pdgf and fgf stimulate wound healing in the genetically
TRANSCRIPT
AmericanJournal ofPathology, Vol. 136, No. 6,June 1990Copyright C American Association ofPatbologists
PDGF and FGF Stimulate Wound Healingin the Genetically Diabetic Mouse
David G. Greenhalgh,* Katherine H. Sprugel,Mark J. Murray,4 and Russell RosstFrom the Department ofSurgery and the University ofWashington Burn Center,* the Department ofPathology,jUniversity ofWashington, and ZymoGenetics, Inc.j,Seattle, Washington
To examine the effects ofrecombinant growth fac-tors in vivo, impaired wound healing was studiedin genetically diabetic C5 7BL/KsJ-db/db mice.Large full-thickness skin wounds made on thebacks of these mice exhibited significant delays inthe entry ofinflammatory cells into the wound, theformation of granulation tissue, and in woundclosure when compared to their nondiabetic lit-termates. Recombinant human platelet-derivedgrowth factor (rPDGF-BB, I or 10 jig), recombi-nanthuman basicfibroblastgrowthfactor (rbFGF,I lug), or combinations of both were applied topi-cally to the woundsfor 5 to 14 days after wound-ing. Diabetic mouse wounds treated with rPDGF-BB or rbFGF had many morefibroblasts and capil-laries in the wound bed at 10 and 21 days than didwounds treated with the vehicle alone. The animalstreated with growth factors also had significantlygreater wound closure at 21 days than thosetreated with the vehicle. Combinations of rPDGF-BB and rbFGF improved all parameters of healingbut not to a greater extent than either growth fac-tor alone. The effectiveness ofrPDGF-BB and rbFGFsuggest that recombinant growth factors may beuseful in the treatment ofpatients with deficientwound repair. (Am J Pathol 1990, 136:1235-1246)
While normal, healthy people rarely have problems withhealing, many medical and surgical complications can beattributed to deficiencies in wound repair. Open woundshave lost the barrier that protects tissues from bacterialinvasion and allows for the escape of vital fluids. Withoutexpeditious healing, infections become more frequent.Most wound complications, such as dehiscence, anasto-motic breakdown, or skin graft loss, are associated withsome form of host impairment such as malnutrition, infec-
tion, diabetes, or treatment with steroids, chemotherapy,or radiation.13
Recently, attempts have been made to improve heal-ing using growth factors. Many in vitro experiments sug-gest that growth factors can act as chemoattractants4-9and mitogens10-14 for the cells involved in wound repair.Growth factors can stimulate angiogenesis, 14-15 extracel-lular matrix production and degradation,1S22 and cytokinerelease.2324 Initial studies of wound repair processes inanimals used partially purified mixtures of growth factorswith some success.2526 Relatively few wound healingstudies have been performed in humans with growth fac-tors. Knighton27 has shown that application of an autolo-gous platelet releasate containing a mixture of growth fac-tors improved the healing of chronic leg ulcers. Improvedhealing in such ulcers has also been reported after appli-cation of bovine platelet extracts.26 The availability oflarger quantities of purified growth factors through bio-technology has enabled new studies in animals and theinitiation of studies in human subjects. Recombinant epi-dermal growth factor (EGF) stimulates an improvementin the healing rate of human skin donor sites.2 EGF3 ortransforming growth factor alpha (TGF-a)31 also improvethe healing of partial-thickness wounds in pigs. In subcu-taneous wound chambers, growth factors have beenfound to increase cellular invasion and fibroplasia.323 At-tempts to improve healing in animals with growth factorsin full-thickness wounds have resulted in observationsvarying from slight improvement37-40 to no effect.41,42 Sev-eral investigators have improved isolated aspects of thenormal healing process but the beneficial effects do notappear to change the overall time required for completewound repair. One explanation for the modest effectsseen after the application of growth factors to wounds innormal animals may be that the healing process alreadyproceeds at a near-optimal rate. Consequently, a moreuseful approach may be to use growth factors in woundsthat demonstrate a clinically relevant healing impairmentsuch as that which occurs in diabetes. Recent reportssuggest that growth factors can reverse some of thedeficits in impaired healing models.34,35,42
Accepted for publication January 5, 1990.Address reprint requests to Katherine H. Sprugel, PhD, ZymoGenet-
ics, Inc., 4225 Roosevelt Way NE, Seattle, WA 98105.
1235

1236 Greenhalgh et alAJPJune 1990, Vol. 136, No. 6
In this report, we present a model of impaired woundhealing in homozygous, genetically diabetic (db/db)mice. These animals develop obesity, insulin resistanceand severe hyperglycemia that resembles human adultonset diabetes. Wound healing in these diabetic mice ismarkedly delayed when compared with their heterozy-gous, nondiabetic littermates. The healing impairment ischaracterized by delayed cellular infiltration and granula-tion tissue formation. In such wounds, topical applicationof recombinant human platelet-derived growth factor(rPDGF-BB) and basic fibroblast growth factor (rbFGF)profoundly stimulate the repair process.
Methods
Animals
Male and female C57BL/KsJ-db/db mice were obtainedfrom Jackson Laboratories (Bar Harbor, ME). The animalswere 8 to 12 weeks old at the start of all experiments.During the experiments the animals were housed one per
cage and maintained in a central animal care facility witha 12-hour light/dark cycle. Water and standard rodent lab-oratory chow were supplied ad libitum. The animal care
facilities were maintained by professionals who followedfederal guidelines, and all procedures were approved bythe University of Washington and ZymoGenetics AnimalCare Committees.
The C57BL/KsJ-db/db mice were chosen becausethey exhibit a series of characteristics similar to those ofhuman adult onset diabetes. The metabolic abnormalitiesresult from a single autosomal recessive mutation on
chromosome 4 (db+).4 Only the homozygous (db+/db+) animals develop diabetes while the heterozygous(db+/+m) littermates show no signs of diabetes or obe-sity. The heterozygotes were used as controls for com-parison with the diabetic homozygotes.
Serum glucose values were obtained in several of theexperiments after anesthetization and before the animalswere killed. Blood was obtained from the retro-orbitalplexus using heparinized capillary tubes. Serum was ana-
lyzed for glucose content using a Beckman Glucose Au-toanalyzer (Beckman Instruments, Towson, MD).
Insulin levels were obtained for some of the mice inheparinized blood samples. The serum was collected, fro-zen at -20° C, and later analyzed for insulin levels byradioimmunoassay.4
Wounding
The animals were anesthetized with a mixture of ketamine(110 mg/kg, Vetalar®, Parke Davis, Morris Plains, NJ) andxylazine (7 mg/kg, Rompun®, Miles Laboratories, Shaw-
nee, KA). The hair on the back was clipped, and the skinwashed with povidone-iodine solution and wiped withsterile water. A template was used to mark a 1.5 X 1.5cm square on the midback and a full-thickness woundcorresponding to the template was made by excising theskin and panniculus carnosus. Tincture Benzoin Com-pound (Paddock Laboratories, Minneapolis, MN) was ap-plied outside the perimeter of the wound and the semiper-meable polyurethane dressing OpSite® (Smith andNephew, Massillon, OH) was placed over the wound andsealed at the edges by the benzoin. The growth factormixture was applied by injecting it through the OpSite witha 27-gauge needle and allowing it to spread over thewound bed. The animals were given 1 ml of subcutane-ous Ringer's solution at completion of the surgical proce-dure.
Growth Factors
Human recombinant PDGF-BB was produced in a yeastexpression system similar to that previously described.45This system secretes the rPDGF-BB into the yeast growthmedium from.which it is purified by ion exchange chroma-tography. The rPDGF-BB used in these studies is morethan 95% pure and was quantitated by amino acid analy-sis. The full-length 155 amino acid form of human rbFGFwas produced by cytoplasmic expression in yeast. TherbFGF was purified from the yeast cytoplasm by acid ex-traction followed by heparin-sepharose chromatogra-phy46 to more than 95% purity and quantitated by aminoacid analysis. The biologic activity of each factor wasmeasured as the ability to stimulate 3H-thymidine incorpo-ration by Swiss 3T3 cells in a mitogenesis assay.47 Valueswere assigned by comparison to standards with knownactivity.
The BB homodimer of rPDGF-BB was used in dosesof 1 and 10 ug/wound/day. The doses used for rbFGFwere 0.4 and 1 isg/day. These doses were chosen basedon the responses described in previous reports36.37 39 andpreliminary dose-response studies. The growth factorswere mixed in a vehicle of 5% polyethylene glycol (PEG)(Carbowax PEG 8000, USP grade, Union Carbide, Dan-bury, CT) in phosphate-buffered saline, lyophilized, andstored at -80° C until the day of use. Mitogenic activityof the preparations was measured after lyophilization.Typically, approximately 20% of the activity was lost dur-ing the processing. The doses referred to in the text arethe prelyophilization values. The vials were prepared andcoded by laboratory personnel who were not involvedwith the histologic evaluation of the wounds. Each animalwas randomly assigned to a coded and blinded treatmentregimen. For each treatment, 0.1 cc of the reconstitutedtreatment mixture (growth factor or vehicle) was injectedthrough the OpSite and over the wound bed. For most of

PDGF and FGF Stimulate Wound Healing 1237AJPJune 1990, Vol. 136, No. 6
the experiments the growth factor was applied daily for 5days starting immediately after wounding. In a few experi-ments, the treatments were given daily for 10 or 14 days.Endotoxin levels were determined in each preparation ofPEG, rPDGF-BB, and rbFGF and were always less than10 pg/ml (QCL 1000. Quantitative Chromogenic Limu-lus Amebocyte Lysate test, Whittaker Bioproducts, Walk-ersville, MD).
