periodontal inflammatory conditions among smokers and never-smokers with and without type 2 diabetes...
TRANSCRIPT

For Peer Review
Periodontal inflammatory conditions among smokers and
never-smokers with and without type 2 diabetes mellitus
Journal: Journal of Periodontology
Manuscript ID: JOP-15-0120.R1
Manuscript Type: Original Article
Date Submitted by the Author: n/a
Complete List of Authors: Javed, Fawad; University of Rochester, Division of General Dentistry; Al-Kheraif, Abdulaziz A.; King Saud University, Applied Medical Sciences Lazo, Karem Salazar; University of Rochester, General Dentistry Fontenla, Virginia Yanez; University of Rochester, General Dentistry Aldosary, Khaled; King Saud University, Division of Restorative Dentistry Alshehri, Mohammed; King Saud University, Division of Restorative and
Implant Dentistry Malmstrom, Hans; University of Rochester, General Dentisry Romanos, Georgios; Stonybrook,
Key Words: Periodontal-systemic disease interactions, Smoking, Diabetes
Journal of Periodontology
For Peer Review
1
Title: Periodontal inflammatory conditions among smokers and never-smokers with and
without type 2 diabetes mellitus
Authors: Fawad Javed,* Abdulaziz A. Al-Kheraif,
† Karem Salazar Lazo,
* Virginia Yanez
Fontenla,* Khalid M. Aldosary,
‡ Mohammed Alshehri,
‡ Hans Malmstrom,
* Georgios E.
Romanosǁ
Affiliations:
* Division of General Dentistry, Eastman Institute for Oral Health, University of Rochester,
Rochester, NY;
† Dental Biomaterials Research Chair, Dental Health Department, College of Applied Medical
Sciences; King Saud University, Riyadh, Saudi Arabia;
‡ Dental Department, King Khalid University Hospital, King Saud University, Riyadh, Saudi
Arabia;
§ Department of Periodontology, School of Dental Medicine, Stony Brook University, NY.
Running title: Periodontal inflammation, smoking and T2DM
One sentence summary: Periodontal inflammatory conditions are comparable among smokers
and never-smokers with T2DM. Among controls, periodontal inflammation is worse among
smokers than never-smokers.
Correspondence: Dr. Fawad Javed, Division of General Dentistry, Eastman Institute for Oral
Health, University of Rochester, Rochester, NY 14642, USA. Email:
Page 1 of 27 Journal of Periodontology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
2
ABSTRACT
Background: There is a dearth of studies regarding the influence of cigarette smoking on
periodontal inflammatory conditions among patients with type 2 diabetes mellitus (T2DM). The
aim of the present study was to assess periodontal inflammatory conditions among smokers and
never-smokers with and without T2DM.
Methods: One hundred individuals (50 patients with T2DM [25 smokers and 25 never-smokers]
and 50 controls [25 smokers and 25 never-smokers]) were included. Information regarding age,
gender, duration and daily frequency of smoking, duration and treatment of diabetes and oral
hygiene was recorded using a questionnaire. Periodontal parameters (plaque index [PI], bleeding
on probing [BOP], probing depth [PD], clinical attachment [CA] loss and marginal bone loss
[MBL]) were measured. Hemoglobin A1c (HbA1c) levels were also recorded.
Results: Mean age, monthly income status and education levels were comparable among
smokers and never-smokers with and without T2DM. Mean HbA1c Levels were significantly
higher among patients with T2DM (8.2±0.1%) compared to controls (4.4±0.3%) (P<0.05).
Smokers in the control group were smoking significantly greater number of cigarettes (15.5±2.5
cigarettes daily) compared to smokers with T2DM (6.2±2.1 cigarettes daily) (P<0.05).
Periodontal parameters were comparable among smokers and never-smokers with T2DM.
Among controls, periodontal parameters (PI [P<0.05], CA loss [P<0.05], PD≥4mm [P<0.05] and
MBL [P<0.05]) were significantly higher in smokers than never smokers. Never-smokers with
T2DM had worse periodontal status than smokers and never-smokers in the control group
(P<0.05).
Page 2 of 27Journal of Periodontology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
3
Conclusion: Periodontal inflammatory conditions are comparable among smokers and never-
smokers with T2DM. Among controls, periodontal inflammation is worse among smokers than
never-smokers.
Key words (MeSH): Alveolar bone loss; Bleeding on probing; Cigarette smoking; Dental
plaque; Inflammation; Type 2 Diabetes Mellitus;
Page 3 of 27 Journal of Periodontology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
4
INTRODUCTION
It is well-established that chronic hyperglycemia is a significant risk factor for
periodontal inflammatory conditions.1-4
Studies3, 5, 6
have shown that clinical parameters of
periodontal inflammation (such as plaque index [PI], bleeding on probing [BOP], probing depth
[PD]≥4mm and clinical attachment [CA] loss are worse among patients with poorly-controlled
type 2 diabetes mellitus (T2DM) as compared to systemically healthy individuals (controls).
