renin-secreting tumor case report
TRANSCRIPT
G Valdés, J M Lopez, P Martinez, H Rosenberg, P Barriga, J A Rodriguez and N OtipkaRenin-secreting tumor. Case report.
Print ISSN: 0194-911X. Online ISSN: 1524-4563 Copyright © 1980 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Hypertension doi: 10.1161/01.HYP.2.5.714
1980;2:714-718Hypertension.
http://hyper.ahajournals.org/content/2/5/714World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://hyper.ahajournals.org//subscriptions/
is online at: Hypertension Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
Request Permissions in the middle column of the Web page under Services. Further information about thisOffice. Once the online version of the published article for which permission is being requested is located, click
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialHypertension Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on July 13, 2014http://hyper.ahajournals.org/Downloaded from by guest on July 13, 2014http://hyper.ahajournals.org/Downloaded from
Case Reports
Renin-Secreting Tumor
Case Report
GLORIA VALDES, M.D., JOSE M. LOPEZ, M.D., PEDRO MARTINEZ, M.D.,
HELMAR ROSENBERG, M.D., PATRICIO BARRIGA, M.D., Jos£ A. RODRIGUEZ, M.D.,
AND NORBERT OTIPKA, M . D .
SUMMARY Renin-secreting tumor, though rare, should be considered in assessing severe hyperreninemic,hypertensive patients. We studied an 18-year-old girl with hypokalemic hyperreninemic hyperaldosteronism.No angiographic lesion could be detected. The plasma renin activity (PRA) of the right/left renal vein was 7 3 .With a presumptive diagnosis of renin-secreting tumor (RST), the patient was operated on, and a corticalnodule was found on the right lower pole. Partial nephrectomy was followed by a rapid fall in PRA (half-life,33-44 min) and normalization of blood pressure (BP). At 3Vi months postoperatJvely, the patient showed nor-motension, normokalemia, normal aldosterone, and slightly elevated PRA unresponsive to postural changesand furosemide treatment. Tumoral PRA secretion responded to postural stimulus, spironolactone use, andnitroprusside-induced hypotension. Neither the high aldosterone excretion nor hyperrenlnemla decreased after3 days of DOCA; this agrees with a previously reported case suggesting the usefulness of this test in thediagnosis of RST. (Hypertension 2: 714-718, 1980)
KEY WORDS • renin-secreting tumor • hyperreninemiadeoxycorticosterone acetate (DOCA) • kidney functionfurosemide > plasma renin activity
hyperaldosteronismspironolactone •
hypokalemia
ELEVEN years after the first case was re-ported by Robertson et al.,1 renin secretingtumor (RST) continues to be a rare cause of
curable hypertension. Initial cases were diagnosed bythe postsurgical histological study,13 and the most re-cent ones have been recognized preoperatively.*11
We describe an additional case in which a presump-tive diagnosis was made preoperatively, facilitatingremoval of the tumor and subsequent rapid andsustained normotension.
Case Report
An 18-year-old white girl was referred to theCatholic University Hospital because of hypertensionof 2 years' duration. Her complaints were headaches,leg cramps, easy fatigability, polydipsia, and nocturia.
From the Departments of Nephrology and Urology, En-docrinology, Radiology, and Pathology, Faculty of Medicine,Catholic University of Chile, Santiago, Chile.
Address for reprints: Gloria Valdes, M.D., LaboratorioNcfrologla, Hospital Cllnico, Universidad Catolica, Marcoleta 347Santiago, Chile.
Received August 7, 1979; revision accepted April 11, 1980.714
Two years before admission, no abnormalities hadbeen detected in renal function, rapid sequence intra-venous pyelogram, and renal arteriogram. At thattime plasma sodium and potassium levels were 138and 3.3 mEq/liter respectively, with a 24-hour urinaryexcretion of sodium 110 mEq and potassium 21 mEq.Guanethidine, methyldopa, and propranolol in com-bination with diuretics were used in maximallytolerated doses and failed to control arterial pressure.
