principles of drainage
TRANSCRIPT

Principles of DrainageHenrik Petrowsky, Stefan Wildi
Introduction
Drains are designated to evacuate intraperitoneal fluid collections. They can be used fordiagnostic, prophylactic, or therapeutic purposes. In upper gastrointestinal surgery,diagnostic drains are mainly placed to assess intraperitoneal fluid collections in order toestablish a diagnosis. These drains are seldom left in place and are, therefore, of minorimportance. In contrast, prophylactic drains placed at the end of an operation are usedfrequently with two intentions: first, to prevent fluid accumulations which could beharmful (i.e., pancreatic juice or bile) or to evacuate fluid collections that can becomeinfected and lead to the formation of intra-abdominal abscesses; second, prophylacticdrains may be used to detect early postoperative complications, such as intra-abdominalbleeding or anastomotic leakage. Sometimes, fluid collections become infected anddevelop into abscesses; the management of these collections requires therapeuticdrainage either by the percutaneous route or by reoperative surgical lavage.
Types of Drain
Drains can be divided into passive and active drains.
Passive Drains
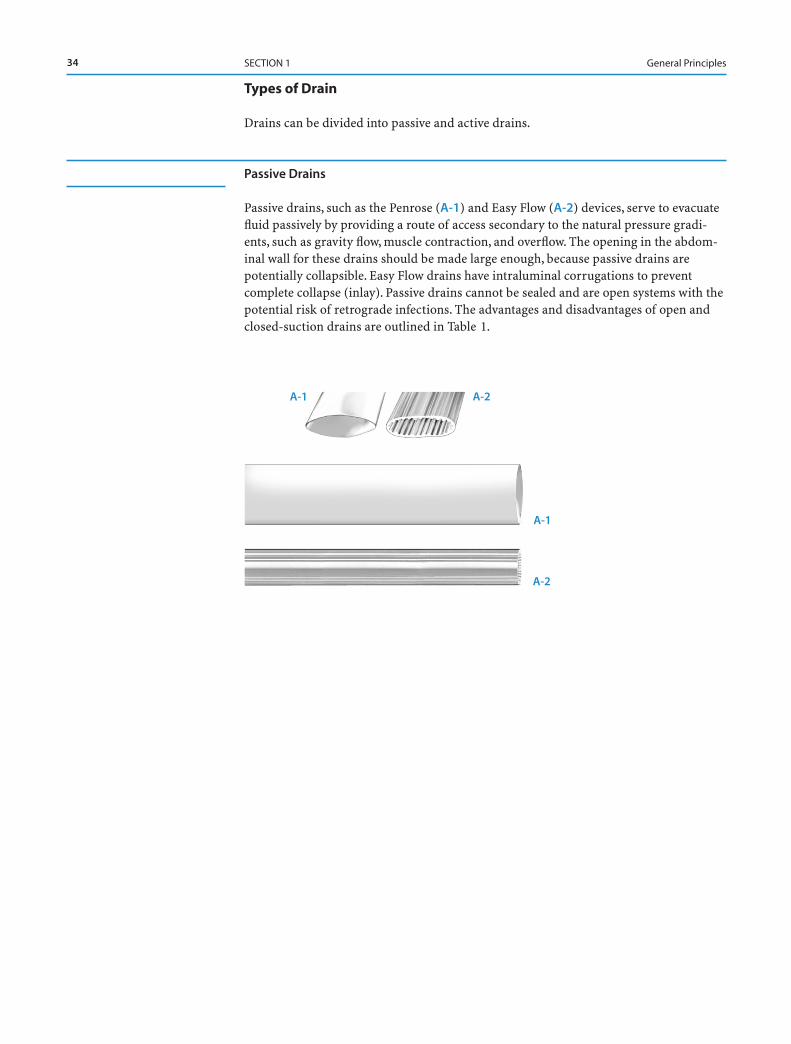
Passive drains, such as the Penrose (A-1) and Easy Flow (A-2) devices, serve to evacuatefluid passively by providing a route of access secondary to the natural pressure gradi-ents, such as gravity flow, muscle contraction, and overflow. The opening in the abdom-inal wall for these drains should be made large enough, because passive drains arepotentially collapsible. Easy Flow drains have intraluminal corrugations to preventcomplete collapse (inlay). Passive drains cannot be sealed and are open systems with thepotential risk of retrograde infections. The advantages and disadvantages of open andclosed-suction drains are outlined in Table 1.
