sims' symptoms in the mind
TRANSCRIPT
Sims’ Symptoms in the Mind

For my father, Jonathan Akinyemi Oyebode (1918–1971)
Femi Oyebode
Content Strategist: Jeremy BowesContent Development Specialist: Helen LengProject Manager: Joanna SouchDesigner: Miles HitchenIllustration Manager: Deena BurgessIllustrator: David Graham
The publisher’s policy is to use paper manufactured from sustainable forests
SIMS’ SYMPTOMS IN THE MINDTextbook of Descriptive Psychopathology
FEMI OYEBODE MBBS, MD, PHD, FRCPSYCHProfessor of Psychiatry & Consultant PsychiatristUniversity of Birmingham, National Centre for Mental HealthBirmingham, UK
F I F T H E D I T I O N
Edinburgh London New York Oxford Philadelphia St Louis Sydney Toronto 2015

© 2015 Elsevier Ltd. All rights reserved.
No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, or any information storage and retrieval system, without permission in writing from the publisher. Details on how to seek permission, further information about the publisher’s permissions policies and our arrangements with organizations such as the Copyright Clearance Center and the Copyright Licensing Agency, can be found at our website: www.elsevier.com/permissions.
This book and the individual contributions contained in it are protected under copyright by the publisher (other than as may be noted herein).
First edition 1988Second edition 1995Third edition 2005Fourth edition 2008Fifth edition 2015
ISBN 978-0-7020-5556-0
British Library Cataloguing in Publication DataA catalogue record for this book is available from the British Library
Library of Congress Cataloging in Publication DataA catalog record for this book is available from the Library of Congress
NoticesKnowledge and best practice in this field are constantly changing. As new research and experience broaden our understanding, changes in research methods, professional practices, or medical treatment may become necessary.
Practitioners and researchers must always rely on their own experience and knowledge in evaluating and using any information, methods, compounds, or experiments described herein. In using such information or methods they should be mindful of their own safety and the safety of others, including parties for whom they have a professional responsibility.
With respect to any drug or pharmaceutical products identified, readers are advised to check the most current information provided (i) on procedures featured or (ii) by the manufacturer of each product to be administered, to verify the recommended dose or formula, the method and duration of administration, and contraindications. It is the responsibility of practitioners, relying on their own experience and knowledge of their patients, to make diagnoses, to determine dosages and the best treatment for each individual patient, and to take all appropriate safety precautions.
To the fullest extent of the law, neither the publisher nor the authors, contributors, or editors, assume any liability for any injury and/or damage to persons or property as a matter of products liability, negligence or otherwise, or from any use or operation of any methods, products, instructions, or ideas contained in the material herein.
Printed in China
Proudly sourced and uploaded by [StormRG] Kickass Torrents | TPB | ET | h33t
v
C O N T E N T S
Preface to the Fifth Edition vii
Additional Materials within Accompanying Electronic Version viii
SECTION ONE Concepts and Method 1
1 Fundamental Concepts of Descriptive Psychopathology 3
2 Eliciting the Symptoms of Mental Illness 19
SECTION TWO Consciousness and Cognition 31
3 Consciousness and Disturbed Consciousness 33
4 Attention, Concentration, Orientation and Sleep 45
5 Disturbance of Memory 59
SECTION THREE Awareness of Reality: Time, Perception and Judgement 73
6 Disorder of Time 75
7 Pathology of Perception 87
8 Delusions and Other Erroneous Ideas 111
9 Disorder of the Thinking Process 139
10 Disorder of Speech and Language 159
11 Insight 175
SECTION FOUR Self and Body 185
12 The Disordered Self 187
13 Depersonalization 205
14 Disorder of the Awareness of the Body 217
15 The Psychopathology of Pain 245
SECTION FIVE Emotions and Action 255
16 Affect and Emotional Disorders 257
17 Anxiety, Panic, Irritability, Phobia and Obsession 279
18 Disorders of Volition and Execution 293
vi Contents
SECTION SIX Variations of Human Nature 315
19 The Expression of Disordered Personality 317
SECTION SEVEN Diagnosis 331
20 Psychopathology and Diagnosis 333
Self-Assessment 1 345
Self-Assessment 2 353
Self-Assessment 1: Answers 359
Self-Assessment 2: Answers 363
Index 367
vii
P R E F A C E T O T H E F I F T H E D I T I O N
Sims’ Symptoms in the Mind has, since its first publication in 1988, become established as theleadingtextbookonclinicalpsychopathology.Inthisnewfifthedition,asinthefourthedition,Ihave retained theoriginal structureof thebookbutmadesomechanges.Thereare shifts inemphasisandnewmaterialinanumberofchapters.Easilyrecognizablemodificationsareevidentinthechaptersondisturbanceofmemory,disorderoftime,pathologyofperception,disorderofspeechandlanguage,affectandemotionaldisorders,anddisordersofvolitionandexecution.Inthemainthesehavebeenpromptedbyadesiretoincorporateadvancesfromneuropsychologyandcognitiveneuroscience.InsomecasesIhaveprovidednovelclassificationsoftheabnormali-tiesunderconsideration.Additionalpathologicalphenomenaaredescribedinvariouschapters.Thesephenomenaincludesuchexperiencesaspalinopsia,palinaptia,teleopsia,pelopsia,akine-topsia,zëitrafferphenomenon,exosomesthesia,synaesthesia,bodyintegritydisorder,vulvodynia,penoscrotodyniaandmanyothers.
Inthisnewedition,Ihavebroughtuptodatemanyoftheconceptsanddescriptionsinvariouschapters.Ihavetriedtoreducetheoverlapinsubjectmatterbutitisimpossibletodoawaywithrepetitionsentirely.Someconcepts,suchaspassivityexperiencesforexample,arebetterunder-stood from different perspectives. However, the main innovation is in the accompanying filmclipsandpodcaststhatextendtherangeofwhatitispossibletoincludeinatextandthatallowmetoillustratecomplexideasbothvisuallyandaurally.OneofthedistinctivefeaturesofSims’ Symptoms in the Mindhasbeenitsuseoffigures,tablesandillustrativecaseexamples.Ihavekepttothisandaddedboxesandadditionalcaseexamplesfromtheclassicalliterature,autobiographi-calnarrativesandfiction.
IhavebeenconsciousofthecentenaryofKarlJaspers’General Psychopathologywhilstpreparingthisneweditionforpublication.Descriptivepsychopathology,asamethod,hasenduredthepast100years.Itisthepre-eminentfoundationforthepracticeofclinicalpsychiatry.Thismethodallowsustoobserveanddescribeabnormalsubjectivephenomenaandbehaviours,andtocatego-rize these inorder to communicatemoreprecisely about theworld thatpatients inhabit.Thecliniciantrainedinthephenomenologicalapproachisallthemoreawareoftheneedforempathicunderstanding, forassuminganatheoretical stance,andfinallyof theprovisional statusofourunderstandingandexplanationsregardingpsychopathology.
I am indebted to many more people than I can list.The Birmingham Philosophy Grouphas been meeting monthly since 1992. Its members continue to influence my thinking aboutpsychiatricphenomenaasdothemembersoftheEuropeanPsychiatricAssociationSectionofPsychopathology including John Cutting, Maria Luisa Figueira, Mircea Lazarescu, MichaelMusalek,GilbertodiPettaandPedroVarandas.Finally,withoutthepatientswhoexperienceandenduretheseabnormalphenomena,andthestudentsandpsychiatrictraineeswhoaskawkwardquestionsandoutofcuriosityenquireintothenatureofthesephenomena,thisbookwoulddefi-nitelybethepoorer.
Femi Oyebode
viii
The searchable full text for ‘Sims’ Symptoms in the Mind 5E’ is available at www.expertconsult.com, accessible via the enclosed pin code. Please follow the instructions on the inside front cover of this book. Additional materials integrated within this enhanced electronic version include:
■ Four patient scenarios (videos with transcripts), exploring:1. auditory verbal hallucinations2. persecutory delusion3. low mood4. obsessive compulsive phenomenon
Look out for alongside the related sections within this book.■ Six author podcasts on the following topics:
1. What is psychopathology?2. What are hallucinations?3. Critique of the nature of delusions4. The nature of obsessions5. The self in psychopathology6. Affect, mood and emotions
Look out for alongside the related sections within this book.■ Interactive question-and-answer sections for each chapter to test your understanding of key
topics.
ADDITIONAL MATERIALS WITHIN ACCOMPANYING ELECTRONIC VERSION
S E C T I O N ONEConcepts and Method

This page intentionally left blank
3
C H A P T E R 1
Fundamental Concepts of Descriptive Psychopathology
SummaryDescriptivepsychopathologyistheprecisedescription,categorizationanddefinitionofabnormalexperiencesasrecountedbythepatientandobservedinhisbehaviour.Itreliesonthemethodofphenomenologybyfocusingonexperiencedphenomenainordertoestablishtheiruniversalcharacter.Theaimistolistenattentively,toaccuratelyobserveandtounderstandthepsychologi-caleventorphenomenonbyempathysothatthecliniciancan,asfaraspossible,knowforhimselfwhatthepatient’sexperiencemustfeellike.
How the mind should be conceived for the purposes of psychopathology, what its faculties, functions or elements are (if there are any), how these can be
distinguished, and how mental disorders can be comprehended by an application of these concepts are philosophical questions.
Manfred Spitzer (1990)
Psychiatry is thatbranchofmedicinethatdealswithmorbidpsychologicalexperiences.Bydefinition,inthemedicalconditionsthatarecentraltopsychiatricpractice,psychologicalphe-nomenaareimportantascauses,symptomsandobservableclinicalsignsandalsoastherapeuticagents.The scopeof psychiatry canbe said to includeminor emotional disturbances that aremeaningfulreactionstoenvironmentalorpsychosocialstress;profoundpsychologicalchangethatisunheraldedbysignificantormeaningfulstress;disturbancesofpersonalitythathaveapervasiveinfluence on behaviour such that the person or others suffer; psychological changes that aredirectlytheconsequencesofdemonstrableorganicbrainchange;andpsychologicalandbehav-iouralconsequencesoftheuseofsubstancessuchasalcohol,cannabis,cocaineorheroin.Inordertodescribe,delineateanddifferentiate these conditions, themorbidpsychologicalphenomenathat constitute the subjective experienceofpatientsneed tobe carefully assessed, elicited andrecorded.This is the territoryofdescriptivepsychopathology. Inotherwords,descriptivepsy-chopathology is concerned with the selection, delimitation, differentiation and description ofparticularphenomenaofexperience,whichthroughtheuseofacceptedterminologybecomebothdefinedandcapableofrepeatedidentification.
Itcanbesaid thatdescriptivepsychopathology is the fundamentalprofessional skillof thepsychiatrist;itis,possibly,theonlydiagnosticskilluniquetothepsychiatrist.Itisconsiderablymore than just carrying out a clinical interview of a patient, or even listening to the patient,althoughitnecessarily involvesbothofthese.Itsaccurateapplicationinvolvesthedeploymentofempathyandunderstanding(weshallreturntotheselater).Ofcourse,fortherationalpracticeofpsychiatrythereisaneedforknowledgeofthebasicneurosciences;appropriatefactualknowl-edge of psychology, sociology and social anthropology is also required.With these, there is a

Keywords:Descriptivepsychopathology,Phenomenology,Norms,Subjectivity.
1—FuNDAMENTAl CONCEPTS OF DESCriPTivE PSyCHOPATHOlOgy 3.e1
4 ONE—CONCEPTS AND METHOD
need for a comprehensive working knowledge of general medicine, especially neurology andendocrinology.Thiscouldbeconsideredtobetheminimumknowledgebasethatisessentialforpractisingpsychiatry.However,itisdescriptivepsychopathologythatprovidesthefoundationofclinical psychiatric practice. The subjective phenomena that are revealed during the clinicalassessment, coupled with observable behaviours, ultimately determine the clinical judgementsthatinfluencetreatmentandmanagementdecisions.
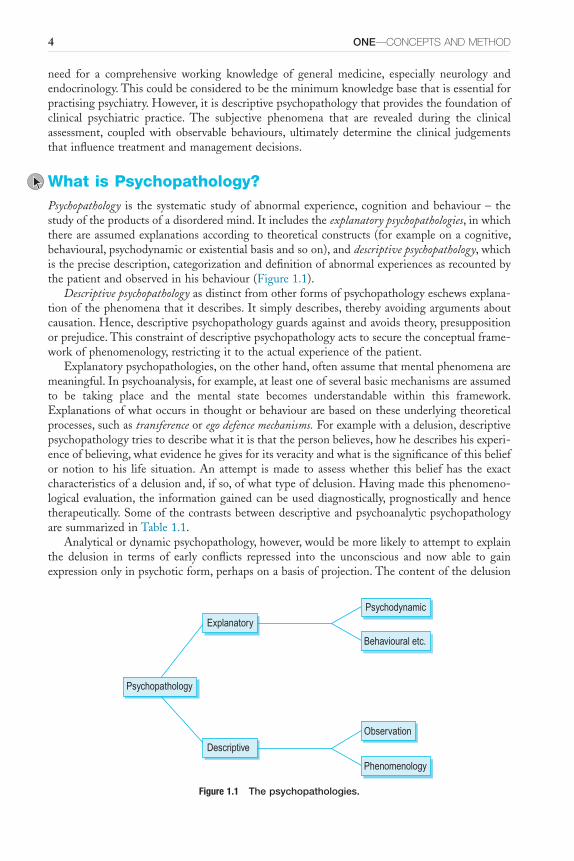
What is Psychopathology?Psychopathology is the systematic studyof abnormalexperience, cognitionandbehaviour– thestudyoftheproductsofadisorderedmind.Itincludestheexplanatory psychopathologies,inwhichthereareassumedexplanationsaccordingtotheoreticalconstructs(forexampleonacognitive,behavioural,psychodynamicorexistentialbasisandsoon),anddescriptive psychopathology,whichistheprecisedescription,categorizationanddefinitionofabnormalexperiencesasrecountedbythepatientandobservedinhisbehaviour(Figure1.1).
Descriptive psychopathologyasdistinctfromotherformsofpsychopathologyeschewsexplana-tionofthephenomenathatitdescribes.Itsimplydescribes,therebyavoidingargumentsaboutcausation.Hence,descriptivepsychopathologyguardsagainstandavoidstheory,presuppositionorprejudice.Thisconstraintofdescriptivepsychopathologyactstosecuretheconceptualframe-workofphenomenology,restrictingittotheactualexperienceofthepatient.
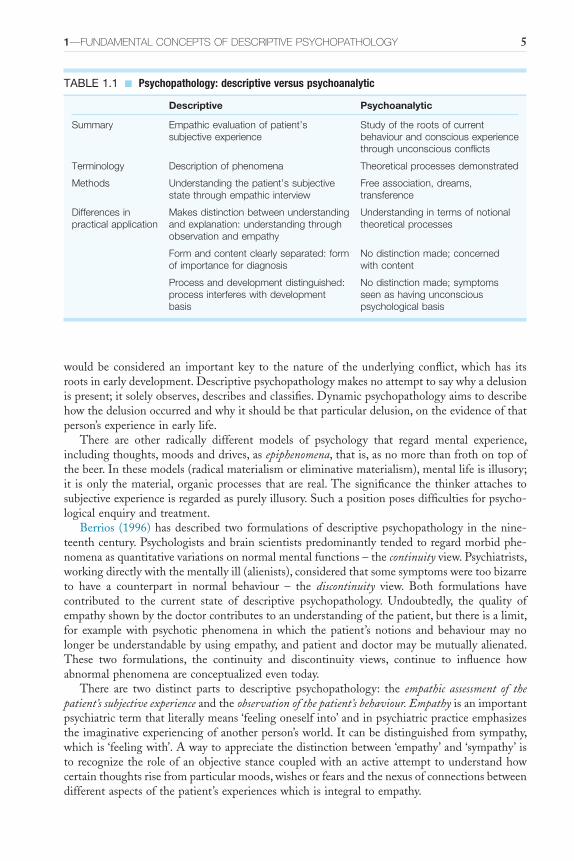
Explanatorypsychopathologies,ontheotherhand,oftenassumethatmentalphenomenaaremeaningful.Inpsychoanalysis,forexample,atleastoneofseveralbasicmechanismsareassumedto be taking place and the mental state becomes understandable within this framework.Explanationsofwhatoccursinthoughtorbehaviourarebasedontheseunderlyingtheoreticalprocesses,suchastransferenceorego defence mechanisms.Forexamplewithadelusion,descriptivepsychopathologytriestodescribewhatitisthatthepersonbelieves,howhedescribeshisexperi-enceofbelieving,whatevidencehegivesforitsveracityandwhatisthesignificanceofthisbeliefornotion tohis life situation.Anattempt ismade to assesswhether thisbeliefhas the exactcharacteristicsofadelusionand,ifso,ofwhattypeofdelusion.Havingmadethisphenomeno-logicalevaluation, the informationgainedcanbeuseddiagnostically,prognosticallyandhencetherapeutically.SomeofthecontrastsbetweendescriptiveandpsychoanalyticpsychopathologyaresummarizedinTable1.1.
Analyticalordynamicpsychopathology,however,wouldbemorelikelytoattempttoexplainthe delusion in terms of early conflicts repressed into the unconscious and now able to gainexpressiononlyinpsychoticform,perhapsonabasisofprojection.Thecontentofthedelusion
Figure 1.1 The psychopathologies.
Explanatory
Descriptive
Psychopathology
Psychodynamic
Behavioural etc.
Observation
Phenomenology
1—FuNDAMENTAl CONCEPTS OF DESCriPTivE PSyCHOPATHOlOgy 5
wouldbe considered an importantkey to thenatureof theunderlying conflict,whichhas itsrootsinearlydevelopment.Descriptivepsychopathologymakesnoattempttosaywhyadelusionispresent;itsolelyobserves,describesandclassifies.Dynamicpsychopathologyaimstodescribehowthedelusionoccurredandwhyitshouldbethatparticulardelusion,ontheevidenceofthatperson’sexperienceinearlylife.
There are other radically different models of psychology that regard mental experience,includingthoughts,moodsanddrives,asepiphenomena,thatis,asnomorethanfrothontopofthebeer.Inthesemodels(radicalmaterialismoreliminativematerialism),mentallifeisillusory;it isonly thematerial,organicprocesses thatare real.Thesignificance the thinkerattaches tosubjectiveexperienceisregardedaspurelyillusory.Suchapositionposesdifficultiesforpsycho-logicalenquiryandtreatment.
Berrios (1996)hasdescribed two formulationsofdescriptivepsychopathology in thenine-teenthcentury.Psychologistsandbrainscientistspredominantlytendedtoregardmorbidphe-nomenaasquantitativevariationsonnormalmentalfunctions–thecontinuityview.Psychiatrists,workingdirectlywiththementallyill(alienists),consideredthatsomesymptomsweretoobizarreto have a counterpart in normal behaviour – the discontinuity view. Both formulations havecontributed to the current state of descriptive psychopathology. Undoubtedly, the quality ofempathyshownbythedoctorcontributestoanunderstandingofthepatient,butthereisalimit,for example with psychotic phenomena in which the patient’s notions and behaviour may nolongerbeunderstandablebyusingempathy,andpatientanddoctormaybemutuallyalienated.These two formulations, the continuity and discontinuity views, continue to influence howabnormalphenomenaareconceptualizedeventoday.
There are two distinct parts to descriptive psychopathology: the empathic assessment of the patient’s subjective experienceandtheobservation of the patient’s behaviour. Empathyisanimportantpsychiatrictermthatliterallymeans‘feelingoneselfinto’andinpsychiatricpracticeemphasizestheimaginativeexperiencingofanotherperson’sworld.Itcanbedistinguishedfromsympathy,whichis‘feelingwith’.Awaytoappreciatethedistinctionbetween‘empathy’and‘sympathy’istorecognizetheroleofanobjectivestancecoupledwithanactiveattempttounderstandhowcertainthoughtsrisefromparticularmoods,wishesorfearsandthenexusofconnectionsbetweendifferentaspectsofthepatient’sexperienceswhichisintegraltoempathy.
TABLE 1.1 ■ Psychopathology: descriptive versus psychoanalytic
Descriptive Psychoanalytic
Summary Empathic evaluation of patient’s subjective experience
Study of the roots of current behaviour and conscious experience through unconscious conflicts
Terminology Description of phenomena Theoretical processes demonstrated
Methods Understanding the patient’s subjective state through empathic interview
Free association, dreams, transference
Differences in practical application
Makes distinction between understanding and explanation: understanding through observation and empathy
Understanding in terms of notional theoretical processes
Form and content clearly separated: form of importance for diagnosis
No distinction made; concerned with content
Process and development distinguished: process interferes with development basis
No distinction made; symptoms seen as having unconscious psychological basis
6 ONE—CONCEPTS AND METHOD
Indescriptivepsychopathology,theconceptofempathyislikeaclinicalinstrumentthatneedstobeusedwith skill tomeasure anotherperson’s internal subjective stateusing theobserver’sown capacity for emotional and cognitive experience as a yardstick. Empathy is achieved byprecise,insightful,persistentandknowledgeablequestioninguntilthedoctorisabletogiveanaccountofthepatient’ssubjectiveexperiencethatthepatientrecognizesashisown.Ifthedoc-tor’saccountofthepatient’sinternalexperienceisnotrecognizedbythepatientashisown,thenthequestioningmustcontinueuntiltheinternalexperienceisrecognizablydescribed.Throughouttheprocess,successdependsonthecapacityofthedoctorasahumanbeingtoexperiencesome-thing likethe internalexperienceof theotherperson, thepatient; it isnotanassessmentthatcouldbecarriedoutbyamicrophoneandcomputer.Itdependsabsolutelyonthesharedcapacityofbothdoctorandpatientforhumanexperienceandfeeling.Itisempathythatallowsthedoctortocometounderstandthepatient’sexperiences.Inthissense,itisempathythatmakesitpossibleforustoknowwhatitislikeforanotherperson,anothersubjectofexperience,tobeinaparticularmentalstate.Whenempathyfailstorenderapatient’ssubjectiveexperienceunderstandable,wecan then talk about that experience as being un-understandable. In other words, the farthestreachesofourintuitivecomprehensionofaphenomenonhavebeenexceeded.
Accurate observation of behaviour is the other component of descriptive psychopathology.Subjectivehumanexperiencebecomesavailabletousforexaminationandexplorationthroughverbalcommunicationbutalsothroughmeaningfulgestures,bodilystance,behaviourandactions.Observationoftheobjectiveexpressionofsubjectiveexperience,thatis,ofbehaviour,isextremelyimportantandisamuchmoreusefulexercisethansimplycountingsymptoms;theslavishuseof a symptom checklist for their presence or absence is often an obstacle to genuine clinicalobservation,ifnottothequalityofdoctor-patientcommunication.Theobjectivitythatisfacili-tatedbychecklistsiscrucial,butthereisaneedalsofortheskilledobservationofbehaviourandforattentiveandfocusedlistening.
Phenomenology and PsychopathologyPsychopathology is concerned with abnormal experience, cognition and behaviour. Descriptive psychopathologyavoidstheoreticalexplanationsforpsychologicalevents.Itdescribesandcatego-rizestheabnormalexperienceasrecountedbythepatientandobservedinhisbehaviour.Initshistoricalcontext,Berrios(1984)definesitasacognitivesystemconstitutedbyterms,assump-tions and rules for its application, ‘the identification of classes of abnormal mental acts’.Phenomenologyisatermthatiscloselyalliedtodescriptivepsychopathology.Ithasalongtradi-tioninphilosophyandisassociatedwiththenameofEdmundHusserl(1859–1938).Itisusuallyusedtodenoteenquiryintoone’sconsciousandintellectualprocesses,eschewinganypreconcep-tionsaboutexternalcausesandpreconceptions.Themethodofphenomenologyaims to focusonexperiencedphenomenainordertoestablishtheiruniversalcharacter.Asusedinpsychiatry,phenomenology involves the elicitation and description of abnormal psychological events, theinternalexperiencesofthepatientandhisconsequentbehaviour.Anattemptismadetolistenattentively, accuratelyobserveandunderstand thepsychological eventorphenomenon so thattheobservercan,asfaraspossible,knowforhimselfwhatthepatient’sexperiencemustfeellike.
Howcanoneusethewordobserveraboutsomeoneelse’sinternalexperience?Thisiswheretheprocessofempathybecomesrelevant.Descriptivepsychopathologythereforeincludessubjec-tiveaspects (phenomenology)andobjectiveaspects (descriptionofbehaviour). It is concernedwiththerichvarietyofhumanexperience,but it isdeliberately limitedin itsscopetowhat isclinicallyrelevant;forexampleitcansaynothingaboutthereligiousvalidityofwhatJames(1902)hascalled‘saintliness’.
Howdoesthisworkinpractice?MrsJenkinscomplainsthatsheisunhappy.Itisthebusinessof descriptive psychopathology both to elicit her thoughts and actionswithout trying to explainthemandtoobserveanddescribeherbehaviour–thelistlesssaggingofhershoulders,thetense
1—FuNDAMENTAl CONCEPTS OF DESCriPTivE PSyCHOPATHOlOgy 7
grippingandwringingofherhands.Phenomenologydemandsaveryprecisedescriptionofexactlyhowshefeelsinsideherself:‘thathorriblefeelingofnotreallyexisting’and‘notbeingabletofeelanyemotion’.
Some psychiatrists have held the method of phenomenology in derision as archaic, hair-splittingorhare-chasingpedantry,butthediagnosticevaluationofsymptomsisataskthatthepsychiatristomitsathisown,andhispatient’s,peril.Studyingphenomenawhetsdiagnostictools,sharpens clinical acumen and improves communication with the patient.The patient and hiscomplaintsdeserveourscrupulousattention.If‘theproperstudyofmankindisman’,theproperstudyofhismentalillnessstartswiththedescriptionofhowhethinksandfeelsinside–‘chaosofthoughtandpassion,allconfused’(Pope,1688–1744).
A cavalier neglect of abnormal phenomena can have serious repercussions for care of thepatient. Eight mentally well researchers were sent separately to twelve admission units inAmericanmentalhospitalsonthepretenceofcomplainingofhearingthesewordssaidaloud:‘empty’,‘hollow’and‘thud’(Rosenhan,1973).Inallcasessaveone,theywerediagnosedassuf-feringfromschizophrenia.Theyproducednofurtherpsychiatricsymptomsafteradmissiontohospitalbut acted asnormally as they could, answeringquestions truthfully except to concealtheirnameandoccupation.Theethicsandgoodsenseoftheexperimentcancertainlybeques-tioned,butwhatcomesoutclearlyisnotthatpsychiatristsshouldrefrainfrommakingadiagnosisbutthattheirdiagnosisshouldbemadeonasoundpsychopathologicalbasis.NeitherRosenhan,norhis colleagues,nor theadmittingpsychiatristsgaveany informationas towhat symptomscould reasonably be required for making a diagnosis of schizophrenia; this requires a methodbasedonpsychopathology(Wing,1978).Withadequateuseofphenomenologicalpsychopathol-ogy,thisfailureofdiagnosiswouldnothaveoccurred.
Jaspers(1959)wrote,‘Phenomenology,thoughoneofthefoundationstonesofpsychopathol-ogy,isstillverycrude’.Oneofthegreatproblemsinusingthismethodisthemuddlednatureofterminology.Almostidenticalideasmaybeassigneddifferentnamesbypeoplefromdifferenttheoreticalbackgrounds,forexampletheplethoraofdescriptionsofhowapersonmayconcep-tualizehimself:self-image,cathexis,bodyawarenessandsoon.
Thereisconsiderableconfusionoverthemeaningofthetermphenomenology.Berrios(1992)hasdescribedfourmeaningsinpsychiatry.
P1 refers to its commonest clinical usage as a mere synonym for ‘signs and symptoms’ (as in ‘phenomenological psychopathology’); this is a bastardized usage, and hence conceptually uninteresting. P2 refers to a pseudo-technical
sense often used in dictionaries and which achieves spurious unity of meaning by simply cataloguing successive usages in chronological order; this approach is
misleading in that it suggests false evolutionary lines and begs important questions relating to history of phenomenology. P3 refers to the idiosyncratic usage started by Karl Jaspers who dedicated his early clinical writings to the
description of mental states in a manner which (according to him) was empathic and theoretically neutral. Finally, P4 refers to a complex
philosophical system started by Edmund Husserl and continued by writers collectively named the ‘Phenomenological Movement’.
(p. 304)
Of these meanings, this chapter, and indeed this book, will concentrate entirely on theJaspersianmeaningofphenomenology,P3ofBerrios. Jaspersdefinesphenomenologyperhaps30to40timesinhiswritingsinsubtlydifferentwaysbutalwaysimplyingthestudy of subjective experience.Walker (1988,1993a,b,1994)has argued, very elegantly, that even though JaspershimselfthoughtthathehadbeeninfluencedbyHusserlandhissystemofphenomenology,thiswasnotinfactso,andhispsychopathologyowedmoretoKantianconceptssuchasformand
8 ONE—CONCEPTS AND METHOD
content.Walker(1995a,b)considersthatJaspersradicallymisconstruedHusserl’sphenomenol-ogy.This view has been rebutted by others (Wiggins etal., 1992).The implication for whatfollowsinthischapter,andintherestofthebook,isthattheconceptofphenomenologyusedherecomesdirectlyfromJaspersandwasprobablyinfluencedbybothKantandHusserl.
Phenomenology,theempathicmethodfortheelicitingofsymptoms,cannotbelearnedfromabook.Patientsarethebestteachers,butitisnecessarytoknowwhatoneislookingfor–thepractical,clinicalaspectsinwhichthepatientdescribeshimself,hisfeelingsandhisworld.Thedoctortriestounravelthenatureofthesufferer’sexperience,tounderstanditwellenoughandtofeelitsopoignantlythattheaccountofhisfindingsevokesrecognitionfromthepatient.Themethodofphenomenologyinpsychiatryisentirelysubjugatedtoitssinglepurposeofrenderingthepatient’sexperienceunderstandable(thisisatechnicalwordinphenomenologyandisdescribedinmoredetailonp.10–12;however,itincorporatesthecapacityforputtingoneselfinthepatient’splace)sothatclassificationandrationaltherapymayproceed.
Itisnottheassimilationofabstrusefactsortheaccumulationofforeigneponymsthatismostdifficultinphenomenology,althougheitherofthesemaybehard:itisthecomprehensionofamethodofinvestigationandtheabilitytousenewconcepts.Inanattempttoavoidtheobscureandobvious,intherestofthischaptersomeoftheseconceptsarediscussed.
ConceptsDISEASE AND ILLNESS
Psychopathologyconcernsitselfwithdisease of the mind,butwhatisdisease?And,howdoesitdifferfromdisorderandillness?Thisisavastsubjectthathasreceiveddiscussionfromphiloso-phers, theologians, administrators and lawyers aswell as fromphysicians.Doctorswho spendmostoftheirworkingtimedealingwithdiseaserarelyaskthisquestionandevenlessfrequentlyattempt toanswer it.Talkofdiseasebydefinition raisesquestionsabout thenatureofhealth.But,anevenmorepressingissueiswhetheritispossibleforthemindtobediseasedinthesamewayormannerthattheliverorthekidneyscanbediseased.Thesequestionsareoutsideofthescopeofthisbookbutitisimportanttobeawareofthevariedapproachesthatdifferentauthori-tiestaketothismatter.Ioutlinethebasicargumentsbelow.
Themostcompellingmodelofadiseaseisthatwhichgroundsamedicalconditionsuchaspulmonarytuberculosisonthebasisofadistinctivemorbidanatomydemonstrableonexamina-tionofthelungsandwhichisindependentofanyparticularobserverandisassumedtobevaluefree.Itisevenbetterifthereisanunderstandingofthedetailedpathophysiology:howthecausa-tiveagent,intuberculosisforinstance,resultsintherecognized,typicalmorbidanatomyofthelungs.Itisobviousfromtheforegoingthatinmostpsychiatricdiseasesnosuchtypicalmorbidanatomyorpathophysiologyhasbeendescribed.
Onthebasisoftheabsenceofdemonstrablephysicallesions,Szasz(1960)arguedthatpsy-chiatricormentaldiseasesdidnotexistandthatonlybehaviouraldevianceandmoralorsocialjudgementswereatplay inpsychiatry.Healsoarguedthat‘mental’ isanabstractconceptandnotanobjective,physicalthingandhenceitcouldnotbediseased.Braindiseases, inhisvieware realbutmentaldiseases are a logical impossibility, and thusSzaszuses the term‘myth’ tocharacterizementaldiseases.
OtherwritersincludingScadding(1967),Kendell(1975),Boorse(1976)andSedgwick(1973)haveput forwardarguments that stand inopposition toSzasz.ScaddingandKendelluse thecombination of statistical deviance and biological disadvantage defined as reduced fertility todeterminewhatadiseaseis.Boorseaddsthatadiseaseisanyconditionthatinterfereswithanyfunction of an organism (and in this view mental functioning counts), which is necessary forits survival and reproduction. Additionally, a disease becomes an illness when it is deemed

1—FuNDAMENTAl CONCEPTS OF DESCriPTivE PSyCHOPATHOlOgy 9
undesirable, a title for special treatment and a valid excuse for particular behaviours. FinallySedgwickmakestheclaimthatalldiseasesstartoffasillnesses,becausethesymptomsarenega-tively valued and hence become a focus of social and moral interest and that in this way thesymptoms later attain disease status. In this account both the so-called physical illnesses andmentalillnessesstartoffasnegativelyvaluedstatesafflictinghumanbeingsandthereisnosharpdistinctiontobedrawnbetweenthem.SeeFulfordetal.(2006)forfurtherelaborationoftheseissues.
It isclear that there isnowidelyacceptedviewabout thestatusof theconditions that fallundertheinterestofpsychiatrists.Asimpledictumistoregarddiseaseaswhatdoctorstreatandillness as what persons suffer from. Although this distinction between normality and disease,healthandillness,isbynomeanstrivial:
A large part of medical ethics and much of the whole underpinning of current medical policy, private and public, are squarely based on the notion of disease
and normality. Left to himself the physician (whether he realizes it or not) can do very well without a formal definition of disease … Unfortunately, the
physician is not left alone to work his common sense. He is attacked from two angles: the predatory consumers and the pretentious advisers.
(Murphy, 1979)
NORMS, NORMAL AND ABNORMAL
Thesubjectofpsychiatryistheperson,notanorgansuchastheliver,kidneyoreventhebrain.Psychiatricdiseasesaredistinctfrommereneurologicaldiseases inthesensethat inneurologythediseaseprocessleavestheself,thepersonhoodofanindividual,intact.Thismeansthatwecanspeakofapersonwhosuffersfrommultiplesclerosisormotorneurondisease.Inpsychiatry,thediseasesafflicttheself;affectthepersoninadeepandnotsuperficialsense.Mooddisordersandschizophreniahaveapervasiveinfluenceonaspectsoftheselfinawaythatstrikesatwhatitmeanstobehuman.
The ability to experience and represent the world; the capacity to inhabit a social worldincludingrecognizingtherulesandconventionsthatoperatetherein;theabilitytoformrelation-shipsandtoimaginetheworldoftheOther;theabilitytocommunicate,touselanguageandtounderstandsymbols,thatistoinhabitaworldofmeanings;thewherewithaltobeanagent,theauthorofone’sownprojectsandthedriveandwilltoact;thecapacitytooperateinaworldofmoralandaestheticvalues;and,thepossibilityofhavinganattitudetotime,anorientationtothefuture;thesemanifoldaspectsofthepersonandmanymoreyettobefullydescribedareinfluenced if not impaired by psychiatric diseases. Our understanding of these higher humanfunctionsistrivial.Abnormalitiesandpathologyinthesedomainsaremanifestinsocialbehaviourandarewithoutindependentorobjectivemarkers.So,talkofnorms,normalityandabnormalityareintegraltoanydiscussionofpsychiatricphenomena,sinceinordertorecognizeimpairmentsintheseareasoffunctionweneedanunderstandingofwhatnormalfunctionentails,butmorefundamentallywhatitmeanstotalkaboutnorms,normalityandabnormality.
ThewordnormalisusedcorrectlyinatleastfoursensesintheEnglishlanguageaccordingtoMowbrayetal. (1979).Theseare thevaluenorm, the statisticalnorm, the individualnormandthetypologicalnorm.Thevaluenormtakestheidealas itsconceptofnormality.Thusthestatement‘Itisnormaltohaveperfectteeth’isusingnormalinavaluesense;inpractice,mostpeoplehavesomethingwrongwiththeirteeth.The statisticalnormis,ofcourse,thepreferreduse; the abnormal is considered to be that which falls outside the average range. If a normalEnglishmanis5feet8inchestall,tobeeither6feet2inchesor5feet2inchestallisequallyabnormalstatistically.
10 ONE—CONCEPTS AND METHOD
Theindividualnormistheconsistentleveloffunctioningthatanindividualmaintainsovertime.Followingbraindamage,apersonmayexperienceadeclineinintelligencethatiscertainlyadeteriorationfromhispreviousindividuallevelbutmaynotrepresentanystatisticalabnormalityfrom that of the general population (for example a decline in intelligence quotient from 125to105).
Typologicalabnormalityisanecessarytermtodescribethesituationinwhichaconditionisregardedasnormalinallthethreemeaningsaboveandyetrepresentsabnormality,perhapsevendisease.TheexamplegivenbyMowbrayetal.istheinfectiveconditionofpinta.ThemottlingoftheskinofthisconditionishighlyprizedbytheSouthAmericanIndianswho‘suffer’fromit, to theextent that‘non-sufferers’ areexcluded fromthe tribe.Thus,having thecondition isnormalinavalue,statisticalandindividualsense,andyetitispathologicalinthesensethatitistheresultofaspirochaetalskininfection.Thepursuitofthinnessbymodelsanddancersinoursocietywouldbeaneverydayexample.
Inaddition,onecantalkabout socialnormsbywhichwemeantherules,conventions,andpractices that determine in specific cultures what behaviours are acceptable and approved of.Theseincludetheetiquette,moresandethicsunderpinningbehaviour.Infactforsomepeople,psychiatricdiseasesarenomorethanbehavioursclassedasdeviantbysocialrulesandpsychiatristsarenomorethansocialpolicemen.
Thereareotherconceptsimplicitindiscussionsofnorms,normalityandabnormality.Thesearewhetherthediscretephenomenaofinteresttopsychopathologistsarecategoricallydifferentfromnormalexperienceorwhetherthedistinctionbetweennormalandabnormalphenomenaaredimensionalinnature.Thedistinctionbeingdrawnhereisoverandbeyondwhetherpsycho-pathologicalphenomenaarestatisticallydeviant.Thequestioniswhethertheanxietyexperiencedbyapsychiatricpatient, forexample, isonlyanexaggerationof thatexperiencedbya‘normal’personorwhetherthereissomethingcategorically/qualitativelydifferentaboutit.
UNDERSTANDING AND UN-UNDERSTANDABLE
Itseemsself-evidentthatunderstandingthepatient’sstory,graspingtheinnerlogicofthenar-rativeandrepresentingtooneselfthepatient’ssubjectiveexperiencesisfundamentaltoclinicalpractice.Understanding,inbothaneverydayandaphenomenologicalsense,cannotbecompleteunless the doctor has a detailed knowledge of the patient’s background culture and specificinformationabouthisfamilyandimmediateenvironment.Neithercanphenomenologyconcen-tratesolelyontheindividualisolatedinamomentoftime.Itmustbeconcernedwiththepersoninasocialsetting;afterall,aperson’sexperienceis largelydeterminedbyhisinteractionswithothers.Itmustalsobeconcernedwiththementalstateandenvironmentoftheindividualbeforetheeventofimmediateinterestandwithwhatoccursafterwards.
The method of phenomenology facilitates communication: its use makes it easier for thedoctor tounderstandhispatient.Thepatient is alsohelped tohave confidence in thedoctor,becauseherealizesthathissymptomsareunderstoodandthereforeacceptedas‘real’.Theprecisedescriptionandevaluationofsymptomsalsohelpscommunicationbetweendoctors.
WilhelmDilthey (1833–1911) argued that thenatural sciences treatnature as objects andforcesthatcanbeexplainedthroughcausallaws.Inotherwords,thegoalofsuchscienceistheformulationofgeneral,universallaws,whereasthehumanities,forexamplehistoryandpsychol-ogy,havethehumansubjectastheirfocusandcausallawsdonotapplyinthesecircumstances.ForDilthey,science‘explains’naturalphenomenabycausalexplanation.Thehumanities‘under-stand’humanpsychicphenomenathroughtheinterpretationofthemeaningstructuresrevealedin texts or through dialogue with another person.This distinction between ‘explanation’ and‘understanding’continuestobeinfluentialinourthinkingeventoday(Phillips,2004).Insciencewecometoknowtheobjectfromoutside,butinthehumanitiesweareableto‘know’thesubjectfrominside.Weareabletorepresenttoourselves,ifnotto‘know’,theinnerlifeofanotherperson
1—FuNDAMENTAl CONCEPTS OF DESCriPTivE PSyCHOPATHOlOgy 11
becausewetoohaveaninnerlife.Weareabletounderstandtheotherpersonthroughthenetworkofmeaningsassociatedwith theirbehaviour.Westartwith thepremise thatbehaviourmeanssomething; that is, it arises with internal consistency from psychological events.Wittgenstein(1953)hasstated,‘Weexplainhumanbehaviourbygivingreasonsnotcauses’.
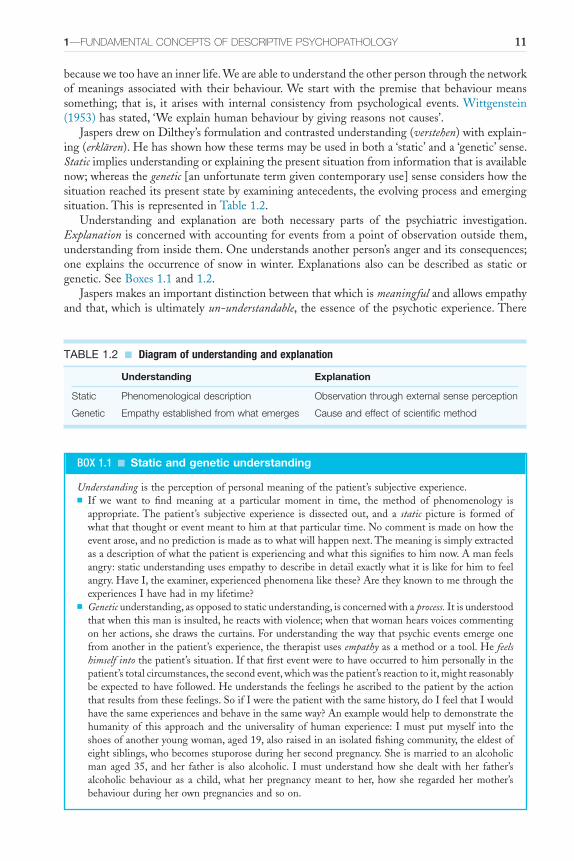
JaspersdrewonDilthey’sformulationandcontrastedunderstanding(verstehen)withexplain-ing(erklären).Hehasshownhowthesetermsmaybeusedinbotha‘static’anda‘genetic’sense.Staticimpliesunderstandingorexplainingthepresentsituationfrominformationthatisavailablenow;whereasthegenetic[anunfortunatetermgivencontemporaryuse]senseconsidershowthesituationreacheditspresentstatebyexaminingantecedents,theevolvingprocessandemergingsituation.ThisisrepresentedinTable1.2.
Understanding and explanation are both necessary parts of the psychiatric investigation.Explanationisconcernedwithaccountingforeventsfromapointofobservationoutsidethem,understandingfrominsidethem.Oneunderstandsanotherperson’sangeranditsconsequences;oneexplains theoccurrenceof snow inwinter.Explanationsalsocanbedescribedas staticorgenetic.SeeBoxes1.1and1.2.
Jaspersmakesanimportantdistinctionbetweenthatwhichismeaningfulandallowsempathyandthat,whichisultimatelyun-understandable,theessenceofthepsychoticexperience.There
TABLE 1.2 ■ Diagram of understanding and explanation
Understanding Explanation
Static Phenomenological description Observation through external sense perception
Genetic Empathy established from what emerges Cause and effect of scientific method
BOX 1.1 ■ Static and genetic understanding
Understandingistheperceptionofpersonalmeaningofthepatient’ssubjectiveexperience.■ If we want to find meaning at a particular moment in time, the method of phenomenology is
appropriate.The patient’s subjective experience is dissected out, and a static picture is formed ofwhatthatthoughtoreventmeanttohimatthatparticulartime.Nocommentismadeonhowtheeventarose,andnopredictionismadeastowhatwillhappennext.Themeaningissimplyextractedasadescriptionofwhatthepatientisexperiencingandwhatthissignifiestohimnow.Amanfeelsangry:staticunderstandingusesempathytodescribeindetailexactlywhatitislikeforhimtofeelangry.HaveI,theexaminer,experiencedphenomenalikethese?AretheyknowntomethroughtheexperiencesIhavehadinmylifetime?
■ Geneticunderstanding,asopposedtostaticunderstanding,isconcernedwithaprocess.Itisunderstoodthatwhenthismanisinsulted,hereactswithviolence;whenthatwomanhearsvoicescommentingonheractions,shedrawsthecurtains.Forunderstandingthewaythatpsychiceventsemergeonefromanotherinthepatient’sexperience,thetherapistusesempathyasamethodoratool.Hefeels himself intothepatient’ssituation.Ifthatfirsteventweretohaveoccurredtohimpersonallyinthepatient’stotalcircumstances,thesecondevent,whichwasthepatient’sreactiontoit,mightreasonablybeexpectedtohavefollowed.Heunderstandsthefeelingsheascribedtothepatientbytheactionthatresultsfromthesefeelings.SoifIwerethepatientwiththesamehistory,doIfeelthatIwouldhavethesameexperiencesandbehaveinthesameway?Anexamplewouldhelptodemonstratethehumanityof this approachand theuniversalityofhumanexperience: Imustputmyself into theshoesofanotheryoungwoman,aged19,alsoraisedinanisolatedfishingcommunity,theeldestofeightsiblings,whobecomesstuporoseduringhersecondpregnancy.Sheismarriedtoanalcoholicmanaged35, andher father is also alcoholic. Imustunderstandhowshedealtwithher father’salcoholic behaviour as a child,whatherpregnancymeant toher,how she regardedhermother’sbehaviourduringherownpregnanciesandsoon.

12 ONE—CONCEPTS AND METHOD
is,thus,alimittounderstandingpsychopathologicalphenomena.Althoughonecanempathizewith the contentofapatient’sdelusionand therebyunderstandhowthatcontentof thebelieforiginated,theoccurrenceofthedelusionitself,isinthismodel,morerecalcitranttoourempathyandunderstanding.Itcanbesaidthatourunderstandingreachesitslimitwhenitconfrontsthefactofthedelusionitself.Forthat,weneedtoappealtocognitivemechanismsorothernaturalscienceprocesses.Weareinneedofscientificexplanation,notpsychologicalunderstanding.
We can understand from a knowledge of the patient’s background why, if her thinking isgoingtobedisorderedinform,thetopicorcontentofthatthinkingshouldbeconcernedwithpersecutionbytheNazis–perhapsbecauseherparentsescapedfromGermanyin1937.Butwecanhavenounderstandingofwhysheshouldbelievesomethingthatisdemonstrablyfalse:thatherpersecutorsareputtingatastelessfluidintoherdrinkingwaterthatmakesherfeelill.Thedelusionitself,aspsychopathologicalform,isun-understandable.Meaningfulconnections,then,show the linkage between different psychological events by understanding how these eventsemergeonefromanotherbyaprocessofempathy.
This is a controversial concept in that it implies that there are aspects of another person’smentallifethatarebeyondourgraspandempathicunderstanding.Itcontradictsanotheraxiomin psychiatric practice, namely that our purpose is to understand another person, and whenunderstanding fails, it calls into question how conscientious and rigorous the psychiatrist hasbeeninthepursuitofgraspingtheinnerlifeofthepatient.
EMPATHY
The classic method in medicine of gaining information about the patient is from the historyand by physical examination.The use of phenomenology in psychiatry is an extension of thehistory,inthatitamplifiesthedescriptionofthepresentcomplainttogivemoredetailedinfor-mation. It is also examination in that it reveals themental state. It isnotpossible forme, thedoctor,toobservemypatient’shallucinationorinanydirectwaytomeasureit.However,whatIcandotocomprehendhimistousethosehumancharacteristicsIholdincommonwithhim:thefactthatweinhabitthesameworldofmeanings,thatwecommunicateinlanguageandthatlikehimIhavearichinner life.It isalsoimportanttobeintellectuallycuriousandgenuinelyinterested in the inner lifeofanotherperson.The inquiries thatarise fromthis stance shouldaimtorecreateforoneselforrepresenttooneself thesubjectiveexperiencesofanotherpersonwiththeaimofunderstandingandmakingsenseofthem.Theaimisthustoexploreandtest,throughdialogue,thepatient’ssubjectiveexperience.Iendeavourtocreateinmyownmindwhathisexperiencemustbelike.IthentesttoseeifIamcorrectinmyreconstructionofhisexperi-encebyaskinghimtoaffirmordenymydescription.Ialsousemyobservationofhisbehaviour– the sad expression of his face or him thumping the desk with his fist – to reconstruct hisexperiences.
Listeningandobservingarecrucialforunderstanding.Greatcaremustbetakenwithaskingquestions.Doctorsnotinfrequentlyidentifysymptomsincorrectlyandcometothewrongdiag-
BOX 1.2 ■ Static and genetic explanation
■ Static explanation is concerned with external sense perception, observing an event, for example‘Iwitnessedthe1999eclipseinPlymouth’.
■ Geneticexplanationconsistsofunravellingcausalconnections;itdescribesachainofeventsandwhytheyfollowthatsequence(‘visualperceptionoftheeclipseistheresultofphysiologicalchangesinmyretina,whichinturnproducechangesinmyoccipitalcortexthatultimatelycausemetoseetheeclipse’).
1—FuNDAMENTAl CONCEPTS OF DESCriPTivE PSyCHOPATHOlOgy 13
nosisbecausetheyhaveaskedleadingquestionswithwhichthepatient,throughhissubmissive-nesstothedoctor’sstatusandhisanxietytocooperate,isonlytoowillingtoconcur.
The method of empathyimpliesusingtheabilitytofeeloneselfintothesituationoftheotherpersonbyproceedingthroughanorganizedseriesofquestions,rephrasingandreiteratingwhennecessaryuntiloneisquitesureofwhatisbeingdescribedbythepatient.Thesequencemightgoasfollows.
Question:‘Youdescribeyourthoughtschanging;whathappenstothem?’Answer:adescriptionofhowhehasarecurringthoughttokillpeopleandthisresultsfrom
apaininhisstomach.Question:(tryingtoisolatetheelementsofhisexperience)‘Whatisyourthoughtofkilling
peoplelike?’(obsession,delusion,fantasy,islikelytobeactedon,etc.).‘Doyoubelievethatyourstomachaffects your thinking?’, ‘Is thisdifferent fromapersonwhoknows that theybecomeirritablewhenhungry?’, ‘Inwhatway is itdifferent fromthat?’,Whatcausesyourpain in thestomach?’
Answer: he describes the details, which will include among irrelevant material the sort ofinformationrequiredfordeterminingwhatsymptomsarepresent.
Question: (the invitation for empathy) ‘Am I right in thinking that you are describing anexperienceinwhichraysarecausingpaininyourstomach,andthatyourstomachinsomewayquiteindependentofyourselfcausesthisthought,whichfrightensyou,thatyoumustkillsome-bodywithaknife?’Thisisanaccountoftherelevantsymptomsthathehasdescribedinlanguageheshouldbeabletorecognizeashisown.
Answer:‘Yes’(wehavethenachievedourgoal);‘No’(thereforeImusttryagaintoelicitthesymptoms,experiencethemformyselfanddescribethembacktohimagain).
Togiveexamplesofwhatthis implies inpractice:howdoI,aclinician,decidewhetheranindividualpatientisdepressedornot?Thisisnotdonebyimitatingamachinethatmightrecordunitsofvocaltoneoroffacialexpression,addinguptoadiagnosisofdepression.Fortheclinicalassessment,Igothroughthefollowingprocess.
■ Iamcapableof feelingunhappy,miserableanddepressedandknowwhat this feeling islikeinsidemyself.
■ IfIwerefeelingasIobservethepatienttobelooking,speaking,actingandsoon,Iwouldbefeelingmiserable,depressedandunhappy.
■ ThereforeIassessthemoodofthepatienttobethatofdepression.Ofcourse,thismentalprocessofdiagnosisisnotusuallyverbalized.Inanotherexample,apatientsays,‘theMartiansaremakingmesayswearwords;itisnotme
doingit’.Empathicquestioningrevealsthefalsebeliefheldbythepatientthatwhenswearwordscome fromhismouthhebelieves that the cause is actually outsidehimself, ‘Martians’, ratherthanfrominsidehimself.Questioningwouldinclude‘DoyouactuallyheartheMartians?HowdoyouknowthatitisMartiansandnooneelse?’andsoon.
Afurther,non-psychoticexamplewouldbea20-year-oldgirlwhohasfaintingattackswhenshe iscriticizedatwork.Theclinicianhas toplacehimorherself,even ifhe isa55-year-oldmanfromadifferentculturalbackground, intoherpositionwithaknowledgenotonlyofhersocialhistorybutalsoofthewaythatshe,inthepresent,perceivesthathistory;onlythenmaythedevelopmentofhersymptomsbecomeunderstandable.Forinstance,whenitisknownaboutheralcohol-abusingfather,therowshehadwithhermotherwhosufferedfromepilepsy,theveryrestrictedculturalbackgroundthattheyexperiencedinanisolatedfishingvillageandhowhermother would have a fit when rows became intolerable, then one may begin to understandsomething of the development of the patient’s own symptom.This is not achieved solely byexplanationasanoutsideobserverbutbyempathicunderstandingandthecapacityforsubjectiveexperiencebythedoctor,whoputshimselfinto,andthereforebecomes,the20-year-oldgirlfortheprocessofthepsychiatricinterview.

14 ONE—CONCEPTS AND METHOD
Itisthepurposeofthephenomenologicalmethodthereforeto(a)describeinnerexperiences,(b) order and classify them and (c) create a reliable terminology. Empathy is also invaluabletherapeuticallyinestablishingarelationshipwiththepatient.Knowingthatthedoctorunder-stands,andiseventosomeextentabletosharehisfeelings,givesthepatientconfidenceandasenseof relief.Thismethodof empathy is alsouseful as awayof extendingknowledgemoregenerallyinthefieldofpsychiatry,asitallowsadiagnosticterminologytobedeveloped.
FORM AND CONTENT
Formandcontentaredistinctinphenomenology.ForJaspers:
form must be kept distinct from content which may change from time to time, e.g., the fact of a hallucination is to be distinguished from its content, whether this is a man or a tree, threatening figures or peaceful landscapes. Perceptions,
ideas, judgements, feelings, drives, self-awareness, are all forms of psychic phenomenon; they denote the particular mode of existence in which content is
presented to us.(Jaspers, 1959)
Thus,likewarpandwoof,formandcontentareessentiallydifferentbutinextricablywoventogether.Onewaytothinkofformistoregarditasthesensemodalityinwhichaperceptionispresentedtousorthecognitivedomaininwhichaparticularaspectofpsychiclifeisexperiencedorenacted.Theformofapsychicexperienceisthedescriptionofitsstructureinphenomenologi-cal terms, for example adelusion,or, asBerrios (1996) says, ‘Form refers to those impersonalaspectsofthementalsymptomsthatguaranteeitsstability intimeandspace;that is, its‘con-stancy’elements’.Viewedinthisway,contentisthesubjectivecolouringoftheexperience.Thepatientisconcernedbecausehebelievesthatpeoplearestealinghismoney.Hisconcernisthat‘peoplearetakingmymoney’,notthat‘Iholdonunacceptablegroundsafalsebeliefthatpeoplearetakingmymoney’.Heisconcernedaboutthecontent.Clearly, formandcontentarebothimportantbutindifferentcontexts.Thepatientisconcernedonlywiththecontent:‘thatIampursuedbytenthousandhockeysticks’.Thedoctor isconcernedwithbothformandcontent,butasaphenomenologistonlywithform,inthiscaseafalsebeliefofbeingpursued.Asfarasformisconcerned,thehockeysticksareirrelevant.Thepatientfindsthedoctor’sinterestinformunintelligibleandadistractionfromwhatheregardsas important,andheoftendemonstrateshisirritation.
InChapter7,apatientisdescribedwhosaid,‘WhenIturnthetapon,Ihearavoicewhis-peringinthewaterpipe,“She’sonherwaytothemoon.Let’shopeshehasasoftlanding”’.Theform of this experience is what demands the attention of the phenomenologist and is usefuldiagnostically.Sheisdescribingaperception;itisanauditoryperceptionandafalseordisorderedauditoryperception.Ithasthecharacteristicsofahallucination,andspecificallyofafunctionalhallucination.This is the form.While thepsychiatrist isbusy clarifying the form, thepatientmightbegettingveryirritatedbecause‘heisnottakinganynoticeofwhatIamsaying’.Sheisworriedthatsheisbeingsenttothemoon.Whatwillhappenwhenshegetsthere?Howwillshe get back?So the content is all-important toher, and thedoctor’s absorptionwith form isincomprehensibleandfrustratingintheextreme.
Theformisdependenton,andisthereforeadiagnostickeyto,theparticularmentalillnessfromwhichthepatientsuffers.Forexample,delusional perceptsoccurinschizophrenia,andwhendemonstratedastheformoftheexperiencetheyindicatethiscondition.Thefindingofavisualhallucinationsuggeststhelikelihoodofanorganicbraindisease(Chapter7).Thenatureofthecontentofthesetwoexamplesisirrelevantincomingtoadiagnosis.Thecontentcanbeunder-stoodbythepatient’slifesituationwithregardtoculture,peergroup,status,sophistication,age,
1—FuNDAMENTAl CONCEPTS OF DESCriPTivE PSyCHOPATHOlOgy 15
sex, life events and geographical location. For example, another patient described himself ashavingbeensenttothemoonandbackduringthenightwithinafortnightofthefirstlandingbymanonthemoon.Describingone’sthoughtsasbeingcontrolledbytelevisionisnecessarilyconfinedtothosepeoplewhohaveseenthatinvention.
Hypochondriacal content can occur in more than one form. It could take the form of anauditoryhallucinationinwhichthepatienthearsavoicesaying‘youhavecancer’.Itcouldbeadelusion, in that he holds with conviction the false belief that he has cancer. It could be anovervaluedidea,inthatthepatienthasaconvictionarisingfrompriorexperienceofamistakendiagnosisofcancer,andthisresultsinhimspendingamajorpartofeverydaycheckingonhishealth. It could be an abnormality of affect that manifests itself in extreme hypochondriacalanxietyorindepressivehypochondriacaldespondency.
The significance of culture and individual variation in ascertaining the detailed complaintofthepatientshouldbestressed.Becausethepsychiatristneedstoassesswhetherthisnotionofthepatientdemonstratesthespecificpsychopathologicalformofdelusion,itdoesnotdiminishtheparallelneedtounderstandthepatient’sphilosophical,religious,politicalandsocialbeliefs,andknowhowtheyfit,orfailtofit,intothepatient’slarger,nationalandmoreintimate,sub-culturalsocialcontexts(Fabrega,2000).
Alongsidetheneedofthepsychiatristtoacquireskillsinpsychopathologyandtheelucidatingofmentalsymptomsistheparallelrequirementforculturaleducationandsensitivity.Bothaspectsarenecessaryforeverypatient-doctorinteraction.Ifanything,thepainstakinganddetailedstudyofphenomenologyincreasestheawarenessoftheculturalcontextandhowitinfluencescognitionandbehaviour.
PRIMARY AND SECONDARY PHENOMENA
Jaspersdiscussesthedifferentmeaningthatcanbegiventothetermsprimaryandsecondarywhenapplied to symptoms.The distinction may be in terms of understanding; what is primary isimmediateandultimateandthereforecannotbefurtherreducedbyunderstanding,forexamplehallucinations.Whatissecondaryiswhatemergesfromtheprimaryinawaythatcanbeunder-stood,forexampledelusionalelaborationarisingfromthehealthypartofthepsycheinresponsetohallucinationsfromtheunhealthypartofthepsyche.Again,theconceptualdistinctionofwhatisprimaryorsecondarymaybedeterminedbythecausalchain, inthatwhatisprimaryistheproximatecausewhilewhatissecondaryisthediscernibledistaleffect:acerebrovascularaccidentcauses sensoryaphasiaandis thereforeprimary; theaphasia is thedistaleffectandis thereforesecondarytothecerebrovascularaccident.
These two distinct meanings of the term primary overlie the crucial distinction betweenmeaningful connections and causal connections. For the avoidance of doubt in physics andchemistry,wemakeobservationsbyexperimentandthenformulatecausalconnectionsandcausallaws, whereas in psychopathology we experience another sort of connection, wherein psychicevents emerge out of one another in a way that can be understood – so-called meaningful connections.
SUBJECTIVITY AND OBJECTIVITY IN PSYCHOPATHOLOGY
Objectivity insciencehascometobereveredastheideal,sothatonlywhat isexternaltothemind is considered to be real, measurable and valuable. This is a mistake, because objectiveassessmentsarenecessarilysubjectivelyvalue-ladeninwhattheobserverchoosestomeasure,andthissubjectiveaspectcanbemademorepreciseandreliable.Therearealwaysvaluejudgementsassociated with both subjective and objective assessments.The process of making a scientificevaluationconsistsofvariousstages:receivingasensorystimulus,perceiving,observing(makingthe percepts meaningful), noting, coding and formulating hypotheses. This is a progressive

16 ONE—CONCEPTS AND METHOD
processofdiscardinginformation,anditisthesubjectivejudgementofwhatinformationisvalu-ablethatdeterminesthesmallamountfromeachstagethatisretainedfortransmissiontothenextpartoftheprocess.‘Thereisnosuchthingasanunprejudicedobservation’(Popper,1974).
Objectiveassessmentsinpsychiatryhavecoveredmanyaspectsoflife.Afewexamplesare,inadditiontomanyphysiologicalmeasures,themeasurementofbodymovements,facialexpression,patients’writings,learningcapacity,responsestoanoperantconditioningprogramme,memoryspan,workefficiencyandevaluationoflogicalcontentofthepatients’statements.Allthesecanbequantifiedandanalyzedobjectively.Subjectiveanalysiscanbemade,forexample,fromfacialexpressionorfromthepatient’sdescriptionofhimself,ofhisownwritingorofhisinnerevents.Whenadoctorsaysaboutapatient‘shelookssad’,heisnotmeasuringthepatient’sfacialexpres-sionin‘unitsofsadness’bysomeobjectiveyardstick.Heisgoingthroughthisprocess:‘IassociateherfacialexpressionwiththeaffectthatIrecognizeinmyselfasfeelingsad;seeingherexpressionmakesmefeelsad’.Rapportisthisqualitythatthepatientestablisheswiththedoctorduringtheclinicalinterview.Inorderforittohappen,thedoctorhastobereceptivetothiscommunication.Hehastobeabletoestablishrapporthimself,tohaveacapacityforhumanunderstanding.Thisisnecessarilyasubjectiveexperienceforthedoctor,butthatisnottosaythatitisunrealoreventhatitcannotbemeasured.Themethodofphenomenologytriestoincreaseourknowledgeofsubjectiveeventssothattheycanbeclassifiedandultimatelyquantified.
Aggernaes (1972) has defined subjectivity and objectivity for immediate everydayexperiences.
When an experienced something has a quality of ‘sensation’, it is also said to have a quality of ‘objectivity’ if the experiencer feels that under favourable
circumstances, he would be able to experience the same something with another modality of sensation than the one giving the quality of sensation. When an
experienced something has a quality of ‘ideation’, i.e., is not being directly sensed at the moment, it is also said to have a quality of ‘objectivity’ if the
experiencer feels that under favourable circumstances, he would nevertheless be able to experience the same something with at least two modalities of sensation.An experienced something has a quality of ‘subjectivity’ if the experiencer feels
that under no circumstances would he be able to experience this something with two or more modalities of sensation.
ThusIcanlookatthetableinfrontofmeasavisualperceptionorIcanturnmyheadandstill fantasize it as avisual image.As I ‘see’ it, ineitherway, the fact that I can imaginebothhearingasoundifIweretohititwithaspoonandbruisingmyknucklesifIweretopunchitconfirmsitsqualityofobjectivity.IfIusemyimaginationtocreateinmymindavisualimageofaChippendalechairthatIhaveneveractuallyseenbutisacompositeofobjectsandpicturesIhaveseen,IknowthatIwillneverbeable to feelorhear thisactualchair; it isasubjectiveimagewithoutexternal,objectivereality.
UNCONSCIOUS EXPERIENCE AND PHENOMENOLOGY
Phenomenologycannotbeconcernedwiththeunconsciousbecausethepatientcannotdescribeit,andsothedoctorcannotempathize.Descriptivepsychopathologyhasnotheoryoftheuncon-scious,nordoesitdenyitsexistence.Strictlyspeakingtheunconsciousissimplyoutsideitstermsof reference, and psychic events are described without recourse to explanations involving theunconscious. Dreams, the contents of hypnotic trance and slips of the tongue are describedaccording to how the patient experienced them, that is, according to how they manifest inconsciousness.
1—FuNDAMENTAl CONCEPTS OF DESCriPTivE PSyCHOPATHOlOgy 17
ORGANIC AND NEURAL SUBSTRATES AND PSYCHOPATHOLOGY
Psychopathologyisthestudyofabnormalmentalprocesses,sothat,evenwhentheorganiccausesofaconditionareknown,psychopathologyremainsinvolvedindescribing,definingandorderingthe symptomaticphenomenaand theexperienceof thepatient rather thanbeingpreoccupiedwithitsneuraloriginorpathophysiology.Thisisnottoimplythatunderlyingneuralmechanismsareunimportant.Tothecontrary,theyareundeniablyimportant.However,theactualsubjectiveexperienceofthepatientisalsoimportantandpsychopathologyconcentratesonthis.
Thereareestablishedlinksbetweendifferentabnormalphenomenaandidentifiableorganicpathologies.However,itisnotwiththeselinksthatpsychopathologyisconcerned,anditsuseful-ness isnotdependentonultimatelyfinding the localization in thebrainof adelusionor anyotherpsychicevent.Early,organicallyorientedpsychiatrists,suchasGriesingerandWernicke,werenotconcernedwiththepsychopathologicalinpsychiatrybutmuchmorewithchartingthediseasedbrain.Thispaidarichdividend,forexampleinelucidatingthenatureandtreatmentofcerebralsyphilis.Similarly,somemodernbehaviouristshavebeenuninterestedinphenomenol-ogy.Phenomenologyisnotultimatelyconcernedwithorganicpathologyorwithbehaviourpersebutwiththepatient’ssubjectiveexperienceofhisworld.
Foralongtime,symptomaticpsychiatryanddescriptivepsychopathologyseemedtohavelostcontactwithorganicpsychiatry,inwhichevidenceofmentalillnessissoughtindiseaseofthebrain.TherehasnowdevelopedwhatMundt(2000)describesasa‘freshwindfromtheexperi-mentalfieldofpsychopathology,neuropsychologyandbiologicalneurosciences’.Thislinkageisstillatanearlystage,butithaspotentialforthefuturestudyofsymptomsandofbrainpathology.Butfortheseinvestigationstosucceedandtocometofruition,athoroughappreciationofpsy-chopathologyisessential.
MIND-BRAIN DUALITY AND PSYCHOPATHOLOGY
Cartesiandualismistheviewthatmindandbodyareseparatesubstances;themindhappenstobeassociatedwithaparticularbody,butisultimatelyself-sufficient,andcapableofindependentexistence.Thisview,expoundedbyRenéDescartes(1596–1650)inwhichhemadeadistinctionbetween the material and physical world and the thinking human mind continues to exertextraordinaryinfluence.Husserl’sphilosophy,phenomenology,aroseoutofHusserl’srejectionofmany of Descartes’ conclusions. There are a number of significant problems with Cartesiandualism,notleasthowanimmaterialsubstancelikethemindcaninfluenceamaterialsubstancelikethebody.
Therearevariedphilosophicalattemptstodealwiththeproblemofdualismandanaccountoftheseisbeyondthescopeofthisbook.Whatisimportantisthatpsychiatryisbedevilledbythisproblem:howtoreconcilethephenomenathatpatientsreportwiththematerialityofthebrain. Is itpossibleorplausible to reducementalevents tophysicalevents in thebrain?And,howfarcanthechangesobservableduringfunctionalMRIscanningbeinterpretedasproductsofcertainmentalphenomena?Phenomenology,asanapproach,avoidsthisdebatebyleavingittooneside(bracketingitasHusserlwouldhavesaid)whilecontinuingtoexplore,investigate,describe,defineandcataloguethementalevents,thephenomena,reportedbypatients.Descriptivepsychopathologyisnotconcernedwithcausesbutwithdescriptionsofexperience.
The philosophy of mind is a thriving area of research, in particular the elucidation of thenatureofmind.Thespecific theoriesareoutside thescopeof thisbook(seeC.McGinn,The Character of Mind: an Introduction to the Philosophy of Mind ).Thatisnottosaythatthosetheoriessuch as Spinoza’s token identity theory, or the type identity theory (also known as reductivematerialism) or eliminative materialism or functionalism are not relevant to psychiatry or toexperimentalpsychopathology,butmerelytoemphasizethatpsychopathologycandevelopintheabsenceofafullandfinaltheoryofthenatureofmind.
18 ONE—CONCEPTS AND METHOD
ReferencesAggernaes A (1972)The experienced reality of hallucinations and other psychological phenomena. Acta
Psychiatrica Scandinavica48,220–38.BerriosGE(1984)Descriptivepsychopathology:conceptualandhistoricalaspects.Psychological Medicine14,
303–13.BerriosGE(1992)Phenomenology,psychopathologyandJaspers:aconceptualhistory.History of Psychiatry
iii,303–27.BerriosGE(1996)The History of Mental Symptoms: Descriptive Psychopathology Since the Nineteenth Century.
Cambridge:CambridgeUniversityPress.BoorseC (1976)What a theory ofmental health shouldbe. Journal of the Theory of Social Behavior 6, 1,
61–84.FabregaH(2000)Culture,spiritualityandpsychiatry.Current Opinion in Psychiatry13,525–30.Fulford KWM, Thornton T and Graham G (2006) Oxford Textbook of Philosophy of Psychiatry. Oxford:
OxfordUniversityPress.JamesW(1902)The Varieties of Religious Experience.London:Penguin.JaspersK(1959)General Psychopathology,7thedn.(transl.HoenigJandHamiltonMW,1963).Manchester:
ManchesterUniversityPress.KendellRE(1975)Theconceptofdiseaseand its implications forpsychiatry.British Journal of Psychiatry
127,305–15.McGinnC(1997)The character of mind: an introduction to the philosophy of mind,2ndedn.Oxford:Oxford
UniversityPress.Mowbray RM, Ferguson Rodger T and Mellor CS (1979) Psychology in Relation to Medicine, 5th edn.
Edinburgh:ChurchillLivingstone.MundtC(2000)Editorial.Psychopathology33,2–4.MurphyEA(1979)Theepistemologyofnormality.Psychological Medicine9,409–15.Phillips J (2004)Understanding/explanation. InRadden J (ed.)The Philosophy of Psychiatry: a Companion.
Oxford:OxfordUniversityPress.PopperK(1974)Unended Quest.Harmondsworth:Penguin.RosenhanDL(1973)Onbeingsaneininsaneplaces.Science179,250–8.ScaddingJG(1967)Diagnosis:theclinicianandthecomputer.Lancetii,877–82.SedgwickP(1973)Illness–mentalandotherwise.Hastings Center Studies1,3,19–40SpitzerM(1990)Whyphilosophy?InSpitzerMandMaherBA(eds.)Philosophy and Psychopathology.New
York:Springer-Verlag.SzaszTS(1960)Themythofmentalillness.American Psychologist15,113–8.WalkerC(1988)Philosophicalconceptsandpractice:thelegacyofKarlJasper’spsychopathology.Current
Opinion in Psychiatry1,624–9.WalkerC(1993a)KarlJaspersasaKantianpsychopathologist.I.Thephilosophicaloriginsoftheconcept
offormandcontext.History of Psychiatry4,209–38.WalkerC(1993b)KarlJaspersasaKantianpsychopathologist.II.TheconceptofformandcontextinJaspers’
psychopathology.History of Psychiatry4,321–48.WalkerC(1994)KarlJaspersandEdmundHusserl:I:theperceivedconvergence.Philosophy, Psychiatry and
Psychology1,117–34.WalkerC(1995a)KarlJaspersandEdmundHusserl:II:thedivergence.Philosophy, Psychiatry and Psychology
2,245–65.WalkerC(1995b)KarlJaspersandEdmundHusserl:III:JaspersasaKantianphenomenologist.Philosophy,
Psychiatry and Psychology2,65–82.WigginsOP,SchwartzMAandSpitzerM(1992)Phenomenology/descriptivepsychiatry: themethodof
Edmund Husserl and Karl Jaspers. In Spitzer M, Uehlein F, Schawartz MA and Mundt C (eds.)Phenomenology, Language and Schizophrenia.NewYork:Springer-Verlag.
WingJK(1978)Clinicalconceptsofschizophrenia.In:WingJK(ed.)Schizophrenia: Towards a New Synthesis.London:AcademicPress.
WittgensteinL(1953)Philosophical Investigation(transl.AnscombeGEM).Oxford:Blackwell.

19
C H A P T E R 2
Eliciting the Symptoms of Mental Illness
SummaryThe clinical assessment of patients, which includes history taking, mental state examination,physicalexaminationandthesynthesisofthefindingsintoadiagnosisthattakesaccountofthepatient’s biological, psychological and social environment, is the basis of psychiatric practice.Withoutit,noadequatetreatmentandfurtherclinicalmanagementispossible.Attheheartofthistaskistheimportanceoffocusingonthepatientasthecentreofclinicalattention,recogniz-ingthevalueofrespectforthedignityofthepatient,andregardingthepatient’snarrativeaccountasvaluable,richandprivileged.Theascendancyofatickboxapproachtoclinicalassessmentistobedeplored.Itfailstograspthatdespitethefactthatassessmentshaveastructuretothem,andthattheyaresystematicinquiries,assessmentsmustbeconductedinaconversationalstyleandinahumanemanner.
Human beings are like parts of a body,Created from the same essence.
When one part is hurt and in pain,The others cannot remain in peace and be quiet.
If the misery of others leaves you indifferentAnd with no feelings of sorrow,
You cannot be called a human being.Sa’adi (thirteenth century), Persian
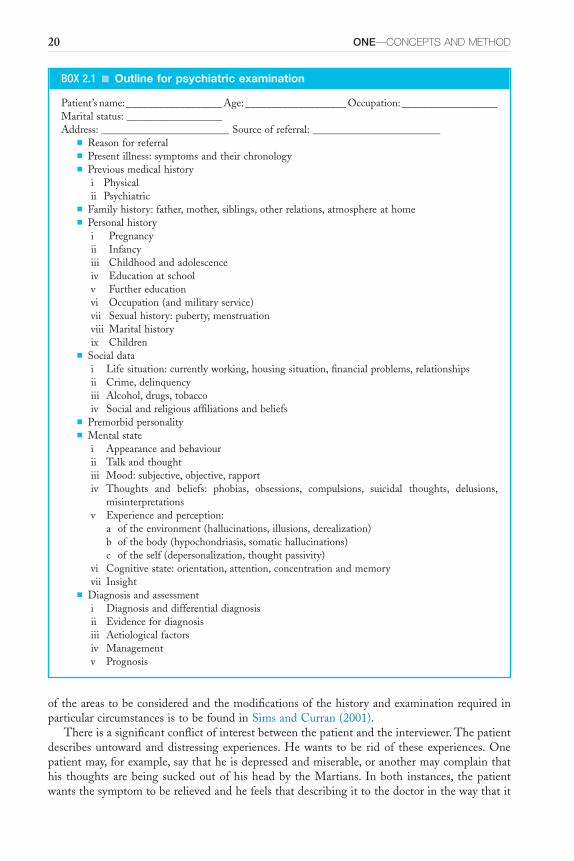
Elicitingthesymptomsandsignsofemotionaldistressinvolvesactivelylisteningtoanarrativeaccountoftheperson’scomplaintsandhisinternalstateandobservingthewholerepertoireofbehaviourandthenreducingthesetoafewsummarizingphrases.Itisadifficulttask,requiringanabilitytolistenandcommunicate,asensitivitytotheneedsandfeelingsofapersonwhoisbewilderedanddistressedandaknowledgeofthepossibleconditionsgivingrisetothecomplaint.Agenuine interest inthehumanconditionanditsmanifoldexpressions,aswellasacuriosityabout intrapsychic experiences, is essential.This cannot be learned from a book alone, but astructureforcasetakingthatsuggestslikelyareasforexplorationisinvaluable.Therearemanycomprehensiveschemes,andtheycanoftenbetracedtoearliertextbookswithonlyslightmodi-fication.AsummaryoftheschemeonwhichthischapterisbasedisshowninBox2.1.Apracticalguidetohistorytakingandevaluationofthementalstate,diagnosis,formulationandmanage-mentisfoundintheHandbook for Trainee Psychiatrists(Rix,1987)andinThe Psychiatric Interview(Carlat,2005).Ausefulapproachtomakingthepatientinformationavailablefordiagnosisandplanning treatment is Making Sense of Psychiatric Cases (Greenberg etal., 1986) and there aremore in-depth texts on the psychiatric interview such as The Psychiatric Interview in Clinical Practice(MacKinnonetal.,2006)andThe First Interview(Morrison,2008).Afurtheraccount

Keywords:Diagnosis,History,MentalStateExamination.
2—ElICITINg THE SyMPTOMS Of MENTAl IllNESS 19.e1
20 ONE—CONCEPTS AND METHOD
BOX 2.1 ■ Outline for psychiatric examination
Patient’sname:__________________Age:___________________Occupation:__________________Maritalstatus:__________________Address:________________________Sourceofreferral:________________________
■ Reasonforreferral■ Presentillness:symptomsandtheirchronology■ Previousmedicalhistory
i Physicalii Psychiatric
■ Familyhistory:father,mother,siblings,otherrelations,atmosphereathome■ Personalhistory
i Pregnancyii Infancyiii Childhoodandadolescenceiv Educationatschoolv Furthereducationvi Occupation(andmilitaryservice)vii Sexualhistory:puberty,menstruationviii Maritalhistoryix Children
■ Socialdatai Lifesituation:currentlyworking,housingsituation,financialproblems,relationshipsii Crime,delinquencyiii Alcohol,drugs,tobaccoiv Socialandreligiousaffiliationsandbeliefs
■ Premorbidpersonality■ Mentalstate
i Appearanceandbehaviourii Talkandthoughtiii Mood:subjective,objective,rapportiv Thoughts and beliefs: phobias, obsessions, compulsions, suicidal thoughts, delusions,
misinterpretationsv Experienceandperception:
a oftheenvironment(hallucinations,illusions,derealization)b ofthebody(hypochondriasis,somatichallucinations)c oftheself(depersonalization,thoughtpassivity)
vi Cognitivestate:orientation,attention,concentrationandmemoryvii Insight
■ Diagnosisandassessmenti Diagnosisanddifferentialdiagnosisii Evidencefordiagnosisiii Aetiologicalfactorsiv Managementv Prognosis
oftheareastobeconsideredandthemodificationsofthehistoryandexaminationrequiredinparticularcircumstancesistobefoundinSimsandCurran(2001).
Thereisasignificantconflictofinterestbetweenthepatientandtheinterviewer.Thepatientdescribesuntowardanddistressingexperiences.Hewants tobe ridof these experiences.Onepatientmay,forexample,saythatheisdepressedandmiserable,oranothermaycomplainthathis thoughtsarebeing suckedoutofhisheadby theMartians. Inboth instances, thepatientwantsthesymptomtoberelievedandhefeelsthatdescribingittothedoctorinthewaythatit
2—ElICITINg THE SyMPTOMS Of MENTAl IllNESS 21
isaffectinghimisthefirststageinachievingthis.Thedoctorneedstolearnalotofthingsfromthepatientthatthelattermayconsiderirrelevant.Sheneedstohaveaprecisedescriptionofthesymptomsandofthepatient’sstateofmind.Sheneedstoknowaboutthecontextofthepatient’ssymptoms,includingthepatient’sdevelopmentalhistory,andabouthisadjustmenttohissocialenvironmentingeneralandtohissymptomsinparticular.Toreturntoourexamples,thedoctorneedstoknownotonlythatthepatientfeelsdepressed;shemustenquireabouttheprecisenatureofthe‘depression’,whatthewordimpliestothepatient,howtheaffectdisturbstheroutineofhislifeandwhetherthereareanyotherassociatedsymptoms.
The person suffering at the hands of the Martians will be only too ready to talk aboutMartians. However, they are largely irrelevant to the interviewer, who is interested in exactlywhattheexperienceof‘thoughtsbeingextracted’entails.Whatisthepatient’sevidencethatthishappens? What other abnormal mental phenomena are experienced?The reader can perhapsunderstandthepatient’s irritationifhecanimaginethat,afterhehadpaidhisgasbill,afinaldemandnoticewithanintimationthathisgassupplywastobecutoffcamethroughthelet-terbox.Onexplainingtotheauthoritiesthathisbillwasalreadypaid,theydidnotapologizeorsaythattheywouldcorrecttheircomputer,buttheystartedinterrogatingtheharassedconsumerastowhyheshouldbesoupsetaboutit,andwhatwashisevidencethathehadbeenespeciallypickedonbytheauthorities.Understandably,thereisapotentialconflictofinterestbetweenthepatient’s wish for relief of symptoms and the doctor’s need to start by making a diagnosis.Acompromiseisnecessary.
Thepatientwillquitequicklytireoftheeffortrequiredtoanswerquestionsthatareaimedat establishing thephenomenological statusof subjective experiences.Several short interviewsarepreferabletoamarathonsession:‘neverasktodaywhatyoucanasktomorrow’.Thismethodshouldencouragetheexaminerto‘bracketout’allpreconceptions,andthepatienttoreflectonhisexperiencesunderguidancefromtheexaminer,whoshouldnotbediggingforphenomenalikeadogatarabbithole.Itisimportantfortheexaminertodistinguishquiteclearlybetweenobservationsandinferences.
Diagnosis and LabellingWhymakeadiagnosis?Themedicalclassificationofdiseasesallowsaclusterofsymptomstobebroughtunderasingletermthatembodiestheessenceofagivencondition.Thediagnostictermcarriesinformationinanefficientmanner.Buttherearedisadvantages,includingtheunreliabilityofdiagnostictermsaswellastheriskofunduelabellingandtheassociatedstigmaofpsychiatricdiagnosis. It is central to the work of a professional that her first task is to carefully collectinformationsothatsheknowsexactlywhatclinicalproblemconfrontsherwithinherprofessionalcompetence,andthereforewhatactionwouldbeappropriate;thisiswhatdiagnosisimplies.Itis true that formanycommonmedicaldiseases suchasdiabetes, thediagnostic termrefers tounderlyingdemonstrablepathophysiology forwhich independentmarkersexist, suchasbloodsugarlevels,etc.Inpsychiatry,practicallyallthemajordisordersarestillrecognizedatasyndromallevel, that isby theclusterof signsandsymptoms thatare thought tobe typicalof thegivendisease.The diagnostic term does not, as yet, refer to any well-described pathophysiology orindeed to any independent or reliable marker.This is a significant problem for the status ofpsychiatricdiseasesasbona fidemedicaldiseases.
Inpsychiatry, amultifactorial approach to theunderstandingof disorder is the rule ratherthan the exception.This is the basis of the biopsychosocial approach topsychiatric disorders.Thismeansthatanarrowdiagnosis,inpurelyorganicorpurelybehaviouralterms,isinadequate.Thediagnosisneedstobemadeinthecontextofanunderstandingofthebiological,psychologi-cal and social antecedents, which in turn determine the biological, psychological and socialmanagementofthecondition.

22 ONE—CONCEPTS AND METHOD
The Psychiatric HistoryThisaccountischieflyinterestedinthewaythattaking the historyshedslightonthemental state.Thenatureandtypeofreferralisnotedandrecorded,forexamplefromageneralpractitionerasanurgentproblem,fromasolicitorforacourtreportandsoon.Afterrecordingthereasonforreferral,thehistorywillusuallybeginwiththepatient’sverbatimdescriptionofhispresent symp-toms,includingthedurationofeachsymptomandanaccountofthedevelopmentoftheillness.Usingthepatient’sownwords isvaluable ingiving insight intohisstateofmindandhowhehimselfviewshissymptoms.Itishelpfulafterreceivingacatalogueofcomplaintstoask‘Whichistheveryworstofall thesesymptoms?Orwhat isyourmainconcern?’Thisrevealshowthepatientconceptualizeshisproblemandalsosuggestsapreliminarytargetfortreatment.
Often, the patient’s history of his present complaint is literally his story; there is nothingwronginrecordingthisinnarrativestyleprovidedthisisaccurate.Achronologicalaccountofthepresentillnessrevealshowthepatientregardsthedevelopmentofhissymptomsaswellasgivinginformationontheactualhistory.Inthehistory,onewantstoknowaboutthesequenceof symptoms and the effects these symptoms had on the patient’s lifestyle, about changes inbehaviourandaboutalterationsinphysicalfunction.Itisappropriateatthispointtonotepsy-chiatricsymptomsofwhichthepatienthasbeenawareinthepastbutforwhichhehasneverconsultedadoctororreceivedtreatment.Theymayhaverelevance inthetotalpictureofhowtheillnessdeveloped,anditisknownthatthemajorityofpeoplewithpsychiatricconditionsofclinicalseveritydonotseekmedicalconsultation,letalonecometotheattentionofapsychiatrist(Andrewsetal.,2001).
Thepatientfeelsittobeinnatelyreasonabletodescribechronologicallyandmeticulouslyhispreviousillnesses,operationsandaccidents.Healsowillappreciatethelogicofgivingdetailsofhospitalandgeneralpracticetreatmentformentalillnessandwillusuallygiveaccurateinforma-tionwithregardtodates,duration,natureoftreatment,inwhathospitalandwhetherhewasanin-patient or out-patient.Treatment received from the family doctor is recalled less well; thedatesarelessreliableandoftenthepatientdoesnotknowwhatwasthenatureoftreatmentorwhatitwasfor.
Thefamily historyisconcernedwithgeneticandenvironmental,pathoplasticfeatures.Historyofmentalillness,suicide,natureoftreatmentandsoonisrelevantforthefirst-degreerelatives(thosesharing50%ofthegeneticmaterialwiththepatient:parents,siblings,children)andmoredistantrelatives.Itisimportanttoknowaboutthequalityofrelationships,emotionalbondingandinterpersonalconflicts,bothforthefamilyinwhichthepatientwasachildandforthefamilyinwhichthepatientmaybeaparent.Relationshipsbetweenindividualmembersofthefamilyaredescribed,andalsothegeneralemotionalatmosphereandsocialandfinancialproblems.Theoccupationsofdifferentfamilymembersgiveinformationaboutthesocialcontext;arecordofhealthmayberelevant,asmayadescriptionoftheirpersonalities.Ofcourse,thefamilyisseenthroughthepatient’seyes;thismeansthatitisnotjustafactualdescriptionbutratheranaccountof theemotional impactthepatient feelshis familyhasmadeonhim.If thehistoryfromthepatientissupplementedbyanaccountfromanotherinformant,thisbiasofthepatient’swillitselfgiveinformationthatmaybeusefulinsubsequenttreatment.
Thepersonal history tracesthestagesofthepatient’sdevelopment,healthandformationofrelationshipsfromconception,birthandinfancythroughchildhood,schoolexperiences,adoles-cenceandfurthereducationtoanoccupational,maritalandsexualhistory.Thefactualdetailsofthese stages need to be recorded, and also the way they have influenced the personality andattitudesofthepatient,howhefeelsaboutthem,howhehasrelatedtootherpeople(forexampleteachersandworkmates)andhowallthesedetailsareconnectedwiththepsychiatriccondition.Thereareatleasttwoprocessesatplayintakingahistory.Thereisthesimplebusinessoftakingafactuallyaccurateaccountofapatient’shistoryofcomplaintsaswellasthefamily,personaland

2—ElICITINg THE SyMPTOMS Of MENTAl IllNESS 23
socialhistory.Inadditiontothisapproach,thereistherequirementtograspthemeaningofthepatient’shistory,thatis,hisstory,inordertounderstandhowheseeshimselfinrelationtotheworldandhowhisdevelopmentandcircumstanceshavebeeninfluentialinprovoking,exacerbat-ing or ameliorating his present illness. The factual history is the foundation of the clinicaldiagnosis.Humanbeingsliveinaworldofmeanings,andthesymbolicandsocialdimensionofthehistoryarethebasisofanadequateandhumaneresponsetothepatient’sillnessanddistress.Accountsthatemphasize,forexample,thefactthatthepatientisanonlychild,apreciouschild,avictimofotherpeople’smaliciousintentions,afighterwhohasstruggledagainsttheodds,oranunluckyindividualforwhomonlyfailureandrejectioncharacterizetheirlifeallsaysomethingaboutthedominantthemes,theprismthroughwhichtheindividualanalyzesandperceivestheworld.So,whilstitisimportanttorecordthefacts,themeaningsandunderstandingthatpatientshaveofthetrajectoryoftheirlifeallcommunicatesomethingthatenrichestheclinicalencounter,andpotentiallymakepossibleadeeperdoctor-patientrelationshipthatshouldbesatisfyingforbothdoctorandpatient.
Premorbid, Previous or Usual PersonalityAssessmentofpersonalityisthemostcomplexandproblematictaskthatapsychiatristfaces.Inclinicalinterviews,thedoctorassessesthepatient’spersonalityusingthreeareasofinformation.First,theexaminerasksthepatienttodescribeindetailhisrelationshipswithotherpeople,hisinterestsandactivities.Second,theexaminerstudiesthewayinwhichthepatientreactstotheexaminerintheinterviewsituation.Third,theexaminertriestohelpthepatienttodescribeanddemonstratewhathe,thepatient,islikeasaperson;howhefeelsinsidehimselfindifferentsitu-ations;andhisinterests,goalsandstandards.
Personalityassessmentisnottheexclusivepreserveofpsychiatristsorpsychologists,butanimportantlearnedskillofmanyprofessionalswhodealwithpeople,forexampleschoolteachers,lawyersandevenbankmanagers,althoughtheirterminologyisdifferent.Personalityisthatpartofaperson,exceptinghisphysical characteristics, thatmakeshim individual, that is,differentfromotherpeople.Personalityisrevealedbyaperson’scharacteristicbehaviour;ifonecanpredicthowhewillreact,whathisbehaviourwillbeinparticularcircumstances,thenthebasisofthatpredictionistheevaluationofhispersonality.Subjectively,personalityisshowninthetotalityofaperson’saimsandgoals,formedofeverythingthathevaluesandtowhichheaspires.Personalityisnotathingbutanabstraction;onewayoflookingathumanbeings.Furthermore,itismulti-dimensionalandisbestdefinedinaction.Verbaldescriptionisunlikelytoexhausttheessenceofanyindividual.Indeed,nodescriptioncanexhausttheessenceofanyindividualperson.Itisatruismthathumanbeingsarefullofpotentialandcontinuetosurpriseandastonishwiththeircapacityforchange,fortransformationandformoralvirtues,whichmaynotbereadilyidentifi-ableonfirstcontact.
Categorizationintonormalandabnormalpersonalityrequiresafurtherlevelofabstraction.Normal,anordinarywordineverydayuse,needstobeusedmorerigorouslyinthiscontext(seeChapter1).Inmedicine,thetermnormalisoftenusedtodenoteastatisticalnorm,thatis,whatoccursinthemajorityofpeople.Equally,thetermisalsousedtomean‘ideal’,inthesenseofadescriptionthatconformstoan‘ideal’type.Inrelationtopersonality,classificationanddefinitionsofpersonalitydisordersdependondeviancefromthenorm,butthedefinitionsdependon‘ideal’descriptionsofpersonalitytypesorbetterstillatypology.Anormalpersonalityconformsthere-fore in its characteristics and the extent to which they are developed with the majority ofmankind.Abnormalpersonalityhassomecharacteristicsdevelopedorunderdevelopedtosuchanextentastobequantitativelydifferentfromthemassofpeople.Inotherwords,abnormalitiesofpersonalityaredifferencesofdegree;thedevianttraitsaresharedincommonwithothersbutexaggeratedinexpression.
24 ONE—CONCEPTS AND METHOD
Intheclinicalinterview,therearevariousareasofdialoguewiththepatientthatarelikelytoleadtousefulinformationfordepictingthedetailandcolouringofhispersonality–thepersonality type.Paintingthepictureanddefiningthetypearebothnecessaryclinicalexercises.Socialrela-tionsareinvestigated.Howdoesherelatetohisfamily?Ishedetachedoroverdependent?Whatsortoffriendshipsdoesheform,withwhatsortofpeople,andaretheycloseknitorsuperficial,withanexclusivefeworanunlimitedcrowd?Howdohisinterestsandleisureactivitiesinvolvehimwithothers?Socialorsolitary,structuredorinformal?Howdoesherelatetobosses,work-matesandemployeesatwork?Ishealeaderorafollower,anorganizeroraloner?Ishepliantor truculent, cooperative, sympathetic or clubbable? His sexual preferences and relationshipsshouldbenoted.
Thenatureofhisinterestsandactivitiesisinformative.Whatdoeshelikedoinginhissparetime?Ifheisinterestedinsport,itisusefultoknowifhecanfeelpartisanandinvolvedandalsowhetherhe is aparticipantor anobserver.Enquiry ismadeofhispreferenceand interests infilmsandliterature:howheobserves,criticizesandenjoysthematerial.Towhatsocialorganiza-tionsdoeshebelong?Religionrequiresmorethanasingleworddesignatingreligiousaffiliationinthecasenotes.Thephenomenologicalmethodisequallyrelevantforthisareaoflife.Whatistheindividual’sself-experienceofhisreligiousbeliefsandhowdotheseinteractwithpsychiatricsymptomatology(Sims,1994)?
Anaccountofhispredominantmood is requested, andwhetherhismood isfluctuatingorstable,responsivetoprecipitantsorendogenous.Charactertraitsimplyadetailedadjectivallist,forexample irritable,reserved, fussyandsoon.Itwill,ofcourse,behelpful tocorroboratehisdescriptionwithanaccountfromanotherperson.Enquiryismadeabouthisattitudesandvalues;hisviewsabouthimselfandhisbody;howheregardsothersclosetohim;hismoregeneralsocialvaluesinreligion,morality,politicsandeconomics;howhefeelseventsoccurandcanbemadetooccur.Driveandenergyandthewaytheseareexpressedinambition,lethargy,effectivenessandpersistenceareanimportantaspectofpersonality.
Studyofhisfantasylifeismade:thefrequencyanddurationofdaydreamsandtheircontent;whether thesearegoal-directedandrealisticordissociatedfromanyexpectationof fulfilment.Dreamsandothersupposedsignsofunconsciouspsychicactivityareuseful,especiallywhenthesubjectattemptstointerpretthem.Wemaycommentonhishabitsofingestion,inhalationandexcretion;whethertheyareregularandtowhatextenthedependsonthisregularity;ifthereisanindicationthatthereshouldbeamoredetailedhistoryandexplorationofcurrenthabitsofeating, smoking,drinkingalcoholandtakingotherdrugs.As thepatientunfolds the facetsofhispersonality,sotheoverallemphasesthatheputsinareasofdescriptionbecomeilluminatinginunderstandinghimasawholeperson.
Differentiation of Personality DisorderAllocatingthepatienttoapersonalitytypewithouttakingintoaccountthe infinitevariabilityofindividualsisquiteinadequate.However,certaincharacteristicstendtooccurtogetherandareof clinical significance. Allocation to a particular category of personality disorder is made onthe relative predominance of these different character traits. Having decided that a certaindefinitetraitortraitsarepresentinthisindividualtoanabnormalextent,doestheabnormalityofpersonalitycausethepersonhimselforotherpeopletosuffer?Thatis,ispersonalitydisorderpresent?
Morethanoneabnormaltypeofpersonalitymaybepresentinanyindividual;theyarenotmutuallyexclusive.Informulatingthepsychiatrichistoryandevaluationofmentalstate,commentonpremorbidpersonalityshouldalwaysbemade,evenifitisonlytostatethatduetotheravagesofthementalillnessitisimpossibletoassesspremorbidstate.Thepredominanttraitsshouldbedescribed,preferablywithverbatimcommentsofthepatienttoillustratethem.Theinterviewer
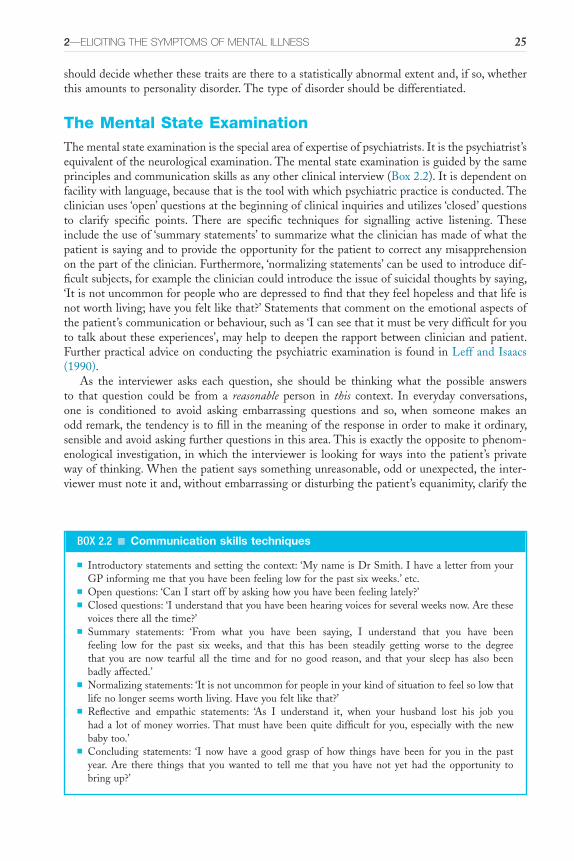
2—ElICITINg THE SyMPTOMS Of MENTAl IllNESS 25
shoulddecidewhetherthesetraitsaretheretoastatisticallyabnormalextentand,ifso,whetherthisamountstopersonalitydisorder.Thetypeofdisordershouldbedifferentiated.
The Mental State ExaminationThementalstateexaminationisthespecialareaofexpertiseofpsychiatrists.Itisthepsychiatrist’sequivalentoftheneurologicalexamination.Thementalstateexaminationisguidedbythesameprinciplesandcommunicationskillsasanyotherclinicalinterview(Box2.2).Itisdependentonfacilitywithlanguage,becausethatisthetoolwithwhichpsychiatricpracticeisconducted.Theclinicianuses‘open’questionsatthebeginningofclinicalinquiriesandutilizes‘closed’questionsto clarify specific points. There are specific techniques for signalling active listening. Theseincludetheuseof‘summarystatements’tosummarizewhattheclinicianhasmadeofwhatthepatientissayingandtoprovidetheopportunityforthepatienttocorrectanymisapprehensiononthepartoftheclinician.Furthermore,‘normalizingstatements’canbeusedtointroducedif-ficultsubjects,forexamplethecliniciancouldintroducetheissueofsuicidalthoughtsbysaying,‘Itisnotuncommonforpeoplewhoaredepressedtofindthattheyfeelhopelessandthatlifeisnotworthliving;haveyoufeltlikethat?’Statementsthatcommentontheemotionalaspectsofthepatient’scommunicationorbehaviour,suchas‘Icanseethatitmustbeverydifficultforyoutotalkabouttheseexperiences’,mayhelptodeepentherapportbetweenclinicianandpatient.FurtherpracticaladviceonconductingthepsychiatricexaminationisfoundinLeffandIsaacs(1990).
As the interviewer asks each question, she should be thinking what the possible answersto that question could be from a reasonable person in this context. In everyday conversations,one is conditioned to avoid asking embarrassing questions and so, when someone makes anoddremark,thetendencyistofillinthemeaningoftheresponseinordertomakeitordinary,sensibleandavoidaskingfurtherquestionsinthisarea.Thisisexactlytheoppositetophenom-enological investigation, inwhichthe interviewer is lookingforways intothepatient’sprivatewayofthinking.Whenthepatientsayssomethingunreasonable,oddorunexpected,theinter-viewermustnoteitand,withoutembarrassingordisturbingthepatient’sequanimity,clarifythe
BOX 2.2 ■ Communication skills techniques
■ Introductorystatementsandsettingthecontext:‘MynameisDrSmith.IhavealetterfromyourGPinformingmethatyouhavebeenfeelinglowforthepastsixweeks.’etc.
■ Openquestions:‘CanIstartoffbyaskinghowyouhavebeenfeelinglately?’■ Closedquestions:‘Iunderstandthatyouhavebeenhearingvoicesforseveralweeksnow.Arethese
voicesthereallthetime?’■ Summary statements: ‘From what you have been saying, I understand that you have been
feeling low for the past six weeks, and that this has been steadily getting worse to the degreethat you are now tearful all the time and for no good reason, and that your sleep has also beenbadlyaffected.’
■ Normalizingstatements:‘Itisnotuncommonforpeopleinyourkindofsituationtofeelsolowthatlifenolongerseemsworthliving.Haveyoufeltlikethat?’
■ Reflective and empathic statements: ‘As I understand it, when your husband lost his job youhada lotofmoneyworries.Thatmusthavebeenquitedifficult for you, especiallywith thenewbabytoo.’
■ Concluding statements: ‘I now have a good grasp of how things have been for you in the pastyear. Are there things that you wanted to tell me that you have not yet had the opportunity tobringup?’

26 ONE—CONCEPTS AND METHOD
innerexperiencepartly revealed.Thiswillentail theuseof theempathicmethoddescribed inChapter1.Oneofthedifficultiesfortheaspiringphenomenologististoknowwhentopursuewhatthepatientrevealsinmoredetail–whentomaketheincisionforthepsychopathologicaloperation.
Wordslimitaswellasliberate.Theclinicalinterviewerneedstobeverycarefulnottorestrainherpatient’sanswersbyimposingtheshacklesofpsychiatrictechnicaljargon.Carefulattentionmust be paid to the patient’s use of language and, as far as possible, the clinician should uselanguagethatmirrorsthepatient’slanguage.Itisimportanttobecertainthatbothclinicianandpatientareusingwordsinthesamesense.Thequestion‘Doyouhearvoices?’isagoodexampleof this.The patient may truthfully answer ‘No’ and yet be suffering from almost continuousauditoryhallucinations.Thisparticularperceptualexperienceismostoftendescribedbypatientsandtheirdoctorsas‘voices’.However,phonemesmaybethoughtofbythepatientinquiteotherterms.Hemaymakenodistinctionatallbetweentheseauditoryperceptions,‘voices’hehearsforwhichanoutsideobserverrealizesthereisanappropriatestimulus,andauditoryhallucina-tions.Hemaybelargelyobliviousoftheformofthecommunicationasauditoryandhallucinatorybecause he is totally absorbed with its content (an order telling him to go to Strasbourg andpreach).Obviously,anotherpatientmayanswerthequestion‘Doyouhearvoices?’truthfullyintheaffirmativeandyethaveaquitedifferentformofphenomenologicalexperiencefromauditoryhallucination(seeChapter7).
Almosteverytechnical termingeneralmedicinehasdiagnosticimplications.Thisisalsotrueinpsychiatry.Asymptommaynotbepathognomonicofacertainconditionbutneverthelessispredominantlyfoundwiththatillness.Ifthedoctorusesthetermperseverationindescribingherpatient’s mental state to a colleague, she is by inference suggesting a diagnosis of an organicpsychiatricstate.If this isnotthediagnosis,shehassomehardexplainingtodoto justifytheuseofthatword.Isitreallyperseverationorjusttherepetitioususeofwordsandphrasesinapersonwhohasintellectualdisabilityandshowspovertyofexpression?Toavoidmisunderstand-ing, it isbesttouse longerdescriptionsuntil the interviewer issurethatthesymptomistrulypresent.
Observationoftheappearanceandbehaviourofthepatientisaninvaluablesupplementtohisself-description.Theobservationsofothers,andat timesother thanthe interview,needtobetakenintoaccount.Astheinterviewproceeds,theinterviewermoredefinitelypursuesherrealintention of finding out the meaning behind the words the patient uses.What is the patientfeeling and experiencing? His own account may be a blind to prevent other people, or evenhimself,seeinghowbadhereallyfeels.Theempathic method isinvaluableinworkingoutwhatheisimplying.Soalsoisacute,insightfulandtrainedobservation.Observationmayrevealwhitelinesacrosstheknucklesofananxiouspersontalkingaboutwhatupsetshimmostandwhichrenders him impotently angry. Empathy allows the observer to employ his own capacity foremotionasadiagnosticandtherapeutictool.Trainingandexperienceareessentialforknowinginwhichareasdelvingwillberewardedwithusefulinformation:howtoaskquestionsthatarecomprehensibletopatientsofdifferentverbalabilitiesandculturalbackgrounds,andwhichwillresultinappropriateanswers;howtoavoiddamagingthepatientstillfurtherwithwell-directedbut brutal questions. Observation and empathy must always be used together in eliciting themental state. Note also the double meaning of the word observant: not only noticing what isgoingonaroundbutalsoconformingwiththeculturalmoresoftheimmediatesociety.Agoodphenomenologistwillbeobservantinbothsensesoftheword.
Systematic EnquiryTheappearance andbehaviour of thepatient areobserved for the clinicalmedical informationtheycarry.Doesthepatientlookill?Ishealert,oriented,fullyconscious,fluctuatinginhismental

2—ElICITINg THE SyMPTOMS Of MENTAl IllNESS 27
state? Are there any behavioural or neurological abnormalities? Observation is also useful forassessingnon-verbalcommunication(Argyle,1975).Fromhisposture,gestures,facialexpressionandsoonhebetrayshisstateofemotion,informationabouthispersonalityandhisattitudetotheobserverandtoothersdespitehissilenceorcontradictoryverbalcommunication.Obviously,observationofbehaviouralsoindicatespsychiatricsymptomatologysuchastics,catatonicmove-ments,possiblehallucinatoryperception,feedingandexcretingdisorders.Posturecanberevealingto theacuteobserver, for instance thepharaonic posture and the slowdeliberatemovementsofheadandneckofthepatientwithschizophrenia.Ifthepatient ismute,observedbehaviour istheonlysourceofclinical information,buttheimportanceofobservationneedstobestressedalsoforthosepatientswhodospeak.Observationmaybevaluabletocorroboratethepatient’scomplaints, to make clear the degree of emotional involvement he has in his symptoms, orsometimestocontradicthisstatement,forexamplethepersonwhomanifestsphysicallyextremeanxietyyetdeniesanyworriesonenquiry.
Talk reveals thought.Listening to and studying thepatient’s utterances is usually themostimportantpartofassessinghismentalstate.Thoughtdisorderandtheinterpretationofabnor-malitiesintheuseofwords,syntaxandassociationofideasarediscussedinmoredetailinChapter9.Theflowoftalkmeritsnotice.Doeshetalkvolublyandeasilyorintaciturnmonosyllables?Doeshe just answer questions or speak spontaneously? Is his conversation appropriate to thesocial context, and is it coherent? Is the train of thought readily distracted?Throughout theinterview,asmuchaspossibleofthepatient’sspeechshouldberecordedverbatim.Thisprovidesaclearerpictureofthisindividualperson’sinnermilieu,andalsothedataofself-experiencewillallowanotherpersontoevaluatethediagnosis.
Astheinterviewerenquiresaboutandformsherownassessmentofmood,shehasthreeareasforexploration:subjectiveandobjectivedescriptionofmoodandevaluationofrapport.Thereismuchmoretomoodthanjustdepressionorelation;thefinernuancesofthisperson’ssubjectiveemotionalexperiencemustbecarefullydugoutliketruffles,usingasensitivenoseanddelicateextraction.Apersonanticipatinganeventmaybeacutelyapprehensive,exquisitelyexcitedbutratheranxious,hopelesslyresignedandsoon;‘afraidofthefuture’isnotanadequatedescription.Moodcanbestudiedforitsdirection(depressionorelation),itsconsistency(stableorlabile),itsappropriateness,itsamplitudeandthedegreeofdiscrepancybetweensubjectivedescriptionandobjectiveobservation.
Ofcourse,thereisreallynosuchthingaswhollyobjectiveassessmentofmood.Thedoctorcommentsonthemoodstateofherpatientfromherobservationofthepatient’sdemeanourandthegeneraltoneofhisconversationduringtheinterview.Shemakesthecomment,‘Heappearsdepressed;heisagitatedandtense’.Infact,thiscommentonherpatient’semotionabbreviatestheempathicprocessthroughwhichshegoestomakethisjudgement.Thedoctorobservesthepatientandpicksupavailablecuesformood,relatingthesetoherexperiencewithotherpatientsandotherpeople throughher life,andultimately toherknowledgeofherownaffectivestate.Herassessment runs ‘If I felthowmypatient looks, speaksandacts, Iwould feelprofoundlydepressedandagitated;heis,onobservation,depressedandagitated.’
Rapport is ausefulmeasureof thepatient’s ability to communicatehis feelings to anotherperson.Theinterviewerneedstomakeherselfintoayardstick,aconstant rapport maker,againstwhich the patient’s ability to make rapport can be measured.To do this, the doctor requiresclinicalexperienceandanobjectivityinwhichsheknowshowshereactsto,andcommunicateswith,manydifferentsortsofpeople.Sheknowsherselfandherowncompetencewellenoughtoexclude this from the assessment of rapport so that, as far as possible, it is only the patient’scapacityforemotionalcommunicationthatisbeingtested.
Theideasandbeliefsthepatientholdsandabnormalities of perceptionheexperiencesareascer-tainedandexploredduringtheinterview.Inordinaryconversation,thereisagreatdealoffillinginoreditingtoeliminatethedeficienciesofcommunication.Apersontalksandcomestoahalt

28 ONE—CONCEPTS AND METHOD
halfway through a sentence for loss of a word.The other person provides the word and thuscontinuestheconversationtobothparties’satisfaction.Thereisatendencyforthosecomingnewtodialoguewith thementally ill tobring into their conversation these socialniceties that areusedtosaveembarrassment.Thedoctortendstonotewhatshethinksthepatientmeanttosay,asifthelatter’sthinkingprocessesweresimilartoherown,ratherthanconcentratingonwhatheactuallysaid.Alotofsignificantpsychopathologyisthusmissed.Delusionsandhallucinationsarenotvolunteeredbythepatientassymptomsfortheobviousreasonthattheyarenotexperi-encedasdifferentfromtherestoftheperson’sthinkingorperceiving.Tothepatient,subjectively,adelusionisindistinguishablefromanyotheridea,ahallucinationisindistinguishablefromanyothernormalperception.Skillininterviewingthereforecomesverymuchinknowingwhentolookforadelusionandhowtomakeacleardistinctionbetweenwhatthepersondescribesasexperienceandwhatitrevealsphenomenologically.
Passivityordelusionsofcontrol,obsessions, compulsionsanddepersonalizationmaybeobviousoronlymadeplainwithsomedifficulty.Itisimportanttotrytocategorizethetypeofexperienceasearlyinthecourseofexposuretoprofessionalenquiryaspossible,becausepatients’explana-tions tend to become contaminated on repeated questioning. When passivity, for example, issuspected,itisgenerallybesttofollowupthecluesrightawayanddecideonceandforallwhetherthesymptomispresent.
Assessmentof the cognitive state includes, at leastbriefly, testing fororientation, attention,concentration and memory. The Mini-Mental State Examination (Folstein etal., 1975) is awidelyused standardizedbedside testof cognitive function that isuseful toadminister in theclinicalsetting.
Thedoctor,fromspecificquestionsandfromtheinterviewingeneral,needstoformanideaof her patient’s attitude to his illness, difficulties and prospects.To what extent does he haveinsightintohiscondition?Anyillnessofsomeseveritywillalterthepatient’sworldandviewoftheworld.Insightassessestheawarenessofthischangebythepatientandtheaccuratelabellingofthischangeasoriginatingfromamental illnessthatrequirestreatment.Insightisthereforehighlycomplexasafunction.Itistheabilityoftheindividualtobeself-awareandtobesensitivetoinnersubjectivechange.Thecapacitytocorrectlyattributethesubjectivepsychologicalchangetopathologicalcausesisevidenceofintactself-awarenessdespiteevidenceofmentalillness.Itispotentiallyanextremelyvaluablepartofthementalstateexamination,asitisassociatedwithcompliance with treatment and also with the likelihood of treatment under compulsion. Insummary,insighthasthreecomponents:recognitionofsubjectivepsychologicalchange,labellingofthischangeaspathologicalinnatureandrecognitionofneedfortreatmentaswellascompli-ancewithtreatment(David,1990;seeChapter11).
Manytextbooksandnumerouspsychiatricinstitutionshavetheirownschemeforpsychiatricinterviewing.This account is a general commentary rather than yet another scheme. Box 2.1containsamemorandumofkeyareastobecoveredinthehistoryandexaminationofapsychiatricpatient.
ReferencesAndrewsG,IssakidisCandCarterG(2001)Theshortfallinmentalhealthserviceutilisation.British Journal
of Psychiatry179,417–25.ArgyleM(1975)Bodily Communication.London:Methuen.CarlatDJ(2005)The Psychiatric Interview,2ndedn.Philadelphia,LippincottWilliams&Wilkins.DavidAS(1990)Insightandpsychosis.British Journal of Psychiatry156,789–808.FolsteinMF,FolsteinSEandMcHughPR(1975)‘Mini-mentalstate’.Apracticalmethodofgradingthe
cognitivestateofpatientsfortheclinician.Journal of Psychiatric Research12,189–98.Greenberg M, Szmuckler G and Tantam D (1986) Making Sense of Psychiatric Cases. Oxford: Oxford
UniversityPress.

2—ElICITINg THE SyMPTOMS Of MENTAl IllNESS 29
Leff JP and Isaacs AD (1990) Psychiatric Examination in Clinical Practice, 3rd edn. Oxford: BlackwellScientific.
MacKinnonRA,MichelsRandBuckleyPJ(2006)The Psychiatric Interview in Clinical Practice.Arlington:AmericanPsychiatricPublishing.
MorrisonJ(2008)The First Interview,3rdedn.London:TheGuildfordPress.RixKJB(1987)Handbook for Trainee Psychiatrists.London:BaillièreTindall.SimsA(1994)‘Psyche’–spiritaswellasmind?British Journal of Psychiatry165,441–6.SimsAandCurranS(2001)Examinationofthepsychiatricpatient.InHennF,SartoriusN,HelmchenH
andLauterH(eds.)Contemporary Psychiatry.Berlin:Springer.

This page intentionally left blank
S E C T I O N TWOConsciousness and Cognition

This page intentionally left blank
33
C H A P T E R 3
Consciousness and Disturbed Consciousness
SummaryConsciousnessisadefiningcharacteristicofanimals,althoughconsciousself-awarenessmaybeparticulartohumanbeings.Abnormalitiesofconsciousnessareproblematicfromaphenomenol-ogypointofviewbecause,bydefinition,self-reportsofpathologicalstatesunlikeself-reportsofconsciousexperiencearenot immunefromerror.Theunconsciousstate isnotprivilegedsincethesubjectisunabletoreportonthenatureandqualityoftheexperienceandeveninsituationswherethereisonlyminimalimpairmentofconsciousness,self-reportsarestillopentoqualifica-tionandquery.Hencetheterminologyisdeterminedbytheobservationofeitherthequantitativedegreeofabnormalityortheapparentqualitativechangesinconsciousstate.Theterminologyisimprecise and often several different terms are used for identical or frankly indistinguishablestates.Inthischaptertermssuchasvigilance,lucidity,cloudingofconsciousness,delirium,stupor,comaandsomeothershavebeenintroducedanddefined.
Psychiatry and neuropathology are not merely two closely related fields, they are but one field in which only one language is spoken and the same laws rule.
Wilhelm Griesinger (1868)
I have always been intrigued by the specific moment when, as we sit awaiting in the auditorium, the door to the stage opens and a performer steps into the light, or, to take the other perspective, the moment when a performer
who waits in semidarkness sees the same door open, revealing the lights, the stage, and the audience … as I reflect on what I have written, I sense that stepping into the light is also a powerful metaphor for consciousness, for the
birth of the knowing mind, for the simple and momentous coming of the self into the world of the mental.
Antonio Damasio (1999)
Onemustbeconscious inorder tobeable toexperience theworld.Sothe logical startingplaceforthestudyofsymptoms,fromasubjectivestandpoint,isthatwhichallowssubjectivitytoexist(consciousness).Untilquiterecently,studiesofconsciousnesswerelookedonwithsus-picionbyneuroscientists,therebyleavingclinicians,bothneurologistsandpsychiatrists,inintel-lectualdarkness.Thishasbeenrectifiedinthepastdecadethroughcombiningandsharingtheperspectivesofdifferentdisciplines:philosophy,psychology,medicineandneurosciences(BockandMarsh,1993).
Althoughit isessential forourclinicalworkconcerningdisturbances inconsciousnessthatweusetheprinciplesofdescriptivepsychopathologyandappliedphenomenology,weneedtobeawareofthelimitations(Dennett,1991).DennetthaspointedoutthatfromDescartesviaLocke,

Keywords: Consciousness,Delirium,Stupor,TwilightState,Automatism.
3—CONSCIOUSNESS AND DISTUrbED CONSCIOUSNESS 33.e1
34 TWO—CONSCIOUSNESS AND COGNITION
BerkeleyandHume,phenomenologyhastendedtodescribeconsciousnessfromthefirstpersonplural: ‘according to longstanding philosophical tradition we all agree on what we find whenwe“lookinside”atourownphenomenology’.Wemaynotallbethesameinside,andevenifweare, we may get it wrong when we try to describe our inner experiences. He also questionsthe purely third person perspective of behavioural psychology and advocates the ‘Method ofHeterophenomenology’.This depends, for its authenticity, on the meticulous precision of thequestionsasked,theobjectivityofrecordingthetranscript(threestenographerspreparingseparatedocumentsfromanaudiotapedinterview),adoptingthe‘intentionalstance’(assumingthatthesubjectofinvestigationwasintendingtomakeastatementaboutsomething)andscopeforclari-fication.Whenthisprocesshasbeenfollowed,thetext‘istakentobethesincere,reliableexpres-sionandtobeasingle,unified subjectofthatverysubject’sbeliefsandopinions’.Itbecomesclearthatthisprocessissimilar,althoughmorehighlystructuredforresearchpurposes,totheseparatestepsinthemethod of empathy,asdescribedinChapter1.
The terminology in this area is appallingly confused. This and subsequent chapters haveattemptedtoclarifythewordsused,sometimesattheexpenseofsacrificingaltogethertermswithalonghistory,andsometimeslumpingasasingleconceptwordsbetweenwhichthereareonlyminutedifferencesofmeaning.Onemajorproblemisthatdifferentdisciplinesusedifferenttermstocoverpartlyoverlappingmeanings.
Conscious and Unconscious ExperiencesCONSCIOUSNESS
Thewordsconsciousness, conscious mindandawarenessareusedveryfreelyinpsychiatrybutoftenwithoutaprecisemeaning.Consciousness‘isastateofawarenessoftheselfandtheenvironment’(Fish, 1967); also, consciousness ‘is to be conscious, to know about oneself and the world’(Scharfetter,1980);and,‘byconsciousness,Isimplymeanthosesubjectivestatesofsentienceorawareness thatendwhenonegoes tosleepatnightor falls intoacoma,ordies,orotherwisebecomes as one would say, unconscious’ (Searle, 1994). Consciousness is characterized by itssubjective nature and privacy. Furthermore, consciousness appears to have a unique quality,termed qualia, that is recalcitrant to any external physical description. This is the particularcharacterofanyobjectofourconsciousexperience,forexampletherednessofthecolourredasweperceiveit.Consciousnessisalsointentional,bywhichwemeanthatit isdirectedtowardsobjects;thatistosaythatconsciousnesshascontent–itisalwaysaboutsomething.Finally,ourconsciousexperience isunified intoawholeandnotgiventous in fragmentsorunintegratedparts.
Theterm,asusedbyclinicians,refersfirsttotheinnerawarenessofexperienceasopposedtothecategorizingofeventsastheyoccur.Second,itreferstothesubjectreactingtoobjectsdelib-erately.Third,itdenotesaknowledgeofaconsciousself.
UNCONSCIOUSNESS
Unconscious, according to Jaspers (1959), ‘means something that is not an inner existence anddoesnotoccurasanexperience;secondly,somethingthatisnotthoughtofasanobjectandhasgoneunregarded;thirdly,itissomethingwhichhasnotreachedanyknowledgeofitself ’.
In clinical practice, the term unconscious is used in three quite different ways that have incommononlythephenomenologicalelementinthatthereisnosubjectiveexperience(Figure3.1).
■ Aperson suffering fromseriousbraindiseasemaybeunconscious; consciousness in thisinstanceisseenasbeingonacontinuum,withanormalstateofconsciousnessatoneendanddeathattheother.
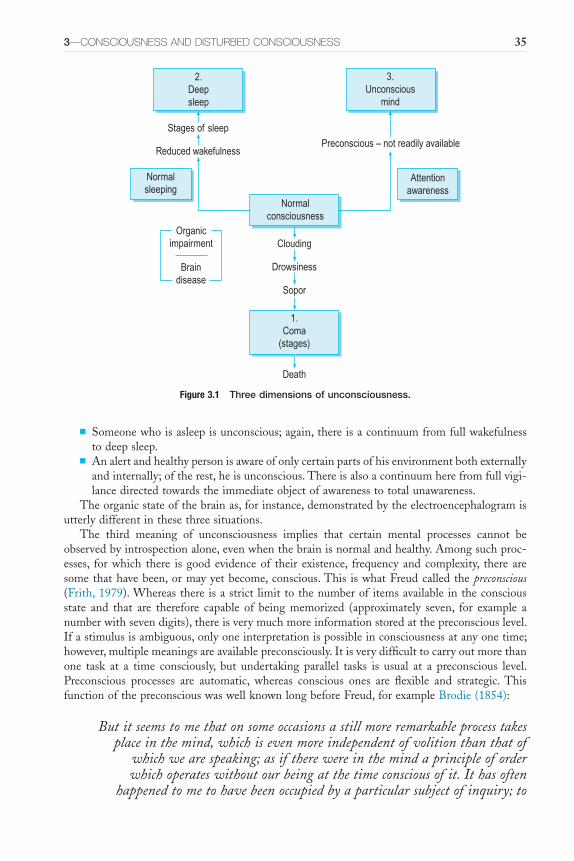
3—CONSCIOUSNESS AND DISTUrbED CONSCIOUSNESS 35
■ Someonewhoisasleepisunconscious;again,thereisacontinuumfromfullwakefulnesstodeepsleep.
■ Analertandhealthypersonisawareofonlycertainpartsofhisenvironmentbothexternallyandinternally;oftherest,heisunconscious.Thereisalsoacontinuumherefromfullvigi-lancedirectedtowardstheimmediateobjectofawarenesstototalunawareness.
Theorganicstateofthebrainas,forinstance,demonstratedbytheelectroencephalogramisutterlydifferentinthesethreesituations.
The third meaning of unconsciousness implies that certain mental processes cannot beobservedbyintrospectionalone,evenwhenthebrainisnormalandhealthy.Amongsuchproc-esses, forwhich there is goodevidenceof their existence, frequency andcomplexity, there aresomethathavebeen,ormayyetbecome,conscious.This iswhatFreudcalledthepreconscious(Frith,1979).Whereasthereisastrict limittothenumberofitemsavailableintheconsciousstate and that are therefore capable of being memorized (approximately seven, for example anumberwithsevendigits),thereisverymuchmoreinformationstoredatthepreconsciouslevel.Ifastimulusisambiguous,onlyoneinterpretationispossibleinconsciousnessatanyonetime;however,multiplemeaningsareavailablepreconsciously.Itisverydifficulttocarryoutmorethanone task at a time consciously, but undertaking parallel tasks is usual at a preconscious level.Preconscious processes are automatic, whereas conscious ones are flexible and strategic. ThisfunctionofthepreconsciouswaswellknownlongbeforeFreud,forexampleBrodie(1854):
But it seems to me that on some occasions a still more remarkable process takes place in the mind, which is even more independent of volition than that of
which we are speaking; as if there were in the mind a principle of order which operates without our being at the time conscious of it. It has often
happened to me to have been occupied by a particular subject of inquiry; to
Figure 3.1 Three dimensions of unconsciousness.
Stages of sleep
Reduced wakefulnessPreconscious – not readily available
Normalconsciousness
3.Unconscious
mind
2.Deepsleep
1.Coma
(stages)
Death
Normalsleeping
Organicimpairment
Braindisease
Clouding
Drowsiness
Sopor
Attentionawareness

36 TWO—CONSCIOUSNESS AND COGNITION
have accumulated a store of facts connected with it; but to have been able to proceed no further. Then, after an interval of time, without any addition to
my stock of knowledge, I have found the obscurity and confusion, in which the subject was originally enveloped, to have cleared away; the facts have all seemed to have settled themselves in their right places, and their mutual relations to have become apparent, although I have not been sensible of
having made any distinct effort for that purpose.
Unconsciousinthesenseaboveisatheorythatpsychiatristsandpsychopathologistshavetoexplain some aspects of observable behaviour. Whereas in the other two senses of the term‘unconscious’,itisthefactthattheindividualisunconscioustotheworld,thatisheisunrousableandunabletoparticipatewiththisawarenessofthesensoryworldintact,thatisatstake.
DIMENSIONS OF CONSCIOUSNESS
Consciousness,then,istheawarenessofexperience.Theremaybeawarenessofobjectsorself-reflection. Awareness of objects includes the capacity to be aware of oneself as an object (seeChapter14); self-reflection refers to the subjective experiencingof self.The threedimensionsofconsciousness(contrastedwithunconsciousness,as inFigure3.1)arevigilance, lucidityandself-consciousness.
Vigilance (Wakefulness)–Drowsiness (Sleep)
Vigilanceistakentomeanthefacultyofdeliberatelyremainingalertwhenotherwiseonemightbedrowsyor asleep.This isnot auniformorunvarying state,but itfluctuates.Factors insidethe individual thatpromotevigilanceare interest, anxiety, extreme fearor enjoyment,whereasboredomencouragesdrowsiness.Thesituation in theenvironmentandtheway the individualperceivesthatsituationalsoaffecttheirpositiononthevigilance–drowsinessaxis.Someabnormalstatesofhealthincreasevigilance,whilemanydiminishit.
Aswellasthecontrastbetweenvigilanceanddrowsiness,therearequalitativedifferencesinthenatureofwakefulness.Thevigilantstateofmindofapersonscanningaradarscreenforapossibleenemyinterceptorisverydifferentfromtheraptattentionofamusicloverlisteningtoasymphony.TheseaspectsofattentionandtheirabnormalitiesarediscussedinChapter4.
Lucidity–Clouding
Consciousnessisinseparablefromtheobjectofconsciousattention:luciditycanbedemonstratedonlyinclarityofthoughtonaparticulartopic.Thesensorium,thetotalawarenessofallinternalandexternalsensationspresentingthemselvestotheorganismatanyparticularmoment,maybeclearorclouded.Obviously,lucidityisnotunrelatedtovigilance:unlessthepersonisfullyawake,hecannotbeclearinconsciousness.
Clouding of consciousness denotes the lesser stages of impairment of consciousness on acontinuum from full alertness and awareness to coma (Lishman, 1997).The patient may bedrowsyor agitated and is likely to showmemorydisturbance anddisorientation. In clouding,mostintellectualfunctionsareimpaired,includingattentionandconcentration,comprehensionand recognition, understanding, forming associations, logical judgement, communication byspeechandpurposefulaction.
Consciousness of Self
Alongsidefullwakefulnessandclearawarenessisanabilitytoexperienceself,andanawarenessofself,thatisbothimmediateandcomplex.ThisisconsideredinmoredetailinChapter12.
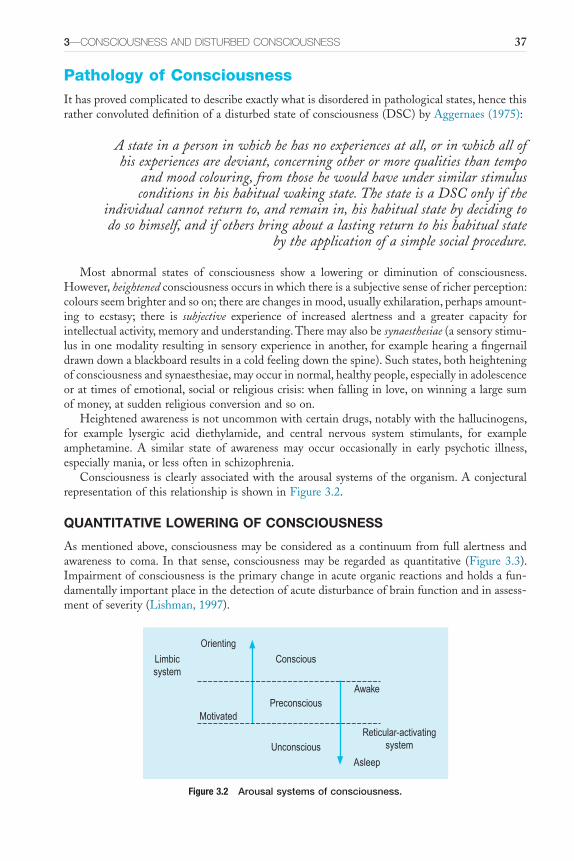
3—CONSCIOUSNESS AND DISTUrbED CONSCIOUSNESS 37
Pathology of ConsciousnessIthasprovedcomplicatedtodescribeexactlywhatisdisorderedinpathologicalstates,hencethisratherconvoluteddefinitionofadisturbedstateofconsciousness(DSC)byAggernaes(1975):
A state in a person in which he has no experiences at all, or in which all of his experiences are deviant, concerning other or more qualities than tempo
and mood colouring, from those he would have under similar stimulus conditions in his habitual waking state. The state is a DSC only if the
individual cannot return to, and remain in, his habitual state by deciding to do so himself, and if others bring about a lasting return to his habitual state
by the application of a simple social procedure.
Most abnormal states of consciousness show a lowering or diminution of consciousness.However,heightenedconsciousnessoccursinwhichthereisasubjectivesenseofricherperception:coloursseembrighterandsoon;therearechangesinmood,usuallyexhilaration,perhapsamount-ing to ecstasy; there is subjective experience of increased alertness and a greater capacity forintellectualactivity,memoryandunderstanding.Theremayalsobesynaesthesiae(asensorystimu-lusinonemodalityresultinginsensoryexperienceinanother,forexamplehearingafingernaildrawndownablackboardresultsinacoldfeelingdownthespine).Suchstates,bothheighteningofconsciousnessandsynaesthesiae,mayoccurinnormal,healthypeople,especiallyinadolescenceorattimesofemotional,socialorreligiouscrisis:whenfallinginlove,onwinningalargesumofmoney,atsuddenreligiousconversionandsoon.
Heightenedawarenessisnotuncommonwithcertaindrugs,notablywiththehallucinogens,for example lysergic acid diethylamide, and central nervous system stimulants, for exampleamphetamine. A similar state of awareness may occur occasionally in early psychotic illness,especiallymania,orlessofteninschizophrenia.
Consciousness isclearlyassociatedwiththearousalsystemsoftheorganism.AconjecturalrepresentationofthisrelationshipisshowninFigure3.2.
QUANTITATIVE LOWERING OF CONSCIOUSNESS
Asmentionedabove,consciousnessmaybeconsideredasacontinuumfromfullalertnessandawareness to coma. In that sense, consciousnessmaybe regarded asquantitative (Figure3.3).Impairmentofconsciousnessistheprimarychangeinacuteorganicreactionsandholdsafun-damentallyimportantplaceinthedetectionofacutedisturbanceofbrainfunctionandinassess-mentofseverity(Lishman,1997).
Figure 3.2 Arousal systems of consciousness.
Orienting
Motivated
Conscious
Unconscious
Asleep
AwakePreconscious
Reticular-activatingsystem
Limbicsystem
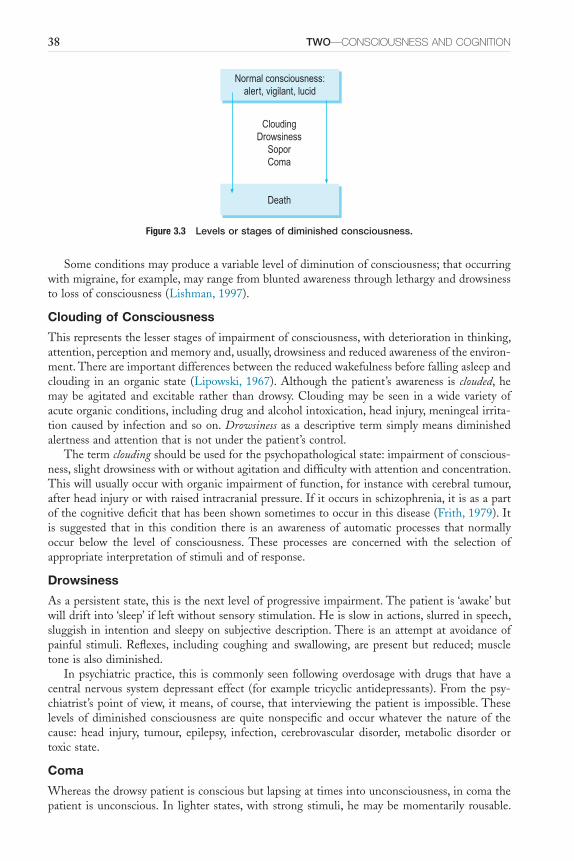
38 TWO—CONSCIOUSNESS AND COGNITION
Figure 3.3 Levels or stages of diminished consciousness.
CloudingDrowsiness
SoporComa
Normal consciousness:alert, vigilant, lucid
Death
Someconditionsmayproduceavariablelevelofdiminutionofconsciousness;thatoccurringwithmigraine,forexample,mayrangefrombluntedawarenessthroughlethargyanddrowsinesstolossofconsciousness(Lishman,1997).
Clouding of Consciousness
Thisrepresentsthelesserstagesofimpairmentofconsciousness,withdeteriorationinthinking,attention,perceptionandmemoryand,usually,drowsinessandreducedawarenessoftheenviron-ment.Thereareimportantdifferencesbetweenthereducedwakefulnessbeforefallingasleepandclouding inanorganic state (Lipowski,1967).Although thepatient’s awareness is clouded,hemaybe agitated and excitable rather thandrowsy.Cloudingmaybe seen in awide varietyofacuteorganicconditions,includingdrugandalcoholintoxication,headinjury,meningealirrita-tioncausedby infectionandsoon.Drowsinessasadescriptive termsimplymeansdiminishedalertnessandattentionthatisnotunderthepatient’scontrol.
Thetermcloudingshouldbeusedforthepsychopathologicalstate:impairmentofconscious-ness,slightdrowsinesswithorwithoutagitationanddifficultywithattentionandconcentration.Thiswillusuallyoccurwithorganicimpairmentoffunction,forinstancewithcerebraltumour,afterheadinjuryorwithraisedintracranialpressure.Ifitoccursinschizophrenia,itisasapartofthecognitivedeficitthathasbeenshownsometimestooccurinthisdisease(Frith,1979).Itis suggested that in this condition there is an awarenessof automaticprocesses thatnormallyoccur below the level of consciousness. These processes are concerned with the selection ofappropriateinterpretationofstimuliandofresponse.
Drowsiness
Asapersistentstate,thisisthenextlevelofprogressiveimpairment.Thepatientis‘awake’butwilldriftinto‘sleep’ifleftwithoutsensorystimulation.Heisslowinactions,slurredinspeech,sluggish in intentionandsleepyonsubjectivedescription.There isanattemptatavoidanceofpainful stimuli.Reflexes, including coughing and swallowing, arepresentbut reduced;muscletoneisalsodiminished.
Inpsychiatricpractice, this iscommonlyseen followingoverdosagewithdrugs thathaveacentralnervoussystemdepressanteffect (forexample tricyclicantidepressants).Fromthepsy-chiatrist’spointofview, itmeans,ofcourse, that interviewingthepatient is impossible.Theselevelsofdiminishedconsciousness arequitenonspecific andoccurwhatever thenatureof thecause: head injury, tumour, epilepsy, infection, cerebrovascular disorder, metabolic disorder ortoxicstate.
Coma
Whereasthedrowsypatientisconsciousbutlapsingattimesintounconsciousness,incomathepatient isunconscious. In lighter states,with strongstimuli,hemaybemomentarily rousable.

3—CONSCIOUSNESS AND DISTUrbED CONSCIOUSNESS 39
Therearenoverbalresponsesorresponsestopainfulstimuli.Therightingresponseofposturehasbeenlost;reflexesandmuscletonearepresentbutgreatlyreduced;breathingisslow,deepandrhythmic;thefaceandskinmaybeflushed.
Inlaterstages,thepatientisnolongerrousable;heisdeeplyunconscious.Distinctstagesofcomahave identifiablephysical signsultimately culminating inbraindeath, but these arenotdiscussedfurtherinthisbook–theyarebeyondpsychiatry(ConferenceofMedicalRoyalCollegesandtheirFaculties,1976).Practicalassessmentofthedepthanddurationofimpairedconscious-nessandcomahasbeenquantifiedonthescaledevisedbyTeasdaleandJennett(1974).
Thesestagesareall thosethatoccurprogressivelyandquantitativelywithloweringofcon-sciousness.Qualitativevariationsarenowdiscussedfurther.
QUALITATIVE CHANGES OF CONSCIOUSNESS
Variousotherorganicdisturbances inbrainfunctionarerecognized.Thesearevirtuallyalwaysassociatedwithsomedegreeofquantitativeimpairment.Theuseofterminologyinthiswholeareaofdiscourseis,unfortunately,verymuddled,withthesametermsometimeshavingdifferentmeaningsandsimilarphenomenabeingdescribedbydifferentwords.
Delirium
Lipowski(1990)definesdeliriumas‘atransientorganicmentalsyndromeofacuteonset,char-acterizedbyglobal impairmentofcognitive functions,a reduced levelofconsciousness,atten-tionalabnormalities, increasedordecreasedpsychomotoractivityandadisordered sleep–wakecycle’.Therecognitionthatthetermdeliriumshouldrefertoasyndromeinvolvingglobaldis-turbancewas incorporated in the Diagnostic and Statistical Manual of Mental Disorders, fourthedition(DSM-IV;AmericanPsychiatricAssociation,1994).InDSM-IV,thetermdescribesadisturbanceofconsciousnessthatisaccompaniedbyachangeincognitionthatcannotbebetteraccountedforbyapre-existingorevolvingdementia.Thereisareductionintheclarityofaware-nessoftheenvironment.Similarly,theICD-10 Classification of Mental and Behavioural Disorders(WorldHealthOrganization,1992)usesthetermdeliriuminagenericandglobalsense:
An etiologically nonspecific syndrome characterized by concurrent disturbances of consciousness and attention, perception, thinking, memory, psychomotor
behaviour, emotion and the sleep-wake cycle.(p. 57)
Subjectiveaccountsofdeliriumarerareandthefewpublisheddescriptionsareopentocriti-cismgiventheestablishedfactthatconsciousness is impairedindeliriumandthedescriptionshavehadtobeconstructedwithhindsight.Nonetheless,Crammer’s(2002)accountconfirmedpartialstatesofarousalduringwhichsomememoryfunctionsandbeliefformationcanbepresent,despite apparent unconsciousness. Inhis comments onCrammer’s account,Fleminger (2002)drewattentiontothefactthattheexperienceofdeliriumisakintodreaming,butthatdeliriumisrememberedwithgreatervividnessthandreams.Also,thatwhereasitistraditionaltoconceiveofdeliriumasbeingadisturbanceofconsciousness,itmightbemoreprofitabletothinkofitasadisturbanceofthesleep-wakecycle.Thisiswhytheexperienceofdeliriumisakintodreamingandwhythereisevidencethatdeliriumismorelikelyinindividualswithsleepdeprivation.
Fluctuation of Consciousness
Fluctuations in consciousness levels are seen in various conditions. It occurs in health, insleepandinfatigue.Inpatientswithepilepsy,thereisfluctuationinrelationtofitsanditmayoccurbefore,duringoraftertheseizures.Alterationsofconsciousness levelaredescribedwiththird-ventricle tumours associated with variations in intracranial pressure (Sim, 1974). In

40 TWO—CONSCIOUSNESS AND COGNITION
deliriousstates,theremaybeconsiderablediurnalfluctuationofconsciousness.Characteristically,the patient becomes more disorientated, disturbed in mood and distracted perceptually withillusionsandhallucinationsinthelateeveningandshowsgreatestluciditymid-morning.Suchvariationofconsciousnesslevelisalsodescribedandobservedwithdrugs,forinstancemescaline,inwhichtheremayalsobefluctuationsoftimesense.
Confusion
The concept of confusion was originally developed in France (confusion mentale) and later inGermany (Verwirrtheit) in the nineteenth century (Berrios, 1981). It is a term, impreciselydefined,referringtosubjectivesymptomsandobjectivesignsindicatinglossofcapacityforclearand coherent thought. It is purely a descriptiveword anddoesnot only apply to cloudingofconsciousness. When physicians, psychiatrists and nurses were asked what confusion meant,markeddiscordancewasfound.Thetermshouldbeusedonlyifclearlydefined(Simpson,1984).Itoccurswithimpairmentofconsciousnessinacuteorganicstatesandwithdisruptionofthoughtprocessesduetobraindamageinchronicorganicstates,butitisalsoseeninnon-organicdis-turbance.Thus,confusionofthinkingmayoccuraspartofthepictureinfunctionalpsychosesandalsoinassociationwithpowerfulemotioninneuroticdisorders.Itshouldthereforebeusedsimplytodescribethesedisturbancesofthoughtandnotasatermpathognomonicoforganicpsychosyndromes.
To simplify, therefore, confusion of thinking canbedescribed as occurring eitherwhen theindividualdescribeshisownthinkingasbeingconfusedorwhentheexternalobserverconsidersthatthethoughtprocessesaredisturbedandconfused.Phenomenologically,therefore,itissimplyadescriptionofthepatient’sself-experienceorthedoctor’sobservation.
OTHER TERMS
Twilight State
A twilight state is a well-defined interruption of the continuity of consciousness (Sims etal.,2000).Itisusuallyanorganicconditionandoccursinthecontextofepilepsy,alcoholism(mania à potu),braintraumaandgeneralparesis;itmayalsooccurwithdissociativestates.Itischaracter-izedby(a)abruptonsetandend;(b)variableduration,fromafewhourstoseveralweeks;and(c) theoccurrenceofunexpectedviolentactsoremotionaloutburstsduringotherwisenormal,quietbehaviour(Lishman,1997).Ifthetermisreservedforthesethreefeaturesincombination,asapsychopathologicalentity,thenitshouldbeusedwhenevertheyconcur,irrespectiveofcause.
Theforensicimplicationsofthisconditionarethereforeimportant,andithasbeenusedasalegaldefenceforviolentbehaviourforwhichthepersonhadsubsequentamnesia.
Consciousnessmaybemarkedlyimpairedorrelativelynormalbetweenepisodes.Theremaybeassociateddream-likestates,delusionsorhallucinations.Itissometimesassociatedwiththetemporallobeseizuresofepilepsy;itmayoccurwithotherorganicstateswithoutepilepsy;similarbehaviourmayoccurinapparenthystericaldissociation;anditisalsodescribedasanacutereac-tiontomassivecatastrophe.Intheforensiccontext,itisimportanttodemonstrate(a)theoccur-renceof similar episodeswith inexplicablebehaviourbefore thekeyhappening and (b)other,objectiveevidenceofphysicalormentalillness.TheGanser state(describedwithmemorydisordersinChapter5)is,inpractice,asortoftwilightstateinwhichtheorganicelementisoftendubious.
Mania à Potu (Pathological Intoxication)
Thisisonetypeoftwilightstatespecificallyassociatedwithalcoholism.Itisimportanttodis-tinguish this syndromeofacutepathological intoxicationwithalcohol fromdeliriumtremens,whichisasymptomofwithdrawal.Keller(1977)hasdefinedmania à potuas:

3—CONSCIOUSNESS AND DISTUrbED CONSCIOUSNESS 41
an extraordinarily severe response to alcohol, especially to small amounts, marked by apparently senseless violent behaviour, usually followed by
exhaustion, sleep and amnesia for the episode. Intoxication is apparently not always involved and for this reason pathological reaction to alcohol is the
preferred term. The reaction is thought to be associated with exhaustion, great strain or hypoglycaemia, and to occur especially in people poorly defended
against their own violent impulses.
Coid(1979)describesfourcomponents:■ theconditionfollowstheconsumptionofavariablequantityofalcohol■ senseless,violentbehaviourthenensues■ thereisthenprolongedsleep■ totalorpartialamnesiaforthedisturbedbehaviouroccurs.Becausethereisoftendoubtastowhetherintoxicationreallyfollowedtheconsumptionof
aninappropriatelysmallamountofalcohol,andbecauseseveraloftheothercausal factorsarediagnosticcategoriesintheirownright(hypoglycaemia,epilepsy),Coidwoulddoawaywiththediagnosticcategoryofpathologicalintoxicationinthedefinitionabove,leavingonlyeitheracutedrunkennessoranotherconditionassociatedwithalcoholintake.
Automatism
Automatismimpliesactiontakingplaceintheabsenceofconsciousness.IthasbeendefinedbyFenwick(1990)asfollows:
An automatism is an involuntary piece of behaviour over which an individual has no control. The behaviour itself is usually inappropriate to the
circumstances, and may be out of character for the individual. It can be complex, co-ordinated, and apparently purposeful and directed, though lacking
in judgement. Afterwards, the individual may have no recollection, or only partial and confused memory, of his actions.
Epilepticautomatismmaybedefinedasastateofcloudingofconsciousnessthatoccursduring,or immediatelyafter, a seizureandduringwhich the individual retainscontrolofpostureandmuscletoneandperformssimpleorcomplexmovementsandactionswithoutbeingawareofwhatishappening(Fenton,1975).Itoccursaspartoftheclinicalpresentationofpsychomotorepilepsy,mostoftenarising fromdischarge in the temporal lobes. Itwasparticularlycommon in thosepatientswithchronicepilepsywhowereresidentinanepilepsycolonyoramentalhospital.
Anauramaybethefirstsignofanepilepticattackwithtemporallobeautomatismandmaybemanifestedasabdominalsensations;feelingsofconfusionwiththinking;sensationselsewhereinthebody,especiallythehead;hallucinationsorillusions(especiallyolfactoryorgustatory);andmotorabnormalitiessuchastoniccontracture,masticatorymovement,salivationorswallowing.
Behaviourduringautomatismisusuallypurposefulandoftenappropriate,forinstancecon-tinuingtodrythedishes.Awarenessoftheenvironmentisimpaired;thepatientappearstobeonlypartlyawareofbeingspokentoanddoesnotreplyappropriately.Initially,activityisdimin-ished,withstaringeyesandslumpedposture;itthenbecomesstereotyped,withrepetitivemove-ments, lip smacking, fumbling andother actions.Finally,more complexpurposeful behaviouroccurs, such as walking about, making irrelevant utterances, removing clothing and so on.Sometimes,thepatientmaycontinue,duringautomatism,withwhateverhewasdoingbefore,forexampledrivinghiscar,althoughthereissubsequentamnesiaandthebehaviourorspeechatthetimeneverappearsentirelynormal.

42 TWO—CONSCIOUSNESS AND COGNITION
Violence is rare during automatism, and when it occurs it usually amounts to resistingrestraint.However,automatismis,rarely,citedasanexplanationforaperson’sviolentandcriminalactionofwhichheisunawareafterwards.Thelegaldefinitionthenbecomes‘Thestateofapersonwho though capable of action, is not conscious of what he is doing… it means unconscious,involuntaryactionand it isadefencebecause theminddoesnotgowithwhat isbeingdone’(Kilmuir,1963).Clearly,whensuchviolentbehaviouroccursautomatismfulfilsthecriteriaforthedefinitionoftwilight stateasdefinedabove.
Speech automatism occurs when there is utterance of identifiable words or phrases at somestageduringtheepilepticattack,ofwhichthepatienthasnomemorylater.Phenomenologically,then,automatismisactionwithoutanyknowledgeofacting,anditisthelatterclaimthatrequirescarefulinvestigation.
Dream-Like (Oneiroid) State
This is an unsatisfactory term not clearly differentiated from twilight state or delirium.Thepatientisdisorientated,confusedandexperienceselaboratehallucinations,usuallyvisual.Thereisimpairmentofconsciousnessandmarkedemotionalchange,whichmaybeterrororenjoymentofthehallucinatoryexperiences;theremayalsobeauditoryortactilehallucinations.Thepatientmayappeartobelivinginadreamworld,andso-calledoccupational deliriumcouldbementionedinthiscontext,forinstancetheship’spettyofficer,admittedtohospitalafteraheadinjuryatsea(associatedwithexcessalcoholintake),whokeptshouting‘Mantheboats’.
Itisimportanttolookforothersymptomsororganicstatestomaketheimportantdistinctionbetweenphysicalillnessandadissociativenon-organiccondition.
Stupor
‘Stupornamesasymptomcomplexwhosecentralfeatureisareductionin,orabsenceof,relationalfunctions:thatis,actionandspeech’(Berrios,1996).Itisdistinctfromcomaanddoesnotlieonacontinuumfromwakefulnesstocoma.Thistermshouldbereservedforthesyndromeinwhichmutism and akinesis occur; that is, the inability to initiate speech or action in a patient whoappearsawakeandevenalert.Itusuallyoccurswithsomedegreeofcloudingofconsciousnessbut does not refer solely to a diminished level.The patient may look ahead or his eyes maywander,butheappearstotakenothingin.
Thissyndromeischaracteristicoflesionsintheareaofthediencephalonandupperbrainstem,andalso the frontal lobe andbasal ganglia, and the termakinetic mutism has sometimesbeenreservedbyneurologiststodescribeamuchmorenarrowlydefinedorganicsyndrome.Ararebutspecificconditioninvolvingthemotorpathwaysintheventralponsiscalledthe locked-in syn-drome,inwhichthereisquadriplegiaandanarthriawithpreservedconsciousnessandverticaleyemovement(PlumandPosner,1972;SmithandDelargy,2005).Itisimportanttorealize,however,thatthesymptomsofakinesisandmutisminaconsciouspatientalsooccurwithschizophrenia,withaffectivepsychoses(bothdepressiveandmanic)andindissociativestates.
Thedifferencebetweenpsychogenic(so-calledfunctional)andneurological(organic)causesofstuporcanbeclinicallyextremelyperplexing.Psychiatricdefinitionshavedemandedthatthecondition occurs when there is ‘a complete absence, in clear consciousness, of any voluntarymovements’(Wingetal.,1974).Ofcourse,itisnotpossibleatthetimeofobservationtoknowwhetherconsciousnessisquiteclearornot;andevenforfunctionalstupors,subsequentamnesiaiscommon.Aphenomenologicaldefinitionofstupormust,therefore,excludethestateofcon-sciousnessofamutepatient,anddiagnosisofstupormustthenbefollowedbyinvestigationofthedifferentialdiagnosiswhichincludesbothorganicandnon-organicconditions.
Sleep Disorders
ThesearediscussedinChapter4.

3—CONSCIOUSNESS AND DISTUrbED CONSCIOUSNESS 43
ReferencesAggernaes A (1975) The concepts: disturbed state of consciousness and psychosis. Acta Psychiatrica
Scandinavica51,119–33.American Psychiatric Association (1994) Diagnostic and Statistical Manual of Mental Disorders, 4th edn.
Washington:AmericanPsychiatricAssociation.Berrios GE (1981) Delirium and confusion in the 19th century: a conceptual history. British Journal of
Psychiatry139,439–49.BerriosGE(1996)The History of Mental Symptoms: Descriptive Psychopathology Since the Nineteenth Century.
Cambridge:CambridgeUniversityPress.BockGRandMarshJ(1993)Experimental and Theoretical Studies of Consciousness.Chichester:JohnWiley.BrodieBC(1854)Psychological Inquiries: in a Series of Essays.London:Longman,Brown,Green&Longman.CoidJ(1979)Maniaàpotu:acriticalreviewofpathologicalintoxication.Psychological Medicine9,709–19.ConferenceofMedicalRoyalCollegesandtheirFaculties(1976)Diagnosisofbraindeath.British Medical
Journalii,1187–8.CrammerJL(2002)Subjectiveexperienceofaconfusionalstate.British Journal of Psychiatry180,71–5.DamasioA(1999)The Feeling of What Happens: Body and Emotion in the Making of Consciousness.London:
WilliamHeinemann.DennettD(1991)Consciousness Explained.London:AllenLane.Fenton GW (1975) Epilepsy and automatism. In Silverstone T and Barraclough B (eds.) Contemporary
Psychiatry,pp.429–39.Ashford:HeadleyBrothers.Fenwick P (1990) Automatism. In Bluglass R and Bowden P (eds.) Principles and Practice of Forensic
Psychiatry.Edinburgh:ChurchillLivingstone.FishF(1967)Clinical Psychopathology.Bristol:JohnWright.FlemingerS(2002)Rememberingdelirium.British Journal of Psychiatry180,4–5.FrithCD(1979)Consciousness,informationprocessingandschizophrenia.British Journal of Psychiatry134,
225–35.GriesingerW(1868)QuotedinZilboorgGandHenryGW(eds.)(1941)A History of Medical Psychology.
NewYork:WWNorton.JaspersK(1959)General Psychopathology(transl.HoenigJandHamiltonMW,1963).Manchester:Manchester
UniversityPress.KellerM(1977)A lexiconofdisablements related toalcohol consumption. InAlcohol Related Disabilities.
Geneva:WorldHealthOrganization.Kilmuir,Viscount(1963)BrattyVAttorneyGeneralforNorthernIrelandAC386;(1961)3WLR965;(1961)
3AllER523.LipowskiZJ(1990)Delirium: Acute Confusional States.Oxford:OxfordUniversityPress.LipowskiZS(1967)Delirium,cloudingofconsciousnessandconfusion.Journal of Nervous Mental Diseases
145,227–55.LishmanWA(1997)Organic Psychiatry: the Psychological Consequences of Cerebral Disorder,3rdedn.Oxford:
BlackwellScientific.PlumFandPosnerJB(1972)Diagnosis of Stupor and Coma,2ndedn.Philadelphia:Davis.ScharfetterC(1980)General Psychopathology: an Introduction.Cambridge:CambridgeUniversityPress.SearleJR(1994)Theproblemofconsciousness.InRevonsuoAandKamppinenM(eds.)Consciousness in
Philosophy and Cognitive Neuroscience.Hillsdale:LawrenceErlbaumAssociates.SimM(1974)Guide to Psychiatry.Edinburgh:ChurchillLivingstone.SimpsonCJ(1984)Doctorsandnursesuseoftheword‘confused’.British Journal of Psychiatry145,441–3.SimsA,MundtC,BernerPandBarockaA(2000)Descriptivephenomenology.InGelderMG,López-Ibor
JJandAndreasenN(eds.)New Oxford Textbook of Psychiatry.Oxford:OxfordUniversityPress.SmithEandDelargyM(2005)Locked-insyndrome.British Medical Journal330,406–9.TeasdaleGandJennettB(1974)Assessmentofcomaandimpairedconsciousness:apracticalscale.Lancet
ii,81–4.Wing JK, Cooper JE and Sartorius N (1974) The Measurement and Classification of Psychiatric Symptoms.
Cambridge:CambridgeUniversityPress.WorldHealthOrganization(1992)The ICD-10 Classification of Mental and Behavioural Disorders: Clinical
Description and Diagnostic Guidelines.Geneva:WorldHealthOrganization.

This page intentionally left blank
45
C H A P T E R 4
Attention, Concentration, Orientation and Sleep
SummaryConsciousness,attention,concentrationandsleepareallinterrelatedphenomena.Inthepreviouschapter,consciousnessanditsabnormalitiesweredescribed.Attentionisoftenlikenedtoabeamoflightthatfocusesonalimitedareaofinterestwithinageneralfield,butitisbesttoconceiveofitasalimitedcapacitychannelthatisdynamicintheselectionandinhibitionofinformationforfurtherprocessing(Broadbent,1958;SmithandKosslyn,2007).Itisimportantforanorgan-ism’sabilitytoengagewithaspectsofitsenvironment.Itisrequiredfororientatingtheorganismwithin its environment. Abnormalities of impairment, therefore, underlie such disparate phe-nomenaasdisorientationandimpairmentofnewlearning.Thesleep-wakecycleisaphysiologicalmechanismthatdeterminesthealterationfromwakefulness,thatis,consciousnessandthespecialtemporarystateofunconsciousnessthatismanifestassleep.Abnormalitiesofthiscycleincludingdisturbancesofamount,quality,etc.aredescribedinthischapter.
Come, Sleep! O Sleep, the certain knot of peaceThe baiting–place of wit, the balm of woe,
The poor man’s wealth, the prisoner’s release,Th’ indifferent judge between the high and low.
Sir Philip Sidney (1554–1586), Astrophel and Stella, sonnet 39
Thetermsattention,concentrationandorientationhaveoftenbeenusedvery loosely. It issuggestedthattheiruseisrestrictedtothefollowing.Attentionistheactiveorpassivefocusingof consciousness on an experience such as sensory inputs, motor programmes, memories orinternal representations. It canbedefinedas theprocess that enhances some informationandinhibits others, thereby allowing us to select some information for further processing (SmithandKosslyn,2007).Theconceptoverlapswiththetermsalertness, awarenessandresponsiveness. Voluntaryattentionoccurswhenthesubjectfocuseshisattentiononaninternalorexternalevent;involuntary when the event attracts the subject’s attention without his conscious effort.Concentration is only one aspect of attention. It involves focused or selective attention. Otheraspects of attention include sustained attention or vigilance, divided attention and alternatingattention.Orientation isanawarenessofone’s setting in timeandplaceandof the realitiesofone’spersonandsituation.Itisnotadiscretefunctionbutiscloselyboundupwithmemoryandtheclarityorcoherenceofthought.
Thischapterisconcernedwithcognitivefunction,butitisnotlimitedtothefunctionsthatare disturbed by organic lesions and covers a wider field than just consciousness and itsdisorders.

