presenting rhythm in sudden deaths temporally proximate to discharge of taser conducted electrical...
TRANSCRIPT

Presenting Rhythm in Sudden DeathsTemporally Proximate to Discharge of TASERConducted Electrical WeaponsCharles D. Swerdlow, MD, Michael C. Fishbein, MD, Linda Chaman, MPH, Dhanunjaya R. Lakkireddy,MD, and Patrick Tchou, MD
AbstractObjectives: Sudden deaths proximate to use of conducted electrical weapons (CEWs) have been attrib-uted to cardiac electrical stimulation. The rhythm in death caused by rapid, cardiac electrical stimulationusually is ventricular fibrillation (VF); electrical stimulation has not been reported to cause asystole orpulseless electrical activity (PEA). The authors studied the presenting rhythms in sudden deaths tempo-rally proximate to use of TASER CEWs to estimate the likelihood that these deaths could be caused bycardiac electrical stimulation.
Methods: This was a retrospective review of CEW-associated, nontraumatic sudden deaths from 2001to 2008. Emergency medical services (EMS), autopsy, and law enforcement reports were requested andanalyzed. Subjects were included if they collapsed within 15 minutes of CEW discharge and the first car-diac arrest rhythm was reported.
Results: Records for 200 cases were received. The presenting rhythm was reported for 56 of 118 sub-jects who collapsed within 15 minutes (47%). The rhythm was VF in four subjects (7%; 95% confidenceinterval [CI] = 3% to 17%) and bradycardia-asystole or PEA in 52 subjects (93%; 95% CI = 83% to 97%).None of the eight subjects who collapsed during electrocardiogram (ECG) monitoring had VF. Only onesubject (2%) collapsed immediately after CEW discharge. This was the only death typical of electricallyinduced VF (2%, 95% CI = 0% to 9%). An additional 4 subjects (7%) collapsed within 1 minute, and theremaining 51 subjects (91%) collapsed more than 1 minute later. The time from collapse to first recordedrhythm was 3 minutes or less in 35 subjects (62%) and 5 minutes or less in 43 subjects (77%).
Conclusions: In sudden deaths proximate to CEW discharge, immediate collapse is unusual, and VF isan uncommon VF presenting rhythm. Within study limitations, including selection bias and the possibil-ity that VF terminated before the presenting rhythm was recorded, these data do not support electricallyinduced VF as a common mechanism of these sudden deaths.
ACADEMIC EMERGENCY MEDICINE 2009; 16:726–739 ª 2009 by the Society for Academic EmergencyMedicine
Keywords: prehospital, out-of-hospital, cardiac arrest
N ontraumatic, sudden deaths of civilians duringinteractions with law enforcement are a publichealth concern.1 The TASER conducted electri-
cal weapon (CEW; TASER International Inc., Scottsdale,AZ) is used increasingly by law enforcement officersbecause of its unique capability to incapacitate violent or
ISSN 1069-6563 ª 2009 by the Society for Academic Emergency Medicine726 PII ISSN 1069-6563583 doi: 10.1111/j.1553-2712.2009.00432.x
From the Division of Cardiology, Cedars Sinai Medical Center (CDS, LC), Los Angeles, CA; the Department of Pathology andLaboratory Medicine, David Geffen School of Medicine at UCLA (MCF), Los Angeles, CA; the Bloch Heart Rhythm Center,University of Kansas Medical Center (DRL), Kansas City, KS; and the Cleveland Clinic (PT), Cleveland, OH.Received December 23, 2008; revisions received February 6 and February 26, 2009; accepted February 27, 2009.Presented at the Heart Rhythm Society Meeting, San Francisco, CA, May 14–17, 2008; and the Heart Rhythm Society meeting,Boston, MA, May 13–16, 2009.Dr. Swerdlow is a member of the TASER International Medical Scientific Advisory Board, which provides advice regarding safetyof conducted electrical weapons. Previously, Drs. Tchou and Lakkireddy performed research funded by TASER International (Refer-ences 9 and 10), but they are not performing such research now. Dr. Fishbein has no potential conflicts. No author has any financialinterest in TASER International or any entity related to this manuscript.Address for correspondence and reprints: Charles Swerdlow, MD; e-mail: [email protected] related commentary appears on page 771.

resisting subjects. Deaths temporally related to use ofCEWs have attracted attention from the media2 andmedical organizations.3
Conducted electrical weapons deliver rapid electricalstimulation at frequency of 15–20 Hz to incapacitate
subjects by causing contraction of skeletal muscles,4
using either two tethered barbed-probe projectiles ortwo closely spaced electrodes on the cartridge of thehand-held unit (‘‘drive-stun’’ mode). In all reported ani-mal experiments and clinical cases of cardiac arrests
Figure 1. Reconstruction of time course using EMS field report (A), law enforcement records (B), and EMS 9-1-1 system phone log(C). Field report (A) indicates that EMS was dispatched after first CEW discharge at 10:46. Accompanying narrative (not shown)states that, after arriving, EMS staged across the road, ‘‘out of the line of sight and gunfire.’’ Law enforcement reports include elec-tronic log of last CEW discharges shown in (B), indicating the last CEW discharge at 10:49:28. Log displays total lifetime number ofCEW discharges, local time, duration of each CEW discharge in seconds, temperature (�C), and percent battery capacity. EMSphone log (C) shows that law enforcement placed an urgent request for EMS at 10:59:13 when subject collapsed (first +). Field log(A) indicates EMS arrived on scene at 11:02 (second asterisk) and records the presenting rhythm as sinus bradycardia at 11:03 (thirdasterisk). Narrative (not shown) states, ‘‘Quick look pads show PEA (sinus brady).’’ In last entry in (C) at 11:03:10, law enforcementon scene confirms arrival of EMS for system operator. Synchronization of time codes indicated that the CEW clock was 5 minutesslow, so the final CEW application occurred at about 10:55. Thus the interval from the last CEW discharge to collapse was4 minutes (10:55 to 10:59). The interval from collapse to presenting rhythm was also 4 minutes (10:59 to 11:03). Names of lawenforcement personnel are redacted. CEW = conducted electrical weapon; ECG = electrocardiogram.
ACAD EMERG MED • August 2009, Vol. 16, No. 8 • www.aemj.org 727
caused by rapid, cardiac electrical stimulation fromother sources, the rhythm has been ventricular fibrilla-tion (VF).5,6 Rapid cardiac stimulation has not beenreported to cause asystole or pulseless electrical activity(PEA).5,7 Thus, investigators have postulated8–14 andmedia reports have implied that deaths proximate touse of CEWs are caused by electrically induced VF.
If CEWs cause death by cardiac stimulation, the initialpostarrest rhythm should be VF, and subjects should col-lapse within 10 seconds after CEW discharge. However,if either collapse is delayed or the initial rhythm is asys-tole or PEA, then electrically induced VF is not the causeof death; thus, cardiac stimulation by the CEW cannot beimplicated as the direct cause of death.
