outcomes of children with severe bronchopulmonary dysplasia who were ventilator dependent at home
TRANSCRIPT

DOI: 10.1542/peds.2012-2990; originally published online August 5, 2013; 2013;132;e727PediatricsVeda L. Ackerman
A. Ioana Cristea, Aaron E. Carroll, Stephanie D. Davis, Nancy L. Swigonski andVentilator Dependent at Home
Outcomes of Children With Severe Bronchopulmonary Dysplasia Who Were
http://pediatrics.aappublications.org/content/132/3/e727.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2013 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at IU Health Medical Library on September 16, 2013pediatrics.aappublications.orgDownloaded from
Outcomes of ChildrenWith Severe BronchopulmonaryDysplasia Who Were Ventilator Dependent at Home
WHAT’S KNOWN ON THIS SUBJECT: Respiratory outcomes ofpatients with bronchopulmonary dysplasia (BPD) range from nooxygen requirement to chronic respiratory failure. Outcomes ofleast severe types of BPD are well described. Limited data exist onoutcomes of patients with BPD-related chronic ventilatordependency.
WHAT THIS STUDY ADDS: Along with a first estimation of theincidence of patients with severe BPD-related chronic respiratoryfailure who were dependent on positive pressure ventilation viatracheostomy at home, we describe their survival rate, liberationfrom positive pressure ventilation, and decannulation.
abstractOBJECTIVE: To describe the incidence and outcomes of children withchronic respiratory failure secondary to severe bronchopulmonarydysplasia (BPD) on chronic positive pressure ventilation (PPV) viatracheostomy at home.
METHODS:We retrospectively reviewed medical charts of patients withsevere BPD who were PPV dependent at home and who were enrolledin a university-affiliated home ventilator program between 1984 and2010. We excluded patients with other comorbidities that couldcontribute to the development of chronic respiratory failure. Wereported the incidence of these children in Indiana and cumulativeincidences of survival, liberation from PPV, and decannulation.
RESULTS: Over 27 years, 628 children were cared for in our home ven-tilator program. Of these, 102 patients met inclusion criteria: 83(81.4%) were alive and 19 (18.6%) were deceased. Sixty-ninepatients (67.6%) were liberated from PPV, and 97.1% of them wereweaned before their fifth birthday, with a median age at liberationof 24 months (interquartile range, 19–33). Similarly, 60 patients(58.8%) were decannulated, of which 96.7% completed this processbefore their sixth birthday, with a median age at decannulation of 37.5months (interquartile range, 31.5–45). The incidence of children withchronic respiratory failure secondary to BPD who were PPV-dependent at home in Indiana was 1.23 per 100 000 live births in1984 and increased to 4.77 per 100 000 live births in 2010.
CONCLUSIONS: Although extreme prematurity associated with severeBPD necessitating PPV at home carries significant risks of morbidityand mortality, successful liberation from mechanical ventilation anddecannulation are likely to occur. Pediatrics 2013;132:e727–e734
AUTHORS: A. Ioana Cristea, MD, MS,a,b Aaron E. Carroll,MD, MS,b Stephanie D. Davis, MD,a Nancy L. Swigonski, MD,MPH,b and Veda L. Ackerman, MDa
aSection of Pediatric Pulmonology, and bChildren’s HealthServices Research, Department of Pediatrics, Indiana UniversitySchool of Medicine, Indianapolis, Indiana
KEY WORDSbronchopulmonary dysplasia, outcome, positive pressureventilation, tracheostomy, home
ABBREVIATIONSBPD—bronchopulmonary dysplasiaHVP—home ventilator programIQR—interquartile rangeIVH—intraventricular hemorrhagePPV—positive pressure ventilation
Dr Cristea conceptualized and designed the study, collected thedata, and drafted the initial manuscript; Dr Carroll carried outthe initial analyses and reviewed and revised the manuscript;Dr Davis provided guidance with study design and criticallyreviewed the manuscript; Dr Swigonski facilitatedcommunication with Indiana State Department of Health andcritically reviewed the manuscript; Dr Ackerman providedguidance with study design and data collection and reviewedand revised the manuscript; and all authors approved the finalmanuscript as submitted.
www.pediatrics.org/cgi/doi/10.1542/peds.2012-2990
doi:10.1542/peds.2012-2990
Accepted for publication May 31, 2013
Address correspondence to A. Ioana Cristea, MD, MS, RileyHospital for Children Indiana University, 705 Riley Hospital Dr. ROC4270, Indianapolis, IN 46202-5225. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2013 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they haveno financial relationships relevant to this article to disclose.
FUNDING: Dr Cristea was supported by a National Institutes ofHealth training grant (T32 HS 017588-04). No other externalfunding was secured for this study. Funded by the NationalInstitutes of Health.
POTENTIAL CONFLICT OF INTEREST: The authors have indicatedthey have no potential conflicts of interest to disclose.