The physical examination showed a young female inno acute distress whose weight was 50 kg and whoseheight was 158 cm. Blood pressure was 220/150 mmHg in both supine and upright position and was notchanged by abdominal palpation. Heart rate wasregular, 80/min supine and 120/min upright. The fun-doscopic examination showed intensely vasocon-stricted arteries with increased light reflex (2+), scarcesmall exudates, and retinal and papillary edema.
Laboratory work-up was performed under balanceconditions on a daily intake of 120 mEq sodium and70 mEq of potassium. All medication had been dis-continued 3 weeks before admission. Plasma andurinary aldosterone were measured by radioim-munoassay;11'1S plasma renin activity (PRA) was
by guest on July 13, 2014http://hyper.ahajournals.org/Downloaded from
RENIN-SECRETING TUMOR/Valdes et al. 715
determined using a commercially available kit fromNew England Nuclear.
Results obtained are the following: hematocrit 42%,BUN 15 mg/dl, creatinine clearance 89 ml/min,plasma creatinine 0.8 mg/dl. The electrocardiogram,serum albumin, total protein, calcium phosphate, uricacid, cholesterol, alkaline phosphatase, LDH, SGOT,and cortisol were all normal, as were urinary 17-hydroxisteroid, 17-ketosteroid, epinephrine andnorepinephrine excretion rates. A renal arteriogramshowed no abnormalities. Maintained hypokalemia,kaliuresis, elevated urinary aldosterone, andhyperreninemia were observed under balance (basal)conditions (table 1). Supine plasma aldosterone con-centration was 13 ng/dl (normal = 3-31.4 ng/dl).Under the same dietary conditions, 3 days of deoxy-corticosterone acetate (DOCA), 10 mg intramuscu-larly twice per day, did not change body weight,arterial pressure, PRA, or urinary aldosterone excre-tion rate (table 1).
The patient was treated for 2 months withspironolactone, 250 mg/day. Although arterial bloodpressure (BP) remained at 220/150 mm Hg she feltconsiderably improved, with disappearance of crampsand fatigue. On readmission to the hospital,laboratory work-up performed under balance con-ditions during spironolactone therapy revealed nor-mokalemia and further increases in PRA and urinaryaldosterone excretion rate (table 1).
Renal venous blood samples were obtained in thesupine position before and after nitroprusside-inducedhypotension (table 2). The PRA ratio of the right/leftrenal vein was 7.3; PRA of the left renal vein was thesame as that of the inferior vena cava in either con-dition. Despite important percentual increments inPRA from both sides after stimulation, identity
TABLE 2. Bilateral Renal Vein Plasma Renin ActivityDuring Basal Conditions and after Sodium Nitroprusside(NPS)—Induced Hypotension
Plasma renin activity (ng/ml/hr)BP PRA RRV
Condition (mm Hg) RRV LRV IVC PRA LRV
Basal 210/150 704 96 96 7.3
NPSinfusion 100/60 1052 132 132 8.0
Increment 49 37 37
RRV = right renal vein; LRVinferior vena cava.
left renal vein; IVC
between the PRA of the left renal vein and inferiorvena cava points to a negligible renin secretion fromthe left kidney.
A working diagnosis of RST of the right kidney wasmade, and at operation a whitish tumor 15 mm indiameter was found in the lower pole; subtotalnephrectomy was done. Surgical exploration ofadrenal glands revealed no abnormalities.
