perceived need of psychological support for taboo obsessions
TRANSCRIPT
Perceived need of psychological support for taboo obsessions in new
parents: A cross-sectional survey
Klara Olofsdotter Lauriab, MSc, Kristina Aspvallab, PhD, Eva Serlachiuscd professor, David
Mataix-Colsd, professor, Christian Rückd, professor, Erik Anderssona, associate professor
a Department of Clinical Neuroscience, Division of Psychology, Karolinska Institutet,
Stockholm, Sweden b Stockholm Health Care Services, Region Stockholm, Stockholm, Swedenc Department of Clinical Sciences, Lunds University, Lund Swedend Centre for Psychiatry Research, Department of Clinical Neuroscience, Karolinska Institutet,
and Stockholm Health Care Services, Region Stockholm, Stockholm, Sweden
Corresponding author: Klara Olofsdotter Lauri, Nobels väg 9, 171 65 Solna, Sweden,
Biographical note: MSc Olofsdotter Lauri is a PhD student, writing a thesis on developing
novel interventions for taboo obsessions. Dr Aspvall is a researcher with a focus on internet-
delivered interventions for children and adolescents with obsessive-compulsive and related
disorders. Professor Serlachius main research interest is internet-delivered interventions for
children and adolescents with mental health issues. Professor Mataix-Cols focus is to
understand the causes and consequences of Obsessive-Compulsive Disorder and Related
Disorders (OCD-RDs) as well as treatment innovation for these conditions. Professor
Christian Rück’s research focuses on the etiology and treatment of psychiatric disorders with
a particular focus on OCD-RDs. Dr Andersson´s main research focus is internet-delivered
treatments for anxiety-related problems as wells as OCD-RDs. He has conducted numerous
trials in this field.
Word count: 3 606
Perceived need of psychological support for taboo obsessions in new
parents: A cross-sectional survey
Previous research has shown that many new parents experience intrusive thoughts about
intentionally harming their child, also known as “taboo obsessions”. These thoughts can for
some parents lead to increased anxiety, depression and have a negative impact on parental
function and quality of life. Taboo obsessions can be stigmatizing and many parents who
could benefit from psychological support do not seek help. One way to increase access to
psychological interventions for new parents could be to deliver the treatment online. Our
research group has developed and evaluated an internet-delivered intervention targeting taboo
obsessions in individuals with a diagnosis obsessive-compulsive disorder (OCD), with
promising results. It is conceivable that the intervention could be helpful to a large proportion
of parents from the general population who struggle with taboo obsessions (i.e. not only
individuals with OCD). In the current study, 594 new parents filled out an online survey about
taboo obsessions and the perceived need for psychological support. Fifty six percent reported
currently experiencing or had previously experienced taboo obsessions. About half (54%)
responded that the taboo obsessions had a negative impact on their self-image. Additionally,
18-19% reported that the intrusive thoughts were difficult to control and/or had a negative
impact on the relationship to the child. Importantly, 51% responded that they would
absolutely or probably like to try online treatments for these intrusive thoughts. Keeping the
limitations of an online survey in mind, the results suggest that an online intervention
targeting taboo obsessions in new parents could be well received.
Keywords: Taboo obsessions, parenthood, psychological support, online intervention.
Data availability statement: The data that support the findings of this study are available upon
reasonable request from the corresponding author, KOL, given that the request comply with
Swedish and EU laws regulating protection of identifiable data.
Funding: This work was funded internally at Karolinska Insitutet.
Introduction
Obsessive-compulsive disorder (OCD) is a common condition during the postpartum period
with prevalence rates ranging from 2.4% to 9% of new parents (Fairbrother et al., 2021;
Goodman, Watson, & Stubbs, 2016; McGuinness, Blissett, & Jones, 2011; Ross & McLean,
2006; Russell, Fawcett, & Mazmanian, 2013). Additionally, up to 65% of new parents
experience subthreshold levels of OCD (Abramowitz, Schwartz, & Moore, 2003; Fairbrother
& Woody, 2008; Miller, Hoxha, Wisner, & Gossett, 2015).
Taboo obsessions are amongst the most common OCD symptoms in new parents
(Abramowitz, Nelson, Rygwall, & Khandker, 2007; Abramowitz et al., 2003; Speisman,
Storch, & Abramowitz, 2011; Starcevic, Eslick, Viswasam, & Berle, 2020; Zambaldi et al.,
2009). Taboo obsessions can be defined as distressing, ego-syntonic, sexual, religious and/or
aggressive intrusive thoughts related to intentionally harming others (e.g. thoughts about
stabbing the baby with a knife; Brakoulias et al., 2013). Taboo obsessions during the
postpartum period are associated with elevated levels of parental stress (Thiséus, Perrin, &
Cervin, 2019), increased rates of depression and anxiety (Boyd & Gannon, 2019; Miller et al.,
2015; Wisner, Peindl, Gigliotti, & Hanusa, 1999), negative impact on quality of life (Gezginç
et al., 2008), and impaired parental function (Challacombe et al., 2016). Many parents are
ashamed of their taboo obsessions and do not seek help due to fear of stigma or potentially
negative consequences, e.g., that they may be deemed unfit as parents (Bayrampour et al.,
2017).
To our knowledge, only two randomized controlled trials (RCT) have evaluated psychological
interventions for OCD symptoms (including taboo obsessions) during the postpartum period.
Timpano, Abramowitz, Mahaffey, Mitchell, and Schmidt (2011) conducted a RCT where they
investigated the effects of a cognitive behavioral prevention program for mothers (n = 38)
compared to an active control intervention (n = 33). Fifty-nine percent of the mothers in this
clinical trial reported taboo obsessions (e.g., sexual or violent obsessions) related to the infant
at one month postpartum. Mothers randomized to the prevention program during pregnancy
had significantly lower levels of OCD symptoms compared to mothers randomized to the
control intervention at 1, 3 and 6 months postpartum. The second study (Challacombe et al.
(2017) investigated the effect of an intensive cognitive behavioral treatment (12 h sessions
over 2 weeks) for new mothers who fulfilled criteria for OCD (N = 34). Forty-one percent of
the sample participants in this trial experienced taboo obsessions associated with harming the
RUNNING HEAD: SURVEY TABOO OBSESSIONS AMONG PARENTS
infant. The treatment was highly effective in reducing OCD symptoms compared to treatment
as usual (between-group effect size: 1.32). Of note, none of the trials specifically focused on
taboo obsessions as the main outcome of interest.
