pattern of utilization of benzodiazepines in patients with hypertension: a pilot study
TRANSCRIPT

Strana 370 VOJNOSANITETSKI PREGLED Volumen 63, Broj 4
Correspondence to: Nevena Divac, School of Medicine, Institute for Pharmacology, Clinical Pharmacology and Toxicolofy Dr. Subotić1, 11000 Belgrade, Serbia and Montenegro, Tel. +381 11 68 44 79, e-mail: [email protected]
O R I G I N A L A R T I C L E UDC: 616.12−008.331.1−085:615.214.22
Pattern of utilization of benzodiazepines in patients withhypertension: a pilot study
Upotreba benzodiazepina kod bolesnika sa hipertenzijom:pilot studija
Nevena Divac*, Slavomir Veljković†, Zorica Nešić*, Radan Stojanović*, MilicaBajčetić*, Zorana Vasiljević‡, Milica Prostran*, Ranka Samardžić*
School of Medicine, *Department of Pharmacology, Clinical Pharmacology and Toxicology,Belgrade; School of Medicine, †Department of Physiology, Niš; Clinical Center of Serbia,
‡Institute for Cardiovascular Diseases, Belgrade
Abstract
Background/Aim. The analysis of drug prescribing in generalpractice in Serbia showed that the use of benzodiazepines ismost frequently associated with hypertension. The aim of thisstudy was to establish the correlation of the characteristics ofpatients with hypertension to antihypertensive drug therapy, andthe intake of benzodiazepines. Methods. A special questionnairewas used for interviewing the patients (n = 171) chronicallytreated for hypertenson. Statistical tests used were χ2-test andStudent's t-test. Results. No differences were noted in terms ofage, gender, education, body weight, smoking habits and bloodpressure (155±4.9/100±2.7 mmHg vs. 160±2.2/105±3.7 mmHg),between the group I (antihypertensive drugs+benzodiazepines:n = 79), and the group II (antihypertensives only: n = 92). Thepatients taking benzodiazepines received a lower number of dif-ferent antihypertensive drugs (2.3±0.09 vs. 2.7±0.10; p < 0.01),but the total antihypertensive drug load was significantly greaterthan in the group II (2.6±0.10 vs. 1.9±0.15 defined daily doses(DDD)/patient/day; p < 0.01). Benzodiazepines were taken foranxiety (62%) and hypertension (21%), rarely for insomnia,mostly once a day, at bedtime. About half the patients took ben-zodiazepines regularly for months or years aware of the risk foraddiction. Diazepam was used by 82% of the patients. The aver-age daily exposure to benzodiazepines was 0.45±0.05DDD/patient/day. The drug was bought without prescription in25% of the patients, and without consulting a physician in 12%of them. Conclusion. The study confirmed a close associationof hypertension with the use of benzodiazepines. The frequentuse of benzodiazepines in the patients with hypertension mightbe caused by an inadequate response to antihypertensive drugtherapy, besides anxiety and insomnia. The therapeutic efficacyof a long-term use of low doses of benzodiazepines in hyperten-sion requires further investigation.
Key words:benzodiazepines; diazepam; hypertension; drugutilization review; family practice.