Moreover, marginal bone loss (MBL) around teeth, a radiographic marker of periodontal
inflammation is also higher among patients with poorly-controlled T2DM than controls.3, 7
An
explanation that has been posed in this regard is that persistent hyperglycemia increases the
formation and accumulation of advanced glycation endproducts (AGEs) in periodontal tissues,
which in turn impairs the chemotactic and phagocytic function of polymorphonuclear leukocytes
(PMNL) and produces proinflammatory cytokines in the serum and gingival crevicular fluid.8, 9
This leads to periodontal inflammation and MBL in patients with T2DM. Furthermore, function
of potential cells involved in immunoinflammatory responses is also sabotaged in a chronic
hyperglycemic state.10
The deleterious effects of tobacco smoking on oral and systemic health are well
documented.11-15
Habitual tobacco smoking has also been associated with an increased
expression of receptors of AGEs in the gingival tissues.16
This in turn jeopardizes the
chemotactic and phagocytic functions of PMNL and provokes a proinflammatory effect by
stimulating the secretion of cytokines and reactive oxygen species that directly cause destruction
of periodontal tissues.17-20
Clinical studies3, 14, 21
have also shown that habitual tobacco smokers
exhibit greater number of sites with plaque accumulation, CA loss and PD (≥ 4mm) as compared
to individual who had never used tobacco in any form. It is however, important to mention that
Page 4 of 27Journal of Periodontology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
5
BOP (a classical marker of periodontal disease activity22
), is masked in tobacco smokers than
never-smokers.3, 21
This most probably occurs as a result of the vasoconstrictive effect of
nicotine on gingival blood vessels.23
Therefore, tobacco smokers may remain unaware of
ongoing periodontal destruction until the inflammatory process reaches a stage where tooth
mobility becomes evident.
Since chronic hyperglycemia and habitual tobacco smoking are significant and
independent risk factors of periodontal disease;3, 21
it is hypothesized that periodontal
inflammatory conditions are more intense among smokers with T2DM as compared to never-
smokers with T2DM. Therefore, the aim of the present study was to assess the periodontal
inflammatory conditions among smokers and never-smoker with and without T2DM.
MATERIALS AND METHODS
Ethical guidelines
The study was approved by the Research Ethics Review committee of the College of
Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia (OR-114-2084). It was
mandatory for all study participants to have read and signed the consent form before being
included in the present investigation.
Eligibility Criteria
The inclusion criteria encompassed the following: (a) Patients with medically diagnosed
T2DM (HbA1c ≥ 6.5%)24
; (b) self-reported controls. The exclusion criteria were: (a) Individuals
Page 5 of 27 Journal of Periodontology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
6
with self-reported systemic diseases other than T2DM (such as human immunodeficiency virus
infection/acquired immunodeficiency syndrome, cardiovascular diseases, renal disease, hepatic
disorder and epilepsy); (b) edentulous individuals; (c) crowding of teeth or occlusal trauma; (d)
habitual alcohol consumers; (e) lactating and/or pregnant individuals; (f) individuals who
reported to have consumed antibiotics, non-steroidal anti-inflammatory drugs and/or steroids
within the past three months; (g) bilateral maxillary and mandibular third molars.
Study participants and groups
Between November 2013 and July 2014, a convenience sample case-control study
involving smokers and never-smokers with and without T2DM was conducted at the College of
Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia. All participants were
recruited from a local residential area in Riyadh, South Arabia. Clinical and radiographic
examinations were performed at the College of Applied Medical Sciences, King Saud
University, Riyadh, South Arabia. All participants who reported to have T2DM were requested
to present their medical records in order to verify the diagnosis of T2DM. Smokers were defined
as individuals who reported to be smoking at least one cigarette daily since at least 1 year.3
Never-smokers were defined as individuals who reported to have never consumed tobacco in any
form.3
Page 6 of 27Journal of Periodontology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
7
Questionnaire
Information regarding gender, age, socioeconomic status (SES), education status
(graduate level education— post-4 year college degree), duration of smoking, number of
cigarettes smoked daily, duration of T2DM, treatment of T2DM recommended by healthcare
provider/s and daily oral hygiene maintenance protocols were collected using a questionnaire. A
trained interviewer (AAK) presented the questionnaire to all participants.
Clinical periodontal parameters
A calibrated and trained investigator (MA) blinded to the study groups performed the
periodontal clinical examinations. The overall k value for intraexaminer reliability was 0.91.
Full-mouth PI,25
BOP,26
PD27
, and CA loss28
were measured at six sites (mesiobuccal, mid-
buccal, distobuccal, distolingual/palatal, mid-lingual/palatal, and mesiolingual/palatal) on all
maxillary and mandibular teeth. A graded probeǁ was used to measure the probing depth to
nearest millimeter.3 Broken down teeth with embedded roots remnants were excluded.