34 SECTION 1 General Principles
A-1 A-2
A-1
A-2
Aktive Drains
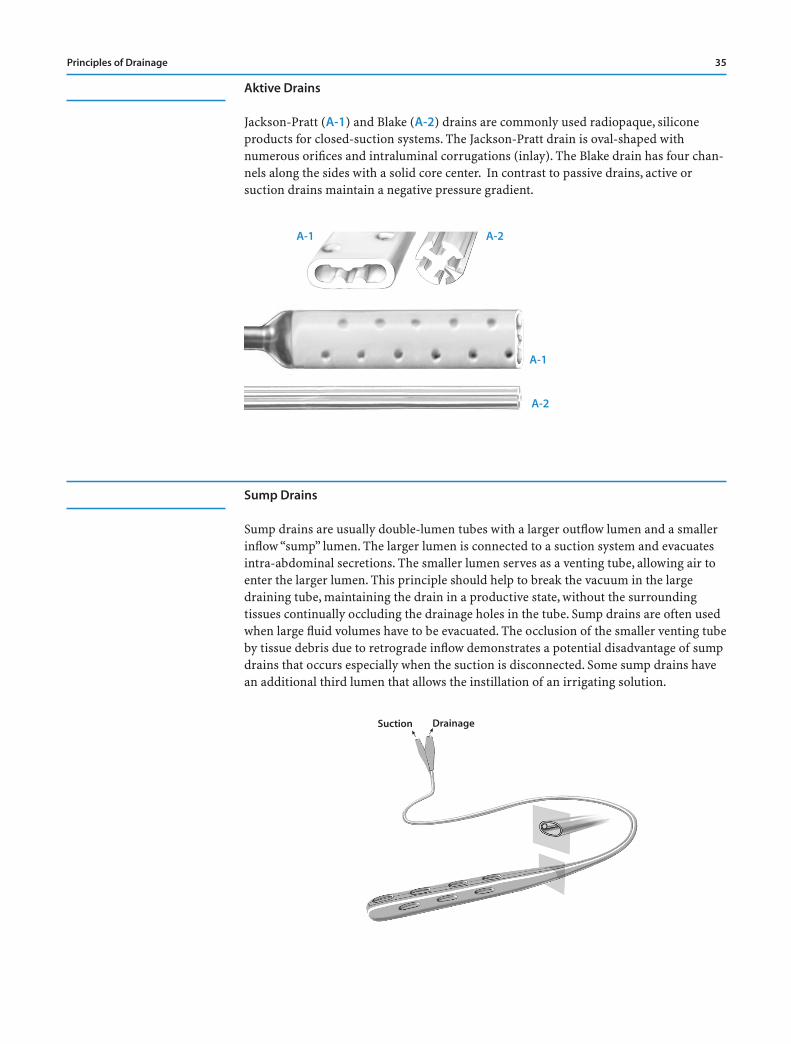
Jackson-Pratt (A-1) and Blake (A-2) drains are commonly used radiopaque, siliconeproducts for closed-suction systems. The Jackson-Pratt drain is oval-shaped withnumerous orifices and intraluminal corrugations (inlay). The Blake drain has four chan-nels along the sides with a solid core center. In contrast to passive drains, active orsuction drains maintain a negative pressure gradient.
Sump Drains
Sump drains are usually double-lumen tubes with a larger outflow lumen and a smallerinflow “sump” lumen. The larger lumen is connected to a suction system and evacuatesintra-abdominal secretions. The smaller lumen serves as a venting tube, allowing air toenter the larger lumen. This principle should help to break the vacuum in the largedraining tube, maintaining the drain in a productive state, without the surroundingtissues continually occluding the drainage holes in the tube. Sump drains are often usedwhen large fluid volumes have to be evacuated. The occlusion of the smaller venting tubeby tissue debris due to retrograde inflow demonstrates a potential disadvantage of sumpdrains that occurs especially when the suction is disconnected. Some sump drains havean additional third lumen that allows the instillation of an irrigating solution.