Apstrakt
Uvod/Cilj. Analiza propisivanja lekova u opštoj praksi u Srbijipokazala je da je primena benzodiazepina najčešće povezana sa te-rapijom hipertenzije. Cilj ovog istraživanja bio je da ustanovi kore-laciju karakteristika bolesnika sa hipertenzijom i njihove antihiper-tenzivne terapije, kao i korišćenja benzodiazepina. Metode. Boles-nici (n = 171) koji su se hronično lečili od hipertenzije intervjuisanisu korišćenjem specijalno pripremljenog upitnika. Korišćene stati-stičke metode bile su χ2 test i Student t test. Rezultati. Izmeđubolesnika grupe I (antihipertenzivni lekovi + benzodiazepini;n = 79) i grupe II (samo antihipertenzivni lekovi; n = 92) nisu na-đene razlike u smislu prosečne starosti, zastupljenosti polova, ni-voa obrazovanja, gojaznosti, pušačkih navika i visine krvnog pritis-ka (155±4,9/100±2,7 mmHg : 160±2,2/105±3,7 mmHg). Bolesnicikoji su uzimali benzodiazepine (grupa I) primali su manji broj anti-hipertenzivnih lekova (2,3±0,09 : 2,7±0,10; p < 0,01), ali je ukupnoopterećenje antihipertenzivnim lekovima kod njih bilo značajnoveće nego kod bolesnika grupe II (2,6±0,10 : 1,9±0,15 definisanihdnevnih doza − DDD/bolesnik/dan; p < 0,01). Bolesnici su uzi-mali benzodiazepine zbog anksioznosti (62%) i hipertenzije (21%),retko zbog nesanice, najčešće u pojedinačnoj dnevnoj dozi i touveče pred spavanje. Oko polovine ispitanika benzodiazepine jeuzimalo redovno, više meseci ili godina, uz obaveštenost o mogu-ćnosti razvoja zavisnosti. Diazepam je lek koji je koristilo 82%bolesnika. Prosečno dnevno opterećenje benzodiazepinima izno-silo je 0,45±0,05 DDD/bolesnik/dan. Bez recepta je benzodiaze-pine nabavljalo 25% bolesnika, a 12% bez ikakve konsultacije salekarom. Zaključak. Rezultati rada potvrđuju da postoji značajnaveza između hipertenzije i primene benzodiazepina. Učestaloj pri-meni benzodiazepina kod bolesnika sa hipertenzijom verovatnodoprinosi i neadekvatan odgovor na antihipertenzivnu terapiju. Te-rapijska efikasnost hronične primene malih doza benzodiazepinakod hipertenzije zahteva dalja istraživanja.
Ključne reči:benzodiazepini; diazepam; hipertenzija; lekovi,korišćenje, izveštaji; medicina, opšta.

Volumen 63, Broj 4 VOJNOSANITETSKI PREGLED Strana 371
Divac N, et al. Vojnosanit Pregl 2006; 63(4): 370–375.
Introduction
An increased use of benzodiazepines (BZDs) has beenrecorded over the past decade in Serbia, with diazepamreaching the first place on the list of the most frequently pre-scribed drugs 1, 2. The analysis of prescribing of BZDs ingeneral practice in Serbia showed that diazepam was mostfrequently prescribed to the patients with hypertension, oftenwithout mentioning any other indication (e.g. anxiety or in-somnia) 1. A long-term use of BZDs associated with hyper-tension has been pointed out in some other studies 3, 4. Al-though a high utilization of BZDs has been correlated tovarious comorbidity and risk factors 5−7, as well as to thedoctors’ prescribing habits 8, the use of BZDs in hyperten-sion remains controversial 9.
The aim the present study was to analyze the pattern ofutilization of BZDs by interviewing the chronically treatedpatients with hypertension. An attempt was made to establisha possible correlation of the intake of BZDs with some char-acteristics of the patients, as well as with the antihyperten-sive drug therapy.
Methods
A questionnaire has been prepared for the assessment ofutilization of BZDs in patients with hypertension. However,exact data on the duration of antihypertensive therapy longerthan 5 years were not available, neither from the records ofpatients nor from the patients directly. Therefore, the patients(n = 171) who claimed to be treated for hypertension be-tween 5 and 10 years approximately were included in thisstudy.
The patients with hypertension were interviewed bythe physicians at the Institute for Nephrology and Haemo-dyalysis, the Clinical Center Niš, and at the Institute forCardiovascular Diseases, the Clinical Center of Serbia,Belgrade.
The first part of the questionnaire included generaldata (age, gender, body weight, education level, smokinghabits) and the blood pressure measured at the check-up.The names, as well as daily doses of all antihypertensivedrugs used by the patients before this visit were recorded.These data were obtained from the patients lists as noted bythe physicians.
The second part of the questionnaire included ques-tions about the use of BZDs in the period before the check-up. These questions were answered by the patients in orderto establish the "real life" pattern of the use of BZDs.
The questionnaire filling-up was anonymous: the pa-tients were informed in advance that their names would notbe recorded.
Based on the usage of BZDs, two groups of patientswere analyzed: the group I included patients treated with an-tihypertensive drugs and BZDs, and the group II includedpatients treated with antihypertensive drugs only.
The general characteristics of patients, as well as theuse of antihypertensive drugs were compared between thegroup I, and the group II.
The therapy for hypertension was analyzed regardingthe type, as well as the number of different antihypertensivedrugs used by each patient per day (monotherapy, 2, 3, 4 or 5drugs per day).
