postnatal estradiol up-regulates lung nitric oxide synthases and improves lung function in...
TRANSCRIPT

Postnatal Estradiol Upregulates Lung
NO Synthases and Improves Lung Function in
Bronchopulmonary Dysplasia
Donald C. McCurnin2,3, Richard A. Pierce4, Brigham C. Willis1, Ling Yi Chang5,
Bradley A. Yoder6, Ivan S. Yuhanna1, Philip L. Ballard7, Ronald I. Clyman7, Nahid Waleh8
William Maniscalco9, James D. Crapo5, Peter H. Grubb10, and Philip W. Shaul1
Division of Pulmonary and Vascular Biology1, Department of Pediatrics,
University of Texas Southwestern Medical Center Department of Pediatrics2, University of Texas Health Science Center at San Antonio,
and the Southwest Foundation for Biomedical Research3 Department of Internal Medicine4, Washington University School of Medicine
Department of Medicine5, National Jewish Medical and Research Center Department of Pediatrics6, University of Utah School of Medicine
Department of Pediatrics7, University of California San Francisco School of Medicine Life Sciences Division8, SRI International, Menlo Park, CA
Department of Pediatrics9, University of Rochester School of Medicine and Dentistry Department of Pediatrics10, Vanderbilt University School of Medicine
Running Head: Estradiol and Bronchopulmonary Dysplasia
Address correspondences to: Philip W. Shaul, Department of Pediatrics, University of
Texas Southwestern Medical Center at Dallas, 5323 Harry Hines Blvd, Dallas, TX. Tel. 214-648-2015, Fax 214-648-2098, email: [email protected].
Support: NIH grants HL63399 and HD30276 (PWS), HL63387 (RAP), HL63397 (JDC),
and HL46691 and HL56061 (RIC). Additional backing was provided by HL52636 (BPD Resource Center) and P51RR13986 for facility support.
Postnatal therapies to prevent bronchopulmonary dysplasia (BPD) in preterm infants are limited. These experiments in a primate model indicate that postnatal estradiol treatment has favorable cardiovascular impact, it enhances pulmonary function and it lowers requirements for ventilatory support in BPD. These effects occur in association with an upregulation of lung NO synthases. Estradiol may be an efficacious postnatal therapy to improve lung function and outcome in preterm infants.
This article has an online data supplement, which is accessible from this issue’s table of
contents online at www.atsjournals.org. 95. Neonatal Lung Disease Word Count: 4397
Page 1 of 56 AJRCCM Articles in Press. Published on January 16, 2009 as doi:10.1164/rccm.200805-794OC
Copyright (C) 2009 by the American Thoracic Society.
ABSTRACT Rationale: Nitric oxide (NO) plays an important role in lung development and perinatal lung
function, and pulmonary NO synthases (NOS) are decreased in bronchopulmonary dysplasia
(BPD) following preterm birth. Fetal estradiol levels increase during late gestation and estradiol
upregulates NOS, suggesting that after preterm birth estradiol deprivation causes attenuated lung
NOS resulting in impaired pulmonary function. Objective: Test the effects of postnatal estradiol
administration in a primate model of BPD over 14 days after delivery at 125 days gestation (term
= 185 days). Methods: Cardiopulmonary function was assessed by echocardiography and whole
body plethysmography. Lung morphometric and histopathologic analyses were performed, and
NOS enzymatic activity and abundance were measured. Measurements and Main Results:
Estradiol caused an increase in blood pressure, and it caused ductus arteriosus closure.
Expiratory resistance and lung compliance were also improved, and this occurred prior to
spontaneous ductal closure. Furthermore, both oxygenation and ventilation indices were
improved with estradiol, and the changes in lung function and ventilatory support requirements
persisted throughout the study period. Whereas estradiol had negligible effect on indicators of
lung inflammation and lung structure assessed after the initial 14 days of ventilatory support, it
caused an increase in lung neuronal and endothelial NOS enzymatic activity. Conclusions: In a
primate model of BPD, postnatal estradiol treatment had favorable cardiovascular impact, it
enhanced pulmonary function, and it lowered requirements for ventilatory support in association
with an upregulation of lung NOS. Estradiol may be an efficacious postnatal therapy to improve
lung function and outcome in preterm infants.
Abstract Word Count: 250 Key Words: airway resistance, compliance, patent ductus arteriosus
1
Page 2 of 56
INTRODUCTION
The signaling molecule nitric oxide (NO), generated by nitric oxide synthase (NOS),
plays a key role in multiple processes in the mature lung(1, 2). In the developing lung, NO
participates in pulmonary vascularization, alveolarization, and airway branching, and NO also
counteracts apoptosis in multiple lung cell types(3-6). In the perinatal period, epithelium-derived
NO is critically involved in the regulation of lung liquid production and of peripheral contractile
elements(7, 8), and NO also mediates pulmonary vasomotor tone(9). In studies of lungs from
fetal baboons, we showed that all three NOS isoforms, neuronal NOS (nNOS), endothelial NOS
(eNOS) and inducible NOS (iNOS), are principally expressed in proximal respiratory epithelium,
and that there are maturational increases in their abundance and in NO production during the
early third trimester(10). Thus, pulmonary NOS expression is upregulated during fetal
development in the primate, and this process may be critical to lung structural development and
airway, parenchymal and pulmonary vascular function in the early postnatal period.
Bronchopulmonary dysplasia (BPD) is a devastating primary complication of premature
birth that develops in the preterm human lung following ventilatory and oxygen support. This
disorder results in disrupted lung maturation and postnatal pulmonary maladaptation. We
previously determined whether there are alterations in NOS in proximal lung and accompanying
changes in NO production in a model of BPD in baboon fetuses delivered at 125d gestation (term
= 185d) and ventilated for 14d. This model best exemplifies the current form of BPD observed
in extremely preterm human infants(11). In contrast to the normal 73% increase in NOS activity
which occurs over the same developmental period in utero, there was an 83% decline in activity
due to decreases in nNOS and eNOS expression. In addition, exhaled NO levels at the time of
preterm birth at 125d gestation were one-third those observed at birth later in the third trimester,
2
Page 3 of 56
and they remained depressed until day of life 11(12). In addition, the administration of inhaled
NO gas (iNO) in the same model improved early pulmonary function. However, with iNO these
improvements were transient and there was negligible impact on ventilatory support
requirements(13). Studies of NOS and iNO in the primate and other animal models of BPD led
to trials of iNO therapy in preterm human infants. Collectively these important trials have
indicated that certain subsets of preterm infants benefit from iNO. However, others do not, and
new postnatal strategies to improve lung function and prevent BPD continue to be needed(14-
17).
The hormone estrogen upregulates nNOS and eNOS and activates NOS enzymatic
activity in diverse tissues and cell types(18-20), including in ovine fetal lung in vivo and in
cultured bronchial epithelial cells and pulmonary artery endothelial cells(20, 21). Fetal plasma
estradiol (E2) levels increase progressively during late gestation, they rise further with the onset
of parturition at term, and then fall in the early postnatal period due to the loss of the placentally-
derived hormone(22, 23). These cumulative observations suggest that there is relative estrogen
deprivation following preterm birth that may adversely impact lung NOS and thereby impair
pulmonary development and function.
In the present investigation we determined the effects of postnatal E2 administration in
the baboon model of BPD that mirrors the current form of the disease in extremely preterm
human infants(11). The baboons were born by cesarean section at 0.67 gestation, which is
comparable to 27 weeks post-conceptual age in humans, and E2 was administered by
subcutaneous pellet beginning at one hour of age. We tested the hypothesis that E2 improves the
pulmonary dysfunction that is due to prematurity and the development of BPD, and that this is
associated with an upregulation of pulmonary NOS. Since estrogen has numerous
3
Page 4 of 56
cardiovascular actions(24), we also determined the effects of postnatal E2 administration on the
pulmonary and systemic circulation and on the status of the ductus arteriosus. In addition,
because the current form of BPD is characterized by abnormal elastin deposition and fewer and
larger alveoli(25, 26), we evaluated the effect of E2 on pulmonary growth and structure.
Furthermore, since estrogen modulates inflammatory responses(27), we assessed the effect of E2
on markers of lung inflammation.
METHODS
Animal Model
Fetal baboons were delivered at 125±2 d gestation (term = 185d) by cesarean section. At
birth the baboons were weighed, sedated, intubated, given 4 cc/kg of surfactant (Survanta,
courtesy of Ross Laboratories, Columbus, OH), and ventilator support was provided for 14d.
Animals were randomly assigned to either the control group which received routine care and
control treatment, or to the estrogen group which received routine care plus E2. Additional detail
on the management of the animals is provided in an online data supplement.
Echocardiography and Pulmonary Function Testing
Echocardiographic studies were performed at 1 and 6 h of age and at 24 h intervals
thereafter. The echocardiograms were done by one of the authors (DM) coincident to the
pulmonary function tests which were performed using the VT1000 body plethysmograph
(Vitaltrends Technology, New York, NY)(13). Dynamic lung compliance and resistance
measurements were made during controlled mechanical breaths, and they were of the respiratory
system as a whole. Since tidal volume can impact measurements of compliance, tidal volume
4
Page 5 of 56
was controlled at 4 - 6 ml/kg, and measured tidal volumes did not differ between study groups.
For data analysis compliance was corrected for body weight.
Postmortem Pressure-Volume Measurements
Immediately prior to termination the animals breathed 100% oxygen for 5 min and the
lungs were degassed by clamping the trachea at end expiration for 2 min. Following the removal
of the lungs from the thoracic cavity en bloc, postmortem quasi-static inflation pressure-volume
measurements were carried out. Additional detail on the method employed is provided in an
online data supplement.
Morphometric-histopathologic Analyses and Assessments of Lung Inflammation
Analyses were performed using the methods previously reported(13, 28). Additional
details are provided in an online data supplement.
Pulmonary Surfactant Analysis
At the end of study a bronchoalveolar lavage (BAL) was done on the left lower lobe with
25 ml of normal saline. Cells were removed by centrifugation and the supernatant was
centrifuged (27,000 × g, 60 min) to yield a large aggregate surfactant pellet and supernatant, and
pulmonary surfactant analysis was performed. Additional details are provided in an online data
supplement.
5
Page 6 of 56
NOS Enzymatic Activity and Expression
NOS enzymatic activity and expression were evaluated in lung parenchymal samples
taken from the proximal 1/3 of the respiratory tree. This approach was taken because the three
NOS isoforms are primarily expressed in the respiratory epithelium of the proximal airways of
the developing primate(10). Additional details are provided in an online data supplement.
Estrogen Receptor Expression
Using previously described methods(29), immunoblot analysis was performed to evaluate
ERα and ERβ expression in the proximal lung of 125d and 140d gestational control animals and
in proximal lung from control- and E2-treated animals. Positive controls consisted of lysates of
COS-7 cells transfected with cDNA for either human ERα or human ERβ.
Statistical Analysis
Differences between gestational control groups were compared by one-way analysis of
variance (ANOVA) followed by Newman-Keuls post hoc testing. Longitudinal between-group
differences in pulmonary and cardiac function parameters over the full course of study were
compared by two-way ANOVA. Repeated measures was not performed for these endpoints
because values for individual animals were occasionally unobtainable due to technical
difficulties or unavailability of the echocardiographer. The inflation and deflation limbs of the
postmortem pressure-volume curves were assessed by separate two-way repeated measures
ANOVAs. OI and VI were assessed by repeated measures ANOVA. Single comparisons
between two groups were performed with nonpaired Student's t tests or Mann-Whitney
6
Page 7 of 56
(nonparametric) for continuous data and by Fisher’s exact test for categorical data. Significance
was accepted at the 0.05 level of probability. All results are expressed as mean±SEM.
RESULTS
Study Groups
To first evaluate developmental changes in fetal serum E2 concentrations during the third
trimester in the baboon, levels were initially measured in additional fetal baboons at 125d, 140d,
160d, or 180d gestation upon euthanization immediately at delivery. E2 levels were determined
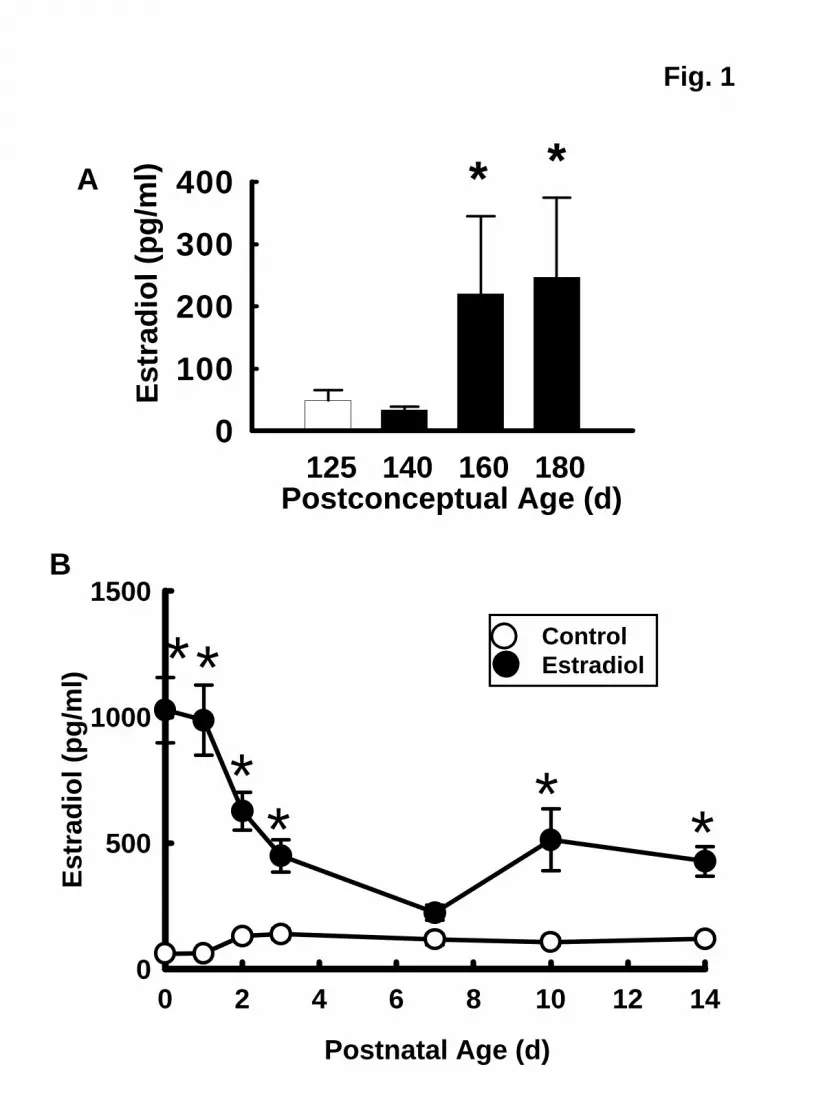
by radioimmunoassay as previously described(30). Fetal serum E2 concentrations rose 5-fold
between 125-140d gestation and 160-180d gestation to achieve mean levels of 250 pg/ml (Fig.