Our research group has recently developed an internet-based psychological intervention
specifically tailored for OCD patients who struggle with taboo obsessions. The intervention
can be described as a therapist-guided online self-help treatment that is divided into chapters
(“modules”) accompanied by audio files and homework exercises. The intervention is
accessed through a secure online-platform where all communication is done online with a
supporting therapist, who provides only minimal guidance and support. The intervention
content is based on cognitive theory where the main focus is to change negative appraisals
related to the obsessions (e.g., “Having these thoughts is a sign that I’m an immoral person”)
to more functional and realistic beliefs (e.g., “It’s just a random thought and it doesn´t say
anything about me as a person”). This cognitive change is achieved through standard CBT
techniques such as behavioral experiments and cognitive restructuring exercises. The
intervention has so far been tested in an open pilot trial with 19 OCD patients. Results
indicated that the intervention was both feasible and acceptable, and a majority of the
participants were able to understand and apply the cognitive model to their own obsessions
(Olofsdotter Lauri et al., submitted manuscript). Additionally, 63% of the participants were
classified as treatment responders at the primary endpoint.
The majority of new parents experience taboo obsessions, which could be viewed as adaptive
and transient (Abramowitz et al., 2003). Furthermore, it is plausible to think that not all
parents whose intrusive thoughts about harming their child are disturbing or persistent may
necessarily meet diagnostic criteria for OCD. The implication is that there may be a
substantial proportion of new parents who would benefit from psychological support and who
may not seek help or even qualify to receive healthcare resources because they do not meet
formal criteria for a mental disorder. We designed an online survey to explore 1) the
frequency and impact of taboo obsessions in a sample of self-recruited parents of infants and
toddlers in Sweden, 2) whether negative appraisals – the hypothesized mechanism of change
in cognitive therapy - could be a relevant factor for intervention in this population, and 3) the
perceived need for an easily scalable self-help intervention for taboo obsessions in new
parents from the general population.
4
RUNNING HEAD: SURVEY TABOO OBSESSIONS AMONG PARENTS
Materials and Methods
Recruitment
The data was collected through an anonymous online survey (software tool: KI survey;
domain: www.jobbigatankar.se). Interested individuals were presented with information about
the study and provided a digital informed consent before getting access to the online survey.
The survey was open to all adults (age 18 and above) in Sweden who self-identified
themselves as being a parent of a child between 0 – 3 years of age.
The participants were recruited through Facebook advertisements. The advertisement stated
that the online survey would inquire about intrusive and disturbing thoughts about
intentionally harming ones child, and that any parent of a child between 0 – 3 years of age
could participate, whether they had experienced these kinds of thoughts or not. It was open
between 1st of April and 17th of May 2021. After having included 300 individuals in the study
(7th of April), only 5 of the respondents were male. In order to get a more diverse sample, we
chose to adjust the Facebook recruitment algorithm to reach males only. After having
included 98 males (14th of May), we set again the algorithm to include all genders.
The study protocol was approved by Swedish Ethical Review Board (2020-06756; Ö8-
2021/3.1).
Online survey content
Overview
The online survey contained questions about demographic characteristics (e.g., gender, age,
number of children, highest education, occupational status), and two questionnaires to assess
obsessions, compulsions and negative appraisals (see Questionnaires below). Additionally,
the survey included four items investigating the impact of taboo obsessions on perceived
control over the obsessions, self-image, social relationships and attachment to one’s child.
The survey also contained one item asking the participants if they had told anybody about
their obsessions (yes/no), and 7 different items assessing healthcare seeking behaviors and
preferences, interest and attitudes to internet-based psychological interventions for taboo
obsessions. The survey took approximately 15 minutes to complete.
5
RUNNING HEAD: SURVEY TABOO OBSESSIONS AMONG PARENTS
Questionnaires
The self-rated version of Parental Thoughts and Behaviors Checklist (PTBC; Abramowitz,
Khandker, Nelson, Deacon, & Rygwall, 2006) was used to investigate severity and impact of
taboo obsessions and related behaviors. The self-rated version of the PTBC has shown good
psychometric properties (Chronbach’s a = 0.91) and a similar factor structure as the PTBC
clinical interview (Thiséus et al., 2019). The questionnaire is divided into two parts. The first
part contains a checklist of 33 examples of intrusive thoughts related to the child and 13
additional related behaviors. In the current study, only the examples containing taboo
thoughts related to the infant and toddler were included (e.g., thoughts about intentionally
drowning the child or stabbing the child to death). The second part of the PTBC contains five
items assessing severity of the obsessions (e.g., ”How much distress do these sensless and
unwanted thougths cause you?”) and five items assessing severity of related behaviors (e.g.,
”How would you feel if prevented from preforming these behaviours/strategies? How anxious
would you become?”). Each item is rated on a 5 point scale (0-4), yielding a total score of 0 –
40 points, with higher scores indicating more severe symptoms.
As negative appraisal of the intrusive thoughts is the hypothesized mechanism of change in
cognitive interventions for taboo obsessions, we used a condensed version of the Personal
Significance Scale (PSS; Rachman, 2003) to investigate if this is a relevant construct also in
the target sample of self-recruited parents of infants and toddlers. The full PSS scale includes
23 statements rated on a 9-point scale (0 = “not at all”, 8 = “definitely”). In order to avoid
participant fatigue, only five items from the full scale PSS were included in the survey. The
items were chosen by first categorizing the full scale into cognitions related to: 1) Personal
significance 2) Fear of acting on the thoughts and 3) Fear of being judged by others.
Subsequently, we chose two items came from category 1 (“Do these thoughts reveal
something important about you?”, “Do these thoughts mean that you are a dangerous
person?”), two items from category 2 (“Do these thoughts mean that you might lose control
and do something awful?”, “Do these thoughts mean that you might go crazy one day?”) and
one item from category 3 (“Would other people condemn or criticize you if they knew about
your thoughts?”). The condensed five-item version showed a strong correlation with the full
scale (r = .86) and a good internal consistency (a = 0.88) in a sample of 19 OCD patients with
taboo obsessions (Olofsdotter Lauri et al., submitted manuscript).
6

RUNNING HEAD: SURVEY TABOO OBSESSIONS AMONG PARENTS
Data analysis
All statistical analyses were conducted in STATA 16.1. Proportion, symptom severity, impact
of taboo obsessions as well as healthcare seeking behaviors and interest in treatment were
investigated using descriptive statistics. Pearson’s correlation was used to assess the
relationship between taboo obsessions and negative appraisals. Chi-square test and one-way
ANOVA were used to investigate if there were any gender differences in respect to symptom
severity of taboo obsessions.
Results
Demographics
A total of 594 new parents completed the online survey. Detailed demographic characteristics
of the participants are presented in Table 1. The majority of the sample were women in their
early thirties with a university degree. About one third of the sample were on parental leave
and one third worked full time. Almost half of the sample had one child aged between 0 – 1
years. One third of the sample reported that they had received a psychiatric diagnosis prior to
the birth of their first child. Seven individuals (1.2%) self-reported having a diagnosis of
OCD. Thirty respondents (9%) had sought treatment for their intrusive thoughts and 17 (5%)
had received treatment.
