pediatric cardiopulmonary resuscitation 2017 - lao space
TRANSCRIPT
Pediatric Cardiopulmonary Resuscitation 2017
Dr LEE Jong-wook–Seoul Project


Dr. Lee Jong-Wook-Seoul Project started in 2011 to promote advanced medical environment of Lao
PDR. Purpose of this project is to build capacities for medical professionals through sharing knowledge,
skills, and capabilities. Over the last seven years, the project has been conducted by Seoul National
University College of Medicine (SNUCM) in cooperation of University of Health Sciences (UHS) of Lao
PDR under the support from Korea Foundation for International Health (KOFIH) and Ministry of Health
and Welfare (MOHW) of Republic of Korea.
It feels as if we just took our first step with the purpose of medical training and clinical reinforcement
for Lao PDR; we are already in process of completing seventh batch. For the last seven years, Dr. Lee
Jong-Wook--Seoul Project took one step further each year. As it made a change one step at a time,
privileged trainees experienced much change as well. In the beginning of the project, most participants
were from medical field. Now, there are trainees from various fields, including dental, nursing, clinical
pathology, medical education, etc. They are conducting number of studies beyond clinical practice.
Primary purpose of this project is training participating professors to strengthen their expertise in
respective fields in order to become excellent adviser for next generation. Expert capability is the most
crucial qualification of an adviser when it comes to student education. SNUCM knows how important
faculty abilities are via first-hand experience obtained through Minnesota Project. The next vital aspect
is proper educational materials. We believe there is nothing more effective than textbooks in Lao for
increasing professionalism of medical doctors in Lao PDR. No matter how much supports are given for
equipment, materials, and Lao PDR environment improvement, well written textbook in their mother
tongue will have far more powerful impact.
This is a textbook for each major, translated in Lao, by sixth batch trainees. Users can read entire
contents in Lao and English; the book contains same materials in original English textbook. I appreciate
all participants who worked hard, day and night, until the book was published. I also want to thank
faculties in central hospitals of Lao for showing endless support for the publication of this book. There
could be few mistranslations since this is the first textbook the faculties have written. Yet, I pray this
will be gradually improved in the sake of valuable education of Lao students.
Letter of Greeting
Hee Young Shin, MD, PhD
Chairman, Steering committee of Dr LEE Jong-wook - Seoul ProjectExecutive Vice President, Seoul National UniversityProfessor, Department of Pediatrics



MD.
Prof. Park June Dong, MD., Ph.D. Associate professor, Department of Pediatrics
Seoul National University College of Medicine
Director
Pediatric Intensive Care Medicine
Seoul National University Hospital
MD
MD II
MD II
1


ooo
1623/1624
3
4

5

AED
AED AED
AED
AED
1
CPR CPR
6
7
8
9

10
11
AED/defibrillator
210
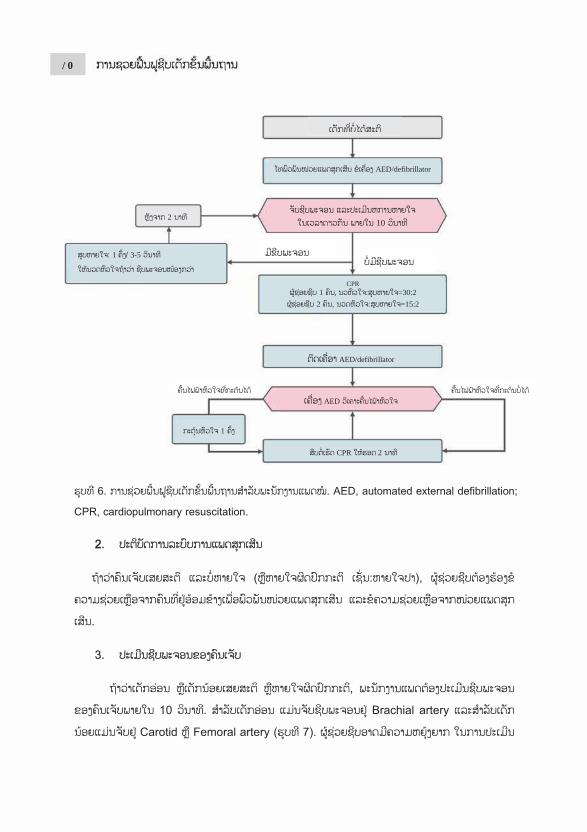
CPR1 , =30:2
2 =15:2
AED/defibrillator
AED
1
CPR 2
1 3-5
12
13
oooo
14
15
16
17
18
19
20

21
22
23

24
25
26

27
28
29
30
31
32
33
34
35
36
37
38

39
40
41
42
43
44

45
46

47
Monitor
Monitor
(ROSC)
48
49
50

51
52

53
54
55
56

57

1. Kim DK, Jhang WK, Ahn JY, Lee JS, Kim YH, Lee B, et al. Part 6. Pediatric advanced life support: 2015 Korean Guidelines for Cardiopulmonary Resuscitation. Clinical and experimental emergency medicine. 2016;3(Suppl):S48-S61.
2. Lee JS, Ahn JY, Kim DK, Kim YH, Lee B, Jhang WK, et al. Part 5. Pediatric basic life support: 2015 Korean Guidelines for Cardiopulmonary Resuscitation. Clinical and experimental emergency medicine. 2016;3(Suppl):S39-S47.
3. Maconochie IK, Bingham R, Eich C, Lopez-Herce J, Thomas R, et al. European Resuscitation Council Guidelines for Resucitation 2015 Section 6. Pediatric life support. Resuscitation. 2015;95:e223-48.
4. Berg MD, Schexnayder SM, Chameides L, Terry M, Donoghue A, Hickey RW, et al. Part 13: pediatric basic life support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation.2010;122(18 Suppl 3):S862-75.
5. Kleinman ME, Chameides L, Schexnayder SM, Samson RA, Hazinski MF, Atkins DL, et al. Part 14: pediatric advanced life support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation.2010;122(18 Suppl 3):S876-908.
6. Clinical and Experimental Emergency Medicine.
Google.com/images.
58
Pediatric basic life support
Pediatric advanced life support

1. Pediatric basic life support 1) Introduction ················································································ 632) Terminology ··············································································· 643) Pbls for lay rescuers ································································ 644) Pbls for healthcare providers ·················································· 695) Foreign-Body airway obstruction (chocking) ························· 766) Resuscitation under special conditions ··································· 777) The Quality Of Bls ·································································· 78
Pediatric advanced life support
1) Basic life support consideration for pediatric advanced life support ·· 792) Vascular access ······································································· 823) Airway ······················································································ 834) CPR Guidelines for newboens with cardiac arrest of cardiac origin · 875) Emergency fluid and medications ······································· 876) Treatment of pulseless arrest ················································ 917) Defibrillators ············································································ 928) Management of torsade de pointes ······································ 949) Specific resuscitation situation ·············································· 9510) Post-CPR management ························································· 9711) Interhospital transportation ················································· 10112) Terminatio of resuscitative efforts ···································· 102


