relevance of braf and extended ras mutational analyses for metastatic colorectal cancer patients
TRANSCRIPT

Page 1 of 8
Critical review
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
For citation purposes: Aprile G, Macerelli M, G De Maglio, Pizzolitto S, Fasola G. Relevance of BRAF and extended RAS mutational analyses for metastatic colorectal cancer patients. OA Molecular Oncology 2013 Dec 25;1(1):7. Co
mpe
ting
inte
rest
s: n
one
decl
ared
. Con
flict
of i
nter
ests
: non
e de
clar
ed.
All
auth
ors
cont
ribut
ed to
con
cepti
on a
nd d
esig
n, m
anus
crip
t pre
para
tion,
read
and
app
rove
d th
e fin
al m
anus
crip
t.A
ll au
thor
s ab
ide
by th
e A
ssoc
iatio
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
Canc
er G
enet
ics
&
Geno
mic
Inst
abili
ty
Relevance of BRAF and extended RAS mutational analyses for metastatic colorectal cancer patients
G Aprile1*, M Macerelli1, G De Maglio2, S Pizzolitto2, G Fasola1
AbstractIntroductionIn the past 15 years, the treatment of advanced colorectal cancer has markedly advanced, leading to a median survival improvement from 1 year with 5-Fluorouracil alone to over 24 months with modern thera-pies. Recently, we have learned that specific genomic alterations have a clear prognostic role and are closely linked to response to specific anti-cancer agents. Specifically, antibod-ies targeting the epidermal growth factor receptor pathway have pro-duced sounding survival improve-ments for advanced colorectal can-cer patients. To optimise their use, however, a more profound knowl-edge of tumour molecular oncology is crucial. In this short viewpoint the authors depict the biological, clinical and economic relevance of v-Raf mu-rine sarcoma viral oncogene homo-logue B1 and extended rat sarcoma mutational analyses when focusing on epidermal growth factor receptor inhibitor-based therapy.ConclusionColorectal cancer patients who are most likely to benefit from epidermal growth factor receptor inhibitors may be selected with a deeper molecular biology, encompassing not only exon 2 Kirsten rat sarcoma viral oncogene homologuemutations (codons 12 and
13), but also neuroblastoma rat sar-coma viral oncogene homologue and BRAF mutational status. This fine-tuning in patients’ selection has pro-duced striking implications.
IntroductionAlthough, colorectal cancer (CRC) still remains a significant healthcare problem, major survival improve-ments have been noted in the past two decades1. More specifically, the life expectancy of patients diag-nosed with advanced, unresectable disease has progressively increased, along with the possibility of receiv-ing all available treatments, includ-ing antiangiogenics and epidermal growth factor receptor inhibitors (EGFR-I)2,3. Between 2008 and 2010, a growing amount of data demon-strated that patients harbouring mutations in codon 12 or 13 on the Kirsten rat sarcoma viral oncogene homologue (KRAS) have a negligi-ble chance to benefit from EGFR-I3, regardless these target drugs were administered alone4,5 or in combi-nation with chemotherapy6,7. This body of information has promptly induced the international commu-nity and the Regulatory Agencies to limit the use of EGFR-I in KRAS wild-type tumours only8. Soon after, this evolving landscape has broadened frenetically beyond KRAS exon 2 mu-tational status9. It was demonstrated that less frequent mutations occur-ring in other KRAS codons, such as codon 61 on exon 3 or codon 146 on exon 4, may also result in impaired EGFR-I efficacy10. Also, v-Raf murine sarcoma viral oncogene homologue B1 (BRAF) mutations seem to limit the benefit from EGFR-I11,12, as may do the loss of phosphatase and tensin
homolog (PTEN) expression13,14. At the same time, many issues regard-ing technical and practical aspects have swiftly raised and have created new challenges. Among these, we list the debates on the optimal method-ology for molecular status assess-ment, the most appropriate site to obtain tissue samples, the testing turnaround time and the need for re-liability of molecular testing, ensured with external and internal quality assessment programmes15. Recently, the huge clinical value of a deeper fo-cusing on tumour molecular biology when deciding the first-line treat-ment strategy has emerged9, render-ing the scenario even more complex than before. How a more profound molecular knowledge, including the analysis of human rat sarcoma (RAS) viral oncogene family, may dramati-cally impact on the molecularly se-lected patients’ outcome when ex-posed to EGFR-I has now reached very compelling evidence, with me-dian improvement in overall survival (OS) surpassing 6 months16.
All these practice-changing shifts have immediately produced sig-nificant consequences and have re-shaped our treatment paradigms. Within the blurred borders of this evolving landscape, the aim of this concise viewpoint is to report and discuss the biological, clinical and economic relevance of the extended molecular testing in CRC patients.
DiscussionThe authors have referenced some of their own studies in this review. These referenced studies have been conducted in accordance with the Declaration of Helsinki (1964) and the protocols of these studies have
* Corresponding authorEmail: [email protected] Department of Medical Oncology, University
and General Hospital, Piazzale S Maria della Misericordia 15, 33100, Udine, Italy
2 Department of Pathology and Molecular Biol-ogy, University and General Hospital, Piazzale S Maria della Misericordia 15, 33100, Udine, Italy
Page 2 of 8
Critical review
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
For citation purposes: Aprile G, Macerelli M, G De Maglio, Pizzolitto S, Fasola G. Relevance of BRAF and extended RAS mutational analyses for metastatic colorectal cancer patients. OA Molecular Oncology 2013 Dec 25;1(1):7. Co
mpe
ting
inte
rest
s: n
one
decl
ared
. Con
flict
of i
nter
ests
: non
e de
clar
ed.
All
auth
ors
cont
ribut
ed to
con
cepti
on a
nd d
esig
n, m
anus
crip
t pre
para
tion,
read
and
app
rove
d th
e fin
al m
anus
crip
t.A
ll au
thor
s ab
ide
by th
e A
ssoc
iatio
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
the EGFR pathway is activated, the tumour phenotype becomes more ag-gressive and may acquire resistance to treatments22. RAS oncogenes have a well-established role in cell growth and proliferation, with its three iso-forms, mainly neuroblastoma rat sarcomal viral oncogene homologue (NRAS) KRAS and Harvey rat sarcoma viral oncogene homologue (HRAS). In CRC, RAS mutations occur in 30%–50% of cases. KRAS is by large the most mutated isoform (35%–45%) followed by NRAS (3%–5%), whereas somatic mutations on HRAS are an-ecdotic events. Also NRAS mutations lead to constitutive activation of the MAPK pathway, and several stud-ies have shown that these mutations predict resistance to EGFR-I23,24. How-ever, over 40% among CRC patients harbouring wild-type KRAS gene fail to respond to EGFR-I25,26.
BRAF mutation is an early event in CRC and there is a high concordance between primary and metastatic tissue. The predominant mutation (90%) is a single-base substitution of valine by glutamic acid at position 600 (V600E) within the activation segment. Since BRAF and KRAS mu-tations are mutually exclusive and BRAF mutations occur in approxi-mately 8% of these patients, the two markers together may identify up to 55% of non-responders27. Products of BRAF gene act as downstream agents of KRAS in the MAPK pathway.
There is growing interest on the analysis of PI3K pathway and PTEN, since activating mutations are frequently detected and may confer a more aggressive clinical behaviour28,29. The usefulness of these biomarkers in the clinical practice, however, is still not validated.
Which method should be preferred to perform the molecular characterisation?Point mutations are the most frequent genotypic alterations in CRC. Molecu-lar analyses of predictive or prognostic biomarkers require standardisation,
been approved by the relevant ethics committees related to the institution in which they were performed. All human subjects, in these referenced studies, gave informed consent to participate in these studies.
