primary vascular tumors of the lungs: a review
TRANSCRIPT

Available online at www.sciencedirect.com
Annals of Diagnostic Pathology 14 (2010) 296–308
Review Article
Primary vascular tumors of the lungs: a reviewAnnikka Weissferdt, MD⁎, Cesar A. Moran, MD
Department of Pathology and Laboratory Medicine, MD Anderson Cancer Center, Houston, TX 77030, USA
Abstract Unlike their counterparts in other organ systems, primary vascular neoplasms of the lung are rare. Most
⁎ Corresponding aE-mail address: aw
1092-9134/$ – see frodoi:10.1016/j.anndiag
of these lesions have only been reported as isolated case studies or small series. When dealing withmalignant lesions, metastasis from extrapulmonary sites will have to be excluded before a primarylocation in the lungs can be confirmed. In this review, the clinicopathologic, immunophenotypical,ultrastructural, and molecular biologic characteristics of primary vascular tumors of the lungs arediscussed. The tumoral conditions that will be addressed include hemangioma, lymphangioma,epithelioid hemangioendothelioma, angiosarcoma, and Kaposi's sarcoma. Their respective differentialdiagnoses will also be discussed.
© 2010 Published by Elsevier Inc.Keywords: Lung; Vascular neoplasms; Immunohistochemistry; Molecular biology; Sarcoma
1. Introduction
Despite being an organ with a rich vascular network, thelung is only uncommonly the primary site for vascularneoplasms. Because of the rarity of these lesions, the clinicaland radiologic features are often mistaken for other, morecommon processes until the vascular nature of the disease isconfirmed by histologic examination. The most commontumors of vascular origin described in the pulmonary systeminclude hemangioma and lymphangioma among the benignlesions and epithelioid hemangioendothelioma, angiosar-coma, and Kaposi's sarcoma among the malignant ones.Before a diagnosis of a primary malignant vascularneoplasm can be rendered, metastasis from extrapulmonarysites will have to be excluded through thorough clinical andradiologic investigations. This review summarizes theprimary vascular neoplasms of the lung with an emphasison the clinicopathologic, immunohistochemical, ultrastruc-tural, and molecular biologic features of these tumors andtheir differential diagnoses.
2. Benign vascular neoplasms
The benign vascular neoplasms of the lung discussed in thisreview include hemangioma and lymphangioma. These
uthor. Tel.: +1 713 563 6786; fax: +1 713 792 [email protected] (A. Weissferdt).
nt matter © 2010 Published by Elsevier Inc.path.2010.03.001
lesions are clinically and radiologically often mistaken formore common intrapulmonary lesions such as cysts, congen-ital malformations, or foci of infection. Hemangiomas arefrequently seen in the soft tissue, skin, and liver and canoccasionally occur in the subglottic region or in themediastinum [1,2]. In the lung, however, these tumors arerare. To date, only 24 cases of pulmonary hemangiomas havebeen described in the English and Japanese literature [3,4].Benign tumors derived from the lymphatic endothelium arecalled lymphangiomas. Solitary lymphangiomas commonlyoccur in the neck, lip, tongue, skin, and soft tissue and onlyrarely in the lung with only 15 cases reported in the Englishliterature to date.
2.1. Clinical features
2.1.1. HemangiomaHemangiomas have been described in patients of all ages
(birth to 84 years) with no specific sex predilection, and bothsolitary and multiple lesions have been reported [3-9]. Patientsare either asymptomatic or present with respiratory symptomssuch as hemoptysis, pneumonia, or cyanosis [10-12].Radiologic examination reveals the presence of a nonspecificcystic lesion ormultiple nodules reminiscent of interstitial lungdisease [3,11]. Hemangiomas may arise anywhere in the lowerrespiratory tract from the lung parenchyma to the airways andthe bronchial tree [13-16]. Although only few hemangiomas ofthe lung have been reported, one case describes an associationwith partial trisomy D, whereas another raises the possibility
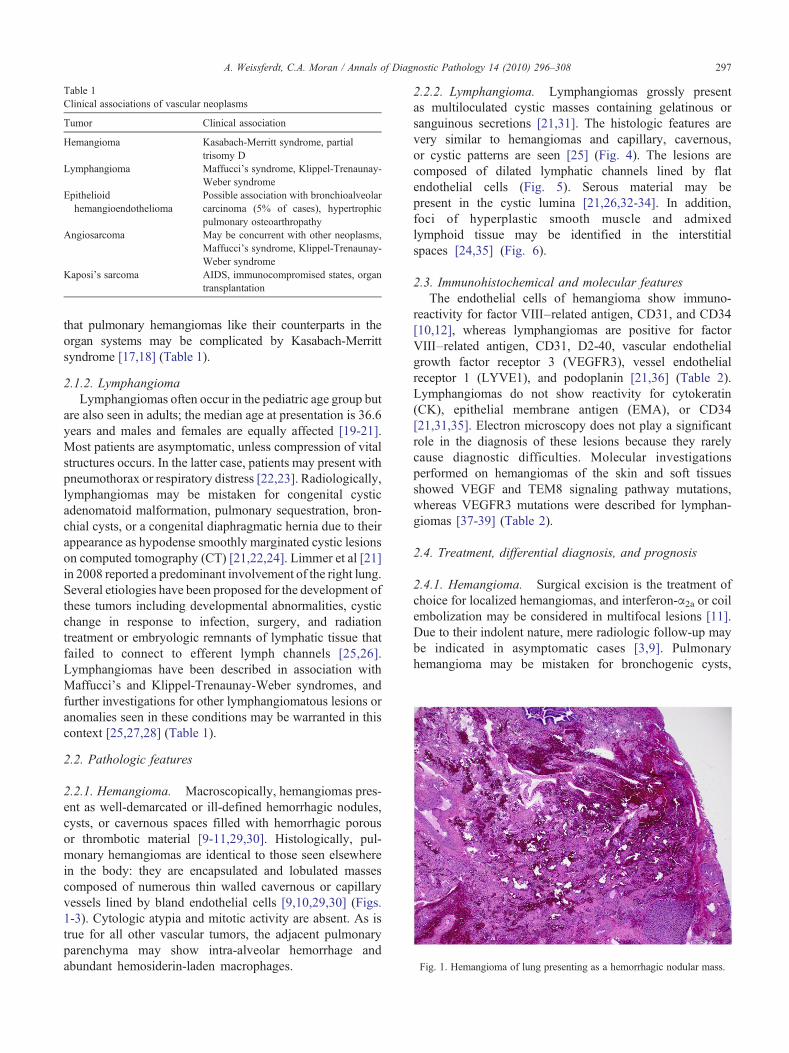
Table 1Clinical associations of vascular neoplasms
Tumor Clinical association
Hemangioma Kasabach-Merritt syndrome, partialtrisomy D
Lymphangioma Maffucci's syndrome, Klippel-Trenaunay-Weber syndrome
Epithelioidhemangioendothelioma
Possible association with bronchioalveolarcarcinoma (5% of cases), hypertrophicpulmonary osteoarthropathy
Angiosarcoma May be concurrent with other neoplasms,Maffucci's syndrome, Klippel-Trenaunay-Weber syndrome
Kaposi's sarcoma AIDS, immunocompromised states, organtransplantation
Fig. 1. Hemangioma of lung presenting as a hemorrhagic nodular mass.
297A. Weissferdt, C.A. Moran / Annals of Diagnostic Pathology 14 (2010) 296–308
that pulmonary hemangiomas like their counterparts in theorgan systems may be complicated by Kasabach-Merrittsyndrome [17,18] (Table 1).
2.1.2. LymphangiomaLymphangiomas often occur in the pediatric age group but
are also seen in adults; the median age at presentation is 36.6years and males and females are equally affected [19-21].Most patients are asymptomatic, unless compression of vitalstructures occurs. In the latter case, patients may present withpneumothorax or respiratory distress [22,23]. Radiologically,lymphangiomas may be mistaken for congenital cysticadenomatoid malformation, pulmonary sequestration, bron-chial cysts, or a congenital diaphragmatic hernia due to theirappearance as hypodense smoothly marginated cystic lesionson computed tomography (CT) [21,22,24]. Limmer et al [21]in 2008 reported a predominant involvement of the right lung.Several etiologies have been proposed for the development ofthese tumors including developmental abnormalities, cysticchange in response to infection, surgery, and radiationtreatment or embryologic remnants of lymphatic tissue thatfailed to connect to efferent lymph channels [25,26].Lymphangiomas have been described in association withMaffucci's and Klippel-Trenaunay-Weber syndromes, andfurther investigations for other lymphangiomatous lesions oranomalies seen in these conditions may be warranted in thiscontext [25,27,28] (Table 1).
2.2. Pathologic features
2.2.1. Hemangioma. Macroscopically, hemangiomas pres-ent as well-demarcated or ill-defined hemorrhagic nodules,cysts, or cavernous spaces filled with hemorrhagic porousor thrombotic material [9-11,29,30]. Histologically, pul-monary hemangiomas are identical to those seen elsewherein the body: they are encapsulated and lobulated massescomposed of numerous thin walled cavernous or capillaryvessels lined by bland endothelial cells [9,10,29,30] (Figs.1-3). Cytologic atypia and mitotic activity are absent. As istrue for all other vascular tumors, the adjacent pulmonaryparenchyma may show intra-alveolar hemorrhage andabundant hemosiderin-laden macrophages.
