randomized trial comparing computer-delivered and face-to-face personalized feedback interventions...
TRANSCRIPT
Journal of Substance Abuse Treatment 43 (2012) 260–267
Brief article
Randomized trial comparing computer-delivered and face-to-facepersonalized feedback interventions for high-risk drinking
among college students
Theodore L. Wagener, (Ph.D.)⁎, Thad R. Leffingwell, (Ph.D.), Joe Mignogna, (Ph.D.),Melissa R. Mignogna, (M.S.), Cameron C. Weaver, (M.S.),
Nathaniel J. Cooney, (M.S.), Kasey R. Claborn, (M.S.)
Oklahoma State University, Oklahoma City, OK
Received 10 May 2011; received in revised form 11 October 2011; accepted 14 November 2011
Abstract
This study evaluated the efficacy of two brief personalized feedback interventions (PFIs) using identical feedback and motivationalinterviewing strategies aimed at reducing alcohol consumption and alcohol-related problems to two control conditions among a sample ofhigh-risk drinking college students. Students (N = 152) were randomly assigned to a computer-delivered PFI with a video interviewer, a face-to-face PFI with a live interviewer, a comprehensive assessment condition, or a minimal assessment-only condition. At 10 weeksposttreatment, the face-to-face PFI significantly reduced weekly drinking quantity and peak and typical blood alcohol concentrationcompared with the comprehensive assessment and minimal assessment-only conditions (d values ranged from 0.32 to 0.61). No significantbetween-group differences were evidenced for the computer-delivered PFI condition, although effect sizes were comparable to other collegedrinking studies using computer-delivered interventions (d values ranged from 0.20 to 0.27). Results provide further support for the use of aface-to-face PFI to help reduce college students' alcohol consumption and suggest that a video interviewer in the context of a computer-delivered PFI is likely a helpful but not necessarily a complete substitute for a live interviewer. © 2012 Elsevier Inc. All rights reserved.
Keywords: College drinking; Brief intervention; Alcohol abuse prevention
1. Introduction
High-risk drinking among college students is a significantpublic health problem for both the drinker and the collegecommunity. Almost 40% of college drinkers meet diagnosticcriteria for either alcohol abuse or dependence (Knight et al.,2002), and 55% of abstainers and non-binge drinkers reportexperiencing two or more secondhand effects of bingedrinking (e.g., physical assault or property damage;Wechsler, Lee, Kuo, & Lee, 2000).
In recent years, a concerted effort has been made toimprove upon and refine effective face-to-face college
⁎ Corresponding author. Centers for Behavioral & Preventive Medicine,The Miriam Hospital & Brown Medical School, CORO Building, Suite 314,One Hoppin St., Providence, RI 02903. Tel.: +1 401 793 8202.
E-mail address: [email protected] (T.L. Wagener).
0740-5472/11/$ – see front matter © 2012 Elsevier Inc. All rights reserved.doi:10.1016/j.jsat.2011.11.001
drinking interventions and develop and test cost-effectiveand easily disseminated computer-delivered interventions tointervene with college drinkers (see Elliot, Carey, & Bolles,2008, for a review). Computer-delivered interventions haveused effective ingredients of face-to-face approaches whilestreamlining the process by eliminating the need for a trainedclinician. Many computer-delivered interventions have usedpersonalized feedback regarding the student's use of alcohol(Barnett, Murphy, Colby, & Monti, 2007; Butler & Correia,2009; Carey, Henson, Carey, & Maisto, 2009; Doumas &Anderson, 2009; Doumas,Workman, Smith,&Navarro, 2011;Neighbors, Larimer, & Lewis, 2004; Neighbors, Lee, Lewis,Fossos, & Walter, 2009; Neighbors, Lewis, Bergstrom, &Larimer, 2006; Leffingwell et al., 2007; Walters, Vader,Harris, Field, & Jouriles, 2009). These computer-deliveredpersonalized feedback interventions (PFIs) confer severaladvantages over face-to-face PFIs, including enhanced

261T.L. Wagener et al. / Journal of Substance Abuse Treatment 43 (2012) 260–267
treatment fidelity, user convenience, efficiency, reducedpersonnel and training requirements, and reduced attritiondue to follow-up no-shows. Further, some data suggest thatparticipants are more likely to acknowledge risky behaviorswhen interacting with a computer and that young peoplefavor assessment and feedback via computer (Kobaket al., 1997; Kypri, Saunders, & Gallagher, 2003). Severalstudies have demonstrated that computer-deliveredfeedback interventions effectively reduce alcohol consump-tion at short-term and long-term follow-up (see Carey, Scott-Sheldon, Elliot, Bolles, & Carey, 2009).
Within the last several years, investigators have begunexamining the comparable efficacy of computer-deliveredPFIs to face-to-face PFIs in the context of a motivationalinterview (e.g., Barnett et al., 2007; Butler & Correia,2009; Carey, Carey, Henson, Maisto, & DeMartini, 2011;Carey et al., 2009; Doumas et al., 2011; Walters et al.,2009). However, only two of these studies (Butler &Correia, 2009; Walters et al., 2009) used identicalfeedback in both the computer-based and face-to-faceinterventions and, therefore, allowed for a more directcomparison of delivery modality on drinking outcomes.However, the results of these two studies are mixed. Forexample, Butler and Correia (2009) compared a face-to-face PFI delivered by a trained graduate clinician with acomputer-based PFI that consisted of a self-paced, text-based, slide presentation. At 4 weeks postintervention,both the computer-delivered intervention and face-to-faceintervention successfully reduced the quantity and fre-quency of alcohol use when compared with an assessment-only control condition. However, Walters et al. (2009),also using identical feedback, found the face-to-faceintervention delivered by one of two doctoral-levelcounselors to be significantly better at reducing alcoholconsumption than a text-based, computer-delivered inter-vention and found no significant difference between thecomputer-delivered intervention and the assessment-onlycontrol condition at the 6-month follow-up.