Which molecular biomarkers should be analysed?Since CRCs have complex and highly heterogeneous genomic profiles that may change over time or evolve un-der treatment pressure17, the Cancer Genome Atlas Network has promoted a more profound molecular knowl-edge of this cancer and has recently published a comprehensive molecu-lar disease characterisation18. To ex-pand the understanding of the dis-ease, pathobiology and its molecular
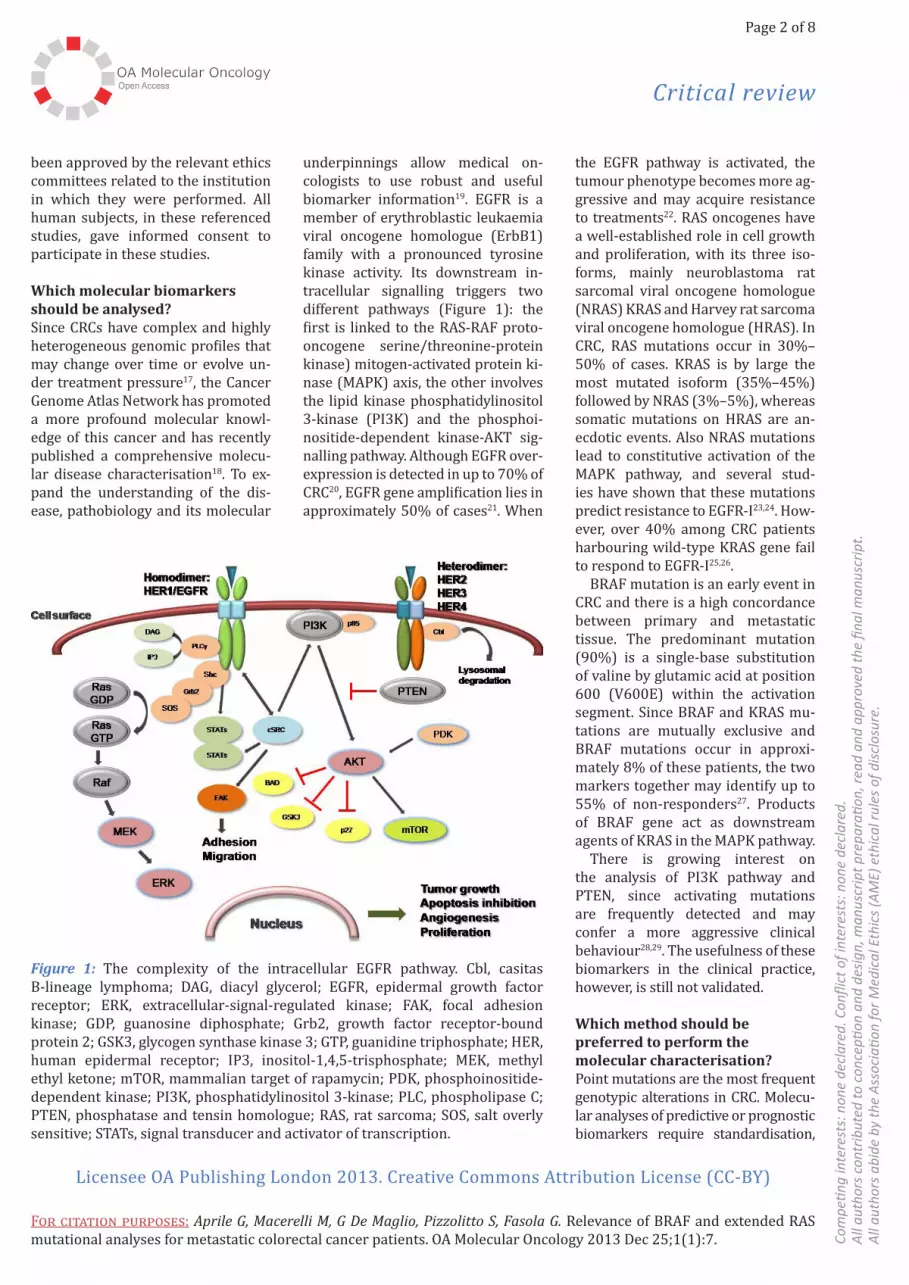
underpinnings allow medical on-cologists to use robust and useful biomarker information19. EGFR is a member of erythroblastic leukaemia viral oncogene homologue (ErbB1) family with a pronounced tyrosine kinase activity. Its downstream in-tracellular signalling triggers two different pathways (Figure 1): the first is linked to the RAS-RAF proto-oncogene serine/threonine-protein kinase) mitogen-activated protein ki-nase (MAPK) axis, the other involves the lipid kinase phosphatidylinositol 3-kinase (PI3K) and the phosphoi-nositide-dependent kinase-AKT sig-nalling pathway. Although EGFR over-expression is detected in up to 70% of CRC20, EGFR gene amplification lies in approximately 50% of cases21. When
Figure 1: The complexity of the intracellular EGFR pathway. Cbl, casitas B-lineage lymphoma; DAG, diacyl glycerol; EGFR, epidermal growth factor receptor; ERK, extracellular-signal-regulated kinase; FAK, focal adhesion kinase; GDP, guanosine diphosphate; Grb2, growth factor receptor-bound protein 2; GSK3, glycogen synthase kinase 3; GTP, guanidine triphosphate; HER, human epidermal receptor; IP3, inositol-1,4,5-trisphosphate; MEK, methyl ethyl ketone; mTOR, mammalian target of rapamycin; PDK, phosphoinositide-dependent kinase; PI3K, phosphatidylinositol 3-kinase; PLC, phospholipase C; PTEN, phosphatase and tensin homologue; RAS, rat sarcoma; SOS, salt overly sensitive; STATs, signal transducer and activator of transcription.

Page 3 of 8
Critical review
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
For citation purposes: Aprile G, Macerelli M, G De Maglio, Pizzolitto S, Fasola G. Relevance of BRAF and extended RAS mutational analyses for metastatic colorectal cancer patients. OA Molecular Oncology 2013 Dec 25;1(1):7. Co
mpe
ting
inte
rest
s: n
one
decl
ared
. Con
flict
of i
nter
ests
: non
e de
clar
ed.
All
auth
ors
cont
ribut
ed to
con
cepti
on a
nd d
esig
n, m
anus
crip
t pre
para
tion,
read
and
app
rove
d th
e fin
al m
anus
crip
t.A
ll au
thor
s ab
ide
by th
e A
ssoc
iatio
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
progression-free survival (PFS) and/or OS in multiple treatment lines, enhancing the possibility for a per-sonalised strategy of treatment. If specific molecular targets for biolog-ic agents are still under discussion, BRAF and extended RAS mutational status analysis have become increas-ingly important to choose the opti-mal upfront therapy.
