sha 078. chylothorax after pediatric cardiovascular surgery
TRANSCRIPT

P.O. Box 2925 Riyadh – 11461KSATel: +966 1 2520088 ext 40151Fax: +966 1 2520718Email: [email protected]: www.sha.org.sa
FULL
LEN
GTH
ART
ICLE
Disclosure: Authors have nothing to disclose with regard tocommercial support.
Received 20 November 2013; revised 11 December 2013; accepted 3January 2014.Available online 13 January 2014
⇑ Corresponding author. Address: Department of Cardiac Sciences(MC: 1420), King Abdulaziz Medical City, P.O. Box 22490, Riyadh 11426,Saudi Arabia. Tel.: +966 501282910; fax: +966 118011111x16971 16855.E-mail addresses: [email protected] (S.R. Ismail), [email protected] (M.S. Kabbani), [email protected] (H.K. Najm), [email protected] (G.A. Shaath), [email protected] (A.M.Z. Jijeh),
[email protected] (O.M. Hijazi).Impact of chylothorax on the early postoperative outcome after pediatriccardiovascular surgery
1016–7315 � 2014 King Saud University. Production and hosting by Elsevier B.V. All rights reserved.
Peer review under responsibility of King Saud University.
URL: www.ksu.edu.sa
http://dx.doi.org/10.1016/j.jsha.2014.01.001 Production and hosting by Elsevier
Sameh R. Ismail a,⇑, Mohamed S. Kabbani a, Hani K. Najm a, Ghassan A. Shaath a,Abdulraouf M.Z. Jijeh a, Omar M. Hijazi a
a King Abdulaziz Medical City, King Saud University for Health Sciences, Department of Cardiac Sciences, National Guard HospitalHealth Affairs, Riyadha Saudi Arabia
Background and aim: Chylothorax is the accumulation of chyle in the pleural cavity, which usually develops afterdisruption of the thoracic duct along its intra-thoracic route. In the majority of cases, this rupture is secondary to trauma(including cardio thoracic surgeries). Chylothorax is a potentially serious complication after cardiovascular surgeriesthat require early diagnosis and adequate management. This study aims to determine the risk factors and the impact ofchylothorax on the early postoperative course after pediatric cardiac surgery.
Methods: A retrospective study of all cases complicated with chylothorax after pediatric cardiac surgery was con-ducted at King Abdulaziz Cardiac Center between January 2007 and December 2009.
Results: There were 1135 cases operated on during the study period. Of these, 57 cases (5%) were complicated bychylothorax in the postoperative period. Thirty patients (54%) were males, while 27 (47%) were females. Ages rangedfrom 4 to 2759 days. The most common surgeries complicated by chylothorax were the single ventricle repair surger-ies (15 cases, 27%); arch repairs (10 cases, 18%); ventricular septal defect repairs (10 cases, 18%); atrioventricular sep-tal defect repairs (7 cases, 12%); arterial switch repair (6 cases, 11%), and others (8 cases, 14%). The intensive care unit(ICU) and the length of hospital stays were significantly longer in the chylothorax group. Additionally, some earlypostoperative parameters such as incidence of sepsis, ventilation time, and inotropes duration and number werehigher in the chylothorax group.
Conclusion: Chylothorax after pediatric cardiac surgery is not a rare complication. It occurs more commonly withsingle ventricle repair and aortic arch repair surgeries, and has a significant impact on the postoperative course andpost operative morbidity.
� 2014 King Saud University. Production and hosting by Elsevier B.V. All rights reserved.
