pulmonary hypertension in preterm infants: prevalence and association with bronchopulmonary...
TRANSCRIPT

Pulmonary Hypertension in Preterm Infants: Prevalence and Associationwith Bronchopulmonary Dysplasia
Hussnain Mirza, MD1, James Ziegler, MD2, Sara Ford, MD2, James Padbury, MD1, Richard Tucker, BA1,
and Abbot Laptook, MD1
Objective To determinewhether early pulmonary hypertension (PH) at 10-14 days of life in preterm infants is asso-ciated with bronchopulmonary dysplasia (BPD) at 36 weeks’ postmenstrual age (PMA).Study design This was a prospective observational cohort study of infants <28 weeks’ gestation. Exclusioncriteria were any major anomaly, genetic syndrome, or death before the initial echocardiogram. Echocardiogramswere performed between 10 and 14 days of life and at 36 weeks’ PMA to assess PH. BPD and its severity weredetermined at 36 weeks PMA by the National Institutes of Health workshop definition.Results FromMarch 2011 to April 2013, of 146 consecutively admitted infants <28 weeks, 120 were enrolled. Oneinfant was excluded, 17 did not consent, and 8 died before undergoing a study echocardiogram. At 10-14 days oflife, 10 infants had early PH (8%). Male sex (56% vs 40%), gestational age (26+2 � 1+2 vs 25+6 � 1+4 weeks), birthweight (837 � 205 g vs 763 � 182 g), and small for gestational age (14% vs 20%) were not significantly differentamong infants with no PH and early PH, respectively. Infants with early PH required >0.3 fraction of inspired oxygenby day 10 of life (70% vs 27%, P < .01). Moderate/severe BPD or death was greater among infants with early PH(90%) compared with no PH (47%, relative risk 1.9, 95% CI 1.43-2.53).Conclusion In this prospective, single-center cohort, early PH was associated with moderate/severe BPD ordeath at 36 weeks’ PMA. (J Pediatr 2014;-:---).
Bronchopulmonary dysplasia (BPD) is the most common complication of prematurity, affecting more than 10 000 in-fants per year in the US.1 Despite recent advances in neonatal care, the incidence of BPD has increased2; however, the“new BPD” differs from the BPD first described in 1967 by Northway et al.3 Rather than fibrosis and scarring of the
lungs, the new BPD is characterized by alveolar simplification and pulmonary vascular hypoplasia or dysplasia.4,5
The risk factors for BPD include mechanical ventilation, oxygen toxicity, inflammation, and pulmonary edema caused byfluid overload or excessive left to right shunting; however, preterm infants without such risk factors can still developBPD.6-8 There is a complex crosstalk between pulmonary alveolar and vascular development.9 A number of studies have foundan association between pulmonary hypertension (PH) and respiratory distress syndrome (RDS)10 or BPD.11
Among infants with BPD, PH has been a well-recognized association or complication.12 In a retrospective study of infantswith BPD, no risk factor for PH associated with BPD was identified on multivariate analysis; however, the role of early PH wasnot assessed.13 PH frequently is associated with severe RDS.14 Subhedar and Shaw15 reported that pulmonary artery pressure(PAP) remained elevated up to 1 year of age among infants with chronic lung disease. These observations raise the possibilitythat PH that occurs in association with severe RDS may not resolve in infants who develop BPD and may persist for years.
The role of early PH as a risk factor for BPD and late-onset PH among extremely premature infants remains unclear. Weconducted a prospective, single-center cohort study to examine the association of early PH with moderate/severe BPD andlate-onset PH or death at 36 weeks’ postmenstrual age (PMA). We hypothesized that echocardiographic evidence of earlyPH (PH between 10 and 14 days of life) is associated with moderate or severe BPD or death at 36 weeks’ PMA. Our secondaryhypothesis was that early PH is associated with late PH or death at 36 weeks’ PMA.
BPD Bronchopulmonary dysplasia
FiO2 Fraction of inspired oxygen
NICU Neonatal intensive care unit
PAP Pulmonary artery pressure
PDA Patent ductus arteriosus
PH Pulmonary hypertension
PMA Postmenstrual age
Methods
This was a prospective, observational cohort study of preterm infants (<28 weeks’ gestation based on obstetric criteria)
admitted to the neonatal intensive care unit (NICU) of Women & InfantsFrom the 1Department of Pediatrics, Women & InfantsHospital/The Alpert Medical School of Brown University;and 2Division of Pediatric Cardiology, Hasbro Children’sHospital/The Alpert Medical School of Brown University,Providence, RI
The authors declare no conflicts of interest.
0022-3476/$ - see front matter. Copyright ª 2014 Elsevier Inc.
All rights reserved.
http://dx.doi.org/10.1016/j.jpeds.2014.07.040
RDS Respiratory distress syndrome
RR Relative risk
sBP Systolic blood pressure
sPAP Systolic pulmonary artery pressure
SpO2 Pulse oximetry
TR Tricuspid regurgitation
VSD Ventricular septal defect
1

THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. -, No. -
Hospital of Rhode Island. With Institutional Review Boardapproval and parental consent, infants were enrolled before14 days of life. We excluded infants with congenital heart dis-ease (except patent ductus arteriosus [PDA], small ventricu-lar septal defect [VSD], atrial septal defect, or patent foramenovale), congenital pulmonary anomaly (cystic adenomatoidmalformation, lobar emphysema, etc), congenital diaphrag-matic hernia, or death before the first study echocardiogram.
