psychosocial adjustment among central american immigrants with disabilities: an exploratory study
TRANSCRIPT

RESEARCH REPORT
Psychosodal Adjustment AmongCentral American Immigrants withDisabilities: An Exploratory Study
S. LISBETH JARAMA
HEIDI REYST
MARILYN RODRIGUEZ
FAYE Z. BELCRAVE
MARIA CECILIA ZEA
George Washington University
This is an exploratory study thai investigated factors influencing the psychoso-
cml adjustment of Central American immigrants with disabilities. The rela-
tionships between stress, and perception of disability seventy and (a) depression
and (b) anxiety were assessed. Furthermore, this study investigated whether so-
cial support moderated the impact of stress and severity of disability on depres-
sion and anxiety. Stress, severity of disability, and social support explained a
high percentage (54 %) of the variance in depression. High levels of stress, in-
creased perceptions of severity of disability, and low social support were associ-
ated with increased depression. The interactions between support and stress
and between support and disability severity did not significantly add to the
original model which predicted depression. Main effects were found for stress,
disability severity, and the interaction between support and disability seventy.
Stress and social support significantly accounted for 31 % of the variance in
anxiety. Increased stress and decreased social support were associated with
greater levels of anxiety. The interaction between support and stress did not sig-
nificantly predict anxiety. Implications of the study in terms of future research
and intervention programs targeting mental health outcomes for Latino immi-
grants with disabilities are discussed. © 1998John Wiley & Sons, Inc.
• stress • social support • severity of disability * Latino immigrants
• This research was supported in part by the Department of Education in a grant (USDE no.
H133G20117) toFaye Z. Belgrave, Principal Investigator.
Reprint requests should be directed to Maria Cecilia Zm, Ph.D., Department of Psychology,
George Washington University, Washington, DC 20052.
Cultural Diversity and Mental Health, Vol. 4, No. 2,115-125 (1998)
© 1998 by John Wiley & Sons, Inc. CCC 1077-341X/98/020115-11

116 J A R A M A E T A
Latino immigrants with disabilities face two
stressors: having a disability and adjusting to
a new culture. High levels of stress have been
associated with negative mental health out-
comes such as depression and anxiety (Turn-
er & McLean, 1989; Weinberger, Tierney,
Booher, & Heiner, 1990). Although there
may be increased stress, poorer mental
health functioning is not inevitable. Social
support may buffer the deleterious effect of
stress. The indirect and direct impact of so-
cial support among persons with disabilities
on outcomes such as depression and anxiety
has been well documented (e.g., Elliot, Her-
rick, Patti, & Witty, 1991; Kelley & Lambert,
1992; Littlefield, Rodin, & Murray, 1990;
Turner & Wood, 1985). This study examined
the relationship between stress, disability
severity, and mental health (i.e., depression
and anxiety) among Latino immigrants with
disabilities. The study also examined the role
of social support in that relationship.
Lazarus and Folkman (1984) defined
stress as external or internal demands that
create a strain on the individual. For Latino
immigrants with disabilities, both disability
status and immigrant status can contribute to
stress and persistent strains. Disability refers
to "any restriction or lack (resulting from im-
pairment) of ability to perform an activity in
the manner or within the range considered
normal for a human being" (World Health
Organization, 1980).
Disability may be a source of ongoing
strain if it renders daily activities difficult and
contributes to the experience of additional
negative life events. As such, persons with dis-
abilities are likely to be at increased risk of
stress. Turner and McLean (1989) state that
"presumably, the elevated difficulty in per-
forming social and occupational roles that
tends to be experienced by disabled individ-
uals constitutes a significant source of en-
during stress that challenges adaptive capac-
ities." Situations in which an individual
perceives that he or she has little or no con-
trol may be stressful (Thompson & Spaca-
pan, 1991). Because of challenges in role
functioning, having a disability may decrease
perceptions of control and create additional
stress.
Being an immigrant and being of a mi-
nority status can be a significant source of
stress in and of itself (Salgado de Snyder, Cer-
vantes, & Padilla, 1990). Latino immigrants
may be at risk of lowered perceptions of con-
trol and high levels of stress resulting from
their immigrant status. Differences in cul-
ture, values, and societal norms of the adopt-
ed country may contribute to feelings of con-
fusion and loss and may make meeting basic
survival needs difficult (Lequerica, 1993).