Keywords:Attention,Concentration,Sleep,Hypersomnia,Parasomnia,Hypnosis.
4—ATTENTION, CONCENTrATION, OrIENTATION AND SlEEp 45.e1

46 TWO—CONSCIOUSNESS AND COGNITION
Attention, Awareness and ConcentrationAttention is adifferent function fromconsciousness, but it is dependenton it.Thus, variabledegreesofattentionarepossiblewithfullconsciousness,butcompleteattentionandconcentra-tionareimpossiblewithdiminishedconsciousness.WilliamJames’(1842–1910)(1890)accountisstillagoodstartingpoint:
Attention is … the taking into possession of the mind, in clear and vivid form, of one out of what seem several simultaneously possible objects or trains
of thought. Focalization, concentration, of consciousness are of its essence.
Therearepassiveandactivemodesofattention.Inpassiveattention,thesubjectrespondsto,forexample,aloudnoise,whereasinactiveattention,anindividual’spriorexpectationsandgoalsdetermineinatop-downfashionwhatisattendedto(seeEysenckandKeane,2010forafullerdescription).Acentralfeatureofattentionisitslimitedcapacity.Thisreferstothefactthatonlysomuchcognitiveprocessingactivitycanbecarriedoutatanyonetime.Attentionalcapacityisusually testedby thedigit span, and although it is a relatively stable feature of attention it ispronetoinfluenceby,forexample,fatigue,depressionandbraininjury.Componentsofattentionincludeorientatingtosensoryevents,detectingsignalsforfocusedprocessing,andmaintaininga vigilant andalert state. It is important to recognize thatknowledge,priorbeliefs, goals andexpectationscanalterthespeedandaccuracyoftheprocessesthatselectmeaningfulordesirableinformationfromtheenvironment.
Therearefourotheraspectsofattention.Focusedor selective attention referstothecapacitytohighlighttheoneortwoimportantstimuliorideasbeingdealtwithwhilesuppressingaware-ness of competing distractions.This aspect of attention is usually referred to as concentration.Serialsevensisusuallyemployedtoassessthisaspectofattention,anditrequiresfocusedatten-tionaswell asothercognitiveprocesses.Sustained attentionorvigilance involves theability tomaintain attentional activity over a period of time. It is usually measured by vigilance tests.Divided attentioninvolvestheabilitytorespondtomorethanonetaskatatimeortomultipleelementswithinatask.Alternating attentionallowsforshiftsinfocusofattentionandtasks(Lezaketal.,2004;Table4.1).
Automaticcognitiveprocesses,thatis,thosethatoccurwithoutintention,thatareinvoluntaryandthatdonotinterferewithotherongoingactivities,existinparallelwiththosethatrequireattentiveprocesses(KolbandWhishaw,1996).Theseautomaticprocessesallowfortheeffortlessextractionoffeaturesofaperceptioninbottom-upfashion,whereasattentiveprocessesallowforthetop-downprocessingofinformation(Figure4.1).
ALTERATION OF THE DEGREE OF ATTENTION
Attentionisdecreasedinnormalpeopleinsleep,dreams,hypnoticstates,fatigueandboredom.Itmaybepathologicallydecreasedinorganicstates,usuallywithloweringofconsciousness,forinstancewithheadinjury,acutetoxicconfusionalstatessuchasdrug-andalcohol-inducedcondi-tions,epilepsy,raisedintracranialpressureandbrainstemlesions.Inpsychogenicstates,attentionmaybealtered,forexamplediminishedinhystericaldissociation.Narrowingofattentionisalsoprominentindepressiveillness,inwhichthemorbidmoodstateresultsinattentionbeinglimitedtoarestrictednumberofthemes–mostlyunhappy.
Aseveredeficitofattentionisaprominentfeatureinthehyperkineticdisordersinchildhood(WorldHealthOrganization,1992)butwhichalsooccurinadultlife(seeChapter3).Observationofthechild’sbehaviourbyadultssuchasparentsorteachersconcentratesonthreeaspects:inat-tention,impulsivenessandhyperactivity.Inattentionisshowninthatthechild,mostoftenaboy
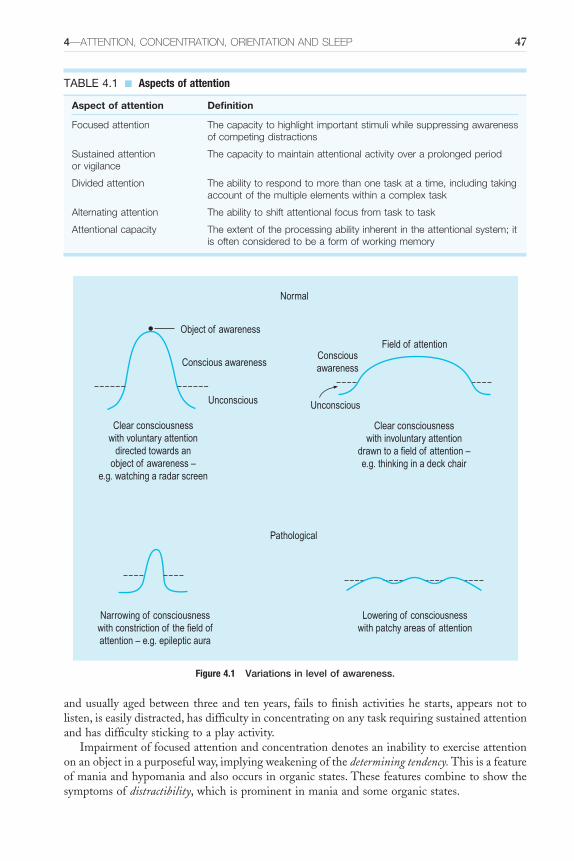
4—ATTENTION, CONCENTrATION, OrIENTATION AND SlEEp 47
TABLE 4.1 ■ Aspects of attention
Aspect of attention Definition
Focused attention The capacity to highlight important stimuli while suppressing awareness of competing distractions
Sustained attention or vigilance
The capacity to maintain attentional activity over a prolonged period
Divided attention The ability to respond to more than one task at a time, including taking account of the multiple elements within a complex task
Alternating attention The ability to shift attentional focus from task to task
Attentional capacity The extent of the processing ability inherent in the attentional system; it is often considered to be a form of working memory
Figure 4.1 Variations in level of awareness.
Clear consciousnesswith voluntary attention
directed towards anobject of awareness –
e.g. watching a radar screen
Clear consciousnesswith involuntary attention
drawn to a field of attention –e.g. thinking in a deck chair
Narrowing of consciousnesswith constriction of the field ofattention – e.g. epileptic aura
Lowering of consciousnesswith patchy areas of attention
Object of awareness
Normal
Pathological
Conscious awareness
Unconscious Unconscious
Field of attentionConsciousawareness
andusuallyagedbetweenthreeandtenyears, fails tofinishactivitieshestarts,appearsnottolisten,iseasilydistracted,hasdifficultyinconcentratingonanytaskrequiringsustainedattentionandhasdifficultystickingtoaplayactivity.
Impairmentoffocusedattentionandconcentrationdenotesaninabilitytoexerciseattentiononanobjectinapurposefulway,implyingweakeningofthedetermining tendency.Thisisafeatureofmaniaandhypomaniaandalsooccursinorganicstates.Thesefeaturescombinetoshowthesymptomsofdistractibility,whichisprominentinmaniaandsomeorganicstates.
48 TWO—CONSCIOUSNESS AND COGNITION
Narrowingofattentionentailstheabilityofthesubjecttofocusonasmallpartofthefieldofawarenessandoccursinconditionsinwhichinvoluntaryattentionisdirectedelsewhere–byhallucinations, by delusions or by strong emotion. After an unprofitable conversation with apatientwithschizophreniainwhichsherepeatedlyignoredquestions,shesaid,‘IwishyouwouldnotinterruptwhenIambeinggivenmyinstructions’.
PSYCHOSIS AND ATTENTION
Schizophreniaisrecognizedasinvolvingdeficitsofattention(Posneretal.,1988).However,thereisconsiderabledifficultyinestablishingwhataspectsofattentionareimpairedinschizophreniabecausethetasksthatareusedtoassessattentionmayinvolveothercognitivefunctions,particu-larlysinceattentioniscloselytiedtoconceptsofworkingmemoryandalsotoexecutivefunction.Current evidence suggests that schizophrenia is associatedwith significant impairment in thecontrolofselection,theabilitytoidentifyandattendtotask-relevantinputs,whereastheremaynotbeimpairmentoftheimplementationofselection–theprocessesthatdeterminetheprocess-ingofrelevantinformationalinputs(LuckandGold,2008).
Ataphenomenological level,Cutting(2011)hasemphasizedthedegree towhichpatientswithschizophreniahaveheightenedattention.Whatremainstobedeterminediswhethertheexperiencesthatarereportedspeaktoactiveorpassiveattention.SeequotationsfromMcGhieandChapman(1961):
‘Things are coming in too fast. I lose my grip of it and get lost. I am attending to everything at once and as a result I do not really
attend to anything.’‘Everything seems to grip my attention although I am not particularly
interested in anything … often the silliest little things that are going on seem to interest me. That’s not even true, they don’t interest me but I find myself
attending to them.’
Itseemslikelythatinschizophrenia,onthebasisofthesereports,thereisagreatersuscep-tibilitytolureswithintheenvironmentthatcapturethepassiveattentionofthepatient.Agoodwaytounderstandthisistoimaginehowasudden,unexpectednoisecapturesourpassiveatten-tion. Itdoes seemas ifpatientswith schizophrenia are in thrall to irrelevant featuresof theirenvironment.
Thereiswell-establishedevidencethatinmooddisorders,includingbipolarmooddisorders,during the acute phase as well as in the euthymic state there are demonstrable impairmentsin sustained attention and working memory (Clark etal., 2002; Marvel and Paradiso, 2004;Thompsonetal.,2005).
Depressedmoodisoftenassociatedwithapreoccupationwithgloomythoughtstosuchanextentthatconcentrationandattentionareimpaired.Thissuggeststhatattention,whetheractiveorpassive, is luredbynegativelyvalued featuresof the individual’s innerorexternalworld. Insuchasituation,misinterpretationsofperceptioninfluencedbythemoodstatefrequentlyarise.Everyhearseisbelievedtobetheretocarrythepatienttothegraveyard,andapassingblackcarisnoticedjustsufficientlytobeconsideredasstrengtheningthisbelief.Similarly,acuteanxietyoftenresults indiminishedattention.Cutting(2011)arguesthat inmooddisorder,what lurestheindividualarepeopleandnotthings,incontrasttoschizophreniawherethereverseistrue.HisexampleisdrawnfromMinkowski:
‘I feel as if when you insist on something I must submit to your will and do what you demand of me … I am caught up in your affairs’.
4—ATTENTION, CONCENTrATION, OrIENTATION AND SlEEp 49
There is aneed todraw thepsychopathologyandcognitivepsychology literature together.In the current state of knowledge it is impossible to see clearly how the patient’s subjectiveexperiencerelatestothefindingsoncognitivetesting.Eventhough,strictlyspeaking,phenom-enology is atheoretical in stance, this does not mean that a severe disjunction ought to existbetweenthedifferentmodesofknowledgeasthereisatpresent.
OrientationOrientationisthecapacityofanindividualtoaccuratelygaugetime,spaceandpersoninhiscurrentsetting.Thisenableshimtomakesenseof,andbeathomein,hisenvironment.Thisisvirtuallythesamefacultyasintellectualgrasp,inthatvariousperceptualcuesareused,andwithcorrectsenseoftimeandplacethepersonisabletocometoappropriateconclusionsfromhiscontext.Amansufferingfromanadvanceddementiawasbeinginterviewedbyadoctorinthepresenceofadozenstudentnurses,whoweretakingnoteswithpenandnotebook.Whenaskedwherehewas,helookedaroundtheratherdingyhospitalclassroomandsaid,‘Well,we’rewaitingtoseethedoctor’.Hehadpickedupcertaincluesthatremindedhimofageneralpractitioner’swaitingroom;hehadtotallymissedthefactthatallthenurseswereinuniform,thattheyweretakingnotesandthathewasbeingaskedformalquestions.Hewasdisorientatedinplaceandinperson.
Orientationintimeislabileandquitereadilydisturbedbyraptconcentration,strongemotionororganicbrainfactors(forexamplealcoholicintoxication).Milderdegreesofdisorientationareshownbyinaccuracyofmorethanhalfanhourforthetimeofdayordurationofinterview.Moreadvancedstatesaredemonstratedwithincorrectdayoftheweek,yearorperiodofday.Yetfurtherdisturbanceisshownwhentheseasonoftheyearisnotknowncorrectly.
Orientation in space is disturbed later in the disease process than time. A patient may beunable tofindhisway,especially inanarea that is relativelynew tohim. Itmay takehimaninordinate length of time to learn his way to the dining table in the ward after admission.Disorientation in time andplace are,when clearly established, evidenceof anorganicmentalstate;theymaybetheearliestsignsinadementingprocess.
Indisorientationforperson,thepatientfailstorememberhisownname.Lossofknowledgeofthepatient’sownnameandidentityoccursataverylatestageoforganicdeterioration.Lossofintellectualgrasp(apprehension)occursinorganicstatesasaformofdisorientation,usuallycombinedwithotherevidenceofdeterioration.Suchapersoncannotunderstandthecontextofhispresentsituationandconnectsoutsideobjectsandeventswithhimself.Disorientationmayoccurwithadisturbanceofconsciousness,attention,perceptionorintelligence.Insevereintel-lectualdefectandseveredisturbancesofmemory,orientationisimpairedevenwhenconscious-nessisclear(Scharfetter,1980).
DISORIENTATION
Orientationmayfluctuateinsomeorganicconditions,forexampleapatientwithanacutetoxicstateassociatedwithcongestivecardiacfailurewasdisorientatedintimeeveryeveningbutquiteclearmentallyinthemorning.
Disorientationintimeandlossofintellectualgrasp(situationaldisorientation)usuallyoccurfirstinaprogressiveillness;disorientationinplaceusuallyoccurslaterand,inperson,lastofall.Disorientation forone’sown identityoccursat a later stage than for thatofotherpeople.Anelderly woman who knew who she was and her previous status as a professor’s wife kept onreferringtoherdaughteras‘thatminxwhocomesineverytimethedoctorvisits’.
Delusions that Mimic Disorientation
Itis,ofcourse,importanttounderstandthephenomenologicaldistinctionbetweendisorientationandadelusionthatresultsinmisinterpretationofplace,ofsituationorofperson.Disorientationisusuallyassociatedwithotherorganicfeatures,suchasloweringofconsciousnessordisturbance

50 TWO—CONSCIOUSNESS AND COGNITION
ofmemory.Delusionsofmisorientationhavethefeaturesofadelusion(Chapter8):apersononthewardmaybelievehimselftobeinprison,andavisitingrelativemaybeconsideredtobeaninterrogatorfromtheGestapo.
Dissociation and Disorientation
Definite, undisputed disorientation is indicative of either an acute organic brain syndrome, ifcoupledwithloweringofconsciousness,orchronicorganicdeterioration.Hystericaldissociationmaymimicthis,however,withapparentdisorientation.Carefulexaminationofthementalstateis likely torevealsuggestivediscrepancies, forexampledisorientationforpersonmaybemuchmoremarkedthanfortime,ormaybebizarretoanexcessiveextent.Apatientisdescribedinthe next chapter who lived in Birmingham, United Kingdom, but who found himself after ahystericalfugueinMontreal.Althoughapparentlydisorientated,heactuallyshowedanabnor-malityofmemoryaspartofadissociativestate.
Sleep DisordersSleep,deep, satisfyingandundisturbed, is conventionallyassociatedwithwell-beingandgoodhealth,asexemplifiedbythequotationwithwhichthischapterbegins;itsabsenceorpoorquality,equally, is held to account for disorder of mood and misery.There is a relationship betweendisturbedsleepandpsychiatricdisorder;mentalillnessmaycauseandmanifestassleepdistur-bance,disturbedsleepmayprecipitatepsychiatricsymptomsorthetwomayoccurtogetherbutindependently.TheInternationalClassificationofSleepDisorderssubsumes85sleepdisordersintosevencategoriesincluding:
1. insomnias;2. sleep-relatedbreathingdisorders;3. thehypersomniasnotduetoabreathingdisorder;4. theparasomnias;5. thesleep-relatedmovementsdisorders;6. othersleepdisorders;and7. isolatedsymptoms,apparentlynormalvariantsandunresolvedissues.ForafulleraccountseeAmericanAcademyofSleepMedicine(2005).Theobjectiveassessmentofsleepisusuallycarriedoutelectrophysiologically.Fivestagesof
sleep can be identified (Rechtschaffen and Kales, 1968). Using an electroencephalogram andelectromyogramoftheexternalocularmuscles,thedurationsofthedifferentstagesarerecorded.It has been shown that rapid eye movement (REM) sleep is associated with dreaming.Withcurrentneuroimagingtechniques, it ispossible,byshowingchanges inregionalcerebralbloodflow,tolocalizeandrepresentvisuallyalteredactivity,especiallyinthemedialthalamus,thatisassociatedwithdifferentstagesofsleepfromrelaxedwakefulnesstotheslow-wavesleepofstage4.Therearealsochanges in thevisualandauditorycortex,possiblyassociatedwithdreaming(Hofle etal., 1997). When considering the quality and duration of sleep and its stages, andwhetherthisamountstoasymptom,itisimportanttotakeintoaccounttheageofthepatient,anymedicationhemaybetakingandwhetherhehassleptduringtheday.Thesubjectiveexperi-ence,asdescribedbythepatient,maybeverydifferentfromtheobjectivefindingsofobservationandmeasurement.Thepsychiatristshouldinvestigatethemeaningofthisdiscrepancyphenom-enologicallyandconsidertheconsequencesfordiagnosisandtreatment.
INSOMNIA
Insomniaimpliessubjectivedissatisfactionwiththedurationorqualityofsleep(Oswald,1981);however, in many psychiatric conditions there is also objective disturbance of sleep. Formally,
4—ATTENTION, CONCENTrATION, OrIENTATION AND SlEEp 51
insomniasaredefinedbydifficultywithsleepinitiationand/ormaintenance,andfinalawakeningsthatoccurearlierthantheestablishedwake-uptime(AhmedandThorpy,2010).Theindividualmaycomplainthatthedurationofsleepistooshort;orthatsleepfeelsbroken,lessrefreshingorinsufficientlydeep;orthatthepatternofsleephaschangedfortheworse.Insomniaismorecommoninwomenandinolderpeopleandismoreoftenassociatedwithafeelingofexcessivemental arousal than bodily disorder. Causes of dissatisfaction include unrealistic expectationsfromtheelderlythattheywillsleepforaslongastheydidwhentheywereyounger,andfromthesedentarythattheywillsleepasdeeplyasafterexhaustingphysicalactivity.
Adiscussionofprimaryinsomniaisoutsidethescopeofthisbook.Itiswellrecognizedthatcomplaintsofsleepingpoorlyarecommon,andoccur inmanypsychiatricdisorders, includingdepression,generalizedanxiety,panicandphobia,hypochondriasisandwithpersonalitydisorders.Theyareamongthemostfrequentsymptomsinanxiety-relateddisordersandaffectivedisorders.Comparingthosepeoplewithneuroseswithanormalpopulation,Jovanovic(1978)foundthatneuroticpatientscomplainedofmorewakefulnessinthefirstthirdofthenight;theyspentmoretime lyingawake inbed, theyawokeduring thenightmore frequently, they spenta relativelyshortperiodindeepsleepandtheirsleepwasmorelikelytobeimpairedbyunfamiliarsurround-ings.Thosewithmajordepressivedisordersufferfromdisturbedsleep,inwhichtheytakelongertofallasleepandspendlesstimeasleepbecauseofperiodsofwakefulnessduringthenightandearlymorningwakening.
Early insomnia,ordifficultyingettingofftosleep,occursinnormalpeoplewhoarearousedthroughanxietyorexcitement.Theirthoughtstendtodwellontheaffect-ladenexperiencesoftheimmediatepastandalsotorehearsewaysofdealingwithproblems.Fatigueisexperienced,but there is also ahigh level of arousal thatprevents thenecessary relaxation andwithdrawalfromperceptionthatisrequiredforsleeping.Late insomniaorearly morning wakeningisparticu-larlycharacteristicofthedepressivephaseofaffectivedisorders.Thepatientmaywakefrequentlyin the night after getting off to sleep satisfactorily and thenceforward sleep only fitfully andlightly.Alternatively,hemaywakeearlyinthemorningandbeunabletogettosleepagain.Theimportantcharacteristicofdepressionisthatthereisamarkedchangeinsleeprhythmfromthenormalpattern for thatperson. Indepression, theearlymorningwakening isoftenassociatedwithmarkeddiurnalityofmood,withthemostseverefeelingsofdespondencyandretardationoccurringintheearlymorning.Thereisalsooftenamarkedreductionofsleeprequirementinmania.
Themeansleeprequirementdiminisheswithincreasingage.Itisusuallyaboutseventoeighthoursthroughthemiddleadultyearsbutismarkedlyreducedfromabout50yearsofageonwards.Withinsomnia,intermediatestagesoflight,restlesssleepoccur.Theseareoftenassociatedwithabnormal experience in the sleepy state, such as hypnagogic and hypnopompic hallucinations(Chapter7).Pseudohallucinationsalsooccur,asdoesvividimagerythatisdifficulttodistinguishfromhallucination.Normally,passage intosleepisrapidandoccurspassivelyratherthanwithactiveintentiontosleep.Wakingisalsonormallyrapid,andtheslowingofthisprocessofbecom-ingawakemaybedescribedasasymptom:acomplaintoffeelingdrowsyandbeingincompetentanduncoordinatedforanexcessivetimeonwakening–inotherwords,sleep drunkennessormoreaccurately confusional arousals from non-REM sleep in which confusion and disorientation,slowedspeechandmentationoccur(Lishman,1997;AhmedandThorpy,2010).Suchpatientsmay sleep for 17 hours or more and always require vigorous stimulation to wake them.Theconditionmaypersistthroughoutlife.
HYPERSOMNIA
Inhypersomniathedefiningcharacteristicisdaytimesleepiness.Thesecasesaremoreoftenseenbyaneurologistthanapsychiatristandarereportedonlybrieflyhere.
52 TWO—CONSCIOUSNESS AND COGNITION
IntheKleine–Levin syndrome,attacksofsomnolenceoccur,usuallyinadolescents.Thecondi-tionisrare.Inearlieraccounts,thepatientsleepsexcessivelybydayandnightbutisrousableasfromnormalsleep.Whenawake,thepatienteatsvoraciously(megaphagia)andmayshowmarkedirritability(Critchley,1962).Morerecentlyithasbecomeclearerthattheconditionischaracter-izedbyrelapsing-remittingepisodesofseverehypersomnia,cognitiveimpairment,apathy,dere-alizationandpsychiatricandbehaviouraldisturbances.Boysaremore frequentlyaffected thangirls.Justoverhalfofpatientshavehyperphagia,arehypersexual(mainlyboys),orhavedepressedmood(mainlygirls),andaboutathirdhaveotherpsychiatricsymptomssuchasanxiety,delusionsorhallucinations.Althoughsomesymptomsaresimilartothoseinpatientswithencephalopathy,imaging and laboratory findings are unremarkable.The first episode of hypersomnia is oftentriggeredbyaninfection,withrelapsesoccurringevery1–12monthsforamedianof14years.Between episodes, patients generally have normal sleep patterns, cognition, mood and eatinghabits. During episodes, electroencephalography might show diffuse or local slow activity.Functional imaging studies have revealed hypoactivity in thalamic and hypothalamic regions,andinthefrontalandtemporallobes(Arnulfetal.,2012).
Narcolepsyisaformofhypersomniaandcanoccureitherwithorwithoutcataplexy.Narcolepticattacksareshortepisodesofsleep(10to15minutes)thatoccurirresistiblyduringtheday;theyusuallybeginduringadolescenceandpersistthroughoutlife.Narcolepsyisoftenassociatedwithcataplexy,duringwhichthesubjectfallsdownbecauseofsuddenlossofmuscletoneprovokedbystrongemotion.Hypnagogic hallucinationsandsleep paralysismayalsooccur,butlesscommonlyso. Narcolepsy is associated with short sleep latency and sleep-onset REM periods.There isusuallyno structuralbraindiseasepresent.Hypnagogichallucinationsareusuallyauditorybutmaybevisualortactile.Theyoccurbetweenwakefulnessandsleep,lesscommonlybetweensleepandwakening (hypopompichallucination).Sleepparalysis is the inability tomoveduring theperiodbetweenwakefulnessandsleep(ineitherdirection).
InthePickwickian syndrome,namedafterthefatboyofThe Pickwick Papers(Dickens,1837),ormorespecificallyobstructive sleep apnoea,profounddaytimesomnolenceisassociatedwithgrossobesityandcyanosisduetohypoventilation.Breathingisperiodicduringsleepandsomnolence,withapnoeicphasesthatmaylastforuptoaminute.
Sustaineddrowsinessmayoccurwithorganiclesionsofthemidbrainorhypothalamusfromvarious causes. Hunger, weight gain, excessive thirst and polyuria may also occur. The mostimportantconditionsgivingrisetosecondaryhypersomniaarebraintumours,neurosarcoidosisandNiemann-PicktypeCdisease.
Hypersomniamayalsooccurasapsychogenicsymptom.Theremaybeastateamountingtohystericalstupor,andotherconversionsymptomsmaybepresent.Otherpatientswithneuroticdisorderscomplainpersistentlyofdaytimesomnolenceandaninabilitytoconcentrate.
PARASOMNIAS
The parasomnias are disorders of arousal and sleep-stage transition that consist of abnormalsleep-relatedmovements,behaviours, emotions,perceptions,dreamingandautonomicnervoussystemfunctioningthataccompanysleep(AhmedandThorpy,2010).Sleepwalkingisanexampleandconsistsofa seriesofcomplexbehavioursarisingduringslow-wavesleepandresulting inwalkingduringaperiodofalteredconsciousness.Itismorecharacteristicofchildrenthanadults,andofmalesmorethanfemales.Activityisusuallyconfinedtoaimlesswanderingandpurposelessrepetitivebehaviourforafewminutes.Thesleepwalkermayreplymono-syllabicallytoquestions,andthereislittleawarenessoftheenvironment,butinjuryisunusual.Frequentlythereisafamilyhistory,andenuresisisoftenassociated.Assleepwalkingoccursindeepsleep(stages3and4),usuallyduringthefirstthirdofthenight,itisunlikelytobetheactingoutofdreams.Itisnotthe same phenomenon as epileptic automatism, which may also result in a person, who is

4—ATTENTION, CONCENTrATION, OrIENTATION AND SlEEp 53
apparentlyasleep,gettingupandwalkingaround.It is important toestablish thediagnosis ineachcase.
Night terrorsalsooccurindeepsleepearlyinthenightandofteninthesameindividualwhosleepwalks. Intense anxiety is manifested, the subject may shout and there is rapid pulse andrespiration.Usually,thereiscompleteamnesiafortheexperienceonwaking.Itisnotthesameexperience as anightmare,because the latter is a typeofdream,occurring in lighter statesofsleep, and is rememberedvividly if thepersonawakes immediatelyafter theexperience.Mostchildrengrowoutofnightterrorsandsleepwalking.
Claimshavebeenmadethatautomatic,violentbehaviourhastakenplaceduringanightterror.Apersonwhocommitsacriminalactwhileasleepisnotconsciousofhisactionsandcannotbeheld legally responsible for them; the lawcalls this sane automatism (Fenwick,1986;EbrahimandFenwick,2010).Iftheact,for instancehomicide, isrememberedbyitsperpetratorasfol-lowingachainofpsychicevents(‘beingchasedbyJapanesesoldiers’),theseimagesaremostlikelytohaveoccurredinthecontextofanightmareandtheactthereforetookplaceonwakingfromthedreamandwouldberegardedasmotivated.Duringthenightmareitself,sleepparalysiswillpreventviolentemotionsbeingactedon.Fortheacttobeconvincinglyascribedtonightterror,neithertheactnoritsantecedentstorylineshouldberememberedandall theevidenceshouldpointtotheindividualbeingasleepatthetime.Previousevidenceofnightterrorandsleepactivityisimportantforcorroboration.
Less known are the reports of sexsomnia in which sexual behaviour occurs during sleep.These cases seem to occur in the setting of disorders of arousal, the so-called non-REMparasomniasthatincludeconfusionalarousal,sleepterror,andsleepwalking;REMsleepbehav-iour disorder; nocturnal partial complex seizures; and obstructive sleep apnoea (Ebrahim andFenwick,2010).
DreamsHowdoesphenomenologyviewdreams,theirsignificanceandtheirinterpretation?First,phe-nomenologycanbeconcernedonlywithwhatisconscious;itcannotcommentonthatwhichisunconscious, although it may infer the existence of unconscious insofar as it explains someobservedbehavioursandphenomena.Second,themeaningbelongstothedreamerandnottoan interpreter or theorist.This has implications for the way in which the phenomenologicalapproachwillbeusedintherapy.
Phenomenologycanmakeacontributiontotheunderstandingofdreaming.Bothbyintro-spectingandbytakingaccountsfrompatientswhileactuallydreaming,weknowthatmemoryisaccurateanddetailed,sometimesverydetailed.Also,theprocessofreasoningisfaultless,bothforwhenbizarreelementsintrudeandalsoforwhentheydonot.Thesebizarreelements,there-fore,demonstrateneitherdeficientmemorynorincapacityforrationalthinking.Theyappeartobepremises –theEuclidean‘let’.Indreaming,fantasyispermittedsothatwhenwesay,ordream,‘letBillSnooks (who lives inHeckmondwike andhasnevermet thePresidentof theUnitedStatesofAmerica)travelonabargedowntheAmazon’;what,then,wouldhappennext?Thisphenomenologicaltheoryofdreamscouldbeexploredexperimentally;ifattitudescanbechangedinconsciousnessbycognitivereprocessing, thentheconstructs thatareused indreamsshouldalsobecapableofchange.
Orthodox sleep (stages 1 to 4) and paradoxical sleep (REM sleep) have been distinguishedfrom each other through the use of sleep electroencephalographic tracings in human subjects(Oswald,1980).Normalreflexactivityoccursinthestagesoforthodoxsleep,butlocalizedactivityis seen in paradoxical sleep while other muscle actions are paralyzed. REMs in paradoxicalsleep are to some extent associated with dreaming. Nightmares are unpleasant dreams; often,the particular horror of a nightmare is that there is nothing the sufferer can do about the

54 TWO—CONSCIOUSNESS AND COGNITION
terrifying experience. Dreaming occurs in REM (paradoxical) sleep, and the transfixedsensation of the nightmare is an accurate representation of the sleep paralysis that occurs inthatphase.
Dreamshavebeenusedtoestablishelaboratepsychiatrictheoriesconcerningtheoriginsofconflict; it is outside the scopeof this book to enter into anydiscussionof this area. It is, ofcourse,atopicthatwasextensivelywrittenaboutbySigmundFreud(1976).Morerecently,themeaningofdreamshasbeenexploredempiricallybyKrameretal.(1976).Dreamsareremem-beredanddescribedasapsychicevent:nightmares(unpleasantdreams)areoftencomplainedofandmaybeaprominentsymptom,forinstanceindepression.Dreamsarehighlycomplexexperi-encesand,sofar,havedefiedadequateanalysisandexplanation.However,certaincharacteristicscanbedescribed.
Thereisalossofsomeofthestructuresofwakingconsciousness,thusthereisalossofself-awarenessandawarenessoftheconfinesofone’sownbody.Themarginbetweenselfandnot-selfbecomesindefinite.Thedreamermaydreamofhimselfmergingortransformingintosomeoneelsewithoutcontradiction.Timesenseisalsolost:thereisnosenseofprogressionofeventsbutonlyimmediateawarenessofthepresent.Eventsoccurringinthedreamincludethoseinwhichthedreamerhimselfisinstrumental.Thereisoftenalossofthesenseofhishavingcircumstanceswithinhiscontrol,andthereisalsoalossofthephysicalandmentalassociationsbetweenthedifferentpartsofawholeexperience.Thereare,therefore,gapsunaccountedforinspaceaswellasintimeandcausation.
Aswellas the lossof temporalandspatialconnections, there isa lossof thepsychologicalassociations between events.There is no progressive sequence of serial ideas or pictures.Thedreamisoftenlikeagroupofshortexcerptsfromverydifferentfilms.
Inadditiontothelossofstructurethatistypicalinthedreamingstate,therearealsoelementsthatdonotoccur inthenormalwakingstate.Thesearebestcalleddreamimages,as theyarenotaccuratelydelusions,hallucinations,falsememoriesorotherabnormalitiesofperceptionorideation characteristic of being awake.These images are more vivid than fantasy and have acharacteristicofimmediacyandimportance,soitisnotsurprisingthatfromthebeginningsoftimepeoplehaveactedontheirdreamsasiftheywereinstructions.
To regard dreaming as a symptom rather than merely a remembered experience, it hastobecomeinvestedwithunpleasantaffect.Apatientmaydescribepleasantdreamsifrequested,buthedoesnot usually complainof these as symptomsor ask for their removal.However, ifthedreamisassociatedwithanxiety,terror,gloomorforeboding,andespeciallyifthecontentorthethemeisrecurrent,itwillbecomplainedofandwillindicateaprevailingaffect;possibly,theareasofconflictthathaveprecipitatedthedistresswillberevealedinthecontentofthedream.Unpleasant dreams in which a part of the traumatic event is re-experienced are a diagnosticfeatureofpost-traumaticstressdisorderfollowingmajordisasterorcatastrophe.
HypnosisIthasbeensuggestedbyMarcuse(1959)thatwe‘definehypnosisbywhatitdoesratherthanbywhatitis’.Atoneextreme,hypnosisisconsideredtobeaverydifferentstateofawarenessfromnormalwakingconsciousness.Attheotherextreme,Merskey(1979)considersthat‘thephenom-enaofhypnosisareidenticalwiththoseofhysteria:theyinvolveself-deceptionandtheproductionofalternativesymptomsorbehaviourtosolveaproblem,evenifnotaconflict’.Merskeyfurthergoesontoproposeasdefinition:
Hypnosis is a manoeuvre in which the subject and hypnotist have an implicit agreement that certain events (e.g. paralysis, hallucinations, amnesias) will
occur, either during a special procedure or later, in accordance with the

4—ATTENTION, CONCENTrATION, OrIENTATION AND SlEEp 55
hypnotist’s instructions. Both try hard to put this agreement into effect and adopt appropriate behavioural rules, and the subject uses mechanisms of
denial to report on the events in accordance with the implicit agreement. This situation is used to implement various motives whether therapeutic or otherwise, on the part of both participants. There is no trance state, no
detectable cerebral physiological change, and only such peripheral physiological responses as may be produced equally by non-hypnotic suggestions or other
emotional changes.
Superficially, hypnosis appears to resemble sleep, but there are no electroencephalographicfindingstodistinguishhypnosisfromotherstatesofrelaxedwakefulness.Thetranceinhypnosisisproduced,therefore,inawakingstatebyonepersononanotherusingsuggestionwithcompli-ance(Marcuse,1959).Ithasbeenclaimedtooccurinnon-humanspecies,butthisstatecannotnecessarilybeconsideredidenticalwithhypnosis.Hypnosishasbeenusedforthecontrolofpain,inthetreatmentofhyperemesisgravidarum,forvarioussexualdifficultiesandespeciallyinthecontrolofanxiety(Waxman,1984).
TheinductionofhypnosisrequirestheimplicitcontractMerskeyimplies.Thesubjectmustbewillingandcooperative;heorsherelaxesandexercisesimagination.Thefieldofconsciousnessisnarrowedtoincludeonlytheinstructionsofthehypnotist.Thesubjectrelinquishessomedegreeofcontroltothehypnotistandacceptsrealitydistortion.Followingthesuccessfulinductionofhypnosis,autohypnosiscanbecomeestablished.Marcuseconsidersthefollowingtobethechar-acteristicsofahypnoticstate:
■ thesubjectceasestomakehisownplans■ attentionisselectivelydirected,forexampletowardsthevoiceofthehypnotist■ realitytestingisdiminishedanddistortionsareaccepted■ suggestibilityisincreased■ thehypnotizedsubjectreadilyenactsunusualroles■ post-hypnoticamnesiaisoftenpresent.Suggestion,forthehypnoticsubject,isstraightforwardandobvious;itdoesnotimplygullibil-
ityorlossofwill-power.Itdescribestheemotionoftrustoccurringwithintheimplicitrelation-shipinwhichthesubjectacceptsthehypnotist’sstatements,actsonhiscommandsanddeniesevidencefromhisownsensesthatwouldcontradictthosestatements.
Acapacityforfantasyisnecessaryforhypnosistotakeplace.Therelaxationthataccompanieshypnosis may progress to normal sleeping, even during a hypnotic session.The alteration inconsciousawarenessoccurring inhypnosis is similar to that indissociative statesbutdifferentfromthefluctuationsofconsciousnessleveloccurringinorganicpsychosyndromes.
Suggestionhasbeenusedtoproducemanyphysicalsequelae,forexampleblisters,alterationsinpulseandbloodpressure,levitationofanarm,opisthotonos,absenceofpainsensationandsoon.Thepsychologicaleffectsareequallyvariableandincludealterationstoperception,cognition,ideation,memoryandaffect.Thesubjectentersadramaticallyalteredstateinwhichhetempo-rarilysurrendersresponsibilityforhisactionstothehypnotist.Inhisturn,thehypnotistretainstheconfidenceof the subjectonlyas longashekeepswithin the limitsofbehaviour that thesubjectfindsacceptable;beyondthis,thesubjectwillrelinquishhisdependentrelationshipandcomeoutofthehypnoticstate.
Hypnosisremainsanenigma.Thereisnowemergingevidenceoftheunderlyingneuralcor-relatesofhypnotizabilityandofthehypnoticstateitself.Thesepointtogreaterfunctionalcon-nectivitybetweentheleftdorsolateralprefrontalcortex,anexecutive-controlregionofthebrain,andthesaliencenetworkcomposedofthedorsalanteriorcingulatecortex,anteriorinsula,amyg-dala and ventral striatum, involved in detecting, integrating, and filtering relevant somatic,

56 TWO—CONSCIOUSNESS AND COGNITION
autonomicandemotionalinformationinhighlyhypnotizablesubjectscomparedtolesshypnotiz-able subjects (Hoeft etal., 2012). As for the hypnotic state itself, during mental imagery forrehabilitationofneurodisability,fMRI-signalincreasesexclusivelyrelatedtohypnosishavebeenobserved inthe leftsuperior frontalcortex, the leftanteriorcingulategyrusand left thalamus.Whilethesuperiorfrontalcortexandtheanteriorcingulatewereactivatedrelatedmoretomove-mentperformancethantoimagery,thethalamuswasactivatedonlyduringmotorimagery.Theseareas represent centralnodesof the saliencenetwork linkingprimaryandhighermotorareas.Thissuggestshypnosisenhancesmotorimagery(Mülleretal.,2012).Muchworkstillneedstobedonetounravelthephysiologyofhypnosis.
ReferencesAhmedIMandThorpyMJ(2010)Classificationofsleepdisorders.InPandi-PerumalSRandKramerM
(eds.)Sleep and Mental Illness.Cambridge:CambridgeUniversityPress.American Academy of Sleep Medicine (2005). International Classification of Sleep Disorders – 2. Chicago:
AmericanAcademyofSleepMedicine.ArnulfI,ThomasJR,andEmmanuelM(2012).Diagnosis,DiseaseCourse,andManagementofPatients
withKleine-LevinSyndrome.Lancet neurology11,10,918–28.BroadbentDE(1958)Perception and communication.London:Pergamon.ClarkL,IversenSDandGoodwinGM(2002)Sustainedattentiondeficitinbipolardisorder.British Journal
of Psychiatry180,313–19.CritchleyM(1962)Periodichypersomniaandmegaphagiainadolescentmales.Brain85,627–56.CuttingJ(2011)A critique of psychopathology.ForestRow:TheForestPublishingCompany.DickensC(1837)The Posthumous Papers of the Pickwick Club.London:Penguin.EbrahimIandFenwickPB(2010).Forensic issuesof sleep inpsychiatricpatients. InPandi-PerumalSR
andKramerM(eds.)Sleep and Mental Illness.Cambridge:CambridgeUniversityPress.EysenckMWandKeaneMT(2010)Cognitive Psychology: A student’s handbook,6thedn.Hove:Psychology
Press.FenwickP(1986)Murderingwhileasleep.British Medical Journal293,574.FreudS(1976)The Interpretation of Dreams(transl.StracheyJ).Harmondsworth:Penguin.HoeftF,GabrieliJDE,Whitfield-GabrieliS,HaasBW,RolandBammerR,MenonVandSpiegelD(2012)
Functionalbrainbasisofhypnotizability.Archives of General Psychiatry69,1064–72.HofleN,PausT,ReutensD,FisetP,GotmanJ,EvansACandJonesBE(1997)Regionalcerebralblood
flow changes as a function of delta and spindle activity during slow wave sleep in humans. Journal of Neurosciences17,4800–8.
JamesW(1890)Principles of Psychology.NewYork:Holt.Jovanovic UJ (1978) Sleep profile and ultradian sleep periodicity in neurotic patients compared with the
correspondingparametersinhealthyhumansubjects.Waking and Sleeping2,47–55.Kolb B and Whishaw IQ (1996) Fundamentals of Human Neuropsychology, 4th edn. Basingstoke: WH
Freeman.KramerM,HlasnyR,JacobsGandRothT(1976)Dodreamshavemeaning?Anempiricalenquiry.American
Journal of Psychiatry133,778–81.LezakMD,HowiesonDBandLoringDW(2004)Neuropsychological Assessment,4thedn.Oxford:Oxford
UniversityPress.LishmanWA(1997)Organic Psychiatry: the Psychological Consequences of Cerebral Disorder,3rdedn.Oxford:
BlackwellScientific.LuckSJandGoldJM(2008)Theconstructofattentioninschizophrenia.Biological Psychiatry64,34–9.MarcuseFL(1959)Hypnosis: Fact and Fiction.Harmondsworth:Penguin.Marvel CL and Paradiso S (2004) Cognitive and neurological impairment in mood disorders. Psychiatric
Clinics North America27,1–17.McGhie A and Chapman J (1961) Disorders of attention and perception in early schizophrenia. British
Journal of Medical Psychology34,103–15.MerskeyH(1979)The Analysis of Hysteria.London:BaillièreTindall.

4—ATTENTION, CONCENTrATION, OrIENTATION AND SlEEp 57
MüllerK,BachtK,SchrammSandSeitzRJ (2012)The facilitatingeffectofclinicalhypnosisonmotorimagery:anfMRIstudy.Behavioral Brain Research231,164–9.
OswaldI(1980)Sleep,4thedn.Harmondsworth:Penguin.OswaldI(1981)Assessmentofinsomnia.British Medical Journal283,874–5.PosnerMI,EarlyTS,ReimanE,PardoPJandDhawanM(1988)Asymmetriesinhemisphericcontrolof
attentioninschizophrenia.Archives of General Psychiatry45,814–21.RechtschaffenAandKalesA(1968)A Manual of Standardized Terminology, Techniques and Scoring System
for Sleep Stages of Human Subjects.Bethesda:USDepartmentofHealth,Education,andWelfare.ScharfetterC(1980)General Psychopathology: an Introduction.Cambridge:CambridgeUniversityPress.Smith EE and Kosslyn SM (2007) Cognitive Psychology: mind and brain. New Jersey: Pearson Prentice
Hall.ThompsonJM,GalagherP,HughesJH,WatsonS,GrayJM,FerrierNandYoungAH(2005)Neurocognitive
impairment in euthymic patients with bipolar affective disorder. British Journal of Psychiatry 186,32–40.
WaxmanD(1984)Psychological Influences and Illness: Hypnosis and Medicine.London:Macmillan.World Health Organization (1992) The ICD-10 Classification of Mental and Behavioral Disorders: Clinical
Description and Diagnostic Guidelines.Geneva:WorldHealthOrganization.

This page intentionally left blank
59
C H A P T E R 5
Disturbance of Memory
SummaryMemoryhasawell-describedanddelineatedarchitecture,namelysensorymemory,short-termmemoryandlong-termmemory.Short-termmemoryisitselfsubdividedintoacentralexecutiveandtheslavesystems,termedvisuospatialscratchpadandthephonologicalloop.Thisarchitec-tureallowsforasystematicunderstandingoftheunderlyingprocessesatplayinmemory.Itishelpfultoconceptualizethememoryprocessesasincludingregistration,retention,retrieval,recallandrecognition.Thesetermsallowforanunderstandingoftheanomaliesthatareexhibitedinorganicimpairmentsofmemory.
Cans’t thou not minister to a mind diseas’d;Pluck from the memory a rooted sorrow;
Raze out the written troubles of the brain;And with some sweet oblivious antidote
Cleanse the stuff ’d bosom of that perilous stuffWhich weighs upon the heart?
William Shakespeare (1606)
Disturbanceofmemoryisalwaysofsignificanceforthesufferer;sometimes,however,forget-tingisequallyimportantandisanactiveprocess,asinthequotationabove.Thatmemorydis-turbance was a specific feature following head injury and other conditions was recognized inneuropsychiatricwritingsinthemid-nineteenthcentury;HughlingsJackson(1887)consideredittobeanintegralpartofdeteriorationinorganicmentalfunctioning.Theearliestdetailedstudyofdisorderedmemory fromapsychological standpointwasbyRibot (1882).Korsakov (1890)subsequentlydescribedhis eponymous condition, pointingout that grossdisorder ofmemorymayoccurinpatientsinwhomotherintellectualfunctionsandjudgementarepreserved.
Mechanisms of MemoryOneofthemajorjustificationsforusingpsychopathologyinthedescriptionofmemorydistur-banceisthatthereexistsnogoodanalogueofmemoryinanimals.Conventionally,disturbanceofmemoryisdescribedbythe lengthoftimeforwhichinformationhasbeenretained.Ifoneconcentratesonthephenomenologicalaspects,theanalysisofexperience,itisinfactquitearbi-trarytomakeadistinctionbetweenmemoryandperceptionastheyarebothstagesininformationprocessing(Weinman,1981).Memorystorageisorganizedinthreeways.
SENSORY MEMORY
Sensorymemoryistheinitialandearlyphaseofmemory.Itholdslargeamountsof incominginformationbriefly.Itisaselectingandrecordingsystemviawhichperceptionsenterthememorysystem(Lezaketal.,2004).Fleetingvisual image,iconicmemory, lastsupto200milliseconds,

Keywords: Memory,Confabulation,GanserState.
5—DISTUrbANCE Of MEMOry 59.e1

60 TWO—CONSCIOUSNESS AND COGNITION
whereas auditory, echoicmemory, lastsup to2,000milliseconds.The information selectedandrecordedatthis levelneedstobefurtherprocessedasshort-termmemoryoritquicklydecaysandislost.
SHORT-TERM MEMORY
Short-termmemoryisconceptualizedasalimitedcapacitysystemthatoperatesasasetofsub-systems.Whileitistheoreticallydistinguishablefromattention,inpracticeitisprofitablyequatedwithasimplespanofattentionlimitedtosixorsevenitemsandlasting15to30secondsunlesstheitemsarerehearsed.BaddeleyandHitch(1974)hypothesizedamodelofworkingmemorycomprisingacentral executive, a visuospatial scratch padandaphonological loop.Inthissystem,thecentral executiveistheattentionalcontrollerassistedbythevisuospatial scratch padthatallowsforthetemporarystorageandmanipulationofvisualandspatialinformation.Thephonological loopholds memory traces of verbal information for a couple of seconds combined with subvocalrehearsal(Baddeley,1986;Baddeley,2002).
LONG-TERM MEMORY
Long-term memory can be conceptualized into two retrieval systems: a declarative system, orexplicitmemory,thatdealswithfactsandeventsandisavailabletoconsciousnessfordeclaration,and a non-declarative or implicit system (Lezak etal., 2004).The declarative system can befurtherdividedinto semantic (factmemory)andepisodic (memoryforspecificautobiographicalincidents)memory.Inotherwords,semantic memoryisthestorageofinformationinpureformwithout specification of time or place (‘General Psychopathology was written by Karl Jaspers’),whereas episodic memory refers to personally experienced events (‘I had a kipper for breakfasttoday’)(Baddeley,1990).Long-termmemorycanholdinformationforperiodsoftimefromafewminutestomanydecades,andthecapacityisverylarge.Forgettingmaybebylossofinfor-mationorfailureofretrieval.Normalforgettingratesaredeterminedbysuchvariablesaspersonalmeaningfulnessofthematerial,conceptualstyleandage.Storagein,andalsoretrievalfrom,thelong-termmemoryisimpairedinthedysmnestic syndromes.Informationisstoredinreorganizedandsometimesdistortedform.
Descriptionof the requirements formemory is chiefly referable to long-termmemoryandcanbesubdividedphenomenologicallyintothefollowingfivefunctions.
■ Registrationorencodingisthecapacitytoaddnewinformationtothememorystore.■ Retentionorstorageistheabilitytomaintainknowledgethatcansubsequentlybereturned
toconsciousness.■ Retrieval isthecapacitytoaccessstoredinformationfrommemorybyrecognition,recall
orimplicitlybydemonstratingthatarelevanttaskisperformedmoreefficientlyasaresultofpriorexperience.
■ Recallistheeffortfulretrievalofstoredinformationintoconsciousnessatachosenmoment.It requires anactive, complex searchprocess. It is influencedbyprimacy (first item)andrecency(lastitem)effects.Thequestion‘WhatisthecapitalofFrance?’requirestherecallfunction.
■ Recognitionistheretrievalofstoredinformationthatdependsontheidentificationofitemspreviously learnedand isbasedoneither remembering (effortful recollection)orknowing(familiarity-basedrecollection).Inthisprocess,astimulustriggersawareness;rememberingorknowingthentakesplace.Thequestion‘WhichofthefollowingisthecapitalofFrance:Paris,LilleorLyon?’teststherecognitionfunction.
Abnormalityofmemorymayoccurinanyoftheseareas.Inotherwords,therecanbeimpair-mentofencoding,impairmentofstorageorimpairmentofretrieval.
5—DISTUrbANCE Of MEMOry 61
Organic Impairment of MemoryMemory disturbances can be separated into those that are psychogenic, sometimes occurringin healthy people, and those that are organic, associated with disease of the brain.The latterare referred to as organic or true amnesias and can be described by the different functions ofmemory.
IMPAIRMENT OF REGISTRATION
In anterograde amnesia, the impairment is usually demonstrated in the failure of retrieval ofinformationencounteredaftertheonsetofaclinicaldisorder.Thisimpairmentofretrievalmay,ofcourse,beduetoproblemsattheregistration(encoding)stage,particularlyinpatientswithKorsakov’ssyndrome.Thereisevidencethatthesepatientsmayhavedifficultyinspontaneouslyencodingthesemanticfeaturesofinformationtoasufficientlevelatinput,andthisfailureresultsinpoormemory(Mayes,2002).Itisthereforeproblemsintheinitialanalysisandrepresentationofinformationandtheinabilitytoselectthesalientsemanticfeaturesofinformationthatunderlieimpairmentofregistration.Inalist-learningtestsituation,forexample,thesemanticfeaturesofthewords,suchasthefactthatthewordsarederivedfromalistofthenamesofflowers,failstoassistthesubjecttoencodethenewinformation.
IMPAIRMENT OF RETENTION
Retrograde amnesiaisthelossofmemoryforeventsprecedingtheonsetofbraininjury.Aswithanterogradeamnesia,thedeficitisdemonstratedintheimpairmentofretrieval,butitisthoughttobeduetoimpairmentofretention(storage),particularlyincasesofcerebraltrauma.Usually,itisofshortdurationoflessthan30minutes.Typically,itfollowsatemporalgradientinwhichnewermemories aremore vulnerable to loss thanolder ones.There is a dissociationbetweenanterogradeandretrogradeamnesiathatsuggeststhattheanatomicalstructuresinvolvedinnewlearningandretrievalofoldmemoriesaredistinct.
IMPAIRMENT OF RETRIEVAL OR RECALL
Retrievalisthecapacitytoaccessinformationfrommemorystores.Impairmentofretrievalcanbe due to a deficit in either direct retrieval, in which a cue elicits a memory automatically, orstrategic (indirect) retrieval, inwhich a cueprovokes a strategic searchprocess that produces aresult.Indirect retrieval,thequestion‘HaveyoueverbeentoLagos?’actsasacuethatelicitsamemoryautomatically.Instrategic retrieval,thequestion‘WhowontheWorldCupbeforethecurrentchampions?’instigatesastrategicprocessthatframesthememoryproblem,initiatesthesearch and constrains it, guiding it towards local, proximal cues that then activate associativememoryprocesses.Thememoryoutputisthenmonitoredforaccuracyandplacedinapropertemporal-spatial context in relation toothermemories (GilboaandMoscovitch,2002).Direct retrieval is thought tobedependentonmedial temporal lobes and related structures,whereasstrategic retrieval is dependenton the ventromedial prefrontal cortex.Confabulation is a goodexampleofaconditionthatisaresultofimpairmentofretrieval.Itresultsfromafaultymemorysystemcreatingfaultycue-memoryassociations,faultysearchstrategiesanddefectivemonitoringoffaultymemories(GilboaandMoscovitch,2002;DeLuca,2009).
IMPAIRMENT OF RECOGNITION
Recognition is the retrieval of stored information that depends on the identification of itemspreviously learned. In episodic memory, that is, memory for events that includes the context,
62 TWO—CONSCIOUSNESS AND COGNITION
time, place and emotions associated with the event, recognition can take the form of eitherconsciousrecollection(remembering)orknowingbasedsimplyonasenseoffamiliarity.This isthe so-called remember-know paradigm, and it proposes a dual process memory system, onerelyingonconsciousrecollectionandtheotherbasedonfamiliarity.Inotherwords,thephenom-enal experience that accompanies the recognition of a previously presented stimulus seems totakeatleasttwoforms.Recognitioncanoccurwhenthestimulusevokessomespecificexperienceinwhichthestimuluswaspreviouslyinvolved,oralternativelythestimulusgivesriseonlytoafeelingof familiaritywithoutanyrecollectiveexperience.A‘remember’ response indicates thatrecognizingthestimulusbringsbacktomindsomeconsciousrecollectionofitsprioroccurrence,whereas a ‘know’ response indicates that recognizing the stimulus is not accompanied by anyconsciousrecollectionofitsprioroccurrence(DallaBarba,1997;Tulving,2000).ImpairmentofrecognitionhasbeendescribedinAlzheimer’sdisease(DallaBarba,1997)andinschizophrenia(Drakefordetal.,2006).
Various Disturbances of MemoryDÉJÀ VU AND RELATED PHENOMENA (IDENTIFYING PARAMNESIA)
Déjà vuisnotprimarilyamemorydisorderbutadisturbanceinwhichtheassociatedfeelingoffamiliarity thatnormallyoccurswithpreviously experiencedeventsoccurswith anovel event,that is, when the event is experienced for the first time. In jamais vu, an experience that thepatientknowshehasexperiencedbeforeisnotassociatedwiththeappropriatefeelingoffamiliar-ity.Thepatientmayalsohavethefeelingthatsomeimportantmemoryisabouttoberecalled,althoughitdoesnotactuallyarrive.
Déjà vuandjamais vuarecommon,normalexperiencesbutmayalsobesignificantsymptomsoftemporallobeepilepsyorcerebrovasculardisorder(Lishman,1998).Anepilepticpatientsaid,‘I feel that I’ve done something terribly wrong’. However, these experiences on their own, orassociatedonlywithvaguefeelingsofdepersonalization,shouldnotbeacceptedasevidenceoftemporallobeepilepsy,asthesesymptomsarealsofrequentlyexperiencedbothinpatientswithanxiety-relateddisordersandinnormalindividuals.
CONFABULATION
Thisisafalsificationofmemoryoccurringinclearconsciousnessinassociationwithanorgani-callyderivedamnesia(Berlyne,1972).Itisprobablybesttoconceiveofconfabulationasaloosetermthatcoversawiderangeofqualitativelydifferentmemoryphenomena.Thetermisusedtodescribemilddistortionsofanactualmemory,suchasintrusions,embellishments,elaborations,paraphrasingorhighfalsealarmratesontestsofanterogradeamnesia.Itcanalsorefertohighlyimplausiblebizarredescriptionsoffalserealitiessuchasclaimingtobeaspacetravellertemporar-ilyresidentonearth(GilboaandMoscovitch,2002;Box5.1).However,itisalsotruethattheterm‘confabulation’hasbeenextended,unhelpfullyinmyview,toinclude:
1. memoryconfabulations;2. confabulations about intentions and actions as can occur in split-brain subjects or in
hemiplegiaoftheleftarmwherethesubjectdeniestheirdisability;3. perceptualconfabulationswhichoccursinAnton’ssyndromecharacterizedbyunawareness
ofblindness;and4. confabulationaboutemotions(seeHirstein,2009forafullerreview).Bonhoeffer(1901)observedthatconfabulationinKorsakov’ssyndromecouldtaketwoforms.■ Confabulationofembarrassmentwasadirectresultofthememorylossanddependedfor
itspresenceonacertainattentivenessandactivity.Thisformofconfabulationismomentary
5—DISTUrbANCE Of MEMOry 63
innature.Thepatient tries to cover an exposedmemory gapby an ad hoc confabulatedexcuserelatingtohisrecentbehaviour.Itdoes,therefore,revealsocialawarenessandsomerealizationoftherequirementsofthesituationintermsofsocialbehaviour.
■ Inothercases,confabulationexceededtheneedsofthememoryimpairment;thepatientdescribesspontaneouslyadventurousexperiencesofafantasticnature.Thespontaneityisakeycharacteristicofthisformofconfabulation.Suchmemorydisturbancemayoccurwithorganicdeteriorationfollowingalcoholabuseandalsointhe‘organicamnesicsyndrome,not induced by alcohol and other psychoactive substances’ (ICD-10; World HealthOrganization, 1992), in which there is severe memory impairment, especially for recentmemory;evidencefordisorderofthebrain;andabsenceofadefectinimmediaterecall,adisturbanceofattentionandconsciousness,andglobalintellectualimpairment.
SuggestibilityisaprominentfeatureoftheconfabulatingpatientandwasconsideredbyPick(1921)tobedependentoncloudingofconsciousness,weakenedjudgementandtheinterplayoffantasy; it may, in fact, closely resemble daydreams. The confabulating patient may producemutuallycontradictorystatementsconsecutivelyandnotmakeanyattempttocorrectthem.Thematerialofconfabulationshasbeenlikenedtodreams(Scheid,1934).Ithasalsobeenexplained,in termsofmemorydisturbance, that confabulations are actual experiences takenoutof theirchronologicalorder(VanderHorst,1932)andthattheindividual’swishesandinterestsguideconfabulationinthesamewayasindreamsandfantasy.
Itseemsprobablethatconfabulationisrelatedtothenormalmechanismsofrecollection.Forexample,saythatalltheownersofacertainmodelofcarwereaskedbythepolice,aspartofalarge-scalemurderhunt,whattheyweredoingonaparticularMondayaboutninemonthsprevi-ously. To answer this question, an individual would have no recollection for that particularMonday,sohewouldrecreateatypicalprogrammewithregularmovementsandtimesofappoint-mentsforaMondayfromaboutthatperiod.Itwouldseemthatthemechanismofsocial confabu-lation isofthatorder.Tothequestion‘Whatdidyoudoyesterday?’,theconfabulatingpatientmightsay,‘Ipushedmybaby in thepramdowntotheofficetoseemyoldworkmates there’.Thiscouldindeedhavehappened12yearspreviouslyaftershehadresignedherjobinthatofficeduringherpregnancy.Thefantastictypeofconfabulationisalsodirectlyassociatedwithmemory.Normally,onehasaclearmemoryofwhichsensationsandeventswereexperiencedandwhichwerefantasized,yetwithconfabulationitisprobablethatdistantfantasiesareremembered,butit is not remembered that they were fantasy rather than reality. Such confabulations, like themomentary type,areautobiographical.Themomentaryorembarrassmentconfabulationisverymuchmorecommonthanthefantastictypeandisatruememorydisplacedinitstimecontext(Berlyne,1972).
Fantastic confabulation with persecutory content has been described by Roth and Myers(1969).Thisisafalsificationofmemoryoccurringinclearconsciousness.Typically,thepatientbelievesothersarestealinghismoneyortryingtodefraudhim.Memoryfalsificationsofvarioustypes occur in schizophrenia, depressive illness, dissocial personality disorder and obsessional
BOX 5.1 ■ Characteristics of confabulation
■ Itisafalselyretrievedmemory,oftencontainingfalsedetailswithinitsowncontext.■ Thepatientisunawarethatheorsheisconfabulatingandoftenunawareoftheexistenceofmemory
deficit.Inotherwords,confabulationsarenotintentionallyproduced.■ Patientsmayactontheirconfabulation,confirmingtheirbeliefinthefalsememory.■ Confabulationismostapparentinautobiographicalmemory.
(FromGilboaandMoscovitch,2002,withpermissionofJohnWiley.)
64 TWO—CONSCIOUSNESS AND COGNITION
states.Themoredefinite,fantasticandgap-fillingfeaturesoforganicconfabulationsarealwaysassociatedwithmemorydefect.
Central to the ideaofconfabulation is thereforeanotionof false reports in thecontextofmemory disorder. At a minimum, it involves both distortions of content as well as temporalcontext. The confabulatory recollection often includes additions, distortions or elaborationswhicheitheractuallyorplausiblyoccurred(DeLuca,2009).
‘Doctor: What did you do today?PatientVR: Today I got up this morning and visited the rehabilitation unit … then I went home and was expecting some material and we received it. Then I came to the rehabilitation institute, no I actually went to Jimsburg
store and we had a small meeting there. Then I came to the hospital and we had lunch and, then met with you …’
(DeLuca, 2009)
Theexamplefirstly illustratescontentdistortion,sincethepatienthadbeeninhospital forseveralmonthswithoutgoinghome,andsecondlyimpairedtemporalcontext,sincethepatienthadownedJimsburgstoremanyyearsbeforeandhadsoldit.
Thecurrentview is thatmemoryconfabulationusuallyderives fromdual lesions taking inbasal forebrain areas and frontal executive systems.These lesions appear to result in impairedstrategic retrieval of memory and disturbed verification/monitoring of the abnormal memoryoutput(DeLuca,2009).
PERSEVERATION
Perseverationusuallyoccursinassociationwithdisturbanceofmemoryandisasignoforganicbrain disease, perhaps the only pathognomonic sign in psychiatry. It occurs with clouding ofconsciousness and is particularly useful in distinguishing this from dissociative abnormalities(Allison,1962).Perseveration isdefinedas a response thatwas appropriate to afirst stimulusbeinggiveninappropriatelytoasecond,differentstimulus.Thismaybedemonstratedverballyorinmotoractivity.Theinterviewer,whileconductingthementalstateexamination,asks‘WhatisthecapitalofItaly?’–‘Rome’,andthensubsequently‘Whatistheobjectthatyouwearthattellsyouthetime?’–‘Rome’.Alternatively,theexaminerasksthepatienttoputhisrighthandonhisleftshoulder,whichhedoescorrectly,andthen,onaskinghimtoputhislefthandonhisleftknee,heagainputshisrighthandonhisleftshoulder.
MEMORY DISTURBANCE AND ELECTROCONVULSIVE THERAPY
Thereisalwayssomememorydisturbanceimmediatelyafterelectroconvulsivetherapy(ECT).This includes impaired learningability,defectiveretrievalandapparent lossofmemorystores.Memoriesofeventsimmediatelyprecedingthetreatments(retrogradeamnesia)aremostlikelytobepermanentlylost,andmorerecentpersonal(autobiographical)memoriesaremorevulnerabletolossthanolderones(CahillandFrith,1995;SternandSackeim,2002).Thereisalsosomeantero-gradeamnesia,withdifficultyinretentionforsomehoursaftertreatment.Defectofmemoryforcurrenteventsataboutthetimeofthetreatmentmaypersistforafewweeksaftercompletingacourseoftreatment.Thismemorydisturbanceissimilartootherorganicamnesicstates.
Theretentiondefect isrelatedtothestrengthanddurationofelectricalstimulationandtothedurationof the seizure.Confusion andmemorydisturbancehavebeen claimed tobe lessafterunilateral,non-dominantECT.Thereisnoevidenceforlossoftheabilitytoacquirenewpatternsofbehaviourorexecuteestablishedones,evenafteralongcourseofECT.
5—DISTUrbANCE Of MEMOry 65
Usingaverywide-rangingbatteryofteststoexamineallareasofcognitivefunction,Weeksetal.(1981)statethatECTdoesnotproducelastingimpairmentwhenusedineverydayclinicalcircumstances. Memory functions tested included recall, releasing rate and recognition in theauditory-verbalandvisuospatialmodalities.Similarly,Fraser(1982)considersthatthememoryloss that follows ECT is minimal and can be detected for only a few hours after treatment.Unilateral placement of electrodes accelerates postictal recovery and shortens the duration ofamnesia(Fraser,1982).Insummary,itseemsnowthatECTdoesnotcausemorethanatem-porarydisturbanceinmemory(Williamsetal.,1990).
MEMORY IMPAIRMENT IN SCHIZOPHRENIA
Earlierwriterstendedtoplaydownthesignificanceofintellectualimpairmentinschizophrenia(Bleuler,1911;Kraepelin,1913).However,decline in intellectualperformance (Rogers,1986),impairment in neuropsychological test batteries (Taylor and Abrams, 1984), sometimes adementia-likesyndrome(LiddleandCrow,1984)andsubstantialmemorydeficit(Cutting,1985;McKenna etal., 1990) have been demonstrated. Memory deficit has been shown not to berestrictedtopatientswithchronicschizophrenia.
Therearedeficitsinlong-termmemory,includingevidenceofimpairedretrievalinbothrecallandrecognition.Thereisalsoevidenceofimpairedshort-termmemory,demonstratedbydeficitof forwarddigit span.Furthermore, there is evidenceof impairmentofworkingmemory andsemantic memory, but procedural or implicit memory is intact.The memory deficit has beenshowntobeassociatedwithseverityandchronicityofillness,andwithnegativesymptomsandformalthoughtdisorder(Tamlynetal.,1992;McKennaetal.,2002).
TEMPORAL LOBE DISORDER
Itisusefultosummarizeatthisstagethepsychopathologicalphenomenaoftemporallobedys-function:disturbanceofmemory,perceptionandaffect.Disorderofmemoryincludesthehip-pocampaldefectsofdiminished storageandaccelerated forgetting;déjà vu and jamais vu alsooccur, as described above.There may be altered states of consciousness such as a fugue, withimpairedregistration.Panoramic recall,inwhichthepatientmayfeelthatheisrapidlyre-enactinglongperiodsofhislife,isalsodescribed.
Affective Disorder of MemoryMemoryisnotonlydisturbedbyorganicdamagetothebrainitself;itisalsoaffectedbyemotion.Thisiscertainlytrueofnormal,healthypeople,inwhomtheaffectivestatestronglyinfluencestheprocessesofrememberingandforgetting.Itisalsotrueofthosewithaffectiveandschizo-phrenicpsychoses,andofneurosesandpersonalitydisorders.Depressionislinkedtoself-reportedmemoryproblems.Thereisalsosubstantialevidenceofanassociationbetweendepressionandgenericmemoryimpairment.Itisthoughtthatmooddisorder,suchasdepression,reducestheamountofcognitiveprocessingresourcesavailableforagiventask,andinthememorydomainthisismanifestasdeficitsintheelaboration,organization,encodingandretrievalofmaterialintoandoutofmemory(DalgleishandCox,2002).Thereisalsoevidenceofmemorybiasforaffec-tivelytonedmaterial,suchthatinformationthathasanemotionalvalenceismorelikelytoberetrieved if it is congruent with the individual’s mood during retrieval. This mood-congruent memory effect is similarbutdistinct from state-dependent memory,whichrefers to thememorybiasformaterialthatislearnedinaparticularmoodandismoreeasilyretrievediftheindividualisinthatsamemoodduringretrieval.

66 TWO—CONSCIOUSNESS AND COGNITION
SELECTIVE FORGETTING
Innormalforgetting,thereislossofordiminishedaccesstorecentlyacquiredandstoredinfor-mation.Ratesof forgettingare influencedby thepersonalmeaningfulnessof the information,theconceptualstyleoftheindividual,thedegreeofprocessingandelaborationoftheinformationandage.Itislikelythatnormalforgettingisdeterminedbydisuseorinterferencebymorerecentlylearnedormorevividmaterialandunderpinnedbyphysiologicalormetabolicprocesses(Lezaketal.,2004).Additionally,therearetwoformsofinterference;proactiveandretroactive.Inproac-tiveinterference,newlylearnedmaterialinterfereswiththerecallofpreviouslylearnedmaterial.Inretroactiveinterference,previouslylearnedmaterialinterfereswiththerecallofnewlylearnedmaterial(seeEysenckandKeane,2010forafullerdiscussion).
Theprocessofrepressionorselective forgetting,however,suggeststhatforgettingisnotsimplydown toerrors in thefilingand retrievalmechanism.Forgetting is subject to the influenceofaffect:whichsensationsareregistered,whatisretainedandforhowlongandwhatinformationis available for recall. InFreud’s (1856–1939) account, traumaticor threateningmemories arekeptoutofconsciousawarenessbythemechanismofrepression.Otherformsofactiveforgettingexist, including motivated forgetting which subsumes repression as an example, and also thedeliberateforgettingofwhereweputourglassesyesterdaywhenwearelookingforthemtoday!Directedforgettingisthetermfortheprocessbywhichweactivelyuseexecutivecontrolproc-esseswithintheprefrontalcortextoforgetitemsthatwedonotwishtorecall.Itisobviousfromtheforegoingthatforgettingisanimportantandnormativeprocess.
FALSIFICATION OF MEMORY
Falsificationofmemoryoccurs tosomeextentbecauseof the interplayofmemorywithaffect.ThiswascommentedonbyNietzsche(1889):‘MemorydeclaresthatIdidthis;Icouldnothavedonethis,saysmypride;andmemorylosestheday’.
Inpseudologia fantastica –fluentplausiblelying–theuntruthfulstatementsareoftengrandioseandextreme.Questionsareansweredwithfluency,andthestoryappearstobebelievedimplicitlybythepseudologichimself.Thisusuallyoccurswithanassociatedpersonalitydisorderofhistri-onicordissocialtype,andoftenwhentheindividual isexperiencingamajor lifecrisissuchasfacingcriminalproceedings.Thepictureisofaveryisolatedperson,withoutfamilyorfriends,driftingintotheaccidentandemergencydepartmentofalargehospitalinastrangecitylateatnight,withstoriesofhisownexploitsandimportanceandtheunfortunatevicissitudeshehasexperienced.Thereisoverlapwiththeso-calledFactitiousDisorder.
Withpersonalitydisordersandalsowithaffectivedisorders,especiallyattimesofheightenedemotion, memory is falsified and distorted, and events and circumstances are misrepresented.Theadviceofdoctorsmaybegrosslymisconstrued.Anophthalmicsurgeonexaminedadepressedpatient’s eyes and informed her that her visual acuity was satisfactory and no treatment wasrequired.Shereportedthistoherpsychiatrist;her‘eyesightwouldbebadforevermoreandthesurgeonhastoldmethatnothingcanbedoneaboutit’.
Memoryimpairmentisaregularfeatureoforganicstates.Whenthereisadefectofreasoningand judgement, falsificationcanoccur.Sothegrandiosedelusionsandmemorydisturbanceofgeneral paresismayresultinfalsificationanddistortionofeventsremembered.Similarly,confabu-lationasintheKorsakovstateisassociatedwithfalsification.
Inschizophrenia,rememberedcircumstancesoftentakeonanewmeaning:‘IrememberlastweekthreeredcarsfollowingmeatthetrafficlightsinStafford…IrealizedthatIhavebecomeinvolvedinpolitics’.Thiswasstatedbyapatientwhohadquitesuddenlycometobelievethatall her actions were being observed and, subsequently, her behaviour controlled. Memory isaccurate, but its significance is distorted. A distinction should be made between delusional
5—DISTUrbANCE Of MEMOry 67
memories, in which the primary delusional experience is a true memory, with delusionalinterpretation, and delusional retrospective falsification. This is a backdating of delusion toa timebeforethepatientwas ill,basedonanadmixtureofrememberedtrueeventsanddelu-sionalelaborationofthemeaningofthoseevents.Thishasbeendescribedbysomeauthoritiesas a form of confabulation (Nathaniel-James and Frith, 1996; McKenna etal., 2009). Intheoriginalstudy,whensubjectswerepresentedwithnarrativesandaskedtorecallthem,con-fabulationwasdefinedasrecallofinformationnotpresentintheoriginalnarrative.Thedegreeof confabulation was related to problems in suppressing inappropriate responses and formalthoughtdisorder.McKennaetal.(2009)concludethat,‘Thereisnodoubtthatthephenomenonofconfabulationcanbeseeninschizophrenia.Itisclearthatitisveryuncommoninaspontane-ousform,andwhenitdoesoccuritalwaysseemstotaketheformofso-calledfantasticconfabu-lation … Simple, momentary, or provoked confabulations, on the other hand, appear to becommonplace.’
Inaccuracyofrecallissometimescalledparamnesia.Aswellasoccurringinthenormalstateandinpersonalitydisorders, it isaprominentfeatureofaffectivedisturbances.Awomanwithdepressiveillnessfalsifiedtheeventsofherlife:‘Iamnotmarried.Mychildrenareillegitimate.Wedonotownthishouse.Wearebankrupt.’Allthesestatementswereuntrue,andthefalsifica-tion of her memory occurred in response to her severe depressive mood. Memory itself wasaccurate,butonremonstratingonanyparticularpointoffact,furtherdepressiveexplanationsofeventswouldbegiven.Forinstance,themarriagelicencewasdescribedasaforgery,andcom-plicatedlegalexplanationsweregivenastowhythehousedidnotbelongtoherandherhusband.In mania, unacceptable events or opinions may be brushed aside as not having occurred andunrealisticgoalspursuedasthoughtherewerenothingtopreventtheirattainment.
PSYCHOGENIC DISTURBANCE OF MEMORY
Cryptamnesiaistheexperienceofnotrememberingthatoneisremembering!Apersonmakesawitty remark, or writes a haunting melody, without realizing that he is quoting (plagiarizing)ratherthanproducingsomethingoriginal.Theprocessisseenwhenwordsorphrasescomeintopopularusageforafewmonthsoryearsbysomeprocessofmassspread,inwhichpeopleusingtheexpressionbelievetheyareintroducinganewidea.
Generally,unpleasantanduncomfortableexperiencesarenotrememberedaccuratelyorcom-pletely–‘forgettingofthedisagreeable’.Thisisadefectofrecallthatcanbeseenasasuccessfuldefence mechanism;ithelpstomaintaintheintegrityoftheperson.However,intheaffect of hope-lessness,reactivationofmemoriesofpreviousfailuresisafrequentreasonforperpetuatingneuroticthinking and behaviour (Engel, 1968). Psychogenic amnesia may appear without any organicdiseasebeingpresent,but thepresentationoforganicbraindisease isalwaysmodifiedbypsy-chogenicfactors(Pratt,1977).
Misnamingobjectsandmomentarylossofmemoryforwordsinhealthysubjectsmayresultfromfaultyretrievalfromshort-andlong-termmemorystoresratherthanfromthepsychoana-lyticexplanationof repression.Sucherrorsmaybecategorizedasacousticor semantic; acousticerrorstendingtooccurinshort-termstoresofupto30secondsandsemanticonesinlong-termstoresaftermorethanfiveminutes(ShalliceandMcGill,1977).
Dissociative (Hysterical) Fugue
The symptoms pertaining to dissociative (conversion) disorders (hysteria) in the International Classification of Diseases (World Health Organization, 1992) are of two types: conversion anddissociation.Indissociation,thereisanarrowingofthefieldofconsciousness,withsubsequentamnesiafortheepisode.Inmanyways,dissociativesymptomsrepresenta layman’s impressionof ‘madness’. In dissociative (hysterical) fugue states, there is narrowing of consciousness,
68 TWO—CONSCIOUSNESS AND COGNITION
wanderingawayfromnormalsurroundingsandsubsequentamnesia.Thepersonappearstobein good contact with his environment and usually behaves appropriately, maintaining basicself-care,althoughhesometimesdisplaysdisinhibition.There isquiteoftenlossof identityorassumptionofanother, false identity.Thedurationof theepisodecanbeveryvariable, fromafew hours to several weeks, and the subject may travel considerable distances. A citizen ofBirmingham,UnitedKingdom,describedastateinwhichhe‘cameto’inacityhedidnotrec-ognizeandwherepeoplewerespeakingFrench.Ashewalkedaboutthestreets,hefoundhewasnearanairportterminaland,tohissurprise,hediscoveredthathewasinMontreal.Germanetohisadventurewasthehistoryofacatastrophicrowandthebreakdownofhismarriage justbeforehe tookoff.Thus the featuresofdissociative fuguearedissociativeamnesia,purposefultravel beyond the usual everyday range and maintenance of basic self-care (World HealthOrganization,1992).
Ganser State
The original paper by Ganser (1898) has been much misunderstood. In it, he described fourcriminalswhoshowedthefollowingsymptoms.
■ Vorbeigehen(‘topassby’)orapproximate answers,describedbyGanserthus:‘Inthechoiceofanswersthepatientappearstodeliberatelypassovertheindicatedcorrectanswerandtoselectafalseone,whichanychildcouldrecognizeassuch’.
■ Cloudingofconsciousnesswithdisorientation.■ ‘Hysterical’stigmata.■ Recenthistoryofheadinjury,typhusorsevereemotionalstress.■ ‘Hallucinations’, auditory and visual (from his description, they are more like
pseudohallucinations).■ Amnesiafortheperiodduringwhichtheabovesymptomsweremanifest.TheGanser state isvery rarely seen inEnglishprisonsbut,when itdoesoccur, it ismore
likelyinthoseawaitingtrialthanthosealreadysentenced(Enoch,1990).Therehasbeenconsiderableargumentastowhetherthisconditionisprimarilyhystericalor
anorganicpsychosis,withdifferentauthorssupportingeachcontention(Latchametal.,1978).Acasethatillustratedboththehysterical(dissociative)andorganicelementswasthatofafemaleuniversity student,aged20years,whoexperiencedhead injurywithconcussionwhen inItaly.Herpremorbidpersonalitywasmarkedlyhistrionicandtheatricaland,attheageof13years,shehad developed a hysterical inability to walk for a few weeks. After transfer from the ItalianhospitaltoBritain,shedemonstratedapproximateanswersthus:
Question:‘WhatisthecapitalofItaly?’Answer:‘Naples.’Question:‘Howmanylegshasacentipede?’Answer:‘Seven.’Thiswasaccompaniedbyinterferenceinthetreatmentofotherpatients,flirtatiousbehaviour
towards male staff, lability of mood and a facetious manner. On serial testing of intellectualfunctionontheWechslerAdultIntelligenceScale,initialtesting12daysafterheadinjuryhadtobeabandoned;afteronemonth,therewasmarkedimpairment,worseforperformancethanforverbal items. Intellectual functionhad eventually returned toherpremorbid, superior level byninemonths.Whitlock(1967)considersthedistinctionbetweentheGanserstateandpseudo-dementia to lie indisturbedconsciousness,present in the formerandnot the latter.However,sometimescloudingofconsciousnessinanorganicstatecannotbedistinguishedfromthealteredmentalstateofdissociativedisorderintheabsenceofotherorganicsigns.
EnochandTrethowan(1979)haveregardedthefourmainfeaturesofGanser’ssyndromeas:■ approximateanswers■ cloudingofconsciousness
5—DISTUrbANCE Of MEMOry 69
■ somaticconversionfeatures■ pseudohallucinations(notalwayspresent).It shouldbenoted thatapproximateanswersarenot the randominaccuraciesof thequick
guessbutresponsesthatappeardeliberatelyjusttohavemissedthecorrectanswer.Theseauthorsregardthesyndromeasahystericaldissociativereactionandhavepointedoutthesimilarityoffeatureswiththoseexhibitedbynormalpeopleaskedtosimulatementaldisorder,thedifferencebeingthattheGansersubjectsweresubsequentlyamnesicfortheirabnormalbehaviour.UngvariandMullen (1997)have classifiedGanser’s syndromewith the controversial groupof reactivepsychosessothatastressfullifeeventistheusualpredisposingfactor.Cutting(2011)hasanovelandoriginalapproachtoGansersyndrome.OnthebasisofexaminationofanumberofcasesincludingtwoofhisownheconcludesthattheGansersyndromeiseitherpartofadepressiveillnessoratransientdisturbanceinthelefthemisphere’slexicalorsemanticknowledge.Cuttingargues that the knowledge deficit demonstrable in Ganser syndrome is not hysterical on anyaccountbutamanifestationofaparticularkindofcognitiveimpairment.
Recovered Memory and False Memory Syndrome
Thisiscurrentlyoneofthemosthotlydebatedissuesinpsychiatryandclinicalpsychology.Thoseworkingwithsurvivorsoftraumaticexperiencesnotedintheirpatientstherecoveryofadditionalmemoriesduringclinicalsessionsafterapparentpsychogenicamnesiaforalongtime;sometimesdecades. Recovered memory has been particularly associated with the return of memory forchildhoodsexualabuse.Brewin(1996)reviewstheevidenceforsucheventsbeing‘forgotten’andthenrecalledaftermanyyearsandthemechanismsthatmayaccountforthisamnesia.Hecon-cludesthatmemoriesmayberecoveredfromtotalamnesiaandtheymaysometimesbeessentiallyaccurate.Equally,such‘memories’maysometimesbeinaccurateinwholeorinpart.
Thetermfalse memory syndromecameintousein1992,whentheFalseMemorySyndromeFoundationwas setup to represent the interestsofparentswhohadbeenaccusedof abusingtheirchildrensexually.IntheopinionofMerskey(1998),sufferersfromfalsememorysyndromeare typically female and are usually participating in some type of psychotherapy.They reportsexualabuse inchildhood,which it is claimedhasbeen forgottenandrecoveredonly inadultlife,havingbeen repressed fromeight to40 years. It is considered that these ‘memories’havebeen implantedduring therapyby aprocessof suggestion similar to that thought tooccur inmultiplepersonalitydisorder.Anothersituationinwhichfalsememorieshavebeenthoughttodevelophasbeeninnurserydaycare,whencaregivershavebeensubjectedtograveandbizarreaccusations.
There is empirical evidence demonstrating that there are differences between individualswhoserecoveredmemorieshavebeenrecalledinsidetherapy,thosewhosememorieswererecalledoutside therapyanda thirdgroupwhosememoriesof abusewere continuous fromchildhoodintoadulthood.Inthefirstgrouptherewas0%corroborativeevidence,whereasfortheothertwogroupsitwas45%and37%.Furthermore,thosewhohadrecoveredmemoriesoutsidetherapywereabletosuppressanxiety-provokingthoughtsrelatingtothoseeventscomparedtothegroupswithrecoveredmemoryfromwithintherapyandthegroupwithcontinuousmemoriessuggestingthatwomenwithrecoveredmemoriesfromoutsidetherapyareespeciallyadeptatsuppressingemotional memories when under laboratory conditions, confirming their liability to remainunaware of traumatic memories for long periods prior to their recovery (Geraerts etal,2007;2008).
ReferencesAllisonRS(1962)The Senile Brain.London:EdwardArnold.BaddeleyAD(1986)Working Memory.Oxford:Clarendon.BaddeleyAD(1990)Human Memory: Theory and Practice.Hove:Erlbaum.

70 TWO—CONSCIOUSNESS AND COGNITION
BaddeleyAD(2002)Thepsychologyofmemory.InBaddeleyAD,KopelmanMDandWilsonBA(eds.)The Handbook of Memory Disorders,pp.3–15.Chichester:JohnWiley.
BaddeleyADandHitchG(1974)Workingmemory.InBowerGA(ed.)RecentAdvancesinLearningandMotivation,vol. 8,pp.47–89.NewYork:AcademicPress.
BerlyneN(1972)Confabulation.British Journal of Psychiatry120,31–9.Bleuler E (1911) Dementia Praecox or the Group of Schizophrenias (transl. Zinkin J, 1950). New York:
InternationalUniversitiesPress.Bonhoeffer K (1901) Die akuten Geisteskrankheiten der Gewohnheitstrinker. Jena: Gustav Fischer. Cited by
BerlyneN(1972).BrewinCR(1996)Scientificstatusofrecoveredmemories.British Journal of Psychiatry169,131–4.CahillCandFrithC(1995)Memoryfollowingelectroconvulsivetherapy.InBaddeleyAD,WilsonBAand
WattsFN(eds.)The Handbook of Memory Disorders.Chichester:JohnWiley.CuttingJC(1985)The Psychology of Schizophrenia.Edinburgh:ChurchillLivingstone.CuttingJC(2011)A Critique of Psychopathology.ForestRow:TheForestPublishingCompany.DalgleishTandCoxSG (2002)Memory and emotionaldisorder. InBaddeleyAD,KopelmanMDand
WilsonBA(eds.)The Handbook of Memory Disorders,2ndedn.Chichester:JohnWiley.Dalla Barba G (1997) Recognition memory and recollective experience in Alzheimer’s disease. Memory
5,657–72.DeLuca J (2009) Confabulation in anterior communicating artery syndrome. In Hirstein W (ed.) Con-
fabulation: views from neuroscience, psychiatry, psychology, and philosophy.Oxford:OxfordUniversityPress.DrakefordJL,EdelstynNM,OyebodeF,SrivastavaS,CalthorpeWRandMurkhejeeT.(2006)Auditory
recognition memory, conscious recollection, and executive function in patients with schizophrenia.Psychopathology39,199–208.
Engel GL (1968) A life setting conducive to illness: the giving up-given up complex. Annals of Internal Medicine69,293–300.
EnochMD(1990)Hysteria,malingering, pseudologia fantastica,Ganser syndrome,prisonpsychosis andMünchausen’ssyndrome.InBluglassRandBowdenP(eds.)Principles and Practice of Forensic Psychiatry.Edinburgh:ChurchillLivingstone.
EnochMDandTrethowanWH(1979)Uncommon Psychiatric Syndromes.Bristol:JohnWright.EysenckMWandKeaneMT(2010)Cognitive Psychology: A student’s Handbook,6thedn.Hove:Psychology
Press.FraserM(1982)ECT: a Clinical Guide.Chichester:JohnWiley.GanserSJM(1898)Apeculiarhystericalstate.Archiv fuer Psychiatrie und Nervenkrankheiten30,633(transl.
SchorerCE,1965,British Journal of Criminology 5,120–6).GeraertsE,Schooler JW,MerckelbachH, JelicicM,HanerBJA, andAmbadarZ (2007)Corroborating
contiuousanddiscontinuousmemoriesofchildhoodsexualabuse.Psychological Science18,564–8.GeraertsE,McNallyRJ,JelicicM,MerckelbachH,andRaymaekersI(2008)Linkingthoughtsuppression
andrecoveredmemoriesofchildhoodsexualabuse.Memory16,22–8.Gilboa A and Moscovitch M (2002) Cognitive neuroscience of confabulation. In Baddeley AD,
Kopelman MD and Wilson BA (eds.) The Handbook of Memory Disorders, 2nd edn. Chichester:JohnWiley.
HirsteinW(2009)Confabulation: views from neuroscience, psychiatry, psychology, and philosophy.Oxford:OxfordUniversityPress.
Jackson JH (1887)Remarkson evolution anddissolutionof thenervous system. InTaylor J (ed.) (1931)Selected Writings of John Hughlings Jackson,vol. 2.London:Hodder&Stoughton.
Korsakov SS (1890) Eine psych. Storung combiniert mit multipler Neuritis. Allgemeine Zeitschrift fuer Psychiatrie 46.
KraepelinE(1913)Dementia Praecox and Paraphrenia(transl.BarclayRM,1919).Edinburgh:Livingstone.Latcham RW,White AC andSimsACP (1978)Ganser syndrome: the aetiological argument. Journal of
Neurology, Neurosurgery and Psychiatry41,851–4.LezakMD,HowiesonDBandLoringDW(2004)Neuropsychological Assessment,4thedn.Oxford:Oxford
UniversityPress.LiddlePFandCrowTS (1984)Agedisorientation in schizophrenia is associatedwithglobal intellectual
impairment.British Journal of Psychiatry144,193–9.
5—DISTUrbANCE Of MEMOry 71
LishmanWA(1998)Organic Psychiatry: the Psychological Consequences of Cerebral Disorder,3rdedn.Oxford:BlackwellScientific.
Lorente-RoviraE,Pomarol-ClotetE,McCarthyRA,BerriosGEandMcKennaPJ(2007)Confabulationinschizophreniaanditsrelationshiptoclinicalandneuropsychologicalfeaturesofthedisorder.Psychological Medicine37,1403–12.
Mayes AR (2002) Anterograde amnesia. In Baddeley AD, Kopelman MD and Wilson BA (eds.) The Handbook of Memory Disorders,2ndedn.Chichester:JohnWiley.
McKennaPJ,TamlynD,LundCE,MortimerAM,HammondSandBaddeleyAD(1990)Amnesicsyn-dromeinschizophrenia.Psychological Medicine20,967–72.
McKennaPJ,OrnsteinTandBaddeleyAD(2002)Schizophrenia. InBaddeleyAD,KopelmanMDandWilsonBA(eds.)The Handbook of Memory Disorders,2ndedn.Chichester:JohnWiley.
MerskeyH(1998)Preventionandmanagementoffalsememorysyndrome.Advances in Psychiatric Treatment4,253–62.
Nathaniel-James DA and Frith CD (1996) Confabulation in schizophrenia: evidence of a new form?Psychological Medicine26,391–9.
NietzscheF(1889)Twilight of the Idols (transl. Hollingdale RS, 1968).Harmondsworth:Penguin.PickA(1921)NeuesZurPsychologiederKonfabulationMsschr.Psychiatria et Neurologia49,314–21.Cited
byBerlyneN(1972).PrattRTC(1977)Psychogeniclossofmemory.InWhittyCWMandZangwillOL(eds.)Amnesia: Clinical,
Psychological and Medicolegal Aspects.London:Butterworth.RibotE(1882)Diseases of Memory: an Essay in the Positive Psychology.London:KegalPaul,Trench.RogersD(1986)Cognitivedisturbances:realorapparent?Psychiatry in Practice5,6–8.RothMandMyersDH(1969)Thediagnosisofdementia.British Journal of Hospital Medicine2,705–17.ScheidW(1934)ZurPathopsychologiedesKorsakowSyndroms.Zeitschrift fuer Neurologie und Psychiatrie
151,346–69.CitedbyBerlyneN(1972).ShakespeareW(1606)Macbeth V,iii,41–6.ShalliceTandMcGillJ(1977)Attentionandpurpose.InRequinJandBertelsonP(eds.)The Origins of
Mixed Errors.NewYork:AcademicPress.SternYandSackeimHA(2002)Neuropsychiatricaspectsofmemoryandamnesia. InYudofskySCand
HalesRE(eds.)American Psychiatric Publishing Textbook of Neuropsychiatry and Clinical Neurosciences,4thedn.Washington:AmericanPsychiatricPublishing.
TamlynD,McKennaPJ,MortimerAM,LundCE,HammondSandBaddeleyAD(1992)Memoryimpair-ment in schizophrenia: its extent, affiliations and neuropsychological character. Psychological Medicine22,101–15.
Taylor MA and AbramsR (1984)Cognitive impairment in schizophrenia. American Journal of Psychiatry141,196–201.
TulvingE (2000)Conceptsofmemory. InTulvingEandCraikFIM(eds.)Oxford Handbook of Memory.Oxford:OxfordUniversityPress.
Ungvari GS and Mullen PE (1997) Reactive psychoses. In Bhugra D and Munro A (eds.) Troublesome Disguises: Underdiagnosed Psychiatric Syndromes.Oxford:BlackwellScience.
Van der Horst L (1932) Ueber die Psychologie des Korsakowsyndroms. Monatsschrift fuer Psychiatrie und Neurologie83,65–84.
WeeksD,FreemanCPLandKendellRE(1981)DoesECTproduceenduringcognitivedeficits?InPalmerRL(ed.)Electroconvulsive Therapy. An Appraisal.Oxford:OxfordUniversityPress.
WeinmanJ(1981)An Outline of Psychology as Applied to Medicine.Bristol:JohnWright.WhitlockFA(1967)TheGansersyndrome.British Journal of Psychiatry113,19–29.WilliamsKM,IaconoWI,RemickRAandGreenwoodP(1990)Dichoticperceptionandmemoryfollowing
electroconvulsivetreatmentfordepression.British Journal of Psychiatry157,366–72.World Health Organization (1992) The ICD-10 Classification of Mental and Behavioral Disorders: Clinical
Description and Diagnostic Guidelines.Geneva:WorldHealthOrganization.

This page intentionally left blank
S E C T I O N THREEAwareness of Reality: Time, Perception and Judgement

This page intentionally left blank
75
C H A P T E R 6
Disorder of Time
SummaryTimeis integraltohowhumanbeingsexperiencetheworld.Althoughit isdifficulttodefine,therearesomeovertaspectssuchasduration,sequence,synchrony,rhythm,past,present,futureorientation and an arrow of time that are easily recognizable and understood by most peoplewithouttheneedforfurtherelaboration.Thereisalsoanimportantrelationshipwithspaceandwithnotionsoftheself.Abnormalitiesoftimeexperiencecanbroadlyspeakingbedividedintothosethataffectobjectivetimeandthosethataffect thesubjectiveaspectsof timeexperience.Therearealsoinfluencesofcircadianrhythms,seasons,monthlycycles,andlifeepochsthatareworthyofnoting.
Space and time are always present in sensory processes. They are not primary objects themselves but they invest all objectivity. Kant calls them ‘forms of
intuition’. They are universal. No sensation, no sensible object, no image is exempt from them. Everything in the world that is presented to us comes to
us in space and time and we experience it only in these terms.Jaspers (1959)
Inthequotationabove,Jaspersdrawsattentiontothewayinwhichhumanbeingsliveinspaceandtimeandhowallsubjectiveexperienceinmediatedbyspaceandtime.Jasperscontinues:
‘If we want to bring these primary things home to ourselves in some neat phraseology we may say that they both represent the sundered existence of
Being, separated from itself. Space is extended being (the side-by-side) and time is sequential being (the one-after-the-other)’.
A sense of time is clearly very central to the concept of self and its relationship with theoutsideworld.Butwhatexactlyistimeandhowisitexperienced?BarbaraAdam(1995)inherbookTime Watchinterviewedanumberofpeopleabouthowtheyexperiencetimeandsometheirresponsesarebothinstructiveandhelpful:
‘How time enters my life? I was born and now I am fifteen years old. We use the word when we ask what time it is. We talk about closing time, lunch-
time, getting up time, and that time is up. What time is, that is more difficult to say. It is not a person, not a thing, not a vegetable. It’s a period and units,
the day chopped up into hours, minutes and seconds. But it also divides the past from the future … The time is now, this very second. But I do not know
what it is we are chopping up into units. I think it’s an illusion since there isn’t anything to be chopped.’

Keywords: Time,CircadianRhythm,Disorientation.
6—DISORDER OF TIME 75.e1

76 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
‘For me time is a dimension within which everything moves and happens. In conjunction with space it is a universal framework. We can’t move through
space without time and vice versa which means that we can’t pass, spend, or allocate time without occupying space. Nothing exists and happens without
time and space.’
Adamherselfemphasizesvariousaspectsoftimeasfollows:
‘Thinking about time, therefore, involves rhythm with variation, a dynamic structure of framing, timing, synchronization, duration, sequence, tempo and
intensity. This cluster of time characteristics is implicated at all levels of being, from the most physical of planetary movements via physiological rhythms to
patterns of social organization, from the taken for granted via the invisible to the obvious, from the imposed via the lived to the culturally constructed.’‘Entailed within those processes is an irreversible unidirectionality, an
arrow of time. There can be no rejuvenation, no unknowing, no reconstitution of pollution back into aeroplane.’
Theseaccountsindicatethattimeisdifficulttodefinebutthattherearesomeovertaspectssuchasduration,sequence,synchrony,rhythm,past,present,futureorientationandanarrowoftime.Thereisalsoanimportantrelationshipwithspaceandwithnotionsoftheself,particularlywithenduringself-identity,thathasbeenremarkeduponbymanythinkersincludingKant(seeCritique of Pure Reason).
Thereisasenseinwhichtimeleavesasignatureonthemostdiverseaspectsofhumanlife,yetinsuchawaythattheinfluenceoftimeisoftenunrecognized.Asidefromtheobvioussuchasovertwaysofmeasuringtime,thereisatimedimensioninmemory, inlanguage(giventherelianceonwordsequenceandorderformanifestmeaning),throughrhythmandnoteorderonmusic, and in all actions including symbolic movements, dance, sports, etc. Covertly, time isinvolvedinsuchconceptsasexpectation,desire,hope,prayerandevendeath.Theselatterideashave evolved from the writings of Eugene Minkowski (1885–1972), a phenomenologicalpsychiatrist.
Disturbanceofsenseoftimeortime-relateddisorderisasensitiveindicatorthatsomethingisgoingwrongeitherintheselforitsmechanisms.Senseoftimeandtime-relateddisordersofbiologicalrhythmwillbeconsideredseparatelyinthischapter.Thereisnowidelyagreedclas-sificationofdisordersof time.However, it ispossible todivide thedisordersof time intotwobroadcategories:disorderofobjectivetimeanddisorderofsubjectivetime(Box6.1).
BOX 6.1 ■ Classification of disorders of time
Disorder of objective time■ Disorderofknowledgeoftime:disorientationintime;agedisorientation■ Disorderofdurationoftime■ Disorderofchronology(temporalorder)
Disorder of subjective time■ Disorderofflowoftime■ Disorderofdirectionoftime■ Disorderofuniquenessoftime■ Disorderofqualityoftime
6—DISORDER OF TIME 77
OBJECTIVE (CLOCK) TIME AND SUBJECTIVE (PERSONAL) TIME
An important distinction is that between objective (clock) time and subjective (personal) time.Objectivetime–chronological,physicalorhistoricaltime–isquantitativeandindependentoftheself.Itdependsonaccuratemeasurementandisobjectivetothedegreethatitissharedwithothersandverifiable.Subjectivetimeistheinner,subjectiveexperienceoftime.Aspectsofbothkindsoftimemaybeaffectedbypsychiatricillnesses.Objectivetimemaybealteredsothattheknowledgeoftime,thatis,theorientationtotimeincludingagedisorientationandappreciationoftimedurationandofchronologymaybeadverselyaffected.Subjectivetimemaybealteredsothat the experience of time duration, flow of time, meaning of time, uniqueness of time andsuccessionoftimemaybeaffected.
BIOLOGICAL RHYTHMS AND TIME
Although our units of time are to some extent arbitrary, natural and biological time operateswithindefiniteperiods.Thefourperiodsthathavethemostrelevancetomentalillnessarecir-cadian rhythms (about24hours–nightandday),monthlycycles, seasonalvariationsand lifeepochs(frombirthtodeath).Alltheserhythmsareimportantforthementalstateintimesofhealthandformthebasisforsuchconditionsasearlymorningwakeningindepression,premen-strualtension,seasonalaffectivedisorderandinvolutionalmelancholia.Manyofthesebiologicalrhythmswithvariationofmoodarebiochemicallymediatedthroughtheendocrinesystem.
Personaltime(andalso,toalesserextent,clocktime)isoftendescribedinrelationtothesebiologicalrhythms.Ourwholenotionoftheprogressionoftimeiscloselyrelatedtoprocessesofphysicalfunction:birth,growthanddecay.
Disorder of Objective TimeAnabilitytoseparateeventsintopast,presentandfuture,eveniflimited;thecapacitytoestimateduration;andtheabilitytoputeventsinthecorrectsequencearenecessaryforintellectualproc-esses to be carried out satisfactorily. Disorder of knowledge of time is closely associated withdisturbanceofconsciousness,attentionandmemory.
DISORIENTATION IN TIME
Disorientationfortimeisdemonstratedbytheinabilitytocorrectlytellthetimewithoutrecoursetoaclock,toindicatethedate,dayandseason.Thisimpairmentiscloselyassociatedwithimpair-ment of attention, concentration, consciousness and memory. It is a feature of delirium anddementia.It isalsoagoodclinicalcriterionfordistinguishingbetweenorganicandfunctionaldisorders (Cutting, 1997).The second abnormality is impairment of the ability to assess theduration of time,andthisisalsodisturbedinorganicstates.
AGE DISORIENTATION
Thetermage disorientationwasfirstusedbyZangwill(1953)inrelationtoKorsakov’ssyndrometodescribea‘fixed,stabledisorientationforage,whichwasimpervioustologicalcorrection’.Age disorientation,nowdefinedasafiveyeardiscrepancybetweenthepatient’sactualageandwhatthepatientstatestobehisownage,hasbeenconsideredtocorrelateclinicallywithintellectualimpairmentinchronicschizophrenia(CrowandStevens,1978).Suchpatientsweremuchlessable thanchronicschizophrenicpatientswithoutagedisorientationtoanswerquestionsaboutdateandthedurationoftime.Theysystematicallyunderestimatedthepresentyearandthedura-tionoftheirstayinhospital,andsometimestheirownage.
78 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
Thisgivesquantitativesupporttotheobservationthatforsomechronicpatients‘timestandsstill’;theyremainintheculturalsetofthetimewhentheydevelopedtheirillness.Suchpatientstendtousetheidiomaticlanguage,singthepopularsongs,wearthemodishclothesandtellthecharacteristicjokesofthetimebeforetheirillnessbecameestablished.Itisamistaketobelievethattheyareindulginginnostalgia;theircultural lifeisstillfirmlyfixedwithinthatparticularperiod.Notonlyinthebackwardofanold-fashionedmentalhospital,butalsoinahostelinthecommunity,thesepatientsliveintheirowntimecapsulewithinvisible,butimpregnable,walls.
DISORDER OF TIME DURATION
Estimationoftimedurationhasbeenstudiedusingvariousmethods,buttheresultshavebeeninconsistent.Objectivemeasuresof estimationof thepassageof time, for example, show thatpatientswithdepressiveillnesstendtounderestimatethepassageof30seconds,onaverage,bysixseconds.Thisiscomparedwithoverestimationofthepassageoftimebynormalcontrolsbyon average 10 seconds (Kuhs etal., 1991).That is to say that depressed patients on averageestimated 30 seconds’ duration as 24 seconds and the normal controls estimated 30 seconds’duration as 40 seconds. In other words, time appeared to flow more slowly for patients withdepressionthanitdidfornormalcontrols.Itisimportanttoemphasizethatthisreferstoestima-tionofthepassageofmomentarytime.Otherinvestigationshavedemonstratedanoverestima-tionoftimedurationindepression(KitamuraandKumar,1984;Munzeletal.,1988).Thereismoreconsensusonthesubjectiveexperienceoftimeindepression(seebelow).
DISORDER OF CHRONOLOGY (TEMPORAL ORDER)
Memoryofthetemporalorderofeventsisanaspectoftimesensethatisoftenignored.Thereis evidence thatpatientswithdiencephalic lesionscomparedwith thosewithmedial temporallobelesionshavedistinctdeficitsintemporalordermemorytasks.Thesepatientsareunabletocorrectlyindicatethetemporalorderoflearnedwordsonalistorthesequenceofpresentationofparticularstimuli.Thishasledtothesuggestionthatdiencephalicstructuresmayhaveafunc-tion in the encoding of temporal information (O’Connor and Verfaellie, 2002). Frontal lobelesionsarealsoassociatedwithimpairmentoffunctionontemporalordertasks.Inadditiontothis,anaspectoftemporalordercoding,namelyfrequencyestimation,whichinvolvesestimatinghowoftenaneventhashappened,isknowntobeimpairedbyleftfrontalbutnottemporallesions(BaldoaandShimamura,2002).
Clinically significant disorders of temporal order for past and current events have beenreported.Thesetaketheformofintactmemoryforautobiographicaleventsbutimpairedappre-ciationofthedurationandtimingoftheseevents.Theseimpairmentsareassociatedwithorganiclesionsinthecingulategyrus,theparietallobesandtheleftanteriorfrontalareas(Cutting,1997).
Disorder of Subjective (Personal) TimeDisorderofsubjectivetime ischaracterizedbyabnormalities inhowtimeisexperienced.Thiscaninvolvetheexperienceof(a)flowoftime,(b)directionoftime,(c)uniquenessoftimeand(d)qualityoftime.Thesedisordersgototheheartofhowtheworldisexperienced.Anyaltera-tioninthewaythattimeisexperiencedwillbydefinitioninfluencetheexperienceoftheobjectiveworldandmaycometoimbueperceptionsoftheobjectiveworldwithanalienhue.
DISORDER OF FLOW OF TIME
Theflow(passage)oftimemayslowdownorspeedup.Insomeinstances,itmaybecomearrestedandstandstill.Tolstoy’s (1895) short storyMaster and Man is true to life–ordeath.LostatnightinaRussiansnowdrift,hischaracter,VasiliiAndreich,
6—DISORDER OF TIME 79
got up and lay down a couple of dozen times. The night seemed it would never end. It must be getting on for morning now, he thought once as he raised
himself and looked around. Let’s have a look at my watch … He could not believe his eyes … It was only ten past twelve. The whole night still lay ahead.
Time, as a modality of personal experience, is disturbed in mood disorders. It has beenobservedbothclinicallyandexperimentallythatthosewithdepressiveillnessfeelthattimepassesslowly(WyrickandWyrick,1977).Lewis(1967)quotesapatientwhowasdepressedwithaffec-tive functional psychosis:
Everything seems very much longer. I should have said it was afternoon, though they say it is midday. They always tell me it is earlier than I think … and it looks as if I’m wrong and I can’t help feeling I’m right … I cannot see
any end to anything, only end to the world.
Theflowoftimecanalsobearrestedsuchthattimeappearstostandstill.Thepatientfeelsthat time is standing still, that in somewayeverything temporalhas come toanend.This isdescribednotuncommonlywithpsychoticdepression.Apatientsays,‘Ihavestoppedbeing,Ihave just stopped,everythingelsehas just stoppedaswell’.The incessant sequentialmarchofeventsnolongerimpressesthepersonwithitsinevitability.
This feeling of time standing still may also be experienced in ecstasy states, in which thepersonmayfeelthatheisexistinginthepast,thepresentandthefutureallatthesametime.Suchstatesmayoccurwithmania,withsomeneuroticconditionsorinnormalpeopleundergoinganexceptionalpsychologicalexperience.
Whenthedisturbanceinthesenseofthepassageoftimeoccursinthesettingofdepression,thedepressedmoodisalsoapparent.AnotherofLewis’(1967)patientssaid,
‘I never know any moment what is going to happen. It’s the most terrible outlook I’ve ever had to look to. It’s all perpetual. I’ve got to suffer perpetually.’
AndoneofMinkowski’s(1970)patientssaid:
‘I continue to live now in eternity; there are no more hours or days or nights. Outside things still go on, the fruits on trees move this way and that. The
others walk to and fro in the room, but time does not flow for me. My watch runs just as before … Sometimes when people run quickly to and fro in the
garden or if the wind stirs up the leaves, I would like to live again as before and be able to run interiorly with them in order that time would pass again.’
Intheseexamples,thepatientsaretryinghardtodescribetheindescribable,theexperienceof timestandingstill. Inaddition to thisexperience there isalso the relatedbutdistinctphe-nomenonof living inthe instantandthis feeling isalliedtothenotionoffinalityand lackofcontinuity:
‘I live in instantaneousness. I don’t have the feeling of continuity anymore … When I finish something, I have the feeling of not being able to do anything
else afterwards and of doing this thing, going to dinner for example, for the last time.’(Minkowski, 1970).
80 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
This last sentence isperhaps thekey to theabnormalpsychopathology. It is theabnormalmoodassociatedwithtimesensethatissignificant,sodepressivein-patientsweresignificantlymorelikelytofeelthattimewaspassingmoreslowlythanhealthy‘control’subjects(KitamuraandKumar,1982).
Inmania,timepassesrapidly,butthepictureisuncertaininschizophrenia(Orme,1966).Theflowoftimeisalsoknowntobeaffectedinorganicbrainconditions.PatientswithKorsakov’ssyndromeunderestimatethepassageoftime,andsubjectswhohavehadthalamotomyexperiencetheflowoftimeasspeededup(Cutting,1997).
AdistinctbutrelateddisturbanceoftheflowoftimeistheZeitrafferphenomenon.Thisisliterallyatime-lapsephenomenon.ItwasfirstdescribedintheGermanliteratureinthe1930s,and Cutting (1997) has now brought it to the attention of the English-speaking world.Thecharacteristicfeaturesare:
1. thespeedinguporslowingdownofevents;2. itsassociationwithincreasedspeed,pitchandvolumeofauditoryperceptions;and3. alterationsinthefluencyofobservedmovements.Theremayalsobevisualhallucinations,anomalousexperienceofspacesuchasdistortionsof
horizontalandverticallines.Thisphenomenoninvariablyoccursinthesettingofacuteorganicbraindiseasesuchascerebrovascularaccident.
TheoriginalcasewasdescribedbyHoffandPotzl(1934,quotedinCutting,1997):
Doctors and nurses were first of all moving with a measured step, conspicuously, as if on a film. Then the tempo of things became very erratic,
sometimes coming at a furious pace, ‘like moving pictures speeded up’ as if the people involved were ‘running a race’ … Music, whose source was to his left,
sounded very loud and very fast, as if ‘several radios were all blaring away together … as if all the instruments wanted to show how much noise they
could make’. Sometimes, other people’s speech seemed excessively fast and incomprehensible ‘as if the doctors and nurses were practising for a world
record’. However, if he were addressed directly, the rate appeared quite normal and he could understand it quite well. It was when someone was speaking away to the left that it sounded most peculiar – shriller, louder and faster
than when to away to the right.
DISORDER OF DIRECTION OF TIME
Itseemssuchafundamentalaspectofourexperienceoftimethatthearrowoftimetravelsfromthepastthroughthepresenttothefuture.Itisincomprehensiblethatanyonecouldexperiencetimeasifeventswerebeingplayedin‘rewindmode’backwards.ThisphenomenonwasreportedbyoneofLewis’patients(1967):
‘Whenever anyone said anything to me, it referred back to some part of my life … One mind was living back and my mind forward.’
AnotherofMinkowski’s(1970)patientssaid:
‘There is no present anymore, only a sense of the past. Is there a future? There used to be, but now it is shrinking. The past is so obtrusive … I’ll give you
an example of what it’s like. I’m like a machine that runs but does not move
6—DISORDER OF TIME 81
from its place. It goes at full speed, but it remains in place. I am like a burning arrow that you hurl before you; then it stops, falls back, and is finally
extinguished as if in a space empty of air. It is hurled backwards.’
DISORDER OF UNIQUENESS OF TIME
Partofourexperienceoftimeisthesenseofuniquenessofthetime,momentaryorotherwise,thatwelivethrough.Thisuniquenessoftimeexperienceisinstantiatedintheuniqueeventsthatpopulatetime.Thismeansthateverymomentisgivenitssingularidentitybythecontext,bytheevents played out in a given place, by particular personalities and by association with specificemotions.Thesecoordinatesoftimestampeachmomentwithitsspecificuniquefeeling.
Thedéjà vu experiencecanbeconceptualizedasanalterationof the feelingofuniquenessthattimeandeventsareinvestedwith.Whenthisisdisrupted,noveleventsandthetimeandplaceinwhichtheyoccurseemfamiliar.Inthisconceptualization,déjà vu istheexperienceofthisfeelingoffamiliarityforeventsandtimesthathavenotbeenpreviouslyencountered.Jamais vuistheabsenceofthisfeelingoffamiliarityforeventsthathavebeenpreviouslyencountered.Inotherwords,evenpreviouslyencounteredsituationsareexperiencedasnovel,thatis,asunique.Althoughitispossibletoconceptualizetheseexperiencesasdisordersoftime,itisprobablymoreappropriatetoregardthemasaspectsofmemorydisturbance(Chapter5).
Déjà vu occurs in the normal state and in pathological conditions. The composer RalphVaughanWilliams,indescribinghisfirsthearingofthetuneusedinDives and Lazarus,explained,‘Ihadthatsenseofrecognition–here’ssomethingwhichIhaveknownallmylife,onlyIdidn’tknowit’(Kennedy,1964).Mostpeoplecanrecallsimilardéjà vuexperiences.Itisalsocommonlyassociatedwithtemporallobeepilepsy.Apatientdescribedhisaurabeforeafitexperiencedinhospital:‘Iwentintothekitchen.ThewindowlookedasifI’dseenitbefore.Ifeltverypeculiar’.Déjà vuandjamais vuarequiteoftendescribedinschizophrenia.
Déjà vuhasbeenproducedwithbrainstimulation.PenfieldandKristiensen(1951)wereabletoreproduceasensationoffamiliaritywithstimulationofabrainelectrodeinepilepticpatients.Thisstimulationclearlyproducedanabnormalityofthefeelingoffamiliarity,notanabnormalityof memory. It was a disturbance of the feeling of recognition that accompanies recall in theprocessofmemory. Janetconsidereddéjà vu tobea formof lossof realityornegationof thepresent (Taylor, 1947), while Freud (1901) regarded it as being associated with the recall ofunconsciousfantasies.
Inamoreextremeform, thedisorderof theuniquenessof timepresentsasreduplication of time.ThetermwasfirstusedbyWeinsteinetal.(1952).Petho(1985)describedacaseinwhichthepatient’scentralsymptomwasthebeliefthatshehadlivedthroughthislifeoncebefore.Thepatientexperiencedareduplicationofeveryevent,andinrelationtoattendingthe1976OlympicGamessaid,‘ItcouldhappenthatIwillgo;Ihaveamemoryof it.ButIalsohaveamemorythatIwon’tgotothoseGamessothatthatmemorywon’tcomebacktome.’
DISORDER OF THE QUALITY OF TIME
Intheseconditions,thenormalexperienceofthequalityoftimeiseitherlostordistortedinsomeway.Whatiscentraltotheseexperiencesisthatthe‘takenforgranted’aspectoftimeisreplacedbyadegreeofalienationfromitsuchthattimebecomessalient,obtrusiveandevenunreal.
Indepersonalizationandderealization, therecanbea lossof thefeelingofreality for timeexperience; theremayalsobealteration in the senseofdurationor in theperspectiveof time(FreemanandMelges,1977).Thepersoncanassessatimespanquiteaccurately,andthereisnolossofmemory.However,hehasno feeling that thingsarehappeningor time ispassing; the

82 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
abnormalityisalwaysoneofexperience.Timeitselftakesonafeelingofunreality,andhefeelsunabletoinitiateaction.
Thisphenomenoncanalsooccurinschizophrenia.OneofCutting’s(1997)patientssaid:
‘Time is somewhat changed. Time isn’t supposed to be the way it is. I don’t know in what way.’
Fischerdescribedanumberofcases(quotedinCutting,1997),ofwhichonesaid:
‘Time stood still. Then it became different. Then it disappeared entirely … Then a new time emerged. This new time was endless, more manifold than
the previous one, hardly deserving the name “time” as we know it. Suddenly it came to me that this time did not only lie in front of and behind me, but
spread out in all directions.’
Biological Rhythms and Their Relation to PsychiatryDaily,thereareprofoundchangesinthebodyandbrainassociatedwiththeexternalrhythmoftheworld.Duringthewakingdayweareactive,andatnightwesleep,recuperateandrepairourbodyparts.Thisbiologicalrhythmisdrivenbyaninternalclock.Theprimaryinternalbodyclockislocatedinthesuprachiasmaticnuclei,aclusterofapproximately100,000neuronslocatedoneither side of the midline above the optic chiasma, about three centimetres above the eyes(Hastings, 1998). There is strong evidence that the clock is an autonomous property of thesuprachiasmatic nuclei, and individual cells, in vitro, continue to fire rhythmically for severalweekswithonlytheslightestdeviationfrom24hours.Itisknownthatthisclockcanbedesyn-chronizedbyjetlag,shiftworkanddepression(Arendt,1995).However,thereisstillagreatdealofignoranceabouttheconnectionswithdifferentmentalillnesses.Inthissection,briefreferenceismadetodaily,monthlyandannualrhythms,andalsototheassociationwiththestageoflife.Amongpsychiatricdisorders,mostinformationisavailableonaffectivedisorderanditsassocia-tionswithdailyandannualrhythms(Thompson,1988).
CIRCADIAN RHYTHMS
Comparinginternaltimewithclocktime,repeatedestimatesoffixedtimespansshowagradualincreaseintimeoftheestimate,suggestingthatthereisaslowingoftheinternalclock.Subjectswereaskedrepeatedlytoguessafixeddurationoftime;theirestimatestartedbybeingslightlylongerthanactualtimeandbecameprogressivelylongerstill.Theintrinsicperiodofthecircadianrhythminhumansisapproximately25hours,butthisisusuallymodifiedbyexternalcuessuchasdaylight(WherandGoodwin,1983).Thishasbeenlikenedtothefindinginvigilanceexperi-ments, inwhichthere isagradualdecreaseofefficiency.Therewasalso foundtobeagreateroverestimationoffixedintervalsinthemorning,ascomparedwithintheafternoon,andthiswasfound to be correlated with body temperature.The internal clock accelerates when the bodytemperatureisraised.
There is considerable circumstantial, but little direct, evidence that circadian rhythms arecausally associated with affective disorders (Thompson, 1984). Early morning wakening anddiurnalvariationinmood,withthemoodmostdepressedintheearlymorning,areconsideredasbiologicalsymptomsofdepressionandhavebeenpostulatedasphase advanceofthesleep–wakecycle;thatis,eachpointoftherhythmoccursearlierthanusualrelativetothelight–darkcycle.Thereisachangeindepressioninthatrapideyemovementsleepoccursearlier,ratherthanlater,
6—DISORDER OF TIME 83
inthenight,andthisalsomaypointtophaseadvanceofthecircadianrhythm.Sleepdeprivationhasbeenusedwithvariablesuccessinthetreatmentofdepression;therehasbeenresearchintothegeneticandfamilialaspectsofsleepdisturbance,intosleepdisordersindepressionandotherneuropsychiatricconditionsandintotherelationshipofsleepdisturbanceindepressionandotherneuroendocrinechanges(LinkowskiandMendlewicz,1993;Vogeletal.,1980).
Althoughdiurnalityofmoodusuallymanifestsitselfbythesubjectfeelingworseintheearlymorning,sometimesthisisreversed.Styron(1991)describesthisforhisownseveredepressiveillness:
‘there was now something that resembled bifurcation of mood: lucidity of sorts in the early hours of the day, gathering murk in the afternoon and evening’.
Indepression,changesofbody temperatureandcortisol levelsover the24hourshavealsobeen interpreted as phase advanceof the circadian rhythm,but the results are equivocal.Theactionofantidepressantdrugsontherhythmhasbeeninvestigatedbylengtheningtheintrinsiccyclesofrest,temperatureandsleep,butagaintheevidenceisnotclear.Corroborationstudiesofairtravellerscrossingtimezoneshavesuggestedthattravelfromeasttowestismorelikelytobeassociatedwithdepression,andfromwesttoeastwithhypomania( JauharandWeller,1982).However, physiological studies of jet lag would not support such an association (Arendt andMarks,1982).
Thinking in relation to circadian rhythms in mood disorders was given further impetusbecauseofthediscoveryofclockgenesandcellularclocks,eventhoughthere isnoconsistentfindingthatdisruptionoftheseclocksexistinmooddisorders(McCarthyandWelsh,2012).Itmaybethatclockgeneexpressionoutsideofthesuprachisamaticnucleus is involvedinmoodregulation(McClung,2007).Thisisamatterforfutureresearch.
Ithasbeensuggestedthattheremaybeashortenedrhythm,oflessthan24hours,inpatientswithlong-termschizophrenia.Abnormalitiesofcircadianrhythmhavealsobeendescribed,butnotfullysubstantiated,inanorexianervosaandinpeoplewithabnormalpersonalities.
MONTHLY CYCLES
Clearly,themostobvioushumanbiologicalrhythmtorecurmonthlyisthemenstrualcycle,andthishasbeenlinkedwithchangesinthementalstate,butpremenstrualsyndromeremainscon-troversialinitsdefinition,managementandpoliticosocialimplications(Bancroft,1993).Similarpsychologicalmoodswingswithamonthlycyclehavebeensoughtinthemalebutnotconvinc-ingly found. Estimates for the frequency of premenstrual syndrome have varied in the generalpopulationbetween30percentand80percentofwomenof reproductiveage (Clare,1982).Psychologicalsymptomsincludelethargy,anxiety,irritabilityanddepression,butmanysymptomsarebothpsychologicalandphysical(headache,feelingbloated,lossofenergy).Itisthetimingratherthanthenatureofthesymptomsthatindicatesthediagnosis,andthereareclearlydifferingconstellationsofcomplaintwithinthesyndrome(Sampson,1989).
MuchnumericaldatahavebeenprovidedbyDalton(1984)tosupportthecontentionthatthereisincreasedpsychopathologyofvarioustypesduringtheeightdaysofthepremenstruumandthemenstrualperiod itself relative to the restof thecycle.Shestated that46percentofemergencypsychiatricadmissions,53percentofattemptedsuicides,47percentofadmissionsfordepressionand47percentofadmissions for schizophreniaofwomenof reproductive ageoccurduring these stages,but thesefigureshavenot yetbeen substantiated.However, reportsofunusualmanifestationsofpremenstrualsyndromeincludedescriptionsofauditoryhallucina-tionsanddelusionsofreferencepresentonlyinthepremenstrualperiod,andhypomanicormanicstatespresentinthe2–3dayperiodbeforetheonsetofmenstruation(HsiaoandLiu,2007).
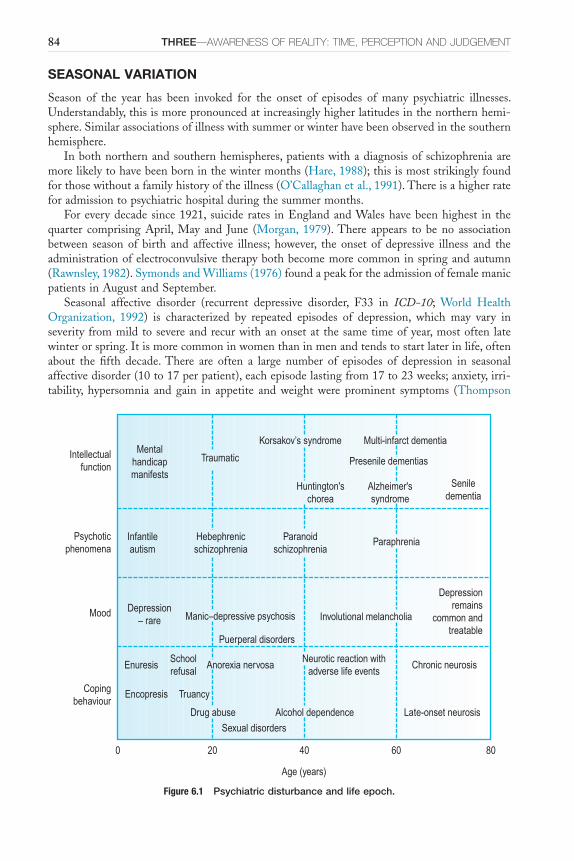
84 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
SEASONAL VARIATION
Season of the year has been invoked for the onset of episodes of many psychiatric illnesses.Understandably,thisismorepronouncedatincreasinglyhigherlatitudesinthenorthernhemi-sphere.Similarassociationsofillnesswithsummerorwinterhavebeenobservedinthesouthernhemisphere.
Inbothnorthernandsouthernhemispheres,patientswithadiagnosisofschizophreniaaremorelikelytohavebeenborninthewintermonths(Hare,1988);thisismoststrikinglyfoundforthosewithoutafamilyhistoryoftheillness(O’Callaghanetal.,1991).Thereisahigherrateforadmissiontopsychiatrichospitalduringthesummermonths.
Foreverydecadesince1921, suicide rates inEnglandandWaleshavebeenhighest in thequarter comprising April, May and June (Morgan, 1979).There appears to be no associationbetween season of birth and affective illness; however, the onset of depressive illness and theadministrationofelectroconvulsivetherapybothbecomemorecommoninspringandautumn(Rawnsley,1982).SymondsandWilliams(1976)foundapeakfortheadmissionoffemalemanicpatientsinAugustandSeptember.
Seasonal affective disorder (recurrent depressive disorder, F33 in ICD-10; World HealthOrganization, 1992) is characterized by repeated episodes of depression, which may vary inseverityfrommildtosevereandrecurwithanonsetat thesametimeofyear,mostoften latewinterorspring.Itismorecommoninwomenthaninmenandtendstostartlaterinlife,oftenabout the fifth decade.There are often a large number of episodes of depression in seasonalaffectivedisorder(10to17perpatient),eachepisodelastingfrom17to23weeks;anxiety,irri-tability, hypersomnia and gain in appetite and weight were prominent symptoms (Thompson
Figure 6.1 Psychiatric disturbance and life epoch.
Intellectualfunction
Psychoticphenomena
Mood
Copingbehaviour
806040200
Age (years)
Mentalhandicapmanifests
Paraphrenia
Seniledementia
Korsakov’s syndrome Multi-infarct dementia
Presenile dementias
Alzheimer'ssyndrome
Huntington'schorea
Infantileautism
Hebephrenicschizophrenia
Paranoidschizophrenia
Depression– rare Manic–depressive psychosis
Puerperal disorders
Involutional melancholia
Depressionremains
common andtreatable
Enuresis
Encopresis
Schoolrefusal
Truancy
Drug abuse
Anorexia nervosa
Sexual disorders
Alcohol dependence
Neurotic reaction withadverse life events
Chronic neurosis
Late-onset neurosis
Traumatic
6—DISORDER OF TIME 85
and Isaacs, 1988).The distinctive symptoms of this condition have been measured using theSeasonalPatternAssessmentQuestionnaire(Thompsonetal.,1988).Itoccursmorefrequentlyinhigherlatitudesinthenorthernhemisphere.InastudyconductedinFinland(Saarijärvietal.,1999),inwhichtheprominentsymptomsincludedlackofenergy,hypersomnia,excessiveeating,weightgainandacravingforcarbohydratesinadditiontootherdepressivesymptoms,therewaslowerprevalenceamongLapps,whoareethnicallyandgeneticallydifferentfromFinnslivingatthesamelatitude.
LIFE EPOCHS
Virtuallythewholeofpsychopathologyismediatedthrough,andinfluencedby,changesinsitu-ationandlifeepoch.Itisimportanttotakeintoaccounttherelativepreponderanceofdifferentfactors:biologicalchange,pressureofsocialcontextandindividualperceptionoflifesituation.Itisoutsidethescopeofthisbooktocharttheseassociationsindetail,butanimpressionisticsketchisofferedinFigure6.1.Thepsychologicaleffectsofimportantlifechangeshavebeenstudiedinprimarycaresituations:birthofthefirstchild( Jewell,1984),startingschool(PittandBrowne,1984),puberty(HoweandPage,1984)andleavingschool(Brown,1984).
Some of the abnormal mental states associated with life changes of female gender couldequallywellbediscussedwithlifeepoch.
ReferencesAdamB(1995)Timewatch: the social analysis of time.Cambridge:PolityPress.ArendtJ(1995)Melatonin and the Mammalian Pineal Gland.London:ChapmanandHall.ArendtJandMarksV(1982)Physiologicalchangesunderlyingjetlag.British Medical Journal284,144–6.Baldoa JV and Shimamura AP (2002) Frontal lobes and memory. In Baddeley AD, Kopelman MD and
WilsonBA(eds.)The Handbook of Memory Disorders,2ndedn.Chichester:JohnWiley.BancroftJ(1993)Thepremenstrualsyndrome–areappraisaloftheconceptandtheevidence.Psychological
Medicine Monograph Supplement24.BrownA(1984)Leavingschool.British Medical Journal288,1884–6.Clare AW (1982) Psychiatric aspects of premenstrual complaint. Journal of Psychosomatic Obstetrics and
Gynaecology1,22–31.CrowTJandStevensM(1978)Agedisorientation inchronic schizophrenics: thenatureof thecognitive
deficit.British Journal of Psychiatry133,137–42.CuttingJ(1997)Principles of Psychopathology: Two Worlds – Two Minds – Two Hemispheres.Oxford:Oxford
UniversityPress.DaltonK(1984)The Premenstrual Syndrome and Progesterone Therapy,2ndedn.London:Heinemann.FreemanAMandMelgesFT(1977)Depersonalizationandtemporaldisintegrationinacutementalillness.
American Journal of Psychiatry134,679–81.FreudS(1901)Thepsychopathologyofeverydaylife.InStandard Edition of the Complete Works of Sigmund
Freud,vol. VI,p.151(transl.StanleyJ,1960).London:HogarthPress.HareE(1988)Temporalfactorsandtrends,includingbirthseasonalityandtheviralhypothesis.InNasrallah
HA(ed.)Handbook of Schizophrenia,vol. 3.Amsterdam:Elsevier.HastingsM(1998)Thebrain,circadianrhythmsandclockgenes.British Medical Journal317,1704–7.HoweCandPageC(1984)Puberty.British Medical Journal288,1809–11.Hsiao MC and Liu C (2007) Unusual manifestations of premenstrual syndrome. Psychiatry and Clinical
Neuroscience61,120–3.JaspersK(1959)General Psychopathology (transl. Hoenig J and Hamilton MW, 1963).Manchester:Manchester
UniversityPress.Jauhar P andWeller MPI (1982) Psychiatric morbidity and time zone changes: a study of patients from
HeathrowAirport.British Journal of Psychiatry140,231–53.JewellMD(1984)Birthofthefirstchild.British Medical Journal288,1584–6.KantI(1781/1929)Critique of Pure Reason(transNKempSmith).London:MacMillanPress.KennedyM(1964)The Works of Ralph Vaughan Williams.London:OxfordUniversityPress.

86 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
KitamuraT and Kumar R (1982)Time passes slowly for patients with depressive state. Acta Psychiatrica Scandinavica65,415–20.
KitamuraTandKumarR(1984)Controlledstudyontimereproductionofdepressivepatients.Psychopathology17,24–7.
Kuhs H, Hermann W, Kammer W andTolle R (1991)Time estimation and the experience of time inendogenousdepression(melancholia):anexperimentalinvestigation.Psychopathology24,7–11.
Lewis A (1967)The experience of time in mental disorder. In Inquiries in Psychiatry, pp. 3–15. London:RoutledgeandKeganPaul.
LinkowskiPandMendlewiczJ (1993)Sleepencephalogramandrhythmdisturbances inmooddisorders.Current Opinion in Psychiatry6,35–7.
McCarthy MJ and Welsh DK (2012) Cellular circadian clocks in mood disorders. Journal of Biological Rhythms27,339–52.
McClungCA(2007)RolefortheClockgeneinbipolardisorder.Cold Spring Harbor Symposium of Quantitative Biology,637–44.
MinkowskiE(1970)Lived Time: phenomenological and psychopathological studies.TranslatedwithintroductionNMetzel.Evanston:NorthwesternUniversityPress.
MorganHG(1979)Death Wishes? The Understanding and Management of Deliberate Self-Harm.Chichester:JohnWiley.
MunzelK,GendnerG,SteinbergRandRaithL(1988)Timeestimationofdepressivepatients:theinfluenceofintervalcontent.European Archives of Psychiatry and Neurological Science237,171–8.
O’CallaghanE,GibsonT,ColohanHA,WalsheD,BuckleyP,LarkinCandWaddingtonJL,(1991)Seasonofbirth in schizophrenia.Evidence for confinementofanexcessofwinterbirths topatientswithoutafamilyhistoryofmentaldisorder.British Journal of Psychiatry158,764–9.
O’ConnorMandVerfaellieM(2002).Theamnesicsyndrome.InBaddeleyAD,KopelmanMDandWilsonBA(eds.)The Handbook of Memory Disorders,2ndedn.Chichester:JohnWiley.
OrmeJE(1966)Timeestimationandthenosologyofschizophrenia.British Journal of Psychiatry112,37–9.PenfieldWandKristiensenK(1951)Epileptic Seizure Patients.Springfield:Thomas.PethoB(1985)Chronophrenia–anewsyndromeinfunctionalpsychosis.Psychopathology18,174–80.PittGandBrowneMJ(1984)Startingschool.British Medical Journal288,1655–7.Rawnsley K (1982) Epidemiology of affective psychoses. In Wing JK and Wing L (eds.) Handbook of
Psychiatry 3: Psychoses of Uncertain Aetiology,pp.129–33.Cambridge:CambridgeUniversityPress.SaarijärviS,LauermaH,HeleniusHandSaarilehtoS(1999)SeasonalaffectivedisordersamongruralFinns
andLapps.Acta Psychiatrica Scandinavica99,95–101.SampsonGA(1989)Premenstrualsyndrome.Baillières Clinical Obstetrics and Gynaecology3,687–704.StyronW(1991)Darkness Visible: a Memoir of Madness.London:JonathanCape.SymondsRLandWilliamsP(1976)Seasonalvariationsintheincidenceofmania.British Journal of Psychiatry
129,45–8.TaylorWS(1947)PierreJanet1859–1947.American Journal of Psychology60,637–45.ThompsonC(1984)Circadianrhythmsandpsychiatry.British Journal of Psychiatry145,204–6.ThompsonC(1988)Biologicalrhythmsandmentalillness.Current Opinion in Psychiatry1,66–71.ThompsonCandIsaacsG(1988)Seasonalaffectivedisorder–aBritishsample:symptomatologyinrelation
tomodeofreferralanddiagnosticsubtype.Journal of Affective Disorders14,1–11.ThompsonC,StinsonD,FernandezM,FineJandIsaacsG(1988)Acomparisonofnormal,bipolarand
seasonal affective disorder subjects using the Seasonal Pattern Assessment Questionnaire. Journal of Affective Disorders14,257–64.
TolstoyL(1895)Master and Man (transl. Foote P, 1977).London:Penguin.Vogel DW, Vogel F, McAbee RS andThurmond AJ (1980) Improvement of depression by REM sleep
deprivation.Archives of General Psychiatry37,247–53.WeinsteinEA,KahnRLandSugarmanLA(1952)Phenomenonofreduplication.Archives of Neurology and
Psychiatry67,808–14.WherTAandGoodwinFK(1983)Circadian Rhythm in Psychiatry.PacificGrove:BoxwoodPress.World Health Organization (1992) The ICD-10 Classification of Mental and Behavioral Disorders: Clinical
Description and Diagnostic Guidelines.Geneva:WorldHealthOrganization.WyrickRAandWyrickLC(1977)Timeexperienceduringdepression.Archives of General Psychiatry14,
1441–3.ZangwillOL(1953)Disorientationforage.Journal of Mental Science99,698–701.

87
C H A P T E R 7
Pathology of Perception
SummaryAbnormalities of perception remain some of the most compelling experiences that patientspresentwith.Theseexperiencesspeaktotheunderlyingstructuresoftheperceptualworldandtheneuralcorrelatesthatmakeperceptionitselfpossible.Sensorydistortionsandfalseperceptionsbetweenthempointtotherelativeimportanceandthedistinctionstobedrawnbetweensensa-tionandperception.Illusion,whichisthemisinterpretationofanormalperception,andhallu-cinations,theperceptionofanobjectintheabsenceofastimulusarethetwomostfrequentlyencounteredfalseperceptionsinclinicalpractice.
For almost seven years – except during sleep – I have never had a single moment in which I did not hear voices. They accompany me to every place
and at all times; they continue to sound even when I am in conversation with other people, they persist undeterred even when I concentrate on other things.
Daniel Schreber (1842–1911)
Disordersofperception,particularlyauditoryhallucinationsor‘hearingvoices’,haveacentralplaceinpsychopathology.Alongwithdelusions(Chapter8),theyarethoughtofassynonymouswithmentalillness.Thisapparentassociationwithmentalillnesshascometoimplythat‘hearingvoices’isasignofseriousmentalillnessandthathallucinationsportendmadness.Inthischapter,thenatureofsensation,perceptionandimageryisdiscussedasapreludetoexaminingthenatureofdisordersofperception.
Sensation and PerceptionSensationisonlythefirststageinreceivinginformationfromoutsidetheself.Thesensorysystemincludesthevisual,auditory,tactile,olfactory,gustatory,kinaestheticandproprioceptivepathways.These pathways deal with the receipt, transformation and transmission of raw and disparatesensorydatafromperipheralreceptorstothecentralnervoussystem.Thetransformationofrawsensorystimuliintosensoryinformationthatisthendecodedintomeaningfulperceptionatthecortical level involvesactiveprocessesthatare influencedbyattention,affect,culturalexpecta-tions,context,priorexperiences,memoryand,most importantly,priorconcepts.It isthereforethecasethatperceptionisnotapassiveprocessbutanactiveonethatinvolvestheconstructionofanexternalworldthatdependsoninternaltemplates.
Muchofwhatweknowaboutsensationandperceptionderivesfromourunderstandingofthevisualsystem.Inthevisualsystem,lightsensationisreceivedbytheretinaandtransformedintoaneuralcodethatistransmittedfromtheretinalganglioncellstotheprimaryvisualcortexviathelateralgeniculatenucleusofthethalamus.Perceptionoccurswhenastimulushasunder-goneprocessingaccordingtoitsform,colour,motionandmeaning.
The distinction between sensation and perception is well illustrated by the dissociationbetweenintactsensationandimpairedperceptionintheagnosias.Invisualobjectagnosia,the

Keywords: Imagery,FormConstants,Synaesthesia,Illusions,Hallucination,Pseudohallucination,Autoscopy.
7—PAThOLOGY OF PERCEPTION 87.e1
88 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
subjectisabletorecognizethatanobjectisinhisfieldofvision(thatis,sensationisintact),buthe is unable to recognizewhat theobject or its function is (impairedperception).This visualmodelofperceptionislikelytohavecounterpartswithintheothersensorysystems.
OliverSachs(1995)recountsthestoryofVirgil,a51-year-oldmanwhohadbeenblindsinceinfancy.Hehadacataractextraction,butthereturnofvisualsensationwasunaccompaniedbyuncomplicatedperception.Virgilwasableto‘pickupdetailsincessantly–butwouldnotbeabletosynthesizethem,toformacomplexperceptionataglance.Thiswasonereasonthecat,visuallywas sopuzzling;hewould see apaw, thenose, the tail, an ear, but couldnot see all of themtogether,seethecatasawhole’.ThiscaseisreminiscentofGregory’spatient(2004),S.B.,whowhenhewasfirstshownalatheafterrecoveringhissight,‘wasquiteunabletosayanythingaboutit,excepthethoughtthenearestpartwasahandle…Hecomplainedthathecouldnotseethecuttingedge,orthemetalbeingworked,oranythingelseaboutit,andappearedratheragitated…S.B.wasallowedtotouchthelathe.Theresultwasstartling…Heranhishandseagerlyoverthe lathe,withhiseyes shut.Thenhestoodbacka littleandopenedhiseyesandsaid:“Nowthat I’ve felt it I can see.”’These two cases underline the distinction between sensation andperceptionandconfirmthat‘wearenotgiventheworld:wemakeourworldthroughincessantexperience,categorization,memory,reconnection’(Sachs,1995).
There are various competing models of the way that recognition is achieved by the visualsystem.Adetaileddescriptionof thesemodels isoutside thescopeof thischapter (seeSmithandKosslyn,2007).Bottom-upprocessingconsistsoftheprimaryprocessesthattransformsensa-tionintotheperceptionofobjectsthathaveform,colour,motionandlocationinspace.Ontheother hand, top-down processes involve the influence of our learned experience of perceivingobjectstonarrowthecompetitionbetweenthepossibleinterpretationsofthesensoryinforma-tion.Thealternativemodelsofthetop-downprocessesthatattempttoexplainobjectrecognition,thatis,perception,arethetemplate-matchingmodel,thefeature-matchingmodel,therecognition-by-componentsmodelandtheconfiguralmodels.
Thetemplate-matchingmodelrequiresaninternaltemplateinmemorytowhichanobjectcanbematched.Theweaknessofthismodelisthatthetemplatemustaccommodateobjectsizeandorientation,forexample,andmuststillberapidandreliable.Thefeature-matchingmodelrequiresonly that adistinct anddiscriminating featureof anobjecton itsownshould specifywhattheobjectis.Treesneedonlybespecifiedbythefactthattheyhaveatrunkandbranches.The exact location of the branches and size of the trunk do not matter.The recognition-by-componentsmodelrequiresaknowledgeofthecorrectarrangementofpartsinthree-dimensionalspace.Thus,irrespectiveoftheperspective,abicycleisstillrecognizedasabicycle.Finally,theconfigural model is a refinement of the recognition-by-components model. It deals with themechanismwherebyindividualexamplesofaclassarerecognized.Thisisthedistinctionbetweendifferentmakesof cars, the variation thatdetermines thatone car is aMercedes andanotherisaVolvo.
IMAGERY
Imageryistheinternalmentalrepresentationoftheworldandisactivelydrawnfrommemory.Imageryunderliesourcapacityformanycrucialcognitiveactivities,suchasmentalarithmetic,mapreading,visualizingandimaginingplacespreviouslyvisitedandrecollectingspokenspeech.Inday-to-daylife,itiscommontoreferto‘seeinginthemind’seyes’or‘hearinginthemind’sears’.Thesetermsrefertoimagery.Jaspers(1962)describedtheformalcharacteristicsofimagesasfollows:
1. imagesarefigurativeandhaveacharacterofsubjectivity;2. theyappearininnersubjectivespace;3. theyarenotclearlydelineatedandcomebeforeusincomplete;

7—PAThOLOGY OF PERCEPTION 89
4. althoughsensoryelementsareindividuallytheequalofthoseinperception,mostlytheyareinsufficient;
5. imagesdissipateandalwayshavetoberecreated;and6. imagesareactivelycreatedandaredependentonourwill(Table7.1).Functionalimagingstudieshavedemonstratedthatthesamecorticalareasareimplicatedin
visual imageryandvisualperception (KosslynandThompson,2003),and transmagnetic reso-nance studieshavealso shown that transmagnetic resonanceapplied repeatedly tovisual areasreducesthecapacityforvisualimagery(Kosslynetal.,1999).Furthermore,behaviouralexperi-ments have shown that participants are able to construct mental images that have perceptualqualitiessuchascolour,size,shapeandorientation.Theseimagesareuneven,withthelevelofdetaildependingonthedegreeofvisualattention(SmithandKosslyn,2007).
Thestudyofimageryremainsacontroversialareawithincognitiveneuroscience.Theoriesofvisualimageryhaveborrowedfromthelanguageandmodelofthecamera;thisisreferredtoasthepictorialordepictiontheoryofmentalimagery.TheforemostproponentofthisapproachisKosslyn.Adetailedaccountof the theoryand itsdifficulties isoutside thescopeof thisbook(seeKosslyn,2004;Pylyshyn,2004).Kosslynarguesthatamentalimageisfigurativelyaccurate,aseachpointoftheimagecorrespondstoeachpointontherepresentedobject.Thismeansthatthereisapoint-to-pointrepresentationsuchthatperformingparticularoperationsontheimagetakesasmuchtimeasitwouldtaketoperformthesameoperationontheobject.Inotherwords,the time to scanamental image is the sameas the time to scan theobject.Pylyshyn,on theother hand, argues that there are decisive differences between retinal or cortical images andmentalimages.
Imageryisimportantforpsychopathologybecauseanunderstandingoftheformalcharacter-isticsornatureofimageryisrequiredforexaminingthenatureofperceptions,hallucinationsandpseudohallucinations.Functionalimagingstudiesandcasereportshaveshownthatthemecha-nismsresponsibleforthevisualperceptionofobjectsandthoseresponsibleforimagerymaybesimilar.Inotherwords,theneuralsubstratesofperceptionandimageryattheveryleastoverlap(Martin, 2006). Ultimately, these investigations may shed light on the mechanisms unitingimageryandabnormalperceptions.
FORM CONSTANTS, EXTENSION AND SYNAESTHESIA
Synaesthesia isa rareconditionthat isnot regardedasanexampleofabnormalexperiencebutnonethelessprovidessomeunderstandingofelementaryperceptualneuralsystemsthatmayhelptoclarifyandilluminatetheproblemofabnormalperception.Synaesthesiacanbedefinedasthe
TABLE 7.1 ■ Formal characteristics of normal perception and imagery
Normal perception Imagery
Perceptions are of concrete reality Images are figurative and have a character of subjectivity
Perceptions occur in external objective space Images appear in inner subjective space
Perceptions are clearly delineated Images are incomplete and poorly delineated
The sensory elements are full and fresh The sensory elements are relatively insufficient
Perceptions are constant and remain unaltered Images dissipate and have to be recreated
Perceptions are independent of our will Images are dependent on our will
(After Jaspers, 1962)

90 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
perceptionof anobject,presented inone sensorymodality, at the same timeas in adifferentsensorymodality.Thisisbestillustratedbygivinganexampleofmusictocolour:
When I listen to music, I see the shapes on an externalized area about 12 inches in front of my face and about one foot high onto which the music is
visually projected. Sounds are most easily likened to oscilloscope configurations – lines moving in colour, often metallic, with height, width and, most
importantly, depth. My favourite music has lines that extend horizontally beyond the ‘screen’ area.
(Cytowic and Eagleman, 2009)
Various forms of synaesthesia have been reported including most commonly grapheme tocolour;timeunittocolour;musicalsoundstocolour;generalsoundstocolour;and,phonemetocolour.Otherformsaresoundstotaste;soundtotouch;visiontotaste;etc.Anotherexampleofsoundtocolour:
One of the things I love about my husband are the colours of his voice and his laugh. It’s a wonderful golden brown, like crisp, buttery toast, which sounds
very odd, I know, but it is very real.(Cytowic and Eagleman, 2009)
Theseexperiencesasdescribedaboveseemtobespatiallyextended,butdifferentfromseeingor imagining. They are experienced close to the body, within limb’s reach, and within ‘peri-personalspace’.Theseexperiencesraisethequestionofhowtheextendedspaceinsynaesthesiaisakintothespaceinwhichhallucinationsareexperienced.Furthermore,thesynaestheticexperi-encesareconsistentovertimeandareelementaryandspecificinnature.Thesensationsdonotevokeelaborateorcomplexperceptions,butratherelementarycolours,shapes,bright-darkcon-figurations,jagged-smoothsensations,etc.areprovoked.Indeed,thereisevidencethatthesensa-tionsareexamplesorelaborationsofForm Constants.Form Constants in thevisualdomainarevariations of tunnels and cones; central radiations; gratings and honeycombs; and spirals.Variations in colour, brightness, symmetry, replication, rotation and pulsation provide furthergradationsofthesubjectiveexperienceofthesepercepts.Whatissignificantisthattheseformconstantsseemtobeapropertyofthevisualcortexitselfandaremorecommonlyexperiencedintheauraphaseofmigraineorinperiodsofsensorydeprivation(seeCytowicandEagleman,2009foramoredetaileddiscussion).
Insummary,synaesthesiaintroducesthepossibilityofunderstandingsomeabnormalpercep-tions as occurring within peri-personal space which is neither like imagery nor like a normalpercept. Inotherwords,a thirdspacemightexist inwhichsomeexperiencessuchas those insynaesthesiatakeplace.Additionally,fundamentalandelementaryfeaturesoftheneuralunder-pinningofperceptionmightbeinvolvedindeterminingtheformofabnormalperception,thatis,thenatureofabnormalperceptionsisnotrandomlydetermined.
PRIVATE SPEECH AND INNER SPEECH
Inadditiontounderstandingthenatureofimagery,extendedspaceandformconstants,thereisaneedtocomprehendwhyauditoryhallucinationshavethesyntacticalstructurethattheyhave,namelycommandformatandsecondandthirdpersonsyntax.AnapproachisVygotsky’s(1896–1934)developmentalmodelof thoughtandspeech.Heproposedthat innerspeechdevelopedfirstfromtheinternalizationofexternaldialogueintoprivatespeechandfinallyintoinnerspeech(Vygotsky,1934/1987;Fernyhough,1996).Achildmight,forexample,beinstructedbyaparent;‘Dothisorthat’andthechildinternalizesthisinstructionintoprivatespeechandlaterintoinner
7—PAThOLOGY OF PERCEPTION 91
speech.Private speech is anovert, spoken language that isnot aimed at communicatingwithothersbut is linkedwith thinking.This transformationofdialogic, external speech into innerspeechprovidesabasisforunderstandingtheubiquityof‘command’auditoryhallucinations.Asimilarcasecanbemadeforsecondandthirdpersonauditoryhallucinations.WhatisimportanthereisthemannerinwhichVygotsky’sclaimlinksthinkingandspeechandalsohowhisbeliefthatinnerspeechandthinkingarebuiltonfragmentaryandcondensedimages,makethephe-nomenologyofverbalhallucinations,inparticular,morecomprehensible.
Abnormal PerceptionWewillnowdivideabnormalperceptionintosensory distortions,inwhicharealperceptualobjectisperceivedinadistortedway,andfalse perceptions,inwhichanewperceptionoccursthatmayormaynotbeinresponsetoanexternalstimulus.Illusions, hallucinationsandpseudohallucinationswillbeincludedunderfalseperceptions.Thepossibilityofaneurologicaldeficitaffectingpercep-tionalsoneedstobeconsidered.
Subjectively,hallucinationissimilartosenseperception:itisexperiencedasanormalpercep-tionanditcanbedistinguishedfromthefantasyelementsthat invest it.Invivid imagery, thewhole experience is imaginary. Pseudohallucination has a close affinity to imagerybut alsohassome aspects that are characteristic of sense perception or hallucination: vividness, definition,constancyandapparentindependencefromvolition.
SENSORY DISTORTIONS
Disturbance of the mental state, with or without organic brain pathology, may cause sensorydistortion.Thisdistortionmayinvolveanyofthecomponentsorelementaryaspectsofpercep-tion,suchasuniqueness,size,shape,colour,location,motionorgeneralquality.Whatissignifi-cant is that theperceivedobject is correctly recognized and identifiedyet there is adeviationfromitscustomaryappearancewithoutprejudicingtheknowledgeofthekindofthingthatitis(Cutting,1997).
Elementary Aspects of Visual Perception
Invisualperception,therecurrenceorprolongationofavisualphenomenonbeyondthecustom-arylimitsoftheappearanceoftherealeventintheworldistermedpalinopsia(Cutting,1997).Critchley(1951)gaveanumberofexamples:acatnoticedinthestreetonedaykeptappearingatvarioustimesandvarioussituationsoverthenextfewdays,andthewords‘PullmanSprings’noticedonthebackofavankeptappearingonothervehiclesoverthenextfewmonths.
Thesizeoftheperceptioncanbeeitherlarger(macropsia)orsmaller(micropsia)thanexpected.Insomecases,therecanbeapparentreductioninonehemifieldofvision(hemimicropsia).Theseanomaliesarecommonintemporallobeepilepsy.Alterationinthecustomaryshapeoftheper-ceivedobjectistermedmetamorphopsia.Usually,thismayinvolvetheappearanceofthingstakingonadifferentaspect:‘Onewomansawpeopleupsidedown,ontheirheads’(Bleuler,1950).Thisisanexampleofinversion.Whenmetamorphopsiaaffectsfaces,itisreferredtoasparaprosopia.Typically,theseperceptualdistortionsoffacesarerapidlyfluctuantanddynamic.Schreber(1955)describeshisexperienceasfollows:‘AtthesametimeIrepeatedlywitnessedthat[somepatients]changedheadsduringtheirstayinthecommonroom;thatistosaywithoutleavingtheroomandwhileIwasobservingthem,theysuddenlyranaboutwithadifferenthead.’Bleuler(1950)alsodescribes,‘Wardmateschangetheirfacestheverymomentthatonelooksatthem’.OneofCutting’spatients(1997)said,‘Manbehindalorrywaspullinghideousfaces’.
Different aspects of colour perception can be affected.The intensity of the colour (visual hyperaesthesia), theactualhueandthequalityofthecolourcanallbeaffected.Cutting(1997)givesseveralexamples:
92 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
1. ‘coloursarebrighter’,‘coloursmorevivid–red,yellow,orangestoodout’;2. ‘black lookedbrownsometimes’, ‘brown lookeddifferent; troublewithpinkas it comes
acrossasgreen’;and3. ‘thiscolourlookslikeanoldblue–somethinghorrible’.Bleuler(1950)describes‘onepatientseeseverythingascolouredred;anotherseeseverything
aswhite’,andJaspers‘Ionlyseeblack;evenwhenthesunisshining,itisstillallblack’.Theseperceptual distortions of colour occur in schizophrenia. In organic conditions, achromatopsia,which is the complete absence of colour, has been described following unilateral or bilateraloccipitallesions,usuallyofthelingualandfusiformgyri.Dyschromatopsiareferstotheperversionofcolourperceptionandoccursfollowingunilateralposteriorlesions.
The spatial location of a perceived object may be distorted. Teleopsia involves the objectappearing faraway,andpelopsia theobjectappearingnearer than it should.Alloaesthesia is thetermforwhentheperceivedobjectisinadifferentpositionfromwhatisexpected,sothatthepatient,forexample,experiencesthetranspositionofobjectsfromlefttoright.
Akinetopsiaistheimpairmentofvisualperceptionofmotioninwhichtheindividualisunabletoperceivethemotionofobjects.Itisveryrareandissaidtofollowbilateralposteriorcorticaldamage.Zeki(1993)quotesZihl’scase:
‘She had difficulty, for example, in pouring tea or coffee into a cup because the fluid appeared to be frozen, like a glacier. In addition, she could not stop
pouring at the right time since she was unable to perceive the movement in the cup (or a pot) when the fluid rose.’
Thegeneralqualityofperceptioncanbeaffected.Thisusuallyinvolvesanindefinablealtera-tioninthevisualappearanceoftheperceivedworldsothateverythingseemsdifferentfromwhatitusedtobe:‘People[look]liketoys–almostdeadandlifeless,carryingoutautomaticmove-mentswithspecialmeaning’(Cutting,1997);‘people lookdead,pale,cold’ (Cutting,1997);‘Afactory-worker seesagrasshopperandbecomesverydisturbedandexcitedat thesightof thisvery strange[myemphasis]andunknownanimal’(Bleuler,1950).Theseexperiencesareexamplesofderealization.Normally,perceptionisaccompaniedbyaffect,whichmaybeafeelingoffamili-arity,ofenjoyment,ofdislike,ofinvolvement,ofproximityandsoon.Thisisusuallyappropriateandsoignored.However,changesinthesefeelingsmaypresentassymptoms,forexample,‘eve-rythinglooksclearbutitalllooksmilesaway’,‘Ifeelinseclusion.Itislikelookingthroughthewrong end of a telescope’.These, and many other feelings, are described under derealization(Chapter13).Thereisafeelingofunrealityintheperceptualfield,analterationinthefeelingsassociatedwiththeobjectsofperception.
Apatientwhoexemplifiedboththelossofintensityofsensationandthechangeinfeelingsassociatedwithperception in thecontextofadepressive illnesswasa23-year-oldSriLankanBuddhistpriest.Followingasessionofmeditation,hebecameveryfrightenedonwakinguptodiscoverthathehadassaultedanotherpriestduringthenight.Inthenextfewdays,hefeltthathehadlostallsensation.Thingshesawandheardhecouldnotunderstandproperly.Hecouldseeonlythethingsthatwerenearby.Hecouldnotgetanysensationsfromhisskin.Hesaidthathecouldnotreadnorunderstand,norfeelsadnessorhappiness.Hesaidthathecouldnotfeelanything:‘all isnumbed,bodyandmind’.Headmittedto feeling low, that lifewasnotworthlivingandthathehadthoughtofendinghis life.Therewasnoneurologicalorotherphysicalabnormality.
Elementary Aspects of Auditory Perception
Theelementaryelementsofauditoryperceptionthatcanbedisturbedincludetheuniquenessofthe experience, the intensity and the spatial position (Cutting, 1997). In palinacousis, the
7—PAThOLOGY OF PERCEPTION 93
uniqueness of a perceptual experience is disturbed and there is persistence of sounds that areheard.Asubjectreturnedtoanswerthedoorseveraltimesduringa30minuteperiodafterthedoorbell had actually rung ( Jacobs etal., 1973).The intensity of auditory perception may bealteredsothat it iseitherheightenedordiminished.Forexample,heighteningintheauditorymodalityiscalledhyperacusis,asymptominwhichthepatientcomplainsofeverythingsoundingabnormally loud, saying, ‘I can’t bear thenoise’.Ordinary conversationmay sound intolerablynoisy, andevenwhisperingat adistancemaybe founduncomfortable.There is,of course,notrueimprovementofauditoryperceptionbutsimplyaloweringofthethresholdatwhichnoisebecomes unpleasant.The symptom occurs in depression, migraine and some toxic states, forexample the hangover following acute alcohol excess.The spatial position of a sound may bedisturbedsothatthesoundappearsasifitwasnearer,furtherordisplacedinposition.
Elementary Aspects of Tactile Perception
Palinaptiaistheexperienceoftactilesensationoutlastingthestimulus,sothatanobjectheldinthehandcontinuestobeperceivedwellafterithasbeendiscarded.Stacy(1987)reportsacaseofapatientwithbiparietallesionswhocouldfeelhertoothbrushinherhand15minutesafterputtingitaway.Thepalinapticexperienceoccurredinthesettingofastereognosisandpalpatoryapraxia.Thepalinaptiacanbeconceivedasacomplexhaptichallucination.Exosomesthesiaisthe‘displacementofcutaneoussensationintoextrapersonalspace’(ShapiroandFink,1952;Shapiroetal., 1952).This is a curious condition in which the individual experiences direct cutaneoustouchsensationasanobjectintheroomthatisdistalfromthembeingtouched.
If the palm of his hand was in contact with some object (bed, table, book) and the dorsum of that pricked with a pin, the patient insisted that the bed or
table had been touched and not his hand. This phenomenon could be elicited only from the hand and only when the palm was in contact with some object.
Thisunusualphenomenoncanbeexperimentallyinduced,andithasbeensuggestedthatthebody image,despite its appearanceofdurability andpermanence, is a transitory internal con-struct that canbe alteredby the stimulus contingencies and correlations that are encountered(RamachandranandHirstein,1998).
It is even possible to ‘project’ tactile sensations onto inanimate objects such as tables and shoes that do not resemble body parts. The subject is asked to place
his right hand below a table surface (or behind a vertical screen) so that he cannot see it. The experimenter then uses his right hand to randomly stroke and tap the subject’s right hand (under the table or behind the screen) and
uses his left hand to simultaneously stroke and tap the table in perfect synchrony … After 10–30 seconds, the subject starts developing the uncanny illusion that the sensations are now coming from the table and that the table
is now part of his body.
Alloaesthesiaisaneurologicalconditionfollowingright-sidedvascularlesionsoftheputamenthatischaracterizedbyasensorystimulusononesideofthebodybeingperceivedonthecon-tralateralside.Itcanalsooccurfollowingspinalcordlesionssuchascervicaltumours,cervicaldischerniationandmultiplesclerosis(Fukutakeetal.,1993;Kawamuraetal.,1987).
Splitting of Perception
Thisratherrarephenomenonisdescribedsometimeswithorganicstatesandalsowithschizo-phrenia:thepatientisunabletoformtheusual,assumedlinksbetweentwoormoreperceptions.
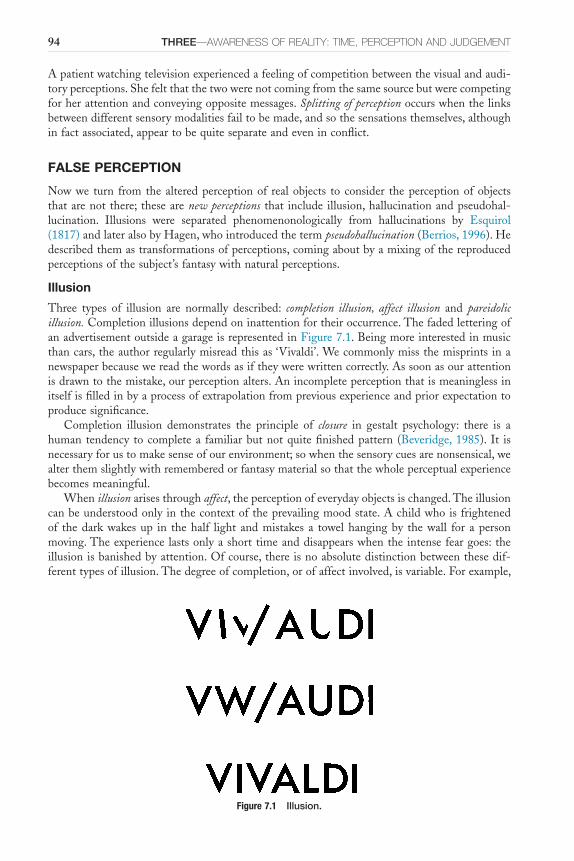
94 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
Apatientwatchingtelevisionexperiencedafeelingofcompetitionbetweenthevisualandaudi-toryperceptions.Shefeltthatthetwowerenotcomingfromthesamesourcebutwerecompetingforherattentionandconveyingoppositemessages.Splitting of perceptionoccurswhenthelinksbetweendifferentsensorymodalitiesfailtobemade,andsothesensationsthemselves,althoughinfactassociated,appeartobequiteseparateandeveninconflict.
FALSE PERCEPTION
Nowwe turn fromthealteredperceptionof realobjects toconsider theperceptionofobjectsthatarenotthere;thesearenew perceptions that includeillusion,hallucinationandpseudohal-lucination. Illusions were separated phenomenonologically from hallucinations by Esquirol(1817)andlateralsobyHagen,whointroducedthetermpseudohallucination(Berrios,1996).Hedescribedthemastransformationsofperceptions,comingaboutbyamixingofthereproducedperceptionsofthesubject’sfantasywithnaturalperceptions.
Illusion
Three types of illusion are normally described: completion illusion, affect illusion and pareidolic illusion.Completionillusionsdependoninattentionfortheiroccurrence.ThefadedletteringofanadvertisementoutsideagarageisrepresentedinFigure7.1.Beingmoreinterestedinmusicthancars,theauthorregularlymisreadthisas‘Vivaldi’.Wecommonlymissthemisprintsinanewspaperbecausewereadthewordsasiftheywerewrittencorrectly.Assoonasourattentionisdrawntothemistake,ourperceptionalters.Anincompleteperceptionthatismeaninglessinitselfisfilledinbyaprocessofextrapolationfrompreviousexperienceandpriorexpectationtoproducesignificance.
Completion illusion demonstrates the principle of closure in gestalt psychology: there is ahuman tendency tocompletea familiarbutnotquitefinishedpattern (Beveridge,1985). It isnecessaryforustomakesenseofourenvironment;sowhenthesensorycuesarenonsensical,wealterthemslightlywithrememberedorfantasymaterialsothatthewholeperceptualexperiencebecomesmeaningful.
Whenillusionarisesthroughaffect,theperceptionofeverydayobjectsischanged.Theillusioncanbeunderstoodonlyinthecontextoftheprevailingmoodstate.Achildwhoisfrightenedof thedarkwakesup in thehalf light andmistakes a towelhangingby thewall for apersonmoving.Theexperiencelastsonlyashorttimeanddisappearswhentheintensefeargoes:theillusionisbanishedbyattention.Ofcourse,thereisnoabsolutedistinctionbetweenthesedif-ferenttypesofillusion.Thedegreeofcompletion,orofaffectinvolved,isvariable.Forexample,
Figure 7.1 Illusion.
7—PAThOLOGY OF PERCEPTION 95
amanlookingthroughadvertisementsforapostfoundajobthathelikedandmisreadthewrittenword‘suitable’fortheillusionalword‘superior …applicantisrequired’.Clearly,thiswasbothanaffective and a completion illusion. Similarly, in the stage of searching that occurs followingbereavement, momentary recognition of the dead person may occur for someone in a crowd.Closeobservationoftheindividualimmediatelydispelsthefeelingoffamiliarity.
Pareidoliaoccursinaconsiderableproportionofnormalpeople.Itmayalsobeprovokedbypsychomimeticdrugs.Typically,imagesareseeninshapesinpareidolicillusion.Forexample,theauthorusedtoseetheheadofaspanielinachiponthefirstpavingstoneofthepathleadingtothehousewherehelivedasachild;theimagewasnotjustadogbutdefinitelyaspaniel.
Pareidolicillusionsarecreatedoutofsensoryperceptsbyanadmixturewithimagination.Thepercept takes on a full and detailed appearance: ‘AVictorian lady with a crinoline and frilledbloomers’.Thepersonexperiencing it, likesomeoneseeingaphotograph,knowsthat it isnottruly there as an object but that it is pictorial. However, he cannot dismiss what he sees.Completionandaffectillusionsoccurduringinattention;theyarebanishedbyattention,whichwill,ifanything,increasetheintensityofpareidolicillusionsastheybecomemoreintricateanddetailed.
Pareidolicillusionoccursinchildrenmorethaninadults.Itshouldbedistinguishedfromthefollowingconditions.
■ Perceptual misinterpretation,thatis,simplymakingamistakeastothenatureofperceptionwithoutthatperceptionbeingparticularlyinfluencedbyemotionmixedwithfantasy.
■ Functional hallucination,whichoccurswhenacertainperceptisnecessaryfortheproductionof a hallucination, but the hallucination is not a transformation of that perception. Forexample,thepatienthearsvoiceswhenthetapisturnedon;hehearsvoicesintherunningwater,butthevoicesandthenoiseofwaterarequitedistinctandcanbeheardseparatelyandsynchronouslylikeanyothervoicethatisheardagainstabackgroundnoise.Theper-ceptionofhearingrunningwaterisnecessarytoproducethehallucination,butthehallu-cinationisnotatransformationofthatperception.
■ Fantastic interpretationsorelaboratedaydreamingcanbeverysimilartopareidolicillusionsand,aswehavealreadydiscussed,thereisalargeadmixtureoffantasyinsuchillusions.
HallucinationHallucinationsare,phenomenologically,themostsignificanttypeoffalseperceptions.Herearefivedefinitionsofhallucination.
■ Aperceptionwithoutanobject(Esquirol,1817).■ Hallucinationsproperarefalseperceptionsthatarenotinanywaydistortionsofrealper-
ceptionsbutspringupontheirownassomethingquitenewandoccursimultaneouslywithandalongsiderealperception( Jaspers,1962).
■ Ahallucinationisanexteroceptiveorinteroceptiveperceptthatdoesnotcorrespondtoanactualobject(Smythies,1956).
■ According to Slade (1976a), three criteria are essential for an operational definition:(a)percept-likeexperienceintheabsenceofanexternalstimulus;(b)percept-likeexperi-encethathasthefullforceandimpactofarealperception;and(c)percept-likeexperiencethatisunwilled,occursspontaneouslyandcannotbereadilycontrolledbythepercipient.ThisdefinitionisderivedfromJasper’sformalcharacteristicsofanormalperception(seeTable7.1).
■ Ahallucinationisaperception without an object(withinarealisticphilosophicalframework)ortheappearance of an individual thing in the world without any corresponding material event(withinaKantianframework),accordingtoCutting(1997).
Oneofthesimplestfactsabouthallucinationsisoftenoneofthemostdifficulttocomprehend.Thatis,whatthedoctorcallsahallucinationisanormal sensory experiencetothepatient.Although
96 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
thestandarddefinitionsofhallucinationimplythat,subjectively,ahallucinationisindistinguish-ablefromanormalpercept,someauthorsarguethathallucinatoryperceptsmaybedistinctfromnormalpercepts (seebelow).Oneof the clues that the sufferer uses to grasp the fact thathemightbehallucinatingisthatthereisnocorroborativeevidencefortheperceptinothermodali-ties.Awomanhearsvoicesgivingacommentaryonheractivity:‘Sheisgoingtothesink.Sheis putting the coffee on’. She sees no one else in the room but recognizes the voices of herneighbours.Shecannotunderstandhowshecanbehearingthem,butsheissoconvincedbytherealityofthevoicesthatshedrawsthecurtainsandtakesthemirrorsoffthewalls.Thereissomeconflictinhermind:shehearsvoicesbutcanseenopersontoaccountforthem.However,sheresolvesthisconflictinwhatisarationalway,assumingthatshebelievesimplicitlyinthegenu-ineness of the perception: ‘someone must have fixed a device or altered my sense of hearing’.Whatisnotableisthatshedoesnotdoubttherealityofthepercept.
Horowitz(1975)hasinvestigatedhallucinationsusingacognitiveapproach,lookingateachofthefollowingfourconstructsintermsofcoding,appraisingandtransforminginformation.
Hallucinations are mental images that (1) occur in the form of images, (2) are derived from internal sources of information, (3) are appraised
incorrectly as if from external sources of information, and (4) usually occur intrusively. Each of these four constructs refers to a separate set of
psychological processes, although together they comprise a holistic experience.
Thisprovidesaconceptualframeworkforinvestigatingthephenomenaofhallucination.This ideahasbeendeveloped furtherbyBentall (1990),who considers thathallucinations
representfaultyjudgementsabouttheoriginoftheirperceptions,tendingtoattributethemtoanexternalsource.Thecontentofhallucinationwasthoughttobeexplained,atleastinpart,bytheneedtodefendtheindividual’sownself-esteem.Hallucinationsmayresultfromafailureofthemetacognitive skills involved indiscriminatingbetween self-generated and external sourcesofinformation.Thisexplanationwasgivenfurthersupportbythefindingthathallucinatorsmoreoftenmisattributedauditorilypresentedanswerstodifficultcluesfromanexperimenterthaneitheradeludedbutnothallucinatedgroupofpatientsornormalcontrolsubjects(Bentalletal.,1991).
Attemptstoexplainhallucinationsbyunderlyingneurochemistryandneuropathologyhavesofarnotmademuchprogress.Anattempthasbeenmadetoincorporateconceptsofbiologicalvulnerabilityandpsychologicalinfluencesintheaetiologyandclinicalpresentationofhallucina-tions,butresearchhasproducednosinglemechanismtoaccountforthem(AsaadandShapiro,1986).
Hallucinations takeplaceat thesametimeasnormalsensorystimuliareperceived.Inthisway, they are unlike dreams, which in fact have more of the characteristics of illusions.Hallucinationsarelikenormalpercepts,ofwhichseveralcanbeperceivedsimultaneouslyorinrapidsuccession.Thus,thepatientcanhearhallucinatoryvoicesatthesametimeasheisseeinghis interviewer and listening to him speak. Hallucination is like after-image, pareidolia or theobservationofanormalsensoryobject,inthatattentionwillnotremoveit.
The sense of reality experienced by patients when they hallucinate has been studied byAggernaes(1972),developingtheconceptsofRasmussen.Hepointedoutsixqualitiesofwhichnormalpeoplecanbeawarewhentheyexperienceasensation,whichalsooccurredinover90percentofaseriesofhallucinations.
■ Withnormalsensation,weareabletodistinguishperceivingwithoursenseorgansfromimaginingthesameobjects;hallucinationssimilarlyareexperiencedassensationandnotasthoughtorfantasy.
■ Whenasubjectexperiencessomething,herealizesitspossiblerelevanceforhisownemo-tions,needsoractions;hallucinationsalsohavethisqualityofbehaviouralrelevance.
7—PAThOLOGY OF PERCEPTION 97
■ Normalsensationhasaqualityofobjectivity,inthattheexperiencerfeelsthatunderfavour-able circumstances he would be able to experience the same something with anothermodalityofsensation;thisisalsotheexperienceofthehallucinator.
■ Anobjectisconsideredtoexistiftheobserverfeelscertainthatitstillexistseventhoughnobodyelseisexperiencingitatthattime;perceivedobjectsandhallucinationssharethisquality.
■ Experienceofobjectperceptionandhallucination is involuntary, in that the experiencerfeelsthatitisimpossibleorextremelydifficulttoalterordismisstheexperiencesimplybywishingtodoso.
■ Normally,theexperiencerisaware,orthroughsimplequestioningbecomesaware,thathisexperience is not simply the result of being in an unusual mental state; this quality ofindependenceispresentwithnormalperceptionandwithhallucination.
Onefurtherqualityofnormalobjectperceptionwasfoundtobeabsentmoreoftenthannotwithhallucination.Thisisthequalityofpublicness,inwhichtheexperiencerwouldbeawarethatanybodyelsewithnormalsensoryfacultieswouldbeabletoperceivethissomething.Often,thehallucinatordoesnotbelievethatotherscouldsharehisexperience(delusionalexplanationmaybegivenforthis).
Clearly,culturalfactorsinfluencethemannerinwhichsubjectsdescribetheirabnormalper-ceptions.IthasbeenclaimedbyAndrade(1988)thatbecausepatientsinIndiaweremorepre-paredtoacceptparanormalexplanationsforphenomena,falseperceptionsor‘truehallucinations’aremore likely tobeascribedwithobjectivityandveridicality.Even if this is so,and it isnotproven,thequalitiesdescribedbyAggernaeswouldstillbeusefulindistinguishinghallucinationfromotherabnormalitiesofperception.
Cutting(1997)hasarguedthathallucinatoryexperiencesarehardlyplausibleeverydayoccur-rences,andthatthereforeitisnotthathallucinatoryperceptsareindistinguishablefromnormalpercepts, but rather that they are taken for realitydespite the fact that they aredistinct fromeverydayreality.Hemakesthepointthat,forexample,Lilliputianhallucinationsindeliriumandcomplexhallucinationsinvolvingcomiccharactersareobviouslynotplausibleperceptionsintherealworldyettheyaretakenasreal!However,Cuttingignoresthefactthatitispreciselybecausehallucinatoryphenomenahavethequalityofanormalexperiencethattheyaretakenforrealitydespitebeing,ashepointsout, implausible.Otherauthors, suchasSpitzer (1994),argue thathallucinations are not like normal perceptions, in that patients can distinguish between realperceptualexperiencesandtheirhallucinatoryexperiences.Thisisonereasonwhypatientsareable to understand the reference to ‘hearing voices’ in interactionswith clinicians; bothpartiesknowwhatthiswayofspeakingstandsfor.Indeed,Wernicke(1906)hadalreadydrawnattentiontothisfactwhenhepointedoutthatthenotionof‘hearingvoices’wasnotinventedbypsychia-trists but rather was used by patients to indicate that somehow their experience was akin tohearingotherpeopletalkbutalsodifferentfromthisaswell.JungingerandFrame(1985)showedthatasubstantialproportionofpatients(40percent)ratedthevoicestheyheardasmoreakinto innerspeechthantoexternalspokenorheardspeech,thusemphasizingthathallucinationsmaynotalwayshavethehallmarkofnormalperception.
AUDITORY HALLUCINATION
An additional video for this topic is available online.
Hallucinationscanoccurinanyoftheareasofthefivespecialsensesandalsowithsomaticsensation.Wewillstartbydiscussingauditory hallucinations,astheyaremostoftenofsupremediagnosticsignificance.Inacuteorganicstates,theauditoryhallucinationsareusuallyunstruc-turedsounds–elementary hallucinations,forexamplethepatienthearswhirringnoisesorrattles,
98 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
whistling,machineryormusic.Often,thenoiseisexperiencedasveryunpleasantandfrightening.Ofinterestaremusicalhallucinations,whichtendtooccurinolderwomenwithdeafnessorbraindiseaseandnohistoryofpsychiatricillness(Berrios,1990).Thereare,therefore,similaritieswithCharlesBonnet’ssyndrome,describedbelowinthesectiononvisualhallucinations.
Hearingvoicesis,ofcourse,characteristicofschizophrenia,butitalsooccursoccasionallyinotherconditions, forexample chronic alcoholic hallucinosisoraffective psychoses.Thesevoicesaresometimescalledphonemes(confusionexists,unfortunately,becausethewordisusedwithatotallydifferentmeaninginlinguistics,inwhichphonemesaretheunitsofspeech-soundfromwhichwords are made). Usually in organic states the phonemes are simple words or short sentences,oftenspokentothepatientinthesecondpersonaseitherperemptoryordersorabusiveremarks.Theseabusiveorimperativephonemesalsooccurinschizophrenia,butothermorecomplicatedspeechisalsoheard;thevoicesmaybesingleormultiple,maleorfemaleorboth,peopleknownandrecognizedbythepatientornotknown.Theyareexperiencedascomingfromoutsidehisheadorhisself.Thevoiceisclear,objectiveanddefiniteandisassumedbythepatienttobeanormal percept that at the same time may be baffling and incomprehensible in its import.Particularlycharacteristicofschizophreniaarevoicesthatsaythepatient’sown thoughts out loud,whichgivearunning commentaryonthepatient’sactionsorvoices,whichargueordiscussvigor-ouslywith each other.Theyrefertothepatientinthethirdperson(Schneider,1959).
In a series of 100 current patients experiencing auditory hallucinations, all of which weredescribedas‘hearingvoices’,61sufferedfromschizophreniaand78fromschizophrenia-relatedconditions (NayaniandDavid,1996).Fifty-twopercentof thepatientshadanexperienceofsadness,and45percentexperiencedchurningorbutterflysensationsinthestomachatorbeforeonset.Mostvoicesspokeinconversationaltones,butafewwhisperedandafewshouted;halfofthesampleheardtheirvoicesthroughtheirearsasexternalstimuli.Mostvoicesweremale,oftenamiddle-agedman,usuallyspeaking inadifferentaccent fromthepatient, forexample‘anupper-classvoice’.Subjectsheardameanof3.2differentvoicesandusuallyknewtheidentityofat leastone; inhalfof thesubjects, thevoicessignifiedforcesofGoodorEvil.Halfof thesubjectswereabletoexertsomecontrolovertheirvoices,andtwo-thirdshaddevelopedcopingmechanismstodealwiththem;highlevelsofdistresswerefoundamongthosewithlittlecontrolandfewmeansofcoping.Themajorityofsubjectsascribedrealitycharacteristicstotheirvoices.Alonghistoryofauditoryhallucinationstendedtobeassociatedwithmorehallucinatedwords,morevoices,agreaterrangeofemotionalexpressionandgrammaticalstyleandgreaterlikelihoodofinterpretingthevoicesdelusionally.
Auditoryhallucinationsinschizophreniaaregenerallyprivateevents,butseveralearlywritersobservedvocalizationsthatcorrespondedwiththecontentofthevoicestakingplaceatthesametimeasthehallucinations.Normalpeopleoccasionallyvocalizetheirownthoughtssotto voce;inthepsychoticequivalentofthis,itseemsthatsometimesthosewithschizophreniaarevocalizingtheirhallucinationsatthesametimeastheyexperiencethem.GreenandPreston(1981)increasedtheaudibilityofthewhispersofsuchapatienttoanintelligiblelevelusingauditoryfeedback.
Sometimes,patientswithschizophreniadescribeabnormalperceptionsinboththevisualandtheauditorymodalities.Theexaminershouldbecarefulnottoassumethattherearebothaudi-toryandvisualhallucinationspresent; theremaybeadifferent form,particularly forthevisualexperience.Amanaged45describedhisexperienceasfollows:‘Ihearmynephewstalking[aboutme].“Heisapoofter[homosexual]andapervert”…Iseethemaswell.ThecurtainsmoveandIknowthatitisthemmovingthem’.Thisisadescriptionofapersecutoryauditoryhallucination,but the visual experience is a delusional interpretation of a normal perception, not a visualhallucination.
Patients’ descriptions of their phonemes vary greatly. Sometimes, patients talk openly andquiteblandlyabouttheir‘voices’.Notuncommonly,apatientmaydenyvoicesbutassertthathehears‘spokenmessages’or‘transmissions’orsomeotherspokensound,anditmaybedifficultto