PEDIATRICS Volume 132, Number 3, September 2013 e727
ARTICLE
at IU Health Medical Library on September 16, 2013pediatrics.aappublications.orgDownloaded from

First characterized by Northway andcolleagues1 in 1967, bronchopulmo-nary dysplasia (BPD) is a known com-plication of prematurity, defined as thepresence of persistent signs and symp-toms of respiratory distress, tachypnea,hypoxemia necessitating supplementaloxygen, and an abnormal chest radio-graph at 36 weeks’ postmenstrual age.2
In recent years, advancements made inthe prevention of BPD, such as prenatalglucocorticoids,3 surfactant use,4 andlung protective ventilation strategies,5,6
have led to changes in the pathologicfindings and clinical course of this con-dition. The “new” BPD is a manifestationof lung immaturity characterized by in-flammation, dysmorphic alveolar andvascular structures, and a decreasedsurface area for gas exchange.7,8
The incidence and prevalence of pa-tients with severe BPD necessitatingpositive pressure ventilation (PPV) athome are unknown. The first estimatesof ventilator-dependent children (,21years of age) in the United States werepublished in the 1980s, with an esti-mated prevalence of 0.7 to 2 per100 000 children9; current state-levelestimates show an increasing preva-lence of home-ventilated children. Forinstance, in Utah the prevalence ofthese children has increased from 5.0per 100 000 in 1996 to 6.3 per 100 000 in2004.10 The 2005Massachusetts censusof children on chronic mechanical re-spiratory support shows a nearlythreefold increase in this population inthe 15-year interval since the last cen-sus.11 In addition, the rate of hospitaldischarges for all children dependenton long-term mechanical ventilationincreased 55% from 2000 to 2006.12
The respiratory outcomes of patientswith BPD range from no oxygen re-quirement to chronic ventilator depen-dency. Various publications13–15 addressthe outcome of the least severe types ofBPD, yet very limited data exist on BPD-related chronic respiratory failure.
Given the limited published outcomedata for children with severe BPD, wesought to define the long-term re-spiratory morbidity of this conditionby evaluating the incidence and out-comes of patients with severe BPD whoneeded chronic PPV via tracheostomyat initial discharge from the hospital.
METHODS
We conducted a retrospective cohortstudy of all patients diagnosedwith BPDwho needed full-time PPV via trache-ostomy at home. These patients werefollowed in the Pediatric PulmonologyClinic Home Ventilator Program (HVP)at Riley Hospital for Children, IndianaUniversity, Indianapolis. This clinic wasfounded in 1984 and is the only com-prehensive clinic of this type in thestate, where children and young adultswho need respiratory support at homeare followed on a regular basis. Themedical care has been very consistent,provided by the same pulmonary andcritical care physician (V.A.), a dedi-cated nurse with special pulmonaryexpertise, respiratory therapists, anda social worker. The HVP team wasusually involved in these patients’ carebefore their discharge from the hos-pital. If the PPV was initiated duringchildhood, that patient is followed inthe HVP clinic, regardless of age. Al-though it follows general principles,the ventilator weaning protocol used inthis clinic is individualized to each pa-tient. Weaning candidates are thosewho are stable at home and thriving.The ventilator settings are slowlyweaned over several months. Weightgain and indirect carbon dioxide levels(obtained via basic metabolic panels)are monitored. When low respiratorysupport is achieved during the day,short off-ventilator trials are initiated.In the months that follow, the time offventilator while awake is gradually in-creased. The patient’s status off venti-lator support while asleep is assessed
through an overnight polysomnogram.If there is no significant hypercarbia,severe desaturation, or tachypnea, nightventilator support is discontinued. Thepatient is seen monthly during weaning.Most patients receive 8 to 12 hours ofskilled nursing per day. Respite care isavailable through specialized pediatricfacilities but not routinely providedthrough the HVP. During the study pe-riod the most common ventilator usedat home was the LP series (Covidien,Mansfield, MA), with transition to theLTV (Pulmonetic Systems, Inc., Minne-apolis, MN) when this type of ventilatorbecame available.
Patients with associated comorbiditiesthat could contribute to the develop-ment of chronic respiratory failurewere excluded from this study; thesecomorbidities include history of chestsurgery and chromosomal, anatomic,metabolic, and neurologic abnormali-ties.We also excluded patientswith BPDwho received a tracheostomy and be-come PPV dependent in a subsequenthospital admission to eliminate otheracute causative factors. Our study wasapproved by the Indiana UniversitySchool of Medicine Institutional ReviewBoard.
