polyarticular and familial chondrocalcinosis
TRANSCRIPT
arthritis and
rheumatism Official J o u r n a l of The American Rheumatism Association
Section of The Arthritis Foundation
Polyarticular and Familial Chondrocalcinosis
Antonio Reginato M., Fernando Valenzuela R., Virginia Martin& C., Gian Passano and Sergio Daza K.
From our series of 72 patients with articular chondrocalcinosis, 37 who presented polyarticular involvement are described. Twenty-eight patients, including 19 aggregated within different family groups, are natives of the Chilob island group. Members of 1 of the 6 families had unusually severe disease with deformities, and 1 had bony ankylosis of multiple joints. Pathologic findings in both the acute and the chronic stages of the joint disease are presented, particularly, some severe changes that have not been described previously.
The excellent reports of Zitnan et al (1-3) and of McCarty et al (4-6) have stim- ulated increasing interest in clinical syn- dromes associated with calcification of joint cartilage. In 1963, Zitnan published a de-
from the Department of Rheumatology, San Juan de Dios Hospital, University of Chile and National Health Service, Santiago, Chile.
ANTONIO RECINATO M., MD: Associate in Rheuma- tology, San Juan de Dios Hospital Providencia 1017, Department 21, Santiago, Chile. FERNANDO VALEN- ZUELA ,R., MD: Assistant Professor of Internal Medicine, University of Chile and Visiting Pro- fessor of Rheumatology, Catholic University of Chile. Chief of Department of Rheurnatology, San Juan de Dim Hospital, Santiago. VIRGINIA MARTIN~Z C., MD: Assistant Pathologist, Hospital San Juan de Dios Hospital, Santiago. GIAN PASSANO, MD: De- partment of Radiology, Regional Hospital, Punta Arenas. SERGIO DAZA K., MD: Assistant Professor of Radiology, University of Chile, Department of Radiology, San Juan de Dios Hospital, Santiago.
Requests for reprints should be addressed to Dr. Reginato 'M.
Submitted for publication Oct 19, 1969: accepted March 7, 1970.
tailed study of 27 patients with chondrocal- cinosis articularis, most of whom had mul- tiple joint involvement and were aggre- gated within specific families. Twenty-one patients were members of 5 families, and 22 were natives of one locality (2). In 1962, McCarty (5) described the "Pseudogout Syndrome" in patients with acute arthritis resembling gout and reported that fluid as- pirated from affected joints contained mi- crocrystals of calcium pyrophosphate dihy- drate (6). I t was readily apparent that the Pseudogout Syndrome was the same dis- ease as articular chondrocalcinosis. Subse- quently, many authors have described large numbers ot patients with calcification in a few joint cartilages, but rarely have they noted any aggregation within family groups (7-11). The few familial cases re- ported involved no more than 1 family (12-16).
Arthritis and Rheumatism, Vol. 13, No. 3 (May-lune 1970) 197
REGINATO ET AL
In 1957, 1,osatla et crl (17) reported the first case of polyal-ticular clioiitliocalcinosis from Chile under the name “generaliLed polyarticular calcinosis.” In 1964, while practicing in Punta Arenas, the southern- most city of the world, one of us found a high incidence of familial polyarticular chondrocalcinosis in patients born in the Chilok Islands. The same natal origin was also noted among patients with this condi- tion who were seen in our Santiago clinic during this period.
The purpose of this report is to summa- rize the study of 37 patients with polyarticu- lar chondrocalcinosis, 28 of whom are na- tives of the ChiloC Islands, including 19 pa- tients from 6 families. In l of these families, the disease was particularly severe, with un- usually extensive involvement of the sym- physis pubis in 4 family members, and bony ankylosis of multiple joints in 1 member. Ankylosis of the joints in chondrocalcinosis has not been noted previously.
MATERIALS AND METHODS Of the 72 patients with chondrocalcinosis whom
we have studied during the past 6 years, 35 had only knee involvement. A clinical description of these patients and many of the 37 with polyarticu- lar involvement has appeared elsewhere (18, 19) . T h e present report will emphasize the ethnic, geographical and familial grouping of these polyar- ticular patients. Diagnosis was based on typical calcifications in multiple articular cartilages in roentgenograms. Utilizing compensated polarized lighmt microscopy, confirmatory evidence was fur- nished when weakly positive mbirefringent crystals of calcium pyrophosphate dihydrate were identified in joint fluids from 16 patients, and in biopsied
. synovial membrane andjor cartilage from 6 (20) . Other laboratory studies included serial lupus
erythematosus (LE) preparations, serum latex fixation, serum calcium, phosphorus, alkaline phos- phatase, uric acid, fasting blood sugar and alka- linization of the urine with NaOH to detect the presence of homogentisic acid. Punch biopsy of the knee was performed with the Cope needle. Surgical biopsies were also obtained from the knee, hip and metatarsophalangeal (MTP) joint of the first toe.
Spccimens were furctl in absolute alcohol. Bone s~iccinicns were partially tlccalcifictl with 57% nitric acid and washed with water for 24 hr before staining. Unstained sections. or sections stained with Van Gieson’s, von Kossa’s, and the PAS atid silver staining technics, were examined by ordinary and compensated polarized light microscopy. .
