cardiopulmonary arrest and resuscitation in landrace/large white swine: a research model
TRANSCRIPT
Cardiopulmonary arrest and resuscitation inLandrace/Large White swine: a research model
T Xanthos1, P Lelovas1, I Vlachos1, N Tsirikos-Karapanos2, E Kouskouni3,D Perrea1 and I Dontas1
1Department of Experimental Surgery and Surgical Research, Medical School University of Athens;2Hippokrateion Hospital, Athens, Medical School; 3Aretaieio General Hospital, University of Athens,Medical School, Greece
Summary
Sudden cardiac death (SCD) is a field of continuous research. In order to answer variousquestions regarding SCD, several animal models have been developed. The aim of thepresent study is to describe our experimental model of inducing cardiac arrest in Landrace/Large White pigs, and then resuscitated according to the International Guidelines onresuscitation. Fifteen Landrace/Large White pigs were anaesthetized and intubated whilespontaneously breathing. The left and right jugular veins, as well as the femoral and thecarotid arteries, were surgically prepared. Induction of cardiac arrest was achieved by usingan ordinary rechargeable lithium battery, through a pacemaker wire inserted into the rightventricle. The typical Advanced Life Support (ALS) protocol was followed, and in case ofrestoration of spontaneous circulation, the animals were further evaluated for 30min. Sevenanimals were successfully resuscitated using this protocol, whereas eight failed resuscitationefforts. Successful resuscitation was contingent on the restoration of the levels of coronaryperfusion pressure and PETCO2 during chest compressions. Among the different waysof inducing cardiac arrest, the ordinary lithium battery is a simple, safe and valuabletechnique. Landrace/Large White pigs’ baseline haemodynamics closely resemble humanhaemodynamics, making the breed a favourable model for resuscitation.
Keywords Swine; cardiopulmonary resuscitation; model
In the 18th century, drowning had theequivalent impact on society that suddendeath has today. In the latter part of thatcentury, scientists throughout Europeestablished humane societies to developresuscitation techniques and to keepregistries of successful and unsuccessfulcases (Stembach et al. 2000). Dr CharlesKite was an active member of the LondonHumane Society, and in 1778 he wrote‘An Essay on the Recovery of theApparently Dead’ in which he wasthe first to differentiate suspended
animation from irreversible death (Eisenberg1994).
From that time forward, the science andart of resuscitation have flourished, andmultiple international organizations, suchas the International Liaison Committee onResuscitation (ILCOR) and the EuropeanResuscitation Council (ERC) were founded.These organizations have tried to establishguidelines on resuscitation, based onconsensus on science, hoping that theycould improve the outcome of cardiac arrestor sudden cardiac death (SCD) (Anonymous1997a, 1998).
Research in the field of sudden deathhas been continuous in the last decade.
Accepted 9 April 2007 r Laboratory Animals Ltd. Laboratory Animals (2007) 41, 353–362
Correspondence: Th Xanthos, 100 Klytemnistras Street,13122, Athens, Greece.Email: [email protected]

Two-thirds of the victims of cardiacarrest are due to cardiovascular disease(Anonymous 1981).
Epidemiologically speaking, cardiac arrestis the suspension of cardiac function in orout of hospital, which is not accompaniedby overt symptoms, or is accompanied bysymptoms lasting less than 1h (Weis 1940,Spain et al. 1960, Kuller 1978, Waller 1985).
In Europe, coronary artery disease (CAD)is responsible for 40% of all deaths in peopleless than 75 years old (Anonymous 2001).The most common cause of death in CADis a lethal arrhythmia, called ventricularfibrillation (VF), which represents 80–90%of out-hospital SCDs (Packer 1985,Anonymous 1997b).
Occlusion of a coronary artery leads toregional ischaemia, which in turn causesintracellular and extracellular acidosis, lossof cellular membrane integrity and loweringof the resting transmembrane potential. Asdepolarization and conduction are slowed,conditions are created for fragmentedelectrical activity and local re-entrantpathways, thereby facilitating the emergenceof VF (Lazzara et al. 1978).
The fact that o5% of human victims ofcardiac arrest survive when cardiac arrestoccurs outside of the hospital promptsvigorous experimental pursuit of a betterunderstanding of the mechanisms andmanagement. The possible therapeuticinterventions suggested by the internationalorganizations are somewhat limited.Defibrillation and epinephrine are the onlyinterventions recommended (Anonymous1997a, 2000). New medications andtechniques are being tried, confirmingdiverging hypotheses. However, it is unethi-cal for these novel interventions to be triedon humans, prior to their application onanimal models (Bulger 1987). In order toreproduce the accurate environment of thislife-threatening situation, different animalmodels have been described (Packer 1985,Hughes 1986, von Planta et al. 1988, Wenzelet al. 1999, Kii et al. 2004, Kofler et al. 2004,Nozari et al. 2004) with multiple methods ofinducing cardiac arrest.
