platelet associated igg may be related with thrombocytopenia in patients with myelodysplastic...
TRANSCRIPT

Pm
SLa
b
c
a
ARRAA
KMTPPG
1
ealtpoiemSdsoac
a
CC
0d
Leukemia Research 36 (2012) 554– 559
Contents lists available at SciVerse ScienceDirect
Leukemia Research
jou rna l h omepa g e: www.elsev ier .com/ locate / leukres
latelet associated IgG may be related with thrombocytopenia in patients withyelodysplastic syndromes
imone Cristina Olenscki Gilli a,b,∗, Samuel de Souza Medinaa,b, Vagner de Castroa,b,uís Gustavo Romani Fernandesa,b, Sara Teresinha Olalla Saada,b,c
Hematology and Hemotherapy Center, University of Campinas, Campinas, BrazilInstituto Nacional de Ciência e Tecnologia do Sangue, Campinas, BrazilDepartment of Clinical Medicine, University of Campinas, Campinas, Brazil
r t i c l e i n f o
rticle history:eceived 8 August 2011eceived in revised form 4 October 2011ccepted 7 October 2011vailable online 29 November 2011
a b s t r a c t
Thrombocytopenia is common in patients with myelodysplastic syndromes (MDS) and immunedestruction of platelets could be an important factor for its occurrence. We prospectively analyzedplatelet-associated IgG (PAIgG) through platelet immunofluorescence test (PIFT), mean platelet vol-ume (MPV), platelet size deviation width (PDW) and glycocalicin index (GCI) of 54 patients withMDS, classified according to the International Prognostic Scoring System (IPSS). Thrombocytopenia
eywords:yelodysplastic syndrome
hrombocytopeniaIFTlatelet indices
(platelet count < 100 × 109/L) was correlated with a higher amount of PAIgG, significantly higher MPVand increased GCI. In addition, worse prognosis IPSS groups were associated with a higher positivity ofPIFT, which could be indicative of advanced disease.
© 2011 Elsevier Ltd. All rights reserved.
lycocalicin index
. Introduction
Myelodysplastic syndromes (MDSs) are a group of hematopoi-tic stem cell disorders characterized by ineffective hematopoeisisnd an increased risk of transformation into acute myelogenouseukemia (AML) [1]. Thrombocytopenia is identifiable in up towo thirds of patients with MDS and severe thrombocytopenia isresent in approximately 10%. The cause of the altered megakary-cytopoiesis in MDS has not yet been elucidated, however studiesndicate that an increased apoptosis of early progenitors, inhibitoryffects of cytokines [2–6], bone marrow fibrosis [7] and immune-ediated mechanisms [5,8,9] might contribute to this process.
everal clinical and immunological studies suggest a significanteregulation of the immune system in the complex pathogene-is of MDS. This deregulation may even promote the progressionf early MDS towards advanced MDS. Although immunologicalbnormalities are frequent in MDS patients, the specific and clinical
onsequences of these phenomena remain unclear.Immune thrombocytopenia (ITP) is an autoimmune diseaseffecting adults and children, in which most patients have
∗ Corresponding author at: Hematology and Hemotherapy Center, University ofampinas. Address: Rua Carlos Chagas, 480. Cidade Universitária “Zeferino Vaz”,ampinas-SP, CEP 13083-970 Brazil. Tel.: +55 19 35218734; fax: +55 19 32891089.
E-mail address: [email protected] (S.C.O. Gilli).
145-2126/$ – see front matter © 2011 Elsevier Ltd. All rights reserved.oi:10.1016/j.leukres.2011.10.003
autoantibodies that accelerate platelet destruction and may alsoimpair megakaryocyte platelet production. Platelet autoantibod-ies may be sensitively determined directly on the platelet surfacein patients with autoimmune-mediated thrombocytopenia [10].The assays for the detection of glycoprotein-specific antibodiessuch as monoclonal antibody-specific immobilization of plateletantigens (MAIPA) are highly specific but less sensitive [11], theyare laborious and require a higher amount of platelets than otherassays for the detection of platelet-associated IgG, such as plateletimmunofluorescence test (PIFT). Platelet immunofluorescence test[12] has been widely used for detection of platelet associated IgG(PAIgG) on the platelet surface (direct PIFT).
Additionally, it has been demonstrated that some morphologicalplatelet indices correlate with the occurrence of immune thrombo-cytopenia and could be of value in discriminating hyperdestructivefrom hypoproductive thrombocytopenia, however little attentionhas been paid to platelet size in one same measurement. Mea-sures of platelet size, such as mean platelet volume (MPV) [13,14],platelet size deviation width (PDW) and platelet large cell ratio (P-LCR) [15] have been known to aid in the differential diagnosis ofthrombocytopenia.