All infants were managed by the clinical teams in the NICUaccording to the local guidelines. Clinical teams targeted anoxygen saturation (SpO2) as close to 90% as possible (lowerand upper alarm limits of 85% and 95%, respectively) andfraction of inspired oxygen (FiO2) was adjusted by the nurses.Study echocardiograms were performed with real-time pulseoximetry. Initial minimum and maximum SpO2, along withthe respective FiO2 values, were recorded during echocardi-ography; however, SpO2 and FiO2 data were not collectedfor clinical echocardiograms. If echocardiography was per-formed for clinical indications, a study echocardiogram wasnot performed, and data were obtained from clinical studies.All study echocardiograms were performed by a pediatricechocardiography technician, a NICU fellow (trained underthe supervision of a pediatric cardiologist), or either of the2 pediatric cardiologists (J.Z., S.F.) on the study team. Inaddition, both pediatric cardiologists were blinded to theclinical status of each infant and either one reviewed eachechocardiogram for the presence and severity of PH. Man-agement in the NICU was otherwise according to the discre-tion of the clinical care teams responsible for the infant.
Right ventricular pressure gradient was estimated bymeasuring the peak velocity of tricuspid regurgitation (TRmax) if there were reproducible holosystolic envelopes. Weused the modified Bernoulli equation to convert Dopplerderived velocity to pressure (pressure gradient between rightventricle and right atrium = 4 � [TR max2]). Systolic PAP(sPAP) was calculated by adding right atrial pressure(5 mm Hg) to estimated right ventricle pressure gradient.In the absence of measureable TR, we relied upon a PDAor VSD gradient to estimate sPAP and identify the severityof PH as described previously. The severity of PH was deter-mined by comparing simultaneously estimated sPAP withsystemic systolic blood pressure (sBP).
PH was categorized as none or mild if the estimated sPAPto sBP ratio was <0.5, moderate if the pulmonary to systemicsystolic ratio was$0.5 but <1, and severe or suprasystemic ifsPAP$ sBP.16 In the absence of TR, PDA, or VSD, sPAP wasestimated by assessing the end-systolic interventricular septalposition at the papillary muscle level in short-axis viewthrough the multiple acoustic windows. PH by septal posi-tion was categorized as follows: normal or mild if the septumwas rounded at end systole, moderate if the septum was flat-tened, and suprasystemic if the septum was bowed into theleft ventricle at end systole.11
Infants with moderate or severe PH on the initial echocar-diogram (10-14 days of life) were classified as having earlyPH. Infants with mild or no PH on the initial echocardio-gram were identified as no PH group. For the purpose of
2
this study, PH identified by echocardiogram at 36 weeks’PMA has been described as late PH. Study echocardiogramfindings, which were deemed noncritical to the clinical careof infants, were not conveyed to the family or the clinicalteams. Potentially important echocardiographic findings(eg, severe PH, hemodynamically significant PDA, hypertro-phic cardiomyopathy with dynamic left ventricular outflowtract obstruction, or cardiac valvular lesions) were revealedto the clinical team. Clinical management of divulged echo-cardiographic findings was at the discretion of providers inthe NICU.BPD was diagnosed if an infant received supplemental ox-
ygen for $28 days. BPD was classified into mild, moderate,or severe forms at 36 weeks’ PMA, as described by Jobe andBancalari.17 Mild BPD was the absence of supplemental oxy-gen, moderate BPD was the need for <0.3 FiO2, and severeBPD was the use of positive pressure ventilation or needfor >0.3 FiO2. The need for continuing oxygen therapy wasdetermined by an O2/room air challenge reduction as out-lined by Walsh et al.18
We calculated sample size using the incidence of moderateor severe BPD at Women & Infants Hospital in 2006 (34%)and an estimated frequency of early PH (15%). To detect a30% increase in moderate/severe BPD secondary to earlyPH, 120 infants were required, using a power of 80% andan alpha of 0.05. Maternal, perinatal, and neonatal datawere collected to characterize the demographic and clinicalcharacteristics of the study cohort. Infants were dichoto-mized based on the presence or absence of early PH at 10-14 days of life. c2 tests were used for categorical variables,and Student t tests were used to compare continuous vari-ables for infants with and without early PH. Bivariate analysiswas performed to identify associations between early PH andstudy outcomes of BPD or late PH at 36 weeks’ PMA. Asso-ciations between early PH and BPD or late PHwere expressedas a relative risk (RR) with 95% CI.
