phenotypic and molecular characterization of community occurring, western samoan phage pattern...
TRANSCRIPT

Journal of Antimicrobial ChemotherapyDOI: 10.1093/jac/dkf242
Page 1 of 7. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
© 2002 The British Society for Antimicrobial Chemotherapy
Phenotypic and molecular characterization of community occurring, Western Samoan phage pattern methicillin-resistant
Staphylococcus aureus
Rajan P. Adhikari1, Gregory M. Cook1, Iain Lamont2, Selwyn Lang3, Helen Heffernan4 and
John M. B. Smith1*
Departments of 1Microbiology and 2Biochemistry, Otago School of Medical Sciences, University of Otago, Dunedin; 3Middlemore Hospital and Diagnostic Medlab, Auckland; 4Institute of Environmental Science and Research,
Porirua, New Zealand
Received 30 May 2002; returned 15 July 2002; revised 10 September 2002; accepted 11 September 2002
In New Zealand, it is estimated that greater than half of the methicillin-resistant Staphylococcusaureus (MRSA) strains recovered from patients belong to what has been termed WesternSamoan phage pattern types 1 and 2 (WSPP1, WSPP2). These strains differ from classical MRSAisolates in terms of their lack of multiresistance and community occurrence, suggesting thatsuch strains possess properties and/or characteristics different from those of other MRSA. Toaddress this hypothesis, 10 WSPP1 and WSPP2 isolates from Western Samoa, New Zealand andAustralia were compared with common hospital MRSA isolates. All WSPP isolates were identicalwith regard to pulsed-field gel electrophoretic pattern of SmaI-digested DNA, coagulase generestriction fragment length polymorphism pattern and localization of mecA to a 194 kb SmaIdigestion fragment. The WSPP strains were no more resistant/sensitive to various environ-mental stresses (e.g. skin fatty acids, UV light, desiccation) compared with hospital epidemicMRSA strains, except for their higher tolerance to salt. In terms of virulence, the WSPP MRSAwere quantitatively better at attaching to the epithelial cell line HEp2, were uniformly egg-yolkopacity factor negative and produced higher levels of haemolytic toxins compared with non-WSPP MRSA isolates.
Keywords: community MRSA, phenotypic and molecular characteristics
Introduction
Methicillin-resistant Staphylococcus aureus (MRSA) havebecome an increasing problem worldwide. MRSA was firstisolated in New Zealand in the mid-1970s, but remaineduncommon until 1986, when a marked increase occurred inthe number of isolates referred to the Communicable DiseaseGroup, Institute of Environmental Science and Research(ESR) at Porirua. Based on data collected from hospital andcommunity diagnostic laboratories, the prevalence of methi-cillin resistance in clinical S. aureus in New Zealand hassteadily risen from 1.1% in 1994 to 6.8% in 2001. In 1995,around half of the MRSA received by ESR belonged to what
was termed Western Samoan phage pattern types 1 and 2 (29/52/52A/80/55/54/77/84/95/96+, WSPP1; 29/81/54/77/84+,WSPP2). In 1997, a complete surveillance involving all hos-pital and community laboratories in New Zealand revealedthat of 2085 MRSA isolated, 76% were of the WSPP type.These were regarded as community based with a predilectionfor Pacific Island races.1–5 By 2000, it was estimated thatalmost 4500 isolates of MRSA were recovered in NewZealand.2 At this time, WSPP strains comprised 61.7% of theisolates, with the next most common (15.4% isolates) strainbeing EMRSA-15. Most (73.4%) of the WSPP isolates wererecovered from community patients, and 73.7% of theEMRSA-15 isolates were from hospital patients. It is worth
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
*Corresponding author. Tel: +64-3-479-7718; Fax: +64-3-479-8540; E-mail: [email protected]
Advance Access published November 1, 2002 by guest on M
arch 25, 2015http://jac.oxfordjournals.org/
Dow
nloaded from
R. P. Adhikari et al.
Page 2 of 7
noting that during the 1990s, New Zealand had an excellentreporting system with almost all diagnostic laboratoriesreferring possible MRSA to ESR.
Although there are difficulties in demonstrating that so-called community MRSA (CMRSA) are not acquired as theresult of a visit to a health care facility, it does seem thatCMRSA are of increasing importance in a number of coun-tries.6–14 In general, such strains have not been multiresistantand often have low methicillin/oxacillin MICs, typically≤64 mg/L. The predilection of such strains for children and/orminority communities has also been a recorded feature in somesurveys.3,5,6,8,9,12,13 In many respects, these CMRSA appearto behave in a similar manner to methicillin-susceptibleS. aureus (MSSA), and can be brought into hospitals andserve as an important source of nosocomial infection. Forsome reason, clindamycin9,10 or gentamicin12 susceptibilityappears to have been taken as an indicator of possible com-munity acquisition.
In New Zealand, the rapid spread of the WSPP clone ofCMRSA throughout the country, and occurrence in patientsdevoid of the risk factors commonly reported for MRSAacquisition,1 suggest that such strains possess properties and/or characteristics different from those of other MRSA. Despitethe increasing problems of WSPP in New Zealand, features ofthe physiology and molecular genetics of this clone are stilllargely unknown. The present study was therefore undertakento compare various characteristics (e.g. toxin production,environmental survival) of WSPP strains from New Zealand,Australia and Western Samoa with those of other MRSAstrains.