The aim of this study is to describe ourexperimental protocol of inducing cardiac
arrest in a swine model. This modelwas successfully resuscitated using theInternational Guidelines (Anonymous2000).
Swine model of cardiopulmonaryresuscitation
Preparation
The experimental protocol was approvedby the General Directorate of VeterinaryServices (permit no. K/227/21-1-2004),according to Greek legislation regardingethical and experimental procedures(Presidential Decree 160/1991, in com-pliance with the EEC Directive 86/609 andLaw 2015/1992 and in conformance with theEuropean Convention ‘for the protection ofvertebrate animals used for experimental orother scientific purposes, 123/1986’). Afterreceiving approval from the Directorate ofVeterinary Services of the Prefecture ofAthens, Attica, Greece, 15 Landrace/LargeWhite piglets of both sexes, aged 10–15weeks and with an average weight of1972kg, all from the same breeder(Validakis, Athens, Greece) were studied.They were housed in single cages. Thearea of the cage was 2m2. The con-ditions in the animal house were 15 airchanges/h, 22721C, relative humidity 55%and light–dark at 06.00 h/18.00 h. Theywere fed a commercial food, the nutrientcontents of which are described inTable 1, and were acclimatized to thelaboratory conditions for a one-weekperiod prior to the experiment. The animalswere fasted overnight but had free accessto water.
Initial sedation in each animal wasachieved with intramuscular ketaminehydrochloride (Merial, Lyon, France) 10mg/kg, midazolam (Roche, Athens, Greece)0.5mg/kg and atropine sulphate (Efar,Athens, Greece) 0.05mg/kg. The marginalauricular vein was then catheterized.Anaesthesia was induced with an intra-venous bolus dose of propofol (2.0mg/kg)via this vein (BD Venflon, Luer-Lok,Helsinborg, Sweden, 20GA 1.26IN 54mL/min). While breathing spontaneously, but
Laboratory Animals (2007) 41
354 T Xanthos et al.

anaesthetized, the pigs were intubated witha 4.5 or 5.0 endotracheal tube (MLTt 4.5 or5.0 Oral 27mm Mallinckrodt Medical,Athlone, Ireland). Correct placement of theendotracheal tube was ascertained withinflation and auscultation of both lungs. Thetracheal tube was secured on the upper jaw;hair was clipped from the ventral thoraxand the head to facilitate the use of self-adhesive electrodes. The animals were thenimmobilized in a supine posture on anoperating table. Additional propofol 1mg/kg,cis-atracurium 0.15mg/kg and fentanyl 4 mg/kg (Janssen, Pharmaceutica, Beerse,Belgium) were administrated immediatelybefore connecting the animals to theautomatic ventilator (ventiPac SimspneuPac, Luton, UK) with 21% oxygen (FiO2
21%). This dose was necessary to ascertaincooperation with the ventilator. Infusion ofpropofol 150mg/kg/min or more, if needed,followed, to maintain adequate anaestheticdepth. Ventilations were delivered with theaid of a volume-controlled ventilator with atotal tidal volume of 15mL/kg. End-tidalPETCO2 was monitored (Nihon KohdenCorp, Bergamo, Italy), and the respiratoryfrequency was adjusted to maintain PETCO2
35–40mmHg.Electrocardiographic (ECG) monitoring
(Mennen Medical, Envoy, Papapostolou,Athens, Greece) was performed, using leadsI, II, III, aVR, aVL, aVF and self-adhesiveelectrodes, to assess the cardiac rhythm,while the heart rate was determined by the
ECG signal. All tracings were recorded onusual ECG thermographic paper.
In order to continuously and non-invasively detect changes in cerebraloxygenation, near infrared spectroscopy(NIRS) was utilized (Somanetics INVOSCerebral Oximeter, Model SPFB PediatricSomasensor SOMANETICS, Papapostolou,Athens, Greece). The optodes of NIRS weremounted on the intact skin covering eachcerebral hemisphere slightly anterior to thecoronal suture to avoid the pig’s frontalsinus, as well as the strong muscular systemof the neck. For optimal spatial resolution,the interoptode distance was set to 5 cm. Thepath length was adjusted according to themanufacturer’s instructions for measure-ments on an intact human skull. Datawere recorded every 10 s after inductionof anaesthesia and for the duration ofcardiopulmonary arrest and resuscitation.The device calculated the relative con-centration changes in Tissue OxygenationIndex (TOI), Tissue HaemoglobinIndex (THI) and cytochrome oxidase(DCytOx).
Pulse oximetry (SpO2) (Vet/Ox Plus 4700,Heska, USA) was also utilized as a meansof peripheral tissue oxygenation and wasmonitored continuously. The pulse oxi-meter was placed on the tongue of theanaesthetized and intubated animal.