Data regarding the cardiac rhythms in deaths proxi-mate to use of CEWs are limited. Our objective was toidentify the first-recorded rhythms in these suddendeaths as an estimate of the initial, cardiac arrestrhythms, to estimate the likelihood that they could becaused by cardiac electrical stimulation.
METHODS
Study DesignThis was a retrospective survey of CEW-associated,nontraumatic sudden deaths identified through an In-ternet search. The study was performed under a letterof assent by the Cedars Sinai Medical Center (LosAngeles, CA) Institutional Review Board.
Study Setting and PopulationWe performed an Internet-based search for deathstemporally proximate to use of TASER CEWs via theGoogle search engine, using key words ‘‘TASER’’ AND‘‘death.’’ Subsequently, we performed searches usingother key words (electronic control device, conductedelectrical weapon, TAZER, electric gun, stun gun) AND‘‘death.’’ Subjects who died suddenly and unexpectedlyafter law enforcement officers discharged a CEW wereincluded based on these prospective criteria: 1) thedischarge was applied to the subject; 2) the subjectbecame unresponsive (‘‘collapsed’’) within 15 minutesof the last discharge; 3) EMS, automatic external
defibrillator (AED), or medical records included acardiac rhythm diagnosis prior to treatment with drugsor defibrillation; and 4) death was not caused byphysical trauma unrelated to the CEW discharge. Weobtained an autopsy report for all subjects who metthese four criteria.
Study ProtocolWe made written requests for records of deathsbetween January 1, 2001, and February 1, 2008, fromappropriate coroners, medical examiners, law enforce-ment agencies, and emergency medical services (EMS)under the Freedom of Information Act. If we receivedno response, we followed-up with a reminder letter andphone call. We specifically requested electrocardio-grams (ECGs), recordings from AEDs, video or audiorecordings, downloads of CEW data, and autopsies.We recorded demographic data from EMS and autopsyreports. Toxicologic data were recorded from autopsyreports whenever available. The CEW model and typeof electrodes were recorded whenever they werereported.4
MeasurementsRhythm Classification The key outcome measure wasthe classification of the first-recorded (presenting)rhythm at cardiac arrest as determined by EMS or anAED. For two cases in which the CEW was dischargedin a hospital, we used physician classification.
The presenting rhythm was recorded from EMSreports as listed: asystole, ‘‘brady’’ (bradycardia), PEA,or VF. In some cases, an AED made the first rhythmclassification of ‘‘shockable’’ or ‘‘nonshockable.’’ Gener-ally, AEDs classify VF and wide-complex tachycardiaswith rates faster than 150–200 beats ⁄ min as ‘‘shock-able’’ and other rhythms as ‘‘nonshockable.’’15 A shock-able rhythm was considered VF. In the five cases inwhich a rhythm was evaluated both by EMS and by anAED, we used the AED classification.
Whenever possible, the EMS and AED rhythm classi-fications were corroborated by review of ECG rhythmstrips or response to rhythm-specific therapy. Resusci-tation to a perfusing rhythm without defibrillation or
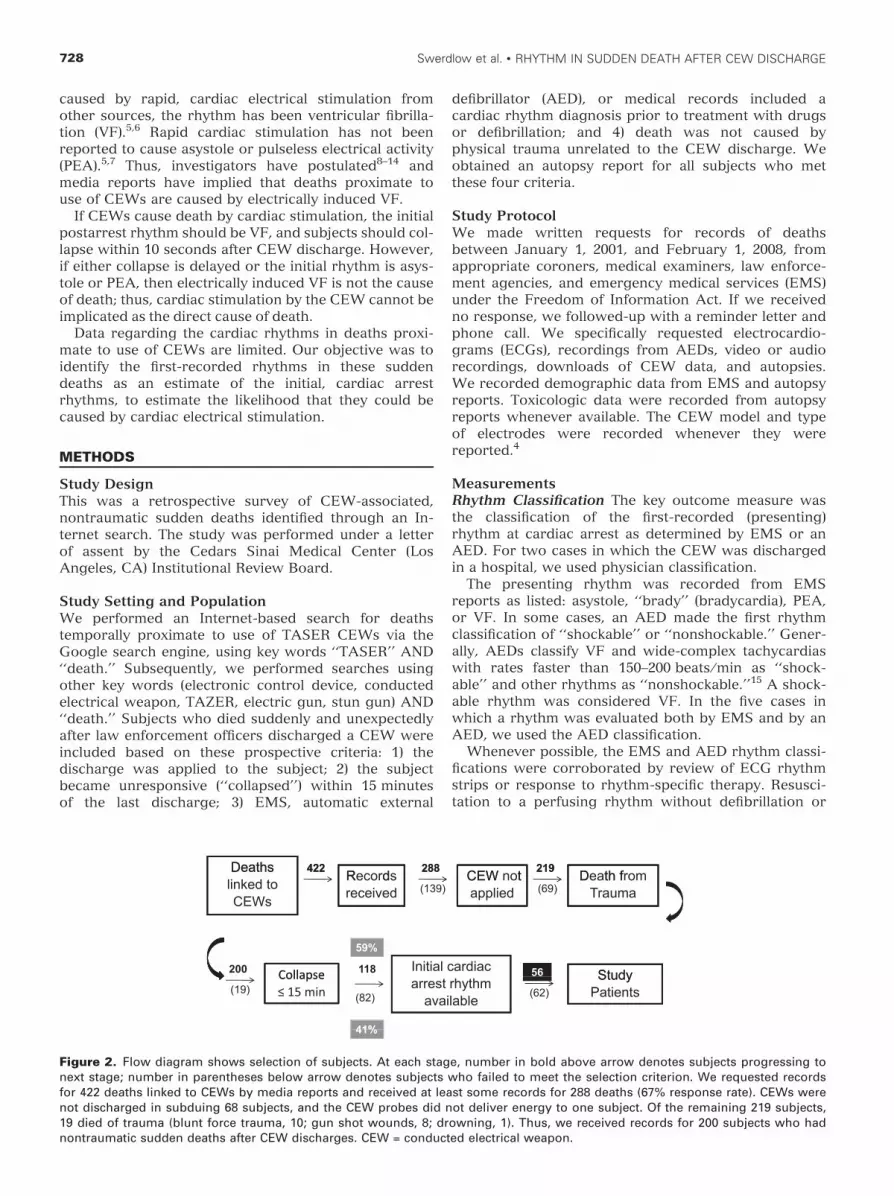
Figure 2. Flow diagram shows selection of subjects. At each stage, number in bold above arrow denotes subjects progressing tonext stage; number in parentheses below arrow denotes subjects who failed to meet the selection criterion. We requested recordsfor 422 deaths linked to CEWs by media reports and received at least some records for 288 deaths (67% response rate). CEWs werenot discharged in subduing 68 subjects, and the CEW probes did not deliver energy to one subject. Of the remaining 219 subjects,19 died of trauma (blunt force trauma, 10; gun shot wounds, 8; drowning, 1). Thus, we received records for 200 subjects who hadnontraumatic sudden deaths after CEW discharges. CEW = conducted electrical weapon.