INTRO
Presponsfor a sefailure likelihocomponbystandsystem, post-carchildrencirculati
High-Qfollowin
Oover thdischargwith Thpediatrifor morfavorab
ODUCTION
Pediatric lie to the pedries of survand shockod of pedia
nents, includder cardiopu
effective ardiac arrest n, prompt aion and goo
uality CPR ng compone
• Star• Push
• Allo• Min
10 s• Giv• Avo
Outcomes fhe past decge improvehe Guidelinec IHCA. Prre than 35 le neurolog
N
ife supportdiatric victimvival procesk. Identifyinatric cardiacding prevenulmonary readvanced licare), and
and effectivod neurolog
improves aents:
rt compressih hard, pusho At leasto At leasto At leastow completnimize interrseconds). e effective b
oid excessiv
from pediatcade. From d from 24%e -Resuscirolonged CP
minutes sgic outcome
Pediatric
t (PBLS) ims with carsses. In chilng childrenc arrest. Thention and eaesuscitationife support integrated p
ve CPR is eic outcome
Fig.1.
a patient’s c
ion within 1h fast: compt 5 cm for adt one third tht one third the chest recoruptions in
breaths thatve ventilatio
tric in-hosp2001 to 2
% to 39%. Ritation progPR is not asurviving to.
c Basic lif
is a major rdiac arrest, dren, Cardi
n with theerefore, the arly recogn
n (CRP), ra(including
post-cardiacessential for.
. pediatric ch
chance of su
10 seconds opress at a radults he depth of he depth of
oil after eachcompressio
t make the con.
pital cardiac2009, rate Recent unp
gram observalways futileo discharge
1623/1624
fe support
componenwhich shou
iac arrest is se problempediatric ch
nition of carapid activati
rapid stabc arrest carer the succe
hain of surviv
urvival. High
of recognitiate of 100 to
f the chest, af the chest, ah compress
ons (try to li
chest rise.
c arrest (IHof pediatri
published 20ved 36% sure, with 12%e and 60%
t
nt of the euld be adequoften secon
ms is essenhain of survrdiac arrestion of the eilization ane (Fig. 1). Sssful recov
val
h-Quality C
ion of cardiao 120/min w
about 5 cm fabout 4 cm fion. mit interrup
CA) have mic IHCA su013 data frorvival to ho
% of patientof those s
emergency uately implndary to res
ntial to redvival comprt, early highemergency nd transportSimilar to avery of spon
CPR compo
ac arrest. with a depth
for childrenfor infants
ption to less
markedly imsurvival to om the AH
ospital dischts who recesurvivors h
medical emented spiration duce the rises five h-quality respond
tation to adults, in ntaneous
ses the
h of
n
s than
mproved hospital
HA’s Get harge for ive CPR
having a
Pediatric basic life support 63
Unlike IHCA, survival from out-hospital cardiac arrest (OHCA) remains poor. Data from 2005-2007 from the Resuscitation Outcomes Consortium, a registry of 11 US and Canadian emergency medical systems, showed age-dependent discharge survival rate of 3.3% for infants, 9.1% for children, and 8.9% for adolescents. More recently published data from this network demonstrate 8.3% survival to hospital discharge across all group.
TERMINOLOGY
The term newly newborn refers to a neonate immediately after delivery. A neonate is an infant within 4 weeks of being born. An infant is a child under 1 year of age (but does not include newly borns) and PBLS guidelines applies to children under 8 years of age except neonates.
Healthcare professionals are those people who look after patients and should have a higher level of training than lay rescuer.
PBLS FOR LAY RESCUERS
Bystander CPR is associated with a better neurological outcome in adults and children.
Rescuers who have been taught adult BLS or the chest compression-only sequence and have no specific knowledge of pediatric resuscitation may use this, as the outcome is worse if they do nothing. However, it is better to provide rescue breath as part of the resuscitation sequence when applied to children as the asphyxia nature of most pediatric cardiac arrests necessitates ventilation as part of effective CPR.
Non-specialists who wish to learn pediatric resuscitation because they have responsibility for children (e.g. teacher, school nurse, lifeguard), should be taught that it is preferable to modify adult BLS.
Historically, the preferred sequence of CPR was A-B-C (Airway-Breathing-Compression). The 2010 AHA Guideline recommended a change to the C-A-B sequence (Compression-Airway-Breathing) to decrease the time to initiation of chest compressions and reduce “no blood flow” time.
The impact of time to first chest compression for C-A-B versus A-B-C sequence has been evaluated. Adult and pediatric manikin studies showed a significantly reduced time to first chest compression with the use of a C-A-B approach compared with an A-B-C approach. Data from 2 of these 3 studies demonstrated that time to first ventilation is delayed by only approximately 6 seconds when using a C-A-B sequence compared with an A-B-C sequence. A flow diagram of PBSL for lay rescuers is shown in Fig. 2
1. Safety of the rescuer and the patient When conducting CPR, the safety of the rescuer and patient must be confirmed at the current location. CPR may carry the risk of transmission of infectious diseases, but the actual risk to the rescuer is extremely low. 2. Determination of the unresponsiveness If an unresponsiveness patient is gasping or not breathing at all, the lay rescuer should understand that the patient is undergoing a cardiac arrest and requires CPR. The rescuer
Pediatric basic life support64
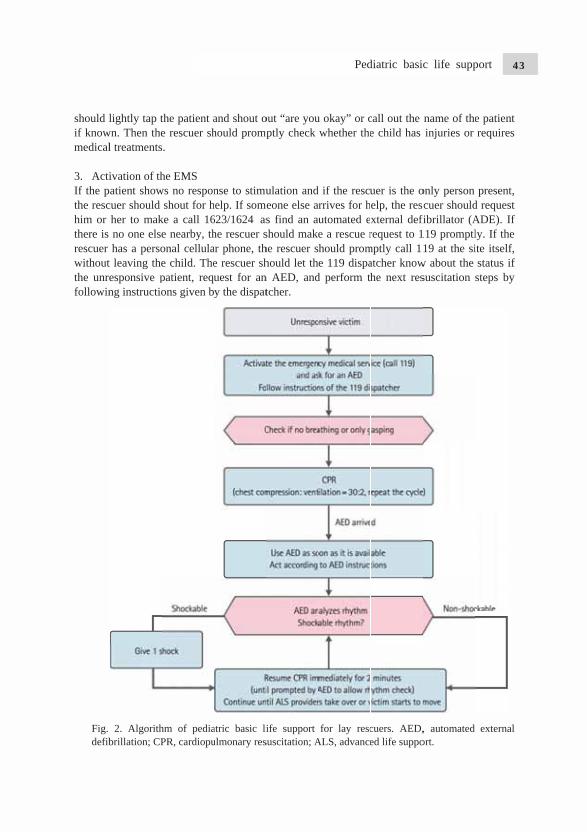
should lif knowmedical 3. ActiIf the pthe reschim or there is rescuer withoutthe unrefollowin
Fig. defib
lightly tap twn. Then thel treatments
ivation of thatient show
cuer should her to makno one elsehas a perso
t leaving theesponsive png instructio
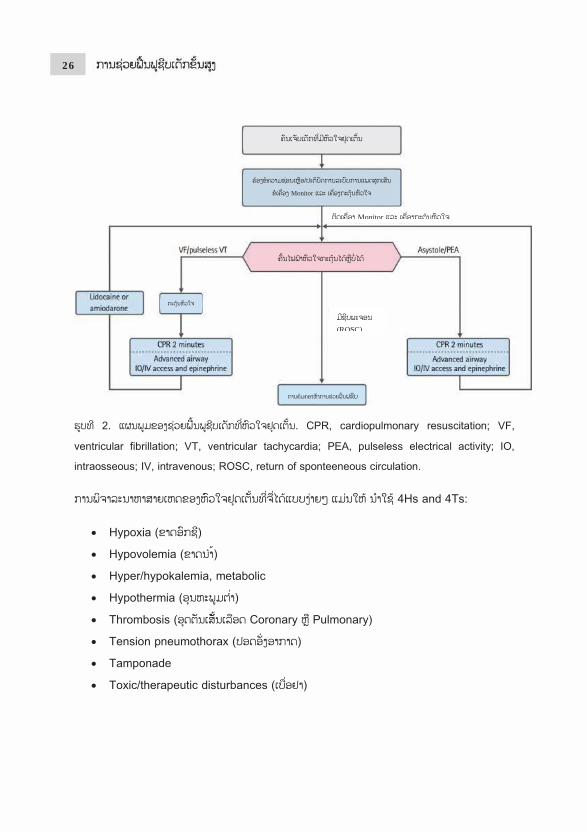
2. Algorithbrillation; CP
the patient ae rescuer shs.
he EMS ws no respon
shout for hke a call 16e nearby, thonal cellulae child. Thepatient, requons given b
hm of pediaPR, cardiopu
and shout ohould promp
nse to stimuhelp. If som623/1624 ashe rescuer sar phone, the rescuer shuest for any the dispat
atric basic liulmonary res
out “are youmptly check
ulation andmeone else a
s find an aushould makehe rescuer should let thn AED, andtcher.
ife support suscitation; A
u okay” or cwhether the
d if the rescurrives for hutomated ee a rescue rhould prome 119 dispa
d perform th
for lay rescALS, advance
call out the e child has
uer is the oelp, the resxternal defirequest to 1
mptly call 1atcher knowhe next res
cuers. AED,ed life suppo
name of theinjuries or
only person cuer should
fibrillator (A119 promptl19 at the si
w about the suscitation
, automated ort.
e patient requires
present, d request ADE). If ly. If the ite itself, status if steps by
external
Pediatric basic life support 65
If the patient shows no response to stimulation and if there are two or more witness, the first rescuer should start CPR immediately and the other should call an EMS and request for an AED.
Most cases of cardiac arrests in children are due to asphyxial arrest rather than VF (ventricular fibrillation). Therefore, if there is only one rescuer without a cellular phone, the rescuer should perform CPR for the first 2 minutes then call EMS and bring a nearby AED. The rescuer should return to the patient as soon as possible and use the AED. If no AED can be found, the rescuer should resume CPR starting with chest compression.
4. Checking patient breathing If a patient is confirmed to be breathing regularly, the child Is not in need of CPR, in such cases, after confirming that there is no evidence of physical injuries, the rescuer should turn the child onto one side and into the recovery position to keep their airway open and reduce the risk of aspiration. The breathing status of the patient should be checked continuously until the arrival of the EMS. If the child tries to change his or her position into a more relaxes d position, the child should be allowed to do so.
If a patient is not responding to stimulation and is not breathing or only gasping (cardiac arrest breathing), CPR should be started. In some cases, patients who are in need of CPR and gasping can be mistaken as having normal breathing. Patients who are gasping should be regulated as not breathing, for which CPR should be started.
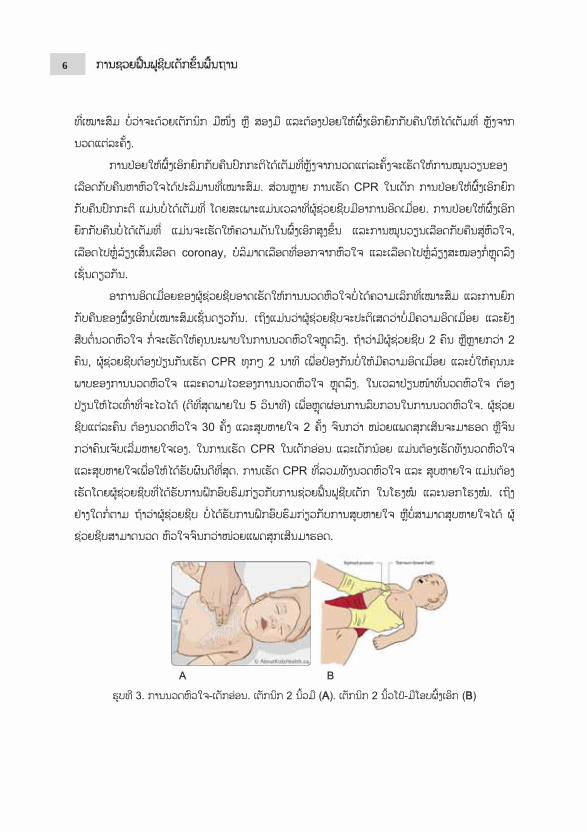
5. Chest compression In CPR, adequate chest compression maintains blood flow to vital organs and increases the possibility of recovery of spontaneous circulation. If a child is neither responding to stimulation nor breathing, the rescuer should immediately perform chest compression 30 times. Chest compression should be performed at a speed of 100-120 per minute and by pressing down at least one-third the depth of the anteroposterior diameter of the rib cage (chest thickness) or 4 cm in infants and 4 to 5 cm in children. It is best to perform chest compression by laying the patient on a flat and hard surface.
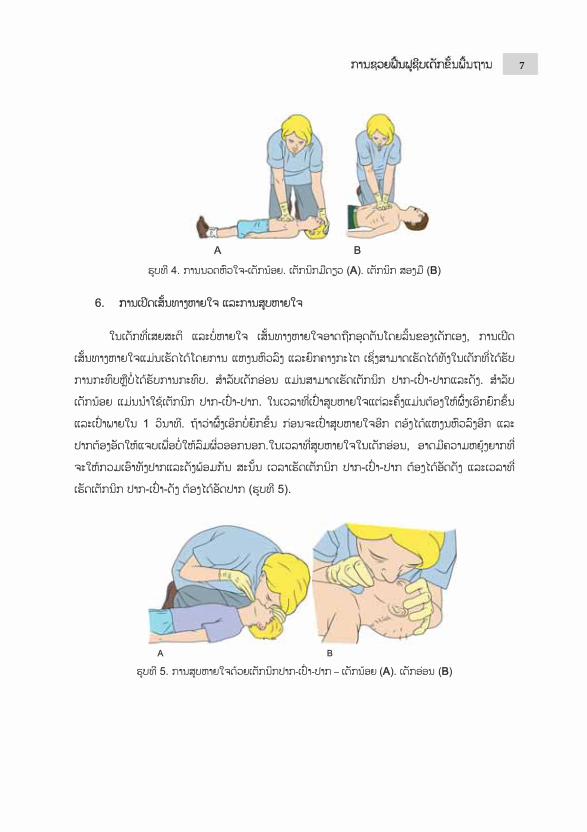
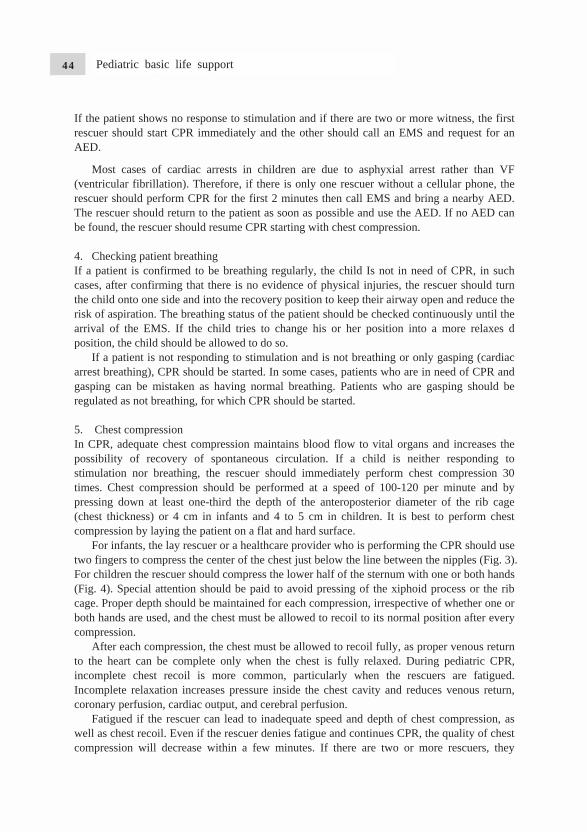
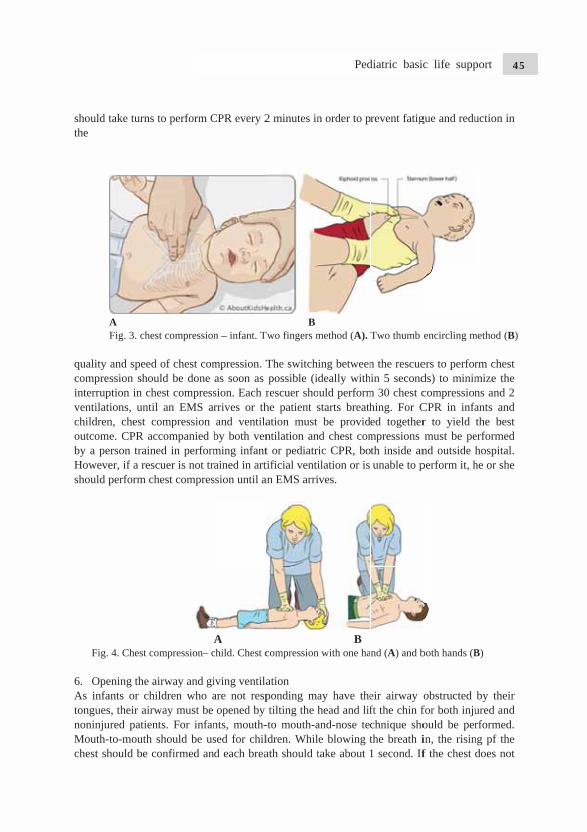
For infants, the lay rescuer or a healthcare provider who is performing the CPR should use two fingers to compress the center of the chest just below the line between the nipples (Fig. 3). For children the rescuer should compress the lower half of the sternum with one or both hands (Fig. 4). Special attention should be paid to avoid pressing of the xiphoid process or the rib cage. Proper depth should be maintained for each compression, irrespective of whether one or both hands are used, and the chest must be allowed to recoil to its normal position after every compression.
After each compression, the chest must be allowed to recoil fully, as proper venous return to the heart can be complete only when the chest is fully relaxed. During pediatric CPR, incomplete chest recoil is more common, particularly when the rescuers are fatigued. Incomplete relaxation increases pressure inside the chest cavity and reduces venous return, coronary perfusion, cardiac output, and cerebral perfusion.
Fatigued if the rescuer can lead to inadequate speed and depth of chest compression, as well as chest recoil. Even if the rescuer denies fatigue and continues CPR, the quality of chest compression will decrease within a few minutes. If there are two or more rescuers, they
Pediatric basic life support66
should tthe
AF
quality compresinterrupventilatichildrenoutcomeby a peHoweveshould p
Fig.
6. OpeAs infatonguesnoninjuMouth-tchest sh
take turns to
A Fig. 3. chest
and speed ossion shoul
ption in cheions, until n, chest coe. CPR acc
erson traineder, if a rescuperform che
4. Chest com
ening the airants or childs, their airwured patientsto-mouth shhould be co
o perform C
compression
of chest comld be done st compressan EMS armpression
companied bd in performuer is not trest compres
mpression– c
rway and gidren who a
way must be s. For infanhould be us
onfirmed an
CPR every 2
n – infant. T
mpression. Tas soon as sion. Each rrrives or thand ventilaby both venming infantained in art
ssion until a
Achild. Chest c
iving ventilaare not respopened by
nts, mouth-sed for child each brea
2 minutes in
BTwo fingers m
The switchipossible (idrescuer shohe patient sation must ntilation ant or pediatritificial ventian EMS arri
compression
ation ponding matilting the h
-to mouth-aldren. Whilath should t
n order to p
method (A).
ing betweendeally withuld performstarts breath
be providnd chest comic CPR, boilation or is ves.
B n with one ha
ay have thehead and lifand-nose tece blowing ttake about 1
revent fatig
Two thumb
n the rescuein 5 second
m 30 chest ching. For Ced togethermpressions th inside anunable to p
nd (A) and b
eir airway ft the chin fchnique shothe breath i1 second. If
gue and redu
encircling m
ers to perfords) to minimcompressionCPR in infar to yield must be pe
nd outside perform it, h
both hands (B
obstructed for both injuould be perin, the risinf the chest
uction in
method (B)
rm chest mize the ns and 2 ants and the best
erformed hospital. he or she
B)
by their ured and rformed.
ng pf the does not
Pediatric basic life support 67
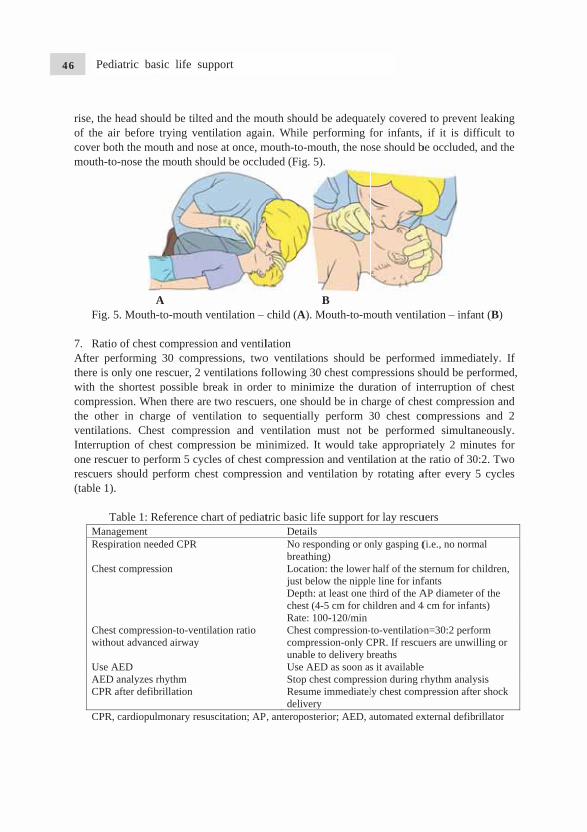
rise, theof the acover bomouth-t
Fig.
7. RatiAfter pthere is with thecompresthe othventilatiInterrupone rescrescuers(table 1)
TManResp
Ches
Cheswith
Use AEDCPR
CPR
e head shouair before toth the mouto-nose the
A 5. Mouth-t
io of chest cerforming only one ree shortest pssion. Whener in chargions. Chest
ption of checuer to perfs should pe).
Table 1: Renagement piration need
st compressi
st compressihout advance
AED D analyzes rhR after defibr
R, cardiopulm
uld be tilted trying ventiuth and nosemouth shou
A to-mouth ve
compression30 compreescuer, 2 vepossible bren there are ge of ventit compressest compresform 5 cycleerform ches
eference cha
ded CPR
on
on-to-ventilad airway
hythm rillation
monary resus
and the moilation againe at once, muld be occlu
entilation –
n and ventilssions, two
entilations foeak in ordetwo rescuerilation to ssion and vssion be mies of chest cst compress
art of pediat
ation ratio
scitation; AP
outh should n. While p
mouth-to-mouded (Fig. 5
child (A). M
lation o ventilationfollowing 30er to minimrs, one shousequentiallyventilation minimized. Itcompressionsion and ve
tric basic lifDetails No respbreathinLocatiojust beloDepth: chest (4Rate: 10Chest ccompreunable tUse AEStop chResumedelivery
, anteroposte
be adequaterforming fouth, the no).
B Mouth-to-m
ns should b0 chest com
mize the duruld be in chy perform 3must not bt would takn and ventintilation by
fe support fo
ponding or onng) on: the lower ow the nipplat least one t
4-5 cm for ch00-120/minompression-ssion-only Cto delivery b
ED as soon ashest compresse immediately erior; AED, a
tely coveredfor infants,
ose should b
mouth ventila
be performmpressions sh
ration of inharge of che30 chest cobe performke approprialation at they rotating a
for lay rescu
nly gasping (
half of the se line for infthird of the Ahildren and 4
to-ventilatioCPR. If rescubreaths s it availablesion during rly chest comp
automated ex
d to prevent if it is dif
be occluded
ation – infa
med immedihould be penterruption est compresompression
med simultaately 2 mine ratio of 30after every
uers
(i.e., no norm
sternum for cfants AP diameter 4 cm for infan
on=30:2 perfouers are unwi
e rhythm analy
mpression afte
xternal defib
t leaking fficult to , and the
ant (B)
iately. If erformed, of chest sion and
ns and 2 aneously. nutes for 0:2. Two 5 cycles
mal
children,
of the nts)
orm illing or
ysis er shock
rillator
Pediatric basic life support68
PBLS F
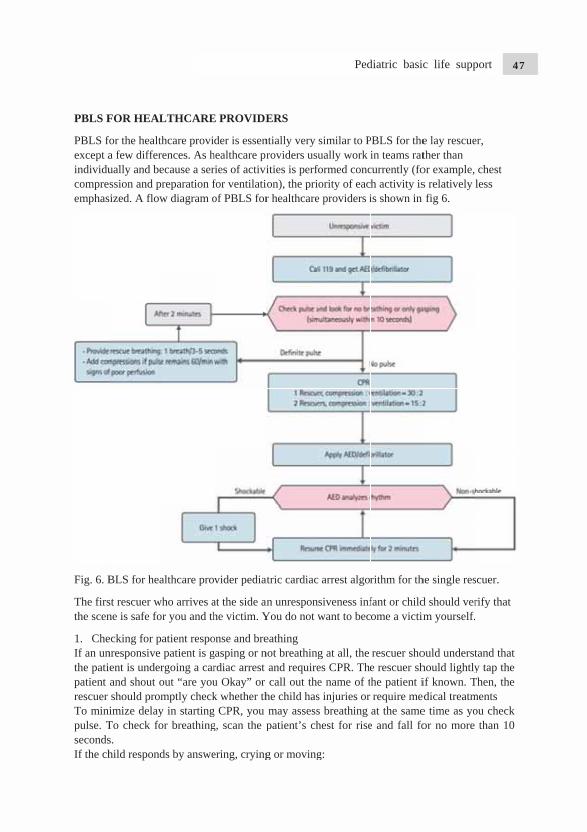
PBLS foexcept aindividucompresemphas
Fig. 6. B
The firsthe scen
1. CheIf an unthe patiepatient rescuer To minipulse. TsecondsIf the ch
FOR HEAL
for the healtha few differually and bession and prized. A flow
BLS for hea
st rescuer wne is safe fo
ecking for pnresponsive ent is underand shout oshould promimize delay
To check fos. hild respond
LTHCARE
hcare proviences. As hecause a serreparation fw diagram o
althcare pro
ho arrives ar you and th
atient respopatient is g
rgoing a carout “are youmptly checky in startingor breathing
ds by answe
E PROVIDE
der is essenhealthcare prries of activifor ventilatiof PBLS for
vider pedia
at the side anhe victim. Y
onse and bregasping or nrdiac arrest u Okay” or k whether thg CPR, you g, scan the p
ering, crying
ERS
ntially very roviders usuities is perfoion), the prior healthcare
atric cardiac
an unresponYou do not w
eathing not breathing
and requirecall out the
he child hasmay assesspatient’s ch
g or moving
similar to Pually work
formed concority of eac
e providers i
arrest algor
siveness infwant to bec
g at all, the es CPR. Thee name of ts injuries or s breathing hest for rise
g:
PBLS for thein teams rat
currently (foh activity isis shown in
rithm for th
fant or childome a victim
rescuer shoe rescuer shhe patient irequire meat the same
e and fall fo
e lay rescuether than or example,s relatively fig 6.
he single res
d should verm yourself.
ould understhould lightlyif known. Tedical treatme time as yoor no more
er,
chest less
scuer.
rify that
tand that y tap the
Then, the ments ou check
than 10
Pediatric basic life support 69
• Ld
• C• R
2. ActiIf the pgasping 3. CheIf an infcheck fbrachialBLS proinfant obeginnin
To pto locate
• Pa
• Ts
Foll
• Pa
• F
Fig.perfo
A
Leave the danger). Check his cReassess hi
ivation of thpatient is neg), the rescu
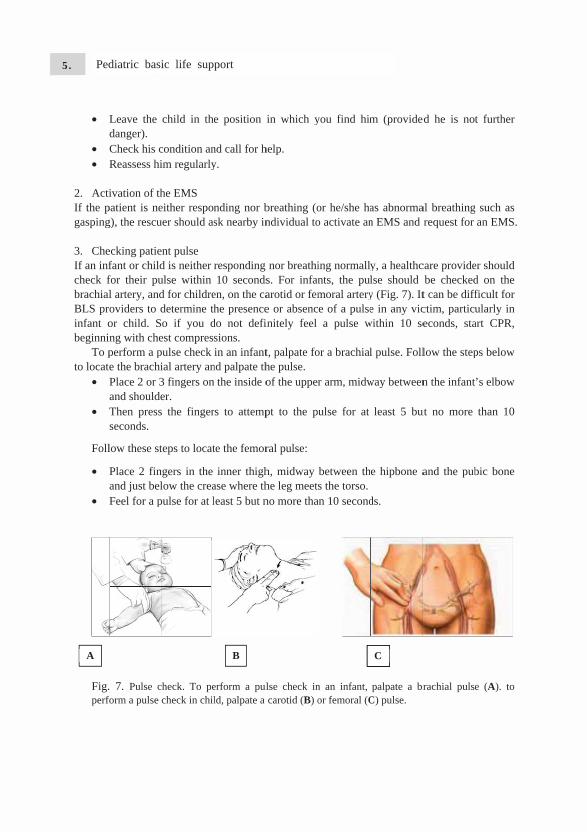
ecking patiefant or childfor their pul artery, andoviders to dor child. Sng with cheperform a pe the brachiPlace 2 or 3and shouldeThen pressseconds.
low these st
Place 2 finand just belFeel for a p
7. Pulse cform a pulse c
child in the
condition anim regularly
he EMS either responuer should as
nt pulse d is neither ulse within d for childredetermine tho if you d
est comprespulse check ial artery an3 fingers oner. the finger
teps to locat
gers in the low the crea
pulse for at l
heck. To pecheck in chil
e position
nd call for hy.
nding nor bsk nearby in
responding 10 seconds
en, on the cahe presence
do not defisions. in an infant
nd palpate thn the inside o
rs to attemp
te the femor
inner thighase where thleast 5 but n
erform a pulld, palpate a
B
in which y
help.
breathing (ondividual to
nor breathis. For infanarotid or feme or absencinitely feel
t, palpate fohe pulse. of the upper
pt to the pu
ral pulse:
h, midway he leg meetsno more tha
lse check incarotid (B) o
you find him
or he/she hao activate an
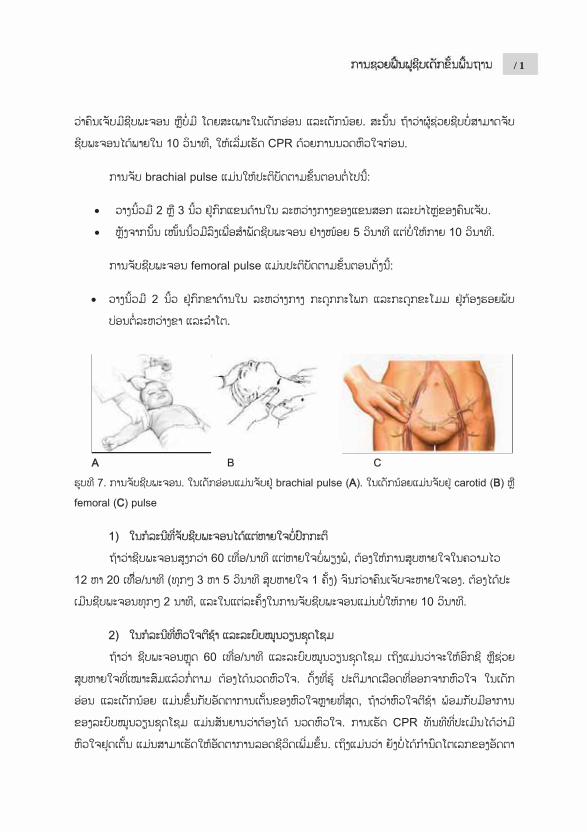
ing normallynts, the pulmoral arterye of a pulsea pulse w
or a brachial
r arm, midw
ulse for at
between ths the torso.
an 10 second
n an infant, or femoral (C
m (provide
as abnorman EMS and
y, a healthclse should y (Fig. 7). Ite in any vic
within 10 se
l pulse. Foll
way between
least 5 bu
e hipbone a
ds.
palpate a brC) pulse.
C
ed he is no
al breathingrequest for
care providebe checkedt can be diffctim, particueconds, sta
low the step
n the infant
ut no more
and the pub
rachial puls
t further
g such as an EMS.
er should d on the ficult for ularly in
art CPR,
ps below
’s elbow
than 10
bic bone
e (A). to
Pediatric basic life support70
1) Case of palpable pulse and inadequate breathing If a pulse is detected to be more than 60 per minute but breathing is inadequate, ventilation should be provided at the speed of 12 to 20 times per minute (1 breath every 3 to 5 seconds) until the return of spontaneous breathing. The pulse should be rechecked every 2 minutes, and each pulse check should not exceed 10 seconds. 2) Case of bradycardia and poor systemic perfusion If the pulse rate is less than 60 per minute and the perfusion status is poor (i.e., pale skin, patches of spots, or cyanosis is observed) even with oxygen and adequate ventilation, chest compression should be performed. As the cardias output of infants and children depends greatly on the heart rate, bradycardia with poor systemic perfusion signals the necessity for chest compression. Performing CPR immediately after the occurrence of cardiac arrest can lead to an increased survival rate. Although the critical value of the heart rate at which chest compression should be performed is not yet clearly defined, chest compression is recommended for a heart rate less than 60 per minute and poor perfusion for the convenience of education and ease of memorization. Assess the flowing to determine signs of poor perfusion:
• Temperature: cool extremities • Altered mental state: continued decline in consciousness/responsiveness • Pulses: weak pulses • Skin: paleness, mottling (patchy appearance), and later cyanosis (turning blue)
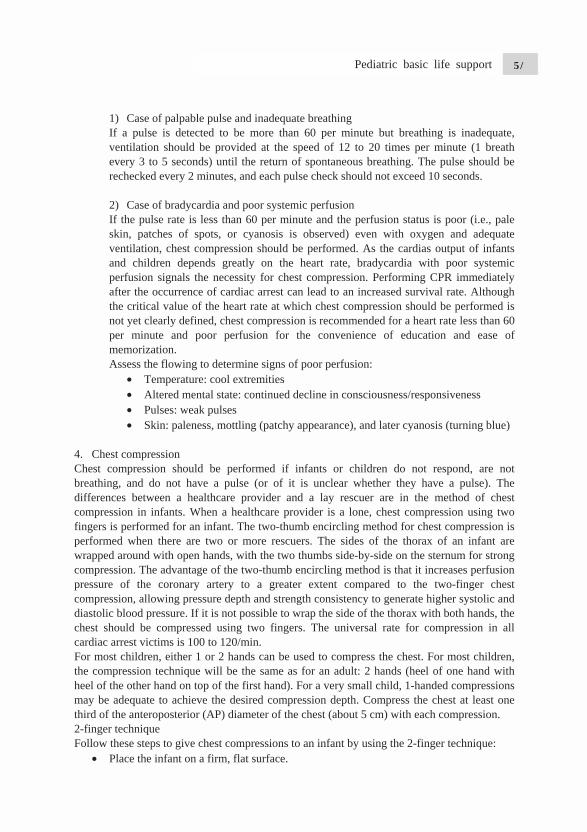
4. Chest compression Chest compression should be performed if infants or children do not respond, are not breathing, and do not have a pulse (or of it is unclear whether they have a pulse). The differences between a healthcare provider and a lay rescuer are in the method of chest compression in infants. When a healthcare provider is a lone, chest compression using two fingers is performed for an infant. The two-thumb encircling method for chest compression is performed when there are two or more rescuers. The sides of the thorax of an infant are wrapped around with open hands, with the two thumbs side-by-side on the sternum for strong compression. The advantage of the two-thumb encircling method is that it increases perfusion pressure of the coronary artery to a greater extent compared to the two-finger chest compression, allowing pressure depth and strength consistency to generate higher systolic and diastolic blood pressure. If it is not possible to wrap the side of the thorax with both hands, the chest should be compressed using two fingers. The universal rate for compression in all cardiac arrest victims is 100 to 120/min. For most children, either 1 or 2 hands can be used to compress the chest. For most children, the compression technique will be the same as for an adult: 2 hands (heel of one hand with heel of the other hand on top of the first hand). For a very small child, 1-handed compressions may be adequate to achieve the desired compression depth. Compress the chest at least one third of the anteroposterior (AP) diameter of the chest (about 5 cm) with each compression. 2-finger technique Follow these steps to give chest compressions to an infant by using the 2-finger technique:
• Place the infant on a firm, flat surface.
Pediatric basic life support 71
• Place 2 fingers in the center of the infant’s chest, just below the nipple line, on the lower half of the breastbone. Do not press the tip of the breastbone.
• Give compressions at a rate of 100 to 120/min. • Compress at least one third of the AP diameter of the infant’s chest (about 4 cm). • At the end of each compression, make sure you allow the chest to fully recoil
(reexpand); do not lean on the chest. Chest compression and chest recoil/relaxation times should be about equal. Minimize interruptions in chest compressions (e.g. to give breaths) to less than 10 seconds.
• After every 30 compressions, open the airway and give 2 breaths each over 1 second. The chest should be rise with each breath.
• After about 5 cycles or 2 minutes of CPR, if you are alone and the emergency response system has not been activated, leave the infant (or carry with you) to activate the emergency response system and retrace the AED.
• Continue compressions and breath un a ratio of 30:2, and use the AED as soon as it is available. Continue until advanced providers take over or the infant begins to breath, move, or otherwise react.
2 Thumb-encircling hands technique Follow these steps to give chest compressions to an infant using the 2 thumb-encircling hands technique:
• Place the infant on a firm, flat surface. • Place the thumbs side by side in the infant’s chest, on the lower half of the
breastbone, the thumbs may overlap in very small infants. Encircle the infant’s chest and support the infant’s back with the fingers of both hands.
• With your hand s encircling the chest, use both thumbs to depress breastbone at a rate of 100 to 12o/min.
• Compress at least one third the AP diameter of the infant’s chest (about 4 cm). • After each compression, complete release the pressure on the breastbone and aloow
the chest recoil completely. • After every 15 compressions, pause briefly for the second rescuer to open the airway
and give 2 breaths, each over 1 second. The chest should rise with each breath. Minimize interruptions in compressions (e.g. to give breaths) to less than 10 seconds.
• Continue compressions and breaths in a ratio of 15:2 (for 2 rescuers). The rescuers providing chest compressions should switch role with another provider about every 5 cycles or 2 minutes to avoid fatigue so that chest compressions remain effective. Continue CPR until the AED arrived, advanced providers take over, or the infant begins to breathe, move or otherwise respond.
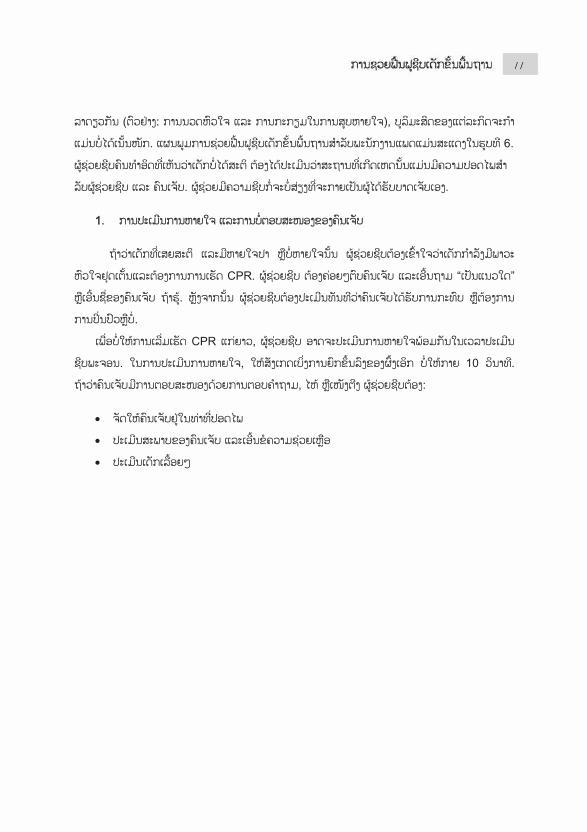
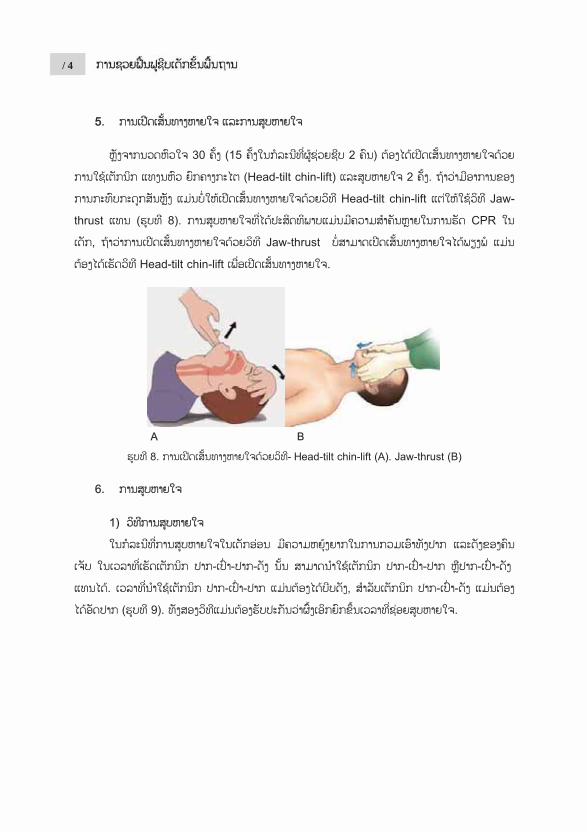
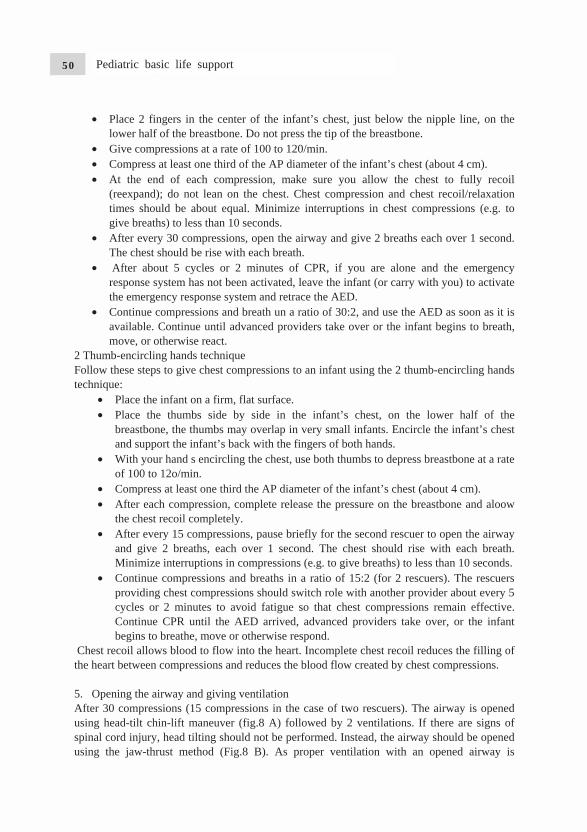
Chest recoil allows blood to flow into the heart. Incomplete chest recoil reduces the filling of the heart between compressions and reduces the blood flow created by chest compressions. 5. Opening the airway and giving ventilation After 30 compressions (15 compressions in the case of two rescuers). The airway is opened using head-tilt chin-lift maneuver (fig.8 A) followed by 2 ventilations. If there are signs of spinal cord injury, head tilting should not be performed. Instead, the airway should be opened using the jaw-thrust method (Fig.8 B). As proper ventilation with an opened airway is
Pediatric basic life support72
extremejaw-thru
Fig.8 A 6. Ven
IoWtb
AF 2Bsrm“Cm
ely importanust is not su
A. Head-tilt ch
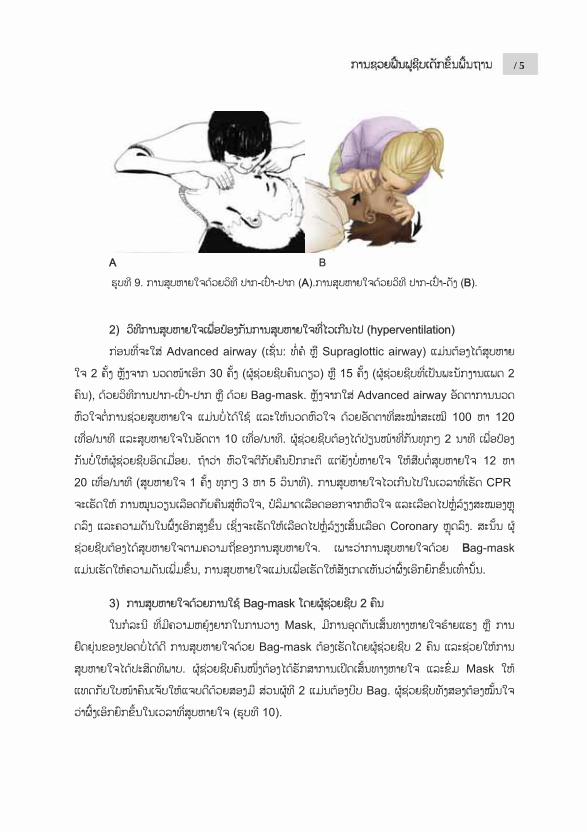
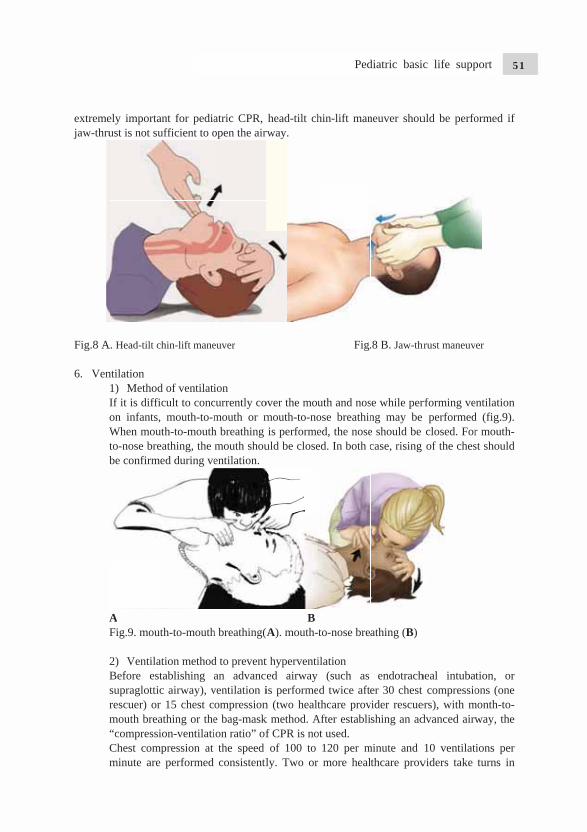
ntilation 1) MethodIf it is difficon infants, When moutto-nose brebe confirme
A Fig.9. mout
2) VentilatBefore estsupraglotticrescuer) or mouth brea“compressiChest compminute are
nt for pediaufficient to o
hin-lift mane
d of ventilaticult to concmouth-to-m
th-to-mouthathing, the ed during ve
th-to-mouth
tion methodtablishing c airway), v
15 chest cathing or theon-ventilatipression at performed
atric CPR, open the air
euver
ion currently comouth or mh breathing mouth shouentilation.
h breathing(
d to preventan advanc
ventilation iompressione bag-maskion ratio” of
the speed consistentl
head-tilt chrway.
over the moumouth-to-nois performe
uld be close
B(A). mouth-t
t hyperventied airway is performen (two healtk method. Af CPR is noof 100 to
ly. Two or
hin-lift man
Fig.
uth and nosose breathined, the noseed. In both c
to-nose bre
ilation (such as
d twice aftethcare prov
After establiot used.
120 per mmore heal
neuver shou
.8 B. Jaw-thr
se while perng may be e should be case, rising
athing (B)
endotracher 30 chest
vider rescueshing an ad
minute and thcare prov
uld be perfo
hrust maneuv
rforming ve performedclosed. Forof the ches
heal intubat compressioers), with mdvanced airw
10 ventilatviders take
ormed if
ver
entilation d (fig.9). r mouth-st should
ation, or ons (one
month-to-way, the
tions per turns in
Pediatric basic life support 73
pI2Cfarpj 3Iourtr
F 4Asptrup 5OrnppO
performing If the perfu20 times peCPR reducflow, and inartery perfurecommendprovide higjust observe
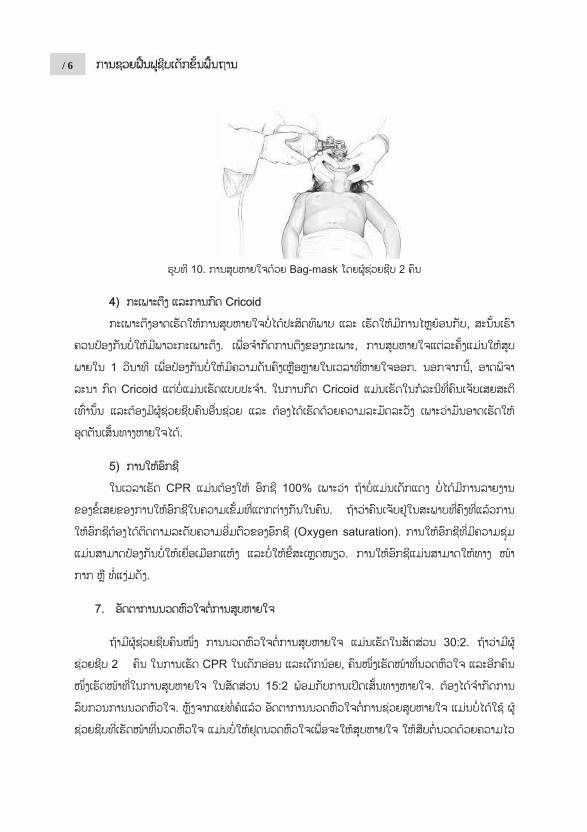
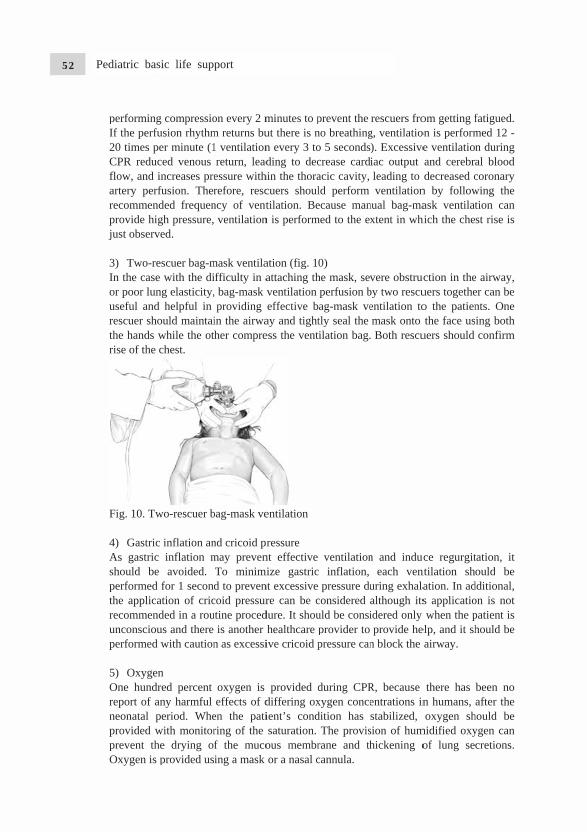
3) Two-resIn the case or poor lunguseful and rescuer shothe hands wrise of the c
Fig. 10. Tw
4) Gastric As gastric should be performed fthe applicatrecommendunconsciouperformed w
5) OxygenOne hundrereport of anneonatal peprovided wprevent theOxygen is p
compressiousion rhythmer minute (1ed venous ncreases pre
fusion. Therded frequengh pressure,ed.
scuer bag-mwith the dig elasticity,helpful in
ould maintaiwhile the otchest.
wo-rescuer b
inflation aninflation mavoided.
for 1 secondtion of cric
ded in a rouus and there with caution
n ed percent ny harmful eriod. Whe
with monitore drying oprovided us
on every 2 mm returns bu1 ventilationreturn, leadessure withrefore, rescncy of vent ventilation
mask ventilaifficulty in a, bag-mask providing
in the airwaher compre
bag-mask ve
nd cricoid pmay prevenTo minimd to prevencoid pressurutine proced
is another n as excessi
oxygen is effects of d
en the patiring of the f the mucoing a mask
minutes to put there is nn every 3 toding to dec
hin the thoracuers shoultilation. Be
n is perform
ation (fig. 1attaching thventilation effective b
ay and tightess the vent
entilation
ressure nt effective
mize gastricnt excessive re can be c
dure. It shouhealthcare pive cricoid p
provided ddiffering oxient’s condsaturation.
ous membror a nasal c
prevent the no breathingo 5 secondscrease cardacic cavity, ld perform ecause man
med to the ex
0) he mask, sevperfusion bag-mask vetly seal the ilation bag.
ventilationc inflation,
pressure duconsidered auld be consiprovider to pressure can
during CPRxygen concedition has
The provisrane and thcannula.
rescuers frog, ventilatio). Excessiveiac output leading to ventilation
nual bag-maxtent in wh
vere obstrucby two rescuentilation tomask onto Both rescu
n and induceach ven
uring exhalaalthough itsidered only provide he
n block the
R, because entrations instabilized,
sion of humhickening o
om getting fon is performe ventilatioand cerebrdecreased c
n by followask ventilat
hich the che
uction in theuers togetheo the patienthe face us
uers should
uce regurgitntilation shation. In ads applicatiowhen the p
elp, and it shairway.
there has n humans, oxygen sh
midified oxyof lung se
fatigued. med 12 - n during al blood coronary wing the tion can st rise is
e airway, er can be nts. One sing both
confirm
tation, it ould be
dditional, on is not patient is hould be
been no after the
hould be ygen can cretions.
Pediatric basic life support74