7—PAThOLOGY OF PERCEPTION 99
decidewhetherthisisarealperceptionoranauditoryhallucination.Thephonemesmaybesoinsistent,compellingandinterestingthatordinaryconversationwiththedoctorisfoundboring,andevenunreal,incomparison.Thevoicesmayformaninsistentbackgroundtolife,soensuringthatalargepartofthepatient’sspeechandbehaviourisoccupiedinansweringandobeyingthevoices. Psychiatric nursing staff often observe that the auditory hallucinations described bypatientsareasrealtothemasanyotherrememberedconversations,andbothhallucinatoryandrealauditoryperceptionsformthememoriesonwhichpatientsbasetheirlifeandbehaviourinthepresent.
Auditoryhallucinationsoccurwhenthereisacombinationofvividmentalimageryandpoorrealitytestingintheauditorymodality(Slade,1976b).Thishasbeeninvestigatedusingabatteryoftestsincludingtheverbal transformation effect.Theword‘tress’wasrepeatedonataperecordertothesubjectsfortenminutes.Afteratime,subjectsbegantohearotherwordsandsyllables.Normal subjectsandpatientswith schizophreniawhowerenotauditorilyhallucinatedusuallyheardwordsthatwerephonetically linkedtotheoriginalmonosyllable,butpatientswhowereauditorilyhallucinatedheardwordsthatwerequitedifferentphoneticallyasoftenasthosethatwerelinked.
Itappearsthatauditoryhallucinationsaredependentonthemeaningfulnessofsensoryinput.Whenvarioustypesofauditoryinputwerepresentedtopatientswithschizophreniawhoexpe-riencedhallucinations,itwasfoundthatitwasnotthedegreeofexternalstimulationthatwasrequiredtodiminishhallucinationsbutthenatureofthestimulusandthedegreeofattentionitreceived.Whenactivemonitoringofmaterialwasrequiredbythesubjectreadingaloudaprosepassageanddecidingthecontentafterwards, thisproducedagreaterdecreaseofhallucinatoryexperiencethananyoftheconditionsinwhichsoundswereplayedtothesubjectthroughear-phones(Margoetal.,1981).Morley(1987)reportedthepsychologicaltreatmentofa30-year-oldmanwithauditoryhallucinations.Distractionbymeansofmusicpresentedbyaportablecassetteproducedatransientreductioninthefrequencyandclarityofhallucinations.Subsequently,thesehallucinationsweretotallyabolishedbytheunilateralplacementofawaxearplug:attentionwasconsideredmore effective thandistraction.Thepatient located thehallucination ‘about a footawayfrommyrightear’,andtheplugwasonlyeffectiveintherightear.
Patientswithschizophreniaexperiencingauditoryhallucinationswerefoundtobeimpairedin cognitive processing in the aspects of tolerance of ambiguity and availability of alternativemeanings.Tolerance of ambiguitywas testedbyasking thepatient to recognizea spokenword,which was obscured by a masking noise of people reading.The masking noise was graduallyreducedinvolumeuntilrecognitionoccurred.Alternative meaningsteststhesubject’sknowledgeoflessfamiliarmeaningsofwords.Thesetwoprocessesreducedthequalityofperception(result-ing in hallucination) by introducing errors of premature judgement without the safeguard ofsubsequentlyconsideredalternatives(HeilbrunandBlum,1984).
Some auditory hallucinations are considered to be ‘first rank symptoms of schizophrenia’(Schneider,1959);theseareaudible thoughts, voicesheardarguingwitheachotherandvoices com-menting on the patient’s behaviour. These three perceptual disturbances, as other first ranksymptoms,eachrepresentamassiveinterferencewiththeboundariesofself-image,thediscrimi-nationofwhatis‘I’fromwhatis‘notI’(Sims,1991).
ThemechanismsusedbypatientswithchronicschizophreniatocopewithpersistentauditoryhallucinationswerediscussedbyFalloon andTalbot (1981).The strategies used to copewithintrusivevoicescouldbeclassifiedaschanges inbehaviour, insensoryoraffectivestateandincognition.Changesinbehaviourincludedalterationofposture,suchaslyingdown,orseekingoutthecompanyofothers.Physiologicalarousalwasalteredtocopewithhallucinationsthroughrelaxationorphysicalexercisesuchasjogging.Cognitivemethodsincludedcontrolofattentionoractivesuppressionofhallucinations.Theseauthorsbelievethatthecommon-senseapplicationofstrategiesusedbypatientscanbebeneficialinthecontrolofthesedistressingsymptoms.
100 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
Finally, there is a vigorous debate about the presence of auditory/verbal hallucinations indisordersotherthanthepsychosessuchasborderlinepersonalitydisordersandalso innormalpopulations(McCarthy-Jones,2012).Thequestionthatremainstobeanswerediswhethertheformoftheseverbalhallucinationsisidenticaltotheformoftheverbalhallucinationsinschizo-phreniaforexample.
VISUAL HALLUCINATION
Visualhallucinationscharacteristicallyoccur inorganic states ratherthaninthefunctionalpsy-choses.A69-year-oldmarriedmanwasreferredtothedutypsychiatristinacasualtydepartmentforassessment.Hesaidthathislifewasatanendandhedeservedtodie,ashehadbeencaughtmasturbatingbyhisdaughter-in-lawandgrandchildrenthatafternoon.Hiswifesaidthatthiswasnottrue;hehadbecomeveryagitatedanddistressedover12hoursandnoonehadvisitedthehousethatday.Duringinterview,hewasintenselyagitatedandputhishandsinfrontofhisface.Heclaimedthathecouldseeclearlyasheetofglasshalfametreinfrontofhim,whichheattemptedtomove.Later,hedescribedseeingdustfallingdowneverywhereandwastryingtocatchit.Hemanifestedcloudingofconsciousness.Adiagnosisofviralencephalitiswasmadeonthebasisof thehistoryofpersistentheadache, theneurological signsand thefindingof lym-phocytosisinthecerebrospinalfluid.
Itisoftendifficulttodecidewhetherthefullcriteriaforthepresenceofahallucinationhavebeenfulfilledinthevisualmodality.Distortionofvisualpercepts,basedoneithersensationofexternalstimuliorinternalinterferencewiththevisualpathway,mayproducedisturbancesthatare similar to those occurring with entirely new perceptions. Sometimes, the account of hisexperiencegivenbythepatientsoundslikeasensorytransformationratherthanahallucination,but thebizarreandcomplexnatureof theexperiencerendersphenomenonologicaldescriptiondifficult.
Visualhallucinationsoccurwithoccipital lobe tumoursinvolvingthevisualcortex,forexampletuberculous granuloma in the left occipital lobe caused a ‘starburst’ effect in the right visualfield (Werring and Marsden, 1999). Hallucinations and other visual disturbances may occurwithotherphysical lesions, suchas loss of colour vision, homonymous hemianopia (lossofhalfofthefieldofvision,thesamehalfinbotheyes;Komel,1985),dyslexia(inabilitytoreadatalevelappropriate to the individual’s age and intelligence), alexia (word blindness) in a dominanthemispherelesionandcortical blindness(blindnessduetoa lesionofthecorticalvisualcentre).They may, as in delirium tremens, be associated with an affect of terror or with an affect ofhilariousabsurdity.Similarvisualhallucinations, illusionsandchanges inmoodoccur inotherformsofdelirium.Visualhallucinationsalsooccurinthepost-concussional state,inepileptic twilight statesandinmetabolicdisturbances,forexamplehepatic failure.Visualhallucinationshavealsobeendescribed inassociationwithvariousdementingprocesses, includingAlzheimer’sdisease(Burns etal., 1990), senile dementia (Haddad and Benbow, 1992), multi-infarct dementia(Cummingsetal.,1987),Pick’sdisease (Ey,1973)andHuntington’s chorea (Lishman,1989).Amongreferralstoapsychogeriatricservice,visualperceptualdisturbanceoccurredin30percentofpatients;therewasastrongcorrelationbetweenthepresenceofvisualhallucinationandeyepathology(BerriosandBrook,1984).Infact,visualhallucinationsarecommoninelderlypatientswith a wide variety of medical conditions and often no psychiatric history (Barodawala andMulley,1997).
Hallucinations have also been described by individuals after sniffing glue and petrol.Thedrugs mescaline and lysergic acid diethylamide are potent causes of visual perceptual change.Visual hallucinations are infinitely variable in their content. They range from quite crudelyformedflashesof lightorcolour(elementaryhallucinations),throughmoreorganizedpatternsand shapes, to complex, full, visual perceptions of people and scenes. Visual and auditory
7—PAThOLOGY OF PERCEPTION 101
hallucinationsmayoccursynchronouslyinorganicstates,forexampleintemporal lobe epilepsyavisualhallucinationofahumanfigurewasalsoheardtospeak.
Withpsychomimeticdrugs, therearealterations in spatialperception, in theperceptionofmovementandintheappreciationofcolour,andvisualillusionsandhallucinationsmayoccur.Visualhallucinationsareveryuncommoninschizophrenia(althoughsomeoftheearlierwritersused the termhallucination forothervisual abnormalities thatoccurred).PersaudandCutting(1991) cautiously refer to ‘anomalousperceptual experiences in thevisualmodality’ in schizo-phrenicpatients,forexample,asinthepatientwhoalthoughstillrecognizingafaceconsidersittobedistorted.Theseauthorsreportfoursuchcasesofperceptualdisturbanceinonevisualfield,alwaystheleftfield.Visualhallucinationsarenotreckonedtooccurinuncomplicatedaffectivepsychoses. It is common in schizophrenia for the patient to describe auditory hallucinationsassociatedwithvisualpseudohallucinations.Althoughthephonemesarecompleteandappeartohave all the characteristics, subjectively, of a normal percept, the visual experiences are ofteninferredonthebasisoftheauditoryhallucinationsandofcontemporaneousdelusions.Itispos-sibletosee,inmostinstances,howpsychoticallydisorderedfantasyaccountsforthecontentofthevisualexperiences.Vividelaboratescenichallucinationshavebeendescribedinoneiroidstatesofschizophrenia.Inthesestates,thereisalsoanalteredstateofconsciousness.
Sometimes, visualhallucinationsdonot appear tobe associatedwithanyotherpsychiatricabnormality.CharlesBonnet’ssyndrome(phantomvisualimages)isaconditioninwhichindi-viduals experience complex visual hallucinations in association with impaired vision withoutdemonstrablepsychopathologyordisturbanceofnormal consciousness (Schultz andMelzack,1991).Althoughmorecommonintheelderly,itcanoccuratanyageandisusuallyassociatedwithcentralorperipheralreductioninvision.Episodesmaylastfromdaystoyears,withimagesofpeople,animals,buildingsandscenerybeingmostfrequentlyreported,theimagesbeingstatic,movinginthevisualfieldoranimated.Clearly,thisconditionisofimportanceinthedifferentialdiagnosis.
InmostcasesofCharlesBonnet’ssyndrome,andinmusicalhallucinosisinthedeaf,towhichit has been likened, there is no demonstrable brain pathology (Fuchs and Lauter, 1992).ThefeaturesofthissyndromehavebeenconsideredbyPodolletal.(1990)tobeasfollows.
■ Elderlypersonswithnormalconsciousnessexperiencevisualhallucinations.■ Noneofthefollowingarepresent:delirium,dementia,organicaffectiveordelusionalsyn-
dromes,psychosis, intoxicationorneurologicaldisorderwith lesionsof thecentralvisualcortex.
■ Thereisreducedvision,resultingfromeyediseaseinmostcases.Hallucinationsinthisconditionarealwayslocatedinexternalspace,areusuallycolouredand
aremuchmorevividanddistinctthanthepatient’simpairedvisionwouldotherwisepermit.Thecontent is elementary in about one-third of cases, such as photisms or geometric patterns.Complexobjectsaremostoftenhumanfigures,lessoftenanimals,plantsandinanimateobjects;theseobjectsmaybefragmentedandmaychangeovertime–figuresglidingthroughtheroom.Theperceptsmaybemodifiablebyvoluntarycontrol,forexampleclosingtheeyelids,andthereisusually insightconcerningtheir‘unreality’.This issometimesassociatedwithfearofmentalillnessandwouldsuggestthatthesephenomenamaybepseudohallucinationsratherthan‘true’hallucinationsinsomecases.
The alcoholic withdrawal syndrome of delirium tremens is a specific form of acute organicsyndromeandischaracterizedbygrosschangesinperception,moodandconsciousnessstate(seeChapter3).Pareidolicoraffectiveillusionsareoftenprodromalindeliriumtremens,andtheseare followed by visual and haptic Lilliputian hallucinations, which are often of little animalsor diminutive men.There is a bizarre intermingling of affect so that the patient experiencesstark terror and, at the same time, a sort of crazy comicalness especially common with thesedisorders.
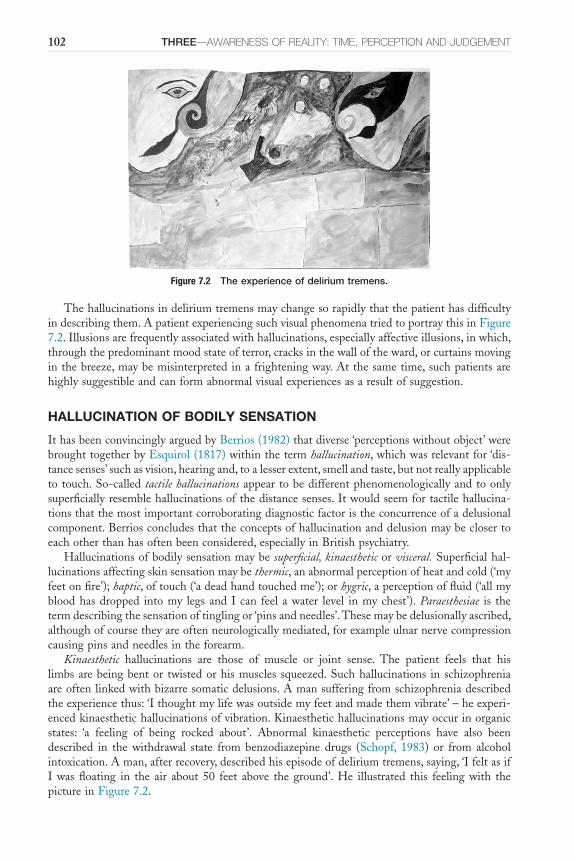
102 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
Thehallucinationsindeliriumtremensmaychangesorapidlythatthepatienthasdifficultyindescribingthem.ApatientexperiencingsuchvisualphenomenatriedtoportraythisinFigure7.2.Illusionsarefrequentlyassociatedwithhallucinations,especiallyaffectiveillusions,inwhich,throughthepredominantmoodstateofterror,cracksinthewalloftheward,orcurtainsmovinginthebreeze,maybemisinterpretedinafrighteningway.Atthesametime,suchpatientsarehighlysuggestibleandcanformabnormalvisualexperiencesasaresultofsuggestion.
HALLUCINATION OF BODILY SENSATION
IthasbeenconvincinglyarguedbyBerrios(1982)thatdiverse‘perceptionswithoutobject’werebroughttogetherbyEsquirol(1817)withinthetermhallucination,whichwasrelevantfor‘dis-tancesenses’suchasvision,hearingand,toalesserextent,smellandtaste,butnotreallyapplicabletotouch.So-calledtactile hallucinationsappeartobedifferentphenomenologicallyandtoonlysuperficiallyresemblehallucinationsofthedistancesenses.Itwouldseemfortactilehallucina-tionsthatthemostimportantcorroboratingdiagnosticfactoristheconcurrenceofadelusionalcomponent.Berriosconcludesthattheconceptsofhallucinationanddelusionmaybeclosertoeachotherthanhasoftenbeenconsidered,especiallyinBritishpsychiatry.
Hallucinationsofbodilysensationmaybesuperficial, kinaestheticorvisceral.Superficialhal-lucinationsaffectingskinsensationmaybethermic,anabnormalperceptionofheatandcold(‘myfeetonfire’);haptic,oftouch(‘adeadhandtouchedme’);orhygric,aperceptionoffluid(‘allmybloodhasdropped intomy legsandIcan feel awater level inmychest’).Paraesthesiae is thetermdescribingthesensationoftinglingor‘pinsandneedles’.Thesemaybedelusionallyascribed,althoughofcoursetheyareoftenneurologicallymediated,forexampleulnarnervecompressioncausingpinsandneedlesintheforearm.
Kinaesthetic hallucinations are those of muscle or joint sense. The patient feels that hislimbsarebeingbentor twistedorhismuscles squeezed.Suchhallucinations inschizophreniaareoftenlinkedwithbizarresomaticdelusions.Amansufferingfromschizophreniadescribedtheexperiencethus:‘Ithoughtmylifewasoutsidemyfeetandmadethemvibrate’–heexperi-encedkinaesthetichallucinationsofvibration.Kinaesthetichallucinationsmayoccurinorganicstates: ‘a feeling of being rocked about’. Abnormal kinaesthetic perceptions have also beendescribed in the withdrawal state from benzodiazepine drugs (Schopf, 1983) or from alcoholintoxication.Aman,afterrecovery,describedhisepisodeofdeliriumtremens,saying,‘IfeltasifIwasfloating in the air about 50 feet above the ground’.He illustrated this feelingwith thepictureinFigure7.2.
Figure 7.2 The experience of delirium tremens.
7—PAThOLOGY OF PERCEPTION 103
Visceralhallucinationsarefalseperceptionsoftheinnerorgans.Thereisonlyalimitedrangeofpossiblevisceral sensation, for examplepain,heaviness, stretchingordistension,palpitationand various combinations of these, such as throbbing. However, the possible range of bizarreschizophrenicfalseperceptionsandinterpretationsislimitless.Onemanbelievedthathecouldfeelsementravellinguphisvertebralcolumnintohisbrain,whereitbecamelaidoutinsheets.
Hallucinationsofbodilysensationarequitecommoninschizophreniaandarealmostalwaysdelusionallyelaborated,oftendelusions of control(Chapters8and9).Haptichallucinationsmaybe experienced as touch (‘like a hand stroking me’) or painful (‘knives stabbing my neck’). Apatientbelievedthatthesmokesensorinthewardwasaninfraredcamera,‘becauseIfeelitwarmonmyneck’.Anotherpatientdescribedahaptichallucinationinwhichsheexperiencedgenitalstimulation that she ascribed to having sexual intercourse simultaneously with ‘both Kennedybrothersallthetime’.Itisimportanttorealizethatthereisbothahallucinatoryandadelusionalcomponentinsuchexperiences.Oneparticularlyunpleasantformofhaptichallucinationiscalledformication(Latin:formica,‘ant’),thesensationoflittleanimalsorinsectscrawlingoverthebodyorjustundertheskin.Thisisespeciallyassociatedwithsomedrugstatesandwithdrawalsymp-toms,forexamplecocaineaddictionandalcoholwithdrawal.Itisoftenassociatedwithdelusions of infestation,butthelattermayoccurwithouthallucination.
OLFACTORY AND GUSTATORY HALLUCINATION
Hallucinationsofsmellandoftastefrequentlyoccurtogether,anditmaybedifficultorimpos-sible todistinguish them fromeachother.This isnot surprising, as a lotofwhat a laypersonascribestotasteisactuallysmell:‘theeucalyptusfragranceofthiswinefromtheBarossaValley’.
Olfactory Hallucinations
Olfactorysensationormemoryisoftenassociatedwithpowerfulemotionalresonances;itisnotsurprising therefore that hallucinations are also invested with a strong affective component.Olfactoryhallucinationsoccurinschizophrenia,inepilepsyandinsomeotherorganicstates.Thepatienthasahallucinationofsmell.Thesmellmayormaynotbeunpleasant,butitusuallyhasaspecialandpersonalsignificance(Aggernaes’qualityofrelevance),forexampleitmaybeassoci-atedwiththebeliefthatpeoplearepumpingapoisonousorananaestheticgasintothehouse,whichthepatientalonecansmell.Sometimes,patientshaveanolfactoryhallucinationrelatingtothemselves:‘Ismellrepulsive,unbearable–likeacorpse, likefaeces’.Thisparticularpatientkilledhimself.He felt thathecreatedsucha stench thathewas intolerable inany reasonablesociety.Sometimes,patientsmisinterpretandovervaluenormalbodyodours.Adelusioninwhichapatientbelieveshimselftosmellmalodorouslywithoutanaccompanyingolfactoryhallucinationisquitecommoninschizophreniaandrelatedparanoidstates.
Olfactoryhallucinationsoccurinepilepsy,especiallyinassociationwithatemporallobefocus,andcommonlyformtheaura(orearliestphase)ofsuchfits.Apatientdescribedasmellofburningrubberregularlyjustbeforehebecameunconscious.Visual,auditory,gustatoryandvisceralhal-lucinationsalsooccurintemporallobeepilepsy.
Gustatory Hallucinations
Gustatory hallucinations occur in various conditions. In schizophrenia, they sometimes occurwithdelusionsofbeingpoisoned.Theremaybeapersistenttaste,forexample‘onions’,‘ametallictaste’orsomemorebizarretypeoftaste.Indepressionandinschizophrenia,theflavouroffoodmaydisappearaltogetherorbecomeunpleasant.Changesingustatoryperceptionmayoccurwithsomeorganicstates,suchastemporallobeepilepsy,andalsowithsomepsychotropicdrugs,forexamplelithiumcarbonateordisulfiram.Itisoftendifficulttodescribehowthisdisturbanceoftasteismediatedand,therefore,whetheritishallucinatoryornot.
104 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
DIFFERENTIATION OF HALLUCINATIONS
Beforedecidingthatapatientishallucinated,thepossibilityofotherperceptualexperiencesmustbeconsidered.Thesearenotnecessarilyofpathologicalsignificance.Thedifferentialdiagnosisofhallucinationincludesillusion,pseudohallucination,hypnagogicandhypnopompicimagesand,ofcourse,vividimageryandnormalperception.
PseudohallucinationsPseudohallucinationisoneoftheleastunderstoodphenomenainpsychopathology.AsBerrios(1996)remarks,‘ithasbeenusedtorefertorealperceptionsperceivedas“unreal”,isolatedhal-lucinationswhichdonotfitintofavoureddiagnoses,sideeffectsofdrugs,withdrawalhallucina-tions,diabetichallucinations,etc’.Berriosgoesontosay:
‘Unrestrained, usage has strayed even wider, pseudohallucinations being sometimes applied to (i) phenomena which meet criteria for hallucinations or
illusions, (ii) hallucinations in people without mental illnesses (e.g., the bereaved), (iii) the false perceptions of people recovering from psychotic
illnesses, (iv) factitious hallucinations in malingerers, and (v) occasionally, normal but unusual perceptions which initially seem to be hallucinations (e.g.,
radio reception in dental amalgam or intracranial shrapnel fragments).’
Furthermore,partoftheconfusionoverthemeaningofthetermpseudohallucinationhasarisenbecauseit isoftenusedintwodifferentandmutuallycontradictoryways,accordingtoKräuplTaylor(1981).Ontheonehand,itreferstohallucinationswithinsight(Hare,1973),andontheotherhand tovivid internal images.Hallucinationswith insightwouldbe thosehallucinatoryexperiences inwhichthesubject isawarethatthehallucinatoryperceptsdonotcorrespondtoexternal reality despite the perceptions being veridical and in external objective space. Vividinternalimagesarethosephenomenathathavealltheclarityandvividnessofanormalperceptexceptthattheyoccurininnersubjectivespace.
Jaspers (1962) identifiedpseudohallucinationas similar tonormalperceptionexcept that itoccurs in inner subjective space. Pseudohallucination shares this characteristic with imagery.In other words, for Jaspers, pseudohallucination is a perceptual experience that is figurativeandoccursininnersubjectivespace,notinexternalobjectivespace.Butithasallthevividnessand clarity of a normal perception and can be retained unaltered. It occurs independently ofthesubject’swillandthereforecannotbedeliberatelyevoked.JaspersderivedthisdescriptionofpseudohallucinationfromKandinsky.
Kandinsky (1849–1889) based his description of pseudohallucination on his own personalexperiences.Hecommittedsuicideattheageof40yearswhileapatientatStNicholasHospital,StPetersburg,wherehehadoncebeenmedicalsuperintendent(Lerneretal.,2001).In1885,hedescribedpseudohallucinationasaseparateformofperceptionfromtruehallucinationandwrote,‘subjectiveperceptionswhichinvividnessandcharacterarerealhallucinationsexceptthattheydonothaveobjectivereality’(quotedinBerrios,1996).Pseudohallucinationscanbeidentifiedinthevisual,auditoryortactilemodalities.
Hare(1973)hasgivenasanexampleofpseudohallucinationthevoiceheardbyanobsessionalordepressedperson.Itisdescribedbythepatientasavoicebutisactuallyrecognizedashisownthoughts.Pseudohallucinationsarenotpathognomonicofanyparticularmentalillness.Apatientwithhistrionicpersonalitydisorder sawa robedfigure at the footofherbed liftinghis indexfingertohismouthtocautionhertosilence.Theimagewassharpandvividbutwasrecognizedasbeingseenwiththeinnereye.Thepatientknewthatthefigurewasnotatthefootofthebed
7—PAThOLOGY OF PERCEPTION 105
andthatotherpeopleintheroomcouldnotseehim.Whenshetriedtorelatethefigureinspacetothebackgroundofherfieldofvision,inthiscasethewallsandcurtainsoftheroom,shereal-izedthatshecouldnotdoso;ithadnodefinitelocationinexternalspace,thatisoutsideherself.
To summarize, the significance of hallucination is that it almost always denotes a morbidmentalstate.Thesignificanceofpseudohallucinationisinitsdifferentialdiagnosisfromhallu-cination,aspseudohallucinationisnotnecessarilypsychopathological.
Other Abnormalities of PerceptionAUTOSCOPY
Autoscopy is theexperienceof seeingan imageofoneself inexternal spaceandknowingthatit is oneself (see also visual hallucination). It is sometimes called the phantom mirror image.It is one of the abnormalities of unity of self described in Chapter 12, but in autoscopy theexperienceisnecessarilyvisual.Likesomanytopicsofconsiderablephenomenologicalinterest,the term autoscopy has been used with different meanings and definitions since its first usebyFéréin1891.Theexperienceconcernshowtheindividualregardstheboundariesofselfandisdiscussedfurtherwithotherdisordersofself-image.Itisbesttoreserveautoscopyforabnor-malitiesofvisualperception involving seeingoneself; ‘visualexperienceswhere subjects seeanimageofthemselvesinexternalspaceviewedfromwithintheirownphysicalbody’(DeningandBerrios,1994).
Althoughthistopichasbeenofconsiderableliteraryinterestovertheyears,clinicalcaseswithdefiniteperceptualabnormalityarenotcommon.DeningandBerrioshavereviewed56cases,53from the literature and three of their own.Males predominated,with a ratio of 2:1, and themeanageofsubjectswas40years.Bothneurologicalandpsychiatricdisorderoccurredinabout60 per cent of cases (different subjects), with epilepsy in approximately one-third. Decreasedconsciousnessoccurredin45percent,deliriumin18percentand9percentofsubjectsweredead within one year. Visual imagery or narcissism was present in one-third of subjects, anddepersonalizationin18percent.Thecommonestpsychiatricdiagnosiswasdepression.Usually,autoscopicepisodeslastedforlessthan30minutes.Almostalways,thesubjectsawhisownface;quiteoften,hewaslyinginbedatthetime.Theexperienceoftenprovokeddistress,fear,anxietyanddepression.Thissubjectiveexperiencewascomplex,withdifferentcomponentsandcausesratherthanunitary.
Negative autoscopy has also been described, in which, for instance, the patient looks in themirrorandseesnoimageatall.
EXTRACAMPINE HALLUCINATION (CONCRETE AWARENESS)
‘Iknowthatthereissomeonebehindmeontherightallthetime;hemoveswhenImove’,‘Ikeeponhearingthemtalkingaboutmydiseasedowninthepostoffice’(halfamileaway)–thesehallucinationsareexperiencedoutsidethelimitsofthesensoryfield,outsidethevisualfieldorbeyondtherangeofaudibility.Theyarenotofdiagnosticimportance,astheyoccurinschizo-phrenia,epilepsyandotherorganicstatesandalsoashypnagogic hallucinationsinhealthypeople.Thephenomenonisquitedefinitelyexperiencedasaperceptionbythepatientandnotjustasabelieforanidea.
HYPNAGOGIC AND HYPNOPOMPIC HALLUCINATION
Theseareperceptionsthatoccurwhilegoingtosleep(hypnagogic)andonwaking(hypnopompic).According to Zilboorg and Henry (1941), hypnagogic hallucinations were first mentioned by

106 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
Aristotle.It isknownthattheconsciousness levelfluctuatesconsiderablyindifferentstagesofsleep,andbothtypesofabnormalperceptionprobablyoccurinaphaseofincreasingdrowsiness:thestructureofthought,feelings,perceptions,fantasiesand,ultimately,self-awarenessbecomesblurredandmergesintooblivion.Theseexperiencesoccurinmanypeopleingoodhealth.Theyarealsodescribedwithnarcolepsy, cataplexyand sleep paralysis toformacharacteristictetradofsymptoms(seeNarcolepsyfordescriptions).Toxic statessuchasgluesniffing,acutefevers(espe-ciallyinchildren),postinfectivedepressive statesandphobicanxietyneurosesareotherconditionsthatmaybeassociatedwiththeseperceptions.
Theperceptionmaybevisual,auditoryortactile.Itissuddeninoccurrence,andthesubjectbelievesthatitwokehimup,forexamplealoudvoiceinthestreetbelowsaying‘worldwar!’,afeelingofsomeonepushinghimoverthebedorseeingamancomingacrossthebedroom.Theimportanceofthesephenomenainpsychopathologyistorecognizetheirnatureandrealizethattheyarenotnecessarilyabnormal,eventhoughtheymaybetrulyhallucinatory.
FUNCTIONAL HALLUCINATION
Thisisthestrangephenomenoninwhichanexternalstimulusisnecessarytoprovokehallucina-tion,butthenormalperceptionofthestimulusandthehallucinationinthesamemodalityareexperiencedsimultaneously.Aschizophrenicpatientheardhallucinatoryvoicesonlywhenwaterwas runningthroughthepipesofhisward.Heheardnophonemes formostof the time,butwhen he heard water rushing through the pipes along the wall he became very distressed byvoicesthattoldhimtodamagehimself.Hewasterrifiedofthecontentofthesevoicesbecausehewasafraidhemightactonthem.Hecouldreadilyseparatethenoiseofwaterfromthevoices,and the latternever occurred apart from the former, butbothperceptionswere recognized asdistinct and real.Another patientheard voiceswhen the radio or televisionwas switchedon,alongsidethebroadcastvoices;hehadpersecutorydelusionsthattheseactivitieswerecarriedoutdeliberatelytoupsethimandhebecameverydistressed,andattimesviolent,asaresult.
REFLEX HALLUCINATION
Asadoctorwaswriting inhiscasenotesduringhis interviewofa femalepatient, shesaid,‘Icanfeelyouwritinginmystomach’.Thepatientsawandheardtheactofwritingandwasquitesurethatitaccountedforthetactilesensationinherabdomen.Astimulusinonesensorymodalityproducingahallucinationinanotheriscalledareflex hallucination.Thisis,infact,ahallucinatoryformofsynaesthesia,mentionedearlierastheexperienceofastimulusimageinonesensemodalitysimultaneouslyproducinganimageinanother,forexamplethefeelingofdiscomfortcausedbyseeingandhearingsomebodyscratchablackboardwiththeirfingernails.Anotherreflexhallu-cinationoccurred inawomanwhoexperiencedpainwhenevercertainwordswerementioned.Functionalandreflexhallucinationsarenotthemselvesofdiagnosticortheoreticalsignificance,but they requirementioning forcompletenessandrecognition inorder to identifyothermoreimportantsymptomswithconfidence.
ABNORMAL IMAGERY
Mentalimagerytasksaredesignedtoassessasubject’scapacityformentalrepresentationoftheperceivedworld.Incasesofhemineglect,therehasbeeninterestinwhethertheobserveddeficitsin imagery are due to inattention or to impairment of mental imagery. Bisiach and Luzzatti(1978) described abnormalities in individuals with hemineglect.Their patients were asked todescribethePiazzadelDuomoinMilanfromtwostandpoints: facingthecathedralandwiththeir backs to the cathedral. From both standpoints, the subjects were unable to describe the
7—PAThOLOGY OF PERCEPTION 107
rightsideofthescenedespitehavingcorrectlydescribeditfromthepreviousstandpoint.Inotherwords,eveninimaginationthementalrepresentationofthepiazzawasunilaterallydeficientforthe right side. In these cases, inattention influenced the capacity for imagery. Guariglia etal.(1993)reportedapatientwithouthemineglect inwhomimpairmentof imagery forobjects intheleftvisualfieldwasdemonstrated.Forthefirsttime,thisshowedthatwithouthemineglect,thatis,visualinattentionforspace,failureofimagerywasstillpossible.
SENSORY DEPRIVATION
Continuingperceptionisnecessaryforconsciousness.Thefieldofsensationvariesallthetimeasindividual sensations in different modalities from the outside world and from inside oneselfcompeteforattention.Consciousnessconsistsoftheintegrationofthischangingfieldtoformacompositeawarenessofoneselfinone’senvironment.Theessentialnatureofsensationhasbeenexploredby studying its absence, as revealedby researchon the effectsof sensorydeprivation(Zubek,1969).Thistopicisonlygivenbriefmention,asitissomewhatperipheraltopsychiatry.
SensorydeprivationwasstudiedusingCanadiancollegestudentsasvolunteers(Bextonetal.,1954).Thesubjects,wearingtranslucentgogglesandgloveswithcardboardcuffs, layonabedinalightbutpartiallysoundproofroom;therewasacontinualbackgroundnoise.Thisexperiencewas found to be extremely unpleasant and, despite being paid, subjects were not prepared toremaininthisstateformorethanthreedays.
Thistechniquehasbeenrefinedsubsequentlytoblotoutexternalsensationsmorecompletely.Various perceptual abnormalities are experienced. Visual hallucinations of varying complexityweredescribed,butfurtherstudyoftheseperceptualchangesresultedintheirbeingconsidered,morecautiously,tobe‘reportedvisualsensations’and‘reportedauditorysensations’(Zuckermann,1969).Thesewereclassifiedinto‘meaninglesssensations’and‘meaningfulintegratedsensations’.Someofthe latteraremore likehallucinatoryexperiences.Dependingonthecompletenessofdeprivation of other sensations, abnormal perception occurs in modalities other than vision.Subjectsshowanalteredaffectivestate:theybecomepanicky,restless,irritableor,alternatively,boredandapathetic.
Despiteconsiderableneuropsychologicalresearchwithvaluablefindingsforinvestigatingthesensoryenvironmentingrowthanddevelopment,developingbraininterconnections,neurochem-istryandneurophysiology,thestudyofsensorydeprivationhasnotsofarmadeasbiganimpacton descriptive psychopathology as was initially expected. There are various difficulties to beaccountedfor.Whatpartoftheeffectsofdeprivationisduetofailureofdevelopmentandwhatto lossofbehaviours already established?Howcanoneuse animalwork to explore subjectivesymptoms? How can one extrapolate from the experience of normal individuals in a highlyabnormalenvironmenttothosewhoarepsychiatricallyill?ManystudiesinsensorydeprivationaredescribedbyRiesen (1975),who links the experimentaldata toneurological functionanddevelopment.
Thedistinctionhasbeenmadebetween sensory deprivation andperceptual deprivation.Thelatterisachievedbyrenderingthesensationspatternlessandmeaningless,ratherthanbyprevent-ing sensations,byusing suchdevices as translucentgoggles andcontinuous ‘white’noise.ThedeleteriouseffectsofsensorydeprivationhavebeenconsideredbySlade(1984)as:
■ inabilitytotoleratethesituation■ perceptualchanges■ intellectualandcognitiveimpairments■ psychomotoreffects■ physiologicalchangesinelectroencephalographandgalvanicskinresponsemeasures.Fantasyisoftenusedasameansofreducingtheunpleasantaffectivecomponentofsensory
deprivation.The subjectmaybecomedisorientedandshow increasingdifficultywithproblem

108 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
solvingandconcentration.Forperceptionandmaintenanceofthenormalstateofconsciousness,itisnecessarytohaveavarietyofsensorystimuliavailableandforthesestimulitobechangeable.Iftheobjectsofperceptiondonotthemselveschange,theobserverwillmovehispointofobser-vationinordertocreatechange.
ReferencesAggernaes A (1972)The experienced reality of hallucinations and other psychological phenomena. Acta
Psychiatrica Scandinavica48,220–38.AndradeC(1988)Freehallucinationsasculturallysanctionedexperience.British Journal of Psychiatry152,
838–9.AsaadGandShapiroB(1986)Hallucinations:theoreticalandclinicaloverview.American Journal of Psychiatry
143,1088–97.BarodawalaSandMulleyGP(1997)Visualhallucinations.Journal of the Royal College of Physicians of London
31,42–8.BentallRP(1990)Theillusionofreality:areviewandintegrationofpsychologicalresearchonhallucinations.
Psychological Bulletin107,82–95.BentallRP,BakerGAandHaversS(1991)Realitymonitoringandpsychotichallucinations.British Journal
of Clinical Psychology30,213–22.BerriosGE(1982)Tactilehallucinations:conceptualandhistoricalaspects.Journal of Neurology, Neurosurgery
and Psychiatry45,285–93.BerriosGE(1990)Musicalhallucinations:ahistoricalandclinical study.British Journal of Psychiatry156,
188–94.BerriosGE(1996)The History of Mental Symptoms: Descriptive Psychopathology Since the Nineteenth Century.
Cambridge:CambridgeUniversityPress.BerriosGEandBrookP(1984)Visualhallucinationsandsensorydelusionsintheelderly.British Journal of
Psychiatry144,662–4.BeveridgeA(1985)Language disorder in schizophrenia.M.Phil.thesis,UniversityofEdinburgh.BextonWH, HeronW and ScottTH (1954) Effects of decreased variation in the sensory environment.
Canadian Journal of Psychology8,70–6.BisiachEandLuzzattiC(1978)Unilateralneglectofrepresentationalspace.Cortex14,129–33.BleulerE(1950)Dementia Praecox or the Group of Schizophrenias(transl.ZinkinJ).NewYork:International
UniversityPress.BurnsA,JacobyRandLevyR(1990)PsychiatricphenomenainAlzheimer’sdisease2.Disordersofpercep-
tion.British Journal of Psychiatry157,76–81.Critchley M (1951) Types of visual perseveration: ‘palinopsia’ and ‘illusory visual spread’. Brain 74,
267–99.CummingsJL,MillerB,HillMAandNeshkesR(1987)Neuropsychiatricaspectsofmulti-infarctdementia
oftheAlzheimertype.Archives of Neurology44,389–93.CuttingJ(1997)Principles of Psychopathology: Two Worlds – Two Minds – Two Hemispheres.Oxford:Oxford
UniversityPress.CytowicREandEaglemanDM(2009)Wednesday is Indigo Blue: Discovering the Brain of Synesthesia.London:
TheMITPress.DeningTRandBerriosGE(1994)Autoscopichallucinations:aclinicalanalysisof56cases.British Journal
of Psychiatry165,808–17.EsquirolJED(1817)Hallucinations (reprinted in Des Maladies Mentales, 1938).Paris:Baillière.EyH(1973)Traité Des Hallucinations.Paris:Masson.FalloonIRHandTalbotRE(1981)Persistentauditoryhallucinations:copingmechanismsandimplications
formanagement.Psychological Medicine11,329–40.FéréC (1891)Note sur leshallucinations autoscopiquesou spéculaires et sur leshallucinations altruistes.
Comptes Rendus Hebdomadaires des Séances et Memoires de la Société de Biologie3,451–3.Fernyhough C (1996) The dialogic: A dialogic approach to the higher mental functions. New Ideas in
Psychology14,47–62.FuchsTandLauterH(1992)CharlesBonnetsyndromeandmusicalhallucinationsintheelderly.InKatona
CandLevyR(eds.)Delusions and Hallucinations in Old Age.London:Gaskell.
7—PAThOLOGY OF PERCEPTION 109
Fukutake T, Kawamura M, Sakakibara R and Hirayama K (1993) Alloaesthesia without impairment ofconsciousnessafterrightputaminalsmallhaemorrhage.Rinsho Shinkeigaku33,130–3.
Green P and Preston M (1981) Reinforcement of vocal correlates of auditory hallucinations by auditoryfeedback:acasestudy.British Journal of Psychiatry139,204–8.
Gregory RL (2004) Recovery from blindness. In Gregory RL (ed.) The Oxford Companion to the Mind,2ndedn.Oxford:OxfordUniversityPress.
GuarigliaC,PadovaniA,PantanoPandPizzamiglioL(1993)Unilateralneglectrestrictedtovisualimagery.Nature364,235–7.
HaddadPMandBenbowSM(1992)Visualhallucinationsasthepresentingsymptomofseniledementia.British Journal of Psychiatry161,263–5.
HareEH(1973)Ashortnoteonpseudohallucinations.British Journal of Psychiatry122,469–76.HeilbrunABandBlumNA(1984)Cognitivevulnerabilitytoauditoryhallucinations:impairedperception
ofmemory.British Journal of Psychiatry144,508–12.HorowitzMJ(1975)Acognitivemodelofhallucinations.American Journal of Psychiatry132,789–95.JacobsL,FeldmanM,DiamondSPandBenderMB(1973)Palinacousis:persistentorrecurringauditory
sensations.Cortex9,211–6.JaspersK (1962)General Psychopathology (transl.Hoenig J andHamiltonMW).Manchester:Manchester
UniversityPress.JungingerJandFrameCL(1985)Self-reportofthefrequencyandphenomenologyofverbalhallucinations.
Journal of Nervous and Mental Diseases173,149–55.KandinskyV(1885)Kritische und klinische.BetrachtungenimGebietederSinnestanschangen.KawamuraM,HitayamaK,ShinoharaY,WatanabeYandSugishitaM(1987)Alloaesthesia.Brain,Feb,
225–36.KomelHW(1985)Complexvisualhallucinationsinthehemianopicfield.Journal of Neurology, Neurosurgery
and Psychiatry48,29–38.KosslynSM(2004)Mentalimagery:depictiveaccounts.InGregoryRL(ed.)The Oxford Companion to the
Mind,2ndedn.Oxford:OxfordUniversityPress.KosslynSMandThompsonWL(2003)Whenisearlyvisualcortexactivatedduringvisualmentalimagery?
Psychological Bulletin129,723–46.KosslynSM,Pascual-LeoneA,FelicianO,CamposanoS,KeenanJP,ThompsonWL,GanisG,SukelKE
andAlpertNM(1999)Theroleofarea17invisualimagery:convergentevidencefromPETandrTMS.Science284,167–70.
KräuplTaylorF(1981)Onpseudohallucinations.Psychological Medicine11,265–72.Lerner V, Kapstan A and Witztum E (2001) The misidentification of Clerambault’s and Kandinsky–
Clerambault’ssyndromes.Canadian Journal of Psychiatry46,441–3.LishmanWA(1989)Organic Psychiatry: the Psychological Consequences of Cerebral Disorder,2ndedn.Oxford:
BlackwellScientific.MargoA,HemsleyDRandSladePD(1981)Theeffectsofvaryingauditoryinputonschizophrenichal-
lucinations.British Journal of Psychiatry139,122–7.MartinGN(2006)Human Neuropsychology.Harlow:PearsonEducation.McCarthy-JonesS (2012)Hearing Voices: The histories, causes and meanings of auditory verbal hallucinations.
Cambridge:CambridgeUniversityPress.MorleyS(1987)Psychologicalmodificationofauditoryhallucinations:distractionversusattention.Behavioral
Psychotherapy15,240–51.Nayani TH and David AS (1996) The auditory hallucination: a phenomenological survey. Psychological
Medicine26,177–89.PersaudRandCuttingJ(1991)Lateralizedanomalousperceptualexperiencesinschizophrenia.Psychopathology
24,365–8.PodollK,SchwartzMandNoth J (1990)CharlesBonnet-Syndrombei einemParkinson-Patientemmit
beidseitigenVisusverlust.Nervenarzt61,52–6.PylyshynZW(2004)Mental imagery. InGregoryRL(ed.)The Oxford Companion to the Mind,2ndedn.
Oxford:OxfordUniversityPress.RamachandranVSandHirsteinW(1998)Theperceptionofphantomlimbs:TheDOHebblecture.Brain
121,1603–30.RiesenAH(1975)The Developmental Neuropsychology of Sensory Deprivation.NewYork:AcademicPress.

110 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
SachsO(1995)An Anthropologist on Mars.London:Picador.Schneider K (1959) Clinical Psychopathology, 5th edn. (transl. Hamilton MW). New York: Grune and
Stratton.Schopf F (1983)Withdrawal phenomena after long-term administration of benzodiazepines: a review of
recentinvestigations.Pharmacopsychiatry16,1–8.SchreberD(1955)Memoirs of My Nervous Illness(transl.MacalpineIandHunterRA).London:Dawson.SchultzGandMelzackR (1991)TheCharlesBonnet syndrome: ‘phantomvisual images’. Perception20,
809–25.ShapiroMFandFinkM(1952)Exosomesthesia:thedisplacementofcutaneoussensationtoextrapersonal
space.Transaction of American Neurological Association56,260–2.ShapiroMF,FinkMandBenderMB(1952)Exosomesthesiaordisplacementofcutaneoussensationinto
extrapersonalspace.Archives of Neurology and Psychiatry68,481–96.SimsACP(1991)Anoverviewof thepsychopathologyofperception:first ranksymptomsasa localizing
signinschizophrenia.Psychopathology24,369–74.SladePD(1976a)Hallucinations.Psychological Medicine6,7–13.SladePD(1976b)Aninvestigationofpsychologicalfactorsinvolvedinthepredispositiontoauditoryhal-
lucinations.Psychological Medicine6,123–32.Slade PD (1984) Sensory deprivation and clinical psychiatry. British Journal of Hospital Medicine 32,
256–60.SmithEEandKosslynSM(2007)Cognitive Psychology: Mind and Brain.UpperSaddleRiver:PrenticeHall.SmythiesJR(1956)Alogicalandculturalanalysisofhallucinatorysense-experience.Journal of Mental Science
102,336.SpitzerM(1994)Thebasisofpsychiatricdiagnosis. InSadler JZ,WigginsOPandSchwartzMA(eds.)
Philosophical Perspectives on Psychiatric Diagnostic Classification.Baltimore:JohnsHopkinsUniversityPress.StacyCB(1987)Complexhaptichallucinationandpalinaptia.Cortex23,337–40.VygotskyLS(1934/1987)Thinking and Speech. The Collected Works of LS Vygotsky,Vol 1.NewYork:Plenum.WernickeC(1906)Grundri der psychiatrie in klinischen vorlesun gen.Leipzig:Thieme.WerringDJandMarsdenCD(1999)Visualhallucinationsandpalinopsiaduetoanoccipitallobetubercu-
loma.Journal of Neurology, Neurosurgery and Psychiatry66,684.ZekiS(1993)A Vision of the Brain.Oxford:Blackwell.ZilboorgGandHenryGW(1941)A History of Medical Psychology.NewYork:Norton.ZubekJP(1969)Sensory Deprivation: Fifteen Years of Research.NewYork:Appleton-Century-Crofts.ZuckermannM(1969)Variablesaffectingdeprivationresults.InZubekJP(ed.)Sensory Deprivation: Fifteen
Years of Research,pp.47–84.NewYork:Appleton-Century-Crofts.

111
C H A P T E R 8
Delusions and Other Erroneous Ideas
SummaryDelusions are false judgements that are held with extraordinary conviction and incomparablesubjectivecertainty,andareimpervioustootherexperiencesandtocompellingcounterargument.Usuallydelusionsareeasilyrecognizedwhenoutofkeepingwiththeindividual’seducationalandsocioculturalbackground.Primarydelusionshavediagnosticsignificancewhereasthecontentofsecondarydelusionsmay signal thenatureof theprimaryabnormalphenomenon fromwhichtheyderive.Overvaluedideasarecomprehensiblebeliefsthatarisefromthehistoryandexperi-encesofanindividual.Theyareheldwithconvictionandmotivatebehaviourthatmaycausethepatientharmandsuffering.
I cannot pretend to agree with him, when I know that his mind is working altogether under a delusion.
Trollope (1869)
AnthonyTrollope,inhisnovelHe Knew He Was Right,describesnotonlythetotallydestruc-tiveeffectofdelusional jealousyonthe individualhimself,butalsotheextraordinarydilemmathisposesforotherpeoplewhocomeintocontactwithhim:whethertohumourtheindividualandriskreinforcement,ortoconfronthimandriskviolence.Fundamentaltoclinicalpracticeinpsychiatry,usingthephenomenologicalorempathicmethod,isobtainingaclearaccountoftheideasornotionsthatthesubject,thepatient,actuallyholds.Althoughdelusionsareoftenreferredtoasbeliefs,thereisagrowingliteraturequestioningwhethertheyarebeliefsatall.False beliefsincludeprimaryandsecondarydelusions,overvaluedideasandsensitive ideasofreference.
Ideas, Beliefs and DelusionsVery rarely does anyone claim to be deluded, and usually what such a patient thought was adelusiondoesnotprovetobeso.Adelusionisafalse,unshakeableideaorbeliefthatisoutofkeepingwiththepatient’seducational,culturalandsocialbackground;itisheldwithextraordi-naryconvictionandsubjectivecertainty.Subjectively,orphenomenologically,itisindistinguish-ablefromatruebelief.AmanwhoisaBachelorofMedicineoftheUniversityofLondonholdsadelusionthathe isbeingusedas‘anenvoyfromMars’.Hebelievesthathe isbothadoctorandanenvoy,andneitherthoughtseemstohimtobedelusionalorimaginary.HelikestoimaginehimselfarichmanwithanestateinGloucestershire.Hehasnottheslightestdifficultyiniden-tifyingthislatterideaasfantasy.Tothemanhimself,adelusionismuchclosertoatruebeliefthanimagination,andthereasonsenlistedtosupportitsveracityareproducedinthesamewaythatapersonwouldproveanyothernotiononwhichhewaschallenged.Normally, fantasy iseasilydistinguishedfromreality,althoughthesubjectmayshowgreatreluctanceinacceptinghisaspirationsas‘merefantasy’.Similarly,thereisusuallyverylittledifficultyfortheexternalobserverindecidingwhetherafalsebeliefisamisinterpretationofthefactsbasedonfalsereasoning,oradelusion.

Keywords: Delusion,DelusionalMisidentificationSyndrome,Koro,OvervaluedIdea.
8—DELUSIONS AND OThER ERRONEOUS IDEAS 111.e1

112 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
MEANING OF DELUSION
TheEnglishworddeludecomesfromLatinandimpliesplayingormocking,defraudingorcheat-ing.TheGermanequivalentWahnisawhim,falseopinionorfancy,andmakesnomorecommentthantheEnglishonthesubjectiveexperience.TheFrenchequivalent,délire,ismoreempathic;it impliestheploughshare jumpingoutofthefurrow(lira),perhapsasimilarmetaphortotheironical‘unhinged’.AsBayneandFernandez(2009)say:
On the face of things, it seems obvious that delusions involve departures – typically, quite radical departures – from the procedural norms of human
belief formation. Delusions stand out as exotic specimens in the garden of belief, as examples of what happens precisely when the mechanisms of belief
formation break down.
Inthischapter,thecomplexityofdelusionsasconcepts,experiencedsymptoms,andabnormalphenomenawillbeexplored,discussedandanalyzed.
Definition of Delusion
An additional video for this topic is available online.
Therecontinues tobemuchdebateandcontroversyabout thedefinitionofdelusions.ThestandardapproachistofollowJaspers’ (1959)claimthatdelusionsaremanifest in judgementsandariseintheprocessofthinkingandjudging.ForJaspers,thecharacteristicsofdelusionsarethat:
1. theyarefalsejudgements;2. theyareheldwithextraordinaryconvictionandincomparablesubjectivecertainty;3. theyareimpervioustootherexperiencesandtocompellingcounterargument;and4. theircontentisimpossible.Eachofthesecriteriahasbeensubjectedtocriticism.Delusionsmaynotbeobjectivelyfalse
insofarasthecontentisconcerned.Thisisbestexemplifiedindelusionaljealousy,wherebythebeliefmaycorrespondtoobjective truthand is thereforenot false.Delusionsmaynotbeheldwithextraordinaryconvictionbut,equally,normalbeliefsmaybeheldwithextraordinaryconvic-tion.Delusionalbeliefsmayalsobeamenabletocounterargument,althoughitisrarethatthisbyitselfwillalterthebelief.Finally,delusionalcontentneednotbeimpossible.
Thereisagrowingbodyofopinionthatdelusionsarenotbeliefsatall.Spitzer(1994),forexample,arguesthiscase.Hemakesthedistinctionbetween‘toknowthat’and‘tobelievethat’.InSpitzer’s view,delusionsmakeknowledge claims rather thanbelief claims. Inotherwords,patients areasserting that they ‘knowsuchand such’ rather than they ‘believe suchand such’,whichiswhydelusionalstatementsareexpressedwithconvictionandcertaintyandnotsubjecttodiscussionandinquiry.Berrios(1996)comestothesameconclusions.Hestatesthat‘delusionsareemptyspeechactswhichassertthemselvesasbeliefs’.Furthermore,hemakesthepointthatthecontentofdelusionsisincidentaltothefactofthephenomenonbeingadelusion.InBerrios’view,thecontentofdelusionsisrandomlychosen;thecontentmerelyreflectswhateverisintheenvironmentatthetimethedelusionisformed.Thecontentislackingininformationalqualityand is not a ‘symbolic expression of anything’.These critiques of the current definitions andunderstandingofdelusionsunderlinethecomplexityof theconceptualstatusofdelusionsandshowthatthereisstillfruitfultheoreticalworktobedoneinpsychopathology.
It is importanttoemphasizethatthetraditionthat locatesdelusionswithinthedomainofthinkingandjudgingderivesverysimplyfromtheneedtodistinguishhallucinations(abnormali-ties of perception) from delusions (abnormalities of thinking and judging). And, in any case
8—DELUSIONS AND OThER ERRONEOUS IDEAS 113
arguingthatdelusionsarenotabnormalitiesofbeliefislikearguingthatchorea(aninvoluntarymovement)isnotanabnormalityofmovementbecausetheobservedmovementsarenotpurpose-fulorintentional.Bortolloti(2010)hascriticallyexaminedtheargumentsagainsttheideathatdelusionsarebeliefsandconcludedthattheseargumentswhichsheclassedasprocedural,epis-temicandagential,applyequallytonormalbeliefs.Shethereforeconcludedthatthere is littlegoodreasontotreatdelusionsasanythingotherthanbeliefs.Withthisinmind,itisprofitabletocontinuetoclassifydelusionsasabnormalbeliefs.
Thedecisiontocallabelieforjudgementdelusionalisnotmadebythepersonholdingthebelief but by an external observer.There can be no phenomenological definition of delusion,becausethepatientislikelytoholdthisbeliefwiththesameconvictionandintensityasheholdsother non-delusional beliefs about himself, or as anyone else holds intensely personal non-delusionalbeliefs.Inthisrespect,delusionsaretoideationwhathallucinationsaretoperception.Subjectively,adelusionissimplyabelief,anotionoranidea.Stoddart’sdefinitionofadelusion(1908);‘ajudgementwhichcannotbeacceptedbypeopleofthesameclass,education,raceandperiodoflifeasthepersonwhoexperiencesit’,hassomeadvantages.However,itcouldincludeasdelusionalfallinginlovewithapersonothersregardasunsuitable,havingaminorityreligiousbelieforholdinganyunusualideawithoutacknowledgingreasonableargumenttothecontrary.
Hamilton(1978)defineddelusionas; ‘a falseunshakeablebeliefwhicharises frominternalmorbidprocesses.Itiseasilyrecognizablewhenitisoutofkeepingwiththeperson’seducationalandculturalbackground.’Thisdefinitionmakesthepointthatabeliefcanbeadelusionevenwhenitisnotoutofkeepingwiththepatient’seducationalandculturalbackground.
Rather than suggest a unitary definition for delusion, Kendler etal. (1983) have proposedseveralpoorlycorrelateddimensionsorvectorsofdelusionalseverity.
■ Conviction: thedegree towhich thepatient isconvincedof the realityof thedelusionalbeliefs.
■ Extension:thedegreetowhichthedelusionalbeliefinvolvesareasofthepatient’slife.■ Bizarreness:thedegreetowhichthedelusionalbeliefsdepartfromculturallydetermined
consensualreality.■ Disorganization:thedegreetowhichthedelusionalbeliefsareinternallyconsistent,logical
andsystematized.■ Pressure:thedegreetowhichthepatientispreoccupiedandconcernedwiththeexpressed
delusionalbeliefs.Twootherdimensionsthatmightalsobeconsideredareasfollows.■ Affective response: the degree to which the patient’s emotions are involved with such
beliefs.■ Deviantbehaviourresultingfromdelusions:patientssometimes,butnotalways,actontheir
delusions.
Primary and Secondary DelusionsTheconfusingsubjectofprimaryandsecondarydelusionsrequiressomeexplanation.Itisprob-ablymostmeaningfultousethetermprimarytoimplythatdelusionisnotoccurringin responseto another psychopathological form such as mood disorder. Secondary delusion is used in thesensethatthefalsebelief isunderstandable inpresentcircumstances–becauseofthepervasivemoodstateorbecauseoftheculturalcontent.
Gruhle (1915)considered thataprimarydelusionwasadisturbanceof symbolicmeaning,notanalterationinsensoryperception,apperceptionorintelligence.Primarydelusionsoccurinschizophreniaandnotinotherconditions;theyincludebothdelusionalperceptionanddelusionalintuition(Cutting,1985).However,delusionalintuitions,notionsorideasarenotpathognomonicofschizophrenia,becauseinanyindividualcasethereistoomuchscopeforarguingwhetherthis

114 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
delusionisindeedprimary,thatis,ultimatelyununderstandable,orsecondaryinnature.Secondarydelusionsoccurinmanyconditionsotherthanschizophreniaandcansometimesbeunderstoodinrelationtotheperson’sbackgroundcultureoremotionalstate.
Wernicke (1906) formulated theconceptofanautochthonous idea, an idea that is ‘native tothesoil’,aboriginal,arisingwithoutexternalcause.Thetroublewithfindingsupposedautoch-thonousorprimarydelusions is that itcanbedisputedwhether theyare trulyautochthonous.Forthisreason,theyarenotconsideredoffirst rankinSchneider’s(1957)classificationofsymp-toms. It is toodifficult todecide inmany caseswhether adelusion is autochthonous.Severalwritershaveclaimedthatalldelusionsareunderstandableifoneknowsenoughaboutthepatient.
The Ultimately Ununderstandable
Jaspers’ detailed exposition of delusion has been carefully reviewed byWalker (1991). Jaspers’conceptsoftheununderstandable,andofmeaningful connections,arerelevanthere.Ifweaskanoffender todescribe thepsychicworld inwhichhe lives–his attitudes,his feelings andhowthese developed through his childhood until now – we may be able to understand his sexualcruelty,whichatfirstseemedquiteincomprehensible:thebehaviourbecomesmeaningfulinthecontextofabusebyhisstepfatherandsurvivingasanadolescentinaharshurbansubculturewithviolence,humiliationandfrustration.However,whenweconsiderthemiddle-agedspinsterwithahistoryofschizophrenia,whobelievesthatmenunlockthedoorofherflat,anaesthetizeherandinterferewithhersexually,wefindanexperiencethatisultimatelynotunderstandable.Wecanunderstand,onobtainingmoredetailsofthehistory,howherdisturbancecentresonsexualexperience,whysheshouldbedistrustfulofmen,herdoubtsaboutherfemininityandherfeel-ingsofsocialisolation.However,thedelusion,herabsoluteconvictionthatthesethingsreallyarehappening to her, that they are true, is not understandable.The best we can do is to try tounderstandexternally,withoutreallybeingabletofeelourselvesintoherposition(genetic empathy,Chapter1),whatsheisthinkingandhowsheexperiencesit.Wecannotunderstandhowsuchanotioncouldhavedeveloped.
Thisisthecoreoftheprimaryorautochthonousdelusion:itisultimately ununderstandable.Thepatientdescribedabovealsobelievedthepolicewereusingraystoobserveher.Onedoesnothavetotrytofindwhichdelusioncamefirst,theanaesthesiaortheobservationbyrays,todecidewhichisprimary;primaryisnotdependentontemporalrelationships.Inthatbothdelu-sionsarenotultimatelyunderstandable,theyarebothprimarydelusions.Adelusioncanstillbeprimaryinthis,Jaspers’,sensealthoughitarisesonthebasisofamemory,anatmosphereoraperception.The protagonist in Gogol’s (1809–1852) Diary of a Madman (Gogol, 1972) says,‘There is aKingofSpain.Hehasbeen foundat last.Thatking isme. Ionlydiscovered thistoday.’Thissuddenandinexplicablebeliefaroseautonomouslyandunpremeditated.Thereafter,itdictatedtheprotagonist’severybehaviourandinfluencedhisviewoftheworld.
How Ideas and Delusions Are Initiated
Adelusionisabelief,anidea,athought,anotionoranintuition,anditarisesinthesametypeofsettingasanyotheridea–inthecontextofaperception,amemoryoranatmosphere–oritmaybeautochthonous,appearingtooccurspontaneously.
Ideasareinitiatedinthefollowingways.■ Anexampleofanideaoccurringonthebasisofapercept:Ismellfoodcookingandthen
formtheideathatIwillgoandeat.■ Ideasmay followmemory: I remember listening toa stringquartetand formthe ideaof
playingacompactdisc.■ Ideasmayariseoutofanatmosphereoramoodstate:Ialreadyfeel irritable,andwhenI
collectmycarfromthegarageanditmakesanunexplainednoiseIbecomeunreasonablyangryandblamethemechanicfornotrepairingitsatisfactorily.

8—DELUSIONS AND OThER ERRONEOUS IDEAS 115
■ Anideamaybeautochthonous.IvisitawardofthehospitalonanafternoonwhenInevernormallygothere.AlthoughIacceptthatallbehaviourhasanexplanationforitsoccur-rence,IdonotknowwhyonthisparticularoccasionIdidthis.Theoreticalexplanationsmaybegivenastowheresuchideascomefrom,forexampletheunconscious,butsubjectivelythey seem to have occurred de novo. Delusions occur in similar settings on the basis ofpercept,memory,atmosphereorde novo –‘outoftheblue’.
Inourdiscussionofprimarydelusions,wewillseehowthesamefoursituationsalsoaccountfortheonsetofdelusions:percept,memory,moodorautochthonous.Inthissense,delusionisanidea.
SECONDARY DELUSIONS
Primarydelusionsdifferfromsecondarydelusionsinthattheformerareultimatelynotunder-standable.Secondarydelusionsareunderstandableinthecontextofotherabnormalphenomenasuchasabnormalmood,abnormalperception,orindeedofaprimaryabnormalbelief.AmanicpatientclaimedtobeMary,QueenofScots.SheacceptedthatthequeeninquestionlivedanddiedcenturiesagobutclaimeddescentfromherandfeltfullyentitledtosaythatshewasMary,QueenofScots.Thebeliefcouldbeunderstood in relation toherelatedandexpansivemoodanddisappearedasheraffectivestatesubsided.Adepressedpatientbelievedthathehadcom-mittedthe‘unforgivablesin’.Discussionandpersuasion,evenwithapersonwhosereligiousviewsherespected,wasofnoavailingivinghimrelief.Thebeliefcouldbeseenasanintegralpartofhisdepressedmood.Depressivedelusionsmayremainaftertreatmenthasresultedinimprove-mentfromretardation,andtheyaccountforsuicideoccasionallyoccurringintherecoveryphaseofdepression.Ithasbeensuggestedthat theremaybeadecline in theprevalenceofdelusionoccurringwithdepressiveillness,butEagles(1983),studyingadmissionstohospitalinEdinburghfrom1892to1982,consideredtheretobenogenuinereduction.
Secondarydelusionscanbedistinguishedfromovervalued ideas(seebelow).Whereassecond-arydelusionsarederivedfromanotherabnormalphenomenon,overvaluedideasarecomprehen-sibleinthelightofthepatient’spersonalhistoryorsomeidentifiablehistoricaleventwhosevaluehasbecomeheightenedforsomereason.Nopriorabnormalphenomenonexplainsthepresenceofanovervaluedidea.
Types of Primary DelusionKurtSchneider(1957)discussesthedilemmaofprimarysymptomsinschizophreniaextremelylucidlybygivingsixdifferentpossiblemeanings for the termprimary,buthestill leavesus indoubtastowhetherthebeliefisprimaryornot.Hemakesitclear,however,thatprimarysymp-tomsarenotthesameasfirst rank symptomsofschizophrenia.Primarysymptomsarethosethatarisewithoutunderstandablecauseinthecontextofthepsychoticillness.Theyarethereforethenecessarymanifestationsoftheunderlyingpsychopathology,inthesamewaythatswellingandrednessareanecessaryconsequenceofphysicaltrauma.Firstranksymptoms,ontheotherhand,are,accordingtoSchneider,simplyausefulempiricallistofsymptomsthatarefoundcommonlyin schizophreniaandnot inother conditions.Describing theirpresencemakesnoclaimas tohowtheyarose.
True delusions, or delusions proper, are distinguished by Jaspers from delusion-like ideas. True delusions become, therefore, synonymous with primary delusions, and delusion-like ideaswith secondary delusions. Delusion-like ideas can be seen to emerge understandably from thepatient’sinternalandexternalenvironment,especiallyfromhismoodstate.Truedelusionscannotbesoexplained;theyarepsychologicallyirreducible.Theyhave,accordingtoJaspers,thefollow-ingtypes:
116 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
1. autochthonousdelusion(delusionalintuition);2. delusionalpercept;3. delusionalatmosphere;and4. delusionalmemory.
AUTOCHTHONOUS DELUSION (DELUSIONAL INTUITION)
Thesearedelusionsthatappeartoarisesuddenly‘outoftheblue’;theyarephenomenologicallyindistinguishablefromthesuddenarrivalofanormalidea.Thepatientgropesforexplanationsfortheoccurrenceofhisdelusioninansweringtheinterviewer’squestion,inthesamewaythatahealthypersonwouldfinditdifficulttoaccountforthearrivalofanyideaifhewereaskedtoexplainit.Thedifferenceliesintheabilityoftheobservertoempathizewith,tounderstand,anon-delusional idea even though itmaybebizarre anddestructive, buthe cannotunderstandhowapersoncanhavecometobelievehisdelusion.
Schneiderregardedthetermdelusional ideaasbasedonoutmodedpsychology,andhefeltitshouldthereforebeabandoned.It isoftenconfusedwithdelusion-like idea,even insometext-books,andthisisanothergoodreasonforabandoningit.Delusional intuitionisperhapsthemostsatisfactorytranslationoftheGermanWahneinfall.Delusionalintuitionoccursasasinglestage,unlikedelusional perception,whichoccursintwostages:perceptionandthenfalseinterpretation.Like delusional perceptions, delusional intuitions are self-referent and usually of momentousimporttothepatient.
DELUSIONAL PERCEPT
This is present when the patient receives a normal perception that is then interpreted withdelusionalmeaningandhas immensepersonal significance. It isafirst rank symptom of schizo-phrenia.Jaspersdelineatedtheconceptofdelusionalpercept,andGruhle(1915)usedthisdescrip-tiontocoveralmostalldelusions–heminimizedtheimportanceofdelusionalintuition.Schneider(1949)consideredtheessenceofdelusionalperceptiontobetheabnormalsignificanceattachedtoa realperceptwithoutanycause that isunderstandable inrationaloremotional terms; it isself-referent,momentous,urgent,ofoverwhelmingpersonalsignificanceand,ofcourse,false.
Itisoftendifficulttodecidewhetheradelusionistrulyadelusionalperceptorisbeingusedtoexplainthesignificanceofcertainobjectsofperceptionwithinadelusionalsystem.Awomansaid,‘everynightbloodisbeinginjectedoutofmyarms[sic]’.Whenaskedforherevidence,sheexplained that shehad littlebrown spotsonher armsand thereforeknew that shewasbeinginjected.Theinterviewerlookedatthespotsonherarms,rolleduphissleeveandshowedherspotsidenticalinappearanceonhisownarm.Hesaidthattheyhadbeenonhisarmaslongashecouldrememberandwerecalled‘freckles’.Sheagreedthatbothsetsofspotslookedsimilarandacceptedhisexplanationofhisownspots,butshestillinsistedthatherfrecklesprovedthatshewasbeinginjectedinhersleep.Thiswasadelusionalpercept.
Anotherexampleofwhatwasprobablyadelusionalperceptcausedconsiderableproblemsinsurgicalmanagement,ultimatelyresultinginthedeathofthepatient(PorterandWilliams,1997).A65-year-oldwomanhadfloodedherhousebyleavingallthetapson.
On admission she was unkempt, with unwashed hair, wearing a dirty dress and vest. She was bringing up bile-stained vomit and was reluctant to be
interviewed. She expressed delusional beliefs that her stomach had been blown up with ether over several weeks and that it was liable to burst as a result of a citizens band radio which was located in her stomach. She believed that the

8—DELUSIONS AND OThER ERRONEOUS IDEAS 117
IRA had been after her for years and experienced auditory hallucinations of voices which she identified as coming from the CB receiver. One ‘voice’ told
her not to let anyone examine her. There was no evidence of an acute confusional state and the diagnosis was consistent with a long-term paranoid
psychosis.On physical examination her abdomen was soft but distended with a hard,
craggy, immobile, central mass. The liver and spleen were of normal size and the kidneys were not palpable. Bowel sounds were loud. A diagnosis of
possible intra-abdominal malignancy was made.
Sherefusedanyinvestigationortreatment.Shedevelopedacuterenalfailureandultimatelydied;asciticfluidrevealedadenocarcinomatouscellsprobablyofovarianorigin.
Anotherpatient,whohadotherdelusionalsymptoms,believedthatmanyofthepatientsinthehospitalwerewell-knowncitizenscunninglydisguisedwithwigs,make-upandfalsebeards.Sherecognizedthattheydidnotlooklikethepeoplewhomshepresumedthemtobebutcon-sidered this to be part of a gigantic hoax, in which she was herself involved, to ‘help peoplespiritually’.Althoughherperceptswerenormalandherinterpretationsdelusional,thiswasnotconsideredtobeadelusionalperceptbutamisinterpretation.Allthecircumstances inher lifewereexplainedbyan immenselycomplicateddelusional system,and theseperceptionshadnoimmediate personal significance beyond the significance that she found in all the objects andeventsaroundher.
In a delusional percept, there is a direct experience of meaning for this particular normalpercept;itisnotsimplyaninterpretationofthispercepttofitinwithotherestablisheddelusionalbeliefs.Delusionalperceptionis, therefore,adirectexperienceofmeaningthatthepatientdidnothavepreviously.Objectsorpersonstakeonnewpersonalsignificancethat isdelusional innature,eventhoughtheperceptionitselfremainsunchanged.Thisisdifferentfromadelusionalmisinterpretation,inwhichthedelusionalsystemaffectsallaspectsofthepatient’slife,andsoeveryeventorperceptionisinterpretedasbeinginvolvedwiththatdelusion.Apatientseesthatadoorknob ismissing; this isnot theprecipitantof immediatenewpersonal significanceofadelusionalnature,rather,itfurtherconfirmsthebeliefhealreadyheldthatpeoplearetryingtotraphimandsubjecthimtovivisection.
Perception, when considering delusional percept, can be understood in quite a wide sense.Thereisnodifference,insubjectiveexperience,betweenperceivinganobjectbymeansofasenseorganandperceivingorunderstanding the senseofwrittenor spokenmessages, although theperceptual routes are different. Thus delusional perception includes delusional significanceattachedtowordsandsentencesaswellastopurelysensoryobjects.Forexample,anin-patientat Rubery Hill Hospital walked to an entrance of the hospital and saw a dilapidated notice:‘RUBE...ILL’.Shesuddenlyrealizedthatthiswasaconcealedmessagejustforher–‘Areyoube(ing)ill?’,thatpeoplewereconcernedtohelpherandthatshewouldgetbetter.Thedelusionalinterpretationwasattachedtothemeaningofthelettersofthenotice.
Therearetwodistinctstagesindelusionalperception:■ theobjectbecomesmeaningfulwithinafieldofsensationsandisperceived;thisisusually
visualperception(Mellor,1991)■ thatobjectbecomesinvestedwithdelusionalsignificance.Thesetwostagesneednotbesimultaneousfortheexperiencetobeadelusionalpercept.On
occasions,theyhavebeenseparatedbyanintervalofyears.Apatientbelievedthathismindwasbeingjammedbyanelectronicdevice.Heclaimedthatthishadstartedwhen,fiveyearsbefore,hehadliftedthetelephonereceiverandheardanunusualclickingnoise.Thedelusionalbeliefhehadheldforonlyafewmonths.

118 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
DELUSIONAL ATMOSPHERE
Forthepatientexperiencingdelusionalatmosphere,hisworldhasbeensubtlyaltered:‘Somethingfunnyisgoingon’,‘Ihavebeenofferedawholeworldofnewmeanings’.Heexperiencesevery-thingaroundhimassinister,portentous,uncanny,peculiarinanindefinableway.Heknowsthathepersonallyisinvolvedbutcannottellhow.Hehasafeelingofanticipation,sometimesevenofexcitement,thatsoonalltheseparatepartsofhisexperiencewillfittogethertorevealsome-thingimmenselysignificant.Thisis, infact,whatusuallyhappens,asdelusionalatmosphereispartoftheunderlyingprocessand,often,thefirstsymptomofschizophreniaandthecontextinwhichafullyformeddelusionalperceptorintuitionarises.Themoodoftheatmosphereisveryimportant,andthisexperienceisoftenreferredtoasdelusional mood.Thepatientfeelsprofoundlyuncomfortable,oftenextremelyperplexedandapprehensive.Whenthedelusionbecomesfullyformed,heoftenappearstoacceptitwithafeelingofrelieffromthepreviousunbearabletensionoftheatmosphere.
Amiddle-agedmanpresentedinitiallyasapsychiatricoutpatientwithapparentobsessionalsymptoms.Hekeptcheckingthathisneighbourscouldnothearwhathewassayinginhishome.Hehadresignedfromseveraljobsbecausehebelievedthathisemployerswouldnotaccepthisreligiousbeliefs.Hefelt thatpeoplearoundhimwerehostileand implacablyopposedtohim,althoughhecouldnotdefinequitehow–hejust‘feltit’.Hekeptmovinghouse,butthefeelingstayedwithhim.Thiscontinuedforseveralyears,andhethenarrivedatacasualtydepartmentclaiming thathisneighbourswere talkingabouthisactionsandcontrollinghis thoughts.Theatmospherehaddevelopedinsidiouslyoveryears,andeventuallyhemanifestedauditory hallucina-tionsandpassivity of thought(seeChapter9).
Germanpsychopathologistsneverusedthetermdelusional atmospherebutalwaysreferredtodelusional mood,accordingtoBerner(1991),butheconsidersthatatmosphereistobepreferred,asitallowsthedistinctiontobemadebetweenacognitive,perceptualdisturbanceprovokinganemotional response and a modification of mood causing a changed perception of the outsideworld.Itisconsideredthatdelusionalatmosphereisacommonendstateresultingfromdifferentpathways:vulnerabilitytocognitivedisturbance,asin‘Bleulerian’schizophrenia;dynamicderail-ment, as in affective disorders such as puerperal depression or psychogenic vulnerability; orwithouteitheroftheothertwo,withstressfullifeevents.Bernerconsidersthatthisstateisnotrestrictedtosufferersofschizophrenia.
The prodromal phases of schizophrenic illnesses are very variable in nature, and oftenanother diagnosis has been given before the definitive symptomatology becomes established.In an instructive review of the literature on the simulation of psychosis, and study of sixpatientswhowerethoughttobefeigningaschizophrenicpsychosis,Hay(1983)commentedonthenatureoffeigned psychosis.Inhisopinion,simulationofschizophreniaisgenerallyaprodromalphaseofaschizophrenicpsychosisoccurringinpeoplewithextremelydeviantpremorbidper-sonalities.Allbutoneofhispatientswerefoundtobesufferingfromschizophreniaatthetimeoffollow-up.
DELUSIONAL MEMORY
Inmuchthesamewaythatdelusionalperceptisadelusionalinterpretationofanormalpercept,delusionalmemory is thedelusional interpretationof anormalmemory.Theseare sometimescalledretrospective delusions.Aneventthatoccurredinthepastisexplainedinadelusionalway.Amanaged50whosementalillnesshadlastedforabouttwoyearsclaimedthathishealthhadbeenpermanently affected since the ageof 16,whenhehadhad ‘anoperation to removehisappendix’.Henowbelievedthattheoperationhadbeenanexcuseto‘implantagoldenconvol-vulus’inhisbowels.
8—DELUSIONS AND OThER ERRONEOUS IDEAS 119
Ifdelusionalmeaningisattachedtoanormalperceptthatisremembered,thisthenbecomesadelusional percept.Ithasthetwocomponentsthatweredescribedasbeingnecessaryfordelu-sional percept: the image of the remembered percept and the attachment to this percept ofdelusionalsignificance.Amarriedwomanrememberedyearspreviouslyseeingamanstandinginapub‘withasadlookonhisface’.She‘realized’,atthestartofherschizophrenicillnesstwoweeksbeforeadmissiontohospital,thathehadbeeninlovewithherthen,andshetriedtolocatehisnameinthetelephonedirectoryandmakecontactagain,feelingthattheywereinvolvedinaspecialrelationship.
Ofcourse,itisamistaketoexpectphenomenologicalsymptomstorevealthemselvestidilyfromthepatient’sconversation.There isnoabsolutedemarcationbetweendelusionalmemoryanddelusionalperceptor intuition.Thepatientdescribesadelusion.Didthisoccuronehour,oneweekortenyearsago?Atwhatpointwillthisbedelusionalmemory,notdelusionalintui-tion?Similarly,thereisnoabsolutedistinctionbetweenanormalevent,perceptionorideathatoccurredinthepastandisrememberedwithadelusionalinterpretation,andadelusionalevent,perceptionorideathatoccurredinthepastandisalsorememberedwithadelusionalinterpreta-tion.Inotherwords, therearetwosensestothetermdelusional memory.There is thesense inwhichanormalmemoryismisinterpretedinthepresent,andanothersenseinwhichtheactualmemoryisitselfafalsememorythatisimbuedwithdelusionalinterpretation.Bothofthesearedelusionalmemories,anditisnotalwayspossibletoknowhowmuchoftheeventwasfactualandhowmuchdelusional.Awomanwithschizophrenia,aged34,described12yearsagopickingupatelephonetoringamanshelikedverymuch:‘Godmovedmyarmandmademeputthetelephoneback’.Itwasnotpossibletodecideexactlywhatpartofthisexperiencewasfactualandwhatdelusional,andatwhattimethedelusionoccurred.
Finedistinctionsare sometimes imposedon theclassificationofprimarydelusionsbut aremore collector’s items than features of useful clinical significance. Delusional awareness is anexperiencethatisnotsensoryinnature,inwhichideasoreventstakeonanextremevividnessas if theyhadadditional reality.Delusional significance is thesecondstageof theoccurrenceofdelusionalperception.Objectsandpersonsareperceivednormallybuttakeonaspecialsignifi-cancethatcannotberationallyexplainedbythepatient.
The Origins of DelusionWhatistheoriginofdelusions?Thisquestiondrivesathowfardelusionsarebydefinitiondif-ferentfromnormalbeliefsand,iftheyaredifferentfromnormalbeliefs,whatthemechanismsarethatareinvolvedintheirdevelopmentandmanifestation.Jaspers’(1959)ownviewwasthatdelusionwasaprimaryphenomenonandthatitimpliesatransformationinthetotalawarenessofreality.Thismeansthatadelusionalbeliefinvolvesandimplicatespracticalactivity,behaviour,themeaningsthatareimmanentinobjects,andradicallytransformsthebasicexperienceoftheworld.Apersonwhoisdeludedthatheis lovedbyacelebrityapproachestheworldwiththiscertaintyandknowledgeandactsaccordingly,bywritingto,telephoningorattemptingtovisitthecelebrity.Thiserroneousbeliefinveststhepatient’sworldwithnewmeanings.Intheseterms,realityliesintheinterpretationof,orthesignificanceattachedto,eventsthatoccurinterpretedinthelightoftheprimaryerroneousbelief.
Anunderstandingofhowdelusionsradicallyalterthepatient’sworldasdescribeddoesnothelpustoexplainhowdelusionsforminthefirstplace.Thefactorsinvolvedindelusionforma-tionhavebeensummarizedbyBrockington(1991);seeBox8.1.
Fish(1967)hasmadeausefulprécisoftheearlierGermantheoriesoftheoriginsofdelusion.Conradproposedfivestagesinthedevelopmentofdelusionalpsychosis.
■ Trema:delusionalmoodrepresentingatotalchangeinperceptionoftheworld.■ Apophany:asearchfor,andthefindingof,newmeaningforpsychologicalevents.
120 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
■ Anastrophy:heighteningofthepsychosis.■ Consolidation:formingofanewworldorpsychologicalsetbasedonnewmeanings.■ Residuum:eventualautisticstate.Gruhle(1915)considereddelusional perceptiontobethemostsignificantformofdelusion,a
normalpercepttakingonanewmeaning.Thisresultsinadisturbedrelationshipoftheunder-standingofevents.Matussekconsideredthatwithdelusionalperceptionthereisachangeeitherinthesignificanceofthewordsusedorintheactualnatureoftheperceptionitself.Thesewriters,andalsoSchneider,regarddelusional perceptionasthekeytounderstandingthenatureofdelu-sionalexperience.
Hagenregardeddelusional atmosphereasprimary,arisingforreasonsunknownandresultinginarearrangementofmeaningsintheworldaroundthepatient,whogropesforananswertothisproblemofunderstandingandfindsitbycreatingadelusion.Itiseasiertobearthecertaintyofadelusionthantheuncertainforebodingoftheatmosphere.Jaspersconsideredthatthereisa subtle change of personality due to the illness itself, and this creates the condition for thedevelopmentofthedelusionalatmosphereinwhichthedelusionalintuitionarises.
Allthesetheoriesassumethatthedelusionisprimaryandultimately not understandableinthesame sense that Jaspers considers the experience of reality to be primary. Experience holds asymbolicimplicationbeyondthefactoftheeventitself;forexamplethedoctorwritingaprescrip-tion forhispatient in the consulting roommeansmuchmore to the latter than if thedoctorweredoodlingonhisprescriptionblock.(ApatientinNorthAfricainthenineteenthcenturyatethewrittenprescriptionhisdoctorgavehim,sogreatwashisconfidencein,andvenerationfor,thedoctor[Sims,1972]).Itseemsthatthesymbolicbeliefattachedtoeventsandperceptionsisalteredindelusion,andthisiswhythepatientdoesnotnecessarilyactonhisdelusions.Thedelusionalatmosphereisnotanessentialprerequisiteforadelusionalintuition,asthelattermayoccurapparentlyde novo.
Somewritershavenottriedtoexplaindelusions,becausetheyfindthemtotally incompre-hensibleandtheyconsiderthattheyaredirectlyduetoanabnormalityofthebrain(Schneider,1949).Bleulerconcentratedonthealteration in affectasprimaryratherthandelusionalatmos-phereorperception.Heconsideredthatheightenedaffectloosensthecapacitytoformassocia-tionsandthus facilitates thearrivalofadelusion.At thebeginningofaschizophrenic illness,thereisextremeaffect,perhapsintheformofanxietyorambivalence,whichthepatientcannotexpress.
Kretschmer(1927)stressedtheimportanceoftheunderlyingpersonality.Hedescribedthesensitive premorbid personalityoccurringinapersonwhoretainsaffect-laden complexesandhasalimitedcapacityforemotionalself-expression.Suchapersonisdrivenpainfullyby,forexample,powerfulsexualfeelings,buthehasgreatdifficultyincommunicatinghispassionandrelatingtootherpeople.Heisverymuchawareofsocialconstraintsandisrigidlycontrolledbyhissuperego.Suchaperson,somewhatrigid,narrow-mindedandsuspiciousinhisviews,readilyformssensitive ideas of reference. A key experiencemayoccur inhis lifecircumstances,andquitesuddenly theseideasbecomestructuredasdelusions of reference.
BOX 8.1 ■ Factors involved in the germination of delusions
■ Disorderofbrainfunctioning■ Backgroundinfluencesoftemperamentandpersonality■ Maintenanceofself-esteem■ Theroleofaffect■ Asaresponsetoperceptualdisturbance■ Asaresponsetodepersonalization■ Associatedwithcognitiveoverload
8—DELUSIONS AND OThER ERRONEOUS IDEAS 121
Agirlwasalwaysshy,reticentandsensitiveatschool.Quiteoften,shewasreluctanttogotoschool.Shewasmeticulousinherattentiontopersonalneatnessandcleanliness.Afterleavingschool,sherememberedvividlyseveraloccasionsasachildwhenshehadfelthumiliated.Attheageof18,whenshewasworkinginafactory,shewasinthewomen’scloakroombroodingbecauseherboyfriendhadtoldherthathewasleavingherforsomeoneelse.Sheheardoneoftheotherwomensay, ‘Ugh,doesn’t she smell?’ Immediately, sheapplied the statement toherself and toexplainherboyfriend’sbehaviour.Fromthenonwards,shewasconvincedthatshesmeltunpleas-ant all the time, although she could smell nothing herself.This delusion dominated her life,preventedhermixingandcausedhergreatdistress.Thisdevelopmentofadelusion(Sensitiver Beziehungswahn)fromsensitiveideasofreference,asthesequeltoakey experience,issometimesseenattheonsetofschizophreniabutisnotcommon.Thekeyexperience,asdemonstratedinthiscase,hastwoimportantqualities.First,ithasparticularappropriatenesstothepatient’sareasofconflictassensitiveideasofreference.Second,itoccursatatimeofmarkedemotionalturmoilanddistress,sothatthepsychicgroundispreparedforacatastrophicevent.
Attempts have been made to find all delusions understandable in relation to the person’sinternal experience or social background.Westphal considered that if one knew all about thepatient,thechangeinhisviewofhimselfandthebeliefthathehadbecomenoticeableinsomeway would explain the delusion (Fish, 1967). Freud’s (1907) theories on the development ofdelusionsalsoattemptedtomakethemultimatelyunderstandable throughthemechanismsofdenial,projectionandsoon.Otherauthorshaveclaimedthatdelusionsareunderstandableinasocialcontext.Laing(1961)consideredtheflightintomadnessasanecessarydefenceagainstahighlydestructivefamily–notonlyunderstandable,butadmirable,andevenworthemulating.
Whenfourdifferentpsychologicaltheorieswereappraisedtoexplainparanoidphenomena,abasis of shame-humiliationwas found tobe themost consistent (Colby, 1977).Winters andNeale (1983) consider that existing theoriesofdelusional thinkingdevelop twomain themes:motivational and defect.The motivational theme explains the arrival of a delusion to explainunusualperceptual experienceor to reduceuncomfortablepsychic states.Defect implies somefundamentalcognitive-attentionaldeficitresultingindelusion.
Thevarietyandrangeofexplanationsadducedastheoriginofdelusionsattesttheextentofourignoranceabouttheultimatenature,structureandderivationofdelusions.Itisprobablywisetoregard‘delusion’asatermdescribingamultitudeofabnormalitiesofthinkingthathavemerelyasuperficialfamilialrelationship.Toemployananalogy,‘delusion’isliketheterm‘ataxia’,atermthathidesseveraldifferentabnormalitiesofmovementwithdifferingunderlyinglesionsandmecha-nisms.Theterm‘delusion’isnotadescriptionofaunitary,homogenousabnormalityofthinking.Itismostlikelyanumbrellatermforacollectionofdisparateabnormalitiesofthinking.
COGNITION AND REASONING IN DELUSION
In trying tounderstand the roleof cognitionand reason indelusion formation, it isprobablyusefultothinkoftheformation,elaborationandpersistenceofdelusionalbeliefsasanexpressionofnumerouscausal influencesconverging;eachexertsadifferent influence in theevolutionofthebelief(Roberts,1992).Theprocessofreasoninginordertocometoconclusionsaboutone’ssituation in the outside environment appears to be altered in those experiencing delusions. A‘jump-to-conclusionsstyle’hasbeendemonstratedindeludedsubjectswhenaskedtoperformaprobabilistic reasoning task (Huqetal., 1988).Thiswas confirmedbyGarety etal. (1991) inshowingthat41percentofdeludedsubjectsbutonly4percentofcontrolsreachedaconclusiononthebasisofonlyoneitemof information.Acommoncauseinabnormalityof informationprocessinghasbeenproposedforthosesubjectswithabnormalreasoningandabnormalpercep-tion;failuretomakeuseofknowledge,previouslyacquired,ofregularitiesintheworld,resultingin over-reliance on information immediately present, may be a factor in delusion formation
122 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
(Garety,1991).Thismodelemphasizesthedeviantnatureofthethinkingprocessthatisassoci-ated with delusions in patients with schizophrenia. In Garety’s model, judgemental processesinvolvedindelusionformationinclude:
1. priorexpectationthatmaybemodifiedbyemotion;2. currentinformationthatwehaveatourdisposal,suchastheinformationreachingusby
wayofourperceptions;and3. thenatureofourinformationprocessingbiasorstyle.Inthismodel,ifperceptualabnormalitiespredominatetheroleofdeviantinformation,then
processingmechanismswillbeunderemphasized.Inotherwords,whendelusionsaresecondarytohallucinations,reasoningshouldremainintact.Theadvantageofthismodelisthatithighlightsthevaryingroutestodelusionformation.
Attribution in Delusion
Analternativepsychologicalexplanationfordelusioncomesfromsocial attribution theory.KaneyandBentall(1989,1992)foundthatdeludedpatientsmadeexcessivelyexternal,stableandglobalattributionsfornegativeevents(‘ThefactthatIbrokemylegprovesyetagainthattheWetherbyfreemasonsaregettingatme’)andexcessivelyinternal,stableandglobalattributionsforpositiveevents(‘EveryonesmilesandnodswhentheyseemebecauseIhavebeensentbyGodtocom-municatewithpeopleaboutevilandIhavealetterfromthePopeasproof ’).Deludedsubjectswereunwilling toattributenegative eventsofwhich theywere thevictim to theirowncause;also,injudgingthebehaviourofotherpeopletheywerereluctanttoattributenegativeeventstothevictimsthemselves.Theseandotherstudiessuggestthatpersecutorydelusionshaveafunctioninprotectingtheindividualfromlowself-esteem(Bentall,1993).
Deluded subjects were considered to evaluate their own causal statements in a distinctivemanner,andthisdifferencefromdepressedsubjectswasgreaterthanthedifferencesinthecausalstatementsthemselves;thatis,thedifferencebetweendeludedandothersubjectsininternalityforpositiveandnegativeeventsdoesnotreflectdifferencesinthecausalstatementsofthesesubjects,butratherdifferences in theirattributions(Kindermanetal.,1992).Onceagain,delusionsarelinkedbothtopersonalmeaningandtoboundariesofself.Thisinvestigationofattributionalstylewas further extended using obvious and opaque tests of attributional style. Deluded subjectsattributednegativeoutcomes toexternalcauses in theobviousor transparent testsbutamorecoverttestingtointernalcauses;thisfurthersupportedthehypothesisthatpersecutorydelusionsfunction as a defence against underlying feelings of low self-esteem (Lyon etal., 1994).Thispsychologicalexplorationisfurthersupportedbytheclinicalstudythatfollows.
Delusion and Meaning in Life
Roberts(1991)hasdevelopedthethesisthatdelusions,inthecontextofschizophrenicillness,maynotthemselvesbeanafflictionorillnessbutanadaptiveresponsetowhateverinitiatesthepsychoticbreak.Agroupofchronicallydeludedsubjectswascomparedwithpreviouslydeludedpatientsnowinremissionandwithtwonon-patientgroups.Persecutorydelusionswerecommoninbothpatientgroups,butgrandioseanderoticdelusionsanddelusionsof specialknowledgeweremostlyfoundinthecurrentlydeludedgroup.Thechronicallydeludedgroupscoredmuchhigher than the remittedpatients forpositivemeaning in life, andmuch lower fordepressionandsuicidalintention.Theyhadaveryhighlevelofperceivedpurposeandmeaninginlife.Itisconsideredthatforsometheformationofdelusionsisadaptiveincombatingpurposelessness,loneliness,senseofinferiority,hopelessness,isolationandpainfulawarenessofbrokenrelation-shipsandprovidesanewsenseofidentity,aclearersenseofdutyandresponsibility,anexperienceoffreedom,protectionfrompasthurts,andachangefromfear,worry,depressionandboredomtowards feeling lively, enthusiastic, interested and peaceful. One patient described this: ‘I’vehadagreattime.I’vegotthisonegreatthoughtinmymindthatIamJesus–that’senough…nothinghurtsmenow,Ineednothingnow.’
8—DELUSIONS AND OThER ERRONEOUS IDEAS 123
Content of DelusionsDelusions are, of course, infinitely variable in their content, but certaingeneral characteristicscommonlyoccur.Unliketheform,whichisdictatedbythetypeofillness,thecontent isdeter-minedbytheemotional,social,culturalandbiographicalbackgroundofthepatient:Napoleonsarenowrareinmentalhospitals;schizophreniasufferersfromtraditionalsocietiesmaydescribetheirthoughtsasbeinginterferedwithbythespiritsoftheirancestorsratherthanbytelevision.As computers and the Internet increasingly affect all aspects of our lives, we are beginningto have described by those with mental illness delusions of control concerning the Internet(Catalanoetal.,1991).
DELUSIONS OF PERSECUTION
Thisisthemostfrequentcontentofdelusion.ItwasdistinguishedfromothertypesofdelusionandfromotherformsofmelancholiabyLasègue(1852).Peoplewhobelievedelusionallythattheirlivesarebeinginterferedwithfromoutsidemoreoftenfeelthistobeharmfulthanbenefi-cial.Avariantontheusualbeliefsofpersecutionormalevolentintentaredelusionsofprejudice:the patient or victim believes that he is being slighted, overlooked, passed over in favour ofsomeoneelse.The interferingagent indelusionsofpersecutionmaybeanimateor inanimate,otherpeopleormachines;itmaybesystems,organizationsorinstitutionsratherthanindividuals.Sometimes, the patient experiences persecution as a vague influence without knowing who isresponsible.
Persecutorydelusionsoccurinmanydifferentconditions:inschizophrenia,inaffectivepsy-chosesofmanicanddepressive typeand inorganic states,bothacuteandchronic.Theaffectassociatedwiththebeliefofpersecutionmayvaryfromaninappropriateindifferenceandapathyinschizophreniatostarkterror,ascommonlyseenindeliriumtremens.
Manic patients with persecutory delusions show gross overactivity and flight of ideas inattemptingtoexpressanddealwiththeirbeliefs.Indepression,thepersecutorydelusionstakeonthecharacteristiccolouringofthedominantmoodstate.Persecutoryovervaluedideasareaprominentfacetofthelitigioustypeofparanoidpersonalitydisorder.
MORBID JEALOUSY AND DELUSION OF INFIDELITY
Morbidjealousy,adisorderofcontentdescribedbyEy(1950),maybemanifestedinvariousforms,forexampleasdelusion,overvaluedidea,depressiveaffectoranxietystate.Thefeelingofjealousy,coupledwithasensethatthelovedobject‘belongstome’and,therefore,‘Ibelongtotheother’,ispartofnormalhumanexperience; it isofsocialvalue inmaritalrelationshipsforpreservingthe family.Various termshavebeenused todescribeabnormal,morbidormalignant jealousy.Kraepelin(1905)usedthetermsexual jealousy.EnochandTrethowan(1979)haveconsidereditimportanttodistinguishpsychoticjealousyfromothertypes,andthisisdependentonthedem-onstrationofadelusion of infidelity.Itissometimesdifficulttodistinguishunderstandablejealousyfromthatwhichisdelusional.
Mullen(1997)classifiedmorbidjealousywithdisorders of passion,inwhichthereisanover-whelmingsenseofentitlementandaconvictionthatothersareabrogatingthesubject’srights:‘Themorbidlyjealousbelievethattheyarethevictimsofaninfidelitythathasdeprivedthemofthefealtywhichistheirdueandtheyaredriventoexposethisdisloyalty,reasserttheircontrolandpunishthetransgression’.Theothertwocategoriesarethequerulant,whoareindignantatinfringementsofrights,andtheerotomanic,whoaredriventoasserttheirrightsoflove.
Delusionofinfidelity,thatis,whenthesubjectunreasonablybelieveshimorherselftobethevictimoftheirpartner’sunfaithfulness,mayoccurwithoutotherpsychoticsymptoms.IthasbeendescribedbyToddandDewhurst(1955)andbyMullen(1990).This is identifiablydelusional

124 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
when thebelief of the spouse is basedondelusional evidence.Suchdelusions are resistant totreatmentanddonotchangewithtime.Apatientwasveryconcernedthathiswifewasbeingunfaithfulwithnumerouspeople, includinghisboss,hergeneralpractitionerandothers.Fouryearslater,despitevarioustreatments,hisbeliefwasunchanged,buthesaid,‘Idon’tblamehernow.SheismuchyoungerthanIamandeveryonedoesthatsortofthing’.Delusionsofjealousyarecommonwithalcoholabuse;forinstance,Shresthaetal.(1985)foundsexualjealousytobepresentin35percentofmenand31percentofwomenwhowerealcoholics.Asjealousyappearedtobejustifiedinsomecases,morbid jealousywasconsideredtobepresentin27percentofmenand15percentofwomen.Delusionaljealousy,oftenassociatedwithimpotence,alsooccursinsomeorganicstates,forexamplethepunchdrunksyndromeofboxersfollowingmultiplecon-trecoupcontusion.Quitefrequently,thespouse,weariedbycontinuedaccusationsof infidelity,doesformanothersexualinvolvement,whichmayresultinanacuteexacerbationinthementalstateofthepatientandfurthermaritalconflict.
Thesexualcontentofthedelusionisobvious;however,Enoch(1991)regardsthenatureoftherelationshipbetweenthetwopartnersasthekeyaspectofthecondition.Jealousyisdirectedtowardsthesexualpartner.Thedeludedpersonisveryattachedto,andoftenemotionallyutterlydependenton,theother;hemayhaveamisplacedsenseofowninghercompletely.Thevictimisoftenmuchmoresexuallyattractivethanthedeludedpartner,forinstanceayoungwifeorasociableandpopularhusband.Thedeludedpersonmayhavebeenpromiscuousinthepastandthereforeresignedlyexpectshisspousetoshowsimilarbehaviour.Hemayhavebecomeimpotentandprojected theblame forhis failureon toher.Hemayhavehomosexual fantasiesdirectedtowardsthemenwithwhomheclaimshiswife isconsorting.Morbid jealousyariseswiththebeliefthatthereisathreattotheexclusivepossessionofhiswife,butthisisjustaslikelytooccurfrom conflicts inside himself, his own inability to love or his sexual interest directed towardssomeoneelseasfromchangingcircumstancesinhisenvironmentorhiswife’sbehaviour.Husbandsorwivesmayshowsexualjealousy,asmaycohabiteesandhomosexualcouples.Crimesofviolencearenotoriously associatedwithmorbid jealousy; violence ismoreoften ventedon thepartnerthanonthesupposedrival,mostoftenbymenonwomen.Morbidjealousymakesamajorcon-tributiontothefrequencyofwifebatteringandisoneofthecommonestmotivationsforhomicide(Mullen,1990).
DELUSIONS OF LOVE
Thedelusionsassociatedwith lovingandbeing lovedarequitedifferent fromthebehaviouralandaffectiveabnormalitiesofnymphomania,thesituationofawomancharacterizedbymorbidoruncontrolledsexualdesire,andsatyriasis,themaleequivalentofexcessivesexualactivity.Boththeselatterconditionsexistinitiallyintheopinionofanexternalcommentator–thedoctor.
Approximatelytwiceasmanyschizophrenicpatientshadsexualpreoccupationsinthemid-twentiethcenturyascomparedwithinthemid-nineteenthcentury(KlafandHamilton,1961).ErotomaniawasdescribedbySirAlexanderMorrison(1848)asbeing:
characterized by delusions … the patient’s love is of the sentimental kind, he is wholly occupied by the object of his adoration, whom, if he approaches, it is
with respect … the fixed and permanent delusions attending erotomania sometimes prompt those labouring under it to destroy themselves or others, for
although in general tranquil and peaceful, the patient sometimes becomes irritable, passionate and jealous.
Erotomania iscommoner inwomenthaninmen,andavarietyhasbeencalled‘oldmaids’insanity’byHart(1921), inwhichpersecutorydelusionsoftendevelop.Thesehavesometimes
8—DELUSIONS AND OThER ERRONEOUS IDEAS 125
beenclassifiedasparanoiaratherthanparanoidschizophrenia;thesedelusionalsymptomssome-times occur in the context of manic-depressive psychosis (Guirguis, 1981).Trethowan (1967)demonstratedthesocialcharacteristicsoferotomania,relatingthepatient’spreviousdifficultiesinparentalrelationshipstothepresenterotomania.
Avariationoferotomaniawasdescribedby,andretainsthenameof,deClérambault(1942).Typically,awomanbelievesaman,whoisolderandofhighersocialstatusthanshe,isinlovewithher.Thevictimhasusuallydonenothingtodeserveherattentionandmaybequiteunawareofherexistence;sometimesheisawell-knownpublicfigurequiteremotefromthepatient.Inacaseoftheauthor’s,thevictimwasapreviousemployerofthepatient.Shebelievedthathewasthefatherofherchild(althoughatanothertimesheagreedthattherehadbeennosexualrela-tionshipwithheremployer).Shealsobelievedthathewassendinghermoney,andshewouldwritelettersthankinghimforhisgenerosityandaffirminghergratitudefortheevidenceofhislove(SimsandWhite,1973).
In a series of 16 erotomanic cases, Mullen and Pathé (1994) tried to distinguish betweenthosecasesinwhichthereisamorbidbeliefinbeinglovedandthosewithmorbidinfatuation.Theyfoundthatinmostcasesbothnotionsweredescribed:amixtureofbeinglovedandlovinginreturn.
DELUSIONAL MISIDENTIFICATION
Delusional misidentification syndromes include a number of discrete but related syndromesthathave incommontheconceptof thedouble.These syndromes includeCapgras’ syndrome(Capgras and Reboul-Lachaux, 1923), Frégoli’s syndrome (Courbon and Fail, 1927), the syn-dromeofintermetamorphosis(CourbonandTusques,1932)andthesyndromeofsubjective doubles(Christodoulou,1978).
Capgras’syndromeisregardedbyEnochandTrethowan(1979)as‘arare,colourfulsyndromeinwhichthepersonbelievesthataperson,usuallycloselyrelatedtohim,hasbeenreplacedbyanexactdouble’.Itisaspecificdelusionalmisidentificationofapersonwithwhomthesubjectusuallyhascloseemotionaltiesandtowardswhomthereisafeelingofambivalenceatthetimeofonset.Thebelief, inCapgras’ syndrome,has thefullcharacteristicsofdelusion(EnochandTrethowan,1979).Thebasic conceptof this syndrome isprominent inall cultures,hence thedelusion is universal (Christodoulou, 1991).Likeotherdelusions,delusion describes the form;thecontentisculture-dependent.Arecentpatientbelievedhismotherhadbeenreplacedbyanimpostorafterfallingthroughatimewarptoaparalleluniverse,andthisexplainedthehorriblethingsthathadhappenedinthepastthreeweeks.
Frégoli’s syndrome is thedelusionalmisidentificationof anunfamiliarperson as a familiarone, even though there is no physical resemblance. The syndrome of intermetamorphosis isthedelusionalbeliefthatothersundergoradicalchangesinphysicalandpsychologicalidentity,culminatinginadifferentpersonaltogether.Thesyndromeofsubjectivedoublesisthedelusionalbeliefintheexistenceofphysicalduplicatesoftheself,andtheseduplicatesareusuallythoughttohavedifferentpsychologicalidentities(seeMoselhyandOyebode,1997,forreview).
InaseriesofcasesreviewedbyBerson(1983),55percent(70patients)wereunquestionablydiagnosedas suffering fromschizophrenia,anda furthereightpatients (totalling61percent)wereprobablysufferingfromschizophrenia;13percentweresufferingfrombipolarmooddis-orderand24percentwereconsideredtohaveanorganicdiagnosis.Of133patients,57percentwerefemale;theagerangewasfrom12to78,withameanof42.8years.Majorityopinionwouldnotfavourdenotingthisasaseparatediseasebutratherasasymptomthatcolourstheclinicalstateanddominatesthesymptomatology.Thefourdifferentvarietiesofdelusionalmisidentifica-tionhaveincommonpsychopathologicallytheformofadelusion.Capgras’syndrome,whenitoccurs in schizophrenia, isbasedonadelusionalpercept (Sims,1986). InCapgras’ syndrome,
126 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
thereisnooutwardchangeintheappearanceoftheobject,andthereisnofalseperception,forthepatientoftenadmitsthatthedoubleexactlyresemblestheoriginal(EnochandTrethowan,1979),butcarefulquestioningusuallyrevealsthattherearedistinguishingstigmata.Sometimespatientswill say,‘Iknowthat it isnotmymotherbecauseshewouldneverstand like that’or‘thispersonmovestooslowlytobemyfather’.
Theambivalencetowardstheobjectofmisidentificationmaybeexpressedinthehistory,withaclearaccountofbothnegativeemotions,suchashostility,fearorcontempt,andaffectionanddependence.Onthosefewoccasionswhenanobject,ratherthanaperson,iswronglyidentified,thatobjecthasimportantemotionalconnotationsforthepatient,forexamplehomeoraletterfromarelative.ThesubjectsofmisidentificationinBerson’s(1983)reviewof133patientscom-prised60spousesandtwolovers;on29occasions,achildorchildren;40parents;24siblings;13therapists; four grandparents; three in-laws; two neighbours; two domestics; and one each offiancé,cousin,stepson,employerandpriest.Oneightoccasions,theselfwasmisidentifiedeithersolelyorwithotherevidenceofthesyndrome;ontwooccasions,animals,andeighttimesinani-mateobjectsweremisidentified.Thus,in31percentofoccasions,thedelusionalmisidentificationreferstoamaritalpartner,andin46percenttoafirst-degreerelative;inonlyfourpercentwasthemisidentificationofthepatienthim-orherself.
There is growing evidence that delusional misidentification syndromes are associated withorganicdisorders, includingdementia,acquiredbrain injury,epilepsyandcerebrovascularacci-dentsin25to40percentofcases,andneuroimagingstudiesrevealassociationwithrighthemi-sphere abnormalities, particularly in the frontal and temporal regions (Edelstyn etal., 1999).Furthermore, neuropsychological investigations have consistently shown impairments of faceprocessing in delusional misidentification syndromes (Edelstyn etal., 1996; Ellis etal., 1993;Oyebodeetal.,1996).Thesefindingsunderpintheassumptionofrighthemisphereabnormalitiesin delusional misidentification syndromes, because the right hemisphere is implicated in faceprocessingandrecognition.
GRANDIOSE DELUSIONS
Primary grandiose delusions occur in schizophrenia.The patient may believe himself to be afamouscelebrityortohavesupernaturalpowers.Hemaybelievehimselftobeinvolvedinsomeveryspecialandsecretmissionaboutwhichhehasnotyetbeenfullybriefedbutinanticipationofwhichheiswaitingwithexcitementforthedénouement.Beliefsofthissortaresometimescalleddelusionsofspecialpurposeandareoftheformofdelusionalintuition.
Expansive or grandiose delusional beliefs may extend to objects. Sometimes a psychoticpatientdemonstratesdelusionsofinventioninwhich,forexample,hebuildsamachinethathebelieves to have special capabilities, considering himself to be a creative prodigy. Secondarygrandiosedelusions,ordelusion-likeideas,occurinmanicstates.ApatientsaidthattherewasnolifeonMarsbecause‘iftherehadbeenIwouldhavebeenabletogetintouchbytelepathyusingmygreatgenius’.Heshowednoevidenceoftruepassivityexperiences.Amanicpatient,mentionedabove,believedthatshewasdescendedfromtheroyalStuartlineandthereforewasactuallyinsomewayMary,QueenofScots.SheinvitedtheQueenandthePrimeMinistertoapartyinherstudentflatbecauseshethoughttheywouldbehonouredtobeinvited:‘Itisonlyfairthattheyshouldhaveaninvitation.’Theexpansiveaffectofmaniacanbeveryclearlyseentorenderthisdelusionunderstandable.
RELIGIOUS DELUSIONS
Religiousdelusionsarecommon.However,theyformedahigherproportionofalldelusionsinthe nineteenth century than in the twentieth century: three times as many patients with
8—DELUSIONS AND OThER ERRONEOUS IDEAS 127
schizophrenia of both sexes had religious preoccupation in the nineteenth century (Klaf andHamilton,1961).Decisionastowhetherbeliefsaredelusionalornotmustrestontheprinciplesdescribedabove;thatis,onthewaythebeliefisheldandtheevidenceproducedinitssupport.Becauseareligiousbeliefisverybizarreandatvariancewiththoseheldbytheinterviewerdoesnotnecessarilymakeitadelusion.Religiousdelusionsmaybegrandioseinnature,forexampleapatientintheUKwhobelievedthatshewasanemissaryofGodtotheBirminghamHousingDepartment.Theymayalsobesecondarytodepressivemood,asinthepatientofEmilKraepelin(1905)quotedatthebeginningofChapter16:‘Icannot liveandIcannotdie,becauseIhavefailedsomuch,Ishallbringmyhusbandandchildrentohell’.
Thereligiousnatureofthedelusionisseenasadisorderofcontentdependentonthepatient’ssocialbackground,interestsandpeergroup.Theformofthedelusionisdictatedbythenatureoftheillness.Soreligiousdelusionsarenotcausedbyexcessivereligiousbelief,orbythewrong-doingthatthepatientattributesascause,buttheysimplyaccentuatethatwhenapersonbecomesmentallyillhisdelusionsreflect,intheircontent,hispredominantinterestsandconcerns.
Sometimes, it can be difficult to make the distinction between religious delusion and theexperienceofanunusual religiousbelieforpractice.Psychiatricmorbiditywouldbesuggestedbythefollowing(Sims,1992).
■ Boththesubjectiveexperienceandtheobservedbehaviourconformwithpsychiatricsymp-toms,thatis,theself-descriptionofthisparticularexperienceisrecognizableasbeingthesymptomatologyofaknownpsychiatricillness–ithastheformofdelusion.
■ Thereareotherrecognizablesymptomsofmentalillnessinotherareasoflife:otherdelu-sions,hallucinations,disturbanceofmood,thoughtdisorderandsoon.
■ Thelifestyle,behaviouranddirectionofpersonalgoalsoftheindividualsubsequenttotheevent or religious experience are consistent with the natural history of mental disorderratherthanwithapersonallyenrichinglifeexperience,compatiblewiththeconditionsinwhichdelusionsoccur.
DELUSIONS OF GUILT AND UNWORTHINESS
Such delusions are common in depressive illness. They often lead to suicide and, rarely, tohomicide,whenthekillingofacloserelativemaybefollowedbythepatient’ssuicide.Affectiveillness may be followed by the killing of children by depressed mothers, or the killing oftheir wife or sometimes also children by husbands; suicide may follow immediately or later(Higgins,1990).
Thebeliefsaboutguiltmaytotallydominatethepatient’sthinking.Anelderlywomanspentthedayrushingroundthehousewringingherhandsandtellingherworriedfamilythatshewaswretched, worthless and only deserved to die. She told her married daughters that they wereillegitimateandthatthehouseshelivedinwasnothersbutstolen,andshetoldherhusbandof30years’ standing that they were not legally married.When it was suggested to her that shecomeintohospital,sheassumedthatshewouldbekilledonarrival,andsheaskedwhetherthiscouldtakeplacethereandthensothatshecouldreceiveherjustdesserts.
DELUSIONS OF POVERTY AND NIHILISTIC DELUSIONS
Delusionsofpovertyarecommonindepression;anelderlypatientbelievedthat‘thenurses’hadbeensystematicallyraidingherpurseandthatshewasdestitute.Cotard’s syndromecontainsfea-turestypicalofpsychoticdepressionintheelderly:nihilisticandhypochondriacaldelusionsthatareoftenbizarre,dramaticandtingedwithgrandiosity;depressedmoodwitheitheragitationorretardation and a completely negative attitude. According to Griesinger (1845), ‘the patientconfusesthesubjectivechangeinhisownattitudetooutsidethings…therealworldseemsto
128 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
the patient to have disappeared completely, or to be dead’.This was graphically depicted byCotard(1882):
I would tentatively suggest the name ‘nihilistic delusions’ (délire de negations) to describe the condition of the patients to whom Griesinger was referring, in
whom the tendency towards negation is carried to its extreme. If they are asked their name or age, they have neither – where were they born? They were not born. Who were their father and mother? They have no father,
mother, wife or children. Have they a headache or pain in the stomach, or any other part of the body? They have no head or stomach and some even have no
body. If one shows them an object, a rose or some other flower they answer, ‘that is not a rose, not a flower at all’. In some cases negation is total.
Nothing exists any longer, not even themselves.
Thecentral character inPatrickMcGrath’snovelSpider said, ‘Iwas contaminatedby it, itshrivelledme,itkilledsomethinginsideme,mademeaghost,adeadthing,inshortitturnedmebad’.Elsewhere,thesamecharactersays,‘asinglepipetakeswaterfrommystomach…andthispipealonedropsthroughthevoidandconnectstothethingbetweenmylegsthathardlyresemblesaformedmaleorganatallanymore’(McGrath,1990).
Nihilisticdelusionsarethereverseofgrandiosedelusions,inwhichoneself,objectsorsitua-tionsareexpansiveandenriched;thereisalsoaperversegrandiosityaboutthenihilisticdelusionsthemselves. Feelings of guilt and hypochondriacal ideas are developed to their most extreme,depressiveforminnihilisticdelusions.
HYPOCHONDRIACAL DELUSIONS
Averydepressedmansaidthathewasfullofwater,thattherewasnothingelseinsidehim,andthathecouldnotpasswaterbutthatifhedidthatwouldbetheendofhim.Hecouldnotdrinkor thewaterwouldflood the room.Other less strikinghypochondriacal beliefs anddelusionsoccurindepression,andSchneider(1920)hasconsideredthatlocatingtheexperienceofdepres-sionasasensationinabodilyorganisequivalenttoa‘firstranksymptom’ofdepressivepsychosis(seeChapter16).Anelderlywomanwithdepression,whohadhadamitralvalvereplacementforrheumaticheartdisease,saidthatshefeltworthlessandhopelessanddescribedherphysicalfunctionsas‘nothingisworking’.
Hypochondriacaldelusionsmayalsooccur inschizophreniaandhave thecharacteristicsofotherschizophrenicideas.Theyaremorelikelytobegivenapersecutorythananihilisticexpla-nation.Thus, a patient believed that his bodily functions were being interfered with by raysemitted fromaplanet and that thiswaspartof aplot to controlhis thoughts andbehaviour.HypochondriacaldelusionsarediscussedfurtherinassociationwithhypochondriasisinChapter14;however,otherfeaturesofhypochondriasis,suchasbodilypreoccupation,diseasephobiaandconvictionofthepresenceofdiseasewithnon-responsetoreassurance,areinfactmorecommonthan delusion (Pilowsky, 1967). Facial pain is described in Chapter 15 and other delusion-like ideasandovervalued ideasof thebody inChapter14.Delusionsconcerning thepatient’soriginsaresometimesdescribedandhavesomeaffinitytohypochondriacaldelusion.Thepatientbelieves,ondelusionalevidence,thatheisnothisparent’schild,orperhapsthatheisofroyalbirth,partanimalorsupernatural.Alternatively,hemaybelievethathedoesnotexistandwasneverborn.
Hypochondriacal delusions are commonly associated with delusional disorder in ICD-10(previouslyknownasparanoia;WorldHealthOrganization,1992).Munro(1988)hasdescribed
8—DELUSIONS AND OThER ERRONEOUS IDEAS 129
delusional disorder as an encapsulated mono-delusional disorder with several subtypes, such aserotomanic,grandiose,jealous,persecutory,somaticandunspecified;theconcepthasdevelopedfromtheoldertermparanoia(Munro,1997).Hehasdescribedthesomatictypeasmonosymp-tomatic hypochondriacal psychosisand,of50cases,thethreemaingroupswere:
■ delusionsofbodyodourandhalitosis■ infestationdelusion(insects,burrowingwormsorforeignbodiesundertheskin)■ delusionsofuglinessormisshapenness(dysmorphicdelusions).Inafactoranalysisofthefeaturesofdelusionaldisorder,fourindependentfactorswereidenti-
fied,suggestingconsiderableheterogeneityofthecondition(Serrettietal.,1999).Thefirstfactorincorporatedcoredepressivesymptoms,whichmaybeeitheradepressivesyndromereactivetostressesderivingfromdelusionalideationoracomorbidmooddisorder,orboth.Otherfactorswerehallucinations,delusionsandsymptomsofirritability.
Thecomplaintwasalwayspresentedwithgreatintensity,andpatientswereutterlyconvincedofthephysicalnatureofthedisorder.Hypochondriacaldelusionsmayalsooccurwithadministra-tionofdrugs,bothprescribedandthoseofabuse.
Koro(Lapierre,1972)isanunusualconditionthathasbeendescribedasanexampleofhypo-chondriacaldelusion.Thisviewisprobablyincorrect.Thefeaturesofkoroinclude:
1. thebeliefthatthepenisisshrinkingintotheabdomen;2. thebeliefthatwhenthepenisdisappearsintotheabdomen,deathwillensue;and3. extremeanxietyaccompanyingthisbelief.Yap (1965) describes this as a culture-bound depersonalization syndrome and considers it
tobeamanifestationofacuteanxietyassociatedwithfolkbeliefsconcerningsexualexhaustion.It has occurred in epidemic proportions among Malays in Singapore (Gwee, 1963) but hasalso been described in individual cases in a French Canadian (Lapierre, 1972), in a WestIndian,aGreekCypriot (AngandWeller,1984)and inanEnglishman (BerriosandMorley,1984).Oyebodeetal.(1986)haveshowninasinglecasestudythatthisbeliefisaccompaniedbyrealpenileshrinkageasmeasuredbyplethysmography.Thissuggeststhatthebeliefisbasedon physiological changes that are likely to be due to anxiety. In essence, the penile changeis similar to tachycardia, hyperhidrosis or other features of sympathetic arousal associatedwithanxiety.
A group of patients who in some respects are intermediate between those suffering fromsomaticdelusionsanddelusionsofinfestationarethosewhoweredescribedbyVidebech(1966)assufferingfromchronicolfactoryparanoidsyndromes;thesehavealsobeenreferredtoashaving‘olfactory reference syndrome’ (Pryse-Phillips, 1971). Characteristically, these patients have afixed and unalterable belief that they smell but do not have hallucinations or other olfactoryexperience.Itisusuallyseeninthecontextofsensitive,paranoidpersonalitydevelopment.Thereisaseverephobicreaction,withthebehaviourofotherpeopleinterpretedasfindingtheirsmelloffensiveandaversive.
Delusions of Infestation
Delusions of infestation have been described by Hopkinson (1970) and by Reilly (1988). InEkbom’s syndrome(Ekbom,1938),thepatientbelievesthatheisinfestedwithsmallbutmacro-scopicorganisms.Thepatient’sexperiencemaytaketheformofatactilehallucinatorystate,adelusionoranovervaluedidea.Theaetiologyisalsovariable.Itisprobablymostcommonasasymptomof circumscribedhypochondriasis in affectivepsychosis, alongwithotherdepressivesymptoms,butitalsooccursinparanoidschizophrenia,inmonosymptomatichypochondriacalpsychosis (delusional disorder), in organic brain syndromes or with neurotically determinedconditions.ThistopicisreviewedbyBerrios(1985)andbyMorris(1991).
Patientshavebelievedthattheyhadaspiderintheirhair,wormsandlicebeneaththeskinor infestation with various insects. The delusion may be accompanied by other depressive
130 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
delusions or overvalued ideas of beingdirty, guilty, unworthyor ill.Thesedelusionsmay alsooccurinschizophrenia,inwhichconditiontheycharacteristicallytakeonabizarrecharacterandareaccompaniedbyotherschizophrenicsymptoms.A49-year-oldmotheroffourchildren,oneofwhosesonshaddevelopedaschizophrenicillness,complainedofrecurrentpaininhervaginathat she explained as being caused by a parasite that had migrated from her stomach, whereithadbeenresponsibleforepigastricpaindiagnosedearlierashiatushernia(McLaughlinandSims,1984).Shedescribed theparasite aswandering throughherbloodstreamandashavingbeenresponsibleforvariousachesandpainsshehadexperiencedinthepast.Sherelatedhavingpassedmultiplesmallredwormsandwormcastsinherfaecesand,ononeoccasion,atwo-inchgreenfrog.
Delusionsof infestationmayoccur inorganicstateswithtactilehallucinations, indeliriumtremensduringalcoholwithdrawalandincocaineaddiction.Theymaybedescribedincerebro-vasculardisease, inseniledementiaand inotherbraindisease,andtheyhavebeenascribedtodisorderofthethalamus.Overvaluedideasanddelusion-likeideasofinfestationsometimesoccurinpeoplewithpersonalitydisorderofanankasticorparanoidtypewithnopsychoticillness.
Characteristically,theseideasoccurinpatientsagedover50years.Typically,thosewithdelu-sionsofinfestationhavealwayshadaparticularconcernforpersonalcleanliness.Sometimes,theconditionisprecipitatedbyaskindiseaseandbecomesadelusionalelaborationofexistingtactilesymptoms.Ithasbeensuggestedthatthesymptomdevelopsinstages:first,abnormalcutaneoussensation;thenanillusiondevelops;and,finally,thefullyformeddelusionofinfestationoccurs.Asmentionedabove,delusionalinfestationisnowviewedasoneformofdelusionaldisorder,inparticularbeingasubtypeofmonosymptomatichypochondriacalpsychosis.
COMMUNICATED INSANITY
LaségueandFalret(1877)described‘la folie à deux (ou folie communiquée)’.Occasionally,adelusion(delusionalintuition)istransferredfromapsychoticpersontooneormoreotherswithwhomthey have been in close association, so that the recipient shares the false belief: the principalacquiresthedelusionfirstandisdominant,theassociatebecomesdeludedthroughassociationwiththeprincipal.Thissituation,inwhichpartnersaccept,supportandshareeachother’sbeliefs,hasbeencalledthepsychosis of association.Theassociateisusuallysociallydeprivedordisadvan-taged,mentallyorphysically.
Gralnick(1942),inareviewoftheEnglishliteratureonfolie à deux,subdividedtheconditionintofourpossiblerelationshipsbetweenprincipalandassociate.
■ Infolie imposée,thedelusionsofamentallyillpersonaretransferredtosomeonewhowasnotpreviouslymentally ill,althoughcharacteristically thevictimhassomesocialorpsy-chologicaldisadvantage.Separationofthepairisoftenfollowedbyremissionofsymptomsintheassociate.
■ Folie communiquéeoccurswhenanormalpersonsuffersacontagionofhisideasafterresist-ing them for a long time. Once he acquires these beliefs, he maintains them despiteseparation.
■ Infolie induite,apersonwhoisalreadypsychoticaddsthedelusionsofacloselyassociatedpersontohisown.
■ Folie simultanéedescribesasituationinwhichtwoormorepeoplebecomepsychoticandsharethesamedelusionalsystemsimultaneously.Ithasbeenconsideredthattheprincipalis always psychotic (Soni and Rockley, 1974), but the associate may or may not bepsychotic.
However,thevalidityofthisclassificationhasbeenquestioned.Itisalsonotofanyparticularclinicalvalue,andthepsychopathologicaldifferencesarequestionable(HughesandSims,1997).
Inacasereportofafamilyaffectedwithfolie à quatre(Simsetal.,1977),theinitiallyreferredpatient believed that a large industrial concern had put ‘bugging’ devices in the walls of his
8—DELUSIONS AND OThER ERRONEOUS IDEAS 131
brother’shouse.Heclaimedthatemployeesofthefirmhadbeenfollowinghimeverywhereandinterferingwithhisownhouse.Hiswifebelievedthis story initiallyandproducedsupposedlycorroborativeevidence.Ayearlater,followinghisin-patienttreatment,shenolongeracceptedtheplotandshebelievedherhusbandtobementallyill.ShewasaveryanxiouspersonwhohadpreviouslyreceivedpsychiatrictreatmentandcamefromafamilyinwhichthreemembershadsufferedfromHuntington’schorea.Whenthepatient’sbrotherwasvisitedathome,itwasfoundthathe, and the sisterwho livedwithhim,bothbelieved in theplot andwerebothcurrentlyreceivingtreatmentforaschizophrenicillnessinwhichfirstranksymptomswerepresent.
Folie à deuxdemonstrateshowthecontentofbeliefisdictatedbysocialandenvironmentalcircumstances,butthepreciseformofthesymptomsvariesaccordingtothenatureoftheillness.Thusthenon-psychoticvictimoffolie imposéewillshowdelusion-likeideas,overvaluedideasormisinterpretationsbutwillnotshow‘true’delusionsordelusionalpercept.
Aninterestingvariationonfolie imposéewasdescribedbyAldridgeandTagg(1998).Thiswasthecaseofa7-year-oldboywhohadpresentedwithspuriouspsychoticsymptomsinducedbylivinginisolationwithhismother,whosufferedfromschizophrenia.Initially,hewaswithdrawn,uncommunicativeandritualistic,withdelayeddevelopment.Atschool,hewasfearfuloftoysandteachers,crouchingunderatable,andwasritualisticconcerningtimekeepingandtoileting,duringwhichhewouldremoveallhisclothingandreverseintothetoilet.Hisonlyspeechwastorepeatthe clock time in a ritualistic way. Foster placement was made with a single mature woman,experiencedwithchildren,andafterayearthisabnormalbehaviourhaddisappearedandhehadmadeprogressconsistentwithhismilddegreeoflearningdisability.
DELUSIONS OF CONTROL
Thesedelusions,otherwiseknownaspassivityormadeexperiences,arediscussedwithdisorderofthinkinginChapter9.
The Reality of DelusionsThedegreetowhichdelusionsinfluencetherealityoftheworldinhabitedbyapatientismostprobablybestjudgedbyhowfarpatientsactontheirbeliefs.Patientswithschizophreniadonotalwaysactontheirdelusions,butquitefrequentlytheydo.AmanwhobelievedthatAmericanbattleshipsweresailingdownthemainstreetofBirmingham,UnitedKingdom(100milesfromthesea)hadtherefinedsocialconsciencetoreportthistothepolice!Personsholdingdelusionsof morbid jealousy are potentially very dangerous: extreme physical violence and murder notuncommonlyoccurinthiscontext.Thepatientwithdepressivedelusionsofguiltandunworthi-nessmaywellactonthembykillinghimself.
Althoughthereisagrowingliteraturecastingdoubtonwhetherdelusionsarefalsebeliefsornot(seeabove),whatisinescapableisthefactthatpatientsdooftenactonthecontentofthesebeliefs.Forpracticalpurposes,thecontentofadelusionisimportantbecauseityieldsinformationaboutthelikelybehaviourofapatient.Inotherwords,thecontentofdelusionsactstomotivatebehaviour,togivereasontoactionandtojustifyconduct;thatis,ithaspredictivepower.Forthisreasonalone,thecontentofdelusionisrelevanttoclinicalpractice.HemsleyandGarety(1986)havecommentedon‘thelackofactionconsequentwithapparentlysincerelyheldbeliefs’while,paradoxically, forensicpsychiatric studieshavegenerally foundthatpsychoticsymptoms,espe-ciallydelusions,arefrequentlyamajorfactorresultingintheoffence(Taylor,1985).Buchanan(1993)hasreviewedthedescriptionsofsituationsinwhichpatientsactontheirdelusions.Heconsidersthatforaffectiveillnesses,bothdelusionalbeliefandactionmaybeconsequentontheabnormalmoodstate.Inothercircumstances,actioncanbeseenasbeingcausedbyacombina-tionof‘belief ’and‘desire’triggeredbyfactorssuchas‘noticings’:beliefclearlyisinfluencedbyoccurrenceofdelusion;desirecorrespondstoconceptssuchasmotivation,driveandinclination;
132 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
noticingisinfluencedbytheperceptualandcognitivechangesofthepsychoticstate.Tayloretal.(1998) conclude for an investigation into violence in a high-security hospital population,‘assymptomswereusuallyafactordrivingtheindexoffence,treatmentappearsasimportantforpublicsafetyas forpersonalhealth’.Theconclusionhere is thatdelusions, likenormalbeliefs,donotnecessarily result in action.Theymaybe expressed yetnot influencebehaviour in anydiscernibleway.But,likenormalbeliefs,theymaymotivatebehaviourinawaythatiscompre-hensiblegiventhecontentofthebelief.
Ingeneral,violentbehaviourinresponsetodelusionsisnotcommon;however,inasampleof83consecutivelyadmitteddeludedsubjects, someaspectof theactionsofhalfof themwascongruentwiththecontentoftheirdelusions(Wesselyetal.,1993).Whenactingonthedelu-sionswasdescribedbythesubjectsthemselves, itwasassociatedwithbeingawareofevidencethat supported their belief and with having actively sought out such evidence; a tendency toreducetheconvictionwithwhichabeliefwasheldwhenthatbeliefwaschallenged;andwithfeelingsad,frightenedoranxiousasaconsequenceofthedelusion(Buchananetal.,1993).
Erroneous IdeationOVERVALUED IDEA
An overvalued idea is an acceptable, comprehensible idea pursued by the patient beyond theboundsof reason.It isusuallyassociatedwithabnormalpersonality.DisordersassociatedwithovervaluedideashavebeenreviewedbyMcKenna(1984),whosedefinitionofovervaluedidea‘referstoasolitary,abnormalbeliefthatisneitherdelusionalnorobsessionalinnature,butwhichispreoccupyingtotheextentofdominatingthesufferer’slife’.Itisovervaluedinthesensethatitcausesdisturbedfunctioningorsufferingtothepersonhimselfortoothers.Thebackgroundonwhichanovervaluedideaisheldisnotnecessarilyunreasonableorfalse.Itbecomessodomi-nantthatallotherideasaresecondaryandrelatetoit:thepatient’swholelifecomestorevolvearoundthisoneidea.Itisusuallyassociatedwithverystrongaffectthattheperson,becauseofhistemperament,hasgreatdifficultyinexpressing.
AccordingtoMcKenna,thetermwasintroducedbyWernicke(1906),whodistinguisheditfromobsession,inthatitwasnotexperiencedsubjectivelyas‘senseless’,andfromdelusion.Jaspersconsideredthatdelusionisqualitativelydifferentfromnormalbelief,witharadicaltransforma-tionofthemeaningattachedtoeventsandincorrigibletoanextentquiteunlikenormalbelief.An overvalued idea, on the contrary, is an isolated notion associated with strong affect andabnormalpersonalityandsimilarinqualitytopassionatepolitical,religiousorethicalconviction.ForJaspers(1959),then,overvaluedideasare‘convictionsthatarestronglytonedbyaffectwhichisunderstandableintermsofthepersonalityanditshistory’.Furthermore,Jasperssays,‘theyareisolatednotionsthatdevelopcomprehensiblyoutofagivenpersonalityandsituation’.Fish(1967)consideredtherewasfrequentlyadiscrepancybetweenthedegreeofconvictionandtheextenttowhichthebeliefdirectedaction.Butthepatientwithanovervaluedideainvariablyactedonit,determinedlyandrepeatedly; it isalmostcarriedoutwiththedriveofan instinct, likenestbuilding. In many respects, these definitions attempt to locate overvalued ideas somewherebetweennormalbeliefsanddelusions.Overvaluedideasdifferfromdelusionsinthattheyarisecomprehensiblyfromwhatweknowaboutthepersonandhissituation.Theyaremorelikepas-sionatepolitical,religiousorethicalconvictionsthannormalbeliefs.Thissuggeststhatthereissomethingabout the tenacityof the conviction thatdistinguishes theseovervalued ideas fromnormalbeliefs,yetthedegreeofconvictionandincorrigibilityisthoughttobelessthanthatofdelusions.Itisobvious,though,thatthedegreeofconvictionisnotasafebasisfordistinguishingbetweendelusionsandover-valued ideas.Asaferapproach is toregardovervaluedascompre-hensibleinthecontextofthepatient’shistoryandlife.

8—DELUSIONS AND OThER ERRONEOUS IDEAS 133
McKenna lists the disorders of content commonly associated with the form of overvaluedidea.ThesearerepresentedinTable8.1.Thepsychopathologyisnotanovervaluedidea inallcasesofeachoftheseconditions;forinstancemorbidjealousymaybedelusionalandhypochon-driasismayoccursecondarytodepressedmood.However,whenanovervaluedideaisfounditisusuallyassociatedwithabnormalpersonality.
Morbid jealousy isoftenmanifestedasanovervalued idea.Ahusbandwas terrifiedthathiswifewasbeingunfaithfultohimbecauseofhercasuallyflirtatiousconduct.Hecheckedonhereverymovement, interrogatedherrepeatedly,examinedherunderwear,employeddetectives tofollowherandmisinterpretedanyinnocentcontactshehadwithothermen.Onexamination,hewasnotdeluded,buttheimportanceheattachedtoinvestigatingandmaintaininghiswife’sfidelity, and the time taken to do this, was excessive, destroyed his family life and lost himhisjob.
The form of the abnormal idea in many of the disturbances of body image, for exampledysmorphophobiaisusuallyanovervaluedidea.Apersonwithparanoid personalitydisorderbecameinvolved in a protracted lawsuit because a farmer ploughed across a public right of way. It isreasonablethathikersgetannoyedwhenafootpathisdestroyed,butthispersontookreasonableirritationtoextremelengthsandconstructedamantraptoeliminatethefarmer.Hisenthusiasmforfootpathshadbecomeanovervaluedidea.
PARANOID IDEAS AND SYNDROMES
Inpsychiatry,thewordparanoidistakentomean‘self-referent’andisnotlimitedtopersecutorydelusions; all delusions aredelusionsof reference in that they relate to thepatienthimself.Apersonwillnotformadelusionalbeliefconcerningsix-inchmenonMarsunlesshehimselfissignificantlyimplicatedinsomeway.Soaparanoiddelusionisadelusionofself-reference,notnecessarilypersecutoryinnature.Aparanoidpersonalitydisorderisthattypeofabnormalper-sonality inwhichtheperson’sreactiontootherpeople isundulyself-referent;aparanoidstate(seeChapter19)includesthosementalstatesinwhichself-referentphenomenaareconspicuous,that is, delusion-like ideas of reference or overvalued ideas predominate. A patient, all of whosedelusionsaregrandioseinnatureandnoneofthempersecutory,maystillbesufferingfrompara-noidschizophrenia.
Althoughprimarydelusionsarecharacteristicofschizophrenia,secondarydelusions(delusion-like ideas)occur inanumberofconditions, forexamplebipolarmooddisorder inbothmanic
TABLE 8.1 ■ Disorders with overvalued ideas
Content of Disorder Abnormality of Personality Reference(s)
Paranoid state: querulous or litigious type
Jaspers (1959), Kraepelin (1905)
Morbid jealousy Ey (1954), Shepherd (1961)
Hypochondriasis Abnormality of personality is usually present with overvalued ideas in all these conditions
Merskey (1979), Pilowsky (1970)
Dysmorphophobia Hay (1970), Munro (1980)
Parasitophobia (Ekbom’s syndrome)
Hopkinson (1973)
Anorexia nervosa Crisp (1980), Dally (1969)
Transsexualism Huxley et al. (1981)
(After McKenna, 1984, with permission.)

134 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
and depressive phases, epilepsy and other organic psychosyndromes, acute drug intoxication,variousalcoholicstatesand,ofcourse,schizophrenia.Thetermparanoidoriginallywassynony-mouswithdelusionalinsanity.Kraepelin(1905)usedthetermmorespecificallytodescribethecondition inwhich therearedelusionsbutnohallucinations.Thepersonality,moodstateandvolitionofthepatient,inKraepelin’sdescription,arewellpreserved.
ReferencesAldridge S and Tagg G (1998) Spurious childhood psychosis induced by schizophrenia in the parent.
Advances in Psychiatric Treatment4,39–43.AngPCandWellerMPI(1984)Koroandpsychosis.British Journal of Psychiatry145,335.Bayne T and Fernandez J (2009) Delusion and self-deception: mapping the terrain. In Bayne T and
Fernandez J (eds.) Delusion and Self-Deception: affective and motivational influences on belief formation.NewYork:PsychologyPress.
BentallRP(1993)Cognitivebiasesandabnormalbeliefs:towardsamodelofpersecutorydelusions.InDavidASandCuttingJC(eds.)The Neuropsychology of Schizophrenia.Hove:LawrenceErlbaum.
BernerP(1991)Delusionalatmosphere.British Journal of Psychiatry159(suppl.14),88–93.BerriosGE(1985)Delusionalparasitosisandphysicaldisease.Comprehensive Psychiatry26,395–403.BerriosGE(1996)The History of Mental Symptoms: Descriptive Psychopathology Since the Nineteenth Century.
Cambridge:CambridgeUniversityPress.BerriosGEandMorleySJ(1984)Koro-likesymptomsinanon-Chinesesubject.British Journal of Psychiatry
145,331–4.BersonRJ(1983)Capgras’syndrome.American Journal of Psychiatry140,969–78.BortolottiL(2010)Delusions and other irrational beliefs.Oxford:OxfordUniversityPress.BrockingtonI (1991)Factors involved indelusion formation.British Journal of Psychiatry159 (suppl.14),
42–5.BuchananA(1993)Actingondelusion:areview.Psychological Medicine23,123–34.BuchananA,ReedA,WesselyS,GaretyP,TaylorP,GrubinDandDunnG(1993)ActingondelusionsII:
thephenomenologicalcorrelatesofactingondelusions.British Journal of Psychiatry163,77–81.CapgrasJandReboul-LachauxJ(1923)L’illusiondessosiesdansundéliresystematiquechronique.Bulletin
de la Societé Clinique de Médicine Mentale11,6–16.CatalanoG,CatalanoMC,EmbiCSandFrantelRL(1991)DelusionsabouttheInternet.Southern Medical
Journal92,609–10.ChristodoulouGN(1978)Syndromeofsubjectivedoubles.American Journal of Psychiatry135,249–51.Christodoulou GN (1991) The delusional misidentification syndromes. British Journal of Psychiatry 159
(suppl.14),65–9.deClérambaultGG(1942)Les psychoses passionelles. Oeuvre psychiatrique.Paris:PressesUniversitaire.Colby KM (1977) Appraisal of four psychological theories of paranoid phenomena. Journal of Abnormal
Psychology86,54–9.CotardJ(1882)Nihilisticdelusions.InHirschSRandShepherdM(eds.)Themes and Variations in European
Psychiatry(transl.RohdeM,1974),pp.353–74.Bristol:JohnWright.CourbonPandFailG(1927)Syndromed’illusiondeFrégolietschizophrenie.Bulletin de la Societé Clinique
de Médecine Mentale15,121–4.CourbonPandTusquesJ(1932)Illusiond’intermétamorphoseetdecharme.Annals Médicopsychologique90,
401–5.CrispAH(1980)Anorexia Nervosa: Let Me Be.London:AcademicPress.CuttingJ(1985)The Psychology of Schizophrenia.Edinburgh:ChurchillLivingstone.DallyP(1969)Anorexia Nervosa.London:Heinemann.EaglesJM(1983)Delusionaldepressivein-patients,1892–1982.British Journal of Psychiatry143,558–63.EdelstynNMJ,RiddochMJ,OyebodeF,HumphreysGWandFordeE(1996)Visualprocessinginpatients
withFregolisyndrome.Cognitive Neuropsychiatry1,103–24.EdelstynNMJ,RiddochMJandOyebodeF(1999)Areviewofthephenomenologyandcognitiveneuro-
psychologicaloriginsoftheCapgrassyndrome.International Journal of Geriatric Psychiatry14,48–59.EkbomK(1938)PraesenilerDermat-zooenwahn.Acta Psychiatrica Scandinavica13,227–59.
8—DELUSIONS AND OThER ERRONEOUS IDEAS 135
EllisHD,dePauwKW,ChristodoulouGN,PapageorgiouL,MilneABandJosephAB(1993)Responsestofacialandnon-facialstimulipresentedtachistoscopicallyineitherorbothvisualfieldsbypatientswiththeCapgrasdelusionandparanoid schizophrenics. Journal of Neurology, Neurosurgery and Psychiatry56,215–9.
EnochD(1991)Delusional jealousyandawarenessof reality.British Journal of Psychiatry159 (suppl.14),52–6.
EnochMDandTrethowanWH(1979)Uncommon Psychiatric Syndromes,2ndedn.Bristol:JohnWright.EyH(1950)Jalousiemorbide.InEtudesPsychiatriques,vol. II.Paris:deBronwen.EyH(1954)Etudes Psychiatriques,vol. II.Paris:Desclée.FishF(1967)Clinical Psychopathology.Bristol:JohnWright.FreudS(1907)Delusionsanddreams inJensen’sgradiva.InStandard Edition of the Complete Psychological
Works,vol. IX(transl.StracheyJ,1959).London:HogarthPress.GaretyP(1991)Reasoninganddelusions.British Journal of Psychiatry159(suppl.14),14–8.GaretyP,HelmsleyDRandWesselyS(1991)Reasoningindeludedschizophrenicandparanoidsubjects:
biases in performance on a probabilistic inference task. Journal of Nervous and Mental Disease 179,194–201.
GogolN(1972)Diary of a Madman and Other Stories(transl.WilksR).London:Penguin.GralnickA(1942)Folieàdeux:thepsychosisofassociation.Areviewof103casesandtheentireEnglish
literature.Psychiatric Quarterly16,230–63.GriesingerW(1845)Mental Pathology and Therapeutics(transl.RobertsonCLandRutherfordJ,1882).New
York:WilliamWoodandCo.GruhleHW(1915)Self-descriptionandempathy.Zeitschrift fuer Gesundheitswesen Neurologie und Psychiatrie
28,148.Guirguis WR (1981) Pure erotomania in manic-depressive psychosis. British Journal of Psychiatry 138,
139–40.GweeAL(1963)Koro–aculturaldisease.Singapore Medical Journal4,119–22.HamiltonM(1978)Fish’s Outline of Psychiatry,3rdedn.Bristol:JohnWright.HartB(1921)The Psychology of Insanity.Cambridge:CambridgeUniversityPress.HayGG(1970)Dysmorphophobia.British Journal of Psychiatry116,399–406.HayGG(1983)Feignedpsychosis–areviewofthesimulationofmentalillness.British Journal of Psychiatry
143,8–10.HemsleyDRandGaretyPA(1986)Theformationandmaintenanceofdelusions:aBayesiananalysis.British
Journal of Psychiatry149,51–6.HigginsJ(1990)Affectivepsychoses.InBluglassRandBowdenP(eds.)Principles and Practice of Forensic
Psychiatry.Edinburgh:ChurchillLivingstone.HopkinsonG(1970)Delusionsofinfestation.Acta Psychiatrica Scandinavica46,111–9.HopkinsonG(1973)Thepsychiatricsyndromeofinfestation.Psychiatrica Clinica6,330–45.HughesTAandSimsACP(1997)Folieàdeux.InBhugraDandMunroA(eds.)Troublesome Disguises:
Underdiagnosed Psychiatric Syndromes.Oxford:BlackwellScientific.HuqSF,GaretyPAandHemsleyDR(1988)Probabilisticjudgementsindeludedandnon-deludedsubjects.
Quarterly Journal of Experimental Psychology40A,801–12.Huxley PJ, Kenna JC and Brandon SC (1981) Partnership in transsexualism, part II.The nature of the
partnership.Archives of Sexual Behavior10,143–60.JaspersK(1959)General Psychopathology(transl.HoenigJandHamiltonMW,1963).Manchester:Manchester
UniversityPress.Kaney S and Bentall RP (1989) Persecutory delusions and attributional style. British Journal of Medical
Psychology62,191–8.KaneySandBentallRP(1992)Persecutorydelusionsandtheself-servingbias:evidencefromacontinuing
judgementtask.Journal of Nervous and Mental Disease180,773–80.KendlerKS,GlaserWMandMorgensternH(1983)Dimensionsofdelusionalexperience.American Journal
of Psychiatry140,466–9.Kinderman P, Kaney S, Morley S and Bentall RP (1992) Paranoia and the defensive attributional style:
deludedanddepressedpatients’attributionabouttheirownattributions.British Journal of Medical Psychology65,371–83.
136 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
KlafFSandHamiltonJG(1961)Schizophrenia:ahundredyearsagoandtoday.Journal of Mental Science107,819–27.
KraepelinE(1905)Lectures on Clinical Psychiatry,3rdedn.(transl.JohnstoneT,1917).NewYork:W.Wood.KretschmerE(1927)Thesensitivedelusionofreference(transl.CandyJ).InHirschSRandShepherdM
(eds.)(1974)Themes and Variations in European Psychiatry.Bristol:JohnWright.LaingRD(1961)The Self and Others.London:Tavistock.LapierreYD(1972)KoroinaFrenchCanadian.Canadian Psychiatric Association Journal17,333–4.LasègueC(1852)citedbyCotardJ(1882)Dudéliredesnégations.Archives de Neurologie Paris4,152–70,
282–96.LaségueCandFalretJ(1877)Lafolieàdeux(oufoliecommuniquée).Annales Médico-psychologique18,321
(transl.MichaudR,1964),supplementtoAmerican Journal of Psychiatry 121,4.LyonHM,KaneySandBentallRP(1994)Thedefensivefunctionofpersecutorydelusions:evidencefrom
attributiontasks.British Journal of Psychiatry164,637–46.McGrathP(1990)Spider.London:Penguin.McKennaPJ(1984)Disorderswithovervaluedideas.British Journal of Psychiatry145,579–85.McLaughlinJAandSimsACP(1984)Co-existenceofCapgrasandEkbomsyndromes.British Journal of
Psychiatry145,439–41.MellorCS(1991)Delusionalperception.British Journal of Psychiatry159(suppl.14),104–7.MerskeyH(1979)The Analysis of Hysteria.London:BaillièreTindall.MorrisM(1991)Delusionalinfestation.British Journal of Psychiatry159(suppl.14),83–7.MorrisonA(1848)Cases of Mental Disease.London:LongmanandS.Highley.Moselhy H and Oyebode F (1997) Delusional misidentification syndromes: a review of the Anglophone
literature.Neurology, Psychiatry and Brain Research5,21–6.MullenP(1990)Morbidjealousyandthedelusionofinfidelity.InBluglassRandBowdenP(eds.)Principles
and Practice of Forensic Psychiatry.Edinburgh:ChurchillLivingstone.Mullen PE (1997) Disorders of passion. In Bhugra D and Munro A (eds.) Troublesome Disguises:
Underdiagnosed Psychiatric Syndromes.Oxford:BlackwellScientific.Mullen PE and Pathé M (1994) The pathological extensions of love. British Journal of Psychiatry 165,
614–23.Munro A (1980) Monosymptomatic hypochondriacal psychosis. British Journal of Hospital Medicine 24,
34–8.MunroA(1988)Monosymptomatichypochondriacalpsychosis.British Journal of Psychiatry153(suppl.2),
37–40.MunroA(1997)Paranoiaordelusionaldisorder.InBhugraDandMunroA(eds.)Troublesome Disguises:
Underdiagnosed Psychiatric Syndromes.Oxford:BlackwellScientific.OyebodeF,JamiesonR,MullaneyJandDavisonK(1986)Koro–apsychophysiologicaldysfunction?British
Journal of Psychiatry148,212–4.OyebodeF,EdelstynNMJ,PatelA,RiddochMJandHumphreysGW(1996)Capgrassyndromeinvascular
dementia: recognition memory and visual processing. International Journal of Geriatric Psychiatry 11,71–3.
PilowskyI(1967)Dimensionsofhypochondriasis.British Journal of Psychiatry113,89–93.Pilowsky I (1970) Primary and secondary hypochondriasis. Acta Psychiatrica Scandinavica 46,
273–85.PorterSandWilliamsC(1997)Psychiatricdilemmas–surgeryandtheMentalHealthAct(1983).Journal
of the Royal Society of Medicine90,327–30.Pryse-PhillipsW(1971)Anolfactoryreferencesyndrome.Acta Psychiatrica Scandinavica47,485–509.ReillyTM(1988)Delusionalinfestation.British Journal of Psychiatry153(suppl.2),44–6.RobertsG(1991)Delusionalbeliefsystemsandmeaninginlife:apreferredreality.British Journal of Psychiatry
159(suppl.14),19–28.RobertsG(1992)Theoriginsofdelusion.British Journal of Psychiatry161,298–308.SchneiderK(1920)Thestratificationofemotionallifeasthestructureofthedepressivestates.Zentralblatt
fuer die gesamte Neurologie und Psychiatrie59,281.SchneiderK(1949)Theconceptofdelusion‘ZumBegriffdesWahns’.Fortschritte der Neurologie-Psychiatrie
17, 26–31 (transl.MarshallH). InHirschSRandShepherdM (eds.) (1974) Themes and Variations in European Psychiatry.Bristol:JohnWright.