728 Swerdlow et al. • RHYTHM IN SUDDEN DEATH AFTER CEW DISCHARGE

antiarrhythmic drugs was considered evidence that therhythm was not VF. Secondary rhythms recorded laterin the resuscitation by EMS were analyzed only as acheck on accuracy of EMS or AED rhythm diagnosis,not to classify the presenting rhythm.
Reconstruction of Time Course.Time From CEW Discharge to Collapse.This interval was calculated from EMS system (9-1-1)
logs, EMS field reports, and law enforcement records(including CEW electronic data logs and timelines incrime reports) whenever we had these data and couldconfirm synchronization of clocks (Figure 1). Theremaining intervals were estimated from narratives ofevents. This interval was usually reported or could beestimated within 1 minute if it was 5 minutes or less.When clock times were not recorded, we used esti-mates based on the key events recorded by lawenforcement: application of handcuffs, the duration ofthe struggle after handcuffs were applied, and whetherthe subject had been assessed and moved from the siteof arrest or encounter after being handcuffed.
.Time From Collapse to First Recorded Rhythm.When EMS or law enforcement personnel who were
already on scene with defibrillators recorded the pre-senting rhythm, we calculated or estimated this intervalfrom time lines in law enforcement records, EMS fieldreports, incident reports of law enforcement officers,and EMS system (9-1-1) logs when available. This inter-val could usually be calculated or estimated within1 minute when EMS was on scene or staged nearby atthe time of collapse. In the remaining cases, the timefrom collapse to call for EMS—or call to EMS to col-lapse, whichever came first—was determined from lawenforcement reports, and the time from the call untilthe rhythm was recorded was taken from EMS fieldreports and phone logs when available (see Figure 1).
A cardiac pathologist, who was blinded to presentingrhythm, reviewed autopsy data for presence and sever-ity of heart disease. Heart weights were normalized forbody height to determine the degree of hypertrophy16:Mild hypertrophy (grade 1) was 101%–125% of normal;moderate hypertrophy (grade 2) was 126%–150% ofnormal, and marked hypertrophy (grade 3) was morethan 150% of normal. Coronary artery disease wasmild if there was less than 50% cross-sectional luminalnarrowing (grade 1), moderate if there was 51%–75%narrowing (grade 2), and severe if there was >75% nar-rowing (grade 3). Left-ventricular dilation and fibrosiswere recorded as present or absent. The overall sever-ity of heart disease (grades 0 to 3) was the sum of thedegrees of hypertrophy and coronary artery disease upto maximum of 3. For example, if a patient had grade 2hypertrophy and grade of coronary artery disease ‡1,the severity of heart disease was assigned grade 3.
Data AnalysisWe used the chi-square test with Yates’ correction orthe unpaired t-test to compare characteristics of studysubjects and subjects who collapsed within 15 minutesbut were not analyzed because of absence of rhythmdata. Severity of cardiac disease was evaluated for cor-relation with the presenting rhythm using Fisher’sexact test.
Table 1Subjects with Nontraumatic Sudden Death After CEW Discharge Who Collapsed Within 15 Minutes (n = 118)
Study Subjects (n = 56) Excluded Subjects (n = 62) p-value
Age, yr (mean ± SD) 37 ± 10 36 ± 9 0.56Sex (M:F) 54:2 61:1 0.46Body mass index (mean ± SD) 30 ± 8 29 ± 6 0.42Stimulants or psychoactive drugs 50 (89%)* 57 (95%)� 0.31CEW electrode type
Probes 36 (64%) 47 (76%) 0.34Drive-stun 12 (21%) 8 (13%)Both 4 (7%) 2 (3%)Unknown 5 (9%) 3 (5%)
CEW = conducted electrical weapon.*Overall, 45 study subjects took illegal drugs (80%) and seven took legal drugs (13%). Illegal drugs included cocaine, 24; meth-amphetamine, 15; phencyclidine (PCP), two; MDMA (ecstasy), three; ephedrine, two; lysergic acid diethylamide (LSD), one; andtetrahydrocannabinol (THC), five. Nine subjects took multiple illegal drugs. Legal drugs included olanzipine, two; mirtazapine,two; promethazine, one; bupropion, one.�Data were available for 60 excluded subjects; percentage of 60 is shown.
Table 2Presenting Cardiac Arrest Rhythm as Classified by EMS (n = 56)
Rhythm n (%) n
No VFAsystole 52 (93) 21 (5)*PEA ‡ 30 beats ⁄ min 11� (3)*Bradycardia < 30 beats ⁄ min 5 (2)*AED—no shock advised 11 (1)*
VFVF 4 (7) 2AED—shock advised 2 (1)*
AED = automatic external defibrillator; PEA = pulseless elec-trical activity; VF = ventricular fibrillation.*Values in parentheses indicate the number of ECG rhythmsconfirmed by the authors.�Two episodes of PEA were also classified by implantablecardiac defibrillator algorithms to not be VT or VF.
ACAD EMERG MED • August 2009, Vol. 16, No. 8 • www.aemj.org 729

RESULTS
SubjectsAll 422 subjects identified by any of the search termsused were found using the terms ‘‘TASER’’ and‘‘death.’’ Figure 2 shows that we received records for200 subjects who had nontraumatic sudden deaths afterCEW discharges. Collapse occurred within 15 minutesin 118 subjects (59%). Of these, 62 subjects wereexcluded because EMS records of the presentingrhythm could not be obtained.
The study population includes the remaining 56 sub-jects. Most were males who were using illegal drugs.The median age was 35 years. Table 1 shows thatdemographic characteristics and CEW electrode typedid not differ significantly between the 56 study sub-jects and the 62 excluded subjects. The TASER CEWmodel was X-26 in 51 study subjects (91%) and 50excluded subjects (81%), M-26 in 2 study subjects (4%),and unknown in 3 study subjects (5%) and 12 excludedsubjects (19%).
Presenting RhythmsTable 2 shows that the presenting rhythm was VF infour subjects (7%; 95% confidence interval [CI] = 3% to17%) and not VF in 52 subjects (93%; 95% CI = 83% to97%). The presenting rhythm was classified by EMSinterpretation in 41 subjects (75%), AED algorithms in13 subjects (23%), and physician interpretation in twosubjects (4%). Figure 3 shows representative EMSrecords of the presenting rhythms.
Corroboration of Rhythm Classifications: ECGRecordingsWe received ECG recordings of presenting rhythms for12 of 56 subjects (21%). EMS personnel classified 10 ofthese rhythms (see Table 2, Figures 3B and 4); AEDsclassified two of these rhythms, one as nonshockable(Figure 5A), and the other as shockable (Figure 5B).Four of seven presenting rhythms confirmed as asystoleby ECG had identifiable QRS complexes with ventricu-lar rates less than 5 beats ⁄ min (Figure 4).