7. Ratio of chest compression and ventilation One rescuer performs chest compression and ventilation at the ratio of 30:2. When two rescuers perform CPR on infants or children, one performs chest compression and the other performs ventilation at the ratio of 15:2, with opening if the airway. The interruption of chest compression for the ventilation should be minimized. After intubation, the ratio of chest compression and ventilation is no longer followed. Instead, the rescuer responsible for chest compression does not stop the compression for ventilation and performs it continuously at the speed of 100 to 120 per minute. The rescuer responsible for ventilation provides ventilation at the speed of 10 times per minute (1 ventilation every 6 seconds). 8. Defibrillation VF may be the cause of sudden cardiac arrest or it may occur during CPR. The sudden collapse of child in the presence of another person (for example, a child who collapse while exercising) that may be caused by VF or pulseless ventricular tachycardia, immediate CPR and prompt defibrillation are necessary in such cases. As VF or pulseless ventricular tachycardia may respond to defibrillation, they are categorized as “shockable rhythms”.
In infants, it is better to use a manual defibrillator by well-trained healthcare provider to give a shock. For defibrillation, the first energy dose is at 2 to 4 J/kg and the second dose is 4 J/kg or higher; the shock should not exceed the maximum dose for adults. If a manual defibrillator is not available, an AED with a pediatric energy attenuator should be used. However, if both a manual defibrillator and an AED with a pediatric energy attenuator are lacking, an AED for adults without an attenuator can be used for infants. Rescuers should minimize the time between chest compression and defibrillation, and resume CPR by restarting chest compression immediately after defibrillation. The use of AED will ensure that rescuers reanalyze the rhythm every 2 minutes, and defibrillation should be performed immediately after chest compression (table 2). 9. Compression-only CPR When sudden cardiac arrest occurs, the oxygen content of the blood is typically adequate to meet oxygen demands of the body for the first few minutes after arrest. So delivering chest compressions is an effective way of distributing oxygen to the heart and brain. In contrast, infants and children who develop cardiac arrest often have respiratory failure or shock that reduces the oxygen content in the blood even before the onset of arrest. As a result, for most infants and children in cardiac arrest, chest compressions alone are not effectives as compressions and breaths for delivering oxygenated blood to the heart and brain for this reason, it is very important to give both compressions and breaths for infants and children during high-quality CPR. Therefore, infant and pediatric CPR accompanies resuscitation comprising ventilation is not possible or the rescuer is not known about how to perform ventilation, compression-only CPR must be performed on its own.
Pediatric basic life support 75
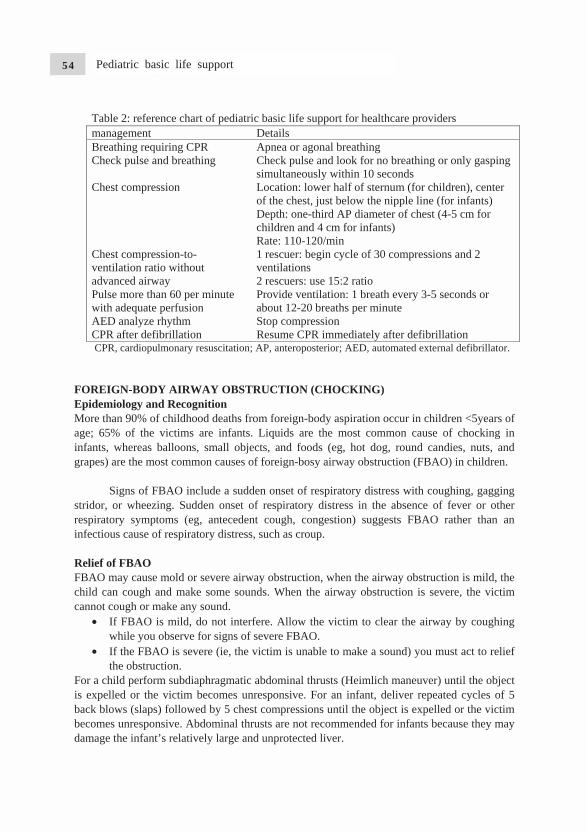
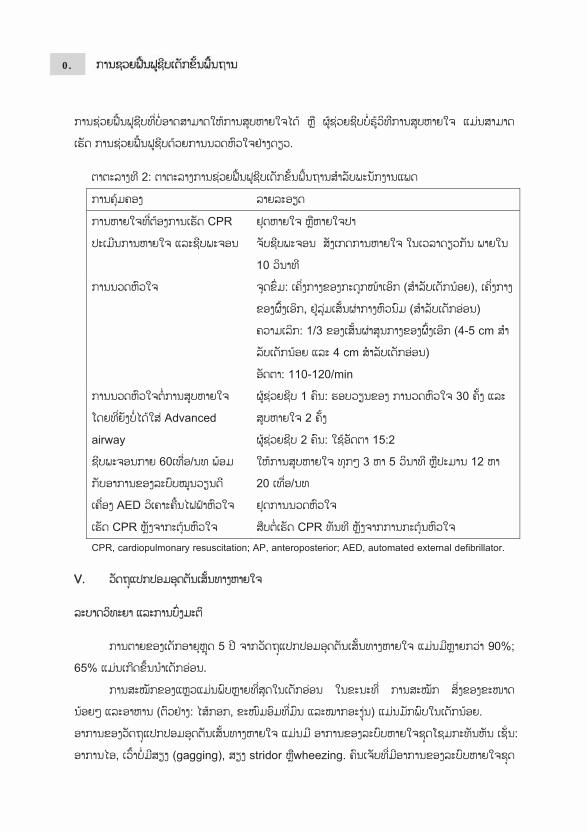
Table 2: reference chart of pediatric basic life support for healthcare providers management Details Breathing requiring CPR Apnea or agonal breathing Check pulse and breathing Check pulse and look for no breathing or only gasping
simultaneously within 10 seconds Chest compression Location: lower half of sternum (for children), center
of the chest, just below the nipple line (for infants) Depth: one-third AP diameter of chest (4-5 cm for children and 4 cm for infants) Rate: 110-120/min
Chest compression-to-ventilation ratio without advanced airway
1 rescuer: begin cycle of 30 compressions and 2 ventilations 2 rescuers: use 15:2 ratio
Pulse more than 60 per minute with adequate perfusion
Provide ventilation: 1 breath every 3-5 seconds or about 12-20 breaths per minute
AED analyze rhythm Stop compression CPR after defibrillation Resume CPR immediately after defibrillation CPR, cardiopulmonary resuscitation; AP, anteroposterior; AED, automated external defibrillator.
FOREIGN-BODY AIRWAY OBSTRUCTION (CHOCKING) Epidemiology and Recognition More than 90% of childhood deaths from foreign-body aspiration occur in children <5years of age; 65% of the victims are infants. Liquids are the most common cause of chocking in infants, whereas balloons, small objects, and foods (eg, hot dog, round candies, nuts, and grapes) are the most common causes of foreign-bosy airway obstruction (FBAO) in children. Signs of FBAO include a sudden onset of respiratory distress with coughing, gagging stridor, or wheezing. Sudden onset of respiratory distress in the absence of fever or other respiratory symptoms (eg, antecedent cough, congestion) suggests FBAO rather than an infectious cause of respiratory distress, such as croup. Relief of FBAO FBAO may cause mold or severe airway obstruction, when the airway obstruction is mild, the child can cough and make some sounds. When the airway obstruction is severe, the victim cannot cough or make any sound.
• If FBAO is mild, do not interfere. Allow the victim to clear the airway by coughing while you observe for signs of severe FBAO.
• If the FBAO is severe (ie, the victim is unable to make a sound) you must act to relief the obstruction.
For a child perform subdiaphragmatic abdominal thrusts (Heimlich maneuver) until the object is expelled or the victim becomes unresponsive. For an infant, deliver repeated cycles of 5 back blows (slaps) followed by 5 chest compressions until the object is expelled or the victim becomes unresponsive. Abdominal thrusts are not recommended for infants because they may damage the infant’s relatively large and unprotected liver.
Pediatric basic life support76
If the vpulse chit but dinto thewith cyminutes RESUS
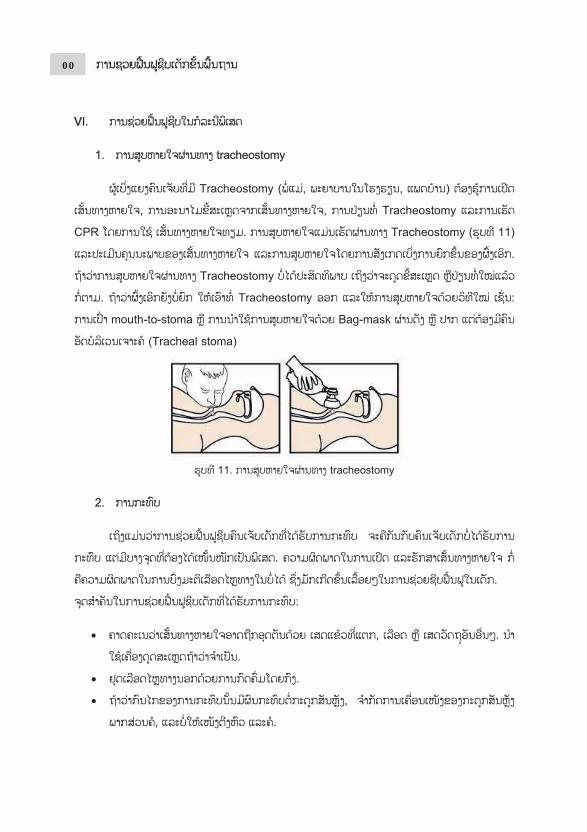
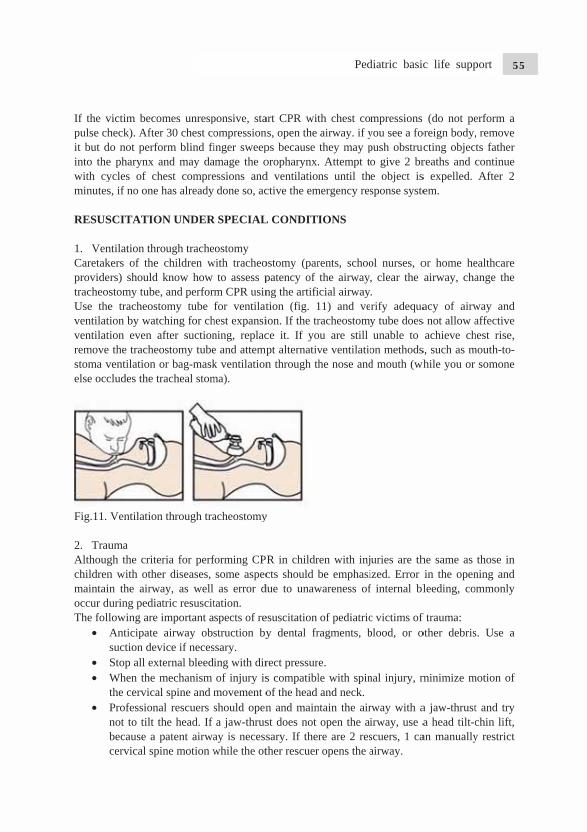
1. VenCaretakprovidetracheosUse theventilativentilatiremove stoma velse occ
Fig.11. 2. TrauAlthougchildrenmaintainoccur duThe foll
• As
•• W
t• P
nbc
victim becoheck). After
do not perfoe pharynx aycles of chs, if no one h
SCITATIO
ntilation throkers of the rs) should stomy tube,e tracheostoion by watcion even athe tracheo
ventilation ocludes the tr
Ventilation
uma gh the critern with othen the airwauring pediatlowing are iAnticipate suction devStop all extWhen the mthe cervicalProfessionanot to tilt thbecause a pcervical spi
mes unrespr 30 chest coorm blind fiand may dahest comprehas already
N UNDER
ough trachechildren wknow how , and performomy tube ching for chafter suctionostomy tubeor bag-maskracheal stom
n through tra
ria for perfr diseases, ay, as well tric resuscitimportant aairway obs
vice if necesternal bleedimechanism l spine and mal rescuers she head. If patent airwaine motion w
ponsive, staompressioninger sweepamage the oessions anddone so, ac
R SPECIAL
ostomy with tracheo
to assess pm CPR usinfor ventilat
hest expansining, replace and attempk ventilationma).
acheostomy
forming CPsome aspecas error d
tation. spects of restruction byssary. ing with dirof injury ismovement oshould opena jaw-thrus
ay is necesswhile the ot
art CPR witns, open the ps because oropharynx.d ventilationctive the em
L CONDITI
ostomy (parpatency of ng the artifition (fig. 1ion. If the trce it. If yopt alternativn through th
y
R in childrcts should b
due to unaw
esuscitation y dental fr
rect pressurs compatiblof the head n and mainst does not sary. If therther rescuer
th chest coairway. if ythey may p. Attempt tons until th
mergency res
IONS
rents, schoothe airway,
icial airway11) and veracheostomyou are still ve ventilatiohe nose and
ren with injbe emphasi
wareness of
of pediatricragments, b
e. le with spinand neck.
ntain the airopen the aire are 2 res
r opens the a
mpressions you see a fopush obstruco give 2 bre object issponse syste
ol nurses, o, clear the . rify adequay tube doesunable to
on methodsd mouth (wh
uries are thized. Error f internal bl
c victims of blood, or o
nal injury, m
rway with airway, use ascuers, 1 caairway.
(do not peoreign body,ucting objecreaths and s expelled. em.
or home heairway, cha
acy of airws not allow aachieve ch
s, such as mwhile you or
he same as in the openleeding, co
f trauma: other debris
minimize m
a jaw-thrusta head tilt-can manually
erform a , remove
cts father continue After 2
ealthcare ange the
way and affective
hest rise, mouth-to-
somone
those in ning and ommonly
s. Use a
motion of
t and try chin lift, y restrict
Pediatric basic life support 77
• To limit spine motion, secure at least the thighs, pelvis, and shoulders to the immobilization board. Because of the disproportionately large size of the head in infants and young children, optimal positioning may require recessing the occiput or elevating the torso to avoid undesirable backboard-induced cervical flexion.
• If possible, transport children with potential for serious trauma to a trauma center with pediatric expertise.
3. Drowning In the case of drowning, the duration of submersion in water is an important factor for the prediction of prognosis. The age, promptness of emergency treatment, form of water (e.g., sea water), water temperature, and the presence or absence of witnesses are not reliable prognosis factors. As the survival rate is relatively high in the case of drowning in ice water even with long submersion durations, the rescue time should be extended in such case. Drowned children must start receiving CPR immediately after being rescued from the water. Rescuers with special training may start ventilation in water. Because chest compression is not efficient in water, it is not usually performed. As there is no evidence that water causes airway obstruction, no time is wasted to pump out water from the lungs of the rescued person. CPR should be started by performing chest compression and the airway is opened, ventilation is performed twice. If the rescuer is alone, 5 cycles of chest compression and ventilation are performed before calling EMS and preparing an AED. If there are two rescuers, one continues CPR while the other activates EMS and prepare an AED. THE QUALITY OF BLS Immediate CPR can improve survival from cardiac arrest in children, but not enough children receive high-quality CPR. We must increase the number of laypersons who learn, remember, and perform CPR, and must improve the quality of CPR provided by lay rescuers and healthcares providers alike. Healthcare systems that deliver CPR should implement processes of the performance improvement. These include monitoring the time required for recognition and activation of emergency medical system, the quality of CPR delivered at the scene of cardiac arrest, other process-of-care measures (e.g. initial rhythm, bystander CPR, and response intervals), and patients outcome up to hospital discharge. This evidence should be used to optimize the quality of CPR delivered.
Pediatric basic life support78