A total exposure to antihypertensive drugs of each indi-vidual patient was expressed as a sum of the number of de-fined daily doses (DDD) of all the antihypertensive drugsregularly used (DDD/patient/day). First, the number of DDDper day for every antihypertensive drug for each patient wascalculated. If a patient was taking two or more antihyperten-sive drugs, the number of DDD of all antihypertensive drugswas added up. Next, for each group of the patients, the aver-age number of DDD of antihypertensive drugs ±standard er-ror of the mean (SEM) was calculated.
The defined daily dose is a widely accepted statisticalunit for measuring drug consumption. It is the amount of adrug which is most often used for the main indication. It isindependent from the mechanism of drug action, from size ofpackage, commercial drug name, in some cases from thepharmaceutical formulation, and from its price 10. Since hy-pertension is the main indication for most drugs used by ourpatients, the use of DDD may be considered as appropriatemeasure of the total antihypertensive drugs load.
The same method was used to express the utilization ofBZD.
For testing the differences between groups, the χ2-testwas performed for nonparametric values and the Student's ttest for parametric values. Only statistically significant dif-ferences (p < 0.05) are shown in the text.
Results
Out of the total number of patients treated for hyperten-sion (n = 171), benzodiazepines were used by 46.2% (n = 79).
There were no significant differences in general char-acteristics of patients (age, gender, education level, bodyweight, smoking habits) between the group that used onlyantihypertensive therapy, and the group that used both, theantihypertensive therapy and the BZD. Also, the values ofarterial blood pressure at the check-up were similar in thesetwo groups (155±4.9 /100±2.7 mmHg in the group I, and160±2.2 / 105±3.7 mmHg in the group II) (Table 1).
Antihypertensive drugs (diuretics, ACE inhibitors, cal-cium antagonists) as monotherapy were prescribed in about22% of the patients in both groups. The polytherapy (dailyuse of 2, 3, 4 or 5 drugs) comprised various combinations ofdiuretics, beta-blockers, calcium channel antagonists andACE inhibitors (Table 2).
The analysis of the prescribed antihypertensive therapyshowed that the patients taking BZDs received significantlysmaller average number of different antihypertensive drugs(2.3±0.09 vs. 2.7±0.10; p < 0.01). However, antihypertensivedrug load expressed as the number of DDD/patient/day, inpatients taking BZDs was significantly greater than in thegroup of patients using BZDs (2.6±0.10 vs. 1.9±0.15DDD/patient/day; p < 0.01) (Table 3).
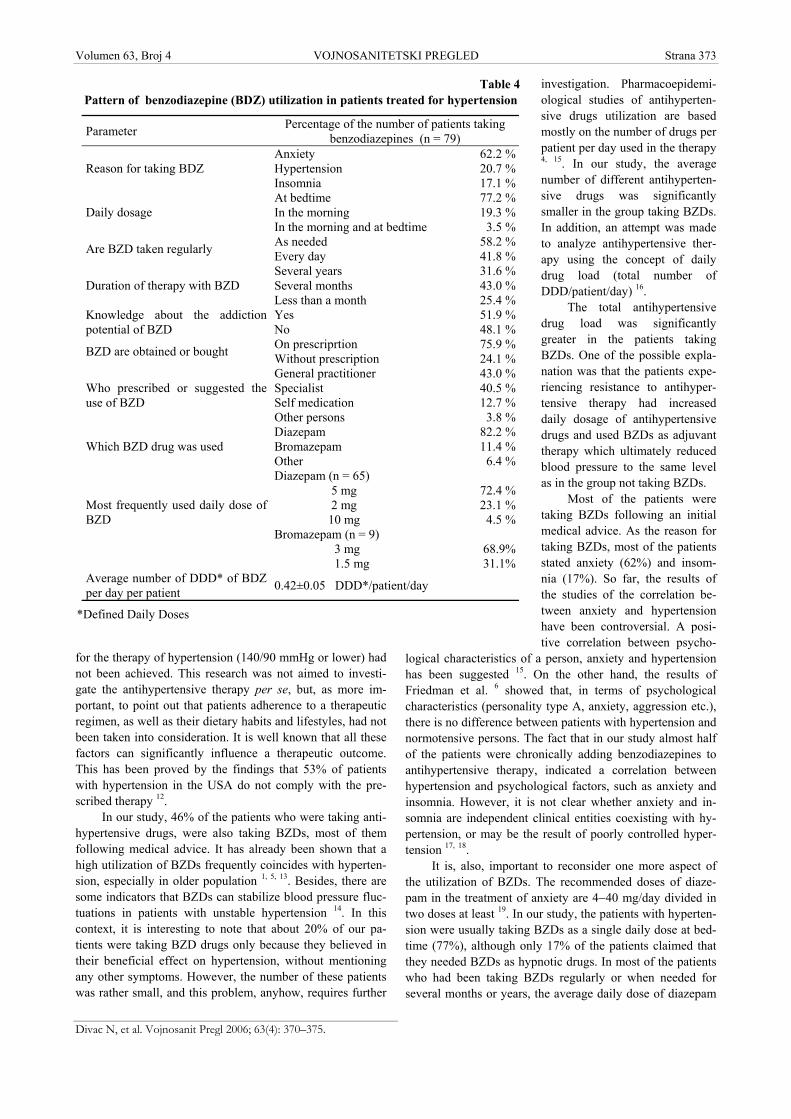
The analysis of patients taking BZDs (group I) showedthat the reason for taking BZDs was most often anxiety and

Strana 372 VOJNOSANITETSKI PREGLED Volumen 63, Broj 4
Divac N, et al. Vojnosanit Pregl 2006; 63(4): 370–375