Figure 3. Representative EMS records. Each panel shows sequential entries with time in the left column. The column indicatingcardiac rhythm (‘‘ECG’’ or ‘‘Rhythm ⁄ Defib’’) has black border added. The first entry in this column is the presenting rhythm. (A)Transition from perfusing sinus rhythm to PEA: a second black border denotes the blood pressure column (‘‘B ⁄ P’’). The presentingrhythm at 18:50 is sinus with a pulse of 76 beats ⁄ min and blood pressure of 99 ⁄ 48 mm Hg. Sequential entries indicate that bloodpressure can no longer be measured and that the rhythm is irregular (‘‘irreg’’) at 18:55 and has a rate of 75–140 beats ⁄ min at 19:04.(B) Asystole. EMS record (top panel) and corresponding initial three-lead ECG rhythm strip (bottom panel). Chest compressions ofcardiopulmonary resuscitation (CPR) are held at arrow. ECG = electrocardiogram.
730 Swerdlow et al. • RHYTHM IN SUDDEN DEATH AFTER CEW DISCHARGE

Figure 4. Sequential ECG rhythm strips during pharmacologic resuscitation from asystole. (A, 00:06:04) Profound bradycardia-asystole recorded when chest compressions were held just before the second dose of epinephrine and atropine. A single wide QRScomplex is recorded at the left; artifact appears at right. (B, 00:06:34): Return of wide-complex rhythm at 43 beats ⁄ min and circula-tion after second doses of epinephrine and atropine. (C) Recorded 5 minutes later (00:11:18): irregular, mostly narrow-complextachycardia without identifiable atrial activity, probably atrial fibrillation.
Figure 5. Rhythms at cardiac arrest. (A and B) First recorded rhythms from AEDs with ECG rhythm strip and AED annotation chan-nel. (A) Initial recording shows bradycardia. Sequential annotations indicate ‘‘Patient Connected’’ and ‘‘Initial Rhythm.’’ The AEDalgorithm then analyzed two rhythm segments and classified the rhythm showing profound bradycardia at 19 beats ⁄ min as‘‘nonshockable.’’ (B) VF (subject 1). The initial recording (not shown) displays artifact from CPR. The tracing shows the first twosegments analyzed, which the AED classifies as ‘‘shockable.’’ (C) Secondary EMS ECG tracing from VF subject 4, 10 minutes afterinitial record, which was not reviewed. Rhythm is shown immediately before and after defibrillation shock (delivered betweendotted vertical lines highlighted by downward facing arrows). Preshock tracing shows an irregular, wide-complex tachycardia withisoelectric baseline and no identifiable atrial activity. Postshock, the rate, irregularity, and morphology of QRS complexes are indis-tinguishable from those in the preshock rhythm. Possible diagnoses include VT and conducted supraventricular arrhythmia withaberrancy (e.g., secondary to hyperkalemia). The lack of effect of defibrillation on the rhythm makes VT less likely. AED = automaticexternal defibrillator; CPR = cardiopulmonary resuscitation; ECG = electrocardiogram; VT = ventricular tachycardia.
ACAD EMERG MED • August 2009, Vol. 16, No. 8 • www.aemj.org 731

Secondary rhythms recorded later in the resuscita-tion by EMS were available for an additional 11 sub-jects (20%). Of the 23 ECG tracings we reviewed (12initial and 11 secondary tracings), we judged the diag-nosis to be accurate in 22 (96%) and inaccurate in onesecondary rhythm (4%). EMS classified this organizedrhythm as VF, but we classified it as PEA (Figure 5C).
Corroboration of EMS Rhythm ClassificationsResponse to Treatment Overall, 17 subjects wereresuscitated to a perfusing rhythm. Sixteen subjectshad return of circulation during pharmacologic resusci-tation, excluding the diagnosis of VF (Figure 4). Pre-senting rhythm classifications in these subjects wereasystole (n = 8), PEA (n = 4), bradycardia less than30 beats ⁄ min (n = 1), and AED nonshockable (n = 3).One subject with an AED shockable rhythm was defib-rillated. Overall, 14 of the 25 rhythms diagnosed asasystole by EMS were corroborated: seven by return ofcirculation during pharmacological resuscitation and 7by review of the ECG.
Subjects with VFTable 3 summarizes these subjects. For subject 1, whocollapsed immediately (subject 6 in Table 4), neitherdrugs nor cardiac disease can be implicated; both thetime course and the electrode location are consistent
with electrically induced VF. In subject 2, neitheris consistent. He was subdued without a CEW, butcollapsed and became unresponsive while walking tothe police car in handcuffs. To determine if he wasfeigning, the arresting officer delivered a 1 seconddrive-stun discharge to the calf. When the subjectremained unresponsive, the officer recognized that hewas in cardiac arrest. In subjects 3 and 4, electrodelocations permit a current path through the heart, butthe time from CEW discharge to collapse excludesimmediate induction of VF. In both cases, subjectswere using stimulant drugs, and subject 3 had cardio-myopathy. We received the initial ECG only for sub-ject 1. In addition, we received a secondary tracing forsubject 4, recorded 10 minutes after the presentingrhythm (Figure 5C). EMS diagnosed it incorrectly asVF.
Time From Last CEW Discharge to CollapseTable 5A summarizes these time intervals for 56 studysubjects. Calculated intervals are listed individually. Theremaining intervals were estimated from narratives ofthe events. Subjects with electrically induced VF wouldbe expected to collapse within 10 seconds. Overall, onlyfive subjects collapsed in the first minute. Of these, onesubject described previously collapsed immediately withVF (Figure 5B). Three of the four remaining subjects
Table 3Subjects in Whom Presenting Rhythm Was VF (n = 4)
Subject Age ⁄ Sex BMI DetailsECGReviewed
Time (min)*
Last CEWDischargeto Collapse
Loss ofPulseto ECG
1 25 ⁄ M 28.4 Police AED Yes Immediate (3–5)
2 41 ⁄ M 28.9 Police AED;‘‘Shockable’’;shocked toperfusingrhythm
No CollapsedbeforeCEWdischarge
(3–5)
3 54 ⁄ M 23.8 EMS-D; collapsedwhile underEMS care
No 8 2
4 18 ⁄ M 19.7 EMS-D� No� 5 6
BMI = body mass index; brady = bradycardia; CAD = coronary artery disease; CEW = conducted electrical weapon; ECG = electro-cardiogram; EMS-D = EMS manual defibrillator; ICD = implantable cardioverter defibrillator; LE = law enforcement records;LSD = lysergic acid dimethylamide; VF = ventricular fibrillation.*Time intervals in parentheses are estimates.�Subsequent ECG diagnosed as VF shows organized tachycardia (Figure 5C).