1A). Seeking to attain the upper range of the concentrations observed in the latter third trimester,
in the studies of postnatal E2 administration the hormone was provided by placement of a 0.5 mg,
21d extended release pellet subcutaneously in the left axilla at 1h of life. Control animals
received a placebo pellet, and a second E2 or control pellet was placed subcutaneously in the
right axilla on day of life 7. The subcutaneous route was selected for E2 administration due to
favorable stability and metabolic fate compared with intravenous or oral forms of estrogen(31,
32).
Nine animals were randomized to the control group and 10 to the E2 treatment group.
There was one death in control animals which occurred at 10d of age, and there was one death in
E2-treated animals at 11d of age, and these were related to coagulase negative staph sepsis.
These animals were excluded from longitudinal analyses. Six of the 8 animals in the control
group and 5 of the 9 in the E2-treated group were born following prenatal betamethasone
treatment, and the remainder were born after prenatal dexamethasone. The birthweights,
7
Page 8 of 56
gestational ages at delivery and number of males versus females were similar in the control and
E2-treated animals (Table 1). There were no differences between groups for daily fluid intake,
daily urine output or daily weights over the course of the study (data not shown).
Serum E2 levels achieved in the control and E2-treated groups are shown in Fig. 1B. With
E2 administration the initial E2 levels were 1000 pg/ml at 6h of life, and they fell to 600 pg/ml on
day 2. By day of life 7 in the treated animals E2 levels were 230 pg/ml and a second E2 pellet
was placed. E2 then rose to concentrations of 400 to 500 pg/ml during the second week of life.
At all timepoints except day of life 7, E2 levels were greater in treated animals than control
animals.
Effect of E2 on Systemic and Pulmonary Hemodynamics
The administration of E2 immediately after birth and continuously throughout the study
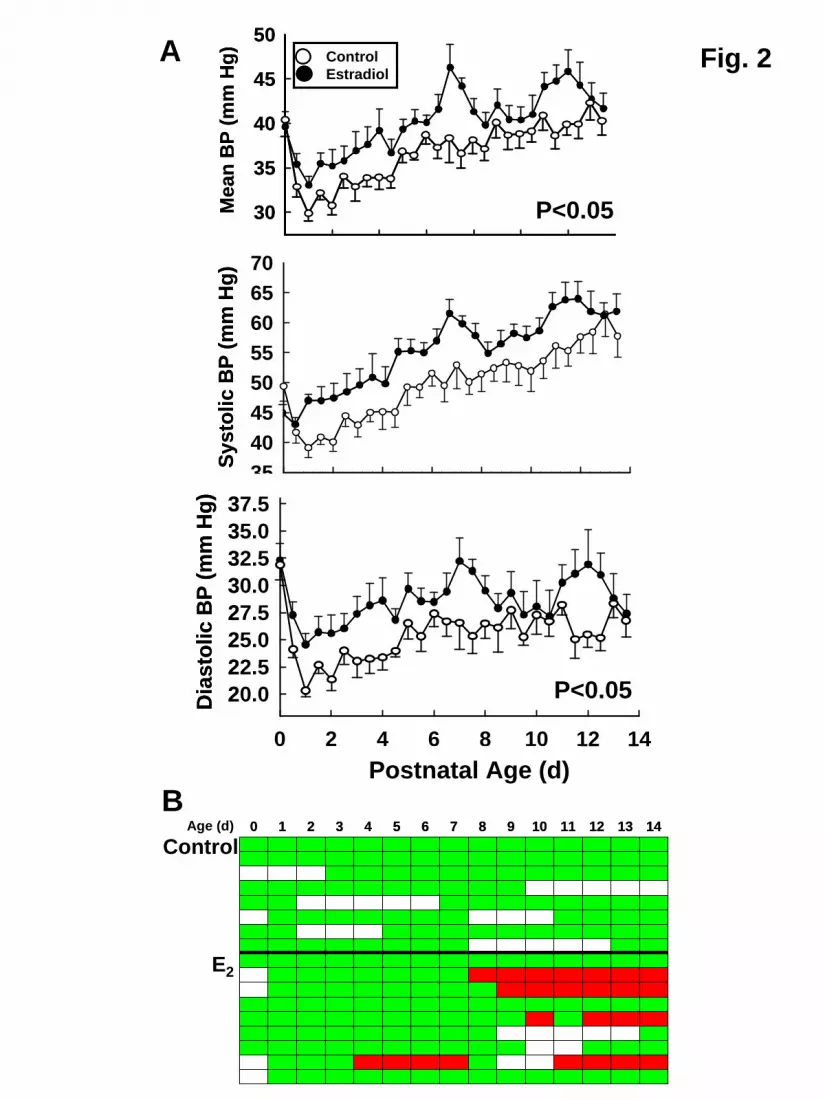
period caused an increase in mean systemic BP (Fig. 2A). Whereas systolic BP did not differ
between study groups, diastolic BP was greater with E2. This led to a lower requirement for
pressor support in the estrogen group in which only 2 of 9 animals required therapy versus 7 of 8
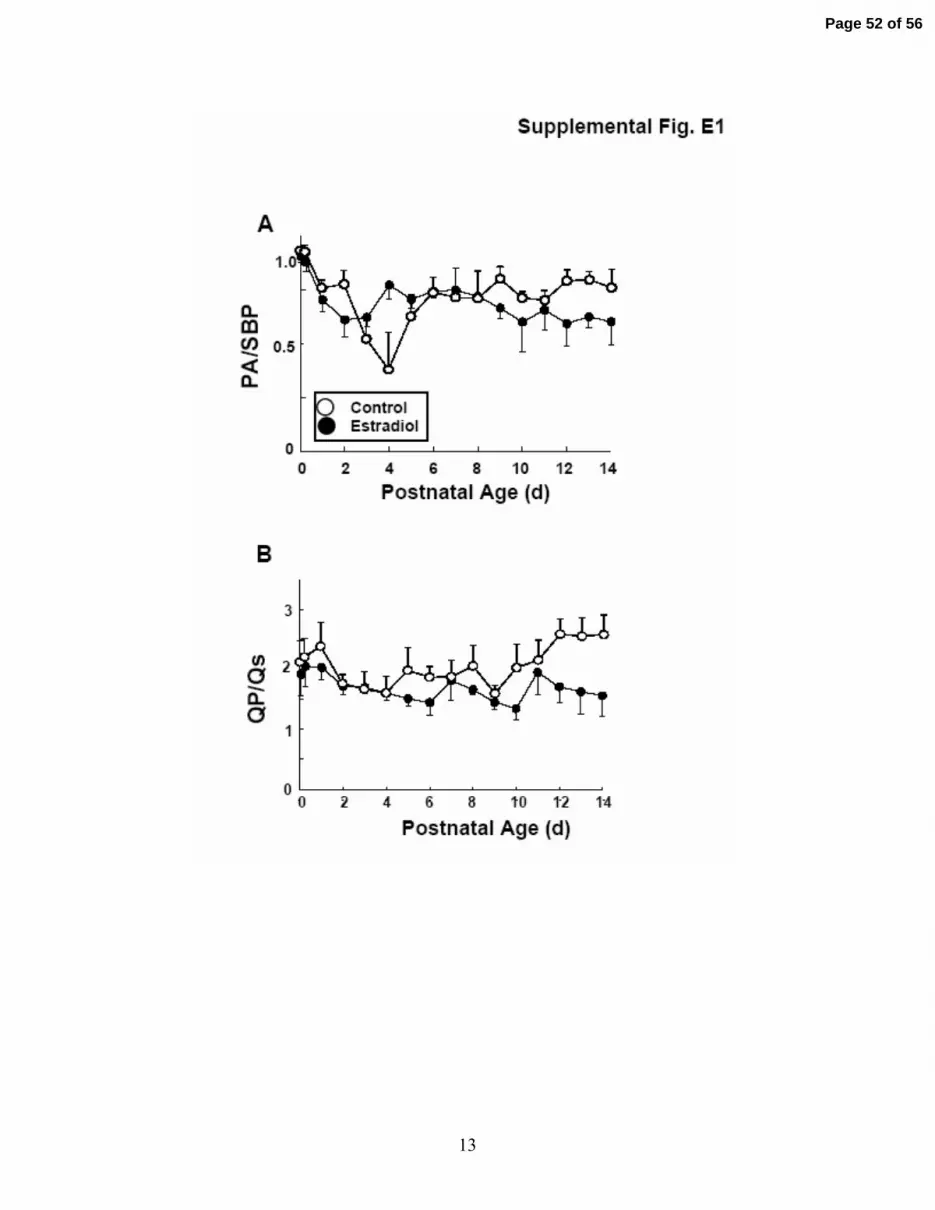
animals in the control group (P=0.01). There were no demonstrable changes in the ratio of the
estimated pulmonary artery pressure to systemic BP or the ratio of pulmonary to systemic blood
flow with E2 administration (See Figure E1A and B, respectively, in the online data supplement).
E2 also altered the incidence of patent ductus arteriosus. Whereas none of the control
animals had spontaneous ductal closure during the 14d study period, 4 of the 9 E2-treated
animals had spontaneous ductal closure by echocardiography (Fig. 2B). In one of these animals
closure was apparent at 4d of age, and in the other 3 animals ductal closure was found at 8 to 11d
of age. The increases in systemic BP with E2 occurred prior to the time of ductal closure (Fig.
8
Page 9 of 56

2A), indicating that the change in BP was due to processes other than the loss of left to right
shunting across the ductus with its spontaneous closure.
Effect of E2 on Pulmonary Function
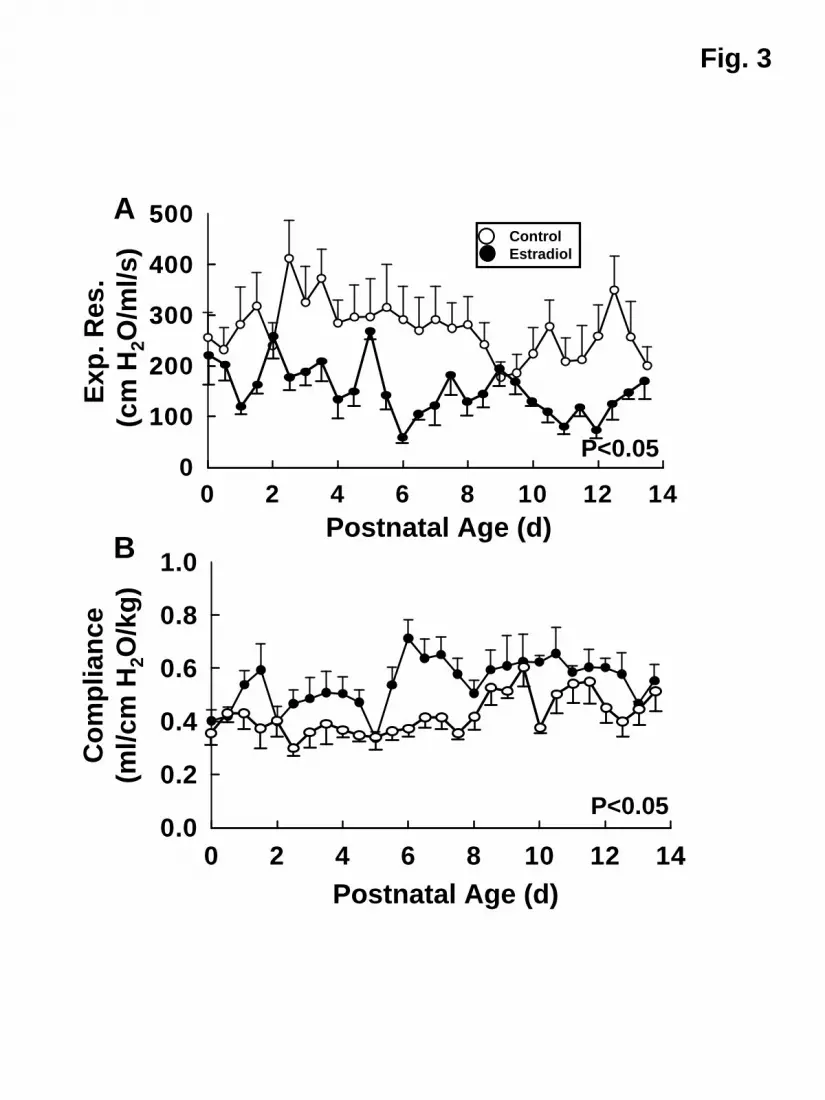
The effect of E2 on pulmonary function is shown in Fig. 3. Expiratory resistance was
lower across the study period in the E2 group (Fig. 3A), and dynamic lung compliance was
increased with E2 (Fig. 3B). To provide an additional assessment of pulmonary function,
postmortem PV curves were performed. During the procedure air leaks occurred in lungs from 3
control animals and from 4 E2-treated animals, and complete analysis was therefore available in
lungs from 5 animals per study group. There was a directional change in both the inflation and
deflation limbs of the PV curves, with shift upward and to the left with E2, and P values were
0.10 and 0.21, respectively (See Figure E2 in the online data supplement). The increase in lung
volume at 35 cm H2O with E2 also approached but did not achieve statistical significance (34±4
versus 48±6 ml/kg for lungs from control and E2 treatment groups, respectively, P=0.07).