Three laboratory methods have been reported to be useful
for the diagnosis of thrombocytopenia. These include reticulatedplatelets (RPs), plasma thrombopoietin (TPO) levels, and plasmaglycocalicin (GC) levels. GC is a carbohydrate-rich hydrophilicfragment. Its levels are significantly reduced in patients with
S.C.O. Gilli et al. / Leukemia Research 36 (2012) 554– 559 555
Table 1Clinical and laboratory characteristic of the studies patients according to IPSS classification.
Platelet counts lower than 100 × 109/L Platelet count 100 × 109/Lor more
No. patients 24 30Low IPSS 6 20INT-1 14 9INT-2 2 –High IPSS 1 –No. male/female 14/10 14/16Age, y, median 62.7 73.0Hb, g/dL. median 9.8 10.5ANC, ×109/L, median (range) 1435 (480–4660) 1765(310–8410)MPV median (range) 9.9(6.9–23.1) 8.3(4.8–12.8)PDW, median (range) 15.3(10.1–21.9) 16.3(14.1–23.5)GC index (range) 3.8(1.4–26.2) 1.1 (0.3–2.8)R direct PIFT-FC test, median (range) 2.1 (0.4–27.8) 1.1 (0.5–4.2)
IPSS indicates International Prognostic Scoring System. Low: low risk, INT: intermediary risk, High: high risk, ANC: absolute neutrophils count, MPV: mean platelet volume,P mmua al ana(
hor(eilai
MpptuntcMi
2
2
HUiTpttMceotta1
2
aeo(Itr
DW: platelet size deviation, GC index: glycocalicin index, R: ratio between patient ind classification of MDS were based on hematological, pathological and chromosomAbbott, Illinois, USA).
ypoplastic thrombocytopenia, but not in patients with normalr increased megakaryocytes [16] suggesting that plasma GC leveleflects the rate of platelet production. In addition, the GC indexplasma GC level normalized for the individual platelet count) islevated in patients with ITP but not in patients with AA, suggest-ng that the GC index reflects the rate of platelet destruction. Plasmaevels of GC could be of relevance to discriminate further betweenn increased destruction of platelets in peripheral blood and anmpaired production by the bone marrow megakaryocytes.
Since it is imperative to know whether thrombocytopenia inDS is mainly due to hypo-production or hyper-destruction of
latelets, as this could possibly imply in important changes inatient care, the aim of the present study was to evaluate prospec-ively the prevalence of platelet antibodies, and determine thesefulness of quantitative PAIgG detection for the differential diag-osis of thrombocytopenia in MDS patients by a combination ofhis highly sensitive direct flow cytometric analysis and the glyco-alicin index, and to assess the convenience of applying PDW andPV measures as indirect markers of hyperdestruction of platelets
n MDS.
. Materials and methods
.1. Patients and platelet indices acquisition
A total of fifty-four consecutive patients with a diagnosis of MDS from theematology and Hemotherapy Center of the University of Campinas (Hemocentro-NICAMP) were enrolled in the study and were fully evaluated after written
nformed consent. The study was approved by the Ethical Committee of UNICAMP.he patients were not subjected to steroids, immunosuppressive therapy or priorlatelet transfusions. The diagnosis and classification of MDS were based on hema-ological, pathological and chromosomal analysis. Patients were grouped accordingo the International Prognostic Scoring System – IPSS [17] which is used to define
DS prognosis. The patients were screened for autoimmune disease and had nolinical or laboratory manifestation of immunological disorder at the time of beingnrolled in the study. All blood samples were prepared and analyzed on the dayf collection. Cell-dyn Sapphire blood cell analyzer (Abbott, Illinois, USA) was usedo measure platelet counts, mean platelet volume (MPV) and platelet size devia-ion width (PDW). The referential ranges at our institute were 6.9–10.6 fL for MPVnd 7.0–11.0 fL for PDW. Thrombocytopenia was defined as a platelet count below00 × 109/L.