Materials and methods
Strains and culture conditions
All isolates used in this study were from the culturecollections of the Department of Microbiology, University ofOtago, and ESR. In addition to control strains, 15 MRSAisolates were included in the comparative investigations—10 WSPP1 or WSPP2 chosen on the basis of geographicalisolation and oxacillin MICs, and five multiresistant hospitalMRSA. MRSA were defined as S. aureus with an oxacillinMIC of ≥4 mg/L. All MICs were determined using Etests(AB Biodisk, Solna, Sweden) as recommended by the manu-facturer. Where required, disc diffusion sensitivity tests werecarried out as described by the NCCLS.15 Other bacterialstrains used in this study were S. aureus strain ATCC 25923as an antimicrobial sensitivity test control, S. aureus strain417 as a mecA-positive control, S. aureus strain 8325-4 (Hla+,Hlb+) and attachment-negative strain S. aureus NCTC 10345(CN56 Wood 46). All strains were maintained on sheepblood agar plates at 4°C with regular subculturing. For long-term storage, strains were stored in skimmed milk (Difco) at–70°C.
PCR, DNA hybridization, pulsed-field gel electrophoresis (PFGE) and restriction fragment length polymorphism (RFLP) of the coagulase gene
All MRSA strains were tested for the presence of mecA byPCR and Southern blot hybridization using standard molecu-lar biology protocols and primers described previously.16–18
The RFLP of the coagulase gene was carried out using themethod described by Goh et al.19
PFGE was carried out as described previously20 using thecontour-clamped homogeneous electric field (CHEF-DRIII)electrophoresis system (Bio-Rad Laboratories, Richmond,CA, USA) at 6 V/cm and 14°C. The Low Range PFG Marker(New England Biolabs, Inc., Beverly, MA, USA) containinglambda concatemers and lambda-digested HindIII fragmentswas used as a size standard. Separated DNA fragments werestained with ethidium bromide and visualized with a UVtransilluminator. The clonality of isolates was judged usingpreviously described criteria from visual comparisons ofbanding patterns of samples run together in the same gel.21
Salt tolerance, and resistance to desiccation, skin fatty acids and ultraviolet radiation
Salt tolerance of the MRSA strains was determined using anagar dilution technique employing different concentrations(0.5–15%) of NaCl incorporated into nutrient agar. Thelowest concentration of NaCl that inhibited colony formationwas interpreted as the MIC of NaCl, as described previ-ously.22
Survival of MRSA strains under different humidities wascarried out using desiccators and a range of relative humid-ities.23 Samples were taken at 7 day intervals and the numberof viable cells remaining on the filter determined by dilutionand plating techniques. Cell viability (survival) was assessedas the number of bacteria remaining as a percentage of thestarting count.
Sensitivity to two free fatty acids was determined by incor-porating the acids into blood agar plates [5% blood in trypticsoy agar (TSA)] to create final fatty acid concentrations in therange 0.025–0.4% for linoleic acid and 1–7% for oleic acid.MICs were determined by identifying the lowest concentra-tion of the fatty acid that inhibited growth after incubation at37°C for 24 h.24
Resistance of each test strain to UV light was observed byspotting 10 µL of an overnight culture (1 × 108 cfu/mL) on tothe surface of sheep blood agar plates followed by exposure(0, 2, 5, 8, 15, 30, 45, 60, 90 and 150 s) to UV light (254 nmwavelength). Plates were then incubated overnight at 37°Cand the presence or absence of growth recorded.
by guest on March 25, 2015
http://jac.oxfordjournals.org/D
ownloaded from
WSPP community MRSA
Page 3 of 7
Production of α- and β-haemolysin toxins, and adherence to HEp2 cells
The quantitative measurement of α- and β-haemolysin toxinproduction was carried out in terms of haemolytic titre asdescribed previously.25 To confirm the presence of the genesencoding α-haemolysin (hla) and β-haemolysin (hlb), PCRand Southern hybridization were carried out as described pre-viously.17,18 The following primers were used: α-haemolysinHLA-1 5′-CTGATTACTATCCAAGAAATTCGATTG-3′and HLA-2 5′-CTTTCCAGCCTACTTTTTTATCAGT-3′,and β-haemolysin HLB-1 5′-GTGCACTTACTGACAAT-AGTGC-3′ and HBL-2 5′-GTTGATGAGTAGCTACCT-TCAGT-3′.26 Strain 8325-4 (Hla+ Hlb+) was used as a positivecontrol for α- and β-haemolysin.25 All PCR products weresequenced to confirm that the correct gene had been ampli-fied. Positive PCR products for hla and hlb were used as DNAprobes for Southern hybridization, as described above.