For measurement of the aortic pressure, anormal saline filled (model 6523, USCI CR,Bart Inc, Papapostolou, Athens, Greece)
Laboratory Animals (2007) 41
Swine model of cardiopulmonary resuscitation 355
Table 1 Nutrient contents of the commercial food used in our laboratory
Total nitrogenous content (%) 20.0 Vitamin A 1300 IU/kgFibre (%) 4.0 Vitamin D3 1560 IU/kgFat (%) 5.0 Vitamin E 53 mg/kgMoisture (%) 12.0 Vitamin B12 26 mg/kgAsh (%) 5.0 Biotin 98 mg/kgCalcium (%) 1.0 Pantothenic acid 12 mg/kgPhosphorus (%) 0.8 Nicotinic acid 19 mg/kgSodium (%) 0.2 Phyllic acid 1 mg/kgLysine (%) 1.0 Vitamin C 17 mg/kgSulphurous amino acid (%) 0.6 Mg 60 mg/kg
Fe 113 mg/kgI 1500mg/kgSe 150mg/kgCu 135 mg/kgCo 1125mg/kg
Form of the food, pellets of 3.5mm
femoral arterial catheter was inserted intothe descending aorta (Mennen Medical,Envoy). Mean arterial pressure (MAP) wasdetermined by the electronic integration ofthe aortic blood pressure waveform. Theinternal jugular vein was surgically prepared(Opticath 5.5 F, 75 cm Abbott, EthiconMersilkt, Athens, Greece). Right atrialpressure and cardiac output (CO) weremeasured by the thermodilution method.For this reason, a 7F, pentalumen,thermodilution-tipped catheter (AbbottCritical Care) was advanced flow-directedinto the pulmonary artery. Conventionalexternal pressure transducers were used(Abbott Critical Care Systems, Transpac IV).Coronary perfusion pressure (CPP) waselectronically calculated as the differencebetween minimal aortic diastolic pressureand the simultaneously measured rightatrial pressure. The second internal jugularvein was also surgically prepared (Figure 1).A 5F flow-directed pacing catheter (Pacelt;100 cm, St Jude Medical, Ladakis, Athens,Greece) was advanced into the apex of theright ventricle. Confirmation of correctplacement was achieved by fluoroscopicimage intensification and by the ventricularectopies recorded on the ECG tracing.Aliquots of 5mL of venous blood werecollected for measurements of neuronspecific enolase (NSE) and S-100, as well asfor troponin I, before induction of VF, after5min of untreated VF and at 60min aftersuccessful resuscitation.
Protocol
VF was induced with a 9V ordinary lithiumbattery. Arrhythmia was confirmedelectrocardiographically and with a suddendrop in the MAP. After induction of VF,the animals were left untreated for 5min.Mechanical ventilation was stoppedcoincident with the onset of cardiac arrest.Resuscitation procedures were started withinspired oxygen concentration 100%,followed by chest compressions for 3min.Compressions were maintained at a rate of100/min with equal compression–relaxationduration. Compression depth was equivalentto 30% of the anteroposterior diameter of thechest. A set of up to three shocks wereinitially given with energies of 2, 2 and 4 J/kg(Figure 2). While the defibrillator wasrecharged, the ECG monitor was observedfor any changes in the rhythm. Blood wasdrawn and adrenaline was peripherallyadministered via the auricular vein. Incase of failure to convert to a cardiacrhythm compatible with pulse, the typicalAdvanced Life Support (ALS) protocol wasperformed, following the 2000 guidelineson resuscitation. This involved furtherdefibrillation with energies of 4, 4 and 4 J/kgand adrenaline administration every 3minin case of failure to convert to a rhythmcompatible with a palpable pulse. If a thirddefibrillation set was required, the energiesadministered were 4, 4 and 4 J/kg. Ourexperimental protocol is shown in Figure 3.Successful resuscitation was defined as thereturn of spontaneous rhythm with a
Laboratory Animals (2007) 41
356 T Xanthos et al.
Figure 1 Surgical preparations of internal jugularvein and carotid artery in our model Figure 2 Defibrillation attempt in the swine model

MAP of at least 60mmHg for a minimumof 5min.
Endpoints of the experiment were definedas either asystole or return of spontaneouscirculation. The animals restoring sponta-neous circulation were monitored for60min, while anaesthesia was main-tained. All animals were euthanized by anintravenous solution of thiopental (2 g).Necropsy was routinely performed afterdeath. Thoracic and abdominal organs wereexamined for gross evidence of traumaticinjuries caused by surgical or resuscitationefforts.
Statistical analysis
Measurements are reported as means7SD. Comparisons between time-basedmeasurements on the same animalsand differences between resuscitated andnon-resuscitated animals were analysedwith analysis of variance (ANOVA)multiple measurements. A P value ofo0.05 was considered statisticallysignificant.
Results
Survival
Seven of 15 animals were successfullyresuscitated. One animal was successfullyresuscitated in the first defibrillationattempt of the first set of defibrillations,whereas two more animals were restoredto spontaneous circulation at the thirddefibrillation attempt of the first set. Threeanimals had circulation restored at the thirddefibrillation attempt of the second set ofdefibrillations, whereas only one animal wassuccessfully resuscitated at the thirddefibrillation set.