RESULTS Of the 37 patients with polyarticular
chondrocalcinosis, 17 were men and 20 women. Ages ranged from 28 to 82 years (mean 53.5 years). Five patients never had
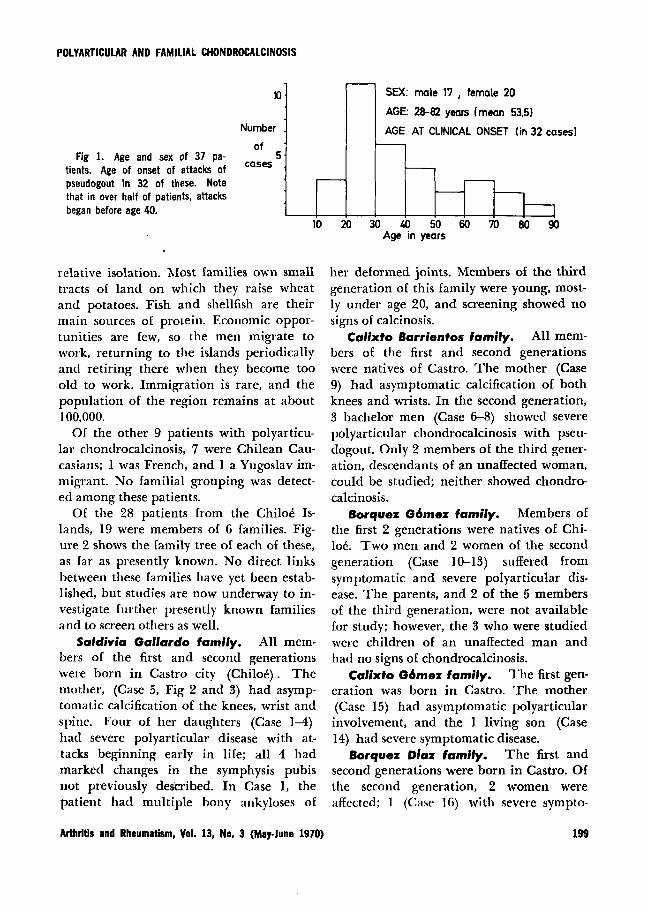
joint symptoms (Case 5, 9, 15, 17 and 36) ; four of these were discovered through fami- ly screening, while the other was associ- ated with secondary hyperparathyroidism. The age of onset of joint symptoms in the remaining 32 patients is charted on Fig 1, which shows that more than half of the pa- tients had become symptomatic before age 40. All of them had suffered multiple at- tacks of pseudogout in more than one joint, ranging from mild attacks in the knees alone to severe and chronic attacks with multiple joint crippling. Of the 15 symptomatic familial patients, 12 had severe polyarthritis with multiple deformi- ties. Of the 17 symptomatic patients not as- sociated with family groups, only 7 had severe polyarticular attacks, and only 1 of these showed marked residual joint defor- mities.
Geographic, Ethnic and Familial Distribution
Twenty-eight of the patients were natives of the Chilo6 Islands, an archipelago lo- cated in the southern part of Chile where a region of islands and fjords begins. Here both summers and winters are cold and hu- mid. The land is largely forested with broad-leaf evergreens. Spaniards settled the area early in the sixteenth century and in- termingled with the natives, giving rise to the “Chilote” race which has persisted in
198 Arthritis and Rheumatism, Vol. 13, No. 3 (MayJune 1970)
POLYARTICULAR AND FAMILIAL CHONDROCALCINOSIS
10 .
Number .
of . Fig 1. Age and sex of 37 Pa- cases 5 . tients. Age of onset of attacks of
pseudogout in 32 of these. Note that in over half of patients, attacks began before age 40.
- SEX: male 17 , female 20
AGE: 28-82 years (mean 53.5)
AGE AT CLINICAL ONSET (in 32 cases) 1
- - - -
relative isolation. Most families own small tracts of land on which they raise wheat and potatoes. Fish and shellfish are their main sources of protein. Economic oppor- tunities are few, so the men migrate to work, returning to the islands periodically and retiring there when they become too old to work. Immigration is rare, and the population of the region remains at about 100,000.
Of the other 9 patients with polyarticu- lar chondrocalcinosis, 7 were Chilean Cau- casians; l was French, and l a Yugoslav im- migrant. No familial grouping was detect- ed among these patients.
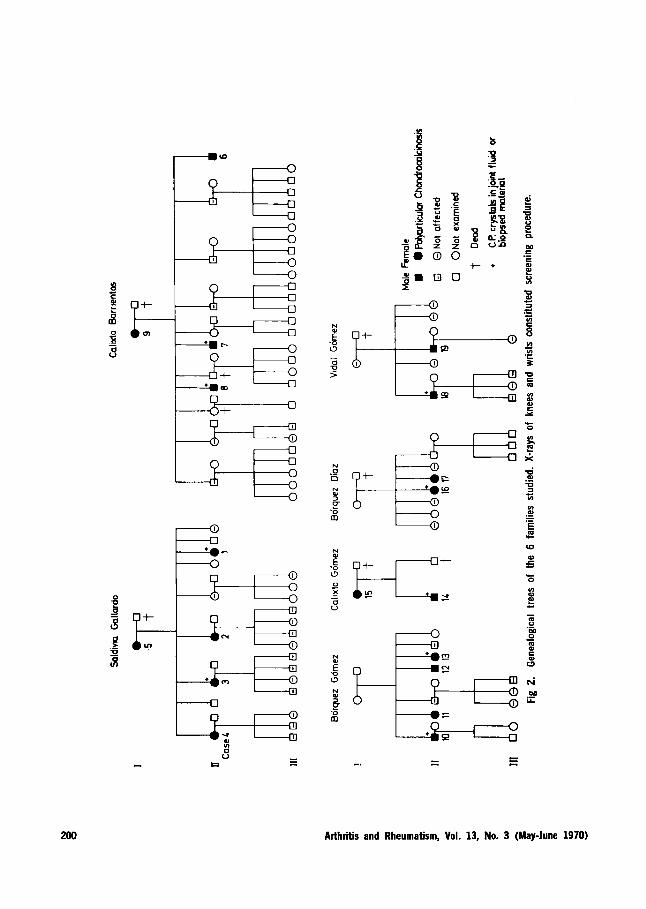
Of the 28 patients from the ChiloC IS- lands, 19 were members of 6 families. Fig- ure 2 shows the family tree of each of these, as far as presently known. No direct links between these families have yet been estab- lished, but studies are now underway to in- vestigate further presently known families and to screen others as well.
Saldivia Gallardo family. All mem- bers of the first and second generations were born in Castro city (ChiloC). The mother, (Case 5 , Fig 2 and 3) had asymp- tomatic calcification of the knees, wrist and spine. Four of her daughters (Case 14) had severe polyarticular disease with at- tacks beginning early in life; all 4 had marked changes in the symphysis pubis not previously described. In Case 1, the patient had multiple bony ankyloses of
her deformed joints. Members of the third generation of this family were young, most- ly under age 20, and screening showed no signs of calcinosis.
Calixto Barrientos family. All mem- bers of the first and second generations were natives of Castro. The mother (Case 9) had asymptomatic calcification of both knees and wrists. In the second generation, 3 bachelor men (Case 6-8) showed severe polyarticular chondrocalcinosis with pseu- dogout. Only 2 members of the third gener- ation, descendants of an unaffected woman, could be studied; neither showed chondro- calcinosis.
Borquez G6mez family. Members of the first 2 generations were natives of Chi- 106. T w o men and 2 women of the second generation (Case 10-13) suffered from symptomatic and severe polyarticular dis- ease. The parents, and 2 of the 5 members of the third generation, were not available for study; however, the 3 who were studied were children of an unaffected man and had no signs of chondrocalcinosis.