Keywords: Chylothorax, Post operative, Pediatric, Cardiac surgery
Abbreviations
ICU intensive care unitTPN total parenteral nutritionRACHS-1 risk adjustment in cardiac surgeryNPO nil per oralMCT medium chain triglyceridesSVC superior vena cavaVSD ventricular septal defectAVSD atrio ventricular septal defectkg kilogramcm centimeterLOHS length of hospital stayH hoursmin minutesno numberCPR cardio-pulmonary resuscitation
FULL LEN
GTH
ARTIC
LE
88 ISMAIL ET ALIMPACT OF CHYLOTHORAX ON THE EARLY POSTOPERATIVE OUTCOME AFTER PEDIATRICCARDIOVASCULAR SURGERY
J Saudi Heart Assoc2014;26:87–92
Introduction
Chyle is a milky colored fluid enriched withemulsified fat (chylomicrons) absorbed by
intestinal cells, transported by lymphatic channelsthat converge to become the thoracic duct, andpassed into the circulation. The diagnosis of chylo-thorax depends on analysis of the pleural fluid,with identification of chylomicrons or high triglyc-eride concentrations [1,2]. Chylothorax is the pres-ence of lymphatic fluid in the pleural space and isusually the result of a leak from the thoracic ductor one of its tributaries along its intra-thoracicroute. The presence of chylothorax can be due tocongenital, traumatic, neoplastic thrombosis ofone of the major neck veins or miscellaneouscauses. Traumatic chylothorax may result fromblunt or penetrating trauma, or occur after varioussurgical procedures. Operative injuries are by farthe most common cause of traumatic chylothorax.Chylothorax complicates different types of car-diac, aortic, esophageal, pulmonary, neck, sympa-thetic nerve, and diaphragmatic operations [2].There are usually 0–10 days between injury ofthe thoracic duct and development of chylothorax.Chylothorax is a potentially life-threateningdisorder that can lead to serious metabolic, immu-nologic and nutritional complications. Initialmanagement is the same regardless of the causeof chylothorax. Low fat diet, total parenteralnutrition (TPN), octreotide, and surgical proce-dures have been described for management [2](See Fig. 1).
Figure 1. Principles of treatment of chylothorax in children.
Aim of the study
The present study aims to determine the inci-dence, risk factors, and the impact of chylothoraxon the early postoperative outcome after pediatriccardiovascular surgery.
Material and methods
PatientsWe conducted a retrospective study of all cases
complicated with chylothorax after pediatric car-diac surgery at King Abdulaziz Cardiac Center be-tween January 2007 and December 2009. Thisgroup of patients was compared to a control groupof pediatric post open heart surgery patients hav-ing similar demographic data and the same riskcategory (Table 1). The design of the study wasbased on a case-matching design by selecting agroup of patients who matched the study patientsin the chylothorax group. The control group wasrandomly selected from our departmental data-base after excluding the patients complicated withchylothorax. They were selected for the samediagnosis, surgical procedures and risk categoryas the group with chylothorax. We used the riskadjustment in cardiac surgery (RACHS-1) methodas described by Jenkins to define the surgical riskcategory for patients with chylothorax and thecontrol group [3,4]. The chylothorax group andthe control group were compared regarding earlypostoperative course, mortality, and post opera-tive complications. We used departmental data-base to collect data, including medical records,progress notes, and patients’ daily chart reviews.