Haemodynamic observations
The baseline haemodynamics of Landrace/Large White pigs are presented in Table 2.There was no difference in the baselinehaemodynamic measurements betweenresuscitated and non-resuscitated animals,as demonstrated in Table 3. MAP beforecardiac arrest ranged from 90 to 95mmHg.MAP over the initial 3min of basic life
Laboratory Animals (2007) 41
Swine model of cardiopulmonary resuscitation 357
Cardiac arrest
Basic life support
Chest compressions –ventilation (oxygen 100%)
1 min chest compressions /ventilation
Adrenaline 0.02 mg/kg (every 3 min)
Advanced life support2 J/kg –2 J/kg –4 J/kg
Defibrillation:
4 J/kg –4 J/kg –4 J/kgDefibrillation:
Figure 3 Experimental flowchart
Table 2 Landrace/Large White baselinehaemodynamics
Parameters Value (SD)
Heart rate (bpm) 116.4178.11Invasive systolic blood
pressure (mmHg)111.72713.61
Invasive diastolic bloodpressure (mmHg)
79.03712.08
Cardiac output (L/min) 5.1270.53Systolic pressure left
ventricle (mmHg)108.96712.06
Diastolic pressure leftventricle (mmHg)
8.8271.81
Systolic pulmonarypressure (mmHg)
21.5173.41
Diastolic pulmonarypressure (mmHg)
11.0373.24
Systolic pressure rightatrium (mmHg)
10.9371.36
Diastolic pressure rightatrium (mmHg)
4.1071.01
Systolic pressure rightventricle (mmHg)
21.2472.16
Diastolic pressure rightventricle (mmHg)
4.2070.72
Pulse oximetry (%) 9571.49Cerebral oximetry (%) 64.5573.88

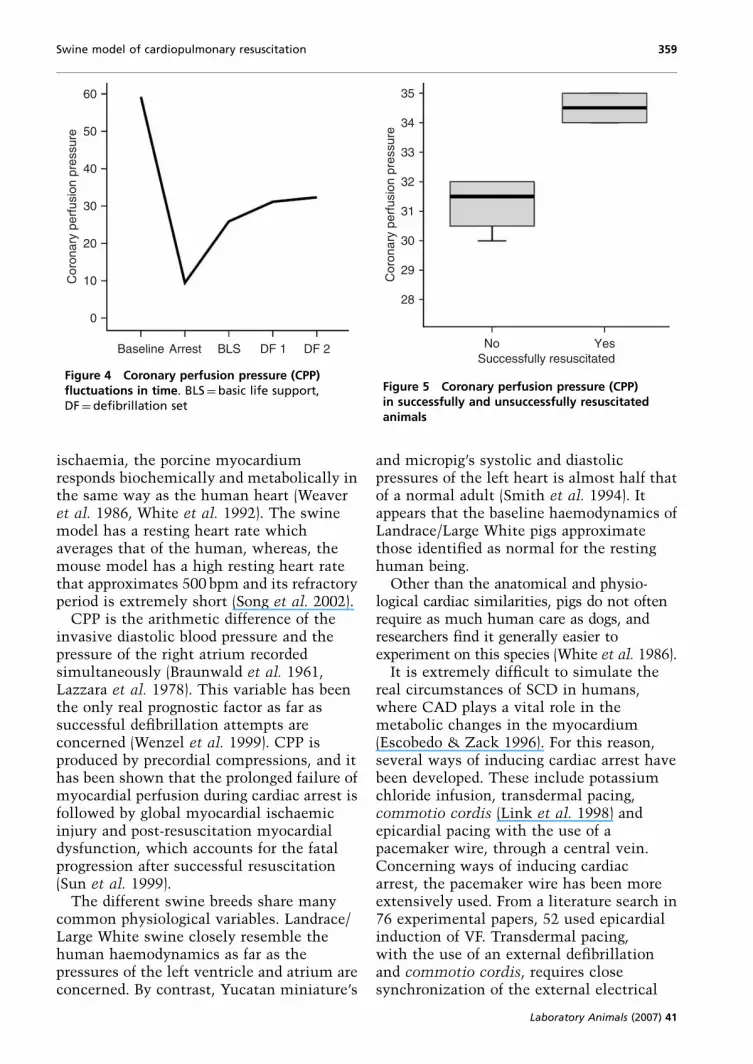
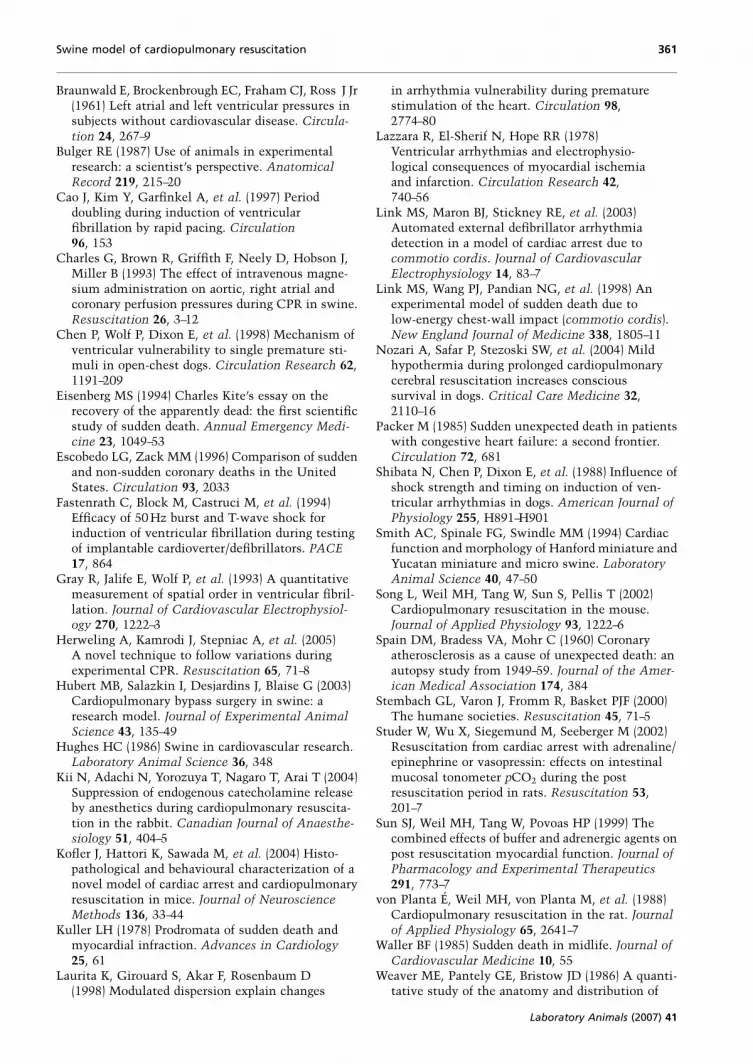
support (BLS) in survivors was 3173mmHgbut only 1075 in non-survivors (Po0.05).CPP fluctuations in time can be seen inFigure 4 for the successfully resuscitatedanimals. CPP fell dramatically after 5min ofuntreated VF, rose to 25mmHg for the BLSperiod and rose further after implementa-tion of the ALS protocol. CPP rose from2473mmHg in the BLS period to3373mmHg in the ALS period (Po0.05).CPP achieved with