The first gen- eration was born in Castro. The mother (Case 15) had asymptomatic polyarticular involvement, and the 1 living son (Case 14) had severe symptomatic disease.
The first and second generations were born in Castro. Of the second generation, 2 women were affected; 1 (Case 16) with severe sympto-
Calixto G6mez family.
Borquez Diaz family.
Arthritis and Rheumatism, Vol. 13, No. 3 (May-lune 1970) 199
W
200 Arthritis and Rheumatism, Vol. 13, No. 3 (May-June 1970)
POLYARTICUIAR AND FAMILIAL CHONDROCALCINOSIS
FAMILY
CASE N'
SEX
b 4
c I7
H
x 34
I1
!E
!L
!L
!1
8
8
7
6
6
>
_ _ ~ ~~~
Saldivia Calixb Mdd W E CASES Gallordo 1 Borrientos I %%
I 2 3 4 5 6 7 8 9 10 11 12 13 I 4 15 16 17 18 19 M 21 22 23 2L 25 26 27 28 29 30 31 32 33 34 35 3kd F F F F F M M M F M F M F H F F F M Y M U F F F F F F M F M F M M M F M M F F
ORIGIN CHILOE ISLANDS I OTHER
~ G E at onset 16 21 30 10 25 36 22 3 29 33 2L 26 31 23 23 25 26 28 L9 57 69 3 L7 I 5 82 19 72 56 67 L7 61 n at study 52 L6 39 36 80 L l U 33 TI LO 38 L1 36 41 72 6L 66 32 28 54 28 30 54 67 75 65 L8 50 02 58 72 64 67 50 66 66 74
Kneecctrtllage I@ 0.0 0 0 0 0 0 0 0000 00 0 0 0 0 0.0 0 0.0 00 0 0 0 0.0 0 0 Wrist
Spphysis Pubis
Hip
Spine
matic polyarticular disease, and the other (Case 17) with asymptomatic polyarticular chondrocalcinosis.
Vidal G6mez family. The maternal grandfather was born in Chilok. Two men of the second generation had severe and symptomatic polyarticular disease. Their children, all under age 10, were unaffected.
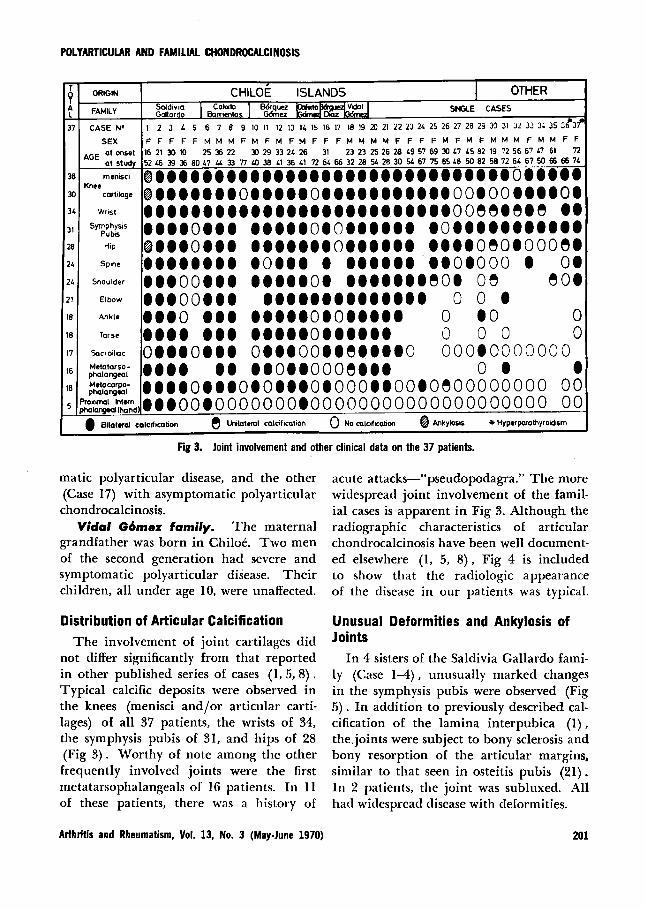
Distribution of Articular Calcification The involvement of joint cartilages did
not differ significantly from that reported in other published series of cases (1, 5, 8). Typical calcific deposits were observed in the knees (menisci and/or articular carti- lages) of all 37 patients, the wrists of 34, the symphysis pubis of 31, and hips of 28 (Fig 3) . Worthy of note among the other frequently involved joints were the first metatarsophalangeals of 16 patients. In 11 of these patients, there was a history of
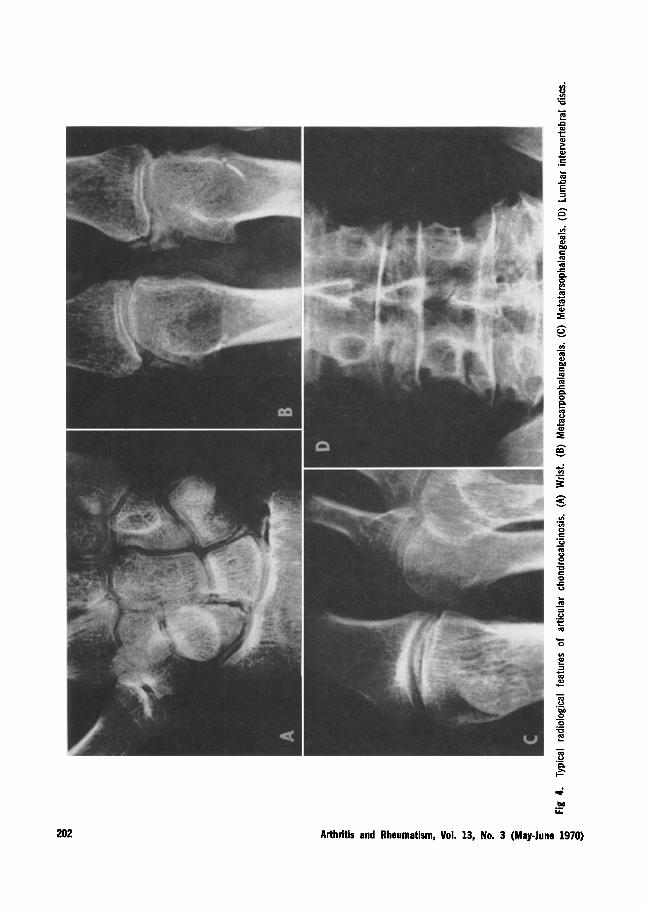
acute attacks-"pseudopodagra." The more widespread joint involvement of the famil- ial cases is apparent in Fig 3. Although the radiographic characteristics of articular chondrocalcinosis have been well document- ed elsewhere (1, 5, 8), Fig 4 is included to show that the radiologic appearance of the disease in our patients was typical.