Radiographic parameter
Full mouth digital bitewing radiographs¶ were taken and were viewed on a calibrated
computer screen# using a software program
**. MBL (defined as the vertical distance from 2 mm
below the cementoenamel junction (CEJ) to the most apical part of marginal bone3) was
measured on all teeth. Surfaces of teeth on which the CEJ or the bone crest were not visible due
to technical reasons (such as dental caries, dental restorations, malocclusion and/or poor
Page 7 of 27 Journal of Periodontology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
8
radiography quality) were excluded. All radiographic assessments were performed by one trained
and calibrated investigator (MA). The overall k value for intraexaminer reliability was 0.89.
Hemoglobin A1c levels
In all groups, HbA1c levels were measured using ion-exchange high-performance liquid
chromatography and expressed as percentages.29
Statistical analysis
Statistical analysis was performed using a software program††
. Clinical and radiographic
periodontal parameters among smokers and never-smokers with and without T2DM were
assessed using one way analysis of variance. Multiple logistic regression analysis was also
performed using a software program††
. This was done evaluate the associations between
periodontal inflammation among smokers and never-smokers with and without T2DM (after
adjustment for tooth brushing habits-confounder). For multiple comparisons, Bonferroni post hoc
adjustment test was used. Power and sample sizes were calculated using a computer software‡‡
.
With inclusion of 50 patients individuals with T2DM [25 smokers and 25 never-smokers] and 50
controls [25 smokers and 25 never-smokers] (assuming a standard deviation of 1.0%), the study
power was estimated to be 85% with a two-sided significance level of 0.05. P-values < 0.05 were
considered statistically significant.
Page 8 of 27Journal of Periodontology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
9
RESULTS
General Characteristics of the study population
In total, 100 individuals (50 patients with T2DM and 50 controls) were included. All
participants were males. The mean age, monthly income status and education levels were
comparable among smokers and never-smokers with and without T2DM. Among patients with
diabetes, the duration of T2DM was 8.5±1.5 years. Among smokers and never-smokers with
T2DM the mean duration of T2DM was 4.6±1.1 years and 10.2±2.5 years, respectively. The
duration of smoking habit among patients with T2DM and controls was 12.6± 4.8 years and
16.4±5.1 years, respectively. Smokers in the control group were smoking significantly greater
number of cigarettes (15.5±2.5 cigarettes daily) compared to smokers with T2DM (6.2±2.1
cigarettes daily) (P<0.05). Seventy-eight percent individuals with T2DM and 88% controls
reported to brush their teeth once daily. None of the participants either with or without T2DM
reported to have ever used dental floss (Table 1).
Hemoglobin A1c
The mean HbA1c Levels were significantly higher among patients with T2DM
(8.2±0.1%) compared to controls (4.4±0.3%) (P<0.05). There was a statistically significant
difference in the mean HbA1c levels among smokers with (7.8±0.4%) and without T2DM
(4.3±0.1%) (P<0.05) (Table1). The mean HbA1c levels were significantly higher among patients
with T2DM (8.2±0.1%) as compared to never-smokers in the control group (4.5±0.1%) (P<0.05).
There was no statistically significance difference in mean HbA1c levels among smokers and
never-smokers with and without T2DM. Never-smokers with T2DM (8.7±0.2%) had a
significantly higher mean HbA1c Levels than smokers in the control group (4.3±0.1%) (P<0.05).
Page 9 of 27 Journal of Periodontology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
10
Among never-smokers with and without T2DM, the mean HbA1c Levels were 8.7±0.2% and
4.5±0.1%, respectively (P<0.05). All patients with T2DM were prescribed conventional
allopathic medications for the management of hypoglycemia. Most of the individuals with and
without T2DM reported to brush their teeth once a day (Table 1).
