dispersed chromatin and inconspicuous nucleoli. The tumor cells showed very little pleomorphism, 1 to 2 mitoses per 10 high-power fields focally (Fig. 4). Necrosis or hemorrhage was not seen in any of the cases.
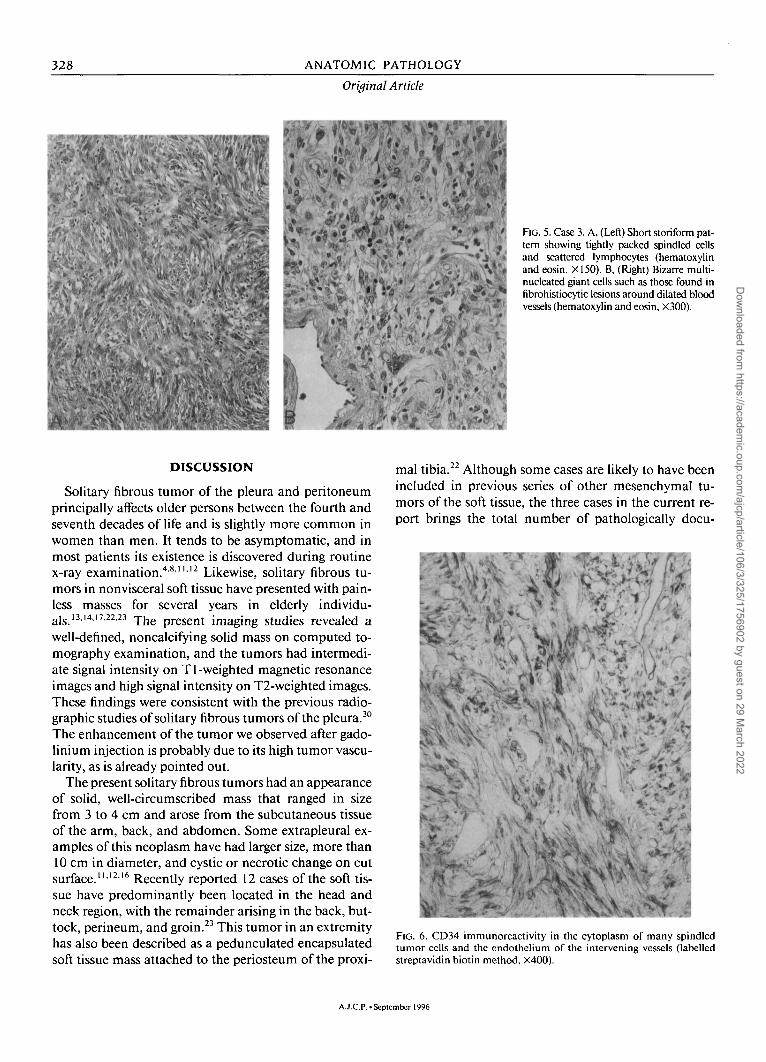
The cellular areas of the tumor exhibited a variety of growth patterns. The most frequent type of histologic pattern consisted of a short storiform or "cartwheel" pattern, that was present in all tumors (Fig. 5A). There were also areas showing a disorganized fascicular and "herringbone" patterns. In some areas of case 2, the spindle cells displayed nuclear palisading. In case 3, bizarre, multinucleated giant cells were scattered around the blood vessels (Fig. 5B). The paucicellular areas often contained abundant myxoid stroma, that was prominent in case 2. Scattered lymphocytes were present and mast cells were also frequently observed in moderate numbers. All tumors showed entrapment of scattered, mature fat cells in the periphery.