hypertension, and rarely insomnia (Table 4). There werenot any clear indications for BZDs prescribing in patients'charts. On the other hand, a dosing regime of BZDs wasmainly once a day, predominantly taken at bedtime. Mostpatients had been using BZDs for sevaral months or years,about one half of the patients regularly, and the other halfwhen needed. Hardly half of them were aware of the risk ofgetting addicted to drugs. Most of the patients took BZDson their doctors' recommendation. Almost one fourth ofpatients used to buy BZDs without prescription. Of all theBZDs on the market, diazepam was used by the majority(83%) of the patients. The exposure to BZDs, expressed asan average number of DDDs of BZDs was 0.45±0.05DDD/patient/day.
Discussion
Our results showed that the patients treated chronicallyfor hypertension with or without BZDs, at the check-up, hadsimilar values of arterial blood pressure, independent fromthe intake of BZDs. Also, between these two groups of pa-tients, there were no significant differences in terms of age,gender, education, smoking habits nor body mass index. Theanalysis of antihypertensive therapy in both groups indicatedthat the therapeutic approach was, generally, in accordancewith the guidelines for antihypertensive therapy 11. On theother hand, the average values of arterial blood pressure atthe check-up (155/100 and 165/105 mmHg) showed that, inboth groups of the patients, the recommended target values
Table 1General characteristics of patients treated with antihypertensive
drugs with and without benzodiazepines
Characteristic
Group I(antihypertensive drugs +
benzodiazepines)(n = 79)
Group II(only antihypertensive drugs)
(n = 92)
Age (years) 52.5±1.2 53.8±1.1Gender (male) (female)
53.2 %46.6 %
58.7%41.3%
Education University Secondary school Primary school
27.5%52.7%19.6%
22.3%48.5%29.2%
SmokersNon-smokers
37.9%62.1%
44.6%55.4%
Body mass index > 30 15.2% 10.9%Arterial blood pressure 155±4.9 / 100±2.7 mmHg 160±2.2 / 105±3.7 mmHg
Table 2Average number of antihypertensive drugs used in therapy of hypertension
Number of antihypertensivedrugs
Group I(antihypertensive drugs + BZD)
n = 79
Group II(only antihypertensives)
n = 92One drug (monotherapy) 18 (22.8%) 20 (21.7%)
ACE inhibitors 10 13β blockers 6 7Ca antagonists 2 0
Two drugs 22 (27.8%) 2 (2.2%)Three drugs 36 (45.6%) 54 (58.7%)Four drugs 3 (3.8%) 16 (17.4%)
Table 3Number of antihypertensive drugs and total antihypertensive drug load expressed
as the number of Defined Daily Doses/day/patient in patients treated with antihypertensive drugswith and without benzodiazepines
ParametersGroup I
(antihypertensive drug + benzodiazepines)(n = 79)
Group II(only antihypertensive drugs)
(n = 92)Average number of antihypertensivedrugs day patient 2.3±0.001* 2.7±0.001†
Average number of DDD of allantihypertensive drugs/day/patient 2.6±0.20* 1.9±0.35†
*p < 0.05; †p < 0.01
Volumen 63, Broj 4 VOJNOSANITETSKI PREGLED Strana 373
Divac N, et al. Vojnosanit Pregl 2006; 63(4): 370–375.