Light microscopy demonstrated a well-defined com-pact tumor composed of ovoidal and fusiform cellswith no atypical cells (fig. 1). Bowie's stain waspositive; no nerve fibers were found with the modifiedChen-Bodian stain.14 The adjacent renal cortex hadarteriolosclerosis with hyalinization and signs of focaland segmental ischemia in 10% of the glomeruli. Thecount of juxtaglomerular cells was normal accordingto Turgeon-Sommers technique.18 Electron micros-copy showed three types of cytoplasmic granules:crystalloid, homogeneous, and fibrillar. The endo-plasmic reticulum was rugged and dilated. Homog-
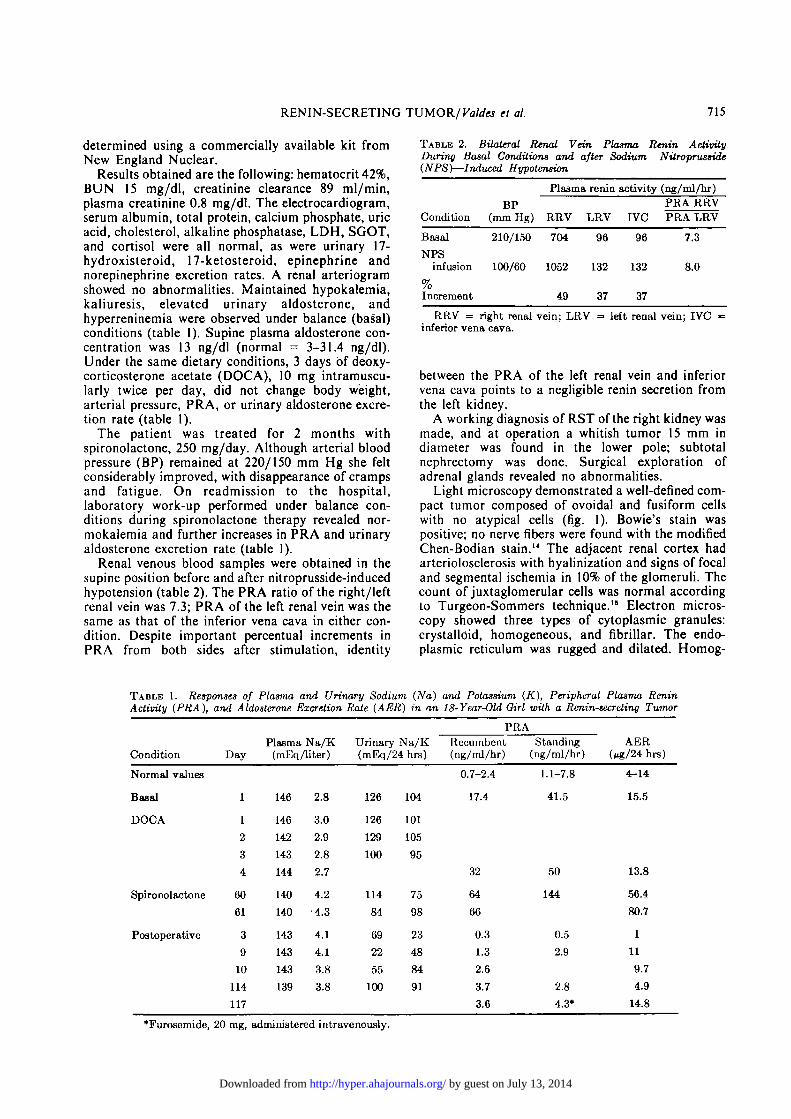
TABLE 1. Responses of Plasma and Urinary Sodium (Na) and Potassium (K), Peripheral Plasma ReninActivity (PRA), and Aldosterone Excretion Rate (AER) in an 18-Year-Old Girl with a Renin-secreting Tumor
Condition
Normal values
Basal
DOCA
Spironolactone
Postoperative
Day
1
1
2
3
4
60
61
3
9
10
114
117
Plasma Na/K(mEq /liter)
146
146
142
143
144
140
140
143
143
143
139
2.8
3.0
2.9
2.8
2.7
4.2
4.3
4.1
4.1
3.8
3.8
Urinary Na/K(mEq/24 hrs)
126
126
129
100
114
84
69
22
55
100
104
101
105
95
75
98
23
48
84
91
PRA
Recumbent(ng/mlAr)
0.7-2.4
17.4
32
64
66
0.3
1.3
2.6
3.7
3.6
Standing(ng/ml/hr)
1.1-7.8
41.5
50
144
0.5
2.9
2.8
4.3*
AER(^g/24 hrs)
4-14
15.5
13.8
56.4
80.7
1
11
9.7
4.9
14.8
*Furosemide, 20 mg, administered intravenously.