Effect of E2 on Ventilatory Support Requirements
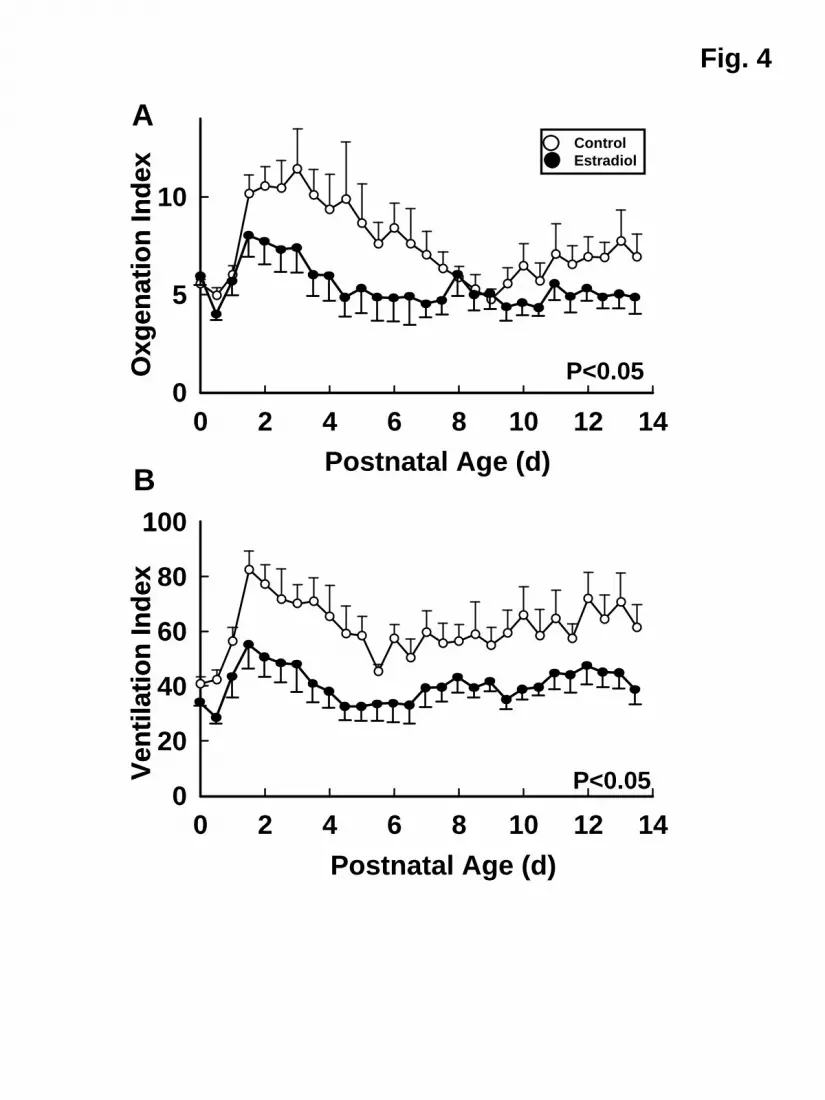
The requirements for ventilatory support are shown in Fig. 4. Oxygenation index over
the course of the 14d study was decreased in the E2-treated animals compared with controls (Fig.
4A), frequently by 30-50%. As impressively, the ventilation index was also lowered throughout
the postnatal period by E2 administration, typically by 40% or more (Fig. 4B).
9
Page 10 of 56
Effect of E2 on Lung Weight, Structure and Inflammation
The weights of the lungs from control and E2-treated animals at the end of the study were
similar (3.6±0.2 and 3.8±0.2% of body weight, respectively). The wet-to-dry weight ratios were
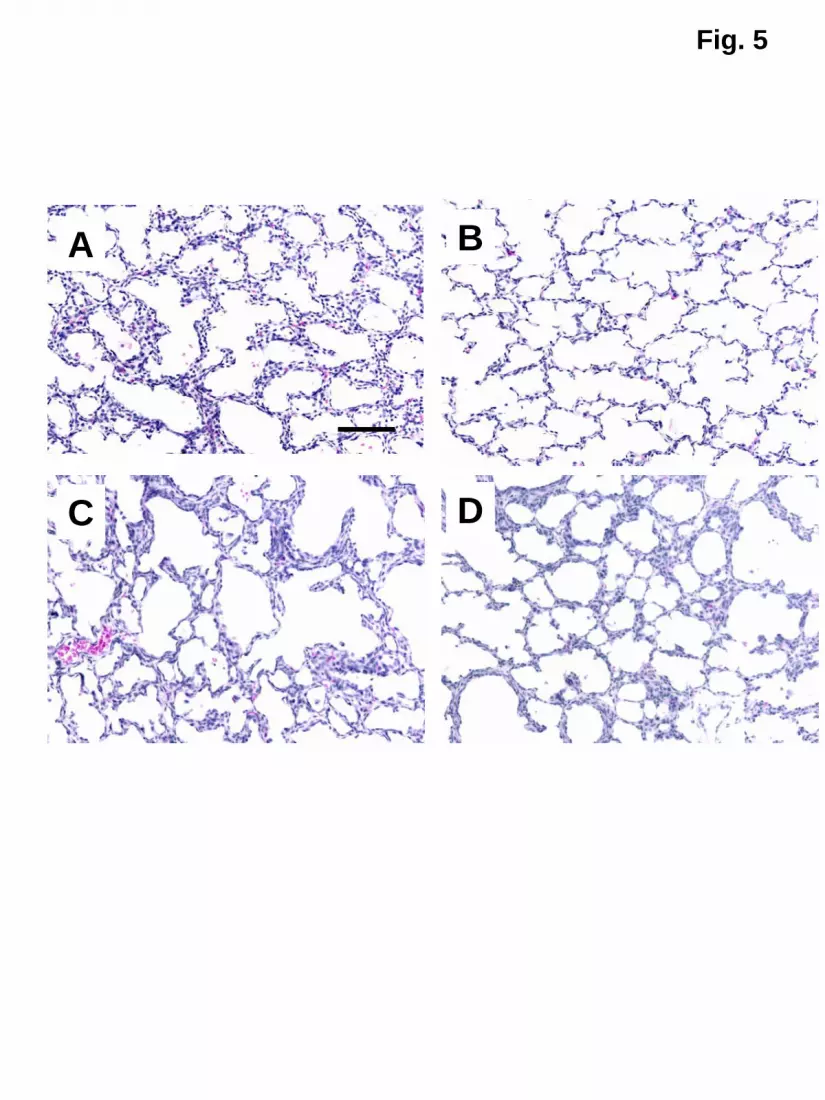
also similar, being 5.13±0.16 and 4.96±0.30, respectively. Representative lungs from 125d
gestation, 140d gestation and control- and E2-treated animals are shown in Fig. 5. With in utero
development between 125d and 140d gestation (Fig. 5A, B), there was thinning of alveolar walls
and increased septation. Compared with fetal lungs at 140d gestation, which is at the same
postconceptual age (Fig. 5B), lungs from control-treated animals on ventilatory support for 14d
had areas with thickened alveolar walls and simplification of the alveolar structures (Fig. 5C): E2
administration did not alter overall lung histology compared to control treatment (Fig. 5D).
Pulmonary morphology was quantitatively compared in the two treatment groups by
skeletonization of alveolar structures and computer-assisted measurements. E2 did not alter
alveolar surface area, the number or length of end segments indicative of secondary crests, or
other determined parameters (Table 2). E2 also did not alter lung vascularization evaluated by
the distribution of PECAM-1 immunostaining of endothelial cells or PECAM-1 abundance, and
VEGF expression or distribution was unchanged (Table E1 in the online data supplement, and
data not shown).
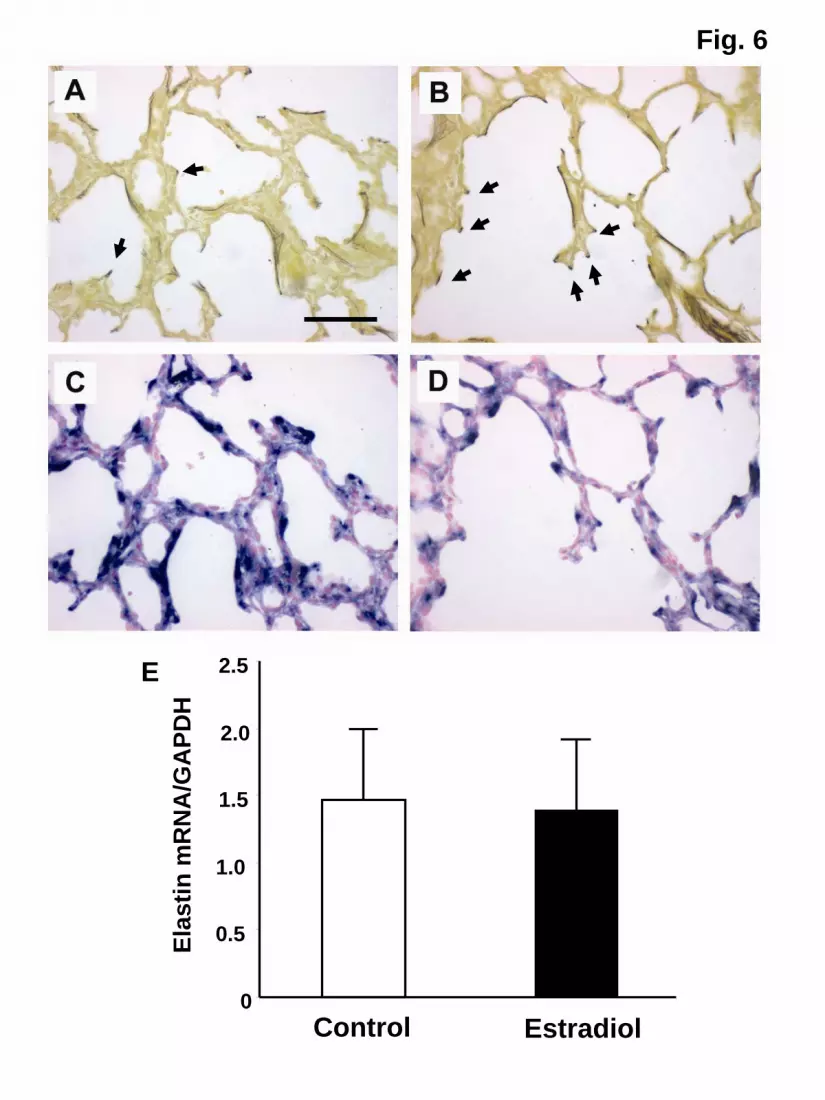
Elastin distribution and levels of expression were evaluated by multiple strategies. Hart’s
staining indicated that elastic fibers were localized to both alveolar walls and septal tips in lungs
of control-treated animals (Fig. 6A) and primarily to emerging septal tips in E2-treated lungs
(Fig. 6B). In situ hybridization on serial sections detected often intense elastin mRNA
expression within alveolar walls and at emerging septae in control-treated animals (Fig. 6C), and
expression was localized primarily to emerging septae in E2-treated animals (Fig. 6D).
10
Page 11 of 56

However, quantitative RT-PCR revealed equal total elastin mRNA abundance in control and E2-
treated lungs (Fig. 6E). Thus, E2 had a modest impact on elastin distribution favoring emerging
septae, but did not alter its overall expression in the lung.
The impact of E2 on lung inflammation was also assessed. TGF-β1 abundance in
tracheal aspirates and terminal BAL samples did not change over the course of development of
BPD in the primate, and it was also similar between control and E2 treatment groups (See Figure
E3 in the online data supplement). In addition, levels of mRNA expression of genes that regulate
inflammation in the lung and are altered in the primate BPD model(28) were not affected by E2
treatment (See Table E1 in the online data supplement).