Salgado de Snyder et al. (1990) found that
female immigrants reported experiencing
high levels of stress because of cultural and
family conflicts.
Padilla, Cervantes, Maldonado, and Gar-
cia (1988) report that among Latinos who
immigrate, language barriers, lowered eco-
nomic status, lack of education and work
skills, and discrimination are significant stres-
sors. Not speaking English and unemploy-
ment were reported as the first and second
most significant stressors by Padilla et al.
(1988). Reentering the work force or enter-
ing the work force for the first time is stress-
ful for any population, including Latinos.
Undocumented immigrant status can also be
a significant source of stress. Mexican and
Central American immigrants reported lhat
immigrant status is the third most difficult
factor in their experience immigrating to the
United States (Padilla et al., 1988).
Among immigrants, having a disabling
condition may increase the burden associat-
ed with migrating to a new country. Special
accommodations may be necessary, and spe-
cialized services from several individuals
and/or agencies may be needed. However,
the experience of coordination with agen-
cies to receive appropriate treatment and ser-
vices may be a new experience for the Latino
immigrant. Along with adapting to a differ-
ent cultural environment, the individual
must also modify that environment to ac-
commodate his or her special needs. The use
of special services for Latinos with disabilities
becomes very difficult because of the inabil-

P S Y C H O S O C I A L A D J U S T M E N T T O D I S A B I L I T Y 117
ity to easily communicate in English, the per-
ception of loss of control, and legal status.
Depression and Anxiety Among Personswith Disabilities
Chronic stress arising from disability status is
positively related to depression among peo-ple with disabilities (Turner & Beiser, 1990).
Turner and Beiser (1990) compared people
with disabilities to people without disabilities
and found that 37% of those with a disability
have a clinically significant level of depressive
symptoms, compared with 12% of those with-
out disabilities. Turner and Wood (1985)
found similar results in a study of adults with
physical disabilities; 34% of subjects with dis-
abilities reported depression. This is nearly
twice the rate found in the general popula-tion. These results suggest that having a dis-
ability increases the probability of becoming
depressed.
Anxiety, another form of distress, has
been linked to high levels of stress (Turner 8c
McLean, 1989). Although anxiety has been
studied with less frequency than depression,
the rates of problematic anxiety levels aresimilar to those of depression with respect to
stress levels. In a study comparing individuals
with disabilities to individuals without dis-
abilities, it was found that 45% of individuals
with a disability exceeded the cutoff score
for problematic levels of anxiety (Turner &McLean, 1989). In contrast, among individu-
als who do not have a disability, 18% had
high levels of anxiety.
A significant correlation between anxiety
and the individual's self-rated impact of ill-
ness and anxiety and the physician's rating ofdisability was found by Kuch and colleagues
(1993). Barrett and colleagues (1988) have
suggested that "high anxiety levels may be as-sociated with concerns about body deterio-ration or mortality." Although not very much
is known about the relationship between dis-
ability and anxiety, there is evidence that ahigher incidence of anxiety does exist amongpersons with disabilities. The literature has
demonstrated that individuals with disabili-
ties are significantly more anxious than the
general population.
The relationship between disability sever-ity and stress is not unequivocal. Some re-
search supports the fact that persons who per-
ceive their disability as severe are likely to
experience increased levels of distress andpoorer mental health outcomes (Jarama,
1996; Kimmel et al., 1995). However, findings
from other studies have not provided sup-port for a relationship between disability
severity and unfavorable outcomes (Eber-
hardt, Larsson, & Nived, 1993; Huber, Ram-
mohan, Bornstein, & Christy, 1993). Thus,
the relationship between level of disability
severity and menial health outcomes is not
conclusive and will be investigated in this
study.
In summary, the literature suggests thathaving a disability can be a stressor that can
lead to unfavorable mental health outcomes.Stressors among Latino immigrants may be
magnified because of minority and ethnic
status. Latino immigrants with disabilities are
therefore at high risk of poor mental health
outcomes such as depression and anxiety.
One factor believed to moderate stress is so-
cial support. There has been limited research
on social support as a moderator of stress for
Latino immigrants with disabilities. This is
the focus of the current study.