2.2.2. Lymphangioma. Lymphangiomas grossly presentas multiloculated cystic masses containing gelatinous orsanguinous secretions [21,31]. The histologic features arevery similar to hemangiomas and capillary, cavernous,or cystic patterns are seen [25] (Fig. 4). The lesions arecomposed of dilated lymphatic channels lined by flatendothelial cells (Fig. 5). Serous material may bepresent in the cystic lumina [21,26,32-34]. In addition,foci of hyperplastic smooth muscle and admixedlymphoid tissue may be identified in the interstitialspaces [24,35] (Fig. 6).
2.3. Immunohistochemical and molecular featuresThe endothelial cells of hemangioma show immuno-
reactivity for factor VIII–related antigen, CD31, and CD34[10,12], whereas lymphangiomas are positive for factorVIII–related antigen, CD31, D2-40, vascular endothelialgrowth factor receptor 3 (VEGFR3), vessel endothelialreceptor 1 (LYVE1), and podoplanin [21,36] (Table 2).Lymphangiomas do not show reactivity for cytokeratin(CK), epithelial membrane antigen (EMA), or CD34[21,31,35]. Electron microscopy does not play a significantrole in the diagnosis of these lesions because they rarelycause diagnostic difficulties. Molecular investigationsperformed on hemangiomas of the skin and soft tissuesshowed VEGF and TEM8 signaling pathway mutations,whereas VEGFR3 mutations were described for lymphan-giomas [37-39] (Table 2).
2.4. Treatment, differential diagnosis, and prognosis
2.4.1. Hemangioma. Surgical excision is the treatment ofchoice for localized hemangiomas, and interferon-α2a or coilembolization may be considered in multifocal lesions [11].Due to their indolent nature, mere radiologic follow-up maybe indicated in asymptomatic cases [3,9]. Pulmonaryhemangioma may be mistaken for bronchogenic cysts,
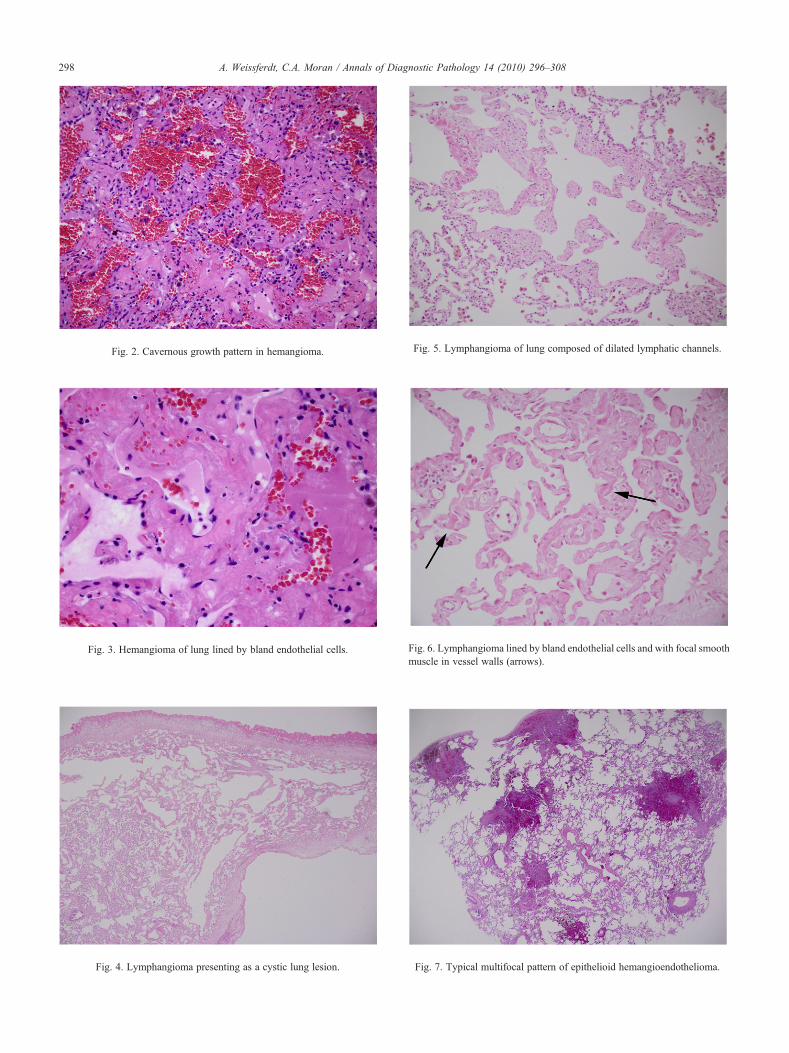
Fig. 2. Cavernous growth pattern in hemangioma.
Fig. 3. Hemangioma of lung lined by bland endothelial cells.
Fig. 4. Lymphangioma presenting as a cystic lung lesion.
Fig. 5. Lymphangioma of lung composed of dilated lymphatic channels.
298 A. Weissferdt, C.A. Moran / Annals of Diagnostic Pathology 14 (2010) 296–308
Fig. 6. Lymphangioma lined by bland endothelial cells and with focal smoothmuscle in vessel walls (arrows).
Fig. 7. Typical multifocal pattern of epithelioid hemangioendothelioma.

Table 2Immunohistochemical and molecular features of vascular neoplasms
Tumor Immunohistochemicalphenotype
Molecular biology
Hemangioma Factor VIII, CD31, CD34 VEGF and TEM8 mutationsLymphangioma Factor VIII, CD31, D2-40, LYVE1, podoplanin VEGFR3 mutationsEpithelioid hemangioendothelioma Factor VIII, CD31, CD34, CK7 in 50% of cases (1;3)(p36.3;q25) or (7;22) translocationsAngiosarcoma Factor VIII, CD31, CD34, CK in epithelioid type K-ras-2 gene mutations; PTEN mutations; up-regulation of p53
protein; chromosomal structural rearrangement and polysomyof chromosome 8; increased expression of VEGFR and mdm-2-protooncogene; gains of chromosomes 5, 8, and 20 and lossesof chromosomes 7, 22, and the Y chromosome
Kaposi's sarcoma CD31, CD34, D2-40, podoplanin, VEGFR3, HHV8 Deletion and translocation of chromosome 3, int-2 oncogeneexpression, overexpression of bcl-2
299A. Weissferdt, C.A. Moran / Annals of Diagnostic Pathology 14 (2010) 296–308
infection, or arteriovenous malformation radiologically andshould be distinguished from pulmonary capillary heman-giomatosis and diffuse neonatal hemangiomatosis at amicroscopic level. Pulmonary capillary hemangiomatosisand diffuse neonatal hemangiomatosis are distinct entitieswith the former presenting as a multifocal angiomatousproliferation associated with pulmonary hypertension andpoor long-term survival and the latter being an often fataldisorder characterized by extensive capillary hemangiomasof the skin and visceral organs. Whereas localizedpulmonary hemangiomas tend to have a favorable outcome,multifocal lesions may cause significant loss of lung functionresulting in a poorer prognosis [11].
2.4.2. Lymphangioma. Because spontaneous regressionhas not been described and the tumors have a tendency torecur if incompletely excised, the therapy of choice forlymphangiomas consists of surgical resection or scler-otherapy [25,40,41]. The differential diagnosis for lym-phangiomas includes localized forms of congenitalpulmonary lymphangiectasia, cystic epithelial tumors,and lymphangioleiomyomatosis [34,42]. Lymphangiectasisis characterized by dilatation of existing lymphatic vesselsrather than an increased number of lymphovascularchannels, and although smooth muscle may be seen inassociation with this disorder, the muscle is generallymore pronounced in lymphangioma [43]. Cystic epithelialtumors normally occur in an older age group, show morepronounced cytologic pleomorphism, an increased mitoticactivity and an epithelial immunophenotype facilitatingdistinction from the benign lymphangioma. Lastly,lymphangioleiomyomatosis is a condition that primarilyoccurs in women of reproductive age. It presents as acystic lung process which is not limited to the lymphaticroutes but rather involves the alveoli and contains arelatively large proportion of smooth muscle [43].Immunohistochemically, the spindle cells in lymphangio-leiomyomatosis express immunoreactivity for estrogen andprogesterone receptors and HMB45, further distinguishingthis lesion from lymphangioma [44-46]. Complete exci-sion of lymphangiomas should be curative with noreported recurrences to date [21].
3. Malignant vascular neoplasms
The malignant neoplasms of vascular origin encounteredin the lungs comprise epithelioid hemangioendothelioma,angiosarcoma, and Kaposi's sarcoma. Epithelioid heman-gioendothelioma was first described as “intravascularbronchioalveolar tumor” by Dail and Liebow in 1975,suggesting that this tumor was of epithelial origin [47].Using ultrastructural techniques, several groups subsequent-ly demonstrated that the lesion was in fact a vascular tumor[48,49]. After Weiss and Enzinger used the term “epithelioidhemangioendothelioma” to describe a similar tumor in thesoft tissue in 1982, it soon became clear that these lesionswere essentially identical and the term “epithelioid heman-gioendothelioma” has since been used to describe thesetumors regardless of their location [50-52]. To date, morethan 80 cases have been described in the lung [53].