Results
Between March 2011 to April 2013, 146 infants of <28 weeks’gestation were admitted to the NICU at Women & InfantsHospital of Rhode Island, and 120 were enrolled. Consentwas declined for 17 infants, and 8 died before undergoingthe initial study echocardiogram. Only 1 infant was excludedbecause of vertebral and chest wall anomalies.The initial echocardiography on 12 � 2 days of life indi-
cated the presence of PH (early PH) in 10 infants (8%) and110 had no PH. All infants with early PH had moderatePH. The diagnosis of early PH (n = 10) was based on TR in2 infants, a PDA gradient in 5, and septal position in 3 in-fants. Because PH had not been diagnosed clinically, specifictreatment for PH was not administered to these infants.Three infants, previously treated with inhaled nitric oxideduring their first week of life because of persistent PH, werenot receiving inhaled nitric oxide at the time of initial studyechocardiogram; only 1 of those 3 infants with persistent PHhad early PH diagnosed on day 14 of life. Maternal
Mirza et al
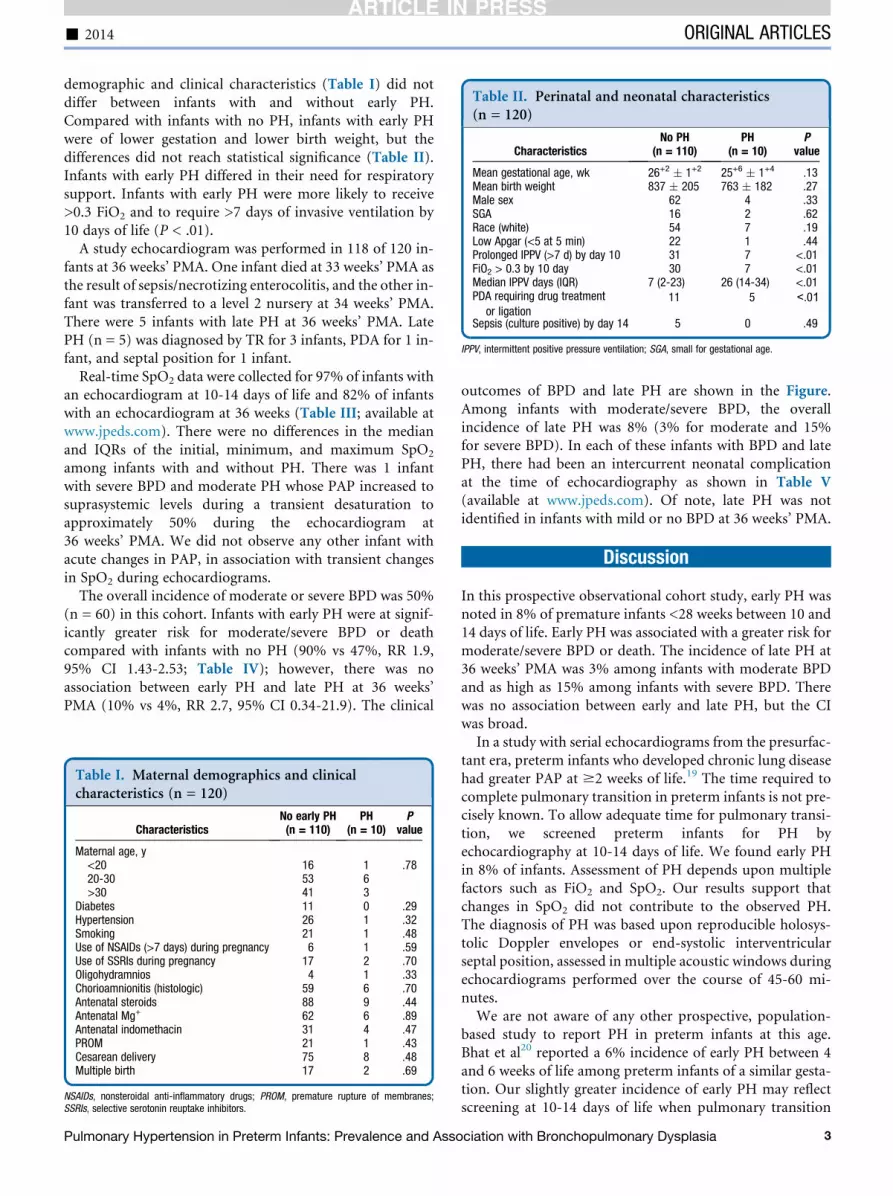
Table II. Perinatal and neonatal characteristics(n = 120)
CharacteristicsNo PH
(n = 110)PH
(n = 10)P
value
Mean gestational age, wk 26+2 � 1+2 25+6 � 1+4 .13Mean birth weight 837 � 205 763 � 182 .27Male sex 62 4 .33SGA 16 2 .62Race (white) 54 7 .19Low Apgar (<5 at 5 min) 22 1 .44Prolonged IPPV (>7 d) by day 10 31 7 <.01FiO2 > 0.3 by 10 day 30 7 <.01Median IPPV days (IQR) 7 (2-23) 26 (14-34) <.01PDA requiring drug treatment
Sepsis (culture positive) by day 14 5 0 .49
IPPV, intermittent positive pressure ventilation; SGA, small for gestational age.
- 2014 ORIGINAL ARTICLES
11 5 <.01 or ligation
demographic and clinical characteristics (Table I) did notdiffer between infants with and without early PH.Compared with infants with no PH, infants with early PHwere of lower gestation and lower birth weight, but thedifferences did not reach statistical significance (Table II).Infants with early PH differed in their need for respiratorysupport. Infants with early PH were more likely to receive>0.3 FiO2 and to require >7 days of invasive ventilation by10 days of life (P < .01).
A study echocardiogram was performed in 118 of 120 in-fants at 36 weeks’ PMA. One infant died at 33 weeks’ PMA asthe result of sepsis/necrotizing enterocolitis, and the other in-fant was transferred to a level 2 nursery at 34 weeks’ PMA.There were 5 infants with late PH at 36 weeks’ PMA. LatePH (n = 5) was diagnosed by TR for 3 infants, PDA for 1 in-fant, and septal position for 1 infant.