precordial compressionaveraged 34.570.7mmHg in survivorscompared with 31.270.9mmHg in non-survivors (Po0.05) as shown in Figure 5.These extremely high levels of CPP, both insurvivors and non-survivors, represent theefficacy of precordial compressions. End-tidal CO2 pressure ( PETCO2 ) decreased froma baseline level of 3074 to 0.6Torr duringcardiopulmonary arrest. It increased to1374Torr during the 3min of BLS inresuscitated animals, but only to 472Torrin non-resuscitated animals (Po0.05). Nostatistically significant difference wasrecorded in any other measured variablebetween the successfully and unsuccessfullyresuscitated animals.
Post-resuscitation period
Several arrhythmias were recorded in theanimals that were successfully resuscitated.One animal had episodes of recurrent VFrequiring further defibrillation attempts.Two animals had episodes of ventriculartachycardia that required the addition of anintravenous beta blocker. Multiple episodesof supraventricular tachycardias wererecorded in all successfully resuscitatedanimals. All those tachycardias areconsistent with the post-resuscitationmyocardial dysfunction.
Necropsy
No evidence of injury to the bony thoraxor abdomen was identified. Minor lungcontusions were observed in two animals inwhich 20min of chest compression failed toreturn spontaneous circulation.
Discussion
This experimental protocol has beendesigned to simulate the real events ofcardiac arrest in humans. It has been shownthat VF is the most common lethalarrhythmia for victims of cardiac arrest(Anonymous 2000). The average time untilarrival of specialized personnel varies, butthe acceptable European Standard is 8min(Anonymous 2000).
This protocol simulates the event of a5min untreated VF, a 3min implementationof the BLS protocol by a bystander rescuerand the arrival of specialized personnelimplementing an approved ALS protocol.