The adherence assay employed a continuous human epi-thelial cell line, HEp2, and was carried out as described byAathithan et al.27 Tryptic soy broth (TSB) cultures of eachstrain were radiolabelled by mixing with 0.925 MBq[3H]thymidine in an orbital shaker (200 rpm) for 18 h at 37°C.The radiolabelled bacteria were then centrifuged and washedtwice in 20 mL of PBS, and the pellet resuspended to anOD540 of 0.4 (∼1 × 108 cells/mL). The specific activity of the3H-labelled bacteria was determined by transferring 100 µLof labelled bacteria into a scintillation vial containing 1 mL ofscintillant, and the radioactivity determined using an LKBWallac Scintillation Counter. Adherence assays were carriedout using fresh HEp2 monolayers in 24-well tissue cultureplates inoculated with 0.5 mL of culture, followed by incuba-tion at 37°C for 2 h. After incubation, the monolayer wasgently washed twice with 1 mL of PBS and then lysed byadding 250 µL of pre-warmed trypsin with incubation at 37°Cfor 15 min. After complete detachment and solubilization ofthe monolayer, the content of each well was transferred to ascintillation vial containing 1 mL of scintillation fluid and theradioactivity determined as above. Percentage adherence wascalculated by applying the following formula: % of adherence= (mean cpm of the lysed monolayer × 100)/(mean cpm of theoriginal bacterial suspension).
Egg-yolk opacity factor
Each isolate was inoculated on to plates of mannitol egg-yolk medium [0.1% beef extract (BBL), 1% peptone 140(Difco), 1% mannitol, 1% NaCl, 2% solution of Phenol Red(12.5 mL/L), 50% saline solution of egg yolk (11 mL/L) and1.5% agar] and incubated for 48 h at 37°C. Any obvious zoneof opacity occurring around the subsequent growth was thenrecorded.
Results
Characterization of the WSPP isolates
Ten WSPP MRSA isolates with varying methicillin MICsfrom New Zealand, Western Samoa and Australia wereincluded in this study (Table 1). All WSPP isolates revealed asimilar biochemical profile using the ID32 STAPH system(Table 1). Variations were observed in the fermentation ofribose and arabinose, acetoin production, the formation ofarginine arylamidase and novobiocin resistance.
The oxacillin MIC for the 10 isolates studied ranged from8 to 128 mg/L (Table 1). All isolates were susceptible togentamicin, erythromycin, ciprofloxacin and co-trimoxazole,except ST94/1208 (resistant to these four antimicrobials) andMR99/692 (resistant to erythromycin). This latter isolate wasalso mupirocin resistant. All isolates were β-lactamase pro-ducers. Clindamycin susceptibility was not tested.
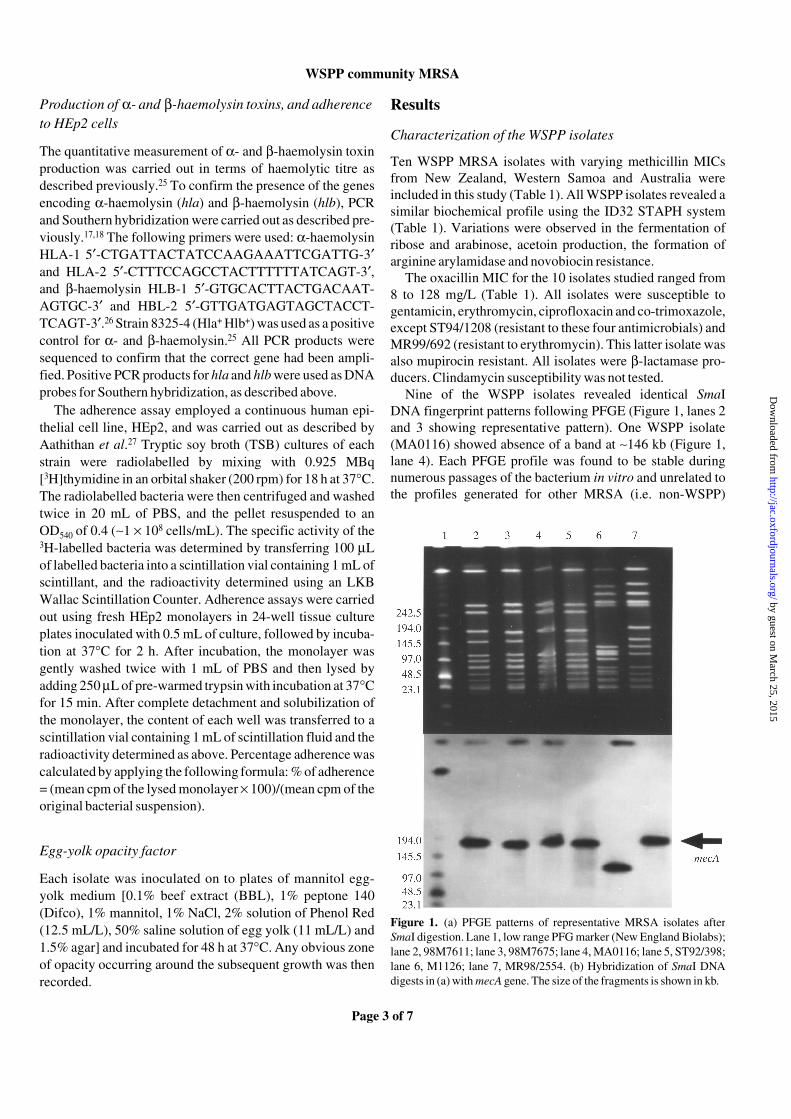
Nine of the WSPP isolates revealed identical SmaIDNA fingerprint patterns following PFGE (Figure 1, lanes 2and 3 showing representative pattern). One WSPP isolate(MA0116) showed absence of a band at ∼146 kb (Figure 1,lane 4). Each PFGE profile was found to be stable duringnumerous passages of the bacterium in vitro and unrelated tothe profiles generated for other MRSA (i.e. non-WSPP)
Figure 1. (a) PFGE patterns of representative MRSA isolates afterSmaI digestion. Lane 1, low range PFG marker (New England Biolabs);lane 2, 98M7611; lane 3, 98M7675; lane 4, MA0116; lane 5, ST92/398;lane 6, M1126; lane 7, MR98/2554. (b) Hybridization of SmaI DNAdigests in (a) with mecA gene. The size of the fragments is shown in kb.