Pediatric Advanced Life Support
In children, secondary pulmonary cardiac arrest, caused by either respiratory or circulation failure, are more frequent than primary arrests caused by arrhythmias. So-called asphyxial arrests or respiratory arrests are more common in young adulthood (e.g. trauma, drowning and poisoning).
Without treatment, the ill/injures child’s initial physiological responses involve compensatory mechanisms. This mean the affected system tries to adapt to the underlying physiological disturbance. So, for the circulatory problem, the initial physiological responses will be the circulatory system, and if there is respiratory problem, then respiratory changes may take place. As things worsen, the other system may become involved as part of the compensatory process. However, the child may continue to deteriorate, leading to decompensated respiratory or circulatory failure. Further physiological deterioration to cardiopulmonary failure may occur with the then inevitable progression to cardiopulmonary arrest. As the outcome from cardiopulmonary arrest in children is poor, identify the preceding stage of circulatory or respiratory failure is a priority as effective early intervention in these stage may be lifesaving.
Another mechanism of cardiac arrest, ventricular fibrillation (VF) or pulseless ventricular tachycardia (VT), is the initial cardiac rhythm in approximately 5% to 15% of pediatric in-hospital and out-of-hospital cardiac arrest, it is reported in up to 27% of pediatric in-hospital arrests at some point during the resuscitation. The incidence of VF/pulseless VT cardiac arrest rise with age. Increasing evidence suggests that sudden unexpected death in young people can be associated with genetic abnormalities in myocyte ion channels resulting in abnormalities in ion flow.
BASIC LIFE SUPPORT CONSIDERATION FOR PEDIATRIC ADVANCED LIFE SUPPORT
1. Collaborative management using a team approach Summoning a pediatric rapid response team or medical emergency team may reduce the risk of respiratory and/or cardiac arrest in hospitalized children outside the intensive care setting. This team should ideally include at least one physician experienced in acute pediatric care and a pediatric nurse, and be called to evaluate a potentially critically ill child already in a pediatric intensive care unit (PICU) or pediatric emergency department (ED).
The ERC writing group recognized that there is national and regional variation in countries as to the composition of such a team but it is clear that processes to detect the early deterioration are likely in reducing the morbidity and mortality of seriously ill and injured children. these processes with subsequent intervention by attending nurses and doctors have a higher priority for implementation than there solely being a rapid response or medical emergency team.
It is important to build an efficient team of healthcare professional that provides advanced life support during cardiopulmonary resuscitation (CPR). The following factors are important in order for these teams to effectively perform CPR: chest compression should be performed immediately after the need for CPR has been established, and ventilation should be performed
Pediatric advanced life support 79
if there is a second rescuer. Breathing is also important for infants or children, and compression-ventilation CPR, rather than compression-only CPR, should be performed inside hospitals. Although the preparation of a ventilation device can delay effective ventilation in some cases, chest compressions should be performed immediately for both infants and children. High-quality CPR within 10 seconds after identifying the cardiac arrest, an adequate compression depth, complete recoil of the chest wall, minimal interruption in the compression, a sufficient chest expansion during the ventilation, and the advanced of hyperventilation. If two rescuers are performing chest compressions and breathing, the third rescuer (if available) should prepare a monitor and defibrillator, establish the medication route(s), and calculate the medication dosage(S). when several rescuers perform CPR, the rescuers should clearly communicate their roles using precise and respectful expressions. 2. Patient on monitoring Many in-hospital patients, especially if there are in an ICU, are monitored and some have an advanced airway and are receiving mechanical ventilation. If the patient has an indwelling arterial catheter, use the wave form as feedback to evaluate hand position and chest compression depth. A minor adjustment of hand position or depth of compression can significantly improve the amplitude of the arterial waveform, reflecting better chest compression-induced stroke volume. The arterial waveform may also be useful identification of return of spontaneous circulation (ROSC). If the patient’s end-tidal CO2 (Petco2) is being monitored. It can be used to evaluate the quality of chest compressions; it can also provide an indication of ROSC. 3. Respiratory failure Respiratory failure can be defined as the body’s inability to maintain adequate blood levels of oxygen and carbon dioxide. Physiological compensatory mechanism may be seen, such as an increase in respiratory rate and heart rate, and increased work of breathing, but these signs are not always present.
The signs of respiratory failure, as feature of those physiological responses, may include: • Respiratory rate outside the normal range for the child’s age-either too fast or too slow. • Initially increased work of breathing, which may progress to inadequate/decreased
work of breathing as the child tries or compensatory mechanism fail. • Additional noised such as stridor, wheezing, crackles, grunting, or the loss of breath
sounds. • Decreased tidal volume marked by shallow breathing, decreased chest expansion or
decrease air entry at auscultation. • Hypoxemia (without/with supplemental oxygen) generally identified by cyanosis but
it is often detectable prior to this by pulse oximetry.
There may be associated signs in other organ systems. Even though the primary problem is respiratory, other organ systems will be involved to try ameliorate the overall physiological disturbance.
• Increasing tachycardia (compensatory mechanism to increase tissue oxygen delivery) • Pallor • Bradycardia (an ominous indicator of the loss of compensatory mechanisms)
Pediatric advanced life support80
• Alternation in the level of consciousness (a sign that compensatory mechanisms are failing ) owing to poor perfusion of the brain)
4. ShockCirculatory failure is characterized by a mismatch between the metabolic demand by the tissues, and the delivery of oxygen and nutrients by the circulation.
Hypotension does not develop during the early phase of shock, which is also called compensated shock or normal pressure shock. Compensated shock presents as a tachycardia, cool and pale extremities, a >2 seconds delay in the capillary refill time, a weak peripheral pulse with a maintained central pulse, and a normal blood pressure. If the compensation mechanism fail, it can result in hypoperfusion of the major organs, reduced consciousness, reduced urine output, metabolic acidosis, tachypnea, weak central pulses, and a change in skin color.
Cardiac output is the product of heart rate and stroke volume. If the stroke volume is decreased due to any cause, the heart rate increases to compensated for the decrease in cardiac output. Sustained sinus tachycardia without other causes can be the first sign of shock, although bradycardia can develop after shock has progressed. Reduction in cardiac output and poor perfusion can decrease the peripheral pressure (intensity or quality), prolong the capillary refill time, and lower the skin temperature despite a warm surrounding temperature. However, the blood vessels of the skin and muscles are inadequately dilated during early septic shock, and the patient may exhibit a palpate peripheral pulse and relatively high skin temperature, despite being in shock.
Learn to integrate the signs of shock because no single sign confirms the diagnosis. For example:
• Capillary refill time alone is not a good indicator of circulatory volume, but a capillary retime >2 seconds is a useful indicator of moderate dehydration when combined with decreased urine output, absent tears, dry mucous membranes, and a generally appearance. Capillary refill time is influenced by ambient temperature, site, and age and its interpretation can be influenced by lighting.
• Tachycardia is a common sign of shock, but it can also result from other causes, such aas pain, anxiety, and fever.
• Pulse are weak in hypovolemic and cardio genic shock, but may be bounding in anaphylactic, neurogenic, and septic shock.
• Blood pressure may be normal in a child with compensated shock but may decline rapidly when the child decompensates. Like the other signs, hypotension must be interpreted within the context of the entire clinical picture.
There are several sources of data that use large populations to identify the 5th percentile for systolic blood pressure at various ages. For purposes of these guidelines, hypotension is defined as a systolic blood pressure:
• full-term infants (0 to 28 days old): a systolic pressure of <60 mmHg • infants (1 to 12 months old): a systolic pressure of <70mmHg • children (1 to 10 years): a systolic pressure of less than (70+[2×age in years]) mmHg • children (>10 years old): a systolic pressure of <90 mmHg.
Pediatric advanced life support 81