Effect of E2 on Pulmonary Surfactant
In an effort to understand the basis for changes in pulmonary function with E2, surfactant-
related parameters were measured in terminal bronchoalveolar lavage samples (See Figure E4 in
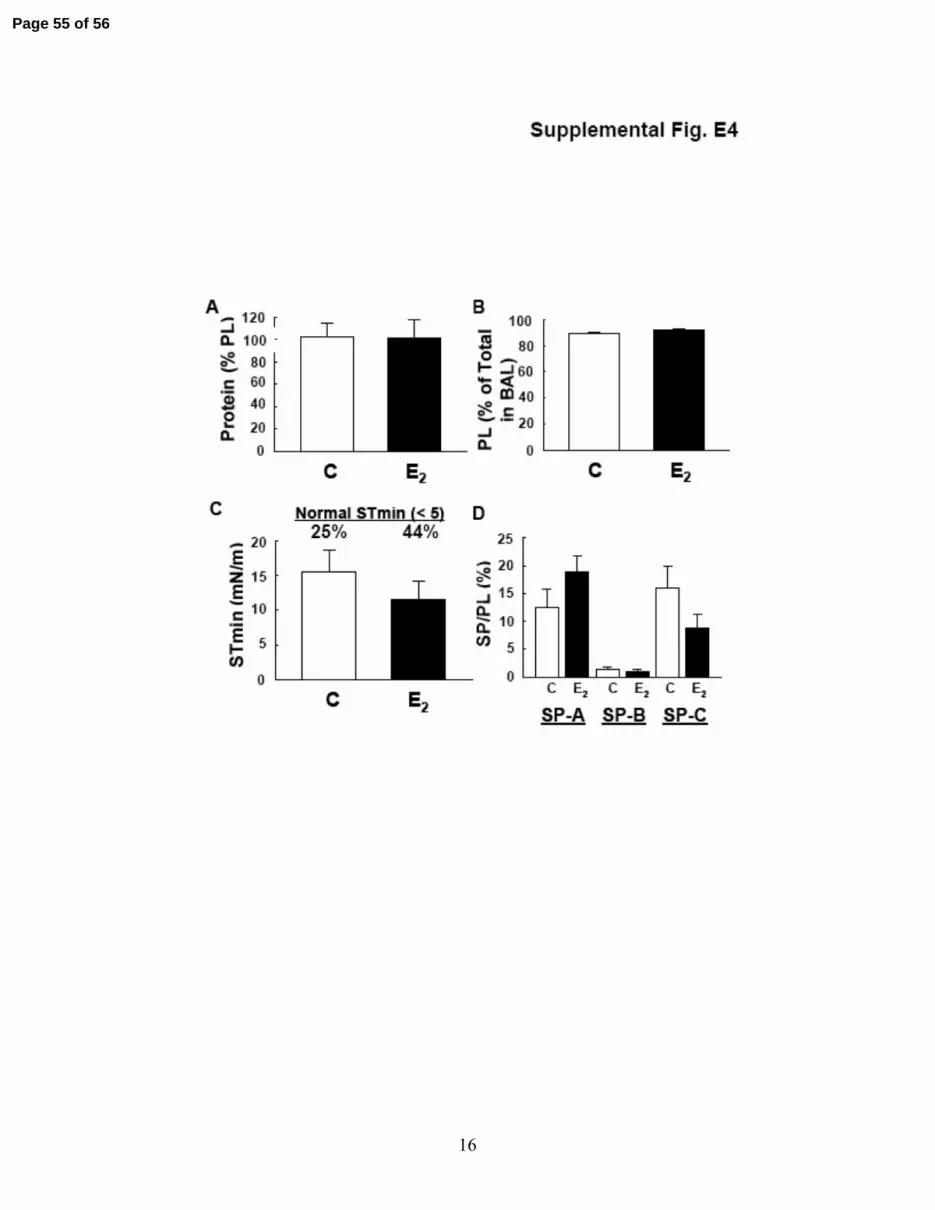
the online data supplement). The total protein and phospholipid contents of the surfactant pellet
were similar in the control and E2 groups (E4A, B, respectively). Mean values for minimal
surface tension were also similar, but there was a directional change suggesting improved surface
tension properties in surfactant from E2-treated animals, with surfactant from 44% of the animals
achieving a normal minimal surface tension of less than 5 mN/m versus 25% in the control group
(Fig. E4C). SP-A, SP-B and SP-C content in the surfactant pellet were unaffected by E2
administration (Fig.E4D).
11
Page 12 of 56
Effect of E2 on Pulmonary NOS and ER
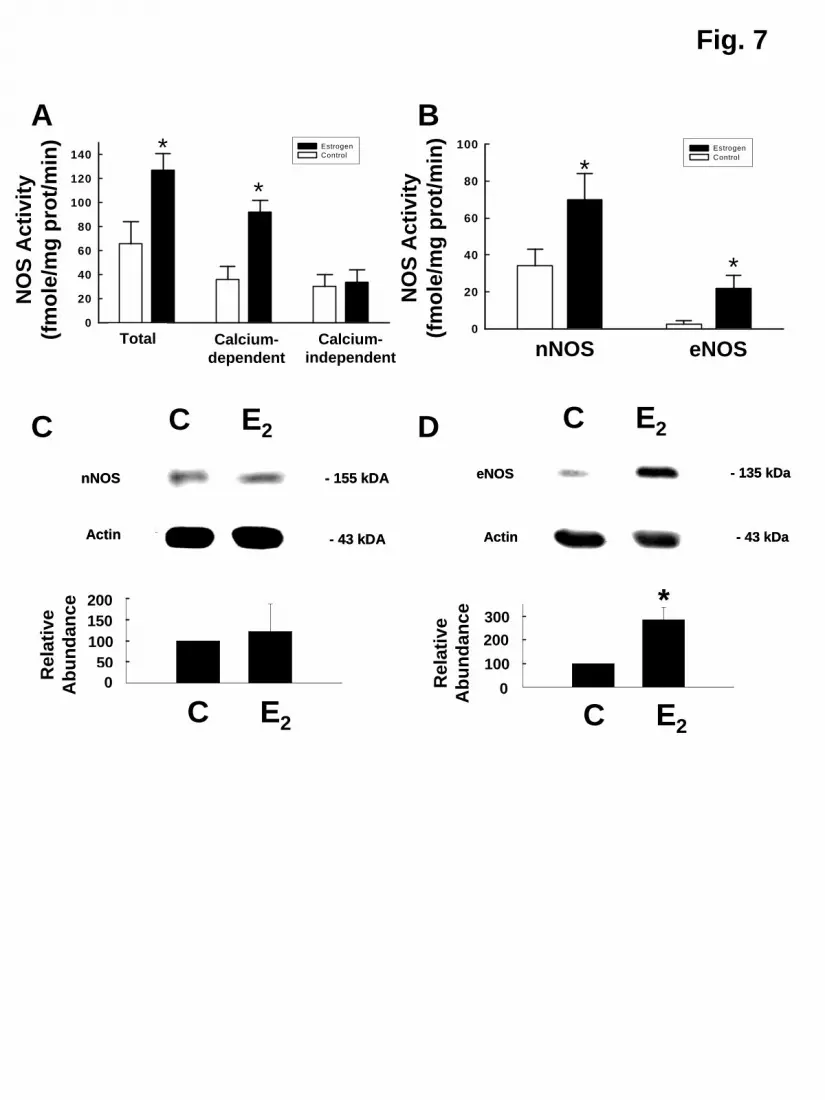
The impact of E2 on pulmonary NOS was first evaluated by determinations of total,
calcium-dependent and calcium-independent NOS enzymatic activity in samples of proximal
lung. Total NOS activity was greater in lungs from E2-treated animals versus controls, and this
was entirely due to greater calcium-dependent activity whereas calcium-independent activity was
unchanged (Fig. 7A). nNOS- and eNOS-derived activity were determined, and nNOS activity
was increased 2-fold with E2 and eNOS activity was increased by over 7-fold (Fig. 7B).
Whereas iNOS protein was not detected by immunoblot analysis in lungs from either study
group (data not shown), nNOS protein was detected and was similar in abundance in lungs from
control and E2-treated animals (Fig. 7C). In contrast, eNOS protein expression was increased by
more than 3-fold with E2 treatment (Fig. 7D), and eNOS mRNA abundance was also increased
by E2 (See Table E1 in the online data supplement).
Having previously shown that estrogen upregulation of eNOS expression is ER-
dependent(33), and that estrogen modifies ERα and ERβ abundance in primary fetal pulmonary
artery endothelial cells(34), the impact of E2 on lung estrogen receptor expression was assessed
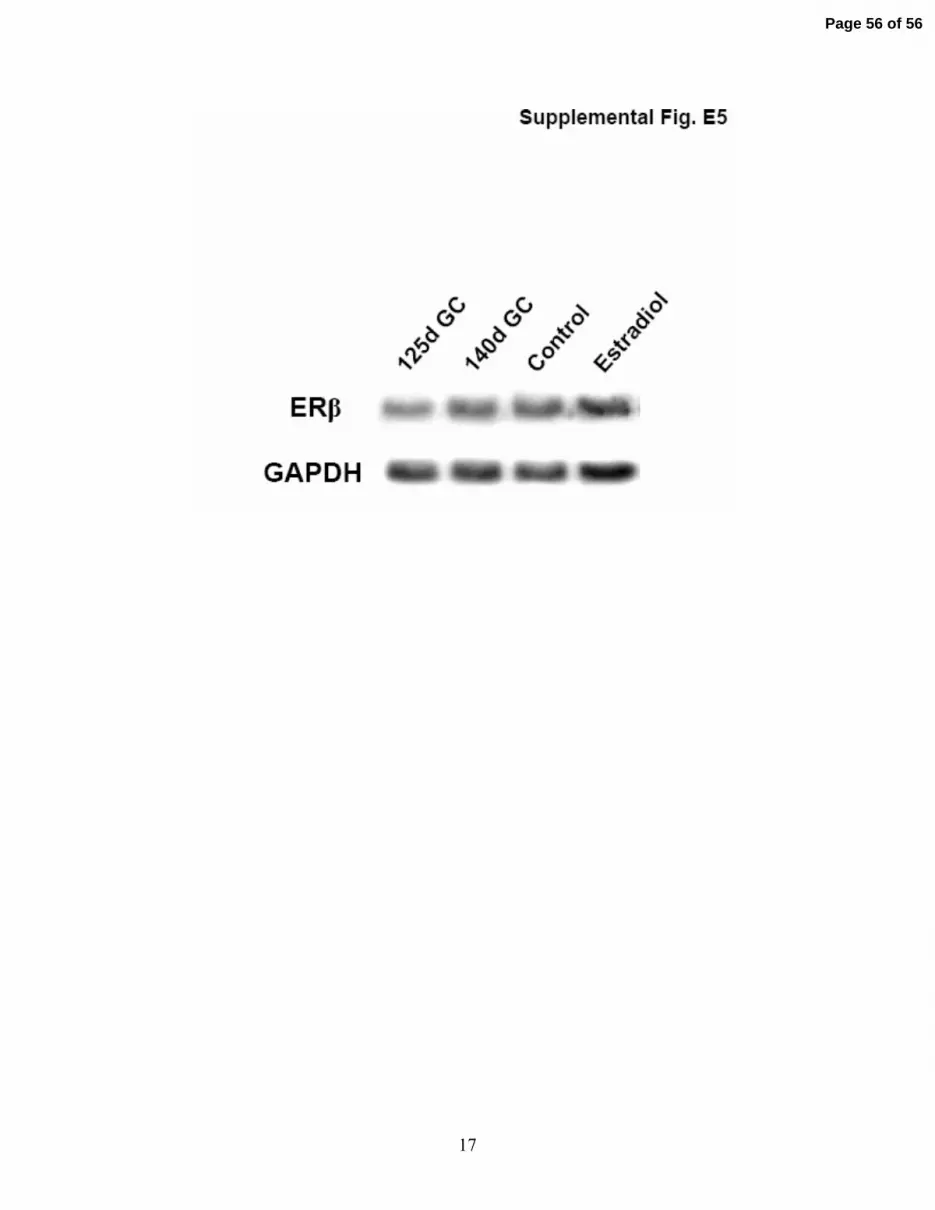
by immunoblot analysis (See Figure E5 in the online data supplement). ERβ protein was
detected in 125d gestation control lung, and the level of expression did not change between 125d
and 140d gestation; ERα protein was not detected (data not shown). ERβ was also readily
detected in lungs from both control and E2-treated animals (Fig. E5) and ERα protein was not
(data not shown), and E2 administration did not modify ERβ abundance.
12
Page 13 of 56
DISCUSSION
With preterm birth early in the third trimester, there is an obligatory decline in circulating
E2 levels that otherwise would increase dramatically during the latter part of gestation in utero.
Since pulmonary NOS is deficient following preterm birth, since E2 upregulates NOS expression
and activity in diverse tissues and cell types, and since NO plays an important role in lung
development and perinatal lung function, we determined the impact of postnatal E2
administration on early postnatal pulmonary status in preterm baboons. We found that the
provision of E2 enhanced pulmonary function and caused a persistent decrease in ventilatory
support requirements. These benefits were associated with an upregulation of both nNOS- and
eNOS-derived NOS enzyme activity in the lung. Thus, postnatal E2 administration has a potent
positive impact on pulmonary status following preterm birth in the primate.
Along with the pulmonary studies, the effect of E2 on systemic hemodynamic status was
evaluated. Postnatal E2 administration caused a persistent elevation in mean systemic BP related
to increased diastolic BP. The E2-treated animals also required pressor support less frequently
than controls, and the disparities in BP between the two groups remained apparent despite the
differences in pressor support. Both endogenous and exogenous estrogens stimulate the hepatic
synthesis of angiotensin that raises aldosterone via activation of the renin-angiotensin system,
and aldosterone causes renal sodium resorption, and these mechanisms may underlie the
hypertension that can occur with oral contraceptive use(35, 36). However, these processes are
unlikely in the present study in which first-pass hepatic metabolism of E2 was avoided with
cutaneous delivery of the hormone(36), and daily weights and urine output were not affected by
E2 treatment. Preterm human infants are at significant risk of hypotension and this is mimicked
in the preterm baboon(37). Although the underlying mechanism is yet to be elucidated, the
13
Page 14 of 56
increase in systemic BP and the lowered requirements for pressor support observed with E2 in
the present study would be of considerable potential clinical benefit.
An additional cardiovascular response observed with postnatal E2 administration was an
increase in the rate of spontaneous closure of the ductus arteriosus. The increases in systemic BP
with E2 occurred considerably earlier than the ductal closure evaluated daily by
echocardiography, indicating that differences in ductal shunting between study groups are most
likely not the cause for the disparities in systemic BP. Although a genetic polymorphism of ERα
has been associated with a lower likelihood of patent ductus arteriosus in preterm male
infants(38), further in-depth investigation will be required to elucidate the mechanisms by which
E2 and ER influence ductal patency. The beneficial impact of E2 on ductal patency would
decrease the need for pharmacologic or surgical closure of the ductus and also the risk of the
multiple significant potential complications that can accompany these interventions(39).