INSERT TABLE 1
Frequency and impact of taboo obsessions
Of the 594 participants, 334 (56%) reported previously having and/or currently experiencing
taboo obsessions related to intentionally harming their child, and 321 (54%) reported
previously having and/or currently engaging in neutralizing behaviors in response to these
intrusions. There were no significant gender differences in experiencing intrusions (X2 (1) =
0.45; p = .504). Participants who had stated gender as other were excluded from analysis due
to the small sample size (n = 6). Half of the sample (n = 167, 50 %) who responded “yes” on
currently/previous taboo obsessions reported they had revealed the content of their intrusive
thoughts to someone.
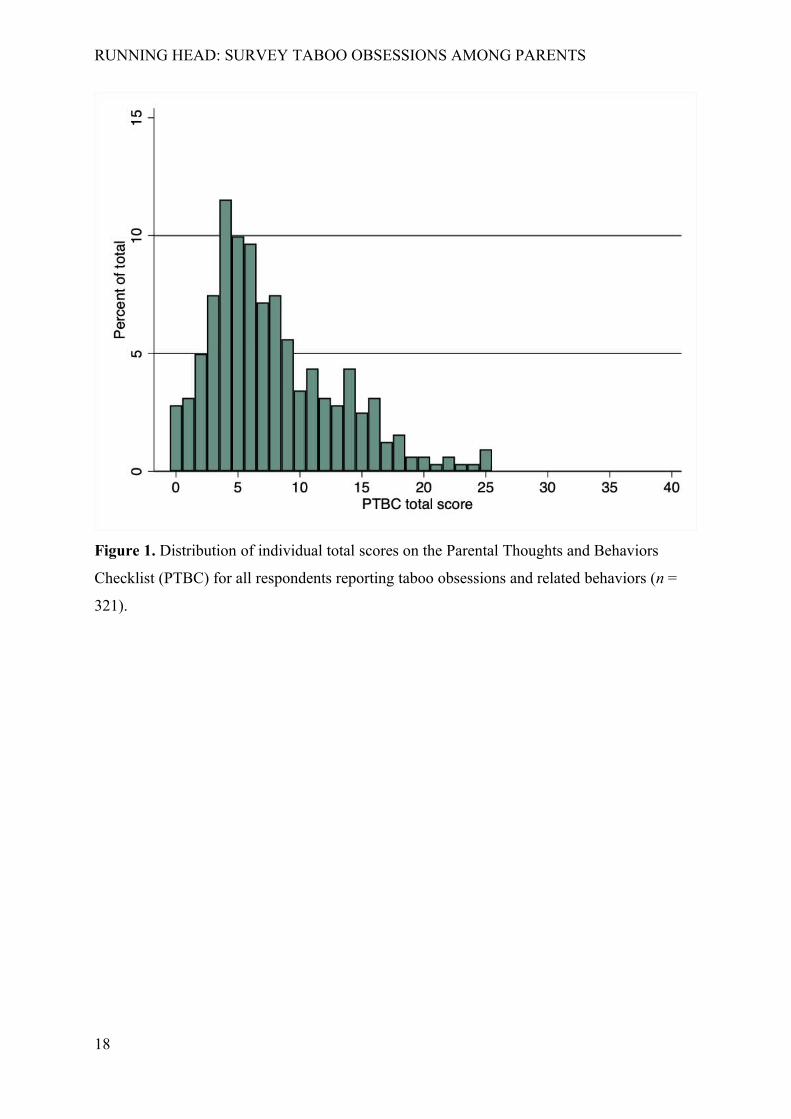
As shown in Figure 1, the majority of the participants (n = 182, 57%) reported a score of 7 or
lower on the PTBC, 108 (33%) reported a score between 8 – 15 points, and 31 (10%) reported
7

RUNNING HEAD: SURVEY TABOO OBSESSIONS AMONG PARENTS
a score of ≥16 points. There were no gender differences in symptom levels (F(1) = 0.15, p
= .67). Participants who had stated gender as other (n = 4) were excluded from the latter
analysis.
INSERT FIGURE 1
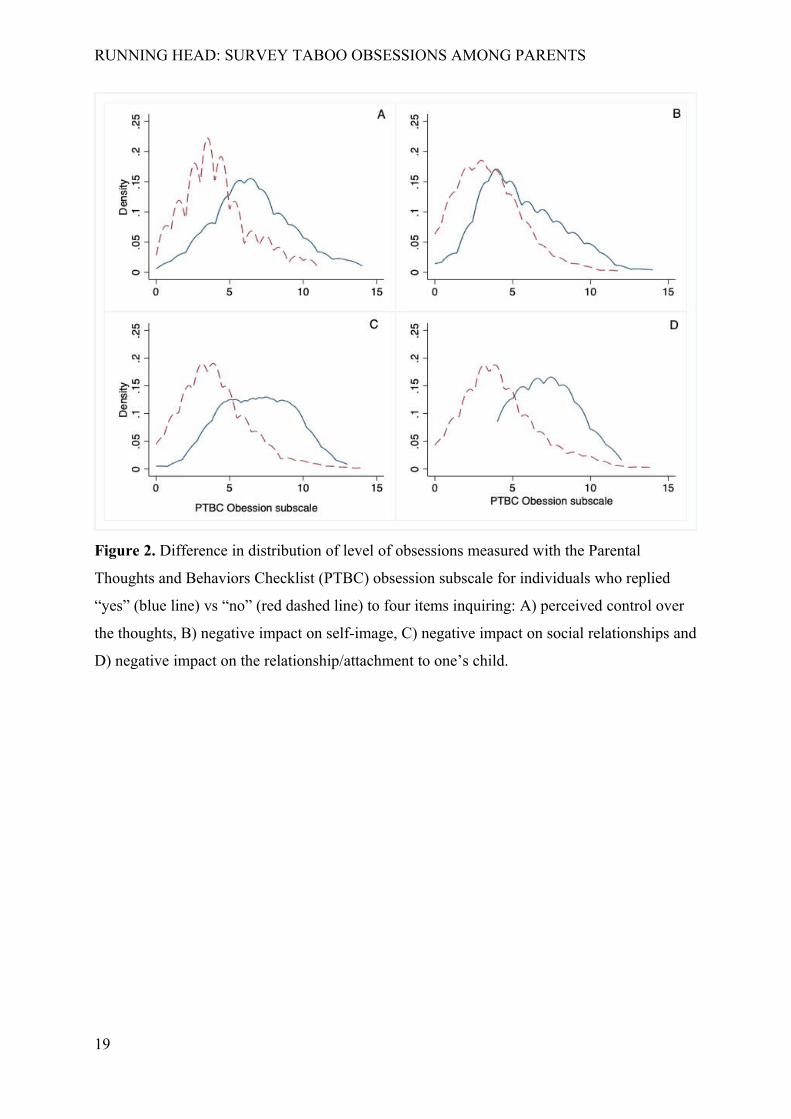
A total of 61 (18%) participants responded that the intrusive thoughts were difficult to control
(PTBC thoughts subscale: M = 6.62, SD = 2.81, median 6, IQR = 5 – 8 vs. individuals who
responded “no” M = 4.12, SD = 2.40, median 4, IQR = 3 – 5). A total of 180 participants
(54%) responded that the taboo thoughts had a negative impact on self-image (PTBC thoughts
subscale: M = 5.51, SD = 2.67, median = 5, IQR = 4 – 7 vs. individuals who responded “no”
M = 3.49, SD = 2.20, median = 3, IQR = 2 – 5). Sixty-four participants (19%) reported that
the intrusive thoughts have had a negative impact on the relationship/attachment to the child
(PTBC thoughts subscale: M = 6.86, SD = 2.53, median = 7, IQR = 5 – 9 vs. individuals who
responded “no” M = 4.03, SD = 2.39, median = 4, IQR = 2 – 5). Finally, 41 participants
(12%) reported a negative impact on the relationship to partner, parents and/or friends (PTBC
thoughts subscale: M = 7.15 (SD = 2.06, median = 7, IQR = 5 – 8 vs. individuals who
responded “no” M = 4.22, SD = 2.54, median = 4, IQR = 3 – 6). Detailed information about
the distribution of scores on the PTBC thoughts subscale is shown in Figure 2.