The choice of the animal model is one ofthe main problems the researcher has toface. There are multiple parameters onehas to consider in designing a model ofcardiopulmonary resuscitation. On review-ing the literature, the animal models thathave been used are: mice, rats, other rodents,cats, dogs, swine and primates. Each specieshas its own advantages. The porcine model,however, is more frequently used. Thereare several reasons for this. Swine cardiacanatomy and physiology closely resemblehumans, as its coronary arteries have only afew lateral epicardial anastomoses (Wyleret al. 1979, Hughes 1986). Further-more, myocardial histology is similar inswine and humans (Hubert et al. 2003). Inaddition, after induction of myocardial
Laboratory Animals (2007) 41
358 T Xanthos et al.
Table 3 Baseline measurements between successfully and unsuccessfully resuscitated animals
Baseline characteristicsVariables Successfully resuscitated Unsuccessfully resuscitated P
Weight (kg) 19.5 19.9 NSSystolic blood pressure (mmHg) 107.9 107.22 NSDiastolic blood pressure (mmHg) 72.2 72.67 NSCPP (mmHg) 58.9 58.33 NSNIRS 66.3 63.3 NS
NS = not significant, CPP = coronary perfusion pressure, NIRS = near infrared spectroscopy
ischaemia, the porcine myocardiumresponds biochemically and metabolically inthe same way as the human heart (Weaveret al. 1986, White et al. 1992). The swinemodel has a resting heart rate whichaverages that of the human, whereas, themouse model has a high resting heart ratethat approximates 500 bpm and its refractoryperiod is extremely short (Song et al. 2002).
CPP is the arithmetic difference of theinvasive diastolic blood pressure and thepressure of the right atrium recordedsimultaneously (Braunwald et al. 1961,Lazzara et al. 1978). This variable has beenthe only real prognostic factor as far assuccessful defibrillation attempts areconcerned (Wenzel et al. 1999). CPP isproduced by precordial compressions, and ithas been shown that the prolonged failure ofmyocardial perfusion during cardiac arrest isfollowed by global myocardial ischaemicinjury and post-resuscitation myocardialdysfunction, which accounts for the fatalprogression after successful resuscitation(Sun et al. 1999).
The different swine breeds share manycommon physiological variables. Landrace/Large White swine closely resemble thehuman haemodynamics as far as thepressures of the left ventricle and atrium areconcerned. By contrast, Yucatan miniature’s
and micropig’s systolic and diastolicpressures of the left heart is almost half thatof a normal adult (Smith et al. 1994). Itappears that the baseline haemodynamics ofLandrace/Large White pigs approximatethose identified as normal for the restinghuman being.
Other than the anatomical and physio-logical cardiac similarities, pigs do not oftenrequire as much human care as dogs, andresearchers find it generally easier toexperiment on this species (White et al. 1986).
It is extremely difficult to simulate thereal circumstances of SCD in humans,where CAD plays a vital role in themetabolic changes in the myocardium(Escobedo & Zack 1996). For this reason,several ways of inducing cardiac arrest havebeen developed. These include potassiumchloride infusion, transdermal pacing,commotio cordis (Link et al. 1998) andepicardial pacing with the use of apacemaker wire, through a central vein.Concerning ways of inducing cardiacarrest, the pacemaker wire has been moreextensively used. From a literature search in76 experimental papers, 52 used epicardialinduction of VF. Transdermal pacing,with the use of an external defibrillationand commotio cordis, requires closesynchronization of the external electrical
Laboratory Animals (2007) 41
Swine model of cardiopulmonary resuscitation 359
Cor
onar
y pe
rfus
ion
pres
sure
0
10
20
30
40
50
60
Baseline Arrest BLS DF 1 DF 2
Figure 4 Coronary perfusion pressure (CPP)fluctuations in time. BLS¼basic life support,DF¼defibrillation set
Successfully resuscitatedYesNo
Cor
onar
y pe
rfus
ion
pres
sure
28
29
30
31
32
33
34
35
Figure 5 Coronary perfusion pressure (CPP)in successfully and unsuccessfully resuscitatedanimals

apparatus with the electrocardiogram, asinduction of cardiac arrest mainly dependson the R-on-T phenomenon (Link et al.2003, Herweling et al. 2005).
Prior studies suggest that various modes ofVF induction may initiate VF by differentelectrophysiological mechanisms (Shibataet al. 1988, Cao et al. 1997, Chen et al. 1998,Laurita et al. 1998). VF was induced (Chenet al. 1998) in a dog model with the use ofpremature stimuli and accounted for thephenomenon by mechanisms of functionalreentry. The influence of T wave shockstrength on the induction of VF was studiedin a dog model (Shibata et al. 1988). Aftershocks of the shortest and longest couplinginterval, for which a response occurred, theactivation pattern was focal, probably froma focus triggered by the shock or micro-reentry. However, shocks that weredelivered during the mid-portion of thevulnerable period after ventricular pacingfibrillation arose, with properties of reent-rant pattern, which is now described as ascroll wave (Winfree 1994, Witowski et al.1998).
During implantable cardiac defibrillator(ICD) testing, several techniques have beenproposed for inducing VF: (1) rapid pacing –typically 50Hz, (2) a high-energy pulsedelivered on the vulnerable period of the Twave (Fastenrath et al. 1994, Bhandari et al.1998) and (3) AC current (Gray et al. 1993).Several studies showed that 50 Hz burststimulation and low-energy T wave shockhave a similar efficacy of inducing VF(Fastenrath et al. 1994, Bhandari et al. 1998).