Immunohistochemical Findings
Neoplastic cells in all cases showed CD34 immunoreac-tivity. CD34 immunoreactivity was characterized by diffuse cytoplasmic staining, often highlighting the slender and elongated cytoplasmic processes of the tumor cells (Fig. 6). CD34 positivity was observed in the endothelium
Vol. 11
tors of Soft Tissue
lining the intervening vascular channels, and this positivity served as an internal control. In the sections that contained adjacent subcutaneous tissue, CD34 positivity was also observed in the small spindle or dendritic cells of the mesenchyme surrounding the vessels, nerves, and sweat glands as well as the normal vascular endothelial cells. Intense immunoreactivity for vimentin was observed in all cases. Approximately 1% of tumor cells in all cases showed nuclear staining for Ki-67. There was no immunoreactivity with antibodies to cytokeratins, desmin, epithelial membrane antigen, alpha-smooth muscle actin, type IV collagen, factor VIII-RAG, and SI00 protein.
Ultrastructural Findings
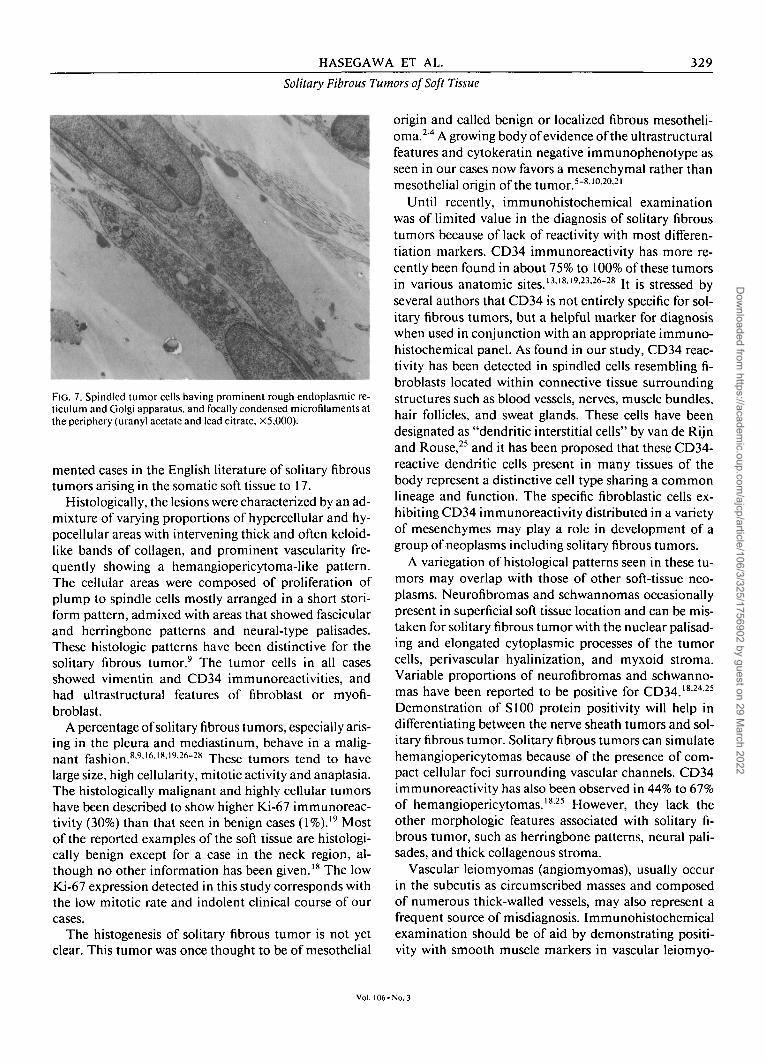
Electron microscopic examination performed in cases 2 and 3 showed similar features in general, composed of polygonal to spindle tumor cells separated by abundant intercellular collagen matrix (Fig. 7). The cells had large nuclei with focal indentations of the nuclear envelope, dispersed, or scattered condensed chromatin, and a few small nucleoli. The cytoplasm contained prominent rough endoplasmic reticulum and Golgi apparatus, and a few mitochondria and pinocytotic vesicles. Some of the cells had intracytoplasmic actin-like microfilaments with focal densities at the periphery and covered by incomplete basal lamina.