Periodontal parameters among smokers and never smokers with and without T2DM
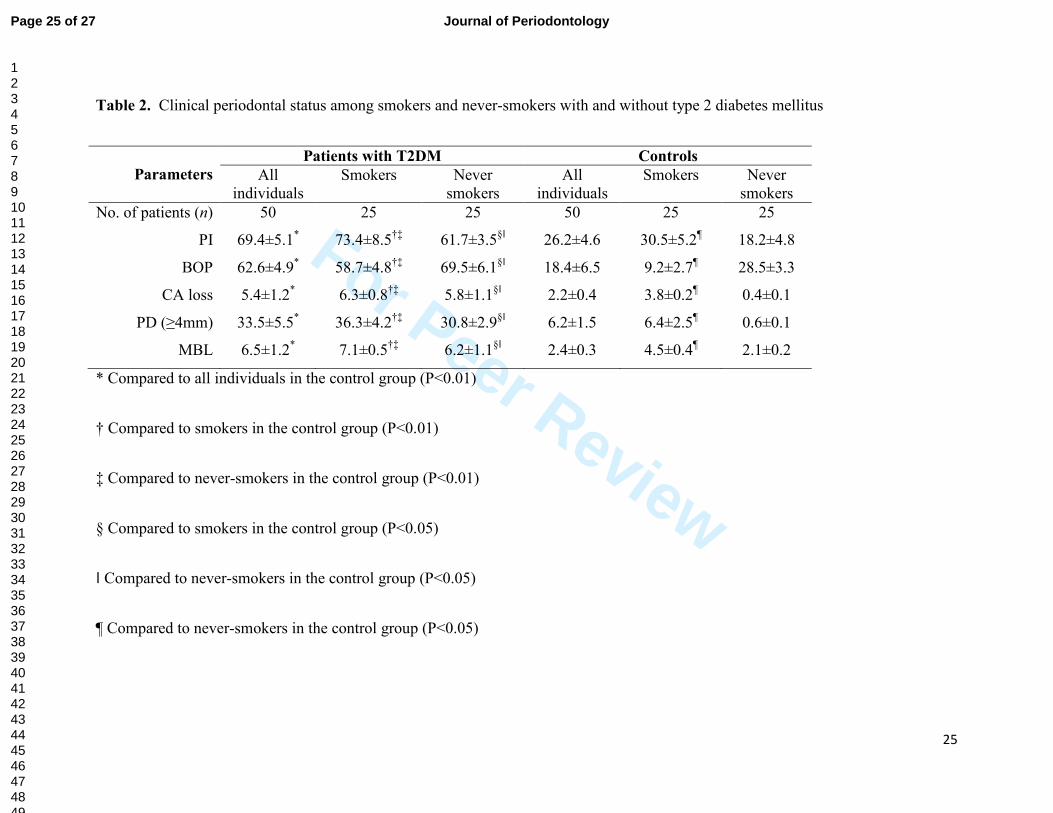
Periodontal parameters (PI [P<0.01], BOP [P<0.01], CA loss [P<0.01], PD≥4mm
[P<0.01] and MBL [P<0.01]) were significantly higher among patients with T2DM than
controls.
Periodontal parameters were significantly higher among smokers with T2DM than
smokers and never-smokers in the control group (PI [P<0.01], BOP [P<0.01], CA loss [P<0.01],
PD≥4mm [P<0.01] and MBL [P<0.01]). Never-smokers with T2DM had worse periodontal
status than smokers and never-smokers in the control group (PI [P<0.05], BOP [P<0.05], CA
loss [P<0.05], PD≥4mm [P<0.05] and MBL [P<0.05]). Among controls, periodontal parameters
(PI [P<0.05], CA loss [P<0.05], PD≥4mm [P<0.05] and MBL [P<0.05]) were significantly
higher in smokers than never-smokers. In the control group, never-smokers demonstrated
significantly greater sites with BOP than smokers (P<0.05). These results are summarized in
Table 2.
Periodontal parameters among smokers and never-smokers with T2DM after stratification for
brushing habits.
Periodontal parameters, PI, BOP, PD≥4mm, CA Loss and the MBL were comparable
among patients with T2DM who brushed their teeth once and twice a day (Figure 1A and 1B).
Page 10 of 27Journal of Periodontology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
11
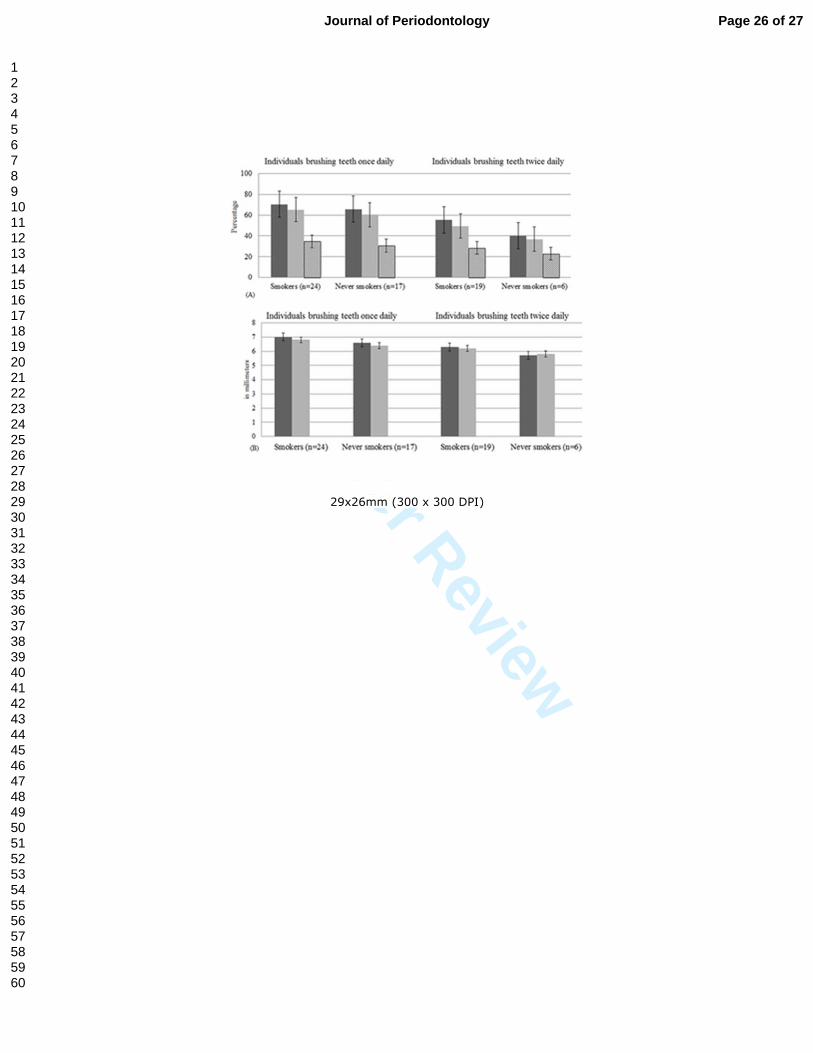
Periodontal parameters among smokers and never smokers in the control group after
stratification for brushing habits.