by guest on July 13, 2014http://hyper.ahajournals.org/Downloaded from
716
FIGURE 1. Tumoral tissue with twosinusoidal vascular structures (S). (Eponand toluidine blue, X 500). i t 71
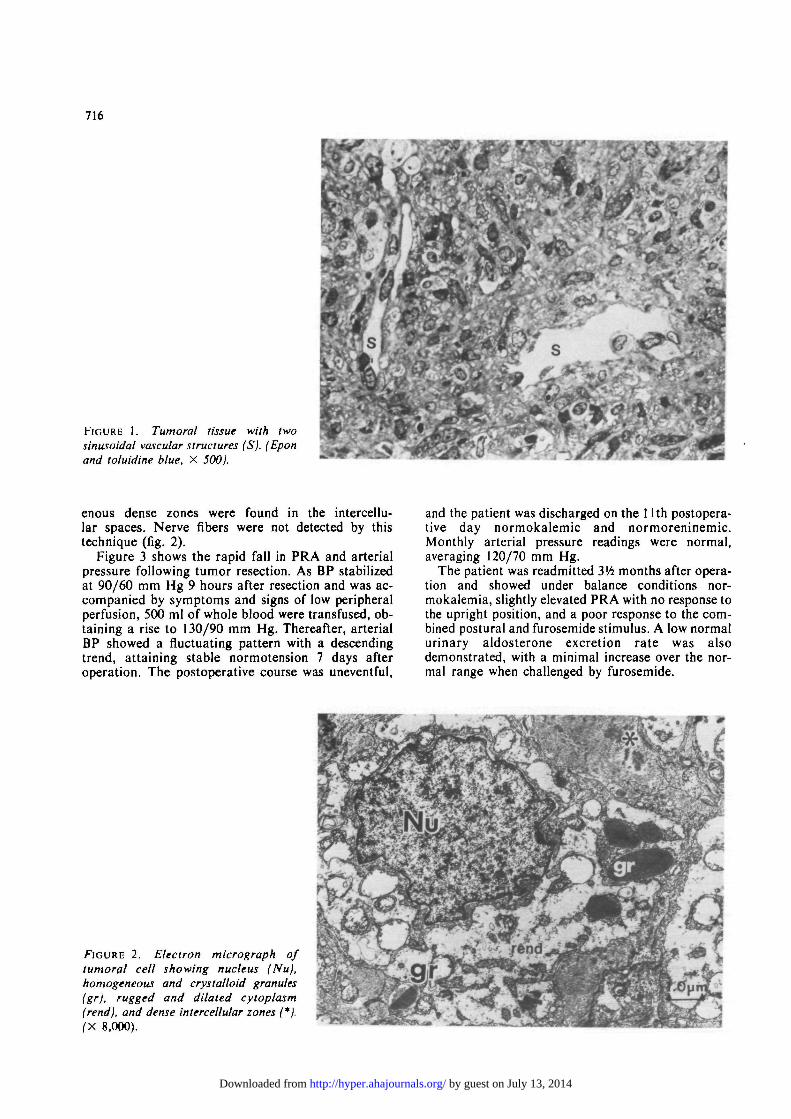
enous dense zones were found in the intercellu-lar spaces. Nerve fibers were not detected by thistechnique (fig. 2).