Wound Analysis
The animals were weighed and the wounds werechecked 3 to 5 times each week. Wounds were consid-ered closed if moist granulation tissue was no longer ap-parent and the wound appeared covered with epithelium.Histologic analysis confirmed the presence of completere-epithelialization under these circumstances.
The edge of the wound was traced onto a glass micro-scope slide and the wound area was determined by pla-nimetry using ImageMeasure® (Microscience, Inc., Fed-eral Way, WA) or Optimas®) (Bioscan, Edmonds, WA).The trace taken immediately after wounding was used asthe reference or original area and all further areas wererecorded as the percentage of the original area. When theanimals were killed, the extent of re-epithelialization wasdetermined by inspection as the border between themoist central, open wound and the dry surroundings. Inthe rare cases in which a scab was present at the end ofthe experiment, the edge of the scab was considered theedge of the re-epithelialization (a conservative interpreta-tion). Wound closure is reported as the percentageclosed and calculated as:
% Closed = [(Area on Day 0
- Open Area on Final Day)/Area on Day 0] X 100
After the final tracing, the entire wound, including amargin of approximately 5 mm of unwounded skin, wasexcised down to the fascia and removed. The wound wasdivided in half and placed in methanol Carnoy's solutionfor histologic analysis. Each histologic specimen was em-bedded in paraffin so that the mid-portion of the woundwas cut in 5-iA sections. The slides were stained with he-matoxylin and eosin or Masson's trichrome for the analy-ses. Each slide was given a histologic score ranging from1 to 12, with 1 corresponding to no healing and 12 corre-sponding to a completely re-epithelialized wound (Table1). The scoring was based on the degree of cellular inva-sion, granulation tissue formation, vascularity, and re-epi-thelialization. The histologic score was assigned sepa-rately by two of the investigators and averaged for analy-sis. Typically the scores of the evaluators were within 1 to2 units of one another. The wounds were also ranked onthe basis of histology from the least healed to the most
Table 1. Scoring ofHistology Sections
Score Criteria
1-3 None to minimal cell accumulation. No granulationtissue or epithelial travel.
4-6 Thin, immature granulation that is dominated byinflammatory cells but has few fibroblasts,capillaries or collagen deposition. Minimalepithelial migration.
7-9 Moderately thick granulation tissue, can range frombeing dominated by inflammatory cells to morefibroblasts and collagen deposition. Extensiveneovascularization. Epithelium can range fromminimal to moderate migration.
10-12 Thick, vascular granulation tissue dominated byfibroblasts and extensive collagen deposition.Epithelium partially to completely covering thewound.
healed for statistical comparisons of the different groups.The code describing each animal's treatment was brokenafter the scoring and ranking were completed by all ob-servers.
Data Analysis
Values are expressed as the mean ± standard error ofthe mean. The Student's t-test was used for comparisonsof biochemical data between the control and diabetic ani-mals. Statistical analysis of the histology rankings wasperformed using the Kruskal-Wallis test,' with individualcomparisons performed by the Dunn's procedure (P< 0.05)49 The data comparing the percentages of woundclosure were compared by analysis of variance (ANOVA)and individual comparisons were performed by Tukey'sprocedure (P < 0.05).5° The analyses were performed us-ing the StatView Il® statistical software package (AbacusConcepts, Inc., Berkeley, CA).
Results
Impaired Wound Healing in theDiabetic Mouse
The C57BL/KsJ-db/db (db/db) mice demonstrated dia-betic characteristics documented in previous reports.4'53The diabetic mice were obese, weighing 40 to 50 g, incontrast to their nondiabetic littermates that weighed 25to 32 g. The diabetics were markedly hyperglycemic withaverage glucose levels of 927 + 35 mg/dl (n = 52) com-pared with 205 ± 8 mg/dl (n = 27) for the nondiabeticanimals (P < 0.0001 by Student's t-test). The hyperglyce-mia produced classic signs of diabetes including polydip-sia, polyuria, and glycosuria. The diabetics had approxi-mately 2.5 times the insulin levels of their nondiabetic lit-termates (diabetic, 48.5 ± 11.0 vs. nondiabetic, 19.7
1238 Greenhalgh et alAJPJune 1990, Vol. 136, No. 6
120
r
c
c0
C._
00R
100
80
60
40
20
0
0 1 0 20 30
Days after Wounding
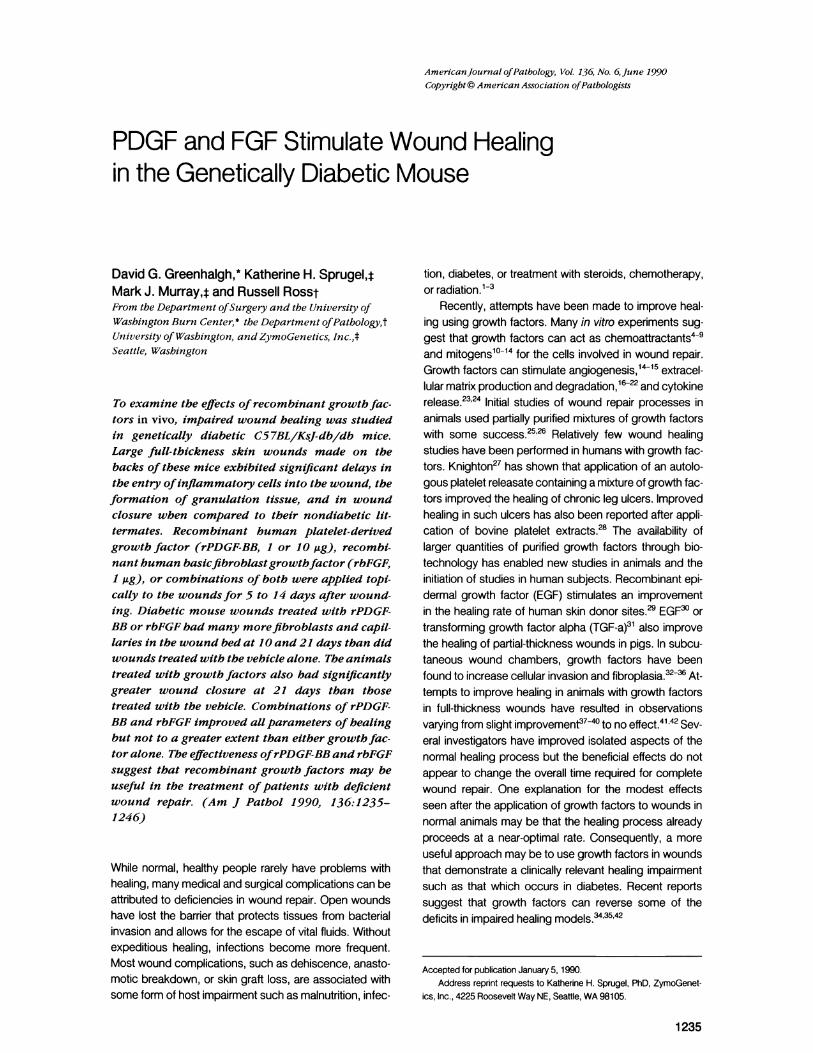
Figure 1. Time course of wound closure in notidiabetic mice. Wound areas were measured immwounding and at various times during the he,Values are presented as percentage of original+ SE, n = 5 to 19), calculated as described in Me
± 3.1 gunits/ml, with n = 15 for both group,
by Student's t-test).Full-thickness wounds were created in t
the anesthetized animals and the exposed -
mediately covered with the semipermeable,dressing OpSite. Both the diabetic and non
mals tolerated the wounding procedure withoNeither of the groups had significant changessumption or weight loss after wounding. Thmained in place until the wound healed. Wevaluated by gross inspection and the edgewound was traced through the OpSite tiwound areas at several time points. On thesis, animals were killed, a final wound area
performed after removal of the OpSite, and thof the wound was preserved for histologic ev
Initial experiments compared the differenchealing between the diabetic and nondiabEThe wounds were inspected and their areas n6 weeks. Histologic sections were obtainedomly chosen animals from both groups atpoints after wounding. The wounds of the nor