Social Support
Despite the numerous barriers for persons
with disabilities, many persons with disabili-
ties are able to maintain a well-adjusted life at
home, at work, and in the community. A fac-
tor that contributes to successful outcomes
among persons with disabilities is social sup-
port (Heller & Swindle, 1983). Social support
includes emotional closeness (intimacy), tan-gible support (material support), appraisal
support (information and advice), esteem
support (feedback that the individual is val-ued by others), and group-belonging support(companionship) (King, Reis, Porter, &

118 J A R A M A E T A L .
Norsen, 1993). These types of support are ex-
pected to buffer the relationship between
stressors and mental health outcomes. Indi-
viduals with high levels of social support are
likely to experience less stress and have bet-
ter mental health outcomes.
Turner and Noh (1988) examined fac-
tors that may buffer the link between stress
and depression in adults with disabilities.
They found that social support and mastery-
were negatively associated with depression,
such that higher feelings of social support
and mastery were associated with lowered
feelings of depression and lowered risk of de-
pressive symptoms.
The nature of the Latino culture, in
which collectivist attitudes arc more preva-
lent than individualistic attitudes, suggests
that social support may be highly beneficial.
In fact, the literature on social support indi-
cates that Latinos use social support and that
this is an important factor in their psycho-
logical and physical well-being (Griffith,
1984; Padilla, Cervantes, Maldonado, & Gar-
cia, 1988; Starrett, Mindel, & Wright, 1983).
Furthermore, social support networks can be
of special value to immigrants, who may not
be acculturated to American culture.
In summary, immigrants who have a dis-
abling condition are at risk of depression and
anxiety from increased slrcssors. The litera-
ture indicates that social support may mod-
erate the relationship between stress and
depression and anxiety. In this study, we ex-
amine how social support, stress, and severi-
ty of disability impact depression and anxiety.
Although models of social support and stress
have been well researched in the literature,
we are interested in the application to Latino
immigrants with disabilities. The following
relationships were hypothesized:
1. Stress and perceived disability severity
will positively correlate with the de-
pendent measures of depression and
anxiety.
2. The impact of stress and of perceived
disability severity on depression and
anxiety will be moderated by social
support.
Methods
Participants
A nonrandom sample of 64 Latinos who were
clients in the Rehabilitation Service Admin-
istration (RSA) in Washington D.C. partici-
pated in the study. There were 27 men and
37 women participants. Most of them origi-
nated from Central America (72%), but
there were a few Dominican (10%) and
South American (17%) participants. Partici-
pants had a variety of disabling conditions
that included physical, chronic illness, neu-
rologic, sensory, emotional, substance abuse,
and cognitive disabilities (Table 1). Sixteen
participants reported not having any disabil-
ity; these participants may have assumed that
a disability meant a visible disability. Howev-
er, one criterion for being clients of RSA is
the presence of a disability.
Procedures
Participants were recruited as part of a larg-
er study that assessed the impact of an inter-
vention program aimed at improving mental
health and employment outcomes among
persons with disabilities. Project staff collab-
orated with the administrators and coun-
selors at RSA to recruit participants. A crite-
rion for participation was that clients be in
job-ready or training status. Clients who met
the study criteria were contacted by their
counselors who provided information about
the study. If clients indicated interest and
were motivated to participate, they were re-
ferred to project staff. The project staff con-
tacted each referral, explained the purpose
of the program, and asked for their partici-pation.
Informed consents were obtained before
data collection. Participants were assured
that their responses would remain coiifiden-

P S Y C H O S O C I A L A D J U S T M E N T T O D I S A B I L I T Y 119
TABLE 1. Descriptive Statistics of Sample
Demographic Characteristics
N %
Age Range: 18-67
Average Age: 32.6
Gender
Women
Men
Education
<12th grade
>12th grade
Marital Status
Single
Married
Divorced
Separated
Living with someone
Type of disability
Physical
Chronic illness
Neurologic
Emotional
Substance abuse
Cognitive
"'None"
37
27
54
9
34
19
1
5
5
20
3
27
1
1
16
57.8
42.2
85.7
14.3
53.1
29.7
1.6
7.8
7.8
40.0
6.0
4.0
14.0
2.0
2.0
32.0
tial and that there would not be negative con-
sequences if they declined to participate. All
measures and informed consents were in
Spanish. At least two persons were available
during date collection to assist participants
with completion of questionnaires if there
were literacy problems. Participants received
a stipend for their participation and tokens
for transportation.
Measures
A comprehensive questionnaire containing
several measures was administered to partic-
ipants. Measures relevant to this study are de-
scribed in the following sections.