INSERT FIGURE 2
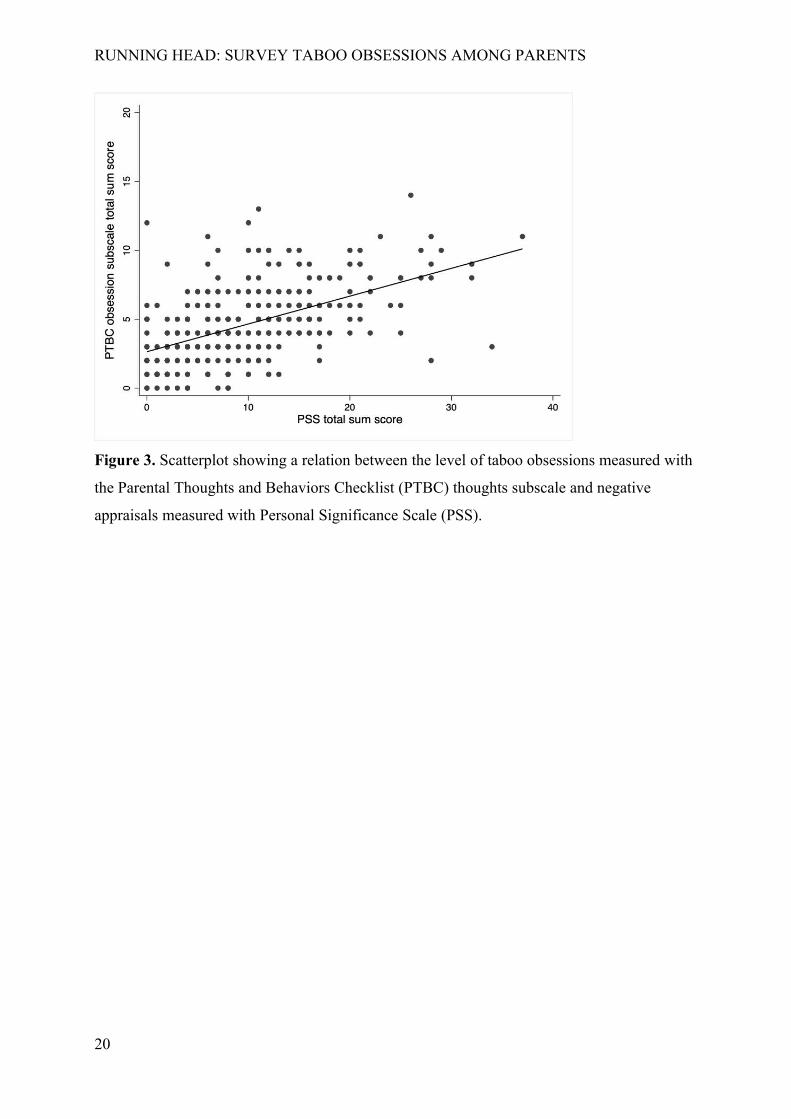
Association between negative appraisals and severity of taboo obsessions
As shown in Figure 3, there was a moderate to strong correlation between scores on the PSS
(negative appraisals) and severity of taboo obsessions assessed with the PTBC (r(320) = .53).
INSERT FIGURE 3
Acceptability of internet-based treatment for taboo obsessions
As shown in Table 2, 420 (71%) participants responded that they would be interested in
receiving psychological support if they would experience taboo obsessions related to their
child. Of these 420 individuals who were positive to psychological treatment, 307 (73%)
responded that would absolutely or probably like to try internet-based psychological treatment
for taboo obsessions. Among individuals who reported a score of ≥16 points on the PTBC (n
8
RUNNING HEAD: SURVEY TABOO OBSESSIONS AMONG PARENTS
= 31) did 26 (84%) respond that they would be interested in psychological support, and 20 of
these individuals (77%) stated that they would absolutely or probably like to try internet-
based psychological treatment. Of the individuals who reported a score of <16 points on the
PTBC (n = 290) did 199 (69%) respond that they would be interested in receiving
psychological support, and of these 199 individuals did 152 (76%) respond that they were
positive towards an internet-based psychological treatment. There were no significant gender
differences in attitude towards psychological treatment (X2 (1) = 0.11, p = 0.746), or in
attitude towards internet-based psychological treatment (X2 (1) = 2.28, p = 0.089).
INSERT TABLE 2
Discussion
The results of this cross-sectional survey showed that the majority of the respondents (56%)
were currently experiencing or had previously experienced taboo obsessions related to their
own child. About one fifth reported difficulties controlling their obsessions and/or that the
obsessions have had a negative impact on the relationship/attachment to their child. As many
as 54% of the respondents experienced the obsessions as having a negative impact on their
self-image. In line with the cognitive model of obsessions, there was a strong association
between severity of taboo obsessions and degree of negative appraisals. An important finding
was that the majority of the sample (71%) reported interest in receiving psychological
treatment for taboo obsessions and 74% of these individuals would definitely or possibly like
to try internet-based psychological treatment.