imals closed completely within 10 to 16 daysto 6 weeks was required for closure to occLbetic animals. After a 2- to 3-day lag, thewounds rapidly contracted to 10% to 20% ofarea within 10 days (Figure 1). The remainingof the original area healed by re-epithelializatigranulation tissue. Wounds created in the i
mals did not show any gross evidence of hefirst 2 to 3 weeks. At as late as 21 days thmained unchanged from their appearance
after wounding. Gradually the wounds de\thema and granulation tissue. The diabetic wtually closed but rarely before 4 weeks, anc
examined had a chronic wound at 90 days.the wounds measured at various times after
the significant delay in diabetic wound closure when com-Nondiabetic pared to those of the nondiabetic animals (Figure 1).Diabetic Histologic evaluation of wounds at various days after
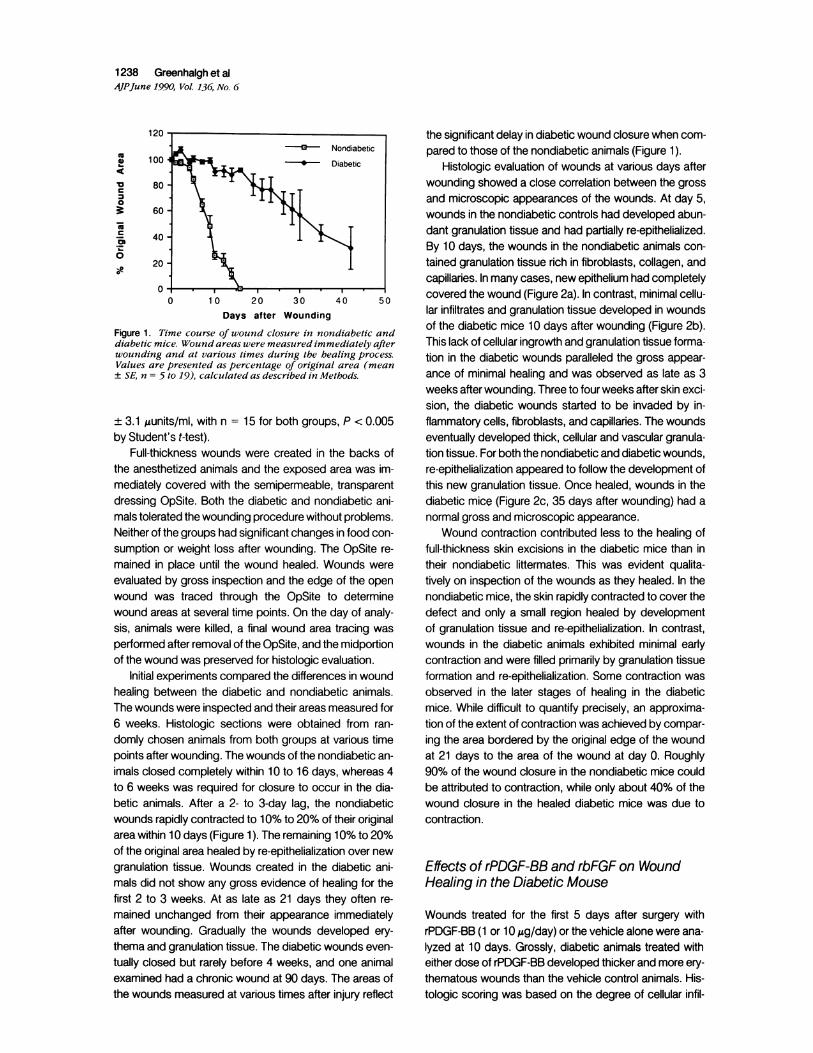
wounding showed a close correlation between the grossand microscopic appearances of the wounds. At day 5,wounds in the nondiabetic controls had developed abun-dant granulation tissue and had partially re-epithelialized.By 10 days, the wounds in the nondiabetic animals con-tained granulation tissue rich in fibroblasts, collagen, andcapillaries. In many cases, new epithelium had completely
I5 O covered the wound (Figure 2a). In contrast, minimal cellu-40 50
lar infiltrates and granulation tissue developed in woundsof the diabetic mice 10 days after wounding (Figure 2b).ildiabetic and
tediately after This lack of cellular ingrowth and granulation tissue forma-aling process. tion in the diabetic wounds paralleled the gross appear-Iarea (meanthods. ance of minimal healing and was observed as late as 3
weeks after wounding. Three to four weeks after skin exci-sion, the diabetic wounds started to be invaded by in-
s, P <0.005 flammatory cells, fibroblasts, and capillaries. The woundseventually developed thick, cellular and vascular granula-
the backs of tion tissue. For both the nondiabetic and diabetic wounds,area was im- re-epithelialization appeared to follow the development of, transparent this new granulation tissue. Once healed, wounds in thediabetic ani- diabetic mice (Figure 2c, 35 days after wounding) had atut problems. normal gross and microscopic appearance., in food con- Wound contraction contributed less to the healing ofe OpSite re- full-thickness skin excisions in the diabetic mice than in/ounds were their nondiabetic littermates. This was evident qualita-of the open tively on inspection of the wounds as they healed. In the
o determine nondiabetic mice, the skin rapidly contracted to cover theday of analy- defect and only a small region healed by developmenttracing was of granulation tissue and re-epithelialization. In contrast,e midportion wounds in the diabetic animals exhibited minimal early(aluation. contraction and were filled primarily by granulation tissue,es in wound formation and re-epithelialization. Some contraction wasetic animals. observed in the later stages of healing in the diabeticneasured for mice. While difficult to quantify precisely, an approxima-Xd from ran- tion of the extent of contraction was achieved by compar-various time ing the area bordered by the original edge of the woundndiabetic an- at 21 days to the area of the wound at day 0. Roughlys, whereas 4 90% of the wound closure in the nondiabetic mice couldur in the dia- be attributed to contraction, while only about 40% of thenondiabetic wound closure in the healed diabetic mice was due totheir original contraction.10% to 20%ion over newdiabetic ani- Effects of rPDGF-BB and rbFGF on Wound,aling for the Healing in the Diabetic Mouserey often re-immediately Wounds treated for the first 5 days after surgery withveloped ery- rPDGF-BB (1 or 10 leg/day) or the vehicle alone were ana-rounds even- lyzed at 10 days. Grossly, diabetic animals treated withone animal either dose of rPDGF-BB developed thicker and more ery-
The areas of thematous wounds than the vehicle control animals. His-injury reflect tologic scoring was based on the degree of cellular infil-
PDGF and FGF Stimulate Wound Healing 1239AJPJune 1990, Vol. 136, No. 6
tration, granulation tissue formation, and re-epithelializa-tion (Table 1). Wounds treated with rPDGF-BB had higheraverage histologic scores (Table 2), which was consistent
Table 2. The Effects of5 Days ofrPDGF-BB Treatmenton Diabetic Wounds Evaluated at 10 Days
Histologic % WoundTreatment* score t closure t N
Vehicle 4.3 ± 0.4 35.8 ± 2.9 201 Ag rPDGF-BB 6.7 ± 0.6§ 46.3 ± 5.6 131Oug rPDGF-BB 7.9 ± 0.3§ 39.0 ± 3.3 8
* Full-thickness skin wounds on diabetic mice were treated with vehi-cle or rPDGF-BB (1 or 10 ug/day) for 5 days.
t Histology scores were assigned to each coded specimen by twoinvestigators using the scale in Table 1. Values are expressed as mean±SEM.
t Values are expressed as mean ± SEM. There were no significantdifferences between groups.
§ P < 0.05 when compared to vehicle treatment by ranking the histo-logic specimens and determining statistical significance using theKruskal-Wallis test with individual comparisons performed using Dunn'sprocedure.
Figure 2. Pbotomicrographs of the midsections of woundsstained withhematoxylint/eosin (original magnigication 33X).a: Nondiabetic wound, day 10: The wound has been exten-sively infiltrated witb inflammatory cells, fibroblasts and bassignificant collagen deposition. Complete reepithelializationindicates that this wound has closed. b: Diabetic wound, day10: In contrast to nondiabetic wounds, very little cellular in-filtration or granulation tissue is seen above the subcutaneousfat. c: Diabetic wound, day 35: Thick, vascular granulationtissue bas been developed in the wound bed. The wound hasclosed. Note that microscopically, this wound appears similarin appearance to the day 10 nondiabetic wounds whichhealed .3 to 4 weeks earlier.