DiagnosisChylothorax was suspected when there was
excessive filling of the pleural cavity after pediat-
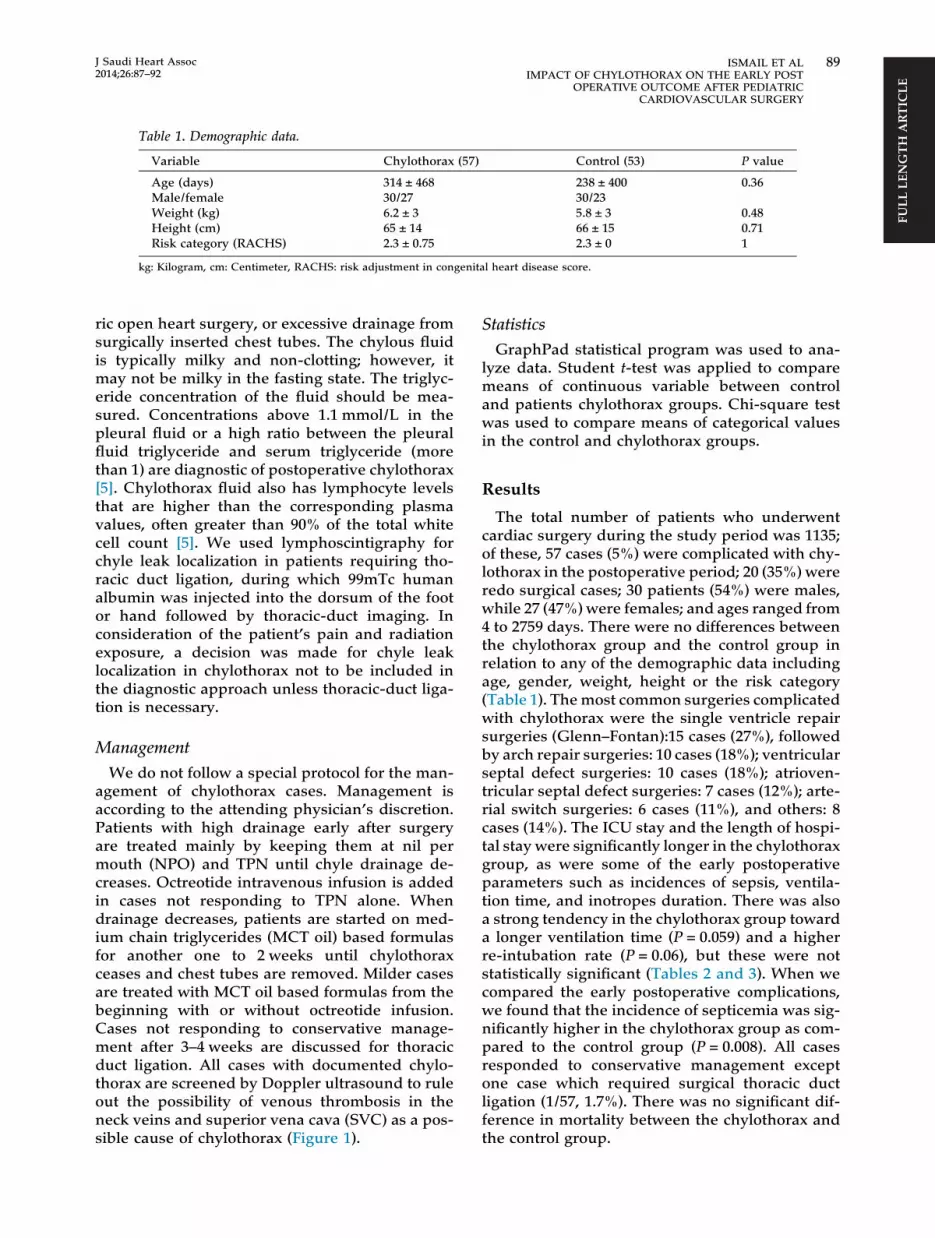
Table 1. Demographic data.
Variable Chylothorax (57) Control (53) P value
Age (days) 314 ± 468 238 ± 400 0.36Male/female 30/27 30/23Weight (kg) 6.2 ± 3 5.8 ± 3 0.48Height (cm) 65 ± 14 66 ± 15 0.71Risk category (RACHS) 2.3 ± 0.75 2.3 ± 0 1
kg: Kilogram, cm: Centimeter, RACHS: risk adjustment in congenital heart disease score.
FULL
LEN
GTH
ART
ICLE
J Saudi Heart Assoc2014;26:87–92
ISMAIL ET AL 89IMPACT OF CHYLOTHORAX ON THE EARLY POST
OPERATIVE OUTCOME AFTER PEDIATRICCARDIOVASCULAR SURGERY
ric open heart surgery, or excessive drainage fromsurgically inserted chest tubes. The chylous fluidis typically milky and non-clotting; however, itmay not be milky in the fasting state. The triglyc-eride concentration of the fluid should be mea-sured. Concentrations above 1.1 mmol/L in thepleural fluid or a high ratio between the pleuralfluid triglyceride and serum triglyceride (morethan 1) are diagnostic of postoperative chylothorax[5]. Chylothorax fluid also has lymphocyte levelsthat are higher than the corresponding plasmavalues, often greater than 90% of the total whitecell count [5]. We used lymphoscintigraphy forchyle leak localization in patients requiring tho-racic duct ligation, during which 99mTc humanalbumin was injected into the dorsum of the footor hand followed by thoracic-duct imaging. Inconsideration of the patient’s pain and radiationexposure, a decision was made for chyle leaklocalization in chylothorax not to be included inthe diagnostic approach unless thoracic-duct liga-tion is necessary.
Management
We do not follow a special protocol for the man-agement of chylothorax cases. Management isaccording to the attending physician’s discretion.Patients with high drainage early after surgeryare treated mainly by keeping them at nil permouth (NPO) and TPN until chyle drainage de-creases. Octreotide intravenous infusion is addedin cases not responding to TPN alone. Whendrainage decreases, patients are started on med-ium chain triglycerides (MCT oil) based formulasfor another one to 2 weeks until chylothoraxceases and chest tubes are removed. Milder casesare treated with MCT oil based formulas from thebeginning with or without octreotide infusion.Cases not responding to conservative manage-ment after 3–4 weeks are discussed for thoracicduct ligation. All cases with documented chylo-thorax are screened by Doppler ultrasound to ruleout the possibility of venous thrombosis in theneck veins and superior vena cava (SVC) as a pos-sible cause of chylothorax (Figure 1).