Angiosarcomas represent less than 1% of all sarcomasand develop most often in the skin, soft tissue, or liver.They may be associated with previous radiation treatment;environmental carcinogens like vinyl chloride, thorotrast,or phenylethyl hydrazine, foreign body material orlymphedema [54-61]. The lungs are more often the siteof metastasis from extrapulmonary tumors, most frequent-ly from the heart and the pulmonary artery trunk [62-65].In the lung, primary angiosarcomas are extremelyuncommon with less than 20 cases reported in the Englishliterature to date.
Before 1981, Kaposi's sarcoma was mainly known as anindolent neoplasm affecting the skin of the lowerextremities of elderly men of Mediterranean or AshkenazieJewish origin [66]. Sporadic disseminated Kaposi's sarco-ma was rare and pulmonary involvement even rarer[67,68]. Kaposi's sarcoma, however, was soon recognizedto be the most common neoplasm in patients with acquiredimmunodeficiency syndrome (AIDS) and in these casesoften presenting with nodal and visceral involvement and amore aggressive behavior [69,70]. As many as 47% to 90%of AIDS patients were found to have Kaposi's sarcomainvolving the lungs at autopsy, but only isolated casereports describe the presence of Kaposi's sarcoma as aprimary pulmonary tumor [71-83].
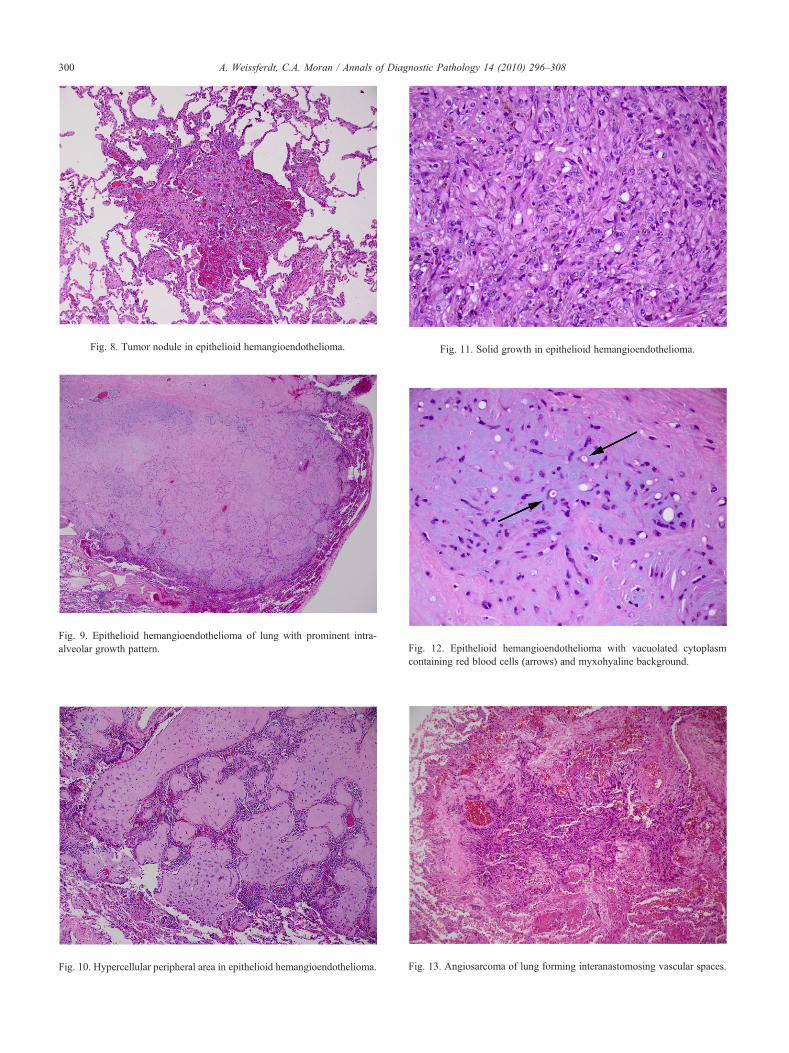
Fig. 8. Tumor nodule in epithelioid hemangioendothelioma.
Fig. 9. Epithelioid hemangioendothelioma of lung with prominent intra-alveolar growth pattern.
Fig. 10. Hypercellular peripheral area in epithelioid hemangioendothelioma.
Fig. 12. Epithelioid hemangioendothelioma with vacuolated cytoplasmcontaining red blood cells (arrows) and myxohyaline background.
Fig. 11. Solid growth in epithelioid hemangioendothelioma.
Fig. 13. Angiosarcoma of lung forming interanastomosing vascular spaces.
300 A. Weissferdt, C.A. Moran / Annals of Diagnostic Pathology 14 (2010) 296–308

301A. Weissferdt, C.A. Moran / Annals of Diagnostic Pathology 14 (2010) 296–308
3.1. Clinical features
3.1.1. Epithelioid hemangioendotheliomaEpithelioid hemangioendothelioma primarily occurs in
younger individuals, with 50% of patients being youngerthan 40 years of age at diagnosis (median age 36 years).Females account for approximately 80% of cases [84-86].Patients are often asymptomatic or present with dyspnea,cough, or pleuritic chest pain. Rare cases are symptomaticwith alveolar hemorrhage and pleural effusions [87-91].Radiologically, epithelioid hemangioendothelioma is char-acterized by multiple small nodular lesions in both lungsmimicking granulomatous or metastatic disease processes.In rare cases, ground glass opacities are identified on CTsuggestive of interstitial lung disease. Epithelioid heman-gioendothelioma is always a multifocal process and com-posed of multiple discrete nodules measuring less than 2cm in diameter [92]. A single case report describes thepresence of pulmonary epithelioid hemangioendotheliomawith hypertrophic pulmonary osteoarthropathy, and ap-proximately 5% of cases have been seen with concurrentbronchioloaveolar carcinoma raising the possibility of anassociation between these lesions [85,87,93] (Table 1).
3.1.2. AngiosarcomaAngiosarcomas affect adults with an age range from 22 to
79 years (mean, 54 years) and a male to female ratio of 3:1.Presenting symptoms include dyspnea, chest pain, hemopty-sis, cough, pulmonary hemorrhage, or hemothorax [94-97].Radiologically, bilateral interstitial or parenchymal infil-trates, pleural effusions, or solid masses are identified, whichmay mimic inflammatory processes or metastatic carcinoma[94,96,98-100]. Tumors arise in the parenchyma, thepulmonary artery trunk, or the bronchus [94,98,101].Although often presenting as a diffuse process, single masslesions may also be seen [95,98,100]. While pulmonaryangiosarcomas may rarely be seen with concurrentmalignant neoplasms of other organ systems, angiosarco-mas of extrapulmonary sites have been described inassociation with Maffucci's and Klippel-Trenaunay-Webersyndromes raising the possibility that patients withpulmonary angiosarcomas may also benefit from furtherinvestigations in this context [102-104] (Table 1).
3.1.3. KaposiTs sarcomaDyspnea, cough, hemoptysis, fatigue, fever or respiratory
failure are the main presenting symptoms in patients withpulmonary Kaposi's sarcoma [67,80,105]. Radiologically,Kaposi's sarcoma is characterized by diffuse reticulonodularpulmonary infiltrates, solitary lung nodules, or pleuraleffusions [71,72,81,106,107]. Often there is central sym-metrical bronchial wall thickening particularly in associationwith septal lines; unusual features include the presence oflarger peripherally located nodules the predominance ofwhich should prompt investigations into a different etiology[69]. Often there is widespread dissemination of disease withinvolvement of the tracheobronchial tree, lung parenchyma,
mediastinal lymph nodes, and the pleura [108,109].Although, most cases of Kaposi's sarcoma of the lungpresent in association with AIDS, cases may also developafter organ transplantation, in association with otherimmunocompromised states and less commonly in healthyindividuals [77,83] (Table 1). Kaposi's sarcoma in AIDS andin transplant patients is closely associated with human herpesvirus 8 (HHV8) infection, and the detection of HHV8-DNAis thought to be highly specific and sensitive for a diagnosisof pulmonary Kaposi's sarcoma adding an importantdiagnostic tool in this setting [110,111].
3.2. Pathologic features
3.2.1. Epithelioid hemangioendotheliomaMacroscopically, epithelioid hemangioendothelioma pre-
sents as multiple nodules with a gray-white cut surface and achondroid appearance. Histologically, epithelioid heman-gioendothelioma is often closely associated with arterioles,venules, and lymphatic vessels and is characterized by thepresence of multiple nodules (Fig. 7 and 8). These tumornodules often display an intra-alveolar growth pattern, hencethe original term of intravascular bronchioalveolar tumor(Fig. 9). The individual nodules often have hypocellularcenters surrounded by rims of more cellular tissue (Fig. 10).The cellular areas are composed of short strands or solidnests of rounded or spindled endothelial cells (Fig. 11). Theyhave central round to ovoid nuclei and intracytoplasmiclumina or vacuoles, which may contain erythrocytes. Thecells are set in a prominent myxochondroid or hyaline stroma(Fig. 12). Overall, the cytologic features are bland withminimal nuclear pleomorphism and virtually no mitoticactivity [92,112]. In the soft tissue, up to one fourth of casesmay display a degree of cytologic atypia, mitotic activity,spindling of cells, or necrosis [112]. These features have notbeen described in primary lung lesions.
