obstetric and neonatal outcome of multifetal pregnancy reduction
TRANSCRIPT
ORIGINAL ARTICLE
Obstetric and neonatal outcome of multifetal
pregnancy reduction
Abdel Baset F. Mohammed a,*, Ibrahim Farid b, Badreldeen Ahmed c,
Ehab Abdel Ghany c
a Departments of Obstetrics and Gynecology, Minia University, Egyptb Departments of Obstetrics and Gynecology, Zagazig University, Egyptc Women’s Hospital, Hamad Medical Corporation, Qatar
Received 27 October 2014; revised 14 January 2015; accepted 25 January 2015
KEYWORDS
Multifetal pregnancy reduc-
tion;
Obstetric and neonatal
outcomes
Abstract Objective: To evaluate obstetric and neonatal outcomes of multifetal pregnancy reduc-
tion (MFPR) in patients with higher order multiple pregnancies (HOMP) compared to those man-
aged expectantly.
Methods: Forty patients with HOMP (quadruplets or more) were included. Seventeen patients
were reduced and 23 patients were non-reduced as per patient’s choice. Obstetric and neonatal out-
come measures were compared.
Results: The mean gestational age at the procedure was 12.8 ± 0.9 weeks. Five cases out of fif-
teen were reduced to triplets and 10 cases were reduced to twins. The mean total volume of KCL
used was 5.4 ± 1.3 ml and the mean number of attempts was 1 ± 0.4. The most frequent compli-
cations were maternal anxiety and abdominal pain (29.4%). The procedure failed in two cases due
to abdominal pain and maternal distress. The differences regarding preterm labor, gestational age at
delivery, mode of delivery and neonatal birth weight were statistically significant. This was in favor
of MFPR procedure.
Conclusion: MFPR procedure seems to be good and acceptable option for patients with HOMP
but not totally safe.
� 2015 The Authors. Production and hosting by Elsevier B.V. on behalf of Middle East Fertility Society.
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-
nd/4.0/).
1. Introduction
The incidence of multifetal pregnancies has increased over the
last few decades – largely a result of assisted reproductive tech-
nology (ART) (1,2). This is significant as the rates of fetal and
maternal complications are higher in multifetal pregnancies,
with this risk increasing with the number of fetuses. This trend
has necessitated the development of fetal reduction to manage
* Corresponding author. Mobile: +20 00974 55458229.
E-mail address: [email protected] (A.B.F. Mohammed).
Peer review under responsibility of Middle East Fertility Society.
Production and hosting by Elsevier
Middle East Fertility Society Journal (2015) xxx, xxx–xxx
Middle East Fertility Society
Middle East Fertility Society Journal
www.mefsjournal.orgwww.sciencedirect.com
http://dx.doi.org/10.1016/j.mefs.2015.01.0011110-5690 � 2015 The Authors. Production and hosting by Elsevier B.V. on behalf of Middle East Fertility Society.This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Please cite this article in press as: Mohammed ABF et al. Obstetric and neonatal outcome of multifetal pregnancy reduction, Middle East Fertil Soc J (2015), http://dx.doi.org/10.1016/j.mefs.2015.01.001

multifetal pregnancies, in order to improve perinatal survival
and reduce maternal risk. Although fetal reduction techniques
have emerged to be effective in improving pregnancy out-
comes, this has been an area of great controversy where ethical
and legal issues have not been clearly addressed (3).
Fetal reduction may be indicated in various circumstances.
In selective termination, (one or more) anomalous fetuses in a
multifetal pregnancy are terminated. In contrast, multifetal
pregnancy reduction (MFPR) reduces the number of fetuses
in gestation in order to improve the chances of healthy survival
in the remaining conceptuses and to reduce the hazards to the
mother (4). Apart from optimization of outcome, fetal reduc-
tion may be conducted for social reasons based on the patient’s
request.