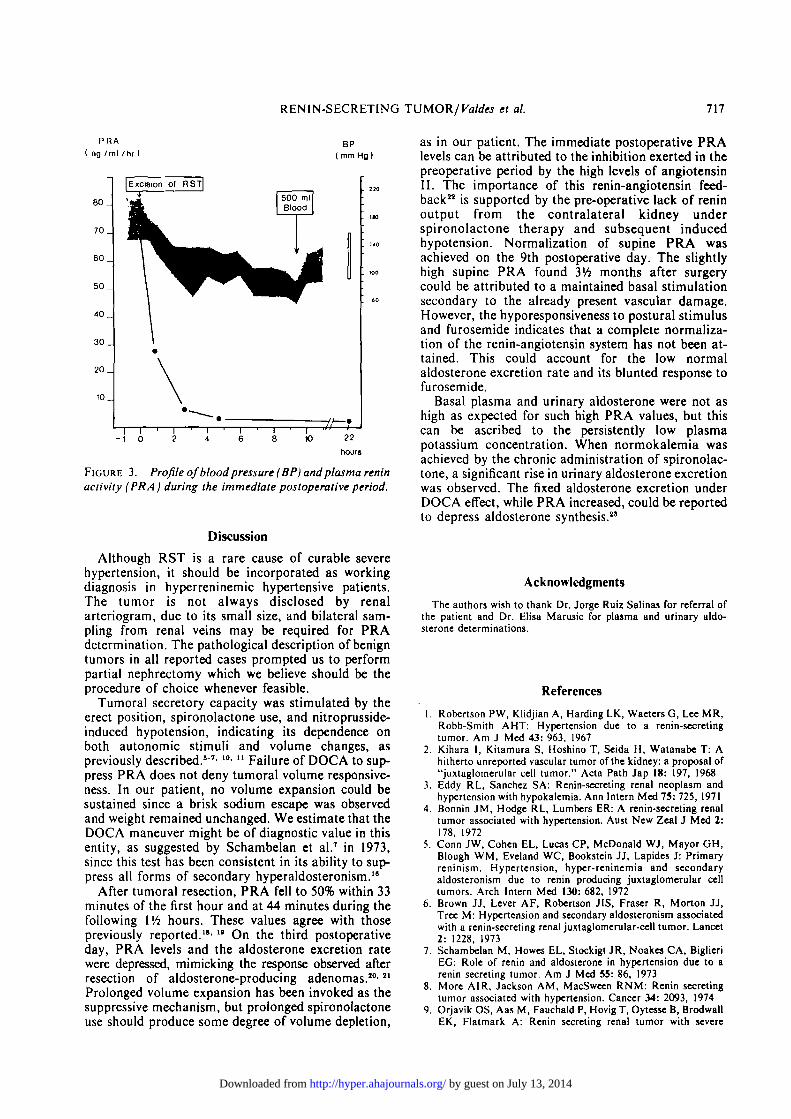
Figure 3 shows the rapid fall in PRA and arterialpressure following tumor resection. As BP stabilizedat 90/60 mm Hg 9 hours after resection and was ac-companied by symptoms and signs of low peripheralperfusion, 500 ml of whole blood were transfused, ob-taining a rise to 130/90 mm Hg. Thereafter, arterialBP showed a fluctuating pattern with a descendingtrend, attaining stable normotension 7 days afteroperation. The postoperative course was uneventful,
and the patient was discharged on the 1 lth postopera-tive day normokalemic and normoreninemic.Monthly arterial pressure readings were normal,averaging 120/70 mm Hg.
The patient was readmitted 3'/6 months after opera-tion and showed under balance conditions nor-mokalemia, slightly elevated PRA with no response tothe upright position, and a poor response to the com-bined postural and furosemide stimulus. A low normalurinary aldosterone excretion rate was alsodemonstrated, with a minimal increase over the nor-mal range when challenged by furosemide.
FIGURE 2. Electron micrograph oftumoral cell showing nucleus (Nu),homogeneous and crystalloid granulesfgr), rugged and dilated cytoplasm(rend), and dense intercellular zones (*).(X 8,000).
by guest on July 13, 2014http://hyper.ahajournals.org/Downloaded from
RENIN-SECRETING TUMOR/Valdcs et al. 717
PRAng /ml /hr)
BP( mm Hg)
6 0 _
70 _
60 _
50 _
40 _
30 _
20 _
10 _
Excision of RST
500 mlBlood
(1
M
\
* "; f- 1 r i r 22
hours
FIGURE 3. Profile ofblood pressure (BP) and plasma reninactivity (PRA) during the immediate postoperative period.