3.2.2. AngiosarcomaIn angiosarcoma, the lungs appear diffusely hemorrhagic
and studded with multiple dark red nodules [95,98]. Thetumors involve particularly the interlobar septa and bronch-ovascular bundles with a predilection to grow along thelymphatic or venous routes. Primary angiosarcomas of thelung have similar histologic growth patterns to those seen inother sites. Low-grade tumors are characterized by irregularinteranastomosing vascular channels dissecting the lungparenchyma (Fig. 13). In contrast to benign vascularneoplasms, these channels are lined by more atypicalendothelial cells that display crowding or hobnailing alongthe vessel walls (Fig. 14). In some areas, the crowding is sopronounced as to form papillary projections similar to thoseseen in papillary endothelial hyperplasia. Further patterns ofgrowth include the formation of capillary, cavernous, or slit-like vascular spaces. In high-grade tumors, the vascularnature of the neoplasms may be difficult to identify. Thesetumors are commonly composed of solid sheets ofepithelioid or spindled tumor cells (Fig. 15). Cytologically,
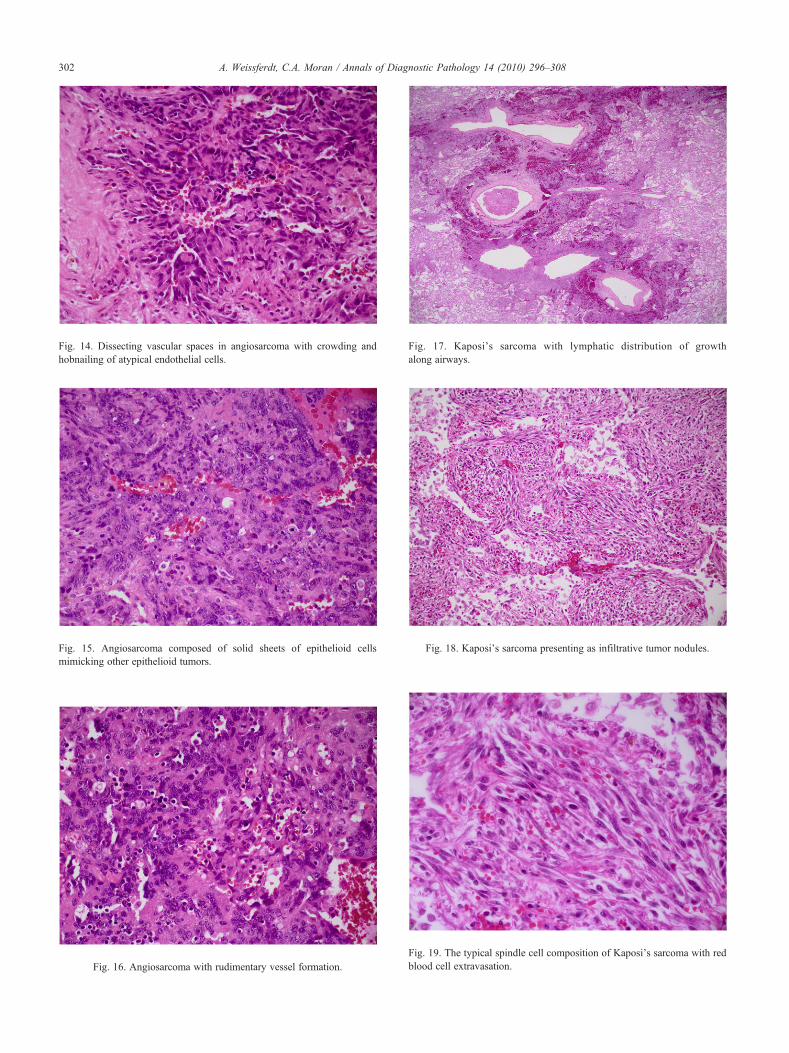
Fig. 15. Angiosarcoma composed of solid sheets of epithelioid cellsmimicking other epithelioid tumors.
Fig. 16. Angiosarcoma with rudimentary vessel formation.
ig. 17. Kaposi's sarcoma with lymphatic distribution of growthFig. 14. Dissecting vascular spaces in angiosarcoma with crowding andhobnailing of atypical endothelial cells.
302 A. Weissferdt, C.A. Moran / Annals of Diagnostic Pathology 14 (2010) 296–308
F
along airways.Fig. 18. Kaposi's sarcoma presenting as infiltrative tumor nodules.
ig. 19. The typical spindle cell composition of Kaposi's sarcoma with redlood cell extravasation.
Fb

303A. Weissferdt, C.A. Moran / Annals of Diagnostic Pathology 14 (2010) 296–308
these cells show obvious malignant features of pleomorphictumor cells with large vesicular and hyperchromatic nuclei,abundant pale cytoplasm, and high mitotic activity. Intracy-toplasmic vacuoles containing red blood cells or rudimentarylumen formation may occasionally be seen facilitatingdistinction from other neoplasms (Fig. 16). The parenchymasurrounding the tumors is often intensely hemorrhagic andmay contain abundant hemosiderin-laden macrophages[94,96,102,113]. Prominent concentric rings of tumoraround intact blood vessels were seen in 1 case [94].
3.2.3. KaposiTs sarcomaMacroscopically, the lung parenchyma in Kaposi's
sarcoma is infiltrated by discrete dark red hemorrhagicnodules with associated intra-alveolar hemorrhage. Endo-bronchial lesions present as multiple dark red raised lesionson bronchoscopy [71,114-116]. The histologic hallmark ofKaposi's sarcoma is its lymphatic distribution with growthalong the septa and infiltration of small airways, pulmonaryarteries, and veins (Fig. 17). The tumor is composed ofspindle cells, inflammatory cells, and red blood cells forminginfiltrative nodular masses of varying size (Fig. 18). Thehistologic spectrum ranges from hypocellular areas in theperiphery of the nodules to cellular areas composed ofspindled tumor cells, nonspecific plump mesenchymal cells,lymphocytes, and plasma cells centrally. The spindle cellshave elongate nuclei, only mild nuclear atypia, densechromatin, and indistinct nucleoli (Fig. 19). Cytoplasmichyaline globules are often conspicuous. The spindle cells arearranged either without a specific pattern or as intersectingfascicles. Cleft-like spaces may be identified containingextravasated red blood cells and hemosiderin. Mitoses areoften present but not plentiful, and necrosis can onlyoccasionally be detected [61,92,117].
3.3. Immunohistochemical, ultrastructural, andmolecular features
Immunohistochemically, epithelioid hemangioendothe-lioma shows the typical phenotype of endothelial cellsdemonstrated by reactivity for factor VIII–related antigen(up to 99% of cases), CD31 (up to 86%), and CD34 (up to94%) [51,118,119]. However, it should be noted that up to50% of cases may show positivity for CK7 so that thismarker may not be helpful in distinguishing hemangioen-dothelioma from certain types of carcinoma [120]. Angio-sarcomas are positive for the endothelial markers factorVIII–related antigen, CD34 and CD31 [121-126]; immuno-reactivity for CK has been identified in a subset of theepithelioid variant of this tumor [127,128]. Immunohisto-chemical characteristics of Kaposi's sarcoma includereactivity of tumor cells for CD34, CD31, D2-40, VEGFR-3, and HHV8 [36,129-135] (Table 2).
Electron microscopy may be helpful in confirming theendothelial nature of epithelioid hemangioendothelioma andangiosarcoma: cellular interdigitations with occasional tightjunctions, pinocytotic vesicles, cytofilaments, intracytoplas-
mic lumina, and Weibel-Palade bodies are typicallyidentified [50,128,136-142]. In contrast to this, ultrastruc-tural investigations are not deemed helpful in the diagnosisof Kaposi's sarcoma [61].
On a molecular level, isolated case reports have described[1,3] (p36.3;q25) or (7;22) translocations in epithelioidhemangioendothelioma of the soft tissue [143,144], butlarger series have yet to be investigated. Studies investigat-ing the molecular events in hepatic and cardiac angiosarco-mas suggest that K-ras-2, p53, ras oncogene, or phosphataseand tensin homolog (PTEN) gene mutations play a role in thedevelopment of these tumors [145-148]. In addition, caseswith chromosomal structural rearrangement and polysomyof chromosome 8 or increased expression of VEGFR andmdm-2-protooncogene have been reported [149,150]. Inangiosarcomas of the soft tissues, abnormal chromosomenumbers have been noted to be characterized by gains ofchromosomes 5, 8, 20, and losses of chromosomes 7, 22, andthe Y chromosome [151,152]. Deletion and translocation ofchromosome 3, int-2 oncogene expression, and overexpres-sion of bcl-2 are cytogenetic alterations observed forKaposi's sarcoma [153-155] (Table 2). Whether thesefindings are true for primary pulmonary vascular tumors isyet to be determined.