for the therapy of hypertension (140/90 mmHg or lower) hadnot been achieved. This research was not aimed to investi-gate the antihypertensive therapy per se, but, as more im-portant, to point out that patients adherence to a therapeuticregimen, as well as their dietary habits and lifestyles, had notbeen taken into consideration. It is well known that all thesefactors can significantly influence a therapeutic outcome.This has been proved by the findings that 53% of patientswith hypertension in the USA do not comply with the pre-scribed therapy 12.
In our study, 46% of the patients who were taking anti-hypertensive drugs, were also taking BZDs, most of themfollowing medical advice. It has already been shown that ahigh utilization of BZDs frequently coincides with hyperten-sion, especially in older population 1, 5, 13. Besides, there aresome indicators that BZDs can stabilize blood pressure fluc-tuations in patients with unstable hypertension 14. In thiscontext, it is interesting to note that about 20% of our pa-tients were taking BZD drugs only because they believed intheir beneficial effect on hypertension, without mentioningany other symptoms. However, the number of these patientswas rather small, and this problem, anyhow, requires further
investigation. Pharmacoepidemi-ological studies of antihyperten-sive drugs utilization are basedmostly on the number of drugs perpatient per day used in the therapy4, 15. In our study, the averagenumber of different antihyperten-sive drugs was significantlysmaller in the group taking BZDs.In addition, an attempt was madeto analyze antihypertensive ther-apy using the concept of dailydrug load (total number ofDDD/patient/day) 16.
The total antihypertensivedrug load was significantlygreater in the patients takingBZDs. One of the possible expla-nation was that the patients expe-riencing resistance to antihyper-tensive therapy had increaseddaily dosage of antihypertensivedrugs and used BZDs as adjuvanttherapy which ultimately reducedblood pressure to the same levelas in the group not taking BZDs.
Most of the patients weretaking BZDs following an initialmedical advice. As the reason fortaking BZDs, most of the patientsstated anxiety (62%) and insom-nia (17%). So far, the results ofthe studies of the correlation be-tween anxiety and hypertensionhave been controversial. A posi-tive correlation between psycho-
logical characteristics of a person, anxiety and hypertensionhas been suggested 15. On the other hand, the results ofFriedman et al. 6 showed that, in terms of psychologicalcharacteristics (personality type A, anxiety, aggression etc.),there is no difference between patients with hypertension andnormotensive persons. The fact that in our study almost halfof the patients were chronically adding benzodiazepines toantihypertensive therapy, indicated a correlation betweenhypertension and psychological factors, such as anxiety andinsomnia. However, it is not clear whether anxiety and in-somnia are independent clinical entities coexisting with hy-pertension, or may be the result of poorly controlled hyper-tension 17, 18.
It is, also, important to reconsider one more aspect ofthe utilization of BZDs. The recommended doses of diaze-pam in the treatment of anxiety are 4−40 mg/day divided intwo doses at least 19. In our study, the patients with hyperten-sion were usually taking BZDs as a single daily dose at bed-time (77%), although only 17% of the patients claimed thatthey needed BZDs as hypnotic drugs. In most of the patientswho had been taking BZDs regularly or when needed forseveral months or years, the average daily dose of diazepam
Table 4Pattern of benzodiazepine (BDZ) utilization in patients treated for hypertension
Parameter Percentage of the number of patients takingbenzodiazepines (n = 79)
Reason for taking BDZAnxietyHypertensionInsomnia
62.2 %20.7 %17.1 %
Daily dosageAt bedtimeIn the morningIn the morning and at bedtime
77.2 %19.3 % 3.5 %
Are BZD taken regularly As neededEvery day
58.2 %41.8 %
Duration of therapy with BZDSeveral yearsSeveral monthsLess than a month
31.6 %43.0 %25.4 %
Knowledge about the addictionpotential of BZD
YesNo
51.9 %48.1 %