Given the mixed findings of the comparative efficacy ofcomputer-delivered PFIs to a face-to-face PFI, this studysought to replicate and extend previous computer-deliveredPFI research by comparing two intervention conditions usingidentical feedback to two control conditions in their capacityto reduce heavy-drinking college students' quantity andfrequency of alcohol use and alcohol-related problems at the10-week follow-up. The two intervention conditions were (a)an interactive computer-delivered PFI that augmented text-based information with a video interviewer designed to guidethe participant through the intervention and enhance interestand engagement, and (b) a face-to-face PFI using amotivational interviewing (MI) style. The two controlconditions were a (a) comprehensive assessment (CA) and(b) minimal assessment-only (MAO) control condition. Thisstudy adds to the previous research examining the compar-ative efficacy of computer-delivered PFIs to face-to-facePFIs by using (a) an all-inclusive computer-delivered PFI
with a video interviewer who served as the same person whoprovided the personalized feedback in the face-to-face PFIcondition (allowing for greater control of therapist effects byincreasing similarity between the two intervention condi-tions), and (b) a CA condition, which allowed for evaluationof measurement reactivity effects on alcohol consumptionbecause of repeated assessments (Murphy et al., 2001). Wehypothesized that from pretreatment to the 10-week follow-up, participants in the two intervention conditions wouldreport significantly greater reductions in alcohol use, peakblood alcohol concentrations (BACs), and alcohol-relatedproblems than those seen in the two control conditions. Wealso hypothesized that participants would find both the face-to-face and computer interventions as acceptable and useful.
2. Method
2.1. Student recruitment and selection
Students were recruited through an online participantpool management system at a large Midwestern universityand identified by answering “yes” to the followingscreening question: “In the last month, have you consumedfive or more drinks (if you are a male) or four or moredrinks (if you are a female) on a single occasion?” Weinvited potential participants via e-mail and requested atelephone number at which they could be contacted.Potential participants who replied were contacted bytelephone and screened to see if they met further inclusioncriteria. Specifically, inclusion criteria were as follows: (a)current enrollment as a college student, (b) between 18 and25 years of age, (c) reported at least one heavy drinkingepisode (5 or more drinks on one occasion for males, 4 ormore for females) in the last month, (d) reported drinking atleast 20 drinks per month on average, and (e) reported atleast one associated negative consequence of that use in thelast month. Further, students were excluded from partici-pating if they were (a) currently in treatment for alcoholabuse or dependence or (b) currently receiving treatment fora psychological or emotional disorder. This study receivedethical approval from our university's institutional reviewboard. For their participation, students received course extracredit for completion of baseline measures and $10 forcompletion of follow-up measures.
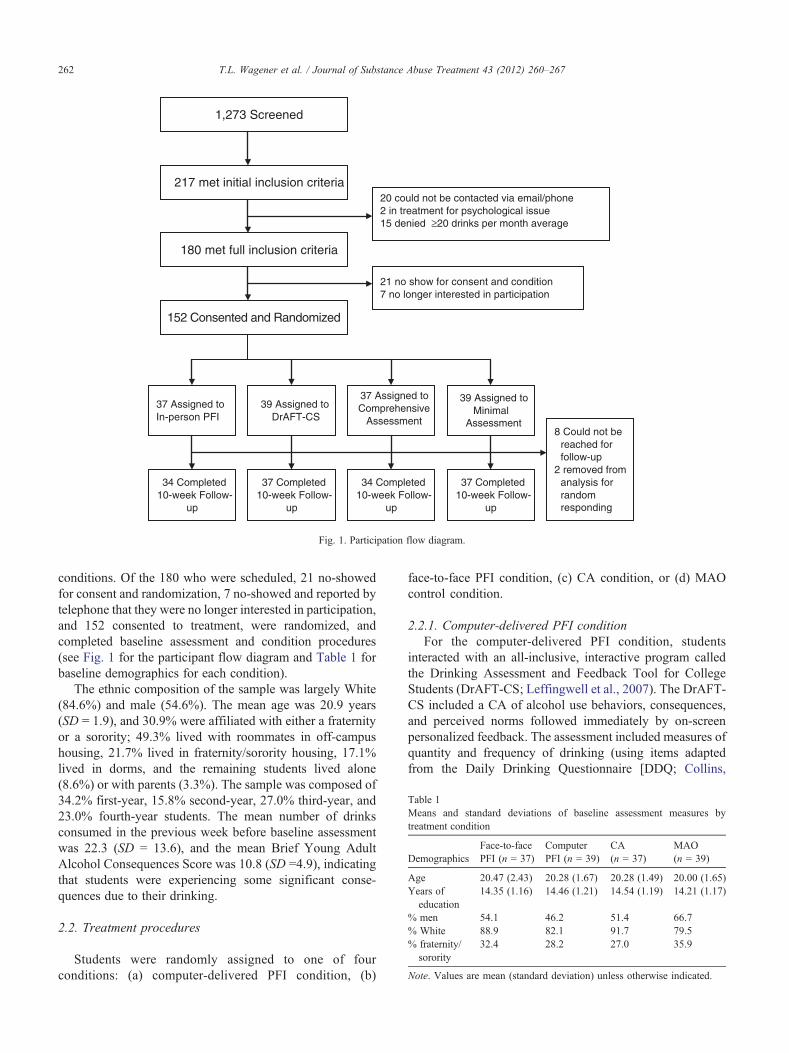
A total of 1,273 students responded to the initial screeningquestion, with 217 meeting initial inclusion criteria andreturning an e-mail to the study coordinator that they wouldbe willing to participate in further screening. Of the 217, 20could not be contacted, 2 were currently in treatment forpsychiatric-related issues, and 15 denied drinking an averageof 20 or more drinks per month, leaving 180 who werescheduled to come into the laboratory and complete baselinemeasures and specific condition procedures. Upon arrival atthe laboratory, students were randomly assigned, using acomputerized random number generator, to one of four
1,273 Screened
217 met initial inclusion criteria
180 met full inclusion criteria
152 Consented and Randomized
20 could not be contacted via email/phone 2 in treatment for psychological issue 15 denied ≥20 drinks per month average
21 no show for consent and condition 7 no longer interested in participation
37 Assigned to In-person PFI
39 Assigned to DrAFT-CS
37 Assigned to Comprehensive
Assessment
39 Assigned toMinimal
Assessment
34 Completed10-week Follow-
up
37 Completed10-week Follow-
up
37 Completed10-week Follow-
up
34 Completed10-week Follow-
up
8 Could not bereached forfollow-up
2 removed from analysis forrandomresponding
Fig. 1. Participation flow diagram.