3.4. Treatment, differential diagnosis, and prognosis
3.4.1. Epithelioid hemangioendotheliomaSurgical excision is the treatment of choice for epithelioid
hemangioendothelioma if disease is limited. Lung transplan-tation may be considered in cases of aggressive tumorgrowth [53]. Unfortunately, both chemotherapy and radia-tion have not proven to be effective in the treatment of thistumor, although antiangiogenic therapy with bevacizumabhas been successful in 1 case [52,87,156,157]. Despite this,epithelioid hemangioendothelioma is considered a low-grademalignant tumor associated with a protracted clinical courseand nonaggressive behavior but metastatic potential [51,52].Life expectancy spans 1 to 20 years with a 5-year survivalrate of 60% [53,158,159]. Factors of poor prognosis includeextensive intrapulmonary and pleural spread, weight loss,anemia, pulmonary symptoms, and hemorrhagic pleuraleffusions [52,53,87]. Partial regression has been described in3 cases, but most patients eventually die of respiratory failuredue to replacement of the pulmonary parenchyma by tumor[86]. It is important to differentiate epithelioid hemangioen-dothelioma from its closest mimics: adenocarcinoma,sarcomas with a chondroid or epithelioid appearance,sclerosing hemangioma, and metastatic cardiac myxoma[87,112]. Adenocarcinomas usually have a glandular growthpattern and show a greater degree of nuclear pleomorphismand increased mitotic activity. Sarcomas may demonstrateprominent intra-alveolar growth, but unequivocal areas ofsarcomatous differentiation as well as cellular pleomorphismand mitotic activity are normally present. Sclerosinghemangioma is a peculiar tumor presenting as an isolated

304 A. Weissferdt, C.A. Moran / Annals of Diagnostic Pathology 14 (2010) 296–308
lung mass; it is composed of bland-looking cells set in asclerotic background. In contrast to epithelioid hemangioen-dothelioma, however, this lesion is more cellular, displays agreater variety of growth patterns, and often contains largetelangiectatic vessels. This tumor fails to stain with thetypical endothelial immunomarkers as described for epithe-lioid hemangioendothelioma. Finally, metastatic cardiacmyxomas, although typically positive for factor VIII–relatedantigen, have a more myxomatous background and anirregular cellular arrangement. These tumors are normallycontained within vascular structures and do not display anintra-alveolar growth pattern. Most of the tumors consideredin the differential diagnosis carry a worse prognosis andrequire different treatment modalities making accuratediagnosis highly important for patient management.
3.4.2. AngiosarcomaCurrent treatment for angiosarcoma consists of systemic
chemotherapy with various combinations of doxorubicin,vincristine, cyclophosphamide, dacarbazine and methotrex-ate and radiotherapy [94,160]. One case report has showntreatment with interleukin-2 to be successful [100]. Theprognosis is generally poor, with survival dates ranging fromless than 1 to 15 months (median, 5.1 months)[94,100,101,160]. The main differential diagnoses includeorganizing thromboemboli and the plexiform lesions ofpulmonary hypertension. These processes have a tendency toform intravascular papillae and anastomosing vascularchannels and may be mistaken for a malignant tumor. Thelack of cytologic atypia, mitoses, and confinement of thelesions to the vascular lumina should help to distinguishthese reactive processes from angiosarcoma. Among theneoplastic lesions, lymphangitis carcinomatosa, pseudo-angiomatous carcinomas, and especially other vascularneoplasms such as Kaposi's sarcoma and epithelioidhemangioendothelioma need to be excluded. Lymphangitiscarcinomatosa is normally associated with a known primarytumor, lacks a vasoformative component, and reacts withepithelial immunohistochemical markers. Pseudoangioma-tous carcinomas likewise should show positivity forepithelial markers and do not react with vascular immuno-histochemical stains. Kaposi's sarcoma is a tumor charac-terized by a proliferation of spindle cells showing prominentextravasation of red blood cells but no blood vesselformation as such. Epithelioid hemangioendotheliomashows a different distribution with a largely intra-alveolargrowth pattern, a conspicuous myxoid background, andbland cytologic morphology.
3.4.3. KaposiTs sarcomaBecause of the tendency for multifocality in Kaposi's
sarcoma, surgical treatment is of limited use and cytotoxicchemotherapy with doxorubicin, bleomycin, vincristin,taxol, or lipososmal doxorubicin is considered the treatmentof choice [72,161,162]. In addition, highly active antire-troviral treatment is thought to be an important component
in the prevention and treatment of Kaposi's sarcoma inpatients with AIDS [163]. Furthermore, targeted antiviraltreatment with zidovudine and immune-response modifiersare thought to be effective but are still at an experimentalstage [164,165]. Radiotherapy plays only a minor role in thepalliation of symptoms and has not shown to be beneficialwith curative intent. The differential diagnosis for Kaposi'ssarcoma of the lung includes entities like angiosarcoma,spindle cell carcinoma, melanoma, and inflammatorylesions like organizing pneumonia. Angiosarcoma formsdefinitive vascular structures and lacks the spindle cellcomponent and red blood cell extravasation seen inKaposi's sarcoma. The lack of red blood cells, prominentinflammatory cells, hyaline globules, and immunoreactivitywith endothelial markers makes a diagnosis of other spindlecell lesions such as carcinoma or melanoma unlikely.Organizing pneumonia, although containing variableamounts of inflammatory or spindle cells, does not havethe growth pattern of Kaposi's sarcoma and does not reactwith the endothelial immunomarkers. Untreated pulmonaryKaposi's sarcoma has a poor prognosis, with a mediansurvival of only 2 to 6 months [71,72,166]; treatment withchemotherapy may increase median survival to up to 10months [161]. The most important factor, however, for theprognosis of patients with pulmonary Kaposi's sarcomaseems to be their serologic HIV status because patients withAIDS are likely to have an accelerated clinical course oftheir disease [92].
References
[1] Shikhani AH, Jones MM, Marsh BR, et al. Infantile subglottichemangiomas. An update. Ann Otol Rhinol Laryngol 1986;95:336-47.
[2] Moran CA, Suster S. Mediastinal hemangiomas: a study of 18 caseswith emphasis on the spectrum of morphological features. HumPathol 1995;26:416-21.
[3] Maeda R, Isowa N, Sumitomo S, et al. Pulmonary cavernoushemangioma. Gen Thorac Cardiovasc Surg 2007;55:177-9.
[4] Capizzani TR, Patel H, Hines MH, Mott RT, Petty JK. A unique caseof a giant congenital pulmonary hemangioma in a newborn. J PediatrSurg 2008;43:574-8.
[5] Harding JR, Williams J, Seal RM. Pedunculated capillary haeman-gioma of the bronchus. Br J Dis Chest 1978;72:336-42.
[6] Mori A, Obata K, Tada T, et al. A case of multiple cavernoushemangiomas of the lung. Gan No Rinsho 1985;31:1433-8.
[7] Wu JM, Lin CS, Wang JN, et al. Pulmonary cavernous hemangio-matosis treated with interferon alfa-2a. Pediatr Cardiol 1996;17:332-4.
[8] Kase M, Sakamoto K, Yamagata T, et al. A case of pulmonarycavernous hemangioma: immunohistological examination revealedits endothelial cell origin. Kyobu Geka 2000;53:1055-7.
[9] Fine SW,Whitney KD.Multiple cavernous hemangiomas of the lung:a case report and review of the literature. Arch Pathol Lab Med2004;128:1439-41.
[10] Galliani CA, Beatty JF, Grosfeld JL. Cavernous hemangioma of thelung in an infant. Pediatr Pathol 1992;12:105-11.
[11] Abrahams NA, Colby TV, Pearl RH, et al. Pulmonary hemangiomasof infancy and childhood: report of two cases and review of theliterature. Pediatr Dev Pathol 2002;5:283-92.
305A. Weissferdt, C.A. Moran / Annals of Diagnostic Pathology 14 (2010) 296–308
[12] Sirmali M, Demirağ F, Aydin E, et al. A pulmonary cavernoushemangioma causing massive hemoptysis. Ann Thorac Surg2003;76:1275-6.
[13] Paul KP, Börner C, Müller KM, et al. Capillary hemangioma of theright main bronchus treated by sleeve resection in infancy. Am RevRespir Dis 1991;143:876-9.
[14] Cohen MC, Kaschula RO. Primary pulmonary tumors in childhood: areview of 31 years' experience and the literature. Pediatr Pulmonol1992;14:222-32.
[15] Kayser K, Zink S, Link B, et al. Endobronchial juvenilehemangioma—a case report of a neonate including immunohisto-chemical monitoring and nuclear, cellular, and vascular morphom-etry. Virchows Arch 2001;438:192-7.
[16] Rose AS, Mathur PN. Endobronchial capillary hemangioma: casereport and review of the literature. Respiration 2008;76:221-4.
[17] Quijano G, Drut R. Multiple congenital infantile hemangiomas of thelung in partial trisomy D. J Clin Pathol 2007;60:943-5.
[18] Kobayashi A, Ohno S, Bando M, et al. Cavernous hemangiomasof lungs and liver in an asymptomatic girl. Respiration 2003;70:647-50.
[19] Bill Jr AH, Sumner DS. A unified concept of lymphangioma andcystic hygroma. Surg Gynecol Obstet 1965;120:79-86.
[20] Kransdorf MJ. Benign soft tissue tumors in a large referralpopulation: distribution of specific diagnoses by age, sex, andlocation. AJR Am J Roentgenol 1994;164:395-402.
[21] Limmer S, Krokowski M, Kujath P. Pulmonary lymphangioma. AnnThorac Surg 2008;85:336-9.
[22] KimWS, Lee KS, Kim I, et al. Cystic intrapulmonary lymphangioma:HRCT findings. Pediatr Radiol 1995;25:206-7.
[23] Drut R, Mosca HH. Intrapulmonary cystic lymphangioma. PediatrPulmonol 1996;22:204-6.
[24] Takahara T, Morisaki Y, Torigoe T, et al. Intrapulmonarycystic lymphangioma: report of a case. Surg Today 1998;28:1310-2.