BZD are obtained or bought On prescriprtionWithout prescription
75.9 %24.1 %
Who prescribed or suggested theuse of BZD
General practitionerSpecialistSelf medicationOther persons
43.0 %40.5 %12.7 % 3.8 %
Which BZD drug was usedDiazepamBromazepamOther
82.2 %11.4 % 6.4 %
Most frequently used daily dose ofBZD
Diazepam (n = 65) 5 mg 2 mg 10 mgBromazepam (n = 9) 3 mg 1.5 mg
72.4 %23.1 % 4.5 %
68.9%31.1%
Average number of DDD* of BDZper day per patient 0.42±0.05 DDD*/patient/day
*Defined Daily Doses

Strana 374 VOJNOSANITETSKI PREGLED Volumen 63, Broj 4
Divac N, et al. Vojnosanit Pregl 2006; 63(4): 370–375
was less than a half of the recommended (defined) daily dosefor the treatment of anxiety. It is well known that the toler-ance to hypnotic effects of BZDs develops after severalweeks of the usage, while anxiolytic effect persists muchlonger. Rickels and Schweizer et al. 20, 21 have shown that allpatients who were taking BZDs over a 8-year period (with-out increasing a dose), expressed some withdrawal symp-toms once the therapy had been abruptly discontinued. About25% of these patients could not stop taking BZDs, becauseof the severity of withdrawal syndrome. A long term, con-stant use of small doses of BZDs indicated their low addic-tive potential in our patients. However, on the basis of thewell known pharmacological and pharmacokinetic charac-teristics of diazepam and other BZDs, it was easy to supposethat a long term use of low single doses of BZDs, at least insome of our patients, could have been prompted by the needto prevent unrecognized mild withdrawal symptoms, whichmight have also been manifested by anxiety, nervousness orinsomnia.
The absolute domination of diazepam over other BZDswas the consequence of its constant availability on the mar-ket, low price and popularity among both the patients anddoctors. Over a 10-year period, the utilization of BZDs dou-bled, whereas the utilization of diazepam alone trebled in
Serbia 1. Art the same time, we noted no significant increasein the use of non-BZD hypnotics, which, together with short-acting anxiolytics have a dominant role in the therapy of in-somnia 22 and anxiety 23 in the developed countries.
About 24% of the interviewed patients buy BZDs with-out prescription, and about 12% have started to take BZDswithout consulting the doctor. The posibility to buy drugswithout prescription and self-medication are common prac-tice in our country 1. The lack of control of drugs on themarket is not rare in the developing countries, and also inthose in transition 22. On the other hand, self-medication is awidespread phenomenon, related to an increasing number ofover-the-counter (OTC) drugs on the market and alternativemethods of healing24.
Conclusion
This study confirmed a close association between hy-pertension and the use of BZDs. It might be that, besidesanxiety and insomnia, an inadequate response to antihyper-tensive drug therapy contribute to the frequent use of BZD inhypertension. However, the therapeutic efficacy of a longterm use of small doses of BZDs in hypertension urges forfurther investigation.
R E F E R E N C E S
1. Divac N, Jašović M, Đukić L, Vujnović M, Babić D, Bajčetić M, etal. Benzodiazepines utilization and self-medication as corre-lates of stress in the population of Serbia. PharmacoepidemiolDrug Saf 2004; 13(5): 315–22.
2. Miljković M, Đukić Lj. Analysis of drug utilization in Serbiaduring years 1996 and 1997. Pharmacoepidemiol Drug Saf2000; 9: 59−64. (Serbian)
3. Zandstra SM, Furer JW, van de Lisdonk EH, Bor JH, Zitman FG,van Weel C. Differences in health status between long-term andshort-term benzodiazepine users. Br J Gen Pract 2002;52(483): 805–8.
4. Yusuff KB, Balogun OB. Pattern of drug utilization among hy-pertensives in a Nigerian teaching hospital. Pharmacoepide-miol Drug Saf 2005; 14(1): 69–74.
5. Alvarez A, Clara JG. Polypharmacotherapy in the elderly hy-pertensive patient. Rev Port Cardiol 1994; 13(7–8): 587–92,563. (Portuguese)
6. Friedman R, Schwartz JE, Schnall PL, Landsbergis PA, Pieper C,Gerin W, et al. Psychological variables in hypertension: rela-tionship to casual or ambulatory blood pressure in men. Psy-chosom Med 2001; 63(1): 19–31.