by guest on March 25, 2015
http://jac.oxfordjournals.org/D
ownloaded from
R. P. Adhikari et al.
Page 4 of 7
(Figure 1, lanes 6 and 7). Coagulase gene RFLP patterns gener-ated from the WSPP isolates were of one type and unrelatedto that of the non-WSPP isolates (Table 1).
The chromosomal location and vicinity of the mecA geneafter SmaI digestion and PFGE of genomic DNA from thedifferent isolates was investigated with a DNA probe that wasinternal to the mecA gene (Figure 1). In all WSPP strains,mecA was localized to a 194 kb SmaI band.
All WSPP were tested for their resistance/sensitivity tovarious environmental stresses and compared with the moreclassical hospital MRSA strains. The MIC of oleic acid for allMRSA isolates examined was >7%. The MIC of linoleic acidranged from 0.3% to 0.4% for all strains and there were nosignificant differences between the WSPP and other MRSAisolates (data not shown). Similarly, percentage survival after15 s exposure to UV light was in the range 0.0001–0.002%for all isolates (data not shown). In the case of salt tolerance,the WSPP isolates appeared consistently more tolerant to saltthan the other MRSA investigated. Inhibitory levels of NaClwere ∼14% for WSPP compared with 6–10% for other MRSA(Table 2).
At relative humidities of 3–84%, all isolates studiedshowed a similar pattern of cell survival with no viable cellsdetected after 35 days of incubation, and therefore WSPPstrains did not appear better adapted to drying than otherstrains of MRSA (data not shown).
All isolates of WSPP studied were found to produce con-sistently high levels of α- and β-haemolysin toxins in theranges 256–4096 and 128–512 haemolytic titre, respectively(Table 2). High-level production of these toxins was not aconsistent feature of the other MRSA studied. All WSPPMRSA were positive for the presence of the hla gene codingfor α-haemolysin toxin production, but were negative for thehlb gene as confirmed by PCR. However, Southern hybrid-ization of genomic DNA with an hlb probe from strain 8325-4(Hla+, Hlb+) demonstrated that all strains were positive for aputative hlb gene (data not shown).
The percentage adherence results and the mean values foreach isolate are shown in Table 2. Mean adherence valuesranged from 1.36% to 13.76% for MRSA isolates. The controlstrain Wood 46 (a known low-adherer) had a value of 1.32%.Analysis of the data using the t-test indicated that as a groupthe WSPP isolates had significantly (P < 0.005) increasedadherence compared with other MRSA.
Of the 15 S. aureus isolates included in the present study,all 10 WSPP were egg-yolk opacity factor negative. All fivenon-WSPP MRSA were egg-yolk positive.
Discussion
The WSPP1 and WSPP2 MRSA were first isolated fromWestern Samoan patients in the Auckland region of New
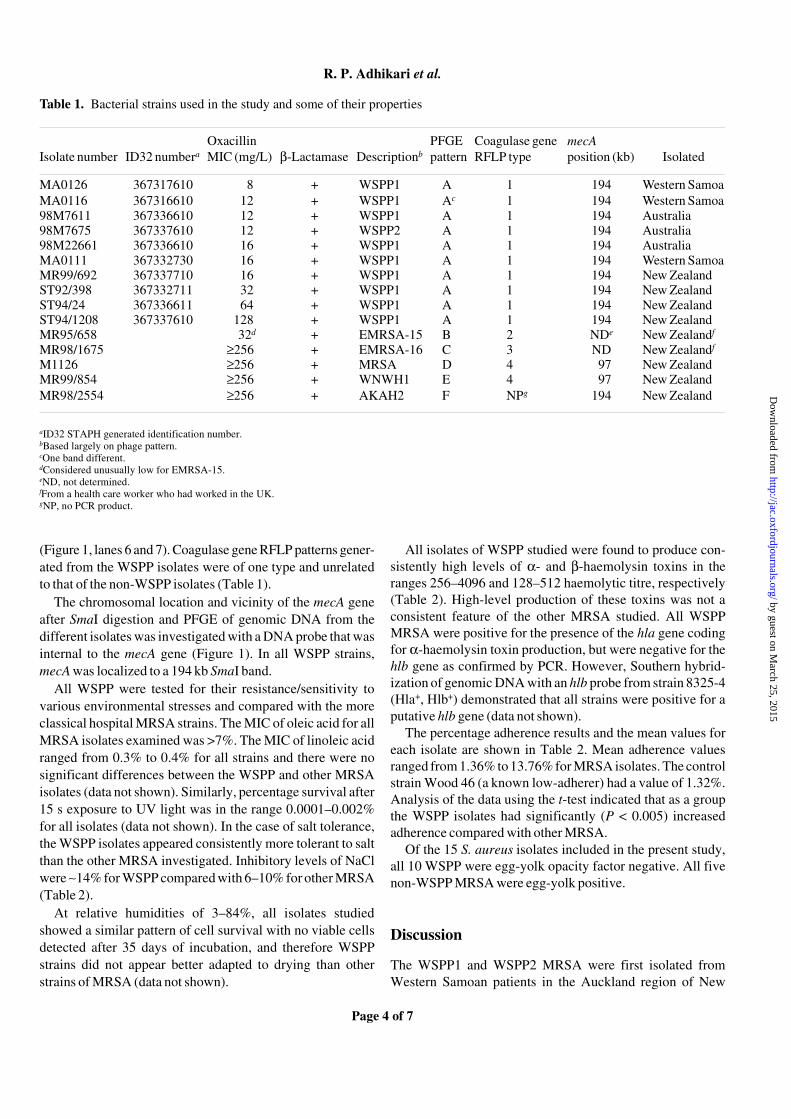
Table 1. Bacterial strains used in the study and some of their properties
aID32 STAPH generated identification number.bBased largely on phage pattern.cOne band different.dConsidered unusually low for EMRSA-15.eND, not determined.fFrom a health care worker who had worked in the UK.gNP, no PCR product.