DEMOGRAPHIC INFORMATION. Demographic
information included age, sex, education,
marital status, and type of disability (Table 1).
Type of disability was assessed by asking par-
ticipants to list their primary disability.
PSYCHOSOCIAL STRESS. The Perceived Stress
Scale (PSS) (Cohen, Kamarck, & Mcrmel-
stain, 1983) was used to assess the degree to
which situations in one's life are appraised as
stressful. The PSS is a general measure of
stress perception. This 14-item scale, which
assesses the frequency of feelings and
thoughts during the preceding month, has
acceptable validity and reliability. Cron-
bach's alpha reliability for the study sample
was .66.
SEVERITY OF DISABILITY. Perception of the
severity of the disability was assessed by ask-
ing participants to rate their disability on a
scale that ranged from "1" a little to "7" very
severe.
SOCIAL SUPPORT. The Personal Resources
Questionnaires-Part I (PRQ) (Brandt & Wein-
crt, 1981, 1987) was used to measure satis-
faction with social support. Participants were

120 I A R A M A E T A L .
presented with problematic/difficult situa-
tions (i.e., finances, loneliness, unemploy-
ment, and urgent needs) and asked whom
they would go to for help for each. They were
asked whether they had needed help for any
of these situations/problems during the past
6 months and how satisfied they felt with the
help received. They responded to a Likert-
typc scale ranging from "6" very satisfied to
"1" very dissatisfied. The PRQ has been used
in a number of studies and has good psycho-
metric properties (Brandt & Weinert, 1981,
1987). Test-retest reliability in a group of 100
adults was .72. Internal consistency reliabili-
ty ranged from .85 to .93. Criteria-related va-
lidity (r = 40) was established by showing a
correlation between the social support mea-
sure and family functioning. The PRQ has
also been used with ethnic minority popula-
tions in other studies (Zea, Belgrave, Town-
send, Jarama, & Banks, 1996). Cronbach al-
pha's internal consistency for the study
sample was .68.
DEPRESSION. The short version of the Beck
Depression Inventory (BDI) (Beck & Beck, 1972)
was used to assess feelings of depression. This
shortened version includes 13 items and has
been demonstrated to be highly correlated
with the long BDI (correlation coefficients
ranging from .89 to .97). It also has high in-
ternal consistency, concurrent validity with
other measures of depression, and construct
validity with psychological, behavioral, and
attitudinal variables related to depression
(Beck, Steer, & Garbin, 1988). In this study
the reliability coefficient was .84.
ANXIETY. The State-Trait Anxiety Inventory
(STAI) (Spielberger, Gorsuch, & Lushene,
1970) was used to assess anxiety. This scale
has been used extensively in research and
clinical practice among persons with psychi-
atric and psychosomatic illnesses as well as
among normal populations. The STAI mea-
sures anxiety as a state and as a trait. In the
present research, the T-Anxiety scale was
used as it reflects stable, long-term anxiety.
The T-Anxiety scale consists of 20 items that
assess how people "generally" feel. In re-
search with working adults, students, and
military recruits, the alpha coefficients for
the T-Anxiety scale were uniformly high, with
a median coefficient of .90 (Spielberger, Gor-
such, Lushene, Vagg, &Jacobs, 1983). Cron-
bach's alpha coefficient for the T-Anxiety of
this sample was .79.
Measures were translated into standard
Spanish by one translator and then back
translated by another translator. The two
English versions were then contrasted to
identify inconsistencies. A panel of four
Spanish-speaking researchers of diverse na-
tionalities reviewed the Spanish version to
ensure that the language was standard and
avoided regionalisms.
Results
Descriptive Statistics
Demographic information on age, sex, edu-
cational level, marital status, and disability
are shown in Table 1. The mean score for de-
pression was 8.83 (SD 7.3); for anxiety, there
was an average score of 2.22 (SO .49). The
mean score of stress for this sample was 3.05
(SD .53); for severity of disability, the mean
score was 1.84 (SD 1.75); and for social sup-
port those scores were 4.4 and 1.48, respec-
tively.
Bivariate Correlations
Initial correlations between the independent
variables and depression indicated that de-
pression was positively related to stress (r =
.65, p < .001) and to perception of severity of
disability (r— .51, p < .001). Depression was
negatively related to satisfaction with social
support (r = —.35, p < .008). Increased
stress, high perception of the severity of dis-
ability', and decreased satisfaction with sup-
P S Y C H O S O C I A L A D J U S T M E N T T O D I S A B I L I T Y 727
port were associated with increased depres-
sion.