8—DELUSIONS AND OThER ERRONEOUS IDEAS 137
SchneiderK(1957)Primaryandsecondarysymptomsinschizophrenia.Fortschritte der Neurologie-Psychiatrie25,487–90(transl.MarshallH).InHirschSRandShepherdM(eds.)(1974)Themes and Variations in European Psychiatry.Bristol:JohnWright.
SerrettiA,LattuadaE,CusinCandSmeraldiE(1999)Factoranalysisofdelusionaldisordersymptomatol-ogy.Comprehensive Psychiatry40,143–7.
ShepherdM(1961)Morbidjealousy:someclinicalandsocialaspectsofapsychiatricsymptom.Journal of Mental Science107,687–753.
Shrestha K, Rees DW, Rix KJB, Hore BD and Faraghere B (1985) Sexual jealousy in alcoholics. Acta Psychiatrica Scandinavica72,283–90.
SimsACP(1972)TheEnglishHospital,Tangier1883–1908.Medical History16,285–90.SimsACP(1986)Thepsychopathologyofschizophreniawithspecialreferencetodelusionalmisidentifica-
tion.InChristodoulouGM(ed.)The Delusional Misidentification Syndromes.Basel:Karger.SimsACP(1992)Symptomsandbeliefs.Journal of the Royal Society of Health112,42–6.Sims ACP and White AC (1973) Co-existence of the Capgras and de Clerambault syndromes – a case
history.British Journal of Psychiatry123,635–8.SimsACP,SalmonsPHandHumphreysP(1977)Folieàquatre.British Journal of Psychiatry130,134–8.SoniSDandRockleyGJ(1974)Socio-clinicalsubstratesof folieàdeux.British Journal of Psychiatry125,
230–5.SpitzerM(1994)Thebasisofpsychiatricdiagnosis. InSadler JZ,WigginsOPandSchwartzMA(eds.)
Philosophical Perspectives on Psychiatric Diagnostic Classification.Baltimore:JohnsHopkinsUniversityPress.StoddartWHB(1908)Mind and its Disorders.London:Lewis.TaylorPJ(1985)Motivesforoffendingamongviolentandpsychiatricmen.British Journal of Psychiatry147,
491–8.TaylorPJ,LeeseM,WilliamsD,ButwellM,DalyRandLarkinE(1998)Mentaldisorderandviolence.
British Journal of Psychiatry172,218–26.Todd J and Dewhurst K (1955) The Othello syndrome. Journal of Nervous and Mental Disease 122,
367–74.TrethowanWH(1967)Erotomania–anolddisorderreconsidered.Alta2,79–86.TrollopeA(1869)He Knew He Was Right.London:Strahan.VidebechT(1966)Chronicolfactoryparanoidsyndromes.Acta Psychiatrica Scandinavica42,183–212.Walker C (1991) Delusion: what did Jaspers really say? British Journal of Psychiatry 159 (suppl. 14),
94–103.WernickeC(1906)Fundamentals of Psychiatry.Leipzig:Thieme.WesselyS,BuchananA,ReedA,CuttingJ,EverittB,GaretyPandTaylorPJ(1993)Actingondelusion1:
prevalence.British Journal of Psychiatry163,69–76.WintersKLandNealeJM(1983)Delusionsanddelusionalthinkinginpsychotics:areviewoftheliterature.
Clinical Psychology Review3,227–53.World Health Organization (1992) The ICD-10 Classification of Mental and Behavioral Disorders: Clinical
Description and Diagnostic Guidelines.Geneva:WorldHealthOrganization.Yap PM (1965) Koro – a culture-bound depersonalization syndrome. British Journal of Psychiatry III,
43–50.

This page intentionally left blank

139
C H A P T E R 9
Disorder of the Thinking Process
SummaryThinking and its processes are little understood. This means that abnormalities of thinkingcannotbeeasilyrelatedtoanyclearlydescribedalreadyestablishednotionofwhatnormalproc-essesareandhowabnormalprocessesdepartfromthesenormalprocesses.Inthischapter,fantasythinking,imaginativethinkingandconceptualthinkingaredescribed.Againstthisbackground,amodelofthinkingdependingontheassociationofideasandgovernedbyadeterminingprin-cipleisdescribed.Thisthenprovidesthebasisforadiscussionofabnormalitiesoftheformofthinking,aparticularlycomplexareaofpsychopathology,asitrequirestheabilitybothtofollowcloselywhatsomeoneissayingandalsotoconcludethatthesequenceofideas,ortheassociationof ideasmaybeawry. In thefinal section,Schneider’sfirst rank symptomsaredescribedwithexamples.
With time and years the individual becomes so lazy in public life that he is not even capable of writing any more. On such a sheet of paper, one can
squeeze many letters if one is careful not to transgress by one ‘square shore’. In such fine weather one should be able to take a walk in the woods. Naturally,
not alone, but with a girl. At the end of the year one always renders the annual accounting. The sun is now in the sky yet it is not yet ten o’clock.
Eugene Bleuler (1857–1939)
Thischapterisconcernedwithdisorderofthinking,andthenextchapterwithdisordersoflanguage.Thinking and thought processes are little understood. Although there is increasinginterestinthesubjectbycognitiveneuroscientists,theirprimaryfocusofstudymisseswhatisofinteresttotheclinicalpsychopathologist,namelythesubjectiveexperienceofthinking,particu-larly as it relates to abnormalities of thinking. Cognitive neuroscientists are interested in thenatureofproblemsolving;inthevariouskindsofreasoning,includinganalogical,inductiveanddeductive;andinthenatureoflogicandbeliefformation.Theseareallimportantsubjectsandcanbeimpairedinpsychiatricdisorders.However,theprocessthatmakestheseaspectsofthink-ing possible; the unique relationship of the subject to his own thoughts, the experience ofthoughtsflowingcoherentlyandtheeffortlessyetgoal-drivendimensionofthinkingthoughtsthatunderpinproblemsolvingandreasoning,ispoorlyunderstoodandresearched.Admittedly,itisdifficulttostudythesubjectiveaspectsofthinking,andmostlyoneisconcernedwithobjec-tivephenomenaofpsychiclife–whatJaspers(1962)calls‘performance’.
Therearetwodistinctaspectsinstudyingdisorderofthinking:thepatient’ssubjectiveaware-ness of his own disturbed thinking patterns and the manifestation of abnormal thinking hebetraysinhisspeech(Chapter10).Thislatteristheexpressionofthoughtanddetermineswhattheobservermaydeduceaboutthepatient’sthinking.Weneedtoenquirealsoabouttheexperi-ence of thinking in the patient’s description of his subjective psychological processes. Formal thought disorder,fromthesubjective,phenomenologicalstandpoint,isabnormalityinthemecha-nismofthinkingdescribedbythepatientintrospectingintohisownprocessesofthought;that

Keywords: Formal Thought Disorder, Circumstantiality, Concrete Thinking, PassivityExperience.
9—DISORDER OF ThE ThINkING PROCESS 139.e1

140 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
is,thepatientdescribesinhisownwordsaprocessofthinkingthatisclearlyabnormaltotheoutsideobserver.
Types of ThinkingTheprocessofthinkingwasdividedbyFish(1967)intothefollowingthreetypes:
■ undirectedfantasythinking–dereistic–autisticthinking■ imaginativethinking■ rationalorconceptualthinking.These three types have slightly different implications for psychopathology, the description
andcategorizationofmorbidprocesses.Theycanbeconsideredasfunctionsofthinking;thatis,theyarethenecessarymechanismsforthinkingtotakeplacebutarenotthemselvesmanifestinthephenomena.Wecancontrastthosephenomena,whicharetheproductsoftheperformanceofthinking,theperceptortheidea,withthefunctionsthatdonotbecomeexplicit.
FANTASY THINKING
Thismaybeofshortduration,forexamplethedaydreambeforegoingtosleep,oritmaybecomeanestablishedwayof life. JaspersquotesMontaigne:‘Plutarchsaysofpeoplewhowaste theirfeelingsonguinea-pigsandpetdogs,thattheloveelementinallofus,ifdeprivedofanyadequateobject,willseekoutsomethingtrivialandfalseratherthanletitselfstayunengaged.Sothepsycheinitspassionspreferstodeceiveitself,oreveninspiteofitselfinventsomenonsensicalobjectratherthangiveupalldriveoraim’.
Fantasy has an important function in the way we all carry out our everyday activities,forinstancewemodelourspeechandbehaviourinimaginationbeforeanimportantencounteror event, and afterwards we rehearse our performance in fantasy to evaluate it and assesswhetherwecouldhavedonebetter (see Imaginative thinking). Inorder tobeable toharnessour imagination constructively,we require the capacity forundirected fantasy and the learnedskilltostructurethoughts.Fantasyalsoallowsapersontoescapefromordenyreality,oralter-nativelytoconvertrealityintosomethingmoretolerableandlessrequiringofcorrectiveaction.A girl aged 20, who had a very deprived childhood and walked the city streets at night as aprostitute,listenedtoavicarbroadcastingonlocalradio.Shestartedtosendhimandhiswifeflowers and cards, made contact with them and began to call them ‘Mum’ and ‘Dad’. Whenquestionedbythepoliceonenight,shegavetheirnamesasnextofkinandsaidtheyreallywereherparents.
Shy, reservedpeople,notsuffering frommental illness,mayusedereistic thinkingtocom-pensateforthedisappointmentsoflife.Bleuler(1911)sawthisisolationfromtherealworldintoautisticthinkingascharacteristicofschizophrenia:‘Theverycommonpreoccupationofyounghebephrenics with “the deepest questions” is nothing but an autistic manifestation’. Fantasy,especiallyinsomewithneurotictraits,maydevelopfromthestageofbeingdeliberateandspo-radic intoanestablishedmode;thepersoncomestobelievethecontentsofhis fantasy,whichbecomesubjectively realandacceptedas fact.Freud, inhis laterwritings,considered that thiswassoinsomeoftheaccountshereceivedfromwomenofanincestuousrelationshipwiththeirfatherduring childhood ( Jones, 1962).However, inhis earlywritingshehad considered thattheyhadexperiencedactualsexualassaultbuthadusedunconsciousmechanismstorepressthisknowledge(IsräelsandSchatzman,1993;Webster,1995).Varioustypesofexperiencecomeintothe category of acting out fantasy, such as pathological lying (pseudologia fantastica), hysterical conversionanddissociation(somaticandpsychologicaldissociativesymptoms)andthedelusion-like ideas occurring in affective psychoses.These last types can be understood as arising from thepatient’saffectiveandsocialsetting.
9—DISORDER OF ThE ThINkING PROCESS 141
Fantasyisusuallyunderstoodtobethecreationofimagesorideasthathavenoexternalreality.However,fantasythinkingmayalsorevealitselfinthedenialofexternalevents.Theobservationsfor which the psychodynamic explanation of ego defence mechanisms have been described arerelevantinthiscontext.Theslipofthetongue,orthe‘forgetting’oftheemotionallyladenwordisnotaccidental;itisaformofself-deception.Theobvious,significant,butunpleasant,objectofperceptionmaybe‘overlooked’,andthisoftenrevealsfantasydenial.Fantasythinkingdeniesunpleasant reality, even though the fantasy itself may also be unpleasant.This rearranging ortransformation of reality is shown by neurotic patients habitually and all people occasionally.Jonathan Swift commented on it thus: ‘When man’s fancy gets astride of his reason; whenimaginationisatcuffswiththesenses;andcommonunderstanding,aswellascommonsense,iskickedoutofdoors,thefirstproselytehemakesishimself ’(Swift,1667–1745).
IMAGINATIVE THINKING
Thetermimaginationcoverspsychologicalstatessuchasfantasy(seeabove),thegenerationofnovelideasandthecreativeoutputsthatconstituteartordiscoveriesinscience.Thereareatleastthreecomponentsofimagination:mentalimagery,counterfactualthinkingandsymbolicrepre-sentation.Mentalimageryreferstotheabilitytocreateimage-basedmentalrepresentationsoftheworld.Counterfactual thinkingrefers to thecapacity todisengagefromreality inorder tothinkofeventsandexperiencesthathavenotoccurredandmayneveroccur.Symbolicrepresenta-tionistheuseofconceptsorimagestorepresentrealworldobjectsorentities(Roth,2004).Thisis,ofcourse,thebasisoflanguage,artandmathematics.
A facetof this typeof thinking that comes fromapsychoanalytic theoretical stance is theconceptofmaternal reverie(Bion,1962).Themother,whileinthesituation,bothphysicalandmental,of ‘holding thebaby’ (Winnicott,1957),hasacapacity for reverieordaydreamingonthebaby’sbehalf;thisusuallyconcernsthefuturehappinessandachievementsofthebaby.Bionwouldregardthisasanecessaryfactorinthehealthydevelopmentoftheself-sensationofthebaby;whenmaternalreveriebreaksdown,forexampleinpuerperaldepression,thebabyexperi-encesthisasdistress.Theprocessofmaternalreverie isclearlyanalogousinsomewaystotheprayersofareligiouspersononanother’sbehalf.
RATIONAL OR CONCEPTUAL THINKING
Problemsolvingandreasoningaretwokeyaspectsofrationalthinking.Problemsolvingisdefinedasthesetofcognitiveprocessesthatweapplytoreachagoalwhenwemustovercomeobstaclestoreachthatgoal,andreasoningisthecognitiveprocessthatweusetomakeinferencesfromknowledgeandtodrawconclusions.Theseaspectsof thinkingaredistinctbutrelated,sothatreasoningcanbeinvolvedinproblemsolving(SmithandKosslyn,2007).Strategiesforproblemsinvolvetheuseofheuristics,thatis,rulesofthumbthatusuallygivethecorrectanswer.Typically,reasoninginvolvesanalogies,inductionordeduction.Analogicreasoninginvolvestheapplicationofsolutionstoalreadyknownproblemstonewproblemswithsimilarcharacteristics.Forexample,ifyoulosethekeystoyourlockedbriefcase,youcanapplytheknowledgetothisnewproblemthatsharp-endedimplementscanbeusedtoopenpadlocks.Inductivereasoningdependsontheuseofspecificknowninstancestodrawaninferenceaboutunknowninstances.Commonly,thisisformulatedasgeneralizingfromasingleinstancetoallinstancesorfromsomemembersofacategoryknowntohaveagivenpropertytootherinstancesofthatcategory.This isknownascategory-basedinduction.Anexampleis‘mycathasfourlegs’,therefore‘allcatshavefourlegs’.Deductive reasoning involves an argument in which if the premises are true, the conclusioncannotbefalse.This isusuallystudiedbywayofsyllogism:(a)allMartiansaregreen, (b)myfatherisaMartian,(c)myfatherisgreen.
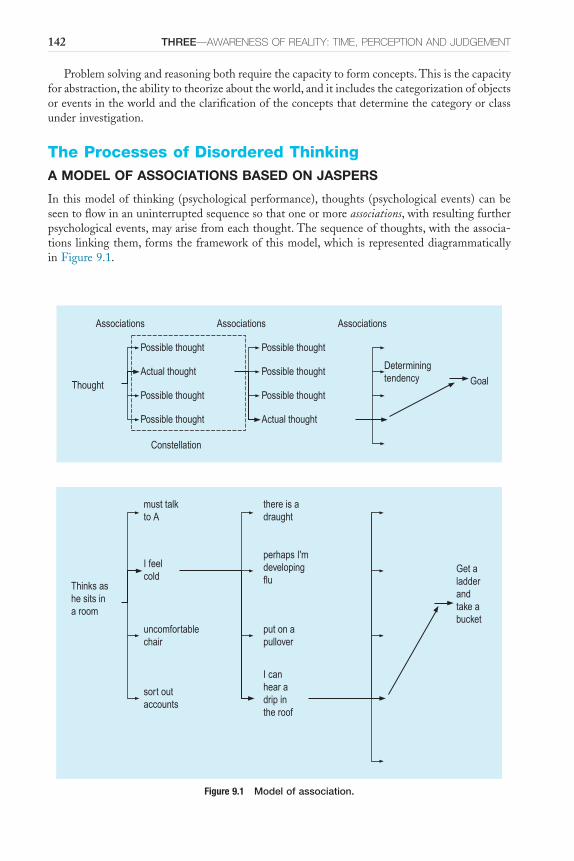
142 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
Problemsolvingandreasoningbothrequirethecapacitytoformconcepts.Thisisthecapacityforabstraction,theabilitytotheorizeabouttheworld,anditincludesthecategorizationofobjectsoreventsintheworldandtheclarificationoftheconceptsthatdeterminethecategoryorclassunderinvestigation.
The Processes of Disordered ThinkingA MODEL OF ASSOCIATIONS BASED ON JASPERS
Inthismodelof thinking(psychologicalperformance), thoughts(psychologicalevents)canbeseentoflowinanuninterruptedsequencesothatoneormoreassociations,withresultingfurtherpsychologicalevents,mayarisefromeachthought.Thesequenceofthoughts,withtheassocia-tionslinkingthem,formstheframeworkofthismodel,whichisrepresenteddiagrammaticallyinFigure9.1.
Figure 9.1 Model of association.
Associations Associations Associations
Possible thought
Actual thought
Possible thought
Possible thought
Possible thought
Possible thought
Possible thought
Actual thought
Thought Goal
Determiningtendency
Constellation
Thinks ashe sits ina room
must talkto A
I feelcold
uncomfortablechair
sort outaccounts
there is adraught
perhaps I'mdevelopingflu
put on apullover
I canhear adrip inthe roof
Get aladderandtake abucket

9—DISORDER OF ThE ThINkING PROCESS 143
Themassofpossibleassociationsresultingfromapsychiceventiscalledaconstellation.Thereare an enormous number of possible associations, but thinking usually proceeds in a definitedirectionforvariousimmediateandcompellingreasons.Thisconsistentflowofthinkingtowardsitsgoalisascribedtothedetermining tendency( Jaspers).Theideaofassociationsisnotintendedtoimplythatonepsychologicaleventevokesanotherbyanautomatic,unintelligent,non-verbalreflex,butthatthethought,whichmaybeexpressedverballyornot,isaconceptthatresultsintheformationofanumberofotherconcepts,oneofwhichisgivenprominencebyoperationofthedeterminingtendency.Thismodelisconjecturalbuthassomevalueinallowingdescriptionoftheabnormalitiesofthinkingandspeechthatoccurinmentalillness.
Weare subjectivelyawareofour thoughtprocessbeinga streamoraflow.Todevelop themetaphor,thoughtsarecapableofaccelerationandslowing,ofeddiesandcalms,ofprecipitousfalls,ofincreasedvolumeofflow,ofblockages.Thisanalogyshouldnotbetakentoofar,asitiswithoutneurophysiologicalbasis,butitisusefulforexaminingcertainabnormalitiesandisbasedonsubjectiveexperience.
ACCELERATION OF THINKING
Accelerationofflowof thinkingoccurs as flight of ideas. In this, there is a logical connectionbetweeneachoftwosequentialideasexpressed.However,thegoalofthinkingisnotmaintainedfor long. It is continuously changing because of the effect of frivolous affect and a very highdegreeofdistractibility.Thedeterminingtendencyisweakened,butassociationsarestillformednormally.The speed of forming such associations, and therefore of the pattern of thought, isgrosslyaccelerated.ThisisdemonstratedinFigure9.2.
Here is anexampleof suchflightof ideas froma femalemanicpatientaged45.She said,‘TheythoughtIwas in thepantryathome…Peekaboo…there’samagicbox.PoordarlingCatherine,youknow,CatherinetheGreat,thefiregrate,I’malwaysupthechimney.Iwanttoscreamwithjoy…Hallelujah!’Discussingthetranscriptofthisconversationwhenhermentalstatehadimproved,thepatientfounditquiteeasytopointoutthelogicalbridgesinherthinkingbetweeneachpairofstatements,buttherewasnosenseofbuildingupanargumentfromthefirsttothefinalstatement.
Markedlydifferentfromthemanicflightofideaswithpressureofspeechandmultiplebutlinkedassociationsistheconfusion psychosisdescribedbyFish(1962).Inthis,thinkingisdisor-deredwhilemoodandpsychomotoractivityareunimpaired.Intheexcitedformofthis,incoher-entpressureofspeechisprominent,thecontextofwhichisoutofkeepingwiththesituation.Theremaybetransient,almostplayful,misidentificationsofpeople;fleetingideasofreference;and auditory hallucinations. In the inhibited state of confusion psychosis, there is poverty ofspeech, almostmutism.Theremay alsobeperplexity, ideas of reference, ideas of significance,illusionsandhallucinations–auditory,visualorsomatic.Thisisusuallyacycloidpsychosisinitspresentation,andotherfeaturesofmanic-depressivepsychosismaybepresent.
Figure 9.2 Abnormal flow of thinking: flight of ideas.
X
X
X
X
X
X

144 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
RETARDATION
Inretardation(suchasoccursindepression),thinking,althoughgoal-directed,proceedssoslowly,withsuchmorbidpreoccupationwithgloomythoughts,thatthepersonmayfailtoachievethosegoals.Thepatientislikelytoshowlittleinitiativeandtobeginneitherplanningnorspontaneousactivity.Whenaskedaquestion,hewillponderoverit,butasnothoughtcomestohimhemakesnoresponse.Eventually,afterconsiderabledelay,theanswerusuallycomes.Hehasdifficultyinmakingdecisionsandinconcentration;thereislossofclarityofthoughtandpoorregistrationofthoseeventsheneedstoremember.Intermsofthemodeloftheflowofthinking,inretarda-tionthereisapovertyintheformationofassociations;seeFigure9.3.
Depression,althoughusuallyassociatedwithretardationofthought,mayoccurwithagitation;theremaybeacomplexsituationwithimpairedconcentrationfromretardationandasubjectiveexperienceof restless, anxious thoughts.Thus,Sutherland (1976), amiddle-agedpsychologistdescribinghisownmentalillness,said,
I contemplated throwing myself off the cross-Channel ferry… We arrived in Naples… and my friends… were upset by my condition while feeling
powerless to help… whilst the others sat at the table I rolled around moaning in the dust. I revisited many of the places I had once loved: the Museo
Nazionale with its magnificent mosaics pillaged from Pompeii, Pompeii itself and Capri. None of them evoked a spark of interest – I stared listlessly and
uncomprehendingly at the pictures in the museum with harrowing thoughts still racing in my mind. I could not guide the children round Pompeii, since I could not concentrate sufficiently to follow the plan. Capri had lost its beauty
and charm. I could not even giggle at the vulgarity of the interior of Axel Munthe’s villa, though the beauty of the formal garden and the magnificent
view of the island and the sea from the belvedere evoked a slight response. The phrase ‘see Naples and die’ echoed through my mind: I was convinced I
would never return alive to England, let alone ever revisit Naples.
ThispossiblecombinationofdepressedaffectandacceleratedactivitycanbeseentoconformquitereadilywithKraepelin’s(1904)descriptionofmixed affective states.
CIRCUMSTANTIAL THINKING
Inbothflightofideasandretardation,affectinfluencesthespeedofthinking:itdictateswhichideatakesprecedenceandcanalsodistortjudgement.Incircumstantial thinking,theslowstreamofthoughtisnotimpededbyaffectbutbyadefectofintellectualgrasp,afailureofdifferentiationofthefigurefromground.Characteristically,thisoccursinpatientswithepilepsy,anditisseeninotherorganicstatesandinmentalretardation.Asomewhatsimilarprocessoccurswithobses-sional personality, but here the excess of detail is introduced anxiously to avoid any possibleomissions: i ’s are dotted, t ’s crossed to such an extent that the process of reaching a goal is
Figure 9.3 Retardation.
X
X
X
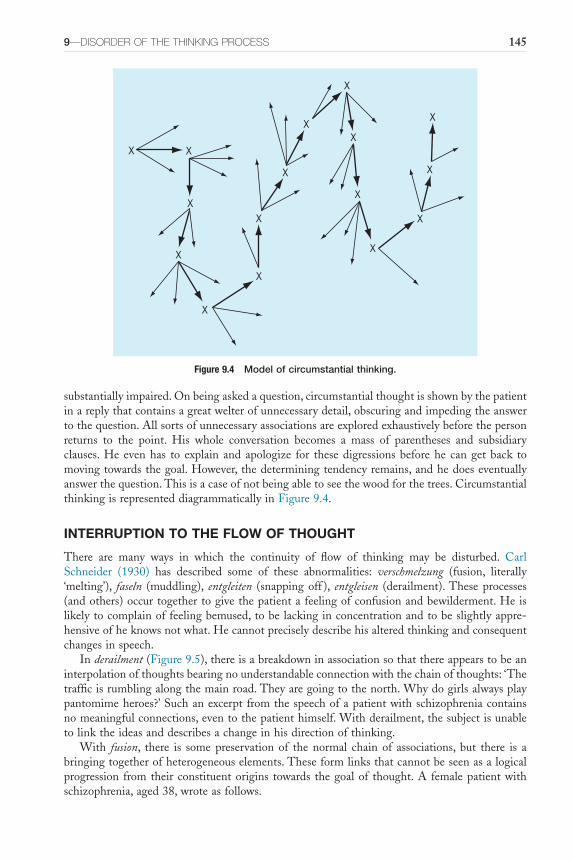
9—DISORDER OF ThE ThINkING PROCESS 145
substantiallyimpaired.Onbeingaskedaquestion,circumstantialthoughtisshownbythepatientinareplythatcontainsagreatwelterofunnecessarydetail,obscuringandimpedingtheanswertothequestion.Allsortsofunnecessaryassociationsareexploredexhaustivelybeforethepersonreturns to the point. His whole conversation becomes a mass of parentheses and subsidiaryclauses.Heevenhas to explain andapologize for thesedigressionsbeforehe cangetback tomovingtowardsthegoal.However,thedeterminingtendencyremains,andhedoeseventuallyanswerthequestion.Thisisacaseofnotbeingabletoseethewoodforthetrees.CircumstantialthinkingisrepresenteddiagrammaticallyinFigure9.4.
INTERRUPTION TO THE FLOW OF THOUGHT
There are many ways in which the continuity of flow of thinking may be disturbed. CarlSchneider (1930) has described some of these abnormalities: verschmelzung (fusion, literally‘melting’), faseln (muddling), entgleiten (snappingoff ), entgleisen (derailment).Theseprocesses(andothers)occurtogethertogivethepatientafeelingofconfusionandbewilderment.Heislikelytocomplainoffeelingbemused,tobelackinginconcentrationandtobeslightlyappre-hensiveofheknowsnotwhat.Hecannotpreciselydescribehisalteredthinkingandconsequentchangesinspeech.
Inderailment(Figure9.5),thereisabreakdowninassociationsothatthereappearstobeaninterpolationofthoughtsbearingnounderstandableconnectionwiththechainofthoughts:‘Thetrafficisrumblingalongthemainroad.Theyaregoingtothenorth.Whydogirlsalwaysplaypantomimeheroes?’Suchanexcerptfromthespeechofapatientwithschizophreniacontainsnomeaningfulconnections,eventothepatienthimself.Withderailment,thesubjectisunabletolinktheideasanddescribesachangeinhisdirectionofthinking.
With fusion, there is some preservation of the normal chain of associations, but there is abringingtogetherofheterogeneouselements.Theseformlinksthatcannotbeseenasalogicalprogression fromtheirconstituentorigins towards thegoalof thought.A femalepatientwithschizophrenia,aged38,wroteasfollows.
Figure 9.4 Model of circumstantial thinking.
X X
X
X
X
X
X
X
X
X
X
X
X
X
X
X
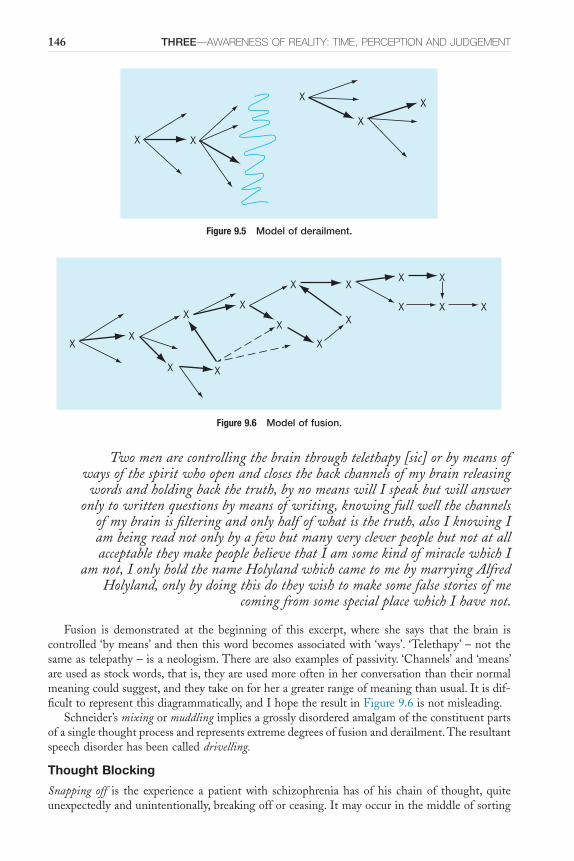
146 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
Two men are controlling the brain through telethapy [sic] or by means of ways of the spirit who open and closes the back channels of my brain releasing
words and holding back the truth, by no means will I speak but will answer only to written questions by means of writing, knowing full well the channels
of my brain is filtering and only half of what is the truth, also I knowing I am being read not only by a few but many very clever people but not at all acceptable they make people believe that I am some kind of miracle which I
am not, I only hold the name Holyland which came to me by marrying Alfred Holyland, only by doing this do they wish to make some false stories of me
coming from some special place which I have not.
Fusion is demonstrated at the beginning of this excerpt, where she says that the brain iscontrolled‘bymeans’andthenthiswordbecomesassociatedwith‘ways’.‘Telethapy’–notthesameastelepathy–isaneologism.Therearealsoexamplesofpassivity.‘Channels’and‘means’areusedasstockwords,thatis,theyareusedmoreofteninherconversationthantheirnormalmeaningcouldsuggest,andtheytakeonforheragreaterrangeofmeaningthanusual.Itisdif-ficulttorepresentthisdiagrammatically,andIhopetheresultinFigure9.6isnotmisleading.
Schneider’smixingormuddlingimpliesagrosslydisorderedamalgamoftheconstituentpartsofasinglethoughtprocessandrepresentsextremedegreesoffusionandderailment.Theresultantspeechdisorderhasbeencalleddrivelling.
Thought Blocking
Snapping off is the experience apatientwith schizophreniahas ofhis chainof thought, quiteunexpectedlyandunintentionally,breakingofforceasing.Itmayoccurinthemiddleofsorting
Figure 9.6 Model of fusion.
XX
X
X X
X
X
X XX
X
X
X XX
X
Figure 9.5 Model of derailment.
X X
X
X
X
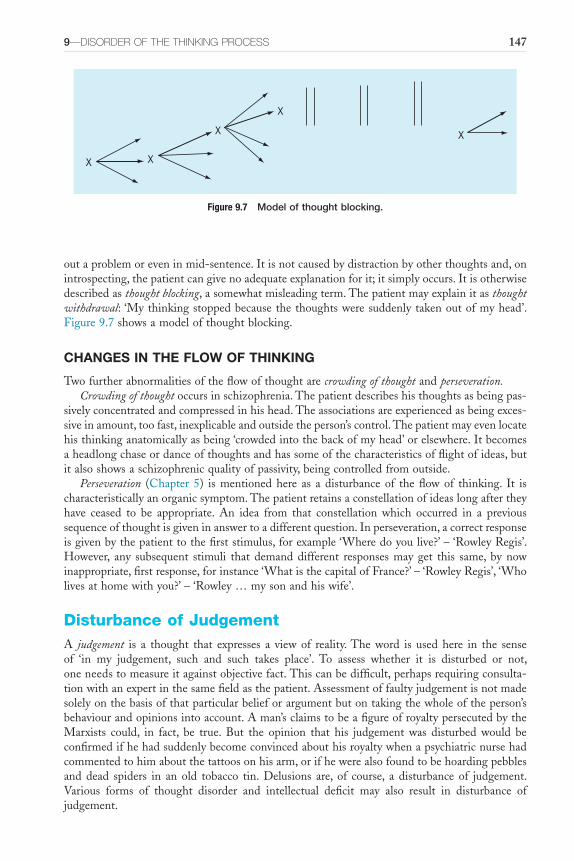
9—DISORDER OF ThE ThINkING PROCESS 147
outaproblemoreveninmid-sentence.Itisnotcausedbydistractionbyotherthoughtsand,onintrospecting,thepatientcangivenoadequateexplanationforit;itsimplyoccurs.Itisotherwisedescribedasthought blocking,asomewhatmisleadingterm.Thepatientmayexplainitasthought withdrawal:‘Mythinkingstoppedbecausethethoughtsweresuddenlytakenoutofmyhead’.Figure9.7showsamodelofthoughtblocking.
CHANGES IN THE FLOW OF THINKING
Twofurtherabnormalitiesoftheflowofthoughtarecrowding of thoughtandperseveration.Crowding of thoughtoccursinschizophrenia.Thepatientdescribeshisthoughtsasbeingpas-
sivelyconcentratedandcompressedinhishead.Theassociationsareexperiencedasbeingexces-siveinamount,toofast,inexplicableandoutsidetheperson’scontrol.Thepatientmayevenlocatehisthinkinganatomicallyasbeing‘crowdedintothebackofmyhead’orelsewhere.Itbecomesaheadlongchaseordanceofthoughtsandhassomeofthecharacteristicsofflightofideas,butitalsoshowsaschizophrenicqualityofpassivity,beingcontrolledfromoutside.
Perseveration (Chapter 5) ismentionedhere as a disturbanceof theflowof thinking. It ischaracteristicallyanorganicsymptom.Thepatientretainsaconstellationofideaslongaftertheyhave ceased to be appropriate. An idea from that constellation which occurred in a previoussequenceofthoughtisgiveninanswertoadifferentquestion.Inperseveration,acorrectresponseisgivenbythepatienttothefirststimulus,forexample‘Wheredoyoulive?’–‘RowleyRegis’.However, any subsequent stimuli that demanddifferent responsesmayget this same, bynowinappropriate,firstresponse,forinstance‘WhatisthecapitalofFrance?’–‘RowleyRegis’,‘Wholivesathomewithyou?’–‘Rowley…mysonandhiswife’.
Disturbance of JudgementA judgement is a thought that expresses a view of reality.The word is used here in the senseof ‘in my judgement, such and such takes place’. To assess whether it is disturbed or not,oneneedstomeasureitagainstobjectivefact.Thiscanbedifficult,perhapsrequiringconsulta-tionwithanexpertinthesamefieldasthepatient.Assessmentoffaultyjudgementisnotmadesolelyonthebasisofthatparticularbelieforargumentbutontakingthewholeoftheperson’sbehaviourandopinionsintoaccount.Aman’sclaimstobeafigureofroyaltypersecutedbytheMarxists could, in fact, be true. But the opinion that his judgement was disturbed would beconfirmedifhehadsuddenlybecomeconvincedabouthisroyaltywhenapsychiatricnursehadcommentedtohimaboutthetattoosonhisarm,orifhewerealsofoundtobehoardingpebblesand dead spiders in an old tobacco tin. Delusions are, of course, a disturbance of judgement.Various forms of thought disorder and intellectual deficit may also result in disturbance ofjudgement.
Figure 9.7 Model of thought blocking.
X X
X
X
X
148 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
DISTURBANCE OF JUDGEMENT AND DELUSION
Thethinkingorpsychologicalperformancerequiredtoproduceadelusionisquiteindependentofintelligence.Itoccurs inclearconsciousnesswithnosignsoforganicdisturbanceofthebrain.Judgementinotherareasoflifeapartfromthedelusioncanbepreserved,andtheveryingenious-nessthepatientusestoexplainanddefendhisdelusionalbeliefdemonstratesthathisessentialcapacitytothinklogicallyislargelyintact;onlythefalselyheldbelief,thefalsepremiseforsubse-quentbeliefsappearsdisordered.Adelusion,inschizophrenia,isnotasimpledefectofreasoning;itsdevelopmentcannotbeunderstoodsolelyinrelationtothepatient’sreallifeexperience.Forinstance,notallthosewithdelusionsofpersecutionhaveanyfirsthandexperienceofbeingperse-cuted.It isanassumptionabouttheworldthepatientinhabits,whichhedoesnotcreatebyaprocessoflogicalconsciousthoughtbutfromfalsepremises.Themechanismunderpinningtheoftenspontaneousdevelopmentofthisfalsepremiseisyettobeunderstood.Thestartingpointsofthethinkingarealready‘deluded’,andthepatientapplieslogictoelaborateandsupporthisbelief.
Wecanunderstandwhythebeliefshouldbewithinthatparticularcontext(associatedwithhismother; relatedto interplanetarytravel),butwecannotexplainhowthe formofaprimarydelusionshouldhaveoccurred.Thisisafundamentaldistinctionfromdelusion-likeideas(sec-ondarydelusions),whichoccur,forexample,inaffectivepsychoses.Inthelatter,wecanseethecontentbeingprogressively influencedbythechangingmoodstatesothat,eventually,thefalsebeliefbecomesalogicaldevelopmentfromtheextremeabnormalityofmood.
Althoughitisusualtodescribedelusionsasdisordersofthoughtcontent,itisimportanttobeawarethatprimarydelusionsarenotmerelytobeunderstoodinthisway.Thewholeprocessof thought inprimarydelusion isdisordered,not just the content. If an ideawere formedondelusionalgrounds–‘IknewthatmywifewasunfaithfulimmediatelyIsawthebulbhadgoneout’(Chapter8)–butthenotionitselfwasnotfalsenorunacceptabletotheperson’speergroup(his wife subsequently admitted to being unfaithful), it would still be a delusion because thenotionwasformedondelusionalevidence.Thereisadifferencebetweendelusionandovervalued ideasinthat,althoughbothmaybeheldwithabsoluteconviction,thelatterisareasonable,pos-siblyeventrue,beliefbutisdominatingconsciousthoughttoanunreasonableextent.
CONCRETE THINKING
Abnormalprocessesofthinkinginschizophreniaandorganicstatesmayresultinaliteralnessofexpressionandunderstanding.Abstractionsandsymbolsareinterpretedsuperficiallywithouttact,finesseoranyawarenessofnuance; thepatient isunable to freehimself fromwhat thewordsliterally mean, excluding the more abstract ideas that are also conveyed.This abnormality isdescribedas concrete thinking.The termwasfirst introducedbyGoldstein (1936). It isusuallytestedforbyproverbinterpretationorbyotherpsychologicaltests,butitiswellacknowledgedthatthesetestsareunreliable.However,itisrecognizableclinically,oftenquitedramatically.Forexample, a femalepatientwith schizophrenia came into the roomfor interviewandpromptlytookhershoesoff,saying,‘IalwaysliketokeepmyfeetonthegroundwhenI’mtalking’.Anotherpatient with long-term schizophrenia was observed by his doctor walking sideways along thehospitalcorridor.Whenaskedwhyhewaswalkinglikethat,hesaidthatitwas‘becauseofthesideeffects’.Andanotherpatientsaid,‘IwasstartingtofeelhighandIdidn’twanttoflyoff,soI’vetiedthesedumb-bellweightsroundmyankle’.
Itisimportanttoemphasizethoughthat,despitethecompellingexamplesofconcretethink-ing above, current thinking is that if anything patients with schizophrenia are more likely tosubscribe toamoreabstract attitude thancontrols (Weiner,1966;Shimkunas,1972;Cutting,2011), so that for examplewhenasked‘inwhatway is a table anda chair alike?’ thepatientsmightanswer‘objectsintheuniverse’.

9—DISORDER OF ThE ThINkING PROCESS 149
PSYCHOLOGICAL THEORIES OF THINKING IN SCHIZOPHRENIA
Thereareanumberofpsychologicaltheoriesthatattempttoexplainthinkinginpatientswithschizophrenia.These theories are hampered by the fact that there are no satisfactory generaltheoriesofthinking.Therearenowconsistentfindingsofdeficitsinattention,workingmemory,recognitionmemoryandexecutivefunctionsinschizophrenia.Theseempiricalfindingsareyetto be integrated into a coherent theory that explains the observed and self-reported thinkingabnormalitiesinthiscondition.
Over-Inclusive Thinking
Thedifferencebetweentheconcretethinkingoforganicpsychosyndromesandthatoccurringinschizophrenia was described by Cameron (1944), who considered that in schizophrenia thepatientisunabletopreserveconceptualboundaries.Thishecalledover-inclusive thinking:ideasthatareonlyremotelyrelatedtotheconceptunderconsiderationbecomeincorporatedwithinitinthepatient’sthinking.Thus,whenasked‘Whatofthefollowingareessentialpartsofaroom:walls,chairs,floor,awindow?’,theover-inclusivepersonwithschizophreniamightinclude‘chair’.This featureofover-inclusivenesscanbe seen inmanyaspectsof schizophrenic thinking,andquestionnaireshavebeendevisedto test for it,particularly involvingsorting tests.The lackofadequateconnectionbetweentwoconsecutivethoughtsiscalledasyndesis.
The concrete thinking of schizophrenia, however, could not be distinguished from that ofotherpsychoticandneuroticpatients(Payneetal.,1970),anditwasfoundtobeassociatedwithintelligence.Over-inclusivethinkingoccurredonlyinabouthalfofthepatientswithschizophre-niatested,usuallythosewhoweremoreacutelyill.Theotherhalf,usuallysufferingfrommorechronicillness,showedmuchmoremarkedretardation.McGhie(1969)foundthatPayne’stestsofover-inclusivenessdidnotselectschizophreniafromsomeotherdiagnoses,forexamplethosewithobsessionalormanicthoughtdisorder,andGathercole(1965)consideredthatthesetestsdemonstratedfluency of associationratherthanover-inclusivethinking.
Ayoungman,whohadsufferedfromschizophreniaforseveralyears,wasknowntohavebeenabusingdrugs recently.To thedoctor’senquiry‘Whatdrugshaveyoubeenusing?’,he replied‘LSD,health foodsandmarijuana’.This isanexampleofover-inclusive thinking.However, itwasvolunteeredspontaneously;hemightwellhavegivenanentirelycorrectresponsetoaformalquestionnairethatdidnottouchonsignificantareasofhisexperience.
IthasbeensuggestedbyChenetal.(1995)thattheremaybeabroadening of category boundary(forexample‘furniture’)withpreservationofinternalcategorystructureinpatientswithschizo-phrenia.Thisresults inrelated issuesthatareactuallyoutsidethecategorybeingprocessedbythepatientinawaythatissimilartothosewithinit.Cutting(2011)arguesthatwhatismostprominentisthatpatientswithschizophreniaovercategorize,findingmanymoreandoftenneed-lesscategoriestosubsumelistswithin.
Aggernaes(Aggernaesetal.,1976)hastakenthistheoryfurtherfromthepracticalandclinicalviewpoint.Heconsidersthatpatientswithschizophreniahavenotpartedfromreality;theyseemtoexperiencetherealworldasbeingrealinthesamewayasnormalpeopledo.However,theirdefectinrealitytestingresultsfromadiffusetendencytoexperiencesomefantasyitemsasbeingrealtoo.
Schizophrenic Inattention and Abnormality of Working Memory: Effect on Performance
McGhie(1969)hasconcentratedonthedisturbanceinthefunctionofattentioninschizophrenicpatients: that they are unable to filter and discount sensory data irrelevant to the task beingperformed.Heshowedthattheperformanceofschizophrenicpatientswasverypoorcomparedwiththatofnormalsubjects,buttheywerenotpronetodistractionbyauditoryorvisualexternal
150 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
stimuli in the way that normal people were. Hebephrenic patients especially showed lessdistractionandalsopoorperceptionandrecallofvisualinformation.Hebephrenicpatientswereconsideredtohavean:
inability to sweep out irrelevant extraneous information… especially where the situation demanded the rapid processing and short term storage of
information. This experience is described subjectively: ‘When people talk to me now it’s like a different kind of language. It’s too much to hold at once. My
head is overloaded and I can’t understand what they say. It makes you forget what you’ve just heard because you can’t get hearing it long enough. It’s all in
different bits that you have to put together in your head – just words in the air unless you can figure it out from their faces.’
TheeffectofthisinattentioninordinarysociallifewaswellobservedbyMorgan(1977)inhisdescriptionofthreeweekslivedincloseproximitytotwochronicschizophrenicpatients:
In the case of Vine our relationship remained just the same, but I did perhaps come to understand his disabilities a little better, and this helped. He would
keep ‘losing his thread’, to some extent in talk but even more noticeably in action. For example, although we went through the sequence of routine tests over 500 times together, he never once completed a sequence without having to be reminded of what came next and what remained to be done each time.
Vine’s other main trouble was a curious one. I would say to him, for example, ‘Let’s do the tests first and then I’d like you to get on with the washing up’,
and I would be surprised when his response to this was to dash off to the sink and start clattering the plates. Eventually I made out that he had some defect of attention. He would often jump like a startled rabbit when he realized he was being addressed anyway, and I think that by the time he had recovered
and collected himself from that, the first half of my sentence had gone and all he heard was the second half. Certainly I found that by inserting a little
preliminary padding, I got a more competent response.Frith(1992)hypothesizesthatthemechanismfordelusionsofcontrolwasalsoresponsible
forthethoughtorlanguageabnormalityinschizophrenia.Inthisscheme,itisafailureofself-monitoring that is responsible for thoughtor languagedisorder.Thus thepatient isunable toeditoutirrelevantorperseveratingphrases,andthisresultsinpoorcommunication.Thereisalsotherelatedpossibilitythatthefundamentalproblemisinplanning.Inthisscheme,thecoherenceofthepatient’sthoughtorlanguageisunderminedbytheabsenceofanexplicitgoalandplan,andfurthermorethereisintrusionofthoughtsthatdonotfitinwiththeoverallgoal,resultingindisorganizedthoughtorlanguage.Insummary,patientswithschizophrenia‘areonlyabletochecktheaccuracyofanutteranceafter[emphasisinoriginal]theyhavemadeit.Itisthereforedifficultforthemtoavoidproducingastringoffaultyutterances,evenduringattemptsatrepair’(Frith,1992).
Liddle (2001) defines the disorganization syndrome as consisting of disjointed thought,emotionandbehaviour.Butthecardinalsymptomsare formal thoughtdisorder, inappropriateaffectandbizarre,erraticbehaviour.Heconcludesthatdisorganizationisassociatedwithslowedperformance inneuropsychological tasks thatdemand selectionbetweencompeting responses,orwitherrorsofcommissionintasksthatrequiresuppressionofaninappropriateresponse.Inhisview,thissuggeststhatthedisorganizationfoundinschizophreniaderivesfromimpairmentoftheneuralcircuitsresponsibleforresponseselectionandinhibition.Thecircuitsinvolvedare
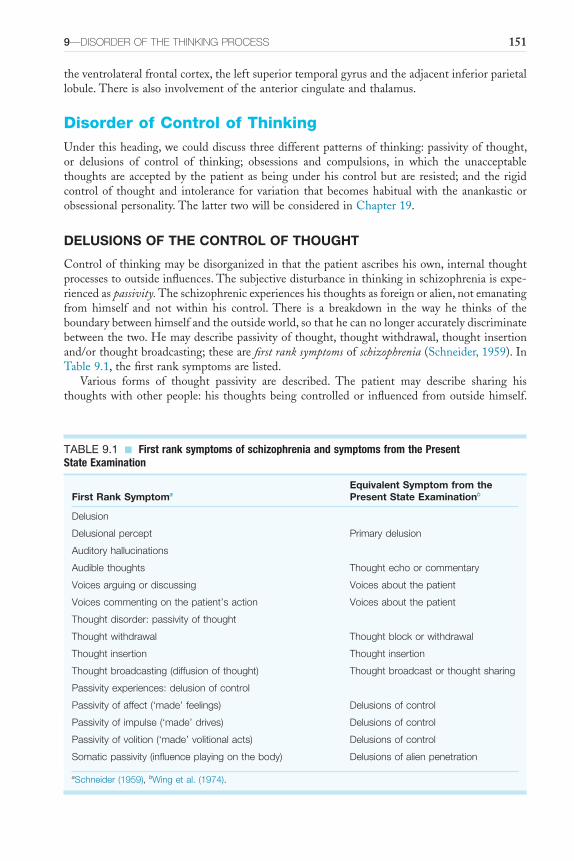
9—DISORDER OF ThE ThINkING PROCESS 151
theventrolateralfrontalcortex,theleftsuperiortemporalgyrusandtheadjacentinferiorparietallobule.Thereisalsoinvolvementoftheanteriorcingulateandthalamus.
Disorder of Control of ThinkingUnderthisheading,wecoulddiscussthreedifferentpatternsofthinking:passivityofthought,or delusions of control of thinking; obsessions and compulsions, in which the unacceptablethoughtsareacceptedby thepatientasbeingunderhiscontrolbutare resisted;andthe rigidcontrolof thought and intolerance for variation thatbecomeshabitualwith the anankasticorobsessionalpersonality.ThelattertwowillbeconsideredinChapter19.
DELUSIONS OF THE CONTROL OF THOUGHT
Controlofthinkingmaybedisorganizedinthatthepatientascribeshisown,internalthoughtprocessestooutsideinfluences.Thesubjectivedisturbanceinthinkinginschizophreniaisexpe-riencedaspassivity.Theschizophrenicexperienceshisthoughtsasforeignoralien,notemanatingfrom himself and not within his control.There is a breakdown in the way he thinks of theboundarybetweenhimselfandtheoutsideworld,sothathecannolongeraccuratelydiscriminatebetweenthetwo.Hemaydescribepassivityofthought,thoughtwithdrawal,thoughtinsertionand/orthoughtbroadcasting;thesearefirst rank symptomsofschizophrenia(Schneider,1959).InTable9.1,thefirstranksymptomsarelisted.
Various forms of thought passivity are described. The patient may describe sharing histhoughtswithotherpeople:his thoughtsbeingcontrolledor influenced fromoutsidehimself.
TABLE 9.1 ■ First rank symptoms of schizophrenia and symptoms from the Present State Examination
First Rank SymptomaEquivalent Symptom from the Present State Examinationb
Delusion
Delusional percept Primary delusion
Auditory hallucinations
Audible thoughts Thought echo or commentary
Voices arguing or discussing Voices about the patient
Voices commenting on the patient’s action Voices about the patient
Thought disorder: passivity of thought
Thought withdrawal Thought block or withdrawal
Thought insertion Thought insertion
Thought broadcasting (diffusion of thought) Thought broadcast or thought sharing
Passivity experiences: delusion of control
Passivity of affect (‘made’ feelings) Delusions of control
Passivity of impulse (‘made’ drives) Delusions of control
Passivity of volition (‘made’ volitional acts) Delusions of control
Somatic passivity (influence playing on the body) Delusions of alien penetration
aSchneider (1959), bWing et al. (1974).

152 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
Thesedelusions of controlareoftenassociatedwithdelusionalexplanationsofhowhisthinkingcould be controlled, for example electronic devices, computers, telepathy. Thought insertion isdescribed,inwhichhebelievesthathisthoughtshavebeenplacedtherefromoutsidehimself.Correspondingly,hemaydescribehisthoughtsbeingtakenawayfromhimselfagainsthiswill:thought withdrawal.Thismaybegivenasanexplanationforthoughtblockingwhenthethoughtsstopandthemindsuddenlygoescompletelyblank.Thoughtinsertionandwithdrawalarefirstranksymptomsofschizophrenia.Thought blockingisnot,asitisdifficulttodecidewhetheritistrulythoughtblockingorsomeformofretardationorotherdifficultywiththinking,andblockingis also subjectively similar to epileptic absences. Thought broadcasting occurs in schizophreniawhenthepatientdescribeshisthoughtsasleavinghimselfandbeingdiffusedwidelyoutofhiscontrol.Italsoisapassivityexperienceandoffirstrank.
Afurthersubjectivesymptomassociatedwiththought,offirstrankimportance,istheexperi-enceofaudible thoughts:hearingone’sownthoughtsoutloud.Thepatientknowsthattheyarehisthoughts,yethehearsthemaudiblywhileheisthinkingthem,justbeforeorjustafter.Thisisofcourseadisorderofperception,anauditoryhallucination(Chapter7).
Wehavediscussedearlierinthechapterfusion,mixing,derailmentandcrowdingofthought,all of which occur in schizophrenia.The resultant confusion causes a loss of ability to thinkclearly,oftendescribedintermsofpassivity.Thepatientmayfeelthathisbrainisreplacedbycottonwoolorconvolutedrubber.Histhoughtsarejumbled,muzzy,vague,blurred:‘Itrytopartmywaythroughthembuttheyareliketreacleandkeeponcomingbackandmakingmestick’.
First Rank Symptoms of Schizophrenia
Firstranksymptomsofschizophreniaarediscussedinthissectionforconvenience,sincemanyofthemareexamplesofdisorderofcontrolorpossessionofthoughts.AccordingtoSchneider,thepresenceofoneormorefirstranksymptomsintheabsenceoforganicdiseasecanbeusedaspositiveevidenceforschizophrenia.Thesesymptomsoffirstrankarenotacomprehensivelistoftheclinicalfeaturesofschizophrenia,forthechangesinaffect,volitionandmotoractivitythatmayoccurintheconditionarenotincludedatall,andmanyothertypesofdelusion,hallucina-tionanddisorderofthinkingoccuralsoinschizophrenia.Forasymptomtoberegardedasfirstrank,itmusthavethefollowingcharacteristics.
■ Itmustoccurwithreasonablefrequencyinschizophrenia.■ Itmustgenerallynotoccurinconditionsotherthanschizophrenia.■ Itmustnotbetoodifficulttodecideifthesymptomisorisnotpresent.There are some symptoms that occur only in schizophrenia but occur too rarely to be of
practicaluseasfirstranksymptoms.Therearemanyfeaturesthatarecharacteristicofschizo-phreniabutmayalsooccurinotherconditions,forexampleunspecifiedauditoryhallucinations,povertyofaffect,over-inclusivethinking.Therearesomesymptomsthatoccuronlyinschizo-phrenia, but there is too much scope for argument as to whether it is, or is not, this precisesymptomforittobevaluedasoffirstrank.Anexampleofthisisaprimary delusion.Someclini-ciansmayregardaparticularbeliefofthepatientasprimarydelusion,whileothersdonot.
Althoughfirstranksymptomsareusedasadiagnosticchecklist,apatientwhoexhibitssevenofthemisnotmoreseverelyillthansomeonewhoshowsthree.Toelicitthemrequiresconsider-ableclinicalexperience; theycannotbecollectedquantitativelybyridingpast thepatientonabicycle!For apsychiatrist touse themclinically, shemustfirst know them.Second, shemustknowhowthispersonfromthissocialandracialbackgroundislikelytodescribeanyparticularfirstranksymptom(‘mythoughtsarecontrolledby…television,by…thespiritsofmydeadancestors’).Third,shemustasktheappropriatedirectquestionsskilfully,withoutputtingwordsinherpatient’smouth.Fourth, shemustbeable to interpret thepatient’sanswersanddecidewhetherafirstranksymptomisbeingdescribed.ThewholeprocessrequiresadextroususeofthephenomenologicalmethodasdescribedinChapter1.

9—DISORDER OF ThE ThINkING PROCESS 153
Therearemanypractisingpsychiatristswhosecommentatthisstageofthediscussionoffirstranksymptomswouldbe‘Whybother?’Theywouldalsoagreethatitisoftendifficulttodiagnoseschizophrenia; that it is importantnottogivethis labeltopeoplewhodonotsufferfromtheillness;andthatitisequallyimportanttotreatthosewhodosufferfromitappropriately,effec-tivelyandasearlyinthecourseofillnessaspossible.
In clinical practice, the eliciting of first rank symptoms could best be seen as a means ofdecidingthedegreeofcertaintythatmaybeattachedtothediagnosis.Inapatientwhoshowsthegeneralfeaturesofschizophrenia(delusion,hallucination,thoughtdisorder,disorderedaffect,volition,motor activity, behaviour, social relationships, life history), thediagnosis ismadebutsome doubts remain. If first rank symptoms are found then, in the absence of clear organicpathology,onecanreckonthatthediagnosishasbeenconfirmed.Someofthefirstranksymptomsarefoundtobelessreliableatfollow-upthanothersasindicatorsofschizophrenia,forexamplevoicesheardarguing (Melloretal.,1981).Oneof theadvantagesoffirst rank symptomsasadiagnostictoolisthat,becauseoftheiremphasisonformratherthancontent,apersonwhoisfeigningmental illness isunlikely toproduce them.They thereforehave a subsidiaryuse as amethodofdistinguishingbetweentrueandsimulated psychosis,forexampleinprisoners.Despitethe value of first rank symptoms indicating schizophrenia when they are present, there areundoubtedlypatientsinwhomtheycannotbeelicited;schizophreniastillremains,tosomeextent,adiagnosisofexclusion(CarpenterandBuchanan,1994).
Examples of First Rank Symptoms
Theonlytypeofdelusionthatisregardedasoffirstrankisadelusional perception,thatis,anormalperception delusionally interpreted and regarded as being highly significant to the patient(Chapter8).Examplesofdelusionalpercept, andofotherfirst rank symptomsas follows, arecitedbyMellor(1970).Delusionalperceptisexemplifiedinthefollowingaccount.
A young Irishman was at breakfast with two fellow lodgers. He felt a sense of unease, that something frightening was going to happen. One of the lodgers
pushed the salt cellar towards him (he appreciated at the same time that this was an ordinary salt cellar and his friend’s intention was innocent). Almost before
the salt cellar reached him he knew he must return home, ‘to greet the Pope, who is visiting Ireland to see his family and to reward them… because Our Lord is going to be born again to one of the women… And because of this they (all the
women) are all born different with their private parts back to front.’(p. 18)
Threetypesofauditoryhallucinationsareregardedasbeingoffirstrank.Theseareaudible thoughts, voices heard arguingandvoices giving a running commentary.Whatismeantbyaudible thoughtsisthepatient’sexperienceofhearinghisownthoughtssaidoutloud.InBritishusage,thesymptomsometimescarriesitsGermanname,Gedankenlautwerden,oritsFrenchone,écho de pensées.Thepatientmayhearpeoplerepeatinghisthoughtsoutloudjustafterhehasthoughtthem,answeringhisthoughts,talkingaboutthemhavingsaidthemaudiblyorsayingaloudwhatheisabouttothinksothathisthoughtsrepeatthevoices.Heoftenbecomesveryupsetatthegross intrusion intohisprivacyandconcerned thathecannotmaintaincontrolof anypartofhimself,notevenhisthoughts.
A 35-year-old painter heard a quiet voice with ‘an Oxford accent’, which he attributed to the BBC. The volume was slightly lower than that of normal
conversation and could be heard equally well with either ear. He could locate

154 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
its source at the right mastoid process. The voice would say, ‘I can’t stand that man, the way he holds his hand he looks like a poof ’ … He immediately
experienced whatever the voice was saying as his own thoughts, to the exclusion of all other thoughts. When he read the newspaper the voice would
speak aloud whatever his eyes fell on. He had not time to think of what he was reading before it was uttered aloud.
(Mellor, 1970: 16)
Voices heard arguing with each other implies twoormorehallucinatory voices quarrellingordiscussingwitheachother.Thepatientusuallyfeaturesinthethirdpersoninthecontentofthesearguing voices.The symptom is not likely to be volunteered spontaneously in this form: thepatientdoesnotactuallysay,‘Ihearvoicesthatargueordiscusswitheachother’.Sothesymptomhastobecautiouslyandsubtlyenquiredfor.
A 24-year-old male patient reported hearing voices coming from the nurse’s office. One voice, deep in pitch and roughly spoken, repeatedly said, ‘G.T. is a
bloody paradox’, and another, higher in pitch, said, ‘He is that, he should be locked up.’ A female voice occasionally interrupted, saying ‘He is not, he is a
lovely man.’(Mellor, 1970: 16)
Hallucinatoryvoices giving a running commentaryonthepatient’sactivitiesoccurandareoffirst rank.The time sequence of the commentary may be such that it takes place just before,duringorafterthepatient’sactivities.Again,thesymptomisnotvolunteeredspontaneouslybutmayquiteoftenbeinferredfromthepatient’scomplaintsagainsthisvoices.Fortheinterviewer,thereisalwaystheproblemofaskingquestionsinsuchawaythatsheis‘let inontheinside’.Sheisaskingquestionsaboutperceptionsthatarequiteobvioustothepatient.Thepatientdoesnotknowthathisparticularperceptionisunique,thatotherpeopledonotsharehisperceptualexperience.Sotheinterviewerhasthedifficultyofaskingquestionsaboutsomethingofwhichshehasnopersonalexperience;thepatienthastoanswerquestionsthat,becauseofhissituation,seemtohavenopoint.Theabnormalthingaboutvoices commentingisthattheyshouldbeexpe-riencedasperceptionsandascomingfromoutsidetheself;manynormalpeoplehavethoughts,recognizedastheirownandcomingfrominsidethemselves,commentingontheiractions:
A 41-year-old housewife heard a voice coming from the house across the road… The voice went on incessantly in a flat monotone describing
everything she was doing, with an admixture of critical comments. ‘She is peeling potatoes, got hold of the peeler, she does not want that potato, she is
putting it back, because she thinks it has a knobble like a penis, she has a dirty mind, she is peeling potatoes, now she is washing them.’
(Mellor, 1970: 16)
Passivityexperiencesarethoseeventsintherealmofsensation,feeling,driveandvolitionthatareexperiencedasmadeorinfluencedbyothers.Theyhavebeenwelldescribedasdelusionsofcontrol,becausethepatient’sexperienceof theeventbeingmadetooccurtakestheformofadelusion. The terms disorders of passivity, made experiences, delusions of control and disorders of personal activity are, inpractice, synonymousand interchangeable.Theevent isexperiencedasalienbythepatientinthatitisnotexperiencedbythepatientashisownbutinsertedintotheself from outside. Passivity experiences of thinking occur as thought withdrawal, thought
9—DISORDER OF ThE ThINkING PROCESS 155
insertionor thoughtbroadcasting. In thought withdrawal, it isbelievedby thepatient thathisthoughtsareinsomewaybeingtakenoutofhismind;hehassomefeelingoflossresultingfromthisprocess.Itmaybecoupledwithotherthoughtpassivityexperiences:
A 22-year-old woman said, ‘I am thinking about my mother, and suddenly my thoughts are sucked out of my mind by a phrenological vacuum extractor,
and there is nothing in my mind, it is empty.’(Mellor, 1970: 16)
In thought insertion, he experiences thoughts thatdonothave the feelingof familiarity, ofbeinghisown,buthefeelsthattheyhavebeenputinhismind,withouthisvolition,fromoutsidehimself.Asinthoughtwithdrawal,thereisclearlyadisturbanceintheself-image,andespeciallyintheboundarybetweenwhatisselfandwhatisnotself;thoughtsthathaveinfactariseninsidehimselfareconsideredtohavebeeninsertedintohisthinkingfromoutside.
A 29-year-old housewife said, ‘I look out of the window and I think the garden looks nice and the grass looks cool, but the thoughts of Eamonn
Andrews come into my mind. There are no other thoughts there, only his …. He treats my mind like a screen and flashes his thoughts onto it like you
flash a picture.’(Mellor, 1970: 17)
In thought broadcasting, thepatientexperienceshis thoughtswithdrawnfromhismindandthen,insomeway,madepublicandprojectedoverawidearea.Theexplanationhegivesforhowthiscanoccurwill,asusualforthecontentofadelusion,dependonhisbackgroundcultureandpredominantinterests:
A 21-year-old student said, ‘As I think, my thoughts leave my head on a type of mental ticker-tape. Everyone around has only to pass the tape through
their mind and they know my thoughts.’(Mellor, 1970: 17)
Obviously,carefulenquirymustbemadeaboutthenatureof‘influence’or‘control’.Thereisaphenomenologicalworldofdifferencebetweenthestatements‘Mythinkingis influencedbymyparentsinasmuchasmythoughtsarecrowdedfromthebackintothefrontofmyhead’–apassivityexperience,and‘WhatIdoisinfluencedbymyfatherinthatIponderwhathewoulddointhecircumstancesandthendothesame’(or‘dotheopposite’)–notpassivity.Allpassivityexperiencesare regardedasfirst ranksymptoms.It isnot reallyofgreat significance todecidewhichtypeofpassivityisdescribed–whetheritis,forexample,passivityofimpulseorofvolition–butitisimportantdiagnosticallytodecidewhetheritisapassivityexperienceornot.Passivity of emotionoccurswhentheaffect that thepatientexperiencesdoesnot seemtohimtobehisown.Hebelievesthathehasbeenmadetofeelit:
A 23-year-old female patient reported, ‘I cry, tears roll down my cheeks and I look unhappy, but inside I have a cold anger because they are using me in this
way, and it is not me who is unhappy, but they are projecting unhappiness onto my brain. They project upon me laughter, for no reason, and you have no
idea how terrible it is to laugh and look happy and know it is not your, but their reaction.’
(Mellor, 1970: 17)
156 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
In passivity of impulse, thepatient experiences adrive,whichhe feels is alien, to carry outsome motor activity. The impulse may be experienced without the subject carrying out thebehaviour.AJewishwoman,aged55,sufferingfromschizophreniasaid,‘Ifeelmyhandgoinguptosalute,andmylipssaying“HeilHitler”…Idon’tactuallysayit…Ihavetotryveryhardtostopmyarmfromgoingup…theyputdrugsinmyfood;thatiswhatmakesithappen’.Ifcarried out, the action is admitted to be the patient’s own, but he feels that the impulse thatprecipitatedhimintodoingitwasnothisown.
A 26-year-old engineer emptied the contents of a urine bottle over the ward dinner trolley. He said, ‘The sudden impulse came over me and I must do it. It was not my feeling, it came into me from the X-ray department, that was
why I was sent there for implants yesterday. It was nothing to do with me, they wanted it done. So I picked up the bottle and poured it in. It seemed
all I could do.’(Mellor, 1970: 17)
Similarly,withpassivity of volitionthepatientfeelsthatitisnothiswillthatcarriedouttheaction.
A 29-year-old shorthand typist described her actions as follows, ‘when I reach my hand for the comb it is my hand and arm which move, and my fingers
pick up the pen, but I don’t control them… I sit there wanting them to move, and they are quite independent, what they do is nothing to do with me … I
am just a puppet who is manipulated by cosmic strings. When the strings are pulled my body moves and I can’t prevent it.’
(Mellor, 1970: 17)
Somatic passivity is thebelief thatoutside influences areplayingon thebody. It isnot thesameashaptichallucination,butitisadelusionalbeliefthatthebodyisbeinginfluencedfromoutsidetheself.Itmayoccurinassociationwithvarioussomatichallucinations.Forexample,akinaesthetichallucinationoccurred,withapassivityexperiencegivenasexplanation,byapatientwhofeltthathishandwasbeingdrawnuptohisface.Hecouldfeelitmovingalthough,infact,itwasmotionless.Somaticpassivitymayalsooccurinassociationwithanormalpercept;theseexperiencesarequitecommoninschizophrenia.
A 38-year-old man had jumped from a bedroom window, injuring his right knee which was very painful. He described his physical experience as,
‘The sun-rays are directed by US army satellites in an intense beam which I can feel entering the centre of my knee and then radiating outwards causing
the pain.’(Mellor, 1970: 16)
Firstranksymptomsareofgeneraluse,diagnostically,inclinicalpractice,andtheyhavealsobeenadaptedforpsychiatricresearch.Themethodofascertainingandmeasuringschizophrenicsymptoms, among other symptoms, developed by Wing etal. (1974) in their Present StateExaminationusesfirstranksymptomsasabasisfordiagnosingschizophrenia.ThePresentStateExaminationprovidestheclinicianwithameansofascertainingwhichsymptomsandsyndromesarepresent.

9—DISORDER OF ThE ThINkING PROCESS 157
Koehler(1979), inareviewofthewaydifferentauthorsdescribethepresenceoffirstranksymptomsintheEnglishliterature,consideredthattheyweresometimesusedinaverynarrowandsometimesaverywidesense.Hemakesthedistinctionbetweenalienationofthoughtandinfluenceofthought,andmakesapleaforclearstatementsontheboundarycriteriaforfirstranksymptomsandthenosologicalbiasattachedto thephenomena.FromthequotedexamplesofMellorabove,alienationisnecessary;thatis,adelusionofcontrolandnotjustanexperienceofinfluenceof thought.Similarly, thoughtbroadcastingwouldbe regardedasoffirst rankwhenthepatientdescribes this ashavingoccurredoutsidehis control, irrespectiveofwhether thesethoughtsaresharedwithothers.Thus,thischapterisrecommendinganarrowuseoffirstranksymptoms. First rank symptoms have been employed to establish the diagnosis; they are notnecessarilyusefulprognostically(BlandandOrn,1980).
This differencebetween alienationor experience of control and influence canbe exempli-fied by the schizophrenic symptom of thought insertion. Thought insertion is more concretethan the insertionof an idea intoone’s thinking.Anormalpersonmay say, ‘mymother gaveme the idea’ or even ‘the idea was put into my head by my mother’. Neither of these isthought insertion. The patient experiencing passivity believes that by some concrete processtheboundariesofhisself involvingthinkingaresoinvadedthathismotherisactuallyplacingthoughts inside his head (Chapter 12), so that he thinks her thoughts, or perhaps she, isthinkinginsidehim.
ReferencesAggernaesA,HaugstedR,MyschetskyA,PaikinHandVitgerJ(1976).Areliableclinicaltechniquefor
investigationoftheexperiencedrealityandunrealityqualitiesconnectedwitheverydaylifeexperiencesinpsychoticandnon-psychoticpersons.Acta Psychiatrica Scandinavica53,241–57.
BionWR(1962)Thepsycho-analyticstudyofthinking.International Journal of Psychoanalysis43,306–10.BlandRCandOrnH(1980)Schizophrenia:Schneider’sfirst-ranksymptomsandoutcome.British Journal
of Psychiatry137,63–8.Bleuler E (1911) Dementia Praecox or the Group of Schizophrenias (transl. Zinkin J, 1950). New York:
InternationalUniversitiesPress.Cameron N (1944) Experimental analysis of schizophrenic thinking. In Kasanin JJ (ed.) Language and
Thought in Schizophrenia.Berkeley:UniversityofCaliforniaPress.CarpenterWTandBuchananRW(1994)Schizophrenia.New England Journal of Medicine330,681–90.ChenEYH,McKennaPJandWilkinsA(1995)Semanticprocessingandcategorizationinschizophrenia.
InSimsA(ed.)Speech and Language Disorders in Psychiatry.London:Gaskell.CuttingJ(2011)A critique of psychopathology.ForestRow:TheForestPublishingCompany.FishFJ(1962)Schizophrenia.Bristol:JohnWright.FishF(1967)Clinical Psychopathology.Bristol:JohnWright.FrithCD(1992)The cognitive neuropsychology of schizophrenia.Hove:LawrenceErlbaumAssociates.Gathercole(1965)Anoteonsometestsofover-inclusivethinking.British Journal of Medical Psychology38,
59–62.GoldsteinK(1936)Themodificationofbehaviourconsequenttocerebrallesions.Psychiatric Quarterly10,
586–610.IsräelsHandSchatzmanM(1993)Theseductiontheory.History of Psychiatry4,23–60.JaspersK (1962)General Psychopathology (transl.Hoenig J andHamiltonMW).Manchester:Manchester
UniversityPress.JonesE(1962)The Life and Work of Sigmund Freud.Harmondsworth:Penguin.KoehlerK(1979)First ranksymptomsofschizophrenia:questionsconcerningclinicalboundaries.British
Journal of Psychiatry134,236–48.KraepelinE(1904)Lectures on Clinical Psychiatry(transl.JohnstonET).NewYork:Hafner.LiddlePF(2001)Disordered Mind and Brain: the Neural Basis of Mental Symptoms.London:Gaskell.McGhieA(1969)Pathology of Attention.Harmondsworth:Penguin.MellorCS(1970)Firstranksymptomsofschizophrenia.British Journal of Psychiatry117,15–23.

158 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
MellorCS,SimsACPandCopeRV(1981)Changesofdiagnosisinschizophreniaandfirstranksymptoms:aneightyearfollow-up.Comprehensive Psychiatry2,184–8.
Morgan R (1977) Three weeks in isolation with two chronic schizophrenic patients. British Journal of Psychiatry131,504–13.
PayneRW,HochbergACandHawksDV(1970)Dichoticstimulationasamethodofassessingthedisorderofattentionofanover-inclusiveschizophrenicpatient.Journal of Abnormal Psychology76,185–93.
Roth I (2004) Imagination. In Gregory RL (ed.) The Oxford Companion to the Mind. Oxford: OxfordUniversityPress.
SchneiderC(1930)Psychologie der Schizophrenie.Leipzig:Thieme.SchneiderK(1959)Clinical Psychopathology,5thedn.(transl.HamiltonMW).NewYork:Grune&Stratton.ShimkunasAM(1972)Conceptualdeficitinschizophrenia:are-appraisal.British Journal of Medical Psychology
45,149–57.SmithEEandKosslynSM(2007)Cognitive Psychology: Mind and Brain.NewJersey:PrenticeHall.Sutherland NS (1976) Breakdown: a Personal Crisis and a Medical Dilemma. London: Weidenfeld &
Nicholson.SwiftJ(1667–1745)Tale of a Tub.London:Dent.WebsterR(1995)Why Freud Was Wrong.London:HarperCollins.WeinerLB(1966)Psychodiagnosis in schizophrenia.NewYork:Wiley.WingJK,CooperJEandSartoriusN(1974)The Measurement and Classification of Psychiatric Symptoms: an
Instruction Manual for the PSE and Catego Program.Cambridge:CambridgeUniversityPress.WinnicottDW(1957)The Child and the Family: First Relationships.London:TavistockPublications.

159
C H A P T E R 10
Disorder of Speech and Language
SummarySpeechistheaspectoflanguagethatcorrespondstothemechanicalandarticulatoryfunctionsthat allow language to be vocalized, whereas language is itself a complex system based on anumberofelementsincludingphonemes,syntacticstructure,semantics,prosodyandpragmatics,alldesignedtoaidcommunicationandtoencodefactsinmemory.Abnormalitiesofspeecharecommon in neurology but rare in psychiatry. Language and thinking disorders are intricatelyaffectedinpsychiatricdisorders,particularly inschizophrenia.Theactualrelationshipbetweenthinkingandlanguageisyettobefullyelucidated.
To speak is not only to utter words, it is to propositionize. A proposition is such a relation of words that it makes one new meaning.
J. Hughlings Jackson (1932)
Itisveryobviousthatthefunctionsofthinkingandspeakingoverlapandcannotbereadilyseparatedfromeachother;atthesametime,theyareclearlydifferent.Thecontentsofthischaptercannotbeconsideredin isolationfromitspredecessor,althoughthisoneconsidersspeechandlanguagefromadifferentperspective.
Maher (1972)proposedamodel thatattempted todemonstrate the linkbetween thinkingandthebehaviourofspeechinlanguage:
conceptualizing the relationship between language and thought. The model might be likened to a typist copying from a script before her. Her copy may
appear to be distorted because the script is distorted although the communication channel of the typist’s eye and hand are functioning correctly.
Alternatively, the original script may be perfect, but the typist may be unskilled, making typing errors in the copy and thus distorting it. Finally, it
is possible for an inefficient typist to add errors to an already incoherent script. Unfortunately, the psychopathologist can observe only the copy
(language utterances): he cannot examine the script (the thought). In general most theorists concerned with schizophrenic language have accepted the first of
the three alternatives, namely that a good typist is transcribing a deviant script. The patient is correctly reporting a set of disordered thoughts. As
Critchley put it: ‘Any considerable aberration of thought or personality will be mirrored in the various levels of articulate speech – phonetic, phonemic,
semantic, syntactic and pragmatic’. The language is a mirror of the thought.(p. 3)
Thescriptis likenedtothoughtandthetypisttolanguage.Mostclinicianshavetakentheview that language closely mirrors thought and see the primary abnormality as the thinking
Keywords: Language,Speech,Aphasia,Mutism,Alogia.
10—DISORDER OF SPEECh AND LANGUAGE 159.e1
160 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
disorder(Beveridge,1985).Disorderedlanguageisthenseenasmerelyareflectionofthisunder-lyingdisturbance,withdiagnosisofthoughtdisorderonlypossibleonthebasisofwhatthepatientsays.Someofthemorerecent linguistictheoriesusedfortheanalysisofschizophrenicspeechcontradicttheprimacyofthinking.
The assumption that language directly mirrors thought can be challenged (Newby, 1995).Thereisatraditionthatarguesthatlanguageitselfstructuresthinkingandconcepts,anddeter-mineshowtheworldisunderstood.ThisviewderivesfromtheworksofEdwardSapir(1884–1939) and Benjamin Whorf (1897–1941). In essence, the Sapir–Whorf hypothesis says thatlanguageinfluencescognition.Thereisverylimitedempiricalsupportforthisview,andPinker(1994)concludesthat‘therepresentationsunderlyingthinking,ontheonehand,andthesen-tencesinalanguage,ontheother,areinmanywaysatcross-purposes.…PeopledonotthinkinEnglishorChineseorApache;theythinkinalanguageofthought.Thislanguageofthoughtprobablylooksabitlikealltheselanguages;presumablyithassymbolsforconcepts,andarrange-mentsofsymbolsthatcorrespondtowhodidwhattowhom’.Thisradicalviewcontradictsthepoint-to-pointrelationshipbetweenlanguageandthoughtimplicitinMaher’sproposition(seeabove)andthelinguisticdeterminismoftheSapir–Whorfhypothesis.
Therelationshipbetweenthinkingandlanguageisascomplicatedfororganicdisordersasitisforschizophrenia:therecanbequitemarkeddisturbanceintheuseoflanguagewithnoappar-ent thoughtdisorder.This is revealed in the rare isolatedabnormalitiesof specific functionoflanguage described in this chapter. An understanding of how the healthy person expressesthoughtsinlanguagecanbeachievedonlybystudyofthenormaldevelopmentoflanguage.Thisis outside the scope of this book but is discussed in relation to perception in Carterette andFriedman(1976).
Languageisbuiltupofanumberofelements.Phonemesarethemostbasicsoundsthatareavailableforuse in language,andanyparticular language,suchasEnglish,usesonlya limitedrepertoireofphonemes.Therepertoireused inEnglishmayshareonlya limitedoverlapwiththatused,forexample,inYoruba.Morphemesareproducedfromphonemesandarethesmallestmeaningfulunitofaword,andcombinationsofmorphemesmakeupwords.Amorphememaybeawordsuchas‘do’or‘un’.Syntax(grammar)istheallowablecombinationofwordsinphrasesandsentencesandincludestherulesthatdeterminewordorder.Semanticsarethemeaningsthatcorrespondtothewordsandincludethemeaningofallpossiblesentences.Prosodyreferstothemodulationofvocalintonationthatinfluencesaccents,andalsotheliteralandemotionalmean-ingsofwordsandsentences.Thepragmaticsof languagearethewaysthat language isusedinpractice.Thisisarelativelynewareaofstudy.Itreferstothemultiplepotentialmeaningsofanyutterance,whichrequiresknowledgeofcontextandof thespeakers for full interpretation.Forexample, the sentence ‘this room is cold’ can have any of several meanings depending on theidentityofthespeaker,thecontextoftheutteranceandwhoisbeingaddressed,thatisthesocialorrelativedistanceoftheaddressee.Itisperhapsimportanttodistinguishbetweenlanguageandspeechforourpurpose.Speechistheaspectoflanguagethatcorrespondstothemechanicalandarticulatoryfunctionsthatallowlanguagetobevocalized.Thus,forlanguagetobecomespeechthevocalcords,thepalate,thelipsandthetongueneedtoperformacomplexandsynchronizeddanceofintricatesteps.Thedissociationbetweenpoorlyarticulatedspeechandintactlanguageindicatesthatthesetwofunctionsareseparate.
Chomsky’stheoryoflanguageisthemostinfluential(Chomsky,1986).Essentially,Chomskyarguedthatlanguageislikeaninstinct,andfurthermorethat‘everysentencethatapersonuttersorunderstandsisabrandnewcombinationofwords,appearingforthefirsttimeinthehistoryoftheuniverse.Thereforealanguagecannotbearepertoireofresponses;thebrainmustcontainarecipeorprogrammethatcanbuildanunlimitedsetofsentencesoutofafinitelistofwords.Theprogrammemaybecalledamentalgrammar’(Pinker,1994).Inadditiontothis,childrenrapidlydevelopthesecomplexgrammarswithoutformalinstruction.Thissuggeststhattheymustbeinnatelyendowedwithaplancommontothegrammarsofalllanguages,auniversalgrammar.
10—DISORDER OF SPEECh AND LANGUAGE 161
Howlanguagedevelops,howwordmeaningislearnedandtheneuropsychologyoflanguageareallareasofincreasingstudy.
Speech DisturbancesThissubjectisdealtwithintextbooksofneurologyandhasbeenreviewedbyCritchley(1995);it is only summarized here. Many abnormalities, such as paraphasia, have both organic andpsychogenic causes (see above);diagnosiswill require fullmedical andpsychiatrichistory andneurologicalandmentalstateexamination.
APHONIA AND DYSPHONIA
Aphoniaisthelossoftheabilitytovocalize;thepatienttalksonlyinawhisper.Dysphoniadenotesimpairmentwithhoarsenessbutwithoutcomplete lossof function. Itoccurswithparalysisoftheninthcranialnerveorwithdiseaseofthevocalcords.
Aphoniamayalsooccurwithoutorganicdiseaseindissociative aphonia,notuncommonasapresentationamongear,noseandthroatoutpatients.Suchapatientmayspeakina‘stagewhisper’;phonationmayfluctuateaccordingtotheresponseofthosethepersonisaddressing.
DYSARTHRIA
Disordersofarticulationmaybecausedbylesionsofthebrainstemsuchasbulbarandpseudo-bulbarpalsy.Itmayalsooccurwithstructuralormusculardisordersofthemouth,pharynx,larynxandthorax.Idiosyncraticdisordersofarticulationaresometimesseeninschizophreniaandalso,perhaps,withpersonalitydisordersconsciouslyproduced.
STUTTERING AND STAMMERING
Thesehaveinthepastbeenenquiredaboutinthepsychiatrichistoryunderneuroticdisturbancesof childhood, along with such behaviour as nail biting. However, psychogenic aetiology hascertainlynowbeenproved,andanyassociationwithneuroticismmaywellbesecondarytothebarriersincommunicationthatstutteringcauses.
LOGOCLONIA
Thisdescribesthespasticrepetitionofsyllablesthatoccurswithparkinsonism(Scharfetter,1980).Thepatientmaygetstuckusingaparticularword.
ECHOLALIA
Thepatientrepeatswordsorpartsofsentencesthatarespokentohimorinhispresence.Thereisusuallynounderstandingofthemeaningofthewords.Itismostoftendemonstratedinexcitedschizophrenicstates,withmentalretardationandwithorganicstatessuchasdementia,especiallyifdysphasiaisalsopresent.
CHANGES IN THE VOLUME AND INTONATION OF SPEECH
Manydepressedpatientsspeakveryquietlywithamonotonousvoice.Manicpatientsoftenspeakloudlyandexcitablywithmuchvariationinpitch.Excitedpatientswithschizophreniamayalsospeakloudly;intonationandstressesonwordsmaybeidiosyncraticandinappropriate.Noneof
162 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
thesemodesofbehaviourhasdiagnosticsignificance.ThespeedandflowoftalkmirrorsthatofthoughtandhasbeendealtwithinChapter9.
UNINTELLIGIBLE SPEECH
Speechmaybeunintelligibleforseveralreasons,andmostoftheabnormalitiesdescribedhere,iftakentoextremes,willresultinincomprehensibility.
■ Dysphasia may be so profound that, although syllables are produced, speech isunintelligible.
■ Paragrammatism(disorderofgrammaticalconstruction)andincoherence of syntaxmayoccurin severaldisorders.Recognizablewordsmaybe soderanged in their sentencesas tobemeaningless–word salad, asoccurs in schizophrenia. Inmania, the speedof associationmaybesorapidastodisruptsentencestructurecompletelyandrenderitmeaningless,whileindepressionretardationmaysoinhibitspeechthatonlyunintelligiblesyllables,oftenofamoaningnature,areproduced.
■ Privatemeaningmayoccurinschizophreniawiththeuseof(a)newwordswithanidiosyn-cratic,personalmeaning–neologisms; (b) stock wordsandphrases inwhichexistingwordsareusedwithspecial individualsymbolicmeaning;or(c)aprivate languagethatmaybespoken(cryptolalia),orwritten(cryptographia).
Organic Disorders of LanguageDysphasicsymptomsareprobablymoreusefulclinicallythananyothercognitivedefectinindi-catingtheapproximatesiteofbrainpathology(Davidetal,2007).However,theauditory,visualandmotormechanismsofspeecharespreadthroughseveraldifferentpartsofthebrain;often,severalfunctionsareaffectedandlesionsareusuallydiffuse,andthusprecisebrainlocalizationisnotoftenpossible.Ninetyper centof right-handedpeoplewithout anybraindamagehavespeech located in the lefthemisphere,and10percenthave righthemisphere speech.Amongthosewhoareleft-handedorambidextrous,64percenthavelefthemispherespeech,20percentrighthemisphereand16percentbilateralspeechrepresentation.
SENSORY DYSPHASIA
Thetermsaphasia anddysphasia areoftenused interchangeably.However,aphasia implies thelossoflanguagealtogether,anddysphasiaimpairmentof,ordifficultywith,language.Dysphasiaisconventionallydividedforclassificationpurposesintosensory(receptive)andmotor(expressive)types.Veryfrequently,thereisaglobalimpairmentoflanguagewithevidenceofimpairmentofbothelements.Table10.1summarizessomeoftheabnormalitiesthatoccurwiththedifferentaspectsoflanguagethatareimpaired.
Pure Word Deafness (Subcortical Auditory Dysphasia)
Inpure word deafness,thepatientcanspeak,readandwritefluently,correctlyandwithcompre-hension.Hecannotunderstandspeech,eventhoughhearingisunimpairedforothersounds;hehearswordsassoundsbutcannotrecognizethemeaningeventhoughheknowsthattheyarewords.Thisisthereforeaformofagnosia(lackofrecognition)forthespokenword.
Pure Word Blindness (Subcortical Visual Aphasia)
Thepatientwithpure word blindness canspeaknormallyandunderstandthespokenword;hecanwritespontaneouslyandtodictationbutcannotreadwithunderstanding(alexia).Thecondi-tionisthereforeagnosic alexia without dysgraphia.Hemayhavemoredifficultywithprintedthan
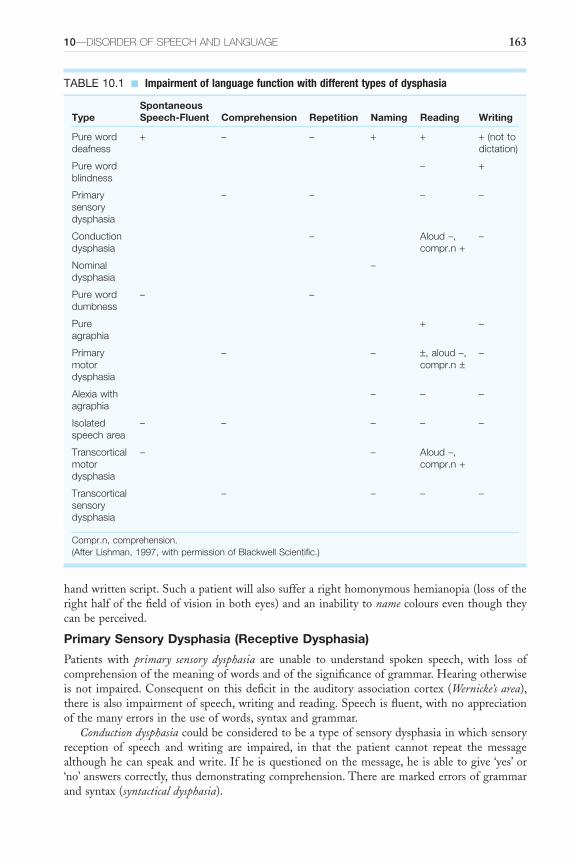
10—DISORDER OF SPEECh AND LANGUAGE 163
handwrittenscript.Suchapatientwillalsosufferarighthomonymoushemianopia(lossoftherighthalfofthefieldofvisioninbotheyes)andaninabilitytonamecolourseventhoughtheycanbeperceived.
Primary Sensory Dysphasia (Receptive Dysphasia)
Patients with primary sensory dysphasia are unable to understand spoken speech, with loss ofcomprehensionofthemeaningofwordsandofthesignificanceofgrammar.Hearingotherwiseisnot impaired.Consequentonthisdeficit in theauditoryassociationcortex (Wernicke’s area),thereisalsoimpairmentofspeech,writingandreading.Speechisfluent,withnoappreciationofthemanyerrorsintheuseofwords,syntaxandgrammar.
Conduction dysphasiacouldbeconsideredtobeatypeofsensorydysphasiainwhichsensoryreception of speech and writing are impaired, in that the patient cannot repeat the messagealthoughhecanspeakandwrite.Ifheisquestionedonthemessage,heisabletogive‘yes’or‘no’answerscorrectly,thusdemonstratingcomprehension.Therearemarkederrorsofgrammarandsyntax(syntactical dysphasia).
TABLE 10.1 ■ Impairment of language function with different types of dysphasia
TypeSpontaneous Speech-Fluent Comprehension Repetition Naming Reading Writing
Pure word deafness
+ – – + + + (not to dictation)
Pure word blindness
– +
Primary sensory dysphasia
– – – –
Conduction dysphasia
– Aloud –, compr.n +
–
Nominal dysphasia
–
Pure word dumbness
– –
Pure agraphia
+ –
Primary motor dysphasia
– – ±, aloud –, compr.n ±
–
Alexia with agraphia
– – –
Isolated speech area
– – – – –
Transcortical motor dysphasia
– – Aloud –, compr.n +
Transcortical sensory dysphasia
– – – –
Compr.n, comprehension.(After Lishman, 1997, with permission of Blackwell Scientific.)
164 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
Nominal Dysphasia
Thepatientwithnominal dysphasiaisunabletoproducenamesandsoundsatwill.Hemaybeabletodescribetheobjectanditsfunctionandtorecognizethenamewhenpresented:apatientdescribedawatchasa‘clockvessel’.Typically,‘empty’nounssuchas‘thing’and‘object’areusedfrequentlywhile‘distinguishing’nounsrarely.Speechisflat,thestructureofsentencesgenerallycorrectandunderstandingunimpaired.
Jargon Dysphasia
Injargon dysphasiaspeechisfluent,butthereissuchgrossdisturbancetowordsandsyntaxthatitisunintelligible.Theintonationandrhythmofspeechareretained.Thisisconsideredaseveretypeofsensorydysphasia;thereisfailuretoevaluatethepatients’ownspeech,inthatpatientsarenotemotionallydisturbedwhenlisteningtorecordingsoftheirowngrosslyimpairedspeech.
MOTOR APHASIA
Pure Word Dumbness
Thepatientwithpure word dumbnessunderstandsspokenspeechandwritingandcanrespondtocomments.Writingispreservedbutspeechisindistinctandcannotbeproducedatwill.Thereisnolocaldisturbanceofmusclesrequiredinspeaking,andthedisabilityisanapraxialimitedtomovementsrequiredforspeech.
Pure Agraphia
Pure agraphia is an isolated inability to write which may also occur with unimpaired speech(agraphia without alexia);thereisnormalunderstandingofwrittenandspokenmaterial.Thisistheequivalentforwritingofpureworddumbnessinspeech.
Primary Motor Dysphasia
Inprimary motor dysphasiathereisdisturbancetotheprocessesofselectingwords,constructingsentencesandexpressingthem.Speechandwritingarebothaffected,andthereisdifficultyincarryingoutcomplexinstructions,eventhoughunderstandingforbothspeechandwritingmaybepreserved.Thepatientfindsitdifficulttochooseandpronouncewords,andspeechishesitantandslow;herecognizeshiserrors,triestocorrectthemandisclearlyupset.Gesturemaybeusedtoreplaceverbalcommunication.Speechisattemptedandrecognizedasspokenwords,butwordsareomitted,sentencesshortenedandperseverationoccurs.
Alexia with Agraphia
Visual aspects of language are construed as being more complex than auditory, in that visualschemataarerequired–‘seeingthewrittenwordinsidehishead’,in additiontoauditory–‘hearingthewordsinone’shead’.Inalexia with agraphia,thepatientisunabletoreadorwrite,butspeak-ingandunderstandingspeecharepreserved.Alexia inthisconditionissimilar tothatofpurewordblindness:thepatientcannotunderstandwordsthatarespeltoutaloud,showingthatheiseffectivelyilliteratebecauseofdisturbanceofthevisualsymbolismoflanguage.
Isolated Speech Area
Impairedcomprehensionmayoccurwithslow,hesitantspeechinanabnormalityinwhichitisassumedthattheanatomicalWernicke’sandBroca’sareasandtheconnectionsbetweenthemareintactbutconnections fromotherpartsof thecortexwith this languagesystemaredisturbed.Twotypes,expressiveandreceptive,aredescribed:transcortical motor dysphasiaandtranscortical sensory dysphasia.

10—DISORDER OF SPEECh AND LANGUAGE 165
Mostfrequently,ofcourse,withdysphasia,thereisamixtureofexpressiveandreceptiveele-mentsandtheclearsyndromescannotbedemonstrated,buttheirsignificanceispartlytheoreticalindemonstratingtherangeofanatomicallesionsandthespecificityofresultantsymptoms.Thisdescriptionhasbeenexclusivelyconcernedwiththesymptoms;precisedescriptionoftheana-tomicallesionsandofassociatedneurologicalsymptomsisoutsideourscope.Itisimportanttodistinguish thephenomenaofdysphasia,perhapswithneologismsanddefectsof syntax, fromthe word salad of schizophrenia with superficially similar defects of language. Verbigerationdescribes the repetition of words or syllables that expressive aphasic patients may use whiledesperatelysearchingforthecorrectword.
MUTISM
Mutism, refraining from speech during consciousness, is an important sign in psychiatricillnesswithanextensivedifferentialdiagnosis.Eliciting thehistory andmental statebecomesimpossible in a mute patient. All the major categories of psychiatric disorder may manifestmutism:learningdisability,organicbraindisease(sometimesdrug-related),functionalpsychosisandneurosisandpersonalitydisorder.Somemorespecificcausesincludedepressiveillness,cata-tonicschizophreniaanddissociativedisorder.Mutismoccursasanessentialelementofstupor(Chapter3),anditisnecessarytoassessthelevelofconsciousnessaspartofafullneurologicalexaminationforallpatientswiththissign.Ifthereisnoloweringofconsciousness,asinfunctionalpsychoses and neuroses, it is likely that the mute patient understands everything that is saidaroundhim.Aswellasspecificbraindisorders,thecausesofstuporincludegeneralmetabolicdisorders that also affect the brain, such as hepatic failure, uraemia, hypothyroidism andhypoglycaemia.
Schizophrenic Language DisorderDefectivecommunicationin languageis thedefiningcharacteristicofschizophreniaaccordingtoCrow(1997),anditisassociatedwithgeneticvariationatthetimelanguagewasacquiredbyHomo sapiens.Theuseoflanguagebypeoplewithschizophreniacandifferfromthatinnormalpeople,andthisdifferencecanbesubtleandunrelatedtopositivesymptomssuchasdelusionsandhallucinations.There isgood reason tobelieve that theabnormalitiesof languageuseareassociatedwiththoughtdisorder.Theprecisenatureofthelanguageabnormalityhassofardefiedclarification,andthisaccountisprovisional; itdescribesthewaysomeofthephenomenahavebeenviewedandconceptualized.Thereisnosingleexplanatorytheorythatunifiesthedisparateabnormalitiesthathavebeenobservedanddescribed.InvestigationintolanguagedisordermaybeascribedtooneofthefourmodelsshowninTable10.2.
TABLE 10.2 ■ Models for investigating language disorder in schizophrenia
Model of Language Technique Employed
Concept of thought disorderBehavioural learning theoryStatistical modelLinguistic model
Psychiatric: clinical description of schizophrenic speechWord association test, multiple choice vocabulary testThe Cloze technique, type : token ratioAnalysis of syntax, cohesion or propositions
(After Beveridge, 1985, with permission.)
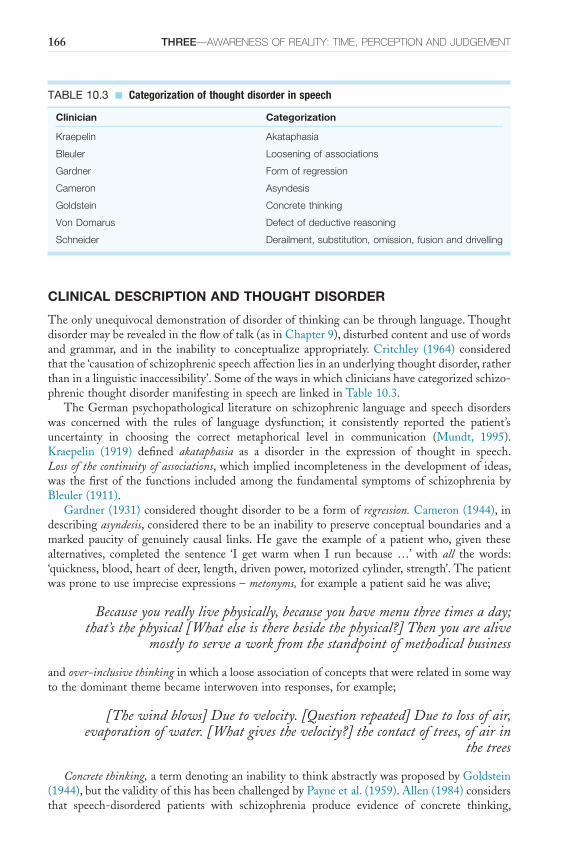
166 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
CLINICAL DESCRIPTION AND THOUGHT DISORDER
Theonlyunequivocaldemonstrationofdisorderofthinkingcanbethroughlanguage.Thoughtdisordermayberevealedintheflowoftalk(asinChapter9),disturbedcontentanduseofwordsandgrammar, and in the inability to conceptualize appropriately.Critchley (1964) consideredthatthe‘causationofschizophrenicspeechaffectionliesinanunderlyingthoughtdisorder,ratherthaninalinguisticinaccessibility’.Someofthewaysinwhichclinicianshavecategorizedschizo-phrenicthoughtdisordermanifestinginspeecharelinkedinTable10.3.
TheGermanpsychopathological literatureonschizophrenic languageandspeechdisorderswas concerned with the rules of language dysfunction; it consistently reported the patient’suncertainty in choosing the correct metaphorical level in communication (Mundt, 1995).Kraepelin (1919) defined akataphasia as a disorder in the expression of thought in speech.Loss of the continuity of associations,whichimpliedincompleteness inthedevelopmentof ideas,was thefirstof the functions includedamongthe fundamental symptomsofschizophreniabyBleuler(1911).
Gardner(1931)consideredthoughtdisordertobeaformofregression.Cameron(1944),indescribingasyndesis,consideredtheretobeaninabilitytopreserveconceptualboundariesandamarked paucity of genuinely causal links. He gave the example of a patient who, given thesealternatives, completed the sentence ‘I get warm when I run because …’ with all the words:‘quickness,blood,heartofdeer,length,drivenpower,motorizedcylinder,strength’.Thepatientwaspronetouseimpreciseexpressions–metonyms,forexampleapatientsaidhewasalive;
Because you really live physically, because you have menu three times a day; that’s the physical [What else is there beside the physical?] Then you are alive
mostly to serve a work from the standpoint of methodical business
andover-inclusive thinkinginwhichalooseassociationofconceptsthatwererelatedinsomewaytothedominantthemebecameinterwovenintoresponses,forexample;
[The wind blows] Due to velocity. [Question repeated] Due to loss of air, evaporation of water. [What gives the velocity?] the contact of trees, of air in
the trees
Concrete thinking,atermdenotinganinabilitytothinkabstractlywasproposedbyGoldstein(1944),butthevalidityofthishasbeenchallengedbyPayneetal.(1959).Allen(1984)considersthat speech-disordered patients with schizophrenia produce evidence of concrete thinking,
TABLE 10.3 ■ Categorization of thought disorder in speech
Clinician Categorization
Kraepelin Akataphasia
Bleuler Loosening of associations
Gardner Form of regression
Cameron Asyndesis
Goldstein Concrete thinking
Von Domarus Defect of deductive reasoning
Schneider Derailment, substitution, omission, fusion and drivelling

10—DISORDER OF SPEECh AND LANGUAGE 167
thinkingwithoutinferringandrestrictedtowhatisexplicitlystated,whilenon-speech-disorderedpatientswithschizophreniadonot.Whenthethematicorganizationofspeechwasanalyzedforpatients with positive speech disorder (incoherence of speech) or negative speech disorder(poverty of speech), there was no difference found: speech-disordered patients, positive aswellasnegative,showedcognitiverestrictionandproducedfewerinferencesthannon-speech-disorderedpatients.
A deficiency in the logic of deductive reasoning in schizophrenia was suggested by VonDomarus (1944). Some of the abnormalities of thinking expressed in speech observed bySchneiderhavebeendiscussedinChapter9.
AnattempthasbeenmadebyAndreasen(1979)toclassifythedescriptionofpatients’cogni-tiveandlinguisticbehaviouronthephenomenademonstratedwithoutmakinginferencesaboutconceptsof‘global’thoughtdisorder;theseabnormalitiesoccurinbothmaniaandschizophrenia.Sometypesofthoughtdisorder,suchasneologismandblocking,occurredtooinfrequentlytohavediagnosticsignificance.However,shefoundhighreliabilitybetweenraterswithmanytypesofthoughtdisorderandalsodiscriminationbetweendifferentpsychoticillnesses.Derailment,lossofgoal,povertyofcontentofspeech,tangentialityandillogicalitywereparticularlycharacteristicofschizophrenia.Derailment implies looseningofassociationsothat ideasslipontoeitheranobliquelyrelated,ortotallyunrelated,theme.Loss of goalisthefailuretofollowachainofthoughtthroughtoitsnaturalconclusion.Poverty of content of speechincludespovertyofthought,emptyspeech,alogia,verbigerationandnegativeformalthoughtdisorder;patients’statementsconveylittleinformationandtendtobevague,over-abstract,over-concrete,repetitiveandstereotyped.Tangentialitymeansreplying toaquestion inanobliqueoreven irrelevantmanner.Illogicalityimpliesdrawingconclusionsfromapremisebyinferencethatcannotbeseenaslogical.
Misuse of Words and Phrases
Thepatientwithschizophreniasometimesshowsmisuseofwordsinthathehas,intheterminol-ogyofKleist(1914),adefectofwordstorage.Hehasarestrictedvocabularyandsouseswordsidiosyncratically to cover a greater range of meaning than they usually encompass.These arecalledstock words or phrases,andtheirusewillsometimesbecomeobviousinalongerconversationinwhichanunusualwordorexpressionmaybeusedseveraltimes.Forexample,apatientused‘dispassionate’asastockword,anduseditfrequentlywithabizarreandidiosyncraticmeaninginthecourseofafewminutes’speech.Awomanwhowasdelusionallyconcernedthatthepolicewere intruding into her private affairs interspersed her conversation, often bizarrely, with theexpression‘confidentiallyspeaking’.
Thisabnormalityappearspartlytoreflectapovertyofwordsandsyntaxandalsoanactivetendencyforwordsorsyllablesbyassociationtointrudeintothoughts,andthereforespeech,soonafterutterance.InthesampleofspeechinChapter9,thefollowingwordscouldbeseenasstimuliandresponses,byintrusion:‘means’–‘ways’,‘opens’–‘closed’,‘holdingbackthetruth’–‘bynomeanswillIspeak’,‘writtenquestions’–‘bymeansofwriting’,‘miracle’–‘Holyland’.Theyalsoappear to be stock words or phrases in that they are used with greater frequency and with agreaterrangeofmeaningthanisnormalandcorrect.
Wordscarryasemantic halo,thatis,theirconstellationofassociationsisgreaterthanjustthedictionarymeaningoftheword.Aboyaged16stealsanapple.IfIcallhim‘atrespasser’,ithasbiblicalassociations;‘acriminal’suggestsagreaterdegreeofviciousnessthantheactionmerits;‘adelinquent’ is readily associatedwithhis youthfulnessbecauseof thephrase ‘juveniledelin-quent’. The constellations of associations in patients are disordered in that they often makeapparentlyirrelevantassociations.Thesemaybeexplainedbymisperceptionofauditorystimuliwithspecificinattention;theactualmediationofassociationsinpatientswithschizophreniamaybe similar to that inhealthypeople.This comes someway toexplainingwhy theassociationsseemappropriatesubjectivelytothepatienthimself,ashedoesnotrealizethathehasmisper-ceived the cue: it seems reasonable tohimbut isquite irrelevant to the interviewer.Toquote
168 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
Maher, ‘What seems to be bizarre is not the nature of the associations that intrude into theutterance,butthefactthattheyintrudeatall’(Maher1972,p.9).
Among the disorders of words, neologism is well recognized. A patient believed that histhoughtswereinfluencedfromoutsidehimselfbyaprocessof‘telegony’.Althoughsuchaworddoesactuallyexist,thepatienthadnonotionofthisnorwhatitmeant.Hecreatedthewordtodescribe a unique experience of his for which no adequate word existed. A 47-year-old malepatient with schizophrenia and expansive mood described himself thus: ‘I am the triplicateactimetric kilophilic telepathic multibillion million genius’ – which does suggest a certaingrandiosity!
TheunintentionalpunsofschizophreniahavebeenexplainedbyChapmanetal.(1964).Ifawordhasmorethanonemeaning,itislikelythatoneusageisdominant.Forexample,themajorityofpeople,inmostcontexts,wouldbemorelikelytousetheword‘bay’torefertoaninletofthesea than to a tree, thenoise ahoundmakes, the colour of ahorse, anopening in awall, thesecondbranchofastag’shorn,anuncomfortableplaceatwhichtostandoreven,phonetically,aTurkishgovernor!Thereisamarkedtendencyinschizophreniatoshowintrusionofthedomi-nantmeaningwhen thecontextdemands theuseofa lesscommonmeaning.Chapmanetal.(1964)usedasentencesuchas‘thetennisplayerleftthecourtbecausehewastired’andaskedpatientswithschizophreniatointerpretitsmeaningwithoneofthreedifferentexplanations:onereferring toa tenniscourt,one toacourtof lawandonealtogether irrelevant.Ananalysisofresponsesshowsthatdominantmeanings,hereacourtoflaw,intrudeintotheresponsesquitefrequently,butintrusionofminormeaningsislessfrequent.
Maherhasdescribeddisorderoflanguageinschizophreniainwhichintrusionoccursthroughclang associationswith the initial syllableof apreviousword: ‘the subterfuge and themistakenplannedsubstitutions’(Maher1972,p.13).Thisisunliketheclangassociationsthatoccurnor-mallyinpoetryandinhumourandalsoinmanicspeech,inwhichtheclangoccursinterminalsyllables.Therepetitivenessofspeechdisorderisalsothoughttobeassociatedwiththeintrusionofassociations:thenormalprocessofeliminatingirrelevantassociationsdoesnottakeplace,sothatawordinaclausewillprovokeassociationsbypun,clangandideationalsimilarity.Whenthatclauseiscompleted,asyntacticallycorrectclausemaythenbeinserted,disruptingmeaningbutdemonstrablyassociatedwiththatpreviouswordoridea.
Maherconsidersthataninabilitytomaintainattentionmayaccountforthelanguagedistur-bancesseeninsomepatients.Disturbedattentionallowsirrelevantassociationstointrudeintospeech,similarlytothedisturbanceaffectingthefilteringofsensoryinput.Inthistheory,normalcoherentspeechisseenastheprogressiveandinstantaneousinhibitionofirrelevantassociationstoeachutterance,andsothedeterminingtendencyproceedswiththeactiveeliminationofthoseassociations thatarenotgoal-directed.This isbutoneofmanypotential explanations for theobservedabnormalities.
Destruction of Words and Grammar
Alogiaisatermusedtodescribenegativethoughtdisorder,orpovertyofthoughtsasexpressedinwords.Correspondingly,paralogiaisusedtodescribepositivethoughtdisorder,ortheintrusionofirrelevantorbizarrethought.Paraphasiaisadestructionofwordswithinterpolationofmoreor lessgarbled sounds.Although thepatient isonlyable toproduce thisnon-verbal sound, itclearlyhassignificanceormeaningtohim.Literal paraphasiaisgrossmisuseofthemeaningofwordstosuchanextentthatstatementsnolongermakeanysense.Verbal paraphasiadescribesthe lossoftheappropriatewordbutthestatementsarestillmeaningful, forexampleapatientdescribedachairas‘afour-leggedsit-up’.
Disturbancesinthewordsandtheirmeaningsaremuchmorecommoninschizophreniathandisturbance of grammar and syntax. However, grammar is also sometimes altered; the loss ofpartsofspeechisdescribedasagrammatism.Adverbsareoccasionallylost,resultingincoarsening
10—DISORDER OF SPEECh AND LANGUAGE 169
andpovertyofsentences,aformoftelegramese.Forexample,‘richtableisworn;thewomanisrichtowrite;sonisalsolamentation’.This,aswellasshowingstock words(rich–lamentation),showslossofpartsofspeech,forexampletheindefinitearticle.Themeaningismoredisjointedthanthegrammar.Paragrammatismoccurswhenthereisamassofcomplicatedclausesthatmakenosense inachievingthegoalof thought.However, the individualphrasesare, in themselves,quitecomprehensible.
Itseemsprobablethattherulesofsyntaxarepreservedinschizophrenialongafteramarkeddisturbanceintheuseofwords,sothat,ifintheprecedingclauseanintrusiveassociationweretoreplacetheword‘rules’,thewordusedwouldprobably,correctly,beanoun.Forinstance,thepatientabovemighthavesaidinthiscontext‘thelamentationsofsyntaxare…’
Inadditiontotheobservedabnormalitiesdescribedabovetherearesuggestionsthatpatientswithschizophreniademonstratelackofuseofcohesivetiesindiscourse(seeMcKennaandOh,2005forafulldiscussion).Cohesivetiesindiscoursearedevicesthatareutilizedtolinksentencestogether, sothatspeech isnotmerelyacollectionofunrelatedsentences.Thereare fourmaintypesofcohesiveties:reference,conjunction, lexical cohesionandellipsis.References inEnglisharepersonalpronounssuchas‘he’,‘she’,‘they’,‘it’;demonstrativesaresuchwordsas‘this’and‘that’;andcomparatives such termsas ‘smaller than’, ‘equal to’, etc. In the following sentences ‘I met Peter yesterday.Hewas wearing a dark suit’.‘He’isareferencetie.Inthesentence‘She went to the High Street this morning and bought some cakes from the supermarket’.‘And’isaconjunctiontie.Alackofuseofcohesivetiesmeansthatthelistenerindialoguewithapatientwithschizophreniacanhavedifficultyfollowingthespeechofthepatient.
PSYCHOGENIC ABNORMALITIES
Andreasen(1979)showedthattheabnormalitiesoflanguagepresentinschizophreniawerealsopresentinmania.Furthermore,McKennaandOh(2005)makethecasethatthereisacontinuumoflanguageorthoughtdisturbancefromschizophreniathroughmooddisordertoorganicdis-orderssuchasepilepsyandfronto-temporaldementia.ThepointthatMcKennaandOhwantto emphasize is that language abnormalities in schizophrenia have a neurological substrate,linkingtheobserveddisturbancestoaphasia,areturntotheideasthatoriginatedwithKleistinthe20thcentury.
Manicspeechhasbeenanalyzed,andthespeechandnumberofassociationsdemonstratedinflight of ideas andpressure of talk is seen in thegreaternumberof cohesive linksoccurring inmanicspeech.Thecontentofdepressivespeechis,ofcourse,influencedbythemoodstate,andsoalsoisthechoiceofwords.Sentencestendtobeshortandhavefewerandsimplerassociations,withretardation.
Hysterical mutismmayoccurasanabnormalreactiontostress.Amanaged35hadbeenunabletotoleratethecontinualnaggingfromhiswifeandhertwosisterswholivedwiththem.Oneday,afterheavydrinkingthepreviousevening,hesmashedhiswife’sfurnitureathomeandthenbecamemutefor24hours.Hewaseventuallyreferredfromtheaccidentandemergencydepart-ment to the psychiatric ward, and speech returned gradually over the next two to three dayswithoutothertreatment.
With the phenomenon of approximate answers (Chapter 5), the patient gives an incorrectanswertoasimplequestion:‘Howmanylegshasasheep?’–‘Five’.Thisis,accordingtoAndersonandMallinson(1941),‘a falseresponseto theexaminer’squestionwheretheanswer,althoughwrong,indicatesthatthequestionhadbeengrasped’.Thissymptommayoccurinanumberofconditions,includingschizophreniainwhichitisoftenassociatedwithfatuousmood;dissociativedisorder,previouslydesignatedhystericalpseudodementia(beforemakingsuchadiagnosis,thewisepsychiatrist thoroughlyexcludesanorganiccause);Ganser’s syndrome;andotherorganicconditions.
170 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
Eccentricandpedanticuseofwordsmaysometimesbeseeninthosewithanankastic personal-ity;obsessionalityobtrudesintothechoiceofwordsandconstructionofsentences.
STATISTICAL MODEL OF LANGUAGE
TheClozeprocedureinvolvesdeletingwordsfromthetranscriptsofspeechandassessingwhetherthe omitted word can be predicted. Maher considered that, in schizophrenia, the greater theseverityoftheillness,thegreateristhedegreeofunpredictabilityoftheutteranceoflanguage.Innormal speech,a largepart of every sentence could be omittedwithout losing themeaning.Forexample,ifthewords‘a…part…couldbe…the’wereomittedfromthelastsentence,themeaningwouldstillbeobvious;ifletterswereomittedfromwords,forinstancenrml spech,themeaningisstillclear.Predictabilityistheabilitytopredictthemissingwordsaccurately;inthissense,schizophrenicsareunpredictableintheirspeech.Theyarelikelytouseunexpectedwordsandphrases.Intheperceptionoflanguage,theschizophrenicpatientislessabletogaininforma-tionfromtheredundancies,bothsemanticandsyntactic,ineverydayspeech.
AsophisticationoftheCloze procedurehasbeeninvestigatedbyNewby(1998).Thisinvolvesthefollowing.
■ ThemodifiedClozeprocedure,inwhichthenatureoftheinsertedwordisnoted,suchasitspartofspeech.
■ InthereverseClozeprocedure,thought-disorderedpatientswereaskedtomakesenseofascriptthathadbeenmutilatedbyinstitutingtheClozeprocedure,forexamplebydeletingeveryfourthorfifthword.Patientswithschizophreniaperformedsignificantlyworsethana control groupof orthopaedicpatients,withmanic-depressivepatients intermediate onbothmodifiedandreverseClozeprocedures.
Schizophrenicspeechisconsideredlesspredictablethannormalspeech,andlackofpredict-ability is more marked with clinically manifest thought disorder (Manschreck etal., 1979).AnexperimentwascarriedoutusingtheClozeprocedure,inwhichraterswereaskedtoassesspassages of schizophrenic ornormal speechwith the fourthorfifthworddeleted.Withfifthworddeletion, thought-disorderedschizophrenic speechwassignificantly lesspredictable thannormalornon-thought-disorderedschizophrenicspeech;thislatterwasnolesspredictablethannormalspeech.
WhetherschizophrenicspeechisreallylessredundantthannormalhasbeenquestionedbyRutter(1979),whowasabletodemonstratenodifference.TheviewthatschizophreniclanguagecanbereducedtosuchsimplemathematicalruleshasbeenrejectedbyMandelbrot(1965).Butstudiesusingthistechniquecontinue,evenifsporadically,anddemonstratethatthespeechandlanguageofpatientswithpsychosismaybelesspredictablethanthatofcontrols(AdewuyaandAdewuya,2006).
Thetype : token ratioisameasureofthenumberofdifferentwordsascomparedwiththetotalnumberofwords(Zipf,1935).Maherconcludedthatthetype:tokenratioofschizophrenicswaslowerthanfornormalsubjects.Thetendencyofschizophrenicpatientstorepeatcertainwordsandusetheminanidiosyncraticwayisreferredtoastheuseofstock words.
LINGUISTIC APPROACHES TO SCHIZOPHRENIA
Variouslinguistictheorieshavebeenappliedtoschizophrenia(forafulldiscussionseeMcKennaandOh,2005).Thesemethodsofanalysisofschizophrenic languageare tentativeanddonotyetcovertherangeofabnormalitiesoccurringinthecondition.Chomsky(1959)proposedthathumansareabletousestringsandcombinationsofwordstheyhaveneverheardbeforethroughuse of a limited set of integrative processes and generalized patterns. However, Moore andCarling(1982)havelabelledChomskyanlinguisticsacontainerviewoflanguage,separatedfrom

10—DISORDER OF SPEECh AND LANGUAGE 171
therealwayusersoflanguageapplyittotheirownmeaningsandcontexts.Individualcasestudieshaveusedtape-recordedinterviewswithpatientswithschizophreniatodemonstratedistinctiveabnormalities.However,on closer analysis suchabnormalities areoften found tooccur in thespeechofnormalpeople,althoughlessfrequently.Afurtherstudyofbilingualpatientsshowedpsychoticsymptomstobepresentintheirnativelanguagebutabsentintheirsecondlanguage.Theproblemofindividualstudiesis,ofcourse,theextenttowhichtheycanbegeneralizedtoallpatientswithschizophrenia.
Syntactical Analysis
Instudiesofspeechanalyzedforsyntax,comparedwithmanicandnormalcontrols,patientswithschizophrenia showed less complex speech, fewer well-formed sentences, more semantic andsyntactic errors and less fluency.There were also marked use of paraphrasias, agrammatisms,anomia,pronounwordproblems,circumlocutions,etc.Theseproblemsseemedtobeassociatedwithageneralintellectualimpairment(McKennaandOh,2005).Suchstudiesdonot,ofcourse,justifytheconclusionthatdifferencesareduedirectlytothediseaseortothoughtdisorder,nordoesittakeintoaccountthesocialcontextoremotionalaspects.However,markeddifferencesareofinterestwhenoneconsidersthatthemajorityofpatientswithschizophreniadonotshowovertdisorderoflanguage.
Propositional Analysis
Thisisaformoftextualanalysisinwhichthetextisbrokendownintoitscomponentproposi-tions,andthesearethenrepresenteddiagrammaticallytoshowthe‘mentalgeometry’(Hoffmanetal.,1982).Normalspeechisconsideredtoproceedasinasingletreediagramwithallbranchesleading from a single key proposition, but psychotic speech more often breaks the ‘rules’ ofpropositionalrelationships.
Observers, listening to the speech of schizophrenic patients, are often struck with itsoddityanddeviance.IthasbeenconsideredbyChaika(1995)thatthisisnotpurelyadeficitofsyntaxbutmoreaphenomenonlikesevereandrepeatedslipsofthetongue,inwhichtheerrorisalapseofexecutivecontrol,alapseofvolition.IthasbeenshownbyMorice(1995)thatwithincreasing complexity of syntax there is an increase in the number of errors in the speech ofschizophrenicpatients;speakersexpressingverysimplesentencesmaderelativelyfewerrors.Oneofhispatientsexpressedthis:‘andcommunicatingordinarilyIcanget lost inthechaosofthelanguage’.
Thisfindingwas confirmedbyThomasandLeudar (1995)using theHunt test, awrittentest in which subjects produce syntactically complex sentences from simple input phrases.Communication-disorderedschizophrenicpatientsmademoreerrorsthannon-communication-disorderedschizophrenicpatientsornormalcontrols,andtheseerrorsweremorelikelytooccurwithmorecomplexsyntacticstructures.Thepatientswerethereforethoughttohaveadiscretefailureoflanguageprocessingthatwasdistinctfromthemoregeneralcognitivedisordersofthecondition.
Althoughthesemethodsarestillexperimental,thepatient’suseoflanguageandsyntaxdoesenable a quantitative method of evaluating the mental state and subjective experience to bedeveloped.Studyoflanguagedisordershouldbeanareainwhichdescriptivepsychopathologycancontributetopsychiatricresearch.
ReferencesAdewuya OA and Adewuya AO (2006) Predictability of speech and language in Nigerian patients with
psychosis:acontrolledstudy.Psychiatric Research143,199–204.AllenHA(1984)Positiveandnegativesymptomsandthethematicorganisationofschizophrenicspeech.
British Journal of Psychiatry144,611–17.
172 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
AndersonWEandMallinsonWP(1941)Psychogenicepisodesinthecourseofmajorpsychoses.Journal of Mental Science87,383–96.
Andreasen NC (1979)Thought, language and communication disorder. Archives of General Psychiatry 36,1315–30.
BeveridgeA(1985)Language disorder in schizophrenia.MPhilthesis,UniversityofEdinburgh.Bleuler E (1911) Dementia Praecox: or the Group of Schizophrenias. New York: International University
Press.CameronN(1944)Experimentalanalysisofschizophrenicthinking.InKasaninJ(ed.)Language and Thought
in Schizophrenia.Berkeley:UniversityofCaliforniaPress.CarteretteGandFriedmanMP(1976)Handbook of Perception Volume VII, Language and Speech.NewYork:
AcademicPress.ChaikaE(1995)Onanalyzingschizophrenicspeech:whatmodelshouldweuse?InSimsACP(ed.)Speech
and Language Disorders in Psychiatry.London:Gaskell.ChapmanLJ,ChapmanJPandMillerGA(1964)Atheoryofverbalbehaviourinschizophrenia.InMaher
BA(ed.)Progress in Experimental Personality Research,vol. 1.NewYork:AcademicPress.ChomskyN(1959)ReviewofSkinner.Language35,26–58.ChomskyN(1986)Knowledge of Language: its Nature, Origin and Use.NewYork:PraegerPublishers.CritchleyM(1964)Theneurologyofpsychoticspeech.British Journal of Psychiatry110,353–64.CritchleyEMR(1995)Growthpoints intheneurologyofspeedandlanguage.InSimsACP(ed.)Speech
and Language Disorders in Psychiatry.London:Gaskell.CrowTJ(1997)IsschizophreniathepricethatHomo sapienspaysforlanguage?Schizophrenia Research28,
127–41.David AS, Fleminger S, Kopelman MD, Lovestone S, Mellers JDC (2007) Lishman’s Organic Psychiatry:
A Textbook of Neuropsychiatry.Chichester:Wiley-Blackwell.GardnerGE(1931)Themeasurementofpsychoticage:apreliminaryreport.American Journal of Psychiatry
10,963–75.GoldsteinK(1944)Methodologicalapproachtothestudyofschizophrenicthoughtdisorder.InKasaninJS
(ed.)Language and Thought in Schizophrenia.Berkeley:UniversityofCaliforniaPress.Hoffman RE, Kirstein L, Stopek S and Cicchetti DV (1982) Apprehending schizophrenic discourse: a
structuralanalysisofthelistener’stask.Brain and Language15,207–33.JacksonJH(1932)Selected Writings of John Hughlings Jackson.London:HodderandStoughton.KleistK(1914)AphasieundGeisteskrankheit.Munchener Medizinische Wochenschrift61,8.KraepelinE(1919)Dementia Praecox and Paraphasia(transl.BarclayBM).Edinburgh:Livingstone.LishmanWA(1997)Organic Psychiatry: the Psychological Consequences of Cerebral Disorder,3rdedn.Oxford:
Blackwell.MaherBA(1972)Thelanguageofschizophrenia:areviewandinterpretation.British Journal of Psychiatry
120,3–17.Mandelbrot B (1965) Information theory and psycholinguistics. In Oldfield RC and Marchall JC (eds.)
(1968)Language.London:PenguinBooks.ManschreckTC,MaherBA,RucklosMEandWhiteMT(1979)Thepredictabilityofthought-disordered
speechinschizophrenicpatients.British Journal of Psychiatry134,595–601.McKennaPandOhT(2005)Schizophrenia Speech: Making Sense of Bathroots and Ponds that Fall in Doorways.
Cambridge:CambridgeUniversityPress.MooreT and Carling C (1982) Understanding Language: Towards a Post-Chomskyan Linguistics. London:
Macmillan.Morice R (1995) Language impairments and executive dysfunction in schizophrenia. In Sims ACP (ed.)
Speech and Language Disorders in Psychiatry.London:Gaskell.MundtC(1995)Conceptsof schizophrenic languagedisorderandrealityassessment inGermanpsycho-
pathology.InSimsACP(ed.)Speech and Language Disorders in Psychiatry.London:Gaskell.NewbyDA(1995)Analysisoflanguage:terminologyandtechniques.InSimsACP(ed.)Speech and Language
Disorders in Psychiatry.London:Gaskell.NewbyD (1998) ‘Cloze’ procedure refined andmodified: ‘modifiedCloze’, ‘reverseCloze’ and theuseof
predictability as a measure of communication problems in psychosis. British Journal of Psychiatry 172,136–41.

10—DISORDER OF SPEECh AND LANGUAGE 173
Payne RW, Matussek P and George EI (1959) An experimental study of schizophrenic thought disor-der.Journal of Mental Science105,627–52.
PinkerS(1994)The Language Instinct.London:PenguinBooks.RutterDR(1979)Thereconstructionofschizophrenicspeech.British Journal of Psychiatry134,356–9.ScharfetterC(1980)General Psychopathology: An Introduction.Cambridge:CambridgeUniversityPress.ThomasPandLeudarI(1995)Syntacticprocessingandcommunicationdisorderinfirstonsetschizophrenia.
InSimsACP(ed.)Speech and Language Disorders in Psychiatry.London:Gaskell.VonDomarusE(1944)Thespecificlawsoflogicinschizophrenia.InKasaninJS(ed.)Language and Thought
in Schizophrenia.Berkeley:UniversityofCaliforniaPress.ZipfGK(1935)The Psychobiology of Language.Boston:HoughtonMifflin.

This page intentionally left blank

175
C H A P T E R 11
Insight
SummaryInsight,inpsychiatry,referstothecapacityofthepatienttorecognizethattheirmentalsymptomsareindicativeofmentalillnessandthatthesesymptomsrequiretreatment.Itisnowknowntobeassociatedwithimpairedcognitivefunction,andpredictspoorcompliancewithtreatmentandhencewithcompulsoryadmissionandtreatmentinhospital.Theunderlyingneuralmechanismofpoorinsightisstartingtobeilluminatedandislinkedmorewidelytodeficitsinself-awareness,self-monitoring,empathyandtheoryofmind.
A man who knows who and what he is, his position in the world, and what the persons and things are around him; who judges according to known, or intelligible rules; and who, if he has singular ideas or singular habits, can
give a reason for his opinions and his conduct; a man who, however wrong he may act, is not misled by any uncontrollable impulse or passion; who does not idly squander his means; who knows the legal consequences of his actions; who can distinguish between unseemly and seemly behaviour, who feels that which
is proper and that which is improper to utter, according to the circumstances in which he is placed; and who reverences the subject and the ministers of
religion; a man who, if he cannot always regulate his thoughts and his temper and his actions, is not continually in the extremes, and if he errs, errs as much
from benevolence and hesitation, as from passion and excitement, and more frequently: lastly, a man who can receive reproof, and acknowledge when he
has needed correction.John Perceval (1840)
Self-awarenessisabasichumanability.Itreferstotheabilitytorecognizeone’sownexistenceandexperienceandtheexistenceandexperienceofothers.Itincludesthefacilityformonitoringtheeventsinone’sownlife,andtheabilitytomakedecisionsaboutthefutureonthebasisofthatknowledge.Furthermore,itinvolvestheabilitytocommunicatethisawarenessofselfandothers tootherhumanbeings (Marková,1987).This characteristicallyhumanability ispartlythesubjectofSophocles’Oedipus the King,inwhichOedipus’questforself-knowledgeresultedinhisdiscoverythathehadkilledhisownfatherandfatheredchildrenbyhisownmother.Theaphorism‘KnowThyself ’wassaidtobe inscribedattheforecourtoftheTempletoApolloatDelphiandinThe Apology,Socratessays,‘Theunexaminedlifeisnotworthlivingforahumanbeing’.These references to self-knowledge in antiquity underline the place of this notion inhumanlife.
Self-awarenessobviouslytakesinmuchmorethananawarenessofillness,butitisplainthatthe psychiatric notion of insight is a subset of the general concept of self-awareness or self-knowledge.Insightasanotionismuchwiderthanjustknowingwhetheroneisillornot,andif so, having a sensible view regarding treatment. It involves our capacities for introspection,

Keywords: Insight,Self-awareness,Self-monitoring,TheoryofMind.
11—INSIGhT 175.e1

176 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
empathyandcommunication;notonlyisitglimpsingourselvesaswereallyarebutalsoourselvesasothersseeus,andthereforeothersastheyreallyarebecausetheygothroughthesamerepertoireofmentalmechanismsthatwedo.Evenforthemostprivateandinternalofinsights,socialsense,thecapacityforrelationships,empathy,knowinghowourbehaviourwillaffecttheemotionsandexperienceofotherpeopleisimportant.Insightisthedirectproductofknowingourselves.Itisaqualitythathasbeenhighlyvaluedbymostmentalhealthclinicians,becauseastronglinkisassumedbetweenhavinginsightandbetterqualityoflife(McGorryandMcConville,1999).
Although, in psychiatry, we concentrate mostly on the narrow meaning of insight withregardtomentalillness,weneedtoretainthisbroaderconcept.Often,ourworkwithpatientsinvolvesushavinginsightintotheirthinkingandbehaviourbecauseofourcapacityforempathyas fellow human beings and also helping them gain insight into themselves and the roots oftheirproblems.
Therelationshipbetweenthiscapacityforinsightinageneralsenseandthepracticalissuesof treatment is very close. A physician suffering from delusional disorder advertised and soldmagnetsforthemedicaltreatmentofarthritisandhayfever.Hestronglybelievedthatthisformoftreatmentwasofunequalledvalueforvirtuallyallmedicalconditions,andhehadphysicallyassaultedapharmacistwhohadtriedtopersuadehimotherwise.Hedecriedthevalidityofthewholeofpsychiatry, ‘because I ama scientist andeverythinghas tobeprovedwithevidence’.Becauseofhislackofinsightintohisownconditionandthenatureofhisbeliefs,itwasimpos-sibletoinitiatetreatment.Hissymptomspersistedlongterm.
Jaspers (1959) has written about the patient’s attitude to his illness under the followingheadings.
1. Understandableattitudestothesuddenonsetofacutepsychosis(perplexity,awarenessofchange).
2. Workingthroughtheeffectsofacutepsychoses.3. Workingthroughtheillnessinchronicstates.4. Thepatient’sjudgementofhisillness.5. Thedeterminationtofallill.6. Theattitudetoone’sownillness:itsmeaningandpossibleimplications.Allthesepointsabove,andespecially3,4and6,involvetheprocessofinsight,theknowledge
ofoneselfwithparticularreferencetoillness.Apersonwhobecomesseriouslyandsuddenlyill,whateverthenatureoftheillness,afterpreviouslyhavingbeenfitformanyyears,isastonishedbyhischangeofhealthstatus.Suchapersonislikelytoundergoaprofoundchangeinselfandbodyimage.Hehasbecomeapersonwho,frombeinghealthyandseeingillnessassomethingthathappenstootherpeople,nowseeshimselfaspotentiallyfrailandvulnerable.Thiscanbepersonallyenrichingandisnotnecessarilyawhollynegativeexperience.
Insight in Clinical PracticeSothatshecanbetterhelpherpatientwithapossiblementalillness,thepsychiatristasksspecificquestionsaboutthepatient’sopinionsconcerninghisillness.Theseincludehisdegreeofacknow-ledgementofillness,hisattitudestoillness,hisunderstandingoftheeffectsofhisillnessonhiscurrentcapabilitiesandfutureprospects.All thisaddsupto theassessmentof insight intohiscondition. Insight is not an absolute; it can vary in its impairment with different facets ofthe condition, for example, a patient could have some limited understanding concerning hisunlikelihoodtoobtainajobcompatiblewithhisqualifications,butvirtuallynounderstandingastohowhispsychoticsymptomsinterferewithrelationships.Thusinsightisnotnowconsideredto be an all-or-none phenomenon, in either clinical evaluation or measurement, but rather adimensionalone,sothatsubjectscanhavedifferentlevelsofawarenessoftheirillness(SurguladzeandDavid,1999).
11—INSIGhT 177
Allmentalillnesseswillalterthepatient’sworldviewandcapacitytocopewithcircumstances.Assessmentof insightmeasures theawarenessof this changeby thepatientandhisability toadapt to the change. Insight is highly complex as a function. It is the understanding of theindividual abouthisown stateofhealth, capacity andworth; it also relates this assessmentofinternalstatetootherpeopleandtheworldoutside.Inotherwords,insightrequiresbothinnerandouterorientation.This aspectof insightbecomesmoreapparent,below, in thediscussionaboutthecontributionofgestaltpsychologytotheconceptualizationofinsight.Insightingestaltpsychologyisorientedtowardsproblemsolvingintheexternalworld,whereasinsightinclinicalpracticeisinner-directed.
David(1990)regardsinsightascomposedofthreedistinct,overlappingdimensions,namely,the recognition of morbid psychological change, the labelling of this change as derivingfrom mental illness and the understanding that this change requires treatment that needs tobe complied with. An assessment schedule was constructed for determining the nature ofinsight, andquantitative lossof insight correlatedwith thedegreeofpsychopathology (Davidetal.,1992).
Oneofthemostfrustratingaspectsofpractisingpsychiatryis,fromthepointofviewofthetreatingprofessional,theapparentinabilityofpatientstorecognizeand/oradmitthattheyarementallyill.Patients,especiallythosewithschizophrenia,oftendenythattheirexperiencesareabnormalandthattheyareunwell.DanielSchreber(1842–1911)describedhisattitudetowardshisauditoryverbalhallucinationsinhisbookMemoirs of My Nervous Illness(Schreber,1955)asfollows:
I noticed therefore with interest that according to Kraepelin’s TEXTBOOK OF PSYCHIATRY (5th edition, Leipzig, 1896, p. 110 ff ) which had been
lent to me, the phenomenon of being in some supernatural communication with voices had frequently been observed before in human beings whose
nerves were in a state of morbid excitation. I do not dispute that in many of these cases one may be dealing with mere hallucinations, as which they are
treated in the mentioned textbook. In my opinion science would go very wrong to designate as ‘hallucinations’ all such phenomena that lack objective reality, and to throw them into the lumber room of things that do not exist.
FurthermoreSchrebercontinues:
Science seems to deny any reality background for hallucinations … In my opinion this is definitely erroneous, at least if so generalized.
ThesequotationsfromDanielSchreberdemonstrateoneofthemostcomplexaspectsofthenatureofinsight.Thisisthecapacitytohaveanattitudetowardsabnormalexperiencesinotherswhereonecanrecognizethemaspathological,buttodenytheabnormalityoftheexperienceinoneself, and to designate it as not being evidence of mental illness. This is so-called double book-keeping.
The resulting refusal to cooperatewith treatment and rehabilitation causes long-term suf-fering for thepatients and their carers. It is this capacityofpatients tounderstand theirownillnessthatisevaluatedclinicallyininsight.Likemanyotherconcepts,terminologicalconfusionexists,withtextbooksdescribinginsightasthepatient’scapacitytoformjudgementsabouttheirown illness and mental state. In recent years, there has been a resurgence of interest in theconcept,withattemptstodefineitreliablyandquantifiablyandtostudyitscorrelates(KumarandSims,1998).

178 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
Overview of the ConceptTheattitudeofthepatienttowardshisillnesshasobviousclinicalimplications,andinsighttriestoassesstheawarenessofthepatientconcerningtheimpacthisillnesshashadonhislifeandhiscapacitytoadapttothechangesbroughtaboutbyit.Asafunction,itishighlycomplexandhastodowithanindividual’sevaluationofhisselfandnon-selfandtheirrelatedness(seeChapter12).Inclinicalpractice,onlycertainaspectsaregivenimportance,suchasthepatient’sawarenessof illness and compliancewithprescribed treatment.The assessmentof insight assumesmoreimportanceinpsychosis,astheincongruencebetweenthepatient’sandothers’viewofhisillnessoftenleadstodifficultieswithtreatment.Theconventioninpsychiatryisthatinsightisunim-pairedinnon-psychoticconditions,butitcanbeseenthatabroaderviewnearertothelexicaldefinitionisrelevantwhenneuroticsymptomshamperthefullrealizationofaperson’spotential.
DEVELOPMENT OF THE CONCEPT
Contributionstothedevelopmentoftheconceptofinsightderivefrompsychopathology,gestaltpsychologyandpsychoanalysis.Ingestaltpsychology,insightisconceivedasasudden,unexpectedsolutiontoaproblem.AccordingtoMarkova(2005),the‘suddenness’specifiesanabruptsolutiontoaproblem,the‘unexpectedness’referstothesurpriseelementoftheeventandtheterm‘solu-tiontoaproblem’signalsthediscretenessoftheeventintime.Inessence,ingestaltpsychology,insightisbydefinitionrelatedtoaspecifictask,aproblemthatstandsinneedofsolutionintheexternalworld.Furthermore,therehasbeenextensivedebatewithingestaltpsychologyaboutthenatureofinsight,whetheritisauniquehumanfacilitythatisalsoaspecificcognitiveskill.Thefactthat,ingestaltpsychology,insightreferstoaproblemintheexternalworlddistinguishesitfromtheconceptofinsightinclinicalpractice.Inclinicalpractice,insightfocusesonunderstand-ingofchangesorhappeningswithinanindividual.
ForJaspers(1959),typicallythepatient’sattitudetohisillnessinvolves‘anawarenessofillness’inwhichthepatient‘expressesafeelingofbeingillandchanged,butthereisnoextensionofthisawarenesstoallhissymptomsnortotheillnessasawhole.Itdoesnotinvolveanyobjectivelycorrectestimateoftheseverityoftheillnessnoranyobjectivelycorrectjudgementofitsparticulartype’.ForJaspers,‘onlywhenallthisispresentandtherehasbeenacorrectjudgementofallthesymptoms and the illness as a whole according to type and severity, can we speak of insight[emphasisinoriginal]’.Thus,forJaspersinsightbecomesmanifestonlywhenthepatientisabletoturnawayfromthecontentofhispsychicexperiencestowardsmakingajudgementaboutitandinquiringintoitscausesandreasons.Lewis’(1934,p.333)definitionofinsightas‘acorrectattitudetomorbidchangeinoneself ’, isarestatementofJaspers’descriptionof insight.Freud(1981)usedtheterminsighttodenoteknowledgeofillnessbut,onthewhole,inpsychoanalytictherapythedevelopmentofadeeperawarenessofselfisconsideredtobethegoaloftreatment.Thisisanotherwayofsayingthatinpsychoanalysis,insightreferstoknowledgeandunderstand-ingofone’sunconsciousmentalprocesses.Thisisamorecomplexnotionofinsight,becauseitinvolvesthepatientacquiringunderstandingoftheunconsciousmotivationsofhisbehaviourand,inthelightofFreud’sstructureofthemind,itsuggestsadegreeofdepthofunderstanding.
David (1990) has proposed that insight is composed of the three overlapping dimensionsdescribedabove.Ithasbeensuggestedthatparallelscanbedrawnbetweenthelossofinsightinpsychiatricpatientsandthelossofawarenessofdiseaseofpartsofthebodyincertainneurologicalconditions.Incorticalblindness,left-sidedhemiplegiafollowingstrokeandamnesicsyndrome,lack of awareness of disease is well recognized.The term anosognosia was coined by Babinski(1857–1932) to refer to the unawareness or denial of hemiplegia seen in patients following astroke.Thereisadifference,though,betweenthelackofinsightseeninpsychiatryandthelackof awareness seen inneurologicaldisease. Inpsychiatry, lackof insight is often attendedby a
11—INSIGhT 179
wider lossof judgementbeyondmerelythesymptomsortheir implicationsforthepatient.Inneurological cases, the lack of awareness is focused on a discrete disability. Nonetheless, eventhoughthe lackof insight inpsychiatryand lackofawarenessofdisease inneurologyarenotidentical,itmaybethatcomparisonsmaypointtopossibleneurobiologicalbasesthattheyshareincommon.
Therearecertainphilosophicalproblemswhenweconsiderinsightinpatientswithpsychosis.Peoplewithoutanypsychiatric illnessvary in their ability toknowthemselvesand theconse-quencesoftheirpersonalities.Becauseatleastsomeconceptualizationsofpsychosisrelyonthelackofinsightasadefiningfeature,discussionconcerningtheconceptcanbecomecircular.Addedtothisisthefactthatvaryingdegreesofinsightcanoccurandthatnon-verbalizationofinsightmaybedifferent fromthe lackof it.Yetanotherproblemis thatapossiblyspeciousmodel inwhicha‘normal’partofthemindiscapableofpassingjudgementonthe‘abnormality’ofanotherparthastobeentertained.Thisworksforaslongastheclinicianrecognizesthatitismerelyawayofspeaking,notnecessarilyanaccuraterepresentationofhowself-monitoringtakesplace.
MEASUREMENT OF INSIGHT
Earlierattempts tomeasure insightcentredon its role inpsychodynamic therapies.TolorandReznikoff (1960) developed a test using hypothetical situations based on common defencemechanisms and found a correlation with intelligence. This test was used by Roback andAbramowitz(1979),whofoundacorrelationinthosewithschizophreniabetweengreatersubjec-tivedistressandbetterbehaviouraladjustment.Thevalidityofthistestforgeneralclinicalworkisaffectedbytheconceptofinsightbeingbasedonpsychodynamicratherthanpsychopathologi-calfeatures.
Anyreliableandvalidmeasureofinsightinclinicalpracticeshouldbebasedonthefollowingfourassumptions:
■ insightiscomplexandmultidimensional■ culturalfactorsneedtobetakenintoaccount■ thelevelofinsightcanvaryacrossthemanymanifestationsofmentalillnesses■ informationaboutthenatureofaperson’sillnessfromsituationsotherthantheinterview
shouldbetakenintoaccount(McGorryandMcConville,1999).McEvoyetal.(1989a)developedaquestionnairetomeasureinsight,definedasthepatient’s
awarenessofthepathologicalnatureofhisexperiencesandalsohisagreementwiththetreatingprofessionalsabouttheneedfortreatment.TheInsightandTreatmentAttitudesQuestionnaire(ITAQ)isavalidated11item,semi-structuredinterviewthatgeneratesascorefrom0(noinsight)to22 (maximum insight).Using thisquestionnaire, they foundno correlationwith aspectsofacutepsychopathology.
The Schedule for Assessment of Insight in Psychosis was published in 1992 (David etal.1992),inwhich,apartfromtherecognitionofmentalillnessandcompliancewithtreatment,theabilitytorelabelunusualmentaleventsaspathologicalwasalsoincluded.Thereweresevenitemswithamaximumpossiblescoreof14andanadditionalitemonhypotheticalcontradiction.
TheScaletoAssessUnawarenessofMentalDisorder(AmadorandStrauss,1993)isamuchmorecomprehensivescalewithsixgeneral itemsandfoursubscales, fromwhichtensummaryscorescanbecalculated.Other scalesavailableare theGlobal InsightScale (Greenfieldetal.,1989)andtheself-reportedInsightScale forPsychosis (Birchwoodetal.,1994).ThescalebyMarkova and Berrios (1991) is more directed to evaluating aspects of self-awareness and lesstoclinicaldefinitionof insightwithregard to illness.This isalso true for theBeckCognitiveInsightScale(Becketal.,2004)whichmeasuresawidernotionofinsight,encompassingpatients’capacityforevaluatingtheiranomalousexperiencesandtheirerroneousinferences.Thescaleiscomposedoftwosubscales:self-reflectivenessandself-certainty.
180 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
Otherapproacheshavebeentousethe‘lackofinsightandjudgement’itemofthePositiveandNegativeSyndromeScale(PANSS;Kayetal.,1987)asasingleglobalmeasureofinsight,andtheuseofpsychopathologyvignettes.McEvoyetal.(1993)usedvignettesthatcastspecificpsychopathologicalfeaturesineverydaylanguagetojudgewhetherpatientsdemonstratedthesefeaturesandthedegreetowhichtheyattributedthemtomentalillness.Theyfoundthatpatientsfailedtoacknowledgenegativesymptomsandfailedtoviewpositivesymptomsasevidenceofmentalillness.
From earlier impressionistic assessments of a global nature, measurement of insight hasmorerecentlyprogressedtotheuseofoperationalizeddefinitionsandstandardizedinstruments.Althoughthedifferentinstrumentsmightbemeasuringdifferentaspectsofacomplexphenom-enon,thereisatleastthefreedomtochooseonetosuitspecificclinicalorresearchaims.Thereisaninversecorrelationbetweeninsight,theseverityofpsychopathologyandpositiveaffectivedisturbance(Sanzetal.,1998).
SCHIZOPHRENIA
Itisnotreallysurprisingthatmostoftheresearchworkontheclinicalcorrelatesofinsighthasbeenonpatientswithschizophrenia.McEvoyetal. (1989a)reportedthat insightasmeasuredbytheITAQdidnotcorrelatewitheithertheseverityofacutepsychopathologyorthechangesin psychopathology with treatment.They speculated whether the mechanisms underlying theproductionofpositivesymptomsanddisturbedinsightwereindependentandwhetherthelatterwasmoreresistanttotheeffectiveuseofneurolepticmedication.Davidetal.(1992)foundthatthe‘totalinsightscore’intheirstudyhadamoderateinversecorrelationwiththePresentStateExamination(Wingetal.,1974)totalscore,whichwasanindicationoftheglobalseverityoftheillness.BothDavidetal.(1992)andMcEvoyetal.(1989b)foundthat,asagroup,involuntary(thatiscompulsorilyadmitted)patientshavelessinsight.Overall,itdoesappearthattherelation-shipbetweenpoorinsightandaspectsofpsychopathologyisnotlinearbutcomplicatedbyotherfactors,includingcompliancewithtreatment.
Insight and Cognitive ImpairmentIthasoftenbeenspeculatedthatpoorinsightmayhaveaneurologicalbasis.LysakerandBell(1994) found that subjects with impaired insight performed more poorly than subjects withunimpairedinsightontheWisconsinCardSortingTest(WCST).TheyusedthePANSSitemof‘lackofinsightandjudgement’tomeasureinsight.Thisitemhadbeenshownbyfactorana-lyticalstudiestobeamemberofthecomponentcomposedofsymptomsofcognitiveimpairmentsuchascognitivedisorganization,poorattention,stereotypedthinkingandpoorabstractthink-ing.However,usingadifferentmethodology,KempandDavid(1996)failedtoshowarelation-shipbetweeninsightandneuropsychologicaldeficits.Itispossiblethatchronicityoftheillnesscouldbeanadditionalvariable,whichpredisposestocognitiveimpairment.Davidetal.(1992)hadfoundarelationshipbetweenaspectsof insightandintellectualperformance.Cuestaetal.(1995) failed to showany relationshipbetween insight andpoorperformanceon theWCST.However,thestudydidnotuseanyofthestandardratingscalestomeasureinsight.Inanotherstudy,Upthegroveetal.(2002)showedthatimpaireddigitspanasameasureofworkingmemorywassignificantlyassociatedwithinsightasmeasuredbyastandardizedmeasure.Additionally,itisbecomingclearerthatinsightcorrelateswithindicesofcognitivefunctionsincludingmeasuresoferrormonitoring,empathyandtheoryofmind(Pegaroetal.,2013;Pijnenborgetal.,2013;Kaoetal.,2013).However,onbalance,theexactnatureandextentoftheserelationshipsisstillunresolved.Asinotherclinicalsituations,therelationshipmaynotbeastraightforwardone,asothervariables,suchasthechronicityofillness,treatmentfactors,andgendermayallbeinvolved.

11—INSIGhT 181
Outcome
Therelationshipbetweeninsightandoutcomeisacomplexone.Firstly,greaterinsightseemstopredicthopelessness,depressionandsuicide(Ampalametal.,2012;BalharaandVerma,2012;Schranketal.,2013).Awarenessoftheadversesocialimplicationsofmentalillnessmaybethemediatingfactorbetweeninsightanddepression(Thomasetal.,2012).
Secondly,McEvoyetal.(1989c)foundthatpatientswithgoodinsightweresignificantlylesslikely toberehospitalizedandtendedtobemorecompliantwithtreatment30daysafterdis-charge;theoverallrelationshipbetweeninsightandoutcomecloselyapproachedstatisticalsig-nificance.Theirmeasureof‘after-careenvironment’,whichaimedtoreflectthedegreetowhichothers’effortswerehelpfullyinvestedinmaintainingthepatientintreatment,wasnotrelatedtoinsight.AmadorandStrauss(1993)alsofoundtheirmeasuresof insighttobecorrelatedwiththecourseoftheillness.
Relatedtotheissueofprognosisandoutcomeiscompliancewithtreatment.Therelationshipbetween poor insight and poor compliance with treatment has been shown by Bartko etal.(1988),Linetal.(1979)andMcEvoyetal.(1989c).
Thebalanceofevidenceseemstobethathigherlevelsofawarenessofhavinganillnessareassociated with better medication compliance and clinical outcome (Amador etal., 1991) inschizophrenia.However, there isa riskofcircularityof logic, in that someof themeasuresofinsightarebasedondefinitionsofinsightthatincludenon-compliance.Moreover,compliancewithprescribedtreatmentisamuchmorecomplexphenomenonaffectedbysocialfactorsandbeliefs about health and sickness (Bebbington, 1995). It is also possible that the relationshipbetweencomplianceanddifferentaspectsofinsightmaybedifferent.Davidetal.(1992)foundthattreatmentcompliancewasnotstronglyrelatedtotheabilitytorecognizeone’sowndelusionsandhallucinationsandtorelabelthemasabnormal.
It is interestingthatpatientsmaycomplywithtreatment,eventhoughtheydonotbelievethemselvestobeill,ifthesocialmilieuisconducive(McEvoyetal.1989b,c).Theroleofhealthbeliefsand illness representation indeterminingcompliancewith treatment is recognized,buthow these interact with insight to influence treatment compliance has yet to be studied.Thedomains of illness representation are identity (the label of the disease), causes (explanatorymodels),timeline(onsetandanticipatedduration),control(beliefthatselfcaninfluenceoutcome)and consequences (functional aswell as other consequences) (Brownlee etal., 2000).What isobvious is that insight is not the only determinant of care-seeking and treatment adherence.McEvoyetal.(1993)proposedthatinsightwouldimprovewithattemptsatpsychosocialreha-bilitation.ThiswasfurtherstudiedbyLysakerandBell (1995)onasampleofpatientswithadiagnosisof schizophreniaor schizoaffectivedisorder.Earlier,Lysakeretal. (1994)had foundinsightasmeasuredbytheitemonPANSStobecorrelatedwithpoorlevelsofworkqualityandparticipationinrehabilitativeprogrammes.Intheirstudyreportedin1995,patientsenrolledinvocationalrehabilitativeprogrammeswerefoundtohaveimprovedinsightafterfivemonths.Thisimprovementwas greater for patientswith comparatively few cognitivedeficits, echoing theirearlier findings regarding a relationship with cognitive impairments. However, the lack of acontrolgrouplimitsthegeneralizabilityofthefindings.Itdoesseemaninterestingsuggestionthatvocationalrehabilitationcanfavourablyaffectinsightintheabsenceofcognitiveimpairment.McEvoyetal.(1993)haveproposedthatenhancedself-esteemfromrehabilitationmayunderlieimprovementininsight.
BIPOLAR DISORDERS
Ghaemietal.(1995)studiedinsightinacutelymanicpatientsusingtheITAQandfoundthatimprovement in insightdidnotcorrelatewith recovery fromother symptoms.However, as inschizophrenia, poor insight was correlated with involuntary admission. Swanson etal. (1995)

182 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
usedthecasevignettemethodtostudyinsightintwogroupsofpatientswithschizophreniaandmania.They foundaqualitativedifferencebetweenmania and schizophrenia, in thatpatientswithschizophreniabutnotmaniahadreducedawarenessoffeaturesoftheir illness.However,althoughthemanicpatientswereawareoftheirsymptoms,theydidnotagreethattheseema-nated from a mental illness. Amador etal. (1994) and Michalakes etal. (1994), on the otherhand,foundnosignificantdifferencebetweenschizophrenicandmanicpatientsonmeasuresofinsight.Theformerfoundthatseverelymanicpatientsweresimilartopatientswithschizophreniaonscoresofinsight,whereasdepressedandschizoaffectivepatientshadmoreinsight.Inconclu-sion,itseemstobethatbothschizophreniaandbipolardisorderpatientshaveimpairedinsightand the mediating factors may be severity of symptoms and cognitive impairment, especiallyworkingmemoryimpairment(Vargaetal.,2007).
CRITICISMS OF THE CONCEPT
Therecentresurgenceofinterestininsighthashaditsshareofcriticism.Medicalanthropologistshavecriticizedtheconceptofinsightforfailingtorecognizethatpeoplecanhavevariouscultur-allyshapedframeworkstoexplaintheirillnesses,allpossiblyvalid.Fromthispointofview,theconceptof insight is ‘Eurocentric and essentially arrogant’ (Perkins andMoodley, 1993), as itdictatesthatpatientsshould,apartfromagreeingthattheyarementallyillandrequiringtreat-ment, also agree to reconstruct their experiences within the terms and concepts of Westernpsychiatry. Johnson andOrrell (1995)have reviewedworkby social scientists on cultural andsocialvariationsinlayperceptionsofmentalillnessandarguethatthesewouldinfluenceinsight.Social and cultural backgrounds influence perceptions of stigma from mental illness and thecongruenceofthepatientswithWesternmedicalviewsofmentalillness.Theabilitytorelabelmentalphenomenaasabnormalmaybe less influencedby social factorswhencomparedwithbeliefs about the causationofmental illness.Although therearevery few studies in this area,evidenceseemstobeemergingthatsocialandculturalfactorsareimportantinthediagnosisofpoorinsight.Forexample,differencesintheethnicbackgroundofthepsychiatristandthepatientappeartoinfluencethejudgementoftheformeraboutinsight( JohnsonandOrrell,1996).
AETIOLOGY OF IMPAIRED INSIGHT
Attempts toexplain thecausationofpoor insighthave focusedon threehypotheses (Amadoretal.,1991;LysakerandBell,1994).Thefirsttwofocusonputativepsychologicalmechanisms.Ithasbeensuggestedthatrefusaltotakeprescribedmedication,implyingpoorinsight,isawilfulpreference for the experience of psychotic phenomenology over drug-induced normality.Thesecondformulationsuggeststhatpatientsdenyillnessatapsychologicalleveltohelpthemcopewithnormallifeastheyrecoverfromapsychosis.Athirdexplanationhassuggestedthatpoorinsightmayhavesomethingtodowithcognitiveimpairment,drawingonsimilaritieswithneu-rologicalconditionssuchasanosognosia.Asmentionedearlier,studieshavefoundasignificantcorrelation between impaired performance on the WCST and poor insight, suggesting thatcognitiveimpairmentsresultingfromfrontallobedeficitsmayunderliepoorinsightinschizo-phrenia.And,afourthexplanationisthatdisruptionofneuralmechanismsandnetworksunderly-ingself-andother-monitoringareinvolved.Inarecentstudy,schizophreniapatientsdemonstratedlessactivationintheposteriorcingulatecortexintheself-andother-reflectionconditionsandlessactivationintheprecuneusintheother-reflectionconditioncomparedwithhealthycontrols.Betterinsightwasassociatedwithgreaterresponseintheinferiorfrontalgyrus,anteriorinsula,andinferiorparietallobuleduringself-reflection.Inaddition,bettercognitiveinsightwasassoci-atedwithhigheractivationinventromedialprefrontalcortexduringself-reflection(vanderMeeretal.,2012).
11—INSIGhT 183
ReferencesAmadorXF,FlumMandAndreasenNC(1994)Awarenessofillnessinschizophreniaandschizoaffective
andmooddisorders.Archives of General Psychiatry51,826–36.AmadorXFandStraussDH(1993)Assessmentofinsightinpsychosis.American Journal of Psychiatry150,
873–9.AmadorXF,StraussDHandYaleSA(1991)Awarenessofillnessinschizophrenia.Schizophrenia Bulletin
17,113–32.Ampalam P, Deepthi R andVadaparty P (2012) Schizophrenia – insight, depression: a correlation study.
Indian Journal of Psychological Medicine34,44–8.BalharaYPandVermaR(2012)Schizophreniaandsuicide.East Asia Archives of Psychiatry22,126–33.BartkoG,HerzogIandZadorG(1988)Clinicalsymptomatologyanddrugcomplianceinschizophrenic
patients.Acta Psychiatrica Scandinavica77,74–6.Bebbington PE (1995)The context of compliance. International Clinical Psychopharmacology 9 (suppl. 5),
45–50.BeckAT,BaruchE,BalterJM,SteerRAandWarmanDM(2004)Anewinstrumentformeasuringinsight:
theBeckCognitiveInsightScale.Schizophrenia Research68,319–29.BirchwoodM,SmithJandDruryV(1994)Aself-reportinsightscaleforpsychosis;reliability,validity,and
sensitivitytochange.Acta Psychiatrica Scandinavica89,62–7.BrownleeS,LeventhalHandLeventhalEA(2000)Regulation,self-regulation,andconstructionoftheself
in themaintenanceofphysicalhealth. InBoekartzM,PintrichPRandZeidnerM(eds.)Handbook of Self-regulation.SanDiego:AcademicPress.
CuestaMJ,PeraltaVandCaroF(1995)Ispoorinsightinpsychoticdisordersassociatedwithpoorperform-anceontheWisconsincardsortingtest?American Journal of Psychiatry152,1380–2.
DavidAS(1990)Insightandpsychosis.British Journal of Psychiatry156,798–808.David AS, Buchanan A, Reed A and Almeida O (1992)The assessment of insight in psychosis. British
Journal of Psychiatry161,599–62.FreudA(1981)Insight: itspresenceandabsenceasafactor innormaldevelopment.InSolintAJ,Eissler
RSandFreudA(eds.)The Psychoanalytic Study of the Child,vol. 36.NewHaven:YaleUniversityPress.GhaemiSN,StollALandPopeHG(1995)Lackofinsightinbipolardisorder:theacutemanicepisode.Journal
of Nervous and Mental Disease183,464–7.GreenfieldD,StraussJSandBowersMB(1989)Insightandinterpretationofillnessinrecoveryfrompsy-
chosis.Schizophrenia Bulletin15,245–52.JaspersK(1959)General Psychopathology(transl.HoenigJandHamiltonMW,1963).Manchester:Manchester
UniversityPress.Johnson S and Orrell M (1995) Insight and psychosis: a social perspective. Psychological Medicine 25,
515–20.JohnsonSandOrrellM(1996)Insight,psychosisandethnicity:acase-notestudy.Psychological Medicine26,
1081–4.KaoYC,LiuYP,LienYJ,LinSJ,LuCW,WangTSandLohCH(2013)Theinfluenceofsexoncognitive
insightandneurocognitivefunctioninginschizophrenia.Progress in Neuropsychopharmacology and Biological Psychiatry44,193–200.
KayS,FiszbeinAandOplerL(1987)ThePositiveandNegativeSyndromeScale(PANSS)forschizophre-nia.Schizophrenia Bulletin13,261–76.
KempRandDavidA(1996)Psychologicalpredictorsofinsightandcomplianceinpsychoticpatients.British Journal of Psychiatry169,444–50.
KumarTMandSimsACP(1998)Insightanditsmeasurementinrelationtopsychosis.Psychiatry Update1,13–8.
LewisA(1934)Thepsychopathologyofinsight.British Journal of Medical Psychology14,332–48.LinIF,SpigaRandFortschW(1979)Insightandadherencetomedicationinchronicschizophrenics.Journal
of Clinical Psychiatry40,430–2.LysakerPandBellM(1994)Insightandcognitiveimpairmentinschizophrenia:performanceonrepeated
administrationsoftheWisconsincardsortingtest.Journal of Nervous and Mental Disease182,656–60.LysakerPandBellM(1995)Workrehabilitationandimprovementsininsightinschizophrenia.Journal of
Nervous and Mental Disease183,103–6.
184 THREE—AWARENESS OF REALITY: TIME, PERCEPTION AND JUDGEMENT
LysakerP,BellMandMilsteinRM(1994)Insightandtreatmentcomplianceinschizophrenia.Psychiatry57,289–93.
MarkováI(1987)Human Awareness: Its Social Development.London:Hutchinson.MarkovaIS(2005)Insight in Psychiatry.Cambridge:CambridgeUniversityPress.Markova IS and Berrios GE (1991) The assessment of insight in clinical psychiatry: a new scale. Acta
Psychiatrica Scandinavica86,159–64.McEvoy JP, Apperson LJ and Appelbaum PS (1989a) Insight in schizophrenia: its relationship to acute
psychopathology.Journal of Nervous and Mental Disease177,43–7.McEvoyJP,ApplebaumPSandAppersonLJ(1989b)Whymustsomeschizophrenicpatientsbeinvoluntar-
ilycommitted?Theroleofinsight.Comprehensive Psychiatry30,13–7.McEvoy JP,FreterSandEverettG(1989c) Insightand theclinicaloutcome in schizophrenia. Journal of
Nervous and Mental Disease177,48–51.McEvoyJP,FreterS,MerrittMandAppersonLJ(1993)Insightaboutpsychosisamongoutpatientswith
schizophrenia.Hospital and Community Psychiatry44,883–4.McGorryPDandMcConvilleSB(1999) Insight inpsychosis: anelusive target.Comprehensive Psychiatry
40,131–42.MichalakesA,SkatasCandCharalambousA(1994)Insightinschizophreniaandmooddisordersandits
relationtopsychopathology.Acta Psychiatrica Scandinavica190,46–9.PegaroLF,DantasCR,BanzatoCEandFuentesD (2013)Correlationbetween insightdimensions and
cognitive functions in patients with deficit or non-deficit schizophrenia. Schizophrenia Research 147,91–4.
PercevalJ(1840)Anarrativeofthetreatmentexperiencedbyagentlemanduringastateofmentalderange-menttoexplainthecausesandthenatureofinsanity.InBatesonG(ed.)Perceval’s Narrative: A Patient’s Account of his Psychosis, 1830–1832.London:HogarthPress.
PerkinsRandMoodleyP(1993)Thearroganceofinsight?Psychiatric Bulletin17,233–4.Pijnenborg GH, Spikman JM, Jeronimus BF and Aleman A (2013) Insight in schizophrenia. European
Archives of Psychiatry and Clinical Neuroscience263,299–307.RobackHBandAbramowitzSI(1979)Insightandhospitaladjustment.Canadian Journal ofPsychiatry24,
233–6.SanzM,ConstableG,Lopez-IborI,KempRandDavidAS(1998)Acomparativestudyofinsightscales
andtheirrelationshiptopsychopathologicalandclinicalvariables.Psychological Medicine28,437–46.Schreber D (1955) Memoirs of My Nervous Illness (trans, edited, with introduction, notes and discussion
MacAlpineIandHunterRA).London:Wm.DawsonandSonsLtd.SchrankB,AmeringM,HayAG,WeberMandSibitzI(2013)Insight,positiveandnegativesymptoms,
hope,depressionandself-stigma:acomprehensivemodelofmutualinfluencesinschizophreniaspectrumdisorders.Epidemiology and Psychiatric Science,29July,1–9(Epub).
SurguladzeS andDavidA (1999) Insight andmajormental illness: anupdate for clinicians.Advances in Psychiatric Treatment5,163–70.
SwansonCL,FreudenreichOandMcEvoyJP(1995)Insightinschizophreniaandmania.Journal of Nervous and Mental Disease193,752–5.
ThomasN,RibauxDandPhillipsLJ(2012)Rumination,depressivesymptomsandawarenessofillnessinschizophrenia.Behavioral Cognitive Psychotherapy,November9,1–13(Epub).
TolorAandReznikoffM(1960)Anewapproachtoinsight:apreliminaryreport.Journal of Nervous and Mental Disease130,286–96.
UpthegroveR,OyebodeF,GeorgeMandHaqueMS(2002)Insight,socialknowledgeandworkingmemoryinschizophrenia.Psychopathology35,341–6.
VanderMeerL,deVosAE,StiekemAP,PijnenborgGH,vanTolMJ,NolenWA,DavidASandAlemanA(2012)Insightinschizophrenia:involvementofself-reflectionnetworks?Schizophrenia Bulletin,October27(Epub).
VargaM,MagnussonA,FlekkoyK,DavidASandOpjordsmoenS(2007)Clinicalandneuropsychologicalcorrelates of insight in schizophrenia and bipolar 1 disorder: does diagnosis matter? Comprehensive Psychiatry48,583–91.
WingJK,CooperJEandSartoriusN(1974)Measurement and Classification of Psychiatric Symptoms.Cambridge:CambridgeUniversityPress.
S E C T I O N FOURSelf and Body

This page intentionally left blank

187
C H A P T E R 12
The Disordered Self
SummaryThe self isaconstruct thathaschanged inmeaningandsignificanceover theyears.Therearefiveputative,formalcharacteristicsoftheself:egovitality,egoactivity,unityoftheselfovertime,self-identityandboundaryoftheself.Theseformalaspectsoftheselfcanbeimpairedbypsy-chiatricdisorders.The senseof vitality canbe impaired toproduce a feelingofdeadness, theextremeexamplebeingnihilisticdelusions. Indisorderofactivity the‘my-ness’ofactions, thesenseofbeinganagentenactingone’swillintheworld,canbedisruptedasoccursinpassivityexperiences.Theunityof theselfover time ismarkedlyaffected inautoscopyanddissociativeidentity disorders. Additionally, disorder of self-identity is illustrated by possession states andphenomenasuchaslycanthropy.Finally,abnormalitiesofthedistinctionbetweenselfandnon-self (disturbance of boundary) is central to our understanding of such diverse experiences inschizophreniaaspassivityexperiences,thoughtinsertionandthoughtwithdrawal.
Often, when I was alone, I sat down on this stone, and then began an imaginary game that went something like this: ‘I am sitting on top of this
stone and it is underneath’. But the stone also could say ‘I’ and think: ‘I am lying here on this slope and he is sitting on top of me’. The question then
arose: ‘Am I the one who is sitting on the stone, or am I the stone on which he is sitting?’ This question always perplexed me, and I would stand up,
wondering who was what now.Jung (1963)
The self was never meant to be a solid object like a stone, a horse, or a weed, nor even a concept to be considered as semantically tantamount to changes in
blood flow or test scores. Of course, patients with disordered minds do sport hurting, afflicted and cursing selves but not as they do carcinomas or broken
legs. Their selves live in the same realm as do their virtues, vices, beliefs and aspirations, and that is where they should remain.
Berrios and Markova (2003)
Ego and SelfThe self is a construct that has changed in meaning and significance since the inception ofHellenisticphilosophy(BerriosandMarkova,2003).Fromthemid-nineteenthcenturyonwards,variousconceptsabouttheselfhavefoundtheirwayintopsychiatrysuchthatincontemporarypsychiatrythereisreckonedtobesomedisturbanceinthewayonethinksaboutandestimatesoneself;this,ofcourse,differsaccordingtothenatureoftheillness.Thereis,however,nocon-sensusonwhatexactly itmeanstobeaself.There isapluralityofconceptions, includingtheecologicalself, the interpersonalself, theextendedself, theprivateselfandtheconceptualself

Keywords: Ego,BodyImage,Self-image,Autoscopy,PossessionState.
12—ThE DiSOrDErED SELF 187.e1
188 FOUR—SELF AND BODY
amongmany(Zahavi,2003).Inthischapter,thetermsegoandselfareusedmoreorlessinter-changeably.Egohastheadvantageofbeingatechnicaltermandthereforemorecircumscribedinitsmeaning;thisisalsoadisadvantagewhenitissimplyoneself,asisusuallyunderstoodandsubjectivelyexperienced,thatisbeingreferredto.
Freud’suseofthewordegoechoesNietzsche(1901):
It is this which sees everywhere deed and doer; this which believes in will as cause in general; this which believes in the ‘ego’ as being, in the ego as
substance, and which projects its belief in the ego-substance on to all things.
Freud(1933)describedegoasstanding‘forreasonandgoodsensewhiletheidstandsfortheuntamedpassions’.Theego:
has been modified by the proximity of the external world with its threat of danger… The poor ego has to serve three severe masters and does what it can
to bring their claims and demands into harmony with one another. These demands are always divergent and often seem incompatible. No wonder that the ego so often fails in this task. Its three tyrannical masters are the external
world, the super-ego and the id.(Freud, 1933)
Self-Concept and Body ImageThebodyisuniqueinthatitisexperiencedbyapersonbothassubjectofexperienceandasanobjectwiththesamematerialityasanyotherphysicalobjectintheworld.ThereisawayinwhichIamsubjectivelyawareofmyownbodythatisdifferentfromhowIexperienceablockofwood.ButIamalsoawarethatmybodyisanobjectintheworld,tobeviewedandevenactedonbyothers.Formostofthetime,wearenotawareofourbodybut,forexampleinextremeanxiety,traumaticpainandsexualexcitement,thereisanawarenessofthebodyasanobject:‘myheartbanging,myfingerthrobbing’.Fortherestofthetimeweassumethepartsofthebodytobeintegrated, and this integratedbody, forpracticalpurposes, coincideswithand is coterminouswith the ‘self ’ of which we are not separately aware and which we take for granted. In otherwords it ismostly in timesofdistressorpain thatwebecomeawareofourbodiesasdistinctfrom ‘ourselves’. It is throughourbody thatwehave contactwith theworldoutsideour self:movementsofthebodyrelateustoexternalspace;ourhandshaveaprehensiletool-likeaspectto them that allow us to grasp objects in the world; and our bodies have a physicality aboutthemthatoccupy space,giveuspresence, locatingus asobjects in theworld.OneofEugeneMinkowski’s(1970)patientssaid:
I don’t want to attach so much attention to my movements, but I am only grub and defaecation. I am only a sort of animal function, and one that
injures himself. I have the feeling of being nothing but living tripe. I have neither sensations nor precise ideas. I have the feeling of being nothing but
vegetative functions, of being nothing but a mass.
Anothersaid:
One day out of two, my body is hard as wood. Today my body is thick like this wall (points to the wall).