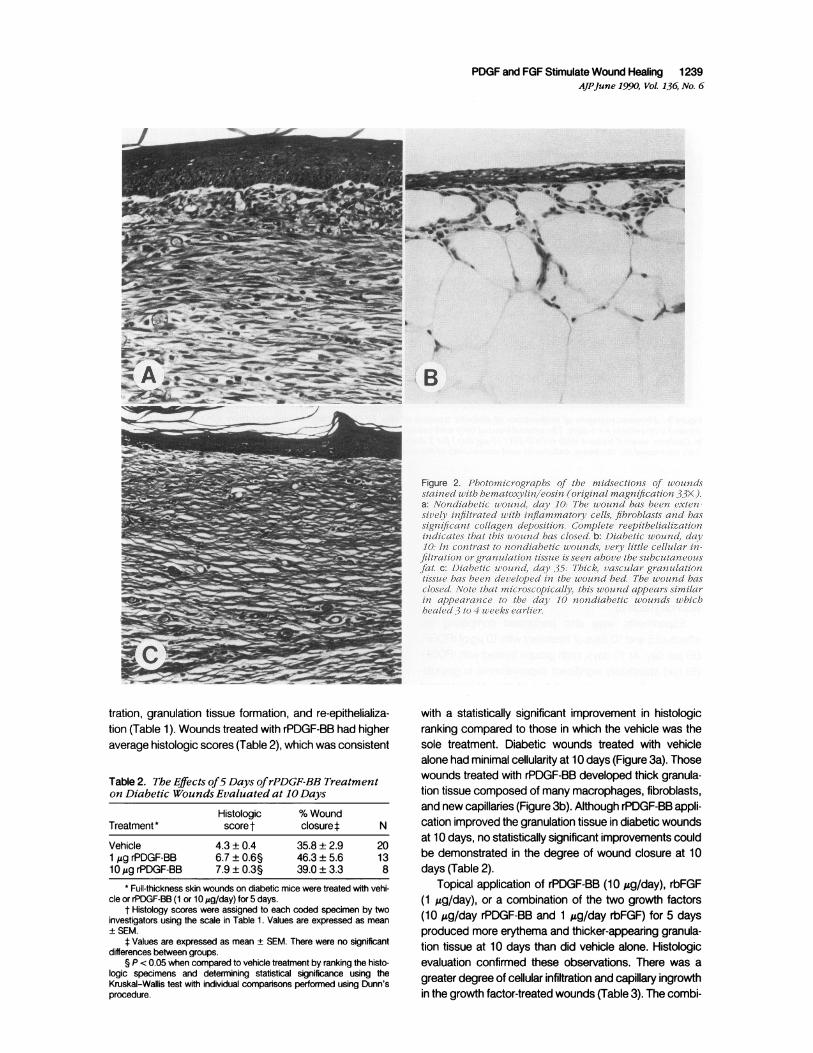
with a statistically significant improvement in histologicranking compared to those in which the vehicle was thesole treatment. Diabetic wounds treated with vehiclealone had minimal cellularity at 10 days (Figure 3a). Thosewounds treated with rPDGF-BB developed thick granula-tion tissue composed of many macrophages, fibroblasts,and new capillaries (Figure 3b). Although rPDGF-BB appli-cation improved the granulation tissue in diabetic woundsat 10 days, no statistically significant improvements couldbe demonstrated in the degree of wound closure at 10days (Table 2).
Topical application of rPDGF-BB (10 pg/day), rbFGF(1 pg/day), or a combination of the two growth factors(10 pg/day rPDGF-BB and 1 pg/day rbFGF) for 5 daysproduced more erythema and thicker-appearing granula-tion tissue at 10 days than did vehicle alone. Histologicevaluation confirmed these observations. There was agreater degree of cellular infiltration and capillary ingrowthin the growth factor-treated wounds (Table 3). The combi-
1240 Greenhalgh et alAJPJune 1990, Vol. 136, No. 6
'A r , ,,~~~~ df-A ~ ~~~~~~~~~~~~~~~~~-
Figure 3. Photomicrographs of midsections of diabetic wounds at day 10 (H&E, original magnification 33X). a: Diabetic woundtreated with vehiclefor5 days: The wound treated only with vehicle has minimal cellular invasion andgranulation tissueformation.b: Diabetic wound treated with rPDGF-BB (10 jg/day)for 5 days: In contrast to vehicle treatment, application ofrPDGF-BB mark-edlj' increased the thickness, cellularity and vascularity ofthe new granulation tissue.
nation of rPDGF-BB and rbFGF did not improve granula-tion tissue formation beyond that of the individual growthfactors. Despite the clear differences in gross and histo-logic appearance in the growth factor-treated animals,there were no statistically significant improvements inwound closure in the growth factor-treated animals whencompared with vehicle-treated animals for 10-daywounds (Table 3).
Experiments were also performed comparing theeffects of 5 and 10 days of treatment with 10 gg of rPDGF-BB per day. At 10 days, both groups treated with rPDGF-BB had statistically significant improvements in granula-tion tissue formation beyond that of the vehicle-treatedwounds (Table 4). Animals treated with rPDGF-BB for 10
Table 3. The Effects of5 Days ofTreatment withrPDGF-BB and/or rbFGFon Diabetic WoundsEvaluated at 10 Days
Histologic % WoundTreatment score t closure t N
Vehicle 2.7 ± 0.3 27.3 ± 3.1 51O,ug rPDGF-BB 6.2 ± 1.0 41.5 ± 4.8 61 jg rbFGF 7.4 ± 0.5§ 48.5 ± 6.5 5rPDGF-BB/rbFGF 7.8 ± 0.7§ 48.3 ± 7.0 6
* Full-thickness skin wounds on diabetic mice were treated with vehi-cle, rPDGF-BB (10 jg/day), rbFGF (1 jig/day), or a combination of bothfor 5 days.
t Histology scores were assigned to each coded specimen by twoinvestigators using the scale in Table 1. Values are expressed as meanSEM.
t Values are expressed as mean ± SEM. There were no significantdifferences between groups.
§ P < 0.05 when compared to vehicle treatment by ranking the histo-logic specimens and determining statistical significance using theKruskal-Wallis test with individual comparisons performed using Dunn'sprocedure.
days exhibited a trend toward a decrease in their woundareas when compared to vehicle-treated mice, but thisdifference lacked statistical significance (Table 4).
By gross observation, many of the wounds developeda distinct red color at 4 to 5 days. After breaking the codewe found that only those animals treated with growth fac-tors developed this erythema. To try to correlate the grossappearance of the wounds with histologic findings,wounds were treated with vehicle or rPDGF-BB (10 ,ug/day) for up to 5 days and animals werer killed at 3, 5, or 7days. At 3 days there were no differences between thetwo treatment groups. By 5 days there were more in-
Table 4. The Effects of5 or 10 Days ofTreatment withrPDGF-BB (10Ag/day) on Diabetic WoundsEvaluated at 10 Days
Histologic % WoundTreatment* score t closure N
Vehicle: 5 days 3.5 ± 0.3 24.4 ± 4.2 6Vehicle: 10 days 4.5 ± 0.5 24.9 ± 4.9 4rPDGF-BB: 5 days 7.3 ± 0.5§ 34.6 ± 3.4 10rPDGF-BB: 10 days 9.1 ± 0.1§1 51.9 ± 2.7 5
* Full-thickness skin wounds on diabetic mice were treated with vehi-cle or rPDGF-BB (10 jig/day) for 5 or 10 days.
t Histology scores were assigned to each coded specimen by twoinvestigators using the scale in Table 1. Values are expressed as mean± SEM.
t Values are expressed as mean ± SEM. There were no significantdifferences between groups.
§ P < 0.05 when compared to vehicle treatment for 5 days by rankingthe histologic specimens and determining statistical significance using theKruskal-Wallis test with individual comparisons performed using Dunn'sprocedure.
I P < 0.05 when compared to vehicle treatment for 10 days by rankingthe histologic specimens and determining statistical significance using theKruskal-Wallis test with individual comparisons performed using Dunn'sprocedure.
PDGF and FGF Stimulate Wound Healing 1241AJPJune 1990, Vol. 136, No. 6
a) Vehicle Treatment:
Day 0
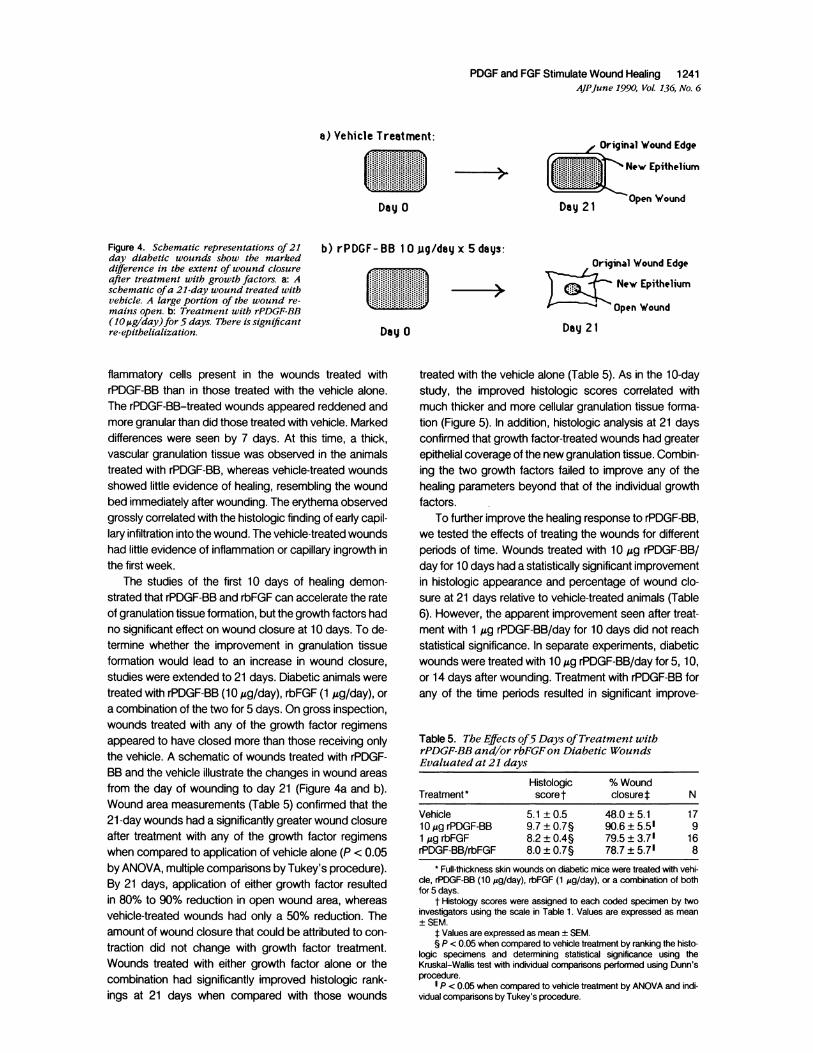
Figure 4. Schematic representations of21 b) rPDGF- BB 1 0 jig/day x 5 days:day diabetic wounds show the markeddifference in the extent of wound closureafter treatment with growth factors. a: A
schematic ofa 21-day wound treated with
vehicle. A large portion of the wound re-
mains open. b: Treatment with rPDGF-BB(10 ug/day)for 5 days. There is significantre-epithelialization. Day 0
Original Wound Edge
New Epithelium
Day 21 Open Wound
Original Wound Edge
New Epithelium
Open Wound
Day 21
flammatory cells present in the wounds treated withrPDGF-BB than in those treated with the vehicle alone.The rPDGF-BB-treated wounds appeared reddened andmore granular than did those treated with vehicle. Markeddifferences were seen by 7 days. At this time, a thick,vascular granulation tissue was observed in the animalstreated with rPDGF-BB, whereas vehicle-treated woundsshowed little evidence of healing, resembling the woundbed immediately after wounding. The erythema observedgrossly correlated with the histologic finding of early capil-lary infiltration into the wound. The vehicle-treated woundshad little evidence of inflammation or capillary ingrowth inthe first week.