StatisticsGraphPad statistical program was used to ana-
lyze data. Student t-test was applied to comparemeans of continuous variable between controland patients chylothorax groups. Chi-square testwas used to compare means of categorical valuesin the control and chylothorax groups.
Results
The total number of patients who underwentcardiac surgery during the study period was 1135;of these, 57 cases (5%) were complicated with chy-lothorax in the postoperative period; 20 (35%) wereredo surgical cases; 30 patients (54%) were males,while 27 (47%) were females; and ages ranged from4 to 2759 days. There were no differences betweenthe chylothorax group and the control group inrelation to any of the demographic data includingage, gender, weight, height or the risk category(Table 1). The most common surgeries complicatedwith chylothorax were the single ventricle repairsurgeries (Glenn–Fontan):15 cases (27%), followedby arch repair surgeries: 10 cases (18%); ventricularseptal defect surgeries: 10 cases (18%); atrioven-tricular septal defect surgeries: 7 cases (12%); arte-rial switch surgeries: 6 cases (11%), and others: 8cases (14%). The ICU stay and the length of hospi-tal stay were significantly longer in the chylothoraxgroup, as were some of the early postoperativeparameters such as incidences of sepsis, ventila-tion time, and inotropes duration. There was alsoa strong tendency in the chylothorax group towarda longer ventilation time (P = 0.059) and a higherre-intubation rate (P = 0.06), but these were notstatistically significant (Tables 2 and 3). When wecompared the early postoperative complications,we found that the incidence of septicemia was sig-nificantly higher in the chylothorax group as com-pared to the control group (P = 0.008). All casesresponded to conservative management exceptone case which required surgical thoracic ductligation (1/57, 1.7%). There was no significant dif-ference in mortality between the chylothorax andthe control group.

Table 2. Comparison of the early post operative data.
Variable Chylothorax (57) Control (53) P value
ICU stay (days) 12 ± 18 5.8 ± 9 0.0259LOHS (days) 37 ± 40 10.4 ± 14 0.0001Bypass time (min) 106 ± 82 112 ± 53 0.65Ventilation time (h) 141 ± 384 40 ± 42 0.059Inotropes duration (h) 107 ± 196 52 ± 43 0.048No. of inotropes >2 18/57 14/53 0.6750
ICU: intensive care unit, LOHS: Length of hospital stay, h: hours, min: Minutes, no: number.
FULL LEN
GTH
ARTIC
LE
Table 3. Comparison of early postoperative complications.
Variable Chylothorax (57) Control (53)) P value
Mortality 3/57 1/53 0.6191Re-intubations 7/57 1/53 0.0618CPR 1/57 1/53 1.000Delayed sterna closure 2/57 1/53 1.000Septicemia 12/57 2/53 0.0086Arrhythmias 6/57 11/53 0.1880Acute renal failure 3/57 1/57 0.6191Pneumothorax 11/57 7/53 0.4466
CPR: cardio-pulmonary resuscitation.
90 ISMAIL ET ALIMPACT OF CHYLOTHORAX ON THE EARLY POSTOPERATIVE OUTCOME AFTER PEDIATRICCARDIOVASCULAR SURGERY
J Saudi Heart Assoc2014;26:87–92
Discussion
Chylothorax in children is not a rare complica-tion after pediatric cardiac surgery, and it is apotentially life threatening complication. Themechanisms of postoperative chylothorax weremostly due to direct trauma to the lymphaticvessels or the thoracic duct and less commonlyto secondary to central venous hypertension aftercavo-pulmonary connection (Glenn or Fontan), orvenous thrombosis [6].
In the present study, we noticed the increasedincidence of chylothorax in redo cases (35%), sin-gle repair cases (27%), aortic arch repairs (18%),ventricular septal defect (VSD) and atrio ventricu-lar septal defect (AVSD) repairs (18%) and (12%),respectively. These numbers were comparable tothe numbers reported by Chan et al., except forthe increased incidence in Tetralogy of Fallot pa-tients in the Chan study, reaching 18% comparedto our incidence of 3.5% [8]. Incidences of chylo-thorax in our study population (5%) are similarto recently reported studies from other centerswith incidences of 4.7% as reported by Cormacket al., [7] 3.8% by Chan et al., [8] and 6% by Seraret al. [9]. This is higher than older studies reporting1% from 1979 to 87 by Allen et al. [10] and 1.1%from 1961 to 1969 by Higgins et al. [11]. This changeis likely due to increased complexity of thepatients, the increased number of single ventriclerepair and the increase in the number of redosurgeries. The mortality of patients complicated
with chylothorax in the present study was 5%and this is similar to previous reports which ran-ged from 6% to 21% [12,13,7].