12—ThE DiSOrDErED SELF 189
Minkowski referred to these experiences as exaggerated materiality in which the patientsdemonstrateanincreasedawarenessofthe‘objectified’aspectofthebodyandrenderingsalientforthecliniciananattitudetothebodythatisnotmanifestinday-to-daylife.
Manydifferenttermsareusedtodescribethewayapersonconceptualizeshimself.Neurologists,neuropsychiatrists,psychoanalystsandpsychologistshaveusedvariouslythetermsbody schema, body concept, body cathexis, body imageandperceived body.Theydescribeapproximatelythesamethingbutwithdifferentnuances.Forexample, self-concept tendstorefer tothefullyconsciousand abstract awareness of oneself, while body image is more concerned with unconscious andphysicalmattersandincludesexperientialaspectsofbodyawareness.Sometimesself-conceptisthesameasbodyconcept,andatothertimesconsciousselfisconceptualizedasbeingindepend-entofits‘cage’,thebody.Thebody schemaimpliesaspatialelementandismorethan,andusuallybiggerthan,thebodyitself.Forinstance,ifyouimagineyourselfonyourwaytowork,automati-callyincludedwithinyourschemaofyourselfareyourclothesandyourspectacles,ifworn.Thebodyschemachangeswithchangingcircumstances.WhenIdrivemycar,Iincorporatewithinmyconceptofmyphysicalsizethewidthofmycar,sothatIamunlikelytoattempttodrivethrough a doorway or up a flight of steps. Spectacles, a cigar, the carpenter’s screwdriver, theblindman’sstickallcontributetothatperson’sconceptofhisselfinaparticularsituation.Cathexisimpliesthenotionofpower,force,libido–perhapsanalogoustoelectricalcharge:theselfthatmakesthingshappen!
Social aspects are obviously important. A man with shoulder-length hair is not usually soendowedthroughneglect;morelikely,itrepresentsadeliberatechoice–howheseeshimselfinhissocialsetting.Itaccordswithhischosenpeergroupandalsodistinguisheshimfromthosefromwhomhewouldwishtobedisassociated.Critchley(1950)hascommentedon‘thatcuriousemotionalstateusuallyknownasbeinginlove’,inwhichthereis‘acompulsivetrendintwobodyimages of opposite sex towards propinquity and contiguity, eventually culminating in a totalfusionormerger’.Asaphenomenologist,onecouldtakeexceptiontoCritchley’smisuseofthetermcompulsive.AccordingtoSchilder(1935),bodyimagesareneverisolated;theyarealwaysencircled by the body images of others. Body images are more closely bound together in theerogenouszonesandaresocialinnature.Ourbodyimageandthewayotherpeopleseeusarenotexclusivelydependentoneachother.Aperson seeshimself and formshis self-image inasocial setting. He sees himself in relation to other people; his view of himself is not totallydependenton,butimportantlyinfluencedby,howanotherindividualseeshim.Itisalsodeter-minedbyhowhebelievesthatpeoplemightseehim.
ThedevelopmentofbodyimagehasbeenneatlysummarizeddiagrammaticallybyBahnson(1969).Heconsidersthatself-imageischangeableandamorphous.Atanyonetime,theindi-vidualperceivesonlyasmallsamplefromagalleryofpossibleself-images.InFigure12.1,themanner inwhich ‘phenomenological selves are superimposedoneachother like the layersof anonion’isdemonstrated.Differentaspectsofself-imagedevelopasthepersonincreasesthescopeand complexity of his relationships.The term ego is not phenomenologically describable, andtherehasbeenargumentthattheselfcannotobserve itself; that is,a thingandwhatobservesthatthingcannotbethesame.However,itisthenatureofselfandegotobeexperiencedaseithersubjectorobject:asmallnuisancelikeamouthulcercanmakemefeeluncomfortable(subjec-tively);Icandescribewhatapersonwithamouthulcerexperiences(objectively).
Self-Image and Non-Verbal CommunicationInasocialrelationship,apersonexpressesviewshehasabouthimself:hiswords,andthewayhesaysthem,conveyhowheviewshisrelationshipwiththeotherpersonandalsohowheseeshimself,forexampletheshopkeeper‘talkingdown’toachild.Probablymoreimportantthanthisverbal manner of expressing, often unconscious, views on how we see ourselves is non-verbal
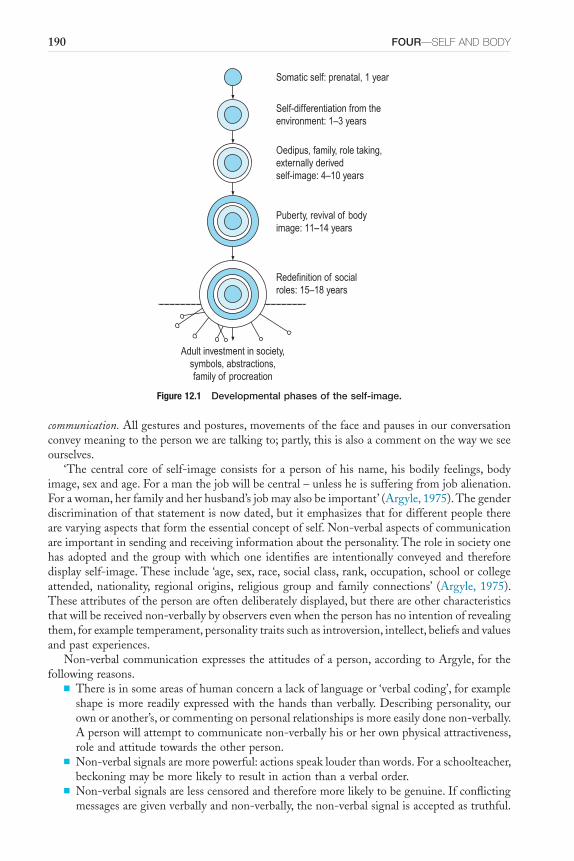
190 FOUR—SELF AND BODY
Figure 12.1 Developmental phases of the self-image.
Somatic self: prenatal, 1 year
Self-differentiation from theenvironment: 1–3 years
Oedipus, family, role taking,externally derivedself-image: 4–10 years
Puberty, revival of bodyimage: 11–14 years
Redefinition of socialroles: 15–18 years
Adult investment in society,symbols, abstractions,family of procreation
communication.Allgesturesandpostures,movementsofthefaceandpausesinourconversationconveymeaningtothepersonwearetalkingto;partly,thisisalsoacommentonthewayweseeourselves.
‘Thecentral coreof self-imageconsists for apersonofhisname,hisbodily feelings,bodyimage,sexandage.Foramanthejobwillbecentral–unlessheissufferingfromjobalienation.Forawoman,herfamilyandherhusband’sjobmayalsobeimportant’(Argyle,1975).Thegenderdiscriminationofthatstatementisnowdated,butitemphasizesthatfordifferentpeopletherearevaryingaspectsthatformtheessentialconceptofself.Non-verbalaspectsofcommunicationareimportantinsendingandreceivinginformationaboutthepersonality.Theroleinsocietyonehasadoptedandthegroupwithwhichone identifiesare intentionallyconveyedandthereforedisplayself-image.Theseinclude‘age,sex,race,socialclass,rank,occupation,schoolorcollegeattended, nationality, regional origins, religious group and family connections’ (Argyle, 1975).Theseattributesofthepersonareoftendeliberatelydisplayed,butthereareothercharacteristicsthatwillbereceivednon-verballybyobserversevenwhenthepersonhasnointentionofrevealingthem,forexampletemperament,personalitytraitssuchasintroversion,intellect,beliefsandvaluesandpastexperiences.
Non-verbalcommunicationexpressestheattitudesofaperson,accordingtoArgyle,forthefollowingreasons.
■ Thereisinsomeareasofhumanconcernalackoflanguageor‘verbalcoding’,forexampleshapeismorereadilyexpressedwiththehandsthanverbally.Describingpersonality,ourownoranother’s,orcommentingonpersonalrelationshipsismoreeasilydonenon-verbally.Apersonwillattempttocommunicatenon-verballyhisorherownphysicalattractiveness,roleandattitudetowardstheotherperson.
■ Non-verbalsignalsaremorepowerful:actionsspeaklouderthanwords.Foraschoolteacher,beckoningmaybemorelikelytoresultinactionthanaverbalorder.
■ Non-verbalsignalsarelesscensoredandthereforemorelikelytobegenuine.Ifconflictingmessagesaregivenverballyandnon-verbally,thenon-verbalsignalisacceptedastruthful.

12—ThE DiSOrDErED SELF 191
■ Somemessages,becauseof social censorship, cannotbemadeexplicit in a social settingandthereforecannotbeverbalizedbutcanbeconveyednon-verballybyappropriateposture,gestureandmovementinspace.Forexample,byfacialexpressionandturningaway,apersonmightsuggestwithoutmaking itexplicit‘Idonot likeyouandamboredwithspeakingtoyou’.
■ Verbalmessagesarepunctuatedandemphasizednon-verbally,forexamplethepauseattheendofaphraseorthecadenceofvoiceused.Theseembellishmentsaddmeaningtotheactualwordsused.
Apersoninteractswithothersbytheuseoflanguage.However,non-verbalsignalsarealsoimportantinexpressingmeaningandconveyingfeelings.Theegotalkswiththebodyaswellaswithwords.
Awareness of the BodyWehaveanawarenessofourselfandanawareness,whichoverlapswiththisbutisslightlydif-ferent,ofourbodies.What is thissenseofbodyimageorawareness?AccordingtoHeadandHolmes (1911), thebody schema is formedas thecompositeexperienceof sensations.Schilder(1935)developedfurthertheimportanceofperceivingsensationsinformingthebodyschema:‘thepictureofourownbodywhichweforminourmind,that istosay,thewayinwhichthebodyappearstoourselves’.Freud(1933)alsowasconcernedwithbodyimageinthedevelopmentofpersonality:‘theegoisfirstlythebodyego’.Clearly,abnormalityofbodyimagemaybetheresultofabnormal sensations,but this isnotalways so.For instance, theabnormalityofbodyimageofanamputeeisdirectlybecauseofthephysicaldamage,butahypochondriacalpatientmayhavenoabnormalsensationsyetbelieveshehascancer.Intranssexualism,amanmayhaveanormalsensoryexperienceofhisbodybutsaysthathehateshisbodyandespeciallyhispenis;hemayfeelthatheisactuallyawomantrappedinsideamalebody(Morris,1974).Hisdisturbedbody image isnot a resultofdisturbed sensation; there is a conflictbetweenego (thewayheexperienceshimselfandthegenderheascribestoit)andbodyimage.ThedistinctionmadeforconveniencebetweenthischapterandChapter14,betweenself-awarenessandawarenessofthebody,isartificial.
Thebodyimagecanbealteredthroughenhancement,diminution(orablation)ordistortion.Itincorporatesmorethanjustthebody,exceptperhapsforthosefewoccasionswhenapersonisbothunclothedandconceptualizinghimselfasnaked: tailorshave longtriedtopersuadeusthat‘clothesmaketheman’.Certainly,theyareaneffectivemeansofnon-verbalcommunication.Clothesgiveussomeinsightintothewayapersonseeshimself(orherself )andalsointhewayhe(orshe)proposestointeractwithotherpeople.Apersoncomplementshismoodandhissocialroleofthemomentinhischoiceofclothes.Hewearsclothes,asashiphoistsaflag,forsignal-ling,andparticularclothesareworntoconveyamessagetosomeonewhocanreadit.Amedicalstudentwearsasuitforanoralexamination,awomanundoesthetopbuttonofherblouseonleavingtheofficefor lunch.Asthepatientcomesintoadoctor’sconsultingroom,hestartstogiveinformationabouthimselffromhisappearancebeforeeitherofthemuttersaword.Apersonwhoseclothesarechosenforhim,asinmentalhospitalsinthepast,presentsapeculiarlybleakandmeaninglessappearance;thisaspectofhisbodyimageisexpressionlessandconveysnothingofhimself.
Disorders of SelfIndescriptivepsychopathology,oneusesthetermego disordersordisorders of selftodescribetheabnormal inner experiences of I-ness and my-ness that occur in psychiatric illness.These mayoccur in thepatient’s stateof inner awareness irrespectiveof any changeshemay show in hisattitude to, or experience of, the world outside himself. Jaspers (1959), with characteristic
192 FOUR—SELF AND BODY
clarity, described self-awareness, that is, the ability todistinguish I from not I, ashaving fourformalcharacteristics.Scharfetter(1981,1995,2003)addedafifthdimensionofego vitalitytothelistandhasmadeacaseforitsinclusionbasedonfactoranalysis.Previously,thischaracteristicwas incorporated within the awareness of activity, which subsumed ‘being’ and ‘existing’ withotherpresentparticiples.Thus,wenowhavethefollowingcharacteristicsofself-awareness:
■ The feeling of awareness of being or existing(egovitality):IknowthatIamaliveandexist,andthisisfundamentaltoawarenessofself.
■ The feeling of awareness of activity (egoactivity):IknowthatIamanagentwhoinitiatesandexecutesmythoughtsandactions.
■ An awareness of unity(egoconsistencyandcoherence):atanygivenmoment,IknowthatIamoneperson.
■ Awareness of identity (ego identity): there is continuity in my biography, physiognomy,gender,genealogicalorigin,etc.;Ihavebeenthesamepersonallthetime.
■ Awareness of the boundaries of self (egodemarcation):Iamdistinct fromotherthingsandbeings andcandistinguishwhat ismyself from theoutside world, and I amawareof theboundarybetweenselfandnon-self.
Thedisordersofinnerexperienceinwhichthesecharacteristicsaredisturbedarenowexploredinmoredetail.WewilldealwiththesefivefunctionsdescribedbyJaspersandScharfetterinorder.
DISORDER OF BEING OR EGO VITALITY
Ineverhavetoaskmyself thequestionas towhetherIexist. It isanassumptionthatImakewithunquestioningcertainty.Iamsosureofthisthatitdoesnotevencomeontotheagendaofdoubtsanduncertainties.MyonlyknowledgethateverythingelseexistsisbasedonthepremisethatIdo.
Being: thepatient’sexperienceofhisveryexistencemaybealtered:‘Idonotexist; there isnothinghere’or‘Iamnotaliveanymore’or‘Iamrotting’.Thisisthecoreexperienceofnihilistic delusions,whichmayoccurinaffectivepsychoses(Chapters8and16).Seebelowforanexample.
I do not sense myself anymore. I do not exist anymore. When someone speaks to me, I feel as if he were speaking to a dead person. I have to look at myself to be sure that it is I. I have the feeling of being an absent person. In sum, I
am a walking shadow. (Minkowski, 1970)
Lesspronouncednihilisticideas(notdelusions)areexperiencedasdepersonalization,analtera-tionof thewayoneexperiencesoneself,which isaccompaniedbya feelingofanalterationorlossofsignificanceforself:‘Ifeelunreal,abitwoozy,asthoughIcan’tbequitecertainofmyselfanymore’.
DISORDER OF ACTIVITY
IdosomethingandknowthatIamdoingit.EverythingIdo,ineverythingIexperience,througheveryeventthatimpingesonme,Iamawarethattheexperiencehastheuniquequalityofbeing mine.‘Itwasincredible.Ipinchedmyselftomakesureitwasreallyhappeningtome’expressesthe relationship we experience between awareness of reality and activity. It is in our actions,includingourthinking,thatwereinforceourselvesconcerningourexistence.
Movingmayshowabnormality,forexampleinthepassivityexperienceordelusionsofcon-trol of patients with schizophrenia (see below). Schreber described several examples of thisexperience:
12—ThE DiSOrDErED SELF 193
The difficulties which were put in my way defy description. My fingers are paralysed, the direction of my gaze is changed in order to prevent my finding
the correct keys, the tempo is quickened by making the muscles of my fingers move prematurely: all these were and still are daily occurrences
and
the bellowing-miracle when my muscles serving the processes of respiration are set in motion by the lower God (Ariman) in such a way that I am forced
to emit the bellowing noises.
Memorizing and imaginingmaybe changed in that thepatientwithdepression feelshe isunable to initiate the act ofmemoryor fantasy; or, alternatively, a patientwith schizophreniafeelsthatthisactivitywhenitoccursisnotinitiatedbyhimbutfromoutsidehimself.Adepressedpatientsaid,‘mymemoryhasgone,Ihavenothoughts,Icannotthinkatall’.
Willingmaybealtered,forexamplethepatientwithschizophreniawhonolongerexperienceshiswillasbeinghisown.Commonly,neuroticpatientsdescribeaninabilitytoinitiateactivity,afeelingofpowerlessness,ofbeinggrounddowninthefaceoflife’svicissitudes.
Someoftheseabnormalitiesofexperienceofone’sownactivitiesarecloselyassociatedwithmood,forexamplethefeelingofthedepressedpatientwhobelievesthatheisincapableofdoinganythingat all: the alterationof self-concept isdirectly linked to themood state.Sometimes,however,itisnottheaffectassociatedwiththechangeofactivitybutthebeliefabouttheinitia-tionoftheactivitythatischanged.Thesearethepassivityexperiences(madeexperiences),whicharediscussedinmoredetailwithotherfirst-ranksymptomsofschizophreniainChapter9.
DISORDER OF SINGLENESS OR EGO CONSISTENCY AND COHERENCE
Inhealth, aperson is integrated inhis thinking andbehaviour so thathe isnot awareofhisfeelingofunity.Thereisanimplicitassumptionthatheisoneperson,andheknowshislimita-tionsandcapabilities.Thisassumptionofunitymaybelostinsomeconditions.Indreams,onesometimesseesoneself,evenperhapswithsomesurprise,inthedrama.Insomeformsoftran-scendentalmeditation,bycarryingoutrepetitivemonotonousactsthesubjectentersaself-inducedtranceinwhichhecanobservehimselfcarryingoutthebehaviour.‘Self ’isboththeobserverandalsotheobjectofobservation(seeBox12.1).
BOX 12.1 ■ Disorders of singleness
■ Therearesixtypesofautoscopy:feelingofpresence,negativeautoscopy,innerautoscopy,autoscopichallucination,outofbodyexperience,heautoscopyproper
■ Feelingofpresenceisadistinctfeelingofthephysicalpresenceofanotherperson■ Negativeautoscopyreferstothefailuretoperceiveone’sownbodyeitherinamirrororwhenlooked
atdirectly■ Innerautoscopyreferstotheexperienceofvisualhallucinationsofinternalorgansinextra-corporeal
space■ Out of body experience is characterizedby theprojectionof anobserving (psychological) self in
extra-personalspaceseeminglytotallydissociatedfromthephysicalbody■ Heautoscopydesignatesaconditioninwhichanindividualseeshisdoubleordoppelgänger

194 FOUR—SELF AND BODY
Autoscopy (Heautoscopy)
Autoscopyisaprofoundlyconceptuallychallengingphenomenoninwhichtheusualindivisibilityoftheselfappearstobecompromised.AccordingtoFish(1967),‘inthisstrangeexperiencethepatientseeshimselfandknowsthatitishe.Itisnotjustavisualhallucinationbecausekinaestheticandsomaticsensationmustalsobepresenttogivethesubjecttheimpressionthatthehallucina-tionishe’.Morerecently,BruggerandRegard(1997)haveidentifiedsixtypesofautoscopy:thefeeling of presence;negative heautoscopy;inner heautoscopy;autoscopic hallucination, out of body experi-ence;andheautoscopy proper.
Inthefeeling of presence,thepatienthasadistinctfeelingofthephysicalpresenceofanotherperson.Novisualperceptionisusuallyreported.Thefeelingofpresencemaybeconfinedtoonehemispaceespeciallywhentheexperienceoccursinassociationwithaseizure.
Negative heautoscopyreferstothefailuretoperceiveone’sownbodyeitherinamirrororwhenlookedatdirectly.Thisphenomenonisoftenassociatedwithdepersonalization.Inner heautoscopyreferstotheexperienceofvisualhallucinationsofinternalorgansinextra-corporealspace(Sollier,1903). Autoscopic hallucination is said to occur when a patient sees an exact mirror image ofhimself,orofhis faceor trunk.Thisexperience isdistinct fromheautoscopy properbecausethepatientdoesnotlocalizehimselfinthepositionofthemirrorimage.Thesehallucinatoryexperi-ences are usually brief, lasting seconds to minutes and followed by flash-like recurrences(Lhermitte,1951;Brugger,2002;Dewhurstetal,1955).
Out of body experiences are characterizedby theprojectionof anobserving (psychological)selfinextra-personalspaceseeminglytotallydissociatedfromthephysicalbody.Inthisphenom-enon, the patient sees himself and the world from a location distinct from his physical body.Therearethreephenomenologicalcharacteristicshere:disembodiment,theimpressionofseeingthe body from a distant and elevated visuo-spatial perspective (the so-called extra-corporealegocentricperspective)andtheimpressionofseeingone’sownbodyfromthiselevatedposition(Anzellottietal,2011).
Heautosocpy proper designates a condition in which an individual sees his double or dop-pelgänger.The double usually appears colourless, can behave independently, and may or maynot mirror the patient’s appearance.There is strong self-identification with the second body,often associated with the experience of existing at and perceiving the world from two placesat the same time (Heydrich and Blanke, 2013). There may be vestibular sensations suchasextremelightnessofthebody,sensationofflying,elevation,rotationandvertigo(Anzellottietal,2011;Blankeetal,2004).There isaNorthEuropeanmyth,sharedbyseveralcountries,thatsomeonemayseehisdouble(‘wraith’,‘fetch’)shortlybeforehisdeath,andithasthereforebecomeasinisteromen(ToddandDewhurst,1962).Theseauthorspresentinterestinghistoricalmaterialtosubstantiatethelinkbetweenperceptualdoppelgängeranddeath.Theusuallegendisthat,asthepersonliesdying,hiswraithfloatsbeforehiseyesandheseeshimselfperformingall themostdisreputable and reprehensible actionsofhis life; they areparadedbeforehimasheexpires.
Thereiscontinuingpopularinterestintheconceptofthedouble.ItisthesubjectofdiversefictionasinThe DoublebyFyodorDostoyevsky(1846),RobertLouisStevenson’sThe Master of Ballantrae(1889),andShusakuEndo’sScandal(1986).Theveryworstfeatureofthedoubleforthesubjecthimself iswell illustrated inWilliamStyron’sDarkness Visible (1991).Theterrible,inextricable involvement of the double with the subject in trying to mortify him, goad him,provokehimtodestroythedoubleand/ordestroyhimself.
the sense of being accompanied by a second self – a wraith-like observer, able to watch with dispassionate curiosity as his companion struggles against the
oncoming disaster, or decides to embrace it … I, the victim-to-be of
12—ThE DiSOrDErED SELF 195
self-murder, was both the solitary actor and lone member of the audience … I watched myself in mingled terror and fascination.
There is growing evidence that autoscopic phenomena occur in association with seizures(Anzellottietal,2011).Furthermore,ithasbeenpostulatedthatautoscopyderivesfromafailureofintegrationofproprioceptive,tactileandvisualinformationaboutthebodyaccompaniedbyvestibulardysfunction (Blanke etal, 2004;Heydrich andBlanke,2013).Theanatomicalbasisandmechanismof autoscopy is yet tobe clarifiedbut there is tentative evidence that the leftposteriorinsularisinvolvedinheautoscopyandrightoccipitalcortexinautoscopichallucination(HeydrichandBlanke,2013).Becauseofthehypothesisthatautoscopyisafailureofintergration,themultimodaljunctionsbetweentheparietalandtemporallobesandbetweentheparietalandoccipitallobeshavebeenimplicated.And,thereisexperimentalworkderivingfromtheapplica-tionof transmagnetic stimulationof the left temporoparietal junction toproduceheautoscopy(doppelgänger)(BlankeandArzy,2005).
Inpractice,thesephenomenacanbeextremelydifficulttoidentifyanddelineate.Thefollow-ingdescriptionbya37-year-old,intelligentmanwithahistoryofepilepsy,receivingtreatmentwithphenobarbitone,isconsideredanexampleofautoscopichallucinationbutanalysishasfea-turesofheautoscopyaswell asout-of–the-bodyexperience.Thepatientheldhishead rigidlywithapparenttorticollistotheright.Ifherotatedittotheleft,therewasmarkedheadnodding,butnotifheturneditfurthertotheright.
I’m standing outside myself on the left hand side but only when I’m sitting down … it comes in short episodes for about 30 seconds … my true self loses
all its senses as all the senses are in my hallucinatory self … the true self is just a shell without any senses … the hallucinatory self can see the true self and
the whole surroundings, and it seems to me as though the hallucinatory self is looking at me and at other things in the room from a position standing to the
left hand side of me, and everything is in the right perspective. If it was occurring now, the hallucinatory self would see you more full face and from
higher up than I see you now because it is standing … I can’t see it or hear it but it can see the side of my head. It seems to be there. I know that it isn’t me
as such. It’s like having a dream and you know that it is a dream. I thought it was a dream but it has occurred when I am fully waking. It seems as clear as
a nightmare at the time but I know afterwards that it is a figment like a very vivid dream but more real than a dream. I would not see a fleck of dust on my
cheek or something like that. The other one is not a different personality.
Whenthisexperienceoccurred,thepatientfeltallsensationwasinthe‘hallucinatoryself ’,includinghearing,seeingandfeelingcold:‘Ifeltcoldonthebackofthehallucinatoryself ’.Therehadbeennoexperienceoftasteorsmell.Therehadbeenanexperienceofaffect.
I was talking to a representative. The hallucinatory self felt sorry for this man because he looked abnormal. It had no feelings for the real self. He looked
abnormal because I had stopped talking and a glazed expression had come into my eye.
AbizarreexampleofautoscopywasreportedbyAmes(1984):theself-shootingofaphantomhead.Thispatientwas suffering fromschizophrenia.Hedescribedseeingandhearingavoicefromanotherheadthatwassetonhisownshoulders,attachedtohisbodyandtryingtodominate

196 FOUR—SELF AND BODY
hisownhead.Hedescribedhimselfashavingtwoheadsbutbelievedthattheotherheadwasactuallythatofhiswife’sgynaecologist,whomhebelievedtobehavinganaffairwithher.Thevoicefromthesecondheadwasthatofthegynaecologist,andtherewerealsothevoicesofJesusandAbrahamaroundhim,conversingwitheachotherandtalkingabouthishavingtwoheads.Thepatienttriedtoremovetheotherheadbyshootingsixshotsatitandthroughhisownpalate,causingextensivedamagetohisbrain.Ameslabelledthisconditionthe‘phenomenonofpercep-tualdelusionalbicephaly’.
Multiple Personality (Dissociative Identity Disorder)
Indissociative(hysterical)states,so-calleddualandmultiplepersonalitieshavebeendescribed(Abse,1982;McDougall,1911;Prince,1905).SlaterandRoth(1969)comment:
A girl who is by turns ‘May’ and ‘Margaret’, may be quiet, studious and obedient as May, and unaware of Margaret’s existence. When she becomes
Margaret, however, she may be gay, headstrong and wilful, and refer to May in contemptuous terms. It seems that these multiple personalities are always artificial productions, the product of the medical attention that they arouse.
Theessenceofmultiplepersonalityistheembodimentofatleasttwopersonalities(identities).Thisphenomenonraisesdoubtsaboutournatural intuitionthatan individualhumanbeingisindivisibleandisanembodiedsingularperson.Prince’saccountgaveavividdescription:
Miss Christine L Beauchamp, the subject of this study, is a person in whom several personalities have become developed; that is to say, she may change
personality from time to time, often from hour to hour, and with each change her character becomes transformed and her memories altered. In addition to
the real, original or normal self, the self that was born and which was intended by nature to be, she may be anyone of the three persons. I say three different, because, although making use of the same body, each nevertheless,
has distinctly different character: a difference manifested by different trains of thought, by different views, and temperament, and by different acquisitive
tastes, habits, experiences, and memories.
InacharacteristiccasestudyofmultiplepersonalitybeforetheconditionsformedicalpracticeintheUnitedStatesresultedinaproliferationofcasesofso-calledmultiplepersonalitydisorder,Larmoreetal.(1977)described‘a35-year-oldwhitewomanofruralKentuckybackground’whohadmadesevensuicideattempts,ofwhichsheclaimedtohavenomemory.‘Shortlyafteradmis-sionahypnotic interviewwasconducted,duringwhichoneof thepersonalitiesspontaneouslyrevealedherselfandgavehintsoftheexistenceofotherpersonalities’.Fourdistinctpersonalitieswereidentified:Faith,‘theprimarypersonality…knownas“thelittleangel”bypersonalityAlicia…kind,lovingandhelpful…hasdifficultyinexpression…anger,andindealingwithcriticism’;Alicia,‘aSatanicagent…claimscontrolovermostofFaith’sphysiologicalfunctions…manifest-ingeitherassaultiveorself-destructivebehaviour’;Alicia–Faith,undertheinfluenceofAlicia,‘hasonlyperipheralawarenessofAliciaandnoknowledgeofFaithorGuardianAngel’;Guardian Angel,‘firstmadeitsappearancefollowingthegrandfather’sdeath…claimstobetheprotectorofFaith’.
Therehasbeenavastoutputofpsychiatric literatureonthesubjectofmultiplepersonalitydisorder, based on the diagnostic criteria of DSM-IIIR (American Psychiatric Association,1987) but often lacking in psychopathological precision. This has been well summarized byFahy(1988):
12—ThE DiSOrDErED SELF 197
Recently there has been a dramatic rise in the number of case reports of multiple personality disorder (MPD)…. A review of the recent literature
reveals a poverty of information on reliability of diagnosis, prognosis, or the role of selection bias. It is argued that iatrogenic factors may contribute to
the development of the syndrome. There is little evidence from genetic or physiological studies to suggest that MPD represents a distinct
psychiatric disorder.
Absestatesthat‘one-wayamnesia’isusualformultiplepersonality;thatis,personalityAisamnesicfortheotherpersonalityB,butthesecond,B,candiscusstheexperiencesofA.Usually,AisinhibitedanddepressedandBisfreerandmoreelated.Theformsofmultiplepersonalityseeninpracticeareusually:
■ simultaneouspartialpersonalities■ successivewell-definedpartialpersonalities■ clusteredmultiplepartialpersonalities.When such patients have been treated in psychotherapy, ingenious explanations are often
givenbypatientandby therapist for theappearanceof theadditionalpersonalities.Althoughthisremainsadisputedarea,anauthoritativeopinionfromMerskey(2000)states:
In this author’s view there is no place for the diagnosis of multiple personality disorder in psychiatry, and the important question is how such a diagnosis
managed to achieve so much prominence in professional circles in North America, although generally not elsewhere.
Lability in the Awareness of Personality
Thelossofunityofselfinschizophreniawasexemplifiedbyapatientwhodescribedhow,everynight,hebecameahorseandtrotteddownWhitehall.Atthesametimeasthiswashappeninginhismind,healsobelievedhewasinWhitehallwatchingthehorse.Thistypeofsymptomhasbeen called lability in the awareness of personality and was described by Bonhoeffer (1907) asoccurringinparanoidpsychosis.
DISORDER OF IDENTITY
IamwhoIwas lastweekor30yearsago;IamwhoIwillbenextweekor in10years’ time.This truism, which we can claim without hesitation, is by no means certain for some peoplesufferingfromschizophreniaorfromorganicstates,fromneurosesorfromdepression,orevenfor somehealthypeople in abnormal situations (seepossession state, below).Thisdisorderofself-awarenessischaracterizedbychangesintheidentityofselfover time.
Apersonwhofeelsthreatenedinhisjobandisafraidofredundancyisnotlikelytofunctionwell,becauseofhisfeelingofimpermanence.Afeeling of continuityforoneselfandone’sroleisa fundamental assumption of life, without which competent behaviour cannot take place. Inhealth,wehavenodoubtsaboutthecontinuityofourselffromourpastintoourpresent.However,patients with schizophrenia sometimes deny that they have always been the same person.Characteristically,thistakestheformofapassivity experience,andthepatientclaimsthatatsometime in thepasthehas been completely changed frombeingoneperson toanother,whomhenowis.Jaspers(1959)givesanaccountofapatientwhosaid,
When telling my story I am aware that only part of my present self experienced all this. Up to 23rd December 1901, I cannot call myself my

198 FOUR—SELF AND BODY
present self; the past self now seems like a little dwarf inside me. It is an unpleasant feeling; it upsets my feelings of existence if I describe my previous
experiences in the first person. I can do it if I use an image and recall that the dwarf reigned up to that date, but since then his past has ended.
Thiscompletealterationinthesenseofidentityisexclusivelypsychotic;thereisabreakinthesenseofidentityofself,andthereisasubjectiveexperienceofsomeonecompletelydifferent,althoughstilldescribedasoneself,‘takingover’.
Afeelingoflossofcontinuity,whichis,however,oflesserintensitythanthepsychoticchangedescribedaboveandwithoutitselementofpassivity,maybeexperiencedinhealthandinneurosesandpersonalitydisorders.Thepersonknowsthatbothpeople,beforeandafter,aretrulyhimself,buthefeelsveryalteredfromwhathewas.Thismayoccurfollowinganoverwhelminglyimpor-tant lifesituationorduringemotionaldevelopmentwithoutanoutsideevent.Forexample,anadolescentmayquitesuddenlyfeelinthecourseofaweek‘asif ’heisquiteadifferentperson.Itshouldbestressedthatthesenseofrealityisneverlosttotheextentthatheactuallybelieveshimselftobeadifferentperson.Inthenon-psychotic,itismorethatthoughtsandfeelingsdonotseemtobeinkeepingwithhimselfashehascometoaccepthimself.
Inthenextchapter,amanisdescribedasdevelopinglong-termdepersonalizationafterexpe-riencingmassivestressatwork,culminatinginanextremelyharassingjourneyinwhichhewasthecardriver.Afterwards,hiswifesaidthathewasneveragainlikethemanshehadmarried,‘butlikehis(non-existent)twinbrother’.Shesaidthat,whereaspreviouslyhewasincisive,wasquick-thinkingandmadethedecisionsinthefamily,nowhelackedself-confidenceandshehadtodoeverything.Neitherpartnerwasinanydoubtthathewasthesameperson,buthiswholedemeanourhadchangedas ifhehadbecomesomeonesimilarbutnotidentical.
Thefeelingoflossofcontinuitycontributestotheinertiaofthepersonwithschizophreniaandtheapathyofthedepressive.Lackofaclearsenseofidentityfromthepastcontinuingintothefutureisastrongdisincentivetoconcertedactivity.Thepatient,withschizophrenia,aspartofdisturbanceofpassivity,mayhavedoubtsabouthiscontinuityfromthepasttothepresent;thedepressive,secondarytodisorderofmood,oftenseesnocontinuationintothefuture:‘eve-rythingisbleak,thereisnothingtolookforwardto’.
Apartofthesenseofcontinuityofself isacceptingthatthechangesinone’stotalstateatpresentaredue to illness.Thisisthecharacteristicusuallydescribedinthementalstateexamina-tionunder the term insight (David, 1990).The individual recognizes thathe is still the samepersonbutthathiscurrentchangeinsubjectivityisduetotheinterveningprocessofillness.
Possession State
ThisisclassifiedinICD-10underdissociative(conversion)disorders(F44)–tranceandposses-sion disorders (F44.3) (World Health Organization, 1992). However, although the trance oralteredstateofconsciousawarenessisaprerequisite,possessionstatedoesnotnecessarilyoccurin the context of dissociative or hysterical disorder. It can occur in normal, healthy people inunusualsituations,eitherasagroupphenomenon(masshypnosis)orindividually;suchacaseisdescribedbelow.Thereisatemporarylossofboththesenseofpersonalidentityandfullawarenessofthesurroundings.Thepersonactsasifhehas,andbelieveshimselftohavebeen,takenoverbyanother–aspirit,aforce,adeityorevenanotherperson.Thedifferencebetweenthosecondi-tions that constitute disorder and those that may be considered as being within a cultural orreligiouscontextaloneisthattheformerareunwanted,causedistresstotheindividualandthosearoundandmaybeprolongedbeyondtheimmediateeventorceremonyatwhichitwasinduced.
Possessionofayoung,entirelyhealthywomanwithahusbandandthreechildrenbytwo‘god-desses’ was witnessed in Sri Lanka.The woman had become a varama, a healer with special

12—ThE DiSOrDErED SELF 199
powers,about2yearspreviously,whenshe‘saw’herdeceasedfather-in-law,whocametoherandsaid that she would have supernatural power to help other people and her own family. Herhusbandhadbecomeaddictedtoarak,alocalspirit,andhisdrinkinghadbythenbroughtthefamilyintoextremeeconomichardship.Afterthisexperience,sheofferedherservicesasahealerand solverofdomesticdifficulties toher village, and severalpeople consultedher eachdayathome,whereshehaddevotedonetinyroomtoasanctuaryandanothertoawaitingroom.Withher husband blowing a buffalo horn repeatedly and herself chanting, she induced a trance inherselfinwhichshespokewithdifferentvoicesaseitheroneoftwofemaledeitiesgivingadvicetoherclients,whichherhusbandinterpreted.Thevillagershadfoundherministrationstobehelpful,itgaveusefuloccupationtoherdelinquenthusbandandshehadcompletelysolvedherownfamily’sfinancialproblemsthroughthegiftsshereceivedforservicesrendered.
A different case, with psychiatric disorder present, was that of a 37-year-old Sri Lankanhousewifewhobelievedherselftobepossessedbyherlong-deadgrandmother;onthreeoccasionsshehadgoneintoatrance,lostcontactwiththeoutsideworldandseentheimageofhergrand-mothercomingclosetoherandtryingtosqueezeherneck.Theseepisodesweredescribedwithfear and distress. She showed symptoms of depressive illness, with poor sleep, early morningwakening, lossofappetiteandweight,anergia, fatigueandfeeling lowinmood;shehadbeenabandonedbyhermotherwhen7yearsold.
Wijesingheetal.(1976)surveyedasemiurbanpopulationof7653peopleinSriLankaandidentified37subjects,9maleand28female,with‘possessiontrancestates’,showingalteredstateofconsciousawareness,behaviourforwhichthesubjectdidnotacknowledgeresponsibility,andhadamnesiafortheperiodofthetrance.Episodes,oftenlastingabout30minutes,wereusuallyprecipitatedeitherbyemotionalstressorculture-boundstimulisuchaswitnessinganexorcismceremony.Duringtrance,subjectsweremostoftenrestlesswithrhythmictremblingofthetrunkand exaggerated gesturing, speech was aggressive and commanding and, typically, mood wasangry;mostoften,thepossessingspiritwasthatofaclosebutdeadrelative.Infemalesespecially,as the condition continued they were increasingly likely to become permanent adepts.Theseauthorsregardedonlyoneoftheirsubjectsassufferingfromschizophrenia,although17of37manifestedactivepsychiatricdisorder,mostlyneuroticinnature.
Possessionandtrancestatesstraddletheboundarybetweennormativebehaviourandabnor-malbehaviourindicativeofadisorder.Moreira-AlmeidaandCardeña(2011)arguethatlackofpersonalsuffering,absenceofsocialorfunctionalimpairment,absenceofpsychiatriccomorbidity,self-controlovertheexperienceandpersonalgrowthallpointinthedirectionofanon-pathologicalspiritualexperience.Itisclearthoughthatpossessionandtrancestatescanoccurinthesettingofindubitableneurologicaldiseasesuchaslesionsinthebasalgangliaandfronto-parietallobes(Basuetal,2002),hencetheneedtohaveanintegrativemodelthatisgroundedinneurosciencebut admits sociocultural processes informed by aspects of how the self is socially constructed(SeligmanandKirmayer,2008).
Jaspers(1959),inwritingaboutdisordersofself-awareness,concernedhimselfwithdisorderofcontentaswellasofform.Indiscussingstatesofpossession,hecommentedontherarecondi-tionoflycanthropy,thepatientbelievingthathehasbeentransformedintoananimal,literallyawolf.LyncathropyhasalonghistoryinWesternsocietiesandidenticalbeliefsoftransformationinto other feared animals such as the fox in Japan, the tiger, hyena and crocodile in China,MalaysiaandIndiaaredocumented(Fahy,1989).Inantiquitytherewasbeliefinthepossibilityofradicalphysicaltransformationofthehumanbodyintothatofawolf.However,recentcasereportshaveadoptedarobustphenomenologicalapproachandidentifythebeliefoftransforma-tionasadelusionofnon-specificvaluebutprincipallyassociatedwithmooddisorders,schizo-phrenia,andoccasionallyorganicbraindisease(Kecketal,1988;Fahy,1989;Kulicketal,1990).Lyncathropyisusuallyatransientbeliefbutoccasionallythebeliefcanbeenduring,lastingformany years (Keck etal, 1988). Koehler etal. (1990) reviewed Jaspers’ work in relation to
200 FOUR—SELF AND BODY
lyncathropyandshowedthatJaspersdifferentiatedbetweenstatesofpossessionpresentingwithanalteredconsciousnessandstatesofpossessioninwhichconsciousnessremainsclear;theformerwereusuallydissociative(hysterical)inorigin,whilethelatterweremoreoftenassociatedwithschizophrenia.This emphasizes the importance for psychiatric diagnosis in assessing psycho-pathologicalform.
DISORDER OF THE BOUNDARIES OF SELF OR EGO DEMARCATION
DisorderoftheboundariesoftheselfreferstothedisturbanceinknowingwhereIendsandnot Ibegins.Abnormalityisnotconfinedtoschizophrenia.Forexample,inlysergicaciddiethylamideintoxicationthefeelingofimpendingegodissolutionassociatedwiththefeelingofself‘slippingaway’withconsiderableanxietyhasbeendescribed(AndersonandRawnsley,1954).Onesubjectputthisas:
I was being disorganized … the world around was looking very distorted indeed … things were pretty rocky so I decided to sit back quietly for a
moment and reassure myself by returning to my own private inner world. As soon as I introspected in this manner I felt to my dismay that ‘I’ myself was
somehow disturbed. The central core of the personality, the ego, the sense of personal identity, was itself fluctuating and, for want of a better
phrase, dissolving.
Anothersubjectsaid,‘IfanyonepresentwentoutoftheroomitfeltasthoughIwerebeingdeprivedofsomething.Ibecamesmaller–definitelyfeltvulnerable’.
Boundaries of Self in Schizophrenia
In schizophrenia, the senseof invasionof self appears tobe fundamental to thenatureof theconditionasitisexperienced;manybutnotallfirst-rank symptomshaveincommonpermeabilityofthebarrierbetweentheindividualandhisenvironment,lossofegoboundaries(Sims,1993).Thereisamergingbetweenselfandnot self ;thisisclearlyportrayedinFigure12.2,paintedbya young schizophrenic patient.The patient is not aware of the disturbance being one of egoboundaries;hedescribesaproblemonlyinasmuchas‘otherpeoplearedoingthingstome,eventsaretakingplaceoutsidemyself ’.Theexternalobserverfindsablurringorlossoftheboundariesofselfthatisnotapparenttothepatienthimself.
Allpassivity experiences falselyattribute functions tonot self influences fromoutside,whichare actually coming from inside the self. This is also true for disorders of the possession ofthought, such as thought insertion and thought withdrawal.Thought broadcasting obviouslyinvolvesprivatethoughtsbecomingpublicwithouttheconsentoractionofthepatient.Thisisanotherexampleofabreakdowninthenormalboundariesofwhatisselfandnon-self.Otherexperiences, such as auditory hallucinations, rely on the patient ascribing internally generatedactivity,thatis,internalspeech,toexternalagencies.
Passivity,delusion of control,isdiscussedinChapter9.Thesubjectiveexperienceofpassivityisadisorderofthedistinctionbetweenwhatisandwhatisnot self.Sensations,emotions,impulsesandactionsthatinobjectiverealitycomefrominsidetheselfareascribedtonot self.
Other Alterations to Boundaries
Instatesofecstasy,therearealsodisturbancesintheboundariesofself(Chapter16).Thepar-ticipant might describe feeling at one with the universe, merging with nirvana, experiencing
12—ThE DiSOrDErED SELF 201
unitywiththesaints,identifyingwiththetreesandflowersoraonenesswithGod.Ecstasystatesoccurinnormalpeopleandinthosewithpersonalitydisorder,aswellasinsufferersfrompsy-chosesandinepilepsy.Inepilepsyitispartoftheauraandischaracterizedbyintensefeelingsofwell-beingandheightenedself-awareness.It isthoughttoemanatefromhyperactivationofthe anterior insula rather than the temporal lobe (Picard andCraig, 2009).This alteration inawarenessof theboundariesofself isdifferent fromthatofschizophreniadescribedabove.Inecstasy,itisanas if experience,anditismediatedaffectively.
ThephenomenondescribedbyJung inhimselfwithwhichthischapterbegins isa lackofdefinitionof theboundariesof self.However, therewasno lossof reality judgement; itwasagame,andJungdid infactknowwhatwashimselfandwhatwasthestone.Inpsychosis, thisability to discriminate is lost. A patient with schizophreia said, ‘I am invaded day and night.Ihavenomoreprivacysincetelevisioncameinsideme’.Anotherpatientbelievedthatwhilehewasinahospitalwardhewashelpingotherpatientsbecausehepermeatedthemedicalstaffandtherebyassistedthemintheirwork.
ReferencesAbseW(1982)Multiplepersonality.InRoyA(ed.)Hysteria.Chichester:JohnWiley.American Psychiatric Association (1987) Diagnostic and Statistical Manual of Mental Disorders, 3rd edn,
revised.Washington:AmericanPsychiatricAssociation.AmesD(1984)Self-shootingofaphantomhead.British Journal of Psychiatry145,193–4.AndersonEWandRawnsleyK(1954)Clinicalstudiesoflysergicdiethylamide.Monatsschrift fuer Psychiatrie
und Neurologie128,38–55.AnzellottiF,OnofriV,MaruottiV,RicciardiL,FranciottiR,BonanniL,ThomasAandOnofrjM(2011)
Autoscopicphenomena:casereportandreviewofliterature.Behavioral and Brain Function7,2.ArgyleM(1975)Bodily Communication.London:Methuen.BahnsonCB(1969)Bodyandself-imagesassociatedwithaudio-visualself-confrontation.Journal of Nervous
and Mental Disease148,262–80.
Figure 12.2 Picture by a young schizophrenic patient.
202 FOUR—SELF AND BODY
BasuS,GuptaSCandAkhtarS(2002)TranceandpossessionlikesymptomsinacaseofCNSlesion:acasereport.Indian Journal of Psychiatry44,65–7.
BerriosGEandMarkovaIS(2003)Theselfandpsychiatry:aconceptualhistory.InKircherTandDavidA(eds.)The Self in Neuroscience and Psychiatry.Cambridge:CambridgeUniversityPress.
BlankeOandArzyS(2005)Theout-of-bodyexperience:disturbedself-processingatthetemporo-parietaljunction.Neuroscientist11,16–24.
BlankeO,LandisT,SpinelliLandSeeckM(2004)Out-of-bodyexperienceandautoscopyofneurologicalorigin.Brain127,243–58.
BonhoefferK(1907)Klinische Beiträge zur Lehre von den Degenerationspsychosen. Alt’s Samml,vol.7,Halle:Marhold.
BruggerP(2002)Reflectivemirrors:perspective-takinginautoscopicphenomena.Cognitive Neuropsychiatry7,179–94.
BruggerPandRegardM(1997)Illusoryreduplicationofone’sownbody:phenomenologyandclassificationofautoscopicphenomena.Cognitive Neuroscience2,19–38.
CritchleyM(1950)Thebodyimageinneurology.Lanceti,335–41.DavidAS(1990)Insightandpsychosis.British Journal of Psychiatry156,798–808.DewhurstKandPearsonJ(1955)Visualhallucinationsoftheselfinorganicdisease.Journal of Neurology,
Neurosurgery and Psychiatry18,53–7.DostoevskyF(1846)The Double(transl.GarnettC,1913).London:Heinemann.EndoS(1986)Scandal(translGesselVC).London:PenguinBooks.FahyTA(1988)Thediagnosisofmultiplepersonalitydisorder:acriticalreview.British Journal of Psychiatry
153,597–606.FahyTA(1989)Lyncathropy:areview.Journal of the Royal Society of Medicine82,37–9.FishFJ(1967)Clinical Psychopathology.Bristol:JohnWright.FreudS (1933)New introductory lecturesonpsychoanalysis. InStandard Edition of the Complete Works of
Sigmund Freud,vol. XXII(transl.StracheyJ,1964).London:HogarthPress.HeadHandHolmesG(1911)Sensorydisturbancesfromcerebrallesions.Brain34,102–254.HeydrichL andBlankeO (2013)Distinct illusory own-bodyperceptions causedbydamage toposterior
insulaandextrastriatecortex.Brain136,790–803.JaspersK(1959)General Psychopathology(transl.HoenigJandHamiltonMWfromtheGerman,7thedn,
1963).Manchester:ManchesterUniversityPress.JungCG(1963)Memories, Dreams, Reflections.London:CollinsRoutledgeandKeganPaul.KeckPEJr,PopeHG,HudsonJI,McElroySLandKulickAR(1988)Lycanthropy:aliveandwellinthe
twentiethcentury.Psychological Medicine18,113–20.KoehlerK,EbelHandVartzopoulosD(1990)Lycanthropyanddemonomania:somepsychopathological
issues.Psychological Medicine20,629–33.KulickAR,PopeHGandKeckPEJr (1990)Lycanthropyandself-identification. Journal of Nervous and
Mental Disease178,134–7.LarmoreK,LudwigAMandCainRL(1977)Multiplepersonality–anobjectivecasestudy.British Journal
of Psychiatry131,35–40.LhermitteJ(1951)Visualhallucinationoftheself.British Medical Journal1,431–4.MinkowskiE(1970)Lived Time: phenomenological and psychopathological studies.(transMetzelN).Evanston:
NorthwesternUniversityPress.McDougallW(1911)Suggestion.EncyclopaediaBritannica.MerskeyH(2000)Conversionanddissociation.InGelderMG,López-IborJJandAndreasenNC(eds.)
New Oxford Textbook of Psychiatry.Oxford:OxfordUniversityPress.Moreira-AlmeidaAandCardeñaE(2011)Differentialdiagnosisbetweennon-pathologicalpsychoticand
spiritualexperiencesandmentaldisorders:acontribution fromLatinAmericanstudies to theICD-11.Revista Brasileira de Psiquiatria33(suppl.1),S21–36.
MorrisJ(1974)Connundrum.London:FaberandFaber.NietzscheF(1901)The Will to Power(transl.KaufmannWandHollingdaleRJ,1968).NewYork:Vintage
Books.PicardF,andCraigAD(2009)Ecstaticepilepticseizures:apotentialwindowontheneuralbasisforhuman
self-awareness.Epilepsy and Behavior16,539–46.PrinceM(1905)The Dissociation of a Personality.NewYork:Longman.

12—ThE DiSOrDErED SELF 203
ScharfetterC(1981)Ego-psychopathology:theconceptanditsempiricalevaluation.Psychological Medicine11,273–80.
ScharfetterC(1995)The Self-experience of Schizophrenics: Empirical Studies of the Ego/Self in Schizophrenia, Borderline Disorders and Depression.Zurich:privatepublication.
ScharfetterC (2003)The self-experienceof schizophrenics. InKircherT andDavidA (eds.) The Self in Neuroscience and Psychiatry.Cambridge:CambridgeUniversityPress.
SchilderP (1935) The Image and Appearance of the Human Body: Studies in the Constructive Energies of the Psyche.London:KeganPaul.
SeligmanRandKirmayerLJ(2008)Dissociativeexperienceandculturalneuroscience:narrative,metaphorandmechanism.Culture, Medicine and Psychiatry32,31–64.
Sims ACP (1993) Schizophrenia and permeability of self. Neurology, Psychiatry and Brain Research 1,133–5.
SlaterEandRothM(1969)Personalitydeviationsandneuroticreactions.InMayer-GrossW,SlaterEandRothM(eds.)Clinical Psychiatry.3rdedn.London:BaillièreTindallandCassell.
SollierP(1903)L’autoscopieinterne.Revue Philosophique55,1–41.StevensonRLB(1889)The Master of Ballantrae.London:Collins.StyronW(1991)Darkness Visible.London:JonathanCape.ToddJandDewhurstK(1962)ThesignificanceoftheDoppelganger(hallucinatorydouble)infolk-loreand
neuropsychiatry.Practitioner188,377–82.WijesingheCP,DissanayakeSAWandMendisN(1976)Possessiontranceinasemi-urbancommunityin
SriLanka.Australia and New Zealand Journal of Psychiatry10,135–9.WorldHealthOrganization(1992)The ICD-10 Classification of Mental and Behavioural Disorders: Clinical
Description and Diagnostic Guidelines.Geneva:WorldHealthOrganization.Zahavi D (2003) Phenomenology of self. In KircherT and David A (eds.) The Self in Neuroscience and
Psychiatry.Cambridge:CambridgeUniversityPress.

This page intentionally left blank

205
C H A P T E R 13
Depersonalization
SummaryDepersonalizationisasubjectivestateofunrealityinwhichthereisafeelingofestrangement,either fromasenseof selfor fromtheexternalenvironment.Frequently, it isaccompaniedbythesymptomofderealization,atermdenotingasimilarfeelingofunrealitywithregardtoaware-nessoftheexternalworld.Thelocalizationofthisfeelingofunrealitytoaselectedpartofthebodyiscalleddesomatization.Theremaybeexperienceofchangesofsizeorquality,forexampleappearing largeor tiny,orempty,ordetachedorfilledwithwateror foam.Deaffectualizationhasbeenusedtodescribetheconsistentlossofthecapacitytofeelemotion,sothatthepersonseemsunabletocry,loveorhate.Theseexperiencesareassociatedwithanxietyandmooddis-orders,organicdiseasesuchasepilepsyandtraumaticbraininjury.Depersonalizationcanalsobetriggeredby theuseofcannabis,hallucinogens,ecstasyandalcohol. It canbeabriefor long-lastingexperience.Itisinvariablydistressingtothepatient.
I may be looking with some degree of attentiveness at a tumbler. As long as I say to myself that this tumbler is a glass or metal vessel made for the purpose
of putting liquid into it and carrying it into one’s lips without upsetting it – as long as I am able to represent the tumbler to myself in a convincing
manner – so long shall I feel that I have some sort of relationship with it, a relationship close enough to make me believe in its existence and also, on a
subordinate level, in my own. But once the tumbler withers away and loses its vitality… reveals itself to me as something with which I have no
relationship, once it appears to me as an absurd object – then from that very absurdity springs boredom, which when all is said and done is simply a kind
of incommunicability and the capacity to disengage oneself from it.(Alberto Moravia, 1960)
Definitions and DescriptionsDepersonalization is the term used to designate a peculiar change in the awareness of self,inwhichthe individual feelsas ifhe isunreal (Sedman,1972). It isbest to reserve theuseofthe word to this as if feeling rather than the experience of unreality that occurs in psychosis.Theas ifprefixisusedbythepatienttodenotethatheisnotusingwordsliterally(howcouldhe know what it would be like not ‘fitting into the world’, as all his experience has been intheworld?).Heisexpressinguncertaintyandpaintingapicture,and‘asif ’isthebestwayhecando it. It has been considered that, after depression and anxiety, depersonalization is the mostfrequentsymptomtooccurinpsychiatry(Stewart,1964)and12monthprevalenceestimatesfordepersonalizationandderealizationinaruralpopulationareputat19.1%and14.4%(Aderibigbeetal.,2001).

Keywords: Depersonalization,Derealization.
13—DEpErSONALizAtiON 205.e1
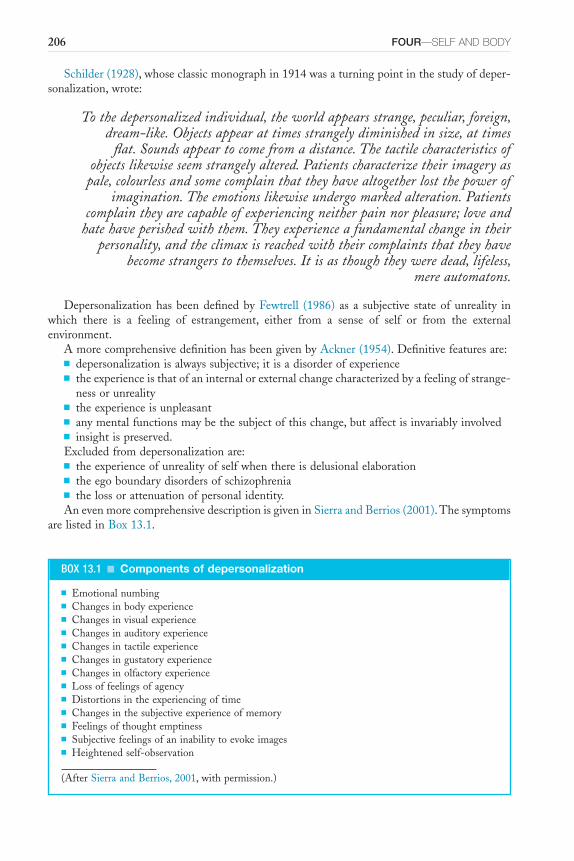
206 FOUR—SELF AND BODY
Schilder(1928),whoseclassicmonographin1914wasaturningpointinthestudyofdeper-sonalization,wrote:
To the depersonalized individual, the world appears strange, peculiar, foreign, dream-like. Objects appear at times strangely diminished in size, at times
flat. Sounds appear to come from a distance. The tactile characteristics of objects likewise seem strangely altered. Patients characterize their imagery as
pale, colourless and some complain that they have altogether lost the power of imagination. The emotions likewise undergo marked alteration. Patients
complain they are capable of experiencing neither pain nor pleasure; love and hate have perished with them. They experience a fundamental change in their
personality, and the climax is reached with their complaints that they have become strangers to themselves. It is as though they were dead, lifeless,
mere automatons.
DepersonalizationhasbeendefinedbyFewtrell (1986) as a subjective stateofunreality inwhich there is a feeling of estrangement, either from a sense of self or from the externalenvironment.
AmorecomprehensivedefinitionhasbeengivenbyAckner(1954).Definitivefeaturesare:■ depersonalizationisalwayssubjective;itisadisorderofexperience■ theexperienceisthatofaninternalorexternalchangecharacterizedbyafeelingofstrange-
nessorunreality■ theexperienceisunpleasant■ anymentalfunctionsmaybethesubjectofthischange,butaffectisinvariablyinvolved■ insightispreserved.Excludedfromdepersonalizationare:■ theexperienceofunrealityofselfwhenthereisdelusionalelaboration■ theegoboundarydisordersofschizophrenia■ thelossorattenuationofpersonalidentity.AnevenmorecomprehensivedescriptionisgiveninSierraandBerrios(2001).Thesymptoms
arelistedinBox13.1.
BOX 13.1 ■ Components of depersonalization
■ Emotionalnumbing■ Changesinbodyexperience■ Changesinvisualexperience■ Changesinauditoryexperience■ Changesintactileexperience■ Changesingustatoryexperience■ Changesinolfactoryexperience■ Lossoffeelingsofagency■ Distortionsintheexperiencingoftime■ Changesinthesubjectiveexperienceofmemory■ Feelingsofthoughtemptiness■ Subjectivefeelingsofaninabilitytoevokeimages■ Heightenedself-observation
(AfterSierraandBerrios,2001,withpermission.)
13—DEpErSONALizAtiON 207
Therelationshipbetweendepersonalizationandvarioustheoreticalaspectsofself-perceptioninphenomenologyhasbeenreviewedbyMellor(1988),whodiscussestheinfluencesofJaspers(1959),Mayer-Gross(1935),Schilder(1920)andSchneider(1958)ontheconcept.Mellorcom-mentson the frequencyof theconditionand thevarietyofdifferentpsychiatric illnesseswithwhichitmaybeassociated.Itmayoccurwithorganicpsychosyndromesincludingtraumaticbraindamage(GrigsbyandKaye,1993),epilepsyandmigraine(Lambertetal.,2002),cannabis,hal-lucinogensandecstasy(Matthewetal.,1993;Simeonetal.,2009).It isassociatedwithmooddisordersandanxietydisordersincludingsocialanxiety(Simeonetal.,1997;Michaletal.,2005).Thedepthofdepressionispositivelycorrelatedwithdepersonalizationandindepressedpatientswithanhedonia,depersonalizationwaspresentin75%ofcases(Zikićetal.,2009).
Althoughthesymptomhasbeendescribedforlonger,thetermwasusedbyHeymans(1904)and by Dugas and Moutier in 1911.The earliest theories implicate the sensory system, butlossofmoodandlossoffeelingswerealsoprominentinearlydescriptions(SierraandBerrios,1997). Frequently, depersonalization is accompanied by the symptom of derealization, a termused by Mapother (1935) to denote a similar change in the awareness of the external world.Depersonalizationandderealizationoftengotogether,becausetheegoanditsenvironmentareexperiencedasonecontinuouswhole.However,inMayer-Gross’cases,aboutaquarterofpatientshaddepersonalizationwithoutderealizationand15percenthadonlyderealization.Thelessapatient takes himself for granted, the more unfamiliar and alien does the world around himbecome(Scharfetter,1980).Ayoungfemalepatientsaid:
I felt as if I didn’t fit into the world … When I saw the moon, I felt I couldn’t cope. One day it wasn’t there and the next it was. I saw it and it
upset me and I went to pieces … I felt I did not want to be alive because I was not related to anything. I just seemed totally out of everything and I
started to cry. I couldn’t cope with the hurt and the pain. I felt I never would feel part of anything.
It is important to realize that depersonalization, the experience, like other non-psychoticphenomena,occursinhealthy,normalpeople.Somepeoplemayhavefeelingsof‘notbeingquitethemselves…lookinginonthemselvesfromtheoutside’andsoon,withoutprovocation.Othersmayhavesuchexperiencesat timesofpowerfulemotionalstimulior lifecrisisofanyvalence:extremehappiness, falling in love, the lossofbereavementor intensefearoranger.Theactualself-descriptionofdepersonalizationissimilarirrespectiveofcontext.
Thereisoneparticularfeaturedescribedbypatientsandnotoccurringinthedepersonaliza-tionthathealthypeople,especiallychildren,mayexperiencespontaneouslyinstatesoffatigue,afterprolongedsleepdeprivationorundersensorydeprivation.Thisisthepatient’sdescriptionoftheexperiencebeingintenselyunpleasantanddistressing(Ackner,1954).Itmaysubjectivelybemuchtheworstsymptominanaffective,reactiveillness.Ayoungmarriedwomansaid:
‘I feel very weird in my head. I have a great deal of torment. My mind will not leave me alone. It’s the surroundings; I cannot get my mind to myself. I felt as though I was going to fall over. I feel as if I’m lost in a fog. I just feel
as if I’m not in my head. I feel numb.’
Thesymptomisdescribedinanumberofdifferentways,anditisoftenimpossibletomakeadistinctionbetweendepersonalizationandderealization:‘everythingseemedtobegoingawayfromme’.ThefivequalitiesoftheexperienceofselfdescribedinChapter12mayeachbeinvolvedin the description of symptoms, although always with this as if character: vitality, activity,
208 FOUR—SELF AND BODY
singleness, identity (continuity) and boundaries or definition. There is virtually always otherevidenceofdisturbanceofmoodpresent:depressionoranxietyorboth.Coupledwiththisisafeelingoflossofself-esteemasaveryprominentsymptom:‘Ifeelunreal,flat,notproperlythere,lessofaperson,asthoughIcan’tgoandgetstuckin’;thatis,thefeelingofunrealityaboutoneselforone’senvironmenthasimplicationsforlackofcompetenceinrelationships.Thepatientnotonlyfeelsunrealbutalso‘detached’;thereisabarriertonormalcommunication.
At this point, it is important to emphasize the distinction between depersonalization as asymptom,occurringassociatedwithmanypsychiatricconditionsornodisorderatall,anddeper-sonalizationasasyndrome.Intheirdetaileddescriptionofthesymptomsofdepersonalizationdisorder,basedonclassicdescriptionsfromauthorsinthenineteenthandearlytwentiethcen-turies,SierraandBerrios(2001)havelistedthefollowingfoursymptomsasmostprevalentfordiagnosis: emotional numbing, changes in visual perception, changes in the experience of thebodyandlossoffeelingsofagency.Inamorerecentstudy,Simeonetal(2008)demonstratedthat the Cambridge Depersonalization Scale (Sierra and Berrios, 2000) yielded five factors:numbing,unrealityof self,perceptual alterations,unrealityof surroundings, and temporaldis-integration.Inadditionpatientswithdepersonalizationappeartohaveimpairedabilitytogener-ate visual imagery compared to normal controls. However in these individuals with impairedimagerytherewasnoassociatedabnormalityofperceptualprocessesasmeasuredbyabatteryofvisualperceptiontests(Lambertetal.,2001).
Thesesymptomsaresometimesincludedwithadescriptionofdepersonalizationbut,forthesake of clarity, should be separated and regarded as different psychopathological phenomena.Disturbancesofbodyimageorschema,disorderofsubjectivetimesense,hypochondriacalpre-occupation,déjà vuphenomenaormetamorphopsia(thedistortionofvisuallyperceivedobjects)maybedescribedbythesameindividualandmayoccurassymptomsofdepersonalizationsyn-drome. Langfeldt’s (1960) inclusion of schizophrenic passivity experiences within the termdepersonalizationisconfusing,andtheseexperiencesshouldbeexcludedfromdepersonalization,bothasasymptomandasadisorder.
SUBJECTIVE EXPERIENCE OF DEPERSONALIZATION
Depersonalizationisdifficultforthedoctortoportray;moreimportant,itisalsoextraordinarilydifficultforthepatienttodescribe.Heoftenprefaceshisattemptsatdescriptionbyembarrassedstatementssuchas‘sometimesIthinkImustbegoingmad’or‘youwillthinkmeverypeculiarwhenItellyouthisdoctor,but…’Thenfollowsahaltingandperplexedlistofdisjointed,unpleas-antexperiencesthatthepatientfeelstobeuniqueandforwhichheisunabletoconstruemeta-phorsthatsatisfyhim.Becauseofhisfailureindescription,hebelievesthatotherswillfindthesesymptomseitherbogusorclearevidenceofimminentmadness,soheomitsthemfromhisinitialaccount even though such symptoms are very common among psychiatric patients and causeenormous suffering. Depersonalization is the symptom the patient has when he experienceshimselfasbeingalteredordeficientinsomemanner;derealizationisitsequivalentwithregardtohis experienceof thingsoutsidehimself, that is, of the externalworld.Because there isnodefiniteandeasilyascertainedboundarycontainingself,itisnotalwayseasytodecidewhetherthe disorder is depersonalization or derealization. Neither is this important: they merge andoverlapandareoftensimplyincludedwithinthetermdepersonalization.
There is always a change in mood with depersonalization: the patient loses the feeling offamiliarityhehasforhimselforfortheworldoutsidehimself.Hemaydescribehimselfasfeelinglikeapuppet:hollow,detachedandstrange;on theoutside;uninvolvedwith life;nothimself;likeaghost,notsolid;astrangertohimself.Heexperiencesa lossofemotion.Similarly,withderealization he may describe his environment as flat, dim in colour, smaller, distant, cloudy,dream-like,still,‘nothingtodowithme’andalsolackinginemotionalsignificance.

13—DEpErSONALizAtiON 209
Depersonalizationiscommon,butyettothepatientsoobscureandunpleasant,that,wheneverthedescriptionofsymptomsisinterruptedbythepatient’sbaffledhesitancy,heshouldbeques-tionedwithpossibledepersonalizationsymptomsinmind.Hisreliefatfindingsomeonepreparedtolisten,andevenperhapsunderstand,isoftenenormous.Schilder(1935)hasdescribedthesesymptomsthus:
In a case of depersonalization the individual feels completely changed from what he was previously. This change is present in the ego (self ) as well as in
the outside world and the individual does not recognize himself as a personality. His actions appear to him as automatic.
He observes his actions and behaviour from the point of view of a spectator. The outside world is foreign and new to him and is not as real as before.
Schilderisusingthewordpersonalityheretorefertothewholeperson,notonlypersonalityinthemodernsenseoftheword.Thischangedawarenessofselfanditsrelationshipswiththeenvironmentisalwaysexperiencedasbeingintenselyunpleasant.
Thelocalizationofthissymptomtoanindividualorganiscalleddesomatization.Therearemanydifferentpossibleparametersintheawarenessofdifferentorgans:changesofsizeorquality,for example appearing large or tiny, or empty, or detached or filled with water or foam.Thepatientmayhaveafeelingofhislegsbeingweightless,offloatingorofsimplybeingunfamiliar.Koro,aculture-bounddisorderdescribedbyYap(1965),issometimesdescribedasanexampleofdepersonalization.Itisprobablybesttoregardthisconditionasaculture-specificmanifestationofacuteanxietyinwhichthepatientbelieveshispenisisshrinkingandfearsthatitwillultimatelydisappear.Whilsttheremaybeassociatedfeelingsofunrealityandofwatchingthedramaasaspectator,theprimaryunderlyingabnormalityisoneofintenseanxiety.
Changeoffeelingconcerningthebodyordepersonalizationmaybeassociatedwithdistortionoftimesense,whenthepassageoftimeappearsalteredinsomeway:‘time,bothpastandpresent,seems quite unreal to me, as if it had never happened and was never going to happen’.Deaffectualizationhasbeenusedtodescribetheconsistentlossofthecapacitytofeelemotion,sothatthepersonseemsunabletocry,loveorhate(Anonymous,1972).
A patient says, ‘I am going mad inside my head’; on further questioning, he is describingfindinghisownmentalprocesses tobe strange.The feelingof familiarity thatoccurswhenapersonperceivespreviouslyknownobjects(openingthefrontdoorathomeandlookinginside)alsooccurswhenoneintrospectsintoone’sownthinking(rememberingorfantasizingmyfronthall).Iknowwhatisthereinmythoughts;IknowwhatIwillthinkaboutanyparticularobject,becauseitisunlikelytobeverydifferentfromwhatIthoughtaboutitlasttime.Ialsoknow,ingeneralterms,whatIwillthinkaboutmyselfbecauseofpastexperience.Itisthisassumedcer-tainty that disappears; the loss of familiarity of oneself occurring in depersonalization, or ofoutsideselfinderealization,issimilartotheabnormalityofthefeelingoffamiliarityoccurringin jamais vu (when there is no sense of previously having seen a well-known object) and itsopposite,déjà vu(whenanunfamiliarobjectorexperienceseemstobefamiliar).Thisassociationbetweenthesubjectiveexperiencesindepersonalizationanddéjà vuphenomena(includingjamais vu)andcommonalityinalterationinthefeelingoffamiliarityhasbeenknownsincetheworkofHeymansatthebeginningofthelastcentury(SnoandDraaisma,1993).
Like other aspects of self-experience, depersonalization has social and situational aspects.Frequently,thepersonfeelsthatheislessabletoaccepthimself,hispersonality,hisbehaviourthanotherpeopleaccepttheirown.Heconsidersthathisfeelingsabouthimself,hislossofreality,isunique.This is abarrier tohisgivinganaccountofhis symptoms, and this in its turn is abarrier to communication in all areas of life. He feels himself to be different, isolated and
210 FOUR—SELF AND BODY
estrangedfromothers.Depersonalizationisanexperiencewithinanindividual,butithascon-siderablesocialconsequences.
Itfrequentlyoccursinattacksthatmaybeofanyduration,fromsecondstomonths.Typically,indepersonalizationdisorderthealteredstatelastsforafewhours,intemporallobeepilepsyforafewminutesandinanxietydisorderforafewseconds.Improvementisusuallyfirstmanifestedin a gradual increase in time free from symptoms rather than a reduction in the symptomsthemselveswhenpresent.But,itcanpresentaswithachronicnon-remittingcourse.
Onsetmaybe insidiousandwithnoknown initiatingcause,or itmaybe in response toatrigger.Themostcommonimmediateprecipitantsareseverestress,depression,panicandmari-juanaingestion(Simeonetal.,2003).Amiddle-agedmanwhodescribedhisdepersonalization‘likesomethingsupernatural–mybodyseparatedfromme–alostfeeling’vividlyrecalledhisfirst attack at the age of 11, when undergoing anaesthesia for the reduction of a fracture.Subsequent attacks felt similar despite the absence of provocation. He had also experiencedattacksofsleepparalysissincetheageof25andhaddiscoveredthatbykeepinghimselfawakeuntilverytiredhewouldfallasleepmorequicklyandthusavoidit.Anothermanwasseverelystressedbyhisquiteunreasonableworkingconditions,hoursofwork,unsympatheticemployeranddifficultcarjourneysinthecourseofhiswork.Earlyonewintermorning,hehadanappall-ingjourneythroughfog,alongcrowdedmotorwaysblockedbyaccidents,andfinallysufferedalapseofrecallfor24hoursinwhichherememberednothingofdrivingtoanothertown,register-inghimself intoahotel,orderingameal,hanginguphisclothes tidilyandgoing tobed.Hisnextmemorywasarrivingatalocalhospitalthenextday.Heremaineddepersonalizedforyearssubsequently,andhiswifedescribedthisas‘he’snotthemanImarried;it’slikehistwinbrother’.
Depersonalization is frequently situational, both in its original context and in its repeatedoccurrences.Factorscommonlyassociatedwithsymptomexacerbationarenegativeaffects,stress,perceivedthreateningsocialinteractionandunfamiliarenvironments(Simeonetal.,2003).Manypolicemenwhowereinvolvedinamajordisasteratafootballgrounddescribeddepersonalizationamongothersymptomsofpost-traumaticstressdisorder,sometimeslastingforyearssubsequently(SimsandSims,1998).Onemandescribedfeeling‘switchedoff…IfeltIwasn’tonthisplanetanymore’.Becausedepersonalizationoccursattimesofgreatstress,itmayoccurintheperpetra-torofantisocialbehaviour,forexampleviolentcrime,aswellasinthevictim.RixandClarkson(1994)giveanaccountofamanwhosavagelyassaultedhiswifewithalargespanner:‘Itwasasifitwasadreamoranightmare.IrealizedlaterwhatIhaddonebutatthetimeitwasasifIwasn’tthere’.Itwasconsideredthatdepersonalizationinthiscasewaslinkedtodissociation,thatalthoughitrepresentedachangeintheindividual’sself-experienceitdidnotaffecthisvolitionorintent.
Although,inthesetwocasesdescribedabove,depersonalizationwasassociatedwithdissocia-tion,itisimportanttoregardthesetwoexperiencesasdistinctphenomena.Empiricalevidencealsosuggeststhattheseexperiencesevenwhenassociatedaredifferentanddonotlieonacon-tinuum(Putnametal.,1996;Simeonetal.,1998).Neitherdoesdepersonalizationoccurwithany greater frequency in chronic dissociative disorders such as dissociative identity disorder,formerlymultiplepersonalitydisorderinDSM-IV(Ross,1997).
Self-inducedepisodesofdepersonalization,asanunpleasant symptom,havebeenrecordedfollowingparticularpatternsofbehaviour.ThusKennedy(1976)describedself-induceddeper-sonalizationpersistingasacomplaintaftertranscendentalmeditationandyoga.
Organic and Psychological TheoriesTheories accounting for theoccurrenceofdepersonalization, includingorganic, psychological,psychoanalytical and those linking it with schizophrenia, were reviewed by Sedman (1970).Depersonalization is regularly cited as a common symptom associated with organic states,
13—DEpErSONALizAtiON 211
especiallytemporallobeepilepsy(SedmanandKenna,1965).ThisisbasedonthecontentionofMayer-Gross(1935)thatdepersonalizationisapreformed functional responseofthebrain,thatis,anon-specificmechanismresultingfrommanydifferentinfluencesonthebrain,occurringinanidiosyncraticwayinindividualsinasimilarmannertoepilepticfitsordelirium.Hewas,inthis,followingtheneurophysiologicalhierarchicalconceptsofHughlingsJackson(1884),whocon-sideredthatthehighestlevelsofcerebralfunctionwerelostfirst,leavinguninterruptedtheactivityoflowerlevels.
Organic theoriespurporting toaccount fordepersonalizationwouldsuggest thatalterationofconsciousnessactsasareleasemechanism.However,Sedman(1970),inreviewingthelitera-ture,showedthat,eveninvariousformsoforganicpsychosyndromes,theincidenceofdeperson-alizationphenomenawassimilartothatfoundinthegeneralpopulation,atbetween25and50percent;inmoreseverechronicorganicpsychosis,theratewaslower.Fromavarietyofstudies,noquantitative relationshiphadbeendemonstratedbetween thedegreeof torpor (that is, thestageonthecontinuumfromfullalertnesstounconsciousness)andthedevelopmentofdeper-sonalization.On studying theperformanceof depersonalized subjects onpsychosomatic tests,theredidnotappeartobeevidencetosupportaspecificrelationshipbetweencloudingofcon-sciousness anddepersonalization.Thereappeared tobemany individualswho,despitevarioustypesofassaultontheirbrains,neverdevelopeddepersonalization.
Fromthisinformation,Sedman(1970)concludedthat:
there may well be a built in preformed mechanism in approximately 40 per cent of the population to exhibit depersonalization; that the factors which
initiate such a response are not specifically those associated with clouding of consciousness; or where clouding of consciousness appears to be playing a part,
it may well be the presence of another common factor that is more relevant.
Thus, the relationship between depersonalization and brain pathology remains unclear.Depersonalizationiscertainlynotpathognomonicoforganicdiseases;infact,thereisnoorganicorpsychoticabnormalityinthevastmajorityofsufferers.
The state of increased alertness observed in depersonalization is considered by Sierra andBerrios(1998)toresultfromactivationofprefrontalattentionalsystemsandreciprocalinhibitionof theanteriorcingulate, leading toexperiencesof ‘mindemptiness’ and‘indifference topain’.Thelackofemotionalcolouring,reportedasfeelingsofunreality,wouldbeaccountedforbyaleft-sided prefrontal mechanism with inhibition of the amygdala. Other authorities describeleft-hemispheric fronto-temporal activation coupled with decreased left caudate perfusion(Hollanderetal.,1992;PhillipsandSierra,2003).
Depersonalization is sometimesassociatedwith self-inducedorganic states.Thus, itoccursfollowing the ingestion of alcohol or drugs, especially psychotomimetics such as lysergic aciddiethylamide(SedmanandKenna,1964),mescaline,marijuanaorcannabis(Szymanski,1981;Carneyetal.,1984;Simeonetal.,2009)andwithsensorydeprivation.Itisalsodescribedasasideeffectwithprescribedpsychotropicdrugssuchasthetricyclicantidepressants,butbecauseof the common association between depersonalization and depression it is difficult always toattributecause.
Neurochemical findings have identified possible involvement of serotonergic, endogenousopioidandglutamatergicNMDApathways.Additionally,thereisevidenceofwidespreadmeta-bolicalterationsinthesensoryassociationcortexaswellasprefrontalhyperactivationandlimbicinhibitioninresponsetoaversivestimuli(Simeon,2004).Furthermore,thereisassociationwithchildhood interpersonal trauma, particularly emotional maltreatment (Simeon etal., 2001;Simeon,2004).

212 FOUR—SELF AND BODY
Depersonalization: Further ConsiderationsSometimestherehasbeenconsiderableconfusionoverwhetherdepersonalizationcanbedistin-guishedfromthedisordersofself-imagedescribedinChapter12asoccurringinschizophrenia.Infact,passivityexperienceshaveevenbeendescribedasavariantofdepersonalization.However,Meyer(1956),ascitedbySedman(1970),hasdistinguishedschizophrenicegodisturbancesfromdepersonalizationonphenomenologicalgrounds;thatis,onthedescriptionbythepatientofhisowninternalexperience.Itis,ofcourse,wellrecognizedthattruedepersonalizationsymptomsdooccurinschizophrenicpatients,especiallyintheearlystagesoftheillness,alongsidedefiniteschizophrenicpsychopathology.
Depersonalizationiscommonlydescribedinmanic-depressivedisorder;however,thesymp-tomsoccuronlyinthedepressivephaseandtherearenoreferencestodepersonalizationoccurringin mania (Sedman, 1970). Anderson (1938) considered that ecstasy states occurring in manic-depressivedisordersweretheobverseofdepersonalizationandthat,whiletheformeroccurredinmania, the latteroccurred indepression.Sedman(1972), inan investigationof threematchedgroups,eachof18subjectswithdepersonalizationanddepressiveandanxietysymptoms,con-sideredthat theresultsstressedthe importanceofdepressedmoodindepersonalization,whileanxietyseemedtocarrynosignificantrelationship.
Manyotherauthorshavestressedthecloseassociationbetweenthesymptomsofdeperson-alizationandanxiety.Forinstance,Roth(1959,1960)describedthephobic anxiety depersonaliza-tion syndrome as a separate nosological entity, but saw it as a form of anxiety on which theadditionalsymptomsaresuperimposedinaparticulargroupofindividuals.Heconsidereddeper-sonalizationtobemorecommonwithanxietythanwithotheraffectivedisorders, forexampledepression.The phobic symptoms are usually agoraphobic in nature.The patient, most oftenfemale,marriedandofteninthethirddecadeoflife,hasagreatfearofbeingconspicuousinanembarrassingway inpublic, for example faintingorbeing taken ill suddenlyonabusor in asupermarket.Fearofleavingthehouseunaccompanieddevelopsfromthis,sothatthepatientisfrightenedofbeingatadistancefromfamiliarsurroundingswithoutsomesupportingfiguretowhomshecanturn.Shemaybeunabletogooutofthehouseatall,evenwithherhusband.Shemayfeelpanickyonherownathomeandsokeepsherchildoffschool,apotentialprecipitatingfactorinsubsequentschoolrefusal.
Thesymptomofdizzinessisaverycommoncomplaintandfrequentlyresultsinreferraltoear,noseandthroatdepartments.FewtrellandO’Connor(1989)discusstwopossiblemodelsfortherelationshipofthisconditiontodepersonalization:onethatdizzinessanddepersonalizationarethesameexperiencedescribeddifferently;theother,abipolarhypothesis,proposesthatthetwo experiences form opposite ends of a dimension describing disturbed self–outside worldrelationships.
Although depersonalization is commonly described in association with agoraphobia, otherphobicstates,panicdisorder,varioustypesofdepressivecondition,post-traumaticstressdisorderandothernon-psychotic conditions, itmayalsoappearasapuredepersonalization syndrome,andDavison(1964)hasdescribedepisodicdepersonalizationinwhichotheraetiologicalfactorsorco-morbiddisordersarenotprominent.
In psychoanalytic theory, depersonalization has taken on a rather different meaning, andthereforetherearedifferentexplanationsforitsorigin.Psychoanalystshavebeenlessconcernedwithdescribing thephenomena than theunderlyingconceptof thealienationof theego.Forexample,intheworkoftheexistentialistschool,astypifiedbyBinswanger(1963),thereisdiscus-sionofthedepersonalization of man.
This depersonalization has by now gone so far that the psychiatrist (even more than the psychoanalyst) can no longer simply say, ‘I’, ‘you’, or ‘he’ wants,

13—DEpErSONALizAtiON 213
wishes etc. the only phrases that would correspond to the phenomenal facts. Theoretical constructs dispose him, rather, to speak instead of my, your, or his Ego wishing something. In this depersonalization we see at work that aspect
of psychiatry’s founding charter that is most at odds with every attempt to establish a genuine psychology. An explanation of this baleful influence need
go no further than the clearly recognized task that psychiatry, since Griesinger, has set itself – namely, to create a psychology that, on the one hand, serves to
bring a reified functional complex into relation with a material ‘organ’ but that, on the other hand, allows this organ itself to be divided into and
understood in terms of its functions.
Thisclearlyisquiteadifferentsenseofthewordthanthephenomenological,withwhichthischapterhasbeenconcerned.
Thedistressingexperienceofdepersonalization,witha feelingofunreality, remainscentralto the description of the disordered self.The disturbance that causes this may be organic orenvironmental,psychoticorexistential.Concernabouttheexperienceofselfandoftheenviron-mentmostcommonlyoccurtogether.
References[Anonymous](1972)Depersonalisationsyndromes[leadingarticle].British Medical Journal4,378.Ackner B (1954) Depersonalization I. Aetiology and phenomenology II. Clinical syndromes. Journal of
Mental Science100,838–72.AderibigbeYA,BlochRMandWalkerWR(2001)Prevalenceofdepersonalizationandderealizationexperi-
encesinaruralpopulation.Social Psychiatry and Psychiatric Epidemiology36,63–9.AndersonEW(1938)Aclinicalstudyofstatesof‘ecstasy’occurringinaffectivedisorders.Journal of Neurology
and Psychiatry1,1–20.Binswanger L (1963) Being-in-the-world. In Selected Papers of Ludwig Binswanger (transl. Needleman J,
1975).London:BasicBooks.CarneyMWP,BacelleLandRobinsonB(1984)Psychosisaftercannabisabuse.British Medical Journal288,
1047.DavisonK (1964) Episodic depersonalisation: observations on sevenpatients. British Journal of Psychiatry
110,505–13.DugasLandMoutierF(1911)La Depersonalisation.Paris:FelixAlcon.FewtrellWD(1986)Depersonalization:adescriptionandsuggested strategies.British Journal of Guidance
and Counselling14,263–9.FewtrellWDandO’ConnorKP(1989)Dizzinessanddepersonalization.Advances in Behaviour Research and
Therapy10,201–18.Grigsby J andKayeK (1993) Incidenceandcorrelatesofdepersonalization followinghead trauma.Brain
Injury7,507–13.Heymans G (1904) Eine Enquête über Depersonalisation und ‘Fausse Reconnaisance’. Zeitschrift fuer
Psychologie36,321–43.Hollander E, Carrasco JL, Mullen LS,Trungold S, DeCaria CM andTowey J (1992) Left hemispheric
activationindepersonalizationdisorder:acasereport.Biological Psychiatry31,1157–62.JacksonJH(1884)Croonianlecturesonevolutionanddissolutionofthenervoussystem.InTaylorJ(ed.)
(1958)Selected Writings of John Hughlings Jackson,vol. II,pp.3–120.London:StaplesPress.JaspersK(1959)General Psychopathology,7thedn.(transl.HoenigJandHamiltonMW,1963).Manchester:
ManchesterUniversityPress.KennedyRB(1976)Self-induceddepersonalizationsyndrome.American Journal of Psychiatry133,1326–8.LambertMV,SeniorC,PhillipsML,SierraM,HunterEandDavidAS(2001)Visualimageryanddeper-
sonalization.Psychopathology34,259–64.LambertMV,SierraM,PhillipsMLandDavidAS(2002)Thespectrumoforganicdepersonalization:a
reviewplusfournewcases.Journal of Neuropsychiatry and Clinical Neuroscience14,141–54.
214 FOUR—SELF AND BODY
LangfeldtG(1960)Diagnosisandprognosisofschizophrenia.Proceedings of the Royal Society of Medicine52,595–6.
MapotherE(1935)citedbyMayer-Gross(1935).MatthewRJ,WilsonWH,HumphreysD,LoweJVandWeitheKE(1993)Depersonalizationaftermari-
juanasmoking.Biological Psychiatry33,431–41.Mayer-GrossW(1935)Ondepersonalisation.British Journal of Medical Psychology15,103–22.MellorCS(1988)Depersonalisationandself-perception.British Journal of Psychiatry153(suppl.2),15–9.MeyerJE(1956)StudienzurDepersonalisation.Psychiatrie et Neurologie(Basel)132,221–32.MichalM,KaufholdJ,GrabhornR,KrakowK,OverbeckGandHeidenreichT(2005)Depersonalization
andsocialanxiety.Journal of Nervous and Mental Diseases193,629–32.MoraviaA(1960)Boredom(translDavidsonA).NewYork:NewYorkReviewBooks.PhillipsMLandSierraM(2003)Depersonalizationdisorder:afunctionalneuroanatomicalperspective.Stress
6,157–65.PutnamFW,CarlsonEB,RossCA,AndersonG,ClarkP,ToremM,BowmanES,CoonsP,ChuJA,Dill
DL,LoewensteinRJandBraunBG(1996)Patternsofdissociationinclinicalandnon-clinicalsamples.Journal of Nervous and Mental Disease184,673–9.
RixKJBandClarkson(1994)Depersonalisationandintent.Journal of Forensic Psychiatry5,409–19.RossC(1997)Dissociative Identity Disorder: Diagnosis, Clinical Features and Treatment of Multiple Personality.
NewYork:JohnWiley.RothM(1959)Thephobicanxiety–depersonalizationsyndrome.Proceedings of the Royal Society of Medicine
52,587–95.RothM(1960)Thephobicanxiety–depersonalizationsyndromeandsomegeneralaetiologicalproblemsin
psychiatry.Journal of Neuropsychiatry1,292–306.ScharfetterC(1980)General Psychopathology: an Introduction.Cambridge:CambridgeUniversityPress.Schilder P (1920) Medizinische Psychologie (transl. Rapaport D, 1953, as Medical Psychologie). New York:
InternationalUniversitiesPress.SchilderP(1928)Depersonalisation.InIntroduction to Psychoanalytic Psychiatry. Nervous and Mental Disease
Monograph series 50.NewYork:WWNorton.SchilderP (1935) The Image and Appearance of the Human Body: Studies in the Constructive Energies of the
Psyche.London:KeganPaul.Schneider K (1958) Clinical Psychopathology, 5th edn. (transl. Hamilton MW). New York: Grune and
Stratton.SedmanG(1970)Theoriesofdepersonalisation:areappraisal.British Journal of Psychiatry117,1–14.SedmanG(1972)Aninvestigationofcertainfactorsconcernedintheaetiologyofdepersonalisation.Acta
Psychiatrica Scandinavica48,191–219.SedmanGandKennaJC(1964)TheoccurrenceofdepersonalisationphenomenaunderLSD.Psychiatrie et
Neurologie (Basel)147,129–37.SedmanGandKenna JC (1965)Depersonalisation in temporal lobe epilepsy and theorganicpsychoses.
British Journal of Psychiatry111,293–9.SierraMandBerriosGE(1997)Depersonalization:aconceptualhistory.History of Psychiatry8,213–29.SierraMandBerriosGE (1998)Depersonalization:neurobiologicalperspectives.Biological Psychiatry44,
898–908.SierraMandBerriosGE(2000)TheCambridgeDepersonalizationScale:anewinstrumentforthemeas-
urementofdepersonalization.Psychiatry Research93,153–64.SierraMandBerriosGE(2001)Thephenomenologicalstabilityofdepersonalization:comparingtheold
withthenew.Journal of Nervous and Mental Diseases189,629–36.SimeonD(2004)Depersonalizationdisorder:acontemporaryoverview.CNS Drugs18,343–54.SimeonD,GrossS,GuralnikO,SteinDJ,SchmeidlerJandHollanderE(1997)Feelingunreal:30cases
ofDSM-IIIRdepersonalizationdisorder.American Journal of Psychiatry154,1107–13.SimeonD,GuralnikO,GrossS,SteinDJ,SchmeidlerJandHollanderE(1998)Thedetectionandmeas-
urementofdepersonalizationdisorder.Journal of Nervous and Mental Diseases186,536–42.SimeonD,GuralnikO,SchmeidlerJ,SirofBandKnutelskaM(2001)Theroleofchildhoodinterpersonal
traumaindepersonalizationdisorder.American Journal of Psychiatry158,1027–33.SimeonD,KozinDS,SegalKandLerchB(2009)Isdepersonalizationdisorderinitiatedbyillicitdruguse
anydifferent?Asurveyof394adults.Journal of Clinical Psychiatry70,1358–64.
13—DEpErSONALizAtiON 215
SimeonD,KozinDS,SegalK,LerchB,DujourRandGiesbrechtT(2008)De-constructingdepersonaliza-tion:furtherevidenceforsymptomclusters.Psychiatry Research157,303–6.
Simeon D, Knutelska M, Nelson D and Guralnik O (2003) Feeling unreal: a depersonalization disorderupdateof117cases.Journal of Clinical Psychiatry64,990–7.
SimsAandSimsD(1998)Thephenomenologyofpost-traumaticstressdisorder:asymptomaticstudyof70victimsofpsychologicaltrauma.Psychopathology31,96–112.
SnoHMandDraaismaD(1993)AnearlyDutchstudyofdéjàvuexperiences.Psychological Medicine23,17–26.
Stewart WA (1964) Panel on depersonalization. Journal of the American Psychoanalytic Association 12,171–86.
SzymanskiHV(1981)Prolongeddepersonalizationaftermarijuanause.American Journal of Psychiatry138,231–3.
Yap PM (1965) Koro – a culture-bound depersonalisation syndrome. British Journal of Psychiatry 111,43–50.
ZikićO,CirićSandMitkovićM(2009)Depressivephenomenology inregardtodepersonalization level.Psychiatria Danubina21,320–6.

This page intentionally left blank

217
C H A P T E R 14
Disorder of the Awareness of the Body
SummaryThe body is the physical manifestation of the individual being. It is the material, corporealinterfacewiththeexternalworld.Theworldisexperiencedthroughthebody’ssenses.Thebody,also,isitselfexperiencedasanobjectintheworld.Inthischapter,weexamine:
1. disordersofbeliefsaboutthebodyincludingbeliefsofillness,diseaseanddeath,2. disordersofbodilyfunction,includingthelossofsensory,motororcognitivefunctionthat
occurintheconversionanddissociativedisorders,3. disordersoftheexperienceofthephysicalcharacteristicsofthebodyandoftheemotional
andaestheticvalue,and4. complexdisordersofthesensoryawarenessofthebodythatalmostexclusivelyderivefrom
neurologicallesions.Even though these abnormal experiences are disparate, what binds them together into a
coherentaspectofpsychopathologyisthatthebodyasexperiencedisattheirheart.
Beside fear and sorrow, ‘sharp belchings, fulsome crudities, heat in the bowels, wind and rumblings in the guts, vehement gripings, pain in the belly and
stomach sometimes after meat that is hard of concoction, much watering of the stomach, and moist spittle, cold sweat.’
Robert Burton (1577–1640), The Anatomy of Melancholia (1628)
To some, ill health isa way to be important,
Others are stoics,a few fanatics,
who won’t feel happy untilthey are cut open.W.H. Auden (1969)
Thephysicalityofthebodyiseverpresent:thereisdensity,mass,movement,action,speed,position,heat,coldandvariousdegreesoftouch,painandsoon.SinceDescartes(1596–1650),the relationship between mind and body has stimulated much investigation and discussion.Descartes’originalclaimwasthatthemindandbodyaredistinctanddifferent;furthermore,thatthemindcanexistwithoutthebody.Thereareother theories thatattempttoaccount for thenatureofmindandbody.Materialisttheoriesproposethatthebodyisallthereis,andvariationsofthesetheoriesaccountformindindifferentways,whereasidealisttheoriesmaketheoppositeclaimthatthemindisallthatexists.Thefactthatmanydescriptionsofmood,cognition,volitionandotherpsychologicalfunctionsareexpressedinphysicalterms–‘aheavyheart’,‘bone-headed’,

Keywords: Hypochondriasis, Disgust, Dysmorphophobia, Body Integrity Identity Disorder,AnorexiaNervosa,MuscleDysmorphia.
14—DiSOrDEr OF thE AwArENESS OF thE BODY 217.e1
218 FOUR—SELF AND BODY
‘gutsanddetermination’,‘apainintheneck’–underlinestheinextricablerelationshipbetweenmindandbodyandemphasizesthedegreetowhichthebodycanbecomeameansofcommu-nicating distress and bodily metaphors used to consciously or unconsciously express feelings.Whetherthesemetaphorsoriginallyderivefromthephysicalmanifestationsofemotionaldistressorwhetherthelanguage,thatis,themetaphor,structurestheexperienceisamootpoint.Whatisclearisthatthereisnoreadydivisionbetweenthesubjectiveexperienceofselfandofbody.Aten-year-oldgirlputthisrelationshipthus:‘Youfeelbetterifyou’vedoneyourhomework;ifyouhaven’tyougetahorriblepaininyourstomach’.Finally,sincethebodyisitselfanobjectintheworld,itinhabitsaworldofvaluesandnormssuchthatthereare‘good’and‘bad’bodies,‘desir-able’and‘undesirable’bodies.Inaddition,asubsetofvaluesisaesthetics,sothatthereare‘beauti-ful’and‘ugly’bodies.Thismeansthat individualsapproachboththeirownandotherpeople’sbodieswithanattitude:theyappraisebodieswithasetofbeliefsandexpectations,formjudge-mentsandacttowardsbodieswithapprovalordisapproval.
Inordertoformacohesiveframeworkforconceptualizingthedisordersofselfandtheverydiverseabnormalitiesofbodyimage,oneneedstoapplythemethodsofdescriptivepsychopathol-ogy.InChapter12,thenatureofselfandthepathologyoftheexperienceofselfwerediscussed.Inthischapter,disordersoftheawarenessofbodyarediscussed.
ClassificationCutting(1997)givesagoodoutlineoftheclassificationofdisordersofawarenessofthebody,whichhasbeenadaptedfor thischapter (Table14.1).Therearedisordersofbeliefsabout thebodyincludingbeliefsofillness,diseaseanddeath(seebelow).Inthisgrouparealsothedisordersofdissatisfactionwiththebody,whichoccurineatingdisorders.Thesedissatisfactionswiththebodyarebestunderstoodasarisingfromnegativecognitiveevaluations,thatis,beliefsaboutthebody.Next,therearedisordersofbodilyfunction,includingthelossofsensory,motororcognitivefunction thatoccurs in thedissociativedisorders.Therearedisordersof theexperienceof thephysicalcharacteristicsofthebody.Theseincludedisordersoftheexperienceofthesize,shape,structureorweightofthebody.And,finally,therearecomplexdisordersofthesensoryexperienceofthebodythatalmostexclusivelyderivefromneurologicallesions.
Disorders of Beliefs About the Body (Bodily Complaint Without Organic Cause)Classificationof thesedisorders isdifficult,partlybecause thesymptomsareobscure inoriginandpartlybecausetherearedifferenttheoreticalbasesforthewordsused.Forexample,conversion hysteriawasusedasatermthatreferredtothepresumedunconsciousconversionofanunaccept-ableaffectintoaphysicalsymptom.Hypochondriasisreferstoaconcernwithsymptomsandwithillnessthattheoutsideobserverregardsasexcessive;thesameamountofconcernorcomplaintassociatedwithpathology that thedoctor regardsas justifying itwouldnotbedeemedhypo-chondriacal.Dysmorphophobiaisaphenomenologicaltermandreferstothesubjectiveexperienceofdissatisfactionwithbodilyshapeorform(Figure14.1).
HYPOCHONDRIASIS
Hypochondriasisdescribesthesubjectiveandundueawarenessofphysicalsymptomswhichareinterpreted as signalling serious illness. It is a symptom and not a disease. There are manydifferentmodesofexpression:minorpainanddiscomfortdominatetheperson’slifeandoccupyhisattention;hemayhaveunreasonablefearsaboutthelikelihoodofdevelopingseriousillness,

14—DiSOrDEr OF thE AwArENESS OF thE BODY 219
andfeelsaneedtotakeexcessiveprecautions;hemaymisinterpretbenignblemishesashavingsinisterpathologicalsignificance.Theseexpressionsofdissatisfactionmayoccurontheirownorinanycombination,andtheycanaffectanybodilysystemorpsychologicalprocess.Hypochondriacalsymptomsareverycommonandusuallytransient.Onlyaminoritycometomedicalattention,andonlyaselectedatypicalproportionoftheseareseenbypsychiatrists.
Thereisadistinctionbetweenillnessfears,whentherearenobodilysymptoms,andthefearsanddistresswhicharenotassociatedwithbodilysymptomsbutmerelyariseoutofthepossibilityofseriousillness.Thisshowstheoverlapbetweenillnessphobias(unreasonablefearofdevelopingillness)andhypochondriasis(preoccupationwithsymptoms).Thereisoftendifficultyindiagnosiswhenapersonwithdemonstrablephysicalpathologycomplainsexcessivelyabouthissymptoms;hiscomplaintsappeartobeoutofproportiontotheanticipatedsufferinganddisabilityoftheillness.Necessaryandentirelyroutinemedicalexaminationandinvestigationtendtoreinforcethepatient’s symptoms.Somatic symptomswithoutorganicpathologyareextremelycommonand may result from misunderstanding the nature and significance of physiological activityaggravatedbyemotion(Kellner,1985).Themechanismsunderlyinghypochondriacalsymptomsincludemisinterpretationofnormalbodilysensations;conversionofunpleasantaffect,especially
TABLE 14.1 ■ Classification of disorders of awareness of the body
Classification Details
Beliefs about the body
Illness and disease Hypochondriacal symptoms
Body dissatisfaction Real and ideal body weight discrepancy
Function of the body
Sensory deficits For example dissociative sensory loss (blindness)
Experience of physical characteristics of the body
Size Microsomatognosia, macrosomatognosia and body image disturbance
Shape ‘My jaws are misshapen’
Colour Skin colour may be experienced as lighter
Structure ‘My lungs are connected to my abdomen’
Weight Feelings of lightness or heaviness
Experience of emotional value of the body
Anosognosic overestimation Exaggeration of body’s strength
Misoplegia Hatred of body part
Dysmorphophobia Feeling of ugliness or defect of body or one of its parts
Experience of sensory awareness of the body and the world
Palinaptia Persistence of sensation beyond the duration of contact with stimuli
Exosomesthesia Cutaneous sensation in extra-personal space
Alloaesthesia Experience of sensation on contralateral side to stimulation
(After Cutting, 1997, p. 317, with permission of Oxford University Press.)
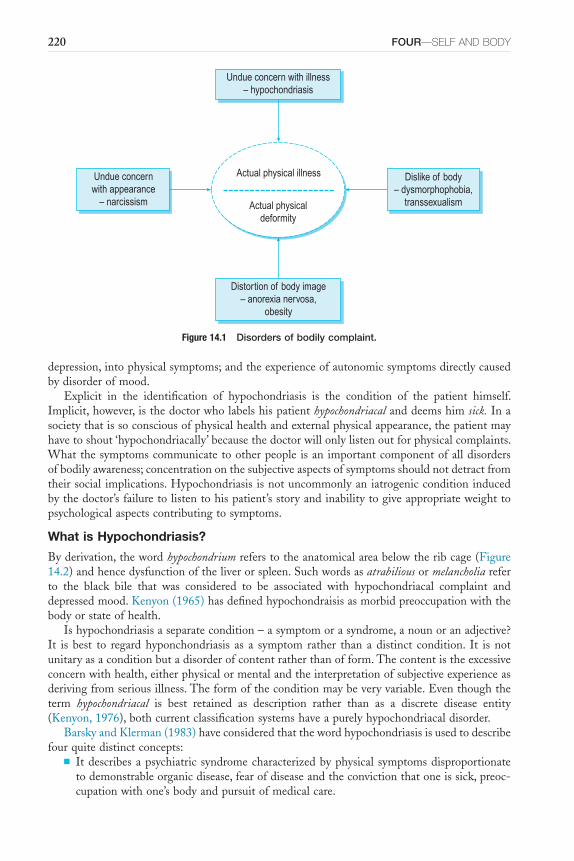
220 FOUR—SELF AND BODY
depression,intophysicalsymptoms;andtheexperienceofautonomicsymptomsdirectlycausedbydisorderofmood.
Explicit in the identification of hypochondriasis is the condition of the patient himself.Implicit,however,isthedoctorwholabelshispatienthypochondriacalanddeemshimsick.Inasocietythatissoconsciousofphysicalhealthandexternalphysicalappearance,thepatientmayhavetoshout‘hypochondriacally’becausethedoctorwillonlylistenoutforphysicalcomplaints.Whatthesymptomscommunicatetootherpeopleisanimportantcomponentofalldisordersofbodilyawareness;concentrationonthesubjectiveaspectsofsymptomsshouldnotdetractfromtheirsocial implications.Hypochondriasisisnotuncommonlyaniatrogenicconditioninducedbythedoctor’sfailuretolistentohispatient’sstoryandinabilitytogiveappropriateweighttopsychologicalaspectscontributingtosymptoms.
What is Hypochondriasis?
Byderivation,thewordhypochondriumreferstotheanatomicalareabelowtheribcage(Figure14.2)andhencedysfunctionoftheliverorspleen.Suchwordsasatrabiliousormelancholiareferto the black bile that was considered to be associated with hypochondriacal complaint anddepressedmood.Kenyon(1965)hasdefinedhypochondraisisasmorbidpreoccupationwiththebodyorstateofhealth.
Ishypochondriasisaseparatecondition–asymptomorasyndrome,anounoranadjective?It is best to regardhyponchondriasis as a symptom rather than adistinct condition. It is notunitaryasaconditionbutadisorderofcontentratherthanofform.Thecontentistheexcessiveconcernwithhealth,eitherphysicalormentalandtheinterpretationofsubjectiveexperienceasderivingfromseriousillness.Theformoftheconditionmaybeveryvariable.Eventhoughtheterm hypochondriacal is best retained as description rather than as a discrete disease entity(Kenyon,1976),bothcurrentclassificationsystemshaveapurelyhypochondriacaldisorder.
BarskyandKlerman(1983)haveconsideredthatthewordhypochondriasisisusedtodescribefourquitedistinctconcepts:
■ Itdescribesapsychiatricsyndromecharacterizedbyphysical symptomsdisproportionatetodemonstrableorganicdisease,fearofdiseaseandtheconvictionthatoneissick,preoc-cupationwithone’sbodyandpursuitofmedicalcare.
Figure 14.1 Disorders of bodily complaint.
Undue concern with illness– hypochondriasis
Dislike of body– dysmorphophobia,
transsexualism
Undue concernwith appearance
– narcissism
Distortion of body image– anorexia nervosa,
obesity
Actual physical illness
Actual physicaldeformity
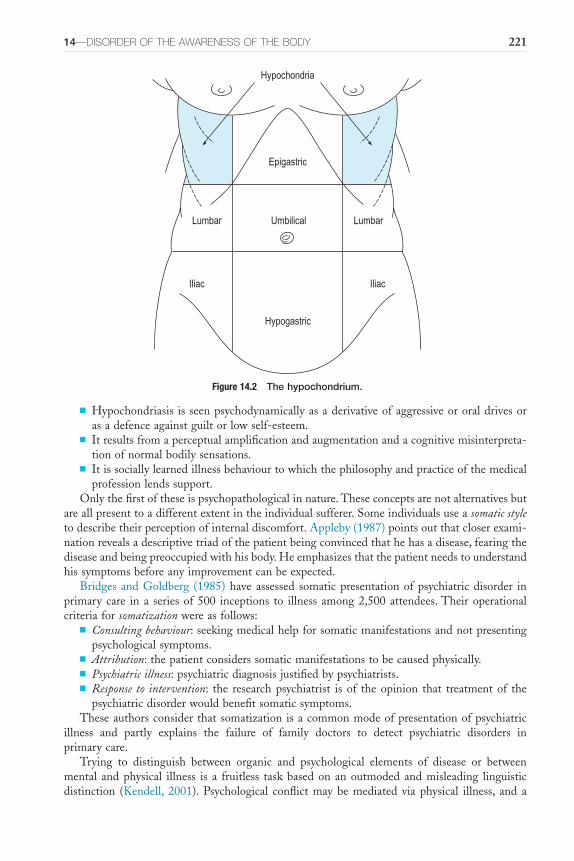
14—DiSOrDEr OF thE AwArENESS OF thE BODY 221
■ Hypochondriasis isseenpsychodynamicallyasaderivativeofaggressiveororaldrivesorasadefenceagainstguiltorlowself-esteem.
■ Itresultsfromaperceptualamplificationandaugmentationandacognitivemisinterpreta-tionofnormalbodilysensations.
■ Itissociallylearnedillnessbehaviourtowhichthephilosophyandpracticeofthemedicalprofessionlendssupport.
Onlythefirstoftheseispsychopathologicalinnature.Theseconceptsarenotalternativesbutareallpresenttoadifferentextentintheindividualsufferer.Someindividualsuseasomatic styletodescribetheirperceptionofinternaldiscomfort.Appleby(1987)pointsoutthatcloserexami-nationrevealsadescriptivetriadofthepatientbeingconvincedthathehasadisease,fearingthediseaseandbeingpreoccupiedwithhisbody.Heemphasizesthatthepatientneedstounderstandhissymptomsbeforeanyimprovementcanbeexpected.
BridgesandGoldberg (1985)haveassessed somaticpresentationofpsychiatricdisorder inprimarycare ina seriesof500 inceptions to illnessamong2,500attendees.Theiroperationalcriteriaforsomatizationwereasfollows:
■ Consulting behaviour:seekingmedicalhelpforsomaticmanifestationsandnotpresentingpsychologicalsymptoms.
■ Attribution:thepatientconsiderssomaticmanifestationstobecausedphysically.■ Psychiatric illness:psychiatricdiagnosisjustifiedbypsychiatrists.■ Response to intervention: the researchpsychiatrist is of theopinion that treatmentof the
psychiatricdisorderwouldbenefitsomaticsymptoms.Theseauthorsconsiderthatsomatizationisacommonmodeofpresentationofpsychiatric
illness and partly explains the failure of family doctors to detect psychiatric disorders inprimarycare.
Trying to distinguish between organic and psychological elements of disease or betweenmental andphysical illness is a fruitless taskbasedonanoutmodedandmisleading linguisticdistinction (Kendell, 2001).Psychological conflictmaybemediated via physical illness, and a
Figure 14.2 The hypochondrium.
Hypogastric
IliacIliac
LumbarLumbar Umbilical
Epigastric
Hypochondria
222 FOUR—SELF AND BODY
physicalillnessresultsinpsychosocialsequelae.Bothsomaticandpsychologicalsymptomsoccur,anditisperfectlypossibleforapatienttohaveahypochondriacalreactiontoaclearlydefinedorganicillness.
Apatientwhoregardshimselfashavingsymptomsofillnesscommunicatesthistorelativesandalsotothedoctorinatacitrequestforbothhelpandlabelling(Parsons,1951).Inordertocometomedicalattention,thepersonhastocarryoutaparticularsetofactions,thatis,undertakeillnessbehaviour(Mechanic,1962,1986).Illnessbehaviourincludesthemannerinwhichsymp-tomsaredifferentiallyperceived,evaluatedandacteduponbydifferentkindsofpeopleandindifferent social situations.Whilst somepeoplemaybeable tomake lightof symptoms, shrugthemoffandavoidseekingmedicalattention,othersmayrespondtotrivialpainanddiscomfortbyreadilyseekingcare.Itisclear,therefore,thatindividualcharacteristicsaswellassocialculturalonesdeterminehowanyoneindividualwillrespondtosymptoms.
Individualdeterminantsofhypochondriasisseemtoincludepreoccupationwithbodilyfunc-tionsorwiththeideaofharbouringanillness,ruminationaboutillness,suggestibility,unrealisticfearofinfection,fascinationwithmedicalinformationandfearofprescribedmedication(Finketal.,2004).Fearofdeathalsoseemstobeanintegralaspectofhypochondriasis(Noyesetal.,2002b),andchildhoodadversity(includingtraumaticeventsandseriousillnessandinjury)andparentalmodellingofillnessbehaviourinchildhoodarevulnerabilityfactors(Noyesetal.,2002a;Kirmayer and Looper, 2006). Anxiety (Olatunji etal., 2009) and disgust (Davey, 2011) alsoappeartounderliehypochondriasis.Disgust,inthiscontext,isconceivedofasadisease-avoidantemotion,anddisgustpropensityandsensitivityareregardedasvulnerabilityfactorsforanumberof disorders including blood-injection-injury phobia and hyponchodriasis. Cyberchondriasis, atermreferringtoexcessiveandrepeatedhealth-relatedsearchesontheInternet,revealsaspectsof hypochondriasis that may have remained covert, namely that behavioural aspects includesearchingforhealthinformationondiagnosedandundiagnoseddisorders,seekingoutdescrip-tions of other people’s experience of illness and using message boards and support groups.However,thesebehavioursonlyprovokemoredistressandanxiety(Museetal.,2012;StarcevicandBerle,2013).
There are very marked cultural differences in the presentation of symptoms of disorderedmood;somatizationofemotionaldistressappliestobothanxietyanddepression(Rack,1982).Thepredominanceofdescriptionofsomaticovermoodsymptomsindepressiveillnesshasbeenreported from India, Pakistan, Bangladesh, Hong Kong, theWest Indies and various Africancountries.Thereasonsforthisincludetheexpectationsthepatienthasofwhatthedoctorcando,theuseofsomaticsymptomsasmetaphorfordistressandthesocialunacceptabilityofpsy-chological symptoms. The Bradford Somatic Inventory has been devised for a multiethniccomparisonofthefrequencyofsomaticsymptoms,theiranatomicallocalizationandtheirasso-ciationwithpsychiatricdisorder(Mumfordetal.,1991).ImmigrantpopulationsfromPakistanintheUnitedKingdomdemonstratemoresomaticsymptomsontheBradfordSomaticInventorycomparedwiththenativepopulation.Thesesymptomsareassociatedwithrecognizableanxietyanddepressionasmeasuredbyvalidatedquestionnaires(Farooqetal.,1995).
Psychopathology of the Hypochondriacal Patient
The contentofhypochondriasis is theexcessiveconcernwithhealth,eitherphysicalormental.PossibleformsoftheconditionarelistedinBox14.1.Theseformsforacontentofconcernaboutcancercanincludethefollowing.
■ Ahallucinatoryvoicemaysaytothepatient,‘youhavecancer,youaremoribund’.■ Asecondary delusionassociatedwithaffectiveillnessmayoccurinwhichthepatientunrea-
sonablybelieveshehascancer;he isquiteunabletoaccepthisdoctor’s reassurance.Thebeliefisunderstandableinrelationtothepatient’soveralldepressedmoodstate.Thatsuchsecondarydelusionscouldbeassociatedwithaffectivepsychoseswasclearlydescribedby

14—DiSOrDEr OF thE AwArENESS OF thE BODY 223
Cotard (1882): ‘she blamed herself and felt guilty. After some months she entertainedhypochondriacaldelusions,believingthatshehadnostomachandthatherorganshadbeendestroyed; sheattributed thesebeliefs to theeffectsofanemeticwhichshehad, in fact,beengiven’.This associationofhypochondriacal andnihilisticdelusionswithdepressivepsychosisintheelderlyhasbeencalledCotard’ssyndrome.
■ Thedelusionmaybeprimaryinnature.Apatientwithschizophreniabelievedthathehadbeen inoculated under a general anaesthetic with a transmissible cancer because othersbelievedhimtobehomosexual.
■ Hypochondriasisoftenmanifestsasanovervalued idea.Suchapersonisconstantlyworriedandconcernedabouttheriskofillnessandtheneedtotakeprecautionsinwaysthathisfriendsfindridiculous,forinstanceinthelengthsthathewillgotoavoidapossiblecar-cinogen.Heconsidersitperfectlyreasonablethatheshouldtakeduecaretomaintainhishealth,butheagreesthathismeasuresareexcessive.Hecannotstophimself,nightorday,from thinking,worryingand trying toprevent illness.Suchanovervalued idea is foundreasonable, or at least not alien to the person’s nature, but preoccupies the mind to anunreasonable extent, in that the whole energy and being becomes directed towards thissingleidea.
■ The hypochondriacal idea may take the form of an obsessional rumination in which thepossibilityofaparticularillnessoraformofwords,as‘Ihavecancer’,mayrecur.Thisisrecognizedasbeingboth ‘alien tomynature’but also ‘coming from insidemyself ’. It isresistedyetoccursrepetitively.
■ Withoutitsamountingtoadelusion,patientsmayoftenhavehypochondriacalsymptomsofanon-specificnatureinthecourseofadepressiveillness.Itmaybepossibletoreassurethemconcerninganyparticularsymptom,butthisdoesnotmakethemfeelbetterintheirmoodnordoesitpreventtheoccurrenceoffurtherhypochondriacalsymptomsintheformofdepressiveruminations.
■ Inthecontextofacuteorchronicanxiety,thepatientmaybepronetomultitudinousworriesconcerningillnessandfearsofillness.Thenormalsensoriumisinterpretedassymptoms;symptomsareinterpretedasseriousillness.Mosthypochondriacalsymptomsoccurinrela-tiontoanxietyanddepression;theotherformsofdisorderaremuchlessfrequent.
The commonest bodily symptoms implicated in hypochondriasis are musculoskeletal; gas-trointestinal,includingindigestion,constipationandotherpreoccupationwithmalfunction;andcentralnervoussystem,includingheadache(Kenyon,1964).Themostcommonlyaffectedpartsof thebodyareheadandneck,abdomenandchest. In16percentofpatients, symptomsarepredominantlyunilateral,andofthese,73percent,accordingtoKenyon,wereleft-sided.Therewasnosignificantphysicalabnormalityfoundin47percentofthoseadmittedtoapsychiatricwardforhypochondriasis.Painwasprominentin70percentofpatients.
Hypochondriasis may be associated with smell; bodily appearance; sexual hypochondria;ear, nose and throat symptoms; and ophthalmological abnormalities (Karseras, 1976) such as
BOX 14.1 ■ Psychopathology of hypochondriasis
■ Hallucination■ Secondarydelusion■ Primarydelusion■ Overvaluedidea■ Obsessionalrumination■ Depressiverumination■ Anxiouspreoccupation
224 FOUR—SELF AND BODY
asthenopia,whichincludessuchcomplaintsasoculardiscomfort,achingeyes,soreness,pressurein or around the eyes, tiredness of eyes, grittiness, chronic redness, feelings that the eyes arepushedoutonstalks,tightnessoftheskinacrossthebridgeofthenoseorprickingoftheskinaroundtheeyes.Photophobiaisacommonhypochondriacalcomplaint,asare‘floaters’–muscaevolitantes,photopsiaandsometimesdiplopia.
Hypochondriacal complaint may relate to psychological symptoms and the fear of mentalillness.Inthiscontext,sleepisofteninvolved,withsubjectivefeelingsofsleepnotoccurringatall,notoccurringinsufficientamountornotbeingofsatisfactoryquality.Fearofmadnessandinevitablepsychiatricdeteriorationiscommonlyassociatedwithacuteanxietydisordersandalsowithdepressiveillness.
Disorders of Bodily Function – Conversion and DissociationPsychopathologyhas,asitssubjectmatter,actualconsciouspsychologicalphenomena.Althoughour main concern is with pathological phenomena, it is also necessary to know what peopleexperienceingeneralandhowtheyexperienceit;inshort,psychopathologyisinterestedinthefullrangeofconsciouspsychologicalphenomena.Theforegoingraisesthequestionofwhetherexperiencesthatarenotinconsciousawareness,suchasthosethatarethesubjectofthissection,caneverbethepropersubjectofpsychopathology,sincetheseexperiencesarenotinconsciousawareness.Theseexperiencesandbehaviourshaveanantiquepedigreeandhave,untilrecently,beendescribedbythetermhysteria.
Themeaningandvalidityof the termhysteriahasbeenarguedabout for centuries (Veith,1965).Slater (1965)wished to reject thediagnosisofhysteriawhile retaining theword as anadjectivetodescribecertaintypesofsymptomsandpersonality.Lewis(1975)summarizedthiscontroversy:‘Themajorityofpsychiatristswouldbehardputtoitiftheycouldnolongermakeadiagnosisof“hysteria”or“hystericalreaction”;andinanycaseatougholdwordlikehysteriadiesveryhard.Ittendstooutliveitsobituarists.’Classically,physicalsymptoms,usuallymimick-ingneurologicaldisturbancessuchasseizures,paralysis,tremors,blindness,andgaitabnormalitiesoccur inthesettingofpsychologicaldistresswithoutaccompanyingexpectedphysicalfindingson examination. The term conversion was used to denote the fact that emotional distress orpsychologicalconflicthadbeenconvertedintophysicalcomplaints.Arelatedtermisdissociation,referringtothedisturbanceofthebasicunityoftheselfresultingintheapparentseparationofaspectsoftheselffromoneanother.Forexample,aseeminglyconsciousindividualmayreportthatsheisunabletorecallvitalaspectsofherbiographydespitehavingnodemonstrableabnor-malitiesofmemory. It isobvious that the termdissociation ismerelyadescriptive concept forsomethingfactuallyexperiencedandencounteredinclinicalpractice,aswellasatheoryforwhathappensintheparticularstate,andthusitprovidesthehypothesisforanobservedclinicalfact.It is a concept that does not describe anything uniform but touches upon modes of extra-consciousexplanatorymechanism.
Theimplicationsthatmaybedrawnfromtheconceptualizationofconversionanddissocia-tionare:
1. thepresentingsymptomsarepsychologicallydetermineddespitebeingphysicalinnature;2. causationisthoughttobeunconsciousandhencethepatientisnotawareofthepsycho-
logicaldeterminants;3. symptomsmaycarrysomesortofadvantagetothepatient,thesocalledprimaryorsec-
ondarygain;and4. thesymptomsoccurbythemediationoftheputativeexplanatorybutill-definedprocesses
ofconversionordissociation.
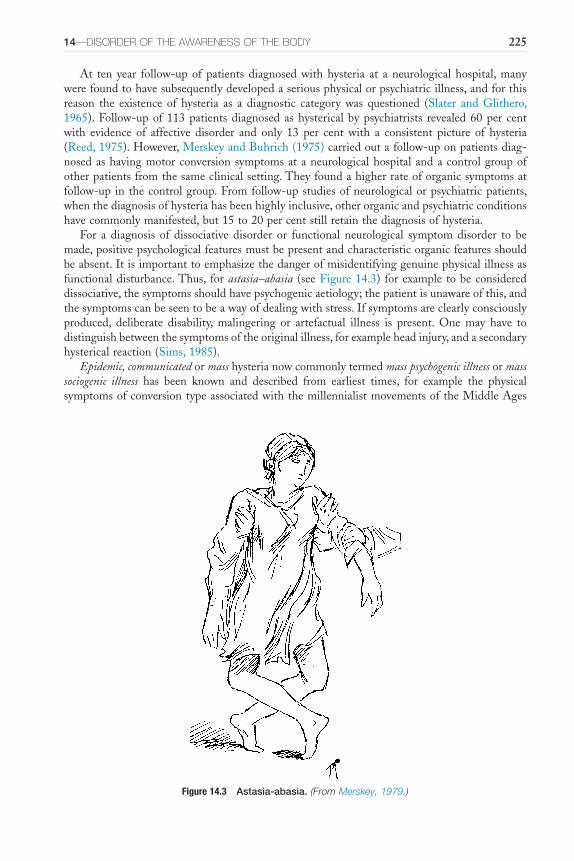
14—DiSOrDEr OF thE AwArENESS OF thE BODY 225
At tenyear follow-upofpatientsdiagnosedwithhysteria at aneurologicalhospital,manywerefoundtohavesubsequentlydevelopedaseriousphysicalorpsychiatricillness,andforthisreason the existence of hysteria as a diagnostic category was questioned (Slater and Glithero,1965).Follow-upof113patientsdiagnosedashystericalbypsychiatrists revealed60per centwith evidence of affective disorder and only 13 per cent with a consistent picture of hysteria(Reed,1975).However,MerskeyandBuhrich(1975)carriedoutafollow-uponpatientsdiag-nosedashavingmotorconversionsymptomsataneurologicalhospitalandacontrolgroupofotherpatientsfromthesameclinicalsetting.Theyfoundahigherrateoforganicsymptomsatfollow-upinthecontrolgroup.Fromfollow-upstudiesofneurologicalorpsychiatricpatients,whenthediagnosisofhysteriahasbeenhighlyinclusive,otherorganicandpsychiatricconditionshavecommonlymanifested,but15to20percentstillretainthediagnosisofhysteria.
For a diagnosis of dissociative disorder or functional neurological symptom disorder to bemade,positivepsychologicalfeaturesmustbepresentandcharacteristicorganicfeaturesshouldbeabsent.Itisimportanttoemphasizethedangerofmisidentifyinggenuinephysicalillnessasfunctionaldisturbance.Thus, forastasia–abasia (seeFigure14.3) forexampletobeconsidereddissociative,thesymptomsshouldhavepsychogenicaetiology;thepatientisunawareofthis,andthesymptomscanbeseentobeawayofdealingwithstress.Ifsymptomsareclearlyconsciouslyproduced, deliberate disability, malingering or artefactual illness is present. One may have todistinguishbetweenthesymptomsoftheoriginalillness,forexampleheadinjury,andasecondaryhystericalreaction(Sims,1985).
Epidemic, communicatedormasshysterianowcommonlytermedmass psychogenic illnessormass sociogenic illness has been known and described from earliest times, for example the physicalsymptomsofconversiontypeassociatedwiththemillennialistmovementsoftheMiddleAges
Figure 14.3 Astasia-abasia. (From Merskey, 1979.)
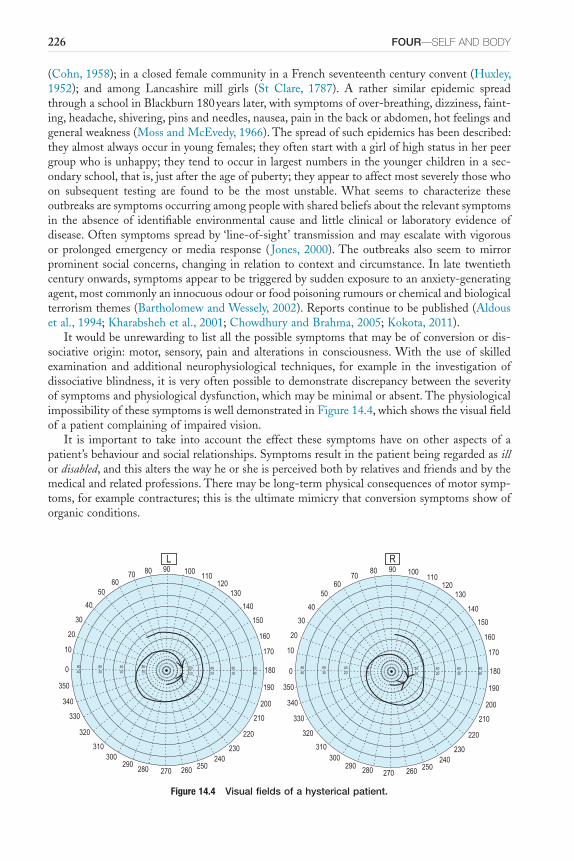
226 FOUR—SELF AND BODY
(Cohn,1958);inaclosedfemalecommunityinaFrenchseventeenthcenturyconvent(Huxley,1952); and among Lancashire mill girls (St Clare, 1787). A rather similar epidemic spreadthroughaschoolinBlackburn180yearslater,withsymptomsofover-breathing,dizziness,faint-ing,headache,shivering,pinsandneedles,nausea,paininthebackorabdomen,hotfeelingsandgeneralweakness(MossandMcEvedy,1966).Thespreadofsuchepidemicshasbeendescribed:theyalmostalwaysoccurinyoungfemales;theyoftenstartwithagirlofhighstatusinherpeergroupwhoisunhappy;theytendtooccurinlargestnumbersintheyoungerchildreninasec-ondaryschool,thatis,justaftertheageofpuberty;theyappeartoaffectmostseverelythosewhoon subsequent testing are found to be the most unstable. What seems to characterize theseoutbreaksaresymptomsoccurringamongpeoplewithsharedbeliefsabouttherelevantsymptomsin the absenceof identifiable environmental cause and little clinical or laboratory evidenceofdisease.Oftensymptomsspreadby‘line-of-sight’transmissionandmayescalatewithvigorousor prolonged emergencyormedia response ( Jones, 2000).Theoutbreaks also seem tomirrorprominentsocialconcerns,changinginrelationtocontextandcircumstance.In latetwentiethcenturyonwards,symptomsappeartobetriggeredbysuddenexposuretoananxiety-generatingagent,mostcommonlyaninnocuousodourorfoodpoisoningrumoursorchemicalandbiologicalterrorismthemes(BartholomewandWessely,2002).Reportscontinuetobepublished(Aldousetal.,1994;Kharabshehetal.,2001;ChowdhuryandBrahma,2005;Kokota,2011).
Itwouldbeunrewardingtolistallthepossiblesymptomsthatmaybeofconversionordis-sociativeorigin:motor, sensory,pain and alterations in consciousness.With theuseof skilledexamination and additionalneurophysiological techniques, for example in the investigationofdissociativeblindness,itisveryoftenpossibletodemonstratediscrepancybetweentheseverityofsymptomsandphysiologicaldysfunction,whichmaybeminimalorabsent.ThephysiologicalimpossibilityofthesesymptomsiswelldemonstratedinFigure14.4,whichshowsthevisualfieldofapatientcomplainingofimpairedvision.
It is important to take into account the effect these symptoms have on other aspects of apatient’sbehaviourandsocialrelationships.Symptomsresultinthepatientbeingregardedasillordisabled,andthisaltersthewayheorsheisperceivedbothbyrelativesandfriendsandbythemedicalandrelatedprofessions.Theremaybelong-termphysicalconsequencesofmotorsymp-toms,forexamplecontractures;thisistheultimatemimicrythatconversionsymptomsshowoforganicconditions.
Figure 14.4 Visual fields of a hysterical patient.
0
350
10
20
30
40
5060
70 80 90 100110
120130
140
150
160
170
180
190
200
210
220
230240
250260270280290
300310
320
330
340
8040
6030
4020
2010
2010
4020
6030
8040
L
0
10
20
30
40
5060
7080 90 100
110120
130
140
150
160
170
180
190
200
210
220
230240
250260270280290300
310
320
330
340
350
8040
6030
4020
2010
2010
4020
6030
8040
R
14—DiSOrDEr OF thE AwArENESS OF thE BODY 227
Classically,moodintheseconditionsisdescribedasbelle indifference.Suchamoodoccurredinagirlaged20withseveredisabilitythathadentailedherusingcrutchesforthepasttwoyears.Shesmiledwithsublimeresignationatherunfortunatesituation,andeveryonearoundherwasrelieved that she accepted her symptom so stoically! However, some patients with conversionsymptoms show higher autonomic arousal than do anxious and phobic patients (Lader andSartorius,1968).
Disorders of the Physical Characteristics and Emotional Value of the Body (Dislike of the Body)This sectiondealswithhow thebody is subjectively experiencedas aphysicalobject thathasboth symbolic and aesthetic value to the individual.These two aspects of a person’s attitudetowards their own body are distinct but interrelated. A distorted subjective experience of thebody,thesocalleddistortionofbodyimage,mayoccurindependentlyofapprovalordisapprovalorindeedofdislikeofthebody.Furthermore,thebodycanbeappraisedasugly,thatisasaes-theticallyunattractive,intheabsenceofdemonstrableabnormalityofbodyimage.
DYSMORPHOPHOBIA (BODY DYSMORPHIC DISORDER)
Many people are dissatisfied with the way they look and, of course, this does not of itselfconstitute a psychiatric symptom. However, unreasonable loathing or excessive preoccupationwithadislikedfeaturemayresultinpsychiatricreferral.Suchpeoplemayshowgeneralizeddisap-proval of their appearance, or it may be concentrated on one feature. Dysmorphophobia wasfirstdefinedbyMorselli(1886)as‘asubjectivefeelingofuglinessorphysicaldefectwhichthepatient feels is noticeable to others, although his appearance is within normal limits’. As themeaningofthetermphobiahaschangedinthepastcentury,Berrios(1996)considersthatdys-morphophobiaisatleastassatisfactoryatermasmodernequivalents.AccordingtoAndreasenandBardach(1977),theprimarysymptomofdysmorphophobiaisthepatient’sbeliefthatheorsheisunattractive.
Dysmorphophobia has been defined, more inclusively, as the primary complaint of someexternalphysicaldefectthoughttobenoticeabletootherpeoplebut,objectively,itsappearancelieswithinnormallimits(Hay,1970).Patientspresentingtoaplasticsurgeonforcosmeticrhi-noplastywere examinedpsychiatrically.Theywere, as agroup,moredisfigured thana controlgroup, and they showed some psychological disturbance in that 40 per cent showed disorderof personality.There was, however, no relationship between the degree of deformity and theamountofpsychologicaldisturbance.HayandHeather (1973)commented thatwhensurgerywascarriedout,thosepatientswithminimaldisfigurementdidaswellasthosewithmoremarkeddefects,bothsubjectively indescriptionof their self-imageandonpsychological testing.Theyconsideredthat thedegreeofdeformitywasnotofmajor importance incomingtoadecisionwithregardtooperation.Patientsreportedmarkedimprovementintheirappearancesixmonthsafterrhinoplasty,andthiswasassociatedwithreductionofpsychiatricsymptomscores(Robinetal.,1988).
Body dysmorphic disorder occurs most frequently in late adolescence; three-quarters ofpatientsarefemaleandmostareeithersingleordivorced(Vealeetal.,1996).Thereisfrequentcomorbiditywithmooddisorder, socialphobia andobsessive-compulsivedisorder, and72percentofcasesmanifestedpersonalitydisorder,usuallyofparanoid,avoidantorobsessive-compulsivetype.Twenty-fourpercentofthisgroupofpatientshadattemptedsuicide.InasimilarAmericanstudy,73percentofpatientsreportedexcessivemirrorchecking,63percentreportedattemptstocamouflagetheir‘deformities’andothersreportedgroomingorskinpicking(Phillipsetal.,
228 FOUR—SELF AND BODY
1993; Phillips etal., 2005). Almost all had severe limitations of their social activities. Mostpatientshadsufferedfromamajormooddisorderand17percenthadmadesuicideattempts.Themostfrequentlyreportedbodyparts,inorderofconcernareskin,hair,nose,stomach,teeth,weight,breasts,buttocks,eyes, thighs,eyebrows, legs, facesizeor shape,chin, lips,arms,hips,cheeksandears(Phillipsetal.,2005).
Thosecomplainingabouttheirface,andespeciallytheirnose,dosoinextremeandexagger-ated terms despite the deformity often being relatively slight. The dissatisfaction with theirappearance and the extent to which they feel others are aware of their disfigurement arequite out of proportion, as are the discomfort and disturbance in function: ‘agonizing pain’and ‘total inability to breathe’. At the same time, the actual description is often quite impre-cise: ‘theskinundermyeyes joinsmynose inafunnyway’(Birtchnell,1988).Becauseoftheextreme degree of reaction they show, they may contemplate radical remedies, for examplewishingtohavetheirnoseamputatedorthreateningtokillthemselves.Dysmorphophobiaisarelativelycommondisturbanceofselfandusuallytakesthepsychopathologicalformofanover-valued idea.
Thecomplaintofdysmorphophobia ismadeby thesubject in relationtoothersbut isnotusuallybasedontheopinionofothers.Soapatientcomplainsofhisnose,orthesmallsizeofherbreasts,andconsidersthatotherswillregardthemasuglyorunattractive.Often,theappear-anceiswellwithinnormal limits,withnodeformity,butthepatient isconvincedthatsurgerywillbebeneficial.Patientsoftenpresentintheirlateteensorearlytwenties.Thereisquiteoftenunderlyingpersonalitydisorderofanankasticordependenttypes;theremaybedepressedmooddisturbanceasareactiontothecomplaint;andsuchpatientsnotinfrequentlytalkof,andattempt,suicide.
A female student, aged 20, was referred to the psychiatric clinic following self-poisoning.When asked her problem, she burst into tears and said, describing the small size of herbreasts:
Basically there is a big difference between me and other girls. I’ve always been self-conscious. I used to pad myself. Even my mother made fun of me. I’ve tried
to convince myself I would change physically. I don’t feel like a total woman. I have to buy clothes that look ridiculous on top. My present boyfriend
I have been going out with for over a year always talks about other girls he has. He went to a dance and danced with another girl, I knew that it
was because she was bigger-busted than me. I was always aware of my figure, that I am not attractive… I detest myself, I hate my body… I don’t like
my boyfriend touching me there, I can’t wear nice clothes, I can’t make the best of what I already have…. even my little sister of 16 has more than I have
ever had.
Itisofinteresttonotethatsurgerycanresultinrestitutionofnormalbodyimage.Inastudyof11youngwomenwithnootherdiseaseandbreastsizenotgrosslyinappropriateforbodysizerequestingreductionmammoplasty,Hollymanetal.(1986)foundthataftersurgerybodyimagehadreturnedtonormal;self-confidence,feelingsaboutfemininityandsexualattractivenesswerealsoenhanced.
Symptomsofdysmorphophobiaaresometimesdescribedbypatientswithschizophrenia.Itmayoccurasthefirstsymptomastheconditiondevelops,andtheclinicianshouldthereforelookcarefullyforsuggestivesymptoms.Itmayalsobepresent intheestablishedcaseandwill thenshowcharacteristicschizophrenicsymptomatology.A19-year-oldAfrican-Caribbeangirl,previ-ouslydiagnosedwithschizophrenia,said:
14—DiSOrDEr OF thE AwArENESS OF thE BODY 229
The Spirit is a man, he feels warm and moves in me. I can’t feel yet. I’ve got to pray for my new body. I’ll have it in March. I will have to look beautiful, I don’t feel beautiful at the moment, I don’t look nice enough. I’ll have a nice
face, nice teeth, red eyebrows, red eyes, pupils red and smooth red lips. My skin will be light and I’ll have long fair thick hair down to my knees. My voice will be different and I’ll have a new tongue. I’ll speak many languages. I’ll
sing too. My brain and my mind will be the same. I’ll have long fingernails, a smaller waist, bigger breasts and my legs will be a bit shapelier. My figure
will change from 33” 24” 35” to 38” 18” 36”.
There is emergingevidence thatvisualprocessingof facesandobjectsmaybe impaired inindividuals with dysmorphic disorder. Abnormalities include inability to identify faces withemotional expressions under experimental conditions (Feusner etal., 2010a) and the use ofgreaterdetail-orientatedandpiecemealprocessingoffacescomparedtocontrols(Feusneretal.,2010b).Impairmentsoffaceprocessingappeartocorrelatewithdemonstrableabnormalitiesinfrontostriatal systems (Feusner etal., 2010c), and regional brain volumes of the left inferiorfrontalgyrusandamygdalaarepositivelycorrelatedwithseverityscoresofdysmorphicdisorder(Feusneretal.,2009).Thesefindingssuggestthat,despitetheabsenceofgrossabnormalitiesofperception,faceandvisualobjectprocessingimpairmentsmayunderliethenegativeevaluationsofthebodythatarecharacteristicofdysmorphophobia.
BODY INTEGRITY IDENTITY DISORDER
This isa rarecondition inwhichthere isanapparentmismatchbetweenthebody imageandthephysicalbody.Patientshaveastrongdesiretochangethephysicalbodysothatitcoincideswiththebodyimage.Themostcommondesireistoamputateamajorlimbortoseverthespinalcordinordertobecomeparalyzed.Patientsarereportedassaying‘Icanfeelexactlywheremylegshouldendandmystumpshouldbegin.Sometimesthislinehurtsorfeelsnumb’or‘mylimbsdonotfeelliketheybelongtome,andshouldnotbethere’(Blometal.,2012).Reportssuggestthat surgery is followedbya feelingofcompleteness,wholenessandsatisfaction.It isperhapssignificant that approximately half of a cohort of patients studied said that they felt sexuallyarousedwhentheysawadisabledpersonresemblingtheirowndesireddisabilityorfeltsexuallyarousedwhenimaginingthemselvesbeingdisabled(Blometal.,2012).
TRANSSEXUALISM
Inthiscondition,thereisadisturbanceofbodyimagewithadisorderofcoregenderidentity,adiscrepancybetweenanatomicalsexandthegenderthepersonascribestohimself.Intranssexual-ism,wearingclothingoftheoppositesex(transvestism)occurs,usually,asameansofpersonalgratificationwithoutgenitalexcitement.Itismuchcommonerinbiologicalmalesthaninfemales,butitoccursinbothsexes.Thesuffererofthisanomalyfeelsheshouldhavebeenoftheothergender, ‘a female spirit trapped in a male body’ (Morris, 1974). In adults, the disturbance ismanifestedbypreoccupationwithgettingridofprimaryandsecondarysexualcharacteristicsandthe request forhormone therapyor surgeryorothermeansof simulating the requiredgender(Green,2000).ThestrengthofthisconvictionisdescribedinConundrumbyJanMorris(1974)withliteraryéclat:‘IwasthreeorperhapsfouryearsoldwhenIrealizedthatIhadbeenbornintothewrongbody,andshouldreallybeagirl…througheachyearmyeveryinstinctseemedto become more feminine, my entombment within the male physique more terrible to me.’Anothertranssexualdescribedhimself:

230 FOUR—SELF AND BODY
I know that I am biologically a man but it is all a horrible freak of nature. Really I am a woman and by some accident I have got a male body. I think
as a woman and have female feelings and interests, and am only comfortable when wearing women’s clothes and in a feminine job. So, genuinely, I am a
woman… I am not against homosexuals although I am not one myself. When I have sex with a man, you must remember that I am really a woman.
Transsexualsdescribetheirfeelingsabouttheirbodyashavingbeenpresentfromearlychild-hood:thefeelingofcomfortand‘rightness’ theyexperiencedwhenwearingtheirsister’sdress,howthey‘fellnaturally’intofemalepursuitsandinterests.Thedifferenceofself-imagefromthebiologicalsexisusually,intheirownaccount,clearlyestablishedbeforepuberty.
The biological basis of transsexualism is uncertain. Blanchard in a series of papers (1989,1991,1993)proposedthatindividualspresentingwithmale-to-femaletranssexualismandwerecharacterizedashavingautogynephilia(sexuallyarousedbythethoughtorimageofthemselvesaswomen)weredistinctfromotherswhowerehomosexualinorientation.Thisclassificationiscontroversialandnotwidelyaccepted(Moser,2010).Thereisevidencethatchromosomalabnor-malitiesarerare(2.9%infemale-to-maletranssexualsand0.6%inmale-to-femaletranssexuals)andincludegonosomalaneuploidy,RobertsoniantranslocationsandKlinefeltersyndrome(Aueretal.,2013).Structuralimaginghasdemonstratedincreasedcorticalthicknessinmale-to-femaletranssexualsbutthesignificanceofthesefindingsisyettobedetermined(Ludersetal.,2012)and diffusion tensor imaging has shown white matter microstructure (superior longitudinalfasciculus,rightanteriorcingulate,rightforcepsminorandrightcorticospinaltract)inuntreatedmale-to-femaletranssexualsthatishalfwaybetweenthatofmaleandfemalecontrols(Ramettietal., 2011). Notwithstanding the fact that the biological basis of transsexualism is yet to beelucidated,whatisincontrovertibleisthatthedissatisfactionwiththebodyandwithsecondarysexualcharacteristicsandgenitaliaisrootedinbrainmechanismsthatunderliegenderidentity.
DISTURBANCE OF EATING AND BODY SIZE
Disturbanceofeatingoccurswithvariousconditions inwhichalterationofbody imageeithercauseseatingdisorderorresultsfromit.Threeconditionswillbediscussed:obesity,anorexiaandbulimianervosa.Onceagain,itisthesubjectiveaspects,theeffectonself-image,thatconcernsushereandnotthephysicalaspects.
Obesity
Obesity has become a major concern in the Western world. Both in Europe and in NorthAmerica,theprevalenceofobesityhasincreasedconsiderablysincethemid-1970s.Between1976and1980 intheUnitedStatesofAmerica,15percentof theadultpopulationaged20to74were obese, whereas by 2003 to 2004 the prevalence had risen to 33 per cent. It is currentlyestimatedat35.7percent(CentresforDiseaseControlandPrevention).Thesetrendsarealsoreplicated in Europe (World Health Organization Regional Office for Europe). Obesity isdefinedasabodymassindexofgreaterthan30kilogramspermetresquared;beingoverweightisabodymassindexofbetween25and29.9kilogramspermetresquared.Thereisalsoconcernabouttheriseofobesityinchildren.Itisnowestimatedthatapproximately17to20percentofchildrenareobese.Theconcernaboutobesityderivesfromtheassociatedhealthrisks;hyperlipi-daemia,insulinresistance,diabetes,hypertension,morbidityandprematuredeatharerecognizedcomplications. Thus, there are national and international health programmes to combat theapparentunrelentingriseintheprevalenceofobesity.
Indiscussionofthebodyimagephenomenaofobesity,Kalucy(1976)considersthatadoles-cenceisthecriticalstageofdevelopmentwhenprimarydisordersofshapeandbodyexperience
14—DiSOrDEr OF thE AwArENESS OF thE BODY 231
appear. Obesity in adolescents in diet-consciousWestern societies results in self-loathing andself-denigration.Thepresenceofanyphysicaldeformityatthisstageoflifeislikelytoprovokerevulsionfromtheself-image;individualsfeelespeciallyphysicallyloathsomewithregardtotheoppositesex.Theymayavoidmirrorsandanyotherreminderoftheirshape.Thereisalsopresentadistortionofbodysizeinthattheyoftenoverestimatetheirsize.Thisisinterestingincompari-sonwithanorexianervosapatients,whoalsooftenoverestimatetheirsizeandwhosebehaviourofdietingandfoodrejectionmaystartwhentheyaremildlyobeseatthetimeofpuberty.
Anorexia Nervosa
This is a condition that in the past was misplaced diagnostically; initially, sufferers wereusually thought to be physically ill. Marcé (1860), however, considered it to be one form ofhypochondriasis.Anorexianervosaisanillnessthatoccursmainlyinyoungwomen;thepropor-tionofmalecasesseenrangesfromonein20toaboutoneintenindifferentseries(DallyandGomez,1979)andtheproportionofboysishigherinchildhood.Thereisafailuretoeat,lowbodyweightandamenorrhoea.IthasbeenconsideredbyCrisp(1975)thatthedisorderispri-marilyaweight phobia,afearofincreasingbodyweight,andnotonlyafeedingdisordersimilartothoseofchildhood.Prominentisthefearoflossofcontrol;ifoneeatsnormally,onewillbeunabletostopandthereforebecomefat.Aswellasanabnormalself-image,therearealsoabnor-mal attitudes towards food, gender and sex. How does the patient with anorexia nervosa seeherself?ItisinpartanarcissisticdisorderaccordingtoBruch(1965),whohascalledit‘thepursuitofthinness’.InthedefinitioninICD-10,bodyimagedistortionisoneoffiveessentialfeatures:‘There isbody imagedistortion in the formofa specificpsychopathologywherebyadreadoffatnesspersistsasanintrusive,overvaluedideaandthepatientimposesalowweightthresholdonhimselforherself ’(WorldHealthOrganization,1992:p.177).Theotherfeaturesare:
■ bodyweightatleast15percentbelowthatexpected■ weightlossisself-induced■ amenorrhoea■ delayedorarrestedpuberty.Anorexia nervosa became more common in the United Kingdom in the latter part of
the twentieth century (Kendell etal., 1973). It is much rarer in, for example, India andother developing countries. This apparent difference in prevalence suggests that it may wellbe linked to social attitudes towards thinness, dieting and slimming. In the Western world,slimness is regarded as beautiful, and dieting may become a social norm that acts as a per-suasivepressureonanimpressionableadolescentfemalewhosebodyweighthasincreasedalittlemorethanaverageatpuberty.Ifthereareotherpsychologicaldifficultiesandsocialconflicts,theslimmingmaygetoutofcontrol.Inotherpartsoftheworld,wheretheaestheticnormsoffemi-ninebeautyarebasedonafulsomebody,thepressuretowardsthinnessislessbutthepressuretowardsobesitymaybegreater.EveninWesternsociety,theprevalenceofanorexianervosaisnot uniform within society but rather is determined by gender, age, socioeconomic class andethnicity.
Patientswithanorexianervosaoftendenytheirthinnessandsometimesclaimtobetoofat.Becauseoftheirextremeconcernovertheirphysicalsizeandweight,atechniquewasdevisedbySladeandRussell(1973)toinvestigatebodilyperceptioninanorexics.Thisinvolvedcomparingrealsizeinsubjects(measuredbyananthropometer)andperceivedsize,whichwasmeasuredbytheobservermovinghorizontallightstoadistancethatthesubjectestimatedasthewidthacrossfour body regions: face, chest, waist and hips.When compared with an age-matched normalcontrol group, anorexic patients significantly overestimated their own perceived width at allregions,withthefacebeingoverestimatedbymorethan50percent.Althoughactuallythinneratthechest,waistandhips,anorexicpatientssawthemselvesasfatterthannormalwomen.Thebodyimagedisturbancecouldnotbeaccountedforbyageneralperceptualdisorder,asanorexics
232 FOUR—SELF AND BODY
werefairlyaccurateatthemeasurementofwidthofwoodenblocksandalsoextremelyaccurateatmeasuringphysicalheight.Theytendedtooverestimatethewidthofotherpeople,butnotbyasmuchasthemselves.Thebodyimagedistortiontendedto lessenaspatientsputonweight,especiallyiftheydidsoslowly.Itwasshownthatagreaterdegreeofbodyimagedisorderhelda worse prognosis. Slade and Russell (1973) considered that ‘patients with anorexia nervosashowafaultyappreciationoftheirownbodyimageinthesensethattheyperceivetheirbodiesaspossessinganexaggeratedgirth’.ItwasfoundbyGarfinkeletal.(1979)thatsomeanorexicsubjectstendtooverestimatebodysizeandthatthisoverestimatewasstableoverayearandnotaffectedbyweightchange.
Experimental work by Button etal. (1977) called into doubt the finding that anorexicsalone overestimate their size while normal females are more accurate and that disturbance ofbodyperception is variable among anorexics.Thisfindinghasnowbeen confirmed in a largemeta-analysisbyCashandDeagle(1997).Bodyimagedisturbancedoesnotappeartobeassoci-ated with other features of either anorexia nervosa or bulimia nervosa and does not help todifferentiatenormalwomen frompatientswith eatingdisorder.Furthermore, attitudinalbodydissatisfaction as measured by questionnaires or self:ideal discrepancy best differentiated thepatients fromthenormalcontrols.Thus, the roleofperceptual sizeestimation inaccuracy, theformalmeasureofbodyimagedistortion,asadiagnosticcriterionofanorexianervosahastobecalledintoquestion.
Slade(1988)hasalsoshownthatnon-anorexicsubjectsoverestimatethedimensionsoftheirbody, especially normal females, neurotic subjects, those who are pregnant and patients withsecondary amenorrhoea. He has contrasted the use of full body techniques (with distortingmirrors,photographs,televisionimages)forinvestigatingthiswithpart of bodymethods(visualsizeestimation,callipers),andhasshownthatrelativelyfixedcognitiveattitudes towardsbodysizewith the formerdemonstrate irrationalbeliefs aboutbody shape,whileamorefluid stateoftheestimationofbodysizedependsmoreonemotionalfactorsthatchangeovertime.Hehasalso shown that themore ‘overfat’ the individual considersherself tobe, themoredissatisfiedshewillbe.
Manyrecentstudieshavebeencarriedoutinsupposedlynormalpopulations.Straumanetal.(1991)studiedtheviewsofselfinalargenumberoffemaleundergraduatesforthefactorstheydescribedas‘actual:idealself-discrepancy’and‘actual:oughtdiscrepancy’.Theyshowedthattheactual:idealdiscrepancycorrelatedwithbodyshapedissatisfaction.Theactual:oughtdiscrepancywas associated with what they described as anorexic-related attitudes and behaviours andactual:idealdiscrepancywithbulimic-relatedattitudesandbehaviours.Gustavsonetal.(1990)investigatedbodyimagedistortionandshoweddifferencesbetweennormalstudentsandthosesuffering from eating disorders. Moore (1988) surveyed 854 females aged between 12 and23yearsfromoutpatientclinics;67percentwerefoundtobedissatisfiedwiththeirweightand54percentwiththeirshape.
Zellneretal.(1989)studiedtheeffectsofeatingabnormalitiesandgenderontheperceptionofdesirablebodyshape,usingfiguredrawingsbytheirsubjects.Theyfoundthatwomendesiretobethinnerthantheythinktheyare,andthatwomenwitheatingdisordersdesiretobethinnerthanthatdegreeof thinnessthat theythinkthatmenwillfindattractive.Steigeretal. (1989)foundthatanorexics,butnotbulimics,exhibitedbody imagedistortion,andthatbodyweightpredicted thedegreeofbody imagedisturbance.Dolanetal. (1990)demonstrateddifferencesbetweenwhite,African-CaribbeanandAsianBritishwomenforsomeofthesymptomsofeatingdisordersbutnodifferencesforbodyimagedisorder.
Supportedbythesestudiesisthefindingofaclearassociationbetweenbodyimagedistur-banceandeatingdisorder.Thisisrelatedinverselytoweight,thatis,thelowertheweightthegreater thedegreeofbody imageabnormality.Thus, ingeneral, thosewithanorexia aremoreaffectedthanthosewithbulimianervosa.