FIG. 4. Case 2. Spindled cells having slender and elongated cytoplasmic processes, and scattered mitotic figures and mast cells in a fibromyxoid background (hematoxylin and eosin, X400).
• No. 3
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/106/3/325/1756902 by guest on 29 M
arch 2022
328 A N A T O M I C P A T H O L O G Y
FIG. 5. Case 3. A, (Left) Short storiform pattern showing tightly packed spindled cells and scattered lymphocytes (hematoxylin and eosin, XI50). B, (Right) Bizarre multinucleated giant cells such as those found in fibrohistiocytic lesions around dilated blood vessels (hematoxylin and eosin, X300).
DISCUSSION
Solitary fibrous tumor of the pleura and peritoneum principally affects older persons between the fourth and seventh decades of life and is slightly more common in women than men. It tends to be asymptomatic, and in most patients its existence is discovered during routine x-ray examination.4-8"'2 Likewise, solitary fibrous tumors in nonvisceral soft tissue have presented with painless masses for several years in elderly individu-als_ i3, i4.17,22.23 y^e p r e s e n t imaging studies revealed a
well-defined, noncalcifying solid mass on computed tomography examination, and the tumors had intermediate signal intensity on T1 -weighted magnetic resonance images and high signal intensity on T2-weighted images. These findings were consistent with the previous radiographic studies of solitary fibrous tumors of the pleura.30
The enhancement of the tumor we observed after gadolinium injection is probably due to its high tumor vascularity, as is already pointed out.
The present solitary fibrous tumors had an appearance of solid, well-circumscribed mass that ranged in size from 3 to 4 cm and arose from the subcutaneous tissue of the arm, back, and abdomen. Some extrapleural examples of this neoplasm have had larger size, more than 10 cm in diameter, and cystic or necrotic change on cut surface."1216 Recently reported 12 cases of the soft tissue have predominantly been located in the head and neck region, with the remainder arising in the back, buttock, perineum, and groin.23 This tumor in an extremity has also been described as a pedunculated encapsulated soft tissue mass attached to the periosteum of the proxi
mal tibia.22 Although some cases are likely to have been included in previous series of other mesenchymal tumors of the soft tissue, the three cases in the current report brings the total number of pathologically docu-
^ar^Vv^?1
Z--*>*%•'* v * , v . * > J * • • -, * . *-• • • ;
JLIati*" FIG. 6. CD34 immunoreactivity in the cytoplasm of many spindled tumor cells and the endothelium of the intervening vessels (labelled streptavidin biotin method, X400).
A.J.C.P.-September 1996
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/106/3/325/1756902 by guest on 29 M
arch 2022
HASEGAWA ET AL. 329
Solitary Fibrous Tumors of Soft Tissue
FIG. 7. Spindled tumor cells having prominent rough endoplasmic reticulum and Golgi apparatus, and focally condensed microfilaments at the periphery (uranyl acetate and lead citrate. X5.000).
mented cases in the English literature of solitary fibrous tumors arising in the somatic soft tissue to 17.
Histologically, the lesions were characterized by an admixture of varying proportions of hypercellular and hy-pocellular areas with intervening thick and often keloid-like bands of collagen, and prominent vascularity frequently showing a hemangiopericytoma-like pattern. The cellular areas were composed of proliferation of plump to spindle cells mostly arranged in a short stori-form pattern, admixed with areas that showed fascicular and herringbone patterns and neural-type palisades. These histologic patterns have been distinctive for the solitary fibrous tumor.9 The tumor cells in all cases showed vimentin and CD34 immunoreactivities, and had ultrastructural features of fibroblast or myofibroblast.
A percentage of solitary fibrous tumors, especially arising in the pleura and mediastinum, behave in a malignant fashion.8-9'6'819-26"28 These tumors tend to have large size, high cellularity, mitotic activity and anaplasia. The histologically malignant and highly cellular tumors have been described to show higher Ki-67 immunoreac-tivity (30%) than that seen in benign cases (1%).19 Most of the reported examples of the soft tissue are histologically benign except for a case in the neck region, although no other information has been given.18 The low Ki-67 expression detected in this study corresponds with the low mitotic rate and indolent clinical course of our cases.