The studies of the first 10 days of healing demon-strated that rPDGF-BB and rbFGF can accelerate the rateof granulation tissue formation, but the growth factors hadno significant effect on wound closure at 10 days. To de-termine whether the improvement in granulation tissueformation would lead to an increase in wound closure,studies were extended to 21 days. Diabetic animals weretreated with rPDGF-BB (10 Ag/day), rbFGF (1 Mg/day), or
a combination of the two for 5 days. On gross inspection,wounds treated with any of the growth factor regimensappeared to have closed more than those receiving onlythe vehicle. A schematic of wounds treated with rPDGF-BB and the vehicle illustrate the changes in wound areas
from the day of wounding to day 21 (Figure 4a and b).Wound area measurements (Table 5) confirmed that the21-day wounds had a significantly greater wound closureafter treatment with any of the growth factor regimenswhen compared to application of vehicle alone (P < 0.05by ANOVA, multiple comparisons by Tukey's procedure).By 21 days, application of either growth factor resultedin 80% to 90% reduction in open wound area, whereasvehicle-treated wounds had only a 50% reduction. Theamount of wound closure that could be attributed to con-
traction did not change with growth factor treatment.Wounds treated with either growth factor alone or thecombination had significantly improved histologic rank-ings at 21 days when compared with those wounds
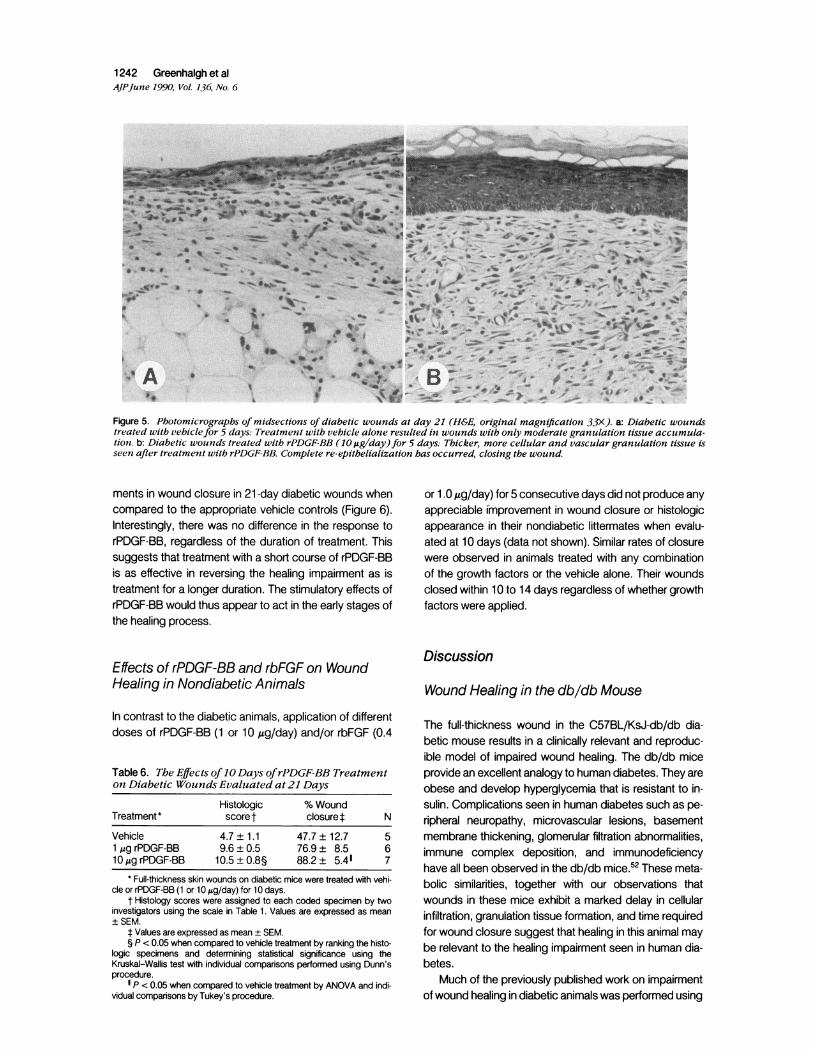
treated with the vehicle alone (Table 5). As in the 1 0-daystudy, the improved histologic scores correlated withmuch thicker and more cellular granulation tissue forma-tion (Figure 5). In addition, histologic analysis at 21 daysconfirmed that growth factor-treated wounds had greaterepithelial coverage of the new granulation tissue. Combin-ing the two growth factors failed to improve any of thehealing parameters beyond that of the individual growthfactors.
To further improve the healing response to rPDGF-BB,we tested the effects of treating the wounds for differentperiods of time. Wounds treated with 10 ,g rPDGF-BB/day for 10 days had a statistically significant improvementin histologic appearance and percentage of wound clo-sure at 21 days relative to vehicle-treated animals (Table6). However, the apparent improvement seen after treat-ment with 1 ,ug rPDGF-BB/day for 10 days did not reachstatistical significance. In separate experiments, diabeticwounds were treated with 10 Mg rPDGF-BB/day for 5, 10,or 14 days after wounding. Treatment with rPDGF-BB forany of the time periods resulted in significant improve-
Table5. The Effects of5 Days ofTreatment withrPDGF-BB and/or rbFGFon Diabetic WoundsEvaluated at 21 days
Histologic % WoundTreatment* score t closuret N
Vehicle 5.1 ±0.5 48.0 ± 5.1 1710O,g rPDGF-BB 9.7 ± 0.7§ 90.6± 5.51 91 gg rbFGF 8.2 ± 0.4§ 79.5 ± 3.71 16rPDGF-BB/rbFGF 8.0 ± 0.7§ 78.7 ± 5.71 8
* Full-thickness skin wounds on diabetic mice were treated with vehi-cle, rPDGF-BB (10 jug/day), rbFGF (1 jug/day), or a combination of bothfor 5 days.
t Histology scores were assigned to each coded specimen by twoinvestigators using the scale in Table 1. Values are expressed as mean+SEM.
t Values are expressed as mean ± SEM.§ P < 0.05 when compared to vehicle treatment by ranking the histo-
logic specimens and determining statistical significance using theKruskal-Wallis test with individual comparisons performed using Dunn'sprocedure.
I P < 0.05 when compared to vehicle treatment by ANOVA and indi-vidual comparisons by Tukey's procedure.
1242 Greenhalgh et alAJPJune 1990, Vol. 136, No. 6
*j~ ; w uv. wS y ab-;75 ~-W U2S - ;F-
,Of~B-w- --V.*A5 k:w _->_*a; ¢arv^.joo*~~~o
Figure 5. Photomicrographs of midsections of diabetic wounds at day 21 (H&E, original magnification 33X). a: Diabetic woundstreated with vehiclefor 5 days: Treatment with vehicle alone resulted in wounds with only moderate granulation tissue accumula-tion. b: Diabetic wounds treated with rPDGF-BB (10 Ag/day)for 5 days: Thicker, more cellular and vascular granulation tissue isseen after treatment with rPDGF-BB. Complete re-epithelialization has occurred, closing the wound.