14—DiSOrDEr OF thE AwArENESS OF thE BODY 233
Aperpetualquestionisthedegreetowhichcultureinfluencesbodyimageandtowhatextentthesocialenvironmenthasasignificantimpactonbodyimage.Thereisevidencethatbodydis-satisfactionisprevalentinfemalesacrossdifferentethnicgroupsinthesamecountryandacrossnational boundaries (Baillie and Copeland, 2013; Angelova and Utermohlen, 2013; Demuthetal., 2013; Santana etal., 2013). There are factors unique to particular settings. So, in theBulgariancontext, faithandtraditionalfastingdifferentiallyaffectedthebehavioursofwomendepending on their pre-existing predisposition to disordered eating. For vulnerable women,fastingactedviareinforcementofasceticismanddietaryrestrainttoinduceweightmanagementin order to achieve a desired thin figure consistent with sociocultural norms (Angelova andUtermohlen,2013).And,intheUnitedStatesofAmerica,EuropeanAmericanwomenendorsed‘a curvy-thin or athletic ideal body’ whereas African American women ‘resisted notions of asingularidealbody’(Webbetal.,2013).Inanelegantstudy,Bagrowiczetal(2013)investigatedasampleofJapanesestudentswhohadrecentlyarrivedinNewYorkcitytoseewhattheinflu-enceofendemicobesitywas.AftertwomonthsinNewYork,theJapanesestudentshadthinnerself-imagebut‘afatterideal-image’andconsequentlylessbodydissatisfaction.Thisstudysuggeststhatsocialenvironmentrapidlyinfluencesidealbodysize.
Itdoesseemthatabnormalityofselfandbodyimageisuniversal ineatingdisorders:‘IeatthereforeIam’.Thereareassociationsbetweenabnormaleating,especiallyinanorexianervosa,andlowbodyweight,withabelieforfearthat‘Iamtoofat’andwithamorepervasivedenialofself.Inattemptingtoinvestigatethefactorsthatinfluencethisoverestimationoftheirbodysizebyanorexicandbulimicwomen,HamiltonandWaller(1993)studiedtheinfluenceofmediaportrayal of idealized female bodies.They concluded that eating-disordered women overesti-matedthemselvessubstantiallymoreafterseeingsuchimagesthanafterseeingphotographsofneutralobjects.Such images in themediadoappear to influence femalebehaviour,at least insomevulnerablepeople.
Strober etal. (1979) assessedperceptionof body size, subjective experienceof body imagedistortionsanddifferentiationofbodyconceptsbyaskingadolescentanorexicpatientsandcon-trols todrawthehumanfiguresoonafter theirhospitaladmissionandsixmonths later.Bothgroupstendedtooverestimatesizeatbothtimes,butexperiencesdenotingestrangementfromthebody,insensitivitytobodysensationsandweaknessofbodyboundariesweremoreprevalentinanorexics,andtheypersistedathighlevelsafterfranksymptomsofweightandeatingdisorderhad subsided.Therewasagreaterdegreeof amorepersistentbody imagedistortion in thosewhovomited.Theseauthorsconsideredthat ‘defectsinbodyimageformationrendertheano-rexic vulnerable to theirmanifestpathology,which is itself activatedbymaturational conflictsuniquetoadolescence’.
Theunderlyingfearof lossofcontrol,andthe incessantneedforvigilanceconcerninganycaloriethatentersthemouth,influencesallotherareasofthepatient’slife.Obsessionaltidinessandcleanlinessmaybemanifested,andalsoanattempttocontrolthebehaviourofotherpeopleathome.Ananorexicpatientcontrolledthebehaviourofherparentsandtwinsisterbythreaten-ingtostarveherselfyetfurtheriftheywouldnotcooperate.Sheweighednotonlyherownfoodbutthatofalltheothermembersofthefamily.Beforeherillness,sheandhersisterbothweighedabout57kg,butasheranorexiaprogressedsheinsistedonhertwineatingherfoodalso,whichthepatientcooked.Asaresult, thepatientdroppedinweighttoabout32kg,whilehersisterreached83kg.
Bulimia Nervosa
ThisconditionwasfirstdescribedbyRussellin1979.Althoughthepatientiscurrentlyofnormalornear-normalweight, there isoftenahistoryofanorexianervosawithweight loss(FairburnandCooper, 1984).Body imagedistortion is also a featureof the condition,with thepatientbelievingherselftobetoofatandtooheavy.
234 FOUR—SELF AND BODY
Thecharacteristic eatingdisorder isofgrosspreoccupationwith food,withepisodicbingeeatingorgorging.This is frequentlycounteredwithself-inducedvomitingandothermethodsofweightreductionsuchasabuseofdrugs,forexamplelaxativesoramphetamine-likedrugs,orvoluntarystarvation.Weight is thusmaintainedwitha fragile stability; sometimesweight lossmayreachanorexicproportions,andsometimestheremaybemildobesitythatisassociatedwithfeelingsofguilt.Thefearofputtingonweightandthedominatingpreoccupationwithfoodisanovervalued idea.
There ismarkeddissatisfactionwith thebody inbulimianervosa that is similar to that inanorexianervosa (CashandDeagle,1997).There is evidence that thedissatisfactionwith thebodyderivesfromcognitiveevaluativedissatisfactionandisnotdependentonsensoryperception,although itmaybe influencedbymood (Gardner andBockenkamp,1996).Various abnormalbehaviours may occur, including alcohol abuse, shoplifting (especially involving stealing food)anddeliberate self-harm.Avarietyof seriousphysical complicationsmay result fromrigorousself-inducedvomitingorpurging.
Underlying factors are particularly centred on doubts concerning femininity (Lacey etal.,1986). Poor relationships with parents, academic striving, parental marital conflict and poorrelationshipswiththepatients’ownpeersalsooccur.Thesepatientsdescribedmajorlifeeventsintheareasofsexualconflict,majorchangesinlifecircumstancesandexperienceofloss.
Muscle Dysmorphia
Muscle dysmorphiaisatermusedtodescribethepathologicalpreoccupationwithmuscularity.Itischaracterizedbypreoccupationwitha)musclesizeandbuild,b)thebeliefthatone’smusclesaretoosmall,c)excessivetimespentingymnasiumweightlifting,d)useofanabolicsteroidsandbulkingdiets,ande)inextremeform,cosmeticsurgeryincludingpectoralimplants.Itissome-timesreferredtoas‘reverse anorexia’or‘bigorexia’(Popeetal.,1997;Choietal.,2002).Theexactnosologicalstatusofmuscledysmorphiaisuncertain.Someauthorshavedescribeditasavariantofbodydysmorphicdisorder (Choi etal., 2002), others as amale variantof anorexianervosa(Murray etal., 2010),whilst othershave commentedon the relationshipwithobsessive com-pulsivedisorder(Chung,2001).Itisprobablybestinthecurrentstateofknowledgetoregarditasaphenomenonthatcanoccurinavarietyofpsychiatricdisordersratherthanasadisorderinitsownright.
Thereisconsistentevidencethatmenwithmuscledysmorphiahavedisturbedbodyimage,disorderedeating,andexcessiveexercising(Murrayetal.,2012).Inweightlifters,itsprevalencehasbeenreportedas13.6%(BeharandMolinari,2010).Bodychecking,whichcanbeconstruedasevidenceofbodydissatisfactioniscommoninmuscledysmorphia(Cafrietal.,2008;Walkeretal.,2009). Incomparison toweightlifterswithoutmuscledysmorphia,patientswithmuscledysmorphiaweremorelikelytohavebodydissatisfaction,abnormaleatingattitudes,useanabolicsteroidsandhaveahistoryofanxietyordepression.Theyalsocomplainedofshameandembar-rassment,poorerqualityoflife,previousattemptedsuicideandtherewasevidenceofimpairedoccupationalandsocialfunctioning(Olivardiaetal.,2000;Popeetal.,2005).
Disorders of the Sensory Awareness of the Body (Organic Changes in Body Image)Disease of, and trauma to, the brain alter the body image in a variety of ways.This is eitherbecauseofdamageoftheconceptualizedobject,forexampleamputationwithphantomlimborblindnessnecessarilyalteringthewayoneperceivesoneself,ordamagetotheprocessofconcep-tualizationitself,forexamplesectionofthecorpuscallosum.Often,ofcourse,thereisscattereddamage,aswitharteriopathyormultiplesclerosis,andthesetwofeaturescannotbeseparated.
14—DiSOrDEr OF thE AwArENESS OF thE BODY 235
Theexpressionbody imageasusedinneurologywasdefinedbyCritchley(1950)asthementalidea that an individualpossesses abouthisownbodyand itsphysical andaesthetic attributes.Visualsensation,tactileimpulsesandproprioceptivestimulicontributetotheformationofbodyimagebutarenotessential; followingtheamputationofa limb,aphantomlimbretainingtheintegrityofthebodyimageoccursinthemajorityofcases.Thebodyimage‘livesonthefringeofawarenessandisbynomeansobtrusiveinordinarycircumstances.Itishoweveravailableandcanbebroughtintoconsciousnessassoonasthestreamofattentionvoluntarilyorinvoluntarilyfocusesuponit’(Critchley,1950).Morbidchangesinthebodyimagemayshowenhancement,diminution(orablation)ordistortion.Inneurology,thetermbody schemaisusedfortheaware-nessofspatialcharacteristicsofone’sownbody,involvingcurrentandprevioussensoryinforma-tion,whilebody experienceismorecomprehensive,includingpsychologicalandsituationalfactorsalso (Cumming, 1988).The parietal lobes play a major role, but the somatoaesthetic afferentsystemandthethalamusarealsoinvolved.
PATHOLOGICAL ACCENTUATION OF BODY IMAGE (HYPERSCHEMAZIA)
Painordiscomfortcausestheaffectedpartof thebodyto loomlarge.Afterdroppingaheavyweightonhisgreattoe,amanfelthisbodytobe‘aninsubstantialshellaroundahugethrobbingtoe’.Suchadescriptionofthepainfulorganseeminglargerinsizeisfrequentfollowingsurgeryand traumatic injury. When size is affected, the body may feel larger (macrosomatognosia).Critchleygivesseveralexamplesofneurologicallesionscausingenhancementofanorgan.
■ Withpartialparalysisof a limb, the affected segmentgives the impressionofbeing tooheavyandtoobig,forexamplewithBrown-Séquardparalysis(unilaterallesionofthespinalcord)thesidewiththepyramidalsignsishyperschematicwhiletheotherside,withlossofpainandtemperaturesensation,isperceivedasnormalinbodyschema.
■ Unilaterally,followingthrombosisoftheposteriorinferiorcerebellarartery.■ Inmultiplesclerosis,againunilaterally.Hyperschemaziamayalsooccurwithperipheralvasculardiseasewhentheaffectedlimbfeels
largerandheavier.Itmayalsooccurinacutetoxicstates.Non-organiccasesoccurwithhypo-chondriasis; in depersonalization states; with dissociation (conversion disorder), for examplepseudocyesis;andalso,occasionally,indreams.
DIMINISHED OR ABSENT BODY IMAGE (HYPOSCHEMAZIA, ASCHEMAZIA)
Thismayoccurwhenafferentandefferentinnervationis lost,forexamplewithtransectionofthespinalcordthepatientmayfeelsawnoffatthewaist.
Hyposchemaziaormicrosomatognosiamayaccompanythesensorydeprivationofweightlessness,for instanceunderwater.With vertigo, thepatientmay feel excessively light, as if floating intheair.
Parietal lobe lesions may result in complicated states of diminution of the body image.Critchley(1950)citesapatientwithembolismoftherightmiddlecerebralartery:
‘It felt as if I was missing one side of my body (the left), but it also felt as if the dummy side was lined with a piece of iron so heavy that I could not move it… I even fancied my head to be narrow, but the left side from the centre felt
heavy, as if filled with bricks’.
At one time he thought that his paralyzed leg belonged to the man in the next bed. Hisbody felt to him half as wide as it should have done. Lying on the left side gave him the
236 FOUR—SELF AND BODY
sensationthathewas‘lyingonavoid’, thathewasattheextremeedgeofthebedandwouldpresentlyfalloff.Intheearlydayshealsofeltthathehadnopenisatall.Onthisaccounthewasclumsywiththeurinalandthebedwasfrequentlysoiled.Hissensationsofowningapenisreturnedquitesuddenlyonemorninginassociationwithanerection,anditafterwardsfeltquitenormal.
Inhemisomatognosia(hemidepersonalization),whichwasdescribedbyL’Hermitte(1939)andisaunilateralmisperceptionofone’sownbody,thepatientbehavesasthoughthelimbsononesidearemissing;thismayoccuraspartofanepilepticauraormigraine.Anosognosiadescribesthelackofawarenessofdisability,whichmay,forinstance,occurwithneglectofahemiplegiclimb.Hemispatial neglectdescribesthosepatientswho,whenaskedtoperformavarietyofbehav-ioural tasks in space, neglect the hemispace contralateral to their lesion (Cumming, 1988).Gerstmann’s syndrome (Gerstmann, 1930) comprises finger agnosia, acalculia, agraphia andright–leftdisorientation.
Again,non-organicconditionssuchasdepersonalizationmayalsoshowdiminutionofbodyimage.Ananxiousanddepersonalizedpatientsaid,‘Idon’tfeelatallthesameperson.SometimesmyheadfeelssonumbwhenIwalktotheshops.IfeelI’velefthalfmybodybehind’.Thiswasclearlyanas ifexperience.
DISTORTION OF THE BODY IMAGE (PARASCHEMAZIA)
Thismayoccurwithenhancementordiminutionofthebodyimage.Itmayoccurwiththeuseofhallucinogenicdrugssuchasmescaline,marijuanaandlysergicaciddiethylamide.Partsofthebodymayfeeldistorted,twisted,separatedfromtherestofthebodyormergedwiththeexternalenvironment.Theseexperiencescanaffecteitherthewholebodyorpartofit,suchasthelimbsorhead.Theshapecanbeexperiencedasmisshapen:‘mylowerjawistwistedandmyteethnolongercloseproperly’or‘myleftarmisshrunkenandgnarled,abitlikeatreetrunk’.Whenthestructureofthebodyisaffected,oftenitistheinternalorgansthatarethefocusofconcern:
‘I assert therefore that on my body, particularly on my bosom, there are present the properties of a nervous system corresponding to a female body and
I am certain that a physical examination would confirm this’
and
‘Food and drink taken simply poured into the abdominal cavity and into the thighs, a process which however unbelievable it may sound, was beyond all
doubt for me as I distinctly remember the sensation.’(Schreber, 1955)
Changesintheexperienceofweightcaninvolveasenseofeitherheavinessorlightness.Withhashish:
the sensations produced were those of exquisite lightness and airiness… I expected to be lifted up and carried away by the first breeze… the walls of my
frame were burst outward and tumbled into ruin, and without thinking what form I wore… I felt that I existed throughout a vast extent of space.
The blood pulsed from my head, sped through uncounted leagues before it reached my extremities; the air drawn into my lungs expanded into seas of
limpid ether, and the arch of my skull was broader than the vault of heaven.
14—DiSOrDEr OF thE AwArENESS OF thE BODY 237
I was a mass of transparent jelly, and a confectioner poured me into a twisted mould.
(Taylor, 1856)
The value attached to the body can be disturbed.This disturbance can vary from strong,positiveovervaluationofthebodyoritspartstoadevaluationofthebodyextendingtodislikeorhatredofit.Inright-sidedhemiparesis,patientscansometimesmaintainthattheirweakarmisinfactstrongerandmoreusefulthanbefore.Thisisreferredtoasanosognosic overestimation(Cutting,1997).Misoplegiaisthehatredofalimbandisassociatedwithleft-sidedparietallesions(Cutting,1997).
Distortionofbodyimagemayoccurwithepilepticauraandalsorarelywithmigraine.
Phantom Limb
Thisoccursimmediatelyfollowingthelossofalimbinvirtuallyallpatients,anditisparticularlycommonfollowingthetraumaticlossofalimboriftherehadbeenapre-existingpainfulcondi-tionofthelimb.Theonsetappearsimmediatelyastheanaesthesiawearsoffinthemajorityofcasesbutmaybedelayedforuptoafewweeksinabout25percentofcases.Thephantommaylastforafewdaysorweeksthengraduallyfadesfromconsciousness.Thereare,however,casesthathavepersistedfordecades.Aswellasoccurringwiththelossofalimb,thistypeofdistortionofbody image is relativelycommonaftersurgical removalofaneye,partsof theface,breasts,therectumorthelarynx.Therearereportsofphantomulcerpainsafterpartialgastrectomyandofmenstrualcrampfollowinghysterectomy.Ifanamputeeexperiencesageneralizedperipheralneuritisinvolvingsensation,paraesthesiaewillalsooccurinthephantomlimb.Theamputeeisawareofthephantomlimbinspaceandalsoexperiencespaininthespaceconceivedasbeingoccupiedbythelimb.
Withtime,thelimbappearstochangeinsize.Theimageshrinks,butunevenly,distaljointsshrinking more slowly than proximal; this is the so called telescoping phenomenon. Thereare several postulated explanations for ‘telescoping’. In loss of the upper limb, telescoping isthoughttooccurbecausethereisover-representationofthehandinthesensorycortex,hencethisistheareafromwhichsensationsurviveslongest.Thereisalsothepossibilitythattelescopingoccursbecausetherepresentationofthelimbintheprimarysomatosensorymapchangesprogres-sively.Thepostureofthephantomisoftensaidtobe‘habitual’,forexamplepartiallyflexedattheelbow,withforearmpronated.The limbcansometimesfeelfixed inanawkwardposition,andthiscancausethepatientdifficulty,forinstanceinwalkingupstairs.Thelimbmayfeeltwistedandpainful.
Thereis increasingliteratureontheplasticityofthesomatosensorysystem,usingphantomlimbasanaturalexperiment todemonstratedeafferentation following lossofa limbandcor-responding reorganization of the somatosensory map (Ramachandran and Hirstein, 1998).Followinglossoftheupperlimb,sensoryinputfromthefaceandupperarmhavebeenshownto invade thehandterritory, suchthat sensorystimulus to the facecanbemislocalized in thephantomlimb.
OrbachandTallent(1965)describedthebodyconceptsofpatientsfivetotenyearsaftertheconstruction of a colostomy. These patients had a conviction that they had been seriouslydamaged.
They believed that their bodily intactness and integrity had been violated. In common with such beliefs many patients on a fantasy level perceived the
operation as a physical or sexual assault. Patients who fantasized the surgery as a sexual assault were supported in this belief by the colostomy stoma, a new opening in the front of the body. Most men regarded this opening as evidence
238 FOUR—SELF AND BODY
of having been feminized, while women often interpreted it as the addition of a second vagina. The bleeding from the stoma reinforced the fantasy of a second vagina because it was interpreted as comparable to menstruation.
Inonefifthofpatients,preoccupationaboutthebodilyprocessesconcernedfoodintakeandelimination was embodied in a replacement concept which attempted to establish equalitybetweenintakeandevacuationbyeatingapproximatelyasmuchashadrecentlybeenevacuated.Amajorityoftheremainingpatientscommunicatedasenseofconfusionaboutthemachineryandfunctioningoftheirbodies.
When colostomy patients were initially studied and reports published, the constriction ofactivityandofthelifespacewasemphasized.Itisnowapparentthattheconstrictionisparalleledbyabodyconceptofbeingdamagedandfragileasaconsequenceoftheinjury.
Mastectomyalso results in relatively severedisturbance in self-conceptandbody image.Apatientdescribedthisas‘Iwillneverbelikebefore…itislikeahole,likeagap…WhenIlieonthatside,it’slikebeingaman’(HopwoodandMaguire,1988).Bodyimageproblemsresultnotonlyfromthelossofbodypartordisfigurementbutalsofromthelossofbodilyfunction.Thedisorderofself-imageisfrequentlyassociatedwithdepressivesymptoms.
Phantom limbpainmaybepsychologicallydetermined (Parkes,1976).Forty-six amputeeswere studied four to eight weeks and 13months after amputation; a third to a half showedmoderatedisturbancetendingtopersistayearlater.
Bodyimagedisturbanceisnotnecessarilyassociatedwithabnormalsensationorperception.Thehypochondriacmaybelievehehascanceralthoughhehasnophysicalsymptoms.Thetrans-sexualexperienceshisbodynormally,buthebelievesthatheisinthewrongbody.Thenarcissistisinordinatelyconcernedwithhisbody;nevertheless,heisquiteaccurateinhisobjectivequan-titativeperceptionofself,thatis,heknowshowlonghisnoseisorhowfarhecanthrowacricketball.Whensensationisabnormalorevendeficientaltogetherinsomemodality,forexamplewithblindnessordeafness,bodyimageisundoubtedlyaltered,butthisalterationdoesnotinanywayimplymentalillness;thealterationofbodyimageisusuallyappropriatetothedisability.
Culture-Bound Disorders of Body ImageVarious culturally determined hysterical conditions have been described by Langness (1967).These conditionshave in commona sudden,dramaticonset related in time to apsychosocialupset.Manifestationsoftheseconditionsaregrosslyunusualbehaviour,volatilemood,transientoccurrencesofalterationsofspeech,depersonalizationwithalteredbodyawarenessandsymptomssomewhat similar to delusions and hallucinations. The course of these conditions is usuallylimitedtoonetothreeweeks,buttheymayrecurwithfurtherepisodes.Theyappeartobemorelikely in thosepredisposedwithhistrionic (hysterical)personalities.Theprecise symptomsareoftenlocalizedtothatparticularcultureanddemonstratehowneuroticsymptomsintheircontentcomply with the expectations of the society in which they occur. For instance, Adair, writingfromBathin1786,describedhowfashioninfluencedthegreatandopulentinthechoiceoftheirdiseasesandconsideredthatQueenAnne’snervousnessresultedinthetransferofsimilarsymp-toms‘toallwhohadtheleastpretensionstorankwithpersonsoffashion’.
SomeoftheculturallylocalizeddisordersofawarenessofthebodyaresummarizedinTable14.2 (fromKiev, 1972).The variability of such syndromes is immense, but thepreoccupationwithbodilyorgansandfunctionsiscommontomanyofthem.Thebizarrenatureofsymptoms,forexamplekoro,inwhichthereisfearofthepenisshrinkingintotheabdomen,isoftenexplainedbyafaultyknowledgeofhumananatomyandphysiologythatseemsnaivetodoctorspractisinginEurope.However,itisnotgenerallyknownhowignorantBritishpatientsareconcerningtheorganizationandfunctionsoftheorganstheycannotsee.Hospitaloutpatientswerecompared
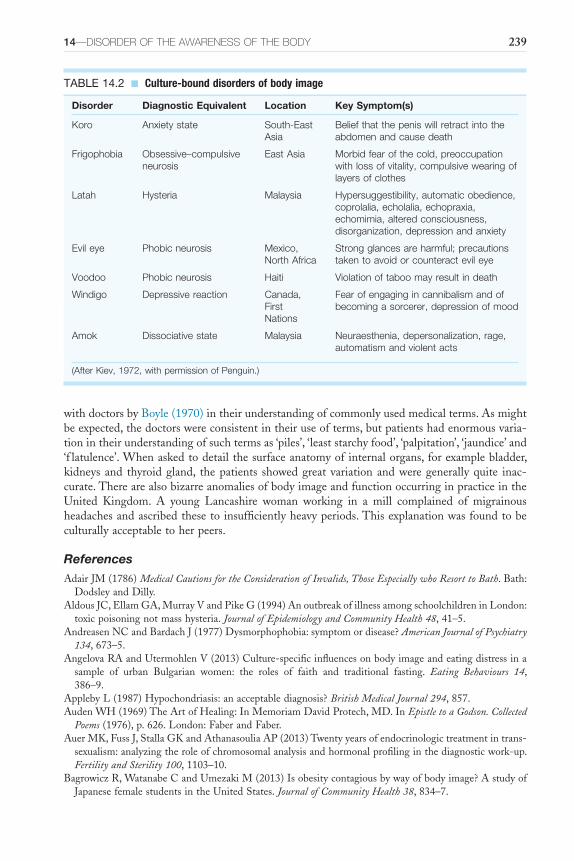
14—DiSOrDEr OF thE AwArENESS OF thE BODY 239
withdoctorsbyBoyle(1970)intheirunderstandingofcommonlyusedmedicalterms.Asmightbeexpected,thedoctorswereconsistentintheiruseofterms,butpatientshadenormousvaria-tionintheirunderstandingofsuchtermsas‘piles’,‘leaststarchyfood’,‘palpitation’,‘jaundice’and‘f latulence’.Whenaskedtodetailthesurfaceanatomyofinternalorgans,forexamplebladder,kidneys and thyroidgland, thepatients showedgreat variationandweregenerallyquite inac-curate.TherearealsobizarreanomaliesofbodyimageandfunctionoccurringinpracticeintheUnited Kingdom. A young Lancashire woman working in a mill complained of migrainousheadachesandascribedthesetoinsufficientlyheavyperiods.Thisexplanationwasfoundtobeculturallyacceptabletoherpeers.
ReferencesAdairJM(1786)Medical Cautions for the Consideration of Invalids, Those Especially who Resort to Bath.Bath:
DodsleyandDilly.AldousJC,EllamGA,MurrayVandPikeG(1994)AnoutbreakofillnessamongschoolchildreninLondon:
toxicpoisoningnotmasshysteria.Journal of Epidemiology and Community Health48,41–5.AndreasenNCandBardachJ(1977)Dysmorphophobia:symptomordisease?American Journal of Psychiatry
134,673–5.AngelovaRAandUtermohlenV(2013)Culture-specificinfluencesonbodyimageandeatingdistressina
sample of urban Bulgarian women: the roles of faith and traditional fasting. Eating Behaviours 14,386–9.
ApplebyL(1987)Hypochondriasis:anacceptablediagnosis?British Medical Journal294,857.AudenWH(1969)TheArtofHealing:InMemoriamDavidProtech,MD.InEpistle to a Godson. Collected
Poems(1976),p.626.London:FaberandFaber.AuerMK,FussJ,StallaGKandAthanasouliaAP(2013)Twentyyearsofendocrinologictreatmentintrans-
sexualism:analyzingtheroleofchromosomalanalysisandhormonalprofilinginthediagnosticwork-up.Fertility and Sterility100,1103–10.
BagrowiczR,WatanabeCandUmezakiM(2013)Isobesitycontagiousbywayofbodyimage?AstudyofJapanesefemalestudentsintheUnitedStates.Journal of Community Health38,834–7.
TABLE 14.2 ■ Culture-bound disorders of body image
Disorder Diagnostic Equivalent Location Key Symptom(s)
Koro Anxiety state South-East Asia
Belief that the penis will retract into the abdomen and cause death
Frigophobia Obsessive–compulsive neurosis
East Asia Morbid fear of the cold, preoccupation with loss of vitality, compulsive wearing of layers of clothes
Latah Hysteria Malaysia Hypersuggestibility, automatic obedience, coprolalia, echolalia, echopraxia, echomimia, altered consciousness, disorganization, depression and anxiety
Evil eye Phobic neurosis Mexico, North Africa
Strong glances are harmful; precautions taken to avoid or counteract evil eye
Voodoo Phobic neurosis Haiti Violation of taboo may result in death
Windigo Depressive reaction Canada, First Nations
Fear of engaging in cannibalism and of becoming a sorcerer, depression of mood
Amok Dissociative state Malaysia Neuraesthenia, depersonalization, rage, automatism and violent acts
(After Kiev, 1972, with permission of Penguin.)
240 FOUR—SELF AND BODY
BaillieLEandCopelandAL(2013)DisorderedeatingandbodyimageinChineseandCaucasianstudentsintheUnitedStates.Eating Behaviors14,314–9.
Barsky AJ and Klerman GL (1983) Overview: hypochondriasis, bodily complaints and somatic styles.American Journal of Psychiatry140,273–83.
BartholomewREandWesselyS(2002)Proteannatureofmasssociogenicillness.British Journal of Psychiatry180,300–6.
BeharRandMolinariD(2010)Muscledysmorphia,bodyimageandeatingbehavioursintwomalepopula-tions.Révista Medica de Chile138,1386–94.
BerriosGE(1996)The History of Mental Symptoms: Descriptive Psychopathology Since the Nineteenth Century.Cambridge:CambridgeUniversityPress.
BirtchnellSA(1988)Dysmorphophobia–acentenarydiscussion.British Journal of Psychiatry153(suppl.2),41–3.
BlanchardR(1989)Theconceptofautogynephiliaandthetypologyofmalegenderdysphoria.Journal of Nervous and Mental Diseases177,616–23.
BlanchardR(1991)Clinicalobservationsandsystematicstudiesofautogynephilia.Journal of Sex and Marital Therapy17,235–51.
BlanchardR(1993)Partialversuscompleteautogynephiliaandgenderdysphoria.Journal of Sex and Marital Therapy19,301–7.
BlomRM,HeenekamRCandDenysD (2012)Body integrity identitydisorder.Public Library of Science One7,e34702.
BoyleCM(1970)Differencebetweenpatients’anddoctors’interpretationofsomecommonmedicalterms.British Medical Journalii,286–9.
BridgesKWandGoldbergDP(1985)SomaticpresentationofDSM-IIIpsychiatricdisorders inprimarycare.Journal of Psychosomatic Research29,563–9.
BruchH(1965)Anorexianervosaanditsdifferentialdiagnosis.Journal of Nervous and Mental Disease141,555–66.
BurtonR(1628)The Anatomy of Melancholia.Oxford:Cripps.ButtonEJ,FransellaFandSladePD(1977)Areappraisalofbodyperceptiondisturbanceinanorexianervosa.
Psychological Medicine7,235–43.CafriG,OlivardiaRandThompsonJK(2008)Symptomcharacteristicsandpsychiatriccomorbidityamong
maleswithmuscledysmorphia.Comprehensive Psychiatry49,374–9.CashTFandDeagleEA(1997)Thenatureandextentofbody-imagedisturbancesinanorexianervosaand
bulimianervosa:ameta-analysis.International Journal of Eating Disorder22,107–25.CentresforDiseaseControlandPrevention.Online.Available:http://www.cdc.gov/obesity/data/adult.html
(AccessedApril2014)ChoiPYL,PopeHGJrandOlivardiaR(2002)Muscledysmorphia:anewsyndromeinweightlifters.British
Journal of Sports Medicine36,375–7.ChowdhuryANandBrahmaA(2005)Anepidemicofmasshysteria inavillage inWestBengal.Indian
Journal of Psychiatry47,106–8.Chung B (2001) Muscle dysmorphia: a critical review of the proposed criteria. Perspective in Biology and
Medicine44,565–74.CohnN(1958)The Pursuit of the Millennium.London:SeckerandWarburg.CotardM(1882)Nihilisticdelusions.InHirschSRandShepherdM(eds.)(1974)Themes and Variations in
European Psychiatry.Bristol:JohnWright.Crisp AH (1975) Anorexia nervosa. In SilverstoneT and Barraclough B (eds.) Contemporary Psychiatry.
Ashford:HeadleyBrothers,150–8.CritchleyM(1950)Thebodyimageinneurology.Lanceti,335–41.CummingWJK(1988)Theneurobiologyof thebodyschema.British Journal of Psychiatry153 (suppl.2),
7–11.CuttingJ(1997)Principles of Psychopathology.Oxford:OxfordUniversityPress.DallyPandGomezJ(1979)Anorexia Nervosa.London:Heinemann.DaveyGC(2011)Disgust:thedisease-avoidanceemotionanditsdysfunctions.Philosophical Transactions of
the Royal Society London. Series B, Biological Sciences366,3453–65.DemuthA,CzerniakUandZiółkowska-ŁajpE(2013)Acomparisonofasubjectivebodyassessmentof
menandwomenofthePolishsocialelite.Homo-Journal of Comparative Human Biology64,398–409.
14—DiSOrDEr OF thE AwArENESS OF thE BODY 241
Dolan B, Lacey JH and Evans C (1990) Eating behaviour and attitudes to weight and shape in Britishwomenfromthreeethnicgroups.British Journal of Psychiatry157(suppl.2),523–8.
FairburnCGandCooperPJ(1984)Theclinicalfeaturesofbulimianervosa.British Journal of Psychiatry144,238–46.
FarooqS,GahirSM,OkyereE,SheikhAJandOyebodeF(1995)Somatization:atransculturalstudy.Journal of Psychosomatic Research39,883–8.
FeusnerJD,BystritskyA,HellemannGandBookheimerS(2010a)Impairedidentityrecognitionoffaceswithemotionalexpressionsinbodydysmorphicdisorder.Psychiatry Research179,318–23.
FeusnerJD,MollerH,AltsteinL,SugarC,BookheimerS,YoonJandHembacherE(2010b)Invertedfaceprocessinginbodydysmorphicdisorder.Psychiatric Research44,1088–94.
Feusner JD, MoodyT, Hembacher E,Townsend J, McKinley M, Moller H and Bookheimer S (2010c)Abnormalities of visual processing and frontostriatal systems in body dysmorphic disorder. Archives of General Psychiatry67,197–205.
Feusner JD,Townsend J, Bystrisky A, Moller H and Bookheimer S (2009) Regional brain volumes andsymptomseverityinbodydysmorphicdisorder.Psychiatry Research172,161–7.
Fink P, Ørnbøl E,ToftT, Sparle KC, Frostholm L and Olesen F (2004) A new, empirically establishedhypochondriasisdiagnosis.American Journal of Psychiatry161,1680–91.
GardnerRMandBockenkampED(1996)Theroleofsensoryandnonsensoryfactorsinbodysizeestima-tionsofeatingdisordersubjects.Journal of Clinical Psychology52,3–15.
Garfinkel PE, Moldofsky H and Garner D (1979) The stability of perceptual disturbances in anorexianervosa.Psychological Medicine9,703–8.
GerstmannJ(1930)Thesymptomsproducedbylesionsofthetransitionalareabetweentheinferiorparietaland middle occipital gyri. In Rottenberg DA and Hochberg FH (eds.) (1977) Neurological Classics in Modern Translation.NewYork:HafnerPress.
GreenR(2000)Genderidentitydisorderinadults.InGelderMG,López-IborJJandAndreasenNC(eds.)New Oxford Textbook of Psychiatry.Oxford:OxfordUniversityPress.
Gustavson CR, Gustavson JC, Pumariega AJ, Reinarz DE, Dameron R, Gustavson AR, PappasT andMcCaulK(1990)Body-imagedistortionamongmaleandfemalecollegeandhighschoolstudents,andeating-disorderedpatients.Perceptual and Motor Skills71(3part1),1003–10.
HamiltonK andWallerG (1993)Media influences onbody size estimation in anorexia andbulimia: anexperimentalstudy.British Journal of Psychiatry162,837–40.
HayGG(1970)Dysmorphophobia.British Journal of Psychiatry116,399–406.HayGGandHeatherBB(1973)Changesinpsychometrictestresultsfollowingcosmeticnasaloperations.
British Journal of Psychology122,89–90.HollymanJA,LaceyJH,WhitfieldPJandWilsonJSP(1986)Surgeryforthepsyche:alongitudinalstudy
ofwomenundergoingreductionmammoplasty.British Journal of Plastic Surgery39,222–4.HopwoodPandMaguireGP(1988)Bodyimageproblemsincancerpatients.British Journal of Psychiatry
153(suppl.2),47–50.HuxleyA(1952)The Devils of Loudon.Harmondsworth:Penguin.JonesTF (2000)Masspsychogenic illness: roleof the individualphysician.American Family Physician15,
2649–53.KalucyRS(1976)Obesity:anattempttofindacommongroundamongsomeofthebiological,psychological
and sociological phenomena of the obesity/overeating syndromes. In Hill OW (ed.) Modern Trends in Psychosomatic Medicine 3.London:Butterworth.
KarserasAG(1976)Psychiatric aspectsofophthalmology. InHowells JG (ed.)Modern Perspectives in the Psychiatric Aspects of Surgery.London:Macmillan.
Kellner R (1985) Functional somatic symptoms and hypochondriasis. Archives of General Psychiatry 42,821–33.
KendellRE (2001)Thedistinctionbetweenmental andphysical illness. British Journal of Psychiatry 178,490–3.
KendellRE,HallDJ,HaileyAandBabigianHM(1973)Theepidemiologyofanorexianervosa.Psychological Medicine3,200–3.
KenyonFE(1964)Hypochondriasis:aclinicalstudy.British Journal of Psychiatry110,478–88.KenyonFE(1965)Hypochondriasis:asurveyofsomehistorical,clinicalandsocialaspects.British Journal
of Medical Psychology38,117–33.

242 FOUR—SELF AND BODY
KenyonFE(1976)Hypochondriacalstates.British Journal of Psychiatry129,1–14.KharabshehS,Al-OtoumH,ClementsJ,AbbasA,Khuri-BulosN,BelbesiA,GaafarTandDellepianeN
(2001)Masspsychogenicillnessfollowingtetanus-diphtheriatoxoidvaccinationinJordan.Bulletin of the World Health Organization79,764–70.
KievA(1972)Transcultural Psychiatry.Harmondsworth:Penguin.Kirmayer LJ and Looper KJ (2006) Abnormal illness behaviour: physiological, psychological and social
dimensionsofcopingwithdistress.Current Opinions in Psychiatry19,54–60.Kokota D (2011)View point: episodes of mass hysteria in African schools – study of literature. Malawi
Medical Journal23,74–7.LaceyJH,CokerSandBirtchnellSA(1986)Bulimia:factorsassociatedwithitsaetiologyandmaintenance.
International Journey of Eating Disorders5,475–87.Lader M and Sartorius N (1968) Anxiety in patients with hysterical conversion symptoms. Journal of
Neurology, Neurosurgery and Psychiatry13,490–5.Langness LL (1967) Hysterical psychosis: the cross-cultural evidence. American Journal of Psychiatry 124,
143–52.LewisAJ(1975)Thesurvivalofhysteria.Psychological Medicine5,9–12.L’HermitteJ(1939)L’image de notre corps.Paris:RevueNouvelleCritique.LudersAE,SánchezFJ,TosunD,ShattuckDW,GaserC,VilainEandTogaAW(2012)Increasedcortical
thicknessinmale-to-femaletranssexualism.Journal of Behavioural and Brain Science2,357–62.MarcéL-V(1860)Noteonaformofhypochondriacaldelusionconsecutivetothedyspepsiasandprincipally
characterized by refusal of food (transl. Blewett A and Bottéro A, 1994). History of Psychiatry 5,273–83.
Mechanic D (1962) Students Under Stress: a Study in the Social Psychology of Adaption. New York:FreePress.
Mechanic D (1986) The concept of illness behaviour: culture, situation and personal predisposition.Psychological Medicine16,1–7.
MerskeyH(1979)The Analysis of Hysteria.London:BaillièreTindall.MerskeyHandBuhrichNA(1975)Hysteriaandorganicbraindisease.British Journal of Medical Psychology
48,359–66.MooreDC(1988)Bodyimageandeatingbehaviourinadolescentgirls.American Journal of Disease of Children
142,1114–8.MorrisJ(1974)Conundrum.London:FaberandFaber.MorselliE(1886)SullaDismorfofobiaesullatafefobia.Bolletino Accademia delle Scienze Mediche di Genova
VI,100–19.MoserC(2010)Blanchard’sautogynephiliatheory:acritique.Journal of Homosexuality57,790–809.MossPDandMcEvedyCP(1966)Anepidemicofover-breathingamongschoolgirls.British Medical Journal
ii,1295–300.MumfordDB,Davington JT,Bhatnagar JS,HussainY,MirzaSandNaraghiMM(1991)TheBradford
Somatic Inventory: a multi-ethnic inventory of somatic symptoms reported by the Indo-PakistanSubcontinent.British Journal of Psychiatrists158,379–86.
MurraySB,RiegerE,HildebrandtT,KarlovL,RussellJ,BoonE,DawsonRTandTouyzSW(2012)Acomparisonofeating,exercise,shape,andweightrelatedsymptomatologyinmaleswithmuscledysmorphiaandanorexianervosa.Body Image9,193–200.
MurraySB,RiegerE,TouyzSWandDeLaGarzaGarciaY(2010)MuscledysmorphiaandtheDSM-VConundrum: Where does it belong? A review paper. International Journal of Eating Disorder 43,483–91.
MuseK,McManusF,LeungC,MehrebianBandWilliamsJM(2012)Cyberchondriasis:factorfiction?ApreliminaryexaminationoftherelationshipbetweenhealthanxietyandsearchingforhealthinformationontheInternet.Journal of Anxiety Disorder26,189–96.
NoyesRJr,StuartS,LangbehnDR,HappelRL,LongleySLandYaglaSJ(2002a)Childhoodantecedentsofhypochondriasis.Psychosomatics43,282–89.
NoyesRJr,StuartS,LongleySL,LangbehnDRandHappelRL(2002b).Hyponchondriasisandfearofdeath.Journal of Nervous and Mental Diseases190,503–9.
OlatunjiBO,DeaconBJandAbramowitzJS(2009)Ishyponchondriasisananxietydisorder?British Journal of Psychiatry194,481–82.
14—DiSOrDEr OF thE AwArENESS OF thE BODY 243
OlivardiaR,PopeHGJrandHudsonJL(2000)Muscledysmorphia inmaleweightlifters:acasecontrolstudy.American Journal of Psychiatry157,1291–96.
OrbachCEandTallentN(1965)Modificationofperceivedbodyandofbodyconcept.Archives of General Psychiatry12,126–35.
ParkesCM(1976)Thepsychologicalreactiontolossofalimb:thefirstyearafteramputation.InHowellsJG(ed.)Modern Perspectives in the Psychiatric Aspects of Surgery.London:Macmillan.
Parsons T (1951) Illness and the role of the physician: a sociological perspective. American Journal of Orthopsychiatry21,452–60.
PhillipsKA,McElroySL,KerkPE,PopeHGandHudsonJI(1993)Bodydysmorphicdisorder:30casesofimaginedugliness.American Journal of Psychiatry150,302–8.
Phillips KA, Menard W, Fav C and Weisberd R (2005) Demographic characteristics, phenomenology,comorbidity, and family history in 200 individuals with body dysmorphic disorder. Psychosomatics 46,317–25.
Pope HG Jr, Griber AJ, Choi P, Olivardia R and Phillips KA (1997) Muscle dysmorphia: an under-recognizedformofbodydysmorphicdisorder.Psychosomatics38,548–57.
PopeCG,PopeHG,MenardW,FayC,OlivardiaRandPhillipsKA(2005)Clinical featuresofmuscledysmorphiaamongmaleswithbodydysmorphicdisorder.Body Image2,395–400.
RackP(1982)Race, Culture and Mental Disorder.London:Tavistock.RamachandranVSandHirsteinW(1998)Theperceptionofphanthomlimbs.TheDOHebblecture.Brain
121,1603–30.RamettiG,CarrilloB,Gómez-GilE,JunqueC,Zubiarre-ElorzaL,SegoviaS,GomezÁandGuillamon
A(2011)Themicrostructureofwhitematter inmale-to-female transsexualsbeforecross-sexhormonaltreatment.ADTIstudy.Journal of Psychiatric Research45,949–54.
ReedJL(1975)Thediagnosisof‘hysteria’.Psychological Medicine5,13–7.RobinAA,Copas JB, JackAB,KaesarACandThomasPJ (1988)Reshaping thepsyche: theconcurrent
improvementinappearanceandmentalstateafterrhinoplasty.British Journal of Psychiatry152,539–43.Russell GFM (1979) Bulimia nervosa: an ominous form of anorexia nervosa. Psychological Medicine 9,
429–48.SantanaML,SilvaRdeC,AssisAM,RaichRM,MachadoMEanddeJPintoE(2013)Factorsassociated
with body image dissatisfaction among adolescents in public schools in Salvador, Brazil. Nutrición Hospitalaria28,747–55.
SchreberD(1955)Memoirs of My Nervous Illness(transl.MacalpineIandHunterRA).London:Dawson.SimsACP(1985)Headinjury,neurosisandaccidentproneness.InTrimbleMR(ed.)Advances in Psychosomatic
Medicine: Neuropsychiatry.Basel:Karger.SladePD(1988)Bodyimageinanorexianervosa.British Journal of Psychiatry153(suppl.2),20–2.SladePDandRussellGFM(1973)Awarenessofbodydimensioninanorexianervosa:cross-sectionaland
longitudinalstudies.Psychological Medicine3,188–99.SlaterE(1965)Diagnosisofhysteria.British Medical Journali,1395–9.Slater E and Glithero E (1965) A follow-up of patients diagnosed as suffering from hysteria. Journal of
Psychosomatic Research9,9–13.StarcevicVandBerleD(2013)Cyberchondria:towardsabetterunderstandingofexcessivehealth-related
Internetuse.Expert Review of Neurotherapeutics13,205–13.StClareW(1787)Country news.InThe Gentleman’s Magazine 57,1,268.CitedbyHunterRandMacalpine
I(1963)Three Hundred Years of Psychiatry.London:OxfordUniversityPress.SteigerH,FraenkelLandLeichnerPP(1989)Relationshipofbody-imagedistortiontosex-roleidentifica-
tions,irrationalcognitions,andbodyweightineating-disorderedfemales.Journal of Clinical Psychology45,61–5.
StraumanTJ,VooklesJ,BerensteinV,ChaikenSandHigginsET(1991)Self-discrepanciesandvulnerabilitytobodydissatisfactionanddisorderedeating.Journal of Personality and Social Psychology61,946–56.
StroberM,GoldenbergI,GreenJandSaxonJ(1979)Bodyimagedisturbanceinanorexianervosaduringtheacuteandrecuperativephase.Psychological Medicine9,695–701.
TaylorB (1856)Thehasheesheater.Putnam’s Monthly Magazine of American Literature, Science and Art8,233–9.
VealeD,BoocockA,GournayK,DrydenW,ShahF,WilsonRandWalburnJ(1996)Bodydysmorphicdisorder:asurveyof50cases.British Journal of Psychiatry169(suppl.2),196–201.

244 FOUR—SELF AND BODY
VeithI(1965)Hysteria: the History of a Disease.Chicago:UniversityofChicagoPress.Walker DC, Anderson DA and HildebrandtT (2009) Body checking behaviours in men. Body Image 6,
164–70.WebbJB,Warren-FindlowJ,ChouYandAdamsL(2013)DoyouseewhatIsee?:Anexplorationofinter-
ethnicidealbodysizecomparisonsamongcollegewomen.Body Image10,369–79.WorldHealthOrganization(1992)The ICD-10 Classification of Mental and Behavioural Disorders: Clinical
Description and Diagnostic Guidelines.Geneva:WorldHealthOrganization.WorldHealthOrganizationRegionalOfficeforEurope.Obesity in Europe.Online.Available:http://www
.euro.who.int/en/health-topics/noncommunicable-diseases/obesity(AccessedApril2014)ZellnerDA,HarnerDEandAdlerRL(1989)Effectsofeatingabnormalitiesandgenderonperceptionsof
desirablebodyshape.Journal of Abnormal Psychology98,93–6.

245
C H A P T E R 15
The Psychopathology of Pain
SummaryPain is an unpleasant experience that involves the conscious awareness of noxious sensations,hurting and aversive feelings associated with actual or potential tissue damage (InternationalAssociationfortheStudyofPain,1994).Itisoftenconceptualizedasamoodstate.Inpsychiatry,pain can present as being heightened, markedly diminished or occurring in the absence ofdemonstrablecause.Themostproblematiccasesarethoseinwhichpainisthefocusofpresentationbutthereisanabsenceofidentifiablephysicalcause.Facialpain,burningmouthsyndrome,vulvodynia,andpsychogenicitchareillustrativeexamplesofthisproblem.
‘ You want to hear of me, my dear? That’s something new, I am sure, when anybody wants to hear of me. Not at all well, Louisa. Very faint and giddy.’
‘Are you in pain, dear mother?’‘I think there’s a pain somewhere in the room,’ said Mrs Gradgrind, ‘but I
couldn’t positively say that I have got it.’Charles Dickens (1854), Hard Times
Since Aristotle, pain has been classified not as a perception but as a mood state, and soexcludedfromthefivesenses.It isconceptuallyamostdifficult topic,hardtodescribeandtocategorize;theonlyaspectthatisclearisthatitrepresentsastateofsubjectivesufferingofthepatient.Butwhatdoeshemeanby‘mypain’?Whereisitandwhatisit?Certainly,themeaningofthepainismorethanthepainitself,andoftenitisthereasonforthesensationbeinginterpretedassuffering.Apatientwithsorenessofthethroatbelievedherselftohaveacancerofthethroat;hermotherhaddiedofthatcondition.Therelationbetweensymptomsandtheirmeaningis not straightforward. Another person believed herself to be suffering from venereal diseasewithouthavingbeen exposed to the risk.But shehadpreviouslybeen successfully treated forHodgkin’sdisease.Shehadnofearsconcerningherfactual,andpotentiallylethal,illnessbutonlyadmittedconsciouslytofearingtheimpossible.
Phenomenologicalaspectsoftheexperienceofpainarenotwellcharted,althoughingeneralmedicinethisis,aboveallothers,theareainwhichphenomenologycouldbemosthelpful:painisasubjectiveexperiencethatoccursonlyinconsciousness(Bond,1976).Thepsychiatristisoftenconfrontedwiththeproblemofwhetherthepainisphysicalormental, organicorfunctional, medicalorpsychiatric,and,ofcourse,theanswerforeachcontrastedpairisoftenboth.Wemaythenberequested toassesshowmuchof thepain ispsychogenic,although this isvirtually impossiblebecause,followingAristotle,painisastateofmind,evenwhenthereissuchanobviouscauseasahaematomaunderthefingernail.
Organic or Psychogenic Pain?The transmission of pain results in a subjective, conscious experience. For an account of theanatomicalbasisforpainandalsothephysiologicalandbiochemicalmechanisms,thereaderis

Keywords: PainAsymbolia,PhantomPain,BurningMouthSyndrome,Vulvodynia.
15—ThE PSYchOPAThOLOgY OF PAiN 245.e1
246 FOUR—SELF AND BODY
referredtoWallandMelzack(1999).Thereisathresholdforpain:lightpressureisperceivedastouch,heavypressureaspain.Anexplanationforthishasbeensuggestedinthegate control theoryof Melzack andWall (1965), who considered that painful stimulation through the thin myelinatedandunmyelinatedfibresresults inpositivefeedbackinthesubstantiagelatinosa;this istransmitted inthe lateralspinothalamictract.However, thisgate isunder the influenceof thehigher centres,which canoverride the local input, asdemonstratedby the effect ofattention:sometimespainisnotfeltwhenattentionisdirectedawayfromtheaffectedsite.Currentbiochemicaltheoriesarealsoimportantinaccountingforthemediationofpain.
Othertheoriesinvolvethestudyofpresynapticandpostsynapticmechanismsinthecentralnervoussystem(Nathan,1980).Electricalstimulationinvarioussitesinthebrainstem,includingthemedullaoblongata,theperiaqueductalgreymatterandthehypothalamusaroundthethirdventricle,mayproduceanalgesia.Endogenousopiatesubstances(endorphins)havebeendiscovered to inhibit nerve fibres reporting noxious events. This was initially discovered followingelectricalstimulationintheperiaqueductalgreymatterofthebrainsteminratsbuthassubsequentlybeendemonstrated inhumans (Bond,1976).Centralnervous systemmechanisms forthe modulation of pain include descending modulatory control and an increasing number ofneurotransmitters,especiallyserotoninandendogenousopioids;itisalmostcertainlytheinteractionofthesedifferentsystemsthatiseffectiveinpainmodulation(FieldsandBasbaum,1994).And, there is increasing understanding of the molecular basis of pain. The role of sodiumchannelsfollowingnerveinjuryandthegenesencodingfortheexpressionofparticularsodiumchannelsinprimarysensoryneuronsisgraduallybeingelucidated(Waxmanetal.,1999;Waxman,1999).
Thetemptationtoregardpainsimplyasanyothersensationcreatescertaindilemmas.Forexample,whatisthesubjectiveexperienceofthepersonwhocomplainsofseverepainwithnoorganicpathologydetectable,orthepersonwithmildpathologywhocomplainsofexcruciatingpain?Howdoesoneassessthepersonwithanapparentlypainfulinjurywhoclaimshedidnotnoticeanypainatthetime?
Purelyorganic,physiologicalterms,andalsopsychological,emotionalwords,havebeenused.Beecher(1959)believedthatpaincouldbedefinedandlistedmanydistinguishedphysiologistsandpsychiatriststosupporthiscase.However,Merskey(1976)considersthatpainisapsychologicalexperience,privatetotheindividualbuttendingtobedescribedintermsofdamagetothebody, and sodefinedpain as ‘anunpleasant experiencewhichweprimarily associatewithtissuedamageordescribeintermsofsuchdamage,orboth’.
Clearly,irrespectiveofthephysicalstimulus,psychologicalfactorsareenormouslyimportantintheappreciationofpain.Forexample,psychological analgesia(educatedornaturalchildbirthinobstetriccare),usingpsychologicalpreparation,explanationandsometimeshypnosis,willresultin5to10percentofsubjectsexperiencinglittleornopain,15to20percentexperiencingonlymoderatepainandintherestpainisnotmodifiedbutfearandanxietyarediminished(Bonica,1994).Doctorshavefrequently,throughneglectingsubjectiveevaluation,missedtheimportantdistinction between the experience of pain and its physical causes (Noordenbos, 1959). Thepatientassumesthathispainindicatesthepresenceofphysicalillness,butpainofvarioustypesis a very common symptom in many psychiatric conditions without there being physicalpathology.
The experience of psychogenic pain has been associated with particular personality types(Engel,1959).Themost importanttraitsofpersonalityassociatedwithpainarethoseofanxiousness, depressiveness and the cyclothymic personality at its depressive pole – hysterical,hypochondriacal and obsessional traits (Bond, 1976). Subjects with such personality traitsdevelopedtoabnormalextentareespeciallylikelytorespondtolifestresseswithpain.Complaintsof pain are common in neurotic disorder, especially with chronic anxiety or hysterical traits(Merskey,1965).
15—ThE PSYchOPAThOLOgY OF PAiN 247
It is important tobeverycareful inattempting todistinguishpainofphysicalorigin fromthatwhichislargelypsychogenic:generalizationscanbedangerous.However,Trethowan(1988)considers that there are certain importantdifferencesbetweenpainofpsychiatric andorganicorigin.Theseareasfollows.
■ Painassociatedwithpsychiatricillnesstendstobemorediffuseandlesswelllocalizedthanpainduetoaphysicallesion.Itspreadswithanonanatomicaldistribution.
■ Painiscomplainedofasaconstantfeature.Itmaybecomeevenmoresevereattimes,butitpersistsunremittingly.Physicalpainsusuallyhavemoredefiniteprovocativeagentsandarerelievedbyspecificmeasures.
■ Psychogenicpainisclearlyseentobeassociatedwithanunderlyingdisturbanceofmoodthatappearstobeprimaryinbothtimeandcausation.
■ Itseemstobemuchmoredifficulttoaccuratelydescribethequalityofpsychogenicpain.Thepatientis innodoubtthatheissuffering,thatthepainisveryunpleasantandthathefeelshecannotbearit.Butincontrasttopainfuldamagetoadefinedorgan,whenpainmaybedescribedasburning(skin),shooting(nerve)orgripping(heartmuscle),thepatientwithnonorganicpaincanfindnoadequatewordsfordescription.
■ Afurtheradditiontothislististhefindingofprogressionoftheseverityandextentofthepain over time – unusual for a purely physically mediated pain without increased tissuedamage(Tyrer,1986).
Pain and Heightened SensationGeneralizedincreaseinsensoryinputmaybeexperiencedaspain.Thisisexemplifiedbyhyperacousia:thepatientcomplainsofnoisesbeinguncomfortablyloud.Thereisnoobjectiveimprovementinhiscapacitytohear,butthethresholdatwhichsoundisperceivedasunpleasantlyloudislowered.Noises,evenanormalspeakingvoice,aredescribedaspainfultolistento.
Withlysergicaciddiethylamide,intensepainmaybeexperiencedinthelimbs,whichseemto the sufferer tobe twistedorcontorted.Similarly, in theearly stagesof thiaminedeficiencytheremaybeincreasedsensitivitytopain.Inthesesituations,thereisanalterationtoperceptionofsensationssothattheyareexperiencedaspain.
Duringconsciousness,thepersonreceivescountlesssensationsfromalloverhisbody,suchasitching,distension,pressure,borborygmi,mildaching,thumping,warmthandsoon.Theseformthesensoriumofthebodyimage;theymakepossiblethelocationofselfinspace.Mostofthesesensationsescapeattentionformostofthetime.However,occasionallythepersonconcentratesandmaytakeactiontoeliminatethesensation–scratchhisearorcrosshis legs.Attentiontosuchsensations, especially if linked toanunpleasantemotion,mayoccasion theexperienceofpain.Noticingthesensationresultsinfear,andthedistressofthisemotionisperceivedaspain.
This would appear to be the explanation for the vital feelings of depression described inChapter16.Vital feelingsare the localizationofdepression inabodilyorgan, complainedof,perhapsaspain,intheheadorchestorelsewhere.Onfurtherquestioning,symptomsaredescribedasbeingunpleasant,painfulpressureorevenafeelingofmiseryanddepressioninthatorgan:morbidinterpretationsofordinarybodilysensations.Thesensationisunpleasantbutnormalandwouldbeignoredinhealth.Withdisorderofaffect,thesensationmaybemorbidlyinterpretedasbeingduetocancer,tuberculosisorvenerealdisease.Thereare,ofcourse,alsoactualphysicalchangesindepression,forexampleslowingofperistalsisanddecreasedgastrointestinalsecretions,andthesemayalsoprovokeunpleasantsensationssuchasspasmandconstipation.
Centralpain(thalamicsyndrome)isexperiencedasaspontaneousburningsensationthatcanbeactivatedbycutaneousstimulationortemperaturechanges.Itcanalsopresentastactileallodynia,coldallodyniaorongoingpain(Greenspanetal.,2004).Itisusuallyintractableandoccursinthesettingofcerebrovascularaccident,multiplesclerosis,syringomyeliaandspinalcordinjury.

248 FOUR—SELF AND BODY
Thecurrenthypothesis isthat itarisesasaresultofdisruptioninthespinothalamicpathwaysassociated with ectopic neuronal discharges and potentially involves adrenergic, GABAergic,glycineandotherneurotransmitters(Devuldeetal.,2002).
Diminished Pain Sensation and Pain CravingIncertainsituations,thereisadecreaseintheperceptionofpain.Pain asymboliaisaconditioninwhichsituationsthatshouldgiverisetopaindonot(SchilderandStengel,1931).Thiscondition can occur as a congenital or an acquired disorder. There are at present five recognizedhereditaryvarieties,usuallyassociatedwithautonomicneuropathiesincludinganhidrosis(Butleretal.,2006).Severalmutationsofnervegrowthfactorhavebeenidentified(Einarsdottiretal.,2004).Acquiredpainasymboliahasalsobeendescribed inpatientswithvascular lesions,predominantlyleftsidedandinvolvingtheinsular(Berthieretal.,1988).Patientswithpainasymbolia show an absent or inadequate response to painful stimuli over the entire body and aninabilityto learnappropriateescapeorprotectiveresponses.Otherfeatures includeanhidrosis,lack of thermal sensitivity, selfmutilation, intellectual disability, recurrent fever secondary toanhidrosisandfailuretothrive(DiasandCharki,2012).Inpatientswithschizophreniaandtheirrelatives,thereisevidenceofelevatedpainthresholdsandpaintolerancedemonstratedbyrelativeinsensitivitytofingerpressure(HooleyandDelgado,2001).Selfdamageofagrossnaturealsooccurssometimesinschizophrenia,forexampleselfcastration.Inothersituations,suchasacutedrunkenness, there isdiminished appreciationdue to the centraldepressant actionof alcohol,andopiatessimilarlyareanalgesicthroughtheiractiononthecentralappreciationofpain.
Attentionisalsoanimportantfactorintheperceptionofpain.Excitementoraggression,asinfootballersorsoldiers,mayrenderthesubjectoblivioustoseriousinjury.Whenawoundhasadvantages to thepatient, for exampleenablinga soldier to leave thebattlefield, it causes lesspainthanwhentheinjuryisseenaswhollydisadvantageous.Variouspsychologicaltechniquescanreducetheexperienceofpain,includinghypnosis,variousstratagemsinchildbirth,placebomedicationand,possibly,acupuncture.Indissociation(conversion),theremaybelocalizedanaesthesiaandanalgesiafortheaffectedlimb,forexamplethepatientmaydescribenoperceptionofpinpricksensation.
Abluntingandpervertingofpainperceptionisdescribedinseverementalretardation,resultingoccasionally ingross selfdamage.Thepatientmaybanghishead so that there is chronichaematoma formation, bite himself or otherwise harm himself repeatedly, causing permanentdamage.Meanwhile,he appears to experiencenopainor evendiscomfort.Selfapplicationofconstricting bands has been described in schizophrenia and organically disordered patients(DawsonButterworthetal.,1969).Thesearemostoftenappliedtotheleftarm;despiteextensivetissuedamage,thepatientdoesnotcomplainofpain.
Selfinflictedharmoccursalsointhoseofdisturbedpersonalitywithoutintellectualdeficiency.Suchbehaviourmay includeskincutting,wrist slashing,skinburning,selfhitting,severeskinscratchingandbonebreaking (McElroyetal.,2000).Thesepatientsareusually female (GraffandMallin,1967),andthebehaviourappearstobelinkedwiththedesiretorelievetensionandalleviatenegativeemotions.There is empirical evidence that itdoes relievenegativeemotions(Klonsky,2007).Thereisalsolimitedevidencethattheselfinjuriousbehaviourhasseveralpossiblegoals:asselfpunishment,toinfluencepersonalrelationships,toreducetendencytodissociationandalsotoinduceintensesensorystimulation(Box15.1).
Pain Without Organic CauseUnfortunately,painisanunpleasantfeaturecommontoalmostallmedicalsettings;itisafrequentcomplaint inmedical, surgical, gynaecological andpsychiatricpractice.Recalcitrant casesmay

15—ThE PSYchOPAThOLOgY OF PAiN 249
bereferredtoapainclinic,andprominentamongsuchreferralsarethoseinwhomnoorganicbasiscanbefoundtoaccountforthecomplaintofpain(Tyrer,1985).Paininthebackandintheheadandface,particularly,isoftenfoundnottobeassociatedwithorganiclesions.From3to 5 per cent of patients, depending on how referrals are made, have measurable psychiatricdisturbance.
There are various possible mechanisms to explain the presence of pain without physicaldisease:autonomicnervousactivitymaybeinterpretedandelaboratedthroughfearofpossibleconsequences,normalsensationsmaybeexperiencedaspainfulinsituationsofstressorinfear,relatively minor pain and discomfort of benign cause may be misinterpreted as being moreominousthanitreallyis.
Classificationofnonorganicpainiscomplex.Aswellasoccurringasaprimarydisturbance,painalsomaybeconspicuouswithhypochondriasis,withsomatizationdisorderand,especially,withdepressioninmooddisorder.InTyrer’sseries,twothirdsofthosepatientswithoutorganiccause and with measurable psychiatric disturbance were diagnosed as suffering from majordepressive disorder.The remainder had personality disorders, anxiety state, hysteria and drugdependence;paraphreniaandorganicbrainsyndromealsooccurred,butrarely(Tyrer,1985).
Painwithoutadequateorganicexplanationisoneofthemostdifficultproblemspsychiatristsarecalledontotreat.Inastudyofpatientswithpainreferredtopsychiatristsinageneralhospital,theheadandneckwasthemostcommonsite,followedbytheback,abdomen,armorleg,rectumorgenitaliaandchest(Pillingetal.,1967).In32percentofthesemedicalandsurgicalpatients,painwasthepresentingcomplaint,anditwasconsideredthatthesepatients‘spoketotheirphysiciansintermsofpainorotherorganicsymptomsratherthananxiety,depressionandthelike’.Intheevaluationofthesignificanceofemotionalfactorsinchronicpain,adequatehistoryandexamination,includingtheassessmentofattributionandtherelationshipwithmoodstate,wasfoundtobemosthelpful(Tyrer,1992);themostusefulquestionnairesweretheHospitalAnxietyandDepressionScale(ZigmondandSnaith,1983)andtheWestHaven–YaleMultidimensionalPainInventory(Kernsetal.,1985).
Itis,ofcourse,whollyunderstandablethatsomeonesufferingpainshouldbemiserableandthatchronicpainortheanticipationofrecurrentpainshouldprovokedepressionofmood.This
BOX 15.1 ■ Examples of self-injurious behaviour
When SHE’s home alone, she cuts herself, slicing off her nose to spite other people’s faces. She always waits and waits for the moment when she can cut herself unobserved. No sooner does the sound of the closing door die down than she takes out her little talisman, the paternal all-purpose razor. SHE peels the blade out of its Sunday coat of five layers of virginal plastic. She is very skilled in the use of blades; after all, she has to shave her father, shave that soft paternal cheek under the completely empty paternal brow, which is now undimmed by any thought, unwrinkled by any will. This blade is destined for HER flesh. This thin, elegant foil of bluish steel, pliable, elastic. SHE sits down in front of the magnifying side of the shaving mirror; spreading her legs, she makes a cut, magnifying the aperture that is the doorway into her body. She knows from experience that such a razor cut doesn’t hurt, for her arms, hands, and legs have often served as guinea pigs. Her hobby is cutting her own body.
Elfriede Jelinek (1988), The Piano Teacher
Late at night I went into the bathroom and took the broken pieces of a razor blade which I had kept. I slashed my wrist again and again, as deeply as I could. I knew perfectly well that it would not kill me, not like the times before. They have been something quite different. As my writing to you comes to a close, the pain is so unbearable inside me that a force of such strength has driven me to inflict a physical pain on myself in the hope of appeasing the other.
Sarah Ferguson (1973), A Guard Within
250 FOUR—SELF AND BODY
isoftensomuchtakenforgrantedthatnostepsaretakentoalleviatethedepressedmoodifthecauseofthepainisobvious.However,iftheperceptionofpainisconsideredtohavetwoseparatecontributions–thesensoryperceptionandtheinvestingaffect–effortstorelievethe latter, ifsuccessful,willproduceaglobaldiminutionofpain.Paincanbeacauseofdepression,andinthissituationtreatmentforthedepressionisappropriate.
PAIN AND LOSS
Thebestknownmodelforthistopicisthephantom limbpainsooftenexperiencedinamputees.Painisexperiencedwithinalimbthatisnotthere;thatis,spatially,painislocatedoutsidethepatient.However,thisisnotahallucination.Thepersonknowsfullwellthathehaslosthislegandthatthefeelingofpainisinsidehimself.Thebodyimagetakesaverylongtimetoadjusttoachangesuchasanamputation,anditmayneverdosofully.RamachandranandHirstein(1998)provideathoroughreviewofthesubject.Thephantomlimbexperienceoccursalmostimmediatelyfollowingthe lossofa limbinthevastmajorityofcases,andtheincidencemaybeevenhigherfollowingatraumaticloss.Inthecaseofsurgicalamputations,phantomsappearassoonastheanaestheticwearsoff.Thephantomispresentforafewdaysorweeksandgraduallyfadesbutmaypersistforyearsorevendecadesinsomepeople.Indeed,somepeopleareabletorecallaphantomlimbatwillafteritsdisappearance.
Phantomsaremostcommonfollowingamputationofanarmoralegbuthavebeenreportedfollowingmastectomiesorremovalofpartsoftheface;evenphantominternalvisceracanproducesensationsofbowelmovementsandflatus.Thepostureofthelimbcanbecomehabitual,aswiththearm,oftenpartiallyflexedattheelbowwithforearmpronated,andwhenthephantomfadesfromconsciousness,especiallywiththeforearm,itbecomesprogressivelyshorteruntilthepatientisleftwithjustthephantomhand.Perhapsmostsurprisingly,childrenwithcongenitallymissinglimbs canexperiencephantoms.Originally, itwas thought that thephantompainwasdue tostumpneuromas,butgiventhatpatientsbornwithoutlimbscanhavephantompain,neuromasdonotseemnecessaryforphantompaintooccur.Thepersistenceofcentralrepresentationoftheamputatedlimbislargelyresponsibleforthephantomillusionandassociatedpain.
PSYCHOGENIC FACIAL PAIN
Ithasbeenknownforalongtimethatmanypatientswithchronicpainatavarietyofsitesdonothaveabnormalphysicalsignsanddonotmanifestseriousorganicillness.Atypical facial painisanespeciallyfrequentandintractableexample,manifestingnoorganicsignsbutcausinggreatsuffering;thepatientisreferredfromsurgeontodentisttopainclinicphysiciantopsychiatrist,often without benefit. Such pain has often been associated with depression. Lascelles (1966)describedaseriesof93patientssufferingfromprolongedfacialpain,ofwhomthemajoritysufferedfromatypical depressionwith intensefatigue, tensionandsleepdisordersuperimposedon‘obsessive’personality;53ofthesepatientsrespondedwelltoantidepressanttherapy.
More recently, Blumer and Heilbronn (1982) have seen chronic, intractable pain withoutorganiccauseasbeingavariantofdepressiveillness.Garveyetal.(1983)investigatedtheassociationbetweenheadacheanddepressionin116patientssufferingfrommajordepressivedisorder.Duringanondepressedperiod,thesepatientsexperiencedasimilarrateforheadachetothatofnondepressivecontrolsubjects,but theyhadamarkedly increasedrateduringdepressiveepisodes.Feinmannetal.(1984)investigatedtheefficacyofanantidepressant,dosulepin(dothiepin),inthetreatmentofpsychogenicfacialpain.Seventyonepercentofpatientswerefreeofsymptomsatnineweeks,comparedwith47percentinaplacebogroup;ata12monthfollowup,81 per cent of patients were painfree. Good prognostic indicators for successful treatmentincludedpainfollowinganadverselifeevent,minimalprevioussurgicalinterventionandfreedom
15—ThE PSYchOPAThOLOgY OF PAiN 251
frompainafternineweeks’treatment.Suchstudieswouldsuggestanassociationbetweenfacialpainwithoutphysicalsignsanddepressiveillness.
BURNING MOUTH SYNDROME
Agroupofheterogeneousskinconditionsthatpresentwithunpleasantskinsensationsincludingitching, burning, stinging or numbness are well recognized as liable to affect face, scalp andperineum.Theseconditionsarepoorlyunderstoodbutdemonstrateaninterplaybetweenneuropathic pain, neuropathic itch, neurology and psychiatric disorders (Gupta and Gupta, 2013).When these conditions affect the oral cavity, it is referred to as “burning mouth syndrome”,a condition characterized by intraoral burning for which no medical or dental cause can beidentified(Ducasseetal.,2013).Theabnormaloralsensationsincludeburning,pricking(pinsandneedles),allodynia(painonbrushingtheteethandgums),tingling,numbness,itchingandsensationofelectricaldischarges(Braudetal.,2013).Thesesensationsoccurprincipallyonthetipofthetongue,thelateralaspectsofthetongue,lips,hardandsoftpalate(Sunetal.,2013)andmayinvolvepainradiatingtothelowerandupperjaws,theinneraspectsofthecheeksandthe gums. Despite normal salivation, patients often complain of xerostomia and dysgeusia.Burningmouthsyndromeseemstooccurmostfrequentlyinperimenopausalfemales(Dahiyaetal.,2013).
VULVODYNIA
Vulvodyniacanbedefinedaspersistent,spontaneous,unwelcomed,intrusiveanddistressingvulvalsensation(MarkosandDinsmore,2013).Itisalittleunderstoodcondition.Afrequentsubtypeistermed‘provokedvestibulodynia’inwhichtheexperiencedpainordiscomfortisprovokedbysexualintercourseratherthanmerelyoccurringspontaneously(Boisetal.,2013).Thereissomeevidencethatvulvodyniaisassociatedwithgeneralizedhyperalgesia.Furthermorethatthereareaugmentedbrain responses to thumbpressure, that is stimulationof an area remote from thevulva, demonstrable within the insula, dorsal midcingulate, posterior cingulate, and thalamuscomparedtonormalcontrols.Thisisinterpretedasshowingaugmentedcentralpainprocessinginvulvodynia(Hampsonetal.,2013).Infocalasopposedtodiffusevulvodynia,whenthepainislocalizedat1and11o’clockittendstobeexperiencedasdeeppainwithinthevestibuleandthepainisprovokedbysexualintercourseandtheinsertionofatampon.Painat5and7o’clockis lesssevere(DondersandBellen,2012).Thereareconsiderableassociatedadverseeffectsonqualityoflifeandonintimaterelationshipswithsexualpartners(Boisetal.,2013;Smithetal.,2013;Xieetal.,2012;Ponteetal.,2009).
Malepatientscanalsopresentwithaconditionsimilartovulvodynia.Thepatientspresentwithburningsensationinthepenisandscrotumandthisconditionistermed‘penoscrotodynia’.Thecurrentproposedclassificationis:generalized,focal,provoked,unprovoked,andmixedtypes(Markos,2011).
PSYCHOGENIC ITCH
Itchandthedesiretoscratchisanormalresponsetoskinsensations.Pruritogenicitch(physiological itch) is transmitted by dedicated afferent neurons much as is pain. Mediators of itchincludethe‘crosstalk’betweendermalMastcellsandadjacentcutaneousafferents.Inaddition,thereareanumberofneuropeptides(neurotensinandsubstancePforexample)involvedintheprocess (Greaves, 2010). Some cases, which are considered to be neuropathic in origin, arethoughttoberelatedtodamagetotheperipheralnervoussystemsuchasinpostherpeticneuralgia,brachioradialpruritus,notalgiaparesthetica,incentralnervousdamagetothespinalcord

252 FOUR—SELF AND BODY
bytumoursanddemyelinatingdiseasesuchasmultiplesclerosis(YosipovitchandSamuel,2008).The itch sensation in these conditions is analogous to neuropathic pain and overlaps withburning, aching and stinging sensations. Psychogenic itch, on the other hand, occurs in theabsenceofaphysicalcauseandisunrelatedtodemonstrablenervedamage.Itcanbeassociatedwithdepressionandobsessivecompulsivedisorder(Calikuşuetal.,2003),anxietyanddelusionsofparasitosis.TheFrenchpsychodermatologygrouphaveproposeddiagnosticcriteriatoincludethefollowingthree:localizedorgeneralizedpruritussinemateria,chronicprurituslastinglongerthansixweeksandtheabsenceofasomaticcause.Inadditionthereshouldbethreeadditionalcriteriafromthefollowingseven:chronologicalrelationshipofprurituswithoneorseverallifeeventsthatcouldhavepsychologicalrepercussions,variationsinintensityassociatedwithstress,nocturnal variations, predominance during rest or inaction, associated psychiatric disorders,improvementinresponsetopsychotropicagentsandimprovementinresponsetopsychotherapy(Miseryetal.,2007).
Pain and SufferingPainisanappropriatestudyforthephenomenologist,inthattheexternalsignsmaybeirrelevantandthesubjectiveexperienceallimportant.Thechiefprobleminassessingpainistheextraordinarydifficultyapatienthasindescribingthequalityofhispain:thegreaterthepsychogeniccomponentofthepain,themoredifficultitistofindtherightwordstodescribeit.Sometimes,itseemsthatpainmaybeneededasaneuroticsolutiontoaneuroticconflict:fortheequilibriumtoremain,itisnecessaryforthepaintoberetained.IthasbeenconsideredbyTrethowan(1988)thatsuchapatient‘isnotsufferingfrompainatall.Whatsheissufferingfromissuffering’.
Therearedifferencesbetweenthepersonsufferingfromorganicallydeterminedpainandthechronicsuffererwithmultiplesymptomswhosepainisconsideredpsychogenic.Thelattertrulysuffersbutdoesnotshowthephysicalcorrelatesofseverepain.Itseemsthatthestateofsufferinginwhichthispersonexistsfindsexpression,donsrespectabilityandcanonlybecommunicatedwhenitistransformedperipherallyintoaspecificpain.Painmayoccurwithlittlesuffering,asintheinjectionof localanaestheticthat,afterthesmallprick,bringsrelief fromaworsepain.Sufferingmayalsooccurwithoutpain,butitmayalsobedescribedaspain,andthismaybethenatureofmanyneuroticcomplaintsofpain.Thistranspositionofaffectiswhollyunderstandablewhenoneconsidersthesemanticsofsuffering.Sufferingofallnonphysicalkinds–indignation,humiliation, disappointment – finds expression in pain terms: taking pains, feeling crushed,bruisedselfesteem,rubbingsaltinthewound,gettingone’sfingersburnt,searingremarks.Itisnotjustthatpainisametaphorforsuffering,butinmanysituationssufferingcanbeexperiencedandexplainedbythesuffereronlyintermsofpain.
Sotheuseofpainwordscanbeconstruedmetaphorically,andtheneuroticpatientmayfollowthistoitslogicalconclusionanddescribeconcretelytheunbearableandhumiliatingsufferingofhisdailyexistenceascomplaintsoflocalizedphysicalpain.Theexperienceofpainisaphysicalsensationthattakesonanaffectivecomponentforitsexpressionandinterpretation.Thisaffectivecomponent–suffering–mayoccurwithoutphysicalperceptionandsometimesstillbeexperiencedbythepersonhimselfaspain.
ReferencesBeecher HK (1959) Measurement of Subjective Responses, Quantitative Effects of Drugs. NewYork: Oxford
UniversityPress.BerthierM,StarkteinSandLeiguardaR(1988)Asymboliaforpain:asensory–limbicdisconnectionsyn
drome.Annals of Neurology24,41–9.BlumerDandHeilbronnM(1982)Chronicpainasavariantofdepressivedisease:thepainpronedisorder.
Journal of Nervous and Mental Diseases70,381–406.
15—ThE PSYchOPAThOLOgY OF PAiN 253
BoisK,BergeronS,RosenNO,McDuffPandGregoireC(2013)Sexualandrelationshipintimacyamongwomenwithprovokedvestibulodyniaandtheirpartners:associationswithsexualsatisfaction,sexualfunction,andpainselfefficacy.Journal of Sexual Medicine10,2024–35.
BondMR(1976)Psychologicalandpsychiatricaspectsofpain.InHowellsJG(ed.)Modern Perspectives in the Psychiatric Aspects of Surgery,pp.109–39.London:Macmillan.
Bonica JJ (1994) Labour pain. InWall PD and Melzack R (eds.) Textbook of Pain, 3rd edn. Edinburgh:ChurchillLivingstone.
BraudA,TouréB,AgboGodeauS,DescroixVandBoucherY(2013)Characteristicsofpainassessedwithvisualanaloguescaleandquestionnaireinburningmouthsyndrome:apilotstudy.Journal of Orofacial Pain27,235–42.
Butler J, Fleming P andWebb D (2006) Congenital insensitivity to pain – review of a case with dentalimplications.Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontics101,58–62.
CalikuşuC,YücelB,PolatAandBaykalC(2003)Therelationofpsychogenicexcoriationwithpsychiatricdisorders:acomparativestudy.Comprehensive Psychiatry44,256–61.
Dahiya P, Kamal R, Kumar M, Niti, Gupta R and Chaudhary K (2013) Burning mouth syndrome andmenopause.International Journal of Preventive Medicine4,15–20.
DawsonButterworth K, Wallen GDP and Gittleson NL (1969) Selfapplied constricting bands.British Journal of Psychiatry115,1255–9.
Devulde R, Crombez E and Mortier E (2002) Central pain: an overview. Acta Neurologica Belgica 102,97–103.
DiasEandCharkiS(2012)Congenitalinsensitivitytopainwithanhidrosis.Journal of Pediatric Neurosciences7,156–7.
DickensC(1854)Hard Times.London:Penguin.Donders G and Bellen G (2012) Characteristics of the pain observed in the focal vulvodynia syndrome.
Medical Hypotheses78,11–4.DucasseD,CourtetPandOlieE(2013)Burningmouthsyndrome:currentclinical,physiopathologic,and
therapeuticdata.Regional Anesthesia and Pain Medicine38,380–90.EinarsdottirE,CarlssonA,MindeJ,ToolanenG,SvenssonD,SoldersG,HolmgrenDandHolmgrenM
(2004)Amutation inthenervegrowthfactorbetagene(NGB)causes lossofpainperception.Human Molecular Genetics13,799–805.
EngelGL(1959)‘Psychogenic’painandthepainpronepatient.American Journal of Medicine26,899.Feinmann C, Harris M and Cawley R (1984) Psychogenic facial pain: presentation and treatment.
British Medical Journal288,436–8.FergusonS(1973)A Guard Within.London:ChattoandWindus.FieldsHLandBasbaumAI(1994)Centralnervoussystemmechanismsofpainmodulation.InWallPD
andMelzackR(eds.)Textbook of Pain,3rdedn.Edinburgh:ChurchillLivingstone.GarveyMJ,SchafferCBandTuasonVB(1983)Relationshipofheadachestodepression.British Journal of
Psychiatry143,544–7.Graff H and Mallin R (1967) The syndrome of the wristcutter. American Journal of Psychiatry 124,
36–42.Greaves MW (2010) Pathogenesis and treatment of pruritus. Current Allergy and Asthma Reports 10,
236–42.GreenspanJD,OharaJ,SarlaniEandLenzFA(2004)Allodyniainpatientswithpoststrokepain(CPSP)
studiedbystatisticalquantitativesensorytestingwithinindividuals.Pain109,357–66.GuptaMAandGuptaAK(2013)Cutaneoussensorydisorder.Seminars in Cutaneous Medicine and Surgery
32,110–8.HampsonJP,ReedBD,ClauwDJ,BhavsarR,GracelyRH,HaefnerHKandHarrisRE(2013)Augmented
centralpainprocessinginvulvodynia.Journal of Pain14,579–89.HooleyJMandDelgadoML(2001)Paininsensitivityintherelativesofschizophrenicpatients.Schizophrenia
Research47,265–73.InternationalAssociationfortheStudyofPain(1994)Classificationofchronicpain:descriptionsofchronic
painsyndromesanddefinitionsofpainterms.Task Force on Taxonomy(suppl.3).Seattle:IASPPress.JelinekE(1988)The Piano Teacher(transl.NeugroschelJ).NewYork:WeidenfeldandNicholson.Kerns RD, Turk DC and Rudy TF (1985) The West Haven–Yale Multidimensional Pain Inventory
(WHYMPI).Pain23,345–56.

254 FOUR—SELF AND BODY
Klonsky(2007)Thefunctionsofdeliberateselfinjury:areviewoftheevidence.Clinical Psychology Review27,226–39.
LascellesRG(1966)Atypicalfacialpainanddepression.British Journal of Psychiatry112,651–9.Markos AR (2011) Dysaesthetic penoscrotodynia: nomenclature, classification, diagnosis and treatment.
International Journal of STD and AIDS22,483–7.MarkosAandDinsmoreW(2013)Persistentgenital arousal and restlessgenitalia: sexualdysfunctionor
subtypeofvulvodynia?International Journal of STD and AIDS24,852–8.McElroySL,ArnoldLMandBeckmanDA(2000)Habitandimpulsecontroldisorders.InGelderMG,
LópezIborJJandAndreasenNC(2000)New Oxford Textbook of Psychiatry.Oxford:OxfordUniversityPress.
MelzackRandWallPD(1965)Painmechanisms:anewtheory.Science150,971.Merskey H (1965)The characteristics of persistent pain in psychological illness. Journal of Psychosomatic
Research9,291.MerskeyH(1976)Thestatusofpain.InHillO(ed.)Modern Trends in Psychosomatic Medicine 3,pp.166–86.
London:Butterworth.Misery L, Alexandre S, Dutray S, Chastaing M, Consoli SG, Audra H, Bauer D, Bertolus S, Callot V,
CardinaudF,CorrinE,FetonDanouN,MaletR,TouboulSandConsoliSM(2007)Functional itchdisorderorpsychogenicpruritus:suggesteddiagnosiscriteriafromtheFrenchpsychodermatologygroup.Acta Dermato Venereologica87,341–4.
NathanP(1980)Recentadvancesinunderstandingpain.British Journal of Psychiatry136,509–12.NoordenbosW(1959)Pain: Problems Pertaining to the Transmission of Nerve Impulses Which Give Rise to Pain.
London:Elsevier.PillingLF,BannickTLandSwensonWM(1967)Psychologicalcharacteristicsofpatientshavingpainasa
presentingsymptom.Canadian Medical Association Journal97,387.PonteM,KlempererE,SahayAandChrenMM(2009)Effectsofvulvodyniaonqualityoflife.Journal of
the American Academy of Dermatology60,70–6.Ramachandran VS and Hirstein W (1998) The perception of phantom limbs. The DO Hebb lecture.
Brain121,1603–30.SchilderPandStengelE(1931)Asymboliaforpain.Archives of Neurology and Psychiatry25,598–600.SmithKB,PukallCFandChamberlainSM(2013)Sexualandrelationshipsatisfactionandvestibularpain
sensitivityamongwomenwithprovokedvestibulodynia.Journal of Sexual Medicine10,2009–23.SunA,WuKM,WangYP,LinHP,ChenHMandChiangCP(2013)Burningmouthsyndrome:areview
andupdate.Journal of Sexual Medicine42,649–55.Trethowan WH (1988) Pain as a psychiatric symptom. In Hall P and Stonier PD (eds.) Perspectives in
Psychiatry.Chichester:JohnWiley.TyrerS(1985)Theroleofthepsychiatrist inthepainclinic.Bulletin of the Royal College of Psychiatrists9,
135–6.TyrerS(1986)Learnedpainbehaviour.British Medical Journal292,1–2.TyrerS(1992)Psychiatricassessmentofchronicpain.British Journal of Psychiatry160,733–41.WallPDandMelzackR(1999)Textbook of Pain,4thedn.Edinburgh:ChurchillLivingstone.WaxmanSG(1999)Themolecularpathophysiologyofpain:abnormalexpressionofsodiumchannelgenes
anditscontributionstohyperexcitabilityofprimarysensoryneurons.Pain(suppl.6),S133–40.WaxmanSG,DibHajjS,CumminsTRandBlackJA(1999)Sodiumchannelsandpain.Proceedings of the
National Academy of Science USA96,7635–9.XieY,ShiL,XiongX,WuE,VeasleyCandDadeC(2012)Economicburdenandqualityoflifeofvul
vodyniaintheUnitedStates.Current Medical Research and Opinion28,601–8.Yosipovitch G and Samuel LS (2008) Neuropathic and psychogenic itch. Dermatology and Therapy 1,
32–41.ZigmondASandSnaithRP(1983)Thehospitalanxietyanddepressionscale.Acta Psychiatrica Scandinavica
67,361–70.
S E C T I O N FIVEEmotions and Action

This page intentionally left blank

257
C H A P T E R 16
Affect and Emotional Disorders
SummaryMooddisturbanceisnotonlyacommonabnormalitypresentingtopsychiatristsbutofconsider-ableimportancebecauseofthesevereconsequencesthatpoorrecognitionortreatmentmayhaveinthelivesofpatients.Itisassociatedwithsuicide,homicide,recklessbehaviourandpotentialsignificantundesirable impactonsocial reputation.Affect isabroadtermthat isusedtocovermood,feeling,attitude,preferencesandevaluations.Inmodernusage,itreferstotheexpressionofemotionasjudgedbytheexternalmanifestationsthatareassociatedwithspecificfeelings;forexample laughter, cryingand fearfulappearance.Mood isamoreprolongedprevailingstateordisposition, whereas emotion is often used to refer to spontaneous and transitory experiencesimilartobutnotidenticaltofeeling,asitneednotincorporatethephysicalaccompanimentsoftheexperience.Abnormalitiesofmoodcanbeclassifiedas:a)morbidstatesofthebasicemotions,includingsadness,happiness,fear,anger,surpriseanddisgustthatcanbeaffectedintheintensity,duration, timing, quality of experience, expression and appropriateness to the object or socialsetting;b)abnormalitiesofthephysiologicalandarousalmechanismsassociatedwithemotions;andc)abnormalitiesofthecognitiveevaluationofthesocialworldandoftheperceptionoftheemotionsofothers.
I wish to inform you that I have received the cake. Many thanks, but I am not worthy. You sent it on the anniversary of my child’s death, for I am not
worthy of my birthday; I must weep myself to death; I cannot live and I cannot die, because I have failed so much, I shall bring my husband and
children to hell. We are all lost; we won’t see each other any more; I shall go to the convict prison and my two girls as well, if they do not make away with
themselves because they were born in my body.A patient of Emil Kraepelin (1905)
Assessingandobservingthestateof,andchangesin,moodisessentialinpsychiatrybutatthesametimerequiresskill.Partoftheproblemhasalwaysbeentheconceptualconfusionandlackofcohesivepsychopathologicaltheorythathastraditionallybeenassociatedwithdisturbanceofaffect (Berrios,1985).Inastudyofpatientswithunsolveddiagnosticproblemsat thetimeofdischargefromhospital,atypicalpsychoticdepressionwasfound,atfollow-up,tobetheconditionmostfrequentlyresponsiblefordoubt(AnsteeandFleminger,1977).Inanotherstudy,depressedaffect was a major cause of somatic problems without physical pathology (Brenner, 1979).However, the termsusedarenot standardized,normutuallyexclusive.Different languages, incontrasttothenamesgiventophysicalobjects,haveanentirelydifferentrangeofdescriptionsofmood,sothatoneisleftwonderingwhetheritisjustthetermsthatdifferindifferentcultures,or perhaps even the experience of emotion itself. So Angst cannot be translated exactly intoEnglishwithasingleequivalentword;neithercandepressionbepreciselytranslatedintoGerman.Thewordfeelingdescribesanactiveexperienceofsomaticsensation,touch,aswellasthepassivesubjectiveexperienceofemotion.Emotion,accordingtoWhybrow(1997),‘isactuallymemory

Keywords: Emotion,Ecstasy,Anhedonia,Alexithymia,Prosody.
16—AffECT AND EMOTIONAl DISOrDErS 257.e1

258 FIVE—EMOTIONS AND ACTION
and feeling intertwined’. Feelings are also personal convictions, predictive forecasts and socialsensibilities.Allthesenuancesofmeaningaresomewhatdifferentfromtheassociationsofthewordmood.
Traditionally,feelinghasbeenusedtodescribeapositiveornegativereactiontoanexperience;it ismarkedbut transitory.Affect isabroadtermthat isusedtocovermood, feeling,attitude,preferences andevaluations. Inpsychiatry, it is customary to limit itsuse to the expressionofemotionas judgedby theexternalmanifestations thatareassociatedwithspecific feelings, forexample laughter, crying or fearful appearance. Mood is a more prolonged prevailing state ordisposition, whereas emotion is often used to refer to spontaneous and transitory experiencesimilartobutnotidenticaltofeeling,asitneednotincorporatethephysicalaccompanimentsoftheexperience.Inpractice,thesetermsareusedmoreorlessinterchangeably,afactthatcontrib-utestomuchconfusion.
Mood describes the state of the self in relation to its environment.There is an enormousrangeofvariationofwhatcouldreasonablybecallednormalmood.Pathologicalmood,thatis,moodfromwhichthepatientsuffersormoodthatcausesdisturbanceorsufferingtoothers,alsovariesagreatdeal,andtheextenttowhichitisacceptabletoothersinitsexpressionisdifferentindifferentsocialcontexts.Theclinicianhastoasktwoquestionsconcerningthemoodofhispatient.First, is thepersonsuffering?Second, is theexpressionofmood inappropriate in thissocial setting? Psychopathology of mood is confined to those situations in which there is anaffirmativeanswertoatleastoneofthesequestions,andtreatmentisdirectedtowardsimprovingthemood.
Likeotherhumancharacteristics,pathologyofmoodarisesinthecontextofadiathesis.Itisthe physical constitution that forms the tendency for developing, for example, a prolapsedintervertebraldisc; in themental realm,personality is closelyassociatedwith the type,qualityanddirectionofmood.So,apersonofcyclothymicpersonalityismorepronetomorbidstatesofelationandexcessiveactivityortaciturndejectionandretardation.
Theories of EmotionThe James–Lange theory of emotion was developed independently by William James(1842–1910) and Carl Lange (1834–1900). Simply, it posits that emotions are the resultof self-awarenessofphysicalandbodilychanges in thepresenceofa stimulus.WilliamJames(1884)wrote:
My theory … is that the bodily changes follow directly the perception of the exciting fact, and that our feeling of the same changes as they occur is the
emotion. Common sense says, we lose our fortune, are sorry and weep; we meet a bear, are frightened and run; we are insulted by a rival, are angry
and strike. The hypothesis here to be defended says that this order of sequence is incorrect … and that the more rational statement is that we feel sorry
because we cry, angry because we strike, afraid because we tremble … Without the bodily states following on the perception, the latter would be
purely cognitive in form, pale, colorless, destitute of emotional warmth. We might then see the bear, and judge it best to run, receive the insult and deem
it right to strike, but we should not actually feel afraid or angry.
This theory was criticized by Walter Cannon (1871–1945) and Philip Bard (1898–1977).Visceral(physiological)responsestostimuliaretooslowtoaccountfortherapidityofemotionsthatariseinthepresenceofappropriatestimuli.Inotherwords,thetimelinessofmyawareness
16—AffECT AND EMOTIONAl DISOrDErS 259
oftheincreasedheartrateanddrymouththatoccurwhenIaminthepresenceofahostilelionisinadequatetoexplainmyfearofthelion.Furthermore,thevisceralresponsestovaryingstimuliaresimilar,yettheemotionsmaybeasdisparateasfear,surprise,joyandsoon.Andinjectionofadrenaline(epinephrine)isaccompaniedbyvisceralchangesbutnotnecessarilybyemotionalchange.Inaddition,animalsthathavespinallesionscontinuetoexperienceemotions.Instead,the Cannon–Bard theory argued that emotion has temporal primacy and that any visceral orbehaviouralchangefollowstheemotion.Inthistheory,Iseeahostilelionandbecomefearful.Myfearfulnessprovokesthetypicalphysiologicalresponseofincreasedheartrateetc.,andtheresultingbehaviouristhatIrunoff.Thistheoryobviouslyleavesnoroomforanycognitiveaspecttotheoriginofemotions.
TheotherinfluentialtheoryisSchachterandSinger’s(1962)two-factortheoryofemotion.Thetworelevantfactorsarephysiologicalarousalandcognition.Inthistheory,anindividualisin a given social context, and he responds to this situation with a physiological arousal.Themeaningattributed to this arousal isdeterminedbyhis cognitions. Ifhis appraisal is that thecontextisthreateningthenhewillfeelfear,butiftheappraisalisthatthesituationisfunnythentheemotionwillbeapositiveone.Thistheoryhasobviousimplicationsfortheclinicalevaluationofdisordersofmood.Itspecifiesthatthesocialcontextisimportant,thatthecognitionsoftheindividualarerelevantand,finally,thatcarefulconsiderationanddescriptionoftheaccompanyingemotionisalsoimportant.
Basic EmotionsEkmanandcolleagues(EkmanandFriesen,1971)haveshownthattherearesixbasicemotionsthatareexpressedintheface:anger,disgust, fear,happiness,sadnessandsurprise.Thesebasicexpressions of emotion are universal. Ekman’s findings were anticipated by Charles Darwin(1872). It isalso thecase thatdespite therebeinguniversals in facialexpressionsofemotions,theseexpressionsarenotuniversalineveryregard.InEkman’sfieldworkinPapuaNewGuineaamongtheForepeople,therewaslittledistinctionbetweensurpriseandfear.Furthermore,itisalsotruethatwhenpeopleexperiencestrongemotionstherearedisplayrulesthatdeterminewhocanshowwhichemotiontowhomandwhen.Culturesalsodifferonwhicheventsarelikelytoproduceparticularemotions.Thisiswellexemplifiedbywhatfoodonecultureregardsasadeli-cacy andwhat another regards as revolting.The importantpoint is that thegeneral theme isuniversal;ingestingsomethingrepulsiveisacausefordisgust(Ekman,1998).
Communication of Mood‘NomanisanIsland,entireof itself ’ ( JohnDonne,1571–1631),and innoareaof life is thismoretruethanthatoffeelings.Ourfeelingsareverymuchaffectedbythosearoundus.Theyareobservableandunderstandabletootherpeople,andthis isnotaccidental; theyareactuallysignalledasanonverbalmessage.Theaffectitselfisnotdirectedtowardsanotherperson,buttheexpressionoftheaffectisconveyedbothdeliberatelyandunintentionallytoothers.
Oneofthemostimportantfindingsinthepastdecadehasbeenthatofmirror neurons.Theseneuronshavebeenfoundinprimatesandbirds,andtheirexistenceinferredinhumans.Mirrorneurons fire when an animal performs an action and also when an animal observes the sameaction performed by another animal. In other words, these neurons mirror the behaviour ofanotheranimal.Inhumans,therelevantneuronsareinthepremotorcortexandinferiorparietalcortex.RizzolattiandFadiga(1998)showedthatinthemacaquemonkeytherearetwodistinctgroupsofneuronsintherostroventralpremotorcortexthatrespondtotheobservationofgraspingobjectsandgraspingactions.Thecanonicalneuronsrespondspecificallytothethree-dimensionalobjects, whereas the mirror neurons respond to the direct observation of the hand actions
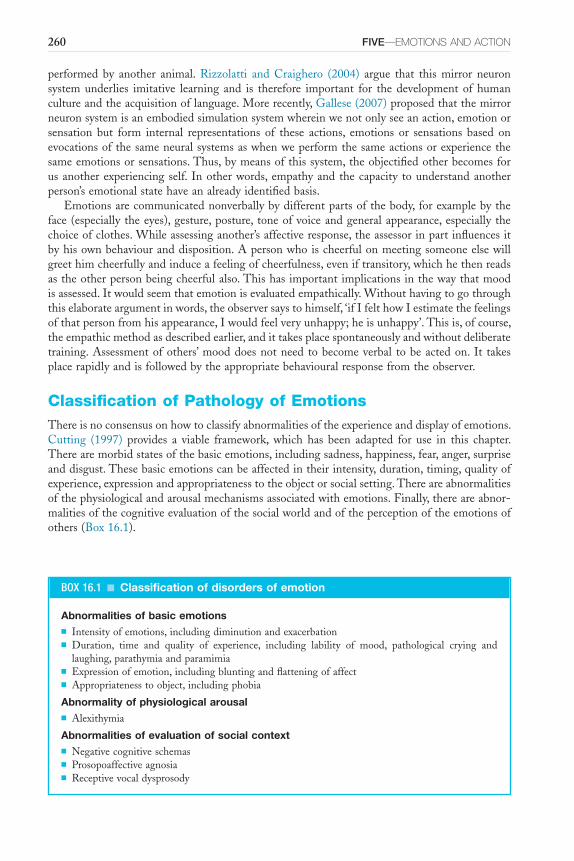
260 FIVE—EMOTIONS AND ACTION
performed by another animal. Rizzolatti and Craighero (2004) argue that this mirror neuronsystemunderlies imitative learning and is therefore important for thedevelopmentofhumancultureandtheacquisitionoflanguage.Morerecently,Gallese(2007)proposedthatthemirrorneuronsystemisanembodiedsimulationsystemwhereinwenotonlyseeanaction,emotionorsensation but form internal representations of these actions, emotions or sensations based onevocationsofthesameneuralsystemsaswhenweperformthesameactionsorexperiencethesameemotionsorsensations.Thus,bymeansofthissystem,theobjectifiedotherbecomesforusanotherexperiencingself. Inotherwords,empathyandthecapacity tounderstandanotherperson’semotionalstatehaveanalreadyidentifiedbasis.
Emotionsarecommunicatednonverballybydifferentpartsofthebody,forexamplebytheface(especially theeyes),gesture,posture, toneofvoiceandgeneralappearance,especially thechoiceofclothes.Whileassessinganother’saffectiveresponse,theassessorinpartinfluencesitbyhisownbehaviouranddisposition.Apersonwhoischeerfulonmeetingsomeoneelsewillgreethimcheerfullyandinduceafeelingofcheerfulness,eveniftransitory,whichhethenreadsastheotherpersonbeingcheerfulalso.Thishasimportantimplicationsinthewaythatmoodisassessed.Itwouldseemthatemotionisevaluatedempathically.Withouthavingtogothroughthiselaborateargumentinwords,theobserversaystohimself,‘ifIfelthowIestimatethefeelingsofthatpersonfromhisappearance,Iwouldfeelveryunhappy;heisunhappy’.Thisis,ofcourse,theempathicmethodasdescribedearlier,andittakesplacespontaneouslyandwithoutdeliberatetraining.Assessmentofothers’mooddoesnotneed tobecomeverbal tobeactedon. It takesplacerapidlyandisfollowedbytheappropriatebehaviouralresponsefromtheobserver.
Classification of Pathology of EmotionsThereisnoconsensusonhowtoclassifyabnormalitiesoftheexperienceanddisplayofemotions.Cutting (1997) provides a viable framework, which has been adapted for use in this chapter.Therearemorbidstatesofthebasicemotions,includingsadness,happiness,fear,anger,surpriseanddisgust.Thesebasicemotionscanbeaffectedintheirintensity,duration,timing,qualityofexperience,expressionandappropriatenesstotheobjectorsocialsetting.Thereareabnormalitiesofthephysiologicalandarousalmechanismsassociatedwithemotions.Finally,thereareabnor-malitiesofthecognitiveevaluationofthesocialworldandoftheperceptionoftheemotionsofothers(Box16.1).
BOX 16.1 ■ Classification of disorders of emotion
Abnormalities of basic emotions■ Intensityofemotions,includingdiminutionandexacerbation■ Duration, time and quality of experience, including lability of mood, pathological crying and
laughing,parathymiaandparamimia■ Expressionofemotion,includingbluntingandflatteningofaffect■ Appropriatenesstoobject,includingphobia
Abnormality of physiological arousal■ Alexithymia
Abnormalities of evaluation of social context■ Negativecognitiveschemas■ Prosopoaffectiveagnosia■ Receptivevocaldysprosody
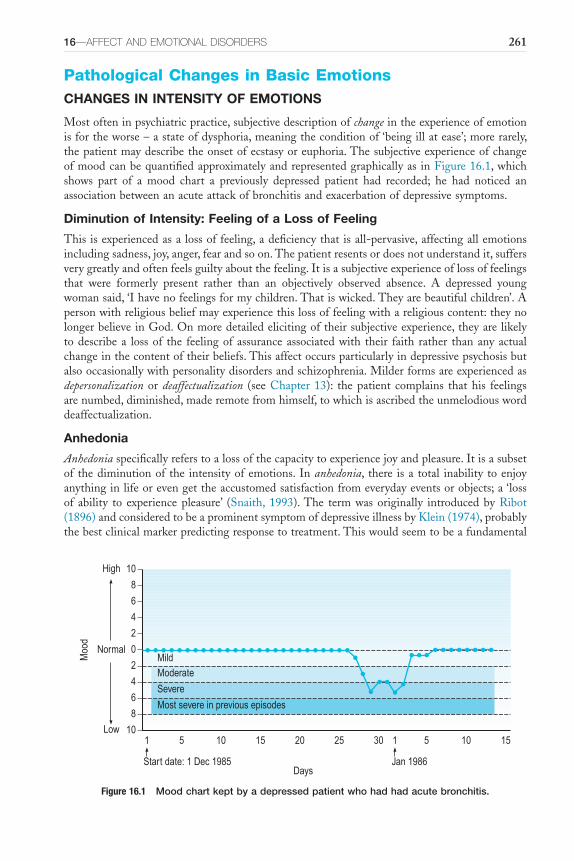
16—AffECT AND EMOTIONAl DISOrDErS 261
Pathological Changes in Basic EmotionsCHANGES IN INTENSITY OF EMOTIONS
Mostofteninpsychiatricpractice,subjectivedescriptionofchangeintheexperienceofemotionisfortheworse–astateofdysphoria,meaningtheconditionof‘beingillatease’;morerarely,thepatientmaydescribetheonsetofecstasyoreuphoria.ThesubjectiveexperienceofchangeofmoodcanbequantifiedapproximatelyandrepresentedgraphicallyasinFigure16.1,whichshows part of a mood chart a previously depressed patient had recorded; he had noticed anassociationbetweenanacuteattackofbronchitisandexacerbationofdepressivesymptoms.
Diminution of Intensity: Feeling of a Loss of Feeling
Thisisexperiencedasalossoffeeling,adeficiencythatisall-pervasive,affectingallemotionsincludingsadness,joy,anger,fearandsoon.Thepatientresentsordoesnotunderstandit,suffersverygreatlyandoftenfeelsguiltyaboutthefeeling.Itisasubjectiveexperienceoflossoffeelingsthat were formerly present rather than an objectively observed absence. A depressed youngwomansaid,‘Ihavenofeelingsformychildren.Thatiswicked.Theyarebeautifulchildren’.Apersonwithreligiousbeliefmayexperiencethislossoffeelingwithareligiouscontent:theynolongerbelieveinGod.Onmoredetailedelicitingoftheirsubjectiveexperience,theyarelikelytodescribea lossof the feelingofassuranceassociatedwith their faith rather thananyactualchangeinthecontentoftheirbeliefs.Thisaffectoccursparticularlyindepressivepsychosisbutalsooccasionallywithpersonalitydisordersandschizophrenia.Milderformsareexperiencedasdepersonalization ordeaffectualization (seeChapter13): thepatient complains thathis feelingsarenumbed,diminished,maderemotefromhimself,towhichisascribedtheunmelodiousworddeaffectualization.
Anhedonia
Anhedoniaspecificallyreferstoalossofthecapacitytoexperiencejoyandpleasure.Itisasubsetof thediminutionof the intensityofemotions.Inanhedonia, there isa total inability toenjoyanythinginlifeorevengettheaccustomedsatisfactionfromeverydayeventsorobjects;a‘lossof ability to experiencepleasure’ (Snaith,1993).The termwasoriginally introducedbyRibot(1896)andconsideredtobeaprominentsymptomofdepressiveillnessbyKlein(1974),probablythebestclinicalmarkerpredictingresponsetotreatment.Thiswouldseemtobeafundamental
Figure 16.1 Mood chart kept by a depressed patient who had had acute bronchitis.
10
10
0
2
4
6
8
2
4
6
8
1 5 10 15 1 5 10 1520 25 30
Normal
Moo
d
High
Low
Start date: 1 Dec 1985 Jan 1986Days
MildModerate
Severe
Most severe in previous episodes

262 FIVE—EMOTIONS AND ACTION
symptomofdepressiveillness.Ahighlyintelligentandperceptivemansufferingfrompsychoticdepressionsaid,‘Ihaveasortofuncannyfeeling.IknowwhatIamreadingisamusingbutIamnotatallamusedbyit’.TheexperiencewasverywelldescribedbyJ.S.Mill(1806–1873):
It was the autumn of 1826. I was in a dull state of nerves, such as everybody is occasionally liable to; unsusceptible to enjoyment or pleasurable excitement;
one of these moods when what is pleasure at other times, becomes insipid or indifferent … In this frame of mind it occurred to me to put the question
directly to myself, ‘suppose that all your objects in life were realized; that all the changes in institutions and opinions which you are looking forward to,
could be completely effected at this very instant: would this be a great joy and happiness to you?’ And an irrepressible self-consciousness distinctly answered,
‘No!’ At this my heart sank within me.(Mill, 1873)
Anhedonia as anexperience is starting tobedeconstructed into its componentparts.Thisdeficitinthecapacitytoexperiencepleasureisnowthoughttoincludeimpairmentsintheproc-esses of reward valuation, decision making, anticipation and motivation. The neural circuitsunderlyingthesereward-relatedmechanismsincludetheventralstriatumandprefrontalcorticalregions(Gaillardetal.,2013;Der-AvakianandMarkou,2012).
Anhedoniaisalsodescribedasasymptominschizophrenia,inwhichitisespeciallylikelytobe social–anabsenceof theability to feelpleasure in relationships (Cutting,1985).There isevidence that the hedonic aspects of olfactory experience may be disturbed in schizophrenia.Malepatientswithschizophreniafailedtoattachtheappropriatehedonicvalencetoapleasantodour,despitecorrectlyperceivingchanges inodour intensity ina studywhere theodourwaspresentedbirhinally.Inastudyinwhichamylacetatewaspresentedunirhinally,bothmalesandfemaleswithschizophreniaunderevaluatedthehedoniccharacteristicsatlowconcentrationsandoverestimated itshedoniccharacteristicsatconcentrations judgedtobeunpleasantbycontrolsandrelatives.Thesepatient-specificfindingswerenotexplicablebymedication,smokinghabitor subjective ratings of odour intensity but rather were associated with increased levels ofanhedonia/asociality(Kamathetal.,2013).Oneoftheparadoxesofanhedoniainschizophreniais thatwhen assessedby ‘trait’measures of affect, there are robust andmarkeddeficits in thereportedexperienceofpleasure.But,whenaffectisassessedin‘themoment’bylaboratorymood-inductionproceduresthereisnoevidenceofanhedonia(Cohenetal.,2011;StraussandGold,2012). The reasons for this disjunction are unclear but may include a) anticipatory hedonicexperiencedeficit,b)affectiveregulationcontrol,c)encoding-retrievaldeficit,d)representationaldeficitande)social-specificdeficits.
Itisthereforelikelythatanhedoniaisnotasingular,homogenousabnormalityinwhichtheinabilitytoexperiencepleasureequallyaffectsallmodalitiesofexperience,butanexperiencethatiscomposedofdifferentcomponentparts.Thisconceptualizationofanhedoniaisgivenfurtheramplificationbyasinglecasereportofselectivelossofemotionalexperienceinlisteningtomusic(Satohetal.,2011).Pleasureindifferentkindsofsensoryexperiencemaybediscreteandopentoselectivedisruption.
Exacerbation of Emotions: Melancholia, Mania, Ecstasy
Inaffectivedisorders,themoodisusuallytheprimaryfocusoftheabnormality.Thepathologyofmoodcanbemanifestasintensificationofsadnessorjoy.Insadness,thismaypresentasfeel-ingsofsadnessandgloom,despondency,despairorhopelessness.Often,theactualexperienceisindescribablebutrecognizedasdifferentincharacterfromnormalsadness.Inotherwords,thecharacterisqualitativelydifferentfromsadnessandakintophysicalpain:

16—AffECT AND EMOTIONAl DISOrDErS 263
I was feeling in my mind a sensation close to, but indescribably different from actual pain.
(William Styron, 1990)
It is a positive and active anguish, a sort of psychical neuralgia wholly unknown to normal life.
(William James, 1902)
WilliamStyron(1990),inhisbookabouthispersonalexperienceofdepression,arguedthatthetermdepressionwasaweakwordfortheexperience.
‘Melancholia’ would appear to be a far more apt and evocative word for the blacker forms of the disorder, but it was usurped by a noun with a bland
tonality and lacking any magisterial presence, used indifferently to describe an economic decline or a rut in the ground, a true wimp of a word for such a
major illness … Nevertheless, for 75 years the word has slithered innocuously through the language like a slug, leaving little trace of its intrinsic
malevolence and preventing, by its insipidity, a general awareness of the horrible intensity of the disease when out of control.
Thepositivefeelingofjoyandpleasurecanalsobeintensified.Jamison(1995)describedherpersonalexperienceofmania:
When you’re high it’s tremendous. The ideas and feelings are fast and frequent like shooting stars and you follow them until you find better
and brighter ones. Shyness goes; the right words and gestures are suddenly there, the power to captivate others a felt certainty. There are interests
found in uninteresting people. Sensuality is pervasive and the desire to seduce and be seduced is irresistible … But somewhere this changes …
Everything previously moving with the grain is now against – you are irritable, angry, frightened, uncontrollable, and enmeshed in the
blackest caves of the mind.
It is clear that thepositive, joyful aspect of the elevationofmood canquickly turn into adysphoricsensationthatisuncomfortableandunwelcome,yetthatisnotavariantofdepression.Euphoriaisastateofexcessiveunreasonablecheerfulness;itmaybemanifestedasextremecheer-fulness,asdescribedaboveinmania,oritmayseeminappropriateandbizarre.Itiscommonlyseeninorganicstates,especiallyassociatedwithfrontallobeimpairment.
Heightenedstatesofhappinesssuchasecstasysometimesoccurinpeoplewithmentalillnessorabnormalityofpersonality.Understandably,mostpsychiatristswritingaboutthemoodstateofecstasyhavedescribeditsoccurrenceinpatientswithpsychosis.Butecstaticexperiencemayalso be reported in association with minor psychiatric symptoms.The patient may describe acalm,exaltedstateofhappinessamountingtoecstasy,althoughthistranquilmoodstateisrela-tivelyuncommonandusuallyshort-lived.Inschizophrenia,ecstaticmoodmaybeassociatedwithexalteddelusions, for example, thechronicpatientwho satplacidlyenrapturedona long-stayward,knowingherself tobetheQueenofHeavenandwaitingforamessengerto informherthatshewastotakeovertheruleoftheworld.Ecstaticstates,usuallywithahistrionicflavour,mayoccurindissociativedisorderandmaybeassociatedwithreligiousstigmata(Simpson,1984).Bizarre,masshystericalphenomena,oftenwithreligiousassociations,areusuallyofthistype,forexampleinthedevilsofLoudunasdescribedbyAldousHuxley(1952).Thesocial,institutional
264 FIVE—EMOTIONS AND ACTION
andgrouppsychologicalprerequisitesforthedevelopmentofepidemicormasshysteria(Sirois,1982)areusuallypresentinthesesituations,andmismanagementisusuallyresponsibleforthedevelopmentfromisolatedhysteriainoneindividualtoanepidemic.Ecstasy,solemnelationorexcessiveexuberantexpansivenessmayalsobeseen inepilepsyand inotherorganicstates, forexampleingeneralparesis.
Characteristicofecstasyisthatitisself-referent;forexample,theflowersofspring‘openforme’.Thereisanalterationoftheboundariesofselfsothatthepersonmayfeel‘atonewiththeuniverse’,orhemay‘emptymyselfofallwill’sothat‘Iamnothingbutfeelings’.Thechangeinegoboundariesdoesnotusuallyhavetheaspectofinterferencewithselfthataccompaniespas-sivity experiences. In ecstasy, the abrogation of self is experienced as being voluntary. Expertknowledgeoftheabnormaldoesnotprecludeignoranceofthenormal,andthepsychiatristcannevergeneralizefromthesampleofpeopleselectivelyreferredtohimtothewholeofmankind.Thisdiscrepancycanbecomeveryobviousintheareaofecstaticandreligious experience.Thereisaneedtoacknowledge,takeintoaccount,haverespectforanduseintreatmentthepatient’sownsubjective experience in this area (Sims, 1994).The psychiatrist sees a most unrepresentativegroupofthosehavingsomeformofreligiousexperience,whichhasbeenconsideredtoamounttoover40percentoftheadultpopulationoftheUnitedStatesofAmerica,moreofwhomaremalesthanfemales,morearestablethanunstableandmorehappythanunhappy.
Theanthropologyofecstasy(Lewis,1971)canbetracedthroughChristianandotherculturesandmakescontactwithrecognizablementalillnessonlyatafewpoints.WilliamJames(1902),in The Variety of Religious Experience, demonstrated the vast extent of the phenomenology ofreligion and showed how unwise it would be to equate the surprising with the pathological.Accountsvaryastotheextentofpsychopathologyamongconvertstoreligiousgroupsandsects;it is probably associatedwith thenatureof thegroup.ThusUngerleider andWellisch (1979)foundnoevidenceofseverementalillnessinonestudy,whileGalanter(1982)describedevidenceof emotional problems among adherents to Divine Light, the Unification Church, Baba andSubud.
Suggestiveindicatorsforestablishingareligiousexperienceasprobablyassociatedwithpsy-chiatricmorbidityare:
■ thephenomenologyoftheexperienceconformswithpsychiatricillness■ thereareotherrecognizablesymptomsofmentaldisturbance■ thelifestyle,behaviouranddirectionofpersonalgoalsofthepersonsubsequenttotheevent
areconsistentwiththenaturalhistoryofmentaldisorderratherthanwithanenrichinglifeexperience
■ suchbehaviourisconsistentwithdisordersintheperson’spersonality.Withthefollowingsigns,theexperienceismorelikelytobeintrinsictotheperson’sbelief
andlesslikelytodenotepsychiatricillness:■ thepersonshowssomedegreeofreticencetodiscusstheexperience,especiallywiththose
heanticipateswillbeunsympathetic;■ itisdescribedunemotionallywithmatter-of-factconvictionandappears‘authentic’;■ thepersonunderstands,allowsforandevensympathizeswiththeincredulityofothers;■ heusuallyconsidersthattheexperienceimpliessomedemandsonhimself;■ the religiousexperienceconformswith thesubject’s recognizable religious traditionsand
peergroup.Ecstatic states can be conceptualized as an altered state of consciousness and can be self-
induced in meditation adepts. Jhanas are an example of such a self-induced meditative statecharacterizedbydimmingoftheawarenessofexternalexperience,fadingofinternalverbaliza-tions,alterationinthesenseofpersonalboundary,intensefocusontheobjectofmeditationandincreaseinjoy.Thisstatehasbeenshowntobeassociatedwiththeactivationofcorticalprocessesandofthenucleusaccumbensinthedopamine/opiodrewardsystem(Hagertyetal.,2013).
16—AffECT AND EMOTIONAl DISOrDErS 265
Intensification of Fear, Anger and Surprise
TheintensificationoffearandangerisdescribedinChapter17.Thesetwobasicemotionscanoccurinpureformbutcanalsocomplicatetheintensificationofsadnessorjoy,sothatitisnotuncommon for depressed or elated mood to be associated with anxiety or irritability. Morbidsurpriseisseeninlatah,aculture-bounddisorderdescribedinMalaysiainwhichthereappearstobeanexaggeratedstartle responsecharacterizedbyamyriadofechophenomena includingecholalia,echopraxiaandechomimia.Thereisalsocoprolalia,automaticobedienceandhypersug-gestibility(Bartholomew,1994).Hyperekplexiaisaheightenedstartlereflexthatoccurseitherasahereditaryneurologicalconditioninvolvingtheinhibitoryglycinereceptor,orasasymptomaticdisorder predominantly of epilepsy in which a surprise stimulus provokes a normal startleresponsethatthentriggersafocal,usuallyfrontallobe,seizure(Meinck,2006).Late-onsetcases,withoutdemonstrablepathology,havebeenreportedinwhichaudiogenic,visualortactilestimulitriggermyoclonicjerkscharacterizedbyeyeblinking,headflexion,abductionoftheupperarms,movementofthetrunkandbendingoftheknees(Hamelinetal.,2004).Inaddition,thestartlereflexcanbeexaggeratedinpost-traumaticstressdisorderandalcoholwithdrawalstates(HowardandFord,1992).
CHANGES IN TIMING, DURATION AND APPROPRIATENESS TO SITUATION
Timing, Duration and Appropriateness to Situation
The timing and duration of emotions are aspects of the emotional expression that determinewhethertheemotionisappropriatetoitscontext.Inpathologicalgrief,thetiminganddurationmaybealteredsuchthatthegriefisdelayedorprolonged.Delayedgriefisinessenceprolonga-tionoftheinitialnumbphase(seebelow).Labilityofmoodinvolvesbothaheighteningoranintensification of emotions accompanied by an instability in the persistence of emotions thatcommunicates itself to the observer as an inappropriateness to the social context. It can alsoappearasashallownessofemotionalexpressiondespitebeingintense,becauseitistransitoryandcanseemnottobedeeplyfelt.Itisoftenasignofbraindamageandisseenfollowingfrontallobeinjuryorcerebrovascularaccident.
Pathologicallaughterorcryingisusuallyanunprovokedemotionthatdoesnothaveanappar-ent object. In other words, the emotion is not related to any identifiable social situation.Pathologicallaughteroccursinepilepsy,inwhichitisknownasgelasticepilepsy,butitmayalsobe associated with acquired brain injury. It is commonly associated with pathological crying,whichisalsoassociatedwithfocalbraininjury.Itisnoteworthythatpathologicalcryingoccursasadiscreteconditionwithoutpathologicallaughter(PoeckandPilleri,1963,quotedinCutting,1997).
Inschizophrenia,Bleuler(1911)describedparathymiaandparamimia.Inparathymia,patientsreacttosadnewswithcheerfulnessorevenlaughter.Thesepatientsmaybecomesadorirritatedbyeventstowhichotherswillreactwithindifferenceorpleasure.Furthermore,thetermpara-thymiaisalsousedforunprovokedorinappropriateburstsoflaughter.Thisparticularaspectofparathymia is similar if not identical topathological laughter. Paramimia refers to the lackofunitybetweenthevariousmodesofexpressionofemotions:
A female catatonic patient approached one of the female attendants whom she liked and told her in the friendliest manner and in her sweetest tone of voice: ‘I really would like to slap your face, people like you are usually called s.o.b.s.’
A woman patient complained bitterly about her ‘voices’ and body-hallucinations; her mouth and her forehead manifested disgust, but her eyes

266 FIVE—EMOTIONS AND ACTION
expressed happy eroticism. After a few minutes the mouth also assumed the expression of happiness while her forehead continued to appear gloomy
and wrinkled.
ABNORMALITIES OF EXPRESSION AND APPROPRIATENESS TO OBJECT
Blunting and Flattening of Feeling
Thetermsbluntingandflatteningareusedinterchangeablytorefertounchangingfacialexpres-sion,decreasedspontaneousmovements,povertyofexpressivegesture,pooreyecontact,affectiveunresponsivityandlackofvocal inflection(Andreasen,1979).Thus,thetermsrefertoacom-positeoffeaturesthatarerelatedbutarenotnecessarilypartofaunifiedabnormality.Bluntingimpliesalackofemotionalsensitivity,suchasthatdisplayedbythegirlwithschizophreniawho,withobviousrelishforthesensationaleffect,tookhervisitorsuptothebedroomtoshowthemhermother,whohadbeendead for 48hours. Flattening is a limitationof theusual rangeofemotionexpressedusuallybyfacialbutalsobodilygestures.Theindividualdoesnotexpressverymuchaffectinanydirection,althoughthatwhichisexpressedisappropriateindirection.Bothbluntingandflatteningoccurinschizophrenia.
Bodily Feelings Associated With Emotion
In the theoriesof emotion,physiological changes suchaspalpitations,drymouth, sweatiness,etc.haveakeydeterminingpartinthelabellingofemotion.Theseandotherchangescanbethesole features of emotional disorder in some individuals.The relationships between mood andsomaticsymptomshavebeendiscussedinChapter14.Inanumberofculturesandlanguages,depression isconsideredtohaveananatomical locationtosuchanextentthat themoodstateandthepartofthebodybecomesynonymous.Melancholialiterallymeans‘blackbile’;similarly,in Urdu the word jee, meaning self, describes the hypochondrium anatomically and comes tomeandepression,thatis,depressionisacentralassaultonthewell-beingoftheself.Changesinbodily feelingare important inanumberofconditions.Physical illness frequentlyprecipitatesa lossof theaccustomedsenseofwell-being.This is subjectivelyexperiencedasageneralizedloweringofvitalityandmaybeassociatedwithotherpsychologicalabnormalities, for instancehypochondriasisordissociation.Inthesesettings,theexpressionofemotionaldisturbanceislikelytoemphasizethephysicalratherthantheemotional:
And thence proceeds wind, palpitation of the heart, short breath, plenty of humidity in the stomach, heaviness of heart and heartache, and intolerable
stupidity and dullness of spirits. Their excrements or stool hard, black to some, and little. If the heart, brain, liver, spleen, be misaffected, as they usually are,
many inconveniences proceed from them, many diseases accompany … those frequent wakings and terrible dreams, intempestive laughing, weeping,
sighing, sobbing, bashfulness, blushing, trembling, sweating, swooning, etc.(Burton, 1577–1650, The Anatomy of Melancholia, 1628)
Vital feelings was a term used by Wernicke (1906) to describe certain somatic symptomsoccurring in the affective psychoses.The word vital comes from the concept of the vital self,whichdescribes thecloserelationshipof thebodytoawarenessofself, thewayweexperienceourbodiesandtheimpressionweconsiderourphysicalpresencemakesonothers.So,vitalfeel-ingsarethosethatmakeusawareofourvitalself.Thesearethefeelingsofmoodthatappearto

16—AffECT AND EMOTIONAl DISOrDErS 267
emanate from thebody itself: localized and somatized affect.For example, depressedpatientscommonlycomplainofheadache.Onmoreinformedenquiry,thepatientmaysay,‘it’snotexactlyapain,butmoreanunbearablefeelingofpressurelikeatightbandaroundthehead’,‘afeelingofmisery,likeablackcloudpressingonmyhead’.Theheadisthecommonestsiteforvitalfeel-ings, but theymay alsooccur in the abdomen– ‘I have adull feeling inmybowels, they areslowing down and blocking’, in the chest – ‘it feels like a weight bearing down on my chest,stoppingmebreathing’,intheeyes–‘everythinglooksblack,darkanddrab;myeyesareheavy,Icannotseeproperly’orinthelegs–‘mylegsareterriblyheavy;IcannotwalkIfeelsoexhausted’.Theymayoccurinotherregionsofthebody,forinstancethebladder,thefeet,thehairandsoon.Thefeaturesthatappeartobeconstantaretheassociationofthe localizedbodysensationwiththeprevailingdepressedmood;thesensationofweight,tension,heaviness,evendepressionintheparticularorgan;andaconsequentlossoffunction–‘Icannotthinkproperly…mybowelsareblocked’.
Schneider(1920)consideredvitalfeelingstobeofparamountdiagnosticsignificanceinde-pressiveillness,equivalenttothefirst-ranksymptomsinschizophrenia,thecoreofcyclothymicdepressionandautonomicinorigin.Heconsideredthesefeelingstobecommonindepression.ItwouldseemthatDupré(1913),writingaboutwhathecalledcoenestopathic states,wasdescribingthesamesymptom:‘Coenestopathicstatesare,indeed,socommonastofigureamongthemostfrequentfeaturesofthepsychoses’.Hedescribedcoenaesthesiaasthe‘deepbutmoreorlessin-definiteawarenessthatwehaveofourownbodiesandthegeneraltoneoffunctionalactivity’.Coenestopathicstatesare‘thedistressingfeelingswhichemanatefromoneorotheroftheco-enesthesicareas…achangeinthenormalqualityofphysicalfeelingincertainpartsofthebody’.Theyare localized,butthere isnolocalpathogenic lesion.Dupréclaimedthatcoenestopathicstateswereautonomous,andnotassociatedwithotherpsychiatricdisorders;but, indescribingtheaffectswithwhichtheyareassociated,heappearstodescribeaffectivedisorders.Themoodofdepressionmaybedescribedasagloballossofvitalityinwhichallfunctionsareaffectedandallperformancesdepressed.
Achangeinvitalfeelingsdoesnotoccuronlyindepression.Thebizarrefeelingsthatapatientwithschizophreniahasabouthisbodyisachangeinthewayheexpresseshimself,oftenfurtherelaboratedbydelusions.Itshouldbenotedthatthetermvitalisusedratherdifferentlyinvital anxiety states. These states have been described (López Ibor, 1966), in which the anxiety isthoughttobeendogenous,developingrelativelyacutelyinpeopleofstablepersonality.
Thedepressivecontentofwhatphenomenologistswouldconsidertobevitalfeelingsvariesverygreatly,forexample‘Ihaveturnedtostone…Ihaveafeelingofdepressioninmychest…itisapain,aknot,aweight…Ihaveacloudonmyhead,afeelingofnothingness’.Burns(1971)commented with regard to respiratory vital feelings, ‘A striking feature of the breathlessnessdescribedbythepatientswithdepressionwasitsfairlysuddenonsetandcessation,correspondingexactlywiththeonsetandresolutionofthedepressiveillness’.
Trethowan (1979) considered that lowering of vitality is fundamental to the experience ofdepressiveillness.Hedescribedthisas‘aloweringofvitalitywhichisall-pervasiveandleadstoamarkedlossofabilityofthesubjecttofunctionashedidbeforehebecameillintermsofbothmindandbody’.
Feelings Attached to the Perception of Objects
Objectsmayevokeanemotionalresponseinanormalperson,forinstanceacomfortablefeelingof familiarity towardsanarmchair inwhichone restsafteranenergeticwalk,orapprehensivedisliketowardsadentist’schair.Thisnormalaffectiveresponsemaybeexaggeratedpathologically.Excessivefeelingsoffearamountingtoterrormayremainassociatedwithobjects.Theobjectstowhichaffect isattachedmaynotonlybephysical, inanimateobjectsbutalsothoughts,and
268 FIVE—EMOTIONS AND ACTION
patterns of thoughts, and people.The occurrence of certain ideas may regularly be associatedwithspecificpathologicalemotion,perhapsresultinginphobia(seeChapter17).Anyobjectofperceptionmaybeinvestedwithidiosyncraticaffect.
Feelings Directed Towards People
These may be disturbed in a number of different ways. Affect may be absent or deadened,increasedandexcessiveordistorted.Itmayalsobeambivalent–bothlovingandhating,rejectingand overprotecting synchronously. A girl described in Chapter 14, suffering from anorexianervosa,wouldtakegreatcaretocookenormousmealsforhertwinsister,towhomshewasveryclose;thesisterbecamegrosslyobesewhilethepatientvanishedalmosttoaskeleton.Inanswertoremonstrationsaboutfeedinghersister,shesaid,‘Ilookhorrible,sosheshouldlookhorribleaswell’.
Free-Floating Emotion
Thisiscommonlydescribedinpsychiatricdisturbance,andinhisoriginaldescriptionofanxietyneurosis,Freud(1895)consideredthattheconditionwascharacterizedbyfree-floatinganxiety.Apowerfulaffectseemstohavenogoalandisassociatedwithnoobject.Thepatientdescribeshimselfas feelinggenerallyanxious,notanxiousaboutanything inparticularbut justanxious.Thisfree-floatinganxietyhassomaticandpsychologicalconcomitants.Itmayseemtobelocal-ized physically in certain areas of the body. Other free-floating affects occur, such as dread,restlessness,tension,gloom,despondency,euphoria,irritabilityandsoon.
Abnormality of Experience and Physiological ActivityAspeculativehypothesis thatclinicianshavefoundhelpful is thetermalexithymia,whichwascoinedbySifneos(1972)todescribeaspecificdisturbanceinpsychicfunctioningcharacterizedby difficulties in the capacity to verbalize affect and elaborate fantasies. This was originallyintroducedtodescribepsychosomaticdisordersoccurringinindividualswithdifficultyexpressingtheiremotions.Thelinkwithabsenceordiminutionoffantasyisaconsistentfinding(NemiahandSifneos,1970).Thecommunicativestyleshowsmarkedlyreducedorabsentsymbolicthink-ingsothatinnerattitudes,feelings,wishesanddrivesarenotrevealed;fewdreamsandapaucityof fantasiesare reported (Taylor,1984).Thinking is literal,utilitarianandconcernedwith theminutiaeofexternalevents.Theseindividualshavegreatdifficultyinrecognizinganddescribingtheirownfeelingsandindiscriminatingbetweenemotionalstatesandbodilysensations.Theyshowastiff,robot-likeexistence,‘almostasiftheyarefollowinganinstructionbook’;theremaybestiffnessofpostureandlackoffacialexpression.Theyshowanimpairedcapacityforempathyintheirinterpersonalrelationships.Alexithymiccharacteristicshavebeenfoundespeciallyamongpatientswithpsychosomaticdisorders,somatoformdisorders,psychogenicpaindisorders,sub-stanceabusedisorders,post-traumaticstressdisorder,maskeddepression,characterneurosesandsexualperversions,butthesefindingshavenotbeenconsistentlyreplicated.
TheTorontoAlexithymiaScale,whichisthemostwidelyusedmeasureofalexithymia,hasfour factors:difficulty in identifyingfeelings,externallyorientedthinking,difficultyexpressingfeelingsandreduceddaydreaming(KirmayerandRobbins,1993).Thedifficultyinidentifyingfeelingsandthedifficultyinexpressingthembothappeartobecorrelatedwithsomatosensoryamplification(Nakaoetal.,2002).Thisprovidessomevalidationoftheideathatalexithymiaisthebasisforexcessivesomatizationandthatthismaybecausedbyundueawarenessofdiscrepantsensationsthatarethenmisconstruedasevidenceofphysicalillness.
Somatizationinpatientswithmentaldisordercanbedefinedastheselectiveperceptionandfocusonthesomaticmanifestationsofthedisorderwithdenialorminimizationoftheaffectiveandcognitivechanges(Katonetal.,1982).Asamethodofexpressionofemotion,itisfrequently
16—AffECT AND EMOTIONAl DISOrDErS 269
reportedintransculturalstudies,especiallyintheIndiansubcontinent,accordingtoRack(1982).Murphy and co-workers (1967) studiedbasic depressive symptomatology in 30 countries andshowedhowculturechangesillnessandthewaydysphoriaisexpressed.Bavington(1981),study-ingdepressioninapredominantlyPathancultureinPakistan,foundsomatizationtobeexpressedin 45 per cent of cases; hypochondriasis was present in 55 per cent, hysterical (dissociative)features in60percent, feelingsofguilt in50percent,paranoid ideas in38percent, suicidalthoughtsin75percent,diurnalvariationin18percent,retardationin50percentandirritabilityin 80 per cent of depressed patients. Bavington explains these somatic ideas by the presenceofvitalfeelingsratherthanpovertyoflanguage.Mumford(1992)foundthatpatientswithpsy-chiatric disorders originating from India and Pakistan typically communicate their distress assomaticsymptoms;somaticpresentationwascommoningeneralhospitalsettingswherepsychi-atricdisorderswereoftenunrecognizedanduntreated.Theuseofsomaticsymptomsandsomaticmetaphortocommunicateemotionaldistressisfoundinalllanguagesandcultures.Complainingofemotionaldysphoriaintermsofsomaticsymptomsmayreflectthelimitationofthemedicalprofessioninlisteningtocomplaintsratherthanapovertyoflanguageorpaucityofverbalexpres-sioninthepatient.
Abnormalities of EvaluationThe relationship between cognitions and emotions is difficult to disentangle. Initially, it wasthoughtthattheemotionalstatedeterminedtheassociatedcognitions.Thus,lowmoodprovokednegativethoughtsabouttheselfandtheworld.However,Beck(Beck1967;Becketal.,1979)proposed that a constellation of cognitive errors initiated or maintained depression. Theseincludedarbitraryinferences,selectiveabstractions,overgeneralizations,magnificationandmini-mization.Furthermore,therewerecognitiveschemas,thatis,underlyingassumptionsabouttheself, the world and the future, that developed from previous experiences and that habituallyinfluencedhoweventsintheworldwereappraisedandthesecouldinducemoodchange,eitherdirectly or via disruption in self-esteem.This proposal is in line with Schachter and Singer’stwo-factortheoryofemotion,inwhichcognitionsplayacentralrole.
Therearealsoabnormalitiesofappraisalofthefacialorvocalexpressionofemotionsinothers.Prosopoaffective agnosiareferstotheselectivedeficiencyinappreciatingtheemotionalexpressiondisplayedinthefaceofothers.Thisabnormalityisdistinctfromprosopagnosia,inwhichonlyrecognitionoffamiliarfacesisimpaired.Itisusuallyassociatedwithacquiredbraindiseaseandhas been reported in frontotemporal dementia, when it is also associated with impairment ofrecognitionofvocalexpressionofemotion(Keaneetal.,2002);followingrightthalamicinfarct(Vuillemieretal.,1998);andinsubjectswithright-sidedlimbicandheteromodalcorticallesions(Weniger and Irle, 2002). It has been reported in autism and Asperger’s syndrome, but it isnot part of a pervasive impairment of face-processing skills (Hofter etal., 2005). In otherwords, it occurs in some patients but not in others and dissociates from impairment of facerecognitionperse.
Prosodicaspectsofspeechsuchaspitch,durationandamplitudearepartof thenonverbalcuesthatmodifythemeaningofthespokenwordandindicatetheemotionalvalueofanutter-ance and the intention of the speaker (Mitchell and Ross, 2013). Expressive emotional prosodyreferstothegenerationofaffectinspeech.Themechanismsareunclearbutarethoughttoincludebilateralbasalgangliainvolvementinmotorproductionofspeechasafunctionofaffectivestateandrightlateralizationofcorticalprocessesinthemonitoringandproductionofacousticspeechparameters(PichonandKell,2013),andthedegreetowhichthere isunilateralright-sidedorbilateralfrontotemporalinvolvementinreceptive emotional prosodyisuncertain(Wittemanetal.,2012).Receptive emotional dysprosodyreferstotheselectivedeficitinrecognizingtheemotionaltone inspeech.This isoftenassociatedwithexpressive emotional dysprosody, the impairmentof

270 FIVE—EMOTIONS AND ACTION
theproductionofemotionaltoneinspeech.BothabnormalitiesarefoundinParkinson’sdisease(Caekebekeetal.,1991;Pell,1996).
Theevolutionaryrelationshipbetweenmusicandlanguageisuncertainbutitisthoughtthatmusic and language may have a common origin as an emotional protolanguage that remainsevident inoverlapping functionsandsharedneural circuitry. Ina studyof12 individualswithcongenital amusia, a disorder characterized by deficits in acoustic and structural attributes ofmusic,amarkedimpairmentinreceptiveemotionalprosodywasdemonstrated;suggestingthatmusic and language share mechanisms that trigger emotional responses to acoustic attributes(Thompsonetal.,2012).
Abnormality of Mood in Bipolar DisorderCertainly since the writings of Kraepelin, the apparently opposite mood states of mania anddepressionhavebeenrecognizedasoccurringinthesameillness–frequentlyatdifferenttimesandstagesoftheillnessinthesamepatient,morerarelyatthesametimeinthesamepatient.Althoughtheyaredescribedseparately,itisimportanttorealizethatthesemoodstatesmayoccurtogether.Maniaanddepressionarenotoppositemoodstates;theyarebothpathological,andtheoppositeofeitherwouldbefreedomfrommorbidemotion.Agitationandoveractivitymayoccurwithdepression, irritabilityanda feelingof frustrationwithmania.Apatient,nowdepressed,havingpreviouslybeenmanic,describedthis:‘Thefirstfinecarelessrapturehasdisappeared.Ifeelmoretiredandmoody’.
Depression of MoodAn additional video for this topic is available online.
CORE EXPERIENCE: PSYCHOLOGICAL AND PHYSICAL
Depressionofmoodisverycommon,anddepressionofsuchpersistenceandintensityastoberegardedas illness frequentlyoccurs.There isconsiderablediscussionas towhat is thecentralcoreofdepression.Ofcourse,argumentsadvocatingbiochemical,psychodynamicorconditioningfactorsasinitiatingcausesarenotmutuallyexclusive.Depressionaffectsvirtuallyallphysicalandpsychologicalfunctions,forexample,usingatachistoscopicmethod,PowellandHemsley(1984)wereabletoshowthatdepressioninfluencedperception.
Theworddepressionisamisnomer,asdepressiveillnessmayoccurwithoutthepatientmakinga complaint of depression as a symptom (depressio sine depressione). For this reason, the termmelancholiamaybepreferred;althoughthisliterallymeans‘blackbile’,ithascometobeacceptedasamedicalillness.ItwasthetermusedbyLewis(1934)inhisclassicdescriptionofdepressivestates in a detailed study of 61 cases; this has influenced all subsequent investigation of thecondition.MelancholiaisthepreferredtermforWhybrow(1997),whoconsidersthatit‘bettercaptures the “veritable tempest in the brain” that marks the experience of inner turmoil andconfusedthinkingasharmonyandemotiondrainaway,oftentobereplacedbyawitheredimita-tionoflife’.
Thesubjectivesymptomsofdepressionareveryvariable.Themoodvariesfromindifferenceandapathytoprofounddejection,despondencyanddespair.Anhedonia,thecompleteinabilitytoexperiencepleasure, isaconstant feature; it isexperiencedas joylessnessandrevealed in facialexpression,speech,behaviour,lifestyleandthepatient’saccountofpersonalexperience.
Aslowingdownoftheabilitytoinitiatethoughtoractionisnotedbytheobserverasretarda-tion.Apatient,describingthisafterrecovery,said,‘itfeelsasiftreaclehasbeenpouredintomyhead throughyourears’.Psychic retardation is experienced subjectivelyasan inability to fulfilnormalobligations, as lossof coping.Theproneness to self-blameoften results in thepatient

16—AffECT AND EMOTIONAl DISOrDErS 271
describinghimselfaslazyandgoodfornothing.Thereisacatastrophicloweringofself-esteemasaprominentcognitivecomponent.
Agitation and purposeless restlessness add to the discomfort and to the inability of thedepressed person to achieve anything.This anxiety and preoccupation with gloomy thoughtsimpairsconcentration.Diurnalvariationofmoodisoftenprominent,withthepatientfeelingathisworst,andperhapsmostsuicidal,whenhewakesearlyinthemorningor,alternatively,some-whatlaterinthemorning.Thedegreeofdepressionandmiserymaysometimessuccessfullybeconcealed; this is thepresentationofdepressio sine depressione (smilingdepression) inapatientwhoappearsnottobedepressedintheconsultingroombutmay,muchtohisdoctor’sdismay,killhimself.Theconcealmentisprobablyconsciousandmaybeassociatedwithhabitualmaskingoftheexpressionofemotionoralternativelyaimedatavoidingtreatment.
Concentration, application and decision making become difficult, painful and sometimesimpossible.Thepersondescribesdifficultyorimpossibilityinfantasyandrecollectionofemotion.Thisisdescribedaslossofmemoryandlossoffeeling.Often,thislossofmentalfunctionmakesthe patient believe he is ‘going mad’ or ‘losing his mind’, a sort of mental hypochondriasis.Physical retardation may become the focus for hypochondriacal beliefs about the body: ‘I amconstipated…mybowelsaretotallyblocked’.Averydepressedmiddle-agedwomandescribedherbodilyfeelingsthus:‘Ihaveafeelinglikehavinganinjectionatthedentist’s.Myfacefeelsnumb,butatthesametimepainfulallover’.
Anxietyisacommonconcomitantwithdepressionandmaycompletelyobscurethelatter.Inagitateddepression,agitationandrestlessnessareextremeandthepatientcarriesaseriousriskofsuicide.Histrionicbehaviourmayalsoobscuretheunderlyingdepressiveillness.Apatientwhowasactuallyprofoundlydepressedkeptpickingherskinandpullingherhair,saying,‘look,Ican’tfeelanythingwhenIdothistomyself ’.
Theaffectofdepressionmaybelocalizedsomaticallyinvitalfeelings(seeabove).Itmaytaketheformofprofoundmiseryordejection.Thereisusuallyafeelingoflossofcapacity,helpless-nessandafeelingthatthepatientcannotcope.Absenceoffeelingsisoftendescribed,oritmaybedescribedasaninexplicablelossoffeelings‘thatoughttobethere’.
Feelingsofguiltandunworthinessareprominentindepressiveillnessoftheendogenoustype.Thishas longbeenknown; forexamplePlutarch, in thefirstcenturyAD,describedaperson:‘Helooksonhimselfasamanwhomthegodshateandpursuewiththeiranger…“Leaveme,”saysthewretchedman,“metheimpious,theaccursed,hatedofthegods,tosuffermypunish-ment.”’(ZilboorgandHenry,1941).Ontheotherhand,Shepherd(1993)considersthatguiltfeelingsdidnotfeaturepredominantlyindepressivestatesdescribedinpre-PuritanEngland.Thepatientmayblamehimselfforhavingallowedhimselftogetintothisstateofmind.Heisfullofself-reproachandrecriminationforallsortsofpeccadilloesfromthedistantpast.Forallthatgoeswrong aroundhimhe takespersonal blame; thismaybeofdelusional intensity.Using ascalefortheevaluationoffeelingsofguilt,itwaspossibletoidentifytwoseparatecomponents:‘delusional’guiltorshame(experiencedinrelationtoone’sactions)and‘affective’guilt(amoregeneralfeelingofunworthiness)(Berriosetal.,1992).Aswellasdelusionsofguiltandunworthi-ness, hypochondriacal and nihilistic delusions are relatively common in depression, especiallywhenitoccursintheelderly.
Delusionsoccur inpsychoticdepression.It is importanttomakethedistinctionbetweenabelief about the state of the world coloured by current mood – ‘I feel that I must have donesomethingtomybrainasIcan’tthinkproperly’,fromanactualdelusionalbelief–‘Ican’tthinkat all, it is impossible, my brain is dead’.The former is a metaphorical statement, the lattera belief held with conviction. In practice, there is often a grey area between frank depressivedelusionsandemotionallyladenviewsoftheworld.
Table16.1showsthefrequencyofsymptoms,howeverslight,indepressiveillnessthatwererecordedquantitativelyusingaratingscalein239menand260women(Hamilton,1989).Itisseenthatanxietyisafrequentsymptomindepressiveillness.
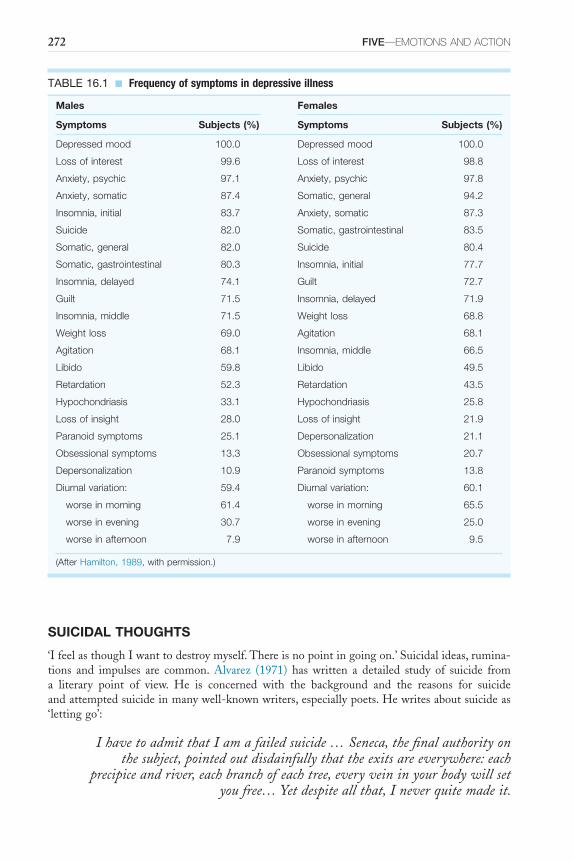
272 FIVE—EMOTIONS AND ACTION
SUICIDAL THOUGHTS
‘IfeelasthoughIwanttodestroymyself.Thereisnopointingoingon.’Suicidalideas,rumina-tions and impulses are common. Alvarez (1971) has written a detailed study of suicide froma literary point of view. He is concerned with the background and the reasons for suicideandattemptedsuicideinmanywell-knownwriters,especiallypoets.Hewritesaboutsuicideas‘lettinggo’:
I have to admit that I am a failed suicide … Seneca, the final authority on the subject, pointed out disdainfully that the exits are everywhere: each
precipice and river, each branch of each tree, every vein in your body will set you free… Yet despite all that, I never quite made it.
TABLE 16.1 ■ Frequency of symptoms in depressive illness
Males Females
Symptoms Subjects (%) Symptoms Subjects (%)
Depressed mood 100.0 Depressed mood 100.0
Loss of interest 99.6 Loss of interest 98.8
Anxiety, psychic 97.1 Anxiety, psychic 97.8
Anxiety, somatic 87.4 Somatic, general 94.2
Insomnia, initial 83.7 Anxiety, somatic 87.3
Suicide 82.0 Somatic, gastrointestinal 83.5
Somatic, general 82.0 Suicide 80.4
Somatic, gastrointestinal 80.3 Insomnia, initial 77.7
Insomnia, delayed 74.1 Guilt 72.7
Guilt 71.5 Insomnia, delayed 71.9
Insomnia, middle 71.5 Weight loss 68.8
Weight loss 69.0 Agitation 68.1
Agitation 68.1 Insomnia, middle 66.5
Libido 59.8 Libido 49.5
Retardation 52.3 Retardation 43.5
Hypochondriasis 33.1 Hypochondriasis 25.8
Loss of insight 28.0 Loss of insight 21.9
Paranoid symptoms 25.1 Depersonalization 21.1
Obsessional symptoms 13.3 Obsessional symptoms 20.7
Depersonalization 10.9 Paranoid symptoms 13.8
Diurnal variation: 59.4 Diurnal variation: 60.1
worse in morning 61.4 worse in morning 65.5
worse in evening 30.7 worse in evening 25.0
worse in afternoon 7.9 worse in afternoon 9.5
(After Hamilton, 1989, with permission.)
16—AffECT AND EMOTIONAl DISOrDErS 273
Theintertwinedthreadsofartisticcreativity,manic-depressiveillnessandsuicidehavebeenexploredbyGoodwinandJamison(1990).
BoththemuseandmadnessasgiftsofthegodshavebeenarecurringthemefromearliesttimesthroughsuchnineteenthcenturypoetsasBrowning,Shelley,ColeridgeandByrontothemodernAmericanpoetssuchasSylviaPlathandAnneSexton,amongwhomtherewasfoundtobeaveryhighprevalenceofmanic-depressiveillnessandmanysuicides.Inherenlighteningstudyofmanic-depressiveillnessandtheartistictemperament,Touched With Fire,Jamison(1993)demonstratesdifferentialratesfordepressiveillnessandsuicideinpoets,artistsandotherwritersandcommentsonthis.
Extrememoodswingsarefrequent,withenthusiasmandcreativityduringelationandstarkdespairwhenthepoetfindshimorherselflackingininspiration.Poetsandalsocreativemusi-cians(Schumann,Wolf,Rachmaninov,Tchaikovsky,etc.)showthispatternespeciallyfrequently,whileitismuchlesscommonamongbiographers–andpresumablywritersoftextbooks.Inthesamewaythatdepressionmayoccurwithoutsuicideorsuicidalideas,suicidemaybecarriedoutwithoutpredisposingpathologicaldepressivemood.
Depressionisregardedasthefinalcommonpathwayleadingtosuicide(VanHeeringenetal.,2000).Theseauthorsimplydepressiontheemotionandnotthediagnosticcategory.Theycon-siderthatpsychological,socialandbiologicalaetiologicalfactors,andtheincreasedratesassoci-atedwithmanypsychiatricdisorders,areallmediatedthroughhopelessnessresultinginsuicidalbehaviour.Thisemotionofhopelessnessarisesfromfeelingdefeatedinsomeimportantareaoflifeandfeelingclosedinwithnopossibleescapeorrescue.Suicidalbehaviouristhena‘cryofpain’,anattempttoescapethesefeelingsofentrapment.
Plansforsuicidemaynotbecarriedoutsolelybecauseofthedegreeofretardation;occasion-ally,electroconvulsivetherapymaylessenretardationafterthreeorfourtreatmentsandtherebyincrease the riskof suicide, because improvement fromdepressionofmood and lowered self-esteembecauseofguiltfeelingshasnotyetoccurred.Deathisoftenwelcomedwithasenseofrelief.Apsychoticallydepressedpatient,whenofferedadmissiontohospital,acceptedwithresig-nation,‘Iwillcomeinandthereyouwillkillme.ItiswhatIdeserve’.Itisfrequentlydescribedafterwardsbytherelativesofsuicidesthatinthedaysorhoursprecedingtheirdeaththeywerehappierandmoretranquilthantheyhadbeenforalongtime.
Homicideofoneormoreofthoseclosetothepatientfollowedbysuicideisarealdangerinasmallminorityofsufferersfromdepressiveillness.Aprofoundlydepressedmanfeltthat lifewasnotworthliving,thathehadfailedcompletelyandthattheworldwasintolerable.Theonlypersonhecaredforwashisfive-year-oldson,andhedidnotwanttocondemnhimtowhatheanticipatedwouldbealifetimeofmisery.Heputhissononthehandlebarsofhisbicycleandrodeoverthequayintotheharbour,intendingtokillthemboth.Theboywasdrownedbutthefatherwasrescued,resuscitatedandchargedwithmurder.Subsequently,herespondedtotreat-mentforhisseveredepressiveillness.
DEPRESSION AND LOSS
Anysocialsituationoftransitionisassociatedwithsomedisturbanceofemotion(Parkes,1971).Depressionistheaffectassociatedwithexperienceofloss.Itisnottheintentionheretoenterintotheoreticalaspectsbuttodiscussthesubjectiveexperience.Parkes(1976)hasdemonstratedhowlossofaperson, lossofa limbandeven lossofahomearestressful insimilarways,andthatthereisamentalprocessgoingoninwhichthepersonis‘makingrealinsidetheselfeventswhichhavealreadyoccurredinrealityoutside’.Thisprocess isassociatedwithmarkedpsychicpain andunhappiness.Anexampleofdepressionassociatedwith the threatof lossof a lovedobject was a taxi driver who owned his own car, which was the only thing he valued in life.Duringanepisodeofprofounddepression,hepolishedthetaxi toperfection, took it intothe
274 FIVE—EMOTIONS AND ACTION
garage, connectedapipe to the exhaustof the car, started the engine andkilledhimself.Thedysphoricmoodassociatedwiththeexperienceoflossisalwaysexacerbatedifthereisanysenseofguiltorself-blameattachedtothecircumstancesoftheloss:‘ifonlyIhadcalledthedoctorintoseeMotherearlier;Ishallneverforgivemyself ’.
Grief
The immediateexperienceof loss is shockandnumbness.Thesuddenlybereavedpersonmaysaythathecannotbelievethatithashappenedtohim.Hejustfeelsnumbandempty.Hemaydescribedepersonalizationfeelings.Thereisatendencytodenythatthelosshashappened.Awomanwasreferredtoasurgeonforalumpinthebreast.Atoperation,themasswasfoundtobemalignantandthebreastwasamputated.Forseveraldaysaftertheoperation,shewasunabletoacceptthatthepainfulareaunderthedressingsignifiedthe lossofherbreastratherthanaminorexcision.
Followingtheinitialshockanddenialcomethepangsofgrief.Thisisanacutefeelingofloss,withanxietyprominent,aswellasgrieving–anxious searching.Theimplicationsoftheexperienceoflossbegintoberealized,andthismaycausethepersonfeelingsofanxietyamountingtopanic:‘HoweveramIgoingtocopewithouthim?’Thesomaticsymptomsofanxietymaybepresentaswellasthepsychological.
Threedistinctpatternsofmorbid grief havebeenobserved(Lieberman,1978):■ phobic avoidance of persons, places or things related to the deceased, combined with
extremeguiltandangeraboutthedeceasedandhis/herdeath■ a total lack of grieving, with anger directed towards others and over-idealization of the
deceased■ physicalillnessandrecurrentnightmaresinvolvingthedeceased.Thesepatternshaverelevancefortreatmentusingthebehavioralmethodofforcedorguided
mourning.Whentheexperienceoflosshasbeenacceptedasareality,depression,theaffectappertaining
toloss,occurs.Thepersonfeelsverylowandhopeless,perhapswiththeloweringofvitalityandapathyofdepression.Hebecomesresignedtohissituationbutseesnowayout:‘thereissimplyno future for me now’. Not surprisingly, this state is often associated with suicidal ideas andimpulses, and there is an increasedmortality fromsuicideandother causes in the sixmonthssubsequenttobereavement(Parkesetal.,1969).
Asthestateofgrievingisresolved,thepersongraduallyovercomesthisdespairinghopeless-ness.There is anattitudeofmind that results in reorganizationand redirection.Hegraduallymakesdecisionsandcarriesoutactivitiesthatdemonstratehisemotionalandintellectualaccept-ance of the loss and intention to continue his life as congenially as possible, although stillrememberingtheloss.Thisstageofresolutionmaybepostponedformanyyears,aswithQueenVictoria’sgrievingforPrinceAlbert.
Parkes (1976) discriminates between the subjective experience of external loss and internal change.Theexternal loss is shownbypining for the lostobject.Anxiety following lossoccursbothinbereavedpeopleandinamputees,andisassociatedwithanxioussearching:abereavedpersonusedtowalkupanddownthestreetwonderingifshewouldseeherhusband,whomsheknewtobedead.Inthesecircumstances,misperceptionofstrangersasbeingthelostrelativemayhappen.Amanwhosefatherhaddiedsomelongtimebeforethoughtheheardhisfather’svoiceinanotherroomandthenrealizeditwashisson.Peoplereturntoplacesassociatedwiththelostpersonorkeeparticlesthatbelongedtothemsacrosanct.
Internalchange,withasenseofmutilation,iscommontopeoplewithdifferenttypesofloss.Amputeesfeelthemselvestobebadlydamagedbothintheirfunctionandintheirself-image.Becauseamanhaslosthisleg,hewillbeunabletocarryouthispreviousactivitiesasbeforeandmayfeelhimselftobelessofaman.Similarly,thewomanwithanamputatedarmmayprefera
16—AffECT AND EMOTIONAl DISOrDErS 275
cosmeticbutuselessprosthesisratherthanamorefunctionalhook.Shemayfeeltheaffronttoherself-imageofamutilatedarmmorethanthelossoffunction.ParkesandNapier(1975)stressthesocialassociationsof loss in theirdiscussionofpreventionandalleviationof theproblemsresultingfromamputation.Widowsalsodescribeafeelingoflosswithinthemselvesduetotheirbereavement; there is,ofcourse,oftenareal lossofstatus.Thoserehousedoftendescribedaninternalchangeonmoving:‘somethingofmewentwhenIlefttheoldhome’.
ManiaManiaisawordwithalonghistory.Hare(1981)considersthattheearlydescriptionsofintel-lectualdeteriorationwithexcitementweremadebecauseoftheassociationwithorganicdeterio-ration from poor general health during the nineteenth century. As the physical health of thepopulationimproved,itwaspossibletodescribeseparateconditionswithdifferentnaturalhis-tories. However, mania still forms a much higher proportion of affective psychoses occurringpuerperallythanofaffectivedisordersoccurringatotherstagesoflife(DeanandKendell,1981).
Mania refers to elation of mood, acceleration of thinking and overactivity. Subjectively,althoughitmaybedescribedasadifferentstatefromnormal,itisrarelycomplainedofbythepatientasasymptom.Ayoung,manicin-patientdescribedhisinternalstatethus:‘Ifeelhyper-suffusedwithexperience…IamdevelopingaclosesecretarialrelationshipwithCamillaBrown(anotheryoungpatient)…Ifeellikearocketwiththebluepaperlit,standinginabottleandjust ready to takeoff ’. Ithasbecomeconventional to refer toallbut themost severecasesassufferingfromhypomania.Thisisunfortunate,asonedoesnotreferto‘hypodepression’andthepersonusingthetermhypomaniaoftengivestheimpressionthatwrongdiagnosisispermissibletoagreaterextentthanifthetermmaniahadbeenused.
Theearlystagesofmaniamaybeexperiencedasenjoyable,even‘wonderful’,andanenormousrelieffromthedepressionthatprecededit.ApatientquotedbyWhybrow(1997)putitthisway:‘IntheearlystagesofmaniaIfeelgood–abouttheworldandeverybodyinit.There’safasterbeat;asenseofexpectationthatmylifewillbefullandexciting’.Forthisreason,thepatientmaybereluctanttotakemedicationortoreporthisconditiontohisdoctor.Lateroninmanicillness,thepatient’sexperienceisusuallydescribedasunpleasantandevenfrightening.
In pure form, it is characterized by excessive cheerfulness, rapid train and association ofthoughtandoveractivity.Thespeedofthinkingandthereadyabilitytoformassociationsresultsin rapid and apparently sparkling conversation (see Chapter 9). Puns and clang associationsabound,forexampleinacasequotedbyBingham(1841):
A fine bold lady, well dressed and well known to the officers of a certain house, ‘a regular madwoman’, as they called her, was brought thither by her friends. She was no sooner announced than every missile and instrument of attack was carefully removed out of her way. She opened the conference by a familiar address to the physician under whose care she had been before and
was going to remain, by saying to him, ‘Well, Doctor M(orrison), but I beg pardon, I forgot whom I was speaking to – it is Sir A(lexander). Well, Sir A—, since I had the pleasure of seeing you last, I have been benighted, and
you have been knighted’.
ReferencesAlvarezA(1971)The Savage God: a Study of Suicide.London:Weidenfeld&Nicolson.AndreasenN (1979)Affectiveflatteningand thecriteria for schizophrenia.American Journal of Psychiatry
136,944–7.

