prognostic relevance of flt3-tkd mutations in aml: the combination matters--an analysis of 3082...
TRANSCRIPT
doi:10.1182/blood-2007-05-091215Prepublished online October 26, 2007;
Ulrike Bacher, Claudia Haferlach, Wolfgang Kern, Torsten Haferlach and Susanne Schnittger matters - an analysis of 3082 patientsPrognostic relevance of FLT3-TKD mutations in AML: the combination
(3716 articles)Clinical Trials and Observations �Articles on similar topics can be found in the following Blood collections
http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#repub_requestsInformation about reproducing this article in parts or in its entirety may be found online at:
http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#reprintsInformation about ordering reprints may be found online at:
http://bloodjournal.hematologylibrary.org/site/subscriptions/index.xhtmlInformation about subscriptions and ASH membership may be found online at:
digital object identifier (DOIs) and date of initial publication. theindexed by PubMed from initial publication. Citations to Advance online articles must include
final publication). Advance online articles are citable and establish publication priority; they areappeared in the paper journal (edited, typeset versions may be posted when available prior to Advance online articles have been peer reviewed and accepted for publication but have not yet
Copyright 2011 by The American Society of Hematology; all rights reserved.20036.the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom

1
Prognostic relevance of FLT3-TKD mutations in AML:
the combination matters - an analysis of 3082 patients
Ulrike Bacher1, Claudia Haferlach2, Wolfgang Kern2, Torsten Haferlach2,
and Susanne Schnittger2*
1Bone Marrow Transplant Unit
University Hospital of Hamburg-Eppendorf
Martinistr. 52
20246 Hamburg, Germany 2MLL - Munich Leukemia Laboratory
Max-Lebsche-Platz 31
81377 Munich, Germany
Corresponding author:
*Susanne Schnittger
MLL, Munich Leukemia Laboratory
Max-Lebsche-Platz 31
81377 Munich
Phone.: 0049 89 990 17 300
Fax: 0049 89 990 17 309
Email: [email protected]
URL : www.mll-online.com
Blood First Edition Paper, prepublished online October 26, 2007; DOI 10.1182/blood-2007-05-091215
Copyright © 2007 American Society of Hematology
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom
2
Abstract
We characterized the mutation status of the FLT3 tyrosine kinase domain (FLT3-TLD)
in 3082 patients with newly diagnosed AML. FLT3-TKD mutations were detected in
147 of 3082 (4.8%) patients. Similar to the FLT3 juxtamembrane domain mutations
(FLT3-LM) there was a high correlation of FLT3-TKD mutations with normal karyotype
(88/1472; 6.0%). FLT3-TKD mutations were most frequent in the AML FAB subtypes
M5b (15/114; 13.2%), M3v (6/51; 11.8%), and M4 (39/484; 8.1%). Similar to FLT3-LM
the FLT3-TKD mutations show elevated peripheral leukocytes as compared to FLT3wt
AML. FLT3-TKD had a high incidence in cases with NPM1 mutations (23/262; 8.8%),
CEPBA mutations (6/76; 7.9%), and NRAS mutations (6/78; 7.7%). FLT3-TKD in
combination with FLT3-LM (17/594 patients; 2.9%) and KITD816 (1/44; 2.3%) was
rare. Unlike the FLT3-LM which are associated with inferior survival, prognosis was
not influenced by FLT3-TKD in the total cohort of 1720 cases, where follow-up data
were available (97 FLT3-TKD; 1623 FLT3-WT). In t(15;17)/PML-RARA with FLT3-
TKD mutations, in FLT3-LM/TKD double mutated, and in MLL-PTD/TKD double
mutated cases prognosis was unfavorably influenced by FLT3-TKD mutations. In
contrast, we found an additional favorable impact of FLT3-TKD on EFS in
prognostically favorable AML with NPM1- or CEPBA mutations.
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom

3
INTRODUCTION
Actual therapy concepts try to modify the intensitity of therapy of acute myeloid
leukemia (AML) in accordance to the individual risk of relapse. Karyotype represents
the strongest prognostic parameter in AML. However, 45% of all AML patients show a
normal karyotype and thus an intermediate prognosis.1-3 As AML with normal
karyotype is considered a heterogeneous disease with respect to molecular aspects,
the definition of suitable molecular markers for the determination of prognosis and for
minimal residual disease (MRD) detection is of increasing importance.
Mutations of the fms-tyrosine kinase (FLT3) were first described in 19974 and account
for the most frequent molecular mutations in AML.5;6 The FLT3 gene is a member of
the class III receptor tyrosine kinase family including c-kit, c-fms, and the platelet-
derived growth factor receptors.6-9 In normal bone marrow FLT3 expression is
restricted to immature hematopoietic progenitor cells and mediates stem cell
proliferation.6;8;10;11
FLT3 length mutations (FLT3-LM or FLT3-ITD for “internal tandem duplication”)
represent one of the most frequent genetic alterations in AML. They show a frequency
of 20%-27% in AML in adults9;12-16 and of 10-16% in childhood cases17;18 and are
associated with progression of myelodysplastic syndrome (MDS) to secondary AML
(s-AML).19 FLT3-LM mostly are represented by internal tandem duplications with/or
insertions or deletions in exons 11 and 12 of the human FLT3 gene on chromosome
13q12, which codes for the juxtamembrane domain of the FLT3 protein. The
mutations are heterogeneous and consist of internal tandem duplications of 6-30
amino acids resulting in an elongated FLT3 protein with constitutive PTK activity.20
These mutations lead to autophosphorylation of the receptor and result in increased
proliferation of AML cells in vitro and to a decrease of apoptosis. Constitutively active
FLT3 mutants have transforming potential in interleukin-3-dependent cells and
activate several signal transduction pathways, including STAT-5 and MAPK.21-24
FLT3-LM are highly associated with normal karyotype, t(15;17)/PML-RARA and
t(6;9)/DEK-CAN,15;16 and are prognostically unfavorable in adults12-16 and in pediatric
patients17;25;26.
In addition to the juxtamembrane domain mutations, mutations in the tyrosine kinase
domain (FLT3-TKD mutations) have been described in AML.7;9;16;27 FLT3-TKD
mutations are small mutations in the activation loop of FLT3 mostly representing point
mutations in codon D835 or deletions of codon I836. They induce constitutive tyrosine
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom
4
phosphorylation leading to activation of the receptor tyrosine kinase and are supposed
to represent gain-of-function mutations.7;22;28-32 Corresponding activation loop
mutations have been reported at position D816 of c-KIT and also in other receptor
tyrosine kinases, e.g. RET.21
Studies on the frequency of FLT3-TKD in AML were performed by Abu-Duhier et al.
(n=97), Yamamoto et al. (n=429), Thiede et al. (n=979), Moreno et al. (n=208), and by
Fröhling et al. in 224 patients with AML showing a normal karyotype.7;9;16;27;33
According to these studies FLT3-TKD show an incidence of 5.8%-7.7% in AML and
thus are less frequent than FLT3-LM.7;9;16;34
Due to the high frequency of FLT3 mutations in AML concentration focuses on the
development of FLT3 inhibitors for treatment of this AML subgroup. A number of
selective FLT3 tyrosine kinase inhibitors have demonstrated in vitro and in vivo
activity.35-39
Because of the low frequency the prognostic significance of FLT3-TKD mutations is
still unclear. In the presented study we analyzed the frequency of FLT3-TKD
mutations in 3082 patients with AML at diagnosis and did correlations to other
biological factors like karyotype, molecular mutations, cytomorphological subtypes,
and leukocyte count. The influence of FLT3-TKD on prognosis was evaluated in detail.
PATIENTS, MATERIAL, AND METHODS
Patients
Bone marrow samples or blood samples from 3082 consecutive patients with AML at
diagnosis were screened for FLT3-TKD mutations.
The range of age was 17.5 years to 91.8 years (median 63.1 years). Of the 3082
patients, 2546 (82.6%) had de novo AML, 334 (10.8%) had secondary AML following
myelodysplastic syndrome (MDS) (s-AML), and 202 (2.0%) had AML following
treatment of a previous malignant disease (t-AML). Patients were treated according to
protocols of the AMLCG study group (80%)40 or according to other intensive AML
therapy protocols. The study was approved by Ethics Committee of participating
institutions and informed consent was provided according to the Declaration of
Helsinki.
Samples were evaluated by cytomorphology, cytochemistry, multiparameter flow
cytometry, cytogenetics, fluorescence in situ hybridization (FISH), and molecular
genetics in parallel.41-44 The cytomorphological classification of AML was performed
according to the FAB classification.45;46 (table 1)
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom

5
Paired samples of 152 patients were compared with respect to the FLT-TKD mutation
status at diagnosis and at relapse.
Molecular analysis
Ficoll, mRNA extraction, cDNA synthesis, mutation analysis for FLT3-LM and control
PCR were performed as previously described (Schnittger Blood 2002). Analysis for
TKD mutations was performed by Lightcycler based melting curve analysis with
forward primer 17F: 5´-CCGCCAGGAACGTGCTTG-3´), reverse primer 17R: 5´-
ATGCCAGGGTAAGGATTCACACC-3´ and hybridization probes FLT3-sensor 5´-
ACTCATGATATCTCGAGCCAATCC-FL-3´ and FLT3-anchor 5´- LCred640-
AAGTCACATATCTTCACCACTTTCCCGT-3´-PH. The PCR reaction was carried out
in a 20 µl reaction volume with each 0.5 µM of forward and reverse primer, 0.75 µM
Hyb-Probes, 4 mM MgCl2 and 2 µl LightCycler-FastStart DNA Master Hybridization
Probes (Roche Diagnostics, Mannheim, Germany). LightCycler data were analyzed
using the LightCycler 3.0 software (Roche Diagnostics, Mannheim, Germany) and the
second derivative maximum method. Each 20 µl reaction contains 2 µl of cDNA, an
equivalent of about 3000 cells. Amplification was performed with 45 cycles using 60°C
annealing temperature. Final melting curve analysis was started at 40°C up to 95°C
with slop of 0.2°C/sec and continuous detection with channel F2/F1 (supplement,
figure 1).
Evaluation of this assay was performed in 100 samples by parallel assessment with
standard PCR, EcoRV restriction enzyme digestion and agarose gel electrophoresis
as was previously described.9
Screening for FLT3-LM, FLT3-TKD, NRAS mutations, and NPM1 mutations was
performed as described elsewhere.16;43;47;48 Mutations of the CEBPA gene were
analyzed by denaturing high performance liquid chromatography (DHPLC) (WAVE,
Transgenomics, Northumberland, USA) with subsequent direct sequencing of
aberrant fragments.
Sequencing analysis
Approximately 100 ng purified PCR products were directly sequenced with 3.3 pmol
primers as described above with BigDye Terminator Cycle Sequencing Kit (Applera,
Weiterstadt, Germany). After initial denaturation at 95 °C for 5 minutes, 25 cycles at
94°C for 15 seconds and 60°C for 4 minutes were performed. Sequence analysis was
performed on an ABI 310 or 3100 Sequence Detection system.
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom
6
Statistical analysis
Overall survival (OS) and event free survival (EFS) were performed according to
Kaplan-Meier. OS was calculated from time of diagnosis to death and EFS from time
of diagnosis to death, documentation of persistent leukemia, or relapse. The
correlation of OS and EFS with other parameters was assessed by Cox regression.
The comparison of survival curves was performed using double sided log rank test.
Comparisons of dichotomous variables between different groups were performed by
use of two-sided Fisher´s exact test. For statistical analysis SPSS (version 12.4)
software (SPSS, Chicago, IL) was used.
Complete remission was defined by <5% blasts in a normocellular bone marrow with
normal levels of peripheral neutrophil and platelet counts.
RESULTS
Frequency of the FLT3-TKD mutation
In total 3082 samples were analysed at diagnosis. Of these 147 were positive for a
FLT3-TKD mutation (4.8%). As estimated from the LightCycler curves and sequence
data 137 had a mutation/wt ratio corresponding to 20-100% of mutated cells. Ten
cases had a TKD/wt ratio of approximately 10%. Lower ratios were not observed. On
the other hand 2935 cases (95.2%) tested negative for a FLT3-TKD mutation.
Sequencing analysis
To further characterize the detected mutations PCR products of cases with low
melting temperatures profiles were directly sequenced. In 10 cases sequencing with a
sensitivity of approximately 10% did not reveal a mutation as the mutated clone as
derived from the melting peak was below 10% of the whole cell population. Of 147
mutated cases 137 (93.2%) could be further characterized. Changes of D835 were
most frequent (122/137; 89.1%). In detail, a change from asparagine to tyrosine
(D835Y) was found in 68/147 cases (49.6%). In 118/122 cases with FLT3-TKD
mutations (96.7%) only one allele was mutated. Compound heterozygotes were found
in 4/122 cases with FLT3-TKD mutations (3.3%) (1. asp > ala / asp > tyr; 2. asp > tyr /
asp > glu; 3. asp > tyr / asp > his; 4. asp > tyr / asp > glu). In one case we found
mutations of both D835 and a ∆I836 (1/137; 0.7%). ∆I836 was observed in 14 cases
(10.2%). (table 2)
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom

7
Biological parameters of patients with FLT3-TKDmut compared to FLT3-TKDwt
The 147 FLT3-TKD mutated cases included 72 males (49.0%) and 75 females
(51.0%), thus revealing no sex difference. Median age of the FLT3-TKD mutated
patients was 59.5 years (range 18.7 - 84.6 years) compared to 63.2 years (range 17.5
- 91.8 years)in the unmutated group (n.s.). Thus, FLT3-TKD mutations were not
significantly correlated with gender or age. The median white blood count (WBC) was
40.0 x 109/L (range: 1.2 x109/L - 332.0 x109/L) in the cohort with FLT3-TKD mutations
compared to 50 x 109/L (range: 1.0 - 840.0 x109/L) in the cohort with FLT3-LM vs. 7.6
x 109/L (range: 115.0 - 462.0 x109/L) in the patients with FLT3- wildtype. Thus, WBC
was significantly higher in FLT3-TKD-mutated than in FLT3wt AML (p<0.001), and
lower than in FLT3-LM (p=0.04).
Correlation of the FLT3-TKD mutation status with AML history
The distribution of FLT3-TKD mutations in de novo AML, s-AML, and t-AML revealed
the highest incidence in de novo AML (135/2546; 5.3%) compared to s-AML (8/334;
2.4%) and t-AML (4/202; 2.0%). Thus, FLT3-TKD mutations were significantly more
frequent in de novo than in s-AML after MDS or precedent chemotherapy (p=0.0101).
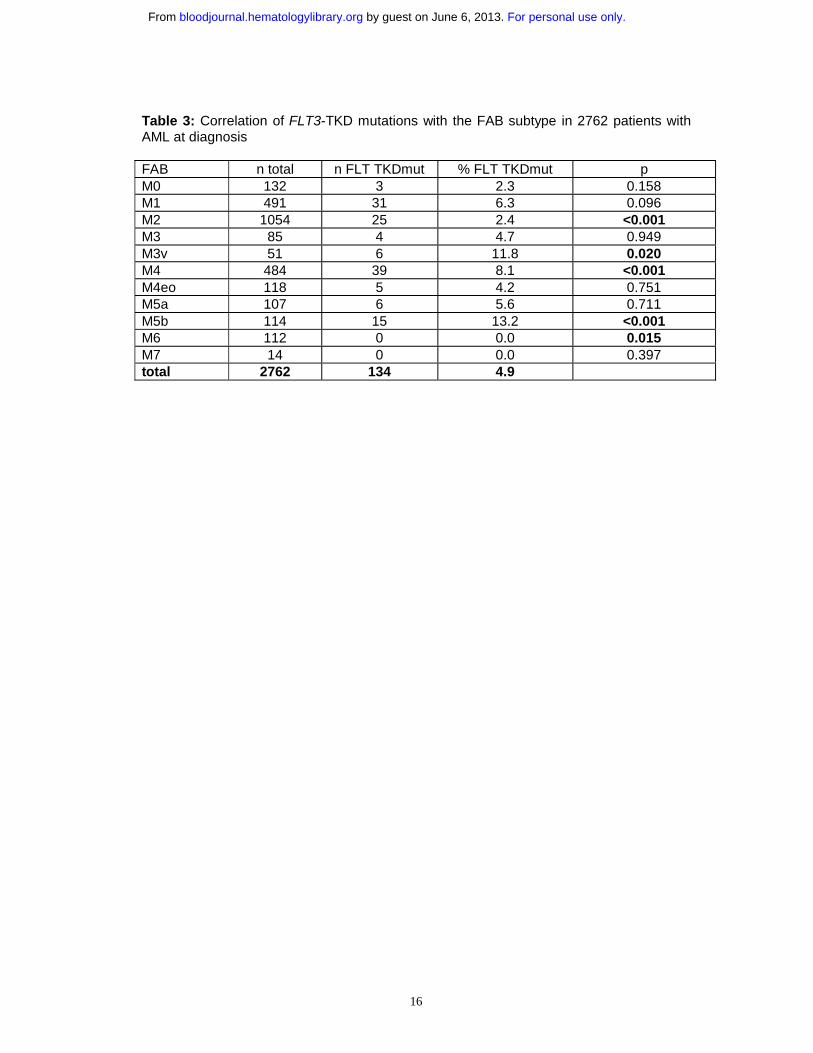
Correlation of the FLT3-TKD mutation status to cytomorphology
The FAB subtype was available in 2762/3082 patients (89.6%) and was correlated to
the FLT3-TKD status. Overall FLT3-TKD mutations were detected in all morphologic
subgroups. They were significantly overrepresented in AML M3v (6/51; 11.8%;
p=0.0204), M4 (39/484; 8.1%; p=0.0003), and M5b (15/114; 13.2%; p<0.0001). In
contrast, they were significantly underrepresented in the subtypes M2 (25/1054) and
M6 (M6: 0/112; 0%; p=0.0147). (table 3)
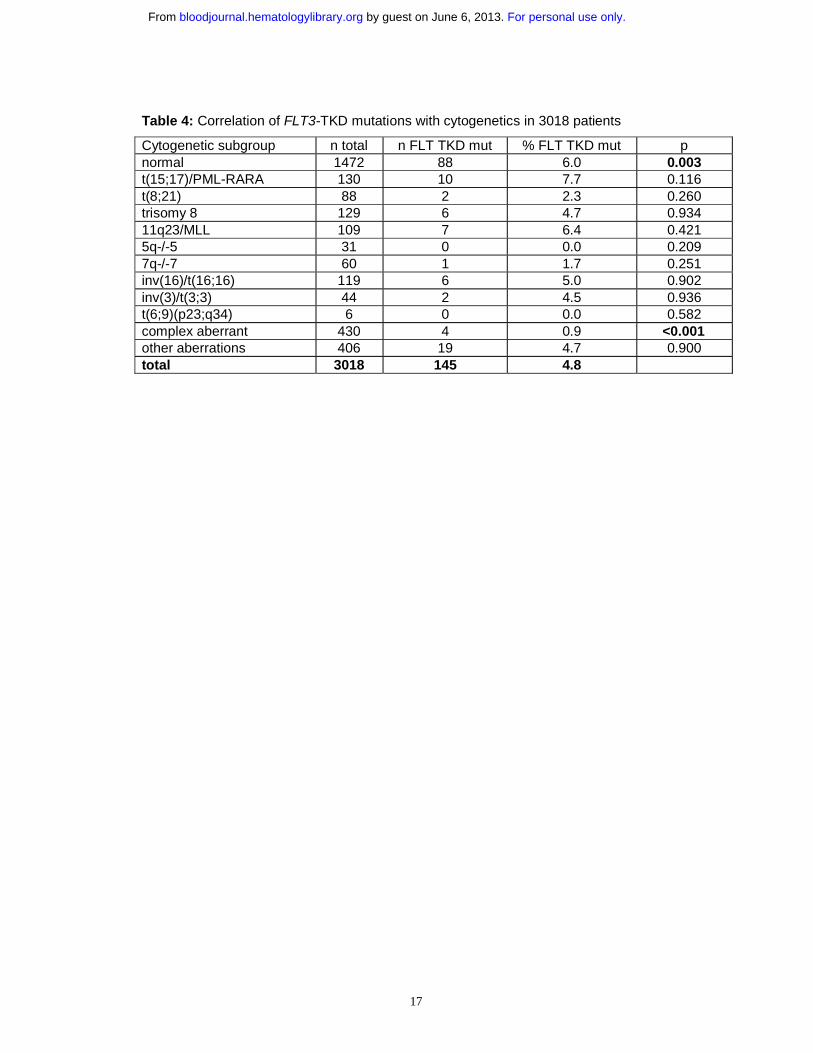
Correlation of the FLT3-TKD mutation status with cytogenetics
Karyotype was available in 3018/3082 cases (97.9%). In 64/3082 cases (2.1%)
karyotype was not available due to a low number of analyzed metaphases. Cases
were grouped into 12 categories: normal karyotype, t(15;17)/PML-RARA,
t(8;21)/AML1-ETO, inv(3)/t(3;3), inv(16)/t(16;16)/CBFB-MYH11, 11q23/MLL, complex
aberrant karyotype (defined by ≥3 chromosomal abnormalities), trisomy 8, 5q- or loss
of chromosome 5, 7q- or loss of chromosome 7, and all others, the so called “other
aberrations”.
FLT3-TKD mutations were observed in all cytogenetic subgroups. However, some
specific associations with distinct cytogenetic subgroups were observed. Compared to
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom

8
the total cohort they were significantly overrepresented in normal karyotype (88/1384;
6.0%; p=0.0033) when compared to the overall cohort. They showed an elevated
frequency in t(15;17)/PML-RARA (10/130; 7.7%); but this association did not reach
significance. In complex aberrant karyotype they were significantly underrepresented
(4/430; 0.9%; p<0.0001). (table 4)
Correlation of the FLT3-TKD mutation status with other molecular markers
The correlation of FLT3-TKD with other molecular markers was analyzed for FLT3-
LM, MLL-PTD, and mutations in NPM1, NRAS, KITD816, and CEPBA. FLT3-TKD
mutations were significantly overrepresented in the patients with NPM1 mutations
(23/262; 8.8%) (p<0.0001). In patients with FLT3-LM they were significantly
underrepresented (17/594; 2.9%; p=0.0066). (table 5)
Stability of the FLT3-TKD in paired samples from diagnosis and relapse
The stability of FLT3-TKD was analyzed by evaluation of 152 paired samples at
diagnosis and relapse. The mutation status was TKDwt/TKDwt at both time points in
139 cases. Four cases revealed an FLT3-TKD mutation at diagnosis as well as at
relapse. Thus, the TKD status was unchanged at diagnosis and relapse in 143 cases
(94.1%). In contrast, nine cases (5.9%) that were FLT3-TKD mutated at diagnosis did
not reveal this mutation at relapse. This meant that of 13 cases that were positive at
diagnosis, 9 (69%) lost the mutation at relapse. Although the limited number of cases
has to be taken into account, this may suggest that FLT3-TKD is a rather unstable
mutation not valid for follow-up studies.
Prognostic significance of the FLT3-TKD mutation
When all patients were taken into account, OS and EFS were not significantly
influenced by the presence of FLT3-TKD mutations (supplement, figure 2 a-2b). This
pattern remained unchanged if all cases with FLT3-LM were excluded (supplement,
figure 2 c-d). We then compared OS and EFS with respect to FLT3-TKD mutations in
different cytogenetic subgroups. In t(8;21), inv16/t(16;16), 11q23/MLL
rearrangements, inv(3)/t(3;3), +8, and in complex aberrant karyotype the influence of
FLT3-TKD could not be determined due to the rare occurrence in these cytogenetic
subgroups. In normal karyotype OS and EFS did not differ significantly in dependence
on FLT3-TKD mutations (supplement, figure 3 a-e). In patients with karyotypes
associated with an intermediate prognosis FLT3-TKD had no prognostic impact as
well (supplement, figures 4a-d). Also when this analysis was restricted to the de novo
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom

9
AML case no prognostic significance could be worked out (supplement, figures 2 e-f
and 3e-f).
In the subgroup with t(15;17) EFS was significantly deteriorated by FLT3-TKD
mutations (p=0.051) (figure 1 b). This became even more evident, when the analysis
was restricted to the cases without FLT3-LM (figure 1 c-d).
Furtheron, we analzyed the prognostic impact of FLT3-TKD mutations in dependence
on FLT3-LM, MLL-PTD, NPM1, and CEPBA. In the NRAS mutated patients the
influence of FLT3-TKD mutations could not be analyzed due to the low incidence in
this subgroup. Kaplan Meier plots showed an unfavorable impact of FLT3-TKD in
prognostically unfavorable groups like FLT3-LM (figure 2) and MLL-PTD (figure 3a-b).
This cooperative adverse effect of FLT3-TKD and MLL-PTD was even stronger, after
the FLT3-LM positive cases had been excluded (figure 3c-d). In contrast there seems
to be a favorable impact in the two subgroups with the favorable markers NPM1
(figure 4a-4b) and CEBPA (figure 5). For NPM1 this cooperative positive effect was
even stronger, when the FLT3-LM mutated cases were excluded. If this analysis was
further broken down to de novo AML, normal karyotype and exclusion of FLT3-LM
mutated cases, FLT3-TKD/NPM1 double mutated cases had a highly significantly
better EFS than sole FLT3-TKD mutated (p=0.010) or FLT3wt/NPM1wt cases
(p=0.028) (figure 4e-f). Because of the limited sample numbers in subgroups a
comparable detailed analysis was not possible for all other mutations.
DISCUSSION
Molecular mutations especially in normal karyotype AML are of increasing importance
for the definition of prognosis in AML. Some mutations have been shown to be
prognostically favorable like NPM148;49 and CEBPA50;51. Others like the MLL-PTD are
unfavorable.52;53 Whereas for the FLT3-LM an association with an unfavorable
prognosis within normal karyotype was clearly established, the prognostic impact of
FLT3-TKD remained unclear, so we did a detailed analysis on 3082 patients with
AML. Although we performed a very specific and sensitive assay which was
potentially able to detect not only the codon 835/836 mutations but covered a total of
17 codons in the TKD domain, the frequency of FLT3-TKD in our study was only
4.8%. This slightly lower frequence when compared to previous studies.9;12;16;27;54
(table 6) might be explained by differences of age as the median age of patients in this
study was 63 years in comparison to (<50 years in comparative studies. Likewise to
the FLT3-LM the FLT3-TKD seem to be more frequently associated with de novo AML
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom

10
rather than with s-AML or t-AML as suggested here and in some previous reports.15;33
Only one analysis found an equal distribution of FLT3-TKD in de novo and in s-AML.27
Like previous studies9;33;54 we found the D835Y mutation being the most frequent
amino acid exchange followed by the D835V and the D835E mutations. Thus, the
mutations are not randomly distributed within the TK domain. The occurrence of two
different TKD mutations in combination was rare in only 3% of all cases at all. This
suggests that a compound heterozygous mutation status does not provide a further
advantage for the leukemic clone.
Similar to AML with FLT3-LM, the FLT3-TKD is clearly associated with higher WBC
when compared to FLT3-wt AML. However, median WBC in FLT3-TKD was lower
than in FLT3-LM which is in accordance to some previous studies,33;54 although others
were not able to show any influence of the FLT3-TKD on peripheral leukocytes.9;27;54
A preliminary analysis of paired samples from diagnosis and relapse suggests low
stability of this mutation. Loss of the FLT3-TKD mutation at relapse was found in 69%
of cases which were positive at diagnosis (6% of all cases). This was in the range of
two previous studies that observed loss in 3%55 and in 8% of the cases, respectively13.
Therefore, it the FLT3-TKD mutations might be less suitable as MRD markers when
compared to other markers. However, this is a matter of future studies. Efforts were
already made to establish a real-time PCR assay for the follow-up of FLT3-TKD
mutations.56
We found a relatively high frequency of FLT3-TKD in t(15;17)/PML-RARA when
compared with the total cohort. This association between the TKD mutations and
acute promyelocytic leukemia (APL) confirmed the results of our previous analysis
which included part of the patients of this study.57 Likewise to the FLT3-LM57 we found
the FLT3-TKD significantly associated with the FAB subtype M3v (11.8%), whereas in
M3 the frequency (4.7%) was comparable to the overall frequency of FLT3-TKD
mutations in AML. In conclusion, this association of the FLT3-LM and of the TKD
mutations with PML-RARA in parallel with the low frequency of other molecular
markers in APL suggests a cooperation of both subtypes of FLT3 mutations with PML-
RARA to cause AML with preference for the cytomorphological M3v subtype.58 Such
cooperation is further emphasized by the previous observation of a higher PML-RARA
expression in FLT3-LM positive patients in comparison to FLT3-LM negative
patients.57
In contrast to the FLT3-LM which are significantly underrepresented in the subgroup
with inv(16)/CBFB-MYH11 (Schnittger et al.: 0%; Thiede et al. 0.6%),15;16 the
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom

11
frequency of FLT3-TKD in inv(16)/CBFB-MYH11 was only slightly lower than the
overall frequency in this study and in previous analyses (this study: 5.0%; Care et al.:
4.8%; Thiede et al.: 5.0%).15;16;59 A recent large study found the TKD mutations even
significantly associated with inv(16).54 Thus, the relationship between the FLT3-TKD
mutations and CBFB-MYH11 is yet not clear. In contrast to FLT3-LM which were
observed in 90% of t(6;9)/DEK-CAN cases,16 the FLT3-TKD mutations were not
detected in this rare entity. In addition, the FLT3-TKD mutations were significantly
underrepresented in AML with complex aberrant karyotype in our study which was in
correspondance to the FLT3-LM being also rare in this cytogenetic subgroup
according to our precedent analysis.15 In conclusion, the FLT3-LM and the TKD
mutations show many parallels with respect to their distribution within the different
cytogenetic AML subgroups – as demonstrated by their association to normal
karyotype, to t(15;17)/PML-RARA preferentially in AML M3v, and by their low
occurrence in complex aberrant karyotype.
Another focus of this analysis was the distribution of the FLT3-TKD mutations within in
AML with different molecular mutations. According to the two hit hypothesis at least
two different mutation types are needed to induce AML. Type I mutations encode
tyrosine kinases and increase proliferation, whereas type II mutations encode
transcription factors and block differentiation.21 The overrepresentation of FLT3-TKD –
being interpreted as type I mutations - in cases with NPM1, CEPBA, and NRAS
mutations (representing type II mutations) in this analysis might support this model.
FLT3-TKD and FLT3-LM seem to differ with respect to their molecular cooperation
partners, as the FLT3-LM were found underrepresented in NRAS mutated cases in
contrast to the overrepresentation of TKD mutations in this subgroup.12 Secondly, the
FLT3-TKD did not differ from the overall frequency in patients with MLL-PTD, whereas
the FLT3-LM were overrepresented in MLL-PTD positive cases.60
Our data support previous suggestions that FLT3-TKD and FLT3-LM show no61 or
rare coincidence9;16;33;62. It was suggested that the FLT3-LM and FLT3-TKD are
caused by totally different underlying mutational mechanisms and in addition do not
cooperate well to amplify any leukemogenic effect. The same seems to be true for
FLT3-TKD and KIT mutations as also these two targets were very rare in this study
The correlation of the FLT3-TKD mutations with cytomorphology allowed further
speculations with respect to their role in leukemogenesis. The association with the
monocytic subtype FAB M5 in this and in previous studies9;16 like the FLT3-LM which
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom

12
show the a similar distribution9;15;16 is indicative for a participation of FLT3 mutations in
monocyte differentiation in AML16;63. It had previously been shown that FLT3 was
continuously expressed during monocyte differentiation, and that FLT3 was needed
for optimal differentiation of monocytes from CD34 positive stem cells.64 In addition,
the underrepresentation of FLT3-TKD mutations in the FAB subtype M6 (own study)16
might be due to the low rate of FLT3-TKD mutations in complex aberrant karyotype,
as AML M6 is correlated with this cytogenetic subgroup.65
With respect to prognosis in the presented study which included 3082 AML cases
there was no influence on OS or EFS in the overall AML population, in de novo AML,
nor in the normal or intermediate karyotype subgroups in accordance with most
previous studies in adults,33;54 in elderly patients,62 and in children26. However, there
are as well reports of a worsened outcome,27 and the metaanalysis of Yanada et al.
on 1160 patients resulted in a significantly worse outcome.66 This is in contrast to a
large recent study which found a significantly improved survival in the patients with
FLT3-TKD mutations.54 Another study showed an inferior outcome in the intermediate
cytogenetic subgroup, whereas there was no impact of the FLT3-TKD mutations on
survival in the poor cytogenetic subgroup.16 These different findings may result from
selection within the cohorts. As we could show the prognostic effect of the FLT3-TKD
is dependend on additional mutations in single patients which came out by detailed
subgroup analyses that have not been performed previously.
Accordingly, if subgroups with defined genetic profiles are regarded a significant
prognostic impact could be worked out. The only cytogenetic subgroup with an
obvious prognosis effect of the FLT3-TKD – a negative one in this case - was
t(15;17)/PML-RARA. Other negative effects were detected in AML with FLT3-LM or
MLL-PTD which are themselves are prognostically unfavorable. Paradoxically in
NPM1 and CEPBA mutated cases, which per se have a favorable prognosis, FLT3-
TKD mutations had a further favorable prognostic impact. These effects were even
stronger when the analysis was restricted to de novo AML or AML without FLT3-LM.
As the case numbers in some of the double mutated groups were rather small -
especially in the FLT3-TKD/CEBPA double mutated group - these finding have to be
taken with caution and should serve mainly as working hypothesis for further studies
within clinical trials.
Different signalling properties of both mutation subtypes were suggested by
Choudhary et al. who showed that FLT3-LM gain a function over ligand-activated
FLT3-wildtype which is not gained by FLT3-TKD mutations.29 Gene expression
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom

13
profiling with microarray analysis showed different gene expression patterns for FLT3-
LM and for FLT3-TKD positive AML.67 The differences between FLT3-TKD and FLT3-
LM regarding the distribution within distinct cytogenetic subgroups, the coincidence
with other molecular markers, and the differences with respect to the prognostic
impact in this and in the precedent studies emphasize the diversity within both
molecular subtypes. In conclusion, FLT3-LM mutations and FLT3-TKD mutations
should be regarded as two biologically and prognostically different mutations within a
single gene.
ACKNOWLEDGEMENT
This investigation was performed in part in the Laboratory for Leukemia Diagnostics;
Medical Department III, (Head: Prof. Dr. W. Hiddemann), Ludwig-Maximilians-
University Munich. We greatly appreciate the excellent technical help of Gudrun
Mellert, Claudia Tschulik, Madlen Fuchs, Theresa Förster, and Nina Leopold. We
would like to thank all participants of the AMLCG study group for sending bone
marrow or blood samples to our laboratory for reference diagnosis and for submitting
clinical data, as part of the patients were treated within the AMLCG study group.
Author Contribution: S.S. was principal investigator. U.B. and S.S. analyzed data
and wrote the manuscript. WK was responsible for immunophenotyping and
contributed in statistical evalualion. TH was responsible for cytomorphology. C.H. was
responsible for cytogenetics. S.S. did the molecular genetic analysis.
Conflict of Interest Disclosure:
CH, WK, TH, and SS in part own the MLL Munich Leukemia Laboratory which is
offering comprehensive leukaemia diagnostics.
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom

14
Tables and figures
Table 1: Characterization of the patient cohort (n=3082)
number of patients (n) percentage (%)
history of AML
de novo AML 2546 82.6
secondary AML (s-AML) 334 10.8
t-AML 202 2.0
total 3082 100.0
cytogenetic subgroup
normal 1472 47.8
t(15;17)* 130 4.2
t(8;21) 88 2.9
trisomy 8 129 4.2
11q23/MLL 109 3.5
5q-/-5 31 1.0
7q-/-7 60 1.9
inv(16)/t(16;16) ** 119 3.9
inv(3)/t(3;3) 44 1.4
t(6;9)(p23;q34) 6 0.2
complex aberrant 430 14.0
other aberrations 400 15.0
total 3018 100.0
FAB subtype
M0 132 4.8
M1 491 17.8
M2 1054 38.2
M3 85 3.1
M3v 51 1.8
M4 484 17.5
M4eo 118 4.3
M5a 107 3.9
M5b 114 4.1
M6 112 4.1
M7 14 0.5
total 2762 100.0
(*136 cases of FAB M3/M3v morphology were associated to 130 cases of t(15;17) in chromosome banding analyses due to additional 6 cryptic PML-RARA rearrangements; **118 cases of FAB M4eo morphology were associated to 119 cases of inv(16)/t(16;16) due to atypical morphology in one case)
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom

15
Table 2: Distribution of point mutations in 137 cases with FLT3-TKD mutations
amino acid exchange number of patients (n)
percentage (%)
D835Y 68 49.6 D835H 20 14.6 D835V 14 10.2 D835E 11 8.0 D835A 3 2.2 D835S 1 0.7 D835N 1 0.7 D835 compound heterozygous: D835Y+D835E D835Y+D835A D835Y+D835H
2 1 1
1.4 0.7 0.7
D835 – total 122 89.1 �I836 14 10.2 D835V and �I836 compound heterozygous
1 0.7
total 137 100.0
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom
16
Table 3: Correlation of FLT3-TKD mutations with the FAB subtype in 2762 patients with AML at diagnosis FAB n total n FLT TKDmut % FLT TKDmut p M0 132 3 2.3 0.158 M1 491 31 6.3 0.096 M2 1054 25 2.4 <0.001 M3 85 4 4.7 0.949 M3v 51 6 11.8 0.020 M4 484 39 8.1 <0.001 M4eo 118 5 4.2 0.751 M5a 107 6 5.6 0.711 M5b 114 15 13.2 <0.001 M6 112 0 0.0 0.015 M7 14 0 0.0 0.397 total 2762 134 4.9
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom
17
Table 4: Correlation of FLT3-TKD mutations with cytogenetics in 3018 patients
Cytogenetic subgroup n total n FLT TKD mut % FLT TKD mut p normal 1472 88 6.0 0.003 t(15;17)/PML-RARA 130 10 7.7 0.116 t(8;21) 88 2 2.3 0.260 trisomy 8 129 6 4.7 0.934 11q23/MLL 109 7 6.4 0.421 5q-/-5 31 0 0.0 0.209 7q-/-7 60 1 1.7 0.251 inv(16)/t(16;16) 119 6 5.0 0.902 inv(3)/t(3;3) 44 2 4.5 0.936 t(6;9)(p23;q34) 6 0 0.0 0.582 complex aberrant 430 4 0.9 <0.001 other aberrations 406 19 4.7 0.900 total 3018 145 4.8
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom

18
Table 5: Correlation of FLT3TKD mutations with other molecular mutations (+: positive mutation status; -: negative mutation status).
molecular mutation
N mutation status
nr. FLT3-TKD mut +
% p
+ 338 12 3.6 FLT3-LM
1051 - 713 57 8.0
0,007
+ 84 6 7.1 MLL-PTD
1044 - 960 64 6.7
0,867
+ 221 20 9.0 NPM1
428 - 207 50 24.2
<0.001
+ 45 4 8.9 CEPBA
363 - 318 25 7.9
0,812
+ 78 3 3.8 NRAS
888 - 810 52 6.4
0,368
+ 44 1 2.3 KITD816
2532 - 2488 118 4.7
0,443
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom

19
Table 6: Frequency of FLT3-TKD mutations in this study and in previous studies
Reference total (n) positive FLT-TKD mutation
status (n)
percentage FLT-TKD mutations
this study 3082 147 4.8% Abu-Duhier et al., 2001 97 7 7.2% Yamamoto et al., 2001 429 30 7.0% Thiede et al., 2002 979 75 7.7% Moreno et al., 2003 208 20 7.7% Andersson et al., 2004 109 (>60 years) 11 10.1% Aurewarakul et al., 2005 256 15 5.8% Wang et al., 2005 143 92 6.3% Mead et al., 2007 1107 127 11% overall 5303 397 7.5%
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom
20
Legends for figures
Figure 1: a) Overall survival and b) event free survival of FLT3-TKD-wiltdtpye (FLT3-wt) versus FLT3-TKD mutated cases (FLT3-TKDmut) in t(15/17)/PML-RARA positive AML. c) Overall survival and b) event free survival of FLT3-TKD-wiltdtpye (FLT3-wt) versus FLT3-TKD mutated cases (FLT3-TKDmut) in t(15/17)/PML-RARA positive AML exclusive all cases that are FLT3-LM mutated. Figure 2: a) Overall survival and b) event free survival of FLT3-TKD-wiltdtpye (FLT3-wt) versus FLT3-TKD mutated cases (FLT3-TKDmut) in dependance on FLT3-LM.
Figure 3: a) Overall survival and b) event free survival of FLT3-TKD-wiltdtpye (FLT3-wt) versus FLT3-TKD mutated cases (FLT3-TKDmut) in dependance on MLL PTD. c) Overall survival and d) event free survival of FLT3-TKD-wiltdtpye (FLT3-wt) versus FLT3-TKD mutated cases (FLT3-TKDmut) in dependance on MLL PTD exclusive all cases that are FLT3-LM mutated. Figure 4: a) Overall survival and b) event free survival of FLT3-TKD-wiltdtpye (FLT3-wt) versus FLT3-TKD mutated cases (FL3T-TKDmut) in dependance on NPM1 mutations. c) Overall survival and d) event free survival of FLT3-TKD-wiltdtpye (FLT3-wt) versus FLT3-TKD mutated cases (FL3T-TKDmut) in dependance on NPM1 mutations all cases that are FLT3-LM mutated. e) Overall survival and f) event free survival of FLT3-TKD-wiltdtpye (FLT3-wt) versus FLT3-TKD mutated cases (FL3T-TKDmut) in dependance on NPM1 mutations exclusive all cases that are FLT3-LM mutated in de novo normal karyotype AML. Figure 5: a) Overall survival and b) event free survival of FLT3-TKD-wiltdtpye (FLT3-wt) versus FLT3-TKD mutated cases (FLT3-TKDmut) in dependance on CEPBA mutations. c) Overall survival and d) event free survival of FLT3-TKD-wiltdtpye (FLT3-wt) versus FLT3-TKD mutated cases (FLT3-TKDmut) in dependance on CEPBA mutations exclusive all cases that are FLT3-LM mutated.
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom

21
Reference List 1. Bloomfield CD, Shuma C, Regal L et al. Long-term survival of patients with acute myeloid
leukemia: a third follow-up of the Fourth International Workshop on Chromosomes in Leukemia. Cancer 1997;80:2191-2198.
2. Grimwade D, Walker H, Oliver F et al. The importance of diagnostic cytogenetics on outcome in AML: analysis of 1,612 patients entered into the MRC AML 10 trial. The Medical Research Council Adult and Children's Leukaemia Working Parties. Blood 1998;92:2322-2333.
3. Slovak ML, Kopecky KJ, Cassileth PA et al. Karyotypic analysis predicts outcome of preremission and postremission therapy in adult acute myeloid leukemia: a Southwest Oncology Group/Eastern Cooperative Oncology Group Study. Blood 2000;96:4075-4083.
4. Kiyoi H, Naoe T, Yokota S et al. Internal tandem duplication of FLT3 associated with leukocytosis in acute promyelocytic leukemia. Leukemia Study Group of the Ministry of Health and Welfare (Kohseisho). Leukemia 1997;11:1447-1452.
5. Gilliland DG, Griffin JD. Role of FLT3 in leukemia. Curr.Opin.Hematol. 2002;9:274-281.
6. Levis M, Small D. Novel FLT3 tyrosine kinase inhibitors. Expert.Opin.Investig.Drugs 2003;12:1951-1962.
7. Abu-Duhier FM, Goodeve AC, Wilson GA et al. Identification of novel FLT-3 Asp835 mutations in adult acute myeloid leukaemia. Br.J.Haematol. 2001;113:983-988.
8. Rosnet O, Buhring HJ, Marchetto S et al. Human FLT3/FLK2 receptor tyrosine kinase is expressed at the surface of normal and malignant hematopoietic cells. Leukemia 1996;10:238-248.
9. Yamamoto Y, Kiyoi H, Nakano Y et al. Activating mutation of D835 within the activation loop of FLT3 in human hematologic malignancies. Blood 2001;97:2434-2439.
10. Lyman SD, Jacobsen SE. c-kit ligand and Flt3 ligand: stem/progenitor cell factors with overlapping yet distinct activities. Blood 1998;91:1101-1134.
11. Rasko JE, Metcalf D, Rossner MT, Begley CG, Nicola NA. The flt3/flk-2 ligand: receptor distribution and action on murine haemopoietic cell survival and proliferation. Leukemia 1995;9:2058-2066.
12. Kiyoi H, Naoe T, Nakano Y et al. Prognostic implication of FLT3 and N-RAS gene mutations in acute myeloid leukemia. Blood 1999;93:3074-3080.
13. Kottaridis PD, Gale RE, Langabeer SE et al. Studies of FLT3 mutations in paired presentation and relapse samples from patients with acute myeloid leukemia: implications for the role of FLT3 mutations in leukemogenesis, minimal residual disease detection, and possible therapy with FLT3 inhibitors. Blood 2002;100:2393-2398.
14. Rombouts WJ, Blokland I, Lowenberg B, Ploemacher RE. Biological characteristics and prognosis of adult acute myeloid leukemia with internal tandem duplications in the Flt3 gene. Leukemia 2000;14:675-683.
15. Schnittger S, Schoch C, Dugas M et al. Analysis of FLT3 length mutations in 1003 patients with acute myeloid leukemia: correlation to cytogenetics, FAB subtype, and prognosis in the AMLCG study and usefulness as a marker for the detection of minimal residual disease. Blood 2002;100:59-66.
16. Thiede C, Steudel C, Mohr B et al. Analysis of FLT3-activating mutations in 979 patients with acute myelogenous leukemia: association with FAB subtypes and identification of subgroups with poor prognosis. Blood 2002;99:4326-4335.
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom
22
17. Meshinchi S, Woods WG, Stirewalt DL et al. Prevalence and prognostic significance of Flt3 internal tandem duplication in pediatric acute myeloid leukemia. Blood 2001;97:89-94.
18. Liang DC, Shih LY, Hung IJ et al. Clinical relevance of internal tandem duplication of the FLT3 gene in childhood acute myeloid leukemia. Cancer 2002;94:3292-3298.
19. Shih LY, Huang CF, Wang PN et al. Acquisition of FLT3 or N-ras mutations is frequently associated with progression of myelodysplastic syndrome to acute myeloid leukemia. Leukemia 2004;18:466-475.
20. Kiyoi H, Towatari M, Yokota S et al. Internal tandem duplication of the FLT3 gene is a novel modality of elongation mutation which causes constitutive activation of the product. Leukemia 1998;12:1333-1337.
21. Gilliland DG. Hematologic malignancies. Curr.Opin.Hematol. 2001;8:189-191.
22. Grundler R, Thiede C, Miething C et al. Sensitivity toward tyrosine kinase inhibitors varies between different activating mutations of the FLT3 receptor. Blood 2003;102:646-651.
23. Hayakawa F, Towatari M, Kiyoi H et al. Tandem-duplicated Flt3 constitutively activates STAT5 and MAP kinase and introduces autonomous cell growth in IL-3-dependent cell lines. Oncogene 2000;19:624-631.
24. Mizuki M, Fenski R, Halfter H et al. Flt3 mutations from patients with acute myeloid leukemia induce transformation of 32D cells mediated by the Ras and STAT5 pathways. Blood 2000;96:3907-3914.
25. Arrigoni P, Beretta C, Silvestri D et al. FLT3 internal tandem duplication in childhood acute myeloid leukaemia: association with hyperleucocytosis in acute promyelocytic leukaemia. Br.J.Haematol. 2003;120:89-92.
26. Kang HJ, Hong SH, Kim IH et al. Prognostic significance of FLT3 mutations in pediatric non-promyelocytic acute myeloid leukemia. Leuk.Res. 2005;29:617-623.
27. Moreno I, Martin G, Bolufer P et al. Incidence and prognostic value of FLT3 internal tandem duplication and D835 mutations in acute myeloid leukemia. Haematologica 2003;88:19-24.
28. Bagrintseva K, Schwab R, Kohl TM et al. Mutations in the tyrosine kinase domain of FLT3 define a new molecular mechanism of acquired drug resistance to PTK inhibitors in FLT3-ITD-transformed hematopoietic cells. Blood 2004;103:2266-2275.
29. Choudhary C, Schwable J, Brandts C et al. AML-associated Flt3 kinase domain mutations show signal transduction differences compared with Flt3 ITD mutations. Blood 2005;106:265-273.
30. Kindler T, Breitenbuecher F, Kasper S et al. Identification of a novel activating mutation (Y842C) within the activation loop of FLT3 in patients with acute myeloid leukemia (AML). Blood 2005;105:335-340.
31. Spiekermann K, Dirschinger RJ, Schwab R et al. The protein tyrosine kinase inhibitor SU5614 inhibits FLT3 and induces growth arrest and apoptosis in AML-derived cell lines expressing a constitutively activated FLT3. Blood 2003;101:1494-1504.
32. Zheng R, Small D. Mutant FLT3 signaling contributes to a block in myeloid differentiation. Leuk.Lymphoma 2005;46:1679-1687.
33. Frohling S, Schlenk RF, Breitruck J et al. Prognostic significance of activating FLT3 mutations in younger adults (16 to 60 years) with acute myeloid leukemia and normal cytogenetics: a study of the AML Study Group Ulm. Blood 2002;100:4372-4380.
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom

23
34. Auewarakul CU, Sritana N, Limwongse C, Thongnoppakhun W, Yenchitsomanus PT. Mutations of the FLT3 gene in adult acute myeloid leukemia: determination of incidence and identification of a novel mutation in a Thai population. Cancer Genet.Cytogenet. 2005;162:127-134.
35. Bali P, George P, Cohen P et al. Superior activity of the combination of histone deacetylase inhibitor LAQ824 and the FLT-3 kinase inhibitor PKC412 against human acute myelogenous leukemia cells with mutant FLT-3. Clin.Cancer Res. 2004;10:4991-4997.
36. George P, Bali P, Annavarapu S et al. Combination of the histone deacetylase inhibitor LBH589 and the hsp90 inhibitor 17-AAG is highly active against human CML-BC cells and AML cells with activating mutation of FLT-3. Blood 2005;105:1768-1776.
37. Gilliland DG. FLT3 Inhibitors in the Treatment of AML. Clin.Adv.Hematol.Oncol. 2004;2:708-710.
38. Tallman MS. New agents for the treatment of acute myeloid leukemia. Best.Pract.Res.Clin.Haematol. 2006;19:311-320.
39. Tickenbrock L, Muller-Tidow C, Berdel WE, Serve H. Emerging Flt3 kinase inhibitors in the treatment of leukaemia. Expert.Opin.Emerg.Drugs 2006;11:153-165.
40. Kern W, Haferlach T, Schoch C et al. Risk-adapted therapy of AML: the AMLCG experience. Ann.Hematol. 2004;83 Suppl 1:S49-S51.
41. Haferlach T, Schoch C, Loffler H et al. Morphologic dysplasia in de novo acute myeloid leukemia (AML) is related to unfavorable cytogenetics but has no independent prognostic relevance under the conditions of intensive induction therapy: results of a multiparameter analysis from the German AML Cooperative Group studies. J.Clin.Oncol. 2003;21:256-265.
42. Kern W, Voskova D, Schoch C et al. Determination of relapse risk based on assessment of minimal residual disease during complete remission by multiparameter flow cytometry in unselected patients with acute myeloid leukemia. Blood 2004;104:3078-3085.
43. Schnittger S, Weisser M, Schoch C et al. New score predicting for prognosis in PML-RARA+, AML1-ETO+, or CBFBMYH11+ acute myeloid leukemia based on quantification of fusion transcripts. Blood 2003;102:2746-2755.
44. Schoch C, Kern W, Schnittger S, Hiddemann W, Haferlach T. Karyotype is an independent prognostic parameter in therapy-related acute myeloid leukemia (t-AML): an analysis of 93 patients with t-AML in comparison to 1091 patients with de novo AML. Leukemia 2004;18:120-125.
45. Bennett JM, Catovsky D, Daniel MT et al. Proposals for the classification of the myelodysplastic syndromes. Br.J.Haematol. 1982;51:189-199.
46. Bennett JM, Catovsky D, Daniel MT et al. Proposed revised criteria for the classification of acute myeloid leukemia. A report of the French-American-British Cooperative Group. Ann.Intern.Med. 1985;103:620-625.
47. Bacher U, Haferlach T, Schoch C, Kern W, Schnittger S. Implications of NRAS mutations in AML: a study of 2502 patients. Blood 2006;107:3847-3853.
48. Schnittger S, Schoch C, Kern W et al. Nucleophosmin gene mutations are predictors of favorable prognosis in acute myelogenous leukemia with a normal karyotype. Blood 2005;106:3733-3739.
49. Falini B, Mecucci C, Tiacci E et al. Cytoplasmic nucleophosmin in acute myelogenous leukemia with a normal karyotype. N.Engl.J.Med. 2005;352:254-266.
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom

24
50. Preudhomme C, Sagot C, Boissel N et al. Favorable prognostic significance of CEBPA mutations in patients with de novo acute myeloid leukemia: a study from the Acute Leukemia French Association (ALFA). Blood 2002;100:2717-2723.
51. Frohling S, Schlenk RF, Stolze I et al. CEBPA mutations in younger adults with acute myeloid leukemia and normal cytogenetics: prognostic relevance and analysis of cooperating mutations. J.Clin.Oncol. 2004;22:624-633.
52. Schnittger S, Kinkelin U, Schoch C et al. Screening for MLL tandem duplication in 387 unselected patients with AML identify a prognostically unfavorable subset of AML. Leukemia 2000;14:796-804.
53. Dohner K, Tobis K, Ulrich R et al. Prognostic significance of partial tandem duplications of the MLL gene in adult patients 16 to 60 years old with acute myeloid leukemia and normal cytogenetics: a study of the Acute Myeloid Leukemia Study Group Ulm. J.Clin.Oncol. 2002;20:3254-3261.
54. Mead AJ, Linch DC, Hills RK et al. FLT3 tyrosine kinase domain mutations are biologically distinct from and have a significantly more favorable prognosis than FLT3 internal tandem duplications in patients with acute myeloid leukemia. Blood 2007;110:1262-1270.
55. Tiesmeier J, Muller-Tidow C, Westermann A et al. Evolution of FLT3-ITD and D835 activating point mutations in relapsing acute myeloid leukemia and response to salvage therapy. Leuk.Res. 2004;28:1069-1074.
56. Scholl S, Krause C, Loncarevic IF et al. Specific detection of Flt3 point mutations by highly sensitive real-time polymerase chain reaction in acute myeloid leukemia. J.Lab Clin.Med. 2005;145:295-304.
57. Kuchenbauer F, Schoch C, Kern W et al. Impact of FLT3 mutations and promyelocytic leukaemia-breakpoint on clinical characteristics and prognosis in acute promyelocytic leukaemia. Br.J.Haematol. 2005;130:196-202.
58. Gilliland DG. FLT3-activating mutations in acute promyelocytic leukaemia: a rationale for risk-adapted therapy with FLT3 inhibitors. Best.Pract.Res.Clin.Haematol. 2003;16:409-417.
59. Care RS, Valk PJ, Goodeve AC et al. Incidence and prognosis of c-KIT and FLT3 mutations in core binding factor (CBF) acute myeloid leukaemias. Br.J.Haematol. 2003;121:775-777.
60. Libura M, Asnafi V, Tu A et al. FLT3 and MLL intragenic abnormalities in AML reflect a common category of genotoxic stress. Blood 2003;102:2198-2204.
61. Abu-Duhier FM, Goodeve AC, Wilson GA et al. FLT3 internal tandem duplication mutations in adult acute myeloid leukaemia define a high-risk group. Br.J.Haematol. 2000;111:190-195.
62. Andersson A, Johansson B, Lassen C et al. Clinical impact of internal tandem duplications and activating point mutations in FLT3 in acute myeloid leukemia in elderly patients. Eur.J.Haematol. 2004;72:307-313.
63. Nakao M, Janssen JW, Erz D, Seriu T, Bartram CR. Tandem duplication of the FLT3 gene in acute lymphoblastic leukemia: a marker for the monitoring of minimal residual disease. Leukemia 2000;14:522-524.
64. Rappold I, Ziegler BL, Kohler I et al. Functional and phenotypic characterization of cord blood and bone marrow subsets expressing FLT3 (CD135) receptor tyrosine kinase. Blood 1997;90:111-125.
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom

25
65. Bacher U, Kern W, Schnittger S et al. Further correlations of morphology according to FAB and WHO classification to cytogenetics in de novo acute myeloid leukemia: a study on 2,235 patients. Ann.Hematol. 2005;84:785-791.
66. Yanada M, Matsuo K, Suzuki T, Kiyoi H, Naoe T. Prognostic significance of FLT3 internal tandem duplication and tyrosine kinase domain mutations for acute myeloid leukemia: a meta-analysis. Leukemia 2005;19:1345-1349.
67. Neben K, Schnittger S, Brors B et al. Distinct gene expression patterns associated with. Oncogene 2005;24:1580-1588.
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom
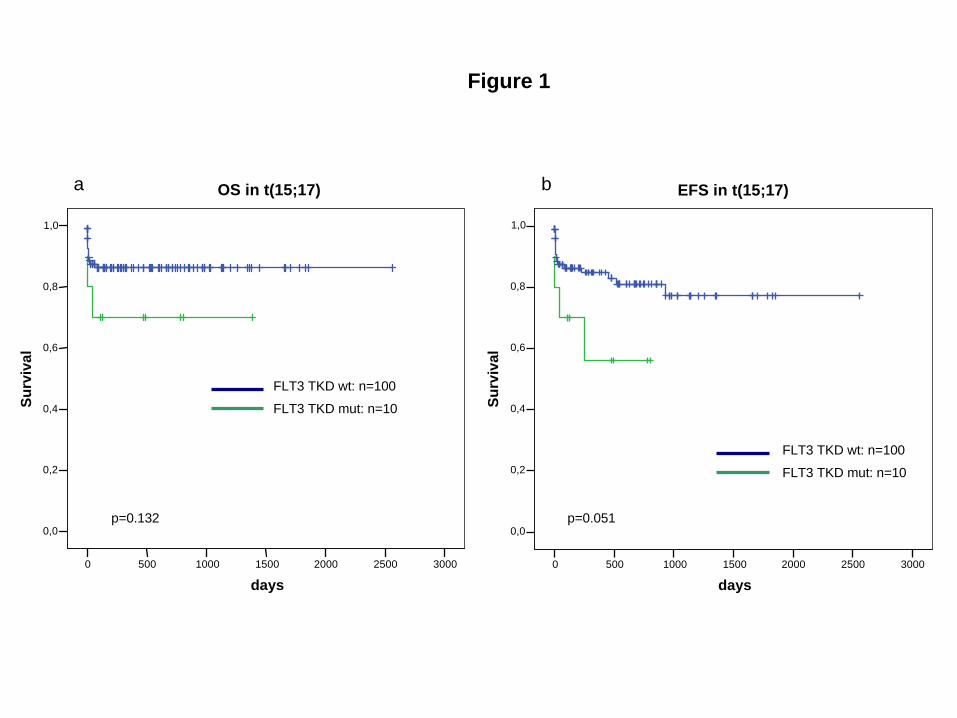
Figure 1
300025002000150010005000
days
1,0
0,8
0,6
0,4
0,2
0,0
Surv
ival
OS in t(15;17)
FLT3 TKD wt: n=100
FLT3 TKD mut: n=10
FLT3 TKD wt: n=100
FLT3 TKD mut: n=10
p=0.132 p=0.051
a b
300025002000150010005000
days
1,0
0,8
0,6
0,4
0,2
0,0
Surv
ival
EFS in t(15;17)
F
or personal use only. by guest on June 6, 2013.
bloodjournal.hematologylibrary.org
From
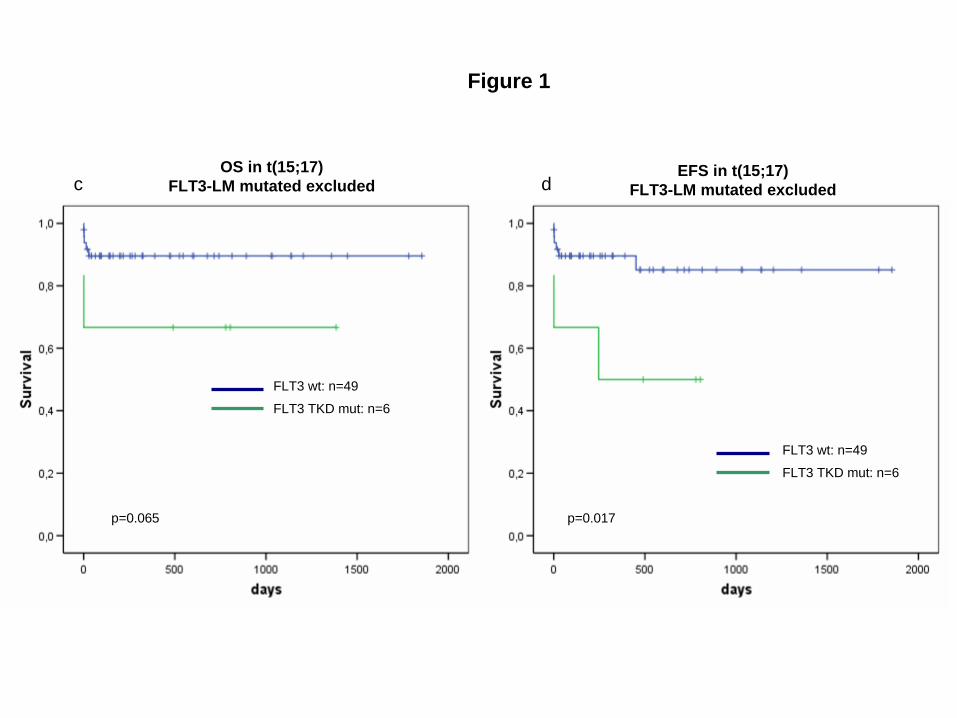
Figure 1
FLT3 wt: n=49
FLT3 TKD mut: n=6
FLT3 wt: n=49
FLT3 TKD mut: n=6
p=0.065 p=0.017
c dOS in t(15;17)
FLT3-LM mutated excludedEFS in t(15;17)
FLT3-LM mutated excluded
F
or personal use only. by guest on June 6, 2013.
bloodjournal.hematologylibrary.org
From
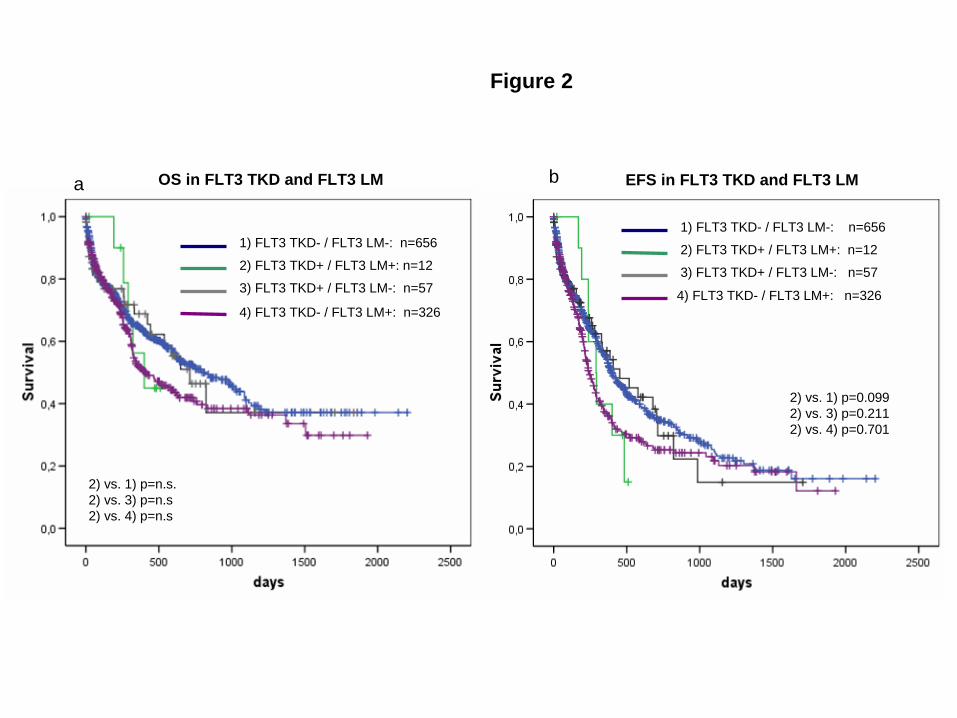
Figure 2
OS in FLT3 TKD and FLT3 LM EFS in FLT3 TKD and FLT3 LM
1) FLT3 TKD- / FLT3 LM-: n=656
2) FLT3 TKD+ / FLT3 LM+: n=12
3) FLT3 TKD+ / FLT3 LM-: n=57
4) FLT3 TKD- / FLT3 LM+: n=326
1) FLT3 TKD- / FLT3 LM-: n=656
2) FLT3 TKD+ / FLT3 LM+: n=12
3) FLT3 TKD+ / FLT3 LM-: n=57
4) FLT3 TKD- / FLT3 LM+: n=326
2) vs. 1) p=n.s.2) vs. 3) p=n.s2) vs. 4) p=n.s
2) vs. 1) p=0.0992) vs. 3) p=0.2112) vs. 4) p=0.701
a b
F
or personal use only. by guest on June 6, 2013.
bloodjournal.hematologylibrary.org
From

Figure 3
1) FLT3 TKD- / MLL PTD-: n=896
2) FLT3 TKD+ / MLL PTD+: n=6
3) FLT3 TKD+ / MLL PTD-: n=64
4) FLT3 TKD- / MLL PTD+: n=78
1) FLT3 TKD- / MLL PTD-: n=896
2) FLT3 TKD+ / MLL PTD+: n=6
3) FLT3 TKD+ / MLL PTD-: n=64
4) FLT3 TKD- / MLL PTD+: n=78
2) vs. 1) p=0.0302) vs. 3) p=0.0202) vs. 4) p=0.152
2) vs. 1) p=0.0202) vs. 3) p=0.0162) vs. 4) p=0.117
a bOS in FLT3-TKD and MLL-PTD OS in FLT3-TKD and MLL-PTD
F
or personal use only. by guest on June 6, 2013.
bloodjournal.hematologylibrary.org
From

Figure 3
1) FLT3 TKD- / MLL PTD-: n=609
2) FLT3 TKD+ / MLL PTD+: n=53) FLT3 TKD+ / MLL PTD-: n=52
4) FLT3 TKD- / MLL PTD+: n=49
1) FLT3 TKD- / MLL PTD-: n=609
2) FLT3 TKD+ / MLL PTD+: n=5
3) FLT3 TKD+ / MLL PTD-: n=52
4) FLT3 TKD- / MLL PTD+: n=49
2) vs. 1) p=0.0202) vs. 3) p=0.0152) vs. 4) p=0.046
1) vs. 3) p=0.0231) vs. 4) p=0.0223) vs. 4) p=0.071
c dOS in FLT3-TKD and MLL-PTD
FLT3-LM mutated excludedEFS in FLT3-TKD and MLL-PTD
FLT3-LM mutated excluded
F
or personal use only. by guest on June 6, 2013.
bloodjournal.hematologylibrary.org
From
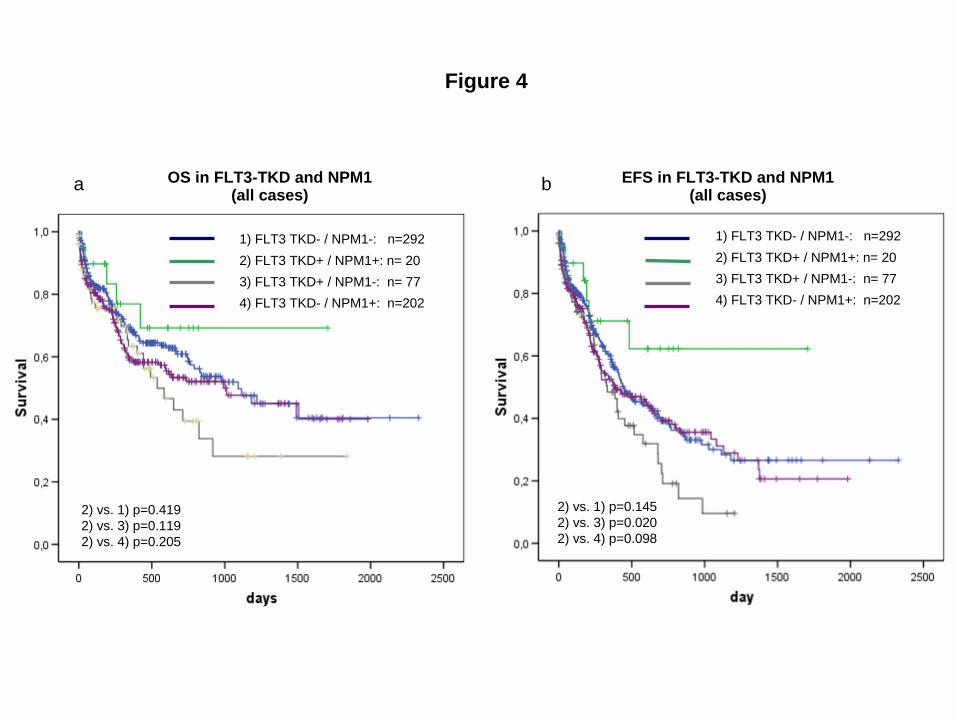
Figure 4
a b
2) FLT3 TKD+ / NPM1+: n= 201) FLT3 TKD- / NPM1-: n=292
3) FLT3 TKD+ / NPM1-: n= 774) FLT3 TKD- / NPM1+: n=202
2) vs. 1) p=0.1452) vs. 3) p=0.0202) vs. 4) p=0.098
2) FLT3 TKD+ / NPM1+: n= 201) FLT3 TKD- / NPM1-: n=292
3) FLT3 TKD+ / NPM1-: n= 774) FLT3 TKD- / NPM1+: n=202
2) vs. 1) p=0.4192) vs. 3) p=0.1192) vs. 4) p=0.205
EFS in FLT3-TKD and NPM1(all cases)
OS in FLT3-TKD and NPM1(all cases)
F
or personal use only. by guest on June 6, 2013.
bloodjournal.hematologylibrary.org
From