In the current study, 9% of the participants had sought treatment for their intrusive obsessions
and 5% had actually received any treatment. Previous research have suggested that women
who suffer from psychiatric symptoms during the postpartum period have difficulties to seek,
receive or complete evidence-based treatments (Goodman & Tyer-Viola, 2010; Smith et al.,
2009). Possible barriers to treatment-seeking among new parents could be shame/stigma,
limited time to spend on therapy, not perceiving one’s problems as sufficiently severe, and
financial barriers (Bayrampour et al., 2017; Maloni, Przeworski, & Damato, 2013;
Woolhouse, Brown, Krastev, Perlen, & Gunn, 2009). There is also evidence suggesting that
individuals with stigmatized conditions are more likely to utilize online resources to receive
help than non-stigmatized conditions (Berger, Wagner, & Baker, 2005), highlighting the
possible benefits of developing and testing a digital solution that can reach the larger
9
RUNNING HEAD: SURVEY TABOO OBSESSIONS AMONG PARENTS
population of parents who struggle with taboo obsessions and who do not necessarily meet
diagnostic criteria for OCD. In our sample, only 7 individuals (1.2%) self-reported having
OCD. An internet-based intervention has the potential to reach individuals who do not have
access to evidence based treatments, for example due to economic limitations and/or long
travel distances to a mental health clinic (Muñoz, 2010; Titov et al., 2020).
Slightly more than half of the total sample reported that they probably or definitely would like
to try an online psychological intervention for taboo obsessions. These results are in line with
a previous survey study investigating the acceptability of online treatments in individuals who
suffer from OCD (Wootton, Titov, Dear, Spence, & Kemp, 2011). Previous trials have found
positive results of internet-based treatments for women experiencing stress, depression and
anxiety in the postpartum period (Lau, Htun, Wong, Tam, & Klainin-Yobas, 2017; Loughnan
et al., 2019; Mu et al., 2021; O'mahen et al., 2014). The results of this survey suggest that it
could be feasible to develop self-guided internet-based psychological interventions for new
parents who experience disturbing and impairing taboo obsessions about harming their
children. A possible risk in developing treatment for, at least partly, a non-diagnostic group is
that it would signal that taboo thoughts are pathological and thereby unintentional
contributing to stigma and over-medicalization. The intervention to be developed in this
project, intends to normalize the taboo obsessions by addressing the negative appraisal and
therefore should be well positioned to mitigate such risks.
The vast majority of research studies on parental taboo obsessions have been conducted on
mothers only. This stands in contrast to previous research showing comparable prevalence
rates of obsessions in fathers (Abramowitz et al., 2007; Abramowitz et al., 2003). The current
study did not find any gender differences in terms of symptom severity, impairment, or
treatment preferences. However, it was generally more difficult to recruit fathers; 84% of the
advertisement budget was spent on reaching men despite only constituting one fifth of the
sample. This overrepresentation of women is line with previous research (Whitaker,
Stevelink, & Fear, 2017); females are generally more favorable attitude towards mental
health treatment, treatment seeking behaviors as well as less perceived stigma towards mental
illness (Eisenberg, Downs, Golberstein, & Zivin, 2009; Mojtabai, 2007). Females sign up for
internet-based psychological assessment and treatment to a larger extent than males (Titov et
al., 2020), and are generally overrepresented in trials investigating internet-based treatments
10

RUNNING HEAD: SURVEY TABOO OBSESSIONS AMONG PARENTS
for depression and anxiety (Etzelmueller et al., 2020). Future clinical trials should investigate
optimal ways to reach and include fathers in such interventions.
The interpretation of the findings from this study are affected by several important limitations.
Firstly, this study is based on a convenience sample recruited via Facebook advertisements.
The majority of participants were highly educated women. Thus, the sample is likely to be
unrepresentative of the full population of new parents in Sweden. For example it is possible
that Facebook users have a more positive attitude towards internet-based treatments than the
population at large. However, the aim in this study was to reach a similar population that may
be interested in participating in a clinical trial of unguided online self-help for taboo
obsessions, i.e., self-referred new parents who are motivated to receive psychological support
for their intrusions. Secondly, all data from this study was based on self-report. It is therefore
possible that some individuals may have undiagnosed OCD or other mental disorders. Future
studies should validate the self-report version of the PTBC against the clinician-rated version.
In conclusion, a majority of a sample of parents, recruited through Facebook advertisements,
experienced taboo obsessions related to harming their child but a very small minority have
sought and/or received treatment. Most participants were positive to the idea of an internet-
based intervention targeting taboo obsessions.
Acknowledgment
We want to express or gratitude to Johan Åhlén for valuable input about the content and
administration of the online survey and David Brandell for support in writing the ethical
application.
References
Abramowitz, J. S., Khandker, M., Nelson, C., Deacon, B., & Rygwall, R. (2006). The role of cognitive factors in the pathogenesis of obsessive–compulsive symptoms: A prospective study. Behaviour research and therapy, 44(9), 1361-1374. doi:10.1016/j.brat.2005.09.011
Abramowitz, J. S., Nelson, C. A., Rygwall, R., & Khandker, M. (2007). The cognitive mediation of obsessive-compulsive symptoms: A longitudinal study. Journal of anxiety disorders, 21(1), 91-104. doi:10.1016/j.janxdis.2006.05.003
Abramowitz, J. S., Schwartz, S., & Moore, K. (2003). Obsessional Thoughts in Postpartum Females and Their Partners: Content, Severity, and Relationship with Depression.