Principles of Drainage 35
A-1 A-2
A-1
A-2
1
Suction1
Drainage
Complete Drainage System
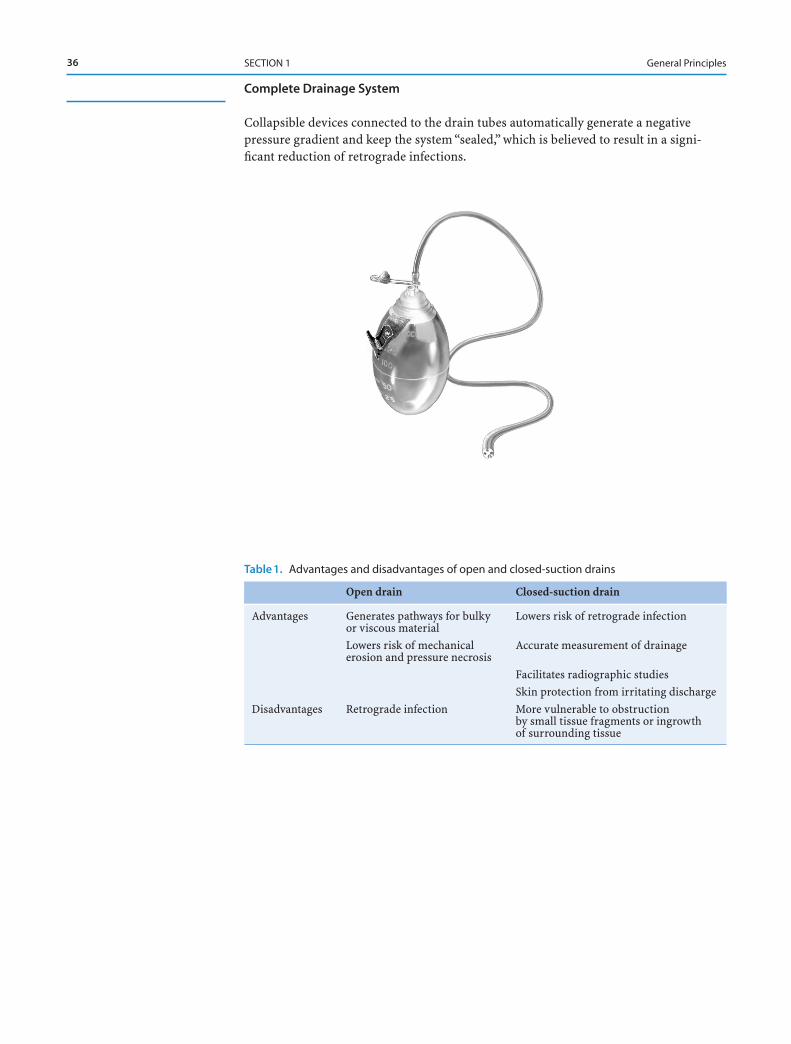
Collapsible devices connected to the drain tubes automatically generate a negative pressure gradient and keep the system “sealed,” which is believed to result in a signi-ficant reduction of retrograde infections.
36 SECTION 1 General Principles
Table 1. Advantages and disadvantages of open and closed-suction drains
Open drain Closed-suction drain
Advantages Generates pathways for bulky Lowers risk of retrograde infectionor viscous materialLowers risk of mechanical Accurate measurement of drainageerosion and pressure necrosis
Facilitates radiographic studiesSkin protection from irritating discharge
Disadvantages Retrograde infection More vulnerable to obstruction by small tissue fragments or ingrowth of surrounding tissue
Prophylactic Drainage