Table 1Means and standard deviations of baseline assessment measures bytreatment condition
DemographicsFace-to-facePFI (n = 37)
ComputerPFI (n = 39)
CA(n = 37)
MAO(n = 39)
Age 20.47 (2.43) 20.28 (1.67) 20.28 (1.49) 20.00 (1.65)Years of
education14.35 (1.16) 14.46 (1.21) 14.54 (1.19) 14.21 (1.17)
% men 54.1 46.2 51.4 66.7% White 88.9 82.1 91.7 79.5% fraternity/
sorority32.4 28.2 27.0 35.9
Note. Values are mean (standard deviation) unless otherwise indicated.
262 T.L. Wagener et al. / Journal of Substance Abuse Treatment 43 (2012) 260–267
conditions. Of the 180 who were scheduled, 21 no-showedfor consent and randomization, 7 no-showed and reported bytelephone that they were no longer interested in participation,and 152 consented to treatment, were randomized, andcompleted baseline assessment and condition procedures(see Fig. 1 for the participant flow diagram and Table 1 forbaseline demographics for each condition).
The ethnic composition of the sample was largely White(84.6%) and male (54.6%). The mean age was 20.9 years(SD = 1.9), and 30.9% were affiliated with either a fraternityor a sorority; 49.3% lived with roommates in off-campushousing, 21.7% lived in fraternity/sorority housing, 17.1%lived in dorms, and the remaining students lived alone(8.6%) or with parents (3.3%). The sample was composed of34.2% first-year, 15.8% second-year, 27.0% third-year, and23.0% fourth-year students. The mean number of drinksconsumed in the previous week before baseline assessmentwas 22.3 (SD = 13.6), and the mean Brief Young AdultAlcohol Consequences Score was 10.8 (SD =4.9), indicatingthat students were experiencing some significant conse-quences due to their drinking.
2.2. Treatment procedures
Students were randomly assigned to one of fourconditions: (a) computer-delivered PFI condition, (b)
face-to-face PFI condition, (c) CA condition, or (d) MAOcontrol condition.
2.2.1. Computer-delivered PFI conditionFor the computer-delivered PFI condition, students
interacted with an all-inclusive, interactive program calledthe Drinking Assessment and Feedback Tool for CollegeStudents (DrAFT-CS; Leffingwell et al., 2007). The DrAFT-CS included a CA of alcohol use behaviors, consequences,and perceived norms followed immediately by on-screenpersonalized feedback. The assessment included measures ofquantity and frequency of drinking (using items adaptedfrom the Daily Drinking Questionnaire [DDQ; Collins,

263T.L. Wagener et al. / Journal of Substance Abuse Treatment 43 (2012) 260–267
Parks, & Marlatt, 1985] and the Frequency–QuantityQuestionnaire [adapted from Cahalan & Cisin, 1968, andreported in Dimeff, Baer, Kivlahan, & Marlatt, 1999]),common problems experienced by college drinkers (RutgersAlcohol Problem Index; White & Labouvie, 1989), levels ofalcohol dependence (Alcohol Dependence Scale; Skinner &Horn, 1984), perceptions of drinking norms (DrinkingNorms Rating Form; Baer, Stacy, & Larimer, 1991),perceptions of alcohol-related risk (Alcohol PerceivedRisks Problems; Duthie, Baer, & Marlatt, 1991), overalllevels of psychological distress (Behavioral Health Screener;Zygowicz & Saunders, 2003), and motivation for change indrinking behaviors (Readiness to Change Questionnaire;Rollnick et al., 1992). The personalized feedback includedquantity and frequency of use; typical and peak bloodalcohol levels achieved on drinking occasions; perceptionsof social norms; dependence criteria; alcohol-related prob-lems experienced; financial and caloric costs of alcohol use;familial risk for alcohol problems; perceptions of risk;alcohol expectancies; psychological problems, such asdepression and anxiety, that may exacerbate or contributeto alcohol abuse; and motivation for changing currentalcohol use. Most students completed the DrAFT-CS inapproximately 45 minutes.
To simulate face-to-face PFIs and enhance interest andengagement in the program, the DrAFT-CS also includes avideo interviewer. The interviewer appears periodically asthe user progresses through the program and offers awelcome message, provides instructions for assessments,offers encouragement, and provides interpretive informationfor feedback screens. This interviewer is a unique componentof the DrAFT-CS that is not found in any other computer-delivered PFIs that are primarily text based. The interviewerwas also designed to provide information in an empathic,nonjudgmental manner consistent with principles of MI(Miller & Rollnick, 2002).