Real-time SpO2 data were collected for 97% of infants withan echocardiogram at 10-14 days of life and 82% of infantswith an echocardiogram at 36 weeks (Table III; available atwww.jpeds.com). There were no differences in the medianand IQRs of the initial, minimum, and maximum SpO2
among infants with and without PH. There was 1 infantwith severe BPD and moderate PH whose PAP increased tosuprasystemic levels during a transient desaturation toapproximately 50% during the echocardiogram at36 weeks’ PMA. We did not observe any other infant withacute changes in PAP, in association with transient changesin SpO2 during echocardiograms.
The overall incidence of moderate or severe BPD was 50%(n = 60) in this cohort. Infants with early PH were at signif-icantly greater risk for moderate/severe BPD or deathcompared with infants with no PH (90% vs 47%, RR 1.9,95% CI 1.43-2.53; Table IV); however, there was noassociation between early PH and late PH at 36 weeks’PMA (10% vs 4%, RR 2.7, 95% CI 0.34-21.9). The clinical
Table I. Maternal demographics and clinicalcharacteristics (n = 120)
CharacteristicsNo early PH(n = 110)
PH(n = 10)
Pvalue
Maternal age, y<20 16 1 .7820-30 53 6>30 41 3
Diabetes 11 0 .29Hypertension 26 1 .32Smoking 21 1 .48Use of NSAIDs (>7 days) during pregnancy 6 1 .59Use of SSRIs during pregnancy 17 2 .70Oligohydramnios 4 1 .33Chorioamnionitis (histologic) 59 6 .70Antenatal steroids 88 9 .44Antenatal Mg+ 62 6 .89Antenatal indomethacin 31 4 .47PROM 21 1 .43Cesarean delivery 75 8 .48Multiple birth 17 2 .69
NSAIDs, nonsteroidal anti-inflammatory drugs; PROM, premature rupture of membranes;SSRIs, selective serotonin reuptake inhibitors.
Pulmonary Hypertension in Preterm Infants: Prevalence and Asso
outcomes of BPD and late PH are shown in the Figure.Among infants with moderate/severe BPD, the overallincidence of late PH was 8% (3% for moderate and 15%for severe BPD). In each of these infants with BPD and latePH, there had been an intercurrent neonatal complicationat the time of echocardiography as shown in Table V(available at www.jpeds.com). Of note, late PH was notidentified in infants with mild or no BPD at 36 weeks’ PMA.
Discussion
In this prospective observational cohort study, early PH wasnoted in 8% of premature infants <28 weeks between 10 and14 days of life. Early PH was associated with a greater risk formoderate/severe BPD or death. The incidence of late PH at36 weeks’ PMA was 3% among infants with moderate BPDand as high as 15% among infants with severe BPD. Therewas no association between early and late PH, but the CIwas broad.In a study with serial echocardiograms from the presurfac-