Pregnancy outcome is improved when higher-order multife-
tal pregnancies [HOMP] are reduced (5). Fetal reduction has
been shown to decrease the incidence of miscarriage, prematu-
rity and low-birth-weight infants. However, fetal reduction
intervention also has inherent risk, with recent series citing
an overall pregnancy loss rate of 4.7% (6). This retrospective
study was conducted to evaluate the obstetric and neonatal
outcomes of MFPR procedure in patients with HOMP com-
pared to those managed expectantly in a local tertiary unit.
2. Patients and methods
This retrospective study was conducted in the Feto-Maternal
Unit (FMU), Women’s Hospital, Hamad Medical Corpora-
tion in Qatar after being accepted from the local research com-
mittee. The study population included all women with HOMP
(quadruplets or more) conceived after ART (ovulation induc-
tion, intra-uterine insemination or in vitro fertilization) during
the period from 2002 to 2012. Women included in this study
were identified using the FMU electronic database. Case
records were reviewed regarding demographic and clinical data
and details of MFPR procedure. Prior to the procedure
patients were counseled and all possible risks were explained
to them. According to patient choice, they were categorized
into those who underwent procedure (reduced group;
n= 17) and those who declined (non-reduced group;
n= 23). A written informed consent was obtained from all
patients who underwent the procedure.
Prior to the procedure, an ultrasound examination was per-
formed to know the number of embryos with heartbeats, to
determine the chorionicity, to establish the relationship of
the gestational sacs to each other and to determine which of
the fetuses are most accessible to needle insertion.
The procedure was performed trans-abdominal (TA) by
injection of 2–3 ml of potassium chloride (2 meq/ml) into the
fetal thorax using a 22 gauge spinal needle under ultrasound
guidance. Potassium chloride was injected slowly so as not
to dislodge the needle tip. The cardiac activity is carefully
observed for at least 2 min and if cardiac activity persists, more
potassium chloride is injected. Asystole was usually seen with-
in 1–2 min of injection of potassium chloride and total proce-
dural time is typically less than five minutes. Additional fetuses
could be reduced with the same needle puncture or, more com-
monly, with a separate needle stick.
The procedure was performed between 12 and 14 weeks of
gestation. Out of the 17 cases, 16 of them were done at the
beginning of the second trimester, and the last one was done
in the first trimester. Selection of fetuses to be reduced was
not based on genetic evaluation, but mainly on chorionicity
and ease of procedure. The fetus (es) reduced are those that
are most easily accessible, usually those closest to the anterior
uterine wall and/or the fundus while those above the cervix
were avoided. Procedures were done by FMU team, not by
single operators.
After the procedure, the patients were observed for one
hour for pain, leaking, bleeding or any other complication
related to the procedure. A repeat ultrasound was performed
one hour after the procedure to confirm asystole in the reduced
fetus (es) and cardiac activity in the non-reduced fetus (es).
All patients were scheduled for ultrasound examination for
fetal well-being and cervical length assessment 2 weeks after
the procedure. Regular follow-up in FMU had been squealed
for them. Maternal data, sonographic findings and MFPR
procedure details were entered into a computer database.
Different outcome measures were compared between the
two groups including miscarriage (pregnancy loss before
24 weeks of gestation), early preterm delivery (prior to
32 weeks of gestation) and median gestational age at delivery.
Data were statistically analyzed. Chi-square, Fischer’s exact
and Mann–Whitney U-tests were used as appropriate to exam-
ine the significance of differences between the two groups for
pregnancy outcomes. Significance was assumed at P < 0.05
and two-tailed P-values are reported.
3. Results
Forty patients with HOMP (quadruplets or more) were identi-
fied and included in this study. Reduced pregnancies (n = 17)
were compared to non-reduced (n = 23) ones regarding differ-
ent outcome measures. All patients underwent the procedure
completed the follow-up in our hospital and included in the
analysis. The demographic and clinical data of patients are
reported in Table 1. There were no significant differences
between the two groups regarding demographic and clinical
data. The range of fetal sacs in both groups was 4–7 in reduced
group and 4–6 in the non-reduced group.