The first author (A.I.C.) reviewed allmedical records for each patient, in-cluding the hospital’s electronic re-cords (Careweb, Regenstrief Institute;Cerner Corporation, Kansas City, MO)and the HVP paper charts. Data ele-ments abstracted were gestationalage, birth weight, gender, race, healthinsurance, date when the patient be-came technology independent, and dateof decannulation. In addition, character-istics of the neonatal intensive care unithospitalization were recorded: morbidity(gastrostomy tube, Nissen procedure,retinopathy of prematurity, severe in-traventricular hemorrhage [IVH] thatnecessitated ventriculoperitoneal shunt,seizures, documented sepsis, inguinalhernia repair, pulmonary hypertension
e728 CRISTEA et al at IU Health Medical Library on September 16, 2013pediatrics.aappublications.orgDownloaded from

[diagnosed by echocardiography], sys-temic hypertension, necrotizing entero-colitis, patent ductus arteriosus), date ofdischarge, and destination after dis-charge (home, foster home, chronic carefacility). All subsequent readmissionswere recorded, along with the main di-agnosis at discharge from the hospital.
Survival status was defined as aliveor deceased. Final respiratory statuswas defined as PPV dependent, weanedoff PPV, or decannulated. Data are pre-sentedasproportionsorasmediansandinterquartile ranges (IQRs). Descrip-tive characteristics were compared byusing Fisher’s exact tests for cate-gorical variables and Mann–Whitney–Wilcoxon rank sum test for continuousvariables.
The incidence of children with severeBPD who were PPV dependent at homewas calculated by dividing the numberofpatientsborn inoneyear into the totalnumber of children born in that par-ticular year, as reported by IndianaState Department of Health vital sta-tistics birth data.16
We constructed Kaplan–Meier survivalcurves and cumulative incidence curvesfor liberation from PPV and decannu-lation. Cox proportional hazards mod-els17 were performed for the outcomesdeath, liberation from PPV, and dec-annulation, using the following cova-riates: birth weight (#750 g or.750 g),gender, race, and severe IVH. Gesta-tional age was not used in this analysisbecause of its very high correlation tobirth weight. Statistical significancewas determined with a P value of .05.Data were analyzed by using SAS soft-ware (version 9.3; SAS Institute, Inc,Cary, NC).
RESULTS
Between 1984 and 2010, 628 childrenreceiving part- or full-time PPV via tra-cheostomy were cared for in the HVP. Asof December 2010, 207 patients followedin this clinic were diagnosed with BPD.
One hundred five (50.7%) of thesepatients were excluded based on theexclusion criteria noted in the Methodssection. Of these, 72 patients had chestsurgery (secondary to tracheoesopha-geal fistula, congenital diaphragmatichernia, or congenital cardiac disease), 8patients had neurologic abnormalities(Chiari malformation, myelomeningo-cele), 7 patients had chromosomal ab-normalities(trisomy21,18,13),4patientshad lung or chest anatomic abnormali-ties (lobar emphysema, hypoplastic lung,thoracic insufficiency syndrome), 3 pa-tients had metabolic disease, 3 patientsbecame ventilator dependent after viralinfection acquired after initial dischargefrom the hospital, 2 patients had con-genital cytomegalovirus infection, and 2patientshad fetal alcohol syndrome. Fourpatients were not followed anymore atour institution: 3 moved out of state ataveryyoungage,whentheywerestill PPVdependent, and 1 patient was liberatedfrom ventilation but still tracheostomydependent.
One hundred two (49.3%) patients whocarried the diagnosis of severe BPDandwere receiving full-time PPV via tra-cheostomy at initial hospital dischargewere included in this study. Thesepatients were intubated at birth orsoon after because of prematurity andrespiratory distress syndrome. Theonly documented indication for tra-cheostomy in this cohort was chronicrespiratory failure necessitating me-chanical ventilation. These patientswere followed for a total of 871 person-years. The characteristics of subjectsgrouped by their survival status areshown in Table 1. Eighty-three (81.4%)of 102 patients were alive and 19(18.6%) were deceased. There were nosignificant differences between thealive and deceased groups, in anydemographic characteristics.
The incidence of children with chronicrespiratory failure secondary to BPDwho were PPV dependent at home in
Indiana was 1.23 per 100 000 live birthsin 1984 and increased to 4.77 per100 000 live births in 2010.
Morbidity during the initial neonatalintensive care unit hospitalization in-cluded the following: 102 (100%) pa-tients received a gastrostomy tube(33.3%alsohadaNissenfundoplication),45 (44.1%)patientswere diagnosedwithretinopathy of prematurity, 26 (25.5%)patients had severe IVH that necessi-tated ventriculoperitoneal shunt, 14(13.7%)patientshadseizures,28(27.4%)patients had documented sepsis, 22(21.5%) patients had inguinal herniarepair, 20 (19.6%) patients had pulmo-nary hypertension, 16 (15.6%) patientshad systemic hypertension, 13 (12.7%)patients were diagnosed with necrotiz-ingenterocolitis, and19 (18.6%)patientshad patent ductus arteriosus, of which11 needed surgical ligation.