tant era, preterm infants who developed chronic lung diseasehad greater PAP at $2 weeks of life.19 The time required tocomplete pulmonary transition in preterm infants is not pre-cisely known. To allow adequate time for pulmonary transi-tion, we screened preterm infants for PH byechocardiography at 10-14 days of life. We found early PHin 8% of infants. Assessment of PH depends upon multiplefactors such as FiO2 and SpO2. Our results support thatchanges in SpO2 did not contribute to the observed PH.The diagnosis of PH was based upon reproducible holosys-tolic Doppler envelopes or end-systolic interventricularseptal position, assessed in multiple acoustic windows duringechocardiograms performed over the course of 45-60 mi-nutes.We are not aware of any other prospective, population-
based study to report PH in preterm infants at this age.Bhat et al20 reported a 6% incidence of early PH between 4and 6 weeks of life among preterm infants of a similar gesta-tion. Our slightly greater incidence of early PH may reflectscreening at 10-14 days of life when pulmonary transition
ciation with Bronchopulmonary Dysplasia 3
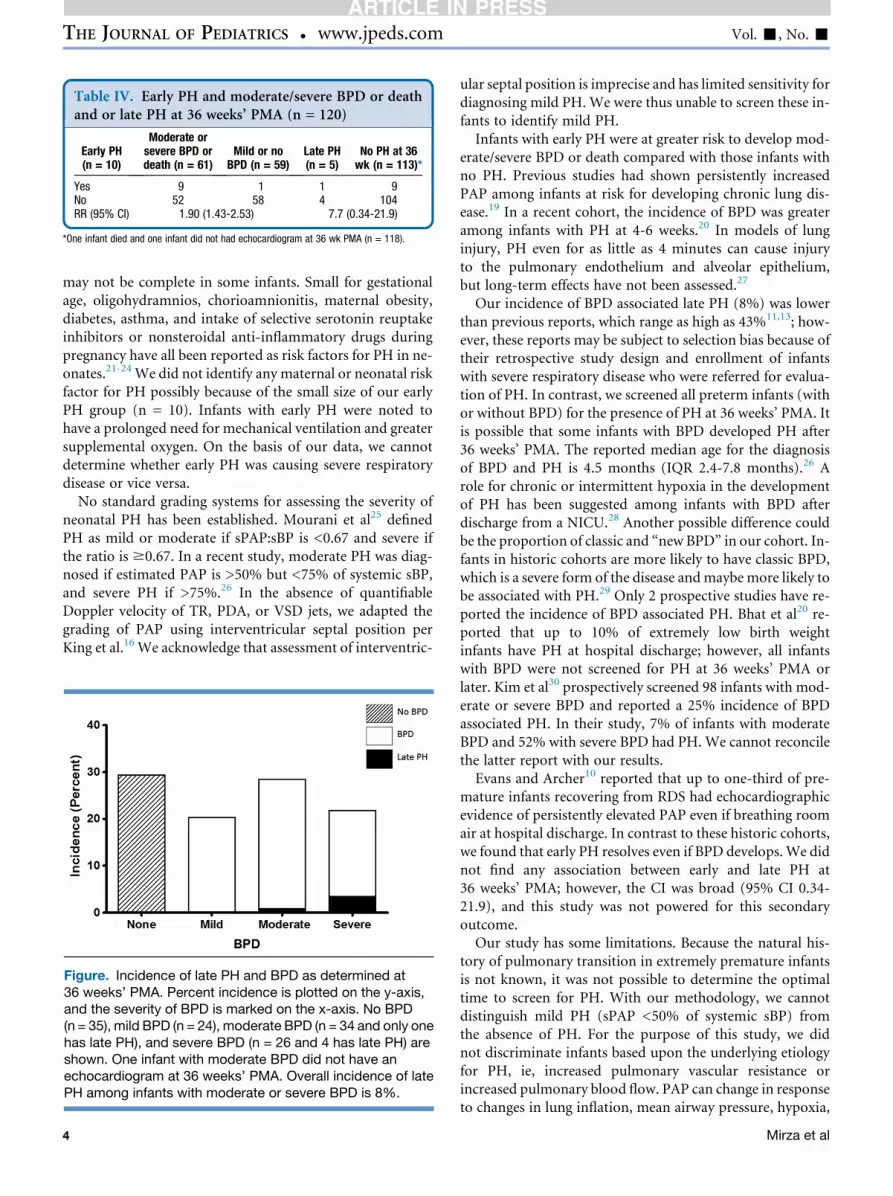
Table IV. Early PH and moderate/severe BPD or deathand or late PH at 36 weeks’ PMA (n = 120)
Early PH(n = 10)
Moderate orsevere BPD ordeath (n = 61)
Mild or noBPD (n = 59)
Late PH(n = 5)
No PH at 36wk (n = 113)*
Yes 9 1 1 9No 52 58 4 104RR (95% CI) 1.90 (1.43-2.53) 7.7 (0.34-21.9)
*One infant died and one infant did not had echocardiogram at 36 wk PMA (n = 118).
THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. -, No. -
may not be complete in some infants. Small for gestationalage, oligohydramnios, chorioamnionitis, maternal obesity,diabetes, asthma, and intake of selective serotonin reuptakeinhibitors or nonsteroidal anti-inflammatory drugs duringpregnancy have all been reported as risk factors for PH in ne-onates.21-24 We did not identify any maternal or neonatal riskfactor for PH possibly because of the small size of our earlyPH group (n = 10). Infants with early PH were noted tohave a prolonged need for mechanical ventilation and greatersupplemental oxygen. On the basis of our data, we cannotdetermine whether early PH was causing severe respiratorydisease or vice versa.
No standard grading systems for assessing the severity ofneonatal PH has been established. Mourani et al25 definedPH as mild or moderate if sPAP:sBP is <0.67 and severe ifthe ratio is $0.67. In a recent study, moderate PH was diag-nosed if estimated PAP is >50% but <75% of systemic sBP,and severe PH if >75%.26 In the absence of quantifiableDoppler velocity of TR, PDA, or VSD jets, we adapted thegrading of PAP using interventricular septal position perKing et al.16 We acknowledge that assessment of interventric-
Figure. Incidence of late PH and BPD as determined at36 weeks’ PMA. Percent incidence is plotted on the y-axis,and the severity of BPD is marked on the x-axis. No BPD(n = 35), mild BPD (n = 24), moderate BPD (n = 34 and only onehas late PH), and severe BPD (n = 26 and 4 has late PH) areshown. One infant with moderate BPD did not have anechocardiogram at 36 weeks’ PMA. Overall incidence of latePH among infants with moderate or severe BPD is 8%.