2.2.2. Face-to-face PFI conditionStudents in the face-to-face PFI condition completed
identical measures as those included in the DrAFT-CS. Theassessment was completed on a computer. Upon completionof the assessment, a printed feedback report was prepared,and the feedback was provided live by a therapist trained inMI. In addition, students in the face-to-face condition wereallowed to take home their feedback report. Because of theenhanced interactivity of the face-to-face PFI condition,most students completed the intervention in 60–90 minutes.
The DrAFT-CS and face-to-face PFI were highly similarin many respects: (a) both used identical assessmentinstruments, presented in the same order, and administeredvia computer; (b) the feedback was virtually identical in bothconditions, with the written feedback report includingidentical content, using the same graphical format, and thesame order of feedback information as the DrAFT-CS; (c)both interventions occurred in the same room in ourlaboratory; and (d) the face-to-face interviewer and video
interviewer in the DrAFT-CS were the same individual.These similarities allowed us to control for many potentialdifferences between the two conditions and rule out rivalhypotheses that may account for any differences betweenintervention conditions.
The face-to-face PFI group received feedback regardingtheir assessment from an advanced graduate student who hadcompleted 30 hours of training in MI and 6 hours of trainingin using the style with this specific feedback intervention.His sessions were recorded and monitored throughout thestudy to ensure that an MI style was consistently followed.As such, the therapist used a nonconfrontational approach,asked open-ended questions, and attempted to create adiscrepancy between values and goals and current alcoholuse. As noted above, this person was also the same personwho provided the video instructions and feedback in theDrAFT-CS, which allows us to control for possible therapisteffects between the two intervention conditions.
2.2.3. The CA conditionStudents in this condition completed baseline and 10-
week follow-up computer-based questionnaires, but alsocompleted the same assessment that was used to generatefeedback in both the face-to-face PFI and DrAFT-CScondition. This condition served as a comparison conditionthat would demonstrate any possible effect that additionalassessment may have on both face-to-face PFI and DrAFT-CS conditions that received one more additional assessmentthan the minimal assessment-only control condition.
2.2.4. The MAO conditionStudents in this condition completed both baseline and
10-week follow-up computer-based questionnaires as de-scribed below.
2.3. Measures
Students completed, via in-laboratory computers, a batteryof self-report questionnaires, which took approximately 15 to20minutes to complete. The scores from these measures wereused as the baseline measures for the analyses and werecompleted again 10 weeks posttreatment, and the scores wereused as follow-up measures for the analyses.
Alcohol consumption was assessed using a modifiedversion of the DDQ (Collins et al., 1985). Students wereasked to think about a typical week in the past month andidentify the typical number of drinks and the typical numberof hours those drinks were consumed on each day of theweek. The DDQ uses reports of standard drinks and waspreceded with instructions regarding how to estimatestandard drinks using examples. Weekly drinking quantitywas calculated by summing the reported number of drinksfor all 7 days of the week. Typical BAC was calculated byfirst determining the students BAC for each day of the weekusing Widmark's formula (Dimeff et al., 1999), then byaveraging the BACs across the week. Peak BAC was
264 T.L. Wagener et al. / Journal of Substance Abuse Treatment 43 (2012) 260–267
calculated by asking students to report the number andduration of their heaviest drinking occasion in the past monthand then combining this information along with their genderand weight, again using Widmark's formula.
2.3.1. Alcohol-related problemsThe Brief Young Adult Alcohol Consequences Ques-
tionnaire (B-YAACQ; Kahler, Strong, & Read, 2005) wasused to assess the students' problems associated with theirdrinking over the previous month. The B-YAACQ is a 24-item measure in which students answer “yes” or “no” toquestions assessing a broad range of alcohol-relatedproblems in both content and severity. Scores range from0 to 24, with a score of 10 indicating that the student is likelyexperiencing some important consequences of his or herdrinking and a score of 15 indicating the likelihood ofalcohol abuse or dependence (Kahler et al., 2005). TheB-YAACQ has shown very high internal reliability (α = .83;Kahler et al., 2005), with similar findings for this study atboth baseline (α = .84) and follow-up (α = .91).
2.3.2. Program Satisfaction QuestionnaireLevel of acceptability and helpfulness for both the
computer-delivered PFI and the face-to-face PFI interventionswas assessed using the Program Satisfaction Questionnaire(PSQ; adapted fromMarlatt et al., 1998). The PSQ is a seven-item questionnaire with questions assessing the level ofagreement or disagreement (i.e., strongly agree, disagree,uncertain, agree, strongly agree) with statements such as, “Iwould recommend this program/interview to a friend” and“The program/interview was nonconfrontational.” PSQ scoresrange can range from −2 to 2, with a score of −2 indicatingstrongly disagree and a score of 2 indicating strongly agree.The internal reliability for the scale was .76 in this study.