[25] Faul JL, Berry GJ, Colby TV, et al. Thoracic lymphangiomas,lymphangiectasis, lymphangiomatosis, and lymphatic dysplasiasyndrome. Am J Respir Crit Care Med 2000;161:1037-46.
[26] Hernanz-Schulman M. Cysts and cystlike lesions of the lung. RadiolClin North Am 1993;31:631-49.
[27] Suringa DW, Ackerman AB. Cutaneous lymphangiomas withdyschondroplasia (Maffucci's syndrome). A unique variant of anunusual syndrome. Arch Dermatol 1970;101:472-4.
[28] Weber PF. Angioma formation in connection with hypertrophy of thelimbs and hemihypertrophy. Br J Dermatol 1907;19:231.
[29] Bowyer JJ, Sheppard M. Capillary haemangioma presenting as a lungpseudocyst. Arch Dis Child 1990;65:1162-4.
[30] Fugo K, Matsuno Y, Okamoto K, et al. Solitary capillaryhemangioma of the lung: report of 2 resected cases detected byhigh-resolution CT. Am J Surg Pathol 2006;30:750-3.
[31] Nagayasu T, Hayashi T, Ashizawa K, et al. A case of solitarypulmonary lymphangioma. J Clin Pathol 2003;56:396-8.
[32] Wada A, Tateishi R, Terazawa T, et al. Case report: lymphangioma ofthe lung. Arch Pathol 1974;98:211-3.
[33] Milovic I, Oluic D. Lymphangioma of the lung associated withrespiratory distress in a neonate. Pediatr Radiol 1992;22:156.
[34] Hilliard RI, McKendry JB, Phillips MJ. Congenital abnormalities of thelymphatic system: a newclinical classification. Pediatrics 1990;86:988-94.
[35] Hamada K, Ishii Y, Nakaya M, et al. Solitary lymphangioma of thelung. Histopathology 1995;27:482-3.
[36] Folpe AL, Veikkola T, Valtola R, et al. Vascular endothelial growthfactor receptor-3 (VEGFR-3): a marker of vascular tumors withpresumed lymphatic differentiation, including Kaposi's sarcoma,kaposiform and Dabska-type hemangioendotheliomas, and a subsetof angiosarcomas. Mod Pathol 2000;13:180-5.
[37] Walter JW, North PE, Waner M, et al. Somatic mutation of vascularendothelial growth factor receptors in juvenile hemangioma. GenesChromosomes Cancer 2002 Mar;33:295-303.
[38] Jinnin M, Medici D, Park L, et al. Suppressed NFAT-dependentVEGFR1 expression and constitutive VEGFR2 signaling in infantilehemangioma. Nat Med 2008;14:1236-46.
[39] Irrthum A, Karkkainen MJ, Devriendt K, et al. Congenital hereditarylymphedema caused by a mutation that inactivates VEGFR3 tyrosinekinase. Am J Hum Genet 2000;67:295-301.
[40] Molitch HI, Unger EC, Witte CL, et al. Percutaneous sclerotherapy oflymphangiomas. Radiology 1995;194:343-7.
[41] Wilson C, Askin FB, Heitmiller RF. Solitary pulmonary lymphan-gioma. Ann Thorac Surg 2001;71:1337-8.
[42] Li YW, Snow J, Smith WL, et al. Localized pulmonary lymphan-giectasia. AJR Am J Roentgenol 1985;145:269-70.
[43] Tazelaar HD, Kerr D, Yousem SA, et al. Diffuse pulmonarylymphangiomatosis. Hum Pathol 1993;24:1313-22.
[44] Berger U, Khaghani A, Pomerance A, et al. Pulmonary lymphangio-leiomyomatosis and steroid receptors. An immunocytochemicalstudy. Am J Clin Pathol 1990;93:609-14.
[45] Ohori NP, Yousem SA, Sonmez-Alpan E, et al. Estrogen andprogesterone receptors in lymphangioleiomyomatosis, epithelioidhemangioendothelioma, and sclerosing hemangioma of the lung. AmJ Clin Pathol 1991;96:529-35.
[46] Bonetti F, Pea M, Martignoni G, et al. Cellular heterogeneity inlymphangiomyomatosis of the lung. Hum Pathol 1991;22:727-8.
[47] Dail DH, Liebow AA. Intravascular bronchioloalveolar tumor. Am JPathol 1975;6a:78 (abstr).
[48] Corrin B, Manners B, Millard M, et al. Histogenesis of the so-called “intravascular bronchioloalveolar tumour”. J Pathol1979;128:163-7.
[49] Weldon-Linne CM, Victor TA, Christ ML, et al. Angiogenic nature ofthe “intravascular bronchioloalveolar tumor” of the lung: an electronmicroscopic study. Arch Pathol Lab Med 1981;105:174-9.
[50] Weiss SW, Enzinger FM. Epithelioid hemangioendothelioma: avascular tumor often mistaken for a carcinoma. Cancer 1982;50:970-81.
[51] Bhagavan BS, Dorfman HD, Murthy MS, et al. Intravascularbronchiolo-alveolar tumor (IVBAT): a low-grade sclerosing epithe-lioid angiosarcoma of lung. Am J Surg Pathol 1982;6:41-52.
[52] Weiss SW, Ishak KG, Dail DH, et al. Epithelioid hemangioendothe-lioma and related lesions. Semin Diagn Pathol 1986;3:259-87.
[53] Bagan P, Hassan M, Le Pimpec Barthes F, et al. Prognostic factorsand surgical indications of pulmonary epithelioid hemangioen-dothelioma: a review of the literature. Ann Thorac Surg 2006;82:2010-3.
[54] Chen KT, Hoffman KD, Hendricks EJ. Angiosarcoma followingtherapeutic irradiation. Cancer 1979;44:2044-8.
[55] Maddox JC, Evans HL. Angiosarcoma of skin and soft tissue: a studyof forty-four cases. Cancer 1981;48:1907-21.
[56] Thomas LB, Popper H. Pathology of angiosarcoma of the liver amongvinyl chloride-polyvinyl chloride workers. Ann NY Acad Sci1975;246:268-77.
[57] Thomas LB, Popper H, Berk PD, et al. Vinyl-chloride-induced liverdisease. From idiopathic portal hypertension (Banti's syndrome) toangiosarcomas. N Engl J Med 1975;292:17-22.
[58] Milby TH. Preventive medicine and public health—epitomes of progress:Vinyl Chloride-Related Cancer. West J Med 1979;130:247-8.
[59] Baxter PJ. The British hepatic angiosarcoma register. Environ HealthPerspect 1981;41:115-6.
[60] Jennings TA, PetersonL,Axiotis CA, et al. Angiosarcoma associatedwithforeign body material. A report of three cases. Cancer 1988;62:2436-44.
[61] Enzinger FM, Weiss SW. Malignant vascular tumors. In: WeissSW, Goldblum JR, editors. Soft tissue tumors. Mosby: Elsevier;2008. p. 703-20.
[62] Glancy DL, Morales Jr JB, Roberts WC. Angiosarcoma of the heart.Am J Cardiol 1968;21:413-9.
[63] Edwards RL, Chalk SM, McEvoy JD, et al. Pulmonary haemorrhagein disseminated cardiac haemangiosarcoma. Br J Dis Chest 1977;71:127-31.
306 A. Weissferdt, C.A. Moran / Annals of Diagnostic Pathology 14 (2010) 296–308
[64] Ali MY, Lee GS. Sarcoma of the pulmonary artery. Cancer 1964;17:1220-4.
[65] Wackers FJ, van der Schoot JB, Hampe JF. Sarcoma of thepulmonary trunk associated with hemorrhagic tendency. A casereport and review of the literature. Cancer 1969;23:339-51.
[66] Cox FH, Helwig EB. Kaposi's sarcoma. Cancer 1959;12:289-98.[67] Dantzig PI, Richardson D, Rayhanzadeh S, et al. Thoracic involvement
of non–African Kaposi's sarcoma. Chest 1974;66:522-5.[68] Epstein DM, Gefter WB, Conard K, et al. Lung disease in
homosexual men. Radiology 1982;143:7-10.[69] Gruden JF, Huang L, Webb WR, et al. AIDS-related Kaposi sarcoma
of the lung: radiographic findings and staging system withbronchoscopic correlation. Radiology 1995;195:545-52.
[70] Mitsuyasu RT, Groopman JE. Biology and therapy of Kaposi'ssarcoma. Semin Oncol 1984;11:53-9.
[71] Meduri GU, Stover DE, Lee M, et al. Pulmonary Kaposi's sarcoma inthe acquired immune deficiency syndrome. Clinical, radiographic,and pathologic manifestations. Am J Med 1986;81:11-8.
[72] Ognibene FP, Steis RG, Macher AM, et al. Kaposi's sarcomacausing pulmonary infiltrates and respiratory failure in the acquiredimmunodeficiency syndrome. Ann Intern Med 1985;102:471-5.
[73] Wallis JM, Hannah J. Pulmonary disease found at autopsy in patientswith the acquired immunodefiencency syndrome (AIDS). Am RevResp Dis 1985;131:A222.
[74] Nesbitt S, Mark PF, Zimmerman HF. Dissemintated visceralidiopathic hemorrhagic sarcoma (Kaposi's disease): report of casewith necropsy findings. Ann Intern Med 1945;22:601-5.