Drain Orifice
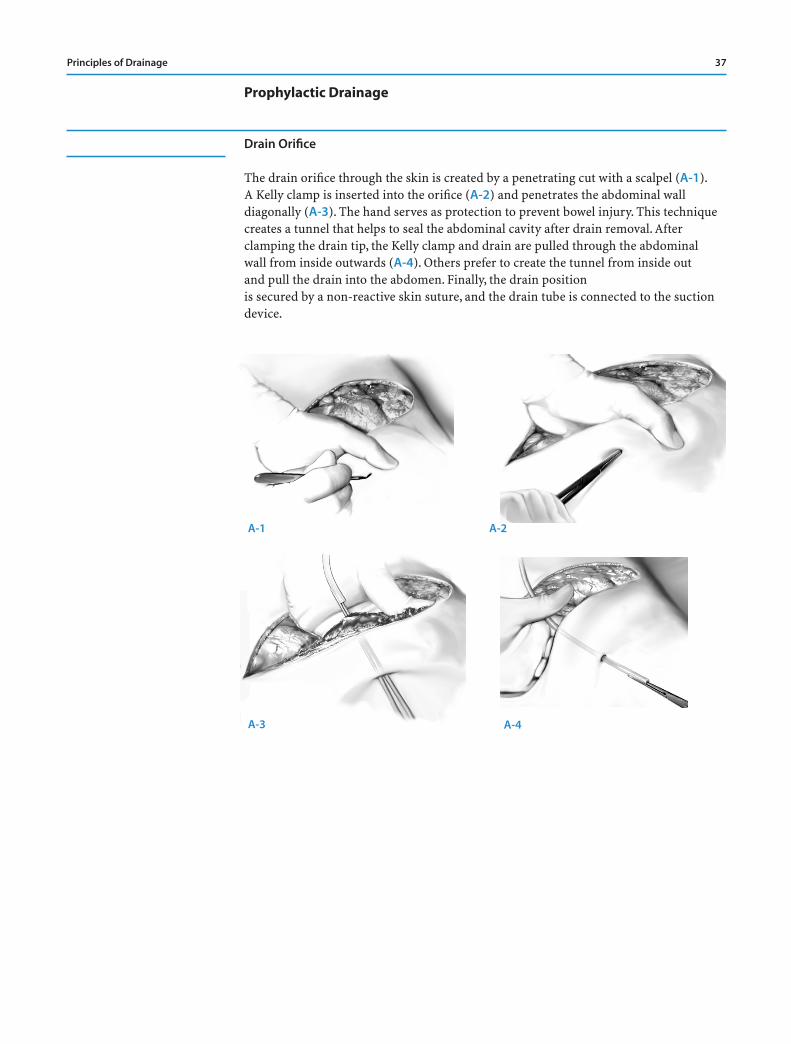
The drain orifice through the skin is created by a penetrating cut with a scalpel (A-1).A Kelly clamp is inserted into the orifice (A-2) and penetrates the abdominal wall diagonally (A-3). The hand serves as protection to prevent bowel injury. This techniquecreates a tunnel that helps to seal the abdominal cavity after drain removal. Afterclamping the drain tip, the Kelly clamp and drain are pulled through the abdominal wall from inside outwards (A-4). Others prefer to create the tunnel from inside out and pull the drain into the abdomen. Finally, the drain position is secured by a non-reactive skin suture, and the drain tube is connected to the suctiondevice.
Principles of Drainage 37
A-1 A-2
A-3 A-4
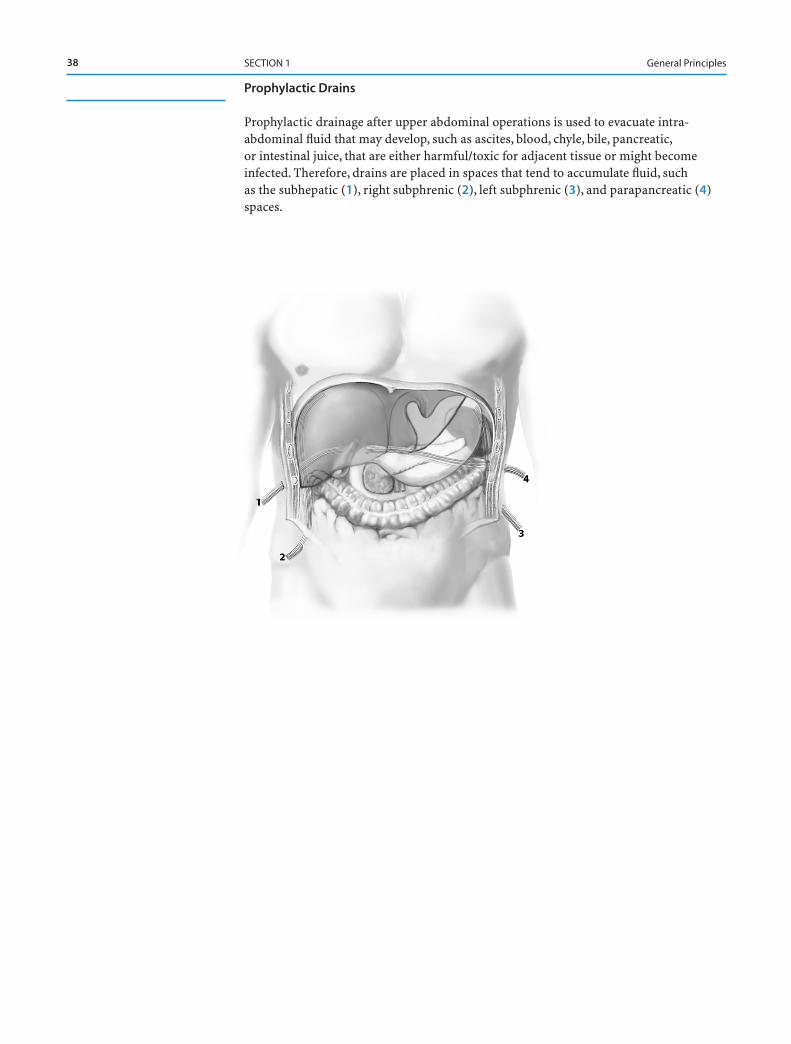
Prophylactic Drains
