psychosocial stress and pregnancy outcome
TRANSCRIPT
Psychosocial Stressand PregnancyOutcome
CALVINJ.HOBEL,MD,AMYGOLDSTEIN,MA,MPH,MFT,and EMILY S. BARRETT, PhD
Department of Obstetrics, Gynecology and Pediatrics, Divisionof Maternal Fetal Medicine, Burns and Allen Research Institute,Cedars Sinai Medical Center, The David Geffen School of Medicineat UCLA, Los Angeles, California
Abstract: This article is intended to help cliniciansbetter understand the ever-expanding body of re-search on whether psychosocial stress (both acuteand chronic) is linked to 2 major adverse pregnancyoutcomes: preterm birth and low birth weight. Wesummarize the existing literature and then reviewassessment tools commonly used to diagnose varioustypes of psychosocial stress, with attention to how andwhen assessments should be made. After discussingthe physiologic mechanisms hypothesized to underliethese relationships, we examine the range of existinginterventions aimed at reducing psychosocial stressand review their efficacy at improving birth outcomes.Future directions for prevention of adverse pregnancyoutcomes are discussed and suggest that an entirelynew approach may be necessary.Key words: stress biology, life events, timing, lifecourse, allostatic load
Introduction—PsychosocialStress and Birth OutcomesDespite efforts to improve birth out-comes, preterm birth and low birthweight(LBW) remain major public health con-cerns, with rates of both increasingsteadily over the last few decades.1 Infantsborn small or preterm have greatlyincreased rates of perinatal morbidityandmortality, and the cost of hospitaliza-tion for preterm and LBW infants in theUnited States is staggering.2 Mountingevidence suggests, moreover, that com-promised fetal development may haveeffects on health and cognition thatstretch through childhood into adult-hood. In other words, infants who surviveare at risk for poor outcomes acrossthe life course and yet our understandingof these adverse pregnancy outcomes re-mains limited. It is estimated that currentscreening methods predict only 60% ofpreterm birth and the prevalence of LBW(>2500 g) has climbed to over 13%
333
Source Support: Miriam Jacobs Chair, Maternal FetalMedicine, Cedars Sinai, NIH R-13 Community ChildHealth Network (2U01 HD044245-04).
Correspondence: Calvin J. Hobel, MD, Departmentof Obstetrics, Gynecology and Pediatrics, Division ofMaternal Fetal Medicine, Burns and Allen ResearchInstitute, Cedars Sinai Medical Center, The DavidGeffen School of Medicine at UCLA, 8635 West 3rdSt, Suite 160W, Los Angeles, CA 90048. E-mail:[email protected]
CLINICAL OBSTETRICS AND GYNECOLOGY / VOLUME 51 / NUMBER 2 / JUNE 2008
CLINICAL OBSTETRICS AND GYNECOLOGYVolume 51, Number 2, 333–348r 2008, Lippincott Williams & Wilkins

among certain ethnic groups in theUnitedStates (NCHS 2000).3 Given the preva-lence of these poor pregnancy outcomesand their potentially serious long-termconsequences, considerable efforts havebeen made to understand the underlyingetiologies.
Both animal models and so-callednatural experiments (eg, the DutchHunger Winter) have implicated stressas a potential contributor to adversepregnancy outcomes. Normally, neuro-endocrine systems respond to acute stress,psychosocial or otherwise, allowing anindividual to adapt and reactto changes in the environment. Whenstress is chronic or excessive, however,these adaptive mechanisms may failand the stress response may even causedisease. As our understanding of stressbiology has grown more sophisticated,it has become increasingly well-acceptedthat biomedical and psychosocial stres-sors alike activate the neuroendocrinestress response. It is hypothesizedthat when the fetal-placental unitis exposed to excessive stressors dur-ing pregnancy, this neuroendocrineresponse may be triggered, resulting inmaternal endocrine changes, acceleratedfetal maturation, preterm birth, andLBW.
With the emergence of better psycho-logic assessment tools and more speci-fic biomarkers of stress in recent years,we can now begin to better addresshow psychosocial stressors may impactfetal development and pregnancy out-comes. On the basis of our currentunderstanding of stress biology, it islikely that a range of psychosocial stres-sors (from the individual-level to thecommunity-level) may affect the func-tion of the fetal-placental unit. If thisis the case, the question then becomeshow we can apply this knowledge tomake practical recommendations thatwill reduce the risks of preterm birthand LBW.
A Review of the Literatureon Psychosocial Stress andPregnancy Outcomes
PSYCHOSOCIAL STRESS ANDPRETERM BIRTH
The large body of research on psychoso-cial stress and preterm birth is rife withconflicting results. Nevertheless there issufficient evidence to suggest a relation-ship between the 2 exists and that muchof the variation is attributable to differingdefinitions and methods of assessment.Although a number of studies, particu-larly the earlier work, have focused onmajor life events, more recent researchhas investigated the role of chronicstressors.
In studies of life events stressors, 2factors have consistently emerged as par-ticularly relevant to the risk of pretermbirth: (1) the timing of the stressor, and (2)the woman’s perception of it. In accor-dance with evidence that women becomeless responsive to stressful stimuli as preg-nancy advances, with some exception,studies show that life events stressors tendto affect birth outcomes most when theyoccur in the first trimester. For example,Glynn et al4 showed that among pregnantwomen exposed to the psychologic effectsof the Northridge earthquake in Califor-nia, only those who experienced it duringthe first trimester showed a significantassociation with a shorter gestationalage at delivery; these women also evalu-ated the earthquake as more upsettingand aversive than women who were intheir second or third trimester at the timeof the earthquake. Similarly, women intheir first trimester who lived in closeproximity to the World Trade Centeron September 11, 2001 showed a slightlyshorter average length of gestation thancontrols, but there was no effect amongwomen who were in their second trime-ster.5 On the other hand, in theirstudy of women who experienced theUkranianChernobyl disaster during early
334 Hobel et al

pregnancy, Levi et al6 found no increasedrisk of preterm labor.
Large-scale, catastrophic life events,such as these, lend themselves to studieson the timing of psychosocial stressors,but the preponderance of studies exam-ines life events occurring on a more in-dividual scale. In most cases, such studiesfocus on the number of events and wo-men’s experience of those events, ratherthan the timing of events.More often thannot, the number or type of life eventsoccurring during pregnancy emerges as aless important predictor of preterm birththan how stressful, negative, or aversivethe experiences were perceived to be.7–9
For instance, Hedegaard et al7 found thatthe occurrence of life events assessedby women as highly stressful was asso-ciated with shorter gestation times, butthe events themselves were not. In fact,the preterm birth risk among women whoexperienced one or more highly stressfulmajor life events was 1.76 times [confi-dence interval (CI)=1.15-2.71] greaterthan that of women who had not experi-enced a highly stressful life event duringpregnancy. In other words, women’sexperience of events during pregnancy iscritically important for understandinghow their bodies respond to such stressorsand by extension, how their pregnanciesare affected. Interestingly, in the after-math of major life events, chronic stres-sorsmay emerge, whether it is copingwiththe death of a loved one, dealing with thefinancial and emotional strain of a naturaldisaster, or adapting to a change in job orresidence. For this reason, although acutestressors and chronic stressors are oftendichotomized in the literature, it may bedifficult to disentangle the effects of the 2.