Unusual Deformities and Ankylosis of Joints
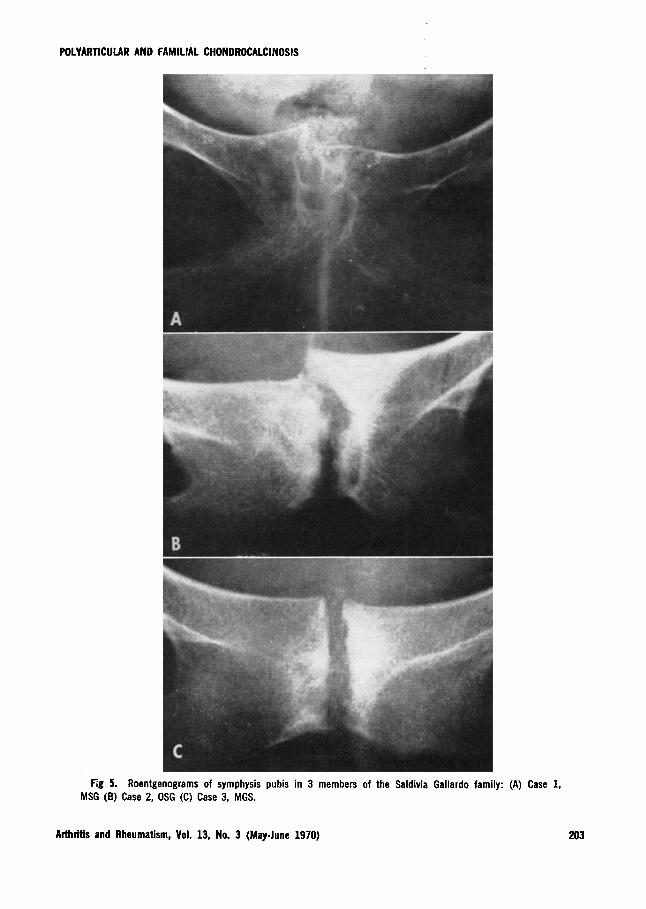
In 4 sisters of the Saldivia Gallardo fami- l y (Case 1 4 ) , unusually marked changes in the symphysis pubis were observed (Fig 5). I n addition to previously described cal- cification of the lamina interpubica (1), the,joints were subject to bony sclerosis and bony resorption of the articular margins, similar to that seen in osteitis pubis (21). In 2 patients, the joint was subluxed. All had widespread disease with deformities.
Arthritis and Rheumatism, Vol. 13, No. 3 (May-lune 1970) 201
202
vi - m c m m c 0
m GI
0 - n e 3 f
vi .- In 0 e GI
m GI
U e 0 c GI
.- - 2
c 0
In E a c m a c
Arthritis and Rheumatism, Vol. 13, No. 3 (May-lune 1970)
POLYARTICULAR AND FAMILIAL CHONDROCALCINOSIS
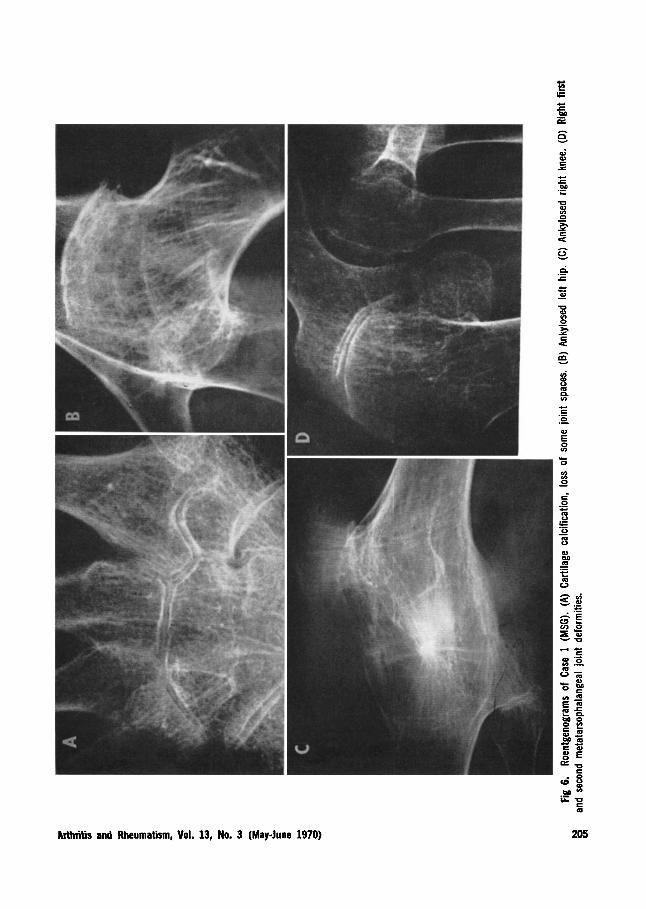
Fig 5. Roentgenograms of symphysis pubis in 3 members of the Saldivia Gallardo family: (A) Case 1, MSG (6) Case 2, OSG (C) Case 3, MGS.
Arthritis and Rheumatism, Vol. 13, No. 3 (May-lune 1970) 203
REGINATO ET AL
I n 1 of these patients (Case 1), the dis- ease led to bony ankylosis of the hips, knees and midtarsal joints. This patient is de- scribed in some detail because of the unique severity of the process. Case 1, MSG, was a 52-year-old woman. Since 1932, a t age 16, she had suffered acute episodes of severe pain with swelling and redness of ankles, knees, elbows and wrists. These at- tacks lasted 2-3 weeks and recurred 3 or 4 times yearly, while mild aching and marked stiffness persisted in the involved joints between acute attacks. At age 31, she was first admitted to a local hospital in Chi- lo6 because of an especially severe attack of polyartliritis involving the hips and first metatarsophalangeal joints. Treatment with phenylbutazone gave only partial re- lief. She was confined to bed for 2 years. She continued to have multiple acute ep- isodes of arthritis in 1 or more joints, with gradually increasing rigidity of the cervical spine, shoulders, elbows, hips and knees. Complete rigidity of both of her hips and knees kept her bedridden since age 44, but she had continuing arthralgias and arthritis of moderate severity in her shoul- ders, elbows, wrists and ankles.