11

RUNNING HEAD: SURVEY TABOO OBSESSIONS AMONG PARENTS
Journal of clinical psychology in medical settings, 10(3), 157-164. doi:10.1023/A:1025454627242
Bayrampour, H., McNeil, D. A., Benzies, K., Salmon, C., Gelb, K., & Tough, S. (2017). A qualitative inquiry on pregnant women's preferences for mental health screening. BMC pregnancy and childbirth, 17(1), 339-339. doi:10.1186/s12884-017-1512-4
Berger, M., Wagner, T. H., & Baker, L. C. (2005). Internet use and stigmatized illness. Socialscience & medicine (1982), 61(8), 1821-1827. doi:10.1016/j.socscimed.2005.03.025
Boyd, C. F. S., & Gannon, K. (2019). How do new/recent mothers experience unwanted harmthoughts related to their newborn? A thematic analysis. Journal of reproductive and infant psychology, 1-13. doi:10.1080/02646838.2019.1657819
Brakoulias, V., Starcevic, V., Berle, D., Milicevic, D., Moses, K., Hannan, A., . . . Martin, A. (2013). The characteristics of unacceptable/taboo thoughts in obsessive-compulsive disorder. Compr Psychiatry, 54(7), 750-757. doi:10.1016/j.comppsych.2013.02.005
Challacombe, F. L., Salkovskis, P. M., Woolgar, M., Wilkinson, E. L., Read, J., & Acheson, R. (2016). Parenting and mother-infant interactions in the context of maternal postpartum obsessive-compulsive disorder: Effects of obsessional symptoms and mood. Infant behavior & development, 44, 11-20. doi:10.1016/j.infbeh.2016.04.003
Challacombe, F. L., Salkovskis, P. M., Woolgar, M., Wilkinson, E. L., Read, J., & Acheson, R. (2017). A pilot randomized controlled trial of time-intensive cognitive–behaviour therapy for postpartum obsessive–compulsive disorder: effects on maternal symptoms,mother–infant interactions and attachment. Psychological medicine, 47(8), 1478-1488.doi:10.1017/S0033291716003573
Eisenberg, D., Downs, M. F., Golberstein, E., & Zivin, K. (2009). Stigma and help seeking for mental health among college students. Med Care Res Rev, 66(5), 522-541. doi:10.1177/1077558709335173
Etzelmueller, A., Vis, C., Karyotaki, E., Baumeister, H., Titov, N., Berking, M., . . . Ebert, D. D. (2020). Effects of Internet-Based Cognitive Behavioral Therapy in Routine Care for Adults in Treatment for Depression and Anxiety: Systematic Review and Meta-Analysis. Journal of medical Internet research, 22(8), e18100-e18100. doi:10.2196/18100
Fairbrother, N., Collardeau, F., Albert, A. Y. K., Challacombe, F. L., Thordarson, D. S., Woody, S. R., & Janssen, P. A. (2021). High Prevalence and Incidence of Obsessive-Compulsive Disorder Among Women Across Pregnancy and the Postpartum. The journal of clinical psychiatry, 82(2). doi:10.4088/JCP.20m13398
Fairbrother, N., & Woody, S. R. (2008). New mothers’ thoughts of harm related to the newborn. Archives of women's mental health, 11(3), 221-229. doi:10.1007/s00737-008-0016-7
Gezginç, K., Uguz, F., Karatayli, S., Zeytinci, E., A kin, R., Güler, Ö., . . . Geçici, Ö. (2008). The impact of obsessive-compulsive disorder in pregnancy on quality of life. International journal of psychiatry in clinical practice, 12(2), 134-137. doi:10.1080/13651500701777363
Goodman, J. H., & Tyer-Viola, L. (2010). Detection, treatment, and referral of perinatal depression and anxiety by obstetrical providers. Journal of women's health, 19(3), 477-490.
Goodman, J. H., Watson, G. R., & Stubbs, B. (2016). Anxiety disorders in postpartum women: A systematic review and meta-analysis. Journal of Affective Disorders, 203, 292-331. doi:10.1016/j.jad.2016.05.033
Lau, Y., Htun, T. P., Wong, S. N., Tam, W. S. W., & Klainin-Yobas, P. (2017). Therapist-supported internet-based cognitive behavior therapy for stress, anxiety, and depressive
12

RUNNING HEAD: SURVEY TABOO OBSESSIONS AMONG PARENTS
symptoms among postpartum women: a systematic review and meta-analysis. Journalof medical Internet research, 19(4), e6712.
Loughnan, S. A., Butler, C., Sie, A. A., Grierson, A. B., Chen, A. Z., Hobbs, M. J., . . . Holt, C. (2019). A randomised controlled trial of ‘MUMentum postnatal’: internet-deliveredcognitive behavioural therapy for anxiety and depression in postpartum women. Behaviour research and therapy.
Maloni, J. A., Przeworski, A., & Damato, E. G. (2013). Web Recruitment and Internet Use and Preferences Reported by Women With Postpartum Depression After Pregnancy Complications. Archives of psychiatric nursing, 27(2), 90-95. doi:10.1016/j.apnu.2012.12.001
McGuinness, M., Blissett, J., & Jones, C. (2011). OCD in the Perinatal Period: Is Postpartum OCD (ppOCD) a Distinct Subtype? A Review of the Literature. Behavioural and cognitive psychotherapy, 39(3), 285-310. doi:10.1017/S1352465810000718
Miller, E. S., Hoxha, D., Wisner, K. L., & Gossett, D. R. (2015). Obsessions and Compulsions in Postpartum Women Without Obsessive Compulsive Disorder. Journal of women's health (Larchmont, N.Y. 2002), 24(10), 825-830. doi:10.1089/jwh.2014.5063
Mojtabai, R. (2007). Americans' attitudes toward mental health treatment seeking: 1990-2003.Psychiatr Serv, 58(5), 642-651. doi:10.1176/ps.2007.58.5.642
Mu, T. Y., Li, Y. H., Xu, R. X., Chen, J., Wang, Y. Y., & Shen, C. Z. (2021). Internet based ‐interventions for postpartum depression: A systematic review and meta analysis. ‐Nursing open, 8(3), 1125-1134.
Muñoz, R. F. (2010). Using evidence-based internet interventions to reduce health disparities worldwide. Journal of medical Internet research, 12(5), e60.
O'mahen, H., Richards, D., Woodford, J., Wilkinson, E., McGinley, J., Taylor, R. S., & Warren, F. (2014). Netmums: a phase II randomized controlled trial of a guided Internet behavioural activation treatment for postpartum depression. Psychological medicine, 44(8), 1675-1689.
Olofsdotter Lauri, K., Aspvall, K., Bagøien Hustad, I., Malmqvist, K., Serlachius, E., Mataix-Cols, D., . . . Andersson, E. (submitted manuscript). A preliminary investigation of a therapist-supported online cognitive intervention for patients with taboo obsessions. Unpublished.
Rachman, S. (2003). The treatment of obsessions: Oxford University Press Oxford.Ross, L. E., & McLean, L. M. (2006). Anxiety disorders during pregnancy and the postpartum
period: A systematic review. The journal of clinical psychiatry, 67(8), 1285-1298. doi:10.4088/JCP.v67n0818
Russell, E. J., Fawcett, J. M., & Mazmanian, D. (2013). Risk of obsessive-compulsive disorder in pregnant and postpartum women: a meta-analysis. The journal of clinical psychiatry, 74(4), 377-385. doi:10.4088/JCP.12r07917
Smith, M. V. D. P. H. M. P. H., Shao, L. M. S., Howell, H. M. S. W. L. C. S. W., Wang, H. M. S., Poschman, K. M. P. H., & Yonkers, K. A. M. D. (2009). Success of mental health referral among pregnant and postpartum women with psychiatric distress. General hospital psychiatry, 31(2), 155-162. doi:10.1016/j.genhosppsych.2008.10.002
Speisman, B. B., Storch, E. A., & Abramowitz, J. S. (2011). Postpartum obsessive‐compulsive disorder. Journal of Obstetric, Gynecologic & Neonatal Nursing, 40(6), 680-690.