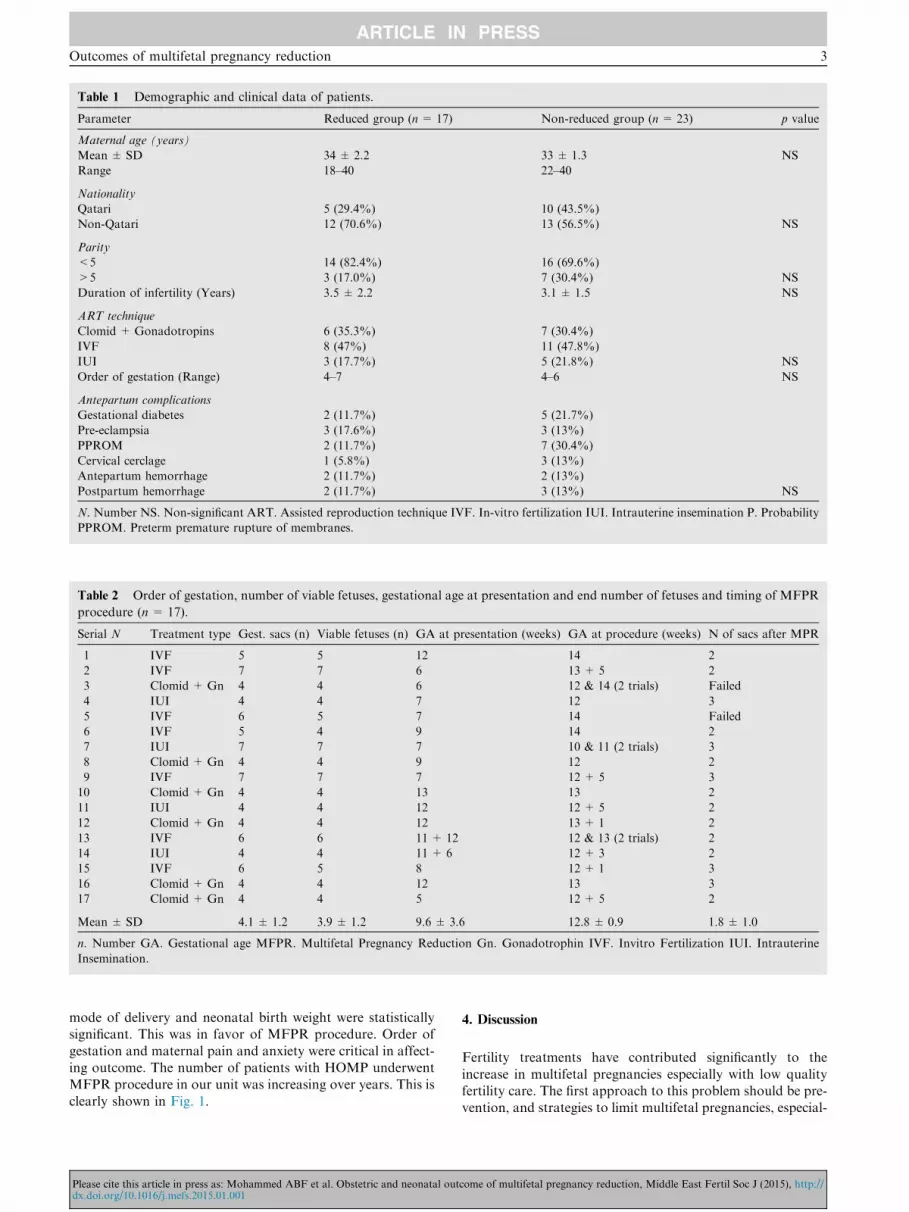
The details of MFPR procedure including the order of ges-
tation, number of viable fetuses at presentation, gestational
age at presentation, timing of the procedure and end number
of fetuses are shown in Table 2. The mean gestational age at
the procedure was 12.8 ± 0.9 weeks. Five cases out of fifteen
were reduced to triplets and 10 cases were reduced to twins.
The method used for MFPR, number of attempts, total vol-
ume of KCL used and possible complications associated with
the procedure were reported in Table 3. The mean total vol-
ume of KCL used was 5.4 ± 1.3 ml and the mean number of
attempts of the procedure was 1 ± 0.4. The most frequent
complications were maternal anxiety and abdominal pain
which occurred in 5 patients (29.4%). The procedure failed
in two cases; the first case after 2 attempts due to abdominal
pain and maternal distress and the second one after only one
attempt due to abdominal pain. Multifetal pregnancy increases
the mother’s risk of developing pregnancy complications.