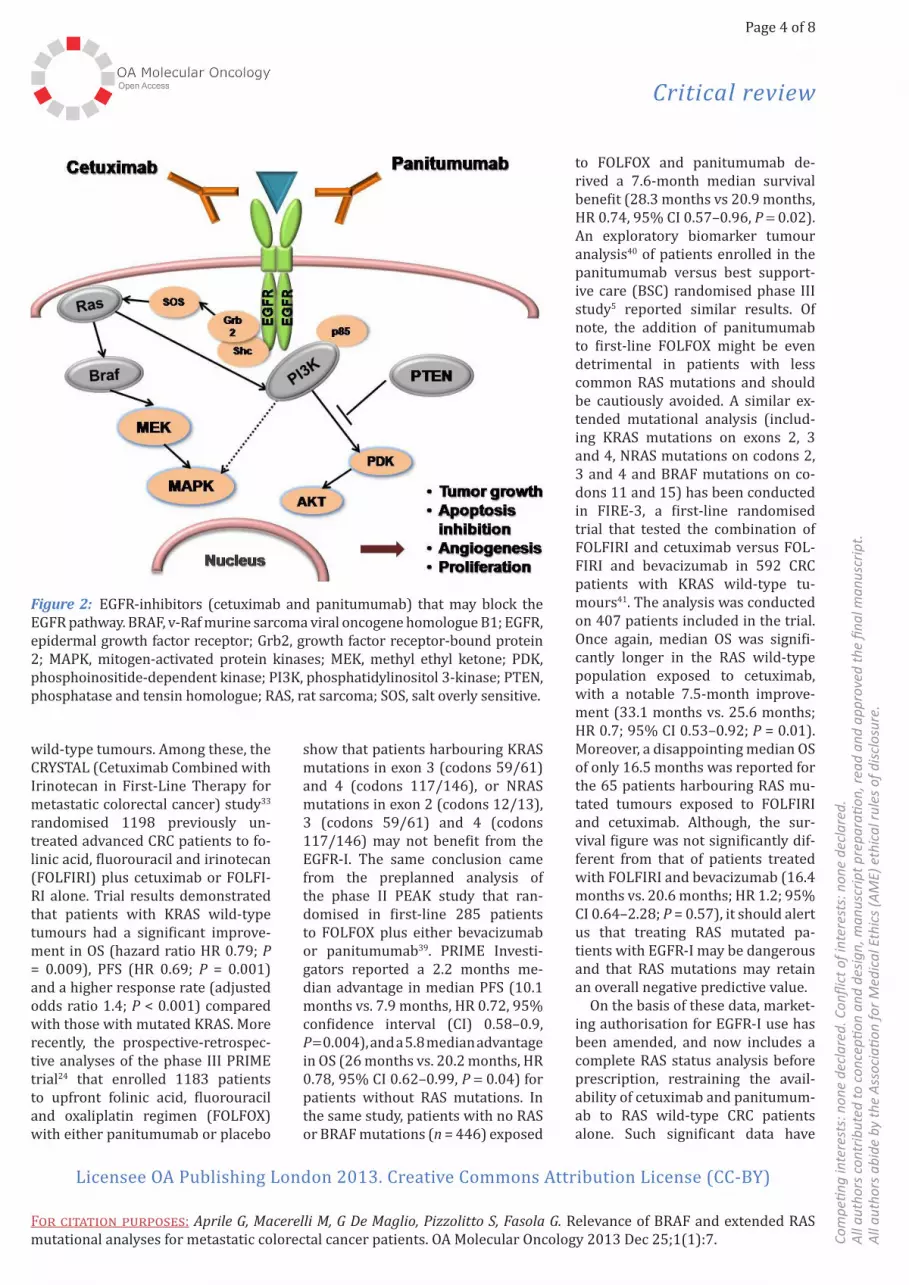
Both cetuximab and panitumum-ab bind to the extracellular domain of EGFR, inhibiting its downstream signal, and have proven efficacy when used upfront in combination with chemotherapy7,33,34 or alone in pretreated patients5,35 (Figure 2). Clinical trials are ongoing to verify if cetuximab could be useful beyond disease progression36 or patients may be rechallenged with the same EGFR-I after a period of time37.
Initial studies have consistently confirmed that CRC patients har-bouring KRAS mutations do not ben-efit from EGFR-I4,5,38. In the following years, a number of randomised tri-als have established that significant response advantages and survival gain for the upfront use of EGFR-I in combination with standard chemotherapy are confined to KRAS
by using very low amounts of DNA with high sensitivity and specific-ity. The major advantage of these next-generation techniques is that KRAS/BRAF/NRAS/PIK3CA muta-tions may be analysed in a single run, instead of using a time-con-suming conventional gene-by-gene approach. Available methodologies for KRAS testing are summarised in Table 1.
Evidence coming from recent randomised clinical trials: Will molecular biomarkers help in selecting patients?While prognostic biomarkers help clinicians to identify patients with a specific disease outcome regardless of received treatments, predictive biomarkers may suggest the most appropriate therapeutic option. Be-yond classical chemotherapeutic agents, patients with metastatic, un-resectable CRC may benefit from an increased list of targeted biologic drugs, including two antiangiogen-ics (bevacizumab, aflibercept), two EGFR-I (cetuximab, panitumumab) and a new orally available multitar-get molecule (regorafenib). All those agents may significantly impact on
accuracy, reproducibility, with ad-equate sensitivity and specificity. Since the introduction of commercial tests for KRAS, Sanger sequencing has been considered the gold standard approach, despite this the technique suffers from a low analytic sensitivity. Preanalytic keypoints that may influ-ence on laboratory results are correct DNA preservation, accurate sample se-lection and precise macrodissection to obtain adequate tumour cells enrich-ment. Analytical sensitivity and speci-ficity are also important, and depend upon the system used. Many studies compared different approaches and defined their reliability in routine clinical practice30,31. Several systems differ for being screening techniques or targeted on known mutations only, for their sensitivity (minimum amount of mutant allele detectable), for the amount of DNA required for the analysis, for the number of mutations they can identify and for being either laboratory-based techniques or com-mercially available diagnostic systems.
New commercially available high-throughput techniques have recently been presented32. They are multiplexed tests that simultane-ously analyse multiple gene panels
Table 1 Overview of main techniques for rat sarcoma and v-Raf murine sarcoma viral oncogene homologue B1 testing used in colorectal cancer
Technique Sensitivity Detected mutations CE-IVD commer-cially available kits
Multiples genes ana-lysed in a single run
Sanger sequencing Low Known and newPyrosequencing Medium Known and new √HRMA Medium Known and newTaqMelt Real Time PCR High Known only √PNA/LNA Clamp High Known onlyASLNAqPCR High Known onlyScorpions ARMS High Known only √Ion Torrent, Ion AmpliSeq™ High Known only √Maldi-TOF, Sequenom ® High Known only √ √ARMS, amplified refractory mutation system; ASLNAqPCR, allele specific locked nucleic acid quantitative polymerase chain reaction; CE-IVD, European economic area in vitro diagnostic; HRMA, high-resolution melting analysis; LNA, locked nucleic acid; Maldi-TOF, matrix-assisted laser desorption / ionisation time-of-flight; PNA, peptide nucleic acid.
Page 4 of 8
Critical review
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
For citation purposes: Aprile G, Macerelli M, G De Maglio, Pizzolitto S, Fasola G. Relevance of BRAF and extended RAS mutational analyses for metastatic colorectal cancer patients. OA Molecular Oncology 2013 Dec 25;1(1):7. Co
mpe
ting
inte
rest
s: n
one
decl
ared
. Con
flict
of i
nter
ests
: non
e de
clar
ed.