The rehospitalization rate for this co-hort was impressive, with a totalnumber of 675 events. The incidence ofrehospitalization was significantlyhigherbeforedecannulation(554vs121events, P , .0001). The most commonreason for rehospitalization was re-spiratory related (358 before dec-annulation versus 67 after decannulation,P , .0001), followed by a need for sur-gical interventions (54 before dec-annulation versus 16 after decannulation,P = .36).
Figure 1 illustrates the Kaplan–Meiersurvival curve for 102 patients withsevere BPD who were discharged onhome PPV, along with the survival in-cidence stratified by birth weight(#750 g or ,750 g). Figure 2 repre-sents the Kaplan–Meier curve showingthe cumulative proportion of livepatients liberated from PPV and dec-annulated. Within the group of patientswho were alive at the end of this study,69 (83.1%) patients were weaned offthe PPV and 60 (72.2%) patients weredecannulated. Sixty-seven (97.1%) of 69patients liberated from PPV were
ARTICLE
PEDIATRICS Volume 132, Number 3, September 2013 e729 at IU Health Medical Library on September 16, 2013pediatrics.aappublications.orgDownloaded from
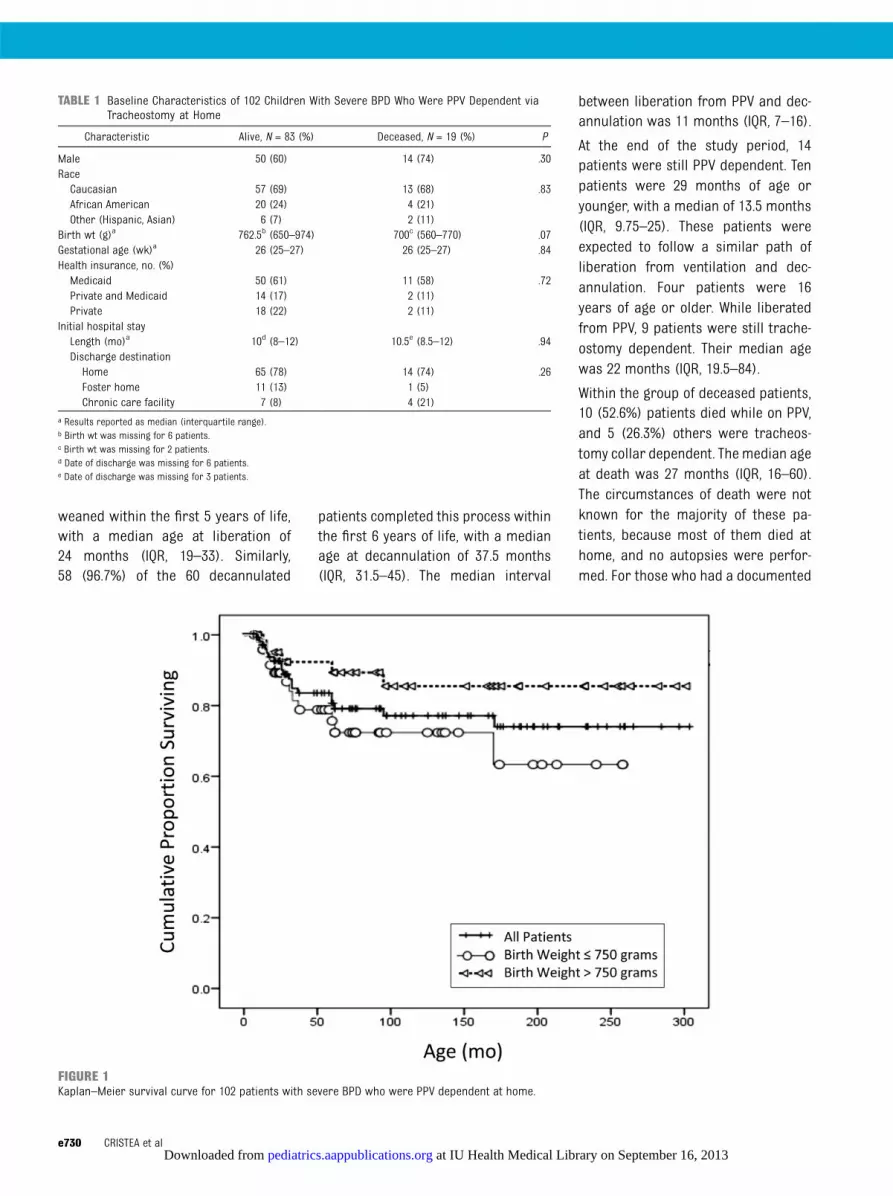
weaned within the first 5 years of life,with a median age at liberation of24 months (IQR, 19–33). Similarly,58 (96.7%) of the 60 decannulated
patients completed this process withinthe first 6 years of life, with a medianage at decannulation of 37.5 months(IQR, 31.5–45). The median interval
between liberation from PPV and dec-annulation was 11 months (IQR, 7–16).