Examination on admission to San Juan de Dios Hospital in 1968 showed an obese middle-aged woman in a fixed recumbent position caused by ankylosis of hips and knees in extension. Her heart, chest and abdomen were normal. No tophi or subcu- taneous nodules were found. Severe muscle atrophy was noted about the shoulders, hips and knees. Neck motion was markedly limited. The right hand had slight ulnar deviation at the metacarpophalangeal (MP) joints; both hands had atrophied interos- seous muscles, and bony enlargement of the proximal IP finger joints, but no re- striction of finger motion. The elbows were contracted in llOo flexion, and the wrists, knees, shoulders, hips and tarsal joints had
complete clinical ankylosis. The ankles had bony enlargement and markedly restricted motion. Multiple MTP joint subluxations and hallux valgus were present on the right foot; hammer toes were found on the left.
Laboratory findings included a leukocy- tosis of 13,6OO/cu mm, normal differential count; Westergren erythrocyte sedimenta- tion rates were 50 and 60 mm/hr. Serum protein electrophoresis showed total pro- tein of 7.7 g/100 ml: albumin 41.60/,, a-1 globulin 3.2%, a-2 globulin 9.6%, p globu- lin 16% and y globulin 29.6%. The pres- ence of homogentisic acid could not be demonstrated in the urine. Serum calcium, phosphorus and alkaline phosphatase were normal. Both the serum latex fixation test and the LE preparations were negative.
Roentgenograms of the joints showed severe and widespread abnormalities. In the shoulders and elbows, marked nar- rowing of joint spaces with lines of calcifi- cation in the remaining cartilages was ob- served. Diffuse osteoporosis and narrowed joint spaces, but no erosions, were seen in the finger and wrist joints (Fig 6A), again with lines of calcification in the cartilages. I n the lumbar intervertebral discs, marked calcification was present (Fig 4D) . Changes in the symphysis pubis were described ear- lier (Fig 5A). Bony ankylosis was observed in both hips (Fig 6B), and marked osteo- porosis with bony ankylosis of tibiofemoral and patellofemoral joints was present in both knees (Fig SC) . Changes in ankle and foot joints were similar to those found in the wrists, but several of the intertarsal joints were ankylosed. A biopsy, taken from the right hip during an angular osteotomy resection, showed an irregular band of par- tially calcified cartilage without articular space. Many weakly positive birefringent crystals could be seen in the periphery of the calcareous deposits (Fig 7) , which were
204 Arthritis and Rheumatism, Vol. 13, No. 3 (May-lune 1970)
F ;c
M E a
e .- h
ai
I
a3 E x
Do .- L.
c. c 0
aa
.- .- 5 In
0
In In 0
c
-
Arthritis and Rheumatism, Vol. 13, No. 3 (MayJune 1970)

REGINATO R M
close to fibrous bone replacing lamellar bone.
Synovial Fluid Findings Synovial fluid was obtained from the
knees of 17 patients, and from the MTP
joint of the great toe in 1. Synovianalysis showed characteristic features of noninflam- matory fluids in 6 chronically effused knees, and of inflammatory fluid in the remainder. Leukocyte counts ranged from 1600 to 42,- OOO/cu mm, roughly in proportion to the
Fig 7. Surgical biopsy' of ankylosed hip, Case 1 (MSG). (top) Acetabular bone (B) above, remaining fibrous cartilage (C), containing multiple calcific deposits (D), and femoral bone (Bl) below. Note absence of joint space. Van Gieson's stain x 10. (bottom) Similar area (acetabulum above, femur below) showing bleck staining of calcific deposits. von Kossa's stain x40.
206 MhWs and Rheumatism, Vol. 13, No. 3 (May-June 1970)

POLYARTICULAR AND FAMILIAL CHONDROCALCINOSIS
acuteness of inflammation noted clinically in the joint. Using compeiisated polarized light microscopy, rhomboid and rod-shaped crystals with weakly positive Iirefringencc were seen in all these fluids. In the acutely inflamed joints, the crystals were found mainly within leukocytes; in fluids from more chronically effused joints the crystals were extracellular.
I n one 72-year-old man (Case 31) seen during his first attack, which involved his right knee and left great toe (pseudopoda- gra) , 2 types of crystals were found in the fluids obtained from both acute joints. Short, rod-like crystals with strongly posi- tive birefringence, and other rod-like crys- tals with strongly negative birefringence were seen. Repeated serum uric acid deter- minations ranged between 4 and 5 mgYb. X-ray photographs of the knee showed thin lines of calcification in the menisci; those of the “bunion joint” showed calcification in the region of the joint capsule. Asympto- matic calcification was noted in x-rays of the symphysis pubis, wrists and elbows.
Histopathologic Studies Needle biopsies of the synovial mem-
brane of the knee were performed during an acute attack in 3 patients (Casc 5, 31, 32). Surgical biopsies of synovial mem- brane and articular cartilage were taken during the chronic stage from the knees of 3 patients (Case 7, 13, 18). A surgical bi- opsy of the hip and of the first MTP joint was done in 1 patient (Case 1).