Isolate number ID32 numberaOxacillin MIC (mg/L) β-Lactamase Descriptionb
PFGE pattern
Coagulase gene RFLP type
mecA position (kb) Isolated
MA0126 367317610 8 + WSPP1 A 1 194 Western SamoaMA0116 367316610 12 + WSPP1 Ac 1 194 Western Samoa98M7611 367336610 12 + WSPP1 A 1 194 Australia98M7675 367337610 12 + WSPP2 A 1 194 Australia98M22661 367336610 16 + WSPP1 A 1 194 AustraliaMA0111 367332730 16 + WSPP1 A 1 194 Western SamoaMR99/692 367337710 16 + WSPP1 A 1 194 New ZealandST92/398 367332711 32 + WSPP1 A 1 194 New ZealandST94/24 367336611 64 + WSPP1 A 1 194 New ZealandST94/1208 367337610 128 + WSPP1 A 1 194 New ZealandMR95/658 32d + EMRSA-15 B 2 NDe New Zealandf
MR98/1675 ≥256 + EMRSA-16 C 3 ND New Zealandf
M1126 ≥256 + MRSA D 4 97 New ZealandMR99/854 ≥256 + WNWH1 E 4 97 New ZealandMR98/2554 ≥256 + AKAH2 F NPg 194 New Zealand
by guest on March 25, 2015
http://jac.oxfordjournals.org/D
ownloaded from
WSPP community MRSA
Page 5 of 7
Zealand during 1992–1993. Whereas Pacific Island groupsoriginally appeared most at risk from WSPP strains, thesestrains are now widespread throughout New Zealand andoccur in all racial populations (although still strongly asso-ciated with Pacific Island people), accounting for >60%(around 2700 isolates from a total of 4500) of all MRSA iso-lated in New Zealand in 2000.2 They are consistently associ-ated with overt skin lesions (abscess or cellulitis) in youngerage groups. In the 2001 New Zealand census, 200 301 (5.4%)of the total population of 3737490 identified themselves asPolynesian.
Our sample of 10 WSPP isolates from New Zealand,Samoa and Australia displayed characteristics consistent withthose found for all other isolates so far examined—identicalmacrorestriction patterns of SmaI-digested DNA, oxacillinMICs in the 8–128 mg/L range, with all susceptible to vanco-mycin and most susceptible to a variety of non-β-lactamantimicrobials such as gentamicin, co-trimoxazole and cipro-floxacin. The most recent (July 2000) local survey in NewZealand revealed that 1.3% of 229 WSPP isolates were resist-ant to two or more classes of antimicrobials in addition toβ-lactams, with >99% still susceptible to chloramphenicol,ciprofloxacin, clindamycin, co-trimoxazole, fusidic acid,gentamicin and tetracycline. Mupirocin resistance was at3.5%.
Apart from New Zealand and Western Samoa, the WSPPclone has been found in Australia;12,13 these isolates were
referred to as gentamicin-sensitive, methicillin-resistantS. aureus (GS-MRSA) in one publication.12 The Australianisolates clearly have identical characteristics to the NewZealand and Western Samoan isolates (Table 1), and as inNew Zealand were first isolated from Polynesians. In theAustralian studies, it was assumed that the strain was intro-duced into Australia from Polynesia via New Zealand,12 oroccurred more commonly (compared with multiresistantMRSA or MSSA) in patients born in New Zealand, Samoa orTonga.13
The possible origins of CMRSA like the WSPP clone isopen to debate. It seems unlikely that they are feral descend-ants of hospital isolates, but more likely represent acommunity MSSA strain that has acquired the mec DNA ele-ment from some other cutaneous staphylococcal species.28
Although it is conceivable that the WSPP clone is of animalorigin (e.g. β-haemolysin toxin producers, egg-yolk opacityfactor negative), the phage patterns of isolates suggest thatthis is unlikely. To some degree, the WSPP clone behaves likethe old phage group I S. aureus, with resistance only topenicillin-type antimicrobials and a predilection for skinabscess/boil formation.