Prophylactic drainage after upper abdominal operations is used to evacuate intra-abdominal fluid that may develop, such as ascites, blood, chyle, bile, pancreatic,or intestinal juice, that are either harmful/toxic for adjacent tissue or might becomeinfected. Therefore, drains are placed in spaces that tend to accumulate fluid, such as the subhepatic (1), right subphrenic (2), left subphrenic (3), and parapancreatic (4)spaces.
38 SECTION 1 General Principles
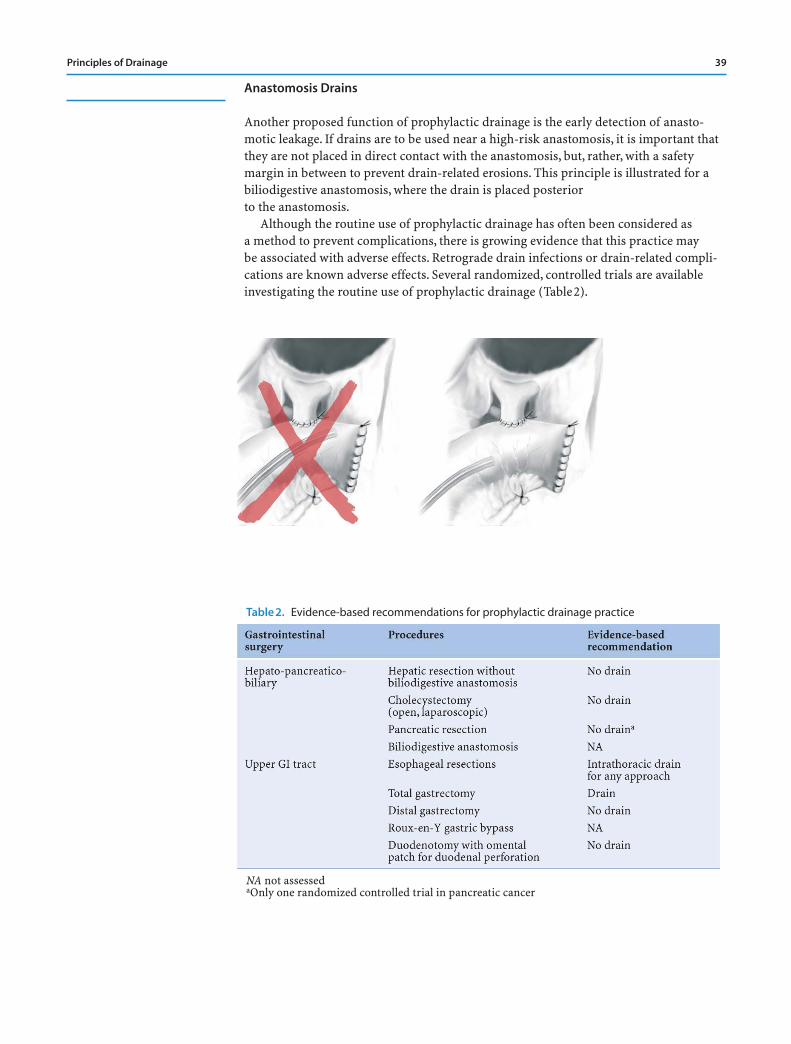
Anastomosis Drains
Another proposed function of prophylactic drainage is the early detection of anasto-motic leakage. If drains are to be used near a high-risk anastomosis, it is important thatthey are not placed in direct contact with the anastomosis, but, rather, with a safetymargin in between to prevent drain-related erosions. This principle is illustrated for abiliodigestive anastomosis, where the drain is placed posterior to the anastomosis.