Unlike life events stress,which is typicallyoperationalized by using a Life Events In-ventory, researchers interested in the effectsof chronic stress may examine a rangeof related exposures, including distress,anxiety, household strain, job stress,daily hassles, negative effect, depression,
pregnancy-related anxiety, coping mechan-isms, and stress of acculturation, as well ascomposite measures of psychosocial andperceived stress. With some exception (seePaarlberg et al for an extensive review),chronically elevated stress levels duringpregnancy, regardless of how they are mea-sured, seem to be associated with increasedrisk of pretermbirth.10 For example, in theirstudy of nearly 6000 women, Hedegaard etal11 found that psychologic distress in week30 (but not week 16) was associated withpreterm delivery; there was a dose-responseeffect, furthermore, whereby the relativerisks of preterm birth for women who ex-perienced moderate and high levels of dis-tress were 1.22 (95% CI=0.84-1.79) and1.75 (95% CI=1.20-2.54), respectively. Si-milarly,Dole et al8 showedadoubled riskofpreterm birth (relative risk=2.1, 95%CI=1.5-3.0) among women with high le-vels of pregnancy-related anxiety and ele-vated risks among women who perceivedhaving experienced racial discrimination(relative risk=1.4, 95% CI=1.0-2.0).Once again in this study, the risk of pretermbirth varied according to the severity of theanxiety.
Psychosocial Stress and LBWAlthough commonly studied togetheras tandem outcomes, preterm birth andLBW due to growth restriction differ inetiology and thus may be affected differ-ently by psychosocial stress. A handful ofstudies suggest that stressful life events areassociated with decreases in birth weightand thus, increased risks of LBW. Mostnotably,Wadhwa et al12 showed that eachunit of life event stress was associatedwitha 55-gram reduction in birth weight andan odds ratio (OR) of 1.32 (CI not given)for LBW. More commonly, however, theimpact of stressful life events on birthweight disappears after controlling forconfounding factors, particularly smok-ing. Tobacco use exerts a strong and well-documented influence on birth weight not
Psychosocial Stress and Pregnancy Outcome 335

only by altering the levels of neurotrans-mitters implicated in stress response, butalso by increasing resistance in the umbi-lical and uterine arteries.13 Given theassociations between stressful life eventsand smoking, it is little surprise that to-bacco use might mediate the relationshipbetween psychosocial stress and birthweight. That there should be few associa-tions found between psychosocial stressand intrauterine growth (and its proxy,birth weight) is not surprising if we con-sider stressful life events to be discrete,acute incidents, rather than indicators orinstigators of chronic stress. Because sizeat birth is the end result of a cumulative9-month process, unless a single stressfulevent has a long-lasting effect onmaternalphysiology resulting in decreased nutri-tion to the fetus, it should not exert asignificant effect on birth weight.
By contrast, the evidence supportinga relationship between chronic indicatorsof psychosocial stress and LBW is morepersuasive. Paarlberg et al14 conducted anextensive review of this literature, con-cluding that the relationship is strongestwhen multiple exposures interact to con-tribute to compromised fetal growth.Indeed many indicators and covariatesof psychosocial stress have been asso-ciated with LBW. In 1 Russian study,for example, perceived stress, living incrowded or shared housing, and excessivepaternal drinking were all associatedwith decreased birth weight.15 Similarly,Pritchard and Teo16 found that expectantmothers who perceived high levels ofhousehold ‘‘strain’’ at 20 weeks of gesta-tion to have an odds ratio of 4.70 (95%CI=1.53-13.38) for LBW, though theresults of this small study are likely con-founded by SES and other complexitiesof assessing the household.
Nevertheless, these studies raise the inter-esting idea that the relationshipsoften foundbetween psychosocial stress and LBW maybe attributable, at least in part, to variationin energetic intake and expenditure. For
instance, expectant mothers who shouldermost of the burden of running a householdor who lack a close relationship with ahusband or partner may experience lessnutritional provisioning by others and agreater workload, both of which could con-tribute to fewer net calories per day, andby extension, reduced maternal and fetalweight gain. In trying to further illuminatethese relationships, it would be useful tomonitor weight gain throughout pregnancyas a standard part of these studies as wellhave women keep daily logs of food intakeand energy expenditure.
Adding further evidence in support ofthis idea, social support has been shownto have positive effects on birth weight ina number of studies. Feldman et al17
found that social support (and other vari-ables) accounted for 31% of the variancein fetal growth in their study (after con-trolling for gestational age). Women whohad multiple types of social support fromdifference sources, in fact, had infantswith the highest birth weight. On the basisof these results and an extensive reviewthe literature on social support and birthweight, they conclude that social supportmay promote higher birth weights byseveral means. In addition to direct mate-rial provisioning of expectant mothers,social support may encourage thesemothers to adopt healthier lifestyles, re-duce their stress levels, and pursue betterprenatal care. As Hoffman and Hatch18
posit more generally, beneficial influencessuch as social support or positive affectmay promote health behaviors and fetalgrowth, while stressors may contribute topoor outcomes through their associationwith negative health behaviors.
Allostatic Load and AdversePregnancy OutcomesEven studies examining the relationshipbetween chronic psychosocial stress andpregnancy outcomes typically only focus
336 Hobel et al
on the 9-month period of gestation. Yetevidence is accumulating to suggest thatadverse pregnancy outcomes such as pre-term birth and LBW may originate longbefore conception. This dramatically dif-ferent perspective on adverse pregnancyoutcomes is an extension of the emergingliterature on allostatic load. Allostaticload provides a measure of the cumula-tive effects of exposure to stressors andphysiologic stress responses over the life-course.19 High allostatic load, as quanti-fied by an index of biomarkers, resultswhen the body’s physiologic responses tochronic stressors are no longer adaptive.To put it simply, allostatic load representsthe build-up of ‘‘wear and tear’’ on thebody, leading to dysfunction, over time.Low SES, experience of racism, exposureto violence, negative health behaviors,loss/trauma, and lack of social supportare just a few of the many stressors thatmay contribute to increased allostaticload and by extension, increased risk ofnegative birth outcomes.