At the end of the study period, 14patients were still PPV dependent. Tenpatients were 29 months of age oryounger, with a median of 13.5 months(IQR, 9.75–25). These patients wereexpected to follow a similar path ofliberation from ventilation and dec-annulation. Four patients were 16years of age or older. While liberatedfrom PPV, 9 patients were still trache-ostomy dependent. Their median agewas 22 months (IQR, 19.5–84).
Within the group of deceased patients,10 (52.6%) patients died while on PPV,and 5 (26.3%) others were tracheos-tomy collar dependent. The median ageat death was 27 months (IQR, 16–60).The circumstances of death were notknown for the majority of these pa-tients, because most of them died athome, and no autopsies were perfor-med. For those who had a documented
TABLE 1 Baseline Characteristics of 102 Children With Severe BPD Who Were PPV Dependent viaTracheostomy at Home
Characteristic Alive, N = 83 (%) Deceased, N = 19 (%) P
Male 50 (60) 14 (74) .30RaceCaucasian 57 (69) 13 (68) .83African American 20 (24) 4 (21)Other (Hispanic, Asian) 6 (7) 2 (11)
Birth wt (g)a 762.5b (650–974) 700c (560–770) .07Gestational age (wk)a 26 (25–27) 26 (25–27) .84Health insurance, no. (%)Medicaid 50 (61) 11 (58) .72Private and Medicaid 14 (17) 2 (11)Private 18 (22) 2 (11)
Initial hospital stayLength (mo)a 10d (8–12) 10.5e (8.5–12) .94Discharge destinationHome 65 (78) 14 (74) .26Foster home 11 (13) 1 (5)Chronic care facility 7 (8) 4 (21)
a Results reported as median (interquartile range).b Birth wt was missing for 6 patients.c Birth wt was missing for 2 patients.d Date of discharge was missing for 6 patients.e Date of discharge was missing for 3 patients.
FIGURE 1Kaplan–Meier survival curve for 102 patients with severe BPD who were PPV dependent at home.
e730 CRISTEA et al at IU Health Medical Library on September 16, 2013pediatrics.aappublications.orgDownloaded from

cause of death in their medical re-cords, 2 deaths were tracheostomyrelated (accidental decannulation), 2deaths were expected (because thepatients had “do not resuscitate”orders), and 2 other deaths were sec-ondary to cardiorespiratory arrest.There was no documentation of deathcaused by ventilator malfunction forany of these patients.
Table 2 provides the hazard ratios andthe 95% confidence intervals for theCox proportional hazards analyses.Patients with a lower birth weight hadgreater odds of an earlier death.
DISCUSSION
This study of 102 children with re-spiratory failure secondary to severeBPD who were discharged from thehospital on PPV represents the largestcohort of such childrenwith the longest
follow-up reported to date. More than80%ofchildrensurvive,andmostof themwere liberated from PPV and decannu-lated. Our data suggest that if a child isnot off PPV by 5 years and decannulatedby6years,heorshe isunlikely tobecomeso (in our study, only 2 [2.4%] patientswere weaned beyond that time period).This information is important for familiesand for health care providers for plan-ning long-term health needs.
In general, children on home mechan-ical ventilation are a heterogeneouspopulation with varied indications forchronic ventilation and severity ofcomorbidities. Earlier studies10,18–23
included a range of subgroups of pa-tients, follow-up periods, geographicsites, and different periods with di-verse technology. Because of thesedifferences, it is difficult to comparepatients’ outcomes across studies. Theincidence of mortality reported in
other studies from different time peri-ods, where patients’ outcomes arereported by the original cause of re-spiratory failure, was higher than18 orsimilar to24 our results. The incidenceand the timing of liberation from homemechanical ventilation are consistentwith those in another study with simi-lar follow-up periods.24
The question of the racial or ethnic andgender disparity in mortality amongpremature infants with BPD remainsopen to interpretation, with studiesreporting conflicting results.25–28 Ourregression analyses showed that race,gender, and IVH necessitating shuntwas not associated with death. Otherraces (Asians and Hispanics) were lesslikely than Caucasians to be liberatedfrom PPV or decannulated, but it isdifficult to speculate on the causal re-lationship, which may include culturaland religious factors that influence
FIGURE 2Cumulative incidence of liberation from PPV and decannulation for 83 alive children with severe BPD.
ARTICLE
PEDIATRICS Volume 132, Number 3, September 2013 e731 at IU Health Medical Library on September 16, 2013pediatrics.aappublications.orgDownloaded from

health care decisions. We also showedthat lower weight was associated withearlier death, a finding supported byearlier studies.29–31
Although several articles32,33 reporta higher readmission rate in the firstyear of life for patients with BPD ingeneral, we could not report thereadmission rate for the first year oflife because the length of the initialhospital stay was very long. This lengthof stay is probably secondary to theneed for extensive caregiver training inventilator and tracheostomy care, aspreviously described.34
We reported the number of hospital-izationsbeforeandafterdecannulation.The rehospitalization rate was signifi-cantly higher before decannulation; themost frequent reason for rehospitali-zation was respiratory related, aspreviously described.35,36 Although noother studies have addressed therehospitalization rates for childrenwith tracheostomy, before and afterdecannulation, several have found thatchildren who are ventilator dependentat home have a higher risk of rehospi-talization than other children.11,12,36–39
The decrease in readmission rate afterdecannulation may be secondary toremoval of the tracheostomy, im-provement in BPD, or both.