Although the routine use of prophylactic drainage has often been considered as a method to prevent complications, there is growing evidence that this practice may be associated with adverse effects. Retrograde drain infections or drain-related compli-cations are known adverse effects. Several randomized, controlled trials are availableinvestigating the routine use of prophylactic drainage (Table2).
Principles of Drainage 39
Table 2. Evidence-based recommendations for prophylactic drainage practice
NA not assessedaOnly one randomized controlled trial in pancreatic cancer
Therapeutic Drainage
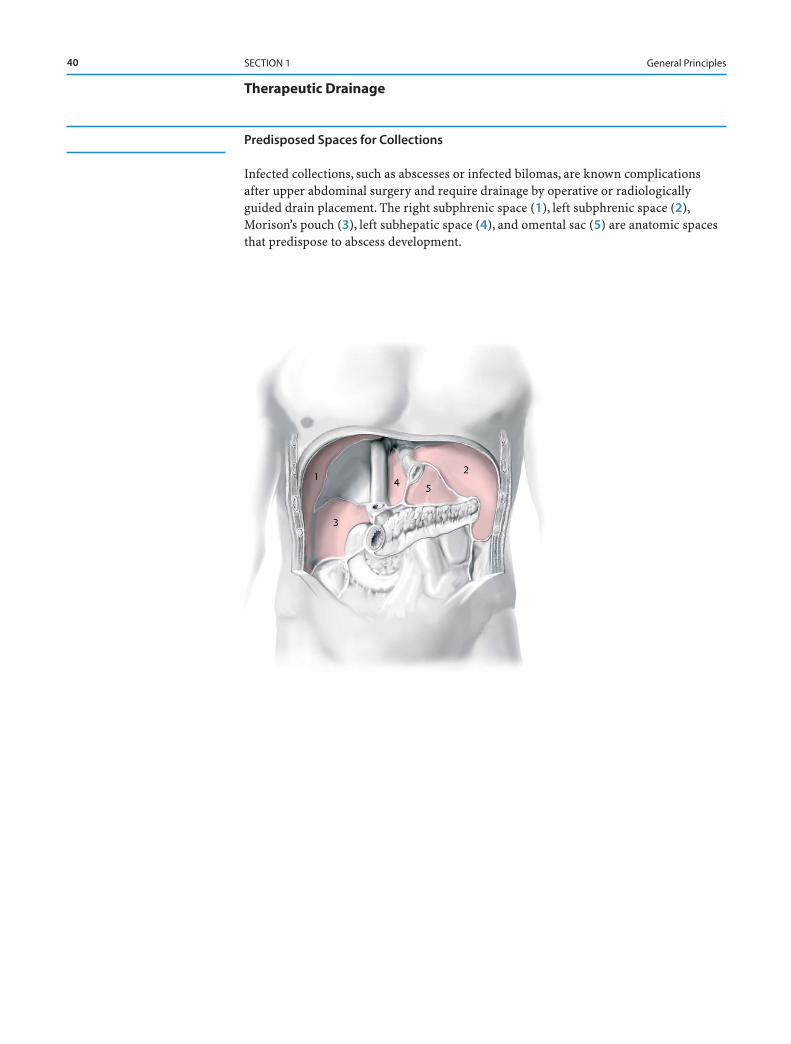
Predisposed Spaces for Collections
Infected collections, such as abscesses or infected bilomas, are known complicationsafter upper abdominal surgery and require drainage by operative or radiologicallyguided drain placement. The right subphrenic space (1), left subphrenic space (2),Morison’s pouch (3), left subhepatic space (4), and omental sac (5) are anatomic spacesthat predispose to abscess development.