Lu andHalfon20 argue that if allostaticload impacts somatic function over thelife course, it follows that reproductivefunction may be similarly affected. Thisperspective is particularly interesting gi-ven that the risk of adverse birth out-comes is exceptionally high amongcertain subpopulations marked by highallostatic load. The racial discrepancy inbirth outcomes, for instance, has beenwell-documented (though not well-under-stood), with infants born to African-American mothers suffering from farhigher rates of preterm birth, perinataldeath, LBW, and very LBW than infantsborn to white mothers.21 These effectsseem to be compounded by maternalage, moreover. For instance, Geroni-mus22 found that the risk of LBW andvery LBW increased 4-fold with ageamong African-American women, butnot white women. These effects, notably,were evident among African-Americanwomen of low and average SES, but
not among African-Americans of highSES.22
Although research on allostatic load asameasure of lifelong chronic stress is in itsinfancy and its relationship to birth out-comes remains largely hypothetical, itmarks a radical shift in how we thinkabout stress and pregnancy outcomes,one which may have dramatic ramifica-tions on how we approach prenatal care.For a more thorough examination ofhow allostatic load may impact preg-nancy outcomes, with particular referenceto racial disparities, see Shannon et al23
and Lu and Halfon.20
Assessing Psychosocial StressGiven the evidence suggesting that a widearray of maternal psychosocial stressorscan contribute to poor pregnancy out-comes, the means by which these variousstressors can be assessed are of particularrelevance to clinicians. The developmentof methods, and more specifically instru-ments used for the assessment of psycho-social stress, has been an area of focus forresearchers over the past several years.Research to date suggests there is indeedsome consensus within the scientific com-munity as to the requisite content areasfor adequate measurement of psychoso-cial stress. This agreement is evidenced bythe overwhelming use of particular tools,or subsets thereof, by researchers in thefield. Those measurements that havedemonstrated staying power due to sus-tained reliability and validity over theyears screen for the following potentiallyproblematic stress variables: life events,anxiety, depression, perceived stress, ra-cism, self-esteem, work or householdstrain, and social support.24,25 Addition-ally, more recent literature suggests thatfuture assessments should also includepregnancy-specific stress and pregnancyintendedness or desirability.26–28
Many instruments, assessing diversestress variables, have yielded significant
Psychosocial Stress and Pregnancy Outcome 337
findings. However, to familiarize clini-cians with the available instruments, weprovide a brief review of those that standout owing to their wide appeal as evi-denced via continued use, whether onlya portion or in its entirety, in the scientificliterature.
LIFE EVENTS INVENTORY
Initially developed by Cochrane andRobertson,29 this self-administered toolis used to assess ‘‘acute’’ stress in personal,family, interpersonal, social, financial,and work-related areas that are not usual-ly everyday occurrences. This inventoryhas served as the springboard from whichseveral other Life Events Inventories havebeen adapted.
STATE-TRAIT ANXIETY INVENTORY
Spielberger et al30 developed this tool toassess levels of anxiety. The assessmentis comprised of items related to howthe respondent ‘‘typically feels.’’ Respon-dents are presentedwith a list of adjectivesand asked to describe and rate their feel-ings, such as nervousness, fright, and ten-sion (on a 4-point Likert scale) in the lastfew days.
EDINBURGH POSTNATALDEPRESSION SCALE
Developed in 1987 byCox and colleagues,this screening tool is unique in that it’s theonly one designed specifically to screenfor postpartum depression. Because thewording of this inventory is quite broad,rather than being geared solely toward thepostpartum period itself (ie, ‘‘I have feltsad or miserable’’), this brief, 10-item,self-administered instrument has alsobecome more widely used in research forthe screening of depression during preg-nancy as well.
CENTER FOR EPIDEMIOLOGICSTUDIES DEPRESSION SCALE
The center for Epidemiologic StudiesDepression Scale is a short (20-item)
self-reporting scale that was designed toassess depression in the general popula-tion by asking respondents to indicatetheir feelings during the past week abouteach item on a 4-point Likert scale.31 Forexample, ‘‘I felt hopeful about the future’’would receive a response of either 1/rarelyor none of the time (less than 1 d), 2/someor a little of the time (1 to 2 d), 3/occa-sionally or amoderate amount of the time(3 to 4 d), or 4/most or all of the time(5 to 7 d).
PERCEIVED STRESS SCALE
Originally published in 1983, this toolembodies a more global assessment ofstress which capturing its chronic natureover time. A short scale (14 items), itassesses the degree to which situationsduring the last month were experiencedas stressful (ie, unpredictable, uncontrol-lable, overwhelming).32
Despite the plethora of instrumentsavailable for the measurement of psycho-social stress, there is no single instrumentthat incorporates what we believe to be allof the crucial components needed foradequate screening of maternal stress. Itis our opinion that development of suchan all-encompassing screening tool wouldbe of considerable benefit to clinicians.Such a user-friendly instrument is essen-tial if we are to move toward practicalapplication of the many years of researchon psychosocial stress and pregnancy out-comes. Additionally, as discussed ingreater detail later in this article, imple-mentation of more routine screening aspart of prenatal care will be important forimproving birth outcomes.
There have been efforts by researchersto combine previously validated tools inlieu of using each individualmeasure in itsentirety.24 This step represents a substan-tial advancement toward what we view asa necessary, multifaceted approach to theassessment of stress. Recently, the Amer-ican College of Obstetricians and Gyne-cologists published its version of a
338 Hobel et al

thorough assessment for psychosocialrisk during pregnancy.33 This 9-itemscreening tool addresses relevant issuessuch as barriers to health care, unstablehousing, unintended pregnancy, nutri-tion, substance use, intimate partner vio-lence, depression, and perceived stress.Nonetheless, we find this screening toolto be incomplete because of its inattentionto other pertinent stress variables such asthe stress of significant life events, workrelated stress, and the presence or absenceof social support.
As part of our strong recommendationfor a single, comprehensive instrument,we present what we consider to be theessential components to target in anystress assessment during pregnancy. Inher PostpartumDepression Predictors In-ventory-Revised (PDPI-R) (2002), Beckidentified 13 predictors or risk factors forpostpartum depression. Although this in-ventory is specifically designed to assessrisk for postpartum depression, its com-ponents include a number of items well-suited for the screening of psychosocialstress during pregnancy. Beck’s design,moreover, is innovative in that it recom-mends periodic revision to include addi-tional significant risk factors as suggestedby recent research and deletion of otherrisk factors that may no longer be ofsignificance. Unlike most other inven-tories, however, the PDPI-R is not aself-reported assessment. It is designedto be conducted as a structured interviewto obtain a more complete picture of thepatient’s problems/experiences. We sug-gest that by combining a number of thosepsychosocial risk indicators with addi-tional items designed to assess other stres-sors such as smoking and nutrition, asufficiently multidimensional screeningtool could be generated.