276 FIVE—EMOTIONS AND ACTION
AnsteeBHandFlemingerJJ(1977)Diagnosis‘uncertain’:afollow-upstudy.British Journal of Psychiatry131,592–8.
BartholomewRE(1994)Disease,disorderordeception?LatahashabitinaMalayextendedfamily.Journal of Nervous Mental Disease182,331–8.
BavingtonJ(1981)Depression in Pakistan.Leeds:TransculturalPsychiatrySociety(UK)Workshop.BeckAT(1967)Depression: Clinical, Experimental and Theoretical Aspects.NewYork:Hoeber.Beck AT, Rush AJ, Shaw BF and Emery G (1979) Cognitive Therapy of Depression. NewYork: Guilford
Press.Berrios GE (1985) The psychopathology of affectivity: conceptual and historical aspects. Psychological
Medicine15,745–58.BerriosGE,BulbenaA,BakshiN,DeningTR,JenawayA,MarkarH,Martin-SantosRandMitchellSL
(1992) Feelings of guilt in major depression: conceptual and psychosomatic aspects. British Journal of Psychiatry160,781–7.
BinghamN(1841)Religious Delusions.London:Hatchard.BleulerE(1911)Dementia Praecox: or the Group of Schizophrenias.NewYork:InternationalUniversityPress.Brenner B (1979) Depressed affect as a cause of associated somatic problems. Psychological Medicine 9,
737–46.BurnsBH(1971)Breathlessnessindepression.British Journal of Psychiatry119,39–45.BurtonR(1628)The Anatomy of Melancholia.Oxford:HenryCripps.CaekebekeJF,Jennekens-SchinkelA,vanderLindenME,BurumaOJandRoosRA(1991)Theinterpreta-
tionofdysprosody inpatientswithParkinson’sdisease.Journal of Neurology, Neurosurgery and Psychiatry54,145–8.
Cohen AS, Najolia GM, Brown LA and Minor KS (2011) The state-trait disjunction of anhedonia inschizophrenia:potentialaffective,cognitiveandsocial-basedmechanisms.Clinical Psychology Review31,440–8.
CuttingJ(1985)The Psychology of Schizophrenia.Edinburgh:ChurchillLivingstone.CuttingJ(1997)Principles of Psychopathology.Oxford:OxfordUniversityPress.DarwinC(1872)The Expression of the Emotions in Man and Animals.London:JohnMurray.DeanCandKendellRE(1981)Thesymptomatologyofpuerperalillness.British Journal of Psychiatry139,
128–33.Der-Avakian A and Markou A (2012)The neurobiology of anhedonia and other reward-related deficits.
Trends in Neurosciences35,68–77.DupréE(1913)LesCénestopathies,MouvementMédical3–22(transl.RohdeM,1974)InHirschSRand
ShepherdM(eds.)Themes and Variations in European Psychiatry.Bristol:JohnWright.Ekman P (1998) Afterword. In Darwin C The Expression of the Emotions in Man and Animals. London:
HarperCollins.EkmanPandFriesenW(1971)Constantsacrossculturesinthefaceandemotion.Journal of Personality and
Social Psychology17,124–9.FreudS(1895)Onthegroundsfordetachingaparticularsyndromefromneurastheniaunderthedescription
‘anxiety neurosis’. In Standard Edition of the Complete Psychological Works of Sigmund Freud, vol. III,pp.90–115.London:HogarthPress.
GaillardR,GourionD,LlorcaPM(2013)Anhedoniaindepression.Encephale39,296–305.GalanterM(1982)Charismatic religious sectsandpsychiatry: anoverview.American Journal of Psychiatry
139,1539–48.Gallese V (2007) Embodied simulation: from mirror neuron systems to interpersonal relations. Novartis
Foundation Symposium278,3–12.GoodwinFKandJamisonKR(1990)Manic-Depressive Illness.NewYork:OxfordUniversityPress.HagertyMR,IsaacsJ,BrasingtonL,ShupeL,FetzEEandCramerSC(2013)Casestudyofecstaticmedita-
tion:fMRIandEEGevidenceofself-stimulatingarewardsystem.Neural Plasticity:653572.Epub.HamelinS,RohrP,KahaneP,MinottiLandVercueilL(2004)Lateonsethyperekplexia.Epileptic Disorders
6,169–72.HamiltonM(1989)Frequencyofsymptomsinmelancholia(depressiveillness).British Journal of Psychiatry
154,201–6.HareE(1981)Thetwomanias:astudyoftheevolutionofthemodernconceptofmania.British Journal of
Psychiatry138,89–99.
16—AffECT AND EMOTIONAl DISOrDErS 277
HofterRL,ManoachDSandBartonJJ(2005)Perceptionoffacialexpressionandfacialidentityinsubjectswithsocialdevelopmentaldisorders.Neurology65,1620–5.
HowardRandFordR(1992)FromthejumpingFrenchmenofMainetoposttraumaticstressdisorder:thestartleresponseinneuropsychiatry.Psychological Medicine22,695–707.
HuxleyA(1952)The Devils of Loudun.London:Chatto&Windus.JamesW(1884)Whatisanemotion?Mind9,188–205.JamesW(1902)The Varieties of Religious Experience: a Study in Human Nature.NewYork:Longmans,Green.JamisonKR(1993)Touched With Fire: Manic-Depressive Illness and the Artistic Temperament.NewYork:Free
Press.JamisonKR(1995)An Unquiet Mind. A Memoir of Moods and Madness.NewYork:Knopf.KamathV,MobergPJ,KohlerCG,GurREandTuretskyBI(2013)Odorhedoniccapacityandanhedonia
inschizophreniaandunaffectedfirst-degreerelativesofschizophreniapatients.Schizophrenia Bulletin39,59–67.
KatonW,KleinmanAandRosenG(1982)Depressionandsomatization:areview.Part1.American Journal of Medicine72,127–35.
Keane J, Calder AJ, Hodges JR and Young AW (2002) Face and emotion processing in frontal variantfrontotemporaldementia.Neuropsychologia40,655–65.
Kirmayer LJ and Robbins JM (1993) Cognitive and social correlates of Toronto Alexithymia Scale.Psychosomatics34,41–52.
KleinDF(1974)Endogenomorphicdepression.Archives of General Psychiatry31,447–54.KraepelinE(1905)Lectures on Clinical Psychiatry,3rded.(transl.JohnstonT,1917).NewYork:W.Wood.LewisA(1934)Melancholia:aclinicalsurveyofdepressivestates.Journal of Mental Science80,277–378.LewisIM(1971)Ecstatic Religion: an Anthropological Study of Spirit Possession and Shamanism.Harmondsworth:
Penguin.LiebermanS(1978)Nineteencasesofmorbidgrief.British Journal of Psychiatry132,159–63.LópezIborJJ(1966)Neuroses as Mood Disorders.Madrid:EditorialGredos.MeinckHM(2006)Startleanditsdisorders.Neurophysiologie Clinique36,357–64.MillJS(1873)Autobiography(ed.RobsonJM,1989).London:Penguin.Mitchell RL, Ross ED (2013) Attitudinal prosody: what we know and the directions for future study.
Neuroscience & Biobehavioral Reviews,37,471–9.Mumford DB (1992) Detection of psychiatric disorders among Asian patients presenting with somatic
symptoms.British Journal of Hospital Medicine47,202–4.MurphyHBM,WittkowerEDandChanceNA(1967)Cross-culturalinquiryintothesymptomatologyof
depression:preliminaryreport.International Journal of Social Psychiatry13,6–15.NakaoM,BarskyAJ,KumanoHandKubokiJ(2002)Relationshipbetweensomatosensoryamplification
andalexithymiainaJapanesepsychosomaticclinic.Psychosomatics43,55–60.NemiahJCandSifneosPE(1970)Affectandfantasyinpatientswithpsychosomaticdisorders.InHillOW
(ed.)Modern Trends in Psychosomatic Medicine 2,pp.26–34.London:Butterworth.ParkesCM(1971)Psycho-socialtransitions:afieldforstudy.Social Science and Medicine5,101–15.ParkesCM(1976)Thepsychologicalreactiontolossofalimb:thefirstyearafteramputation.InHowells
JG(ed.)Modern Perception in the Psychiatric Aspects of Surgery,pp.515–33.London:Macmillan.ParkesCM,BenjaminBandFitzgeraldRG(1969)Brokenheart:astatisticalstudyofincreasedmortality
amongwidows.British Medical Journal i,740–3.ParkesCMandNapierMM(1975)Psychiatricsequelaeofamputation.InSilverstoneTandBarraclough
B(eds.)Contemporary Psychiatry,pp.440–6.Ashford:HeadleyBrothers.PellMD(1996)OnthereceptiveprosodiclossinParkinson’sdisease.Cortex32,693–704.PichonSandKellCA(2013)Affectiveandsensorimotorcomponentsofemotionalprosodygeneration.The
Journal of Neuroscience33,1640–50.PoeckKandPilleriaG(1963)Pathologisches Lachen und Weinen.OrellFüssli:ArtInstitut.Powell M and Hemsley DR (1984) Depression: a breakdown of perceptual defence? British Journal of
Psychiatry145,358–62.RackP(1982)Race, Culture and Mental Disorder.London:Tavistock.RibotT(1896)La Psychologie des Sentiments.Paris:FélixAlcan.Rizzolatti G and Craighero L (2004) The mirror-neuron system. Annual Review of Neuroscience 27,
169–92.
278 FIVE—EMOTIONS AND ACTION
RizzolattiGandFadigaL(1998)Graspingobjectsandgraspingactionmeanings:thedualroleofmonkeyrostroventralpremotorcortex(area5).Novartis Foundation Symposium218,81–95.
Satoh M, NakaseT, Nagata K andTomimoto H (2011) Musical anhedonia: selective loss of emotionalexperienceinlisteningtomusic.Neurocase17,410–7.
Schachter S and Singer J (1962) Cognitive, social and physiological determinants of emotional state.Psychological Review69,379–99.
SchneiderK(1920)Thestratificationofemotionallifeandthestructureofthedepressivestates.Zeitschrift fuer Gesundheitswesen Neurologie und Psychiatrie59,281.
Shepherd M (1993) Historical epidemiology and the functional psychoses. Psychological Medicine 23,301–4.
SifneosPE(1972)Short-term Psychotherapy and Emotional Crisis.Cambridge:HarvardUniversityPress.SimpsonCJ(1984)Thestigmata:pathologyormiracle?British Medical Journal289,1746–8.SimsA(1994)‘Psyche’–spiritaswellasmind?British Journal of Psychiatry165,441–6.SiroisF(1982)Epidemichysteria.InRoyA(ed.)Hysteria,pp.101–16.Chichester:JohnWiley.Snaith RP (1993) Anhedonia: a neglected symptom of psychopathology. Psychological Medicine 23,
957–66.Strauss GP and Gold JM (2012) A new perspective on anhedonia in schizophrenia. American Journal of
Psychiatry169,364–73.StyronW(1990)Darkness Visible: A Memoir of Madness.London:Cape.Taylor G (1984) Alexithymia: concept, measurement and implications for treatment. American Journal of
Psychiatry141,725–32.ThompsonWF,MarinMMandStewartL(2012)Reducedsensitivitytoemotionalprosodyincongenital
amusiarekindlesthemusicalprotolanguagehypothesis.Proceedings of the National Academy of Sciences USA109,19027–32.
TrethowanWH(1979)Affectivedisorders.InTrethowanWH(ed.)Psychiatry,4thedn.London:BaillièreTindall.
UngerleiderJTandWellischDK(1979)Coercivepersuasion(brainwashing),religiouscults,anddeprogram-ming.American Journal of Psychiatry136,279–82.
VanHeeringenK,HawtonKandWilliamsJMG(2000)Pathwaystosuicide:anintegrativeapproach.InHawton K and Van Heeringen K (eds.) The International Handbook of Suicide and Attempted Suicide.Chichester:JohnWiley.
VuillemierP,Ghika-SchmidF,BogousslavskyJ,AssalGandRegliF(1998)Persistentrecurrenceofhypo-maniaandprosoaffectiveagnosiainapatientwithrightthalamicinfarct.Neuropsychiatry, Neuropsychology and Behavioral Neurology11,40–4.
Weniger G and Irle E (2002) Impaired facial affect recognition and emotional change in subjects withtransmodalcorticallesions.Cerebral Cortex12,258–68.
WernickeC(1906)Fundamentals of Psychiatry.Leipzig:Thieme.WhybrowPC(1997)A Mood Apart: Depression, Mania and Other Afflictions of the Self.NewYork:BasicBooks.WittemanJ,VanHeuvenVJandSchillerNO(2012)Hearingfeelings:aquantitativemeta-analysisonthe
neuroimagingliteratureofemotionalprosodyperception.Neuropsychologia50,2752–63.ZilboorgGandHenryGW(1941)A History of Medical Psychology.NewYork:Norton.
279
C H A P T E R 17
Anxiety, Panic, Irritability, Phobia and Obsession
SummaryResponsetostressisanintegralaspectofhumanexistence,andthealarmreactionsetsthecontextfor an understanding of anxiety and anxiety-related disorders. Hence free-floating anxietyincludesexperientialfeaturesofthealarmreactionbutmarkedoutasabnormalbytheintensity,the prolonged duration, the trivial nature of the triggering events and finally by the sociallydisruptiveanddisablingnatureoftheexperience.Anxietycanbefocusedonaspecifiedobjectorsituationandthisistermedphobia,itcanoccurasparoxysmalandepisodicattacksasinpanic,oritcanbediscomfortingifunregulatedasinobsessive-compulsivephenomena.
Montanus speaks of one that durst not walk alone from home for fear that he should swoon or die. A second fears every man he meets will rob him, quarrel
with him or kill him. A third dares not venture to walk alone, for fear he should meet the devil, a thief, be sick; fears all old women as witches; and
every black dog or cat he sees he suspecteth to be a devil; every person comes near him is malificiated; every creature, all intend to hurt him, seek his ruine;
another dares not go over a bridge, come near a pool, rock, steep hill, lye in a chamber where cross beams are for fear he be tempted to hang, drown or
precipitate himself. If he be in a silent auditory, as at a sermon, he is afraid he shall speak aloud, at unawares, something undecent, unfit to be said. If he
be locked in a close room, he is afraid of being stifled for want of air, and still carries bisket, aquavitae, or some strong waters about him for fear of deliquiums, or being sick; or if he be in a throng, middle of a church,
multitude, where he may not well get out, though he sit at ease he is certase affected. He will freely promise, undertake any business beforehand; but when it comes to be performed he dares not adventure, but fears an infinite number
of dangers, disasters, etc.…They are afraid of some loss, danger, that they shall surely lose their lives, goods, and all they have; but why they know not.
Robert Burton (1621)
Responsetostress isanintegralaspectofhumanexistence.Butwhatisstress?Thereareatleastthreeconceptualizationsofstress:stressasastimulus;stressasaresponse;andstressasaninteraction.Thenotionofstressasastimulusismodelledontheassumptionthatitisanexternalfactorthataffectsanindividual,whereasstressasaresponselocatesthestresswithintheindi-vidual.This latter notion was developed by Selye (1907–1982), who defined stress as a ‘non-specificresponseofthebodytoanydemandmadeuponit’(Selye,1956).ThenotionofstressasaninteractionbuiltonSelye’sworkandwasdevelopedbyLazarus(1922–2002):

Keywords: Anxiety,Panic,Phobia,Obsession,Compulsion,Irritability.
17—ANxIETy, PANIC, IrrITAbIlITy, PhObIA AND ObSESSION 279.e1
280 FIVE—EMOTIONS AND ACTION
A particular relationship between the person and the environment that is appraised by the person as taxing or exceeding his or her resources and
endangers his or her well being.(Lazarus and Folkman, 1984)
Selye’sGeneralAdaptationSyndromedescribesthestressresponseascomprisingthreestages:alarmreaction,resistanceandexhaustion.Thealarmreaction,typicallytermedtheflight-or-fightresponse,involvesautonomicarousalmediatedbyreleaseofcatecholaminesandisexperiencedasfear,palpitationsorreadinessforaction,amongstotherthings.Intheeventthatthestressorpersists, there is decreased release of catecholamines and a switch to release of glucocorticoidhormonesduring the resistancephase.And,finally incontextsof chronic stress, exhaustion istheresultwiththepotentialforhypoglycaemiaanddeath.
AnunderstandingofSelye’sGeneralAdaptationSyndrome,particularlythephysiologicalandexperiential aspects of the alarm reaction (flight-or-fight response) sets anxiety and anxiety-relatedemotionaldisturbanceincontext.Thefiveabnormalphenomenaofthischapterarerela-tivelycommonhumanexperiencesandcanbeconstruedasemanatingfromdisturbancesoftheregulationofanxiety.Abnormalityinthiscontextismarkedoutbytheseverityandintensityoftheexperience,prolongedduration,occurrenceinreactiontowhatcouldbeconsideredaninad-equatesituationalstressandthedeleteriousanddisablingeffectonsocialfunctioning.Eachofthese phenomena has a normal, even necessary, aspect: it is appropriate to be anxious at thebeginningofaspeechinpublic;itisnormalforaparenttoexpressirritabilitywhenan8-year-oldsonbreaksawindow–itisanecessarylearningexperienceforhim;fearisnecessaryforcopingwhen an individual suddenly discovers him or herself to be surrounded by poisonous snakes;meticulouscheckingandcheckingagainisanimportantpartoflearningtobeacompetentairlinepilot;evenpanicisnormal,inastatisticalsense,insomesituationsofextrememassdisaster.
Inanymodernconsiderationofanxietydisorders,anxiety,panicandphobiawouldbeincludedbothasstatesofemotionandasdistinctsyndromes(NoyesandHoehn-Saric,1998).Irritabilityisadistinctandimportantmoodstatethatoccursinseveraldifferentconditions,andobsessionis both an individual symptom and an essential feature of obsessive-compulsive disorder.Superficially,obsessionandcompulsioncanseemunrelatedtoanxietybutbothcanbeconstruedasmeansofregulatinganxiety.
Patients may have insight and present themselves as suffering from ‘phobia’, ‘obsession’ or‘anxiety state’.However, the laymeaningofeachof these terms is significantlydifferent fromtheir psychiatric use, and it will be more usual for the clinician to diagnose the state from adescriptionofthemoodorthoughtprocess.
AnxietyAnxietyisauniversalandnormalemotion.Itisanecessaryandadaptiveresponseoftheorgan-ismtostress.It isclearthat levelsofarousalrelatetotheefficiencyofanorganism’sabilitytorespondappropriatelytoatask:toolittlearousalandexcessivearousalarebothassociatedwithpoorperformance(thisistheYerkes-DodsonLaw)(YerkesandDodson,1908).LaderandMarks(1971)havediscussedthefeaturesofanxietyintermsoftheemotionbeingnormalorpathologi-cal. In rather concrete terms, amanwhodiscovers thathe is sharing afieldwith a bull feelsacutelyanxiousandrunsattopspeedforthegate;if,sixweekslater,whenbackinthecity,hehasapanicattackandhastoliedownbecausesomeonementionsapartofthecitycalledtheBullring,hisresponseisclearlymaladaptiveandhisanxietypathological.
Anxietymayalso,arbitrarily,bepolarizedbetween stateand trait (SimsandSnaith,1988).Anxietystateisthequalityofbeinganxiousnow,atthisparticulartime,probablyasareactiontoprovokingcircumstances.Anxietytraitisthetendencyoveralongtime,perhapsthroughout
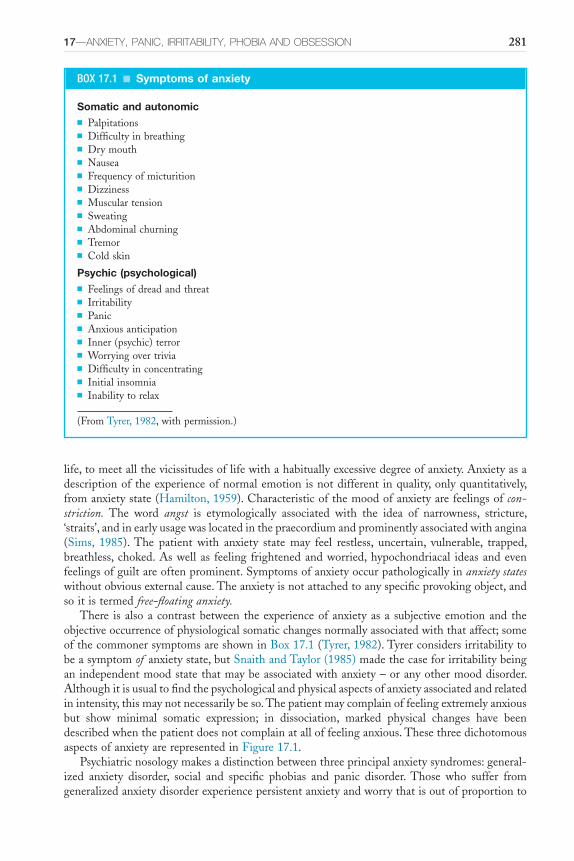
17—ANxIETy, PANIC, IrrITAbIlITy, PhObIA AND ObSESSION 281
life,tomeetallthevicissitudesoflifewithahabituallyexcessivedegreeofanxiety.Anxietyasadescriptionoftheexperienceofnormalemotionisnotdifferent inquality,onlyquantitatively,fromanxietystate(Hamilton,1959).Characteristicofthemoodofanxietyarefeelingsofconstriction. The word angst is etymologically associated with the idea of narrowness, stricture,‘straits’,andinearlyusagewaslocatedinthepraecordiumandprominentlyassociatedwithangina(Sims, 1985).The patient with anxiety state may feel restless, uncertain, vulnerable, trapped,breathless,choked.Aswellas feeling frightenedandworried,hypochondriacal ideasandevenfeelingsofguiltareoftenprominent.Symptomsofanxietyoccurpathologicallyinanxiety stateswithoutobviousexternalcause.Theanxietyisnotattachedtoanyspecificprovokingobject,andsoitistermedfreefloating anxiety.
There isalsoacontrastbetween theexperienceofanxietyasa subjectiveemotionand theobjectiveoccurrenceofphysiologicalsomaticchangesnormallyassociatedwiththataffect;someofthecommonersymptomsareshowninBox17.1(Tyrer,1982).Tyrerconsidersirritabilitytobeasymptomof anxietystate,butSnaithandTaylor(1985)madethecaseforirritabilitybeinganindependentmoodstatethatmaybeassociatedwithanxiety–oranyothermooddisorder.Althoughitisusualtofindthepsychologicalandphysicalaspectsofanxietyassociatedandrelatedinintensity,thismaynotnecessarilybeso.Thepatientmaycomplainoffeelingextremelyanxiousbut show minimal somatic expression; in dissociation, marked physical changes have beendescribedwhenthepatientdoesnotcomplainatalloffeelinganxious.ThesethreedichotomousaspectsofanxietyarerepresentedinFigure17.1.
Psychiatricnosologymakesadistinctionbetweenthreeprincipalanxietysyndromes:general-ized anxiety disorder, social and specific phobias and panic disorder. Those who suffer fromgeneralizedanxietydisorderexperiencepersistentanxietyandworrythatisoutofproportionto
BOX 17.1 ■ Symptoms of anxiety
Somatic and autonomic■ Palpitations■ Difficultyinbreathing■ Drymouth■ Nausea■ Frequencyofmicturition■ Dizziness■ Musculartension■ Sweating■ Abdominalchurning■ Tremor■ Coldskin
Psychic (psychological)■ Feelingsofdreadandthreat■ Irritability■ Panic■ Anxiousanticipation■ Inner(psychic)terror■ Worryingovertrivia■ Difficultyinconcentrating■ Initialinsomnia■ Inabilitytorelax
(FromTyrer,1982,withpermission.)
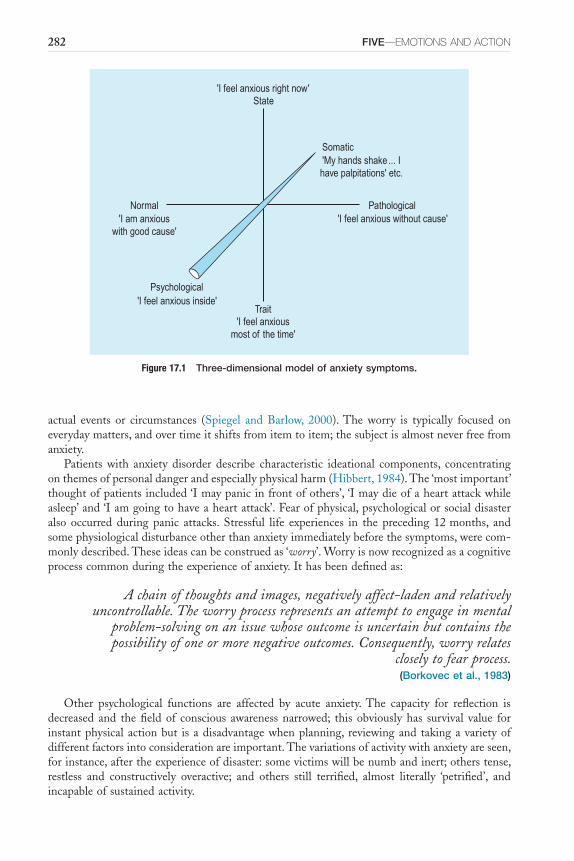
282 FIVE—EMOTIONS AND ACTION
Figure 17.1 Three-dimensional model of anxiety symptoms.
'I feel anxious right now'
'I feel anxious without cause''I am anxiouswith good cause'
'I feel anxiousmost of the time'
'I feel anxious inside'
'My hands shake... Ihave palpitations' etc.
State
Somatic
Trait
Psychological
PathologicalNormal
actual events or circumstances (Spiegel and Barlow, 2000).The worry is typically focused oneverydaymatters,andovertimeitshiftsfromitemtoitem;thesubjectisalmostneverfreefromanxiety.
Patients with anxiety disorder describe characteristic ideational components, concentratingonthemesofpersonaldangerandespeciallyphysicalharm(Hibbert,1984).The‘mostimportant’thoughtofpatientsincluded‘Imaypanicinfrontofothers’,‘Imaydieofaheartattackwhileasleep’and‘Iamgoingtohaveaheartattack’.Fearofphysical,psychologicalorsocialdisasteralso occurred during panic attacks. Stressful life experiences in the preceding 12months, andsomephysiologicaldisturbanceotherthananxietyimmediatelybeforethesymptoms,werecom-monlydescribed.Theseideascanbeconstruedas‘worry’.Worryisnowrecognizedasacognitiveprocesscommonduringtheexperienceofanxiety.Ithasbeendefinedas:
A chain of thoughts and images, negatively affectladen and relatively uncontrollable. The worry process represents an attempt to engage in mental
problemsolving on an issue whose outcome is uncertain but contains the possibility of one or more negative outcomes. Consequently, worry relates
closely to fear process.(Borkovec et al., 1983)
Other psychological functions are affected by acute anxiety.The capacity for reflection isdecreased and thefieldof conscious awarenessnarrowed; this obviouslyhas survival value forinstantphysicalactionbut isadisadvantagewhenplanning, reviewingand takingavarietyofdifferentfactorsintoconsiderationareimportant.Thevariationsofactivitywithanxietyareseen,forinstance,aftertheexperienceofdisaster:somevictimswillbenumbandinert;otherstense,restless and constructively overactive; and others still terrified, almost literally ‘petrified’, andincapableofsustainedactivity.
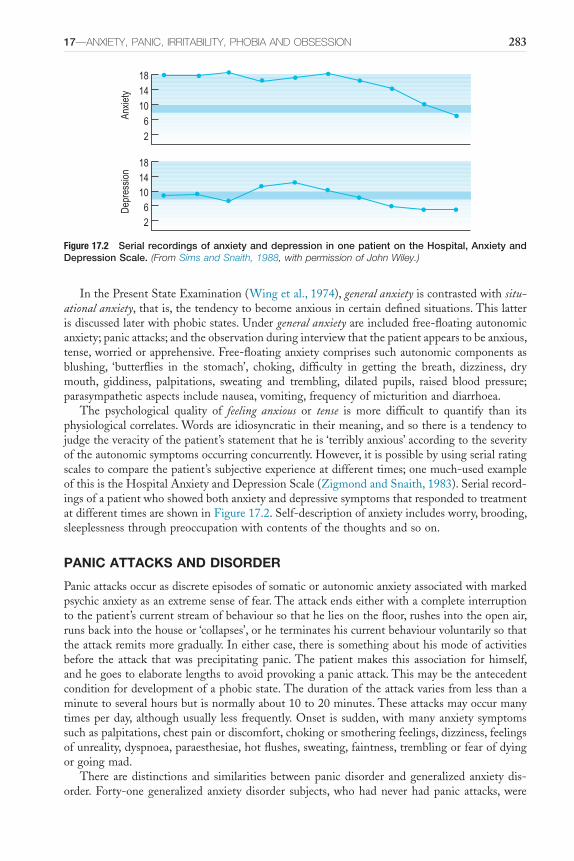
17—ANxIETy, PANIC, IrrITAbIlITy, PhObIA AND ObSESSION 283
InthePresentStateExamination(Wingetal.,1974),general anxietyiscontrastedwithsituational anxiety,thatis,thetendencytobecomeanxiousincertaindefinedsituations.Thislatterisdiscussedlaterwithphobicstates.Undergeneral anxietyareincludedfree-floatingautonomicanxiety;panicattacks;andtheobservationduringinterviewthatthepatientappearstobeanxious,tense,worriedorapprehensive.Free-floatinganxietycomprisessuchautonomiccomponentsasblushing, ‘butterflies in the stomach’, choking, difficulty in getting the breath, dizziness, drymouth, giddiness, palpitations, sweating and trembling, dilated pupils, raised blood pressure;parasympatheticaspectsincludenausea,vomiting,frequencyofmicturitionanddiarrhoea.
The psychological quality of feeling anxious or tense is more difficult to quantify than itsphysiologicalcorrelates.Wordsareidiosyncraticintheirmeaning,andsothereisatendencytojudgetheveracityofthepatient’sstatementthatheis‘terriblyanxious’accordingtotheseverityoftheautonomicsymptomsoccurringconcurrently.However,itispossiblebyusingserialratingscalestocomparethepatient’ssubjectiveexperienceatdifferenttimes;onemuch-usedexampleofthisistheHospitalAnxietyandDepressionScale(ZigmondandSnaith,1983).Serialrecord-ingsofapatientwhoshowedbothanxietyanddepressivesymptomsthatrespondedtotreatmentatdifferenttimesareshowninFigure17.2.Self-descriptionofanxietyincludesworry,brooding,sleeplessnessthroughpreoccupationwithcontentsofthethoughtsandsoon.
PANIC ATTACKS AND DISORDER
Panicattacksoccurasdiscreteepisodesofsomaticorautonomicanxietyassociatedwithmarkedpsychicanxietyasanextremesenseoffear.Theattackendseitherwithacompleteinterruptiontothepatient’scurrentstreamofbehavioursothatheliesonthefloor,rushesintotheopenair,runsbackintothehouseor‘collapses’,orheterminateshiscurrentbehaviourvoluntarilysothattheattackremitsmoregradually.Ineithercase,thereissomethingabouthismodeofactivitiesbefore the attack thatwasprecipitatingpanic.Thepatientmakes this association forhimself,andhegoestoelaboratelengthstoavoidprovokingapanicattack.Thismaybetheantecedentconditionfordevelopmentofaphobicstate.Thedurationoftheattackvariesfromlessthanaminutetoseveralhoursbutisnormallyabout10to20minutes.Theseattacksmayoccurmanytimesperday,althoughusually less frequently.Onset is sudden,withmanyanxiety symptomssuchaspalpitations,chestpainordiscomfort,chokingorsmotheringfeelings,dizziness,feelingsofunreality,dyspnoea,paraesthesiae,hotflushes,sweating,faintness,tremblingorfearofdyingorgoingmad.
Therearedistinctionsand similaritiesbetweenpanicdisorder andgeneralizedanxietydis-order.Forty-onegeneralized anxietydisorder subjects,whohadneverhadpanic attacks,were
Figure 17.2 Serial recordings of anxiety and depression in one patient on the Hospital, Anxiety and Depression Scale. (From Sims and Snaith, 1988, with permission of John Wiley.)
181410
Anxi
ety
62
181410
Dep
ress
ion
62

284 FIVE—EMOTIONS AND ACTION
compared with 71 subjects with panic disorder (Noyes etal., 1992).The generalized anxietydisordersubjectshadanearlier,moregradualonsetofsymptomsandmoreoftensufferedfromsimplephobias,whilethepanicdisordersubjectstendedtoreportdepersonalizationandagora-phobia.Ingeneral,thosewithpanicdisorderhadamoreseveredegreeofillnessandweremorelikelytogiveahistoryofmajordepression.
There is growing recognition that there are at least two discrete and distinct experientialsubtypes of panic disorder: a respiratory type that is characterized by fear of dying, chestpainanddiscomfort,shortnessofbreath,paraesthesiasandthesensationofchoking;andanon-respiratorytype.Therespiratorysubtypeisassociatedwithspontaneouspanicexperienceratherthansituationallyinducedpanic.Furthermore,itismorelikelytobeprovoked,inchallengetests,byinhalationof35%carbondioxideorbyhyperventilationproducinghypocapnicalkalosis(FreireandNardi,2012).
PHOBIC STATES
Phobias,orunreasonablefears,havebeendescribedformanycenturies.Forexample,BenjaminRush(1798)definesphobiaas‘afearofanimaginaryevil,oranunduefearofarealone’andthenproducesalistof18phobias,partlyhumorouslyintended;thisisreproducedinBox17.2.Agoraphobia was originally described by Westphal (1871); this condition, literally ‘fear of themarketplace’,causesveryseveredisability.AnimalphobiashavebeencontrastedbyMarks(1970):
If ever we are tempted to think that all phobic states are a unity which reflects the same disorder and aetiology, we can quickly dispel this illusion
simply by looking at the startling contrast between animal phobias and agoraphobias. These two conditions differ radically in onset, course, symptomatology, response to treatment and psychological measures.
Solyometal.(1986)dividedthesymptomatologyof199patientsintothreecategories:ago-raphobia(80patients),socialphobia(47patients)andsimplephobia(72patients).Agoraphobia
BOX 17.2 ■ Species of phobia according to Rush (1798)
■ Thecatphobia■ Theratphobia■ Theinsectphobia■ Theodourphobia■ Thedirtphobia■ Therumphobia■ Thewaterphobia■ Thesolophobia■ Thepowerphobia■ Thefactionphobia■ Thewantphobia■ Thedoctorphobia■ Thebloodphobia■ Thethunderphobia■ Thehomephobia■ Thechurchphobia■ Theghostphobia■ Thedeathphobia

17—ANxIETy, PANIC, IrrITAbIlITy, PhObIA AND ObSESSION 285
included‘fearofleavinghome,ofbeingaloneathomeoronthestreet,incrowds,oftravellingbycar,busortrain’.Socialphobiainvolvedanxietyinsocialsituations.Simplephobiadescribedasinglebut life-disruptingfear, suchasofanimals,heights,disease,aeroplanes, insectsandsoon.Whatiscommontoallthesephobicexperiencesisthatthefearisintenseandpersistentandthatfurthermoreitisprovokedbyexposureortheanticipationofexposuretocuesthatareclearlydiscernibleandcircumscribedobjectsorsituations.
A more comprehensive subdivision of phobic states is contained in Box 17.3 from Marks(1969).As agoraphobia literallymeans ‘fearof themarketplace’, this is frequently appropriatenowadays,asoftenthemostphobicsituationforsuchpeopleisinthesupermarket.Agoraphobiais, infact,aheterogeneouscollectionofdisordersandnotanentity; thepatientdoesnotonlyfearathrongofpeoplebuthasmultipleavoidanceresponsestomanydifferentstimuli(Snaith,1991).Itincludesboththosewhohaveafearofbeingunderpublicscrutiny,andthereforewhoavoidpublicplaces,andthosewithillnessfearsineitherapublicplacewheretheybecomenotice-ableoranexposedplacewheretheywillnotbeabletoreceivehelp.
Socialphobiasarecommonconditionsthathavebeenrelativelyneglectedoverrecentyears(Swinson,1992).Theyareparticularlylikelytooccurinassociationwithotherdisordersofmoodorothertypesofanxiety.Thereareavarietyofdifferentmanifestations,butsocialphobiacanbe considered tobe an extremevariantof shyness.However, avoidance ismore typical of theestablished disorder. It is characterized by excessive fear, self-consciousness and avoidance ofsocialsituationsduetothepossibilityofembarrassmentorhumiliation.Typicallythefearfocusesonsituationswherethereisthepossibilityofpublicperformancesuchaspublicspeaking,eatinginpublic,signingadocumentunderscrutiny,orformen,urinatinginapublictoilet.
Illnessphobiaisdifferentfromhypochondriacalpreoccupationinthat,withtheformer,avoid-anceoccurs.Thusthecriteriaforphobia,accordingtoMarks(1969),are:
■ fearisoutofproportiontothedemandsofthesituation■ itcannotbeexplainedorreasonedaway■ itisnotundervoluntarycontrol■ thefearleadstoanavoidanceofthefearedsituation.A28-year-oldmarriedwomansaid,
My fear problems are worst… I am afraid of catching cancer. I am afraid of catching it from the hospital [radiotherapy hospital] 1 mile away… I bought
a scarf from a shop and the assistant frightened me… the look of her, she hardly had any hair and looked very old… I thought I had caught it from her
and so I had to wash the house. I cleaned the whole house and it made me
BOX 17.3 ■ Subdivisions of phobic neurosis
Phobias of external stimuli■ Agoraphobia■ Socialphobias■ Animalphobias
Phobias of internal stimuli■ Illnessphobias■ Obsessivephobias■ Miscellaneousspecificphobias
(AfterMarks,1969,withpermission.)
286 FIVE—EMOTIONS AND ACTION
poorly. I had to move house because of the hospital and I cannot go back to that shop ever again.
There is also some relationship between phobias, especially agoraphobia, and depression(Schapiraetal.,1970).Persistent fearandforeboding,oftenofasituationalnature,mayoccurwithotherdepressivesymptoms.Phobicstates,asalsopanicdisorder,mayrespondtoantidepres-santtherapy.
Phobiasareoverpoweringandcompellingintheirnature,dominatingthewholeoflife.Likeobsessions, they are repetitive, resistedunsuccessfully, regardedby the subject as senseless andirrationalbutatthesametimeascomingfrominsideofhimorherself.Someauthorsthereforedescribethemasobsessional fears.Oftencompulsivebehaviour,suchashandwashing,arisesoutofaphobia,forinstancefearofdirtandcontamination.Prominentinthesubject’sdescriptionofhisphobiaisthatheiscontrolledbyit,thatthefearissomethingfrominsidehimself(innowaycontrolledfromoutside).
ANXIETY IN OTHER DISORDERS
Obviously, most consideration of anxiety and its different forms and manifestations has beengiven in the context of the anxiety disorders. However, anxiety is a common symptom and isfrequentlyapartofotherillnesses,bothpsychiatricandphysical.Amongstpsychiatricconditions,themostfrequentcomorbidityiswithdepressiveillness;mostpatientswithdepressionhavesomeanxietysymptoms,mostofthosewithmoresevereanxietydisordersalsohavesomefeelingsofdepression.Anxietyisafrequentsymptomintheprodromalstagesofschizophreniaandisalsoassociatedwith relapse (TarrierandTurpin,1992).Anxietyoftenoccurswithorganicpsycho-syndromes,bothexacerbatingtherestlessnessofacuteorganicpsychosyndromesordeliriumandmanifestingasanadditionalcauseofsubjectivedistressinchronicorganicstatesordementia.
Anxiety is an understandable reaction to physical illness and its consequent distress, pain,physicalandsocialdisabilityandthreattolife(SimsandSnaith,1988).Inthefollowingcondi-tions,itmayalsobeadirectexpressionofthemorbidprocess:hypoglycaemia,hyperthyroidism,phaeochromocytoma,carcinoidsyndrome,somecardiacand ictaldisordersandstatesofwith-drawal frompsychoactive substances.These conditions thereforeneed tobe considered in thedifferentialdiagnosisofanxiety,andthecomponentofanxietyintheirsymptomatologymustbedealtwithintheirtreatment.
IrritabilityIrritabilityofthepatientmaybeobservedbyothersorexperiencedsubjectivelydirectedtowardsothers(outward)ortowardstheself(inward).Irritability,outwardlyexpressed,isconsideredtobeadisorderofmood in itsownrightand independentofanxiety,depressionorothermoodstate(SnaithandTaylor,1985):‘Outwardlyexpressedirritabilityisanindependentmooddisorderandnotmerelyonewhichissymptomaticofstatesofdepressionoranxiety’.Outwardlyexpressedirritability is particularly commonly associated with puerperal mood disorder, while inwardlydirectedirritabilitywasdescribedinthosewithobsessive–compulsivedisorder.IntheIrritability,DepressionandAnxietyScale,twosubscalesweredevelopedforirritability(Snaithetal.,1978):outwardlydirected irritabilityand inwardlydirected irritability.SnaithandTaylor (1985)havedefinedirritabilityforuseinthecontextofpsychopathologyas:
Irritability is a feeling state characterized by reduced control over temper – which usually results in irascible verbal or behavioural outbursts, although
the mood may be present without observed manifestation. It may be

17—ANxIETy, PANIC, IrrITAbIlITy, PhObIA AND ObSESSION 287
experienced as brief episodes, in particular circumstances, or it may be prolonged and generalized. The experience of irritability is always unpleasant
for the individual and overt manifestation lacks the cathartic effect of justified outbursts of anger.
It isaprominent symptominpost-traumatic stressdisorder, inwhich it is listedasoneofthe symptoms of increased arousal. Relatives described an individual survivor of disaster: ‘Hehas completely changed his character. He has become nasty tempered and swears at us allthetime.’
Theseverityofirritabilityprobablyhasaninversecorrelationwithage;itoccursinbothmenandwomen.Itisusefultomakeadistinctionbetweenthesubjectivemoodofirritabilityandtheobservationofviolentbehaviour,althoughthesemayoverlap.Severeirritabilitymaycausecon-siderabledistresstopatients,relativesandhealthcareprofessionals;theremaybenootherpsy-chiatricsymptomatologypresent.Thefactorsthatpredisposetoirritabilityarenotclearlyknown.‘The stateof irritability isprimarily amoodwhichmaybe translated intobehaviour’ (Snaith,1991).
Obsessions and CompulsionsAn additional video for this topic is available online.
Thereisnonecessaryassociationbetweenobsessions,orobsessive–compulsivedisorder,andanxietyoranytypeofanxietydisorder.Isolatedobsessionsorobsessive–compulsivedisordermayoccur with or without anxiety; with or without depression; and with or without personalitydisorder,anankasticorotherwise.Itisadistinctandseparatephenomenon.
The patient may be troubled by thoughts that he knows to be his own but that he findsrepetitiveandstrange;hefindsheisunabletopreventtheirrepetition.Theseobsessionalthoughtshave, according toLewis (1936), threeessential features: a feelingof subjective compulsion, aresistancetoitandthepreservationofinsight.Thesefeaturesdistinguishobsessionfromvolun-taryrepetitiveactsandsocialceremonies.Thewordobsessionisusuallyreservedforthethoughtandcompulsionfortheact.Thesuffererknowsthatitishisownthought(oract),thatitarisesfrom within himself and that it is subject to his own will whether he continues to think (orperform)it;hecandecidenottothinkitonthisparticularoccasion(butitdoesandwillrecur).Heistormentedbythefearofwhatmayhappenifhedisturbstheroutine.Thereisnodistur-banceof consciousnessorof theawarenessof thepossessionofhisown thought.Thepersonusually functions satisfactorily in other areas of his life uncontaminated by the obsessionalthought,butastheobsessionsbecomemoreseverethereisincreasingsocialincapacityandmiserythatcangrosslydisrupthiswholelifestyle.
JohnBunyan,inhispoignantautobiographyGrace Abounding to the Chief of Sinners(1666),describesgross,obsessionalthoughtsandruminationsthatareconnectedwith,butcanbeclearlyseparatedfrom,hisunderlyingreligiousbeliefs.Forexample:
33. Now you must know, that before this I had taken much delight in ringing, but my Conscience beginning to be tender, I thought that such a
practice was but vain, and therefore forced myself to leave it, yet my mind hankered, wherefore I should go to the Steeple house, and look on: though I
durst not ring. But I thought this did not become Religion neither, yet I forced my self and would look on still; but quickly after, I began to think, How, if
one of the bells should fall: then I chose to stand under a main Beam that lay

288 FIVE—EMOTIONS AND ACTION
over thwart the Steeple from side to side thinking there I might stand sure; But then I should think again, Should the Bell fall with a swing, it might first hit the Wall, and then rebounding upon me, might kill me for all this
Beam; this made me stand in the Steeple door, and now thought I, I am safe enough for if a Bell should fall, I can slip out behind these thick walls, and so
be preserved not withstanding.34. So after this, I would yet go to see them ring, but would not go further
than the Steeple door; but then it came into my head, how if the Steeple it self should fall, and this thought, (it
may fall for ought I know) would when I stood and looked on, continually so shake my mind, that I durst not stand at the Steeple door any longer, but was
forced to fly, for fear it should fall upon my head.(p. 13)
The obsessional symptom and the religious belief expressed in this passage are not the samephenomenologically,althoughtheyareinterconnected.Thenatureoftheobsessionalthoughtisdemonstrated in theway thatBunyan felt compelled to think through this elaborate chainofarguments;heresistedhisideas,butunsuccessfully.Thereisnolackofinsightintoitsbeinghisownbehaviour.Thebehaviourwascompulsiveinthatitwastheactingoutofambivalent,obses-sionalnotions.Thereismorethanahintofunderlyingobsessionalpersonality, for instanceinthenumberingoftheparagraphs.
Amidwife,aged32,keptthinkingaftershehadfinishedherspellofdutyathospitalthatshemighthavepushedanairwaydownthethroatofababythatshehaddelivered.Shewouldtele-phonethewardrepeatedlytocheckthattheinfantwaswell.Shefrequentlymadesurethatherdog’scollarwassecurewhenshewasoutwalking incaseheescapedandwaskilledbytraffic.Whenalittleboyandhismothervisitedherhome,shegavehimaglassof‘pop’.However,shehadtodrinkwhatshehadjustpouredoutforhimherself,althoughshedislikedit,tomakesureit reallywaspopandnot somethingharmful.Theaccumulationofmoreandmoresymptomseventuallypreventedherfromworkingorcarryingoutanyreasonablesociallife.Sheknewthatthesewereherownnotions,thattheywerestupid,butshecouldnotstopherselfthinkingandperformingthem.
The compulsive behaviour often provokes further anxiety in the patient, the need both toperform the action and to preserve social acceptability. Although wide areas of life are oftenimplicatedincompulsiverituals,itisoftenstrikinghowtheobsessionalpersonomitsotherareasfromhisobsessionality.Thepatientwhoexcoriateshishandsbyexcessivewashinganddevotesasubstantialportionofeachdaytothepursuitofcleanlinessmaydrivetoworkinadirtyandill-servicedcarandworkinanuntidyoffice!Thedilemmaofobsessionalsymptomsremainsthattheyarebothreckonedaspartofthepatient’sownbehaviourandresistedunsuccessfully,thatis,theyareundervoluntarycontrolbutnotaltogetherexperiencedasvoluntary.Thepatienthasanawarenessthatthisparticularactorthoughtisvoluntaryandcanberesisted,withdifficulty,buttheoverallpatternofthinkingorbehavingisexperiencedsubjectivelyasinevitable–it isulti-matelyfutiletostruggle.Theactionsometimes‘appearstobeagainstthewillofthepatient,andoftenseemstohavethequalityofdisgustorrepulsion;thisurgetodosomethingyettoberepelledbyit,issaidtobeasingularcharacteristicoftheobsessionalstate’(Beech,1974).
Obsessionmayoccurasthoughts,images,impulses,ruminationsorfears;compulsionsasacts,rituals,behaviours.Schneider’sdefinition(1959)emphasizesthatthereisnolossofcontactwithreality:‘Anobsessionoccurswhensomeonecannotgetridofacontentofconsciousness,althoughwhenitoccursherealizesthatitissenselessoratleastthatitisdominatingandpersistingwithoutcause’.Thus,hallucinations,delusionsandmooddisturbancescannotbeobsessionalinform;they
17—ANxIETy, PANIC, IrrITAbIlITy, PhObIA AND ObSESSION 289
arenotexperiencedassenseless,nor isthereanattempttogetridofthem.Thecravingofanalcoholicforhisbeverageortheabnormaldriveofsexualdeviationisnotcompulsiveinastrictsense.Theydonotcontravene theperson’swill, althoughhemaydislikehimself intensely forhavingsuchwishes.
Obsessionalideasmaybesimpleorcomplicated.Atuneorafewmusicalnotesmaybecomerepetitive andbe resisted,or a sequenceofwords, for example ‘theBritishSocialistParty’,bereiterated irritatingly inside the person’s head. The obsessions or compulsions may be morecomplexandritualistic, forexampleapatientwhotried to shut thecardooraftergettingoutfoundthisverydifficultbecausehewasafraidthattheactofshuttingwouldproduceunpleasant,obscene,repetitivethoughts.Forthisreason,hehadtogotoelaboratelengthstoputthecarinacertainplace,checkallthedoorsbeforegettingout,checkthemallagainaftergettingoutandturnthekeywhilelookinginaparticulardirection.
Theimagesofobsessionalthinkingmaybevividbutarealwaysknownbythepatienttobeproductsofhisownmind.TheseimageshavebeenconsideredbyDeSilva(1986)tobeoneoffourtypes.
1. The obsessional image depicts repetitively the unwanted intrusive cognition – images ofbloodflowing,injuriesandsoon.
2. The compulsive image depicts compulsive behaviour by rectifying either an obsessionalimage–thewomanwhosawcorpsesincoffinsandhadtoimaginethesamepeoplestand-ing–oranindependentcompulsiveimage.
3. Thedisaster image affects compulsive checkerswhomaynotonly fear thatdisasterwilloccurunlesstheycheckbutalso‘see’thedisasterhappeninginfantasy–thehouseburningdownifthegastapsarenotturnedoff.
4. Thedisruptive imagemayintrudewhilecompulsiveritualsarebeingcarriedoutandneces-sitatetheritualbeingrecommenced.
Ruminationsareoftenpseudophilosophical,irritatinglyunnecessary,repetitiveandachievenoconclusion.Apriesthasaninnerimpulsetoutterswearwordsinchurch,oramotheranimpulsetoharmherchild–bothquitefrequentcomplaintsofobsessionalpatients.Reassurancethathewillnotharmhimselforothersoractontheimpulsescanbegiventotheobsessional,provideditistrulyobsessionalinform,thatheisnotconcurrentlydepressedandthatthereisnotcoexist-ingdissocialpersonalitydisorder.
Theconstituentelementsofobsessive-compulsiveexperiencearesaidtoinclude:1. atriggerwhichisaneventorcuethatsetsoffanobsession,afeelingofdiscomfort,ora
compulsiveurge;2. anobsessionitself;3. adiscomfortthatisexperiencedasageneralunease,tensionorasenseofguilt;4. acompulsiveurgeordrivetocarryoutaparticularbehaviour;5. discomfortreduction;6. fearsofdisaster that thepatientbelieveswill tocomepassbut thatcanbeavoidedby
engagingincompulsivebehaviour;7. inflatedsenseofresponsibilityevenforeventsoverwhichthepatienthasnocontrol;8. reassurance-seekingbehaviour;9. avoidanceofstimuliorsituationsthatmaytriggerobsessionsorcompulsions;
10. disruptionofsocialfunctioningbecauseofthelongandcomplicatedcompulsionswhichareoftentimeconsumingandexhausting;and
11. resistance–whichhasalreadybeendiscussedabove(deSilva,2003).Obsessionsoccur inthecontextofobsessive-compulsivedisorderasthemajorsymptomof
the condition. However, they also occasionally occur in other circumstances. The depressedpatient with obsessional (anankastic) personality may show obsessions and compulsions thatclearwhenhisillnessistreated.Obsessionalstatesaremorecommonwhenobsessionalpersonal-

290 FIVE—EMOTIONS AND ACTION
ity ispresent,but thispersonality type isnotaprerequisite.Obsessional symptomsmayoccurin schizophrenia, when they usually have a bizarre character. Apparent obsessional symptomsmay arise de novo in an older person, associated with an organic psychosyndrome. However,theelementofresistancecharacteristicofobsessionalityisusuallynotpresent.Itseemsthatthepersoncarriesoutrepetitivebehaviourinordertocopewiththeuncertaintiesofhislifecausedby his failing memory and performance. Repetition and stereotyped behaviour in those withlearningdisabilityhassometimesbeenlabelledcompulsive;however,thisispsychopathologicallyincorrect,asthereisnoresistanceorconflictofurgeandrepulsion.Similarly,repetitivenessandstickinessofthinkingoccurwithepilepsy,followingheadinjuryandwithotherorganicstates,butagain,thisisnottrulyobsessionalinnature.
Thereisastrikingsimilaritybetweentheclinicalpresentationofobsessive-compulsivedis-orderinchildrenandadolescentsandinadults(Swedoetal.,1989).In70consecutivejuvenilepatients,washingandgrooming,repeating,checkingandtouchingritualswerethemostfrequentcompulsions, and obsessions were contamination fears, concerns about disasters happening tothepatient or those close tohim, symmetry and scrupulousness.Although the conditionwasfrequentlyfamilial,theactualpresentingsymptomswerenotsharedbyrelatives,evenbymonozy-gotictwins.
Thereissomeevidencethattherearecategoriesofobsessive-compulsivefearsandbehavioursthatareassociatedwithparticulartypesofthreat,orthreatdomains.Theseare:aggressivethreatdomain,which concerns fears aboutone’swellbeingand thatof lovedones;physical securitythreat that relates to the immediate home environment and includes checking, symmetry,and ‘just right’ symptoms; environmental cleanliness threat domain which relates to personalhygieneandcleanlinessandincludescontaminationfearsandwashingandcleaningrituals;and,privation threat domain and relates to essential resources and includes hoarding behaviours(Mathews,2009).
Theroleofdisgustinthepsychopathologyofanxietydisorders,andprincipallyinobsessionsandcompulsionsisgraduallybeingexaminedandunderstood.Disgustcanbeconsideredasanadaptivesystemthatevolvedtomotivatedisease-avoidantbehaviours.Itisarguedthatitarosetofacilitatetherecognitionofobjectsandsituationsassociatedwithriskofdiseaseandtodrivehygienicbehaviour.Furthermore,disgustassumedaroleinregulatingsocialbehaviourbyactingtomarkprohibitedanddisapprovedbehavioursasunacceptable. In this regard,disgustcanbeconceptualizedasastrongandvisceralemotionthatcanarousepowerfulaffectiveandbehaviouralresponses.Obsessionsandcompulsionscanbeunderstoodinthisschemaasdisordersofdisgustsystems:patientspresentwithcontaminationfears,sufferfromintrusivethoughtsofcontamina-tion, engage in excessive sanitation and disinfection of self and the environment (for a fullerexplorationanddiscussionoftheplaceofdisgustinpsychopathologyseeCurtis,2011).
ReferencesBeechHR(1974)Obsessional States.London:Methuen.BorkovecTD, Robinson E, PruzinskyT and DePree JA (1983) Preliminary exploration of worry: some
characteristicsandprocesses.Behaviour Research and Therapy21,9–16.Bunyan J (1666) Grace Abounding to the Chief of Sinners: or, a Brief and Faithful Relation of the Exceeding
Mercy of God in Christ, to his Poor Servant John Bunyan (ed. Sharrock R, 1962), p. 13. Oxford: OxfordUniversityPress.
BurtonR(1621)The Anatomy of Melancholy, What It Is. With All the Kinds, Causes, Symptomes, Prognostickes, and Several Cures of it by Democritus Junior.Oxford:Cripps.
Curtis V (2011) Why disgust matters. Philosophical Transactions of the Royal Society of London. Series B: Biological Sciences366,3478–90.
DeSilvaP(1986)Obsessional-compulsiveimagery.Behaviour Research and Therapy24,333–50.DeSilvaP(2003)Thephenomenologyofobsessive-compulsivedisorder.InMenziesRGanddeSilvaP(eds.)
Obsessivecompulsive disorder: theory, research and treatment,pp.20–36.Chichester,JohnWileyandSons.
17—ANxIETy, PANIC, IrrITAbIlITy, PhObIA AND ObSESSION 291
FreireRCandNardiAE(2012)Panicdisorderandtherespiratorysystem:clinicalsubtypeandchallengetests.Revista Brasileira de Psiquiatria34,s1,32–41.
Hamilton M (1959)The assessment of anxiety states by rating. British Journal of Medical Psychology 32,50–5.
HibbertGA(1984)Ideationalcomponentsofanxiety:theiroriginandcontent.British Journal of Psychiatry144,613–24.
LaderMHandMarksIM(1971)Clinical Anxiety.London:Heinemann.LazarusRSandFolkmanS(1984)Stress, Appraisal, and Coping.NewYork:Springer.LewisAJ(1936)Problemsofobsessionalillness.Proceedings of the Royal Society of Medicine29,325–36.MarksIM(1969)Fears and Phobias.London:Heinemann.MarksIM(1970)Theclassificationofphobicdisorders.British Journal of Psychiatry116,377–86.Mathews CA (2009) Phenomenology of obsessive-compulsive disorder. In Antony MA and Stein MB
(eds.)Oxford Handbook of Anxiety and Related Disorders,pp.56–64.Oxford:OxfordUniversityPress.NoyesRandHoehn-SaricR(1998)The Anxiety Disorders.Cambridge:CambridgeUniversityPress.NoyesR,WoodmanC,GarveyMJ,CookBL,SuelzerM,ClancyJandAndersonDJ(1992)Generalized
anxietydisorderversuspanicdisorder.Distinguishingcharacteristicsandpatternsofcomorbidity.Journal of Nervous and Mental Disease180,369–79.
RushB(1798)Onthedifferentspeciesofphobia.The Weekly Magazine of Original Essays, Fugitive Pieces, and Interesting Intelligence, Philadelphia. In Hunter R and McAlpine I (1963) Three Hundred Years of Psychiatry 1535–1860,pp.669–70.London:OxfordUniversityPress.
Schapira K, KerrTA and Roth M (1970) Phobias and affective illness. British Journal of Psychiatry 117,25–32.
Schneider K (1959) Clinical Psychopathology, 5th edn. (transl. Hamilton MW). New York: Grune andStratton.
SelyeH(1956)The Stress of Life.NewYork:McGraw-Hill.SimsACP(1985)Anxietyinhistoricalperspective.British Journal of Clinical Practice Supplement38,4–9.SimsACPandSnaithP(1988)Anxiety in Clinical Practice.Chichester:JohnWiley.SnaithP(1991)Clinical Neurosis,2ndedn.Oxford:OxfordUniversityPress.SnaithRPandTaylorCM(1985)Irritability:definition,assessmentandassociatedfactors.British Journal of
Psychiatry147,127–36.SnaithRP,ConstantopoulosAA,JardineMYandMcGuffinP(1978)Aclinicalscalefortheselfassessment
ofirritability,anxietyanddepression.British Journal of Psychiatry132,164–71.Solyom L, Ledwige B and Solyom C (1986) Delineating social phobia. British Journal of Psychiatry 149,
464–70.SpiegelDAandBarlowDH(2000)Anxietydisorders.InGelderM,Lépez-IborJJandAndreasenNC(eds.)
New Oxford Textbook of Psychiatry.Oxford:OxfordUniversityPress.SwedoSE,RapoportJL,LeonardH,LenaneMandCheslowD(1989)Obsessive-compulsivedisorderin
childrenandadolescents.Archives of General Psychiatry46,335–41.SwinsonRP(1992)Phobicdisorders.Current Opinion in Psychiatry5,238–44.TarrierNandTurpinG(1992)Psychosocialfactors,arousalandschizophrenicrelapse.Thepsychophysiologi-
caldata.British Journal of Psychiatry161,3–11.TyrerP(1982)Anxiety.British Journal of Hospital Medicine27,109–16.WestphalC(1871)DieAgoraphobie:eineneuropathischeErscheinung.Archiv fuer Psychiatrie und Nerven
Krankheiten3,138–61.Wing JK, Cooper JE and Sartorius N (1974) The Measurement and Classification of Psychiatric Symptoms.
Cambridge:CambridgeUniversityPress.YerkesRM,DodsonJD(1908)Therelationofstrengthofstimulustorapidityofhabit-formation.Journal
of Comparative Neurology and Psychology18,459–82.ZigmondASandSnaithRP(1983)TheHospitalAnxietyandDepressionScale.Acta Psychiatrica Scandinavica
67,361–70.

This page intentionally left blank

293
C H A P T E R 18
Disorders of Volition and Execution
SummaryIn this chapter, the experience of contentless non-directional urge; natural instinctual drivedirected towards some target and the volitional act with a consciously conceived goal and anawarenessofhowtoachieveitanditsconsequencesarediscussed.Abnormalitiesofurge,instinct,driveandwillaresomeofthemostcomplex inpsychopathology.Needisastrivingtowardsaparticularobject,stateoractionthatisexperiencedasadesire.Driveisaninclinationtosatisfycertainprimary,thatis, innate,needsandasactivity,theindividual’sbasicmodeofexpression.Instinctisaninnatepatternofbehaviourthatleadstodrivesatisfaction.Willisagoal-directedstrivingorintentionbasedoncognitivelyplannedmotivation.Disturbancesofthesebasicaspectsofbehaviouroccur inbothorganicand‘functional’psychiatricdisordersandaremanifest inavarietyofways,includingimpairmentsofappetites,impulsivity,aggression,motordisordersandgrossbehaviouralabnormalities.
For I know that in me (that is, in my flesh,) dwellethno good thing; for to will is present with me; but how to
perform that which is good I find not.For the good that I would I do not: but the evil which
I would not, that I do.Now if I do that I would not, it is no more I that
do it, but sin that dwelleth in me.I find then a law, that, when I would do good,
evil is present with me…But I see another law in my members, warring againstthe law of my mind, and bringing me into captivity to
the law of sin which is in my members.The Epistle of Paul the Apostle to the Romans (1662)
This is themostunsatisfactorysubjectarea inclinicalpsychopathology.Thedissatisfactionderivespartlyfromthelossofinterestinthesubjectsincetheendofthenineteenthcenturyandthelackofconceptualclaritythathasresultedfromtheimpoverishedliteraturebutalsobecauseoftheinherentcomplexityofthesubject.AsBerrios(1996)putit,‘The“will”nolongerplaysaroleinpsychiatryandpsychology.Ahundredyearsago,however,itwasanimportantdescriptiveandexplanatoryconcept,namingthehuman“power,potencyorfaculty”toinitiateaction’.Thedistinctionsbetweenrelatedbutdistinctconceptssuchasinstinct,urge,impetus,impulse,drive,motivation,will,involuntaryandvoluntarymovementsandresponsibilityhaveuntilveryrecentlyceasedtoberegardedaspropersubjectsofinquiry.Adistinctioncancorrectlybuttheoreticallybedrawnbetweentheinstinctandthusdesiretocarryoutanactioninordertosatisfyaparticularneed,thedriveandmotivationtoeffecttheactionandthewilltoexecutetheaction.Allthesearedifferentfromtheendproduct,theobservableactionorbehaviouritself(Figure18.1).

Keywords: Urge,Will,Drive,Movement,Behaviour.
18—DISOrDErS Of VOlITION AND ExECuTION 293.e1
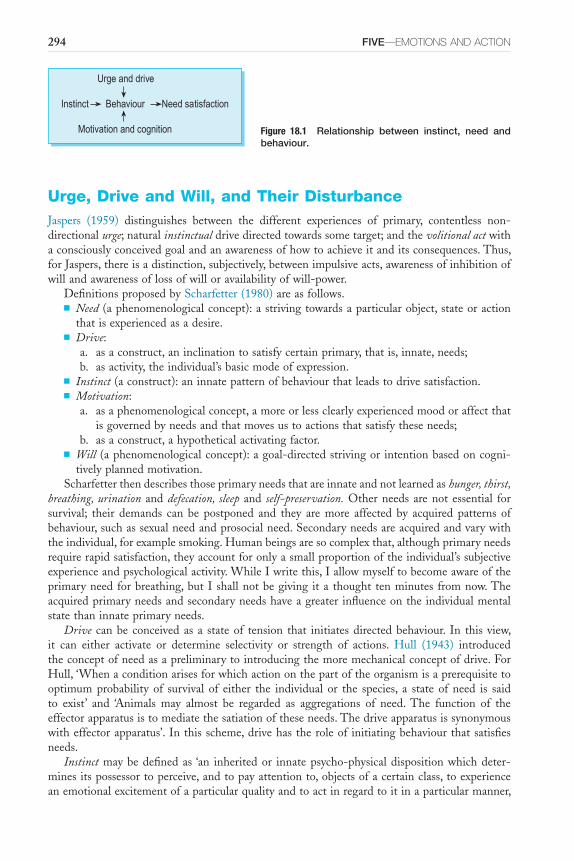
294 FIVE—EMOTIONS AND ACTION
Urge, Drive and Will, and Their DisturbanceJaspers (1959) distinguishes between the different experiences of primary, contentless non-directionalurge;naturalinstinctualdrivedirectedtowardssometarget;andthevolitional actwithaconsciouslyconceivedgoalandanawarenessofhowtoachieveitanditsconsequences.Thus,forJaspers,thereisadistinction,subjectively,betweenimpulsiveacts,awarenessofinhibitionofwillandawarenessoflossofwilloravailabilityofwill-power.
DefinitionsproposedbyScharfetter(1980)areasfollows.■ Need(aphenomenologicalconcept):astrivingtowardsaparticularobject,stateoraction
thatisexperiencedasadesire.■ Drive:
a. asaconstruct,aninclinationtosatisfycertainprimary,thatis,innate,needs;b. asactivity,theindividual’sbasicmodeofexpression.
■ Instinct(aconstruct):aninnatepatternofbehaviourthatleadstodrivesatisfaction.■ Motivation:
a. asaphenomenologicalconcept,amoreorlessclearlyexperiencedmoodoraffectthatisgovernedbyneedsandthatmovesustoactionsthatsatisfytheseneeds;
b. asaconstruct,ahypotheticalactivatingfactor.■ Will (aphenomenologicalconcept):agoal-directedstrivingor intentionbasedoncogni-
tivelyplannedmotivation.Scharfetterthendescribesthoseprimaryneedsthatareinnateandnotlearnedashunger, thirst,
breathing, urination anddefecation, sleep and self-preservation.Otherneedsarenotessential forsurvival; their demands can be postponed and they are more affected by acquired patterns ofbehaviour,suchassexualneedandprosocialneed.Secondaryneedsareacquiredandvarywiththeindividual,forexamplesmoking.Humanbeingsaresocomplexthat,althoughprimaryneedsrequirerapidsatisfaction,theyaccountforonlyasmallproportionoftheindividual’ssubjectiveexperienceandpsychologicalactivity.WhileIwritethis,Iallowmyselftobecomeawareoftheprimaryneedforbreathing,butI shallnotbegiving ita thought tenminutes fromnow.Theacquiredprimaryneedsandsecondaryneedshaveagreaterinfluenceontheindividualmentalstatethaninnateprimaryneeds.
Drive canbe conceivedas a stateof tension that initiatesdirectedbehaviour. In this view,it can either activate or determine selectivity or strength of actions. Hull (1943) introducedtheconceptofneedasapreliminarytointroducingthemoremechanicalconceptofdrive.ForHull,‘Whenaconditionarisesforwhichactiononthepartoftheorganismisaprerequisitetooptimumprobability of survival of either the individual or the species, a state of need is saidto exist’ and ‘Animals may almost be regarded as aggregations of need.The function of theeffectorapparatusistomediatethesatiationoftheseneeds.Thedriveapparatusissynonymouswitheffectorapparatus’.Inthisscheme,drivehastheroleof initiatingbehaviourthatsatisfiesneeds.
Instinctmaybedefinedas ‘an inheritedor innatepsycho-physicaldispositionwhichdeter-minesitspossessortoperceive,andtopayattentionto,objectsofacertainclass,toexperienceanemotionalexcitementofaparticularqualityandtoactinregardtoitinaparticularmanner,
Figure 18.1 Relationship between instinct, need and behaviour.
Urge and drive
Instinct Behaviour Need satisfaction
Motivation and cognition
18—DISOrDErS Of VOlITION AND ExECuTION 295
oratleasttoexperienceanimpulsetoact’(McDougall,1908).ForFreud,instinct‘appearsasaborderlineconcept,beingboththementalrepresentativeofthestimuliemanatingfromwithinandpenetrating to themind, andat the same timeameasureof thedemandmadeupon theenergyofthelatterinconsequenceofitsconnectionwiththebody’(Freud,1915).
Motivation,asaphenomenologicalconcept,isreadilyunderstoodbythelaymanbutisulti-matelytautologous:‘IdoitbecauseIammotivated’,‘Iammotivatedtodoit’.However,itisaconceptthatinpsychiatryandpsychologywecannotdowithout.Ithasbothanemotionalaspectaswellasacognitiveaspect.Inotherwords,itincludesthepleasurablerewardsthatgovernandregulatebehaviouraswellasthereasonsprofferedforbehaviour.Thereare intrinsicaswellasextrinsicmotivatingfactors.Intrinsicfactorsarethosethatareinternaltotheperson,andextrinsicfactors are those, such as supermarket reward cards, that are external incentives to behave inparticularways.Thus,thetermmotivationrefersnotonlytothegoaltowardswhichbehaviouris directed but also to emotional states that set it off as well as those that act to reward thebehaviour.Italsoreferstothereasons,justificationsorexplanationsofanaction.
Similarly,willisanecessaryconceptbutwehavegreatdifficultyincomprehendingit.ThomasReid(1710–1796),founderoftheScottishSchoolofCommonSense,regardedthewillasthepowertoputintoeffectourvoluntaryactions.ForReid(1863),‘allourpowerisdirectedbyourwill,wecanformnoconceptionofpower,properlysocalled,thatisnotunderthedirectionofwill.Andthereforeourexertions,ourdeliberations,ourpurposes,ourpromises,areonlyinthingsthatdependuponourwill.Our advices, exhortations, and commands, areonly in things thatdependuponthewillofthosetowhomtheyareaddressed.Weimputenoguilttoourselves,nortoothers,inthingswherethewillisnotconcerned’.Otherauthoritiesmakesimilarpointsbutemphasizedifferentaspectsofwill:‘Willhasaconsciouslyconceivedgoalandisaccompaniedwithanawarenessofthenecessarymeansandconsequences.Itimpliesdecisionmakingability,intentionandresponsibility’( Jaspers,1959).Hence,theoriesofwillhaveimplicationsfornotionsofmoralresponsibility,forwhatbeinganagententailsandforanydescriptionofguilt,shameandpunishment.
There are more modern attempts to clarify and delineate the phenomenology of will.Metzinger(2006)makesthepointthattheexperientialcontentofwillisfundamentallydifficultto pin down, what he terms ‘thin’ and evasive’ characteristics of the phenomenal content ofwill.Bythis,hemeansthefact that‘will’ lackssensoryconcretenessunlikesayvisionortaste;that the awareness of the process of ‘willing’ something is intermittent and not functionallystable;thatepisodesof‘will’arenottemporallysegmentedandareinherentlyfuzzy;andfinallythattheintendedgoalof‘will’isoftenlessthanclear.Toamplifythesepoints,BayneandLevy(2006)write:
We typically experience our actions as purposive. We do not simply find ourselves walking towards a door and, on the basis of this, form the belief that we must be intending to open it; instead, we experience ourselves as
walking towards the door in order to open it. The sense of goal-directedness can operate at a number of levels. For example, one might experience oneself: walking towards a door in order to open it; opening the door in order to feed the dog; and feeding the dog in order to keep him quiet. The phenomenology
of a single action can include the nested purposes for which the action is being performed.
The range of definitions and understandings of the various terms underlines the intrinsiccomplexityofthesubjectareaandthecurrentabsenceofaunifyingtheoryormodelformakingsenseofthesubject.
296 FIVE—EMOTIONS AND ACTION
Abnormalities of Need, Instinct, Motivation and WillIn termsof the self-descriptionof the subject, anyof the followingphenomenological abnor-malitiesresultinginobserveddisturbanceofvolitionmayoccur.Theremaybeadisturbanceofneed, which may involve hunger, thirst, exploratory behaviour or sleep. An absence of hungercan result in anorexia occurring in chronic physical illness, an increase in hunger causinghyperphagia in Kleine–Levin syndrome and a perversion in pica. Abnormality of thirst cantake the form of increased thirst in lithium-induced polydipsia (diabetes insipidus) or ofcompulsivewaterdrinkinginpsychosis(Singhetal.,1985),whichcanresultinhyponatraemia.Abnormalityofexploratorybehaviourcantaketheformofdiminution,whichismanifestaslackofcuriosityandexplorationoftheenvironment.Thiscanbefoundinschizophreniaanddepres-sion.Exploratorybehaviourcanbeincreasedinmania.Abnormalitiesofsleeparecommonandvaried.Therearedifferentpatternsofinsomnia,includinginitialinsomnia,whichismoreoftenassociatedwithanxiety-baseddisorders,andearlymorningwakening,whichischaracteristicofdepression. Hypersomnia can occur in narcolepsy, Kleine–Levin syndrome and Pickwickiansyndrome.
Abnormality of drive can involve diminution, increase or perversion. Diminution of drivetowardsprimaryneedsoccursinschizophreniaanddepression,andisprobablyindistinguishablefromabnormalitiesofneed.It ismanifestasanabsenceoftheactivatingtensionthatinitiatesbehaviourandisobservableasapathy.Exacerbationofdrivetosatisfysexualneedismostpromi-nent in mania but can occur as part of Kleine–Levin syndrome or indeed following acquiredbrain injury or in L-dopa-induced hypersexuality in Parkinson’s disease. If drive determinesstrengthandselectivityofgoalofbehaviour,thenperversionofdrivewillincludesuchconditionsasfetishism.
Abnormality of motivation may involve diminution or exacerbation. In schizophrenia anddepression,thepleasurableintrinsicmotivationthatactsasincentiveforbehaviourmaybelost.This is most accurately described as anhedonia, the absence of pleasure in relation to usuallypleasurableactivities.Inmania, itmaybe increasedsothatmundaneactivitiesbecomeundulyfascinatingandrewarding.Disorderofmotivationcanalsobeunderstoodasinvolvingtheabnor-malitiesofreasoning,justificationandexplanation,asdescribedinthepsychoanalyticalliterature.Thisisoutsidethescopeofthisbook.
Disturbanceofwillcanbemanifestaslossofvolition.AsJeannerod(2006)putit,disorderofvolitionshouldonlyrefertothosepathologicalconditionsinwhichtheabilitytomakechoices,toexpresspreferences,orpossiblytoexperiencepleasureandfreedominmakingthesechoicesorexpressingthesepreferencesisaffected.Thiscantaketheformofimpairmentofthewilltoactinschizophreniaandseveredepression.Itisdifficulttodistinguishbetweenabsenceofneed,drive,motivationorwill.Theobservableendresultislackofactionintheabsenceofanymotorabnormalityimpairingaction.Otherabnormalitiesofwillincludeindecisivenessindepression,ambivalenceorambitendencyinschizophrenia.Theseabnormalitieshave,attheircore,contrast-ingconceivedgoalswithoscillatingdecisionmakingthatisobservableasindecisionoralternatingandcontrastedmotorbehaviours.Passivityexperiencesarebydefinitionabnormalitiesofvolition(Box18.1).Failureofvolitionasaresultofinabilitytoexperiencepleasure,thatis,asaresultofanhedoniahasbeendiscussedelsewhere(Chapter16).
ORGANIC CAUSES
Biologicaldrives suchas appetite, sleepand thirst are locatedanatomically inandaround themidbrain.Localizeddiseaseinthisarea,ofeitherastructuralorbiochemicalnature,isthereforelikelytoresultindisturbanceofdriveandhencevolition.Hormonal,metabolicandneurophysio-logicalmechanismsaffectvolition.Thus,theneedforfood,expressedinhungerandresultingin

18—DISOrDErS Of VOlITION AND ExECuTION 297
seekingfood,isaffectedbythestateoffullnessofthegastrointestinaltract,bythesecretionofinsulinfromthepancreasandbysensoryinnervationofthegutwall,aswellasbyregulationina putative ‘appetite centre’. Physical illnesses have both a specific and a generalized effectonvolition.
Excessiveappetite(bulimia)mayoccurwithconditionssuchastumouraffectingthehypotha-lamusandresultingrossobesity,obesitymaybeassociatedwithhypoventilationandexcessivesleeping(hypersomnia)inthePickwickiansyndrome(Burwelletal.,1956),periodicsomnolenceandintensehungerwithvoraciousover-eatingoccurintheKleine–Levinsyndrome(Critchley,1962).Excessivethirstandfluidintake(polydipsia)occurwithdiseaseoftheposteriorpituitaryor the kidney (nephrogenic diabetes insipidus, for example, with lithium treatment). Loss ofappetite(anorexia)mayoccurwithlocalizeddiseaseofthemidbrain,resultinginseverecachexia;however,weightlossismuchmorecommonasageneralfeatureofanyseveredebilitatingphysicalillness.
DISTURBANCE OF VOLITION IN SCHIZOPHRENIA
Inschizophrenia,thedisturbanceofvolitionismuchmoreatthelevelofmotivationorwillthanofneed.Theremaybeabnormalityofappetitewithpolyphagiaandconsequentobesity,asoccursinsomechronicschizophrenicpatients;however,thisisnotusual.Patientswithschizophreniawhobelievethattheirfoodisbeingpoisonedmayrefrainfromeatingasaconsequence;thatis,
BOX 18.1 ■ Classification of abnormalities of need, drive, motivation and will
Abnormalities of need
Appetite■ Absenceinanorexia■ Increase,ashyperphagiainKleine–Levinsyndrome■ Perversioninpica
Thirst■ Increaseindiabetesinsipidus,resultinginpolydipsiaand,incompulsivewaterdrinking,resultingin
hyponatraemia
Exploratory Behaviour■ Decreaseinschizophreniaanddepression■ Increaseinmania
Sleep■ Decreaseinanxietyanddepressivedisorders■ IncreaseinhypersomniainKleine–LevinsyndromeandPickwickiansyndrome
Abnormalities of drive■ Decreaseinschizophreniaanddepression■ Increaseinmania■ Perversioninfetishism
Abnormalities of motivation■ Diminution,resultinginanhedoniaindepressionandschizophrenia■ Increaseinmania
Abnormalities of will■ Absenceorloss,resultinginapathyinschizophreniaanddepression■ Oscillatingwill,resultinginindecisiveness,ambivalenceorambitendency■ Anomalouswillinpassivityexperiencesandmadeactions
298 FIVE—EMOTIONS AND ACTION
ofcourse,adeliberateactofwill.Themoreconspicuousdisturbance,however,isloss of volitionthatresultsinwithdrawalfromnormalsocialinteraction,forinstancelackofmotivationtoobtainandcontinueinemploymentordiminishedsexualdriveresultingindecreasedfecundity,espe-ciallyinmaleschizophrenicpatients.
This symptom was described by Bleuler (1911) as disturbance of initiative, according toLehmann(1967). It isalso recognizedamongthesocallednegative symptomsofwhatCrow(1980)hasdesignatedtype2schizophrenia.Thenegative traits –emotionalapathy,slownessofthoughtandmovement,underactivity,lackofdrive,povertyofspeechandsocialwithdrawal–area major barrier to effective rehabilitation in chronic schizophrenic patients (Wing, 1978).Althoughpositivesymptoms, suchasdelusions,hallucinationsandthoughtdisorder,aremoreconspicuous,especiallyintheearlierstagesofaschizophrenicillness,theprognosisisprobablyaffectedtoagreaterextentbythelossofvolition.
Andreasenhasdevelopedaninstrumentformeasuringthenegativesymptomsofschizophre-nia,theScalefortheAssessmentofNegativeSystems(Andreasen1982,1989).Itisveryobviousthatthepatient’squalityoflifeandalsothatofhiscarerisimpairedbytheconsequencesofthesenegativesymptoms,especiallyflatnessofaffectandlossofvolition.Whatisnotsocleariswhetherhehasasubjectiveawarenessofthesesymptomsorwhetherhesuffersasaresultofthem.Seltenetal.(1993)havedevelopedaself-ratingscale,theSubjectiveExperienceofNegativeSymptoms,tomeasurethesubjectiveexperienceofaffectiveflattening,alogia,avolitionandapathy,anhedoniaandasocialityandimpairedattention;thescalelooksatawareness,causalattribution,disruptionanddistress.
DISTURBANCE OF VOLITION IN MOOD DISORDERS
Abnormalitiesofvolitioninaffectiveillnessesareassociatedwithabnormalityofactivity,retarda-tion being prominent in depression and overactivity in mania. In depression, motivation isimpairedratherthanwill.Aseverelydepressedmanagingdirectorcontinuedtoworryabouthisplansforhiscompany,buthefoundhimselfunabletomakehimselfdoanythingaboutit.Lossofmotivationoccursalongsidelossofotheraffect.Anhedonia(seeChapter16)orlossofabilitytoexperienceenjoymentisaprominentsymptomindepressiveillness(Snaith,1993)whichalsooccurs inschizophrenia.Depressedpatientsnormallydescribe lossof interest intheirprevioushobbiesandenjoymentsinlife.Thisanhedoniacanbeconstruedaspartofthelossofmotivationtocarryouttheseactivities.Suchpatientsalsodescribelackofappetiteandlossofallinterestinfood;thismayresultinmarkedlossofweight.
A45-year-oldmalepatient,previouslyhighlysuccessfulasasalesman,developedsevereandpersistentdepressivesymptoms(Sims,1994).Asaresult, twoyearspriortoadmissionhehadlefthisjob,hishome,hiswifeandhistwochildrenanddriftedaroundthecountry,beingadmit-tedforshortperiodsoftimetoseveralpsychiatrichospitals.Hedescribedhissubjectivestate:‘Ifeelveryanxious,uncomfortableanddepressed. It is likehaving the sameperson in the samebodyasme.Itisliketwodifferentpeopleinsideonebody.Onepersonisholdingback–that’slike me.The other person is trying to let go – the other is different, quite strong’. ‘Me’ wasdescribed as ‘frightened, depressed, unsure’, and the ‘other person’ as ‘confident, affable, a greatsalesman’.‘Self ’andhis‘otherself ’arecomparedinFigure18.2.Whenhewashealthy,hewasenergetic,extrovertandabletofunctionwellinapressuredsituation.Whenhebecamedepressed,hewasmiserable,unsureofwhattodo,frightenedandlackinginallenergyforanysortofactiv-ity.Whendepressed,hesaw‘self ’asbeinghisrealidentityand‘otherself ’as‘likeafantasy’.
Inmania,commonlythereisincreasedactivity,asubjectivefeelingofgreaterenergy,effective-nessandself-confidence;suchapersonmayinitiateallsortsofnewprojects.Manicpatientsarepronetodrinktoomuchalcohol,buttheydonotusuallyovereat,perhapsbecausetheyarereadilydistractedandtendtointerrupttheirmealswithothernewenterprises.Suchpeopledescribeit
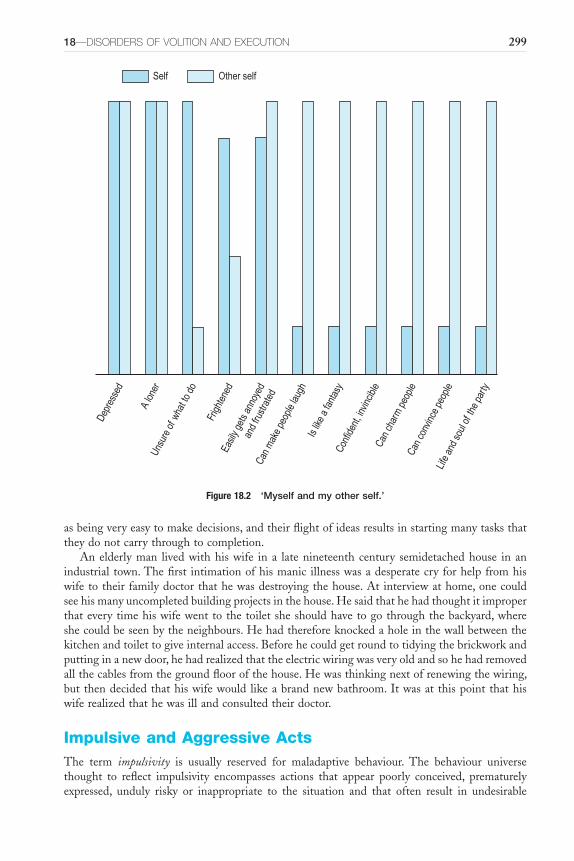
18—DISOrDErS Of VOlITION AND ExECuTION 299
asbeingveryeasytomakedecisions,andtheirflightofideasresultsinstartingmanytasksthattheydonotcarrythroughtocompletion.
Anelderlyman livedwithhiswife ina latenineteenthcentury semidetachedhouse inanindustrialtown.Thefirst intimationofhismanicillnesswasadesperatecryforhelpfromhiswifetotheirfamilydoctorthathewasdestroyingthehouse.Atinterviewathome,onecouldseehismanyuncompletedbuildingprojectsinthehouse.Hesaidthathehadthoughtitimproperthateverytimehiswifewenttothetoiletsheshouldhavetogothroughthebackyard,whereshecouldbeseenbytheneighbours.Hehadthereforeknockedaholeinthewallbetweenthekitchenandtoilettogiveinternalaccess.Beforehecouldgetroundtotidyingthebrickworkandputtinginanewdoor,hehadrealizedthattheelectricwiringwasveryoldandsohehadremovedallthecablesfromthegroundfloorofthehouse.Hewasthinkingnextofrenewingthewiring,butthendecidedthathiswifewould likeabrandnewbathroom.Itwasatthispointthathiswiferealizedthathewasillandconsultedtheirdoctor.
Impulsive and Aggressive ActsThe term impulsivity is usually reserved for maladaptive behaviour. The behaviour universethought to reflect impulsivity encompasses actions that appear poorly conceived, prematurelyexpressed, unduly risky or inappropriate to the situation and that often result in undesirable
Figure 18.2 ‘Myself and my other self.’
Depr
esse
d
A lon
erUn
sure
of w
hat t
o do
Frigh
tene
dEa
sily g
ets a
nnoy
edan
d fru
strat
edCa
n m
ake
peop
le lau
ghIs
like
a fa
ntas
yCo
nfide
nt, in
vincib
leCa
n ch
arm
peo
pleCa
n co
nvinc
e pe
ople
Life
and
soul
of th
e pa
rty
Self Other self
300 FIVE—EMOTIONS AND ACTION
consequences.Whensuchactionshavepositiveoutcomes,theytendnottobeseenassignsofimpulsivitybutas indicatorsofboldness,quickness, spontaneity, courageousnessorunconven-tionality (Daruna and Barnes, 1993). Eysenck (1993) distinguishes between impulsivity andventuresomeness as follows: ‘Our concept of impulsiveness and venturesomeness can best bedescribedbyanalogytoadriverwhosteershiscararoundablindbendonthewrongsideoftheroad.AdriverwhoscoreshighonImpneverconsidersthedangerhemightbeexposinghimselftoandisgenuinelysurprisedwhenanaccidentoccurs.ThedriverwhoscoreshighonVent,ontheotherhand,considersthepositioncarefullyanddecidesconsciouslytotaketherisk.’
Impulsive actsare‘executedforcefullywithnodeliberationorreflection,undertheinfluenceof a compellingpressure that restricts the subject’s freedomofwill.Since reflective controlorconsiderationislacking,theconsequencesofsuchactsarenotthoughtoutortakenintoconsid-eration’ (Scharfetter, 1980). It will be seen that this is not an all-or-nothing phenomenon.Voluntary inhibitions will be present to a varying extent from completely preventing the act,modifyingitordelayingittonotexistingatall,whentheacttakesplaceunrestrained.
Inthepastdecadetherehasbeenincreasinginterestinimpulsivityasaconceptaswellasindefininganumberofimpulsecontroldisorders.Impulsivityisseenasapredispositiontowardsrapid,unplannedreactionstointernalorexternalstimuliandwithoutdueregardtothenegativeconsequencesof theseactions for the impulsive individualor forothers (Moelleretal.,2001).Theessentialelementsarepredisposition,rapidunplannedactionandlackofregardforconse-quences.This suggests that the term isnowbeingused to identifya trait rather than isolatedbehaviour that is associatedwithanepisodeof illness.Thecurrentpsychological literature, inturn,focusesonbehaviouristconceptsthatarederivedfromexperimentalanimalmodels.Theseschemesidentifythefeaturesofimpulsivityas:
1. perseveranceofbehavioursdespitepunishment;2. preferenceforasmallbutimmediaterewardoveradelayedlargerreward;and3. makingprematureresponses,orbeingunabletopreventaresponseinaresponsedisinhibi-
tionattentionalparadigm.Onceagain,theseconceptualizationsofimpulsivitysuggestthatimpulsivityisatrait.Ontheotherhand,theolderpsychiatricliteraturefocusedonimpulsivebehaviouraspartof
episodes of illness: ‘of all the morbid desires, the violent impulse [my emphasis] to muscularactivity, to bodily movement, is particularly to be noticed, as it is seen, especially in states ofmania, as a constantnecessity to restlessmotionhither and thither,beatingabout, screaming,etc.,astatewhichfrequentlyinvolvestheinjuryanddestructionofwhatiswithinreachofthepatient,withouthishavinganydefinitepurposeindoingso’and‘theinvoluntarynatureoftheseacts; the patient often complains that he cannot resist the desire; and further these acts havesomethinginstinctiveinthemannerinwhichtheyshowthemselves;theycomeoninfitswithlucidintervals,theyarefrequentlyaccompaniedbyothersymptomsofderangement’(Griesinger,1845). Bleuler (1911) distinguishes between impulsive acts and compulsive acts: ‘The actionappears tohimassomethingbeyondhisvoluntarycontrol.…Thepatientdoessomethinghedoesnotwanttodo;howeverhedoesnotofferanyresistance.’Thus,inthisview,itisresistancetotheimpulsetoactthatdefinescompulsion.
Disordersofimpulsecontrolincludeimpairmentofcontrolresultingindisinhibitionandcanbe manifest in acquired brain injury, schizophrenia, mania, episodic dyscontrol syndrome andantisocialandemotionallyunstablepersonalitydisorders.Excessivecontrolofimpulsescanresultin inhibited behaviour and lack of spontaneity, present in anxiety-related disorders includingavoidantpersonalitydisorder.
Aggression is defined as ‘a verbal or physical attack on other living creatures or things’(Scharfetter,1980),andaggressivenessasareadinesstobeaggressive.Ingeneralethologicalterms,this is required by animals for survival and by humans to cope with individual conflicts andproblems in their society. However, in a more restricted psychopathological sense, aggression

18—DISOrDErS Of VOlITION AND ExECuTION 301
involvesdeliberateorrecklessdamageanddestructionandisaccompaniedbynegativeemotionssuchasanger,fear,despair,spiteorrage.
ThetwoconceptsofaggressionthatScharfettercontrastsareaninnate driveandanacquired response.TheformertheoryisfollowedbothbyethologistssuchasLorenz(1963)andinclassicalpsychoanalysisinthewritingsofFreudandofAdler(1929);ifaggressionisaninnatedrive,itmustfindsomeformofexpression.Learningtheorywouldsupposethataggressionisanacquiredreactioninresponsetoexternalstimuli,especiallytheexpressionofothers’aggressivebehaviour,anditisreinforcedbythesuccessitachieves.
Examplesofimpulsiveactsfollow.
We had a party. On the way home I was seized by an idea out of the blue – swim across the river in your clothes. It was not so much a compulsion to be reckoned with but simply one, colossal, powerful impulse. I did not think for a
minute but jumped straight in… only when I felt the water did I realize it was most extraordinary conduct and I climbed out again. The whole incident
gave me a lot to think about. For the first time something inexplicable, something quite sporadic and alien, had happened to me.
(Jaspers, 1923)
A 19-year-old was hospitalized for mutism. She sat motionless for prolonged periods, disinterested in her surroundings, although she appeared alert… She
ate and moved slowly but was not stiff. On the second day, suddenly and without warning, she leapt from the chair and grabbed the throat of a
passing therapist, severely damaging the therapist’s thyroid.(Fink and Taylor, 2003)
He complained of headaches, was irritable, and occasionally exploded in a rage with minimal or trivial precipitants. Destruction of property occurred,
including holes punched in walls and furniture broken plus poorly coordinated assaults on family members and some neighbours.
(Benson and Blumer, 1982)
Although impulsivity is often demonstrated by aggression, this is not invariably the case.Gambling,misuseof substances, sexual acts associatedwithdisinhibition and stealing arebutsomeofthebehavioursthatcanoccurimpulsively.
PSYCHOPATHOLOGY OF IMPULSIVE AND AGGRESSIVE BEHAVIOUR
Criminal acts may arise from delusions of one kind and another, from hallucinations of the various senses, from loss of control, which may act in
various different ways; the most difficult point of all to decide upon is the so called impulsive insanity, in which a patient loses self-control, and commits
an act, the details of which he remembers, but which he truthfully says he was unable to prevent. Such insane impulses undoubtedly do occur, and I have
been consulted by patients who have told me that loss of control of this kind would come upon them like a storm, and that they would seek shelter
anywhere to avoid the danger which might arise to themselves or others. It is

302 FIVE—EMOTIONS AND ACTION
simple enough when these impulses occur in persons who have suffered from mental unsoundness, but it is much more difficult when the only evidence of
insanity is the existence of these impulses; for it may be said that they are but the result of uncontrolled pleasure of power, which is common to all. I should
hesitate before accepting impulses, unless I had evidences of insanity in other members of the family, or neuroses such as neuralgia or epilepsy in the
patient himself.(Savage, 1886)
Thereisnothingthatis likelytoresult inreferraltopsychiatricservicesmorequicklythanthepublicexhibitionofinexplicableimpulsiveandaggressiveacts.Also,thereisnothingmorelikely to be labelled as madness by the lay public. In practice, such public behaviour is quitecommonlyassociatedwithmentalillness.Inastudyofmentallydisturbedpeoplecomingtotheattentionofthepolice,therewasatendencyforsuchpeopletocreatetheirdisturbancenearthecity centre rather than at theperiphery.Of the situations resulting in the involvement of thepolice,assaultanddamagewerefrequent,butitwasthebizarrenessofthebehaviourthatmarkedthepersonasbeingmentallyill;forexampleamanwhoprofferedawindscreenwiperasfarefortravellingonabus,orawomanwhopresentedherselfmuteatahostel.Onsubsequentadmissiontohospital,diagnosiswaspredominantlyofpsychotic illness(57percent),withschizophreniaaccountingfor40percent(SimsandSymonds,1975).
Excessiveaggression,andespeciallyunprovoked inappropriateormisdirectedaggression, ismuch more often presented for psychiatric evaluation than a pathological lack of aggressivebehaviour.However,thelattermayalsobeamanifestationofillness.Excessiveaggressionmaybeconsideredbothinrelationtotheunderlyingpsychiatricillnessandaccordingtothespecificnatureofthebehaviour.
DIMINISHED AGGRESSION
Decreasedaggressivenessmayaccompanyreduceddrive;itisseensometimesinorganic,psychoticandpsychogenicdisturbance.It is frequentlyassociatedwithapathy inacuteorganicdisorderssuch as encephalitis, or in progressive dementia, although irritability and fractiousness mayalsooccur.Generalizeddebilitatingphysicalillnessisnormallyaccompaniedbylistlessnessandapathy.
Inschizophrenia,aggressionisusuallymarkedlyreduced,withlackofvolitionandfailuretoinitiate any directed activity; however, unprovoked violence may also occasionally occur. Indepressivepsychosisalso,reducedaggressionismuchthemostcommonpresentation;however,homicide, quite often associated with suicide, is certainly described among severely depressedindividualswithdepressivedelusions.
Aconsistentlylowlevelofaggressivenessmayoccurasapersonalitycharacteristic,forexamplewithdependentdisorderofpersonality.Itmaybeseenaspartofaneuroticreactionorduringadverselifesituations,forinstancewiththegriefofbereavementortheunhappinessoffeelinglonely.Acertaindegreeofaggressionisnecessaryformanyofthesocialactivitiesofnormallife,and its absence impairs functioning. Pathological lack of aggression is closely associated withdisorderofvolition.
Disturbance of Movement and BehaviourBehaviouralandmovementdisturbancesmayhavecrucialdiagnosticsignificance,especiallywhenthereisdifficultywithverbalexplanation.However,astheemphasisofthisbookisonsubjective

18—DISOrDErS Of VOlITION AND ExECuTION 303
description of abnormality, these disorders are discussed only briefly.The distinction betweenmovement and behaviour is arbitrary, as will be shown, especially when schizophrenia isconsidered.
DISTURBANCE OF MOVEMENT
Movementmaybe increasedor speededup, reducedor sloweddown,or itmay showvariousqualitativeabnormalities.Someofthesedisordersofmovementareinvoluntaryandareappro-priatelyregardedasneurological,somearevoluntarybutcarriedoutunconsciouslyandsomearedeliberateactions(ofthewill).Thewordsusedmostlydescribetheobjectivecharacteristicsoftheactiontoanoutsideobserver,notthesubjectiveexperienceoftheactor.
These disorders of movement are now considered briefly, starting with abnormalities ofincreasedmovement–agitation andhyperactivity, anddecreasedmovement– retardation.Themovement disorders of some psychiatric conditions are then described.There are psychiatricsequelaeofprimarymovementdisordersincludingparkinsonism,andoftenthereisdisorderofmovementassociatedwithconditionsthatareprimarilypsychiatric.
Agitation
Agitation implies mental disturbance causing physical restlessness and increased arousal; it isphenomenologically a description of a subjective mood state associated with and resulting inphysical expression.Thepatientmaydescribehis affect as ‘feeling agitated’, andbothhe andtheexternalobserverseemotorrestlessnessasbeinglogicallyconnectedwiththis.Itisdemon-strated in many different mental states; pathologically, it may occur with affective psychoses,with schizophrenia, with organic psychosyndromes such as senile dementia or with neuroticand personality disorders, especially states of anxiety. Agitation is quite often a symptom ofphysicalillness,forexamplehyperthyroidismorhypoparathyroidism.Itisanimportantcompo-nentof some statesof severedepressive illness.Although retardation ismore commonly seenwith‘endogenousdepression’ormelancholia,agitationmayoccur,eitherwithoutretardationinalternating phase with retardation, or concurrently with retardation in a mixed affective state. Agitated depressionisanoldtermforonevariantofaseveredepressiveepisodewithorwithoutpsychoticcomponent.Itisalternativelyknownasmelancholia.Thepracticalclinicalimportanceofthismoodstateensuesfromthefactthat,whereassuicidalimpulsesmaybepreventedfromexpression by retardation, agitation with restlessness may render such behaviour more likely.An early response to treatment following electroconvulsive treatment or effective antidepres-sant medicationmayresult in thepatientbecoming less retardedandthereforeatgreater riskofsuicide.
Hyperactivity
Thisdescribesthestateinwhichthereisincreasedmotoractivity,possiblywithaggressiveness,over-talkativenessoruncoordinatedphysicalactivity.Thetermisdescriptiveofbehaviourratherthanofasubjectivepsychologicalstate.Restlessnessispoorlydefinedinthepsychiatricliteratureandhasdiverseandmultitudinouscauses (SachdevandKruk,1996).Restlesshyperactivityorhyperkinesismayoccurwithavarietyofdifferentphysicalassaultsonthebrainbutisespeciallyprominentasasequeltoheadinjuryinchildren,inwhomitmaybeassociatedwithimpulsivedisobedienceandexplosiveoutburstsofangerandirritability(Blacketal.,1969);itisalsoassoci-atedwithchildhoodepilepsywhenthereisbraindamage.
Overrecentyears,theconditionofattentiondeficit/hyperactivitydisorder,previouslydescribedasoccurringonlyinchildren,hasbeendiagnosedinadults;thechildhooddisorderdoessome-timespersistintoadultlife,buttheprevalenceofthedisorderinadulthoodislowcomparedwiththatinchildhood(Sachdev,1999).Thereisapatternofpersistentinattentioninallareasoflife,

304 FIVE—EMOTIONS AND ACTION
overactivity with fidgeting and restlessness and impulsivity with impatience and difficulty indelayingresponses.Thesepsychologicalcharacteristicsresultindisturbedbehaviourinallareasoflife.Inadultlife,therearepersistentdifficultiesinrelationships,usuallyapoorworkrecordandsometimesalsoacriminalrecord.Theindividualisparticularlydistractibleandpronetobedisruptiveinagroupsetting.
Considerablecomorbidityinchildrenoccurswithconductdisorder,oppositionaldeficitdis-order,moodandanxietydisordersandmentalretardation(Biedermanetal.,1991).Between30and70percentofchildrenwhoarediagnosedashavingADHDwillcontinuetoshowsymptomsof the condition as adults (Bellak and Black, 1992). In a study of adults with ADHD, bothgendershadthemanifestationsoftheconditionbutfemales,whounlikethesituationinchild-hoodwereinthemajority,hadhigherratesofdepression,anxietydisordersandconductdisorderthannormalcontrolsubjects(Biedermanetal.,1994).Thisisclearlyaconditiontowhichthosepractisingingeneraladultpsychiatrywillhavetopaymoreattentioninfuture,anditisworthyofmoredetailedpsychopathologicalstudy.
Retardation
Retardationhastwoquitedifferentmeaningsinpsychiatry.Motor retardation,thesenseinwhichitisusedhere,impliesslownessoftheinitiation,executionandcompletionofphysicalactivity;it is frequentlyassociatedwithretardationof thought, forexample inseveredepressive illness.Thepatientsubjectivelydescribeshimselfashavingdifficultywiththinking–‘mythoughtsareslowedup’–andalsowithinitiatingandcarryingoutspontaneousactivity.Mental retardationisasynonymformentalhandicap,mentalsubnormalityorlearningdisability.Itisanunfortunatetermas,althoughthere is intellectualdeficit, theremaybenophysical slowness; in fact, theremaybeoveractivity,especially ifthereiscoexistingbraindamage.Also,thesufferer isunlikelytocomplain,subjectively,ofslownessinthethinkingprocess.
Retardationissoprominentasymptomofthesevereendogenoustypeofdepressionthatinthepastitwasusedtonamethecondition,retarded depression.Thereisrestrictedmovement,astatic posture of dejection and decrease of muscular tone. Gesticulation is reduced, as is theemotionalcomponentoffacialexpression.
Retardationwithslownessofmotoractivityisalsoseenwithothercausesofmentalslowness,as invariousorganicpsychosyndromesandwithphysical illnesses.Theextremeof retardation–novoluntarymovementatall–isknownasakinesisandoccurswithmutenessinstupor.
Disorder of Movement in Schizophrenia
For the sake of convenience, three types of abnormality may be recognized in schizophrenia:isolatedabnormalitiesofmovementandposture,whicharenowdiscussed;morecomplexpatternsofdisorderedbehaviour,describedlaterinthechapter;andthepresumedeffectsonmovementoftheantipsychoticdrugs,whichareoftenusedinlargedosagesandforalongtimeinschizo-phrenia.Extrapyramidalsideeffectsaredescribedlaterinthischapter,butbriefmentionshouldbemadeoftheneuroleptic malignant syndrome,withrapidonsetofseveregeneralizedmuscularhypertonicitywithhyperpyrexiaandakineticmutismandautonomicdisturbance;deathoccursinabout15percentofsufferers(Kellam,1987).Someoftheoddmotordisordersthatoccuraredescribedfirst,andthenthedisturbancesofchronicschizophreniaarementioned.
Isolated Disorders of Movement and Posture
Catatoniameansastateofincreasedtoneinmusclesatrest,abolishedbyvoluntaryactivitiesandthereby distinguished from extrapyramidal rigidity. The syndrome catatonic schizophrenia wasoriginally described by Kahlbaum (1873) and is characterized by the presence of the motordisordersdescribedbelow.InreviewingKahlbaum’sconcept,Johnson(1993)considerscatatonia,the ‘tension insanity’, to be a neuropsychiatric syndrome caused by a large variety of organic

18—DISOrDErS Of VOlITION AND ExECuTION 305
diseaseprocessesmanifestingascatalepsywithanabnormalmentalstate.It isverydifficulttoclassify the precise nature of the odd and abnormal posture in catatonic schizophrenia. Waxy flexibility(flexibilitascerea)andpsychological pillowoccurbutarebothrareconditions.Inwaxyflexibility,whenthelimbsofthepatientareputintoanyposturebytheinterviewertheywillberetainedinthatpositionforasustainedperiod(aminuteormore).Psychologicalpillow,whenthesupinepatient’sheadismaintainedafewinchesabovethebed,maycontinueforhours.Instereotypy,abizarreuncomfortable-lookingposturealsomayberetainedforsomehours.
Theveryvariedsymptomsofcatatoniaalwaysinvolvemotoractivityandposture.Theremaybehyper-orhypoactivity,mutism,stereotypicalposturingandmovement,waxyflexibility,stuporand uncontrollable excitement (Fink, 1993). Some variants of catatonia are lethal (pernicious) catatonia,withhighfever,rigidityandextremehyperactivityand/orstupor;neuroleptic malignant syndrome,withrigidity,fever,autonomicinstabilityandstupor,associatedwiththeuseofanti-psychoticdrugs;periodic catatonia,characterizedbyperiodsofexcitementfollowedbycatatonicstupor;manic excitement,withconfusion;andstuporinthecontextofdelirium.Itisnowrecog-nizedthatcatatonicmovementdisturbanceispresentindisordersotherthanschizophreniaandhasbeenmostrecentlyidentifiedinanti-NMDARencephalitisandinself-injuriousbehavioursinautisticspectrumdisorderinchildhood(Fink,2013).
Thereare two typesofabnormalmovement in schizophrenia: idiosyncratic voluntary move-ments or mannerisms and spontaneous involuntary movements. Mannerisms are shown in odd,stilted,voluntarymovementsandpatternsofbehaviour.Thepatientmayclaimtobeunawareoftheseactsorexplainthemintermsofhisdelusions.
Itissometimesdifficulttodistinguishmannerismsfromthepurposelessmovementsorpos-turesthatarenotgoal-directedbutarecarriedoutinanunvaryingwayinanyindividualpatient.Itisimportanttoattempttodistinguisheitherofthesetypesofmovementfromtheabnormalmovements of parkinsonian syndromes, which occur quite frequently in schizophrenic patientstreated with typical (first generation) antipsychotic drugs. Grimacing is a common feature inschizophrenia; Schnauzkrampf (literally ‘snout spasm’) is a characteristic facial expression inwhichthenoseandlipsaredrawntogetherinapout.
Abnormality of the execution of movement may result from the internal experiences of theschizophrenicpatient.Attimes,heresistsstimuli,forexampletheinterviewer’srequesttoraisehis right arm, and shows negativism. At other times, he demonstrates excessive complianceamounting toautomatic obedience:notonlydoeshe raisehis rightarmbuthe raises theotherarmandthenstandsupwithbotharmsraisedindramaticresponsetotherequest.Thisalter-nation of cooperation and opposition produces the diffident, unpredictable behaviour ofambitendency.
Obstructionistheequivalentintheflowofactiontothoughtblockingintheflowofspeech.Whilecarryingoutamotoract,thepatientstopsstillinhistracks.Afterapause,hecontinueswiththeactorhemayproceedtodosomethingelse.Usually,hecannotaccountforhisobstruc-tionbutmaydosointermsofpassivity:‘myactionwasstopped’.
Abnormalmovementsmanifestedintheinteractionwiththeinterviewermayrevealexcessivecooperationoropposition.Mitgehen, echopraxia, automatic obedienceandadvertencearesymptomsofexcessivecooperation.InMitgehen(literally,German,‘togowith’),theinterviewercanmovethepatient’s limbsorbodybydirectinghimwithfingertippressure, ‘as ifonewasmovingananglepoiselamp’accordingtoHamilton(1984).Whenthepatientimitatestheinterviewer’severyaction, the symptom is called echopraxia; this occurs despite the doctor asking him not to.Automatic obedience denotes a condition in which the patient carries out every command in aliteral,concretefashion,likeanautomaton.Todemonstratethesesymptomsofexcessivecoopera-tion,thepatientshouldbeaskedtoresisttheinterviewer.Mitgehenandechopraxiastilloccur.This inability to accede to instructions to resist occurs with forced grasping. The interviewerpresentshishandtobeshakenbutatthesametimeasksthepatientnottoshakeit;everytime
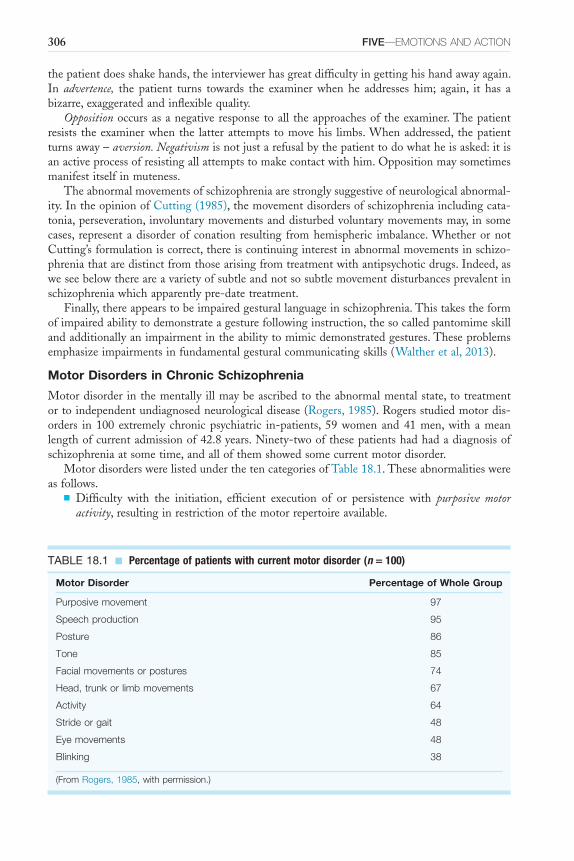
306 FIVE—EMOTIONS AND ACTION
thepatientdoesshakehands,theinterviewerhasgreatdifficultyingettinghishandawayagain.In advertence, the patient turns towards the examiner when he addresses him; again, it has abizarre,exaggeratedandinflexiblequality.
Oppositionoccursasanegativeresponsetoall theapproachesof theexaminer.Thepatientresists theexaminerwhenthe latterattempts tomovehis limbs.Whenaddressed, thepatientturnsaway–aversion. Negativismisnotjustarefusalbythepatienttodowhatheisasked:itisanactiveprocessofresistingallattemptstomakecontactwithhim.Oppositionmaysometimesmanifestitselfinmuteness.
Theabnormalmovementsofschizophreniaarestronglysuggestiveofneurologicalabnormal-ity.IntheopinionofCutting(1985),themovementdisordersofschizophreniaincludingcata-tonia,perseveration, involuntarymovementsanddisturbedvoluntarymovementsmay, insomecases, represent adisorderof conation resulting fromhemispheric imbalance.WhetherornotCutting’sformulationiscorrect,thereiscontinuinginterestinabnormalmovementsinschizo-phreniathataredistinctfromthosearisingfromtreatmentwithantipsychoticdrugs.Indeed,asweseebelowthereareavarietyofsubtleandnotsosubtlemovementdisturbancesprevalentinschizophreniawhichapparentlypre-datetreatment.
Finally,thereappearstobeimpairedgesturallanguageinschizophrenia.Thistakestheformofimpairedabilitytodemonstrateagesturefollowinginstruction,thesocalledpantomimeskillandadditionallyanimpairmentintheabilitytomimicdemonstratedgestures.Theseproblemsemphasizeimpairmentsinfundamentalgesturalcommunicatingskills(Waltheretal,2013).
Motor Disorders in Chronic Schizophrenia
Motordisorderinthementally illmaybeascribedtotheabnormalmentalstate,totreatmentortoindependentundiagnosedneurologicaldisease(Rogers,1985).Rogersstudiedmotordis-orders in 100 extremely chronic psychiatric in-patients, 59women and41men,with ameanlengthofcurrentadmissionof42.8years.Ninety-twoofthesepatientshadhadadiagnosisofschizophreniaatsometime,andallofthemshowedsomecurrentmotordisorder.
MotordisorderswerelistedunderthetencategoriesofTable18.1.Theseabnormalitieswereasfollows.
■ Difficulty with the initiation, efficient execution of or persistence with purposive motor activity,resultinginrestrictionofthemotorrepertoireavailable.
TABLE 18.1 ■ Percentage of patients with current motor disorder (n = 100)
Motor Disorder Percentage of Whole Group
Purposive movement 97
Speech production 95
Posture 86
Tone 85
Facial movements or postures 74
Head, trunk or limb movements 67
Activity 64
Stride or gait 48
Eye movements 48
Blinking 38
(From Rogers, 1985, with permission.)
18—DISOrDErS Of VOlITION AND ExECuTION 307
■ Speech production,with22patientsusuallymute;25neverinitiatingspontaneousconversa-tion;53showing‘outbursts’of shouting, singingor talking;and51 inarticulateorbarelyaudibleatinterview.
■ Postureand■ tone,with a tendency toflexionassociatedwithvaryingdegreesof rigidity and typically
affectingtheheadorneck.■ Abnormal movementorposturesoforofacial muscles,withrapidorslowcontractionsofdif-
ferentmusclegroups.■ Abnormalmovementsof thehead, trunkor limbs,whichmightbebrief, jerkyandsemi-
purposiveinquality.■ Abnormal activitymightoccurinoutburstsorcontinuouslywithbehaviour,suchashitting
outatothers,stamping,touchingorfollowingotherpeople.■ Strideorgaitmightshowshuffling,slowness,notswingingthearms,orturningwithhead
andneck‘inonepiece’.■ Conjugatedeviationof theeyes,oftenupand laterallywithdeviationof thehead in the
samedirection.■ Blinkingmarkedlyincreasedordecreasedinrate,sometimesin‘bursts’.Ninety-eight of these100patientshadhadmotordisorder recordedprior to1955, before
therewasanytreatmentwithneurolepticdrugs.Therewasconsiderablevariabilitybetweenthetypeofmotordisorderrecordedbefore1955andobservedcurrently.Disorderofeyemovements,tone, gait and blinking were recorded less commonly in the past. Movement disorder in thisgroupofpatientswascomparedbetweenthosecurrentlyreceivingneurolepticdrugs;thosenottreatedforonemonth,oneyearorfiveyears;andthoseneverhavingreceivedmedication.Withthepossibleexceptionoffacialmovements,whichweremorefrequentinthosehavingreceivedtreatment in the past year, there was no difference in the frequency of abnormal movements.In addition to the description of abnormal movements above, overflow movements havebeendescribed.Thesearedefinedasinvoluntarymovementsthattendtoaccompanyvoluntarymovementsandarerecognizedasneurologicalsoftsignsandarethoughttobecharacteristicofschizophrenia(D’Agatietal,2012).
Motor Disorder in Brain Disease
The disturbance of basal ganglia resulting in parkinsonian symptoms has two main causes ofrelevancetopsychiatry:Parkinson’sdiseaseandsymptomssecondarytoexposuretopsychotropicdrugs.Someofthemotorsymptomsaresimilarinthesetwoconditions,buttheoverallclinicalpicturediffers.
Parkinson’s Disease. InParkinson’sdisease,aswellasmotorsymptoms,thereareoftensensory,autonomic and psychiatric abnormalities. Parkinson’s original description in 1817 implied anabsenceofperceptual(asopposedtosensory)abnormalityanddoesnotcommenton‘psychiatricstatus’,whichwouldthenhavebeenanunknownconcept.
Primaryorsecondarysensoryabnormalitiesmayoccur,andtheremaybeautonomicunder-or overactivity. However, the most conspicuous symptoms are in motor function: slowing ofemotional and voluntary movement (Walton, 1985); muscular rigidity; akinesia; tremor; anddisordersofgait,speechandposture.Thereisnotnecessarilyanymentalchange;however,depres-sion is very common (Mindham, 1970), intellectual deterioration may occur and personalitydisorderissometimesassociated.Psychoticepisodeshavealsobeendescribed.Agraphicdescrip-tion of the symptoms and subjective experience of parkinsonism is given in Sacks’ account,Awakenings(1973).
Extrapyramidal Side Effects of Antipsychotic Drugs. TheextrapyramidalmovementdisordersproducedbyantipsychoticdrugsaredescribedindetailbyMarsdenetal.(1986).Theseinclude
308 FIVE—EMOTIONS AND ACTION
drug-induced parkinsonism with the classic parkinsonian triad of muscle rigidity, tremor andakinesia,andalsosuchsymptomsasabnormalitiesofgait,speech,andposture;excessivesaliva-tion; difficulty with swallowing; the characteristic facies; and greasy skin. Akinesia varies frombeingmild indegree(dyskinesia),withan immobile,blank,expressionless face; limitedmove-mentswithlossofsuchassociatedmotoractivityasthearmsswingingwhenwalking;andlackofspontaneity;tomoresevereandgeneralizedabsenceofmovement–thismaystartsoonafterbeginningantipsychoticmedication.Cogwheelrigidityand‘pillrolling’ofthefingers,tremorofthehandsorperiorbital tremormayoccurbutare lesscommonthanakinesia.ExtrapyramidalsideeffectsofantipsychoticdrugsarelistedinBox18.2(fromGervinandBarnes,2000).
Akathisia, motor restlessness, occurs frequently. There is a subjective experience of motorunease,withafeelingofbeingunabletositstill,aneedtogetupandmoveaboutandtostretchthe legs, tap the feet, rock thebody (Box18.3).Akathisiamayoccurat the same timeas theakinesiaofdrug-inducedparkinsonismandpresentsthecontrastingstateofasubjectiveurgetomoveandphysicalimpairmentofmovement.Inordertodistinguishakathisiafromothercausesofinnerrestlessness,restlessnessofthelegsshouldbefoundtobeespeciallyprominent.
Acute dystonic reactions include a variety of intermittent or sustained muscular spasms andabnormalpostures.Dystoniahasbeendefined as ‘a syndromedominatedby sustainedmusclecontractions,frequentlycausingtwistingandrepetitivemovements,orabnormalpostures’(Fahnetal.,1987).Theremaybeprotrusionofthetongue,grimacing,oculogyriccrises,blepharospasm,
BOX 18.2 ■ Extrapyramidal side effects of antipsychotic drugs
Acute movement disorders■ Parkinsonism■ Acuteakathisia■ Acutedystonia
Chronic movement disorders■ Tardivedystonia■ Chronicakathisia■ Tardivedyskinesia
(FromGervinandBarnes,2000,withpermission.)
BOX 18.3 ■ Subjective components of akathisia
Commonly experienced■ Senseofinnerrestlessness■ Mentalunease■ Unrestordysphoria■ Feelingunabletokeepstill■ Anirresistibleurgetomovethelegs■ Mountinginnertensionwhenrequiredtostandstill
Less commonly experienced■ Tensionanddiscomfortinthelimbs■ Paraesthesiaeandunpleasantpullingordrawingsensationsinthemusclesofthelegs
(FromGervinandBarnes,2000,withpermission.)
18—DISOrDErS Of VOlITION AND ExECuTION 309
torticollis,opisthotonusandotherhyperkineticexaggeratedactionsof the face,head, trunkorlimbs.Owens(1990)hasconsideredthemajorclinicaltypesofdystoniatobeacutedystonias,oculogyricspasms,focaldystoniasincludingtorticollis,blepharospasm,writer’scrampandotheroccupationaldystonias,andlaryngopharyngealdystonia,segmentaldystonias,generalizeddysto-nia,drug-related(symptomatic)dystoniasandpsychogenicdystonia.
Thefrequencyofassociationofsocalledtardivedyskinesia,inwhichrepetitive,purposelessmovementsofthefacialmuscles,mouthandtongueoccur(sometimeswithchoreoathetoticlimbmovementandrespiratorygrunting)withexposuretopsychotropicdrugs isdisputed.There isnodoubtthatfaciobuccolinguomasticatorydyskinesiaoccursinmanychronic,especiallyelderly,psychoticpatientsonneurolepticmedication,butisitcausallyconnectedwithdrugs?Thewordtardive is used, as the syndrome was considered to be a late consequence of drug treatment;however, there are casesdescribed inpatientswhohavenever receivedneurolepticdrugs, andthepreciserelationshipremains tobeelucidated– itmaybesimplya latestageof the illness.In practice, the extrapyramidal symptoms secondary to medication are difficult to evaluateand measure by severity – problematic in accounting for aetiologically but important in thesatisfactorytreatmentofthepatient.Atathreeyearfollow-upofpsychiatricpatientsreceivingantipsychoticmedication,orofacialdyskinesiaincreasedfrom39percentto47percentofthesample,withafewindividualsdevelopingthedisorderanewandafewremitting(Barnesetal.,1983).Therewasanassociationbetweendyskinesiaandageover50yearsandthepresenceofakathisia,butnonewiththeuseofantipsychoticdrugs;infact,thoseonhighdosagewereunlikelytohavethecondition.ThesedyskinesicsymptomsalsooccurinHuntington’schoreaandinsenilechorea.
Huntington’s Chorea
This isahereditarycondition, inheritedasaMendeliandominant,whichmanifestsusually inearly middle life and is characterized by choreiform movements and dementia. Jerky, rapid,involuntarymovementsstart inthefaceandupperlimbs.Dysarthriaanddisordersofgaitcanalso occur before intellectual impairment develops. The progressive dementia, with inertiaand apathy, may be accompanied by irritability and occasional outbursts of excited behaviour.Occasionally,thedementiaoccursasthefirstsignoftheillness.
Variouspsychologicalabnormalitieshavebeendescribedintheprodromalstagebeforemani-festationofchoreaanddementia.Thesemaybeanxiety,reactivedepressionandthefeaturesofpersonality disorder, especially antisocial behaviour. It is not known if this is truly an earlysymptomof the illness or part of thepsychosocial reaction to this appalling anddoom-ladencondition.
Tics and Gilles De La Tourette’s Syndrome
Ticsarerapid,repetitive,coordinatedandstereotypedmovements,mostofwhichcanbemim-icked,andareusually reproduced faithfullyby the individual (Macleod,1987). InGillesde laTourette’s syndrome,multiple ticsareaccompaniedby forcedvocalizations thatoften take theformofobscenewordsorphrases–coprolalia(Lishman,1997).Theconditionstartsinchildhood,under the age of 16; there are multiple motor tics and unprovoked loud utterances that mayamounttoshoutedobscenities.
Theconditionismorecommoninboysthaningirlsandusuallystartsbetweentheagesoffiveandeightwithsimpletics.Thevocalizationsusuallybeginasunrecognizablesoundsbutmayprogressto‘four-letter’swearwords.Bothticsandutterancesarelikelytooccurwithemotionalstress.Thesubjectoftentriesdesperatelyhardnottovocalizetheword,andthismaybeaccom-panied by considerable anxiety. An interesting study compared adult sufferers with depressedadults and normal controls on measures of obsessionality, depression and anxiety (Robertsonetal.,1993).GillesdelaTourette’ssyndromesufferersscoredashighasdepressivesonmeasures

310 FIVE—EMOTIONS AND ACTION
ofobsessionalitybutwereintermediatebetweenthemandnormalsubjectsforbothdepressionandanxiety.
DISTURBANCE OF BEHAVIOUR
There is no clear demarcation between disturbance of movement and of behaviour, and thedistinctionmadehereisarbitrary.Thuswithparkinsonism,andtoanevengreaterextentcatatonicschizophrenia,an individualabnormalmovementmaybeelaborated intoanabnormalpatternofbehaviour.
Behavioural Disorders of Schizophrenia
Disorderofmovementischaracteristicofcatatonia,inwhichthepatientmaybecomeimmobi-lizedinoneattitudebecauseofincreasedmuscletoneatrest;itisusuallyseeninschizophreniabuthasbeendescribedwithfrontallobetumourandsomeotherorganicconditions.Thereareabnormalitiesofpostureandofmovement,frequentlyshownintheactionsmadeinrelationtoanotherperson–theinterviewer.Thus,inwaxy flexibilitythepostureofthelimbsissodescribedbecauseitismaintainedindefinitelyafterbeingmanipulatedintothatattitudebytheobserver.Behaviour,thecompositeofmovements,mayalsobeabnormal,andthisischaracteristicofcata-tonic schizophrenia,withmore than justone isolatedabnormalityofposture. Ithasoftenbeencommented that the incidence of catatonic schizophrenia has markedly declined. However,Mahendra(1981)hasqueriedtheexistenceofcatatonicschizophreniaasaconditionwithclassicKraepelinianschizophrenicfeaturesandcatatoniainthesamepatient.Hebelievesmanyofthepatients with catatonia suffered from neurological disease, perhaps postencephalitis, followingepidemicandendemicviralinfections.Ifthiswereso,thepresumedassociationbetweenschizo-phreniaandcatatoniawasaccidental.
Onecouldmakeavastcatalogueofthebizarre,andsometimesunpleasant,behaviourdem-onstratedbypatientswith chronic schizophrenia,but thiswouldneverbe exhaustive.Certaintypesofbehaviourpatternaredescribedherewithexamples.Schizophrenicstuporoccurs,althoughrarely.Thepatientismuteandakinetic,althoughfromthealertnessoftheeyesandtheoccasionalexcursion into abrupt activity or speech he is clearly conscious. It can be distinguished fromdepressiveormanicstuporbytheobviousabnormalitiesofmoodinthestuporoftheaffectivepsychoses.Apatientwithschizophreniasatmuteandmotionlesswithherarmsheldinstereo-typed, twistedposture forhoursata time.This symptomisalmostneverseennowadayswithadequatetreatmentofschizophrenicsymptoms.
Negativism, as described above under motor disorders, may influence the behaviour of thepatientsubstantially.Aschizophrenicpatientwasinterviewedinprison.Hewasbroughttothedoorofthedoctor’sexaminationroom.Whenthedoctorinvitedhimtoenter,hetooktwostepsbackwards.Togethimtoenter,thedoctorhadtoaskhimtogoaway.Whenthedoctorputhishandouttoshakehands,thepatientputhishandbehindhisbackandreversedbehindthedesk.Hewouldnotsitdownuntilhewaspolitelyaskedtoremainstanding.
Excitementmayoccurassociatedwithcatatoniabutcanalsobeseenwithoutthisstate;some-times,apatient ismuteandmotionless fora timeand thenunpredictablybecomesoveractiveandaimlesslydestructive.Achronicschizophrenicpatient,normallycalm,wouldsuddenlyandunaccountablyrushheadlongacrossthewardandchargeheadfirstintothewall.Onoccasionthisbehaviourwasdirectedatawindow,andhehadcuthimselfseverelyontheglassinthepast.
Impulsive behaviour may not always be manifested as excitement; it may be carried out incontradistinctiontothepatient’shabitualbehaviour.Anormallyrespectableandtranquilelderlyfemale patient would suddenly and unpredictably make sexual assaults on unsuspecting malevisitorstothehospital.
18—DISOrDErS Of VOlITION AND ExECuTION 311
Hoarding is a common feature in chronic schizophrenics and is not confined to those ininstitutions.Apatientusedtoputinsectsandpiecesofrubbishfoundaroundthehospital,suchascigaretteendsandsmallpiecesofstring,intoasmalltin.Shedidnotappeartouseherassort-mentbutwasconstantlycollectingmoreitems.
Water intoxicationduetogrosslyexcessivewaterdrinkinghasbeendescribedinschizophrenia,althoughitmayoccur,butmuchlesscommonly,inalmostanypsychiatricdisorder(Ferrier,1985).The symptom ispotentiallydangerous (Singhet al.,1985)andcaneven result indeath fromhyponatraemia,oftenassociatedwithconvulsions.Thewaterdrinkingmaybeexplainedbythepatientintermsofdelusions,ortheremaybeafailureofthenormalthirst-fluidintakehomeo-staticmechanism,orboth.
Theremaybe mannerisms and idiosyncrasies of behaviour aswell as of singlemovements.One totallymutemale chronicpatientused to retire to the topof a remote staircase above award,whereheingeniouslyanddelicatelycutkeysthatwouldopenanydoorinthehospital.Hewouldexchangetheseforcigaretteswithotherpatients,despiteremainingutterlysilent.
Grossself-neglecthasbeendescribed,especiallyamongelderlyreclusiveswhohavesometimesbeenwelleducated,intelligentandwealthy.Thissyndromehas,ratherunfortunately,beencalledtheDiogenessyndromeaftertheGreekphilosopherwhorejectedsocialnormsandworldlyluxu-ries(Clarketal.,1975).AnearlycasewasdescribedbyDanielHackTuke(1874)ofaricholdman,‘madLucas’,whodiedinafilthystate,half-nakedandaloneinhisdecayingmansion.Heremainedasahermitfor25years,continuallyterrifiedthathisyoungerbrotherwouldseizehishouseandkillhim.Heandsimilarreclusesusuallysufferfromaparanoidschizophrenicillness,althoughthetermDiogenessyndromeitselfispurelydescriptive(Aquilina,1992).
Multitudinousotherformsofabnormalbehaviouraremanifestedinschizophrenia.Flagrantstealingoccurs,sometimeswithamanneristicflavour,suchasthehospitalin-patientwho‘stole’bedsprings, much to the discomfort of the occupants. Unprovoked aggression and ‘nastiness’sometimes occur. Patients may exhibit childish naughtiness or grotesque dirtiness, and self-immolationandsuicidehaveoccasionallyoccurred.Thismaytakeplaceinobediencetoauditoryhallucinationsoraspartofadelusion.Onepatientregularlyheardavoicethatinstructedhimtojumpoutofthewindow;hewaspreventedonmanyoccasionsbutfinallytookthereinforcedwindowframeswithhiminleapingtohisdeath.
Behavioural Signs of Emotional Disturbance
Psychiatristshave learnedthattheymust listen totheirpatients; it isalso importanttoobservethem and form useful, testable hypotheses from these observations. Internal medicine has,traditionally,madegreatdiagnosticuseofphysicalsigns,andpsychiatryalsowoulddowell touse behavioural signs as possible indicators, not positive proof, of psychological disturbance.Trethowan (1977) has noted, in addition to the evidence for catatonia and parkinsonism, thefollowingbehavioural,asopposedtoneurological,signs,whichmaybeofvaluediagnosticallyinpsychiatry.
■ The handshakemaybelimpandlifeless,asintheasthenicadolescentorsuffererfromsimpleschizophrenia,orvice-likeinmania.Thehandoftheschizophrenicpatientwithnegativismmaybewithdrawnwhentheintervieweroffershis,orthemanicorpersonalitydisorderedpatientmayinsistonshakinghands,contrarytothedoctor’sintention.
■ Other forms of hand behaviourthatmaybesignificantincludebittenorpickednails,clenchedhandswithblanchedknucklesandrestlessfidgetingwiththefingers;allthesemayindicateacuteorchronicanxiety.Heavilycigarette-stainedfingersobviouslyreflectthelargenumberofcigarettessmokedandtheextenttowhicheachcigaretteisconsumed;thismaydem-onstrate a degree of tension.Tremor may reveal alcoholism with alcohol withdrawal. In‘Trethowan’sweddingringsign’,awomanduringhistorytakingunconsciouslyrevealshermaritaldifficultiesbyconstantlyslidingherweddingringonandoffherfinger.

312 FIVE—EMOTIONS AND ACTION
■ The feetmaybeusedforrestlesspacinginagitateddepression.Akathisia,asdescribedonp. 308, with an inability to keep the feet still, may indicate excessive medication withphenothiazinedrugs.
■ Depressive facies and posture sometimes lead to diagnosis before the patient speaks.Thepatientmaybe slumped in thechairwithafixedexpressionofunmitigatedgriefonhisfaceandaprominent‘crow’sfoot’betweentheeyebrows.Trethowan(1977)hascommentedonthegreatlyreducedblinkratewithseverelyretardeddepressives.
■ Clothinginmaniamaybedistinctiveandsuggestiveofboththediagnosisandthehyper-eroticism that sometimes accompanies it. Hair, make-up and dress may be unequivocaldemonstrationsofmanicmood:‘ThusStella,normallyafairlymodestgirl,appearedonedayinmyconsultingroomwearinganallblackoutfitconsistingofnetstockings,amini-skirtwhichextendedbarelytovulvalevel,andatopwithsodeepacleavageasalmosttoexposeherumbilicus.Asifthiswerenotenoughshehadstuffedherred,whiteandbluejubileepantiesintothetopofheropenhandbag,foralltosee’(Trethowan,1977).
■ Stroking the cheekmaybeanindicatorofemotionaldistress,asdescribedbyGillett(1986):‘During the initialhistory takingandassessment, therewasoneover-ridingly importantemotiveissue,asevidentfromobservationofherbodylanguagesigns.Whenshespokeofher son dying at the age of three, her body stiffened, the muscle tension in her faceincreased,asiftryingtostifleexpression,lacrimationincreased(thoughonlyjustpercep-tibly),andhervoice rose inpitchandwavered.She then lightly strokedher rightcheekwiththetipofherfore-finger,asifwipingawayanimaginarytear–acommonsignwhichusuallyindicatesadesiretocryatthesametimeasawishnottoshowit’.
This list is far fromexhaustive.Thepoint is thatcliniciansshoulduse theireyesandtheirpreviousclinicalexperiencetoformhypothesesinobservationthattheycansubsequentlytestinthehistoryorexaminationofmentalstate.
ReferencesAdlerA(1929)Problems of Neuroses.London:KeganPaul,Trench,Trubner.AndreasenNC(1982)Negative symptoms in schizophrenia.Definitionand reliability.Archives of General
Psychiatry39,784–8.AndreasenNC(1989)ScalefortheAssessmentofNegativeSystems(SANS).British Journal of Psychiatry
155(suppl.7),53–8.AquilinaC(1992)Diogenessyndrome.Psychiatric Bulletin16,573.BarnesTRE,KidgerTandGoreSM(1983)Tardivedyskinesia:athreeyearfollow-upstudy.Psychological
Medicine13,71–81.BayneTandLevyN(2006)Thefeelingofdoing:deconstructingthephenomenologyofagency.InSebanz
NandPrinzW(eds.)Disorders of Volitionpp.49–68.Massachusetts,MITPress.Bellak L and Black RB (1992) Attention-deficit hyperactivity disorder in adults. Clinical Therapeutics 14,
138–47.Benson DF and Blumer D (1982) Psychiatric Aspect of Neurologic Disease, vol. 2. New York: Grune and
Stratton.BerriosGE(1996)The History of Mental Symptoms.Cambridge:CambridgeUniversityPress.BiedermanJ,FaraoneSV,SpencerT,WilensT,MickEandLapeyKA(1994)Genderdifferencesinasample
ofadultswithattentiondeficithyperactivitydisorder.Psychiatry Research53,13–29.BiedermanJ,NewcornJandSprichS(1991)Comorbidityofattentiondeficithyperactivitydisorderwith
conduct,depressive,anxiety,andotherdisorders.American Journal of Psychiatry148,564–77.BlackP,JeffriesJJ,BlumerD,WellnerAandWalkerAE(1969)Thepost-traumaticsyndromeinchildren.
InWalkerAE,CavenessWFandCritchleyM(eds.)The Late Effects of Head Injury.Springfield:Thomas.Bleuler E (1911) Dementia Praecox or the Group of Schizophrenias (transl. Zinkin J, 1950). New York:
InternationalUniversitiesPress.BurwellCS,RobinED,WhaleyRDandBickelmannAG(1956)Extremeobesityassociatedwithalveolar
hypoventilation–aPickwickiansyndrome.American Journal of Medicine21,811–8.
18—DISOrDErS Of VOlITION AND ExECuTION 313
ClarkANG,ManikarGDandGrayI(1975)Diogenessyndrome:aclinicalstudyofgrossneglect inoldage.Lanceti,366–73.
CritchleyM(1962)Periodichypersomniaandmegaphagiainadolescentmales.Brain85,627–56.CrowTJ(1980)Molecularpathologyofschizophrenia:morethanonediseaseprocess?British Medical Journal
280,66–8.CuttingJ(1985)The Psychology of Schizophrenia.Edinburgh:ChurchillLivingstone.D’AgatiE,CasarelliL,PitziantiM,PasiniA (2012)Neuroleptic treatments andoverflowmovements in
schizophrenia:aretheyindependent?Psychiatry Research200,970–6.DarunaJHandBarnesPA(1993)Aneurodevelopmentalviewofimpulsivity.InMcCownWG,JohnsonJL
and Shure MB (eds.) The Impulsive Client: Theory, Research and Treatment. Washington: AmericanPsychologicalAssociation.
EpistleofPaultheApostletotheRomans(1662),Chapter7,18–23,AuthorizedVersion.EysenckSGB(1993)The17:developmentofameasureofimpulsivityanditsrelationshiptothesuperfactors
ofpersonality.InMcCownWG,JohnsonJLandShureMB(eds.)The Impulsive Client: Theory, Research and Treatment.Washington:AmericanPsychologicalAssociation.
FahnS,MarsdenCDandCalneB(1987)Classificationandinvestigationofdystonia.InMarsdenCDandFahnRS(eds)Movement Disorders 2.London:Butterworth.
FerrierIN(1985)Waterintoxication.British Medical Journal291,1594–6.Fink M (1993) Catatonia: a treatable disorder, occasionally recognized. Directions in Psychiatry 13,
1–8.FinkM(2013)Rediscoveringcatatonia:thebiographyofatreatablesyndrome.Acta Psychiatrica Scandinavica
Supplement441,1–47.Fink M and Taylor MA (2003) Catatonia: a Clinician’s Guide to Diagnosis and Treatment. Cambridge:
CambridgeUniversityPress.FreudS(1915)Instinctsandtheirvicissitudes.InCollected Papers,vol.4.London:HogarthPress.Gervin M and Barnes TRE (2000) Assessment of drug-related movement disorders in schizophrenia.
Advances in Psychiatric Treatment6,332–41.Gillett R (1986) Short term intensive psychotherapy – a case history. British Journal of Psychiatry 148,
98–100.Griesinger W (1845) Mental Pathology and Therapeutics (transl. Robertson CL and Rutherford J, 1882).
NewYork:WilliamWoodandCo.HamiltonM(1984)Fish’s Schizophrenia,3rdedn.Bristol:Wright.HullCL(1943)Principles of Behaviour.NewYork:Appleton-Century-Crofts.JaspersK(1923)General Psychopathology(transl.HoenigJandHamiltonMW,1963)Manchester:Manchester
UniversityPress.JaspersK(1959)General Psychopathology,7thedn.(transl.HoenigJandHamiltonMW,1963).Manchester:
ManchesterUniversityPress.JeannerodM(2006)Fromvolitiontoagency:themechanismofactionrecognitionanditsfailures.InSebanz
NandPrinzW(eds.)Disorders of Volition,pp.175–92.Massachusetts:MITPress.JohnsonJ(1993)Catatonia:thetensioninsanity.British Journal of Psychiatry162,733–8.KahlbaumKL(1873)DieKatatonie,oderdasSpannungsIrresein.InCatatonia(transl.LeviYandPridan
T,1973).Baltimore:JohnsHopkinsUniversityPress.KellamAMP(1987)Theneurolepticmalignantsyndrome,socalled:asurveyoftheworldliterature.British
Journal of Psychiatry150,752–9.Lehmann HE (1967) Schizophrenia. In Freedman AM and Kaplan HI (eds.) Comprehensive Textbook of
Psychiatry.Baltimore:WilliamsandWilkins.LishmanWA(1997)Organic Psychiatry,3rdedn.Oxford:BlackwellScientific.LorenzK(1963)On Aggression(transl.LatzkeM,1966).London:Methuen.Macleod J (1987) Davidson’s Principles and Practice of Medicine, 13th edn. Edinburgh: Churchill
Livingstone.MahendraB(1981)Wherehaveallthecatatonicsgone?Psychological Medicine11,669–71.MarsdenCD,MindhamRHSandMacKayAVP(1986)Extrapyramidalmovementdisordersproducedby
antipsychotic drugs. In Bradley PB and Hirsch SR (eds.) The Psychopharmacology and Treatment of Schizophrenia.Oxford:OxfordUniversityPress.
McDougallW(1908)An Introduction to Social Psychology.London:Methuen.

314 FIVE—EMOTIONS AND ACTION
MetzingerT(2006)Consciousvolitionandmentalrepresentation:towardamorefine-grainedanalysis.InSebanzNandPrinzW(eds.)Disorders of Volition,pp.19–48.Massachusetts:MITPress.
Mindham RHS (1970) Psychiatric symptoms in Parkinsonism. Journal of Neurology, Neurosurgery and Psychiatry33,188–91.
MoellerFG,BarrattES,DoughertyDM,SchmitzJMandSwannAC(2001)Psychiatricaspectsofimpulsiv-ity.American Journal of Psychiatry158,1783–93.
OwensDGC(1990)Dystonia–apotentialpsychiatricpitfall.British Journal of Psychiatry156,620–34.ReidT(1863)InHamiltonW(ed.)The Works of Thomas Reid.Edinburgh:MaclachlanandStewart.RobertsonMM,ChannonS,BakerJandFlynnD(1993)ThepsychopathologyofGillesde laTourette’s
syndrome:acontrolledstudy.British Journal of Psychiatry162,114–7.RogersD(1985)Themotordisordersofseverepsychiatricillness:aconflictofparadigms.British Journal of
Psychiatry147,221–32.Sachdev P (1999) Attention deficit hyperactivity disorder in adults [editorial]. Psychological Medicine 29,
507–14.SachdevPandKrukJ(1996)Restlessness:theanatomyofaneuropsychiatricsymptom.Australian and New
Zealand Journal of Psychiatry30,38–53.SacksOW(1973)Awakenings.London:Duckworth.SavageG(1886)Insanity and Allied Neuroses: Practice and Clinical.London:Cassell.ScharfetterC(1980)General Psychopathology: an Introduction.Cambridge:CambridgeUniversityPress.SeltenJ-PCJ,SijbenNES,vandenBoschRJ,Omloo-VisserJandWarmerdamH(1993)TheSubjective
ExperienceofNegativeSymptoms:aself-ratingscale.Comprehensive Psychiatry34,192–7.SimsA(1994)Myselfandmyotherself:the‘doublephenomenon’inneuroticdisorders.InSenskyT,Katona
CandMontgomeryS(eds)Psychiatry in Europe: Directions and Developments.London:Gaskell.SimsACPandSymondsRL(1975)Psychiatricreferralsfromthepolice.British Journal of Psychiatry127,
171–8.Singh S, Padi MH, Bullard H and Freeman H (1985)Water intoxication in psychiatric patients. British
Journal of Psychiatry146,127–31.SnaithRP(1993)Anhedonia:aneglectedsymptomofpsychopathology.Psychological Medicine23,957–66.TrethowanWH(1977)Psychiatry’sphysicalsigns.World Medicine November16,19–21.TukeDH(1874)ThehermitofRedCoats’Green.Journal of Mental Science20,361–72.WaltherS,VandellingenT,MüriR,StrikWandBohlhalterS(2013)Impairedpantomimeinschizophrenia:
associationwithfrontallobe.Cortex49,520–27.WaltonJ(1985)Brain’s Diseases of the Nervous System,9thedn.Oxford:OxfordUniversityPress.WingJK(1978)Reasoning About Madness.Oxford:OxfordUniversityPress.
S E C T I O N SIXVariations of Human Nature
This page intentionally left blank
317
C H A P T E R 19
The Expression of Disordered Personality
SummaryPersonalityistheuniquewaythatanindividualexpresseshimself.Itincludeshischaracteristicgait,hismodeofexperiencingtheworldandreactingtoit.Histypicalaffectiveresponses,hisconductandmoralattitude,whatvaluesguidehimandwhathedoes,whathecreatesandhowheacts.Abnormalitiesofpersonalityontheotherhandareenduringpatternsofexperienceandbehavioraffectingcognition,affect,interpersonalfunctioning,andimpulsecontrolthatareinflex-ible,pervasive,and lead toclinically significant impairment. It is important toemphasise thatthe types of abnormal personality currently described are at most tentative and inconclusiveattemptstorenderinwordscomplexaspectsofhumanfunctioning.Thecategorieshaveclinicalutilitybutareproblematicformanyreasonsincludinglackofreliability,validityandinstabilityovertime.
But the impressions and actions of human beings are not solely the result of their present circumstances, but the joint result of those circumstances and of the characters of the individuals: and the agencies which determine human
character are so numerous, (nothing which has happened to the person throughout life being without its portion of influence), that in the aggregate they are never in any two cases exactly similar. Hence, even if our science of
human nature were theoretically perfect, that is, if we could calculate any character as we can calculate the orbit of any planet, from given data; still, as
the data are never all given, nor even precisely alike in different cases, we could neither make positive predictions, nor lay down universal propositions.
John Stuart Mill (1811)
MillinaSystem of Logicasquotedabovestatessuccinctlythedifficultyofformingatheoryofpersonality that is useful in clinical practice in predicting behaviour. Nonetheless, theories ofpersonalityabound.Jaspers’(1913)definitionofpersonalityisasgoodaplacetostartasanyotherdefinition
‘We see the personality in the particular way an individual expresses himself, in the way he moves, how he experiences and reacts to situations, how he
loves, grows jealous, how he conducts his life in general, what needs he has, what are his longings and aims, what are his ideals and how he shapes them,
what values guide him and what he does, what he creates and how he acts. In short, personality is the term we to the individually differing and
characteristic totality of meaningful connections in any one psychic life’

Keywords:Personality,PersonalityDisorder,ParanoidPersonalityDisorder,SchizoidPersonalityDisorder,DissocialPersonalityDisorder,EmotionallyUnstablePersonalityDisorder,HistrionicPersonalityDisorder,AnakasticPersonalityDisorder,Anxious(Avoidant)PersonalityDisorder,DependentPersonalityDisorder.
19—THE ExPRESSION OF DISORDERED PERSONAlITy 317.e1
318 SIX—VARIATIONS OF HUMAN NATURE
Thereisanimplicitbuterroneousnotionthatadescriptionofpersonalitysomehowcapturesallthatthereistosayaboutaperson.Reflectionmakesobviousthatitisimpossibletodescribethetotalityofanyhumanbeinginasingle,simpleterm.Furthermore,asJaspersremarked‘Thepersonalityasunderstoodisnotwhatanindividualactuallyisbutanempiricalandinconclusivephenomenon’ that is limited in itsscopepreciselybecausehumanbeingsare freetoact intheworld and ‘at any moment freedom can have birth and give everything a different meaning’.Descriptions of personality, in other words, are tentative and fragile.The individual’s life andchoicesarenotfixedandpre-determinedbyanydescriptionthatwemayhave.Everyindividualhasaninfiniterealityandpotential.Ourfeebleattemptsatdescriptionaremainlytomakecom-municationbetweenpractitionersefficient.
Attemptsatclassifyingpersonalityfallintotwomaincategories:nomotheticandidiographic.The nomothetic approach assumes that human beings only vary to the degree in which theyshare certain traits or personality dimensions. On the other hand, the idiographic approachassumesthathumanbeingsareuniqueindividualsandthetheoriesherepointtothecharacter-isticsthatmakeindividualsuniqueanddistinctive.Sadly,thereisagulfbetweenpsychologicalpersonalitytheoriessuchasthatbyfiguressuchasGordonAllport(1897–1967),HansEysenck(1916–1997),andRaymondCattell(1905–1998)andtheapproachthatisfavouredbypsychia-tristswhichdealspredominantlywithabnormalitiesofpersonality.
Thetermpersonality disorderisanabstractionbuiltonseveraltenuoustheories.Itisanuntidyconcept,butitcarriesclinicalusefulness.Thewayinwhichthetermhasbeendevelopedanditsrelationship with neurosis is dealt with elsewhere (Sims, 1983).The intention here is only todiscusstheeffectsthatdifferenttypesofpersonalityhaveonactionsandbehaviour.Theclinicianbuildsonaprofileforpersonalitydisorder.Thisleadstoacharacteristicpatternofbehaviourthatallowsus,tosomeextent,topredicthisfutureactionsandtodescribewhatmakesthisindividualdifferent.Theclinicaldesignationofpersonalityispurelydescriptiveandcarriesnotheoreticalimplications,otherwisethereisalogicalflawindescribingpersonalitytypeintermsofconsistentbehaviour and at the same time claiming the type accounts fordefinitepatterns of behaviour.Acuteanddetailedobservationofthecharacteristicsofpersonalityanditsevaluationisausefulpsychiatricskillthathas,regrettably,beenmuchneglectedformanyyears.
Thesecharacteristicsofbehaviour,includingthecapacityforandnatureofrelationshipswithotherpeople,arebroughttogethertodescribetraitsorpersonality types;obviously,tobeclinicallyrelevantthesetraitsmusthaveimplicationsforthefunctioningoftheindividual.Thedistinctionbetweentrait,thepredispositionassociatedwithpersonality,andstate,thecurrentmentalcondi-tion,isveryimportant.Theseclassificationsofpersonalitydisorder,basedonsuchlistsoftraits,werecategorizedbySchneider(1923)andmorerecentlyinICD-10(WorldHealthOrganization,1992) and in DSM-V (American Psychiatric Association, 2013). Certain characteristics haveclinicalsignificance,suchasthedegreetowhichthepersonisawareofthefeelings,andissensi-tivetothejudgements,ofotherpeople.Abnormalpersonalityisfoundwhenapersonalitytraitconsidered to be clinically significant is present to either too small or too great an extent toconform statistically with the mass of mankind.The concepts of personality and personalitydisorder were discussed by Tantam (1988), and more recently personality disorder has beenreviewedbyTyrerandStein (1993).Thereareconsiderableproblemswith thedescriptionsoftypesofpersonalitydisorders.Themostsignificantarethelackofspecificityinthedefinitionsofpersonalitydisorders,theexcessivecomorbidityamongpersonalitydisorders,thequestionablevalidityoftheidentifiedcategoriesandtheinstabilityofthesediagnostictermsovertime(Skodol,2012). Furthermore, it is recognized that part of the problem with the current classificationsystemistheunsatisfactorynatureofpersonalitytypologiesandtheneedforanintegrationofdimensional thinking into how personality and personality disorder are conceptualized. Thisdevelopmentinthinkingaboutpersonalitydisordersisalsodrawingattentiontotheneedtobasediscussions about personality disorder on what is understood about normal personality traits.
19—THE ExPRESSION OF DISORDERED PERSONAlITy 319
ThishasledtoanevaluationoftheFive-Factormodelofpersonalityasapotentialfoundationforatheoryofabnormalpersonality(Widigeretal.,2012).TheFive-Factormodelofpersonalityincludesneuroticism,extraversion,openness,agreeablenessandconscientiousnessastherelevantfactors.Thehopeisthatanintegrationofnormalandabnormalpersonalitywithinacommonhierarchicalstructurewouldallowforamorepreciseandindividualizeddescriptionofperson-ality structure for each individual (Widiger etal., 2012) but this hope is not widely shared(Paris,2013).
Abnormality of personality has been described in terms of trait. What then is personality disorder?HereSchneider’sdefinitionisagoodstartingpoint:‘Personalitydisorderispresentwhenthat abnormality of personality causes either the patient himself or other people to suffer’(Schneider,1958).Alternatively,fromDSM-IV(APA,1994):‘Anenduringpatternofexperienceandbehaviouraffectingcognition,affect, interpersonalfunctioningandimpulsecontrolthatisinflexible,pervasiveandleadstoclinicallysignificantimpairment’.
■ AhighlyconscientiousandmeticulousPostOfficesorterwaspromotedtoforemansorteraftermanyyears’reliableservice.Theappropriateresponsemighthavebeentobepleasedattheincreasedpayandtospendthefirstweek’sincrementbeforereceivingit.However,thismanwasfearfulaboutthepromotion.Heworriedthathemightnotbeabletocopewiththejob,thathemightnotbeabletopersuadethemeninhischargetosortletterstohisownhighstandards,thathewouldnotbeabletomixsociallywithhissuperiorsandequals, thathewouldmakea foolofhimselfandthatotherpeoplewould laughathim.Hebecamemiserable,anxiousandlackingconfidence,andhehadtostopwork.Becauseofhisabnormal,obsessional(anankastic)personality,herespondedtothestressofpromo-tionbybecomingacutelydistressedanddevelopingneuroticdepressivesymptoms.
■ Ablandandplausible confidence trickster extractedwithout compunction themeansofsubsistencefromanelderlywidow.Hispsychopathicbluntingofappreciationforthewayotherswouldexperiencehisbehaviourandtheirconsequentfeelingsresultedinhimcausingsufferingtoothers.
Personalityabnormalityisapartoftheindividual’sconstitution.Whetherornotitmanifestsaspersonalitydisorderdependstoaconsiderableextentonsocialcircumstances.Ahighlyabnor-malpersonalitythatinonesituationmaybeconsideredcriminalpsychopathyandbepossessedbyaconvictedprisoner,inanothersituationwillbethedrivingforceinahighlysuccessfulandrelativelycreativepoliticalrevolutionary.Personalityinanindividualcannotbedivorcedfromitssocialandculturalsetting.Indeed,somehavearguedthatthepersonalitydisorderconstructsthatwecurrentlyutilizearederivedfromandcalibratedagainstWesternmiddle-classculturalnorms(Mulder,2012).
Having ascertained whether personality disorder is present, its type should be categorizedusinganacceptedsystem.However,acautionisneededhere.Itisoftenextremelydifficulttofitpeopleintoarbitrarycategoriesofpersonality,andthewholetopicofclassificationisstillhighlyunsatisfactory.Itmaybemuchbettertouseafewdescriptivesentencesforthepersonality,andprobablyitisbesttocombinedescriptionwithcategorization.ThesystemsusedinICD-10andDSM-V canbe recommended; the typological classificationofpersonalitydisorder introducedbyTyrerandAlexander(1979)wasalsosatisfactorybuthasnotbeenwidelyused.Table19.1isacompositeoftheseclassifications.Theyallstartfromthesamebases:thedefinitionofpersonal-ity,theevaluationofabnormalityandtheobservationofcertaininfluentialandregularlyoccurringtraits.Tyrer and Alexander’s five discrete categories of abnormal personality followed from acluster analysis of personality data and is therefore a simplification of ICD-9 (World HealthOrganization,1977),whichitselfwasbasedoriginallyonSchneider.DSM-IVandDSM-VhavecertaindifferenttermsthathaveprovedimportantinAmericanpsychiatry,althoughtheyarenotnecessarilyfoundhelpfulelsewhere.Theseincludenarcissisticpersonalitydisorder,whichisdis-cussedlaterinthischapter;avoidant,whichissimilartoanxiouspersonalitydisorderinICD-10;
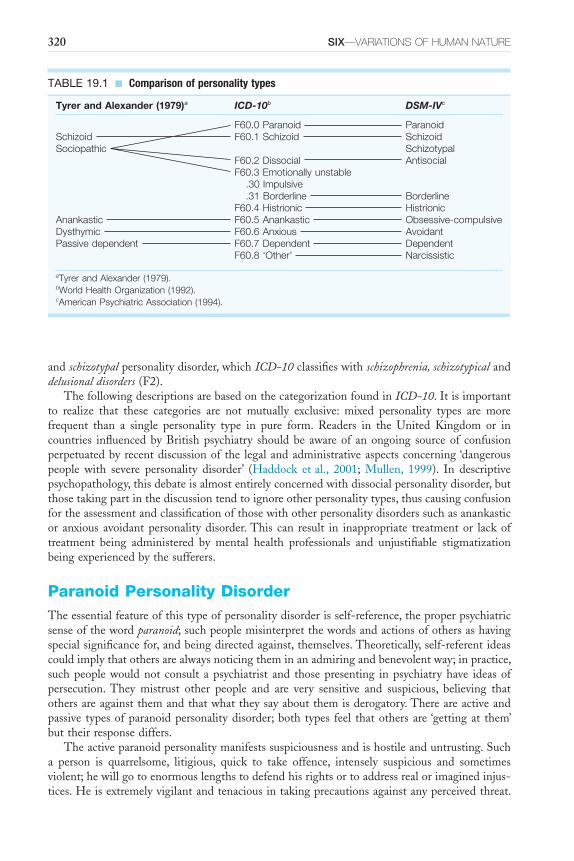
320 SIX—VARIATIONS OF HUMAN NATURE
andschizotypalpersonalitydisorder,whichICD-10classifieswithschizophrenia, schizotypicalanddelusional disorders(F2).
ThefollowingdescriptionsarebasedonthecategorizationfoundinICD-10.Itisimportantto realize that these categories are not mutually exclusive: mixed personality types are morefrequent than a single personality type in pure form. Readers in the United Kingdom or incountries influencedbyBritishpsychiatry shouldbe awareof anongoing sourceof confusionperpetuatedbyrecentdiscussionof the legalandadministrativeaspectsconcerning‘dangerouspeople with severe personality disorder’ (Haddock etal., 2001; Mullen, 1999). In descriptivepsychopathology,thisdebateisalmostentirelyconcernedwithdissocialpersonalitydisorder,butthosetakingpartinthediscussiontendtoignoreotherpersonalitytypes,thuscausingconfusionfortheassessmentandclassificationofthosewithotherpersonalitydisorderssuchasanankasticor anxious avoidantpersonalitydisorder.This can result in inappropriate treatmentor lackoftreatment being administered by mental health professionals and unjustifiable stigmatizationbeingexperiencedbythesufferers.
Paranoid Personality DisorderTheessentialfeatureofthistypeofpersonalitydisorderisself-reference,theproperpsychiatricsenseofthewordparanoid;suchpeoplemisinterpretthewordsandactionsofothersashavingspecialsignificancefor,andbeingdirectedagainst,themselves.Theoretically,self-referentideascouldimplythatothersarealwaysnoticingtheminanadmiringandbenevolentway;inpractice,suchpeoplewouldnot consult apsychiatrist and thosepresenting inpsychiatryhave ideasofpersecution.They mistrust other people and are very sensitive and suspicious, believing thatothersareagainstthemandthatwhattheysayaboutthemisderogatory.Thereareactiveandpassive typesofparanoidpersonalitydisorder;both types feel thatothersare‘gettingat them’buttheirresponsediffers.
Theactiveparanoidpersonalitymanifestssuspiciousnessandishostileanduntrusting.Sucha person is quarrelsome, litigious, quick to take offence, intensely suspicious and sometimesviolent;hewillgotoenormouslengthstodefendhisrightsortoaddressrealorimaginedinjus-tices.Heisextremelyvigilantandtenaciousintakingprecautionsagainstanyperceivedthreat.
TABLE 19.1 ■ Comparison of personality types
Tyrer and Alexander (1979)a ICD-10b DSM-IVc
F60.0 Paranoid ParanoidSchizoid F60.1 Schizoid SchizoidSociopathic Schizotypal
F60.2 Dissocial AntisocialF60.3 Emotionally unstable .30 Impulsive .31 Borderline BorderlineF60.4 Histrionic Histrionic
Anankastic F60.5 Anankastic Obsessive-compulsiveDysthymic F60.6 Anxious AvoidantPassive dependent F60.7 Dependent Dependent
F60.8 ‘Other’ Narcissistic
aTyrer and Alexander (1979).bWorld Health Organization (1992).cAmerican Psychiatric Association (1994).
19—THE ExPRESSION OF DISORDERED PERSONAlITy 321
Thisisthesortofpersonwhowillmarchfearlesslyacrossafieldofyoungcornbecauseheseesthereisapublicrightofwayonhismapandthefarmerhasnorighttoviolatethis.Theyrepudi-ateblameandmayberegardedbyothersasdevious,schemingandsecretive.Suchapersonisintenselyjealousofwhatheregardsashisownbelongings,whichmaybepeopleaswellasobjects,andhespendsalotoftimeplanningto‘gethisownback’.Hemaybeself-importantandfanati-cal.Morbidjealousymaybeshown,andsuchapersonmaybeinvolvedinactsofviolencebecauseofimaginedinjustice.Suchapersonalitymayfindcreativeexpressioninsocialandpoliticallifebut is likely tobeverydestructivewithin the family.Apatientcommentedon this ruefully, ‘Ihavescarcely talked tomywife for the last tenyears’,becauseofhis successionofcourtcasesagainstthosewithwhomhecameintocontact.
Apersonwithpassiveparanoidpersonalityfacestheworldfromapositionofsubmissionandhumiliation.Heassumesthatwhateverhappenstohimwillbedamaging.Liketheactivetype,heissuspicious,sensitiveandself-referentandmisconstruescircumstancesandotherpeople.Hebelievesthatotherpeoplewilldislikehimandthattheywillultimatelylethimdown.However,heaccepts‘theslingsandarrowsofoutrageousfortune’passively,bowingtotheinevitable;heisvulnerable and frequently feels humiliated and unable to initiate any assertive activity. Otherpeopletendtotakeadvantageofhim,thusfulfillinghispessimisticexpectations.
A frequentmanifestationofpsychopathologywithin thecontextofparanoidpersonality isthepresenceofanovervaluedidea(Chapter8).This,alternativelydescribedasafixedidea(idéefixe),isabeliefthatmightseemreasonablebothtothepatientandtootherpeople.However,itcomestocompletelydominatetheperson’sthinkingandlife,andinsteadoftestingitsvalidityhetendstoconsiderthateverycircumstanceoflifesubstantiatesit;itbecomesthebasisforactionthatissometimesaggressiveorself-destructive.Itisquitedistinctphenomenologicallyfrombothdelusionandobsessional ideas.
Schizoid Personality DisorderThispersonalitydisorder is characterizedby a lackofneed for, anddefect in, the capacity toformsocialrelationships.Suchpeopleshowwithdrawalfromsocialinvolvement;emotionalcool-nessanddetachment;andindifferencetothepraise,criticismandfeelingsofotherpeople.
Theseindividualsare‘loners’withadisinclinationtomix,andtheyappearsomewhataloof.Theylacktenderfeelings,havelittleinterestinsexualexperienceandarenotinterestedinthecompanyofothers.Theyarenotdepressedinmood,noraretheyshyorsensitivetowardsotherpeople,buttheyaresolitaryandprefernottobeinvolvedinsocialoccupations.Theirinterestsandhobbiesusuallytendtoincreasetheirisolationfromotherpeople,astheyaremoreinterestedinthings,objectsandmachines.
Close relativesmaycomplainof the subject’semotionaldetachment,an inability to inspirestrongfeelingsinothers,alackofanyrealsenseofpleasure,oddnessandeccentricityandcallousindifferencetoothers’suffering.Inafollow-upofformerschizoidsubjects,theywerefoundtousepsychologicalconstructslessthanacontrolgroup,andthispointedtotheschizoidindividual’slackofempathy(Chicketal.,1979).
Thosewithschizoidpersonalityandpoorsocialadjustmenthavebeenconsideredmorelikelytodevelopschizophrenia.Inalargestudybasedonthepreviouspersonalityassessmentof50,054malerecruits to theSwedisharmy,aspectsofpersonalitywere foundtoberisk factors for thesubsequentdevelopmentofschizophrenia(Malmbergetal.,1998).
Dissocial Personality DisorderThe essential, phenomenological abnormality of dissocial (asocial, antisocial or psychopathic)personalitydisorderisprimarilyoneofempathy.Thereisadefectinthecapacitytoappreciate
322 SIX—VARIATIONS OF HUMAN NATURE
otherpeople’sfeelings,especiallyincomprehendinghowotherpeoplefeelabouttheconsequencesofthisperson’sownactions.Thispersonalitytype,orabnormality,includesthosepeopleconsid-eredtosufferfrompsychopathicpersonalitywithinthemeaningoftheMentalHealthAct,1983(Bluglass,1983).Anormalpersonispreventedmostofthetime,byshameorbyhiscapacityforempathy, fromcarryingoutunpleasant actions towardsotherpeople.Hedoesnotwant tobedislikedandfeelsverykeenlyhowitwouldbepassivelytobetherecipientofsuchbehaviour.Itisthisinabilitytofeelforhimselfthediscomfortthatothersexperienceasaresultofhisantisocialactivitiesthatappearstobeabsentinthepsychopath.DespitesuchcomprehensivedescriptionsasthatofCleckley(1941),inThe Mask of Sanity,andothers,therearestillconsiderabledoubtsas towhether thispersonality type formsadistinct categoryornot, and if itdoes,whether itshouldbeconsideredwithinoroutsidepsychiatry.ThisissuccinctlyexpressedbyWooton(1959):psychopathsare‘extremelyselfishpersonsandnooneknowswhatmakesthemso’.
Theconfusionofterminologyisexplainedpartlybythevariednatureofpresentation;partlybytheconflictingdesiresofprofessionalsnottostigmatizeandalsonottocastblameonthosewhocannotcontrol theiractions;andpartlyby the requirementsofclassification fordifferentprofessionalgroupsandsettings–lawyers,criminologists,psychiatrists,psychologistsandsoon.Acomprehensiveaccountofdiagnosticissues,developmentalhistoryandmethodsoftreatmentistobefoundinDolanandCoid(1993).
Theconceptofmoral derangementwas introducedbyBenjaminRush (1812), andofmoral insanitybyPrichard(1835),whoconsideredthistooccuramongcriminalswhoshowedlossoffeeling,ofcontrol,andofethicalsense,equivalenttomentaldiseasebutatadifferentlevel.Itisimportant to stress that not all psychopaths are criminal, nor are all criminals psychopathic.Henderson (1939)described creative, inadequate andaggressive psychopathy, citingLawrenceofArabiaasanexampleofacreativepsychopath.Dissocialpersonalitydisorder,withconspicuouslackofconscienceandhumansympathy,isfoundmoreofteninmalesthaninfemales.
Thispersonalitydisorder shouldnotbediagnosedunless the subject isagedover18years.However, inchildhoodoradolescencemanyof the followingmayhavebeendemonstratedbythepersonsubsequentlydiagnosedasdissocial:truancy,expulsionorsuspensionfromschoolformisbehaviour, delinquency, running away from home, persistent lying, repeated casual sexualintercourse,repeateddrunkenness,substanceabuse,theft,vandalism,schoolperformancebelowexpectation,repeatedviolationofrulesathomeandschoolandfighting.Ofcourse,suchbehav-iourmayoccurinnormalchildren,especiallywithsocialdeprivation,butitistheirpersistenceandthepresenceofsomanyofthesesignsofdisturbedbehaviourthatmaypredictsubsequentpsychopathy.There isalsodebateconcerningthemanifestationofattentiondeficitdisorder inchildhoodandsubsequentantisocialbehaviourinyoungadultlife(Hinshaw,1994).
Suchapersonmaybemeaninglesslycruel,callous,aggressiveandemotionallycold,rejectingsocialnormsand showing irresponsibility inhis relationships.He isoftenunable tomaintainconsistencyatwork,withfrequentunemployment,changesofoccupation,absenteeismandpoorrelationships.Similarly,thereareunsatisfactoryrelationshipswithsexualpartners,withahistoryof several separations or divorces, promiscuity with heterosexual or homosexual preferences,desertion and repeated marital arguments. Poor parenting results in conspicuous physical andpsychologicalproblemsamonghischildren,andtheindividual’saggressivenessmayresultinchildabusewithnon-accidentalinjury.Asheages,heislesslikelytobeinconflictwiththelawandlesslikelytobeviolent,buthisaffectionlessinabilitytoseetheconsequencesofhisactionsandthewayotherpeoplesufferbecauseofthem,remainsdestructivewithinthefamilyandinotherinstitutions.There is a failure to accept society’snormsas regards socialbehaviour,drugs andalcoholandpersonalproperty.Alengthycriminalrecordisfrequentlyseen,ashefailstolearnfromhis experiences (Craft, 1966).Suchapersonmay feelmiserable andeven suicidalwhendiscoveredinanunacceptableact,butthisdoesnotamounttothenormalsenseoffeelingguilt.Thereisafailuretoidentifywiththevictim.
19—THE ExPRESSION OF DISORDERED PERSONAlITy 323
ThedefinitionofpsychopathyproposedbyWhiteley(1975)isasfollows:thepsychopathisanindividual:
1. whopersistentlybehavesinawaythatisnotinaccordwiththeacceptedsocialnormsofthecultureortimesinwhichhelives;
2. whoappearstobeunawarethathisbehaviourisseriouslyatfault;and3. whoseabnormalitycannotbereadilyexplainedasresultingfromthe‘madness’wecom-
monlyrecognizenorfrom‘badness’alone.Failuretoplanaheadandfailuretohonourobligations,forexamplematrimonialorfinancial
commitments,arerepeated.Thereisadisregardfortruthandalsoforsafety,bothfortheindi-vidualhimselfandforothers.
Emotionally Unstable Personality DisorderIMPULSIVE TYPE
Thispersonalitydisorderisnotoftenencountered.Theessentialfeatureisliabilitytointemperateanduncontrolledoutburstsofmood,mostfrequentlyviolentangerbutoccasionallyinconsolablegrief,extremeanxietyoruproarioushilarity. It isusuallyaggressiveness thatbrings individualswiththisdisordertotheattentionofthepsychiatrist;withveryslightprovocation,theymayhavebecomeirritableandonoccasionsviolent.Theyaretreatedwithextremecircumspectionbyotherpeople,and their illhumour thereforebecomes reinforcedas itenables themtoget theirownway.Theymayexploitotherpeople’sfearsofthemtoachievetheirobjectives,forexamplethearbitrarilyviolenthusbandwhosewifeiscompletelydominatedbyhimthroughfear.Suchper-sonalitiesaredisruptiveandunpopular.
Thosewiththispersonalitystructurebehavenormallyformostofthetimeandonlyoccasion-allyexplodeinimpulsiveirritability,whichismorecommoninyoungerpeopleandmayappearineithersex(SnaithandTaylor,1985).InthesystemofclassificationadvocatedbyTyrerandAlexander,thispersonalitytypeisnotretainedasdistinctbutcombinedwithparanoidandasocialpersonalitytoformacategoryofsociopathic personality disorder.
BORDERLINE TYPE
This very confuseddiagnostic termhasbeenusedvariously todescribe agroupof apparentlyneuroticallydisturbedpatientswhobecamepsychoticwhileundergoingpsychoanalysis;anendur-ing, unstable and vulnerable personality structure; and a group of patients who ‘almost’ hadschizophrenia(Anonymous,1986).Itisconsideredthatatleastfiveofthefollowingshouldbepresentforthediagnosistobemade(DSM-V;AmericanPsychiatricAssociation,2013):
■ franticeffortstoavoidrealorimaginedabandonment■ apatternofunstableandintenseinterpersonalrelationships■ identitydisturbanceinareassuchasself-image,genderidentityorlong-termgoals■ impulsivityorunpredictabilityinareasthatarepotentiallyself-damaging■ recurrentsuicidalbehaviour,gesturesorthreatsorself-mutilatingbehaviour■ affectiveinstabilityduetoamarkedreactivityofmood■ chronicfeelingsofemptiness■ inappropriateintenseangerordifficultyincontrollinganger■ transient,stress-relatedparanoidideationorseveredissociativesymptoms.Althoughpsychodynamicallyinclinedpsychiatristshaveusedthiscategoryextensively,there
appearstobenophenomenologicalthreadlinkingtheverydifferentcriteriathatarerequiredforits diagnosis. Carrasco and Lecic-Tosevski (2000) have described it as the most controversialof all personality disorders and ‘best understood as a heterogeneous syndrome manifested by
324 SIX—VARIATIONS OF HUMAN NATURE
egosyntonic affective instability and impulsivity (behavioural dys-control) and propensity tocognitive-perceptualdistortionsinthecontextofchronicallyunstableinterpersonalrelationships’.Bothgeneticfactorsandearlychildhoodadversityareimplicatedinitsaetiologywithimplica-tionsfortheneuralcircuitsthatregulateaffect,behaviourandcognition(Hooleyetal.,2012).
Histrionic Personality DisorderThewordhistrionic isderivedfrom‘playingonthestage’; it isabettertermthanhysterical forthisdisorder,whichischaracterizedbytheatricalbehaviour,cravingforattentionandexcitement,excessivereactiontominoreventsandoutburstsofmood,especiallytempertantrums.Insum-marizingthedescriptionsof22differentauthors,DeAlarcon(1973)foundthegreatestagree-mentforhystericalpersonalitydisorderinthefollowingfeatures:histrionicbehaviour,egocentricity,emotionallability,excitability,dependency,suggestibilityandseductiveness.
Characteristicofthedisturbanceofhistrionicpersonalityisthenatureofrelationships,withlimitedabilitytoexperienceprofoundaffectandcommunicatesuchfeelings.Thereisashallow-nessandlabilityofemotion,andthisisseenbyothersas lackingingenuineness,eventhoughtheyaresuperficiallycharming–‘thelifeandsouloftheparty’.Theyformexcellentandrapidacquaintanceshipswithnewpeople,buttheyhavegreatdifficultysustainingacloselong-term,mutuallyrewarding,exclusiverelationship.
Mood is fluctuating and inconsistent, and they display towards other people a craving forattention,affectionandappreciation.Theyareseenasegocentric,self-indulgentandinconsider-ateofothers.Thereisoftenextremebutsuperficialinvolvementwithmanydifferentpeopleinashortspaceoftime,andsuchapersonisseenasbeingmanipulative,vainanddemanding;themanipulativenessisoftenineffectualandself-destructive.Theyareoftensuperficiallyfoundveryattractiveandachievetheirshort-termgoalswhilebeingunabletosustain long-termrelation-ships; for instance marriage frequently ends in divorce.They may be dependent and helpless,constantly seeking reassurance and the approval of others. Gestures of deliberate self-harm,hysterical conversion symptoms and abuse of alcohol and other drugs are common. Reactivedepressionisalsofrequentlyencountered,especiallywhenabreakdownofrelationshipsoccurs.Inahospitalstudyofthosewithhystericalpersonalitydisorder,Thompson(1980)found83percentofsubjectstobefemale;therewasaclearassociationwithneuroticdepression,overdosage,self-mutilation,abuseofalcoholandahistoryofcriminalityandsometimesviolence.TyrerandAlexanderdonot regardthisasadistinctpersonalitydisorderbutcombine itwithdependentpersonalitydisorderinacategoryofpassive dependence.
Anankastic Personality DisorderAnankasticpersonalitytraitsinmoderateamountarevaluableinsocietyandforthesuccessoftheindividual;theyarefrequentlyobservedinprofessionalssuchaslawyersordoctors.However,when these are developed to an abnormal extent and interfere with the person’s functioning,personalitydisorderispresentandischaracterizedbyperfectionism,rigidity,sensitivity,indeci-siveness,alackofcapacitytoexpressstronglyfeltemotionandexcessiveconscientiousness.Theanankast’s pervading sense of insecurity is associated with extreme self-doubt and feelings ofsensitivityconcerninghowotherpeopleviewhim.
Perfectionismandexcessiveattentiontodetailinterferewiththeoverallgraspofsubjectsorsituations.Thereisgrosspreoccupationwithrules,efficiency,trivialdetails,proceduresandpro-tocol.Onepatientwasmakinglistsofthelistsshehadpreviouslysetherself.Shecouldnotthrowawayalistuntileverythingonithadbeencompletedand,assomeoftheitemsonthelistswerethings that shewished to remindherself todo regularly, shewas accumulating such an ever-increasingnumberoflistsastobeunmanageable.Efficiencyandperfectionareaimedat,butthe

19—THE ExPRESSION OF DISORDERED PERSONAlITy 325
excessivelydetailedmannerinwhichtheattempttoachievethemismadeunderminesthepos-sibilityofsuccess.Often,extremeorderlinessinoneareaofliferesultsinchaosinanother,forexamplethemedicalpractitionerwhokeptthetopofhisdeskinimmaculatetidinessbuttippedallhiscasenotesandotherpapersintothebackofhiscar.
Rigidity inpatternsofbehaviour ischaracteristic.Theindividualvaluesaccuracyandthor-oughnesshighlyandrespectsotherobsessionalpeopleforthesequalities.Hetendstokeepfixedtimesandlivetoaregularprogramme,alteredonlywiththegreatestmisgivings.Theseconstraintsareextendedtootherpeopleinthatheinsiststhattheysubmittohiswayofdoingthings.Thereisoftena lackofawarenessof the feelings inothersevokedbyhisbehaviour.ThisanankasticcontrolofotherpeopleistypifiedbyMrsOgmore-PritchardinDylanThomas’Under Milk Wood(1954),who imposesonherdeadhusband thedictum‘Imustputmypyjamas in thedrawermarkedpyjamas…Imusttakemycoldbathwhichisgoodforme’.
Theanankast is extremely sensitive to thecriticism, realor suspected,ofotherpeople; theslightestcensureis‘takenverymuchtoheart’.Thisawarenessofotherpeople’sopinionmakeshimaconformist,notpreparedtostepoutofline,alwayswishing‘tokeepupwiththeJoneses’.Heisrigid,formalandself-controlled,notonlyinhispublicbusinessbutalsoathomeandwithhis more intimate relationships. Insecurity about his abilities and his relationships makes theanankast indecisive.Hedoubtshisowncapacityandonlytooeasily finds himself agreeing insecret with those who criticize him. He vacillates and has great difficulty inmakingchoices,constantly lookingatsituationsfromdifferentpointsofview,‘weighinguptheprosandcons’.Heoftenfindshimselfinapositionofambivalenceandmayovercompensateforthisindecisive-nessbymakingarbitrarydecisionsthatthenbecomeimmutable on insufficient evidence, or hemay compensate for his legalistic rigidity by flaunting thelawostentatiously.Eveninthis,hisbasic obsessionality and perfectionism are still manifest.The anankast finds the initiation orcompletion of any activity very difficult, but hard work is highly prized, and he is thereforepreparedtocarryonthemiddlepartofthetaskindefinitely.
Theobsessional’sneedfor formality,andhis feelingsofsensitivityabouthowotherpeopleviewhim,resultsinrestrictedabilitytoexpresstenderemotion.Heisundulyconventional,seriousandformal.Stinginessmaybeshownbothwithmoneyandwiththeexpressionoffeelings.Suchapersonactuallyexperiencesverystrongaffectbutisquiteunabletoexpressthisappropriatelytowardsotherpeople.
Thedifferentfacetsoftheanankasticpersonalitydisorderare,ofcourse,interlocked.Astraitsofpersonality,theyareseenveryfrequently,notleastamongmembersofthemedicalprofession.However,developedasapersonalitydisorder, thiswayof lifemaybe incapacitating,especiallythe indecisiveness and inability to express strong emotion. Depression, obsessive-compulsivedisorder,eatingdisorderandhypochondriasisarenotuncommonlyassociatedwiththisabnor-malityofpersonality(SamuelsandCosta,2012).
Anxious (Avoidant) Personality DisorderThisisadisorderoftrait,whileanxietydisorderisadisorderofstate(seeChapter17).Thereisoftenfree-floatinganxietythatisexacerbatedbyanyovertpredisposingcause.Suchpeopleoftenfindthepublicsideoflife,forexampleatwork,verymuchmorestressfulthantheprivateside,withinthefamily.Traitanxietyispresentwhenthedevelopmentoftheindividual’spersonalityresultsinsomelevelofabnormalanxietybeingapersistentbackgroundpartoftheirconstitution(SimsandSnaith,1988);thiscouldalternativelybedescribedasanxioustemperamentoranxiety-pronepersonality.Suchpeopledescribethemselvesas‘bornworriers’.
Thispersonalitydisorder is characterizedbypersistentandpervasive feelingsof terrorandapprehension;abeliefthatoneissociallyinept,unattractiveorinferior;excessivepreoccupationwithcriticismandrejectionbyothers;hesitancyinnewsocialrelationships;restrictionoflifestyle
326 SIX—VARIATIONS OF HUMAN NATURE
because of the need for security; and avoidance of those social situations that might provokedisapproval(ICD-10;WorldHealthOrganization,1992).
Dependent Personality DisorderThedependentpersonalityischaracterizedbyfeelingsofinadequacyconcerningselfanddepend-enceonotherpeople.Thereisgrosslackofself-confidence,initiativeanddrive.Suchapersonisunabletoreacttothechangingdemandsoflifeandallowsotherpeople,sometimesoneotherperson, to assume responsibility for major areas of life. He may function reasonably well andappearinconspicuouswhencarriedalongthroughlifebyadominantcloserelationship.However,whenexternalstressoccurshelacksconfidence,isunabletocopeandcraveslong-termsupportandencouragementfromrelatives,aclosefriend,hisfamilydoctor,hissocialworker,hisminister,hisemployerorhissurroundingsocialorganizations.Hemay,forexample,flourishinthearmedforcesbutbeunabletoadjusttocivilianlife.
Suchpeopletendtogothroughlifewithonedominantdependentrelationship;foraman,thismaybeinitiallyhismotherandsubsequentlyhiswife,whotakesoverhismother’srole.Crisesresultinginpsychiatricreferralmayoccurwhenaparentdiesorbecomesincapable,hismarriagebreaksdown,heloseshisjob,afterdetectionincrimeorfollowingphysicalillness.Itisusuallyonlyaftersuchsituationsthatapersonwiththistypeofpersonalitydisordercomestotheatten-tionof the caringprofessions.Dependenceamounts topassive compliancewith theaimsanddemandsofthemoredominantpartner.Thereisalackofvigourinmaintainingaimsandgoalsandinattemptingtoachievethese.Theymaydescribethemselvesasdepressed,butitismoreafeelingof inertiaandan inability tocopewith theirproblems than the symptomsofaffectivedisorder.Originally, thispersonalitydisorderwas conceptualizedas arisingoutofproblematicearlyparent-child relationshipsbutpathologicaldependency isnow seen as stemming fromaperceptionof the‘self ’asweakaccompaniedby thebelief thatotherpeoplearecomparativelycompetentandconfident.Asaresultofthistheindividualbecomespreoccupiedwithobtainingandmaintainingrelationshipswithpotentialcaregivers(Bornstein,2012).
Persistent Mood DisordersIn ICD-9 (WorldHealthOrganization, 1977), these conditionswere classified asdisorder ofpersonality. However, in ICD-10 they have been listed as a subcategory of affective disordersbecause they are genetically related to mood disorders and sometimes respond to the samemethodsoftreatment.Theyareretainedinthischapterbecausetheyconformwiththepsycho-pathology of personality disorders. Akiskal (1993) has made a convincing case for depressivepersonalitytobereturnedtothegenericcategoryofpersonalitydisordersratherthanbeingclas-sifiedwithaxis 1 mood (affective) disorders.There is apersistent lifelongabnormalityofmood,notamountingtoillness,asopposedtothosereactiveorendogenousdisturbancesofaffectthatareofshorterdurationandareregardedasillness.Themostfrequenttypesofaffectivepersonalitydisorder show excessive lability of mood or persistent depressive stance towards life. Otherabnormalitiesofpersonalitymayoccur,suchaspersistenthypomania,buttheserarelypresenttothepsychiatrist.
Thosewithcyclothymiashowmarkedfluctuationsofmood,forinstanceforadayoraweekthey may be optimistic, energetic, creative and garrulous, then for a period they may becomegloomy, morose, taciturn and unable to turn themselves to any useful activity. These cyclesmaybelinkedtootherbiologicalrhythmssuchasthemenstrualcycle;theymay,however,appearout of the blue, apparently unprovoked. A premorbid cyclothymic personality is thought topredisposetomanic-depressivepsychosis.Certainly,GoodwinandJamison(1990),inastudyof
19—THE ExPRESSION OF DISORDERED PERSONAlITy 327
manic-depressiveillnessandcreativity,foundthatamongpoetsespeciallytherewasanexcessofcyclothymicpersonality,depressiveillnessandsuicide.
Dysthymiaismanifestedbyall-pervasiveandpermanentgloomandapprehension.Itleadstothediagnosticquandary‘isthisdepressivestateordepressivetrait?’Suchpeopleareusuallygentleandsensitive;theytakethemselvesandtheiractivitiesseriously;theyareoftensafety-consciousand hypochondriacal. An acquaintance with this personality structure coined aphorisms thatrevealedhismentalstate,suchas‘thereisnosituationinlifesobadastobeincapableoffurtherdeterioration’or‘everysilverlininghasitscloud’.
Other Personality DisordersDSM-V(AmericanPsychiatricAssociation,1994)includestwootherpersonalitydisorders.Theyaredescribedbelow,inbrief,forcompleteness.
NARCISSISTIC PERSONALITY DISORDER
This iscategorizedbyagrandiosesenseofself-importanceoruniqueness;preoccupationwithfantasiesofunlimitedsuccess,power,brilliance,beautyorideallove;anexhibitionisticneedforconstantattentionandadmiration;indifference,angerorhumiliationinresponsetocriticismorindifference fromothers;andcharacteristicdisturbances in interpersonal relationships, suchasfeelingsof entitlement to special favours, takingadvantageofotherpeople, relationshipswithothers that alternate between the extremes of over-idealization and devaluation and lack ofempathy.
AVOIDANT PERSONALITY DISORDER
Thispersonalitydisorderis,infact,veryclosetotheanxiouspersonalitydisorderofICD-10;itischaracterizedbyexcessivesensitivitytorejection,humiliationorshame.Thereisunwillingnesstoenterintoarelationshipunlessthepersonreceivesstrongguaranteesofuncriticalacceptance.Thereissocialwithdrawal,despiteaneedforaffectionandacceptance,andthepersonhasverylowself-esteem,devaluinghisownachievementsandisveryawareofhispersonalshortcomings.Suchpeopleareexquisitelysensitivetothewaytheybelieveotherswillreacttothem.
In DSM-V, thehelpful notionof three clusters of personality types is basedondescriptivesimilarities.ClusterA includesparanoid, schizoid and schizotypal personality disorders. InclusterBareantisocial, borderline, histrionic and narcissistic personality disorders.ClusterCcontainsavoid-ant, dependent and obsessive-compulsive personality disorders. Inpractice, of course, patientsmayshow features from different clusters, and the validity of this subclassification is still beingquestioned.
Whyisatextonpsychopathologyconcernedwithpersonalityclassificationanddisorder?Theaccurateobservationanddelineationofpersonalitycharacteristicsisvaluableinclinicalpracticefordiagnosis,prognosisandtherationalplanningoftreatment.Theskillsofatrainedpsycho-pathologistareideallysuitedtotheobservationofconsistentpersonalitytraitsandforminganopinionunprejudicedbypreconceivedtheoreticalconsiderations.
References[Anonymous] (1986) Management of borderline personality disorders [leading article]. Lancet ii,
846–7.Akiskal HS (1993) Proposal for a depressive personality (temperament). In Tyrer P and Stein G (eds.)
Personality Disorder Reviewed.London:Gaskell.
328 SIX—VARIATIONS OF HUMAN NATURE
American Psychiatric Association (1994) Diagnostic and Statistical Manual of Mental Disorders, 4th edn.Washington:AmericanPsychiatricAssociation.
American Psychiatric Association (2013) Diagnostic and Statistical Manual of Mental Disorders, 5th edn.Washington:AmericanPsychiatricAssociation.
BluglassRS(1983)A Guide to the Mental Health Act, 1983.Edinburgh:ChurchillLivingstone.BornsteinRF(2012)Dependentpersonalitydisorder.InWidigerTA(ed.)The Oxford Handbook of Personality
Disorders.Oxford:OxfordUniversityPress.CarrascoJLandLecic-TosevskiD(2000)Specifictypesofpersonalitydisorder.InGelderM,López-Ibor
JJandAndreasenNC(eds.)New Oxford Textbook of Psychiatry.Oxford:OxfordUniversityPress.ChickJ,WaterhouseLandWolffS(1979)Psychologicalconstruinginschizoidchildrengrownup.British
Journal of Psychiatry135,425–30.CleckleyHM(1941)The Mask of Sanity.London:Kingston.CraftM(1966)Psychopathic Disorders.Oxford:PergamonPress.DeAlarconRD(1973)Hysteriaandhystericalpersonalitydisorder.Psychiatric Quarterly47,258–75.Dolan B and Coid J (1993) Psychopathic and Antisocial Personality Disorders: Treatment and Research
Issues.London:Gaskell.GoodwinFKandJamisonKR(1990)Manic-depressive Illness.NewYork:OxfordUniversityPress.HaddockA,SnowdenP,DolanM,Parker JandReesH(2001)Managingdangerouspeoplewithsevere
personalitydisorder:asurveyofforensicpsychiatrists’opinions.Psychiatric Bulletin25,293–6.HendersonDK(1939)Psychopathic States.NewYork:Norton.HinshawSP(1994)Attention Deficits and Hyperactivity in Children.ThousandOaks:SagePublications.HooleyJM,ColeSHandGirondeS(2012)Borderlinepersonalitydisorder.InWidigerTA(ed.)The Oxford
Handbook of Personality Disorders.Oxford:OxfordUniversityPress.Jaspers K (1913 and 1963) General Psychopathology (transl. Hoenig J and Hamilton MW). Manchester:
ManchesterUniversityPress.MalmbergA,LewisG,DavidAandAllebeckP(1998)Premorbidadjustmentandpersonality inpeople
withschizophrenia.British Journal of Psychiatry172,308–13.MillJS(1811)A System of Logic Volume II,3rdedn.London:JohnW.Parker.MulderRT (2012)Cultural aspects ofpersonalitydisorder. InWidigerTA (ed.)The Oxford Handbook of
Personality Disorders.Oxford:OxfordUniversityPress.Mullen PE (1999) Dangerous people with severe personality disorder. British Medical Journal 319,
1146–7.ParisJ(2013)The intelligent clinician’s guide to the DSM-5.Oxford:OxfordUniversityPress.PrichardJC(1835)A Treatise on Insanity and Other Disorders Affecting the Mind.London:Sherwood,Gilbert
andPiper.RushB(1812)Medical Inquiries and Observations Upon the Diseases of the Mind.Philadelphia:Kimberand
Richardson.Samuels J, Costa PT (2012) Obsessive-compulsive personality disorder. InWidigerTA (ed.) The Oxford
Handbook of Personality Disorders.Oxford:OxfordUniversityPress.SchneiderK(1923and1958)Psychopathic Personalities.(transl.HamiltonMW).London:Cassell.SchneiderK(1958)Clinical Psychopathology,5thedn.(transl.HamiltonMW,1959).NewYork:Gruneand
Stratton.SkodolAE(2012)DiagnosisandDSM-5:workinprogress.InWidigerTA(ed.)The Oxford Handbook of
Personality Disorders.Oxford:OxfordUniversityPress.SimsACP(1983)Neurosis in Society.Basingstoke:Macmillan.SimsAandSnaithR(1988)Anxiety in Clinical Practice.Chichester:JohnWiley.SnaithRPandTaylorCM(1985)Irritability:definition,assessmentandassociatedfactors.British Journal of
Psychiatry147,127–36.TantamD(1988)Personalitydisorders.InGranville-GrossmanK(ed.)Recent Advances in Clinical Psychiatry,
no.6.Edinburgh:ChurchillLivingstone.ThomasD(1954)Under Milk Wood.London:Dent.Thompson DJ (1980) A comprehensive study of hysterical personality disorder. MSc Thesis, University of
Manchester.Tyrer P and Alexander J (1979) Classification of personality disorder. British Journal of Psychiatry 135,
163–7.