Starcevic, V., Eslick, G. D., Viswasam, K., & Berle, D. (2020). Symptoms of Obsessive-Compulsive Disorder during Pregnancy and the Postpartum Period: a Systematic Review and Meta-Analysis. Psychiatr Q. doi:10.1007/s11126-020-09769-8
13

RUNNING HEAD: SURVEY TABOO OBSESSIONS AMONG PARENTS
Thiséus, J., Perrin, S., & Cervin, M. (2019). Intrusive thoughts and compulsive behaviors in postpartum women: Psychometric properties of the Parental Thoughts and Behaviors Checklist. Psychiatry research, 278, 194-198. doi:10.1016/j.psychres.2019.06.015
Timpano, K. R., Abramowitz, J. S., Mahaffey, B. L., Mitchell, M. A., & Schmidt, N. B. (2011). Efficacy of a prevention program for postpartum obsessive–compulsive symptoms. Journal of Psychiatric Research, 45(11), 1511-1517. doi:10.1016/j.jpsychires.2011.06.015
Titov, N., Dear, B. F., Nielssen, O., Wootton, B., Kayrouz, R., Karin, E., . . . Staples, L. G. (2020). User characteristics and outcomes from a national digital mental health service: an observational study of registrants of the Australian MindSpot Clinic. The Lancet. Digital health, 2(11), e582-e593. doi:10.1016/S2589-7500(20)30224-7
Whitaker, C., Stevelink, S., & Fear, N. (2017). The Use of Facebook in Recruiting Participants for Health Research Purposes: A Systematic Review. J Med Internet Res, 19(8), e290. doi:10.2196/jmir.7071
Wisner, K. L., Peindl, K. S., Gigliotti, T., & Hanusa, B. H. (1999). Obsessions and compulsions in women with postpartum depression. The journal of clinical psychiatry, 60(3), 176-180. doi:10.4088/JCP.v60n0305
Woolhouse, H., Brown, S., Krastev, A., Perlen, S., & Gunn, J. (2009). Seeking help for anxiety and depression after childbirth: results of the Maternal Health Study. Archives of women's mental health, 12(2), 75-83.
Wootton, B. M., Titov, N., Dear, B. F., Spence, J., & Kemp, A. (2011). The acceptability of Internet-based treatment and characteristics of an adult sample with obsessive compulsive disorder: an Internet survey. PLoS One, 6(6), e20548.
Zambaldi, C. F., Cantilino, A., Montenegro, A. C., Paes, J. A., de Albuquerque, T. L. C., & Sougey, E. B. (2009). Postpartum obsessive-compulsive disorder: prevalence and clinical characteristics. Comprehensive psychiatry, 50(6), 503-509. doi:10.1016/j.comppsych.2008.11.014
14

RUNNING HEAD: SURVEY TABOO OBSESSIONS AMONG PARENTS
Table 1. Demographic characteristics of the sample (N = 594)
Variable
Gender, n (%)
Female 490 (82%)
Male 98 (17%)
Other 6 (1%)
Age
Mean (SD) 33.90 (4.67)
Min-Max 21 - 57
Age, youngest child
Mean (SD) 1.10 (0.84)
Min-Max 0 - 3
Number of children, n (%)
1 277 (47%)
2 236 (40%)
3 62 (10%)
4 11 (2%)
5 or more 8 (1%)
Occupational status, n (%)
Parental leave 208 (35%)
Full-time work 221 (37%)
Part-time work 96 (16%)
Full-time sick leave 7 (1.5%)
Student 50 (8%)
Unemployed 5 (1%)
Other 7 (1.5%)
Highest education, n (%)
Primary school 7 (1%)
High school 48 (8%)
Higher education, not university 36 (6%)
University < 3 years 38 (7%)
University > 3 years 435 (73%)
Postgraduate education 30 (5%)
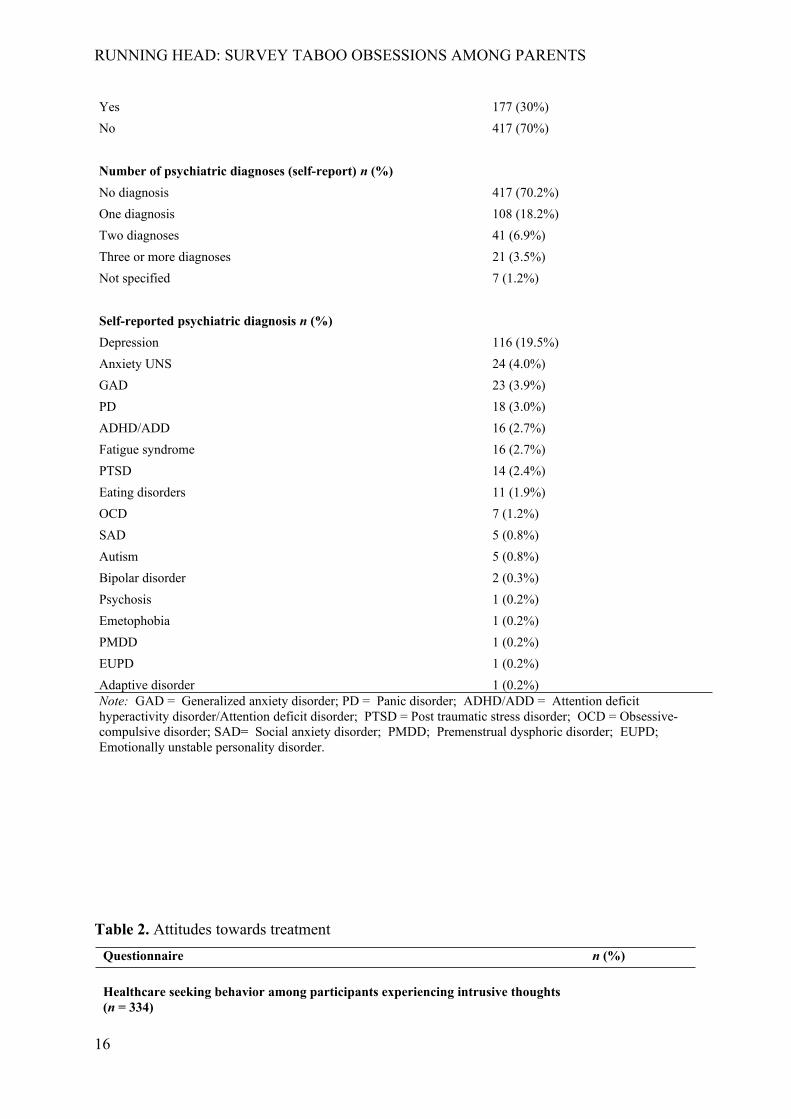
Psychiatric diagnosis prior to the first child? n (%)
15
RUNNING HEAD: SURVEY TABOO OBSESSIONS AMONG PARENTS
Yes 177 (30%)
No 417 (70%)
Number of psychiatric diagnoses (self-report) n (%)
No diagnosis 417 (70.2%)
One diagnosis 108 (18.2%)
Two diagnoses 41 (6.9%)
Three or more diagnoses 21 (3.5%)
Not specified 7 (1.2%)
Self-reported psychiatric diagnosis n (%)
Depression 116 (19.5%)
Anxiety UNS 24 (4.0%)
GAD 23 (3.9%)
PD 18 (3.0%)
ADHD/ADD 16 (2.7%)
Fatigue syndrome 16 (2.7%)
PTSD 14 (2.4%)
Eating disorders 11 (1.9%)
OCD 7 (1.2%)
SAD 5 (0.8%)
Autism 5 (0.8%)
Bipolar disorder 2 (0.3%)
Psychosis 1 (0.2%)
Emetophobia 1 (0.2%)
PMDD 1 (0.2%)
EUPD 1 (0.2%)
Adaptive disorder 1 (0.2%) Note: GAD = Generalized anxiety disorder; PD = Panic disorder; ADHD/ADD = Attention deficit hyperactivity disorder/Attention deficit disorder; PTSD = Post traumatic stress disorder; OCD = Obsessive-compulsive disorder; SAD= Social anxiety disorder; PMDD; Premenstrual dysphoric disorder; EUPD; Emotionally unstable personality disorder.