The primary physiologic effects of E2 on the lung were to cause improvements in both
dynamic lung compliance and expiratory resistance in the early postnatal period. The degrees
and durations of these improvements surpass those obtained previously in the preterm baboon
model with interventions including the administration of a superoxide dismutase mimetic, a
modulator of prolyl hydrolase that impacts HIF-related processes, and inhaled NO gas(13, 40,
41). Although attempts to generate postmortem PV curves were complicated by air leaks in the
lungs of some animals, the available data provide further evidence of improved lung function
with postnatal E2 administration.
The improvements in pulmonary function caused by postnatal E2 administration likely
underlie the decline in ventilatory support requirements reflected by long-term diminutions in
both the oxygenation and ventilation indices. It is notable that this beneficial impact of postnatal
14
Page 15 of 56
E2 was apparent in the setting of maternal prenatal steroid treatment, which is the current clinical
strategy in routine use that best optimizes the pulmonary status of the preterm infant(42).
E2 had negligible impact on pulmonary morphology, specifically secondary crest/end
segment formation and vascularization. However, this may be due to the timing of the
assessment of these parameters at 2 weeks of life, which is early in the postnatal period. Later
impact on lung structure is possible because there were albeit modest but consistent E2-induced
changes in elastin distribution favoring localization to emerging septae at 2 weeks of age.
Studies in postnatal rats and mice indicate that E2 modulates alveolar formation and
regeneration(43, 44), and ER and progesterone receptor blockade during late gestation in piglets
causes impaired alveolar formation and fluid clearance(45). However, aromatase inhibition
during the latter half of baboon pregnancy that lowered umbilical venous E2 levels by 95% did
not alter fetal lung growth or alveolarization(46). Considering the improvements in pulmonary
function and support requirements that we observed in the first two weeks with E2 treatment, and
the benefits on lung structure that can be found after 28d in this model if ventilatory support is
lessened(11, 47), additional studies including long-term assessments of lung morphology are
now warranted to determine the ultimate impact of postnatal E2 administration on the developing
lung.
Lung inflammation was also evaluated to determine the potential basis for the observed
effects of E2 on lung function. TGF-β1 levels in tracheal aspirates and terminal BAL were
unchanged during the course of BPD development in the primate and were also unaffected by E2,
and there were no effects of E2 on the expression of genes regulating lung inflammation.
Surfactant-related parameters were also assessed in terminal BAL, and no changes were apparent
with E2. The latter findings are consistent with prior observations that aromatase inhibition
15
Page 16 of 56
during the latter half of baboon pregnancy did not alter lung SP-A or SP-B expression(46).
Thus, there were no observed changes in lung inflammation or surfactant status with postnatal E2
treatment.
Since E2 upregulates NOS expression and enzymatic activity in numerous tissues and cell
types(18-20), changes in lung NOS activity and expression that would be favorable to pulmonary
function were anticipated. Increases in calcium-dependent nNOS-derived enzymatic activity
were found in the lungs of E2-treated animals, and there were even greater increases in eNOS-
derived activity. In contrast, iNOS-derived, calcium-independent activity was unaltered. There
was no demonstrable change in nNOS protein expression with E2, and this may reflect the
greater sensitivity of the enzyme activity assay to discern alterations in enzyme abundance.
However, eNOS protein and mRNA expression were increased by E2 paralleling the rise in
eNOS-derived activity, and this mirrors the known capacity of the hormone to upregulate eNOS
gene expression in numerous model systems(20). Thus, the beneficial changes in lung function
induced by E2 were associated with upregulation of NOS enzyme activity, and the pleiotropic
functions of NO in pulmonary cells may be operative in this intervention. From a therapeutic
standpoint, the ability to upregulate endogenous pulmonary NOS may be more favorable that the
provision of exogenous NO, which benefits only certain subpopulations of preterm infants at risk
for BPD(14-17). Additional potential mechanism of action of E2, including the nongenomic
activation of eNOS that is independent in changes in enzyme abundance and other processes that
do not involve NO(20), should be queried in future experiments.
BPD occurs in over 20% of the more than 50,000 preterm infants born in the U.S. each
year with birthweights < 1500g(48), causing considerable morbidity and mortality, and
additional strategies are needed to combat the disorder. In the animal model that best
16
Page 17 of 56

exemplifies the human condition, we have found that postnatal transcutaneous E2 administration
following preterm birth caused persistent improvements in pulmonary function and a decrease in
ventilatory support requirements in association with lung NOS upregulation. In a recently-
reported small trial by Trotter and colleagues, intravenous E2 and progesterone treatment in
preterm infants tended to decrease the incidence of BPD. In addition, their work to date suggests
potential added benefits on bone mineralization, retinopathy of prematurity, and neurologic
outcome(49-51), lending further credence to the concept of postnatal estrogen treatment. In our
model there were also favorable impacts on hypotension and PDA that are also key
complications of prematurity. As such, estrogen-based therapies for BPD and other
complications of prematurity should now be further developed.
As future studies of postnatal E2 treatment for BPD are contemplated either in animal
models or in humans, full consideration must be given to the possible effects of estrogen on
nonpulmonary development including that related to reproductive health(52). Fortunately, in the
studies of E2 and progesterone replacement in preterm infants, Trotter and coworkers found that
changes in vaginal cytology and mammary and uterine growth were no greater than those that
would have occurred in utero, and they ceased when replacement was discontinued(53).
Furthermore, if necessary, systemic actions of estrogen can potentially be obviated by the use of
E2 in aerosolized form(54). Thus, after decades of consideration of estrogen treatment to prevent
diseases in the postmenopausal period, the hormone now has the potential to ameliorate a
devastating condition at the extreme opposite end of the age spectrum.
17
Page 18 of 56

ACKNOWLEDGMENTS
The authors are indebted to Dr. J. Coalson and V. Winter, without whom the studies
could not have been performed. The authors also thank all the personnel that support the BPD
Resource Center: the animal husbandry group led by Drs. D. Carey and M. Leland, the NICU
staff (H. Martin, S. Ali, D. Correll, L. Kalisky, L. Nicley, R. Degan, S. Gamez), the Wilford Hall
Medical Center neonatal fellows and D. Catland, NNP, who assist in the care of the animals, and
the UTHSCSA pathology staff (L. Buchanan, H. Dixon, A. Schreiner) who perform necropsies
and obtain biological specimens. The authors also thank M. Dixon for assistance in the
preparation of the manuscript.
18
Page 19 of 56
REFERENCES
1. Barnes PJ. Nitric oxide and airway disease. Ann. Med. 1995;27:389-393.
2. Gaston B, Drazen JM, Loscalzo J, Stamler JS. The biology of nitrogen oxides in the
airways. Am. J. Respir. Crit Care Med. 1994;149:538-551.
3. Balasubramaniam V, Tang JR, Maxey A, Plopper CG, Abman SH. Mild hypoxia impairs
alveolarization in the endothelial nitric oxide synthase (eNOS) deficient mouse. Am. J.
Physiol Lung Cell Mol. Physiol 2003;284:L964-L971.
4. Young SL, Evans K, Eu JP. Nitric oxide modulates branching morphogenesis in fetal rat
lung explants. Am. J. Physiol Lung Cell Mol. Physiol 2002;282:L379-L385.
5. Tang ZL, Wasserloos KJ, Liu X, Stitt MS, Reynolds IJ, Pitt BR, St Croix CM. Nitric oxide
decreases the sensitivity of pulmonary endothelial cells to LPS-induced apoptosis in a zinc-
dependent fashion. Mol. Cell Biochem. 2002;234-235:211-217.
6. Edwards YS, Sutherland LM, Murray AW. NO protects alveolar type II cells from stretch-
induced apoptosis. A novel role for macrophages in the lung. Am. J. Physiol Lung Cell
Mol. Physiol 2000;279:L1236-L1242.
7. Cummings JJ. Nitric oxide decreases lung liquid production in fetal lambs. J. Appl. Physiol
1997;83:1538-1544.
8. Khassawneh MY, Dreshaj IA, Liu S, Chang CH, Haxhiu MA, Martin RJ. Endogenous
nitric oxide modulates responses of tissue and airway resistance to vagal stimulation in
piglets. J. Appl. Physiol 2002;93:450-456.
9. Shaul PW. Nitric oxide in the developing lung. Adv. Pediatr. 1995;42:367-414.
19
Page 20 of 56
10. Shaul PW, Afshar S, Gibson LL, Sherman TS, Kerecman JD, Grubb PH, Yoder BA,
McCurnin DC. Developmental changes in nitric oxide synthase isoform expression and
nitric oxide production in fetal baboon lung. Am. J. Physiol Lung Cell Mol. Physiol
2002;283:L1192-L1199.
11. Coalson JJ, Winter VT, Siler-Khodr T, Yoder BA. Neonatal chronic lung disease in
extremely immature baboons. Am. J Respir. Crit Care Med. 1999;160:1333-1346.
12. Afshar S, Gibson LL, Yuhanna IS, Sherman TS, Kerecman JD, Grubb PH, Yoder BA,
McCurnin DC, Shaul PW. Pulmonary NO synthase expression is attenuated in a fetal
baboon model of chronic lung disease. Am. J. Physiol Lung Cell Mol. Physiol
2003;284:L749-L758.
13. McCurnin DC, Pierce RA, Chang LY, Gibson LL, Osborne-Lawrence S, Yoder BA,
Kerecman JD, Albertine KH, Winter VT, Coalson JJ, Crapo JD, Grubb PH, Shaul PW.
Inhaled NO improves early pulmonary function and modifies lung growth and elastin
deposition in a baboon model of neonatal chronic lung disease. Am J Physiol Lung Cell
Mol. Physiol 2005;288:L450-L459.
14. Schreiber MD, Gin-Mestan K, Marks JD, Huo D, Lee G, Srisuparp P. Inhaled nitric oxide
in premature infants with the respiratory distress syndrome. N. Engl. J Med.
2003;349:2099-2107.
15. Van Meurs KP, Wright LL, Ehrenkranz RA, Lemons JA, Ball MB, Poole WK, Perritt R,
Higgins RD, Oh W, Hudak ML, Laptook AR, Shankaran S, Finer NN, Carlo WA, Kennedy
KA, Fridriksson JH, Steinhorn RH, Sokol GM, Konduri GG, Aschner JL, Stoll BJ,
D'Angio CT, Stevenson DK. Inhaled nitric oxide for premature infants with severe
respiratory failure. N. Engl. J Med. 2005;353:13-22.
20
Page 21 of 56
16. Kinsella JP, Cutter GR, Walsh WF, Gerstmann DR, Bose CL, Hart C, Sekar KC, Auten
RL, Bhutani VK, Gerdes JS, George TN, Southgate WM, Carriedo H, Couser RJ, Mammel
MC, Hall DC, Pappagallo M, Sardesai S, Strain JD, Baier M, Abman SH. Early inhaled
nitric oxide therapy in premature newborns with respiratory failure. N. Engl. J. Med.
2006;355:354-364.
17. Ballard RA, Truog WE, Cnaan A, Martin RJ, Ballard PL, Merrill JD, Walsh MC, Durand
DJ, Mayock DE, Eichenwald EC, Null DR, Hudak ML, Puri AR, Golombek SG, Courtney
SE, Stewart DL, Welty SE, Phibbs RH, Hibbs AM, Luan X, Wadlinger SR, Asselin JM,
Coburn CE. Inhaled nitric oxide in preterm infants undergoing mechanical ventilation. N.
Engl. J. Med. 2006;355:343-353.
18. Gingerich S, Krukoff TL. Estrogen modulates endothelial and neuronal nitric oxide
synthase expression via an estrogen receptor beta-dependent mechanism in hypothalamic
slice cultures. Endocrinology 2005;146:2933-2941.
19. Han G, Ma H, Chintala R, Miyake K, Fulton DJ, Barman SA, White RE. Nongenomic,
endothelium-independent effects of estrogen on human coronary smooth muscle are
mediated by type I (neuronal) NOS and PI3-kinase-Akt signaling. Am. J. Physiol Heart
Circ. Physiol 2007;293:H314-H321.
20. Chambliss KL, Shaul PW. Estrogen Modulation of Endothelial Nitric Oxide Synthase.
Endo. Rev. 2002;23:665-686.
21. Parker TA, Kinsella JP, Galan HL, Le Cras TD, Richter GT, Markham NE, Abman SH.
Prolonged infusions of estradiol dilate the ovine fetal pulmonary circulation. Pediatr. Res.
2000;47:89-96.
21
Page 22 of 56
22. Robertson HA, Dwyer RJ, King GJ. Oestrogens in fetal and maternal fluids throughout
pregnancy in the pig and comparisons with the ewe and cow. J. Endocrinol. 1985;106:355-
360.
23. Gelly C, Sumida C, Gulino A, Pasqualini JR. Concentrations of oestradiol and oestrone in
plasma, uterus and other tissues of fetal guinea pigs: their relationship to uptakeand specific
binding of [3H] oestradiol. J. Endocrinol. 1981;89:71-77.
24. Klouche M. Estrogens in human vascular diseases. Ann. N. Y. Acad. Sci. 2006;1089:431-
443.
25. Husain AN, Siddiqui NH, Stocker JT. Pathology of arrested acinar development in
postsurfactant bronchopulmonary dysplasia. Hum. Pathol. 1998;29:710-717.
26. Thibeault DW, Mabry SM, Ekekezie II, Truog WE. Lung elastic tissue maturation and
perturbations during the evolution of chronic lung disease. Pediatrics 2000;106:1452-1459.
27. Nilsson BO. Modulation of the inflammatory response by estrogens with focus on the
endothelium and its interactions with leukocytes. Inflamm. Res. 2007;56:269-273.
28. McCurnin D, Seidner S, Chang LY, Waleh N, Ikegami M, Petershack J, Yoder B,
Giavedoni L, Albertine KH, Dahl MJ, Wang ZM, Clyman RI. Ibuprofen-induced patent
ductus arteriosus closure: physiologic, histologic, and biochemical effects on the premature
lung. Pediatrics 2008;121:945-956.