Major practice changes occurred dur-ing the 27 years of the study.3–6 We didsecondary analyses (data not shown)to test whether practice changeswere associated with changes in our
outcomes. Our data showed that morepatients with severe BPD who neededprolonged PPVat homewere born after1996, when prenatal corticosteroidsand surfactant became widely used.Statistical comparisons were madebetween the groups of patients bornbefore or during versus after 1996.There were no significant differencesbetween these subgroups of patients,with the exception of the length of theinitial hospital stay, which was shorterfor those born after 1996 (P = .01).These findings are probably secondaryto the major changes in the manage-ment of premature babies, which led tothe improved survival of smaller, lessmature infants in the 1990s.29
Our study has several limitations. First,this is a retrospective chart review, andwe focus on the diagnosis of severeBPDas the only cause of respiratory failurein these patients. Second, we wereunable to evaluate neurocognitive out-comes. Third, we could not identify thecause of death for several of the de-ceased patients. Fourth, during thestudy period only a few types of homeventilators were used, to ensure con-sistency in careprovidedby respiratorycare practitioners both at home and inthe hospital setting. We cannot com-ment on other types of ventilatorsavailable for use at home. Furthermore,we are reporting one institution’s ex-perience and recognize that commonpractices may be different at othercenters. The methods described hereshould not be considered the standard
but rather one starting point for eval-uation and improvement of the qualityof care for these patients. Finally, ourincidence data may be underestimatedbecause they are based on our groupof patients and state birth rate, possi-bly ignoring children who live closer tothe state borders and receiving care inneighboring states.
The decision to take a baby home fromthe hospital with significant techno-logical support comes with significantemotional burden for families. Ourstudy provides new outcome data tosupport parents’ and medical teams’decisions in caring for premature in-fants with severe BPD who need ventila-tory support at home. Multi-institutionaloutcome research with better stratifica-tion of factors that can influence mor-tality and successful weaning protocolsfrom PPV and decannulation are needed.Home ventilator programs should pro-vide quality assurance and frequentmonitoring not only for survival but forliberation from ventilation and dec-annulation to optimize care, minimizehealth care costs, and ensure that theclinical outcomes are comparable withthose of other institutions.
CONCLUSIONS
Extreme prematurity associated withsevere BPD necessitating PPV at homecarries significant risks of morbidityand mortality. However, successful lib-eration from PPV and decannulation islikely to occur. Before this study, therewere no long-term outcome data on themortality and morbidity associatedwith home ventilation of children withsevere BPD. This study offers valuableinformation thatwill enable health careprovidersand families tobetterplan forthe medical care of these vulnerableinfants. Prospective multicenter stud-ies are necessary to elucidate thetrends in outcomes of children withsevere BPD and to standardize the careprovided to these children.
TABLE 2 Cox Proportional Hazards Model of Death, Liberation From PPV and Decannulation,Controlling for Gender, Race, Birth Wt, and IVHa
Variable Death Liberation From PPV Decannulation
GenderFemale versus male 0.41 (0.13, 1.30) 0.72 (0.25, 2.03) 0.82 (0.37, 1.79)
RaceAfrican American versus Caucasian 0.76 (0.21, 2.79) 1.11 (0.30, 4.10) 1.14 (0.44, 2.99)Other versus Caucasian 3.35 (0.68, 16.59) 7.54 (2.36, 24.12) 5.51 (2.05, 14.83)
Birth wt#750 g vs .750 g 0.34 (0.12, 0.99) 1.20 (0.46, 3.13) 0.55 (0.26, 1.17)
IVH 0.97 (0.33, 2.82) 1.33 (0.47, 3.78) 1.00 (0.47, 2.13)a Results reported as hazard ratio (95% confidence interval).
e732 CRISTEA et al at IU Health Medical Library on September 16, 2013pediatrics.aappublications.orgDownloaded from

ACKNOWLEDGMENTS
We thank the Pediatric PulmonologyChart Room Staff for their assistancein retrieving the medical charts for
these patients. We thank Dr Zhangheng
Yu and Mr James Slaven, Indiana Uni-
versity Department of Biostatistics,
for guidance in data analysis. We thank
MsMichele Starkey of the Indiana State
Department of Health, Epidemiology Re-
source Center, for helping us retrieve
the number of live births in our state.