Table 3 also demonstrates the maternal complications encoun-
tered during pregnancy after MFPR procedure.
Different obstetric outcome measures were compared
between the two groups (Table 4). The differences regarding
incidence of preterm labor, median gestational age at delivery,
2 A.B.F. Mohammed et al.
Please cite this article in press as: Mohammed ABF et al. Obstetric and neonatal outcome of multifetal pregnancy reduction, Middle East Fertil Soc J (2015), http://dx.doi.org/10.1016/j.mefs.2015.01.001
mode of delivery and neonatal birth weight were statistically
significant. This was in favor of MFPR procedure. Order of
gestation and maternal pain and anxiety were critical in affect-
ing outcome. The number of patients with HOMP underwent
MFPR procedure in our unit was increasing over years. This is
clearly shown in Fig. 1.
4. Discussion
Fertility treatments have contributed significantly to the
increase in multifetal pregnancies especially with low quality
fertility care. The first approach to this problem should be pre-
vention, and strategies to limit multifetal pregnancies, especial-
Table 1 Demographic and clinical data of patients.
Parameter Reduced group (n = 17) Non-reduced group (n = 23) p value
Maternal age (years)
Mean ± SD 34 ± 2.2 33 ± 1.3 NS
Range 18–40 22–40
Nationality
Qatari 5 (29.4%) 10 (43.5%)
Non-Qatari 12 (70.6%) 13 (56.5%) NS
Parity
<5 14 (82.4%) 16 (69.6%)
>5 3 (17.0%) 7 (30.4%) NS
Duration of infertility (Years) 3.5 ± 2.2 3.1 ± 1.5 NS
ART technique
Clomid + Gonadotropins 6 (35.3%) 7 (30.4%)
IVF 8 (47%) 11 (47.8%)
IUI 3 (17.7%) 5 (21.8%) NS
Order of gestation (Range) 4–7 4–6 NS
Antepartum complications
Gestational diabetes 2 (11.7%) 5 (21.7%)
Pre-eclampsia 3 (17.6%) 3 (13%)
PPROM 2 (11.7%) 7 (30.4%)
Cervical cerclage 1 (5.8%) 3 (13%)
Antepartum hemorrhage 2 (11.7%) 2 (13%)
Postpartum hemorrhage 2 (11.7%) 3 (13%) NS
N. Number NS. Non-significant ART. Assisted reproduction technique IVF. In-vitro fertilization IUI. Intrauterine insemination P. Probability
PPROM. Preterm premature rupture of membranes.
Table 2 Order of gestation, number of viable fetuses, gestational age at presentation and end number of fetuses and timing of MFPR
procedure (n= 17).
Serial N Treatment type Gest. sacs (n) Viable fetuses (n) GA at presentation (weeks) GA at procedure (weeks) N of sacs after MPR
1 IVF 5 5 12 14 2
2 IVF 7 7 6 13 + 5 2
3 Clomid + Gn 4 4 6 12 & 14 (2 trials) Failed
4 IUI 4 4 7 12 3
5 IVF 6 5 7 14 Failed
6 IVF 5 4 9 14 2
7 IUI 7 7 7 10 & 11 (2 trials) 3
8 Clomid + Gn 4 4 9 12 2
9 IVF 7 7 7 12 + 5 3
10 Clomid + Gn 4 4 13 13 2
11 IUI 4 4 12 12 + 5 2
12 Clomid + Gn 4 4 12 13 + 1 2
13 IVF 6 6 11 + 12 12 & 13 (2 trials) 2
14 IUI 4 4 11 + 6 12 + 3 2
15 IVF 6 5 8 12 + 1 3
16 Clomid + Gn 4 4 12 13 3
17 Clomid + Gn 4 4 5 12 + 5 2
Mean ± SD 4.1 ± 1.2 3.9 ± 1.2 9.6 ± 3.6 12.8 ± 0.9 1.8 ± 1.0
n. Number GA. Gestational age MFPR. Multifetal Pregnancy Reduction Gn. Gonadotrophin IVF. Invitro Fertilization IUI. Intrauterine
Insemination.