Ideally, the goal would be for womenand their care providers to address theseissues of stress before pregnancy. How-ever, as this does not consistently occurand the optimal time to intervene for any
particular stress variables is yet unclear,we propose screening for stress once pertrimester during pregnancy for a total of 3screenings. Table 1 outlines the significantstress variables to include in a Stress InPregnancy Assessment based on the cur-rent literature.
Physiologic MechanismsUnderlying the RelationshipBetween Psychosocial Stressand Pregnancy Outcomes
PRETERM BIRTH
Hobel discusses the biologic mechanismsand pathways by which stress may leadto preterm birth. In the nonpregnantstate, the hypothalamic-pituitary-adrenal(HPA) modulates the subjects’ responseto an environmental stressor.25 The prin-cipal molecular regulator of the HPAaxis, corticotrophin-releasing hormone(CRH), is frequently referred to as themediator of the stress response. When
TABLE 1. Components of the ideal compre-hensive approach to the assess-ment of stress during pregnancy.It should be performed during eachtrimester of pregnancy
Stress in Pregnancy Assessment
Stress variablesSignificant life events (such as bereavement orother significant loss, moving)Mental health issues (current symptoms orhistory of depression, anxiety, or other mental/emotional disorder)WorkRacism/discriminationDaily hasslesSocial supportChronic stressPoor nutrition (food frequency, food insecurity)Tobacco usePregnancy-specific stressPregnancy desirability
Psychosocial Stress and Pregnancy Outcome 339
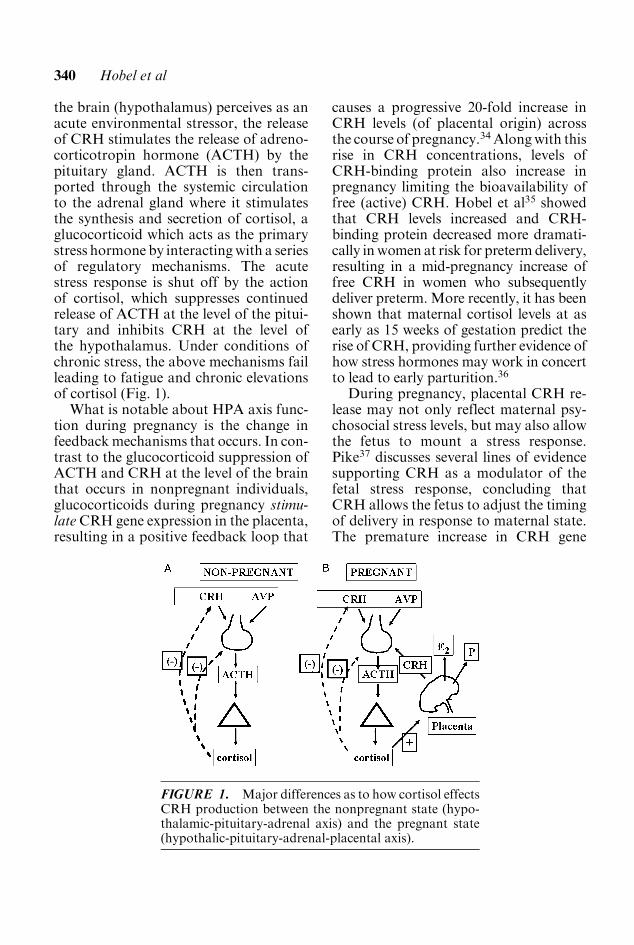
the brain (hypothalamus) perceives as anacute environmental stressor, the releaseof CRH stimulates the release of adreno-corticotropin hormone (ACTH) by thepituitary gland. ACTH is then trans-ported through the systemic circulationto the adrenal gland where it stimulatesthe synthesis and secretion of cortisol, aglucocorticoid which acts as the primarystress hormone by interactingwith a seriesof regulatory mechanisms. The acutestress response is shut off by the actionof cortisol, which suppresses continuedrelease of ACTH at the level of the pitui-tary and inhibits CRH at the level ofthe hypothalamus. Under conditions ofchronic stress, the above mechanisms failleading to fatigue and chronic elevationsof cortisol (Fig. 1).
What is notable about HPA axis func-tion during pregnancy is the change infeedbackmechanisms that occurs. In con-trast to the glucocorticoid suppression ofACTH and CRH at the level of the brainthat occurs in nonpregnant individuals,glucocorticoids during pregnancy stimu-lateCRH gene expression in the placenta,resulting in a positive feedback loop that
causes a progressive 20-fold increase inCRH levels (of placental origin) acrossthe course of pregnancy.34Alongwith thisrise in CRH concentrations, levels ofCRH-binding protein also increase inpregnancy limiting the bioavailability offree (active) CRH. Hobel et al35 showedthat CRH levels increased and CRH-binding protein decreased more dramati-cally inwomen at risk for pretermdelivery,resulting in a mid-pregnancy increase offree CRH in women who subsequentlydeliver preterm. More recently, it has beenshown that maternal cortisol levels at asearly as 15 weeks of gestation predict therise of CRH, providing further evidence ofhow stress hormones may work in concertto lead to early parturition.36
During pregnancy, placental CRH re-lease may not only reflect maternal psy-chosocial stress levels, but may also allowthe fetus to mount a stress response.Pike37 discusses several lines of evidencesupporting CRH as a modulator of thefetal stress response, concluding thatCRH allows the fetus to adjust the timingof delivery in response to maternal state.The premature increase in CRH gene
FIGURE 1. Major differences as to how cortisol effectsCRH production between the nonpregnant state (hypo-thalamic-pituitary-adrenal axis) and the pregnant state(hypothalic-pituitary-adrenal-placental axis).