VASCULAR ACCESS
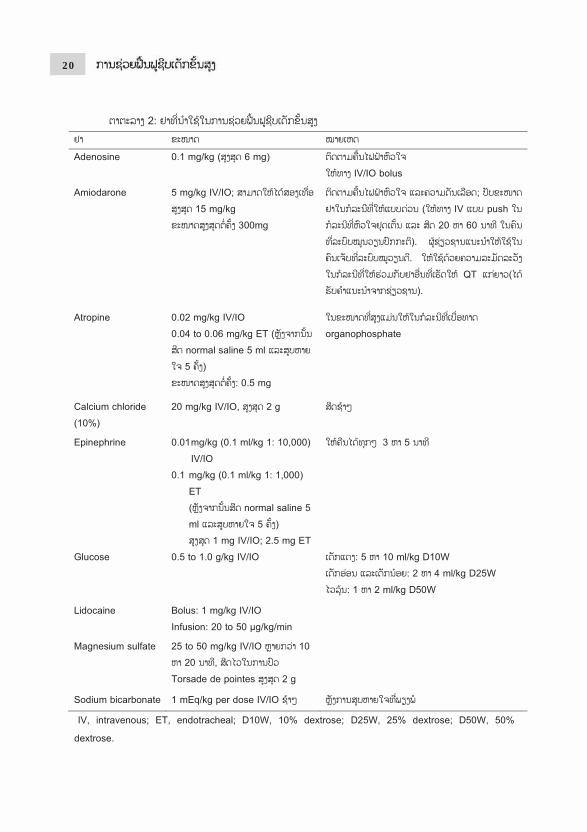
Vascular access is essential to enable drugs and fluid to be give, and blood samples obtained. Venous access can be difficult to establish during resuscitation of an infant or child. In critically ill children, whenever venous access is not readily attainable, intraosseous access should be considered early, especially if the child is in cardiac arrest or decompensated circulatory failure. In any case, in critically ill children, if attempts at establishing intravenous (IV) access are unsuccessful after one minute, insert an intra-osseous (IO) needle instead. Intraosseous (IO) access IO access is a rapid, safe, and effective route to give drugs, fluids and blood products. The onset of action and time to achieve adequate plasma drug concentrations are similar to that achieve via the central venous route. Bone marrow samples can be used to cross match for blood type or group for chemical analysis and for blood gas measurement (the values may be comparable to central venous blood gases if no drug has been injected in the cavity). However, these bone marrow samples can damage auto-analyzers and should be used preferably in a cartridge analyzer. After taking blood samples, flush each given drug with a bolus normal saline to ensure dispersal beyond the marrow cavity, and to achieve faster distribution to the central circulation. Inject large boluses of fluid using manual pressure or a pressure bag. Maintain IO access until definitive IV access has been established. Venous Access Intravenous access and other route. Peripheral IV access provides plasma concentration of drugs and clinical responses equivalent to central or IO access. The intramuscular route is preferred for the administration of adrenaline in anaphylaxis. Other routes are useful for different circumstances e.g. intranasal, buccal etc. but are beyond the remit of these guidelines. Central venous lines provide more secure long-term access but, compared with IO or peripheral IV access, offer no advantages during resuscitation. Endotracheal Drug AdministrationVascular access (IO or IV) is the preferred method for drug delivery during CPR, but if it is not possible, lipid-soluble drugs, such as lidocaine, epinephrine, atropine, and naloxone (mnemonic “LEAN”) can be administered via an endotracheal tube. However, the effects may not be uniform with tracheal as compared with intravenous administration. One study of children in cardiac arrest demonstrated similar ROSC and survival rates regardless of the method of drug delivery, while three studies of adults in cardiac arrest demonstrated reduced ROSC and survival to hospital discharge with tracheal administration of epinephrine compared to vascular delivery. If CPR is in progress, stop chest compressions briefly, administer the medications, and follow with a flush of at least 5 ml of normal saline and 5 consecutive positive-pressure ventilations. Optimal endotracheal doses of medications are unknown; in general expert consensus recommends doubling or tripling the dose of lidocaine, atropine, naloxone given via the ETT. For epinephrine, a dose ten times of the intravenous dose (0.1mg/kg or 0.1 ml/kg of 1:1000 concentrate) is recommended (see table) The effectiveness of endotracheal epinephrine during cardiac arrest is controversial. Some studies showed it to be as effective as vascular administration while other studies Have not
Pediatric advanced life support82

found it to be as effective. Animal studies suggested that a higher dose of epinephrine is require for endotracheal than for intravenous administration because the lower dose epinephrine concentration achieved when the drug is delivery by the endotracheal route may produce predominant transient peripheral 2–adrenergic vasodilating effects. These effects can be detrimental, and cause hypotension, lower coronary artery perfusion pressure and flow, and a reduced potential for ROSC. Non-lipid-soluble drugs (eg, sodium bicarbonate and calcium) may injure the airway; they should not be administered via the endotracheal route. AIRWAY
Oropharyngeal and Nasopharyngeal Airways
Oropharyngeal and nasopharyngeal airways help maintain an open by displacing the tongue or soft palate from the pharyngeal air passage. Oropharyngeal airways are used in unresponsive victims who do not have gag reflex. Make sure to select the correct size: an oropharyngeal airway that is too small may push the base of the tongue father into the airway; one that is too large may obstruct the airway.
Nasopharyngeal airways can be used in children who do have a gag reflex. Pay careful attention to proper diameter and length. A nasopharyngeal airway that is too short may not maintain an open airway, while one that is too long may obstructed easily by secretions. It may therefore require frequent suctioning.
Laryngeal Mask Airway (LMA)
Although several supraglottic devices have been used in children, clinical studies of devices other than the LMA in pediatric patients are limited. When bag-mask ventilation is unsuccessful and when endotracheal intubation is not possible, the LMA is accepted when used by experienced providers to provide a patent airway and support ventilation. LMA insertion is associated with a higher incidence of complication in young children compared to older children and adults.
Oxygen
It is reasonable to ventilate with 100% oxygen during CPR because there is insufficient information on the optimal inspired oxygen concentration. Once the circulation is restored, monitor system oxygen saturation. It may be reasonable to, when the appropriate equipment is available, to titrate oxygen administration to maintain the oxyhemoglobin saturation 94%. Provided appropriate equipment is available, once ROSC is achieved, adjust the Fio2 to the minimum centration needed to achieve an arterial oxyhemoglobin saturation at least 94%, with the goal of avoiding hyperoxia while ensuring adequate oxygen delivery. Since an arterial oxyhemoglobin saturation of 100% may correspond to a PaO2 anywhere between ~80 and 500mmHg, in general it is appropriate to wean the Fio2 when saturation is 100%, provided the oxyhemoglobin saturation can be maintained 94%. Remember that adequate oxygen delivery requires not only adequate arterial oxyhemoglobin saturation but also adequate hemoglobin concentration output.
Pulse Oximetry
Pediatric advanced life support 83