40 SECTION 1 General Principles
Catheters
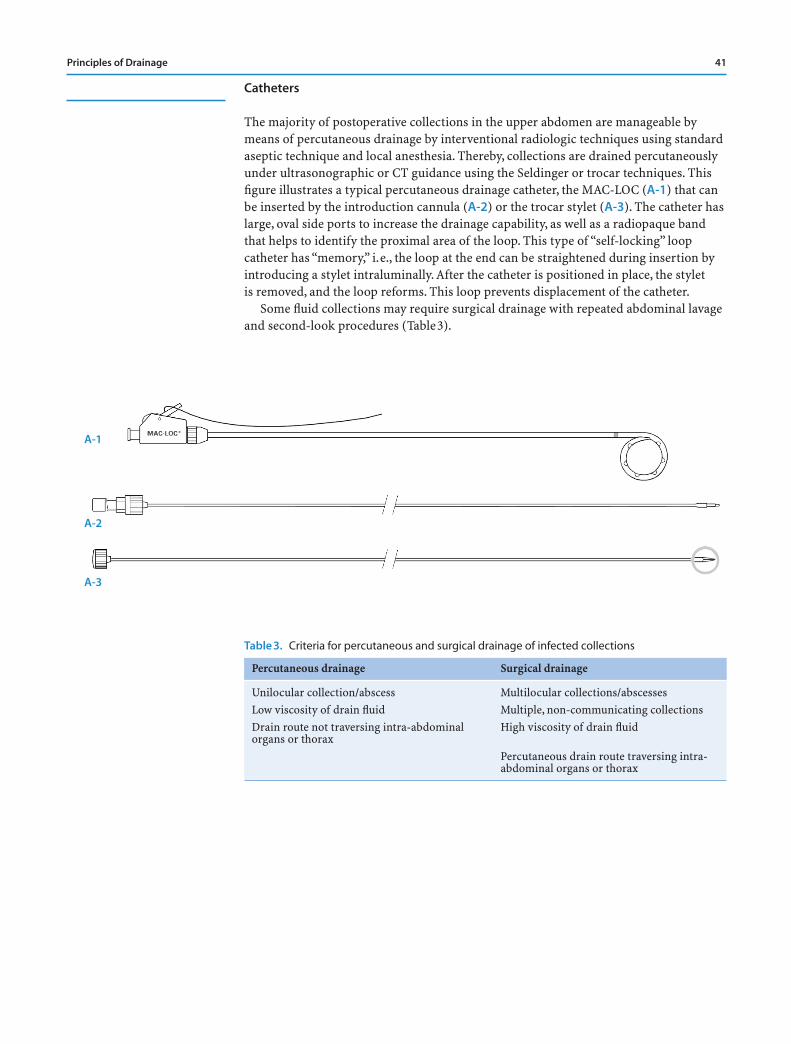
The majority of postoperative collections in the upper abdomen are manageable bymeans of percutaneous drainage by interventional radiologic techniques using standardaseptic technique and local anesthesia. Thereby, collections are drained percutaneouslyunder ultrasonographic or CT guidance using the Seldinger or trocar techniques. Thisfigure illustrates a typical percutaneous drainage catheter, the MAC-LOC (A-1) that canbe inserted by the introduction cannula (A-2) or the trocar stylet (A-3). The catheter haslarge, oval side ports to increase the drainage capability, as well as a radiopaque bandthat helps to identify the proximal area of the loop. This type of “self-locking” loopcatheter has “memory,” i.e., the loop at the end can be straightened during insertion byintroducing a stylet intraluminally. After the catheter is positioned in place, the stylet is removed, and the loop reforms. This loop prevents displacement of the catheter.
Some fluid collections may require surgical drainage with repeated abdominal lavageand second-look procedures (Table3).
Principles of Drainage 41
Table 3. Criteria for percutaneous and surgical drainage of infected collections
Percutaneous drainage Surgical drainage
Unilocular collection/abscess Multilocular collections/abscessesLow viscosity of drain fluid Multiple, non-communicating collectionsDrain route not traversing intra-abdominal High viscosity of drain fluidorgans or thorax
Percutaneous drain route traversing intra-abdominal organs or thorax
A-1
A-2
A-3
42
Tricks of the Senior Surgeon
■ Whenever indicated, always use closed drain systems and keep drains as short as possible to minimize the risk of retrograde infections.
■ Place drains near but never in direct contact to the anastomotic sutures toprevent drain-induced erosions or drain-induced anastomotic leaks.
■ When drains are not productive, do not rely on them! Drains could be occludedor obstructed by adjacent tissue.
■ Try to position intraperitoneal drains such that the drain does not rub against or lie in direct contact with blood vessels or hollow organs in an attempt toprevent drain erosions.
SECTION 1 General Principles