29. Chambliss KL, Yuhanna IS, Anderson RG, Mendelsohn ME, Shaul PW. ERbeta has
nongenomic action in caveolae. Mol. Endocrinol. 2002;16:938-946.
30. Albrecht ED, Aberdeen GW, Pepe GJ. The role of estrogen in the maintenance of primate
pregnancy. Am. J. Obstet. Gynecol. 2000;182:432-438.
22
Page 23 of 56
31. Koh KK, Yoon BK. Controversies regarding hormone therapy: Insights from inflammation
and hemostasis. Cardiovasc. Res. 2006;70:22-30.
32. Kuhl H. Pharmacology of estrogens and progestogens: influence of different routes of
administration. Climacteric. 8 Suppl 2005;1:3-63.
33. MacRitchie AN, Jun SS, Chen Z, German Z, Yuhanna IS, Sherman TS, Shaul PW.
Estrogen upregulates endothelial nitric oxide synthase gene expression in fetal pulmonary
artery endothelium. Circ. Res. 1997;81:355-362.
34. Ihionkhan CE, Chambliss KL, Gibson LL, Hahner LD, Mendelsohn ME, Shaul PW
Estrogen causes dynamic alterations in endothelial estrogen receptor expression. Circ Res
2002;91:814-820.
35. Hormones and cardiovascular health in women. Hum. Reprod. Update. 2006;12:483-97
36. Ashraf MS, Vongpatanasin W. Estrogen and hypertension. Curr. Hypertens. Rep.
2006;8:368-376.
37. Yoder B, Martin H, McCurnin DC, Coalson JJ. Impaired urinary cortisol excretion and
early cardiopulmonary dysfunction in immature baboons. Pediatr. Res. 2002;51:426-432.
38. Derzbach L, Treszl A, Balogh A, Vasarhelyi B, Tulassay T, Rigo JJ. Gender dependent
association between perinatal morbidity and estrogen receptor-alpha Pvull polymorphism.
J. Perinat. Med. 2005;33:461-462.
39. Chorne N, Leonard C, Piecuch R, Clyman RI. Patent ductus arteriosus and its treatment as
risk factors for neonatal and neurodevelopmental morbidity. Pediatrics 2007;119:1165-
1174.
23
Page 24 of 56
40. Chang LY, Subramaniam M, Yoder BA, Day BJ, Ellison MC, Sunday ME, Crapo JD. A
catalytic antioxidant attenuates alveolar structural remodeling in bronchopulmonary
dysplasia. Am. J Respir. Crit Care Med. 2003;167:57-64.
41. Asikainen TM, Chang LY, Coalson JJ, Schneider BK, Waleh NS, Ikegami M, Shannon
JM, Winter VT, Grubb P, Clyman RI, Yoder BA, Crapo JD, White CW. Improved lung
growth and function through hypoxia-inducible factor in primate chronic lung disease of
prematurity. FASEB J. 2006;20:1698-1700.
42. Jobe AH. Indications for and questions about antenatal steroids. Adv. Pediatr. 2002;49:227-
243.
43. Massaro D, Clerch LB, Massaro GD. Estrogen receptor-alpha regulates pulmonary alveolar
loss and regeneration in female mice: morphometric and gene expression studies. Am. J.
Physiol Lung Cell Mol. Physiol 2007;293:L222-L228.
44. Morani A, Barros RP, Imamov O, Hultenby K, Arner A, Warner M, Gustafsson JA. Lung
dysfunction causes systemic hypoxia in estrogen receptor beta knockout (ERbeta-/-) mice.
Proc. Natl. Acad. Sci. U. S. A 2006;103:7165-7169.
45. Trotter A, Ebsen M, Kiossis E, Meggle S, Kueppers E, Beyer C, Pohlandt F, Maier L,
Thome UH. Prenatal estrogen and progesterone deprivation impairs alveolar formation and
fluid clearance in newborn piglets. Pediatr. Res. 2006;60:60-64.
46. Pepe GJ, Ballard PL, Albrecht ED. Fetal lung maturation in estrogen-deprived baboons. J.
Clin. Endocrinol. Metab 2003;88:471-477.
47. Thomson MA, Yoder BA, Winter VT, Martin H, Catland D, Siler-Khodr TM, Coalson JJ.
Treatment of immature baboons for 28 days with early nasal continuous positive airway
pressure. Am. J. Respir. Crit Care Med. 2004;169:1054-1062.
24
Page 25 of 56
48. Fanaroff AA, Stoll BJ, Wright LL, Carlo WA, Ehrenkranz RA, Stark AR, Bauer CR,
Donovan EF, Korones SB, Laptook AR, Lemons JA, Oh W, Papile LA, Shankaran S,
Stevenson DK, Tyson JE, Poole WK. Trends in neonatal morbidity and mortality for very
low birthweight infants. Am. J. Obstet. Gynecol. 2007;196:147-148.
49. Trotter A, Maier L, Grill HJ, Kohn T, Heckmann M, Pohlandt F. Effects of postnatal
estradiol and progesterone replacement in extremely preterm infants. J. Clin. Endocrinol.
Metab 1999;84:4531-4535.
50. Trotter A, Bokelmann B, Sorgo W, Bechinger-Kornhuber D, Heinemann H, Schmucker G,
Oesterle M, Kohntop B, Brisch KH, Pohlandt F. Follow-up examination at the age of 15
months of extremely preterm infants after postnatal estradiol and progesterone replacement.
J. Clin. Endocrinol. Metab 2001;86:601-603.
51. Trotter A, Maier L, Kron M, Pohlandt F. Effect of oestradiol and progesterone replacement
on bronchopulmonary dysplasia in extremely preterm infants. Arch. Dis. Child Fetal
Neonatal Ed 2007;92:F94-F98.
52. Jones LA, Hajek RA. Effects of estrogenic chemicals on development. Environ. Health
Perspect. 1995;103 Suppl 7:63-67.
53. Trotter A, Maier L, Kohn T, Bohm W, Pohlandt F. Growth of the uterus and mammary
glands and vaginal cytologic features in extremely premature infants with postnatal
replacement of estradiol and progesterone. Am. J. Obstet. Gynecol. 2002;186:184-188.
54. Studd J, Pornel B, Marton I, Bringer J, Varin C, Tsouderos Y, Christiansen C. Efficacy and
acceptability of intranasal 17 beta-oestradiol for menopausal symptoms: randomised dose-
response study. Aerodiol Study Group. Lancet 1999;353:1574-1578.
25
Page 26 of 56

FIGURE LEGENDS
Figure 1. A. Fetal E2 levels increase in the latter half of the third trimester of primate pregnancy.
Serum E2 was measured in fetal baboons at 125d, 140d, 160d, or 180d gestation upon
euthanization immediately at delivery. Values are mean±SEM, n=6/group. *P<0.05 vs 125d
gestation. B. Subcutaneous E2 administration raises serum levels in the immediate postnatal
period. The hormone was provided postnatally to preterm baboons delivered by cesarean section
at 125d gestation by placement of a 0.5 mg, 21d extended release pellet subcutaneously in the
left axilla at 1h of life. Control animals received a placebo pellet, and a second E2 or control
pellet was placed subcutaneously in the right axilla on day of life 7. Serum levels were
determined at 6h of life and at 1, 2, 3, 7, 10 and 14d of age. Values are mean±SEM, n=8 and 9
for control and E2-groups, respectively. *P<0.05 vs control.
Figure 2. Postnatal E2 administration increases systemic blood pressure and causes closure of the
ductus arteriosus. A. Systemic mean, systolic and diastolic blood pressures were measured via
an arterial catheter. B. Ductal patency was determined by echocardiography. Green indicates an
open ductus, red indicates a closed ductus, and white indicates that an echocardiogram was not
performed. Values are mean±SEM, n=8 and 9 for control and E2-groups, respectively.
Statistical comparisons of BP between groups were made by repeated measures ANOVA, and
ductal patency was compared by two-way ANOVA. P<0.05 for mean BP, diastolic BP and
ductal patency.
Figure 3. Postnatal E2 administration causes improvements in pulmonary function. Expiratory
resistance (A, cmH2O/ml/s) and compliance (B, ml/cm H2O/kg) were measured by whole body
plethysmography. Reported values are for the respiratory system as a whole. Values are
mean±SEM, n = 8 and 9 for control and E2 groups, respectively. Statistical comparisons were
Page 27 of 56
made between groups by two-way ANOVA. P<0.05 for expiratory resistance and for
compliance.
Figure 4. Postnatal E2 administration causes improvements in oxygenation index (A) and
ventilation index (B). Values are mean±SEM, n = 8 and 9 for control and E2 groups,
respectively. Statistical comparisons were made between groups by two-way ANOVA (p<0.05
for Panel A and for Panel B).
Figure 5. Representative lungs from 125d gestation (A), 140d gestation (B) and control- and E2-
treated animals (C and D, respectively). Magnification = 20X, bar = 100 um.
Figure 6. Impact of postnatal E2 administration on elastin distribution and expression. Hart’s
staining indicated that elastic fibers were localized to both alveolar walls and septal tips (arrows)
in lungs of control-treated animals (A) and primarily to emerging septal tips in E2-treated lungs
(B). In situ hybridization on serial sections similarly detected often intense elastin mRNA
expression within alveolar walls and at emerging septae in control-treated animals (C), and
expression was localized primarily to emerging septae in E2-treated animals (D). Findings in A-
D are representative of those in 4-5 animals/group, magnification = 200X, bar = 50 um. E.
Elastin mRNA expression was evaluated by quantitative RT-PCR. Values are mean±SEM,
n=6/group.
Figure 7. Postnatal E2 administration upregulates lung nNOS and eNOS enzymatic activity.
Using arginine-to-citrulline conversion, total, calcium-dependent and calcium-independent NOS
activity was measured in proximal lung (A). nNOS-derived and eNOS-derived enzymatic
activity was also quantified (B). nNOS (C) and eNOS (D) protein abundance was evaluate by
immunoblot analysis. In C and D, upper panels display representative immunoblots for NOS and
actin, and cumulative findings for NOS abundance relative to actin in lungs from 6 animals per
Page 28 of 56

group are shown in lower panels. Values are mean±SEM, *P<0.05 vs control.