All
auth
ors
cont
ribut
ed to
con
cepti
on a
nd d
esig
n, m
anus
crip
t pre
para
tion,
read
and
app
rove
d th
e fin
al m
anus
crip
t.A
ll au
thor
s ab
ide
by th
e A
ssoc
iatio
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
to FOLFOX and panitumumab de-rived a 7.6-month median survival benefit (28.3 months vs 20.9 months, HR 0.74, 95% CI 0.57–0.96, P = 0.02). An exploratory biomarker tumour analysis40 of patients enrolled in the panitumumab versus best support-ive care (BSC) randomised phase III study5 reported similar results. Of note, the addition of panitumumab to first-line FOLFOX might be even detrimental in patients with less common RAS mutations and should be cautiously avoided. A similar ex-tended mutational analysis (includ-ing KRAS mutations on exons 2, 3 and 4, NRAS mutations on codons 2, 3 and 4 and BRAF mutations on co-dons 11 and 15) has been conducted in FIRE-3, a first-line randomised trial that tested the combination of FOLFIRI and cetuximab versus FOL-FIRI and bevacizumab in 592 CRC patients with KRAS wild-type tu-mours41. The analysis was conducted on 407 patients included in the trial. Once again, median OS was signifi-cantly longer in the RAS wild-type population exposed to cetuximab, with a notable 7.5-month improve-ment (33.1 months vs. 25.6 months; HR 0.7; 95% CI 0.53–0.92; P = 0.01). Moreover, a disappointing median OS of only 16.5 months was reported for the 65 patients harbouring RAS mu-tated tumours exposed to FOLFIRI and cetuximab. Although, the sur-vival figure was not significantly dif-ferent from that of patients treated with FOLFIRI and bevacizumab (16.4 months vs. 20.6 months; HR 1.2; 95% CI 0.64–2.28; P = 0.57), it should alert us that treating RAS mutated pa-tients with EGFR-I may be dangerous and that RAS mutations may retain an overall negative predictive value.
On the basis of these data, market-ing authorisation for EGFR-I use has been amended, and now includes a complete RAS status analysis before prescription, restraining the avail-ability of cetuximab and panitumum-ab to RAS wild-type CRC patients alone. Such significant data have
show that patients harbouring KRAS mutations in exon 3 (codons 59/61) and 4 (codons 117/146), or NRAS mutations in exon 2 (codons 12/13), 3 (codons 59/61) and 4 (codons 117/146) may not benefit from the EGFR-I. The same conclusion came from the preplanned analysis of the phase II PEAK study that ran-domised in first-line 285 patients to FOLFOX plus either bevacizumab or panitumumab39. PRIME Investi-gators reported a 2.2 months me-dian advantage in median PFS (10.1 months vs. 7.9 months, HR 0.72, 95% confidence interval (CI) 0.58–0.9, P = 0.004), and a 5.8 median advantage in OS (26 months vs. 20.2 months, HR 0.78, 95% CI 0.62–0.99, P = 0.04) for patients without RAS mutations. In the same study, patients with no RAS or BRAF mutations (n = 446) exposed
wild-type tumours. Among these, the CRYSTAL (Cetuximab Combined with Irinotecan in First-Line Therapy for metastatic colorectal cancer) study33 randomised 1198 previously un-treated advanced CRC patients to fo-linic acid, fluorouracil and irinotecan (FOLFIRI) plus cetuximab or FOLFI-RI alone. Trial results demonstrated that patients with KRAS wild-type tumours had a significant improve-ment in OS (hazard ratio HR 0.79; P = 0.009), PFS (HR 0.69; P = 0.001) and a higher response rate (adjusted odds ratio 1.4; P < 0.001) compared with those with mutated KRAS. More recently, the prospective-retrospec-tive analyses of the phase III PRIME trial24 that enrolled 1183 patients to upfront folinic acid, fluorouracil and oxaliplatin regimen (FOLFOX) with either panitumumab or placebo
Figure 2: EGFR-inhibitors (cetuximab and panitumumab) that may block the EGFR pathway. BRAF, v-Raf murine sarcoma viral oncogene homologue B1; EGFR, epidermal growth factor receptor; Grb2, growth factor receptor-bound protein 2; MAPK, mitogen-activated protein kinases; MEK, methyl ethyl ketone; PDK, phosphoinositide-dependent kinase; PI3K, phosphatidylinositol 3-kinase; PTEN, phosphatase and tensin homologue; RAS, rat sarcoma; SOS, salt overly sensitive.
Page 5 of 8
Critical review
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
For citation purposes: Aprile G, Macerelli M, G De Maglio, Pizzolitto S, Fasola G. Relevance of BRAF and extended RAS mutational analyses for metastatic colorectal cancer patients. OA Molecular Oncology 2013 Dec 25;1(1):7. Co