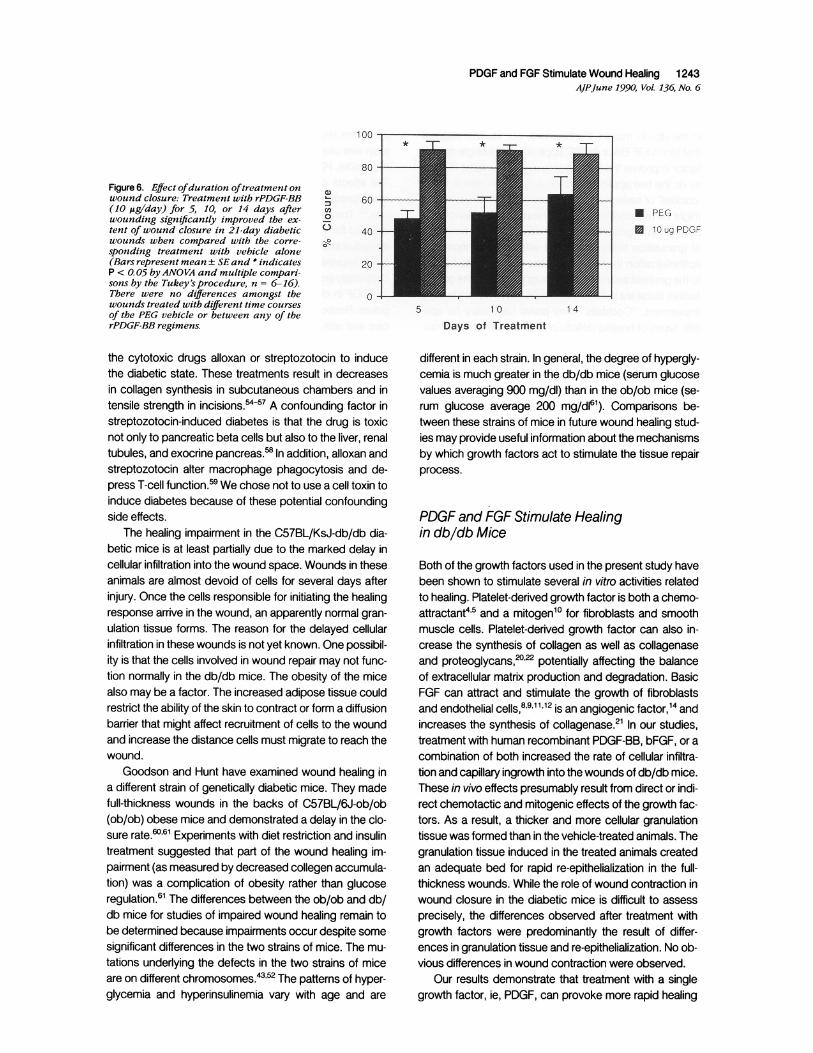
ments in wound closure in 21-day diabetic wounds whencompared to the appropriate vehicle controls (Figure 6).Interestingly, there was no difference in the response torPDGF-BB, regardless of the duration of treatment. Thissuggests that treatment with a short course of rPDGF-BBis as effective in reversing the healing impairment as istreatment for a longer duration. The stimulatory effects ofrPDGF-BB would thus appear to act in the early stages ofthe healing process.
Effects of rPDGF-BB and rbFGF on WoundHealing in Nondiabetic Animals
In contrast to the diabetic animals, application of differentdoses of rPDGF-BB (1 or 10 ,g/day) and/or rbFGF (0.4
Table 6. The Effects of10 Days ofrPDGF-BB Treatmenton Diabetic Wounds Evaluated at 21 Days
Histologic % WoundTreatment* scoret closuret N
Vehicle 4.7 ± 1.1 47.7 ± 12.7 51 jg rPDGF-BB 9.6 ± 0.5 76.9 ± 8.5 610,g rPDGF-BB 10.5 ± 0.8§ 88.2 ± 5.41 7
* Full-thickness skin wounds on diabetic mice were treated with vehi-cle or rPDGF-BB (1 or 10 jg/day) for 10 days.
t Histology scores were assigned to each coded specimen by twoinvestigators using the scale in Table 1. Values are expressed as mean+SEM.
t Values are expressed as mean ± SEM.§ P < 0.05 when compared to vehicle treatment by ranking the histo-
logic specimens and determining statistical significance using theKruskal-Wallis test with individual comparisons performed using Dunn'sprocedure.
I P < 0.05 when compared to vehicle treatment by ANOVA and indi-vidual comparisons by Tukey's procedure.
or 1.0 ,ug/day) for 5 consecutive days did not produce anyappreciable improvement in wound closure or histologicappearance in their nondiabetic liftermates when evalu-ated at 10 days (data not shown). Similar rates of closurewere observed in animals treated with any combinationof the growth factors or the vehicle alone. Their woundsclosed within 10 to 14 days regardless of whether growthfactors were applied.
Discussion
Wound Healing in the db/db Mouse
The full-thickness wound in the C57BL/KsJ-db/db dia-betic mouse results in a clinically relevant and reproduc-ible model of impaired wound healing. The db/db miceprovide an excellent analogy to human diabetes. They areobese and develop hyperglycemia that is resistant to in-sulin. Complications seen in human diabetes such as pe-ripheral neuropathy, microvascular lesions, basementmembrane thickening, glomerular filtration abnormalities,immune complex deposition, and immunodeficiencyhave all been observed in the db/db mice.52 These meta-bolic similarities, together with our observations thatwounds in these mice exhibit a marked delay in cellularinfiltration, granulation tissue formation, and time requiredfor wound closure suggest that healing in this animal maybe relevant to the healing impairment seen in human dia-betes.
Much of the previously published work on impairmentof wound healing in diabetic animals was performed using
PDGF and FGF Stimulate Wound Healing 1243AJPJune 1990, Vol. 136, No. 6
100
80 -
Figure 6. Effect ofduration oftreatment onwound closure: Treatment with rPDGF-BB ; 60(10 fig/day) for 5, 10, or 14 days after enwounding significantly improved the ex- °tent of wound closure in 21-day diabetic C 40wounds when compared with the corre-sponding treatment with vehicle alone(Bars represent mean ± SEand * indicates 20P < O. 05 byANOVA and multiple compari-sons by the Tukey's procedure, n = 6-16).There were no differences amongst the 0wounds treated with different time coursesof the PEG vehicle or between any of therPDGF-BB regimens.
the cytotoxic drugs alloxan or streptozotocin to inducethe diabetic state. These treatments result in decreasesin collagen synthesis in subcutaneous chambers and intensile strength in incisions.-5457 A confounding factor instreptozotocin-induced diabetes is that the drug is toxicnot only to pancreatic beta cells but also to the liver, renaltubules, and exocrine pancreas.58 In addition, alloxan andstreptozotocin alter macrophage phagocytosis and de-press T-cell function.59 We chose not to use a cell toxin toinduce diabetes because of these potential confoundingside effects.
The healing impairment in the C57BL/KsJ-db/db dia-betic mice is at least partially due to the marked delay incellular infiltration into the wound space. Wounds in theseanimals are almost devoid of cells for several days afterinjury. Once the cells responsible for initiating the healingresponse arrive in the wound, an apparently normal gran-ulation tissue forms. The reason for the delayed cellularinfiltration in these wounds is not yet known. One possibil-ity is that the cells involved in wound repair may not func-tion normally in the db/db mice. The obesity of the micealso may be a factor. The increased adipose tissue couldrestrict the ability of the skin to contract or form a diffusionbarrier that might affect recruitment of cells to the woundand increase the distance cells must migrate to reach thewound.
Goodson and Hunt have examined wound healing ina different strain of genetically diabetic mice. They madefull-thickness wounds in the backs of C57BL/6J-ob/ob(ob/ob) obese mice and demonstrated a delay in the clo-sure rate.60'6' Experiments with diet restriction and insulintreatment suggested that part of the wound healing im-pairment (as measured by decreased collegen accumula-tion) was a complication of obesity rather than glucoseregulation.6' The differences between the ob/ob and db/db mice for studies of impaired wound healing remain tobe determined because impairments occur despite somesignificant differences in the two strains of mice. The mu-tations underlying the defects in the two strains of miceare on different chromosomes.43'52 The patterns of hyper-glycemia and hyperinsulinemia vary with age and are
* _1T * I
5 10
* PEG
* 10 ug PDGF
1 4
Days of Treatment
different in each strain. In general, the degree of hypergly-cemia is much greater in the db/db mice (serum glucosevalues averaging 900 mg/dl) than in the ob/ob mice (se-rum glucose average 200 mg/di6"). Comparisons be-tween these strains of mice in future wound healing stud-ies may provide useful information about the mechanismsby which growth factors act to stimulate the tissue repairprocess.
PDGF and FGF Stimulate Healingin db/db Mice
Both of the growth factors used in the present study havebeen shown to stimulate several in vitro activities relatedto healing. Platelet-derived growth factor is both a chemo-attractant4-5 and a mitogen'0 for fibroblasts and smoothmuscle cells. Platelet-derived growth factor can also in-crease the synthesis of collagen as well as collagenaseand proteoglycans,2022 potentially affecting the balanceof extracellular matrix production and degradation. BasicFGF can attract and stimulate the growth of fibroblastsand endothelial cells,8 9 '1 2is an angiogenic factor,'4 andincreases the synthesis of collagenase.2' In our studies,treatment with human recombinant PDGF-BB, bFGF, or acombination of both increased the rate of cellular infiltra-tion and capillary ingrowth into the wounds of db/db mice.These in vivo effects presumably result from direct or indi-rect chemotactic and mitogenic effects of the growth fac-tors. As a result, a thicker and more cellular granulationtissue was formed than in the vehicle-treated animals. Thegranulation tissue induced in the treated animals createdan adequate bed for rapid re-epithelialization in the full-thickness wounds. While the role of wound contraction inwound closure in the diabetic mice is difficult to assessprecisely, the differences observed after treatment withgrowth factors were predominantly the result of differ-ences in granulation tissue and re-epithelialization. No ob-vious differences in wound contraction were observed.