Outcomes of multifetal pregnancy reduction 3
Please cite this article in press as: Mohammed ABF et al. Obstetric and neonatal outcome of multifetal pregnancy reduction, Middle East Fertil Soc J (2015), http://dx.doi.org/10.1016/j.mefs.2015.01.001

ly HOMP, should be practiced by all physicians who treat
women for infertility (7).
Multifetal pregnancy reduction should be considered for
any pregnancy with three or more fetuses, as there is good evi-
dence that it improves pregnancy outcome for survivors. But it
must be emphasized that this still is fraught with dangers to
pregnancy and not always accepted when compared to single-
ton pregnancy resulting from good quality fertility care. In
fact, an International Federation of Gynecologists and Obste-
tricians (FIGO) Committee Report stated that, ‘‘Multiple
pregnancy of an order of magnitude higher than twins involves
great danger for the woman’s health and also for her fetuses,
which are likely to be delivered prematurely with a high risk
of either dying or suffering damage’’ and ‘‘where such preg-
nancies arise, it may be considered ethically preferable to
reduce the number of fetuses rather than to do nothing’’ (8).
The rate of MFPR Procedure increased steadily in
Women’s hospital, Hamad Medical Corporation over the last
few years since the establishment of FMU at 2002 as a com-
mon sequel of overly aggressive infertility therapy, increased
patient and physician awareness of the availability of the pro-
cedure and lack of guidelines appears to have contributed to
more aggressive infertility treatments and more subsequent
MFPR procedures. Recently, local Hospital guidelines on fer-
tility care were developed but still not well implemented and
not reflected on prevention of HOMP.
All patients included in this study had suffered from infer-
tility for a significant time ranging from one to four years.
Table 3 The method used for MFPR, number of attempts, volume of KCL used and possible complications associated with the
procedure.
Case N Method used KCL volume (ml) N of
attempts
Reason
of failure
Procedure related
complications
Maternal complications
1 TA 4 1 Nil Preterm labor
2 TA 5 1 Nil APH 26 weeks
3 TA Unknown 2 Maternal distress Maternal pain – failed Miscarriage 15 weeks
4 TA 5 2 Nil Severe PET, IUGR in twin who
shares the placenta with the reduced twin
5 TA 4 1 Painful procedure Maternal pain – failed Severe PET, PPH
6 TA 4 1 Nil PPROM and preterm labor
7 TA 6 2 Maternal pain Severe hyper emesis
8 TA 4 1 Nil Nil
9 TA 10 1 Nil GDM, preterm labor
10 TA 3 1 Nil PET
11 TA 3 2 Nil IGTT
12 TA 4 2 Miscarriage 17 weeks
13 TA 4 2 Maternal pain exhaustion PPROM, APH, preterm labor
14 TA 3.5 1 Nil Nil
15 TA 3 1 Nil Preterm labor
16 TA 3 1 Nil Preterm labor 24 weeks
17 TA 3 1 Maternal pain Nil
N. Number TA. Transabdominal PPROM. Preterm premature rupture of membranes APH. Antepartum hemorrhage PPH. Postpartum
hemorrhage PET. Pre-eclampsia GDM. Gestational diabetes IGTT. Impaired GTT. IUGR. Intrauterine growth restriction.
Table 4 Obstetric outcome measures in the two groups.