Correlations between the independent
variables and anxiety indicated that anxietywas positively related to stress (r — .44, p <
.008) and negatively related to satisfaction
with social support (r = .41, p < .02). Therewas no relationship between anxiety and dis-
ability severity. Increased stress and de-
creased satisfaction with support were associ-
ated with increased anxiety.Correlations between demographic vari-
ables and depression and anxiety were com-puted. There were no significant associations
between demographic variables and depres-
sion and anxiety.
Hierarchical Regression Analyses
Multivariate analyses were conducted to ex-amine whether stress, perception of severity
of disability, and satisfaction with social sup-
port predicted depression and anxiety. Sepa-
rate hierarchical multiple regressions were
performed in which stress, perception of the
severity of disability, and satisfaction with so-
cial support were entered simultaneously in
the first step. Two-way interactions betweensupport and stress and between support and
perception of the severity of disability were
examined. Two separate analyses were con-
ducted in which each interaction was entered
in the second step. Demographic variables
(i.e., gender, education) were not entered in
the model because they were not significant
at the bivariate level.
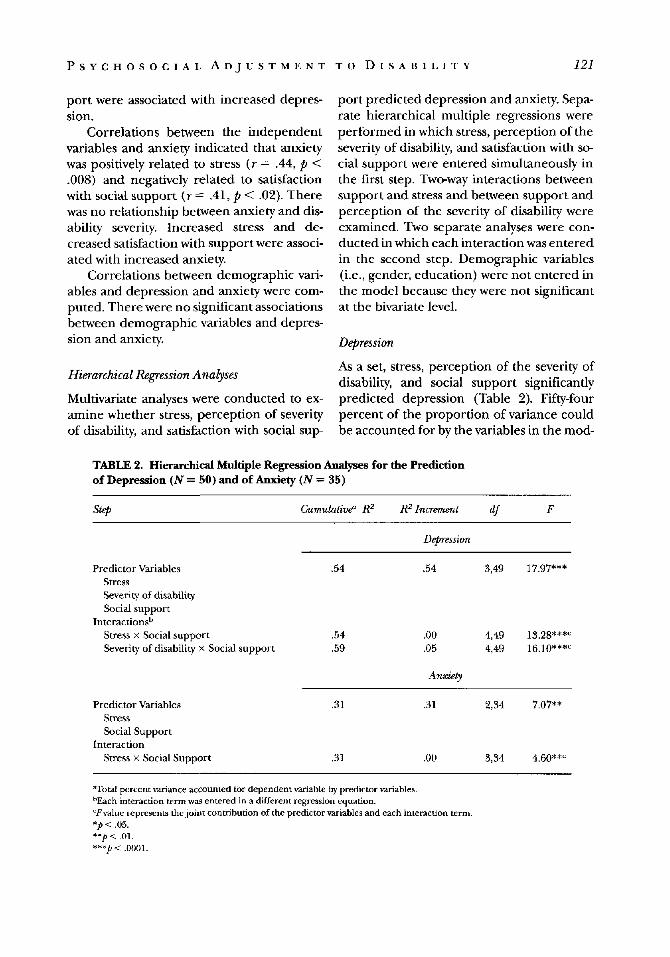
Depression
As a set, stress, perception of the severity of
disability, and social support significantly
predicted depression (Table 2). Fifty-four
percent of the proportion of variance could
be accounted for by the variables in the mod-
TABLE 2. Hierarchical Multiple Regression Analyses for the Prediction
of Depression (JV = 50) and of Anxiety (N = 35)
Step
Predictor Variables
Cumulative" R2
.54
R2 Increment df F
Depression
.54 3,49 17.97***
Stress
Severity of disability
Social support
Interactions1*
Stress x Social support
Severity of disability x Social support
Predictor Variables
Stress
Social Support
Interaction
Stress x Social Support
.54
.59
.31
.00
.05
Anxiety
.31
4,49
4,49
2,34
13.28***c
16.10**»
7.07**
.31 3,34 4.60**
aTota! percent variance accounted tor dependent variable by predictor variables.hEach interaction term was entered in a different regression equation.lvalue represents the joint contribution of the predictor variables and each interaction term.*p < .05.