.2. Direct platelet immunofluorescence test (PIFT-FC)
For the determination of platelet associated IgG (PAIgG) blood samples werenalyzed by direct PIFT (platelet immunofluorescence test) and results werexpressed as a ratio R (patient immunofluorescence/positive control immunoflu-
rescence). Briefly, 5 × 106 platelets from patients were incubated with fluoresceinFITC)-conjugated Polyclonal affinity isolated F(ab′)2 Fragment Rabbit Anti-HumangG, (DakoCytomationTM – Glostrup – Denmark) diluted 1:20 for 30 min at roomemperature in the dark. This sample was then washed with PBS/EDTA 1% andessuspended in 500 �L buffer. Reading – 10,000 events – was performed in anofluorescence direct PIFT test/positive control immunofluorescence. The diagnosislysis and the blood samples were analyzed by Cell-dyn Sapphire blood cell analyzer
FACScalibur (Becton-Dickenson, San Jose, California) flow cytometer. A positive testwas defined by fluorescence ≥2 standard deviation – sd – from negative control andinconclusive test by fluorescence ≥1 sd, < 2 sd from negative control.
2.3. Plasma glycocalicin assay
Plasma glycocalicin (GC) was measured by commercially available enzymeimmunoassay (EIA) (Takara Shuzo, Ohtsu, Japan). Briefly, 200 �L of the sam-ples of rich platelet plasma (RPP) were added to a microtiter plate precoatedwith anti-GC monoclonal antibody. After washing, anti-GC antibody was addedand the GC concentration from the patients’ samples was calculated from thecorresponding standard curve. Since GC levels are dependent on the plateletcount, the GC index (GCI) was calculated using the following formula: GC(�g/mL) × 250 × 103/individual platelet count (/�L), as proposed by Steinberg et al.[16]. According to the literature, we considered 0.7 ± 0.2 as the normal value of GCI[18].
2.4. Statistical analysis
Statistical analysis was performed to compare platelet count with MPV,PDW, glycocalicin index, and direct PIFT. Statistical analysis was performed usingKruskal–Wallis nonparametric analysis of variances and the Wilcoxon 2 sample test.Spearman rank correlation was used for assessing correlations between continuousvariables. P < 0.05 was considered statistically significant.
3. Results
3.1. Prevalence of thrombocytopenia in MDS patients
According to the IPSS classification, there were 26 casesclassified as low-risk, 23 cases intermediate-1 risk, 3 casesintermediate-2 risk and 1 case was classified as high-risk; onepatient was not classified. The median platelet count in the sam-ples was 120.5 × 109/L (ranging from 6.7 to 708.0 × 109/L), mean153.3 ± 131.4 × 109/L. Twenty four patients (44.4%) had plateletcounts <100 × 109/L. Data of patients are summarized in Table 1.
3.2. MPV was significantly higher in patients withthrombocytopenia