340 Hobel et al
expression can activate a series of endo-crine events, both autocrine and para-crine, to prepare the fetus and uterus forparturition. Elevated CRH levels fromthe placenta enter fetal circulation andsignal the now mature fetal pituitary-adrenal axis to further produce andsecrete ACTH, cortisol, and dehydro-epiandrosterone, an estrogen precursor.The positive feedback loop between thefetal adrenal gland and placental produc-tion ofCRHunderlies the exponential risein placental CRH and estrogens, 2 impor-tant mediators of labor. Early activationof CRH gene expression in the placentaprovides a mechanism whereby these ma-turational events could occur early in thecase of preterm labor. McGregor et al38
identified an early estriol surge occurringapproximately 3 weeks before pretermdelivery. Such interactions between ma-
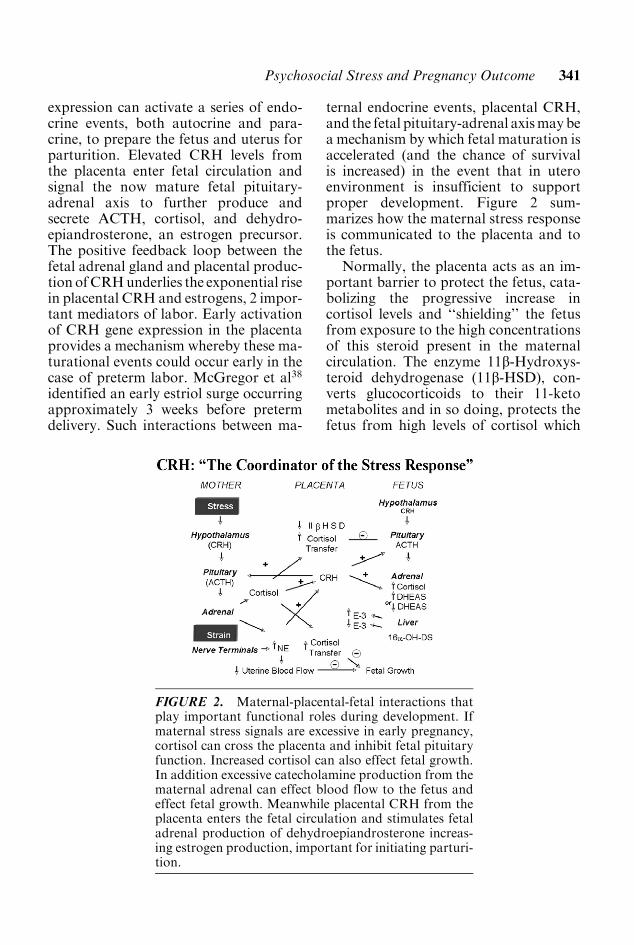
ternal endocrine events, placental CRH,and the fetal pituitary-adrenal axismaybea mechanism by which fetal maturation isaccelerated (and the chance of survivalis increased) in the event that in uteroenvironment is insufficient to supportproper development. Figure 2 sum-marizes how the maternal stress responseis communicated to the placenta and tothe fetus.
Normally, the placenta acts as an im-portant barrier to protect the fetus, cata-bolizing the progressive increase incortisol levels and ‘‘shielding’’ the fetusfrom exposure to the high concentrationsof this steroid present in the maternalcirculation. The enzyme 11b-Hydroxys-teroid dehydrogenase (11b-HSD), con-verts glucocorticoids to their 11-ketometabolites and in so doing, protects thefetus from high levels of cortisol which
FIGURE 2. Maternal-placental-fetal interactions thatplay important functional roles during development. Ifmaternal stress signals are excessive in early pregnancy,cortisol can cross the placenta and inhibit fetal pituitaryfunction. Increased cortisol can also effect fetal growth.In addition excessive catecholamine production from thematernal adrenal can effect blood flow to the fetus andeffect fetal growth. Meanwhile placental CRH from theplacenta enters the fetal circulation and stimulates fetaladrenal production of dehydroepiandrosterone increas-ing estrogen production, important for initiating parturi-tion.
Psychosocial Stress and Pregnancy Outcome 341
could initiate early/premature matura-tion. Nonetheless, the fetus can be inad-vertently exposed to excessive cortisollevels through 2 main pathways: (1) whenlevels of cortisol are greatly elevated earlyin pregnancy (before 20wk) before 11b-HSD is functional or (2) when 11b-HSDfails to convert cortisol to cortisone be-cause of a genetic defect in this enzymesystem.39
LBW
The physiologic mechanisms by whichmaternal stress increases the risk forLBW are less clear than for preterm birth.LBW is defined as birth weight less than2500 g irrespective of gestational age. It
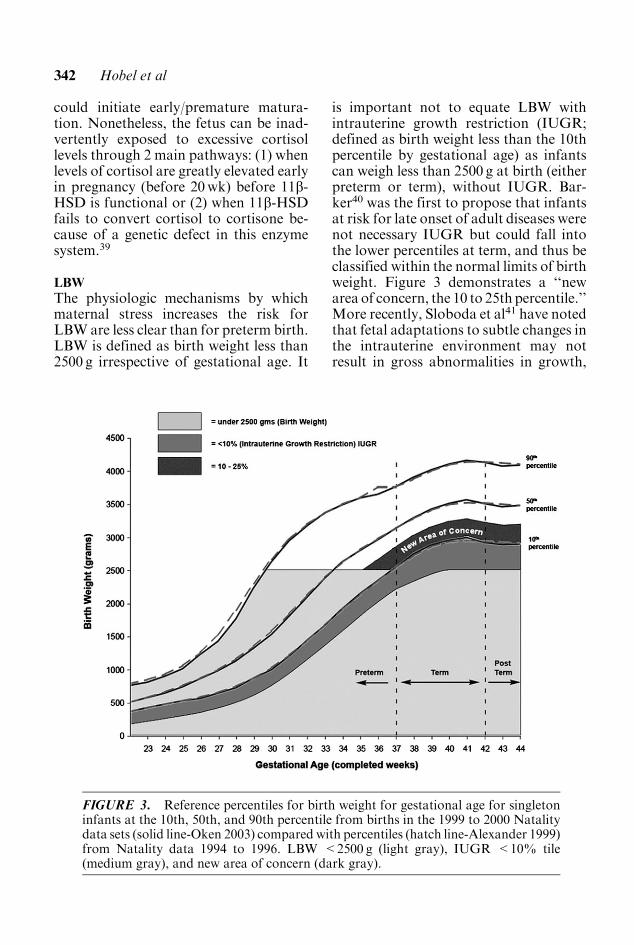
is important not to equate LBW withintrauterine growth restriction (IUGR;defined as birth weight less than the 10thpercentile by gestational age) as infantscan weigh less than 2500 g at birth (eitherpreterm or term), without IUGR. Bar-ker40 was the first to propose that infantsat risk for late onset of adult diseases werenot necessary IUGR but could fall intothe lower percentiles at term, and thus beclassified within the normal limits of birthweight. Figure 3 demonstrates a ‘‘newarea of concern, the 10 to 25th percentile.’’More recently, Sloboda et al41 have notedthat fetal adaptations to subtle changes inthe intrauterine environment may notresult in gross abnormalities in growth,
FIGURE 3. Reference percentiles for birth weight for gestational age for singletoninfants at the 10th, 50th, and 90th percentile from births in the 1999 to 2000 Natalitydata sets (solid line-Oken 2003) compared with percentiles (hatch line-Alexander 1999)from Natality data 1994 to 1996. LBW <2500 g (light gray), IUGR <10% tile(medium gray), and new area of concern (dark gray).
342 Hobel et al

but may still predispose an individualto subtle changes in endocrine functionslater in life.
It is probable that at least 3 pathwayslead to the pathophysiology of LBW.First, as depicted in Figure 2, maternalstress is thought to lead to the release ofcatecholamines which can reduce uterineperfusion, potentially limiting the amountof substrate delivered to the fetus. Thusvia mechanisms described in greaterdetail by Hobel,25 under chronic stress,prolonged exposure to catecholaminescould contribute to reduced fetal growth.Recently Justus et al42 have shown thatmaternal smoking, a known predictor ofLBW, results in the significantly eleva-tions of both catecholamines and all 3HPA axis hormones (CRH, ACTH, andcortisol).