Presumably the WSPP clone originated in Samoa andwas readily disseminated amongst individuals because of theliving conditions found in that country. Thirty-two of 110(29%) adults passing through the front door of a hospital inWestern Samoa were colonized with S. aureus, including
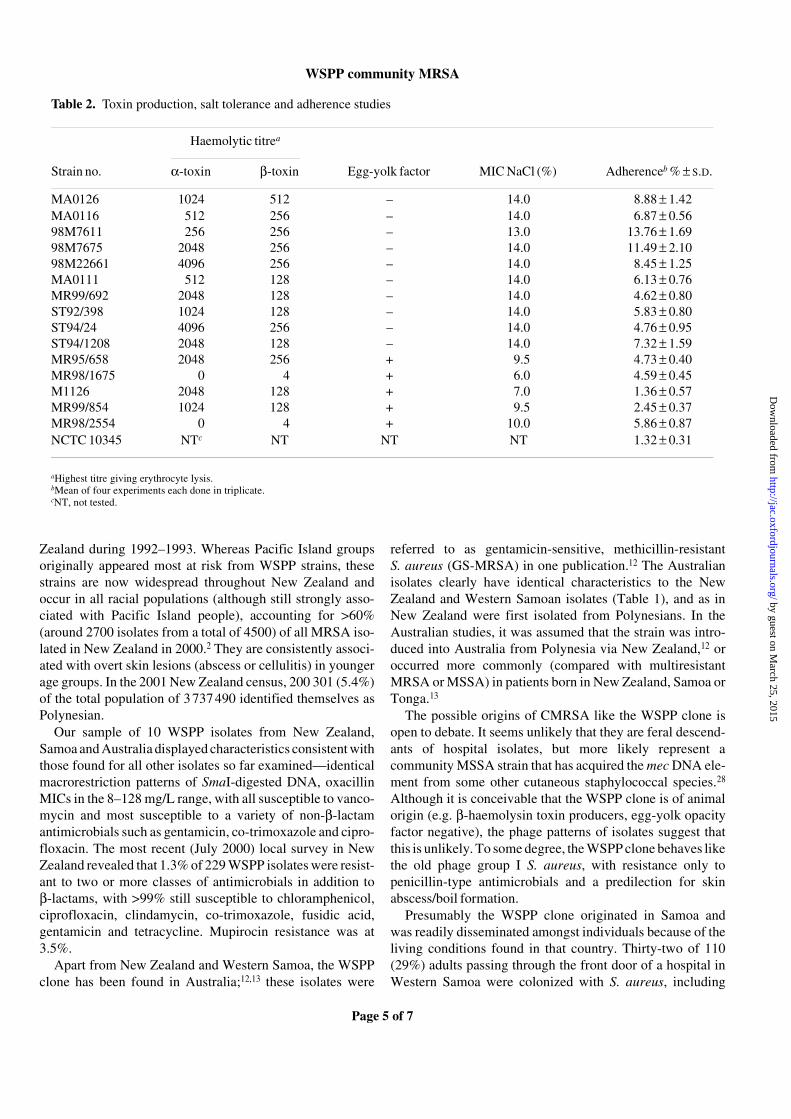
Table 2. Toxin production, salt tolerance and adherence studies
aHighest titre giving erythrocyte lysis.bMean of four experiments each done in triplicate.cNT, not tested.
Haemolytic titrea
Strain no. α-toxin β-toxin Egg-yolk factor MIC NaCl (%) Adherenceb % ± S.D.
MA0126 1024 512 – 14.0 8.88 ± 1.42MA0116 512 256 – 14.0 6.87 ± 0.5698M7611 256 256 – 13.0 13.76 ± 1.6998M7675 2048 256 – 14.0 11.49 ± 2.1098M22661 4096 256 – 14.0 8.45 ± 1.25MA0111 512 128 – 14.0 6.13 ± 0.76MR99/692 2048 128 – 14.0 4.62 ± 0.80ST92/398 1024 128 – 14.0 5.83 ± 0.80ST94/24 4096 256 – 14.0 4.76 ± 0.95ST94/1208 2048 128 – 14.0 7.32 ± 1.59MR95/658 2048 256 + 9.5 4.73 ± 0.40MR98/1675 0 4 + 6.0 4.59 ± 0.45M1126 2048 128 + 7.0 1.36 ± 0.57MR99/854 1024 128 + 9.5 2.45 ± 0.37MR98/2554 0 4 + 10.0 5.86 ± 0.87NCTC 10345 NTc NT NT NT 1.32 ± 0.31
by guest on March 25, 2015
http://jac.oxfordjournals.org/D
ownloaded from

R. P. Adhikari et al.
Page 6 of 7
2.7% with WSPP MRSA.2 Clearly there is no barrier to itscolonization and spread amongst other people of any raceshould the opportunity for spread occur. The high salttolerance of the WSPP clone probably helps in this respect,as would the ability to adhere to cell surfaces. In general,studies27,29 attempting to correlate adherence with epidemic-ity and spread amongst MRSA strains have reported nosignificant differences in the abilities of epidemic MRSA,other MRSA and MSSA to adhere to human nasal epithelialcells, HEp-2 cells or to other cultured cell lines. In ourinvestigations, the WSPP MRSA as a group appeared toadhere significantly better to HEp-2 cells than did all otherMRSA studied. This finding is possibly related in some wayto the unique mec DNA element (Staphylococcus cassettechromosome mec) found in WSPP MRSA (data not shown).