REFERENCES
1. Northway WH Jr, Rosan RC, Porter DY. Pul-monary disease following respirator therapyof hyaline-membrane disease. Broncho-pulmonary dysplasia. N Engl J Med. 1967;276(7):357–368
2. Bancalari E, Abdenour GE, Feller R, GannonJ. Bronchopulmonary dysplasia: clinicalpresentation. J Pediatr. 1979;95(5 pt 2):819–823
3. Roberts D, Dalziel S. Antenatal cortico-steroids for accelerating fetal lung matu-ration for women at risk of preterm birth.Cochrane Database Syst Rev. 2006;3(3):CD004454
4. Soll RF. Prophylactic natural surfactantextract for preventing morbidity and mor-tality in preterm infants. Cochrane Data-base Syst Rev. 2000;(2):CD000511
5. Carlo WA, Finer NN, Walsh MC, et al;SUPPORT Study Group of the Eunice KennedyShriver NICHD Neonatal Research Network.Target ranges of oxygen saturation in ex-tremely preterm infants. N Engl J Med. 2010;362(21):1959–1969
6. Vento M, Moro M, Escrig R, et al. Pretermresuscitation with low oxygen causes lessoxidative stress, inflammation, and chroniclung disease. Pediatrics. 2009;124(3).Available at: www.pediatrics.org/cgi/con-tent/full/124/3/e439
7. Rojas MA, Gonzalez A, Bancalari E, Claure N,Poole C, Silva-Neto G. Changing trends inthe epidemiology and pathogenesis ofneonatal chronic lung disease. J Pediatr.1995;126(4):605–610
8. Charafeddine L, D’Angio CT, Phelps DL. Atyp-ical chronic lung disease patterns in neo-nates. Pediatrics. 1999;103(4 pt 1):759–765
9. US Congress OTA. Technology DependentChildren: Hospital vs. Home Care. Vol NTISorder #PB87-194551. Office Technology As-sessment Archive: Federation of AmericanScientists. Washington, DC: US GovernmentPrinting Office; 1987
10. Gowans M, Keenan HT, Bratton SL. Thepopulation prevalence of children receivinginvasive home ventilation in Utah. PediatrPulmonol. 2007;42(3):231–236
11. Graham RJ, Fleegler EW, Robinson WM.Chronic ventilator need in the community:a 2005 pediatric census of Massachusetts.
Pediatrics. 2007;119(6). Available at: www.pediatrics.org/cgi/content/full/119/6/e1280
12. Benneyworth BD, Gebremariam A, Clark SJ,Shanley TP, Davis MM. Inpatient health careutilization for children dependent on long-term mechanical ventilation. Pediatrics.2011;127(6). Available at: www.pediatrics.org/cgi/content/full/127/6/e1533
13. Singer L, Yamashita T, Lilien L, Collin M,Baley J. A longitudinal study of develop-mental outcome of infants with broncho-pulmonary dysplasia and very low birthweight. Pediatrics. 1997;100(6):987–993
14. Short EJ, Klein NK, Lewis BA, et al. Cognitiveand academic consequences of broncho-pulmonary dysplasia and very low birthweight: 8-year-old outcomes. Pediatrics.2003;112(5). Available at: www.pediatrics.org/cgi/content/full/112/5/e359
15. Schmidt B, Asztalos EV, Roberts RS,Robertson CM, Sauve RS, Whitfield MF;Trial of Indomethacin Prophylaxis in Pre-terms (TIPP) Investigators. Impact ofbronchopulmonary dysplasia, brain injury,and severe retinopathy on the outcome ofextremely low-birth-weight infants at 18months: results from the trial of in-domethacin prophylaxis in preterms.JAMA. 2003;289(9):1124–1129
16. Indiana State Department of Health. Avail-able at: www.in.gov/isdh/19095.htm. Acc-essed December 17, 2012
17. Vittinghoff E, McCulloch CE. Relaxing therule of ten events per variable in logisticand Cox regression. Am J Epidemiol. 2007;165(6):710–718
18. Schreiner MS, Downes JJ, Kettrick RG, Ise C,Voit R. Chronic respiratory failure in infantswith prolonged ventilator dependency.JAMA. 1987;258(23):3398–3404
19. Fields AI, Coble DH, Pollack MM, Kaufman J.Outcome of home care for technology-dependent children: success of an indepen-dent, community-based case managementmodel. Pediatr Pulmonol. 1991;11(4):310–317
20. Wheeler WB, Maguire EL, Kurachek SC,Lobas JG, Fugate JH, McNamara JJ. Chronicrespiratory failure of infancy and child-hood: clinical outcomes based on un-derlying etiology. Pediatr Pulmonol. 1994;17(1):1–5
21. Edwards EA, O’Toole M, Wallis C. Sendingchildren home on tracheostomy dependentventilation: pitfalls and outcomes. Arch DisChild. 2004;89(3):251–255
22. Appierto L, Cori M, Bianchi R, et al. Homecare for chronic respiratory failure inchildren: 15 years experience. PaediatrAnaesth. 2002;12(4):345–350
23. Fraser J, Henrichsen T, Mok Q, Tasker RC.Prolonged mechanical ventilation as a con-sequence of acute illness. Arch Dis Child.1998;78(3):253–256