Through a second pathway, even briefperiods of exposure to glucocorticoidscan affect fetal growth. In short, consider-able evidence fromanimalmodels demon-strates that fetal exposure to elevatedlevels of glucocorticoids alters fetalgrowth and has additional long-termeffects on cardiovascular and metabolicfunction.41 The human fetus can beexposed to excessive glucocorticoids in2 ways. First, elevated endogenous ma-ternal cortisol levels caused by stress earlyin pregnancy could affect fetal growth.Secondly, the use of glucocorticoids forfetal lung maturation could also inhibitfetal growth. In the latter instance, sec-ondary synthetic glucocorticoids are be-lieved to decrease the levels of placental11b-HSDwhich, as noted above, preventsthe passage of cortisol across the placenta.Large-scale, randomized controlled trialsare needed to evaluate the effects of syn-thetic glucocorticoid administration dur-ing pregnancy on long-term outcome ofchildren.
The availability of substrate from themother may be a third pathway throughwhich LBW can occur. Substrate avail-ability is determined at 3 levels. First,
maternal dietary habits are critical.Adequate nutrition during pregnancy isclearly essential, but even dietary patternsbefore pregnancy may play an importantrole in programming fetal growth duringpregnancy.43 Appetite, food frequencypatterns, and the timing of weight gainall play an important role in fetal growthand may be affected by psychosocialstress. Second, the delivery of substrateto the fetal-placental unit is also impor-tant. Smoking, for example, may impactfetal growth by causing the excessive re-lease of catecholamines, thereby limitingsubstrate delivery and increasing the me-tabolic rate in the mother, while simulta-neously suppressing appetite. Third, theability of the uterine arteries to deliveradequate substrate to the fetus may belimited. Atherosclerosis of the uterinearteries, commonly found in women withvarious forms of hypertension, can alsoeffect fetal growth. Thus, at multiplelevels altered nutrient availability tothe fetus can result in inadequate fetalgrowth. Clinical assessment at all 3 levelsis possible and interventionsmay decreasethe risk of poor fetal growth.
What Interventions areAvailable to Reduce Stress inPregnant Women and ImproveBirth Outcomes?Given the prevalence of preterm birth,LBW, and the suite of associated post-natal problems, there has been a greatdeal of interest in intervention strategies,especially among high-risk mothers. As acomplement to standard pharmacologicand nutritional approaches to preventingadverse pregnancy outcomes, interven-tions specifically aimed at reducing stresslevels among expectant mothers have gar-nered attention. Despite this interest,however, there has been a decided lackof rigorous scientific research into theefficacy of such interventions and the
Psychosocial Stress and Pregnancy Outcome 343

current body of research offers surpris-ingly few recommendations for clinicians.Thus far, intervention studies aimedspecifically at stress reduction havepromoted 3 main approaches: physicalrelaxation and meditation, assessmentand education, and counseling and socialsupport.
The literature on physical, stress-alleviating interventions, albeit limited,has yielded promising results. Womenrandomly assigned to a yoga group hadoffspring with higher mean birth weight,a decreased incidence of preterm birth,and fewer birth complications (includingintrauterine growth retardation) thanwomen assigned to a walking group.44
In a separate study, pregnant women as-signed to a single session of passive oractive relaxation showed a decrease instate anxiety and heart rate as well as areduction in cortisol levels.45 A similarstudy of high-anxiety pregnant womenparticipating in a 7-week applied relaxa-tion training program showed a decreasedincidence of LBW compared with a con-trol group, but no different in pretermbirth rates. It remains unknown whetherinterventions promoting relaxation resultin a long-lasting decrease in stress reactiv-ity and HPA axis activation or wouldhave an impact on birth outcomes in alarger-scale study; however, these preli-minary results are suggestive.
A second category of interventionsfocuses on assessing psychosocial stresslevels in expectant mothers, particularlythose at high-risk, and then directingthem toward the appropriate resourcesand services. This approach has shownsome success, particularly in a large-scalestudy of women on Medicaid in Califor-nia which found that those who received apsychosocial assessment in each trimesterhad half the risk of having preterm birth(OR=0.53; CI=0.40-0.72) or LBWinfants (OR=0.49; CI=0.34-0.71)compared with those who did not. Theseoutcomes, furthermore, were not depen-
dent on the qualifications of the provideror the practice setting type.46 Similarly, astudy of low-income pregnant womenshowed that receiving more than 45 min-utes of psychosocial services was asso-ciated with a reduced risk of LBW.47 Itis unclear, from these studies alone; how-ever, what aspect of the assessment andservices is responsible for the vastlyimproved outcomes. For instance, didwomen who received assessments everytrimester pursue more follow-up care?Did a single episode of psychosocial ser-vices somehow significantly lower stresslevels or change behavior? Or, equallyprobable, is there something intrinsicallydifferent about those who seek frequentprenatal psychosocial assessments andcounseling?
The third category of interventions fo-cuses on social support and is the direc-tion that has attracted the most researchby far. Unfortunately, the preponderanceof evidence suggests that providing socialsupport to high-risk pregnant womenaffords little, if any, protection againstpreterm delivery and LBW. Two exten-sive reviews of the literature on inter-ventions come to similar conclusions:whereas observational studies of pregnantwomen and their support networks oftenhave positive findings, randomized con-trolled trials have met with little suc-cess.18,48 That is to say, although womenwith established social support networktend to have a reduced risk of adversepregnancy outcomes, providing socialsupport services (such as home visits andphone calls from midwives or ‘‘familyworkers’’) to women at risk does notproduce this same protective effect. Per-haps the most obvious explanation is thatit is impossible to emulate the well-estab-lished relationships and support given bya network of friends and family in arandomized trial. But it is also plausiblethat these trials fail because the high-riskwomen recruited into them have intrinsicbiologic or pervasive psychosocial risk
344 Hobel et al

factors that are not addressed by simplesocial support. Finally, these interventionstudies are subject to the same issues ofassessment discussed earlier, namely thatrather than focusing solely on acute stres-sors (as assessed by a life events checklist),researchers need to take a broader, morelong-term view of stress, looking atchronic stressors (eg, crowding, lack ofresources, marital strain) and individual-level traits and experiences (eg, perceivedstress, resilience, and commitment to thepregnancy), as well as community-levelstressors (eg, safety, access to resources).