The WSPP isolates were found to be high level α- andβ-haemolysin toxin producers (as determined by assays usedhere and the presence of hla and hlb) in comparison with theother S. aureus isolates tested; this may positively influencethe ability of such isolates to initiate joint/bone infections.25
α-Haemolysin toxin is a pore-forming haemolytic andmembrane-damaging toxin,30 whereas β-haemolysin toxin isproduced by a large number of S. aureus strains, especiallythose of animal origin.31 Our results indicate that α-haemo-lysin toxin production is a consistent feature of WSPP iso-lates, and may in part be responsible for their association withovert cutaneous lesions. All WSPP MRSA were positive forthe presence of the hla gene, but the hlb gene could only bedetected by Southern hybridization. This result suggested thatthe primers used here to amplify hlb were not homologous tothe hlb gene of the WSPP MRSA. Moreover, despite theWSPP isolates being able to produce β-haemolysin toxin, allwere egg-yolk opacity factor negative, suggesting that theβ-haemolysin toxin produced by the WSPP isolates maydiffer from that of other S. aureus isolates. Further work willbe required to determine how this toxin differs in WSPPMRSA strains.
In conclusion, WSPP1 and WSPP2 strains are now themost common type of MRSA found in New Zealand popula-tions. In the main, these non-multiresistant strains appear tobe associated with community-acquired cutaneous lesions,rather than being hospital acquired as is the case for mostMRSA in other countries. WSPP strains are especiallycommon in Polynesian populations and younger age groups.We have shown WSPP MRSA from Western Samoa and NewZealand to be identical to Australian isolates (GR-MRSA)and all of the isolates are likely to represent a single clone.These highly toxigenic, salt tolerant and egg-yolk-negativestrains are clearly clonally related. The WSPP strains as agroup show increased adherence to tissue culture cells com-pared with other MRSA, and this may relate to their increasedfitness and the relative success of this clone.
Acknowledgements
The financial assistance of the Otago Medical ResearchFoundation and the Deans Fund, Otago School of MedicalSciences is gratefully acknowledged. R.P.A. was the recipientof a New Zealand Official Development Assistance (NZODA)Study Award.
References
1. Smith, J. M. B. (1998). Emerging problems of antibiotic resistantbacteria. New Zealand Medical Journal 111, 441–4.
2. Lang, S., Taylor, S. & Morris, A. (2001). Community-acquiredmethicillin-resistant Staphylococcus aureus. Antibiotics and Chemo-therapy 5, 12–3.
3. Mitchell, J. M., MacCulloch, D. & Morris, A. J. (1996). MRSA inthe community. New Zealand Medical Journal 109, 411.
4. Riley, D., MacCulloch, D. & Morris, A. J. (1998). Methicillin-resistant S. aureus in the suburbs. New Zealand Medical Journal111, 59.
5. Rings, T., Findlay, R. & Lang, S. (1998). Ethnicity andmethicillin-resistant S. aureus in South Auckland. New ZealandMedical Journal 111, 151.
6. Ayliffe, G. A. (1997). The progressive intercontinental spreadof methicillin-resistant Staphylococcus aureus. Clinical InfectiousDiseases 24, Suppl. 1, S74–9.
7. Herold, B. C., Immergluck, L. C., Maranan, M. C., Lauderdale,D. S., Gaskin, R. E., Boyle-Vavra, S. et al. (1998). Community-acquired methicillin-resistant Staphylococcus aureus in childrenwith no identified predisposing risk. Journal of the American MedicalAssociation 279, 593–8.
8. Maguire, G. P., Arthur, A. D., Boustead, P. J., Dwyer, B. &Currie, B. J. (1998). Clinical experience and outcomes of community-acquired and nosocomial methicillin-resistant Staphylococcusaureus in a northern Australian hospital. Journal of Hospital Infec-tion 38, 273–81.
9. Gorak, E. J., Yamada, S. M. & Brown, J. D. (1999). Community-acquired methicillin-resistant Staphylococcus aureus in hospitalizedadults and children without known risk factors. Clinical InfectiousDiseases 29, 797–800.
10. Frank, A. L., Marcinak, J. F., Daisy Mangat, P. & Schrecken-berger, P. C. (1999). Increase in community-acquired methicillin-resistant Staphylococcus aureus in children. Clinical InfectiousDiseases 29, 935–6.
11. Kak, V. & Levine, D. P. (1999). Editorial response: community-acquired methicillin-resistant Staphylococcus aureus infections—where do we go from here? Clinical Infectious Diseases 29, 801–2.
12. Nimmo, G. R., Schooneveldt, J., O’Kane, G., McCall, B. &Vickery, A. (2000). Community acquisition of gentamicin-sensitivemethicillin-resistant Staphylococcus aureus in southeast Queens-land, Australia. Journal of Clinical Microbiology 38, 3926–31.