4
ular septal position is imprecise and has limited sensitivity fordiagnosing mild PH. We were thus unable to screen these in-fants to identify mild PH.Infants with early PH were at greater risk to develop mod-
erate/severe BPD or death compared with those infants withno PH. Previous studies had shown persistently increasedPAP among infants at risk for developing chronic lung dis-ease.19 In a recent cohort, the incidence of BPD was greateramong infants with PH at 4-6 weeks.20 In models of lunginjury, PH even for as little as 4 minutes can cause injuryto the pulmonary endothelium and alveolar epithelium,but long-term effects have not been assessed.27
Our incidence of BPD associated late PH (8%) was lowerthan previous reports, which range as high as 43%11,13; how-ever, these reports may be subject to selection bias because oftheir retrospective study design and enrollment of infantswith severe respiratory disease who were referred for evalua-tion of PH. In contrast, we screened all preterm infants (withor without BPD) for the presence of PH at 36 weeks’ PMA. Itis possible that some infants with BPD developed PH after36 weeks’ PMA. The reported median age for the diagnosisof BPD and PH is 4.5 months (IQR 2.4-7.8 months).26 Arole for chronic or intermittent hypoxia in the developmentof PH has been suggested among infants with BPD afterdischarge from a NICU.28 Another possible difference couldbe the proportion of classic and “new BPD” in our cohort. In-fants in historic cohorts are more likely to have classic BPD,which is a severe form of the disease andmaybe more likely tobe associated with PH.29 Only 2 prospective studies have re-ported the incidence of BPD associated PH. Bhat et al20 re-ported that up to 10% of extremely low birth weightinfants have PH at hospital discharge; however, all infantswith BPD were not screened for PH at 36 weeks’ PMA orlater. Kim et al30 prospectively screened 98 infants with mod-erate or severe BPD and reported a 25% incidence of BPDassociated PH. In their study, 7% of infants with moderateBPD and 52% with severe BPD had PH. We cannot reconcilethe latter report with our results.Evans and Archer10 reported that up to one-third of pre-
mature infants recovering from RDS had echocardiographicevidence of persistently elevated PAP even if breathing roomair at hospital discharge. In contrast to these historic cohorts,we found that early PH resolves even if BPD develops.We didnot find any association between early and late PH at36 weeks’ PMA; however, the CI was broad (95% CI 0.34-21.9), and this study was not powered for this secondaryoutcome.Our study has some limitations. Because the natural his-
tory of pulmonary transition in extremely premature infantsis not known, it was not possible to determine the optimaltime to screen for PH. With our methodology, we cannotdistinguish mild PH (sPAP <50% of systemic sBP) fromthe absence of PH. For the purpose of this study, we didnot discriminate infants based upon the underlying etiologyfor PH, ie, increased pulmonary vascular resistance orincreased pulmonary blood flow. PAP can change in responseto changes in lung inflation, mean airway pressure, hypoxia,
Mirza et al

- 2014 ORIGINAL ARTICLES
and inadequate mechanical ventilation. We did not performchest radiographs or arterial blood gases concurrent withechocardiographic assessment of PH. Therefore, we cannotcomment on the adequacy of lung expansion or optimizedventilation. Echocardiography is not the gold standard for as-sessing PAP. Mourani et al25 have raised questions about thequantitative assessment of PH by echocardiographycompared with cardiac catheterization. Nonetheless, otherexpert opinions have endorsed echocardiography as a reliabletool for the diagnosis of PH in infants with BPD.31,32 Despitelimitations, echocardiography remains the most feasible andwidely used choice for PH screening in extremely preterm in-fants.
Our study has strengths that include its prospective designand a predetermined sample size to test our primary hypoth-esis. Because we are the regional referral center for neonatalcare in southern New England, this is a representative,population-based cohort. In this study, extremely prematureinfants were universally screened for early (10-14 days of life)and late PH (36 weeks’ PMA) to report early and late PH in-cidences. We monitored SpO2 and FiO2 at the time of echo-cardiographic assessment for PH. To decrease interobservervariability, 1 of only 2 pediatric cardiologists on our researchteam reviewed all study echocardiograms without knowledgeof the clinical status of the patient.
Some experts have recommended universal screening forPH in extremely premature infants with severe respiratory dis-ease or infants with moderate or severe BPD20,26; however, theoptimal timing for this screening has not been determined.33
Furthermore, whether early recognition and intervention totreat PH in extremely premature infants can decrease the inci-dence of adverse outcomes, including BPD, is unknown.Further research is needed to determine the optimal time forPH screening and to assess potential benefits of treating earlyPH in extremely premature infants. n
We are thankful to the Division of Pediatric Cardiology at HasbroChildren’s Hospital for their continued support and guidance, NICUservice teams, and families who have enrolled their infants in thisstudy.
Submitted for publication Dec 26, 2013; last revision received Jul 3, 2014;
accepted Jul 23, 2014.
Reprint requests: Abbot Laptook, MD, Department of Pediatrics, Women &
Infants Hospital of Rhode Island, Providence, RI 02905. E-mail: alaptook@
wihri.org
References
1. Stenmark KR, Abman SH. Lung vascular development: implications for
the pathogenesis of bronchopulmonary dysplasia. Annu Rev Physiol
2005;67:623-61.
2. Stoll BJ, Hansen NI, Bell EF, Shankaran S, Laptook AR, Walsh MC, et al.
Neonatal outcomes of extremely preterm infants from the NICHD
Neonatal Research Network. Pediatrics 2010;126:443-56.
3. Northway WH Jr, Rosan RC, Porter DY. Pulmonary disease following
respirator therapy of hyaline-membrane disease. Bronchopulmonary
dysplasia. N Engl J Med 1967;276:357-68.
4. Coalson JJ. Pathology of new bronchopulmonary dysplasia. Semin Neo-
natol 2003;8:73-81.
Pulmonary Hypertension in Preterm Infants: Prevalence and Asso
5. Bland RD. Neonatal chronic lung disease in the post-surfactant era. Biol
Neonate 2005;88:181-91.
6. Rojas MA, Gonzalez A, Bancalari E, Claure N, Poole C, Silva-Neto G.
Changing trends in the epidemiology and pathogenesis of neonatal
chronic lung disease. J Pediatr 1995;126:605-10.
7. Charafeddine L, D’Angio CT, Phelps DL. Atypical chronic lung disease
patterns in neonates. Pediatrics 1999;103:759-65.
8. Jobe AJ. The new BPD: an arrest of lung development. Pediatr Res 1999;
46:641-3.