MPV was significantly higher in patients with plateletcount <100 × 109/L (median, min–max: 9.93, 6.9–23.1 vs 8.32,4.88–12.83; p < 0.001, Wilcoxon rank sum test with continuitycorrection), and platelet count was significantly different amongpatients with MPV below the lower limit of normal, within thenormal range of MPV, and with MPV above the upper limit of nor-mal (median, min–max: 183.5 × 109/L, 135.0–261.0; 120.5 × 109/L,
20.3–708.0; 28.5 × 109/L, 6.7–267.0; p = 0.01, Kruskal–Wallis ranksum test). In addition, an inverse correlation between the num-ber of platelets and the MPV value was demonstrated (p < 0.001,r = −0.45, Spearman’s rank correlation rho) (Fig. 1). Taken together,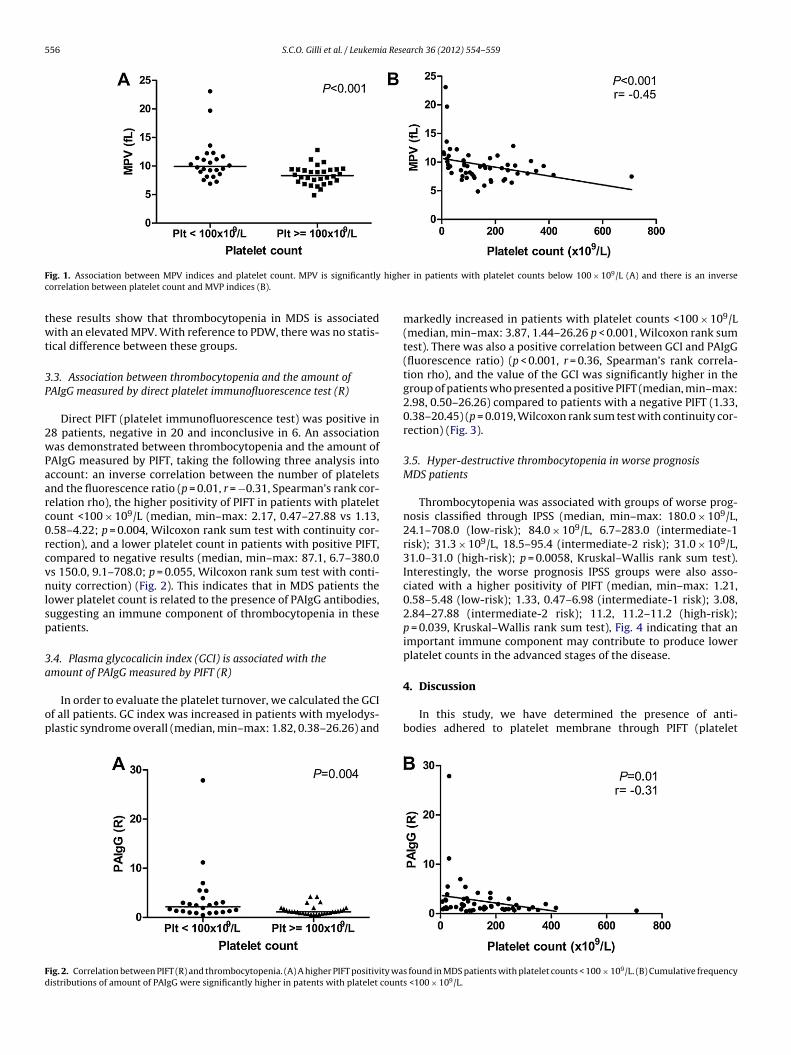
556 S.C.O. Gilli et al. / Leukemia Research 36 (2012) 554– 559
F highec
twt
3P
2wPaarc0rcvnlsp
3a
op
Fd
ig. 1. Association between MPV indices and platelet count. MPV is significantlyorrelation between platelet count and MVP indices (B).
hese results show that thrombocytopenia in MDS is associatedith an elevated MPV. With reference to PDW, there was no statis-
ical difference between these groups.
.3. Association between thrombocytopenia and the amount ofAIgG measured by direct platelet immunofluorescence test (R)
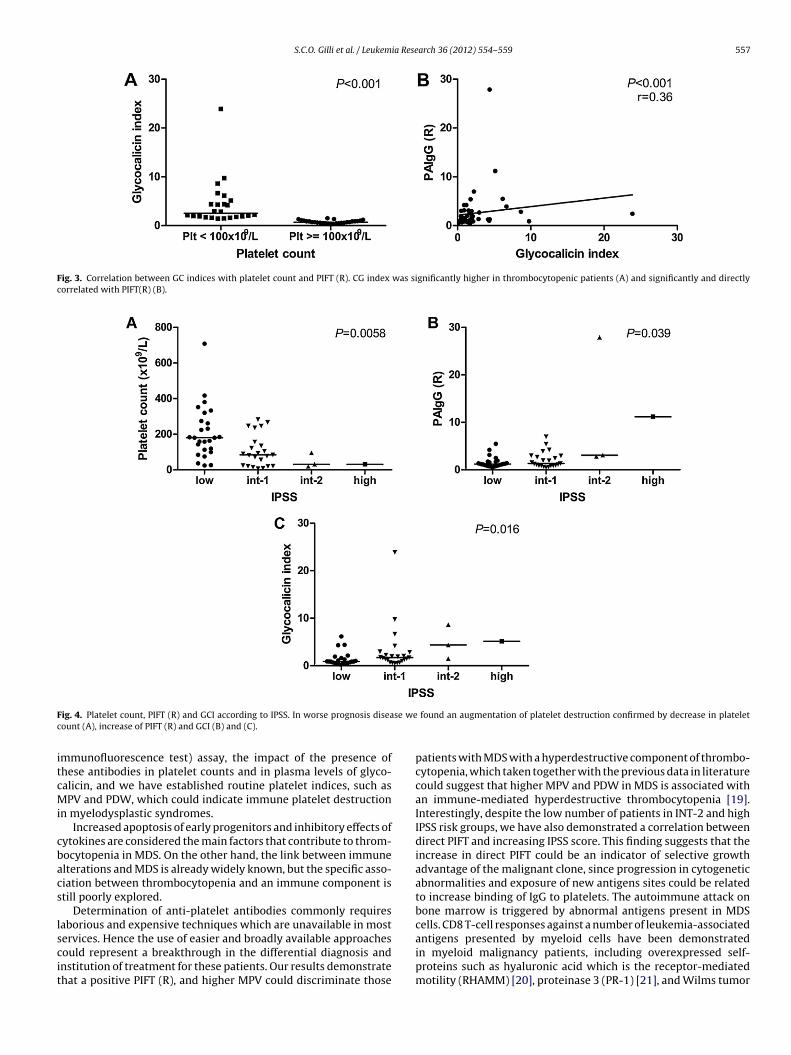
Direct PIFT (platelet immunofluorescence test) was positive in8 patients, negative in 20 and inconclusive in 6. An associationas demonstrated between thrombocytopenia and the amount of
AIgG measured by PIFT, taking the following three analysis intoccount: an inverse correlation between the number of plateletsnd the fluorescence ratio (p = 0.01, r = −0.31, Spearman’s rank cor-elation rho), the higher positivity of PIFT in patients with plateletount <100 × 109/L (median, min–max: 2.17, 0.47–27.88 vs 1.13,.58–4.22; p = 0.004, Wilcoxon rank sum test with continuity cor-ection), and a lower platelet count in patients with positive PIFT,ompared to negative results (median, min–max: 87.1, 6.7–380.0s 150.0, 9.1–708.0; p = 0.055, Wilcoxon rank sum test with conti-uity correction) (Fig. 2). This indicates that in MDS patients the
ower platelet count is related to the presence of PAIgG antibodies,uggesting an immune component of thrombocytopenia in theseatients.
.4. Plasma glycocalicin index (GCI) is associated with themount of PAIgG measured by PIFT (R)
In order to evaluate the platelet turnover, we calculated the GCIf all patients. GC index was increased in patients with myelodys-lastic syndrome overall (median, min–max: 1.82, 0.38–26.26) and
ig. 2. Correlation between PIFT (R) and thrombocytopenia. (A) A higher PIFT positivity waistributions of amount of PAIgG were significantly higher in patents with platelet count