mpe
ting
inte
rest
s: n
one
decl
ared
. Con
flict
of i
nter
ests
: non
e de
clar
ed.
All
auth
ors
cont
ribut
ed to
con
cepti
on a
nd d
esig
n, m
anus
crip
t pre
para
tion,
read
and
app
rove
d th
e fin
al m
anus
crip
t.A
ll au
thor
s ab
ide
by th
e A
ssoc
iatio
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
are among the possible solutions to bend the cost curve. Recently, a 20% increase in cancer drug expenditures was reported in the United States, mainly caused by the introduction of novel targeted therapies47. Moreo-ver, 90% of the new cancer drugs approved by the Food and Drug Ad-ministration in the last 5 years ex-ceeded 20,000 USD for 12 weeks of treatment48, rising controversies on their cost-effectiveness. Since 2009, both the American Society of Clini-cal Oncology and the European Soci-ety of Medical Oncology have recom-mended that advanced CRC patients who are candidates for EGFR-I ther-apy have their tumours tested for KRAS mutations. Accordingly, Regu-latory Agencies asked for the test before EGFR-I prescription. Never-theless, health economic evaluations of the procedure conducted with cost-utility studies and cost-effective analyses seemed initially unconvinc-ing. In the molecular unselected pop-ulation, a National Cancer Institute of Canada prospective cost-effective analysis of cetuximab compared with best supportive care alone for pre-treated CRC patients enrolled in the CO.17 trial49 showed an unacceptable incremental cost-effectiveness ratio close to 200,00 USD per with the in-cremental cost-utility ratio of 300,00 USD per quality-adjusted life-year (QALY) gained50. When repeating such economic analyses in the KRAS wild-type population, the incremen-tal cost-effectiveness ratio life-year gained and the incremental cost-utility ratio per QALY gained figures, although reduced by approximately 40%, still remained above the gener-ally accepted threshold of 100,000 USD per QALY50. A Japanese cost-effective analysis brought to similar conclusions51. With the improve-ments in technology and the addition of BRAF mutational analysis testing, the results might be more favour-able, as more recent cost-effective analyses52–55 and a large literature re-view of cost-effective and cost-utility
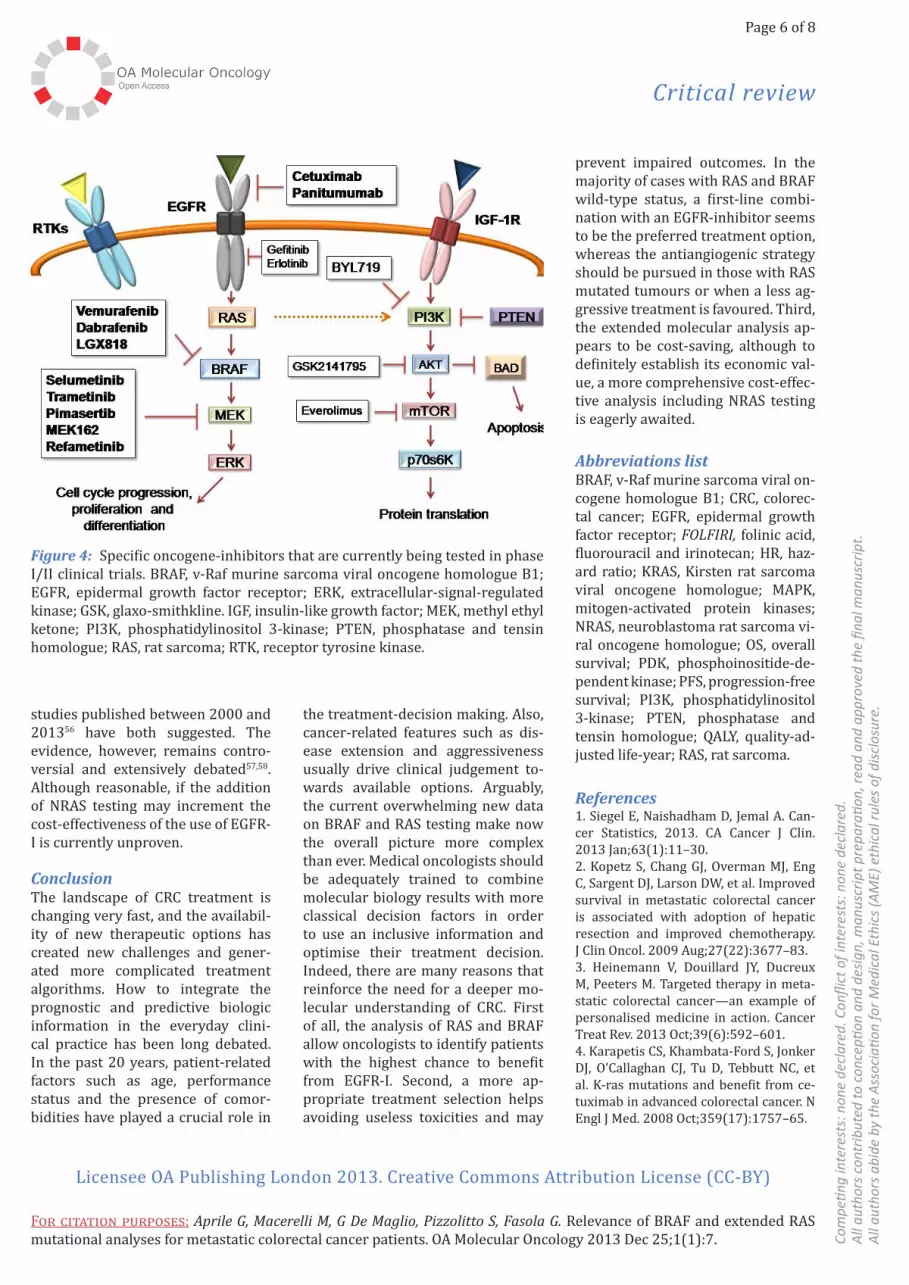
impact on tumour growth are being tested (Figure 4). While phase II tri-als are ongoing to verify if a combi-nation of BRAF-I and MEK-I (methyl ethyl ketone Inhibitor) or EGFR-I may overcome this hurdle and proteasome inhibitors (such as bortezomib) are being tested at a preclinical level45, an upfront intense treatment encom-passing 5-Fluorouracil, oxaliplatin, irinotecan and bevacizumab may be useful for CRC patients harbouring BRAF mutations46.
Cost-effectiveness of rat sarcoma and v-Raf murine sarcoma viral on-cogene homologue B1 testing: Are we moving towards a more rational use of the epidermal growth factor receptor-I?
The increasing burden of cancer is producing growing costs that signifi-cantly impact on healthcare expen-ditures, and value-based approaches
immediately shrunk the population, but this enriched cohort certainly includes those who may benefit the most and, importantly, exclude those who may have detrimental effects.
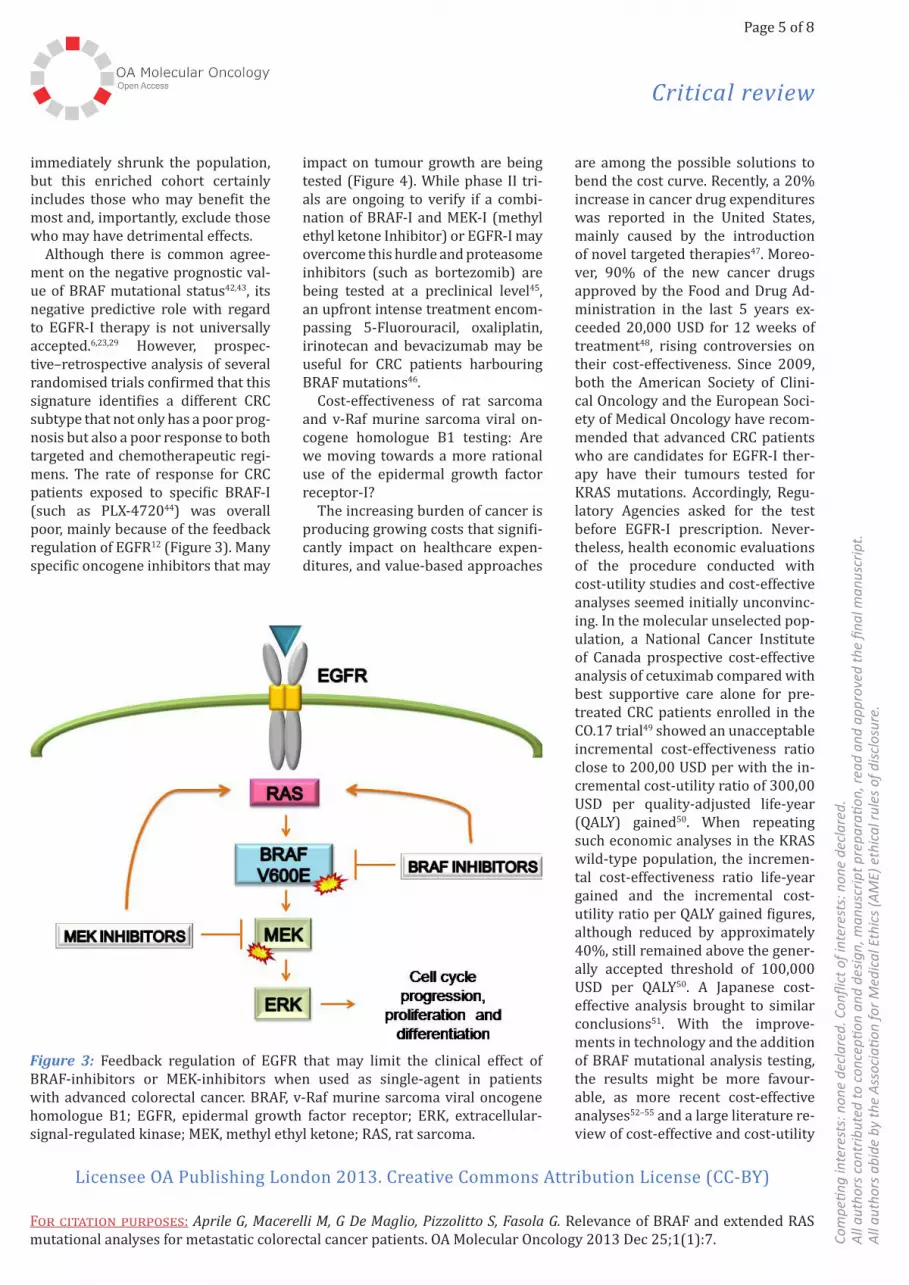
Although there is common agree-ment on the negative prognostic val-ue of BRAF mutational status42,43, its negative predictive role with regard to EGFR-I therapy is not universally accepted.6,23,29 However, prospec-tive–retrospective analysis of several randomised trials confirmed that this signature identifies a different CRC subtype that not only has a poor prog-nosis but also a poor response to both targeted and chemotherapeutic regi-mens. The rate of response for CRC patients exposed to specific BRAF-I (such as PLX-472044) was overall poor, mainly because of the feedback regulation of EGFR12 (Figure 3). Many specific oncogene inhibitors that may
Figure 3: Feedback regulation of EGFR that may limit the clinical effect of BRAF-inhibitors or MEK-inhibitors when used as single-agent in patients with advanced colorectal cancer. BRAF, v-Raf murine sarcoma viral oncogene homologue B1; EGFR, epidermal growth factor receptor; ERK, extracellular-signal-regulated kinase; MEK, methyl ethyl ketone; RAS, rat sarcoma.