24. Edwards JD, Kun SS, Keens TG. Outcomesand causes of death in children on homemechanical ventilation via tracheostomy:an institutional and literature review. JPediatr. 2010;157(6):955–959
25. Petrova A, Mehta R, Anwar M, Hiatt M, HegyiT. Impact of race and ethnicity on the out-come of preterm infants below 32 weeksgestation. J Perinatol. 2003;23(5):404–408
26. Rowley DL. Framing the debate: can pre-natal care help to reduce the black–whitedisparity in infant mortality? J Am MedWomens Assoc. 1995;50(5):187–193
27. Avery ME, Tooley WH, Keller JB, et al. Ischronic lung disease in low birth weightinfants preventable? A survey of eightcenters. Pediatrics. 1987;79(1):26–30
28. Horbar JD, McAuliffe TL, Adler SM, et al.Variability in 28-day outcomes for very lowbirth weight infants: an analysis of 11neonatal intensive care units. Pediatrics.1988;82(4):554–559
29. Fanaroff AA, Hack M, Walsh MC. The NICHDNeonatal Research Network: changes inpractice and outcomes during the first 15years. Semin Perinatol. 2003;27(4):281–287
30. Ambalavanan N, Van Meurs KP, Perritt R,et al; NICHD Neonatal Research Network,Bethesda, MD. Predictors of death orbronchopulmonary dysplasia in preterminfants with respiratory failure. J Perinatol.2008;28(6):420–426
31. Stoll BJ, Hansen NI, Bell EF, et al; EuniceKennedy Shriver National Institute of ChildHealth and Human Development NeonatalResearch Network. Neonatal outcomes ofextremely preterm infants from the NICHDNeonatal Research Network. Pediatrics.2010;126(3):443–456
ARTICLE
PEDIATRICS Volume 132, Number 3, September 2013 e733 at IU Health Medical Library on September 16, 2013pediatrics.aappublications.orgDownloaded from

32. Furman L, Baley J, Borawski-Clark E, AucottS, Hack M. Hospitalization as a measure ofmorbidity among very low birth weightinfants with chronic lung disease. J Pediatr.1996;128(4):447–452
33. Gunville CF, Sontag MK, Stratton KA, RanadeDJ, Abman SH, Mourani PM. Scope andimpact of early and late preterm infantsadmitted to the PICU with respiratory ill-ness. J Pediatr. 2010;157(2):209–214
34. O’Brien JE, Dumas HM, Haley SM, et al.Clinical findings and resource use of infants
and toddlers dependent on oxygen andventilators. Clin Pediatr (Phila). 2002;41(3):155–162
35. Berry JG, Graham DA, Graham RJ, et al.Predictors of clinical outcomes and hospi-tal resource use of children after trache-otomy. Pediatrics. 2009;124(2):563–572
36. Kun SS, Edwards JD, Ward SL, Keens TG.Hospital readmissions for newly dis-charged pediatric home mechanical venti-lation patients. Pediatr Pulmonol. 2012;47(4):409–414
37. Jardine E, O’Toole M, Paton JY, Wallis C.Current status of long term ventilation ofchildren in the United Kingdom: question-naire survey. BMJ. 1999;318(7179):295–299
38. Cushman DG, Dumas HM, Haley SM, O’BrienJE, Kharasch VS. Re-admissions to inpatientpaediatric pulmonary rehabilitation.Pediatr Rehabil. 2002;5(3):133–139
39. Al-Samri M, Mitchell I, Drummond DS,Bjornson C. Tracheostomy in children:a population-based experience over 17years. Pediatr Pulmonol. 2010;45(5):487–493
e734 CRISTEA et al at IU Health Medical Library on September 16, 2013pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2012-2990; originally published online August 5, 2013; 2013;132;e727PediatricsVeda L. Ackerman
A. Ioana Cristea, Aaron E. Carroll, Stephanie D. Davis, Nancy L. Swigonski andVentilator Dependent at Home
Outcomes of Children With Severe Bronchopulmonary Dysplasia Who Were
ServicesUpdated Information &
tmlhttp://pediatrics.aappublications.org/content/132/3/e727.full.hincluding high resolution figures, can be found at:
References
tml#ref-list-1http://pediatrics.aappublications.org/content/132/3/e727.full.hat:This article cites 37 articles, 14 of which can be accessed free
Subspecialty Collections
gy_subhttp://pediatrics.aappublications.org/cgi/collection/pulmonoloPulmonology
_subhttp://pediatrics.aappublications.org/cgi/collection/home_careHome Carethe following collection(s):This article, along with others on similar topics, appears in
Permissions & Licensing
tmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2013 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at IU Health Medical Library on September 16, 2013pediatrics.aappublications.orgDownloaded from