For experimental induction of cardiacarrest, different electrical devices were used,such as direct connection to alternating ordirect current (Charles et al. 1993, Studeret al. 2002). However, this connection couldinvolve potential dangers for the researchers,although there are no recorded incidents ofelectrocution from experimental research.The ordinary lithium battery seems saferand extremely efficient in inducing cardiacarrest. The mechanisms by which VF isinduced, using the ordinary lithium battery,are similar to the delivery of the low-energyT wave shock, using electrical current. Toour knowledge, there are no experimental
studies that induced VF with an ordinaryrechargeable lithium battery.
Conclusion
Landrace/Large White pigs are a favourableswine breed for experimentation on cardiacarrest. CPP, which is the real prognosticfactor for successful resuscitation iscomparable in humans and Landrace/LargeWhite pigs. Among the different ways ofinducing VF, the ordinary rechargeablebattery is extremely easy and efficient to use.
References
Anonymous (1981) Report of the Working Group on
Arteriosclerosis of the National Heart, Lung and
Blood Institute (Vol. 2): Patient Oriented Research
Fundamental and Applied, Sudden Cardiac Death.
Department of Health, Education andWelfare, NIH
Publication No. 82-2035. Washington DC:
Government Printing Office, 114–122Anonymous (1997a) Advanced Life Support Working
Group of the International Liaison Committee
on Resuscitation, an advisory statement by the
Advanced Life Support Working Group of the
International Liaison Committee on Resuscitation.
Resuscitation 34, 113–15Anonymous (1997b) Consensus statement of the Joint
Steering Committees of the unexplained cardiac
arrest registry Europe and of the idiopathic ven-
tricular fibrillation registry of the United States,
survivors of out-of-hospital cardiac arrest with
apparently normal heart: need for definition and
standardize clinical evaluation. Circulation 95,
265–72Anonymous (1998) The 1998 European Resuscitation
Council Guidelines for Adult Advanced Life
Support. In: European Resuscitation Council
Guidelines for Resuscitation (Bossaert L, ed).
Amsterdam: Elsevier, 36–47Anonymous (2000) The American Heart Association
in collaboration with the International Liaison
Committee Resuscitation (ILCOR), Resuscitation
and Emergency Cardiovascular Care an Interna-
tional consensus on Science. Resuscitation 46,
135–62Anonymous (2001) Advanced Life Support Course
Provider Manual. 4th edn. London: Resuscitation
Council UKBhandari A, Isber N, Estioko M, et al. (1998) Effect of
low-energy shocks for induction of ventricular
fibrillation in patients with implantable cardio-
verter defibrillators. Journal of Electrocardiology
31, 31–7
Laboratory Animals (2007) 41
360 T Xanthos et al.
Braunwald E, Brockenbrough EC, Fraham CJ, Ross J Jr(1961) Left atrial and left ventricular pressures insubjects without cardiovascular disease. Circula-
tion 24, 267–9Bulger RE (1987) Use of animals in experimental
research: a scientist’s perspective. Anatomical
Record 219, 215–20Cao J, Kim Y, Garfinkel A, et al. (1997) Period
doubling during induction of ventricularfibrillation by rapid pacing. Circulation
96, 153Charles G, Brown R, Griffith F, Neely D, Hobson J,
Miller B (1993) The effect of intravenous magne-sium administration on aortic, right atrial andcoronary perfusion pressures during CPR in swine.Resuscitation 26, 3–12
Chen P, Wolf P, Dixon E, et al. (1998) Mechanism ofventricular vulnerability to single premature sti-muli in open-chest dogs. Circulation Research 62,1191–209
Eisenberg MS (1994) Charles Kite’s essay on therecovery of the apparently dead: the first scientificstudy of sudden death. Annual Emergency Medi-
cine 23, 1049–53Escobedo LG, Zack MM (1996) Comparison of sudden
and non-sudden coronary deaths in the UnitedStates. Circulation 93, 2033
Fastenrath C, Block M, Castruci M, et al. (1994)Efficacy of 50Hz burst and T-wave shock forinduction of ventricular fibrillation during testingof implantable cardioverter/defibrillators. PACE
17, 864Gray R, Jalife E, Wolf P, et al. (1993) A quantitative
measurement of spatial order in ventricular fibril-lation. Journal of Cardiovascular Electrophysiol-
ogy 270, 1222–3Herweling A, Kamrodi J, Stepniac A, et al. (2005)
A novel technique to follow variations duringexperimental CPR. Resuscitation 65, 71–8
Hubert MB, Salazkin I, Desjardins J, Blaise G (2003)Cardiopulmonary bypass surgery in swine: aresearch model. Journal of Experimental Animal
Science 43, 135–49Hughes HC (1986) Swine in cardiovascular research.