r in patients with platelet counts below 100 × 109/L (A) and there is an inverse
markedly increased in patients with platelet counts <100 × 109/L(median, min–max: 3.87, 1.44–26.26 p < 0.001, Wilcoxon rank sumtest). There was also a positive correlation between GCI and PAIgG(fluorescence ratio) (p < 0.001, r = 0.36, Spearman’s rank correla-tion rho), and the value of the GCI was significantly higher in thegroup of patients who presented a positive PIFT (median, min–max:2.98, 0.50–26.26) compared to patients with a negative PIFT (1.33,0.38–20.45) (p = 0.019, Wilcoxon rank sum test with continuity cor-rection) (Fig. 3).
3.5. Hyper-destructive thrombocytopenia in worse prognosisMDS patients
Thrombocytopenia was associated with groups of worse prog-nosis classified through IPSS (median, min–max: 180.0 × 109/L,24.1–708.0 (low-risk); 84.0 × 109/L, 6.7–283.0 (intermediate-1risk); 31.3 × 109/L, 18.5–95.4 (intermediate-2 risk); 31.0 × 109/L,31.0–31.0 (high-risk); p = 0.0058, Kruskal–Wallis rank sum test).Interestingly, the worse prognosis IPSS groups were also asso-ciated with a higher positivity of PIFT (median, min–max: 1.21,0.58–5.48 (low-risk); 1.33, 0.47–6.98 (intermediate-1 risk); 3.08,2.84–27.88 (intermediate-2 risk); 11.2, 11.2–11.2 (high-risk);p = 0.039, Kruskal–Wallis rank sum test), Fig. 4 indicating that animportant immune component may contribute to produce lowerplatelet counts in the advanced stages of the disease.
4. Discussion
In this study, we have determined the presence of anti-bodies adhered to platelet membrane through PIFT (platelet
s found in MDS patients with platelet counts < 100 × 109/L. (B) Cumulative frequencys <100 × 109/L.
S.C.O. Gilli et al. / Leukemia Research 36 (2012) 554– 559 557
Fig. 3. Correlation between GC indices with platelet count and PIFT (R). CG index was significantly higher in thrombocytopenic patients (A) and significantly and directlycorrelated with PIFT(R) (B).
F se wec
itcMi
cbacs
lscit
ig. 4. Platelet count, PIFT (R) and GCI according to IPSS. In worse prognosis diseaount (A), increase of PIFT (R) and GCI (B) and (C).
mmunofluorescence test) assay, the impact of the presence ofhese antibodies in platelet counts and in plasma levels of glyco-alicin, and we have established routine platelet indices, such asPV and PDW, which could indicate immune platelet destruction
n myelodysplastic syndromes.Increased apoptosis of early progenitors and inhibitory effects of
ytokines are considered the main factors that contribute to throm-ocytopenia in MDS. On the other hand, the link between immunelterations and MDS is already widely known, but the specific asso-iation between thrombocytopenia and an immune component istill poorly explored.