19—THE ExPRESSION OF DISORDERED PERSONAlITy 329
TyrerPandSteinG(1993)Personality Disorder Reviewed.London:Gaskell.WhiteleyJS(1975)Thepsychopathandhistreatment.InSilverstoneTandBarracloughB(eds.)Contem-
porary Psychiatry.Ashford:HeadleyBrothers.WidigerTA,SamuelDB,Mullins-SweattS,GoreWLandCregoC(2012)Anintegrationofnormaland
abnormal personality structure: the five-factor model. In Widiger TA (ed.) The Oxford Handbook of Personality Disorders.Oxford:OxfordUniversityPress.
WootonBF(1959)Social Science and Social Pathology.London:AllenandUnwin.World Health Organization (1977) International Statistical Classification of Diseases, Injuries and Causes of
Death,9threvision.Geneva:WorldHealthOrganization.WorldHealthOrganization(1992)The ICD-10 Classification of Mental and Behavioural Disorders: Clinical
Description and Diagnostic Guidelines.Geneva:WorldHealthOrganization.
This page intentionally left blank
S E C T I O N SEVENDiagnosis
This page intentionally left blank

333
C H A P T E R 20
Psychopathology and Diagnosis
SummaryDiagnosisallowsthenaming,thedefining,andidentificationofasingularmaladysothatitcanbecome an object for consideration, comparison, explanation and control. It is therefore self-evidentthatthediagnosticprocessisfundamentaltothepracticeofpsychiatry.Theimportanceandrelevanceofpsychopathologyisthatitistheconstellationofabnormalphenomenathatareelicitedbytheclinical interview,reinforcedbythephenomenologicalapproach,thatconstitutepsychiatricsyndromes.Inotherwords,psychopathology is thefoundationuponwhichclinicalpsychiatryisbuilt.
‘There’s glory for you!’ ‘I don’t know what you mean by “glory”,’ Alice said. ‘I meant, there’s a nice knock-down argument for you!’ ‘But “glory” doesn’t mean “a nice knock-down argument”,’ Alice objected. ‘When I use a word,’ Humpty
Dumpty said in a rather scornful tone, ‘it means just what I choose it to mean, – neither more nor less.’
Lewis Carroll (1872), Through the Looking Glass
Diagnosisismuchmorethanawordpluckedoutoftheairandpinnedontoahapless‘patient’.Itconveysmeaningabouttheantecedentsofthepresentstate,aboutotherconditionsthataresimilarand,most importantofall,aboutwhat is likelytohappeninthefutureand,therefore,whatshouldbedoneaboutit.Diagnosisisameansofcommunicationbetweendoctors;itshouldencompassafullformulation(seeChapter2)ratherthanjustasinglewordusedinanidiosyn-craticmanner.
Theimportanceofmakingadiagnosis,andtherangeofdiagnoses,isasgreatinpsychiatryasintherestofmedicine;theconceptualdifferencesbetweendifferentdiagnosticcategoriesareactuallygreater,asmental disorders includesituational, social,emotionalandpsychologicaldis-turbanceaswellasphysicalillness.Understandably,mostofthemedicalillnessesthathavebeendescribedarebasedonsignsorsymptoms;thisistruealsoforpsychiatry.Thereis,therefore,avery close association between the observation and classification of ‘symptoms in the mind’(Burton,1621)andpsychiatricdiagnosis.
Theimportancewithwhichdiagnosisisregardedinpsychiatryhasdevelopedalongsidetheintroductionofeffectiveremediesformanyconditions.TherehasbeenasubstantialchangeintheattitudeofpsychiatristssinceStengelwrotein1959thattherewas‘almostgeneraldissatisfac-tionwiththestateofpsychiatricclassification,nationalandinternational’.Muchoftheprogressmadehasarisendirectly fromthemorecarefulapplicationofdescriptivepsychopathology, forinstance Kendell (1975). Schwartz and Wiggins (1987) have shown that in order to make adiagnosis an experienced clinician uses a mechanism of typification: ‘This more fundamentalcapacitytorecognizevariousmentaldisordersarises,notthroughmasteringconceptualdefini-tions,butratherthroughdirectlyencounteringindividualpatientswhomanifestthesedisorders.Through such direct encounters we learn the typical forms of the various mental disorders.

Keywords:Diagnosis,Health.
20—PSychOPAthOlOGy AND DIAGNOSIS 333.e1
334 SEVEN—DIAGNOSIS
We learn what is distinctive to each condition and how to distinguish these conditions fromone another’.This process of ‘typification’ seeks to recognize what is emblematic of differentconditions,whatisunusualbutyetrepresentative,andwhatisuntypicalandsohighlyunusualas tobeuncharacteristic.Thus, thedetailed examinationof psychopathological functions thatforms the substanceof this text is aprerequisite to this, thefirst step for clinicaldiagnosis inpsychiatry.
Abnormal phenomena, then, are the foundation of the diagnostic process. And diagnosisallowsthenaming,thedefining,andidentificationofasingularmaladysothatitcanbecomeanobjectforconsideration,comparison,explanationandcontrol(Sadler,2004).
In general medicine, diagnosis is based on the complete clinical process: detailed historytaking,examinationofthepatientandcarryingoutappropriatespecialinvestigations.Thisistruealso forpsychiatry.However,becauseof the limitationsof its subject, thisbookdoesnotdealwithphysicalexaminationnorwithphysical(radiological,laboratory)orpsychological(psycho-metric)investigations.
Concepts of Health and PsychopathologyThelatePeterSedgwick(1981)madetheimportantpointthat‘diseaseisahumaninvention…therearenoillnessesordiseasesinnature’,hencethequotationatthebeginningofthischapter.Herightlypointedoutthathumanbeingsdescribepotatoblightasadiseasesolelybecausetheywanttogrowpotatoes:‘ifmanwishedtocultivateparasites(ratherthanpotatoes)therewouldbeno“blight”butsimplythenecessaryfodderingoftheparasitecrop’.Sedgwickclaimedthatitwasthehumansocialmeaningattachedtothefractureofaseptuagenarianfemurthatconstitutedillnessordisease.
Out of his anthropocentric self-interest, man has chosen to consider as ‘illness’ or ‘diseases’ those natural circumstances which precipitate the death (or the
failure to function according to certain rules) of a limited number of biological species; man himself, his pets and other cherished livestock, and the plant
varieties he cultivates for gain or pleasure.
Suchargumentspointustothefactthatmedicineisnot‘objective,scientific’appliedbiologybut isnecessarilyvalue-laden.This is trueof thedisruptionof the internalstate that‘patients’bringas‘complaints’tothedoctor,andtruealsoofthosecomplaintsthatthedoctorregardsas‘symptoms’.ForSedgwick(1982),alldiseasesstartasillnessstatesrecognizedassuchbecauseofthenegativevalueattachedtothesymptomsorcomplaints.
Allillness, whether conceived in localized bodily terms or within a larger view of human functioning, expresses both a social value judgement
(contrasting a person’s condition with certain understood and accepted norms) and an attempt at explanation (with a view to controlling the disvalued
condition).
Anotherviewoftheeffectofsocialvaluesonthepresentationofillnessisthenotionofthesick roleasdevelopedbyTalcottParsons(1902–1979)(1951a).Whatevertheunderlyingcausesofconditions,therolethatthesubjecthimself,thepatient,choosestoplayandtherolethatisforcedonhimbythosearoundhimbecauseofhis illnessarehighlysignificant inthewayhissymptomsmanifest.Parsons(1951b)arguedthathealth is included inthefunctionalneedsoftheindividualmemberofsociety,sothatfromthepointofviewofthefunctioningofthesocial

20—PSychOPAthOlOGy AND DIAGNOSIS 335
system, too lowageneral levelofhealth,or toohighan incidenceof illness, isdysfunctional.Disease in this formulation incapacitates theeffectiveperformanceof social roles and there isthereforesocial interest in thealleviationofdisease.Toput this inanotherway,disease isnotpurely or merely a natural phenomenon but a state of disturbance of the total human being,includingthestateoftheorganismasabiologicalsystemandofhispersonalandsocialadjust-ments,includinghisabilitytofulfilsocialroles.
This approach introduces the notion that behavioural deviance itself can be the source ofdisease.But,howissuchdeviancetoberecognizedanddefined?Socialdeviancecanberecog-nizedbyself-definition.The individualmaycometoholdthebelief thathehasaproblemortheremaybeasocietalreactionthatindicatesthatanindividual’sbehaviourconstitutesaproblem.Societalreactionofthistypemightoccurwhenacommunitycomestorecognizeaperson’sinabil-ityorreluctancetorespondinaparticularexpectedway.AccordingtoDavidMechanic(1968),‘theviewtakenof thedeviantdepends in largepartontheframeofreferenceof theobserverand the extent to which the deviant appears to be able or willing to control his responses.The evaluator views the act within the context of what he believes the actor’s motivation tobe.Iftheactionappearsreasonableintermsoftheassumedmotivationoftheactor,thereisaverygoodchancethatdeviantbehaviourwillbedefinedintermsofthegoodness–badnessdimen-sion.Ifthebehaviourappearstobepeculiarandatoddswithexpectationsofhowareasonablepersonmightbemotivated, suchbehaviour ismore likely tobe characterized in termsof thesicknessdimension’.Theproblemwiththisisself-evident.Diseasedefinitioninthisformulationseems significantly prone to error, to subjective judgement, and liable to be used as a tool ofsocialcontrol.
Withregardtoself-definitionofillness,peopledifferinthewaytheyperceive,evaluateandacton,orfailtoacton,thesymptomstheyexperience.Mechanic(1986)hascalledthis illness behaviour.This is influencedby the salienceof the complaint, thedegree towhich itdisturbssocial roles, the folk understanding of the seriousness and consequences of the complaint orimplieddisease,andthecompetingclaimsontheperson’stimeandresources.
Somaticorpsychologicalsymptomsdo,ofcourse,frequentlyoccurwithoutanyevidenceoforganicdisease.Whenattemptingtodescribeandclassifysuchsymptoms,itishelpfultoestablishaphenomenologicalbasis;conditionsarerecognizedbecauseoftheparticularcharacteristicsofthepatient’scomplaints,notbecauseofsomepresumedtheoreticalnotionofcause.Thebizarrelengthsthatresultfromtheapplicationofapreformedtheoryofdiseaseaetiologytosymptoms,ratherthandevelopingfromsymptomstotheory, isadmirablyillustratedinEngelhardt’s(1981)essay‘The disease of masturbation’. Inthenineteenthcentury,masturbationwaswidelybelievedtoproducemanysignsandsymptomsincludingdyspepsia,constrictionoftheurethra,epilepsy,blindness,vertigo,lossofhearing,headache,impotence,lossofmemory,insanity,cardiacarrhyth-mia,rickets,leucorrhoeainwomen,conjunctivitisandgeneralizedweakness,anditwasheldtobeadangerousdiseaseentity.
Lewis(1953)pointedoutthatmentalillnesscouldbecharacterizedintermsofpsychopathol-ogy:‘disturbanceofpartfunctionsaswellasgeneralefficiency’.Part functionsrefertothedifferentaspectsofpsychologicalexperienceandbehaviourdescribedinpreviouschapters:memory,per-ception, forming beliefs and so on.Thus Lewis saw a disturbance in perception, for examplehallucination,asareasonforestablishingacaseofmentalillness–onpsychopathologicalgrounds.ThisapproachantedatedChristopherBoorse’scontributiontoourunderstandingofthenatureof mental disorders. His distinction between disease and illness is deservedly influential. Hearguedthatanorganismishealthytothedegreethatitisnotdiseased.And,hedefinedadiseaseasatypeofinternalstateofanorganismthatinterfereswithsomefunctionthatcontributestosurvivalandreproduction.Inaddition,thatthediseasestateisnotsimplyinthenatureofthespecies;i.e.,itiseitheratypicalofthespeciesor,iftypical,mainlyduetoenvironmentalcauses.Diseasesbecome illnessesonlywhentheysatisfycertain further,andnormative,conditions.A
336 SEVEN—DIAGNOSIS
diseaseisanillnessonlyifitisseriousenoughtobeincapacitating,andthereforeisregardedasundesirable,a title for special treatmentandavalidexcuse fornormallycriticizablebehaviour.For Boorse, mental functions such as perceptual processing, intelligence, and memory clearlyserve to provide information about the world that can guide effective action. Drives serve tomotivate it. Anxiety and pain function as signals of danger, language as a device for culturalco-operationandcognitiveenrichment,andsoon.Heconcludes:‘itseemscertainthatafewoftherecognizedmentaldisordersaregenuinediseases,whethermentalorphysical.Evenwithoutanyknowledgeoftherelevantfunctionalsystems,onecansometimesinferinternalmalfunctionimmediatelyfrombiologicallyincompetentbehaviour’.Finally,Boorsethoughtthatdiseasesarewhatdoctorstreatandillnessesarewhatpeoplesufferfrom(Boorse,1976).
Use of Symptoms to Form Diagnostic CategoriesThe relationship between signs and symptoms in psychiatry was discussed in Chapter 1.Traditionally,symptomshavebeendividedintothosecausingsufferingandpain(distress)andthosecausinglossoffunction(disability).Whentheonlydisharmonyisbetweentheindividualandhissociety,thedisturbanceisnotregardedasmentalillness.Forthegreatmajorityofmentaldisorders, diagnostic classification is made according to the profile of symptoms presented.Exceptionstothisare:
1. when the aetiology is known, for example dementia in human immunodeficiency virusdisease;
2. when the genetic basis and structural pathology are known, for example Huntingtondisease;and
3. when cause is hypothesized to result from a process without conclusive evidence, forexampledissociativefugue.
Descriptivepsychopathologyisalmostatheoreticalinnatureandthusallowsthedevelopmentofagenerallydescriptivediagnosticterminology.
Symptoms are collected into constellations that commonly occur together to form thesyndromes of mental illness. It is usual to make a distinction between illness, with a definiteonset after normal health, and the lifelong characteristics of learning disability or personalitydisorder.
Another fundamentaldistinctionoftenmadebypsychiatristsandbasedultimatelyonpsy-chopathologyisthatbetweenpsychosesandneuroses.Psychoses‘aremajormentalillness.Theyareexceedinglyhardtodefinealthoughtheyareusuallysaidtobecharacterizedbyseveresymptoms,suchasdelusionsandhallucinations,andbylackofinsight’(Gelderetal.,1983);thereislossofcontactwithreality.Itisprobablethattheeverydayuseoftheconceptofpsychosisbycliniciansisbasedonthenotionof‘unitarypsychosis’;thedevelopmentofthisconcepthasbeendiscussedbyBerriosandBeer(1994).Neurosis‘isapsychologicalreactiontoacuteorcontinuousperceivedstress, expressed in emotion or behaviour ultimately inappropriate in dealing with that stress’(Sims,1983:3);phenomenologicalcharacteristicsheldincommonbyneuroticpatientsincludedisturbancesofself-image,oftheexperienceofrelationshipsand,often,bodilysymptomswithoutorganiccause (Sims,1983).Although the termneurosishas fallenoutof favour, theconceptsthatthetermreferstoarestillimportantasorganizingprinciples:anunderstandablereactiontostress; the emotionaldisturbance is a variantofnormal response,possiblyonly exaggerated indegreeandintensity;aconditioninwhichinsightisretained;and,finallytheextentofdisruptiontopersonalityandself-identityisminimal.
Psychiatricdiagnosis isoftenhierarchical,organic syndromes takingprecedenceover func-tionalpsychoses, theseoverneuroses andneurosesover situationalor adjustment reactions.Apatient with schizophrenia and super-added anxiety will usually receive only the diagnosis ofschizophrenia. This can be a considerable disadvantage in practice for planning treatment
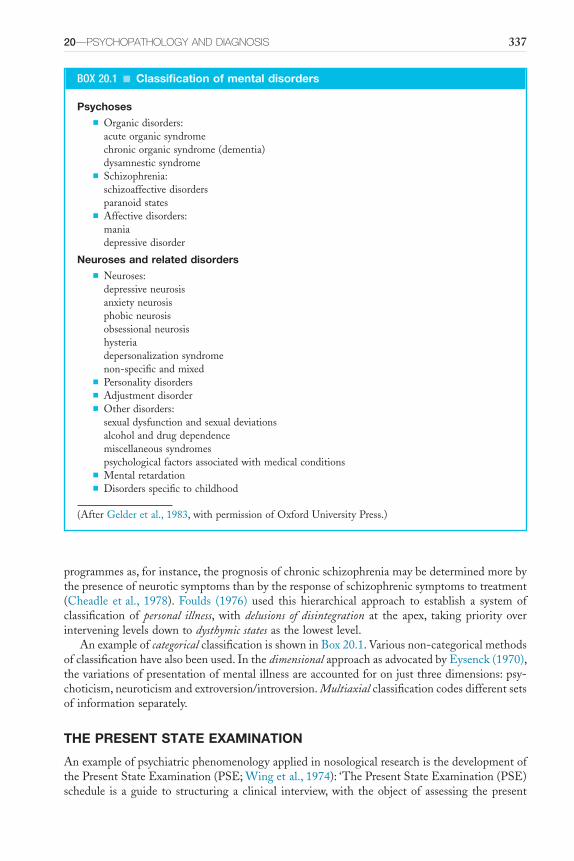
20—PSychOPAthOlOGy AND DIAGNOSIS 337
programmesas,forinstance,theprognosisofchronicschizophreniamaybedeterminedmorebythepresenceofneuroticsymptomsthanbytheresponseofschizophrenicsymptomstotreatment(Cheadle etal., 1978). Foulds (1976) used this hierarchical approach to establish a system ofclassificationof personal illness,with delusions of disintegration at the apex, takingpriority overinterveninglevelsdowntodysthymic statesasthelowestlevel.
AnexampleofcategoricalclassificationisshowninBox20.1.Variousnon-categoricalmethodsofclassificationhavealsobeenused.InthedimensionalapproachasadvocatedbyEysenck(1970),thevariationsofpresentationofmentalillnessareaccountedforonjustthreedimensions:psy-choticism,neuroticismandextroversion/introversion.Multiaxialclassificationcodesdifferentsetsofinformationseparately.
THE PRESENT STATE EXAMINATION
AnexampleofpsychiatricphenomenologyappliedinnosologicalresearchisthedevelopmentofthePresentStateExamination(PSE;Wingetal.,1974):‘ThePresentStateExamination(PSE)schedule is aguide to structuringa clinical interview,with theobjectof assessing thepresent
BOX 20.1 ■ Classification of mental disorders
Psychoses■ Organicdisorders:
acuteorganicsyndromechronicorganicsyndrome(dementia)dysamnesticsyndrome
■ Schizophrenia:schizoaffectivedisordersparanoidstates
■ Affectivedisorders:maniadepressivedisorder
Neuroses and related disorders■ Neuroses:
depressiveneurosisanxietyneurosisphobicneurosisobsessionalneurosishysteriadepersonalizationsyndromenon-specificandmixed
■ Personalitydisorders■ Adjustmentdisorder■ Otherdisorders:
sexualdysfunctionandsexualdeviationsalcoholanddrugdependencemiscellaneoussyndromespsychologicalfactorsassociatedwithmedicalconditions
■ Mentalretardation■ Disordersspecifictochildhood
(AfterGelderetal.,1983,withpermissionofOxfordUniversityPress.)
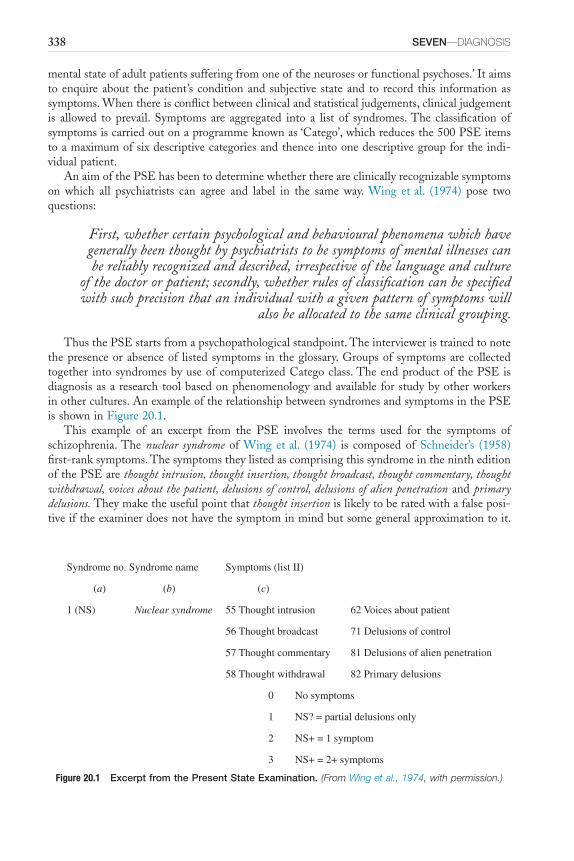
338 SEVEN—DIAGNOSIS
mentalstateofadultpatientssufferingfromoneoftheneurosesorfunctionalpsychoses.’Itaimstoenquireabout thepatient’s conditionandsubjective stateand to record this informationassymptoms.Whenthereisconflictbetweenclinicalandstatisticaljudgements,clinicaljudgementis allowed to prevail. Symptoms are aggregated into a list of syndromes.The classification ofsymptomsiscarriedoutonaprogrammeknownas‘Catego’,whichreducesthe500PSEitemstoamaximumofsixdescriptivecategoriesandthenceintoonedescriptivegroupfortheindi-vidualpatient.
AnaimofthePSEhasbeentodeterminewhetherthereareclinicallyrecognizablesymptomson which all psychiatrists can agree and label in the same way. Wing etal. (1974) pose twoquestions:
First, whether certain psychological and behavioural phenomena which have generally been thought by psychiatrists to be symptoms of mental illnesses can be reliably recognized and described, irrespective of the language and culture
of the doctor or patient; secondly, whether rules of classification can be specified with such precision that an individual with a given pattern of symptoms will
also be allocated to the same clinical grouping.
ThusthePSEstartsfromapsychopathologicalstandpoint.Theintervieweristrainedtonotethepresenceorabsenceof listedsymptoms in theglossary.Groupsofsymptomsarecollectedtogether intosyndromesbyuseofcomputerizedCategoclass.TheendproductofthePSEisdiagnosisasaresearchtoolbasedonphenomenologyandavailableforstudybyotherworkersinothercultures.AnexampleoftherelationshipbetweensyndromesandsymptomsinthePSEisshowninFigure20.1.
This example of an excerpt from the PSE involves the terms used for the symptoms ofschizophrenia.The nuclear syndrome ofWing etal. (1974) is composed of Schneider’s (1958)first-ranksymptoms.ThesymptomstheylistedascomprisingthissyndromeinthenintheditionofthePSEarethought intrusion, thought insertion, thought broadcast, thought commentary, thought withdrawal, voices about the patient, delusions of control, delusions of alien penetrationandprimary delusions.Theymaketheusefulpointthatthought insertionislikelytoberatedwithafalseposi-tiveiftheexaminerdoesnothavethesymptominmindbutsomegeneralapproximationtoit.
Figure 20.1 Excerpt from the Present State Examination. (From Wing et al., 1974, with permission.)
Syndrome no. Syndrome name Symptoms (list II)
(a) (b) (c)
1 (NS) Nuclear syndrome 55 Thought intrusion 62 Voices about patient
56 Thought broadcast 71 Delusions of control
57 Thought commentary 81 Delusions of alien penetration
58 Thought withdrawal 82 Primary delusions
0 No symptoms
1 NS? = partial delusions only
2 NS+ = 1 symptom
3 NS+ = 2+ symptoms
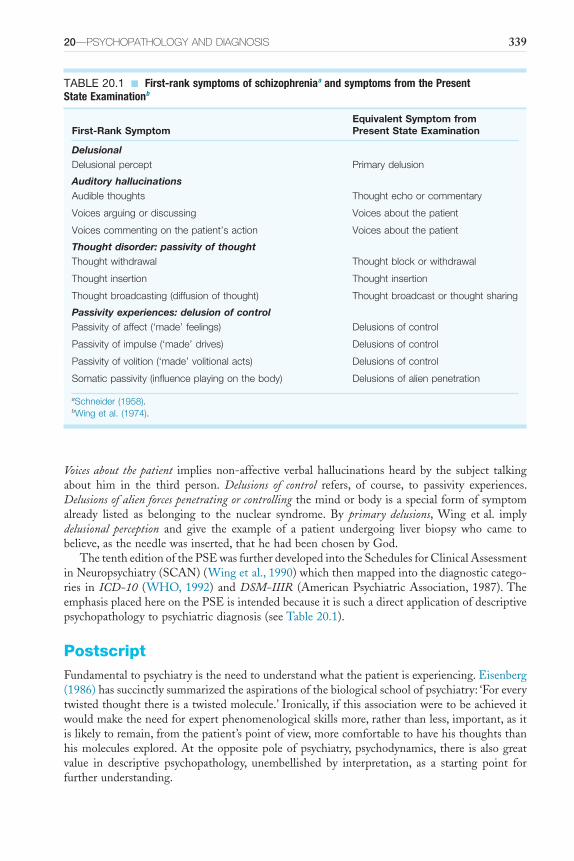
20—PSychOPAthOlOGy AND DIAGNOSIS 339
Voices about the patient impliesnon-affective verbalhallucinationsheardby the subject talkingabout him in the third person. Delusions of control refers, of course, to passivity experiences.Delusions of alien forces penetrating or controllingthemindorbodyisaspecialformofsymptomalready listed as belonging to the nuclear syndrome. By primary delusions, Wing etal. implydelusional perception and give the example of a patient undergoing liver biopsy who came tobelieve,astheneedlewasinserted,thathehadbeenchosenbyGod.
ThetentheditionofthePSEwasfurtherdevelopedintotheSchedulesforClinicalAssessmentinNeuropsychiatry(SCAN)(Wingetal.,1990)whichthenmappedintothediagnosticcatego-ries in ICD-10 (WHO,1992) andDSM-IIIR (AmericanPsychiatricAssociation,1987).TheemphasisplacedhereonthePSEisintendedbecauseitissuchadirectapplicationofdescriptivepsychopathologytopsychiatricdiagnosis(seeTable20.1).
PostscriptFundamentaltopsychiatryistheneedtounderstandwhatthepatientisexperiencing.Eisenberg(1986)hassuccinctlysummarizedtheaspirationsofthebiologicalschoolofpsychiatry:‘Foreverytwistedthoughtthereisatwistedmolecule.’Ironically,ifthisassociationweretobeachieveditwouldmaketheneedforexpertphenomenologicalskillsmore,ratherthanless,important,asitislikelytoremain,fromthepatient’spointofview,morecomfortabletohavehisthoughtsthanhismoleculesexplored.At theoppositepoleofpsychiatry,psychodynamics, there isalsogreatvalue in descriptive psychopathology, unembellished by interpretation, as a starting point forfurtherunderstanding.
TABLE 20.1 ■ First-rank symptoms of schizophreniaa and symptoms from the Present State Examinationb
First-Rank SymptomEquivalent Symptom from Present State Examination
DelusionalDelusional percept Primary delusion
Auditory hallucinationsAudible thoughts Thought echo or commentary
Voices arguing or discussing Voices about the patient
Voices commenting on the patient’s action Voices about the patient
Thought disorder: passivity of thoughtThought withdrawal Thought block or withdrawal
Thought insertion Thought insertion
Thought broadcasting (diffusion of thought) Thought broadcast or thought sharing
Passivity experiences: delusion of controlPassivity of affect (‘made’ feelings) Delusions of control
Passivity of impulse (‘made’ drives) Delusions of control
Passivity of volition (‘made’ volitional acts) Delusions of control
Somatic passivity (influence playing on the body) Delusions of alien penetration
aSchneider (1958).bWing et al. (1974).
340 SEVEN—DIAGNOSIS
USES OF PSYCHOPATHOLOGY
IthasbeensaidofWilliamofOckham,whosocourageouslynavigatedthemurkyanddangerouswatersofmedievalphilosophyandscience,thathewas‘anempiricistrefusingtostretchknowl-edgebeyondtheboundsofascertainableexperience’(Leff,1958).Thisisthepositionofdescrip-tivepsychopathology:aimingnot todrawconclusionsbeyondthesubjectiveexperienceof thepatientanditsjudiciousexplorationbytheinterviewer.Everypsychiatristusesphenomenologytosomeextent,butitisamuchmorevaluabletoolifusedrigorously.
Thefourpracticalapplicationsofdescriptivepsychopathology,then,areasfollows.■ Communication.Itenablesclinicianstospeakandwritetoeachotherabouttheproblems
oftheirpatientsinamutuallycomprehensibleway.Thisisclearlyofvaluebothinclinicalpracticeandforresearch.
■ Diagnosis.Psychiatricdiagnosisisbasedtoaconsiderableextentonpsychopathology,andthisiswhollyappropriate,especiallyuntilthereismoreevidenceforaetiologyandunderly-ingpathologyforthedifferentconditions.
■ Therapy.The method of empathy, that is using phenomenology to explore the patient’ssubjectiveexperience,isarationalwayofestablishingatherapeuticrelationship.Itenablesthe therapist to understand the subjective experience of his patient and will give thepatient confidence in further entrusting the secrets of his internal environment to thetherapist.
■ The law.Descriptivepsychopathology is theonlyreasonablewayofdeterminingwhat ismentalillnessandwhatarethedifferencesbetweenmentalillnesses,fromaforensicpointofview.Mutualenlightenmentintheareabetweenthelawandpsychiatry,wherethereisatpresentsomuchmisunderstanding,will result fromacleareracknowledgementofthevalueofpsychopathologybylawyersanddoctors.
Thepatient’ssymptoms,hissufferings,arealogicalstartingpointforthedoctor’ssympathy,curiosityandtherapeuticendeavour.Tostartelsewhereturnsmedicineonitsheadand,ultimately,onearrivesinatopsy-turvyworldlikeSamuelButler’sErewhon(1872),where‘illnessofanysortisconsidered…tobehighlycriminalandimmoral;andthatIwasliable,forcatchingcold,tobehadupbeforetheMagistratesandimprisonedforaconsiderableperiod…’and‘ifamanforgesacheque,orsetshishomeonfireorrobswithviolencefromaperson,ordoesanysuchthingsthatarecriminalinourowncountry,heiseithertakentoahospitalandiscarefullytendedatthepublicexpense,orifhewasingoodcircumstances,heletsitbeknowntoallhisfriendsthatheissufferingfromaseverefitofimmorality…andtheycomeandvisithimwithgreatsolici-tude…’Youmaythinkthisistoofar-fetched;however,thelesspleasantaspectsofthiscertainlyappeartohavebeenthesituationforsomeofthedissidentsinpsychiatriccustodyinthepreviousUSSR(BlochandReddaway,1977).
Theultimateaimofpsychiatryisnot,ofcourse,knowledge,buttohelppeopletofunctionandfeelbetter;phenomenologyisavaluabletherapeutictool.Ideally,itgivesthepatient,inhisdoctor,apersonwhounderstandswhatheisfeelingbutdoesnottrytoexplaincausesintermsoftheory,whichthepatientmayfindunconvincing.Thepatientoftenhasagreatsenseofreliefwhenthedoctor,howeverfalteringly,describesbacktohimthesymptoms,ortheinternalexperi-ence,thathe,thepatient,hasfoundsodifficulttodescribe.
NEED FOR RESEARCH
Psychopathologywasintroducedintopsychiatrybeforethecurrentemphasisonquantification,populationsurveysandexperimentalmethod.Itisnowimperativebothforthefurtherdevelop-mentofdescriptivepsychopathologyand,moreimportantly,forcontinuedprogressinpsychiatricresearch that more rigorous research methods be applied. Phenomenology has a place in

20—PSychOPAthOlOGy AND DIAGNOSIS 341
psychiatric research that has not yet been fully exploited. It forms a logical bridge betweenresearchfindingsemanatingfromclinicalandappliedpsychologyandtheincreasingknowledgeofdisorderedneuroanatomy–physiologyandchemistry–thatisresultingfrommoresophisti-cated methods of neuroimaging and assay. This is the direction that research in descriptivepsychopathologyshouldgo.
Investigationoftheexperienceoftheindividualhastobelinkedtoanunderstandingofhisbiology, and it is also important to assess how normal phenomena are distributed within thepopulation.Thescientificbasesofpsychiatryinclude,aswellasbiologicalandbehaviouralsci-ences,epidemiologyandphenomenology.Recognitionofhomogeneityincludesboththesymp-tomswithinanindividualpatientandthefeaturesofanaffectedpopulation.ThePSEhasbeendiscussedearlierasamethodofquantifyingpsychopathologicalinformation.
Tointroduceexperimentalmethodsintoresearchindescriptivepsychopathologywillsome-timesinvolvesinglecasestudiesinwhichvariablesthathavebeenevaluatedphenomenologicallyarealtered.Forexample,GreenandPreston(1981)amplifiedthequietwhisperingofachronicschizophrenicpatientduringthetimehewasauditorilyhallucinated.Hewhisperedatthesametimeasheheardvoices,andthecontentofhisvocalizationcorrespondedtowhatthevoiceswerereportedtohavesaid,thusdemonstratingthedisturbanceofboundariesofselffoundinschizo-phrenia.Thistypeofinvestigationhasbeenextendedfurther,andthereareseveralexamplesinthisbook,forexampleinChapters7and8.Therehasbeenadangerinthatsomeotherpsycho-logical studies,notquotedhere,haveusedphenomenology impreciselyandhencevitiated thesignificanceoftheirfindings.
Aninterestingdevelopmentinresearchbasedondescriptivepsychopathologyistheapplica-tionof particular psychological techniques to specificphenomenological entities.Examples ofthisaretheuseofcognitivebehaviourtherapyinthetreatmentofpersistentauditoryhallucina-tions(Bentalletal.,1994)andmoregeneralapplicationofpsychologicalinterventionsinschizo-phrenia(HaddockandLewis,1996).
It is important thatprogress in the treatmentofpatients and in research that advances inbiologicalaspectsofpsychiatryareassistedbyaccuratepsychiatricdiagnosisbasedonphenom-enologythatisbothreliable(thatis,capableofreproductionbythesameintervieweratadifferenttime,orbydifferentinterviewers)andquantifiable.Neverweretheskillsoftheclinicalphenom-enologistmorenecessaryormorelikelytoyieldbeneficialresultsbothinunderstandingandintherapy.The introductionof improvedneuropsychiatricmethodsof investigation increases theneed for reliable findings from descriptive psychopathology rather than rendering it obsolete.Jaspers(1959)commented,‘phenomenology,thoughoneofthefoundationstonesofpsychopa-thology,isstillverycrude’.Thisisstilltrue,butitisnowhightimethatdescriptivepsychopa-thologybecamemoresophisticated.
Phenomenologytakesthedoctor’sartanddisciplineofobservationinsidehispatient’smind.DavidHume(1804)describedtheabsenceofphysicalexaminationinmedicineinhisessay‘Of Polygamy and Divorces’.He tellsof thephysicianbrought into theGrandSignior’s seraglio inConstantinople.
He was not a little surprised, in looking along a gallery, to see a great number of naked arms standing out from the sides of the room. He could not
imagine what this could mean; till he was told that those arms belonged to bodies, which he must cure, without knowing any more about them than
what he could learn from the arms. He was not allowed to ask a question of the patient, or even of her attendants, lest he might find it necessary to
enquire concerning circumstances which the delicacy of the seraglio allows not to be revealed. Hence physicians in the east pretend to know all diseases from

342 SEVEN—DIAGNOSIS
the pulse, as our quacks in Europe undertake to cure a person merely from seeing his water.
Psychiatrymustnowcomeoutoftheseraglioanduseallavailableinformationintheserviceofitspatients,includingphenomenology,fordiagnosis,forunderstandingandfortreatment.
ReferencesBentallRP,HaddockGandSladePD(1994)Cognitivebehaviourtherapyforpersistentauditoryhallucina-
tions:fromtheorytotherapy.Behaviour Psychotherapy25,51–6.BerriosGEandBeerD(1994)Thenotionofunitarypsychosis:aconceptualhistory.History of Psychiatry
V,13–36.BlochSandReddawayP(1977)Russia’s Political Hospital.London:Gollancz.Boorse C (1976) What a theory of mental health should be. Journal of the Theory of Social Behaviour 6,
61–84.BurtonR(1621)The Anatomy of Melancholy, What it is. With all the Kinds, Causes, Symptoms, Prognostickes,
and Severall Cures of it by Democritus Junior.Oxford:Cripps.ButlerS(1872)Erewhon.London:Cape.CarrollL(1872)Through the Looking Glass, and What Alice Found There.London:Macmillan.Cheadle AJ, Freeman HL and Korer J (1978) Chronic schizophrenic patients in the community. British
Journal of Psychiatry132,221–7.Eisenberg L (1986) Mindlessness and brainlessness in psychiatry. British Journal of Psychiatry 148,
497–508.Engelhardt HT (1981) The disease of masturbation: values and the concept of disease. In Caplan AL,
EngelhardtDTandMcCartneyJJ(eds.)Concepts of Health and Disease.Reading:Addison-Wesley.Eysenck HJ (1970) A dimensional system of psychodiagnosis. In Mahrer AR (ed.) New Approaches to
Personality Classification,pp.169–207.NewYork:ColumbiaUniversityPress.FouldsGA(1976)The Hierarchical Nature of Personal Illness.London:AcademicPress.GelderM,GathDandMayouR(1983)Oxford Textbook of Psychiatry.Oxford:OxfordUniversityPress.GreenPandPrestonM(1981)Reinforcementofvocalcorrelatesofauditoryhallucinationsusingauditory
feedback:acasestudy.British Journal of Psychiatry139,204–8.HaddockGandLewisSW(1996)Newpsychologicaltreatmentsinschizophrenia.Advances in Psychiatric
Treatment2,110–6.HumeD(1804)Essays and Treaties on Several Subjects,vol.1.Edinburgh:BellandBradfute.JaspersK(1959)General Psychopathology,7thedn.(transl.HoenigJandHamiltonMW,1963).Manchester:
ManchesterUniversityPress.KendellRE(1975)The Role of Diagnosis in Psychiatry.Oxford:Blackwell.LeffG(1958)Medieval Thoughts.Harmondsworth:Penguin.LewisAJ(1953)Healthasasocialconcept.British Journal of Sociology4,109–24.MechanicD(1968).Medical Sociology.NewYork:TheFreePress.Mechanic D (1986) The concept of illness behaviour: culture, situation and personal predisposition.
Psychological Medicine16,1–7.Parsons T (1951a) Illness and the role of the physician: a sociological perspective. American Journal of
Orthopsychiatry21,452–60.ParsonsT(1951b).The Social System.NewYork:TheFreePress.SadlerJZ(2004)Values and Psychiatric Diagnosis.Oxford:OxfordUniversityPress.SchneiderK(1958)Clinical Psychopathology,5thedn.(transl.HamiltonMW,1959).NewYork:Gruneand
Stratton.SchwartzMAandWigginsOP(1987)Typifications:thefirststepforclinicaldiagnosisinpsychiatry.Journal
of Nervous and Mental Disease175,65–77.SedgwickP(1981)Illness–mentalandotherwise.InCaplanAL,EngelhardtHTandMcCartneyJJ(eds.)
Concepts of Health and Disease: Interdisciplinary Perspectives,pp.119–30.Reading:Addison-Wesley.SedgwickP(1982)Psycho politics.NewYork:HarperandRow.

20—PSychOPAthOlOGy AND DIAGNOSIS 343
SimsACP(1983)Neurosis in Society.London:Macmillan.StengelE(1959)Classificationofmentaldisorders.Bulletin of the World Health Organization21,601–3.Wing JK, Babor T, Brugha T, Burke J, Cooper E, Giel R, Jablenski A, Regier D and Sartorius N
(1990)SCAN:Schedules forClinicalAssessment inNeuropsychiatry.Archives of General Psychiatry47,589–93.
WingJK,CooperJEandSartoriusN(1974)The Measurement and Classification of Psychiatric Symptoms: an Instruction Manual for the PSE and Category Program.Cambridge:CambridgeUniversityPress.
WorldHealthOrganization(1992)The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Description and Diagnostic Guidelines.Geneva:WorldHealthOrganization.

This page intentionally left blank
345
S E L F - A S S E S S M E N T 1
Instructions
Each set of numbered items is followed by five lettered options. Select the ONE lettered option that is BEST in each case.
Chapter 1Descriptivepsychopathologyis:
a) Thestudyofegodefencemechanismsthatunderliebehaviourchangeb) Concernedwiththeselection,delimitation,differentiationanddescriptionofabnormalpsycho-
logicalphenomenac) Directlytheoutcomeofanalyzingthecontentofdreamsd) Amethodofdescribingtheinteractionbetweendoctorsandpatientse) Anintrospectivesystemofunderstandinganddescribingabnormalcognitions
Empathyindescriptivepsychopathologyis:a) Achieved by precise, insightful, persistent and knowledgeable exploration of the patient’s
experienceb) Acommunicationtechniqueaimedatputtingthepatientathiseasec) Meta-communicationd) Thebasisofsympathyforthepatient’ssituatione) Anaspectoftransference
Theterm‘understanding’inpsychopathology:a) DerivesfromFreud’sstructuraltheoryofthepsycheb) Describesthecausalmechanismsunderlyingabnormalexperiencesc) Hasnolimitinthecapacitytodescribeandcomprehendexperienced) DerivesfromDilthey’sconceptionofthedistinctionbetweenthesciencesandhumanitiese) Hasnoplaceincontemporarypsychiatry
Chapter 2SpecificcommunicationskilltechniquesincludethefollowingEXCEPT:
a) Summarystatementsb) Attentivelisteningc) Normalizingstatementsd) Loopedquestionse) Openquestions
AspectsofobservationofappearanceandbehaviourincludethefollowingEXCEPT:a) Postureb) Gesturec) Talkd) Facialexpressione) Self-hygiene
AssessmentofinsightinvolvesthefollowingdomainsEXCEPT:a) Fluencyoftalkb) Recognitionofsubjectivepsychologicalchangec) Attributionofthechangetopathologyd) Recognitionofneedfortreatmente) Compliancewithtreatment
346 Self-ASSeSSment 1
Chapter 3AutomatismischaracterizedbythefollowingEXCEPT:
a) Involuntarybehaviourb) Behaviourthatisinappropriatetothecircumstancesc) Complexandcoordinatedbehaviourd) Unimpairedjudgemente) Apparentlypurposefulanddirectedbehaviour
Mania à potuisasyndromecharacterizedbythefollowingEXCEPT:a) Insomniab) Totalorpartialamnesiafortheaberrantbehaviourc) Alcoholconsumptiond) Senselessviolencee) Prolongedsleep
DeliriumisaconditioncharacterizedbythefollowingEXCEPT:a) Insidiousonsetb) Globalimpairmentofcognitivefunctionsc) Reducedlevelofconsciousnessd) Impairedattentione) Disorderedsleep-wakecycle
Chapter 4Dreams:
a) Occurinnon-REMsleepb) Areassociatedwithparalysisc) Involveanaccentuationofself-awarenessd) Involveconsolidationofspatialandtemporalconnectionse) Aresynonymouswithnightterror
Kleine–Levinsyndromeischaracterizedby:a) Severehypersomniab) Sleepparalysisc) ShortREMlatencyd) Hypnogogichallucinationse) Cataplexy
Attention:a) Isthefocusingofconsciousnessonanyaspectofexperienceb) Issynonymouswithconcentrationc) Involvesdisinhibitionofmemoryd) Isdistinctfromvigilancee) Reliessolelyonactiveprocesses
Chapter 5ThefollowingareTRUEofconfabulationEXCEPT:
a) Itisafalsememoryb) Itisassociatedwithorganicamnesiac) Itcaninvolveembellishmentofactualmemoriesd) Itistypically‘fantastic’innaturee) Suggestibilityisaprominentfeature
Short-termmemory:a) Isanunlimitedcapacitysystemb) Comprisesofacentralactionsystemc) Involvesa‘phonologicalloop’thatholdsmemorytracesforuptofiveminutesd) Involvesavisuospatialscratchpadthatallowsformanipulationofvisualinformatione) Cannotbedistinguishedfromattention
Self-ASSeSSment 1 347
LongtermmemoryfunctionsincludethefollowingEXCEPT:a) Registrationb) Retentionc) Repressiond) Retrievale) Recall
Chapter 6Formalcharacteristicsoftimeinclude:
a) Durationb) Sequencec) Synchronyd) Rhythme) Bi-directionality
Déjàvuexperienceisanexampleofabnormalityof:a) Rhythmb) Senseofuniquenessoftimec) Timedurationd) Temporalordere) Directionoftime
FeaturesofseasonalaffectivedisorderincludethefollowingEXCEPT:a) Hypersomniab) Insomniac) Cravingforcarbohydratesd) Overeatinge) Lethargy
Chapter 7AbnormalitiesoftheelementaryaspectsofvisualperceptionincludethefollowingEXCEPT:
a) Palinopsiab) Macropsiac) Hemacropsiad) Palinacousise) Achromatopsia
Insynaesthesia:a) Theperceptionofasensoryobjectispresentedinanothersensorymodalityb) Theperceptionoccursinperi-personalspacec) Musictocolourtransformationsoccurd) ElaborationofFormConstantsisafeaturee) Emotionaldistressisacommonaccompaniment
FormalcharacteristicsofimagesincludethefollowingEXCEPT:a) Imagesarenotclearlydelineatedb) Imageshaveacharacterofobjectivityc) Imagesappearininnersubjectivespaced) Imagesareactivelycreatede) Imagesdissipaterapidlyandhavetobere-created
Chapter 8Thefollowingareexamplesofprimarydelusions:
a) Autochthonousdelusionsb) Delusionalperceptc) Persecutorydelusionsd) Delusionalatmospheree) Delusionalmemory
348 Self-ASSeSSment 1
Secondarydelusionsare:a) Secondarytootherabnormalexperiencesb) Understandableinthelightofthepatient’ssocialcontextc) Notheldwithconvictiond) Amenabletocounterargumente) Transient
Delusionsareexamplesof:a) Perseverationb) Impairmentofconsciousnessc) Falseperceptiond) Falsebeliefse) Autoscopy
Chapter 9Schneider’sFirstRankSymptomsincludethefollowingEXCEPT:
a) Somatichallucinationsb) Audiblethoughtsc) Passivityexperiencesd) Thoughtwithdrawale) Thoughtinsertion
Delusionsofcontrolofthoughtinclude:a) Thoughtbroadcastingb) Thoughtechoc) Thoughtinsertiond) Thoughtwithdrawale) Thoughtblocking
Theterm‘circumstantiality’refersto:a) Flightofideasb) Looseningofassociationc) Concretethinkingd) Over-inclusivethinkinge) Impedanceofflowofthinkingbyunnecessarydetail
Chapter 10RecognizedabnormalitiesoflanguageinschizophreniaincludethefollowingEXCEPT:
a) Lackofuseofcohesivetiesb) Alogiac) Neologismd) Clangassociationse) Telegony
TheClozetechniqueisameasureof:a) Predictabilityofspeechb) Theproportionofthenumberofdifferentwordstothetotalnumberofwordsc) Cohesivetiesd) Rulesofpropositione) Fluencyoflanguage
Primarysensorydysphasiais:a) Theinabilitytoproducenamesorsoundsatwillb) Agrossdisturbanceofwordsandsyntaxresultinginunintelligiblespeechc) Adisorderofindistinctspeechd) Thelossofcomprehensionofthemeaningofwordse) Theinabilitytoreadwithunderstanding
Self-ASSeSSment 1 349
Chapter 11InsightinschizophreniahasbeenshowntobepositivelycorrelatedwiththefollowingEXCEPT:
a) Thelikelihoodofdevelopingdepressionb) Thelikelihoodofhospitalizationsc) Compliancewithtreatmentd) Long-termoutcomee) Workingmemory
ValidmeasuresofinsightmusttakeintoconsiderationthefollowingEXCEPT:a) Themultidimensionalaspectofinsightb) Therelationshipofinsighttoaffectc) Theinfluenceofculturalfactorsd) Thevariationofinsightacrossdifferentsymptomdomainse) Theaddedvalueofbehaviouralobservations
InsightinvolvesallofthefollowingEXCEPT:a) Awarenessofchangeb) Recognitionofillnessinothersc) Attributionofchangetoillnessd) Recognitionoftheneedfortreatmente) Co-operationwithtreatment
Chapter 12AutoscopycaninvolveallofthefollowingEXCEPT:
a) Feelingofpresenceb) Failuretoperceiveselfinamirrorc) Visualhallucinationofinternalorganswithinbodilyspaced) Visualhallucinationofexactcopyoftheselfinmirrorimagee) Projectionoftheobservingselfinextra-personalspace
Egovitalityis:a) Awarenessofbeinganagentb) Awarenessofunityandcoherenceofselfc) Awarenessofbeingd) Awarenessofcontinuityofselfovertimee) Awarenessofboundariestotheself
Nihilisticdelusionisanexampleof:a) Disorderofegoboundaryb) Disorderofcontinuityofselfovertimec) Disorderofactivityd) Disorderofvitalitye) Disorderofunityofself
Chapter 13DefinitivefeaturesofdepersonalizationincludethefollowingEXCEPT:
a) Theexperienceispleasantb) Thereisafeelingofstrangenessc) Itisasubjectiveexperienced) Insightispreservede) Itcanaffectbodilysensation
350 Self-ASSeSSment 1
DepersonalizationhasshowntoconsistofanumberofcomponentsincludingthefollowingEXCEPT:a) Perceptualalterationb) Unrealityofsurroundingsc) Temporalintegrationd) Unrealityofselfe) Emotionalnumbing
DepersonalizationisknowntobeassociatedwiththefollowingEXCEPT:a) LSDb) Cannabisc) Mescalined) Sensorydeprivatione) Narcolepsy
Chapter 14IndividualdeterminantsofhypochondriasisincludethefollowingEXCEPT:
a) Feelingsofdisgustb) Preoccupationwithbodilyfunctionc) Seriousillnessorinjuryinchildhoodd) Fearofinfectione) FascinationwiththeInternet
Masspsychogenicillness:a) Occursmostcommonlyinyoungmalesb) Oftenstartsinachildoflowstatusinthepeergroupc) Affectsmostseverelythemostadjustedpeopled) Symptomsspreadbyline-of-sighttransmissione) Isunaffectedbymediaresponse
Theconceptsof‘conversion’and‘dissociation’suggest:a) Thatphysicalsymptomscanonlyhaveanorganicbasisb) Thatcausationisunconsciousc) Thatsymptomscarrynoobviousadvantageforthepatientd) Thatsymptomsareunlikelytobepsychologicallymeaningfule) Thatthepatientisactingapart
Chapter 15Painasymbolia:
a) Presentswithabsentpainresponseb) Isassociatedwithincreasedthermalsensitivityc) Isassociatedwithhyperhidrosisd) Presentswithself-stimulatione) Isusuallyanacquireddisorderfollowingvascularlesions
Painassociatedwithpsychopathologyis:a) Betterlocalizedb) Clearlydelineatedalongrecognizedneuroanatomicaldistributionc) Easyforthepatienttodescribed) Constantandunremittinge) Tendstobeprovokedbydefiniteagents
Centralpain(thalamicsyndrome):a) Presentswithacuttingsensationb) Isactivatedbycutaneousstimulationc) Presentsashypoalgesiad) Isunaffectedbytemperaturechangee) Doesnotpresentwithallodynia
Self-ASSeSSment 1 351
Chapter 16Alexithymiarefersto:
a) Inabilitytoexperiencepleasureb) Reactingtosadnewswithlaughterc) Absenceofunitybetweendifferentmodesofexperienceofemotionsd) Inabilitytoverbalizeaffectandelaboratefantasye) Selectivedeficiencyincorrectlyappraisingvocalexpressionofemotion
Ekman’sbasicemotionsincludeallthefollowingEXCEPT:a) Angerb) Disgustc) Feard) Jealousye) Sadness
Moodisdefinedas:a) Apositiveornegativereactiontoanexperienceb) Aprolongedprevailinginnerstateorpredispositionc) Aspontaneousandtransitoryexperienceinresponsetoanexperienced) Theexternalbehaviouralmanifestationofinnerstatee) Anevaluativeattitudetowardsanobject
Chapter 17TherespiratorysubtypeofpanicdisorderischaracterizedbyallthefollowingEXCEPT:
a) Fearofdyingb) Chestpainanddiscomfortc) Shortnessofbreathd) Provocationbyinhalationof35%carbondioxidee) Inducedbyspecificsituations
Selye’sGeneralAdaptationSyndromeincludesoneofthefollowingstages:a) Shockandnumbnessb) Sadnessc) Guiltandhostilityd) Flight-or-fightresponsee) Resolution
TheconstituentelementsofobsessivecompulsivephenomenonincludeallthefollowingEXCEPT:a) Inflatedsenseofresponsibilityevenforeventsoverwhichthepatienthasnocontrolb) Avoidanceofcueslikelytotriggerobsessionc) Fearofdisasterthatthepatientbelieveswillcometopassd) Resistancee) Increaseddiscomfortfollowingcompulsiveact
Chapter 18AbnormalmovementincatatoniaincludeallthefollowingEXCEPT:
a) Waxyflexibilityb) Psychologicalpillowc) Stereotypyd) Cataplexye) Mitgehen
Motivationcanbedefinedas:a) Innatedispositionthatdetermineswhatobjectstoattendtointheworldb) Astatethatinitiatesdirectedactionc) Astrivingtowardsanobjectthatisexperiencedasadesired) Arewardsystemthatgovernsandregulatesbehavioure) Thepowertoputintoeffectvoluntaryaction
352 Self-ASSeSSment 1
ImpulsivityinvolvesallthefollowingEXCEPT:a) Predispositiontowardsrapid,unplannedactionb) Lackofregardforconsequencesc) Preferencefordelayedlargerrewardoversmallbutimmediaterewardd) Perseveranceofbehaviourdespitepunishmente) Inabilitytopreventresponseinresponsedisinhibitionattentionalparadigm
Chapter 19Paranoidpersonalitydisordercanbedefinedasadisorderinwhich:
a) Anindividualmistrustsothersandisundulysuspiciousb) Thereisalackofneedforanddefectincapacitytoformrelationshipsc) Adefectinempathyisevidentd) Uncontrollableoutburstsofintemperateanduncontrolledmoodoccurse) Theatricalbehaviourandcravingforattentionoccurs
InDependentPersonalityDisorderthefollowingfeaturesalloccurEXCEPT:a) Lackofselfconfidenceb) Perfectionisticdispositionc) Cravingforsupportandencouragementofothersd) Difficultyincopingwithchangingdemandsoflifee) Presenceofadominantcloserelationship
The following conditions have been shown to be frequently associated with anankastic personalitydisorderEXCEPT:
a) Eatingdisorderb) Hypochondriasisc) Alcoholdependencesyndromed) Obsessivecompulsivedisordere) Recurrentdepressivedisorder
Chapter 20IllnessbehaviourisinfluencedbyallthefollowingEXCEPT:
a) Salienceofthecomplaintb) Extentofdisturbanceofsocialrolesc) Culturalunderstandingoftheseriousnessofthecomplaintd) Competingclaimsonthesufferer’sresourcese) Theunderlyingbiologyofthecondition
All the following individuals have made contributions to our understanding of health and diseaseEXCEPT:
a) ChristopherBoorseb) AaronBeckc) PeterSedgwickd) TalcottParsonse) DavidMechanic
PracticalapplicationsofpsychopathologyincludeallthefollowingEXCEPT:a) Communicationbetweencliniciansb) Cognitiveneuroscienceresearchc) Diagnosisd) Nosologye) Therapy
353
S E L F - A S S E S S M E N T 2
Instructions
Each set of matching questions consists of a list of ten lettered options (A–J) followed by four numbered items. For each numbered item, select the appropriate lettered option. Each lettered option may be selected only once.
Chapters 3 and 4A. ConfusionB. ComaC. DeliriumD. DisorientationE. HypersomniaF. InsomniaG. OneiroidstateH. ParasomniaI. StuporJ. Twilightstate
1. A75-year-oldfemalepatientisfoundwanderingthestreets.Onexaminationshedoesnotknowthedate,day,time,season,placewheresheisorherownaddress.
2. An18-year-oldmalepatientpresentswithahistoryofseveralandirresistibleperiodsofdrowsi-nessduringtheday.Atnighthereportsperiodswhenheisfullyawakebutunabletomovehislimbs.
3. Thepartnerofa25-year-oldmalepatientaccompanieshimtotheoutpatientappointment.Shereportsthathetalksinhissleep,wandersaimlesslyinthebedroomforafewminutesatnightandthathehasnorecollectionoftheseincidents.
4. A47-year-oldfemalepatientwithahistoryofrecurrentdepressionisadmittedinamutestate.She is immobilebut fully conscious andalert.She is able tomake eye contactbutdoesnotrespondtoanyattemptatverbalcommunication.
Chapter 5A. AnterogradeamnesiaB. ConfabulationC. CryptamnesiaD. DissociativefugueE. FalsememoryF. GanserstateG. PerseverationH. PseudologiafantasticaI. RecoveredmemoryJ. Retrogradeamnesia
1. A20-year-oldmalepatientwasinvolvedinaroadtrafficaccident.Hesustainedaheadinjury.He was only able to recall events that happened approximately five minutes before thecollision.
2. A20-year-oldmalepatientpresentedinprisonwhilstonremand.WhenexaminedherespondedtoquestionsaboutthedateandthecapitalofFrancewithapproximateanswers,disorientationfortimeandplace.
354 Self-aSSeSSment 2
3. A45-year-oldmalepatientwasinvolvedinanaccidentatworkwherehesustainedaseriousheadinjuryandlostconsciousness.Onregaininghisconsciousnesshecouldonlyrecalleventsthathappenedapproximately36hoursaftertheincident.
4. A57-year-oldmalepatientwithanestablishedhistoryofimpairmentofshort-termmemoryinthecontextofalcoholabuserespondedtoquestionsaboutwhathehadspentthepreviousdaywithobjectivelyfalseaccountsthatincludedembellishmentsandintrusionsfrompreviousoccasions.
Chapter 7A. ImageryB. PalinopsiaC. MacropsiaD. MicropsiaE. ParaprosopiaF. AlloaesthesiaG. PelopsiaH. DyschromatopsiaI. TeleopsiaJ. Metamorphopsia
1. A45-yearmanpresentswithacomplaintthathefirstsawablackcatatthecornerwherehisdrivejoinedthemainstreet.Afterthis,forthenext72hoursorso,hekeptseeingthesamecatatvarioustimesandsituations.Whatisthetermforthisexperience?
2. A19-year-oldmanwitharecentdiagnosisofschizophreniacomplainedthatthefacesofpeoplelookingathimwouldsuddenlylookdifferent,asiftheywerepullingfacesathim.Sometimes,thefaceswouldappearsinister,lopsidedandstrange.Whatisthetermforthisexperience?
3. A25-year-oldfemalepatientwithahistoryofcomplexfocalseizurescomplainedofscenesandobjectsbecomingsmallerbeforeaseizure.Whatisthisexperiencetermed?
4. A25-year-oldmalepatientcomplainedthatobjectslookfaraway.Hefoundthissurprisinganddistressing.Whatisthisexperiencetermed?
Chapter 8A. DelusionalperceptB. DelusionalintuitionC. DelusionalmemoryD. DelusionalatmosphereE. SecondarydelusionF. Over-valuedideaG. DelusionofloveH. DelusionalmisidentificationI. DelusionofpersecutionJ. Delusionaljealousy
1. A20-year-oldmalepatientwasadmittedintohospitalfollowinganattackuponhisfather.Hereportedthathisfatherhadbeenreplacedbyarobotwholookedalmostexactlylikehimbutwasdefinitelynothim.Hefearedthatthis‘robot’hadmalignintentionsandthathislifewasindanger.Whatisthisbeliefcalled?
2. A40-year-oldfemalepatientcomplainedthatherlocalpriestwassendinghersecretmessages,declaringhisfeelingsforher.Shecomplainedthatalthoughhewasthefatherofherchildhewasyettovisitthem.
3. A21-year-oldfemalepatientsuddenlybecameconvincedthatshewastherightfulheirtothethroneofNorway.ShewasnotNorwegianbybirthorancestry.Whenaskedthereasonforthisbelief, shesaidthatshehadsuddenlycometothisrealization.Shedeniedanyotherunusualexperience.
Self-aSSeSSment 2 355
4. A54-year-oldmalepatientwith a longstandinghistoryof schizophrenia reportedpersistentandstressfulauditoryverbalhallucinationsofderogatoryandthreateningcontent.ThevoiceswouldoftentellhimthathedeservedtobekilledandthatnewimmigrantsintohislocalareafromRomaniaweregoingtomurderhim.Hethenheldafirmbeliefthathewasatriskfromimmigrants,particularlyRomanians.Thisbeliefwasheldwithconvictionandwasimpervioustocounterargument.
Chapter 9A. FantasythinkingB. ImaginativethinkingC. ConceptualthinkingD. CircumstantialthinkingE. ThoughtblockF. ConcretethinkingG. Over-inclusivethinkingH. ThoughtinsertionI. ThoughtwithdrawalJ. Audiblethought
1. A 21-year-old male university student described spending a lot of time thinking about thefuture,aboutthepossibilityofbecomingafamousmusician,becomingrichandabletoliveinamansioninFlorida.
2. A25-year-oldfemalepatient,newlyadmittedintohospitalcomplainedthatherthoughtswerebeing interfered with. She was particularly distressed by the experience of having thoughtsmanipulatedandtakenfromher.
3. Inatest,a19-year-oldpatientwithadiagnosisofschizophreniarespondedtoaquestioninthefollowingway:‘Whichofthefollowingareessentialpartsofaroom:walls,chairs,floor,window?’‘Chairs’.
4. A57-year-oldfemalepatientsaid:‘IwasstartingtofeelhighsoItieddumb-bellweightsroundmyankle’.
Chapter 10A. AphoniaB. LogocloniaC. EcholaliaD. ParagrammatismE. NominaldysphasiaF. AsyndesisG. MetonymH. JargonaphasiaI. ReceptivedysphasiaJ. Neologism
1. A 65-year-old right-handed male patient, who was recovering from a left-sided stroke, wasunabletofollowtheverbalcommand:‘Takethepaperwithyourlefthand,folditintwoandputitonthefloor’.
2. A25-year-oldpatientsaid,‘Phlogonshave invadedmy lungs turningfirst sidewaysandnowmedways’.
3. A64-year-oldmalepatientwithalongstandinghistoryofschizophreniarepliedtothequestion,‘Whathaveyougotinyourcup?’‘Afluidthatwhilstbeingcolourlessturnsdarkonbrewing’.
4. A72-year-oldmalepatientwithadiagnosisofParkinsondiseasesaid,‘I’mstar…,star…,start-ingtothinkofmo…,mo…,mo…,movinghouse’.
356 Self-aSSeSSment 2
Chapter 14A. MisoplegiaB. DysmorphophobiaC. PalinaptiaD. AlloaesthesiaE. ExosomesthesiaF. MicrosomatognosiaG. MacrosomatognosiaH. MuscledysmorphiaI. ParaschemaziaJ. Aschemazia
1. A23-year-oldmalepatientpresentedwiththebeliefthathismusclesweretoosmall,apreoc-cupationwithphysicalbuild,excessiveexercisinganddisturbedeating.
2. A56-year-oldfemalepatientcomplainedofhatingherlefthand.Althoughitlookednormal,shesaidthatshehateditandhadalwayswishedthatitwasdifferentinsize,shapeandfeel.
3. A 27-year-old male patient presented with a longstanding belief that his face was ugly, inparticularhisnosethathethoughtwasfartoolargeandcrooked.Objectively,hisnosewasnotexcessivelylargeorcrooked.
4. A40-year-oldfemalepatientpresentedwiththecomplaintthatshecouldcontinuetofeelhertoothbrushinherhandsforupto15minutesaftersheusedit.
Chapter 16A. AnhedoniaB. EcholaliaC. HyperekplexiaD. CoenaesthesiaE. ProsopoaffectiveagnosiaF. ReceptiveemotionaldysprosodyG. CyclothymiaH. EcstasyI. EchomimiaJ. Alexithymia
1. An8-year-oldmalepatientpresentedwithahistoryofheightenedstartlereflexcharacterizedbyeyeblinking,headflexion,abductionoftheupperarms,movementofthetrunkandbendingofthekneesinresponsetoaloudnoise.
2. A40-year-oldfemalepatientwithahistoryofrecurrentdepression,andcurrentlydepressed,gaveahistoryofinabilitytoexperiencepleasureinherusualhobbiesandinterestsaswellasageneralinabilitytoexperienceanyfeeling.
3. A36-year-oldmalepatientpresentedtothelocaldentalhospitalwithanachingpaininbothsidesofthelowerjawradiatingtothetemporo-mandibularjointsandtotheneck.Inresponseto thequestion, ‘Howare you feeling in your spirits?’, he seemedpuzzled and asked for thequestiontoberepeated.Hethensaid,‘MybodyisheavyandIamachingallover’.
4. A75-year-oldmalepatientwithadiagnosisofParkinsondiseasespokeinamonotonousvoice.Inadditionheseemednottorecognizetheemotionalmeaningofvariationsintoneofvoice.
Chapter 17A. AnxietyB. AnankasticpersonalityC. CompulsionD. DisgustE. Irritability
Self-aSSeSSment 2 357
F. PanicG. PhobiaH. ObsessionI. RuminationJ. Socialphobia
1. A32-year-oldfemalepatientpresentedwithdiscreteepisodesofintenseandextremefear.2. A23-year-oldfemalepatientpresentedwithexcessivefear,self-consciousnessandavoidanceof
socialsituationsduetothepossibilityofembarrassmentorhumiliation.3. A 27-year-old male accountancy trainee presented with a history of repetitive and intrusive
thoughts about cleanliness and hygiene, which were associated with increasing tension andworry, and which he recognized as his own thoughts. He tried to resist these thoughts, butfoundthattheybecameevenmoreurgentandintrusive.
4. A32-year-oldfemalepatient,whohadrecentlygivenbirth,presentedwithasixweekhistoryoftemperoutbursts,feelingsofhostilitytowardsherhusband,anunpleasantfeelingofdistressandimpatiencewithherchildren.
Chapter 18A. AkathisiaB. AnhedoniaC. CatatoniaD. DriveE. ImpulsivityF. InstinctG. Kleine–LevinsyndromeH. MotivationI. UrgeJ. Will
1. A21-year-oldmalerecentlydiagnosedwithschizophreniaandtreatedwithrisperidonecom-plainsofmotorrestlessness,inneragitationandaninabilitytositstill.
2. A17-year-oldmalepatient isbroughttotheattentionofhisgeneralpractitionerbecausehenewly recognized a problem with gambling, drinking excessively and misusing cannabis. Inadditionhe is reportedasprone to losinghis temperand liable to say thingswhichhe laterregrets.
3. A21-year-oldmalepatientpresentedwithahistoryofepisodesofexcessivesleeping(amount-ing to up 15hours a day), excessive eating, increased sexual libido, low mood and transientpersecutorybeliefs.
4. A28-yearfemalepatientpresentedforthefirsttimewithmarkedlyslowedmovements,some-timesresultingin immobility,strangeposturesandmuteness.Onexaminationsheallowsherupperlimbstobeputinuncomfortableposturesthatsheholdsforlongperiodsoftime.

This page intentionally left blank
359
S E L F - A S S E S S M E N T 1 : A N S W E R S
Chapter 1Descriptivepsychopathologyis:
b) Concernedwith the selection,delimitation,differentiation anddescriptionof abnormalpsychologicalphenomena(seepage3)
Empathyindescriptivepsychopathologyis:a) Achievedbyprecise,insightful,persistentandknowledgeableexplorationofthepatient’s
experience(seepage5)Theterm‘understanding’inpsychopathology:
d) DerivesfromDilthey’sconceptionofthedistinctionbetweenthesciencesandhumanities(seepage10)
Chapter 2SpecificcommunicationskilltechniquesincludethefollowingEXCEPT:
d) Loopedquestions(seepage25)AspectsofobservationofappearanceandbehaviourincludethefollowingEXCEPT:
c) Talk(seepage26)AssessmentofinsightinvolvesthefollowingdomainsEXCEPT:
a) Fluencyoftalk(seepage28)
Chapter 3AutomatismischaracterizedbythefollowingEXCEPT:
d) Unimpairedjudgment(seepage41)Mania à potuisasyndromecharacterizedbythefollowingEXCEPT:
a) Insomnia(seepage40)DeliriumisaconditioncharacterizedbythefollowingEXCEPT:
a) Insidiousonset(seepage39)
Chapter 4Dreams:
b) Areassociatedwithparalysis(seepage53)Kleine–Levinsyndromeischaracterizedby:
a) Severehypersomnia(seepage52)Attention:
a) Isthefocusingofconsciousnessonanyaspectofexperience(seepage45)
Chapter 5ThefollowingareTRUEforconfabulationEXCEPT:
d) Itistypically‘fantastic’innature(seepage62)
360 Self-ASSeSSment 1: AnSwerS
Short-termmemory:d) Involvesavisuospatialscratchpadthatallowsformanipulationofvisualinformation(see
page60)Long-termmemoryfunctionsincludethefollowingEXCEPT:
c) Repression(seepage60)
Chapter 6Formalcharacteristicsoftimeinclude:
e) Bi-directionality(seepage76)Déjàvuexperienceisanexampleofabnormalityof:
b) Senseofuniquenessoftime(seepage81)FeaturesofseasonalaffectivedisorderincludethefollowingEXCEPT:
b) Insomnia(seepage84)
Chapter 7AbnormalitiesoftheelementaryaspectsofvisualperceptionincludethefollowingEXCEPT:
d) Palinacousis(seepage91)Insynaesthesia:
e) Emotionaldistressisacommonaccompaniment(seepage89)FormalcharacteristicsofimagesincludethefollowingEXCEPT:
b) Imageshaveacharacterofobjectivity(seepage88)
Chapter 8Thefollowingareexamplesofprimarydelusions:
c) Persecutorydelusions(seepage123)Secondarydelusionsare:
a) Secondarytootherabnormalexperiences(seepage115)Delusionsareexamplesof:
d) Falsebeliefs(seepage112)
Chapter 9Schneider’sFirstRankSymptomsincludethefollowingEXCEPT:
a) Somatichallucinations(seepage151)Delusionsofcontrolofthoughtinclude:
b) Thoughtecho(seepage151)Theterm‘circumstantiality’refersto:
e) Impedanceofflowofthinkingbyunnecessarydetail(seepage114)
Chapter 10RecognizedabnormalitiesoflanguageinschizophreniaincludethefollowingEXCEPT:
e) Telegony(seepage165)TheClozetechniqueisameasureof:
a) Predictabilityofspeech(seepage170)Primarysensorydysphasiais:
d) Thelossofcomprehensionofthemeaningofwords(seepage163)
Self-ASSeSSment 1: AnSwerS 361
Chapter 11InsightinschizophreniahasbeenshowntobepositivelycorrelatedwiththefollowingEXCEPT:
b) Thelikelihoodofhospitalizations(seepage180)ValidmeasuresofinsightmusttakeintoconsiderationthefollowingEXCEPT:
b) Therelationshipofinsighttoaffect(seepage179)InsightinvolvesallofthefollowingEXCEPT:
b) Recognitionofillnessinothers(seepage176)
Chapter 12AutoscopycaninvolveallofthefollowingEXCEPT:
c) Visualhallucinationofinternalorganswithinbodilyspace(seepage194)Egovitalityis:
c) Awarenessofbeing(seepage192)Nihilisticdelusionisanexampleof:
d) Disorderofvitality(seepage192)
Chapter 13DefinitivefeaturesofdepersonalizationincludethefollowingEXCEPT:
a) Theexperienceispleasant(seepage206)Depersonalization has shown to consist of a number of components including the followingEXCEPT:
c) Temporalintegration(seepage206)DepersonalizationisknowntobeassociatedwiththefollowingEXCEPT:
e) Narcolepsy(seepage52)
Chapter 14IndividualdeterminantsofhypochondriasisincludethefollowingEXCEPT:
e) FascinationwiththeInternet(seepage220)Masspsychogenicillness:
d) Symptomsspreadbyline-of-sighttransmission(seepage225)Theconceptsof‘conversion’and‘dissociation’suggest:
b) Thatcausationisunconscious(seepage224)
Chapter 15Painasymbolia:
a) Presentswithabsentpainresponse(seepage248)Painassociatedwithpsychopathologyis:
d) Constantandunremitting(seepage247)Centralpain(thalamicsyndrome):
b) Isactivatedbycutaneousstimulation(seepage247)
Chapter 16Alexithymiarefersto:
d) Inabilitytoverbalizeaffectandelaboratefantasy(seepage268)
362 Self-ASSeSSment 1: AnSwerS
Ekman’sbasicemotionsincludeallthefollowingEXCEPT:d) Jealousy(seepage259)
Moodisdefinedas:b) Aprolongedprevailinginnerstateorpredisposition(seepage257)
Chapter 17TherespiratorysubtypeofpanicdisorderischaracterizedbyallthefollowingEXCEPT:
e) Inducedbyspecificsituations(seepage284)Selye’sGeneralAdaptationSyndromeincludesoneofthefollowingstages:
d) Flight-or-fightresponse(seepage280)The constituent elements of obsessive compulsive phenomenon include all the followingEXCEPT:
e) Increaseddiscomfortfollowingcompulsiveact(seepage289)
Chapter 18AbnormalmovementincatatoniaincludeallthefollowingEXCEPT:
d) Cataplexy(seepage304)Motivationcanbedefinedas:
d) Arewardsystemthatgovernsandregulatesbehaviour(seepage295)ImpulsivityinvolvesallthefollowingEXCEPT:
c) Preferencefordelayedlargerrewardoversmallbutimmediatereward(seepage300)
Chapter 19Paranoidpersonalitydisordercanbedefinedasadisorderinwhich:
a) Anindividualmistrustsothersandisundulysuspicious(seepage320)InDependentPersonalityDisorderthefollowingfeaturesalloccurEXCEPT:
b) Perfectionisticdisposition(seepage326)ThefollowingconditionshavebeenshowntobefrequentlyassociatedwithanankasticpersonalitydisorderEXCEPT:
c) Alcoholdependencesyndrome(seepage324)
Chapter 20IllnessbehaviourisinfluencedbyallthefollowingEXCEPT:
e) Theunderlyingbiologyofthecondition(seepage335)AllthefollowingindividualshavemadecontributionstoourunderstandingofhealthanddiseaseEXCEPT:
b) AaronBeck (well-known topsychiatrists as creatorof cognitivebehavioral therapyandnotanauthorityonconceptofillnessanddisease)
PracticalapplicationsofpsychopathologyincludeallthefollowingEXCEPT:d) Nosology(seepage340)
363
S E L F - A S S E S S M E N T 2 : A N S W E R S
Chapters 3 and 41. A75-year-oldfemalepatientisfoundwanderingthestreets.Onexaminationshedoesnot
knowthedate,day,time,season,placewheresheisandherownaddress.D. Disorientation(seepage49)
2. An 18-year-old male patient presents with a history of several and irresistible periods ofdrowsinessduringtheday.Atnighthereportsperiodswhenheisfullyawakebutunabletomovehislimbs.
E. Hypersomnia(seepage52)3. Thepartnerofa25-year-oldmalepatientaccompanieshimtotheoutpatientappointment.
Shereportsthathetalksinhissleep,wandersaimlesslyinthebedroomforafewminutesatnightandthathehasnorecollectionoftheseincidents.
H. Parasomnia(seepage52)4. A47-year-old femalepatientwith ahistoryof recurrentdepression is admitted in amute
state.Sheisimmobilebutfullyconsciousandalert.Sheisabletomakeeyecontactbutdoesnotrespondtoanyattemptatverbalcommunication.
I. Stupor(seepage52)
Chapter 51. A20-year-oldmalepatientwasinvolvedinaroadtrafficaccident.Hesustainedheadinjury.
He was only able to recall events that happened approximately five minutes before thecollision.
J. Retrogradeamnesia(seepage61)2. A 20-year-old male patient presented in prison whilst on remand. When examined he
respondedtoquestionsaboutthedateandthecapitalofFrancewithapproximateanswers,disorientationfortimeandplace.
F. Ganserstate(seepage68)3. A45-year-oldmalepatientwasinvolvedinanaccidentatworkwherehesustainedaserious
headinjuryandlostconsciousness.Onregaininghisconsciousnesshecouldonlyrecalleventsthathappenedapproximately36hoursaftertheincident.
A. Anterogradeamnesia(seepage61)4. A57-year-oldmalepatientwithanestablishedhistoryofimpairmentofshort-termmemory
inthecontextofalcoholabuserespondedtoquestionsaboutwhathehadspentthepreviousdaywithobjectivelyfalseaccountsthatincludedembellishmentsandintrusionsfrompreviousoccasions.
B. Confabulation(seepage62)
Chapter 71. A45-yearmanpresentswithacomplaintthathefirstsawablackcatatthecornerwherehis
drivejoinedthemainstreet.Afterthis,forthenext72hoursorso,hekeptseeingthesamecatatvarioustimesandsituations.Whatisthetermforthisexperience?
B. Palinopsia(seepage91)
364 Self-ASSeSSment 2: AnSwerS
2. A 19-year-old man with a recent diagnosis of schizophrenia complained that the faces ofpeople looking athimwould suddenly lookdifferent, as if theywerepulling faces athim.Sometimes, the faces would sinister, lopsided and strange. What is the term for thisexperience?
E. Paraprosopia(seepage91)3. A25-year-oldfemalepatientwithahistoryofcomplexfocalseizurescomplainedofscenes
andobjectsbecomingsmallerbeforeaseizure.Whatisthisexperiencetermed?D. Micropsia(seepage91)
4. A25-year-oldmalepatientcomplainedthatobjectslookedfaraway.Hefoundthissurprisinganddistressing.Whatisthisexperiencetermed?
G. Pelopsia(seepage92)
Chapter 81. A20-year-oldmalepatientwasadmittedintohospitalfollowinganattackuponhisfather.
Hereportedthathisfatherhadbeenreplacedbyarobotwholookedalmostexactlylikehimbutwasdefinitelynothim.Hefearedthatthis‘robot’hadmalignintentionsandthathislifewasindanger.Whatisthisbeliefcalled?
H. Delusionalmisidentification(seepage125)2. A40-year-oldfemalepatientcomplainedthatherlocalpriestwassendinghersecretmessages,
declaringhisfeelingsforher.Shecomplainedthatalthoughhewasthefatherofherchildhewasyettovisitthem.
G. Delusionoflove(seepage124)3. A21-year-old femalepatient suddenlybecameconvinced that shewas the rightfulheir to
thethroneofNorway.ShewasnotNorwegianbybirthorancestry.Whenaskedthereasonforthisbelief,shesaidthatshehadsuddenlycometothisrealization.Shedeniedanyotherunusualexperience.
B. Delusionalintuition(seepage116)4. A54-year-oldmalepatientwithalongstandinghistoryofschizophreniareportedpersistent
andstressfulauditoryverbalhallucinationsofderogatoryandthreateningcontent.ThevoiceswouldoftentellhimthathedeservedtobekilledandthatnewimmigrantsintohislocalareafromRomaniaweregoingtomurderhim.Hethenheldafirmbeliefthathewasatriskfromimmigrants,particularlyRomanians.Thisbeliefwasheldwithconvictionandwasimpervioustocounterargument.
E. Secondarydelusion(seepage113)
Chapter 91. A21-year-oldmaleuniversitystudentdescribedspendinga lotof timethinkingaboutthe
future,aboutthepossibilityofbecomingafamousmusician,becomingrichandabletoliveinamansioninFlorida.
A. Fantasythinking(seepage140)2. A 25-year-old female patient, newly admitted into hospital complained that her thoughts
were being interfered with. She was particularly distressed by the experience of havingthoughtsmanipulatedandtakenfromher.
I. Thoughtwithdrawal(seepage155)3. Inatest,a19-year-oldpatientwithadiagnosisofschizophreniarespondedtoaquestionin
thefollowingway:‘Whichofthefollowingareessentialpartsofaroom:walls,chairs,floor,window?’‘Chairs’.
G. Over-inclusivethinking(seepage149)
Self-ASSeSSment 2: AnSwerS 365
4. A57-year-old femalepatient said: ‘Iwas starting to feelhigh so I tieddumb-bellweightsroundmyankle’.
F. Concretethinking(seepage148)
Chapter 101. A65-year-oldright-handedmalepatient,whowasrecoveringfromaleft-sidedstroke,was
unabletofollowtheverbalcommand:‘Takethepaperwithyourlefthand,folditintwoandputitonthefloor’.
I. Receptivedysphasia(seepage163)2. A25-year-oldpatientsaid,‘Phlogonshaveinvadedmylungsturningfirstsidewaysandnow
medways’.J. Neologism(seepage168)
3. A64-year-oldmalepatientwithalongstandinghistoryofschizophreniarepliedtotheques-tion, ‘What have you got in your cup?’ ‘A fluid that whilst being colourless turns dark onbrewing’.
G. Metonym(seepage166)4. A 72-year-old male patient with a diagnosis of Parkinson disease said, ‘I’m star…, star…,
startingtothinkofmo…,mo…,mo…,movinghouse’.B. Logoclonia(seepage161)
Chapter 141. A23-year-oldmalepatientpresentedwiththebeliefthathismusclesweretoosmall,apreoc-
cupationwithphysicalbuild,excessiveexercisinganddisturbedeating.H. Muscledysmorphia(seepage234)
2. A 56-year-old female patient complained of hating her left hand. Although it lookednormal,shesaidthatshehateditandhadalwayswishedthatitwasdifferentinsize,shapeandfeel.
A. Misoplegia(seepage237)3. A27-year-oldmalepatientpresentedwith a longstandingbelief thathis facewasugly, in
particularhisnosethathethoughtwasfartoolargeandcrooked.Objectively,hisnosewasnotexcessivelylargeorcrooked.
B. Dysmorphophobia(seepage227)4. A40-year-old femalepatientpresentedwiththecomplaint thatshecouldcontinueto feel
hertoothbrushinherhandsforupto15minutesaftersheusedit.C. Palinaptia(seepage219)
Chapter 161. An8-year-oldmalepatientpresentedwithahistoryofheightenedstartlereflexcharacterized
by eye blinking, head flexion, abduction of the upper arms, movement of the trunk andbendingofthekneesinresponsetoaloudnoise.
C. Hyperekplexia(seepage265)2. A40-year-oldfemalepatientwithahistoryofrecurrentdepression,andcurrentlydepressed,
gaveahistoryofinabilitytoexperiencepleasureinherusualhobbiesandinterestsaswellasageneralinabilitytoexperienceanyfeeling.
A. Anhedonia(seepage261)3. A36-year-oldmalepatientpresentedtothelocaldentalhospitalwithanachingpaininboth
sidesofthelowerjawradiatingtothetemporo-mandibularjointsandtotheneck.Inresponse
366 Self-ASSeSSment 2: AnSwerS
tothequestion,‘Howareyoufeelinginyourspirits?’,heseemedpuzzledandaskedforthequestiontoberepeated.Hethensaid,‘MybodyisheavyandIamachingallover’.
J. Alexithymia(seepage268)4. A75-year-oldmalepatientwithadiagnosisofParkinsondiseasespokewithamonotonous
voice.Inadditionheseemednottorecognizetheemotionalmeaningofvariationsintoneofvoice.
F. Receptiveemotionaldysprosody(seepage269)
Chapter 171. A32-year-oldfemalepatientpresentedwithdiscreteepisodesofintenseandextremefear.
F. Panic(seepage283)2. A23-year-oldfemalepatientpresentedwithexcessivefear,self-consciousnessandavoidance
ofsocialsituationsduetothepossibilityofembarrassmentorhumiliation.J. Socialphobia(seepage285)
3. A27-year-oldmaleaccountancytraineepresentedwithahistoryofrepetitiveandintrusivethoughtsaboutcleanlinessandhygiene,whichwereassociatedwith increasingtensionandworry,andwhichherecognizedashisownthoughts.Hetriedtoresistthesethoughts,butfoundthattheybecameevenmoreurgentandintrusive.
H. Obsession(seepage287)4. A32-year-oldfemalepatient,whohadrecentlygiven,birthpresentedwithasixweekhistory
oftemperoutbursts,feelingsofhostilitytowardsherhusband,anunpleasantfeelingofdistressandimpatiencewithherchildren.
E. Irritability(seepage286)
Chapter 181. A 21-year-old male recently diagnosed with schizophrenia and treated with risperidone
complainsofmotorrestlessness,inneragitationandaninabilitytositstill.A. Akathisia(seepage308)
2. A17-year-oldmalepatientisbroughttotheattentionofhisgeneralpractitionerbecausehenewlyrecognizedaproblemwithgambling,drinkingexcessivelyandmisusingcannabis.Inadditionheisreportedaspronetolosinghistemperandliabletosaythingswhichhelaterregrets.
E. Impulsivity(seepage299)3. A21-year-oldmalepatientpresentedwithahistoryofepisodesofexcessivesleeping(amount-
ingtoup15hoursaday),excessiveeating,increasedsexuallibido,lowmoodandtransientpersecutorybeliefs.
G. Kleine–Levinsyndrome(seepage296)4. A 28-year female patient presented for the first time with markedly slowed movements,
sometimesresultinginimmobility,strangeposturesandmuteness.Onexaminationsheallowsherupperlimbstobeputinuncomfortableposturesthatsheholdsforlongperiodsoftime.
C. Catatonia(seepage304)
367
Pagenumbersfollowedby‘f ’indicatefigures,‘t’indicatetables,and‘b’indicateboxes.
AAbnormalpersonality,23,318–319Abnormality,9–10
typological,10Abstractions,142Achromatopsia,92Acquiredbraininjury,ofdelusional
misidentification,126Activity
disorderof,192–193inpersonalityassessment,24physiological,abnormalityof,268–269
Actual:idealself-discrepancy,232Actual:oughtdiscrepancy,232Adolescents
dissocialpersonalitydisorder,322obesity,230–231obsessive-compulsivedisorder,290
Adrenaline(epinephrine),258–259Advertence,305–306Affect
alterationin,delusions,120blunting,266definitionof,257–258difficultiesinthecapacitytoverbalize,268ofhopelessness,67perceptionassociated,92selectiveforgettingassociated,66
Affectillusions,94–95Affect-ladencomplexes,120Affectivedisorders,257–278
circadianrhythmsassociatedwith,82–83exacerbationofemotions,262–264falsificationofmemory,66volitionaldisturbances,298
Affectivepsychoses,auditoryhallucinations,98Affectiveresponse,todelusions,113After-image,96Age
disorientationin,77–78severityofirritability,287
Aggernaes,A.consciousness,disturbedstateof,37defectinrealitytestinginschizophrenia,149hallucinationsvs.perceptiondefects,96–97subjectivityandobjectivity,16
I N D E X
Aggression,300–301diminished,302excessive,302innatedriveandacquiredresponse,301
Aggressiveacts,299–302Aggressivebehaviours
inemotionallyunstablepersonalitydisorder,323psychiatricillnessand,302psychopathology,301–302inschizophrenia,302
Aggressivenessdecreased,302definition,300–301
Agitation,144,303indepression,303inphysicalillness,303
Agnosia,162prosopoaffective,269visualobject,87–88
Agnosicalexiawithoutdysgraphia,162–163Agoraphobia,212,284Agrammatism,168–169Agraphia
alexiawith,164pure,164
Akataphasia,166Akathisia,308,357,366
dyskinesiaassociation,309subjectivecomponents,308b
Akinesia,307–308Akinesis,304Akineticmutism,42Akinetopsia,92Alcohol
craving,288–289diminishedpainsensation,248mania,298–299pathologicalintoxication,40–41withdrawalstates,exaggeratedstartlereflex,265
Alcoholabuse,delusionsofjealousyand,123–124Alcoholichallucinosis,chronic,98Alertness,45
increased,depersonalisation,211Alexia,100,162–163
withagraphia,164withoutdysgraphia,162–163
Alexithymia,351,356,361,366Alloaesthesia,92–93,219tAlogia,168Alteration,depersonalisationtheories,211
368 Index
Alzheimer’sdisease,visualhallucination,100Ambiguity,toleranceof,99Ambitendency,305Amnesia
anterograde,61dissociative(hysterical)fugue,67–68one-way,197organic(true),61psychogenic,67retrograde,61
Amnesicsyndrome,178–179Amok,239tAmputee/amputation
bodyimage,234grief,274phantomlimb,237,250
Analgesia,psychological,246Analogicreasoning,141Analytical(dynamic)psychopathology,4–5Anankasticpersonalitydisorder,324–325,352,
362Anankasticpersonalitytraits,324Anastrophy,120Anger,intensificationof,265Angst,280–281Anhedonia,261–262,270,296,356,365
indepression,298Animalphobias,284Anorexia,297Anorexianervosa,231–233Anosognosia,178–179,236Anosognosicoverestimation,237Anterogradeamnesia,354,363Antipsychoticdrugs,extrapyramidalsideeffects,
307–309,308bAntisocialbehaviour,322Antisocial(dissocial)personalitydisorder,321–322Anxiety,280–286
acute,282characteristicof,280–281depersonalisation,212free-floating,280–281general,283inhypochondriasis,222–223normal,280inotherdisorders,286pathological,280self-description,283situational,283stressassociated,280symptomsof,280–281,281b
three-dimensionalmodel,282fAnxietydisorders,286
depersonalisation,210ideationalcomponents,282
Anxietystates,280–281Anxiousfeeling,283Anxiouspersonalitydisorder,327Anxioussearching,ingrief,274Apathy,ofdepression,274Aphasia,162
motor,164–165subcorticalvisual,162–163
Aphonia,161dissociative,161
Apophany,119Appearanceofpatient,observationof,26,345,
359Appetite
abnormalities,297bexcessive,297loss(anorexia),297inschizophrenia,297–298
‘Appetitecentre,’296–297Apprehension(lossofintellectualgrasp),49Approximateanswers,68,169Argyle,M.,non-verbalcommunication,190–191Arousal,physiological,abnormalitiesof,260bArousalsystems,ofconsciousness,37f‘Asif ’feeling,205Aschemazia,235–236Asocial(dissocial)personalitydisorder,321–322Associations
clang,168constellationof,167–168modelsbasedonJaspers,142–143,142fpsychosisof,130ofthoughts,lossofcontinuityof,166
Astasia-abasia,225,225fAsthenopia,223–224Asyndesis,149,166Atmosphere
delusional,118ideasarisingfrom,114
Atrabilious,220Attention,46–49,346,359
alterationofdegreeof,46–48alternating,46,47tcapacity,46,47tdeficits,48divided,46,47tfocused/selective,46,47tinvoluntary,45narrowingof,46inpainperception,248psychosisand,48–49sustained(vigilance),46,47tvoluntary,45
Attentiondeficit/hyperactivitydisorder,303–304Attitudinalbodydissatisfaction,232
Index 369
Attributionindelusion,122hypochondriasis,221
Atypicalfacialpain,250Auditoryhallucinations,15,97–100
conditionsassociatedwith,98delusionalatmospheremanifestingas,118elementary,97–98inmentalstateexamination,26persecutory,98schizophrenia,341
Auditoryperception,14Aura,epileptic,41Autochthonousdelusions,116Autochthonousidea,114Autogynephilia,230Autohypnosis,55Automaticcognitiveprocesses,46Automaticobedience,305–306Automatism,41–42,346,359
epileptic,41,52–53sane,53
Autoscopy(heautoscopy),105,194–196,349,361
Aversion,306Avoidantpersonalitydisorder,325–327Awareness,46–49
delusional,119ofexperience,36heightened,37inner,191–192ofpersonality,labilityin,197variationsinlevelof,47f
BBehaviours
aggressive.seeAggressivebehavioursantisocial,322duringautomatism,41characteristic,personalityrevealedby,23indescriptivepsychopathology,4,4fdeviant,duetodelusions,113disturbance,310–312
schizophrenia,310–311exploratory,abnormalities,296,297bmaladaptive,299–300observationof,5–6,26,345,359relationshiptoneedandinstinct,294fviolent.seeViolentbehaviours(violence)
Being,disorderof,192Beliefs,111–113
aboutthebody,disordersof,218–224,220fassessmentof,27–28delusional,112
false,111delusionsas,131–132
folk,129non-delusional,113religious.seeReligiousbeliefssymbolic,120
Belleindifference,227Bereavement,feelingofloss,274–275Berner,P.,delusionalatmosphere,118Berrios,G.E.
delusions,112pseudohallucinations,104
Bias,informant,22Bigorexia,234Biologicaldisadvantage,8–9Biologicalrhythms,77
andpsychiatry,82–85Bipolardisorders
insightand,181–182moodin,abnormalityof,270
‘Blackbile,’266Blindness
bodyimage,234cortical,100,178–179pureword,162–163
Blunting,offeeling,266Bodilyfeelings,associatedwithemotion,266–267Bodilyfunction,disordersof,224–227Bodilysensation,hallucinationof,102–103Body
disordersofthephysicalcharacteristics/emotionalvalueof,227–234
dissatisfaction,bulimianervosa,234experience,235physicalityof,217–218size,disturbanceof,230–234
Bodyawareness,191disorderof,217–244
classificationof,218,219tsensory,234–238
Bodycathexis,189Bodychecking,234Bodyclock,primaryinternal,82Bodyconcept,189Bodydysmorphicdisorder.seeDysmorphophobiaBodyimage,188–189,235
culture-bounddisordersof,238–239,239tdevelopmentof,189,190fdiminished/absent,235–236distortion,233,236–238disturbance,238organicchangesin,234–238pathologicalaccentuationof,235sensoriumof,247socialaspects,189
370 Index
Bodyintegrityidentitydisorder,229Bodyschema,189,235Borderlinetypepersonalitydisorder,323–324Bottom-upprocessing,visualrecognition,88Braintrauma,40
retrogradeamnesia,61Brainstemlesions,dysarthria,161Broca’sarea,164Bulimia,297Bulimianervosa,233–234Burningmouthsyndrome,251
CCannabis,depersonalisation,211Cannon-Bardtheoryofemotion,258–259Capacity,forinsight,176Capgras’syndrome,125Cartesiandualism,17Casevignettemethod,181–182Cataplexy,52Catatonia,304–305,310,351,357,362,366
lethal(pernicious),305Catatonicschizophrenia,304–305,310Catego,classificationofsymptoms,337–338Category-basedinduction,141Categoryboundary,broadeningof,149Centralexecutive,short-termmemory,60Cerebrovascularaccidents
delusionalmisidentification,126intime-lapsephenomenon,80
CharlesBonnet’ssyndrome,101Cheek,stroking,312Children
attentiondeficit/hyperactivitydisorder,303–304
dissocialpersonalitydisorder,322non-accidentalinjury,322
Chomsky’stheoryoflanguage,160–161Chronology,disorderof,78Circadianrhythms,82–83Circumstantiality,348,360Cleanliness,obsessional,288Closure,principle,completionillusionand,
94Clothing
choice,bodyimageand,191inmania,312
Clozeprocedure,170modified,170reverse,170
Clozetechnique,348,360Cocaineaddiction,130Coenaesthesia,267Coenestopathicstates,267
Cognition(s)indelusions,121–122emotions,relationship,259,269languagerelationship,160
Cognitiveimpairment,insightand,180–182Cognitiveprocessing,impairment,inauditory
hallucinations,99Cognitivestate,assessmentof,28Cohesiveties(links),169Coid,J.,maniaàpotu,components,41Colostomy,bodyimageafter,238Colourperception,91–92Colourvision,lossof,100Coma,38–39Communicatedinsanity,130–131Communication
descriptivepsychopathologyapplication,340
ofemotions,260phenomenologyinvolving,10skillsandtechniques,345,359
mentalstateexamination,25bforunderstandingofpatient’ssymptoms,10
Compliancewithtreatment,insightand,181Comprehensionofspeech,disordersof,163tCompulsions,assessmentof,28Compulsions/compulsivebehaviours,287–290
nolackofinsight,288Compulsiveideas,explanationfordoubling,
189Compulsiveimage,289Concentration,46–49Conceptualthinking,141–142Concretethinking,148,355,365Confabulation,62–64,346,354,359,363
characteristics,63bofembarrassment,62–63fantastic,63
persecutorycontent,63–64momentary,63schizophrenia,63–64social,63
Configuralmodel,88Conflictofinterest,20–21Confusion,40Confusionpsychosis,143Consciousness,34
arousalsystemsof,37fchangesof,qualitative,39–40cloudingof,36,38definition/meaningof,34dimensionsof,36diminished,levels(stages)of,38fdisturbed,33–43fluctuationof,39–40
Index 371
heightened,37intentional,34limittonumberofitemsin,35loweringof,quantitative,37–39pathologyof,37–42ofself,36
Consolidation,delusionorigin,120Constellation
ofassociations,143ofsymptoms,336
Constriction,inanxiety,280–281Consultingbehaviour,hypochondriasis,221Content
ofdelusions,131–132disorder,inmorbidjealousy,123ofexperience,14–15hypochondriacal,15
Continuity,feelingof,197Continuityview,5Conversion,67–68,224–227,361
conceptof,350Conversionhysteria,218Copingbehaviour,andlifeepoch,84fCoprolalia,309Cortisol,levelof,changesindepression,83Cotard’ssyndrome,127–128Counterfactualthinking,141Creative,inadequateandaggressivepsychopathy,
322Criminalpsychopathy,319Crowdingofthought,147Cryptamnesia,67Cryptographia,162Cryptolalia,162Cues,formemoryretrieval,61Culturalfactors
bodyimagedisorders,238–239,239temotions,259hallucinations,97insight,182
Cutting,J.hallucinations,95pathologyofemotions,260
Cyberchondriasis,222Cycloidpsychosis,143Cyclothymia,326–327Cyclothymicpersonality,258
DDaydreams,63
pareidolicillusionsvs.,95personalityassessment,24
Deaffectualisation,209,261Decision-making,mania,298–299
Defencemechanismsdefectofmemoryrecall,67ego,4
Déjàvu,62,81,209,347,360brainstimulationand,81temporallobedisorder,65intemporallobeepilepsy,81
Delirium,39,346,359definitionof,39occupational,42
Deliriumtremens,visualhallucination,100,102fDelusions,111–137,348,360
actingon,132affectiveresponseto,113ofalienforcescontrolling,338–339assessmentof,27–28attributionin,122autochthonous,116characteristicsof,112cleanlinessinvolvement,130cognitionandreasoningin,121–122communicatedinsanityand,130–131contentof,123–131ofcontrol,28,103,150–152,154–155,338–339
internetinvolvement,123ofthought,348,360
defect,theme,121definitionof,112–113delusion-likeideasvs.,115–116deviantbehaviourdueto,113disturbanceof,148dysmorphic,129factorsinvolvedin,120basfalsebeliefs,131–132asfalsejudgements,111grandiose,126ofguilt,127inhypochondriasis,223ofinfestation,129–130ofinfidelity,123–124ofintegration,336–337oflove,124–125,354,364andmeaninginlife,122meaningof,112–113mimickingdisorientation,49–50ofmisorientation,49–50motivationaltheme,121nihilistic,127–128,349,361originsof,119–122
factorsinvolved,119Garety’smodel,121–122Germantheories,119–120
overvaluedideavs.,132paranoid,133patient’sviewof,27–28
372 Index
ofpersecution,123ofpoverty,127–128primary,113–115,338–339,347,360
typesof,115–119realityof,131–132ofreference,133religious,126–127retrospective,118secondary.seeDelusion-likeideas(secondary
delusions)sexualcontentof,124ofunworthiness,127violentbehaviourinresponseto,132
Delusion-likeideas(secondarydelusions),133–134,140,148,222–223,348,355,360,364
Delusionalatmosphere,118Delusionalawareness,119Delusionaldisorder,128–129Delusionalevidence,128Delusionalidea,116Delusionalintuition,354,364Delusionaljealousy,123–124Delusionalmemory,66–67,118–119
delusionalretrospectivefalsificationvs.,66–67Delusionalmisidentification,125–126,354,364Delusionalmisinterpretation,117Delusionalmood,118Delusionalperception,120,153Delusionalpercepts,14–15,116–117
examplesof,153Delusionalretrospectivefalsification,66–67Delusionalsignificance,119Dementia
ofdelusionalmisidentification,126disorientation,49
Dependentpersonalitydisorder,326,352,362Depersonalisation,192,205–215,350,361
alterationofconsciousness,211anxiety,212assessmentof,28componentsof,206b,350,361considerations,212–213definitions/descriptions,205–210definitivefeaturesof,349,361indepression,212derealisationwith,207diminutionofintensity,261dissociationassociated,210dizziness,212drugscausing,211fatiguein,207manic-depressive,212moodchangewith,208onset,210
organicandpsychologicaltheories,210–211personality,209aspreformedfunctionalresponse,210–211psychoanalytictheory,212self-inducedepisodes,210self-perceptionrelationship,207socialandsituationalaspects,209–210subjectiveexperience,208–210assymptom,207timesensedistorted,209
Depersonalisationsyndrome,129,208,212culture-bound,koro,209symptoms,208
Depictiontheory,ofmentalimagery,89Depressiosinedepressione,270Depression,144,257–258,270,274
agitated,303anhedonia,298atypical,250biologicalrhythmdisorderin,82–83circadianrhythmchangesin,83clinicalassessment,13coreexperience(psychological/physical),
270–271delusions
ofguiltandunworthiness,127hypochondriacal,128ofpersecution,123ofpoverty,127–128religious,126–127
depersonalisation,212emotionsof,265andloss,273–275memoryimpairment,65moodchart,261fmotivationimpairment,298passageoftimedisorders,78posture,312preoccupationwithgloomythoughts,48reactive,histrionicpersonalitydisorder,324retardation,298,304smiling,271suicidalthoughtsin,272–273symptomsof,frequencyof,272tvitalfeelingsof,247
Depressivefacies,312Derailment,inthinking,145,146f,167Derealisation,92,208
depersonalisationwith,207timeexperienceloss,81
Descriptivepsychopathology,336,345,359applicationsof,340behaviourdescriptionin,4,4fcontinuityanddiscontinuityviews,5definitionof,3–4
Index 373
egodisordersandselfdisorders,191–192empathyin,3–4,6,345fundamentalconceptsof,3–18mind-brainduality,17organicandneuralsubstrates,17phenomenologyand,6–8research,340–341unconsciousexperience,16understandingin,345vs.psychoanalytic,5t
Desomatization,209Determiningtendency,47,143Diabetesinsipidus,nephrogenic,297Diagnosis,psychiatric,21
definitionof,333descriptivepsychopathologyapplication,340hierarchical,336–337importanceof,333postscript,339–342PresentStateExamination,283psychopathologyand,333–343symptomstoformdiagnosticcategories,
336–339Diencephaliclesions,inchronologydisorders,
78Digitspan,180Disasterimage,289Discontinuityview,5Diseases,definition,8–9Disgust,222,290Disinhibition,300Disorderedself.seeSelf,disordersofDisorganisationsyndrome,150–151Disorientation,49–50,353,363
inage,77–78delusionsmimicking,49–50dissociationand,50hysterical,50ofidentity,49forperson,49situational,49intime,49,77
Disruptiveimage,289Dissocialpersonalitydisorder,321–323Dissociation,67–68,140,224–227,361
inanxiety,281conceptof,350depersonalisationassociation,210disorientationand,50
Dissociativedisorders,depersonalisationas,210
Dissociative(hysterical)fugue,67–68Distractibility,47Distraction,auditoryhallucinationreduction,
99
Dizziness,depersonalisationand,212Doppelgänger,194Dosulepin(dothiepin),250–251Doublebook-keeping,177Dream-like(oneiroid)state,42Dreams,24,53–54,193,346,359
inREMsleep,53–54unpleasant,53–54
Drive,294–295abnormalities,296,297b
organiccauses,296–297biological,296–297definition,294diminution,296exacerbation,296innate,aggressive,301
Drivelling,146Drowsiness,36,38
incloudingofconsciousness,38Drugs
antipsychotic,extrapyramidalsideeffects,307–309,308b
depersonalisationdueto,211visualhallucinationsdueto,101
DSM-IV(DiagnosticandStatisticalManualofMentalDisorders,fourthedition)
delirium,39personalitydisorders,319,320t
Duality,mind-brain,17Dynamic(analytical)psychopathology,4–5Dysarthria,161Dyschromatopsia,92Dyskinesia,tardive,akathisiaassociation,309Dyslexia,100Dysmnesticsyndromes,60Dysmorphicdelusions,129Dysmorphophobia,133,218,219t,220f,227–229,
356,365abnormalitiesin,229complaintof,228
Dysphasia,162conduction,163jargon,164motor,162
primary,164transcortical,164
nominal,164receptive,163sensory,162–164
primary,163transcortical,164
subcorticalauditory,162syntactical,163types,163t
Dysphonia,161
374 Index
Dysphoria,emotional,261Dysprosody
expressiveemotional,269–270receptiveemotional,269–270,356,366
Dysthymia,327Dystonia,308–309Dystonicreactions,acute,308–309
EEating,disturbanceof,230–234Echolalia,161Echopraxia,305–306Ecstasy,200–201,262–264
anthropologyof,264characteristicof,264inmania,212
Ecstaticexperiences,religiousexperiencesvs.,264
Ego,187–188disturbances,schizophrenia,212Freud’sconcept,188pluralityofconceptions,187–188
Egoactivity,192–193Egoboundaries
changein,ecstasy,264loss,200
Egoconsistency,193–197,193bEgodefencemechanisms,4,141Egodemarcation,197–201Egovitality,192,349,361Ekbom’ssyndrome,129Ekman’sbasicemotions,351,362Electroconvulsivetherapy(ECT),memory
disturbance,64–65Emotions
abnormalitiesofappropriateness,266–268abnormalitiesofevaluation,269–270abnormalitiesofexpression,266–268basictypesof,259
pathologicalchangesin,260bodilyfeelingsassociatedwith,266–267changesinintensity,261–265changesintiming,duration,andappropriateness
tosituation,265–266cognitionrelationship,269culturalinfluences,259
definition,257–258definitionof,257disordersof,257–278exacerbationof,262–264expression,shallownessof,265free-floating,268lability,histrionicpersonalitydisorder,324nonverbalcommunicationof,260
pathologicalchangesin,261–268classificationof,260
inpsychiatry,258theoriesof,258–259
Emotionaldetachment,inschizoidpersonalitydisorder,321
Emotionaldisordersbehaviouralsigns,311–312classificationof,260b
Emotionaldistress,symptomsandsignsof,eliciting,19–20
Emotionalnumbness,208,274Emotionalsensitivity,lackof,266Emotionallyunstablepersonalitydisorder,323–324
borderlinetype,323–324impulsivetype,323
Empathy,12–14,359assessmentofsubjectiveexperience,5indescriptivepsychopathology,3–5,345genetic,114lackof,schizoidpersonalitydisorder,321meaningfulunderstanding,11–12method,13,26therapeutictool,14
Endorphins,246Epidemichysteria,263–264Epilepsy
ofdelusionalmisidentification,126ecstasyin,263–264fluctuationofconsciousness,39–40gelastic,265pathologicallaughter/cryingin,265
Epilepticaura,41bodyimagedistortion,237
Epiphenomena,5Erotomania,124–125Erroneousideas,delusionsand,111–137Euphoria,263Evileye,239tExcitement,inschizophrenia,310Execution,disordersof,293–314Exosomesthesia,93,219tExpansive(grandiose)delusionalbeliefs,126Experience
abnormalityof,268–269formandcontent,14–15subjectivityandobjectivityin,15–16
Explanation,11staticandgenetic,12bunderstandingvs.,11t
Explanatorypsychopathology,4Exploratorybehaviour,abnormalities,296,297bExpressiveemotionaldysprosody,269–270Expressiveemotionalprosody,269–270
Index 375
FFaceprocessing,impairmentsof,229Facialexpression,unchanging(bluntingoffeeling),
266Facialpain,atypical,250Faciobuccolinguomasticatorydyskinesia,309Factualhistory,22–23Falseidentity,67–68Falsememorysyndrome,69Falsification
delusionalretrospective,66–67memory.seeMemory,falsification
Familiarityfeelingof,208
lossof,depersonalisation,208knowingbasedon,61–62
Familyhistory,22Fantasticinterpretations,pareidolicillusionsvs.,
95Fantasy,111
capacityfor,55dream,53explanationfordoubling,193inhypnosis,55
Fantasylife,studyof,personalityassessment,24Fantasythinking,140–141,355,364
andsexualassault,140Fatigue,depersonalisationassociated,207Fear
ofdeath,222illness,285intensificationof,265obsessional,286performance,285
Feature-matchingmodel,88Feelings
anxious,tense,283attachedtoperceptionofobjects,267–268bluntingof,266definitionof,257–258directedtowardpeople,268flatteningof,266lossof,261
Fenwick,P.,automatismdefinition,41Five-Factormodel,ofpersonality,318–319Fixedidea,321Flattening,offeeling,266Flightofideas,143,143f,169
mania,298–299Flowofthought,interruptionto,145–147Fluencyofassociation,149Folieàdeux,131Foliecommuniquée,130Folieimposée,130Folieinduite,130
Foliesimultanée,130Forcedgrasping,305–306Forgetting,60
ofdisagreeable,67influenceofaffect,66rates,66selective,66
Form,14–15definitionof,14
Formconstants,90Formalthoughtdisorder,139–140Formication,103Free-floatingemotion,268Frégoli’ssyndrome,125Freud,S.
dreams,54insight,178instinct,294–295
Frigophobia,239tFrontallobelesions,chronology(temporalorder),
disorderof,78Fullbodytechniques,232Functionalimaging,visualimagery,89Functionalneurologicalsymptomdisorder,
225Fusion,ofthoughts,145,146f
GGanserstate,40,68–69,353,363Ganser’ssyndrome,featuresof,68–69Generalparesis,40,263–264
falsificationofmemory,66Generalizedanxietydisorder,281–282
panicdisordervs.,283–284Genuineness,lacking,inhistrionicpersonality
disorder,324Gerstmann’ssyndrome,236Gestaltpsychology,insightconcept,178Gesticulation,reducedinretardation,304Gestures,164
non-verbalcommunication,189–190,260GillesdelaTourette’ssyndrome,309–310GlobalInsightScale,179Grammar,160
destructionof,inschizophrenia,168–169mental,160–161
Grammaticalconstruction,disorderof(paragrammatism),162
Grandiosedelusions,126Grief,274–275
delayed,265morbid,patternsof,274pathological,265
Grimacing,305
376 Index
Guiltdelusionsof,127feelingsof
indepression,271eatingdisorder,234
Gustatoryhallucination,103
HHallucination,91,95–104
autoscopic,194characteristics,95cognitiveapproachtoinvestigation,96conceptsofRasmussen,96–97culturalfactors,97elementary,97–98extracampine,105functional,14,106
pareidolicillusionvs.,95gustatory,103haptic,103hygric,102hypnagogic,51–52,105–106hypnopompic,51,105–106kinaesthetic,102Lilliputian,97musical,97–98normalperceptsrelationship,95–96asnormalsensoryexperience,95–96olfactory,103reflex,106thermic,102visceral,103visual.seeVisualhallucinations
Handbehaviour,311Handwashing,286Handshake,311Hangover,92–93Happiness,heightenedstatesof,263–264Headinjury
hyperactivityafter,303obsessionalbehaviour,289–290
Healthconceptsof,334–336normal,9–10
Healthbeliefs,181Heautoscopyproper,194Hebephrenicpatients,schizophrenia,149–150Hemianopia,homonymous,162–163Hemidepersonalisation,236Hemimicropsia,91Hemiplegia,left-sided,178–179Hemisomatognosia,236Hemispatialneglect,236Heterophenomenology,methodof,33–34
History,takingof,22family,22past,22personalhistory,22–23
Histrionicbehaviourindepression,271ecstaticstateof,263–264
Histrionicpersonalitydisorder,104–105,324Hoarding,schizophrenia,311Homicide,delusionsofguilt,127Homonymoushemianopia,100HospitalAnxietyandDepressionScale,283,
283fHunger,296Hunttest,171Huntington’schorea,309Hyperacousia,247Hyperactivity,303–304
restless,303Hyperacusis,92–93Hyperekplexia,265,356,365Hyperkinesis,303Hyperkineticdisordersinchildhood,46–47Hyperschemazia,235Hypersomnia,51–52,296,353,363Hypnosis,54–56
fantasyin,55inductionof,55
Hypochondriacaldelusions,128–130Hypochondriacalpsychosis,monosymptomatic,
129Hypochondriasis,128,218–224,220f,361
contentof,222–223determinantsof,350psychopathologyof,222–224,223b
Hypochondrium,220,221f,266Hypomania,275Hyposchemazia,235–236Hysteria,224,249
conversion,218epidemic,263–264mass,263–264symptoms,67–68visualfieldsofpatientwith,226f
Hystericalconversion,140
II-ness,191–192ICD-9,persistentmooddisorders,326ICD-10
delirium,39delusionaldisorders,128–129persistentmooddisorders,326personality,319–320
Index 377
‘Ideal,’normalas,23Ideas,111–113
assessmentof,27–28delusion-like,115–116delusional,116fixed,321ofpersecution,320self-referent,320
Ideation,16erroneous,132–134
Idéefixe,321Identity
disorderof,197–200temporaryloss,198
Illness,8–9behaviour,335fear,285aslossofwell-being,266personal,336–337physical,anxietyin,286
Illnessbehaviour,222,352,362Illogicality,167Illusion,94–95,94f
affect,94–95completion,94pareidolic,95
Imagery,88–89abnormal,106–107characteristicsof,88–89,89tvisual,89vivid,91
Imagescharacteristicsof,360formalcharacteristicsof,347vividinternal,pseudohallucinations,104
Imagination,141Impulse
insane,301–302resistance,300
Impulsecontroldisorders,300excessivecontrol,300
Impulsiveacts,294,299–302examples,301violent,300voluntaryinhibitions,300
Impulsivebehaviour,300emotionallyunstablepersonalitydisorder,
323psychopathology,301–302inschizophrenia,310
Impulsiveinsanity,301–302Impulsivity,300,352,357,362,366
features,300venturesomenessversus,299–300
Inattention,children,46–47
Infestations,delusionsof,129–130Infidelity,delusionof,123–124Informationprocessing,abnormality,delusions,
121–122Innerheautoscopy,194Insanity
communicated,130–131moral,322
Insight,175–184,349,361assessmentof,28,176–177,345inbipolardisorders,181–182capacity,176inclinicalpractice,176–177cognitiveimpairmentand,180–182compliancewithtreatment,179,181concept,178–180
criticisms,182development,178–179Gestaltpsychology,178socialandculturalfactors,182
intoillness,176impaired,aetiology,182intellectualperformanceand,180lackof,178–179measurement,179–180neurologicalbasis,180inschizophrenia,180assudden,unexpectedsolutiontoproblem,
178treatmentaffectedby
outcome,181validmeasuresof,349,361
InsightandTreatmentAttitudesQuestionnaire(ITAQ),179
InsightScaleforPsychosis,179Insomnia,50–51
early,51late,51
Instinctabnormalities,296–299definition,294relationshiptoneedandbehaviour,294f
Instinctualdrive,294Insulin,296–297Intellectualfunction,andlifeepoch,84fIntellectualgrasp,loss(apprehension),49Intellectualperformance,insightand,180Intentionalstance,33–34
consciousnessand,34Interests
loss,indepression,298inpersonalityassessment,24
Interviewsshort,21speechandthoughtassessment,27
378 Index
Irritability,286–287,357,366andanxiety,286outwardlyexpressed,286severityandageaffecting,287
Itchpruritogenic,251–252psychogenic,251–252
JJamaisvu,62,81,209
temporallobedisorder,65James-Langetheoryofemotion,258Jaspers,K.
delusions,132disorderofidentity,197hallucination,95imagesandimagery,88–89insight,176phenomenology,7pseudohallucinations,104self-awareness,191–192timedisorders,75unconsciousness,34understandingvs.explaining,11urge,instinctualdriveandvolitionalact,294
Jealousy,morbid,123–124,320–321Jee,266Jetlag,82Judgement,147
disturbanceof,147–151false,delusionsas,111
‘Jump-to-conclusions’style,121–122
KKeyexperience,delusionsorigin,120Kleine-Levinsyndrome,52,296–297,346,357,
359,366Knowing,rememberingvs.,61–62Koro,129,209,238–239,239tKorsakov’ssyndrome,61
confabulation,62–63passageoftimedisorders,80
Kraepelin,Emilreligiousdelusions,126–127sexualjealousy,123
LLabelling,ofdisorders,21Language
Chomsky’stheoryof,160–161disordersof,159–173
organic,162–165
pragmatics,160psychogenicabnormalities,169–170statisticalmodelof,170
Latah,239t,265Law,descriptivepsychopathologyapplication,340Learningdisability,anxietyin,289–290Learningtheory,301Lifeepochs,85
psychiatricdisturbanceand,84fListening,forunderstandingofpatient’ssymptoms,
12–13Locked-in-syndrome,42Logoclonia,161,355,365‘Loners,’321Long-termmemory,347,360Loss
anddepression,273–275external,subjectexperience,274
Lovebeing‘inlove,’189delusionsof,124–125
Lucidity-clouding,36Lycanthropy,199–200Lying,fluentplausible(pseudologiafantastica),66Lysergicaciddiethylamide
depersonalisation,211painsensationincreased,247
MMacropsia,91Macrosomatognosia,235Madeexperiences,154–155Maher,BA,inlanguagedisorders,168Mania
affectandemotionaldisorderin,275clothing,312exacerbationofemotions,262–264falsificationofmemory,67flightofideas,298–299grandiosedelusion-likeideas(secondary
delusions),126insight,181–182joyandpleasurefeelingsof,263motivationabnormality,296passageoftimedisorders,80speech,162volitionaldisturbance,298–299
Maniaàpotu(pathologicalintoxication),40–41,346,359
Manic-depressivedisorder,depersonalisation,212
Manic-depressivepsychosis,143Manipulativeness,histrionicpersonalitydisorder,
324
Index 379
Mannerisms,305,311Masshypnosis,198Masspsychogenicillness,225–226,350,361Masssociogenicillness,225–226Mastectomy,238Masturbation,335Maternalreverie,141Meaning,alternativetests,99Meaningfulconnections,15
delusionsand,114Medialthalamus,sleepstagesand,50Megaphagia,52Melancholia,220,262–264,266,270,303
delusionsofpersecutionvs.,123Memory
acoustic,errors,67bias,inaffectivedisorder,65cueforretrieval,61declarative(explicit),60delusional,66–67,118–119disturbanceof,59–71
ECTand,64–65psychogenic,67–69
dualprocesssystem,61–62echoic,59–60episodic(autobiographicalincidents),60–62false,delusionalmemoryas,119falsification,66–67
see alsoConfabulationiconic,59–60impairment/disorder
affective,65–69organic,61–62inschizophrenia,65temporallobedisorder,65see alsoAmnesia
implanted,falsememorysyndrome,69long-term,60,347
functions,60lossforwords,67mechanisms,59–60mood-congruent,65non-declarative(implicit),60recall,60
impairment,61inaccuracy,67panoramic,65
recognition,60impairment,61–62
recovered,69registration/encoding,60
impairment,61retention,60
defectinducedbyECT,64impairment,61
retrieval,60direct,61impairment,61indirect(strategic),61
semantic(factmemory),60errors,67
sensory,59–60short-term,60,346state-dependent,65storage,60working,60
Menstrualcycle,83Mentalarousal,excessive,ininsomnia,50–51Mentalillness,8–9
classification,337bcategoricalvs.dimensional,337
elicitingsymptomsof,19–29onsetafternormalhealth,336syndromes,336
Mentalimagery,89,141auditoryhallucinations,99
Mentalimages,hallucinationas,96Mentalretardation,304
diminishedpainsensation,248Mentalstate,22
examination,25–26Mescaline
depersonalisation,211visualhallucinationdueto,100–101
Metamorphopsia,91Metonyms,166,355,365Micropsia,91,354,364Microsomatognosia,235Mind,philosophyof,17Mini-MentalStateExamination,28Mirrorneurons,259–260Misidentification,delusional,125–126Misnamingobjects,67Misoplegia,219t,237,356,365Mitgehen,305–306Mixedaffectivestates,144,303Mixedpersonalitytypes,320Mixing,146Monthlycycles,83Mood,351,362
abnormalitiesof,classificationof,257inbipolardisorder,abnormalityof,270communicationof,259–260definitionof,257delusional,118depersonalisation,208indepression,270–275disturbance,257diurnalityof,83elevationof,263
380 Index
histrionicpersonalitydisorder,324labilityof,265lifeepochand,84fnormal,258persistentdisorders,326–327inpersonalityassessment,24inpsychiatry,258subjectiveandobjectivedescriptionsof,27swings
extreme,suicidalthoughtsin,273inpremenstrualsyndrome,83
Moodchart,261fMooddisorders
circadianrhythmsin,83inflowoftimedisorders,79
Moralderangement,322Moralinsanity,322Morphemes,160Motivation,351,362
abnormalities,296–299,297binschizophrenia,297–298
definition,294intrinsicandextrinsicfactors,295
Motordisorders,306–307see alsoMovement,disturbancesinbraindisease,307–309inParkinson’sdisease.seeParkinson’sdisease
Mourning,forced/guided,274Movement,disturbances,303–310
agitation.seeAgitationincatatonia,304–305inexecutionofmovement,305hyperactivity,303–304isolateddisordersofmovement,304–306obstructionofflowofaction,305inschizophrenia,304,306–307
see alsoMotordisordersMuddling,146Multiplepersonality(dissociativeidentitydisorder),
196–197Muscledysmorphia,234,356,365Mutism,165
akinetic,42hysterical,169instupor,42
My-ness,191–192Myoclonicjerks,265
NNailbiting,161Naming,impairmentoflanguagefunction,163tNarcissism,105Narcissisticpersonalitydisorder,327Narcolepsy,52
Needabnormalities,296–299,297bdefinition,294primary/innate,294relationshiptoinstinctandbehaviour,294fsecondary,294
Negativeheautoscopy,194Negativetraits,ofschizophrenia,298Negativism,306
inschizophrenia,305Neologism,162,167–168,355,365Neuroanatomy,340–341Neurolepticmalignantsyndrome,304–305Neuromas,stump,250Neuropsychiatricmethods,341Neurosis
andstress,336vs.psychosis,336
Nightterrors,53Nightmares,53–54Nihilisticdelusions,127–128,192,349Non-accidentalinjury,children,322Non-verbalcommunication,260
assessment,26–27self-imageand,189–191
Norm,9–10individual,10social,10statistical,9value,9
Normal,definitionof,9,23Normalpersonality,23‘Normalisingstatement,’25Nuclearsyndrome,338–339Nymphomania,124
OObesity,230–231,297
schizophrenia,297–298Objectiveassessments,16Objective(clock)time,77
disorderof,76b,77–78Objectivity,15–16
definitionof,16ofnormalsensation,97
Object(s),delusionalmisidentification,126Observant,26Observation
ofappearanceandbehaviour,5,26forunderstandingofpatient’ssymptoms,12–13
Observer,6Obsession,287–290,357,366
assessmentof,28definitionof,287
Index 381
religiousbeliefsand,288inschizophrenia,289–290
Obsessional(anankastic)personality,289–290Obsessionalideas,289Obsessionalimage,289Obsessionalrumination,223Obsessive-compulsivedisorder,287Obsessivecompulsivephenomenon,elementsof,
351,362Obstruction,offlowofaction,305Obstructivesleepapnoea,52Occipitallobetumours,visualhallucinationswith,
100‘Oldmaids’insanity,124–125Olfactoryparanoidsyndromes,129‘Olfactoryreferencesyndrome,’129Oneiroidstates,visualhallucination,101Opposition,tomovement,306Organicamnesicsyndrome,63Organicbraindisease,acute,intime-lapse
phenomenon,80Organicpain,psychogenicpainvs.,245–247Organicpsychiatry,symptomaticpsychiatryvs.,17Organicpsychosyndromes,anxietyin,286Orientation,49–50
definitionof,49inspace,49intime,49
Orthodoxsleep,53–54Outofbodyexperiences,194‘Outoftheblue,’delusions,116Over-inclusivethinking,149,166,355,364Overactivity,inmania,298Overvaluedideas,132–133,148,223,228,234
disordersofcontentassociated,133tmorbidjealousyas,133inparanoidpersonalitydisorder,133,321
PPain
associatedwithpsychopathology,361attentionand,245–246atypicalfacial,250centralnervoussystemmodulationof,246central(thalamicsyndrome),247–248,350,361craving,248definitionof,245depressionand,249diminishedsensation,248gatecontroltheory,245–246andheightenedsensation,247–248lossand,250non-organic,classificationof,249organicorpsychogenic,245–247
perception,245phenomenologicalaspectsof,245inpsychiatricillness,247psychopathology,245–254,350recalcitrant,248–249subjectiveexperience,252andsuffering,252thresholdfor,245–246transmissionof,245–246withoutorganiccause,248–252
Painasymbolia,248,350,361acquired,248
Palinacousis,92–93Palinaptia,93,219t,356,365Palinopsia,91,354,363Panic,357,366Panicattacks,283–284Panicdisorder,283–284
generalizedanxietydisordervs.,283–284respiratorysubtypeof,351,362
Panoramicrecall,65Paradoxicalsleep(REMsleep),53–54Paraesthesiae,102Paragrammatism,162,168–169Paralogia,168Paramimia,265Paramnesia,67Paranoia,128–129Paranoid,133,320Paranoidideas,133–134Paranoidpersonalitydisorder,320–321,352,362
active,320–321passive,321
Paraphasia,168literal,168verbal,168
Paraprosopia,91,354,364Paraschemazia,236–238Parasomnias,52–53,353,363Parathymia,265Pareidolia,95Parietallobes,235
lesions,inhyposchemazia,235Parkinsoniansyndromes,305Parkinson’sdisease,307
exacerbationofdrive,296Partfunctions,335–336Passivedependence,324Passivity,28
disordersof,154–155ofemotion,155experiences,197
first-ranksymptomsofschizophrenia,154–155
asvolitionabnormality,296
382 Index
ofimpulse,156somatic,156ofthought,151
indelusionalatmosphere,118ofvolition,156
Pathologicallying,140Pelopsia,92,354,364Penilechange,hypochondriacaldelusions,129Penoscrotodynia,251Perceivedbody,189Perception,14
abnormalitiesof,87,91–95assessment,27–28falseperception,94–95sensorydistortions,91–94
auditory,14elementaryaspectsof,92–93
characteristicsof,89tfalse,94–95meaningindelusion,117misinterpretation,pareidolicillusionsvs.,95ofobjects,feelingattachedto,267–268pathologyof,87–110qualityof,92sensationand,87–91splittingof,93–94tactile,elementaryaspectsof,93visual,89
Perceptualdelusionalbicephaly,195–196Perfectionism,324–325Periodiccatatonia,305Persecution,ideas,320Perseveration,26,64,147Persistentmooddisorders,326–327Personalactivity,disordersof,154–155Personalhistory,22–23Personality
abnormal,23assessmentof,23definitionof,23depersonalisation,209double,194labilityinawarenessof,197multiple,196–197normalvs.abnormal,23premorbid(previous/usual),23–24sensitivepremorbid,120
Personalitydisorders,317–329anankastic,324–325anxious(avoidant),325–326avoidant,327classificationsof,318–319definition,319dependent,326differentiationof,24–25
dissocial,321–323falsificationofmemory,66histrionic,324mixed,320schizoid,321sociopathic,323theoryof,317
Personalitytraits,324Personalitytype,24Phantomhead,195–196Phantomlimb,237–238,250
bodyimage,235pain,238
Phenomenologicalselves,189Phenomenology,340–341
definitionof,6confusionover,7
diagnosticuse,14methodof,7
communicationfacilitation,10andpsychopathology,6–8purposeof,14
Phobias,284animal,284indepression,286illness,285simple,284–285social,284–285speciesof,284b
Phobicanxietydepersonalisationsyndrome,212Phobicneurosis,subdivisionsof,285bPhobicstates,284–286Phonemes,98,160Phonologicalloop,short-termmemory,60Photophobia,223–224Phrases,misuseof,inschizophrenia,167–168Pickwickiansyndrome,52Pictorialtheory,ofmentalimagery,89Pinta,10Plagiarising,cryptamnesiaand,67Polydipsia,297PositiveandNegativeSyndromeScale(PANSS),
180Possessionstate,198–200
andtrance,198Post-traumaticstressdisorder
irritabilityin,287startlereflex,exaggeratedin,265unpleasantdreams,54
Posture,26–27incatatonia,304–305incatatonicschizophrenia,304–305isolateddisordersof,304–306non-verbalcommunication,189–190pharaonic,26–27
Index 383
Poverty,delusionsof,127–128Preconsciousprocesses,35Premenstrualsyndrome,83Presence,feelingof,194PresentStateExamination(PSE),156,283,
337–339first-ranksymptomsofschizophreniaand,339t‘totalinsightscore’and,180
Primarydelusions,148,152,347Primarysensorydysphasia,348,360Problemsolving,141Prognosis,insightand,181Propositionalanalysis,171Prosody,160Prosopoaffectiveagnosia,269Pseudohallucinations,51,91,94,104–105Pseudologiafantastica,66,140Psychiatricexamination,outlinefor,20bPsychiatrichistory,22–23Psychiatricillness,221Psychiatry
biologicalschoolof,339definitionof,3scopeof,3
Psychoanalysis,insight,178Psychoanalyticpsychopathology
vs.descriptive,5tPsychoanalytictheory,depersonalisation,212Psychodynamics,339Psychogenicabnormalities,inschizophrenic
languagedisorder,169–170Psychogenicpain
facial,250–251organicpainvs.,245–247
Psychogenicsymptom,hypersomnia,52Psychologicalpillow,304–305Psychologicaltechniques,applicationof,341Psychomimeticdrugs,visualhallucinationsdueto,
101Psychopathicpersonalitydisorder,321–322Psychopathology,4–6,4f
conceptsof,334–336definitionof,4descriptive.seeDescriptivepsychopathologyanddiagnosis,333–343explanatory,4increased,inpremenstrualperiod,83mind-braindualityand,17organicandneuralsubstrates,17phenomenologyand,6–8practicalapplicationsof,352,362usesof,340
Psychopathycreative,inadequateandaggressive,322definitionof,323
Psychosisofassociation,130attentionand,48–49feigned,118insightofpatient’s,178
Psychosocialrehabilitation,insightimproving,181Psychoticphenomena,lifeepochand,84fPublicness,normalobjectperceptionand
hallucination,97Puns,unintentional,inschizophrenia,168Purewordblindness,162–163Pureworddeafness,162
QQualia,34Questions
empathic,13leading,12–13inmentalstateexamination
‘closed,’25‘open,’25
RRapideyemovement(REM)sleep,50Rapport,16,27
evaluationof,27Rasmussen,conceptsof,96–97Rationalthinking,141–142Reading,disordersof,163tReality
ofdelusions,131–132senseof,hallucinationsand,96–97
Realitytesting,poor,auditoryhallucinations,99Reasoning,141
deductive,141inschizophrenia,167
inductive,141Receptivedysphasia,355,365Receptiveemotionaldysprosody,269–270,356,
366Receptiveemotionalprosody,269–270Recognition-by-componentsmodel,88Reference
delusion-likeideasof,133delusionsof,120sensitiveideasof,120
Referenceties,169Referral
psychiatric,impulsiveandaggressivebehaviour,302
psychiatric,natureandtypeof,22Regression,thoughtdisorderas,166Religiousbeliefs,religiousdelusionsvs.,126–127
384 Index
Religiousdelusions,126–127Religiousexperiences
indicatorsfor,264vs.ecstaticexperiences,264
Remember-knowparadigm,61–62Remembering,61–62Repetitionofspeech,disordersof,163tResearch,psychiatric,340–341Residuum,120Resolution,274Responsetointervention,221Responsiveness,45Retardation,144,144f,149
indepression,270,298,304mental.seeMentalretardationmotor,304psychic,270
Retrogradeamnesia,353,363Reverseanorexia,234Rewards,motivationand,295Rituals,compulsive,288Ruminations,289
obsessional,223
SSachs,O.,visualperception,88Sadness,affectivedisorders,262Sapir-Whorfhypothesis,inlanguage,160Satyriasis,124ScalefortheAssessmentofNegativeSystems,
298ScaletoAssessUnawarenessofMentalDisorder,
179Schachter-Singer’stwo-factortheoryofemotion,
259ScheduleforAssessmentofInsightinPsychosis,
179Schizoidpersonalitydisorder,321Schizophrenia
abnormalitiesoflanguagein,348,360anhedoniain,262anxiety,286auditoryhallucinations,98,341behaviouraldisorders,310–311Bleulerian,118bluntingoffeelingin,266boundariesofself,200,201fchronic,inagedisorientation,77circadianrhythmabnormalities,83cloudingofconsciousness,38concretethinking,166–167confabulationin,63–64deductivereasoningin,deficiency,167delusionalpercept,116
delusionshypochondriacal,128ofinfestation,129–130oflove,124
diminishedpainsensation,248egodisturbances,212first-ranksymptomsof,116,151–153,151t,
200examplesof,153–157PresentStateExamination,339t
flatteningoffeelingin,266insightand,180–182,349,361languagedisorderin,165–171
modelsforinvestigating,165tlinguisticapproachesto,170–171memoryimpairment,65motordisorder,306–307
categories,306tmovementdisorder,304negativetraits,298paranoid,133parathymiaandparamimiain,265primarysymptomsin,115prodromalphases,118psychologicaltheoriesofthinkingin,149–151qualityoftimedisorder,82riskinschizoidpersonalitydisorder,321seasonalvariationand,84speech,170
lackofpredictability,170thoughtdisordersin,170
symptoms,7thoughtdisordersin
andclinicaldescription,166–169destructionofwords/grammar,168–169misuseofwords/phrases,167–168inspeech,166ttypesof,167
volitionaldisturbances,297–298Schizophrenicinattention,149–151Schizotypalpersonalitydisorders,327Schnauzkrampf,305Schneider,Kurt
delusionalidea,116firstranksymptoms,115
Schneider’sFirstRankSymptoms,348,360Searching,stage,afterbereavement,94–95Seasonalaffectivedisorder,84–85,347,360SeasonalPatternAssessmentQuestionnaire,84–85Seasonalvariations,84–85Self,187
abrogation,inecstasy,264boundaries
disorderof,200–201inschizophrenia,200,201f
Index 385
consciousnessof,36continuity,lossof,198disordersof,187–203misidentification,126and‘other,’298,299f
Self-concept,188–189Self-deception,141Self-esteem,feelingoflossof,207–208Self-image
centralcore,190andnon-verbalcommunication,189–191
Self-inducedvomiting,234Self-inflictedharm,248Self-injuriousbehaviour,248,249bSelf-monitoring,failureof,150Self-outsideworldrelationships,disturbed,212Self-perception,depersonalisationrelationship,
207‘Self-referent,’133Self-referentideas,320Selye’sGeneralAdaptationSyndrome,351,362Semantichalo,towords,167–168Semantics,160Sensation
experiencing,bodyschema,191andperception,87–91
Sensorium,36ofthebodyimage,247
Sensorydeprivation,107–108Sensorydistortions,91–94Sensoryexperience,normal,95–96Serialsevenstest,46Sexsomnia,53Sexualabuse,childhood,recoveredmemories,69Sexualneed,exacerbation,296Shame-humiliation,121Shiftwork,82Short-termmemory,346,360Sickrole,334–335Simulatedpsychosis,153Singleness,disorderof,193–197,193bSituationalaspects,depersonalisation,209–210Sleep,45–57
abnormalitiesofneedfor,296,297bdeprivation,82–83drunkenness,51objectiveassessmentof,50paralysis,52REM,50requirements,51stagesof,50
Sleepdisorders,50–53hypersomnia,51–52insomnia,50–51parasomnias,52–53
Sleep-wakecycle,phaseadvanceof,82–83Sleepwalking,52–53Snappingoff,146–147Socialaspects,depersonalisation,209–210Socialcensorship,191Socialcontext,ofemotions,abnormalitiesof,
260bSocialdeprivation,322Socialfactors,insight,182Socialphobia,357,366Sociopathicpersonalitydisorder,323Somaticpassivity,156Somatization,221,268–269Space,senseof,75Speech
assessmentof,27automatism,42disorderof,159–173flightofideas,169fluency,disordersof,163themisphereassociatedwith,162hesitant,164indistinct,164inner,90–91intonationchanges,161–162isolatedareafor,164–165inmania,162povertyofcontentof,167pressureof,169private,90–91repetitionof,163tunintelligible,162volumeof,changesin,161–162
Spinothalamicpathways,disruptionin,247–248
Spitzer,M.,delusionsvs.beliefs,112Spontaneousinvoluntarymovements,in
schizophrenia,305Spontaneousspeech-fluent,disordersof,163tStammering,161Startlereflex,heightened,265State,318–319
vs.trait,280–281,325Stereotypy,304–305Stockwords/phrases,167–170
exampleof,167Stress
abnormalreaction,hystericalmutism,169andanxiety,280
Structuralimaging,230Stupor,42,165,353,363
psychogenicvs.neurologicalcauses,42Stuttering,161Subjectiveanalysis,16Subjectivedoubles,syndromeof,125
386 Index
Subjectiveexperienceheightenedconsciousness,37studyof,7–8
SubjectiveExperienceofNegativeSymptoms,scale,298
Subjective(personal)time,77disorderof,76b
Subjectivity,15–16definitionof,16
Suffering,252painand,252
Suggestibility,63Suicidalthoughts,depression,272–273Suicide
delusionsofguiltandunworthiness,127rateof,seasonalvariationand,84
‘Summarystatements,’inmentalstateexamination,25
Suprachiasmaticnuclei,biologicalrhythmcontrolin,82
Surpriseintensificationof,265morbid,265
Symbolicrepresentation,141Sympathy,5Symptomaticpsychiatry,organicpsychiatryvs.,17Symptoms
classificationof,337–338constellationsof,336diagnosticcategoriesformedfrom,336–339eliciting,19–29present,22primaryvs.secondary,15understanding,10–12
Synaesthesiae,37,89–90,347,360Syndromes,336Syntacticalanalysis,171Syntax,160
incoherenceof,162Systematicenquiry,26–28
TTactilehallucinations,102Tangentiality,167Technicalterm,diagnosticimplicationsof,26Telegramese,168–169Teleopsia,92Telescopingphenomenon,237Temperature,body,changesindepression,83Template-matchingmodel,88Temporallobedisorder
déjàvu,65jamaisvu,65memoryimpairment,65
Temporallobeepilepsydéjàvu,62,81twilightstateand,40visualhallucination,100–101
Temporalorder,disorderof,78‘Tensioninsanity,’304–305Thalamicsyndrome,247–248Therapy,descriptivepsychopathologyapplication,
340Thinking
accelerationof,143autistic,140changesintheflowof,147circumstantial,144–145,145fconcrete,166–167confusionof,40disorderofthecontrolof,151–157functionsof,140imaginative,141andlanguage,relationshipbetween,160over-inclusive,166performanceof,140process,disorderof,139–158typesof,140–142
Thirst,abnormalities,296,297bThoughts
alienationof,157assessmentof,27audible,152–153blocking,146–147,147f,151–152,167broadcasting,151–152,155coherent,40disorders,27influenceof,157insertion,151–152,155,157,338–339lossofgoal,167withdrawal,146–147,151–152,154–155,355,
364Thoughtdisorder,inspeech,categorizationof,166tTics,309–310Time
biologicalrhythmsand,77,82–85characteristicsof,360chronology,disordersof,78directionof,disorderof,80–81disorderof,75–86
classificationof,76bobjective(clock)time,77–78subjective(personal)time,78–82
disorientation,49durationof,disorderof,78flowof,disorderof,78–80formalcharacteristicsof,347objective(clock),77
disorderof,77–78
Index 387
qualityof,disorderof,81–82reduplicationof,81subjective(personal),77
disorderof,78–82uniquenessof,disorderof,81
Time-lapsephenomenon,80Timesense,75
alteration,depersonalisationandderealisation,81–82
distortion,depersonalisation,209loss,indreams,54
‘Timestandsstill,’observationof,78Top-downprocess,visualrecognition,88Torpor,211Traits,318–319
anxiety,280–281negative,ofschizophrenia,298personality,324statevs.,325vs.state,280–281
Trance,self-induced,193Transcendentalmeditation,193,210Transference,4Transsexualism,229–230
bodyimage,191Transvestism,229Travel,purposeful,dissociative(hysterical)fugue,
67–68Trema,119Tricyclicantidepressants,depersonalisationdueto,
211Twilightstate,40Two-factortheoryofemotion,259Type:tokenratio,170Typification,333–334TyrerandAlexander’spersonalitydisorder,
319–320
UUnconsciousexperience,phenomenologyand,
16Unconsciousstate,33Unconsciousness,34–36
definition,34threedimensionsof,35f
Understandableexperience,primarydelusions,114
Understandingindescriptivepsychopathology,3–4,345explanationvs.,11tofindividual’shealthanddisease,352,362ofpatient’ssymptoms,10–12inpsychopathology,359staticandgenetic,11b
Unityawarenessof(egoconsistencyandcoherence),
193lackof,inexpressionofemotions,265lossof,inschizophrenia,197
Un-understandableexperience,6Unworthiness
delusionsof,127feelingsof,indepression,271
Urge,non-directional,294
VVenturesomeness,299–300Verbalcoding,190Verbalmessages,191Verbigeration,165Vertigo,hyposchemaziawith,235Vigilance-drowsinessaxis,36Vigilance(wakefulness),36Vignettes,psychopathology,180Violentbehaviours(violence)
associatedwithdelusions,132duringautomatism,42depersonalisationafter,210emotionallyunstablepersonalitydisorder,
323irritabilityleadingto,287morbidjealousy,124twilightstateand,42
Violentimpulse,300Visualhallucinations,14–15,100–102
auditoryhallucinationsand,101elementary,100–101organicstatesassociated,100
Visualhyperaesthesia,91–92Visualobjectagnosia,87–88Visualperception
colour,91–92elementaryaspectsof,91–92
abnormalities,347,360ofmotion,92sizeabnormalities,91spatiallocation,92
Visualpseudohallucinations,101Visualsystem
recognitionin,88sensationandperception,87–91
Visuospatialscratchpad,short-termmemory,60
Vitalanxietystates,267Vitalfeelings,266–267
indepression,247sites/regionsofbody,266–267
Vitalself,266–267
388 Index
Vocationalrehabilitation,insightimproving,181Voices,hearing,338–339
arguing,154givingarunningcommentary,154schizophrenia,98
Volitionaffectiveillnessesof,298disorders,293–314disturbance
inmooddisorders,298–299inschizophrenia,297–298
loss,296–298Volitionalact,294Voluntarymovements,idiosyncratic,in
schizophrenia,305Vomiting,self-induced,234Voodoo,239tVorbeigehen,68Vulvodynia,251
WWahneinfall(delusionalintuition),116Waterintoxication,schizophrenia,311Waxyflexibility,304–305,310WechslerAdultIntelligenceScale,68Weightphobia,231Well-being,loss,266Wernicke’sarea,164
deficitof,163
Will,294–295abnormalities,296–299,297b
inschizophrenia,297–298concept,295definition,294
Windigo,239tWisconsinCardSortingTest(WCST),180Words
blindness,pure,162–163choice,inmentalstateexamination,26deafness,pure,162destructionof,inschizophrenia,168–169dumbness,pure,164intrusionof,168lossofmemoryfor,67misuseof,inschizophrenia,167–168predictability,170semantichaloto,167–168stock.seeStockwords/phrases
Wordsalad,165Workingmemory,abnormalityof,149–151Writing,disordersof,163t
YYoga,210
ZZeitrafferphenomenon,80