If the patient has a perfusing rhythm, monitor oxyhemoglobin saturation continuously with a pulse oximeter because clinical recognition of hypoxemia is not reliable. Pulse oximetry may, however, also be unreliable in patients with poor peripheral perfusion, carbon monoxide poisoning, or methemoglonemia.
Bag-mask ventilation
Bag-mask ventilation is relatively effective and safe in cases of out-of-hospital CPR, compared to endotracheal intubation. Select an adequate size of mask, open the airway properly, complete attach the mask to the face, and maintain a sufficient respiratory rate and pressure to ensure that the chest rise properly. Hyperventilation can reduce blood flow to the brain and heart, as it increases intrathoracic pressure, reduce venous return, and reduces cardiac output. In additional, hyperventilation can cause air trapping in patients with peripheral airway collapse and barotrauma. Excessive inspiratory pressure can cause gastric inflation, which can lead to reflux of the stomach contents and pulmonary aspiration. In infants and children without an inserted advanced airway, perform two breaths after every 30 compressions (or after every 15 compressions of there are rescuers). Stop compressions during the breathing, which should be performed for approximately 1 second per breath. Breaths should be performed every 6 seconds (10 per minutes) without interruption of the chest compressions if an advanced airway is inserted. Perform breathing only every 3 to 5 seconds (12 to 20 per minute) if ROSC is achieved but respiration is inadequate. The ventilation rate should be increased when the patient is young.
Two-person bag-mask ventilation
Perform two-person bag-mask ventilation when there are two rescuers. This technique is especially helpful when a patient has airway collapse or low pulmonary compliance, or when the rescuer cannot completely attach the bag to the patient’s face. During two-person bag-mask ventilation, one rescuer holds the mask to the face while lifting the patient’s chin with both hands. While the other rescuer compresses the bag. Both rescuers should frequently confirm that the patient’s chest is expanding properly.
Endotracheal intubation
Significant training is needed to successfully perform endotracheal intubation in infants and children, because they have a unique tracheal structure. Compared to adults, children’s tongues are relatively large, their airways are more flexible, the tip of their epiglottis is located at a relatively high and anterior portion if the neck, and their airway is smaller. 1. Size of the pediatric endotracheal tube Among children who weigh <35 kg, even with a relatively short stature, determining the endotracheal tube (ETT)’s size based on height is more accurate than using their age (e.g., using a Broselow resuscitation tape). However, also prepare tubes that are 0.5 mm larger and smaller in internal diameter (ID) than the calculated tube size, regardless of the presence or absence of a cuff. If resistance is felt during the intubation, use the 0.5 mm smaller tube. If there is significant air leakage at the glottis, the 0.5 mm large tube or a cuffed tube should be
Pediatric advanced life support84

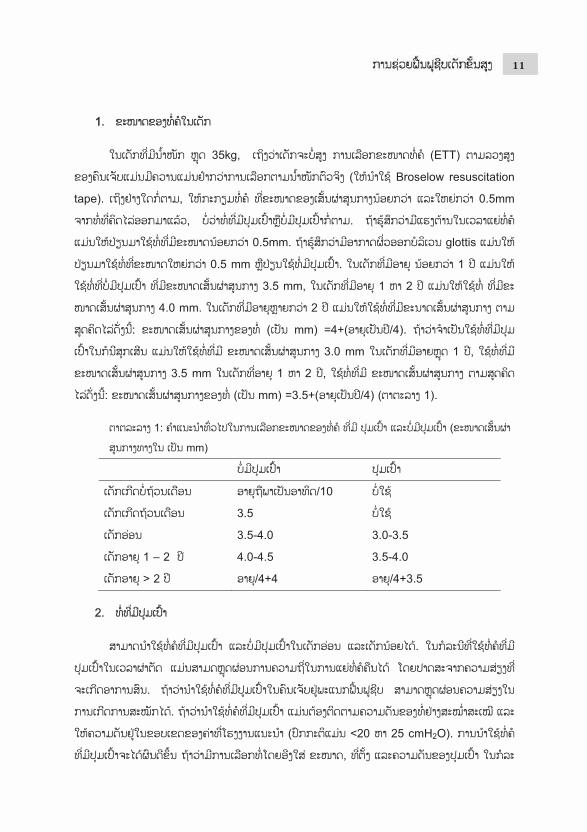
used. For an un-cuffed tube, use a tube with an ID of 3.5 mm for infants who are <1year old, and a 4.0 mm tube for children who are 1 to 2 years old. For children who are > 2 years old, use the following formula: ID of the un-cuffed tube (in mm) =4+(age in years/4). If a cuffed tube must be used in an emergency, use a tube with an ID of 3.0 mm for children who are <1year old, and 3.5 mm tube for children who are 1 to 2 years old. For children who are >2 years old, use the following formula: ID of the cuffed tube (in mm) =3.5+(age in years/4) (table 1).
Table 1: general recommendation for cuffed and uncuffed tracheal tube sizes (internal diameter in mm) Uncuffed Cuffed Premature neonates Gestational age in
weeks/10 Not used
Full term neonates 3.5 Not used Infants 3.5-4.0 3.0-3.5 Child 1 – 2 y 4.0-4.5 3.5-4.0 Child > 2 y Age/4+4 Age/4+3.5
2. Cuffed ETT Both cuffed and un-cuffed tube can be used for endotracheal intubation in infants and children. If a cuffed tube is used during surgery, the frequency of reintubation can be reduced without an increased risk of complications. Using a cuffed tube in the intensive care unit (ICU) can reduce the risk of aspiration. If a cuffed tube is used, the cuff’s pressure should be constantly monitored and the manufacturer’s recommended pressure should be maintained (usually <20 to 25 cmH2O). a cuffed tube can be more effective if it is selected based on the size, location, and pressure of the cuff in case with low pulmonary compliance, high airway resistance, or significant air leakage at the glottis area.
3. Endotracheal intubation Prepare a suction catheter, bag-mask, oxygen, and stylet before the intubation. The tip of the stylet not pass the tip of the tube. Applying a water-based lubricant or sterile distilled water to the tip of the stylet may make it easier to remove the intubation. Also prepare a functioning handle, blades, an extra light bulb, extra batteries, capnometry, tape to fix the tube, and gauze to clean the patient’s face.
Perform endotracheal intubation after oxygen administration unless the patient is in cardiac arrest. Assisted ventilation can be performed if the patient’s respiratory effort is insufficient. It should be performed with the preparation of a secondary method for maintaining the airway, in anticipation of intubation failure. Immobilize the cervical vertebrae to prevent spinal injury during the intubation in case that involve severe trauma to the head, neck or other areas. The procedure duration should not exceed 30 seconds, as hypoxia or ischemic injury can occur due to inadequate or delayed intubation. Monitor the patient’s heart rate and oxygen saturation (using pulse oximetry) while performing endotracheal intubation. Stop the procedure and wait until the patient’s condition improves, while providing oxygen using bag-mask, if the patient develops bradycardia (<60/min), a change in skin color or blood circulation status, or oxygen saturation below the normal level. In cases of pediatric
Pediatric advanced life support 85
cardiac arrest, the endotracheal intubation should not be delayed to set up pulse oximetry, which cannot function properly if the pulse is not palpable.
Use either straight or curved laryngoscope blades. Once the tip of a straight blade passes the epiglottis, place it at the entrance of the vocal cords, lift the base of the tongue, and swipe the blade anteriorly to lift the epiglottis. Of a curved blade is used, anteriorly adjust the location of the tongue’s base after the tip of the blade is placed in the epiglottic vallecula. At that point, the laryngoscope blade or handle should not be used as a lever, and direct pressure on the lips or gum should be avoided.
The glottis entrance should be exposed for ideal endotracheal intubation. To simplify the intubation in infants and children, align the pharynx by placing a pillow under the patient’s head with the chin in the sniffing position. For infants or children who are <2 years old, it is acceptable to lay them flat without a pillow to perform intubation through the mouth.
The depth of the ETT intubation can be calculated using the following formula: intubation depth (in cm) = the tube’s ID (in cm) ×3. For children who are >2 years old, the formula is: intubation depth (in cm) = (the children’s age in years/2) +12.
4. Checking the tube’s location The correct location of the tube cannot be verified using only clinical signs such as chest wall movement or vapor inside the tube. The tube’s location should be checked immediately after intubation, re-fixing the tube, transfer, and patient movement. The signs of a correct tube location are:
• Movement of the bilateral chest wall and symmetrical breathing sound in both lungs, and particularly in the axillary areas
• The absence of gastric inflation sounds • Appropriate end-tidal CO2 (end-tidal carbon dioxide, ETCO2) • Adequate oxygen saturation while perfusion is maintained. However, oxygen
saturation can be maintained for appropriately 3 minutes after hyperoxygenation despite poor ventilation
• Laryngoscopic evidence that the tube is placed between the vocal cords • Chest radiography findings that confirm the tube is correctly located
For immobilization of the tube, the tube should be fixed in a neutral position to prevent the tube from sliding deeper if the patient’s neck flexes, or sliding out if the patient’s neck extends. If the patient’s condition suddenly deteriorates while they are intubated, consider the following possibilities (mnemonic DOPE):
• Displacement of the tube • Obstruction of the tube • Pneumothorax • Equipment failure
5. Capnometry or capnography If possible, verify the location of the ETT using capnometry for all age group and in all circumstances, including the pre-hospital, emergency room, ICU ward, operation room, or transfer setting. However, this method cannot detect whether a tube is placed in the right main bronchus, despite the appearance of color changes or the proper waveform. Because ETCO2
Pediatric advanced life support86
may not be detected during cardiac arrest, even if the tube is properly located, the tube’s location must be checked using a laryngoscope.
• If the capnometry is contaminated by gastric contents or an acidic drug, the color persists as the acidic color and does not accurately reflect the ventilation
• When epinephrine is intravenously infused, pulmonary perfusion is temporarily reduced and the ETCO2 value can decrease below the critical value
• If there is severe airway occlusion, such as moderate asthma or pulmonary edema, the exhalation of CO2 can decrease below the critical value
• In cases with air leakage at the glottis region, the CO2 is diluted and may not be detected, due to the insufficient ventilation
CPR GUIDELINES FOR NEWBOENS WITH CARDIAC ARREST OF CARDIAC ORIGINRecommendation for infants differ from those for the newly born (ie, in the delivery room and during the first hours after birth) and newborns (during their initial hospitalization and in the NICU). The compression-to-ventilation ratio differs (newly born and newborns – 3:1; infant two rescuers -15:2) and how to provide ventilations in the presence of an advanced airway differs (newly born and newborns – pause after 3 compressions; infants – no pause for ventilations). This presence a dilemma for healthcare providers who may also care for newborns outside the NICU. Because there are no definitive scientific data to help resolve this dilemma, for ease of training we recommend that newborns (intubated or not) who require CPR in the newborn nursery or NICU receive CPR using the same as for the newly born in the delivery room (ie, 3:1 compression-to-ventilation ratio with a pause for ventilation). Newborns who require CPR in other stings (eg, prehospital, ED, PCIU, etc.), should receive CPR according to infant guidelines: 2 rescuers provide continuous chest compressions with asynchronous ventilations if an advanced airway is in place and a 15:2 ventilation-to-compression ratio no advanced airway is in place. It is reasonable to resuscitate newborns with a primary cardiac etiology of arrest, regardless of location, according to infant guidelines, with emphasis on chest compressions.
EMERGENCY FLUID AND MEDICATIONS
Estimating weight
In the out-of-hospital setting, a child’s weight is often unknown, and even experienced personnel may not be able to estimate it accurately. Tapes with precalculated doses printed at various patient lengths have been clinically validated and are more accurate than age-based methods in the prediction of body weight. Body habitus may also be an important consideration.
Medication dose calculation
To calculate the dose of resuscitation medications, use the child’s weight if it is known. If the child’s weight is unknown, it is reasonable to use a body length tape with precalculated doses.
It is unclear if an adjustment in the calculation of resuscitation medications is needed in obese children. use of the actual body weight in calculation of the drugs doses in obese patients may
Pediatric advanced life support 87

result in potentially toxic doses. Length-based tapes estimate the 50th percentile weight for length (ideal body weight), which may theoretically, result in inadequate doses of some medications in obese patients. Despite these theoretical considerations, there are no data regarding the safety or efficacy of adjusting the doses of resuscitation medications in obese patients. Therefore, regardless of the patient’s habitus, use the actual body weight for calculating initial resuscitation drug doses or use a body length tape with precalculated doses.
For subsequent doses of resuscitation dugs in both non-obese and obese patients, expert providers may consider adjusting doses to achieve the desired therapeutic effect. In general, the dose administered to a child should not exceed the standard dose recommended for adult patients.
MEDICATIONS THAT ARE USED FOR PALS (TABLE 2) 1. AdenosineAdenosine temporarily block atrioventricular (AV) node conduction and interrupts the re-entrant mechanism. Adenosine is recommended for the treatment of supraventricular tachycardia (SVT). The half-life of adenosine is very short (10s), which gives it a broad safety range. Large doses should be administered through a peripheral vein compared to a central vein, although adenosine can be also administered intraosseously. Additional normal saline should be provided immediately after an intravenous (IV) infusion of adenosine to help the adenosine rapidly enter the central circulation. Adenosine must be used with caution in asthmatics, second or third degree AV block, long QT syndromes and in cardiac transplant recipients. 2. AmiodaroneAmiodarone delays conduction in the AV node, prolong the refractory period and QT interval, and slows ventricular conduction. However, amiodarone should be infused as the patient’s condition allows, and their blood pressure should be monitored. The appropriate infusion rate is relatively slow if there is a pulse, and is relatively fast in case of cardiac arrest or VF. Hypotension can develop due to vasodilation during the administration, and its magnitude is related to the administration rate. This effect is less frequent when amiodarone is administered as a liquid form. An electrocardiogram (ECG) should be used to monitor for administration-related complications, such as bradycardia, AV block, and torsade de pointes. Special care should be taken during the coadminiatration of other medications that can prolong the QT interval. The half-life of amiodarone can reach 40 days, so any related adverse effect(s) may last a prolonged duration. 3. AtropineAs a parasympathetolytic agent, atropine increase cardiac rhythm and AV conduction. Atropine is administered as an IV or intraosseous (IO) infusion, with no minimum dose, in pediatric case with a risk of severe bradycardia during emergency endotracheal intubation. However, routine atropine administration is not recommended for infants and children if emergency endotracheal intubation is necessary. Large doses of atropine should be administered in cases of nerve gas poisoning or organophosphate poisoning.
Pediatric advanced life support88

4. CalciumThe routine administration of calcium during cardiac arrest does not improve the patient’s prognosis, and routine administration is not recommended as life support for Patients who are in asystole. Calcium is used to treat proven hypocalcemia or hyperkalemia, especially in patients with hemodynamic dysfunction. A decrease in the level of ionized calcium is relatively common in severely ill children, and especially in children with sepsis. Calcium should be considered for treating hypermagnesemia or over dose with a calcium channel blocker. The most common formation of calcium for children is 100% calcium chloride, as it has a higher bioavailability than calcium gluconate, and this solution should be infused through a central vein due to the risk of peripheral vein injury. An IV infusion of calcium should be administered over 10 to 20 seconds for patients in cardiac arrest and over 5 to 10 minutes for patients with a perfusing rhythm. 5. EpinephrineEpinephrine is an intrinsic catecholamine that strongly stimulates the alpha and beta adrenergic receptors of the sympathetic nerves. Epinephrine’s most significant pharmacological action during cardiac arrest is vasoconstriction caused by activation of alpha adrenergic receptors. This increases the aortic diastolic pressure and the perfusion pressure of successful CPR. During compressions, the increased perfusion pressure in the coronary artery increases the oxygen supply to the heart. Epinephrine also improves the rate of successful defibrillation by increasing the VF amplitude and myocardial contraction, which stimulate spontaneous contraction.
The most common rhythms during pediatric cardiac arrest are asystole and bradycardia, and epinephrine can provide a perfusing rhythm in these patients. The epinephrine can be administered using an IV/IO infusion, or through the ETT in pediatric patients with symptomatic bradycardia who do not respond to effective assisted ventailation or oxygen supply. However, it is important to monitor the oxygen supply and circulation, because catecholamine activity can be reduced by acidosis or hypoxia. If the initial dose of epinephrine is not effective, it should be repeatedly administered every 3 to 5 minutes during CPR.
Although epinephrine can be absorbed when it is administered using an ETT, the absorbed amount and serum concentration cannot be predicted. Therefore, a continuous IV infusion of epinephrine can be helpful once ROSC is achieved. Epinephrine’s hemodynamic effects are related to its dosage, with low dose (0.3 g/kg/min) Prominently resulting in beta adrenergic
activity and higher doses (> 0.3 g/kg/min) predominantly causing vasoconstriction due to both beta and alpha adrenergic activities. It is preferable to administer epinephrine via the central circulation, as extravasation of epinephrine can lead to local ischemia, tissue damage, and necrosis. Similar to other catecholamine, epinephrine is inactivated in alkali solution and should not be mixed to with sodium bicarbonate. Epinephrine can be administered during CPR for infants and children who are in cardiac arrest, although there is insufficient evidence regarding the effects of other vasopressors.
Pediatric advanced life support 89