Determination of anti-platelet antibodies commonly requiresaborious and expensive techniques which are unavailable in most
ervices. Hence the use of easier and broadly available approachesould represent a breakthrough in the differential diagnosis andnstitution of treatment for these patients. Our results demonstratehat a positive PIFT (R), and higher MPV could discriminate thosefound an augmentation of platelet destruction confirmed by decrease in platelet
patients with MDS with a hyperdestructive component of thrombo-cytopenia, which taken together with the previous data in literaturecould suggest that higher MPV and PDW in MDS is associated withan immune-mediated hyperdestructive thrombocytopenia [19].Interestingly, despite the low number of patients in INT-2 and highIPSS risk groups, we have also demonstrated a correlation betweendirect PIFT and increasing IPSS score. This finding suggests that theincrease in direct PIFT could be an indicator of selective growthadvantage of the malignant clone, since progression in cytogeneticabnormalities and exposure of new antigens sites could be relatedto increase binding of IgG to platelets. The autoimmune attack onbone marrow is triggered by abnormal antigens present in MDScells. CD8 T-cell responses against a number of leukemia-associated
antigens presented by myeloid cells have been demonstratedin myeloid malignancy patients, including overexpressed self-proteins such as hyaluronic acid which is the receptor-mediatedmotility (RHAMM) [20], proteinase 3 (PR-1) [21], and Wilms tumor
5 ia Rese
anirlbo
aMilapaein
sbDomwfsan
pg
cHaotamubJruo
ntibnaatPrdtp(tMuas
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
58 S.C.O. Gilli et al. / Leukem
ntigen 1 (http://www.ncbi.nlm.nih.gov/gene/7490) [22], and alsoeoantigens created by chromosomal translocations [23] would be
nvolved in this process. These autoimmune abnormalities couldeflect the presence of an incipient immune response against theeukemic phenotype, though insufficient to prevent its evolutiony deregulation of other interactions such as increased frequencyf Tregs and decreased function of NK cells [24].
Wang et al. demonstrated the presence of plasma specificutoantibodies against platelet GP II b/III a and GP Ib/IX inDS patients using a modified monoclonal antibody specific
mmobilization platelet antigen assay (MAIPA), indicating a corre-ation of patient thrombocytopenia with immune factors and thatutoantibody-mediated platelet destruction may be involved in theathogenesis of MDS [25]. The use of a test by flow cytometrys PIFT would be easier to run and could suggest the pres-nce of antibodies to platelets adhered with clinical significancen an initial screening of MDS patients with thrombocytope-ia.
Antiplatelet antibody assays, such as the monoclonal antibody-pecific immobilization of platelet antigens, are relatively specificut not very sensitive and appear to be only semiquantitative.espite the specificity of PIFT, it will always remain lower than thatf MAIPA, therefore quantitative PIFT is not intended as a replace-ent for GP-specific tests. However, in MDS patients who presentith thrombocytopenia, especially those requiring platelet trans-
usion, we recommend the quantitative PIFT as a highly sensitivecreening test, as suggested by other authors [26], since GP-specificntibodies have rarely been detected in cases where the PIFT wasegative.
Supporting our hypothesis of increased platelet destruction inatients with MDS, Barsam et al. [27] recently described a higherlycocalicin index in IPT patients.
An important application of our study is the possibility oforticosteroid therapy in thrombocytopenic patients with MDS.owever, immunosuppressive treatment may fail because, inddition to the presence of antibodies against platelets, megakary-poiesis failure exits and therefore only immunosuppressiveherapy is not enough. Some options to be taken into account are thessociations with agents that increase platelet count, stimulatingegakaryopoiesis and thereby increasing thrombopoiesis as the
se of thrombopoietin receptor agonists (TPO-A), which increaseslood levels of transforming growth factor-� [28], activates theAK/STAT and MAPK signaling pathways, and increases bone mar-ow precursor proliferation and platelet production [29,30] or these of monoclonal antibody anti-Fc RIII that inhibits the destructionf antibody-coated platelets [31].