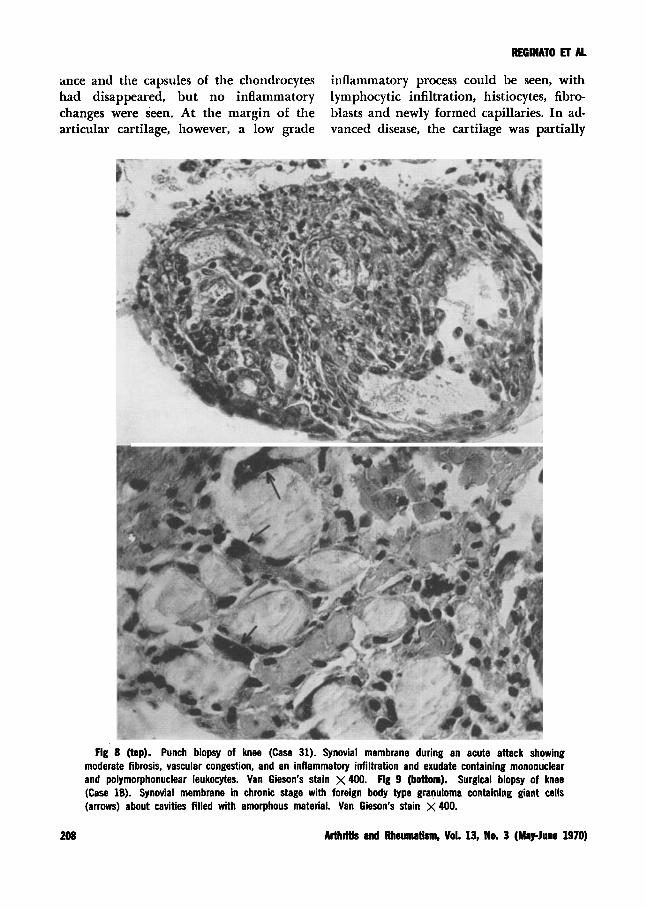
Synovial membrane in an acute at- tack. Findings in all 3 specimens were similar. Proliferation of the lining cells of the synovial membrane, vascular congestion, fibrosis and inflammatory infiltration as well as the presence of polymorphonuclear leukocytes, lymphocytes and other mon- onuclear cells were noted. A fibrinous ex- udate covering the synovial memhrane con-
tained a1)uiitlant synovial cells, polynior- phonuclear and mononuclear leukocytes. Polymorphonuclear leukocytes predomi- nated, both i n the synovial infiltrate and the overlying exudate (Fig 8) . Unstained sections (which had been fixed in absolute alcohol) were examined under compen- sated polarized light. These sections were found to contain rod-like and rhomboidal crystals, having a weakly positive bire- fringence, imbedded both in the synovial membrane and the exudate. Such crystals were located in the interstitium of the con- nective tissue, in the cytoplasm of the poly- morphonuclear leukocytes and also in the fibrin network.
Synovial membrane in the chronic stage. After the patient had had repeated attacks and had developed persistent joint symptoms, the process was regarded as chronic. Specimens from such joints showed increased fibrosis, continued infiltration of mononuclear cells and a foreign body type of granuloma with giant cells surrounding spaces filled with a material that appeared amorphous with van Gieson’s stain (Fig 9) . This material was also found in the cyto- plasm of the giant cells, staining deeply and showing a finely granular and fibrillar structure by the von Kossa method.
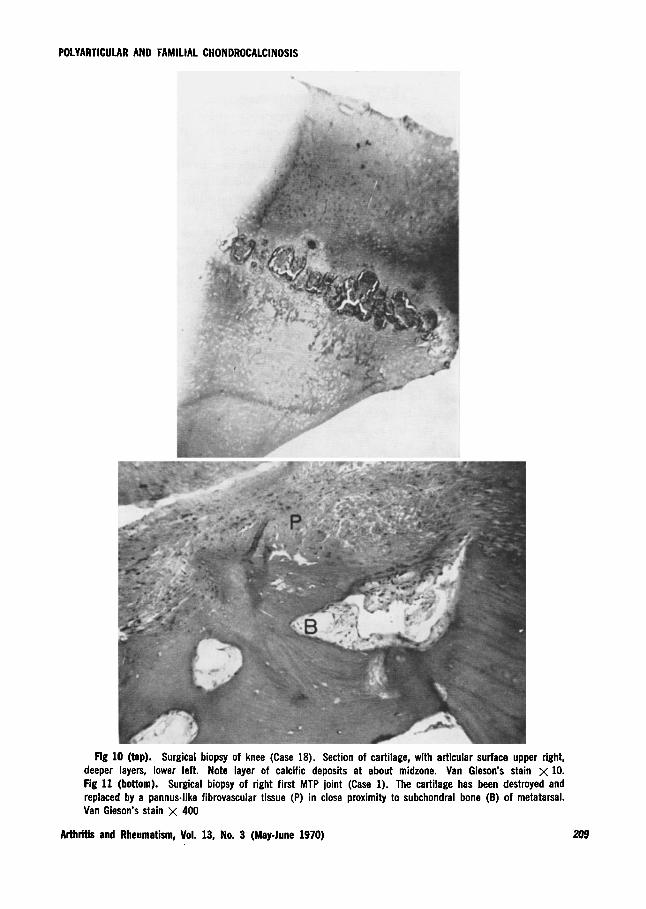
Cartilage in the chronic stage. Mac- roscopically, the cartilage appeared to be imbedded with minute chalky beads, and in some areas, larger deposits formed plaques. These areas contained crystals of calcium pyrophosphate when seen under compensated polarized light. Such deposits were most numerous in areas of greatest friction or in the center of cartilages or fibrocartilages. In less damaged joints, the crystalline deposits were found within the midzone of cartilage in a layer parallel to the surface (Fig 10). In cartilage adjacent to crystalline deposits, degeneration was evident: the matrix had a fibrillar appear-
Arthritis and Rheumatism, Vol. 13, No. 3 (May-lune 1970) 207
ance and the capsules of the chondrocytes inflammatory process could be seen, with had disappeared, but no inflammatory lymphocytic infiltration, histiocytes, fibro- changes were seen. At the margin of the blasts and newly formed capillaries. In ad- articular cartilage, however, a low grade vanced disease, the cartilage was partially
Fig 8 (top). Punch biopsy of knee (Case 31). Synovial membrane during an acute attack showing moderate fibrosis, vascular congestion, and an inflammatory infiltration and exudate containing mononuclear and polyrnorphonuclear leukocytes. Van Gieson’s stain X 400. Fig 9 (bottom). Surgical biopsy of knee (Case 18). Synovial membrane in chronic stage with foreign body type granuloma containing giant cells (arrows) about cavities filled with amorphous material. Van Gieson’s stain x 400.
208 Arthritis and Rheumatism, Vol. 13, No. 3 (May-June 1970)
POLYARTICULAR AND FAMILIAL CHONDROCALCINOSIS
Fig 10 (top). Surgical biopsy of knee (Case 18). Section of cartilage, with articular surface upper right, deeper layers, lower left. Note layer of calcific deposits at about midzone. Van Gieson's stain x 10. Fig 11 (bottom). Surgical biopsy of right first MTP joint (Case 1). The cartilage has been destroyed and replaced by a pannus-like fibrovascular tissue (P) in close proximity to subchondral bone (B) of metatarsal. Van Gieson's stain x 400
Arthritis and Rheumatism, Vol. 13, No. 3 (MayJune 1970)
REGINATO ET A 1
or even totally destroyed, being replaced by granulation tissue containing giant cells about the deposits of calcium pyrophos- phate crystals. The ankylosed hip of one of the patients (Case 1) (Fig 7A) is unique because the acetabulum and femoral head were welded together by a fibrocartilag- inous tissue encrusted with deposits of cal- cium pyrophosphate crystals. Such deposits stained black with von Kossa’s stain (Fig 7B).