The histogenesis of solitary fibrous tumor is not yet clear. This tumor was once thought to be of mesothelial
origin and called benign or localized fibrous mesothelioma.2"4 A growing body of evidence of the ultrastructural features and cytokeratin negative immunophenotype as seen in our cases now favors a mesenchymal rather than mesothelial origin of the tumor.5"8'I0'20'21
Until recently, immunohistochemical examination was of limited value in the diagnosis of solitary fibrous tumors because of lack of reactivity with most differentiation markers. CD34 immunoreactivity has more recently been found in about 75% to 100% of these tumors in various anatomic sites.131819'2326"28 It is stressed by several authors that CD34 is not entirely specific for solitary fibrous tumors, but a helpful marker for diagnosis when used in conjunction with an appropriate immunohistochemical panel. As found in our study, CD34 reactivity has been detected in spindled cells resembling fibroblasts located within connective tissue surrounding structures such as blood vessels, nerves, muscle bundles, hair follicles, and sweat glands. These cells have been designated as "dendritic interstitial cells" by van de Rijn and Rouse,25 and it has been proposed that these CD34-reactive dendritic cells present in many tissues of the body represent a distinctive cell type sharing a common lineage and function. The specific fibroblastic cells exhibiting CD34 immunoreactivity distributed in a variety of mesenchymes may play a role in development of a group of neoplasms including solitary fibrous tumors.
A variegation of histological patterns seen in these tumors may overlap with those of other soft-tissue neoplasms. Neurofibromas and schwannomas occasionally present in superficial soft tissue location and can be mistaken for solitary fibrous tumor with the nuclear palisading and elongated cytoplasmic processes of the tumor cells, perivascular hyalinization, and myxoid stroma. Variable proportions of neurofibromas and schwannomas have been reported to be positive for CD34.'8-24'25
Demonstration of SI00 protein positivity will help in differentiating between the nerve sheath tumors and solitary fibrous tumor. Solitary fibrous tumors can simulate hemangiopericytomas because of the presence of compact cellular foci surrounding vascular channels. CD34 immunoreactivity has also been observed in 44% to 67% of hemangiopericytomas.18'25 However, they lack the other morphologic features associated with solitary fibrous tumor, such as herringbone patterns, neural palisades, and thick collagenous stroma.
Vascular leiomyomas (angiomyomas), usually occur in the subcutis as circumscribed masses and composed of numerous thick-walled vessels, may also represent a frequent source of misdiagnosis. Immunohistochemical examination should be of aid by demonstrating positivity with smooth muscle markers in vascular leiomyo-
Vol. 106-No. 3
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/106/3/325/1756902 by guest on 29 M
arch 2022

330 ANATOMIC PATHOLOGY
Original Article
mas. Solitary fibrous tumors of the breast have been described to show morphologic similarities to so-called myofibroblastomas arising in the same region,16 and muscular differentiation with actin and/or desmin im-munophenotypes, along with CD34 positivity.13
The frequent storiform pattern coupled with the occasional presence of bizarre giant cells seen in solitary fibrous tumors may raise the question of benign or malignant fibrous histiocytoma in the differential diagnosis. However, the present tumors are histologically distinguishable from malignant fibrous histiocytoma on the basis of a low mitotic rate, and the absence of nuclear atypia and areas of necrosis. Benign fibrohistiocytic tumors having histologic appearances similar to their cutaneous counterparts have been known to occur in subcutaneous and deep soft tissues.31 They present as painless, circumscribed masses, and have a more consistent storiform pattern and fewer secondary elements such as xanthoma cells. The tumors occasionally display myxoid change or hyalinization in the stroma, and a hemangio-pericytoma-like vascular pattern. From these morphologic features, the distinction between solitary fibrous tumor and fibrous histiocytoma could be difficult in some instances. Immunohistochemical absence of CD34 in fibrous histiocytomas serves to separate these two le-sions.