Among individuals who brushed their teeth once and twice daily, PI (P<0.01), PD≥4mm
(P<0.01) and MBL (P<0.01) were significantly higher among smokers than never-smokers.
Never-smokers showed significantly greater number of sites with BOP (P<0.01) than smokers
regardless of their daily tooth brushing frequency (Figure 2A and 2B).
DISCUSSION
The present study was based on the hypothesis that periodontal inflammatory conditions
are worse among smokers with T2DM than never-smokers with T2DM. This was mainly
speculated due to the fact that both hyperglycemia and habitual smoking enhance the formation
and accumulation of AGEs in the periodontal tissues, which jeopardize periodontal health.9
16
Interestingly, in the present study, clinical and radiologic parameters of periodontal inflammation
(PI, BOP, PD [≥4mm], CA loss and MBL, respectively) were comparable among smokers and
never-smokers with T2DM. It is pertinent to note that all individuals with T2DM (smokers and
never-smokers) included in the present investigation had poorly-controlled T2DM (HbA1c
≥6.5%). It is known that persistent hyperglycemia is associated with increased formation and
accumulation of AGEs in the periodontal tissues. Therefore, it is likely that AGEs produced and
accumulated in the periodontal tissues of smokers and never-smokers with T2DM were
comparable. This could be an explanation for the similar periodontal inflammatory parameters
among smokers and never-smokers with T2DM.
Page 11 of 27 Journal of Periodontology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
12
Among controls, PI, PD (≥4mm), CA loss and MBL were worse in smokers than never
smokers; however, sites with BOP were more often manifested in never-smokers as compared to
smokers. These results are in accordance with previous studies.3, 14
A precise mechanism by
which habitual smoking increases periodontal inflammation is poorly understood. However, it
has been reported that smoking induces endothelial dysfunction, which may initiate an
inflammatory response in the vascular walls.30
This inflammatory response is mediated by pro-
inflammatory cytokines (such as IL-6, and tumor necrosis factor alpha) and adhesion
molecules.30
Serum levels of immunoglobulin (Ig) G (particularly IgG2, an important antibody
against gram-negative periodontal microbes), have also been reported to be lower in smokers
than never-smokers, thereby making them more susceptible to develop periodontal disease. 31, 32
It is noteworthy that a suppressed BOP among smokers (most likely due to the vasoconstrictive
effect of nicotine on gingival blood vessels 23
) may make them unaware of the ongoing
periodontal destruction sometimes until the stage where tooth mobility becomes evident (as a
result of profound MBL). It is therefore imperative for healthcare providers to educate patients
about the detrimental effect of smoking on oral health. In addition, routine community-based
smoking awareness programs are also warranted for patient/community education purposes.
It is well-known that advancing age3, poor education status
3 and underprivileged SES
3
are significant risk-factors of periodontal inflammatory conditions. In this regard, these factors
may be considered as confounders while assessing periodontal inflammatory conditions among
smokers and never-smokers with and without T2DM. It is emphasized that in the present study,
mean age, graduate level education (post-four year college degree) status and SES were
comparable in smokers and never-smokers among individuals with and without T2DM. It was
therefore perceived that the only parameter that may have influenced the periodontal
Page 12 of 27Journal of Periodontology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
13
inflammatory conditions among smokers and never-smokers with and without T2DM was daily
tooth brushing frequency. After stratification of data with reference to daily tooth brushing
protocols (once and twice daily ), it was observed that periodontal parameters (PI, BOP, PD≥4
mm, CA loss and MBL) remained comparable among smokers and never-smokers with T2DM
(Figure 1A and 1B). This outcome also suggests that chronic hyperglycemia seems to be the
most likely factor that influenced periodontal inflammation in patients with T2DM and the role
of smoking in this regard was rather secondary. Among controls, there was no significant
difference in periodontal parameters in patients who either brushed their teeth once or twice daily
(Figure 2A and 2B). These results are in accordance with the study by Attin and Hornecker33
,
which reported that tooth brushing once daily is sufficient to maintain oral health and to prevent
periodontal inflammation.