Parameter Reduced group (n= 17) Nonreduced group (n = 23) P value
Miscarriage (<24 weeks)
N% 2 (11.7%) 3 (13%)
GA 16 ± 2.5 17.3 ± 3.5 NS
Preterm labor 10 (58.8%) 20 (87%) <0.001
GA at time of delivery
Median 35.6 ± 2.5 31.6 ± 1.9 <0.01
Range 26–39 24–35
Mode of delivery
Normal Delivery 5/17 (29.4%) 0
Cesarean section 10/17 (58.8%) 20/23 (87%) <0.001
Neonatal birth weight 1916 ± 320 1320 ± 280 <0.05
IUGR 3 (17.6%) 6 (26.1%) NS
Cerebral palsy 1 (5.8%) 3 (13%) NS
Neonatal mortality 2 (11.7%) 1 (4.3%) NS
N. Number P. Probability IUGR. Intrauterine growth restriction GA. Gestational age.
4 A.B.F. Mohammed et al.
Please cite this article in press as: Mohammed ABF et al. Obstetric and neonatal outcome of multifetal pregnancy reduction, Middle East Fertil Soc J (2015), http://dx.doi.org/10.1016/j.mefs.2015.01.001

The patients and their husbands have three difficult options to
choose; Termination of the pregnancy and start a new one
which is an unlikely choice for a couple who has suffered years
of infertility and is probably going through great emotional and
financial expenses. A second choice is to continue the HOMP,
accepting the high possibility of having a miscarriage or a very
preterm delivery and the increased risk for perinatal mortality
and morbidity. The third option is the MFPR, where the num-
ber of fetuses is reduced in order to lower the likelihood of pre-
term delivery and optimize the chance of a successful outcome.
In a multichorionic pregnancy, the fetus (es) reduced are
those that are most easily accessible, usually those closest to
the anterior uterine wall and/or the fundus. The fetus above
the cervix is avoided whenever possible because of a hypo-
thetical increased risk for infection or uterine irritability if that
fetus was reduced. However, if a fetus has a lagging crown
rump length, a significantly smaller sac, markers of aneu-
ploidy, or an obvious anomaly, then that fetus is preferentially
reduced since these findings are associated with adverse preg-
nancy outcome (miscarriage, fetal aneuploidy) (8,9). In this
study, MFPR was not done selectively, as we do not have
the ability of genetic testing. It was based on chorionicity
and ease of the technique.
The majority of centers, which perform the technique, uti-
lize TA approach with intra-thoracic injection of potassium
chloride under ultrasound guidance (10,11). All procedures
in our unit were performed utilizing TA approach. A trans-cer-
vical or a trans-vaginal approach can be used, but both have
been associated with increased post-procedural pregnancy loss
rates when compared with the TA approach; therefore, these
approaches are usually reserved for situations in which the
TA approach is not technically feasible (9).
Maternal pain and anxiety were the main complications
related to the procedure in this study. It was noted in five
patients and the procedure was abandoned to another session.
The procedure failed in two patients because of this pain. The
procedure was done without local anesthesia or sedation. This
may be a favorable option to avoid maternal pain and anxiety
and increase chance of success of the procedure. Other compli-
cations encountered were not related to the procedure but
related to the risks of multifetal pregnancy.
Regarding the timing of the procedure, sixteen of our
patients had the procedure done at the beginning of the second
trimester and one was done in the first trimester. The literature
reviews say fetal reduction in most centers is performed
between 10 and l4 weeks’ gestation. Before 10 weeks it is tech-
nically more difficult because of the small size of the fetuses
and greater distance from the maternal abdominal wall to
the fetuses. If fetal reduction was performed too late the risk
of preterm labor may be higher (12). To verify it, Lynch and
Berkowitz (13) in 1993, after reporting two hundred completed
cases say there is no advantage in delaying the procedure
beyond the l2th week of gestation, because if all fetuses are
alive and are of appropriate size at that time, spontaneous loss-
es are not likely in the next few weeks. Moreover the later in
pregnancy the termination is not recommended, the more
probable it is that fetal resorption will be incomplete, and
may be the rare chance, that maternal disseminated intravascu-
lar coagulation will develop.
The results of the present study suggest favorable obstetric
outcomes after MFPR procedure in terms of incidence of pre-
term labor, median gestational age at delivery, mode of deliv-
ery and neonatal birth weight. This was in agreement with
previous studies and meta-analysis (6,13–19). However, the
risk of miscarriage before 24th gestational week following
MFPR has been a controversial issue. While an earlier study
reported that risk of miscarriage was increased after the proce-
dure (20), a more recent review reported similar risk of preg-
nancy loss before 24 weeks for reduced and non-reduced
pregnancies (21). Our findings are in accordance with the latter
report and with a recent study mostly with similar results (22).