**/»<.01.***£<.0001.

122 J A R A M A E T A L .
el (F= 17.97, p < .0001). The individual con-
tribution of variables when controlling for
each other showed that stress was a stronger
predictor (F= 16.37,p< .001) than percep-
tion of severity of disability (F = 6.40, p <
.01). Social support did not make a unique
contribution to the model.
The two-way interactions between sup-
port and stress and support and severity of
disability were tested in separate regression
equations. Each interaction was entered in
the second step along with the predictor vari-
ables. The models containing each interac-
tion term did not significantly add to the
original model that contained the predictor
variables. However, when each variable was
controlled for each other, there was a unique
contribution of the interaction between so-
cial support and severity of disability (F =
5.36, p < .03). Increased perception of sever-
ity of disability was related to high levels of
depression when social support was low.
Anxiety
Stress and social support were entered as a
block in the first step. Perception of severity
of disability was not entered in this step be-
cause it was not significant at the bivariatc lev-
el. Stress and social support were significant
predictors of anxiety'. The individual contri-
bution of stress and social support when con-
trolling for the other was also significant (F
= 6.56, p < .02, and F= 5.11, p .03, respec-
tively). Thirty-one percent of the proportion
of variance could be accounted for by the
variables in the model (F = 7.07, p < .003).
Although the model that included the inter-
action between support and stress was signif-
icant, the interaction did not significantly
add to the original model.
Discussion
This was an exploratory study that examined
the relationships between stress, perceived
severity of disability, social support, and de-
pression and anxiety among Central Ameri-
can immigrants with disabilities. The role of
social support in moderating the impact of
stress and severity of disability on depression
and anxiety was also explored.
Stress, severity of disability, and social
support jointly explained a large percentage
(54%) of the variance in depression. High
levels of stress, coupled with increased per-
ceptions of severity of the disability, and a
nonexistent or ineffective social support net-
work were associated with increased depres-
sion among Central American immigrants
with disabilities. Stress made the greatest
unique contribution to depression, followed
by perceptions of the severity of disability.
These findings are consistent with those re-
ported in other studies, which have found
stress and disability severity to correlate sig-
nificantly with depression among persons
with disabilities (Turner & Beiser, 1990;
Turner & McLean, 1989; Turner & Wood,
1985). In addition, increased perceptions of
disability' severity resulted in depression
when satisfaction with social support was low.
A significant proportion (31%) of anxiety
experienced by Central Americans with dis-
abilities can be explained by increased stress
and decreased social support. Although pre-
liminary, these findings contribute to the
sparse literature research assessing the rela-
tionship between stress and anxiety among
persons with disabilities. Latino immigrants
with disabilities experience great levels of
anxiety because of their increased stress.
There are several stressors unique to this
population such as immigrant status, uproot-
ing from culture of origin, the language bar-
rier, and limited employment opportunities,
which contribute directly to anxiety. The
study findings are consistent with the few
studies that have found stress to be related
to anxiety among persons with disabilities
(Burlewetal., 1995; Turner & McLean, 1989).Perception of disability severity con-
tributed to depression, but not to anxiety.
Perhaps for this population, other stressors
play a more insidious role in generating anx-
iety than perception of disability severity.
Among study participants, not having ade-
quate social support contributed to in-
creased anxiety. However, the impact of

P S Y C H O S O C I A L A D J U S T M E N T T O D I S A B I L I T Y 123
stress on anxiety was not moderated by social
support. The small sample size available for
these analyses may have contributed to this
lack of effects.It is of interest that there was a finding of
a direct impact of social support on anxiety
and not on depression. This finding suggests
that the experience of anxiety may be inde-
pendent of depression for this population.
The findings underscore the role of satisfac-tion with social support on mental health
among Latino immigrants with disabilities.Social support can directly relieve the dis-
tress from anxiety or may serve a protective
function when there is depression. Social
support may significantly reduce anxiety feel-
ings regardless of the level of stress experi-
enced. Likewise, satisfaction with one's social
network may be critical to protect persons
from feeling depressed when they have high
perceptions of severity of disability.Despite the significant findings, this is an
exploratory study that has some limitations.