Our results demonstrate that treatment with a singlegrowth factor, ie, PDGF, can provoke more rapid healing
I~~~~~~~~~~~~~~~~~

1244 Greenhalgh et alAJPJune 1990, Vol. 136, No. 6
in the db/db mouse. Furthermore, our studies suggestthat for rPDGF-BB or rbFGF, application of a single growthfactor improves the healing process to the same degreeas do the two applied together. A common view is that a'cocktail' of several growth factors with different activitiesmight be required for complete healing. For instance, ap-plication of a growth factor that stimulates the formationof granulation tissue combined with one that increasesepithelialization might be expected to accelerate healingto the greatest extent. Our data suggest that some growthfactors alone are sufficient to completely reverse a healingimpairment. "Cocktails" may prove necessary for spe-cific types of healing deficits or may be useful in optimiz-ing healing responses, but in the db/db mouse a benefi-cial response can clearly be achieved with a single factor.Similar in vivo responses to growth factors that have adifferent spectrum of in vitro activities might be explainedif each factor were to initiate or affect a common pathwayleading to healing. Further understanding of the mecha-nism of healing impairment in the db/db mouse and howgrowth factors reverse this defect may aid in understand-ing clinical problems of healing in human diabetes.
Application of rPDGF-BB or bFGF for a relatively briefperiod (5 days) had the same effect as did applicationfor 10 or 14 days. Apparently chemotactic and mitogenicstimulation by PDGF at the early stages of healing triggersthe repair process, allowing a return to a more normal rate.Extending the growth factor treatment beyond this earlytime provides no additional improvement of healing. As acorollary, this finding suggests that in the db/db mice thehealing deficit is related to the early, cellular phase ofwound repair. Once the cells arrive in the wound, healingmay proceed without additional significant delay.
While rbFGF appeared to be more effective at a lowerdose than rPDGF-BB in these experiments, we are cau-tious about interpreting this as a difference in potency be-tween the factors. Rigorous dose-response studies havenot been performed with these growth factors in thismodel. The doses used were based on reports from otherlaboratories373.40,4l and our own preliminary dose-re-sponse studies. In addition, the pharmacokinetics of thefactors in the wound space are not known. Differentialbinding to extracellular matrix components or differentsusceptibility to degradation could affect the concentra-tion of active growth factor available to stimulate a re-sponse. PDGF and bFGF, with different molecularweights, isoelectric points, and binding proteins probablyhave different pharmacokinetics in the wounds.
Other investigators have examined the effects ofgrowth factors in different impaired wound healingmodels. In two animal models, conflicting results havebeen reported when looking at changes in cellularity andcollagen accumulation in subcutaneous chambers. Whenthe chemotherapeutic agent doxorubicin was used to im-pair granulation tissue accumulation, PDGF did not im-
prove the response, but TGF-f did.' When streptozo-tocin was used to impair healing in a subcutaneous cham-ber model, PDGF restored responses to normal levels.'The effects of TGF-/3 and PDGF have been studied inmethylprednisolone-impaired healing of linear incisions inrats.6' Transforming growth factor ,3 but not PDGF in-creased the breaking strength of incisions in the steroid-treated animals. In our studies, rPDGF-BB was very effec-tive in improving healing in genetically diabetic mice withchronically impaired wounds. The variability of responsesto PDGF in different studies highlights several importantpoints. Responses to a given growth factor vary with spe-cies and with the underlying cause of the healing impair-ment. A single factor may not be effective in improving alltypes of impaired healing. Animals with impaired healinginduced by drugs may be more prone to variation in thedegree of impairment between individuals than animals inwhich the impairment has a genetic basis. There may beadvantages to comparing different factors in the samemodel in the future.
In vitro studies have provided insight into the actionsof growth factors under relatively simple and controlledconditions, suggesting the possible usefulness of suchfactors in tissue repair. In a wound, the interactionsamong the various cell types, the extracellular matrix, andthe many cytokines present are complex and still incom-pletely understood, so the growth factors may not behaveas predicted from in vitro studies. In addition, healthy or-ganisms heal wounds so rapidly that changes in healingcan be hard to measure. Models of impaired wound heal-ing present opportunities to see pronounced growth fac-tor effects and offer the potential to explore the mecha-nisms by which the factors act.
References
1. Schrock TR, Deveney CW, Dunphy JE: Factors contributingto leakage of colonic anastomoses. Ann Surg 1973, 177:513-518
2. Poole GU Jr: Mechanical factors of abdominal closure. Theprevention of fascial dehiscence. Surgery 1985, 97:631-639
3. Irvin GL, Robinson DS, Hubbard S: Operative risks in pa-tients with colorectal cancer. Am Surg 1985, 51:418-422
4. Seppa H, Grotendorst G, Seppa S, Schiffman E, Martin GR:Platelet-derived growth factor is chemotactic for fibroblasts.J Cell Biol 1982, 92:584-588
5. Deuel TF, Senior RM, Huang JS, Griffin GL: Chemotaxis ofmonocytes and neutrophils to platelet-derived growth factor.J Clin Invest 1982, 69:1046-1049
6. Wahl SM, Hunt DA, Wakefield LM, McCartney-Francis N,Wahl LM, Roberts AB, Spom MB: Transforming growth fac-tor beta induces monocyte chemotaxis and growth factorproduction. Proc Natl Acad Sci USA 1987, 84:5788-5792
7. Postlethwaite AE, Keski-Oja MB, Moses HL, Kang AH: Stim-ulation of the chemotactic migration of human fibroblasts by
PDGF and FGF Stimulate Wound Healing 1245AJPJune 1990, Vol. 136, No. 6
transforming growth factor fd. J Exp Med 1987, 165:251-256
8. Terranova VP, DiFlorio R, Lyall RM, Hic S, Friesel R, MaciagT: Human endothelial cells are chemotactic to endothelialcell growth factor and heparin. J Cell Biol 1985, 101:2330-2334
9. Senior RM, Huang SS, Griffin GL, Huang JS: Brain-derivedgrowth factor is a chemoattractant for fibroblasts and astro-glial cells. Biochem Biophys Res Commun 1986,141:67-72
10. Bowen-Pope DF, Ross R: Platelet-derived growth factor. ll.Specific binding to cultured cells. J Biol Chem 1982, 257:5161-5171
11. Roberts AB, Anzano MA, Wakefield LM, Roche NS, SternDF, Sporn MB: Type fd transforming growth factor: A bifunc-tional regulator of cellular growth. Proc Natl Acad Sci USA1985, 82:119-123
12. Bohlen P, Baird A, Esch F, Ling N, Gospodarowicz D: Isola-tion and partial molecular characterization of pituitary fibro-blast growth factor. Proc Natl Acad Sci USA 1984, 81:5364-5368
13. Gospodarowicz D, Moran JS: Mitogenic effect of fibroblastgrowth factor on early passage cultures of human and mu-rine fibroblasts. J Cell Biol 1975, 66:451-457
14. Gospodarowicz D, Neufeld G, Schweigerer L: Molecular andbiological characterization of fibroblast growth factor, an an-giogenic factor which also controls the proliferation anddifferentiation of mesoderm and neuroectoderm derivedcells. Cell Differentiation 1986,19:1-17
15. Schreiber AB, Winkler ME, Derynck R: Transforming growthfactor-a: A more potent angiogenic mediator than epidermalgrowth factor. Science 1986, 232:1250-1253
16. Roberts AB, Sporn MB, Assoian RK, Smith JM, Roche NS,Wakefield LM, Heine Ul, Liotta LA, Falanga V, Kehrl JH,Fauci AS: Transforming growth factor type d3: rapid inductionof fibrosis and angiogenesis in vivo and stimulation of colla-gen formation in vitro. Proc Natl Acad Sci USA 1986, 83:4167-4171
17. Narayanan SA, Page RC: Biosynthesis and regulation oftype V collagen in diploid human fibroblasts. J Biol Chem1983, 58:11694-11699
18. Ignotz RA, Massague J: Transforming growth factor-: stimu-lates the expression of fibronectin and collagen and theirincorporation into the extracellular matrix. J Biol Chem 1986,261: 4337-4345