732 Swerdlow et al. • RHYTHM IN SUDDEN DEATH AFTER CEW DISCHARGE

who collapsed in the first minute had non-VF rhythms.They were involved in protracted, grappling struggleswith multiple law enforcement officers, who used mul-tiple probe and drive-stun discharges as well asrepeated applications of pepper spray and baton strikesuntil the subjects collapsed. Each subject collapsedmore than 5 minutes after the last probe discharge, butwithin 1 minute of the last of more than 10 drive-stundischarges to the back or extremities. In all three sub-jects, non-VF rhythms were recorded within 5 minutesof collapse (EMS-diagnosed asystole, EMS-diagnosedPEA, and AED-diagnosed nonshockable rhythm). Thefourth subject, who received only drive-stun dischargesand had AED-diagnosed nonshockable rhythm, wasresuscitated pharmacologically to sinus tachycardia,which is extremely unlikely in terminal asystole thatdegenerates from VF.
Time From Collapse to First Recorded RhythmTable 5B summarizes these intervals: immediate ineight subjects (14%) who were under observation onECG monitors at the time of collapse, 3 minutes or lessin 27 additional subjects (48%), 3 to 5 minutes in eightsubjects (14%), 6 to 10 minutes in four subjects (7%),and unknown in nine subjects (16%). Overall, the inter-val was 3 minutes or less in 35 subjects (62%) and5 minutes or less in 43 subjects (77%). The prevalence
of short intervals is explained by two factors: 1) EMS isoften dispatched before law enforcement because thesubject’s erratic behavior suggests a psychiatricproblem, and 2) law enforcement often calls for EMS atthe onset of an altercation or after the first CEWdeployment. None of the eight subjects who collapsedwhile on ECG monitors had VF as the presentingrhythm.
Cardiac DiseaseAutopsy reports were available for all study subjects.Three autopsies indicated that subjects had been trea-ted for heart disease, including two with nonischemiccardiomyopathy who had been treated with primary-prevention implantable cardioverter-defibrillators(ICDs).
Figure 6 summarizes postmortem findings. Sevensubjects (14%) had marked hypertrophy, and one sub-ject (2%) had severe coronary artery disease. Overall,heart disease was classified as marked in 14 subjects(25%) and moderate in 11 subjects (20%).
DISCUSSION
Our principal finding is that, in sudden death proximateto discharge of CEWs, VF is an uncommon presentingrhythm and collapse is rarely immediate.
Electrodesand No. ofDischarges Electrode Locations Drugs Cardiac Pathology
Probes,3 · 5 sec
Anterior chest: 1midline lowerchest, 1 superiorto medial leftclavicle
None None
Drive stun,1 · 1 sec
Right calf Cocaine Extensive anterior,septal, and inferiorinfarction; 3-vesselCAD (80–90%stenosis)
Probes,2 · 5 sec
Chest slightly to leftof midline: 1near level ofnipple, 1 atcostophrenicmargin
Methamphetamine Marked left-ventricularhypertrophy andenlargement; 50%left anteriordescendingcoronary arterystenosis
Probes,2 · 5 sec
Left chest slightlymedial to nipple:1 just belownipple and 1 nearcostophrenicmargin
Methamphetamine,MDMA
None
ACAD EMERG MED • August 2009, Vol. 16, No. 8 • www.aemj.org 733

Studies of Arrest-related DeathsSudden deaths of civilians temporally proximate tointeractions with law enforcement were describedbefore use of CEWs.17,18 Most reported subjects wereagitated young males, often chronic and acute users ofstimulant or psychoactive drugs, who collapsed whilebeing restrained.19–23 A recent European publicationconfirms the international nature of this problem.24
Initial studies focused on methods of restraining orsubduing subjects,17,23 providing few data regarding car-diac rhythms. Hick et al.25 reported on cardiac arrestsafter restraint in five agitated and violent subjects notassociated with use of CEWs. The presenting rhythmwas asystole or PEA in four subjects and VF in one sub-ject; all subjects had extreme metabolic acidosis. Strattonet al.19 reported 13 delirious subjects who died afterbeing restrained. The rhythm was asystole or PEA in allthree subjects who received CEW discharges and in nineof 10 subjects who did not receive discharges.
Cardiac Effects of CEWsBecause rapid cardiac electrical stimulation can causecardiac arrest by inducing VF,5,6 studies on suddendeath after discharges of CEWs have focused on therisk of electrically induced VF.8–13 Under some experi-mental conditions, CEWs can induce VF in animalsusing probe discharges across the anterior chest;8,13,14
but they have not been reported to induce VF or anyother arrhythmias in human volunteers.26,27 There isuncertainty regarding how results of these studiesrelate to sudden death after tactical exposure toCEWs: VF thresholds for external electrical stimula-tion may differ between smaller, anesthetized animalsand larger, awake humans. The controlled conditionsof research in humans do not duplicate the stressesof tactical interactions, and volunteers, usually lawenforcement officers, differ from decedents, whooften use street drugs and are typically in less robustphysical condition.
Table 4Subjects in Whom Presenting ECG Record Was Reviewed (n = 12)
Subject Age ⁄ Sex BMIRhythm (ECGType)
Time (min)*
Last CEWDischarge toCollapse
Loss ofPulse toECG
1 22 ⁄ M 18.7 Sinus brady19 beats ⁄min (EMS-D)
5 6
2 47 ⁄ M 28.4 Asystole (EMS-D) 7 0 (inambulance)
3 34 ⁄ M 30.0 PEA (hospitalmonitor)
5 0 (onmonitor)
4 21 ⁄ M 26.5 Asystole (EMS-D) 13 2 (EMSon scene)
5 62 ⁄ M 45.1 Sinus brady 18beats ⁄min (EMS-D)
(3–5), (3–5) (2–3) EMSon scene
6 25 ⁄ M 28.4 VF (police AED) Immediate (3–5) PoliceAED
7 53 ⁄ M 32.0 PEA (EMS-D; ICDinterrogation)
(2–3) (2–3) EMS onscene
8 40 ⁄ M 31.5 Asystole (EMS-D) 1, (4–6) 8
9 32 ⁄ M 25.4 PEA (EMS-D) (2–3) (2–3) EMSon scene
10 17 ⁄ M 21.1 Asystole (EMS-D) (3–5) (2–3) EMSon scene
11 34 ⁄ M 34.4 PEA (EMS-D) (8–12) 0 On Monitor12 45 ⁄ M 27.0 Asystole EMS ED (1), (4–8) (1–3) EMS
on scene
BMI = body mass index; brady = bradycardia; CAD = coronary artery disease; CEW = conducted electrical weapon; EMS-D = EMSmanual defibrillator; ICD = implantable cardioverter defibrillator; LE = law enforcement records; LSD = lysergic acid dimethyla-mide; PEA = pulseless electrical activity; VF = ventricular fibrillation.*Time intervals in parentheses are estimates. If both probes and drive-stun modes were used, first interval is from last drive stunand second interval is from last probe discharge.�Number in parentheses is number of electrodes over anterior left chest.