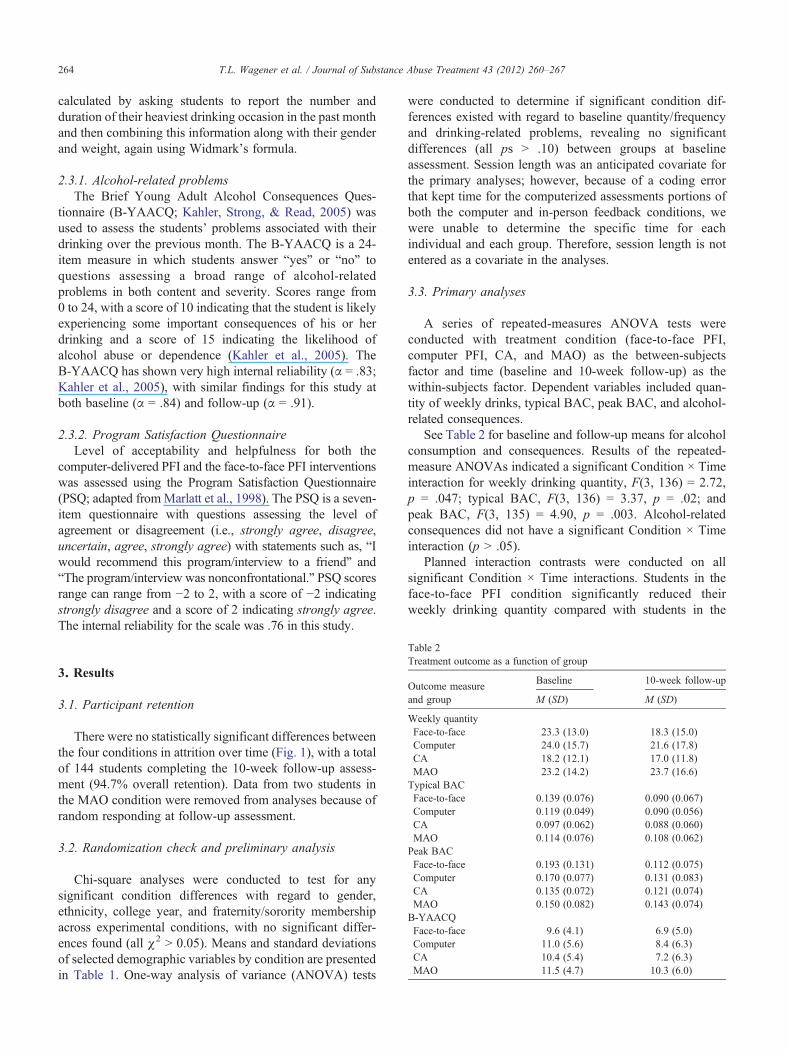
Table 2Treatment outcome as a function of group
Outcome measureand group
Baseline 10-week follow-up
M (SD) M (SD)
Weekly quantityFace-to-face 23.3 (13.0) 18.3 (15.0)Computer 24.0 (15.7) 21.6 (17.8)CA 18.2 (12.1) 17.0 (11.8)MAO 23.2 (14.2) 23.7 (16.6)Typical BACFace-to-face 0.139 (0.076) 0.090 (0.067)Computer 0.119 (0.049) 0.090 (0.056)CA 0.097 (0.062) 0.088 (0.060)MAO 0.114 (0.076) 0.108 (0.062)Peak BACFace-to-face 0.193 (0.131) 0.112 (0.075)Computer 0.170 (0.077) 0.131 (0.083)CA 0.135 (0.072) 0.121 (0.074)MAO 0.150 (0.082) 0.143 (0.074)B-YAACQFace-to-face 9.6 (4.1) 6.9 (5.0)Computer 11.0 (5.6) 8.4 (6.3)CA 10.4 (5.4) 7.2 (6.3)MAO 11.5 (4.7) 10.3 (6.0)
3. Results
3.1. Participant retention
There were no statistically significant differences betweenthe four conditions in attrition over time (Fig. 1), with a totalof 144 students completing the 10-week follow-up assess-ment (94.7% overall retention). Data from two students inthe MAO condition were removed from analyses because ofrandom responding at follow-up assessment.
3.2. Randomization check and preliminary analysis
Chi-square analyses were conducted to test for anysignificant condition differences with regard to gender,ethnicity, college year, and fraternity/sorority membershipacross experimental conditions, with no significant differ-ences found (all χ2 N 0.05). Means and standard deviationsof selected demographic variables by condition are presentedin Table 1. One-way analysis of variance (ANOVA) tests
were conducted to determine if significant condition dif-ferences existed with regard to baseline quantity/frequencyand drinking-related problems, revealing no significantdifferences (all ps N .10) between groups at baselineassessment. Session length was an anticipated covariate forthe primary analyses; however, because of a coding errorthat kept time for the computerized assessments portions ofboth the computer and in-person feedback conditions, wewere unable to determine the specific time for eachindividual and each group. Therefore, session length is notentered as a covariate in the analyses.
3.3. Primary analyses
A series of repeated-measures ANOVA tests wereconducted with treatment condition (face-to-face PFI,computer PFI, CA, and MAO) as the between-subjectsfactor and time (baseline and 10-week follow-up) as thewithin-subjects factor. Dependent variables included quan-tity of weekly drinks, typical BAC, peak BAC, and alcohol-related consequences.
See Table 2 for baseline and follow-up means for alcoholconsumption and consequences. Results of the repeated-measure ANOVAs indicated a significant Condition × Timeinteraction for weekly drinking quantity, F(3, 136) = 2.72,p = .047; typical BAC, F(3, 136) = 3.37, p = .02; andpeak BAC, F(3, 135) = 4.90, p = .003. Alcohol-relatedconsequences did not have a significant Condition × Timeinteraction (p N .05).