Available data on MFPR, do not support an increase in the
risk of miscarriage before 24 weeks when MFPR is performed
by experienced operators and when compared with those who
declined the procedure. It is suggested that the resorbing dead
fetoplacental tissue rather than the procedure itself could cause
increased risk of pregnancy loss before 24th gestational week
following the procedure (20).
Since a favorable obstetric outcome is reported in our study
when compared to those who declined the procedure, it
appears that the mechanism causing the spontaneous loss of
one embryo did not affect the growth of remaining embryos
and pregnancy outcome. A uterine factor causing embryonic
loss is unlikely to be present in this situation. The presence
of a uterine factor could be expected to cause the loss of other
remaining embryos as well (21).
The management of multifetal pregnancy is difficult. While
fetal reduction is a possible management option, it should not
be utilized as a safety net in fertility treatment. Prevention of
HOMPs must be the primary objective. In addressing complex
medical issues such as fetal reduction, knowledge of the rele-
vant ethical and legal implications besides medical skill compe-
tency are important. Nevertheless, while knowledge makes for
good medical practice, it is the upholding of compassion,
fidelity and humanity as common denominators across time
and cultures that should be the ethical aspirations of health
professionals (3,23).
This study has limitations in terms of small number of
patients as HOMP is rare and fetal reduction for a couple suf-
fered from infertility for long time is a difficult choice. Another
limitation also is the absence of control group from singleton
or twin pregnancy for comparison regarding pregnancy
outcome.
Figure 1 Number of MPR procedures over the years.
Outcomes of multifetal pregnancy reduction 5
Please cite this article in press as: Mohammed ABF et al. Obstetric and neonatal outcome of multifetal pregnancy reduction, Middle East Fertil Soc J (2015), http://dx.doi.org/10.1016/j.mefs.2015.01.001
In conclusion, MFPR procedure seems to be good and
acceptable option for patients with HOMP but not totally safe.
Patients should be thoroughly counseled before the procedure.
Local hospital guidelines should be implemented to limit the
number of embryos transferred and avoid occurrence of
HOMP in the first place. A large randomized controlled study
is recommended.
Conflict of interest
The authors report no conflict of interests.
Acknowledgments
The authors thank all members of Fetomaternal Unit, WH,
HMC; Dr Najat Kenyab, Dr Najah Saleh, Dr Zeina Al Man-
souri, Dr Sawsan Al Obaidy, Dr Abdallah Al Ibrahim, Dr
Mariam Bleushi.
References
(1) Chia KS, Lee JJ, Cheung P, et al. Twin births in Singapore: a
population-based study using the National Birth Registry. Ann
Acad Med Singapore 2004;33:195–9.
(2) Bebbington M. Selective reduction in multiple gestations. Best
Pract Res Clin Obstet Gynaecol 2014;28(2):239–47.
(3) Cheong MA, Kian CS. Application of legal principles and
medical ethics: multifetal pregnancy and fetal reduction. Singa-
pore Med J 2014;55(6):298–301. http://dx.doi.org/10.11622/
smedj.2014077.
(4) Howie PW. Selective reduction: medical aspects. In: Templeton
AA, Cuisine DJ, editors. Reproductive medicine and the law.
London: Churchill Livingstone; 1990. p. 25–32.
(5) Evans MI, Dommergues M, Wapner RJ, et al. International,
collaborative experience of 1789 patients having multifetal
pregnancy reduction: a plateauing of risks and outcomes. J Soc
Gynecol Investig 1996;3:23–6.
(6) Stone J, Eddleman K, Lynch L, Berkowitz RL. A single center
experience with 1000 consecutive cases of multifetal pregnancy
reduction. Am J Obstet Gynecol 2002;187:116–7.
(7) American college of obstetricians and gynecologists. ACOG
Committee opinion no. 553: multifetal pregnancy reduction.