Page 6 of 8
Critical review
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
For citation purposes: Aprile G, Macerelli M, G De Maglio, Pizzolitto S, Fasola G. Relevance of BRAF and extended RAS mutational analyses for metastatic colorectal cancer patients. OA Molecular Oncology 2013 Dec 25;1(1):7. Co
mpe
ting
inte
rest
s: n
one
decl
ared
. Con
flict
of i
nter
ests
: non
e de
clar
ed.
All
auth
ors
cont
ribut
ed to
con
cepti
on a
nd d
esig
n, m
anus
crip
t pre
para
tion,
read
and
app
rove
d th
e fin
al m
anus
crip
t.A
ll au
thor
s ab
ide
by th
e A
ssoc
iatio
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.the treatment-decision making. Also, cancer-related features such as dis-ease extension and aggressiveness usually drive clinical judgement to-wards available options. Arguably, the current overwhelming new data on BRAF and RAS testing make now the overall picture more complex than ever. Medical oncologists should be adequately trained to combine molecular biology results with more classical decision factors in order to use an inclusive information and optimise their treatment decision. Indeed, there are many reasons that reinforce the need for a deeper mo-lecular understanding of CRC. First of all, the analysis of RAS and BRAF allow oncologists to identify patients with the highest chance to benefit from EGFR-I. Second, a more ap-propriate treatment selection helps avoiding useless toxicities and may
studies published between 2000 and 201356 have both suggested. The evidence, however, remains contro-versial and extensively debated57,58. Although reasonable, if the addition of NRAS testing may increment the cost-effectiveness of the use of EGFR-I is currently unproven.
ConclusionThe landscape of CRC treatment is changing very fast, and the availabil-ity of new therapeutic options has created new challenges and gener-ated more complicated treatment algorithms. How to integrate the prognostic and predictive biologic information in the everyday clini-cal practice has been long debated. In the past 20 years, patient-related factors such as age, performance status and the presence of comor-bidities have played a crucial role in
Figure 4: Specific oncogene-inhibitors that are currently being tested in phase I/II clinical trials. BRAF, v-Raf murine sarcoma viral oncogene homologue B1; EGFR, epidermal growth factor receptor; ERK, extracellular-signal-regulated kinase; GSK, glaxo-smithkline. IGF, insulin-like growth factor; MEK, methyl ethyl ketone; PI3K, phosphatidylinositol 3-kinase; PTEN, phosphatase and tensin homologue; RAS, rat sarcoma; RTK, receptor tyrosine kinase.
prevent impaired outcomes. In the majority of cases with RAS and BRAF wild-type status, a first-line combi-nation with an EGFR-inhibitor seems to be the preferred treatment option, whereas the antiangiogenic strategy should be pursued in those with RAS mutated tumours or when a less ag-gressive treatment is favoured. Third, the extended molecular analysis ap-pears to be cost-saving, although to definitely establish its economic val-ue, a more comprehensive cost-effec-tive analysis including NRAS testing is eagerly awaited.
Abbreviations listBRAF, v-Raf murine sarcoma viral on-cogene homologue B1; CRC, colorec-tal cancer; EGFR, epidermal growth factor receptor; FOLFIRI, folinic acid, fluorouracil and irinotecan; HR, haz-ard ratio; KRAS, Kirsten rat sarcoma viral oncogene homologue; MAPK, mitogen-activated protein kinases; NRAS, neuroblastoma rat sarcoma vi-ral oncogene homologue; OS, overall survival; PDK, phosphoinositide-de-pendent kinase; PFS, progression-free survival; PI3K, phosphatidylinositol 3-kinase; PTEN, phosphatase and tensin homologue; QALY, quality-ad-justed life-year; RAS, rat sarcoma.
References1. Siegel E, Naishadham D, Jemal A. Can-cer Statistics, 2013. CA Cancer J Clin. 2013 Jan;63(1):11–30.2. Kopetz S, Chang GJ, Overman MJ, Eng C, Sargent DJ, Larson DW, et al. Improved survival in metastatic colorectal cancer is associated with adoption of hepatic resection and improved chemotherapy. J Clin Oncol. 2009 Aug;27(22):3677–83.3. Heinemann V, Douillard JY, Ducreux M, Peeters M. Targeted therapy in meta-static colorectal cancer—an example of personalised medicine in action. Cancer Treat Rev. 2013 Oct;39(6):592–601.4. Karapetis CS, Khambata-Ford S, Jonker DJ, O’Callaghan CJ, Tu D, Tebbutt NC, et al. K-ras mutations and benefit from ce-tuximab in advanced colorectal cancer. N Engl J Med. 2008 Oct;359(17):1757–65.

Page 7 of 8
Critical review
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
For citation purposes: Aprile G, Macerelli M, G De Maglio, Pizzolitto S, Fasola G. Relevance of BRAF and extended RAS mutational analyses for metastatic colorectal cancer patients. OA Molecular Oncology 2013 Dec 25;1(1):7. Co
mpe
ting
inte
rest
s: n
one
decl
ared
. Con
flict
of i
nter
ests
: non
e de
clar
ed.
All
auth
ors
cont
ribut
ed to
con
cepti
on a
nd d
esig
n, m
anus
crip
t pre
para
tion,
read
and
app
rove
d th
e fin
al m
anus
crip
t.A
ll au
thor
s ab
ide
by th
e A
ssoc
iatio
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
mutations on the efficacy of cetuximab plus chemotherapy in chemotherapy-refractory metastatic colorectal cancer: a retrospective consortium analysis. Lan-cet Oncol. 2010 Aug;11(8):753–62.24. Douillard JY, Oliner KS, Siena S, Tab-ernero J, Burkes R, Barugel M, et al. Panitumumab-FOLFOX4 treatment and RAS mutations in colorectal cancer. N Engl J Med. 2013 Sep;369(11):1023–34.25. Linardou H, Dahabreh IJ, Kanaloupiti D, Siannis F, Bafaloukos D, Kosmidis P, et al. Assessment of somatic k-RAS muta-tions as a mechanism associated with resistance to EGFR-targeted agents: a systematic review and meta-analysis of studies in advanced non-small-cell lung cancer and metastatic colorectal cancer. Lancet Oncol. 2008 Oct;9(10):962–72.26. Bardelli A, Siena S. Molecular mecha-nisms of resistance to cetuximab and panitumumab in colorectal cancer. J Clin Oncol. 2010 Mar;28(7):1254–61.27. Di Nicolantonio F, Martini M, Molinari F, Sartore-Bianchi A, Arena S, Saletti P, et al. Wild-type BRAF is required for re-sponse to panitumumab or cetuximab in metastatic colorectal cancer. J Clin Oncol. 2008 Dec;26(35):5705–12.28. Sartore-Bianchi A, Martini M, Moli-nari F, Veronese S, Nichelatti M, Artale S, et al. PIK3CA mutations in colorectal can-cer are associated with clinical resistance to EGFR-targeted monoclonal antibodies. Cancer Res. 2009 Mar;69(5):1851–7.29. Laurent-Puig P, Cayre A, Manceau G, Buc E, Bachet JB, Lecomte T, et al. Analy-sis of PTEN, BRAF, and EGFR status in determining benefit from cetuximab therapy in wild-type KRAS metastatic co-lon cancer. J Clin Oncol. 2009 Dec;27(35): 5924–30.30. Gonzalez de Castro D, Angulo B, Gomez B, Mair D, Martinez R, Suarez-Gauthier A, et al. A comparison of three methods for detecting KRAS muta-tions in formalin-fixed colorectal cancer specimens. Br J Cancer. 2012 Jul;107(2): 345–51.31. Deeb KK, Sram JP, Gao H, Fakih MG. Mul-tigene assays in metastatic colorectal can-cer. J Natl Compr Canc Netw. 2013 Sep;11 (Suppl 4):S9–17.32. Han SW, Kim HP, Shin JY, Jeong EG, Lee WC, Lee KH, et al. Targeted sequencing of cancer-related genes in colorectal cancer using next-generation sequencing. PLoS One. 2013 May;8(5):e64271.