The definition of an immune component in thrombocytope-ia has been recently explored in myelodysplasia and, in practice,he diagnosis of antibodies against plateles is extremely importantn this disease, since thrombocytopenia is supposedly related toone marrow failure. Thus, the diagnosis of the immune compo-ent avoids unnecessary transfusions in MDS and could guide theppropriate treatment. The use of sophisticated methods as MAIPAssay often delays or even fails to diagnose the cause of immunehrombocytopenia in this group of patients. We believe that directIFT used as a sensitive screening test associated with the MPV testepresents an applicable and easy method to suggest the immuneestruction of platelets in patients with MDS, providing a diagnos-ic change and changes in the conduct adopted in the treatment ofatients. Thus, we propose that the combination of a platelet indexMPV) and a highly sensitive and easy to perform screening test forhe detection of PAIgG (PIFT) could be applied to select a subset of
DS patients in which we would be able to prevent the overuse ofnnecessary platelet transfusions and who could be candidate forn immunosuppressive therapeutic approach validated in clinicaltudies.
[
arch 36 (2012) 554– 559
References
[1] Layton DM, Mufti GJ. Myelodysplastic syndromes: their history, evolution andrelation to acute myeloid leukaemia. Blut 1986;53:423–36.
[2] Brada S, de Wolf J, Hendriks D, Esselink M, Ruiters M, Vellenga E. The supportiveeffects of erythropoietin and mast cell growth factor on CD34+/CD36− sortedbone marrow cells of myelodysplasia patients. Blood 1996;88:505–10.
[3] Brada SJ, de Wolf JT, Hendriks DW, Smit JW, Vellenga E. CD34+/CD36− cells frommyelodysplasia patients have a limited capacity to proliferate but can differ-entiate in response to Epo and MGF stimulation. Leukemia 1998;12:882–6.
[4] Hofmann WK, Kalina U, Koschmieder S, Seipelt G, Hoelzer D, OttmannOG. Defective megakaryocytic development in myelodysplastic syndromes.Leukemia & lymphoma 2000;38:13–9.
[5] Mufti GJ, Figes A, Hamblin TJ, Oscier DG, Copplestone JA. Immunologicalabnormalities in myelodysplastic syndromes I. Serum immunoglobulins andautoantibodies. British Journal of Haematology 1986;63:143–7.
[6] van de Loosdrecht AA, Vellenga E. Myelodysplasia and apoptosis: new insightsinto ineffective erythropoiesis. Medical Oncology (Northwood, London, Eng-land) 2000;17:16–21.
[7] Lambertenghi-Deliliers G, Annaloro C, Oriani A, Soligo D. Myelodysplasticsyndrome associated with bone marrow fibrosis. Leukemia & lymphoma1992;8:51–5.
[8] Hall AG, Proctor SJ, Saunders PW. Increased platelet associated immunoglob-ulin in myelodysplastic syndromes. British Journal of Haematology1987;65:245–6.
[9] Billstrom R, Johansson H, Johansson B, Mitelman F. Immune-mediated compli-cations in patients with myelodysplastic syndromes—clinical and cytogeneticfeatures. European Journal of Haematology 1995;55:42–8.
10] von dem Borne AE, Vos JJ, van der Lelie J, Bossers B, van Dalen CM. Clinicalsignificance of positive platelet immunofluorescence test in thrombocytopenia.British Journal of Haematology 1986;64:767–76.
11] Hebbar M, Kaplan C, Caulier MT, Wattel E, Morel P, Wetterwald M, et al. Lowincidence of specific anti-platelet antibodies detected by the MAIPA assay inthe serum of thrombocytopenic MDS patients and lack of correlation betweenplatelet autoantibodies, platelet lifespan and response to danazol therapy.British Journal of Haematology 1996;94:112–5.
12] von dem Borne AE, Verheugt FW, Oosterhof F, von Riesz E, de la Riviere AB,Engelfriet CP. A simple immunofluorescence test for the detection of plateletantibodies. British Journal of Haematology 1978;39:195–207.
13] Illes I, Pfueller SL, Hussein S, Chesterman CN, Martin JF. Platelets in idiopathicthrombocytopenic purpura are increased in size but are of normal density.British Journal of Haematology 1987;67:173–6.
14] Rajantie J, Javela K, Joutsi-Korhonen L, Kekomaki R. Chronic thrombocytope-nia of childhood: use of non-invasive methods in clinical evaluation. EuropeanJournal of Haematology 2004;72:268–72.