Discussion
Although RST is a rare cause of curable severehypertension, it should be incorporated as workingdiagnosis in hyperreninemic hypertensive patients.The tumor is not always disclosed by renalarteriogram, due to its small size, and bilateral sam-pling from renal veins may be required for PRAdetermination. The pathological description of benigntumors in all reported cases prompted us to performpartial nephrectomy which we believe should be theprocedure of choice whenever feasible.
Tumoral secretory capacity was stimulated by theerect position, spironolactone use, and nitroprusside-induced hypotension, indicating its dependence onboth autonomic stimuli and volume changes, aspreviously described.07' 10' u Failure of DOCA to sup-press PRA does not deny tumoral volume responsive-ness. In our patient, no volume expansion could besustained since a brisk sodium escape was observedand weight remained unchanged. We estimate that theDOCA maneuver might be of diagnostic value in thisentity, as suggested by Schambelan et al.7 in 1973,since this test has been consistent in its ability to sup-press all forms of secondary hyperaldosteronism.18
After tumoral resection, PRA fell to 50% within 33minutes of the first hour and at 44 minutes during thefollowing Vh hours. These values agree with thosepreviously reported.1'1 " On the third postoperativeday, PRA levels and the aldosterone excretion ratewere depressed, mimicking the response observed afterresection of aldosterone-producing adenomas.10'21
Prolonged volume expansion has been invoked as thesuppressive mechanism, but prolonged spironolactoneuse should produce some degree of volume depletion,
as in our patient. The immediate postoperative PRAlevels can be attributed to the inhibition exerted in thepreoperative period by the high levels of angiotensinII. The importance of this renin-angiotensin feed-back22 is supported by the pre-operative lack of reninoutput from the contralateral kidney underspironolactone therapy and subsequent inducedhypotension. Normalization of supine PRA wasachieved on the 9th postoperative day. The slightlyhigh supine PRA found 3Vi months after surgerycould be attributed to a maintained basal stimulationsecondary to the already present vascular damage.However, the hyporesponsiveness to postural stimulusand furosemide indicates that a complete normaliza-tion of the renin-angiotensin system has not been at-tained. This could account for the low normalaldosterone excretion rate and its blunted response tofurosemide.
Basal plasma and urinary aldosterone were not ashigh as expected for such high PRA values, but thiscan be ascribed to the persistently low plasmapotassium concentration. When normokalemia wasachieved by the chronic administration of spironolac-tone, a significant rise in urinary aldosterone excretionwas observed. The fixed aldosterone excretion underDOCA effect, while PRA increased, could be reportedto depress aldosterone synthesis."
Acknowledgments
The authors wish to thank Dr. Jorge Ruiz Salinas for referral ofthe patient and Dr. Elisa Mamsic for plasma and urinary aldo-sterone determinations.