A limitation of the present study is that all individuals that agreed to participate in the
present investigation were males. Although females were also invited to participate in the present
study; none of them volunteered. It is known that hormonal changes and postmenopausal state
influences periodontal health status. It is therefore likely that female smokers with T2DM in the
postmenopausal phase may exhibit variation in the expression of periodontal disease activity as
compared to male smokers with T2DM.34
Furthermore, in the present study, controls were
smoking almost twice as many cigarettes (~15 cigarettes daily) as compared to patients with
T2DM (~6 cigarettes daily). It is tempting to hypothesize that diabetic smokers who smoke
approximately 15 cigarettes a day may exhibit more intense periodontal inflammation as
compared to never-smokers with T2DM. However, further randomized controlled trials are
warranted to assess a dose-dependent relationship between smoking, periodontal disease and
T2DM.
Page 13 of 27 Journal of Periodontology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
14
CONCLUSION
Periodontal inflammatory conditions are comparable among smokers and never-smokers
with T2DM. Among controls, periodontal inflammation is worse among smokers than never-
smokers.
Page 14 of 27Journal of Periodontology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
15
LEGENDS
Table 1. Sociodemographic characteristics of the study participants
Table 2. Clinical periodontal status among smokers and never-smokers with and without type 2
diabetes mellitus
Figure 1. (A) Plaque index (dark grey bars), bleeding on probing (light grey bars) and probing
depth (≥4mm) (striped bars) among smokers and never-smokers with type 2 diabetes mellitus
after stratification for brushing habits. (B) Clinical attachment loss (dark grey bars) and
marginal bone loss (light grey bars) among smokers and never-smokers with type 2 diabetes
mellitus after stratification for brushing habits.
Figure 2. (A) Plaque index (dark grey bars), bleeding on probing (light grey bars) and probing
depth (≥4mm) (striped bars) among smokers and never-smokers in the control group after
stratification for brushing habits. (B) Clinical attachment loss (dark grey bars) and marginal bone
loss (light grey bars) among smokers and never-smokers in the control group after stratification
for brushing habits. *P<0.01 †P<0.01 ‡P<0.01 §P<0.01 ǁP<0.01 ¶P<0.01
Page 15 of 27 Journal of Periodontology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
16
FOOT NOTES
ǁ Hu-Friedy, Chicago, IL.
¶ Ektaspeed plus; Kodak, Rochester, NY.
# Samsung SyncMaster digital TV monitor, Suwon City, Gyeonggi-do, Korea.
** Image Tool 3.0, Department of Dental Diagnostic Science, University of Texas Health
Science Center, San Antonio, TX.
†† SPSS v.18, IBM, Chicago, IL.
‡‡ nQuery Advisor 6.0, Statistical Solutions, Saugas, MA.
Page 16 of 27Journal of Periodontology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
17
ACKNOWLEDGEMENTS
The authors extend their appreciation to the Research Center, College of Applied Medical
Sciences and Deanship of Scientific Research at King Saud University, Saudi Arabia for funding
this research. The authors also thank the Visiting Professor Program at King Saud University,
Saudi Arabia for supporting this research project.
Page 17 of 27 Journal of Periodontology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
18
Conflict of interest and financial disclosure
The authors declare that they have no conflict of interest and there was no external source of
funding for the present study.
Page 18 of 27Journal of Periodontology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
19
REFERENCES
1. Friesen LR, Walker MP, Kisling RE, Liu Y, Williams KB. Knowledge of risk factors and
the periodontal disease-systemic link in dental students' clinical decisions. J Dent Educ
2014;78:1244-1251.
2. Haseeb M, Khawaja KI, Ataullah K, Munir MB, Fatima A. Periodontal disease in type 2
diabetes mellitus. J Coll Physicians Surg Pak 2012;22:514-518.
3. Javed F, Nasstrom K, Benchimol D, Altamash M, Klinge B, Engstrom PE. Comparison
of periodontal and socioeconomic status between subjects with type 2 diabetes mellitus
and non-diabetic controls. J Periodontol 2007;78:2112-2119.
4. Chee B, Park B, Bartold PM. Periodontitis and type II diabetes: a two-way relationship.
Int J Evid Based Healthc 2013;11:317-329.
5. Javed F, Klingspor L, Sundin U, Altamash M, Klinge B, Engstrom PE. Periodontal
conditions, oral Candida albicans and salivary proteins in type 2 diabetic subjects with
emphasis on gender. BMC Oral Health 2009;9:12.
6. Javed F, Altamash M, Klinge B, Engstrom PE. Periodontal conditions and oral symptoms
in gutka-chewers with and without type 2 diabetes. Acta Odontol Scand 2008;66:268-
273.