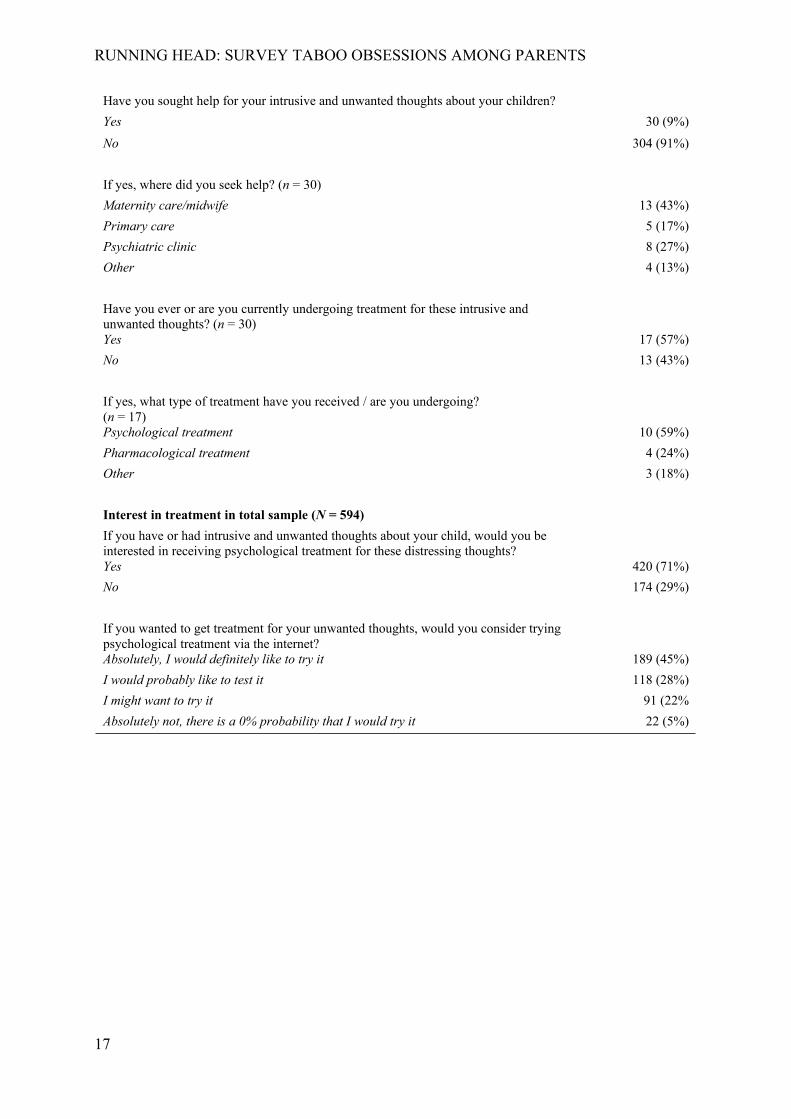
Table 2. Attitudes towards treatment
Questionnaire n (%)
Healthcare seeking behavior among participants experiencing intrusive thoughts (n = 334)
16
RUNNING HEAD: SURVEY TABOO OBSESSIONS AMONG PARENTS
Have you sought help for your intrusive and unwanted thoughts about your children?
Yes 30 (9%)
No 304 (91%)
If yes, where did you seek help? (n = 30)
Maternity care/midwife 13 (43%)
Primary care 5 (17%)
Psychiatric clinic 8 (27%)
Other 4 (13%)
Have you ever or are you currently undergoing treatment for these intrusive and unwanted thoughts? (n = 30)Yes 17 (57%)
No 13 (43%)
If yes, what type of treatment have you received / are you undergoing? (n = 17)Psychological treatment 10 (59%)
Pharmacological treatment 4 (24%)
Other 3 (18%)
Interest in treatment in total sample (N = 594)
If you have or had intrusive and unwanted thoughts about your child, would you be interested in receiving psychological treatment for these distressing thoughts?Yes 420 (71%)
No 174 (29%)
If you wanted to get treatment for your unwanted thoughts, would you consider trying psychological treatment via the internet?Absolutely, I would definitely like to try it 189 (45%)
I would probably like to test it 118 (28%)
I might want to try it 91 (22%
Absolutely not, there is a 0% probability that I would try it 22 (5%)
17
RUNNING HEAD: SURVEY TABOO OBSESSIONS AMONG PARENTS
Figure 1. Distribution of individual total scores on the Parental Thoughts and Behaviors
Checklist (PTBC) for all respondents reporting taboo obsessions and related behaviors (n =
321).
18
RUNNING HEAD: SURVEY TABOO OBSESSIONS AMONG PARENTS
Figure 2. Difference in distribution of level of obsessions measured with the Parental
Thoughts and Behaviors Checklist (PTBC) obsession subscale for individuals who replied
“yes” (blue line) vs “no” (red dashed line) to four items inquiring: A) perceived control over
the thoughts, B) negative impact on self-image, C) negative impact on social relationships and
D) negative impact on the relationship/attachment to one’s child.
19
RUNNING HEAD: SURVEY TABOO OBSESSIONS AMONG PARENTS
Figure 3. Scatterplot showing a relation between the level of taboo obsessions measured with
the Parental Thoughts and Behaviors Checklist (PTBC) thoughts subscale and negative
appraisals measured with Personal Significance Scale (PSS).
20