Given the somewhat discouragingresults of the limited body of work oninterventions to reduce psychosocialstress and improve birth outcomes, it isdifficult to make simple, unequivocal re-commendations to clinicians. The mostpromising approaches would include psy-chosocial assessment in every trimesteras part of standard care for all expectantmothers. Ideally, clinicians should be pre-pared to follow-up on these assessmentswith referrals to and information on spe-cific local resources available to pregnantwomen, including food stamps programs,Special Supplementation Nutrition Pro-gram for Women, Infants, and Children(WIC), women’s shelters, medical assis-tance programs, smoking cessationprograms, and counseling services. Re-laxation therapies, ranging from yoga tomeditation may also be of benefit andclinicians are advised to make informa-tion on accessible, low-cost options avail-able to their patients.
Identifying and trying to reduce psy-chosocial stress levels in expectantmothers may also exert indirect effectson pregnancy outcomes by influencinghealth behaviors. For example, as dis-cussed, one of the strongest predictors ofboth LBW and preterm birth is smoking.Given that smoking is often linked tostress and depression, helping pregnantwomen to reduce their psychosocial stressload may also promote smoking cessa-
tion. For this reason, questions on andcounseling related to tobacco use shouldbe included in standard psychosocialassessments during pregnancy.
Similarly, stress can influence eatinghabits, which in turn, impact fetal growthand risk of preterm birth. Strong evidencehas emerged, for instance, that fasting orskipping meals periodically during preg-nancy is associated with preterm birth,most likely due to the resulting increasein maternal CRH levels (reviewed inHobel and Culhane43). Interventions toreduce psychosocial stress may have theancillary impact of normalizing food in-take and improving eating habits, therebyreducing the risk of preterm birth.Although changing health behaviors isnot necessarily the primary goal of psy-chosocial stress interventions, it can onlyhelp improve pregnancy outcomes. Phy-sicians should include questions regardinghealth behaviors (including smoking, sub-stance use, and nutrition) in every trimesteras part of standard prenatal care.
What is the Future forPreventing Adverse BirthOutcomes Associated WithPsychosocial Stress?Unfortunately, what emerges from re-search to date is that the current systemof prenatal care is inadequate to improveoutcomes in the high-riskwomen atwhichthey are primarily directed. Rather thanthe current approach, aimed at identify-ing and treating pregnancies that are al-ready considered high-risk, an emphasison primary prevention would shift thefocus to how we can create environmentsand support systems that promote healthywomen and by extension, healthy preg-nancies. From this perspective, the seedsfor a healthy pregnancy are sown longbefore conception and are dependenton women’s health care throughout life.As Lu and Halfon20 suggest, to improve
Psychosocial Stress and Pregnancy Outcome 345

pregnancy outcomes, women’s healthcare needs to be integrated across the lifecourse, from ‘‘womb to tomb.’’ Interest-ingly, from this perspective, althoughprenatal interventions aimed at reducingpsychosocial stress occur too late to haveany immediate effect on pregnancy out-come, theremay bemore long-term, inter-generational benefits.
Returning to the concept of allostaticload, if women’s health across the lifecourse contributes to their likelihood ofhaving a successful pregnancy, it followsthat stressors and risk factors throughoutlife can have a significant, cumulativeeffect as well. With physiology and stressreactivity thus shaped over the course ofdecades, the idea of limiting prenatal careto the 9 months immediately before birthseems insufficient. Compounding the pro-blem is that while current pregnancyinterventions tend to address single riskfactors, evidence suggests that both LBWand preterm birth are complex, multifac-torial outcomes, deriving from a combi-nation of exposures interacting atdifferent points across the life course.Given these complicating factors, it is nowonder that most efforts to improve birthoutcomes have failed thus far.
Ultimately, major research, publichealth, and policy initiatives beyond thepurview of individual clinicians will needto be implemented to effect this transitionto a life course perspective on pregnancyand adverse outcomes. Ideally, implemen-tation of this perspective would lead togreater longitudinal and contextual inte-gration of clinical and public health inter-ventions. Such an approach is essentialfor narrowing the well-documentedand insufficiently unexplained racial dis-parities in birth outcomes that often putminority children at an early life disad-vantage. Greater attention to women’shealth across the life course would likelynot only improve birth outcomes, further-more, but would promote intergenera-tional health and have positive effects
on the broader health of families andcommunities.
References1. Mathews TJ, Menacker F, MacDorman
MF. Infant mortality statistics from the2002 period.MonVital Stat Rep. 2004;53:1–29.
2. Russell RB, Green NS, Steiner CA, et al.Cost of hospitalization for preterm andlow birth weight infants in the UnitedStates. Peds. 2007;120:e1–e9.
3. Goldenberg RL, Iams JD, Mercer BM,et al. The preterm prediction study: thevalue of new vs. standard risk factors inpredicting early and all spontaneous pre-term births. NICHD MFMU Network[see comment].AmJPubHealth. 1998;88:233–238.
4. Glynn LM, Wadhwa PD, Dunkel-Schet-ter C, et al. When stress happens matters:effects of earthquake timing on stressresponsivity in pregnancy [see comment].Am J Obstet Gynecol. 2001;184:637–642.
5. Lederman SA, Rauh V, Weiss L, et al.The effects of the World Trade Centerevent on birth outcomes among termdeliveries at three lower Manhattan hos-pitals.EnvironHealth Perspectt 2004;112:1772–1778.
6. Levi R, Lundberg U, Hanson U, et al.Anxiety during pregnancy after the Cher-nobyl accident as related to obstetricoutcome. J Psychosom Obstet Gynaecol.1989;10:221–230.
7. HedegaardM, Henriksen TB, Sacher NJ,et al. Do stressful life events affect dura-tion of gestation and risk of pretermdelivery? Epidemiology. 1996;7:339–345.
8. Dole N, Savitz DA, Hertz-Picciotto I,et al. Maternal stress and preterm birth.Am J Epidemiol. 2003;157:14–24.
9. Lobel M, Dunkel-Schetter C, ScrimshawSC. Prenatal maternal stress and prema-turity: a prospective study of socioecono-mically disadvantaged women. HealthPsychol. 1992;11:32–40.
10. Paarlberg KM. Psychosocial factorsand pregnancy outcome: a review withemphasis on methodological issues.J Psychosom Res. 1995;29:563–595.
346 Hobel et al
11. Hedegaard M, Henriksen TB, Sabroe S,et al. Psychological distress in pregnancyand preterm delivery [see comment]. BrMed J. 1993;307:234–239.
12. Wadhwa PD, Sandman CA, Porto M,et al. The association between prenatalstress and infant birth weight and gesta-tional age at birth: a prospective investi-gation. Am J Obstet Gynecol. 1993;169:858–865.
13. Albuquerque CA, Smith KR, Johnson C,et al. Influence of maternal tobaccosmoking during pregnancy on uterine,umbilical and fetal cerebral artery bloodflows. Early Hum Develop. 2004;80:31–42.