Figure 4
2) FLT3 TKD+ / NPM1+: n= 161) FLT3 TKD- / NPM1-: n=238
3) FLT3 TKD+ / NPM1-: n= 634) FLT3 TKD- / NPM1+: n=112
2) vs. 1) p=0.2902) vs. 3) p=0.0752) vs. 4) p=0.250
c d EFS in FLT3-TKD and NPM1(excluded all FLT3-LM+ cases)
OS in FLT3-TKD and NPM1(excluded all FLT3+ cases)
2) FLT3 TKD+ / NPM1+: n= 161) FLT3 TKD- / NPM1-: n=238
3) FLT3 TKD+ / NPM1-: n= 634) FLT3 TKD- / NPM1+: n=112
2) vs. 1) p=0.0692) vs. 3) p=0.0082) vs. 4) p=0.011
F
or personal use only. by guest on June 6, 2013.
bloodjournal.hematologylibrary.org
From
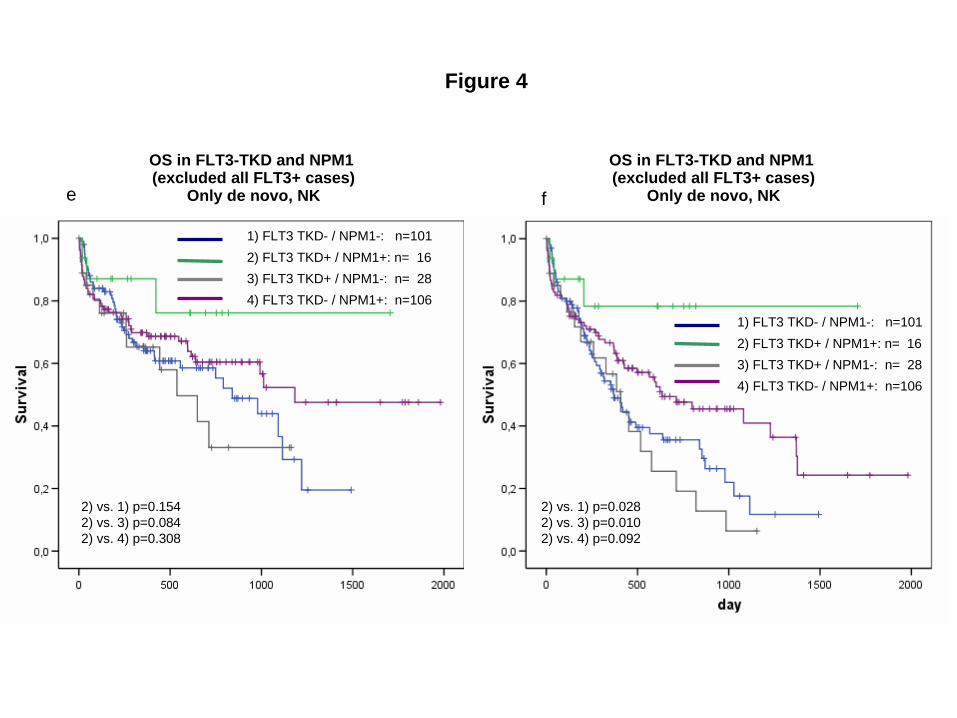
Figure 4
e f
2) vs. 1) p=0.1542) vs. 3) p=0.0842) vs. 4) p=0.308
2) FLT3 TKD+ / NPM1+: n= 161) FLT3 TKD- / NPM1-: n=101
3) FLT3 TKD+ / NPM1-: n= 284) FLT3 TKD- / NPM1+: n=106
OS in FLT3-TKD and NPM1 (excluded all FLT3+ cases)
Only de novo, NK
OS in FLT3-TKD and NPM1 (excluded all FLT3+ cases)
Only de novo, NK
2) FLT3 TKD+ / NPM1+: n= 161) FLT3 TKD- / NPM1-: n=101
3) FLT3 TKD+ / NPM1-: n= 284) FLT3 TKD- / NPM1+: n=106
2) vs. 1) p=0.0282) vs. 3) p=0.0102) vs. 4) p=0.092
F
or personal use only. by guest on June 6, 2013.
bloodjournal.hematologylibrary.org
From

Figure 5
2) FLT3 TKD+ / CEBPA+:n=4
1) FLT3 TKD- / CEBPA-: n=293
3) FLT3 TKD+ / CEBPA-: n=25
4) FLT3 TKD- / CEBPA+: n=41
2) FLT3 TKD+ / CEBPA+:n=4
1) FLT3 TKD- / CEBPA-: n=293
3) FLT3 TKD+ / CEBPA-: n=25
4) FLT3 TKD- / CEBPA+: n=41
2) vs. 1) p=0.0932) vs. 3) p=0.0372) vs. 4) p=0.124
2) vs. 1) p=0.1202) vs. 3) p=0.0742) vs. 4) p=0.204
a b
F
or personal use only. by guest on June 6, 2013.
bloodjournal.hematologylibrary.org
From
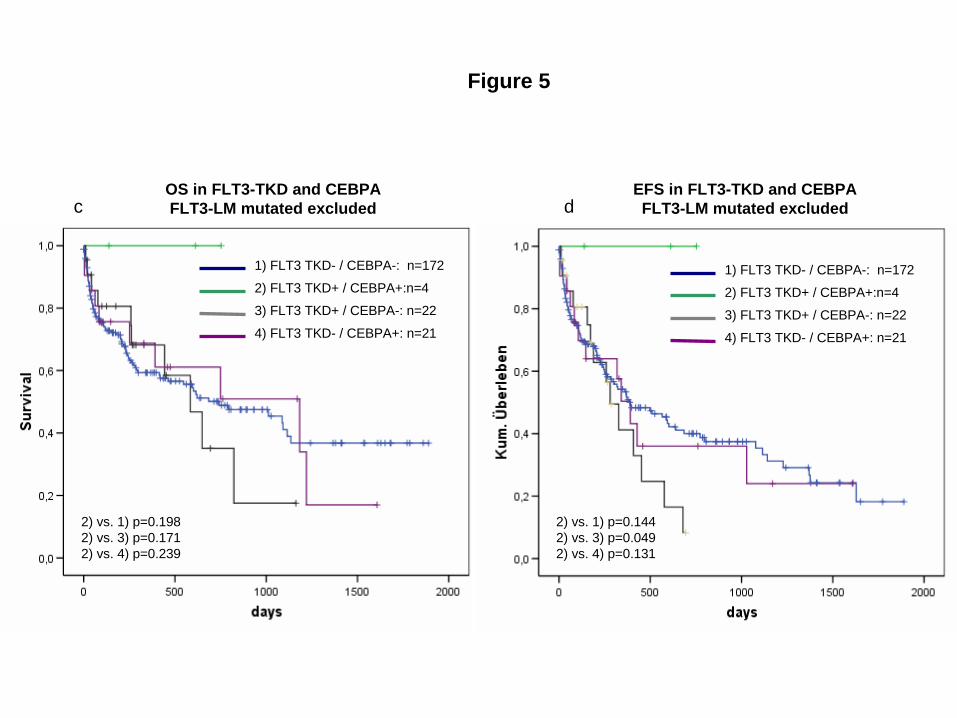
Figure 5
2) FLT3 TKD+ / CEBPA+:n=4
1) FLT3 TKD- / CEBPA-: n=172
3) FLT3 TKD+ / CEBPA-: n=22
4) FLT3 TKD- / CEBPA+: n=21
2) FLT3 TKD+ / CEBPA+:n=4
1) FLT3 TKD- / CEBPA-: n=172
3) FLT3 TKD+ / CEBPA-: n=22
4) FLT3 TKD- / CEBPA+: n=21
c dOS in FLT3-TKD and CEBPAFLT3-LM mutated excluded
EFS in FLT3-TKD and CEBPAFLT3-LM mutated excluded
2) vs. 1) p=0.1982) vs. 3) p=0.1712) vs. 4) p=0.239
2) vs. 1) p=0.1442) vs. 3) p=0.0492) vs. 4) p=0.131
F
or personal use only. by guest on June 6, 2013.
bloodjournal.hematologylibrary.org
From