Spindle cell lipoma may occur as a circumscribed, painless, firm nodule in the subcutis of the posterior neck and shoulder of middle-aged male patients as in our case 2.32 It is composed of a mixture of mature fat cells and uniform spindle cells that are closely associated with a mucoid matrix and bundles of collagen. In view of the recent report of CD34 expression in a variety of cell types and tumors including giant cell angiofibromas,33 it is not surprising that spindle cell lipoma is also CD34 positive (unpublished observation). However, the entrapped adipocytes seen in our cases form a minor component at the periphery of the tumors. Spindle cell lipoma usually lacks other specific histologic features for solitary fibrous tumors, as described subsequently.
In summary, solitary fibrous tumors seem to represent distinct mesenchymal neoplasms that should be included into a group of benign fibro/myofibroblastic tumors of the soft tissue. Awareness of the different histologic patterns as well as the classic appearance that they may exhibit plus attention to their unusual location other than the pleura and macroscopic features are therefore important for accurate diagnosis.
REFERENCES
1. Klemperer P, Rabin CB. Primary neoplasm of the pleura: A report of five cases. A rch Pathol 1931; 11:385-412.
2. Stout AP, Murray MR. Localized pleural mesothelioma: Investigation of its characteristics and histogenesis by the method of tissue culture. Arch Pathol 1942; 34:951-964.
3. Kawai T, Mikata A, Torikata C, et al. Solitary (localized) pleural mesothelioma: A light- and electron-microscopic study. Am J Surg Pathol 1978;2:365-375.
4. Briselli M, Mark EJ, Dickersin GR. Solitary fibrous tumors of the pleura: Eight new cases and review of 360 cases in the literature. Cancer 1981;47:2678-2689.
5. Bu'rrig K, Kastendieck H. Ultrastructural observations on the histogenesis of localized fibrous tumours of the pleura (benign mesothelioma). VirchowsArch 1984;403:413-424.
6. Said JW, Nash G, Banks-Schlegel S, Sassoon F, Shintaku IP. Localized fibrous mesothelioma: An immunohistochemical and electron microscopic study. Hum Pathol 1984; 15:440-443.
7. Dervan PA, Tobin B, O'Connor M. Solitary (localized) fibrous mesothelioma: Evidence against mesothelial cell origin. Histopa-thology 1986; 10:867-875.
8. England DM, Hochholzer L, McCarthy MJ. Localized benign and malignant fibrous tumors of the pleura: A clinicopathologic review of 223 cases. Am J Surg Pathol 1989; 13:640-58.
9. Moran CA. Suster S, Koss MN. The spectrum of histologic growth patterns in benign and malignant fibrous tumors of the pleura. Semin Diagn Pathol 1992; 9:169-80.
10. El-Naggar AK, Ro JY, Ayala AG, Ward R, Ordonez NG. Localized fibrous tumor of the serosal cavities: Immunohistochemical, electron-microscopic, and flow-cytometric DNA study. Am J Clin Pathol 1989;92:561-65.
11. Young RH, Clement PB, McCaughey WTE. Solitary fibrous tumors (fibrous mesotheliomas) of the peritoneum: A report of three cases and a review of the literature. Arch Pathol Lab Med 1990;114:493-95.
12. Goodlad JR. Fletcher CDM. Solitary fibrous tumour arising at unusual sites: Analysis of a series. Histopathologv 1991; 19:515— 22.
13. Damiani S. Miettinen M, Peterse JL, Eusebi V. Solitary fibrous tumour (myofibroblastoma) of the breast. Virchows Archiv 1994;425:89-2.
14. Cameselle-Teijeiro J. Varela-Duran J, Fonseca E, Villanueva JP, Sobrinho-Simoes M. Solitary fibrous tumor of the thyroid. Am J Clin Pathol 1994; 101:535-38.