[75] LoringWE,Wolman SR. Idiopathic multiple hemorrhagic sarcoma oflung (Kaposi's sarcoma). NY State J Med 1965;65:668-76.
[76] Mesmin F, Gomes H, Behar C, et al. Lymphoblastic leukaemia andKaposi's sarcoma. Pediatr Radiol 1979;8:185-7.
[77] Misra DP, Sunderrajan EV, Hurst DJ, et al. Kaposi's sarcoma of thelung: radiography and pathology. Thorax 1982;37:155-6.
[78] Friedman-Kien AE, Laubenstein LJ, Rubinstein P, et al. Disseminat-ed Kaposi's sarcoma in homosexual men. Ann Intern Med 1982;96:693-700.
[79] Kornfeld H, Axelrod JL. Pulmonary presentation of Kaposi'ssarcoma in a homosexual patient. Am Rev Respir Dis 1983;127:248-9.
[80] Bach MC, Bagwell SP, Fanning JP. Primary pulmonary Kaposi'ssarcoma in the acquired immunodeficiency syndrome: a cause ofpersistent pyrexia. Am J Med 1988;85:274-5.
[81] Roux FJ, Bancal C, Dombret MC, et al. Pulmonary Kaposi'ssarcoma revealed by a solitary nodule in a patient withacquired immunodeficiency syndrome. Am J Respir Crit CareMed 1994;149:1041-3.
[82] Huang L, Schnapp LM, Gruden JF, et al. Presentation of AIDS-related pulmonary Kaposi's sarcoma diagnosed by bronchoscopy.Am J Respir Crit Care Med 1996;153:1385-90.
[83] Martinez S, McAdams HP, Youens KE. Kaposi sarcomaafter bilateral lung transplantation. J Thorac Imaging2008;23:50-3.
[84] Rock MJ, Kaufman RA, Lobe TE, et al. Epithelioid hemangioen-dothelioma of the lung (intravascular bronchioloalveolar tumor) in ayoung girl. Pediatr Pulmonol 1991;11:181-6.
[85] Kitaichi M, Nagai S, Nishimura K, et al. Pulmonary epithelioidhaemangioendothelioma in 21 patients, including three with partialspontaneous regression. Eur Respir J 1998;12:89-96.
[86] Einsfelder B, Kuhnen C. Epithelioid hemangioendothelioma of thelung (IVBAT)-clinicopathological and immunohistochemical analy-sis of 11 cases. Pathologe 2006;27:106-15.
[87] Dail DH, Liebow AA, Gmelich JT, et al. Intravascular, bronchiolar,and alveolar tumor of the lung (IVBAT). An analysis of twentycases of a peculiar sclerosing endothelial tumor. Cancer 1983;51:452-64.
[88] Miettinen M, Collan Y, Halttunen P, et al. Intravascular bronchio-loalveolar tumor. Cancer 1987;60:2471-5.
[89] Bevelaqua FA, Valensi Q, Hulnick D. Epithelioid hemangioendothe-lioma. A rare tumor with variable prognosis presenting as a pleuraleffusion. Chest 1988;93:665-6.
[90] Carter EJ, Bradburne RM, Jhung JW, et al. Alveolar hemorrhagewith epithelioid hemangioendothelioma. A previously unreportedmanifestation of a rare tumor. Am Rev Respir Dis 1990;142:700-1.
[91] Struhar D, Sorkin P, Greif J, et al. Alveolar haemorrhage with pleuraleffusion as a manifestation of epithelioid haemangioendothelioma.Eur Respir J 1992;5:592-3.
[92] Wick MR, Leslie KO, Cerilli LA, Mills SE. Sarcomas andsarcomatoid neoplasms of the lungs and pleural surfaces. In: LeslieKO, Wick MR, editors. Practical pulmonary pathology. A diagnosticapproach. Churchill Livingstone Elsevier; 2005. p. 465-517.
[93] Ledson MJ, Convery R, Carty A, et al. Epithelioid haemangioen-dothelioma. Thorax 1999;54:560-1.
[94] Yousem SA. Angiosarcoma presenting in the lung. Arch Pathol LabMed 1986;110:112-5.
[95] Segal SL, Lenchner GS, Cichelli AV, et al. Angiosarcoma presentingas diffuse alveolar hemorrhage. Chest 1988;94:214-6.
[96] Pandit SA, Fiedler PN, Westcott JL. Primary angiosarcoma of thelung. Ann Diagn Pathol 2005;9:302-4.
[97] Campione A, Forte G, Luzzi L, et al. Pulmonary angiosarcomapresenting as spontaneous recurrent hemothorax. Asian CardiovascThorac Ann 2009;17:84-5.
[98] Spragg RG, Wolf PL, Haghighi P, et al. Angiosarcoma of the lungwith fatal pulmonary hemorrhage. Am J Med 1983;74:1072-6.
[99] Primack SL, Hartman TE, Lee KS, et al. Pulmonary nodules and theCT halo sign. Radiology 1994;190:513-5.
[100] Kojima K, Okamoto I, Ushijima S, et al. Successful treatment ofprimary pulmonary angiosarcoma. Chest 2003;124:2397-400.
[101] Palvio DH, Paulsen SM, Henneberg EW. Primary angiosarcoma ofthe lung presenting as intractable hemoptysis. Thorac CardiovascSurg 1987;35:105-7.
[102] Ott RA, Eugene J, Kollin J, et al. Primary pulmonary angiosarcomaassociated with multiple synchronous neoplasms. J Surg Oncol1987;35:269-76.
[103] Davidson TI, Kissin MW, Bradish CF, et al. Angiosarcoma arisingin a patient with Maffucci syndrome. Eur J Surg Oncol 1985;11:381-4.
[104] Ploegmakers MJ, Pruszczynski M, De Rooy J, et al. Angiosarcomawith malignant peripheral nerve sheath tumour developing in apatient with Klippel-Trénaunay-Weber syndrome. Sarcoma 2005;9:137-40.
[105] Sadaghdar H, Eden E. Pulmonary Kaposi's sarcoma presenting asfulminant respiratory failure. Chest 1991;100:858-60.
[106] Stover DE, White DA, Romano PA, et al. Spectrum of pulmonarydiseases associated with the acquired immune deficiency syndrome.Am J Med 1985;78:429-37.
[107] Davis SD, Henschke CI, Chamides BK, et al. Intrathoracic Kaposisarcoma in AIDS patients: radiographic-pathologic correlation.Radiology 1987;163:495-500.
[108] Stats D. The visceral manifestations of Kaposi's sarcoma. J Mt SinaiHosp 1946;12:971-83.
[109] Zibrak JD, Silvestri RC, Costello P, et al. Bronchoscopic andradiologic features of Kaposi's sarcoma involving the respiratorysystem. Chest 1986;90:476-9.
[110] Chang Y, Cesarman E, Pessin MS, et al. Identification of herpesvirus-like DNA sequences in AIDS-associated Kaposi's sarcoma. Science1994;266:1865-9.
[111] Tamm M, Reichenberger F, McGandy CE, et al. Diagnosis ofpulmonary Kaposi's sarcoma by detection of human herpes virus8 in bronchoalveolar lavage. Am J Respir Crit Care Med 1998;157:458-63.
[112] Enzinger FM, Weiss SW. Hemangioendothelioma: vascular tumorsof intermediate malignancy. In: Weiss SW, Goldblum JR, editors.Soft tissue tumors. Mosby Elsevier; 2008. p. 681-702.
307A. Weissferdt, C.A. Moran / Annals of Diagnostic Pathology 14 (2010) 296–308
[113] Sheppard MN, Hansell DM, Du Bois RM, et al. Primary epithelioidangiosarcoma of the lung presenting as pulmonary hemorrhage. HumPathol 1997;28:383-5.
[114] Pitchenik AE, Fischl MA, Saldana MJ. Kaposi's sarcoma of thetracheobronchial tree. Clinical, bronchoscopic, and pathologicfeatures. Chest 1985;87:122-4.
[115] Garay SM, Belenko M, Fazzini E, et al. Pulmonary manifestations ofKaposi's sarcoma. Chest 1987;91:39-43.
[116] Hanson PJ, Harcourt-Webster JN, Gazzard BG, et al. Fibreopticbronchoscopy in diagnosis of bronchopulmonary Kaposi's sarcoma.Thorax 1987;42:269-71.
[117] Purdy LJ, Colby TV, Yousem SA, et al. Pulmonary Kaposi'ssarcoma. Premortem histologic diagnosis. Am J Surg Pathol 1986;10:301-11.
[118] Bollinger BK, Laskin WB, Knight CB. Epithelioid hemangioen-dothelioma with multiple site involvement. Literature review andobservations. Cancer 1994;73:610-5.
[119] Makhlouf HR, Ishak KG, Goodman ZD. Epithelioid hemangioen-dothelioma of the liver: a clinicopathologic study of 137 cases.Cancer 1999;85:562-82.
[120] Miettinen M, Fetsch JF. Distribution of keratins in normal endothelialcells and a spectrum of vascular tumors: implications in tumordiagnosis. Hum Pathol 2000;31:1062-7.
[121] Mukai K, Rosai J, Burgdorf WH. Localization of factor VIII-relatedantigen in vascular endothelial cells using an immunoperoxidasemethod. Am J Surg Pathol 1980;4:273-6.