734 Swerdlow et al. • RHYTHM IN SUDDEN DEATH AFTER CEW DISCHARGE

Present StudyTo the best of our knowledge, this is the first system-atic analysis of the presenting rhythm in sudden deathproximate to use of CEWs. Of those collapsing within15 minutes, the presenting rhythm was VF in only fourof 56 study subjects (7%).
The time sequence and electrode location are bothconsistent with electrically induced VF in one subject(subject 1), and neither drug use nor cardiac diseaseprovides alternative explanations. To the best of ourknowledge, this is the first reported fatality suggestiveof CEW-induced VF.
Conversely, both the time sequence and the electrodelocation are inconsistent with VF in subject 2. Electrodelocations in subjects 3 and 4 could have placed theheart in the current pathway, but delays from CEWdischarge to collapse exclude direct electrical inductionof VF. Electrical induction of an intermediate arrhyth-mia, such as ventricular tachycardia (VT) or atrial fibril-lation, is possible. However, electrical induction ofstable VT that degenerates to VF is rare, especially in a
structurally normal heart (subject 4),6 and degenerationof atrial fibrillation to VF is rare, except in unusualcases of ventricular preexcitation (Wolff-Parkinson-White syndrome).
Results in the Context of Prior StudiesThe low incidence of VT ⁄ VF in our subjects is similarto that reported in small studies of subjects who weresubdued without CEWs.19,25 Our data confirm andexpand the only known previous report of cardiacarrest rhythms associated with CEWs, in which Strat-ton reported no VF in three subjects.19 Our 12 subjectswith initial ECG records is the largest group reportedwith validated rhythms in sudden deaths after CEWdischarge. Our eight subjects who collapsed duringECG monitoring is the only group in whom the initial,cardiac arrest rhythm had been recorded after CEWdischarges.
These results focus attention on the paradoxically highprevalence of asystole and PEA in nontraumatic suddendeaths after extreme stress or exertion during law
SourceData forTime
Electrodes andNo. ofDischarges
Electrodes toAnteriorChest� Drugs
MedicalConditions
LE, EMS Probes · 1 Yes (1) Marijuana
LE, EMSvideo
Probe · 3 No Cocaine, alcohol
Medicalrecord
Drive stun · 3 No Cocaine
LE, EMSvideo�
Probes anddrive stun ·multiple
No LSD, MDMA
LE, EMS Probes · 2;drive stun ·multiple
No None Hypertensivecardiomyopathy;moderate CAD; heatexhaustion;schizophrenia
LE Probes · 3 Yes (2) None
LE, EMS Probes ·unknown
No Methamphetamine Dilatedcardiomyopathy;ICD
LE, EMS,9-1-1 log
Probes ·multiple &drive stun · 1
No Methamphetamine Hypertensivecardiomyopathy
LE, EMS Probes · 5 No Cocaine
LE, EMS Probes · 2 No None Schizophrenia
P EMS No Cocaine, marijuanaP EMS Probes · 1 and
drive stun · 1No Cocaine,
methamphetamineHypertensivecardiomyopathy;schizophrenia
ACAD EMERG MED • August 2009, Vol. 16, No. 8 • www.aemj.org 735

enforcement interactions.28 In combination with similardemographic and drug use profiles, they raise the possi-bility that the principal mechanism may be related tocharacteristics of the subject and the struggle. Metabolicacidosis and alterations of the central nervous systemhave been proposed, but not confirmed, as contributoryfactors. Experimental evidence does not suggest a mech-
anism by which CEWs contribute. Specifically, probedischarges cause little acidosis,29 and drive-stun dis-charges should cause less. But we cannot exclude aCEW contribution by mechanisms yet unknown.
LIMITATIONS
Likelihood of Underdiagnosis of VFDespite extensive efforts to obtain ECG records of theinitial cardiac arrest rhythm, we succeeded in only 12cases. It is unlikely many more ECGs could be obtainedretrospectively, and unexpected sudden death after tac-tical discharges of CEWs is too rare for a prospectivestudy. The largest known study30 reported no atraumat-ic deaths within 15 minutes of CEW discharges in 996consecutive subjects.
However, the fact that we reviewed ECGs in only 12subjects requires us to consider the possibility that ourmethods failed to identify a significant number of sub-jects with electrically induced VF, because either EMSmisinterpreted ‘‘fine’’ VF as ‘‘flatline’’ asystole or VFterminated before the initial ECG recording.
Likelihood of Misdiagnosis of VF as Asystole Fivelines of evidence suggest a low rate of misdiagnosis.First, misdiagnosis of VF as asystole is rare, either byEMS31 or AEDs.15 For example, emergency medicaltechnicians analyzing a single ECG lead misdiagnosedVF as asystole in only three of 118 cardiac arrestpatients.31 Second, the prevalence of VF is low in casesfor which the EMS diagnosis is corroborated: of the 12subjects for whom we reviewed ECG rhythm strips, VF
Table 5Time Intervals: Calculated From Reported Data or Estimated From Narratives of Events
Collapse Relative to EventsNo. of
Subjects
No. WithCalculatedIntervals
CalculatedIntervals(min)
No. WithEstimatedIntervals
EstimatedIntervals (min)
A. Time From Last CEW Discharge to CollapseImmediate 1 1 0 0 NABefore handcuffs 5 5 0.5, 1, 1, 1, 5 0 NAAfter handcuffs, before beingmoved on siteStopped struggling aftercuffs
8 5 2, 3, 3, 4, 7 3 2–3
Struggled forseveral minutes
18 8 4, 4, 5, 6, 6, 6, 7, 8 10 3–5
Moved on sitebefore collapse
24 7 7, 8, 8, 10, 10, 12, 15 17 6–15
Total 56 26 30
B. Time from Collapse to First Recorded RhythmSubject on ECG monitor underobservation*
8 8 0, 0, 0, 0, 0, 0, 0, 0 0 NA
EMS with defibrillator onscene, witnessed collapse
23 8 1, 1, 2, 2, 2, 2, 2, 2 15 1–3
Law enforcement usedon-scene AED
4 1 3 3 3–5
EMS staged adjacent to scene 4 4 3, 3, 4, 4 0 NAEMS in route 11 6 3, 5, 5, 6, 7, 8 5 UnknownEMS called after collapse 6 2 5, 10 4 UnknownTotal 56 29 27
AED = automatic external defibrillator; CEW = conducted electrical weapon; ECG = electrocardiogram; NA = not applicable.*Six subjects were under EMS observation and two subjects were in hospital EDs under physician observation.
Figure 6. Histogram showing heart disease found at autopsy.Gross fibrosis and left-ventricular (LV) dilation were recordedas present (+) or absent ()). Coronary artery disease, hypertro-phy, and overall heart disease were graded on a scale of 1 to 3.PEA = pulseless electrical activity; VF = ventricular fibrillation.