14. Paarlberg KM, Vingerhoets AJ, Passch-ier J, et al. Psychosocial predictors oflow birthweight: a prospective study.Br J Obstet Gynaecol. 1999;106:834–841.
15. Grjibovski A, Bygren LO, Svartbo B,et al. Housing conditions, perceivedstress, smoking, and alcohol: determi-nants of fetal growth in Northwest Rus-sia. Acta Obstet Gynecol Scand. 2004;83:1159–1166.
16. Pritchard CW, Teo PY. Preterm birth,low birthweight and the stressfulness ofthe household role for pregnant women.Soc Sci Med. 1998;38:89–96.
17. Feldman PJ, Dunkel-Schetter C, SandmanCA, et al. Maternal social support predictsbirth weight and fetal growth in humanpregnancy. Psychosom Med. 2000;62:715–725.
18. Hoffman S, Hatch MC. Stress, socialsupport and pregnancy outcome: a reas-sessment based on recent research [Re-view] [144 refs]. Paediatr PerinatEpidemiol. 1996;10:380–405.
19. Stewart JA. The detrimental effects ofallostasis: allostatic load as a measureof cumulative stress [Review] [140 refs].J Physiol Anthropol. 2006;25:133–145.
20. Lu MC, Halfon N. Racial and ethnicdisparities in birth outcomes: a life-courseperspective [see comment] [Review]. [124refs]. M Child Health J. 2003;17:13–30.
21. Minino AM, Arias E, Kochanek KD,et al. Deaths: final data for 2000. NatlVital Stat Rep. 2002;50:1–119.
22. Geronimus AT. Black/white differencesin the relationship of maternal age to
birthweight: a population-based test ofthe weathering hypothesis. Soc Sci Med.1996;42:589–597.
23. Shannon M, King TL, Kennedy HP.Allostasis: a theoretical framework forunderstanding and evaluating perinatalhealth outcomes [Review] [78 refs].JOGNN. 2007;36:125–134.
24. Goldenberg RL, Hickey CA, Cliver SP,et al. Abbreviated scale for the assessmentof psychosocial status in pregnancy:development and evaluation.Acta ObstetGynecol Scand. 1997;165S:19–29.
25. Hobel CJ. Stress and preterm birth [Re-view] [159 refs]. Clin Obstet Gynecol.2004;47:856–880.
26. DiPietro JA, Ghera MM, Costigan K,et al. Measuring the ups and downsof pregnancy stress. J Psychosom ObstetGynecol. 2004;25:189–201.
27. Dominguez TP, Schetter CD, MancusoR, et al. Stress in African American preg-nancies: testing the roles of various stressconcepts in prediction of birth outcomes.Ann Behav Med. 2005;29:12–21.
28. Messer LC, Dole N, Kaufman JS, et al.Pregnancy intendedness, maternal psy-chosocial factors and preterm birth. MatChild Health J. 2005;9:403–412.
29. CochraneR,RobertsonA. The life eventsinventory: a measture of the relative se-verity of psychosocial stressors. J Psycho-som Res. 1973;17:135–139.
30. Spielberger CD, Gorusch TC, LusheneRE. The State Trait Anxiety Inventory.Palo Alto, CA: Consulting PsychologistsPress; 1970.
31. Radloff L. A self-report depression scalefor research in the general population.Appl Psych Meas. 1997;1:385–401.
32. Cohen S, Kamarck T, Mermelstein R.A global measure of perceived stress.J Health Soc Behav. 1983;24:385–396.
33. The American College of Obstetriciansand Gynecologists. Psychosocial risk fac-tors: perinatal screening and intervention.ACOG Comm Opin. 2006;108:469–477.
34. Challis JR, Sloboda D, Matthews SG,et al. The fetal placental hypothalamic-pituitary-adrenal (HPA) axis, parturitionand post natal health [Review][39 refs]. Mol Cell Endocrinol. 2001;185:135–144.
Psychosocial Stress and Pregnancy Outcome 347
35. Hobel CJ, Arora CP, Korst LM. Cortico-trophin-releasing hormone and CRH-bindingprotein.Differencesbetweenpatientsat risk for preterm birth and hypertension.Ann N Y Acad Sci. 1999;897:54–65.
36. Sandman CA, Glynn L, Schetter CD,et al. Elevated maternal cortisol early inpregnancy predicts third trimester levelsof placental corticotropin releasinghormone (CRH): priming the placentalclock. Peptides. 2006;27:1457–1463.
37. Pike I. Maternal stress and fetal re-sponses: evoluntionary perspectiveson preterm delivery. J Human Biol. 2005;17:55–65.
38. McGregor JA, Jackson GM, LachelinGC, et al. Salivary estriol as risk assess-ment for preterm labor: a prospectivetrial. Am J Obstet Gynecol. 1995;173:1337–1342.
39. Seckl JR, Cleasby M, NyirendaMJ. Glu-cocorticoids, 11beta-hydroxysteroiddehydrogenase, and fetal programming[Review] [74 refs]. Kidney Int. 2000;57:1412–1417.
40. Barker DJ. Fetal origins of coronaryheart disease [Review] [38 refs]. BrMed J.1995;311:171–174.
41. Sloboda DM, Challis JR, Moss TJ, et al.Synthetic glucocorticoids: antenatal ad-ministration and long-term implications[Review] [193 refs]. Curr Pharm Des.2005;11:1459–1472.
42. Justus K, Arora C, Sandhu M, et al. Theeffect of smoking on the time course
release of catecholamines and corticotro-pin releasing hormone (CRH), adreno-corticotropin hormone (ACTH) andcortisol in pregnancy. J Soc GynecolInvest. 2005;2:S368A.
43. Hobel C, Culhane J. Role of psycho-social and nutritional stress on poorpregnancy outcome [Review] [120 refs].J Nutr. 2003;133(5 Suppl 2):1709S–1717S.
44. Narendran S, Nagarathna R, NarendranV, et al. Efficacy of yoga on pregnancyoutcome. J Altern Complementary Med.2005;11:237–244.
45. Teixeira J, Martin D, Prendiville O,et al. The effects of acute relaxation onindices of anxiety during pregnancy.J Psychosom Obstet Gynecol. 2005;26:271–276.
46. Wilkinson DS, Korenbrot CC, Greene J.A performance indicator of psycho-social services in enhanced prenatal careof Medicaid-eligible women [see com-ment]. Matern Child Health J. 1998;2:131–143.
47. Zimmer-Gembeck MJ, Helfand M. Lowbirthweight in a public prenatal care pro-gram: behavioral and psychosocial riskfactors and psychosocial intervention.Soc Sci Med. 1996;43:187–197.
48. Kramer MS, Goulet L, Lydon J, et al.Socio-economic disparities in pretermbirth: causal pathways and mechanisms.Paediatr Perinat Epidemiol. 2001;15S2:104–123.
348 Hobel et al