9. Morrisey EE, Cardoso WV, Lane RH, Rabinovitch M, Abman SH, Ai X,
et al. Molecular determinants of lung development. Ann Am Thorac Soc
2013;10:S12-6.
10. Evans NJ, Archer LN. Doppler assessment of pulmonary artery pressure
and extrapulmonary shunting in the acute phase of hyaline membrane
disease. Arch Dis Child 1991;66:6-11.
11. Khemani E, McElhinney DB, Rhein L, Andrade O, Lacro RV,
Thomas KC, et al. Pulmonary artery hypertension in formerly premature
infants with bronchopulmonary dysplasia: clinical features and out-
comes in the surfactant era. Pediatrics 2007;120:1260-9.
12. Collaco JM, Romer LH, Stuart BD, Coulson JD, Everett AD, Lawson EE,
et al. Frontiers in pulmonary hypertension in infants and children with
bronchopulmonary dysplasia. Pediatr Pulmonol 2012;47:1042-53.
13. An HS, Bae EJ, Kim GB, Kwon BS, Beak JS, Kim EK, et al. Pulmonary
hypertension in preterm infants with bronchopulmonary dysplasia.
Korean Circ J 2010;40:131-6.
14. Gill AB, Weindling AM. Raised pulmonary artery pressure in very low
birthweight infants requiring supplemental oxygen at 36 weeks after
conception. Arch Dis Child Fetal Neonatal Ed 1995;72:F20-2.
15. Subhedar NV, Shaw NJ. Changes in pulmonary arterial pressure in pre-
term infants with chronic lung disease. Arch Dis Child 2000;82:F243-7.
16. King M, Braun H, Goldblatt A, Liberthson R, Weyman A. Interventric-
ular septal configuration as a predictor of right ventricular systolic hy-
pertension in children: a cross-sectional echocardiographic study.
Circulation 1983;68:68-75.
17. Jobe AH, Bancalari E. Bronchopulmonary dysplasia. Am J Respir Crit
Care Med 2001;163:1723-9.
18. Walsh M, Engle W, Laptook A, Kazzi SN, Buchter S, RasmussenM, et al.
Oxygen delivery through nasal cannulae to preterm infants: can practice
be improved? Pediatrics 2005;116:857-61.
19. Gill AB, Weindling AM. Pulmonary artery pressure changes in the very
low birthweight infant developing chronic lung disease. Arch Dis Child
1993;68:303-7.
20. Bhat R, Salas AA, Foster C, Carlo WA, Ambalavanan N. Prospective
analysis of pulmonary hypertension in extremely low birth weight in-
fants. Pediatrics 2012;129:e682-9.
21. Chambers CD, Hernandez-Diaz S, VanMarter LJ, Werler MM, Louik C,
Jones KL, et al. Selective serotonin-reuptake inhibitors and risk of persis-
tent pulmonary hypertension of the newborn. N Engl J Med 2006;354:
579-87.
22. Hernandez-Diaz S, Van Marter LJ, Werler MM, Louik C, Mitchell AA.
Risk factors for persistent pulmonary hypertension of the newborn. Pe-
diatrics 2007;120:e272-82.
23. Williams MC, Wyble LE, O’Brien WF, Nelson RM, Schwenke JR,
Casanova C. Persistent pulmonary hypertension of the neonate and
asymmetric growth restriction. Obstet Gynecol 1998;91:336-41.
24. Woldesenbet M, Perlman JM. Histologic chorioamnionitis: an occult
marker of severe pulmonary hypertension in the term newborn. J Peri-
natol 2005;25:189-92.
25. Mourani PM, Sontag MK, Younoszai A, Ivy DD, Abman SH. Clinical
utility of echocardiography for the diagnosis and management of pul-
monary vascular disease in young children with chronic lung disease. Pe-
diatrics 2008;121:317-25.
26. del Cerro MJ, Sabate Rotes A, Carton A, Deiros L, Bret M, Cordeiro M,
et al. Pulmonary hypertension in bronchopulmonary dysplasia: clinical
findings, cardiovascular anomalies and outcomes. Pediatr Pulmonol
2014;49:49-59.
27. West JB, Tsukimoto K, Mathieu-Costello O, Prediletto R. Stress failure
in pulmonary capillaries. J Appl Physiol 1991;70:1731-42.
ciation with Bronchopulmonary Dysplasia 5

THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. -, No. -
28. Berkelhamer SK, Mestan KK, Steinhorn RH. Pulmonary hypertension in
bronchopulmonary dysplasia. Semin Perinatol 2013;37:124-31.
29. Bancalari E, Claure N. Definitions and diagnostic criteria for broncho-
pulmonary dysplasia. Semin Perinatol 2006;30:164-70.
30. Kim DH, Kim HS, Choi CW, Kim EK, Kim BI, Choi JH. Risk factors for
pulmonary artery hypertension in preterm infants with moderate or se-
vere bronchopulmonary dysplasia. Neonatology 2012;101:40-6.
6
31. Abman SH. Monitoring cardiovascular function in infants with chronic
lung disease of prematurity. Arch Dis Child 2002;87:F15-8.
32. Farquhar M, Fitzgerald DA. Pulmonary hypertension in chronic
neonatal lung disease. Paediatr Respir Rev 2010;11:149-53.