Page 29 of 56
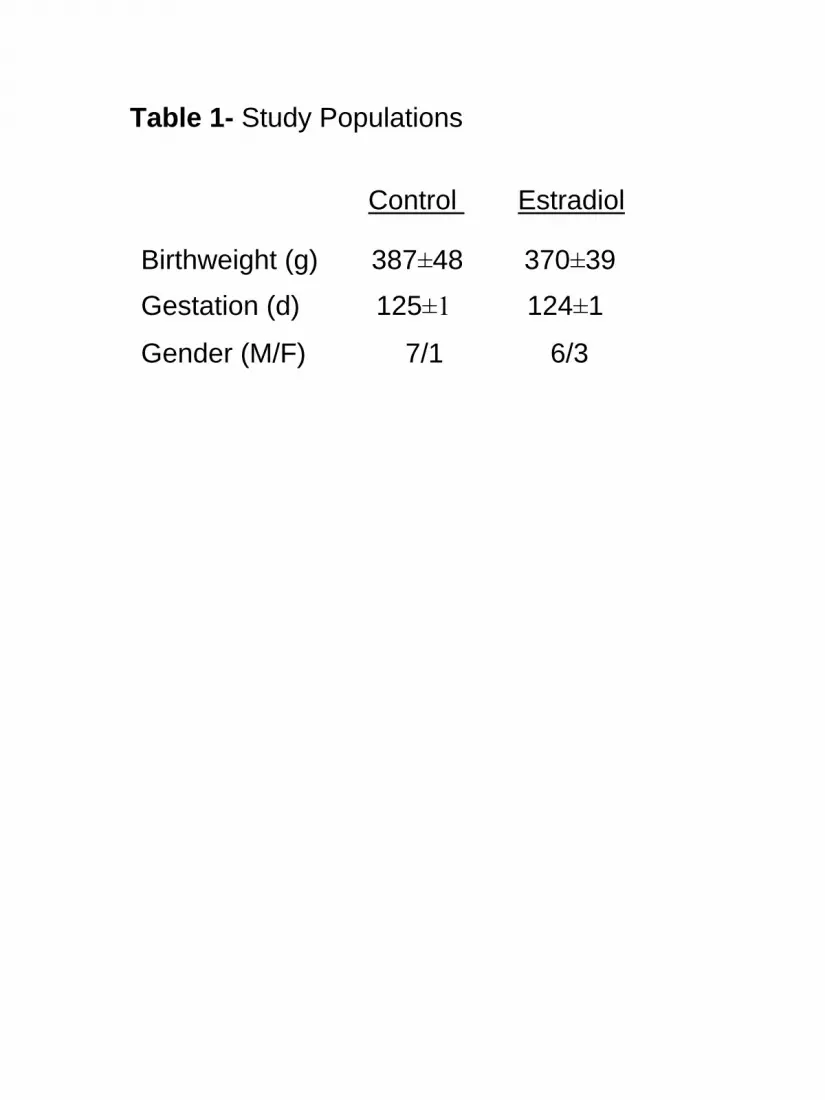
Table 1- Study Populations
Birthweight (g) 387±48 370±39
Gestation (d) 125±1 124±1
Gender (M/F) 7/1 6/3
Control Estradiol
Page 30 of 56
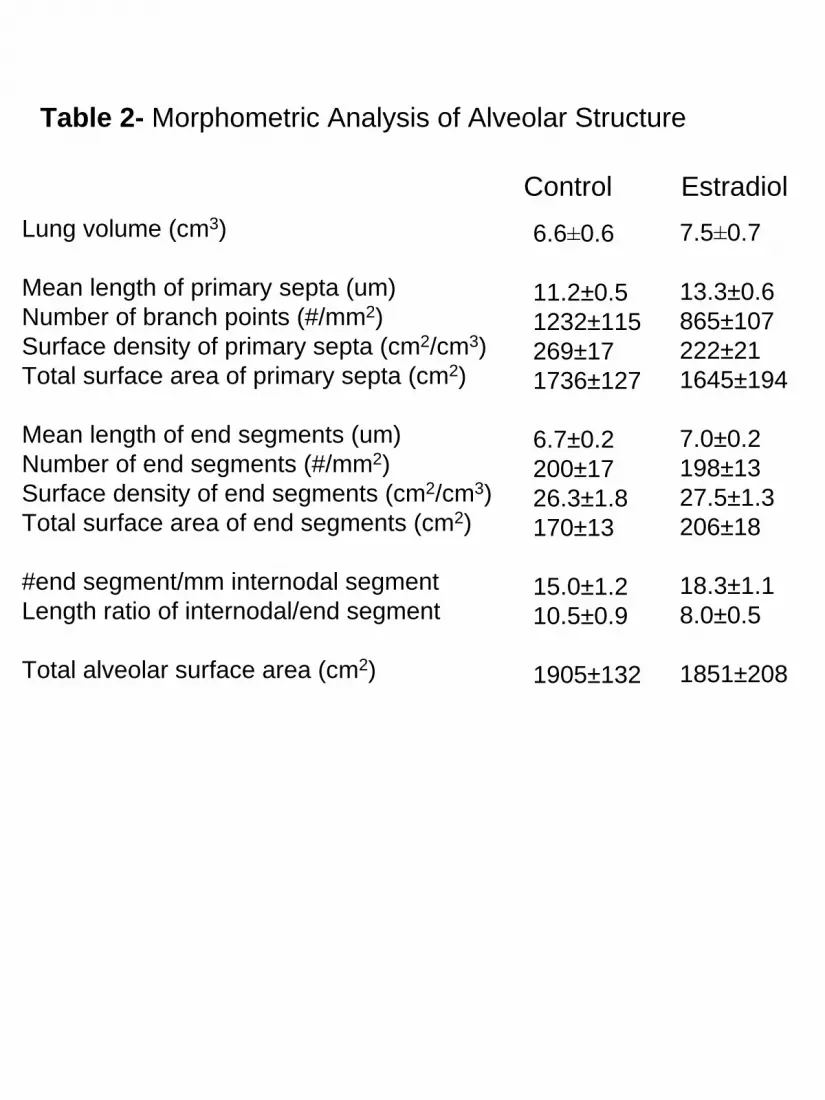
Table 2- Morphometric Analysis of Alveolar Structure
Lung volume (cm3)
Mean length of primary septa (um)Number of branch points (#/mm2)Surface density of primary septa (cm2/cm3)Total surface area of primary septa (cm2)
Mean length of end segments (um)Number of end segments (#/mm2)Surface density of end segments (cm2/cm3)Total surface area of end segments (cm2)
#end segment/mm internodal segmentLength ratio of internodal/end segment
Total alveolar surface area (cm2)
Control Estradiol
6.6±0.6
11.2±0.51232±115269±171736±127
6.7±0.2200±1726.3±1.8170±13
15.0±1.210.5±0.9
1905±132
7.5±0.7
13.3±0.6865±107222±211645±194
7.0±0.2198±1327.5±1.3206±18
18.3±1.18.0±0.5
1851±208
Page 31 of 56
0
100
200
300
400 *
125 140 160 180Postconceptual Age (d)
Estr
adio
l(pg
/ml) *
Fig. 1
0 2 4 6 8 10 12 140
500
1000
1500EstrogenPlacebo
Estr
adio
l (pg
/ml)
Postnatal Age (d)
**
** * *
ControlEstradiolControlEstradiol
A
B
Page 32 of 56
0 2 4 6 8 10 12 14
30
35
40
45
50
Mea
n B
P (m
m H
g)0 2 4 6 8 10 12 14
30
35
40
45
50
Mea
n B
P (m
m H
g)
Days0 2 4 6 8 10 12 14 16
Syst
olic
BP
(mm
Hg)
35.0
37.5
40.0
42.5
45.0
47.5
50.0
52.5
55.0
57.5
60.0
62.5
65.0
67.5
70.0
0 2 4 6 8 10 12 143540455055606570
Syst
olic
BP
(mm
Hg)
Days0 2 4 6 8 10 12 14 16
Syst
olic
BP
(mm
Hg)
35.0
37.5
40.0
42.5
45.0
47.5
50.0
52.5
55.0
57.5
60.0
62.5
65.0
67.5
70.0
0 2 4 6 8 10 12 143540455055606570
Syst
olic
BP
(mm
Hg)
0 2 4 6 8 10 12 14
20.022.525.027.530.032.535.037.5
Dia
stol
ic B
P (m
m H
g)
0 2 4 6 8 10 12 14
20.022.525.027.530.032.535.037.5
Dia
stol
ic B
P (m
m H
g)
Postnatal Age (d)
A
B
ControlEstradiolControlEstradiol
P<0.05
P<0.05
Fig. 2
Age (d)Control
E2
14131211109876543210 14131211109876543210
Page 33 of 56
0 2 4 6 8 10 12 140
100
200
300
400
500
Exp.
Res
.
0 2 4 6 8 10 12 140
100
200
300
400
500
Exp.
Res
.
0 2 4 6 8 10 12 140.0
0.2
0.4
0.6
0.8
1.0
Com
plia
nce/
Kg
0 2 4 6 8 10 12 140.0
0.2
0.4
0.6
0.8
1.0
Com
plia
nce/
Kg
Fig. 3
A
BPostnatal Age (d)
Postnatal Age (d)
ControlEstradiolControlEstradiol
P<0.05
P<0.05
Com
plia
nce
(ml/c
m H
2O/k
g)Ex
p. R
es.
(cm
H2O
/ml/s
)
Page 34 of 56
0 2 4 6 8 10 12 140
20
40
60
80
100
Vent
ilatio
n In
dex
0 2 4 6 8 10 12 140
20
40
60
80
100
Vent
ilatio
n In
dex
0 2 4 6 8 10 12 140
5
10
Oxg
enat
ion
Inde
x
0 2 4 6 8 10 12 140
5
10
Oxg
enat
ion
Inde
xA
Fig. 4
Postnatal Age (d)
Postnatal Age (d)
B
ControlEstradiolControlEstradiol
P<0.05
P<0.05
Page 35 of 56
A B
C D
Fig. 5
Page 36 of 56
0
0.5
1.0
1.5
2.0
2.5
Control Estradiol
Elas
tinm
RN
A/G
APD
H
E
Fig. 6
Page 37 of 56
0
20
40
60
80
100
120
140EstrogenControl
Total Calcium Calcium depenedent independent
*
NO
S A
ctiv
ity
(fm
ole/
mg
prot
/min
) *
0
20
40
60
80
100 EstrogenControl
nNOS eNOS
*
NO
S A
ctiv
ity
(fm
ole/
mg
prot
/min
)
*
0
5 0
1 0 0
1 5 0
2 0 0
Con E2
Rel
ativ
e A
bund
ance
nNOS
Actin - 43 kDA
Control Estradiol
- 155 kDA
0
5 0
1 0 0
1 5 0
2 0 0
Con E2
Rel
ativ
e A
bund
ance
nNOS
Actin - 43 kDA
Control Estradiol
- 155 kDA
Actin
eNOS - 135 kDa
- 43 kDa
Rel
ativ
e A
bund
ance
0
1 0 0
2 0 0
3 0 0*
Con E2
Control Estradiol
Actin
eNOS - 135 kDa
- 43 kDa
Rel
ativ
e A
bund
ance
0
1 0 0
2 0 0
3 0 0*
Con E2
Control Estradiol
Fig. 7
A B
C D
NO
S A
ctiv
ity(fm
ole/
mg
prot
/min
)
NO
S A
ctiv
ity(fm
ole/
mg
prot
/min
)
Total Calcium-dependent
Calcium-independent nNOS eNOS
C E2 C E2
C E2 C E2
200150100500
300200100
0
Rel
ativ
eA
bund
ance
Rel
ativ
eA
bund
ance
Page 38 of 56

Postnatal Estradiol Upregulates Lung
NO Synthases and Improves Lung Function in
Bronchopulmonary Dysplasia
Donald C. McCurnin, Richard A. Pierce, Brigham C. Willis, Ling Yi Chang,
Bradley A. Yoder, Ivan S. Yuhanna, Philip L. Ballard, Ronald I. Clyman, Nahid Waleh
William Maniscalco, James D. Crapo, Peter H. Grubb, and Philip W. Shaul
ONLINE DATA SUPPLEMENT
Page 39 of 56
ONLINE DATA SUPPLEMENT
METHODS
Animal Model
All animal studies were performed at the Southwest Foundation for Biomedical Research
Primate Center in San Antonio, TX. Pregnancies in baboons (Papio papio) were timed with
cycle dates, and fetal growth parameters were obtained from prenatal ultrasound examinations
performed at 70 and 100d estimated fetal gestation. Mirroring current clinical practice in
humans, all animals received antenatal steroids. Initially 12 mg of betamethasone was given IM
every 24h beginning 48h prior to delivery. However, due to a world-wide shortage of
betamethasone which restricted its use to humans only, dexamethasone (6 mg IM every 12h
beginning 48h prior to delivery) was substituted until betamethasone again became available.
Following birth at 125±2 d gestation (term = 185d) by cesarean section and initial
stabilization, ventilation was provided for 14d with a humidified, pressure-limited, time-cycled
infant ventilator (InfantStar, Infrasonics, San Diego, CA) or a 3100A high frequency oscillatory
ventilator (kindly provided by Sensormedics, Yorba Linda, CA) when necessary. Pulse
oximeters were kindly provided by Masimo Corporation (Irving, CA). Details of animal care
have been published elsewhere(1, 2).
Ventilatory Management
The ventilatory approach entailed a strategy to maintain tidal volumes at 4 - 6 ml/kg as
determined by a VitalTrends body plethysmograph system (VT1000, Vitaltrends Technology,
New York, NY) and to generate adequate chest motion by clinical examination. There was
1
Page 40 of 56
rigorous targeting of arterial blood gas parameters to PaCO2 values ranging from 45 to 55 torr
and PaO2 levels between 55 and 70 torr. In an attempt to minimize exposure to high FiO2, if the
PaO2 level was above target goals, FiO2 was weaned until < 0.40 and then modifiers of mean
airway pressure or FiO2 were decreased as tolerated. If PaO2 was below target guidelines, a
chest radiograph was obtained to evaluate lung inflation. Adjustments in mean airway pressure
were made to minimize underinflation or overinflation of the lung. If lung inflation was deemed
adequate, FiO2 alone was adjusted.
Levels of ventilatory and oxygen support were assessed by determinations of
oxygenation index and ventilation index. The formula utilized for oxygenation index (OI) was:
OI = mean airway pressure (cm/H2O) X FiO2 X 100/ PaO2
The formula for ventilation index (VI) was:
VI = peak inspiratory pressure X ventilator rate X PaCO2/ 1000
Hemodynamic Support
Significant hypotension was defined as a transduced mean blood pressure < 28 mm Hg
accompanied by either increasing base deficit or decreasing urine output. Hypotension was
initially treated with additional volume supplementation (20 ml/kg over 1h) and the use of
dopamine (5-20 ug/kg/min). Dobutamine was added (4-10 ug/kg/min) if mean pressure was not
restored to > 28 mm Hg. In those animals where dobutamine appeared to exacerbate
hypotension, epinephrine (0.2-1.0 ug/kg/min) was used in lieu of or as an additional inotrope. If
this approach failed to improve mean blood pressure within 2 h, then a stress dose of
hydrocortisone (1.0 mg/kg) was administered at 6 h intervals until either mean blood pressure
increased to > 28 mm Hg or a maximum of 4 doses of hydrocortisone were received. Once mean
2
Page 41 of 56
blood pressure was stable for > 12 h, pressor support was weaned in reverse to the order it was
initiated.
Echocardiography
2-D, m-mode and Doppler echo studies were performed with a ND 256-8 Biosound
echocardiographic system (Genoa, Italy) equipped with an 8 MHz mechanical transducer.
Postmortem Pressure-Volume Measurements
Postmortem quasi-static inflation pressure-volume measurements were carried out by
inflating the lungs in a stepwise manner (5 cm H2O increments) to a pressure of 20 cm H2O. At
each increment, the pressure was held for 30 sec and volume was recorded. The lungs were then
inflated to 35 cm H2O for 1 min and maximal lung volume was recorded. A deflation limb
pressure-volume curve was also generated by reducing pressure in steps of 5 cm H2O, with
stabilization at each step, and recording of the corresponding volumes(2).
Morphometric-histopathologic Analyses
To quantifiably assess alveolarization, digital image analysis of the lung parenchyma was
performed using the methods previously reported(2). The number and length of primary septal
segments and of secondary crests that develop in alveoli and are quantified as end segments were
tallied and analyzed. The following specific parameters were also evaluated: number of branch
points, numerical frequency of primary septal segments and end segments per mm2 of alveolar
area, total surface area of primary septal segments and end segments, the number of end
3
Page 42 of 56
segments per mm of internodal segment, the length ratio of internodal segment to end segment,
and total alveolar surface area.
To evaluate capillary density, lung sections were immunostained for PECAM-1 (platelet
endothelial cell adhesion molecule, CD31, Dako Corporation, Via Real, CA), an endothelial cell
marker, and PECAM immunoblot analysis was also performed. VEGF mRNA was also
quantified by real-time quantitative PCR and riboprotection assay, and its localization was
assessed by in situ hybridization(3, 4).
To evaluate elastin deposition, sections of paraformaldehyde-fixed, paraffin-embedded
lung were deparaffinized and hydrated, and stained by Hart’s method as previously described.