This study reports an impact of chylothorax onpostoperative morbidity in the form of a signifi-cant increase in ICU stay, length of hospital stay,and on some early postoperative parameters likethe significant increase in the incidence of sepsis,ventilation time, and inotropes duration. Therewas also a strong tendency in the chylothoraxgroup toward a longer ventilation time (P = 0.059)and a higher re-intubation rate (P = 0.06) but itwas not statistically significant (Tables 2 and 3).The increased incidence of sepsis can be ex-plained by the increased ICU stay and the needfor TPN which requires insertion of a central ve-nous access for long duration, continuous chesttube drainage, and nutritional loss. Immunosup-pression increases risk for sepsis, and thereforeregular bacteriological screening is useful in theearly treatment of opportunistic infections. Therisk of fulminant or fungal infections is wellknown [14,15]. Unfortunately, there is little datato guide treatment of postoperative chylothorax,leading to wide practice variation. Most publishedpediatric studies are limited to small case seriesand case reports [13]. All our study cases re-sponded to medical management including chesttube drainage, TPN, octreotide, and MCT oil-based formulas, except one case requiring thoracicduct ligation (1/57, 1.7%). The optimal manage-ment of a chylothorax is unclear because no
FULL
LEN
GTH
ART
ICLE
J Saudi Heart Assoc2014;26:87–92
ISMAIL ET AL 91IMPACT OF CHYLOTHORAX ON THE EARLY POST
OPERATIVE OUTCOME AFTER PEDIATRICCARDIOVASCULAR SURGERY
prospective studies exist to guide therapy; and dif-ferent protocols and strategies are applied in dif-ferent centers. Chest tube placement is typicallyperformed in patients with a postsurgical chylo-thorax or in those with chylothoraces that rapidlyre-accumulate [16]. Fasting with TPN or a reducedfat diet decreases the flow of chyle through thethoracic duct and allows spontaneous closure ofa thoracic duct leak. Dietary exclusion of long-chain triglycerides avoids their conversion intomonoglycerides and free fatty acids, which aretransported as chylomicrons to the intestinallymph ducts. A reduced fat diet may be supple-mented with medium chain triglycerides (MCTs),which are absorbed directly into intestinal cellsand transported directly to the liver via the portalvein, thus bypassing the thoracic duct. MCTs arecommercially available as MCT oil [17]. In resis-tant cases, surgery is indicated and in our seriesone case required thoracic duct ligation, and thepatient survived. Most authors agree that surgeryshould be reserved for failure of medical treat-ment [19,20]. To date, there has been no agree-ment on how long to wait for the success of themedical treatment. Some authors recommend sur-gery within 5–7 days to limit the morbidity andmortality associated with the operation [21,22,5].Others recommend waiting longer, about 2 weeksor even more to give medical treatment a suffi-cient chance [8,24,25]. Two surgical strategies pre-dominate: direct wound ligature or en massesupradiaphragmatic ligature. For non-traumaticcauses, other methods have been developedwhich are indicated in very rare cases: pleuroper-itoneal shunt, pleurectomy, pleurodesis, or evenradiotherapy [18]. There are other modalities intreatment such as pleurodesis, pleurectomy, bio-logic glue, pleuroperitoneal shunts, and others[13,26]. Pleurodesis has been recommended forrefractory chylothorax that did not respond tomedical or surgical intervention [26]. Someauthors recommend fenestrating the diaphragmor creating pleura-peritoneal windows [26]. Noneof our patients required these procedures andthe vast majority responded to conservative man-agement or thoracic duct ligation with no need forfurther interventions recommended for severerefractory cases. Our study has limitations as aretrospective study, with a small number of pa-tients, possibility of bias during selection of thecontrol group, and lack of hemodynamic data ofboth groups especially those with single ventriclerepair. We recommend further studies avoidingthese limitations.
References
[1] Hillerdal G. Chylothorax and pseudochylothorax. EurRespir J 1997;10(5):1157–62.
[2] Romero S. Nontraumatic chylothorax. Curr Opin PulmMed 2000;6(4):287–91.
[3] Jenkins KJ, Gauvreau K. Center-specific differences inmortality: preliminary analyses using the risk adjustmentin congenital heart surgery (RACHS-1) method. J ThoracCardiovasc Surg 2002;124(1):97–104.