While we expected social support, stress, anddisability severity to precede depression and
anxiety, this may not have been the case. De-
pression and anxiety may have unfavorably
influenced participants' perceptions of sup-
port, disability severity, and stress, law sup-
port, increased perceptions of the severity of
disability, and increased stress may resultfrom a depressive and/or anxious view. An
important caveat relates to the generalizabil-
ity of the study results. The sample was takenfrom a state rehabilitation agency in Wash-
ington, DC. These individuals may have been
different from others who are not affiliated
with a state rehabilitation agency. For exam-
ple, participants may have been more moti-
vated because they were clients at this
agency; or they may have been clients be-cause they needed more services.
Another limitation of this research is the
small sample size, which limited the power of
analyses. The use of self-report measures isanother limitation.
Future research is needed to continue toaddress the relationship between stress, per-
ceived severity of disability, social supportand anxiety and depression. Using a larger
and more heterogeneous sample may con-
tribute to better generalizability of findings.
Objective measures, such as independent rat-
ings of disability severity by rehabilitationprofessionals, could be used to complement
the more subjective self-reported perception
of disability severity. Perhaps focusing on onespecific disability instead of disabilities in
general would also yield different results. An-
other interesting research possibility would
be to assess the relationship between stress,
severity of disability, and social support, and
their impact on other outcomes such as
health behaviors, morbidity and mortality,and vocational outcomes. Evaluating whether
differences exist between nonimmigrant andimmigrant Latinos is also an interesting ex-
tension of the present research.
Clinical Implications
The findings provide some suggestions and
issues to address when designing interven-
tions. An effective intervention for Latino
immigrants with disabilities should consider
individual perceptions of stress and of the
severity of the disability. Strategies aimed atcognitive restructuring, improving coping
skills, and improving self-efficacy may proveeffective. For example, to change detrimen-
tal perceptions of severity of disability, learn-ing to think of one's disabling condition in
more adaptive ways through cognitive re-
structuring could be effective. Also, stressmanagement training, which teaches effec-
tive coping skills, may be helpful in reducing
stress. Finally, intervention programs mayemphasize the use and development of social
networks as effective resources to alleviate or
prevent the experience of anxiety and distress.
References
Barrett, D. H., Wisotzek, I. E., Abel, G. G.,
Rouleau, J. L., Platt, A. F., Pollard, W. E., &
Eckman, J. R. (1988). Assessment of psy-
chosocial functioning of patients with sickle
cell disease. Southern Medical Journal, 81,
745-750.

124 J A R A M A E T A T . .
Beck, A. T., & Beck, R. W. (1972). Screening de-
pressed patients in family practice: A rapid
technique. Postgraduate Medicine, 52, 81-85.
Beck, A. T., Steer, R. A., & Garbin, M. G. (1988).
Psychometric properties of the Beck Depres-
sion Inventory: Twenty-five years of evalua-
tion. Clinical Psychology Review, 8, 77-100.
Brandt, P., & Weinert, C. (1981). The PRQ: A social
support measure. NursingResource, 30,277-278.
Brandt, P., & Weinert, C. (1987). The personal re-
source questionnaire. Available from Mon-
tana State University College of Nursing.
Cohen, S., Kamarck, T, & Mermelstein, R. (1983).
A global measure of perceived stress, journal
of Health and Social Behaviirr, 24, 385-396.
Eberhardt, K., Larsson, B., & Nived, K. (1993). Psy-
chological reactions in patienls wilh early
rheumatoid arthritis. Patient Education and
Counseling, 20, 93-100.
Elliott, T. R., Herrick, S. M., Patti, A. M., & Witty,
T. E. (1991). Assertiveness, social support,
and psychological adjustment following spinal
cord injury. Behaviour Research and Therapy, 29,
485-493.
Griffith, J. (1984). Emotional support providers
and psychological distress among Anglo and
Mexican Americans. Community Mental Health
Journal, 20, 182-201.
Heller, K., £ Swindle, R. W. (1983). Social net-
works, perceived social support, and coping
with stress. In Felner, R. D., Jason, L. A., Mori-
tangu, J. N., & Farber, S. S. (Eds.), Preventive
Psychology: Theory, Research, and Practice (pp.
87-103). New York: Pergamon Press.
Huber, S. J., Rammohan, K. W., Bornstein, R. A.,
& Christy, J. A. (1993). Depressive symptoms
are not influenced by severity of multiple
sclerosis. Neuropsychiatry, Neuropsychology, and
Behavioral Neurology, 6, 177-180.
Jarama, S. L. (1996). A model ofpsychosodal adjust-
ment, to disability among African Americans. Un-
published doctoral dissertation, The George
Washington University, Washington, DC.