Subchondraf bone in the chronic stage. Trabeculae were sparse in the subchondral bone. I n some areas, the fibrovascular tis- sue which had replaced the cartilage was close to the lamellar bone (Fig 7A and 11) , perhaps, encroaching on it.
Biochemical Studies Serum calcium, phosphorus and alkaline
phosphatase levels were within norpal lim- its, except in those instances where abnor- mal values (Case 36 and 37) and the subse- quent search for parathyroid adenomas (Case 37) confirmed hyperparathyroidism. Serum uric acid, fasting blood sugar and tests for homogentisic acid in urine were all normal or negative, as were lupus erythematosus cell preparations. The serum latex fixation test was negative in 10 patients, and posi- tive at only 1:20 in 5.
DISCUSSION
Calcific deposits in articular cartilage have been described in conjunction with: various joint disorders including gout (22, 23) , rheumatoid arthritis (23), osteoar- thritis (24) and joint trauma (25); meta- bolic diseases such as primary hyperparathy- roidism (26), ochronosis (27) or hemo- chromatosis (28) ; vitamin D intoxication (29) ; and senescence (24). Whether such calcific deposits are part of the primary disorder in these conditions, has not been
definitely established. In our patients, at least in most cases, it would seem that the calcifications could be primary, affecting a few joints in elderly patients and multiple joints in the younger patients, particularly. the familial cases. In the latter patients, the condition would appear to be an heredi- tary disorder, possibly, the result of a meta- bolic defect (2) .
The clinical features of our total series of patients have been reported in detail else- where (18, 19). In many ways, these fea- tures are similar to those found in the extensive reports of others already cited. However, in our patients the incidence of chondrocalcinosis of the first MTP joint and “pseudopodagra” is higher, and the severity of joint involvement, even to the point of ankylosis, is more marked. Case 1, patient MSG, with multiple joint anky- loses, represents the most severe form of the disease yet described. I n this case, we feel that the disease is primary chondrocalcino- sis for the following reasons: (1) the typical history of recurrent attacks of pseudogout of increasing severity beginning at age 16; (2) the characteristic calcifications ob- served in the roentgenograms of the nonankylosed joints, with narrowing of the joint space‘and a lack of bony erosions (Fig 6A) ; (3) the discovery of a band of fibrocar- tilage encrusted with nests of calcium pyro- phosphate crystals forming a bridge be- tween femoral head and acetabular bone in the ankylosed hip (Fig 7) ; (4) the biopsy €rom the first toe joint which showed a fibrovascular tissue lacking some features of the pannus of rheumatoid arthritis (Fig 11) , but replacing the cartilage and a p pearing to invade the subchondral bone; (5) the absence of biochemical abnormali- ties, the negative test for rheumatoid factor and negative lupus erythematosa cell prepa- rations which tend to rule out other joint diseases; (6) the incidence of chondro-
210 Arthritis and Rheumatism, Vol. 13, No. 3 (MapJune 1970)
POLYARTICULAR AND FAMILIAL CHONDROCALCINOSIS
calcinosis in the family, including the mother’s asymptomatic polyarticular in- volvement and the 3 sisters’ severe, sympto- matic and diffuse chondrocalcinosis. In 1 of the patient’s sisters, crystals of typical a p pearance were found in synovial mem- brane and synovial fluid obtained by biopsy during an acute attack; none of the sisters showed signs of even seronegative rheuma- toid arthritis.
The marked changes in the symphysis pubis in these 4 sisters, which resembled that of osteitis pubis in roentgenographic appearance, have not been described else- where in patients with chrondrocalcinosis. These changes occurred in the absence of any history or detection of bladder infec- tion or surgery.
Pathologic data from biopsies of the joints of our patients, which range from the early acute stage to the late chronic stages, may help to explain how the acute synovitis of pseudogout could lead to severe joint destruction and even ankylosis. Ly- sosomal proteases, or other products re- leased from leukocytes during the repeated episodes of inflammation, could readily damage cartilage (30). The deposit of calci- um pyrophosphate crystals in the midzone of cartilage would certainly alter its resilience to stress, if not its viability, pre- disposing its superficial layers in areas sub- ject to friction to degeneration and frag- mentation. At the margins of the cartilage, we have noted granulomatous inflamma- tion resembling somewhat the pannus of rheumatoid arthritis, but with foreign body giant cells about the deposits of calcium py- rophosphate in the synovium. Similar changes, rarely including bony ankylosis, have also been described in gout (31, 32) .
Our patients with polyarticular chondro- calcinosis closely resemble those w h o Zit- nan (1) describes under the name, “chon- drocalcinosis articularis familialis.” Our
family studies, like those of others (2, 12), do not yet allow us to form conclusions about the mechanism of genetic transmis- sion of this disease. Because the relatives of our patients are scattered over southern Ar- gentina and Chile, we have been unable to obtain a more complete study of the oldest generations. Furthermore, there is still no more sensitive indicator of the disease than x-ray studies of joints to assist in perform- ing family surveys. Since all members of the third generation in our groups were under 20 years of age, they were too young to show positive x-ray changes. If a more sensitive indicator, such as a missing or ab- normal enzyme, could be found, family screening would be greatly facilitated.
Early studies of pyrophosphate phos- phohydrolase activity in the synovial fluid of such patients as well as urinary excre- tion of pyrophosphate are of great interest (33,34), particularly, since depressed activ- ity of the enzyme has been demonstrated in a number of chondrocalcinosis patients (34). Although this finding suggests an en- zymatic inborn error of metabolism, more data are needed.
We are continuing our population studies of chondrocalcinosis in the CliiloP Islands in an effort to determine the real incidence of the disease there, and to com- plete the family trees of our patients. The possible influence of the genetic factors of populations-consanguinity, migration fe- cundity-and racial and environmental fac- tors is being studied. Genetic markers- blood groups and coloring-and their cor- relation with chondrocalcinosis are also being investigated.