Laboratory Animal Science 36, 348Kii N, Adachi N, Yorozuya T, Nagaro T, Arai T (2004)
Suppression of endogenous catecholamine releaseby anesthetics during cardiopulmonary resuscita-tion in the rabbit. Canadian Journal of Anaesthe-
siology 51, 404–5Kofler J, Hattori K, Sawada M, et al. (2004) Histo-
pathological and behavioural characterization of anovel model of cardiac arrest and cardiopulmonaryresuscitation in mice. Journal of Neuroscience
Methods 136, 33–44Kuller LH (1978) Prodromata of sudden death and
myocardial infraction. Advances in Cardiology
25, 61Laurita K, Girouard S, Akar F, Rosenbaum D
(1998) Modulated dispersion explain changes
in arrhythmia vulnerability during prematurestimulation of the heart. Circulation 98,2774–80
Lazzara R, El-Sherif N, Hope RR (1978)Ventricular arrhythmias and electrophysio-logical consequences of myocardial ischemiaand infarction. Circulation Research 42,740–56
Link MS, Maron BJ, Stickney RE, et al. (2003)Automated external defibrillator arrhythmiadetection in a model of cardiac arrest due tocommotio cordis. Journal of Cardiovascular
Electrophysiology 14, 83–7Link MS, Wang PJ, Pandian NG, et al. (1998) An
experimental model of sudden death due tolow-energy chest-wall impact (commotio cordis).New England Journal of Medicine 338, 1805–11
Nozari A, Safar P, Stezoski SW, et al. (2004) Mildhypothermia during prolonged cardiopulmonarycerebral resuscitation increases conscioussurvival in dogs. Critical Care Medicine 32,2110–16
Packer M (1985) Sudden unexpected death in patientswith congestive heart failure: a second frontier.Circulation 72, 681
Shibata N, Chen P, Dixon E, et al. (1988) Influence ofshock strength and timing on induction of ven-tricular arrhythmias in dogs. American Journal of
Physiology 255, H891–H901Smith AC, Spinale FG, Swindle MM (1994) Cardiac
function and morphology of Hanford miniature andYucatan miniature and micro swine. LaboratoryAnimal Science 40, 47–50
Song L, Weil MH, Tang W, Sun S, Pellis T (2002)Cardiopulmonary resuscitation in the mouse.Journal of Applied Physiology 93, 1222–6
Spain DM, Bradess VA, Mohr C (1960) Coronaryatherosclerosis as a cause of unexpected death: anautopsy study from 1949–59. Journal of the Amer-
ican Medical Association 174, 384Stembach GL, Varon J, Fromm R, Basket PJF (2000)
The humane societies. Resuscitation 45, 71–5Studer W, Wu X, Siegemund M, Seeberger M (2002)
Resuscitation from cardiac arrest with adrenaline/epinephrine or vasopressin: effects on intestinalmucosal tonometer pCO2 during the postresuscitation period in rats. Resuscitation 53,201–7
Sun SJ, Weil MH, Tang W, Povoas HP (1999) Thecombined effects of buffer and adrenergic agents onpost resuscitation myocardial function. Journal ofPharmacology and Experimental Therapeutics
291, 773–7von Planta E, Weil MH, von Planta M, et al. (1988)
Cardiopulmonary resuscitation in the rat. Journalof Applied Physiology 65, 2641–7
Waller BF (1985) Sudden death in midlife. Journal ofCardiovascular Medicine 10, 55
Weaver ME, Pantely GE, Bristow JD (1986) A quanti-tative study of the anatomy and distribution of
Laboratory Animals (2007) 41
Swine model of cardiopulmonary resuscitation 361

coronary arteries in swine in comparison withother animals and man. Cardiovascular Research
20, 907–17Weis S (1940) Instantaneous ‘physiologic’ death. New
England Journal of Medicine 223, 793Wenzel V, Linder KH, Krismer AC, Miller AE,
Voelckel WG, Lingau W (1999) Repeated adminis-tration of vasopressin but not epinephrine main-tains coronary perfusion pressure after earlyand late administration during prolongedcardiopulmonary resuscitation in pigs. Circulation
99, 1379–84White FC, Carroll SM, Magnet A (1992) Coronary
collateral development in swine after coronary
artery occlusion. Circulation Research 71,1450–500
White FC, Roth DM, Bloor CM (1986) The pig as amodel for myocardial ischemia and exercise.Laboratory Animal Science 36, 351–6
Winfree A (1994) Electrical turbulence in three-dimensionless heart muscle. Science 266, 1003–6
Witowski F, Leon L, Penkoske P, et al. (1998)Spatiotemporal evolution of ventricular fibrilla-tion. Nature 392, 78–81
Wyler F, Rutishauser M, Stalder G (1979) Distributionof cardiac output and organ blood flow in theminipig, an experimental animal for haemodynamicresearch. European Journal of Cardiology 10, 327
Laboratory Animals (2007) 41
362 T Xanthos et al.