33. Ambalavanan N, Mourani P. Pulmonary hypertension in broncho-
pulmonary dysplasia. Birth Defects Res A Clin Mol Teratol 2014;
100:240-6.
Mirza et al
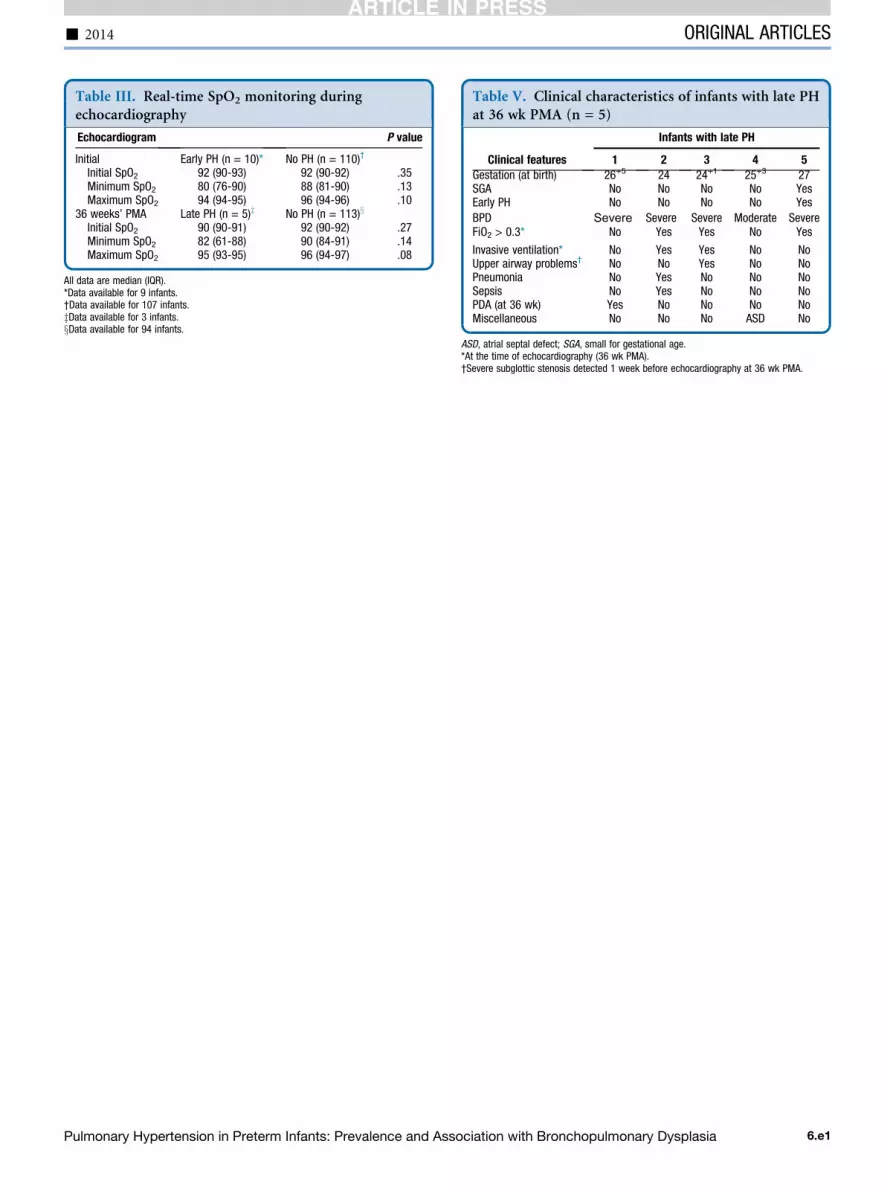
Table III. Real-time SpO2 monitoring duringechocardiography
Echocardiogram P value
Initial Early PH (n = 10)* No PH (n = 110)†
Initial SpO2 92 (90-93) 92 (90-92) .35Minimum SpO2 80 (76-90) 88 (81-90) .13Maximum SpO2 94 (94-95) 96 (94-96) .10
36 weeks’ PMA Late PH (n = 5)z No PH (n = 113)x
Initial SpO2 90 (90-91) 92 (90-92) .27Minimum SpO2 82 (61-88) 90 (84-91) .14Maximum SpO2 95 (93-95) 96 (94-97) .08
All data are median (IQR).*Data available for 9 infants.†Data available for 107 infants.zData available for 3 infants.xData available for 94 infants.
Table V. Clinical characteristics of infants with late PHat 36 wk PMA (n = 5)
Clinical features
Infants with late PH
1 2 3 4 5
Invasive ventilation* No Yes Yes No NoUpper airway problems† No No Yes No NoPneumonia No Yes No No NoSepsis No Yes No No NoPDA (at 36 wk) Yes No No No NoMiscellaneous No No No ASD No
ASD, atrial septal defect; SGA, small for gestational age.*At the time of echocardiography (36 wk PMA).†Severe subglottic stenosis detected 1 week before echocardiography at 36 wk PMA.
- 2014 ORIGINAL ARTICLES
Pulmonary Hypertension in Preterm Infants: Prevalence and Association with Bronchopulmonary Dysplasia 6.e1
Gestation (at birth) 26+5 24 24+1 25+3 27SGA No No No No YesEarly PH No No No No Yes
BPD Severe Severe Severe Moderate SevereFiO2 > 0.3* No Yes Yes No Yes