13. Gosbell, I. B., Mercer, J. L., Neville, S. A., Crone, S. A., Chant,K. G., Jalaludin Bin, B. et al. (2001). Non-multiresistant andmultiresistant methicillin-resistant Staphylococcus aureus incommunity-acquired infections. Medical Journal of Australia 174,627–30.
by guest on March 25, 2015
http://jac.oxfordjournals.org/D
ownloaded from

WSPP community MRSA
Page 7 of 7
14. Chambers, H. F. (2001). The changing epidemiology ofStaphylococcus aureus? Emerging Infectious Diseases 7, 178–82.
15. National Committee for Clinical Laboratory Standards. (2000).Performance Standards for Antimicrobial Disk SusceptibilityTests—Seventh Edition: Approved Standard M2-A7. NCCLS, Villa-nova, PA, USA.
16. de Lencastre, H., Couto, I., Santos, I., Melo-Cristino, J., Torres-Pereira, A. & Tomasz, A. (1994). Methicillin-resistant Staphylo-coccus aureus disease in a Portuguese hospital: characterization ofclonal types by a combination of DNA typing methods. EuropeanJournal of Clinical Microbiology and Infectious Diseases 13, 64–73.
17. Geha, D. J., Uhl, J. R., Gustaferro, C. A. & Persing, D. H.(1994). Multiplex PCR for identification of methicillin-resistantStaphylococcus aureus in the clinical laboratory. Journal of ClinicalMicrobiology 32, 1768–72.
18. Sambrook, J., Fritsch, E. F. & Maniatis, T. (1998). MolecularCloning: A Laboratory Manual, 2nd edn. Cold Spring HarborLaboratory Press, Cold Spring Harbor, NY, USA.
19. Goh, S. H., Byrne, S. K., Zhang, J. L. & Chow, A. W. (1992).Molecular typing of Staphylococcus aureus on the basis ofcoagulase gene polymorphisms. Journal of Clinical Microbiology30, 1642–5.
20. Matushek, M. G., Bonten, M. J. & Hayden, M. K. (1996). Rapidpreparation of bacterial DNA for pulsed-field gel electrophoresis.Journal of Clinical Microbiology 34, 2598–600.
21. Tenover, F. C., Arbeit, R. D., Goering, R. V., Mickelsen, P. A.,Murray, B. E., Persing, D. H. et al. (1995). Interpreting chromosomalDNA restriction patterns produced by pulsed-field gel electro-phoresis: criteria for bacterial strain typing. Journal of ClinicalMicrobiology 33, 2233–9.
22. Jones, E. M., Bowker, K. E., Cooke, R., Marshall, R. J., Reeves,D. S. & MacGowan, A. P. (1997). Salt tolerance of EMRSA-16 andits effect on the sensitivity of screening cultures. Journal of HospitalInfection 35, 59–62.
23. Mary, P., Dupuy, N., Dolhem-Biremon, C., Defives, C. &Tailliez, R. (1994). Differences among Rhizobium meliloti andBradyrhizobium japonicum strains in tolerance to desiccation andstorage at different humidities. Soil Biology and Biochemistry 26,1125–32.
24. Lacey, R. W. & Lord, V. L. (1981). Sensitivity of staphylococci tofatty acids: novel inactivation of linolenic acid by serum. Journal ofMedical Microbiology 14, 41–9.
25. Nilsson, I.-M., Hartford, O., Foster, T. & Tarkowski, A. (1999).Alpha-toxin and gamma-toxin jointly promote Staphylococcusaureus virulence in murine septic arthritis. Infection and Immunity67, 1045–9.
26. Jarraud, S., Mougel, C., Thioulouse, J., Lina, G., Meugnier, H.,Forey, F. et al. (2002). Relationships between Staphylococcusaureus genetic background, virulence factors, agr groups (alleles),and human disease. Infection and Immunity 70, 631–41.
27. Aathithan, S., Dybowski, R. & French, G. L. (2001). Highlyepidemic strains of methicillin-resistant Staphylococcus aureus notdistinguished by capsule formation, protein A content or adherenceto HEp-2 cells. European Journal of Clinical Microbiology andInfectious Diseases 20, 27–32.
28. Wielders, C. L. C., Vriens, M. R., Brisse, S., de Graaf-Miltenbury, L. A. M., Troelstra, A., Fleer, A. et al. (2001). Evidenceof in-vivo transfer of mecA DNA between strains of Staphylococcusaureus. Lancet 357, 1674–5.
29. Duckworth, G. J. & Jordens, J. Z. (1990). Adherence andsurvival properties of an epidemic methicillin-resistant strain ofStaphylococcus aureus compared with those of methicillin-sensitivestrains. Journal of Medical Microbiology 32, 195–200.
30. Harshman, S., Boquet, P., Duflot, E., Alouf, J. E., Montecucco,C. & Papini, E. (1989). Staphylococcal alpha-toxin: a study ofmembrane penetration and pore formation. Journal of BiologicalChemistry 264, 14978–84.
31. Dinges, M. M., Orwin, P. M. & Schlievert, P. M. (2000). Exo-toxins of Staphylococcus aureus. Clinical Microbiology Reviews 13,16–34.
by guest on March 25, 2015
http://jac.oxfordjournals.org/D
ownloaded from