Obstet Gynecol. 2013;121(2 Pt 1):405–12.
(8) FIGO Committee for the Ethical Aspects of Human Reproduc-
tion and Women’s Health. Ethical recommendations on multiple
pregnancy and multifetal reduction. Int J Gynaecol Obstet
2006;92(3):331.
(9) Evans MI, Goldberg JD, Dommergues M, Wapner RJ, Lynch L,
Dock BS, Horenstein J, Golbus MS, Rodeck CH, Dumez Y.
Efficacy of second-trimester selective termination for fetal abnor-
malities: international collaborative experience among the world’s
largest centers. Am J Obstet Gynecol 1994;171(1):90–4.
(10) Itskovits-Eldor J, Drugan A, Levron J, Thaler I, Bromdes J.
Trans-vaginal embryo aspiration a safe method for selective
reduction in multiple pregnancies. Fertil Steril 1992;58:3515.
(11) Berkowitz RL, Lynch L, Lapiski R, Bergh P. First trimester
trans-abdominal multifetal pregnancy reduction: a report of two
hundred completed cases. Am J Obstet Gynecol 1993;69:1711.
(12) Berkowitz RL, Lynch L, Chitkara V. Selective reduction of
multifetal pregnancy in the first trimester. N Engl J Med
1988;3l8:1043–7.
(13) Lynch L, Berkowitz RL. Maternal serum alpha-fetoprotein and
coagulation profiles after multifetal pregnancy reduction. Am J
Obstet Gynecol 1993;169:987–90.
(14) Wimalasundera RC, Trew G, Fisk NM. Reducing the incidence
of twins and triplets. Best Pract Res Clin Obstet Gynaecol
2003;17(2):309–13.
(15) Evans MI, Berkowitz RL, Wapner RJ, Carpenter RJ, Goldberg
JD, Ayoub MA, Horenstein J, Dommergues M, Brambati B,
Nicolaides KH, Holzgreve W, Timor-Tritsch IE. Improvement in
outcomes of multifetal pregnancy reduction with increased
experience. Am J Obstet Gynecol 2001;184(2):97–9.
(16) Britt DW, Evans MI. Information-sharing among couples con-
sidering multifetal pregnancy reduction. Fertil Steril
2007;87(3):490–4.
(17) Stone J, Ferrara L, Kamrath J, Getrajdman J, Berkowitz R,
Moshier E, Eddleman K. Contemporary outcomes with the latest
1000 cases of multifetal pregnancy reduction (MPR). Am J Obstet
Gynecol 2008;199(4):406.e1.
(18) Sebire NJ, Sherod C, Abbas A, Snijders RJM, Nicolaides KH.
Preterm delivery and growth restriction in multifetal pregnancies
reduced to twins. Hum Reprod 1997;12(1):173–5.
(19) Badreldeen Ahmed, Al Nuggar Eman, Spalldi Barisic Lura.
Selective feticide – lessons learned and future challenges.
Gynaecol Perinatol 2009;18(4):78–82.
(20) Papageorghiou AT, Avgidou K, Bakoulas V, Sebire NJ, Nico-
laides K. Risks of miscarriage and early preterm birth in
trichorionic triplet pregnancies with embryo reduction versus
expectant management: new data and systematic review. Hum
Reprod 2006;21(7):1912–7.
(21) Wimalasundera R. Selective reduction and termination of
multiple pregnancies. Semin Fetal Neonatal Med 2010;15:327–35.
(22) Skiadas CC, Missmer SA, Benson CB, Acker D, Racowsky C.
Spontaneous reduction before 12 weeks’ gestation and
selective reduction similarly extend time to delivery in in vitro
fertilization of trichorionic–triamniotic triplets. Fertil Steril
2011;95:596–9.
(23) Cohen MH. Toward a bioethics of compassion. Ind L Rev
1995;28:667–8.
6 A.B.F. Mohammed et al.
Please cite this article in press as: Mohammed ABF et al. Obstetric and neonatal outcome of multifetal pregnancy reduction, Middle East Fertil Soc J (2015), http://dx.doi.org/10.1016/j.mefs.2015.01.001