Counterstaining was with tartrazine (yellow)(5). Elastin mRNA distribution was assessed by in
situ hybridization, and abundance was evaluated by quantitative RT-PCR (5).
Analyses of Lung Inflammation
TGF-β1 abundance in tracheal aspirates and terminal BAL samples obtained at postnatal
ages of 1, 3, 6-7, 9-11 and 14 d was quantified by ELISA (R&D System, Minneapolis, MN) and
was normalized to total protein content measured using the NanoDrop 1000 Protein A280
Application (Thermo Scientific, Wilmington, DE). mRNA expression of genes involved in
inflammation and remodeling in the lung, as well as vascular behavior, was evaluated at 14d by
quantitative RT-PCR as previously described(6). Total RNA was isolated from lung samples
and the TaqMan Universal PCR master mix of PE Applied Biosystems (Foster City, CA) was
used to quantify gene expression. Taqman probes were designed using the Primer Express
program and labeled with fluorophores FAM (6-caboxy-fluorescein) and TAMRA (6 carboxy-
tetramethyl-rhodamine) as reporter and quencher dyes, respectively. An ABI PRISM 7700
4
Page 43 of 56
Sequence detection system was used to determine the cycle threshold (CT). Reactions were
carried out in triplicates, and data were analyzed using the Sequence Detector version 1.6.3
program. Malate dehydrogenase (MDH) was used as an internal control to normalize the data.
We previously compared transcript abundance in lungs from BPD animals at 14d postnatal age
and 140d gestation fetuses of equal postconceptual age, and found that there were significant
differences in RNA expression for COX2, TGF β3, TNFα and VEGF, but not for several other
genes involved with lung inflammation, remodeling and vascular development and function
(e.g., CD14, CD154, COX1, E-selectin, ET-1, IL-1. IL-6, IL-8, interferon gamma, MMP-2, -3,
or -9, TGFβ1, VCAM-1). We therefore analyzed COX2, TGF β3, TNFα and VEGF mRNA
expression in lungs from140d gestation fetuses and control and E2 treatment groups. In addition,
since eNOS protein abundance was altered by E2 treatment in the current study, eNOS mRNA
abundance was also evaluated.
Pulmonary Surfactant Analysis
Analyses were performed as previously described(7). Protein and PL content were
determined and the remaining pellet was diluted to 1.5 mg PL/mL for pulsating bubble
surfactometery, with minimal surface tension (STmin, <5 mN/m defined as normal) of primary
interest. Due to the limited amount of available BAL, a single determination of surfactant
function was made for each animal; the coefficient of variation for 10 replicate determinations of
STmin in a pooled sample was 6%. SP-A, SP-B, and SP-C content were analyzed by Western
immunoblotting and quantitative immunodot assays.
5
Page 44 of 56

NOS Enzymatic Activity and Expression
NOS enzymatic activity was measured in proximal lung samples from control and E2-
treated animals. Prior studies demonstrated that the majority of NOS expression and activity in
fetal baboon lung resides in the proximal respiratory epithelium(8). Activity derived from
calcium-dependent nNOS and eNOS versus calcium-independent inducible NOS (iNOS) was
distinguished. In addition, nNOS- and eNOS-related enzymatic activity was delineated by
measurement of calcium-dependent activity in the absence versus presence of the nNOS-specific
antagonist S-methyl-L-thiocitrulline (SMTC, 10 8M). Immunoblot analyses were also
performed to evaluate NOS isoform abundance, using alpha actin as the loading control(9).
6
Page 45 of 56
REFERENCES
E1. Coalson JJ, Winter VT, Siler-Khodr T, Yoder BA. Neonatal chronic lung disease in
extremely immature baboons. Am. J Respir. Crit Care Med. 1999;160:1333-1346.
E2. McCurnin DC, Pierce RA, Chang LY, Gibson LL, Osborne-Lawrence S, Yoder BA,
Kerecman JD, Albertine KH, Winter VT, Coalson JJ, Crapo JD, Grubb PH, Shaul PW.
Inhaled NO improves early pulmonary function and modifies lung growth and elastin
deposition in a baboon model of neonatal chronic lung disease. Am J Physiol Lung Cell
Mol. Physiol 2005;288:L450-L459.
E3. Maniscalco WM, Watkins RH, Roper JM, Staversky R, O'Reilly MA. Hyperoxic ventilated
premature baboons have increased p53, oxidant DNA damage and decreased VEGF
expression. Pediatr. Res. 2005;58:549-556.
E4. Pierce RA, Joyce B, Officer S, Heintz C, Moore C, McCurnin D, Johnston C, Maniscalco
W. Retinoids increase lung elastin expression but fail to alter morphology or angiogenesis
genes in premature ventilated baboons. Pediatr. Res. 2007;61:703-709.
E5. Pierce RA, Albertine KH, Starcher BC, Bohnsack JF, Carlton DP, Bland RD. Chronic lung
injury in preterm lambs: disordered pulmonary elastin deposition. Am. J. Physiol
1997;272:L452-L460.
E6. McCurnin D, Seidner S, Chang LY, Waleh N, Ikegami M, Petershack J, Yoder B,
Giavedoni L, Albertine KH, Dahl MJ, Wang ZM, Clyman RI. Ibuprofen-induced patent
ductus arteriosus closure: physiologic, histologic, and biochemical effects on the premature
lung. Pediatrics 2008;121:945-956.
7
Page 46 of 56
E7. Ballard PL, Gonzales LW, Godinez RI, Godinez MH, Savani RC, McCurnin DC, Gibson
LL, Yoder BA, Kerecman JD, Grubb PH, Shaul PW. Surfactant composition and function
in a primate model of infant chronic lung disease: effects of inhaled nitric oxide. Pediatr.
Res 2006;59:157-162.
E8. Shaul PW, Afshar S, Gibson LL, Sherman TS, Kerecman JD, Grubb PH, Yoder BA,
McCurnin DC. Developmental changes in nitric oxide synthase isoform expression and
nitric oxide production in fetal baboon lung. Am. J. Physiol Lung Cell Mol. Physiol
2002;283:L1192-L1199.
E9. Afshar S, Gibson LL, Yuhanna IS, Sherman TS, Kerecman JD, Grubb PH, Yoder BA,
McCurnin DC, Shaul PW. Pulmonary NO synthase expression is attenuated in a fetal
baboon model of chronic lung disease. Am. J. Physiol Lung Cell Mol. Physiol
2003;284:L749-L758.
8
Page 47 of 56

Supplemental Table E1: Real Time PCR measurements of genes involved in inflammation,
lung remodeling and vascular behavior. ΔCT(MDH-gene) = difference in cycle threshold (CT)
between the expression of the housekeeping gene Malate dehydrogenase (MDH) and the gene of
interest. Each unit of ΔCT(MDH-gene) represents a 2-fold increase in a gene’s mRNA
abundance. The more negative the ΔCT(MDH-gene), the fewer the number of starting copies of
a gene (mRNA). n= number of separate animals used. Values are mean±SEM, n=11, 8 and 7 for
140d gestatation fetus, control and estradiol groups. * p<0.05 versus 140d gestation fetus. #
p<0.05 versus control group.
9
Page 48 of 56
SUPPLEMENTAL FIGURE LEGENDS
Figure E1: Postnatal E2 administration does not modify pulmonary artery pressure (PAP) or the
ratio of pulmonary to systemic blood flow (Qp/Qs). A. PAP was estimated noninvasively by
measuring the peak velocity of the patent ductus arteriosus jet, and the ratio of PAP to systemic
arterial pressure (SAP) was calculated. B. Left and right ventricular output was calculated from
the mean velocity and used to determine Qp/Qs.
Figure E2: Impact of postnatal E2 administration on postmortem pressure-volume
measurements. Quasi-static inspiratory pressure-volume measurements were performed up to 20
cm H2O, lung volume at maximal distending pressure of 35 cm H2O was recorded, and
expiratory curves were also generated. Values are mean±SEM, n = 5 for control and E2 groups.
Separate two-way ANOVA analysis of the inflation and deflation limbs yielded P = 0.10 and
0.21, respectively. Comparison of the lung volumes at 35 cm H2O yielded P=0.07.
Figure E3: Bronchoalveolar lavage TGFβ1 levels are not altered during the development of
BPD in the primate model, and they are not affected by E2 treatment. Values normalized to total
protein content are shown as mean±SEM, and n=8 and 9 for control (open bars) and E2 groups
(closed bars), respectively.
Figure E4: Postnatal E2 administration does not modify pulmonary surfactant. A large
aggregate surfactant pellet was prepared from terminal BAL, protein (A) and PL content (B)
were quantified, and the remaining pellet underwent pulsating bubble surfactometery to
determine minimal surface tension (C). Normal minimal surface tension, defined as <5 mN/m,
was observed in 25% and 44% of control and E2 treated animals, respectively. SP-A, SP-B, and
SP-C content were also analyzed (D). Values are mean±SEM, n=8 and 9 for control and E2
groups, respectively.
10
Page 49 of 56

Figure E5: Postnatal E2 administration does not modify lung ER expression. Immunoblot
analyses were performed for ERα and ERβ on lungs from 125d gestation and 140d gestation
control lung and from lungs from both control- and E2-treated animals. Equal protein loading
was confirmed by immunoblotting for GAPDH. ERβ protein was detected in all samples, and its
abundance did not change with fetal development between 125 and 140d gestation or with E2
treatment. ERα protein was not detected in any groups. Results shown are representative of 4
independent experiments.
11
Page 50 of 56
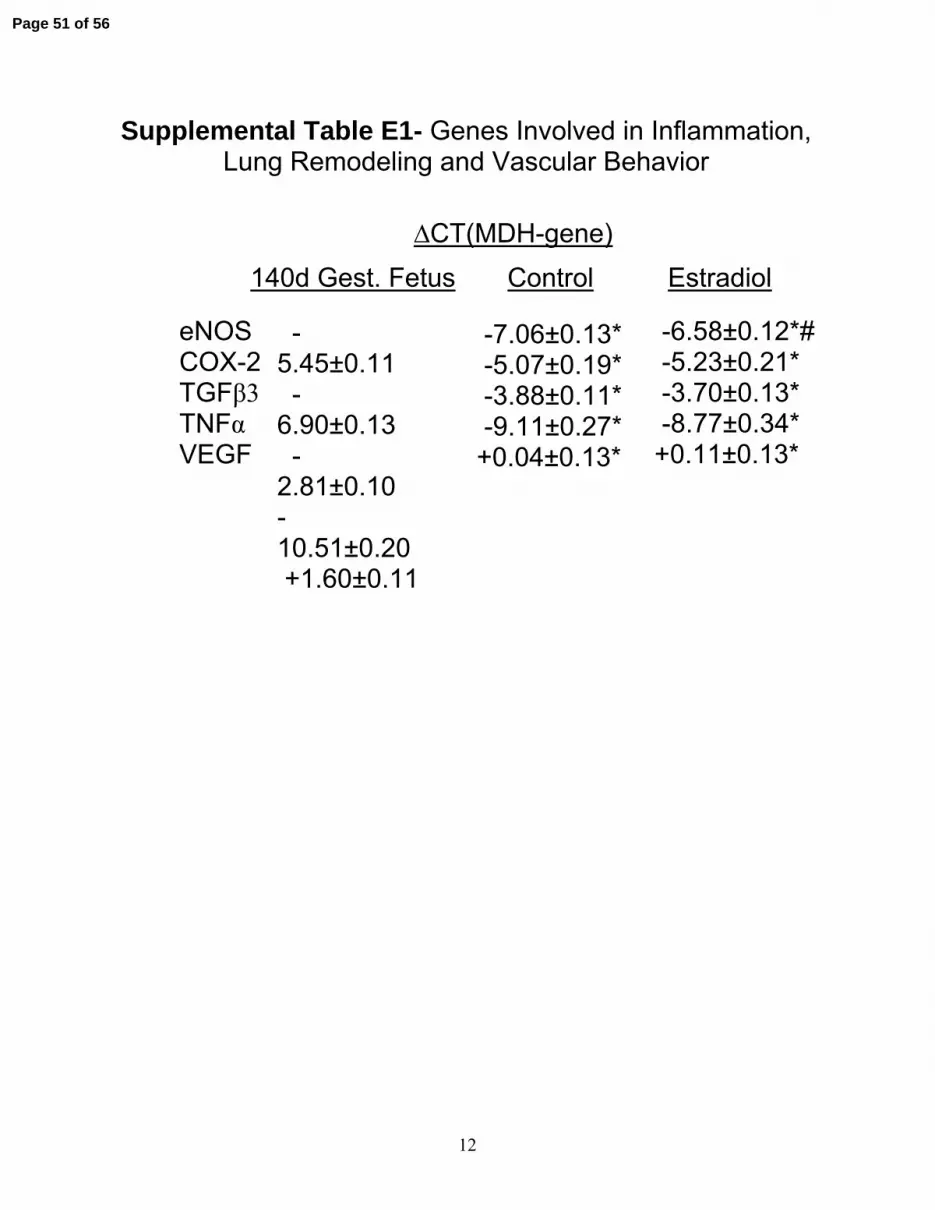
Supplemental Table E1- Genes Involved in Inflammation,Lung Remodeling and Vascular Behavior
∆CT(MDH-gene)140d Gest. Fetus Control Estradiol
-7.06±0.13* -5.07±0.19* -3.88±0.11* -9.11±0.27* +0.04±0.13*
-6.58±0.12*# -5.23±0.21* -3.70±0.13* -8.77±0.34* +0.11±0.13*
eNOS COX-2 TGFβ3 TNFα VEGF
-5.45±0.11 -6.90±0.13 -2.81±0.10 -10.51±0.20 +1.60±0.11
12
Page 51 of 56
13
Page 52 of 56

14
Page 53 of 56

15
Page 54 of 56
16
Page 55 of 56
17
Page 56 of 56