[122] Burgdorf WH, Mukai K, Rosai J. Immunohistochemical identifica-tion of factor VIII-related antigen in endothelial cells of cutaneouslesions of alleged vascular nature. Am J Clin Pathol 1981;75:167-71.
[123] Sehested M, Hou-Jensen K. Factor VII related antigen as anendothelial cell marker in benign and malignant diseases. VirchowsArch A Pathol Anat Histol 1981;391:217-25.
[124] Guarda LA, Ordonez NG, Smith Jr JL, et al. Immunoperoxidaselocalization of factor VIII in angiosarcomas. Arch Pathol Lab Med1982;106:515-6.
[125] DeYoung BR, Swanson PE, Argenyi ZB, et al. CD31 immuno-reactivity in mesenchymal neoplasms of the skin and subcutis:report of 145 cases and review of putative immunohistologicmarkers of endothelial differentiation. J Cutan Pathol 1995;22:215-22.
[126] Orchard GE, Zelger B, Jones EW, et al. An immunocytochemicalassessment of 19 cases of cutaneous angiosarcoma. Histopathology1996;28:235-40.
[127] Fletcher CD, Beham A, Bekir S, et al. Epithelioid angiosarcoma ofdeep soft tissue: a distinctive tumor readily mistaken for an epithelialneoplasm. Am J Surg Pathol 1991;15:915-24.
[128] Meis-Kindblom JM, Kindblom LG. Angiosarcoma of soft tissue: astudy of 80 cases. Am J Surg Pathol 1998;22:683-97.
[129] Nadji M, Morales AR, Ziegles-Weissman J, et al. Kaposi's sarcoma:immunohistologic evidence for an endothelial origin. Arch PatholLab Med 1981;105:274-5.
[130] Weninger W, Partanen TA, Breiteneder-Geleff S, et al. Expression ofvascular endothelial growth factor receptor-3 and podoplaninsuggests a lymphatic endothelial cell origin of Kaposi's sarcomatumor cells. Lab Invest 1999;79:243-51.
[131] Kahn HJ, Bailey D, Marks A. Monoclonal antibody D2-40, a newmarker of lymphatic endothelium, reacts with Kaposi's sarcoma and asubset of angiosarcomas. Mod Pathol 2002;15:434-40.
[132] Patel RM, Goldblum JR, Hsi ED. Immunohistochemical detection ofhuman herpes virus-8 latent nuclear antigen-1 is useful in thediagnosis of Kaposi sarcoma. Mod Pathol 2004;17:456-60.
[133] CheukW, Wong KOY, Wong CSC, et al. Immunostaining for humanherpesvirus 8 latent nuclear antigen-1 helps distinguish Kaposisarcoma from its mimickers. Am J Clin Pathol 2004;121:335-42.
[134] Hammock L, Reisenauer A, Wang W, et al. Latency-associatednuclear antigen expression and human herpesvirus-8 polymerasechain reaction in the evaluation of Kaposi sarcoma and other
vascular tumors in HIV-positive patients. Mod Pathol 2005;18:463-8.
[135] Fukunaga M. Expression of D2-40 in lymphatic endothelium ofnormal tissues and in vascular tumours. Histopathology 2005;46:396-402.
[136] Rosai J, Sumner HW, Kostianovsky M, et al. Angiosarcoma of theskin. A clinicopathologic and fine structural study. Hum Pathol1976;7:83-109.
[137] Waldo ED, Vuletin JC, Kaye GI. The ultrastructure of vasculartumors: additional observations and a review of the literature. PatholAnnu 1977;12:279-308.
[138] Eggleston JC. The intravascular bronchioloalveolar tumor and thesclerosing hemangioma of the lung: misnomers of pulmonaryneoplasia. Semin Diagn Pathol 1985;2:270-80.
[139] Holden CA, Spaull J, Das AK, et al. The histogenesis ofangiosarcoma of the face and scalp: an immunohistochemical andultrastructural study. Histopathology 1987;11:37-51.
[140] Mackay B, Ordóñez NG, Huang WL. Ultrastructural and immuno-cytochemical observations on angiosarcomas. Ultrastruct Pathol1989;13:97-110.
[141] Corrin B, Dewar A, Simpson CG. Epithelioid hemangioendotheliomaof the lung. Ultrastruct Pathol 1996;20:345-7.
[142] Vasquez M, Ordóñez NG, English GW, Mackay B. Epithelioidhemangioendothelioma of soft tissue: report of a case withultrastructural observations. Ultrastruct Pathol 1998;22:73-8.
[143] Boudousquie AC, Lawce HJ, Sherman R, et al. Complex transloca-tion [7;22] identified in an epithelioid hemangioendothelioma.Cancer Genet Cytogenet 1996;92:116-21.
[144] Mendlick MR, Nelson M, Pickering D, et al. Translocation t(1;3)(p36.3;q25) is a nonrandom aberration in epithelioid hemangioen-dothelioma. Am J Surg Pathol 2001;25:684-7.
[145] Przygodzki RM, Finkelstein SD, Keohavong P, et al. Sporadic andThorotrast-induced angiosarcomas of the liver manifest frequentand multiple point mutations in K-ras-2. Lab Invest 1997;76:153-9.
[146] Marion MJ, Froment O, Trépo C. Activation of Ki-ras gene by pointmutation in human liver angiosarcoma associated with vinyl chlorideexposure. Mol Carcinog 1991;4:450-4.
[147] De Vivo I, Marion MJ, Smith SJ, et al. Mutant c-Ki-ras p21 protein inchemical carcinogenesis in humans exposed to vinyl chloride. CancerCauses Control 1994;5:273-8.
[148] Tate G, Suzuki T, Mitsuya T. Mutation of the PTEN gene in a humanhepatic angiosarcoma. Cancer Genet Cytogenet 2007;178:160-2.
[149] Zu Y, Perle MA, Yan Z, et al. Chromosomal abnormalities and p53gene mutation in a cardiac angiosarcoma. Appl ImmunohistochemMol Morphol 2001;9:24-8.
[150] Zietz C, Rössle M, Haas C, et al. MDM-2 oncoprotein over-expression, p53 gene mutation, and VEGF up-regulation inangiosarcomas. Am J Pathol 1998;153:1425-33.
[151] Mandahl N, Jin YS, Heim S, et al. Trisomy 5 and loss of the Ychromosome as the sole cytogenetic anomalies in a cavernoushemangioma/angiosarcoma. Genes Chromosomes Cancer 1990;1:315-6.
[152] Schuborg C, Mertens F, Rydholm A. Cytogenetic analysis of fourangiosarcomas from deep and superficial soft tissue. Cancer GenetCytogenet 1998;100:52-6.
[153] Popescu NC, Zimonjic DB, Leventon-Kriss S, et al. Deletion andtranslocation involving chromosome 3 (p14) in two tumorigenicKaposi's sarcoma cell lines. J Natl Cancer Inst 1996;88:450-5.
[154] Huang YQ, Li JJ, Moscatelli D, et al. Expression of int-2 oncogene inKaposi's sarcoma lesions. J Clin Invest 1993;91:1191-7.
[155] Simonart T, Degraef C, Noel JC, et al. Overexpression of Bcl-2 inKaposi's sarcoma–derived cells. J Invest Dermatol 1998;111:349-53.
[156] Emery RW, Fox AL, Raab DE. Intravascular bronchioloalveolartumour. Thorax 1982;37:472-3.
[157] Belmont L, Zemoura L, Couderc LJ. Pulmonary epithelioid haeman-gioendothelioma and bevacizumab. J Thorac Oncol 2008;3:557-8.

308 A. Weissferdt, C.A. Moran / Annals of Diagnostic Pathology 14 (2010) 296–308
[158] Cronin P, Arenberg D. Pulmonary epithelioid hemangioendothe-lioma: an unusual case and a review of the literature. Chest 2004;125:789-93.
[159] Schattenberg T, Pfannschmidt J, Herpel E, et al. Bilateral surgicalresection in pulmonary epitheloid hemangioendothelioma. ThoracCardiovasc Surg 2007;55:199-200.
[160] Patel AM, Ryu JH. Angiosarcoma in the lung. Chest 1993;103:1531-5.
[161] Gill PS, Akil B, Colletti P, et al. Pulmonary Kaposi's sarcoma:clinical findings and results of therapy. Am J Med 1989;87:57-61.
[162] Stewart S, Jablonowski H, Goebel FD, et al. Randomized comparativetrial of pegylated liposomal doxorubicin versus bleomycin and vincristinein the treatment of AIDS-related Kaposi's sarcoma. International
Pegylated Liposomal Doxorubicin Study Group. J Clin Oncol 1998;16:683-91.
[163] International Collaboration on HIV and Cancer. Highly activeantiretroviral therapy and incidence of cancer in human immuno-deficiency virus–infected adults. J Natl Cancer Inst 2000;92:1823-30.
[164] Wick MR. Kaposi's sarcoma unrelated to the acquired immunode-ficiency syndrome. Curr Opin Oncol 1991;3:377-82.
[165] Cadranel J, Naccache J, Wislez M, et al. Pulmonary malignanciesin the immunocompromised patient. Respiration 1999;66:289-309.
[166] Kaplan LD, Hopewell PC, Jaffe H, et al. Kaposi's sarcoma involvingthe lung in patients with the acquired immunodeficiency syndrome.J Acquir Immune Defic Syndr 1988;1:23-30.