Planned interaction contrasts were conducted on allsignificant Condition × Time interactions. Students in theface-to-face PFI condition significantly reduced theirweekly drinking quantity compared with students in the

265T.L. Wagener et al. / Journal of Substance Abuse Treatment 43 (2012) 260–267
MAO condition, F(1, 136) = 7.80, p = .006, d = 0.48.Although approaching significance, no significant differ-ence was found between the face-to-face condition and theCA in weekly drinking quantity, F(1, 136) = 3.41, p =.067. Students in the face-to-face PFI condition signifi-cantly reduced their typical BAC compared with studentsin both the CA, F(1, 136) = 6.43, p = .012, d = 0.43, andthe MAO conditions, F(1, 136) = 8.03, p = .005, d =0.49. Finally, students in the face-to-face PFI conditionsignificantly reduced their peak BAC compared withstudents in the computer-delivered PFI, F(1, 135) = 3.99,p = .048, d = 0.35; CA, F(1, 135) = 9.57, p = .002,d = 0.53; and MAO conditions, F(1, 135) = 12.32, p =.001, d = 0.61. Baseline to follow-up change in peak BACwas the only significant difference between the face-to-faceand computer-delivered PFIs.
Examination of the baseline to follow-up change scoresindicates that students in the face-to-face condition reducedtheir weekly drinking quantity by an average of five drinks(20%), whereas students in the computer and CA conditionsreduced their quantity by 2.4 drinks (10%) and 1.2 drinks(7%), respectively. Students in the MAO condition increasedin their weekly drinking quantity by 0.5 drinks. Students in theface-to-face condition reduced their typical BAC by 35%, ascompared with 24%, 9%, and 4% for students in thecomputer, CA, and MAO conditions, respectively. Studentsin the face-to-face condition reduced their peak BAC by 42%,as compared with 23%, 10%, and 5% for students in thecomputer, CA, and MAO conditions, respectively. Althoughdifferences between groups regarding alcohol-related conse-quences were not statistically significant, students in the face-to-face condition reduced their B-YAACQ scores by 28%,whereas students in the computer, CA, and MAO conditionsreduced their scores by 24%, 31%, and 10%, respectively.
Students in both the face-to-face and computer-deliveredfeedback conditions rated the interventions as acceptable andhelpful. No significant difference was found between theface-to-face (M = 1.37, SD = 0.37) and the computerizedcondition (M = 1.25, SD = 0.47).
4. Discussion
This study is the first to investigate the use of an all-inclusive computer-delivered PFI with a video interviewer as ameans of intervening with college drinkers. This study wasfurther strengthened by the use of the CA condition, allowingfor measurement of the effects of repeated assessment onstudent alcohol consumption. It was hypothesized thatidentical personalized feedback delivered via computer orthrough face-to-face interaction would significantly reduceoverall alcohol use and hazardous consumption comparedwithtwo control conditions (CA and MAO). Students found bothfeedback conditions to be helpful and acceptable. However,consistent with Walters et al. (2009), significant reductions inalcohol consumption compared with controls were evidenced
only for the face-to-face intervention and not the computer-delivered intervention at follow-up. However, with theexception of peak BAC, no significant differences werefound between the face-to-face and the computer-deliveredintervention. These results lend further support for the use of aface-to-face personalized feedback to affect significant re-ductions in college drinking and suggest that a videointerviewer in the context of a computer-delivered PFI ishelpful but not necessarily a complete substitute for a liveinterviewer. Specifically, face-to-face feedback led to signif-icant reductions in weekly drinking quantity and peak andtypical BAC comparedwith both control conditions and, in thecase of peakBAC, computerized feedback. All effects betweenthe face-to-face condition and the MAO condition were in themedium range (d values = 0.48–0.61), and compared with CAwere in the small to medium range (d values = 0.32–0.53).However, the intervention condition did not influence changesin students' alcohol-related consequences.
Although the sample size was small for a four-groupdesign, thus limiting the power to detect small effect sizes(observed power ranged from 0.27 to 0.90), it is unclear whythis specific computer-delivered condition (i.e., DrAFT-CS)did not perform as well as in previous studies. In a previousstudy (Leffingwell et al., 2007) using the same computerizedPFI with a similar student sample, and compared with aMAOcondition, students in the computerized PFI reduced theirtotal drinks per week by approximately seven drinks at1-month follow-up, six drinks at 4-month follow-up, andnine drinks at 6-month follow-up. In this study, studentsreduced their weekly drinking quantity by two drinks.Nonetheless, in this study, observed effect sizes of thecomputerized PFI compared with MAO (d values rangedfrom 0.20 to 0.27) were comparable to other college drinkingstudies using computerized PFIs, with d values ranging from0.09 to 0.28 (for meta-analysis, see Carey et al., 2009). Thesefindings are also consistent with more recent studiescomparing computer versus face-to-face personalized feed-back approaches (i.e., Carey et al., 2011; Doumas et al., 2011),indicating that there appears to be a small but consistent trendfavoring face-to-face intervention producing larger effects thancomputer-based interventions for college drinkers.
It was thought that the video interviewer in the currentcomputerized PFI would serve as a useful proxy in place of aface-to-face interview by providing encouragement andinterpretive information for feedback and emphasizingpersonal responsibility for change. However, in light of thecurrent findings, it appears that a video interviewer in itscurrent form is not a sufficient replacement for a liveinterviewer. One possibility is that students in the face-to-facecondition may have processed the information more deeplybecause of being exposed to the feedback longer (60–90minutes in the face-to-face versus approximately 45 minutesin the computerized) leading to better retention and hencebetter drinking outcomes (Jouriles et al., 2010). However,Butler and Correia (2009) also had a large discrepancy in timebetween the computer-based condition (M = 11.1 minutes)

266 T.L. Wagener et al. / Journal of Substance Abuse Treatment 43 (2012) 260–267
and the face-to-face feedback condition (M = 41.0 minutes)but found both interventions to be more effective than controlbut with no significant differences between each other.Another possibility is that meeting with a live interviewermay have increased the validity of the feedback, made thefeedback seem more important, provided the student anopportunity to resolve ambivalence that they may have beenexperiencing regarding their drinking behavior, or moresignificantly influenced their norm perceptions (Doumas,Workman, Smith, &Navarro, 2011). Future research needs tobe conducted to evaluate these possibilities.