7. Lagnaoui R, Moore N, Longy-Boursier M, Baumevieille M, Begaud B.Benzodiazepine use in patients hospitalized in a department ofinternal medicine: frequency and clinical correlates. Pharmaco-epidemiol Drug Saf 2001; 10(6): 531–5.
8. Boixet M, Batlle E, Bolibar I. Benzodiazepines in primary healthcare: a survey of general practitioners prescribing patterns.Addiction 1996; 91(4): 549–56.
9. Franchi F, Puddu GM. The heart and central nervous system.Benzodiazepines in cardiovascular psychosomatic medicine.Clin Ter 1990; 134(5): 307–12. (Italian)
10. WHO Collaborating Center for Drug Statistics MethodologyATC/DDD. [updated 2006 Nov 11]. Available from:www.whocc.no/atcddd
11. Izhar M, Bakris G. Hypertension. In: Conn HF, Rakel RE, edi-tors. Conn's Current Therapy 2002. Latest Approved Methodsof Treatment for the Practicing Physician. Philadelphia: W.B.Saunders Company; 2002. p. 319−33.
12. Nelson EC, Stason WB, Neutra RR, Solomon HS. Identification ofthe noncompliant hypertensive patient. Prev Med 1980; 9(4):504–17.
13. Kruse W, Rampmaier J, Frauenrath-Volkers C, Volkert D, Wank-muller I, Micol W, et al. Drug-prescribing patterns in old age. Astudy of the impact of hospitalization on drug prescriptionsand follow-up survey in patients 75 years and older. Eur J ClinPharmacol 1991; 41(5): 441–7.
14. Dmitriev KV, Fedorova VI, Nedostup AV. Clonazepam in thetreatment of labile arterial hypertension in the elderly. TerArkh 2001; 73(3): 58–61. (Russian)
15. Ohene Buabeng K, Matowe L, Plange-Rhule J. Unaffordable drugprices: the major cause of non-compliance with hypertensionmedication in Ghana. J Pharm Pharm Sci 2004; 7(3): 350–2.
16. Marić N. Đorđević A, Samardžić R, Jašović-Gašić M. Antipsychot-ics − towards unified dosage comparison. Psihijat Dan 2000;32(2−3): 95−103. (Serbian)
17. Markovitz JH, Matthews KA, Kannel WB, Cobb JL, D'Agostino RB.Psychological predictors of hypertension in the FraminghamStudy. Is there tension in hypertension? JAMA 1993; 270(20):2439–43.
18. Rostrup M, Ekeberg O. Awareness of high blood pressure influ-ences on psychological and sympathetic responses. J Psycho-som Res 1992; 36(2): 117–23.
19. Holister LE. Treatment of psychiatric disorders. In: CarruthersSG, Hoffman BB, Melmon KL, Nierenberg DW, editors. Melmonand Morrelli's Clinical Pharmacology. 4th ed. New York:McGraw Hill; 2000. p. 489−528.
20. Rickels K, Schweizer E, Case WG, Greenblatt DJ. Long-termtherapeutic use of benzodiazepines. I. Effects of abrupt dis-continuation. Arch Gen Psychiatry 1990; 47(10): 899–907.

Volumen 63, Broj 4 VOJNOSANITETSKI PREGLED Strana 375
Divac N, et al. Vojnosanit Pregl 2006; 63(4): 370–375.
21. Schweizer E, Rickels K, Case WG, Greenblatt DJ. Long-termtherapeutic use of benzodiazepines. II. Effects of gradual ta-per. Arch Gen Psychiatry 1990; 47(10): 908–15.
22. Rayon P, Serrano-Castro M, del Barrio H, Alvarez C, Montero D,Madurga M, et al. Hypnotic drug use in Spain: a cross-sectionalstudy based on a network of community pharmacies. SpanishGroup for the Study of Hypnotic Drug Utilization. AnnPharmacother 1996; 30(10): 1092–100.
23. Skaer TL, Robinson L, Sclar RS. Anxiety disorders in the USA,1990 to 1997 − Trend in Complaint, Diagnosis, Use of Phar-macotherapy and Diagnosis of Comorbid Depression. ClinDrug Invest 2000; 20(4): 237−44.
24. Pilsczek FH. Survey of drugs sold in pharmacies in Afghani-stan. Pharmacoepidemiol Drug Saf 1999; 8(1): 45–9.
The paper was received on Jun 20, 2005.