7. de Oliveira Diniz CK, Correa MG, Casati MZ, et al. Diabetes mellitus may increase bone
loss after occlusal trauma and experimental periodontitis. J Periodontol 2012;83:1297-
1303.
Page 19 of 27 Journal of Periodontology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
20
8. Javed F, Al-Askar M, Al-Hezaimi K. Cytokine profile in the gingival crevicular fluid of
periodontitis patients with and without type 2 diabetes: a literature review. J Periodontol
2012;83:156-161.
9. Gurav AN. Advanced glycation end products: a link between periodontitis and diabetes
mellitus? Curr Diabetes Rev 2013;9:355-361.
10. Mealey BL. Periodontal disease and diabetes. A two-way street. J Am Dent Assoc
2006;137 Suppl:26S-31S.
11. Nakanishi R, Berman DS, Budoff MJ, et al. Current but not past smoking increases the
risk of cardiac events: insights from coronary computed tomographic angiography. Eur
Heart J 2015 doi: 10.1093/eurheartj/ehv013 [Epub ahead of print].
12. Wang J, Qiu M, Xu Y, et al. Long noncoding RNA CCAT2 correlates with smoking in
esophageal squamous cell carcinoma. Tumour Biol 2015 doi: 10.1007/s13277-015-3220-
x [Epub ahead of print].
13. Al-Amad SH, Awad MA, Nimri O. Oral cancer in young Jordanians: potential
association with frequency of narghile smoking. Oral Surg Oral Med Oral Pathol Oral
Radiol 2014;118:560-565.
14. Javed F, Al-Askar M, Samaranayake LP, Al-Hezaimi K. Periodontal disease in habitual
cigarette smokers and nonsmokers with and without prediabetes. Am J Med Sci
2013;345:94-98.
15. Javed F, Bashir Ahmed H, Romanos GE. Association between environmental tobacco
smoke and periodontal disease: a systematic review. Environ Res 2014;133:117-122.
Page 20 of 27Journal of Periodontology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
21
16. Biswas SK, Mudi SR, Mollah FH, Bierhaus A, Arslan MI. Serum soluble receptor for
advanced glycation end products (sRAGE) is independently associated with cigarette
smoking in non-diabetic healthy subjects. Diab Vasc Dis Res 2013;10:380-382.
17. Breitling LP, Yang R, Korn B, Burwinkel B, Brenner H. Tobacco-smoking-related
differential DNA methylation: 27K discovery and replication. Am J Hum Genet
2011;88:450-457.
18. Katz J, Yoon TY, Mao S, Lamont RJ, Caudle RM. Expression of the receptor of
advanced glycation end products in the gingival tissue of smokers with generalized
periodontal disease and after nornicotine induction in primary gingival epithelial cells. J
Periodontol 2007;78:736-741.
19. Katz J, Caudle RM, Bhattacharyya I, Stewart CM, Cohen DM. Receptor for advanced
glycation end product (RAGE) upregulation in human gingival fibroblasts incubated with
nornicotine. J Periodontol 2005;76:1171-1174.
20. Palmer RM, Scott DA, Meekin TN, Poston RN, Odell EW, Wilson RF. Potential
mechanisms of susceptibility to periodontitis in tobacco smokers. J Periodontal Res
1999;34:363-369.
21. Javed F, Al-Kheraif AA, Al Amri MD, et al. Periodontal status and whole salivary
cytokine profile among smokers and never-smokers with and without prediabetes. J
Periodontol 2015 doi: 10.1902/jop.2015.140593:1-15 [Epub ahead of print].
22. Gutweniger CA. Gingival bleeding as an indication of periodontal disease. J Oreg Dent
Assoc 1983;52:37-39.
23. Clarke NG, Shephard BC. The effects of epinephrine and nicotine on gingival blood flow
in the rabbit. Arch Oral Biol 1984;29:789-793.
Page 21 of 27 Journal of Periodontology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
22
24. American Diabetes Association. Standards of medical care in diabetes--2011. Diabetes
Care 2011;34 Suppl 1:S11-61.
25. Ainamo J, Bay I. Problems and proposals for recording gingivitis and plaque. Int Dent J
1975;25:229-235.
26. Muhlemann HR, Son S. Gingival sulcus bleeding--a leading symptom in initial gingivitis.
Helv Odontol Acta 1971;15:107-113.
27. Armitage GC, Svanberg GK, Loe H. Microscopic evaluation of clinical measurements of
connective tissue attachment levels. J Clin Periodontol 1977;4:173-190.
28. Genco RJ, Grossi SG, Ho A, Nishimura F, Murayama Y. A proposed model linking
inflammation to obesity, diabetes, and periodontal infections. J Periodontol
2005;76:2075-2084.
29. Ozcelik F, Yiginer O, Arslan E, et al. Association between glycemic control and the level
of knowledge and disease awareness in type 2 diabetic patients. Pol Arch Med Wewn
2010;120:399-406.