15] Kaito K, Otsubo H, Usui N, Yoshida M, Tanno J, Kurihara E, et al. Platelet sizedeviation width, platelet large cell ratio, and mean platelet volume have suffi-cient sensitivity and specificity in the diagnosis of immune thrombocytopenia.British Journal of Haematology 2005;128:698–702.
16] Steinberg MH, Kelton JG, Coller BS. Plasma glycocalicin. An aid in the classifi-cation of thrombocytopenic disorders. The New England Journal of Medicine1987;317:1037–42.
17] Greenberg P, Cox C, LeBeau MM, Fenaux P, Morel P, Sanz G, et al. Internationalscoring system for evaluating prognosis in myelodysplastic syndromes. Blood1997;89:2079–88.
18] Houwerzijl EJ, Blom NR, van der Want JJ, Louwes H, Esselink MT, Smit JW,et al. Increased peripheral platelet destruction and caspase-3-independentprogrammed cell death of bone marrow megakaryocytes in myelodysplasticpatients. Blood 2005;105:3472–9.
19] Numbenjapon T, Mahapo N, Pornvipavee R, Sriswasdi C, Mongkonsritra-goon W, Leelasiri A, et al. A prospective evaluation of normal mean plateletvolume in discriminating hyperdestructive thrombocytopenia from hypopro-ductive thrombocytopenia. International Journal of Laboratory Hematology2008;30:408–14.
20] Greiner J, Schmitt A, Giannopoulos K, Rojewski MT, Gotz M, Funk I, et al.High-dose RHAMM-R3 peptide vaccination for patients with acute myeloidleukemia, myelodysplastic syndrome and multiple myeloma. Haematologica2010;95:1191–7.
21] Molldrem JJ, Lee PP, Wang C, Champlin RE, Davis MM. A PR1-human leukocyteantigen-A2 tetramer can be used to isolate low-frequency cytotoxic T lympho-cytes from healthy donors that selectively lyse chronic myelogenous leukemia.Cancer Research 1999;59:2675–81.
22] Cilloni D, Saglio G. WT1 as a universal marker for minimal residual diseasedetection and quantification in myeloid leukemias and in myelodysplastic syn-drome. Acta Haematologica 2004;112:79–84.
23] Bosch GJ, Joosten AM, Kessler JH, Melief CJ, Leeksma OC. Recognition of BCR-ABL positive leukemic blasts by human CD4+ T cells elicited by primary in vitroimmunization with a BCR-ABL breakpoint peptide. Blood 1996;88:3522–7.
24] Molldrem JJ, Caples M, Mavroudis D, Plante M, Young NS, Barrett AJ. Antithy-mocyte globulin for patients with myelodysplastic syndrome. British Journalof Haematology 1997;99:699–705.
25] Wang JD, Pan XL, Yin Z, Sun JH, Kong GX, Chen YJ, et al. Expression of specificantibodies against platelet glycoproteins in patients with mds and its signif-icance. Zhongguo shi yan xue ye xue za zhi/Zhongguo bing li sheng li xuehui=Journal of Experimental Hematology/Chinese Association of Pathophys-iology 2007;15:95–8.

ia Rese
[
[
[
[
[
S.C.O. Gilli et al. / Leukem
26] Hagenstrom H, Schlenke P, Hennig H, Kirchner H, Kluter H. Quantification ofplatelet-associated IgG for differential diagnosis of patients with thrombocy-topenia. Thrombosis and Haemostasis 2000;84:779–83.
27] Barsam SJ, Psaila B, Forestier M, Page LK, Sloane PA, Geyer JT, et al. Platelet
production and platelet destruction: assessing mechanisms of treatment effectin immune thrombocytopenia. Blood 2011;117:5723–32.28] Olsson B, Andersson PO, Jernas M, Jacobsson S, Carlsson B, Carlsson LM, et al.T-cell-mediated cytotoxicity toward platelets in chronic idiopathic thrombo-cytopenic purpura. Nature Medicine 2003;9:1123–4.
[
arch 36 (2012) 554– 559 559
29] Cines DB, McKenzie SE, Siegel DL. Mechanisms of action of therapeutics in idio-pathic thrombocytopenic purpura. Journal of Pediatric Hematology/Oncology2003;25(Suppl. 1):S52–6.
30] Kuter DJ. New thrombopoietic growth factors. Blood 2007;109:
4607–16.31] Clarkson SB, Bussel JB, Kimberly RP, Valinsky JE, Nachman RL, UnkelessJC. Treatment of refractory immune thrombocytopenic purpura with ananti-Fc gamma-receptor antibody. The New England Journal of Medicine1986;314:1236–9.