References
Robertson PW, Klidjian A, Harding LK, Waeters G, Lee MR,Robb-Smith AHT: Hypertension due to a renin-secretingtumor. Am J Mcd 43: 963, 1967Kihara I, Kitamura S, Hoshino T, Seida H, Watanabe T: Ahitherto unreportcd vascular tumor of the kidney: a proposal of"juxtaglomerular cell tumor." Acta Path Jap 18: 197, 1968Eddy RL, Sanchez SA: Renin-secreting renal neoplasm andhypertension with hypokalemia. Ann Intern Med 75: 725, 1971Bonnin JM, Hodge RL, Lumbers ER: A renin-secreting renaltumor associated with hypertension. Aust New Zeal J Med 2:178, 1972Conn JW, Cohen EL, Lucas CP, McDonald WJ, Mayor GH,Blough WM, Eveland WC, Bookstein JJ, Lapides J: Primaryreninism. Hypertension, hypcr-reninemia and secondaryaldosteronism due to renin producing juxtaglomerular celltumors. Arch Intern Med 130: 682, 1972Brown JJ, Lever AF, Robertson JIS, Fraser R, Morton JJ,Tree M: Hypertension and secondary aldosteronism associatedwith a renin-secreting renal juxtaglomerular-cell tumor. Lancet2: 1228, 1973Schambelan M, Howes EL, Stockigt JR, Noakes CA, BiglieriEG: Role of renin and aldosterone in hypertension due to arenin secreting tumor. Am J Med 55: 86, 1973More AIR, Jackson AM, MacSween RNM: Renin secretingtumor associated with hypertension. Cancer 34: 2093, 1974Orjavik OS, Aas M, Fauchald P, Hovig T, Oytesse B, BrodwallEK, Flatmark A: Renin secreting renal tumor with severe
by guest on July 13, 2014http://hyper.ahajournals.org/Downloaded from
718 HYPERTENSION VOL 2, No 5, SEPTEMBER-OCTOBER 1980
hypertension. Acta Med Scand 197: 329, 197510. Takahashi T, Miura T, Sue A, Saito K, Sakaue M, Yamagata
Y, Fukuchi S, Sato Z, Hirai T, Terashima K, Oka K, Imai Y:A case of juxtaglomerular cell tumor diagnosed preoperatively.Nephron 17: 483, 1976
11. Mirman A, Leckie BJ, Fourcade JC, Baldet P, Navratil H,Barjon P: Blood pressure, rcnin-angiotensin system and urinarykallikrein in a case of juxtaglomerular cell tumor. Am J Med65: 527, 1978
12. Underwood RH, Williams GH: The simultaneous measure-ment of aldosterone, cortisol and corticosterone in humanperipheral plasma by displacement analysis. J Lab Clin Med79: 848, 1972
13. Sealey JE, Buhler FR, Laragh JH, Manning El, Bmnner HR:Aldosterone excretion. Physiological variations in manmeasured by radioimmunoassay or double isotope dilution.Circ Res 31: 367, 1972
14. Luna LG: Manual of Histological Staining Methods of theArmed Forces Institute of Pathology. New York, McGrawHill, 1968
15. Turgeon C, Sommers SC: Juxtaglomerular cell counts andhuman hypertension. Am J Pathol 38: 227, 1961
16. Biglieri EG, Schambelan M, Stockigt JR: Hypertension andhyperaldosteronism: discriminating value of desoxycor-
ticosterone acetate (DOCA) testing. Clin Res 20: 163, 197217. Barajas I, Bennet CM, Connor G, Linstrom RR: Structure of a
juxtaglomerular cell tumor: the presence of a neural compo-nent. A light and electron microscopic study. Lab Invest 37:357, 1977
18. Devaux CJ, Mennard JH, Alexandre JM, Idatte P, Meyer P,Milliez P: Variations in renin and its substrate after binephrec-tomy. Lancet 1: 300, 1968
19. Hannon RC, Deruyck RP, Joosens JB, Amery AK:Disappearance rate of endogenous renin from the plasma afterbilateral nephrectomy in humans. J Clin Endocrinol Metab 29:1420, 1969
20. Bigheri EG, Slayton PA, Silen WS, Galante M, Forsham PH:Postoperative studies of adrenal function in primaryaldosteronism. J Clin Endocrinol Metab 26: 553, 1966
21. Schambelan M, Stockgit JR, Biglieri EG: Recovery of reninand aldosterone after removal of an aldosterone producingadenoma (APA) (abstr A589). In Abstracts IV InternationalCongress Series 256: 234, 1972
22. De Champlain J, Genest J, Veyrat R, Boucher R: Factors con-trolling renin in man. Trans Assoc Am Physicians 78:135, 1965
23. Himathogkam T, Dluhy RG, Williams GH: Potassium-aldosterone-rcnin interrelationships. J Clin Endocrinol Metab41: 153, 1975
by guest on July 13, 2014http://hyper.ahajournals.org/Downloaded from