expression and KRAS mutations on pri-mary tumors and metastases in the prediction of benefit from cetuximab plus irinotecan for patients with meta-static colorectal cancer. J Clin Oncol. 2009 Jun;27(16):2622–9.14. Mao C, Liao RY, Chen Q. Loss of PTEN expression predicts resistance to EGFR-targeted monoclonal antibodies in pa-tients with metastatic colorectal cancer. Br J Cancer. 2010 Mar;102(5):940.15. Malapelle U, Carlomagno C, de Luca C, Bellevicine C, Troncone G. KRAS testing in metastatic colorectal carcinoma: chal-lenges, controversies, breakthroughs and beyond. J Clin Pathol. 2014 Jan;67(1):1–9.16. Casagrande M, Cremolini C, Loupa-kis F, Aprile G. A perspective on the cur-rent management of advanced colorectal cancer. Future Oncol. 2013 Nov;9(11): 1687–91.17. Budinska E, Popovici V, Tejpar S, D’Ario G, Lapique N, Sikora KO, et al. Gene expression patterns unveil a new level of molecular heterogeneity in colorectal cancer. J Pathol. 2013 Sep;231(1):63–76.18. Cancer Genome Atlas Network. Comprehensive molecular portraits of human breast tumours. Nature. 2012 Oct;490(7418):61–70.19. Custodio A, Feliu J. Prognostic and predictive biomarkers for epidermal growth factor receptor-targeted therapy in colorectal cancer: beyond KRAS mu-tations. Crit Rev Oncol Hematol. 2013 Jan;85(1):45–81.20. Goldstein NS, Armin M. Epidermal growth factor receptor immunohis-tochemical reactivity in patients with American Joint Committee on Cancer Stage IV colon adenocarcinoma: implica-tions for a standardized scoring system. Cancer. 2001 Sep;92(5):1331–46.21. Cappuzzo F, Finocchiaro G, Rossi E, Jänne PA, Carnaghi C, Calandri C, et al. EGFR FISH assay predicts for response to cetuximab in chemotherapy refractory colorectal cancer patients. Ann Oncol. 2008 Apr;19(4):717–23.22. Grimminger PP, Danenberg P, Dellas K, Arnold D, Rödel C, Machiels JP, et al. Biomarkers for cetuximab-based neo-adjuvant radiochemotherapy in locally advanced rectal cancer. Clin Cancer Res. 2011 May;17(10):3469–77.23. De Roock W, Claes B, Bernasconi D, De Schutter J, Biesmans B, Fountzilas G, et al. Effects of KRAS, BRAF, NRAS, and PIK3CA
5. Amado RG, Wolf M, Peeters M, Van Cutsem E, Siena S, Freeman DJ, et al. Wild-type KRAS is required for panitu-mumab efficacy in patients with meta-static colorectal cancer. J Clin Oncol. 2008 Apr;26(10):1626–34.6. Van Cutsem E, Köhne CH, Láng I, Fol-precht G, Nowacki MP, Cascinu S, et al. Cetuximab plus irinotecan, fluorouracil, and leucovorin as first-line treatment for metastatic colorectal cancer: updated analysis of overall survival according to tumor KRAS and BRAF mutation status. J Clin Oncol. 2011 May;29(15):2011–9.7. Douillard JY, Siena S, Cassidy J, Tab-ernero J, Burkes R, Barugel M, et al. Ran-domized, phase III trial of panitumumab with infusional fluorouracil, leucovorin, and oxaliplatin (FOLFOX4) versus FOL-FOX4 alone as first-line treatment in patients with previously untreated meta-static colorectal cancer: the PRIME study. J Clin Oncol. 2010 Nov;28(31):4697–705.8. Ciardiello F, Tejpar S, Normanno N, Mer-cadante D, Teague T, Wohlschlegel B, Van Cutsem E. Uptake of KRAS mutation test-ing in patients with metastatic colorectal cancer in Europe, Latin America and Asia. Target Oncol. 2011 Sep;6(3):133–45.9. Aprile G, Lutrino SE, Ferrari L, Casa-grande M, Bonotto M, Ongaro E, Puglisi F. Evidence-based appraisal of the upfront treatment for unresectable metastatic colorectal cancer patients. World J Gas-troenterol. 2013 Dec;19(46):8474–88.10. Loupakis F, Ruzzo A, Cremolini C, Vin-cenzi B, Salvatore L, Santini D, et al. KRAS codon 61, 146 and BRAF mutations pre-dict resistance to cetuximab plus irinote-can in KRAS codon 12 and 13 wild-type metastatic colorectal cancer. Br J Cancer. 2009 Aug;101(4):715–21.11. Fornaro L, Baldi GG, Masi G, Allegrini G, Loupakis F, Vasile E, et al. Cetuximab plus irinotecan after irinotecan failure in elderly metastatic colorectal cancer patients: clinical outcome according to KRAS and BRAF mutational status. Crit Rev Oncol Hematol. 2011 Jun;78(3): 243–51.12. Prahallad A, Sun C, Huang S, Di Nicol-antonio F, Salazar R, Zecchin D, et al. Unresponsiveness of colon cancer to BRAF(V600E) inhibition through feed-back activation of EGFR. Nature. 2012 Jan;483(7387):100–3.13. Loupakis F, Pollina L, Stasi I, Ruzzo A, Scartozzi M, Santini D, et al. PTEN

Page 8 of 8
Critical review
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
For citation purposes: Aprile G, Macerelli M, G De Maglio, Pizzolitto S, Fasola G. Relevance of BRAF and extended RAS mutational analyses for metastatic colorectal cancer patients. OA Molecular Oncology 2013 Dec 25;1(1):7. Co
mpe
ting
inte
rest
s: n
one
decl
ared
. Con
flict
of i
nter
ests
: non
e de
clar
ed.