736 Swerdlow et al. • RHYTHM IN SUDDEN DEATH AFTER CEW DISCHARGE

was present in only one (8%). If we include subjects inwhom an AED evaluated the rhythm (12 additional sub-jects), an ICD did not detect VF (one additional subject),and return of circulation occurred after pharmacologicresuscitation (10 additional subjects), the prevalence ofVF was two in 35 (6%). Third, of the 23 total initial andsubsequent ECG tracings reviewed, only one had a mis-diagnosis; but in this case, VF was not underdiagnosed,but rather diagnosed in error (Figure 5C). Fourth, fourof seven rhythms strips that were diagnosed as asystoleand reviewed by the authors had at least one discernableQRS complex (Figure 4, top panel) rather than true flat-line. Fifth, 14 of the 25 rhythms diagnosed as asystole byEMS were corroborated by ECG or return of circulationduring pharmacologic resuscitation. Some of theremaining 11 episodes probably had QRS complexes,reducing the likelihood of misdiagnosing ‘‘fine’’ VF.
Likelihood of Presenting Rhythm Differing From Ini-tial Rhythm Of greatest concern is the likelihood thatVF terminated before the rhythm was recorded. How-ever, three considerations suggest that this is unlikely tohave significantly altered our observed prevalence of VF.
First, in most subjects, the time from collapse torhythm determination was short relative to the likelyduration of VF. The duration of human VF required fordegeneration to asystole has not been studied for ethi-cal reasons. However, in pigs and dogs, electricallyinduced VF persists for at least 10 minutes.32 Rarecases in which ICDs have failed to terminate VF indi-cate that human VF can persist for more than 30 min-utes.33 Relative to the 10 minute time frame, the timefrom collapse to rhythm determination in sudden deathafter CEW discharge is short: 3 minutes or less in 62%of subjects and 5 minutes or less in 77%. This occurredbecause EMS usually was on scene, nearby, or en routeprior to the subject’s collapse.
Second, if VF degenerated to asystole, we wouldexpect a greater fraction of VF episodes to degeneratewith longer intervals from collapse to rhythm determi-nation, resulting in an inverse correlation between theinterval and the prevalence of VF. But the reverseoccurred: VF was recorded in none of the eight sub-jects who had cardiac arrests during continuous ECGmonitoring, one of the remaining 27 subjects (4%)whose rhythms were recorded in the first 3 minutesafter collapse, and three of 21 subjects (14%) in whomthe time from collapse to rhythm determination wasgreater than 3 minutes or unknown.
Third, bradycardia or asystole may have degeneratedto VF before the rhythm was recorded, offsetting anydegeneration of VF to asystole. Although VF lasts forminutes before degeneration to asystole, a single longpause usually precipitates bradycardia-dependentVF.34,35 This must be considered given the inverse rela-tionship between the time from collapse and preva-lence of VF.
Time Course and Current Pathway in ElectricallyInduced VF Any estimate of the likelihood of underdiag-nosing VF must consider both the time course, which istypically immediate for electrically induced VF,6 and theelectrode type and location, because CEW discharges in
animals have induced VF only using probe electrodesover the anterior chest.8–13 These considerations lead usto focus on subjects who collapsed with non-VF rhythmsrapidly after CEW discharges through probe electrodes,but the only subject who collapsed in the first minuteafter a probe CEW discharge had VF. Drive-stun dis-charges have not been reported to induce VF in animals,even when delivered directly over the heart.11 Thus thelow detected prevalence of VF in our study is consistentwith the observation that, in 98% of subjects, the timecourse or current pathway is atypical of electricallyinduced VF in animal experiments.
Method of Identifying SubjectsThe Internet search method has been used infrequentlyin medical research36 because confidentiality of patientdata is protected. We could use it in this study becausesudden deaths after CEW discharges attract mediaattention, and media reports often include the names ofdecedents.
Our method identified only those subjects whosedeaths were reported publically and detected by thesearch terms used. Once subjects were identified, ouraccess to data depended on cooperation of differentlaw enforcement and EMS agencies with the Freedomof Information Act. A national database of in-custodysudden deaths would facilitate identifying subjects andreduce sample bias inherent in our method.
We do not know if our study subjects are representa-tive of those who die suddenly after CEW discharges.However, our subjects had demographic and drug-useprofiles similar to those of subjects we excludedbecause of insufficient data, subjects identified by pro-spective study of nonfatal use of CEWs by law enforce-ment,30,37 and subjects in prior reports of suddendeaths during law enforcement interactions—eitherassociated21 or unassociated with use of CEWs.18,19,24
At autopsy, the overall incidence of moderate andmarked heart disease was 45%, not statistically differ-ent from the 54% reported for subjects who diedwithin 24 hours of CEW discharge21 (p = 0.50). Theseconsiderations suggest that our subjects are in fact rep-resentative, but do not exclude undetected bias.
Our methods did not identify subjects who wereresuscitated from cardiac arrests and survived to bedischarged from the hospital. However, the fraction ofsubjects who were resuscitated to a perfusing rhythmwas not statistically different for VF and non-VF pre-senting rhythms: one of four subjects (25%) versus 16of 52 subjects (31%; p = 1.00). This suggests thatrhythms in subjects who survived to be discharged andthose who died would have a similar distribution.
In summary, study subjects represent only a smallfraction of sudden deaths proximate to CEW dis-charges. Although the method of selecting them intro-duced bias, there is no evidence that this biasinfluenced the distribution of presenting rhythms; how-ever, we cannot exclude this possibility.
CONCLUSIONS
In sudden deaths after conducted electrical weapon dis-charge, collapse is rarely immediate, and VF is an
ACAD EMERG MED • August 2009, Vol. 16, No. 8 • www.aemj.org 737

uncommon presenting rhythm. Only one death wassuggestive of electrically induced VF. Except for theeight subjects who collapsed during electrocardiogrammonitoring, our estimates of initial cardiac arrestrhythms are subject to the limitations discussed, andwe do not know if selection bias limits extrapolation ofour findings to subjects identified by another strategy.With these qualifications, our data do not support elec-trically induced VF as a common mechanism of suddendeath after conducted electrical weapon discharge. Thespecific mechanisms for most of these deaths remainunknown.
References
1. Mumola C. Arrest-related Deaths in the UnitedStates, 2003–2005. Bureau of Justice Statistics Spe-cial Report. 2007; (NCJ 219534).
2. Berenson A. As police use of Tasers soars, questionsover safety emerge. New York Times. July 18,2004.
3. American Medical Assoication House of Delegates.Resolution 401 (A-08). Available at: http://www.ama-assn.org/ama1/pub/upload/mm/471/401.doc. Acces-sed July 10, 2008.