19. Chua CC, Geiman DE, Keller GH, Ladda RL: Induction ofcollagenase secretion in human fibroblasts by growth pro-moting factors. J Biol Chem 1985, 260:5213-5216
20. Bauer EA, Cooper TW, Huang JS, Altman J, Deuel TF: Stimu-lation of in vitro human skin collagenase expression by plate-let-derived growth factor. Proc Natl Acad Sci USA 1985, 82:4132-4136
21. Edwards DR, Murphy G, Reynolds JJ, Whitham SE, Doch-erty AJP, Angel P, Heath JK: Transforming growth factorbeta modulates the expression of collagenase and metallo-proteinase inhibitor. EMBO J 1987, 6:1899-1904
22. Savage K, Siebert E, Swann D: The effect of platelet-derivedgrowth factor on cell division and glycosaminoglycan syn-thesis by skin and scar fibroblasts. J Invest Dermatol 1987,89:93-99
23. Raines EW, Dower SK, Ross R: Interleukin-1 mitogenic activ-ity for fibroblasts and smooth muscle cells is due to PDGF-AA. Science 1989,243:393-396
24. Hajjar KA, Hajjar DP, Silverstein RL, Nachman RL: Tumornecrosis factor-mediated release of platelet-derived growthfactor from cultured endothelial cells. J Exp Med 1987,166:235-245
25. Knighton DR, Hunt TK, Thakral KK, Goodson WH: Role ofplatelets and fibrin in the healing sequence. An in vivo studyof angiogenesis and collagen synthesis. Ann Surg 1982,196:379-388
26. Buntrock P, Jentzsch KD, Heder G: Stimulation of woundhealing using brain extract with fibroblast growth factor(FGF) activity. Exp Path 1982, 21:46-53
27. Knighton DR, Fiegel VD, Austin LL, Ciresi KF, Butler EL:Classification and treatment of chronic nonhealing wounds.Successful treatment with autologous platelet-derivedwound healing factors (PDWHF). Ann Surg 1986, 204:322-330
28. Carter DM, Balin AK, Gottlieb AB, Eisinger M, Lin A, PrattL, Sherbany A, Caldwell D: Clinical experience with crudepreparations of growth factors in healing of chronic woundsin human subjects. In Barbul A, Pines E, Caldwell M, HuntTK, eds. Growth Factors and Other Aspects of Wound Heal-ing: Biological and Clinical Implications. New York, Alan R.Liss, 1988, pp 303-317
29. Brown GL, Nanney LB, Griffin J, Cramer AB, Yancey JM,Curtsinger LJ 1II, Holtzin L, Schultz GS, Jurkiewicz NJ, LynchJB: Enhancement of wound healing by topical treatmentwith epidermal growth factor. New Engl J Med 1989, 321:76-79
30. Brown GL, Curtsinger L Ill, Brightwell JR, Ackerman DM,Tobin GR, Polk HC Jr, George-Nascimento C, ValenzuelaP, Schultz GS: Enhancement of epidermal regeneration bybiosynthetic epidermal growth factor. J Exp Med 1986,163:1319-1324
31. Schultz GS, White M, Mitchell R, Brown G, Lynch J, TwardzikDR, Todaro GJ: Epithelial wound healing enhanced by trans-forming growth factor-a and vaccinia growth factor. Science1987, 235:350-352
32. Davidson JM, Klagsbrun M, Hill KE, Buckley A, Sullivan R,Brewer PS, Woodward SC: Accelerated wound repair, cellproliferation, and collagen accumulation are produced by acartilage-derived growth factor. J Cell Biol 1985,100:1219-1227
33. Fourtanier AY, Courty J, Muller E, Courtois Y, Prunieras M,Barritault D: Eye-derived growth factor isolated from bovineretina and used for epidermal wound healing in vivo. J InvestDermatol 1986, 87:76-80
34. Lawrence WT, Sporn MB, Gorschboth C, Norton JA, Gro-tendorst GR: The reversal of an Adriamycin® induced heal-ing impairment with chemoattractants and growth factors.Ann Surg 1986, 203:142-147
35. Grotendorst GR, Martin GR, Pencev D, Sodek J, Harvey AK:Stimulation of granulation tissue formation by platelet-de-rived growth factor in normal and diabetic rats. J Clin Invest1985,76:2323-2329
36. Sprugel KH, McPherson JM, Clowes AW, Ross R: Effects ofgrowth factors in vivo. 1. Cell ingrowth into porous subcuta-neous chambers. Am J Pathol 1987, 129:601-613
1246 Greenhalgh et alAJPJune 1990, Vol. 136, No. 6
37. Pierce GF, Mustoe TA, Senior RM, Reed J, Griffin GL, Tho-mason A, Deuel TF: In vivo incisional wound healing aug-mented by platelet-derived growth factor and recombinantc-sis gene homodimeric proteins. J Exp Med 1988, 167:974-987
38. Mustoe TA, Pierce GF, Thomason A, Gramates P, SpornMB, Deuel TF: Accelerated healing of incisional wounds inrats induced by transforming growth factor-3. Science 1987,237:1333-1336
39. McGee GS, Davidson JM, Buckley A, Sommer A, Wood-ward SC, Aquino AM, Barbour R, Demetriou AA: Recombi-nant basic fibroblast growth factor accelerates wound heal-ing. J Surg Res 1988, 45:145-153
40. Lynch SE, Nixon JC, Colvin RB, Antoniades HN: Role ofplatelet-derived growth factor in wound healing: Synergisticeffects with other growth factors. Proc Natl Acad Sci USA1987,84:7696-7700
41. Leitzel K, Cano C, Marks JG Jr, Lipton A: Growth factorsand wound healing in the hamster. J Dermatol Surg Oncol1985,11:617-622
42. Woost PG, Brightwell J, Eiferman RA, Schultz GS: Effect ofgrowth factors with dexamethasone on healing of rabbit cor-neal stromal incisions. Exp Eye Res 1985, 40:47-60
43. Coleman DL: Obese and Diabetes: Two mutant genes caus-ing diabetes-obesity syndromes in mice. Diabetologia 1978,14:141-148
44. Morgan CR, Lazarow A: Immunoassay of insulin: Two anti-body system plasma levels of normal, subdiabetic and dia-betic rats. Diabetes 1963,12:115-126
45. Kelly JD, Raines EW, Ross R, Murray MJ: The B chain ofPDGF alone is sufficient for mitogenesis. EMBO J 1985, 4:3339-3405
46. Lobb R, Sasse J, Sullivan R, Shing Y, D'Amore P, JacobsJ, Klagsbrun M: Purification and characterization of heparin-binding endothelial cell growth factors. J Biol Chem 1986,261:1924-1928
47. Raines EW, Ross R: Purification of human platelet derivedgrowth factor. Meth Enzymol 1985,109:749-773
48. Linton M, Gallo PS Jr, Logan CA: The Practical Statistician:A Simplified Handbook of Statistics. Monterey, CA, Brooks/Cole Publishing Co., 1975, pp 107-111
49. Daniel WW: Applied Nonparametric Statistics. Boston, MA,Houghton Mifflin Co., 1978, pp 211-214
50. Linton M, Gallo PS Jr, Logan CA: The Practical Statistician:A Simplified Handbook of Statistics. Monterey, CA, Brooks/Cole Publishing Co., 1975, pp 316-323
51. Mordes JP, Rossini AA: Animal models of diabetes. Am JMed 1981, 70:353-360
52. Coleman DL: Diabetes-obesity syndromes in mice. Diabetes1982, 31 (Suppl): 1-6
53. DeBray-Sachs M, Dardenne M, Sai P, Savino W, QuiniouMC, Boillot D, Gepts W, Assan R: Anti-islet immunity andthymic dysfunction in the mutant diabetic C57BL/KsJ db/db mouse. Diabetes 1983, 32:1048-1054
54. Goodson WH Ill, Hunt TK: Studies of wound healing in exper-imental diabetes mellitus. J Surg Res 1977, 22:221-227
55. Gottrup F, Andreassen TT: Healing of incisional wounds instomach and duodenum: The influence of experimental dia-betes. J Surg Res 1981, 31:61-68
56. Seifter E, Rettura G, Padawer J, Stratford F, Kambosos D,Levenson SM: Impaired wound healing in streptozotocin dia-betes. Prevention by supplemental vitamin A. Ann Surg1981,194:42-50
57. Yue DK, McLennan S, Marsh M, Mai YW, Spaliviero J, Del-bridge L, Reeve T, Turtle JR: Effects of experimental diabe-tes, uremia, and malnutrition on wound healing. Diabetes1987,36:295-299
58. Rerup CC: Drugs producing diabetes through damage ofthe insulin secreting cells. Pharmacol Rev 1970, 22:485-518
59. Goodson WH ll, Hunt TK: Wound healing and the diabeticpatient. Surg Gynecol Obstet 1979,149:600-608
60. Goodson WH ll, Hunt TK: Deficient collagen formation byobese mice in a standard wound model. Am J Surg 1979,138:692-694
61. Goodson WH ll, Hunt TK: Wound collagen accumulation inobese hyperglycemic mice. Diabetes 1986, 35:491-495
62. Pierce GF, Mustoe TA, Lingelbach J, Masakowski VR, Gra-mates P, Deuel TF: Transforming growth factor # reversesthe glucocorticoid-induced wound healing deficit in rats:Possible regulation in macrophages by platelet-derivedgrowth factor. Proc Natl Acad Sci USA 1989, 86:2229-2233
Acknowledgments
The authors thank their colleagues in the yeast expression, pro-tein chemistry, and bioassay groups at ZymoGenetics for pro-duction and characterization of the recombinant growth factorsused herein, Paul Goodwin and Megan Lantry for their able tech-nical assistance, and Margo Rogers for preparing the manu-script. Thanks also go to the laboratory of Daniel Porte Jr., M.D.for performing the insulin radioimmunoassays. Finally, the au-thors appreciate the helpful discussions with Drs. David Heim-bach and Joe Leibovich. DGG was supported in part by theNorthwest Burn Foundation.