6. Glucose Infants have low stored levels of glucose, and a high demand for glucose. Furthermore, infants can readily develop hypoglycemia if they have a condition that requires an increases energy supply (e.g., shock). Therefore, glucose levels should be closely monitored using a rapid bedsides test in cases of coma, shock, or respiratory failure. Once hypoglycemia has been conformed, it should be treated using a glucose-containing fluid. Two to four milliliters of 25% glucose solution (250mg/ml) per kilogram providers 0.5 to 1.0 g/kg of glucose, and 5 to 10 ml of 10% glucose solution (100mg/ml) also provides a similar amount of glucose. It is preferable to treat hypoglycemia using a continuous infusion of a glucose solution, as osmotic diuresis can be caused by a sudden increase in the plasma oncotic pressure after a single administration of a hypertonic glucose solution. The current recommendation is to maintain euglycemia during the CPR and to prevent hypoglycemia after the CPR, as there are no data regarding whether hyperglycemia is advantageous or harmful after cardiac arrest.
7. LidocaineLidocaine reduces myocardial automaticity and prevents ventricular arrhythmia. But it can depress the myocardium, and reduced circulation, causing drowsiness, disorientation, muscle twitching, and seizure. Amiodarone and lidocaine can be used in infants and children with VF and pulseless VT that does not respond to defibrillation. Nevertheless, there is a significant possibility of adverse effect(s) in cases with a low cardiac output, abnormal hepatic function, or abnormal renal function. 8. MagnesiumMagnesium is only administered to patients with proven hypomagnesium and torsade de pointes. A rapid Iv infusion (for few minutes) of magnesium sulfate is recommended for torsade de pointes, regardless of its cause. Magnesium causes vasodilation, and hypotension can develop when it is rapidly infused. 9. Sodium bicarbonate In most studies, the routine administration of sodium bicarbonate has not improved the post-arrest prognosis. Adequate ventilation, oxygen supply, and effective recovery of systemic perfusion (to correct tissue ischemia) should be the primary concerns in pediatric cardiac arrest, because respiratory failure is an important cause in these cases. Once effective ventilation has been confirmed, and epinephrine with compressions has been started to maximize circulation, the administration of sodium bicarbonate can be considered in cases of a prolonged cardiac arrest. Sodium bicarbonate is also recommended for patients with symptomatic hyperkalemia, hypermagnesemia, and overdose with tricyclic antidepressants or other sodium channel blockers. If indicated, sodium bicarbonate is administered as an IV or IO infusion, and a diluted solution can be used to prevent increased oncotic pressure in neonate. Although there is no evidence that a diluted solution is beneficial in infants or children. The appropriate dose of sodium bicarbonate can be determined using blood gas analysis. Because catecholamines are inactivated by sodium bicarbonate, and calcium forms a precipitate when it is mixed with sodium bicarbonate, 5 to 10 ml of normal saline should be used to flush the IV line after administered sodium bicarbonate.
Pediatric advanced life support90
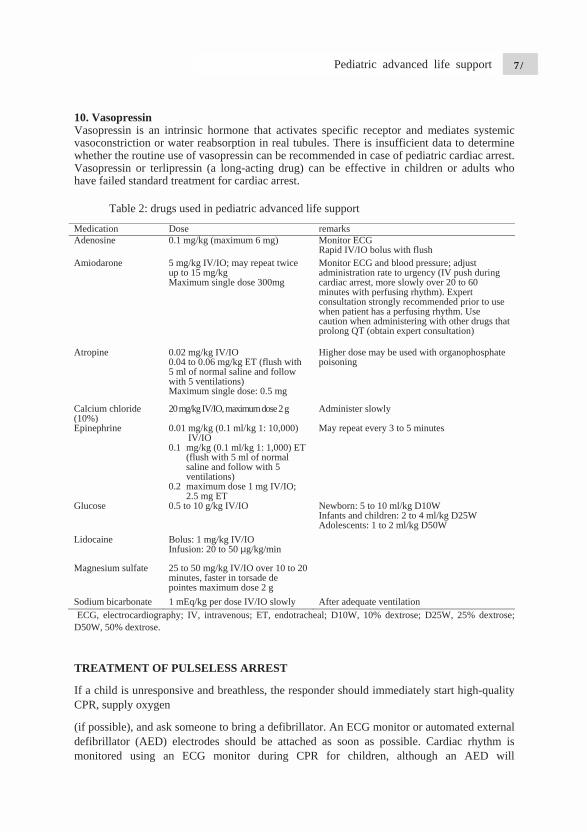
10. Vasopressin Vasopressin is an intrinsic hormone that activates specific receptor and mediates systemic vasoconstriction or water reabsorption in real tubules. There is insufficient data to determine whether the routine use of vasopressin can be recommended in case of pediatric cardiac arrest. Vasopressin or terlipressin (a long-acting drug) can be effective in children or adults who have failed standard treatment for cardiac arrest.
Table 2: drugs used in pediatric advanced life support
Medication Dose remarksAdenosine 0.1 mg/kg (maximum 6 mg) Monitor ECG
Rapid IV/IO bolus with flush Amiodarone 5 mg/kg IV/IO; may repeat twice
up to 15 mg/kg Maximum single dose 300mg
Monitor ECG and blood pressure; adjust administration rate to urgency (IV push during cardiac arrest, more slowly over 20 to 60 minutes with perfusing rhythm). Expert consultation strongly recommended prior to use when patient has a perfusing rhythm. Use caution when administering with other drugs that prolong QT (obtain expert consultation)
Atropine 0.02 mg/kg IV/IO 0.04 to 0.06 mg/kg ET (flush with 5 ml of normal saline and follow with 5 ventilations) Maximum single dose: 0.5 mg
Higher dose may be used with organophosphate poisoning
Calcium chloride (10%)
20 mg/kg IV/IO, maximum dose 2 g Administer slowly
Epinephrine 0.01 mg/kg (0.1 ml/kg 1: 10,000) IV/IO
0.1 mg/kg (0.1 ml/kg 1: 1,000) ET (flush with 5 ml of normal saline and follow with 5 ventilations)
0.2 maximum dose 1 mg IV/IO; 2.5 mg ET
May repeat every 3 to 5 minutes
Glucose 0.5 to 10 g/kg IV/IO Newborn: 5 to 10 ml/kg D10W Infants and children: 2 to 4 ml/kg D25W Adolescents: 1 to 2 ml/kg D50W
Lidocaine Bolus: 1 mg/kg IV/IO Infusion: 20 to 50 g/kg/min
Magnesium sulfate 25 to 50 mg/kg IV/IO over 10 to 20 minutes, faster in torsade de pointes maximum dose 2 g
Sodium bicarbonate 1 mEq/kg per dose IV/IO slowly After adequate ventilation ECG, electrocardiography; IV, intravenous; ET, endotracheal; D10W, 10% dextrose; D25W, 25% dextrose; D50W, 50% dextrose.
TREATMENT OF PULSELESS ARREST
If a child is unresponsive and breathless, the responder should immediately start high-quality CPR, supply oxygen
(if possible), and ask someone to bring a defibrillator. An ECG monitor or automated external defibrillator (AED) electrodes should be attached as soon as possible. Cardiac rhythm is monitored using an ECG monitor during CPR for children, although an AED will
Pediatric advanced life support 91
automatically notify the rescuer if the patient has a shockable rhythm (VF or pulseless VT) or a non-shockable rhythm (asystole or pulseless electrical activity [PEA]). Temporary interrupting the compression may be necessary to check the rhythm. Asystole or wide QRS bradycardia is the most common rhythms during asphyxia cardiac arrest. Although VF or PEA dose not frequently occur in infants or children, there is a high probability of VF-induced cardiac arrest in case of sudden witnessed cardiac arrest among older children (Fig. 2).
1. Non-shockable rhythm (asystole/PEA) The definition of PEA is the presence of organized electrical activity, such as a low and wide QRS, without a palpable pulse. There can be a normal heart rate without a pulse and with poor tissue perfusion during the early stage of suddenly impaired cardiac output. This condition is more reversible than asystole and use to be known as electromechanical dissociation. Minimize any interruption in the compression and continue CPR. The second rescuer should establish an IV or IO line and administer epinephrine at 0.01 mg/kg (0.1 ml/kg in a 1: 10,000 solution) during the CPR, and the same dose should be administered every 3 to 5 minutes. High-dose epinephrine does not improve the survival rate, and can cause harm, although it may be considered in exceptional cases, such as case of overdose with beta blockers. If an advanced airway has been placed, the first rescuer should perform constant compression at a rate of 100 to 120 per minute, and the second rescuer should provide breaths every 6 seconds (approximately 10 per minute). The rescuer(s) who are performing the compression should switch approximately every 2 minutes, while minimizing the interruption, to provide optimal compression quality and rate, and to avoid compression-induced fatigued. During this period, the rhythm should be monitored while minimizing any interruption of the compressions. If the rhythm is non-shockable, CPR should be continued with epinephrine administration until there is evidence of ROSC or a decision is made to cease CPR. If the rhythm changes to a shockable rhythm, immediate compressions and defibrillation should always be performed, and the rhythm should be reached after 2 minutes of CPR. The period between stopping or restarting the compressions and the defibrillation should be minimized, find reversible cause(s) and correct them.
2. Shockable rhythm (VF/pulses VT) Defibrillation is the most important treatment for VF, and provides an overall survival rate of approximately 17% to 20%. The resulting survival rate is higher for primary VF, compared to secondary VF, and the survival rate after adult cardiac arrest decreases by 7% to 10% for every 1-minute delay in starting CPR and defibrillation. The survival rate is highest when high-quality CPR is performed with minimal interruptions during the early stage of cardiac arrest. The output of defibrillations is better when the rescuer minimized the time between the compressions and defibrillation.
DEFIBRILLATORS
As AED can detect the pediatric heart rhythm, they should be installed in facilities that treat children with a risk of arrhythmia or cardiac arrest. The ideal defibrillator can adjust the energy dose for children.
Pediatric advanced life support92

1. ElecA manusome mapproprshould nadhesivthem onyear oldweigh <
2. InteSelf-adhon the psaline, u
3. EleThe melectrodleft lowthe hearcontact,the patie
4. EneThe lowinfant omonophthe secomaximuhighest
5. AEDVF can an eneryear old
ctrode size ual defibrillmanual defiriate electronot contact
ve electrodento the chesd or weigh <10 kg.
erfacehesive electpatient’s cheultrasound g
ectrode placmanufacture’des of an AE
wer rib, laterrt between , and there ient’s trunk
ergy dosewer energy dor children hasic or bipond recommum adult doenergy in th
Dsbe accurate
rgy attenuatd. An AED
lator typicalfibrillators hode should each other,s should be
st. The adult 10 kg, an
trodes have est. Howevgel, or alcoh
cement’s recommED or monial to the lefthe electrodis no benefi(fig. 1).
Fig
dose for effare unkno
hasic defibrmended dosose. If therehe energy s
ely detectedting device,with an ene
lly has diffehave self-abe selected
, and the spe completelt size of elend the pedia
pre-applieder, electrodhol are not a
endations tor/defibrill
ft nipple) andes. The eleit to placing
g. 1. Paddle
fective defibown. The frillators if tse is 4 J/kg
is no exactelector whe
d by most AE, a manual ergy attenua
erent sizes adhesive eled based on
pace betweely attached ectrodes (8 tatric size is
d electrode de gel must appropriate
should be lator. Manu
nd the right uectrodes mug the electro
position fo
brillation anfirst recommthere the infg, and any st energy do
en escalating
EDs in childefibrillato
ating device
of electrodeectrodes. In
n the patienen the two e
to the patito 10 cm) iss used for in
gel on the ibe applied replacemen
followed ual electrodeupper quadrust be firmlodes on the
or defibrillat
nd the uppermended enfant or childsubsequent
ose meter ong the dose.
dren of all aor is performe can be use
es for adultn pediatric
nt’s chest sielectrodes shent’s chest s used for chnfants who
interface thfor manual
nts.
when plaes are placedrant of the cly applied toanterior an
tion – child
r limit for sergy dose d exhibits Vdose shoul
n the defibr
ages. If the med for chied unless a m
ts and childcases, the
ize. The elhould 3 cby firmly
hildren whoare < 1 yea
hat should belectrodes.
acing self-ad at the apechest, whicho maintain
nd posterior
safe defibrilis 2 to 4
VF or pulseld never exrillator, use
AED does hildren who manual defi
dren, and e largest lectrodes cm. Self-pressing o are 1 ar old or
be placed Normal
adhesive ex (at the h locates a strong sides of
llation in J/kg for less VT/ ceed the the next
not have are < 1
ibrillator
Pediatric advanced life support 93
is available. If both an AED with an energy attenuating device and a manual defibrillator are unavailable, an AED without an energy attenuating device can be used in children. 6. Integrating defibrillation and CPR CPR should be performed until the defibrillator is prepared and defibrillation is feasible, and the compression should be re-started immediately after the defibrillation. It is ideal to only interrupt the compressions for checking cardiac rhythm, performing defibrillation, and breathing before placing an advanced airway. Once the rhythm has been evaluated, start and continue the compressions until the defibrillator is charged, even in case with a shockable rhythm. The first defibrillation (2 to 4J/kg) should be started as soon as possible, and CPR with compression should be immediately re-started after the defibrillation. It is very important to minimize the interval between starting or stopping the compressions and the defibrillation. Continue CPR for approximately 2 minutes, although this sequence may be changed based on an expert’s opinion if the environment can facilitate continuous invasive monitoring (e.g., in a hospital). An IV or IO line can be established if there are enough rescuers. Rhythm should be checked after 2 minutes of CPR, and the defibrillator should be charged at 4 J/kg. if shockable rhythm persists, defibrillation should be applied at 4 J/kg, and the algorithm for asystole/PEA should be followed if a non-shockable rhythm is observed. Resume the compression immediately after the second defibrillation, and continue CPR for approximately 2 minutes. Epinephrine should be administered at 0.01 mg/kg (0.1 ml/kg in a 1: 10,000 solution) every 3 to 5 minutes during the CPR. If there is a third rescuer, epinephrine should be prepared before checking the rhythm and administered as soon as possible. The rescuer who is in charge of the defibrillator should prepare the third defibrillator charge before checking the ECG rhythm (4J/kg and < 10 J/kg or the maximum adult dose). If there is a shockable rhythm, an additional defibrillation should be administered (>4 J/kg and <10 J/kg or the maximum adult dose), and CPR should be immediately resumed. If the defibrillation is unsuccessful, amiodarone or lidocaine should be administered while continuing the CPR. The algorithm for pulseless cardiac arrest is always followed if there is a non-shockable rhythm. If an advanced airway is placed, one rescuer should continue compression at a rate of 100 to 120 per minute, and the second rescuer should perform breathing every 6 seconds (10 per minute). If there are two or more rescuers, they should switch every 2 minutes to prevent compression-induced fatigued and to maintain adequate compression rate and quality. If there is an organized rhythm at 2 minutes after the defibrillation, check the pulse to determine whether it is a perfusing rhythm. ROSC is predicted if the ETCO2 rapidly increases during the compressions or the monitored arterial waveform increases. If both ROSC and a pulse are achieved, post-CPR management can be started. However, if VF re-develops after successful defibrillation, CPR should be re-started and defibrillations should be attempted with the dose which achieved successful defibrillation. Find and correct any other reversible causes. MANAGEMENT OF TORSADE DE POINTES
Torsade de pointe is polymorphic VT and is associated with a prolonged QT interval. A prolonged QT interval can develop due to congenital conditions or drug toxicity, and is associated with class 1A antiarrhythmic drugs (procainamide, quinine and disopyramide), class III antiarrhythmic drugs (sotalol and amiodarone), tricyclic antidepressants, digoxin, and drug interactions. Torsade de pointe typically progresses to VF or VT. Therefore, if pulseless
Pediatric advanced life support94
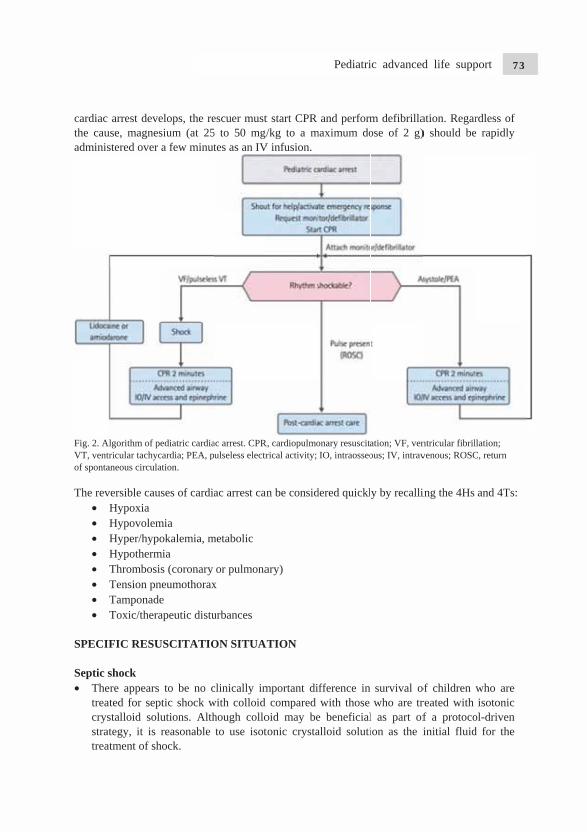
cardiac the cauadminis
Fig. 2. AlVT, ventrof sponta The rev
• H• H• H• H• T• T• T• T
SPECIF
Septic s• The
treatcrysstrattreat
arrest deveuse, magnesstered over a
lgorithm of pericular tachyc
aneous circulat
versible causHypoxia HypovolemHyper/hypoHypothermThrombosisTension pneTamponadeToxic/thera
FIC RESU
shockre appears ted for septstalloid solutegy, it is rtment of sh
elops, the resium (at 25a few minut
ediatric cardiaardia; PEA, ption.
ses of cardia
mia okalemia, m
mia s (coronary eumothoraxe apeutic distu
USCITATIO
to be no ctic shock wutions. Althreasonable ock.
escuer must5 to 50 mg/tes as an IV
ac arrest. CPRulseless electr
ac arrest can
metabolic
or pulmonax
urbances
ON SITUA
clinically imwith colloid hough colloto use isot
t start CPR /kg to a m
V infusion.
R, cardiopulmorical activity;
n be consid
ary)
ATION
mportant dicompared
oid may betonic crysta
and performmaximum do
onary resuscitaIO, intraosseo
dered quickl
fference in with those
e beneficialalloid soluti
m defibrillaose of 2 g)
ation; VF, venous; IV, intrav
y by recalli
survival owho are tr
l as part ofion as the i
ation. Regar) should be
ntricular fibrilvenous; ROSC
ing the 4Hs
of children reated with f a protocoinitial fluid
rdless of e rapidly
llation; C, return
and 4Ts:
who are isotonic
ol-driven d for the
Pediatric advanced life support 95