4. Kroll M. Crafting the perfect shock. IEEE Spectrum.2007; 44:27–30.
5. Reilly J. Cardiac sensitivity to electrical stimulation.In: Reilly J, ed. Applied Bioelectricity: From Electri-cal Stimulation to Electrical Pathology. New York,NY: Springer-Verlag, 1998, pp 194–239.
6. Ideker RE, Dosdall DJ. Can the direct cardiac effectsof the electric pulses generated by the TASER X26cause immediate or delayed sudden cardiac arrestin normal adults? Am J Forensic Med Pathol. 2007;28:195–201.
7. Olson W. Electrical safety. In: Webster J, ed.Medical Instrumentation Application and Design.New York, NY: John Wiley & Sons, 2009.
8. Dennis AJ, Valentino DJ, Walter RJ, et al. Acuteeffects of TASER X26 discharges in a swine model.J Trauma. 2007; 63:581–90.
9. Jauchem JR, Sherry CJ, Fines DA, Cook MC. Acido-sis, lactate, electrolytes, muscle enzymes, and otherfactors in the blood of Sus scrofa following repeatedTASER exposures. Forensic Sci Int. 2006; 161:20–30.
10. Lakkireddy D, Wallick D, Ryschon K, et al. Effectsof cocaine intoxication on the threshold for stungun induction of ventricular fibrillation. J Am CollCardiol. 2006; 48:805–11.
11. Lakkireddy D, Wallick D, Verma A, et al. Cardiaceffects of electrical stun guns: does position ofbarbs contact make a difference? Pacing Clin Elec-trophysiol. 2008; 31:398–408.
12. McDaniel WC, Stratbucker RA, Nerheim M, BrewerJE. Cardiac safety of neuromuscular incapacitatingdefensive devices. Pacing Clin Electrophysiol. 2005;28(Suppl 1):S284–7.
13. Nanthakumar K, Billingsley IM, Masse S, et al. Car-diac electrophysiological consequences of neuro-muscular incapacitating device discharges. J AmColl Cardiol. 2006; 48:798–804.
14. Wu JY, Sun H, O’Rourke AP, et al. Taser dart-to-heart distance that causes ventricular fibrillation inpigs. IEEE Trans Biomed Eng. 2007; 54:503–8.
15. MacDonald R, Swanson J, Mottley J, Weinstein C.Performance and error analysis of automated exter-nal defibrillator use in the out-of-hospital setting.Ann Emerg Med. 2001; 38:262–7.
16. Zeek P. Heart weight I: The weight of the normalhuman heart. Arch Pathol. 1942; 34:820–32.
17. Reay DT, Eisele JW. Death from law enforcementneck holds. Am J Forensic Med Pathol. 1982; 3:253–8.
18. Reay DT. Death in custody. Clin Lab Med. 1998;18:1–22.
19. Stratton SJ, Rogers C, Brickett K, Gruzinski G. Fac-tors associated with sudden death of individualsrequiring restraint for excited delirium. Am JEmerg Med. 2001; 19:187–91.
20. Stratton SJ, Rogers C, Green K. Sudden death inindividuals in hobble restraints during paramedictransport. Ann Emerg Med. 1995; 25:710–2.
21. Strote J, Hutson HR. Taser use in restraint-relateddeaths. Prehospital Emerg Care. 2006; 10:447–50.
22. Mirchandani HG, Rorke LB, Sekula-Perlman A,Hood IC. Cocaine-induced agitated delirium, force-ful struggle, and minor head injury. A further defi-nition of sudden death during restraint. Am JForensic Med Pathol. 1994; 15:95–9.
23. Pollanen MS, Chiasson DA, Cairns JT, Young JG.Unexpected death related to restraint for exciteddelirium: a retrospective study of deaths in policecustody and in the community. Can Med Assoc J.1998; 158:1603–7.
24. Martinez-Selles M. Sudden death after police deten-tion in young males in Spain. A new syndrome witha possible cardiovascular origin [abstract]. EurHeart J. 2008; 29(suppl):644.
25. Hick JL, Smith SW, Lynch MT. Metabolic acidosisin restraint-associated cardiac arrest: a case series.Acad Emerg Med. 1999; 6:239–43.
26. Ho JD, Dawes DM, Reardon RF, et al. Echocardio-graphic evaluation of a TASER-X26 application inthe ideal human cardiac axis. Acad Emerg Med.2008; 15:838–44.
27. Vilke GM, Sloane C, Levine S, Neuman T, CastilloE, Chan TC. Twelve-lead electrocardiogram moni-toring of subjects before and after voluntary expo-sure to the Taser X26. Am J Emerg Med. 2008;26:1–4.
28. Ornato JP, Peberdy MA. The mystery of bradyasys-tole during cardiac arrest. Ann Emerg Med. 1996;27:576–87.
29. Ho JD, Dawes DM, Bultman LL, Moscati RM,Janchar J, Miner JR. Prolonged TASER use onexhausted humans does not worsen markers ofacidosis. Am J Emerg Med. 2009; 27:413–418.
30. Bozeman W, Hauda II W, Heck J, Graham D,Martin B, Winslow J. Safety and injury profile ofconducted electrical weapons used by law enforce-ment officers against criminal suspects. Ann EmergMed. 2009; 53:480–489 .
31. Cummins RO, Austin D Jr. The frequency of ‘occult’ventricular fibrillation masquerading as a flat line in
738 Swerdlow et al. • RHYTHM IN SUDDEN DEATH AFTER CEW DISCHARGE

prehospital cardiac arrest. Ann Emerg Med. 1988;17:813–7.
32. Allison JS, Qin H, Dosdall DJ, et al. The transmuralactivation sequence in porcine and canine left ven-tricle is markedly different during long-durationventricular fibrillation. J Cardiovasc Electrophysiol.2007; 18:1306–12.
33. Veltmann C, Borggrefe M, Schimpf R, Wolpert C.Fatal inappropriate ICD shock. J Cardiovasc Elec-trophysiol. 2007; 18:326–8.
34. Kay GN, Plumb VJ, Arciniegas JG, Henthorn RW,Waldo AL. Torsade de pointes: the long-shortinitiating sequence and other clinical features:observations in 32 patients. J Am Coll Cardiol.1983; 2:806–17.
35. Taylor E, Berger R, Hummel JD, et al. Analysis ofthe pattern of initiation of sustained ventricular ar-rhythmias in patients with implantable defibrilla-tors. J Cardiovasc Electrophysiol. 2000; 11:719–26.
36. Ho J, Miner J, Reardon R, Heegaard W, ReardonR. Unexpected arrest-related deaths in America: 12months of open source surveillance. West J EmergMed. 2009; in press.
37. Eastman AL, Metzger JC, Pepe PE, et al.Conductive electrical devices: a prospective, popu-lation-based study of the medical safety of lawenforcement use. J Trauma. 2008; 64:1567–72.
ACAD EMERG MED • August 2009, Vol. 16, No. 8 • www.aemj.org 739