30. Ojima M, Hanioka T. Destructive effects of smoking on molecular and genetic factors of
periodontal disease. Tob Induc Dis 2010;8:4.
31. Quinn SM, Zhang JB, Gunsolley JC, Schenkein HA, Tew JG. The influence of smoking
and race on adult periodontitis and serum IgG2 levels. J Periodontol 1998;69:171-177.
32. Tomar SL, Asma S. Smoking-attributable periodontitis in the United States: findings
from NHANES III. National Health and Nutrition Examination Survey. J Periodontol
2000;71:743-751.
33. Attin T, Hornecker E. Tooth brushing and oral health: how frequently and when should
tooth brushing be performed? Oral Health Prev Dent 2005;3:135-140.
Page 22 of 27Journal of Periodontology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
23
34. DeBaz C, Shamia H, Hahn J, Mithani S, Sadeghi G, Palomo L. Periodontitis impacts
quality of life in postmenopausal women. Climacteric 2015 doi:
10.3109/13697137.2014.996124:1-6 [Epub ahead of print].
Page 23 of 27 Journal of Periodontology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
24
Table 1. Sociodemographic characteristics of the study participants
Parameters
Patients with T2DM Controls
All
individuals
Smokers Never
smokers
All
individuals
Smokers Never
smokers
No. of patients (n) 50 25 25 50 25 25
Gender (Male) 50 25 25 50 25 25
Mean age (in years) 52.6±3.8 50.6±1.8 54.1±3.2 50.5±2.4 48.5±4.8 55.6±5.5
Duration of T2DM (in years) 8.5±1.5 4.6±1.1 10.2±2.5 — — —
Duration of smoking (in years) 12.6±4.8 12.6±4.8 — 16.4±5.1 16.4±5.1 —
No. of cigarettes smoked daily (n) 6.2±2.1
6.2±2.1* — 15.5±2.5 15.5±2.5 —
Monthly income (in USD) 525±85.4 498.7±90.6
598.5±75.5
585±88.6 530.6±54.7 627±58.8
Graduate level education status (%) 40% 16% 24% 41% 19% 22%
Mean Hemoglobin A1c (±SD) 8.2±0.1† 7.8±0.4
‡§ 8.7±0.2
ǁ¶ 4.4±0.3 4.3±0.1 4.5±0.1
Treatment of T2DM
Allopathic 100% 100% 100% — — —
Homeopathic — — — — — —
Others — — — — — —
Daily tooth brushing
Once daily 78% 80% 76% 88% 92% 84%
Twice daily 22% 20% 24% 12% 8% 16%
Three times or more — — — — — —
Have you ever used a dental floss?
Yes — — — — — —
No 100% 100% 100% 100% 100% 100% *Compared to smokers in the control group (P<0.05)
† Compared to all individuals in the control group (P<0.05)
‡ Compared to smokers in the control group (P<0.05)
§ Compared to never-smokers in the control group (P<0.05)
ǁ Compared to smokers in the control group (P<0.05) ¶ Compared to never-smokers in the control group (P<0.05)
Page 24 of 27Journal of Periodontology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
25
Table 2. Clinical periodontal status among smokers and never-smokers with and without type 2 diabetes mellitus
Parameters
Patients with T2DM Controls
All
individuals
Smokers Never
smokers
All
individuals
Smokers Never
smokers
No. of patients (n) 50 25 25 50 25 25
PI 69.4±5.1* 73.4±8.5
†‡ 61.7±3.5
§ǁ 26.2±4.6 30.5±5.2
¶ 18.2±4.8
BOP 62.6±4.9* 58.7±4.8
†‡ 69.5±6.1
§ǁ 18.4±6.5 9.2±2.7
¶ 28.5±3.3
CA loss 5.4±1.2* 6.3±0.8
†‡ 5.8±1.1
§ǁ 2.2±0.4 3.8±0.2
¶ 0.4±0.1
PD (≥4mm) 33.5±5.5* 36.3±4.2
†‡ 30.8±2.9
§ǁ 6.2±1.5 6.4±2.5
¶ 0.6±0.1
MBL 6.5±1.2*
7.1±0.5†‡
6.2±1.1§ǁ
2.4±0.3 4.5±0.4¶ 2.1±0.2
* Compared to all individuals in the control group (P<0.01)
† Compared to smokers in the control group (P<0.01)
‡ Compared to never-smokers in the control group (P<0.01)
§ Compared to smokers in the control group (P<0.05)
ǁ Compared to never-smokers in the control group (P<0.05)
¶ Compared to never-smokers in the control group (P<0.05)
Page 25 of 27 Journal of Periodontology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
29x26mm (300 x 300 DPI)
Page 26 of 27Journal of Periodontology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
28x24mm (300 x 300 DPI)
Page 27 of 27 Journal of Periodontology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960