ACKNOWLEDGMENTS
The authors are indebted to Dr. A. Reid and Dr. Joseph Lee Hollander for their helpful assistance in the preparation of this manuscript.
Arthritis and Rheumatism, Vol. 13, No. 3 (May-lune 1970) 211
REGINATO I3 AL
They are also grateful to Dr. Padding Phelps and Dr. Daniel J. McCarty for their suggestions.
13. Aschoff H, Bom P, Schoen E, et al: Heredi- tate Chondrocalcinosis Articularis: Unter-
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
1 I .
12.
REFERENCES
Zitnan D, Sitaj S: Chondrocalcinosis articu- laris. I. Clinical and radiological study. Ann Rheum Dis 22: 142-151, 1963 Valsik J, Zitnan D, Sitaj S: Chondrocal- cinosis articularis. 11. Genetic study. Ann Rheum Dis 22:153-157, 1963 Zitnan D, Sitaj S, Huttl S, et al: 111. Physio- pathological study. Ann Rheum Dis 22:
McCarty DJ, Hollander JL: Identifications of urate crystals in gouty synovial fluid. A n n Intern Ned 54:452-460, 1961 McCarty DJ, Kohn NN, Faires JS: Signifi- cance of calcium phosphate crystals in synovial fluid of arthritis patientx pseudo- gout syndrome. I. Clinical aspects. Ann Intern hled 56:711-737, 1962 McCarty DJ, Gatter RA: Pseudogout syn-
drome (articular chondrocalcinosis). Bull Rheum Dis 14:322, 1964 McCarty DJ: Pseudogout, Arthritis and Al- lied Conditions. Edited by JL Hollander. Philadelphia, Lea & Febiger, 1966, p 947- 964 Moskowitz R, Katz D: Chondrocalcinosis and chondrocalciosynovitis (pseudogout syn- drome). Amer J h k d 43:322, 1967 Currey HLF, Key JJ, Mason RM, et al: Significance of radiological calcification of joint cartilage. Ann Rheum Dis 26:295, 1966 Solnica J, Hubault A, Kahn, MF: Les chon- drocalcinoses articulaires. Etude clinique, biologique, eristalographique et Ctiologique. A propos de 36 observations personnelles. Rev Rhum 33:93, 1966 Serre H, Simon L, Sany J: A propos de la chondrocalcinose articulaire difusse. Les circonstances etiologiques d’apres trente cas personellment observes. Rev Rhum 32:425, 1965 Moskowitz R, Katz D: Chondrocalcinosis (pseudogout syndrome). A family study. JAMA 188:867, 1964
158-1 70, 1963
suchung einer Familie. Humangenetik 3: 98, 1966
14. S i s J, Guiika V, Srubar Y: DBlsi pozorovini nhkolika ptipado polyartikularni rodidinne chondrokalciriosy. Vnitrni Lkk 12:74, 1966
15. Louyot P, Barthelme P, Peterschmitt J, et al: Chondro-calcinose articulaire diffuse ii caractere familial. J Radio1 Electr 46:64, 1965
16. Van der Korst JK: Familial joint chondro- calcinosis (Pseudogout syndrome) . Folia Med Neerl 9:48, 1966
17. Losada M, Cox FL, Rodriguez JV, et al: Generalized articular calcinosis. Report of a case. Ann Rheum Dis 16:454-455, 1957
18. Valenzuela F, Reginato A, Ponce H, et al: Las mlltiples facetas clinicas de la condro- calcinosis. IV Congress0 Panamericano de Reumatologia. Ciudad de Mexico. Excerpta Med 143:112, 1967
19. Reginato A, Valenzuela F, Martinez V, et al: Chondrocalcinosis articularis. Rev Med Chile 97:421, 1969
20. Phelps P, Steele AD, McCarty DJ: Com- pensated polarized light microscopy: identi- fication of crystals in synovial fluids from gout and pseudogout. JAMA 203:508, 1968
21. Valenzuela F, Contreras V, Lackington C: Osteitis pubis not following urological op- erations. Arch Interam Rheumatol 6274, 1963
22. Dodds NJ, Steimbach HL: Gout associated with calcification of cartilage. New Eng J Med 275~745, 1966
13. Good AE, Rapp R: Chondrocalcinosis of the knee with gout and rheumatoid ar- thritis. New Erig J Med 277:286, 1967
24. Bocher J, Mankin HL, Berk RN, et al: Prevalence of calcified meniscal cartilage in elderly persons. New Eng J Med 272:1093, 1965
2.5. Weaver JB: Calcification and ossification of menisci. J Hone Joint Surg 24A:873, 1942
26. Bywaters E, Dixon A, Scott J: Joint lesions of hyperparathyroidism. Ann Rheum Dis 22:171, 1963
27. O’Brien WM, La Du NB, Bunim JJ: Bio-
212 Arthritis and Rheumatism, Vol. 13, No. 3 (May-lune 1970)

POLYARTICULAR AND FAMILIAL CHONDROCALCINOSIS
chemical, pathologic and clinical aspects of alcaptonuria, ochronosis and ochronotic arthropathy. Review of world literature (1584-1962). Amer J Med 34:813, 1963
28. Schumacher HR: Arthritis with synovial iron deposition in a patient with hemo- chromatosis. Arthritis Rheum 7:41, 1964
29. Swoboda W: Die Rontgensymptomatik der Vitamin htoxikation in Kindesalter. Forstchr Roentgenstr 77:534, 1952
30. Moses J'M, Ebert RH, Graham RC: Patho- genesis of inflammation. 1. The production of an inflammatory substance from rabbit granulocytes in vitro and its relationships to leucocyte pyrogen. J Exp Med 120:57,
Arthritis and Rheumatism, Vol. 13, No. 3 (May-June 1970)
1964 31. Ludwig AO, Bennett GA, Bauer W: A rare
manifestation of gout: widespread ankylosis simulating rheumatoid arthritis. Ann Intern Med 11 : 1248, 1938
32. Graham RH, Barnes CG, Mason Khf: Bony ankylosis in gout. Ann Rheum Dis 27:67, 1968
33. Good AE, Starkweather WH: Synovial fluid pyrophosphohydrolase (PPPH) in pseudo- gout, gout and rheumatoid arthritis. Ar- thritis Rheum 12:298, 1969
34. Pflug M. McCarty DJ, Kawahara F: Basal urinary pyrosphosphate excretion in pseu- dogout. Arthritis Rheum 12:228, 1969
213