[4] Jenkins KJ, Gauvreau K, Newburger JW, Spray TL, MollerJH, Iezzoni LI. Consensus-based method for riskadjustment for surgery for congenital heart disease. JThorac Cardiovasc Surg 2002;123(1):110–8.
[5] Merrigan BA, Winter DC, O’Sullivan GC. Chylothorax. BrJ Surg 1997;84(1):15–20.
[6] Efrati O, Barak A. Pleural effusions in the pediatricpopulation. Pediatr Rev 2002;23(12):417–26.
[7] Cormack BE, Wilson NJ, Finucane K, West TM. Use ofmonogen for pediatric postoperative chylothorax. AnnThorac Surg 2004;77(1):301–5.
[8] Chan EH, Russell JL, Williams WG, Van Arsdell GS, ColesJG, McCrindle BW. Postoperative chylothorax aftercardiothoracic surgery in children. Ann Thorac Surg2005;80(5):1864–70.
[9] Sersar SI. Predictors of prolonged drainage of chylothoraxafter cardiac surgery: single centre study. Pediatr Surg Int2011;27(8):811–5.
[10] Allen EM, van Heeckeren DW, Spector ML, Blumer JL.Management of nutritional and infectious complications ofpostoperative chylothorax in children. J Pediatr Surg1991;26(10):1169–74.
[11] Higgins CB, Mulder DG. Chylothorax after surgery forcongenital heart disease. J Thorac Cardiovasc Surg1971;61(3):411–8.
[12] Bond SJ, Guzzetta PC, Snyder ML, Randolph JG.Management of pediatric postoperative chylothorax. AnnThorac Surg 1993;56(3):469–72 [discussion 472–3].
[13] Beghetti M, La Scala G, Belli D, Bugmann P, Kalangos A,Le Coultre C. Etiology and management of pediatricchylothorax. J Pediatr 2000;136(5):653–8.
[14] Franksson C, Lundgren G, Magnusson G, Ringdén O.Drainage of thoracic duct lymph in renal transplantpatients. Transplantation 1976;21(2):133–40.
[15] Ferguson MK, Little AG, Skinner DB. Current concepts inthe management of postoperative chylothorax. AnnThorac Surg 1985;40(6):542–5.
[16] Wasmuth-Pietzuch A, Hansmann M, Bartmann P,Heep A. Congenital chylothorax: lymphopenia andhigh risk of neonatal infections. Acta Paediatr2004;93(2):220–4.
[17] Jensen GL, Mascioli EA, Meyer LP, Lopes SM, Bell SJ,Babayan VK, et al.. Dietary modification of chylecomposition in chylothorax. Gastroenterology1989;97(3):761–5.
[18] Nair SK, Petko M, Hayward MP. Aetiology andmanagement of chylothorax in adults. Eur J CardiothoracSurg 2007;32(2):362–9.
[19] Alexiou C, Watson M, Beggs D, Salama FD, Morgan WE.Chylothorax following oesophagogastrectomy formalignant disease. Eur J Cardiothorac Surg1998;14(5):460–6.
[20] Orringer MB, Bluett M, Deeb GM. Aggressive treatment ofchylothorax complicating transhiatal esophagectomywithout thoracotomy. Surgery 1988;104(4):720–6.
[21] Wemyss-Holden SA, Launois B, Maddern GJ.Management of thoracic duct injuries afteroesophagectomy. Br J Surg 2001;88(11):1442–8.
[22] Chalret du Rieu M, Baulieux J, Rode A, Mabrut JY.Management of postoperative chylothorax. J Visc Surg2011;148(5):e346–52.

FULL LEN
GTH
ARTIC
LE
92 ISMAIL ET ALIMPACT OF CHYLOTHORAX ON THE EARLY POSTOPERATIVE OUTCOME AFTER PEDIATRICCARDIOVASCULAR SURGERY
J Saudi Heart Assoc2014;26:87–92
[23] Marts BC, Naunheim KS, Fiore AC, Pennington DG.Conservative versus surgical management ofchylothorax. Am J Surg 1992;164(5):532–4.
[24] Fahimi H, Casselman FP, Mariani MA, van Boven WJ,Knaepen PJ, van Swieten HA. Current management of
postoperative chylothorax. Ann Thorac Surg2001;71(2):448–50 [discussion 450–1].
[25] Liu CS, Tsai HL, Chin TW, Wei CF. Surgical treatment ofchylothorax caused by cardiothoracic surgery in children. JChin Med Assoc 2005;68(5):234–6.