15. Yousem SA. Flynn SD. Intrapulmonary localized fibrous tumor: Intraparenchymal so-called localized fibrous mesothelioma. Am J Clin Pathol 1988;89:365-69.
16. WitkinGB, Rosai J. Solitary fibrous tumor of the mediastinum: A report of 14 cases. Am J Surg Pathol 1989; 13:547-57.
17. Dorfman DM, To K, Dickersin GR, Rosenberg AE, Pilch BZ. Solitary fibrous tumor of the orbit. Am J Surg Pathol 1994; 18:281-7.
18. Westra WH, Gerald WL, Rosai J. Solitary fibrous tumor: Consistent CD34 immunoreactivity and occurrence in the orbit. Am J Surg Pathol 1994; 18:992-98.
19. Hanau CA, Miettinen M. Solitary fibrous tumor: Histological and immunohistochemical spectrum of benign and malignant variants presenting at different sites. Hum Pathol 1995;26:440-49.
20. Witkin GB, Rosai J. Solitary fibrous tumor of the upper respiratory tract: A report of six cases. Am J Surg Pathol 1991; 15:842-48.
21. Zukerberg LR, Rosenberg AE, Randolph G, Pilch BZ, Goodman ML. Solitary fibrous tumor of the nasal cavity and paranasal sinuses. Am J Surg Pathol 1991; 15:126-30.
22. O'Connell JX, Logan PM, Beauchamp CP. Solitary fibrous tumor of the periosteum. Hum Pathol 1995;26:460-62.
23. Suster S, Nascimento AG, Miettinen M, Sickel JZ, Moran CA. Solitary fibrous tumors of soft tissue: A clinicopathologic and immunohistochemical study of 12 cases. Am J Surg Pathol 1995;19:1257-266.
24. Weiss SW, Nickoloff BJ. CD-34 is expressed by a distinctive cell population in peripheral nerve, nerve sheath tumors, and related lesions. Am J Surg Pathol 1993; 17:1039-045.
A.J.C.P.- September 1996
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/106/3/325/1756902 by guest on 29 M
arch 2022

HASEGAWA ET AL. 331
Solitary Fibrous Tumors of Soft Tissue
25. van de Rijn M, Rouse R. CD34: A review. AppI Immunohislochem 1994;2:71-0.
26. Renshaw AA, PinkusGS, Corson JM. CD34and AE1/AE3: Diagnostic discriminants in the distinction of solitary fibrous tumor of the pleura from sarcomatoid mesothelioma. AppI Immunohislochem 1994;2:94-02.
27. van de Rijn M, Lombard CM, Rouse RV. Expression of CD34 by solitary fibrous tumors of the pleura, mediastinum, and lung. Am J Surg Pathol 1994; 18:814-20.
28. Flint A, Weiss SW. CD-34 and keratin expression distinguishes solitary fibrous tumor (fibrous mesothelioma) of pleura from desmoplastic mesothelioma. Hum Pathol 1995;26:428-31.
29. Takahashi K, Yamaguchi H, Ishizeki J, Nakajima T, Nakazato Y. Immunohistochemical and immunoelectron micro
scopic localization of S-100 protein in the interdigitating reticulum cells of the human lymph node. Virchows Arch 1981;37:125-35.
30. George JC. Benign fibrous mesothelioma of the pleura: MR findings. Am J Roentgenol 1993; 160:204-05.
31. Fletcher CDM. Benign fibrous histiocytoma of subcutaneous and deep soft tissue: A clinicopathologic analysis of 21 cases. Am J Surg Pathol 1990; 14:801-09.
32. Enzinger FM, Weiss SW. Soft Tissue Tumors, ed 3. St. Louis: Mosby, 1995.
33. Dei Tos AP, Seregard S, Calonje E, Chan JKC. Fletcher CDM. Giant cell angiofibroma: A distinctive orbital tumor in adults. Am J Surg Pathol 1995; 19:1286-293.
Vol. 106-No. 3
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/106/3/325/1756902 by guest on 29 M
arch 2022