• Monitoring the central venous (superior vena cava) oxygen saturation (Scvo2) may be useful to titrate therapy in infants and children with septic shock. Protocol-driven or “goal-directed” therapy, with a target ScvO2 70% appears to improve patient survival in severe sepsis.
• Early assisted ventilation may be considered as part of a protocol-driven strategy for septic shock.
• Etomidate has been shown to facilitate endotracheal intubation in infants and children with minimal hemodynamic effect, but do not use it routine in pediatric patients with evidence of septic shock. Adrenaline suppression is seen after administration of etomidate in children and adults. In children and adults with septic shock, etomidate administration is associated with a higher mortality rate.
Hypovolemic Shock • Use an isotonic crystalloid (eg, lactate Ringer’s solution or normal saline) as the initial
fluid for the treatment of shock. There is no added benefit in using colloid (eg, albumin) during the early phase of resuscitation.
• Treat signs of shock with a bolus of 20ml/kg of isotonic crystalloid even if blood pressure is normal. Crystalloids may have an associated survival benefit over colloid for children with shock secondary to general trauma, traumatic brain injury, and burns. There is no evidence to support the use of a specific isotonic crystalloid. Give additional boluses (20ml/kg) if systemic perfusion fails to improve. There are insufficient data to make a recommendation for or against use of hypertonic saline for shock associated with head injuries or hypovolemia.
• There is insufficient evidence in infants and children to make a recommendation about the best timing or extent of volume resuscitation for children with hemorrhagic shock following trauma.
• There is growing evidence to prefer the use of balanced crystalloids as these induce less hyperchloraemic acidosis. In-life threatening hypovolemic shock, as may be seen in rapid blood loss in trauma, limiting the use of crystalloids in favor of a regime of massive blood transfusion may be required. There are varying regime of combining plasma, platelets and other blood products in delivering massive blood transfusion, so the regime used should be according to local protocols. Similarly, in other type of shock, when multiple boluses of crystalloids are given, timely blood products should be considered to treat dilutional effects. Avoid glucose containing solutions unless there is hypoglycemia. Monitor blood glucose levels and avoid hypoglycemia; infants and children are particularly prone to hypoglycemia.
TraumaSome aspect of trauma resuscitation require emphasis because improperly performed resuscitation is a major cause of preventable pediatric deaths.Common errors in pediatric trauma resuscitation include failure to open and maintain the airway, failure to provide appropriate fluid resuscitation, and failure to recognize and treat internal bleeding. Involve a qualified surgeon early and, if possible, transport a child with multisystem trauma to a trauma center with pediatric expert. The following are special aspects of trauma resuscitation:
Pediatric advanced life support96

• When the mechanism of injury is compatible with cervical spinal injury, restrict motion of the cervical spine and avoid traction or movement of the head and neck. Open and maintain the airway with a jaw thrust, and do not tilt the head.
• If the airway cannot be opened with jaw thrust, use a head tilt-chin lift because you must establish a patent airway. Because of the disproportionately large head of infants and young children, optimal positioning may require recessing the occiput or elevate the torso to avoid undesirable backboard-induced cervical flexion.
• Do not routinely hyperventilation even in case of head injury. Intentional brief hyperventilation may be used as a temporizing rescue therapy if there are signs of impending brain herniation (eg, sudden rise in measured intracranial pressure, dilation of one or both pupils with decreased response to light, bradycardia, and hypertension).
• Suspect thoracic injury in all thoraco-abdominal trauma, even in the absence of external injuries. Tension pneumothorax, hemothorax, or pulmonary contusion may impair oxygenation and ventilation.
• If the patient has maxillofacial trauma or if you suspect a basilar skull fracture, insert an orogastric rather than a nasogastric tube.
• In the very select circumstances of children with cardiac arrest from penetrating trauma with short transport times, consider performing resuscitative thoracotomy.
• Consider intra-abdominal hemorrhage, tension pneumothorax, pericardial tamponade, and spinal cord injury in infants and children, and intracranial hemorrhage in infants as a cause of shock.
POST-CPR MANAGEMENT
Post-CPR management should begin immediately after ROSC in patients who had shock, respiratory failure, and cardiac arrest. The purposes of post-CPR management are to: (1) maintain brain function, (2) avoid secondary organ damage, (3) correct the cause(s) of cardiac arrest, and (4) prepare for the next treatment step with an optimal hemodynamic status. Because the patient’s condition can deteriorate after a short period of temporary stabilization, the patient should be frequently monitored. Thoroughly determine whether the airway is secure, oxygen is supplied, and ventilation and perfusion are stabilized. Look for evidence of trauma and reevaluate the patient’s neurological condition during the examination. Check for any history of allergy, disease, medication, or vaccination and evaluate the patient’s renal and hepatic function (dysfunction can indirectly effect the patient’s prognosis).
1. Management of the respiratory system After children have received CPR, oxygen should be supplied until adequate oxygenation and proper oxygen caring capacity is achieved, as measured using pulse oximetry or direct arterial blood gas analysis. High-dose oxygen should be administered if there are symptoms of significant respiratory distress (e.g., anxiety, breathing impairment, cyanosis, or hypoxemia), and endotracheal intubation with mechanical ventilation can be performed. If the intubated patient experiences a sudden deterioration, consider the possibility if displacement or obstruction of the ETT, pneumothorax, or mechanical errors. Analgesics or sedatives can be used for anxious patients if these factors are confirmed to be absent. However, careful attention is warranted, as seizures can be masked by the use of a neuromuscular blocker.
Pediatric advanced life support 97
A target arterial CO2 partial can be established and maintained based on the patient’s specific condition after ROSC is achieved. There is no evidence that hypercapnia or hypocapnia are more beneficial than eucapnia for improving the patient’s survival rate and quality of life. Oxygen should be supplied to provide proper oxygenation for intubated patients, and the respiratory rate should be maintained at 30 to40 per minute for infants and 20 t0 30 for children. A sufficient tidal volume will cause the chest to visibly rise. Once mechanical ventilation is started, the tidal volume should be maintained at 6 ml/kg, which should cause the chest visibly rise and yield respiratory sound at the periphery of the lung that can be detected using auscultation. A valued of approximately 3 to 6 cmH2O should be used for positive end-expiratory pressure, although a higher value can be used if the functional residual capacity is reduced and the lung has collapsed. Arterial blood gas analysis should be performed at 10 to 15 minutes after early mechanical ventilation, and it is recommended that normal arterial oxygen partial pressure be maintained unless there is a specific reason for deviation. Cardiac anomalies in children should be evaluate via echocardiography immediately after CPR, as the proper oxygen saturation can vary based on the patient’s hemodynamic status and congenital heart disease(s). nasogastric or orogastric tube insertion is needed, as gastric inflation can cause discomfort and ventilation impairment. 2. Cardiovascular management Because circulatory failure can develop after recovery from cardiac arrest, continuous or frequent evaluation of the cardiovascular system should be performed to rapidly detect any decreased cardiac output or the development of shock. Inadequate tissue perfusion cab result in a prolonged capillary refill time, a reduced or absent peripheral pulse, a change in consciousness, cold extremities, tachycardia a decrease urine output, and hypotension. An insufficient administration of fluid after CPR can cause a reduction in the cardiac output or shock that develops secondary to the reduced peripheral vascular resistance and myocardial stunning. Heart rate, blood pressure, and oxygen saturation should be constantly monitored after CPR and blood pressure should be monitored using an intra-arterial catheter (if possible) inpatients with cardiovascular dysfunction. Because hypotension can frequently occur during the period of ROSC after CPR, and this condition is associated with a poor prognosis, the systolic pressure should be maintained at or above the fifth age-specific percentile, and IV fluid or inotropic agents should be administered. Urine output is a significant indicator of internal organ perfusion, and should be monitored using a urine catheter in patients with hemodynamic dysfunction. The IO route should be removed once a secure IV line is established.
3. Drugs to maintain cardiac output Myocardial impairment and vascular instability frequently occur after recovery from cardiac arrest. After CPR, systemic and pulmonary vascular resistance usually increase during the early phase, except in cases of septic shock. Cardiovascular function also constantly change after CPR, as it exhibits a hyperdynamic status during the early phase, which subsides towards a gradual weakening of cardiac function. Therefore, if abnormal cardiovascular function is observed or suspected after CPR, an adequate dose of vasoactive drug(s) should be
Pediatric advanced life support98

administered to improve cardiac function and tissue perfusion. The selection and dose of the drug(s) should be based on the individual patient’s status, and should be administered using an accurate IV route.
1) EpinephrineEpinephrine is used to treat shock for any reason, which does not respond to fluid administration and exhibits extremely low systemic perfusion. As a strong vasoconstrictor, epinephrine increases systemic vascular resistance and heart rate through its chronotropic activity. Epinephrine can be administered during bradycardia with hemodynamic changes that do not respond to oxygen and mechanical ventilation. Low-dose epinephrine (0.3 g/kg/min) works as a strong inotropic agent and reduces systemic vascular resistance by activating beta adrenergic receptors. If the dose is increased to >0.3 g/kg/min, epinephrine exerts both an inotropic effect and increases systemic vascular resistance by activating the vascular alpha adrenergic receptors. As epinephrine’s effects vary according to the dose in different patients, the dose must be frequently adjusted to achieve its intended effect. Epinephrine is more effective than dopamine in patients with severe circulatory compromise, and especially in infants. 2) DopamineDopamine has beta and alpha sympathomimetic effects through a direct dopaminergic effect and an indirect stimulatory effect on norepinephrine secretion. The dose of dopamine must be frequently adjusted when it is used to treat shock with low systemic vascular resistance and no respond to fluid administration. Although it barely affects the systemic hemodynamic status at low dose (0.5 to 2 g/kg/min), dopamine typically increases the blood flow to the heart and intestine, and increases cardiac output and blood pressure in neonates. At dose of >0.5 g/kg/min, dopamine induces cardiac beta adrenergic receptor activity, which induces the secretion of norepinephrine from the cardiac sympathetic nerve. However, dopamine’s ability to stimulate myocardial and vascular contraction can be reduced in some cases, such as chronic heart failure patients with depletion of myocardial norepinephrine, and infants who are < 1 month old with incomplete development of the cardiac sympathetic nerve. At dose of > 20 g/kg/min, dopamine induces excessive vasoconstriction and renovascular dilation disappears. Therefore, epinephrine or dobutamine are recommended in case where > 20 g/kg/min of dopamine would be needed to increase myocardial contraction. Dopamine is a catecholamine that can be partially inactivated in alkali solutions, and should not be mixed with bicarbonate. 3) DobutamineDobutamine is a synthetic catecholamine that exerts relatively selective effects on the beta-1 adrenergic receptor, and has minimal effects on the beta-2 adrenergic receptor. Therefore, dobutamine is a relatively selective inotrope that can increase myocardial
Pediatric advanced life support 99
contraction and reduce systemic vascular resistance. Dobutamine is effective for increasing cardiac output and blood pressure in infants and children. In particular, dobutamine can be used to treat secondary reduction in cardiac output due to decreased myocardial function, such as in the post-cardiac arrest situation. Tachycardia and premature ventricular contractions can occur at high doses of dobutamine. 4) NorepinephrineNorepinephrine is a neurotransmitter that is secreted from the sympathetic nerve, and is a strong inotrope that it works on the peripheral alpha and beta sympathetic nerve to induce strong myocardial and peripheral vascular contractions. The alpha sympathomimetic effect is predominant at the standard dose. As norepinephrine is a strong vasoconstrictor, it can be used to treat septic shock that does not respond to fluid infusion and exhibits low systemic vascular resistance, spinal shock, and anaphylaxis. The infusion rate may be adjusted according to the patient’s blood pressure and perfusion status. 5) NitroprussideNitroprusside is a vasodilator that induces the local production of nitric oxide an all blood vessels. At the therapeutic dose, it has no direct effects on myocytes, and increases cardiac output by reducing the resistance of the systemic and pulmonary blood vessels. The combination of nitroprusside and inotropes can be used in patients with severe hypertension or reduced cardiac output due to reduced myocardial function and increase vascular resistance. However, it should not be used if the blood volume is reduced, as it can cause severe hypotension. Nitroprusside is rapidly metabolized and should be constantly infused with a dextrose solution, and should not be mixed with normal saline. Level of thiocyanate should be monitored in cases with prolonged use, and especially when the infusion rate is > 2 g/kg/min. 6) Inodilators Inodilators, such as amrinone and milrinone, are used for patients with reduced cardiac function or increases resistance of the systemic and pulmonary blood vessels. Similar to vasodilators inodilators do not increase the myocardial oxygen demand, increase the cardiac output, and have minimal effect on the heart rate. Hypotension is not common if the circulating blood volume is adequate, but can occur due to vasodilation if there is an inadequate circulating blood volume. Therefore, fluid administration may be necessary to counteract vasodilation after drug administration.
4. Nervous system management The primary purpose of CPR is to maintain brain function, and care must be taken to prevent secondary damage to the nervous system after CPR. Hyperventilation has a negative effect on the prognosis of the nervous system, as its effect both cardiac function and cerebral perfusion. Short periods of intentional hyperventilation are acceptable in cases with signs of brain herniation, such as a sudden increase in intracranial pressure, mydriasis without a light reflex, bradycardia, or hypertension. Target temperature management can be considered for
Pediatric advanced life support100
unconscious infants or children with ROSC after cardiac arrest. The body temperature should not be allowed to drop below 32 C, or to increase above 37.5 C, even if target temperature management is not performed. As fever has a negative effect on the recovery of brain function, it should be actively treated by using an antipyretic drug and an external cooling method. Tremors can occur at low temperature, and can be prevented using a sedative. Neuromuscular blockade can be used if necessary, although it can mask a seizure, and continuous electroencephalogram monitoring can be used to detect seizures. Although ab adequate cooling and rewarming method has not been established, the body temperature should not increase at a rate of > 0.5 C every 2 hours, unless there is another reason for rapid rewarming. 5. Renal system management The prerenal condition that is caused by hydration or inadequate perfusion, and/or ischemic injuries in the kidney(s), can reduce urine output (infants and children: < 1 ml/kg/hr, adolescents: < 30 ml/hr). Avoid using drud with renal toxicity until the patient’s renal function has been confirmed, and adjusted the dose of drugs that undergo renal excretion. 6. Gastrointestinal system management In cases with no bowel sounds, abdominal distention, or required mechanical ventilation, performed nasogastric or orogastric intubation to prevent or treat gastric inflation. However, nasogastric intubation is prohibited in patients with facial injuries or basal skull fractures, because the tube can enter the cranium. 7. Factors predicting prognosis The survival rate is higher in cases with a pupillary reflex within 24 hours after CPR, compared to that in cases that do not fulfill this criterion, and there are reports that a poor prognosis may be predicted by increased level of neuron-specific enolase and S100 calcium-binding protein B. Although there are no established predictors of neurological and survival outcomes in children with ROSC, these outcomes may be predicted by pupillary reflex, neuron-specific enolase and S100 calcium-binding protein B levels. Furthermore, electroencephalogram results within 7 days after cardiac arrest may help predict neurologic outcomes, but the outcomes cannot be predicted using only electroencephalogram results. INTERHOSPITAL TRANSPORTATION
Ideally postresuscitation care should be provided by a trained team from a pediatric tertiary care facility. Contact such a team as early as possible during the resuscitation attempt and coordianate transportation with the receiving unit. Transport team members should be trained and experienced in the care of critically ill and injured children and supervised by a pediatric emergency medicine or pediatric critical care physician. The mode of transport and composition of the team should be established for each system based on the care required by each patient. Monitor exhaled CO2 (qualitative colorimetric detector or capnography) during interhospital or intrahospital transport of intubated patients.
TERMINATIO OF RESUSCITATIVE EFFORTS
Pediatric advanced life support 101

Pediatric advanced life support102
TERMINATIO OF RESUSCITATIVE EFFORTS
There are no reliable predictors of outcome to guide when to terminate resuscitative efforts in children.
Clinical variables associated with survival included length of CPR, number of doses of epinephrine, age, witnessed versus unwitnessed cardiac arrest, and the first and subsequent rhythm. None of these association, however, predict outcome. witnessed collapse, bystander CPR, and a short interval from collapse to arrival of professionals improve the chance of a successful resuscitation. Intact survival has been documented after unusually prolonged in-hospital resuscitation.
Team
Compile and translate
Vilaphone PHAYMANY, MD. PCIU, Children’s Hospital
Advisor
Prof. Park June Dong, MD., PhD Associate professor
Department of Pediatrics
Seoul National University College of Medicine
Director
Pediatric Intensive Care Medicine
Seoul National University Hospital
Editors
Sommanikhone PHANGMANIXAY, MD. Pediatrician
Director of Children’s Hospital
Ministry of Health
Vice Chair of Department of Pediatric
Faculty of Medicine, University of Health
Science
Bandith SOUMPHONPHAKDY, MD. Pediatric Infectious Disease Subspecialist
Vice Chair of Department of Pediatric
Faculty of Medicine, University of Health
Science
Neonatal-Pediatric Intensive Care unit
Mahosot Hospital, Ministry of Health
Sonephet SAYSOULIGNO, MD. Pediatric Hemato-oncology Subspecialist
Head of Hematology Department, Children’s
Hospital, Ministry of Health
Pediatric advanced life support 103

References
1. Kim DK, Jhang WK, Ahn JY, Lee JS, Kim YH, Lee B, et al. Part 6. Pediatric advanced life support: 2015 Korean Guidelines for Cardiopulmonary Resuscitation. Clinical and experimental emergency medicine. 2016;3(Suppl):S48-S61.
2. Lee JS, Ahn JY, Kim DK, Kim YH, Lee B, Jhang WK, et al. Part 5. Pediatric basic life support: 2015 Korean Guidelines for Cardiopulmonary Resuscitation. Clinical and experimental emergency medicine. 2016;3(Suppl):S39-S47.
3. Maconochie IK, Bingham R, Eich C, Lopez-Herce J, Thomas R, et al. European Resuscitation Council Guidelines for Resucitation 2015 Section 6. Pediatric life support. Resuscitation. 2015;95:e223-48.
4. Berg MD, Schexnayder SM, Chameides L, Terry M, Donoghue A, Hickey RW, et al. Part 13: pediatric basic life support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation.2010;122(18 Suppl 3):S862-75.
5. Kleinman ME, Chameides L, Schexnayder SM, Samson RA, Hazinski MF, Atkins DL, et al. Part 14: pediatric advanced life support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation.2010;122(18 Suppl 3):S876-908.
6. The figures of algorithm were authorized by Clinical and Experimental Emergency Medicine. The figures were copied from Google.com/images.
Pediatric advanced life support104
Pediatric Cardiopulmonary Resuscitation 2017