In light of these findings, several limitations areacknowledged in this study. First, although consistent withthe population at the university where this study wasconducted, our sample consisted of a disproportionatenumber of White students, possibly limiting the generaliz-ability of the findings. Second, the small sample size made itdifficult to detect potential differences between the face-to-face and the computer conditions as well as the computer andcontrol conditions on measures of alcohol consumption.Third, the relatively short 10-week follow-up period isanother limitation of this study. Previous research has shownthat the differences between students receiving feedbackversus those completing assessment-only tend to degradewith increased time (e.g., Carey, Carey, Maisto, & Henson,2006). Fourth, we relied on self-reported drinking as our mainoutcome. Although the absence of collateral verification ofself-reported drinking consumption potentially leads tobiased reporting, a recent meta-analysis indicated littleevidence of biased reporting in college drinkers (Borsari &Muellerleile, 2009). Fifth, although having all of the face-to-face feedback provided by one graduate clinician helped toeliminate potential therapist effects between the computerand face-to-face conditions, and thereby eliminating apotential confound, this feature of the study also potentiallylimits the generalizability of our results.
Given recent research by Jouriles et al. (2010), futureinvestigations of computerized interventions might benefitfrom having students reread or attempt to recall the feedbackfollowing the initial computer-delivered feedback, therebyhelping students better retain the information and possiblycreating better drinking outcomes. In addition, given thatprevious studies have shown that other computer-basedcollege drinking interventions (e.g., e-Chug and Alcoho-lEdu) are superior to assessment-only controls (e.g., Hustad,Barnett, Borsari, & Jackson, 2010) future investigations ofthe DrAFT-CS should evaluate the benefit of the videointerviewer. It may be possible that the video interviewer hadan iatrogenic effect, and, therefore, removing its presencefrom the intervention would strengthen the program's effectson drinking.
Acknowledgments
Study funding was provided by the Oklahoma Depart-ment of Mental Health and Substance Abuse Services
Science to Service Grant (T. Wagener, PI). Dr. Wagener issupported by Grant T32-HL-076134-05 (R. Wing, PI) fromthe National Heart Blood and Lung Institute. Developmentof the DrAFT-CS intervention was supported by a grant fromthe Oklahoma Center for the Advancement of Science andTechnology Health Research Program (T. Leffingwell, PI).
References
Baer, J. S., Stacy, A., & Larimer, M. (1991). Biases in the perception ofdrinking norms among college students. Journal of Studies on Alcohol,52, 580–586.
Barnett, N. P., Murphy, J. G., Colby, S. M., & Monti, P. M. (2007). Efficacyof counselor vs. computer-delivered intervention with mandated collegestudents. Addictive Behaviors, 32, 2529–2548.
Borsari, B., & Muellerleile, P. (2009). Collateral reports in the collegesetting: A meta-analytic integration. Alcoholism: Clinical and Experi-mental Research, 33, 826–838.
Butler, L. H., & Correia, C. J. (2009). Brief alcohol intervention with collegestudent drinkers: Face-to-face versus computerized feedback. Psychol-ogy of Addictive Behaviors, 23, 163–167, doi:10.1037/a0014892.
Cahalan, D., & Cisin, I. H. (1968). American drinking practices: Summaryof findings from a national probability sample: II. Measurement ofmassed versus spaced drinking. Quarterly Journal of Studies onAlcohol, 29, 642.
Carey, K. B., Carey, M. P., Henson, J. M., Maisto, S. A., & DeMartini, K. S.(2011). Brief alcohol interventions for mandated college students:Comparison of face-to-face counseling and computer-delivered in-terventions. Addiction, 106, 528–537.
Carey, K. B., Carey, M. P., Maisto, S. A., & Henson, J. M. (2006). Briefmotivational interventions for heavy college drinkers: A randomizedcontrolled trial. Journal of Consulting and Clinical Psychology, 74,943–954.
Carey, K. B., Henson, J. M., Carey, M. P., &Maisto, S. A. (2009). Computerversus face-to-face intervention for students violating campus alcoholpolicy. Journal of Consulting and Clinical Psychology, 77, 74–87, doi:10.1037/a0014281.
Carey, K. B., Scott-Sheldon, L. A. J., Elliott, J. C., Bolles, J. R., & Carey, M.P. (2009). Computer delivered interventions to reduce college studentdrinking: A meta-analysis. Addiction, 104, 1807–1819.
Collins, R. L., Parks, G. A., & Marlatt, G. A. (1985). Social determinants ofalcohol consumption: The effects of social interaction and model statuson the self-administration of alcohol. Journal of Consulting and ClinicalPsychology, 53, 189–200, doi:10.1037/0022-006X.53.2.189.
Dimeff, L. A., Baer, J. S., Kivlahan, D. R., & Marlatt, G. A. (1999). BriefAlcohol Screening and Intervention for College Students (BASICS): Aharm reduction approach. Guilford Press.
Doumas, D. M., & Anderson, L. (2009). Reducing alcohol use in first-yearuniversity students: Evaluation of a Web-based personalized feedbackprogram. Journal of College Counseling, 18, 18–32.
Doumas, D. M., Workman, C. R., Smith, D., & Navarro, A. (2011).Reducing high-risk drinking in mandated college students: Evaluation oftwo personalized normative feedback interventions. Journal of Sub-stance Abuse Treatment, 40, 376–385.