All
auth
ors
cont
ribut
ed to
con
cepti
on a
nd d
esig
n, m
anus
crip
t pre
para
tion,
read
and
app
rove
d th
e fin
al m
anus
crip
t.A
ll au
thor
s ab
ide
by th
e A
ssoc
iatio
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
CO.17 trial. J Natl Cancer Inst. 2009 Sep;101(17):1182–92.51. Shiroiwa T, Motoo Y, Tsutani K. Cost-effectiveness analysis of KRAS testing and cetuximab as last-line therapy for colorectal cancer. Mol Diagn Ther. 2010 Dec;14(6):375–84.52. Blank PR, Moch H, Szucs TD, Schwen-kglenks M. KRAS and BRAF mutation analysis in metastatic colorectal can-cer: a cost-effectiveness analysis from a Swiss perspective. Clin Cancer Res. 2011 Oct;17(19):6338–46.53. Vijayaraghavan A, Efrusy MB, Göke B, Kirchner T, Santas CC, Goldberg RM. Cost-effectiveness of KRAS testing in metastat-ic colorectal cancer patients in the United States and Germany. Int J Cancer. 2012 Jul;131(2):438–45.54. Königsberg R, Hulla W, Klimpfinger M, Reiner-Concin A, Steininger T, Büchler W, et al. Clinical and economic aspects of KRAS mutational status as predictor for epider-mal growth factor receptor inhibitor thera-py in metastatic colorectal cancer patients. Oncology. 2011 Jan;81(5–6): 359–64.55. Lange A, Prenzler A, Frank M, Kirstein M, Vogel A, von der Schulenburg JM. A systematic review of cost-effectiveness of monoclonal antibodies for metastatic colorectal cancer. Eur J Cancer. 2014 Jan;50(1):40–9.56. Hoyle M, Peters J, Crathorne L, Jones-Hughes T, Cooper C, Napier M, Hyde C. Cost-effectiveness of cetuximab, cetuxi-mab plus irinotecan, and panitumumab for third and further lines of treatment for KRAS wild-type patients with meta-static colorectal cancer. Value Health. 2013 Mar–Apr;16(2):288–96.57. Hoyle M, Crathorne L, Peters J, Jones-Hughes T, Cooper C, Napier M, et al. The clinical effectiveness and cost-effectiveness of cetuximab (mono- or combination chem-otherapy), bevacizumab (combination with non-oxaliplatin chemotherapy) and panitu-mumab (monotherapy) for the treatment of metastatic colorectal cancer after first-line chemotherapy (review of technology appraisal No.150 and part review of tech-nology appraisal No. 118): a systematic re-view and economic model. Health Technol Assess. 2013 Apr;17(14):1–237.58. Behl A, Goddard K, Flottemesh TJ, Veenstra D, Meenan RT, Lin JS, Maciosek MV. Cost-effectiveness analysis of screen-ing for KRAS and BRAF mutations in met-astatic colorectal cancers. J Natl Cancer Inst. 2012 Dec;104(23):1785–95.
41. Stintzing S, Jung A, Rossius L, Modest DP, Fischer von Weikersthal L, Decker T, et al. Analysis of KRAS/NRAS and BRAF mutations in FIRE-3: A randomized phase III study of FOLFIRI plus cetuxi-mab or bevacizumab as first-line treat-ment for wild-type (WT) KRAS (exon 2) metastatic colorectal cancer (mCRC) patients. In: European Cancer Congress; Amsterdam, Netherlands; 28 September 2013. (Abstract LBA17).42. Roth AD, Tejpar S, Delorenzi M, Yan P, Fiocca R, Klingbiel D, et al. Prognostic role of KRAS and BRAF in stage II and III resected colon cancer: results of the translational study on the PETACC-3, EO-RTC 40993, SAKK 60-00 trial. J Clin On-col. 2010 Jan;28(3):466–74.43. Tran B, Kopetz S, Tie J, Gibbs P, Jiang ZQ, Lieu CH, et al. Impact of BRAF muta-tion and microsatellite instability on the pattern of metastatic spread and progno-sis in metastatic colorectal cancer. Can-cer. 2011 Oct;117(20):4623–32.44. Oikonomou E, Koc M, Sourkova V, An-dera L, Pintzas A. Selective BRAF V600E inhibitor PLX4720, requires TRAIL assis-tance to overcome oncogenic PIK3CA re-sistance. PLoS One. 2011 Jun;6(6):e21632.45. Zecchin D, Boscaro V, Medico E, Ba-rault L, Martini M, Arena S, et al. BRAF V600E Is a Determinant of Sensitivity to Proteasome Inhibitors. Mol Cancer Ther. 2013 Dec;12(12):2950–61.46. Loupakis F, Cremolini C, Salvatore L, Masi G, Sensi E, Schirripa M, et al. FOLFOXI-RI plus bevacizumab as first-line treatment in BRAF mutant metastatic colorectal can-cer. Eur J Cancer. 2014 Jan;50(1):57–63.47. Hoffman JM, Shah ND, Vermeulen LC, Doloresco F, Grim P, Hunkler RJ, et al. Projecting future drug expendi-tures—2008. Am J Health Syst Pharm. 2008 Feb;65(3):234–53.48. Bach PB. Limits on Medicare’s abil-ity to control rising spending on cancer drugs. N Engl J Med. 2009 Feb;360(6): 626–33.49. Jonker DJ, O’Callaghan CJ, Karapetis CS, Zalcberg JR, Tu D, Au HJ, et al. Cetuxi-mab for the treatment of colorectal cancer. N Engl J Med. 2007 Nov;357(20):2040–8.50. Mittmann N, Au HJ, Tu D, O’Callaghan CJ, Isogai PK, Karapetis CS, et al; Aus-tralasian Gastrointestinal Interest Group. Prospective cost-effectiveness analysis of cetuximab in metastatic colorectal cancer: evaluation of National Cancer Institute of Canada Clinical Trials Group
33. Van Cutsem E, Köhne CH, Hitre E, Zaluski J, Chang Chien CR, Makhson A, et al. Cetuximab and chemothera-py as initial treatment for metastatic colorectal cancer. N Engl J Med. 2009 Apr;360(14):1408–17.34. Stintzing S, Fischer von Weikersthal L, Decker T, Vehling-Kaiser U, Jäger E, Heintges T, et al. FOLFIRI plus cetuximab versus FOLFIRI plus bevacizumab as first-line treatment for patients with metastat-ic colorectal cancer-subgroup analysis of patients with KRAS: mutated tumours in the randomised German AIO study KRK-0306. Ann Oncol. 2012 Jul;23(7):1693–9.35. Cunningham D, Humblet Y, Siena S, Khayat D, Bleiberg H, Santoro A, et al. Cetuximab monotherapy and cetuximab plus irinotecan in irinotecan-refractory metastatic colorectal cancer. N Engl J Med. 2004 Jul;351(4):337–45.36. Ciardiello F. Molecular profiling of the CAPRI GOIM trial in KRAS wild type (wt) metastatic colorectal cancer (mCRC) patients (pts): cetuximab + FOLFIRI fol-lowed by FOLFOX4 ± cetuximab. Late breaking abstract LBA 31. In: European Cancer Congress; Amsterdam, Nether-lands; 29 September 2013.37. Santini D, Vincenzi B, Addeo R, Garufi C, Masi G, Scartozzi M, et al. Cetuximab rechallenge in metastatic colorectal can-cer patients: how to come away from acquired resistance? Ann Oncol. 2012 Sep;23(9):2313–8.38. Lièvre A, Bachet JB, Boige V, Cayre A, Le Corre D, Buc E, et al. KRAS mutations as an independent prognostic factor in patients with advanced colorectal can-cer treated with cetuximab. J Clin Oncol. 2008 Jan;26(3):374–9.39. Schwartzberg LS, Rivera F, Karthaus M, Fasola G, Canon JL, Hecht JR, et al. PEAK (study 20070509): A randomized phase II study of mFOLFOX6 with either panitumumab or bevacizumab as first-line treatment in patients with unresecta-ble wild-type KRAS metastatic colorectal cancer. In: Gastrointestinal Cancers Sym-posium; 26 January 2013 (Abstract 446).40. Patterson SD, Peeters M, Siena S, Van Cutsem E, Humblet Y, Van Laethem JL, et al. Comprehensive analysis of KRAS and NRAS mutations as predictive biomark-ers for single agent panitumumab (pmab) response in a randomized, phase III met-astatic colorectal cancer (mCRC) study (20020408) 2013 ASCO Annual Meeting; J Clin Oncol. 2013;31(Suppl; Abstract 3617).