Kelley, S. D. M., & Lambert, S. S. (1992). Family
support in rehabilitation: A review of re-
search, 1980-1990. Rehabilitation Counseling
Bulletin, 56,98-119.
Kimmel, P. L., Peterson, R. A., Weihs, K. L., Sim-
mens, S. J., Boyle, D. N., Cruz, L, Umana, W.
O., Alleyne, S., &Veis,J. H. (1995). Aspects of
quality of life in hemodialysis patients. Jour-
nal of the American Society of Nephrology, 6,
1418-1426.
King, K. B., Reis, H. X, Porter, L. A,, & Norsen, L.
H. (1993). Social support and long-term re-
covery from coronary artery surgery: Effects
on patients and spouses. Health Psychology, 12,
56-63.
Kuch, K, Cox, B., Evans, R. J., Watson, P. C., &
Bubela, C. (1993). To what extent do anxiety
and depression interact with chronic pain.
Canadian Journal of Psychiatry, 38, 36-38.
Lazarus, R. S., & Folkman, S. (1984). Stress, ap-
praisal, and coping. New York: Springer.
Lequerica, M. (1993). Stress in immigrant families
with handicapped children: a child advocacy
approach. American Journal of Orthopsychiatry,
63, 545-552.
Littlefield, C. H., Rodin, G. M., & Murray, M. A.
(1990). Influence of functional impairment
and social support on depressive symptoms in
persons with diabetes. Health Psychology, 9,
737-749.
Padilla, A. M., Cervantes, R. C., Maldonado, M., &
Garcia, R. E. (1988). Coping responses to psy-
chosocial stressors among Mexican and Cen-
tral American immigrants. Journal of Commu-
nity Psychology, 16, 418-427.
Salgado de Snyder, V. N., Cervantes, R. C., & Padil-
la, A. M. (1990). Gender and ethnic differ-
ences in psychosocial stress and generalized
distress among Hispanics. SexRoles, 22,441-453.
Spiclbcrgcr, C. D., Gorsuch, R. L., & Lushene, R.
E. (1970). Manual far the State-Trait Anxiety In-
ventory (Self-Evaluation Questionnaire). Palo
Alto, CA: Consulting Psychologists Press.
Spielberger, C. D., Gorsuch, R. L., Lushene, R. E.,
Vagg, P. R., & Jacobs, G. A. Manual for the State-
Trait Anxiety Inventory (Forms Y) (Self-Evalua-
tion (Questionnaire). Palo Alto, CA: Consulting
Psychologists Press, 1983.
Starrett, R. A., Mindel, C. H., & Wright, R. (1983).
Influence of support systems on the use of so-
cial services by the Hispanic elderly. Social
Work Research and Abstracts, 10, 35-40.
Turner, J. R., £ fleiser, M. (1990). Major depres-
sion and depressive symptomatology among
the physically disabled. Nervous and Mental
Disease, 178, 343-350.
Turner, J. R., & McLean, P. D. (1989). Physical dis-
ability and psychological distress. Rehabilita-
tion Psychology, 34, 225-242.

P S Y C H O S O C I A L A D J U S T M E N T T O D I S A B I L I T Y 125
Turner, J. R., & Noh, S. (1988). Physical disability
and depression: A longitudinal analysis. Jour-
nal of Health and Social Behavior, 29, 23-37.
Turner, R. J., & Wood, D. W. (1985). Depression
and disability: The stress process in a chroni-
cally strained population. Research in Commu-
nity and Mental Health, 5, 77-109.
Thompson, S. C., & Spacapan, S. (1991). Percep-
tions of control in vulnerable populations.
Journal of Social Issues, 47, 1-21.
Weinberger, M., Tierney, W. M., Booher, P., & Hin-
er, S. L. (1990). Social support, stress and
functional status in patients with osteoarthri-
tis. Social Science and Medicine, 30, 503-508.
World Health Organization. (1980). International
classification of impairments, disabilities, and
handicaps: A manual of classification relating to
the consequences of disease. Geneva: World
Health Organization.
Zea, M. C., Belgrave, F. Z., Tovmsend, T. G., Jara-
ma, S. L., & Banks, S. R. (1996). The influ-
ence of social support and active coping on
depression among African Americans and
Latinos with disabilities. Rehabilitation Psy-
chology 41, 223-242.