Duthie, D. A., Baer, J. S., & Marlatt, G. A. (1991). High risk status andpersonal risk perception for alcohol problems among college students.Poster presented at the Association for the Advancement of BehaviorTherapy, New York.
Elliot, J. C., Carey, K. B., & Bolles, J. R. (2008). Computer-basedinterventions for college drinking: A qualitative review. AddictiveBehaviors, 33, 994–1005, doi:10.1016/j.addbeh.2008.03.006.
Hustad, J. T. P., Barnett, N. P., Borsari, B., & Jackson, K. M. (2010). Web-based alcohol prevention for incoming college students: A randomizedcontrolled trial. Addictive Behaviors, 35, 183–189.

267T.L. Wagener et al. / Journal of Substance Abuse Treatment 43 (2012) 260–267
Jouriles, E. N., Brown, A. S., Rosenfield, D., McDonald, R., Croft, K.,Leahy, M. M., & Walters, S. T. (2010). Improving the effectiveness ofcomputer-delivered personalized drinking feedback interventions forcollege students. Psychology of Addictive Behaviors, 24, 592–599.
Kahler, C. W., Strong, D. R., & Read, J. P. (2005). Toward efficient andcomprehensive measurement of the alcohol problems continuum incollege students: The brief young adult alcohol consequences question-naire. Alcoholism: Clinical and Experimental Research, 29,1180–1189, doi:10.1097/01.ALC.0000171940.95813.A5.
Knight, J. R., Wechsler, H., Kuo, M., Seibring, M., Weitzman, E. R., &Schuckit, M. A. (2002). Alcohol abuse and dependence among U.S.college students. Journal of Studies on Alcohol, 63, 263–270.
Kobak, K. A., Taylor, L. v., Dottl, S. L., Greist, J. H., Jefferson, J. W.,Burroughs, D., et al. (1997). A computer-administered telephoneinterview to identify mental disorders. JAMA: Journal of the AmericanMedical Association, 278, 905–910.
Kypri, K., Saunders, J. B., & Gallagher, S. J. (2003). Acceptability ofvarious brief intervention approaches for hazardous drinking amonguniversity students. Alcohol and Alcoholism, 38, 626–628.
Leffingwell, T., Hopper, R., Mignogna, J., Jackson, M., Leedy, M., & Lack,C. (2007). A randomized trial of a computerized multimedia feedbackintervention for high-risk drinking among college students. Posterpresented at the annual meeting of the Society of Behavioral Medicine,Washington, DC.
Marlatt, G. A., Baer, J. S., Kivlahan, D. R., Dimeff, L. A., Larimer, M. E.,Quigley, L. A., et al. (1998). Screening and brief intervention for high-risk college student drinkers: Results from a 2-year follow-upassessment. Journal of Consulting and Clinical Psychology, 66,604–615, doi:10.1037/0022-006X.66.4.604.
Miller, W. R., & Rollnick, S. (2002). Motivational interviewing: Preparingpeople for change (2nd ed.). Guilford Press.
Murphy, J. G., Duchnick, J. J., Vuchinich, R. E., Davison, J. W., Karg, R. S.,Olson, A. M., et al. (2001). Relative efficacy of a brief motivationalintervention for college student drinkers. Psychology of AddictiveBehaviors, 15, 373–379, doi:10.1037/0893-164X.15.4.373.
Neighbors, C., Larimer, M. E., & Lewis, M. A. (2004). Targetingmisperceptions of descriptive drinking norms: Efficacy of a computer-delivered personalized normative feedback intervention. Journal ofConsulting and Clinical Psychology, 72, 434–447, doi:10.1037/0022-006X.72.3.434.
Neighbors, C., Lee, C. M., Lewis, M. A., Fossos, N., & Walter, T. (2009).Internet-based personalized feedback to reduce 21st-birthday drinking:A randomized controlled trial of an event-specific prevention interven-tion. Journal of Consulting and Clinical Psychology, 77, 51–63, doi:10.1037/a0014386.
Neighbors, C., Lewis, M. A., Bergstrom, R. L., & Larimer, M. E. (2006).Being controlled by normative influences: Self-determination as amoderator of a normative feedback alcohol intervention. HealthPsychology, 25, 571–579, doi:10.1037/0278-6133.25.5.571.
Rollnick, S., Heather, N., Gold, R., & Hall, W. (1992). Development of ashort ‘readiness to change' questionnaire for use in brief, opportunisticinterventions among excessive drinkers. British Journal of Addiction, 87,743–754.
Skinner, H. A., & Horn, J. L. (1984). Alcohol Dependence Scale: Usersguide. Toronto, Canada: Addiction Research Foundation.
Walters, S. T., Vader, A. M., Harris, T. R., Field, C. A., & Jouriles, E. N.(2009). Dismantling motivational interviewing and feedback for collegedrinkers: A randomized clinical trial. Journal of Consulting and ClinicalPsychology, 77, 64–73, doi:10.1037/a0014472.
Wechsler, H., Lee, J. E., Kuo, M., & Lee, H. (2000). College binge drinkingin the 1990s: A continuing problem: Results of the Harvard School ofPublic Health 1999 College Alcohol Study. Journal of AmericanCollege Health, 48, 199–210.
White, H. R., & Labouvie, E. W. (1989). Towards the assessment ofadolescent problem drinking. Journal of Studies on Alcohol, 50,30–37.
Zygowicz, K. M., & Saunders, S. M. (2003). A behavioral health screeningmeasure for use with young adults in primary care settings. Journalof Clinical Psychology in Medical Settings, 71–77, doi:10.1023/A:1023351203497.